Suicid e Suicidal behavior / parasuicide Self injury Risky behavior

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Suicide Suicidal
behavior / parasuicide
Self injury
Risky behavior

הנעשית פעולהאו התנהגותלמוות כוונהמתוך לגרום
עצמי

Self-Injurious Behavior
Self-injury (also known as self-harm, self-mutilation,
self-abuse and self-inflicted violence) is a compulsion or impulse to inflict physical wounds on one's own body, motivated by a need to cope with unbearable psychological distress or regain a sense of emotional balance. The act is usually carried out without suicidal, sexual or decorative intent.
» (Sutton & Others, 2000)
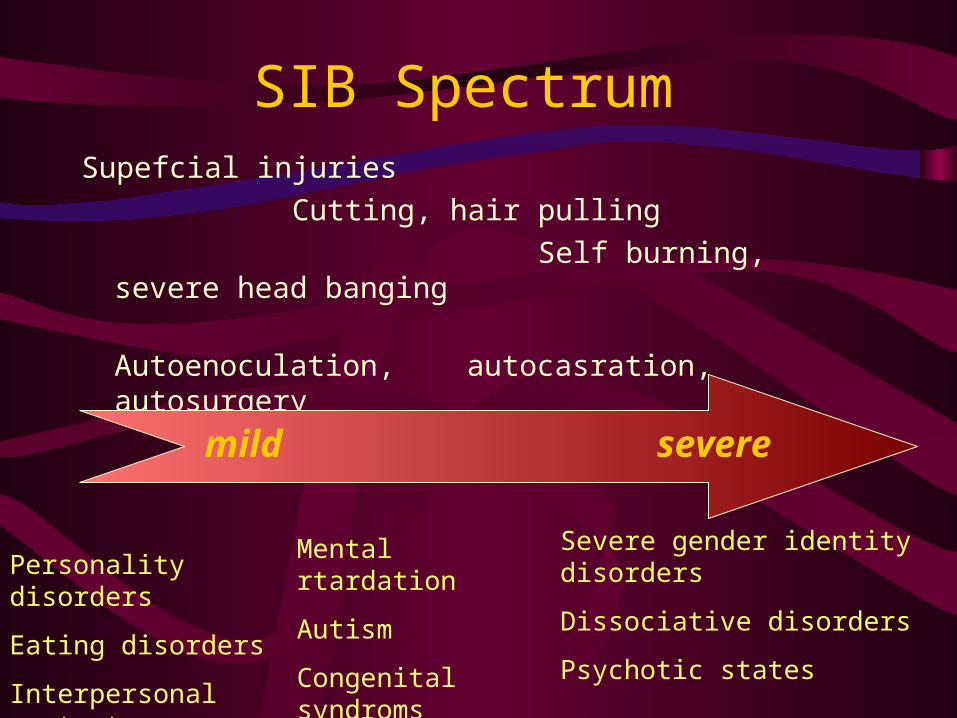
SIB SpectrumSupefcial injuries Cutting, hair pulling Self burning, severe head banging Autoenoculation,
autocasration, autosurgery
mild severe
Personality disorders
Eating disorders
Interpersonal context
Mental rtardation
Autism
Congenital syndroms
Severe gender identity disorders
Dissociative disorders
Psychotic states

Epidemiology of SIB
• Prevalence:– 1:600 general population, – 400-1400:100,000
• 40.5% of laxative-abusing bulimics
• 14% of mentally retarded
• Gender differences uncertain, appears to be more prevalent in women.

Neurobiology of SIB
• Animal models:– Dopamin activation: L-DOPA induces SIB via
activation 0f D1 receptor. Selective D1 antagonists reduce autoagression
– Opioids activation: sufentanil induced autoagression.
– Serotonin depletion: p-chlorophenilalanine increases agression and autoagressin

Neurobiology of SIB
• Human studies:– Lesch-Nyhan Syndrom: decreased level of dopamine
and thyrosine hysroxolase in atopsied brains.
– Cornelia-De-Lange Syndrom: Depressed Blood serotonin.
– Suicide attempters: decreased CSF 5-HIAA, reduced prolactin response to fenfluramine.
– Opioid dysregulation: increased plasma enkephalin in SIB patients, incread CSF endorphins in SIB autistics.

Different Meanings of SIB• Expression of intense emotions.• Impulse, self regulation, self control.• Distraction from psychic pain.• Self (or others) punishment, atornmement.• Feeling , excitement.• Reenactment of trauma.• A cry for help.• Psycholgical or secondary gains.

גישות לאובדנות
פילוסופית / ערכית: סוגיה אקזיסטנציאלית •
סוציולוגית: בעיה באינטגרציה, ניכור•
פסיכולוגית: תוקפנות והרס עצמי•
רפואית / פסיכיאטרית: הפרעה נפשית•

Integration )-(
Integration )+(
Regulation )+(
Regulation )-(
anomiaegiosm
altriosmfatalism

העובדות המטרידות
כמיליון אנשים מתאבדים מדי שנה ברחבי העולם.•
הבדלים גיאוגרפיים משמעותיים .•
עליה בהיקף ההתאבדויות, חיקוי, "הידבקות".•
משמעויות חמורות בכל קבוצות הגיל.•
הטרוגניות, גורמי סיכון רבים, יכולת ניבוי מועטה.•
ערך מוגבל לגישות המניעה הראשונית.•
מחיר גבוה, השקעה מערכתית דלה•

SUICIDE: A MULTI-FACTORIAL EVENT
Neurobiology
Severe MedicalIllness
Impulsiveness
Access To Weapons
Hopelessness
Life Stressors
Family History
SuicidalBehavior
Personality Disorder/Traits
Psychiatric IllnessCo-morbidity
Psychodynamics/Psychological Vulnerability
Substance Use/Abuse
Suicide

Facing the facts…• Suicide is considered to be the second leading cause of death among college
students.
• Suicide is the second leading cause of death for people aged 24-34.
• Suicide is the third leading cause of death for people aged 10-24.
• Suicide is the fourth leading cause of death for adults between the ages of 18 and 65.
• Suicide is highest in white males over 85.
(48.42/100,000, 2004)

טווח ההתנהגויות האובדניותטווח ההתנהגויות האובדניות
מחשבות התאבדות
התאבדות איומי
מחוות אובדניים
ניסיונות התאבדות
התאבדות
משבר אובדנימשבר אובדני
סיכון גורמיפרטניים
סיכון גורמימצביים
אמצעי זמינותמשאבי קטל
התמודדות
תמך מקורות
מעכבים גורמים
, נפשיות הפרעותאימפולסיביות
דמוגרפיה, תורשה
, : אובדנים חיים ארועי , חוק, בעיות דחיה
, בעיות, הגירה אבטלה , . טירונות, כשלון בריאות
כליאה,.
ותופעת חיקויהאשכולות.

Demographic male; widowed, divorced, single; increases with age; white
Psychosocial lack of social support; unemployment; drop in socio-economic status; firearm access
Psychiatric psychiatric diagnosis; comorbidity
Physical Illness malignant neoplasms; HIV/AIDS; peptic ulcer disease; hemodialysis; systemic lupus erthematosis; pain syndromes; functional impairment; diseases of nervous system
Psychological Dimensions
hopelessness; psychic pain/anxiety; psychological turmoil; decreased self-esteem; fragile narcissism & perfectionism
Behavioral Dimensions
impulsivity; aggression; severe anxiety; panic attacks; agitation; intoxication; prior suicide attempt
Cognitive Dimensions
thought constriction; polarized thinking
Childhood Trauma
sexual/physical abuse; neglect; parental loss
Genetic & Familial
family history of suicide, mental illness, or abuse
Risk factors
•Children in the home, (except postpartum psychosis)
•Pregnancy
•Deterrent religious beliefs
•Life satisfaction
•Reality testing ability
•Positive coping skills
•Positive social support
•Positive therapeutic relationship
Protective factors

התרחיש האובדני התרחיש האובדני
כאב נפשי בלתי נסבל•
הכפשה עצמית•
“היצרות” החשיבה•
בדידות וניכור•
חוסר תקווה•
היעלמות כפתרון יחיד•


המאפיינים השכיחים 10בהתאבדויות
המניע הנפוץ בהתאבדויות הוא מציאת פתרון.המטרה השכיחה בהתאבדויות היא הפסקת המודעות.
הגירוי המשותף להתאבדויות הנו כאב נפשי בלתי נסבל.גורם הדחק המשותף בהתאבדויות הנו צורך פסיכולוגי מתוסכל.
הרגש השכיח בהתאבדויות הנו חוסר תקווה וחוסר אונים.המצב הקוגניטיבי האופייני להתאבדויות הוא אמביבלנטיות.
המצב התפיסתי האופייני להתאבדויות הוא צמצום.הפעולה האופיינית להתאבדויות הנה הסתלקות.
ההתנהגות הבין-אישית השכיחה בהתאבדויות הנה ביטוי הכוונה.העקביות האופיינית להתאבדויות הנה בדפוסי התמודדות
מתמשכים.

High Risk Strategies
While 90% of suicide are considered to be due to mental
disorders, about half have never been in contact with MH services1
Suicide risk is extremely high immediately after discharge from a
psychiatric hospital, and for the first year after deliberate self
harm. In these groups, it takes 385 / 500 cases to treat in order to
prevent one suicide.
Major changes in suicide rates are most likely to result from
population strategies rather then high-risk strategies
Effective interventions for deliberate self - harm patients are
probably the best high-risk strategies
1 Vassilas & Morgan, BMJ 19932 Lewis, Hawton & Jones, BJPsy 1997
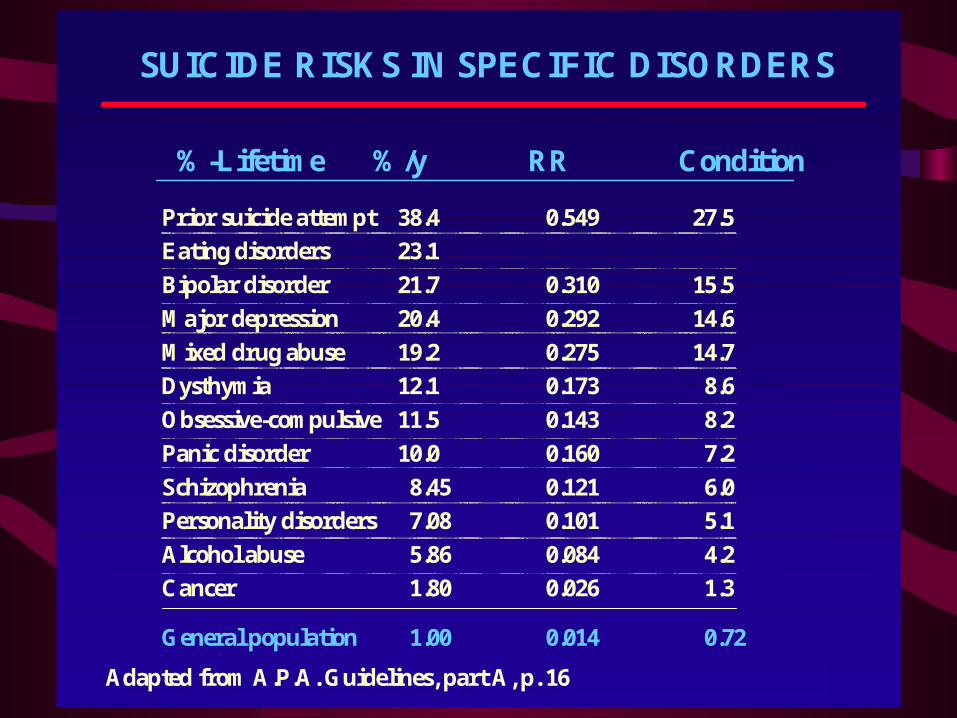
SUICIDE RISKS IN SPECIFIC DISORDERS
Prior suicide attempt 38.4 0.549 27.5
Eating disorders 23.1
Bipolar disorder 21.7 0.310 15.5
Major depression 20.4 0.292 14.6
Mixed drug abuse 19.2 0.275 14.7
Dysthymia 12.1 0.173 8.6
Obsessive-compulsive 11.5 0.143 8.2
Panic disorder 10.0 0.160 7.2
Schizophrenia 8.45 0.121 6.0
Personality disorders 7.08 0.101 5.1
Alcohol abuse 5.86 0.084 4.2
Cancer 1.80 0.026 1.3
General population 1.00 0.014 0.72
ConditionRR%/y%-Lifetime
Adapted from A.P.A. Guidelines, part A, p. 16

Disorders Correlated With Suicidal Behavior
Mood Disorders (15 percent lifetime risk of suicide) A. The absence of psychosis does not imply safety. B. A misleading reduction of anxious or depressed affect can occur
in some patients who have resolved their ambivalence by deciding to commit suicide.
C. The likelihood of suicide within 1 year is increased when the patient exhibits: Panic attacks, Psychic anxiety, Anhedonia, Alcohol abuse .
D. The likelihood of suicide during the ensuing 1-5 years is increased when the patient exhibits: Increased hopelessness, Suicidal ideation, History of suicide attempts.
Developed by the Suicide Risk Advisory Committee of the Risk Management Foundation of the Harvard Medical Institutions in 1996.

Disorders Correlated With Suicidal Behavior
Panic Disorder (7-15 percent lifetime risk of suicide) A. Suicide rate may be similar to that of mood
disorders B. Greater likelihood is correlated with more severe
illness or comorbidity C. Suicide does not necessarily occur during a panic
attack D. Demoralization or significant loss increase the
likelihood of suicide E. Agitation may increase the likelihood of
translating impulses into action

Disorders Correlated With Suicidal Behavior
Schizophrenia (10 percent lifetime risk of suicide)
A. Suicide is relatively uncommon during psychotic episodes B. The relationship between command hallucinations and actual
suicide is not clearly causal C. Suicidal ideation occurs in 60-80 percent of patients D. Suicide attempts occur in 30-55 percent of patients E. Suicide potential is increased by:
a. Good premorbid functioning b. Early phase of illness c. Hopelessness or depression d. Recognition of deterioration, e.g., during a post-psychotic depressed
phase

Disorders Correlated With Suicidal Behavior
Alcoholism (3 percent lifetime risk of suicide) A. Abusers of alcohol/drugs comprise 15-25 percent of suicides
B. Alcohol is associated with nearly 50 percent of all suicides
C. Increased suicide potential in an alcoholic patient correlates with:
a. Active substance abuse
b. Adolescence
c. Second or third decades of illness
d. Comorbid psychiatric illness
e. Recent or anticipated interpersonal loss
D. Substance abuse can represent self treatment to blunt the anxiety or mood disturbance associated with a masked, comorbid psychiatric disorder

Disorders Correlated With Suicidal Behavior
Borderline Personality Disorder (7 % lifetime risk of suicide)
A. Much higher risk associated with comorbidity, especially with mood disorder and substance abuse
B. Psychopathology associated with increased risk: a. Impulsivity, hopelessness/despair b. Antisocial features (with dishonesty) c. Interpersonal aloofness ("malignant narcissism") d. Self-mutilating tendencies e. Psychosis with bizarre suicide attempts
C. Psychopathology associated with diminished risk: a. Infantile personality (with hysterical features) b. Masochistic personality
The Neurobiology of suicide risk
• Suicidal behavior has neurobiological
determinants independent of the psychiatric
illness with which it is associated.
• Vulnerability to act on suicide impulses results
from the interaction between triggers or
precipitants and the threshold for suicidal
behavior
• Studies found decreased serotonin activity in the
prefrontal cerebral cortex of suicide victims.
J.J. Mann, 1999

Familial Transmission of Suicidality:
Risk factor for suicide is transmitted in
families independently of transmission of
major depression or psychosis, but not
independently of impulsive aggression.
Brent DA et al, Arch J Psych 1996:1145-1152

התאבדויות במניעת כשל גורמי
קושי בזיהוי אנשים בסיכון.
רתיעה מקבלת עזרה נפשית.
חוסר נגישות לסוכנויות התערבות.
אפקטיביות נמוכה של שיטות התערבות.
טיפול מפוצל או בלתי מתואם.
מיקוד מקצועי צר.
בעיות סביב קביעת אחריות ואשמה.

Areas to Evaluate in Suicide Assessment
Psychiatric
Illnesses
Comorbidity, Affective Disorders, Alcohol / Substance Abuse, Schizophrenia, Cluster B Personality disorders.
History Prior suicide attempts, aborted attempts or self harm; Medical diagnoses, Family history of suicide / attempts / mental illness
Individual strengths /
vulnerabilities
Coping skills; personality traits; past responses to stress; capacity for reality testing; tolerance of psychological pain
Psychosocial situation
Acute and chronic stressors; changes in status; quality of support; religious beliefs
Suicidality and Symptoms
Past and present suicidal ideation, plans, behaviors, intent; methods; hopelessness, anhedonia, anxiety symptoms; reasons for living; associated substance use; homicidal ideation
Adapted from APA guidelines, part A, p. 4

The assessment of suicidality is an active process during which clinicians evaluate:
a. Suicidal intent and lethality b. Dynamic meanings and motivation for suicide c. Presence of a suicidal plan d. Presence of overt suicidal/self-destructive behavior e. The patient's physiological, cognitive, and affective
states f. The patient's coping potential g. The patient's epidemiological risk factors
The Detection of Suicidality

The Detection of SuicidalitySuicide-specific questions
1. Are suicidal thoughts/feelings present?
2. What form does the patient's wish for suicide take?
3. What does suicide mean to the patient?
4. Has the patient lost or anticipates losing an essential sustaining
relationship?
5. Has the patient lost or anticipates losing his/her main reason for
living?
6. How far has the suicide planning process proceeded?
7. Have suicidal behaviors occurred in the past?
8. Has the patient engaged in self-mutilating behaviors?
9. Does the patient's mental state increase the potential for
suicide?

10. Are depression and/or despair present?
11. Does the patient's physiologic state increase the potential for suicide?
12. Is the patient vulnerable to painful affects such as aloneness, self-contempt, murderous rage, shame, or panic?
13. Are there recent stresses in the patient's life?
14. What are the patient's capacities for self-regulation?
15. Is the patient able/competent to participate in treatment?
16. Loss of coping mechanism?
17. Are epidemiological risk factors present?
The Detection of Suicidality (cont.)

Treatment Planning
Treatment planning takes into account:
• The patient's potential for suicide,
• Capacity to form a treatment alliance,
• Range of available treatment alternatives
from outpatient follow-up to
hospitalization with constant observation.

• Collect Data Before Treatment Planning
• Identify a Range of Treatment Alternatives
Weigh the risks and benefits of each alternative,
including the alternative "no treatment."
• Involve the Patient and Family in the Treatment
Planning Process to the Degree Possible
• Consider pharmacotherapy.
Treatment Planning (cont.)
• Contracts Will Not Guarantee the Patient's Safetycontracts can give staff a false sense of security and interfere with a thorough suicide assessment.
• Choose Appropriate Levels of Observation, Supervision, and Privileges.
• The treatment team may decide to tolerate short term risk to foster long-term growth.
• Documentation should make clear the choices and rationale.
• Assess the risk of continued hospitalization
Treatment Planning (cont.)
Related Documents











