Sugammadex Clinical advantages in neuromuscular reversal Geoff Muller Puerto Vallarta Feb 2018

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SugammadexClinical advantages in neuromuscular reversal
Geoff MullerPuerto Vallarta
Feb 2018

Conflicts of Interest
• None to declare
NMB + Anticholinesterase + Anticholinergic

NMB + Anticholinesterase + Anticholinergic
Poison + Antidote + Antidote-to-the-antidote

NMB + Anticholinesterase + Anticholinergic
Poison + Antidote + Antidote-to-the-antidote


Learning objectives
• Review the use of neuromuscular blockers• Problems with traditional neuromuscular reversal• Pharmacology of sugammadex• Clinical advantages• Practical considerations
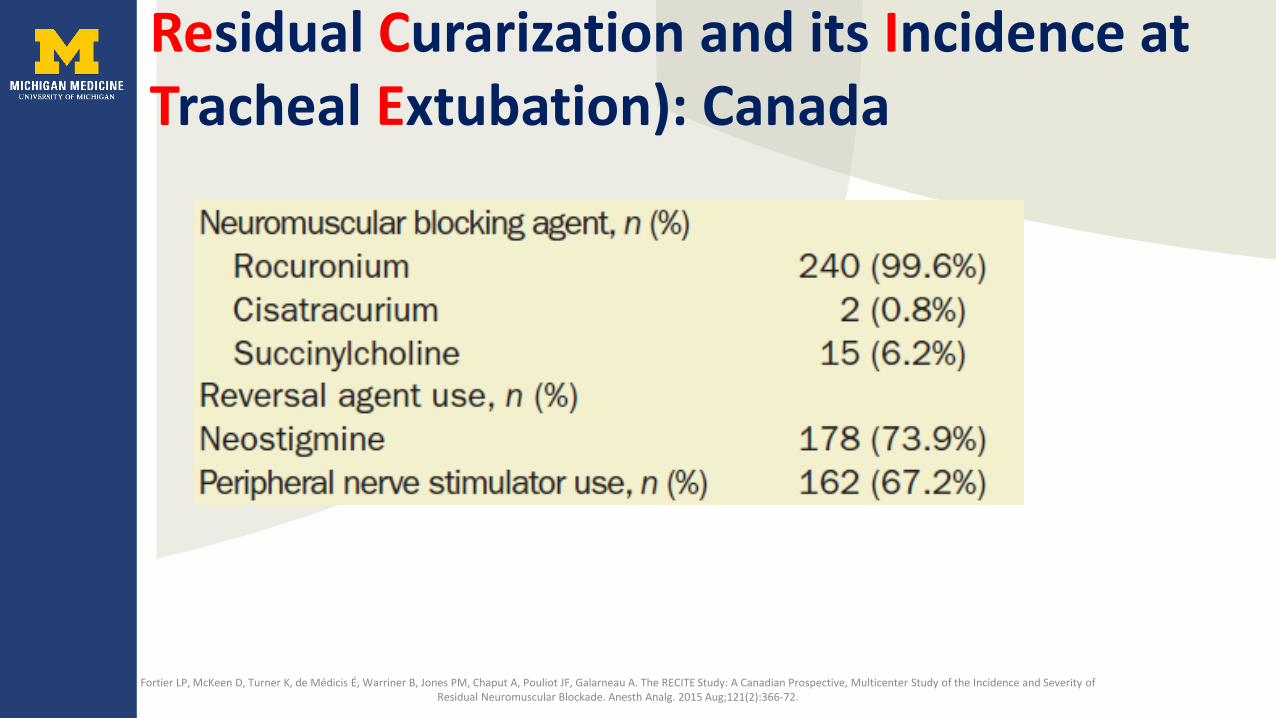
Residual Curarization and its Incidence at Tracheal Extubation): Canada
Fortier LP, McKeen D, Turner K, de Médicis É, Warriner B, Jones PM, Chaput A, Pouliot JF, Galarneau A. The RECITE Study: A Canadian Prospective, Multicenter Study of the Incidence and Severity of Residual Neuromuscular Blockade. Anesth Analg. 2015 Aug;121(2):366-72.
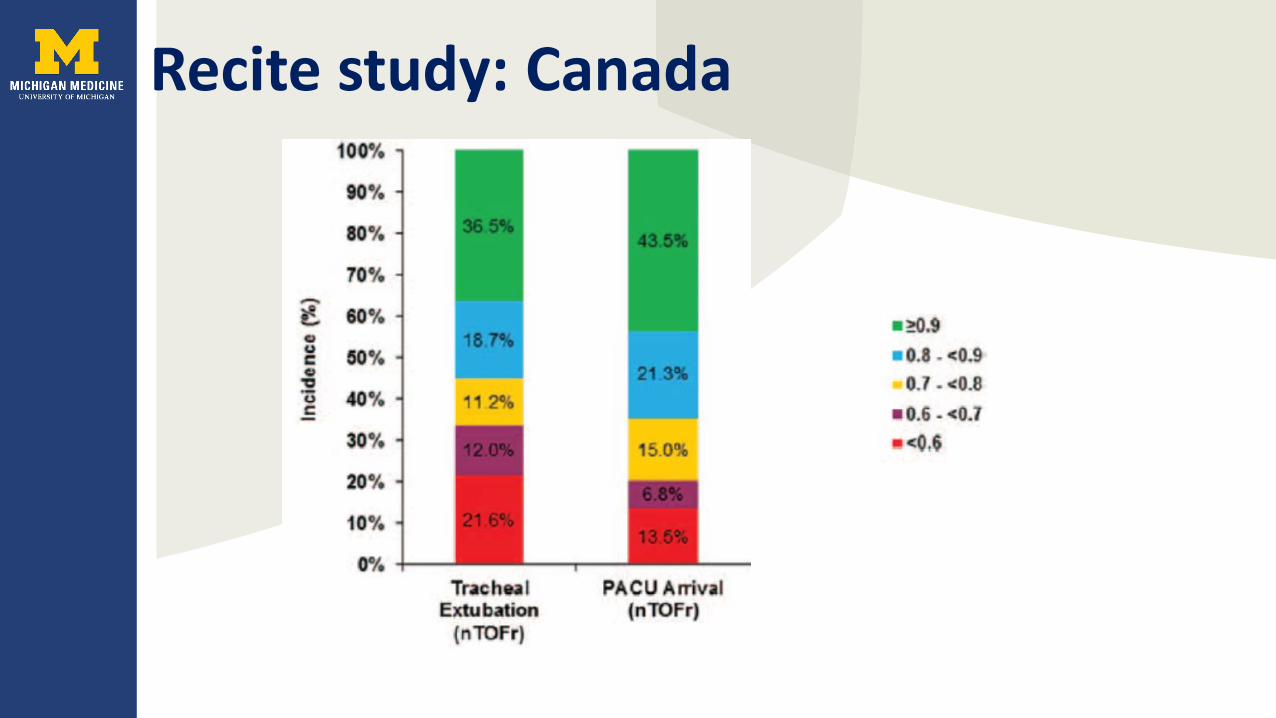
Recite study: Canada

Learning objectives
• Review of usage neuromuscular blockers• Problems with traditional neuromuscular reversal• Pharmacology of sugammadex• Clinical advantages• Practical considerations
Why are we so bad at NMB reversal?
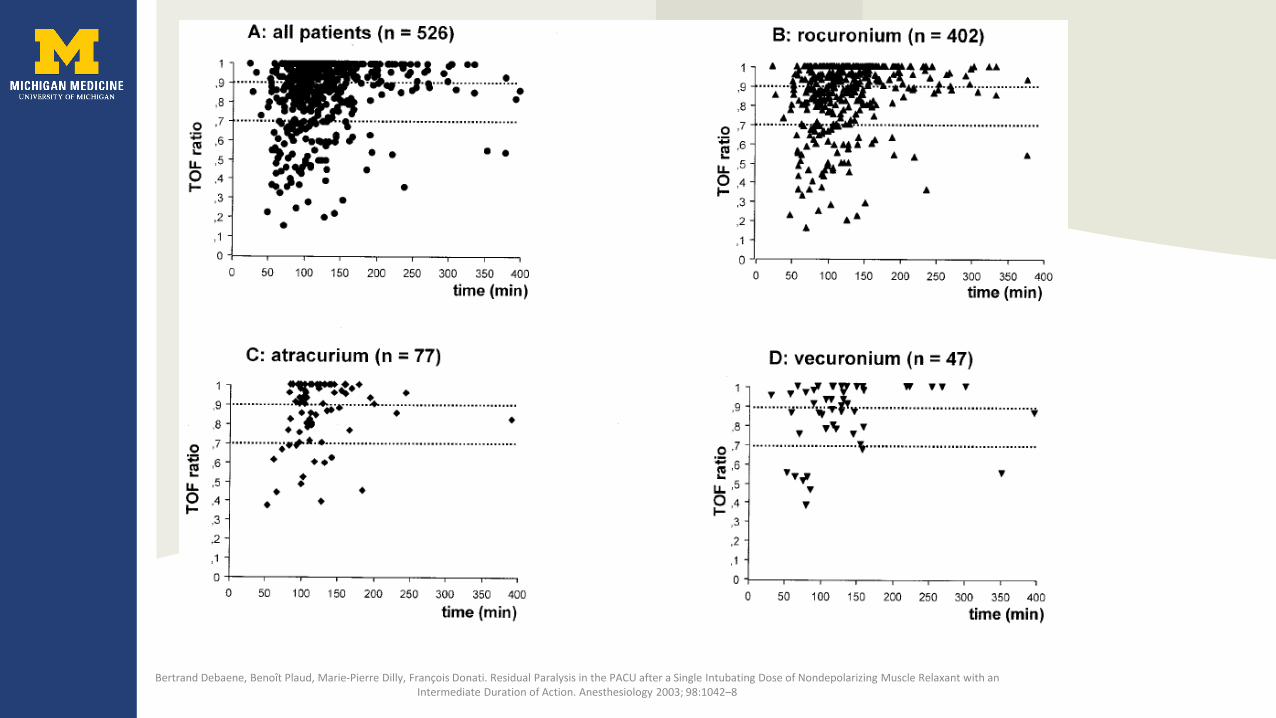
Bertrand Debaene, Benoît Plaud, Marie-Pierre Dilly, François Donati. Residual Paralysis in the PACU after a Single Intubating Dose of Nondepolarizing Muscle Relaxant with an Intermediate Duration of Action. Anesthesiology 2003; 98:1042–8
Bertrand Debaene, Benoît Plaud, Marie-Pierre Dilly, François Donati. Residual Paralysis in the PACU after a Single Intubating Dose of Nondepolarizing Muscle Relaxant with an Intermediate Duration of Action. Anesthesiology 2003; 98:1042–8

Kirkegaard H, Heier T, Caldwell JE: Efficacy of tactile guided reversal from cisatracurium-induced neuromuscular block. Anesthesiology 2002; 96:45–50
TOF>0.9
TOF 0.8-0.9
TOF 0.7-0.8
TOF<0.7
TOF 0.9
TOF 0.8TOF 0.7
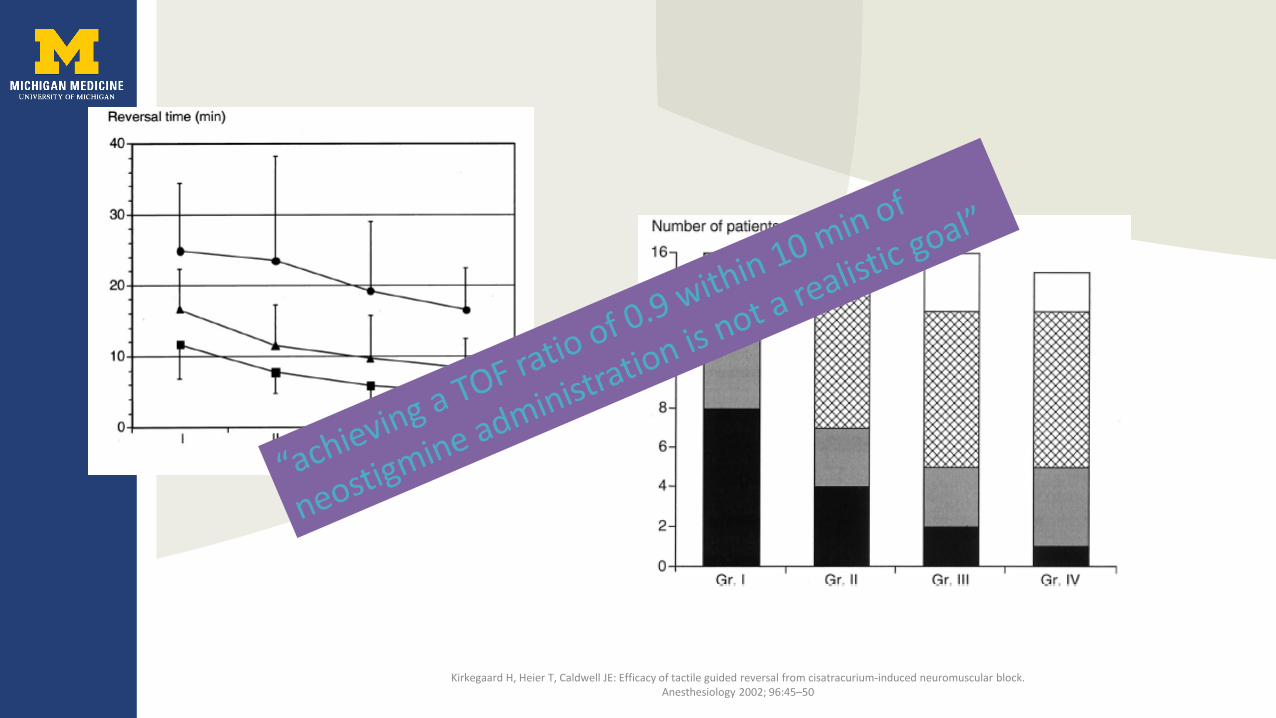
Kirkegaard H, Heier T, Caldwell JE: Efficacy of tactile guided reversal from cisatracurium-induced neuromuscular block. Anesthesiology 2002; 96:45–50
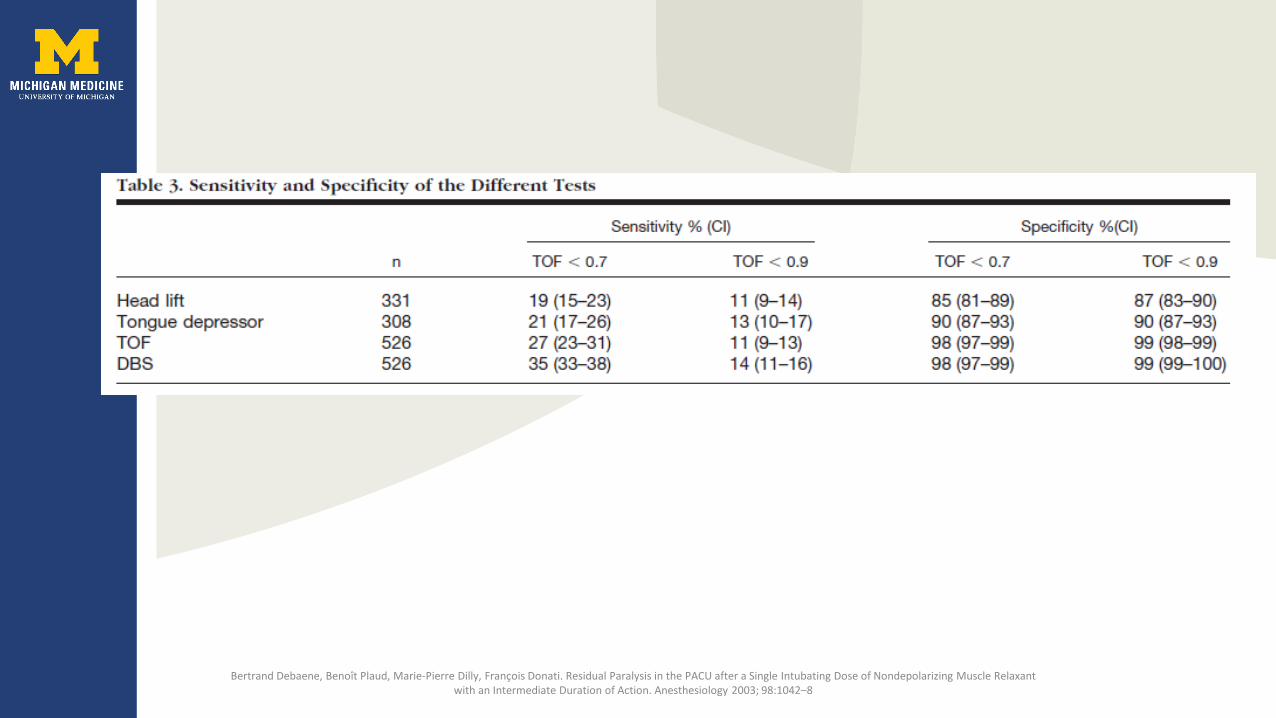
Why are we so bad at NMB reversal?
• Insufficient monitoring• Wide interindividual variation in pharmacokinetics• Low sensitivity of detecting residual block• Time to recovery to TOF ratio >0.9


So what?

Residual Neuromuscular block (RNMB) - Airway
• 6/14 with residual block aspirated (TOF ratio <0.9)
Eriksson LI, Sundman E, Olsson R, Nilsson L, Witt H, Ekberg O, Kuylenstierna R. Functional assessment of the pharynx at rest and during swallowing in partially paralyzed humans: simultaneous videomanometry and mechanomyography of awake human volunteers. Anesthesiology. 1997 Nov;87(5):1035-43.

RNMB - Airway• 6/14 with residual block aspirated (TOF ratio <0.9)• Normal• Volunteers • Young (22-44yrs)• No reflux or airway disease• No surgery• No other drugs (vecuronium)
Eriksson LI, Sundman E, Olsson R, Nilsson L, Witt H, Ekberg O, Kuylenstierna R. Functional assessment of the pharynx at rest and during swallowing in partially paralyzed humans: simultaneous videomanometry and mechanomyography of awake human volunteers. Anesthesiology. 1997 Nov;87(5):1035-43.
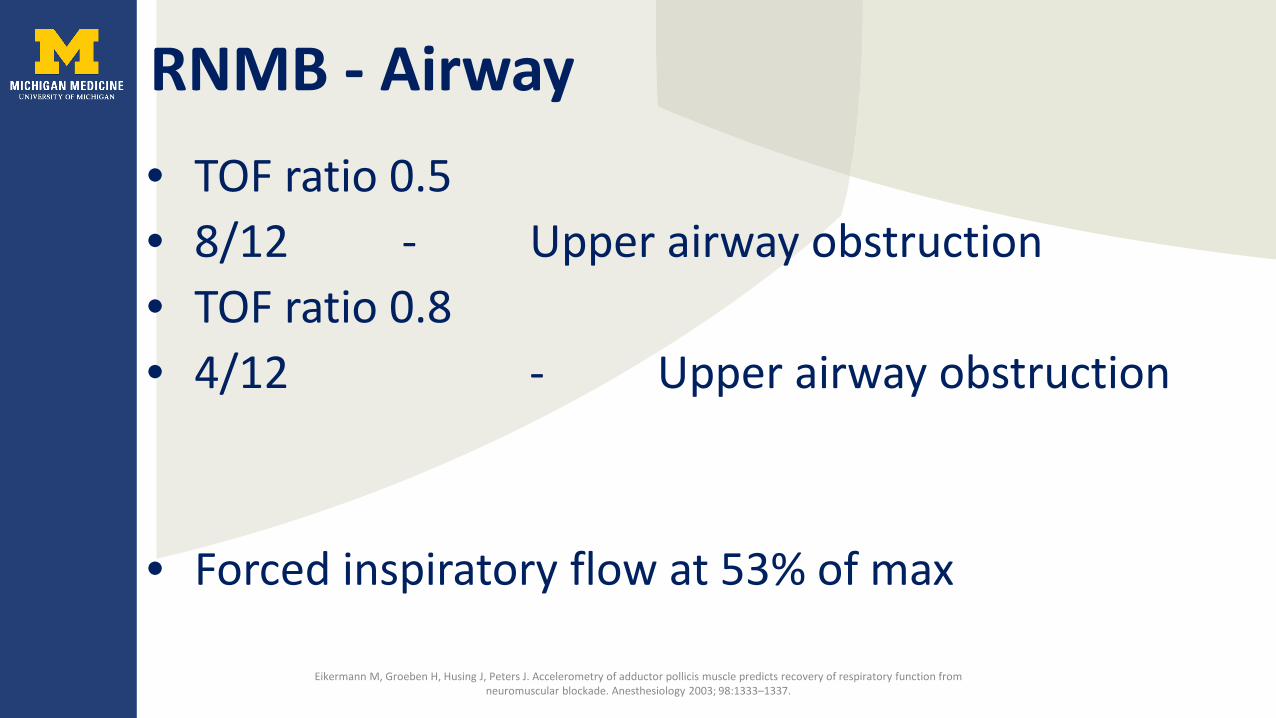
RNMB - Airway• TOF ratio 0.5• 8/12 - Upper airway obstruction• TOF ratio 0.8• 4/12 - Upper airway obstruction
• Forced inspiratory flow at 53% of max
Eikermann M, Groeben H, Husing J, Peters J. Accelerometry of adductor pollicis muscle predicts recovery of respiratory function from neuromuscular blockade. Anesthesiology 2003; 98:1333–1337.

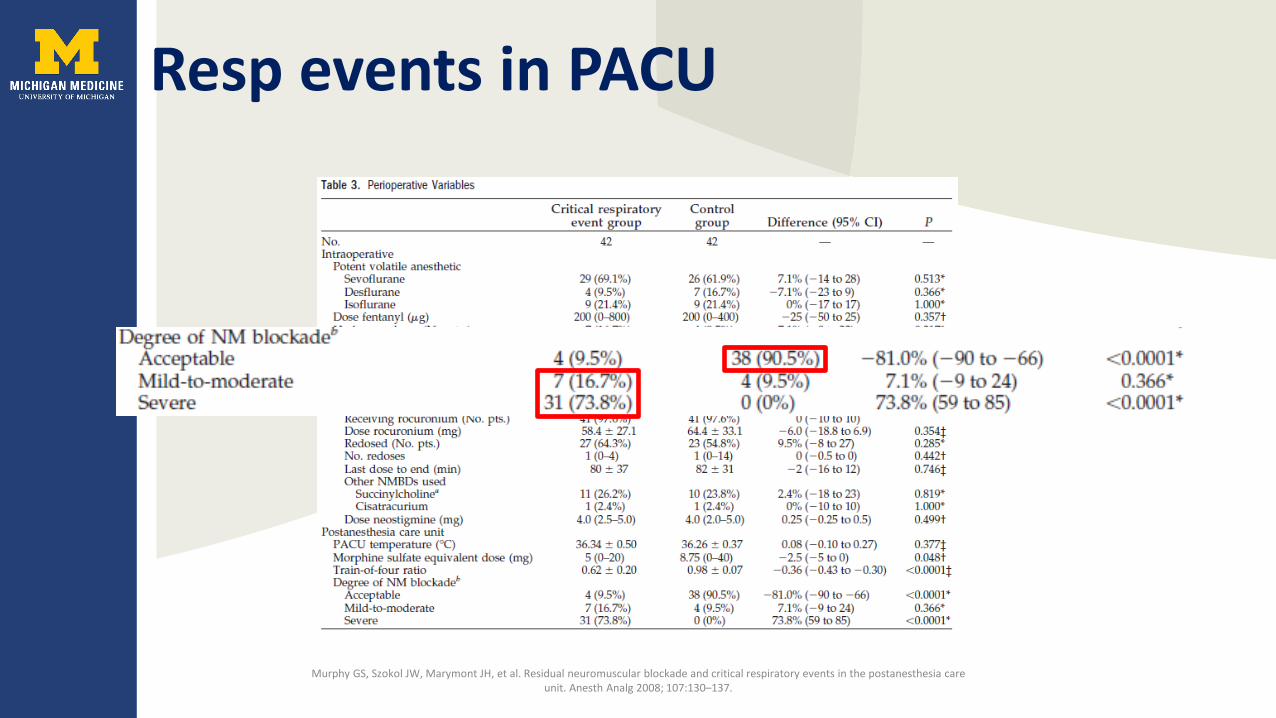
Resp events in PACU
Murphy GS, Szokol JW, Marymont JH, et al. Residual neuromuscular blockade and critical respiratory events in the postanesthesia care unit. Anesth Analg 2008; 107:130–137.

Resp events in PACU
Murphy GS, Szokol JW, Marymont JH, et al. Residual neuromuscular blockade and critical respiratory events in the postanesthesia care unit. Anesth Analg 2008; 107:130–137.
Resp events in PACU
Murphy GS, Szokol JW, Marymont JH, et al. Residual neuromuscular blockade and critical respiratory events in the postanesthesia care unit. Anesth Analg 2008; 107:130–137.
Is there a better way?
Learning objectives
• Review of usage neuromuscular blockers• Problems with traditional neuromuscular reversal• Pharmacology of sugammadex• Clinical advantages• Practical considerations

Cyclodextrins
• Cyclic oligosaccharide• 6-α,7-β, 8-γ• Febreze – beta cyclodextrin, traps odor molecules• Emulsifier, cholesterol free products, sweeteners,
medications

Sugammadex
• EU 2009• Japan 2010• FDA approval Dec 2015

Sugammadex (Sugar gamma cyclodextrin)
• Synthetic modified cyclodextrin• γ cyclodextrin – 8 monomer ring structure • 6-glucopyranoside units• Side chain to fit rocuronium

Sugammadex
• Toroidal shape
Sugammadex
• Toroidal shape• Donut shape• Encapsulates aminosteroid NMB
Sugammadex
• Toroidal shape• Donut shape• Encapsulates aminosteroid NMB
– Pancuronium– Vecuronium– Rocuronium– Pipecuronium

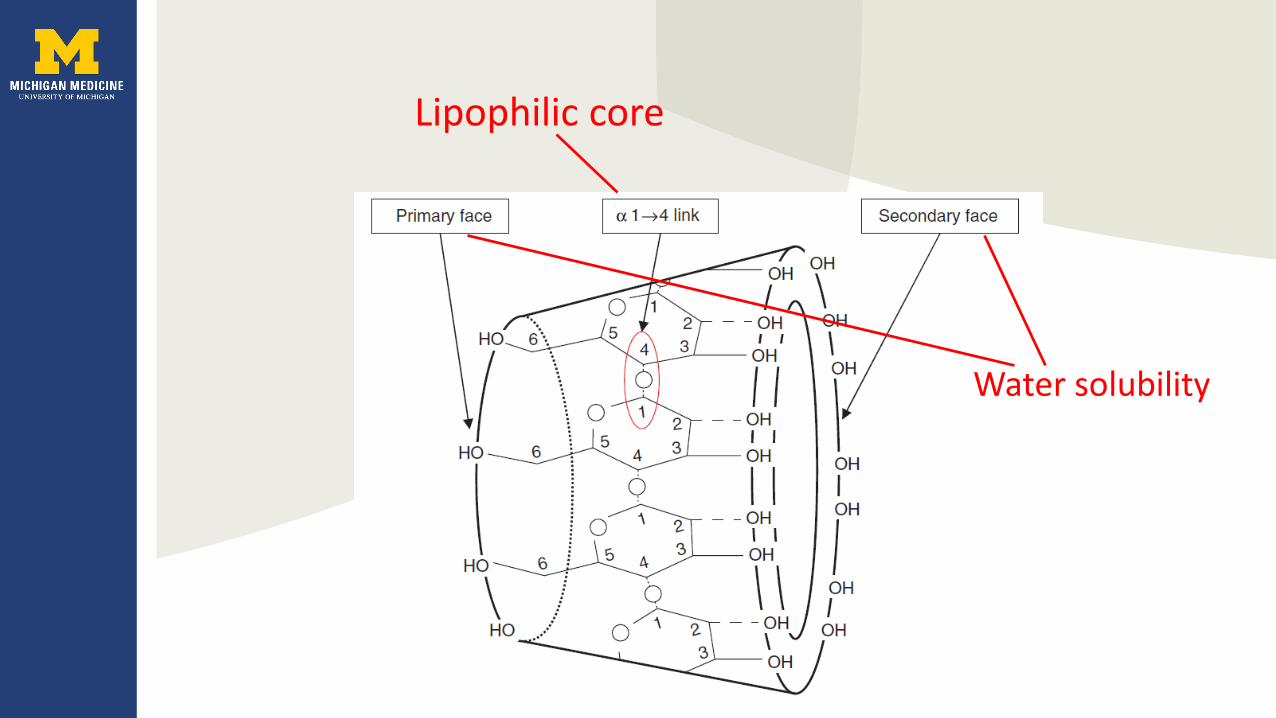
Lipophilic core
Water solubility

Pharmacodynamics
• No receptor effects

Pharmacodynamics
• No receptor effects• No muscarinic (cholinergic) effects

Pharmacokinetics
• Terminal Elimination half life 100-136mins• Clearance approaches GFR• Administered dose excreted in urine over 24hrs• Increases Rocuronium renal excretion from 26 to
76%• No plasma protein binding

Interactions – hormonal contraception• Binds to progestogens • Women taking hormonal contraceptives:
– continue taking hormonal contraceptive– alternate non-hormonal contraceptive for 7 days
• Toremifene (Fareston) SERM –– Can displace NMB– Recovery from NMB may be delayed
Interactions• Also binds:
– Cortisone– Atropine– Remifentanil– Verapamil– Fusidic acid
– Flucloxacillin
Interactions• Also binds:
– Cortisone– Atropine– Remifentanil– Verapamil– Fusidic acid– Flucloxacillin - ≥500 mg should be avoided for 6 h after
sugammadex

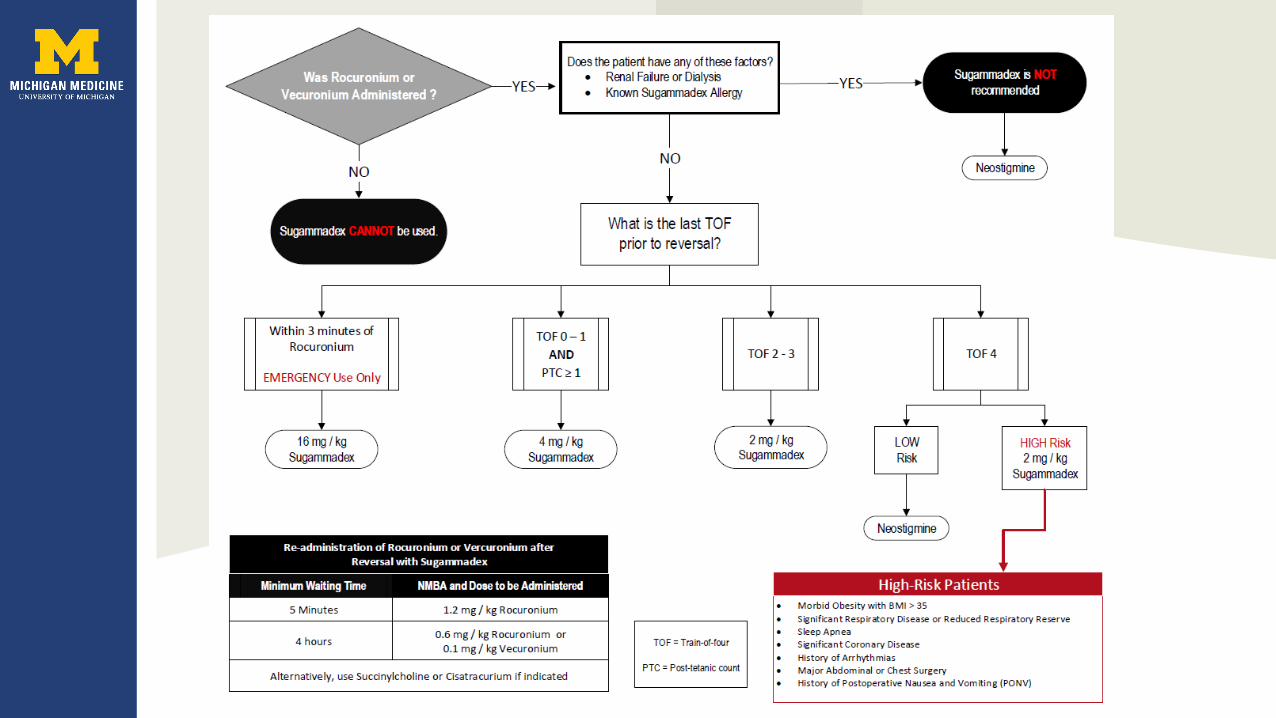
Variable Dosing
• Rocuronium and Vecuronium:• TOF 0 and ≥ PTC 1-2 twitches 4mg/kg• TOF ≥ 2/4 twitches 2mg/kg
• Rocuronium RSI (1.2mg/kg) 16mg/kg

Side effects
• Marked bradycardia, asystole• Dysgeusia – distortion of taste• Allergic reactions• Erythematous rash
Learning objectives
• Review of usage neuromuscular blockers• Problems with traditional neuromuscular reversal• Pharmacology of sugammadex• Clinical advantages• Disadvantages
Clinical scenarios• Preplanned early reversal in short procedures
where succinyl choline is contraindicated• Instead of neostigmine in neuromuscular or resp
disease• Unplanned early reversal – CICO • Instead of neostigmine for time saving• Instead of neostigmine for side effect avoidance
Gibbs NM, KAm PCA. Anaesthesia and Intensive Care, Vol. 40, No. 2, March 2012
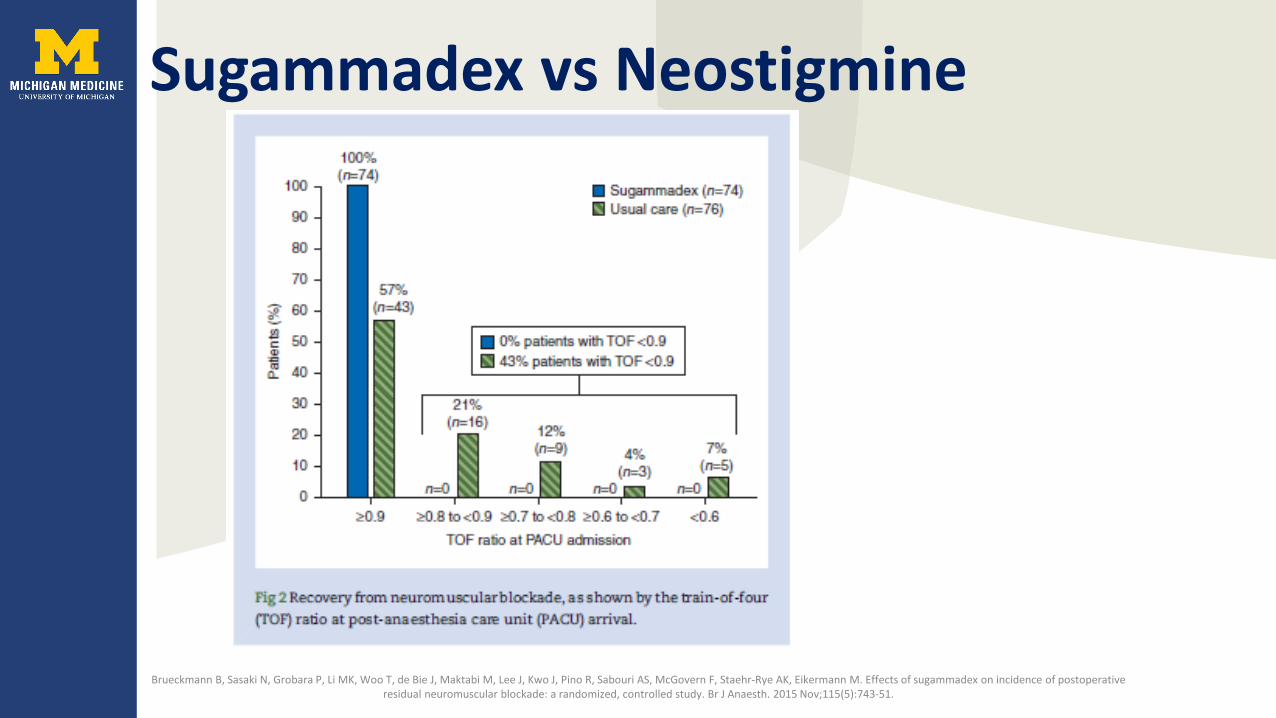
Sugammadex vs Neostigmine
Brueckmann B, Sasaki N, Grobara P, Li MK, Woo T, de Bie J, Maktabi M, Lee J, Kwo J, Pino R, Sabouri AS, McGovern F, Staehr-Rye AK, Eikermann M. Effects of sugammadex on incidence of postoperative residual neuromuscular blockade: a randomized, controlled study. Br J Anaesth. 2015 Nov;115(5):743-51.

Sugammadex vs Neostigmine
Brueckmann B, Sasaki N, Grobara P, Li MK, Woo T, de Bie J, Maktabi M, Lee J, Kwo J, Pino R, Sabouri AS, McGovern F, Staehr-Rye AK, Eikermann M. Effects of sugammadex on incidence of postoperative residual neuromuscular blockade: a randomized, controlled study. Br J Anaesth. 2015 Nov;115(5):743-51.

Sugammadex vs Neostigmine
• Twitch = 2 • 2mg/kg sugammadex vs 50mcg/kg neostigmine
– 1.96 vs 12.86 mins• PTC 1-5• 4mg/kg sugammadex vs 70mcg/kg neostigmine
– 2.9 vs 48.8 mins
Hristovska AM, Duch P, Allingstrup M, Afshari A. Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults. Cochrane Database Syst Rev. 2017 Aug 14;8:CD012763.
RSI recovery vs succinyl choline
• T1 recovery to 90% - 6.2 vs 10.9 mins• T4:T1 90% recovery 2.2 mins after sugammadex
Lee C, Jahr JS, Candiotti KA, Warriner B, Zornow MH, Naguib M. Reversal of profound neuromuscular block by Sugammadex administered three minutes after rocuronium: a comparison with spontaneous recovery from suxamethonium. Anesthesiology 2009; 110: 1020–5.

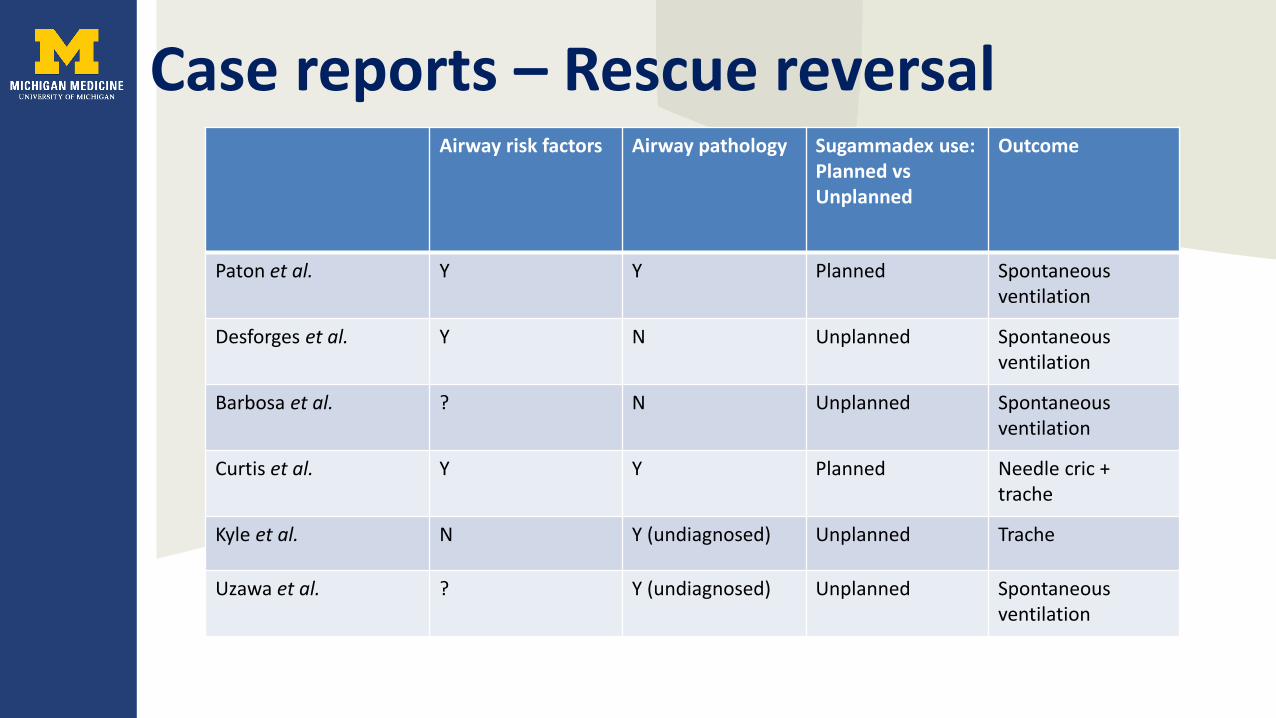
Case reports – Rescue reversalAirway risk factors Airway pathology Sugammadex use:
Planned vs Unplanned
Outcome
Paton et al. Y Y Planned Spontaneousventilation
Desforges et al. Y N Unplanned Spontaneousventilation
Barbosa et al. ? N Unplanned Spontaneousventilation
Curtis et al. Y Y Planned Needle cric + trache
Kyle et al. N Y (undiagnosed) Unplanned Trache
Uzawa et al. ? Y (undiagnosed) Unplanned Spontaneousventilation
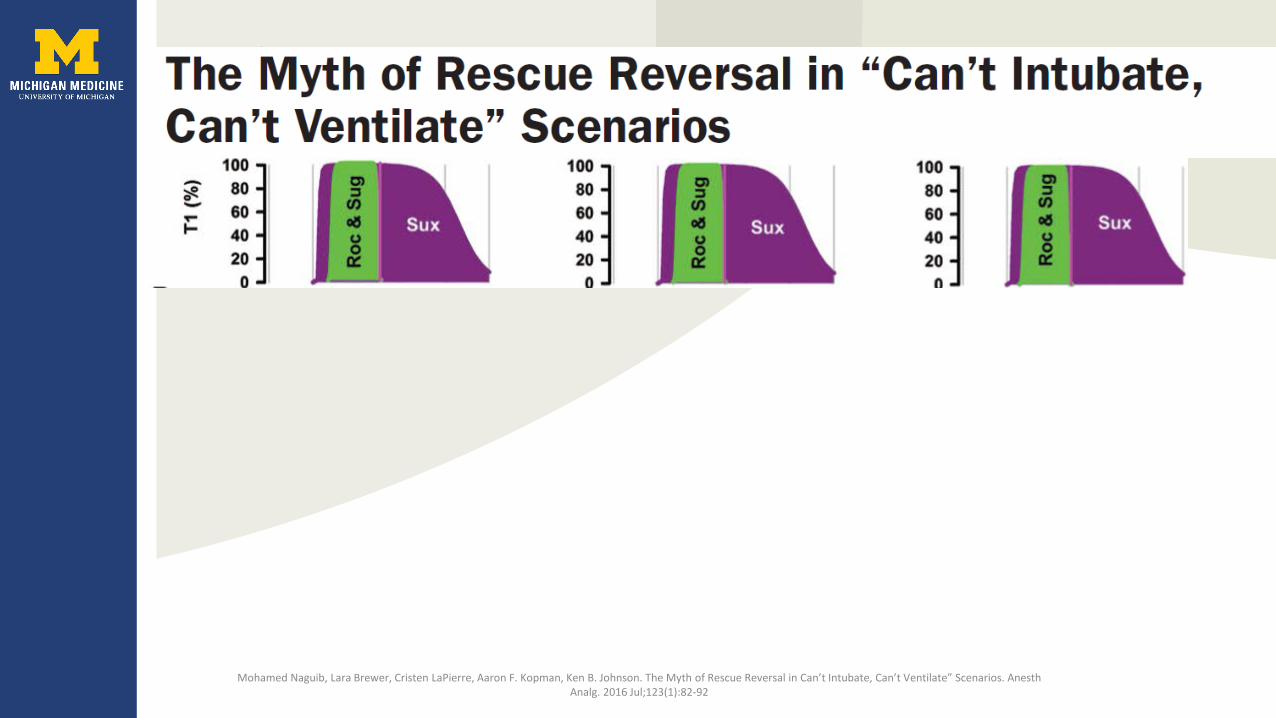
CICO
Mohamed Naguib, Lara Brewer, Cristen LaPierre, The Myth of Rescue Reversal in Can’t Intubate, Can’t Ventilate” Scenarios. Anesth Analg. 2016 Jul;123(1):82-92
Aaron F. Kopman, Ken B. Johnson.

CICO
Mohamed Naguib, Lara Brewer, Cristen LaPierre, Aaron F. Kopman, Ken B. Johnson. The Myth of Rescue Reversal in Can’t Intubate, Can’t Ventilate” Scenarios. Anesth Analg. 2016 Jul;123(1):82-92

CICO

Practical considerations for CICO• Availability
– In OR– Quantity
• Dosage• Multiply X 16• Draw up and administer• (Manikin simulation study - 6.7mins)
Bisschops MMA, Holleman C, Huitink JM. Can sugammadex save a patient in a simulated “cannot intubate, cannot ventilate” situation? Anaesthesia 2010; 65:936-941.
Short procedures – deep paralysis
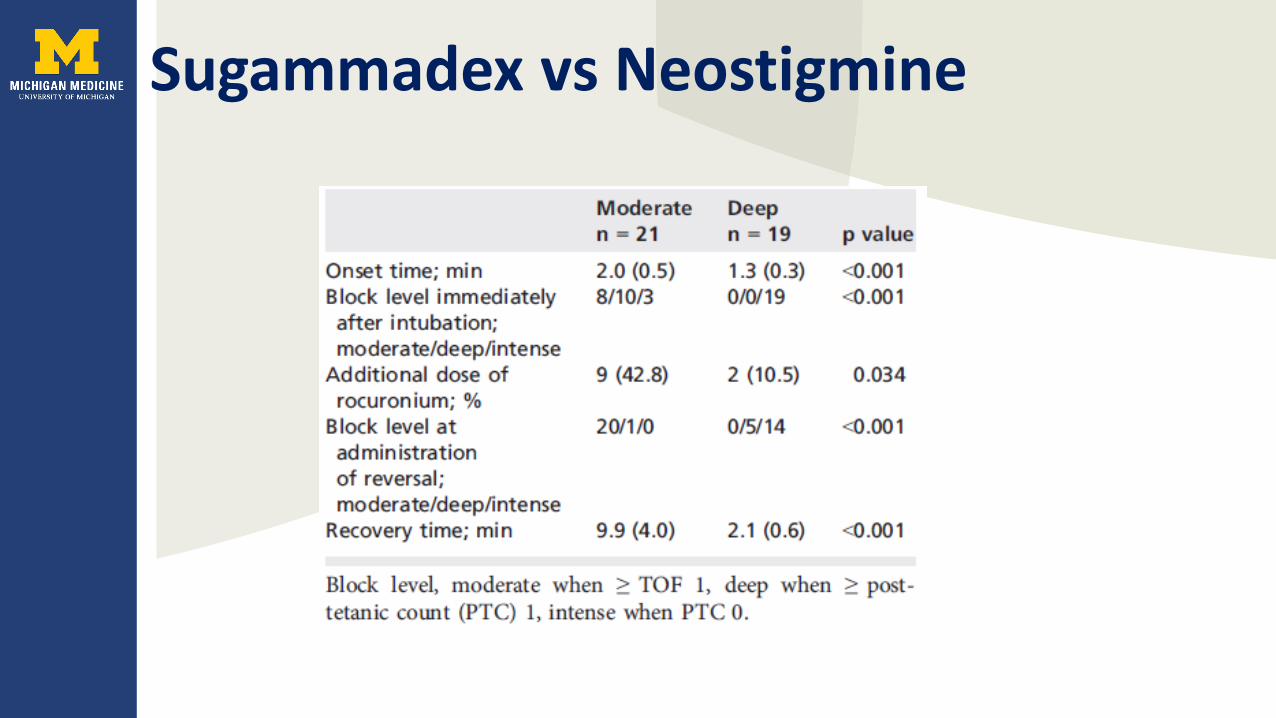
Sugammadex vs Neostigmine
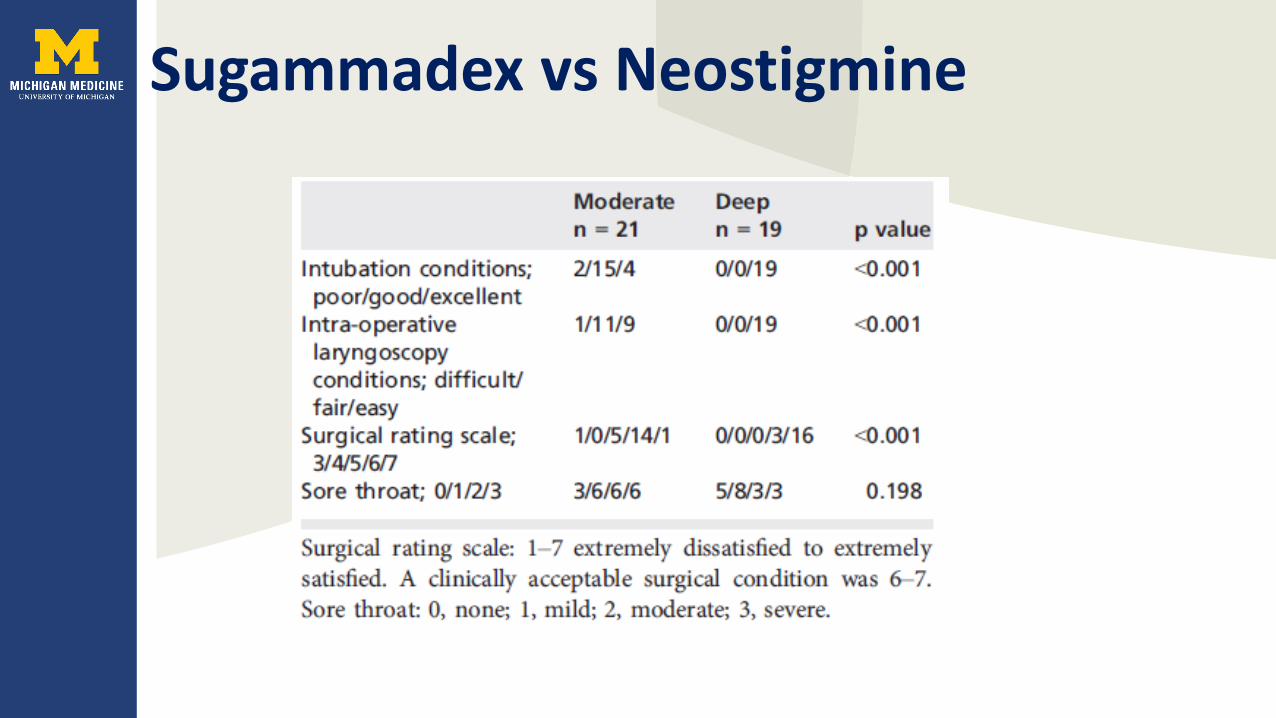
Sugammadex vs Neostigmine
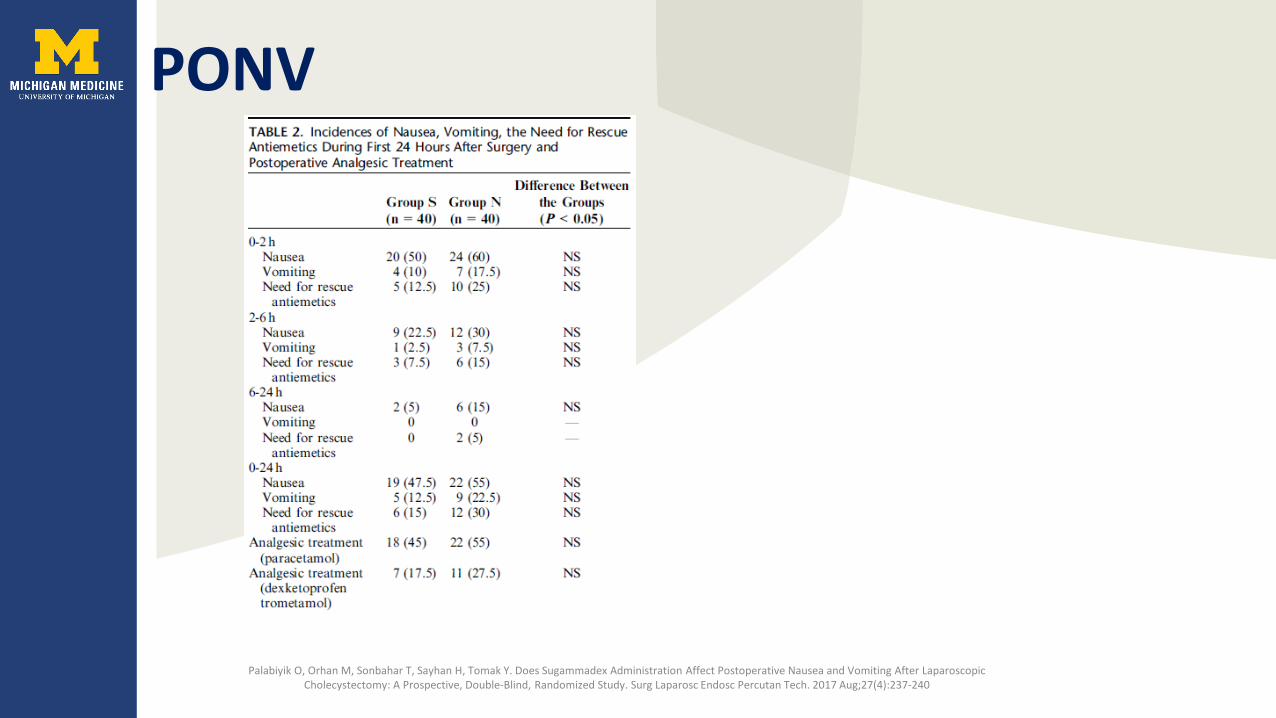
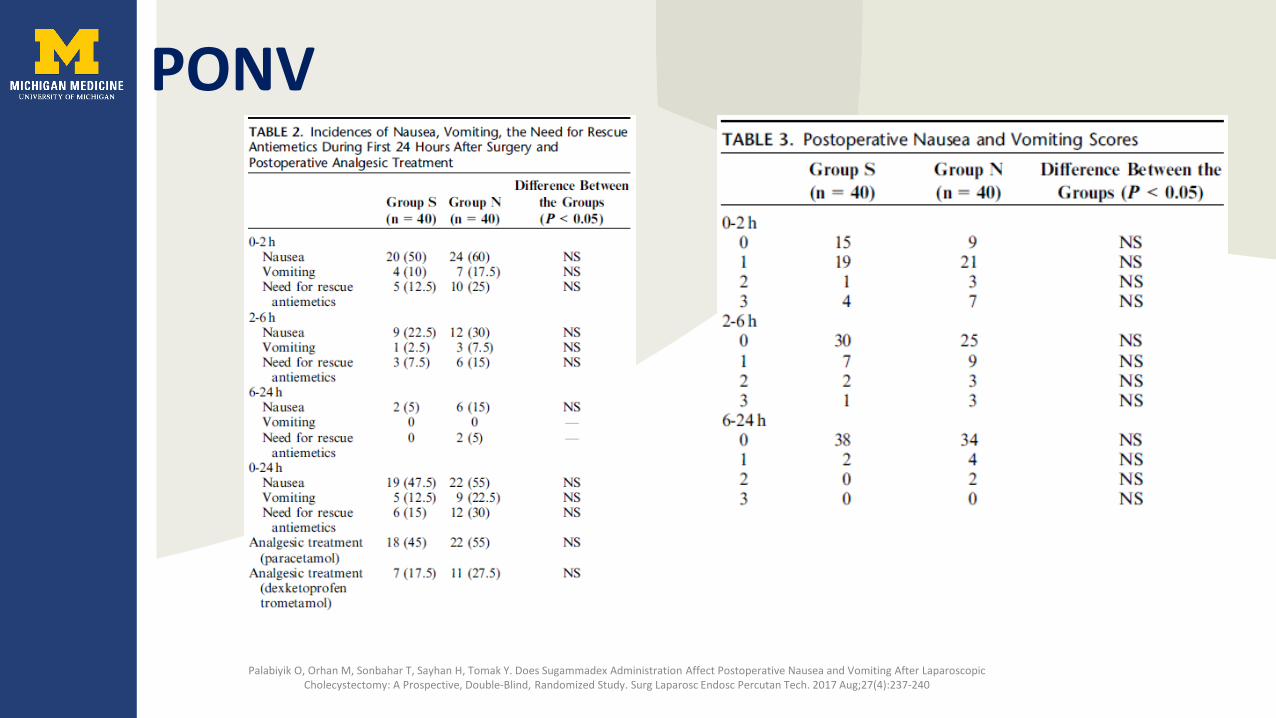
PONV
Palabiyik O, Orhan M, Sonbahar T, Sayhan H, Tomak Y. Does Sugammadex Administration Affect Postoperative Nausea and Vomiting After Laparoscopic Cholecystectomy: A Prospective, Double-Blind, Randomized Study. Surg Laparosc Endosc Percutan Tech. 2017 Aug;27(4):237-240
PONV
Palabiyik O, Orhan M, Sonbahar T, Sayhan H, Tomak Y. Does Sugammadex Administration Affect Postoperative Nausea and Vomiting After Laparoscopic Cholecystectomy: A Prospective, Double-Blind, Randomized Study. Surg Laparosc Endosc Percutan Tech. 2017 Aug;27(4):237-240

Carron M, Zarantonello F, Tellaroli P, Ori CA. Efficacy and safety of sugammadex compared to neostigmine for reversal of neuromuscular blockade: a meta-analysis of randomized controlled trials. J Clin Anesth. 2016 Dec;35:1-12.

Hristovska AM, Duch P, Allingstrup M, Afshari A. Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults. Cochrane Database Syst Rev. 2017 Aug 14;8:CD012763.

Learning objectives
• Review of usage neuromuscular blockers• Problems with traditional neuromuscular reversal• Pharmacology of sugammadex• Clinical advantages• Practical considerations
Residual block after sugammadex
• Incidence TOFR <0.9– No reversal - 13.0%– Neostigmine - 23.9%– Sugammadex - 4.3% (1.7-9.4%)
Kotake Y, Ochiai R, Suzuki T, Ogawa S, Takagi S, Ozaki M, Nakatsuka I, Takeda J. Reversal with sugammadex in the absence of monitoring did not preclude residual neuromuscular block. Anesth Analg 2013;117:345–51.
Residual block after sugammadex
• TOFR <0.9– No reversal - 13.0%– Neostigmine - 23.9%– Sugammadex - 4.3% (1.7-9.4%)
Kotake Y, Ochiai R, Suzuki T, Ogawa S, Takagi S, Ozaki M, Nakatsuka I, Takeda J. Reversal with sugammadex in the absence of monitoring did not preclude residual neuromuscular block. Anesth Analg 2013;117:345–51.

Residual block after sugammadex• 6 cases in literature• Issues:
– Under-dosing– Not using TOF guidance– Larger doses (infusions)– Hypothermia
• 1 case appeared to be a genuine outlierLe Corre F, Nejmeddine S, Fatahine C, et al. Recurarization after sugammadex reversal in an obese patient. CanJ Anesth2011;58:944–947.
Murata T, Kubodera T, Ohbayashi M, et al. Recurarization after sugammadex following a prolonged rocuronium infusion for induced hypothermia. Can J Anesth 2013; 60:508–9.Özel F, Altunkan AA, Azizoğlu M. Postoperative Respiratory Failure in a Patient with Undiagnosed Myastenia Gravis. Turk J Anaesthesiol Reanim. 2016 Apr;44(2):108-10.
Failure of sugammadex to reverse rocuronium-induced neuromuscular blockade. Eur J Anaesthesiol 2014; 31:708–721Bellod A, March X, Hernandez C, Villalonga A. Delayed recurarisation after sugammadex reversal. Eur J Anaesthesiol 2014; 31:710–712.
Ortiz-Gómez JR, Palacio-Abizanda FJ, Fornet-Ruiz I.
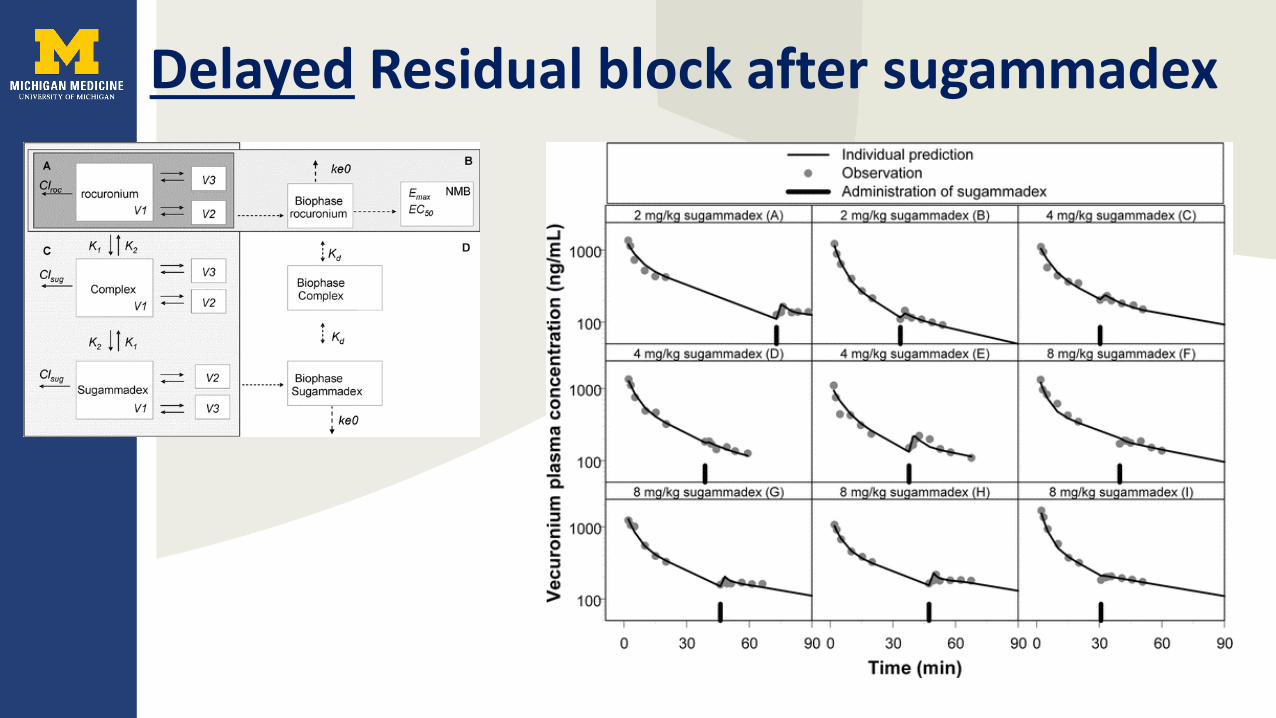
Delayed Residual block after sugammadex

Delayed Residual block after sugammadex

Sugammadex to treat anaphylaxis to rocuronium• NMBs are the most common causal agents in
anesthesia (55-69%)• Allergen is the quarternary ammonium ion• Sugammadex encapsulates free allergen• Slows/halts immunologic process

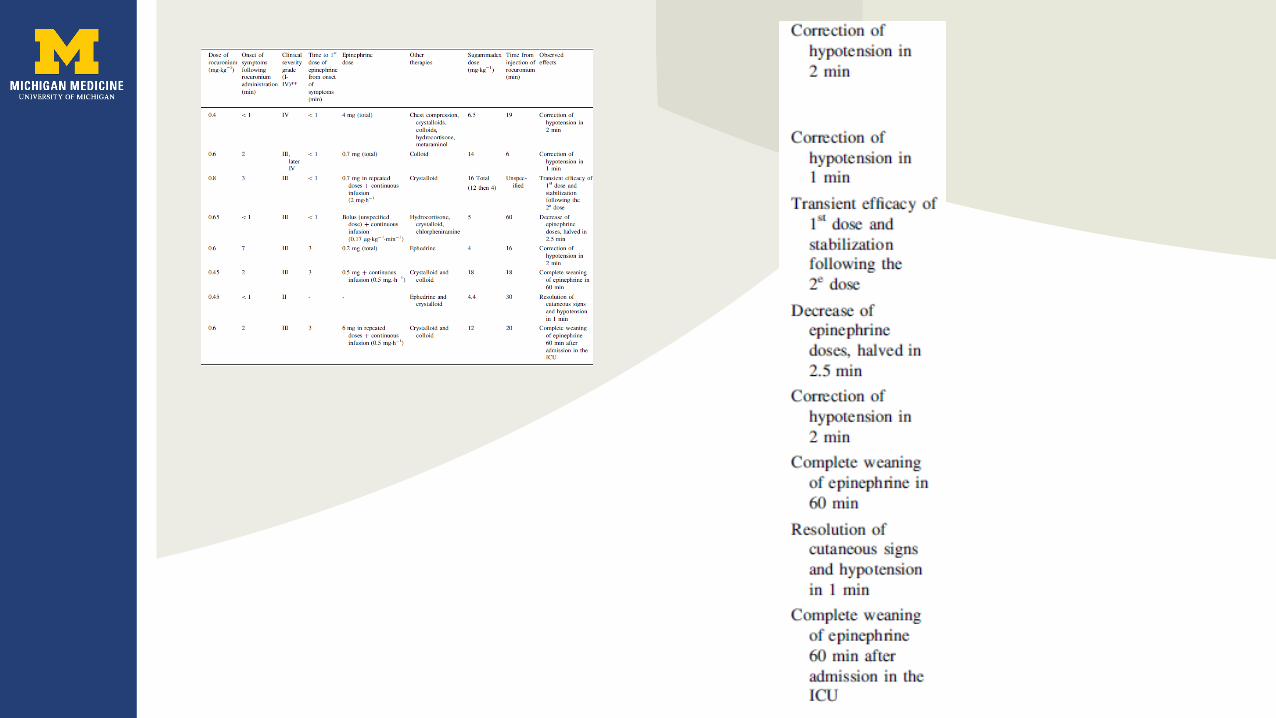

Treatment for Roc anaphylaxis - not so simple• Some of the epitope might protrude from complex• Incorrect causative agent in 1/3 of cases• Sugammadex vs IgE – which has great affinity for
rocuronium
Jones PM, Turkstra TP. Mitigation of rocuronium-induced anaphylaxis by sugammadex: the great unknown. Anaesthesia 2010; 65:89-90.
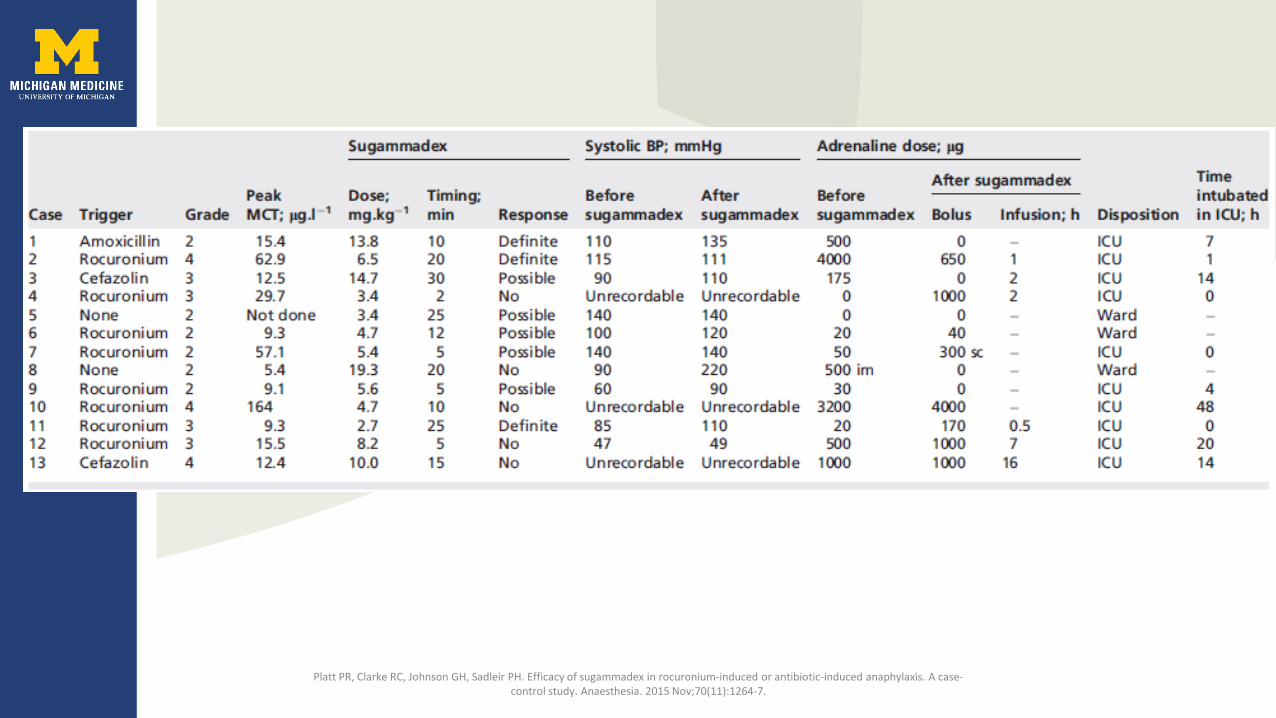
Platt PR, Clarke RC, Johnson GH, Sadleir PH. Efficacy of sugammadex in rocuronium-induced or antibiotic-induced anaphylaxis. A case-control study. Anaesthesia. 2015 Nov;70(11):1264-7.


Anaphylaxis to sugammadex• Japanese study: Hypersensitivity 0.22%; Anaphylaxis 0.039%
(n=15479)– Same rate as rocuronium or succinylcholine
• Skin prick testing• No commercially available IgE assays• Average person consumes 4g of gamma-cyclodextrin daily• Oral sensitization resulting in anaphylaxis to “first” exposure• Symptoms might develop after extubation
– Reintubation
Ue KL, Kasternow B, Wagner A, Rutkowski R, Rutkowski K. Sugammadex: An emerging trigger of intraoperative anaphylaxis. Ann Allergy Asthma Immunol. 2016 Dec;117(6):714-716.Miyazaki Y, Sunaga H, Kida K, Hobo S, Inoue N, Muto M, Uezono S. Incidence of Anaphylaxis Associated With Sugammadex. Anesth Analg. 2017 Oct 19.

Anaphylaxis to sugammadex-rocuronium complex• Allergies to:
– Rocuronium– Sugammadex– Complex
• 2 cases in literature
Yamaoka M, Deguchi M, Ninomiya K, Kurasako T, Matsumoto M. A suspected case of rocuronium-sugammadex complex-induced anaphylactic shock after cesarean section. J Anesth. 2017 Feb;31(1):148-151.
Ho G, Clarke RC, Sadleir PH, Platt PR. The First Case Report of Anaphylaxis Caused by the Inclusion Complex of Rocuronium and Sugammadex. A Case Rep. 2016 Nov 1;7(9):190-192.
Renal failure
• Sugammadex is entirely renally excreted• Hepatic elimination of rocuronium eliminated once
bound to sugammadex • Plasma clearance complex = GFR (120 ml/min).• High-flux dialysis effective in removing
Kopman AF. Sugammadex: A Revolutionary Approach to Anesthesiology 2006; 104:631–2

Pharmacokinetics in renal failure
Staals LM, Snoeck MM, Driessen JJ, van Hamersvelt HW, Flockton EA, van den Heuvel MW, Hunter JM. Reduced clearance of rocuronium and sugammadex in patients with severe to end-stage renal failure: a pharmacokinetic study. Br J Anaesth. 2010 Jan;104(1):31-9.

Renal failure
Panhuizen IF, Gold SJ, Buerkle C, Snoeck MM, Harper NJ, Kaspers MJ, van den Heuvel M, Hollmann MW. Efficacy, safety and pharmacokinetics of sugammadex 4 mg kg-1 for reversal of deep neuromuscular blockade in patients with severe renal impairment. Br J Anaesth. 2015 May;114(5):777-84.

Renal failure
Panhuizen IF, Gold SJ, Buerkle C, Snoeck MM, Harper NJ, Kaspers MJ, van den Heuvel M, Hollmann MW. Efficacy, safety and pharmacokinetics of sugammadex 4 mg kg-1 for reversal of deep neuromuscular blockade in patients with severe renal impairment. Br J Anaesth. 2015 May;114(5):777-84.
• No adverse effects related to sugammadex• Six renal patients had measurable rocuronium concentrations at Day7• No recurrence of NMB• Prolonged sugammadex exposure in renal failure –
• current safety data insufficient • recommend against using sugammadex in renal failure

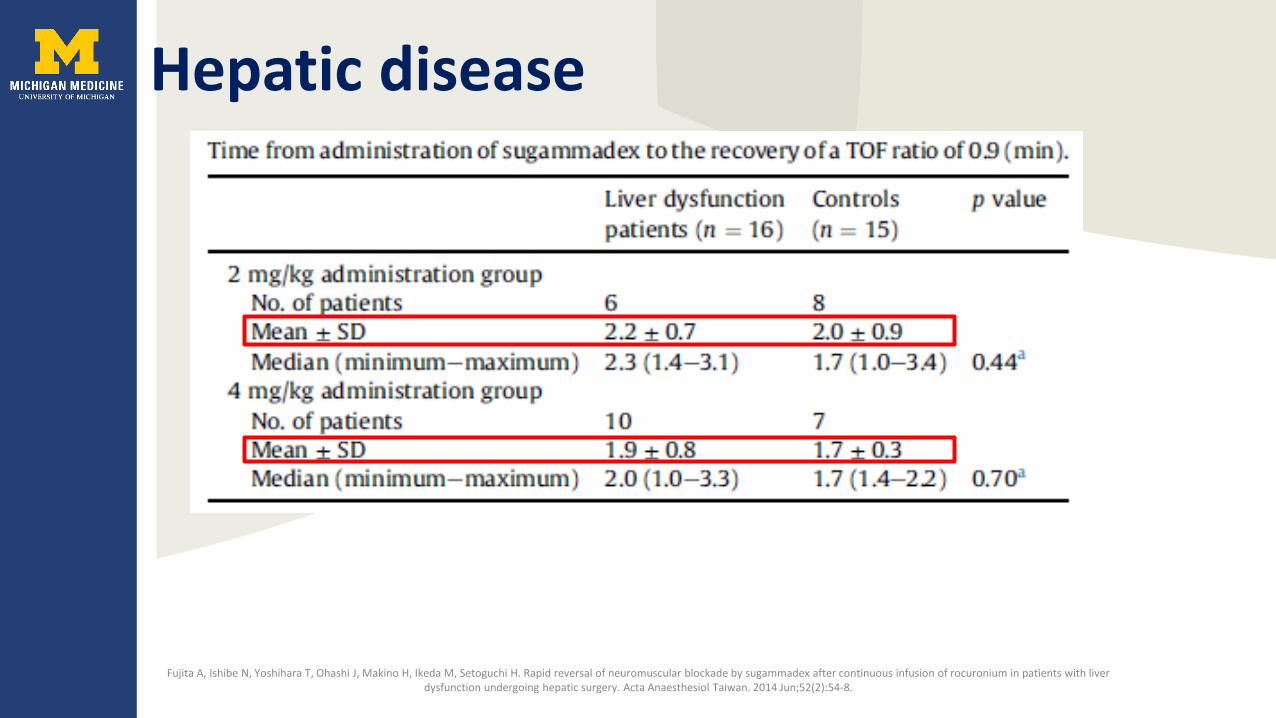
Hepatic disease
• Reappearance of T1:• 49.1 mins (liver dysfunction)• 33.3 mins (controls)• P=0.016
Fujita A, Ishibe N, Yoshihara T, Ohashi J, Makino H, Ikeda M, Setoguchi H. Rapid reversal of neuromuscular blockade by sugammadex after continuous infusion of rocuronium in patients with liver dysfunction undergoing hepatic surgery. Acta Anaesthesiol Taiwan. 2014 Jun;52(2):54-8.
Hepatic disease
Fujita A, Ishibe N, Yoshihara T, Ohashi J, Makino H, Ikeda M, Setoguchi H. Rapid reversal of neuromuscular blockade by sugammadex after continuous infusion of rocuronium in patients with liver dysfunction undergoing hepatic surgery. Acta Anaesthesiol Taiwan. 2014 Jun;52(2):54-8.

Dosing in obesity
• Roc and sugammadex IBW dosing • Further 2mg/kg if TOFR <0.9 in 3mins• 2nd dose in:
– 39.5% with PTC 0-2– 23.4% in ≥2 twitches
• Recommended real body weight dosing
Llauradó S, Sabaté A, Ferreres E, Camprubí I, Cabrera A. Sugammadex ideal body weight dose adjusted by level of neuromuscular blockade in laparoscopic bariatric surgery. Anesthesiology. 2012 Jul;117(1):93-8.

Dosing in obesity
• Pooled data from 27 trials• 1418 patients• BMI >30• All dosed according to actual body weight• No correlation between recovery time and BMI
(average 1.9 mins)
Monk TG, Rietbergen H, Woo T, Fennema H. Use of Sugammadex in Patients With Obesity: A Pooled Analysis. Am J Ther. 2017 Sep/Oct;24(5):e507-e516.

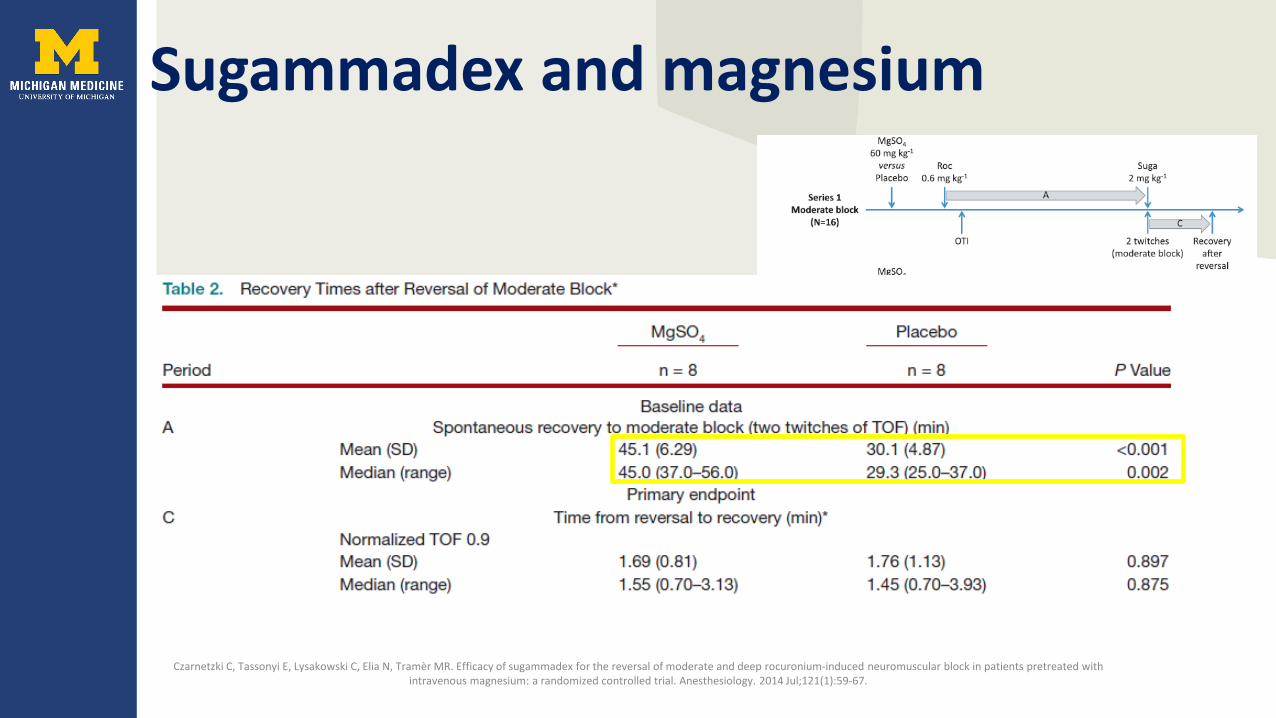
Sugammadex and magnesium
Czarnetzki C, Tassonyi E, Lysakowski C, Elia N, Tramèr MR. Efficacy of sugammadex for the reversal of moderate and deep rocuronium-induced neuromuscular block in patients pretreated with intravenous magnesium: a randomized controlled trial. Anesthesiology. 2014 Jul;121(1):59-67.
Sugammadex and magnesium
Czarnetzki C, Tassonyi E, Lysakowski C, Elia N, Tramèr MR. Efficacy of sugammadex for the reversal of moderate and deep rocuronium-induced neuromuscular block in patients pretreated with intravenous magnesium: a randomized controlled trial. Anesthesiology. 2014 Jul;121(1):59-67.

Sugammadex and magnesium
Czarnetzki C, Tassonyi E, Lysakowski C, Elia N, Tramèr MR. Efficacy of sugammadex for the reversal of moderate and deep rocuronium-induced neuromuscular block in patients pretreated with intravenous magnesium: a randomized controlled trial. Anesthesiology. 2014 Jul;121(1):59-67.
Pediatrics• Interaction with dexamethasone N=60• Effective: 3 trials n=180 vs neostigmine• Open label n=42 (oncology) , n=14 (Congenital
cardiac)• Case reports
– Neuromyopathic disease– Neonates
• Dosing unchanged
Tobias JD. Current evidence for the use of sugammadex in children. Paediatr Anaesth. 2017 Feb;27(2):118-125.
Bleeding
• No interaction with platelet function with/without aspirin
• aPTT and PT(INR) increase
de Kam PJ, El Galta R, Kruithof AC, Fennema H, van Lierop MJ, Mihara K, Burggraaf J, Moerland M, Peeters P, Troyer MD. No clinically relevant interaction between sugammadex and aspirin on platelet aggregation and coagulation parameters. Int J Clin Pharmacol Ther. 2013 Dec;51(12):976-85.

Bleeding
• Hip and knee replacements with thromboprophylaxis
• Randomized, blinded to neostigmine / sugammadex
• n=1184
Rahe-Meyer N, Fennema H, Schulman S, Klimscha W, Przemeck M, Blobner M, Wulf H, Speek M, McCrary Sisk C, Williams-Herman D, Woo T, Szegedi A. Effect of reversal of neuromuscular blockade with sugammadex versus usual care on bleeding risk in a randomized study of surgical patients. Anesthesiology. 2014 Nov;121(5):969-77.



Safety• Toxicology seems very safe (food studies)• Kids
– Not FDA approved• Pregnancy:
– no human data except in cesarean section– Placental transfer - 6%– Almost non-teratogenic in animals
• Breast feeding– Present in rat milk– Oral absorption very low
• QTc unchanged / normal

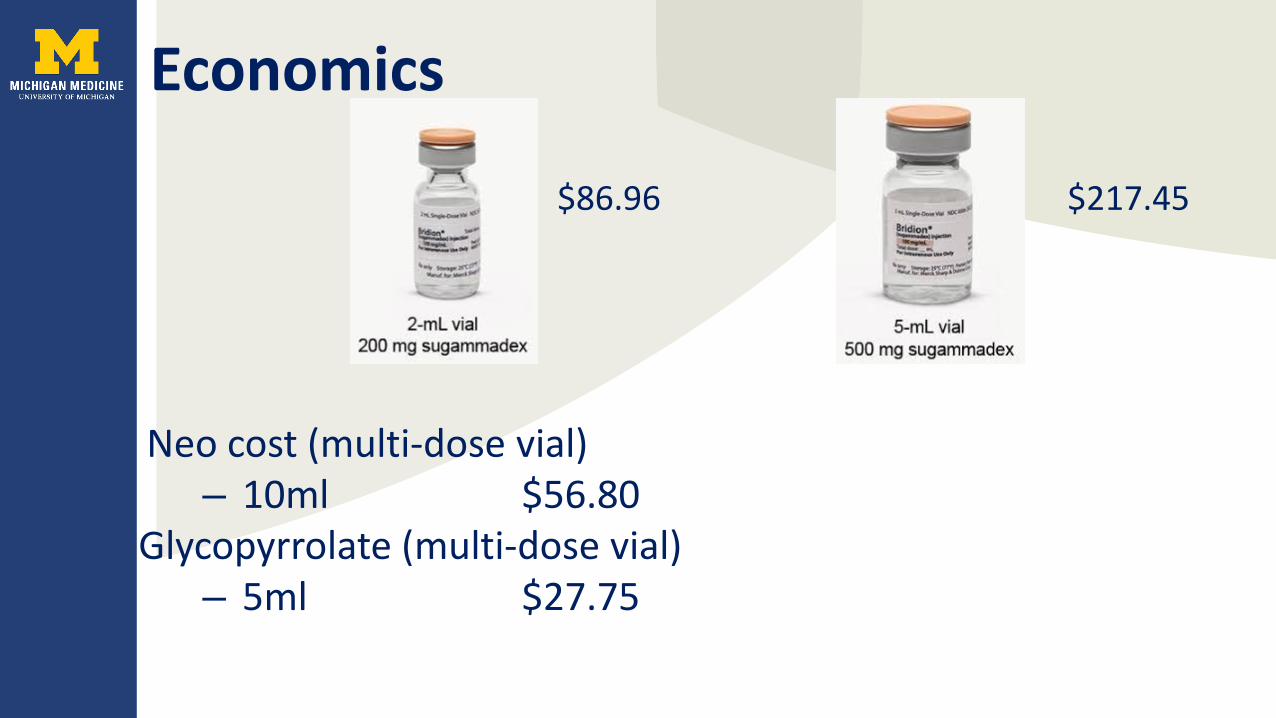
Economics
Economics
Neo cost (multi-dose vial)– 10ml $56.80
Glycopyrrolate (multi-dose vial)– 5ml $27.75
$86.96 $217.45
Economics
• 70kg patient• Sugammadex $86.96• Neo+Glyco $28.40 + $19.43 =$47.83

Economics• End of surgery to OR discharge:
– 9.1 mins - sugammadex– 13.9 - neostigmine
• Max:– 22 mins - sugammadex– 72 mins - neostigmine
• No difference in PACU stay
Putz L, Dransart C, Jamart J, Marotta ML, Delnooz G, Dubois PE. Operating room discharge after deep neuromuscular block reversed with sugammadex compared with shallow block reversed with neostigmine: a randomized controlled trial. J Clin Anesth. 2016 Dec;35:107-113.
Reduces frustration
• Waiting an hour for twitches to returnor
• Ventilation in PACURemember about 10 minutes ago when I said we had 3 hrs left … well surprisingly we have finished
Dexter F, Coffin S, Tinker JH. Decreases in anesthesia-controlled time cannot permit one additional surgical operation to be reliably scheduled during the workday. Anesth Analg. 1995 Dec;81(6):1263-8.



Economics• Combination reversal:
– 4mg/kg sugammadex – vs – 2mg/kg + Neostigmine 50mcg/kg + Glyco
10mcg/kg• 50% reduction in 200mg ampoules for patients 52-
100kg• Non-inferior reversal
Aouad MT, Alfahel WS, Kaddoum RN, Siddik-Sayyid SM. Half dose sugammadex combined with neostigmine is non-inferior to full dose sugammadex for reversal of rocuronium-induced deep neuromuscular blockade: a cost-saving strategy. BMC Anesthesiol. 2017 Apr 11;17(1):57.

Outcome benefits
• Cochrane review: 10 studies (n= 959)• Serious adverse events:
– RR 0.54; 95%CI 0.13-2.25 GRADE: low quality• No mortality data
Hristovska AM, Duch P, Allingstrup M, Afshari A. Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults. Cochrane Database Syst Rev. 2017 Aug 14;8:CD012763.
Summary
• Sugammadex:– Reverses any depth of block– Variable dosing – Can eliminate postoperative weakness

Questions?
Related Documents











