REVIEW Surgical management of intratemporal lesions A. BOZORG GRAYELI, H. EL GAREM, D. BOUCCARA & O. STERKERS Otolaryngology/Head and Neck Surgery Department, Ho ˆpital Beaujon, Clichy, France Accepted for publication 1 May 2001 BOZORG GRAYELI A ., EL GAREM H ., BOUCCARA D . & STERKERS O . (2001) Clin. Otolaryngol. 26, 357–366 Surgical management of intratemporal lesions In order to evaluate the decisional elements in the surgical strategy of deep-seated and/or extensive intratemporal lesions, a retrospective review of cases followed up between 1985 and 1996 in our department was undertaken. Eighty-one adult patients presenting temporal bone lesions located or extending beyond the middle ear limits excluding vestibular schwannomas and surgically treated were included. The population comprised 38 men and 43 women (mean age: 43 years, range: 17–81). Pre-, intra- and postoperative data were collected from medical files. The principal factors influencing the choice of the surgical approach were the location of the lesion and its presumed aggressiveness, the tumour involvement of the internal carotid artery and the labyrinth on preoperative imaging, and the preoperative hearing loss. A coherent algorithm based on these factors can be proposed for the surgical management of intratemporal lesions. High quality preoperative imaging is mandatory for the surgical planning. Keywords intratemporal tumour surgical approach strategy Extensive intratemporal lesions have always raised surgical difficulties because of the complex anatomy of the temporal bone and the multitude of tumour extension possibilities. 1 The main objective of the surgical treatment is the complete eradication of the lesion with minimal morbidity. However, owing to the vicinity of vital structures such as the carotid artery and many cranial nerves, this objective is not achieved in all cases. 1 To improve the surgical access to different temporal bone regions, and to reduce postoperative sequelae, many surgical approaches and their variants have been described. 2,3 The choice of the surgical approach and its adaptation to individual cases is based principally on a precise radiological work-up. In addition to imaging data, preoperative neurological and audiovestibular status, and the patient’s general condition, influence the therapeutic strategy. 3 The aim of this study was to evaluate the decisional factors in the management of intratemporal lesions and to define a strategic algorithm for their surgical treatment. Material and methods population A retrospective study of 81 consecutive cases of intratemporal lesions, located or extending beyond the middle ear limits and undergoing surgery between 1985 and 1996 in our depart- ment, was undertaken. Intracanalicular vestibular schwanno- mas were excluded from this study. The population comprised 38 men and 43 women (sex ratio ¼ 1.7). The mean age was 41 years (ranging from 16 to 60). The mean follow-up period was 27 months (ranging from 2 to 94 months). Sixty-six cases were operated on for the first time (81%) and 15 were treated surgically for recurrence (19%). Clin. Otolaryngol. 2001, 26, 357–366 # 2001 Blackwell Science Ltd 357 Correspondence: Alexis Bozorg Grayeli, M.D., Ph.D., Service d’Oto-Rhino-Laryngologie, Ho ˆpital Beaujon, 100 Boulevard Ge ´ne ´ral Leclerc, F-92118, Clichy Cedex, France (e-mail: [email protected]).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
REVIEW
Surgical management of intratemporal lesions
A. BOZORG GRAYELI, H. EL GAREM, D. BOUCCARA & O. STERKERSOtolaryngology/Head and Neck Surgery Department, Hopital Beaujon, Clichy, France
Accepted for publication 1 May 2001
B O Z O R G G R AY E L I A. , E L G A R E M H. , B O U C C A R A D. & S T E R K E R S O.
(2001) Clin. Otolaryngol. 26, 357–366
Surgical management of intratemporal lesions
In order to evaluate the decisional elements in the surgical strategy of deep-seated and/or extensive intratemporal
lesions, a retrospective review of cases followed up between 1985 and 1996 in our department was undertaken.
Eighty-one adult patients presenting temporal bone lesions located or extending beyond the middle ear limits
excluding vestibular schwannomas and surgically treated were included. The population comprised
38 men and 43 women (mean age: 43 years, range: 17–81). Pre-, intra- and postoperative data were collected
from medical files. The principal factors influencing the choice of the surgical approach were the location of
the lesion and its presumed aggressiveness, the tumour involvement of the internal carotid artery and the labyrinth
on preoperative imaging, and the preoperative hearing loss. A coherent algorithm based on these factors can
be proposed for the surgical management of intratemporal lesions. High quality preoperative imaging is
mandatory for the surgical planning.
Keywords intratemporal tumour surgical approach strategy
Extensive intratemporal lesions have always raised surgical
difficulties because of the complex anatomy of the temporal
bone and the multitude of tumour extension possibilities.1 The
main objective of the surgical treatment is the complete
eradication of the lesion with minimal morbidity. However,
owing to the vicinity of vital structures such as the carotid
artery and many cranial nerves, this objective is not achieved
in all cases.1
To improve the surgical access to different temporal bone
regions, and to reduce postoperative sequelae, many surgical
approaches and their variants have been described.2,3 The
choice of the surgical approach and its adaptation to individual
cases is based principally on a precise radiological work-up.
In addition to imaging data, preoperative neurological and
audiovestibular status, and the patient’s general condition,
influence the therapeutic strategy.3
The aim of this study was to evaluate the decisional factors
in the management of intratemporal lesions and to define a
strategic algorithm for their surgical treatment.
Material and methods
populat ion
A retrospective study of 81 consecutive cases of intratemporal
lesions, located or extending beyond the middle ear limits and
undergoing surgery between 1985 and 1996 in our depart-
ment, was undertaken. Intracanalicular vestibular schwanno-
mas were excluded from this study. The population comprised
38 men and 43 women (sex ratio ¼ 1.7). The mean age was
41 years (ranging from 16 to 60). The mean follow-up period
was 27 months (ranging from 2 to 94 months). Sixty-six cases
were operated on for the first time (81%) and 15 were treated
surgically for recurrence (19%).
Clin. Otolaryngol. 2001, 26, 357–366
# 2001 Blackwell Science Ltd 357
Correspondence: Alexis Bozorg Grayeli, M.D., Ph.D., Serviced’Oto-Rhino-Laryngologie, Hopital Beaujon, 100 BoulevardGeneral Leclerc, F-92118, Clichy Cedex, France(e-mail: [email protected]).
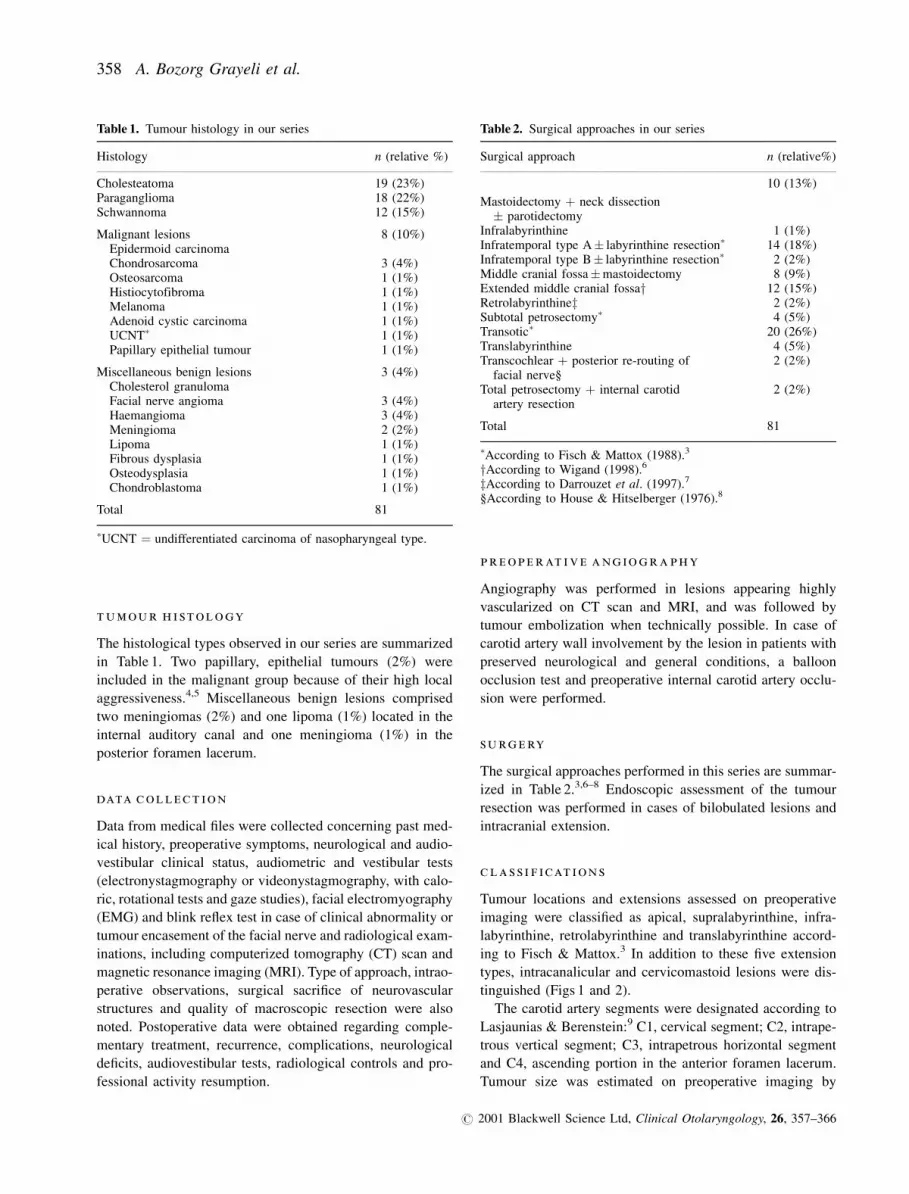
tumour h i stology
The histological types observed in our series are summarized
in Table 1. Two papillary, epithelial tumours (2%) were
included in the malignant group because of their high local
aggressiveness.4,5 Miscellaneous benign lesions comprised
two meningiomas (2%) and one lipoma (1%) located in the
internal auditory canal and one meningioma (1%) in the
posterior foramen lacerum.
data collect ion
Data from medical files were collected concerning past med-
ical history, preoperative symptoms, neurological and audio-
vestibular clinical status, audiometric and vestibular tests
(electronystagmography or videonystagmography, with calo-
ric, rotational tests and gaze studies), facial electromyography
(EMG) and blink reflex test in case of clinical abnormality or
tumour encasement of the facial nerve and radiological exam-
inations, including computerized tomography (CT) scan and
magnetic resonance imaging (MRI). Type of approach, intrao-
perative observations, surgical sacrifice of neurovascular
structures and quality of macroscopic resection were also
noted. Postoperative data were obtained regarding comple-
mentary treatment, recurrence, complications, neurological
deficits, audiovestibular tests, radiological controls and pro-
fessional activity resumption.
pr e ope r at i v e ang iogr a phy
Angiography was performed in lesions appearing highly
vascularized on CT scan and MRI, and was followed by
tumour embolization when technically possible. In case of
carotid artery wall involvement by the lesion in patients with
preserved neurological and general conditions, a balloon
occlusion test and preoperative internal carotid artery occlu-
sion were performed.
su rg e ry
The surgical approaches performed in this series are summar-
ized in Table 2.3,6–8 Endoscopic assessment of the tumour
resection was performed in cases of bilobulated lesions and
intracranial extension.
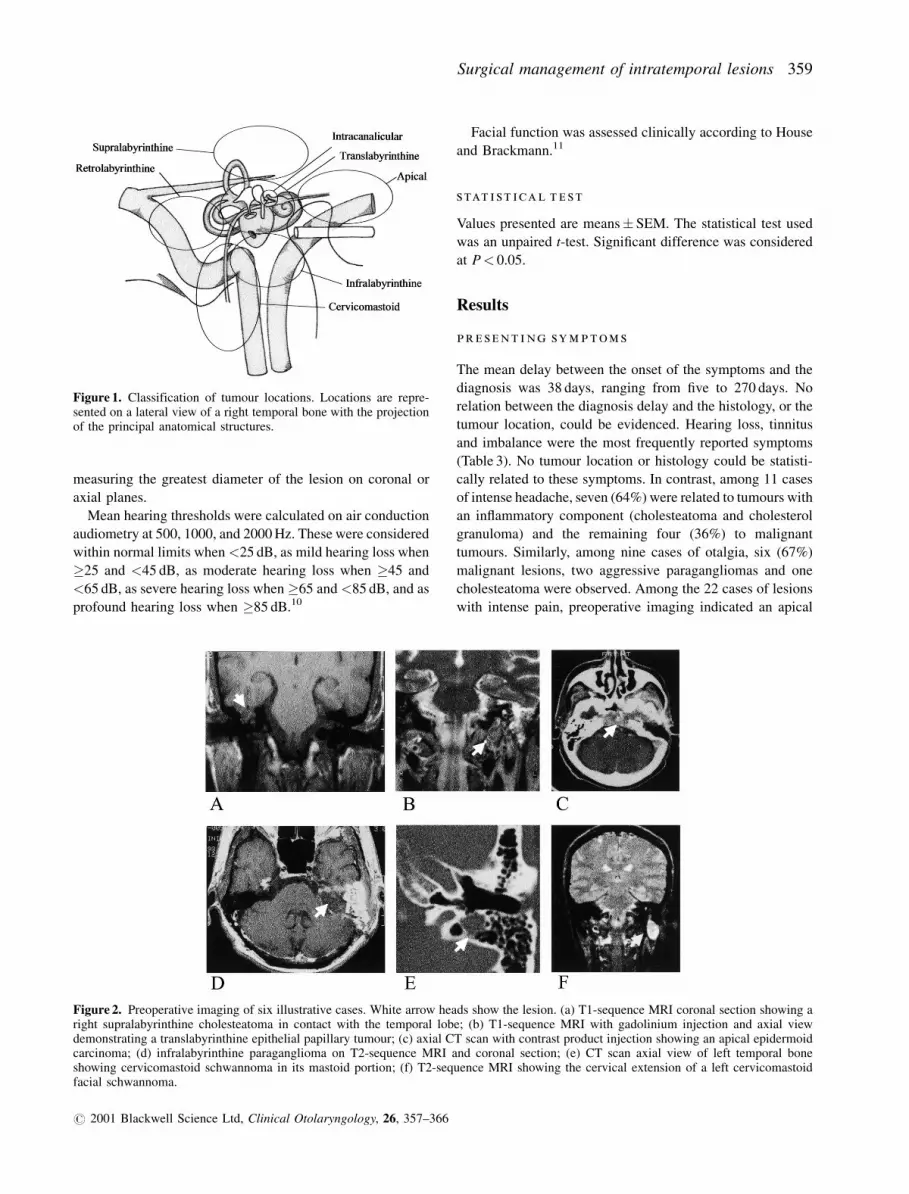
cla s s i f icat i on s
Tumour locations and extensions assessed on preoperative
imaging were classified as apical, supralabyrinthine, infra-
labyrinthine, retrolabyrinthine and translabyrinthine accord-
ing to Fisch & Mattox.3 In addition to these five extension
types, intracanalicular and cervicomastoid lesions were dis-
tinguished (Figs 1 and 2).
The carotid artery segments were designated according to
Lasjaunias & Berenstein:9 C1, cervical segment; C2, intrape-
trous vertical segment; C3, intrapetrous horizontal segment
and C4, ascending portion in the anterior foramen lacerum.
Tumour size was estimated on preoperative imaging by
Table 1. Tumour histology in our series
Histology n (relative %)
Cholesteatoma 19 (23%)Paraganglioma 18 (22%)Schwannoma 12 (15%)
Malignant lesionsEpidermoid carcinoma
8 (10%)
Chondrosarcoma 3 (4%)Osteosarcoma 1 (1%)Histiocytofibroma 1 (1%)Melanoma 1 (1%)Adenoid cystic carcinoma 1 (1%)UCNT� 1 (1%)Papillary epithelial tumour 1 (1%)
Miscellaneous benign lesionsCholesterol granuloma
3 (4%)
Facial nerve angioma 3 (4%)Haemangioma 3 (4%)Meningioma 2 (2%)Lipoma 1 (1%)Fibrous dysplasia 1 (1%)Osteodysplasia 1 (1%)Chondroblastoma 1 (1%)
Total 81
�UCNT ¼ undifferentiated carcinoma of nasopharyngeal type.
Table 2. Surgical approaches in our series
Surgical approach n (relative%)
Mastoidectomy þ neck dissection� parotidectomy
10 (13%)
Infralabyrinthine 1 (1%)Infratemporal type A� labyrinthine resection� 14 (18%)Infratemporal type B� labyrinthine resection� 2 (2%)Middle cranial fossa�mastoidectomy 8 (9%)Extended middle cranial fossay 12 (15%)Retrolabyrinthinez 2 (2%)Subtotal petrosectomy� 4 (5%)Transotic� 20 (26%)Translabyrinthine 4 (5%)Transcochlear þ posterior re-routing of
facial nerve§2 (2%)
Total petrosectomy þ internal carotidartery resection
2 (2%)
Total 81
�According to Fisch & Mattox (1988).3
yAccording to Wigand (1998).6
zAccording to Darrouzet et al. (1997).7
§According to House & Hitselberger (1976).8
358 A. Bozorg Grayeli et al.
# 2001 Blackwell Science Ltd, Clinical Otolaryngology, 26, 357–366
measuring the greatest diameter of the lesion on coronal or
axial planes.
Mean hearing thresholds were calculated on air conduction
audiometry at 500, 1000, and 2000 Hz. These were considered
within normal limits when <25 dB, as mild hearing loss when
�25 and <45 dB, as moderate hearing loss when �45 and
<65 dB, as severe hearing loss when �65 and <85 dB, and as
profound hearing loss when �85 dB.10
Facial function was assessed clinically according to House
and Brackmann.11
stat i st ical t e st
Values presented are means� SEM. The statistical test used
was an unpaired t-test. Significant difference was considered
at P< 0.05.
Results
pr e s ent i ng symptom s
The mean delay between the onset of the symptoms and the
diagnosis was 38 days, ranging from five to 270 days. No
relation between the diagnosis delay and the histology, or the
tumour location, could be evidenced. Hearing loss, tinnitus
and imbalance were the most frequently reported symptoms
(Table 3). No tumour location or histology could be statisti-
cally related to these symptoms. In contrast, among 11 cases
of intense headache, seven (64%) were related to tumours with
an inflammatory component (cholesteatoma and cholesterol
granuloma) and the remaining four (36%) to malignant
tumours. Similarly, among nine cases of otalgia, six (67%)
malignant lesions, two aggressive paragangliomas and one
cholesteatoma were observed. Among the 22 cases of lesions
with intense pain, preoperative imaging indicated an apical
Figure 1. Classification of tumour locations. Locations are repre-sented on a lateral view of a right temporal bone with the projectionof the principal anatomical structures.
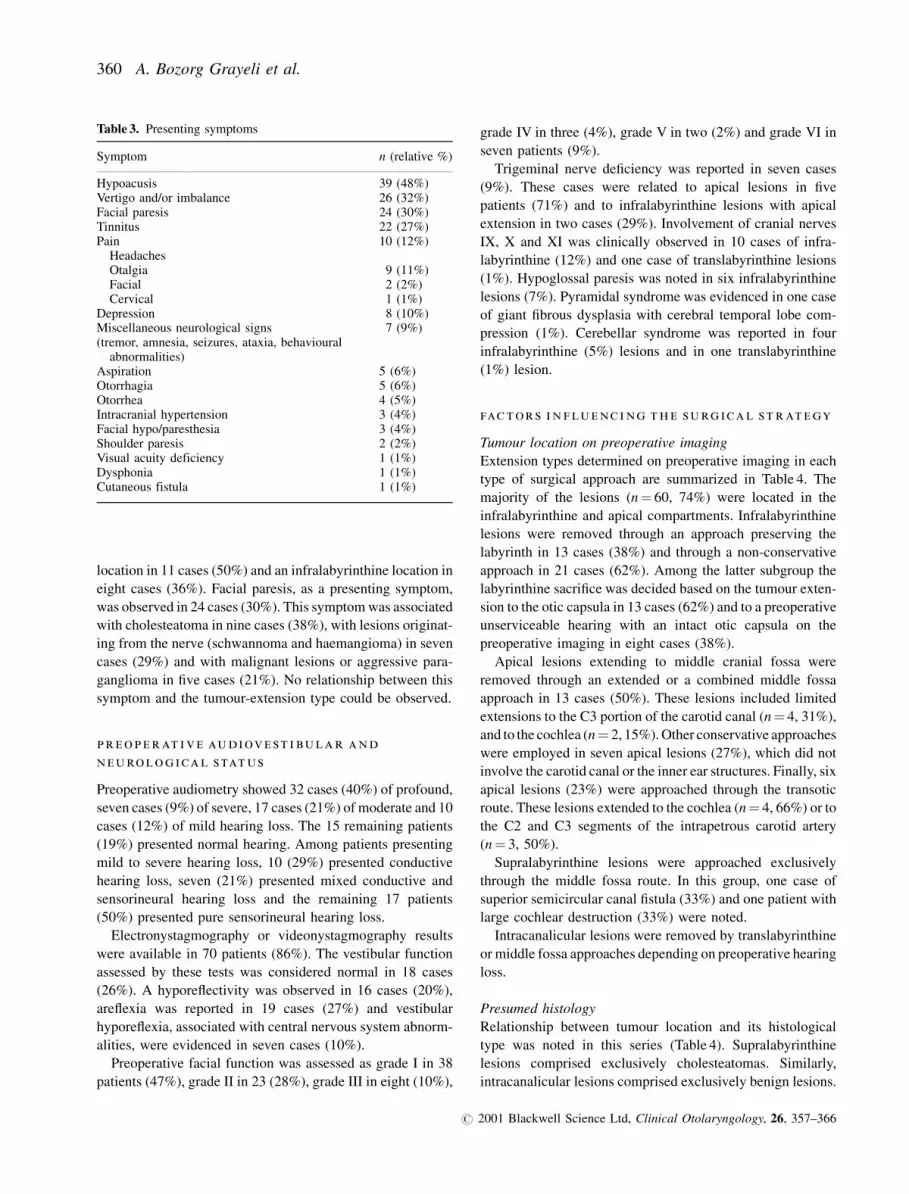
Figure 2. Preoperative imaging of six illustrative cases. White arrow heads show the lesion. (a) T1-sequence MRI coronal section showing aright supralabyrinthine cholesteatoma in contact with the temporal lobe; (b) T1-sequence MRI with gadolinium injection and axial viewdemonstrating a translabyrinthine epithelial papillary tumour; (c) axial CT scan with contrast product injection showing an apical epidermoidcarcinoma; (d) infralabyrinthine paraganglioma on T2-sequence MRI and coronal section; (e) CT scan axial view of left temporal boneshowing cervicomastoid schwannoma in its mastoid portion; (f) T2-sequence MRI showing the cervical extension of a left cervicomastoidfacial schwannoma.
# 2001 Blackwell Science Ltd, Clinical Otolaryngology, 26, 357–366
Surgical management of intratemporal lesions 359
location in 11 cases (50%) and an infralabyrinthine location in
eight cases (36%). Facial paresis, as a presenting symptom,
was observed in 24 cases (30%). This symptom was associated
with cholesteatoma in nine cases (38%), with lesions originat-
ing from the nerve (schwannoma and haemangioma) in seven
cases (29%) and with malignant lesions or aggressive para-
ganglioma in five cases (21%). No relationship between this
symptom and the tumour-extension type could be observed.
pr e ope r at i v e audiov e st i bular and
n eurolog ical status
Preoperative audiometry showed 32 cases (40%) of profound,
seven cases (9%) of severe, 17 cases (21%) of moderate and 10
cases (12%) of mild hearing loss. The 15 remaining patients
(19%) presented normal hearing. Among patients presenting
mild to severe hearing loss, 10 (29%) presented conductive
hearing loss, seven (21%) presented mixed conductive and
sensorineural hearing loss and the remaining 17 patients
(50%) presented pure sensorineural hearing loss.
Electronystagmography or videonystagmography results
were available in 70 patients (86%). The vestibular function
assessed by these tests was considered normal in 18 cases
(26%). A hyporeflectivity was observed in 16 cases (20%),
areflexia was reported in 19 cases (27%) and vestibular
hyporeflexia, associated with central nervous system abnorm-
alities, were evidenced in seven cases (10%).
Preoperative facial function was assessed as grade I in 38
patients (47%), grade II in 23 (28%), grade III in eight (10%),
grade IV in three (4%), grade V in two (2%) and grade VI in
seven patients (9%).
Trigeminal nerve deficiency was reported in seven cases
(9%). These cases were related to apical lesions in five
patients (71%) and to infralabyrinthine lesions with apical
extension in two cases (29%). Involvement of cranial nerves
IX, X and XI was clinically observed in 10 cases of infra-
labyrinthine (12%) and one case of translabyrinthine lesions
(1%). Hypoglossal paresis was noted in six infralabyrinthine
lesions (7%). Pyramidal syndrome was evidenced in one case
of giant fibrous dysplasia with cerebral temporal lobe com-
pression (1%). Cerebellar syndrome was reported in four
infralabyrinthine (5%) lesions and in one translabyrinthine
(1%) lesion.
factors i n flu enc i ng th e surg ical st r at egy
Tumour location on preoperative imaging
Extension types determined on preoperative imaging in each
type of surgical approach are summarized in Table 4. The
majority of the lesions (n¼ 60, 74%) were located in the
infralabyrinthine and apical compartments. Infralabyrinthine
lesions were removed through an approach preserving the
labyrinth in 13 cases (38%) and through a non-conservative
approach in 21 cases (62%). Among the latter subgroup the
labyrinthine sacrifice was decided based on the tumour exten-
sion to the otic capsula in 13 cases (62%) and to a preoperative
unserviceable hearing with an intact otic capsula on the
preoperative imaging in eight cases (38%).
Apical lesions extending to middle cranial fossa were
removed through an extended or a combined middle fossa
approach in 13 cases (50%). These lesions included limited
extensions to the C3 portion of the carotid canal (n¼ 4, 31%),
and to the cochlea (n¼ 2, 15%). Other conservative approaches
were employed in seven apical lesions (27%), which did not
involve the carotid canal or the inner ear structures. Finally, six
apical lesions (23%) were approached through the transotic
route. These lesions extended to the cochlea (n¼ 4, 66%) or to
the C2 and C3 segments of the intrapetrous carotid artery
(n¼ 3, 50%).
Supralabyrinthine lesions were approached exclusively
through the middle fossa route. In this group, one case of
superior semicircular canal fistula (33%) and one patient with
large cochlear destruction (33%) were noted.
Intracanalicular lesions were removed by translabyrinthine
or middle fossa approaches depending on preoperative hearing
loss.
Presumed histology
Relationship between tumour location and its histological
type was noted in this series (Table 4). Supralabyrinthine
lesions comprised exclusively cholesteatomas. Similarly,
intracanalicular lesions comprised exclusively benign lesions.
Table 3. Presenting symptoms
Symptom n (relative %)
Hypoacusis 39 (48%)Vertigo and/or imbalance 26 (32%)Facial paresis 24 (30%)Tinnitus 22 (27%)Pain
Headaches10 (12%)
Otalgia 9 (11%)Facial 2 (2%)Cervical 1 (1%)
Depression 8 (10%)Miscellaneous neurological signs(tremor, amnesia, seizures, ataxia, behavioural
abnormalities)
7 (9%)
Aspiration 5 (6%)Otorrhagia 5 (6%)Otorrhea 4 (5%)Intracranial hypertension 3 (4%)Facial hypo/paresthesia 3 (4%)Shoulder paresis 2 (2%)Visual acuity deficiency 1 (1%)Dysphonia 1 (1%)Cutaneous fistula 1 (1%)
# 2001 Blackwell Science Ltd, Clinical Otolaryngology, 26, 357–366
360 A. Bozorg Grayeli et al.

Infralabyrinthine lesions comprised 17 over the 18 paragan-
gliomas (94%) in our series. The remaining infralabyrinthine
lesions were principally composed of caudal nerve schwan-
nomas and malignant lesions.
Paragangliomas necessitated large surgical exposure
through infratemporal, transotic or total petrosectomy in 13
cases (87%). In contrast, the majority of cholesteatomas,
schwannomas and other benign lesions were managed by
approaches preserving the labyrinthine structures.
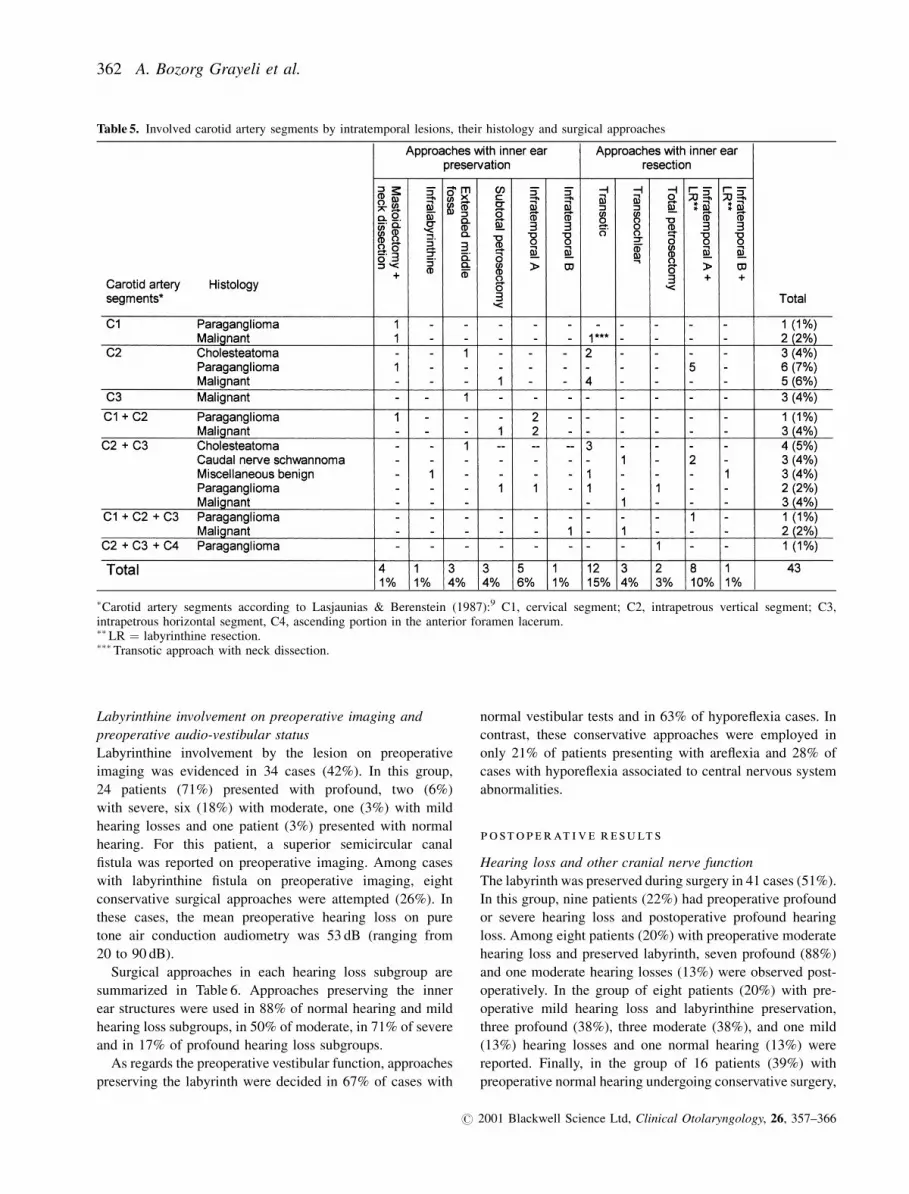
Carotid artery involvement
Tumour involvement of different carotid artery segments for
different tumour types and surgical approaches is summarized
in Table 5. The majority of paragangliomas (13 out of 18,
72%) and malignant lesions (12 out of 18, 66%) encased the
cervical or intrapetrous carotid artery. Carotid artery was
sacrificed in two extensive paragangliomas removed by total
petrosectomy (2%). In contrast, the carotid canal involvement
was observed in a low proportion of cholesteatomas (four out
of 19, 21%). The involvement of the cervical portion of the
carotid artery, which was only observed in paragangliomas
and malignant tumours, necessitated a cervical dissection
associated to the temporal bone approach.
Tumour size on preoperative imaging
Mean tumour size was 38� 2.4 mm. Lesion size was related to
its location. Translabyrinthine lesions measured 59� 12.4 mm
and were larger than infralabyrinthine (39� 2.1 mm), apical
(37� 3.5 mm) and cervicomastoid lesions (35� 5.0 mm)
(P< 0.05). Infralabyrinthine lesions were larger than supra-
labyrinthine lesions (25� 2.9 mm) (P< 0.05). The only
retrolabyrinthine lesion measured 25 mm and was similar to
supralabyrinthine lesions in size. Intracanalicular lesions
represented the smallest lesions in comparison with all
other locations with a mean diameter of 11.0� 1.35 mm
(P< 0.05).
Tumour size on preoperative imaging appeared to be related
to its aggressiveness. Malignant and epithelial papillary
lesions measured 46� 4.6 and 53� 7.5 mm respectively.
These tumour types had a larger diameter than cholesteatomas
(33� 2.1 mm) and schwannomas (33� 3.0 mm) (P< 0.05).
Paragangliomas’ mean diameter (41� 3.5 mm) was inter-
mediate between malignant lesions and cholesteatomas and
was not significantly different from these two groups. The
mean diameter of miscellaneous benign lesions, to the exclu-
sion of a giant fibrous dysplasia which measured 150 mm in its
greatest diameter, was 24� 4.1 mm. This group had the
smallest diameter in comparison with malignant lesions
(P< 0.01), epithelial papillary lesions, paragangliomas and
cholesteatomas (P< 0.05).
The diameter of lesions for which a labyrinthine preserva-
tion was decided (31� 2.1 mm) was smaller than the diameter
of those for which the labyrinth was sacrificed (46� 3.9 mm)
(P< 0.01).
Table 4. Surgical approaches in different tumour types and locations
�LR ¼ labyrinthine resection.
# 2001 Blackwell Science Ltd, Clinical Otolaryngology, 26, 357–366
Surgical management of intratemporal lesions 361
Labyrinthine involvement on preoperative imaging and
preoperative audio-vestibular status
Labyrinthine involvement by the lesion on preoperative
imaging was evidenced in 34 cases (42%). In this group,
24 patients (71%) presented with profound, two (6%)
with severe, six (18%) with moderate, one (3%) with mild
hearing losses and one patient (3%) presented with normal
hearing. For this patient, a superior semicircular canal
fistula was reported on preoperative imaging. Among cases
with labyrinthine fistula on preoperative imaging, eight
conservative surgical approaches were attempted (26%). In
these cases, the mean preoperative hearing loss on pure
tone air conduction audiometry was 53 dB (ranging from
20 to 90 dB).
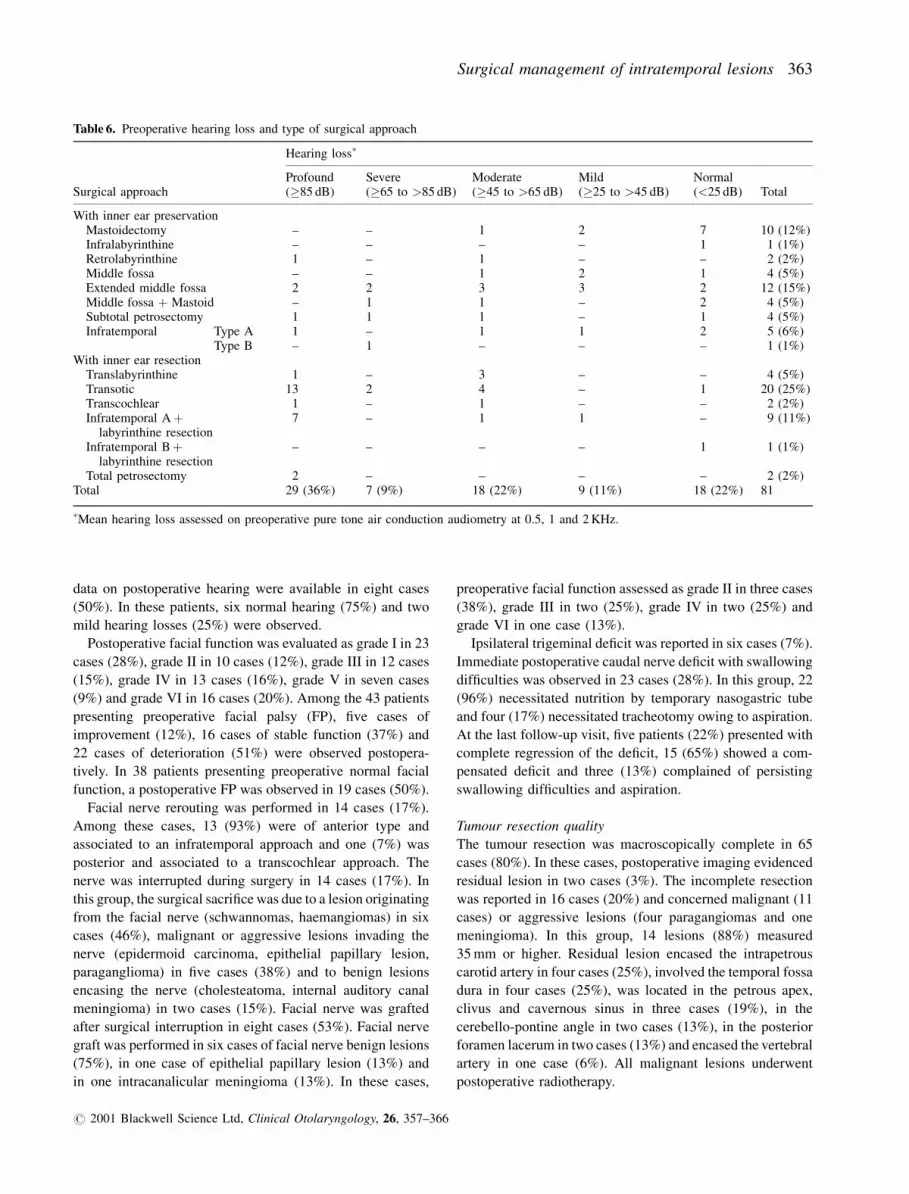
Surgical approaches in each hearing loss subgroup are
summarized in Table 6. Approaches preserving the inner
ear structures were used in 88% of normal hearing and mild
hearing loss subgroups, in 50% of moderate, in 71% of severe
and in 17% of profound hearing loss subgroups.
As regards the preoperative vestibular function, approaches
preserving the labyrinth were decided in 67% of cases with
normal vestibular tests and in 63% of hyporeflexia cases. In
contrast, these conservative approaches were employed in
only 21% of patients presenting with areflexia and 28% of
cases with hyporeflexia associated to central nervous system
abnormalities.
po stope r at i v e r e sult s
Hearing loss and other cranial nerve function
The labyrinth was preserved during surgery in 41 cases (51%).
In this group, nine patients (22%) had preoperative profound
or severe hearing loss and postoperative profound hearing
loss. Among eight patients (20%) with preoperative moderate
hearing loss and preserved labyrinth, seven profound (88%)
and one moderate hearing losses (13%) were observed post-
operatively. In the group of eight patients (20%) with pre-
operative mild hearing loss and labyrinthine preservation,
three profound (38%), three moderate (38%), and one mild
(13%) hearing losses and one normal hearing (13%) were
reported. Finally, in the group of 16 patients (39%) with
preoperative normal hearing undergoing conservative surgery,
Table 5. Involved carotid artery segments by intratemporal lesions, their histology and surgical approaches
�Carotid artery segments according to Lasjaunias & Berenstein (1987):9 C1, cervical segment; C2, intrapetrous vertical segment; C3,intrapetrous horizontal segment, C4, ascending portion in the anterior foramen lacerum.�� LR ¼ labyrinthine resection.��� Transotic approach with neck dissection.
# 2001 Blackwell Science Ltd, Clinical Otolaryngology, 26, 357–366
362 A. Bozorg Grayeli et al.
data on postoperative hearing were available in eight cases
(50%). In these patients, six normal hearing (75%) and two
mild hearing losses (25%) were observed.
Postoperative facial function was evaluated as grade I in 23
cases (28%), grade II in 10 cases (12%), grade III in 12 cases
(15%), grade IV in 13 cases (16%), grade V in seven cases
(9%) and grade VI in 16 cases (20%). Among the 43 patients
presenting preoperative facial palsy (FP), five cases of
improvement (12%), 16 cases of stable function (37%) and
22 cases of deterioration (51%) were observed postopera-
tively. In 38 patients presenting preoperative normal facial
function, a postoperative FP was observed in 19 cases (50%).
Facial nerve rerouting was performed in 14 cases (17%).
Among these cases, 13 (93%) were of anterior type and
associated to an infratemporal approach and one (7%) was
posterior and associated to a transcochlear approach. The
nerve was interrupted during surgery in 14 cases (17%). In
this group, the surgical sacrifice was due to a lesion originating
from the facial nerve (schwannomas, haemangiomas) in six
cases (46%), malignant or aggressive lesions invading the
nerve (epidermoid carcinoma, epithelial papillary lesion,
paraganglioma) in five cases (38%) and to benign lesions
encasing the nerve (cholesteatoma, internal auditory canal
meningioma) in two cases (15%). Facial nerve was grafted
after surgical interruption in eight cases (53%). Facial nerve
graft was performed in six cases of facial nerve benign lesions
(75%), in one case of epithelial papillary lesion (13%) and
in one intracanalicular meningioma (13%). In these cases,
preoperative facial function assessed as grade II in three cases
(38%), grade III in two (25%), grade IV in two (25%) and
grade VI in one case (13%).
Ipsilateral trigeminal deficit was reported in six cases (7%).
Immediate postoperative caudal nerve deficit with swallowing
difficulties was observed in 23 cases (28%). In this group, 22
(96%) necessitated nutrition by temporary nasogastric tube
and four (17%) necessitated tracheotomy owing to aspiration.
At the last follow-up visit, five patients (22%) presented with
complete regression of the deficit, 15 (65%) showed a com-
pensated deficit and three (13%) complained of persisting
swallowing difficulties and aspiration.
Tumour resection quality
The tumour resection was macroscopically complete in 65
cases (80%). In these cases, postoperative imaging evidenced
residual lesion in two cases (3%). The incomplete resection
was reported in 16 cases (20%) and concerned malignant (11
cases) or aggressive lesions (four paragangiomas and one
meningioma). In this group, 14 lesions (88%) measured
35 mm or higher. Residual lesion encased the intrapetrous
carotid artery in four cases (25%), involved the temporal fossa
dura in four cases (25%), was located in the petrous apex,
clivus and cavernous sinus in three cases (19%), in the
cerebello-pontine angle in two cases (13%), in the posterior
foramen lacerum in two cases (13%) and encased the vertebral
artery in one case (6%). All malignant lesions underwent
postoperative radiotherapy.
Table 6. Preoperative hearing loss and type of surgical approach
Surgical approach
Hearing loss�
Profound(�85 dB)
Severe(�65 to >85 dB)
Moderate(�45 to >65 dB)
Mild(�25 to >45 dB)
Normal(<25 dB) Total
With inner ear preservationMastoidectomy – – 1 2 7 10 (12%)Infralabyrinthine – – – – 1 1 (1%)Retrolabyrinthine 1 – 1 – – 2 (2%)Middle fossa – – 1 2 1 4 (5%)Extended middle fossa 2 2 3 3 2 12 (15%)Middle fossa þ Mastoid – 1 1 – 2 4 (5%)Subtotal petrosectomy 1 1 1 – 1 4 (5%)Infratemporal Type A 1 – 1 1 2 5 (6%)
Type B – 1 – – – 1 (1%)With inner ear resection
Translabyrinthine 1 – 3 – – 4 (5%)Transotic 13 2 4 – 1 20 (25%)Transcochlear 1 – 1 – – 2 (2%)Infratemporal Aþ
labyrinthine resection7 – 1 1 – 9 (11%)
Infratemporal Bþlabyrinthine resection
– – – – 1 1 (1%)
Total petrosectomy 2 – – – – 2 (2%)Total 29 (36%) 7 (9%) 18 (22%) 9 (11%) 18 (22%) 81
�Mean hearing loss assessed on preoperative pure tone air conduction audiometry at 0.5, 1 and 2 KHz.
# 2001 Blackwell Science Ltd, Clinical Otolaryngology, 26, 357–366
Surgical management of intratemporal lesions 363

A recurrence was observed in five patients (6%). The mean
delay of recurrence detection after surgery was 26 months,
extremes ranging from 20 to 38 months. These recurrences
concerned two cholesteatomas and one adenoid cystic carci-
noma of the petrous apex, and two paragangliomas located in
infralabyrinthine and translabyrinthine regions.
Postoperative morbidity and mortality
Local or general infectious complications occurred in seven
cases (9%). They were managed medically in all cases.
Cerebrospinal fluid leak by the incision or as rhinorrhea
was noted in 13 cases (16%). These patients were treated
medically in 10 cases (12%) and necessitated surgical revision
in three cases (4%).
Three cases of postoperative ischaemic cerebral accident
were reported (4%). In one case (1%), this complication
occurred after the resection of a giant fibrous dysplasia with
temporal lobe compression. The two remaining cases (3%)
with extensive intratemporal and intracranial paragangliomas
presented with a fatal ischaemic neurological complication
during the immediate postoperative period. Other neurologi-
cal complications (seizures, intracranial hypertension and
brainstem compression by abdominal fat graft) were observed
in three cases (4%). These complications were regressive after
medical or surgical treatment. Patients who underwent inter-
nal carotid artery ligation did not present neurological com-
plications. Two patients (2%) died from a malignant tumour
evolution.
Information concerning postoperative professional activity
resumption was available in 46 cases (57%). Among these
cases, 30 patients (65%) resumed anterior professional
activity.
Postoperative mortality and morbidity was related to
tumour size. Lesions measured 90� 30.5 mm in patients
deceased by postoperative complication, 60� 20.0 mm in
patients deceased by tumour evolution, 44� 4.5 mm in con-
valescent patients at the last follow-up examination, and
32� 2.1 mm in patients having resumed their professional
activity at the last follow-up visit. No significant difference
was evidenced in the lesion’s size between patients deceased
by complication and those deceased by tumour evolution.
Tumour size in these two groups was larger than those in
convalescent and professionally active patients (P< 0.01 and
P< 0.001). Patient having resumed professional activity had
smaller lesions than convalescent patients at last follow-up
visit (P< 0.02). Follow-up duration was not significantly
different between convalescent and active patients (19� 5.9
and 21� 3.4 months respectively).
Discussion
Intratemporal extensive lesions represent a heterogeneous
pathologic entity as different tumour types and locations make
each case a unique situation. Despite this heterogeneity, the
surgical strategy for these lesions follow general rules that can
be highlighted.2
The aim of this retrospective study was to assess different
decisional elements in the surgical treatment of extensive
intratemporal lesions in the light of postoperative results
and to deduce an algorithm for the surgical approach.
The location of the lesion evaluated by preoperative
imaging represents the major decisional factor in the choice
of the surgical approach.2,3 The tumour location indicates
the possible involved neurovascular structures and is
helpful in predicting the type of the lesion.12 Consequently,
this data is the basis of many proposed classifications for
intratemporal lesions.2,13 The classification that we have
used in our series was first proposed by Fisch & Mattox,3
based on clinical observations and temporal bone cell
tract anatomy that offers a low resistance to tumour invasion.1
This classification subdivides the petrous pyramid into
four compartments around the labyrinthine block: apical,
supralabyrinthine, infralabyrinthine and retrolabyrinthine.
In addition, the translabyrinthine subgroup was assigned to
large lesions destroying the labyrinthine structures and
extending to the cerebellopontine angle. In order to include
all the possible locations for intratemporal lesions, intracanali-
cular and cervicomastoid lesions were also distinguished in
our series. Although this classification leads to a coherent
algorithm for the surgical strategy, it does not take in account
the extensions of the lesion to principal neurovascular
structures such as the internal carotid artery, the middle fossa
dura, the labyrinth or the facial nerve. As observed in our
series, this type of information is crucial in predicting the
functional results and the possible complications, and directly
influences the surgical approach.
The presumed tumour histology based on preoperative
imaging also influences the surgical strategy. In our series,
this information was deduced from the location, the imaging
characteristics, and clinical data including past medical his-
tory, preoperative symptoms and rapidity of evolution. The
tumour types encountered in our series can be divided into
three categories:4
1. Benign lesions with a slow growth, not invading the
adjacent neurovascular structures and presenting a low
recurrence risk after complete macroscopic resection. In
our series, this group is mainly represented by apical
cholesteatomas for which surgical strategy has been
reported,14 but also comprises schwannomas, cholesterol
granulomas, lipomas, haemangiomas and osteoblastomas.
2. Aggressive benign lesions comprising paragangliomas
and chordomas in our series. This group includes
benign lesions presenting at least one of the following
characteristics: rapid growth, invasion of neurovascular
structures, high recurrence risk after complete macroscopic
resection, and possibility of malignant transformation with
# 2001 Blackwell Science Ltd, Clinical Otolaryngology, 26, 357–366
364 A. Bozorg Grayeli et al.
metastasis. These lesions necessitated large surgical access
in order to control involved vessels and extensions.
3. Primary malignant or metastatic lesions with maximal
aggressiveness (rapid regional extension, adjacent structure
invasion and metastasis). These lesions necessitated the
largest surgical access possible with important resection
margins and complementary radiotherapy. This group
mainly included middle ear carcinomas, but also malignant
melanoma, sarcomas, adenoid cystic carcinomas, and
undifferentiated carcinoma of nasopharyngeal type invad-
ing the petrous apex in our series. Considering their high
potential of local invasion, papillary epithelial tumours can
also be included in this group.5
The tumour size in our series was related to its location and
aggressiveness and influenced the labyrinthine preservation.
Lesions measuring 35 mm or higher constituted the majority
of incomplete resection cases. Moreover, the lesion’s size was
related to postoperative mortality and morbidity. Many clas-
sifications take this parameter in account to determine the
surgical attitude and the prognosis.2,3
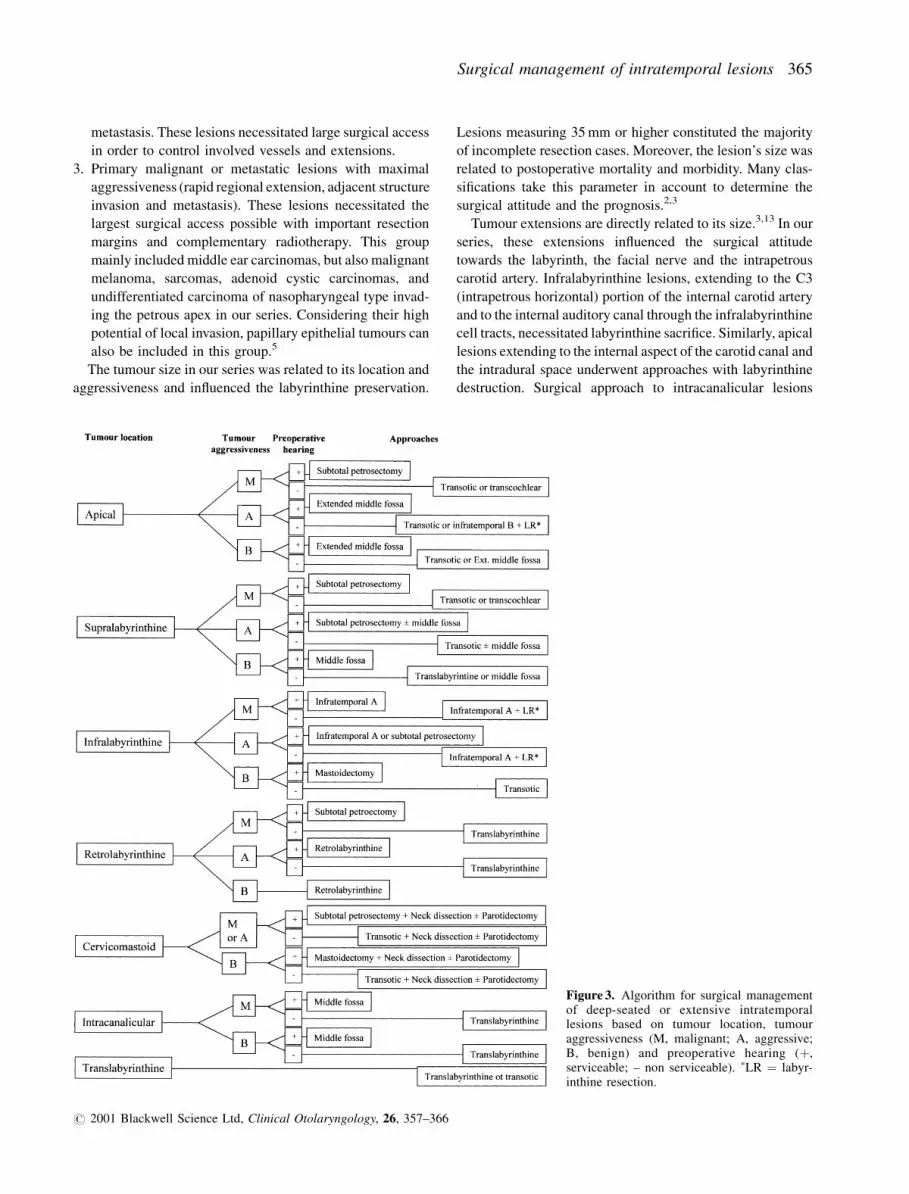
Tumour extensions are directly related to its size.3,13 In our
series, these extensions influenced the surgical attitude
towards the labyrinth, the facial nerve and the intrapetrous
carotid artery. Infralabyrinthine lesions, extending to the C3
(intrapetrous horizontal) portion of the internal carotid artery
and to the internal auditory canal through the infralabyrinthine
cell tracts, necessitated labyrinthine sacrifice. Similarly, apical
lesions extending to the internal aspect of the carotid canal and
the intradural space underwent approaches with labyrinthine
destruction. Surgical approach to intracanalicular lesions
Figure 3. Algorithm for surgical managementof deep-seated or extensive intratemporallesions based on tumour location, tumouraggressiveness (M, malignant; A, aggressive;B, benign) and preoperative hearing (þ,serviceable; – non serviceable). �LR ¼ labyr-inthine resection.
# 2001 Blackwell Science Ltd, Clinical Otolaryngology, 26, 357–366
Surgical management of intratemporal lesions 365

mainly depended on the extension of the lesion to the fundus
and the preoperative hearing function. Supralabyrinthine and
cervicomastoid lesions could be treated by conservative sur-
gical approaches owing to their type of extension. Suprala-
byrinthine lesions extended towards the middle fossa and
cervicomastoid lesions towards the stylomastoid forman.
The surgical attitude in our series based on tumour location
and aggressiveness, and the inner ear involvement on pre-
operative imaging is summarized in Fig. 3.
The functional results in our series could not be directly
compared to other series owing to differences in the tumour
types, locations and extensions.15–17 The poor auditory prog-
nosis in our series was mainly as a result of the tumour
destruction of the cochlea or the tumour extension to the
C3 portion of the intrapetrous carotid artery that necessitated
the cochlear sacrifice. Incomplete resection was observed
principally in aggressive tumours and its proportion in our
series was similar to that reported by Briner et al. (17%).16
Malignant lesions had a high mortality despite aggressive
surgical treatment in our series. In other series, this mortality
rate is reported to be 44% and 80%, 18 and 30 months after
surgery respectively.13,15 The rate of postoperative complica-
tions (28%) and consequent mortality (4%) in our series was
also similar to that reported in the literature.1,12,15 The possible
occurrence of fatal complications in the treatment of such
lesions underlines the importance of a complete preoperative
assessment of the lesion and the patient’s general condition.
In conclusion, the location and the size of the lesion, its
presumed aggressiveness, the internal carotid artery involve-
ment on preoperative imaging and the degree of preoperative
hearing loss were the principal decisional elements for the
choice of the surgical approach and the conservation of
the labyrinth in our series. Thus, a high quality preoperative
imaging is mandatory in the surgical planning for extensive
intratemporal lesions.
References
1 LEONETTI J.P., SMITH P.G., KLETZKER G.R. et al. (1996)Invasion patterns of advanced temporal bone malignancies.Am. J Otol. 17, 438–442
2 HIRSCH B.E, SEKHAR L.N. & KAMERE D.B. (1993) Transtem-poral and infratemporal approach for benign tumors of jugularforamen and temporal bone. In Surgery of Cranial Base Tumors,pp. 267–289. Raven Press, New York
3 FISCH U. & MATTOX D. (1988) Subtotal petrosectomy, transoticapproach to the cerebellopontine angle, infratemporal fossaapproach type A, and infratemporal fossa approach type B. InMicrosurgery of the Skull Base, pp. 4–609. Theime MedicalPublishers, New York
4 NAGER G.T. (1993) Tumours of the brain, nerve sheath,meninges, brain, and other space occupying lesions of thetemporal bone. In Pathology of the Ear and Temporal Bone, pp.515–895. Williams & Wilkins, Baltimore
5 FEGHALI J.G., LEVIN R.J., LLENA J. et al. (1995) Aggressivepapillary tumors of the endolymphatic sac: clinical and tissueculture characteristics. Am. J. Otol. 16, 778–782
6 WIGAND M.E. (1998) The enlarged middle fossa approach to thecerebello-pontine angle. Technique and indications. Rev. Lar-yngol. Otol. Rhinol. 119, 159–162
7 DARROUZET V., GUERIN J., AOUAD N. et al. (1997) The widenedretrolabyrinthine approach: a new concept in acoustic neuromasurgery. J. Neurosurg. 86, 812–821
8 HOUSE W.F. & HITSELBERGER W.E. (1976) The transcochlearapproach to the skull base. Arch. Otolaryngol. Head Neck Surg.,102, 334–342
9 LASJAUNIAS P. & BERENSTEIN A. (1987) Carotid artery. InSurgical Neuroangiography, pp. 2–11. Springer–Verlag, Berlin
10 STELMACHOWICZ P.G. & GORGA M.P. (1992) Auditory functiontests. In Otolaryngology: Head and Neck Surgery, pp. 2699–2717. Mosby-Year Book, St. Louis
11 HOUSE J.W. & BRACKMANN D.E. (1985) Facial nerve gradingsystem. Otolaryngol. Head Neck Surg. 3, 184–193
12 CONSTANTINO P.D. & JANECKA I.P. (1993) Cranial base surgery.In Head and Neck Surgery: Otolaryngology, pp. 1411–1430.Lippincott, Philadelphia
13 POMERANZ S., SEKHAR L.N., JANECKA I.P. et al. (1993)Classification, technique and results of surgical resection ofpetrous bone tumors. In Surgery of Cranial Base Tumors, pp.317–335. Raven Press, New York
14 BOZORG GRAYELI A., MOSNIER I., EL GAREM H. et al. (2000)Extensive intratemporal cholesteatoma: surgical strategy. Am. J.Otol. 21, 774–781
15 SEKHAR L.N., POMERANZ S., JANECKA I.P. et al. (1992)Temporal bone neoplasms: a report on 20 surgically treatedcases. J. Neurosurg. 76, 578–587
16 BRINER H.R., LINDER T.E., PAUW B. et al. (1999) Long termresults of surgery for temporal bone paragangliomas. Laryngo-scope 109, 577–583
17 POE D.S., JACKSON G., GLASSCOCK M.E. et al. (1991) Longterm results after lateral cranial base surgery. Laryngoscope 101,372–378
# 2001 Blackwell Science Ltd, Clinical Otolaryngology, 26, 357–366
366 A. Bozorg Grayeli et al.
Related Documents