Membranous bronchioles and connective tissue network of normal and emphysematous lungs E. K. VERBEKEN, M. CAUBERGHS, AND K. P. VAN DE WOESTIJNE Laboratorium voor Pathologische Ontleedkunde I and Laboratorium voor Pneumologie, Universitaire Ziekenhuizen St. Rafae ¨l en Gasthuisberg, B-3000 Leuven, Belgium Verbeken, E. K., M. Cauberghs, and K. P. Van de Woestijne. Membranous bronchioles and connective tissue network of normal and emphysematous lungs. J. Appl. Physiol. 81(6): 2468–2480, 1996.—Three-dimensional recon- structions of the septal system of normal human lungs revealed that airways course within the interlobular septa, i.e., between the two blades formed by the peripheral bound- aries of adjacent lobuli of whatever order, and enter the supplied pulmonary unit at its side. This is not in keeping with the classic view of a peripheral airway in the center of a lung unit and submitted to radial traction by attached alveolar septa. The basic design of the lung fibrous scaffold appears to be in conformity with the laws of fractal geometry. Similar reconstructions in centrilobular emphysema dis- closed tortuosities of both intra-acinar and interlobular septa, with consequent distortions of the corresponding intraseptal bronchioles and collapse of lung units of different sizes. It is suggested that in centrilobular emphysema competition for space, besides intrinsic airways narrowing because of in- flammation and loss of elastic recoil, is a cause of flow limitation. airway obstruction; emphysema; fibrous septa; fractals; com- petition for space IN THE CONVENTIONAL DESCRIPTION of the morphology of the lung, the latter is divided into successively smaller and smaller cone-shaped units surrounded by a septum and centered around a bronchovascular bundle. In this design, the smallest pulmonary unit completely sur- rounded by a septum is the secondary lobule (27). It contains three to five acini, which are the basic units participating in gas exchange. In contrast to the lob- ules, individual acini cannot be recognized by gross examination. In a previous study (26), we prepared serial histological sections of blocks of lung tissue from normal, senile, and emphysematous lungs to recon- struct the peripheral airway tree in three dimensions. Unexpectedly, these reconstructions showed that bron- chi and bronchioles coursed within a septum and entered the supplied pulmonary unit at its side. To understand the relationship between classic inter- lobular septa and the septa containing an airway, which we observed, a reconstruction of the total septal system in three dimensions was attempted and pro- jected onto the corresponding airway tree. First, nor- mal lungs were examined. In a second step, reconstruc- tions were performed from lungs with centrilobular emphysema, in an attempt to relate the loss of the orderly appearance of the parenchyma in the latter condition to the construction principle of the normal lung. MATERIALS AND METHODS The study was performed on excised human lungs obtained at autopsy: two normal lungs and four lungs with centrilobu- lar emphysema were investigated. The lungs were perfused intrabronchially for 72 h with a 10% Formalin solution at a pressure of 2.5–3.0 kPa. This type of slow fixation was found to fix the lung at a volume close to total lung capacity (26). Because lobular septa are barely visible by light micros- copy in normal lungs, we developed a technique to better visualize these septa. A barium gelatine suspension was prepared by suspending 1.5 g of gelatine powder in 3 ml of water and heating it to 40°C. To this gel, 37 ml of barium sulfate, also at 40°C (Micropaque, Guerbet, Brussels, Bel- gium), were added. With a 22-gauge needle, 5–10 ml of this suspension were injected in the subpleural parenchyma at five or more locations chosen randomly on both lateral and medial sides of each normal lung. The gelatine stiffens when coming in contact with the Formalin-filled tissue at room temperature, thus allowing further processing for histology. The barium suspension mostly demarcated a pulmonary unit of variable size at the pleural surface, although spilling over of the contrast medium in an adjacent area was frequently observed. Three injected peripheral tissue blocks contiguous to the pleura were resected from the two normal lungs. In the emphysematous lungs, the injection procedure was not used. Five tissue blocks contiguous to the pleura were selected at random from the four lungs. Zones of marked destruction (bullae) were avoided, however. All tissue blocks were serially sectioned. Sections were cut parallel to the pleural surface and stained with Masson’s trichrome; 1,500–2,000 serial sections, 4 μm thick, correspond- ing to 7.7–10.3 mm in depth of peripheral lung tissue [taking into account the shrinkage during processing: 0.78 for each dimension (24)] were prepared. To reach the level of the cartilagenous bronchi, one block from an emphysematous lung was cut into 20-μm-thick sections; 1,700 serial sections were examined, corresponding to 43.5 mm of peripheral lung tissue. The serial sections represent, after correction for shrinkage, an average tissue block volume of 2.40 cm 3 for normal lungs and 6.55 cm 3 for emphysematous lungs. In the latter, larger tissue blocks were taken, with the purpose of examing more lobuli. From these serial sections, both the peripheral airway tree and the parenchymal septa were reconstructed. An order number was attributed to each airway by using Horsfield’s counting method (12), with order 1 corresponding to the terminal bronchioles (TB). Two TB meet to form an order 2 membranous bronchiole (MB 2 ), and so on. If two branches of differing order meet, the numbering is continued from the highest order of the two meeting branches. Bifurcations were found to be dichotomous (26). The most distal cartilage in the airway tree was located at the bifurcations. Accordingly, in keeping with Von Hayek (27), we called MB the daughter branches originating at the level of a cartilagenous bifurcation, with the mother branch being a bronchus. 0161-7567/96 $5.00 Copyright r 1996 the American Physiological Society 2468

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Membranous bronchioles and connective tissue networkof normal and emphysematous lungs
E. K. VERBEKEN, M. CAUBERGHS, AND K. P. VAN DE WOESTIJNELaboratorium voor Pathologische Ontleedkunde I and Laboratorium voor Pneumologie,Universitaire Ziekenhuizen St. Rafael en Gasthuisberg, B-3000 Leuven, Belgium
Verbeken, E. K., M. Cauberghs, and K. P. Van deWoestijne. Membranous bronchioles and connective tissuenetwork of normal and emphysematous lungs. J. Appl.Physiol. 81(6): 2468–2480, 1996.—Three-dimensional recon-structions of the septal system of normal human lungsrevealed that airways course within the interlobular septa,i.e., between the two blades formed by the peripheral bound-aries of adjacent lobuli of whatever order, and enter thesupplied pulmonary unit at its side. This is not in keepingwith the classic view of a peripheral airway in the center of alung unit and submitted to radial traction by attachedalveolar septa. The basic design of the lung fibrous scaffoldappears to be in conformity with the laws of fractal geometry.Similar reconstructions in centrilobular emphysema dis-closed tortuosities of both intra-acinar and interlobular septa,with consequent distortions of the corresponding intraseptalbronchioles and collapse of lung units of different sizes. It issuggested that in centrilobular emphysema competition forspace, besides intrinsic airways narrowing because of in-flammation and loss of elastic recoil, is a cause of flowlimitation.
airway obstruction; emphysema; fibrous septa; fractals; com-petition for space
IN THE CONVENTIONAL DESCRIPTION of the morphology ofthe lung, the latter is divided into successively smallerand smaller cone-shaped units surrounded by a septumand centered around a bronchovascular bundle. In thisdesign, the smallest pulmonary unit completely sur-rounded by a septum is the secondary lobule (27). Itcontains three to five acini, which are the basic unitsparticipating in gas exchange. In contrast to the lob-ules, individual acini cannot be recognized by grossexamination. In a previous study (26), we preparedserial histological sections of blocks of lung tissue fromnormal, senile, and emphysematous lungs to recon-struct the peripheral airway tree in three dimensions.Unexpectedly, these reconstructions showed that bron-chi and bronchioles coursed within a septum andentered the supplied pulmonary unit at its side.To understand the relationship between classic inter-
lobular septa and the septa containing an airway,which we observed, a reconstruction of the total septalsystem in three dimensions was attempted and pro-jected onto the corresponding airway tree. First, nor-mal lungs were examined. In a second step, reconstruc-tions were performed from lungs with centrilobularemphysema, in an attempt to relate the loss of theorderly appearance of the parenchyma in the lattercondition to the construction principle of the normallung.
MATERIALS AND METHODS
The study was performed on excised human lungs obtainedat autopsy: two normal lungs and four lungs with centrilobu-lar emphysema were investigated. The lungs were perfusedintrabronchially for 72 h with a 10% Formalin solution at apressure of 2.5–3.0 kPa. This type of slow fixation was foundto fix the lung at a volume close to total lung capacity (26).Because lobular septa are barely visible by light micros-
copy in normal lungs, we developed a technique to bettervisualize these septa. A barium gelatine suspension wasprepared by suspending 1.5 g of gelatine powder in 3 ml ofwater and heating it to 40°C. To this gel, 37 ml of bariumsulfate, also at 40°C (Micropaque, Guerbet, Brussels, Bel-gium), were added. With a 22-gauge needle, 5–10 ml of thissuspension were injected in the subpleural parenchyma atfive or more locations chosen randomly on both lateral andmedial sides of each normal lung. The gelatine stiffens whencoming in contact with the Formalin-filled tissue at roomtemperature, thus allowing further processing for histology.The barium suspension mostly demarcated a pulmonary unitof variable size at the pleural surface, although spilling overof the contrast medium in an adjacent area was frequentlyobserved. Three injected peripheral tissue blocks contiguousto the pleura were resected from the two normal lungs. In theemphysematous lungs, the injection procedure was not used.Five tissue blocks contiguous to the pleura were selected atrandom from the four lungs. Zones of marked destruction(bullae) were avoided, however.All tissue blocks were serially sectioned. Sections were cut
parallel to the pleural surface and stained with Masson’strichrome; 1,500–2,000 serial sections, 4 µm thick, correspond-ing to 7.7–10.3 mm in depth of peripheral lung tissue [takinginto account the shrinkage during processing: 0.78 for eachdimension (24)] were prepared. To reach the level of thecartilagenous bronchi, one block from an emphysematouslung was cut into 20-µm-thick sections; 1,700 serial sectionswere examined, corresponding to 43.5 mm of peripheral lungtissue. The serial sections represent, after correction forshrinkage, an average tissue block volume of 2.40 cm3 fornormal lungs and 6.55 cm3 for emphysematous lungs. In thelatter, larger tissue blocks were taken, with the purpose ofexaming more lobuli. From these serial sections, both theperipheral airway tree and the parenchymal septa werereconstructed. An order number was attributed to eachairway by using Horsfield’s counting method (12), with order1 corresponding to the terminal bronchioles (TB). Two TBmeet to form an order 2 membranous bronchiole (MB2), andso on. If two branches of differing order meet, the numberingis continued from the highest order of the two meetingbranches. Bifurcations were found to be dichotomous (26).The most distal cartilage in the airway tree was located at thebifurcations. Accordingly, in keeping with Von Hayek (27), wecalled MB the daughter branches originating at the level of acartilagenous bifurcation, with the mother branch being abronchus.
0161-7567/96 $5.00 Copyright r 1996 the American Physiological Society2468

An additional tissue block was resected from a normal lungat the level of the lobar bronchi and sectioned serially: 1,500sections were prepared.
RESULTS
Reconstruction of the septa from a normal lung. InFig. 1, a subpleural pentagonal area is shown, corre-sponding to a secondary lobule (27). After injection, thebarium sulfate filled only one-half of the pentagonbecause of the presence of a thin septum between theinjected and the noninjected areas. A histological sec-tion of the corresponding area, ,1 mm under thepleura, is presented in Fig. 2. It shows that thenoninjected one-half of the pentagon is divided into twoareas of equal size, A and B, by a septum perpendicularto the one separating the injected from the noninjectedarea. Similarly, the injected area is divided by a septuminto two parts, C and D. These septa are recognizedbecause of their continuity rather than because of theirthickness. At deeper levels, these thin septa are lessregular, apparently because of alveolar outpouchings,and thus difficult to follow. Also larger parts of theseptum delineating the pentagon at the pleural surfaceare lost in the depth of the lung. In fact, we were unableto reconstruct the septa starting from the pleura, evenwhen guided by the barium sulfate. We were moresuccessful in reconstructing the septa starting from theopposite side, namely from the depth of the lung. Itturned out that each airway bifurcation appeared togenerate systematically a septum, the reconstruction ofthe septa thus necessitating a three-dimensional recon-struction of the airway tree. This reconstruction ispresented schematically in Fig. 3, A and B. Figure 3Aschematizes the last generations of bronchi, the MB,and the first generation of respiratory bronchioles (RB)as well as the relationship between the airway bifurca-
Fig. 1. Pleural view of septal architecture. After injection in themiddle of a secondary lobule, one-half of lobule appears to be injectedwith barium sulfate (areas C andD). Fact that areas A and B are freeof contrast medium and sharply demarcated from C and D suggestsexistence of a septum between AB and CD.
Fig. 2. Subpleural section (no. 70) showinghistology of area corresponding to Fig. 1. Aseptum is seen between AB and CD. Inaddition, in both injected and noninjectedareas of pentagon, a thin transversal sep-tum is visualized (arrows). Arrowhead indi-cates a septum generated by bronchi B1 andB1? (see Fig. 3 for further description).
2469RECONSTRUCTION OF PULMONARY SEPTA

tions and the origin of septa. Figure 3B shows the sameairway tree in relation to the supplied parenchymalvolumes. The drawing emphasizes that airways coursewithin septa corresponding to the outer walls of twoadjacent parenchymal units. Figures 4, 5, 6, and 7group a selection of the serial sections between the lastgenerations of bifurcating bronchi (section 1400) andthe peripheral parenchyma (level 338). At level 1400,the outline of the pentagon is only partly seen. Abronchus is bifurcating into a branch that leaves thetissue block (B1?) and a bronchus, B1 (Fig. 3A). Carti-lage is found at the bifurcation. At level 1300, B1branches into an airway, the order of which is notdefined (MB3?), and a MB of the third order (MB3). It isMB3 that supplies the pentagon. Remarkably, MB3enters the corresponding lung unit not at its center butat its side. At level 1250 (not shown), a side branchoriginates, classified as a second-order MB (MB2E),which will supply area E (Fig. 3B). MB2E penetratesdeeper into the parenchyma, separating area E fromareas A and B by a septum parallel to the pleuralsurface and, hence, parallel to the serial sections. Sucha septum, because it is not perfectly flat, will not bevisualized in one single histological section.After its bifurcation at level 1250, the second daugh-
ter branch of MB3 proceeds as MB2. It can be seen thatthe bifurcation of the airways traces a septum, whichwe therefore called a ‘‘branching’’ septum. This septumis projected on the pleural surface (as part of thepentagon, at the level of A and between A andD).The septum ‘‘actively’’ traced by MB3? and MB3
(prolonged byMB2) continues into a septum (betweenBand C) that completes the separation between thenoninjected and the injected areas, AB and CD, respec-tively. This is a second type of septum that is notpositioned between two bifurcating airways but, on thecontrary, between an airway and a vein and separatesthe volumes B and C. We called this an ‘‘extended’’septum. At level 640, MB2 branches into two first-orderMB (MB1), again tracing a branching septum betweenthe two airways (part of the septum separating A fromB and D from C) and prolonged by extended septa,
Fig. 3. A: schematic reconstruction of membranous (MB) and respira-tory bronchioles (RB) and corresponding septa of pentagon. Septaoriginating at airway bifurcations are shaded. No distinction is madehere between branching and extended septa (see further). MB1, MB2,MB3, 1st, 2nd, and 3rd order of MB, respectively; B1, bronchus of 1storder; ?, unknown order; RBA, RBB, RBC, RBD, RB supplying areas Aand B, C and D, respectively. Bifurcation of bronchi B1-B1? generatesa septum (not shaded) partially seen on Fig. 2, not related topentagon. Bifurcation of MB3?-MB3 (continued by MB2) generates aseptum projected on pleural surface as a septum demarcating a smallpart of pentagon and as a second septum between A and D.Separation MB1-MB1 is at origin of a septum partly separating areasB-C from A-D. B: volume units of pentagon and corresponding MBand RB. Lung units A, B, C and D are supplied by 1st-order RB: RBA,RBB, RBC, and RBD, respectively. Figure emphasizes intraseptalcourse of airways. x-Axis, no. of sections starting from pleura.Asterisks point to presence of cartilage.
Fig. 4. Selected serial sections are projected onto a schematicdrawing of peripheral airway tree. Level closest to pleural surfacecorresponds to level 338 of Fig. 7. See Figs. 5–7 for photographs andcorresponding drawings of sections.
2470 RECONSTRUCTION OF PULMONARY SEPTA

Fig. 5. Selected photographs and corresponding drawings of serial sections. At level 1400, a bronchus is branchinginto B1 and B1?. Contrast material is filling lumen of B1 and of B1?; there is also somematerial inside parenchyma. V,veins within septa, limiting (partly) pentagon (drawing: thin continuous lines). a, Artery. At level 1300, B1 branchesinto MB3 and MB3? and MB2E into MB1E and MB1E (supplying volume E). Arrow indicates onset of a branchingseptum (thick line on drawing) generated by bifurcation B1? and B1. Level 1100 shows location of MB2 between abranching septum (thick line on drawing) and extended septum (dotted line on drawing). Arrows point at persistentbranching septa, generated at previous bifurcations. Periphery of pentagon (thin lines on drawing) and separationAB-CD are now completely demarcated.
2471RECONSTRUCTION OF PULMONARY SEPTA

Fig. 6. Selected photographs and corresponding drawings of serial sections. At level 640, MB2 bifurcates into twoMB1, creating a septum (arrowhead) clearly shown at level 550. At level 500 (not shown), MB1 divides into RBA andRBB, supplying volumes A andB, respectively.Anew branching septum perpendicular to septum separatingA andB(not indicated in Fig. 3) appears, clearly shown at level 438 (arrowhead) (extended part of it is seen to left of RBA).Septum traced by MB1 persists (double arrowhead), as does its extended septum (thick arrow). Latter is blurredbecause of alveolar outpouchings. (Masson’s trichrome.)
2472 RECONSTRUCTION OF PULMONARY SEPTA
completing the separation between A and B and D andC, respectively.The volumes A, B, C, and D are supplied by further
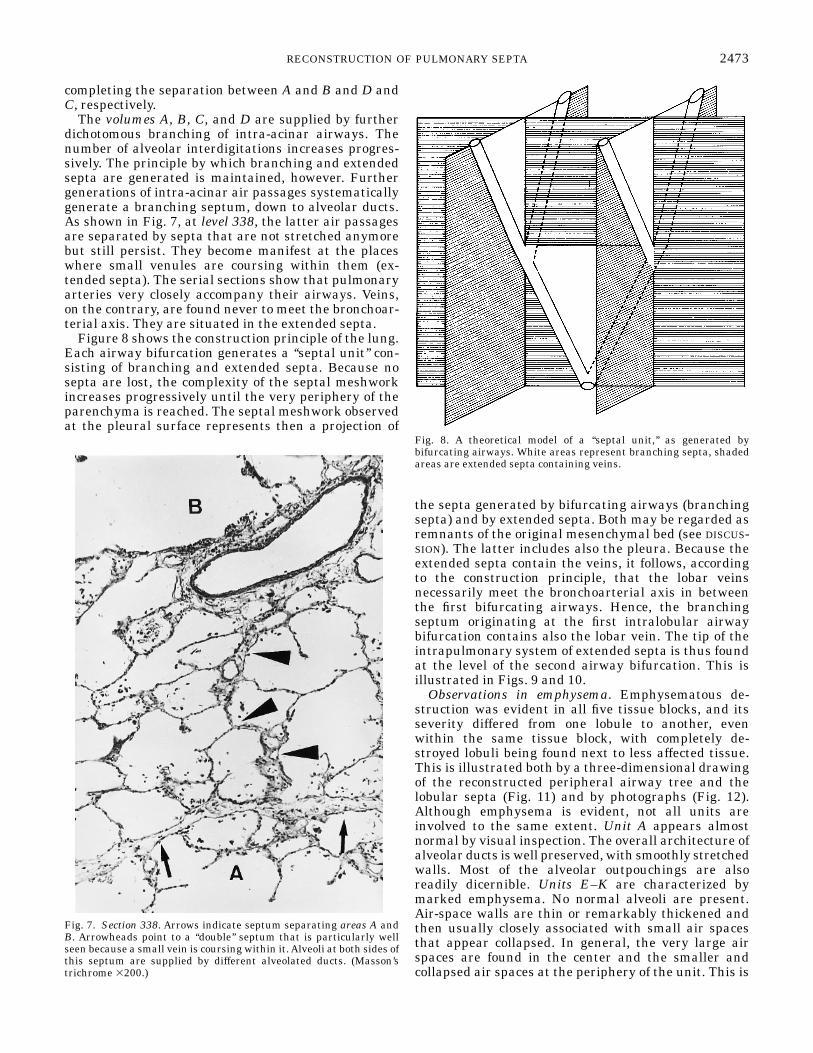
dichotomous branching of intra-acinar airways. Thenumber of alveolar interdigitations increases progres-sively. The principle by which branching and extendedsepta are generated is maintained, however. Furthergenerations of intra-acinar air passages systematicallygenerate a branching septum, down to alveolar ducts.As shown in Fig. 7, at level 338, the latter air passagesare separated by septa that are not stretched anymorebut still persist. They become manifest at the placeswhere small venules are coursing within them (ex-tended septa). The serial sections show that pulmonaryarteries very closely accompany their airways. Veins,on the contrary, are found never to meet the bronchoar-terial axis. They are situated in the extended septa.Figure 8 shows the construction principle of the lung.
Each airway bifurcation generates a ‘‘septal unit’’ con-sisting of branching and extended septa. Because nosepta are lost, the complexity of the septal meshworkincreases progressively until the very periphery of theparenchyma is reached. The septal meshwork observedat the pleural surface represents then a projection of
the septa generated by bifurcating airways (branchingsepta) and by extended septa. Both may be regarded asremnants of the original mesenchymal bed (see DISCUS-SION). The latter includes also the pleura. Because theextended septa contain the veins, it follows, accordingto the construction principle, that the lobar veinsnecessarily meet the bronchoarterial axis in betweenthe first bifurcating airways. Hence, the branchingseptum originating at the first intralobular airwaybifurcation contains also the lobar vein. The tip of theintrapulmonary system of extended septa is thus foundat the level of the second airway bifurcation. This isillustrated in Figs. 9 and 10.Observations in emphysema. Emphysematous de-
struction was evident in all five tissue blocks, and itsseverity differed from one lobule to another, evenwithin the same tissue block, with completely de-stroyed lobuli being found next to less affected tissue.This is illustrated both by a three-dimensional drawingof the reconstructed peripheral airway tree and thelobular septa (Fig. 11) and by photographs (Fig. 12).Although emphysema is evident, not all units areinvolved to the same extent. Unit A appears almostnormal by visual inspection. The overall architecture ofalveolar ducts is well preserved, with smoothly stretchedwalls. Most of the alveolar outpouchings are alsoreadily dicernible. Units E–K are characterized bymarked emphysema. No normal alveoli are present.Air-space walls are thin or remarkably thickened andthen usually closely associated with small air spacesthat appear collapsed. In general, the very large airspaces are found in the center and the smaller andcollapsed air spaces at the periphery of the unit. This is
Fig. 7. Section 338. Arrows indicate septum separating areas A andB. Arrowheads point to a ‘‘double’’ septum that is particularly wellseen because a small vein is coursing within it.Alveoli at both sides ofthis septum are supplied by different alveolated ducts. (Masson’strichrome 3200.)
Fig. 8. A theoretical model of a ‘‘septal unit,’’ as generated bybifurcating airways. White areas represent branching septa, shadedareas are extended septa containing veins.
2473RECONSTRUCTION OF PULMONARY SEPTA

particularly manifest in units E, G, J, and K. Disrup-tion of thickened walls of enlarged air spaces is alsoclearly seen (in particular in units G and K in Fig. 12,bottom). Units B, C, and D are also emphysematous,although to a lesser extent than the units E–K. Air-space septa are not stretched as in normal lungs butrather tortuous on transsection (particularly in C).Unit B appears collapsed.In contrast to normal lungs, MB are tortuous and
stenotic in all emphysematous lungs (Fig. 12). Al-though some chronic inflammatory infiltration is pres-ent locally, luminal narrowing, even extreme stenosis,is observed without inflammation or any noticeablefibrosis, as shown in Fig. 13. Extremely narrowed TBopen into enlarged RB. No inflammation or fibrosis ofthe bronchiolar wall is seen.
DISCUSSION
The model. During lung development, the airwaytree branches by dichotomy in an originally compactmesenchymal bed, the splanchnopleuric mesenchym(10). As illustrated in Fig. 8, this branching processcreates well-defined planes in that original matrix,with each new pair of sister branches of airways beingat the origin of a newly oriented plane. The latter can bepartitioned into a septum situated in between the sisterairways and an outward extension of that septum. Thetwo parts of the septum differ in their topographicrelation with the pulmonary vessels. The outer part is
systematically positioned in between airways and veins.Arteries appear to course mostly next to the airway.This topographic relationship justifies the distinctionbetween the outer part as being a venous septum andthe inner part as being a bronchoarterial septum.Because the latter septum is defined by the process ofairway branching during lung development, we pro-pose the term ‘‘branching septum.’’ The outer part thencorresponds to the remnants of the progressively vanish-ing original mesenchymal bed, thus representing anextension to the periphery of the branching septum.Hence the term ‘‘extended’’ septum. The ‘‘branching’’septa constitute awell-defined three-dimensionalmesh-work, as judged from the observation that veins andarteries do not meet, except at the lung hilus. At thehilus, the origin of the branching septal system mustnecessarily meet the insertion of the extended septalsystem. This particular point is shown in Fig. 9.In the classic model of the connective tissue network
of the lungs, three components are distinguished: theaxial, peripheral, and alveolar septal fibers (28, 30).The axial fibers form a sheath along the airwaysextending from the hilus along the bronchi and bronchi-oles down to the alveolar ducts. The peripheral fibersare connected to the pleura and form the interlobularsepta between parenchymal units of various orders(from acini to segments), providing an anchoring pointfor the alveolar septal fibers. The interlobular septacontain the pulmonary veins and lymphatics and ex-tend centrally toward the bronchial walls. There, theperipheral fiber system forms the peribronchiumaroundthe bronchus and the pulmonary arteries. Axial andperipheral fiber tracts are, in turn, connected by anetwork of fibers in the alveolar septa, anchored at oneend to the fiber net of the alveolar ducts (axial system)and at the other end to fibers running between adjacentalveolar ducts, which are the most distal extension ofthe peripheral fiber system. The alveolar septal fibersystem is the major support system for the pulmonarycapillaries. Because the three fiber systems are intercon-nected, a fibrous scaffold is formed, which supports thelung. Pressures across the lung are transmitted insidethis fibrous continuum, from the pleura via the paren-chyma toward the airways, ensuring the patency of theintrapulmonary airways.In contrast to the conventional description of the
fibrous scaffold of the lungs, the present model stressesthe continuity of the various components of the support-ing fibrous system, with the branching septa contain-ing airways and arteries being prolonged laterally andtoward the pleura or larger intrapulmonary septa bythe ‘‘extended’’ septa containing veins and lymphatics.The extended septa correspond to the peripheral fibersystem, the axial system is contained in the branchingsepta. The alveolar septal fiber system corresponds tothe most distal part of that continuum, generated bythe alveolar ducts in the mesenchymal matrix. Becausethe intra-acinar air passages are lined with alveoli, thedistal septa between adjacent intra-acinar passagesmay be blurred by interdigitating alveoli. At this level,septa are more a concept than an anatomic reality.
Fig. 9. Model of tip of intrapulmonary system of extended septa.White areas are branching septa, shaded area represents an ex-tended septum. Levels a, b, and c are shown in correspondingphotographs of Fig. 10. Veins (V) and pulmonary arteries (A) meet atlevel of lobar bronchi (B).
2474 RECONSTRUCTION OF PULMONARY SEPTA

Although the construction principle is maintained, itsanatomic expression is hardly visible, thus reducingthe model rather to a conceptual framework in normallungs. This explains why it has been stated that thesmallest lung unit defined anatomically is a lung lobe,because a lobe is enwrapped more or less completely by
visceral pleura (30); and, furthermore, why the defini-tion of smaller pulmonary units, such as an acinus or alobulus, is determined more by functional consider-ations than by the anatomy (8). Earlier, Von Hayek (27)pointed out that lobules were not always demar-cated by septa at the surface of a lung lobe or in the
Fig. 10. Selected photographs and corresponding drawings at levels a, b, and c in Fig. 9. Branching septa (thickcontinuous lines on drawing) are arrowheaded. Extended septum (arrow, dotted line on drawing) in which veincourses is partially blurred because of alveolar outpouchings (arrow on drawing). Vein V is meeting A1 at level cbranching septum, thus merging into extended septum (shaded area on drawing).
2475RECONSTRUCTION OF PULMONARY SEPTA

depth of a lobe. Large parts of the surfaces facing theinterlobular fissures often showed no divisions intolobules. Septa in adult lungs may thus vary widely intheir composition, from thick fibrous plates to a fewextracellular fibers, with their presence being markedonly (in the case of extended septa) by the course of avein. Because the alveolar ducts and alveoli are locatedat the periphery of units of whatever size, collateralventilation at the interalveolar level (5) may occurbetween units of various order, even those supplied bydifferent segmental bronchi.The general construction principle of the lung is
characterized by the fact that it is invariant when thescale is changed, whether we are dealing with a lung‘‘unit’’ supplied by a cartilageneous bronchus (Fig. 3) oran alveolar duct (Fig. 7). The principle by whichbranching bronchoarterial and extended venous septaare formed at all levels in the lung is in keeping withthe fundamental notions of fractal geometry. The latterdeals with the geometry of hierarchies. When growthoccurs without a change in shape of the organ, as is thecase of the growing lung, the shape may be preservedbecause the organ’s inner structure grows and in-creases in dimension without changes in shape andbranching pattern of its comprising elements. Manynatural patterns appear too complex, fragmented, andirregular to be described in terms of classic three-dimensional Euclidean geometry and, therefore, ap-pear ‘‘amorphous.’’ This problem has been dealt with byMandelbrot (17) thanks to the use of fractal dimen-sions, i.e., noninteger dimensions. As outlined by Wei-bel (28, 29), fractal properties can be attributed to thepulmonary airways and vessels. This study suggeststhat the basic design pattern of lung tissue may alsofollow the laws of fractal geometry.Implications for peripheral airways. The classic rep-
resentation of the fibrous tissue of the lung as anetwork attached at the periphery of the airway, an-chored between two more rigid frameworks, and thussubmitting the peripheral airway to radial tractionappears to be an incomplete picture of the lung anatomy.
According to the present results, the airways enterthe unit that they supply at its side, with the alveoli ofthe unit being generated by the daughter branches ofthe supplying airway. The alveolar septa, seen asalveolar attachments (AA) of the MB, are attached tothe outer side of the blades formed by the interlobularsepta, rather than to the airway wall itself.Accordingly,the AA do not necessarily correspond to the amount ofsupport provided directly by the connective tissuenetwork to theMB. This may have consequences for thepermeability of the peripheral airways in emphysema.As early as in 1957, Leopold and Gough (14) observedmarked airway narrowing of the bronchioles supplyingthe emphysematous spaces. These authors suggestedthat, besides an anatomic narrowing of the bronchiolescaused by inflammation in their walls, these airwaysgot kinked or compressed during expiration ‘‘becausethey pass unsupported into the emphysematous tis-sue.’’ As an expression of this support, Anderson andForaker (1) counted the number of AA on MB; thatnumber was reduced in emphysema and proportionalto bronchiolar lumen size. This observation was con-firmed by others in emphysematous patients and insmokers (13, 15, 16, 21, 22). AA were inversely relatedto the emphysema score (15, 19, 21) and to the elasticrecoil pressure of the lungs (21, 22). Functional airwayobstruction detected clinically or expressed by a reduc-tion of forced expiratory volume in 1 s (FEV1) wascorrelated with the severity of emphysema (9, 13, 18,19) and a reduction of the diameter of the MB (d) (9, 20,26) or of AA (13, 19, 21). The separate contribution ofthese factors to airflow obstruction was evaluated bymeans of multiple-regression analysis. Berend andThurlbeck (2) observed on excised human lungs a jointrelationship between maximal expiratory flow at agiven elastic recoil pressure (5 cmH2O) and both inflam-mation score of the small airways and emphysemascore. This suggests that emphysema, apart from itseffect on elastic recoil, also influences expiratory flowby another mechanism. Similarly, when FEV1 wasrelated to pathological (including scores of small-air-way inflammation and fibrosis) and morphometric in-dexes of small airways (d, AA), the severity of emphy-sema turned out to be the most important factor forobstruction, with none of the bronchiolar variableshaving a significant value in predicting the reduction ofventilatory function (9, 19). Apparently, an inflamma-tory thickening of bronchiolar walls or a loss of alveolarattachments or even a decrease of small-airway diam-eter was related to airflow obstruction only because ofits correlation with emphysema. This conclusion wasnot confirmed by recent structure-function studies.Hogg et al. (11) and Gelb et al. (6, 7) observed only veryweak or no correlations between airflow limitationmeasured in vivo and both severity of emphysema andinflammatory scores of small airways in resectionspecimens (11) or on computerized tomography lungscans [completed by pathological examinations (7)].Accordingly, the relationship between increase in pe-ripheral airway resistance or airflow limitation andsmall-airway diameter observed in excised emphysema-
Fig. 11. Schematic reconstruction of peripheral airway tree, paren-chyma, and corresponding septa in a lung with centrilobular emphy-sema. As in Fig. 3A, septa originating at airway bifurcations areshaded, and their extensions are white. *Presence of cartilage.Except for A, areas B–K are supplied by terminal bronchioles (orderMB1).
2476 RECONSTRUCTION OF PULMONARY SEPTA

Fig. 12. Photographs of 2 serial sections (top: section 1200, deepest level of drawing; bottom: section 1060, mostperipheral level of drawing) used for reconstruction of Fig. 11. Area A is close to normal. Intra-acinar septa arestretched as in normal lungs. Emphysema is worst in areas E, F, G, J, and K. Unit B is almost totally collapsed.Intra-acinar septa are tortuous, especially in areas B and C, and focally in area D. Unit C is collapsed to a lesserextent. Collapse of distal intra-acinar units such as alveolar ducts is marked in severely affected regions (arrows).
2477RECONSTRUCTION OF PULMONARY SEPTA

tous lungs (25, 26) does not appear to be a directconsequence of emphysema itself or of airway wallinflammation. Apparently, another mechanism respon-sible for peripheral airway narrowing is operating.
In this respect, we observed collapse of units ofdifferent sizes in the emphysematous lungs, resultingin tortuous septa of corresponding order. This is manifestboth at the level of intra-acinar air passages and of MB
Fig. 13. Noninflammatory stenosis of peripheral air-ways in emphysema. Extremely narrowed terminalbronchioles are opening (arrowheads) into abnormallyenlarged air spaces: A 312.5; B 3100; C 3400. Ex-tended septa (arrows) of both terminal bronchiolespersist. Wall of terminal bronchioles is not inflamed orfibrotic (C).
2478 RECONSTRUCTION OF PULMONARY SEPTA

(Fig. 12, area B). Bends in the septa are accompaniedby corresponding deformations of the airways coursingin those septa. Accordingly, local airway stenosis mightresult from a competition for space between enlargedemphysematous air spaces and the surrounding struc-tures, to the extent that all structures of a lung unit areconstrained to a fairly fixed volume because the expan-sion of the lung is limited by its own fibrous scaffoldincluding the pleura and, finally, by the chest wall. Insuch a system, expansion of one structure may result incompression and deformation of adjacent structures,depending on the relative compressibility of thesestructures.Besides the inflammatory narrowing of nonrespira-
tory bronchioles described in smokers and in pulmo-nary emphysema (3, 4, 9, 11, 32), a concurring nonin-flammatory stenosis may be found, related tocompression by the enlarged air spaces. Air-space en-largement will be the cause of airway narrowing only inthe presence of competition for space. The relationshipbetween the severity of emphysema and the degree offlow limitation is thus indirect. Thus the observedcorrelations may be weak (6, 7, 11).Two other observations can be explained by the
mechanism of competition for space. 1) In keeping withLinhartova et al. (16), we observed that focal airwaynarrowing in emphysema is marked mainly in the MB,is less pronounced in the bronchi with discontinuousintramural cartilagenous support, and virtually absentin the larger bronchi (26). 2) Wilson et al. (31) docu-mented a smaller percent change with lung deflation ofthe diameter of small airways (ID ,1 mm) in emphyse-matous lungs compared with normal lungs and withlarger airways in the same emphysematous lungs.Conversely, we measured during inflation an increasein peripheral airway resistance at recoil pressuresexceeding 0.8 kPa in emphysematous, but not in nor-mal, lungs (26). In the presence of compression of theperipheral airways by enlarged air spaces, the narrow-ing will be proportional to the compressibility of theairway walls and will increase with further inflation ofthe air spaces (or further stiffening of the fibrousscaffold).
We thank G. Verbeeck for secretarial assistance, K. Konings and J.Brebels for histotechnical support, and A. Vandormael for his photo-graphic work. Finally, we thank L. Brullemans for his elegantdrawings. We are indebted to Prof. Dr. P. Burri (Bern) for his criticalevaluation of the results and his valuable comments.
Address for reprint requests: E. K. Verbeken, Laboratory ofPathology I, U. Z. St. Rafael, Minderbroedersstraat 12, B-3000Leuven, Belgium.
Received 10 July 1995; accepted in final form 18 July 1996.
REFERENCES
1. Anderson, A. E., Jr., and A. G. Foraker. Relative dimensionsof bronchioles and parenchymal spaces in lungs from normalsubjects and emphysematous patients. Am. J. Med. 32: 218–226,1962.
2. Berend, N., and W. M. Thurlbeck. Correlations of maximumexpiratory flow with small airway dimensions and pathology. J.Appl. Physiol. 52: 346–351, 1982.
3. Bosken, C. H., B. R. Wiggs, P. D. Pare, and J. C. Hogg. Smallairway dimensions in smokers with obstruction to airflow. Am.Rev. Respir. Dis. 142: 563–570, 1990.
4. Cosio, M., H. Ghezzo, J. C. Hogg, R. Corbin, M. Loveland, J.Dosman, and P. T. Macklem. The relations between structuralchanges in small airways and pulmonary function tests. N.Engl. J. Med. 298: 1277–1281, 1978.
5. Delaunois, L. Anatomy and physiology of collateral respiratorypathways. Eur. Respir. J. 2: 893–904, 1989.
6. Gelb, A. F., J. C. Hogg, N. L. Muller, M. J. Schein, J. Kuei,D. P. Tashkin, J. D. Epstein, J. Kollin, R. H. Green, N.Zamel, W. M. Elliott, and L. Hadjiaghai. Contribution ofemphysema and small airways in COPD. Chest 109: 353–359,1996.
7. Gelb, A. F., M. Schein, J. Kuei, D. P. Tashkin, N. L. Muller,J. C. Hogg, J. D. Epstein, and N. Zamel. Limited contributionof emphysema in advanced chronic obstructive pulmonary dis-ese. Am. Rev. Respir. Dis. 147: 1157–1161, 1993.
8. Haefeli-Bleuer, B., and E. R. Weibel. Morphometry of thehuman pulmonary acinus. Anat. Rec. 220: 401–414, 1988.
9. Hale, K. A., S. L. Ewing, B. A. Gosnell, and D. E. Niewoe-hner. Lung disease in long-term cigarette smokers with andwithout chronic air-flow obstruction. Am. Rev. Respir. Dis. 130:716–721, 1984.
10. Hamilton, W. J., and H. W. Mossman. Human Embryology.Prenatal Development of Form and Function (4th ed.). Balti-more, MD: Williams &Wilkins, 1972.
11. Hogg, J. C., J. L.Wright, B. R.Wiggs, H. O. Coxson,A. OpazoSaez, and P. D. Pare. Lung structure and function in cigarettesmokers. Thorax 49: 473–478, 1994.
12. Horsfield, K. Pulmonary airways and blood vessels consideredas confluent trees. In: The Lung: Scientific Foundations, editedby R. G. Crystal, J. B. West, P. J. Barnes, N. S. Cherniack, andE. R. Weibel. NewYork: Raven, 1991, p. 721–727.
13. Lamb, D.,A.McLean,M. Gillooly, P.M.Warren, G.A. Gould,andW.MacNee.Relation between distal air space size, bronchio-lar attachments, and lung function. Thorax 48: 1012–1017, 1993.
14. Leopold, J. G., and J. Gough. The centrilobular form ofhypertrophic emphysema and its relation to chronic bronchitis.Thorax 12: 219–235, 1957.
15. Linhartova, A., A. E. Anderson, Jr., and A. G. Foraker.Radial traction and bronchiolar obstruction in pulmonary emphy-sema. Arch. Pathol. 92: 384–391, 1971.
16. Linhartova, A., A. E. Anderson, Jr., and A. G. Foraker.Further observations on luminal deformity and stenosis ofnonrespiratory bronchioles in pulmonary emphysema. Thorax32: 53–59, 1977.
17. Mandelbrot, B. B. The Fractal Geometry of Nature. New York:Freeman, 1993.
18. Mitchell, R. S., R. E. Stanford, J. M. Johnson, G. W. Silvers,G. Dart, and M. S. George. The morphologic features of thebronchi, bronchioles, and alveoli in chronic airway obstruction: aclinicopathologic study.Am. Rev. Respir. Dis. 114: 137–145, 1976.
19. Nagai, A., I. Yamawai, T. Takizawa, and W. M. Thurlbeck.Alveolar attachments in emphysema of human lungs. Am. Rev.Respir. Dis. 144: 888–891, 1991.
20. Petty, T. L., G. W. Silvers, and R. E. Stanford. Small airwaydimension and size distribution in human lungs with an in-creased closing capacity. Am. Rev. Respir. Dis. 125: 535–539,1982.
21. Petty, T. L., G. W. Silvers, and R. E. Stanford. Radial tractionand small airways disease in excised human lungs. Am. Rev.Respir. Dis. 133: 132–135, 1986.
22. Saetta, M., H. Ghezzo, W. D. Kim, G. E. Angus, N. S. Wang,M. King, and M. G. Cosio. Loss of alveolar attachments insmokers. Am. Rev. Respir. Dis. 132: 894–900, 1985.
23. Snider, G. L., J. Kleinerman, W. M. Thurlbeck, and Z. H.Bengali. The definition of emphysema. Am. Rev. Respir. Dis.132: 182–185, 1985.
24. Van Brabandt, H., M. Cauberghs, E. K. Verbeken, P. Moer-man, J.M. Lauweryns, andK. P. VandeWoestijne. Partition-
2479RECONSTRUCTION OF PULMONARY SEPTA
ing of pulmonary impedance in excised human and canine lungs.J. Appl. Physiol. 55: 1733–1742, 1983.
25. Verbeken, E. K., M. Cauberghs, J. M. Lauweryns, and K. P.Van de Woestijne. Anatomy of membranous bronchioles innormal, senile, and emphysematous human lungs. J. Appl.Physiol. 77: 1875–1884, 1994.
26. Verbeken, E. K., M. Cauberghs, I. Mertens, J. Clement, J.Lauweryns, and K. P. Van de Woestijne. Tissue and airwayimpedance of excised normal, senile, and emphysematous lungs.J. Appl. Physiol. 72: 2343–2353, 1992.
27. Von Hayek, H. Die Menschliche Lunge. Berlin: Springer, 1953.[English translation by V. E. Krahl. NewYork: Hafner, 1960.]
28. Weibel, E. R. Functional morphology of lung parenchyma. In:Handbook of Physiology. The Respiratory System. Mechanics of
Breathing. Bethesda, MD: Am. Physiol. Soc., 1986, sect. 3, vol.III, pt. 1, chapt. 8, p. 89–111.
29. Weibel, E. R. Fractal geometry: a design principle for livingorganisms. Am. J. Physiol. 261 (Lung Cell. Mol. Physiol. 5):L361–L369, 1991.
30. Weibel, E. R., and H. Bachofen. The fiber scaffold of lungparenchym. In: The Lung: Scientific Foundations, edited by R. G.Crystal, J. B. West, P. J. Barnes, N. S. Cherniack, and E. R.Weibel. NewYork: Raven, 1991, p. 787–794.
31. Wilson, A. G., G. R. Massarella, and N. B. Pride. Elasticproperties of airways in human lungs post mortem. Am. Rev.Respir. Dis. 110: 716–729, 1974.
32. Wright, J. L., L. M. Lawson, P. D. Pare, S. Kennedy, S.Wiggs, and J. C. Hogg. The detection of small airways disease.Am. Rev. Respir. Dis. 129: 989–994, 1984.
2480 RECONSTRUCTION OF PULMONARY SEPTA
Related Documents











