DR BA SHI RU AMI NU Surgical site infections

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 1/78
D R B AS H IR U A M IN U
Surgical site infections
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 2/78
outline
y Introduction
y Definition
y Historical perspective
y
Epidemiology y pathogenesis
y aetiology
y Classification
y
Clinical featuresy Management
y conclusion

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 3/78
introduction
y Surgical site infections continue to be a majorchallenge
y in spite of various advances in science
y It is responsible for significant increase in mortality ,morbidity &hospital stay
y This means more expenditure

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 4/78
definitions
y Infection occurring at site of operation or surgicaltract within thirty days of surgery or one year ff
implant surgerys

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 5/78
Historical perspective
y Edwin smith(circa 1600 bc), ebers papyrus(circa1534)
y Hippocrates (460ad-377bc)
y Galen laudable pus theory

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 6/78
14th century at the time of ambrose pare(1510-1590)
y Koch (1843-1910) recognized septic foci as result of microbial growth
y Semmelweis(1818-1865) reduction in puerperalsepsis

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 7/78
y Pasteur revolutionarized concept of wound infection
y Lister(1827-1912) used carbolic acid
y Antoine depagne(1862-1925) reintroduced
debridment & delayed closure
y Alexander fleming(1881-1955)of penicillin

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 8/78
y Halsted introduced rubber gloves to his scrub nurse who allergic to materials used in sterilizinginstruments
y His student J. bloodgood made it routine use

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 9/78
epidemiology
y frequency of SSI difficult to monitor
y A survey by WHO infections varying from 3-21%, with wound infections accounting for 5-34% of the
total.y The 2002 report (NINSS) Oct 97 and Sept 2001,
shows rates of 10% costing1 billion pounds annually.
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 10/78
y 75% of deaths in surgical patients is related to SSI
y Actual estimates difficult to make here due to paucity of data

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 11/78
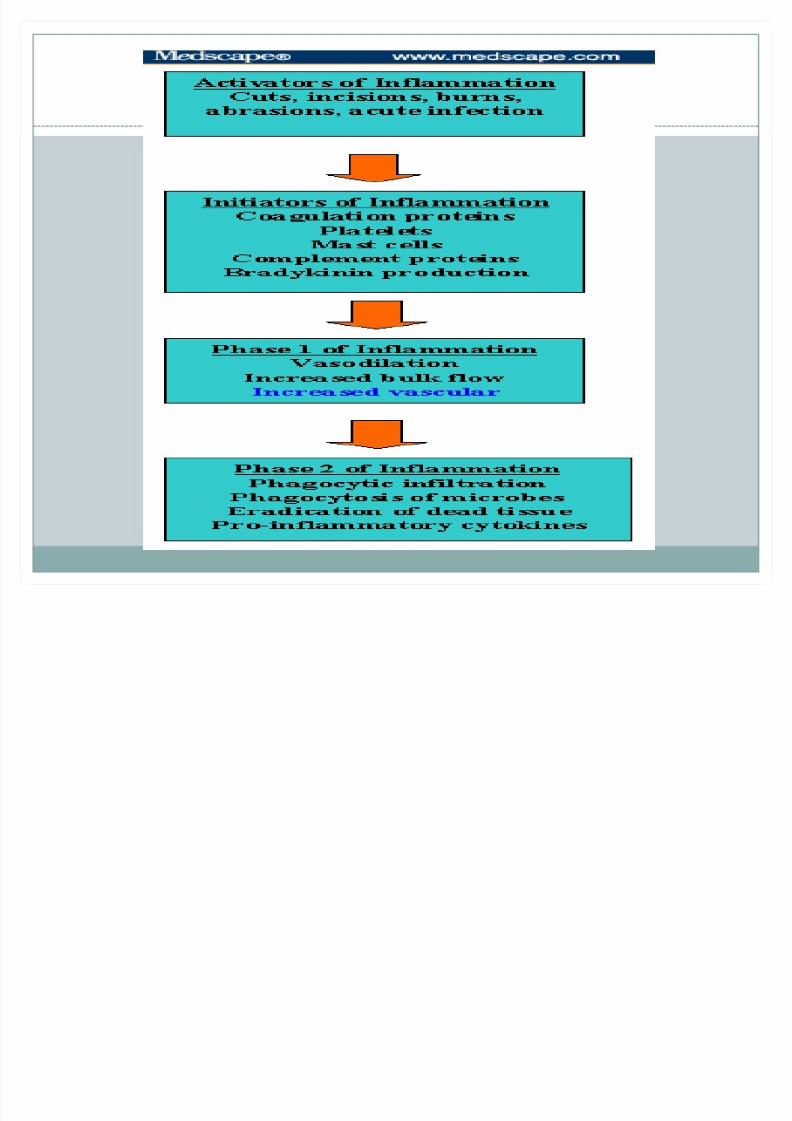
pathogenesis
y With incision on skin 5 critical initiators of inflammatory response are activated
y Coagulation proteins
y platelets
y part of the hemostatic mechanism
y herald the onset of inflammation.
y
Mast cells ,complement proteins
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 12/78

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 13/78
y bradykinin is produced from protein precursors.
y The net effect of 5 factors is vasodilation andincreased blood flow

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 14/78
y products from 5 initiators result in nonspecificchemoattractant signals,
y mast cells produce specific chemokine signals that
"draw" specific neutrophil, monocyte, etc

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 15/78
y The point is that tissue injury initiates mobilizationof phagocytes into the wound before contaminationoccurs
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 16/78
aetiology
y All surgical wounds are contaminated
y most cases, infection does not develop because hostdefenses are efficient
y A complex interplay between host, microbial, andsurgical factors
y ultimately determines prevention or establishmentinfection.
y Factors that affect surgical wound healing areclassified below

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 17/78
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 18/78
microbiology
y Microbial factors are;
y the dose of inoculum,
y virulence,
y Microenvironment
y impaired host defenses
y patient's own endogenous flora

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 19/78
y The traditional microbial concentration is bacterialcounts higher than 10,000 organisms per gram of tissue (or in the case of burned sites, organisms per
cm2
of wound).

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 20/78
y largest inoculum is structure ordinarily heavily colonized eg bowel.
y distal small intestine and colon have large concn of
bacteria with 103 - 104 bacteria/mL of distal small bowel content,
y 105 - 106 bacteria/mL in the right colon, and 1010 -1012 bacteria/g of stool in the rectosigmoid colon.

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 21/78
y Large amts also present in stomach of older patients with hypo- or achlorhydria.
y Significant concn in biliary tract when patients are
over 70 years of agey or have obstructive jaundice etc

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 22/78
y Procedures in female genital tract will encounter 106
- 107 bacteria/mL.
y Procedures in oropharynx, lung, or urinary tract
have significant contaminantsy Notably, SSIs are generally consequence of intra
operative contamination
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 23/78
y The most bacteria responsible for SSIs Staphylococcus aureus.
y The emergence of resistant strains considerably
increased burden of morbidity and mortality
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 24/78
y skin and mucosal surfaces ; gram-positive cocci(notably staphylococci)
y G-ve aerobes and anaerobic bacteria contaminateskin in the groin/perineal areas.
y Contaminants in GIT surgery are bowel flora
y which include g-ve bacilli (eg, E coli ), g+s,enterococci

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 25/78
y G+ particularly staph & strep are main exogenousflora in SSIs.
y Sources of such pathogens include ;
y surgical/hospital personnely intra operative circumstances, instruments,
operating room air.
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 26/78
y Methicillin resistant Staphylococcus aureus (MRSA)
y MRSA colonize skin ,body of individual withoutcausing sickness,
y this way, it can be passed on to other individuals
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 27/78
y Systemic factors include;
y age, malnutrition, hypovolemia, poor tissueperfusion
y obesity, diabetes, steroids,y Immuno suppressants.
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 28/78
y Wound characteristics include;
y nonviable tissue in wound; hematoma;
y foreign material, including drains and sutures;
y dead space; poor skin prep +shaving
y and preexistent sepsis (local or distant).

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 29/78
y Operative chrxs include poor surgical technique;
y lengthy operation (>2 h);
y intraoperative contamination, eg theater staff and
instrumentsy inadequate theater ventilation;

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 30/78
y prolonged preop stay
y hypothermia.
y The type of procedure is a risk factor.

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 31/78

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 32/78

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 33/78
Vacuum-assisted wound closure
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 34/78
classification
y Various classifications
y traditional developed in wake of uv light study of 1964
y Primarily to provide clinical estimate of inoculum of bacteria
y does not take into cognisance factors like;
y virulence, host defences, microenvironment of the wound
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 35/78
y Clean Wounds
y does not enter into a colonized viscus or lumen
y eg elective inguinal hernia repair
y SSI risk is minimal
y common pathogen is Staphylococcus aureus
y SSI rates is 2% or less
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 36/78
y Clean-Contaminated Wounds
y enters colonized viscus or cavity under elective
y contaminants are endogenous bacteria
y Eg sigmoid colectomy wounds contain E coli and Bacteroides fragilis

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 37/78
y Elective intestinal resection, pulmonary resection,gynecologic procedures, and head-neck cancer op inoropharynx are examples
y Infection rates in the range of 4% to 10%

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 38/78
y Contaminated Wounds
y gross contamination present in absence of obviousinfection.
y eg laparotomy for penetrating injury +intestinalspillage
y contaminants bacteria introduced by gross soilage
y Infection rates greater than 10%
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 39/78
y Dirty Wounds
y active infection is already present
y Abdominal exploration for acute bacterial peritonitis
and intra-abdominal abscess are examplesy Pathogens those of active infection
y Unusual pathogens are seen
y
Esp if infection occurred in hospital or nursing homesetting

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 40/78
y US CDC developed the NNIS Risk Index system
y member hospitals report cumulative data.
y A risk index developed to include ;
y traditional wound classification system definedabove and additional variables.
y This simplified risk index has a range from 0 to 3points.
y A point is added to the patient's risk index for eachof the following 3 variables:

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 41/78
y This simplified risk index has a range from 0 to 3points.
y A point is added to the patient's risk index for each
of the following 3 variables

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 42/78
y 1 point - the patient had operation classified as eithercontaminated or dirty.
1 point - the patient has an ASA preoperativeassessment score of 3, 4, or 5
1 point - the duration of operation exceeds the 75th
percentile

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 43/78
y standard T point (75% percentile) determined fromNNIS database
y the T point defined as length of time in hours that
represents the 75th percentile of procedures

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 44/78
y Table 1. Ph ysical Status Classification f or Surgical Patients
y Class I A patient in normal health
y Class II A patient with mild systemic diseaseresulting in no functional limitations
y Class III A patient with severe systemic disease thatlimits activity, but is not incapacitating

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 45/78
y Class IV A patient with severe systemic disease thatis a constant threat to life
y Class V A moribund patient not likely to survive 24
hours
O i T i (h )
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 46/78
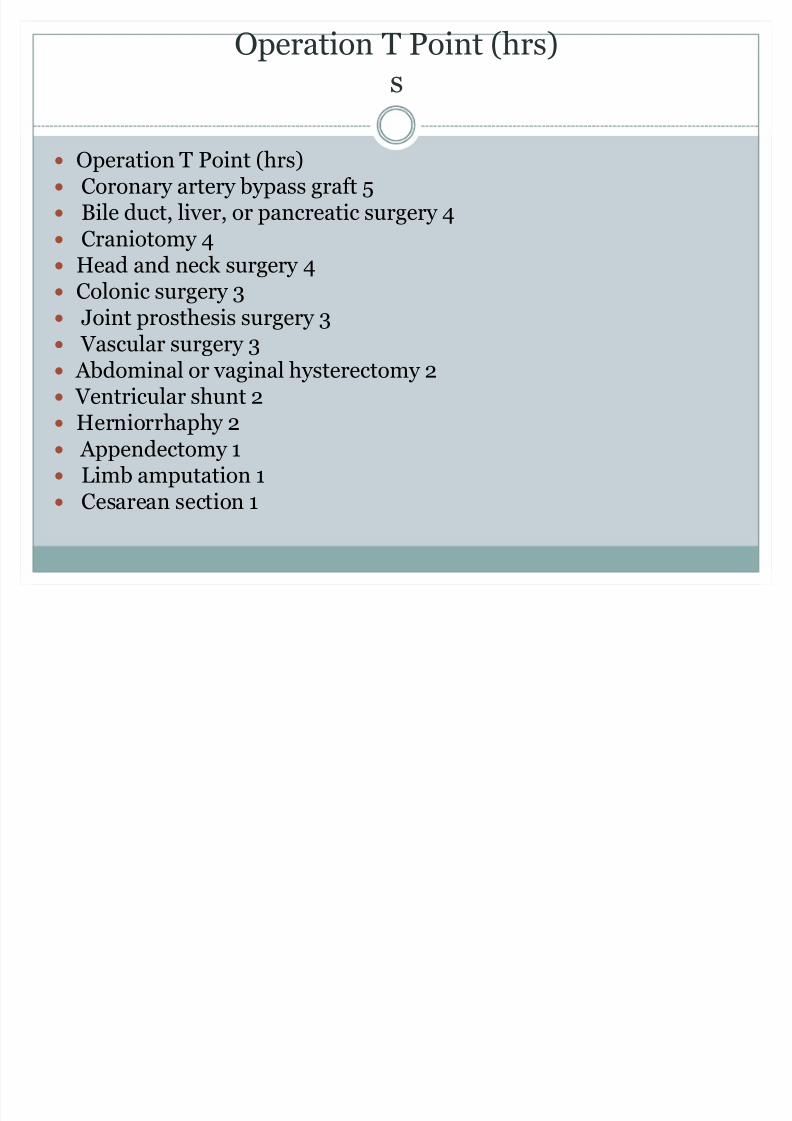
Operation T Point (hrs)s
y Operation T Point (hrs)y Coronary artery bypass graft 5y Bile duct, liver, or pancreatic surgery 4y Craniotomy 4y Head and neck surgery 4y Colonic surgery 3y Joint prosthesis surgery 3y Vascular surgery 3y Abdominal or vaginal hysterectomy 2y Ventricular shunt 2
y Herniorrhaphy 2y Appendectomy 1y Limb amputation 1y Cesarean section 1

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 47/78
y newer definitions of superficial incisional SSI, deepincisional SSI, and organ space SSI
y This methodology, + NNIS Risk Index, allows
recognition of SSI rates + classification of severity.y Reporting of data stratified by risk and severity

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 48/78
S fi i l I i i l SSI

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 49/78
Superficial Incisional SSI
y Occurs within 30 days after the operation;
y Involves only the skin or subcutaneous tissue; and
y At least 1 of the following:
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 50/78
Purulent drainage (culture documentation not required)
Organisms isolated from fluid/tissue of superficial incision
At least 1 sign of inflammation (eg, pain or tenderness,induration, erythema, local warmth of the wound)

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 51/78
y Deep Incisional SSIy Occurs within 30 days of operation or within 1 year if an
implant is present;
y Involves deep soft tissues (eg, fascia and/or muscle) of the incision; and
y At least 1 of the following:
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 52/78
y Purulent drainage from deep incision minus organ/spaceinvolvement
Fascial dehiscence or fascia separated by the surgeon
Deep abscess identified by during reoperation,histopathology, radiologically
Surgeon declares deep incisional infection is present.

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 53/78

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 54/78
Wound is deliberately opened by the surgeon
Surgeon or attending physician declares the wound infected.
Organ/Space SSI

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 55/78
Organ/Space SSI
y Organ/Space SSI
y Occurs within 30 days of operation or within 1 year if animplant is present;
y Involves structures not opened or manipulated operation
y At least 1 of the following:

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 56/78
y Purulent drainage from a drain placed by a stab wound
y Organisms isolated from organ/space by aseptic culturing technique
y
Identification of abscess in the organ/space by direct examination,during reoperation, or by histopathologic or radiologic examination
y Diagnosis of organ/space SSI by surgeon

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 57/78
w ound grading Southampton system
0 ± normal healing
1 ± normal healing with mild bruising/erythema
2 ±
Erythema + other signs of inflammation3- Clear or heamoserous discharge
4- Pus
5-Deep or severe wound infection with or without
tissue breakdown

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 58/78
ASEPSIS wound score
y A dditional treatment Antibiotic for wound infection 10Drainage of pus under LA 5Debridement of wound under GA 10
Serous discharge Daily 0-5Erythema Daily 0-5Purulent exudation Daily 0-10Separation of deep tissues Daily 0-10Isolation of bacteria 10
Stay greater than 14 days 5

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 59/78
Clinical features
y Most have been mentioned along line
y Local features which vary depending on stage, type
y Erythema , swelling, discharge, gaping wound,
dehiscencey Systemic symtoms; fever, weight loss from increased
catabolic loss
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 60/78
Major w ound infectiondefined as a wound that either discharge significantquantity of pus spontaneously or secondary procedure to drain it +/- systemic signs
Minor w ound infectionsthis may discharge pus or infected serous fluid butnot excessive s
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 61/78
Systemic manifestations
y Sepsis is the systemic manifestation of adocumented infection
y SIRS is the body systemic response to an infected wound
y MODS is the effect that the infection has on the whole body
y MSOF is the end stage of uncontrolled MODS

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 62/78
management
y Detailed history y Thorough physical examinationy Relevant investigations
Gram stain
Culture (both aerobic and anaerobic)Sensitivity testing Antigen and antibody testingDetecting of RNA and DNA sequencingPCR

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 63/78
y Staining methods;Gram stain
y Staining for fungal elements
y Culture techniques
y Fungal cultures can be requested

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 64/78
y Isolation of single colonies allows further growthand identification of the specific organism.
y Sensitivity testing then follows mainly for aerobic
organisms.y Newer techniques ELISA, radioimmunoassay

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 65/78
y Detection of antibody in host sera
y Detection of RNA or DNA sequences by Northern,Southern, or Western blotting, respectively
y Polymerase chain reaction (PCR)y FBC, FBS, U/E,SERUM PROTEINS

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 66/78
y Imaging Studies
y Ultrasound can be applied to the infected woundarea to assess whether any collection needs drainage.
y MRI, CT SCAN
TREATMENT

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 67/78
TREATMENT
Local-Drainage
-DebridementSystemic
-resuscitation-appropriate antibiotics
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 68/78
prevention
yPrinciples
ySpecific 1- removal of source of infection
2 - block transfer
3 - increase patient resistance
General 1- Infrastructure
theatre design
2 - Administrative policiesantibiotic policies
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 69/78
y patients to shower and scrub the surgical site withantiseptic soap
y dont shave or clipp evening before operation.
y Nicks and scrapes result in colonizationy Depilatory agents recommended
y occasionally result in a hypersensitivity

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 70/78
y The presence of open skin wounds or infection of thehands or arms of the surgeon makes postponementof the operation desirable.
y
If the patient has any preexisting infection, SSI will be more likely.

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 71/78
y Prevention in the OR begins with the skinpreparation
y The site is cleansed with chlorhexidine or
povidone iodine.y Isopropyl alcohol has excellent antiseptic qualities
but is undesirable because of its flammability

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 72/78
y Povidone iodine should be allowed to dry before theincision
y use of caps, gowns, masks, and sterile surgical
gloves.y Double gloving prevents blood "strike through" onto
the surgeon's hands
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 73/78
y Avoid blood ,fluid breakthrough especially onsurgeon's forearms
y Avoid wet drapes
y replace soaked gown &drapes.y Wide areas of skin prep around surgical site reduces
risk of breakthrough
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 74/78
y Gas sterilization of instruments after thoroughcleansing of any particulate matter
y Bowel prep
y Achieving hemostasis at the surgical site isimportant

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 75/78
y process of controlling bleeding may itself increaseinfection.
y HB in soft tissues or wound space Is potent stimulus
to microbial multiplicationy exuberant use of electro cautery leaves necrotic
tissue

8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 76/78
y Prophylactic antibioticsReduces incidence of post-op wound infections
Directed against likely bacteria
Given 30-60mins before operation
Repeated if operation >4hours
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 77/78
± Incision should destroy as little tissue as possible(incisionmade through entire skin layer)
- Tissue plane divided with few passes of the knife always
beginning a new pass in the depths of the wound ± Ensure bleeding has stopped before closing wound
8/9/2019 Surgical Site Infections (2)
http://slidepdf.com/reader/full/surgical-site-infections-2 78/78
Avoid wound edge desication
Proper wound edge apposition
Use of few sutures
Related Documents











