Stress ECG:- Role in Arrhythmia Diagnosis DR SHOMU BOHORA ASSOCIATE PROFESSOR UN MEHTA INSTITUTE OF CARDIOLOGY AND RESEARCH CENTRE AHMEDABAD CONSULTANT ELECTROPHYSIOLOGIST VADODARA INDIA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Stress ECG:- Role in Arrhythmia Diagnosis
D R S H O M U B O H O R A
A S S O C I A T E P R O F E S S O R
U N M E H T A I N S T I T U T E O F C A R D I O L O G Y A N D
R E S E A R C H C E N T R E
A H M E D A B A D
C O N S U L T A N T E L E C T R O P H Y S I O L O G I S T
V A D O D A R A
I N D I A
Introduction
Stress test TMT DSE Isoprenaline
Indications Dyspnea on exertion Fatigue on exertion Palpitations on exertion Syncope on exertion Chest pain on exertion Ectopics for prognostication Asymptomatic patients
Ectopics Sick sinus CHB congenital WPW
Which arrhythmias can come during TMT Bradycardia
Bundle branch block AV block Sinus dysfunction
Ectopics Atrial and Ventricular
Tachycardia Atrial fibrillation NSVT/VT/Torsades/V Fib Atrial tachycardia
Other ECG findings Long QT Ischemia
Precautions while interpreting arrhythmia
Linked median (Computer average) vs Raw rhythm
VPC’s may mimic VT on linked median and VPC’s may not be seen on linked median.
Raw rhythm ideal, but may have artifacts
Placement of leads is different
Hence we cannot comment on morphology of arrhythmia accurately.
Defibrillator to be present in the place
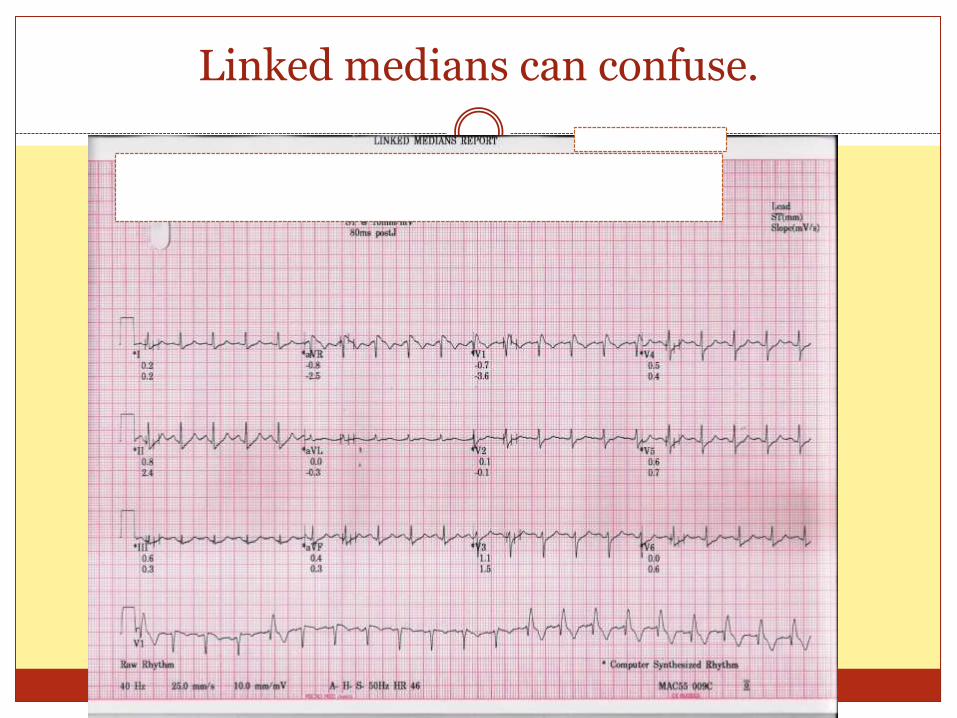
Linked medians can confuse.
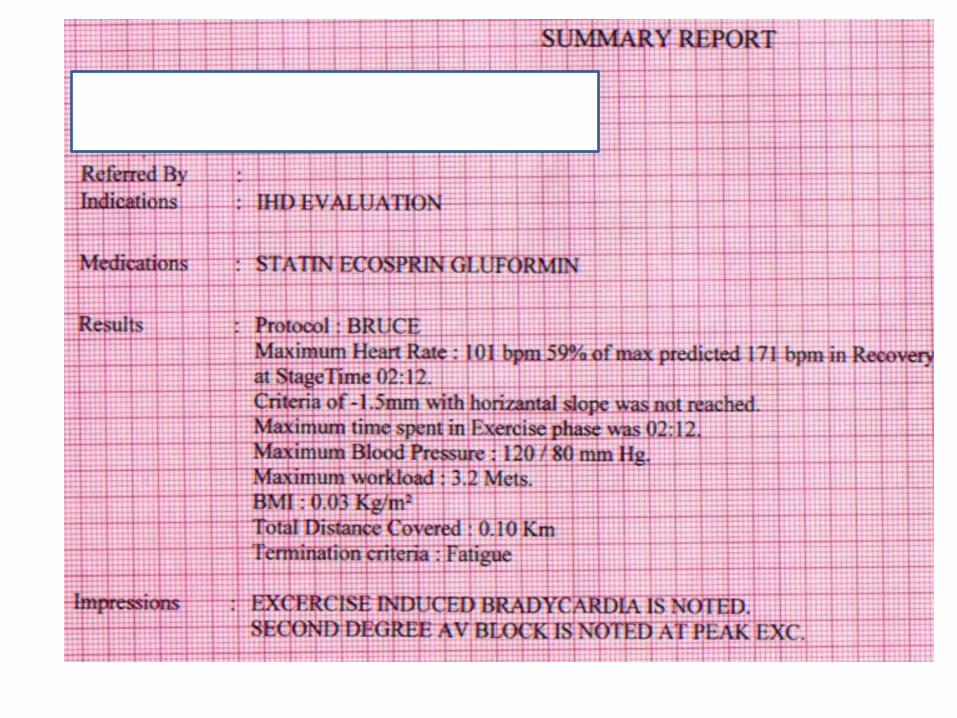
Stress test with outcome being bradycardia
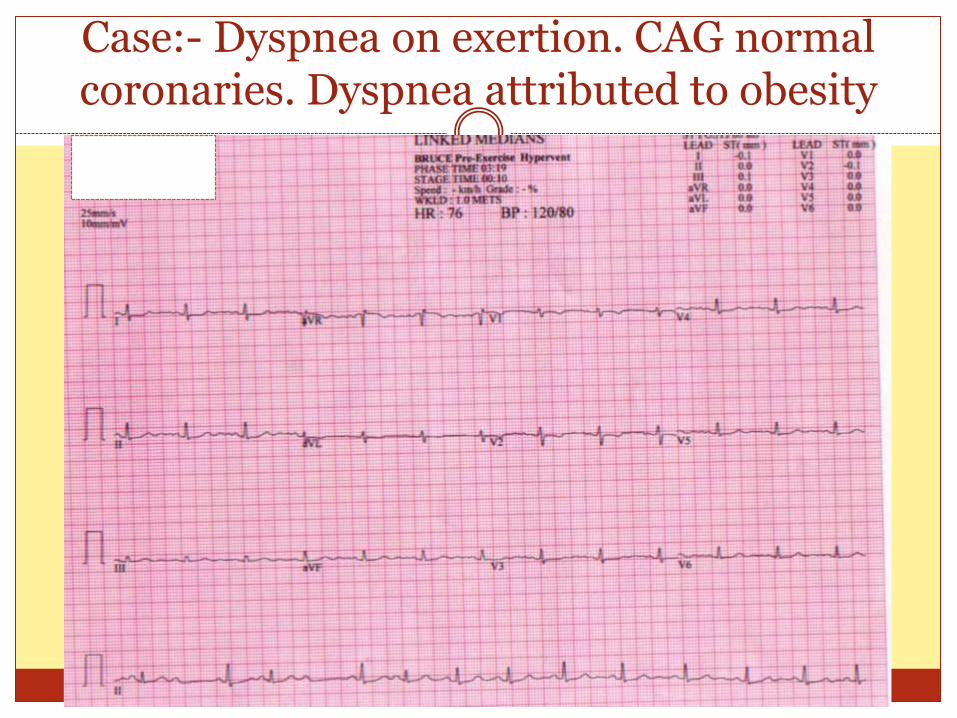
Case:- Dyspnea on exertion. CAG normal coronaries. Dyspnea attributed to obesity
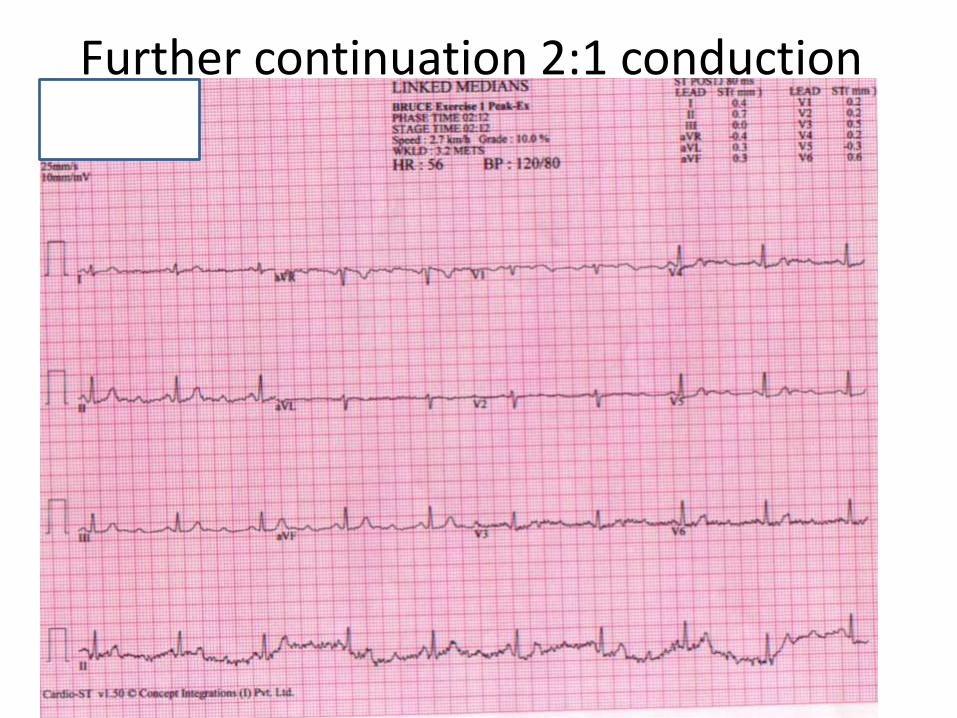
Further continuation 2:1 conduction
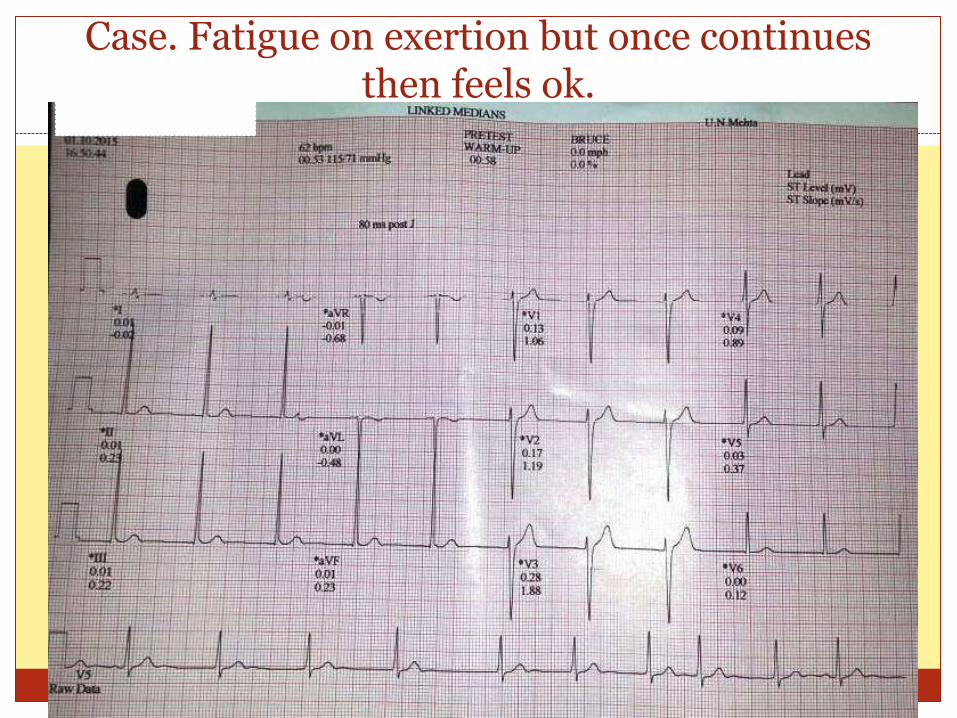
Case. Fatigue on exertion but once continues then feels ok.
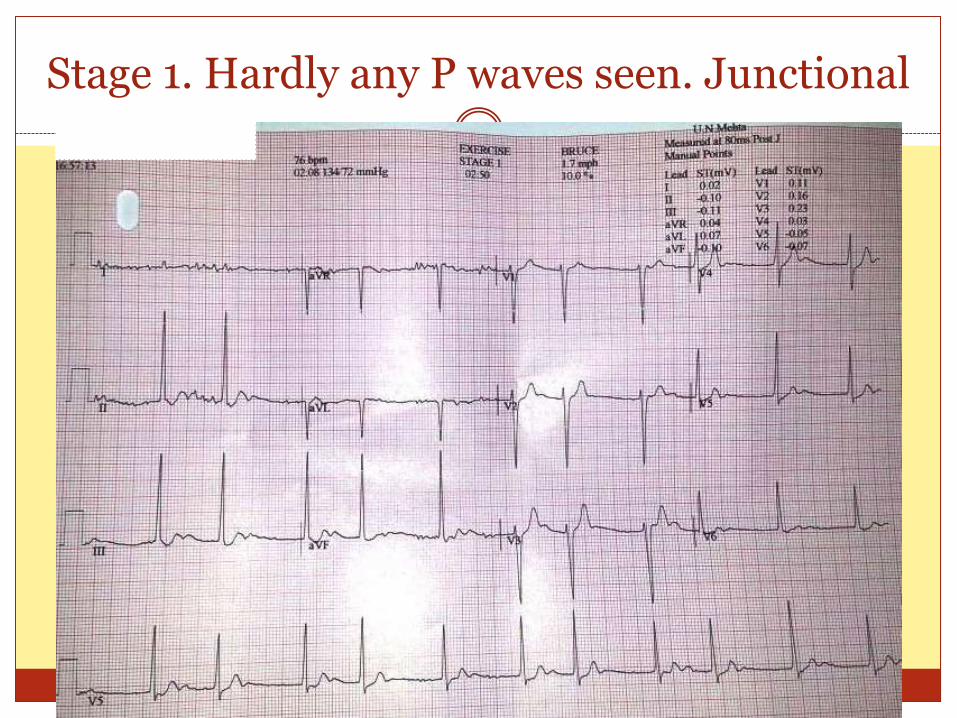
Stage 1. Hardly any P waves seen. Junctional
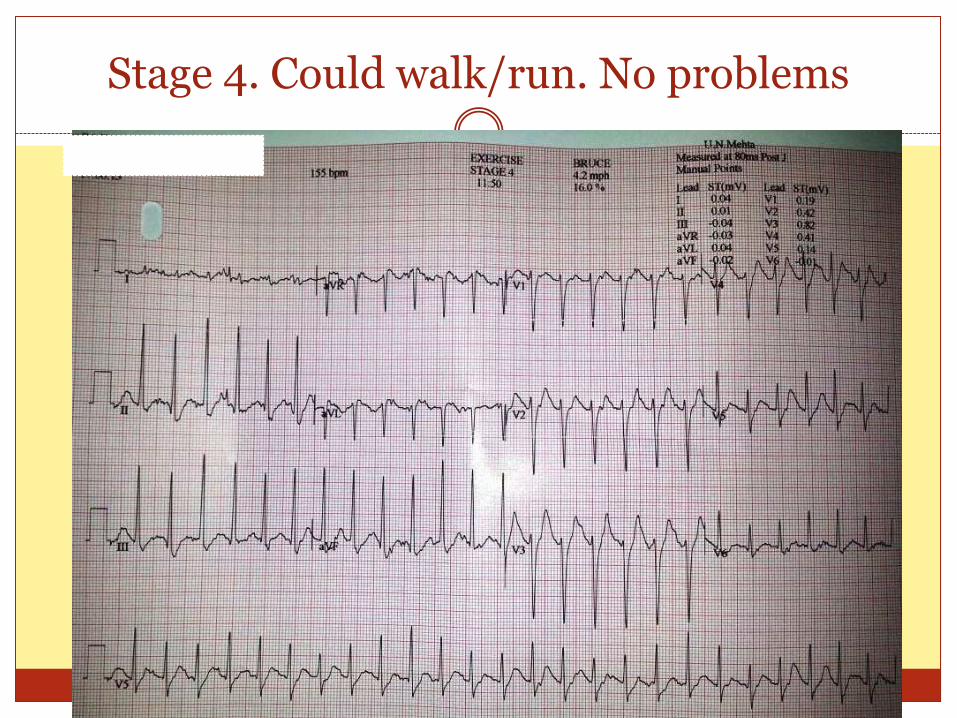
Stage 4. Could walk/run. No problems
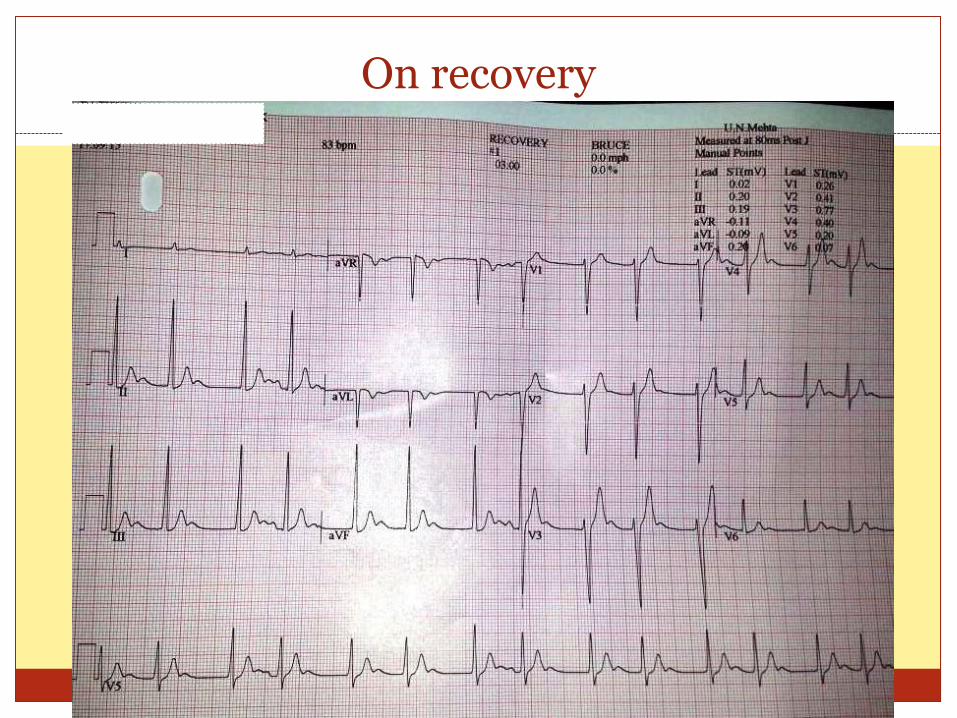
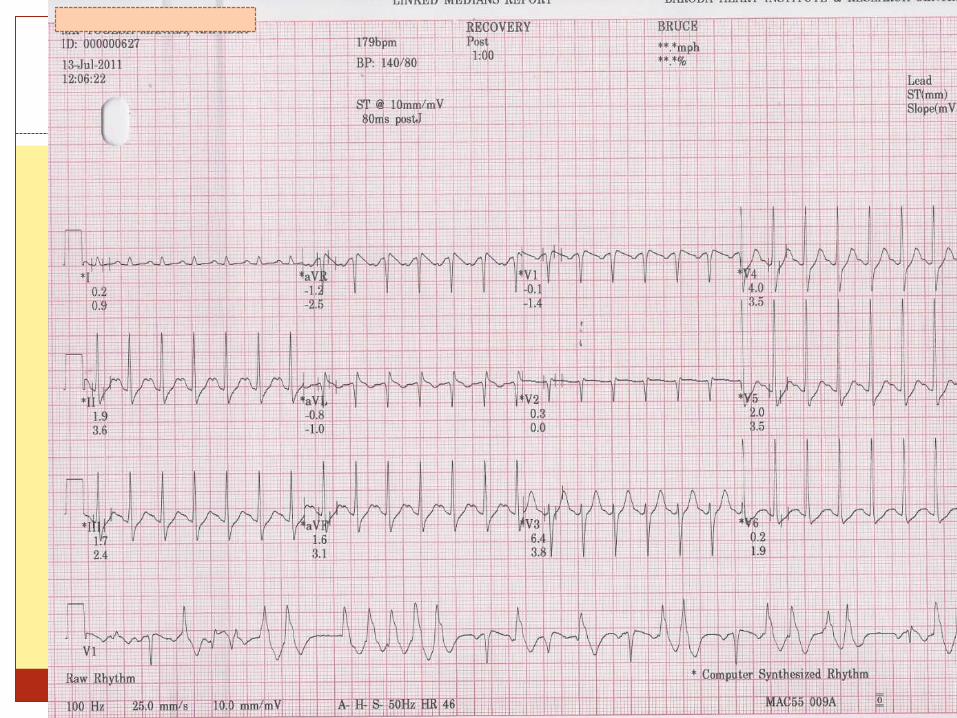
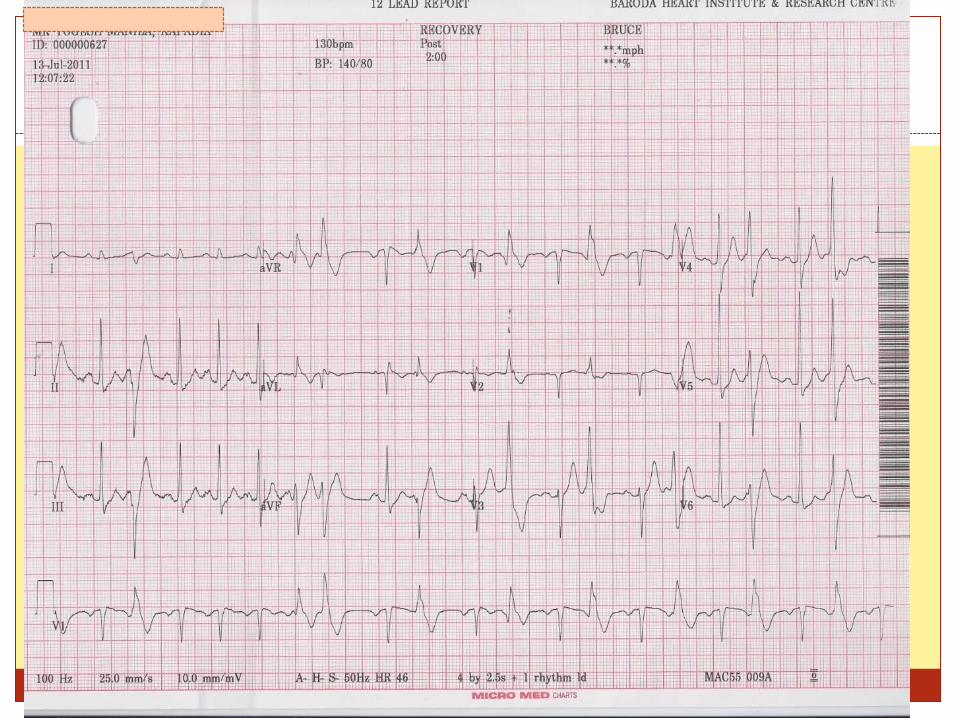
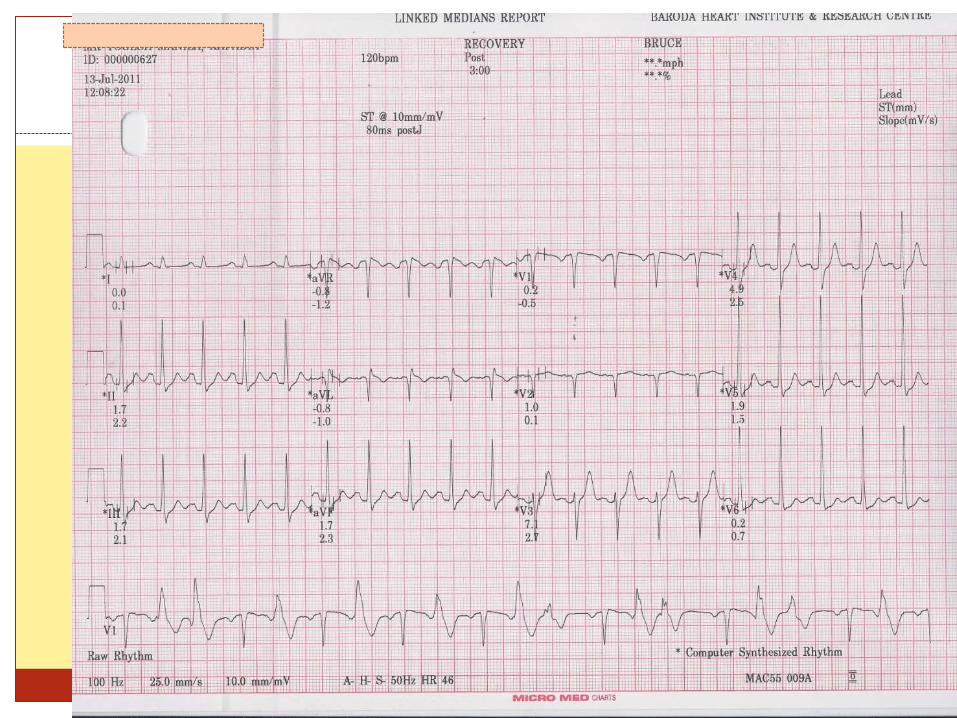
On recovery
TMT/Stress test in assessment of bradycardia
Exercise tolerance in Sinus bradycardia and asymptomatic CHB (congenital) with narrow QRS Target heart rate achieved or not
If patient becomes symptomatic
Any sudden decrease in heart rates
Pacemaker indications Symptoms
Long pauses
Sudden decrease in rates at increasing exercise
Failure to achieve target heart rates not an indication
Stress test and atrial arrhythmia on test
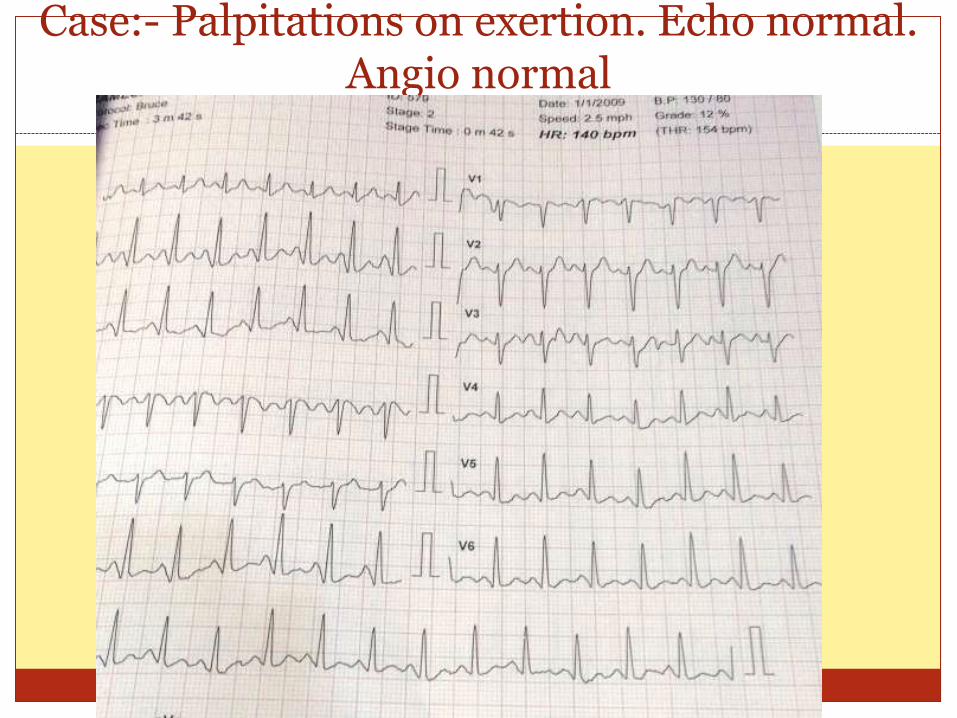
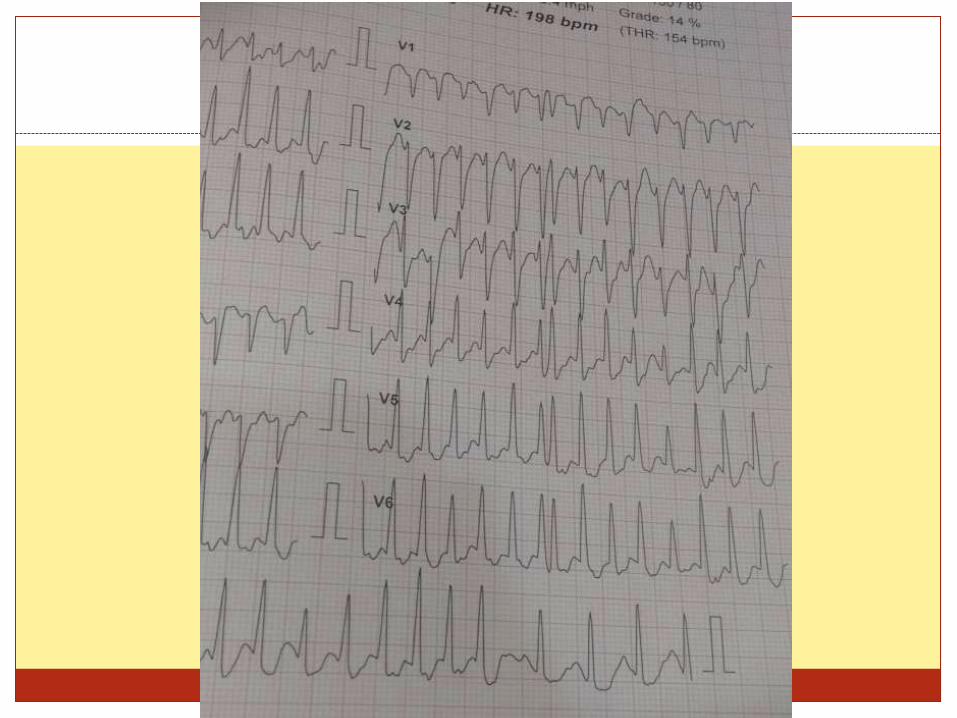
Case:- Palpitations on exertion. Echo normal. Angio normal
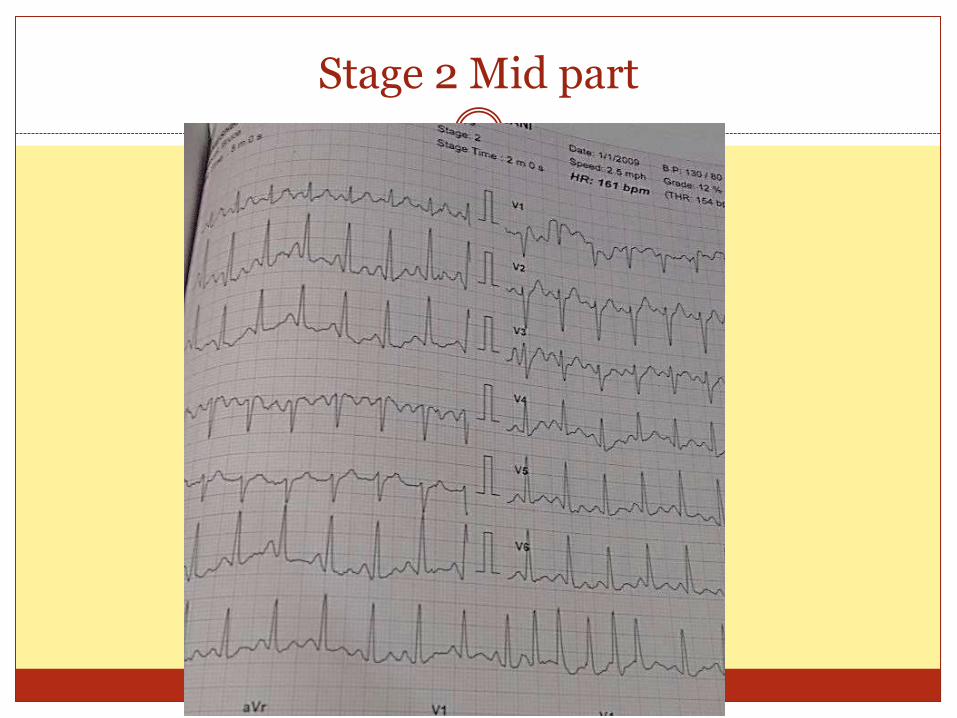
Stage 2 Mid part
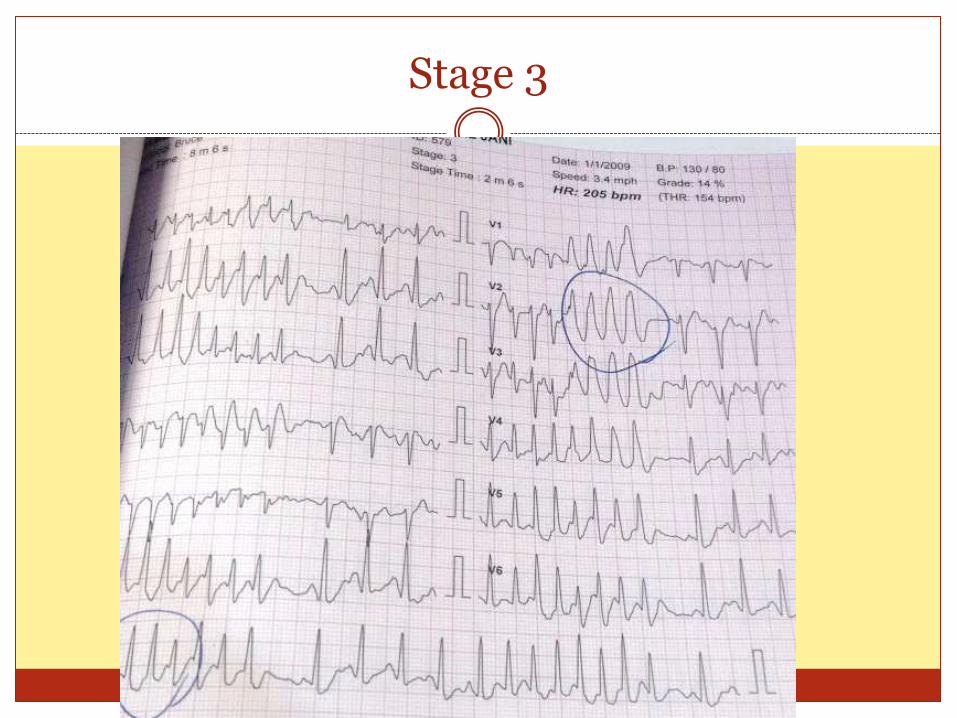
Stage 3
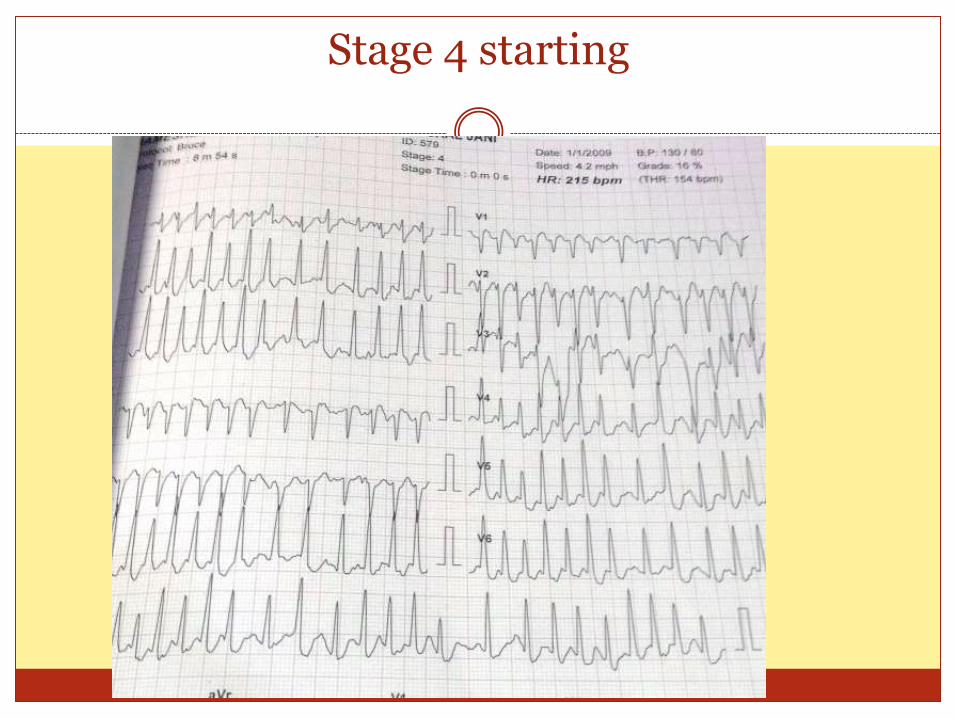
Stage 4 starting
Up to 6% of patients may develop atrial arrhythmia
More likely to have CAD
Atrial arrhythmias may reflect underlying left atrial enlargement and ventricular dysfunction.
Exercise-induced SVT is not a marker for latent heart disease but is a marker for AF or paroxysmal SVT
(8 times) during the follow-up period.
H E A L T H Y
R E F E R R A L P A T I E N T S W I T H C O M P L A I N T S
C A D
H E A R T F A I L U R E
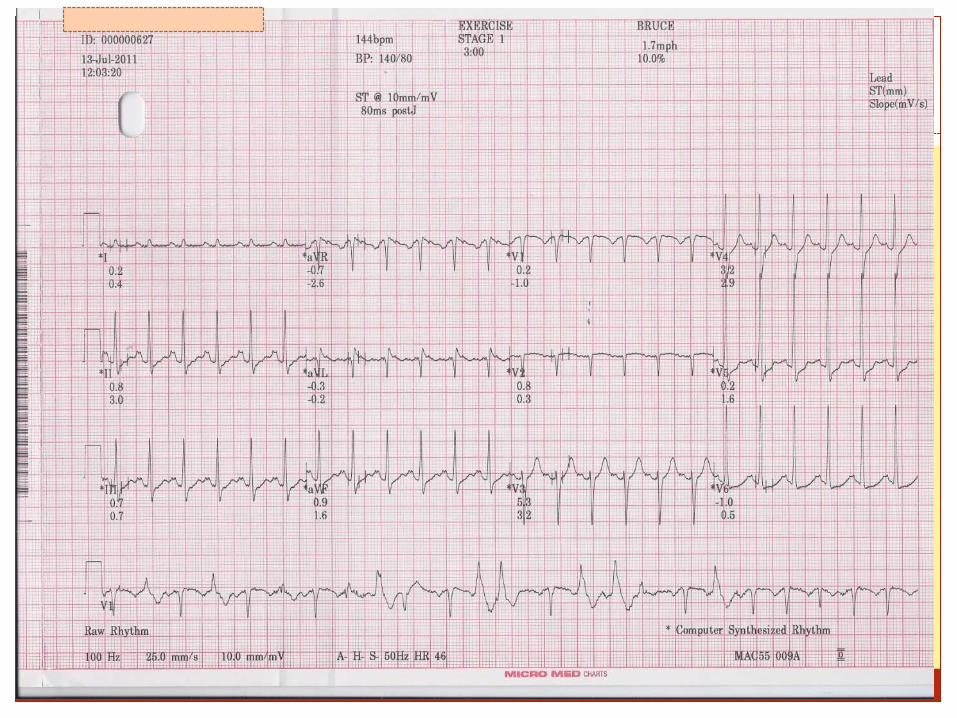
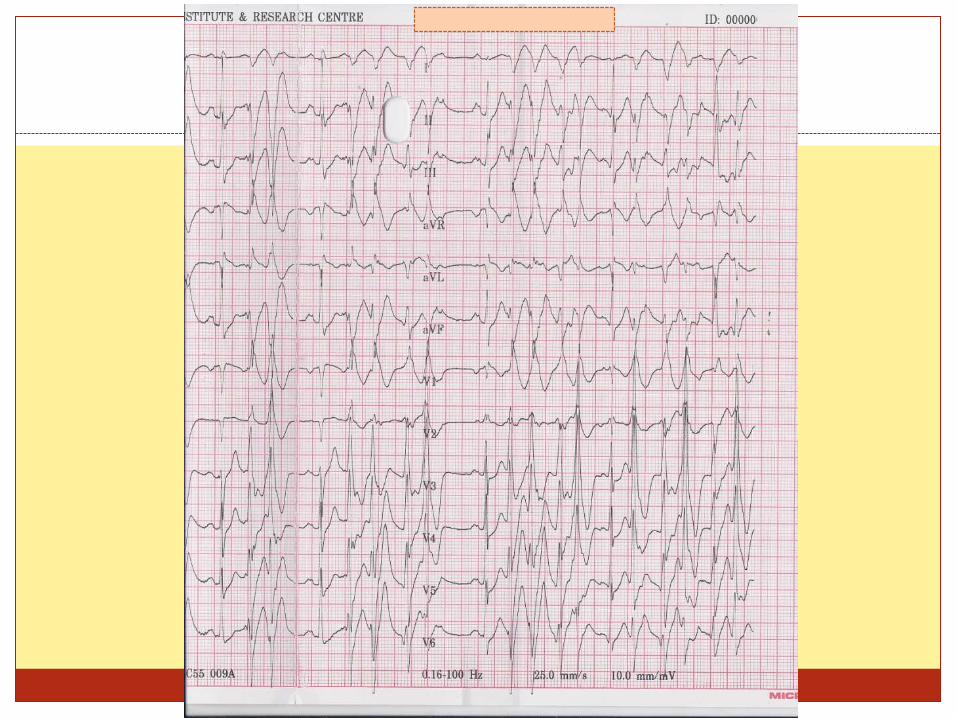
Stress test and ventricular arrhythmia seen on testing
When to say it is exercise induced arrhythmia
Exercise-induced arrhythmias are defined as frequent PVCs at near-maximal or maximal exercise, or 3 consecutive PVCs or more occurring at any time.
Frequent PVCs were defined as 10 or more PVCs out of any 50 consecutive beats.
10% in 30 seconds
presence of 7 or more PVCs per minute,
Ventricular bigeminy or trigeminy,
Exercise test–induced ventricular arrhythmias were noted in 2.1% of this apparently healthy population with no CAD/SHD
With CAD 10-19% may have Ventricular arrhythmia
More common with LV dysfunction and heart failure
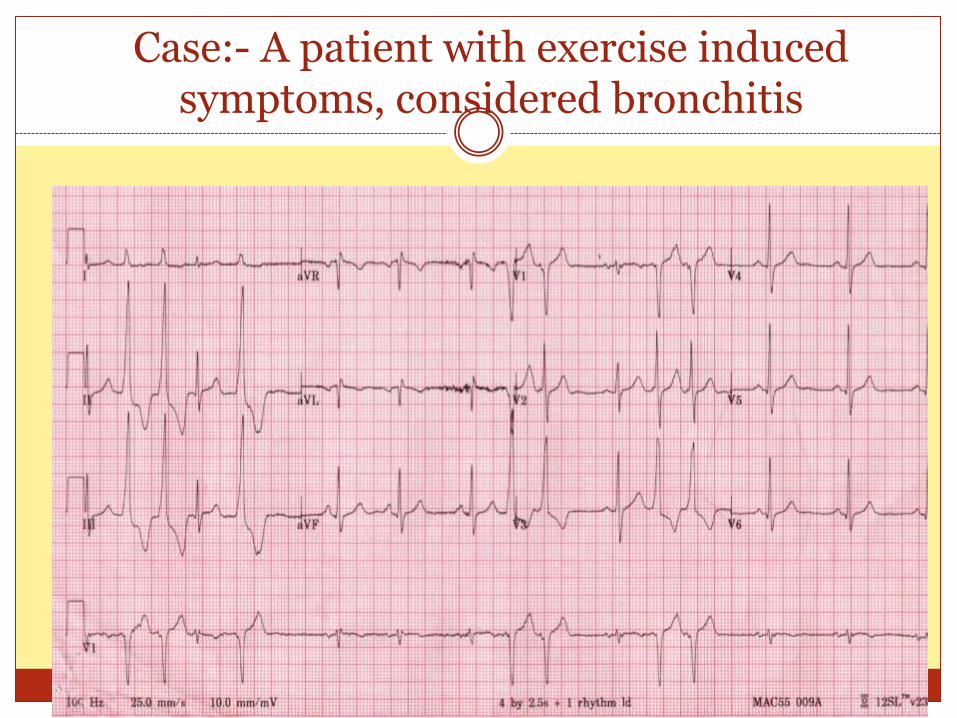
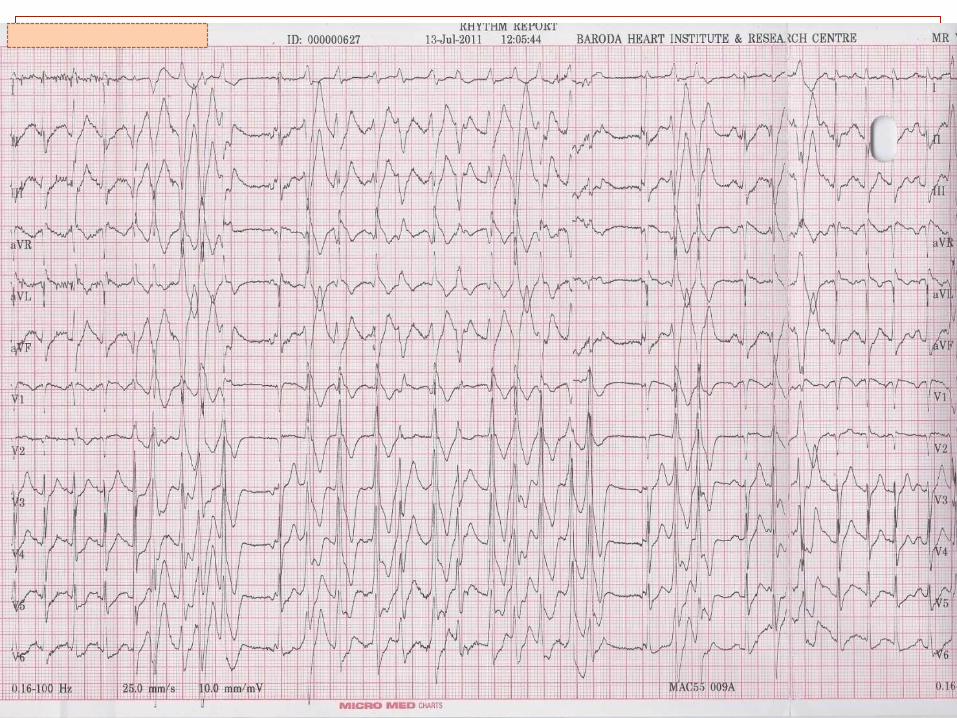
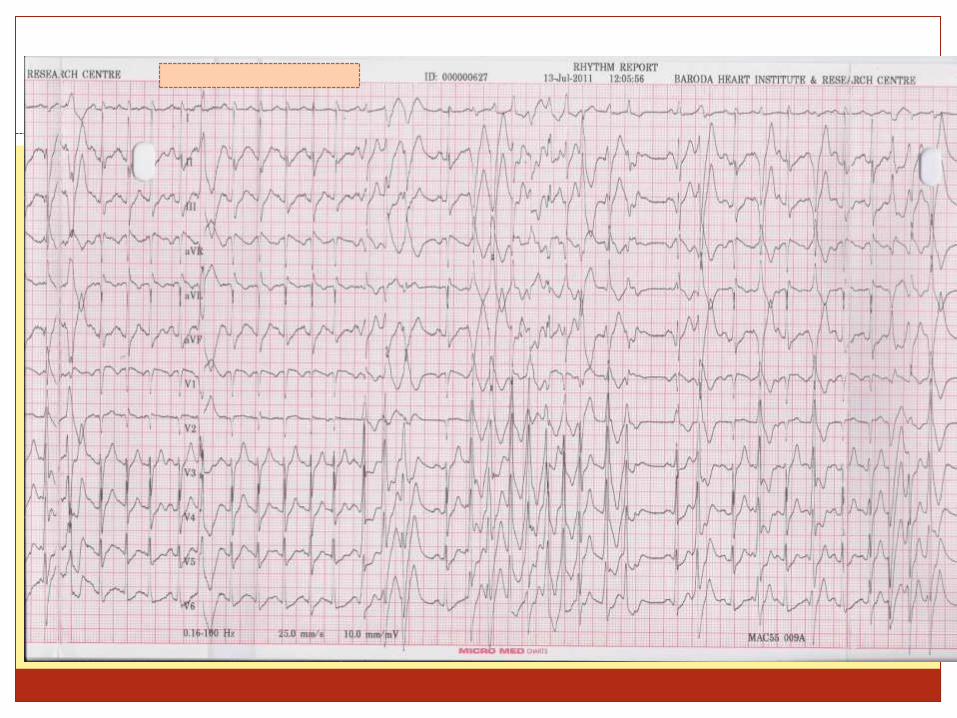
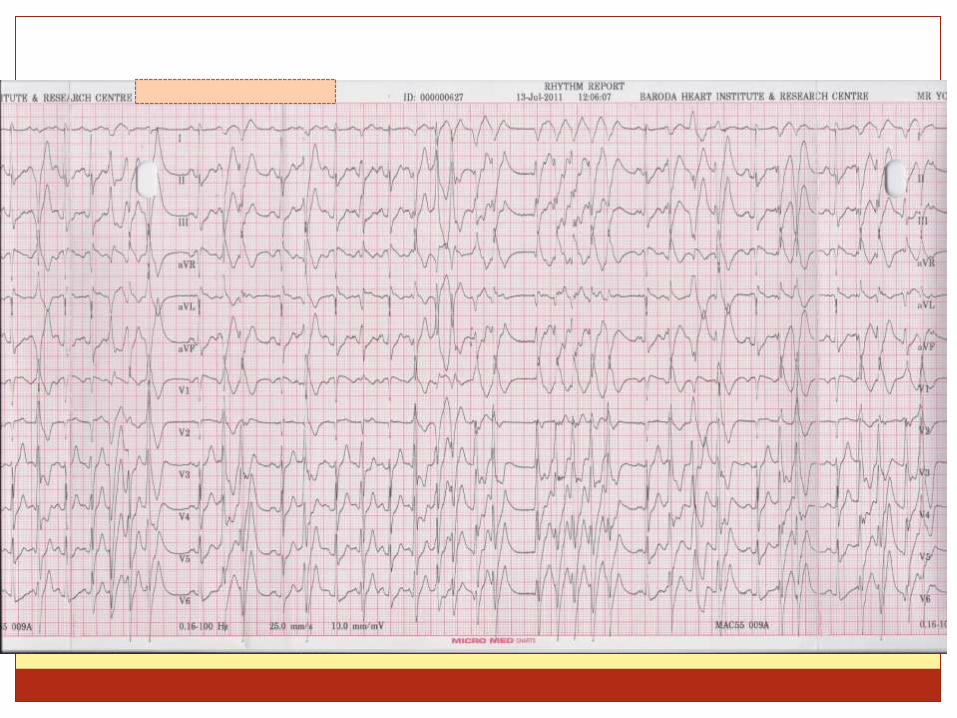
Case:- A patient with exercise induced symptoms, considered bronchitis
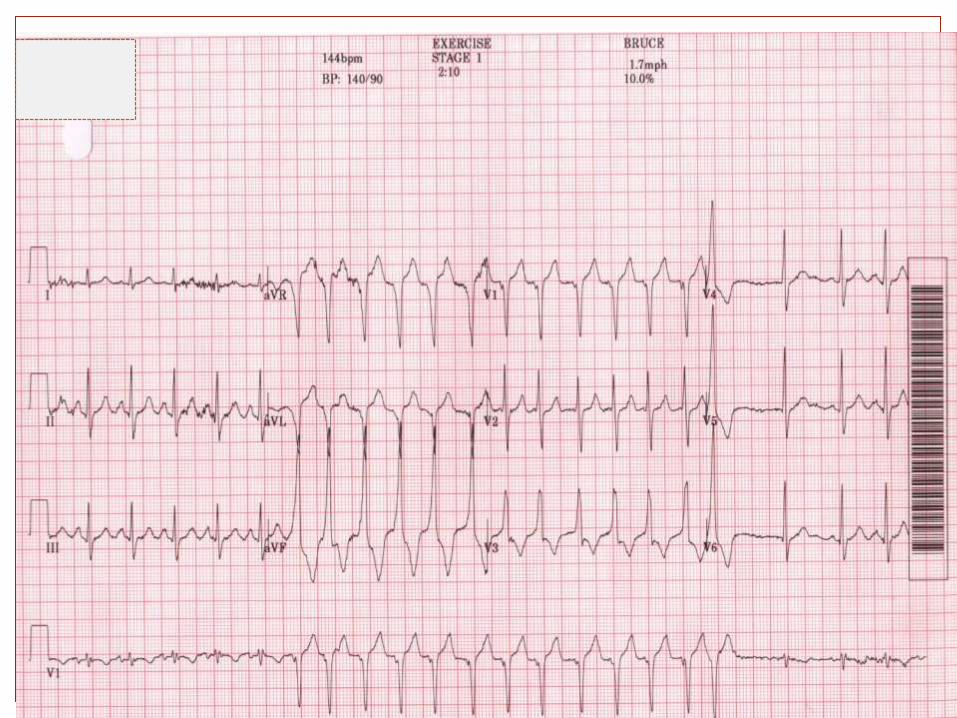
Hence made him do a TMT and ->
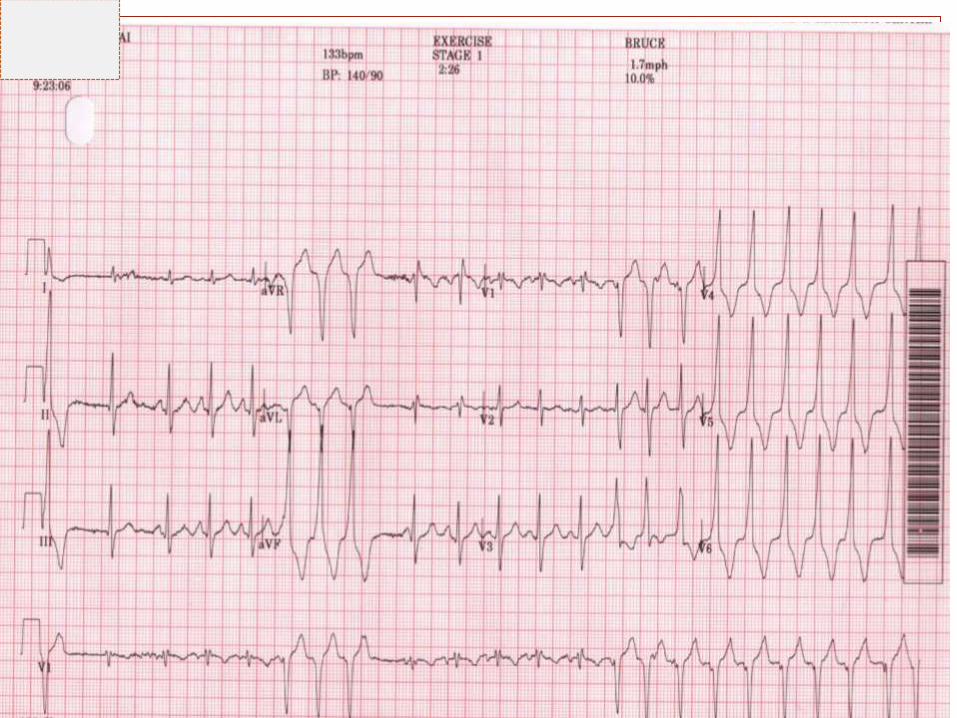
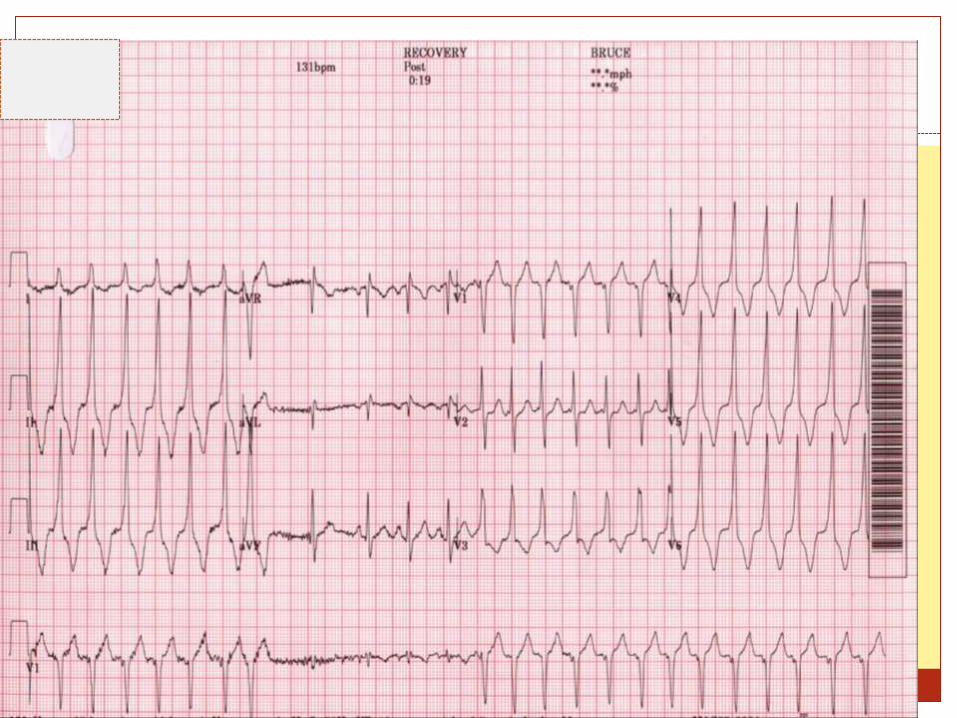
Diagnosis
Outflow tract ventricular tachycardia.
Options of treatment
Drugs
EPS and RFA ablation
Treated with ablation
No complaints on follow up
Case
14 year old boy with history of atypical chest pain.
? Palpitations/DOE on exertion
ECG baseline 0k.
ECHO frequent PVC however no significant finding
TMT
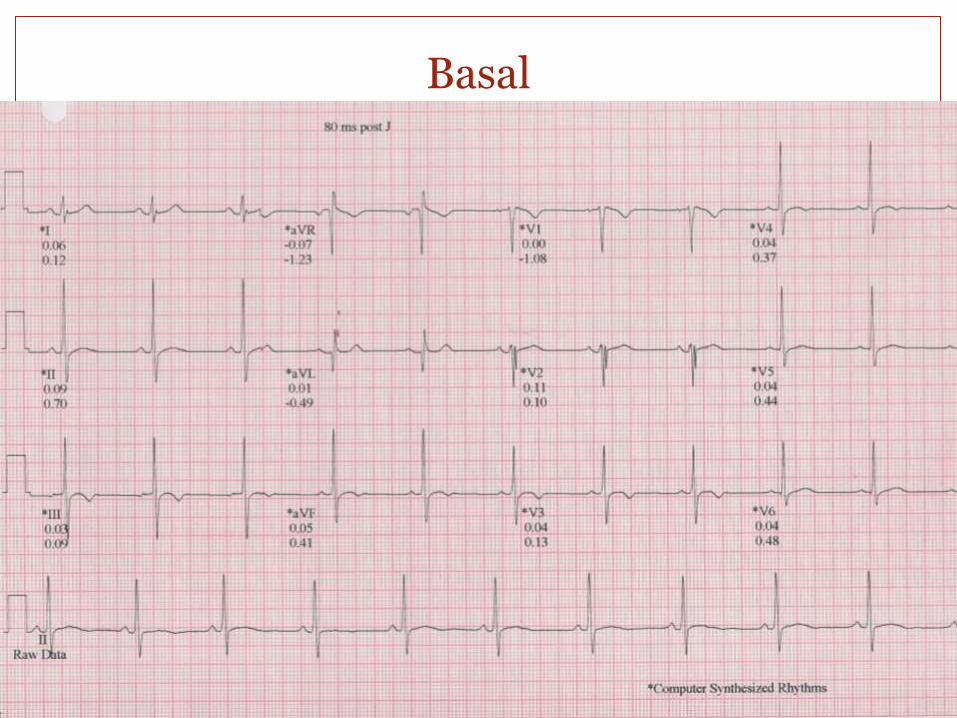
Basal
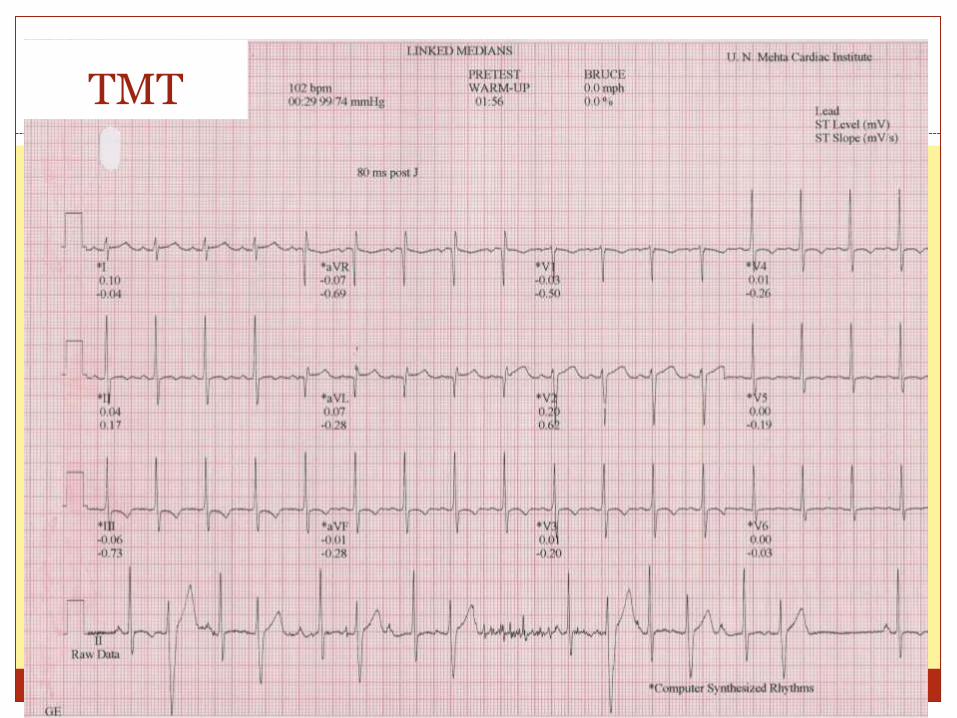
TMT
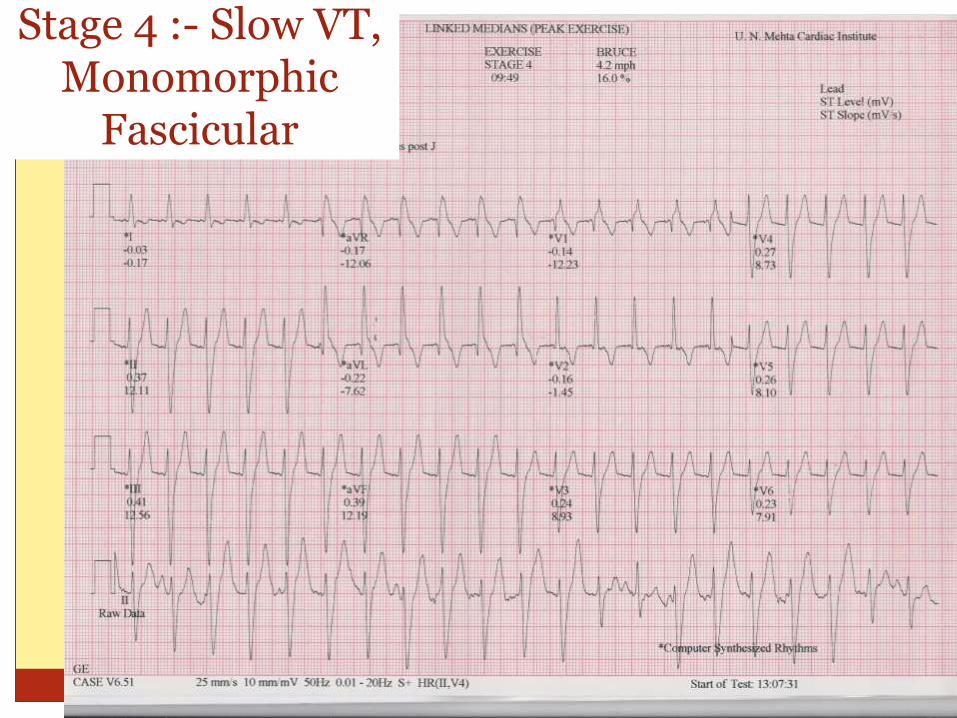
Stage 4 :- Slow VT, Monomorphic
Fascicular
Options
Investigations
Holter
Cardiac MRI
If elderly CAG is required
Family screening for arrhythmic cardiomyopathies
Treatment
Drugs
EPS & RFA
CASE
A 56 year old gentleman with history of exertion
induced lightheadedness with blackness in front of
eyes, breathlessness, and palpitations
k/c/o mod MR on medications for the same.
Irregular treatment. Stopped treatment for a month
? Familial retinal problem.
Clinically murmur of MR.
Right eye perception of light only.
Otherwise no s/o failure
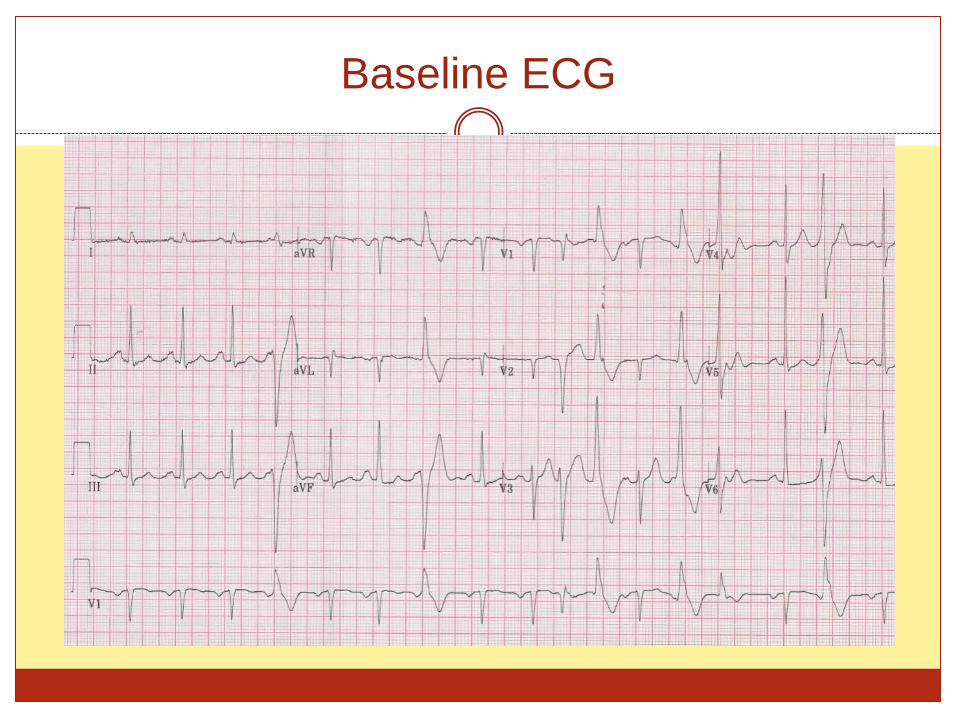
Baseline ECG

Diagnosis
CAD ?
MR /MVP related
Idiopathic
Genetic (CPVT/ATS/Long QTS)
Investigations CAG
Cardiac MRI
Genetic testing
Therapy For polymorphic arrhythmia EPS not generally an option
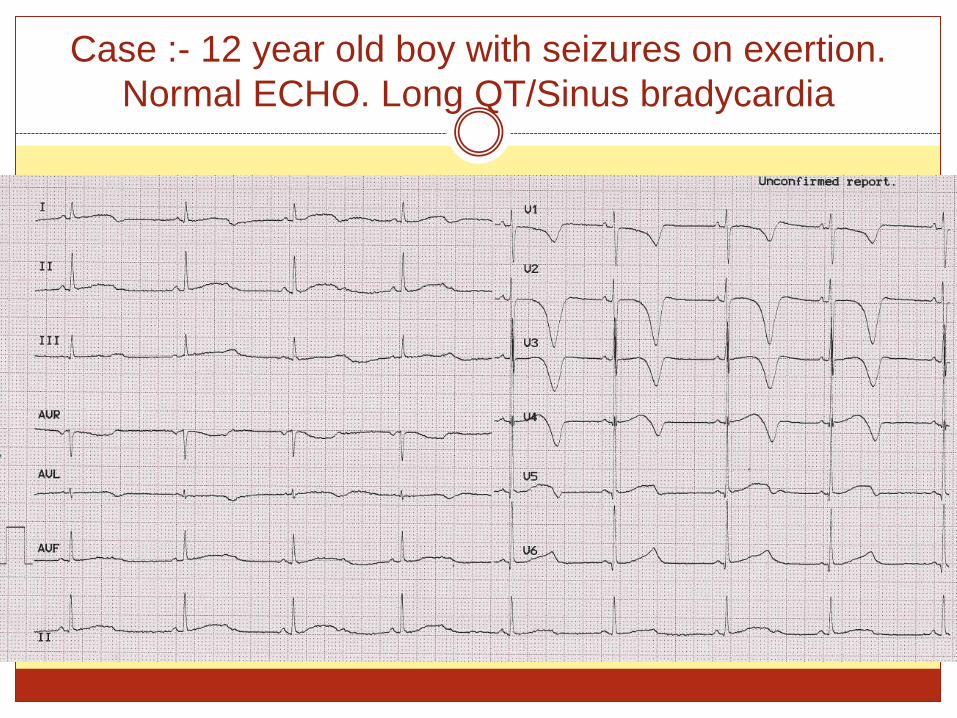
Case :- 12 year old boy with seizures on exertion.
Normal ECHO. Long QT/Sinus bradycardia
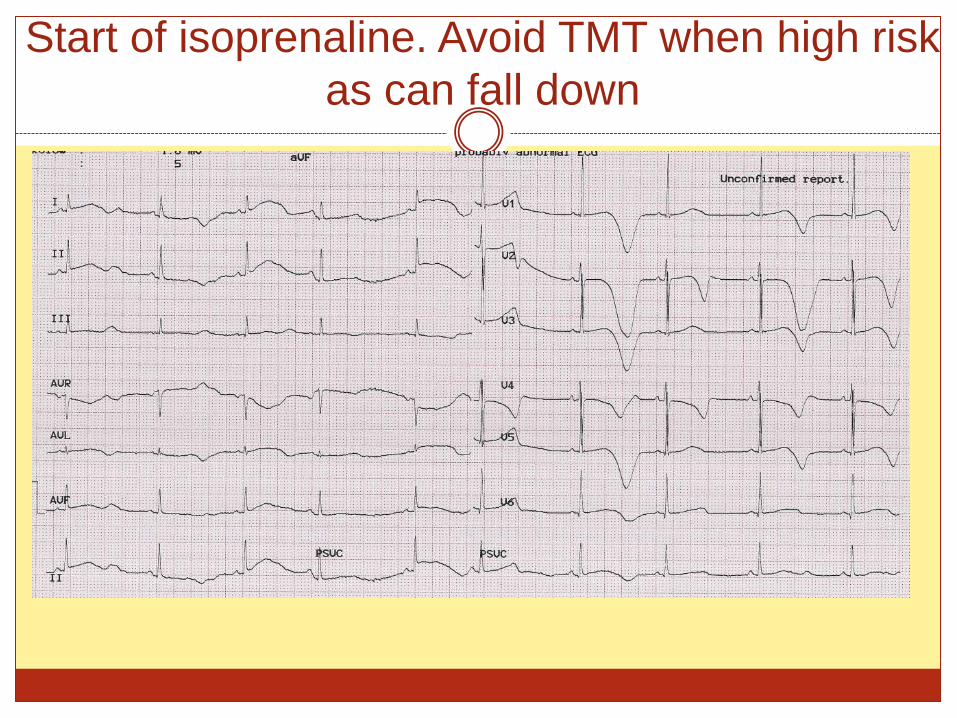
Start of isoprenaline. Avoid TMT when high risk
as can fall down
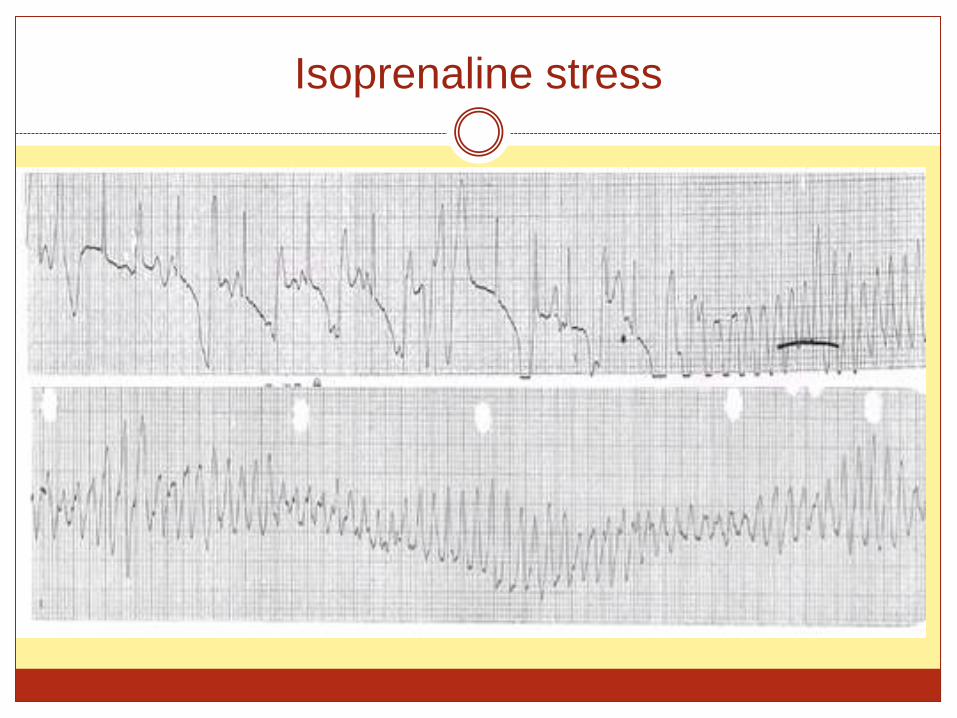
Isoprenaline stress
Case
25 year old lady with exertional syncope.
Recurrent.
Family history of SCD in younger brother and similar
episodes in sister
Now pregnant.
Echo normal
Holter normal
Cannot make exercise as pregnant.
Hence isoprenaline test
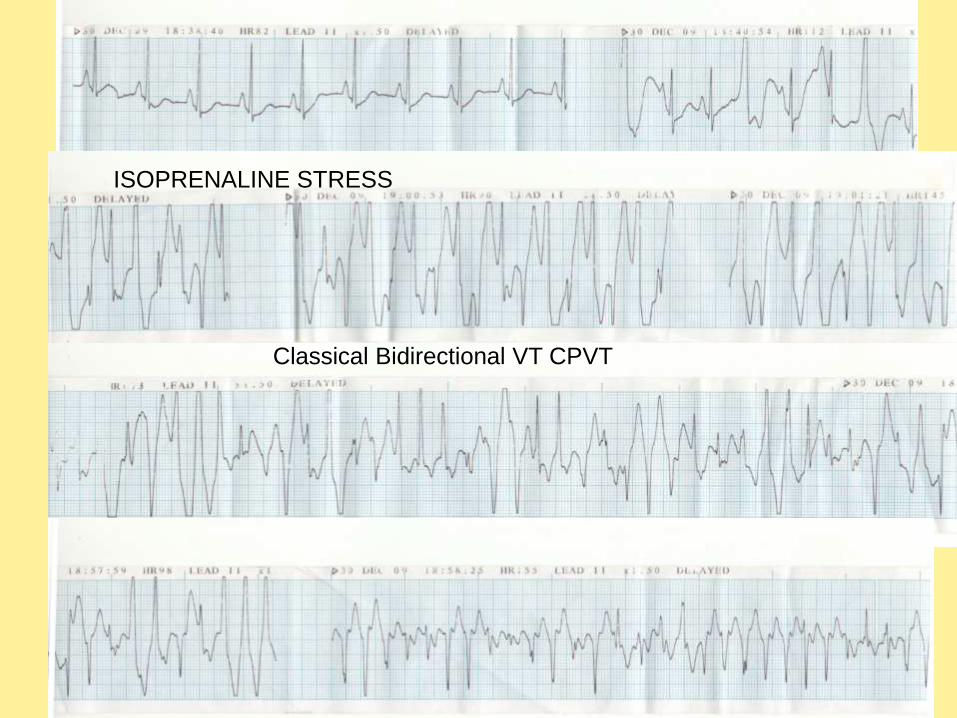
ISOPRENALINE STRESS
Classical Bidirectional VT CPVT
Exercise induced Ventricular arrhythmia
Idiopathic VT Outflow tract VT
Fascicular VT
Channelopathy/Cardiomyopathy LQTS 1/ATS
CPVT
ARVC
Saini et al :- Ventricular arrhythmia is reproducible in patients known to have serious arrhythmias. Excluding infrequent single ventricular premature complexes, the reproducibility of a test with positive outcome was 76%.
Faris et al:- Subjects whose arrhythmias are reproducible may form a group more likely to develop clinical cardiovascular disease in long-term follow-up studies.
Ventricular arrhythmia in CAD
on stress test
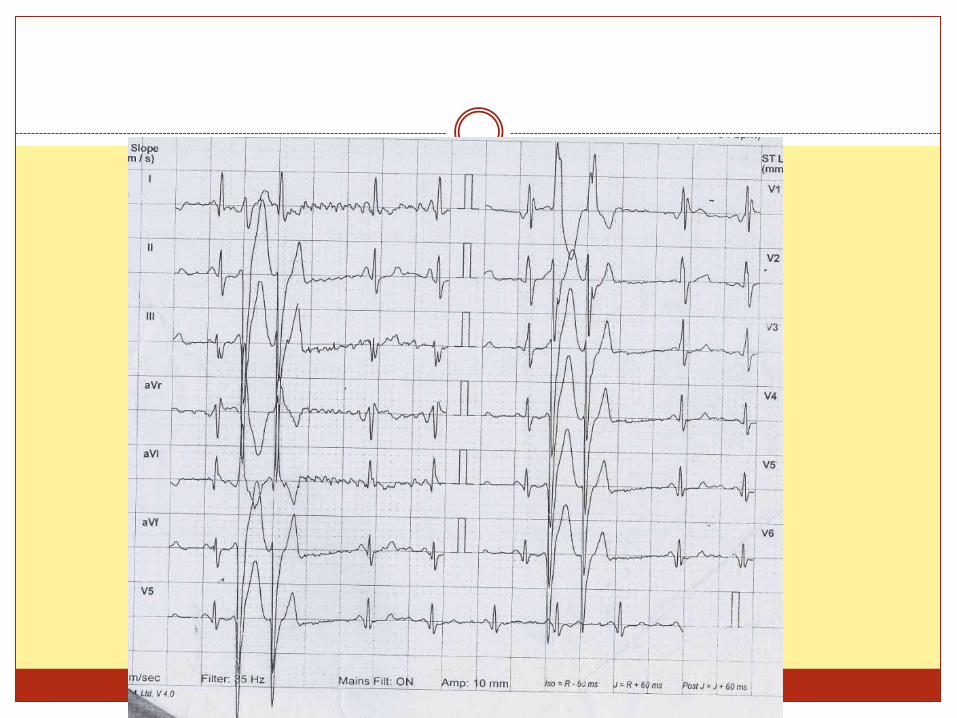
Case
62 year old gentleman with chest pain on exertion
while doing treadmill since a week
Recent history of giddiness while doing Treadmill at
home
Active gentleman
Baseline ECG RBBB, LAD
Good LV function
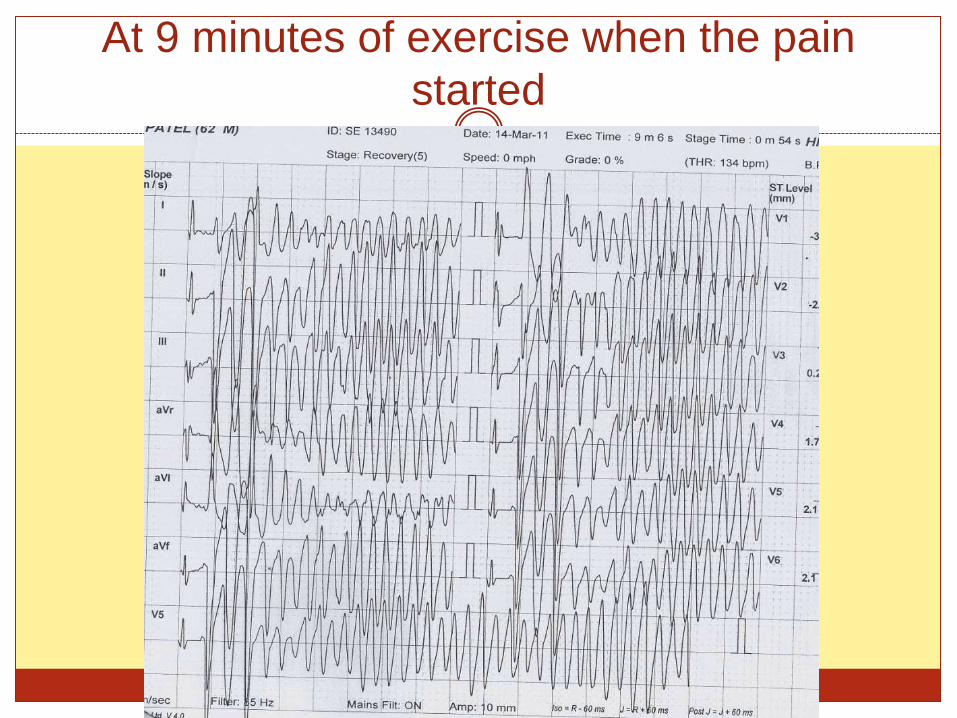
At 9 minutes of exercise when the pain
started
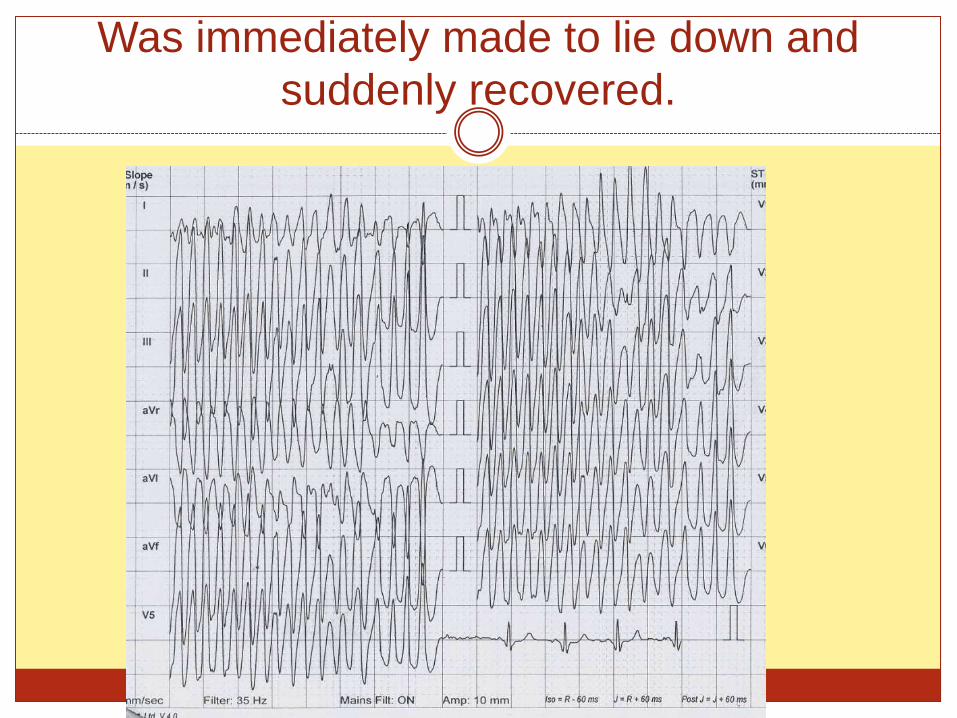
Was immediately made to lie down and
suddenly recovered.
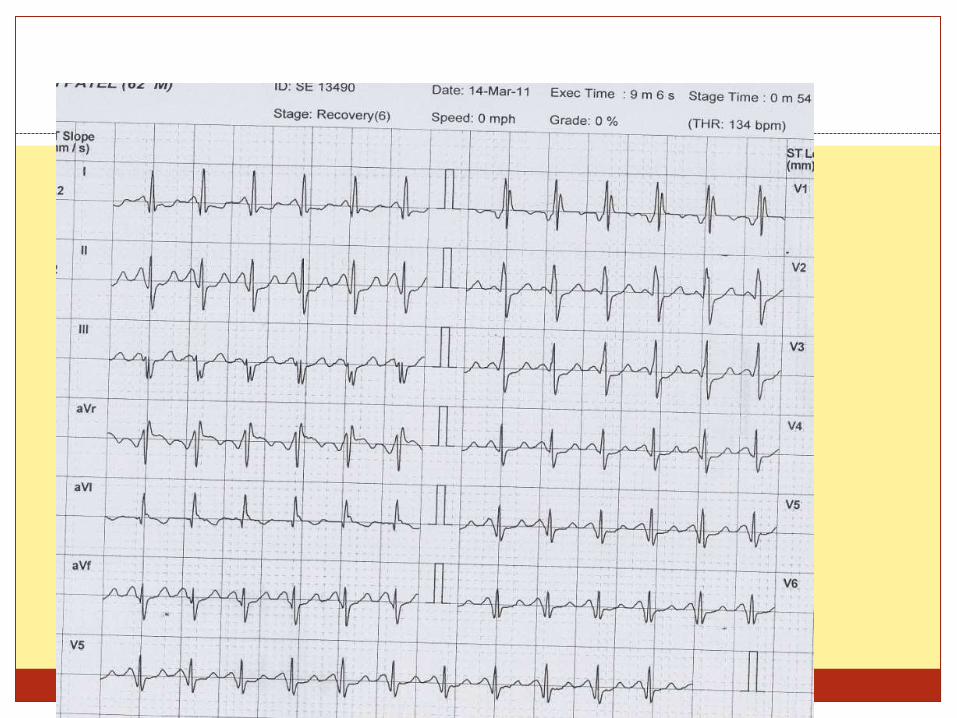
Admitted
CAG suggestive of triple vessel disease
Critical LAD and RCA disease
CABG done
Further need for testing.
Yes to rule out arrhythmic cardiomyopathy
Elhendy et al showed that exercise test–induced ventricular arrhythmias occurred in 146 (10%) of patients evaluated. Greater prevalence of abnormal exercise echocardiographic
findings and ischemia on exercise echocardiography, greater increase in wall motion score index with exercise, and a greater percentage of abnormal segments with exercise
Mc Henry et al showed that Patients with 3-vessel CAD and left ventricular wall motion
abnormalities were found to have a significantly greater prevalence of arrhythmia
Milanes et al showed that 4% had ventricular arrhythmia 79% of patients with ventricular fibrillation or tachycardia had an
abnormal ST response as well.
ST elevation is very arrhythmogenic while depression is not.
Recovery phase arrhythmia more dangerous
Stress test in HCM patients
Prior used for hemodynamic as well as arrhythmia
induction.
With better diagnostics like Holter and genetic
assessment, less useful.
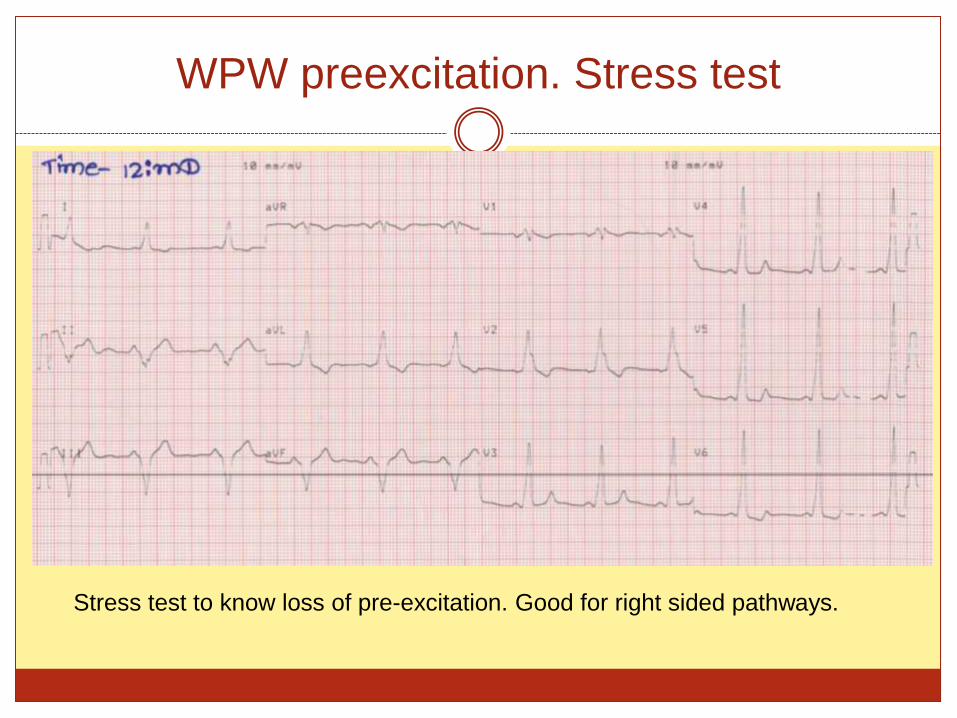
WPW preexcitation. Stress test
Stress test to know loss of pre-excitation. Good for right sided pathways.
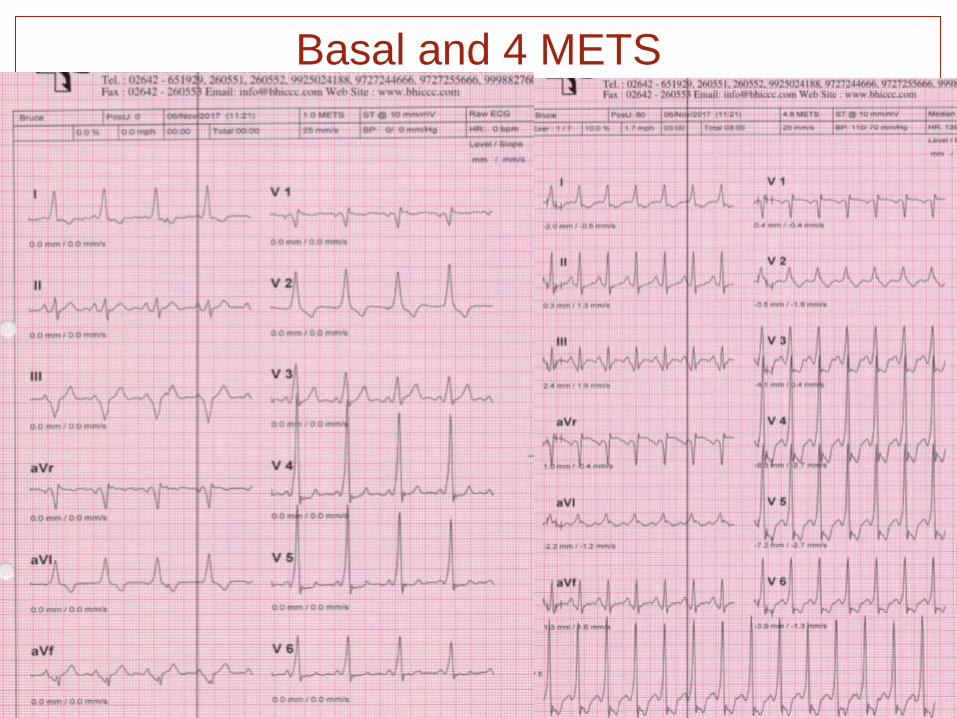
Basal and 4 METS
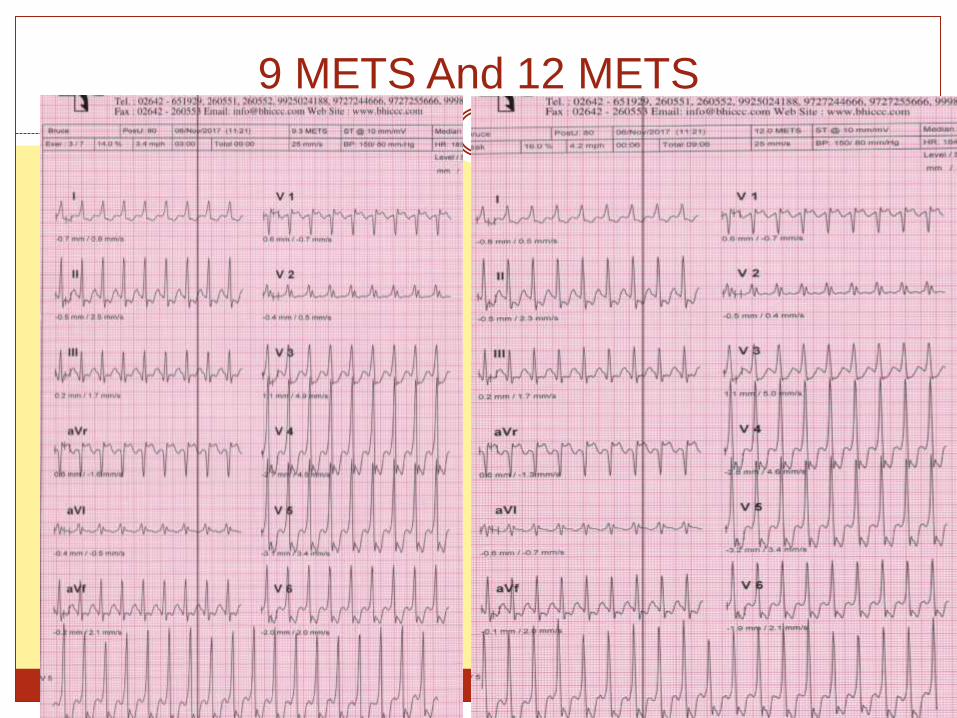
9 METS And 12 METS
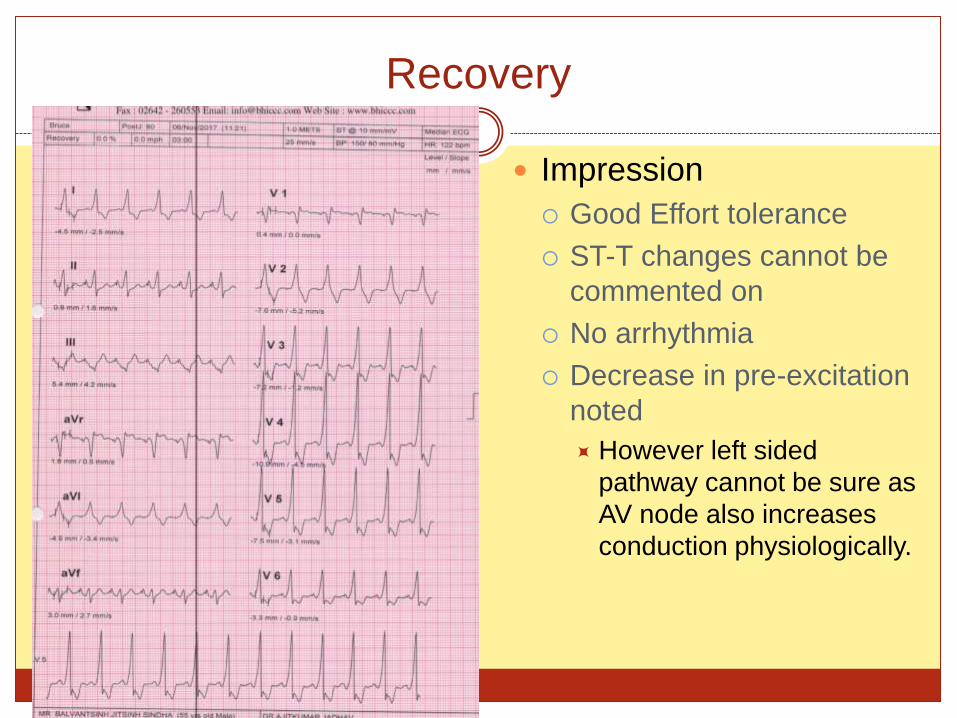
Recovery
Impression
Good Effort tolerance
ST-T changes cannot be
commented on
No arrhythmia
Decrease in pre-excitation
noted
However left sided
pathway cannot be sure as
AV node also increases
conduction physiologically.
Summarizing
Stress test is integral in testing for arrhythmia and should be advised in patients with symptoms on exertion especially in young patients.
Stress test helps in diagnosis and treatment of bradycardia and tachycardia both.
Risk stratification of asymptomatic patients with VPC and SHD can be done using stress test
Appropriate precautions should be taken while doing stress test in patients with suspected arrhythmia
WELCOME
ISECON 2018
FEBRUARY 17TH AND 18TH
VADODARA
GUJARAT
Thank you
Related Documents











