Suits and Cases: Potential Pitfalls in the management of Poisoned Patients John Kashani DO St. Josephs Regional Medical Center New Jersey Poison Center

Suits and Cases: Potential Pitfalls in the management of Poisoned Patients John Kashani DO St. Josephs Regional Medical Center New Jersey Poison Center.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Suits and Cases: Potential Pitfalls in the management of
Poisoned Patients
John Kashani DO
St. Josephs Regional Medical Center
New Jersey Poison Center
Case 1
• An 18 year old female, with a past medical history significant for asthma and depression, presents to the ED for shortness of breath
• She has a respiratory rate of 34, is diaphoretic, is actively vomiting and appears confused
Case 1
• Her blood pressure is 90/54, Heart rate is 150 and a rectal temperature is 102
.
farenheit and pulse oximetry is 99% on supplemental oxygen
• Her mother states that this is the worst asthma attack she has ever had
• She is emergently intubated
Case 1
• Shortly after being intubated she seizes and develops ventricular fibrilation
• Despite your best efforts she dies
• An autopsy is requested by the family
• A post mortem salicylate level was 150mg/dL
Introduction
• Salicylates are the most widely used analgesic, anti-pyretic and anti-inflamatory and is the standard for the comparison and evaluation of others
• Because salicylates are so widely available the potential for misuse is often underappreciated

Introduction
• The physician taking care of the salicylate intoxicated patient must be familiar with the pathophysiology, pharmakokinetics, potential pitfalls, and treatment options
Sources of Salicylates
• Found in Willow bark (Salix alba vulgaris)• Available in a multitude of
formulas/preparations– Over-the-counter (pepto-bismol)– Topical preparation (wart removal)– Combinations (excedrin, fiorinal,
percodan)– Other (oil of wintergreen)
Pharmakokinetics
• Peak levels – Regular preparations – Enteric coated– Liquids preparations– Overdose
• Distribution• Metabolism• Excretion
Distribution
• Volume of distribution (Vd)
– Apparent volume the drug is dissolved in
– Measured in Liters or Liters/Kg
• not a real volume

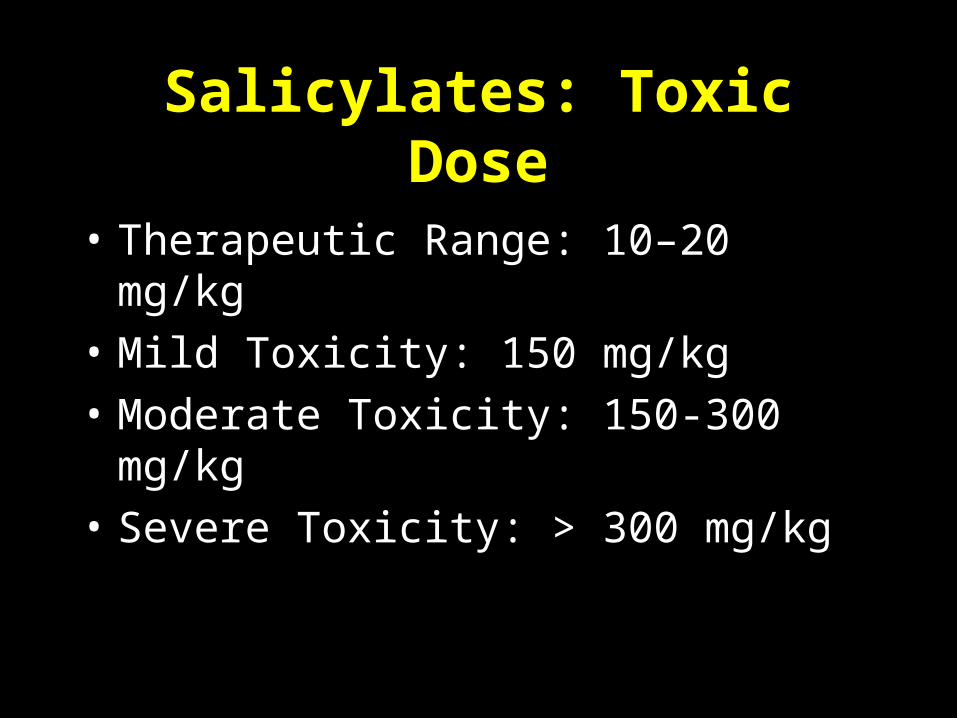
Salicylates: Toxic Dose
• Therapeutic Range: 10–20 mg/kg
• Mild Toxicity: 150 mg/kg
• Moderate Toxicity: 150-300 mg/kg
• Severe Toxicity: > 300 mg/kg

Inflamatory Mediators
• Inhibits cyclooxygenase
– Decrease in prostaglandins
– Increase leukotrienes
• Increases microvascular permeability
acetyl-CoA
oxaloacetate citrate
isocitrate
-ketoglutarate
succinyl-CoAsuccinate
fumarate
malateNAD+
NADH
NAD+
NADH
NAD+
NADH
FAD
FADH2
pyruvate
CO2
CO2
CO2
NAD+
NADH
matrix
Glucose
Pyruvate Lactate
2 ATP
ALT
Muscle
Alanine
Liver
Alanine
Pyruvate
Glucose
NH2
Urea6 ATP
4 ATP
X
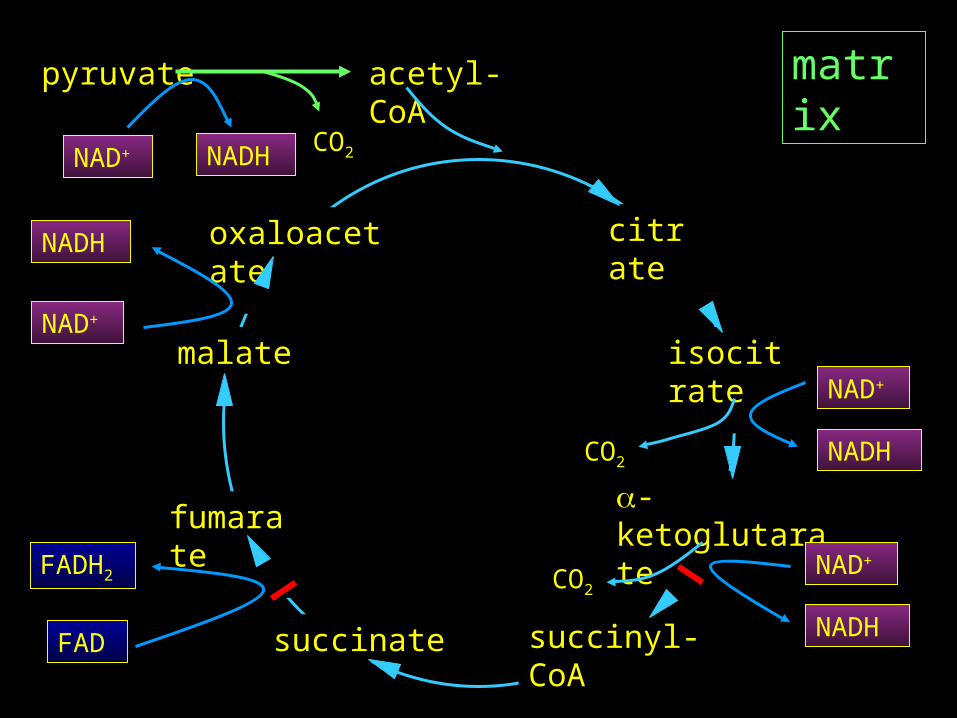
Respiration
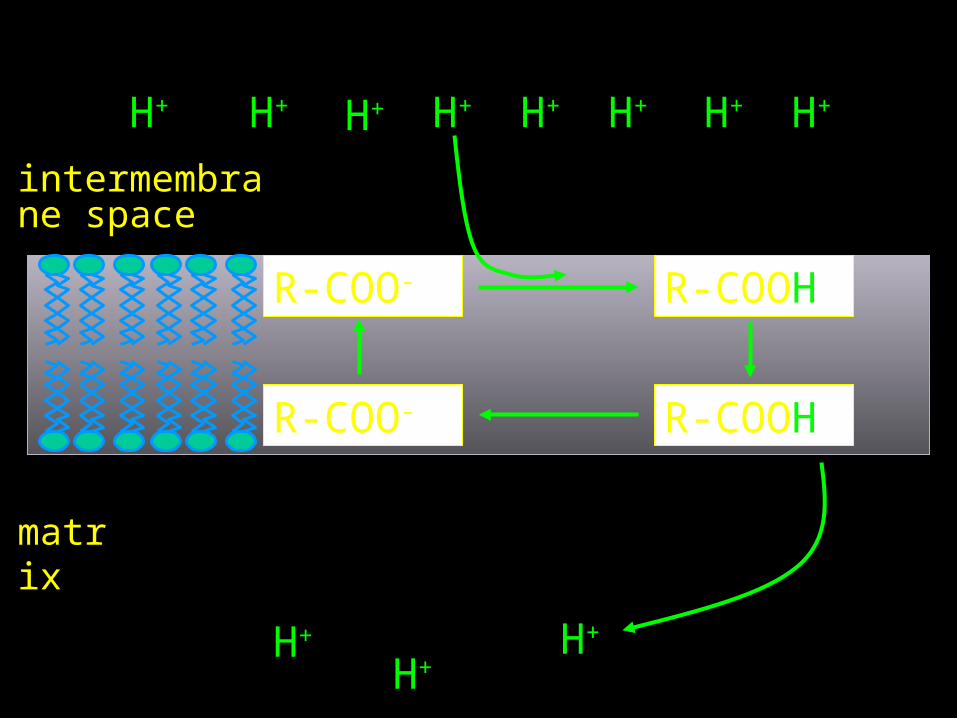
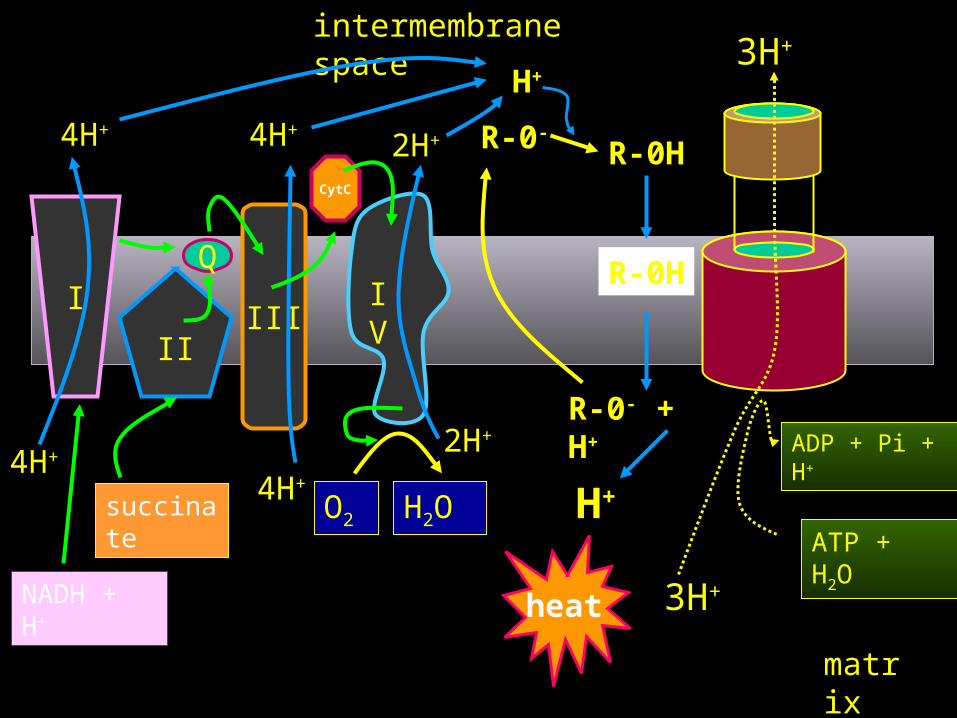
• Uncouples oxidative phosphorylation– Disrupts hydrogen ion gradient– Unable to generate ATP using electron
transport• Increased oxygen consumption,
increased heat production, increased metabolic rate, decreased ATP production, increased CO2 production
R-COOH
matrix
intermembrane space
H+ H+ H+ H+ H+ H+ H+ H+
H+ H+
H+
R-COOHR-COO-
R-COO-
I
matrix
intermembrane space
II
Q
4H+
4H+
III
4H+
4H+
IV
CytC
O2 H2O
2H+
2H+
succinate
NADH + H+
ATP + H2O
ADP + Pi + H+
3H+
3H+
R-0H
R-0H
R-0- + H+
H+
R-0-
H+
heat
Metabolic
• Increased lipolysis
• Increased production of ketones
– Ketonuria present in almost all overdose patients
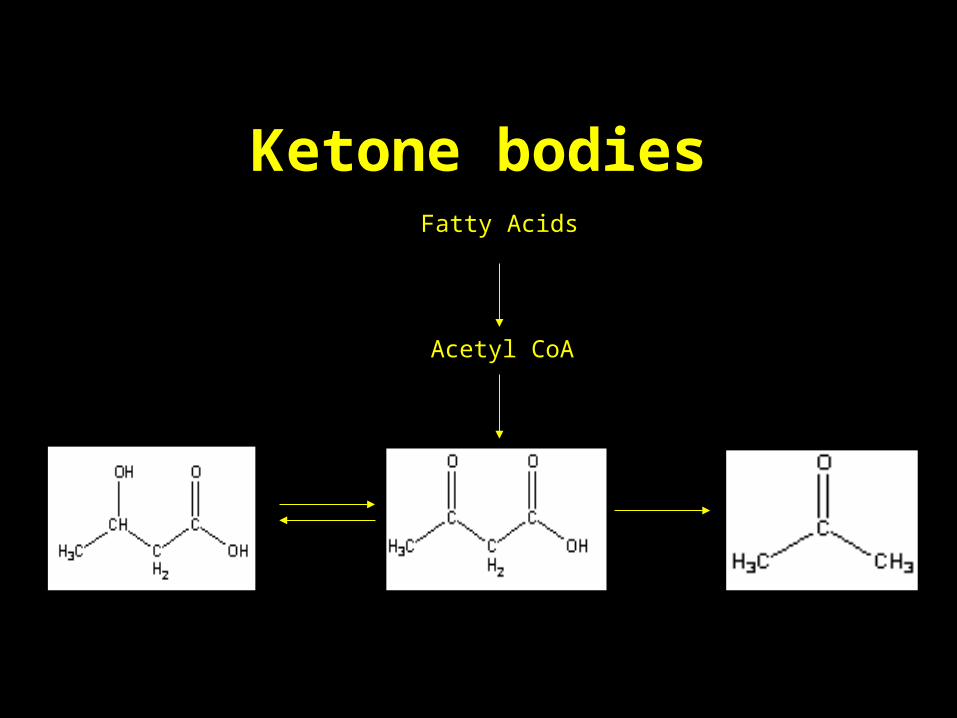
Ketone bodies
Acetyl CoA
Fatty Acids
Metabolic
• Hyperglycemia in acute setting
– Glycogenolysis
– May cause glucosuria
• Hypoglycemia may subsequently develop
Metabolic
• Causes a respiratory alkalosis
– Due to respiratory center stimulation
– Increase in respiratory rate and depth
Hematologic
• Platelet dysfunction• Inhibition of Vitamin K dependent
clotting factors• II, VII, IX, X, Protein C, Protein S
• Hypoprothrombinemia
Gastrointestinal Effects
• Nausea
• Vomiting
• Gastritis
• Pylorospasm
Neurologic• Occurs from metabolic derangements and
salicylate CNS levels– Agitation, irritability– Tinnitus
• Occurs at levels of 20-45 mg/dL– Lethargy

Laboratories
• Salicylate Level
– An Level of 100 mg/dL is extremely worrisome (impending doom)
– Chronic Levels of > 30 mg/dL are concerning
• Difficulty in interpretation due to variable Vd

Laboratories
• Levels should be obtained every 1 to 2 hours until downward trend is observed
• Do not rely on a single level• Levels < 20mg/dl and a downward trend
can be medically cleared
Case 2
• A 35 year old male presents to the emergency department for profound weakness, bradycardia and emesis
• An I stat potassium is 8.5mg/dL and an EKG show a sine wave pattern
• IV Calcium chloride is administered and he develops ventricular fibrilitation shortly thereafter
Case 2
• Despite your best efforts he dies
• The wife said he has no medical problems, but was recently doing a “cleansing diet” that included herbal teas
Introduction
• Digitalis and digitalis like cardiac glycosides (DG’s) are found in a variety plants, toads and pharmaceutical agents
• Dried powders and extracts have been used for centuries for medicinal agents and as arrow poisons








Pharmacokinetics
• Peak serum concentrations occur in minutes with IV dosing and 1-2 hours after an oral dose
• The VD is initially small and increases following a two phase compartment model– Higher in infants and neonates and
lower in the elderly

Pharmacokinetics
• Tissue distribution takes 6-12 hours
• Digoxin crosses the placenta with fetal levels approaching that of the mother
• Elimination
– Hepatic metabolism
– Urinary excretion of unchanged drug
Pathophysiology
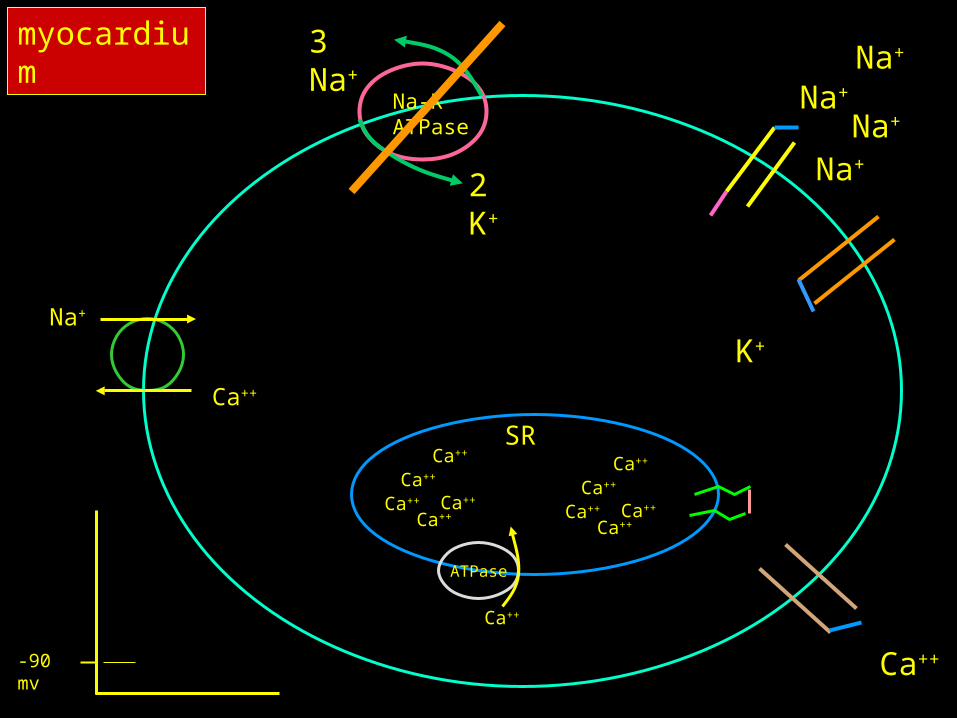
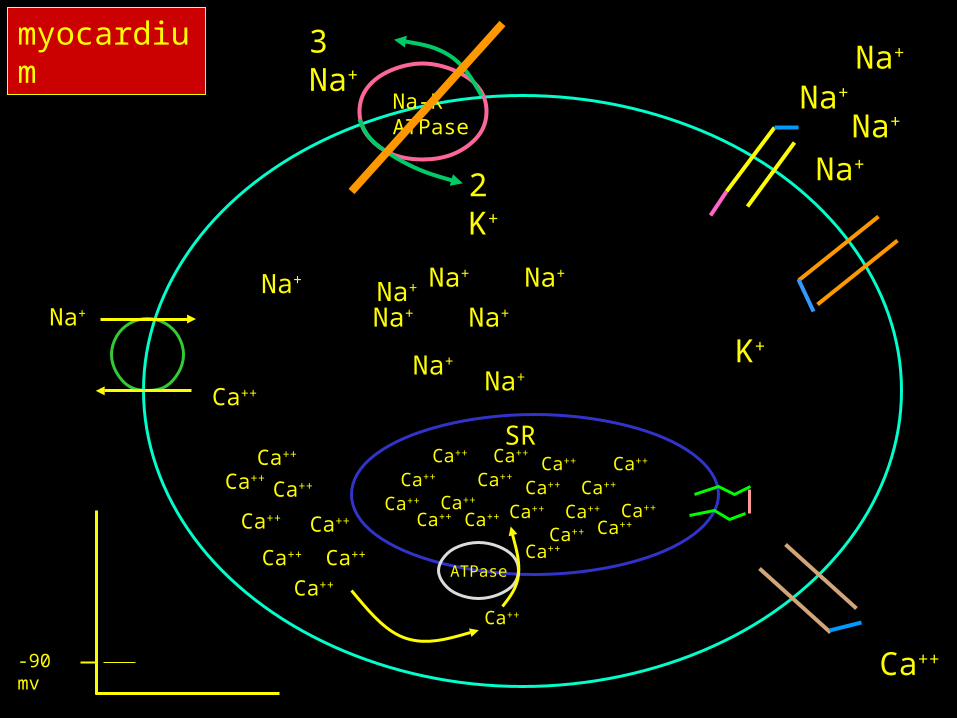
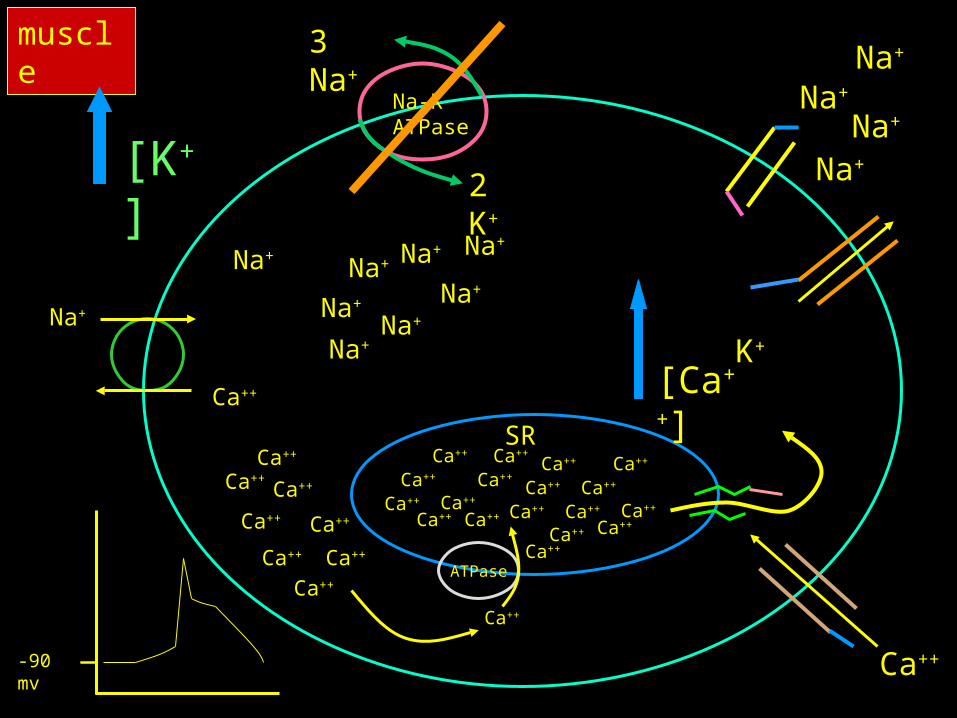
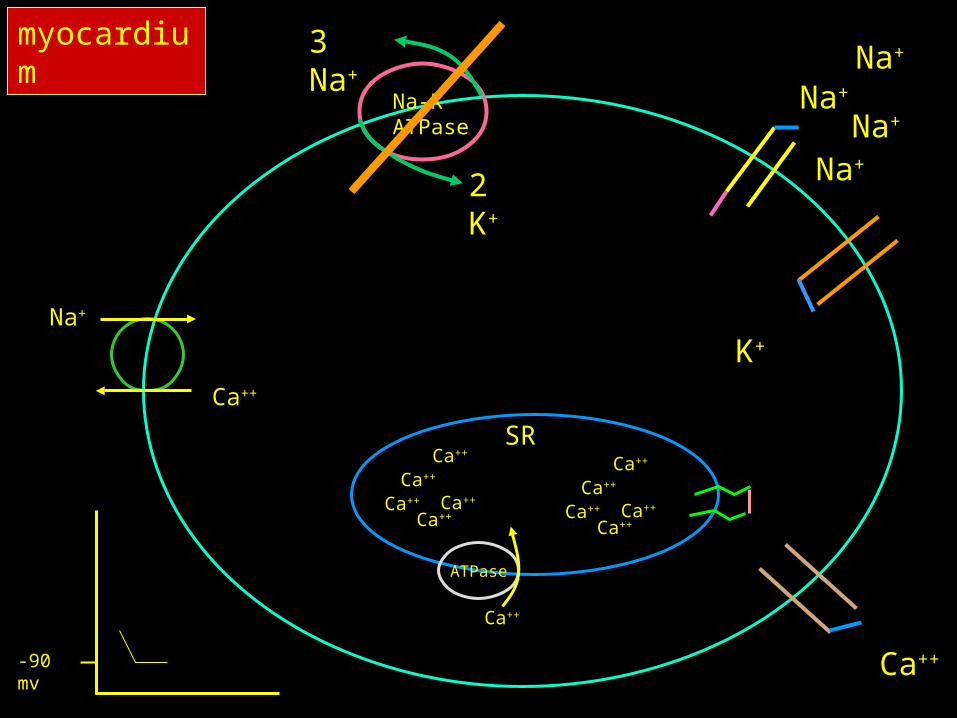
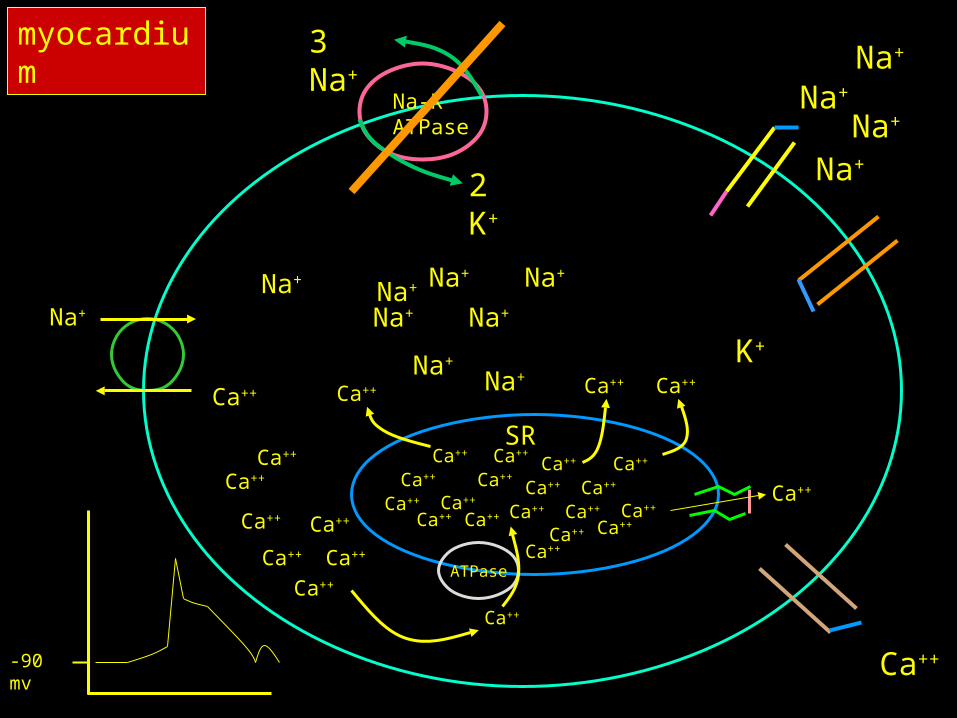
• Cardiac glycosides inhibit the sodium potassium atp-ase
– Responsible for pumping two sodium ions out of the cell for every two potassium ions in to the cell
3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Ca++
Na+

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Na+
Na+
Ca++
Na+
3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Na+

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
[Ca++]Ca++
Na+
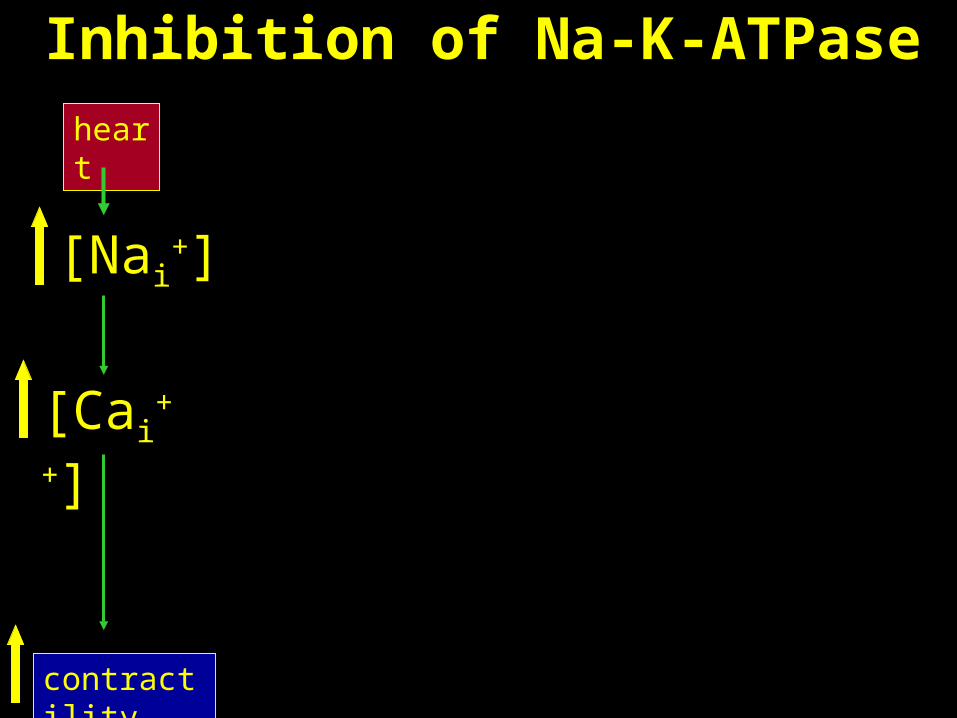
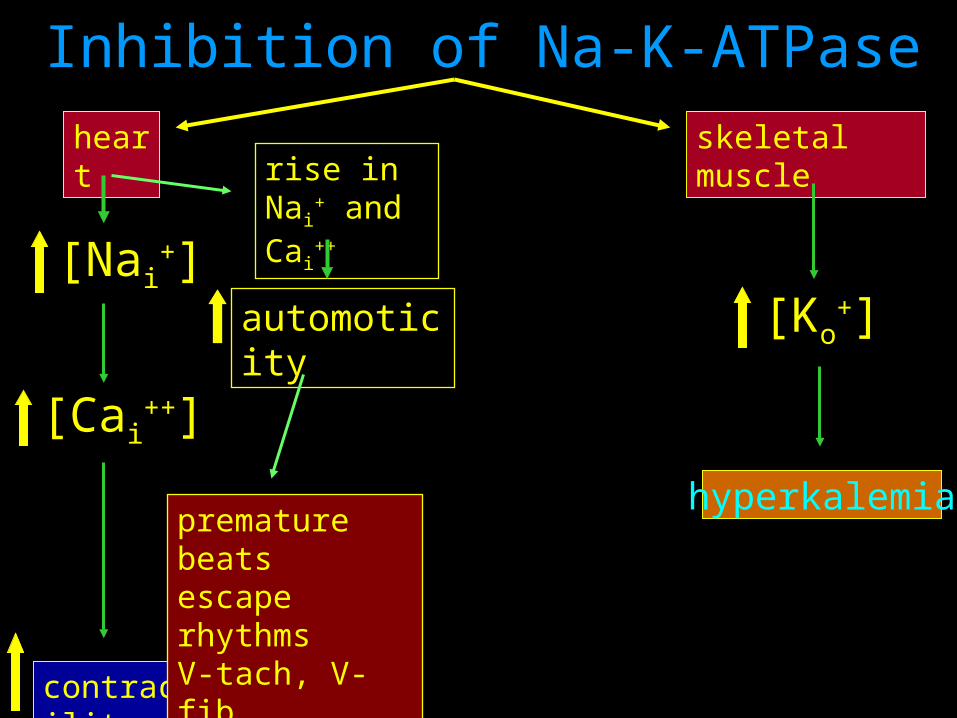
Inhibition of Na-K-ATPase
[Nai+]
[Cai++]
heart
contractility
3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
muscle
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
[Ca++]
[K+]
Ca++
Na+
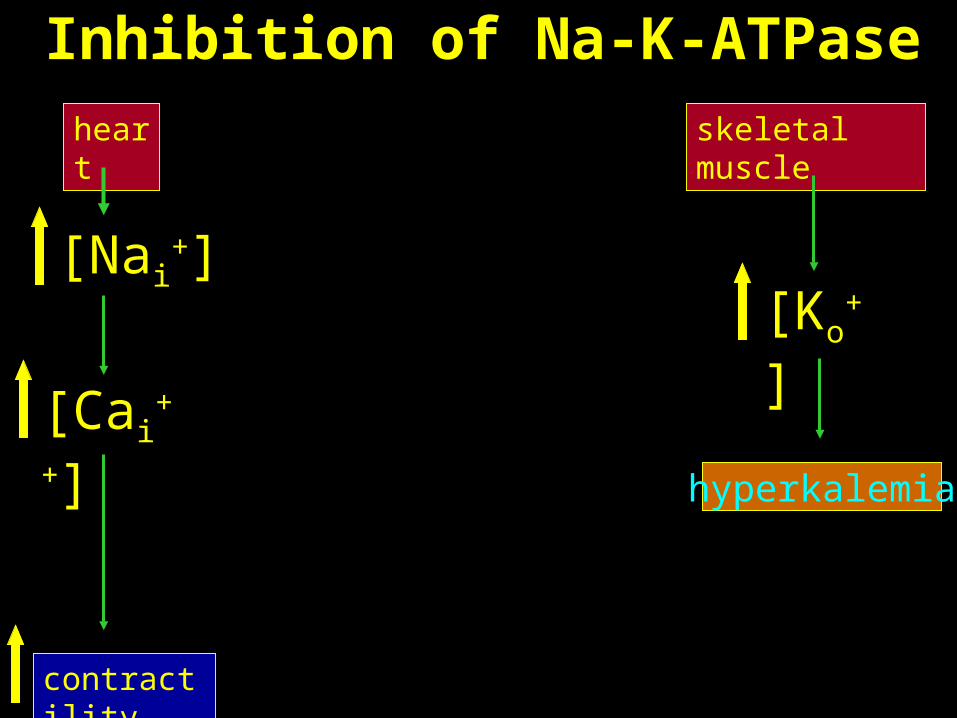
Inhibition of Na-K-ATPase
[Nai+]
[Ko+]
hyperkalemia
[Cai++]
skeletal muscleheart
contractility
3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Ca++
Na+

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
Ca++ Ca++
Ca++
Ca++
Na+
3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
Ca++ Ca++
Ca++
Ca++
Na+

-90 mv
premature beat or ectopic focus
increased automoticity
late afterdepolarizations
Inhibition of Na-K-ATPase
[Nai+]
[Ko+]
hyperkalemia
[Cai++]
skeletal muscleheart
contractility
automoticity
premature beatsescape rhythmsV-tach, V-fib
rise in Nai+
and Cai++
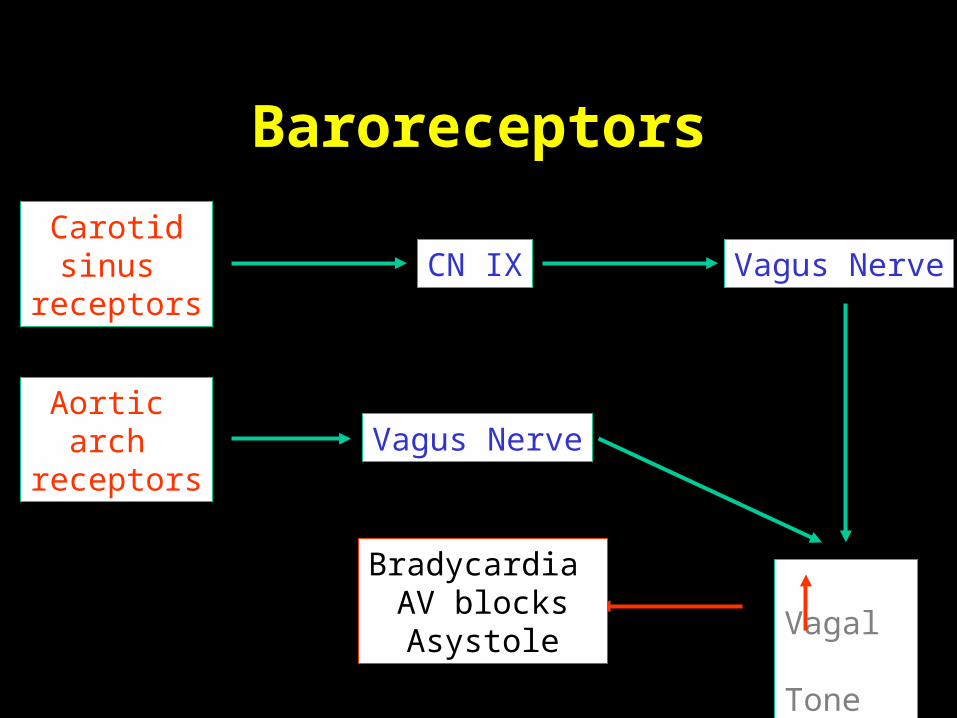
Baroreceptors
Carotidsinus
receptorsCN IX Vagus Nerve
Aortic arch
receptors
Vagal Tone
Bradycardia AV blocksAsystole
Vagus Nerve
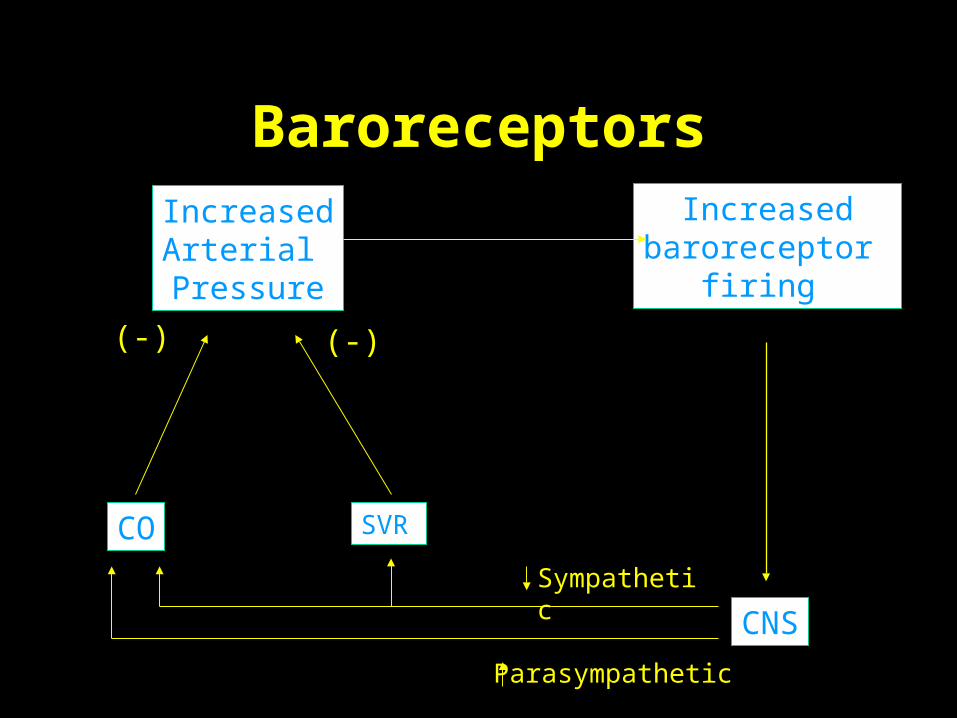
Increasedbaroreceptor
firing
CNS
Parasympathetic
Sympathetic
SVRCO
IncreasedArterial
Pressure
(-)(-)
Baroreceptors
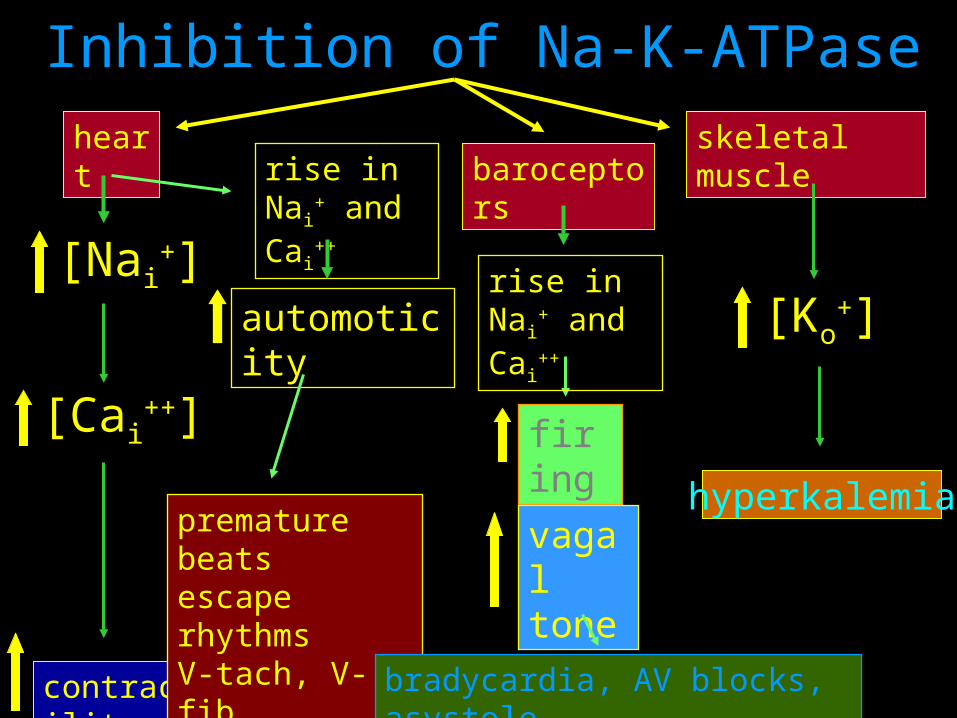
Inhibition of Na-K-ATPase
[Nai+]
[Ko+]
hyperkalemia
[Cai++]
skeletal muscleheart
contractility
premature beatsescape rhythmsV-tach, V-fib
firing
baroceptors
vagal tone
bradycardia, AV blocks, asystole
automoticity
rise in Nai+
and Cai++
rise in Nai+
and Cai++

Devils Advocate
• Treatment of Hyperkalemia in a patient with unrecognized digitalis toxicity
– 80 yr old female presents to the ED with AMS, hyperkalemia and bradycardia
– Treated with intravenous pacing and IV calcium chloride
J Toxicol Clin Toxicol. 2003;41(4):373-6
Devils Advocate
• A toxicological Surprise
– A 42 year old man was admitted to a medical service for CP, nausea and vomiting
– Heart rate was 35, EKG showed total AV block
– Potassium was 5.7mmol/L
Lancet. 2000 Oct 21;356(9239):1406.
Devils Advocate
• He was treated for a myocardial infarction
• A transvenous pacer was inserted with an increase in his heart rate to 70 BPM
• A serum digoxin level was 365ng/mL (therapeutic range 10-30)
Lancet. 2000 Oct 21;356(9239):1406.
Digoxin in herbal Supplements
• Digoxin Toxicity in a 26 year-old woman taking a herbal dietary supplement
– Presented to an ED with chest pain
– Initially her heart rate was 70 BPM and BP was 112/59
– Her heart rate dropped to 39 and BP dropped to 59/36J Am Osteopath Assoc. 2001 Aug;101(8):444-6

Digoxin in herbal Supplements
• EKG showed the absence of P waves
• She was given a NS fluid bolus and placed in the trendelenberg position
• Her BP and heart returned to her original baseline
• A digoxin level was 0.9ng/mL
J Am Osteopath Assoc. 2001 Aug;101(8):444-6

Digoxin in herbal Supplements
• She confessed to consuming a tea that contained:
– Skullcap herb, wood betony herb, black cohosh root, hops flowers, valerian root and cayenne pepper fruit
J Am Osteopath Assoc. 2001 Aug;101(8):444-6
Case 3
• A 36 year old female, with a past medical history for depression and chronic back pain, presents to the ED for back pain
• She states that Demerol is the only medication that relieves her pain
• Reluctantly, you write an order for Demerol
Case 3
• Two hours after the administration of Demerol she develops tachycardia, AMS and myoclonus
• You believe that she developed serotonin syndrome
• A NGT is placed in preparation for the administration of cyproheptadine

Case 3
• She has a self limited seizure, vomits and has a decrease in her O2 sat
• She is intubated using etomidate and succinylcholine
• A post intubation x-ray shows a right upper lobe consolidation
• She dies on hospital day 6 from complications of aspiration pneumonia

Serotonin Syndrome
• Drug Induced Disorder• Variable alterations in
– cognition-behavior– neuromuscular activity– autonomic nervous system function
• Increased CNS serotonin neurotransmission at 5-HT1A and 5-HT2A receptors
Serotonin Receptors
• The largest and most diverse of all neurotransmitter systems– 5HT1 – 5HT7
• Each receptor class may contain many subclasses
• 5HT1A - presynaptic and postsynaptic• 5HT1D - presynaptic and postynaptic
5HT2A - postsynaptic
Serotonin Syndrome
• No gender predilection
• Idiosyncratic in nature
• Patients are not more likely to develop SS following an overdose than they are while taking therapeutic doses
• SS is a diagnosis of exclusion
Precipitants
– Addition of second serotonergic drug usually at therapeutic doses
– Increasing primary drug
• Inherited / Acquired
– Reduction in endothelial MAOA activity
– Genetic variation

Serotonergic Agents
• Inhibit 5-HT uptake
• Enhances 5-HT release
• Inhibits 5-HT breakdown
• Metabolized to 5-HT
• 5-HT1A agonist
• Enhances 5-HT receptor response to stimulation

L-tryptophan
5-hydroxytrytophan
5-HT
TPH
AAD
5-HT
5-HT receptors 1-7
MAO
5-HIAA
5-HT1A, D
-
X
X

Inhibit 5-HT Uptake
• Specific SRIs• Non-specific SRIs - clomipramine, trazodone• TCAs• Meperidine• Dextromethorphan• Pentazocine• Tramadol• Dexfenfluramine
Enhance 5-HT Release
• Lithium
• Levodopa, dopamine
• MDMA
• Cocaine
• Amphetamines
• Fenfluramine
• Dexfenfluramine
5-HT1 Agonists
• LSD
• Buspirone
• Sumatriptan
• Dihydroergotamine
Serotonergic Agents
• Inhibits 5-HT breakdown
– MAOIs
• Metabolized to 5-HT
– Tryptophan
• Enhances 5-HT1A receptor response to stimulation
– Lithium
Drug Combinations
• All MAOI combinations• Dextromethorphan and SSRI• Lithium and SSRI• Trazodone and SSRI• Tramadol and SSRI• Trazodone and Buspirone• Selegiline and SSRIs or TCAs• Switching from 1 SSRI to another SSRI
Serotonin Syndrome Associated with Monotherapy
• Clomipramine
• Fluvoxamine
• Venlafaxine
• MDMA
• Sertraline

Clinical Manifestations
• Cognitive and behavioral
– Confusion (54%)
– Agitation (35%)
– Coma (28%)
– Hypomania (15%)
– Seizures (14%)
– Hallucinations (6%)Mills K. Serotonin Syndrome A Clinical Update. Critical Care Clinics, Volume 13:4 Oct 1997

Clinical Manifestations
• Autonomic Dysfunction
– Blood Pressure Lability (47%)
– Hyperthermia (46%)
– Diaphoresis (46%)
– Tachycardia (41%)
– Mydriasis (26%)
– Diarrhea (12%) Mills K. Serotonin Syndrome A Clinical Update. Critical Care Clinics, Volume 13:4 Oct 1997
Clinical Manifestations
• Neuromuscular Abnormalities– Myoclonus (57%) – Hyperreflexia (55%) – Rigidity (49%)– Tremor (49%) – Incoordination (38%) – Shivering (25%) – Nystagmus (13%)– Seizures (14%)
Mills K. Serotonin Syndrome A Clinical Update. Critical Care Clinics, Volume 13:4 Oct 1997

Sternbach’s Suggested Diagnostic Criteria
• Coincidental with the addition of or increase in known serotonergic agents to an established medications regimen - at least 3 of the following– agitation, diaphoresis, diarrhea, fever,
hyperreflexia, incoordination, MS changes, myoclonus, shivering, tremor
• Other etiologies (infections, metabolic, withdrawal) have been ruled out
• A neuroleptic agent has not been started or increased in dosage
Other Criteria
• Hegerl Criteria
• Dursun Criteria
• Randomski Criteria
• Mills Criteria
• Hunters Decision Rules
• MOFO Criteria
Time course
• Usually abrupt
• Occurring within hours after initiation of new serotonergic agent
• 2/3 of cases resolves within 24 hours
Treatment
• Five basic management principles
– Supportive care
– Discontinue serotinergic agents
– Anticipate potential complications
– Administer antiserotinergic agents
– Reassess the need for reinstituting pharmacotherapy

Treatment
• Antipyretics are generally ineffective
• Benzodiazepines are the initial choice for relieving muscle spasm
• No specific antidotes for SS
• Most symptoms resolve in 12 – 24 hours
Cyproheptadiene
• Cyproheptadine (periactin)
– Most consistently effective
– Blocks postsynaptic 5HT1A and 5HT2
receptors
– Only available orally (syrup, tablet)
– Also has antimuscarinic and antihistaminc properties
Case 4
• A 54 year old male presents to the ED with a rash that has been getting progressively worse over that past week and a half
• He also offers complaints of chills, nausea, vomiting and diarrhea
• Past medical history is significant for seizure disorder and hypertension


Case 4
• His medications include phenytoin and lisinopril
• He is febrile with a temperature of 102.c, tachycardic at a ventricular rate of 130, hypotensive with a sys BP of 80, RR 24
• His white count is 28,000 with a left shift, HG: 19, HCT: 45, Platelets 52

Case 4
• Na+ 156, K+ 5.4, Cl- 92, NaHco3- 12,
• BUN: 60, CR 5.2 and glucose is 220
• His LFTS are markedly elevated and he has a creatinine of 3.2
• His phenytoin level 0.5mcg/mL
• He is loaded with IV phenytoin in the ED
Case 4
• One hour after the administration of phenytoin he drops his blood pressure and becomes apneic
• He is subsequently intubated and is transferred to the ICU
• He dies on Hospital day 7 from multi-system organ failure
Introduction
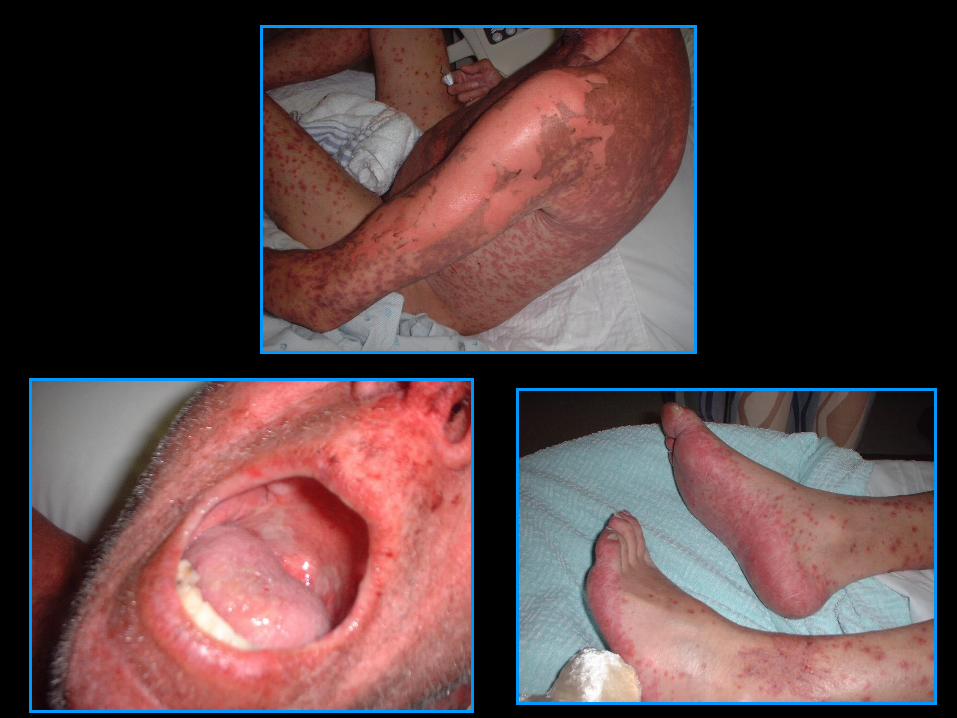
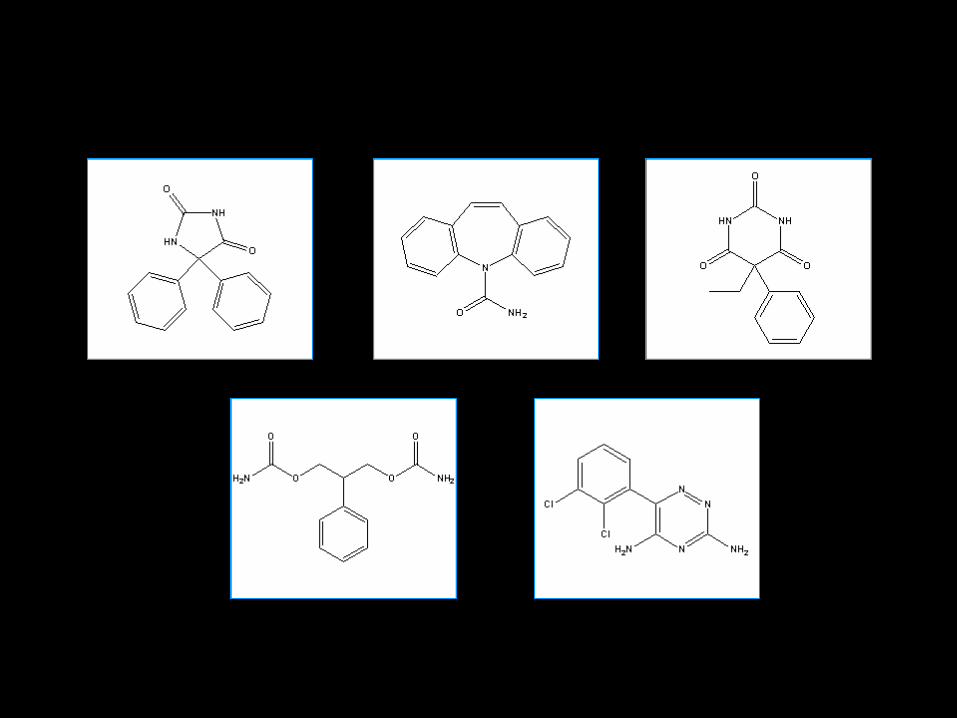
• Anticonvulsant hypersensitivity syndrome (ACHS) is a rare, potentially fatal multisystem disorder that occurs after exposure to phenytoin, carbamazepine, phenobarbital, felbamate and lamotrigine
Signs and Symptoms
• ACHS commonly begins within one to four weeks after starting therapy, but may present as late as three months
• ACHS may occur within hours of a previously sensitized individual
• ACHS is not related to the dose or serum concentration

Signs and Symptoms
• Most commonly ACHS begins with a fever, followed by a rash and variable degrees of lymphadenopathy
• The fever usually ranges from 38 – 40.C
• The Rash may develop concurrently or shortly after the fever
Signs and Symptoms
• The Rash is commonly described as an exanthem with or without pruritus
• The upper extremities, face and trunk are usually first affected
• Periorbital edema, exudative tonsillitis, pharyngitis, oral ulcerations and conjunctivitis may be seen
Signs and Symptoms
• Rarely, more severe skin reactions may occur (SJS, TEN, EM)
– Usually in the setting of repeated exposures or continued use
• Tender lymphadenopathy is commonly seen
Signs and Symptoms
• The Liver is the most common organ involved
• The CNS, heart, lungs, renal system and thyroid gland may be involved– Patients may present with elevated
transaminases, alkaline phosphatase, PT and bilirubin
• The hepatitis is usually mild and anicteric

Signs and Symptoms
• The degree of hepatitis is related to the time between the onset of symptoms and the discontinuation of the offending agent
• Liver biopsies reveal periportal inflammation with or without necrosis
• The majority of patients recover within a few weeks
Signs and Symptoms
• Hematologic abnormalities – Lymphocytosis – Leukocytosis– Eosinophilia– Anemia– Leukopenia – Thrombocytopenia– Aplastic anemia

Pathophysiology
• The anticonvulsants implicated in ACHS all have in common an aromatic benzene ring that is metabolized by cytochrome p450 to an arene oxide
• Arene oxides are highly electrophilic and covalently bind to macromolecules to disrupt cellular function

Pathophysiology
• Arene oxides may also form neoantigens that trigger an immunologic response
• These metabolites are highly unstable and under normal conditions can be detoxified by one of several routes

Diagnosis
• Usually based on history of drug exposure and clinical examination
– Atypical lymphocytes
– Eosinophilia
– Elevated liver enzymes
– hyperbilirubinemia

Treatment
• The mainstay of treatment is discontinuation of the offending agent and supportive care
• Severe skin reactions are best managed in a burn center
• Strict attention must be paid to maintaining fluid and electrolyte balance
Thank You
Related Documents










