496 SAMJ VOL 75 20 MAY 1989 9. Kato H, Koike S, Yamamoto M, Iro Y, Yano E. Coronary aneurysms in infants and young children with acute febrile mucocutaneous lymph node syndrome. J Pedialr 1975; 86: 892-898. 10. Karo H, lchinose E, Yoshioka F el af. Fate of coronary artery aneurysms in Kawasaki disease: serial coronary angiography and long-term follow up srudy. AmJ Cardiol1982; 49: 1758-1766. 11. Rowley AH, Gonzaleng-Crussi F, Gidding SS, Duffy CE, Shulman ST. Incomplete Kawasaki disease wirh coronary artery involvement. J Pedialr 1987; 110: 409-413. 12. Nakano H, Saito A, Ueda K, Nojima K. Oinical characteristics of myo- cardial infarction following Kawasaki disease: report of II cases. J Pedialr 1986; 108: 198-203. 13. Karo H, lchinose E, Kawasaki T. Myocardial infarction in Kawasaki disease: clinical analysis in 195 cases.J Pediacr 1986; 108: 923-927. 14. Karen G, Lavi S, Rose V, Rowe R. Kawasaki disease: review of risk factors for coronary aneurysms. J Pedialr 1986; 108: 388-392. 15. Kiramura S, Kawashina Y, Kawachi K el al. Left ventricular function in patients with coronary arteritis due to acute febrile mucocutaneous lymph node syndrome or related diseases. AmJ Cardiol1977; 40: 156-164. 16. Kohr R.M.. Progressive asympromatic coronary artery disease as a late faral sequela of Kawasaki disease. J Pedialr 1986; 108: 256-259. 17. Sasagwi Y, Kato H. Regression of aneurysms in Kawasaki disease: a pathological srudy.J Pedialr 1982; 100: 225-231. 18. Karen G, Rose V, Lavi S el af. Possible efficacy of high dose salicylates in reducing coronary involvement in Kawasaki disease. JAMA 1985; 254: 767-769. 19. Furusho K, Kanaiya T, Nakano H ec al. High-dose intravenous gamma globulin therapy for Kawasaki disease. Lanal 1984; 2: 1055-1058. 20. Newburger JW, Takahashi M, Bums JC el al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med 1986; 315: 341-347. 21. Corrigan 11. Kawasaki disease and the plight of the platelet. AmJ Dis Child 1986; 140: 1223-1224. 22. Burns JC, Glode MP, Oarke SH, Wiggins J, Harhaway WE. Coagulopathy and platelet activation in Kawasaki syndrome: identification of patients with high risk for developing coronary artery aneurysms. J Pediacr 1984; 105: 206-211. 23. Pollack P. Anticoagulation in Kawasaki disease (Correspondence). Am J Dis Child 1987; 141: 713-714. 24. Bum DM, Pollack P, Bianco JA. Inrravenous streptokinase in an infant with Kawasaki's disease complicated by acute myocardial infarction. Pediacr Cardiol 1986; 6: 307-311. 25. TIMI Srudy Group. The thrombolysis in myocardial infarction (TIMI) trial. N Engl J Med 198"; 313: 932-936. 26. Pritchard SL, Culham JAG, Rogers PC]. Low-dose fibrinolytic therapy in infants.J Pediacr 1985; 106: 594-598. Subjective pulsatile tinnitus cured by carotid endarterectomy A case report H. D. LOUWRENS, J. BOTHA, D. M. VAN DER MERWE A 70-year-old woman with unilateral pulsatile tinnitus was relieved of the complaint after carotid endarterectomy. Internal carotid artery stenosis presenting with pulsatile tinnitus is rare. Endarterectomy can relieve symptoms if the correct diagnosis is made. S AIr Med J 1989; 75: 496-497. Case report An otherwise healthy 70-year-old woman with unilateral tinni- tus was referred to Tygerberg Hospital by her general practi- tioner. The tinnitus, confined to the left ear, was accentuated by bending forward and by reclining at night. In the absence of environmental noise, the 'bicycle pumping' in the left ear was more troublesome. The patient volunteered that the noise was synchronous with her heartbeat. On examination a loud systolic murmur, localised to the left carotid bifurcation, was detectable. Duplex Doppler examina- tion confirmed the presence of a type D2 stenosis of the left Departments of Surgery and Otorhinolaryngology, Uni- versity of Stelienbosch and Tygerberg Hospital, Parow- valiei, CP H. D. LOUWRENS, M.B. CH.B., M.MED. (CHIR.), F.CS. (S.A.) J. BOTHA, M.B. CH.B. Panorama Medical Centre, Rothschild Boulevard, Parow, CP D. M. VAN DER MERWE, M.B. CH. B., M.MED. (CHIR.), F.CS. (S.A.), F.R.C.S. Accepted 6 July 1988. internal carotid artery (80 - 99%) and a D 1 stenosis of the right internal carotid artery (50 - 79%). However, no murmur was detectable over the right carotid bifurcation. The ultrasono- graphic fmdings on the Doppler scan were confIrmed by carotid angiography (Fig. 1). The diagnosis of pulsatile tinnitus was one of exclusion of other causes made by the Department of Otorhinolaryngology. Endarterectomy of the left internal carotid artery completely relieved the patient's symptoms, which have not recurred. Discussion Pulsatile tinnitus, a rare symptom of carotid artery stenosis, is the perception of sounds synchronous with the heartbeat. Accurate diagnosis of pulsatile tinnitus is important since it is usually amenable to therapy and progression of the underlying disease can be detrimental to health. l Except for intraluminal arterial irregularities, other arterial causes of tinnitus include arteriovenous shunts and arterio-arterial shunts of various sorts. Non-arterial causes are: cervical venous hum; elevated cardiac output; heart murmurs; abnormalities of the jugular bulb; elevated intracranial pressure; vascular neoplasms of the internal ear; and primary intratemporal bone meningiomas. Careful assessment of the patient is mandatory before carotid endarterectomy can be considered. 0ne approach l to a defInite diagnosis by way of exclusion of other possible causes might consist of otoscopic examination and audiological assessment followed by computed tomography of the head. Should these tests prove negative and papilloedema is present, a lumbar puncture should be performed carefully to exclude raised intracranial pressure. Finally, an arteriogram will confirm the

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

496 SAMJ VOL 75 20 MAY 1989
9. Kato H, Koike S, Yamamoto M, Iro Y, Yano E. Coronary aneurysms ininfants and young children with acute febrile mucocutaneous lymph nodesyndrome. J Pedialr 1975; 86: 892-898.
10. Karo H, lchinose E, Yoshioka F el af. Fate of coronary artery aneurysms inKawasaki disease: serial coronary angiography and long-term follow upsrudy. AmJ Cardiol1982; 49: 1758-1766.
11. Rowley AH, Gonzaleng-Crussi F, Gidding SS, Duffy CE, Shulman ST.Incomplete Kawasaki disease wirh coronary artery involvement. J Pedialr1987; 110: 409-413.
12. Nakano H, Saito A, Ueda K, Nojima K. Oinical characteristics of myocardial infarction following Kawasaki disease: report of II cases. J Pedialr1986; 108: 198-203.
13. Karo H, lchinose E, Kawasaki T. Myocardial infarction in Kawasakidisease: clinical analysis in 195 cases.J Pediacr 1986; 108: 923-927.
14. Karen G, Lavi S, Rose V, Rowe R. Kawasaki disease: review of risk factorsfor coronary aneurysms. J Pedialr 1986; 108: 388-392.
15. Kiramura S, Kawashina Y, Kawachi K el al. Left ventricular function inpatients with coronary arteritis due to acute febrile mucocutaneous lymphnode syndrome or related diseases. AmJ Cardiol1977; 40: 156-164.
16. Kohr R.M.. Progressive asympromatic coronary artery disease as a late faralsequela of Kawasaki disease. J Pedialr 1986; 108: 256-259.
17. Sasagwi Y, Kato H. Regression of aneurysms in Kawasaki disease: apathological srudy.J Pedialr 1982; 100: 225-231.
18. Karen G, Rose V, Lavi S el af. Possible efficacy of high dose salicylates inreducing coronary involvement in Kawasaki disease. JAMA 1985; 254:767-769.
19. Furusho K, Kanaiya T, Nakano H ec al. High-dose intravenous gammaglobulin therapy for Kawasaki disease. Lanal 1984; 2: 1055-1058.
20. Newburger JW, Takahashi M, Bums JC el al. The treatment of Kawasakisyndrome with intravenous gamma globulin. N Engl J Med 1986; 315:341-347.
21. Corrigan 11. Kawasaki disease and the plight of the platelet. AmJ Dis Child1986; 140: 1223-1224.
22. Burns JC, Glode MP, Oarke SH, Wiggins J, Harhaway WE. Coagulopathyand platelet activation in Kawasaki syndrome: identification of patients withhigh risk for developing coronary artery aneurysms. J Pediacr 1984; 105:206-211.
23. Pollack P. Anticoagulation in Kawasaki disease (Correspondence). Am J DisChild 1987; 141: 713-714.
24. Bum DM, Pollack P, Bianco JA. Inrravenous streptokinase in an infant withKawasaki's disease complicated by acute myocardial infarction. PediacrCardiol 1986; 6: 307-311.
25. TIMI Srudy Group. The thrombolysis in myocardial infarction (TIMI)trial. N EnglJ Med 198"; 313: 932-936.
26. Pritchard SL, Culham JAG, Rogers PC]. Low-dose fibrinolytic therapy ininfants.J Pediacr 1985; 106: 594-598.
Subjective pulsatile tinnitus cured bycarotid endarterectomyA case report
H. D. LOUWRENS, J. BOTHA, D. M. VAN DER MERWE
A 70-year-old woman with unilateral pulsatile tinnitus wasrelieved of the complaint after carotid endarterectomy. Internalcarotid artery stenosis presenting with pulsatile tinnitus israre. Endarterectomy can relieve symptoms if the correctdiagnosis is made.
S AIr Med J 1989; 75: 496-497.
Case report
An otherwise healthy 70-year-old woman with unilateral tinnitus was referred to Tygerberg Hospital by her general practitioner. The tinnitus, confined to the left ear, was accentuatedby bending forward and by reclining at night. In the absenceof environmental noise, the 'bicycle pumping' in the left earwas more troublesome. The patient volunteered that the noisewas synchronous with her heartbeat.
On examination a loud systolic murmur, localised to the leftcarotid bifurcation, was detectable. Duplex Doppler examination confirmed the presence of a type D2 stenosis of the left
Departments of Surgery and Otorhinolaryngology, University of Stelienbosch and Tygerberg Hospital, Parowvaliei, CPH. D. LOUWRENS, M.B. CH.B., M.MED. (CHIR.), F.CS. (S.A.)
J. BOTHA, M.B. CH.B.
Panorama Medical Centre, Rothschild Boulevard, Parow,CPD. M. VAN DER MERWE, M.B. CH. B., M.MED. (CHIR.), F.CS. (S.A.),
F.R.C.S.
Accepted 6 July 1988.
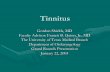
internal carotid artery (80 - 99%) and a D 1 stenosis of the rightinternal carotid artery (50 - 79%). However, no murmur wasdetectable over the right carotid bifurcation. The ultrasonographic fmdings on the Doppler scan were confIrmed bycarotid angiography (Fig. 1).
The diagnosis of pulsatile tinnitus was one of exclusion ofother causes made by the Department of Otorhinolaryngology.
Endarterectomy of the left internal carotid artery completelyrelieved the patient's symptoms, which have not recurred.
Discussion
Pulsatile tinnitus, a rare symptom of carotid artery stenosis, isthe perception of sounds synchronous with the heartbeat.Accurate diagnosis of pulsatile tinnitus is important since it isusually amenable to therapy and progression of the underlyingdisease can be detrimental to health. l Except for intraluminalarterial irregularities, other arterial causes of tinnitus includearteriovenous shunts and arterio-arterial shunts of varioussorts. Non-arterial causes are: cervical venous hum; elevatedcardiac output; heart murmurs; abnormalities of the jugularbulb; elevated intracranial pressure; vascular neoplasms of theinternal ear; and primary intratemporal bone meningiomas.
Careful assessment of the patient is mandatory before carotidendarterectomy can be considered. 0ne approach l to a defInitediagnosis by way of exclusion of other possible causes mightconsist of otoscopic examination and audiological assessmentfollowed by computed tomography of the head. Should thesetests prove negative and papilloedema is present, a lumbarpuncture should be performed carefully to exclude raisedintracranial pressure. Finally, an arteriogram will confirm the

Fig. 1. Riglit carotid system.
presumed diagnosis and exclude other arterial and non-arterialcauses.
The acrual reduction in surface diameter necessary to producea bruit varies greatly and depends on the character of theplaque, which in turn -determines the amount of turbulentflow present. In our patient significant stenoses were presentin both internal carotid arteries but there was bruit andtinnitus only on the left.
The probable mechanism which caused pulsatile tinnitus inthis patient was the conduction of sound energy by the skulJ.2Since the source of energy generation was in close proximityto the skull, the physiological mechanisms responsible for theattenuation of normal body sounds were inadequate to copewith this abnormal body sound. Consequently, the murmurwas perceived as pulsatile tinnitus especially in the absence ofambient noise.
After endarterectomy, both bruit and symptoms disappearedsimultaneously.
SAMT VOL 75 20 MEI 1989 497
Fig. 2. Left carotid system.
We thank Professor D. F. du Toit for critical review of themanuscript.
REFERENCES
l. Levine SB. Puls.tile tinnitus. Laryngoscope 1987; 97: 401-406.2. B.l1anryne J, Groves J. Diseases of rhe Ear, Nose and Throat. 4th ed.
London: Bunerworths, 1979: 96-98.
Related Documents








![Annals of Clinical Case Reports Case Report · artery. When characterized by pulsatile tinnitus, may indicate a neurological pathology [6]. Because of the pulsatile nature of tinnitus,](https://static.cupdf.com/doc/110x72/5fc6c321266a1328af21a56b/annals-of-clinical-case-reports-case-artery-when-characterized-by-pulsatile-tinnitus.jpg)

