Team Surgency Supporting time-critical combat care during mass casualty response Week 0: Problem: Developing the capability for forward deployment of robotic telesurgery in order to reduce the ‘Golden Hour’ critical time window with early surgical intervention Solution: Solve signal latency for robotic telesurgery Week 10: Problem: Addressing triage and treatment bottlenecks during mass casualty situations at a Role 1 Battalion Aid Station Solution: improve situational awareness and intra-BAS communication 90+ Interviews

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
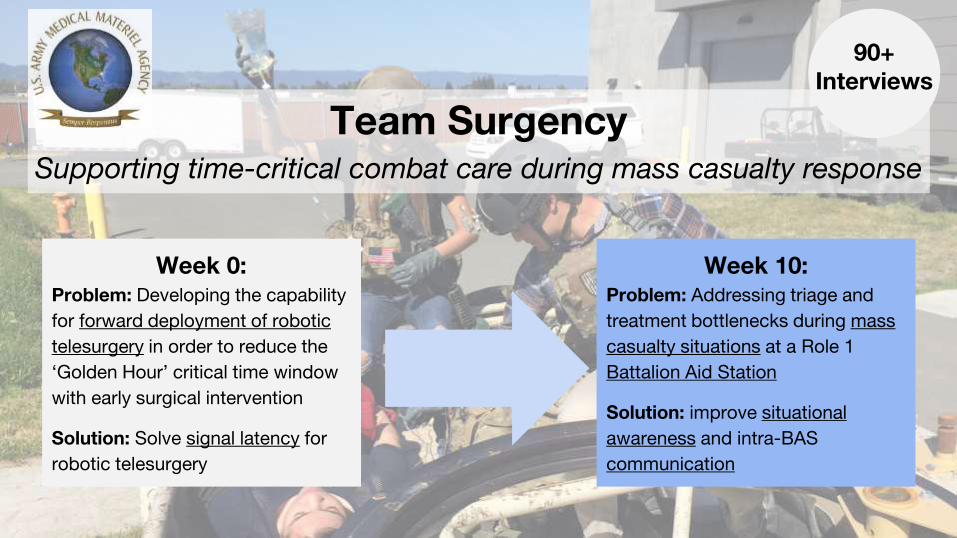
Team SurgencySupporting time-critical combat care during mass casualty response
Week 0:Problem: Developing the capability
for forward deployment of robotic
telesurgery in order to reduce the
‘Golden Hour’ critical time window
with early surgical intervention
Solution: Solve signal latency for
robotic telesurgery
Week 10:Problem: Addressing triage and
treatment bottlenecks during mass
casualty situations at a Role 1
Battalion Aid Station
Solution: improve situational
awareness and intra-BAS
communication
90+ Interviews

Chris SebastianSoftware Engineering &
Product
Andrew DeClerckMachine Learning &
Software Engineering
Negin BehzadianAnalog Circuit Design &
Signals
Abbey CutchinTissue Engineering & Orthopedic Surgery
Mentors and Sponsors
Rafi HoltzmanDr. Steve HongAmanda Love, USAMMA
The Team
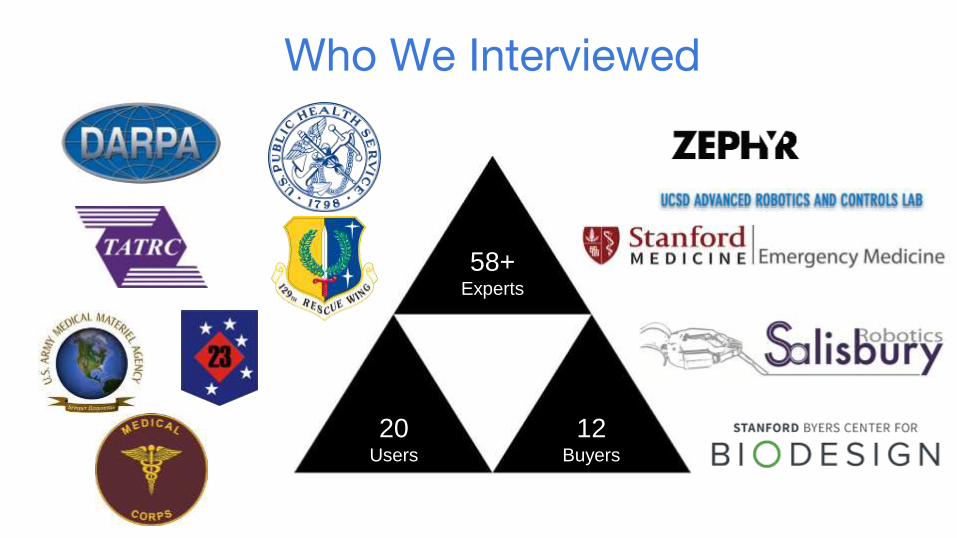
Who We Interviewed
58+Experts
20Users
12Buyers

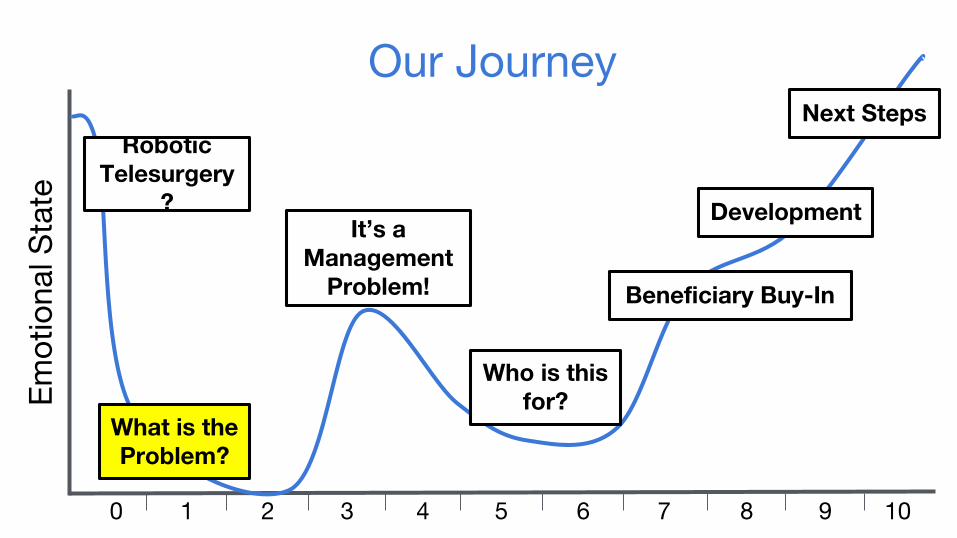
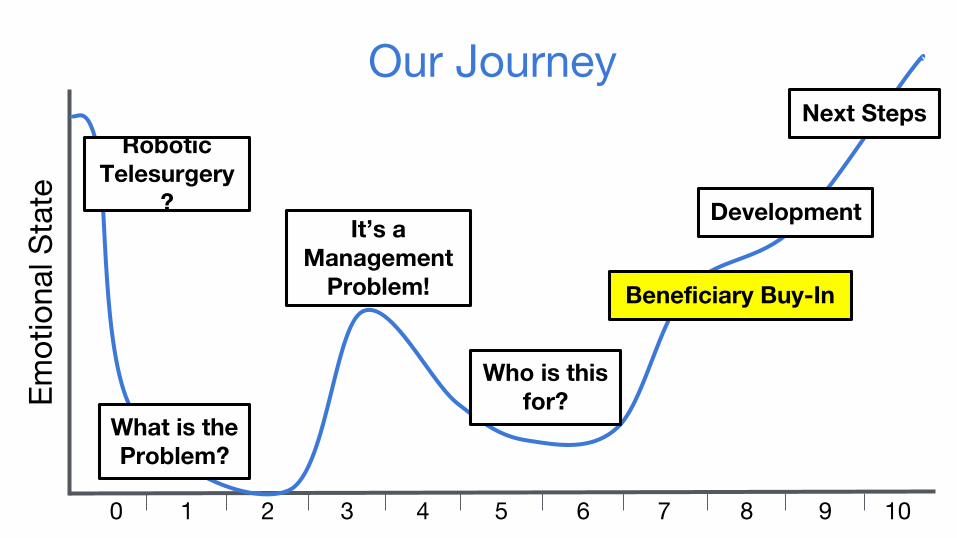
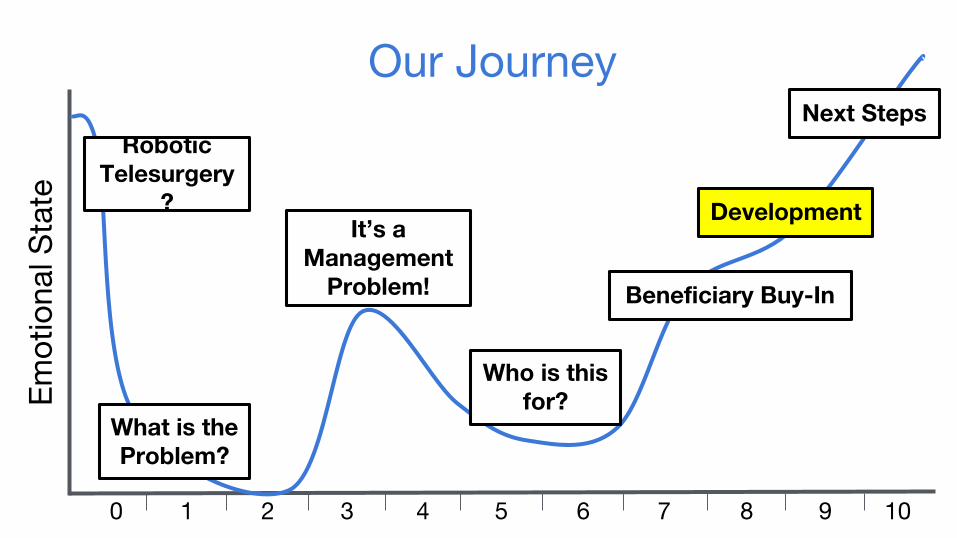
0 1 2 3 4 5 6 7 8 9
Em
otio
nal S
tate
10
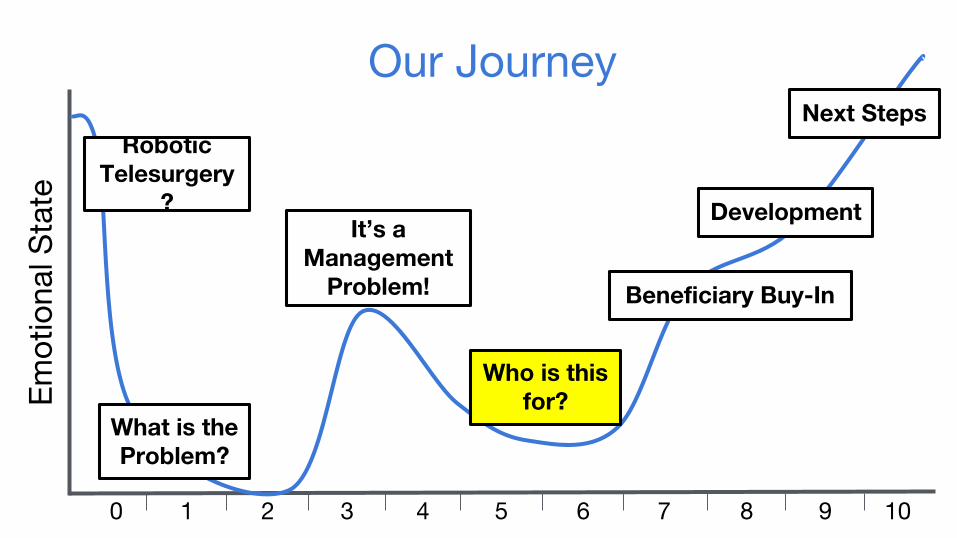
Robotic Telesurgery
?
What is the Problem?
It’s a Management
Problem!
Who is this for?
Beneficiary Buy-In
Development
Next Steps
Our Journey
Develop capability for robotic telesurgery that would allow
physicians to provide time-critical treatments for injured patients from
remote geographic distances.
The Original Challenge
“People are scared to move a daVinci down a hallway, let alone
use it on the battlefield”- Anonymous Stanford Hospital Trauma Surgeon
0 1 2 3 4 5 6 7 8 9
Em
otio
nal S
tate
10
Robotic Telesurgery
?
What is the Problem?
It’s a Management
Problem!
Who is this for?
Beneficiary Buy-In
Development
Next Steps
Our Journey
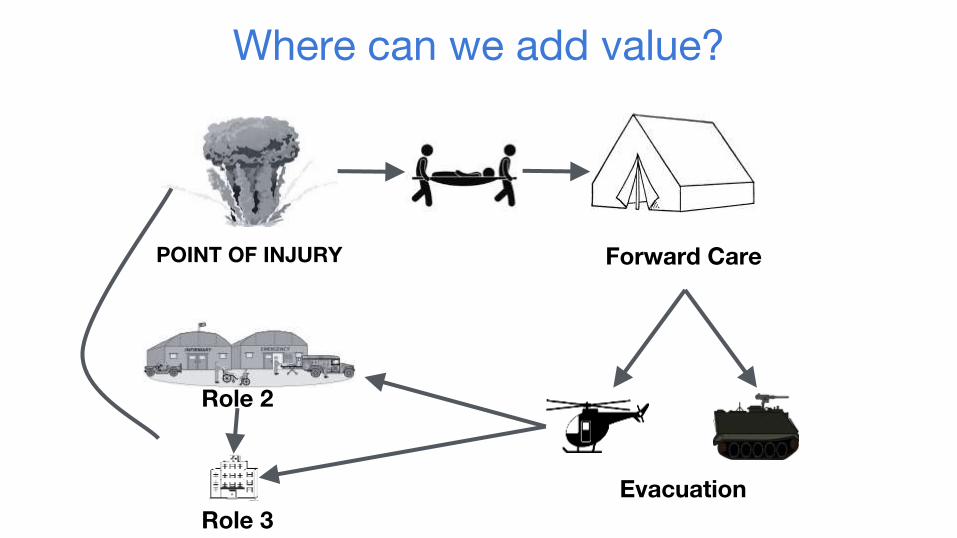
Where can we add value?
Evacuation
Forward CarePOINT OF INJURY
Role 2
Role 3

Visit to 129th Rescue Wing at Moffett Airfield
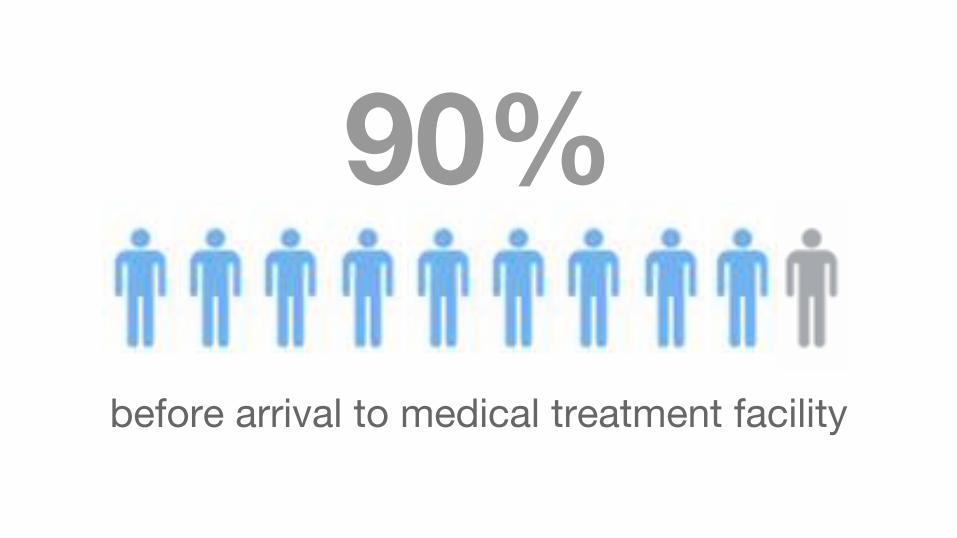
90%
before arrival to medical treatment facility
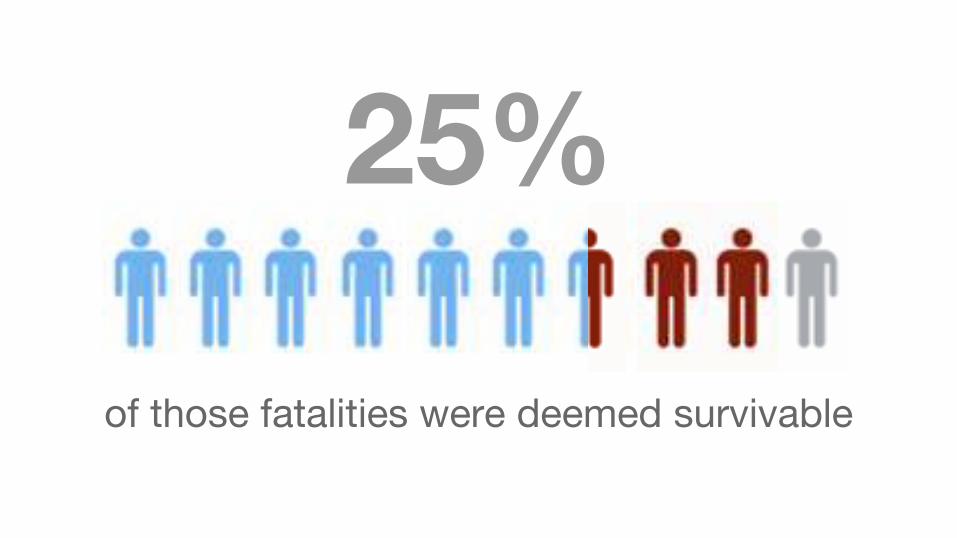
25%
of those fatalities were deemed survivable
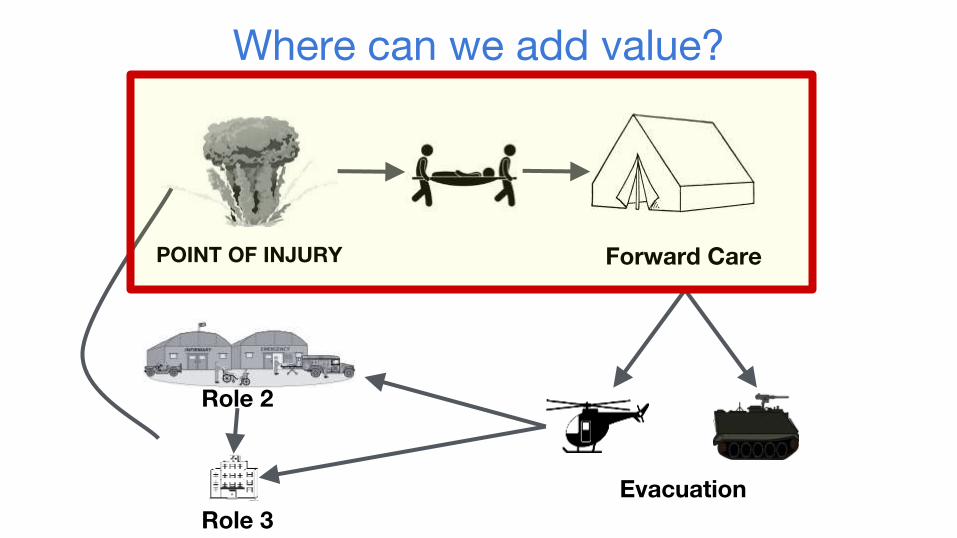
Where can we add value?
Evacuation
Forward CarePOINT OF INJURY
Role 2
Role 3

“[Mass casualty triage] is not a patient care problem, it’s a management problem.”
- 129th Rescue Wing Pararescuer

0 1 2 3 4 5 6 7 8 9
Em
otio
nal S
tate
10
Robotic Telesurgery
?
What is the Problem?
It’s a Management
Problem!
Who is this for?
Beneficiary Buy-In
Development
Next Steps
Our Journey

Civilian Mass Casualty Training Simulation

“It’s a waste of time to try and diagnose — it’s all about
prioritization.”- Timothy Browder, MD; Stanford Trauma Surgery

Justin
Roberto
Davis
Clute
Nicolas
Lozano
MVP 1.0
A Potential Solution for Automating Pre-Evacuation Mass Casualty Prioritization
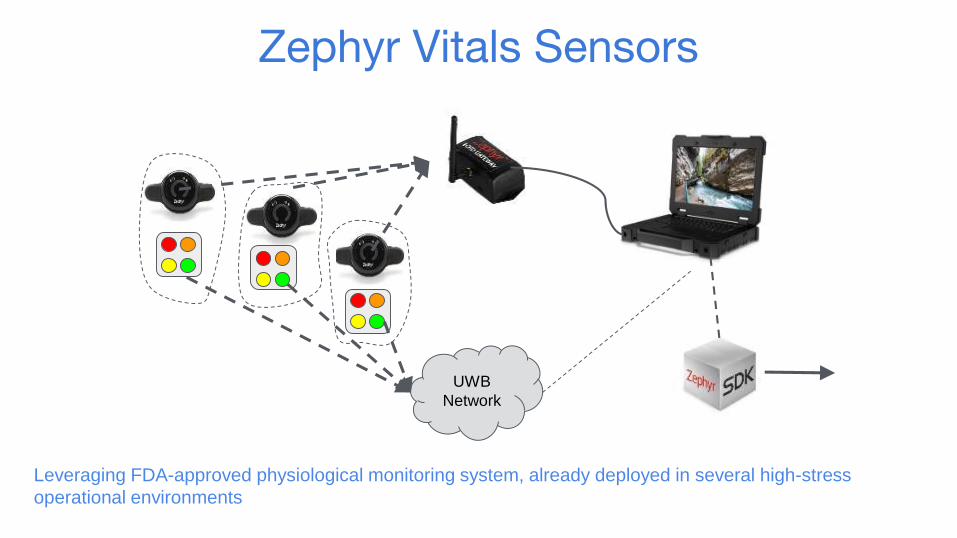
UWB
Network
Zephyr Vitals Sensors
Leveraging FDA-approved physiological monitoring system, already deployed in several high-stress
operational environments

“The first time extensive triage takes place is at the Battalion Aid
Station.”- LtCol Hasseltine, former Commanding Officer, 2d
Battalion, 7th Marines,1st Marine Divison
0 1 2 3 4 5 6 7 8 9
Em
otio
nal S
tate
10
Robotic Telesurgery
?
What is the Problem?
It’s a Management
Problem!
Who is this for?
Beneficiary Buy-In
Development
Next Steps
Our Journey
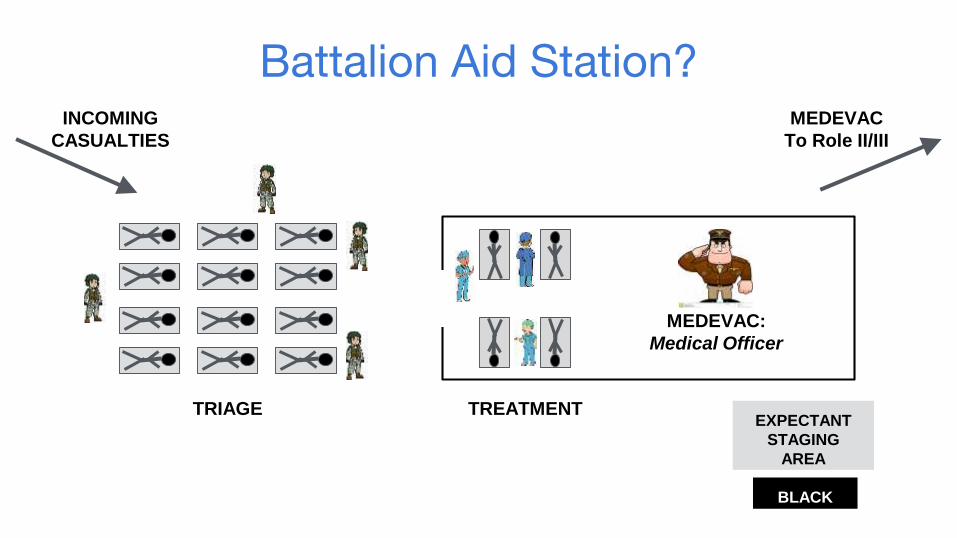
Battalion Aid Station?
EXPECTANT
STAGING
AREA
BLACK
MEDEVAC:
Medical Officer
TRIAGE TREATMENT
INCOMING
CASUALTIES
MEDEVAC
To Role II/III
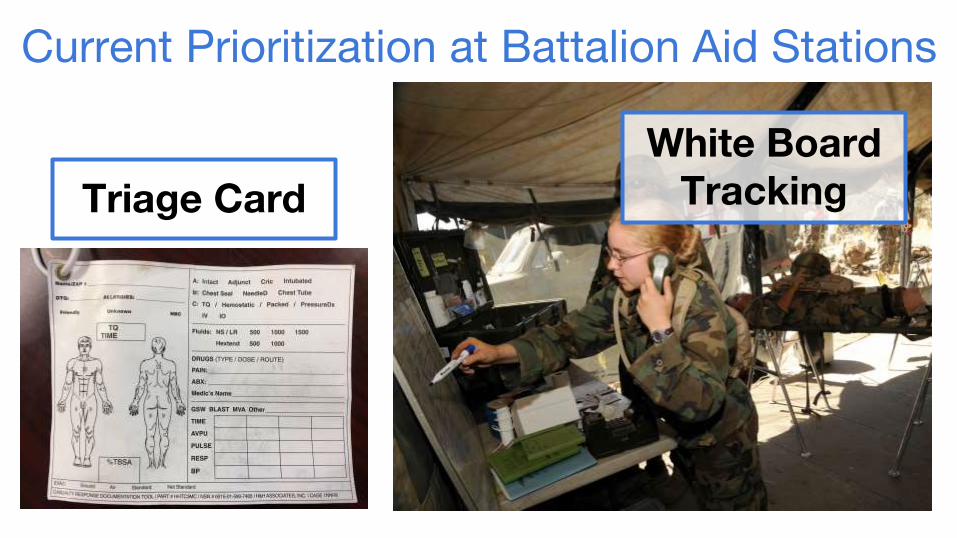
Current Prioritization at Battalion Aid Stations
White Board TrackingTriage Card
“There is a continuous stream of communication at a BAS supporting triage, treatment, and EVAC of casualties across medical and tactical personnel. This chain could easily break down in the chaos of a
mass cal.”- MAJ Michael Holloway, former BAS Physician Assistant
0 1 2 3 4 5 6 7 8 9
Em
otio
nal S
tate
10
Robotic Telesurgery
?
What is the Problem?
It’s a Management
Problem!
Who is this for?
Beneficiary Buy-In
Development
Next Steps
Our Journey

MVP 2.1: Triage Manager Interface

MVP 2.2: Physician Assistant Interface
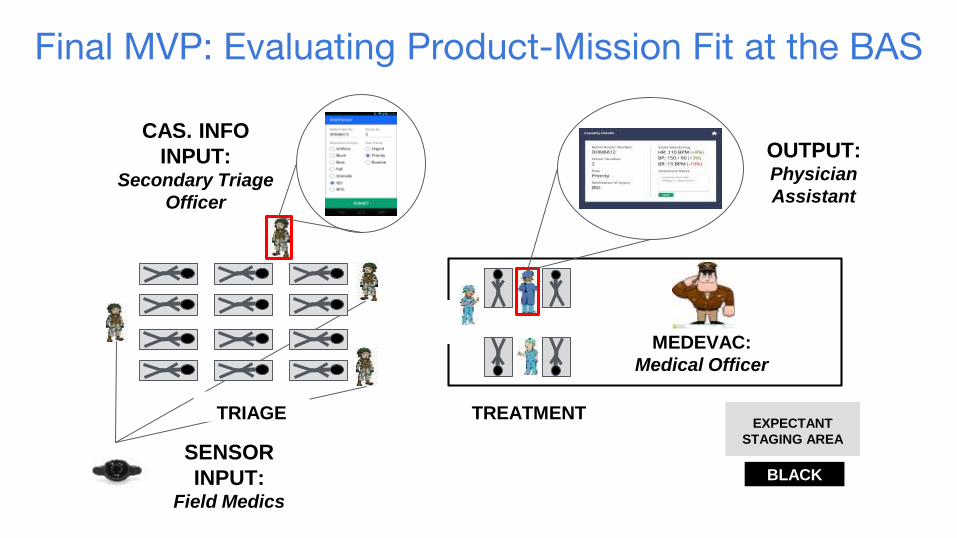
Final MVP: Evaluating Product-Mission Fit at the BAS
TRIAGE TREATMENT
CAS. INFO
INPUT:Secondary Triage
Officer
OUTPUT:Physician
Assistant
EXPECTANT
STAGING AREA
BLACK
SENSOR
INPUT:Field Medics
MEDEVAC:
Medical Officer
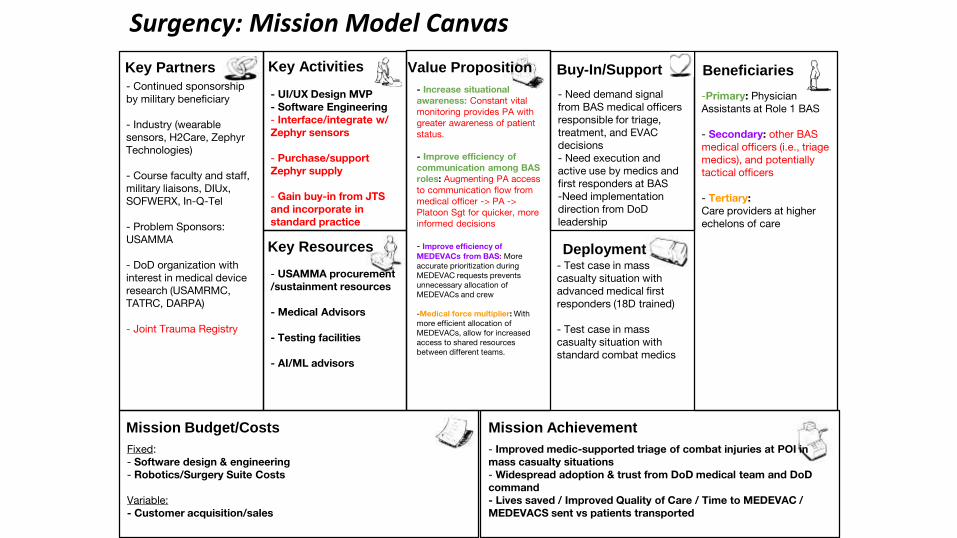
Surgency: Mission Model Canvas
- UI/UX Design MVP- Software Engineering- Interface/integrate w/ Zephyr sensors
- Purchase/support Zephyr supply
- Gain buy-in from JTS and incorporate in standard practice
- Continued sponsorship by military beneficiary
- Industry (wearable sensors, H2Care, Zephyr Technologies)
- Course faculty and staff, military liaisons, DIUx, SOFWERX, In-Q-Tel
- Problem Sponsors: USAMMA
- DoD organization with interest in medical device research (USAMRMC, TATRC, DARPA)
- Joint Trauma Registry
-Primary: Physician Assistants at Role 1 BAS
- Secondary: other BAS medical officers (i.e., triage medics), and potentially tactical officers
- Tertiary: Care providers at higher echelons of care
- Increase situational awareness: Constant vital monitoring provides PA with greater awareness of patient status.
- Improve efficiency of communication among BAS roles: Augmenting PA access to communication flow from medical officer -> PA -> Platoon Sgt for quicker, more informed decisions
- Improve efficiency of MEDEVACs from BAS: More accurate prioritization during MEDEVAC requests prevents unnecessary allocation of MEDEVACs and crew
-Medical force multiplier: With more efficient allocation of MEDEVACs, allow for increased access to shared resources between different teams.
- Improved medic-supported triage of combat injuries at POI in mass casualty situations- Widespread adoption & trust from DoD medical team and DoD command- Lives saved / Improved Quality of Care / Time to MEDEVAC / MEDEVACS sent vs patients transported
- Test case in mass casualty situation with advanced medical first responders (18D trained)
- Test case in mass casualty situation with standard combat medics
Fixed:- Software design & engineering- Robotics/Surgery Suite Costs
Variable:- Customer acquisition/sales
- USAMMA procurement /sustainment resources
- Medical Advisors
- Testing facilities
- AI/ML advisors
- Need demand signal from BAS medical officers responsible for triage, treatment, and EVAC decisions- Need execution and active use by medics and first responders at BAS-Need implementation direction from DoD leadership
Beneficiaries
Mission AchievementMission Budget/Costs
Buy-In/Support
Deployment
Value PropositionKey Activities
Key Resources
Key Partners
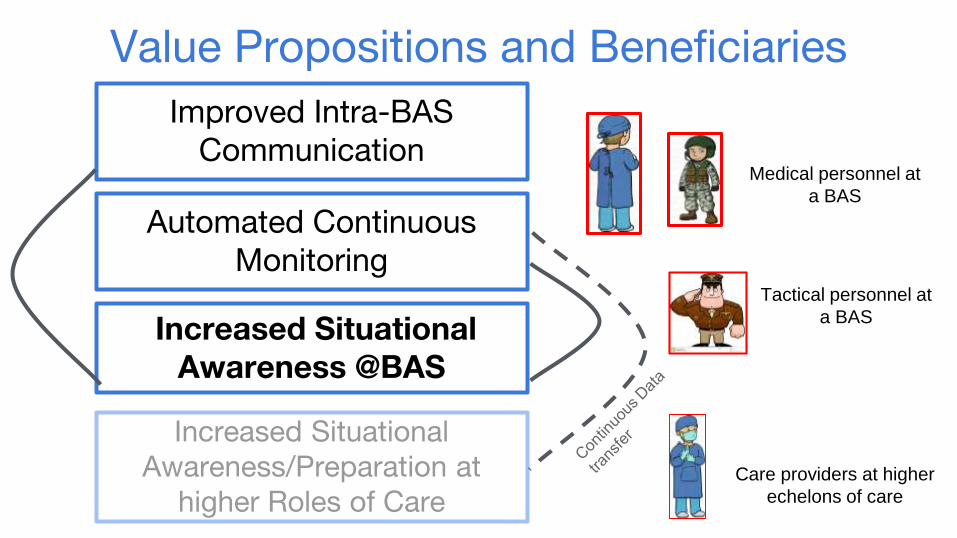
Value Propositions and Beneficiaries
Automated Continuous Monitoring
Improved Intra-BAS Communication
Increased Situational Awareness @BAS
Medical personnel at
a BAS
Care providers at higher
echelons of care
Increased Situational Awareness/Preparation at
higher Roles of Care
Tactical personnel at
a BAS
“I have dozens of anecdotes of patients that have died or had poor outcomes, because the number of
casualties overwhelmed capability to monitor or treat...”
- LtCol DeLellis, Deputy Surgeon at the United States Army Special Operations Command
“...active monitoring would likely have changed the outcome, for
the better, for many of those patients.”
- LtCol DeLellis, Deputy Surgeon at the United States Army Special Operations Command

Mission Achievement:
Save lives deemed survivable, where they are often lost
0 1 2 3 4 5 6 7 8 9
Em
otio
nal S
tate
10
Robotic Telesurgery
?
What is the Problem?
It’s a Management
Problem!
Who is this for?
Beneficiary Buy-In
Development
Next Steps
Our Journey

Development - Data Entry Application
Development - PA Interface

Development - PA Interface

Testing our Final MVP: 23rd Marine Regiment

“[The MVP] would effectively eliminate the standard 15 minute interval
between vital re-measurements by enabling continuous vitals monitoring.”
- 23rd Marine Regiment Corpsman

0 1 2 3 4 5 6 7 8 9
Em
otio
nal S
tate
10
Robotic Telesurgery
?
What is the Problem?
It’s a Management
Problem!
Who is this for?
Beneficiary Buy-In
Development
Next Steps
Our Journey
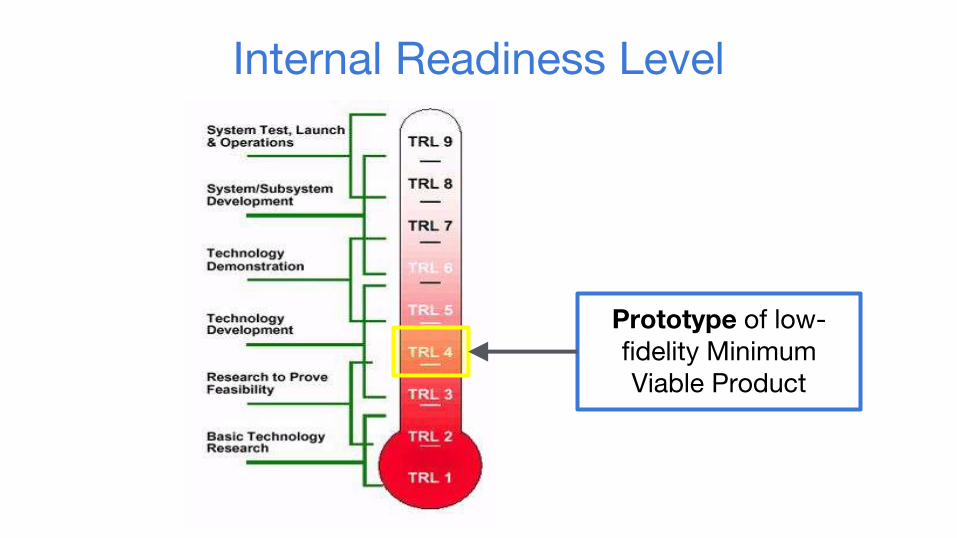
Internal Readiness Level
Prototype of low-fidelity Minimum Viable Product
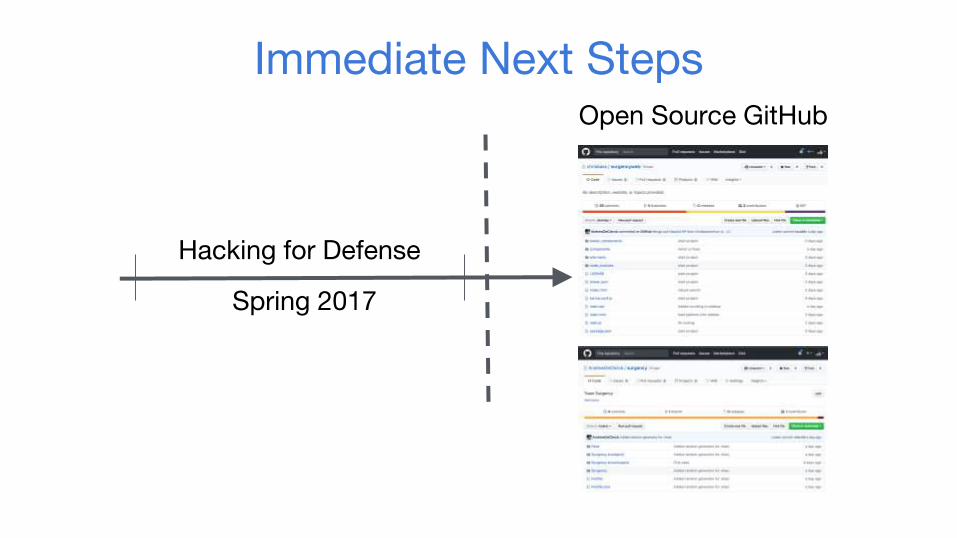
Immediate Next Steps
Hacking for Defense
Spring 2017
Open Source GitHub
Where do we go from here?- Secure funding sources for further development i.e. the
AAMTI Award
- Interface with Zephyr biopatch sensors
- Work with USAMMA to develop formal requirement upon MVP screening
- Explore field testing with a unit in a frequent deployment cycle i.e. the 101st Airborne
Acknowledgements:- USAMMA: Amanda Love, Jay Wang, Nita Grimsley- TATRC: Daniel Kral, James Beach, Nathan Fisher
- Mentors: Steven Hong, David Zinn, George Hasseltine, Seth Krummrich, Rafi Holtzman, Tammer Barkouki
- MVP Feedback: Stephen DeLellis, Jeffrey Oliver, Michael Holloway, Erwin Villeros
Related Documents











