Clinical Endocrinology Edited by J. A. H. Wass P. H. Baylis and S. Franks Editorial Assistant J. S. Bevan Medical Statistician T. Butler Volume 41 1994 BLACKWELL SCIENTIFIC PUBLICATIONS OXFORD LONDON EDINBURGH BOSTON MELBOURNE PARIS BERLIN VIENNA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical Endocrinology Edited by J. A. H. Wass P. H. Baylis and S. Franks
Editorial Assistant J. S. Bevan
Medical Statistician T. Butler
Volume 41
1994
BLACKWELL SCIENTIFIC PUBLICATIONS OXFORD LONDON EDINBURGH BOSTON
MELBOURNE PARIS BERLIN VIENNA
Osney Mead, Oxford 0X2 OEL 25 John Street, London WC I N 2BL 23 Ainslie Place, Edinburgh EH 3 6AJ 238 Main Street, Cambridge, MA 02142, USA PO Box 378, Carlton South, Victoria 3053, Australia Arnette Blackwell SA, 1, rue de Lille, 75007 Paris, France Blackwell Wissenschafts-Verlag GmbH, Kurfüstendamm 57, 10707 Berlin, Germany Blackwell MZV, Feldgasse 13, A-1238 Wien, Austria
© 1994 Blackwell Scientific Publications Ltd. Authorization to photocopy for internal or personal use or the internal or personal use of specific clients is granted by Blackwell Scientific Publications Ltd for libraries and other users registered with the Copyright Clearance Center (CCC) Transactional Reporting Service, provided that the base fee of $10.50 per copy is paid directly to the CCC, 222 Rosewood Drive, Suite 910, Danvers, MA 01923, USA. This consent does not extend to other kinds of copying, such as copying for general distribution for advertising or promotional purposes, for creating new collective works or for resale. Special requests should be addressed to the Editor. 0300-0664/94/$ 10.50.
ISSN 0300-0664
Typeset and printed at Alden Press Limited, Oxford and Northampton, Great Britain

Clinical Endocrinology (1994) 41, iii-viii
Contents
Volume 41, Number 1, July 1994
1 Review The role of growth hormone in male infertility: Z . S H O H A M , Y . Z A L E L and H . S . J A C O B S
7 Commentary Prediction of post-partum thyroiditis: A . P . W E E T M A N
9 Serum thyroglobulin: an early indicator of autoimmune post-partum thyroiditis: A . B . P A R K E S ,
E . G . B L A C K , H . A D A M S , R . J O H N , C . J . R I C H A R D S ,
R . H A L L and J . H . L A Z A R U S
15 Prediction of post-partum Graves' thyrotoxicosis by measurement of thyroid stimulating antibody in early pregnancy: Y . H I D A K A , H . T A M A K I , Y . I W A T A N I ,
H . T A D A , N . M I T S U D A and N . A M I N O
21 Amylin/islet amyloid polypeptide expression in medullary carcinoma of the thyroid: correlation with the expression of the related calcitonin/CGRP genes: M . A L E V I Z A K I , K . D A I , S . I . G R I G O R A K I S , S . L E G O N
and A . S O U V A T Z O G L U
27 Seasonal variation in the diagnosis of Graves' disease: S. A . W E S T P H A L
31 Effect of FK-506 on xenografted human Graves' thyroid tissue in severe combined immunodeficient mice: N . Y O S H I K A W A , G . A R R E A Z A , T . M U K U T A ,
E . R E S E T K O V A , N . M I L L E R , C . J A M I E S O N ,
M . N I S H I K A W A , M . I N A D A and R . V O L P E
41 Renal leak of calcium in post-menopausal osteoporosis: B . E . C N O R D I N , M . H O R O W I T Z ,
A . N E E D and H . A . M O R R I S
47 Effect of bisphosphonate therapy and parathyroidectomy on the urinary excretion of galactosylhydroxylysine in primary hyperparathyroidism: v. L O C A S C I O , v. B R A G A ,
F . B E R T O L D O , P . B E T T I C A , A . F . P A S I N I , L . S T E F A N I
and L . M O R O
53 A hormonal and radiological evaluation of adrenal gland in patients with acute or chronic pulmonary tuberculosis: F . K E L E S T I M U R , Y . Ü N L Ü , M . O Z E S M I
and i . T O L U
57 Gonadal function and response to human chorionic and menopausal gonadotrophin therapy in male patients with idiopathic hypogonadotrophic hypogonadism: J . M . w. K I R K , M . O . S A V A G E ,
D . B . G R A N T , P - M . G . B O U L O U X and G . M . B E S S E R
65 Less acidic forms of luteinizing hormone are associated wtih lower testosterone secretion in men on haemodialysis treatment: R . M I T C H E L L , C . B A U E R F E L D ,
F . S C H A E F E R , K . S C H Ä R E R and w. R . R O B E R T S O N
75 Characterization of 24-hour growth hormone secretion in acromegaly: implications for diagnosis and therapy: K . K . Y . H O and A . J . W E I S S B E R G E R
85 The ratio between serum levels of insulin-like growth factor ( IGF)- I and the I F G binding proteins (IGFBP-1, 2 and 3) decreases with age in healthy adults and is increased in acromegalic patients: A . J U U L , K . M A I N ,
w. F . B L U M , J . L I N D H O L M , M . B . R A N K E and
N . E . S K A K K E B / E K
95 Determinants of clinical outcome and survival in acromegaly: c. R A J A S O O R Y A , I . M . H O L D A W A Y ,
P . W R I G H T S O N , D . J . S C O T T and H . K . I B B E R T S O N
103 Treatment with octreotide and bromocriptine: an open pharmacodynamic interaction study: L . F R E D S T O R P ,
K . K U T Z and s. . W E R N E R
109 Low dose continuously infused growth hormone results in increased lipöprotein(a) and decreased low density lipoprotein cholesterol concentrations in middle-aged men: J . O S C A R S S O N , M . O T T O S S O N , O . W I K L U N D ,
P . M Ä R I N , K . V I K M A N - A D O L F S S O N , P . B J Ö R N S T O R P
and s. E D E N
117 Relation between growth hormone and Cortisol spontaneous secretion in children: c. E . M A R T I N E L L I
and A . c. M O R E I R A
123 Endocrinology audit A n audit of the insulin tolerance test in adult subjects in an acute investigation unit over one year: s. L . J O N E S , P . J . T R A I N E R ,
L . P E R R Y , J . A . H . W A S S , G . M . B E S S E R and
A . G R O S S M A N
129 C a s e report Congenital euthyroid goitre with impaired thyroglobulin transport: Y . O H Y A M A , T . H O S O Y A ,
T . K A M E Y A , N . S U Z U K I , s. N A K A M U R A ,
K . K A Z A H A R I , K . S H I B A Y A M A , Y . Y O K O T A and
N . M A T S U U R A
137 Letter to the Editors 138 Book review
Volume 41, Number 2, August 1994
139 Rev iew 5a-Reductase inhibitors and prostatic disease: F . H . S C H R Ö D E R
149 Commentary Wherefore art thou brown fat?: R . J U N G
151 Commentary Inhibin as a tumour marker: H . G . B U R G E R
iii
iv Contents
155 Inhibin as a marker for hydatidiform mole: a comparative study with the determinations of intact human chorionic gonadotrophin and its free /?-subunit: Y . B A D O N N E L , F . B A R B E , H . L E G A G N E U R ,
E . P O N C E L E T and M . S C H W E I T Z E R
163 Radiation and neuroregulatory control of growth hormone secretion: A . L . O G I L V Y - S T U A R T ,
W . H . B . W A L L A C E and S . M . S H A L E T
169 Comparative effects of G H , I G F - I and insulin on serum sex hormone binding globulin: M . G A F N Y ,
A . S I L B E R G E L D , B . K L I N G E R , M . W A S S E R M A N and
Z . L A R O N
177 Glycoprotein hormone a-subunit secretion in prolactinomas and in non-functioning adenomas: relation with the tumour size: A . W A R N E T ,
i . P O R S O V A - D U T O I T , N . L A H L O U , D . S E R E T - B E G U E ,
E . L A J E U N I E , P . C H A N S O N , F . W O L M A N T , G . L O T ,
P - J . G U I L L A U S S E A U and M . R O G E R
185 Expression patterns of messenger ribonucleic acids encoding prohormone convertases (PC2 and PC3) in human pituitary adenomas: K . H A S H I M O T O , M . K O G A ,
H . K O U H A R A , N . A R I T A , T . H A Y A K A W A ,
T . K I S H I M O T O and B . S A T O
193 Serum lactogens possessed normal bioactivity in patients with lactation insufficiency: v. H . L I V I N G S T O N E ,
P . W . G O U T , S . D . C R I C K M E R , K . F O X and J . C . P R I O R
199 Hypothalamic-pituitary ageing: progressive increase in FSH and L H concentrations throughout the reproductive life in regularly menstruating women: N . A . A H M E D E B B I A R Y , E . A . L E N T O N and I . D . C O O K E
207 Osmoregulation of vasopressin and thirst: comparison of 20% mannitol with 5% saline as osmotic stimulants in healthy man: E . M . G . P H I L L I P S , T . B U T L E R and P . H . B A Y L I S
213 Hyperinsulinaemia and N a + , K + -ATPase activity in thyrotoxic periodic paralysis: A . C H A N , R . S H I N D E ,
c. c. C H O W , c. s. C O C K R A M and R . S W A M I N A T H A N
217 Insulin sensitivity and insulin clearance in cystic fibrosis patients with normal and diabetic glucose tolerance: S. L A N N G , B . T H O R S T E I N S S O N , M . E . R 0 D E R ,
j . N E R U P and c. K O C H
225 Insulin-like growth factor binding protein 1 response to acute insulin induced hypoglycaemia in Type 1 diabetes: J . D . Q U I N , B . M . F I S H E R , A . C . M A C C U I S H ,
G . H . B E A S T A L L , M . S M A L L , J . M . P . H O L L Y and
A . M . C O T T E R I L L
231 A prospective study of the prevalence of clear-cut endocrine disorders and polycystic ovaries in 350 patients presenting with hirsutism or androgenic alopecia: J . B . O ' D R I S C O L L , H . M A M T O R A ,
J . H I G G I N S O N , A . K A N E and D . C . A N D E R S O N
237 Oestrogen formation in genital and non-genital skin fibroblasts cultured from patients with hypospadias: P . S T A I B , N . K A U , G . R O M A L O and H - U . S C H W E I K E R T
245 Comparison of changes in bone mineral in idiopathic and secondary osteoporosis following therapy with cyclical disodium etidronate and high dose calcium: supplementation: s. M . O R M E , M . S I M P S O N ,
S . P . S T E W A R T , B . O L D R O Y D , C . F . W E S T M A C O T T ,
M . A . S M I T H and P . E . B E L C H E T Z
251 Malignancy-associated hypercalcaemia: resolution of controversies over vitamin D metabolism by a pathophysiological approach to the syndrome: D . H . S C H W E I T Z E R , N . A . T . H A M D Y , M . F R Ö L I C H ,
A . H . Z W I N D E R M A N and S . E . P A P A P O U L O S
257 C a s e report Calcitonin-producing insulinoma: clinical, immunocytochemical and cytogenetical study: M . J . G . M . B U G A L H O , L . R O Q U E , L . G . S O B R I N H O ,
A . H O O G , J . F . M . N U N E S , J . M . M . A L M E I D A ,
C . N . L E I T Ä O , J . R . S A N T O S , M . C . P E R E I R A ,
M . A . S A N T O S and J . S O A R E S
261 C a s e report Secondary hypoadrenalism presenting with hypercalcaemia: s. D . V A S I K A R A N , G . A . T A L L I S
and w. J . B R A U N D
263 Commentary M . D A V I E S
265 Notices
Volume 41, Number 3, September 1994
267 Rev iew Endocrine adaptation to intensive physical training during growth: G . E . T H E I N Z
273 Commentary Glucocorticoid induced osteoporosis: C . G E N N A R I
275 Effect of treatment on established osteoporosis in young women with amenorrhoea: B . G U L E K I L ,
M . c. D A V I E S and H . s. J A C O B S
283 Is a low skinfold thickness an indicator of osteoporosis?: s. M . O R M E and p. E . B E L C H E T Z
289 Whole body composition and regional bone mass in women with insulin-dependent diabetes mellitus: j . E . C O M P S T O N , E . M . S M I T H , C . M A T T H E W S and
P . S C H O F I E L D
295 High dose topical calcipotriol consistently reduces serum parathyroid hormone levels: J . F . B O U R K E .
J . B E R T H - J O N E S , R . M U M F O R D , S . J . I Q B A L and
P . E . H U T C H I N S O N
299 Suramin in adrenocortical cancer: limited efficacy and serious toxicity: w. A R L T , M . R E I N C K E , L . S I E K M A N N ,
w. W I N K E L M A N N and B . A L L O L I O

Contents v
309 Postural Stimulation test in patients with aldosterone producing adenomas: T . F E L T Y N O W S K I ,
H . I G N A T O W S K A - S W I T A L S K A , B . W O C I A L ,
J . L E W A N D O W S K I , J . C H O D A K O W S K A and
W . J A N U S Z E W I C Z
315 Glucose and fat metabolism in adults with growth hormone deficiency: F . S A L O M O N , R . C . C U N E O ,
A . M . U M P L E B Y and P . H . S Ö N K S E N
323 Body composition in active acromegaly during treatment with octreotide: a double-blind, placebo-controlled cross-over study: T . B . H A N S E N ,
J . G R A M , p. B J E R R E , C . H A G E N and J . B O L L E R S L E V
331 Age as a determinant of the impact of growth hormone therapy on predicted adult height: z. H Ö C H B E R G ,
E . L E I B E R M A N , H . L A N D A U , R . K O R E N and
Z . Z A D I K
337 Metabolic effects of growth hormone administered subcutaneously once or twice daily to growth hormone deficient adults: T . L A U R S E N , J . O . L . J O R G E N S E N and J . S . C H R I S T I A N S E N
345 The effect of growth hormone replacement on serum lipids, lipoproteins, apolipoproteins and cholesterol precursors in adult growth hormone deficient patients: D . L . R U S S E L L - J O N E S , G . F . W A T T S , A . W E I S S B E R G E R ,
R . N A O U M O V A , J . M Y E R S , G . R . T H O M P S O N and
P. H . S Ö N K S E N
351 Serum insulin-like growth factor I in a random population sample of men and women: relation to age, sex, smoking habits, coffee consumption and physical activity, blood pressure and concentrations of plasma lipids, fibrinogen, parathyroid hormone and osteocalcin: K . L A N D I N - W I L H E L M S E N ,
L . W I L H E L M S E N , G . L A P P A S , T . R O S E N , G . L I N D S T E D T ,
P A . L U N D B E R G and B - Ä . B E N G T S S O N
359 Age-related and gender-related occurrence of pituitary adenomas: T . M I N D E R M A N N and c. B . W I L S O N
365 Prevalence of thyroid hormone autoantibodies in healthy subjects: s. S A K A T A , M . M A T S U D A , T . O G A W A ,
H . T A K U N O , 1. M A T S U I , H . S A R U I and K . Y A S U D A
371 Impaired prolactin response to arginine in patients with hyperthyroidism: E . C I C C A R E L L I , M . Z I N I , s. G R O T T O L I ,
P . R A Z Z O R E , I . P O R T i O L i and R . V A L C A V I
375 Thyroid function and thyroid size in normal pregnant women living in an iodine replete area: A . B E R G H O U T ,
E . E N D E R T , A . R O S S , H . V . H O G E R Z E I L , N . J . S M I T S
and W . M . W I E R S I N G A
381 Susceptibility to autoimmune thyroiditis in Down's syndrome is associated with the major histocompatibility class I I D Q A 0301 allele: L . B . N I C H O L S O N , F . S . W O N G , D . L . E W I N S , J . B U T L E R ,
A . H O L L A N D . A . G . D E M A I N E and A . M . M C G R E G O R
385 Audit in Endocrinology Imaging in endocrinology: use of a potential methodology for audit consensus development: M . J . D A V I E S and T . A . H O W L E T T
391 C a s e report Multiple spuriously abnormal thyroid function indices due to heterophilic antibodies: T . M . F I A D , J . D U F F Y and T . J . M C K E N N A
397 C a s e report A case of hepatoma associated with hypoglycaemia and overproduction of I G F - I I (E-21): beneficial effects of treatment with growth hormone and intrahepatic adriamycin: s. J . H U N T E R ,
W . H . D A U G H A D A Y , M . E . C A L L E N D E R ,
J . A . M C K N I G H T , E . M . M C I L R A T H , J . D . T E A L E
and A . B . A T K I N S O N
402 Commentary Non-islet-cell tumour hypoglycaemia: J . Z A P F
403 Book review 404 Notices
Volume 41, Number 4, October 1994
405 Commentary The investigation of hypercalcaemia: I . R . R E I D
407 Parathyroid hormone and parathyroid hormone-related protein in the investigation of hypercalcaemia in two hospital populations: J . W A L L S , W . A . R A T C L I F F E ,
A . H O W E L L and N . J . B U N D R E D
415 Familial isolated primary hyperparathyroidism: M . K A S S E M , X . Z H A N G , S . B R A S K , E . F . E R I K S E N ,
L . M O S E K I L D E and T . A . K R U S E
421 Bone metabolism during anti-thyroid drug treatment of endogenous subclinical hyperthyroidism: A . H . M U D D E , A . J . H . M . H O U B E N and
A . C . N . K R U S E M A N
425 Bone mineral density in thyroxine treated females with or without a previous history of thyrotoxicosis: J . F R A N K L Y N , J . B E T T E R I D G E , R . H O L D E R , J . D A Y K I N ,
J . L I L L E Y and M . S H E P P A R D
433 Increased insulin sensitivity in patients with aldosterone producing adenoma: M . I S H I M O R I ,
N . T A K E D A , S. O K U M U R A , T . M U R A I , H . I N O U Y E and
K . Y A S U D A
439 Mineralocorticoid and glucocorticoid status in idiopathic haemochromatosis: c. H . W A L S H ,
A . L . M U R P H Y , S . C U N N I N G H A M and T . J . M C K E N N A
445 Augmented 17a-hydroxyprogesterone response to A C T H stimulation as evidence of decreased 21-hydroxylase activity in patients with incidentally discovered adrenal tumours ('incidentalomas'): T . S E P P E L and R . S C H L A G H E C K E
vi Contents
453 Development and validation of a radioimmunoassay for follistatin in human serum: c. P . G I L F I L L A N and D . M . R O B E R T S O N
463 Serum lipoprotein lipid profile in women with the polycystic ovary syndrome: relation to anthropometric, endocrine and metabolic variables: J . H O L T E , T . B E R G H ,
c. B E R N E and H . L I T H E L L
473 The independent effects of polycystic ovary syndrome and obesity on serum concentrations of gonadotrophins and sex steroids in premenopausal women: J . H O L T E , T . B E R G H , G . G E N N A R E L L I and L . W I D E
483 Evaluation of maternal serum immunoreactive inhibin as a first trimester marker of Down's syndrome: E . M . W A L L A C E , L . M . H A R K N E S S , S . B U R N S and
W . A . L I S T O N
487 Treatment with GHRH(1-29)NH 2 in children with idiopathic short stature induces a sustained increase in growth velocity: J . M . w. K I R K , P . J . T R A I N E R ,
W . H . M A J R O W S K I , J . M U R P H Y , M . O . S A V A G E and
G . M . B E S S E R
495 Inverse correlation between insulin-like growth factor binding protein-1 and insulin in patients with acromegaly during treatment with the somatostatin analogue octreotide: L . F R E D S T O R P , S . W E R N E R ,
P . B A N G and K . H A L L
503 Effects of insulin-like growth factor-I on growth hormone and prolactin secretion and cell proliferation of human somatotrophinomas and prolactinomas in vitro: s. L . A T K I N , A . M . L A N D O L T , P . F O Y ,
R . V . J E F F R E Y S , L . H I P K I N and M . C . W H I T E
511 The severity of growth hormone deficiency in adults with pituitary disease is related to the degree of hypopituitarism: A . T . T O O G O O D , C . G . B E A R D W E L L
and s. M . S H A L E T
517 Loss of the normal relationships between growth hormone, growth hormone-binding protein and insulin-like growth factor-I in adolescents with insulin-dependent diabetes mellitus: K . L . C L A Y T O N ,
J . M . P . H O L L Y , L . M . S . C A R L S S O N , J . J O N E S ,
T . D . C H E E T H A M , A . M . T A Y L O R and
D . B . D U N G E R
525 Endocrine profiles during administration of the new non-steroidal anti-androgen Casodex in prostate cancer: J . V E R H E L S T , L . D E N I S , P . V A N V L I E T ,
H . V A N P O P P E L , J . B R A E C K M A N , P . V A N C A N G H ,
J . M A T T E L A E R , D . D ' H U L S T E R and C H . M A H L E R
531 C a s e report Neonatal primary hyperparathyroidism masked by vitamin D deficiency: K . M E E R A N ,
M . H U S A I N , M . P U C C I N I , H . S C O T T , C . D I O N I S I - V I C I ,
D . R . H A R V E Y , J . L Y N N and R . V . T H A K K E R
535 C a s e report Intrapulmonary shunting causing hypoxaemia in a case of carcinoid syndrome: A . H U S S A I N , E . T . Y O U N G , J . D . G R E A V E S ,
P . J . H A M M O N D , J . M . B . H U G H E S , S . C . W A L L I S
and s. R . B L O O M
538 Commentary M . T . S E Y M O U R
539 Rapid communicat ion Growth hormone releasing activity by intranasal administration of a synthetic hexapeptide (hexarelin): z. L A R O N , J . F R E N K E L ,
I . G I L - A D , B . K L I N G E R , E . L U B I N , P . W U T H R I C H ,
F . B O U T I G N O N , V . L E N G E R T S and R . D E G H E N G H I
Volume 41, Number 5, November 1994
543 Voluntary support for pituitary patients 545 Rev iew Lymphocytic traffic and homing into target
tissue and the generation of endocrine autoimmunity: P . P O Z Z I L L I , P . C A R O T E N U T O and G . D E L I T A L A
555 Commentary Ovarian stromal hypertrophy: A . K Y E L - M E N S A H and H . S . J A C O B S
557 Ovarian stromal hypertrophy in hyperandrogenic women: D . D E W A I L L Y , Y . R O B E R T , I . H E L I N ,
Y . A R D A E N S , P . T H O M A S - D E S R O U S S E A U X ,
L . L E M A I T R E and P . F O S S A T I
563 Luteinizing hormone secretion and hypoandrogenaemia in critically i l l men: effect of dopamine: G . V A N D E N B E R G H E , F . D E Z E G H E R ,
P . L A U W E R S and J . D . V E L D H U I S
571 Androgen suppressive effect of G n R H agonist in ovarian hyperthecosis and virilizing tumours: M - M . P A S C A L E , M . P U G E A T , M . R O B E R T S , H . R O U S S E T ,
H . D E C H A U D , N . D U T R I E U X - B E R G E R and
J . T O U R N I A I R E
577 Identification of olfactory dysfunction in carriers of X-linked Kallmann's syndrome: J . M . W . K I R K ,
D . B . G R A N T , M . O . S A V A G E , G . M . B E S S E R and
P . - M . G . B O U L O U X
581 Two mutations causing vitamin D resistant rickets: modelling on the basis of steroid hormone receptor DNA-binding domain crystal structures: A . R . R U T , M . H E W I S O N , K . K R I S T J A N S S O N , B . L U I S I ,
M . R . H U G H E S and J . L . H . O ' R I O R D A N
591 Optimal frequency of administration of Pamidronate in patients with hypercalcaemia of malignancy: S . J . W I M A L A W A N S A
597 Does acromegaly really predispose to an increased prevalence of gastrointestinal tumours?: s. D . L A D A S ,
N . C . T H A L A S S I N O S , G . I O A N N I D E S and
S . A . R A P T I S
Contents vii
603 Serum lipoproteins in acromegaly before and 6-15 months after transsphenoidal adenomectomy: J . O S C A R S S O N , O . W I K L U N D , K - E . J A K O B S S O N ,
B . P E T R U S O N and B . - Ä . B E N G T S S O N
609 Growth hormone administration stimulates energy expenditure and extrathyroidal conversion of thyroxine to triiodothyronine in a dose-dependent manner and suppresses circadian thyrotrophin levels: studies in GH-deficient adults: J . O . L . J O R G E N S E N , J . M O L L E R ,
T . L A U R S E N , H . 0 R S K O V , J . S . C H R I S T I A N S E N and
J . W E E K E
615 Short and long-term cardiovascular effects of growth hormone therapy in growth hormone deficient adults: L . T H U E S E N , J . O . L . J 0 R G E N S E N , J . R . M Ü L L E R ,
B . 0 . K R I S T E N S E N , N . E . S K A K K E B J E K , N . V A H I and
J . S . C H R I S T I A N S E N
621 Endogenous and stimulated G H secretion, urinary G H excretion, and plasma I G F - I and I G F - I I levels in prepubertal children with short stature after intrauterine growth retardation: w. J . D E W A A L ,
A . c. s. H O K K E N - K O E L G A , T H . S T I J N E N ,
S . M . P . F . D E M U I N C K K E I Z E R - S C H R A M A ,
s. L . s. D R O P and T H E D U T C H W O R K I N G
G R O U P O N G R O W T H H O R M O N E
631 I G F - I treatment of adult patients with Laron syndrome: preliminary results: z. L A R O N and B . K L I N G E R
639 The effect of growth hormone replacement on Cortisol metabolism and glucocorticoid sensitivity in hypopituitary adults: J . U . W E A V E R ,
L . T H A V E N T H I R A N , K . N O O N A N , J . M . B U R R I N ,
N . F . T A Y L O R , M . R . N O R M A N and J . P . M O N S O N
649 Inhibition of growth hormone release after the combined administration of G H R H and GHRP-6 in patients with Cushing's syndrome: A . L E A L - C E R R O ,
A . P U M A R , E . G A R C I A - G A R C I A , C . D I E G U E Z and
F . F . C A S A N U E V A
655 An audit of selected patients with non-functioning pituitary adenoma treated by transsphenoidal surgery without irradiation: K . M . B R A D L E Y , C . B . T . A D A M S ,
C . P . s. P O T T E R , D . W . W H E E L E R , P . J . A N S L O W and
c. w. B U R K E
661 Abnormal response of luteinizing hormone beta subunit to thyrotrophin-releasing hormone in patients with non-functioning pituitary adenoma: P . G I L - D E L - A L A M O , K . S . I . P E T T E R S S O N ,
K . S A C C O M A N N O , A . S P A D A , G . F A G L I A and
P . B E C K - P E C C O Z
667 Evidence for the effect of antibodies to TSH receptors on the thyroid ultrasonographic volume in patients with Graves' disease: M . R I E U , A . R A Y N A U D , A . R I C H A R D ,
s. L A P L A N C H E , B . S A M B O R and J - L . B E R R O D
673 Turner's syndrome with X-isochromosome and Hashimoto's thyroiditis: M . D E K E R D A N E T , J . L U C A S ,
F . L E M E E and M . L E C O R N U
677 Corticotrophin-releasing factor immunostaining is present in placenta and fetal membranes from the first trimester onwards and is not affected by labour or administration of mifepristone: E . S . C O O P E R ,
A . N . B R O O K S , M . R . M I L L E R and i . A . G R E E R
685 C a s e report Hyperthyroidism associated with metastatic thyroid carcinoma: F . H . S T E F F E N S E N and N . A A . A U N S H O L T
689 C a s e report Growth hormone deficiency coupled with hypogonadism in AIDS: T . T . C . N G , I . P . M . O ' C O N N E L L and E . G . L . W I L K I N S
693 Commentary J M . P A R K I N
695 Letters to the Editors 699 Book rev iews 700 Notices 700 Erratum
Volume 41, Number 6, December 1994
701 Endocr ine Investigation S e r i e s 702 A Registry for R e s i s t a n c e to Thyroid Hormone 703 Endocr ine Investigation Investigation of obesity:
P . G . K O P E L M A N
709 Commentary Cabergoline: an advance in dopaminergic therapy: J . S . B E V A N and J . R . E . D A V I S
713 Commentary Radioiodine therapy of non-toxic multinodular goitre: D . G L I N O E R
715 Acute changes in thyroid volume and function following 1 3 1 1 therapy of multinodular goitre: B . N Y G A A R D , J . F A B E R and L . H E G E D Ü S
719 Ultrasound guided percutaneous ethanol injection in the treatment of cystic thyroid nodules: G . V E R D E ,
E . P A P I N I , C . M . P A C E L L A , C . G A L L O T T I , S . D E L P I A N O ,
S . S T R A D A , R . F A B B R I N I , G . B I Z Z A R R I , R . R I N A L D I ,
c. P A N U N Z I and D . G E L L I
725 Variability of serum thyroglobulin levels is determined by a major gene: L . D . K . E . P R E M A W A R D H A N A ,
S . S . S . L O , D . I . W . P H I L L I P S , L . M . P R E N T I C E and
B . R E E S S M I T H
731 Dopamine and the sick euthyroid syndrome in critical illness: G . V A N D E N B E R G H E , F . D E Z E G H E R and p. L A U W E R S
739 Oral progestogen-only contraception may protect against loss of bone mass in breast-feeding women: L . E . C A I R D , V . R E I D - T H O M A S , W . J . H A N N A N , S . G O W
and A . F . G L A S I E R
viii Contents
747 Bone mineral density and metabolism in premenopausal women taking L-thyroxine replacement therapy: M . G A R T O N , I . R E I D , N . L O V E R I D G E ,
S . R O B I N S , L . M U R C H I S O N , G . B E C K E T T and D . R E I D
757 Eighty-six cases of Addison's disease: M - F . K O N G and w. J E F F C O A T E
763 Amplification of nocturnal melatonin secretion in women with functional secondary amenorrhoea: relation to endogenous oestrogen concentration: Y . O K A T A N I and Y . S A G A R A
771 Serum inhibin during lactation: relation to the gonadotrophins and gonadal steroids: H . G . B U R G E R ,
J . P . C . H E E , P . M A M E R S , M . B A N G A H , M . Z I S S I M O S
and p. i . M C C L O U D
779 Serotoninergic control of gonadotrophin and prolactin secretion in women: u. U L R I C H , I . N O W A R A and W . G . R O S S M A N I T H
787 Effects of follicular phase exercise on luteinizing hormone pulse characteristics in sedentary eumenorrhoeic women: N . I . W I L L I A M S ,
J . W . M C A R T H U R , B . A . T U R N B U L L , B . A . B U L L E N ,
G . S . S K R I N A R , I . Z . B E I T I N S , G . M . B E S S E R , L . H . R E E S ,
I . G I L B E R T , D . C R A M E R , L . P E R R Y and D . S . T . P E D O E
795 Dissociation of adrenal androgen and Cortisol secretion in Cushing's syndrome: s. K . C U N N I N G H A M and T . J . M C K E N N A
801 The effect of recombinant I G F - I on anterior pituitary function in healthy volunteers: p. J . T R A I N E R ,
J . H O L L Y , S . M E D B A K , L . H . R E E S and G . M . B E S S E R
809 p53 gene mutations in pituitary adenomas: rare events: A . L E V Y , L . H A L L , W . A . Y E U D A L L and S . L . L I G H T M A N
815 Gsa and Gi2o: mutations in clinically non-functioning pituitary tumours: E . A . W I L L I A M S O N , M . D A N I E L S ,
S . F O S T E R , W . F . K E L L Y , P . K E N D A L L - T A Y L O R and
P . E . H A R R I S
821 Quinagolide efficacy and tolerability in hyperprolactinaemic patients who are resistant to or intolerant of bromocriptine: L . V I L A R and C . W . B U R K E
827 C a s e report Adrenocorticotrophin-independent
unilateral macronodular adrenal hyperplasia occurring with myelolipoma: an unusual cause of Cushing's syndrome: P . J . J E N K I N S , S . L . C H E W , D . G . L O W E ,
R . H . R E Z N E K and J . A . H . W A S S
831 C a s e report Primary hyperparathyroidism masked by antituberculous therapy-induced vitamin D deficiency: C . S . K O V A C S , G . J O N E S and E . R . Y E N D T
837 Commentary: E . B . M A W E R
839 Let ters to the Editors 841 Book rev iews 843 Notices 844 R e f e r e e s 846 Erratum 847 Author index 857 Subject index

Clinical Endocrinology (1994) 41, 299-307
Suramin in adrenocortical cancer: limited efficacy and serious toxicity
Wiebke Arlt*, Martin Re incke* , Lothar S iekmannt , Werner Winkelmannt and Bruno Allolio* Departments of *lnternal Medicine, Julius-Maximilians-
University, Würzburg, ^Clinical Biochemistry, Friedrich-
Wilhelms-University, Bonn, and pnternal Medicine II,
University of Cologne, Cologne, Germany
(Received 14 December 1993; returned for revision 31 January 1994; finally revised 1 March 1994; accepted 17 March 1994)
S u m m a r y
O B J E C T I V E No satisfactory treatment for adrenocort ical c a r c i n o m a ( A C C ) is avai lable . We investigated the effic a c y and toxicity of suramin in the treatment of metastatic A C C s i n c e suramin h a s been recently reported to be active a s a s ingle agent therapy for patients with A C C and prostatic c a r c i n o m a .
D E S I G N We col lected data on 9 patients with metastatic A C C treated with suramin in four centres in G e r m a n y between 1987 and 1992. PAT IENTS Nine patients (5 women, 4 men; age range 32 -67 y e a r s ) w e r e included. B iochemica l ev idence of steroid e x c e s s w a s found in 6/9, in three leading to cl inical symptoms (hypertension, hyperglycaemia, hirsutism, gynaecomast ia ) .
M E A S U R E M E N T S Tumour r e s p o n s e s were a s s e s s e d by radiological and b iochemical evaluation. Other investigations included regular measurements of blood cel l counts , coagulat ion, hepatic and renal function para meters , and s e r u m suramin concentrat ions. R E S U L T S The patients rece ived cumulat ive d o s e s ranging from 8-2 to 30*2 g suramin over per iods of 1 -15 months. 3/9 ach ieved a partial r esponse , 2/9 d i s e a s e stabilization and 4/9 exper ienced progress ive d i s e a s e . Tumour r e s p o n s e s were transient. Suramin treatment w a s without direct influence on steroid e x c e s s . S e r i o u s side-effects included coagulopathy (6/9), thrombocytopenia (6/9), polyneuropathy (2/9) and al lergic skin reac tions (4/9); the death of two patients w a s possibly related to suramin therapy. Both toxicity and tumour r e s p o n s e were strongly assoc i a ted with s e r u m level or cumulat ive dose of suramin .
Correspondence: Professor Dr. B. Allolio, Medizinische Universitätsklinik, Josef-Schneider-Str. 2, D-97080 Würzburg, Germany.
C O N C L U S I O N S (1) S u r a m i n is of antineoplastic efficacy in the treatment of metastat ic adrenocort ical carc inoma. (2) The cl inical u s e of s u r a m i n i s limited by a narrow therapeutic window with the risk of ser ious and possibly lethal toxicity at o n e ext reme, and loss of efficacy at the other. Strict monitoring of s u r a m i n s e r u m levels is mandatory a iming at l eve ls between 200 and 250mg/ l . Suramin should not be c o n s i d e r e d a s first-line treatment for metastatic adrenocort ica l c a r c i n o m a . (3) To improve treatment options in adrenocort ica l carc inoma a s well a s for further investigation on the usefu lness of suramin, controlled prospect ive tr ials a r e urgently needed.
Adrenocortical carcinoma (ACC) is a rare neoplasm with
high malignancy. Because of its low incidence, well designed
prospective therapeutic trials involving large numbers of
patients are lacking. Thus treatment has not been
standardized and the prognosis is usually poor. Most
patients with metastatic disease are treated with mitotane,
an adrenolytic drug, introduced into clinical use by
Bergenstal et al. (1960). I t has never been proved that the
use of mitotane in patients wi th A C C leads to significant
prolongation of life and the drug is associated with
significant side-effects (Luton et al, 1990). Since trials with
cytotoxic chemotherapy or radiotherapy did not improve
treatment results and even patients who responded
experienced only transient palliative effects (Johnson &
Greco, 1986; Percarpio & Knowlton, 1976), other treatment
options for adrenocortical cancer are urgently needed.
Suramin, a polysulphonated naphthylurea, has been used
successfully in the treatment of African sleeping sickness
since 1923. In 1986 its clinical use as an anti-HIV agent
revealed remarkable adrenotoxicity leading to adreno
cortical insufficiency (Levine et al, 1986; Kaplan et al.,
1987). In contrast, we recently found that lower doses of
suramin in sleeping sickness improve the adrenocortical
function which had been impaired by acute parasitic disease
(Reincke et al, 1994). In animal experiments with Cynomol-
gus monkeys adrenocortical destruction with lymphocytic
infiltration was seen after the administration of suramin
(Feuillan et al, 1987).
These findings led to the use o f suramin in the treatment
of ACC. In recent studies, the therapeutic efficacy of
suramin as a single agent was shown in patients with ACC
(Stein et al., 1989; LaRocca et al., 1990a) and with prostatic
299
300 W. Ar It et al. Cl in ica l Endoc r i no logy (1994) 41
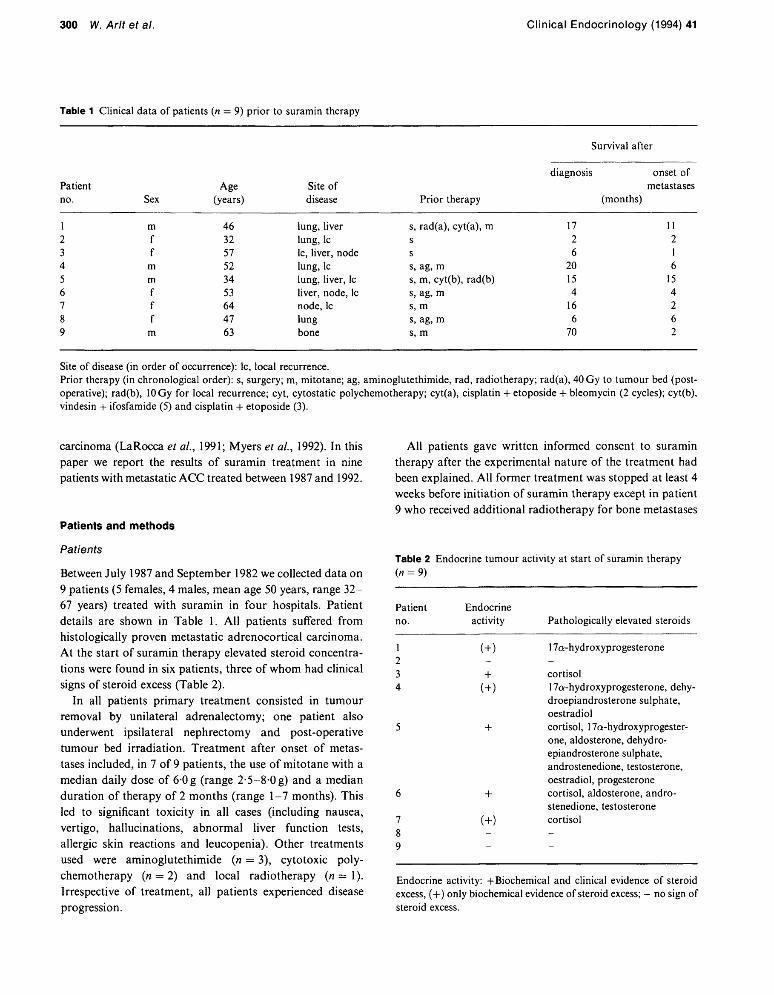
Table 1 Clinical data of patients (n = 9) prior to suramin therapy
Survival after
diagnosis onset of Patient Age Site of metastases no. Sex (years) disease Prior therapy (months)
1 m 46 lung, liver s, rad(a), cyt(a), m 17 11 2 f 32 lung, lc s 2 2 3 f 57 lc, liver, node s 6 1 4 m 52 lung, lc s, ag, m 20 6 5 m 34 lung, liver, lc s, m, cyt(b), rad(b) 15 15 6 f 53 liver, node, lc s, ag, m 4 4 7 f 64 node, lc s, m 16 2 8 f 47 lung s, ag, m 6 6 9 m 63 bone s, m 70 2
Site of disease (in order of occurrence): lc, local recurrence. Prior therapy (in chronological order): s, surgery; m, mitotane; ag, aminoglutethimide, rad, radiotherapy; rad(a), 40 Gy to tumour bed (postoperative); rad(b), 10 Gy for local recurrence; cyt, cytostatic polychemotherapy; cyt(a), cisplatin + etoposide + bleomycin (2 cycles); cyt(b), vindesin + ifosfamide (5) and cisplatin + etoposide (3).
carcinoma (LaRocca et al., 1991; Myers et al., 1992). In this paper we report the results of suramin treatment in nine patients with metastatic ACC treated between 1987 and 1992.
Patients and methods
Patients
Between July 1987 and September 1982 we collected data on 9 patients (5 females, 4 males, mean age 50 years, range 32-67 years) treated with suramin in four hospitals. Patient details are shown in Table 1. A l l patients suffered from histologically proven metastatic adrenocortical carcinoma. At the start of suramin therapy elevated steroid concentrations were found in six patients, three of whom had clinical signs of steroid excess (Table 2).
In all patients primary treatment consisted in tumour removal by unilateral adrenalectomy; one patient also underwent ipsilateral nephrectomy and post-operative tumour bed irradiation. Treatment after onset of metastases included, in 7 of 9 patients, the use of mitotane with a median daily dose of 6 0 g (range 2-5-8-0g) and a median duration of therapy of 2 months (range 1-7 months). This led to significant toxicity in all cases (including nausea, vertigo, hallucinations, abnormal liver function tests, allergic skin reactions and leucopenia). Other treatments used were aminoglutethimide (n = 3), cytotoxic polychemotherapy (n = 2) and local radiotherapy (n = 1). Irrespective of treatment, all patients experienced disease progression.
A l l patients gave written informed consent to suramin therapy after the experimental nature of the treatment had been explained. A l l former treatment was stopped at least 4 weeks before initiation of suramin therapy except in patient 9 who received additional radiotherapy for bone metastases
Table 2 Endocrine tumour activity at start of suramin therapy (« = 9)
Patient Endocrine no. activity Pathologically elevated steroids
1 (+) 1 -
17a-hydroxyprogesterone
z 3 + Cortisol
4 (+) 17a-hydroxyprogesterone, dehy-droepiandrosterone sulphate, oestradiol
5 + Cortisol, 17a-hydroxyprogester-one, aldosterone, dehydro-epiandrosterone sulphate, androstenedione, testosterone, oestradiol, progesterone
6 + Cortisol, aldosterone, androstenedione, testosterone
7 (+) 8 9
Cortisol
Endocrine activity: -(-Biochemical and clinical evidence of steroid excess, (+) only biochemical evidence of steroid excess; - no sign of steroid excess.

Cl in i ca l E n d o c r i n o l o g y (1994) 41 Suramin in adrenocortical cancer 301
during the first 4 weeks of his suramin regimen. Two of the nine patients (nos 2 and 3) were treated with suramin after surgery without having received additional therapy for metastases encouraged by very promising initial results in two patients in this series (Allolio et al., 1989a; Baldus et al., 1990) and in the series of the N I H group (Stein, personal communication, 1987; Stein et al., 1989; LaRocca et al, 1990a). Both patients were suffering from rapidly progressing disease.
Before initiation of suramin therapy all patients were in a general state equivalent to a Karnofsky index of at least 50. A l l patients had normal coagulation parameters, platelet counts above 120 x 109/1 and sufficient renal and hepatic function as assessed by a creatinine clearance above 0-7 ml/s and a serum total bilirubin concentration below 25 /rniol/1. In patients 4-9 maximum motor conduction velocity measurements in upper and lower limbs showed values within the normal range.
Treatment
Suramin (Germanin, Bayer, FRG) was diluted in 0-9% saline solution and administered intravenously.
On day 0 all patients received a test dose of 200 mg suramin in a bolus injection in order to minimize the risk of anaphylactic reactions. Five patients (nos 1-4, 9) received suramin by bolus injections according to a dose regimen similar to standard therapy in sleeping sickness patients (Hawking, 1978) but achieving a higher cumulative dose during a shorter period. As more data on the toxicity and on target serum concentrations of suramin became available (Stein et al, 1989), the schedule was changed and in patients 5-8 suramin was given by continuous infusion (0-35 g/m 2
body surface/day during 10-16 days) aiming at suramin serum levels around 200mg/l. After the initial course treatment was interrupted for 14 days in all patients and maintenance doses were then given in weekly to two-weekly intervals depending on serum suramin concentrations.
Baseline and follow-up studies
Al l patients were evaluated prior to therapy and thereafter at regular intervals (4-8 weeks) by chest X-ray, abdominal sonography, and chest and abdominal computed tomography. Additionally they underwent serial ophthalmological examinations including slit lamp studies. In patients 4-9 monthly measurements of maximum motor conduction velocity in upper and lower limbs were performed. Weekly laboratory studies included blood cell counts, coagulation tests (partial thromboplastin time, prothrombin time (given
as Quick value) and thrombin time) as well as renal and hepatic function parameters.
Serum suramin concentration
Serum suramin levels were determined by high-performance liquid chromatography (HPLC) using the method reported by Klecker and Collins (1985) with minor modifications. Measurements were carried out at least twice weekly during the treatment.
Response criteria
A tumour response to suramin was defined as complete (complete response, CR) i f there was no sign of measurable disease for at least 6 months. Partial response (PR) was equivalent to a more than 25% decrease, and progressive disease (POD) to a more than 25% increase of the radiologically measurable extent of disease. Stable disease (SD) was defined as < 25% increase or decrease of measurable disease.
Statistical analysis
Linear and exponential regression analyses were used to determine the correlation between blood or coagulation parameters and suramin serum level or cumulative dose. A correlation was considered statistically significant with a P value less than 005.
Resu l ts
During treatment periods varying from 1 to 15 months cumulative doses o f suramin ranging from 8-2 to 30-2 g were administered (see Table 3).
Efficacy
Three patients achieved a partial response (PR) during suramin therapy. Almost complete disappearance of multiple lung metastases was observed for 5 months in patient 1 and for 7 months in patient 8. In the third patient an extensive vertebral bone lesion (maximum diameter 8 cm) decreased in size by more than 50%. This patient also received local radiotherapy during the first 4 weeks of suramin treatment. There may have been an additive effect but regression of the lesion only became apparent 3 months after cessation of radiation therapy suggesting that the tumour regression was induced largely by continuous suramin therapy. Two of the nine patients showed transient disease stabilization (SD) during suramin treatment and
302 W. Arlt et al. Cl in ica l E n d o c r i n o l o g y (1994) 41
Table 3 Suramin therapy and tumour response (n — 9)
Suramin therapy
max. serum levels Survival
after start serum continuously cumulative duration of suramin
Pat. Tumour level ^200g/ml dose of therapy therapy no. response (mg/1) for ^ 4 weeks (g) (months) (months)
1 PR(5) 476 + 24-7 7 8 8 PR(7) 361 + 30-2 15 > 36 9 PR(5) 232 + 18-2 8 9 4 SD(3) 283 + 261 5 12 6 SD(1) 246 - 116 1 2 7 POD 199 - 100 1 2 2 POD 169 - 11-5 2 3 5 POD 93 - 12-3 1 1 3 POD 64 — 8-2 1 1
Tumour response: PR, partial response; SD, stable disease; POD, progressive disease (definitions see 'Response criteria')- Duration of response (months) is given in parentheses.
was paralleled by a decline in elevated 17a-OH-progesterone levels, returning to elevated levels after relapse. In none of the five other patients with steroid-secreting tumours was an influence of suramin on steroid production detected.
Treatment was terminated in two patients (1 PR, 1 SD) because of major toxicity (see below), in three patients because of relapse after initial tumour response (2 PR, 1 SD) and in four patients because of lack of response to suramin treatment. Relapse occurred in two of the three patients with PR after a period of at least 4 weeks with serum suramin levels continuously below 100 mg/1. In both cases reinduction therapy leading to serum concentrations above 200 mg/1 was without effect on tumour progression. Two patients (nos 4 and 8) with initial response to suramin received additional cytotoxic polychemotherapy after they had relapsed. However, no tumour regression was found. The survival after initiation of suramin therapy varied between 1 and more than 36 months (median 9 months); patient 8 is still alive despite progressive disease.
Toxicity (see Table 4)
Renal and hepatic function impairment was only mild and transient: elevation of serum alkaline phosphatase (4/9) and albuminuria (2/9) were reversible during ongoing treatment. Elevation of serum creatinine (177^mol/l) was seen in the patient with unilateral nephrectomy (patient 1) and was reversible after cessation of treatment.
A coagulopathy with a prolongation of partial thromboplastin time (PTT) and an alteration of prothrombin time
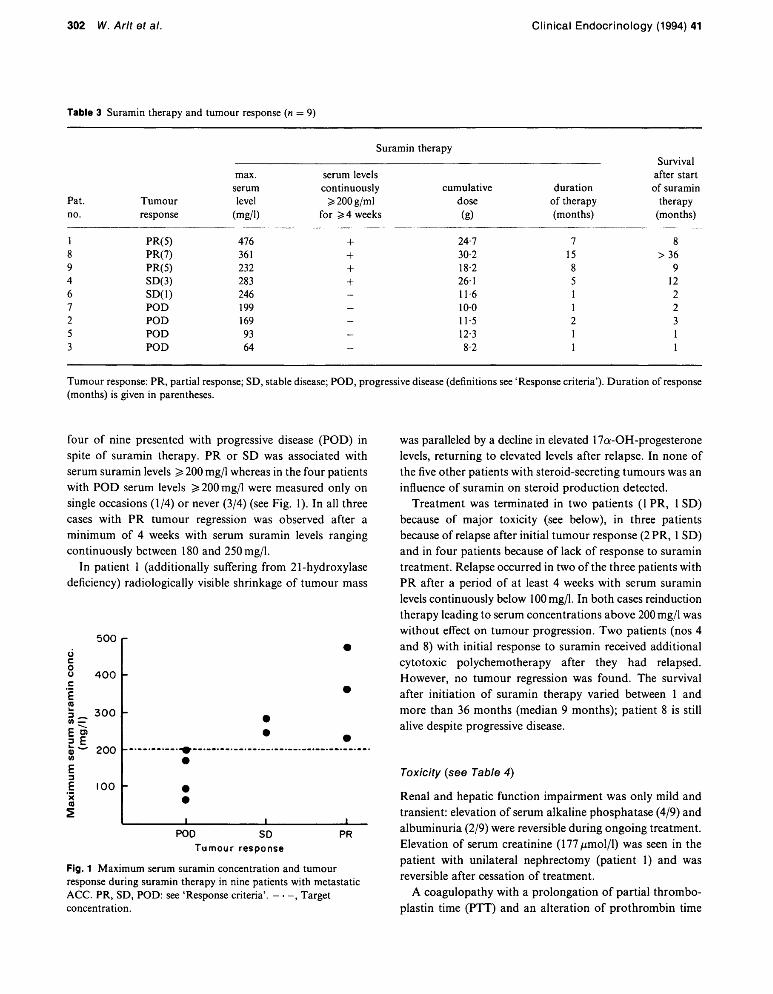
four of nine presented with progressive disease (POD) in spite of suramin therapy. PR or SD was associated with serum suramin levels ^ 200 mg/1 whereas in the four patients with POD serum levels ^ 200 mg/1 were measured only on single occasions (1/4) or never (3/4) (see Fig. 1). In all three cases with PR tumour regression was observed after a minimum of 4 weeks with serum suramin levels ranging continuously between 180 and 250 mg/1.
In patient 1 (additionally suffering from 21-hydroxylase deficiency) radiologically visible shrinkage of tumour mass
u c o u
E (0
500
4 0 0 -
3 0 0 -
I? ; w 200
E
£ X (0 2
100 -
POD SD Tumour response
PR
Fig. 1 Maximum serum suramin concentration and tumour response during suramin therapy in nine patients with metastatic ACC. PR, SD, POD: see 'Response criteria'. , Target concentration.
Cl in i ca l E n d o c r i n o l o g y (1994) 41 Suramin in adrenocortical cancer 303
Table 4 Toxicity during suramin therapy (« = 9) and association with mode of administration, serum concentration or cumulative dose of suramin
Toxicity n Association
Renal function impairment albuminuria 2 (> 0-2g/day) creatinine elevation 1 (> 133/xmol/l)
Hepatic dysfunction alkaline phosphatase elevation (> 200 U/l) 4
Coagulopathy 6 serum level Myelotoxicity
thrombocytopenia 6 cumulative dose (< 120 x 109/1) haemoglobin decrease 2 cumulative dose? (> 30g/l)
Neurological disorders paraesthesia and/or dysgeusia 3 bolus injection polyneuropathy 2 including
sensorimotor Guillain-Barre-like syndrome 1 serum level motor polyneuropathy 1 cumulative dose?
Skin reactions generalized exanthema 3 bolus injection (n = 2) toxic epidermal necroeysis 1
Vortex keratopathy 3 cumulative dose?
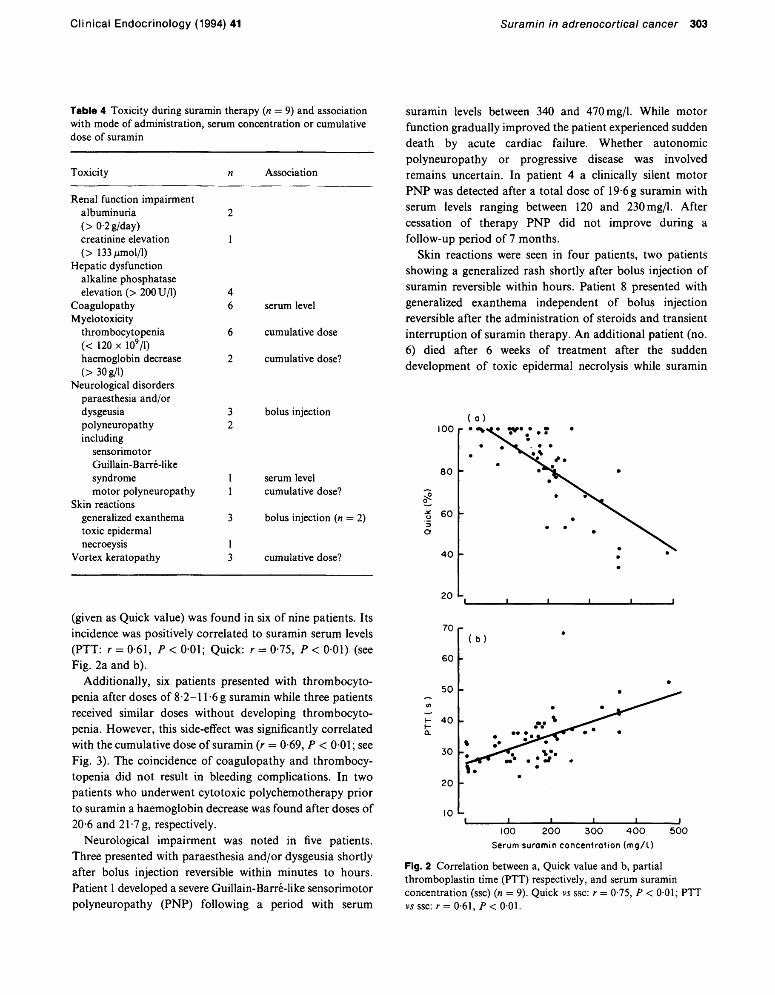
(given as Quick value) was found in six of nine patients. Its incidence was positively correlated to suramin serum levels (PTT: r = 0-61, P < 0 0 1 ; Quick: r = 0 75, P < 001) (see Fig. 2a and b).
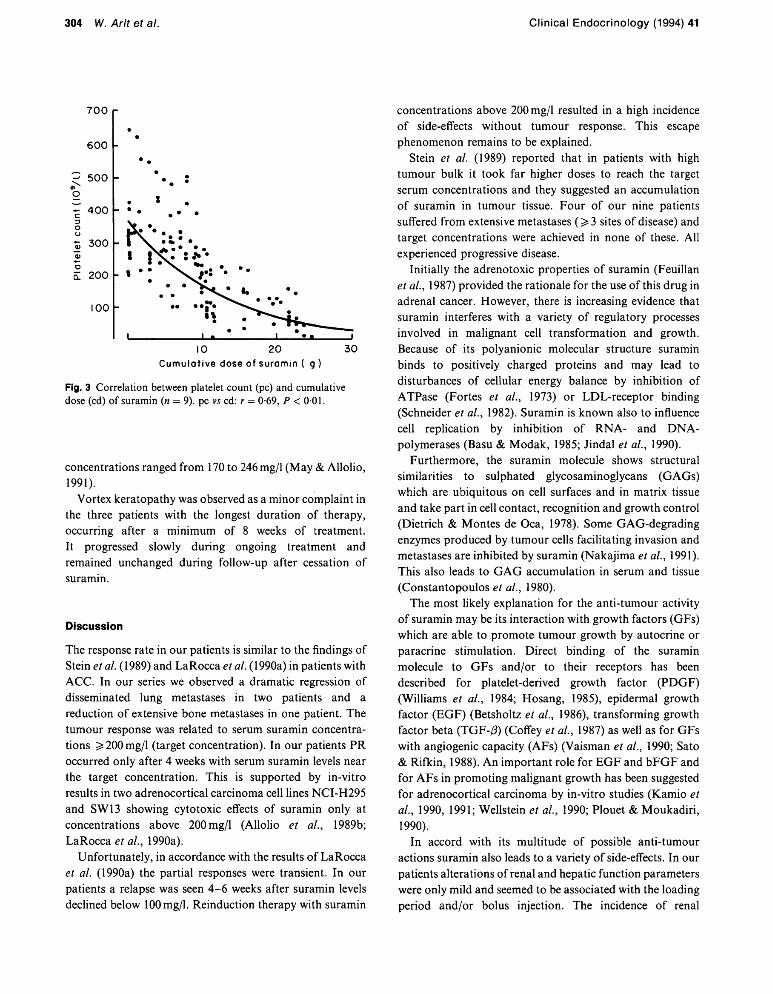
Additionally, six patients presented with thrombocytopenia after doses of 8-2-11 -6 g suramin while three patients received similar doses without developing thrombocytopenia. However, this side-effect was significantly correlated with the cumulative dose of suramin (r = 0-69, P < 0 0 1 ; see Fig. 3). The coincidence of coagulopathy and thrombocytopenia did not result in bleeding complications. In two patients who underwent cytotoxic polychemotherapy prior to suramin a haemoglobin decrease was found after doses of 20-6 and 21-7 g, respectively.
Neurological impairment was noted in five patients. Three presented with paraesthesia and/or dysgeusia shortly after bolus injection reversible within minutes to hours. Patient 1 developed a severe Guillain-Barre-like sensorimotor polyneuropathy (PNP) following a period with serum
suramin levels between 340 and 470mg/l. While motor function gradually improved the patient experienced sudden death by acute cardiac failure. Whether autonomic polyneuropathy or progressive disease was involved remains uncertain. In patient 4 a clinically silent motor PNP was detected after a total dose of 19-6 g suramin with serum levels ranging between 120 and 230mg/l. After cessation of therapy PNP did not improve during a follow-up period of 7 months.
Skin reactions were seen in four patients, two patients showing a generalized rash shortly after bolus injection of suramin reversible within hours. Patient 8 presented with generalized exanthema independent of bolus injection reversible after the administration of steroids and transient interruption of suramin therapy. A n additional patient (no. 6) died after 6 weeks of treatment after the sudden development o f toxic epidermal necrolysis while suramin
( o )
2 0 -
10 L
< i 1 1 1 i 100 2 0 0 3 0 0 4 0 0 5 0 0
Serum suramin concentration ( m g / l )
Fig. 2 Correlation between a, Quick value and b, partial thromboplastin time (PTT) respectively, and serum suramin concentration (ssc) (n = 9). Quick vs ssc: r = 0-75, P < 0-01; PTT vsssc: r = 0-61, P < 001.
304 W. Arlt et al. Cl in ica l E n d o c r i n o l o g y (1994) 41
7 0 0 -
6 0 0 -4
? 500 -
- 4 0 0 - • •
I0 20 30 Cumulative dose of suramin ( g )
Fig. 3 Correlation between platelet count (pc) and cumulative dose (cd) of suramin (n - 9). pc vs cd: r - 0-69, P < 001.
concentrations ranged from 170 to 246 mg/1 (May & Allolio, 1991).
Vortex keratopathy was observed as a minor complaint in the three patients with the longest duration of therapy, occurring after a minimum of 8 weeks of treatment. It progressed slowly during ongoing treatment and remained unchanged during follow-up after cessation of suramin.
Discuss ion
The response rate in our patients is similar to the findings of Stein et al. (1989) and LaRocca et al. (1990a) in patients with ACC. In our series we observed a dramatic regression of disseminated lung metastases in two patients and a reduction of extensive bone metastases in one patient. The tumour response was related to serum suramin concentrations ^ 200 mg/1 (target concentration). In our patients PR occurred only after 4 weeks with serum suramin levels near the target concentration. This is supported by in-vitro results in two adrenocortical carcinoma cell lines NCI-H295 and SW13 showing cytotoxic effects of suramin only at concentrations above 200 mg/1 (Allolio et al., 1989b; LaRocca et al, 1990a).
Unfortunately, in accordance with the results of LaRocca et al. (1990a) the partial responses were transient. I n our patients a relapse was seen 4-6 weeks after suramin levels declined below 100 mg/1. Reinduction therapy with suramin
concentrations above 200 mg/1 resulted in a high incidence of side-effects without tumour response. This escape phenomenon remains to be explained.
Stein et al. (1989) reported that in patients with high tumour bulk it took far higher doses to reach the target serum concentrations and they suggested an accumulation of suramin in tumour tissue. Four of our nine patients suffered from extensive metastases ( ^ 3 sites of disease) and target concentrations were achieved in none of these. A l l experienced progressive disease.
Initially the adrenotoxic properties of suramin (Feuillan et al., 1987) provided the rationale for the use of this drug in adrenal cancer. However, there is increasing evidence that suramin interferes with a variety of regulatory processes involved in malignant cell transformation and growth. Because of its polyanionic molecular structure suramin binds to positively charged proteins and may lead to disturbances of cellular energy balance by inhibition of ATPase (Fortes et al., 1973) or LDL-receptor binding (Schneider et al, 1982). Suramin is known also to influence cell replication by inhibition of RNA- and D N A -polymerases (Basu & Modak, 1985; Jindal et al., 1990).
Furthermore, the suramin molecule shows structural similarities to sulphated glycosaminoglycans (GAGs) which are ubiquitous on cell surfaces and in matrix tissue and take part in cell contact, recognition and growth control (Dietrich & Montes de Oca, 1978). Some GAG-degrading enzymes produced by tumour cells facilitating invasion and metastases are inhibited by suramin (Nakajima et al., 1991). This also leads to G A G accumulation in serum and tissue (Constantopoulos et al., 1980).
The most likely explanation for the anti-tumour activity of suramin may be its interaction with growth factors (GFs) which are able to promote tumour growth by autocrine or paracrine stimulation. Direct binding of the suramin molecule to GFs and/or to their receptors has been described for platelet-derived growth factor (PDGF) (Williams et al., 1984; Hosang, 1985), epidermal growth factor (EGF) (Betsholtz et al., 1986), transforming growth factor beta (TGF-/3) (Coffey et al., 1987) as well as for GFs with angiogenic capacity (AFs) (Vaisman et al., 1990; Sato & Rifkin, 1988). An important role for EGF and bFGF and for AFs in promoting malignant growth has been suggested for adrenocortical carcinoma by in-vitro studies (Kamio et al., 1990, 1991; Wellstein et al., 1990; Plouet & Moukadiri , 1990).
In accord with its multitude of possible anti-tumour actions suramin also leads to a variety of side-effects. In our patients alterations of renal and hepatic function parameters were only mild and seemed to be associated with the loading period and/or bolus injection. The incidence of renal

Cl in ica l E n d o c r i n o l o g y (1994) 41 Suramin in adrenocortical cancer 305
dysfunction noted by Stein et al. (1989) was far higher (10/ 10) than in our patients (2/9); this may be explained by the fact that all patients presented by Stein et al. had undergone unilateral nephrectomy (in our patients only 1/9). Other mild side-effects possibly related to transient peaks of suramin concentration after bolus injection were generalized rash (2/9) and paraesthesiae (3/9).
A serious toxicity positively correlated with suramin serum concentration was coagulopathy seen in six of our nine patients. Similar to Hörne et al. (1988) significant changes of clotting parameters became measurable at suramin serum levels around 250mg/l. We found an involvement of both intrinsic and extrinsic clotting systems. Home et al. (1988) studied plasma from suramin treated patients and found an accumulation of the GAGs heparan sulphate and dermatan sulphate exhibiting a heparin-like anticoagulant activity. In a recent study Hörne et al. (1992) found direct inhibitory effects of suramin on procoagulant proteins (factors X I I , X I , V I I I , X , V) explaining the involvement of the intrinsic clotting system. Such direct effects have already been described by Eisen and Loveday (1973) who also found an anti-thrombin activity of suramin. In contrast to the patients reported by Stein et al. (1989) no significant bleeding complications were observed in our patients. A correlation between tumour response and incidence of suramin-induced coagulopathy (Stein et al., 1989) was also not seen in our patients. Another toxicity associated with G A G accumulation was vortex keratopathy. I t resulted in minor complaints but may bear the risk of visual function impairment as histological examination of lens epithelia and retinal cells from suramin treated patients revealed significant G A G accumulation (Holland et al., 1988). In our patients keratopathy seemed to be related to the cumulative dose of suramin.
The incidence of myelotoxicity during suramin treatment also seemed to depend on cumulative dose. A specific accumulation of suramin in bone marrow cells has been described repeatedly and may lead to direct interference of the drug with haemopoietic growth factors as is known for heparan sulphate (Buys et al, 1978; Constantopoulos et al, 1980; Roberts et al, 1980; Roberts et al, 1988). This suggests that suramin induced myelotoxicity will be reversible paralleling tissue clearance. Suramin related thrombocytopenia may also be caused by complement activation following the formation of drug-antibody complexes; a case of severe immune mediated thrombocytopenia has been reported recently by Seidman et al. (1993).
Another possibly immune mediated toxicity is Guillain-Barre-like Polyneuropathie syndrome (GBS) which developed in one of our patients while serum suramin
concentrations varied between 300 and 400mg/l. LaRocca et al. (1990b) found a 40% risk of GBS in patients with serum concentrations above 350mg/l and noted a good response to plasmapheresis. In one additional patient we observed a clinically silent motor polyneuropathy slowly progressing with increasing cumulative dose of suramin, an association that has not been described yet.
A n immunosuppressive influence of the drug was proposed by O'Donnell et al. (1992) who described two patients who developed keratoacanthoma during suramin therapy. As a possible mechanism for immunosuppression Mills et al. (1990) described an inhibitory effect of suramin on the interleukin-2 binding to lymphoid cells possibly leading to altered proliferation and differentiation.
In our series allergic skin reactions were frequent (4/9) and may be serious, as one patient experienced a lethal toxic epidermal necrolysis (May & Allolio, 1991). A history of drug-induced allergic skin reactions was reported by three of the four symptomatic patients and perhaps should be considered an exclusion criterion for suramin treatment. In a recent letter Falkson and Rapoport (1992) suggested the administration of 200 mg hydrocortisone preceding each suramin injection and reported promising reduction of allergic skin reactions. As Wilks et al. (1991) demonstrated in vitro, combination treatment with steroids and suramin may also support the anti-tumour efficacy by increased inhibition of angiogenesis.
The incidence of serious side-effects (polyneuropathy and coagulopathy) associated with serum suramin concentrations above 300mg/l and the anti-tumour activity of suramin being found to depend on serum concentrations above 200 mg/1, demonstrate a narrow therapeutic window. This suggests mandatory strict serum level monitoring during suramin therapy.
Suramin treatment is hampered by the unique pharmacokinetic characteristics of the drug: an extremely strong protein binding (99-7%), an extensive lysosomotropic tissue accumulation (>90%), and a lack of metabolism leading to a slow renal clearance and a plasma half-life of 44-54 days (Buys et al, 1978; Collins et al, 1986). Recent studies suggested a computer-assisted Bayesian approach for development of individualized dosing schemes (Scher et al, 1992; Cooper et al, 1992; van Rijswijk et al, 1992).
The use of suramin in combination therapies may lead to a dose reduction and thereby to a reduction of toxicity and/ or an enhancement of anti-tumour efficacy. Vierhapper et al. (1989) reported on a patient with ACC presenting with partial response during combined treatment with suramin and mitotane. Furthermore, there are in-vitro data suggesting synergistic activities of suramin with cytotoxic drugs like cyclophosphamide (Osswald & Youssef, 1979) and tumour

306 W. Arlt et al. Cl in ica l E n d o c r i n o l o g y (1994) 41
necrosis factor alpha (Fruehauf et al., 1990). Another possibility for avoiding toxicity may be the use of structural analogues of suramin (Baghdiguian et al., 1990; 1991).
In conclusion, suramin is of limited efficacy in patients with metastatic adrenocortical carcinoma and its use is complicated by a high incidence of serious toxicity. The unique properties of suramin demand further research. A t the moment it is not a first-line treatment for metastatic adrenocortical carcinoma. Controlled prospective trials are urgently needed to improve the treatment options for this malignancy.
Acknowledgements
We are grateful to Dr M . Baldus, Ludwigshafen, Professor Dr J. Beyer, Mainz, and Dr T. Geer, Schwäbisch-Hall, for allowing us to analyse the data from one of their patients.
BA is supported by the Deutsche Forschungsgemeinschaft (AI 203/4-1).
References
Allolio, B., Reincke, ML, Jaursch-Hancke, C , Arlt, W. & Winkelmann, W. (1989a) Treatment of metastatic adrenocortical carcinoma with suramin. Deutsche Medizinische Wochenschrift, 114, 381-384.
Allolio, B., Reincke, M., Jaursch-Hancke, C, Deuss, U., Siekmann, L., Arlt, W., Hoewner, C, Schulte, H.M. & Winkelmann, W. (1989b) Adrenotoxic properties of suramin in vitro and in vivo. Endocrinology, 124 (Suppl.), 672 (abstr.).
Baghdiguian, S., Nickel, P. & Fantini, J. (1991) Double screening of suramin derivatives on human colon cancer cells and on neural cells provides new therapeutic agents with reduced toxicity. Cancer Letter, 60, 213-219.
Baghdiguian, S., Nickel, P., Marvaldi, J. & Fantini, J. (1990) A suramin derivative induces enterocyte-like differentiation of human colon cancer cells without lysosomal storage disorder. Anticancer Drugs, 1, 59-66.
Baldus, M., Allolio, B. & Brass, H. (1990) Suramin—ein neues therapeutisches Prinzip in der Behandlung des metastasierten Nebennierenkarzinoms. Internist, 31, 719-722.
Basu, A. & Modak, M.J. (1985) Observations on the suramin-mediated inhibition of cellular and viral DNA polymerases. Biochemical and Biophysical Research Communications, 128, 1395-1402.
Bergenstal, D.M., Hertz, R., Lipsett, M B . & Moy, R.H. (1960) Chemotherapy of adrenocortical cancer with o,p'DDD. Annals of Internal Medicine, 53, 672-682.
Betsholtz, C, Johnsson, A., Heldin, C.H. & Westermark, B. (1986) Efficient reversion of simian sarcoma virus-transformation and inhibition of growth factor-induced mitogenesis by suramin. Proceedings of the National Academy of Sciences, USA, 83, 6440-6444.
Buys, C.H.C.M., Bourma, J.W., Gruber, M. & Wisse, E. (1978) Induction of lysosomal storage disease by suramin. Naunyn-Schmiedeberg's Archives of Pharmacology, 304, 183-190.
Coffey, R.J., Leof, E.B., Shipley, G.D. & Moses, H.L. (1987) Suramin inhibition of growth factor receptor binding and mitogenicity in AKR-2B cells. Journal of Cellular Physiology, 132, 143-148.
Collins, J.M., Klecker, R.W., Yarchoan, R., Lane, H.C., Gauci, A.S., Redfield, R.R., Broder, S. & Myers, C.E. (1986) Clinical pharmacokinetics of suramin in patients with HTLV-III/LAV infection. Journal of Clinical Pharmacology, 26, 22-26.
Constantopoulos, G., Rees, S., Cragg, B.G., Barranger, J.A. & Brady, R.O. (1980) Experimental animal model for mucopolysaccharidosis: suramin-induced glycosaminoglycan and sphingo-lipid accumulation in the rat. Proceedings of the National Academy of Sciences, USA, 77, 3700-3704.
Cooper, M.R., Lieberman, R., LaRocca, R.V., Gernt, P.R., Weinberger, M.S., Headlee, D.J., Kohler, D.R., Goldspiel, P.R., Peck, C.C. & Myers, C.E. (1992) Adaptive control with feed-back strategies for suramin dosing. Clinical Pharmacology and Therapeutics, 52, 11-23.
Dietrich, CP. & Montes de Oca, H. (1978) Surface sulfated mucopolysaccharides of primary and permanent mammalian cell lines. Biochemical and Biophysical Research Communications, 80, 805-812.
Eisen, V. & Loveday, C. (1973) Effects of suramin on complement, blood clotting, fibrinolysis and kinin formation. British Journal of Pharmacology, 49, 678-687.
Falkson, G. & Rapoport, B.L. (1992) Lethal toxic epidermal necrolysis during suramin treatment. European Journal of Cancer, 28A, 1294.
Feuillan, P., Raffeid, M., Stein, CA., Lipford, N. , Rehnquist, D., Myers, C.E., LaRocca, R.V. & Chrousos, G.P. (1987) Effects of suramin on the function and structure of the adrenal cortex in the Cynomolgus monkey. Journal of Clinical Endocrinology and Metabolism, 65, 153-158.
Fortes, P.A.G., Ellory, J.C. & Lew, V.L. (1973) Suramin: a potent ATPase inhibitor which acts on the inside surface of the sodium pump. Biochimica et Biophysica Acta, 318, 262-272.
Fruehauf, J.P., Myers, C.E. & Sinha, B.K. (1990) Synergistic activity of suramin with tumor necrosis factor alpha and doxorubicin on human prostate cancer cell lines. Journal of the National Cancer Institute, 82, 1206-1209.
Hawking, F. (1978) Suramin: with special reference to onchocerciasis. Advances in Pharmacology and Chemotherapy, 15, 289-322.
Holland, E.J., Stein, C.A., Palestine, A.G., LaRocca, R.V., Chan, C.C, Kuwabara, T., Myers, C.E., Thomas, R., Mcatee, N. & Nussenblatt, R.N. (1988) Suramin keratopathy. American Journal of Ophthalmology, 106, 216-220.
Home, M.K., Stein, CA., LaRocca, R.V. & Myers, C.E. (1988) Circulating glycosaminoglycan anticoagulants associated with suramin treatment. Blood, 71, 273-279.
Hörne, M.K., Wilson, O.J., Cooper, M., Gralnick, H.R. & Myers, C.E. (1992) The effect of suramin on laboratory tests of coagulation. Thrombosis and Haemostasis, 67, 434-439.
Hosang, M. (1985) Suramin binds to platelet-derived growth factor and inhibits its biological activity. Journal of Cellular Biochemistry, 29, 265-273.
Jindal, H.K., Anderson, C.W., Davis, R.G. & Vishnawata, J.K. (1990) Suramin affects DNA synthesis in HeLa cells by inhibition of DNA polymerases. Cancer Research, 50, 7754-7757.
Johnson, D.H. & Greco, F.A. (1986) Treatment of metastatic adrenal cortical carcinoma with cisplatin and etoposide (VP-16). Cancer, 58, 2198-2202.
Cl in i ca l E n d o c r i n o l o g y (1994) 41 Suramin in adrenocortical cancer 307
Kamio, T., Shigematsu, K., Sou, H., Kawai, K. & Tsuchiyama, H. (1990) Immunohistochemical expression of epidermal growth factor receptors in human adrenocortical carcinoma. Human Pathology, 21, 277-282.
Kamio, T., Shigematsu, K., Kawai, K. & Tsuchiyama, H. (1991) Irnmunoreactivity and receptor expression of insulin-like growth factor I and insulin in human adrenal tumors. An immunohistochemical study of 94 cases. American Journal of Pathology, 138, 83-91.
Kaplan, L.D., Wolfe, P.R., Volberding, P.A., Feorino, P., Levy, J.A., Abrams, D., Kipror, D., Wong, R., Kaufman, L. & Gottlieb, M.S. (1987) Lack of response to suramin in patients with AIDS and AIDS-related complex. American Journal of Medicine, 82, 615-620.
Klecker, R.W. & Collins, J.M. (1985) Quantification of suramin by reverse-phase ion-pairing high-performance liquid chromatography. Journal of Liquid Chromatography, 8, 1685-1696.
LaRocca, R.V., Cooper, M.R., Uhrich, M., Danesi, R., Walther, M.M., Linehan, W.M. & Myers, C.E. (1991) Use of suramin in treatment of prostatic carcinoma refractory to conventional hormonal manipulation. Urologie Clinics of North America, 18, 123-129.
LaRocca, R.V., Meer, J., Gilliatt, R.W., Stein, C.A., Cassidy, J., Myers, C.E. & Dalakas, M.C. (1990b) Suramin-induced polyneuropathy. Neurology, 40, 954-960.
LaRocca, R.V., Stein, C.A., Danesi, R., Jamis-Dow, C.A., Weiss, G.H. & Myers, C.E. (1990a) Suramin in adrenal cancer: Modulation of steroid production, cytotoxicity in vitro, and clinical antitumor effect. Journal of Clinical Endocrinology and Metabolism, 71, 497-504.
Levine, A.M., Gill, P.S., Cohen, J., Hawkins, J.G., Formenti, S.C., Aguilar, S., Meyer, P.R., Krailo, M., Parker, J. & Rasheed, S. (1986) Suramin antiviral therapy in the acquired immunodeficiency syndrome. Clinical, immunological, and virological results. Annals of Internal Medicine, 105, 32-37.
Luton, J.P., Cerdas, S., Billaud, L., Thomas, G., Guilhaume, B., Bertagna, X., Laudat, M.H., Louvel, A., Chapuis, Y., Blondeau, P., Bonnin, A. & Bricaire, H. (1990) Clinical features of adrenocortical carcinoma, prognostic factors, and the effect of mitotane therapy. New England Journal of Medicine, 322, 1195— 1201.
May, E. & Allolio, B. (1991) Fatal toxic epidermal necrolysis during suramin therapy. European Journal of Cancer, 27, 1338.
Mills, G.B., Zhang, N. , May, C, Hill, M. & Chung, A. (1990) Suramin prevents binding of interleukin 2 to its cell surface receptor: a possible mechanism for immunosuppression. Cancer Research, 50, 3036-3042.
Myers, C.E., Cooper, M., Stein, C.A., LaRocca, R.V., Walther, M.M., Weiss, G., Choyke, P., Dawson, N. , Steinberg, S. & Uhrich, M.M. (1992) Suramin: a novel growth factor antagonist with activity in hormone-refractory metastatic prostate cancer. Journal of Clinical Oncology, 10, 875-877.
Nakajima, M., Dechavigny, A., Johnson, C.E., Hamada, J., Stein, CA. & Nicolson, G.L. (1991) Suramin. A potent inhibitor of melanoma heparanese and invasion. Journal of Biological Chemistry, 266, 9661-9666.
O'Donnell, B.P., Dawson, N.A., Weiss, R.B., Myers, C.E. & James, W.D. (1992) Suramin-induced skin reactions. Archives of Dermatology, 128, 75-79.
Osswald, H. & Youssef, M. (1979) Suramin enhancement of the chemotherapeutic actions of cyclophosphamide or adriamycin of
intramuscularly implanted Ehrlich carcinoma. Cancer Letters, 6, 337-343.
Percarpio, B. & Knowlton, A.H. (1976) Radiation therapy of adrenocortical carcinoma. Acta Radiologica Therapy Physics Biology, 15, 288-292.
Plouet, J. & Moukadiri, H. (1990) Characterization of the receptor to vasculotropin on bovine adrenal cortex-derived capillary endothelial cells. Journal of Biological Chemistry, 265, 22071-22074.
Reincke, M., Heppner, C, Petzke, F., Allolio, B., Arlt, W., Mbulamberi, D., Siekmann, L., Vollmer, D., Winkelmann, W. & Chrousos, G.P. (1994) Impairment of adrenocortical function associated with increased plasma tumor necrosis factor-alpha and interleukin-6 concentrations in African trypanosomiasis. Neuro-immunomodulation, 1, 14-22.
Roberts, R., Gallagher, J., Spooner, E., Allen, T.D., Bloomfield, F. & Dexter, T.M. (1988) Heparan sulphate bound growth factors: a mechanism for stromal cell mediated haemopoiesis. Nature, 332, 376-377.
Sato, Y. & Rifkin, D.B. (1988) Autocrine activities of basic fibroblast growth factor: regulation of endothelial cell movement, plasminogen activator synthesis, and DNA synthesis. Journal of Cell Biology, 107, 1199-1205.
Scher, HJ., Jodrelli, D.J., Iversen, J.M., Curley, T., Tong, W., Egorin, M.J. & Forrest, A. (1992) Use of adaptive control with feedback to individualize suramin dosing. Cancer Research, 52, 64-70.
Schneider, W.J., Beisiegel, U., Goldstein, J.L. & Brown, M.S. (1982) Purification of the low density lipoprotein receptor, an acidic glycoprotein of 164,000 molecular weight. Journal of Biological Chemistry, 257, 2664-2672.
Seidman, A.D., Schwartz, M., Reich, L. & Scher, H.J. (1993) Immune-mediated thrombocytopenia secondary to suramin. Cancer, 71, 851-854.
Stein, C.A., LaRocca, R.V., Thomas, R., Mcatee, N. & Myers, C.E. (1989) Suramin: An anticancer drug with a unique mechanism of action. Journal of Clinical Oncology, 7, 499-508.
Van Rijswijk, R.E., Van Loenen, A.C., Wagstaff, J., Meijer, E. Lopez, R., Van Groeningen, C.J., Heimans, J.J. & Pinedo, H.M. (1992) Suramin: rapid loading and weekly maintenance regimens for cancer patients. Journal of Clinical Oncology, 10, 1788-1794.
Vaisman, N., Gospodarowicz, D. & Neufeld, G. (1990) Characterization of the receptors for vascular endothelial growth factor. Journal of Biological Chemistry, 265, 19461-19466.
Vierhapper, H., Nowotny, P., Mostbeck, G. & Waldhäusl, W. (1989) Effect of suramin in a patient with adrenocortical carcinoma. Lancet, i , 1207-1208.
Wellstein, A., Lupu, R., Zugmaier, G., Flamm, S.L., Cheville, A.L., Delli-Bovi, P., Basilico, C, Lippman, M.E. & Kern, F.G. (1990) Autocrine growth stimulation by secreted Kaposi fibroblast growth factor but not by endogenous basic fibroblast growth factor. Cell Growth and Differentiation, 1, 63-71.
Wilks, J.W., Scott, P.S., Vrba, L.K. & Cocuzza, J.M. (1991) Inhibition of angiogenesis with combination treatment of angiostatic steroids and suramin. International Journal of Radiation Biology, 60, 73-77.
Williams, L.T., Tremble, P.M., Lavin, M.F. & Sunday, M.E. (1984) Platelet-derived growth factor receptors form a high affinity state in membrane preparations. Kinetics and affinity cross-linking studies. Journal of Biological Chemistry, 259, 5287— 5294.
Related Documents