CONTINUING EDUCATION Surgical Risk Factors in Geriatric Perioperative Patients MARIE BASHAW, MS, RN, NEA-BC, CNOR; DANA N. SCOTT, BSN, RN 2.9 www.aorn.org/CE Continuing Education Contact Hours indicates that continuing education contact hours are available for this activity. Earn the contact hours by reading this article, reviewing the purpose/goal and objectives, and completing the online Examination and Learner Evaluation at http://www.aorn.org/CE. A score of 70% correct on the examination is required for credit. Participants receive feed- back on incorrect answers. Each applicant who successfully completes this program can immediately print a certificate of completion. Event: #12520 Session: #0001 Fee: Members $14.50, Nonmembers $29 The contact hours for this article expire July 31, 2015. Purpose/Goal To educate perioperative nurses about surgical risk factors in older adults undergoing surgical interventions. Objectives 1. Describe the changes associated with aging. 2. Discuss the nurse’s role in caring for geriatric patients in the OR. Accreditation AORN is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. Approvals This program meets criteria for CNOR and CRNFA recertifi- cation, as well as other continuing education requirements. AORN is provider-approved by the California Board of Registered Nursing, Provider Number CEP 13019. Check with your state board of nursing for acceptance of this activity for relicensure. Conflict of Interest Disclosures Marie Bashaw, MS, RN, NEA-BC, CNOR, and Dana N. Scott, BSN, RN, have no declared affiliations that could be perceived as posing potential conflicts of interest in the publication of this article. The behavioral objectives for this program were created by Helen Starbuck Pashley, MA, BSN, RN, CNOR, clinical editor, and Susan Bakewell, MS, RN-BC, director, Perioper- ative Education. Ms Starbuck Pashley and Ms Bakewell have no declared affiliations that could be perceived as posing potential conflicts of interest in the publication of this article. Sponsorship or Commercial Support No sponsorship or commercial support was received for this article. Disclaimer AORN recognizes these activities as continuing education for registered nurses. This recognition does not imply that AORN or the American Nurses Credentialing Center approves or endorses products mentioned in the activity. doi: 10.1016/j.aorn.2011.05.025 58 j AORN Journal July 2012 Vol 96 No 1 Ó AORN, Inc, 2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
CONTINUING EDUCATION
Surgical Risk Factors in GeriatricPerioperative PatientsMARIE BASHAW, MS, RN, NEA-BC, CNOR; DANA N. SCOTT, BSN, RN 2.9
www.aorn.org/CE
Continuing Education Contact Hoursindicates that continuing education contact hours are
available for this activity. Earn the contact hours by reading
this article, reviewing the purpose/goal and objectives, and
completing the online Examination and Learner Evaluation
at http://www.aorn.org/CE. A score of 70% correct on the
examination is required for credit. Participants receive feed-
back on incorrect answers. Each applicant who successfully
completes this program can immediately print a certificate of
completion.
Event: #12520
Session: #0001
Fee: Members $14.50, Nonmembers $29
The contact hours for this article expire July 31, 2015.
Purpose/GoalTo educate perioperative nurses about surgical risk factors in
older adults undergoing surgical interventions.
Objectives
1. Describe the changes associated with aging.
2. Discuss the nurse’s role in caring for geriatric patients
in the OR.
AccreditationAORN is accredited as a provider of continuing nursing
education by the American Nurses Credentialing Center’s
Commission on Accreditation.
58 j AORN Journal � July 2012 Vol 96 No 1
ApprovalsThis program meets criteria for CNOR and CRNFA recertifi-
cation, as well as other continuing education requirements.
AORN is provider-approved by the California Board of
Registered Nursing, Provider Number CEP 13019. Check with
your state board of nursing for acceptance of this activity for
relicensure.
Conflict of Interest DisclosuresMarie Bashaw, MS, RN, NEA-BC, CNOR, and Dana N. Scott,
BSN, RN, have no declared affiliations that could be perceived
as posing potential conflicts of interest in the publication of
this article.
The behavioral objectives for this program were created
by Helen Starbuck Pashley, MA, BSN, RN, CNOR, clinical
editor, and Susan Bakewell, MS, RN-BC, director, Perioper-
ative Education. Ms Starbuck Pashley and Ms Bakewell have
no declared affiliations that could be perceived as posing
potential conflicts of interest in the publication of this article.
Sponsorship or Commercial SupportNo sponsorship or commercial support was received for this
article.
DisclaimerAORN recognizes these activities as continuing education for
registered nurses. This recognition does not imply that AORN
or the American Nurses Credentialing Center approves or
endorses products mentioned in the activity.
doi: 10.1016/j.aorn.2011.05.025
� AORN, Inc, 2012
P
Surgical Risk Fac
tors in GeriatricPerioperative PatientsMARIE BASHAW, MS, RN, NEA-BC, CNOR; DANA N. SCOTT, BSN, RN 2.9www.aorn.org/CE
ABSTRACT
The geriatric population is growing in number, and risk factors commonly seen in
this population of patients can seriously affect the outcomes of surgical interven-
tions. Identification of surgical risk factors (eg, hearing and vision loss, inadequate
nutrition, preexisting conditions) and early intervention by the perioperative nurse
to plan for, correct, or accommodate physical limitations often can minimize or
eliminate problems and potential complications. AORN J 96 (July 2012) 59-71. �AORN, Inc, 2012. doi: 10.1016/j.aorn.2011.05.025
Key words: geriatric surgical risk factors, geriatric patients, risk factors.
ersons 65 years of age and older make up
the fastest growing segment of the world’s
population (Figure 1).1 This increase can be
attributed to healthier lifestyles, better preventative
care, and advances in health care.2 In addition, be-
cause of advances in health care, geriatric patients,
once considered poor candidates for surgery because
of complex comorbidities and advancing age, are
now considered appropriate surgical patients.3
Preexisting conditions and normal changes
related to aging, however, can result in perioper-
ative complications in the geriatric patient. The
seriousness of the complication depends on the
patient’s specific preexisting condition or aging
changes. Early intervention, including postponing
the surgical procedure for patients with modifiable
risk factors, may reduce morbidity and mortality
rates in the geriatric surgical patient population.4
CHANGES SPECIFIC TO GERIATRICPATIENTS
Aging affects every body system to some extent,
with some systems more seriously affected than
doi: 10.1016/j.aorn.2011.05.025
� AORN, Inc, 2012
others. In general, aging affects the older adults’
ability to process information and to interpret
and physically navigate their environment. This
in turn affects how older adults experience surgery
and, without careful planning for nursing care
(Table 1), can alter the outcomes of any surgery
the patient undergoes.
Hearing and Vision
Changes in vision occur in older adults and include
decreased visual acuity because of lens thickening
and decreased light sensitivity.2 Aging also changes
the ear and hearing of older adults. This includes
an increase in cerumen accumulation, which can
block the ear canal and reduce hearing, and sensory
hair cell loss and organ of Corti atrophy, which
also affect the ability to hear.2
Hearing and vision losses can prevent geriat-
ric patients from understanding preoperative and
postoperative instructions.5 To ensure that the pa-
tient can understand this information, the nurse
should assess the patient for hearing deficits and
whether he or she uses assistive devices (eg,
July 2012 Vol 96 No 1 � AORN Journal j 59
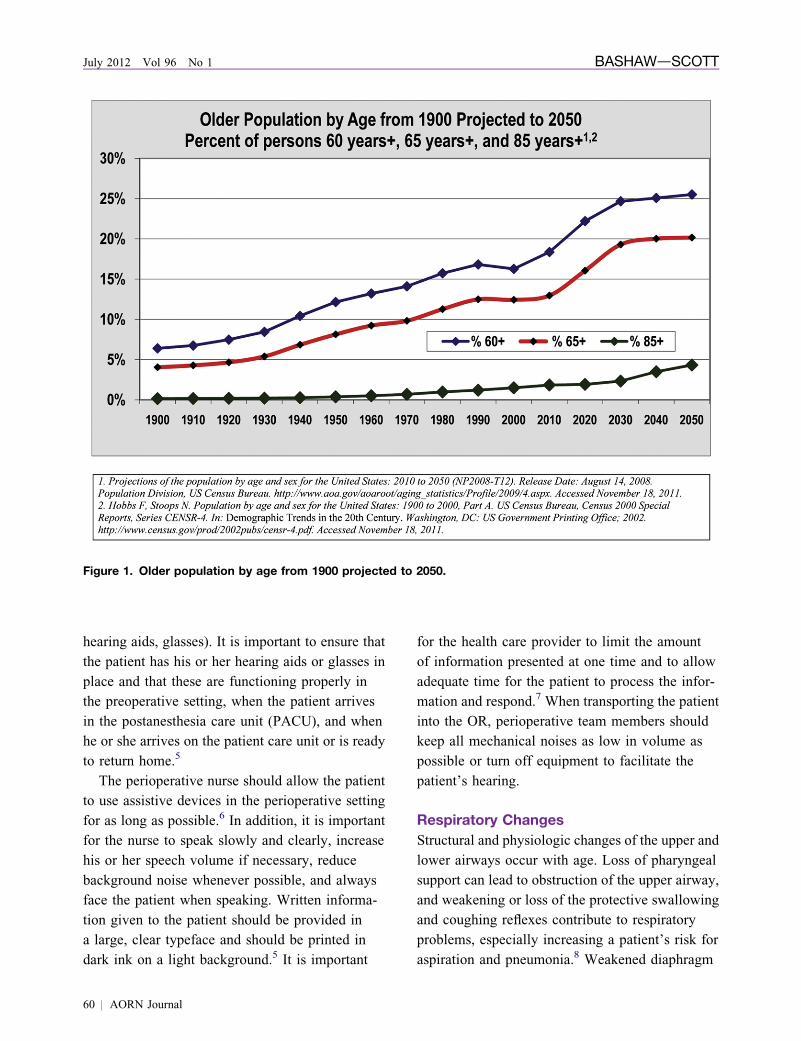
Figure 1. Older population by age from 1900 projected to 2050.
July 2012 Vol 96 No 1 BASHAWdSCOTT
hearing aids, glasses). It is important to ensure that
the patient has his or her hearing aids or glasses in
place and that these are functioning properly in
the preoperative setting, when the patient arrives
in the postanesthesia care unit (PACU), and when
he or she arrives on the patient care unit or is ready
to return home.5
The perioperative nurse should allow the patient
to use assistive devices in the perioperative setting
for as long as possible.6 In addition, it is important
for the nurse to speak slowly and clearly, increase
his or her speech volume if necessary, reduce
background noise whenever possible, and always
face the patient when speaking. Written informa-
tion given to the patient should be provided in
a large, clear typeface and should be printed in
dark ink on a light background.5 It is important
60 j AORN Journal
for the health care provider to limit the amount
of information presented at one time and to allow
adequate time for the patient to process the infor-
mation and respond.7 When transporting the patient
into the OR, perioperative team members should
keep all mechanical noises as low in volume as
possible or turn off equipment to facilitate the
patient’s hearing.
Respiratory Changes
Structural and physiologic changes of the upper and
lower airways occur with age. Loss of pharyngeal
support can lead to obstruction of the upper airway,
and weakening or loss of the protective swallowing
and coughing reflexes contribute to respiratory
problems, especially increasing a patient’s risk for
aspiration and pneumonia.8 Weakened diaphragm
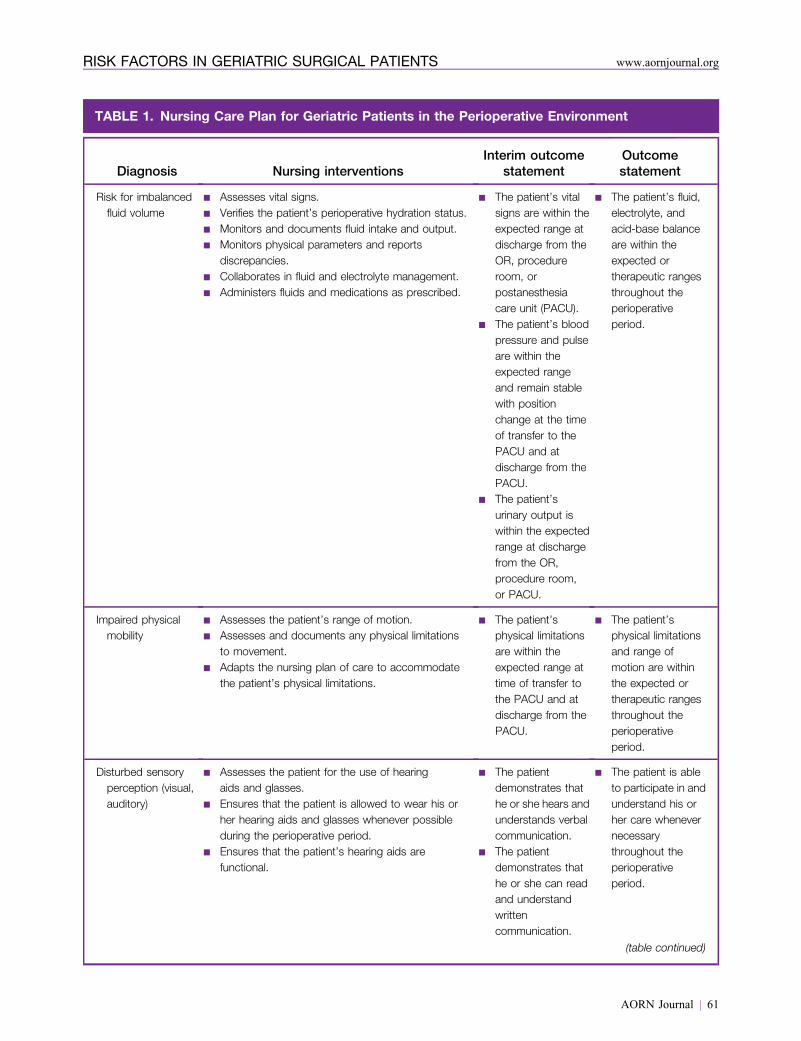
TABLE 1. Nursing Care Plan for Geriatric Patients in the Perioperative Environment
Diagnosis Nursing interventionsInterim outcome
statementOutcomestatement
Risk for imbalancedfluid volume
n Assesses vital signs.n Verifies the patient’s perioperative hydration status.n Monitors and documents fluid intake and output.n Monitors physical parameters and reports
discrepancies.n Collaborates in fluid and electrolyte management.n Administers fluids and medications as prescribed.
n The patient’s vitalsigns are within theexpected range atdischarge from theOR, procedureroom, orpostanesthesiacare unit (PACU).
n The patient’s bloodpressure and pulseare within theexpected rangeand remain stablewith positionchange at the timeof transfer to thePACU and atdischarge from thePACU.
n The patient’surinary output iswithin the expectedrange at dischargefrom the OR,procedure room,or PACU.
n The patient’s fluid,electrolyte, andacid-base balanceare within theexpected ortherapeutic rangesthroughout theperioperativeperiod.
Impaired physicalmobility
n Assesses the patient’s range of motion.n Assesses and documents any physical limitations
to movement.n Adapts the nursing plan of care to accommodate
the patient’s physical limitations.
n The patient’sphysical limitationsare within theexpected range attime of transfer tothe PACU and atdischarge from thePACU.
n The patient’sphysical limitationsand range ofmotion are withinthe expected ortherapeutic rangesthroughout theperioperativeperiod.
Disturbed sensoryperception (visual,auditory)
n Assesses the patient for the use of hearingaids and glasses.
n Ensures that the patient is allowed to wear his orher hearing aids and glasses whenever possibleduring the perioperative period.
n Ensures that the patient’s hearing aids arefunctional.
n The patientdemonstrates thathe or she hears andunderstands verbalcommunication.
n The patientdemonstrates thathe or she can readand understandwrittencommunication.
n The patient is ableto participate in andunderstand his orher care whenevernecessarythroughout theperioperativeperiod.
(table continued)
AORN Journal j 61
RISK FACTORS IN GERIATRIC SURGICAL PATIENTS www.aornjournal.org
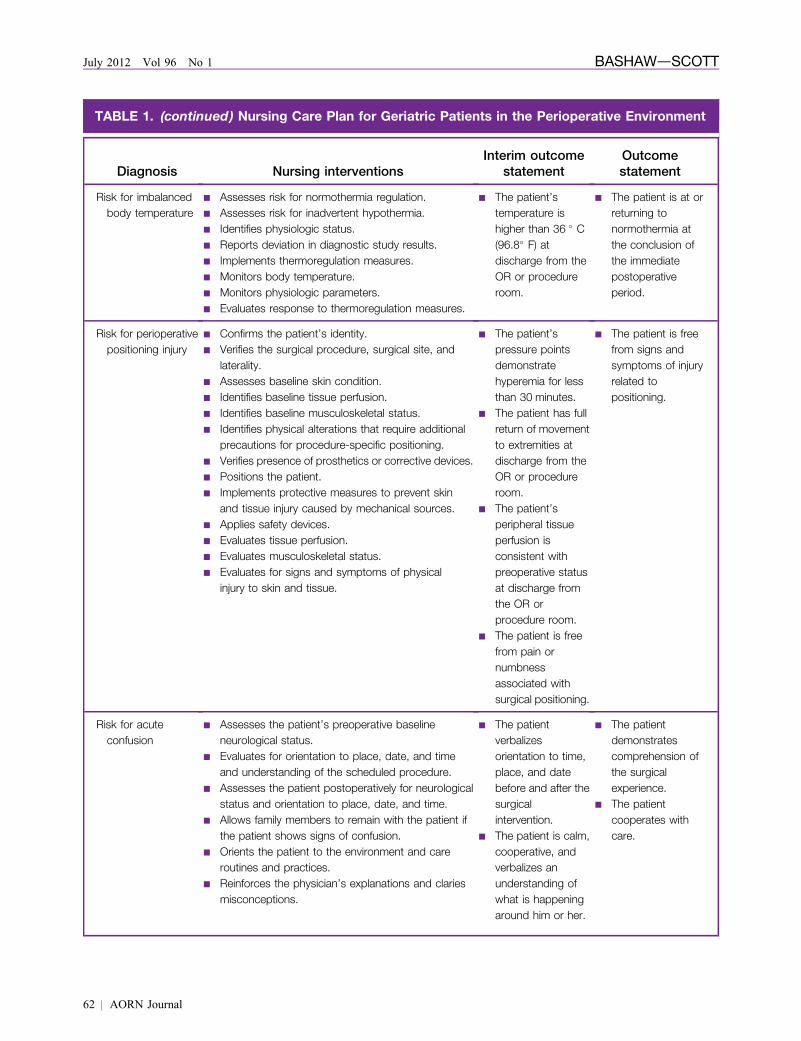
TABLE 1. (continued) Nursing Care Plan for Geriatric Patients in the Perioperative Environment
Diagnosis Nursing interventionsInterim outcome
statementOutcomestatement
Risk for imbalancedbody temperature
n Assesses risk for normothermia regulation.n Assesses risk for inadvertent hypothermia.n Identifies physiologic status.n Reports deviation in diagnostic study results.n Implements thermoregulation measures.n Monitors body temperature.n Monitors physiologic parameters.n Evaluates response to thermoregulation measures.
n The patient’stemperature ishigher than 36 � C(96.8� F) atdischarge from theOR or procedureroom.
n The patient is at orreturning tonormothermia atthe conclusion ofthe immediatepostoperativeperiod.
Risk for perioperativepositioning injury
n Confirms the patient’s identity.n Verifies the surgical procedure, surgical site, and
laterality.n Assesses baseline skin condition.n Identifies baseline tissue perfusion.n Identifies baseline musculoskeletal status.n Identifies physical alterations that require additional
precautions for procedure-specific positioning.n Verifies presence of prosthetics or corrective devices.n Positions the patient.n Implements protective measures to prevent skin
and tissue injury caused by mechanical sources.n Applies safety devices.n Evaluates tissue perfusion.n Evaluates musculoskeletal status.n Evaluates for signs and symptoms of physical
injury to skin and tissue.
n The patient’spressure pointsdemonstratehyperemia for lessthan 30 minutes.
n The patient has fullreturn of movementto extremities atdischarge from theOR or procedureroom.
n The patient’speripheral tissueperfusion isconsistent withpreoperative statusat discharge fromthe OR orprocedure room.
n The patient is freefrom pain ornumbnessassociated withsurgical positioning.
n The patient is freefrom signs andsymptoms of injuryrelated topositioning.
Risk for acuteconfusion
n Assesses the patient’s preoperative baselineneurological status.
n Evaluates for orientation to place, date, and timeand understanding of the scheduled procedure.
n Assesses the patient postoperatively for neurologicalstatus and orientation to place, date, and time.
n Allows family members to remain with the patient ifthe patient shows signs of confusion.
n Orients the patient to the environment and careroutines and practices.
n Reinforces the physician’s explanations and clariesmisconceptions.
n The patientverbalizesorientation to time,place, and datebefore and after thesurgicalintervention.
n The patient is calm,cooperative, andverbalizes anunderstanding ofwhat is happeningaround him or her.
n The patientdemonstratescomprehension ofthe surgicalexperience.
n The patientcooperates withcare.
62 j AORN Journal
July 2012 Vol 96 No 1 BASHAWdSCOTT

TABLE 1. (continued) Nursing Care Plan for Geriatric Patients in the Perioperative Environment
Diagnosis Nursing interventionsInterim outcome
statementOutcomestatement
Risk for pain n Assesses the patient for pain control.n Administers pain medication as prescribed.n Implements pain guidelines.n Implements alternative methods of pain control.n Evaluates the patient’s response to pain
management interventions.
n The patient is ableto describe andreport his or herpain.
n The patientverbalizes controlof pain.
n The patientcooperates withthe plan of care.
n The patient displaysa relaxed bodyposition.
n The patient doesnot display signsof discomfort(eg, grimacing,guarding, agitation,weeping).
n The patientdemonstrates anability to cope.
n The patient’s vitalsigns are improvedor equal topreoperativevalues.
n The patient is freefrom signs andsymptoms of pain.
RISK FACTORS IN GERIATRIC SURGICAL PATIENTS www.aornjournal.org
function can lead to lung atelectasis and pneumonia
after surgery.8 Forty percent of all surgical com-
plications and 20% of deaths related to surgery
in the geriatric population are the result of respi-
ratory complications, including those related to
reduced elasticity of the chest wall and decreased
vital capacity.5
Preoperative fasting allows for gastric emptying
and reduces aspiration risk during induction and
emergence from anesthesia; therefore, it is impor-
tant for the nurse to ascertain the patient’s NPO
status.9 Lying in the supine position can restrict
movement of the patient’s diaphragm, thus im-
peding air flow.10 This position is often required
for surgery; however, proper positioning (eg,
elevating the head and chest) can reduce respira-
tory problems.
In the PACU and on the patient care unit,
frequent turning (eg, every two hours) improves
the patient’s gas exchange and reduces the risks
of respiratory complications.8 Encouraging the
patient to cough and breathe deeply after sur-
gery helps maintain proper lung function, and
providing oral hygiene for the patient on me-
chanical ventilation helps to prevent postopera-
tive pneumonia.5 Minimizing sedation, whenever
possible, and instituting weaning protocols for
patients on mechanical ventilation and prophy-
lactic treatment for stress ulcers have been
found to reduce the incidence of postoperative
pneumonia.11
Cardiovascular and Circulatory Changes
Age-related cardiovascular and circulatory sys-
tem changes include stiffening of the walls of
large arteries from atherosclerosis, which in turn
leads to an increase in systolic pressure and
peripheral vascular resistance.12 Over time, this
AORN Journal j 63

July 2012 Vol 96 No 1 BASHAWdSCOTT
results in thickened ventricular walls and hyper-
trophy of the ventricles.12 Careful perioperative
positioning is crucial in reducing the risk of ves-
sel damage. According to Millsaps,10 prolonged
or improper positioning “can cause the greatest
amount of damage to the cardiovascular sys-
tem,”10(p62) and proper positioning can minimize
cardiac problems from pressure on or obstruction
of a vessel.
Acute and chronic cardiovascular conditions
put older patients at higher risk for adverse surgical
outcomes. For example, heart blocks can cause
cardiac arrest during surgery5; however, the use
of beta blockers has been shown to reduce this risk.
Geriatric patients also have changes in stroke
volume, conduction, and degeneration of heart
valves.12 The perioperative nurse should assess an
older patient for signs of heart failure and closely
monitor for electrocardiogram changes.12 Proper
positioning during surgery can minimize cardiac
problems and reduce bleeding by preventing
venous congestion.10
Deep Vein Thrombosis
Deep vein thrombosis (DVT) can occur in any
surgical patient; however, risk factors increase
when a patient
n is older than 40 years,
n is obese,
n experiences prolonged immobility,
n undergoes general anesthesia for more than two
hours,
n has varicose veins, or
n is a smoker.13
Geriatric patients are at increased risk for DVT
because they often have several of these risk
factors.5 To minimize this risk for an elderly
patient, the perioperative nurse can implement
several safety measures. He or she can maintain
the patient’s body in proper alignment and ad-
minister DVT prophylaxis medications (eg,
heparin, enoxaparin) or ask about their adminis-
tration if they are not ordered, perform range
64 j AORN Journal
of motion exercises, and apply antiembolism
stockings.5 The use of sequential compression
devices with thigh-high or foot pumps also helps
blood return to the heart and reduces the risk
of pooling of the blood in the lower extremities
and DVT.6
Musculoskeletal System
As people age, they experience progressive loss of
muscle strength and muscle mass. Posture can be
affected by bone loss and increased bone break-
down because of osteoporosis, which can increase
older patients’ risk of fractures. Mobility and range
of motion are lost because of tissue elasticity changes,
joint breakdown, and stiffness. In addition, many
older patients have long-standing issues of chronic
pain from arthritis, neuralgias, and ischemic disor-
ders, making pain assessment a necessary part of
nursing care.14
Gastrointestinal System
Geriatric patients have an increased risk of pep-
tic ulcer disease. The gastric mucosa of older
patients has a reduced capacity to resist damage
from nonsteroidal anti-inflammatory drugs and
from Helicobacter pylori.2 Older patients often
have impaired dentition, decreased saliva produc-
tion, and decreased peristalsis.2,6 Age-related
slowing of peristalsis, low fiber and fluid intake,
medications, and sedentary lifestyles put elderly
patients at risk for constipation.2 Preoperative
fasting can lead to dehydration, which has been
shown to increase postoperative nausea and
vomiting.15 The nurse should assess the patient
for signs and symptoms of
n fluid or electrolyte imbalance,
n nausea and vomiting,
n constipation, and
n diarrhea.
If any of these is present, the nurse should admin-
ister appropriate medications to relieve symptoms6
and should encourage fluids and mobility to help
prevent constipation.16
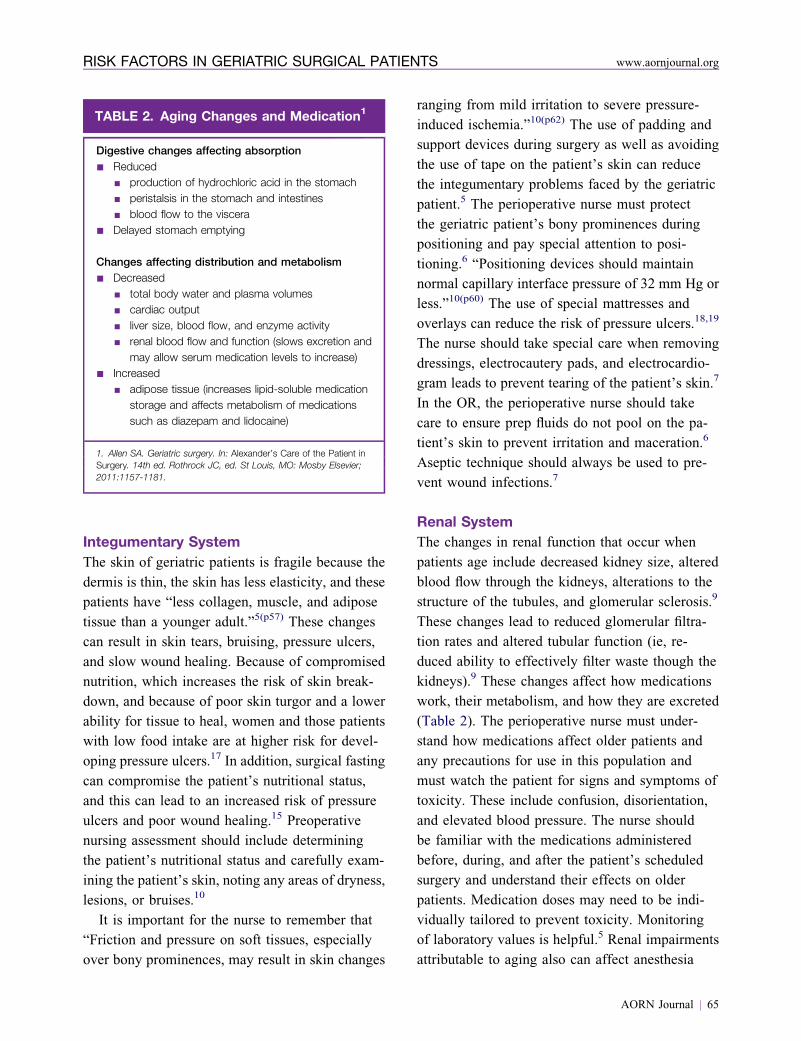
TABLE 2. Aging Changes and Medication1
Digestive changes affecting absorption
n Reducedn production of hydrochloric acid in the stomachn peristalsis in the stomach and intestinesn blood flow to the viscera
n Delayed stomach emptying
Changes affecting distribution and metabolism
n Decreasedn total body water and plasma volumesn cardiac outputn liver size, blood flow, and enzyme activityn renal blood flow and function (slows excretion and
may allow serum medication levels to increase)n Increased
n adipose tissue (increases lipid-soluble medicationstorage and affects metabolism of medicationssuch as diazepam and lidocaine)
1. Allen SA. Geriatric surgery. In: Alexander’s Care of the Patient inSurgery. 14th ed. Rothrock JC, ed. St Louis, MO: Mosby Elsevier;2011:1157-1181.
RISK FACTORS IN GERIATRIC SURGICAL PATIENTS www.aornjournal.org
Integumentary System
The skin of geriatric patients is fragile because the
dermis is thin, the skin has less elasticity, and these
patients have “less collagen, muscle, and adipose
tissue than a younger adult.”5(p57) These changes
can result in skin tears, bruising, pressure ulcers,
and slow wound healing. Because of compromised
nutrition, which increases the risk of skin break-
down, and because of poor skin turgor and a lower
ability for tissue to heal, women and those patients
with low food intake are at higher risk for devel-
oping pressure ulcers.17 In addition, surgical fasting
can compromise the patient’s nutritional status,
and this can lead to an increased risk of pressure
ulcers and poor wound healing.15 Preoperative
nursing assessment should include determining
the patient’s nutritional status and carefully exam-
ining the patient’s skin, noting any areas of dryness,
lesions, or bruises.10
It is important for the nurse to remember that
“Friction and pressure on soft tissues, especially
over bony prominences, may result in skin changes
ranging from mild irritation to severe pressure-
induced ischemia.”10(p62) The use of padding and
support devices during surgery as well as avoiding
the use of tape on the patient’s skin can reduce
the integumentary problems faced by the geriatric
patient.5 The perioperative nurse must protect
the geriatric patient’s bony prominences during
positioning and pay special attention to posi-
tioning.6 “Positioning devices should maintain
normal capillary interface pressure of 32 mm Hg or
less.”10(p60) The use of special mattresses and
overlays can reduce the risk of pressure ulcers.18,19
The nurse should take special care when removing
dressings, electrocautery pads, and electrocardio-
gram leads to prevent tearing of the patient’s skin.7
In the OR, the perioperative nurse should take
care to ensure prep fluids do not pool on the pa-
tient’s skin to prevent irritation and maceration.6
Aseptic technique should always be used to pre-
vent wound infections.7
Renal System
The changes in renal function that occur when
patients age include decreased kidney size, altered
blood flow through the kidneys, alterations to the
structure of the tubules, and glomerular sclerosis.9
These changes lead to reduced glomerular filtra-
tion rates and altered tubular function (ie, re-
duced ability to effectively filter waste though the
kidneys).9 These changes affect how medications
work, their metabolism, and how they are excreted
(Table 2). The perioperative nurse must under-
stand how medications affect older patients and
any precautions for use in this population and
must watch the patient for signs and symptoms of
toxicity. These include confusion, disorientation,
and elevated blood pressure. The nurse should
be familiar with the medications administered
before, during, and after the patient’s scheduled
surgery and understand their effects on older
patients. Medication doses may need to be indi-
vidually tailored to prevent toxicity. Monitoring
of laboratory values is helpful.5 Renal impairments
attributable to aging also can affect anesthesia
AORN Journal j 65

July 2012 Vol 96 No 1 BASHAWdSCOTT
and the patient’s fluid and electrolyte balance.5,6
Anesthesia effects include
n decreased respiratory function,
n disorientation,
n being slow to wake up after the completion of
surgery,
n a slow return of baseline cognitive status, and
n low blood pressure.
The nurse should be aware that older patients may
need to be reoriented to where they are, to breathe
deeply, and to move slowly when getting up to
avoid a drop in blood pressure and that they must
have assistance when getting out of bed because
they may feel light-headed and dizzy and are at
increased risk for a fall. Patients may need to be
repeatedly reminded of these issues.
Maintaining an older patient’s fluid and elec-
trolyte balance during surgery can be challenging.
Fluid shifts in older adults can lead to impaired
respiratory function and swelling in the extremities.
The nurse should carefully monitor all fluids that
are administered on the field and all fluid output
(eg, blood loss, urine output). The nurse should
report any unusual discrepancies to the anesthesia
care provider and the surgeon and document them
on the OR record.
Nervous System
Normal changes in the central nervous system of
geriatric patients, such as short-term memory loss
and difficulty in processing information and prob-
lem solving, can affect perioperative teaching and
patient care. Geriatric patients also are susceptible
to postoperative problems such as delirium, con-
fusion, and depression.5 As many as 20% of geri-
atric patients experience postoperative delirium,20
which has been associated with increased morbidity
and mortality.20
Delirium manifests as patients not knowing who
they are, where they are, or what the nurses are
doing to help them.20 They become suspicious of
the people around them and believe that caregivers
are trying to harm them. They are not compliant
66 j AORN Journal
with care and are at risk for injuring themselves.
The greater risk of injury increases patients’ overall
morbidity and mortality risk. Patients who are
delirious can become harmful to themselves and
others, whereas confused patients usually are not.
When an older adult patient is confused, the nurse
should be able to reorient the patient and help the
patient comply with what the nurse asks him or
her to do. Nurses must monitor a patient experi-
encing delirium closely and, if necessary, have
someone stay with the patient at all times. As a last
resort, orders for restraints may be required to
keep the patient from harming himself or herself.
The presence of depression and delirium may affect
the patient’s postoperative recovery or ability to
provide self-care.5
Depressed patients are oriented and aware of
their surroundings but do not respond quickly and
sometimes do not respond at all to requests from the
nurse to participate in their own care.20 For example,
a patient may not want to perform deep breathing,
coughing, and turning exercises or sit in a chair or go
for a walk. This can lead to respiratory complica-
tions. Patients who are depressed understand what is
being asked of them but, because of the depression,
do not want to participate in self-care. Delirious
patients, in contrast, do not understand what they
are being asked to do and therefore do not comply.
Failure to comply, regardless of its reasons, can lead
to postoperative complications and increased length
of stay in the hospital.20 The nurse may be able to
prevent postoperative delirium by assessing the
patient for risk factors that include cognitive, hear-
ing, and vision impairments; sleep deprivation;
immobility; and dehydration and planning patient
care to accommodate any deficits.20
Cognitive impairment. Preoperatively, it is
important for the nurse to assess the geriatric
patient for the cognitive ability to “perform [any]
behavior that is essential to the procedure.”7(p37)
The nurse should include family members or
caregivers in patient teaching with the patient’s
permission. If the patient appears unable to follow

RISK FACTORS IN GERIATRIC SURGICAL PATIENTS www.aornjournal.org
directions or is unable to perform self-care tasks
that will be required after surgery, the nurse should
assess family members or caregivers for the ability
to perform these tasks. In instances where the
patient has no support system, the nurse may need
to ask for discharge planning to ensure that the
patient is discharged to an appropriate care facility
until able to care for himself or herself. Nursing
interventions for cognitive impairment include
providing stimulating activities; ensuring frequent
interaction with personnel; and orienting the patient
to time, place, and date.20 Allowing a family mem-
ber to stay with the patient whenever possible also
can be helpful.
Visual and hearing impairments. Auditory
or visual impairments can seriously affect the
patient’s ability to understand what is being said
or see his or her environment. This affects the
patient’s ability to provide self-care and can
contribute to confusion and delirium. If a patient
requires the use of hearing aids or glasses, these
should be available to the patient for as long as
possible in the perioperative setting and should be
working properly.20 If the hearing or visual aids
must be removed, they should handled carefully
and returned to the patient as soon as possible in
the postoperative setting.
Sleep deprivation. To prevent sleep depriva-
tion, health care providers should schedule surgery,
medications, testing, and care activities so that they
do not interrupt the patient’s sleep and should
provide nonpharmacological sleep aids such as
warm milk, relaxation activities, soothing music,
and noise reduction if needed.20 The perioperative
nurse should be aware that the anxiety of an ap-
proaching surgery may have altered the patient’s
sleep pattern and may pose a risk for postoperative
delirium. The perioperative nurse can provide
a calm, soothing environment in the preoperative
holding area. Allowing family members to remain
with the patient until the time of surgery and
providing a hand massage, soft music, or a dark-
ened environment can help the patient relax.
Immobility. Prolonged bedrest can cause pres-
sure on the nerves and atrophy of the muscles.
When patients do attempt to get up, their extremi-
ties do not respond as rapidly as before, which
increases the risk of falling. If a patient believes
he or she is going to fall and becomes afraid to try,
this initiates a downward spiral.
In surgery, prolonged positioning can result in
nerve and tissue damage, and because of the effects
of the surgery or prolonged hospitalization, the
same types of immobility problems can result.
Reassurance by the nurse and one or two persons
who can assist the patient with ambulating can
decrease his or her fears and facilitate postoperative
recovery. The nurse should help the patient ambu-
late as soon as possible. The use of devices such
as indwelling urinary catheters that could restrict
a patient’s ability to move should be avoided.20
Dehydration. Preoperative fasting will have
altered the patient’s normal intake and output. The
nurse should assess the patient’s regular intake and
output patterns, assess his or her current NPO
status, and review the patient’s blood urea nitrogen
levels and creatinine ratios for signs of dehydration
and closely monitor them during surgery.20 Any
apparent deficits should be reported to the anes-
thesia care provider, the surgeon, and postoperative
caregivers.
Nerve injury. Injury to nerves can occur when
there is pressure caused by incorrect positioning.10
The brachial plexus, radial nerves, sciatic nerves,
and popliteal nerves are prone to pressure injury
in geriatric patients. Being aware of a patient’s
particular risks helps caregivers determine when
and where to provide extra protection.10 The nurse
should assess the patient for numbness or tingling
of the extremities10 as well as mobility issues and
any areas of skin breakdown or bruising. These
should be documented and discussed with the
surgical team. Because of limitations in mobility
associated with aging, the surgical team may need
to modify positioning and should take particular
care not to hyperextend joints or use undue force
AORN Journal j 67

July 2012 Vol 96 No 1 BASHAWdSCOTT
when positioning the patient for surgery.21 When
placing the patient in the supine position, the
patient’s arms should be positioned on arm boards
at less than a 90-degree angle from the body, and
the patient’s palms should face up to prevent ul-
nar nerve damage.21 When tucking the patient’s
arms at his or her sides is required, the nurse
should place the patient’s palms facing inward and
support the elbows to avoid compression on the
ulnar nerve; the patient’s fingertips should be
checked to ensure that any repositioning of the
OR bed does not trap them.21 Bony prominences
should be carefully padded, and heels should be
elevated off the mattress if possible to avoid un-
due pressure.20 The patient’s head should be in
a neutral position.21
Pain. Contrary to popular belief, older adults
do not have higher pain thresholds than younger
adults,6 and pain is not a natural outcome of
aging.22 Elderly patients, however, may appear to
have less pain because they may be reluctant to
report it to the nurse or will underreport the in-
tensity of their pain. Older adults often believe
that pain must be endured or that if they report
having pain, they will be “labeled as a ‘bad’
patient.”14(p1160) Elderly patients often use words
such as aching, soreness, or discomfort to describe
what they are feeling.22 These words are considered
“softening” words and may poorly describe the
magnitude of the pain the patient is experiencing,
resulting in unrelieved or poorly relieved pain.22
Unrelieved pain can cause many postoperative
complications, including hypertension, tachy-
cardia, depression, anxiety, sleep disturbances,
immune dysfunction, weight loss, urinary reten-
tion, atelectasis, fluid imbalance, constipation,
weakness, fatigue, confusion, glucose intolerance,
and fluid overload.16 “Pain may actually hasten
death by increasing physiological stress, decreas-
ing mobility, and contributing to pneumonia and
thromboemboli.”23(p79)
The nurse should assess the patient’s pain level
and treat it. Ideally, pain medication should be
68 j AORN Journal
administered regularly in the immediate postoperative
period to prevent the patient’s pain from recur-
ring.2,6 If the patient is unable to report pain be-
cause of delirium or dementia, the nurse should
observe him or her for other indications of pain,
including
n restlessness,
n facial expressions (eg grimacing, frowning),
n posturing,
n guarding,
n aggression,
n withdrawal,
n appetite changes, or
n mental status changes (eg, increased confusion,
crying, irritability).2
If these symptoms of pain are observed, the nurse
should administer pain medication as symptoms
present to reduce potential complications. The
nurse can also institute complementary and alter-
native therapies for pain treatment, including
n therapeutic touch,
n massage therapy,
n distraction,
n guided imagery,
n aromatherapy, and
n the use of hot or cold packs if ordered by the
physician.2
Thermoregulation. During surgery, any patient
can experience hypothermia. Heat can be lost be-
cause of the use of cool IV and irrigation fluids,
lower ambient room temperature in the OR, and
mechanical ventilation and through radiation, con-
vection, conduction, and evaporation.14 Hypo-
thermia can lead to increased postoperative pain
and bleeding, immune system compromise, medi-
cation metabolism delay, and impaired wound
healing. The normal physiologic response to hy-
pothermia is shivering and vasoconstriction.14
Shivering increases oxygen consumption, cardiac
output, and carbon dioxide production.16 Vaso-
constriction shunts blood from the extremities to
the core body organs in an attempt to conserve
PATIENT EDUCATION
Surgery and the Older Adult
OverviewPreexisting conditions and normal aging can cause
complications in the older adult patient who requires
surgery. The seriousness of the complication de-
pends on your specific preexisting conditions and
the planned surgery. Please let your caregivers know
about any preexisting conditions you may have and
any problems you may have had with surgery in
the past.
Hearing and eyesight problemsIf you are hard of hearing or require the use of
hearing aids or glasses, remember to bring them
with you to the hospital and let caregivers know that
you need them to see or hear well. This will help
ensure that you get the information you need for
a successful outcome to your surgery. If you have
a hard time hearing what a caregiver is saying, ask
him or her to speak up or repeat the information.
Ask the caregiver to explain anything you do not
understand. If you cannot read the postoperative
instructions that are given to you, ask your caregiver
to read them to you. If a caregiver is speaking too
rapidly or using words you do not understand, ask
him or her to slow down or further explain the in-
formation. Caregivers may ask you to demonstrate
that you can follow postoperative instructions.
When you are away from familiar surroundings,
you may feel confused or disoriented. If possible,
have a family member come with you to help you
adjust to the hospital environment. If you become
confused, remember that this is not unusual and ask
caregivers or family members to help orient you.
PainPain is a normal result of surgery; however, it can be
relieved by medication and other treatments. Pro-
viding pain relief is important to prevent other
complications. It is important for you to tell your
caregivers if you are experiencing pain and whether
medications or other treatments to relieve it have
been successful. Do not minimize what you are
experiencing or worry that you are bothering your
caregivers. Do not wait until you are in a lot of pain
to ask for relief.
MedicationsTell your caregivers about any medications you are
taking and why; this includes over-the-counter med-
ications, herbs, or vitamins. If it is hard for you to
remember, bring a written medication list with you to
the hospital. Let caregivers know if there are any
medications that you cannot take and why.
Skin, muscles, and jointsLet your caregivers know if you have any bruising,
cuts, or other skin damage so that they can take
precautions to protect these areas. Also let your
caregivers know if you have problems with arthritis,
stiffness, or other mobility issues. Your caregiver
may ask you to move these joints so that any move-
ment restrictions can be identified and caregivers can
take extra care to prevent injury during surgery.
TemperatureLet your caregivers know if you are cold or would
like more blankets. This will help them ensure that
you do not have complications from being cold.
ResourcesHow to prepare for surgery. Women to Women.
http://www.womentowomen.com/womenshealth/
howtoprepareforsurgery.aspx. Accessed April 4,
2012.
Preparing the older adult for surgery and anesthesia.
Mosby’s NursingConsult. http://www.nursingconsu
lt.com/nursing/journals/10899472/full-text?issn¼10899472&full_text¼html&article_id¼483748&
spid¼15433640&iphub_return¼http%3A%2F%
2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%
2FS1089947204002941%3Fshowall%3Dtrue. Ac-
cessed April 4, 2012.
AORN Journal j 69
RISK FACTORS IN GERIATRIC SURGICAL PATIENTS www.aornjournal.org

July 2012 Vol 96 No 1 BASHAWdSCOTT
heat.14 Older patients, however, havemore difficulty
regulating their body temperature and surgical
procedures place them at increased risk for hypo-
thermia because of their decreased ability to vaso-
constrict and shiver.14
The nurse can increase the ambient room
temperature of the OR to reduce radiant heat loss
and use temperature regulating blankets and head
coverings to reduce the risk of heat loss from
radiation and convection.6,14 Warmed irrigation
fluids should be used on the sterile field and the
circulating nurse should use warmed prep solutions
(if the manufacturer supports this) to reduce heat
loss and ensure that the patient is not lying in prep
solution or on wet linen, which could increase heat
loss. Anesthesia care providers should use fluid
warmers for IV solutions. The patient’s feet should
be kept warm with socks if possible.14
SURGICAL RISK
Age alone is not a contraindication for surgery;
however, certain situations and conditions increase
surgical risk for the geriatric population. For ex-
ample, surgery performed on an emergent basis or
surgery involving the heart, chest, or abdominal
cavity and that lasts more than 3.5 hours increases
the risk of complications significantly.14 The
American Society of Anesthesiologists Physical
Status Classification System24 helps to categorize
a patient’s anesthetic risk. A patient with a classi-
fication of III, IV, or V (ie, presence of preexisting
disease of increasing severity) and who is older
than 75 years is at an increased level of surgical
and anesthetic risk and requires careful assessment
and planning to prevent complications.14,24
CONCLUSION
Perioperative nurses must be aware of the surgi-
cal risk factors for geriatric patients and the phys-
iologic and cognitive changes associated with
aging and how they affect patients undergoing
surgery. Careful patient assessment, addressing and
correcting issues perioperatively when possible,
70 j AORN Journal
and planning for care can provide a safer, more
successful surgical experience for the geriatric
patient.
References1. Projected future growth of the older population. 2010.
Department of Health and Human Services Administra-
tion on Aging. http://www.aoa.gov/AoARoot/Aging_
Statistics/future_growth/future_growth.aspx#age. Ac-
cessed November 21, 2011.
2. Tabloski PA. Gerontological Nursing. 2nd ed. Upper
Saddle River, NJ: Pearson Education, Inc; 2010.
3. Swann J. Fall prevention is everyone’s responsibility.
Nurs Resid Care. 2008;10(6):294-297.
4. Harari D, Martin F, Buttery A, O’Neill S, Hopper A.
The older persons’ assessment and liaison team “OPAL”:
evaluation of comprehensive geriatric assessment in
acute medical inpatients. Age Ageing. 2007;36(6):
670-675.
5. Dunn D. Preventing perioperative complications in an
older adult. Nursing. 2004;34(11):36-42.
6. Doerflinger D. Older adult surgical patients: presentation
and challenges. AORN J. 2009;90(2):223-244.
7. Westhead C. Perioperative nursing management of the
elderly patient. Can Oper Room Nurs J. 2007;25(3):34.
8. Bergman SA, Coletti D. Perioperative management of the
geriatric patient. Part I: respiratory system. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod. 2006;102(3):
e1-e6.
9. Ekstein M, Gavish D, Ezri T, Weinbroum A. Monitored
anaesthesia care in the elderly: guidelines and recom-
mendations. Drugs Aging. 2008;25(6):477-500.
10. Millsaps C. Pay attention to patient positioning! RN.
2006;69(1):59-63.
11. Turrentine F, Wang H, Simpson V, Jones R. Surgical risk
factors, morbidity, and mortality in elderly patients. J Am
Coll Surg. 2006;203(6):865-877.
12. Bergman SA, Coletti D. Perioperative management of the
geriatric patient. Part II: cardiovascular system. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;
102(3):e7-e12.
13. Recommended practices for the prevention of deep vein
thrombosis. In: Perioperative Standards and Recom-
mended Practices. Denver, CO: AORN, Inc; 2012:
353-363.
14. Allen SA. Geriatric surgery. In: Rothrock JC, ed. Alex-
ander’s Care of the Patient in Surgery. 14th ed. St Louis,
MO: Mosby Elsevier; 2011:1157-1181.
15. Millar E. Reducing the impact of pre-operative fasting
on patients. Kai Tiaki Nurs New Zealand. 2009;15(5):
16-18.
16. Lewis S, Heitkemper M, Dirksen S, O’Brian P, Bucher L.
Medical-Surgical Nursing: Assessment and Management
of Clinical Problems. 7th ed. St Louis, MO: Mosby
Elsevier; 2007.
17. Lindgren M, Unosson M, Krantz A, Ek A. Pressure ulcer
risk factors in patients undergoing surgery. J Adv Nurs.
2005;50(6):605-612.
18. Sewchuk D, Padula C, Osborne E. Prevention and early
detection of pressure ulcers in patients undergoing
cardiac surgery. AORN J. 2006;84(1):75-96.
RISK FACTORS IN GERIATRIC SURGICAL PATIENTS www.aornjournal.org
19. Feuchtinger J, de Bie R, Dassen T, Halfen RA. 4-cm
thermoactive viscoelastic foam pad on the operating
room table to prevent pressure ulcer during cardiac
surgery. J Clin Nurs. 2006;15(2):162-167.
20. Bergman SA, Coletti D. Perioperative management of
the geriatric patient. Part III: delirium. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod. 2006;102(3):
e13-e16.
21. Recommended practices for positioning the patient in the
perioperative setting. In: Perioperative Standards and
Recommended Practices. Denver, CO: AORN, Inc; 2012:
421-443.
22. Mauk KL. Gerontological Nursing: Competencies
for Care. Boston, MA: Jones and Bartlett Publishers;
2010.
23. Paice JA, Fine PG. Pain at the end of life. In: Ferrell B,
Coyle N, eds. Textbook of Palliative Nursing. New York,
NY: Oxford University Press; 2001:76-90.
24. ASA Physical Status Classification System. American
Society of Anesthesiologists. http://www.asahq
.org/clinical/physicalstatus.htm. Accessed November
18, 2011.
Marie Bashaw, MS, RN, NEA-BC, CNOR, is
a clinical assistant professor and associate di-
rector of the Master’s in Nursing Administration
Program at Wright State University, Dayton, OH.
Ms Bashaw has no declared affiliation that could
be perceived as posing a potential conflict of
interest in the publication of this article.
Dana N. Scott, BSN, RN, is a recent bachelor
of science in nursing graduate and is currently
enrolled in a master’s degree program at Wright
State University, Dayton, OH. Ms Scott has no
declared affiliation that could be perceived as
posing a potential conflict of interest in the
publication of this article.
AORN Journal j 71
EXAMINATION
CONTINUING EDUCATION PROGRAM2.9
www.aorn.org/CESurgical Risk Factors in GeriatricPerioperative Patients
PURPOSE/GOAL
72
To educate perioperative nurses about surgical risk factors in older adults under-
going surgical interventions.
OBJECTIVES
1. Describe the changes associated with aging.
2. Discuss the nurse’s role in caring for geriatric patients in the OR.
The Examination and Learner Evaluation are printed here for your conven-
ience. To receive continuing education credit, you must complete the Exami-
nation and Learner Evaluation online at http://www.aorn.org/CE.
QUESTIONS
1. Hearing and vision losses that occur in the geri-
atric patient include
1. lens thickening.
2. increased light sensitivity.
3. increased cerumen production.
4. sensory hair cell loss.
5. organ of Corti atrophy.
a. 1, 4, and 5 b. 2, 3, and 4
j AORN Journal
c. 1, 3, 4, and 5 d. 1, 2, 3, 4, and 5
2. To help a patient understand preoperative
and postoperative instructions, the nurse
should
1. make sure that a patient who uses hearing
aids and glasses is able to use them as long as
possible.
2. increase speech volume, if necessary, and
face the patient when speaking.
3. limit the amount of information given at one
time.
� July 2012 Vol 96 No 1
4. provide written materials printed in light ink
on a dark background.
a. 1 and 2 b. 3 and 4
c. 1, 2, and 3 d. 1, 2, 3, and 4
3. Respiratory system changes seen in older adult
patients include
1. loss of pharyngeal support.
2. decreased risk of aspiration.
3. weakened diaphragm function.
4. weakening or loss of swallowing and
coughing reflexes.
a. 1 and 3 b. 2 and 4
c. 1, 3, and 4 d. 1, 2, 3, and 4
4. Acute and chronic cardiovascular conditions that
place older patients at risk for negative surgical
outcomes include
1. heart block.
2. changes in stroke volume and cardiac
conduction.
3. degeneration of heart valves.
� AORN, Inc, 2012
CE EXAMINATION www.aornjournal.org
4. stiffening of the walls of large arteries.
5. increases in systolic pressure and peripheral
vascular resistance.
a. 1 and 2 b. 3, 4 and 5
c. 1, 2, 3 and 4 d. 1, 2, 3, 4, and 5
5. Surgical fasting can lead to increased risk of
pressure ulcers and wound healing.
a. true b. false
6. Renal changes caused by aging affect how
___________ are processed by geriatric patients.
a. foods b. blood products
c. medications d. instructions
7. The nurse can help prevent postoperative delirium
by planning perioperative care after assessing
1. cognitive impairment.
2. hearing and vision impairments.
3. sleep deprivation.
4. immobility.
5. dehydration.
a. 1 and 2 b. 4 and 5
c. 1, 3, and 5 d. 1, 2, 3, 4, and 5
8. The nurse should help the patient ambulate as
soon as possible and avoid the use of devices such
as indwelling urinary catheters that could restrict
the patient’s ability to move.
a. true b. false
9. Older patients require careful nursing assessment
and may appear to have less pain because they
a. have difficulty feeling pain because of age-
related changes.
b. are reluctant to report pain or underreport it.
c. have higher pain thresholds.
d. are used to pain.
10. Surgical procedures place older patients at
increased risk for hypothermia because of their
bodies’ decreased abilities to vasoconstrict and
shiver.
a. true b. false
AORN Journal j 73
LEARNER EVALUATION
CONTINUING EDUCATION PROGRAM2.9
www.aorn.org/CESurgical Risk Factors in GeriatricPerioperative Patients
This evaluation is used to determine the extent to
which this continuing education program met
your learning needs. Rate the items as described
below. The Learner Evaluation is printed here for your
convenience. To receive continuing education credit,
you must complete the Learner Evaluation online at
http://www.aorn.org/CE.
OBJECTIVES
To what extent were the following objectives of this
continuing education program achieved?
1. Describe the changes associated with
aging. Low 1. 2. 3. 4. 5. High
2. Discuss the nurse’s role in caring for geriatric
patients in the OR.
Low 1. 2. 3. 4. 5. High
CONTENT
3. To what extent did this article increase your
knowledge of the subject matter?
Low 1. 2. 3. 4. 5. High
4. To what extent were your individual objectives
met? Low 1. 2. 3. 4. 5. High
5. Will you be able to use the information from this
article in your work setting? 1. Yes 2. No
6. Will you change your practice as a result of reading
this article? (If yes, answer question #6A. If no,
answer question #6B.)
74 j AORN Journal � July 2012 Vol 96 No 1
6A. How will you change your practice? (Select all that
apply)
1. I will provide education to my team regarding
why change is needed.
2. I will work with management to change/
implement a policy and procedure.
3. I will plan an informational meeting with
physicians to seek their input and acceptance
of the need for change.
4. I will implement change and evaluate the
effect of the change at regular intervals until
the change is incorporated as best practice.
5. Other: ______________________________
6B. If you will not change your practice as a result
of reading this article, why? (Select all that
apply)
1. The content of the article is not relevant to my
practice.
2. I do not have enough time to teach others
about the purpose of the needed change.
3. I do not have management support to make
a change.
4. Other: ______________________________
7. Our accrediting body requires that we verify
the time you needed to complete the 2.9 continuing
education contact hour (174-minute) program:
_________________________________
� AORN, Inc, 2012
Related Documents











