Suicide Prevention And Health Care August 31, 2017 Presented by: Adrienne Shilton, Steinberg Institute Victor Ojakian, NAMI Santa Clara County and Advocate

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Suicide Prevention And Health Care
August 31, 2017
Presented by:
Adrienne Shilton, Steinberg InstituteVictor Ojakian, NAMI Santa Clara County and
Advocate
The Steinberg Institute is dedicated to advancing sound public policy and inspiring leadership on the issues of mental health.
We believe that brain health is the under-attended issue of our time.
We: Bring together stakeholders and
nontraditional partners on key issues to discuss and establish shared priorities
Identify and coordinate strategic opportunities to advance sound policy and implement cutting-edge programs and services
Address complex disputes and resolve challenges, resulting in improved outcomes
In the US, 44,000 people die by suicide each year, most because of untreated mental illness.
Each year, more than 200 college students in California take their lives.
This loss of life is tragic and preventable.
We are committed to changing this story.
My story begins when my son took his life in 2004. I do not believe anything prepares a person to lose a loved one to suicide, particularly the death of a family member with a non-diagnosed mental health condition.
The intimacy you have with your loved one can mask recognition of some subtle behaviors and make it difficult to believe your loved one would harm themselves.
Often it is suggested parents do something more to recognize signs in their children, as if this is a simple task. Just provide some teaching or tell them the signs and symptoms they should look for. It is not that simple or easy.
What Do The Numbers Mean – Data
As a public health matter, suicide involves a spectrum of activity: ◦ Suicidal thoughts (ideation), suicide planning, suicide attempts, and completed
deaths
How significant are the occurrences: ◦ An estimated 9.4 million Americans (aged 18 or older):serious thoughts of suicide◦ 2.7 million made a suicide plan and 1.1 million attempted suicide◦ 42,826 completed suicides The NSDUH Report: Suicidal Thoughts and Behaviors Among Adults (2014) https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR2-2014/NSDUH-FRR2-2014.pdf/
California suicides are increasing and the 2014 data is: ◦ Attempts: 48,531◦ Deaths: 4,119 suicides◦ California suicide rate:10.64 Source for California suicide and suicide attempt data: Epicenter database
http://epicenter.cdph.ca.gov/ReportMenus/CustomTables.aspx
The one percent (1%) fallacy: ◦ Suicides equal about 1% of our population as if that is insignificant ◦ Suicides far outnumber homicides
The CDC issued a report comparing 2014 with 1999 rates of suicides by females and male at various age intervals:
All gender and aged categories showed an increase in rates The average annual percent increase in the age-adjusted suicide rate was about 1% per
year from 1999 through 2006 but increased to 2% per year from 2006 through 2014. Highest suicide rates: ◦ 45-64 yr. old females in both 1999 (6.0 per 100,000) and 2014 (9.8) and second-
largest percent increase (63%) since 1999. ◦ Women aged 75 and over decreased by 11% from 1999 through 2014, declining from
4.5 to 4.0 per 100,000◦ Females aged 10–14: largest percent increase (200%), 150 suicides in 2014, tripling
from 0.5 per 100,000 in 1999 to 1.5 in 2014. ◦ Since 1999 females aged 15–24, 25–44, and 65–74 suicides rates increased between
31% and 53%. ◦ Males aged 75 and over had their suicide rate decreased by 8%, from 42.4 per
100,000 in 1999 to 38.8 in 2014. ◦ Males aged 45–64: second-highest suicide rate in 2014 and the largest percent
increase (43%) in rates, increasing from 20.8 in 1999 to 29.7 in 2014.
Increase in Suicide in the United States, 1999–2014 Sally C. Curtin, M.A., Margaret Warner, Ph.D., and Holly Hedegaard, M.D., M.S.P.H. https://www.cdc.gov/nchs/data/databriefs/db241.pdf
Other sources of local/regional data: Review your county Medial Examiner/Coroners’ Office annual death report
Work with Medical Examiner/Coroners’ Office to produce an analysis report on local suicides◦ Analysis of 2009-2011 Suicide Data of Santa Clara County
https://www.sccgov.org/sites/bhd/partners/workgroups/SuicidePrevention/Documents/Analysis%20of%202009-2011%20Suicide%20Data%20of%20SCC%2011-8.pdf
County Death Review Panel data
Get crisis call center data, if available◦ Attempts and ideation by age, gender, race/ethnicity etc.◦ Be aware of other support functions they offer
Emergency call center (9-1-1) data: 1056 and 1056a calls
Training: See Locating and Understanding Data for Suicide Prevention (SPRC)
http://training.sprc.org/enrol/index.php?id=2
Californians’ Attitudes About Suicide Prevention
California Statewide Awareness of Suicide - 2012 (part three of California Situational Overview for Suicide Prevention http://emmresourcecenter.org/resources/situational-overview-suicide-prevention-2011 A telephone survey of 2,003 Californian of diverse backgrounds on suicide attitudes and
knowledge
Some results: Over Fifty-one percent (51.2%) of Californians: a personal experience with suicide
Individuals with warning sign knowledge: Review an informational website (82%); call a crisis line (85.6%); provide a phone number or other resource (93.5%); express concern (94.7%); express concern to others (92.5%)
Some attitudes measured: Suicide is preventable (73.9%); individuals know warning signs (70%); understand there are more deaths by suicide than homicide (34.5%); take suicide talk seriously (59.4%); able to discuss suicide with loved one (77.5%); express concern about suicidal behavior (89.9%)
What To Look For – Warning Signs, Risk, And Protective Factors
There are three key “identifiers” commonly -- risk factors, warning signs and protective factors.
The American Foundation for Suicide Prevention(AFSP) defines each as follows: ◦ Risk factors: Risk factors are characteristics or conditions that increase the
chance that a person may try to take their life. The more risk factors, the higher the risk. They classify them as health, environmental, or historic factors. https://www.afsp.org/understanding-suicide/suicide-risk-factors
◦ Warning signs: People who kill themselves exhibit one or more warning signs, either through what they say or what they do. The more warning signs, the greater the risk. Three subcategories are provided talk, behavior, and mood. https://www.afsp.org/preventing-suicide/suicide-warning-signs
◦ Protective factors: They reduce the likelihood of suicide. They enhance resilience and may serve to counterbalance risk factors. http://www.sprc.org/sites/sprc.org/files/library/srisk.pdf
◦ Is your ER using the Emergency Nurses Association poster: http://www.sprc.org/sites/default/files/migrate/library/ER_SuicideRiskPosterVert2.pdf
What Actions Can Be Taken – Strategies, Assessments, and Interventions
Primary care providers : ◦ Seventy-six percent (76%) of individuals who die by suicide see PCP in the prior
month◦ Ninety percent (90%) of individuals who die by suicide see a PCP sometime in
the last year ◦ These same individuals were more than twice as likely to have seen their PCPthan a mental health professional in the year and month prior to their suicide.
Emergency Rooms and hospitals: ◦ Often the setting for involuntary detentions◦ Provide intervention services
Psychiatric Emergency Services or Emergency Psychiatric Services facilities: initial evaluation of possibly suicidal individuals
Contact With Mental Health and Primary Care Providers Before Suicide: A Review of the Evidence http://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.159.6.909
Suicide Prevention Strategies in Primary Care include:
Training staff to recognize and respond to warning signs of suicide
Universal screening and aggressive treating for depression
Screening for suicidality in patients with key risk factors:
Educating patients about warning signs for suicide
Restricting means for lethal self‐harm
Suicide prevention toolkit for rural primary care, page 6 http://www.sprc.org/resources-programs/suicide-prevention-toolkit-rural-primary-care
Suicide risk assessment should have key elements, including: Assess risk factors (chart/poster in upcoming slide)
Suicide Inquiry: thoughts/plan /intent/access to means◦ Asking a person/patient directly if they are suicidal ◦ Sample question: Have you ever tried to kill yourself or attempt suicide?
Assess protective factors◦ Mitigate risk in a person with moderate to low suicide risk
Clinical judgment◦ Assessment is complex when multiple patient conditions exist (including medical,
mental health and substance use conditions◦ Assessment and intervention of suicidal patients chart available
http://www.sprc.org/sites/default/files/PCPocketCard.pdf
Document◦ Patient history imperative◦ Follow-up inquiries necessary
Suicide prevention toolkit for rural primary care, page 10 http://www.sprc.org/resources-programs/suicide-prevention-toolkit-rural-primary-care
Suicide Prevention Interventions in Primary Care: Primary Care Suicide Prevention Practice Model
http://www.sprc.org/sites/default/files/Intervention_Scheme.pdf
Referrals:
Treatment of psychiatric symptoms, including depression and seversanxiety
Strengthening the support network:
Developing a safety plan (example in slides)
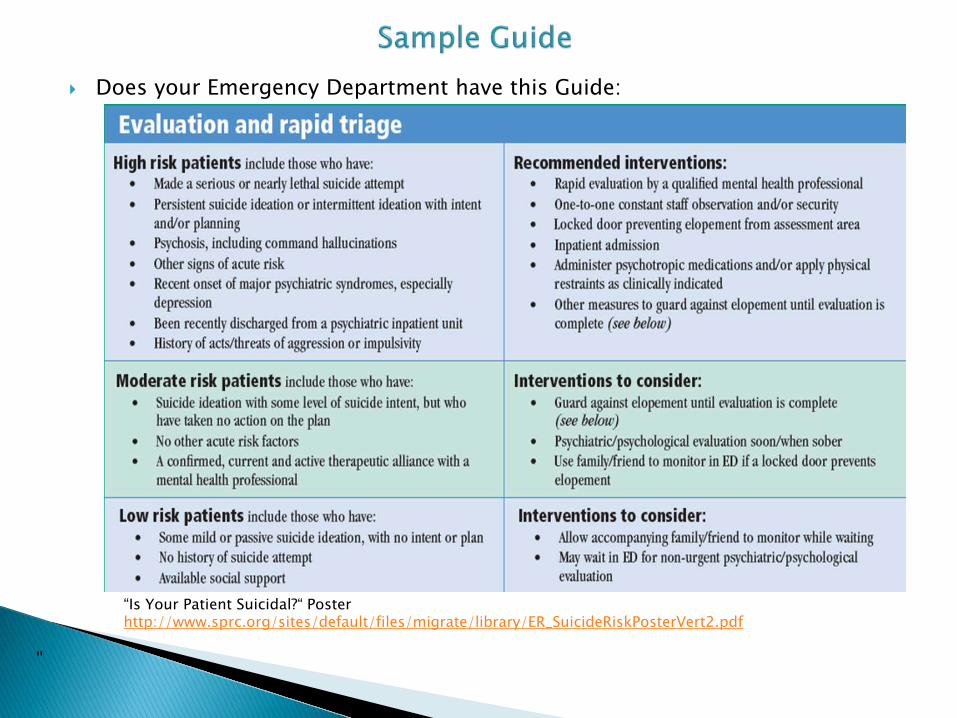
Does your Emergency Department have this Guide:
“Is Your Patient Suicidal?“ Poster http://www.sprc.org/sites/default/files/migrate/library/ER_SuicideRiskPosterVert2.pdf
"
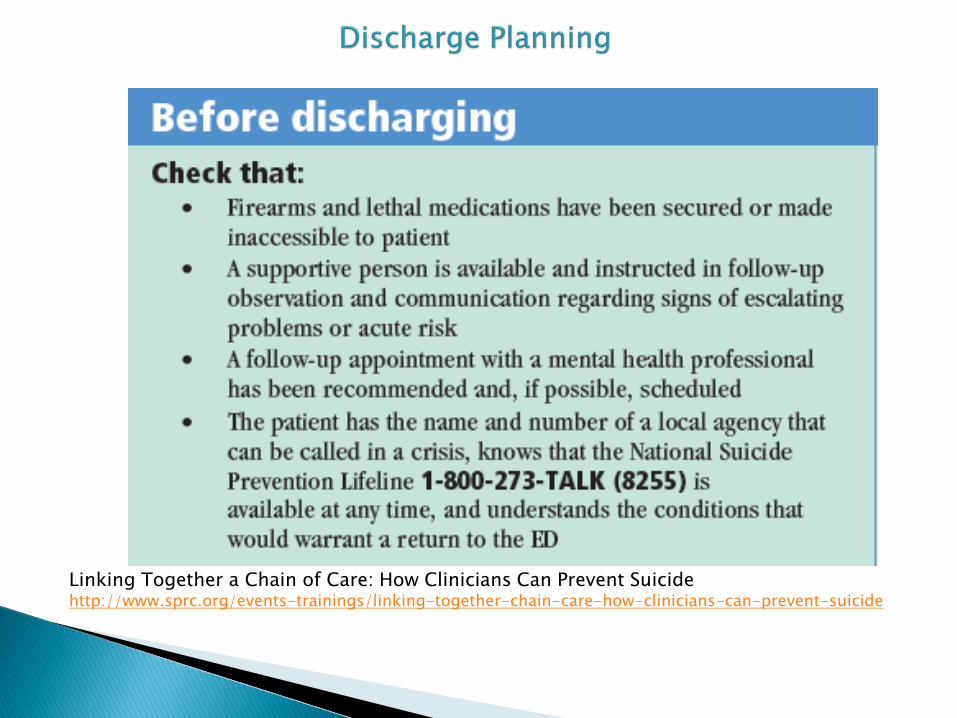
Linking Together a Chain of Care: How Clinicians Can Prevent Suicide http://www.sprc.org/events-trainings/linking-together-chain-care-how-clinicians-can-prevent-suicide
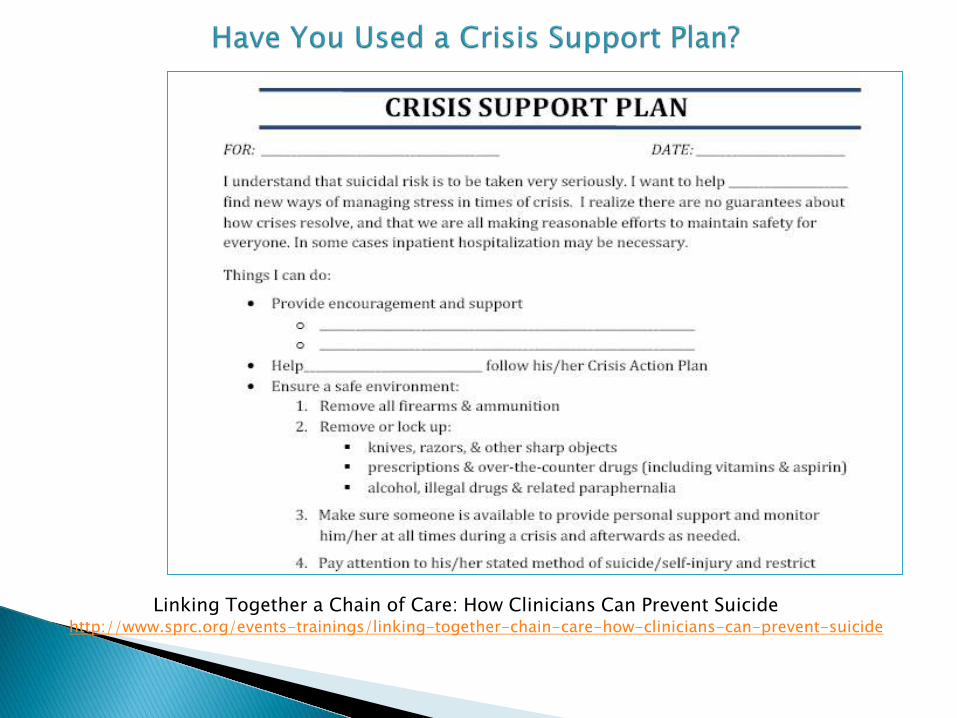
Linking Together a Chain of Care: How Clinicians Can Prevent Suicide http://www.sprc.org/events-trainings/linking-together-chain-care-how-clinicians-can-prevent-suicide

Toolkits, Tools, and Resources
Take advantage of available, free, suicide prevention toolkits tailored to the health care environment including but not limited to:◦ An exception: K-12 Toolkit for Mental Health Promotion & Suicide Prevention
http://www.heardalliance.org/help-toolkit/#web
◦ Suicide prevention toolkit for rural primary care http://www.sprc.org/resources-programs/suicide-prevention-toolkit-rural-primary-care
◦ Collaborative Safety Planning to Reduce Risk in Suicidal Patients: A Key Component of the Zero Suicide Model http://suicideprevention-icrc-s.org/collaborative-safety-planning-reduce-risk-suicidal-patients-key-component-zero-suicide-model?utm_source=Weekly+Spark+8%2F11%2F17&utm_campaign=Weekly+Spark+August+11%2C+2017&utm_medium=email
◦ Initiative on Depression and Primary Care https://www.amerihealthcaritasla.com/pdf/provider/behavioral-health/depression-toolkit-adolescent-questionnaire.pdf
◦ Assessing and Treating Suicidal Behaviors and Practice Guidelines For The Assessment and Treatment of Patients With Suicidal Behaviors (American Psychiatric Association) http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/suicide-guide.pdf and http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/suicide.pdf
Tools:
Seven Cups of Tea: https://www.7cups.com/. Free, anonymous and confidential online text chat with trained listeners, online therapists & counselors
Treatment and discharge plans for suicidal patients:
Patient Safety Plan Template http://www.sprc.org/sites/default/files/Brown_StanleySafetyPlanTemplate.pdf
My3App http://my3app.org/
SAFE-T Pocket Card: Suicide Assessment Five-Step Evaluation and Triage for Clinicians https://store.samhsa.gov/product/SAFE-T-Pocket-Card-Suicide-Assessment-Five-Step-Evaluation-and-Triage-for-Clinicians/SMA09-4432
Resources: Linking Together a Chain of Care: How Clinicians Can Prevent Suicide
http://www.sprc.org/events-trainings/linking-together-chain-care-how-clinicians-can-prevent-suicide
A Resource Guide for Implementing the 2007 Patient Safety Goals on Suicide by The Joint Commission http://www.sprc.org/sites/default/files/migrate/library/jcsafetygoals.pdf
◦ Question, Persuade, and Refer (QPR) https://www.qprinstitute.com/
◦ LivingWorks trainings: SafeTALK https://www.livingworks.net/programs/safetalk/ Applied Suicide Intervention Skills Training (ASIST)
https://www.livingworks.net/programs/asist/ For availability contact: Kathleen S. Snyder, MSW, California Representative
LivingWorks Education at 916.316.2076 [email protected]
◦ Talk Saves Lives https://afsp.org/our-work/education/talk-saves-lives-introduction-suicide-prevention/
◦ Break Free From Depression http://www.childrenshospital.org/centers-and-services/boston-childrens-hospital-neighborhood-partnerships-program/break-free-from-depression-program
◦ Mental Health First Aid https://www.mentalhealthfirstaid.org
Local NAMI affiliate including the Provider Education class https://www.nami.org/Find-Support/NAMI-Programs/NAMI-Provider-Education
There are a plethora of organizations and websites. Here are a few:
Each Mind Matters: http://www.eachmindmatters.org/spw2017/ HEARD Alliance http://www.heardalliance.org/ American Association of Suicidology (AAS) http://www.suicidology.org/ American Foundation for Suicide Prevention (AFSP) https://afsp.org/ American Psychiatric Association (APA) https://www.psychiatry.org/patients-
families/suicide-prevention American Psychiatric Nurses Association (APNA)
https://www.apna.org/i4a/pages/index.cfm?pageID=5684 American Psychological Association (APA)
http://www.apa.org/search.aspx?query=suicide+prevention&fq=ClassificationFilt%3a%22Suicide%22
Center for Disease Control (CDC) https://www.cdc.gov/ National Action Alliance for Suicide Prevention (Action Alliance)
http://actionallianceforsuicideprevention.org/ National Institute of Mental Health (NIMH)
https://www.nimh.nih.gov/search.jsp?query=suicide+prevention+ National Suicide Prevention Lifeline (NSPL) https://suicidepreventionlifeline.org/ Suicide Prevention Resource Center (SPRC) http://www.sprc.org/

How Can I Help Now?
Laws can ensure or promote actions and change our culture!
Current California Legislation of interest:◦ AB 917 (Arambula) regarding college suicide prevention. This bill would
dramatically change the way we care for students by mandating that colleges and universities adopt and implement a suicide prevention policy on every campus with information on signs and symptoms of suicide ideation as well as information on how to access local, state and federal resources. https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201720180AB917. AB 917 will be a two year bill.
◦ AB 89 (Levine) regarding suicide prevention training for psychologists: All California psychologists would be required to have six hours of training in suicide assessment, treatment, and management. http://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201720180AB89 . AB 89 is on the Governor’s desk.
◦ AB 1315 (Mullin) which would shift our paradigm of care from fail-first to care first, and incentivize counties to expand evidence based early intervention programs. https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201720180AB1315 . AB 1315 is in Senate Appropriations.
Related Documents











