J. Clin. Endocrinol. Metab. published online Apr 6, 2010; , doi: 10.1210/jc.2009-2032 A. M. Middelkoop, Alberto M. Pereira and Johannes A. Romijn Jitske Tiemensma, Nieke E. Kokshoorn, Nienke R. Biermasz, Bart-Jan S. A. Keijser, Moniek J. E. Wassenaar, Huub Disease Subtle Cognitive Impairments in Patients with Long-Term Cure of Cushing's Society please go to: http://jcem.endojournals.org//subscriptions/ or any of the other journals published by The Endocrine Journal of Clinical Endocrinology & Metabolism To subscribe to Copyright © The Endocrine Society. All rights reserved. Print ISSN: 0021-972X. Online

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
J. Clin. Endocrinol. Metab. published online Apr 6, 2010; , doi: 10.1210/jc.2009-2032
A. M. Middelkoop, Alberto M. Pereira and Johannes A. Romijn Jitske Tiemensma, Nieke E. Kokshoorn, Nienke R. Biermasz, Bart-Jan S. A. Keijser, Moniek J. E. Wassenaar, Huub
Disease
Subtle Cognitive Impairments in Patients with Long-Term Cure of Cushing's
Society please go to: http://jcem.endojournals.org//subscriptions/ or any of the other journals published by The EndocrineJournal of Clinical Endocrinology & MetabolismTo subscribe to
Copyright © The Endocrine Society. All rights reserved. Print ISSN: 0021-972X. Online

Subtle Cognitive Impairments in Patients withLong-Term Cure of Cushing’s Disease
Jitske Tiemensma, Nieke E. Kokshoorn, Nienke R. Biermasz, Bart-Jan S. A. Keijser,Moniek J. E. Wassenaar, Huub A. M. Middelkoop, Alberto M. Pereira,and Johannes A. Romijn
Departments of Endocrinology and Metabolism (J.T., N.E.K., N.R.B., B.-J.S.A.K., M.J.E.W., A.M.P., J.A.R.)and Neurology (H.A.M.M.), Leiden University Medical Center, 2300 RC Leiden, The Netherlands
Context and Objective: Active Cushing’s disease is associated with cognitive impairments. Wehypothesized that previous hypercortisolism in patients with Cushing’s disease results in irrevers-ible impairments in cognitive functioning. Therefore, our aim was to assess cognitive functioningafter long-term cure of Cushing’s disease.
Design: Cognitive assessment consisted of 11 tests, which evaluated global cognitive functioning,memory, and executive functioning.
Patients and Control Subjects: We included 74 patients cured of Cushing’s disease and 74 controlsmatched for age, gender, and education. Furthermore, we included 54 patients previously treatedfor nonfunctioning pituitary macroadenomas (NFMA) and 54 controls matched for age, gender,and education.
Results: Compared with NFMA patients, patients cured from Cushing’s disease had lower scores onthe Mini Mental State Examination (P � 0.001), and on the memory quotient of the WechslerMemory Scale (P � 0.050). Furthermore, patients cured from Cushing’s disease tended to recallfewer words on the imprinting (P � 0.013), immediate recall (P � 0.012), and delayed recall (P �
0.003) trials of the Verbal Learning Test of Rey. On the Rey Complex Figure Test, patients cured fromCushing’s disease had lower scores on both trials (P � 0.002 and P � 0.007) compared with NFMApatients. Patients cured from Cushing’s disease also made fewer correct substitutions on the Letter-Digit Substitution Test (P � 0.039) and came up with fewer correct patterns on the Figure FluencyTest (P � 0.003) compared with treated NFMA patients.
Conclusions: Cognitive function, reflecting memory and executive functions, is impaired inpatients despite long-term cure of Cushing’s disease. These observations indicate irreversibleeffects of previous hypercortisolism on cognitive function and, thus, on the central nervoussystem. These observations may also be of relevance for patients treated with high-dose ex-ogenous glucocorticoids. (J Clin Endocrinol Metab 95: 0000 – 0000, 2010)
Cushing’s disease is characterized by excessive exposureto cortisol. Despite curative treatment, cardiovascu-
lar morbidity and mortality remain increased in these pa-tients (1, 2). In addition, despite long-term cure of Cush-ing’s disease, these patients have persistent physical andpsychological complaints, associated with decreased qual-ity of life parameters (3).
Patients with active Cushing’s disease and Cushing’ssyndrome have cognitive impairments, especially in thememory domain. Previous studies reported impairmentsin memory, visual and spatial information, reasoning, ver-bal learning, and language performance (4–10). Struc-tures important in cognitive functioning, like the hip-pocampus and cerebral cortex, are rich in glucocorticoid
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2010 by The Endocrine Societydoi: 10.1210/jc.2009-2032 Received September 22, 2009. Accepted March 8, 2010.
Abbreviations: HADS, Hospital Anxiety and Depression Scale; MMSE, Mini Mental StateExamination; MQ, memory quotient; NFMA, nonfunctioning pituitary macroadenoma.
O R I G I N A L A R T I C L E
E n d o c r i n e C a r e
J Clin Endocrinol Metab, June 2010, 95(6):0000–0000 jcem.endojournals.org 1
J Clin Endocrin Metab. First published ahead of print April 6, 2010 as doi:10.1210/jc.2009-2032
Copyright (C) 2010 by The Endocrine Society

receptors and are therefore particularly vulnerable tothe glucocorticoid excess present in Cushing’s disease(7). Starkman et al. (11) reported that 27% of the pa-tients with active Cushing’s syndrome fell outside the95% confidence intervals for normal subject hippocam-pal formation volume and that hippocampal formationvolume and performance on cognitive tests were positivelyrelated. In accordance, many other studies in humans andanimal models have documented that prolonged, in-creased endogenous or exogenous exposure to glu-cocorticoids may have long-lasting adverse effects onbehavioral, psychiatric, and cognitive functions, due tofunctional and, over time, structural alterations in specificbrain target areas including the hippocampus (11–16). Af-ter treatment, all patients in the study by Starkman et al.(17) showed an increase in hippocampal formation vol-ume, and half of the patients also showed an increase incognitive function test scores. In contrast, other studiesfound no improvements in cognitive functioning within 1yr after treatment (18, 19). Some studies reported im-paired cognitive functioning in patients with treated Cush-ing’s disease (6, 18–20). However, these studies includedonly small numbers of subjects (n � 35), and patients weretested relatively shortly (i.e. within the first 12–18 months)after cure of Cushing’s disease. Therefore, it is presentlyunclear to which extent impairments in cognitive func-tioning remain present in patients with much longer du-ration of cure of Cushing’s disease.
We hypothesized that previous hypercortisolism in pa-tients with Cushing’s disease results in irreversible impair-ments in cognitive functioning. Therefore, we evaluatedcognitive functioning in patients after long-term cure forCushing’s disease and compared these data with those ofage- and sex-matched controls as well as with those ofpatients treated for nonfunctioning pituitary macroad-enomas (NFMA) and matched controls.
Subjects and Methods
SubjectsWe included four groups of subjects: 1) patients cured from
Cushing’s disease and 2) gender-, age-, and education-matchedcontrol subjects and 3) patients previously treated for NFMAand 4) gender-, age-, and education-matched control subjects.The inclusion of these additional control groups was necessarybecause patients with Cushing’s disease and NFMA differ withregard to age and gender.
We invited all patients in remission after treatment for Cush-ing’s disease in our institution to participate (n � 153). Eachpatient was asked to provide a control person of comparable age,gender, and education. Patients and their controls were evalu-ated at the same time. Patients who did not respond were en-couraged by phone to participate. The response rate was 93%.Eighty-five patients were willing to participate, of whom 74 pa-
tients actually participated in all cognitive tests. Fifty-seven pa-tients preferred not to participate, whereas 11 patients did notrespond. The characteristics of patients who participated in thetests and those who did not participate were carefully compared.There were no differences in clinical characteristics between bothgroups. Reasons for not participating were distance to our in-stitution, participation in other studies, old age, and debilitatingdisease.
The diagnosis of Cushing’s disease had been established byclinical signs and symptoms and by biochemical tests includingincreased urinary excretion rates of free cortisol, decreased over-night suppression by dexamethasone (1 mg) and, since 2004,elevated midnight salivary cortisol values in addition to sup-pressed ACTH levels. All patients were treated by transsphenoi-dal surgery, if necessary followed by repeat surgery and/or ra-diotherapy. Cure of Cushing’s disease was defined by normalovernight suppression of plasma cortisol levels (�100 nmol/liter) after administration of dexamethasone (1 mg) and normal24-h urinary excretion rates of cortisol (�220 nmol/24 h). Hy-drocortisone independency was defined as a normal cortisol re-sponse to CRH or insulin tolerance test. Patients were followedat our department with yearly intervals, and pituitary hormonesubstitution was prescribed in accordance with the results ofyearly evaluation. Persistent cure of Cushing’s disease was doc-umented by normal values of a dexamethasone (1 mg) suppres-sion test, urinary cortisol excretion rates, and midnight salivarycortisol levels before participation in the current study.
In addition, we invited 132 patients with NFMA to partici-pate in the study and to provide a control person (see above). Theresponse rate was 94%. Fifty-four had undergone transsphenoi-dal surgery and participated in all cognitive tests. There were nodifferences in clinical characteristics between participants andnonparticipants.
Pituitary function was assessed at yearly intervals. In patientswho were glucocorticoid dependent after treatment, recovery ofthe pituitary-adrenal axis was tested twice a year. The dose ofhydrocortisone was on average 20 mg/d divided into two to threedosages. After withdrawal of hydrocortisone replacement for24 h, a fasting morning blood sample was taken for the mea-surement of serum cortisol concentrations. Patients with serumcortisol concentration less than 120 nmol/liter were consideredglucocorticoid dependent, and hydrocortisone treatment was re-started. Patients with serum cortisol levels of 120–500 nmol/literwere tested by ACTH stimulation tests (250 �g). A normal re-sponse to ACTH stimulation was defined as a stimulated cortisolhigher than550nmol/liter. In case the cortisol response toACTHwas normal the patients were tested by insulin tolerance test orCRH stimulation test. In case the cortisol responses to these testswere less than 550 nmol/liter, hydrocortisone treatment was re-started. Evaluation of GH deficiency was done by insulin toler-ance test or arginine-GHRH test only in patients under the ageof 70 yr and only after at least 2 yr of remission. Patients with aninadequate stimulation of GH by one of these tests were treatedwith recombinant human GH, aiming at IGF-I levels between 0and �2 SD values. In addition, the twice-yearly evaluation con-sisted of measurement of free T4 and testosterone (in male pa-tients). If results were below the lower limit of the respectivereference ranges, substitution with L-T4 and/or testosterone wasstarted. In the case of amenorrhea and low estradiol levels inpremenopausal women, estrogen replacement was provided. Pa-tient and treatment characteristics were collected from the pa-tient records.
2 Tiemensma et al. Cognitive Impairments in Cushing’s Disease J Clin Endocrinol Metab, June 2010, 95(6):0000–0000

Twelve percent of the controls were treated for hypertensionwith appropriate blood pressure control (i.e. �140/90 mmHg)without evidence of hypertensive organ damage. Four percent ofthe controls were treated for type 2 diabetes mellitus with gly-cosylated hemoglobin levels less than 7% and without evidenceof organ damage.
Inclusion criteria for the current study were age older than 18yr and remission defined by strict biochemical criteria at the timeof study. Patients with present or previous drug or alcohol abuseor with neurological problems, not related to Cushing’s diseaseor NFMA, were excluded. The protocol was approved by theMedical Ethics Committee, and written informed consent wasobtained from all subjects.
Study designA single study visit was planned, during which each subject of
the two patient groups and the two control groups underwentanamnesis and performed the cognitive tests.
Cognitive evaluationEleven cognitive tests were to be completed to assess the full
spectrum of cognitive functioning. A functional classificationwas used to subdivide the tests into the cognitive domains globalcognitive functioning, memory, and executive functioning (21).
To measure global cognitive functioning, the Mini MentalState Examination (MMSE) was used. This is a 30-point ques-tionnaire to assess cognition, with a higher score reflecting betterperformance (22).
Memory was measured with the Wechsler Memory Scale,resulting in a memory quotient (MQ) based on scores in var-ious subscales (23). The Verbal Learning Test of Rey, to mea-sure verbal memory and learning, consists of three trials.Number of correctly recalled words was counted for each trial(24). The Rey Complex Figure, which measures drawing andvisual memory, consists of two trials. A higher score indicatesbetter visual memory (25).
Executive functioning was measured with the Trail MakingTest (26), which measures psychomotor functioning andvisuoconceptual tracking. Time used for both tests and numberof mistakes were counted. The Stroop Color-Word Test (27)measures interference. Number of correct and wrong responseswere counted. The Letter-Digit Substitution Test (28) measuresmental flexibility and speed of information processing. Numberof correctly substituted letters and errors within 60 sec werecounted. The Digit-Deletion Test measures selective attentionand concentration. Number of correctly deleted digits and thenumber of missed digits in 3 min were counted. The Figure Flu-ency Test measures the ability to produce new figures and as-sesses nonverbal mental flexibility and fluency (29). The numberof correct figures, percentage of repeats, and percentage ofwrong figures were counted. The FAS Test employs the letters F,A, and S and measures verbal mental flexibility and fluency (30).The number of correctly produced words and percentage of re-peats and errors were counted. Furthermore, the SynonymsSubtest of the Groninger Intelligence Test-2 was used, with ahigher score indicating better performance (31).
The Hospital Anxiety and Depression Scale (HADS) was usedto measure anxiety and depression. The HADS consists of 14items on a 4-point scale. Both anxiety and depression subscalescores range from 0–21 points. Higher scores indicate more se-vere anxiety and/or depression. A total score higher than 13
points on both subscales together is used to characterize subjectsas anxious or depressed (32, 33).
Statistical analysisData were analyzed using SPSS for Windows version 16.0.2
(SPSS Inc., Chicago, IL). All data are reported in tabular form,expressed as mean � SD. The primary analysis comprised thecomparison of the results between patients cured from Cushing’sdisease and their matched controls and between the patients withNFMA and their matched controls. Groups were compared us-ing a general linear mixed model, with the matched patient-control couples as random factor. Secondary analysis comprisedthe comparison of results in relation to patient and treatmentcharacteristics. To compare patients treated for Cushing’s dis-ease and for NFMA, mean and SD scores for each cognitive testwere calculated for each control group, and subsequently, Z-scores were calculated for each patient group in relation to theirappropriate control group. A general linear model was used tocompare the Z-scores, with postoperative additional radiother-apy, hydrocortisone usage, and hypopituitarism as fixed factors.Independent variables affecting cognitive functioning in patientscured from Cushing’s disease were explored by stepwise linearregression analysis. The standardized �-coefficients of this anal-ysis were reported. To check the appropriateness of assumptionsfor each statistical analysis, we used Levene’s test, Durbin-Watson test, histograms, and scatter plots. All assumptions weremet, except for the independence assumption for parametricdata. We therefore used nonparametric tests to analyze the clin-ical characteristics of patients vs. controls (McNemar test, Fried-man ANOVA, and Wilcoxon signed-ranks test). The level ofsignificance was set at P � 0.05.
Results
Patient characteristics
Patients treated for Cushing’s disease (Table 1)All 74 patients were treated by transsphenoidal sur-
gery, and 20 patients (27%) received additional radio-therapy because of persistent disease after surgery. Themean duration of remission was 13 � 13 yr (range 1–51yr). The number of years in remission was calculated fromthe date of curative transsphenoidal surgery or, in case ofpersistent postoperative disease, from the date of the nor-malization of the biochemical tests after postoperative ra-diotherapy. Any degree of hypopituitarism was present in43 patients (58%), and hydrocortisone replacement wasgiven to 38 patients (51%). There were no differencesbetween patients and controls with respect to age, gender,and education. We asked all patients whether they expe-rienced limitations with respect to memory and/or exec-utive functioning. Sixty-two percent reported memoryproblems, and 47% reported problems in executivefunctioning.
All patients with Cushing’s disease also completed theHADS questionnaire. The mean scores for the depression
J Clin Endocrinol Metab, June 2010, 95(6):0000–0000 jcem.endojournals.org 3

subscale were 5.6 � 4.7 and for the anxiety subscale 5.0 �4.7, resulting in total HADS scores of 10.5 � 8.8. This iswell below the cutoff score of 13 (32, 33), which indicatesthat there is, on average, no clinical depression or anxietyin this cohort of Cushing’s disease patients.
Patients treated for nonfunctioning pituitarymacroadenomas (Table 2)
All patients (n � 54) were treated by transsphenoidalsurgery, and 24 patients (44%) received postoperative ra-diotherapy. Fifty patients (93%) required treatment forpituitary insufficiency, and hydrocortisone replacementtherapy was given to 31 patients (57%). There were nodifferences between patients and controls with respect toage, gender, and education. Thirty-nine percent reported
memory problems, and 24% reported problems in exec-utive functioning.
Cognitive function
Patients with Cushing’s disease vs. matched controls(Table 3)
Patients with long-term cure of Cushing’s disease didnot perform worse on measures of global cognitive func-tioning. However, these patients showed a lower MQ onthe Wechsler Memory Scale compared with controls (P �0.015), especially in the subtests concentration (P �0.023), visual memory (P � 0.013), and associative learn-ing (P � 0.023). Furthermore, patients recalled fewerwords than controls in the immediate and delayed recall
TABLE 1. Clinical characteristics of patients cured from Cushing’s disease and matched controls
Cushing’s disease (n � 74) Matched controls (n � 74) P valueGender (male/female) 13/61 13/61 1.00Age (yr), mean � SD 52 � 13 52 � 13 0.26Education (n)
Low 29 28 0.28Average 19 22High 26 24
Transsphenoidal surgery (n) 74 (100%) NA NAPostoperative radiotherapy (n) 20 (27%) NA NADuration of remission (yr), mean � SD 13 � 13 NA NADuration of follow-up (yr), mean � SD 16 � 12 NA NAHypopituitarism (n)
Any axis 43 (58%) NA NAGH 26 (35% NA NALH/FSH 19 (26%) NA NATSH 24 (32%) NA NAADH 11 (15%) NA NA
Hydrocortisone substitution (n) 38 (51%) NA NA
NA, Not applicable.
TABLE 2. Clinical characteristics of the patients treated for nonfunctioning pituitary macroadenomas and matchedcontrols
NFMA (n � 54) Matched controls (n � 54) P valueGender (male/female) 30/24 30/24 1.00Age (yr), mean � SD 61 � 11 59 � 11 0.06Education (n)
Low 18 21 0.90Average 21 15High 15 18
Transsphenoidal surgery (n) 54 (100%) NA NAPostoperative radiotherapy (%) 24 (44%) NA NADuration of follow up (yr), mean � SD 15 � 12 NA NAHypopituitarism (n)
Any axis 50 (93%) NA NAGH 40 (74%) NA NALH/FSH 32 (59%) NA NATSH 33 (61%) NA NAADH 6 (11%) NA NA
Hydrocortisone substitution (%) 31 (57%) NA NA
NA, Not applicable.
4 Tiemensma et al. Cognitive Impairments in Cushing’s Disease J Clin Endocrinol Metab, June 2010, 95(6):0000–0000
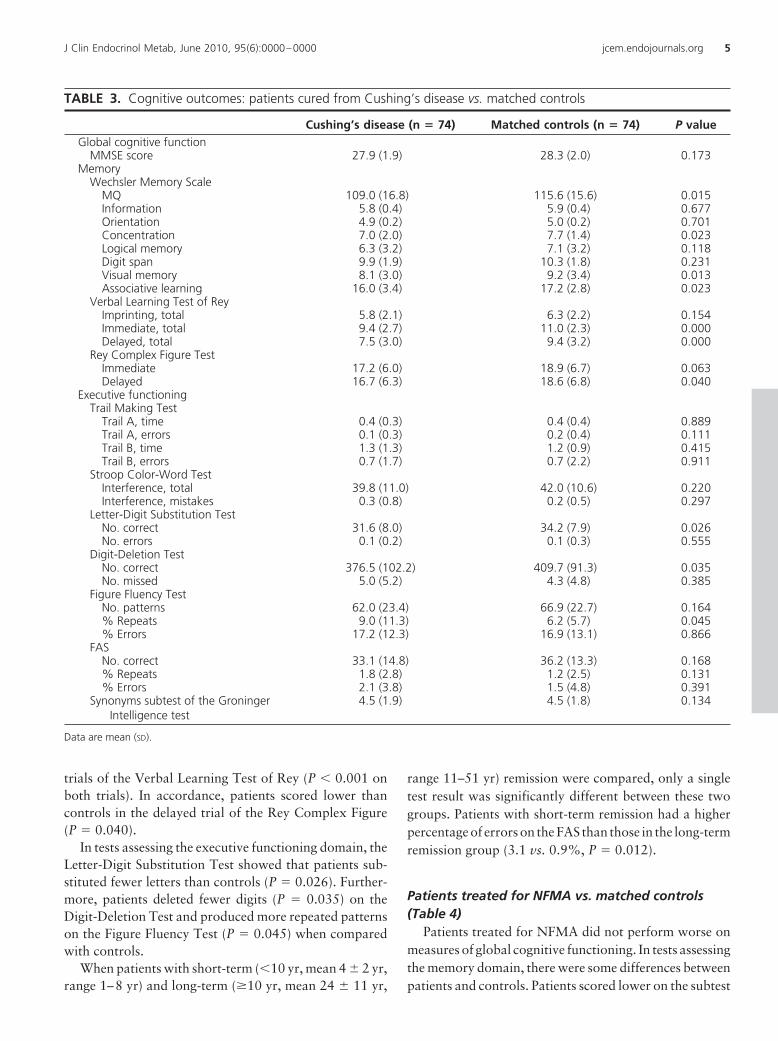
trials of the Verbal Learning Test of Rey (P � 0.001 onboth trials). In accordance, patients scored lower thancontrols in the delayed trial of the Rey Complex Figure(P � 0.040).
In tests assessing the executive functioning domain, theLetter-Digit Substitution Test showed that patients sub-stituted fewer letters than controls (P � 0.026). Further-more, patients deleted fewer digits (P � 0.035) on theDigit-Deletion Test and produced more repeated patternson the Figure Fluency Test (P � 0.045) when comparedwith controls.
When patients with short-term (�10 yr, mean 4 � 2 yr,range 1–8 yr) and long-term (�10 yr, mean 24 � 11 yr,
range 11–51 yr) remission were compared, only a singletest result was significantly different between these twogroups. Patients with short-term remission had a higherpercentage of errors on the FAS than those in the long-termremission group (3.1 vs. 0.9%, P � 0.012).
Patients treated for NFMA vs. matched controls(Table 4)
Patients treated for NFMA did not perform worse onmeasures of global cognitive functioning. In tests assessingthe memory domain, there were some differences betweenpatients and controls. Patients scored lower on the subtest
TABLE 3. Cognitive outcomes: patients cured from Cushing’s disease vs. matched controls
Cushing’s disease (n � 74) Matched controls (n � 74) P valueGlobal cognitive function
MMSE score 27.9 (1.9) 28.3 (2.0) 0.173Memory
Wechsler Memory ScaleMQ 109.0 (16.8) 115.6 (15.6) 0.015Information 5.8 (0.4) 5.9 (0.4) 0.677Orientation 4.9 (0.2) 5.0 (0.2) 0.701Concentration 7.0 (2.0) 7.7 (1.4) 0.023Logical memory 6.3 (3.2) 7.1 (3.2) 0.118Digit span 9.9 (1.9) 10.3 (1.8) 0.231Visual memory 8.1 (3.0) 9.2 (3.4) 0.013Associative learning 16.0 (3.4) 17.2 (2.8) 0.023
Verbal Learning Test of ReyImprinting, total 5.8 (2.1) 6.3 (2.2) 0.154Immediate, total 9.4 (2.7) 11.0 (2.3) 0.000Delayed, total 7.5 (3.0) 9.4 (3.2) 0.000
Rey Complex Figure TestImmediate 17.2 (6.0) 18.9 (6.7) 0.063Delayed 16.7 (6.3) 18.6 (6.8) 0.040
Executive functioningTrail Making Test
Trail A, time 0.4 (0.3) 0.4 (0.4) 0.889Trail A, errors 0.1 (0.3) 0.2 (0.4) 0.111Trail B, time 1.3 (1.3) 1.2 (0.9) 0.415Trail B, errors 0.7 (1.7) 0.7 (2.2) 0.911
Stroop Color-Word TestInterference, total 39.8 (11.0) 42.0 (10.6) 0.220Interference, mistakes 0.3 (0.8) 0.2 (0.5) 0.297
Letter-Digit Substitution TestNo. correct 31.6 (8.0) 34.2 (7.9) 0.026No. errors 0.1 (0.2) 0.1 (0.3) 0.555
Digit-Deletion TestNo. correct 376.5 (102.2) 409.7 (91.3) 0.035No. missed 5.0 (5.2) 4.3 (4.8) 0.385
Figure Fluency TestNo. patterns 62.0 (23.4) 66.9 (22.7) 0.164% Repeats 9.0 (11.3) 6.2 (5.7) 0.045% Errors 17.2 (12.3) 16.9 (13.1) 0.866
FASNo. correct 33.1 (14.8) 36.2 (13.3) 0.168% Repeats 1.8 (2.8) 1.2 (2.5) 0.131% Errors 2.1 (3.8) 1.5 (4.8) 0.391
Synonyms subtest of the GroningerIntelligence test
4.5 (1.9) 4.5 (1.8) 0.134
Data are mean (SD).
J Clin Endocrinol Metab, June 2010, 95(6):0000–0000 jcem.endojournals.org 5
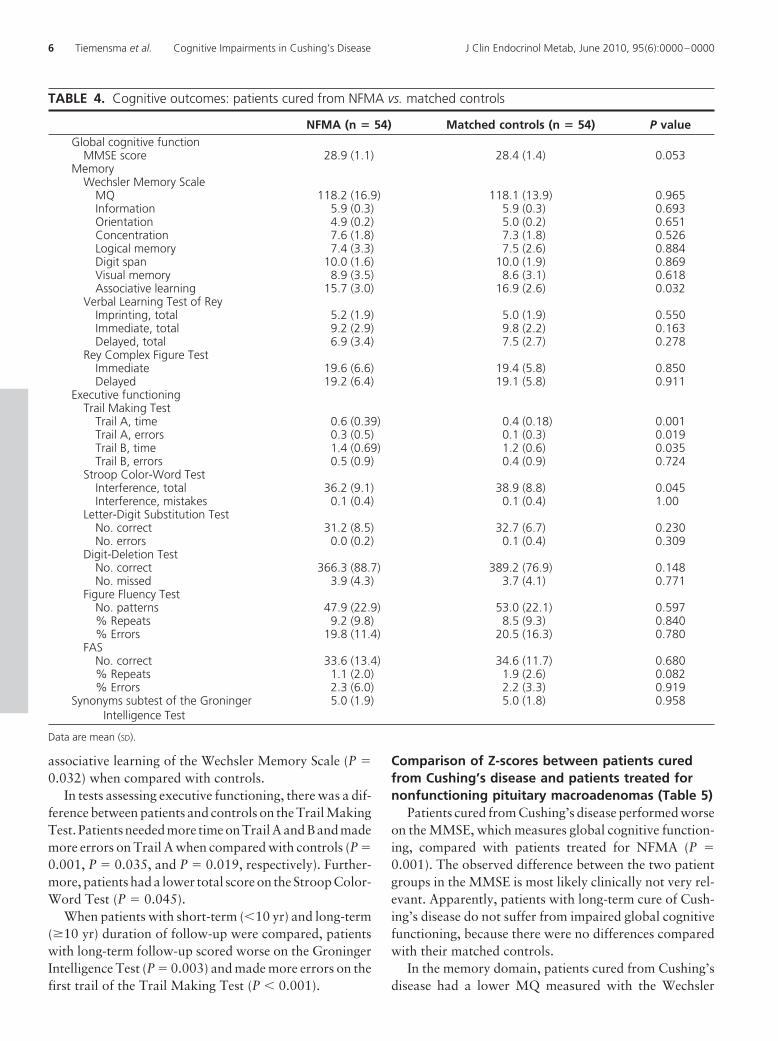
associative learning of the Wechsler Memory Scale (P �0.032) when compared with controls.
In tests assessing executive functioning, there was a dif-ference between patients and controls on the Trail MakingTest. Patients needed more time on Trail A and B and mademore errors on Trail A when compared with controls (P �0.001, P � 0.035, and P � 0.019, respectively). Further-more, patients had a lower total score on the Stroop Color-Word Test (P � 0.045).
When patients with short-term (�10 yr) and long-term(�10 yr) duration of follow-up were compared, patientswith long-term follow-up scored worse on the GroningerIntelligence Test (P � 0.003) and made more errors on thefirst trail of the Trail Making Test (P � 0.001).
Comparison of Z-scores between patients curedfrom Cushing’s disease and patients treated fornonfunctioning pituitary macroadenomas (Table 5)
Patients cured from Cushing’s disease performed worseon the MMSE, which measures global cognitive function-ing, compared with patients treated for NFMA (P �0.001). The observed difference between the two patientgroups in the MMSE is most likely clinically not very rel-evant. Apparently, patients with long-term cure of Cush-ing’s disease do not suffer from impaired global cognitivefunctioning, because there were no differences comparedwith their matched controls.
In the memory domain, patients cured from Cushing’sdisease had a lower MQ measured with the Wechsler
TABLE 4. Cognitive outcomes: patients cured from NFMA vs. matched controls
NFMA (n � 54) Matched controls (n � 54) P valueGlobal cognitive function
MMSE score 28.9 (1.1) 28.4 (1.4) 0.053Memory
Wechsler Memory ScaleMQ 118.2 (16.9) 118.1 (13.9) 0.965Information 5.9 (0.3) 5.9 (0.3) 0.693Orientation 4.9 (0.2) 5.0 (0.2) 0.651Concentration 7.6 (1.8) 7.3 (1.8) 0.526Logical memory 7.4 (3.3) 7.5 (2.6) 0.884Digit span 10.0 (1.6) 10.0 (1.9) 0.869Visual memory 8.9 (3.5) 8.6 (3.1) 0.618Associative learning 15.7 (3.0) 16.9 (2.6) 0.032
Verbal Learning Test of ReyImprinting, total 5.2 (1.9) 5.0 (1.9) 0.550Immediate, total 9.2 (2.9) 9.8 (2.2) 0.163Delayed, total 6.9 (3.4) 7.5 (2.7) 0.278
Rey Complex Figure TestImmediate 19.6 (6.6) 19.4 (5.8) 0.850Delayed 19.2 (6.4) 19.1 (5.8) 0.911
Executive functioningTrail Making Test
Trail A, time 0.6 (0.39) 0.4 (0.18) 0.001Trail A, errors 0.3 (0.5) 0.1 (0.3) 0.019Trail B, time 1.4 (0.69) 1.2 (0.6) 0.035Trail B, errors 0.5 (0.9) 0.4 (0.9) 0.724
Stroop Color-Word TestInterference, total 36.2 (9.1) 38.9 (8.8) 0.045Interference, mistakes 0.1 (0.4) 0.1 (0.4) 1.00
Letter-Digit Substitution TestNo. correct 31.2 (8.5) 32.7 (6.7) 0.230No. errors 0.0 (0.2) 0.1 (0.4) 0.309
Digit-Deletion TestNo. correct 366.3 (88.7) 389.2 (76.9) 0.148No. missed 3.9 (4.3) 3.7 (4.1) 0.771
Figure Fluency TestNo. patterns 47.9 (22.9) 53.0 (22.1) 0.597% Repeats 9.2 (9.8) 8.5 (9.3) 0.840% Errors 19.8 (11.4) 20.5 (16.3) 0.780
FASNo. correct 33.6 (13.4) 34.6 (11.7) 0.680% Repeats 1.1 (2.0) 1.9 (2.6) 0.082% Errors 2.3 (6.0) 2.2 (3.3) 0.919
Synonyms subtest of the GroningerIntelligence Test
5.0 (1.9) 5.0 (1.8) 0.958
Data are mean (SD).
6 Tiemensma et al. Cognitive Impairments in Cushing’s Disease J Clin Endocrinol Metab, June 2010, 95(6):0000–0000
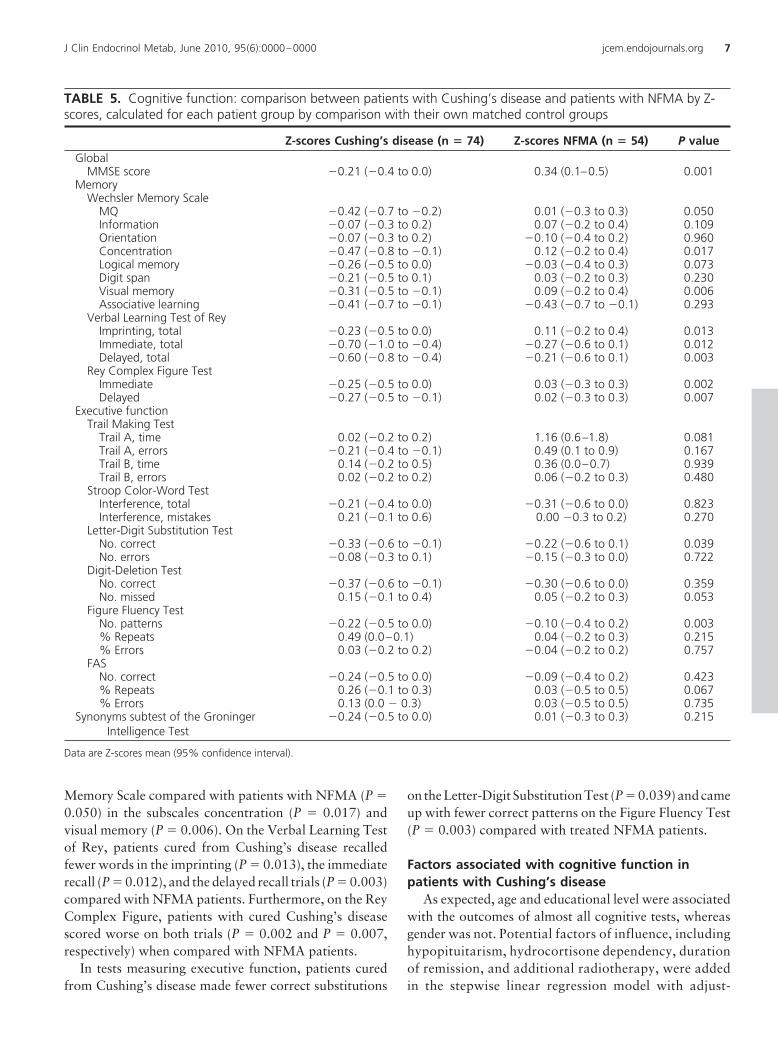
Memory Scale compared with patients with NFMA (P �0.050) in the subscales concentration (P � 0.017) andvisual memory (P � 0.006). On the Verbal Learning Testof Rey, patients cured from Cushing’s disease recalledfewer words in the imprinting (P � 0.013), the immediaterecall (P � 0.012), and the delayed recall trials (P � 0.003)compared with NFMA patients. Furthermore, on the ReyComplex Figure, patients with cured Cushing’s diseasescored worse on both trials (P � 0.002 and P � 0.007,respectively) when compared with NFMA patients.
In tests measuring executive function, patients curedfrom Cushing’s disease made fewer correct substitutions
on the Letter-Digit Substitution Test (P � 0.039) and cameup with fewer correct patterns on the Figure Fluency Test(P � 0.003) compared with treated NFMA patients.
Factors associated with cognitive function inpatients with Cushing’s disease
As expected, age and educational level were associatedwith the outcomes of almost all cognitive tests, whereasgender was not. Potential factors of influence, includinghypopituitarism, hydrocortisone dependency, durationof remission, and additional radiotherapy, were addedin the stepwise linear regression model with adjust-
TABLE 5. Cognitive function: comparison between patients with Cushing’s disease and patients with NFMA by Z-scores, calculated for each patient group by comparison with their own matched control groups
Z-scores Cushing’s disease (n � 74) Z-scores NFMA (n � 54) P valueGlobal
MMSE score �0.21 (�0.4 to 0.0) 0.34 (0.1–0.5) 0.001Memory
Wechsler Memory ScaleMQ �0.42 (�0.7 to �0.2) 0.01 (�0.3 to 0.3) 0.050Information �0.07 (�0.3 to 0.2) 0.07 (�0.2 to 0.4) 0.109Orientation �0.07 (�0.3 to 0.2) �0.10 (�0.4 to 0.2) 0.960Concentration �0.47 (�0.8 to �0.1) 0.12 (�0.2 to 0.4) 0.017Logical memory �0.26 (�0.5 to 0.0) �0.03 (�0.4 to 0.3) 0.073Digit span �0.21 (�0.5 to 0.1) 0.03 (�0.2 to 0.3) 0.230Visual memory �0.31 (�0.5 to �0.1) 0.09 (�0.2 to 0.4) 0.006Associative learning �0.41 (�0.7 to �0.1) �0.43 (�0.7 to �0.1) 0.293
Verbal Learning Test of ReyImprinting, total �0.23 (�0.5 to 0.0) 0.11 (�0.2 to 0.4) 0.013Immediate, total �0.70 (�1.0 to �0.4) �0.27 (�0.6 to 0.1) 0.012Delayed, total �0.60 (�0.8 to �0.4) �0.21 (�0.6 to 0.1) 0.003
Rey Complex Figure TestImmediate �0.25 (�0.5 to 0.0) 0.03 (�0.3 to 0.3) 0.002Delayed �0.27 (�0.5 to �0.1) 0.02 (�0.3 to 0.3) 0.007
Executive functionTrail Making Test
Trail A, time 0.02 (�0.2 to 0.2) 1.16 (0.6–1.8) 0.081Trail A, errors �0.21 (�0.4 to �0.1) 0.49 (0.1 to 0.9) 0.167Trail B, time 0.14 (�0.2 to 0.5) 0.36 (0.0–0.7) 0.939Trail B, errors 0.02 (�0.2 to 0.2) 0.06 (�0.2 to 0.3) 0.480
Stroop Color-Word TestInterference, total �0.21 (�0.4 to 0.0) �0.31 (�0.6 to 0.0) 0.823Interference, mistakes 0.21 (�0.1 to 0.6) 0.00 �0.3 to 0.2) 0.270
Letter-Digit Substitution TestNo. correct �0.33 (�0.6 to �0.1) �0.22 (�0.6 to 0.1) 0.039No. errors �0.08 (�0.3 to 0.1) �0.15 (�0.3 to 0.0) 0.722
Digit-Deletion TestNo. correct �0.37 (�0.6 to �0.1) �0.30 (�0.6 to 0.0) 0.359No. missed 0.15 (�0.1 to 0.4) 0.05 (�0.2 to 0.3) 0.053
Figure Fluency TestNo. patterns �0.22 (�0.5 to 0.0) �0.10 (�0.4 to 0.2) 0.003% Repeats 0.49 (0.0–0.1) 0.04 (�0.2 to 0.3) 0.215% Errors 0.03 (�0.2 to 0.2) �0.04 (�0.2 to 0.2) 0.757
FASNo. correct �0.24 (�0.5 to 0.0) �0.09 (�0.4 to 0.2) 0.423% Repeats 0.26 (�0.1 to 0.3) 0.03 (�0.5 to 0.5) 0.067% Errors 0.13 (0.0 � 0.3) 0.03 (�0.5 to 0.5) 0.735
Synonyms subtest of the GroningerIntelligence Test
�0.24 (�0.5 to 0.0) 0.01 (�0.3 to 0.3) 0.215
Data are Z-scores mean (95% confidence interval).
J Clin Endocrinol Metab, June 2010, 95(6):0000–0000 jcem.endojournals.org 7

ments for age and education. We calculated regressioncoefficients for test outcomes that were associated withduration of remission, which might indicate the poten-tial for improvement.
Global cognitive functioning was not associated withany of the variables. In the memory domain, the WechslerMemory Scale MQ was positively associated with dura-tion of remission (� � 0.276; P � 0.017). In the executivefunction domain, the number of missed digits on the Digit-Deletion Test was positively associated with duration ofremission (� � 0.245; P � 0.041) and additional radio-therapy (� � 0.361; P � 0.002). Furthermore, the numberof correct patterns in the Figure Fluency Test was nega-tively associated with hypopituitarism (� � �0.278; P �0.012) and hydrocortisone dependency (� � �0.230; P �0.040). The percentage of mistakes in the Figure FluencyTest was positively associated with hydrocortisone depen-dency (� � 0.224; P � 0.048). The percentage of mistakeson the FAS Test was inversely associated with duration ofremission (� � �0.254; P � 0.034).
There was a significant correlation between the out-come on the Wechsler Memory Scale (MQ) and dura-tion of remission (r � 0.236; P � 0.049). There was alsoa significant correlation between the number of misseddigits on the Digit-Deletion Test and duration of remis-sion (r � 0.245; P � 0.041), and the percentage ofmistakes on the FAS and duration of remission (r ��0.254; P � 0.034).
Discussion
This study demonstrates that cognitive function is im-paired in patients despite long-term cure of Cushing’s dis-ease. These patients reported impairments in memory indaily life, which was confirmed by cognitive functioningtests. The performance was decreased in certain aspects ofexecutive functioning and several memory tasks com-pared with matched controls. These impairments were notmerely related to pituitary disease in general, because thesepatients with long-term cure of Cushing’s disease also re-vealed impaired cognitive function compared with pa-tients previously treated for NFMA. These observationsindicate irreversible effects of previous hypercortisolismon cognitive function and, thus, on the central nervoussystem.
The outcomes of the cognitive tests are in general af-fected by many factors, including age, gender, and edu-cational level. Because the controls and patients were per-fectly matched, these potentially confounding factors didnot influence our results or conclusions. We do not thinkthat our results can be explained to a large extend by thedifference in gender distribution between both patient
groups. First, patients with long-term cure of Cushing’sdisease had impaired cognition compared with gender-matched controls. Second, we used Z-scores derived fromthe comparisons between patients and appropriatelymatched controls to compare the patients with curedCushing’s disease with patients treated for NFMA, be-cause the gender differences were too large between thesetwo patients groups to justify a direct comparison.
Several clinical characteristics influenced outcomeparameters. Hypopituitarism was associated with mildlyimpaired executive functioning. Hydrocortisone depen-dency and additional radiotherapy were negativelyassociated with memory and executive functioning,whereas the duration of remission positively influencedmemory and executive functioning. These findings do notinvalidate our conclusions, because these factors were alsopresent in patients treated for NFMA, who in general hadbetter performances compared with the patients curedfrom Cushing’s disease.
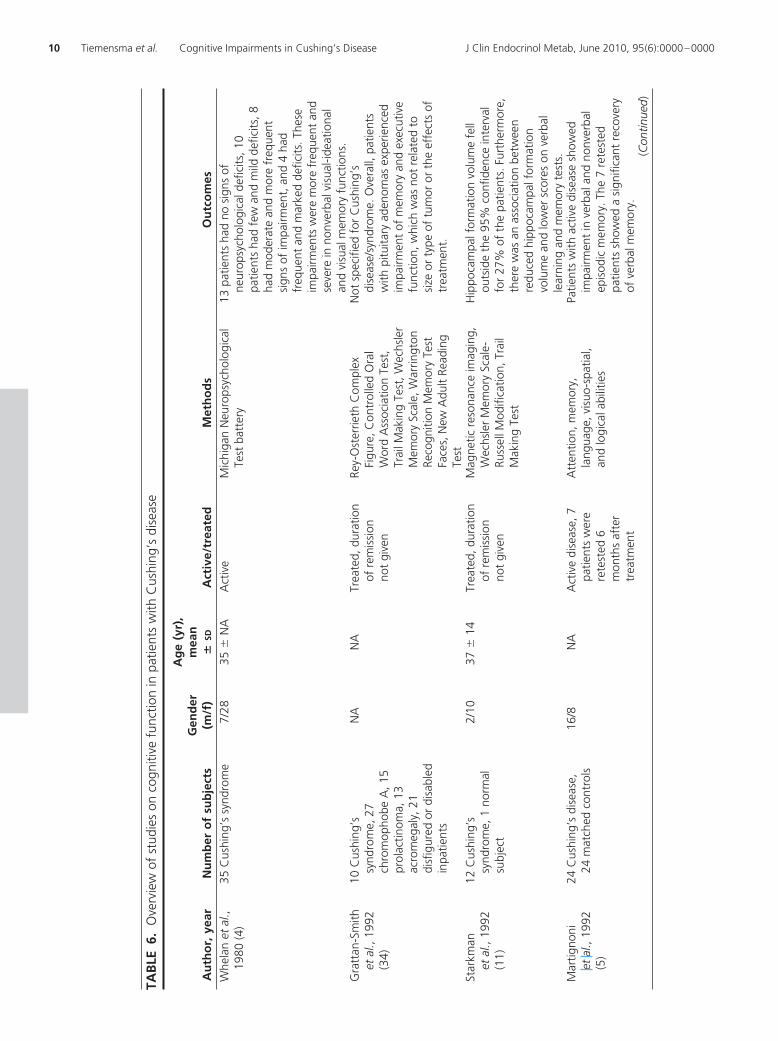
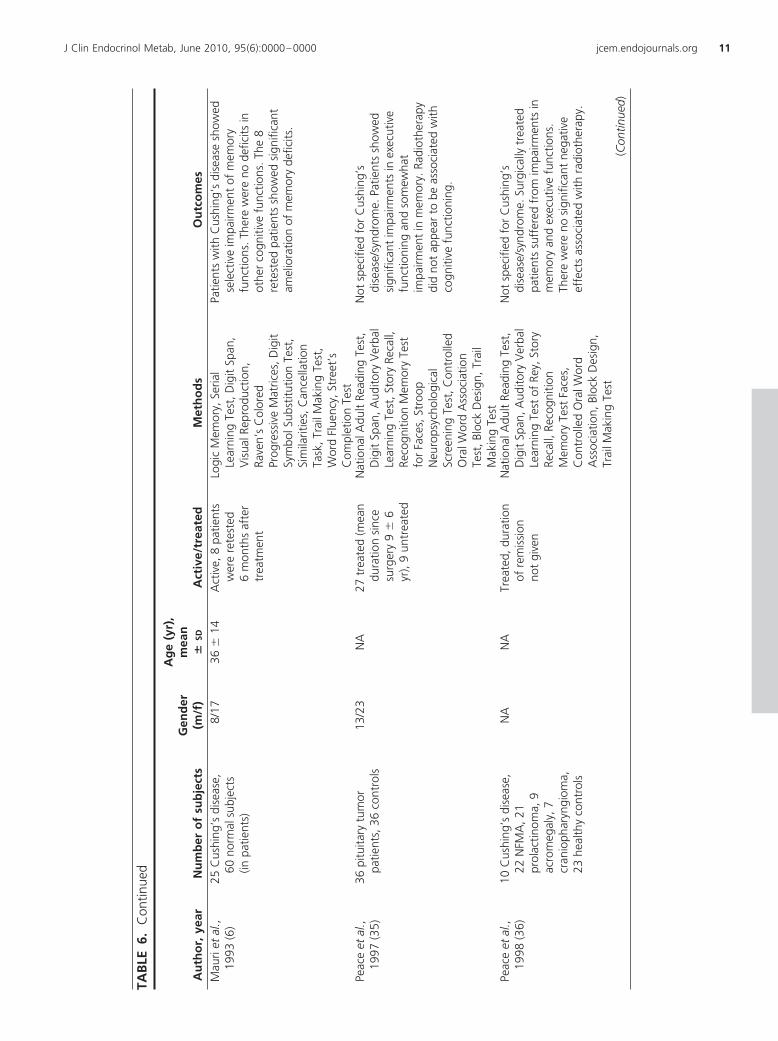
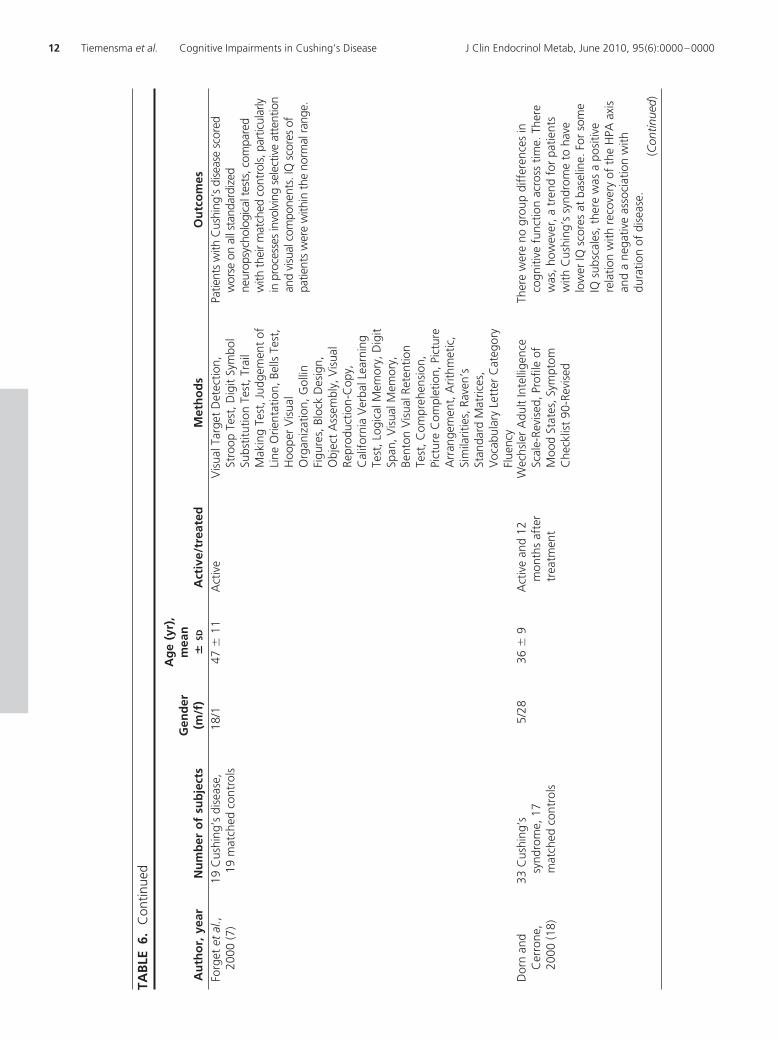
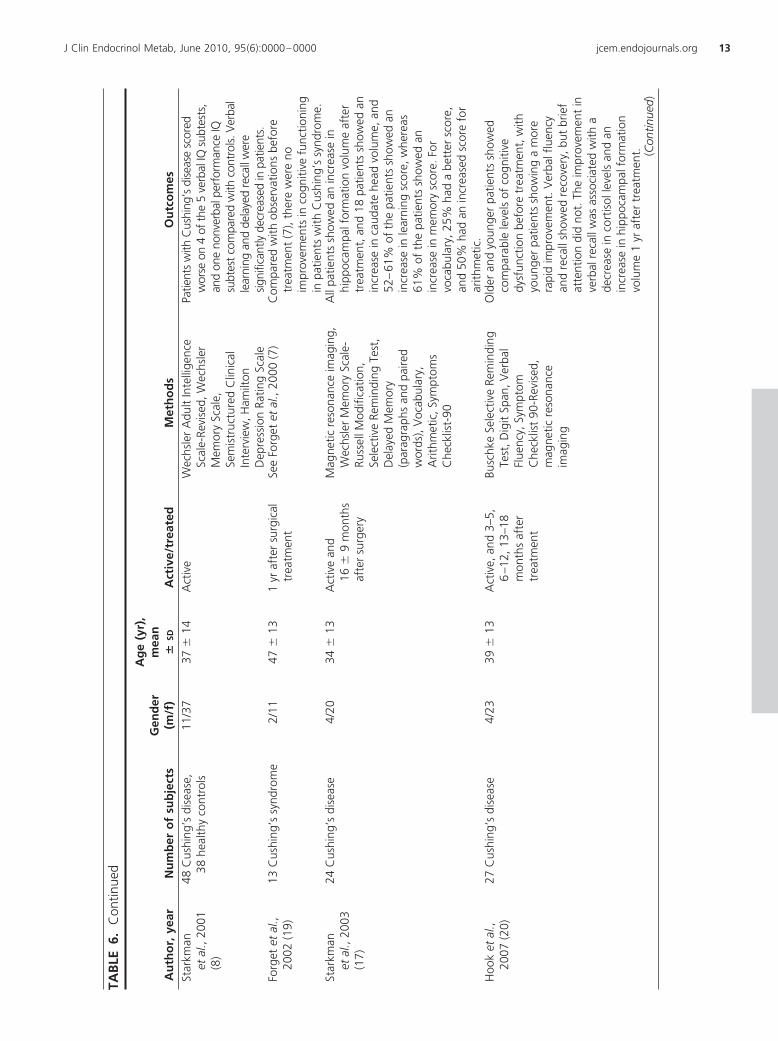
Table 6 summarizes all studies on the effect of Cush-ing’s disease and syndrome on cognitive functions, includ-ing the effects of treatment. Our observations extend thoseof previous studies. Four previous studies studied cogni-tive functioning in treated Cushing’s disease patients, witha total of 98 patients and 77 controls. In the first study,patients with treated Cushing’s disease (n � 27) showedimprovement of verbal fluency and recall within 18months of follow-up, whereas brief attention did notchange. This indicates that some but not all of the effectsof previous glucocorticoid excess are reversible (20). Thesecond study showed that there were no differences be-tween patients (n � 33) and matched controls in IQ duringactive disease and 12 months after treatment. There was,however, a positive relation for some subscales of the IQtest and recovery of the hypothalamic-pituitary-adrenalaxis. There was also a negative association between someIQ subscales and duration of disease (18). The third studyshowed that 1 yr after surgical treatment, high levels ofcortisol caused long-lasting impairments in attention,visuospatial processing, memory, reasoning, and verbalfluency in patients with Cushing’s syndrome (n � 13) (19).Furthermore, the last study observed that patients withCushing’s disease (n � 25) showed selective impairmentsin memory functions. After treatment, the eight patientswho were retested showed amelioration of these memoryimpairments (6). Our study indicates that patients withlong-term cure of Cushing’s disease have impaired scoresof memory and to a lesser extent in executive functionscompared with both matched controls and treated NFMApatients. Our study differs in several respects from theprevious studies. First, the number of patients included inour study was relatively large compared with the previous
8 Tiemensma et al. Cognitive Impairments in Cushing’s Disease J Clin Endocrinol Metab, June 2010, 95(6):0000–0000

studies. Second, the duration of cure was very long in ourstudy compared with previous studies. Third, we com-pared the patients with long-term cure of Cushing’s dis-ease both with matched controls and with patients previ-ously operated for NFMA. From the studies summarizedin Table 6, including our present study, the notion emergesthat active Cushing’s disease is associated with cognitiveimpairment and that treatment of Cushing’s disease re-sults in some but not complete recovery of cognitiveimpairment.
Several other studies evaluated the effects of pituitaryadenomas, including ACTH-producing adenomas, onexecutive functioning and memory but did not specifythe differences between different pituitary adenomas(34–36). Therefore, these studies do not permit any con-clusion with respect to the specific effects of Cushing’sdisease compared with the effects of other pituitary ade-nomas on cognitive function.
Prolonged glucocorticoid excess modifies neurotrans-mitter function and neuronal structure of the central ner-vous system (7, 11). In rodents, chronic exposure to highlevels of glucocorticoids impairs hippocampal long-termpotentiation (12) and decreases hippocampal synapticplasticity (13). In humans, endogenous active Cushing’sdisease is associated with cognitive impairment (6, 7, 20).The hippocampus is one of the most sensitive structures inthe brain for glucocorticoids and is crucial in cognitivefunction (37). The persistent impairments in cognitivefunction in patients with previous Cushing’s disease mightbe explained by irreversible effects of previous glucocor-ticoid excess on the central nervous system, especially thehippocampus. Additional studies, including functionalmagnetic resonance imaging and postmortem analyses ofthe central nervous system, are required to evaluate theeffects of previous glucocorticoid excess on brain areas ofinterest.
Patients with long-term cure of Cushing’s disease are aunique, monofactorial model to study the long-term ef-fects of glucocorticoid exposure. The results of the currentstudy may also apply to patients previously treated withhigh-dose glucocorticoids for nonendocrine diseases. Inaddition, the results might also be of relevance for patientswith chronically increased glucocorticoid levels in condi-tions like depression (38, 39).
In the review process of the manuscript, there was con-cern with respect to the presentation of the data withoutadjustments for multiple comparisons. Simply defined,these adjustments test for no effects in all the primaryendpoints undertaken vs. an effect in one or more of thoseendpoints. This is a difficult methodological issue becausethere are divergent views on the need for statistical ad-justment for multiplicity. This is also reflected in the
Lancet papers by Schulz and Grimes (40, 41), who advo-cate a restrictive approach toward adjustments for mul-tiple comparisons. If we consider our own data and if weassume that the differences would mostly reflect false-pos-itive results, it is to be expected that the positive significantresults would have been randomly distributed among thedifferent variables. However, this is not the case, as shownin Tables 3 and 4. Moreover, there are several argumentsthat cortisol excess can indeed cause irreversible effects onthe central nervous system (see above). We designed thisstudy inourpatients cured fromCushing’sdiseasewith theprimary aim to evaluate cognitive function in detail, inview of the documented abnormalities in previous studiesand those observed in experimental animal studies. In-deed, the main results of our study point toward similaradverse effects of previous Cushing’s disease documentedin previous studies, although these had a different studydesign. According to Schulz and Grimes (40, 41), statis-tical adjustments somewhat rescue the positive results ofscattershot analyses. However, we performed a targetedevaluation and analysis focused on cognitive function re-lated to previous Cushing’s disease rather than a scatter-shot analysis of cognitive functions in general. Therefore,in our opinion, our data should not be neglected merelybecause of the absence of adjustments for multiple com-parisons. Moreover, this would carry the serious risk ofmissing an important association between previous Cush-ing’s disease and cognitive impairments.
A limitation of the present study was the cross-sectionalstudy design. Consequently, we do not have any informa-tion on premorbid functions, the effects of active Cush-ing’s disease, and the extent of reversibility of the dis-turbed parameters. Nonetheless, these limitations do notinvalidate our observations that patients with long-termcure have subtle impairments in cognitive function com-pared with matched controls and with patients treatedsimilarly for NFMA. It might be argued that potential biasmay have been introduced by the selection of the controlsby the patients. In previous studies, we used similarly se-lected controls and compared the responses of thesematched controls with those obtained from publishedDutch control populations for several questionnaires (in-cluding HADS, Nottingham Health Profile, Multidimen-sional Fatigue Index, and Short Form) (3, 42, 43). In gen-eral, the conclusions obtained in the matched controlsubjects were in agreement with the literature-based ref-erence data. In the present study, the self-selection ofcontrols enabled a perfect match for an additional pa-rameter, i.e. socioeconomic status, an important deter-minant of the outcomesof thequestionnaires, inaddition toage, gender, and education. Moreover, we used the samemethod of selection of controls for both groups of patients.
J Clin Endocrinol Metab, June 2010, 95(6):0000–0000 jcem.endojournals.org 9
TAB
LE6.
Ove
rvie
wof
stud
ies
onco
gniti
vefu
nctio
nin
patie
nts
with
Cus
hing
’sdi
seas
e
Au
tho
r,ye
arN
um
ber
of
sub
ject
sG
end
er(m
/f)
Ag
e(y
r),
mea
n�
SDA
ctiv
e/tr
eate
dM
eth
od
sO
utc
om
esW
hela
net
al.,
1980
(4)
35C
ushi
ng’s
synd
rom
e7/
2835
�N
AA
ctiv
eM
ichi
gan
Neu
rops
ycho
logi
cal
Test
batt
ery
13pa
tient
sha
dno
sign
sof
neur
opsy
chol
ogic
alde
ficits
,10
patie
nts
had
few
and
mild
defic
its,8
had
mod
erat
ean
dm
ore
freq
uent
sign
sof
impa
irmen
t,an
d4
had
freq
uent
and
mar
ked
defic
its.T
hese
impa
irmen
tsw
ere
mor
efr
eque
ntan
dse
vere
inno
nver
balv
isua
l-ide
atio
nal
and
visu
alm
emor
yfu
nctio
ns.
Gra
ttan
-Sm
ithet
al.,
1992
(34)
10C
ushi
ng’s
synd
rom
e,27
chro
mop
hobe
A,1
5pr
olac
tinom
a,13
acro
meg
aly,
21di
sfig
ured
ordi
sabl
edin
patie
nts
NA
NA
Trea
ted,
dura
tion
ofre
mis
sion
not
give
n
Rey-
Ost
errie
thC
ompl
exFi
gure
,Con
trol
led
Ora
lW
ord
Ass
ocia
tion
Test
,Tr
ailM
akin
gTe
st,W
echs
ler
Mem
ory
Scal
e,W
arrin
gton
Reco
gniti
onM
emor
yTe
stFa
ces,
New
Adu
ltRe
adin
gTe
st
Not
spec
ified
for
Cus
hing
’sdi
seas
e/sy
ndro
me.
Ove
rall,
patie
nts
with
pitu
itary
aden
omas
expe
rienc
edim
pairm
ent
ofm
emor
yan
dex
ecut
ive
func
tion,
whi
chw
asno
tre
late
dto
size
orty
peof
tum
oror
the
effe
cts
oftr
eatm
ent.
Star
kman
etal
.,19
92(1
1)
12C
ushi
ng’s
synd
rom
e,1
norm
alsu
bjec
t
2/10
37�
14Tr
eate
d,du
ratio
nof
rem
issi
onno
tgi
ven
Mag
netic
reso
nanc
eim
agin
g,W
echs
ler
Mem
ory
Scal
e-Ru
ssel
lMod
ifica
tion,
Trai
lM
akin
gTe
st
Hip
poca
mpa
lfor
mat
ion
volu
me
fell
outs
ide
the
95%
conf
iden
cein
terv
alfo
r27
%of
the
patie
nts.
Furt
herm
ore,
ther
ew
asan
asso
ciat
ion
betw
een
redu
ced
hipp
ocam
palf
orm
atio
nvo
lum
ean
dlo
wer
scor
eson
verb
alle
arni
ngan
dm
emor
yte
sts.
Mar
tigno
niet
al.,
1992
(5)
24C
ushi
ng’s
dise
ase,
24m
atch
edco
ntro
ls16
/8N
AA
ctiv
edi
seas
e,7
patie
nts
wer
ere
test
ed6
mon
ths
afte
rtr
eatm
ent
Att
entio
n,m
emor
y,la
ngua
ge,v
isuo
-spa
tial,
and
logi
cala
bilit
ies
Patie
nts
with
activ
edi
seas
esh
owed
impa
irmen
tin
verb
alan
dno
nver
bal
epis
odic
mem
ory.
The
7re
test
edpa
tient
ssh
owed
asi
gnifi
cant
reco
very
ofve
rbal
mem
ory.
(Con
tinue
d)
10 Tiemensma et al. Cognitive Impairments in Cushing’s Disease J Clin Endocrinol Metab, June 2010, 95(6):0000–0000
TAB
LE6.
Con
tinue
d
Au
tho
r,ye
arN
um
ber
of
sub
ject
sG
end
er(m
/f)
Ag
e(y
r),
mea
n�
SDA
ctiv
e/tr
eate
dM
eth
od
sO
utc
om
esM
auri
etal
.,19
93(6
)25
Cus
hing
’sdi
seas
e,60
norm
alsu
bjec
ts(in
patie
nts)
8/17
36�
14A
ctiv
e,8
patie
nts
wer
ere
test
ed6
mon
ths
afte
rtr
eatm
ent
Logi
cM
emor
y,Se
rial
Lear
ning
Test
,Dig
itSp
an,
Vis
ualR
epro
duct
ion,
Rave
n’s
Col
ored
Prog
ress
ive
Mat
rices
,Dig
itSy
mbo
lSub
stitu
tion
Test
,Si
mila
ritie
s,C
ance
llatio
nTa
sk,T
rail
Mak
ing
Test
,W
ord
Flue
ncy,
Stre
et’s
Com
plet
ion
Test
Patie
nts
with
Cus
hing
’sdi
seas
esh
owed
sele
ctiv
eim
pairm
ent
ofm
emor
yfu
nctio
ns.T
here
wer
eno
defic
itsin
othe
rco
gniti
vefu
nctio
ns.T
he8
rete
sted
patie
nts
show
edsi
gnifi
cant
amel
iora
tion
ofm
emor
yde
ficits
.
Peac
eet
al.,
1997
(35)
36pi
tuita
rytu
mor
patie
nts,
36co
ntro
ls13
/23
NA
27tr
eate
d(m
ean
dura
tion
sinc
esu
rger
y9
�6
yr),
9un
trea
ted
Nat
iona
lAdu
ltRe
adin
gTe
st,
Dig
itSp
an,A
udito
ryV
erba
lLe
arni
ngTe
st,S
tory
Reca
ll,Re
cogn
ition
Mem
ory
Test
for
Face
s,St
roop
Neu
rops
ycho
logi
cal
Scre
enin
gTe
st,C
ontr
olle
dO
ralW
ord
Ass
ocia
tion
Test
,Blo
ckD
esig
n,Tr
ail
Mak
ing
Test
Not
spec
ified
for
Cus
hing
’sdi
seas
e/sy
ndro
me.
Patie
nts
show
edsi
gnifi
cant
impa
irmen
tsin
exec
utiv
efu
nctio
ning
and
som
ewha
tim
pairm
ent
inm
emor
y.Ra
diot
hera
pydi
dno
tap
pear
tobe
asso
ciat
edw
ithco
gniti
vefu
nctio
ning
.
Peac
eet
al.,
1998
(36)
10C
ushi
ng’s
dise
ase,
22N
FMA
,21
prol
actin
oma,
9ac
rom
egal
y,7
cran
ioph
aryn
giom
a,23
heal
thy
cont
rols
NA
NA
Trea
ted,
dura
tion
ofre
mis
sion
not
give
n
Nat
iona
lAdu
ltRe
adin
gTe
st,
Dig
itSp
an,A
udito
ryV
erba
lLe
arni
ngTe
stof
Rey,
Stor
yRe
call,
Reco
gniti
onM
emor
yTe
stFa
ces,
Con
trol
led
Ora
lWor
dA
ssoc
iatio
n,Bl
ock
Des
ign,
Trai
lMak
ing
Test
Not
spec
ified
for
Cus
hing
’sdi
seas
e/sy
ndro
me.
Surg
ical
lytr
eate
dpa
tient
ssu
ffer
edfr
omim
pairm
ents
inm
emor
yan
dex
ecut
ive
func
tions
.Th
ere
wer
eno
sign
ifica
ntne
gativ
eef
fect
sas
soci
ated
with
radi
othe
rapy
.
(Con
tinue
d)
J Clin Endocrinol Metab, June 2010, 95(6):0000–0000 jcem.endojournals.org 11
TAB
LE6.
Con
tinue
d
Au
tho
r,ye
arN
um
ber
of
sub
ject
sG
end
er(m
/f)
Ag
e(y
r),
mea
n�
SDA
ctiv
e/tr
eate
dM
eth
od
sO
utc
om
esFo
rget
etal
.,20
00(7
)19
Cus
hing
’sdi
seas
e,19
mat
ched
cont
rols
18/1
47�
11A
ctiv
eV
isua
lTar
get
Det
ectio
n,St
roop
Test
,Dig
itSy
mbo
lSu
bstit
utio
nTe
st,T
rail
Mak
ing
Test
,Jud
gem
ent
ofLi
neO
rient
atio
n,Be
llsTe
st,
Hoo
per
Vis
ual
Org
aniz
atio
n,G
ollin
Figu
res,
Bloc
kD
esig
n,O
bjec
tA
ssem
bly,
Vis
ual
Repr
oduc
tion-
Cop
y,C
alifo
rnia
Ver
balL
earn
ing
Test
,Log
ical
Mem
ory,
Dig
itSp
an,V
isua
lMem
ory,
Bent
onV
isua
lRet
entio
nTe
st,C
ompr
ehen
sion
,Pi
ctur
eC
ompl
etio
n,Pi
ctur
eA
rran
gem
ent,
Arit
hmet
ic,
Sim
ilarit
ies,
Rave
n’s
Stan
dard
Mat
rices
,V
ocab
ular
yLe
tter
Cat
egor
yFl
uenc
y
Patie
nts
with
Cus
hing
’sdi
seas
esc
ored
wor
seon
alls
tand
ardi
zed
neur
opsy
chol
ogic
alte
sts,
com
pare
dw
ithth
eirm
atch
edco
ntro
ls,pa
rtic
ular
lyin
proc
esse
sin
volv
ing
sele
ctiv
eat
tent
ion
and
visu
alco
mpo
nent
s.IQ
scor
esof
patie
nts
wer
ew
ithin
the
norm
alra
nge.
Dor
nan
dC
erro
ne,
2000
(18)
33C
ushi
ng’s
synd
rom
e,17
mat
ched
cont
rols
5/28
36�
9A
ctiv
ean
d12
mon
ths
afte
rtr
eatm
ent
Wec
hsle
rA
dult
Inte
llige
nce
Scal
e-Re
vise
d,Pr
ofile
ofM
ood
Stat
es,S
ympt
omC
heck
list
90-R
evis
ed
Ther
ew
ere
nogr
oup
diff
eren
ces
inco
gniti
vefu
nctio
nac
ross
time.
Ther
ew
as,h
owev
er,a
tren
dfo
rpa
tient
sw
ithC
ushi
ng’s
synd
rom
eto
have
low
erIQ
scor
esat
base
line.
For
som
eIQ
subs
cale
s,th
ere
was
apo
sitiv
ere
latio
nw
ithre
cove
ryof
the
HPA
axis
and
ane
gativ
eas
soci
atio
nw
ithdu
ratio
nof
dise
ase.
(Con
tinue
d)
12 Tiemensma et al. Cognitive Impairments in Cushing’s Disease J Clin Endocrinol Metab, June 2010, 95(6):0000–0000
TAB
LE6.
Con
tinue
d
Au
tho
r,ye
arN
um
ber
of
sub
ject
sG
end
er(m
/f)
Ag
e(y
r),
mea
n�
SDA
ctiv
e/tr
eate
dM
eth
od
sO
utc
om
esSt
arkm
anet
al.,
2001
(8)
48C
ushi
ng’s
dise
ase,
38he
alth
yco
ntro
ls11
/37
37�
14A
ctiv
eW
echs
ler
Adu
ltIn
telli
genc
eSc
ale-
Revi
sed,
Wec
hsle
rM
emor
ySc
ale,
Sem
istr
uctu
red
Clin
ical
Inte
rvie
w,H
amilt
onD
epre
ssio
nRa
ting
Scal
e
Patie
nts
with
Cus
hing
’sdi
seas
esc
ored
wor
seon
4of
the
5ve
rbal
IQsu
btes
ts,
and
one
nonv
erba
lper
form
ance
IQsu
btes
tcom
pare
dw
ithco
ntro
ls.V
erba
lle
arni
ngan
dde
laye
dre
call
wer
esig
nific
antly
decr
ease
din
patie
nts.
Forg
etet
al.,
2002
(19)
13C
ushi
ng’s
synd
rom
e2/
1147
�13
1yr
afte
rsu
rgic
altr
eatm
ent
See
Forg
etet
al.,
2000
(7)
Com
pare
dw
ithob
serv
atio
nsbe
fore
trea
tmen
t(7
),th
ere
wer
eno
impr
ovem
ents
inco
gniti
vefu
nctio
ning
inpa
tient
sw
ithC
ushi
ng’s
synd
rom
e.St
arkm
anet
al.,
2003
(17)
24C
ushi
ng’s
dise
ase
4/20
34�
13A
ctiv
ean
d16
�9
mon
ths
afte
rsu
rger
y
Mag
netic
reso
nanc
eim
agin
g,W
echs
ler
Mem
ory
Scal
e-Ru
ssel
lMod
ifica
tion,
Sele
ctiv
eRe
min
ding
Test
,D
elay
edM
emor
y(p
arag
raph
san
dpa
ired
wor
ds),
Voc
abul
ary,
Arit
hmet
ic,S
ympt
oms
Che
cklis
t-90
All
patie
nts
show
edan
incr
ease
inhi
ppoc
ampa
lfor
mat
ion
volu
me
afte
rtr
eatm
ent,
and
18pa
tient
ssh
owed
anin
crea
sein
caud
ate
head
volu
me,
and
52–
61%
ofth
epa
tient
ssh
owed
anin
crea
sein
lear
ning
scor
e,w
here
as61
%of
the
patie
nts
show
edan
incr
ease
inm
emor
ysc
ore.
For
voca
bula
ry,2
5%ha
da
bett
ersc
ore,
and
50%
had
anin
crea
sed
scor
efo
rar
ithm
etic
.H
ook
etal
.,20
07(2
0)27
Cus
hing
’sdi
seas
e4/
2339
�13
Act
ive,
and
3–5,
6–1
2,13
–18
mon
ths
afte
rtr
eatm
ent
Busc
hke
Sele
ctiv
eRe
min
ding
Test
,Dig
itSp
an,V
erba
lFl
uenc
y,Sy
mpt
omC
heck
list
90-R
evis
ed,
mag
netic
reso
nanc
eim
agin
g
Old
eran
dyo
unge
rpa
tient
ssh
owed
com
para
ble
leve
lsof
cogn
itive
dysf
unct
ion
befo
retr
eatm
ent,
with
youn
ger
patie
nts
show
ing
am
ore
rapi
dim
prov
emen
t.V
erba
lflu
ency
and
reca
llsh
owed
reco
very
,but
brie
fat
tent
ion
did
not.
The
impr
ovem
ent
inve
rbal
reca
llw
asas
soci
ated
with
ade
crea
sein
cort
isol
leve
lsan
dan
incr
ease
inhi
ppoc
ampa
lfor
mat
ion
volu
me
1yr
afte
rtr
eatm
ent. (C
ontin
ued)
J Clin Endocrinol Metab, June 2010, 95(6):0000–0000 jcem.endojournals.org 13
TAB
LE6.
Con
tinue
d
Au
tho
r,ye
arN
um
ber
of
sub
ject
sG
end
er(m
/f)
Ag
e(y
r),
mea
n�
SDA
ctiv
e/tr
eate
dM
eth
od
sO
utc
om
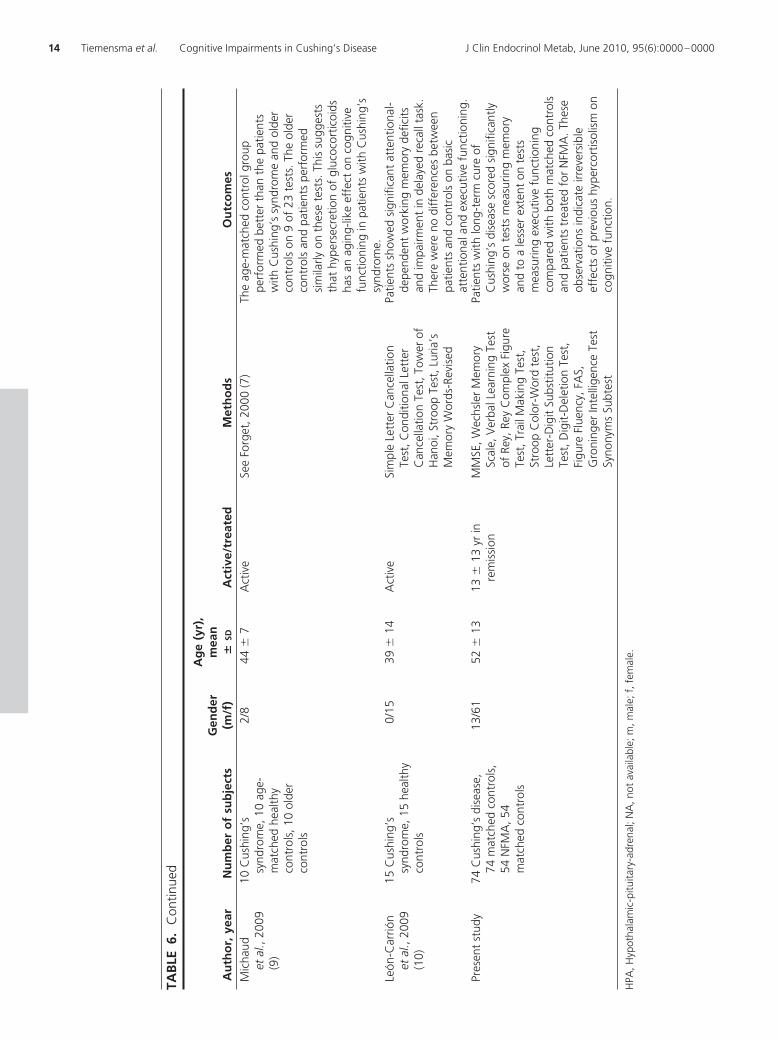
esM
icha
udet
al.,
2009
(9)
10C
ushi
ng’s
synd
rom
e,10
age-
mat
ched
heal
thy
cont
rols
,10
olde
rco
ntro
ls
2/8
44�
7A
ctiv
eSe
eFo
rget
,200
0(7
)Th
eag
e-m
atch
edco
ntro
lgro
uppe
rfor
med
bett
erth
anth
epa
tient
sw
ithC
ushi
ng’s
synd
rom
ean
dol
der
cont
rols
on9
of23
test
s.Th
eol
der
cont
rols
and
patie
nts
perf
orm
edsi
mila
rlyon
thes
ete
sts.
This
sugg
ests
that
hype
rsec
retio
nof
gluc
ocor
ticoi
dsha
san
agin
g-lik
eef
fect
onco
gniti
vefu
nctio
ning
inpa
tient
sw
ithC
ushi
ng’s
synd
rom
e.Le
ón-C
arrió
net
al.,
2009
(10)
15C
ushi
ng’s
synd
rom
e,15
heal
thy
cont
rols
0/15
39�
14A
ctiv
eSi
mpl
eLe
tter
Can
cella
tion
Test
,Con
ditio
nalL
ette
rC
ance
llatio
nTe
st,T
ower
ofH
anoi
,Str
oop
Test
,Lur
ia’s
Mem
ory
Wor
ds-R
evis
ed
Patie
nts
show
edsi
gnifi
cant
atte
ntio
nal-
depe
nden
tw
orki
ngm
emor
yde
ficits
and
impa
irmen
tin
dela
yed
reca
llta
sk.
Ther
ew
ere
nodi
ffer
ence
sbe
twee
npa
tient
san
dco
ntro
lson
basi
cat
tent
iona
land
exec
utiv
efu
nctio
ning
.Pr
esen
tst
udy
74C
ushi
ng’s
dise
ase,
74m
atch
edco
ntro
ls,
54N
FMA
,54
mat
ched
cont
rols
13/6
152
�13
13�
13yr
inre
mis
sion
MM
SE,W
echs
ler
Mem
ory
Scal
e,V
erba
lLea
rnin
gTe
stof
Rey,
Rey
Com
plex
Figu
reTe
st,T
rail
Mak
ing
Test
,St
roop
Col
or-W
ord
test
,Le
tter
-Dig
itSu
bstit
utio
nTe
st,D
igit-
Del
etio
nTe
st,
Figu
reFl
uenc
y,FA
S,G
roni
nger
Inte
llige
nce
Test
Syno
nym
sSu
btes
t
Patie
nts
with
long
-ter
mcu
reof
Cus
hing
’sdi
seas
esc
ored
sign
ifica
ntly
wor
seon
test
sm
easu
ring
mem
ory
and
toa
less
erex
tent
onte
sts
mea
surin
gex
ecut
ive
func
tioni
ngco
mpa
red
with
both
mat
ched
cont
rols
and
patie
nts
trea
ted
for
NFM
A.T
hese
obse
rvat
ions
indi
cate
irrev
ersi
ble
effe
cts
ofpr
evio
ushy
perc
ortis
olis
mon
cogn
itive
func
tion.
HPA
,Hyp
otha
lam
ic-p
ituita
ry-a
dren
al;N
A,n
otav
aila
ble;
m,m
ale;
f,fe
mal
e.
14 Tiemensma et al. Cognitive Impairments in Cushing’s Disease J Clin Endocrinol Metab, June 2010, 95(6):0000–0000

Even though the selection procedure may have inducedsome, but unknown, bias, the data indicate that there weredifferences in outcome parameters between both groups ofpatientswith the similar selectionmethodof controls.There-fore, the outcomes are not a consequence of the study designor the selection procedure of the control subjects but, rather,of the long-term consequences of Cushing’s disease.
In summary, there are subtle impairments in cognitivefunction in patients during long-term follow-up after cureof Cushing’s disease compared with NFMA patients andmatched controls. The greatest impairment was present inmemory, although executive functioning was also af-fected. This impairment in cognitive function after treat-ment of Cushing’s disease is not merely the result of pitu-itary disease in general and/or its treatment but includesspecific elements most likely caused by the irreversible ef-fects of previous glucocorticoid excess on the central ner-vous system.
Acknowledgments
Address all correspondence and requests for reprints to:J. Tiemensma, MSc., Department of Endocrinology and Met-abolic Diseases C4-R, Leiden University Medical Center, P.O. Box9600, 2300 RC Leiden, The Netherlands. E-mail: [email protected].
Disclosure Summary: The authors have nothing to disclose.
References
1. Colao A, Pivonello R, Spiezia S, Faggiano A, Ferone D, Filippella M,Marzullo P, Cerbone G, Siciliani M, Lombardi G 1999 Persistenceof increased cardiovascular risk in patients with Cushing’s diseaseafter five years of successful cure. J Clin Endocrinol Metab 84:2664–2672
2. Dekkers OM, Biermasz NR, Pereira AM, Roelfsema F, van AkenMO, Voormolen JH, Romijn JA 2007 Mortality in patients treatedfor Cushing’s disease is increased, compared with patients treatedfor nonfunctioning pituitary macroadenoma. J Clin EndocrinolMetab 92:976–981
3. van Aken MO, Pereira AM, Biermasz NR, van Thiel SW, HoftijzerHC, Smit JW, Roelfsema F, Lamberts SW, Romijn JA 2005 Qualityof life in patients after long-term biochemical cure of Cushing’s dis-ease. J Clin Endocrinol Metab 90:3279–3286
4. Whelan TB, Schteingart DE, Starkman MN, Smith A 1980 Neuro-psychological deficits in Cushing’s syndrome. J Nerv Ment Dis 168:753–757
5. Martignoni E, Costa A, Sinforiani E, Liuzzi A, Chiodini P, MauriM, Bono G, Nappi G 1992 The brain as a target for adrenocorticalsteroids: cognitive implications. Psychoneuroendocrinology 17:343–354
6. Mauri M, Sinforiani E, Bono G, Vignati F, Berselli ME, Attanasio R,Nappi G 1993 Memory impairment in Cushing’s disease. Acta Neu-rol Scand 87:52–55
7. Forget H, Lacroix A, Somma M, Cohen H 2000 Cognitive declinein patients with Cushing’s syndrome. J Int Neuropsychol Soc6:20–29
8. Starkman MN, Giordani B, Berent S, Schork MA, Schteingart DE
2001 Elevated cortisol levels in Cushing’s disease are associated withcognitive decrements. Psychosom Med 63:985–993
9. Michaud K, Forget H, Cohen H 2009 Chronic glucocorticoid hy-persecretion in Cushing’s syndrome exacerbates cognitive aging.Brain Cogn 71:1–8
10. Leon-Carrion J, Atutxa AM, Mangas MA, Soto-Moreno A, PumarA, Leon-Justel A, Martín-Rodriguez JF, Venegas E, Domínguez-Morales MR, Leal-Cerro A 2009 A clinical profile of memory im-pairment in humans due to endogenous glucocorticoid excess. ClinEndocrinol (Oxf) 70:192–200
11. Starkman MN, Gebarski SS, Berent S, Schteingart DE 1992 Hip-pocampal formation volume, memory dysfunction, and cortisollevels in patients with Cushing’s syndrome. Biol Psychiatry 32:756 –765
12. Foy MR, Stanton ME, Levine S, Thompson RF 1987 Behavioralstress impairs long-term potentiation in rodent hippocampus. BehavNeural Biol 48:138–149
13. Bodnoff SR, Humphreys AG, Lehman JC, Diamond DM, Rose GM,Meaney MJ 1995 Enduring effects of chronic corticosterone treat-ment on spatial learning, synaptic plasticity, and hippocampal neu-ropathology in young and mid-aged rats. J Neurosci 15(1 Pt 1):61–69
14. Bourdeau I, Bard C, Forget H, Boulanger Y, Cohen H, Lacroix A2005 Cognitive function and cerebral assessment in patients whohave Cushing’s syndrome. Endocrinol Metab Clin North Am 34:357–369, ix
15. Fietta P, Fietta P, Delsante G 2009 Central nervous system effects ofnatural and synthetic glucocorticoids. Psychiatry Clin Neurosci 63:613–622
16. Brown ES 2009 Effects of glucocorticoids on mood, memory, andthe hippocampus. Treatment and preventive therapy. Ann NY AcadSci 1179:41–55
17. Starkman MN, Giordani B, Gebarski SS, Schteingart DE 2003 Im-provement in learning associated with increase in hippocampal for-mation volume. Biol Psychiatry 53:233–238
18. Dorn LD, Cerrone P 2000 Cognitive function in patients with Cush-ing syndrome: a longitudinal perspective. Clin Nurs Res 9:420–440
19. Forget H, Lacroix A, Cohen H 2002 Persistent cognitive impairmentfollowing surgical treatment of Cushing’s syndrome. Psychoneu-roendocrinology 27:367–383
20. Hook JN, Giordani B, Schteingart DE, Guire K, Giles J, Ryan K,Gebarski SS, Langenecker SA, Starkman MN 2007 Patterns of cog-nitive change over time and relationship to age following successfultreatment of Cushing’s disease. J Int Neuropsychol Soc 13:21–29
21. Lezak MD 1995 Neuropsychological assessment. 3rd ed. NewYork: Oxford University Press
22. Folstein MF, Folstein SE, McHugh PR 1975 “Mini-mental state.” Apractical method for grading the cognitive state of patients for theclinician. J Psychiatr Res 12:189–198
23. Wechsler D, Stone CP 1945 Wechsler Memory Scale. New York:Psychological Corporation
24. Rey A 1958 L’examin Clinique en Psyhcologie. Paris: Presses Uni-versitaires de France
25. Rey A 1941 L’examen psychologique dans les cas d’encephalopathietraumatique. Arch Psychol 28:286–340
26. Reitan R 1956 Trail making test: manual for administration, scor-ing, and interpretation. Bloomington, IN: Indiana University
27. Stroop J 1935 Studies of interference in serial verbal reactions. J ExpPsychol 18:643–662
28. van der Elst W, van Boxtel MP, van Breukelen GJ, Jolles J 2006 TheLetter Digit Substitution Test: normative data for 1,858 healthyparticipants aged 24–81 from the Maastricht Aging Study (MAAS):influence of age, education, and sex. J Clin Exp Neuropsychol 28:998–1009
29. Regard M, Strauss E, Knapp P 1982 Children’s production on verbaland non-verbal fluency tasks. Percept Mot Skills 55:839–844
30. Benton AL, Hamsher Kd 1976 Multilingual Aphasia Examination.Iowa City, IA: University of Iowa
J Clin Endocrinol Metab, June 2010, 95(6):0000–0000 jcem.endojournals.org 15
31. Luteijn F, Ploeg FAEvd 1983 Manual Groninger Intelligence Test.Lisse, The Netherlands: Swets, Zeitlinger
32. Spinhoven P, Ormel J, Sloekers PP, Kempen GI, Speckens AE, VanHemert AM 1997 A validation study of the Hospital Anxiety andDepression Scale (HADS) in different groups of Dutch subjects. Psy-chol Med 27:363–370
33. Zigmond AS, Snaith RP 1983 The hospital anxiety and depressionscale. Acta Psychiatr Scand 67:361–370
34. Grattan-Smith PJ, Morris JG, Shores EA, Batchelor J, Sparks RS1992 Neuropsychological abnormalities in patients with pituitarytumours. Acta Neurol Scand 86:626–631
35. Peace KA, Orme SM, Thompson AR, Padayatty S, Ellis AW,Belchetz PE 1997 Cognitive dysfunction in patients treated for pi-tuitary tumours. J Clin Exp Neuropsychol 19:1–6
36. Peace KA, Orme SM, Padayatty SJ, Godfrey HP, Belchetz PE 1998Cognitive dysfunction in patients with pituitary tumour who havebeen treated with transfrontal or transsphenoidal surgery or medi-cation. Clin Endocrinol (Oxf) 49:391–396
37. McEwen BS 2008 Central effects of stress hormones in health and
disease: understanding the protective and damaging effects of stressand stress mediators. Eur J Pharmacol 583:174–185
38. Yehuda R 2002 Post-traumatic stress disorder. N Engl J Med 346:108–114
39. Wolkowitz OM, Burke H, Epel ES, Reus VI 2009 Glucocorti-coids: mood, memory, and mechanisms. Ann NY Acad Sci 1179:19 – 40
40. Schulz KF, Grimes DA 2005 Multiplicity in randomised trials I:endpoints and treatments. Lancet 365:1591–1595
41. Schulz KF, Grimes DA 2005 Multiplicity in randomised trials II:subgroup and interim analyses. Lancet 365:1657–1661
42. Biermasz NR, van Thiel SW, Pereira AM, Hoftijzer HC, van HemertAM, Smit JW, Romijn JA, Roelfsema F 2004 Decreased quality oflife in patients with acromegaly despite long-term cure of growthhormone excess. J Clin Endocrinol Metab 89:5369–5376
43. Dekkers OM, van der Klaauw AA, Pereira AM, Biermasz NR,Honkoop PJ, Roelfsema F, Smit JW, Romijn JA 2006 Quality of lifeis decreased after treatment for nonfunctioning pituitary macroad-enoma. J Clin Endocrinol Metab 91:3364–3369
16 Tiemensma et al. Cognitive Impairments in Cushing’s Disease J Clin Endocrinol Metab, June 2010, 95(6):0000–0000
Related Documents











