81 81 Successful nonsurgical retreatment of resected teeth associated with persistent periapical lesion by placing triple Antibiotic paste and mineral trioxide aggregate apical plug - A case report Sumanthini.M.V. # Vanitha.U.Shenoy # Rupali Deshmukh # Rahul Kumar # ABSTRACT This article describes the nonsurgical management of traumatized teeth that had undergone apisectomy and associated with a large periapical lesion. A combination of antibacterial drugs consisting of metronidazole, ciprofloxacin and minocycline was used for root canal disinfection. The common problem encountered with this drug combination is tooth discoloration due to minocycline. Adhesive restoration was used to address this problem. Mineral trioxide aggregate apical plug was placed in the lateral incisor that had undergone unsuccessful root resection. On two year follow up the patient was asymptomatic and intraoral periapical radiograph showed successful healing with complete resolution of the periradicular lesion. Key words: Discolouration, mineral trioxide aggregate, retreatment, triple antibiotic paste. # Department of Conservative Dentistry and Endodontics, MGM Dental College and Hospital, Navi Mumbai Introduction Endodontic surgery with root end resection often leaves a canal with an apex that is large in diameter creating an open apex. 1 In the event of failure subsequent orthograde retreatment may be indicated. It is difficult to obtain a fluid tight apical seal in such teeth with open apices by using the conventional endodontic treatment methods due to absence of an apical barrier, against which obturation material can be compacted. Traditionally, multiple-visit apexification with calcium hydroxide (CH) was the treatment of choice in teeth with open apex, which would induce formation of an apical hard tissue barrier. Although successful, it takes anywhere from 3 to 18 months for the creation of physiologic hard tissue barrier. 2 The disadvantages of this technique is multiple treatment appointments, coronal leakage, and increased susceptibility of tooth fracture. 3,4 An alternative technique for apexification with CH is to seal the open apical foramen with mineral trioxide aggregate (MTA) apical plug. Considerable success has been reported recently with this technique in treating permanent teeth with immature apices which is attributed to its ability to induce periradicular tissue regeneration, biocompatibility, good sealing ability and enables treatment to be completed in a short frame of time. 5 MTA has been found to be an appropriate material for apical sealing of mature root canals with open apex as a result of over instrumentation, resorption or former apisectomy. 6,7 The major causative role of microorganisms in the pathogenesis of persistent periapical diseases is well documented and considered to be ENDODONTOLOGY ENDODONTOLOGY ENDODONTOLOGY ENDODONTOLOGY ENDODONTOLOGY Volume: 25 Issue 2 December 2013 Case Report

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8181
Successful nonsurgical retreatment of resected teethassociated with persistent periapical lesion by placing tripleAntibiotic paste and mineral trioxide aggregate apical plug- A case report
Sumanthini.M.V. #Vanitha.U.Shenoy #Rupali Deshmukh #Rahul Kumar #
ABSTRACT
This article describes the nonsurgical management of traumatized teeth that had undergone apisectomy and associated
with a large periapical lesion. A combination of antibacterial drugs consisting of metronidazole, ciprofloxacin and
minocycline was used for root canal disinfection. The common problem encountered with this drug combination is
tooth discoloration due to minocycline. Adhesive restoration was used to address this problem. Mineral trioxide
aggregate apical plug was placed in the lateral incisor that had undergone unsuccessful root resection. On two year
follow up the patient was asymptomatic and intraoral periapical radiograph showed successful healing with complete
resolution of the periradicular lesion.
Key words: Discolouration, mineral trioxide aggregate, retreatment, triple antibiotic paste.
# Department of Conservative Dentistry and Endodontics, MGM Dental College and Hospital, Navi Mumbai
Introduction Endodontic surgery with root end resection
often leaves a canal with an apex that is large in
diameter creating an open apex.1 In the event of
failure subsequent orthograde retreatment may be
indicated. It is difficult to obtain a fluid tight apical
seal in such teeth with open apices by using the
conventional endodontic treatment methods due to
absence of an apical barrier, against which
obturation material can be compacted.
Traditionally, multiple-visit apexification with
calcium hydroxide (CH) was the treatment of choice
in teeth with open apex, which would induce
formation of an apical hard tissue barrier. Although
successful, it takes anywhere from 3 to 18 months
for the creation of physiologic hard tissue barrier.2
The disadvantages of this technique is multiple
treatment appointments, coronal leakage, and
increased susceptibility of tooth fracture.3,4 An
alternative technique for apexification with CH is
to seal the open apical foramen with mineral
trioxide aggregate (MTA) apical plug. Considerable
success has been reported recently with this
technique in treating permanent teeth with
immature apices which is attributed to its ability to
induce periradicular tissue regeneration,
biocompatibility, good sealing ability and enables
treatment to be completed in a short frame of time.5
MTA has been found to be an appropriate material
for apical sealing of mature root canals with open
apex as a result of over instrumentation, resorption
or former apisectomy.6,7
The major causative role of microorganisms
in the pathogenesis of persistent periapical diseases
is well documented and considered to be
ENDODONTOLOGYENDODONTOLOGYENDODONTOLOGYENDODONTOLOGYENDODONTOLOGY Volume: 25 Issue 2 December 2013 Case Report

8282
polymicrobial. A combination of antimicrobial
drugs consisting of metronidazole, ciprofloxacin and
minocycline has been shown to be very effective in
eliminating endodontic pathogens in vitro and in
vivo. In combination, these drugs were able to
consistently sterilize all samples.8Among the
components of the mixture, minocycline, a
semisynthetic derivative of tetracycline has the
potential to induce tooth discolouration.9
Anticipating this, as a precaution, adhesive
restorative techniques need to be adopted from the
beginning of commencement of treatment in order
to prevent discolouration from occurring.
The following case report describes nonsurgical
endodontic retreatment of teeth that had undergone
apical root resection and was associated with a
persistent large periradicular lesion.
Case ReportA 26 year old female patient was referred to
Department of conservative dentistry and
endodontics, with a chief complaint of pain and
swelling in maxillary left central incisor (21) and
maxillary left lateral incisor (22) since one month.
The patient gave a history of root canal treatment in
the 21, 22 and maxillary left canine (23) followed
by surgical root resection in 21 and 22. Clinical
examination revealed an intraoral, labial swelling
and sinus tract at the apex of 21 [Fig 1a]. The access
cavities were restored with tooth coloured
restorations. Tooth number 22 was tender on
percussion and 23 were asymptomatic. Maxillary
right central incisor (11) had a mesial angle fracture
involving enamel and tested vital. Intraoral
periapical radiograph revealed large periapical
rarefactions in 21 and 22, obturation in both teeth
were below acceptable standards and the root ends
were resected [Fig 1b]. A Gutta percha cone is
radiographically seen tracing the source of infection
to 21[Fig 1c]. In view of the signs and symptoms
Fig 1a: Preoperative intraoral picture of maxillary left central andlateral incisors with swelling and sinus tract apical to maxillary leftcentral incisor, mesioangle fracture in maxillary right central incisor.
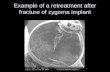
Fig 1b: Preoperative intraoral periapical radiograph revealing largeperiapical lesion in relation to maxillary left central and lateral incisors,obturation not meeting acceptable standards and resected root apex
Fig 1c: Intraoral periapical radiograph showing gutta-percha conetracing the sinus tract to the root apex of 21.
SUMANTHINI.M.V., VANITHA.U.SHENOY, RUPALI DESHMUKH, RAHUL KUMAR

8383
presented, a diagnosis of acute exacerbation of
chronic alveolar abscess was arrived at. Non-
surgical retreatment of the involved teeth was
planned. Patient’s medical history was
noncontributory.
All the clinical steps were performed under
rubber dam isolation (Hygienic Dental Dam,
Colténe Whaledent, Germany). The coronal
restorations and gutta-percha root canal filling was
removed from 21 and 22. Pus exuded through the
canal of 22, canal was irrigated with normal saline
to facilitate drainage. A loose sterile cotton pledget
was placed in the pulp chambers of both teeth
followed by thin closed dressing of zinc oxide
eugenol (DPI, Mumbai, India). Patient was recalled
the following day; her acute symptom of pain had
subsided. Canals were re-entered, working length
established by radiographic method [Fig 1d]. Root
canals were cleaned and shaped with hand files by
step back technique to a #60 ISO size K file (Mani
INC, Japan). During instrumentation, the canals
were copiously irrigated with 5% sodium
hypochlorite (NaOCl) (Trifarma, Thane, India)
intermittently. A thick paste of CH (Deepashree
Fig 1d: Working length radiograph, note the lack of apical stop inmaxillary left lateral incisor
Products, Ratnagiri, India) and saline was packed
within the canal and temporized with zinc oxide
eugenol cement. The CH dressing was changed
every week for 3 weeks.
As the symptoms of pain and swelling were
not alleviated, triple antibiotic paste (TAP) was
considered for the intracanal dressing, consisting
of ciprofloxacin 250mg (Ciplox, Cipla Ltd, Mumbai,
India) metronidazole 400mg (Flagyl, Abbott Health
care private limited, Thane, Maharashtra, India ) and
minocycline 100mg (Minoz, Ranbaxy Laboratories
Limited, India) after obtaining patient’s consent.
Prior to the placement of the paste (TAP), adhesive
restoration was placed in the pulp chamber. The
root canal orifices of teeth 21 and 22 were blocked
with a large gutta percha point. The pulp chamber
was etched with 37 %phosphoric acid (SS White,
Dental Pvt.Ltd. England) for 15 seconds and rinsed
with water. A total etch adhesive (Tetric N-Bond,
Ivoclar Vivadent, Liechtenstien) was applied
according to manufacturer’s instructions, followed
by placement of composite resin( Tetric N-Ceram,
Ivoclar Vivadent, Schaan, Liechtenstien) on the
internal walls of the pulp chamber and light cured.
Hundred milligrams of each drug was obtained
after removal of the enteric coating. The drugs were
pulverized in sterile mortar and pestle separately
and mixed in 0.5 ml of propylene glycol (Desmo
exports limited, Mumbai, India) in a sterile dappen
dish. The TAP was freshly prepared just prior to
insertion in the canal. It was placed in the canals
using lentulospirals (Mani INC, Japan) 1mm short
of the working length and 2 mm short of the canal
orifice. A cotton pledget was placed and the access
cavity sealed with Glass ionomer cement (Type II
GC Universal restorative, Tokyo, Japan). The paste
SUCCESSFUL NONSURGICAL RETREATMENT OF RESECTED TEETH ASSOCIATED WITH PERSISTENT PERIAPICALLESION BY PLACING TRIPLE ANTIBIOTIC PASTE AND MINERAL TRIOXIDE AGGREGATE APICAL PLUG : A CASE REPORT

8484
was changed every month for a period of three
months, after which the symptoms of pain and
swelling resolved. On examination, sinus tract had
healed, soft tissues were healthy and the teeth
showed no signs of discoloration due to
minocycline (Fig 2a). The antibiotic medication was
removed with K- files and irrigation with
5%NaOCl. Root canal of tooth 21was dried with
sterile paper points (Dentsply Maillefer Ballaigues,
Switzerland), obturated with gutta-percha (Dentsply
Maillefer Ballaigues, Switzerland) and AH Plus
(Dentsply Detrey Konstanz, Germany) sealer by
lateral compaction technique (Fig 2b). In 22, due to
the absence of an apical stop, MTA (ProRoot,
Dentsply Maillefer, Ballaigues, Switzerland) apical
plug was placed. MTA was mixed with sterile water
as per manufacturer’s instructions and placed in
small increments using prefitted modified finger
Fig 2a: Intraoral photograph showing no discoloration due tominocycline in maxillary left central and left lateral incisor
Fig 2b: Intraoral periapical radiograph of MTA apical plug placed inmaxillary left lateral incisor and obturation of maxillary central incisor
pluggers and the butt end of gutta-percha to a
thickness of 5mm. A radiograph was taken to
confirm the dense placement of MTA plug [Fig 2b].
A moist sterile cotton pledget was placed in the
canal and access cavity sealed with a zinc oxide
eugenol temporary filling. After 24 hours, the
temporary filling and cotton pellet were removed.
Set of MTA was checked gently with a K-file and
the remaining pulp space was obturated with AH
Plus and gutta-percha by lateral compaction
technique [Fig 2c]. Post endodontically, the access
Fig 2c: Immediate post obturation radiograph
Fig 2d: 3month recall radiograph
SUMANTHINI.M.V., VANITHA.U.SHENOY, RUPALI DESHMUKH, RAHUL KUMAR

8585
cavities of 21, 22 and the mesial angle fracture in
11 were restored with light cured resin composite
restoration. Patient was recalled for checkup at
regular intervals of 3, 6, 12 and 24 months.
Radiographs and clinical photographs revealed
complete healing and patient has been symptom
free [Fig 2d, 3a, b, c, d].
DiscussionInadequate cleaning and obturation of root
canals is the major cause of endodontic failure. As
with the present case, the intra oral radiograph
revealed that canal preparation and the orthograde
Fig 3a: 6 month recall radiograph
Fig 3b: 12 month recall radiograph
obturation was unsatisfactory hence nonsurgical
retreatment was opted though the teeth had
undergone surgical resection. In such canals
significant portions of root canal walls probably are
left untouched and this might have jeopardized
optimal healing of the periradicular tissues.
Complete elimination of bacteria by instrumentation
alone is unlikely to occur. Therefore some form of
root canal disinfection is necessary to eliminate
residual microorganisms. CH is an effective
intracanal medicament, owing to its high alkalinity.
We chose to place CH medicament as symptoms
did not resolve, probably due to limited antibacterial
spectrum10 and the reduced efficacy of CH in
retreatment cases11, the treatment protocol was
changed and TAP was used instead after obtaining
patient consent.
Fig 3c: 24 month recall radiograph revealing healing of periapical tissues.
Fig 3d: 24 month photograph demonstrates no discoulortation postoperatively and satisfactory soft tissue healing, mesial angle fracture
of 11 restored with resin composite restoration
SUCCESSFUL NONSURGICAL RETREATMENT OF RESECTED TEETH ASSOCIATED WITH PERSISTENT PERIAPICALLESION BY PLACING TRIPLE ANTIBIOTIC PASTE AND MINERAL TRIOXIDE AGGREGATE APICAL PLUG : A CASE REPORT

8686
The local application of antibacterial drugs
represents one of the means of eradicating bacteria
in root canal treatment. A study by Sato et al found
that combination of antibacterial drugs comprising
of metronidazole, ciprofloxacin and minocycline
was effective in killing bacteria in the deep layers
of root canal dentine, capable of sterilizing carious
lesions, necrotic pulp and infected root dentin of
deciduous teeth.12 Several reports in recent times
have demonstrated its successful application in
regenerative endodontic treatment13, retreatment14,
root fracture15 and in healing of large periradicular
lesions.16 Nevertheless, caution has to be exercised
when we attempt to locally apply systemic
antibiotic drugs as this may cause development of
resistant species of microbes. Though there have
been no reports of any side effects, care should be
taken if patients are sensitive to chemicals or
antibiotics.
Various agents such as saline, sterile distilled
water and macrogol combined with propylene
glycol have been used as a vehicle for preparing
the antibiotic mixture. The antibiotic paste used in
the presented case consisted of 100mg of each of
the three drugs namely ciprofloxacin, metronidazole
and minocycline in a total volume of 0.5 ml of
pharmaceutical carrier propylene glycol. Propylene
glycol is a clear colourless, odourless liquid. Its
wide application in endodontics as a vehicle for
intracanal medicaments is attributed to its well
documented antibacterial action against
microorganism and its consistency which improves
the handling qualities of the paste. Also propylene
glycol, though viscous, has a low surface tension
which enables it to penetrate through dentinal
tubules when used as a vehicle.17
Of the three antibiotics, minocycline is often
reported to cause green-grey or blue-grey intrinsic
tooth discoloration. Minocycline is a semi synthetic
derivative of tetracycline and is a broad spectrum
antibiotic, effective against gram positive and
negative bacteria. The literature shows no theory
that conclusively illustrates the mechanism of
minocycline staining. Discolouration may be due
to minocycline binding to calcium ions via chelation
to form an insoluble complex and is incorporated
into tooth matrix causing discoloration.18 According
to ‘intrinsic theory’ minocycline is bound only by
those tissues with a high affinity for it such as dental
pulp, dentin, and bone which are collagenous.
Once in the tissues, the minocycline is oxidized
and subsequently transformed to a coloured
product. Pigment deposits from discoloured teeth
when examined microscopically and histologically
suggest the presence of iron and hemosiderin, a
minocycline degradation product, chelates with iron
to form an insoluble complex. The pigment contains
a quinone –like structure which is the main
contributor to its colour.19 Minocycline cannot stain
the tooth matrix unless it comes in contact with
coronal dentin.9The discolouration caused by
minocycline cannot be rectified satisfactorily by
bleaching techniques alone, depending on the
severity of cases the clinician may have to resort to
indirect veneers or even crowns. Inspite of its
potential draw back minocycline is incorporated
in the antibiotic mixture since it (minocycline) is
the most effective component of the antibiotic
mixture against E.faecalis.20
The discoloration can be best prevented by
bonding the pulp chamber with a two-step etch and
rinse dentin bonding system and composite resin
SUMANTHINI.M.V., VANITHA.U.SHENOY, RUPALI DESHMUKH, RAHUL KUMAR

8787
restoration, there by sealing the dentinal tubules.9, 21 This prevents contact between the antibiotic
medicament and the dentin. Following the above
method, in the present study, discolouration due to
minocycline was prevented in the treated teeth, 21
and 22 (fig 2a, 3d). The paste application should
terminate to a level cervical to the canal orifice and
completely removed from the access cavity. Also
the access cavity should be adequately sealed with
a suitable adhesive restoration, else moisture
contamination could lead to leaching of the paste
and subsequent discoloration of the tooth. After the
placement of triple antibiotic paste, we chose to
restore access cavity with type II Glass ionomer
cement as an intermediate restoration between the
appointments. Glass ionomer cement being truly
chemically bonded to the tooth structure could have
played a significant role in preventing discoloration
of the coronal tooth structure.
In this case, the resected 22 presented an
abnormally large diameter or misshapen apical
foramen due to the retrograde preparation
previously completed. Endodontic obturation
techniques rely on the presence of an apical barrier
against which obturation material can be placed.
In these cases placement of an apical plug of MTA
followed by conventional obturation is the current
treatment of choice.1 The results of the retrospective
study of treatment outcome conducted by Mente et
al suggest placing 4mm apical MTA plug in open
apical foramina yielded a predictable outcome at
par with outcomes expected in conventionally root
filled teeth with undisturbed apical constriction.7
In the case presented a 5mm thick MTA apical
plug was placed which is the recommended
thickness to provide adequate apical seal against
bacterial microleakage .22 MTA is has excellent
sealing properties in the presence of moisture,
induces regeneration of cementum, periodontal
ligament and bone.5,23The favorable biologic
properties of MTA in human periapical tissues are
attributed to the production of bone morphogenic
protein-2 and transforming growth factor beta-
1.24The release of hydroxyl ions, sustained high
pH of 12.5 for extended periods of time, formation
of a mineralized interstitial layer might contribute
to its antibacterial properties.23 MTA inhibits the
growth of Enterococcous faecalis and yeasts such
as Candida albicans prevalent in root canal failures
and refractory endodontic disease.25,26
In the case presented, considering all the merits
of MTA, we concluded that placing an apical plug
of MTA would best address the problem of lack of
apical constriction secondary to root resection. The
6, 12 and 24 month follow up radiographs
demonstrated complete healing of the periapical
lesion and new hard tissue formation in the apical
area.
ConclusionThe outcome in this case suggests that failing
surgically resected teeth can be successfully
retreated nonsurgically by using a combination of
antibiotic drugs for canal disinfection. In order that
no tooth discoloration occurs, adhesive restorative
materials should be used to seal the dentine surface
while applying the minocycline based intracanal
medicament.
MTA apical plug can be considered a viable
option in resected teeth that can possibly reduce
the indications for endodontic resurgery.
SUCCESSFUL NONSURGICAL RETREATMENT OF RESECTED TEETH ASSOCIATED WITH PERSISTENT PERIAPICALLESION BY PLACING TRIPLE ANTIBIOTIC PASTE AND MINERAL TRIOXIDE AGGREGATE APICAL PLUG : A CASE REPORT

8888
References :
1. Stéphane S and Wihelm-Joseph P. Clinical Success inEndodontic Retreatment. Paris: Quintessence Int, 2007.p.122.
2. Ingle IJ, Bakland KL, Baumgartner C J. Ingle’sEndodontics6th edition. Ontario: BC Decker Inc,2008: 1337.
3. Andreasen JO, Munksgaard EC, Bakland KL. Comparisonof fracture resistance in root canals of immature sheep teethafter filling with calcium hydroxide or MTA. DentTraumatol2006; 22:154-6.
4. Doyon EG, Dhumsha T, Anthony von Fraunhofer J.Fracture resistance of human root dentin exposed tointracanal calcium hydroxide. J Endod2005;31:895-897.
5. Roberts HW, Jeffery MT, Berzins DW, Charlton DG. Mineraltrioxide aggregate material use in endodontic treatment: Areview of literature. Dent Mater 2008;24:149-64.
6. Hayashi M, Shimizu A, Ebisu S. MTA for obturation ofmandibular central incisors with open apices: case report. JEndod 2004;30:120-122.
7. Mente J, Hage N, Pfefferle T, Koch MJ, Dreyhaupt J, StaehleHJ, Friedman S. MTA apical plugs in teeth with open apicalforamina: A retrospective analysis of treatment outcome. JEndod 2009;35:1354-58.
8.Hoshino E,Kurihara-Ando N, Sato I, Uematsu H, Sato M, KotaK, Iwaku M. In-vitro antibacterial susceptibility of bacteria takenfrom infected root dentine to a mixture of ciprofloxacin,metronidazole and minocycline. Int Endod J 1996;29:125-30.
9. Kim J, Kim Y, Shin S, Park J, Jung I. Tooth Discoloration ofimmature permanent incisor associated with triple antibiotictherapy: A Case Report. J Endod 2010;36:1086-91.
10. Siqueira JF, Loupes HP. Mechanisms of antimicrobialactivity of calcium hydroxide: A Critical Review. Int Endod J1999;32:361-9.
11. Ingle IJ, Bakland KL, Baumgartner C J. Ingle’sEndodontics6th edition. Ontario:BC Decker Inc,2008; 1201.
12. Sato I, Kurihara-Ando N, Kota K, Iwaku M, Hoshino E.Sterilization of infected root canal dentine by topicalapplication of a mixture of ciprofloxacin, metronidazole andminocycline in situ. Int Endod J 1996;29:118-24.
13. Akgun OM, Atlun C, Guven G.Use of triple antibioticpaste as a disinfectant for a traumatized immature tooth witha periapical lesion: a case report. Oral Surg Oral Med OralPathol Oral Radiol Endod 2009;108:e62-e65.
14. Kusgoz A, Yildirim T, Er K, Arslan I. Retreatment of aresected tooth associated with a large periradicular lesion by
using a triple antibiotic paste and mineral trioxide aggregate:a case report with a thirty month follow-up. J Endod 2009;35:1603-6.
15. Er K, ªelik D, Taºdemir T, Yildirim T. Treatment ofhorizontal root fractures using a triple antibiotic paste andmineral trioxide aggregate: A case report. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2009; 108:e63-e66.
16. Özan Ü, Er K. Endodontic treatment of a large cyst- likeperiradicular lesion using a combination of antibiotic drugs:A case report. J Endod 2005; 31:898-900.
17. Cruz EV, Kota K, Huque J, Iwaku M, Hoshino E.Penetration of propylene glycol into dentine. Int Endod J.2002;35: 330–336.
18. Tanase S, Tsuchiya H, Yao J, Ohmoto S, Takagi N, YoshidaS. Reversed-phase ion-pair chromatographic analysis oftetracycline antibiotics: application to discolored teeth. JChromatogr B Biomed Sci Appl. 1998;706:279–285.
19. Cheek CC, Heymann OH. Dental and Oral DiscolorationsAssociated with Minocycline and Other Tetracycline Analogs.J of Esthetic Dent 1999;11:43-48.
20. Adl A, Shojaee SN, Motamedifar MA. Comparisonbetween the Antimicrobial Effects of Triple Antibiotic Pasteand Calcium Hydroxide against Enterococcus faecalis.Iranian Endodontic Journal 2012;7(3):149-155.
21. Reynolds K, Johnson JD, Cohenca N. Pulprevascularization of necrotic bilateral bicuspids using amodified novel technique to eliminate potential coronaldiscoloration: A Case Report, Int Endod J 2009;42:84-92.
22. Al-Kahtani A, Shostad S, Schifferle R, Bhambhani S. Invitro evaluation of micro leakage of an orthograde apicalplug of mineral trioxide aggregate in permanent teeth withsimulated immature apices. J Endod 2005; 31:117-9.
23. Bogen G, Kuttler S. Mineral trioxide aggregate obturation:A review and case series. J Endod 2009; 35:777-790.
24. Guven G, Cehreli CZ, Ural A, Serdar AM, Basak F. Effectof Mineral trioxide aggregate cements on transforming growthfactor â-1 and bone morphogenic protein production byhuman fibroblast inn vitro. J Endod 2007;33:447-450.
25. Eldeniz AU, Hadimli HH, Ataoglu H, Ørstavik D.Antibacterial effect of selected root-end filling materials. JEndod 2006; 32: 345–349.
26. Al-Nazhan S, Al-Judai A. Evaluation of antifungal activityof mineral trioxide aggregate. J Endod 2003; 29: 826–827.
SUMANTHINI.M.V., VANITHA.U.SHENOY, RUPALI DESHMUKH, RAHUL KUMAR
Related Documents