Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Surgery of the Gasserian Ganglion, withDemonstration and Report of
Two Cases.
Stenographic report made at the meeting of the Mississippi Valley MedicalAssociation, at St. Paul, Minn., September 15,1896.
J. B. MURPHY, M. D.,CHICAGO, ILL.
REPRINTED FROM WESTERN MEDICAL REVIEW, OCTOBER, 1896.
LINCOLN:Western Medical Review Publishing Co.


SURGERY OF THE GASSERIAN GANGLION,WITH DEMONSTRATION AND REPORTOF TWO CASES.*
J. B. MURPHY, M. DCHICAGO, ILL.
In speaking of the surgery of the gasserianganglion, I will confine my remarks largely to thetechnique of the more recent operation, after re-viewing some of the results of operations whichhave preceded or led to the operation which isadopted at the present time. The gasserian gan-glion, situated, as it is, on the petrous portion ofthe temporal bone, is in a very inaccessible posi-tion. It is desirable in some cases to remove thisganglion for the purpose of curing intractableneuralgias of the facial nerve, or what is com-monly known as migraine. As you know, allmethods of treatment by internal medication withall the varieties of anodynes, and more recentlythe medical treatment now in vogue, large dosesof castor oil, have failed. If a case had been re-lieved by the anodyne treatment, it was only tem-porary, and was followed by another attack ofincreased intensity. The operations for its reliefmay be classified as follows: 1. Division of thebranches of the trifacial in the face or mouth.2. Division of the nerves at the base of the cra-nium (Kroenlein). 3. Extraction of the ganglionfrom the base (Rose). 4. Intradural extraction ofthe ganglion (Horsley). 5. Extradural excisionof ganglion (Hartley-Krause). The operationmost effectual and least dangerous before thepresent one (Kroenlein’s) consisted of division ofthe zygomatic process, turning it down with the
* Stenographic report made at the meeting of the Mississippi Valley MedicalAssociation, at St. Paul, Minn., September 15, 1896.

2
most important muscle, dividing the coronoid pro-cess of the inferior maxillary, dividing the tempo-ral muscle and reflecting it upon the cranium,finally dividing the nerve at the base of the cra-nium, that is, dividing the third branch of thenerve at the foramen ovale and the second branchat the foramen rotundum. The operation wasalmost as extensive and, if not as dangerous, wasmore difficult than the operation for the removalof the ganglion itself. The results with this oper-ation were only temporary relief in a very largeproportion of cases; for that reason it was deemedadvisable to attack the nerve within the cranium.Dr. Rose, of London, in 1890, was the first to openthe cranium from the base. He followed the sameprocedure as Kroenlein, making a division of theparts mentioned, passing into the base of the cra-nium at the foramen ovale, and chiseling out anopening sufficiently large to permit of the extrac-tion of the ganglion through the opening. Theopening was necessarily small, consequently theoperator had very imperfect light, and it was veryuncertain whether the ganglion was extracted intoto in any of these operations. The Rose methodwas performed, I think, for the first time in Amer-ica by Dr. Edmund Andrews of Chicago. He hasperformed the operation three times. On accountof the difficulty and dangers of this operation,coupled with the uncertainty of incomplete ex-traction of the ganglion, it was necessary to aban-don the procedure. The next method was devisedby Victor Horsley, of London (1891), who reasonedthat as the ganglion was situated between thetwo layers of the dura, with its roots on the innerside of the dura at the base, it could best bereached by incising the dura and elevating theconvolutions. In the Horsley operation an open-ing should be made in the cranium above the zygo-matic arch, with a horseshoe-shaped osteoplasticflap; finally incise the dura and elevate it with a

3
retractor, as I show you here. Pass this longcurved retractor beneath the convolutions andgently elevate the brain, so that the ganglion andmotor root on the inner side can be reached andextracted from the side of the medulla. We canreadily see that this is a difficult procedure, as thebrain is not a resisting substance and the retract-ors tear or lacerate the brain tissue before theganglion is exposed at its base. The operationwas performed by Horsley with a fatal termi-nation.
In the latter part of 1891 Frank Hartley, ofNew York, conceived the idea of attacking theganglion from within the cranium and withoutthe dura. This is the operation to which I shalldirect your attention to-day, and is the one whichI will perform, with the assistance of Dr. Mayo,so that you may see how readily the ganglion androot of the nerve can be reached and extracted bythis method.
We will next consider the dangers of the opera-tions. In the operation from the base (Rose’s op-eration) the dangers were found to be hemorrhageand infection; in the majority of fatal cases foundin the literature on the subject, infection was dueto injury to the eiistachian tube, as the channelwhich the surgeon follows in getting to the baseof the cranium at the foramen ovale is in closeproximity to that tube. The mortality of the op-eration was eighteen per cent. In Horsley’s oper-ation there was danger from hemorrhage, infec-tion, and mutilation and laceration of the brain.He performed the operation once and the patientdied six hours after.
We will now consider briefly the technique ofthe Hartley operation. In this operation, afterwe have made our incision through the skin andexposed the bone, we chisel an opening throughthe cranium, and if we have a De Yilbiss instru-ment we can remove as large a piece of the era-

4
nium as we desire, in a very short time. Thechisel of Hartley or Krause's saw, which is veryconvenient, may be used. The De Vilbiss instru-ment lias the advantage that it does not cut thedura when the instrument is pressed; when itis opened it pushes the dura out of the operativefield. Last week I used it in excising a large de-pression in the skull. It worked admirably and
Fig. I.—Primary incision.
saved time. Make an omega incision (see Fig. 1)in the flap and cut the bone so that the base of theother incision will be just above the zygoma; ele-vate the bone and its fractures below the level ofthe zygoma. Press the Kocher blunt dissector be-tween the dura and bone, lift the bone gently, andpush the dura back. As soon as this is done weare liable to have hemorrhage from the middle

5
meningeal artery. Should this occur we can com-press the bone with forceps or push the artery intothe canal and introduce a catgut plug. The hem-orrhage from the dura is considerable when theflap is elevated. The flap is now turned down andallowed to remain. As soon as the bleeding hasceased, pass the linger along beneath the dura,gently elevating it until the base of the fossa isreached. At this stage there is profuse hemor-rhage from the vena santorini and the arteriameningea media. This artery occasionally entersthe base through a separate foramen, and has beenruptured in elevating the dura from the bone.Whenever rupture takes place the foramen shouldbe packed with catgut and allowed to remain.The venous hemorrhage may be so excessive thatit may become necessary to stop the operation atthis point and plug the fossa with gauze, allowingit to remain three days before completing the op-eration. Excessive hemorrhage was encounteredin three of Dr. Keen’s cases. The doctor, in com-menting on the cases, stated that he introduced apiece of gauze sixteen by twenty inches, which didnot produce sufficient pressure on the brain tocause unpleasant symptoms. As soon as the baseis exposed, introduce the retractor, which holdsup the dura. As the specimen is passed around,notice the foramen ovale where the inferior max-illary division finds exit, and just in front of itthe foramen rotundum for the superior maxillarydivision. After both openings have been exposed,divide the layer of the dura between the two divi-sions of tlie nerve, allowing the periosteal portionto remain attached to the bone beneath the rootsof the nerves. The upper layer can then be ele-vated from the surface of the nerves and ganglionwith very little danger of perforating it. This isa very important point in the operation. Proceedalong the upper surface of the nerve to the gan-glion, which is situated between the two layers of

6
the dura, one beneath and the other above. Assoon as this point is reached the blunt dissectoris used to elevate the dura; with it separate thetwo layers of the dura, following along up thenerve. Peel the dura off until the ganglion isthoroughly exposed. After the dura is peeled offa short distance it may possibly be torn; therewill then be an escape of cerebro-spinal fluid. Ifthe sinus be torn the hemorrhage will be profuse.Control it with the finger or with a compress onthe retractor. Cleanse the cavity with a spongeuntil the parts become dry. With two of theseretractors the sinus can be readily compressed iftorn. The opening in the dura can be compressedin the same manner to suppress the flow of cere-bro-spinal fluid. If necessary the optic divisionof the nerve can be removed ; it is difficult, as it issituated in the wall of the cavernous sinus. Ifan endeavor be made to remove the optic divisionfrom the cavernous sinus, the chances are thesinus will be opened and hemorrhage will follow,thus compelling the suspension of the operationfor the time being, to be completed at another sit-ting. As soon as the ganglion is exposed, passthe blunt hooks which we have for that purposeunder the roots of the nerves, elevate the nerves,and make considerable traction from the openingstoward the center. As soon as the roots are thor-oughly drawn in and divided close to the foramen,elevate the ganglion from its fossa and grasp itwith a pair of large hemostatic forceps. I havefound the eight-inch forceps of Billroth good forthis purpose. The nerves being divided, the dis-tal ends are pushed out of the foramina. This isdone to lessen the possibility of subsequent regen-eration of nerve tissue in case the ganglion isnot completely removed. When the roots are di-vided remove the booklets which have been usedfor the purpose of elevating; separate the rootsand the ganglion from the periosteal portion of

7
the dura by gently elevating it; make a turn anda half of the Billroth forceps on the ganglion andthe motor root will come in one mass with theganglion.
In the first case which I operated I was an-noyed considerably by hemorrhage. It retardedme for five or six minutes after I had the nerve ex-posed and had placed the forceps on the ganglion.As soon as the hemorrhage was under control Iproceeded and the nerve was extracted.
This method is very advantageous, as it affordsan excellent view of the field of operation. I likethe position suggested by Keen, i. e., placing thepatient on the back and operating from the side.In this position we can have a strand of gauze inthe lower part of the wound, which will siphonthe blood out as rapidly as it appears. When theganglion is extracted it should be examined to seeif it has all been removed. The ganglion is not alarge body; it is much smaller than is generallysupposed. In some of the recorded cases a partof the ganglion was removed. This should notoccur if the dura be retracted sufficiently with theblunt dissector. In both of my cases the perma-nent arrest of hemorrhage was produced with aplug of gauze, which was removed forty-eighthours after the operation through a small openingleft in the bone. The osteoplastic flap was re-placed and retained by periosteal and cutaneoussutures. In the second there was some escape ofcerebro-spinal fluid when the gauze was extracted;the provisional suture which was inserted at thetime of the operation was tied and prevented thefurther loss of fluid. The danger of injury to thebrain is not great. The danger from sepsis whenthe dura has been lacerated is considerable; inthese cases the drain should always be used. Itis surprising in such cases how quickly patientsrally from the operation. The first patient onwhom I operated left the hospital two weeks after

8
the operation. The first operation consumedforty-two minutes, the second fifty-seven. This isan operation of considerable anxiety, because weare at a disadvantage in controlling hemorrhage;if the carotid be injured its control is almost im-possible.
As to the results obtained from operative inter-ference: There have been fifty-seven cases col-lected up to date, and of this number there werefive deaths. Two of the patients were seventyyears of age. One died shortly after the opera-tion as a result of shock, the other six days afterthe operation, without any special symptoms.Nothing was revealed post-mortem to account forthe patient’s'death. For an operation which af-fords relief from such great suffering the mor-tality is small, one in eleven, and an idea of thesuffering of these patients can only be gatheredfrom those who are afflicted. They are willing toundergo any operation in the hope of obtainingrelief. One of my patients, when informed of thedangers of the operation, expressed himself as fol-lows: “Anything you can get out of this betterthan death is clear profit.”
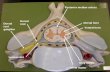
Fig. 2 shows the line of complete anesthesiathree weeks after the operation.
Recent reports from 1113- cases show that therehas been no return of the neuralgia, and neitherhave they suffered from ocular symptoms.
Mrs. Kate M., Lincoln Neb.; housewife; age53. Family history; Mother 85 years old, living,and health}-; father deceased, the result of an ac-cident; two sisters are living and enjoying goodhealth; husband and one boy are well. Patientenjoyed excellent health until sixteen years ago,when she was attacked with the present trouble.Was married at the age of twenty. Had onechild; no miscarriages nor abortions. Never suf-fered from gout, rheumatism, nor any kind of dis-ease. Had sustained no injury to the head. Had

not suffered from severe emotional excitement normental over-taxation previous to present illness.Menstniatiou normal.
Present history: Sixteen years ago, after a hardday’s work, patient was attacked with a “stroke”or “shock” which prostrated her to the floor. The“shock” consisted of a severe sharp pain in the
Fig. '1. — of complete anesthesia.
entire right side of the face. The pain was in-tense and lasted about ten minutes. She couldnot open her jaws and remained for a time asthough completely paralyzed. This was the onsetof the attacks of chronic neuralgia for which shenow seeks relief. The “attacks” occurred everyfew hours in the beginning, but for the last sixyears a spasmodic contraction of the muscles of

10
the right wide of the face, with closure of the righteye, accompanied by intense pain, occurs everyfifteen or twenty minutes, day and night. Ex-citement, pressure on the face, or a slight draughtwill bring on an attack. In the interval betweenthe attacks the face is painful. The right halfof the tongue appears to be the most painful spot.For that reason conversation is carried on in a lowmuttering tone, and has to be interrupted fre-quently when the attacks come on.
Examination.—No deformities or irregulari-ties in the head or face; sight normal; nose freefrom obstruction. Teeth on the right side had allbeen extracted with the hope of relieving the neu-ralgia. No defect in the mouth or fauces; exter-nal meatus and drum normal. Heart and lungsnormal; no irregularity in abdominal organs; pel-vic organs normal; urine normal; no enlargementof glands; epitrochlear glands normal. The areaof pain extends from right superciliary ridgedown the entire right side of the face to the lowermargin of mandible, from the anterior border ofthe ear forward to the middle line of the forehead,nose, lips, and tongue. An electrode placed overany part of the face produced intense pain.
The patient’s condition was really pitiable, andwhen on the table, before the anesthetic was ad-ministered, she said: “Doctor, promise me thatyou will do one of two things; either cure me ofthis neuralgia or kill me.”
Operation.—The patient was operated uponDecember 24th, 1895; chloroform was used. Thehead was placed in a somewhat elevated positionand turned to the side. The details of the opera-tion were as described above. The evening afterthe operation the patient was conscious and shesaid she was entirely relieved from pain, sufferingonly from the soreness at the position of thewound. Forty-eight hours after the operationthe gauze packing was removed. A small quan-

tin* of serum, blood and detritus escaped, but nocerebro-spinal fluid. Tlie patient expressed greatrelief after the gauze was extracted, as she saidthe pressure seemed to be taken out of her head.At no time did her temperature reach 100 degrees.Her improvement was very rapid. She was ableto sit up in a week and in two weeks left thehospital. The accompanying cut shows the lineof incision and also the line of anesthesia threeweeks after the operation. A letter from the pa-tient, dated August 20th, states that she has hadno return of pain. The only inconvenience ex-perienced is the absence of sensation on the rightside of the face.
John G., Ossian, Iowa; male, age 52; German;merchant; married; several children, all well.Received a bullet wound in the army. Enjoyedexcellent health up to seven years ago, when hebegan to have attacks of pain on the right side ofthe face. In the winter time he would have themevery day, or at the most, every second day. Insummer he might go for a week without an at-tack. The last winter they increased very muchin severitv and duration.
He is of phlegmatic temperament; respondsslowly to questions; appears to be suffering fromsome mental disturbance. Complains of pain inan area about the size of a dollar above the rightsuperciliary ridge. When the “attack” is on thepain extends over the greater portion of the face.
Eyes, nose, mouth, and ears normal; has somedigestive disturbance; lungs and heart normal;urine negative.
Date of operation, April 9th, 1896. Incisionthe same as described above. In this case thedura was opened and a considerable quantity ofcerebro-spinal fluid escaped. The packing waswithdrawn seventy-two hours after operation.That was also followed by a discharge of cerebro-spinal fluid, which was stopped by tying the pro-

visional suture. The patient made a rapid recov-ery; the numbness of his face annoyed him con-siderable. There was no pain after the operation.The ganglion and root were removed in one mass:it was given to Dr. Evans for examination.
Information received from patient August 14thstates that he is not suffering from pain and en-joys excellent health since the operation. Inneither of the patients was there any inconven-ience expressed from the loss of sensibility in theeye. Convalescence was rapid; the patient wasup and about the room in a week and left the hos-pital three weeks after the operation.


Related Documents