Suicide prevention strategies. A systematic review Mann JJ et al., JAMA 2005, 294: 2064-2074. Asbtract Conclusions: „Physician education in depression recognition and treatment and restricting access to lethal methods reduce suicide rates. Other interventions need more evidence of efficacy”.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Suicide prevention strategies.A systematic review
Mann JJ et al., JAMA 2005, 294: 2064-2074.
AsbtractConclusions: „Physician education in
depression recognition and treatment andrestricting access to lethal methodsreduce suicide rates. Other interventions need more evidence of efficacy”.


Medical contact before suicide (%)
GPs Psychiatrists
• 3 months 47-73 -----
• 4 weeks 34-66 18-21
• 1 week 18-40 9-11
- Medical contact: Females > males- Suicide victims: 65-80 % are males
Pirkis and Burgess, Brit J Psychiat 1998, 173:462-474. Andersen et al, Acta Psychiat Scand 2000, 102:126-134.



Suicide prevention strategies –Competence of healthcare (1)
I. Patient-oriented prespective (targetinghigh-risk groups)
• Elimination of acute suicide danger (emergency admission, crisis/hotline services, etc.)
• Improving the diagnosis and treatment of mental disorders (depression)
• Education of doctors, patients, relatives• Aftercare of persons with high risk
__________________________________________________

Pharmacotherapy of depressed suicidal patients
The rate of antidepressant/mood stabilizerpharmacotherapy (and ECT) amongsuicide victims/attempters is 10 – 32 % (adequate + inadequate)
Rihmer et al,J Affect Disord, 1990, 18: 221-225.Isometsa et al, Amer J Psychiat, 1994, 151: 530-536.Isometsa et al, Amer J Psychiat, 1994; 151: 1020-2024.Marzuk et al, Amer J Psychiat, 1995, 152: 1520-1522.Suominen et al, Amer J Psychiat, 1998; 155: 1778-1780.Oquendo et al, Amer J Psychiat, 1999, 156: 190-194.Isacsson, Acta Psychiat Scand, 2000, 102: 113-117.Henriksson et al, Acta Psychiat Scand 2001, 103: 301-306.Dhossche et al, Arch Intern Med, 2001, 161: 991-994Balázs et al,J Affect Disord. 2003, 76: 113-119.Leon et al, J Clin Psychiat, 2007; 68: 1399-1405.Almási et al,BMC Psychiatry, 2009; 9: 45-53.

Treatment of suicidal people around the world
• 6 continents, 21 counrties• Nationally representative samples• 109.381 persons (55.302 analysed)• Past year suicidal behaviour:
- ideation: 2.5 %- attempt: 0.7 %
• Only 40% have received treatment
Bruffaerts et al, Brit J Psychiat, 2011; 199: 64-70.
Low-income counrties: 17 % --- high income countries: 56%

The role of pharmacotherapy in suicide prevention of psychiatric patients

Acute and long-term pharmacotherapy of patients with unipolar and bipolar
major mood disorders (ADs, MSs, APs)
Risk reduction of:• Suicide 82 % (60 - 95 %)• Suicide attempts 72 % (40 - 93 %)
Leon et al, Amer J Psychiat, 1999, 156: 195-201.Baldessarini et al, Bipol Disord, 2006; 8: 625-639.Angst et al, J Affect Disord, 2002; 68: 167-181.Montgomery et al, Int Clin Psychopharmacol, 2003; 18 (S-1): 1-9.Yerevanian et al, Acta Psychiat Scand, 2004; 110: 452-458.Kessing et al, Arch Gen Psychiat, 2005; 62: 860-866.Sondergard et al, Arch Suic Res, 2007; 11: 163-175.Yerevanian et al, J Affect Disord, 2007; 103: 5, 13, 23.Sondergard et al, Bipol Disord, 2008; 10: 87-94.Pompili et al, Expert Rev Neurother, 2009; 9: 109-136.

Antidepresants and suicidal behaviour in unipolar depression
Risk-reduction (%)
Suicide Suic. att.
• Angst et al, 2002 67 -• Yerevaninan et al, 2004 95 85• Sondergard et al, 2007 84 -
Angst et al, J Affect Disord, 2002; 68: 167-181.Yerevanian et al, Acta Psychiat Scand, 2004; 110: 452-548.Sondergard et al, Arch Suic Res, 2007; 11: 163-175.
______________________________
____________________________________________________________________
____________________________________________________________________

Meta-Analysis:Lithium vs. Suicides &Attempts inBipolar Disorder
Baldessarini et al. Bipol Disord, 2006: 8: 625-639.
________
31 studies, 33.340 pts
Risk reduction: 80%
Ss vs SAs andRCTs vs Open studies:similar results
0.01 0.1 1 10 100 1000
Risk Ratio (RR; 95%CI)
Overall RR
Gonzalez-Pinto et al. 2005Angst et al. 2005
Yerevanian et al. 2003Goodwin et al. 2003
Calabrese et al. 2003*Bowden et al. 2003*
Rucci et al. 2002Coryell et al. 2001Kallner et al. 2000
Brodersen et al. 2000Bauer et al. 2000*Tondo et al. 1998
Coppen & Farmer 1998Bocchetta et al. 1998
Greil et al. 1996, 1997a,b*Nilsson 1995
Koukopoulos et al. 1995Sharma & Markar 1994
Lenz et al. 1994Felber & Kyber 1994
Rihmer et al. 1993Müller-Oerlinghausen et al. 1992
Modestin & Schwarzenbach 1992Nilsson & Axelsson 1990
Lepkifker et al. 1985Hanus & Zapletalek 1984Venkoba-Rao et al. 1982
Ahlfors et al. 1981Poole et al. 1978
Kay & Petterson 1977Prien et al. 1974*
Pooled RR(4.91)
_______________ *

Fig 2 Forest plot showing meta-analysis of suicides in randomised trials comparing lithium with placebo or with active comparators.
Cipriani A et al. BMJ 2013;346:bmj.f3646
©2013 by British Medical Journal Publishing Group
48 RCTs
6674 pts
OR forsuicide,Li vs other.
0.13
(0.03-0.66)

Guzzetta et al, J Clin Psychiat, 2007; 68: 380-383.
8 studies, 329 patients
Risk reduction:S: 85 %S+SA: 88.5%
0.1 1 10
Risk Ratio (95%CI)
Tondo et al. 2006
Bauer et al. 2000
Coppen & Farmer 1998
Bocchetta et al. 1998
Greil et al. 1996
Müller-Oerlinghausen et al. 1992
Lepifker et al. 1985
Bech et al. 1976
Pooled RR2.01 (1.81–2.22)
Lithium Treatment: Reduced Suicidal Risk in Recurrent Unipolar Major Depression

Prophylactic lithium treatment and suicidal behaviour in 167 recurrent
(UP and BP) depressives with one or more suicide attempt before lithium
Number of SAs per year Decrease Non SAbefore Li during Li (%) (%)
Excellent resp. 0,26 0,02 92* 93(n = 45)Moderate resp. 0,27 0,06 78** 83(n = 81)Poor resp. 0,33 0,10 70** 49(n = 41)* p = 0,001** p = 0,007
Ahrens and Müller-Oerlinghausen, Pharmacopsychiat. 2001, 34: 132-136

0.1 1 10 100
Relative Risk (RR; 95%CI)
Pooled
Collins & McFarland 2007 [VPA+CBZ]
Yerevanian et al. 2003 [VPA+CBZ]
Goodwin et al. 2003 [VPA+CBZ]
Calabrese et al. 2003 [LTG]
Bowden et al. 2003 [LTG]
Greil et al. 1997 [CBZ]
Pooled RR2.86 [2.29–3.57]
Suicidal Risk in BPD: Lithium vs. Anticonvulsants
[Baldessarini & Tondo 2007]
Baldassarini and TondoPharmacopsychiatry, 2008; 41: 1-4.

Quendo et al, Amer J Psychiat, 2011; 168: 1050-1056.
Lithium, valproate and suicidality in MDD. A 2.2-year long follow-up

Suicide rates in patients with depressive disorders for three different treatment era
Treatment era No of Sample Mean SR*studies size
• Pretreatment era 10 6332 6.3(1900-1939)
• ECT era 8 5992 5.7(1940-1959)
• Antidepressant era 26 47664 3.3(1960-1992)
1993-2010 ???
* per 1000 person-year, p = 0,001 O’Leary et al, J Clin Psych, 2001, 62: 804-811
___________________________________________________
- 48%
IIIIIII

Treatment ofSuicide Risk inSchizophrenia
0.1 1 10Odds Ratio (95%CI)
Pooled OR
Modestin et al. 2005
Meltzer et al. 2003
Sernyak et al. 2001
Munro et al. 1999
Reid et al. 1998
Walker et al. 1997
Meltzer & Okayli 1995
Pooled OR(4.64; p<0.0001)
Clozapine vs. Suicidal Risk
Hennen & Baldessarini Schizophrenia Res 2005; 73: 13 9–145; Baldessarini 2006 ]

Antidepressants, benzodiazepines and suicide risk in schizophrenia
• 2.588 Finish patients with schizophrenia• 4 year follow-up• 35 patients completed suicides (1.35%)• Among patients who used also
antidepressants the suicide risk was 85%lower
• Benzodiazepine use was associated with marked increase of suicidality (283%, protocol violation, withdraval syndrome, confunding by indication)
Tiihonen et al, Arch Gen Psychiat, 2012; 69: 476-483.
Mostly temazepam, diazepam and oxaepam but no suicide on alprazolam, nitrazepamand chloridazepoxide ! Comorbid substance-use disorders were not detected !

AD vs AD+BZD in short-term treatment of major depression
• Meta-analysis of 9 RCTs (1979-1998,n=679, in-and outpatients with MDD)
• In the AD+BZD group (vs AD+PLAC group):fewer drop-outs (- 37%)more early responders at (+ 41-63%)
• Comparing with AD + PL group responders in the AD+BZD group:
week 1 + 63%week 2 + 41%week 4 + 38%week 6-8 + 6%
Furukawa et al. J. Affect. Disord.2001,65:173-7.

Fluoxetine vs fluoxetine + clonazepam in short-term treatment of major
depression
FLU FLU+CLON20-40 mg 20-40 and
0,5-1 mgN=25 N=25
---------------------------------------------------------------• Responders
day 7 4% 32%day 14 12% 32%day 56 56% 76%
---------------------------------------------------------------Smith et al. J. Affect. Dis. 2002,70: 251-259.

Insomnia, major depression and suicide
• In patients with MDE insomnia is a powerful suicide risk factor
• In patients with MDE hypersomnia is a suicide protective factor
Fawcett et al, Amer J Psychiat, 1990; 147: 1189-1194.Taylor et al, Behav Sleep Med, 2003; 1: 227-247.McGirr et al, J Affect Disord, 2007; 97: 203-209.
McGirr et al, J Affect Disord, 2007; 97: 203-209.

Evaluation of the HAM-D17 following eszopiclone treatment in patients with
insomnia co-morbid with major depressive disorder or GAD (n=545)
• Conclusions: „Treatment of insomnia with eszopiclone co-therapy was associated with significant improvement in HAM-D17 scores relative to fluoxetine or escitalopram monotherapy in patients with insomnia comorbid with MDD or GAD, even after removal of insomnia items from the scale”
Montgomery et al, Int. J. Psychopharmacol, 2008; 11: S1, p.306.

• Fluoxetine + eszopiclone therapy in major depression resulted in significantly higher response/remission rates than fluoxetine monotherapy. This beneficial effect was more than the simple reflexion of improved sleep.
Fava et al, Biol Psychiat, 2006; 59: 1052-1060.

Fava et al, Biol Psychiat, 2006; 59: 1052-1060.
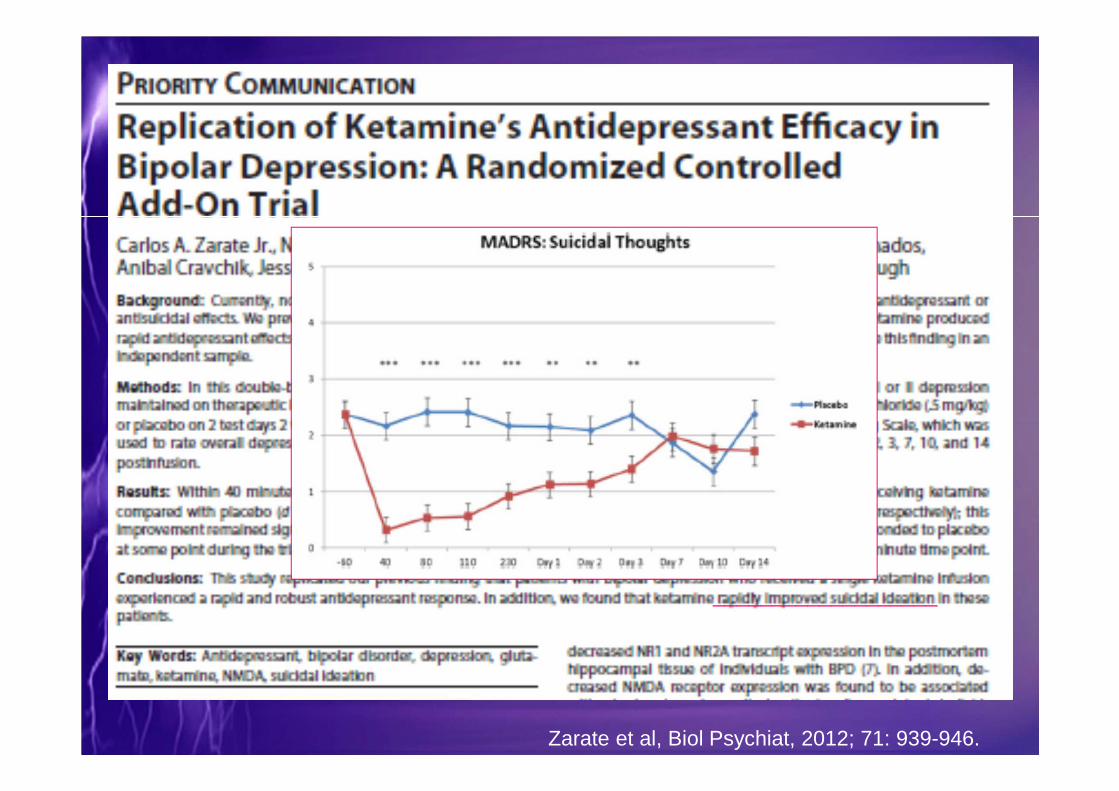
Zarate et al, Biol Psychiat, 2012; 71: 939-946.
___________________

Psychotherapy for depression, suicidality and hopelessness
• Systematic review and meta-analysis• 13 studies (616 patients, MDD, DD)• Outcome measures: suicidal ideation
and hopelessness• Suicidality (and hopelessness) in
depressed patients can not be significantly reduced with psychotherapy for depression
Cuijpers et al, J Affect Disord, 2013; 144: 183-190.

Antidepressants, psychotherapy and suicidality in pediatric depression (FDA RCTs)
Rate of suicide attempt and ideation (there were no completed suicides in these trials)
*Whittington et al., Lancet, 2004, 363, 1341-1345**Bridge et al., Amer J Psychiat, 2005, 162, 2173-2175
%
Antidepressants* (n=1208)
Placebo* (n=1054)
Psychotherapy** (n=88)
15
10
54.7%
2.4%
12.5%

The role of GPs in suicide prevention
• The majority of depressives areseen/diagnosed /treated by GPs
• GP contact is very common (40-60%) 4 weeks before the suicide
• The rate of recognized/treated depression in primary care is quite low (20-50%)
Luoma et al, Amer J Psychiat, 2002; 159: 909-916.Berardi et al, Psychother Psychosom, 2005; 74: 225-230.
Rihmer, Curr Opin Psychiat, 2007; 20: 17-22.

The Gotland Study
13
11 11
54
10
13
10
1312
9
56
109
0
2
4
6
8
10
12
14
1981 82 83 84 85 86 87 88 89 90 91 92 93 94 95
Number of suicide victims on Gotland between 1981-1995
Mean number of victims between 1969–1980: 14.5 (8–20)
Rutz et al., IJCP, 1997; 1: 39–46
GPeducation GP
education
ADs: 1981= 5.8 � 1996 = 28.9 DDD/1000/year (5 x)
620
183
0
100
200
300
400
500
600
700
2000 2000
500
182
2001
-19,4%
-0,01%
2001
471
196
2002
Chi² (one-tailed):2000 versus 2001; p< 0,052000 versus 2002; p< 0,012000 versus 2003; p< 0,01
-24,0%
+7,7%
2002 2003
173
-5,5%
2003
420-32,2%
The Nuremberg StudySuicidal acts, Nuremberg - Wuerzburg
Sui
cida
lact
s
Nuremberg (intervention) Würzburg (cotrol)
Baseline, intervention and follow up
Hegerl et al, Psychol Med, 2006; 36: 1225-1234.
The Jamtland Study
Jamtland Sweden• Mean suicide rate’
1970 - 1994 27.7 25.01995 - 2002 17.3 17.6
change - 36% - 30%• Antidepressants’’
1995 21.6 27.52002 56.4 57.2
change + 161% +108%
Henriksson and Isacsson, Acta Psychiat Scand, 2006, 114: 159-167.
‘ per 100.000/year, ‘’ DDD/1000 persons/day
N
50
40
30
’96 ’97 ’98 ’99 ’00 ’01 ’02 ’03 ’04 ‘05
36
50
41
51
4243
34
42
37
30
N
50
40
30
’96 ’97 ’98 ’99 ’00 ’01 ’02 ’03 ’04 ‘05
36
50
41
51
4243
34
42
37
30
The Hungarian GP-based suicideprevention study
Before GP trainingmean 44,0 / year
After GP trainingmean 37,2 / year
Before GP trainingmean 44,0 / year
After GP trainingmean 37,2 / year
- 15 %
x
x
x
x
x
x
x
Szántó et al,AGP, 2007:64. 914-920.
(+ 34 lifes)
10.6
30.4

N
50
40
30
’96 ’97 ’98 ’99 ’00 ’01 ’02 ’03 ’04 ‘05
36
50
41
51
4243
34
42
37
30
Yearly number of suicides and ADs in Kiskunhalas region (1996 – 2000 vs 2001 –
2005)
Before GP training mean 44,0 / year
After GP training mean 37,2 / year
- 15 %
10.6x
30.4x
x
x
x
x
x
(+34 lifes)
Szántó et al,AGP, 2007:64: 914-920.
ADs(DDD/1000/day)

The role of psycho-social interventions in suicide prevention

Standard psychotherapy plus intensive care for suicide attempters - RCT
ATTEMPTERS CONTR
(N=258) (N=258)
• Suicide attempt rate 7,7 13,9x
at month 12, (%)
• Suicide rate 3,1 3,6
at month 12, (%)
• Suicide or suicide attempt 10,7 17,4xx
rate at month 12, (%)
x p = 0,07 xx p = 0,056van Heeringen et al: Psychol.Med. 25:963-970, 1995

January 2008Danuta Wasserman 35
WHO Brief intervention and contact study -
18-month follow-up• RCT multi-center based intervention study SUPRE-MISS (2002-
2005)
• BIC = An 1 hour consultation in combination with discharge after a suicide attempt and afterwards nine further follow-up contacts – 1,2,4 7,11 weeks, and 4,6,12 och 18 months after a suicide attempt - with a doctor, psychologist or nurse
1867 suicide attemptpatients after randomisation
TAU = 945Treatment as usual
BIC = 922(Brief intervention and contact) +TAU
Fleischmann et al, Bulletin of the WHO, 2008; 86: 703-709.
Suicide:N = 18,2.2 %
Suicide:N = 2,0.2 %

Suicide prevention strategies –Competence of healthcare (2)
II. Public-oriented prespective (targetinggeneral population/specific subpopulations)
• Community suicide prevention programs -Gatekeeper training (GPs, teachers, priests,social workers, civil organizations..)
• Decresig negative attitudes regarding mental disorders and suicide and showing that mental illnesses can be successfully treated and suicide is preventable
• Responsible media reporting of suicide
___________________________________________________

TeleHelp – TeleCheck Service and Suicide Mortality
• A telephone helpline and emergency
response service
• 18.641 old people (≥ 65 yrs) in Veneto
region, Italy
• Follow-up periode: 1988 – 1998
• Number of suicides: observed = 6
expected = 20,86
• SMR for suicide: 29 (71% reduction)De Leo et al: Brit J Psychiat, 2002, 181:226-229, 2002

Suicides and suicide attempts in the Vienna subway system, 1984-1990,
before and after the introduction of reporting guid elines
39
19 15
8
0
5
10
15
20
25
30
35
40
1984-1987/I 1987/II-1990
suicides (n)suicide attempts (n)
Sonneck et al: Soc.Sci.Med. 38:453-457, 1994

Suicide prevention strategies –Competence of community leaders
• Restricting means of access (domestic/car exhaust gas, guns, pesticides, less toxic medicines)
• More restrictive alchol/drug policy• Improving well-beeing in general (incl.
decreasing unemployment)• Increasing support of health/social services• Supporting family life/cohesion
Rihmer et al, Curr Opin Psychiat, 2002; 15: 83-87.
____________________________________________________

Co-operationwith GPs
(e.g trainingsessions, video,phone hotline)
Support for high riskgroups and self help
activities
Cooperation withmultipliers
e.g. media, priests,teachers, geriatric
caregivers etc.
Publicrelation
campaign
4-level action programme
Hegerl, 2010

To implement the 4 level approach, you need a local/regional network
Association ofmedical doctors
PsychiatricHospital
Psychotherapists
GeneralPractitioners
Health insurancefunds
Schools
Churches andsocial services
Police/Military Forces Local health
authorities
Crisisintervention
centres
Self-helf groups
Geriatric care
Hegerl, 2010

Non-pharmacological health-care interventions for reducing suicide risk
• Crisis intervention• Intensive aftercare of suicidal patients• Problem-solving psychotherapy• TeleHelp-TeleCheck services• Decreasing access to means• Appropriate media policy
King et al, Brit J Psychiat, 2001; 178: 531-536.Motto and Bostrom, Psychiat Serv, 2001; 52: 828-833.Van Heeringen et al, Psychol Med, 1995; 25: 963-970.Linehan et al, Arch Gen Psychiat, 1993; 50: 971-974.DeLeo et al, Brit J psychiat, 2002; 226-229.

Rates of Suicide Attempts During 4 Weeks After Initial Antidepressant Prescriptiona
aBars indicate 95% confidence intervals.
Simon et al., Amer J Psychiat 2006, 163:41-47
Suicide attempts 4 weeks after starting ADs

Rates of Suicide Attempts During the 4 Weeks Before and 4 Weeks After Initial Antidepressant Prescriptiona
aBars indicate 95% confidence intervals.
Suicide attempts 4 weeks before and after starting ADs
Simon et al, Amer J Psychiat, 2006; 163: 41-47.

Why suicidal behaviour in depressed patients receiving ADs is still high in the
first few days/weeks of the AD treatment ?
• Lack of action of ADs (no change or spontaneous worsening of depression)- Resolution: close observation, removing lethal means, crisis intervention, anxiolysis, sedation (sleep !, BZPs), lithium, 2GAPs
• Worsening of depression due to AD in (potentially) bipolar depressives via inducing and/or aggravating depressive mixed states/agitation- Resolution: co-therapy: MSs, BZDs, 2GAPs
(quetiapine, olanzapine, MSs alone or in combination)

Why is suicide mortality still so high in the population?
• Low proportion of depressed/psychiatric patients are treated
• High rate of nonadherence• Lacking psychoeducation/psychotherapy• Low access to healthcare in some countries or
subpopulations• Increasing negative public attitude regarding
psychiatry, depression, and antidepressants• Internet propagation of suicide (!)• Increasing alcohol consumption• Negative psycho-social factors (unemployment) show
increasing tendency• Media coverage of mental disorders/suicide is not
optimal

Suicide rates and antidepressants in Italy and Hungary
6 x
- 51%
- 25%3 x
Gusmao et al, PLoSOne, 2013

Antidepresants and suicidal behaviour

Antidepressants and suicidality in adult population – RC drug trials
--------------------------------------------------------
All summay reports of FDA phase 2-3 (adult)RCTs on antidepressants (N=48.277)
Annual rate ( % ) Suicide Suicide attempt
• Antidepr. 0,6-0,9 2,8-6,3
• Placebo 0,4-0,5 2,7-6,7---------------------------------------------------------------
Kahn et al. 2000, 2001, 2003.

SSRIs and venlafaxine in childhood depression: Review of published and
unpublished RCTs--------------------------------------------------------
• 2262 patients with MDE (6-18 yrs)• No single patient committed suicide !• Rate ( % ) of suicidal attempts+intention:
Active treatm. Placebo • Fluoxetine 9/249 (3,6) 8/209 (3,8)• Paroxetine 14/378 (3,7) 7/285 (2,5)• Sertraline 5/189 (2,6) 2/184 (1,1)• Citalopram 15/210 (7,1) 7/197 (3,5)• Venlafaxine 14/182 (7,7) 1/179 (0,6)• TOTAL 57/1208 (4,7) 25/1054 (2,4)Whittington et al, Lancet, 2004, 363:1341-1345.

Suicidal behaviour and ideation in RCTs on ADs in unipolar MDD as a
function of age372 RCTs, 99,839 patients
OR• Children 2.22• 18-24 yr 1.55• 25-30 yr 1.00• 31-64 yr 0.77• 65 yr and over 0.39• All adults 0.84
Friedman and Leon, NEJM, 2007; 356: 2343-2346.
___________

Risk of suicidality in RCTs on ADs
• 99,231 major depressed and other patients incl. nonpsychiatric indications
OR of suicdal behaviour
• 18 - 24 yr 2.30• 25 – 64 yr 0.87• 65 yr and over 0.06
Stone et al, BMJ, 2009; 339: b2880
_______________________________
The risk of suic. behav. in nonpsychiatric indications was exremely low !

Barbui et al, CMAJ, 2009; 180: 291-297.
SSRIs and suicide in unipolar depression: Review of the observational studies
__________________________________________________________
_________
______
_____
x
x
x

Antidepressants and suicidal behaviour
In the cases of unrecognized/covert bipolarity, antidepressant monotherapy (unprotected by mood-stabilizers or atypical antipsychotics) in „unipolar” depression can result in:
- response/remission (rare)- hypomanic/manic switch (common)- rapid cycling/destabilization (common)- nonresponse (common)- worsening (via inducing/aggravating mixed depression
and increasing the risk of suicidal behaviour) (rare)
Koulopoulos et al, Clin Neuropsychopharmacol, 1992; 15 (S1): 626.627.Rihmer and Akiskal, J Affect Disord, 2006; 94: 3-13.Rihmer, Curr Opin Psychiat, 2007, 20: 17-22.


Int J Psychopharmacol, 2013; 33: 449-452.

Antidepressant-induced suicidal ideation and bipolarity
• 269 inpatients with Major Depressive Episode (6% bipolar depression)
• No SI: 130 pts• Non-TESI: 117• TESI: 22• Rate of TESI
bipolar depression: 26.7%nonbipolar depression: 7.1%
p = 0.025
Musil et al, Eur Neuropsychopharmacol, 2013; 23: 663-674.
TESI: Treatment emergent suicidal ideation

Inpatients with MDE and treatment resistance
• 269 inpatients with MDE • Rate of treatment resistant depression:
- TESI (n=22) 27 %- non TESI (n=117) 4 %- nonsuicidal pts. (n=130) 18 %
TESI: Treatment emergent suicidal ideation
Musil et al, Eur Neuropsychopharmacol, 2013; 23: 663-674.

Augmentation with MSs in resistant unipolar major depression
• 256 strictly diagnosed unipolar major depr.• 23 % (59/256) had at least one
agugmentation with MSs (Lithium, CBZ, valpromide)
• Responders: 30% (18/59)• Nonresponders: 70% (41/59)• Clinical profile of responders:
younger age, shorter episodes, „activated depression” (less retard., more agitation), suicidal tendencies, cyclothymic/hyperthymic temperament
Hantouche et al. J Affect Disord, 2005, 84: 243-249.

Antidepressants and suicidal behaviour in RCTs on unipolar
depression
EXCLUDED:Acutely suicidal, very severe, comorbid,noncompliant, and officially (DSM-IV orICD-10) diagnosed Bipolar I and II pts
INCLUDED:Subsyndromal bipolar, and bipolar spectrum disorder patients, and agitated depressives resulting in about 30 % covert bipolarity in these „unipolar” patients
x therefore no detectable anti-suicidal effect is expected
x

%30
20
10
3%1.5%
Suicidality (attempts + suicides) and AD treatment in UP MDE
RCTsExcl. suic. pts
+100%
Before/without ADs
On ADs

%30
20
10
30%
3%1.5%
6%
Real life studiesIncl. suic. pts
RCTsExcl. suic. pts
-80%
+100%
Before/without ADs
On ADs
Suicidality (attempts + suicides) and AD treatment in UP MDD

Conclusions
• Untreated major mood disorders (schizophrenia and substance-use disorders) markedly increases the risk of suicidal behaviour particularly in severe bipolar (mixed) depresion
• As the majority of mood disorder patients never complete suicide, other (personality and psychosocial) factors play also a role
• Suicide risk factors are additive in their nature• Suicide risk is predictable with good chance• Effective acute and long-term treatment of psychiatric patients
(Li, MS, ADs, APs, ANXLs) significantly reduces the risk of suicidal behaviour
• MS is the key component in the acute and long-term treatment of bipolar disorders
• AD monotherapy in bipolar depression (incl. subthreshold forms) can worsen depression and resulting in suicidal behaviour
• Supportive psychotherapy is allways needed and supplementary specific psychosocial interventions further improve the results
Related Documents











