1 TECHNISCHE UNIVERSITÄT MÜNCHEN Klinik für Anaesthesiologie, Klinikum rechts der Isar Sugammadex and Neostigmine Dose-finding Study for Reversal of Residual Neuromuscular Block (SUNDRO-Study) Stefan Schaller Vollständiger Abdruck der von der Fakultät für Medizin der Technischen Universität München zur Erlangung des akademischen Grades eines Doktors der Medizin genehmigten Dissertation. Vorsitzender: Univ.-Prof. Dr. E. J. Rummeny Prüfer der Dissertation: 1. Priv.-Doz. Dr. H. Fink 2. Univ.-Prof. Dr. P. Tassani-Prell Die Dissertation wurde am 12.07.2011 bei der Technischen Universität München eingereicht und durch die Fakultät für Medizin am 18.09.2013 angenommen.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
TECHNISCHE UNIVERSITÄT MÜNCHEN
Klinik für Anaesthesiologie, Klinikum rechts der Isar
Sugammadex and Neostigmine Dose-finding Study for
Reversal of Residual Neuromuscular Block
(SUNDRO-Study)
Stefan Schaller
Vollständiger Abdruck der von der Fakultät für Medizin der Technischen Universität
München zur Erlangung des akademischen Grades eines
Doktors der Medizin
genehmigten Dissertation.
Vorsitzender: Univ.-Prof. Dr. E. J. Rummeny
Prüfer der Dissertation: 1. Priv.-Doz. Dr. H. Fink
2. Univ.-Prof. Dr. P. Tassani-Prell
Die Dissertation wurde am 12.07.2011 bei der Technischen Universität München eingereicht
und durch die Fakultät für Medizin am 18.09.2013 angenommen.

2
Ich weiß, dass ich nichts weiß.
(Sokrates)

3
Table of Contents List of Abbreviations .................................................................................................................. 4 1 Introduction ........................................................................................................................ 5
1.1 Historical View and Safety ........................................................................................ 5 1.2 Muscle Relaxants ....................................................................................................... 6 1.3 Postoperative Residual Curarization (PORC) ............................................................ 7 1.4 Reversal of Muscle Relaxants .................................................................................... 7
1.4.1 Overview ............................................................................................................ 7 1.4.2 Cholinesterase Inhibitors .................................................................................... 7 1.4.3 Encapsulator Sugammadex ................................................................................ 9
1.5 Aims of the Study ..................................................................................................... 11 2 Materials and Methods ..................................................................................................... 12
2.1 Study Design and Patient Selection ......................................................................... 12 2.2 Procedure .................................................................................................................. 12 2.3 Data Management and Statistical Analysis .............................................................. 14
3 Results .............................................................................................................................. 16 3.1 Demographics ........................................................................................................... 16 3.2 Efficacy .................................................................................................................... 16 3.3 Safety ........................................................................................................................ 22
4 Discussion ........................................................................................................................ 24 5 Abstract ............................................................................................................................ 28 6 Literature .......................................................................................................................... 29 7 Acknowledgments ............................................................................................................ 34 8 Curriculum Vitae .............................................................................................................. 35

4
List of Abbreviations AE Adverse Event AIC Akaike Information Criterion ASA American Society of Anesthesiology COO- Carboxy-group CRE Critical Respiratory Event ECG Electrocardiogram Max Maximum min Minutes Min Minimum mio Million ml Milliliter MRC Medical Research Council n.e. not estimable NMT Neuro Muscular Transmission PORC Postoperative Residual Curarization PTC Post-Tetanic Count SAE Serious Adverse Event smPC Summary of Product Characteristics SUNDRO Sugammadex and Neostigmine Dose-finding Study for Reversal of
Residual Neuromuscular Block TOF Train-of-Four

5
1 Introduction
1.1 Historical View and Safety
Over the last years there has been tremendous improvement in patient safety as regards
anesthesia. This is reflected by a reduction of intraoperative mortality from approximately 1
in 10,000 in the 1980s to under 1 in 100,000 in the year 2000 (Gibbs 2005, p. 616; Hovi-
Viander 1980, p. 483; Lagasse 2002, p. 1609; Lienhart 2006, p. 1087). This improvement
may be credited not only to technical advances like intraoperative high-tech monitoring or
ventilation machines (Auroy 2009, p. 366) as well as structured training programs, but also to
pharmacological advances like short acting substances. These contributing factors to the
aforementioned improvement have led to a concept of (so-called) “balanced anesthesia”
(Tonner 2005, p. 475), a concept which connotes the combination of an anesthetic, an
analgesic and a muscle relaxant so as to induce (and maintain) general anesthesia. The
combination of different substances thereby reduces each substance’s individual amount and
consequently the unwanted effects otherwise implicated by these substances.
An integral element of (the concept of) balanced anesthesia are muscle relaxants. They
improve intubation conditions (Mencke 2003, p. 1049; Schlaich 2000, p. 720; Sparr 1997, p.
1300) and might even contribute to depth of anesthesia (Bonhomme 2007, p. 456). During the
overall improvement on patient safety it became evident that the ratio of intra- to post-
operative mortality is 1 to 1000 (Fink 2007, p. 1127; Henderson 2007, p. 1103); a
development which caused the researches to focus on potential unintended (and undesirable)
effects of muscle relaxation. A pharmacological action of muscle relaxation, beyond its
intended effect for induction of anesthesia and intraoperative surgical conditions, defined as
postoperative residual curarization (PORC) (Cammu 2002, p. 129; Debaene 2003, p. 1042;
Hayes 2001, p. 312; McCaul 2002, p. 766) can cause the following effects:
(1) respiratory insufficiency (Murphy 2008, p. 130),
(2) impaired upper airway function (Eikermann 2006, p. 937),
(3) increased risk of aspiration (Sundman 2000, p. 977), as well as (consecutively)
(4) the risk of postoperative pulmonary complications (Berg 1997, p. 1095).

6
1.2 Muscle Relaxants
Muscle relaxation improves intubation conditions, which in turn lead to reduced postoperative
hoarseness and injuries of the vocal cords (Lieutaud 2003, p. 121; Masso 2006, p. 249;
Mencke 2003, p. 1049). Since airway injuries are a frequent cause for claims against
anesthesiologists (Cass 2004, p. 47), muscle relaxation is an imperative for modern balanced
anesthesia including intubation. In addition, muscle relaxants may potentially improve
surgical conditions – although there are no supporting studies available to date.
Muscle relaxants can be divided into:
1. depolarizing muscle relaxants (e.g. succinylcholine) and
2. nondepolarizing muscle relaxants
a. benzylisoquinolones (e.g. atracurium, cisatracurium and mivacurium)
b. aminosteroidal muscle relaxants (e.g. rocuronium, vecuronium and
pancuronium) (Blobner 2009, p. 105)
Succinylcholine (structurally a di-acetylcholine molecule) mimics the effect of acetylcholine
at the neuromuscular junction. It depolarizes the post-synaptic membrane, leading to an initial
fasciculation. Succinylcholine is the only depolarizing muscle relaxant in clinical use.
However, it has numerous unwanted effects such as life-threatening hyperkalemia, malignant
hyperthermia, as well as increased intraocular, gastric, and cerebral pressure (Blobner 2009,
p. 112).
Non-depolarizing muscle relaxants act by inducing a competitive blockade of the
acetylcholine receptor of the neuromuscular junction, thus inhibiting any physiologic
neuromuscular transmission.
The effects of muscle relaxants are evaluated by neuromuscular monitoring. Most frequently
a train-of-four stimulation pattern is used. For two seconds, four 2 Hz stimuli are applied to a
peripheral nerve, with the evoked muscle contraction recorded. The fourth contraction is then
set into relation to the first contraction, resulting in a train-of-four ratio. Complete muscle
paralysis occurs at a train-of-four ratio of zero. Recovery to a train-of-four ratio of 0.9 is
considered to be sufficient functional recovery by today’s standard.

7
1.3 Postoperative Residual Curarization (PORC)
Although textbooks suggest muscle relaxants to have a predictable duration of effect
clinically, there is a wide inter-individual difference in duration of action, which leads to high
rates of PORC (Maybauer 2007, p. 12). PORC is defined as a train-of-four (TOF) ratio below
0.9 and is a common but largely underestimated problem. PORC leads to respiratory
insufficiency, impaired upper airway function and increased risk of aspiration, which leads to
an increased incidence of postoperative pulmonary complications if not treated properly.
In 1979 Viby-Mogensen showed (Viby Mogensen 1979, p. 539) that 42% of patient
admissions in the recovery room suffered from PORC (in those days defined as a TOF ratio
below 0.7). Unfortunately, patient safety has not improved as regards PORC, as in 2003 60%
of the patients in the recovery room still suffered PORC with a TOF ratio below 0.9 (Debaene
2003, p. 1042). Clinically, there is a high incidence of Critical Respiratory Events (CRE) in
patients with PORC (Murphy 2008, p. 130). However, clinical tests per se are not sufficient to
identify PORC. The only way to identify PORC and thereby effectively treat patients is by
neuromuscular monitoring (Baillard 2005, p. 622). And once PORC is identified, the residual
effects of muscle relaxants need to be reversed.
1.4 Reversal of Muscle Relaxants
1.4.1 Overview
Drugs used to reverse the effects of neuromuscular blocking drugs are divided into:
1. Antagonists
2. Encapsulators
1.4.2 Cholinesterase Inhibitors
Presynaptically released acetylcholine is degraded by acetylcholine esterase into acetate and
choline. Both choline and acetate are transported back into the presynaptic nerve terminal and
re-used to synthesize acetylcholine. Acetylcholine esterase is mostly located in the
extracellular matrix of the neuromuscular junction. As a result, most of the released

8
acetylcholine is degraded right after its release. Inhibition of acetylcholine esterase therefore
increases the concentration of acetylcholine in the neuromuscular junction. Due to the
competitive mechanism of non-depolarizing muscle relaxants, an increase in acetylcholine
leads to a higher possibility of the agonist to bind at the receptor location, leading to restored
neuromuscular transmission. (Fink 2004, p. 573)
Two acetylcholine esterase inhibitors are currently used in Germany for reversal of
neuromuscular block:
1. neostigmine
2. pyridostigmine
Physiostigmine is not used to reverse neuromuscular block, since it crosses the brain-blood-
barrier. Its application is limited to act as a therapeutic agent for a central anticholinergic
syndrome.
Antagonists, however, have certain limitations. After blocking all present acetylcholine
esterase an additional dose of cholinesterase inhibitors will not produce a further effect
(ceiling effect). Therefore, a deep neuromuscular block cannot be antagonized with
acetylcholine esterase inhibitors. Secondly, acetylcholine esterase inhibitors do not selectively
act at the neuromuscular junction. They also increase acetylcholine in the autonomous
nervous system, leading to several side effects – in particular, bradycardia, rise in intraocular
pressure, increased bowel movement, increased contraction of the gall bladder, ureter and
detrusor muscle, relaxation of the bladder sphincter and increased sudoral secretion.
Therefore, acetylcholine esterase inhibitors are usually combined with parasympatholytic
drugs (e.g. atropine or glycopyrronium bromide) to decrease these unwanted side effects.
Parasympatholytic drugs, however, exert unwanted effects of their own, such as tachycardia
or dry mouth.
Neostigmine, which was used in this study, has a quaternary ammonium structure and is a
peripheral acting reversible cholinesterase inhibitor. It is not lipophilic and therefore does not
cross the blood brain barrier. It is poorly reabsorbed after oral intake, but is quickly
distributed after intravenous application. After application, a high concentration can be
measured in the liver and muscle tissue. Elimination half time after intravenous application
occurs between 24 and 80 minutes, a duration which increases under impaired renal function
(Blobner 2008, p. 342).

9
Recommended doses of neostigmine for reversal of neuromuscular block vary from 20-
70 µg/kg bodyweight (Blobner 2009, p. 115). A ceiling effect is observed at approximately
60-80 µg/kg. Maximal antagonistic effect of neostigmine occurs in approximately ten
minutes. The recommended combination of neostigmine with a parasympatholytic agent is
1:2.5 for atropine or 1:5 for glycopyrronium bromide. In this study, glycopyrronium bromide
is used as it (in addition) does not cross the blood-brain-barrier and thus has a lower incidence
for postoperative cognitive deficits compared to atropine.
1.4.3 Encapsulator Sugammadex
Sugammadex is a modified γ-cyclodextrin which has been developed to reverse rocuronium
bromide-induced neuromuscular block. It has been available in Germany since October 2008.
Cyclodextrins are cyclic oligosaccharide molecules, which are known for their capability to
encapsulate lipohilic molecules. Cyclodextrins are divided into α-, β- and γ-cyclodextrins
dependent on their assembly of six, seven or eight glucose molecules. Characteristically, they
have a cylindrical form with a lipophilic cavity and a hydrophilic exterior part. Liphophilic
molecules can be encapsulated in the cavity and transported to a hydrophilic environment.
Sugammadex, however, is a synthetic γ-cyclodextrin where every sixth carbohydroxyl-group
is replaced by a thioether-side-chain with a negatively charged carboxy-group (COO-). This
leads to a larger cavity and allows encapsulating the muscle relaxants rocuronium (and, to a
lesser effective degree, vecuronium) (Bom 2009, p. 29; Welliver 2009, p. 49).
Encapsulation of rocuronium or vecuronium occurs in two phases:
1. After intravenous injection, all intravasal rocuronium/vecuronium-molecules are
encapsulated and by that, pharmacologically inactivated. This results in a
concentration gradient between plasma and extravasal space (including the
neuromuscular junction).
2. All extravasal rocuronium/vecuronium molecules are recruited back into the
bloodstream where they are immediately encapsulated and inactivated.
The binding shows a high stability based on electrostatic interaction between the positively
charged azotic molecules of rocuronium/vecuronium and the negatively charged carboxy-
groups of sugammadex. Van der Waals forces play a minor role in this interaction. The

10
association-dissociation-rate of sugammadex and rocuronium is 25,000,000 to 1 – meaning,
while 25 million molecules of rocuronium are encapsulated, only one molecule dissociates
from sugammadex within the same time (Bom 2009, p. 30; Welliver 2009, p. 52). The
rocuronium-sugammadex complex is highly stable under alternating conditions as regards
temperature or pH, and is eliminated entirely via the kidney (normally within 8 hours).
Interestingly, the primary hepatic elimination of rocuronium is in this way replaced by a renal
elimination (together with sugammadex). Its elimination half-life period is approximately 100
minutes, calculated at a plasma clearance equal to the glomeric filtration rate of 120 ml/min
(Naguib 2007, p. 577; Sparr 2009, p. 69).
Because of the 1:1 interaction of the encapsulation, the reversal depends on adequate dosage.
The following doses are recommended in the Summary of Product Characteristics when used
for a reversal of rocuronium-induced block:
a. appearance of second twitch of TOF-stimulation (T2>0): 2 mg/kg
b. 1-2 post-tetanic counts after five seconds of tetanic stimulation (PTC 1-2): 4 mg/kg
c. immediate reversal of rocuronium-induced block: 16 mg/kg
Under these dosages, a TOF-ratio of 0.9 will be reached within two minutes on average (Sparr
2009, p. 70).
Compared to antagonists (like neostigmine) cyclodextrins have no intrinsic effect. Their most
common side effects consist in anesthetic complications (such as grimacing or coughing
against the intratracheal tube), intraoperative awareness, allergic reactions, or dysgeusia.
In pharmaco-kinetic/pharmaco-dynamic modeling, no interaction was found for 300
compounds commonly used during anesthesia. However, three drugs are identified where
interaction may occur (Sparr 2009, p. 73):
1. Toremifene (an orally administered non-steroidal Selective Estrogen Receptor
Modulator used for treatment of metastatic breast cancer)
2. Flucloxacillin (a narrow spectrum beta-lactam penicillin)
3. Fusidic acid (a steroidal bacteriostatic agent)

11
Since progesterones and estrogens show some affinity for sugammadex, clinically relevant
interaction with hormonal contraceptives could not be excluded.
1.5 Aims of the Study
Previous dose finding studies were restricted to immediate reversals of 1.2 mg/kg rocuronium
or to reversals of very deep (post tetanic count of 1-2) or deep (T2 > 0) rocuronium or
vecuronium neuromuscular blockade. In a clinical setting, however, residual neuromuscular
paralysis occurs more frequently at much lower levels, as not every anesthetized patient
requires deep neuromuscular blockade for the complete surgical procedure. Unfortunately, no
dose recommendation is provided for any level of neuromuscular blockade beyond T2 > 0.
Since, however, rocuronium encapsulation by sugammadex is a 1:1 molecule interaction, it
seems feasible that shallow neuromuscular blocks would require less sugammadex.
In addition, those studies also showed that neostigmine is not effective to reverse profound or
deep neuromuscular blockade. This is due to the nature of competitive neuromuscular
blocking, where – even if all acetylcholine esterase in the junction is inhibited – there is still
too few of it in the neuromuscular junction to reverse a deep neuromuscular block. However,
neostigmine is widely used as reversal agent of residual neuromuscular block.
The primary aim of the study was to find the doses of neostigmine and sugammadex able to
reverse a residual neuromuscular block from a train-of-four ratio (TOF) of 0.5 to TOF 0.9
within two minutes on average and no more than five minutes for 95% of all patients.
The secondary goal of the study was to obtain the dose for a less accelerated reversal –
meaning, five minutes on average, and the upper time limit being 10 minutes for 95% of the
patient population.

12
2 Materials and Methods
2.1 Study Design and Patient Selection
This single center, randomized, parallel-group, double-blinded study was approved by the
ethics committee of the medical faculty of the “Technische Universität München” and the
Federal Institute for Drugs and Medical Devices (“Bundesanstalt für Arzneimittel und
Medizinprodukte”) of Germany. The study is listed under the acronym SUNDRO
(NCT00895609 and EudraCT 2008-008239-27).
Patients were included after informed written consent. Inclusion criteria were: age between 18
and 65 years, American Society of Anesthesiology physical status (ASA) I to III, and
scheduled for elective surgery under general anesthesia with rocuronium for endotracheal
intubation. Patients were excluded if they were expected to have a difficult airway, known
neuromuscular disease, significant hepatic or renal dysfunction, family history of malignant
hyperthermia, known allergy to one of the drugs used in this protocol, intake of any
medication which may interact with muscle relaxants, as well pregnant women or women
who were breast feeding. In addition, patients were not included if they were included in
another clinical study in the past 30 days.
Ninety-nine patients were randomly assigned to receive either sugammadex at doses of
0.0625 mg/kg, 0.125 mg/kg, 0.25 mg/kg, 0.5 mg/kg, and 1.0 mg/kg or neostigmine at doses of
5 µg/kg, 8 µg/kg, 15 µg/kg, 25 µg/kg, and 40 µg/kg in a mixture with 1 µg glycopyrrolate /
5 µg neostigmine or saline (n = 9 per dose group).
2.2 Procedure
An intravenous cannula was inserted into a forearm vein and standard anesthesia monitoring
(non-invasive blood pressure, ECG and oxygen saturation) established on arrival in the
operating room. Anesthesia was induced with propofol (2-3 mg/kg) and fentanyl (0.1-
0.2 µg/kg) and maintained with propofol and remifentanil according to the clinical need and
preference of the anesthesiologist. Patients received a laryngeal mask and were artificially
ventilated to keep the arterial oxygen saturation ≥ 96% and to maintain normocapnia. Body
temperature was maintained ≥ 35.0°C.
Neuromuscular monitoring was carried out according to international consensus guidelines
(Fuchs-Buder 2007, p. 789), using evoked electromyography of the adductor pollicis muscle

13
using the NMT module in a S/5 GE Datex Light monitor (GE Datex Medical Instrumentation,
Inc., Tewksbury, MA). In brief, the forearm was immobilized and surface skin electrodes
were placed over the ulnar nerve proximal to the wrist. Following calibration, the ulnar nerve
was stimulated with supramaximal TOF stimulation at 15-s intervals and the evoked
electromyogram of the adductor pollicis muscle was recorded. Neuromuscular transmission
and its suppression were described by parameters related to the TOF stimulation patterns, i.e.,
the response to the four stimulations (T1, T2, T3, and T4) related to the baseline values and the
ratio of the fourth twitch response, T4, to the first, T1, of a TOF complex (TOF ratio). Skin
temperature was measured at the site of the neuromuscular measurements and maintained
≥ 32.0°C using heating blankets.
Following three minutes of stabilization of the electromyography recording, 0.6 mg/kg
rocuronium was injected. At T1 = 0 the trachea was intubated. During surgery, maintenance
doses of 0.1-0.2 mg/kg rocuronium were injected according to clinical need.
When the surgical procedure did not require further neuromuscular block, spontaneous
recovery from the neuromuscular block was allowed to a TOF ratio of 0.5. At this point, the
study medication was injected according to the randomization. Neuromuscular monitoring
was continued until a stable TOF ≥ 0.9. At the end of surgery and emergence of anesthesia the
awake patient was extubated. Any decrease in the TOF ratio below 0.8 had to be recorded as
reoccurrence of neuromuscular block. Heart rate and blood pressure were recorded before and
2, 5, 10, and 20 min after the injection of the study medication.
Patients were kept in the recovery room for a minimum of 60 min. Oxygen saturation,
respiration rate, heart rate and blood pressure were routinely monitored. Any signs of
reoccurrence of muscle weakness were recorded. Therefore at several time points (every 15
min and before discharge from the recovery room) the patients’ levels of consciousness (i.e.,
awake and oriented, arousable with minimal stimulation, or responsive only to tactile
stimulation) were assessed. Cooperative patients were asked to open their eyes for 5 seconds,
perform a 5-s head lift test, a 5-s arm lift test and were asked to swallow a bolus of 20 ml
plain water. Then a test for general muscle weakness was performed using the Medical
Research Council (MRC) Scale: 0 - no movement, 1 - flicker is perceptible in the muscle, 2 -
movement only if gravity eliminated, 3 - can move limb against gravity, 4 - can move against
gravity & some resistance exerted by examiner, 5 - normal power. These postoperative

14
clinical assessments were performed by the blinded safety assessor. The study was finished
for a patient after discharge from the recovery room to the regular ward.
The anesthesiologist of the patient and the safety assessor also monitored all patients for
adverse events (AE), including serious AEs (SAE). However, if there was doubt about
classification the safety assessor had to decide the coding of the AE or SAE. AEs were
defined as drug related if the investigator considered them to be definitely, probably or
possibly related to the study drug.
2.3 Data Management and Statistical Analysis
Recovery from neuromuscular block induced by rocuronium was studied in the per-protocol
population (i.e., all treated patients without any major protocol violations). Safety data were
studied in all patients who received a dose of the study drug.
The primary study aim was to estimate a dose of sugammadex or neostigmine to accelerate
the time between start of administration of the respective study drug at TOF = 0.5 to
TOF 0.9 to an average time of two min with an upper limit of five min for 95% of the
patients. Secondary aim of the study were to estimate the doses of sugammadex and
neostigmine for a less advanced acceleration of the reversal, i.e. an average time of five min
and upper time limit of 10 min for 95% of patients.
Separate dose–response relationships were estimated from the available data for each reversal
agent. To explore the relationship between the dose of sugammadex or neostigmine and
recovery from neuromuscular block (TOF ratio to 0.9), several models have been tested in
order to describe the data with the model that fits best. We tested mono-(Puhringer 2008, p.
188; Sorgenfrei 2006, p. 669; Sparr 2007, p. 935) and bi-exponential models with the
recovery time to a TOF ratio ≥ 0.9 (t) in linear or logarithmic scale.
doseaeaadoset 321 (1)
doseaeaadoset 321ln (2)
doseadosea eaeaadoset 53421 (3)
doseadosea eaeaadoset 53421ln (4)
Additionally, we analyzed the data using fractional polynomials (FP) developed by Royston
and Altman (Royston 1994, p. 429), consisting of one (= FP1) or two degrees (= FP2) :

15
pdoseaadosetFP 211 : (5)
pdoseaadosetFP 211 ln : (6)
dosedoseadoseaa
doseadoseaadosetFP
pp
pp
ln
:
321
3212
21
(7)
dosedoseadoseaa
doseadoseaadosetFP
pp
pp
ln
ln:
321
3212
21
(8)
Since the models are not nested they were compared by applying the adjusted R2 ( = R2adj):
1
111 22
rn
nRR adj
with R2adj the value for the fit of the model and k the number of parameters in the model
excluding the intercept. The model with the largest R2adj is considered to be the best and was
used for further evaluations.

16
3 Results
3.1 Demographics
The study drug was injected in 99 patients. With five patients, major protocol violations
occurred: with one patient the neostigmine was incompletely injected due to a leaking venous
cannula, with four patients electromyographic response was instable. Since these violations
might have affected the primary and secondary aims, the respective data were omitted
resulting in a per protocol population of 94 patients.
Groups did not differ significantly regarding age, weight, height, sex and ASA physical
status: age was 42 ± 14 years, height 173 ± 10 cm, weight 76 ± 16 kg, 46 females and 53
males, 48 patients were classified as ASA physical status I, 44 as ASA II, and 7 as ASA III.
3.2 Efficacy
The median time to recover to a TOF ratio of 0.9 after injection of the study drug decreased
from 19 min (placebo) to 2.0 minutes with 40 µg/kg neostigmine (table 1) and to 1.0 min with
1.0 mg/kg sugammadex (table 2). No signs of re-curarization in any patient were observed
during the TOF monitoring or at the clinical testing of the patient in the recovery room.

17
3.2.1.1.1.1 Table 1: Time interval from administration of various doses of neostigmine
or placebo at Train-of-four (TOF) Ratio of 0.5 to 0.7, 0.8, or 0.9.
*Placebo values are also presented in table 2. Per-protocol population
Placebo* Neostigmine. Dose Group
5 µg/kg 8 µg/kg 15 µg/kg 25 µg/kg 40 µg/kg
n = 9 n = 8 n = 8 n = 9 n = 9 n = 8
Reversal – to TOF ³ 0.7
Median [min] 5.9 2.7 1.9 1.5 1.3 1.1
(Min - Max) [min] (3.5 - 9.8) (1.8 - 3.5) (1.5 - 2.3) (1.2 - 2.5) (1.0 - 2.3) (0.7 - 1.5)
Reversal – to TOF ³ 0.8
Median [min] 10 4.9 2.8 2.3 1.8 1.4
(Min - Max) [min] (7.2 - 16) (3.3 – 6.0) (2.5 - 3.3) (1.7 - 3.7) (1.2 - 3.2) (1.2 - 2)
Reversal – to TOF ³ 0.9
Median [min] 19 9.3 5.3 4.0 3.2 2.0
(Min - Max) [min] (12 – 33) (5.8 - 15) (3.5 - 8.7) (2.8 – 6.0) (1.7 - 6.2) (1.7 - 4.2)

18
3.2.1.1.1.2 Table 2: Time interval from administration of various doses of sugammadex
or placebo at Train-of-four (TOF) Ratio of 0.5 to 0.7, 0.8, or 0.9.
*Placebo values are also presented in table 1. Per-protocol population
Placebo* Sugammadex. Dose Group
0.06 mg/kg 0.12 mg/kg 0.25 mg/kg 0.5 mg/kg 1.0 mg/kg
n = 9 n = 9 n = 7 n = 9 n = 9 n = 9
Reversal – to TOF ³ 0.7
Median [min] 5.9 1.3 1.0 1.0 0.7 0.8
(Min - Max) [min] (3.5 - 9.8) (0.8 - 2.8) (0.7 – 1.7) (0.7 - 1.7) (0.7 – 1.0) (0.7 – 1.0)
Reversal - TOF ³ 0.8
Median [min] 10 2.5 1.2 1.0 1.0 1.0
(Min - Max) [min] (7.2 - 16) (1.0 - 4.7) (0.7 – 3.0) (1.0 – 2.0) (0.7 - 1.2) (0.7 - 1.3)
Reversal - TOF ³ 0.9
Median [min] 19 7.8 2.3 1.7 1.3 1.0
(Min - Max) [min] (12 – 33) (2.0 - 13) (1.0 – 11) (1.0 – 4.0) (0.8 – 2.0) (0.7 - 1.5)

19
The best fit of the relationship between the neostigmine dose and the time between
administration at TOF = 0.5 to recovery of TOF 0.9 was revealed by the bi-exponential
model using the time in logarithmic scale (model 4) with the highest adjusted regression
coefficient R2 = 0.814 (table 3). Based on this estimate, the dose of neostigmine is calculated
to be 50 µg/kg for an average recovery time of two min (extrapolation) and 34 µg/kg for an
upper limit of five min for the 95% patients’ population (primary endpoint) or 11 µg/kg for an
average recovery time of five min and 10 µg/kg for an upper limit of 10 min for 95% of
patients (secondary endpoint).
Table 3: Dose estimations for neostigmine using several mathematical models.
n.e. not estimable [ ] estimate of the value required extrapolation
Model t scale R2 Para-
metersAdjusted
R2
Dose estimate [µg/kg] for ...
Meant = 2 min
95% of patientst < 5 min
Meant = 5 min
95% of patients
t < 10 min
(primary endpoint) (secondary endpoint)
mono-exponential
linear 0,805 3
0,797 n.e. n.e. 10 14 logarithmic 0,816 0,808 n.e. 41 10 10
bi-exponential
linear 0,807 4
0,795 [60] n.e. 11 17 logarithmic 0,825 0,814 [50] 34 11 10
fractional polynomas (1 degree)
linear 0,789 3 0,780 [60] n.e. 14 26 logarithmic 0,806 0,797 40 32 13 13
fractional polynomas (2 degrees)
linear 0,807 5
0,791 [130] n.e. 11 16 logarithmic 0,825 0,810 [70] 35 10 9
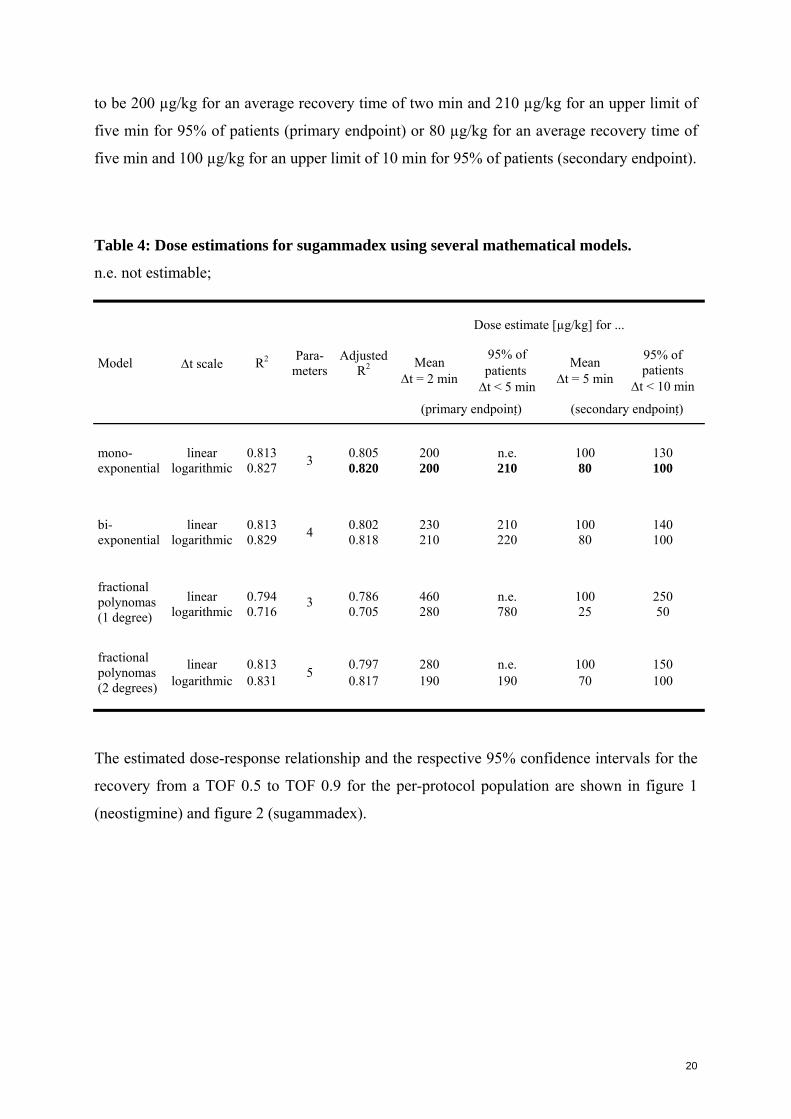
The best fit of the relationship between the sugammadex dose and the time between
administration at TOF = 0.5 to recovery of TOF 0.9 was revealed by the mono-exponential
model using the time in logarithmic scale (model 2) with the highest adjusted regression
coefficient R2 = 0.820 (table 4). Based on this estimate the dose of sugammadex is calculated
20
to be 200 µg/kg for an average recovery time of two min and 210 µg/kg for an upper limit of
five min for 95% of patients (primary endpoint) or 80 µg/kg for an average recovery time of
five min and 100 µg/kg for an upper limit of 10 min for 95% of patients (secondary endpoint).
Table 4: Dose estimations for sugammadex using several mathematical models.
n.e. not estimable;
Model t scale R2 Para-
metersAdjusted
R2
Dose estimate [µg/kg] for ...
Meant = 2 min
95% of patientst < 5 min
Meant = 5 min
95% of patients
t < 10 min
(primary endpoint) (secondary endpoint)
mono-exponential
linear 0.813 3
0.805 200 n.e. 100 130 logarithmic 0.827 0.820 200 210 80 100
bi-exponential
linear 0.813 4
0.802 230 210 100 140 logarithmic 0.829 0.818 210 220 80 100
fractional polynomas (1 degree)
linear 0.794 3 0.786 460 n.e. 100 250 logarithmic 0.716 0.705 280 780 25 50
fractional polynomas (2 degrees)
linear 0.813 5
0.797 280 n.e. 100 150 logarithmic 0.831 0.817 190 190 70 100
The estimated dose-response relationship and the respective 95% confidence intervals for the
recovery from a TOF 0.5 to TOF 0.9 for the per-protocol population are shown in figure 1
(neostigmine) and figure 2 (sugammadex).

21
Mean
Mean ± 1.96 SD
0
5
10
15
20
25
30
35
40
0 5 10 15 20 25 30 35 40 45
2
50
Figure 1: Neostigmine bi-exponential fit
Neostigmine Dose [µg/kg]
Tim
e fr
om a
dmin
istr
atio
n of
IP to
TO
F
0.9
(m
in)

22
3.3 Safety
Clinical muscle function tests and evaluation of consciousness revealed no difference between
groups at any time during postoperative period in the recovery room. At arrival, 13% of the
79 cooperative patients were not able to keep the eyes open for 5s, 6% were not able to lift the
head for 5s, 4% were not able to lift the arm for 5s, 13% were not able to swallow 20 ml of
water without difficulties, and 46% of the cooperative patients had not reached normal muscle
strength (MRC scale). After 60 min in the recovery room all patients were cooperative and
did not show any clinical sign of muscle weakness.
After administration of study medication one or more adverse events were reported in 48
patients (table 5). The majority of AEs were classified as mild or moderate. The three most
often observed AEs were postoperative shivering, bradycardia, and hypotension.
Postoperative shivering was treated with 25-50 mg meperidine, bradycardia was treated with
Tim
e fr
om a
dmin
istr
atio
n of
IP to
TO
F
0.9
(m
in)
Sugammadex Dose [µg/kg]
Mean
Mean ± 1.96 SD
0
10
15
20
25
30
35
0 100 200 300 400 500 600 700 800 900 1000 1100
40
5
2
Figure 2. Sugammadex mono-exponential fit

23
0.2 mg glycopyrrolate, and hypotension with 0.5 – 2.0 ml Akrinor (vasopressor available in
Germany consisting of theophylline, ephedrine, caffeine and norepinephrine). No dose-
response relationship was observed.
Table 5: Incidence of Adverse Events for all Groups after Administration of
Neostigmine, Sugammadex or Placebo.
SAE = Serious Adverse Event * p < 0.05 compared to sugammadex groups
Neostigmin Placebo Sugammadex
Hypertension 1 (2%) 0 1 (2%)
Bradycardia 12 (27%)* 0 1 (2%)
Hypoglycemia 0 1 (11%) 0
Hypokalemia 1 (2%) 1 (11%) 0
Hypocalcemia 1 (2%) 1 (11%) 1 (2%)
Hypotension 3 (7%) 4 (44%) 5 (11%)
Desaturation < 90 % 3 (7%) 0 0
Paresthesia N. ulnaris 0 1 (11%) 0
Postoperative Nausea and Vomiting 0 2 (22%) 2 (5%)
Postoperative Shivering 11 (25%) 0 8 (18%)
Tachycardia 2 (5%) 0 1 (2%)
Anesthetic complications
(intraoperative cough/movement) 1 (2%) 0 1 (2%)
Acute lung failure (SAE) 1 (2%) 0 0
At least 1 AE 28 (64%)* 4 (44%) 16 (36%)
One patient developed acute lung failure 63 h postoperatively. This adverse event was
categorized to be severe and possibly related to the study medication of 5 µg/kg neostigmine.
The patient was known to have a restrictive lung disorder (vital capacity of 1.9 l, i.e. 35 % of
normal) after bleomycine chemotherapy. None of the patients discontinued the study because
of a (serious) AE.

24
4 Discussion Sugammadex as well as neostigmine was able to reverse a rocuronium-induced residual
neuromuscular block at a TOF ratio of 0.5 in a dose-dependent manner. Best fit modeling of
the dose response relationship revealed 0.21 mg/kg sugammadex and 34 µg/kg neostigmine to
be able to accelerate the recovery from TOF = 0.5 to TOF 0.9 in an average of two min or,
at least, in five min in 95% of all treated patients. Incidence of adverse events was
significantly higher in neostigmine treated patients. It is important to note, that no patient
showed any sign of recurarization following every tested dose of the two reversal agents.
Quintessentially for any dose finding study is the statistical model to calculate the requested
dose. The published dose finding studies for sugammadex used a mono-exponential approach
with the recovery times in linear scale (de Boer 2007, p. 239; Groudine 2007, p. 555;
Puhringer 2008, p. 188; Sorgenfrei 2006, p. 667; Sparr 2007, p. 935). This approach assumes
that only one process, e.g. encapsulation of rocuronium, is responsible for the recovery
kinetics and, in addition, that this process follows linear characteristics. Before ruling out
alternative mathematical relations this assumption cannot be transferred to the data of our
study, especially for the much more complex acting neostigmine reversal groups. Therefore,
we additionally analyzed bi-exponential models with the time to recovery of the TOF ratio to
0.9 (t) in linear or logarithmic scale as well as fractional polynomials consisting of one, two
or more degrees (Royston 1994, p. 429). Our results confirmed the notion that a logarithmic
scale may improve the fitting of the models because all models using the recovery times in
logarithmic scale showed higher R2adj and more homogeneous variances at each dose
fulfilling one of the assumptions of any regression analysis.
The decision which model fits the observed values best was performed based on the linear
least square technique and an adjustment of R² in order to address the different number of free
variables. An alternative approach the AIC criterion proposed by Akaike has the disadvantage
that only models using the same type of values for the dependent variable can be compared
(Akaike 1973, p. 267).
In addition to the highest correlation coefficient, the extrapolation of the model to high doses
of the reversal agents influenced our decision which model fits best. The results obtained
from the sugammadex dose finding study at reappearance of T2 (Sorgenfrei 2006, p. 667)
suggest the existence of a dose that is able to reverse even deeper neuromuscular blocks than

25
the TOF of 0.5 within an average time of two min or in five min in 95% of the patients (Jones
2008, p. 816; Sorgenfrei 2006, p. 667). Accordingly, models that cannot estimate a respective
dose are in contradiction to the published data and have to be rejected; in addition, such
models do not reflect the observation of the 1 mg/kg and 0.5 mg/kg sugammadex subgroups
of this investigation.
The three models with the highest adjusted R² and an estimate for the dose according to our
endpoints were the mono-exponential, the bi-exponential, and the fractional polynomial with
two degrees, all using the recovery times in logarithmic scale. Based on these models the dose
to reverse a residual rocuronium-induced neuromuscular block at TOF = 0.5 with
sugammadex is considered to be between 0.19 mg/kg and 0.22 mg/kg, resulting in a
recommendation to test 0.25 mg/kg in a comparative study with a larger number of patients,
expecting a recovery time of 1.7 min with a 95% tolerance interval of 0.7 min to 4.3 min.
In this study we did not observe any clinical or monitoring related sign of residual paralysis or
re-curarization. This is important to note since we have tested doses between 0.0625 and 1.0
mg/kg sugammadex. Especially in the low dose sugammadex groups, one can assume that
there are not enough sugammadex molecules present to encapsulate all rocuronium molecules
expected to be in the patients’ body at TOF 0.5. Accordingly, we must assume that –
irrespectively of the complete recovery of the TOF ratio with doses below 1.0 mg/kg
sugammadex – unbound rocuronium is still available (Bom 2002, p. 265; Robertson 2005,
p. 4). In other words, fast recovery is not only caused by the encapsulation with sugammadex
but also by the margin of safety of the neuromuscular transmission (Paton 1967, p. 59).
Therefore, neuromuscular monitoring to control the sufficient reversal effect is mandatory,
even when the suggested dose of 0.25 mg/kg is used at a TOF ratio of 0.5.
Analogously rigorous claims regarding the quality of reversal cannot be postulated as regards
neostigmine, as that drug has neither the potential to withdraw muscle relaxants from
neuromuscular cleft (owing to its indirect and therefore limited antagonism, (Bartkowski
1987, p. 594) nor an onset of action which merits expecting a recovery time averaging below
3 min (Calvey 1979, p. 149). In accordance, only one model was able to define a dose being
able to reverse the neuromuscular function within an average of two min. As a result, it seems
to be more relevant to base the primary endpoint upon a recovery to TOF > 0.9 of the 95%
population within five min. Although a dose recommendation influenced by this decision still
meets clinical needs, it marks another difference between the two study arms.

26
The three models with the highest adjusted R² of the neostigmine dose-response relationship
were the same as for sugammadex: the mono-exponential model, the bi-exponential model,
and the fractional polynomial model with two degrees, using recovery times in logarithmic
scale. Based on these models and the knowledge about the onset time of neostigmine, the
dose to reverse a residual rocuronium-induced neuromuscular block at TOF = 0.5 is
considered between 34 µg/kg and 41 µg/kg, resulting in a recommendation to test 40 µg/kg in
a comparative study with a larger number of patients, expecting a recovery time of 2.4 min
with a 95% tolerance interval of 1.2 min to 4.6 min.
Less advanced accelerations of neuromuscular recovery have been defined for the secondary
endpoint. Since 95% of the placebo treated patients recovered within 25 min there is still an
acceleration of recovery of 15 min if reversal agents shorten the recovery time to 10 min.
Based on the same criteria applied at the primary endpoint, the dose recommendations for a
recovery between TOF 0.5 and 0.9 within an average of five min and an upper confidence
limit of 10 min were found to be 10 µg/kg neostigmine and 0.1 mg/kg sugammadex,
respectively. The recommended neostigmine dose is in accordance with the recent findings of
Fuchs-Buder et al. who suggested 10-20 µg/kg to be sufficient for a reversal of a shallow
atracurium-induced neuromuscular block, defined at a TOF ratio of 0.4 or 0.6 (Fuchs-Buder
2010, p. 34).
This study was neither designed nor powered to address any side effect comparisons. Due to
safety issues, the side effects were documented and are presented descriptively. The number
of patients showing at least one side effect following the study drug was significantly lower in
the summarized sugammadex groups. With the exception of the higher incidence of
bradycardia (heart rate < 40 beats/min) following neostigmine there was no systematic
observation. The latter, however, is a well-known cholinergic side effect, which appeared
even though neostigmine was administered as a premix with glycopyrronium (ratio 1:5).
Bradycardia could be controlled in every patient with an additional dose of 0.2 mg
glycopyrronium.
Interestingly, postoperative shivering was observed after neostigmine or sugammadex in
respectively 18% and 25 % of patients, but not in the placebo treated patient and not in the
low dose subgroups of neostigmine (5 µg/kg) and sugammadex (0.0625 mg/kg). Further
investigation may be meaningful to elucidate whether an effective or fast reversal of
neuromuscular blocking agents increases the risk of postoperative shivering.

27
This study represents a third degree of incomplete recovery from rocuronium-induced
neuromuscular block. Deep block defined as PTC 1-2 (Groudine 2007, p. 555), moderate
block defined as reappearance response of the second twitch following train-of-four
stimulation (Sorgenfrei 2006, p. 667), and residual block at TOF = 0.5 as shown in this study
require decreasing doses of sugammadex in order to achieve the same result, i.e. TOF > 0.9
within approximately two min. This relationship between depth of block and sugammadex
demand in conjunction with the very fast onset of its reversal effect suggests that titration of
sugammadex based on quantitative neuromuscular monitoring might be possible. Additional
dose finding studies, e.g. at TOF = 0.2, may help to estimate the appropriate dose at a block
between reappearance of T2 and TOF 0.5. Since we were able to identify an effective
neostigmine dose at TOF 0.5 below the maximum recommended 70 µg/kg, it also appears
reasonable to test neostigmine at lower TOF values, addressing the question at which TOF
value the ceiling effect of neostigmine becomes relevant.
In conclusion, sugammadex 0.25 mg/kg and neostigmine 40 µg/kg effectively reverse a
rocuronium-induced residual neuromuscular block of TOF 0.5 in a comparable manner.

28
5 Abstract Introduction: Sugammadex is very effective to rapidly reverse moderate or deep
rocuronium-induced neuromuscular blockade. However, the dosage of sugammadex to
reverse residual neuromuscular block at the end of surgery (a phenomenon in clinical practice
more widespread than the aforementioned) is still unknown. This study therefore compares
the efficacy of sugammadex and neostigmine in various doses at a train-of-four (TOF) ratio of
0.5.
Methods: After IRB approval and written informed consent, 99 patients (ASA physical status
I-III) aged between 18 and 65 years were anaesthetized with propofol, remifentanil, and
rocuronium. Neuromuscular monitoring was performed by calibrated electromyography. At
recovery of the TOF-ratio to 0.5, patients were randomized to receive either sugammadex
(0.0625, 0.125, 0.25, 0.5 or 1.0 mg/kg) or neostigmine (5, 8, 15, 25 or 40 µg/kg) or saline (n =
9 per group). The time between injection of the drug under study and TOF ≥ 0.9 was
measured. Several mathematical models (mono-exponential, bi-exponential, and fractional
polynomial) were tested in order to describe the data with the model that best fits the data
using the recovery time in logarithmic or linear scale. The effective doses were calculated by
interpolation of the regression models.
Results: 0.21 mg/kg sugammadex is able to reverse a TOF ratio of 0.5 to ≥ 0.9 at an average
time of two min – and within five min for 95 % of patients in the best fitting model. 34 µg/kg
neostigmine is able to reverse a TOF ratio of 0.5 to ≥ 0.9 within five minutes for 95 % of
patients. No re-curarization was observed.
Conclusions: Sugammadex 0.25 mg/kg and neostigmine 40 µg/kg effectively reverse a
rocuronium-induced residual neuromuscular block of TOF 0.5 in a comparable manner.

29
6 Literature 1. Akaike, H.: ed. Information theory and an extension of the maximum likelihood
principle. Budapest: Akademiai Kiado, 1973: 267-281. (Petrov, B.N., Csaki, F., ed. 2nd
International Symposium on Information Theory; vol
2. Auroy, Y., Benhamou, D., Péquignot, F., Bovet, M., Jougla, E., Lienhart, A.:
Mortality related to anaesthesia in France: analysis of deaths related to airway
complications*. Anaesthesia 64 (2009) 366-370
3. Baillard, C., Clec'h, C., Catineau, J., Salhi, F., Gehan, G., Cupa, M., Samama, C.M.:
Postoperative residual neuromuscular block: a survey of management. Br J Anaesth 95
(2005) 622-626
4. Bartkowski, R.R.: Incomplete reversal of pancuronium neuromuscular blockade by
neostigmine, pyridostigmine, and edrophonium. Anesth Analg 66 (1987) 594-598
5. Berg, H., Roed, J., Viby-Mogensen, J., Mortensen, C.R., Engbaek, J., Skovgaard,
L.T., Krintel, J.J.: Residual neuromuscular block is a risk factor for postoperative
pulmonary complications. A prospective, randomised, and blinded study of postoperative
pulmonary complications after atracurium, vecuronium and pancuronium. Acta
Anaesthesiol Scand 41 (1997) 1095-1103
6. Blobner, M., Frick, C.G., Busley, R.: Muskelrelaxanzien und ihre Antagonisten In: "Die
Anästhesiologie", Rossaint, R., Werner, C., Zwißler, B. (Ed.), Springer Medizin Verlag,
Heidelberg, 2008, 2. Ed., p. 321-347.
7. Blobner, M., Frick, C.G., Diefenbach, C.: Muskelrelaxanzien und deren Antagonisten:
Pharmakologie und neuromuskuläres Monitoring In: "Anästhesiologie", Kochs, E.,
Adams, H., Spies, C. (Ed.), Georg Thieme Verlag KG, Stuttgart, 2009, 2. Ed., p. 105-122.
8. Bom, A., Bradley, M., Cameron, K., Clark, J.K., Van Egmond, J., Feilden, H.,
MacLean, E.J., Muir, A.W., Palin, R., Rees, D.C., Zhang, M.Q.: A Novel Concept of
Reversing Neuromuscular Block: Chemical Encapsulation of Rocuronium Bromide by a
Cyclodextrin-Based Synthetic Host. Angew Chem Int Ed Engl 41 (2002) 265-270
9. Bom, A., Hope, F., Rutherford, S., Thomson, K.: Preclinical pharmacology of
sugammadex. J Crit Care 24 (2009) 29-35
10. Bonhomme, V., Hans, P.: Muscle relaxation and depth of anaesthesia: where is the
missing link? Br J Anaesth 99 (2007) 456-460
11. Calvey, T.N., Wareing, M., Williams, N.E., Chan, K.: Pharmacokinetics and
pharmacological effects of neostigmine in man. Br J Clin Pharmacol 7 (1979) 149-155

30
12. Cammu, G., de Baerdemaeker, L., den Blauwen, N., de Mey, J.-C., Struys, M.,
Mortier, E.: Postoperative residual curarization with cisatracurium and rocuronium
infusions. Eur J Anaesthesiol 19 (2002) 129-134
13. Cass, N.M.: Medicolegal claims against anaesthetists: a 20 year study. Anaesth Intensive
Care 32 (2004) 47-58
14. de Boer, H.D., Driessen, J.J., Marcus, M.A., Kerkkamp, H., Heeringa, M., Klimek,
M.: Reversal of rocuronium-induced (1.2 mg/kg) profound neuromuscular block by
sugammadex: a multicenter, dose-finding and safety study. Anesthesiology 107 (2007)
239-244
15. Debaene, B., Plaud, B., Dilly, M.P., Donati, F.: Residual paralysis in the PACU after a
single intubating dose of nondepolarizing muscle relaxant with an intermediate duration
of action. Anesthesiology 98 (2003) 1042-1048
16. Eikermann, M., Blobner, M., Groeben, H., Rex, C., Grote, T., Neuhauser, M.,
Beiderlinden, M., Peters, J.: Postoperative upper airway obstruction after recovery of the
train of four ratio of the adductor pollicis muscle from neuromuscular blockade. Anesth
Analg 102 (2006) 937-942
17. Fink, A.S., Hutter, M.M., Campbell Jr, D.C., Henderson, W.G., Mosca, C., Khuri,
S.F.: Comparison of Risk-Adjusted 30-Day Postoperative Mortality and Morbidity in
Department of Veterans Affairs Hospitals and Selected University Medical Centers:
General Surgical Operations in Women. Journal of the American College of Surgeons 204
(2007) 1127-1136
18. Fink, H., Blobner, M., Martyn, J.: Neuromuscular Blocking Agents and Reversal Drugs
In: "Anesthetic Pharmacology: Physoiologic Principles and Clinical Practice", Evers,
A.S., Maze, M. (Ed.), Elsevier Inc., HongKong, 2004, 1. Ed., p. 573-598.
19. Fuchs-Buder, T., Claudius, C., Skovgaard, L.T., Eriksson, L.I., Mirakhur, R.K.,
Viby-Mogensen, J.: Good clinical research practice in pharmacodynamic studies of
neuromuscular blocking agents II: the Stockholm revision. Acta Anaesthesiol Scand 51
(2007) 789-808
20. Fuchs-Buder, T., Meistelman, C., Alla, F., Grandjean, A., Wuthrich, Y., Donati, F.:
Antagonism of low degrees of atracurium-induced neuromuscular blockade: dose-effect
relationship for neostigmine. Anesthesiology 112 (2010) 34-40
21. Gibbs, N., Rodoreda, P.: Anaesthetic mortality rates in Western Australia 1980-2002.
Anaesth Intensive Care 33 (2005) 616-622

31
22. Groudine, S.B., Soto, R., Lien, C., Drover, D., Roberts, K.: A randomized, dose-
finding, phase II study of the selective relaxant binding drug, Sugammadex, capable of
safely reversing profound rocuronium-induced neuromuscular block. Anesth Analg 104
(2007) 555-562
23. Hayes, A.H., Mirakhur, R.K., Breslin, D.S., Reid, J.E., McCourt, K.C.: Postoperative
residual block after intermediate-acting neuromuscular blocking drugs. Anaesthesia 56
(2001) 312-318
24. Henderson, W.G., Khuri, S.F., Mosca, C., Fink, A.S., Hutter, M.M., Neumayer, L.A.:
Comparison of Risk-Adjusted 30-Day Postoperative Mortality and Morbidity in
Department of Veterans Affairs Hospitals and Selected University Medical Centers:
General Surgical Operations in Men. Journal of the American College of Surgeons 204
(2007) 1103-1114
25. Hovi-Viander, M.: Death associated with anaesthesia in Finland. Br J Anaesth 52 (1980)
483-489
26. Jones, R.K., Caldwell, J.E., Brull, S.J., Soto, R.G.: Reversal of profound rocuronium-
induced blockade with sugammadex: a randomized comparison with neostigmine.
Anesthesiology 109 (2008) 816-824
27. Lagasse, R.S.: Anesthesia Safety: Model or Myth?: A Review of the Published Literature
and Analysis of Current Original Data. Anesthesiology 97 (2002) 1609-1617
28. Lienhart, A., Auroy, Y., Pequignot, F., Benhamou, D., Warszawski, J., Bovet, M.,
Jougla, E.: Survey of Anesthesia-related Mortality in France. Anesthesiology 105 (2006)
1087-1097
29. Lieutaud, T., Billard, V., Khalaf, H., Debaene, B.: Muscle relaxation and increasing
doses of propofol improve intubating conditions. Canadian Journal of Anesthesia / Journal
canadien d'anesthésie 50 (2003) 121-126
30. Masso, E., Sabate, S., Hinojosa, M., Vila, P., Canet, J., Langeron, O.: Lightwand
Tracheal Intubation with and without Muscle Relaxation. Anesthesiology 104 (2006) 249-
254
31. Maybauer, D.M., Geldner, G., Blobner, M., Puhringer, F., Hofmockel, R., Rex, C.,
Wulf, H.F., Eberhart, L., Arndt, C., Eikermann, M.: Incidence and duration of residual
paralysis at the end of surgery after multiple administrations of cisatracurium and
rocuronium. Anaesthesia 62 (2007) 12-17
32. McCaul, C., Tobin, E., Boylan, J.F., McShane, A.J.: Atracurium is associated with
postoperative residual curarization. Br J Anaesth 89 (2002) 766-769

32
33. Mencke, T., Echternach, M., Kleinschmidt, S., Lux, P., Barth, V., Plinkert, P.K.,
Fuchs-Buder, T.: Laryngeal morbidity and quality of tracheal intubation: a randomized
controlled trial. Anesthesiology 98 (2003) 1049-1056
34. Murphy, G.S., Szokol, J.W., Marymont, J.H., Greenberg, S.B., Avram, M.J.,
Vender, J.S.: Residual neuromuscular blockade and critical respiratory events in the
postanesthesia care unit. Anesth Analg 107 (2008) 130-137
35. Naguib, M.: Sugammadex: another milestone in clinical neuromuscular pharmacology.
Anesth Analg 104 (2007) 575-581
36. Paton, W.D., Waud, D.R.: The margin of safety of neuromuscular transmission. J
Physiol Lond 191 (1967) 59-90
37. Puhringer, F.K., Rex, C., Sielenkamper, A.W., Claudius, C., Larsen, P.B., Prins,
M.E., Eikermann, M., Khuenl-Brady, K.S.: Reversal of profound, high-dose
rocuronium-induced neuromuscular blockade by sugammadex at two different time
points: an international, multicenter, randomized, dose-finding, safety assessor-blinded,
phase II trial. Anesthesiology 109 (2008) 188-197
38. Robertson, E.N., Driessen, J.J., Booij, L.H.: Pharmacokinetics and pharmacodynamics
of rocuronium in patients with and without renal failure. Eur J Anaesthesiol 22 (2005) 4-
10
39. Royston, P., Altman, D.: Regression using fractional polynomials of continuous
covariates: parsimonious parametric modelling (with Discussion). Appl Stat 43 (1994)
429-467
40. Schlaich, N., Mertzlufft, F., Soltesz, S., Fuchs-Buder, T.: Remifentanil and propofol
without muscle relaxants or with different doses of rocuronium for tracheal intubation in
outpatient anaesthesia. Acta Anaesthesiol Scand 44 (2000) 720-726
41. Sorgenfrei, I., Norrild, K., Larsen, P., Stensballe, J., Ostergaard, D., Prins, M., Viby-
Mogensen, J.: Reversal of rocuronium-induced neuromuscular block by the selective
relaxant binding agent sugammadex: a dose-finding and safety study. Anesthesiology 104
(2006) 667-674
42. Sparr, H.J., Booij, L.H., Fuchs-Buder, T.: [Sugammadex. New pharmacological
concept for antagonizing rocuronium and vecuronium]. Anaesthesist 58 (2009) 66-80
43. Sparr, H.J., Leo, C., Ladner, E., Deusch, E., Baumgartner, H.: Influence of
anaesthesia and muscle relaxation on intubating conditions and sympathoadrenal response
to tracheal intubation. Acta Anaesthesiol Scand 41 (1997) 1300-1307

33
44. Sparr, H.J., Vermeyen, K.M., Beaufort, A.M., Rietbergen, H., Proost, J.H., Saldien,
V., Velik-Salchner, C., Wierda, J.M.: Early reversal of profound rocuronium-induced
neuromuscular blockade by sugammadex in a randomized multicenter study: efficacy,
safety, and pharmacokinetics. Anesthesiology 106 (2007) 935-943
45. Sundman, E., Witt, H., Olsson, R., Ekberg, O., Kuylenstierna, R., Eriksson, L.I.: The
incidence and mechanisms of pharyngeal and upper esophageal dysfunction in partially
paralyzed humans: pharyngeal videoradiography and simultaneous manometry after
atracurium. Anesthesiology 92 (2000) 977-984
46. Tonner, P.H.: Balanced anaesthesia today. Best Pract Res Clin Anaesthesiol 19 (2005)
475-484
47. Viby Mogensen, J., Chraemer Jorgensen, B., Ording, H.: Residual curarization in the
recovery room. Anesthesiology 50 (1979) 539 - 541
48. Welliver, M., McDonough, J., Kalynych, N., Redfern, R.: Discovery, development, and
clinical application of sugammadex sodium, a selective relaxant binding agent. Drug Des
Devel Ther 2 (2009) 49-59

34
7 Acknowledgments I would like to thank Professor Dr. Dipl-phys. Eberhard Kochs, chair and director of the
Klinik für Anaesthesiologie at the Technische Universität München, for his unlimited support
not only for this study but also for my further research interests.
I am very grateful to Professor Dr. Manfred Blobner, Klinik für Anaesthesiologie at the
Technische Universität München. His research enthusiasm sparked my interest for clinical
research. He also thought me the importance of critical scientific thinking and debate.
This study could not have been completed without my mentor, Associate Professor Dr.
Heidrun Fink, who guided me through all the ups and downs and who supported me at all
times. I owe her a debt of gratitude for her unconfined mentorship for my research career and
her friendship.
I would also like to extend my thanks to Professor Kurt Ulm, Institut für Medizinische
Statistik und Epidemiologie, Klinikum rechts der Isar, Technische Universität München for
his advice regarding the mathematical approach and statistical analysis used in this thesis and
Stefan Koller, Richard Hofmann and Volkmar Lautscham for their help with linguistic
problems.
Sincere thanks to Professor Dr. Josef Smolle, Professor Dr. Gilbert Reibnegger and Professor
Dr. Walther Wegscheider who inspired me during my studies.
Last but not least, my wholehearted gratitude and thanks go to my mother and brother. My
professional and scientific career would not have been possible without their loving support
and their unconditional help.

35
8 Curriculum Vitae Name: Stefan Schaller
Date of birth: 23rd January 1980
Place of birth: Graz, Austria
1. Education
1986 – 1990 Volksschule Kepler (elementary school), Graz, Austria
1990 – 1998 BRG Keplerstrasse (secondary school), Graz, Austria
final examination (“Matura”) overall grade 1.0
2. University
1999-2007 Medical University of Graz
2001 First part of viva voce (overall grade-point-average 1.0)
2004 Second part of viva voce (overall grade-point-average 1.0)
2007 Third part of viva voce (overall grade-point-average 1.0)
2004 6-month ERASMUS scholarship awarded by the EU, Amsterdam
Netherlands (overall grade-point-average 1.0)
2006 Rotation at the department of Emergency Medicine, SUNY Downstate,
New York City, USA
Since July 2007 Resident
Klinik für Anaesthesiologie
Klinikum rechts der Isar
Technische Universität München
Related Documents











