Subclinical seizures in children diagnosed with localization-related epilepsy: Clinical and EEG characteristics Cigdem I. Akman a,b, * , Maria A. Montenegro a , Susan Jacob a , Karen Eck a , Danielle McBrian a , Claudia A. Chiriboga b , Marc C. Patterson b,1 a Comprehensive Epilepsy Center, Department of Neurology, Columbia University College of Physician and Surgeons, New York, NY, USA b Division of Pediatric Neurology, Department of Neurology, Columbia University College of Physician and Surgeons, New York, NY, USA article info Article history: Received 30 March 2009 Revised 8 June 2009 Accepted 13 June 2009 Available online 25 July 2009 Keywords: Localization-related epilepsy Children Subclinical seizure abstract Objective: Subclinical seizures (SCSs) are characterized by paroxysmal rhythmic epileptiform discharges that evolve in time and space in the absence of objective clinical manifestation or report of a seizure. The aim of this study was to evaluate the frequency and characteristics of SCSs in children with localization- related epilepsy (LRE). Methods: The results of video/EEG monitoring were reviewed to identify patients with SCS. We identified 187 children diagnosed with LRE, in 32 of whom SCSs were reported in the EEG recording. Results: SCSs were reported only in the children who had received a diagnosis of either symptomatic or cryptogenic LRE. All children had a history of clinical seizure(s). The ictal onset of SCSs was most frequent from the temporal and frontal lobes. SCSs were lateralized to the left hemispheres in 19, right hemisphere in 8, and both hemispheres independently in 5 children. SCSs were more often reported in young chil- dren, and associated with a history of developmental delay, infantile spasms, and frequent seizures. EEG abnormalities included background slowing and lack of normal sleep architecture in addition to the epileptiform activity. Seizure freedom was reported less often in children with SCSs. Six patients sei- zure free at the time of the admission were found to have SCSs. Conclusion: Subclinical seizures are not uncommon in children with LRE, in particular, with younger age, developmental disability, and medically refractory clinical course. Video/EEG monitoring will be informa- tive in selected children with LRE to assess the seizure frequency more accurately. Ó 2009 Elsevier Inc. All rights reserved. 1. Introduction The main objective of the treatment of children with epilepsy is to improve quality of life by achieving complete seizure control without medication side effects. Although most children become seizure free after introduction of the first antiepileptic drug (AED), a substantial proportion continue to have seizures refrac- tory to AED treatment [1]. Eyewitness descriptions of seizures by caregivers or parents for individuals with epilepsy are essential to optimize AED treatment based on the frequency and features of clinical events. In younger children or those with neurological disability, the identification of seizures even by experienced caregivers may pose challenges be- cause of their often subtle clinical features [2,3]. Failure to identify seizures may compromise the efficacy of medical treatment. Video/ EEG monitoring has emerged as an essential diagnostic tool to im- prove patient care by optimizing seizure control, particularly for children diagnosed with epilepsy by differentiation of seizures from other paroxysmal events. This diagnostic tool has refined our understanding of the semiology and electrographic findings of various epilepsy syndromes [4]. An electrographic seizure consists of a paroxysmal rhythmic pattern of epileptiform activity that evolves in time and location and defines an EEG pattern [5], whereas subclinical seizures (SCSs) describe the absence of subjective and objective clinical features associated with an electrographic seizure (ES) [6]. In clinical prac- tice, these descriptions are often used interchangeably to imply lack of clinical manifestations with apparent electrographic seizure on EEG recording. Therefore, it is essential to recognize ictal EEG findings and distinguish from the interictal epileptiform discharges to identify an ES or SCS. In children, SCSs are reported frequently in newborns or children presenting with acute neurological illness. Application of 1525-5050/$ - see front matter Ó 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.yebeh.2009.06.026 * Corresponding author. Address: Pediatric Neurology, Texas Children’s Hospital, Baylor College of Medicine, 6621 Fannin Street, 1250 CC, Houston, TX 77030, USA. Fax: +1 832 822 1717. E-mail address: [email protected] (C.I. Akman). 1 Present address: Division of Child and Adolescent Neurology, Department of Neurology, Mayo Clinic, Rochester, MN, USA. Epilepsy & Behavior 16 (2009) 86–98 Contents lists available at ScienceDirect Epilepsy & Behavior journal homepage: www.elsevier.com/locate/yebeh

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Epilepsy & Behavior 16 (2009) 86–98
Contents lists available at ScienceDirect
Epilepsy & Behavior
journal homepage: www.elsevier .com/locate /yebeh
Subclinical seizures in children diagnosed with localization-related epilepsy:Clinical and EEG characteristics
Cigdem I. Akman a,b,*, Maria A. Montenegro a, Susan Jacob a, Karen Eck a, Danielle McBrian a,Claudia A. Chiriboga b, Marc C. Patterson b,1
a Comprehensive Epilepsy Center, Department of Neurology, Columbia University College of Physician and Surgeons, New York, NY, USAb Division of Pediatric Neurology, Department of Neurology, Columbia University College of Physician and Surgeons, New York, NY, USA
a r t i c l e i n f o
Article history:Received 30 March 2009Revised 8 June 2009Accepted 13 June 2009Available online 25 July 2009
Keywords:Localization-related epilepsyChildrenSubclinical seizure
1525-5050/$ - see front matter � 2009 Elsevier Inc. Adoi:10.1016/j.yebeh.2009.06.026
* Corresponding author. Address: Pediatric NeuroloBaylor College of Medicine, 6621 Fannin Street, 1250Fax: +1 832 822 1717.
E-mail address: [email protected] (C.I. Akman)1 Present address: Division of Child and Adolescen
Neurology, Mayo Clinic, Rochester, MN, USA.
a b s t r a c t
Objective: Subclinical seizures (SCSs) are characterized by paroxysmal rhythmic epileptiform dischargesthat evolve in time and space in the absence of objective clinical manifestation or report of a seizure. Theaim of this study was to evaluate the frequency and characteristics of SCSs in children with localization-related epilepsy (LRE).Methods: The results of video/EEG monitoring were reviewed to identify patients with SCS. We identified187 children diagnosed with LRE, in 32 of whom SCSs were reported in the EEG recording.Results: SCSs were reported only in the children who had received a diagnosis of either symptomatic orcryptogenic LRE. All children had a history of clinical seizure(s). The ictal onset of SCSs was most frequentfrom the temporal and frontal lobes. SCSs were lateralized to the left hemispheres in 19, right hemispherein 8, and both hemispheres independently in 5 children. SCSs were more often reported in young chil-dren, and associated with a history of developmental delay, infantile spasms, and frequent seizures.EEG abnormalities included background slowing and lack of normal sleep architecture in addition tothe epileptiform activity. Seizure freedom was reported less often in children with SCSs. Six patients sei-zure free at the time of the admission were found to have SCSs.Conclusion: Subclinical seizures are not uncommon in children with LRE, in particular, with younger age,developmental disability, and medically refractory clinical course. Video/EEG monitoring will be informa-tive in selected children with LRE to assess the seizure frequency more accurately.
� 2009 Elsevier Inc. All rights reserved.
1. Introduction
The main objective of the treatment of children with epilepsy isto improve quality of life by achieving complete seizure controlwithout medication side effects. Although most children becomeseizure free after introduction of the first antiepileptic drug(AED), a substantial proportion continue to have seizures refrac-tory to AED treatment [1].
Eyewitness descriptions of seizures by caregivers or parents forindividuals with epilepsy are essential to optimize AED treatmentbased on the frequency and features of clinical events. In youngerchildren or those with neurological disability, the identification ofseizures even by experienced caregivers may pose challenges be-
ll rights reserved.
gy, Texas Children’s Hospital,CC, Houston, TX 77030, USA.
.t Neurology, Department of
cause of their often subtle clinical features [2,3]. Failure to identifyseizures may compromise the efficacy of medical treatment. Video/EEG monitoring has emerged as an essential diagnostic tool to im-prove patient care by optimizing seizure control, particularly forchildren diagnosed with epilepsy by differentiation of seizuresfrom other paroxysmal events. This diagnostic tool has refinedour understanding of the semiology and electrographic findingsof various epilepsy syndromes [4].
An electrographic seizure consists of a paroxysmal rhythmicpattern of epileptiform activity that evolves in time and locationand defines an EEG pattern [5], whereas subclinical seizures (SCSs)describe the absence of subjective and objective clinical featuresassociated with an electrographic seizure (ES) [6]. In clinical prac-tice, these descriptions are often used interchangeably to implylack of clinical manifestations with apparent electrographic seizureon EEG recording. Therefore, it is essential to recognize ictal EEGfindings and distinguish from the interictal epileptiform dischargesto identify an ES or SCS.
In children, SCSs are reported frequently in newborns orchildren presenting with acute neurological illness. Application of

Fig. 1. EEG demonstrates (Patient 11) the multifocal spike discharges in the right hemisphere at baseline. At the onset of SCS, the rhythmic spike discharges are seen in theright mid temporal region (T4), subsequently spread to the adjacent temporal region (F8 and T6). Bipolar montage, low frequency filter = 1 Hz; high frequency filter = 70 Hz,sensitivity 7 lV/mm.
C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98 87

88 C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98
prolonged video/EEG recording to monitor the course of acute ill-ness led to this discovery [7–9]. However, the question remainsunanswered whether SCSs are reported more often in children asan age-related phenomenon reflecting limited communicationskills attributable to immaturity or as the consequence of an acuteneurological insult in critically ill children. The clinical significanceof SCSs and its importance for long term outcome in children withepilepsy and acute neurological insult remain unknown.
The true frequency of SCSs in patients with localization-relatedepilepsy (LRE) is unknown. Sperling and O’Connor examined thefrequency of SCSs in adult patients with partial epilepsy whounderwent video/EEG recording with intracranial electrodes [10].In this study, we aimed to examine the frequency of SCSs in chil-dren with LRE and to identify the associated clinical features ofthese children who were admitted for epilepsy monitoring in a ter-tiary care center in the absence of acute neurological illness.
2. Methods
This retrospective study was designed to review the clinical his-tory and video/EEG recordings of children who were diagnosedwith LRE and underwent video/EEG monitoring between January
Fig. 2. EEG (Patient 13) demonstrates the spike discharges in semi-rhythmic pattern in th(T5) with increased frequency. Bipolar montage, low frequency filter = 1 Hz; high frequ
2004 and December 2006. The study was approved by the institu-tional review board.
EEG recording was performed with electrode placement accord-ing to the 10–20 international electrode system. Inferior temporalelectrodes (F9, T9, P9, F10, T10, and P10) were added, when indi-cated. EEG activity was digitally recorded referentially to P1/P2or A1/A2 electrodes. For patients who underwent an epilepsy sur-gery evaluation, AED doses were reduced as an activation methodto enhance the likelihood of capturing typical clinical seizures.Throughout video/EEG monitoring, seizures were annotated byparents, caregivers, physicians, nurses, or EEG technologists acti-vating an alarm button linked to the electroencephalograph. Vi-deo/EEG files were reviewed by a board-certifiedneurophysiologist to report EEG findings during sleep and wakeful-ness and interictal and ictal states as part of the routine evaluation.These EEG and video clips were saved and stored under the pa-tient’s name in a secured EEG database.
We reviewed the clinical records and EEG files of the childrenwho had SCSs on EEG recording and compared them with the clin-ical and EEG characteristics of the children diagnosed with LREonly. Required inclusion criteria included (1) elective admissionto the video/EEG monitoring unit with the diagnosis of LRE, (2)age between 1 month and 18 years, (3) established diagnosis of
e left mid temporal region (T3) which later spreads to the adjacent temporal regionency filter = 70 Hz, sensitivity 7 lV/mm.
C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98 89
LRE, and (4) clinical follow-up for 12 months or longer. Patientswith an unclear epilepsy diagnosis or diagnosis of epilepticencephalopathy (i.e., Lennox–Gastaut syndrome, Dravet’s syn-drome) were excluded from the study. Two authors (C.I.A. andM.A.M.) reviewed the clips of recorded video/EEG files or entireEEG files (if available) independently. Video files and EEG reportswere reviewed systematically to identify clinical reports of an auraor other subtle clinical features. If any clinical symptom was re-ported (1) subjectively by the child or (2) objectively by the par-ents and recorded by video monitoring that demonstrated asubtle clinical change such as behavioral arrest or arousal fromsleep at the time of ictal EEG findings, this event was considereda clinical seizure.
The EEG background characteristics, frequency, and location ofepileptiform discharges at interictal phase, at the onset of SCSand/or habitual seizure, and duration of subclinical seizures werereviewed. Absence of alpha rhythm or posterior reactive rhythmand presence of sustained focal or generalized slowing were ac-cepted as abnormal EEG background during wakefulness; absenceof spindles or persistent asynchrony and/or asymmetry of spindles(unless compatible with patient’s age) were defined as abnormalsleep architecture. The definition of ES was applied when a runof rhythmic epileptiform activity evolved in time and space
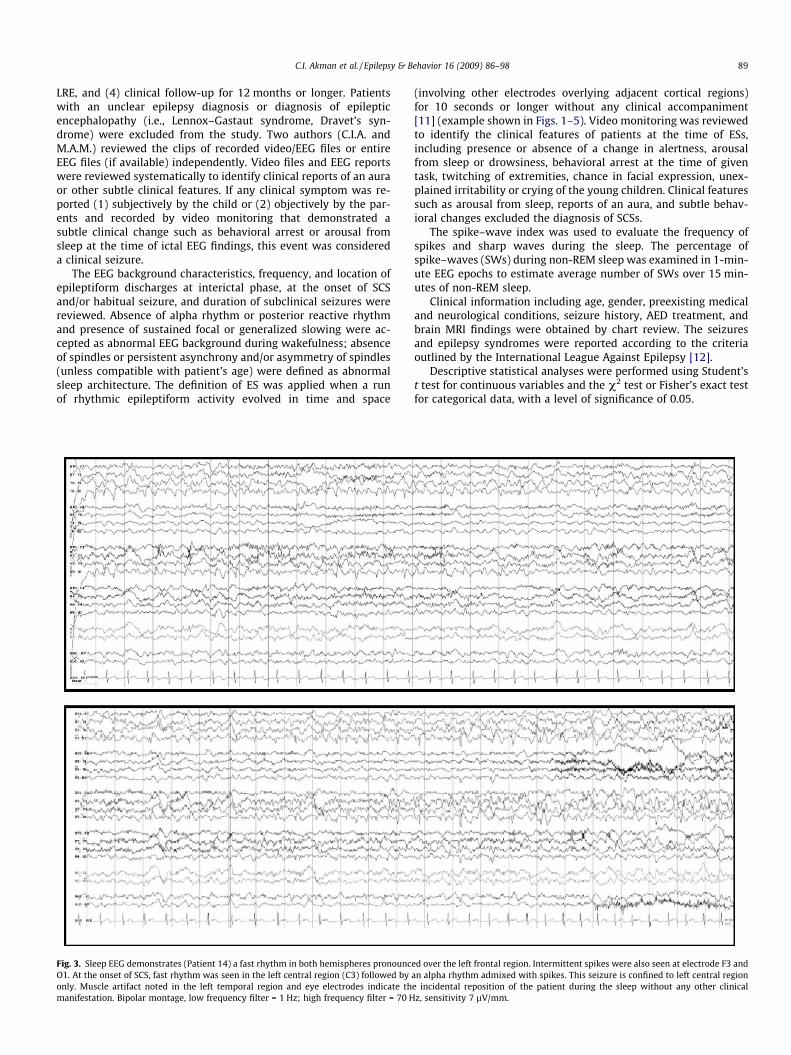
Fig. 3. Sleep EEG demonstrates (Patient 14) a fast rhythm in both hemispheres pronouncO1. At the onset of SCS, fast rhythm was seen in the left central region (C3) followed byonly. Muscle artifact noted in the left temporal region and eye electrodes indicate thmanifestation. Bipolar montage, low frequency filter = 1 Hz; high frequency filter = 70 H
(involving other electrodes overlying adjacent cortical regions)for 10 seconds or longer without any clinical accompaniment[11] (example shown in Figs. 1–5). Video monitoring was reviewedto identify the clinical features of patients at the time of ESs,including presence or absence of a change in alertness, arousalfrom sleep or drowsiness, behavioral arrest at the time of giventask, twitching of extremities, chance in facial expression, unex-plained irritability or crying of the young children. Clinical featuressuch as arousal from sleep, reports of an aura, and subtle behav-ioral changes excluded the diagnosis of SCSs.
The spike–wave index was used to evaluate the frequency ofspikes and sharp waves during the sleep. The percentage ofspike–waves (SWs) during non-REM sleep was examined in 1-min-ute EEG epochs to estimate average number of SWs over 15 min-utes of non-REM sleep.
Clinical information including age, gender, preexisting medicaland neurological conditions, seizure history, AED treatment, andbrain MRI findings were obtained by chart review. The seizuresand epilepsy syndromes were reported according to the criteriaoutlined by the International League Against Epilepsy [12].
Descriptive statistical analyses were performed using Student’st test for continuous variables and the v2 test or Fisher’s exact testfor categorical data, with a level of significance of 0.05.
ed over the left frontal region. Intermittent spikes were also seen at electrode F3 andan alpha rhythm admixed with spikes. This seizure is confined to left central regione incidental reposition of the patient during the sleep without any other clinicalz, sensitivity 7 lV/mm.

90 C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98
3. Results
A total of 1203 video/EEG monitoring studies were performedon 746 children. The diagnosis of LRE was identified in 222 pa-tients, 35 of whom were excluded from the study because of his-tory of a single seizure without adequate follow-up (n = 13) andunclear epilepsy diagnosis (n = 22). The clinical and EEG features
Fig. 3 (cont
of 188 patients (age: 8.2 ± 4.6 years) with a confirmed diagnosisof LRE are reported here.
3.1. Children with LRE and SCSs
Subclinical seizures were reported in 32 children (age:6.8 ± 5.1 years) who were younger than the others in the LRE
inued)

C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98 91
group. Seizure onset also occurred at a younger age in this group(P < 0.05) (Table 1).
The epilepsy diagnosis was established on the basis of etiologyas symptomatic LRE in 22 children (Table 1). MRI was reported asnormal in 5 (15.6%) and suggested the diagnosis of cortical dyspla-sia in 12 (37.5%) children. The diagnostic workup failed to revealunderlying etiology for epilepsy diagnosis in 10 children who wereidentified as having cryptogenic LRE. None of the children in thisgroup received the diagnosis of idiopathic epilepsy. History ofWest syndrome was reported in 10 children (31.3%); in 26 children(83.9%), there were various degrees of delay in developmentalmilestones (at least in one area), which were significantly morefrequent than in the children without SCSs on EEG recordings. Sei-zures were also reported more frequently in children with SCSs(Table 2).
The majority of the children were on two or more AEDs at thetime of admission. Nineteen children were on treatment withtwo or more AEDs. Three children had history of prior epilepsy sur-gery. Six children were seizure free at the time of video/EEG mon-itoring. The indications for video/EEG monitoring for these sixchildren were (1) to identify the nature of recent-onset behavioralproblems (three children), (2) to confirm the efficacy of AED treat-ment (two children), and (3) to follow up the incidental finding of asingle electrographic seizure that was captured on a 30-minuteEEG recording (one child).
Fig. 4. Sleep EEG (Patient 18) demonstrates asymmetry between hemispheres at baselinedischarges at electrode C3, T3 and F3. At the onset of SCS, a fast rhythm is seen in the lefspread to the adjacent parietal and posterior temporal regions (P3 and P7). This SCS enfrequency filter = 1 Hz; high frequency filter = 70 Hz, sensitivity 7 lV/mm.
3.1.1. EEG findings for patients with SCSsThere was no disagreement between the two reviewers on EEG
findings. Duration of SCSs ranged from 10 to 300 seconds (48 ± 59seconds). In 14 (44%) children, SCSs had not been observed in pre-vious video/EEG recordings (Table 3). After SCSs were reported, fol-low-up video/EEG monitoring was available in 21 children. SCSscontinued to occur in 14 (14/21, 66.5%) despite the adjustment ofAED treatment. SCSs were captured during sleep in 15, duringwakefulness in 14, and in both sleep and wakefulness in 3 children.SCS onset was reported in the temporal or frontal lobe in 10 chil-dren each, rolandic region in 4, central region or vertex in 5, occip-ital region in 2, and parietal region in 1. SCSs were lateralizedmostly to the left hemisphere in 19, right hemisphere in 8, andboth hemispheres independently in 5 children. Habitual seizureswere documented for 27 (81%) children, lateralized to the left sidein 17 (53%), right side in 9 (28%), and both sides in 1 patient. Local-ization of SCSs was congruent with the ictal onset of the habitualclinical seizures. Of the remaining five children with SCSs whosehabitual seizures were not recorded, four children had interictaldischarges reported in the same location where ictal onset of SCSswas identified. One child had no interictal discharges on EEGrecordings. In six children, epileptiform discharges were frequentlyseen during sleep and constituted more than 50% of non-REM sleeprecording. Background slowing was reported in 10 children andabnormal sleep architecture in 7. Bilateral or unilateral appearance
. High amplitude slow waves are present in the left hemisphere admixed with spiket occipital region (O1) admixed with irregular spike discharges which subsequentlyds with a run of slow waves in the left posterior quadrant. Bipolar montage, low

Fig. 4 (continued)
92 C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98

Fig. 4 (continued)
C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98 93
of epileptiform discharges did not differ between the groups of pa-tients with SCSs and LRE only.
3.2. Children with LRE and no SCSs
In this group, 156 children were identified (mean age: 8.5 ± 4.5,age at seizure onset: 5.0 ± 3.9 years). Twenty children were not onany AED treatment (13%). The diagnosis of idiopathic LRE (benignfocal epilepsy of childhood) was established in 13 (8.3%), andsymptomatic LRE in 75 (48.3%) children. Most common MRI abnor-malities included cortical dysplasia in 20, periventricular encepha-lomalacia in 17, remote vascular insult in 10, hydrocephalus in 5,mesial temporal sclerosis in 5, and tuberous sclerosis complex in5. Other abnormalities reported were Dandy Walker malformation,low-grade glioma, delayed or abnormal myelination pattern ofwhite matter, arachnoid cyst, chronic subdural hematoma, andagenesis of corpus callosum. MRI was normal in 63 children(40.4%). A history of West syndrome was reported in 10 children(6.4%), and developmental delay in 78 children (50.6%) (Table 2).
3.2.1. EEG findings of LRE onlySeizures were captured during either recent or previous EEG
recordings in 70 children. In this group, 21 children had ictal onsetin the temporal lobe, 27 in the frontal lobe, 6 in the rolandic region,6 in the central region or vertex, 8 in the occipital lobe, and 2 in theparietal lobe. Ictal onset lateralized to the right hemisphere in 41(58.6%), left hemisphere in 21 (30%), and both hemispheres in 8(11.4%) children. Epileptiform discharges constituting >50% ofnon-REM sleep recording were recognized in 13 children only.Baseline EEG abnormalities such as abnormal sleep architectureand background slowing were reported rarely in this group.
Abnormal sleep architecture (P = 0.004) and background slow-ing (P = 0.001) were seen more often in children presenting withSCSs. Unilateral or bilateral appearance of interictal epileptiformdischarges and frequency of spike-and-wave discharges duringsleep were not significant in children with SCSs compared withchildren without SCSs (P > 0.05).
4. Discussion
This article describes the prevalence of SCSs in children with fo-cal epilepsy who were electively admitted to the pediatric epilepsymonitoring unit of a tertiary care center over a 2-year period. Wefind that SCSs occur more often in young children, children withdevelopmental delay, and children with cortical malformations.Furthermore, clinical seizures are frequent and seizure freedomis achieved less often in children presenting with SCSs.
Clinical reports of seizure frequency may underestimate thetrue frequency of seizures for adults diagnosed with LRE. In thisstudy we also found that the clinical features of seizures may re-main unrecognized in children despite close clinical observationby parents. A higher incidence of SCSs was described in newbornsor children with critical illness [7,9]. Our results also confirm thatSCSs or seizures with subtle clinical features may occur as young asthe newborn period and infancy. A higher frequency of SCSs at ayounger age underlines the challenge of reporting seizures accu-rately in young children. The difficulty in recognizing the behav-ioral changes associated with seizures, particularly in infants, isone of the challenges faced by parents and physicians [4]. The nat-ural limitation of young age or neurological disability may compro-mise the ability to assess accurately the change in consciousness orsomatic manifestations during a focal seizure.

Fig. 5. Sleep EEG (Patient 19) demonstrates the onset of SCS arising from the right anterior temporal region (F8) with a spread only to central and parietal region (C4 and P4).Bipolar montage, low frequency filter = 1 Hz; high frequency filter = 70 Hz, sensitivity 7 lV/mm.
94 C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98
The children with frequent seizures appeared to have SCSs moreoften in this study. This finding suggests that SCSs may be morefrequent in intractable epilepsy and may be more often associatedwith SCSs besides younger age. We were also interested in whetherelectrographic seizures represent a different seizure pattern. To an-swer this question, we compared the EEG findings in SCSs with theEEG findings in habitual seizures with a clinical accompaniment.We found that EEG findings were congruent regardless of the pres-ence or absence of clinical symptoms [6]. This finding may impli-cate that a SCS is a seizure arising from the same epileptogeniczone and remains underreported because of the factors affectingthe seizure self-report. Therefore ‘‘subclinical seizure” would bemore appropriate terminology rather than ‘‘electrographic”or:asymptomatic” seizures to describe this phenomenon in thepediatric age group.
In our study, six children were diagnosed with SCSs despite theclinical report of seizure freedom. Three children were referred forvideo/EEG monitoring for further evaluation because of behavioraldisturbances of recent onset. However, all children had a previoushistory of clinical seizures and we did not note any child present-ing with SCSs only without previous history of clinical seizures.Furthermore, we noted that cortical dysplasia was seen as the mostcommon underlying cause for seizures in children presenting withSCSs. This observation suggests that children with frequent sei-
zures and cortical dysplasia are at risk for SCSs. The intrinsic epi-leptogenesis and propensity for electrographic seizures constitutea main characteristic and electrographic hallmark for cortical dys-plasia (Otsuba H, 2005).
The clinical significance of SCSs in behavior and cognition is thesubject of continuing debate. The effects of brief electroencephalo-graphic paroxysms on cognitive performance were first demon-strated during 3-Hz generalized SW discharges [13,14].Preliminary studies of focal spikes were not designed to detectsubtle and transient disruptions of function and, not surprisingly,found that the effects of focal paroxysmal discharges were negligi-ble [15].
The occurrence of neuronal loss after prolonged seizures isfirmly established [16]. However, the consequences of recurrentbrief seizures are yet to be clarified. Seizures early in life maybe followed by lifelong impairment of certain cognitive andbehavioral functions [17]. Interictal spikes—particularly if fre-quent and widespread—can impair cognitive abilities throughinterference with waking learning and memory consolidationduring sleep [18]. Mild cognitive impairment is frequently seenin patients with refractory epilepsy. For some patients, suchimpairment can adversely affect their psychosocial functioningin daily life, which can be even more debilitating than the sei-zures [19–22]. A study using functional brain MRI demonstrated

Fig. 5 (continued)
C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98 95
that the impairment of blood oxygen level associated with SCSs ofa few seconds did not return to baseline for up to 30 seconds[23]. These lines of evidence support a potential impact of SCSsin a spectrum of the problems encountered in children withLRE. About one-half of children with interictal discharges mayshow transient cognitive impairment during these events ifappropriately evaluated [19,20]. Predominantly left-sided dis-charges are associated with poor performance on reading, andright-sided discharges with poor performance on visual spatialtasks [24]. In addition, posterior focal spikes transiently impair vi-sual perception [25,26].
Our aim in this study was to examine the frequency and charac-teristics of SCSs in children diagnosed with focal epilepsy. How-ever, we realized that it would be difficult to estimate theprevalence accurately. Approximately half of the children (43%)in this cohort presented first time with SCSs and did not have sim-ilar ictal EEG findings previously, and more than half of these chil-dren continued to have the same EEG features on subsequentrecordings. Follow-up video/EEG recording is impractical and notcost-effective to monitor SCSs for every child diagnosed withLRE. However our results suggest that video/EEG monitoring wouldadd important information to identify SCSs despite the clinical re-ports of seizure freedom in children. Although our study mightsuggest that children with idiopathic LRE are not at risk for SCSs,our result may reflect a selection bias based on the patient referral
to a tertiary care center. Additionally, most children with idio-pathic LRE routinely undergo a brief EEG recording rather than vi-deo/EEG monitoring.
Although complete control of SCSs is probably desirable, thereis no clear guideline whether this EEG pattern warrants modifi-cation of AED regimen. Refractory seizures often require highdoses of AEDs, which may themselves cause cognitive dysfunc-tion. The number of AEDs that caused toxicity and the age at sei-zure onset are predictors of ultimate IQ; therefore, total seizurecontrol should not be achieved at the price of repeated episodesof drug toxicity in younger children [27–29]. Further prospectivestudies are needed to establish the benefit of more aggressiveAED treatment to achieve complete control of SCSs in patientswith LRE.
This study has a number of limitations. The retrospective naturemakes it difficult to obtain information regarding the clinical fea-tures of seizures. Prospective studies are needed to address thequestion of whether SCSs play a role in cognitive and seizure out-come and warrant modification of treatment in children with adiagnosis of chronic epilepsy.
In conclusion, our findings suggest that seizures without obvi-ous clinical manifestations may occur quite frequently in childrenwith LRE, in particular younger children and children with devel-opmental disability, a history of infantile spasms, and cortical dys-plasia. Therefore, prolonged video/EEG monitoring is useful in

Table 1Clinical features of children with SCSs.a
Patient Gender/age Age at firstseizure
Age at SCSiagnosis
History ofinfantile spasm
Seizurefrequency
Seizuretypes
No. of AEDs atdiagnosis of SCSs
Neurologicalexamination
Neuroimaging Diagnosis
1 M/5 years 6 months 5 years No Seizure free CPS, GTC 0 DD Mild diffuse cortical atrophy Cryptogenic2 M/11 years 4 months 11 years Yes Seizure free CPS 1 DD Normal Cryptogenic3 M/2 years 2 months 4 months No Daily CPS, GTC 2 DD PMG Symptomatic (PMG)4 M/10 years 9 years 12 years No Daily CPS 3 DD Normal Cryptogenic5 F/8 years 6 years 7 years No Daily CPS, GTC 2 Normal FCD Symptomatic (FCD)6 F/6 months 1 day 5 months No Daily CPS, SPS 3 DD NA Symptomatic (perinatal complications)7 M/15 months 2 days 7 months No Daily SPS 2 DD Normal Cryptogenic8 M/10 years 8 years 9 years No Seizure free CPS, SPS 1 DD Multiple hamartomas and PVH Symptomatic (TSC)9 F/17 years 16 years 17 years No Weekly CPS, GTC 0 Normal Normal Cryptogenic
10 M/16 years 13 years 16 years No Monthly CPS, GTC 2 Normal Increased signal of inferior temporal cortex Cryptogenic11 M/2 years 7 months 10 months No Daily CPS 2 DD Hemimegalencephaly Symptomatic (hemimegalencephaly)12 F/6 years 5 years 5 years No Seizure free CPS 1 DD Encephalomalacia and R hippocampus atrophy Symptomatic (HSV encephalitis)13 F/5 years 3 months 4 years No Daily CPS 3 DD Multiple hamartomas, PVH Symptomatic (TSC)14 M/8 years 4 months 8 years No Daily CPS, GTC 2 DD Macrocephaly Mild diffuse atrophy Cryptogenic15 M/17 years 2 years 11 years No Seizure free CPS 1 Normal R porencephalic cyst Cryptogenic16 F/12 years 1 year 10 years No Seizure free CPS 2 Normal L temporal Symptomatic (DNET)17 M/2 years 8 months 2 years No Weekly CPS, GTC 2 DD L temporal lobe low-grade tumor Symptomatic (DNET)18 F/7 years 5 years 7 years No Weekly CPS, SPS 2 DD Hypotonia Encephalomalacia Symptomatic (encephalitis)19 F/6 years 6 months 6 years No Weekly CPS, GTC,SE 2 DD R temporal lobe CD and MTS Symptomatic20 M/7 years 6 years 7 years No Monthly CPS 1 DD Chiari I malformation Cryptogenic21 F/7 years 6 years 6 years No Monthly CPS, SPS 1 DD FCD Symptomatic (FCD)22 M/8 years 6 years 7 years No Daily CPS, FSE, GTC 1 DD Macrocephaly Normal Cryptogenic23 M/17 years 1 year 16 year No Daily CPS, GTC 3 DD PVL Symptomatic (HIE)24 F/2 years 6 months 2 years Yes Weekly CPS, SPS 1 DD Multiple hamartomas and PVH Symptomatic (TSC)25 M/9 years 6 years 7 years No Yearly SPS, CPS 1 R hemiparesis L hemiatrophy Symptomatic (perinatal complications)26 M/3 years 1 day 1.5 years Yes Daily CPS, GTC, 1 DD PVL Symptomatic (Perinatal complications)27 F/14 months NA 13 months No Daily CPS 4 DD Microcephaly Diffuse cortical atrophy Cryptogenic28 M/7 years 3 months 6 years Yes Daily CPS, GTC 3 DD Lissencephaly Symptomatic29 M/6 years 2 years 6 years No Weekly CPS 2 DD PVL Symptomatic (Perinatal complications)30 F/1 year 2 days 1 year Yes Daily CPS 1 Normal FCD Symptomatic (FCD)31 F/12 years NA 10 years Yes NA CPS, GTC 2 Normal FCD Symptomatic (FCD)32 F/4 years 5 days 4 month No Daily CPS, SPS, GTC 3 DD Hemimegalancephaly Symptomatic
a L, left; R, right; MTS, mesial temporal sclerosis; DD, developmental delay; DNET, dysembryoplastic neuroepithelial tumor; FCD, focal cortical dysplasia; HSV, herpes simples virus; NA, not available; PVH, periventricularheterotopia; SCS, subclinical seizures; TS, tuberous sclerosis; PMG, polymicrogyria; CPS, complex partial seizures; SPS, simple partial seizures; GTC, generalized tonic clonic seizures; SE, status epilepticus; FS, E, febrile statusepilepticus; PVL, periventricular leucomalacia.
96C.I.A
kman
etal./Epilepsy
&Behavior
16(2009)
86–98

Table 2Demographic and clinical data for children with SCSs versus those without SCSs.a
Data SCSs (n = 32) No SCSs (n = 155) P
Age, years (mean ± SD)b 6.8 ± 5.1 8.5 yr ± 4.5 0.056Age at seizure onset, years (mean ± SD)b 3.5 ± 4.0 5.0 ± 3.9 0.044Male/female ratio 18/14 87/68 0.563Duration of epilepsy, years (mean ± SD) 3.2 ± 3.5 3.6 ± 3.8 0.651Past history of infantile spasms, n (%)b 10 (31.3) 6 (3.9) <0.001Developmental delay, n (%)b 26 (83.9) 78 (50.6) 0.001Seizure frequency, n (%)
Daily 6(18.7) 12 (7) 0.684Weeklyb 14 (43.8) 26 (16.6) 0.02Monthlyb 5 (15.6) 52 (33) 0.02
Seizure freedom, n (%)b 0 (0) 21 (13.7%) 0.014MRI findings, n (%)b
Normal 5 (7.4) 63 (40.4) 0.005Cortical dysplasia 12 (37.5) 20(12.8) 0.003
a SCSs, subclinical seizures.b P < 0.05.
Table 3EEG findings in patients with SCSs.a
Patient Background SCSs/days Ictal onset Interictal EEG Maximalwavefrequency(Hz)
SCSduration(s)
Follow-up Previousvideo/EEGwithoutSCSs?
1 Abnormal 70/2 days L temporal L and R temporal 1 60 No follow-up No2 Abnormal 1/1 day Occipital (bilateral) Multifocal 1 32 No follow-up Yes3 Abnormal >100/6 days R frontocentral R frontal and
L frontal3–4 20–120 18 months—SCSs No
4 Normal 40/6 days L frontal L frontal 2 60–120 12 months—SCSs Yes5 Normal 33/1 day R frontal R frontal 3–4 120–300 18 months—SCSs No6 Abnormal 38/4 days L and R centrotemporal Multifocal 2 10–11 1 month—SCSs Yes7 Abnormal 21/6 days L + R frontal, L + R temporal,
L occipitalMultifocal 6 120 3 and 8 months—no Yes
8 Normal >100/1 day L frontoparietal L frontal 3 10 8 months—SCSs (11, 13, and15 months—no SCSs)
No
9 Normal 90/1 day L temporal L temporal 1.5–2 10–60 No follow-up No10 Abnormal >100/5 days R posterior quadrant Multifocal 3 270 No follow-up No11 Abnormal 66/1 day R temporal R temporal 6–7 60–70 1 month—SCSs (3, 5 and
12 months—no SCSs)No
12 Abnormal >100/2 days R posterior quadrant Multifocal 2–3 15 6, 9, 11, and 18 months—SCSs Yes13 Abnormal 20/1 day L temporal L temporal b 20–30 2 and 11 months—SCSs No14 Abnormal 6/2 days L fronto-temporal Multifocal 5 10 No follow-up Yes15 Normal 1/1 day L frontal L frontal 3 10 3 and 10 months—SCSs Yes16 Normal 6/1 day L temporal L temporal 2 10 30 months—SCSs No17 Normal 2/7 days L temporal L temporal 2 15 No follow-up Yes18 Abnormal >100/2 days Bifrontal Multifocal 4 5–10 18 and 24 months—SCSs Yes19 Normal >100/3 days R posterior quadrant R frontal,
R parietal4 20–30 No follow-up Yes
20 Normal >100/2 days L frontal L frontal 2 10–15 7 months—no SCSs No21 Normal 5/18 days L and R frontal L and R frontal 2.5 15 9 and 13 months—no SCSs Yes22 Abnormal 20/2 days L temporal L temporal 2–3 10–70 10, 14 and 20 months—no SCSs No23 Normal 16/6 days L temporal L temporal 1 20–50 No No24 Normal 1/1 day R temporal R temporal, R
frontal1–2 40 5 months—no SCSs Yes
25 Abnormal 2/1 day R and L temporal Multifocal 6 10–15 24 months—still having SCSs No26 Abnormal 7/3 days L and R hemisphere Multifocal 8 10–120 6 and 12 months—SCSs
(24 months—no SCSs)No
27 Abnormal >100/8 days R parasagital R parasagital 2–3 NA 1 month—SCSs No28 Abnormal 8/3 days L temporal Multifocal 5–7 60 1 month—still having SCSs No29 Abnormal 1/9 days R posterior quadrant R parietal, L
hemisphere2 120 No follow-up No
30 Normal 10/2 days L central L central 4 30 No follow-up No31 Abnormal 3/5 days L posterior quadrant L posterior
quadrant4 20 4, 12, 19, and 27 months—no SCSs Yes
32 Abnormal 1/10 days R temporal, R occipital R posteriorquadrant
5–7 110 Seizure free after hemispherectomy Yes
a SCSs, subclinical seizures; L, left; R, right.b 1 Hz PLEDs (periodic laterilized epileptiform discharges)-like followed by 3–4 Hz.
C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98 97
selected patients to estimate seizure frequency more accurately.Prospective studies are needed to assess the consequences of SCSson clinical outcome and the role of treatment for children.
Conflict of interest statement
The authors do not have any conflicts of interest to disclose.

98 C.I. Akman et al. / Epilepsy & Behavior 16 (2009) 86–98
Acknowledgement
The authors thank Dr. J. Riviello for his review and comments onthis study and article.
References
[1] Sillanpaa M, Jalava M, Kaleva O, Shinnar S. Long-term prognosis of seizureswith onset in childhood. N Engl J Med 1998;338:1715–22.
[2] Korff CM, Nordli Jr DR. The clinical-electrographic expression of infantileseizures. Epilepsy Res 2006;70(Suppl. 1):S116–31.
[3] Korff CM, Nordli Jr DR. Epilepsy syndromes undetermined whether focal orgeneralized in infants. Epilepsy Res 2006;70(Suppl. 1):S105–9.
[4] Nordli Jr DR, Bazil CW, Scheuer ML, Pedley TA. Recognition and classification ofseizures in infants. Epilepsia 1997;38:553–60.
[5] Chong DJ, Hirsch LJ. Which EEG patterns warrant treatment in the critically ill?Reviewing the evidence for treatment of periodic epileptiform discharges andrelated patterns. J Clin Neurophysiol 2005;22:79–91.
[6] Sperling MR, O’Connor MJ. Auras and subclinical seizures: characteristics andprognostic significance. Ann Neurol 1990;28:320–8.
[7] Jette N, Claassen J, Emerson RG, Hirsch LJ. Frequency and predictors ofnonconvulsive seizures during continuous electroencephalographicmonitoring in critically ill children. Arch Neurol 2006;63:1750–5.
[8] Scher MS. Controversies regarding neonatal seizure recognition. EpilepticDisord 2002;4:139–58.
[9] Tay SK, Hirsch LJ, Leary L, Jette N, Wittman J, Akman CI. Nonconvulsive statusepilepticus in children: clinical and EEG characteristics. Epilepsia2006;47:1504–9.
[10] Zangaladze A, Nei M, Liporace JD, Sperling MR. Characteristics and clinicalsignificance of subclinical seizures. Epilepsia 2008;49:2016–21.
[11] Granner MA, Lee SI. Nonconvulsive status epilepticus: EEG analysis in a largeseries. Epilepsia 1994;35:42–7.
[12] Commission on Classification and Terminology of the International LeagueAgainst Epilepsy. Proposal for revised classification of epilepsies and epilepticsyndromes. Epilepsia 1989;30:389–99.
[13] Matsuoka H, Okuma T, Ueno T, Saito H. Impairment of parietal corticalfunctions associated with episodic prolonged spike-and-wave discharges.Epilepsia 1986;27:432–6.
[14] Tizard B, Margerison JH. The relationship between generalized paroxysmalE.E.G. discharges and various test situations in two epileptic patients. J NeurolNeurosurg Psychiatry 1963;26:308–13.
[15] Tassinari CA, Rubboli G. Cognition and paroxysmal EEG activities: from a singlespike to electrical status epilepticus during sleep. Epilepsia2006;47(Suppl. 2):40–3.
[16] Holmes GL. Seizure-induced neuronal injury: animal data. Neurology2002;59:S3–6.
[17] Sayin U, Sutula TP, Stafstrom CE. Seizures in the developing brain causeadverse long-term effects on spatial learning and anxiety. Epilepsia2004;45:1539–48.
[18] Holmes GL, Lenck-Santini PP. Role of interictal epileptiform abnormalities incognitive impairment. Epilepsy Behav 2006;8:504–15.
[19] Aldenkamp A, Arends J. The relative influence of epileptic EEG discharges,short nonconvulsive seizures, and type of epilepsy on cognitive function.Epilepsia 2004;45:54–63.
[20] Aldenkamp AP, Beitler J, Arends J, van der Linden I, Diepman L. Acute effects ofsubclinical epileptiform EEG discharges on cognitive activation. Funct Neurol2005;20:23–8.
[21] Binnie CD, Marston D. Cognitive correlates of interictal discharges. Epilepsia1992;33(Suppl. 6):S11–7.
[22] Shackleton DP, Kasteleijn-Nolst Trenite DG, de Craen AJ, Vandenbroucke JP,Westendorp RG. Living with epilepsy: long-term prognosis and psychosocialoutcomes. Neurology 2003;61:64–70.
[23] Kobayashi E, Hawco CS, Grova C, Dubeau F,Gotman J. Widespread andintenseBOLDchanges during brief focal electrographic seizures. Neurology 2006;66:1049–55.
[24] Kasteleijn-Nolst Trenite DG. Transient cognitive impairment during subclinicalepileptiform electroencephalographic discharges. Semin Pediatr Neurol1995;2:246–53.
[25] Shewmon DA, Erwin RJ. The effect of focal interictal spikes on perception andreaction time: I. General considerations. Electroencephalogr Clin Neurophysiol1988;69:319–37.
[26] Shewmon DA, Erwin RJ. Focal spike-induced cerebral dysfunction is related tothe after-coming slow wave. Ann Neurol 1988;23:131–7.
[27] Bourgeois BF. Determining the effects of antiepileptic drugs on cognitivefunction in pediatric patients with epilepsy. J Child Neurol 2004;19(Suppl.1):S15–24.
[28] Bourgeois BF, Prensky AL, Palkes HS, Talent BK, Busch SG. Intelligence inepilepsy: a prospective study in children. Ann Neurol 1983;14:438–44.
[29] Trimble MR. Antiepileptic drugs, cognitive function, and behavior in children:evidence from recent studies. Epilepsia 1990;31(Suppl. 4):S30–4.
Related Documents











