Abstract—The correction of dento-facial deformity often requires combined surgical and orthodontic therapy. Poor facial appearance and functional difficulties are the motivating factors for seeking treatment in patients with Class III skeletal anomalies. This presentation aims to show the surgical and orthodontic procedure in correcting Class III patients. Keywords—skeletal anomalies, orthognathic surgery, class III malocclusion. I. INTRODUCTION During the last few decades our profession has witnessed an intense interest in the treatment of facial deformities.[1,2,3,4] Orthognathic surgery has become an acceptable treatment plan for patients with various maxillofacial deformities with pleasing results. The rehabilitation of severe Class III adult patients requires a complex interdisciplinary orthodontic and orthognathic approach. The interdisciplinary team provides the professional opinion and guidance for diagnosis of the problem, selection of orthodontic and surgical treatment plan.[5,6] This presentation aims to show the surgical and orthodontic procedure in correcting complexe Class III patients with long faces. The goals of combined surgical and orthodontic treatment are: • to improve facial and dental aesthetics • a functional, balanced and stable occlusion • a satisfied patient. The management protocol for facial deformity should comprise the: • History • Clinical examination • Investigations • Initial diagnosis • Treatment plan • Presurgical orthodontics • Final treatment plan • Surgery • Postsurgical orthodontics. • Retention. When appropriate, restorative dentistry, psychological intervention or support and speech therapy will be required[7]. II. CASE REPORT A 19 year old male patient presented to the orthodontist requesting a better dental and facial appearance. The medical and familial history were not significant in determining the etiological factor. Facial features consisted of large lower facial height, lack of malar proeminence, concave profile, prognathic mandible, retruded maxilla. Intraoral findings were also significant: severe class III malocclusion, large openbite, midline shift, protrusion of lower incisors, posterior crossbite. The lateral cephalogram was analysed with the Cephx software and revealed: • Extremely large lower face height • Retruded maxilla • Retruded upper incisors • Large intercincisal angle(139.34°) • Mandible forward to maxilla(concave profile) • Class III skeletal relationship(ANB – 6.18°) • Severe high angle associated with openbite • Upper lip retrusion. Fig.1 Initial facial situation. Large lower facial height, lack of malar proeminence, concave profile. Surgical-Orthodontic Treatment in Class III Skeletal Anomalies Eduard Gîdea Paraschivescu, Camelia Szuhanek Faculty of Dental Medicine, University of Medicine and Pharmacy “Victor Babes” Timisoara, ROMANIA [email protected], [email protected] Proceedings of the World Medical Conference ISBN: 978-1-61804-036-7 227

Surgical-Orthodontic Treatment in Class III Skeletal …[email protected] Dr.Camelia Szuhanek was born in Timisoara, Romania, on 25th of November 1975. She is a specialist
Mar 10, 2020
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Abstract—The correction of dento-facial deformity often
requires combined surgical and orthodontic therapy. Poor
facial appearance and functional difficulties are the motivating
factors for seeking treatment in patients with Class III skeletal
anomalies. This presentation aims to show the surgical and
orthodontic procedure in correcting Class III patients.
Keywords—skeletal anomalies, orthognathic surgery, class
III malocclusion.
I. INTRODUCTION
During the last few decades our profession has witnessed an
intense interest in the treatment of facial deformities.[1,2,3,4]
Orthognathic surgery has become an acceptable treatment plan
for patients with various maxillofacial deformities with
pleasing results. The rehabilitation of severe Class III adult
patients requires a complex interdisciplinary orthodontic and
orthognathic approach. The interdisciplinary team provides the
professional opinion and guidance for diagnosis of the
problem, selection of orthodontic and surgical treatment
plan.[5,6]
This presentation aims to show the surgical and orthodontic
procedure in correcting complexe Class III patients with long
faces.
The goals of combined surgical and orthodontic treatment
are:
• to improve facial and dental aesthetics
• a functional, balanced and stable occlusion
• a satisfied patient.
The management protocol for facial deformity should
comprise the:
• History
• Clinical examination
• Investigations
• Initial diagnosis
• Treatment plan
• Presurgical orthodontics
• Final treatment plan
• Surgery
• Postsurgical orthodontics.
• Retention.
When appropriate, restorative dentistry, psychological
intervention or support and speech therapy will be
required[7].
II. CASE REPORT
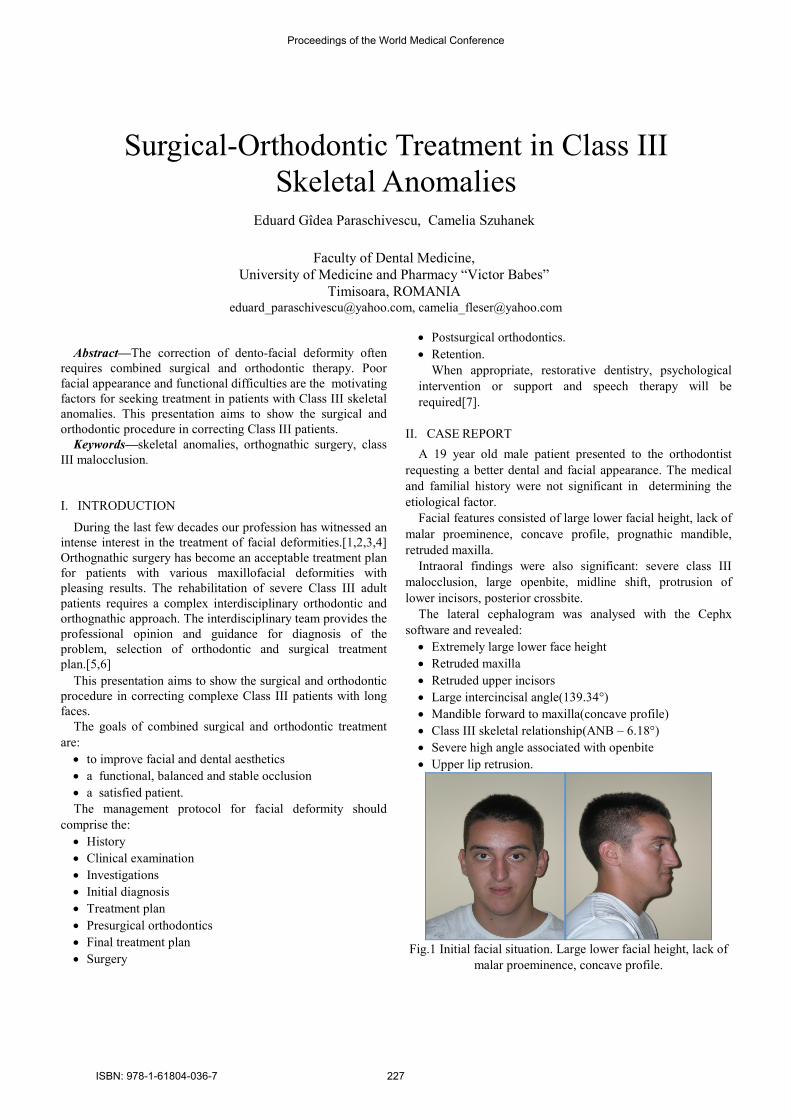
A 19 year old male patient presented to the orthodontist
requesting a better dental and facial appearance. The medical
and familial history were not significant in determining the
etiological factor.
Facial features consisted of large lower facial height, lack of
malar proeminence, concave profile, prognathic mandible,
retruded maxilla.
Intraoral findings were also significant: severe class III
malocclusion, large openbite, midline shift, protrusion of
lower incisors, posterior crossbite.
The lateral cephalogram was analysed with the Cephx
software and revealed:
• Extremely large lower face height
• Retruded maxilla
• Retruded upper incisors
• Large intercincisal angle(139.34°)
• Mandible forward to maxilla(concave profile)
• Class III skeletal relationship(ANB – 6.18°)
• Severe high angle associated with openbite
• Upper lip retrusion.
Fig.1 Initial facial situation. Large lower facial height, lack of
malar proeminence, concave profile.
Surgical-Orthodontic Treatment in Class III
Skeletal Anomalies
Eduard Gîdea Paraschivescu, Camelia Szuhanek
Faculty of Dental Medicine,
University of Medicine and Pharmacy “Victor Babes”
Timisoara, ROMANIA [email protected], [email protected]
Proceedings of the World Medical Conference
ISBN: 978-1-61804-036-7 227
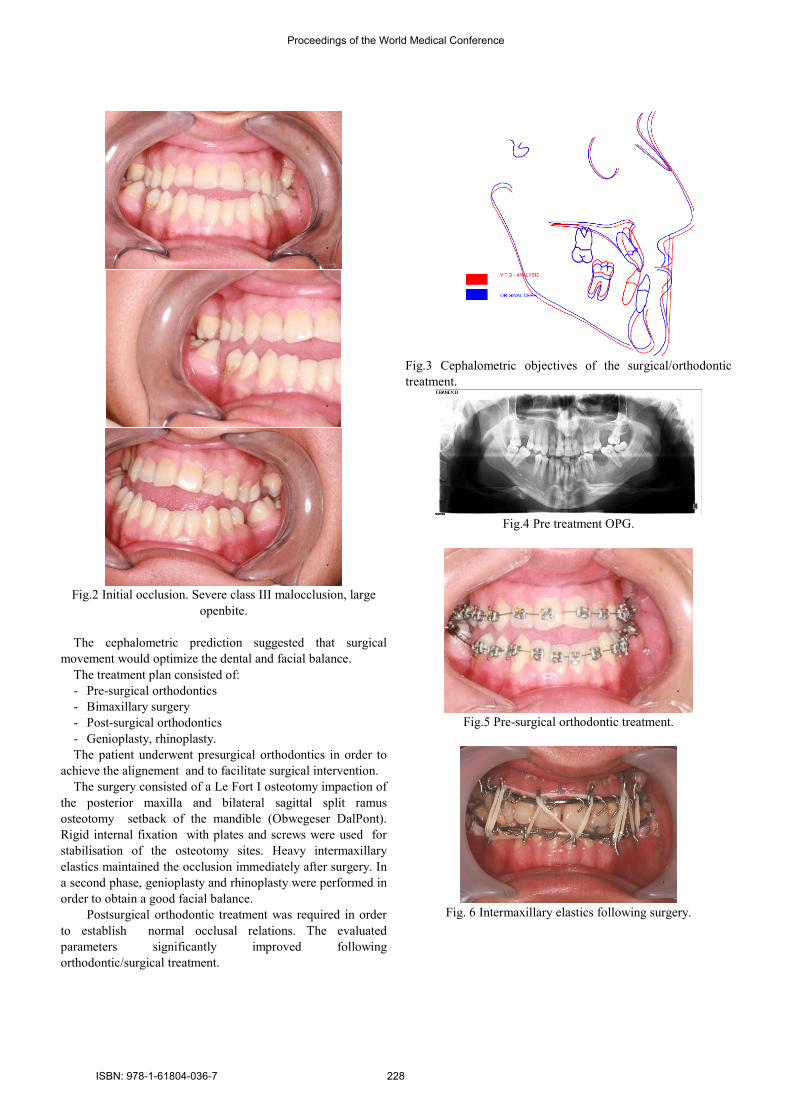
Fig.2 Initial occlusion. Severe class III malocclusion, large
openbite.
The cephalometric prediction suggested that surgical
movement would optimize the dental and facial balance.
The treatment plan consisted of:
- Pre-surgical orthodontics
- Bimaxillary surgery
- Post-surgical orthodontics
- Genioplasty, rhinoplasty.
The patient underwent presurgical orthodontics in order to
achieve the alignement and to facilitate surgical intervention.
The surgery consisted of a Le Fort I osteotomy impaction of
the posterior maxilla and bilateral sagittal split ramus
osteotomy setback of the mandible (Obwegeser DalPont).
Rigid internal fixation with plates and screws were used for
stabilisation of the osteotomy sites. Heavy intermaxillary
elastics maintained the occlusion immediately after surgery. In
a second phase, genioplasty and rhinoplasty were performed in
order to obtain a good facial balance.
Postsurgical orthodontic treatment was required in order
to establish normal occlusal relations. The evaluated
parameters significantly improved following
orthodontic/surgical treatment.
Fig.3 Cephalometric objectives of the surgical/orthodontic
treatment.
Fig.4 Pre treatment OPG.
Fig.5 Pre-surgical orthodontic treatment.
Fig. 6 Intermaxillary elastics following surgery.
Proceedings of the World Medical Conference
ISBN: 978-1-61804-036-7 228
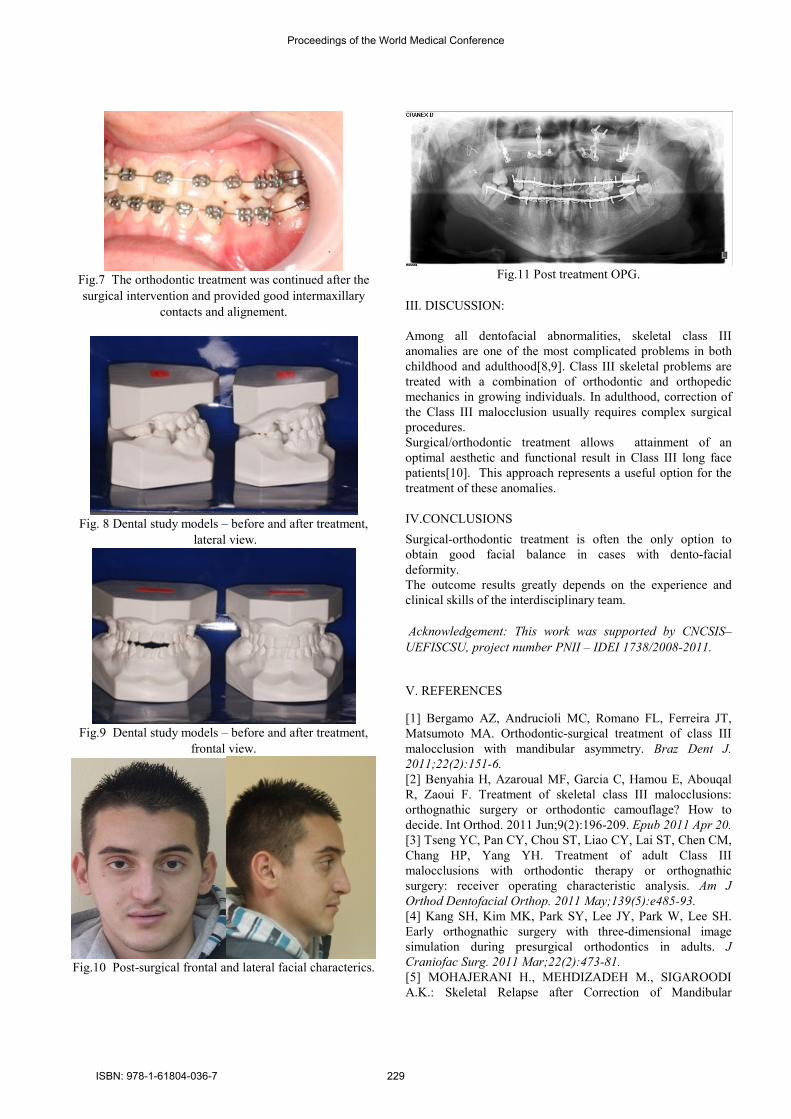
Fig.7 The orthodontic treatment was continued after the
surgical intervention and provided good intermaxillary
contacts and alignement.
Fig. 8 Dental study models – before and after treatment,
lateral view.
Fig.9 Dental study models – before and after treatment,
frontal view.
Fig.10 Post-surgical frontal and lateral facial characterics.
Fig.11 Post treatment OPG.
III. DISCUSSION:
Among all dentofacial abnormalities, skeletal class III
anomalies are one of the most complicated problems in both
childhood and adulthood[8,9]. Class III skeletal problems are
treated with a combination of orthodontic and orthopedic
mechanics in growing individuals. In adulthood, correction of
the Class III malocclusion usually requires complex surgical
procedures.
Surgical/orthodontic treatment allows attainment of an
optimal aesthetic and functional result in Class III long face
patients[10]. This approach represents a useful option for the
treatment of these anomalies.
IV.CONCLUSIONS
Surgical-orthodontic treatment is often the only option to
obtain good facial balance in cases with dento-facial
deformity.
The outcome results greatly depends on the experience and
clinical skills of the interdisciplinary team.
Acknowledgement: This work was supported by CNCSIS–
UEFISCSU, project number PNII – IDEI 1738/2008-2011.
V. REFERENCES
[1] Bergamo AZ, Andrucioli MC, Romano FL, Ferreira JT,
Matsumoto MA. Orthodontic-surgical treatment of class III
malocclusion with mandibular asymmetry. Braz Dent J.
2011;22(2):151-6.
[2] Benyahia H, Azaroual MF, Garcia C, Hamou E, Abouqal
R, Zaoui F. Treatment of skeletal class III malocclusions:
orthognathic surgery or orthodontic camouflage? How to
decide. Int Orthod. 2011 Jun;9(2):196-209. Epub 2011 Apr 20.
[3] Tseng YC, Pan CY, Chou ST, Liao CY, Lai ST, Chen CM,
Chang HP, Yang YH. Treatment of adult Class III
malocclusions with orthodontic therapy or orthognathic
surgery: receiver operating characteristic analysis. Am J
Orthod Dentofacial Orthop. 2011 May;139(5):e485-93.
[4] Kang SH, Kim MK, Park SY, Lee JY, Park W, Lee SH.
Early orthognathic surgery with three-dimensional image
simulation during presurgical orthodontics in adults. J
Craniofac Surg. 2011 Mar;22(2):473-81.
[5] MOHAJERANI H., MEHDIZADEH M., SIGAROODI
A.K.: Skeletal Relapse after Correction of Mandibular
Proceedings of the World Medical Conference
ISBN: 978-1-61804-036-7 229

Prognathism by Bilateral Sagittal Split Ramus Osteotomy,
Journal of Dentistry, Tehran University of Medical Sciences,
Tehran, Iran (2009; Vol. 6, No.3), 2008
[6] Nout E, Koudstaal MJ, Wolvius EB, Van der Wal KG.
Additional orthognathic surgery following Le Fort III and
monobloc advancement. Int J Oral Maxillofac Surg. 2011
Jul;40(7):679-84. Epub 2011 Mar 12.
[7] Liao YF, Chiu YT, Huang CS, Ko EW, Chen YR.
Presurgical orthodontics versus no presurgical orthodontics:
treatment outcome of surgical-orthodontic correction for
skeletal class III open bite. Plast Reconstr Surg. 2010
Dec;126(6):2074-83.
[8] Takahashi H., Furuta H., Moriyama S. : Assessment of
three bilateral sagittal split osteotomy techniques with respect
to mandibular biomechanical stability by experimental study
and finite element analysis simulation; Med.Bull. Fukuoka
Univ.: 36(3), 181-192, 200.9
[9] Tompach PC, Wheeler JJ,: Orthodontic considerations in
orthognathic surgery, Int. J Adult Orthoganth. Surg. 1995
[10] Szuhanek C., Paraschivescu E. - Interdisciplinary
surgical-orthodontic treatment of class III long face patients.
87th European Orthodontic Society Congress, 19-23th of June
2011, Istanbul, Turkey.
Consultant Dr. Gidea Paraschivescu
Eduard,PhD - born in
Bucharest,Romania, on 27th of
September 1970. Specialist in Cranio-
Maxillo-Facial Surgery, with 17 years of
experience, currently employed as
Assistant Professor at the "Victor
Babes" University of Medicine and
Pharmacy, Timisoara, Romania and part
time at the Municipal Hospital
Timisoara, as consultant CMF Surgeon.
Author and co-author of several books and articles, published
in Romania and abroad and over 50 papers in oral presentation
at national and international conferences and congresses. Chief
surgeon of the Cleft Children International Humanitarian
Mission in Niger, Africa, where he founded a Center of
Excellence in Cleft Lip and Palate Surgery.
Main fields of interest - orthognathic surgery, cleft surgery,
plastic surgery, oncology.
Dr.Camelia Szuhanek was born in
Timisoara, Romania, on 25th of
November 1975. She is a specialist in
Orthodontics and Dentofacial
Orthopedics and received her DDS,
MSc and PhD degrees at the Faculty
of Dental Medicine, University of
Medicine and Pharmacy “Victor
Babes” Timisoara. She is currently an
Assistant Professor at the Department of Orthodontics and the
director of a research project on orthodontic biomechanics at
the University of Medicine and Pharmacy “Victor Babes”
Timisoara. She published over 140 articles in the field of
orthodontics. Dr.Szuhanek maintains a private practice
limited to orthodontics in Timisoara, Romania. Her main
research interests are biomechanics, numerical analysis,
lingual orthodontics, multidisciplinary treatment and skeletal
anchorage.
e-mail: [email protected]
Proceedings of the World Medical Conference
ISBN: 978-1-61804-036-7 230
Related Documents