This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

E
Se
JF
a
b
RA
NSf
0d
pilepsy Research (2010) 89, 310—318
journa l homepage: www.e lsev ier .com/ locate /ep i lepsyres
urgical outcomes in lesional and non-lesionalpilepsy: A systematic review and meta-analysis
osé F. Téllez-Zentenoa,∗, Lizbeth Hernández Ronquilloa,arzad Moien-Afshari a, Samuel Wiebeb
Department of Medicine, Division of Neurology, University of Saskatchewan, Saskatoon, CanadaDepartment of Clinical Neurosciences. University of Calgary, Alberta, Canada
eceived 17 October 2009; received in revised form 5 January 2010; accepted 13 February 2010vailable online 15 March 2010
KEYWORDSEpilepsy surgery;Non-lesional epilepsy;MRI;Histopathology;Surgical outcomes
SummaryPurposes: To provide evidence-based quantitative summary estimates of seizure outcomes inpatients with non-lesional and lesional epilepsy treated with surgery, and to assess the consis-tency of results among published studies.Methods: An exhaustive literature search identified articles published since 1995, describingoutcomes according to lesional status in patients of any age who underwent resective epilepsysurgery. Two reviewers independently assessed study eligibility and extracted the data. Dis-agreements were resolved through discussion. Random effects meta-analyses were used afterassessing the dataset for heterogeneity.Results: Forty articles fulfilled eligibility criteria and described outcomes in 697 patients withnon-lesional epilepsy and 2860 patients with lesional epilepsy. Overall, the odds of being seizure-free after surgery were 2.5 times higher in patients with lesions on MRI or histopathology (OR2.5, 95%CI 2.1, 3.0, p < 0.001). In patients with temporal lobe epilepsy surgery the odds were2.7 times higher in those with lesions (OR 2.7, 95%CI 2.1, 3.5, p < 0.001). In patients withextratemporal epilepsy surgery the odds were 2.9 higher in those with lesions (OR 2.9, 95%CI
1.6, 5.1, p < 0.001). Outcomes were similar in children, adults, and studies that used MRI orhistopathology to identify lesions.Discussion: Overall, the odds of seizure freedom after surgery are two to three times higherin the presence of a lesion on histopathology or MRI. The results are clinically and statisticallysignificant, consistent across various subgroups, and quite homogeneous across studies.© 2010 Elsevier B.V. All rights reserved.∗ Corresponding author at: Department of Medicine, Division ofeurology, Royal University Hospital, 103 Hospital Drive, Box 26,askatoon, SK, Canada S7N 0W8. Tel.: +1 306 966 8011;ax: +1 306 966 8008.
E-mail address: [email protected] (J.F. Téllez-Zenteno).
Introduction
The success of epilepsy surgery is directly related to ourability to localize and resect or disconnect precisely theepileptogenic cortex. The process of localization (Blume,1986) generally requires good quality imaging studies, e.g.,
920-1211/$ — see front matter © 2010 Elsevier B.V. All rights reserved.oi:10.1016/j.eplepsyres.2010.02.007

Surgical outcomes in lesional and non-lesional epilepsy: A systematic review and meta-analysis 311
magnetic resonance imaging (MRI) and expert interpretation(Duncan, 1997) to identify resectable lesions such as mesialtemporal sclerosis, gliotic tissue, malformations of corti-cal development, tumors and other circumscribed anomalies(Cascino, 2008). Although advances in structural and func-tional MRI allow for identification of subtle lesions, 20—30%of patients with temporal epilepsy and 20—40% of those withextratemporal epilepsy have no clear lesion on MRI (Carne etal., 2004; Hong et al., 2002; Kutsy, 1999). This is importantbecause cohort studies of predictors of surgical outcomeoften report better outcomes in patients with demonstratedMRI lesions than in those without relevant MRI abnormalities.For example, Berkovic et al. (1995) found that in patientswith temporal lobe epilepsy surgery, 62—80% of those witha lesion identified on MRI became seizure-free, comparedwith 36% of the non-lesional (NL) patients. Other studiesincluding temporal and extratemporal epilepsy surgery havereported similar findings (Ferrier et al., 1999; Jeha et al.,2006; Stavem et al., 2004; Wieshmann et al., 2008).
The presence or absence of a lesion can be based on MRIor on histopathological analysis (Sinclair et al., 2001). How-ever, clinicians use MRI findings to make decisions aboutsurgery, estimate probabilities of outcome, and counselpatients regarding prognosis and surgery. Accordingly moststudies refer to MRI findings when describing lesional (LE)and NL cases (Siegel et al., 2001).
We performed a systematic review and meta-analysis ofthe evidence comparing surgical outcomes in LE and NLpatients. Our aim was to provide clinicians with a scien-tifically valid and coherent summary of the best currentevidence, to provide a best estimate of surgical successrates in both patient groups, and to assess possible causesof variation in published results.
Methods
Data sources
A medical librarian performed a comprehensive literature search ofthe Medline®, Embase®, Index Medicus®, and Cochrane databases(Medline search strategy in Appendix A). Studies from previousmeta-analyses were revised in full text to identify relevant arti-cles (Engel et al., 2003; McIntosh et al., 2001; Tellez-Zenteno etal., 2005, 2007). We also searched bibliographies of reviews, origi-nal articles and book chapters, and consulted experts about otherstudies. To obtain a more homogeneous and up to date dataset, wefocused on full-length articles published in English between January1995 and December 2007.
Study selection, classification and data gathering
Two reviewers independently applied the following study inclusioncriteria: (a) reports of ≥5 patients of any age undergoing resec-tive epilepsy surgery, (b) outcomes reported after at least 1 yearof follow-up, (c) quantitative report of seizure and other out-comes, (d) description of type of surgery and number of patientsundergoing each intervention, and (e) description of surgical out-comes in LE and in NL patients in the same study, thus allowingfor direct comparisons. We excluded studies with any overlap-ping patient populations from the same centre, and those inwhich outcomes for LE or NL patients were not reported in thesame study. We further classified studies by surgical topogra-phy into: (a) those reporting temporal and extratemporal surgery,
(b) those reporting temporal lobe surgery, and (c) those report-ing extratemporal surgery (e.g., occipital, parietal, or frontal).LE and NL cases were defined according to MRI findings or byhistopathology. Lesions were defined as anomalies considered bythe authors as directly relevant for the epileptogenic process.Finally, studies of adults and children were analyzed separately.We used the seizure outcome definition provided by authors ineach study. Most commonly, this referred to seizure freedom dur-ing the last recorded follow-up, without specifying duration ofseizure freedom. For the purpose of this analysis, patients withEngel I outcomes were considered seizure-free. Two reviewers inde-pendently abstracted all data, resolving disagreements throughdiscussion.
Analysis
Studies were the unit of analysis. Some articles contributed morethan one study to the analysis, e.g., they provided separate reportson MRI and histopathology or on more than one surgical topography.We used Comprehensive Meta-Analysis V2® for all meta-analyses,and Statistics with Confidence® to obtain exact 95% confidenceintervals (95%CI) around proportions. We assessed the data forheterogeneity by visual analysis of the forest plots, and quantita-tively using the Q-statistic. In the absence of heterogeneity, theproportions of seizure-free patients in each category were pooledusing the random effects model, which was a more conservativeanalysis in this dataset. We used odds ratios (OR) to comparepooled proportions of seizure-free patients in LE and NL stud-ies.
Results
Evidence base
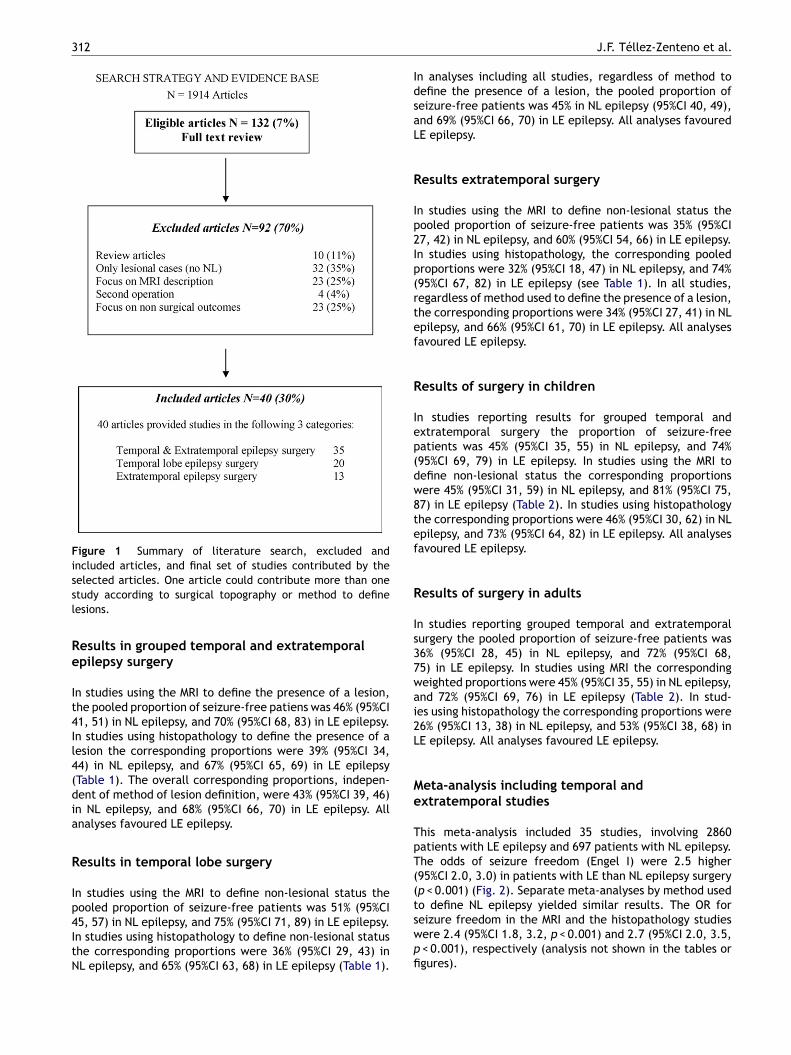
The literature search yielded 1914 citations, of which 132(7%) were potentially eligible and were examined in fulltext independently by two reviewers (Fig. 1). Of these, 92(70%) articles were excluded and 40 (30%) were included inthe meta-analysis. Of the 40 articles included, 28 reportedon 35 studies describing surgical outcomes of temporal andextratemporal surgeries, 17 reported on 20 studies of tem-poral lobe epilepsy surgery, and 12 reported on 13 studies ofextratemporal epilepsy surgery (Appendix B). Visual analysisof forest plots revealed no substantial clinical heterogene-ity; the point estimate of all but two studies was in the samedirection. The Q-statistic for all meta-analysis revealed nostatistically significant heterogeneity (p-values ranged from0.12 to 0.59). Accordingly, we performed the correspondingmeta-analyses.
Prevalence of non-lesional epilepsy surgery
The overall prevalence of patients with NL epilepsy in allsurgical studies was 26%, but it was significantly higher inpatients with extratemporal surgery (45%), than in thosewith temporal or grouped temporal and extratemporalsurgery (24% each, p < 0.001). The prevalence also variedby the method used to define NL epilepsy. It was sig-nificantly higher in cases defined by MRI (44%) than byhistopathology (16%) (p < 0.001). Lastly, the prevalence wassignificantly higher in children (31%) than in adults (21%)(p < 0.001).
312 J.F. Téllez-Zenteno et al.
Figure 1 Summary of literature search, excluded andincluded articles, and final set of studies contributed by thessl
Re
It4Il4(dia
R
Ip4ItN
In analyses including all studies, regardless of method todefine the presence of a lesion, the pooled proportion ofseizure-free patients was 45% in NL epilepsy (95%CI 40, 49),and 69% (95%CI 66, 70) in LE epilepsy. All analyses favouredLE epilepsy.
Results extratemporal surgery
In studies using the MRI to define non-lesional status thepooled proportion of seizure-free patients was 35% (95%CI27, 42) in NL epilepsy, and 60% (95%CI 54, 66) in LE epilepsy.In studies using histopathology, the corresponding pooledproportions were 32% (95%CI 18, 47) in NL epilepsy, and 74%(95%CI 67, 82) in LE epilepsy (see Table 1). In all studies,regardless of method used to define the presence of a lesion,the corresponding proportions were 34% (95%CI 27, 41) in NLepilepsy, and 66% (95%CI 61, 70) in LE epilepsy. All analysesfavoured LE epilepsy.
Results of surgery in children
In studies reporting results for grouped temporal andextratemporal surgery the proportion of seizure-freepatients was 45% (95%CI 35, 55) in NL epilepsy, and 74%(95%CI 69, 79) in LE epilepsy. In studies using the MRI todefine non-lesional status the corresponding proportionswere 45% (95%CI 31, 59) in NL epilepsy, and 81% (95%CI 75,87) in LE epilepsy (Table 2). In studies using histopathologythe corresponding proportions were 46% (95%CI 30, 62) in NLepilepsy, and 73% (95%CI 64, 82) in LE epilepsy. All analysesfavoured LE epilepsy.
Results of surgery in adults
In studies reporting grouped temporal and extratemporalsurgery the pooled proportion of seizure-free patients was36% (95%CI 28, 45) in NL epilepsy, and 72% (95%CI 68,75) in LE epilepsy. In studies using MRI the correspondingweighted proportions were 45% (95%CI 35, 55) in NL epilepsy,and 72% (95%CI 69, 76) in LE epilepsy (Table 2). In stud-ies using histopathology the corresponding proportions were26% (95%CI 13, 38) in NL epilepsy, and 53% (95%CI 38, 68) inLE epilepsy. All analyses favoured LE epilepsy.
Meta-analysis including temporal andextratemporal studies
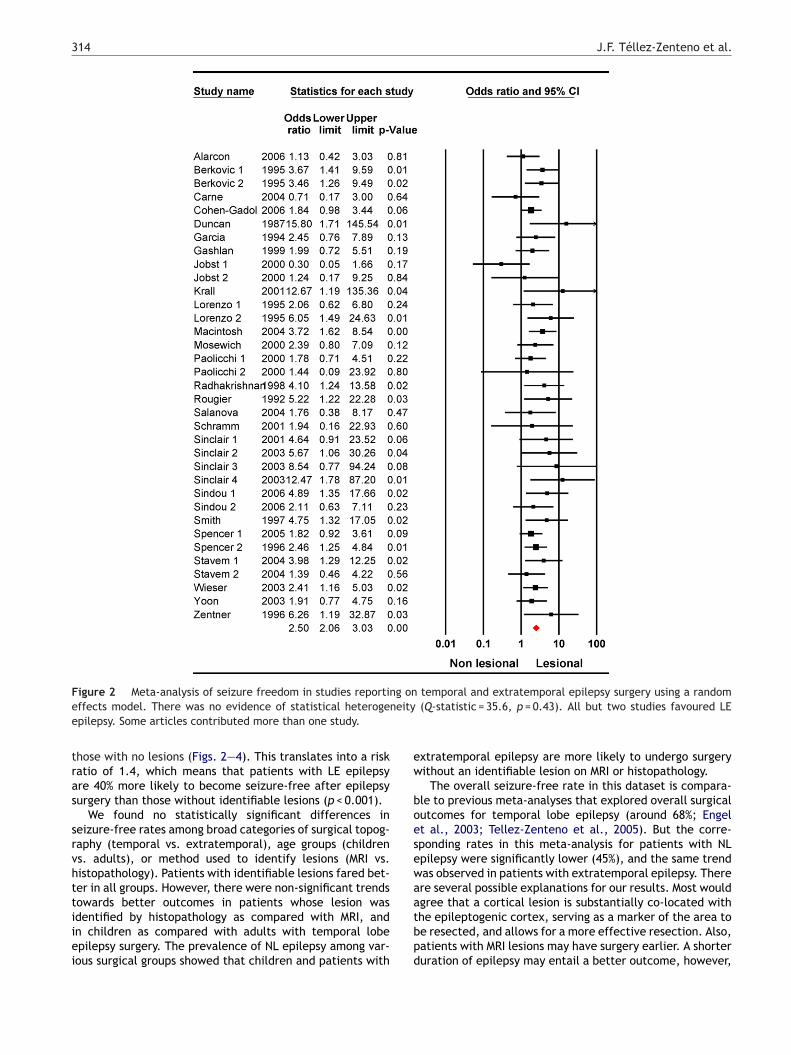
This meta-analysis included 35 studies, involving 2860patients with LE epilepsy and 697 patients with NL epilepsy.The odds of seizure freedom (Engel I) were 2.5 higher(95%CI 2.0, 3.0) in patients with LE than NL epilepsy surgery(p < 0.001) (Fig. 2). Separate meta-analyses by method usedto define NL epilepsy yielded similar results. The OR for
elected articles. One article could contribute more than onetudy according to surgical topography or method to defineesions.
esults in grouped temporal and extratemporalpilepsy surgery
n studies using the MRI to define the presence of a lesion,he pooled proportion of seizure-free patiens was 46% (95%CI1, 51) in NL epilepsy, and 70% (95%CI 68, 83) in LE epilepsy.n studies using histopathology to define the presence of aesion the corresponding proportions were 39% (95%CI 34,4) in NL epilepsy, and 67% (95%CI 65, 69) in LE epilepsyTable 1). The overall corresponding proportions, indepen-ent of method of lesion definition, were 43% (95%CI 39, 46)n NL epilepsy, and 68% (95%CI 66, 70) in LE epilepsy. Allnalyses favoured LE epilepsy.
esults in temporal lobe surgery
n studies using the MRI to define non-lesional status theooled proportion of seizure-free patients was 51% (95%CI
5, 57) in NL epilepsy, and 75% (95%CI 71, 89) in LE epilepsy.n studies using histopathology to define non-lesional statushe corresponding proportions were 36% (95%CI 29, 43) inL epilepsy, and 65% (95%CI 63, 68) in LE epilepsy (Table 1).seizure freedom in the MRI and the histopathology studieswere 2.4 (95%CI 1.8, 3.2, p < 0.001) and 2.7 (95%CI 2.0, 3.5,p < 0.001), respectively (analysis not shown in the tables orfigures).
Surgical outcomes in lesional and non-lesional epilepsy: A systematic review and meta-analysis 313
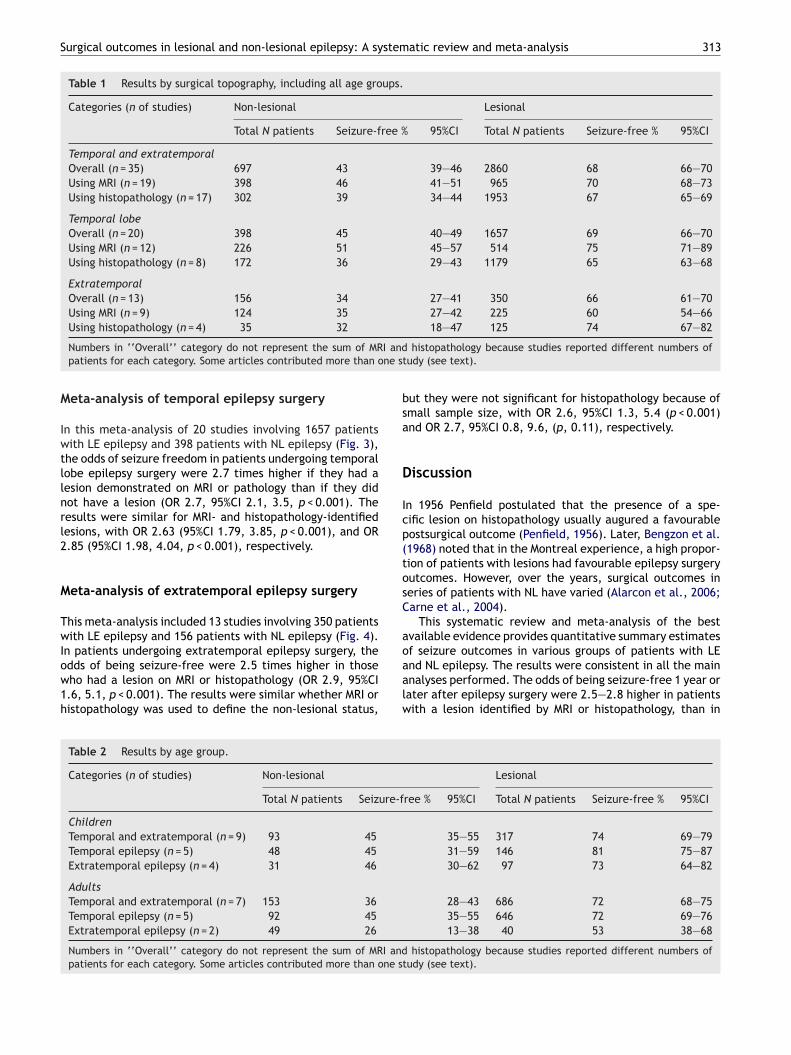
Table 1 Results by surgical topography, including all age groups.
Categories (n of studies) Non-lesional Lesional
Total N patients Seizure-free % 95%CI Total N patients Seizure-free % 95%CI
Temporal and extratemporalOverall (n = 35) 697 43 39—46 2860 68 66—70Using MRI (n = 19) 398 46 41—51 965 70 68—73Using histopathology (n = 17) 302 39 34—44 1953 67 65—69
Temporal lobeOverall (n = 20) 398 45 40—49 1657 69 66—70Using MRI (n = 12) 226 51 45—57 514 75 71—89Using histopathology (n = 8) 172 36 29—43 1179 65 63—68
ExtratemporalOverall (n = 13) 156 34 27—41 350 66 61—70Using MRI (n = 9) 124 35 27—42 225 60 54—66Using histopathology (n = 4) 35 32 18—47 125 74 67—82
Numbers in ‘‘Overall’’ category do not represent the sum of MRI and histopathology because studies reported different numbers ofpatients for each category. Some articles contributed more than one study (see text).
Meta-analysis of temporal epilepsy surgery
In this meta-analysis of 20 studies involving 1657 patientswith LE epilepsy and 398 patients with NL epilepsy (Fig. 3),the odds of seizure freedom in patients undergoing temporallobe epilepsy surgery were 2.7 times higher if they had alesion demonstrated on MRI or pathology than if they didnot have a lesion (OR 2.7, 95%CI 2.1, 3.5, p < 0.001). Theresults were similar for MRI- and histopathology-identifiedlesions, with OR 2.63 (95%CI 1.79, 3.85, p < 0.001), and OR2.85 (95%CI 1.98, 4.04, p < 0.001), respectively.
Meta-analysis of extratemporal epilepsy surgery
This meta-analysis included 13 studies involving 350 patientswith LE epilepsy and 156 patients with NL epilepsy (Fig. 4).In patients undergoing extratemporal epilepsy surgery, theodds of being seizure-free were 2.5 times higher in thosewho had a lesion on MRI or histopathology (OR 2.9, 95%CI1.6, 5.1, p < 0.001). The results were similar whether MRI orhistopathology was used to define the non-lesional status,
but they were not significant for histopathology because ofsmall sample size, with OR 2.6, 95%CI 1.3, 5.4 (p < 0.001)and OR 2.7, 95%CI 0.8, 9.6, (p, 0.11), respectively.
Discussion
In 1956 Penfield postulated that the presence of a spe-cific lesion on histopathology usually augured a favourablepostsurgical outcome (Penfield, 1956). Later, Bengzon et al.(1968) noted that in the Montreal experience, a high propor-tion of patients with lesions had favourable epilepsy surgeryoutcomes. However, over the years, surgical outcomes inseries of patients with NL have varied (Alarcon et al., 2006;Carne et al., 2004).
This systematic review and meta-analysis of the bestavailable evidence provides quantitative summary estimatesof seizure outcomes in various groups of patients with LEand NL epilepsy. The results were consistent in all the mainanalyses performed. The odds of being seizure-free 1 year orlater after epilepsy surgery were 2.5—2.8 higher in patientswith a lesion identified by MRI or histopathology, than in
Table 2 Results by age group.
Categories (n of studies) Non-lesional Lesional
Total N patients Seizure-free % 95%CI Total N patients Seizure-free % 95%CI
ChildrenTemporal and extratemporal (n = 9) 93 45 35—55 317 74 69—79Temporal epilepsy (n = 5) 48 45 31—59 146 81 75—87Extratemporal epilepsy (n = 4) 31 46 30—62 97 73 64—82
AdultsTemporal and extratemporal (n = 7) 153 36 28—43 686 72 68—75Temporal epilepsy (n = 5) 92 45 35—55 646 72 69—76Extratemporal epilepsy (n = 2) 49 26 13—38 40 53 38—68
Numbers in ‘‘Overall’’ category do not represent the sum of MRI and histopathology because studies reported different numbers ofpatients for each category. Some articles contributed more than one study (see text).
314 J.F. Téllez-Zenteno et al.
Figure 2 Meta-analysis of seizure freedom in studies reporting on temporal and extratemporal epilepsy surgery using a randomeffects model. There was no evidence of statistical heterogeneity (Q-statistic = 35.6, p = 0.43). All but two studies favoured LEepilepsy. Some articles contributed more than one study.
those with no lesions (Figs. 2—4). This translates into a riskratio of 1.4, which means that patients with LE epilepsyare 40% more likely to become seizure-free after epilepsysurgery than those without identifiable lesions (p < 0.001).
We found no statistically significant differences inseizure-free rates among broad categories of surgical topog-raphy (temporal vs. extratemporal), age groups (childrenvs. adults), or method used to identify lesions (MRI vs.histopathology). Patients with identifiable lesions fared bet-ter in all groups. However, there were non-significant trendstowards better outcomes in patients whose lesion wasidentified by histopathology as compared with MRI, andin children as compared with adults with temporal lobeepilepsy surgery. The prevalence of NL epilepsy among var-ious surgical groups showed that children and patients with
extratemporal epilepsy are more likely to undergo surgerywithout an identifiable lesion on MRI or histopathology.
The overall seizure-free rate in this dataset is compara-ble to previous meta-analyses that explored overall surgicaloutcomes for temporal lobe epilepsy (around 68%; Engelet al., 2003; Tellez-Zenteno et al., 2005). But the corre-sponding rates in this meta-analysis for patients with NLepilepsy were significantly lower (45%), and the same trendwas observed in patients with extratemporal epilepsy. Thereare several possible explanations for our results. Most wouldagree that a cortical lesion is substantially co-located withthe epileptogenic cortex, serving as a marker of the area tobe resected, and allows for a more effective resection. Also,patients with MRI lesions may have surgery earlier. A shorterduration of epilepsy may entail a better outcome, however,

Surgical outcomes in lesional and non-lesional epilepsy: A systematic review and meta-analysis 315
Figure 3 Meta-analysis of seizure freedom in studies reporting on temporal epilepsy surgery using a random effects model. Therewas no evidence of statistical heterogeneity (Q-statistic = 18.1, p = 0.47). All but two studies favoured LE epilepsy. Some articlescontributed more than one study.
this requires further exploration (McIntosh et al., 2004).The lower chance of success in patients with NL epilepsycould be associated with a multifocal seizure onset, fail-ure of scalp and intracranial EEG to accurately identify theepileptogenic area, and the presence of subcortical seizuregenerators (Salanova et al., 2005; Siegel et al., 2004; Wyleret al., 1989). New imaging techniques such as high definitionMRI, diffusion tensor imaging, and the various modalities offunctional imaging are expected to improve not only the cer-tainty and precision of epilepsy surgery (Cascino, 2008), butalso its outcomes.
Strengths of this meta-analysis include the steps takento ensure validity and reliability of the data, the selectionof controlled studies (i.e., those reporting outcomes in bothLE and NL patients in the same study), and the achieve-ment of a relatively homogeneous group of studies thatallowed for meaningful pooling of data and summary esti-mates. Selecting studies that report outcomes on LE andNL patients from the same program or center contributedto avoiding noise in the analyses. However, readers shouldalso consider some weaknesses of this meta-analysis wheninterpreting and applying the results. We are limited bythe data available in the primary studies. First, there ismethodological variability among studies, e.g., in the defi-nitions and methods of outcome assessment and reporting,
in patient selection, and in the nature of interventions. Yet,as in previous meta-analyses of epilepsy surgery, it is reas-suring to encounter homogeneous and consistent findingsacross studies, which lend validity to the results. Second,the data do not allow us to explore other factors in addi-tion to lesional status that could influence seizure outcomes.Conceivably, lesional status interacts with other variablesto influence prognosis. On the other hand, the robustnessof the results across all analyses supports the notion thatlesional status is a reliable prognostic indicator of seizureoutcomes in epilepsy surgery. Finally, we have not exploredother important outcomes, such as quality of life, mood,and psychosocial outcomes. Data on these variables is muchmore limited and more difficult to summarize meaningfully.Nonetheless, seizure outcome is a strong predictor of theseoutcomes.
Our results should not be used to foster skepticismtowards surgery in patients without a lesion on MRI whoare otherwise good surgical candidates. It is important topoint out that nearly half of these patients achieved seizurefreedom with surgery. Furthermore, lesions may also beidentified a posteriori, through histopathological analysis,and these patients also have better outcomes. A non-lesionalMRI does not negate surgery. On the other hand, our resultssupport the importance of obtaining high quality, expertly

316 J.F. Téllez-Zenteno et al.
Figure 4 Meta-analysis of seizure freedom in studies reporting on extratemporal epilepsy surgery using a random effects model.There was no evidence of statistical heterogeneity (Q-statistic = 17.9, p = 0.12). Only three studies favoured NL epilepsy. Somearticles contributed more than one study.
interpreted MRI in evaluating patients for surgery. Theseresults play an important role in counseling patients and inprognosticating surgical outcomes.
Acknowledgements
This research was supported by research grant from the Uni-versity of Saskatchewan and the Royal University HospitalFoundation, Saskatoon, Saskatchewan.
Appendix A. Literature search strategy
First step:‘‘Epilepsy/surgery’’ [MeSH] OR (‘‘epilepsy’’ [TW] AND
‘‘surgery’’ [TW])
Second step:‘‘Incidence’’ [MESH] OR ‘‘Mortality’’ [MESH] OR ‘‘mortality’’
[SH] OR ‘‘Follow-Up Studies’’ [MESH] OR ‘‘Prognosis’’[MeSH:NOEXP] OR ‘‘prognos*’’ [TW] OR ‘‘predict*’’ [TW] OR
‘‘course’’ [TW] OR ‘‘outcome’’ [TW] OR ‘‘psychology’’[TW] OR ‘‘Quality of Life’’ [MeSH] OR ‘‘Quality of Life’’ [TW]
OR memory [TW] OR ‘‘Survival Analysis’’[MH:NOEXP]
Third step:‘‘Randomized controlled trial’’ [PTYP] OR ‘‘random*’’ [TW]
OR (‘‘double’’[TW] AND ‘‘blind*’’ [TW]) OR ‘‘placebo’’
[TW] OR ‘‘drug therapy’’ [SH] OR ‘‘therapeutic use’’[SH:NOEXP] OR ‘‘cohort studies’’ [MESH] OR ‘‘risk’’ [MESH]OR
(‘‘odds’’ [TW] AND ‘‘ratio*’’ [TW]) OR (‘‘relative’’ [TW] AND‘‘risk’’ [TW]) OR ‘‘case—control*’’ [TW] OR ‘‘case—control
studies’’ [MESH]
Fourth step: LimitsPublication Year 1995—2007HumanJournal article
Appendix B. Articles contributing to thesystematic review
Analysis of grouped temporal and extratemporal epilepsy(Alarcon et al., 2006; Berkovic et al., 1995; Carne et al., 2004;
Cohen-Gadol et al., 2006; Duncan and Sagar, 1987; Garcia etal., 1994; Gashlan et al., 1999; Jobst et al., 2000; Kral etal., 2001; Lorenzo et al., 1995; McIntosh et al., 2004;Mosewich et al., 2000; Paolicchi et al., 2000; Radhakrishnanet al., 1998; Rougier et al., 1992; Salanova et al., 2004;Schramm et al., 2001; Sinclair et al., 2001, 2003, 2004;Sindou et al., 2006; Smith et al., 1997; Spencer, 1996;Spencer et al., 2005; Stavem et al., 2004; Wieser et al.,2003; Yoon et al., 2003; Zentner et al.,1996)

Surgical outcomes in lesional and non-lesional epilepsy: A systematic review and meta-analysis 317
Analysis of temporal epilepsy(Alarcon et al., 2006; Berkovic et al., 1995; Carne et al., 2004;
Duncan, 1997; Garcia et al., 1994; Gashlan et al., 1999;McIntosh et al., 2004; Paolicchi et al., 2000; Radhakrishnanet al., 1998; Salanova et al., 2004; Sinclair et al., 2001,2003, 2004; Sindou et al., 2006; Spencer et al., 2005;Stavem et al., 2004; Wieser et al., 2003)
Analysis of extratemporal epilepsy(Alarcon et al., 2006; Gashlan et al., 1999; Jobst et al., 2000;
Kral et al., 2001; Lorenzo et al., 1995; Mosewich et al.,2000; Paolicchi et al., 2000; Schramm et al., 2001; Sinclairet al., 2001, 2003, 2004; Smith et al., 1997)
References
Alarcon, G., Valentin, A., Watt, C., Selway, R.P., Lacruz, M.E.,Elwes, R.D., Jarosz, J.M., Honavar, M., Brunhuber, F., Mullatti,N., Bodi, I., Salinas, M., Binnie, C.D., Polkey, C.E., 2006. Isit worth pursuing surgery for epilepsy in patients with normalneuroimaging? J. Neurol. Neurosurg. Psychiatry 77, 474—480.
Bengzon, A.R., Rasmussen, T., Gloor, P., Dussault, J., Stephens, M.,1968. Prognostic factors in the surgical treatment of temporallobe epileptics. Neurology 18, 717—731.
Berkovic, S.F., McIntosh, A.M., Kalnins, R.M., Jackson, G.D.,Fabinyi, G.C., Brazenor, G.A., Bladin, P.F., Hopper, J.L., 1995.Preoperative MRI predicts outcome of temporal lobectomy: anactuarial analysis. Neurology 45, 1358—1363.
Blume, W.T., 1986. Principles of clinical investigation of surgicalpatients. Int. Anesthesiol. Clin. 24, 47—73.
Carne, R.P., O’Brien, T.J., Kilpatrick, C.J., MacGregor, L.R., Hicks,R.J., Murphy, M.A., Bowden, S.C., Kaye, A.H., Cook, M.J., 2004.MRI-negative PET-positive temporal lobe epilepsy: a distinct sur-gically remediable syndrome. Brain 127, 2276—2285.
Cascino, G.D., 2008. Neuroimaging in epilepsy: diagnostic strategiesin partial epilepsy. Semin. Neurol. 28, 523—532.
Cohen-Gadol, A.A., Wilhelmi, B.G., Collignon, F., White, J.B.,Britton, J.W., Cambier, D.M., Christianson, T.J., Marsh, W.R.,Meyer, F.B., Cascino, G.D., 2006. Long-term outcome of epilepsysurgery among 399 patients with nonlesional seizure foci includ-ing mesial temporal lobe sclerosis. J. Neurosurg. 104, 513—524.
Duncan, J.S., 1997. Imaging and epilepsy. Brain 120 (Pt 2), 339—377.Duncan, J.S., Sagar, H.J., 1987. Seizure characteristics, pathology,
and outcome after temporal lobectomy. Neurology 37, 405—409.Engel Jr., J., Wiebe, S., French, J., Sperling, M., Williamson, P.,
Spencer, D., Gumnit, R., Zahn, C., Westbrook, E., Enos, B.,2003. Practice parameter: temporal lobe and localized neocor-tical resections for epilepsy: report of the Quality StandardsSubcommittee of the American Academy of Neurology, in asso-ciation with the American Epilepsy Society and the AmericanAssociation of Neurological Surgeons. Neurology 60, 538—547.
Ferrier, C.H., Engelsman, J., Alarcon, G., Binnie, C.D., Polkey, C.E.,1999. Prognostic factors in presurgical assessment of frontal lobeepilepsy. J. Neurol. Neurosurg. Psychiatry 66, 350—356.
Garcia, P.A., Laxer, K.D., Barbaro, N.M., Dillon, W.P., 1994.Prognostic value of qualitative magnetic resonance imaginghippocampal abnormalities in patients undergoing temporallobectomy for medically refractory seizures. Epilepsia 35,520—524.
Gashlan, M., Loy-English, I., Ventureyra, E.C., Keene, D., 1999.Predictors of seizure outcome following cortical resection inpediatric and adolescent patients with medically refractoryepilepsy. Childs Nerv. Syst. 15, 45—50.
Hong, K.S., Lee, S.K., Kim, J.Y., Lee, D.S., Chung, C.K., 2002. Pre-surgical evaluation and surgical outcome of 41 patients with non-lesional neocortical epilepsy. Seizure 11, 184—192.
Jeha, L.E., Najm, I.M., Bingaman, W.E., Khandwala, F., Widdess-Walsh, P., Morris, H.H., Dinner, D.S., Nair, D., Foldvary-Schaeffer,N., Prayson, R.A., Comair, Y., O’Brien, R., Bulacio, J., Gupta,A., Luders, H.O., 2006. Predictors of outcome after temporallobectomy for the treatment of intractable epilepsy. Neurology66, 1938—1940.
Jobst, B.C., Siegel, A.M., Thadani, V.M., Roberts, D.W., Rhodes,H.C., Williamson, P.D., 2000. Intractable seizures of frontal lobeorigin: clinical characteristics, localizing signs, and results ofsurgery. Epilepsia 41, 1139—1152.
Kral, T., Kuczaty, S., Blumcke, I., Urbach, H., Clusmann, H.,Wiestler, O.D., Elger, C., Schramm, J., 2001. Postsurgical out-come of children and adolescents with medically refractoryfrontal lobe epilepsies. Childs Nerv. Syst. 17, 595—601.
Kutsy, R.L., 1999. Focal extratemporal epilepsy: clinical features.EEG patterns, and surgical approach. J. Neurol. Sci. 166, 1—15.
Lorenzo, N.Y., Parisi, J.E., Cascino, G.D., Jack Jr., C.R., Marsh,W.R., Hirschorn, K.A., 1995. Intractable frontal lobe epilepsy:pathological and MRI features. Epilepsy Res. 20, 171—178.
McIntosh, A.M., Kalnins, R.M., Mitchell, L.A., Fabinyi, G.C., Briell-mann, R.S., Berkovic, S.F., 2004. Temporal lobectomy: long-termseizure outcome, late recurrence and risks for seizure recur-rence. Brain 127, 2018—2030.
McIntosh, A.M., Wilson, S.J., Berkovic, S.F., 2001. Seizure outcomeafter temporal lobectomy: current research practice and find-ings. Epilepsia 42, 1288—1307.
Mosewich, R.K., So, E.L., O’Brien, T.J., Cascino, G.D., Sharbrough,F.W., Marsh, W.R., Meyer, F.B., Jack, C.R., O’Brien, P.C., 2000.Factors predictive of the outcome of frontal lobe epilepsysurgery. Epilepsia 41, 843—849.
Paolicchi, J.M., Jayakar, P., Dean, P., Yaylali, I., Morrison, G., Prats,A., Resnik, T., Alvarez, L., Duchowny, M., 2000. Predictors ofoutcome in pediatric epilepsy surgery. Neurology 54, 642—647.
Penfield, W., 1956. Epileptogenic lesions. Acta Neurol. Psychiatr.Belg. 56, 75—88.
Radhakrishnan, K., So, E.L., Silbert, P.L., Jack Jr., C.R., Cascino,G.D., Sharbrough, F.W., O’Brien, P.C., 1998. Predictors of out-come of anterior temporal lobectomy for intractable epilepsy:a multivariate study. Neurology 51, 465—471.
Rougier, A., Dartigues, J.F., Commenges, D., Claverie, B., Loiseau,P., Cohadon, F., 1992. A longitudinal assessment of seizure out-come and overall benefit from 100 cortectomies for epilepsy. J.Neurol. Neurosurg. Psychiatry 55, 762—767.
Salanova, V., Markand, O., Worth, R., 2004. Temporal lobe epilepsy:analysis of patients with dual pathology. Acta Neurol. Scand.109, 126—131.
Salanova, V., Markand, O., Worth, R., 2005. Temporal lobe epilepsy:analysis of failures and the role of reoperation. Acta Neurol.Scand. 111, 126—133.
Schramm, J., Kral, T., Grunwald, T., Blumcke, I., 2001. Surgicaltreatment for neocortical temporal lobe epilepsy: clinical andsurgical aspects and seizure outcome. J. Neurosurg. 94, 33—42.
Siegel, A.M., Cascino, G.D., Meyer, F.B., McClelland, R.L., So, E.L.,Marsh, W.R., Scheithauer, B.W., Sharbrough, F.W., 2004. Resec-tive reoperation for failed epilepsy surgery: seizure outcome in64 patients. Neurology 63, 2298—2302.
Siegel, A.M., Jobst, B.C., Thadani, V.M., Rhodes, C.H., Lewis, P.J.,Roberts, D.W., Williamson, P.D., 2001. Medically intractable,localization-related epilepsy with normal MRI: presurgical eval-uation and surgical outcome in 43 patients. Epilepsia 42,883—888.
Sinclair, D.B., Aronyk, K., Snyder, T., McKean, J., Wheatley, M.,Bhargava, R., Hoskinson, M., Hao, C., Colmers, W., 2003. Pedi-atric temporal lobectomy for epilepsy. Pediatr. Neurosurg. 38,192—205.
Sinclair, D.B., Aronyk, K., Snyder, T., McKean, J.D., Wheatley, M.,Gross, D., Bastos, A., Ahmed, S.N., Hao, C., Colmers, W., 2004.

318 J.F. Téllez-Zenteno et al.
Extratemporal resection for childhood epilepsy. Pediatr. Neurol.30, 177—185.
Sinclair, D.B., Wheatley, M., Aronyk, K., Hao, C., Snyder, T.,Colmers, W., McKean, J.D., 2001. Pathology and neuroimaging inpediatric temporal lobectomy for intractable epilepsy. Pediatr.Neurosurg. 35, 239—246.
Sindou, M., Guenot, M., Isnard, J., Ryvlin, P., Fischer, C., Mau-guiere, F., 2006. Temporo-mesial epilepsy surgery: outcome andcomplications in 100 consecutive adult patients. Acta Neurochir.(Wien.) 148, 39—45.
Smith, J.R., Lee, M.R., King, D.W., Murro, A.M., Park, Y.D., Lee,G.P., Loring, D.W., Meador, K.J., Harp, R., 1997. Results oflesional vs. nonlesional frontal lobe epilepsy surgery. Stereotact.Funct. Neurosurg. 69, 202—209.
Spencer, S.S., 1996. Long-term outcome after epilepsy surgery.Epilepsia 37, 807—813.
Spencer, S.S., Berg, A.T., Vickrey, B.G., Sperling, M.R., Bazil, C.W.,Shinnar, S., Langfitt, J.T., Walczak, T.S., Pacia, S.V., 2005.Predicting long-term seizure outcome after resective epilepsysurgery: the multicenter study. Neurology 65, 912—918.
Stavem, K., Bjornaes, H., Langmoen, I.A., 2004. Predictors ofseizure outcome after temporal lobectomy for intractableepilepsy. Acta Neurol. Scand. 109, 244—249.
Tellez-Zenteno, J.F., Dhar, R., Hernandez-Ronquillo, L., Wiebe, S.,2007. Long-term outcomes in epilepsy surgery: antiepilepticdrugs, mortality, cognitive and psychosocial aspects. Brain 130,334—345.
Tellez-Zenteno, J.F., Dhar, R., Wiebe, S., 2005. Long-term seizureoutcomes following epilepsy surgery: a systematic review andmeta-analysis. Brain 128, 1188—1198.
Wieser, H.G., Ortega, M., Friedman, A., Yonekawa, Y., 2003. Long-term seizure outcomes following amygdalohippocampectomy. J.Neurosurg. 98, 751—763.
Wieshmann, U.C., Larkin, D., Varma, T., Eldridge, P., 2008. Pre-dictors of outcome after temporal lobectomy for refractorytemporal lobe epilepsy. Acta Neurol. Scand. 118, 306—312.
Wyler, A.R., Hermann, B.P., Richey, E.T., 1989. Results of reopera-tion for failed epilepsy surgery. J. Neurosurg. 71, 815—819.
Yoon, H.H., Kwon, H.L., Mattson, R.H., Spencer, D.D., Spencer, S.S.,2003. Long-term seizure outcome in patients initially seizure-free after resective epilepsy surgery. Neurology 61, 445—450.
Zentner, J., Hufnagel, A., Ostertun, B., Wolf, H.K., Behrens,E., Campos, M.G., Solymosi, L., Elger, C.E., Wiestler, O.D.,Schramm, J., 1996. Surgical treatment of extratemporalepilepsy: clinical, radiologic, and histopathologic findings in 60patients. Epilepsia 37, 1072—1080.
Related Documents