Osama Elazouni etl al. 421 Study of The Occurrence of Abnormal Involuntary Movements after Cerebral Stroke Osama M.M.A. Elazouni 1 , Amal SE Elmotayam 1 , Karam Selim 1 , Said A. Elmonem 2 Departments of Neurology 1 , Radiology 2 , Zagazig University ABSTRACT Introduction: Abnormal involuntary movements (AIM) following cerebral stroke were reported after lesions in certain areas of the brain, but most of these studies were case reports or series of patients with a given type of abnormal movement or anatomical lesion. Aim of The Work: The aim is to study pattern of occurrence of AIM that may occur after cerebral stroke and their relationship to the cause of stroke, clinical and personal data of patients as well as sites of lesions based on imaging studies. Patients and Methods: Thirty four patients with AIM after cerebral strokes were included in this study. These patients were selected suffering first ever clinical stroke, with negative history of previous attacks. These patients were subjected to medical history taking, and thorough neurological examination. The type of AIM was evaluated by more than one of the authors separately with consultation of every case. Clinical follow up of these AIM was done using abnormal involuntary movements scale (AIMS) for detection of improvement or deterioration of these abnormal movements. Also clinical follow up of the motor power, sensory deficits, cerebellar manifestations etc was done. Follow up was done every two weeks in the first month and every month afterward and patients were followed up for at least a year after onset of AIM. Patients that died or did not comply with the study were excluded, also patients with previous history of AIM before onset of stroke were excluded as well. All patients were subjected to CT brain in the acute stage of stroke and those that had normal CT in the acute stage were resubjected to CT or MRI brain. Another 3 cases of central thalamic ischemic lesions, authors came across while doing this research, were included and studied as previously. Results: Thirteen (38.2%) of patients suffered chorea, while only 4 (11.7%) suffered parkinsonism and patients with tremor and dystonia were 9 (26.4%), and 8 (23.5%) respectively. Group of patients with chorea were found significantly (P<0.05) the elder among the other groups. The shortest mean interval time between onset of stroke and development of AIM was that for chorea with statistical significant difference (P<0.05). Most of the patients with AIM were grade 4 and 5 on MRC scale, and of moderate to severe affection of proprioceptive sensation and ataxia. Although lesions of the thalamus and/or basal ganglia were found common in these patients, good percent of patients were found suffering lesions in other areas of the brain. Central thalamic lesion was accompanied with contralateral hypothesis, chorea, and ataxia. Summary and Conclusion: Correlation between site of lesion and type of AIM could be difficult to establish. Although thalamic and basal ganglion lesions are common underlying cause for AIM, these AIM could occur in a good percentage after lesions in other areas of the brain and that could be due to concurrent ataxia and proprioceptive sensory impairment beside reasonable motor strength. Finally, pathogenesis of AIM needs more speculation and more scrutinized analysis of imaging studies with paying more attention to functional brain imaging studies. (Egypt J. Neurol. Psychiat. Neurosurg., 2007, 44(2): 421-435) INTRODUCTION Abnormal involuntary movements (AIM) caused by cerebral strokes were reported 1-6 . These reported involuntary movements are in the form of chorea 7-11 , tremor 12-15 , dystonia 16-20 , parkinsonism 21-25 , and myoclonus 26 , as well as hemiballismus 27 , and all have been associated with both cerebral infarctions and haemorrhages. AIM may be part of acute clinical manifestation of stroke 9,14,15,27,28 or delayed in onset with progressive course 12,13,19 . Previous studies attributed AIM (dystonia, myoclonus, tremor) to

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Osama Elazouni etl al.
421
Study of The Occurrence of Abnormal Involuntary
Movements after Cerebral Stroke
Osama M.M.A. Elazouni1, Amal SE Elmotayam
1, Karam Selim
1, Said A. Elmonem
2
Departments of Neurology1, Radiology2, Zagazig University
ABSTRACT
Introduction: Abnormal involuntary movements (AIM) following cerebral stroke were reported after lesions in
certain areas of the brain, but most of these studies were case reports or series of patients with a given type of
abnormal movement or anatomical lesion. Aim of The Work: The aim is to study pattern of occurrence of AIM that
may occur after cerebral stroke and their relationship to the cause of stroke, clinical and personal data of patients as
well as sites of lesions based on imaging studies. Patients and Methods: Thirty four patients with AIM after cerebral
strokes were included in this study. These patients were selected suffering first ever clinical stroke, with negative
history of previous attacks. These patients were subjected to medical history taking, and thorough neurological
examination. The type of AIM was evaluated by more than one of the authors separately with consultation of every
case. Clinical follow up of these AIM was done using abnormal involuntary movements scale (AIMS) for detection of
improvement or deterioration of these abnormal movements. Also clinical follow up of the motor power, sensory
deficits, cerebellar manifestations etc was done. Follow up was done every two weeks in the first month and every
month afterward and patients were followed up for at least a year after onset of AIM. Patients that died or did not
comply with the study were excluded, also patients with previous history of AIM before onset of stroke were excluded
as well. All patients were subjected to CT brain in the acute stage of stroke and those that had normal CT in the acute
stage were resubjected to CT or MRI brain. Another 3 cases of central thalamic ischemic lesions, authors came
across while doing this research, were included and studied as previously. Results: Thirteen (38.2%) of patients
suffered chorea, while only 4 (11.7%) suffered parkinsonism and patients with tremor and dystonia were 9 (26.4%),
and 8 (23.5%) respectively. Group of patients with chorea were found significantly (P<0.05) the elder among the
other groups. The shortest mean interval time between onset of stroke and development of AIM was that for chorea
with statistical significant difference (P<0.05). Most of the patients with AIM were grade 4 and 5 on MRC scale, and
of moderate to severe affection of proprioceptive sensation and ataxia. Although lesions of the thalamus and/or basal
ganglia were found common in these patients, good percent of patients were found suffering lesions in other areas of
the brain. Central thalamic lesion was accompanied with contralateral hypothesis, chorea, and ataxia. Summary and
Conclusion: Correlation between site of lesion and type of AIM could be difficult to establish. Although thalamic and
basal ganglion lesions are common underlying cause for AIM, these AIM could occur in a good percentage after
lesions in other areas of the brain and that could be due to concurrent ataxia and proprioceptive sensory impairment
beside reasonable motor strength. Finally, pathogenesis of AIM needs more speculation and more scrutinized
analysis of imaging studies with paying more attention to functional brain imaging studies. (Egypt J. Neurol. Psychiat. Neurosurg., 2007, 44(2): 421-435)
INTRODUCTION
Abnormal involuntary movements (AIM)
caused by cerebral strokes were reported1-6.
These reported involuntary movements are in the
form of chorea7-11, tremor
12-15, dystonia
16-20,
parkinsonism21-25, and myoclonus
26, as well as
hemiballismus27, and all have been associated
with both cerebral infarctions and haemorrhages.
AIM may be part of acute clinical manifestation
of stroke9,14,15,27,28
or delayed in onset with
progressive course12,13,19. Previous studies
attributed AIM (dystonia, myoclonus, tremor) to

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
422
lesions of various structures including the striato-
pallidal complex, the mesencephalon, and the
thalamus10,29,30. In the thalamus, lesions associated
with movement disorders have been described in
the ventrolateral, ventral posterolateral, and
paramedian territories10,29,31,32
. Some other studies
of the thalamic lesions that are responsible for
dystonia have attributed lesion to the subnuclei of
the thalamus33. The basal ganglia (caudate,
putamen, globus pallidus, subthalamic nucleus,
and substantia nigra) are a complex
interconnected link of several nuclear groups
within the brain and brainstem. They are involved
in parallel modular loops that leave and return to
the cortex much modulated and processed. They
receive afferents from many motor and limbic
areas to process motor information, and they
modulate the excitement level of the thalamus
motor nuclei that project to motor cortices. Basal
ganglia circuitry have two major pathways: the
direct and the indirect. The indirect pathway
includes a connection via the glutamatergic
subthalamic nucleus. Both pathways are in
balance and affect level of excitation of the motor
thalamus and its effect on the output of the
cerebral cortex. Diminished inhibitory output via
the direct pathway of the basal ganglia allows for
facilitation of the thalamic neurons. Increased
inhibition via the indirect pathways leads to
suppression of thalamic neurons. Altered output
or imbalance of these inhibitory pathways in the
diseased brain can account for the hyperkinesias
or hypokinesia as in Parkinson's disease34. Details
of the movement disorders were often lacking as
most of these studies were case reports or series of
patients with a given type of anatomical lesion.
The aim of this work is to study pattern of
occurrence of AIM that may occur after cerebral
stroke and their relationship to the cause of stroke,
clinical and personal data of patients as well as
sites of lesions based on imaging studies.
PATIENTS AND METHODS
Thirty four patients, suffered involuntary
movements after cerebral stroke, were included in
this study which was carried out in the ICU and
neurology outpatient clinic, in Zagazig university
hospitals from the period from July 2003 to June
2006. All patients selected were suffering first
ever clinical stroke with negative history of
previous attacks. This patients were subjected to
thorough neurological examination in the acute
stage and the medical history was obtained. The
type of AIM was evaluated by more than one of
the authors separately with final consultation
about every case. Clinical follow up included
reporting onset or disappearance of AIM and
calculation of the time from onset of cerebral
stroke to beginning of AIM, also period from
onset to disappearance of these AIM,
improvement of motor power, sensory deficit, and
cerebellar manifestations. Patients that did not
comply with follow up, and those died before
follow up period, were excluded. Also patients
with history of previous AIM before onset of
stroke were excluded as well. Some of the patients
were followed up from the beginning especially
those who showed evidence of beginning
abnormal movements in early post-stroke period
or whom suffered lesions in areas suspected to
develop AIM (thalamus, basal ganglia,
mesencephalon). Other group of patients affected
later and they were studied retrospectively and
then followed up as well. These patients were
followed up every two weeks in the first month,
and every month afterward. The patients were
followed up for at least a year after onset of AIM.
Definitions of AIM used by the authors were the
followings: Dystonia, sustained contractions of
both agonist and antagonist muscles frequently
causing twisting and repetitive movements or
abnormal postures35; Myoclonus, brief sudden
shock like jerks that may be caused not only by
active muscle contractions (positive myoclonus)
but also by lapses of muscle contraction (negative
myoclonus)36; Chorea, involuntary continuous
abrupt rapid brief unsustained irregular
movements that flow randomly from one body
part to another. Patients frequently incorporate
movements into semipurposeful activities36;
Tremor, rhythmic oscillatory involuntary
movements of a body part37; and Parkinsonism,

Osama Elazouni etl al.
423
the presence of bradykinesia and at least one of
the following: muscle rigidity, rest tremor, or
postural instability38. Ballismus (or hemiballismus
if unilateral) is a condition in which large scale,
violent, flail-like or ballistic movements occur39.
Dystonia, chorea and tremor, were defined focal if
affect single part of the body; segmental in case
two or more adjacent parts affected; multifocal,
more than one part of the body; and unilateral in
ipsilateral affection of arm and leg, as well as
generalized form. Sense of position and
movement were graded based on Nathan et al.40
and Davidoff41 findings into minimal (loss of the
sense of position in small finger or toes),
moderate (loss of sense of position and movement
in small finger or toes), severe (loss of sense of
position or movement in thumb or big toe). Motor
strength was assessed and followed up and graded
as I to V using the Medical Research Council
scale (MRC)42. Ataxia if present was graded as
mild (slight dysmetria on approaching the target,
or ataxia observed on reinforcement, resistance
applied by examiner on the volar surface of the
patient's forearm on doing finger to nose test),
Severe (severe oscillation of the arm from start of
movement with decomposition of movement and
severe overshooting, sometimes complete inability
to execute the act on finger to nose test).
Moderate is the grade between mild and severe43.
In follow up severity of AIM was assessed using
abnormal involuntary movement scale (AIMS)44,
this scale allows rating facial and oral movements,
extremity movements, trunk movements, and
global judgements of the severity of AIM, as well
as dental status. This scale allows global
judgements of the severity of abnormal
movements, incapacitation and also patient's
awareness of the abnormal movements. Score 1:
for none, 2: for minimal or extreme normal, and 3,
4, 5 for mild, moderate, and severe respectively.
Imaging studies:
All the patients were subjected to CT brain
in the acute stage of stroke, but patients who
showed AIM and their previous CT scans were
negative (CT brain scanning within first 72
hours), these patients were re-subjected to CT or
MRI brain imaging studies.
Finally, results were collected and data base
processing was done using statistical package of
social sciences (SPSS) version 0.845. Chi-Squared
Test was used for qualitative variables and
ANOVA test to compare group means of
quantitative variables and the results were
considered significant if P-value <0.05, while P-
value >0.05 indicates non significant and P‹0.001
highly significant values.
RESULTS
Thirty four patients suffered AIM after
cerebral strokes were included in this study. The
relationships were done between AIM to personal
data of patients (age and gender), clinical
findings, pattern of cerebral stroke, time interval
between onset of stroke and appearance and
disappearance of AIM, and analysis of these
abnormal movements, as well as description of
AIM reported in extra three cases of rare central
thalamic infarction we came across while doing
this study. The results of this study were as
follow:
Relationship between AIM and clinical
parameters of the patients in the form of muscle
strength, manifestation of proprioceptive
sensation, and ataxia were studies (Tables 2, 3 and
4).
Cases of chorea, tremor, and dystonia, as
well as parkinsonism were analysed separately in
relation to anatomical lesions evidenced by
imaging studies and the results were as shown in
tables (5), (6), (7) and (8). Although lesion of the
thalamus or basal ganglia are common among
these patients, good percentage of patients were
found suffering lesions in other areas of the brain
(Tables 5, 6, 7 and 8).
Central thalamic lesion: Three patients of
age 43, 57, and 65 year old were included in the
study and had unilateral central thalamic infarcts
(one right lesion and two on the left side). One of
these patients was known hypertensive with
medical treatment Bisoprolol fumarate 5mg once

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
424
daily, but his blood pressure on admission was
210/120. The other two cases showed high blood
pressure on admission (210/120 & 180/110) but
their relatives denied any history. Blood sugar
estimation was abnormal in random samples for
all patients. Lipid profiles for all the three patients
was abnormal (abnormally high LDL, low HD).
All these patients were admitted with low
conscious level, contralateral hemiparesis, and
hypoesthesia. On follow up these patients
regained full consciousness within few days but
cognition was impaired. Within 2 weeks, motor
power improved to grade 4 but two patients had
developed contralateral chorea and hemiataxia.
Table 1. AIM versus demographic data, and type of stroke, as well as time interval between onset of stroke
and AIM appearance and improvement.
Chorea Tremor Dystonia Parkinsonism
Number and percent of patients
Mean age of patients
Gender of patients Male
Female
Patients of ischemic stroke
Patients of hemorrhagic stroke
Hemorrhagic infarct or combined
Mean time to develop AIM (days)
Improvement of AIM Partial
(No and % of patients) Total
None
13 (38.2%)
67.69±5.99*
5 (38.46%)
8 (61.54%)
4 (30.8%)
8 (61.5%)
1 (7.7%)
7.61±4.44*
9 (69.23%)
1 (7.69%)
3 (23.08%)
9 (26.4%)
53.77±6.01
7 (77.78%)
2 (22.22%)
3 (33.3%)
5 (55.6%)
1(11.1%)
23.22±9.43
6 (66.66%)
2 (22.22%)
1 (11.12%)
8 (23.5%)
46.5±10.9
6 (75.00%)
2 (25.00%)
3 (37.5%)
5 (62.5%)
0
29.25±13.44
6 (75.00%)
2 (25.00%)
None
4 (11.7%)
56.75±4.03
1 (25.00%)
3 (75.00%)
4 (100%)
None
0
125.00±73.82
None
None
4 (100.00%)†
* statistically significant difference (P<0.05), ANOVA.
† statistically significant difference (P<0.05), Chi-Squared Test.
Table 2. Relationship between AIM and muscle strength (MRC scale).
Muscle strength Grade 0 Grade 1 Grade 2 Grade 3 Grade 4 Grade 5
No. & % of patients
Chorea:
Tremor:
Dystonia:
Parkinsonism:
0
0
0
0
0
0
0
0
1 (7.7%)
0
0
0
0
2 (22.2%)
0
0
9 (69.2%)
7 (77.8%)
8 (100.00%)
2 (50.00%)
3 (23.1%)
0
0
2 (50.00%)
Chi-Squared Test, x2 = 14.72, P = 0.09 (non significant).
Table 3. Relationship between AIM and severity of sensory affection.
Sensory Affection Normal Mild Moderate Severe
No. & % of patients
Chorea:
Tremor:
Dystonia:
Parkinsonism:
0
0
0
1 (25%)
1 (7.7%)
0
1(12.5%)
1 (25%)
7 (53.8%)
3 (33.33%)
3 (37.5%)
2 (50%)
5 (38.5%)
6 (66.7%)
4 (50%)
0
Chi-Squared Test, x2 = 13.21, P = 0.15 (non significant).
Osama Elazouni etl al.
425
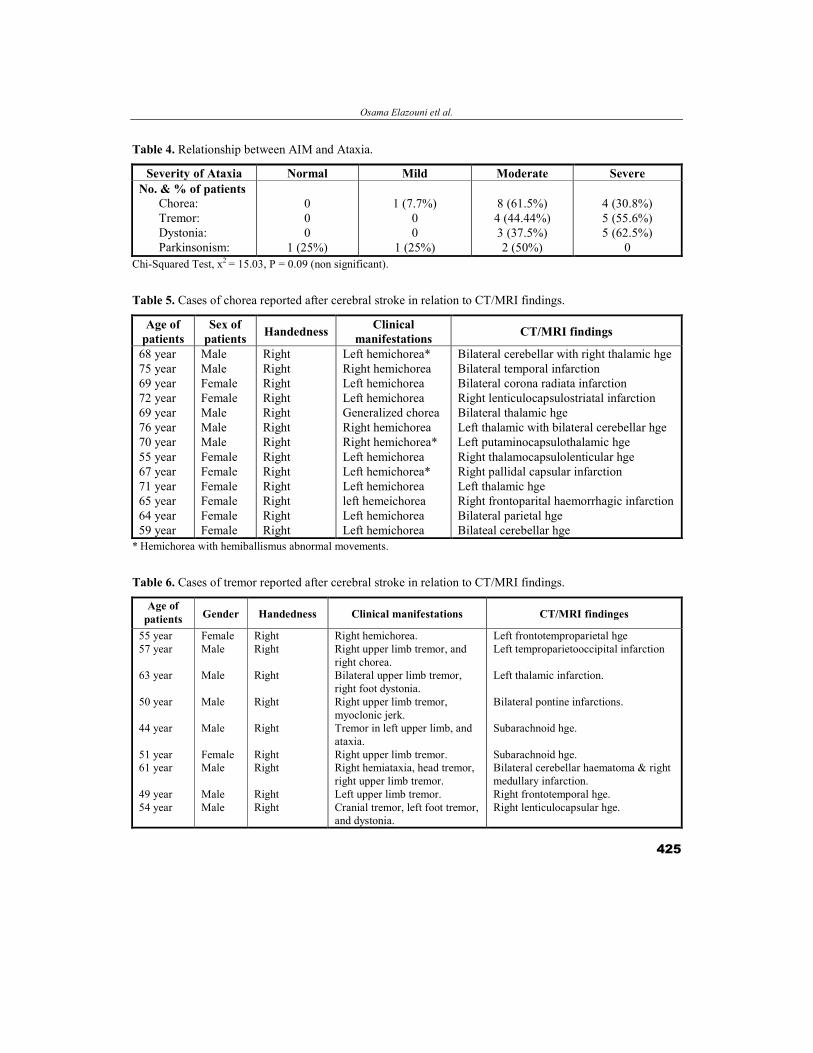
Table 4. Relationship between AIM and Ataxia.
Severity of Ataxia Normal Mild Moderate Severe
No. & % of patients
Chorea:
Tremor:
Dystonia:
Parkinsonism:
0
0
0
1 (25%)
1 (7.7%)
0
0
1 (25%)
8 (61.5%)
4 (44.44%)
3 (37.5%)
2 (50%)
4 (30.8%)
5 (55.6%)
5 (62.5%)
0
Chi-Squared Test, x2 = 15.03, P = 0.09 (non significant).
Table 5. Cases of chorea reported after cerebral stroke in relation to CT/MRI findings.
Age of
patients
Sex of
patients Handedness
Clinical
manifestations CT/MRI findings
68 year
75 year
69 year
72 year
69 year
76 year
70 year
55 year
67 year
71 year
65 year
64 year
59 year
Male
Male
Female
Female
Male
Male
Male
Female
Female
Female
Female
Female
Female
Right
Right
Right
Right
Right
Right
Right
Right
Right
Right
Right
Right
Right
Left hemichorea*
Right hemichorea
Left hemichorea
Left hemichorea
Generalized chorea
Right hemichorea
Right hemichorea*
Left hemichorea
Left hemichorea*
Left hemichorea
left hemeichorea
Left hemichorea
Left hemichorea
Bilateral cerebellar with right thalamic hge
Bilateral temporal infarction
Bilateral corona radiata infarction
Right lenticulocapsulostriatal infarction
Bilateral thalamic hge
Left thalamic with bilateral cerebellar hge
Left putaminocapsulothalamic hge
Right thalamocapsulolenticular hge
Right pallidal capsular infarction
Left thalamic hge
Right frontoparital haemorrhagic infarction
Bilateral parietal hge
Bilateal cerebellar hge
* Hemichorea with hemiballismus abnormal movements.
Table 6. Cases of tremor reported after cerebral stroke in relation to CT/MRI findings.
Age of
patients Gender Handedness Clinical manifestations CT/MRI findinges
55 year
57 year
63 year
50 year
44 year
51 year
61 year
49 year
54 year
Female
Male
Male
Male
Male
Female
Male
Male
Male
Right
Right
Right
Right
Right
Right
Right
Right
Right
Right hemichorea.
Right upper limb tremor, and
right chorea.
Bilateral upper limb tremor,
right foot dystonia.
Right upper limb tremor,
myoclonic jerk.
Tremor in left upper limb, and
ataxia.
Right upper limb tremor.
Right hemiataxia, head tremor,
right upper limb tremor.
Left upper limb tremor.
Cranial tremor, left foot tremor,
and dystonia.
Left frontotemproparietal hge
Left temproparietooccipital infarction
Left thalamic infarction.
Bilateral pontine infarctions.
Subarachnoid hge.
Subarachnoid hge.
Bilateral cerebellar haematoma & right
medullary infarction.
Right frontotemporal hge.
Right lenticulocapsular hge.

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
426
Table 7. Cases of dystonia reported after cerebral stroke in relation to CT/MRI findings.
Age of
patients Gender Handedness
Clinical
Manifestations CT/MRI findings
43 year
35 year
43 year
41 year
50 year
71 year
48 year
41 year
Male
Male
Female
Male
Male
Male
Male
Female
Right
Right
Right
Right
Right
Right
Right
Right
Generalized dystonia.
Left hemidystonia.
Left upper limb dystonia.
Oromandibular, and left cervical
dystonia.
Left upper limb dystonia.
Dystonia in left foot.
Right hemidystonia.
Left foot dystonia, and left hemitremor.
Bilateral cerebellar ischaemia.
Bilateral pontine infarctions.
Right temporal infarction.
Right frontoparietal hge.
Right temporal hge.
Right thalamic hge.
Left lenticulocapsulothalamic hge.
Right lenticulocapsular hge.
Table 8. Cases of parkinsonism reported after ischemic cerebral stroke in relation to CT/MRI findings.
Age of
patients Gender Handedness Clinical manifestations CT/MRI findings
57 years
60 years
59 years
51 years
Male
Female
Female
Female
Right
Right
Right
Right
Right hemiparkinsonism*
Right hemiparkinsonism**
Right hemiparkinsonism***
Left hemiparkinsonism****
Left frontoparital infarction
Left lenticulocapsular infarction
Left mesencephalic ischemic lesion
Right striatocapsular infarction * Right hemiparkinsonism more prominent in upper limb (rigidity, bradykinesia, and postural tremor). ** Right hemiparkinsonism more prominent on the lower limb in the form of rigidity, and bradykinesia. *** Right hemiparkinsonism in the form of rigidity, bradykinesia, and rest tremor. **** Left hemiparkinsonism, more prominent in the upper limb, in the form of rigidity and bradykinesia, hemidystonic
movements were reported as well.
Fig. (1): Axial brain CT showing right and left central thalamic lacunar infarctions.

Osama Elazouni etl al.
427
Fig. (2): Axial T1 and T2 weighted images reveal left anterior thalamic and capsular infarctions.
Fig. (3): Axial CT brain showing right frontoparietal haemorrhagic infarction with incomplete effacement of
the frontal horn of lateral ventricle of female patient presented with left hemichoreic movements.

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
428
DISCUSSION
Most of the AIM reported in this study were
cases of chorea followed in frequency by tremor
and dystonia, and the least reported pattern was
parkinsonism. The mean age of patients with
chorea was significantly (P<0.05) higher than
other patients, whereas, patients who suffered
dystonia were the youngest group. This finding
came to agree with a clinical evidence that brain
damage early in life most probably leads to
dystonia rather than other abnormal movement
disorders, an example is that young onset
Parkinson's disease tends to present with dystonia
rather than parkinsonism46, and this might be a
result of changes in neuronal development related
to age or brain plasticity as demonstrated in
experimental focal cortical lesions inducing
changes in the adjacent cortex and in the
contralateral hemisphere47.
The interval between onset of stroke and
development of chorea was the shortest among all
other AIM and the difference was statistically
significant (P<0.05). On the other hand, the time
interval for parkinsonism to develop was the
longest with mean time ± SD. 125.00±73.82 days
as shown in the table (1). The reason for the delay
in occurrence of AIM, remains speculative. This
delay may reflect the time required for the
unbalanced successful recovery of the motor
function and subsequent development of
pathological neuronal circuitry, or it may indicate
the time required for the possible changes in
neuronal synaptic activities13,48,49
. Another
explanation for the delay in appearance of
parkinsonism is due to deafferentation (indicated
by secondary or transsynaptic degeneration) or
certain functional changes in neuronal activities
and their connecting structures15.
Most of the patients suffering chorea, tremor,
and dystonia, have improved partially, but few of
them either showed complete resolution of these
abnormal movement or have not improved at all.
The partial or complete recovery might be a result
of a plastic reorganization or reinnervation with
partial or complete regaining of their functions15,47.
In this study, reported clinical manifestations
of patients with AIM showed that most of the
patients had reasonable muscle strength, grade 4,
on MRC scale, and moderate to severe affection
of proprioceptive sensation and ataxia as shown
in tables (2), (3) and (4). Despite these values
could not reach statistical significant level, we
may consider these values near significance or
border line and that might be due to paucity of the
cases. These findings made us hypothesize that
reasonable motor power accompanied with
manifest affection of the proprioceptive sensation
and moderate to severe ataxia are important to
develop AIM. In support to this hypothesis,
results of the previously published studies of
Chollet et al.50, and Lee and van Donkelaar51, that
showed the functional recovery of motor
dysfunction is related to a plastic reorganization
of the motor cortex or activation of the uncrossed
pyramidal pathways from the opposite
hemisphere. In the presence of persistent failure of
original proprioceptive and cerebellar inputs, the
newly organized proprioceptive-cerebellar-motor
integrative system should be unstable or even
misdirected. In addition, it has shown that
development of dystonia is related to
proprioceptive sensory dysfunction52,53,54
, and also
in Tinazzi et al.55 study they reported enhanced
cortical somatosensory evoked potentials in
patients with dystonia. Morover, in experimental
study with monkeys subjected to cerebellar injury,
Mackel56 found that compensation of cerebellar
deficits was considerably impaired if the sensory
cortex was concomitantly removed. From all these
previous data, one can suggest that decreased
proprioceptive sensory input may result in
excessive cortical activation and impair cerebellar
function in coordination of the movements and all
that could play a role in the pathogenesis of AIM.
Chorea: Most of the cases of chorea, had
underling thalamic lesion (6 patients, 46.1%),
followed in frequency by lesions in lentiform
nucleus and neighbouring structures (4 patients,
30.8%), whereas surface lesions (frontal, parietal, &
temporal), were reported in 3 patients (23.1%).
Only one patient had lesion in corona radiate and

Osama Elazouni etl al.
429
another patient suffered cerebellar lesion alone as
shown in the table (5). Based on the previous data,
one can conclude that most of cases of chorea in
this study are due to deep lesions particularly in
thalamus and lentiform nucleus with contralateral
development of chorea. In spite of this previous
finding, more than quarter of patients had lesions in
other regions so we can suggest that although most
of the cases of chorea are due to lesions in thalamus
or lentiform nucleus, lesions in other regions as
cortical areas (temporal, frontal, parietal),
cerebellum, and corona radiate, could be
incriminated in the pathogenesis of chorea. Our
finding came to agree with that of Dewey and
Jankovic9, and Lee and Marsden10, that reported the
most frequent lesion in cases of chorea is thalamic
lesion, and Chang, et al.11, that found lentiform
nucleus lesions were common cause of chorea.
Through reduction of inhibitory output of the
globus pallidus on the thalamus10, lesions in the
thalamus and lentiform nuclei presumably leads to
excess excitatory output to the cortex with
subsequent contralateral hyperkinetic movements30.
Hemiballismus: Rather than subthalamus, we
found in this study that ballismus movement was
present in patients having lesion in thalamus,
putamin, globus pallidus and neighbouring
structures as shown in table (5). This finding could
be explained based on previous studies9,10,30
, that
attributed hemiballismus movement after
subthalamus lesion to reduction of the inhibitory
output of the globus pallidus on the thalamus by
diminishing the normal excitatory drive to the
internal segment of the globus pallidus, and this
disinhibition gives rise to excessive excitatory drive
to the cortex which is expressed as a contralateral
hyperkinetic movement. From this previous data,
one can report that subthalamus, globus pallidus,
and thalamus, all of them are involved in
pathogenesis of ballismus movement.
Tremor: Tremor reported in this study were
mainly intention type and most of them in the
upper limb, 5 (55.5%) patients out of 9 had both
resting and intention pattern, and all the patients
had postural element but to varying degrees.
Cortical lesions were reported in 3 patients
(33.3%), in agreement with Kim in 1992, 1994,
and 200112,57,58
, who reported upper limb tremor,
especially of the hand in patients with cortical
lesion. Kim in 1992, and 1994 has suggested that
cortical strokes may modulate the sensorimotor
circuitry and produce movement disorders. Other
patients with tremor had thalamic, pontine,
medullary, and cerebellar lesions as well as
subarachnoid haemorrhage. This finding match
with results reported by previous studies59,60,61
,
that posterior thalamic lesion including thalamic
infarction, haemorrhage, traumatic brain injury,
infection, or neoplasm, was reported as well as
dentatorubrothalamic tract involvement to cause
intention tremor. Subarachnoid haemorrhage itself
or its complications (hydrocephalic lesion), might
induce its tremogenic effect via global
compromise of brain functions or secondary
hydrocephalic changes with dilatation of
ventricles and subsequent compression of
structures adjacent to ventricular system as basal
ganglia, thalamus, etc.
Dystonia: As far as dystonia is concerned,
our patients who suffered dystonia have lesions in
different regions of the brain rather than basal
ganglia, as cortical lesions (frontal, parietal,
temporal), thalamus, lenticulocapsular, cerebellar,
and pontine lesions as shown in the table (7). This
finding shows that brain lesions behind the later
development of dystonia in this study, were not
confined to basal ganglia as the previously
established, indisputable evidence of the link
between basal ganglia and dystonia29,62,63. Our
results showed that lentiform nucleus lesion was
reported in 2 (25%) cases of dystonia. This
contrast with either Alarcón et al.64, that found
lentiform nucleus lesions the most frequent in
dystonia and we also contrast with Russman et
al.65, that reported no case of dystonia in their
patients with lentiform nucleus lesions. This
discrepancy might be due to paucity of the cases
or that the studies done were based on different
selection criteria either of the type of movement
disorder or the anatomical sites of the lesions.
Recently, Le Ber et al.66 have suggested that
dystonia at least in their patients, arises from

Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
430
dysfunction of the cerebellum. This suggestion
based on their patients' brain MRI that revealed
prominent atrophy of the cerebellum without
obvious abnormalities of the basal ganglia. This
suggestion challenged traditional views of the
anatomy of dystonia which focus predominantly
on the basal ganglia. The link between the basal
ganglia and dystonia is supported by CT and MRI
studies that have repeatedly linked dystonia with
focal lesions of the basal ganglia29. PET and other
functional imaging techniques have also revealed
abnormal function of basal ganglia even when
focal lesions are not apparent62,63. Although Le
Ber and colleagues have acknowledged in the end
of their study that the cerebellar atrophy may be
unrelated to dystonia and that additional basal
ganglia defects may have escaped detection, some
other evidence for primary role of the cerebellum
in the genesis of dystonia have emerged. An
autopsy study established a link between cervical
dystonia and tumours of the cerebellum and in
some cases it improved or disappeared after
tumour removal67. Neuroimaging studies have
shown the most frequent abnormalities among
patients with cervical dystonia are in the
cerebellum or its afferents68. Thalamic lesions can
cause limb dystonia and the responsible lesions
occur most frequently in subnuclei linked to the
cerebellum, not the basal ganglia, and an effective
surgical target for deep brain stimulation in
dystonia also involves the thalamic regions
connected with the cerebellum3,10.
Parkinsonism: The authors have got 4
patients suffering contralateral parkinsonism after
lesions in basal ganglia and cortical lesion
(frontoparietal infarction). Parkinsonian
manifestations were not isolated in all the cases
but combined with hemidystonia and postural
tremor in two of them. Previous studies have
suggested two forms of vascular parkinsonism:
one form with acute onset associated with basal
ganglionic infarction and the other form is
insidious and progressive possibly associated with
diffuse subcortical white matter ischaemia22,69.
This approach neither explain our patient with
frontoparital infarction nor that of Kims' patients58
that had anterior cerebral artery territory
infarction lesion underlying later development of
parkinsonism. Despite, previous authors have
attributed vascular parkinsonism to the lesions of
the basal ganglia in the striatum or lentiform
nucleus whether unilateral24,25 or bilateral22,70.
Other authors have showed that vascular
parkinsonian symptoms could be due to vascular
lesions disrupting the interconnecting fibre tracts
between the basal ganglia, the thalamus, and the
motor cortex that leads to disruption not only of
sensorimotor integration22,23,24
, but also of
descending reticular pathways to the major centres
of the brain stem23. The parkinsonian symptoms
could be due to vascular lesions disrupting the
interconnecting fibre tracts between the basal
ganglia, the thalamus, and the motor cortex that
leads to disruption not only of sensorimotor
intergeration, but also of descending reticular
pathways to the major centres of the brain
stem22,23,24
. None of our patients showed evidence
of improvement even those with lesion in basal
ganglia in contrast to Tolosa and Santamarǐa
study71.
Central thalamic lesion: Central thalamic
infarction is rare among other infarcts of the
thalamus31,72. Low conscious level could be due to
affection of adjacent structures as dorsomedian
nucleus (DM), and intralaminar nuclei (IL) that
may together play an important role in
maintaining wakefulness73. Sensory deficit is
related to affection of ventroposterolateral (VPL)
nucleus31,72 but this nucleus is mainly affected in
the posterior lateral thalamic lesion74 but that
could be due to affection of the adjacent part of
this nucleus. Ventrolateral (VL) nucleus affection
in these cases was the underlying cause of
hemiataxia reported75. From all these previous
data, one can report that central thalamic lesion is
associated with combination of neuropsychiatric
manifestations due to affection of adjacent nuclei
in anteromedian and posterolateral areas of the
thalamus. Study of a large number of these
patients would help to clarify neuropsychiatric
manifestations linked to this lesion more
accurately.

Osama Elazouni etl al.
431
In summary, the authors reported that
correlation between site of lesion and type of AIM
could be difficult to establish. Although lesions
that involved the thalamus and basal ganglia most
commonly cause movement disorders on the
contralateral side, involvement of basal ganglia or
thalamic lesion was not the case in all the patients
of AIM, as lesions in some other regions of the
brain were found linked to AIM. Accepted models
of basal ganglia circuitry do not fit well with
clinical observations. Most of the patients with
AIM had suffered a manifest proprioceptive
sensory impairment, and ataxia in contrast to
motor strength which was affected to a lesser
degree. Therefore, authors conclude that although
thalamic and neighbouring basal ganglion lesions
are the common lesions underlying later
development of contralateral AIM after cerebral
stroke, these AIM could occur in a good
percentage after lesions in other areas of the brain
and that could be due to concurrent ataxia and
proprioceptive sensory impairment beside
reasonable motor strength, or the CT or MRI
might be neither show the full extent of pathology
nor the functional effects of such lesions,
furthermore concurrent or previous ischemic
lesions might be not detected by current imaging
techniques. Finally, pathogenesis of AIM needs
more speculation and more scrutinized analysis of
imaging studies with paying more attention to
functional brain imaging studies.
REEFRENCES
1. Cho C, Samkoff LM. A lesion of the anterior
thalamus producing dystonic tremor of the hand.
Arch Neurol. 2000;57:1353-1355.
2. Münchau A, Mathen D, Cox T, et al. Unilateral
lesions of the globus pallidus: report of four
patients presenting with focal or segmental
dystonia. J Neurol Neurosurg Psychiatry
2000;69:494-498.
3. Lehéricy S, Grand S, Pollak P, et al. Clinical
characteristics and topography of lesions in
movement disorders due to thalamic lesions.
Neurology 2001;57:1055-1066.
4. Kim JS. Delayed onset mixed involuntary movements after thalamic stroke: Clinical, radiological and pathophysiological findings. Brain 2001; Vol.124, No.2:299-309.
5. Carrera E, Michel P, Bogousslavsky J. Anteromedian, central, and posterolateral infarcts of the thalamus: Three variant types. Stroke 2004;35:2826.
6. Cerrato P, Grasso M, Azzaro C, et al. Palatal myoclonus in a patient with a lateral thalamic infarction. Neurology 2005;64:March (1 of 2):924-925.
7. Jones HR, Baker RA, Kott S. Hypertensive putaminal haemorrhage presenting with hemichorea. Stroke 1985;16:130-1.
8. Tabaton M, Mancardi G, Loeb C. Generalized chorea due to bilateral small deep cerebral infarcts. Neurology 1985;35:588-9.
9. Dewey RB, Jankovic J. Hemiballism-hemichorea: clinical and pharmacological findings in 21 patients. Arch Neurol 1989;46:862-7.
10. Lee MS, Marsden CD. Movement disorders following lesions of the thalamus or subthalamuic region. Mov Disord 1995;9:493-507.
11. Chang MH, Chiang HT, Lai PH, et al. Putaminal petechial haemorrhage as the cause of chorea: a neuroimaging study. J Neurol Neurosurg Psychiatry 1997; 63: 300-303.
12. Kim JS. Delayed onset hand tremor caused by cerebral infarction. Stroke 1992;23:292-4.
13. Ghika J, Bogousslavsky J, Henderson J, et al. The 'jerky dystonic unsteady hand': a delayed motor syndrome in posterior thalamic infarctions. J Neurol 1994;241:537-42.
14. Otto S, Buttner T, Schols L, et al. Head tremor due to bilateral thalamic and midbrain infarction. J Neurol 1995;242:608-11.
15. Miwa H, Hatori K, Kondo T, et al. Thalamic tremor: case reports and implications of the tremor: generating mechanism. Neurology 1996; 46: 75-9.
16. Obeso JA, Gimenez-Roldán S. Clinico-pathological correlation in symptomatic dystonia. Adv Neurol 1988; 50:113-22.
17. Moiho ES, Factor SA. Basal ganglia infarction as a possible cause of cervical dystonia. Mov Disord 1993; 8: 213-16.
18. Jacob PC, Pratap CR. Blepharospasm and jaw closing dystonia after parietal infarcts. Mov Disord 1995;10:794-802.
19. Schwartz MC, De Deyn PP, Van den Kerchove M, et al. Cervical dystonia as a probable consequence of focal cerebral lesion. Mov Disord 1995;10:797-8.
Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
432
20. Muñoz JE, Tolosa E, Saiz A, et al. Upper limb dystonia secondary to a mid-brain hemorrhage. Mov Disord 1996;11:96-9.
21. Chang CM, Yu YL, Ng HK, et al. Vascular pseudoparkinsonism. Acta Neurol Scand 1992;86:588-92.
22. Winikates J, Jankovic J. Clinical correlates of vascular parkinsonism. Arch Neurol 1999; 56:98-102.
23. Kulisevsky J, Avila A, Berthier ML. Bipolar affective disorder and unilateral Parkinsonism after a brainstem infarction. Mov Disord 1995;10:802
24. Kulisevsky J, Berthier ML, Avila A, et al. Unilateral Parkinsonism and stereotyped movements following a right lenticular infarction. Mov Disord 1996;11:752-4.
25. Fénélon G, Houéto JL. Unilateral Parkinsonism following a large infarct in the territory of the lenticulostriate arteries. Mov Disord 1997;12:1086-90.
26. Gatto EM, Zurrú MC, Rugilo C, et al. Focal myoclonus associated with posterior thalamic hematoma. Mov Disord 1998;13:182-4.
27. Srinivas K, Rao VM, Subbulaskshmi N, et al. Hemiballism after striatal haemorrhage. Neurology 1987;37:1428-9.
28. Kurlan R, Shoulson I. Differential diagnosis of facial chorea. In: Jankovich J, Tolosa e, eds. Advances in Neurology, Facial Dyskinesias. New York: Raven Press, 1988;49.
29. Marsden CD, Obeso JA, Zarranz JJ, et al. The anatomical basis of symptomatic hemidystonia. Brain 1985;108:463-483.
30. Bhatia KP, Marsden CD. The behavioural and motor consequences of focal lesions of the basal ganglia in man. Brain 1994;117:859-879.
31. Bogousslavski J, Regli F, Uske A. Thalamic infarcts: clinical syndrome, etiology, and prognosis. Neurology 1988;38:837-848.
32. Pettigrew LC, Jankovic J. Hemidystonia: a report of 22 patients and a review of the literature. J Neurol Neurosurg Psychiatry 1985;48:650-657.
33. Lehéricy S, Vidailhet M, Dormont D, et al. Striatal and thalamic dystonia: an MR anatomo-clinical study. Arch Neurol 1996;53:241-250.
34. Parent A, Hazrati LM. Functional anatomy of the basal ganglia. I. The cortico-basal ganglia-thalamo-cortical loop. Brain Res Revs 1995; 20: 91-127.
35. Jankovic J, Fahn S: Dystonic disorders. In Jankovic J, Tolosa E (eds): Parkinson's Disease and Movement Disorders, 3rd ed. Baltimore, Williams & Wilkins, 1998.
36. Marsden CD, Fahn S (eds). Movement disorders 3. London, Butterworths, 1993.
37. Findley LJ. Tremors: differential diagnosis and pharmacology. In: Jankovic J, Tolosa E, eds. Parkinson's disease and movement disorders. Baltimore, Munich: Urban and Schwartzenberg, 1988.
38. Hughes AJ, Daniel SE, Kilford L, et al. Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico-pathological study. J Neurol Neurosurg Psychiatry 1992;55:181-4.
39. Parent A, Hazrati LN. Functional anatomy of the basal ganglia II. The place of subthalamic nucleus and external pallidum in basal ganglia circuitry. Brain Res Rev 1995;20:128-154.
40. Nathan PW, Smith MC, Cook AW. Sensory effects in man of lesions of the posterior columns and of some other afferent pathways. Brain 1986;109:1003.
41. Davidoff RA. The dorsal columns. Neurology 1989;39:1377.
42. Medical Research Council memorandum No. 45 (superseding war memorandum No. 7). Aids to the examination of the peripheral nervous system. London, Her Majesty's Stationery Office, 1976, quoted from; Haerer AF. DeJong's The Neurologic Examination (5th edition); J.B. Lippincott Company 1992: (333-374).
43. Haerer AF. DeJong's The Neurologic Examination (5th edition); J.B.Lippincott Company 1992: (393-401).
44. Psychopharmacology Research Branch, NIMH. Abnormal involuntary movement scale (AIMS). In: Guy W, ed ECDEU Assessment Manual for Psychopharmacology, revised DHEW Pub No (ADM) 76-338, Rockville, MD: National Institute of Mental Health, 1976, 534-37, quoted from; Burns A, Lawlor B, Craig S. Assessment Scales in old age Psychiatry. Martin Dunitz 1999; pp. 221-223.
45. Dean AG, Dean G, Colmbeir D. EP1-INFO, Data Processing, Statistics and Epidemiology, Soft Ware Computer, package on microcomputer CDC, Atlanta, USA, 2000.
46. Quinn NP. Parkinsonism and dystonia, pseudo-Parkinsonism and pseudodystonia. Adv Neurol 1993;60:540-3.
47. Johansson BB. Brain plasticity and stroke rehabilitation: The Willis lecture. Stroke 2000;31:223-30.
48. Louis ED, Lynch T, Ford B, et al. Delayed onset cerebellar syndrome. Arch Neurol 1996; 53: 450-4.
Osama Elazouni etl al.
433
49. Scott BL, Jankovic J. Delayed onset progressive
movement disorders after static brain lesions.
Neurology 1996;46:68-74.
50. Chollet F, DiPiero V, Wise RJ, et al. The
functional anatomy of motor recovery after stroke
in humans: a study with positron emission
tomography. Ann Neurol 1991;29:63-71.
51. Lee RG, van Donkelaar P. Mechanisms
underlying functional recovery following stroke.
Can J Neurol Sci 1995;22:257-63.
52. Ghika J, Regli F, Growdon JH. Sensory
symptoms in cranial dystonia: a potential role in
the etiology? J Neurol Sci 1993;116:142-7.
53. Hallett M. Is dystonia a sensory disorder?. Ann
Neurol 1995;38:139-40.
54. Byl NN, Merzenich MM, Jenkins WM. A
primate genesis model of focal dystonia and
repetitive strain injury: I. Learning-induced
dedifferentiation of the representation of the hand
in the primary somatosensory cortex in adult
monkeys. Neurology 1996;47:508-20.
55. Tinazzi M, Frasson E, Polo A, et al. Evidence for
an abnormal cortical sensory processing in
dystonia: selective enhancement of lower limb
P37-N50 somatosensory evoked potential. Mov
Disord 1999;14:473-80.
56. Mackel R. The role of the monkey sensory cortex
in the recovery from cerebellar injury. Exp Brain
Res 1987;66:638-52.
57. Kim JS. Writing tremor after discrete cortical
infarction. Stroke 1994;25:2280-2.
58. Kim JS. Involuntary movements after anterior
cerebral artery territory infarction. Stroke
2001;32:258-61.
59. Ferbert A, Gerwig M. Tremor due to stroke. Mov
Disord. 1993;8:179-182.
60. Miwa H, Hatori K, Kondo T, et al. Thalamic
tremor: case reports and implications of the
tremor-generating mechanism. Neurology
1996;46:75-79.
61. Deuschl G, Krack P. Tremors: differential
diagnosis, neurophysiology, and pharmacology.
In: Jankovic J, Tolusa E, eds. Parkinson's Disease
and Movement Disorders. 3rd ed. Philadelphia,
Pa: Williams & Wilkins; 1998:419-452.
62. Eidelberg D, Moeller JR, Antonini A, et al.
Functional brain networks in DYT1 dystonia.
Ann Neurol 1998; 44:303-312.
63. Muenier S, Lehericy S, Garnero L, et al.
Dystonia: lessons from brain mapping.
Neuroscientist 2003;9:76-81.
64. (64) Alarcón F, Zijlmans JCM, Dueñas G, et al.
Post-stroke movement disorderes: report of 56
patients. J Neurol Neurosurg and Psychiatry
2004;75:1568-1574.
65. Russman H, Vingerhoets F, Ghika J, et al. Acute
infarction limited to the lenticular nucleus:
clinical, etiologic, and topographic features. Arch
Neurol 2003;60:351-5.
66. Le Ber I, Clot F, Vercueil L, et al. Predominant
dystonia with marked cerebellar atrophy: a rare
phenotype in familial dystonia. Neurology
2006;67:1769-1773.
67. Krauss JK, Seeger W, Jankovic J. Cervical
dystonia associated with tumours of the posterior
fossa. Mov Disord 1997;12:443-447.
68. LeDoux MS, Brady KA. Secondary cervical
dystonia associated with structural lesions of the
central nervous system. Mov Disord 2002;18:60-
69.
69. Zijlmans JC, Thijssen HO, Vogels OJ, et al. MRI
in patients with suspected vascular parkinsonism.
Neurology 1995;45:2183-8.
70. Murrow RW, Schweiger GD, Kepes JJ, et al.
Parkinsonism due to a basal ganglia lacunar state:
clinicopathological correlation. Neurology
1990;40:897-900.
71. Tolosa E, Santamaría J. Parkinsonism and basal
ganglia infarcts. Neurology 1984;34:1516-18.
72. Steinke W, Sacco RL, Mohr JP, et al. Thalamic
stroke. Arch Neurol. 1992;49:703-710.
73. Bassetti C, Mathis J, Gugger M, et al.
Hypersomnia following paramedian thalamic
stroke: a report of 12 patients. Ann Neurol.
1996;39:471-480.
74. Paciaroni M, Bogousslavsky J. Pure sensory
syndromes in thalamic stroke. Eur Neurol.
1998;39:211-217.
75. Boiten J, Lodder J. Ataxic hemiparesis following
thalamic infarction. Stroke. 1990;21:339-340.
Egypt J. Neurol. Psychiat. Neurosurg. Vol. 44 (2) – July 2007
434
ــ+ ا#*()ـــ&%ا#"!
� ا����������� � درا�� ��وث ا���آ�ت ا��إراد�� ا������ �� ا���
: �$��� #" ا�!�
������� ������ � � ��� �������� ������� � � ������ �������� ����� ���� ����� �� ���� ��� ��
�������� ����� ���� �� ����� � ! �� �� � "�# ���� �$ ���� %�& #�� ������ � ! '( � ���� ��)�����
*��# +�� �$ ���� %�& �� ,���� �#� � ��%#� -& ����� �$ ��.�#�� .
: '�ف �" ا�!� ا�
���)����� ������� ������ � � 0���� -& ������ �������� ����� ���� �! ����� � ! 1�.� �� 2�3�� ��
��� ��)����� ������ "�#� �������� ����� � ! ���� ���$� ,���� ������ ���� ��� ��� ����� � ! ��$�# ��� ��
4����� �%5. �� 2�6# �������� �7� 0��5� -�89�� ,������ 0��5� ����#�5��� ������� ����� � ! ���$ ����
��$� 9�� ������ 05$ ���� � ,���� ������ ����� :#.��� ����.
:(�ق ا�!�
��$ ����� � ! ����43 �)����� ������� ������ � � ������ �������� ����� ���� �� ��#� � ���� '� ��� �
0���� 1+;!� 0��5� ��$� 9� � ����#�5�� �<+� 05$ 1�#� =� � 0��>� *�5� ������ :��� 05$ 0���� 1+;! ���8�
#� '3� ���� '� ��� ���� �������� ����� '3�& 3( �� �� �� '! 1+;!� 0��>� *�?�� -& ������ 0�� '3�� '� �� ���
� 1+;! �� ������� ,���� ��)����� ������ ���� ,��� ����� � '3��& '� ��� =�� � � �������� ����� '3�& 3( �� �
'�� ���� 0����� �� ��8@� �7� '3� ����� -�%�� ,����� �� =�� �)� ��)����� ������ "�#� ����� � ! ����
! ��� �����+ ���� ������ �� �� �� 0���� �� ���� �� �� �� �5����� � ������ *��� ������� �� �8� '� �� ��� ������ �
-��� 0���� 1+;! "��8� '� ��� *���� � ! ��� ��&�� �� :
• �!��� �#$ '3��&�� �� �� 0���� �� -�%�� ,����� 05$ ������ �#���� -�� �� 6�3.5� ���9 0��#�5�� B�&
0��5� -$��� C����. � ����� '� ��� � �! -�& ��7����� �� ��#7� D�% �$ �������� ����� � ! "�# B�89�
������ :����� '��8����� ������ � ! � ����� -<�3#�� B�89�5� E�85� *�9��+� '7 ��� 05$ F� ������
��� ������� ������ *���� ��� �� 0��5� ����#�5��� ������ � ���� ����� ������ �������� E���8+� ����� ���
��3( � � ��>� 05$ '�$ *��� 39 �� *�& =� � � '7 ��>� 39�� -& ��$���� �� � ������ � ! �� ��� -�� ��
����� � ! .
• ��$� 9� ����),��� 05$ -��%�#H� ��# �� �� %�� � 9� ( ��$� ��� ��)����� ������� ������ � � 0��>� *�?�� -&
� � 0���� � �� ������ � ! ��$= ������ J��� '� �.
��6���� ,��� ��3� ��%#� �%5. �� *��# +�� ��7 05$ ������ 5��9� ���� , # '3��5$ ��.� ���� :�?
������� ������.
Osama Elazouni etl al.
435
�+* ا�!� , :
���+L M<��#�� ����� 3(� :
• 0���� �� N��# ���38.2 % �5�9�� ��� 0#� � #�� 0���� �� ���# ���� ������ �������� ������ ������
P�$��11.7%
• � �$��.��� -���� ���#��� 05$>� �! ������ �������� ����� 0�� ��$� %���� ��<���� ��+� � D�?�.
• � D��?� ��� -!� ������ �������� ����� ����� ���8�� =5� -! ������5�� ����� ����� *�� %���� ���
�$�.��� ���� �$ ��<���� ��+�
• P�$�� �59�� 0�� �� ��� 1�?9 '�� '� ��<���� ��+� � D�?�
• ���� ������ �������� 0���� '( � �.� 05$ ��#�� ������ ����4 ��.� �#��� ������ *���� :���� 05$
*���9 � �%���� -�� �� E��8+�� ������ '!7Q�
• ������� ��� ����# �.� �� ���$���� *��#�� �� 08��� ��3��� ��%#� -& 0��5� ��)����� ������ R��. ��� '�
�>� ��9��� ������ �7� D%�#��� � ! E�8���� ,����.�� ,��)���� ,������# �� �� 2�6# ����� ��?58�� , �����
,�8��� ,=�� �) � ,��� "6. �����
• E���8+� ������ ������ �������� ������ ������ �� 08��� ��3�5� ��6���� ��%#���� �%5.� �������� 0����
-�� ��.
: �/.- ا�!�
� ���� ��� ���$ ��.�� �� S � ����>� � � -& ���� �� ���� ������ �������� ����� "�#� ,��� -& �����
�� +� �������� ���5� R<�9�� S���� -! ���$���� *��#�� �� 08��� ��3��� ��%#�� ������ �� �� ')�� 05$� T��� �)�
�� ,��� �� C8� ����� -& ������ �� ��#�� 0���� 1+;! �� ���# ���� ������ -��$ E��8� ����� =�� ��?� ���
����� � ! ���� 1�� S���� ���� �� ���� � !� -���� 6�3.�� -& �%��� ����� R� *���9 �� �%���� �.�� ����$
������� ����+� E�8 ,��� ����� -& .�8��� � 0�� E���� �������� ����� ���� ��?�� ���� �� ����� ���� 0�� �7��
���$+� �� � (#�� R� ��$� 9�� ����5� D����� ��5���� � ���� �� ������0�� ��?�(��� ��$� 9�� ������.
Related Documents











