STREAMLINING HMIS REPORTING AT BUMANYA HEALTH SUB DISTRICT IN KALIRO DISTRICT By NANYONJO ROSETTE GENEVIEVE MEDIUM TERM FELLOW 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
STREAMLINING HMIS REPORTING AT BUMANYA HEALTH
SUB DISTRICT IN KALIRO DISTRICT
By
NANYONJO ROSETTE GENEVIEVE
MEDIUM TERM FELLOW
2013

Table of contents
Contents
Declaration ............................................................................................................................................... i
Fellow’s role in project implementation .................................................................................................. ii
Acknowledgements ................................................................................................................................ iii
Acronyms ............................................................................................................................................... iv
Abstract .................................................................................................................................................. v
1.0 Introduction and Background ............................................................................................................ 1
2.0 Literature review ............................................................................................................................... 2
3.0 Statement of the problem ................................................................................................................. 3
4.0 Justification ....................................................................................................................................... 3
5.0 Conceptual framework ...................................................................................................................... 4
6.0 Project objectives .............................................................................................................................. 5
Project Goal......................................................................................................................................... 5
7.0 Methodology ..................................................................................................................................... 5
8.0 Project implementation ..................................................................................................................... 8
9.0 Project achievements/outcomes...................................................................................................... 10
10.0 Lessons learned: ............................................................................................................................ 12
11.0 Challenges experienced and how they were overcome .................................................................. 12
12.0 Conclusions: .................................................................................................................................. 12
13.0 Recommendations: ........................................................................................................................ 13
14.0 Next steps...................................................................................................................................... 13
15.0 References: .................................................................................................................................... 13

List of Figures
Figure 1: Conceptual framework ...............................................................................................................
Figure 2 MoH Official facilitating training for In charges ........................................................................... 9
Figure 3: Status of health facilities submitting reports to HSD ............................................................... 10
Figure 4: Status of records management before project implementation .............................................. 11
Figure 5: Status of records management after project implementation ................................................ 11
List of Tables
Table 1: CQI project team ........................................................................................................................ 6
Table 2: Multi voting results ................................................................................................................... 7
3: Theme selection matrix ...................................................................................................................... 7

i
Declaration
I Rosette Genevieve Nanyonjo do hereby declare that this end-of-project report entitled
“Streamlining HMIS reporting at Bumanya Health Sub District in Kaliro District” has been
prepared and submitted in fulfilment of the requirements of the Medium-term Fellowship
Program at Makerere University School of Public Health and has not been submitted for any
academic or non-academic qualifications elsewhere.
Signed …………………………………… Date …………………….
Rosette Genevieve Nanyonjo, Medium-term Fellow
Signed Date …………………….
James Kakooza, Institution Mentor
Signed ………………………………………….. Date ……………………..
Dr. Benson Tumwesigye, Academic Mentor

ii
Fellow’s role in project implementation
This project was initiated by the Fellow together with Kaliro District and Bumanya Health Sub
District Staff. Since Kaliro District is one of the districts supported by Strengthening
Decentralization for Sustainability (SDS) Programme, it was easy to work with them. The
fellow introduced the concept of Continuous Quality Improvement (CQI) to the District Health
Team (DHT) and the Health Sub District (HSD) staff at Bumanya. The Health Management
Information System (HMIS) Focal Person together with the District Biostatistician were selected
to participate in project implementation. The Fellow initiated the idea of solving an HMIS
reporting problem to the DHT and HSD staff and led the process for problem identification,
development of counter measures, identification of practical methods and support supervision
during implementation of the project. The Fellow was not directly involved in implementation
but supervised the process and coached and mentored health facility staff in how to use the Plan
Do Check and Act (PDCA) approach to problem identification and thereafter the team
implemented the project.

iii
Acknowledgements
I wish to thank God for enabling the team to complete this project successfully.
I would like to thank Makerere School of Public Health – Centre for Diseases Control (MakSPH-
CDC) Fellowship Program for selecting me to be part of this Program. Special thanks to Mr.
Matovu KB Joseph for continuously guiding me.
To the SDS Programme for the support rendered to ensure smooth implementation of the Project.
Special thanks to Ms Ella Hoxha, Chief of Party, and Mr James Kakooza, my Institutional
Mentor.
I would also like to thank Dr. Benson Tumwesigye, my Academic Mentor, for his continuous
support and guidance.
Not forgetting the staff of Bumanya HSD and Kaliro DHO’s Office, Jafali Muhamed, Dr. Allan
Katamba and Joshua Mugweri, you were a wonderful team to work with.
Fellow CQI Fellows, thanks for the positive feedback during class time.

iv
Acronyms
CQI Continuous Quality Improvement
DHIS District Health Information System
DHO District Health Officer
DHT District Health Team
HMIS Health Management Information System
HSD Health Sub District
HUMC Health Unit Management Committee
HU Health Unit
MIS Management Information Systems
MRO Medical Records Officer

v
Abstract 1.0 Introduction: The Health Management Information Systems (HMIS) reporting guidelines
require that health facilities submit complete reports to the Health Sub District (HSD) for entry
into District Health Information System (DHIS2). In 2012, none of the 19 health facilities
submitted reports to the HSD as required. This was due to the difficulty in accessing the HSD as
compared to the District and there was no data management system at the HSD. The purpose of
this project was to initiate the process of submitting reports to the HSD with the aim of
increasing the percentage of health facilities submitting reports to HSD from 0% to 100% in 5
months.
2.0 Project Description: This project involved 3 interrelated components: (i) orientation of in-
charges on HMIS reporting tools and guidelines, health facility in-charges were also sensitized
about the importance of submitting reports to the HSD); (ii) establishment of a data management
system at HSD (i.e. filing cabinets, files & a register for incoming reports were put in place) and
(iii) training of HSD Medical Records Officer (MRO) in data management and facilitation with
internet modem for data entry into the District Health Information System 2(DHIS)).
3.0 Project Outcomes: The number of Health Facilities that submitted reports to the HSD
increased from 0 (0%) in May 2013 to 7/19 (37%) in September 2013. The target of 100% could
not be achieved because of lack of compliance by the HSD MRO which was very crucial in the
implementation of this project. Nevertheless, the level of achievement attained helped to improve
the ability of the HSD to provide feedback to the health facilities through the Health Unit
Management Committees to improve reporting and other service delivery indicators.
vi
4.0 Lessons learned: While HMIS reporting guidelines emphasize the need for health facilities
to report through HSD than directly to the district, they don’t empower the HSD to demand
health facilities to report to them prior to reporting to the district
5.0 Recommendations: The reporting system needs to be configured in such a way that it only
allows reports into DHIS2 that have been initially entered at the HSD.

1
1.0 Introduction and Background
Bumanya HSD is located in Kaliro District and is the only HSD in the district. Kaliro District
has 20 health facilities and only one HSD to which all the health facilities report. Bumanya is
one of the oldest health facilities in the district and serves a high population as it provides
services equivalent to a hospital in the district. As an HSD, it’s mandated by the Ministry of
Health (MoH) to perform certain key functions such as receiving HMIS reports from the lower
health facilities, data quality control, and ensuring data entry into the DHIS2 among others.
Despite the fact that the HSD is mandated to perform the above mentioned functions, it hasn’t
been doing so for instance as in the case of reporting where the health facilities were submitting
the reports directly to the District instead of the HSD hence the need for an intervention.
Strengthening Decentralization for Sustainability (SDS) is a 5 year USAID funded program
aiming at improving results and sustainability of decentralized service delivery, in Health and
HIV/AIDS, at Local Government levels in Uganda. Among the functional areas that SDS
focuses on is Management Information Systems for Health and Community Based Services
where HMIS is key. It also builds capacity of District personnel to utilize data from the existing
MIS like HMIS to make management decisions to improve service delivery.SDS supported
districts to develop District Management Improvement Plans and Kaliro district as one of the
districts supported, highlighted a gap in HMIS reporting that required support. It’s for this
reason that Kaliro was selected to benefit from this project.

2
2.0 Literature review
The HMIS is a set of integrated components and procedures organized with an objective of
generating information which will improve health care management decisions at all levels of the
health system. It is also a routine monitoring system that plays a specific role in the monitoring
and evaluation process which is intended to provide warning signals through the use of
indicators.The main goal of HMIS is to provide quality information to support decision-making
at all levels of the health care system in Uganda (MoH, HMIS Manual, 2010)
All reports generated at the health facility have to be submitted to the HSD and DHO by the 7th
of the following month. During health facility meetings, performance review should focus on
timeliness, completeness and accuracy of the submitted reports. These reports are to be
discussed during the quarterly HUMC meetings. The HSD is required to review the HSD
performance based on the HMIS as the routine reporting system. The HSD Health Information
Assistant shall be responsible for compilation of the administrative and service delivery reports.
All weekly, monthly, quarterly and annual reports from health facilities should be compiled into
a single HSD report (MOH, M&E Plan for Health Sector, 2011)
According to the MoH M&E plan, the HSD Health Information Assistant is responsible for
receiving all health unit data (including those from private providers) in the HSD, enter all health
unit data info the DHIS2, analyzing the quality of HMIS reports received and ensuring follow up
for incompleteness and delays, compiling all reports into a single HSD reports, analyzing the
data for discussion by the HSD team for decision making, forward HSD report to DHO, provide
quarterly feed-back on data management to health units among others

3
3.0 Statement of the problem
The Ministry of Health reporting guidelines require that health facilities submit complete reports
to the HSD thereafter the HSD enters the data into the DHIS2 and analyses data to provide
feedback to improve performance of the health facilities. The health team observed that there
was inadequate HMIS reporting in Bumanya HSD as indicated by the report which showed that
out of the 19 health facilities none reported as required. This was not in line with the MoH
reporting guidelines which require that all health facilities should submit HMIS reports to the
HSD.
Despite the fact that the district had trained health facility in charges and records assistants in
HMIS reporting, the performance remained poor. This limited the HSD from undertaking its
responsibilities including checking the data for completeness, accuracy and timeliness, compiling
it and entering it into DHIS2 as well as analysing and providing feedback to health facilities. It’s
in this interest therefore, that this project aimed to streamline HMIS reporting at Bumanya HSD
as it’s the only HSD in the district responsible for 19 health facilities.
4.0 Justification
Reporting on health indicators through the HMIS is mandatory for all districts as it enables the
Ministry monitor progress and assess where the service delivery gaps are basing on the HMIS
data. MoH developed HMIS guidelines to be followed to ensure compete reporting is done and
in the right flow from the health facilities, consolidated at the HSD& entered into DHIS2 and
sent to the District for final submission.
Kaliro District had a challenge of untimely reporting into DHIS2 and one of the root causes was
because the District Bio Statistician was overwhelmed with entering all the data yet it’s supposed

4
to be entered at the HSD which was not happening. Some of the reasons as to why there were
these significant reporting gaps could be due to long distance from the health facilities to the
HSD, the HSD information assistant not being aware of his roles and the HSD not having a clear
data management system in place. It’s for this reason that the problem of inadequate reporting to
HSD was ranked the highest by the team.
5.0 Conceptual framework
From Figure 1 above, it can be observed that inadequate HMIS reporting by health facilities is
mainly caused by the difficulty in accessing the HSD due to long distances, no clear data
management system at the HSD and limited knowledge about the MoH reporting guidelines by
the health facility records staff. A data management system was set up at the HSD and the HSD
Medical Records Officer was trained in data management (including entry and recording), filing
cabinets and files were procured and all health facility records staff were trained in MoH
reporting guidelines and oriented about the importance of submitting reports to the HSD.
Figure 1: Conceptual framework
Limited knowledge
about MoH
reporting
guidelines
Inadequate
HMIS
reporting by
health
facilities
Lack of filing
cabinets and files
at HSD
Improved data
management
at HSD
Increased
submission of
complete
reports to HSD
Timely and
complete
entry into
DHIS2
No clear data
management
system at HSD
Limited
accessibility to HSD
due to long
distances
Train HSD records
Officer in data
management
Train HU records
staff in MoH
report guidelines
Sensitize HU
records staff in
importance of
reporting to HSD
5
The interventions mentioned above significantly increased the number of health facilities
submitting complete reports to the HSD. By establishing a data management system at the HSD
and training the HSD Records Officer in data management improved the capacity of the HSD to
file the incoming reports, records them and provide feedback to health facilities for
completeness, timeliness and accuracy on the reports submitted. This also improved the capacity
of the HSD Records Officer to enter the submitted data into DHIS2 as required. This project
therefore aimed at streamlining reporting in accordance with the MoH/HMIS reporting
guidelines which helped in improving timely and compete data entry into DHIS2.
6.0 Project objectives
Project Goal
The purpose of this project was to initiate the process of submitting reports to the HSD with the
aim of increasing the percentage of HFs submitting reports to HSD from 0% to 100% in 5
months.
Specific Objectives
To train all health facility In charges on HMIS reporting guidelines in the first 2 months
To strengthen the data management system at the HSD by August 2013
7.0 Methodology
CQI Project team formation
The CQI fellow held a series of meetings with various stakeholders from the project initiation to
its completion. Some of the people met included SDS Programme Institutional Supervisors, the
DHO, District Biostatistician, HSD In-Charge and the HSD Records Officer. During the initial
meeting with the District and HSD staff, the Fellow introduced the concept of CQI and the

6
members present accepted to be part of the team and hence a concrete team of 5 members was
formed as shown in table 1 below:
Table 1: CQI project team
No. Name Position
1. Rosette Nanyonjo Fellow/ M&E Specialist
2. Baker Serwambala SDS M&E Specialist (Former CQI Fellow)
3. Dr. Katamba Allan Bumanya HSD In charge
4. Jafali Muhammed District Bio statistician
5. Mugweri Joshua HMIS Focal person/HSD Records assistant
The team comprised 3 members from Kaliro District which included the HSD In-Charge, HSD,
Records Officer and the District Bio Statistician. In addition, 2 staff members from SDS
including a fellow and an alumni member from the CQI 2011 Fellowship group and colleague.
Problem Identification
In order to come up with the problem to be addressed, various steps were taken and these
included; a brainstorming session on a number of challenges faced by the District Health Office.
Some of the problems included late HMIS reporting, poor quality of reports, inaccurate
department reports, inadequate reporting by health facilities, no data analysis, limited data use
and feedback, poor filing system and others. The key problems that were zeroed on are shown in
the table below:
7
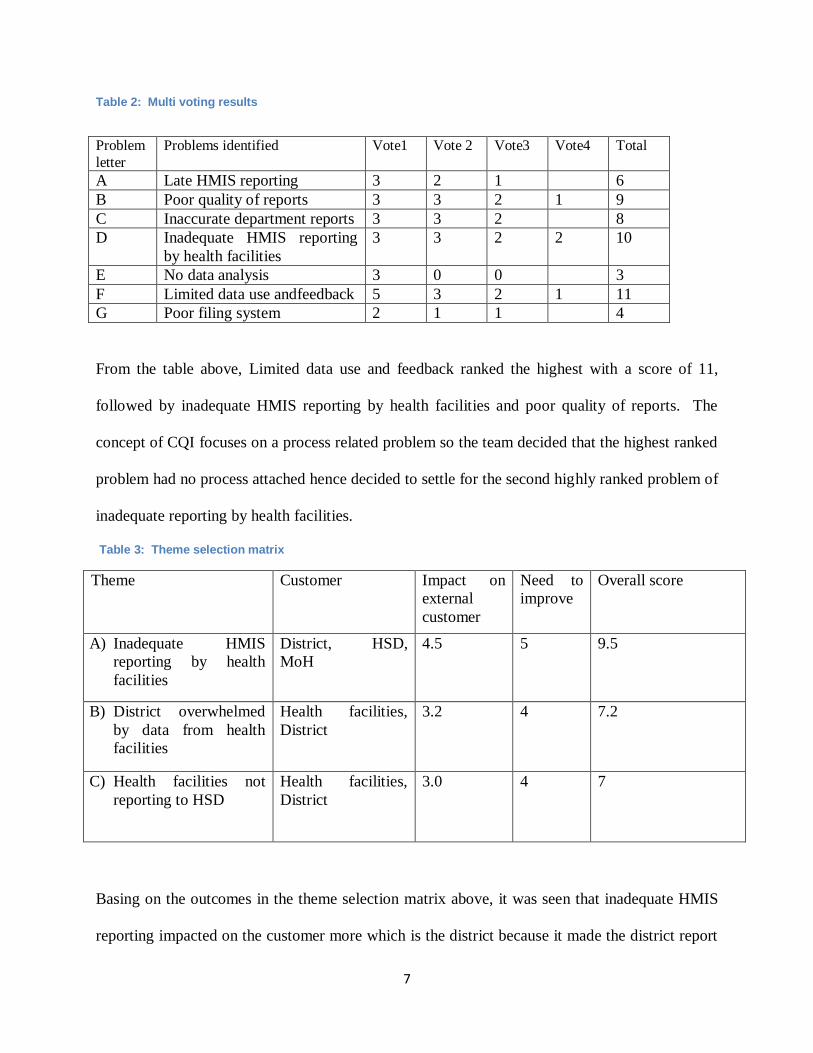
Table 2: Multi voting results
Problem
letter
Problems identified Vote1 Vote 2 Vote3 Vote4 Total
A Late HMIS reporting 3 2 1 6
B Poor quality of reports 3 3 2 1 9
C Inaccurate department reports 3 3 2 8
D Inadequate HMIS reporting
by health facilities
3 3 2 2 10
E No data analysis 3 0 0 3
F Limited data use andfeedback 5 3 2 1 11
G Poor filing system 2 1 1 4
From the table above, Limited data use and feedback ranked the highest with a score of 11,
followed by inadequate HMIS reporting by health facilities and poor quality of reports. The
concept of CQI focuses on a process related problem so the team decided that the highest ranked
problem had no process attached hence decided to settle for the second highly ranked problem of
inadequate reporting by health facilities.
Table 3: Theme selection matrix
Theme Customer Impact on
external
customer
Need to
improve
Overall score
A) Inadequate HMIS
reporting by health
facilities
District, HSD,
MoH
4.5 5 9.5
B) District overwhelmed
by data from health
facilities
Health facilities,
District
3.2 4 7.2
C) Health facilities not
reporting to HSD
Health facilities,
District
3.0 4 7
Basing on the outcomes in the theme selection matrix above, it was seen that inadequate HMIS
reporting impacted on the customer more which is the district because it made the district report

8
late and also the HSD because it can’t do its work if the health facilities don’t report adequately.
The conclusion therefore was that there was need to streamline reporting by the health facilities
at the HSD level.
8.0 Project implementation
Counter measures were selected by the team members basing on the root cause analysis and
practical methods were identified for each counter measure. The project then focused on
implementing the following counter measures; ensuring health facilities report to HSD, putting in
place a data management system at the HSD, training the HSD Records Officer in data management,
providing filing cabinets and files and conducting regular review meetings to assess the progress of the
project implementation as well as providing feedback to health facilities through the health unit
management committee.
Orientation of in-charges on HMIS reporting tools and guidelines
Health facility Incharges and records assistants were trained in June as the first activity for the project.
The objective of this training was to orient staff on MoH/HMIS reporting guidelines and sensitize them
about the importance of submitting reports to the HSD. Twenty Five staff were trained from all the 20
health facilities in the district and this was done with the aid of a facilitator from Ministry of Health and
Kaliro District Bio Statistician.

9
Figure 2: MoH Official facilitating training for In charges
Establishment of a data management system at the HSD
The HSD had never received any reports from the health facilities hence they didnt have a data
management system in place. Filing cabinets were procured, files for all health facilities and a register to
record in coming reports for timeliness, completeness and accuracy was also put in place.All files were
filed as they were sent to the HSD.
Training of the HSD Medical Records Officer on data management.
Th HSD MRO was trained in basic data management skills. These included recording incoming reports
and filing. An internet modem was purchased to enable the HSD MROenter the data into the DHIS2 as
required by the Ministry.
10
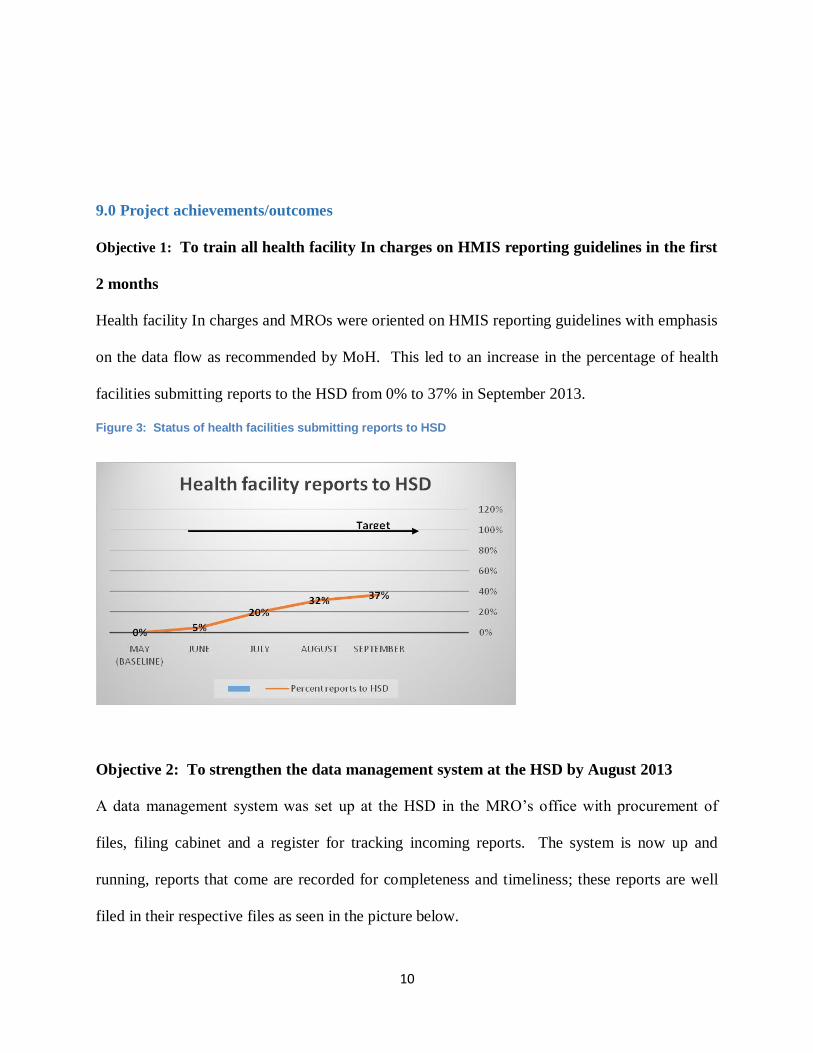
9.0 Project achievements/outcomes
Objective 1: To train all health facility In charges on HMIS reporting guidelines in the first
2 months
Health facility In charges and MROs were oriented on HMIS reporting guidelines with emphasis
on the data flow as recommended by MoH. This led to an increase in the percentage of health
facilities submitting reports to the HSD from 0% to 37% in September 2013.
Figure 3: Status of health facilities submitting reports to HSD
Objective 2: To strengthen the data management system at the HSD by August 2013
A data management system was set up at the HSD in the MRO’s office with procurement of
files, filing cabinet and a register for tracking incoming reports. The system is now up and
running, reports that come are recorded for completeness and timeliness; these reports are well
filed in their respective files as seen in the picture below.
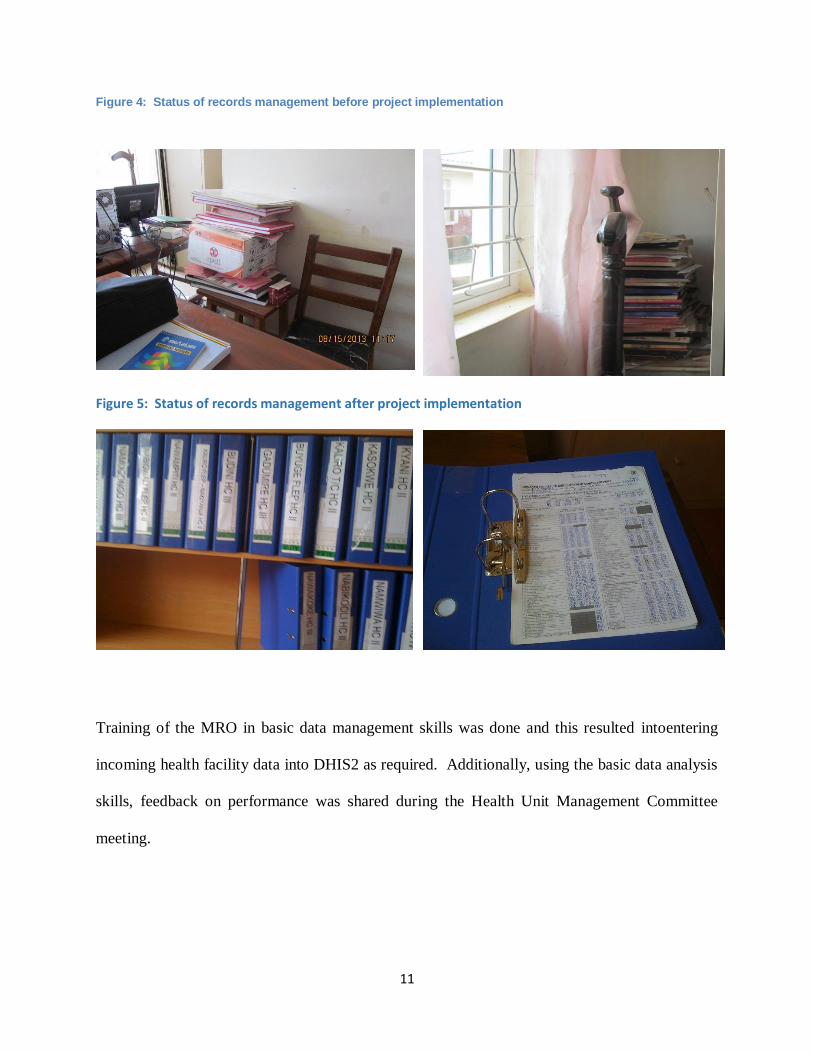
11
Figure 4: Status of records management before project implementation
Figure 5: Status of records management after project implementation
Training of the MRO in basic data management skills was done and this resulted intoentering
incoming health facility data into DHIS2 as required. Additionally, using the basic data analysis
skills, feedback on performance was shared during the Health Unit Management Committee
meeting.

12
10.0 Lessons learned:
While HMIS reporting guidelines emphasize the need for Health facilities to report
through HSD than directly to the district, they don’t empower the HSD to demand HFs to
report to them prior to reporting to the district
Compliance by the HSD MRO is key for improving HMIS reporting.
Data sharing is an informative way of providing feedback that can lead to improved
performance.
The target of 100% could not be achieved because it was too ambitious.
11.0 Challenges experienced and how they were overcome
Challenge Solution
1. Non-compliance of HSD MRO Involved Management to take action
2. Distance to HSD too long compared to
district hence limiting facilities from
submitting reports to HSD
Health units were encouraged to submit 2
copies to district to be picked by HSD MRO
3. Inadequate supply of HMIS triplicated
reporting tools hindered submission of
2 copies
Advised the DHO to lobby MoH and
Implementing Partners for more reporting
tools
12.0 Conclusions:
In conclusion, all the steps that were taken to implement the project from multi voting, theme
selection, root cause analysis, identification of counter measures, practical methods and
outcomes were key in ensuring successful implementation of the project. This led to results like
increase in the health facilities reporting to the HSD as required by MoH, a functional data
management system at the HSD and increased knowledge by the HSD MRO in data management
which will ensure that this practice stays on even after the project ended. Unfortunately the
target of 100% was not achieved because it was too ambitious and other challenges.

13
13.0 Recommendations:
The reporting system needs to be configured in such a way that it only allows reports into
DHIS2 that have been initially entered at the HSD. This way all facilities will ensure to
submit reports to the HSD.
MakSPH – CDC Fellowship Program to lobby with MoH to pilot a revised system in a
few districts with a similar challenge to see if there will be a significant change.
Recommend that SDS incorporates supporting HMIS reporting in supported districts that
have similar challenges with continuous technical assistance.
Ministry of Health to design some quality improvement indicators to be used to monitor
districts with similar reporting challenges
14.0 Next steps
Kaliro District Health Team to continue supporting and supervising the HSD to ensure
the data management system is functional and data entry into DHIS2 is done.
15.0 References:
1) Ministry of Health (2010), The Health Management Information System, Volume 1:
Health Unit Procedure Manual.
2) Ministry of Health (2011), Monitoring and Evaluation Plan for Health Sector, Strategic &
Investment Plan 2010/11 – 2014/15
Related Documents











