Superinfection and the evolution of resistance to antimalarial drugs Eili Y. Klein 1,3, *, David L. Smith 3,4,5 , Ramanan Laxminarayan 2,3 and Simon Levin 1 1 Department of Ecology and Evolutionary Biology, and 2 Princeton Environmental Institute, Princeton University, Princeton, NJ 08544, USA 3 Center for Disease Dynamics Economics and Policy, Washington, DC 20036, USA 4 Department of Epidemiology, and 5 Malaria Research Institute, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21205, USA A major issue in the control of malaria is the evolution of drug resistance. Ecological theory has demon- strated that pathogen superinfection and the resulting within-host competition influences the evolution of specific traits. Individuals infected with Plasmodium falciparum are consistently infected by multiple parasites; however, while this probably alters the dynamics of resistance evolution, there are few robust mathematical models examining this issue. We developed a general theory for modelling the evolution of resistance with host superinfection and examine: (i) the effect of transmission intensity on the rate of resist- ance evolution; (ii) the importance of different biological costs of resistance; and (iii) the best measure of the frequency of resistance. We find that within-host competition retards the ability and slows the rate at which drug-resistant parasites invade, particularly as the transmission rate increases. We also find that biological costs of resistance that reduce transmission are less important than reductions in the duration of drug- resistant infections. Lastly, we find that random sampling of the population for resistant parasites is likely to significantly underestimate the frequency of resistance. Considering superinfection in mathematical models of antimalarial drug resistance may thus be important for generating accurate predictions of interventions to contain resistance. Keywords: Plasmodium falciparum; malaria; superinfection; drug resistance; evolution 1. INTRODUCTION More than a century ago, the Nobel prize-winning German scientist Paul Ehrlich predicted that pathogens subjected to drugs would evolve resistance [1]. The conjecture has been proven true so often and in so many contexts that it can be regarded as Ehrlich’s Law. There is, nevertheless, uncer- tainty about virtually every other question of academic or public health interest—in particular, the role of superinfec- tion, defined as the simultaneous infection with multiple strains of the same pathogen, and its influence on the evolution of drug resistance. Even though superinfection has been shown to alter the evolution of specific traits, particularly virulence [2 – 4], a robust theory of the effect of superinfection on the evolution of drug resistance is still lacking. This is important in the study of malaria, because superinfection, with the concomitant increase in within-host competition, is likely to change the dynamics of resistance evolution and have ramifications for control efforts. Here, we extend some of the classic models in malaria to consider the consequences of within-host competition among drug-sensitive and drug-resistant Plasmodium falciparum malaria parasites, the species of malaria associated with the highest levels of morbidity and mortality. Early studies of P. falciparum malaria suggested that high rates of exposure to malaria could result in simul- taneous infection with multiple parasites, termed superinfection [5]. This was not conclusively confirmed until the 1970s [6], but it is now known that P. falciparum malaria infections are typically composed of several genetically distinct lineages, called the multiplicity of infection (MOI), even in areas of low transmission [7]. Because of the complexity of the parasite’s life cycle, in which parasite meiosis and recombination occurs in the mosquito, genetic and phenotypic variation between clonal P. falciparum populations can be significant, which can impact their competitive ability. Antimalarial drug resistance is encoded by mutations in, or changes to, the copy number of genes relating to the drug’s target or influx –efflux pumps that affect intra- parasitic concentrations of the drug [8]. These changes, which are beneficial in the presence of drugs, also have a biological fitness cost to the parasite, lowering its competitiveness [9,10]. In the presence of therapy, the drug-resistant parasites have an advantage. Removal of the drug exposes the parasites to increased competition and can lead to a decline in the frequency of resistance- conferring mutations, as occurred in Malawi after the country stopped using chloroquine (CQ) [11]. However, in areas with lower transmission (and lower MOI and lower rates of competition), the frequency of resistance has declined at a slower rate [12]. Thus, understanding how superinfection affected historical examples of resist- ance to the former first-line antimalarial drugs CQ and * Author for correspondence ([email protected]). Electronic supplementary material is available at http://dx.doi.org/ 10.1098/rspb.2012.1064 or via http://rspb.royalsocietypublishing.org. Proc. R. Soc. B (2012) 279, 3834–3842 doi:10.1098/rspb.2012.1064 Published online 11 July 2012 Received 9 May 2012 Accepted 20 June 2012 3834 This journal is q 2012 The Royal Society

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Proc. R. Soc. B (2012) 279, 3834–3842
* Autho
Electron10.1098
doi:10.1098/rspb.2012.1064
Published online 11 July 2012
ReceivedAccepted
Superinfection and the evolution ofresistance to antimalarial drugs
Eili Y. Klein1,3,*, David L. Smith3,4,5, Ramanan Laxminarayan2,3
and Simon Levin1
1Department of Ecology and Evolutionary Biology, and 2Princeton Environmental Institute,
Princeton University, Princeton, NJ 08544, USA3Center for Disease Dynamics Economics and Policy, Washington, DC 20036, USA
4Department of Epidemiology, and 5Malaria Research Institute,
Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21205, USA
A major issue in the control of malaria is the evolution of drug resistance. Ecological theory has demon-
strated that pathogen superinfection and the resulting within-host competition influences the evolution
of specific traits. Individuals infected with Plasmodium falciparum are consistently infected by multiple
parasites; however, while this probably alters the dynamics of resistance evolution, there are few robust
mathematical models examining this issue. We developed a general theory for modelling the evolution of
resistance with host superinfection and examine: (i) the effect of transmission intensity on the rate of resist-
ance evolution; (ii) the importance of different biological costs of resistance; and (iii) the best measure of the
frequency of resistance. We find that within-host competition retards the ability and slows the rate at which
drug-resistant parasites invade, particularly as the transmission rate increases. We also find that biological
costs of resistance that reduce transmission are less important than reductions in the duration of drug-
resistant infections. Lastly, we find that random sampling of the population for resistant parasites is likely
to significantly underestimate the frequency of resistance. Considering superinfection in mathematical
models of antimalarial drug resistance may thus be important for generating accurate predictions of
interventions to contain resistance.
Keywords: Plasmodium falciparum; malaria; superinfection; drug resistance; evolution
1. INTRODUCTIONMore than a century ago, the Nobel prize-winning German
scientist Paul Ehrlich predicted that pathogens subjected to
drugs would evolve resistance [1]. The conjecture has been
proven true so often and in so many contexts that it can
be regarded as Ehrlich’s Law. There is, nevertheless, uncer-
tainty about virtually every other question of academic or
public health interest—in particular, the role of superinfec-
tion, defined as the simultaneous infection with multiple
strains of the same pathogen, and its influence on the
evolution of drug resistance. Even though superinfection
has been shown to alter the evolution of specific traits,
particularly virulence [2–4], a robust theory of the effect
of superinfection on the evolution of drug resistance is
still lacking. This is important in the study of malaria,
because superinfection, with the concomitant increase in
within-host competition, is likely to change the dynamics
of resistance evolution and have ramifications for control
efforts. Here, we extend some of the classic models
in malaria to consider the consequences of within-host
competition among drug-sensitive and drug-resistant
Plasmodium falciparum malaria parasites, the species of
malaria associated with the highest levels of morbidity
and mortality.
r for correspondence ([email protected]).
ic supplementary material is available at http://dx.doi.org//rspb.2012.1064 or via http://rspb.royalsocietypublishing.org.
9 May 201220 June 2012 3834
Early studies of P. falciparum malaria suggested that
high rates of exposure to malaria could result in simul-
taneous infection with multiple parasites, termed
superinfection [5]. This was not conclusively confirmed
until the 1970s [6], but it is now known that P. falciparum
malaria infections are typically composed of several
genetically distinct lineages, called the multiplicity of
infection (MOI), even in areas of low transmission [7].
Because of the complexity of the parasite’s life cycle, in
which parasite meiosis and recombination occurs in the
mosquito, genetic and phenotypic variation between
clonal P. falciparum populations can be significant,
which can impact their competitive ability.
Antimalarial drug resistance is encoded by mutations
in, or changes to, the copy number of genes relating to
the drug’s target or influx–efflux pumps that affect intra-
parasitic concentrations of the drug [8]. These changes,
which are beneficial in the presence of drugs, also have
a biological fitness cost to the parasite, lowering its
competitiveness [9,10]. In the presence of therapy, the
drug-resistant parasites have an advantage. Removal of
the drug exposes the parasites to increased competition
and can lead to a decline in the frequency of resistance-
conferring mutations, as occurred in Malawi after the
country stopped using chloroquine (CQ) [11]. However,
in areas with lower transmission (and lower MOI and
lower rates of competition), the frequency of resistance
has declined at a slower rate [12]. Thus, understanding
how superinfection affected historical examples of resist-
ance to the former first-line antimalarial drugs CQ and
This journal is q 2012 The Royal Society

no. d
rug-
resi
stan
t par
asite
s
0,0 1,0 2,0 3,0
0,1 1,1 2,1
0,2 1,2
0,3
drug use
no. drug-sensitive parasites
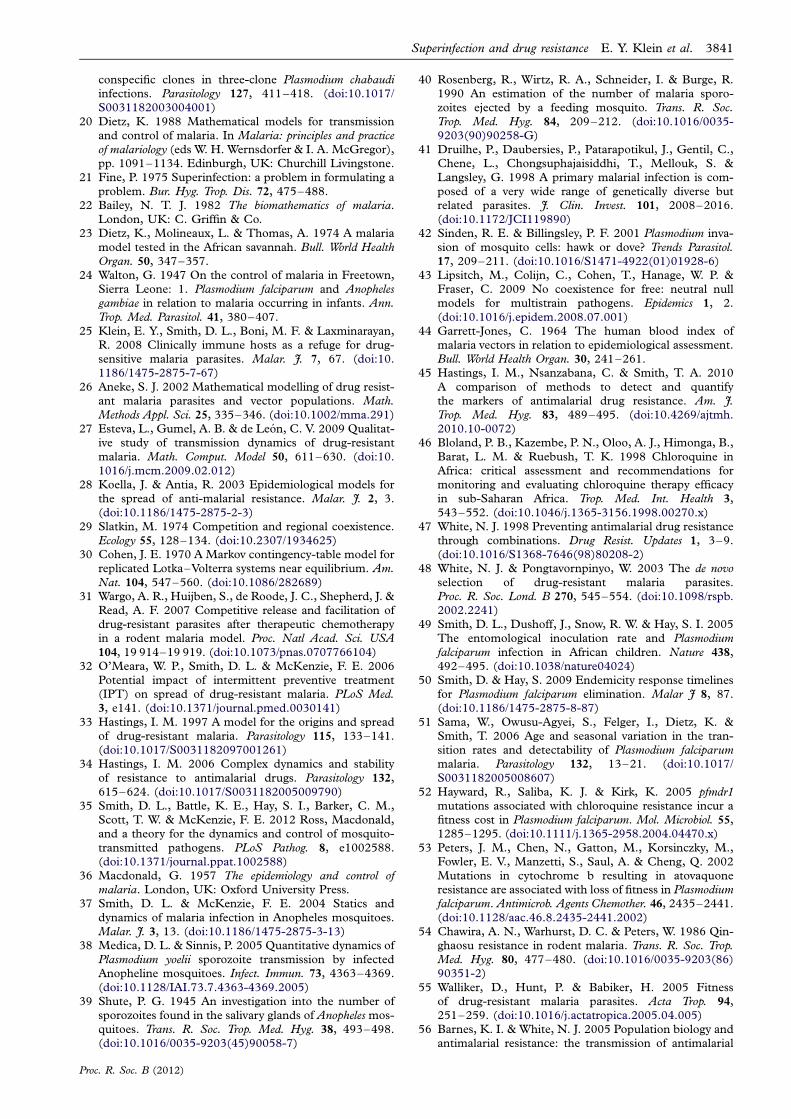
Figure 1. The MOI model with sensitive and resistant types.
The state variables describe the proportion of the populationwith a given MOI for both drug-sensitive and drug-resistantparasites, and the solid lines show changes that are the resultof transmission and clearance. Antibiotic use (dashed lines)reduces the MOI of drug-sensitive parasites, but not drug-
resistant ones. Biological costs of resistance are introducedas an increased propensity to clear or a reduced propensityto transmit drug-resistant types.
Superinfection and drug resistance E. Y. Klein et al. 3835
sulphadoxine-pyrimethamine (SP) is of great interest for
understanding the factors that are likely to be important
for the evolution of resistance to artemisinin-class drugs
and to the artemisinin combination therapies that are
now the first-line treatment for falciparum malaria in
much of the world.
The existing mathematical theory describing the evol-
ution of resistance is poorly developed with respect to
superinfection and within-host competition. Models of
superinfection in other organisms [2,3] either have
assumed that a dominant strain could displace another
pathogen and take over the host, but not vice versa, or
have not allowed for transmission from coinfected states
[13,14]. Neither of these approaches is biologically rel-
evant in malaria, where superinfection is the rule rather
than the exception, and evidence from the field [15,16]
and murine models [17–19] has demonstrated the
impact of within-host competition on the survival and
transmissibility of genetically distinct malaria clones.
In malaria, the mathematical theory of superinfection
was developed by Walton, Macdonald, Irwin, Dietz and
Bailey [5,20–24]. Their models allow for superinfection,
meaning that multiple genetically distinct clones coinfect a
host, and were developed to aid in matching assumptions
of the transmission rate with clearance rates. Although the
models generally fit the data on prevalence better than the
assumption that additional infections have no effect on the
clearance rate [20], epidemiological models of this type
have not been applied to problems of within-host compe-
tition and drug resistance, where it is often assumed
that individuals are infected by either drug-resistant or
drug-sensitive parasites only [25–27].
In their model of antimalarial resistance, Koella &
Antia [28] assume that individuals can be superinfected
by both drug-resistant and drug-sensitive infections (het-
erotypic) but not by two drug-resistant or drug-sensitive
types (homotypic). They assume that individuals with
heterotypic infections transmit both parasites at the
same rate regardless of the composition of drug-resistant
and drug-sensitive parasites in the population. This
significantly biases transmission, particularly when resist-
ance is first emerging, and drug-resistant parasites
are rare. As has been shown in species coexistence
models [29,30], the only way that one species can exclude
another is if there is significant competition in superin-
fected hosts, and in malaria, there is strong evidence
that drug-resistant and drug-sensitive parasites compete
in a host, and removing one will increase the fitness
advantage of the other [31]. Because the full costs of com-
petition are not embedded in the model (i.e. individuals
cannot be multiply infected by the same type of parasite),
when the fitness cost of resistance is low (but not zero),
the model predicts coexistence even when there is no
treatment in the population [28], a result that is not bio-
logically plausible (see electronic supplementary material,
appendix SI).
In this paper, using a general formulation of malaria
superinfection, we present a general theory for the evol-
ution of resistance when superinfection occurs. Building
on population genetics models for malaria [32–34] as
well as past epidemiological models [25], the approach
presented here allows for an examination of some of the
basic questions involved in how competition affects
the spread of drug resistance in different environments.
Proc. R. Soc. B (2012)
Our model provides a new way of thinking about model-
ling antimalarial drug resistance, incorporating many
of the concepts that are in common use in malaria
epidemiology today [35], and suggests ways to better
understand the important control points and identify
new directions for future research.
2. METHODS(a) Superinfection model
To model the evolution of resistance with superinfection, we
modified a Markov chain model for superinfection and clear-
ance to include clinical malaria and antimalarial drugs; the
original model was developed for malaria [22]. MOI (the
number of pathogens per host individual) increases as new
infections occur, but decreases as they clear. The state vari-
ables in the model represent the fraction of the population
that has a given MOI: Xi denotes the fraction of hosts with
an MOI of i. We have extended the model to track the
MOI of sensitive and resistant types (figure 1). Let Xi,j
denote the fraction of the population with i sensitive and j
resistant strains. The equations are formulated so thatPi;j Xi;j ¼ 1, and hence the sum of the time derivativesPi;j
_Xi;j ¼ 0. Thus, the values of the state variables describe
the joint distribution of resistant and sensitive phenotypes in
a population.
(b) Entomology
The dynamics of infection in the model follow a notation
similar to that of single-infection models by Macdonald
[36], as modified by Smith & McKenzie [37]. Vectorial
capacity (V ), the number of infectious bites by a mosquito
over its lifetime, is given by the formula V ¼ ma2e2gn/g,
where m denotes the number of mosquitoes per human
and a is the number of bites on humans per mosquito per

3836 E. Y. Klein et al. Superinfection and drug resistance
day. The instantaneous death rate is g (e2g is the probability
of a mosquito surviving 1 day) and n is the number of days
required for sporogony.
The daily entomological inoculation rate (EIR), the
number of infectious bites per person per day, is calculated
as the product of vectorial capacity and the fraction of mos-
quitoes that are infectious (P/(1 þ aP/g)), where P is the
proportion of the bites on the infected human population
that infect mosquitoes, assuming transmission efficiency c
from humans to mosquitoes (P ¼ cXi,j, where i = 0 or j =
0). The force of infection, or happenings rate (h), is bEIR,
where b, the infectivity rate, is the fraction of bites on
humans that produce a patent infection.
(c) Competition and a biological cost of resistance
The model ignores fluctuations in the abundance of parasites
within a host, but competition is naturally incorporated into
the model as a transmission bottleneck at the mosquito. In
the absence of any biases, the probability of a mosquito trans-
mitting either a resistant or a sensitive parasite is a function of
the proportion of each type ingested (assuming there is no
preference for selfing). We assume that resistant genotypes
in each gamete in the mosquito are lower than the proportion
of the resistant genotypes in the human infection; thus, the
parameter l weighs all the factors that could produce a bio-
logical cost of resistance in the dynamics of parasites from
hepatocyte to gametocyte.
The number of genotypes that are transmitted by each
infectious bite is limited both by the number of ookinetes
that have contributed sporozoites, and by the number of
liver-stage schizonts that arise from each infectious bite.
The proportion of sporozoites in a mosquito’s salivary
glands injected during a feeding event is typically small
[38–40], though the number of genetically distinct sporo-
zoites injected is unclear [41]. Because the bottlenecks
inherent within the system are likely to make the infection
of an individual with a large number of genetically diverse
sporozoites an uncommon event [42], we assume that each
mosquito transmits the offspring of only one gamete,
regardless of the MOI of the host that infected it.
Because competition for transmission occurs only when
a mosquito bites an individual with a mixed infection,
the overall probability that an individual sporozoite in the
next generation is sensitive (~Xw) or resistant (~X r) can be
represented as
~Xw ¼X
i
Xj
i2 þ lij
ði þ ljÞ2Xi;j ð2:1aÞ
and
~X r ¼X
i
Xj
ðljÞ2 þ lij
ði þ ljÞ2Xi;j ; ð2:1bÞ
where l , 1 (see electronic supplementary material, appen-
dix SII for derivation). Thus, the frequency of resistance in
new infections is ~X r=ð ~Xw þ ~X rÞ, and the force of infection
for sensitive (hw) and resistant (hr) parasites is defined as
hw ¼ h~Xw
~X r þ ~Xw
� �ð2:2aÞ
and
hr ¼ h~X r
~X r þ ~Xw
� �: ð2:2bÞ
Proc. R. Soc. B (2012)
We also assume that resistant parasites face an additional
cost in clearance. This is denoted by q, where qi,j ¼ [(i þ j)/j]a
and a . 0. Thus, a describes the bias in the proportion of
cleared parasites that are drug-resistant, relative to the fre-
quency of drug-resistant types among all types in a host.
While numerous reports have presented evidence of fitness
costs of resistance in malaria [10–12], there is no clear
understanding of how these costs are paid [10]. However,
as the resistance alleles are seemingly lost at a much higher
rate in high-transmission areas relative to low-transmission
areas [11,12], we assume that within-host competition is
the most important driver, and thus drug-resistant parasites
are assumed to have a biased clearance rate only when in
competition with drug-sensitive parasites.
(d) Clinical infections and drug use
Drug use is assumed to be associated with clinical symptoms
(primarily fever), which develop at rate c. The rate at which
clinical symptoms arise is independent of MOI. A fraction, r,
of symptomatic patients are assumed to use drugs and suc-
cessfully clear all sensitive parasites. The drug usage rate is
assumed to be constant over each simulation, but is varied
among simulations as noted. Treatment of resistant parasites
is assumed to be ineffective.
(e) Equations
The dynamics of the state variable, Xi,j, which denotes the
fraction of the population with i sensitive and j resistant
strains, are thus described by the following set of coupled
ordinary differential equations.
The equation describing the change in the proportion of
uninfected hosts (i ¼ 0, j ¼ 0) is
_X0;0 ¼ �hX0;0 þ r1;0X1;0 þ r0;1X0;1 þXNi¼1
rcXi;0; ð2:3aÞ
where r is the recovery rate of an infection consisting of i sen-
sitive and j resistant strains, h is the force of infection, c is the
rate that clinical symptoms develop, and r is the fraction of
those patients that are treated and clear the infection
successfully.
For individuals infected only with drug-sensitive clones
(i . 0, j ¼ 0),
_Xi;0 ¼ �hXi;0 � ri;0Xi;0 þ riþ1;0Xiþ1;0 þ ri;1qi;1Xi;1
þ hwXi�1;0 � rcXi;0; ð2:3bÞ
where q is the reduction in the duration of infection owing
to the biological cost of resistance, and hw is the force of
infection for drug-sensitive parasites.
For individuals infected only with drug-resistant clones
(i ¼ 0, j . 0),
_X0; j ¼ �hX0; j � r0; jX0; j þ r0; jþ1X0; jþ1 þ r1; jX1; j
þ hrX0; j�1 þXNi¼1
rcXi; j ; ð2:3cÞ
where hr is the force of infection for drug-resistant parasites.
For individuals infected with both drug-sensitive and
drug-resistant clones (i . 0, j . 0),
_Xi; j ¼� hXi; j � ri; jXi; j þ riþ1; jXiþ1; j þ ri; jþ1qi; jþ1Xi; jþ1
þ hwXi�1; j þ hrXi; j�1 � rcXi; j : ð2:3dÞ
The equations are constrained such that the model has a
‘triangular’ formulation (as in figure 1).

Superinfection and drug resistance E. Y. Klein et al. 3837
(f) Triangularity and the neutrality condition
The model presupposes coexistence in the parasite population
of a large number of distinct genotypes, but it considers com-
petition solely between drug-sensitive and drug-resistant
parasites, which differ both genetically and phenotypically.
To describe the effect of competition on the evolution of resist-
ance, it was necessary to establish that the model satisfied
general principles of ecological and population genetic neu-
trality as described by Lipsitch et al. [43]. These principles
note that the models of competition between genotypically
different but phenotypically similar strains should meet two
criteria: (i) the relative fraction of infected and uninfected
hosts should not depend on the frequency of either strain;
and (ii) the relative frequency of both strains should remain
stable for all time greater than zero. In other words, the struc-
ture of the model should not, in and of itself, generate
coexistence of indistinguishable strains, but mechanisms that
could induce coexistence should be introduced explicitly.
These principles suggest that the prior superinfection model
published by Koella & Antia [28] needs modification because,
as formulated, the model structure itself promotes coexistence.
In the electronic supplementary material, appendix SI, we
describe a model with similar properties to the Koella &
Antia superinfection model, in which homotypic superinfec-
tion was not allowed, and rigorously demonstrate that
coexistence is always an outcome of the model, even when
the resistant strain has a fitness cost.
To ensure that coexistence in our model of superinfection,
described earlier, is not an artefact of the model formulation,
we analysed a special case of the general form of the model,
in which the maximum MOI was two. In this case, the model
allows for both heterotypic superinfection and homotypic
superinfection. Numerical simulations confirm that in the
absence of drug treatment, drug-resistant parasites can neither
invade nor persist when they have a cost of resistance. We also
found that in the absence of either drug pressure or a biological
cost of resistance, the model is neutrally stable, provided
the transmission rate and the recovery rate of each type in a
heterotypic superinfection are exactly equal to each type
in a homotypic superinfection. In other words, the rate that
individuals become doubly infected with either the same type
or a different type must be equal, and the transmission rate of
heterotypic and homotypic infections must be the same regard-
less of strain composition, with an equal rate of transmission of
each type from heterotypic infections. Thus, the model in this
form does not predict coexistence when there is no specific
mechanism promoting its spread.
Both conditions remain true as MOI increases, provided
that the model structure maintains a triangular formulation
in which every possible combination of the maximum MOI
is included (i.e. in a model with a maximum MOI of three,
all possible states where the MOI is equal to three must be
possible: X3,0 and X2,1 and X1,2 and X0,3). Otherwise, the
model structurally creates a niche that allows for coexistence.
All our numerical simulations were done using a general
form of the model with the triangularity condition in place
and in which the maximum MOI was 30. Parameters used
in simulations were consistent with malaria epidemiologi-
cal literature [35,37,44], and are listed in the electronic
supplementary material, table S1.
(g) Frequency of resistance
We employ two measures of the frequency of resistance in
complex infections: (i) the fraction of the population that is
Proc. R. Soc. B (2012)
infected by at least one resistant strain, 1�P
i Xi;0; and
(ii) the fraction of the parasite load that is resistant,Pij j=ði þ jÞXi ; j: The former is important because it tracks
nearly exactly with the frequency that a treated clinical infec-
tion is resistant, which is the measure by which resistance is
often tracked in a population [45,46]. On the other hand, the
latter is particularly useful when discussing the role that
asymptomatic infections play in the spread of resistance.
3. RESULTSThe model is based on the ideas of malaria superinfection
as first laid out by Walton [24] and Macdonald [5] and
written down in equation form by Bailey [22]. However,
unlike previous models of drug resistance in malaria
[25,28], we explicitly model the effect of within-host
competition between drug-resistant and drug-sensitive
parasites. This allows for an examination of the impor-
tance of different types of fitness costs as well as how
competition affects the rate at which resistance spreads
across differential transmission rates.
To evaluate the model, we ran the system to equilibrium
without resistance and then introduced resistance at a low
frequency (1027). At low transmission rates (an annual
EIR of approximately one or less), the model predicts
that drug-resistant parasites will invade and spread,
and eventually dominate the drug-sensitive parasites.
However, as the transmission rate increases, the ability of
drug-resistant parasites to competitively exclude drug-
sensitive parasites decreases (see electronic supplementary
material, figure S1). This is because the mean MOI
increases with the intensity of transmission, measured in
terms of either vectorial capacity or EIR, and so compe-
tition increases. Thus, at low transmission rates, most
individuals are infected with approximately one infection
only, and the influence of within-host competition is
limited. As the mean MOI increases, it becomes more
difficult for resistant parasites to invade because competition
within the host increases, overcoming the ability of resistant
parasites to spread when they are rare. This is consistent with
historical suggestions that resistance to the former first-line
malaria drugs, CQ and SP, both emerged from areas of
low or unstable transmission [47,48]. Changing the drug
treatment rate for any particular transmission level increases
the competitive ability of resistant parasites, allowing them to
invade even when within-host competition increases at
higher transmission levels.
The model also predicts that superinfection modu-
lates coexistence. This result depends on the biological
fitness costs as well as the treatment rate. At high treatment
rates (80% of clinical infections treated), the drug-resistant
parasite competitively excludes the drug-sensitive parasite
at all fitness costs at low transmission. As the transmission
rate increases (annual EIR approx. 7), coexistence can
occur over a large range of fitness costs—even where the
fitness cost of clearance is zero (figure 2). At higher
transmission rates (annual EIR approx. 25), the range
over which coexistence is possible contracts. Lowering
the treatment rate (20% of clinical cases treated) shifts
the results and allows for coexistence at lower transmis-
sion rates, and shrinks the parameter range over which
coexistence can occur at higher transmission rates
(see electronic supplementary material, figure S2).

fitness cost of clearance (%)
013
2434
4350
56fitness cost
of transmission (%)7563
5343
per
cent
res
ista
nt
0204060
80
100
fitness cost of clearance (%)
013
2434
4350 fitness cost
of transmission (%)6343
2713
0
0204060
80
100
per
cent
res
ista
nt(a)
(b)
Figure 2. Fitness costs and coexistence. The cost of resist-ance can occur through either transmission or clearance.The transmission cost is measured as the relative differencein the contribution of resistant and sensitive parasites to
transmission when in equal abundance. The fitness cost ofclearance is measured as the reduction in the rate of clear-ance of a resistant parasite relative to a sensitive parasitewhen in competition. Thus, when there is little or no costof clearance but a significant cost of transmission, the
result is coexistence. As the transmission rate is increased(b), the parameter space over which coexistence can occuris abrogated. In addition, there are significant differences inthe range of each parameter over which coexistence canoccur. Areas of coexistence are marked by low to moderate
fitness costs of clearance and high costs of transmission.In fact, in low-transmission areas, resistant parasites cancoexist with sensitive parasites even when there is no fitnesscost of clearance. (a) Moderate transmission is defined as an
annual EIR of approximately 7, and (b) high transmission isan annual EIR of approximately 25. The treatment ratewas assumed to be 80%.
0 0.2 0.4 0.6
0
0.02
0.04
0.06
0.08
0.10
log of vectorial capacity
resi
stan
ce f
requ
ency
Figure 3. Measuring the frequency of resistance. There are
multiple ways to calculate the frequency of resistance in apopulation: (i) the prevalence of resistance (the fraction ofindividuals infected with a resistant parasite); (ii) the fractionof clinical infections that fail treatment; and (iii) the resist-ance load (the proportion of the parasite population that is
resistant). Depending on the measurement, the frequencyof resistance could be wildly different. To measure thesedifferences, we calculated the resistance load at the point intime when the percentage of clinical infections that faildrug treatment reached 10%. Although both measures
increase nearly concurrently at low transmission rates, astransmission increases (and thus so does competition), thefraction of the parasite population (dashed line) that is resist-ant soon peaks and then begins to fall, even as the proportion
of clinical infections harbouring resistant parasites (solidline) increases.
3838 E. Y. Klein et al. Superinfection and drug resistance
The fitness of drug-resistant parasites is proportional
to both the average duration of an infection and the ability
to transmit. The former is a function only of within-host
competition, whereas the latter is a function of both
within-host and among-host competition, because trans-
mission potential is a function of both transmissibility to
a susceptible vector (a function of competition between
clones within the host) and the propensity for infectious
vectors to infect a new host (the relative fraction of each
type). Results from the model suggest that resistant para-
sites can invade even with significant fitness costs of
transmission, but not when the fitness cost of clearance
increases significantly. This suggests that the ability to
remain competitively infectious within hosts is a stronger
determinant of the invasion capacity of drug-resistant
Proc. R. Soc. B (2012)
parasites than their probability of transmission at any
single event.
Competition also affects the rate that resistance
spreads in a population. At low transmission rates,
increasing the transmission intensity increases the rate
that resistance spreads in a population because, as noted
earlier, most infected individuals have an MOI of one
and there is no competition. Thus, the ability of drug-
resistant parasites to competitively exclude drug-sensitive
parasites increases as transmission increases. However, as
the average MOI increases and competition begins to
inhibit the ability of the drug-resistant parasite to exclude
drug-sensitive parasites, the rate at which resistance
spreads in a population decreases—or, stated another
way, the waiting time for resistance to reach a certain
threshold value grows longer (electronic supplementary
material, figure S3). This change is rapid at first, but as
the transmission rate continues to increase, the rate of
increase slows.
Superinfection also affects how the frequency of resist-
ance is calculated. Although the prevalence of resistance
(the fraction of infected people that harbour at least one
resistant parasite) increases concomitantly with the fraction
of the population that harbours at least one resistant para-
site, the resistance load (the proportion of types that are
resistant) changes at a different rate (figure 3). As the trans-
mission intensity increases, the resistance load increases at
a rate that is similar to the other measures. However, the
rate of increase slows after a point and then falls, while

Superinfection and drug resistance E. Y. Klein et al. 3839
the prevalence of resistance continues to increase. At
high transmission levels, this spread can be more than five
percentage points different when the fraction of clinical
infections reaches 10 per cent.
4. DISCUSSIONA prior model of superinfection in malaria with
drug-resistant and drug-sensitive parasites assumes that
heterotypic superinfection is possible but homotypic super-
infection is not [28]. However, this assumption means that
coexistence will always occur (see electronic supplementary
material, appendix SI). The structure of this prior model
[28] is also similar to earlier models of species coexistence
[29,30], which always predict coexistence unless there is
some type of competition in individuals heterotypically
superinfected. Thus, coexistence is an artefact of the math-
ematical model, not a generic property of the underlying
biological process.
In this paper, we replace those assumptions with a
model that implements a more robust competition frame-
work that allows for a thorough examination of the effect
of competition on the spread of drug-resistant malaria
parasites in an epidemiological context. We found general
conditions for the evolution of resistance as the outcome
of within- and among-host competition between two
classes of parasite types with differing fitness; the con-
ditions depend on competition, drug pressure and the
biological cost of resistance.
Results from a general model demonstrate that the
estimate of disease prevalence as a function of the trans-
mission rate was qualitatively similar to that found in
other models [5] and similar to estimates of the same
relationship in the field [49–51]. Our results also support
earlier studies showing a strong relationship between the
fitness cost of resistance and transmission [25,33].
When the fitness cost of resistance is low, drug-resistant
parasites are able to invade and spread across all trans-
mission levels. However, as the fitness cost of resistance
increases, the ability of drug-resistant parasites to invade
and spread is reduced. One possible reason previously
suggested for this relationship is that the parasite is exposed
to a higher level of drug pressure per infection in low-
transmission areas because a higher fraction of infections
in these areas result in clinical symptoms [33]. Our results
suggest that the low force of infection when recolonization
of infected individuals is rare plays a significant role in
low-transmission areas as well. After drug use eliminates
drug-sensitive parasites, individuals harbouring resistant
parasites are less likely to be recolonized by drug-sensitive
parasites, reducing within-host competition.
Although a biological cost of resistance has been
measured in in vitro experiments [52,53] and estimated
from the field [11,12], reductions in the competitive abil-
ity of the parasite are not expected to be equal across
different axes of competition. This has significant biologi-
cal and epidemiological importance. On the basis of
in vitro experiments in which CQ-resistant parasites had
an estimated 25 per cent loss of fitness per generation
[52], as well as murine models demonstrating slower
growth of drug-resistant parasites in the mouse [54,55],
it has been suggested that mutations conferring resistance
decrease the reproductive efficiency of the parasite and
slow growth [10]. The end result of the lower growth
Proc. R. Soc. B (2012)
rate is assumed to be a decrease in the probability of a
parasite being transmitted when a mosquito feeds on
blood because of the lower relative numbers of gameto-
cytes. A similar mechanism is also presumed to affect
the duration of infection; however, evidence on the rela-
tive cost of resistance on clearance is lacking, particular
in relation to transmissibility. We found that although
the reductions in transmission probability were impor-
tant, the ability to persist in an infection may be a more
important measure of the resistant parasite’s competi-
tive ability, particularly in lower-transmission settings.
These results can be partly explained by the vast time-
scale differences between these processes. Because the
time from infection of a susceptible mosquito to infection
of a human is an order of magnitude faster than the dur-
ation of infection, the benefit of increasing the duration of
infection is significantly greater than the benefit of
increasing infectiousness within an infection. The result
is that resistant parasites can invade even with significant
fitness costs of transmission, but not when the fitness cost
of clearance increases significantly.
Because the parasite has evolved an extremely long
duration of infection to maximize transmission opportu-
nities and can transmit efficiently at very low densities
[56], it is not surprising that the effect of changes in the
clearance rate is more pronounced on the viability of
drug-resistant parasites than on reductions in trans-
mission. However, the effect on attempts to control the
spread of resistance is important. Recent evidence has
shown the emergence of a delayed clearance phenotype
to the drug artemisinin in western Cambodia [57],
which has led to calls for implementing a resistance
containment strategy. Our results suggest that interven-
tions that can shorten the duration of infection for
resistant parasites, such as mass drug administration or
mass screening and treating, may be more beneficial
than has been recognized by earlier models that ignored
superinfection [58].
Within-host competition can also produce coexistence
of the two different parasite phenotypes at the population
level. Coexistence can occur when the relative advantage
of the sensitive parasite, measured as transmission poten-
tial over recovery rate, is greater in mixed infections.
However, the parameter range over which coexistence
can occur is altered by the transmission rate. At low
transmission rates, competition is lessened between
different phenotypes as well as with the same phenotypes.
Individuals with drug-resistant parasites can then be
easily reinfected because they have only a few parasites.
Thus, if drug-sensitive parasites have an advantage in
mixed infections, the result for a fixed treatment rate
will be a greater tendency to coexist. On the other
hand, as the transmission rate increases, individuals who
are treated with drugs are likely to harbour multiple
drug-resistant parasite clones. In this case, the invasion
capability of drug-sensitive parasites is reduced, making
the range over which coexistence can occur smaller.
In terms of designing control strategies, the time until
resistance reaches a critical level, which is critically influ-
enced by the transmission and treatment rates, may be a
more important measure than the final equilibrium level
of resistance. Currently, there is no standardized method-
ology for assessing the frequency of resistance, though it is
generally measured as the proportion of a type specimen

3840 E. Y. Klein et al. Superinfection and drug resistance
isolated from a clinical infection that did not adequately
respond to treatment [46]. However, screening surveys
of the human population using in vitro tests to determine
resistance of a type specimen has also been suggested as a
means to ascertain the frequency of resistance in the
population [59]. These sampling mechanisms are not
identical when individuals have complex infections,
and it is important to understand how these sampling
differences may end up measuring radically different
quantities. In high-transmission areas, when the fre-
quency of resistance is low, complex infections will
primarily consist of drug-sensitive parasites. Because
sampling is imperfect, the probability of false negatives
(i.e. at least one resistant parasite is present but was not
detected) is high [45], which suggests that random
screening surveys as a measure of resistance in higher-
transmission areas may result in biased results. This is
probably also true when withdrawing a drug. For
instance, even though the detection of CQ-resistant
mutations has dropped to undetectable levels in Malawi
[11,60], the complexity of malaria infections suggests
that drug-resistant parasites may still be present at low fre-
quencies and that the reintroduction of CQ may be
followed by a rapid resurgence in resistant infections.
In this model of malaria superinfection, which was
extended to incorporate competition between drug-sensi-
tive and drug-resistant parasites, our results are limited to
examining only the axis of competition between drug-
resistant and drug-sensitive phenotypes. The evolution
of antimalarial drug resistance is obviously a complicated
process involving superinfection and many interacting
processes, including immunity [25], the patterns of
drug use and heterogeneous biting [49]. The results of
this simple model clearly demonstrate that within-host
competition is a significant component in the emergence
and spread of drug resistance even at lower transmission
rates. Models that examine the best ways to control or
contain the emergence of resistance must take account
of superinfection and a variable degree of within-host
competition across the spectrum of transmission. In par-
ticular, the assumption of a blanket fitness cost of
resistance is less reasonable when the duration of infec-
tion dominates the probability that resistance will
spread. Future studies in this area will include how het-
erogeneous biting by the mosquito vector changes the
dynamics of competition, particularly in low-transmission
areas, and how host immunity interacts with virulence to
change the dynamics of the emergence of drug resistance.
This work was funded by Princeton University’s HealthGrand Challenges Program. This publication was alsomade possible by grant no. 1R01GM100471-01 from theNational Institute of General Medical Sciences (NIGMS)at the National Institutes of Health. Its contents are solelythe responsibility of the authors and do not necessarilyrepresent the official views of NIGMS. E.Y.K. wassupported by Princeton University (Harold W. DoddsFellowship). D.L.S. is funded by the RAPIDD program ofthe Science and Technology Directorate, Department ofHomeland Security, and the Fogarty International Center,National Institutes of Health.
REFERENCES1 Ehrlich, P. 1913 Address in pathology, ON CHE-
MIOTHERAPY. Delivered before the Seventeenth
Proc. R. Soc. B (2012)
International Congress of Medicine. Br. Med. J. 2,353–359. (doi:10.1136/bmj.2.2746.353)
2 Levin, S. & Pimentel, D. 1981 Selection of intermediate
rates of increase in parasite–host systems. Am. Nat. 117,308–315. (doi:10.1086/283708)
3 Nowak, M. A. & May, R. M. 1994 Superinfection andthe evolution of parasite virulence. Proc. R. Soc. Lond.B 255, 81–89. (doi:10.1098/rspb.1994.0012)
4 van Baalen, M. & Sabelis, M. W. 1995 The dynamics ofmultiple infection and the evolution of virulence. Am.Nat. 146, 881. (doi:10.1086/285830)
5 Macdonald, G. 1950 The analysis of infection rates in
diseases in which superinfection occurs. Trop. Dis. Bull.47, 907–915.
6 McKenzie, F. E., Smith, D. L., O’Meara, W. P., Riley,E. M., Rollinson, D. & Hay, S. I. 2008 Strain theory ofmalaria: the first 50 years. Adv. Parasitol. 66, 1–46.
(doi:10.1016/S0065-308X(08)00201-7)7 Paul, R., Hackford, I., Brockman, A., Muller-Graf, C.,
Price, R., Luxemburger, C., White, N., Nosten, F. &Day, K. 1998 Transmission intensity and Plasmodiumfalciparum diversity on the northwestern border of
Thailand. Am. J. Trop. Med. Hyg. 58, 195–203.8 White, N. J. 2004 Antimalarial drug resistance. J. Clin.
Invest. 113, 1084–1092.9 Felger, I. & Beck, H.-P. 2008 Fitness costs of resistance
to antimalarial drugs. Trends Parasitol. 24, 331–333.
(doi:10.1016/j.pt.2008.05.004)10 Babiker, H. A., Hastings, I. M. & Swedberg, G. 2009
Impaired fitness of drug-resistant malaria parasites: evi-dence and implication on drug-deployment policies.
Expert Rev. Anti-Infect. Ther. 7, 581–593. (doi:10.1586/eri.09.29)
11 Laufer, M. K., Thesing, P. C., Eddington, N. D.,Masonga, R., Dzinjalamala, F. K., Takala, S. L.,Taylor, T. E. & Plowe, C. V. 2006 Return of chloroquine
antimalarial efficacy in Malawi. N Engl. J. Med. 355,1959–1966. (doi:10.1056/NEJMoa062032)
12 De-quan, L. et al. 1995 Changes in the resistance of Plas-modium falciparum to chloroquine in Hainan, China. Bull.World Health Organ. 73, 483–486.
13 Levin, S. A. 1983 Some approaches to the modelling of co-evolutionary interactions. In Coevolution (ed. M. Ntecki),pp. 21–65. Chicago, IL: University of Chicago Press.
14 Levin, S. A. 1983 Coevolution. Lect. Notes Biomath. 52,328–334. (doi:10.1007/978-3-642-87893-0_41)
15 Daubersies, P., Sallenave-Sales, S., Magne, S., Trape,J. F., Contamin, H., Fandeur, T., Rogier, C.,Mercereau-Puijalon, O. & Druilhe, P. 1996 Rapid turn-over of Plasmodium falciparum populations in
asymptomatic individuals living in a high transmissionarea. Am. J. Trop. Med. Hyg. 54, 18–26.
16 Arnot, D. 1998 Clone multiplicity of Plasmodium falci-parum infections in individuals exposed to variablelevels of disease transmission. Trans. R. Soc. Trop. Med.Hyg. 92, 580–585. (doi:10.1016/S0035-9203(98)90773-8)
17 Taylor, L. H., Walliker, D. & Read, A. F. 1997 Mixed-genotype infections of malaria parasites: within-hostdynamics and transmission success of competing
clones. Proc. R. Soc. Lond. B 264, 927–935. (doi:10.1098/rspb.1997.0128)
18 Snounou, G., Jarra, W., Viriyakosol, S., Wood, J. C. &Brown, K. N. 1989 Use of a DNA probe to analyse thedynamics of infection with rodent malaria parasites con-
firms that parasite clearance during crisis is predominantlystrain- and species-specific. Mol. Biochem. Parasitol. 37,37–46. (doi:10.1016/0166-6851(89)90100-x)
19 De Roode, J., Read, A., Chan, B. & Mackinnon, M. 2003Rodent malaria parasites suffer from the presence of
Superinfection and drug resistance E. Y. Klein et al. 3841
conspecific clones in three-clone Plasmodium chabaudiinfections. Parasitology 127, 411–418. (doi:10.1017/S0031182003004001)
20 Dietz, K. 1988 Mathematical models for transmissionand control of malaria. In Malaria: principles and practiceof malariology (eds W. H. Wernsdorfer & I. A. McGregor),pp. 1091–1134. Edinburgh, UK: Churchill Livingstone.
21 Fine, P. 1975 Superinfection: a problem in formulating a
problem. Bur. Hyg. Trop. Dis. 72, 475–488.22 Bailey, N. T. J. 1982 The biomathematics of malaria.
London, UK: C. Griffin & Co.23 Dietz, K., Molineaux, L. & Thomas, A. 1974 A malaria
model tested in the African savannah. Bull. World HealthOrgan. 50, 347–357.
24 Walton, G. 1947 On the control of malaria in Freetown,Sierra Leone: 1. Plasmodium falciparum and Anophelesgambiae in relation to malaria occurring in infants. Ann.Trop. Med. Parasitol. 41, 380–407.
25 Klein, E. Y., Smith, D. L., Boni, M. F. & Laxminarayan,R. 2008 Clinically immune hosts as a refuge for drug-sensitive malaria parasites. Malar. J. 7, 67. (doi:10.1186/1475-2875-7-67)
26 Aneke, S. J. 2002 Mathematical modelling of drug resist-ant malaria parasites and vector populations. Math.Methods Appl. Sci. 25, 335–346. (doi:10.1002/mma.291)
27 Esteva, L., Gumel, A. B. & de Leon, C. V. 2009 Qualitat-ive study of transmission dynamics of drug-resistant
malaria. Math. Comput. Model 50, 611–630. (doi:10.1016/j.mcm.2009.02.012)
28 Koella, J. & Antia, R. 2003 Epidemiological models forthe spread of anti-malarial resistance. Malar. J. 2, 3.
(doi:10.1186/1475-2875-2-3)29 Slatkin, M. 1974 Competition and regional coexistence.
Ecology 55, 128–134. (doi:10.2307/1934625)30 Cohen, J. E. 1970 A Markov contingency-table model for
replicated Lotka–Volterra systems near equilibrium. Am.Nat. 104, 547–560. (doi:10.1086/282689)
31 Wargo, A. R., Huijben, S., de Roode, J. C., Shepherd, J. &Read, A. F. 2007 Competitive release and facilitation ofdrug-resistant parasites after therapeutic chemotherapyin a rodent malaria model. Proc. Natl Acad. Sci. USA104, 19 914–19 919. (doi:10.1073/pnas.0707766104)
32 O’Meara, W. P., Smith, D. L. & McKenzie, F. E. 2006Potential impact of intermittent preventive treatment(IPT) on spread of drug-resistant malaria. PLoS Med.3, e141. (doi:10.1371/journal.pmed.0030141)
33 Hastings, I. M. 1997 A model for the origins and spreadof drug-resistant malaria. Parasitology 115, 133–141.(doi:10.1017/S0031182097001261)
34 Hastings, I. M. 2006 Complex dynamics and stability
of resistance to antimalarial drugs. Parasitology 132,615–624. (doi:10.1017/S0031182005009790)
35 Smith, D. L., Battle, K. E., Hay, S. I., Barker, C. M.,Scott, T. W. & McKenzie, F. E. 2012 Ross, Macdonald,and a theory for the dynamics and control of mosquito-
transmitted pathogens. PLoS Pathog. 8, e1002588.(doi:10.1371/journal.ppat.1002588)
36 Macdonald, G. 1957 The epidemiology and control ofmalaria. London, UK: Oxford University Press.
37 Smith, D. L. & McKenzie, F. E. 2004 Statics and
dynamics of malaria infection in Anopheles mosquitoes.Malar. J. 3, 13. (doi:10.1186/1475-2875-3-13)
38 Medica, D. L. & Sinnis, P. 2005 Quantitative dynamics ofPlasmodium yoelii sporozoite transmission by infectedAnopheline mosquitoes. Infect. Immun. 73, 4363–4369.
(doi:10.1128/IAI.73.7.4363-4369.2005)39 Shute, P. G. 1945 An investigation into the number of
sporozoites found in the salivary glands of Anopheles mos-quitoes. Trans. R. Soc. Trop. Med. Hyg. 38, 493–498.(doi:10.1016/0035-9203(45)90058-7)
Proc. R. Soc. B (2012)
40 Rosenberg, R., Wirtz, R. A., Schneider, I. & Burge, R.1990 An estimation of the number of malaria sporo-zoites ejected by a feeding mosquito. Trans. R. Soc.Trop. Med. Hyg. 84, 209–212. (doi:10.1016/0035-9203(90)90258-G)
41 Druilhe, P., Daubersies, P., Patarapotikul, J., Gentil, C.,Chene, L., Chongsuphajaisiddhi, T., Mellouk, S. &Langsley, G. 1998 A primary malarial infection is com-
posed of a very wide range of genetically diverse butrelated parasites. J. Clin. Invest. 101, 2008–2016.(doi:10.1172/JCI119890)
42 Sinden, R. E. & Billingsley, P. F. 2001 Plasmodium inva-
sion of mosquito cells: hawk or dove? Trends Parasitol.17, 209–211. (doi:10.1016/S1471-4922(01)01928-6)
43 Lipsitch, M., Colijn, C., Cohen, T., Hanage, W. P. &Fraser, C. 2009 No coexistence for free: neutral nullmodels for multistrain pathogens. Epidemics 1, 2.
(doi:10.1016/j.epidem.2008.07.001)44 Garrett-Jones, C. 1964 The human blood index of
malaria vectors in relation to epidemiological assessment.Bull. World Health Organ. 30, 241–261.
45 Hastings, I. M., Nsanzabana, C. & Smith, T. A. 2010A comparison of methods to detect and quantifythe markers of antimalarial drug resistance. Am. J.Trop. Med. Hyg. 83, 489–495. (doi:10.4269/ajtmh.2010.10-0072)
46 Bloland, P. B., Kazembe, P. N., Oloo, A. J., Himonga, B.,
Barat, L. M. & Ruebush, T. K. 1998 Chloroquine inAfrica: critical assessment and recommendations formonitoring and evaluating chloroquine therapy efficacyin sub-Saharan Africa. Trop. Med. Int. Health 3,
543–552. (doi:10.1046/j.1365-3156.1998.00270.x)47 White, N. J. 1998 Preventing antimalarial drug resistance
through combinations. Drug Resist. Updates 1, 3–9.(doi:10.1016/S1368-7646(98)80208-2)
48 White, N. J. & Pongtavornpinyo, W. 2003 The de novoselection of drug-resistant malaria parasites.Proc. R. Soc. Lond. B 270, 545–554. (doi:10.1098/rspb.2002.2241)
49 Smith, D. L., Dushoff, J., Snow, R. W. & Hay, S. I. 2005The entomological inoculation rate and Plasmodiumfalciparum infection in African children. Nature 438,492–495. (doi:10.1038/nature04024)
50 Smith, D. & Hay, S. 2009 Endemicity response timelinesfor Plasmodium falciparum elimination. Malar J 8, 87.(doi:10.1186/1475-2875-8-87)
51 Sama, W., Owusu-Agyei, S., Felger, I., Dietz, K. &Smith, T. 2006 Age and seasonal variation in the tran-sition rates and detectability of Plasmodium falciparummalaria. Parasitology 132, 13–21. (doi:10.1017/
S0031182005008607)52 Hayward, R., Saliba, K. J. & Kirk, K. 2005 pfmdr1
mutations associated with chloroquine resistance incur afitness cost in Plasmodium falciparum. Mol. Microbiol. 55,1285–1295. (doi:10.1111/j.1365-2958.2004.04470.x)
53 Peters, J. M., Chen, N., Gatton, M., Korsinczky, M.,Fowler, E. V., Manzetti, S., Saul, A. & Cheng, Q. 2002Mutations in cytochrome b resulting in atovaquoneresistance are associated with loss of fitness in Plasmodiumfalciparum. Antimicrob. Agents Chemother. 46, 2435–2441.
(doi:10.1128/aac.46.8.2435-2441.2002)54 Chawira, A. N., Warhurst, D. C. & Peters, W. 1986 Qin-
ghaosu resistance in rodent malaria. Trans. R. Soc. Trop.Med. Hyg. 80, 477–480. (doi:10.1016/0035-9203(86)90351-2)
55 Walliker, D., Hunt, P. & Babiker, H. 2005 Fitnessof drug-resistant malaria parasites. Acta Trop. 94,251–259. (doi:10.1016/j.actatropica.2005.04.005)
56 Barnes, K. I. & White, N. J. 2005 Population biology andantimalarial resistance: the transmission of antimalarial

3842 E. Y. Klein et al. Superinfection and drug resistance
drug resistance in Plasmodium falciparum. Acta Trop. 94,230–240. (doi:10.1016/j.actatropica.2005.04.014)
57 Dondorp, A. M., Yeung, S., White, L., Nguon, C.,
Day, N. P. J., Socheat, D. & von Seidlein, L. 2010 Arte-misinin resistance: current status and scenarios forcontainment. Nat. Rev. Microbiol. 8, 272–280. (doi:10.1038/nrmicro2331)
58 Pongtavornpinyo, W., Yeung, S., Hastings, I., Dondorp,
A., Day, N. & White, N. 2008 Spread of anti-malarialdrug resistance: mathematical model with implicationsfor ACT drug policies. Malar. J. 7, 229. (doi:10.1186/1475-2875-7-229)
Proc. R. Soc. B (2012)
59 Picot, S., Olliaro, P., de Monbrison, F., Bienvenu, A. L.,Price, R. N. & Ringwald, P. 2009 A systematic review andmeta-analysis of evidence for correlation between mol-
ecular markers of parasite resistance and treatmentoutcome in falciparum malaria. Malar. J. 8, 89. (doi:10.1186/1475-2875-8-89)
60 Laufer, M. K., Takala-Harrison, S., Dzinjalamala,F. K., Stine, O. C., Taylor, T. E. & Plowe, C. V.
2010 Return of chloroquine-susceptible falciparummalaria in Malawi was a reexpansion of diverse sus-ceptible parasites. J. Infect. Dis. 202, 801–808. (doi:10.1086/655659)
Related Documents











