Strategies to Reduce Adverse Events of Invasive Coronary Procedures Craig Phillip Juergens (MBBS (Hons), FRACP, FACC, FCSANZ) Conjoint Associate Professor South Western Sydney Clinical School The University of New South Wales Publications submitted in fulfilment of the requirement for the degree of Doctor of Medicine (MD) by published work UNSW South Western Sydney Clinical School Faculty of Medicine The University of New South Wales Sydney, NSW, Australia 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Strategies to Reduce Adverse
Events of Invasive Coronary
Procedures
Craig Phillip Juergens
(MBBS (Hons), FRACP, FACC, FCSANZ)
Conjoint Associate Professor
South Western Sydney Clinical School
The University of New South Wales
Publications submitted in fulfilment of the requirement for the degree of
Doctor of Medicine (MD) by published work
UNSW
South Western Sydney Clinical School
Faculty of Medicine
The University of New South Wales
Sydney, NSW, Australia
2013
THE UNIVERSITY OF NEW SOUTH WALES
Sunmmc or Family name: Juergens Fii'.H name: Craig
Thesis/Dissertation Sheet
Abbreviation for degree as given in the University calendar: Doctor of Medicine (MD) by publishrd work School: South Western Sydney Clinical School
Title: Stnttegies to Reduce Adverse I~ vents of Invasive Coronary Procedures
Other namc/s: Phillip
Faculty: Medicine
I have and continue to be enthusiastically involved in Cardiology Research, particularly with respect to strategies to reduce the adverse outcomes of invasive coronary procedures, I present a body of work which specifically addresses a number of areas related to the practice of interventional cardiology including the use of varying contrast agents during invasive coronary procedures; sheath management techniques relating to the use of vascular closure devices, sheath removal practices, differing sheath sizes; the use of antithrombotic agents during and after the procedure; the reporting and management of campi ications and outcomes of large stent registries monitoring outcomes of differing types of coronary stents, Percutaneous coronary intervention remains a rapidly evolving field and I believe I have made a significant contribution to improving the outcomes of patients who undergo this procedure.
Declaration relating to disposition of project thesis/dissertation
I hereby grant to the University of New South Wales or its agents the right to archive and to make available my thesis or dissertation in whole or in part in the University libraries in a!! fOrms of media, now or here a ncr known, subject to the provisions of the Copyright Act I 968. I retain all property rights, such as patent rights. I also retain the right to usc in future works (such as articles or books) all or part of this thesis or dissertation
I also authorise University Microfilms to use the 350 word abstract of my thesis in Dissertation Abstracts International (this is applicable to doctoral theses only).
s.;guoturc .•.... ;b.. ~--··········· ...... A .. ~·.· ......· ... \.................... Datc.l.?.lt/.z:.o.! 1-... (Jvu···· .. · (~~--~~ss 'The University recognises that there may be exceptional circumstances requiring restrictions on copying or cond1tions on usc. Requests fOr restriction for a period of up to 2 years must be made in writing. Requests for a longer period of restriction may be considered in exceptional circumstances and require the ap mlVal of the Dean of Graduate Research
FOR OFFICE USE ONLY Bate of completion of requirements fo1· Award:
Originality Statement
I hereby declare that this submission is my own work and to the best of my
knowledge it contains no materials previously published or written by another person,
or substantial prop01tions of material which have been accepted for the award of any
other degree or diploma at the University of New South Wales or any other
educational institution, except where due acknowledgement is made in the thesis. Any
contribution made to the research by others, with whom l have worked at the
University of New South Wales or elsewhere, is explicitly acknowledged in the thesis.
l also declare that the intellectual content of this thesis is the product of my own work,
except to the extent that assistance from others in the project's design and conception
or in style, presentation and linguistic expression is acknowledged.
Signed: ............... ~······················
Name: Craig P. Juergens
Date: ............ !.~/~./??/1-. ............................ .
Copyright Statement
'I hereby grant the University of New South Wales or its agents the right to archive and to make available my thesis or dissertation in whole or part in the University libraries in all forms of media, now or here after known, subject to the provisions of the Copyright Act 1968. I retain all proprietary rights, such as patent rights. I also retain the right to use in future works (such as articles or books) all or part of this thesis or dissertation. I also authorise University Microfilms to use the 350 word abstract of my thesis in Dissertation Abstract International (this is applicable to doctoral theses only). I have either used no substantial portions of copyright material in my thesis or I have obtained permission to use copyright material; where permission has not been granted I have applied/will apply for a patiial restriction of the digital copy of my thesis or dissetiation.'
Signed: ............... ~······················· Name: Craig P. Juergens
Date: .............. e/1/2..011: .............................. .
Authenticity Statement
'I certify that the Library deposit digital copy is a direct equivalent of the final officially approved version of my thesis. No emendation of content has occurred and if there are any minor variations in formatting, they are the result of the conversion to digital format.'
Signed: ............. -6&························· Name: Craig P. Juergens
Date: .............. f.?.h/. Z. .0 !.f.. ............................. .
1
ABSTRACT
I have been, and continue to be enthusiastically involved in Cardiology
research, particularly with respect to strategies to reduce the adverse outcomes of
invasive coronary procedures. I present a body of work which specifically addresses a
number of areas related to the practise of interventional cardiology including the use
of varying contrast agents during invasive coronary procedures; sheath management
techniques relating to the use of vascular closure devices, sheath removal practices,
differing sheath sizes; the use of antithrombotic agents during and after the procedure;
the reporting and management of complications and outcomes of large stent registries
monitoring outcomes of differing types of coronary stents. Percutaneous coronary
intervention remains a rapidly evolving field and I believe I have made a significant
contribution to improving the outcomes of patients who undergo this procedure.
2
TABLE OF CONTENTS
Abstract………………………………………………………………………………1
Brief Curriculum Vitae, Craig Phillip Juergens…………………………………..3
Introduction………………………………………………………………………….4
Chapter 1
Contrast Studies……………………………………………………...………9
Chapter 2
Arterial Access Studies………………………………………………...……23
Chapter 3
Antithrombotic Agents…………………………………………………...…38
Use of unfractionated heparin……………………………………...38
Antiplatelet agents…………………………………………………..42
Glycoprotein IIb/IIIa antagonists………………………………….47
Chapter 4
Reporting and management of complications………………………….…69
Peri-procedural myocardial infarction……………………………69
Aortic dissection…………………………………………………….71
Chapter 5
Stent Registries……………………………………………………………...77
Conclusion…………………………………………………………………………..82
Bibliography of papers as part of MD submission……………………………..…83
Additional Publications not forming part of thesis……………………………….86
3
Brief Curriculum Vitae, Craig Phillip Juergens
MB BS (Hons), University of NSW 1987
Basic Physician Trainee,
Royal North Shore Hospital, Sydney 1989-91
Cardiology Trainee,
Royal Prince Alfred Hospital, Sydney 1992-1993
Fellowship of Royal Australasian College of Physicians 1993
Research Fellow,
Royal Prince Alfred Hospital, Sydney 1994-1995
Interventional Cardiology Fellow,
Stanford University Medical Centre, Stanford California USA 1995-1997
Senior Staff Specialist,
Liverpool Hospital, Sydney 1997-present. Head of Department 2011-present
Fellow of American College of Cardiology, 1999
Fellow Cardiac Society of Australia and New Zealand, 2004
Conjoint Associate Professor UNSW, 2006-present
4
INTRODUCTION
This submission for MD by publication concerns strategies that identify and
try to reduce the adverse events that may occur after coronary interventional
procedures. I have had a strong interest throughout my medical career in research in
Cardiology and particularly the subspecialty of Interventional Cardiology. After
undertaking an Interventional Cardiology Fellowship at Stanford University in the
USA, I returned to establish the Interventional Cardiology service at Liverpool
Hospital, Sydney which has grown in the space of 15 years to be one of the busiest
such units in Australia. As well as being actively involved in the training of
interventional cardiologists from Australia, I have supervised the training of Fellows
from around the world from countries including Myanmar, Malaysia, China, England,
New Zealand and Singapore.
I have had a particular interest into the procedural aspects of invasive coronary
procedures. This area is often not studied in a rigorous scientific fashion due to the
lack of industry support. To date there have been many trials published with respect to
the use of stenting versus coronary artery bypass surgery or medical therapy; and
balloon angioplasty versus bare metal stenting versus drug eluting stents. However
there is a paucity of data on the more routine aspects of the procedure including
sheath management and to a lesser extent, the type of contrast used. Initially the type
of anticoagulants used during and after the procedure were not subjected to rigorous
scientific assessment. There is also limited data assessing the long term outcomes of
any particular type of stent due to the rapid obsolescence of each device. Research
around definitions of periprocedural myocardial infarction is a rapidly changing field
due to the prompt uptake of new cardiac biomarkers and approaches to the
management of rare complications are also not well researched due to the fact they
5
occur uncommonly and unpredictably, which prevents assessment in the context of a
controlled clinical trial. I believe my research represents a somewhat unique
contribution as it focuses on the less well studied areas of interventional Cardiology
and provides a substantial advancement of knowledge in these areas.
I have compiled a body of work, covered by this thesis, which specifically
addresses each of these areas including:
1. Use of varying contrast agents during invasive coronary procedures
2. Sheath management including use of vascular closure devices, sheath
removal techniques and differing sheath sizes
3. Use of antithrombotic agents during and after the procedure
4. Reporting and management of complications
5. Participation in large registries monitoring outcomes of differing types of
bare metal stents
My personal contribution to the research discussed above has generally been
to lead the research from its inception to its conclusion. This has included the
formation of the hypothesis and aims of the study, the assembly of teams and
collaborators and the conduct and reporting of the research. The majority of the work
has been performed at my current institution in the Department of Cardiology,
Liverpool Hospital, Sydney, Australia. I acknowledge and am very grateful for the
contributions of my colleagues who are listed with each individual work. For work
where I was not senior or first author, I have sought and obtained permission from the
senior authors to reproduce this work as part of my thesis.
6
Structure of Thesis
The five broad themes of my research are discussed in separate sections; use
of contrast agents, sheath management after coronary procedures, use of varying
antithrombotic agents during percutaneous coronary intervention, reporting and
management of complications in the cardiac catheterisation laboratory and
participation in large registries of coronary stents.
I have included 21 publications as part of this thesis but have published a
further 33 articles as listed in the additional publication section of this submission. As
of February 2013, my overall body of work has been cited 334 times, with the 21
publications used as part of the thesis cited 161 times. Given six of these thesis papers
were published after 2010, I would expect the citations to increase over time.
According to Scopus ® my calculated h index is 10. A number of my publications
have been cited in review articles and have been included in meta-analyses. My work
has been acknowledged in local and international guidelines with papers cited in “A
position statement of the Society of Cardiovascular Angiography and
Interventions”[1]; “European Society of Urogenital Radiology contrast media safety
committee guidelines”[2]; “the 2011 American College of Cardiology
Foundation/American Heart Association/Society of Cardiovascular Angiography and
Interventions guidelines for percutaneous coronary intervention”[3]; the “Italian
Society for Haemostasis and Thrombosis guidelines for the management of bleeding
and of invasive procedures in patients with platelet disorders and/or
thrombocytopaenia”[4] and the “Australian clinical practice guidelines to improve
care for people undergoing percutaneous coronary interventions”[5].
Each section contains a discussion of my research and places it in the context
of the theme and its significance amongst the published literature. The references

7
relevant to each section are listed at the end of the chapter, followed by copies of each
paper.
8
Introduction References
1. Klein LW, Sheldon MW, Brinker J, et al. The use of radiographic contrast media
during PCI: a focused review. A position statement of the Society of Cardiovascular
Angiography and Interventions. Catheter Cardiovasc Interv 2009;74:728-746.
2. Stacul F, van der Molen AJ, Reimer P, et al. Contrast induced nephropathy:
updated ESUR contrast media committee guidelines. Eur Radiol 2011;21:2527-2541.
3. Levine GN, Bates ER, Blakenship JC, et al. 2011 ACCF/AHA/SCAI guideline for
percutaneous coronary intervention: a report of the American College of Cardiology
Foundation/American Heart Association task force on practice guidelines and the
Society for Cardiovascular Angiography and Interventions. Circulation
2011;124:e574-e651.
4. Tosetto A, Balduini CL, Cattaneo M, et al. Management of bleeding and of
invasive procedures in patients with platelet disorders and/or thrombocytopaenia:
Guidelines of the Italian Society for Haemostasis and Thrombosis (SISET). Thromb
Res 2009;124:e13-e18.
5. Rolley JX, Salamonson Y, Wensley C, Dennison CR, Davidson PM. Nursing
clinical practice guidelines to improve care for people undergoing percutaneous
coronary interventions. Aust Crit Care 2011; 24:18-38.
9
CHAPTER 1
CONTRAST STUDIES
Introduction.
Contrast media are essential components of the performance of angiography
and percutaneous coronary intervention (PCI). Contrast induced nephropathy (CIN) is
one of the most important complications of interventional coronary procedures. Less
frequent, but occasionally life threatening, is the occurrence of allergic reactions.
There is data that suggests differing classes of contrast agents are associated with
divergent incidences of allergic reactions or CIN.
Paper 1(Heart Lung Circ 2005;14:172-177)
Non-ionic low osmolar contrast agents have been shown to decrease the
incidence of adverse reactions associated with diagnostic procedures when compared
to high osmolar ionic compounds [1-4]. Allergic reactions also appear to occur more
frequently in patients receiving low osmolarity ionic compounds when compared to
non-ionic compounds [5,6]. Non-ionic compounds are also more affordable in the
Australian market. However, studies in vitro have shown that non-ionic low osmolar
agents have less inherent anticoagulant activity than ionic agents [7,8] and a number
of randomised clinical trials have supported the conclusion that the ionic low osmolar
compound ioxaglate is associated with fewer ischaemic complications of coronary
intervention than are non-ionic agents [9,10]. Consequently in our environment, there
were patients who “followed on” from their diagnostic angiogram to a coronary
10
intervention who received two different classes of agents in rapid succession during
the same procedure, as we felt ioxaglate would result in fewer ischaemic
complications in this context. On review of the literature it was apparent that there
was no data concerning the safety of “mixing” different classes of contrast agents and
so we sought to determine whether this practice resulted in more adverse clinical
events than would a policy of continuing the same type of contrast agent. This formed
the basis of my first contrast paper; Paper 1. We found that combining ionic and non-
ionic contrast agents in the same procedure was not associated with any more adverse
reactions than using an ionic contrast agent alone and that the ionic contrast agent
ioxaglate was associated with the majority of allergic reactions. We concluded that
using the non-ionic agent iopromide alone for coronary intervention was associated
with the lowest risk of an adverse event.
Context and Implications
This work was initiated and completed by the author at Liverpool hospital and
remains the only paper to my knowledge specifically addressing the issue of
combining differing contrast agents. As a consequence of this study we stopped using
ioxaglate in our catheterisation laboratory.
Impact on literature
According to Scopus ®, this article has been cited at least five times since publication
from a journal with an impact factor of 1.196. It has been cited in the “Position
statement of the Society of Cardiovascular Angiography and Interventions” on the use
of radiographic contrast media during PCI [11].
11
Paper 2 (Intern Med J 2009;39:25-31)
Apart from limiting the amount of contrast given, there have been a number of
interventions designed to reduce the risk of CIN, including hydration with saline [12]
or sodium bicarbonate [13], and periprocedural hemofiltration [14]. The antioxidant
N-acetylcysteine (NAC) in combination with prehydration has been shown in a
number of studies to reduce CIN in patients with chronic renal insufficiency [15-19].
Other studies however have either shown no benefit [20], or a dose effect [21].
Despite the disparate views on the efficacy of NAC, due to its low cost and toxicity
many operators routinely prescribe it with prehydration in patients at high risk for
CIN.
Iodixanol is an iso-osmolar, dimeric, non-ionic contrast medium, which has
been shown to have reduced general toxicity when compared to low-osmolar contrast
mediums [22,23]. Two trials [24,25] in patients at high risk for developing CIN
concluded that nephropathy was reduced in patients receiving iodixanol rather than
low-osmolar contrast medium. Many operators switched to using this agent based on
these studies. However we noted that other measures to reduce the risk of CIN were
not controlled for in these studies. Whilst one study mandated prehydration prior to
contrast exposure [25], in the other, hydration was recommended but not required
[24]. The use of NAC was either given in a small number of patients [24] or was an
exclusion criterion [25] in these studies. Only one of these studies [24] collected
serum creatinine levels beyond day 2. It is possible that longer follow up, adequate
hydration and the routine use of NAC may have altered the outcome of these studies.
We therefore performed a randomised, prospective, double-blind multicentre
study comparing the nephrotoxicity of iodixanol with that of iopromide in patients
12
with impaired renal function who had received mandated prehydration and oral NAC
prior to a coronary angiographic and/or interventional procedure. We aimed to
determine whether the use of iso-osmolar iodixanol is less nephrotoxic than low-
osmolar iopromide when patients are adequately prehydrated and have received N-
acetylcysteine (NAC).
Paper 2 demonstrated that there remains a high incidence of CIN at both days
2 and 7 despite prehydration and routine NAC in patients with pre-existing renal
dysfunction undergoing a coronary interventional procedure. We concluded that
whilst underpowered, our study suggested that when other renoprotective measures
are controlled for, the choice of contrast agent becomes less important.
Context and Implications
This work, which was supported by a Health Research Foundation Sydney Southwest
Grant (Project No. 2004.10.11), was initiated and completed by the author at
Liverpool hospital. Other sites were approached by the author to make this a
multicentre study. As a consequence of this study, Liverpool Hospital and the centres
involved with the trial have changed their practise with respect to the type of contrast
used along with the usual attempts to limit the total volume administered.
Impact on literature
According to Scopus ®, this article has been cited fourteen times since publication
from a journal with a 5 year impact factor of 1.674, including as part of a meta-
analysis on this topic and in the updated European Society of Urogenital Radiology
contrast media safety guidelines [26].
13
Paper 3(Med J Aust 2011;195:268-269)
There is a paucity of prospective randomised controlled trials involving the
long term follow up of patients who have developed CIN after invasive coronary
procedures to determine the late effects on renal function and outcomes in relation to
dialysis and mortality. As a consequence we chose to report the long term follow up
of the patients enrolled in our initial study. This forms the basis of Paper 3, where
our primary end point was the incidence of persistent renal impairment. This was
defined using standard definitions and we accounted for the coefficient of variation of
creatinine and also the age related decline in glomerular filtration rate (GFR). The
secondary end point was a composite of death and need for dialysis.
At a median follow up of 43 months, we found a high rate of persisting renal
dysfunction in patients who developed CIN early after invasive coronary procedures
and concluded that physicians should be alert to this complication.
Context and Implications
This work continued on from our previous study and was initiated and completed by
the author at Liverpool hospital. One of the original sites did not provide long term
data so were excluded, but the overall conclusions emphasised our need for ongoing
diligence in following these complex patients.
Impact on literature
This work was submitted to the Medical Journal of Australia as a full article but the
reviewers suggested resubmitting as a Letter to the Editor which we ultimately did in
order to ensure publication in a reasonable impact general medical journal. According
to Scopus ®, this article has not yet been cited from a journal with a 5 year impact
factor of 3.101.
14
Paper 4 (J Am Coll Cardiol 2010;56:525-526)
I was approached by collaborators at the Baker IDI Heart and Diabetes
Institute in Melbourne, Australia to use the population data from paper 2, to serve as a
contemporaneous comparison group for a cohort of 26 patients whom they treated
with a coronary sinus aspiration catheter. This new device was evaluated for the first
time in this paper ( Paper 4) to assess the feasibility of coronary sinus blood removal
during coronary angiography and intervention, using a unique vacuum aspiration
assisted aspiration system with the specific intent of reducing the systemic appearance
of radiographic contrast and thus to the kidneys. We concluded that removal of
contrast laden blood from the coronary sinus attenuates the incidence of
nephrotoxicity in patients with pre-existing renal impairment undergoing invasive
coronary procedures.
Context and Implications
Whilst the work with the coronary sinus aspiration catheter was conducted by the
Baker IDI Heart and Diabetes Institute as part of a single arm multicentre trial, the
data from our original study provided a necessary comparator group to evaluate this
new technology. I provided input into the analysis of the data and assisted in the
drafting of the manuscript. The first and senior authors have been contacted and are
supportive of me using this article as part of my thesis.
Impact on literature
This article was only published in 2010 and according to Scopus ®, has been cited
once from a journal with a 5 year impact factor of 13.065.
15
Chapter 1 References
1. Bettman MA, Higgins CB. Comparison of an ionic with a non-ionic contrast agent
for cardiac angiography: Results of a multicenter trial. Invest Radiol 1985;20:S70-74.
2. Wolf GL, Arenson RL, Cross AP. A prospective trial of ionic vs non-ionic contrast
agents in routine clinical practice: comparison of adverse effects. AJR 1989;152:939-
944.
3. Barrett BJ, Parfrey PS, McDonald JR, Hefferton DM, Reddy ER, McManamon PJ.
Nonionic low osmolality versus ionic high osmolality contrast material for
intravenous use in patients perceived to be at high risk: randomised trial. Radiology
1992;183:105-110.
4. Katayama H, Yamaguchi K, Kozuka T, Takashima T, Seez P, Matsuura K. Adverse
reactions to ionic and non-ionic contrast media: a report from the Japanese committee
on the safety of contrast material. Radiology 1990;175:621-628.
5. Schrader R, Esch I, Ensslen R, et al. A randomized trial comparing the impact of a
non-ionic (Iomeprol) versus an ionic (Ioxaglate) low osmolar contrast medium on
abrupt vessel closure and ischemic complications after coronary angioplasty. J Am
Coll Cardiol 1999;33:395-402.
6. Lasser EC, Lyon SG, Berry CC. Reports on contrast media reactions: analysis of
data from reports to the US Food and Drug administration. Radiology 1997;203:605-
610.
7. Stormorken H, Skalpe IO, Testart MC. Effect of various contrast media on
coagulation, fibrinolysis and platelet function: an in vitro study and in vivo study.
Invest Radiol 1986;21:348-354.
16
8. Belleville J, Baquet J, Paul J, Clendinnen G, Elroy R. In vitro study of the
inhibition of coagulation induced by different radiocontrast molecules. Thromb res
1985;38:149-162.
9. Grines CL, Schreiber TL, Savas V, et al. A randomized trial of low osmolar ionic
versus nonionic contrast media in patients with myocardial infarction or unstable
angina undergoing percutaneous transluminal coronary angioplasty. J Am Coll
Cardiol 1996;27:1381-1386.
10. Piessens JH, Stammen F, Vrolix MC, et al. Effects of ionic versus a nonionic low
osmolar contrast agent on the thrombotic complications of coronary angioplasty.
Cathet Cardiovasc Diagn 1993;28:99-105.
11. Klein LW, Sheldon MW, Brinker J, et al. The use of radiographic contrast media
during PCI: a focused review. A position statement of the Society of Cardiovascular
Angiography and Interventions. Catheter Cardiovasc Interv 2009;74:728-746.
12. Solomon R, Werner C, Mann D, D’Elia J, Silva P. Effects of saline, mannitol and
furosemide on acute decreases in renal function induced by radiocontrast agents. N
Engl J Med 1994;331:1416-1420.
13. Merten GJ, Burgess WP, Gray LV, et al. Prevention of contrast induced
nephropathy with sodium bicarbonate: a randomized controlled trial. JAMA
2004;291:2328-2334.
14. Marenzi G, Marana I, Lauri G, et al. The prevention of radiocontrast agent
induced nephropathy by hemofiltration. N Engl J Med 2003;349:1333-1340.
15. Tepel M, van der Giet M, Schwarzfeld C, Laufer U, Liermann D, Zidek W.
Prevention of radiographic contrast agent induced reductions in renal function by
acetylcysteine. N Eng J Med 2000;343:180-184.
17
16. Shyu KG, Cheng JJ, Kuan P. Acetylcysteine protects against acute renal damage
in patients with abnormal renal function undergoing a coronary procedure. J Am Coll
Cardiol 2002;40:1383-1388.
17. Diaz-Sandoval LJ, Kosowsky BD, Losordo DW. Acetylcysteine to prevent
angiography related renal tissue injury (the APART trial). Am J Cardiol 2002;89:356-
358.
18. Briguori C, Colombo A, Airoldi F, et al. N-acetylcysteine versus fenoldopam
mesylate to prevent contrast agent associated nephrotoxicity. J Am Coll Cardiol
2004;44:762-765.
19. Marenzi G, Assanelli E, Marana I, et al. N-acetylcysteine and contrast induced
nephropathy in primary angioplasty. N Engl J Med 2006;354:2773-2782.
20. Goldenberg I, Shechter M, Matetzky S, et al. Oral acetylcysteine as an adjunct to
saline hydration for the prevention of contrast induced nephropathy following
coronary angiography: a randomized controlled trial and review of the current
literature. Eur Heart J 2004;25:212-218.
21. Briguori C, Colombo A, Violante A, et al. Standard vs double dose of N-
acetylcysteine to prevent contrast agent associated nephrotoxicity. Eur Heart J
2004;25:206-211.
22. Grynne BH, Nossen JO, Bolstad B, Borch KW. Main results of the first
comparative clinical studies on Visipaque. Acta Radiol Suppl 1995;399:265-270.
23. Davidson CJ, Laskey WK, Hermiller JB, et al. Randomized trial of contrast media
utilization in high-risk PTCA: the COURT trial. Circulation 2000;101:2172-2177.
24. Aspelin P, Aubry P, Fransson SG, Strasser R, Willenbrock R, Berg KJ.
Nephrotoxic effects in high-risk patients undergoing angiography. N Eng J Med
2003;348:491-499.
18
25. Jo SH, Youn TJ, Koo BK, et al. Renal toxicity evaluation and comparison
between visipaque (iodixanol) and hexabrix (ioxaglate) in patients with renal
insufficiency undergoing coronary angiography: The RECOVER study: a randomized
controlled trial. J Am Coll Cardiol 2006;48:924-930.
26. Stacul F, van der Molen AJ, Reimer P, et al. Contrast induced nephropathy:
updated ESUR contrast media committee guidelines. Eur Radiol 2011;21:2527-2541.

19
PAPER 1
Reprinted from Heart Lung and Circulation 2005;14:172-177 with
permission from Elsevier
ORIG
INALARTICLE
Original Article
Adverse Reactions of Low Osmolar Non-Ionicand Ionic Contrast Media When
Used Together or Separately DuringPercutaneous Coronary Intervention
Craig P. Juergens, FRACPa,∗, Aye Mi Khaing, MRCPb,Geraldine J. McIntyre, RNa, Dominic Y.C. Leung, PhD, FRACPa,
Sidney T.H. Lo, FRACPa, Clyne Fernandes, FRACPa andAndrew P. Hopkins, FRACPa
a Department of Cardiology, Liverpool Hospital, Locked Bag 7103, Elizabeth Street, Liverpool, NSW 2170 Australiab Cardiac Medical Unit, Yangon General Hospital, Myanmar
C
Background: Due to perceived advantages in the use of non-ionic contrast agents for diagnostic angiography and ionicagents for percutaneous coronary intervention (PCI), patients often receive various combinations of both types of agents.
Aim: To assess potential adverse effects of non-ionic and ionic contrast media when used together or separately duringpercutaneous coronary intervention.
Methods: We retrospectively evaluated the outcomes of 532 patients undergoing percutaneous coronary interventionin our institution. Patients were divided into two groups: those that underwent diagnostic angiography and “follow on”PCI; and those that underwent “planned” PCI. The groups were subdivided on the basis of the use of the ionic agentioxaglate or the non-ionic agent iopromide during PCI. The frequency of allergic reactions and major adverse cardiacevents (MACE) were noted.
Results: With respect to the “follow on” group, allergic reactions occurred in 9 of 150 patients (6.0%) who receivedthe combination of ioxaglate and iopromide versus 1 of 93 (1.1%) who only received iopromide (p= 0.094). There wasno difference with respect to MACE [6 (4.0%) ioxaglate and iopromide versus 4 (4.3%) iopromide alone, p= 1.00]. In the“planned” group, 7 of 165 patients (4.2%) receiving ioxaglate had an allergic reaction as opposed 0.0% (0 of 124 patients)in the iopromide group (p= 0.021). All contrast reactions weremild. The incidence of aMACEwas similar in both groups[1 (0.6%) ioxaglate versus 2 (1.6%) iopromide, p= 0.579]. The incidence of allergic reactions was similar if ioxaglate wasused alone or in combination with iopromide (p= 0.478).
Conclusions: Whilst combining ionic and non-ionic contrast agents in the same procedure was not associated with anymore adverse reactions than using an ionic contrast agent alone, the ionic contrast agent ioxaglate was associated withthe majority of allergic reactions. With respect to choice of contrast agent, using the non-ionic agent iopromide alone forcoronary intervention is associated with the lowest risk of an adverse event.
(Heart Lung and Circulation 2005;14:172–177)© 2005 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society of Australia and New
Zealand. Published by Elsevier Inc. All rights reserved.
Keywords. Ioxaglate; Iopromide; Angioplasty; Complications
Introduction
ontrastmedia are essential components of the perfor-mance of percutaneous coronary intervention (PCI),
but their contribution to complications occurring dur-ing these procedures has been debated. Non-ionic lowosmolar contrast agents have been shown to decrease
∗ Corresponding author. Tel.: +61 2 9828 3074; fax: +61 2 9828 3054.E-mail address: [email protected] (C.P. Juergens).
the incidence of adverse reactions associated with diag-nostic procedures when compared to high osmolar ioniccompounds.1–4 Allergic reactions also appear to occurmore frequently in patients receiving low osmolarity ioniccompounds when compared to non-ionic compounds.5,6
Studies in vitro have shown that non-ionic low osmolaragents have less inherent anticoagulant activity than ionicagents.7,8 A few randomised clinical trials have supportedthe conclusion that the ionic low osmolar compound
© 2005 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society ofAustralia and New Zealand. Published by Elsevier Inc. All rights reserved.
1443-9506/04/$30.00doi:10.1016/j.hlc.2005.06.013

ORIG
INALARTICLE
Heart Lung and Circulation Juergens et al. 1732005;14:172–177 Contrast and percutaneous coronary intervention
ioxaglate is associatedwith fewer ischaemic complicationsof coronary intervention than are non-ionic agents.9,10
Based on theperceivedbetter tolerability and cheaper costof non-ionic agents in our environment, our laboratoryroutinely uses these compounds for diagnostic angiog-raphy and reserves the ionic agent, ioxaglate, for percu-taneous coronary interventions. This policy meant thatmany patients who “followed on” from their diagnosticprocedures to coronary interventions received two differ-ent classes of agents in rapid succession during the sameprocedure. Due to a lack of data concerning the safety of“mixing” different classes of contrast agents, we sought todetermine whether this practice resulted in more adverseclinical events than would a policy of continuing the sametype of contrast agent. In order to establish a baselinerisk of adverse reactions, we ascertained the incidenceof such events in patients undergoing “planned” percu-taneous coronary intervention that received exclusivelyeither ioxaglate or iopromide (the non-ionic agent).
Materials and Methods
Study PopulationAll 532 patients who underwent PCI from January 2001to February 2002 in our institution were included inthe study. We performed a retrospective analysis of ourprospective, observational percutaneous coronary inter-vnsetpifld7ibifcotaeadul(iclGofict
nary intervention directly after the diagnostic angiogram.All patients received iopromideduring thediagnostic pro-cedure and either iopromide or ioxaglate during the coro-nary intervention. The second group of patients had theirdiagnostic angiogram (using iopromide) performed sometime before their “planned” percutaneous coronary inter-vention. This groupwas divided into two subgroups basedon whether or not they received iopromide or ioxaglateduring their coronary intervention. Finally, we comparedthe incidence of allergic reactions in patientswho receivedioxaglate alone or in combination with iopromide.
Procedural VariablesThenumber of attempted lesions, stent usage, fluoroscopytime, volume of contrast media used and use of glycopro-tein IIb/IIIa antagonists were recorded for each patient.
Study EndpointsThe primary endpoint was the development of an allergicreaction requiring treatment with H1 and H2 antagonists,corticosteroids or catecholamines.Allergic reactions couldinclude cutaneousmanifestationsofurticariawithorwith-out pruritus, erythema, maculopapular rash, conjunctivalsymptoms and facial or peripheral angioneurotic oedema.This data was obtained from the database and where nec-essary correlations were obtained from the clinical record.The secondary endpoint was a composite of cardiovas-
ctwbrditCtatcstfc
SAtcacvMfs
R
D“
ention database. Three operators using standard tech-iques performed all coronary interventions during thetudy period and patients’ details were prospectivelyntered into our database. It is our policy for patientso receive at least 300mg of aspirin within 24h of therocedure and to continue on 100–150mg daily after thentervention. Intracoronary stent implantations were per-ormed using standard techniques of high-pressure bal-oon inflations and patients generally received a loadingose of 300mg of clopidogrel (if not previously on it) and5mg daily thereafter for 4 weeks. Heparin was admin-stered as a weight-adjusted dose. Patients routinely hadlood drawn for creatine kinase (CK) enzyme (and MBsoenzyme) the morning after the procedure and morerequently if there was a reason to suspect an adverseardiac event. Data on the occurrence of thrombotic stentcclusion (TSO), emergency target vessel revascularisa-ion (TVR) and periprocedural myocardial infarction (MI)re routinely collected in our institution prospectively andntered into our database. In addition, the occurrence ofllergic reactions is noted and routinely entered into ouratabase. As is the policy of our institution, all patientsndergoing diagnostic coronary angiography received theowosmolarnon-ionicmonomercontrast agent iopromideUltravist, Schering, Berlin, Germany). During coronaryntervention the choice of contrast mediumwas at the dis-retion of the operator and all patients received either theow osmolar ionic dimer compound ioxaglate (Hexabrix,uerbet, Paris, France) or iopromide. For the purposef this study we divided patients into two groups. Therst group comprised patients who underwent diagnosticoronary angiography and “follow on” coronary interven-ion, which was defined as unplanned percutaneous coro-
ular death, non-fatal myocardial infarction and urgentarget vessel revascularisation at 30 days. Urgent TVRas defined as the occurrence of emergency coronaryypass surgery or repeat PCI of the treated vessel forecurrent ischaemia within 30 days of the initial proce-ure. Non-fatal myocardial infarction was defined as anncrease in the creatinekinase concentration to three timeshe upper limit of normal with a concomitant rise in theK–MB isoenzyme above the upper limit of normal orhe appearance of new Q waves after the procedure. Ifpatient reached more than one cardiac endpoint, onlyhe most severe endpoint was counted as a major adverseardiac event (MACE) for the final analysis. Thrombotictent occlusion was defined as angiographically provenotal occlusion (TIMI flow <2), or flow-limiting thrombusormation inside the stentwithin 30days after initially suc-essful stenting.
tatistical Analysisll values are reported as mean±one standard devia-ion unless otherwise stated. Categorical variables areompared with χ2-test or Fischer’s exact test as appropri-te. Continuous variables with a normal distribution areompared with unpaired Student’s t-test and continuousariables not normally distributed are compared with theann–WhitneyWilcoxon test. Statistical analysiswas per-ormed using SPSS for Windows (version 10). Statisticalignificance was defined as a two-tailed p value of <0.05.
esults
uring the study period there were 243 patients who hadfollow on” PCI. Of these 93 received iopromide alone
ORIG
INALARTICLE
174 Juergens et al. Heart Lung and CirculationContrast and percutaneous coronary intervention 2005;14:172–177
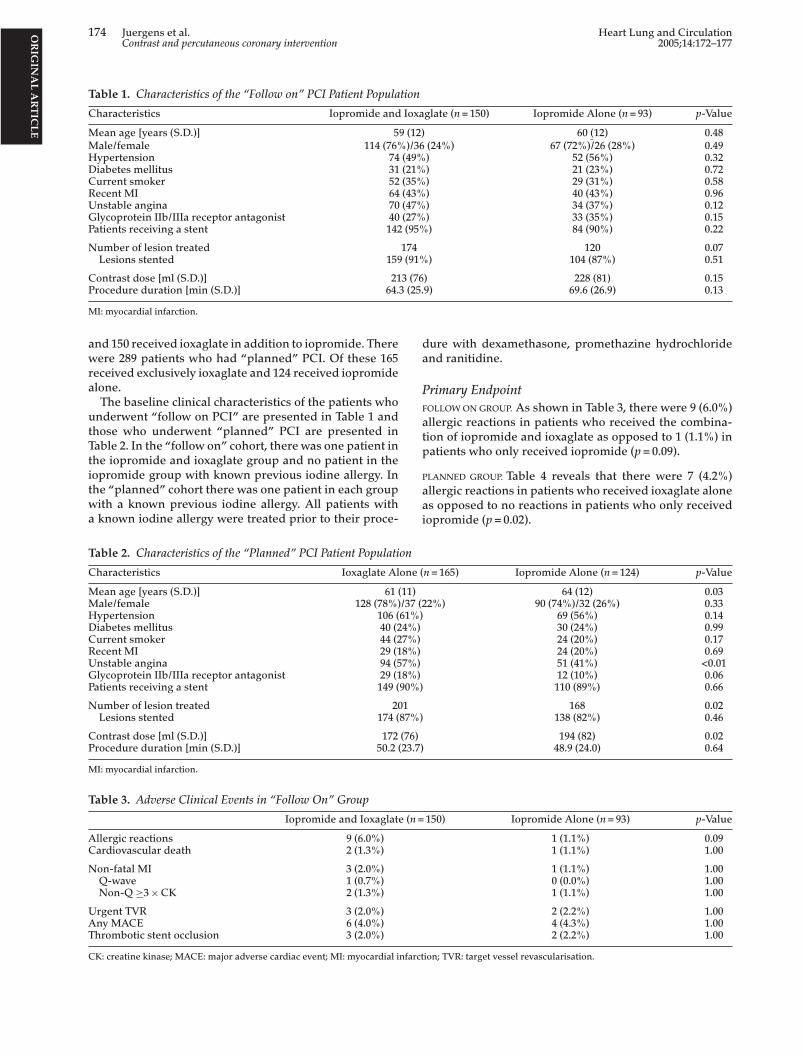
Table 1. Characteristics of the “Follow on” PCI Patient Population
Characteristics Iopromide and Ioxaglate (n= 150) Iopromide Alone (n= 93) p-Value
Mean age [years (S.D.)] 59 (12) 60 (12) 0.48Male/female 114 (76%)/36 (24%) 67 (72%)/26 (28%) 0.49Hypertension 74 (49%) 52 (56%) 0.32Diabetes mellitus 31 (21%) 21 (23%) 0.72Current smoker 52 (35%) 29 (31%) 0.58Recent MI 64 (43%) 40 (43%) 0.96Unstable angina 70 (47%) 34 (37%) 0.12Glycoprotein IIb/IIIa receptor antagonist 40 (27%) 33 (35%) 0.15Patients receiving a stent 142 (95%) 84 (90%) 0.22
Number of lesion treated 174 120 0.07Lesions stented 159 (91%) 104 (87%) 0.51
Contrast dose [ml (S.D.)] 213 (76) 228 (81) 0.15Procedure duration [min (S.D.)] 64.3 (25.9) 69.6 (26.9) 0.13
MI: myocardial infarction.
and 150 received ioxaglate in addition to iopromide. Therewere 289 patients who had “planned” PCI. Of these 165received exclusively ioxaglate and 124 received iopromidealone.The baseline clinical characteristics of the patients who
underwent “follow on PCI” are presented in Table 1 andthose who underwent “planned” PCI are presented inTable 2. In the “follow on” cohort, there was one patient inthe iopromide and ioxaglate group and no patient in theiopromide group with known previous iodine allergy. Inthe “planned” cohort there was one patient in each groupwith a known previous iodine allergy. All patients witha known iodine allergy were treated prior to their proce-
dure with dexamethasone, promethazine hydrochlorideand ranitidine.
Primary EndpointFOLLOWONGROUP. As shown in Table 3, there were 9 (6.0%)allergic reactions in patients who received the combina-tion of iopromide and ioxaglate as opposed to 1 (1.1%) inpatients who only received iopromide (p= 0.09).
PLANNED GROUP. Table 4 reveals that there were 7 (4.2%)allergic reactions in patients who received ioxaglate aloneas opposed to no reactions in patients who only receivediopromide (p= 0.02).
Table 2. Characteristics of the “Planned” PCI Patient Population
Characteristics Ioxaglate Alone (n= 165) Iopromide Alone (n= 124) p-Value
Mean age [years (S.D.)] 61 (11) 64 (12) 0.03Male/female 128 (78%)/37 (22%) 90 (74%)/32 (26%) 0.33Hypertension 106 (61%) 69 (56%) 0.14Diabetes mellitus 40 (24%) 30 (24%) 0.99Current smoker 44 (27%) 24 (20%) 0.17Recent MI 29 (18%) 24 (20%) 0.69Unstable angina 94 (57%) 51 (41%) <0.01Glycoprotein IIb/IIIa receptor antagonist 29 (18%) 12 (10%) 0.06Patients receiving a stent 149 (90%) 110 (89%) 0.66
Number of lesion treated 201 168 0.02Lesions stented 174 (87%) 138 (82%) 0.46
Contrast dose [ml (S.D.)] 172 (76) 194 (82) 0.0223.7)
(n=
Procedure duration [min (S.D.)] 50.2 (
MI: myocardial infarction.
Table 3. Adverse Clinical Events in “Follow On” Group
Iopromide and Ioxaglate
Allergic reactions 9 (6.0%)Cardiovascular death 2 (1.3%)
Non-fatal MI 3 (2.0%)Q-wave 1 (0.7%)Non-Q ≥3×CK 2 (1.3%)
Urgent TVR 3 (2.0%)
Any MACE 6 (4.0%)Thrombotic stent occlusion 3 (2.0%)CK: creatine kinase; MACE: major adverse cardiac event; MI: myocardial infarct
48.9 (24.0) 0.64
150) Iopromide Alone (n= 93) p-Value
1 (1.1%) 0.091 (1.1%) 1.00
1 (1.1%) 1.000 (0.0%) 1.001 (1.1%) 1.00
2 (2.2%) 1.00
4 (4.3%) 1.002 (2.2%) 1.00ion; TVR: target vessel revascularisation.
ORIG
INALARTICLE
Heart Lung and Circulation Juergens et al. 1752005;14:172–177 Contrast and percutaneous coronary intervention
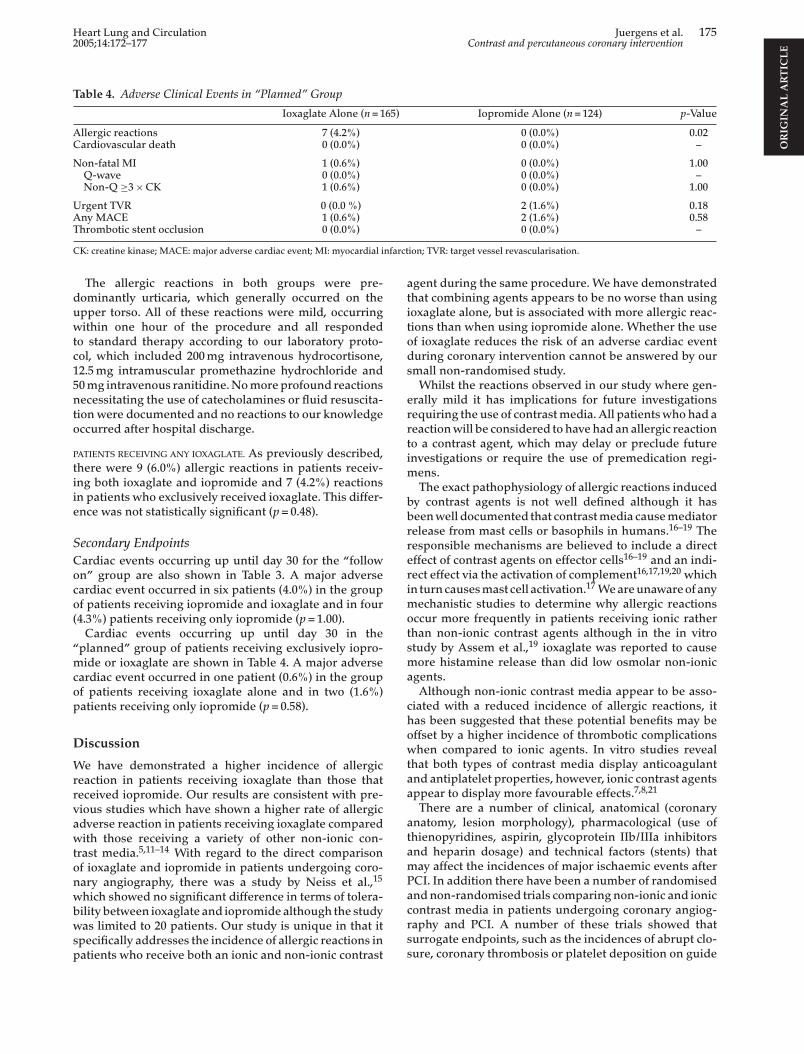
Table 4. Adverse Clinical Events in “Planned” Group
Ioxaglate Alone (n= 165) Iopromide Alone (n= 124) p-Value
Allergic reactions 7 (4.2%) 0 (0.0%) 0.02Cardiovascular death 0 (0.0%) 0 (0.0%) –
Non-fatal MI 1 (0.6%) 0 (0.0%) 1.00Q-wave 0 (0.0%) 0 (0.0%) –Non-Q ≥3×CK 1 (0.6%) 0 (0.0%) 1.00
Urgent TVR 0 (0.0 %) 2 (1.6%) 0.18Any MACE 1 (0.6%) 2 (1.6%) 0.58Thrombotic stent occlusion 0 (0.0%) 0 (0.0%) –
CK: creatine kinase; MACE: major adverse cardiac event; MI: myocardial infarction; TVR: target vessel revascularisation.
The allergic reactions in both groups were pre-dominantly urticaria, which generally occurred on theupper torso. All of these reactions were mild, occurringwithin one hour of the procedure and all respondedto standard therapy according to our laboratory proto-col, which included 200mg intravenous hydrocortisone,12.5mg intramuscular promethazine hydrochloride and50mg intravenous ranitidine.Nomoreprofound reactionsnecessitating the use of catecholamines or fluid resuscita-tion were documented and no reactions to our knowledgeoccurred after hospital discharge.
PATIENTS RECEIVING ANY IOXAGLATE. As previously described,there were 9 (6.0%) allergic reactions in patients receiv-ing both ioxaglate and iopromide and 7 (4.2%) reactionsin patients who exclusively received ioxaglate. This differ-ence was not statistically significant (p= 0.48).
Secondary EndpointsCardiac events occurring up until day 30 for the “followon” group are also shown in Table 3. A major adversecardiac event occurred in six patients (4.0%) in the groupof patients receiving iopromide and ioxaglate and in four(4.3%) patients receiving only iopromide (p= 1.00).Cardiac events occurring up until day 30 in the
“planned” group of patients receiving exclusively iopro-mide or ioxaglate are shown in Table 4. A major adversecop
D
Wrrvawtonwbwsp
agent during the same procedure. We have demonstratedthat combining agents appears to be no worse than usingioxaglate alone, but is associated with more allergic reac-tions than when using iopromide alone. Whether the useof ioxaglate reduces the risk of an adverse cardiac eventduring coronary intervention cannot be answered by oursmall non-randomised study.Whilst the reactions observed in our study where gen-
erally mild it has implications for future investigationsrequiring the use of contrastmedia. All patientswhohad areactionwill be considered to havehad an allergic reactionto a contrast agent, which may delay or preclude futureinvestigations or require the use of premedication regi-mens.The exact pathophysiology of allergic reactions induced
by contrast agents is not well defined although it hasbeenwell documented that contrastmedia causemediatorrelease from mast cells or basophils in humans.16–19 Theresponsible mechanisms are believed to include a directeffect of contrast agents on effector cells16–19 and an indi-rect effect via the activation of complement16,17,19,20 whichin turncausesmast cell activation.17Weareunawareofanymechanistic studies to determine why allergic reactionsoccur more frequently in patients receiving ionic ratherthan non-ionic contrast agents although in the in vitrostudy by Assem et al.,19 ioxaglate was reported to causemore histamine release than did low osmolar non-ionica
chowtaa
atamPacrss
ardiac event occurred in one patient (0.6%) in the groupf patients receiving ioxaglate alone and in two (1.6%)atients receiving only iopromide (p= 0.58).
iscussion
e have demonstrated a higher incidence of allergiceaction in patients receiving ioxaglate than those thateceived iopromide. Our results are consistent with pre-ious studies which have shown a higher rate of allergicdverse reaction in patients receiving ioxaglate comparedith those receiving a variety of other non-ionic con-rast media.5,11–14 With regard to the direct comparisonf ioxaglate and iopromide in patients undergoing coro-ary angiography, there was a study by Neiss et al.,15
hich showed no significant difference in terms of tolera-ility between ioxaglate and iopromide although the studyas limited to 20 patients. Our study is unique in that itpecifically addresses the incidence of allergic reactions inatients who receive both an ionic and non-ionic contrast
gents.Although non-ionic contrast media appear to be asso-iated with a reduced incidence of allergic reactions, itas been suggested that these potential benefits may beffset by a higher incidence of thrombotic complicationshen compared to ionic agents. In vitro studies revealhat both types of contrast media display anticoagulantnd antiplatelet properties, however, ionic contrast agentsppear to display more favourable effects.7,8,21
There are a number of clinical, anatomical (coronarynatomy, lesion morphology), pharmacological (use ofhienopyridines, aspirin, glycoprotein IIb/IIIa inhibitorsnd heparin dosage) and technical factors (stents) thatay affect the incidences of major ischaemic events afterCI. In addition there have been a number of randomisedndnon-randomised trials comparing non-ionic and ionicontrast media in patients undergoing coronary angiog-aphy and PCI. A number of these trials showed thaturrogate endpoints, such as the incidences of abrupt clo-ure, coronary thrombosis or platelet deposition on guide

ORIG
INALARTICLE
176 Juergens et al. Heart Lung and CirculationContrast and percutaneous coronary intervention 2005;14:172–177
wires, were less frequent with ionic contrast agents.10,22,23
In terms of direct comparison of ioxaglate and iopro-mide, there has been a small study of patients undergoingabdominal and femoral angiography,24 which looked at anumber of haemostatic parameters in vivo. The authorsfound that both agents caused activation of the coagu-lation system and platelets and there was no differencein the degree of activation between the two agents. Thesmall study of patients undergoing coronary angiographyby Neiss et al.,15 did not specifically address thromboticcomplications of contrast use.When it comes to clinicallymore relevantmajor adverse
events there are conflicting data concerning the useof ioxaglate in coronary interventions. In a number ofrandomised9,10 and non-randomised trials,25 the use ofioxaglate was associated with a reduction in thromboticevents afterpercutaneous coronary intervention. Ina largenon-randomised trial by Scheller et al.,25 the authorsfound ahigher rate of both acute and subacute stent occlu-sion in patients receiving non-ionic contrast agents whencompared to ioxaglate. They also found a lower incidenceof the combined clinical endpoint of target lesion revas-cularisation, coronary artery bypass surgery and deathin the group who received ioxaglate (16.3% versus 22.9%,p= 0.001). Whilst a large study of nearly 4000 patients, thisstudy is limited by its non-randomised nature, the use ofsix different non-ionic contrast agents and slight differ-
ioxaglate over iopromide with respect to a reduction inmajor ischaemic complications of percutaneous coronaryintervention.
Study LimitationsOur study has a number of limitations inherent in retro-spective observational reports. Patients in this study werenot randomised either to the use of contrast agent or asto whether they would have “follow on” PCI or “planned”PCI. The diagnosis of an allergic reaction is rather sub-jective and open to bias, however, it has always been ourpolicy to document such events prospectively at the timeof the percutaneous coronary intervention. In addition,our observations are only applicable to the index hospi-tal admission and wemay have missed late reactions. Theionic and non-ionicmonomers appear to induce late onsetallergy-like reactions with equal frequency28 and there-fore would have potentially affected both groups equally.Notably, this typeof reaction is considered tobe rarely life-threatening as opposed to acute reactions and is possiblyof less clinical relevance. It is also possible that allergicreactions were related to other medications although thetiming ismore likely to reflect the choice of contrast agent.We routinely perform a creatine kinase measurement
the morning after a percutaneous coronary interventionand more frequently if there is clinical suspicion of anadverse cardiac event. It is possible, however, that wemay
ences between the groups compared. Of note we foundno difference in the rate of thrombotic stent occlusionbetween our groups although our study is too small todrawanydefinite conclusionswith this respect to this end-point.In contrast, a number of trials have shown no differ-
ence between ionic or non-ionic contrast media5,14,26,27
with respect to major ischaemic events. In the largest ran-domised trial published to date, Schrader et al.5 evaluatedthe outcomes of 2000 patients undergoing PCI. Patientsreceived either iomeprol (non-ionic) or ioxaglate (ionic)according to a randomised double-blind protocol. The fre-quency of re-occlusions necessitating repeat angioplastyand the rate of major ischaemic complications includingemergencybypass surgery andmyocardial infarctionwerenot significantly different in either group. The authorsof this study concluded that the observed in vitro differ-ences between non-ionic and ionic contrastmedia seem tobe insignificant under clinical conditions. More recently,two large multicentre studies of patients undergoing PCIhave compared the isosmolar non-ionic dimer iodixanol toioxaglate.14,27 In the study byDavidson et al.,27 therewas alow incidenceof in-hospital adverse events inbothgroups,and the iodixanol cohort actually experienced the pri-mary composite clinical outcomes less frequently than theioxaglate group (5.4% versus 9.5%, respectively; p= 0.027).In the larger study by Bertrand et al.,14 therewas no differ-ence in 2 day or 1 month major adverse cardiac events ineither group. These studies suggest that, using contempo-rary techniques, non-ionic agentsmay potentially be safer(or at leastnoworse), than ionic agents.Thedatapresentedin our study, whilst non-randomised, support the conclu-sions that there is no apparent major advantage of using
havemissed small rises in creatine kinase,whichmayhaveinfluenced the number of myocardial infarcts diagnosed.Whilst our study groups were well matched in the “fol-
low on” group, there were some significant differencesin the “planned” PCI cohort. There was a higher dose ofcontrast utilised in the iopromide group, however, we doc-umented more allergic reactions in the ioxaglate group.As this is a retrospective study we did not collect data
on other potential adverse events related to contrast usesuch nausea and vomiting, renal failure and other poten-tially thromboembolic events including stroke or systemicinfarction, which may have impacted on our results.
Conclusions
Whilst combining ionic and non-ionic contrast agents inthe same procedure was not associated with any moreadverse reactions than using an ionic contrast agent alone,the ionic contrast agent ioxaglate was associated with themajorityof allergic reactions.With respect to choiceof con-trast agent, using the non-ionic agent iopromide alone forcoronary intervention is associated with the lowest risk ofan adverse event.
References
1. Bettman MA, Higgins CB. Comparison of an ionic with anon-ionic contrast agent for cardiac angiography: results ofa multicenter trial. Invest Radiol 1985;20:70–4.
2. Wolf GL, Arenson RL, Cross AP. A prospective trial of ionicvs. non-ionic contrast agents in routine clinical practice: com-parison of adverse effects. AJR 1989;152:939–44.
3. Barrett BJ, ParfreyPS,McDonald JR,HeffertonDM,ReddyER,McManamon PJ. Nonionic low osmolality versus ionic high

ORIG
INALARTICLE
Heart Lung and Circulation Juergens et al. 1772005;14:172–177 Contrast and percutaneous coronary intervention
osmolality contrast material for intravenous use in patientsperceived to be at high risk: randomised trial. Radiology1992;183:105–10.
4. Katayama H, Yamaguchi K, Kozuka T, Takashima T, Seez P,MatsuuraK.Adverse reactions to ionic andnon-ionic contrastmedia: a report from the Japanese committee on the safety ofcontrast material. Radiology 1990;175:621–8.
5. Schrader R, Esch I, Ensslen R, Fach WA, Merle H, Scherer D,et al. A randomized trial comparing the impact of a non-ionic(Iomeprol) versus an ionic (Ioxaglate) low osmolar contrastmedium on abrupt vessel closure and ischemic complicationsafter coronary angioplasty. J Am Coll Cardiol 1999;33:395–402.
6. Lasser EC, Lyon SG, Berry CC. Reports on contrast mediareactions: analysis of data from reports to the US Food andDrug administration. Radiology 1997;203:605–10.
7. Stormorken H, Skalpe IO, Testart MC. Effect of various con-trast media on coagulation, fibrinolysis and platelet function:an in vitro study and in vivo study. Invest Radiol 1986;21:348–54.
8. Belleville J, Baquet J, Paul J, Clendinnen G, Elroy R. In vitrostudy of the inhibition of coagulation induced by differentradiocontrast molecules. Thromb Res 1985;38:149–62.
9. Grines CL, Schreiber TL, Savas V, Jones DE, Zidar FJ, Gan-gadharan V, et al. A randomized trial of low osmolar ionicversus nonionic contrast media in patients with myocardialinfarctionorunstable anginaundergoingpercutaneous trans-luminal coronaryangioplasty. JAmCollCardiol 1996;27:1381–6.
10. Piessens JH, Stammen F, Vrolix MC, Glazier JJ, Benit E, DeGeest H, et al. Effects of ionic versus a nonionic low osmolarcontrast agent on the thrombotic complications of coronaryangioplasty. Cathet Cardiovasc Diagn 1993;28:99–105.
15. Neiss AC, Barth P, Chastin I, Erdmann E. Comparison ofsodium-meglumine ioxaglate and iopromide in coronaryangiography. Ann Radiol 1989;32:49–53.
16. Laroche D, Aimone-Gastin I, Dubois F, Huet H, Gerard P,VergnaudM-C, et al. Mechanisms of severe, immediate reac-tions to iodinatedcontrastmaterial.Radiology1998;209:183–90.
17. Ring J, Arroyave CM, Frizler MJ, Tan EM. In vitro histamineand serotonin release by radiographic contrast media (RCM):complement dependent and independent release reactionand changes in ultrastructure of human blood cells. Clin ExpImmunol 1978;32:105–18.
18. Younger RE, Herrod HG, Lieberman PL, Trouy RL, CrawfordLV. Characteristics of diatrizoate-induced basophil histaminerelease. J Allergy Clin Immunol 1986;77:94–100.
19. Assem ESK, Bray K. The release of histamine from humanbasophils by radiological contrast agents. Br J Radiol1983;56:647–52.
20. KolbWP, Lang JH, Lasser EC. Nonimmunologic complementactivation in normal human serum induced by radiographiccontrast media. J Immunol 1978;121:1232–8.
21. Sane DC,Moser TL, Bashore TM,Wagner CL, Greenberg CS.Diatrizoate-containing contrast media inhibit platelet aggre-gation by disrupting fibrinogen binding. Coron Artery Dis1991;2:389–96.
22. EsplugasE,CequierA, Jara F,Mauri J, Soler T, Sola J, et al. Riskof thrombosis during coronary angioplasty with low osmolal-ity contrast media. Am J Cardiol 1991;68:1020–4.
23. Qureshi NR, den Heijer P, Crijns HJGM. Percutaneous coro-nary angioscopic comparison of thrombus formation duringpercutaneous coronary angioplasty with ionic and nonionic
11. Gertz EW, Wisneski JA, Miller R, Knudtson M, Robb J, Dra-gatakis L, et al. Adverse reactions of low osmolality contrastmedia during cardiac angiography: a prospective randomizedmulticenter study. J Am Coll Cardiol 1992;19:899–906.
12. Fransson SG, Stenport G, Andersson M. Immediate lateadverse reactions in coronary angiography: a comparisonbetween iodixanol and ioxaglate. Acta Radiol 1996;37:218–22.
13. Sutton AGC, Finn P, Grech ED, Hall JA, Stewart MJ, Davies A,et al. Early and late reactions after the use of iopamidol 340,ioxaglate 320, and iodixanol 320 in cardiac catheterisation.AmHeart J 2001;141:677–83.
14. Bertrand ME, Esplugas E, Piessens J, Rasch W. For the visi-paque in percutaneous transluminal coronary angioplasty[VIP] trial investigators. Influence of a non-ionic, iso-osmolarcontrast medium (iodixanol) versus an ionic, low-osmolarcontrast medium (ioxaglate) on major adverse cardiac eventsin patients undergoing percutaneous transluminal coronaryangioplasty. A multicenter, randomised, double-blind study.Circulation 2000;101:131–6.
low osmolality contrast media in unstable angina. Am J Car-diol 1997;80:700–4.
24. Hoffmann JJML, Tielbeek AV, Krause W. Haemostatic effectsof low osmolar non-ionic and ionic contrast media: a doubleblind comparative study. Br J Radiol 2000;73:248–55.
25. Scheller B, Hennen B, Pohl A, SchiefferH,Markwirth T. Acuteand subacute stent occlusion: risk reduction by ionic contrastmedia. Eur Heart J 2001;22:385–91.
26. Lembo NJ, King III SB, Roubin GS, Black AJ, Douglas Jr JS.Effects of nonionic versus ionic contrast media on complica-tions of percutaneous transluminal coronary angioplasty. AmJ Cardiol 1991;67:1046–50.
27. Davidson CJ, Laskey WK, Hermiller JB, Harrison JK, MatthaiJr W, Vlietstra RE, et al. Randomized trial of contrast mediautilisation in high risk PTCA. The COURT trial. Circulation2000;101:2172–7.
28. PedersenSH, SvalandMG,ReissA-L,AndrewE. Late allergy-like reactions following vascular administration of radiogra-phy contrast media. Acta Radiol 1998;39:344–8.

20
PAPER 2
Reprinted from Internal Medical Journal 2009;39:25-31 with permission
from “John Wiley and Sons”

ORIGINAL ARTICLE
Nephrotoxic effects of iodixanol and iopromide in patients withabnormal renal function receiving N-acetylcysteine and hydrationbefore coronary angiography and intervention: a randomized trialC. P. Juergens,1 J. P. Winter,1 P. Nguyen-Do,1 S. Lo,1 J. K. French,1 H. Hallani,2 C. Fernandes,2 N. Jepson3
and D. Y. C. Leung1
1Department of Cardiology, Liverpool Hospital, University of New South Wales, 2Department of Cardiology, Nepean Hospital and3Department of Cardiology, Prince of Wales Hospital, Sydney, New South Wales, Australia
Key words
contrast, nephropathy, iopromide, iodixanol.
Correspondence
Craig P. Juergens, Department of Cardiology,
Liverpool Hospital, Elizabeth Street, Locked
Bag 7103, Liverpool BC, NSW 1871, Australia.
Email: [email protected]
Received 27 September 2007; accepted
14 January 2008.
doi:10.1111/j.1445-5994.2008.01675.x
Abstract
Background: The use of contrast agents during coronary intervention can
result in nephropathy, particularly in patientswith renal dysfunction.We aimed
to determine whether the use of iso-osmolar iodixanol is less nephrotoxic than
that of low-osmolar iopromide when patients are adequately prehydrated and
have received N-acetylcysteine.
Methods: We conducted a randomized, double-blind, multicentre study of
patients with impaired renal function undergoing a coronary interventional
procedure. Primary end-point was the incidence of contrast-induced nephro-
pathy (CIN) on day 2, defined as an increase in serum creatinine concentration
of �44 lmol/L (0.5 mg/dL) or by a relative increase of �25% from baseline.
Secondary end-points included peak increase in serum creatinine between
baseline and day 7.
Results: Of 191 patients recruited, 15% (95% CI: 8–22) of the patients
receiving iopromide and 12% (95%CI: 5–19) of the patients receiving iodixanol
developed CIN (95% CI of the difference: 13 to27, P = 0.56). When including
peak serum creatinine on day 7, CIN developed in 23% of patients receiving
iopromide and in 27%of patients receiving iodixanol (95%CI of the difference:
8 to216, P = 0.48). The peak increase in serum creatinine concentration at day
7was similar in both groups (patients receiving iopromide, 18.4 ± 24.4 lmol/L,
vs patients receiving iodixanol, 21.9 ± 24.2 lmol/L; P = 0.33).
Conclusion: There remains a high incidence of CIN despite prehydration and
routine use of N-acetylcysteine in patients with pre-existing renal dysfunction
undergoing coronary interventional procedures. Although our study is under-
powered, iodixanol was not associated with a statistically significant lower
incidence of CIN when compared with iopromide.
Introduction
Contrast-induced nephropathy (CIN) is one of the most
important complications of interventional coronary pro-
cedures. High-risk patients for CIN include those with pre-
existing renal dysfunction, particularly diabetic nephro-
pathy, and patients receiving higher doses of contrast
agents.1,2 It is usually defined as an absolute increase in
the serum creatinine concentration of at least 44 lmol/L
(0.5 mg/dL) or by a relative increase of at least 25% from
the baseline value within 48 h of contrast administra-
tion.3–6 Generally, the serum creatinine peaks on days 2
to 5 after exposure to contrast and returns to baseline
Funding: The study was supported by Health Research Founda-
tion Sydney Southwest Grant (Project No. 2004.10.11).
Potential conflicts of interest: None
Internal Medicine Journal 39 (2009) 25–31
ª 2008 The Authors
Journal compilation ª 2008 Royal Australasian College of Physicians 25

within 2 weeks.6–10 Although it is generally reversible,
it can occasionally lead to chronic renal failure, need
for transient dialysis and increased morbidity and
mortality.7,9,11–13
There have been several interventions designed to
reduce the risk of CIN, including hydration with saline14
or sodium bicarbonate,15 and periprocedural haemofiltra-
tion.16 The anti-oxidant N-acetylcysteine (NAC) in com-
bination with prehydration has been shown in several
studies to reduce CIN in patients with chronic renal insuf-
ficiency.4,17–20 Other studies, however, have either shown
no benefit21 or a dose effect.22 Despite the disparate views
on the efficacy of NAC, because of its low cost and toxicity,
many operators routinely prescribe it with prehydration
in patients at high risk for CIN.
Large clinical studies have shown that the use of low-
osmolar contrast medium substantially reduce the risk of
CIN in high-risk patients compared with the use of high-
osmolar contrast agents.1,23–25 Iodixanol is an iso-osmolar,
dimeric, non-ionic contrast medium, which has been
shown to reduce general toxicity when compared with
low-osmolar contrast mediums.26,27 Two trials in patients
at high risk for developing CIN concluded that nephro-
pathy was reduced in patients receiving iodixanol rather
than patients receiving low-osmolar contrast medium
treatment.5,28 Although one study mandated prehydra-
tion before contrast exposure,28 in the other study, hydra-
tion was recommended but not required.5 The use of NAC
was either given in a small number of patients5 or was an
exclusion criteria28 in these studies. Only one of these
studies5 collected serum creatinine levels beyond day 2.
It is possible that longer follow up, adequate hydration
and the routine use of NACmay have altered the outcome
of these studies.
We carriedout a randomized, prospective, double-blind,
multicentre study comparing the nephrotoxicity of iodix-
anolwith that of iopromide in patientswith impaired renal
function who had received mandated prehydration and
oral NAC before a coronary angiographic and/or interven-
tional procedure.
Methods
Study patients
Patients were eligible for the study if they were older
than 18 years, were undergoing coronary angiography or
percutaneous coronary intervention (PCI), had a stable
serum creatinine concentration above 130 lmol/L (meas-
ured within 3 months) or a calculated creatinine clear-
ance of <60 mL/min, according to the Cockcroft and
Gault formula. Exclusion criteria were pregnancy,
history of anaphylactic reaction to iodinated contrast
medium, treatment with contrast agents within 7 days,
known allergies to NAC, cardiogenic shock, current
dialysis, conditions or circumstances that precluded
adequate hydration or planned postcontrast dialysis.
Patients on metformin had it withheld on the day of
and for 48 h postprocedures or until the creatinine
normalized, whichever was later. The protocol was
approved by the institutional review board of each
hospital, and all patients provided written informed
consent.
Study design
This is an investigator-initiated study conducted in three
centres in Sydney, Australia. Patients were randomized to
receive either the low-osmolar contrast agent, iopromide
(Schering, Berlin, Germany), or the iso-osmolar agent,
iodixanol (Amersham Health, Amersham, UK). Both
agents are non-ionic and have an iodine concentration
of 370 mg/mL. Randomization was carried out at one site,
by means of sealed envelopes containing the patients’
assigned contrast agent. The person carrying out random-
ization was independent of the investigators, and the type
of contrast agent was then conveyed to a member of the
nursing staff in the appropriate cardiac catheterization
laboratory. Contrast was then loaded into an injector by
cardiac catheterization laboratory staff so that patients and
operators were blinded to the type of contrast used. Four
doses ofNACwere givenorally (600 mgb.i.d.), starting the
day before contrast administration. Saline (0.9%) was
given intravenously so that patients received at least
500 mL before the procedure. For outpatients, this was
given over at least 2 h. Patients also received 130 mL/h for
at least 3 h postprocedure in addition to liberal oral fluid
intake. The follow-up periodwas 7 days. Serum creatinine
wasmeasured immediately before contrast administration
(after prehydration) and on days 2 and 7. This was carried
out either in hospital or as an outpatient by their primary
care physician. All serum creatinine levels were deter-
mined in a blinded fashion by local laboratories. Patients
were questioned regarding adverse events during the
7-day follow-up period.
The primary end-point was the incidence of CIN,
defined as an absolute increase in the serum creatinine
concentration of at least 44 lmol/L (0.5 mg/dL) or by
a relative increase of at least 25% from the baseline value
on day 2. Secondary end-points were the number of
patients with CIN on day 2 or 7 and a peak increase in
serumcreatinine of 88 lmol/L (1.0 mg/dL) on either day 2
or 7. We also assessed the peak increase in the serum
creatinine between baseline and days 2 through 7. The
incidence of other reactions to both contrast agents was
also examined.
Juergens et al.
26ª 2008 The Authors
Journal compilation ª 2008 Royal Australasian College of Physicians
Statistical analysis
Based on the study of Jo et al.,28 we hypothesized that if
iodixanol would result in a 9% absolute reduction (17 vs
8%) in the incidence of CIN when compared with iopro-
mide, a sample size of 210 patients per arm would be
needed to have a power of 80% to detect such a difference
at a Type I error of 5% (two sided). All results are quoted as
mean ± 1 SD unless otherwise stated. The primary and
secondary end-points are presented as point estimates
with the 95% confidence interval. Continuous variables
were compared by unpaired Student’s t-test, and categor-
ical variables were compared with v2-test or Fisher’s exacttest where appropriate. Multivariate logistic regression
analysis (forward selection), maximal likelihood ratio
method, was used to identify independent predictors for
the development of the primary end-point. Statistical
significance was defined as a two-tailed P value of <0.05.
Results
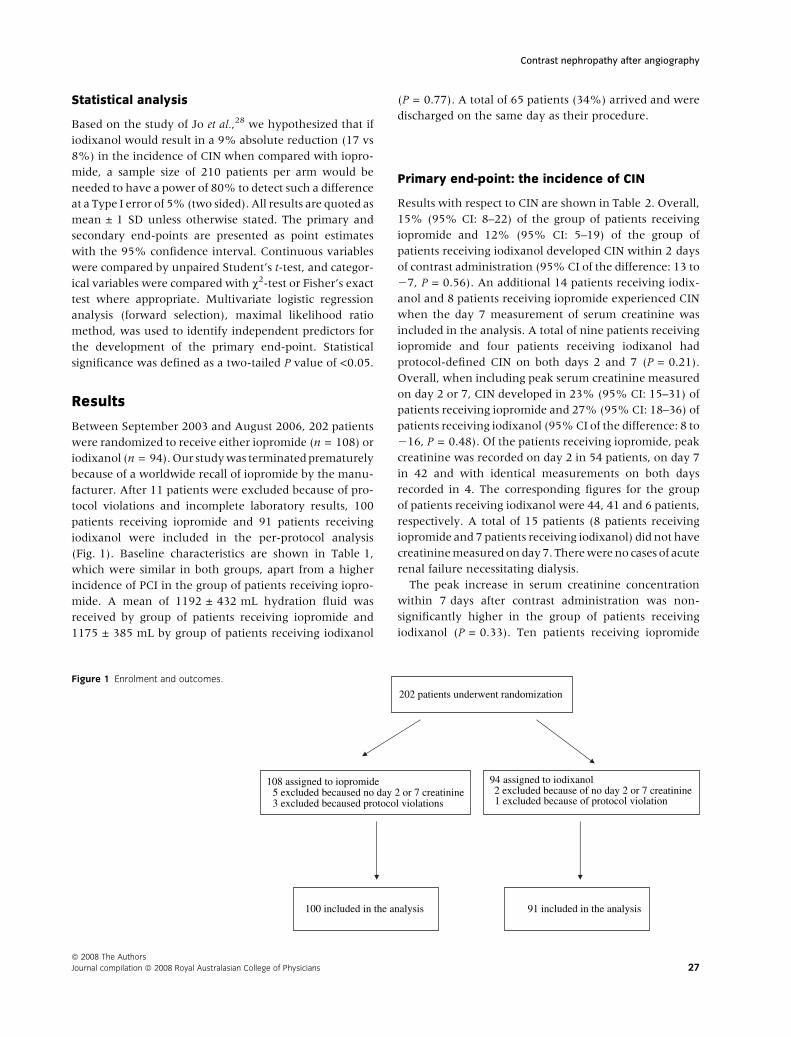
Between September 2003 and August 2006, 202 patients
were randomized to receive either iopromide (n = 108) or
iodixanol (n = 94).Our studywas terminatedprematurely
because of a worldwide recall of iopromide by the manu-
facturer. After 11 patients were excluded because of pro-
tocol violations and incomplete laboratory results, 100
patients receiving iopromide and 91 patients receiving
iodixanol were included in the per-protocol analysis
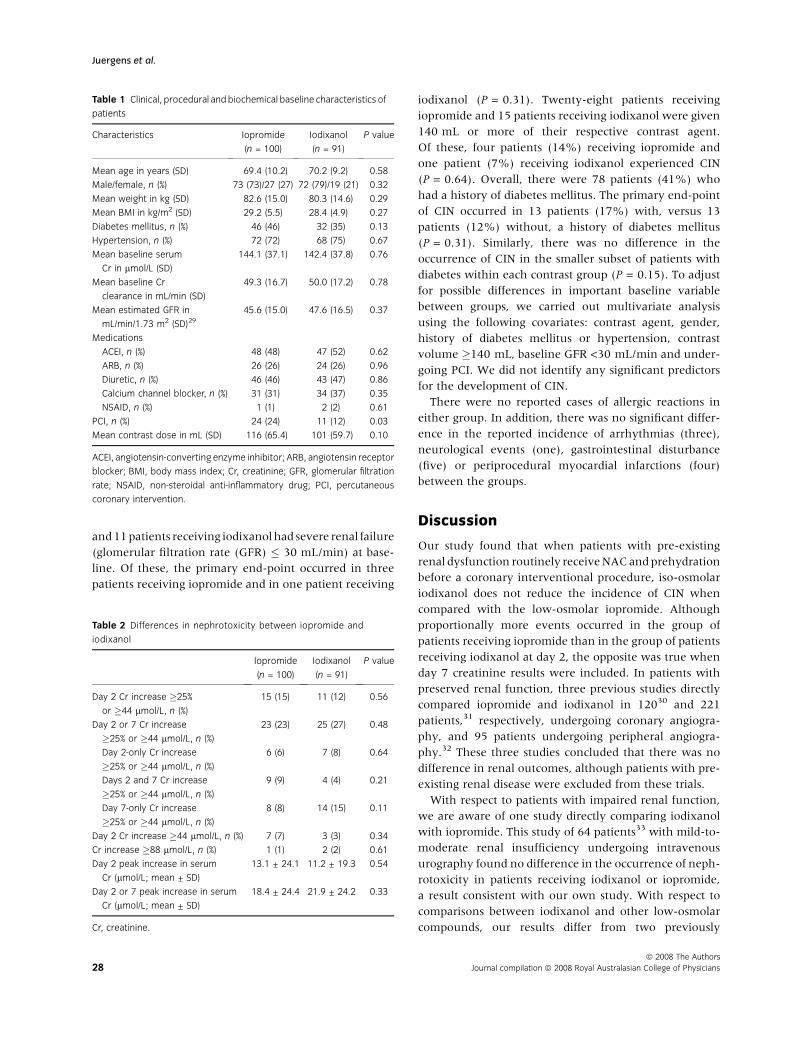
(Fig. 1). Baseline characteristics are shown in Table 1,
which were similar in both groups, apart from a higher
incidence of PCI in the group of patients receiving iopro-
mide. A mean of 1192 ± 432 mL hydration fluid was
received by group of patients receiving iopromide and
1175 ± 385 mL by group of patients receiving iodixanol
(P = 0.77). A total of 65 patients (34%) arrived and were
discharged on the same day as their procedure.
Primary end-point: the incidence of CIN
Results with respect to CIN are shown in Table 2. Overall,
15% (95% CI: 8–22) of the group of patients receiving
iopromide and 12% (95% CI: 5–19) of the group of
patients receiving iodixanol developed CIN within 2 days
of contrast administration (95% CI of the difference: 13 to
27, P = 0.56). An additional 14 patients receiving iodix-
anol and 8 patients receiving iopromide experienced CIN
when the day 7 measurement of serum creatinine was
included in the analysis. A total of nine patients receiving
iopromide and four patients receiving iodixanol had
protocol-defined CIN on both days 2 and 7 (P = 0.21).
Overall, when including peak serum creatinine measured
on day 2 or 7, CIN developed in 23% (95% CI: 15–31) of
patients receiving iopromide and 27% (95% CI: 18–36) of
patients receiving iodixanol (95%CI of the difference: 8 to
216, P = 0.48). Of the patients receiving iopromide, peak
creatinine was recorded on day 2 in 54 patients, on day 7
in 42 and with identical measurements on both days
recorded in 4. The corresponding figures for the group
of patients receiving iodixanol were 44, 41 and 6 patients,
respectively. A total of 15 patients (8 patients receiving
iopromide and 7 patients receiving iodixanol) did not have
creatininemeasuredonday7. Therewereno cases of acute
renal failure necessitating dialysis.
The peak increase in serum creatinine concentration
within 7 days after contrast administration was non-
significantly higher in the group of patients receiving
iodixanol (P = 0.33). Ten patients receiving iopromide
202 patients underwent randomization
100 included in the analysis 91 included in the analysis
108 assigned to iopromide
3 excluded becaused protocol violations5 excluded becaused no day 2 or 7 creatinine
94 assigned to iodixanol 2 excluded because of no day 2 or 7 creatinine1 excluded because of protocol violation
Figure 1 Enrolment and outcomes.
Contrast nephropathy after angiography
ª 2008 The Authors
Journal compilation ª 2008 Royal Australasian College of Physicians 27
and11patients receiving iodixanolhad severe renal failure
(glomerular filtration rate (GFR) � 30 mL/min) at base-
line. Of these, the primary end-point occurred in three
patients receiving iopromide and in one patient receiving
iodixanol (P = 0.31). Twenty-eight patients receiving
iopromide and 15 patients receiving iodixanol were given
140 mL or more of their respective contrast agent.
Of these, four patients (14%) receiving iopromide and
one patient (7%) receiving iodixanol experienced CIN
(P = 0.64). Overall, there were 78 patients (41%) who
had a history of diabetes mellitus. The primary end-point
of CIN occurred in 13 patients (17%) with, versus 13
patients (12%) without, a history of diabetes mellitus
(P = 0.31). Similarly, there was no difference in the
occurrence of CIN in the smaller subset of patients with
diabetes within each contrast group (P = 0.15). To adjust
for possible differences in important baseline variable
between groups, we carried out multivariate analysis
using the following covariates: contrast agent, gender,
history of diabetes mellitus or hypertension, contrast
volume �140 mL, baseline GFR <30 mL/min and under-
going PCI. We did not identify any significant predictors
for the development of CIN.
There were no reported cases of allergic reactions in
either group. In addition, there was no significant differ-
ence in the reported incidence of arrhythmias (three),
neurological events (one), gastrointestinal disturbance
(five) or periprocedural myocardial infarctions (four)
between the groups.
Discussion
Our study found that when patients with pre-existing
renal dysfunction routinely receiveNACandprehydration
before a coronary interventional procedure, iso-osmolar
iodixanol does not reduce the incidence of CIN when
compared with the low-osmolar iopromide. Although
proportionally more events occurred in the group of
patients receiving iopromide than in the group of patients
receiving iodixanol at day 2, the opposite was true when
day 7 creatinine results were included. In patients with
preserved renal function, three previous studies directly
compared iopromide and iodixanol in 12030 and 221
patients,31 respectively, undergoing coronary angiogra-
phy, and 95 patients undergoing peripheral angiogra-
phy.32 These three studies concluded that there was no
difference in renal outcomes, although patients with pre-
existing renal disease were excluded from these trials.
With respect to patients with impaired renal function,
we are aware of one study directly comparing iodixanol
with iopromide. This study of 64 patients33 with mild-to-
moderate renal insufficiency undergoing intravenous
urography found no difference in the occurrence of neph-
rotoxicity in patients receiving iodixanol or iopromide,
a result consistent with our own study. With respect to
comparisons between iodixanol and other low-osmolar
compounds, our results differ from two previously
Table 1 Clinical, procedural and biochemical baseline characteristics of
patients
Characteristics Iopromide
(n = 100)
Iodixanol
(n = 91)
P value
Mean age in years (SD) 69.4 (10.2) 70.2 (9.2) 0.58
Male/female, n (%) 73 (73)/27 (27) 72 (79)/19 (21) 0.32
Mean weight in kg (SD) 82.6 (15.0) 80.3 (14.6) 0.29
Mean BMI in kg/m2 (SD) 29.2 (5.5) 28.4 (4.9) 0.27
Diabetes mellitus, n (%) 46 (46) 32 (35) 0.13
Hypertension, n (%) 72 (72) 68 (75) 0.67
Mean baseline serum
Cr in lmol/L (SD)
144.1 (37.1) 142.4 (37.8) 0.76
Mean baseline Cr
clearance in mL/min (SD)
49.3 (16.7) 50.0 (17.2) 0.78
Mean estimated GFR in
mL/min/1.73 m2 (SD)29
45.6 (15.0) 47.6 (16.5) 0.37
Medications
ACEI, n (%) 48 (48) 47 (52) 0.62
ARB, n (%) 26 (26) 24 (26) 0.96
Diuretic, n (%) 46 (46) 43 (47) 0.86
Calcium channel blocker, n (%) 31 (31) 34 (37) 0.35
NSAID, n (%) 1 (1) 2 (2) 0.61
PCI, n (%) 24 (24) 11 (12) 0.03
Mean contrast dose in mL (SD) 116 (65.4) 101 (59.7) 0.10
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor
blocker; BMI, body mass index; Cr, creatinine; GFR, glomerular filtration
rate; NSAID, non-steroidal anti-inflammatory drug; PCI, percutaneous
coronary intervention.
Table 2 Differences in nephrotoxicity between iopromide and
iodixanol
Iopromide
(n = 100)
Iodixanol
(n = 91)
P value
Day 2 Cr increase �25%
or �44 lmol/L, n (%)
15 (15) 11 (12) 0.56
Day 2 or 7 Cr increase
�25% or �44 lmol/L, n (%)
23 (23) 25 (27) 0.48
Day 2-only Cr increase
�25% or �44 lmol/L, n (%)
6 (6) 7 (8) 0.64
Days 2 and 7 Cr increase
�25% or �44 lmol/L, n (%)
9 (9) 4 (4) 0.21
Day 7-only Cr increase
�25% or �44 lmol/L, n (%)
8 (8) 14 (15) 0.11
Day 2 Cr increase �44 lmol/L, n (%) 7 (7) 3 (3) 0.34
Cr increase �88 lmol/L, n (%) 1 (1) 2 (2) 0.61
Day 2 peak increase in serum
Cr (lmol/L; mean ± SD)
13.1 ± 24.1 11.2 ± 19.3 0.54
Day 2 or 7 peak increase in serum
Cr (lmol/L; mean ± SD)
18.4 ± 24.4 21.9 ± 24.2 0.33
Cr, creatinine.
Juergens et al.
28ª 2008 The Authors
Journal compilation ª 2008 Royal Australasian College of Physicians

studies5,28 that suggested that iodixanol reduced the inci-
dence of CINwhen comparedwith iohexol5 or ioxaglate.28
Our results are consistent, however, with the 414-patient
randomized study of Solomon et al.34 that showed no
difference in the rate of CIN between iopromide and
iodixanol in patients with chronic kidney disease. Simi-
larly, a recent Swedish registry analysis of more than
57 000 patients with longer term follow up showed
ahigher incidence of renal failure after iodixanol usewhen
compared with ioxaglate or iohexol.35
The incidence of CIN at day 2 in our study was not
statistically different between the group of patients receiv-
ing iopromide (15%) and iodixanol (12%). The observed
rate in our group of patients receiving iodixanol is higher
than that reported in the studies of Jo et al. (7.9%)28 and
Aspelin et al.5 (3%), although the latter study did not
include increases in baseline creatinine of greater than
25% as an end-point. The fact that we examined our
baseline creatinine after a period of hydration may have
resulted in an apparent higher incidence of CIN when
compared with other studies, particularly that of Jo et al.28
where the baseline creatinine was taken before prehydra-
tion. Conversely, the incidence of CIN in the group of
patients receiving iopromide in our study was lower than
the corresponding groups of these other studies, 1728 and
26%,5 respectively.
With respect to study population, the group of patients
receiving iodixanol in our study had a higher baseline
creatinine (142 lmol/L) than those in the other two stud-
ies, 1325 and 122 lmol/L,28 although creatinine clearance
was similar between all three studies. Patients in our study
were generally older and had a higher incidence of dia-
betes mellitus than those in the study of Jo et al.,28
although the age of patients in our study was similar to
that of patients in the study of Aspelin et al. in which all
patients had diabetes mellitus. Another potentially import-
ant difference was that our study patients on iodixanol
received less contrast volume (101 mL) during their index
procedure than those in the other two studies at 1635 and
204 mL,28 respectively.
Patients in our study routinely received prehydration
with intravenous saline (0.9%) before their procedure.
The study of Jo et al.28 specified that patients receive
hydrationbefore andafter angiography,whereas the study
of Aspelin recommended, but not required, that patients
receive a combination of oral and intravenous hydration
periprocedurally. This study reported that patients
received between 934 and 977 mL of intravenous hydra-
tion, compared with 1174–1192 mL received by patients
in our study. Although the administration of fluids is
recommended to reduce the risk of CIN,36 there are incon-
sistent data with respect to the optimal fluid regimen for
prehydration. One trial showed benefit of giving intrave-
nous saline for 24 h, beginning 12 h before administration
of contrast medium,37 although another study showed
that intravenous fluids for 12 h was superior to the use
of oral fluids.38 The trial of Solomon et al.14 confirmed that
in patients with chronic renal insufficiency undergoing
coronary angiography, hydration with 0.45% saline pro-
vided better protection against worsening renal function
than did hydration in combination with mannitol or
furosemide. Our prehydration regimen facilitated day-
only procedures in 34% of cases as prehydration could
be commencedwithin 2 h of the procedure. It is likely that
mandated hydration as part of our protocol contributed to
the equivalent outcomes for the differing types of contrast
agents.
Another difference between our trial and the aforemen-
tioned trails was in the use of NAC that was mandated in
our study design but excluded in the study of Jo et al.28 and
was only given to 8.5% of patients in the study of Aspelin
et al.5 The first placebo-controlled, randomized trial of
prophylactic oral administration of NAC together with
intravenous hydration in patients with chronic renal
insufficiency receiving iopromide showed a significant
reduction in CIN (2 vs 21%, P = 0.01).4 Subsequent stud-
ies have showed inconsistent results, with some confirm-
ing a benefit17–20 and others suggesting no benefit.21
Another trial22 suggested that a higher dose of NAC
(1200 mg orally b.i.d.) was superior to standard dose
(600 mg b.i.d.) in preventing CIN, particularly when high
volumes of contrast agents (�140 mL) are used. The
increase in creatinine of at least 44 lmol/L (0.5 mg/dL)
at 48 h was the end-point used in the majority of NAC
trials.4,17,19–22 In these trials, thenumber of patients reach-
ing this end-point in the NAC arms (800–2400 mg orally
daily) ranged between 2 and 11%, whereas in the control
arms, CIN occurred in between 8 and 24.6% of patients.
This particular end-point occurred in 7% of patients
receiving iopromide and 3% of patients receiving iodix-
anol in our study, suggesting a beneficial effect of the
protocol-mandated use of NAC as seen in the earlier
studies.
A strength of our study was the measurement of serum
creatinine on day 7 in the majority of patients, which
resulted in proportionately more patients receiving iodix-
anol than patients receiving iopromide (27 vs 23%)meet-
ing the primary end-point definition of CIN. There are few
studies that report renal function beyond a few days after
contrast exposure, although a number of investigators
have suggested that serum creatinine may not peak until
4–5 days after contrast administration.6,39,40 Our results
are consistent with this view as we observed numerically
more eventswhenwe includedmeasurements of the day 7
creatinine. The studyof Pugh et al.32 is particularly relevant
to our study as they concluded that creatinine clearance
Contrast nephropathy after angiography
ª 2008 The Authors
Journal compilation ª 2008 Royal Australasian College of Physicians 29

returned to baseline more quickly with iopromide than
with iodixanol. We believe that future trials in CIN pre-
vention should measure serum creatinine at day 7 and
perhaps beyond, as in 43% of patients in our study, the
peak creatinine was actually observed at this time-point.
Our study has a number of limitations including the
small patient numbers, and consequently, it is underpow-
ered to detect a clinically meaningful difference between
the two contrast agents if in truth one existed. The number
of patients enrolled, however, exceeds that of a number of
important contrast studies.4,5,14,15 Our study excluded
patients requiring primary or rescue coronary interven-
tion and others unable to receive adequate hydration,
therefore limiting the generalizability of our findings.
The volume of contrast used was lower than that used
in other similar trials, but this dose is generally adequate to
carry out diagnostic angiography or non-complex PCI that
was carried out in 18%of our study patient population.5,28
In summary, our trial shows that there remains a high
incidence of CIN at both days 2 and 7, despite prehydration
and routine use of NAC in patients with pre-existing renal
dysfunction undergoing a coronary interventional pro-
cedure. Although the power of our study is limited by
its early termination,we conclude that theuse of iodixanol
was not associated with a statistically significant lower
incidence of CIN when compared with iopromide, with
differing trends observed at 48 h and 7 days after the
procedure.
Acknowledgement
We acknowledge our clinical research nurses, fellows,
radiographers and catheter laboratory nursing staff for
their assistance in completing this study.
References
1 Rudnick MR, Goldfarb S, Wexler L, Ludbrook PA, Murphy
MJ, Halpern EF et al. Nephrotoxicity of ionic and nonionic
contrast media in 1196 patients: a randomised trial.
Kidney Int 1995; 47: 254–61.
2 Cigarroa RC, Lange RA, Williams RH, Hillis LD. Dosing of
contrast material to prevent contrast nephropathy in
patients with renal disease. Am J Med 1989; 86: 649–52.
3 Barrett BJ, Parfrey PS. Prevention of nephrotoxicity induced
by radiocontrast agents. N Eng J Med 1994; 331: 1449–50.
4 TepelM, van der GietM, Schwarzfeld C, Laufer U, Liermann
D, Zidek W. Prevention of radiographic contrast agent
induced reductions in renal function by acetylcysteine.
N Eng J Med 2000; 343: 180–84.
5 Aspelin P, Aubry P, Fransson SG, Strasser R, Willenbrock R,
Berg KJ. Nephrotoxic effects in high-risk patients
undergoing angiography. N Eng J Med 2003; 348: 491–9.
6 McCullough PA, Adam A, Becker CR, Davidson C, Lameire
N, Stacul F et al. Epidemiology and prognostic implications
of contrast induced nephropathy. Am J Cardiol 2006; 98:
5K–13.
7 MarenziG, LauriG,Assanelli E, Campodonico J,MetrioMD,
Marana I et al. Contrast induced nephropathy in patients
undergoing primary angioplasty for acute myocardial
infarction. J Am Coll Cardiol 2004; 44: 1780–85.
8 MaederM, KleinM, Fehr T, Rickli H. Contrast nephropathy:
review focusing on prevention. J Am Coll Cardiol 2004;
44: 1763–71.
9 Manske CL, Sprafka JM, Strony JT. Contrast nephropathy
in azotemic diabetic patients undergoing coronary
angiography. Am J Med 1990; 89: 615–20.
10 Rich MW, Crecelius CA. Incidence, risk factors, and clinical
course of acute renal insufficiency after cardiac
catheterisation in patients 70 years of age or older:
a prospective study. Arch Intern Med 1990; 150: 1237–42.
11 Gruberg L, Mehran R, Dangas G, Mintz GS, Waksman R,
Kent KM et al. Acute renal failure requiring dialysis after
percutaneous coronary interventions. Catheter Cardiovasc
Interv 2001; 52: 409–16.
12 McCullough PA, Wolyn R, Rocher LL, Levin RN, O’Neill
WW. Acute renal failure after coronary intervention:
incidence, risk factors, and relationship to mortality.
Am J Med 1997; 103: 368–75.
13 Rihal CS, Textor SC, Grill DE, Berger PB, Ting HH, Best PJ
et al. Incidence and prognostic importance of acute renal
failure after percutaneous coronary intervention. Circulation
2002; 105: 2259–64.
14 Solomon R, Werner C, Mann D, D’Elia J, Silva P. Effects of
saline, mannitol and furosemide on acute decreases in renal
function induced by radiocontrast agents.NEngl JMed1994;
331: 1416–20.
15 Merten GJ, Burgess WP, Gray LV, Holleman JH, Roush TS,
Kowalchuk GJ et al. Prevention of contrast induced
nephropathy with sodium bicarbonate. JAMA 2004;
291: 2328–34.
16 Marenzi G, Marana I, Lauri G, Assanelli E, Grazi M,
Campodonico J et al. The prevention of radiocontrast agent
induced nephropathy by hemofiltration.N Engl J Med 2003;
349: 1333–40.
17 Shyu KG, Cheng JJ, Kuan P. Acetylcysteine protects against
acute renal damage in patients with abnormal renal
function undergoing a coronary procedure. J Am Coll Cardiol
2002; 40: 1383–8.
18 Diaz-Sandoval LJ, Kosowsky BD, Losordo DW.
Acetylcysteine to prevent angiography related renal tissue
injury (the APART trial). Am J Cardiol 2002; 89: 356–8.
19 Briguori C, Colombo A, Airoldi F, Violante A, Castelli A,
Balestrieri P et al. N-acetylcysteine versus fenoldopam
mesylate to prevent contrast agent associated
nephrotoxicity. J Am Coll Cardiol 2004; 44: 762–5.
20 Marenzi G, Assanelli E, Marana I, Lauri G, Campodonico J,
Grazi M et al. N-acetylcysteine and contrast induced
Juergens et al.
30ª 2008 The Authors
Journal compilation ª 2008 Royal Australasian College of Physicians
nephropathy in primary angioplasty. N Engl J Med 2006;
354: 2773–82.
21 Goldenberg I, Shechter M, Matetzky S, Jonas M, Adam M,
Pres H et al. Oral acetylcysteine as an adjunct to saline
hydration for the prevention of contrast induced
nephropathy following coronary angiography. Eur Heart J
2004; 25: 212–18.
22 Briguori C, ColomboA,ViolanteA,Balestrieri P,Manganelli
F, Elia PP et al. Standardvs double doseofN-acetylcysteine to
prevent contrast agent associatednephrotoxicity.EurHeart J
2004; 25: 206–11.
23 Taliercio CP, Vlietstra RE, Ilstrup DM, Burnett JC, Menke
KK, Stensrud SL et al. A randomized comparison of the
nephrotoxicity of iopamidol and diatrizoate in high risk
patients undergoing coronary angiography. J AmColl Cardiol
1991; 17: 384–90.
24 Lautin EM, Freeman NJ, Schoenfeld AH, Bakal CW,
Haramiti N, Friedman AC et al. Radiocontrast-associated
renal dysfunction: a comparison of lower-osmolality and
conventional high-osmolality contrast media. AJR Am J
Roentgenol 1991; 157: 59–65.
25 Barrett BJ, Carlisle EJ. Metaanalysis of the relative
nephrotoxicity of high and low osmolality iodinated
contrast media. Radiology 1993; 188: 171–8.
26 Grynne BH, Nossen JO, Bolstad B, Borch KW. Main results
of the first comparative clinical studies on Visipaque.
Acta Radiol Suppl 1995; 399: 265–70.
27 Davidson CJ, Laskey WK, Hermiller JB, Harrison JK,
Matthai W, Vliestra RE et al. Randomized trial of contrast
media utilization in high-risk PTCA: the COURT trial.
Circulation 2000; 101: 2172–7.
28 Jo SH, Youn TJ, Koo BK, Park J-S, Kang H-J, Cho Y-S et al.
Renal toxicity evaluation and comparison between
visipaque (iodixanol) and hexabrix (ioxaglate) in patients
with renal insufficiency undergoing coronary angiography.
J Am Coll Cardiol 2006; 48: 924–30.
29 Levey AS, Bosch JP, Breyer Lewis J, Greene T, Rogers N,
Roth D. A more accurate method to estimate glomerular
filtration rate from serum creatinine: a new prediction
equation. Ann Intern Med 1999; 130: 461–70.
30 Manninen H, Tahvanainen K, Borch KW, Wallen T,
Soimakallio S, Matsi P, et al. Iodixanol, a new non-ionic,
dimeric contrast medium in cardioangiography:
a double-masked, parallel comparison with iopromide.
Eur Radiol 1995; 5: 364–70.
31 Feldkamp T, Baumgart D, Elsner M, Herget-Rosenthal S,
Pietruck F, Erbel R et al. Nephrotoxicity of iso-osmolar
versus low-osmolar contrast media is equal in low risk
patients. Clin Nephrol 2006; 66: 322–30.
32 Pugh ND, Sissons GRJ, Ruttley MST, Berg KJ, Nossen JO,
Eide H. Iodixanol in femoral arteriography (phase III):
a comparative double-blind parallel trial between iodixanol
and iopromide. Clin Radiol 1993; 47: 96–9.
33 CarraroM,Malalan F,AntonioneR, Stacul F, CovaM, Petz S
et al. Effects of a dimeric vs a monomeric nonionic contrast
mediumon renal function in patientswithmild tomoderate
renal insufficiency: a double-blind, randomised clinical trial.
Eur Radiol 1998; 8: 144–7.
34 SolomonRJ,NatarajanMK,Doucet S, SharmaSK, Staniloae
CS,Katholi RE et al. Cardiac angiography in renally impaired
patients (CARE) study. A randomised double-blind trial of
contrast-induced nephropathy in patients with chronic
kidney disease. Circulation 2007; 115: 3189–96.
35 Liss P, Persson PB, Hansell P, Lagerqvist B. Renal failure
in 57925 patients undergoing coronary procedures using
ios-osmolar or low-osmolar contrast media. Kidney Int
2006; 70: 1811–17.
36 Barrett BJ, Parfrey PS. Preventing nephropathy induced by
contrast medium. N Engl J Med 2006; 354: 379–86.
37 Trivedi HS,Moore H, Nasr S, Aggarwal K, Agrawal A, Goel P
et al. A randomized prospective trial to assess the role of
saline hydration on the development of contrast
nephrotoxicity. Nephron Clin Pract 2003; 93: C29–34.
38 Bader BD, Berger ED, Heede MB, Silberbaur I, Duda S,
Risler T et al. What is the best hydration regimen to prevent
contrast media-induced nephrotoxicity? Clin Nephrol 2004;
62: 1–7.
39 MacNeill BD, Harding SA, Bazari H, Patton KK,
Colon-Hernadez P, deJoseph D et al. Prophylaxis of
contrast-induced nephropathy in patients undergoing
coronary angiography. Catheter Cardiovasc Interv 2003;
60: 458–61.
40 Vogt B, Ferrari P, Schoenholzer C, Marti H-P, Mohaupt M,
Wiederkehr M et al. Prophylactic hemodialysis after
radiocontrast media in patients with renal insufficiency is
potentially harmful. Am J Med 2001; 111: 692–8.
Contrast nephropathy after angiography
ª 2008 The Authors
Journal compilation ª 2008 Royal Australasian College of Physicians 31

21
PAPER 3
Reprinted from The Medical Journal of Australia 2011;195:268-269 with
permission from The Medical Journal of Australia

Letters
MJA 195 (5) · 5 September 2011268
Contrast induced nephropathy in patients with pre-existing renal impairment undergoing invasive coronary procedures — a long-term follow-upTO THE EDITOR: Contrast induced nephropathy (CIN) is one of the most important and frequent complications of invasive coronary procedures.1 We have previously reported a multicentre randomised trial comparing use of iso-osmolar and low osmolar contrast agents (iopromide and iodixanol, respectively) in patients with pre-
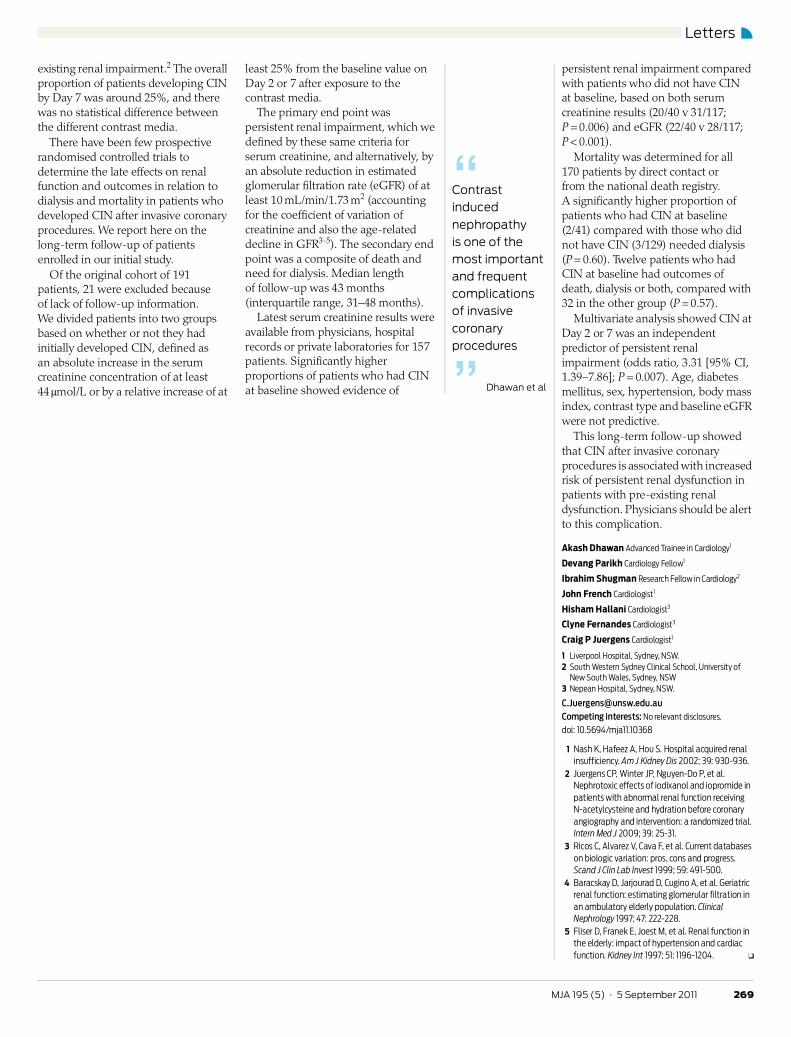
Letters
269MJA 195 (5) · 5 September 2011
existing renal impairment.2 The overall proportion of patients developing CIN by Day 7 was around 25%, and there was no statistical difference between the different contrast media.
There have been few prospective randomised controlled trials to determine the late effects on renal function and outcomes in relation to dialysis and mortality in patients who developed CIN after invasive coronary procedures. We report here on the long-term follow-up of patients enrolled in our initial study.
Of the original cohort of 191 patients, 21 were excluded because of lack of follow-up information. We divided patients into two groups based on whether or not they had initially developed CIN, defined as an absolute increase in the serum creatinine concentration of at least 44 μmol/L or by a relative increase of at
least 25% from the baseline value on Day 2 or 7 after exposure to the contrast media.
The primary end point was persistent renal impairment, which we defined by these same criteria for serum creatinine, and alternatively, by an absolute reduction in estimated glomerular filtration rate (eGFR) of at least 10 mL/min/1.73 m2 (accounting for the coefficient of variation of creatinine and also the age-related decline in GFR3-5). The secondary end point was a composite of death and need for dialysis. Median length of follow-up was 43 months (interquartile range, 31–48 months).
Latest serum creatinine results were available from physicians, hospital records or private laboratories for 157 patients. Significantly higher proportions of patients who had CIN at baseline showed evidence of
persistent renal impairment compared with patients who did not have CIN at baseline, based on both serum creatinine results (20/40 v 31/117; P = 0.006) and eGFR (22/40 v 28/117; P < 0.001).
Mortality was determined for all 170 patients by direct contact or from the national death registry. A significantly higher proportion of patients who had CIN at baseline (2/41) compared with those who did not have CIN (3/129) needed dialysis (P = 0.60). Twelve patients who had CIN at baseline had outcomes of death, dialysis or both, compared with 32 in the other group (P = 0.57).
Multivariate analysis showed CIN at Day 2 or 7 was an independent predictor of persistent renal impairment (odds ratio, 3.31 [95% CI, 1.39–7.86]; P = 0.007). Age, diabetes mellitus, sex, hypertension, body mass index, contrast type and baseline eGFR were not predictive.
This long-term follow-up showed that CIN after invasive coronary procedures is associated with increased risk of persistent renal dysfunction in patients with pre-existing renal dysfunction. Physicians should be alert to this complication.
Akash Dhawan Advanced Trainee in Cardiology1
Devang Parikh Cardiology Fellow1
Ibrahim Shugman Research Fellow in Cardiology2
John French Cardiologist1
Hisham Hallani Cardiologist3
Clyne Fernandes Cardiologist3
Craig P Juergens Cardiologist1
1 Liverpool Hospital, Sydney, NSW.2 South Western Sydney Clinical School, University of
New South Wales, Sydney, NSW3 Nepean Hospital, Sydney, NSW.
[email protected] interests: No relevant disclosures.
doi: 10.5694/mja11.10368
1 Nash K, Hafeez A, Hou S. Hospital acquired renal insufficiency. Am J Kidney Dis 2002; 39: 930-936.
2 Juergens CP, Winter JP, Nguyen-Do P, et al. Nephrotoxic effects of iodixanol and iopromide in patients with abnormal renal function receiving N-acetylcysteine and hydration before coronary angiography and intervention: a randomized trial. Intern Med J 2009; 39: 25-31.
3 Ricos C, Alvarez V, Cava F, et al. Current databases on biologic variation: pros, cons and progress. Scand J Clin Lab Invest 1999; 59: 491-500.
4 Baracskay D, Jarjourad D, Cugino A, et al. Geriatric renal function: estimating glomerular filtration in an ambulatory elderly population. Clinical Nephrology 1997; 47: 222-228.
5 Fliser D, Franek E, Joest M, et al. Renal function in the elderly: impact of hypertension and cardiac function. Kidney Int 1997; 51: 1196-1204. ❏
“Contrast induced nephropathy is one of the most important and frequent complications of invasive coronary procedures
” Dhawan et al

22
PAPER 4
Reprinted from the Journal of the American College of Cardiology
2010;56:525-526 with permission from Elsevier

doi:10.1016/j.jacc.2010.01.065 2010;56;525-526 J. Am. Coll. Cardiol.
Kaye James Blake, Robert Whitbourn, H. Omar Farouque, Terence Pertile, and David M. Stephen J. Duffy, Peter Ruygrok, Craig P. Juergens, Horst Sievert, Mark Richards,
After Coronary Angiography and InterventionRemoval of Contrast Media From the Coronary Sinus Attenuates Renal Injury
This information is current as of July 27, 2010
http://content.onlinejacc.org/cgi/content/full/56/6/525located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by on July 27, 2010 content.onlinejacc.orgDownloaded from
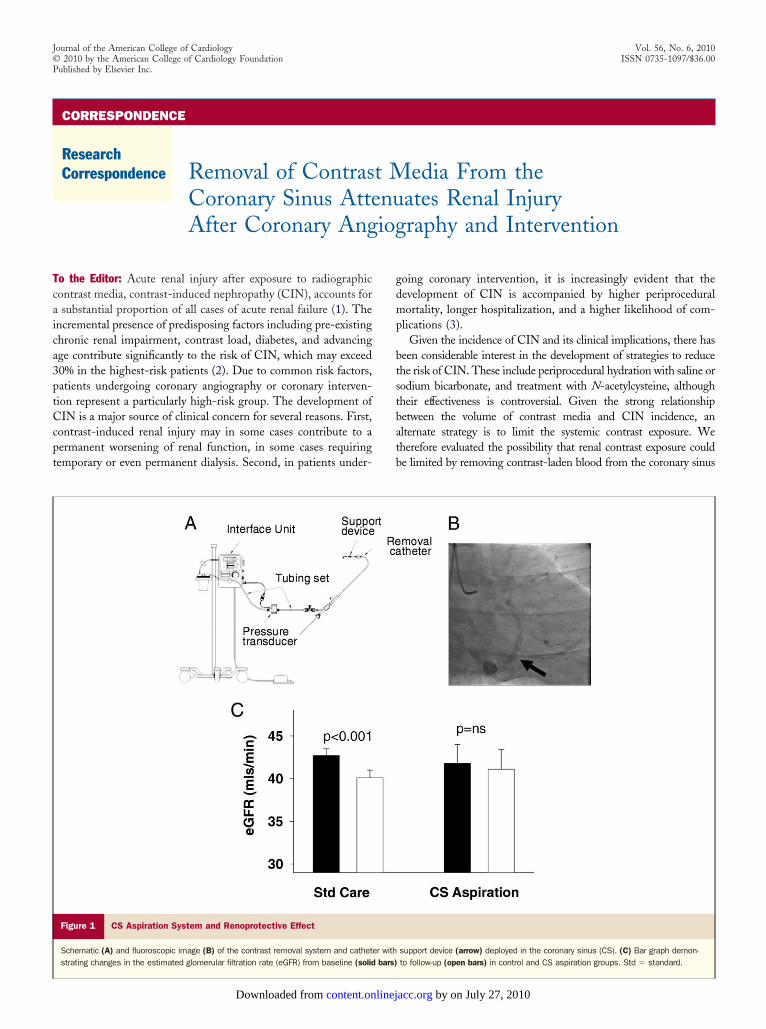
Tcaica3ptCcpt
Journal of the American College of Cardiology Vol. 56, No. 6, 2010© 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00Published by Elsevier Inc.
CORRESPONDENCE
ResearchCorrespondence Removal of Contrast Media From the
Coronary Sinus Attenuates Renal Injury
After Coronary Angiography and Interventiongdmp
btstbatb
o the Editor: Acute renal injury after exposure to radiographicontrast media, contrast-induced nephropathy (CIN), accounts forsubstantial proportion of all cases of acute renal failure (1). The
ncremental presence of predisposing factors including pre-existinghronic renal impairment, contrast load, diabetes, and advancingge contribute significantly to the risk of CIN, which may exceed0% in the highest-risk patients (2). Due to common risk factors,atients undergoing coronary angiography or coronary interven-ion represent a particularly high-risk group. The development ofIN is a major source of clinical concern for several reasons. First,
ontrast-induced renal injury may in some cases contribute to aermanent worsening of renal function, in some cases requiringemporary or even permanent dialysis. Second, in patients under-
Figure 1 CS Aspiration System and Renoprotective Effect
Schematic (A) and fluoroscopic image (B) of the contrast removal system and cathetstrating changes in the estimated glomerular filtration rate (eGFR) from baseline (solid
content.onlinejDownloaded from
oing coronary intervention, it is increasingly evident that theevelopment of CIN is accompanied by higher periproceduralortality, longer hospitalization, and a higher likelihood of com-
lications (3).Given the incidence of CIN and its clinical implications, there has
een considerable interest in the development of strategies to reducehe risk of CIN. These include periprocedural hydration with saline orodium bicarbonate, and treatment with N-acetylcysteine, althoughheir effectiveness is controversial. Given the strong relationshipetween the volume of contrast media and CIN incidence, anlternate strategy is to limit the systemic contrast exposure. Weherefore evaluated the possibility that renal contrast exposure coulde limited by removing contrast-laden blood from the coronary sinus
support device (arrow) deployed in the coronary sinus (CS). (C) Bar graph demon-to follow-up (open bars) in control and CS aspiration groups. Std � standard.
er withbars)
by on July 27, 2010 acc.org

(c
faOwacavc1Ofiogp(setdmothIt0e(bmCcmitd
traieTtc
SPCHMJRHT*
*BPSMAE
PcBEKOSChf
R
1
2
3
4
DAGiaTfi
Wdi(sp(A
526 Correspondence JACC Vol. 56, No. 6, 2010August 3, 2010:525–30
CS) during and immediately after the intracoronary injection ofontrast media.
We report here the initial experience with a system developedor the aspiration of contrast media from the CS during coronaryngiography and intervention (CINCOR Contrast Removal System,sprey Medical, St. Paul, Minnesota). The primary aim of the studyas to evaluate the safety and efficacy of this approach, and second-
rily we examined its ability to limit the decline in renal function afterontrast exposure. A purpose-designed 11-F CS aspiration catheternd CS support device were placed via a 14-F right internal jugularein sheath. The CS was successfully cannulated with the aspirationatheter in 31 of 41 patients. The mean time to cannulate the CS was1.1 � 9.3 min. There were no device-related serious adverse events.ur cohort included 26 patients with an estimated glomerular
ltration rate (eGFR) of �60 ml/min that were evaluated for renalutcomes (5 pilot-phase patients had normal renal function). In thisroup, there was no change in eGFR from baseline to 72 host-procedure (41.8 � 2.2 ml/min to 41.1 � 2.3 ml/min, p � 0.55)Fig. 1). By comparison, a matched comparator cohort of 148tandard care patients (4) receiving a similar contrast load experi-nced a significant decrease in the eGFR from 42.7 � 0.8 ml/mino 40.1 � 0.9 ml/min (p � 0.001) at 48 h. There was a greater netecrease in the eGFR in the comparator group: �2.5 � 0.5l/min versus �0.7 � 1.2 ml/min, p � 0.05. The average amount
f blood collected by CS aspiration was 169 � 15 ml per patient, andhis resulted in a clinically small but statistically significant decrease inemoglobin from 12.3 � 0.2 g/dl to 11.7 � 0.2 g/dl (p � 0.01).n 65 standard care patients with a baseline eGFR �40 ml/min,he eGFR fell from 33.1 � 0.7 ml/min to 31.7 � 0.8 ml/min (p �.003), whereas in those with concomitant CS aspiration and anGFR �40 ml/min (n � 11), there was no change in the eGFR30.7 � 1.6 ml/min to 31.4 � 1.8 ml/min, p � 0.42). Theetween-group difference in the eGFR response was �1.5 � 0.5l/min versus �0.5 � 0.7 ml/min (p � 0.05). In patients undergoingS aspiration, we quantified the extent of radiographic contrast
apture. Unlike other experimental studies of CS capture, we directlyeasured the concentration of iodine in the collected material using
nductively coupled plasma-optical emission spectroscopy. CS con-rast aspiration resulted in the recapture of 32 � 3% of theelivered contrast, ranging from 6% to 64%.
Taken together, the present study provides supportive evidence ofhe safety and feasibility of a CS-based aspiration system for theemoval of radiographic contrast in patients undergoing coronaryngiography and intervention. Our data also provide a preliminaryndication that the collection of contrast from the CS reduces systemicxposure and, in conjunction, attenuates expected nephrotoxicity.hese data warrant further evaluation in a large-scale randomized trial
o evaluate the capacity of CS contrast capture to reduce the risk ofontrast-induced nephropathy and its complications.
tephen J. Duffy, MD, PhDeter Ruygrok, MDraig P. Juergens, MDorst Sievert, MDark Richards, MD
ames Blake, MDobert Whitbourn, MD. Omar Farouque, MD, PhDerence Pertile, PhD
David M. Kaye, MD, PhD s
content.onlinejDownloaded from
Heart Failure Research Groupaker IDI Heart and Diabetes Institute.O. Box 6492t Kilda Road Centralelbourne, Victoria 8008ustralia-mail [email protected]
doi:10.1016/j.jacc.2010.01.065
lease note: Dr. Sievert has received study honoraria, travel expenses, and/oronsulting fees from Access Closure, AGA, Angiomed, Ardian, Arstasis, Avinger,ridgepoint, CardioKinetix, CardioMEMS, Coherex, CSI, EndoCross, EndoTex,pitek, Evalve, ev3, FlowCardia, Gore, Guidant, Lumen Biochemical, Kensey Nash,yoto Medical, Lutonix, Medinol, Medtronic, NCD, NMT, OAS, Occlutech,sprey, Ovalis, Pathway, PendraCare, Percardia, pfm, Remon, Rox Medical, Sadra,
orin, Spectranetics, SquareOne, Viacor, and Velocimed; and has stock options inardiokinetix, Access Closure, Velocimed, CoAptus, Lumen Biomedical, and Co-erex. Dr. Pertile is an employee and stockholder of Osprey Medical. Dr. Kaye is aounder and stockholder of Osprey Medical.
EFERENCES
. McCullough PA. Contrast-induced acute kidney injury. J Am CollCardiol 2008;51:1419–28.
. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score forprediction of contrast-induced nephropathy after percutaneous coronaryintervention: development and initial validation. J Am Coll Cardiol2004;44:1393–9.
. McCullough PA, Wolyn R, Rocher LL, Levin RN, O’Neill WW.Acute renal failure after coronary intervention: incidence, risk factors,and relationship to mortality. Am J Med 1997;103:368–75.
. Juergens CP, Winter JP, Nguyen-Do P, et al. Nephrotoxic effects ofiodixanol and iopromide in patients with abnormal renal functionreceiving N-acetylcysteine and hydration before coronary angiographyand intervention: a randomized trial. Intern Med J 2009;39:25–31.
Letters to the Editor
istinct Patterns ofutoantibodies Against-Protein–Coupled Receptors
n Chagas’ Cardiomyopathynd Megacolonheir Potential Impact
or Early Risk Assessmentn Asymptomatic Chagas’ Patients
e demonstrated in the Journal (1) that patients with Chagas’isease suffering from cardiomyopathy and megacolon show pos-tivity of autoantibodies directed to the beta1-adrenoreceptorAAB), beta2-AAB, and muscarinergic2-receptor (M2-AAB). Aubset of nearly 35% of asymptomatic Chagas’ patients alsoresented with AAB patterns indicative of either cardiomyopathybeta1-AAB and M2-AAB) or megacolon (beta2-AAB and M2-AB). Because the numbers of AAB positive but asymptomatic
ubjects paralleled the epidemiological data for the percentage of
by on July 27, 2010 acc.org

doi:10.1016/j.jacc.2010.01.065 2010;56;525-526 J. Am. Coll. Cardiol.
Kaye James Blake, Robert Whitbourn, H. Omar Farouque, Terence Pertile, and David M. Stephen J. Duffy, Peter Ruygrok, Craig P. Juergens, Horst Sievert, Mark Richards,
After Coronary Angiography and InterventionRemoval of Contrast Media From the Coronary Sinus Attenuates Renal Injury
This information is current as of July 27, 2010
& ServicesUpdated Information
http://content.onlinejacc.org/cgi/content/full/56/6/525including high-resolution figures, can be found at:
References
http://content.onlinejacc.org/cgi/content/full/56/6/525#BIBLat: This article cites 4 articles, 2 of which you can access for free
Rights & Permissions
http://content.onlinejacc.org/misc/permissions.dtltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://content.onlinejacc.org/misc/reprints.dtl
Information about ordering reprints can be found online:
by on July 27, 2010 content.onlinejacc.orgDownloaded from
23
CHAPTER 2
ARTERIAL ACCESS STUDIES
Introduction
Vascular access site complications result in significant morbidity after
coronary interventional procedures, with an incidence of 0.5 -16.8% [1-3] of cases.
Initially vascular sheaths were removed by manual compression either by hand or
with external compression devices such as the Femostop™. Despite the universal
need for vascular sheath removal at the end of a coronary interventional procedure,
there is a paucity of data around the process by which this occurs. There is little
prospective published data on procedural factors such as sheath size which may
predict adverse events and the cardiovascular consequences of such events during
sheath removal. In addition, a number of vascular closure devices have been
developed in a bid to shorten haemostasis times and possibly reduce vascular
complications although their utilisation has not been fully evaluated.
Paper 5 (Catheter Cardiovasc Interv 2004;63:166-170)
The Angioseal™ is one such vascular closure device which has been
developed, and whilst a number studies have sought to address the incidence of
vascular complications comparing various vascular closure devices [4-12], there is
little published data addressing patient tolerance and resource implications of using
the Angioseal™ and Femostop™ devices. The Angioseal™ is a sheath-deployed,
bioabsorbable, haemostatic closure device that allows sheath removal at the end of the
24
procedure whilst patients are still systemically anticoagulated. Alternatively, the
Femostop™ is an external compression device, which is cheaper but is applied after
the effects of intraprocedural anticoagulation have dissipated resulting in delays in
time to haemostasis, ambulation and discharge when compared to the Angioseal™.
Furthermore, the delay in the removal of the sheath and prolonged period of
compression with the Femostop™ may result in more patient discomfort than would
occur using the Angioseal™ device. Paper 5 sought to specifically compare patient
tolerance and the resource implications of using the Angioseal™ and Femostop™
devices.
We found that femoral access site closure using the Angioseal™ device
resulted in a slight delay in removal from the angiography suite and a higher
disposable cost. However, patients receiving the Angioseal™ achieved haemostasis
faster, were able to ambulate sooner and reported less pain than those patients who
received assisted manual compression with the Femostop™ device, outcomes which
may justify the small incremental cost involved.
Context and Implications
This work was initiated and completed by the author at Liverpool hospital in
collaboration with the department of Vascular surgery. It was the first paper to
specifically address patient tolerance and resource implication of these two commonly
used devices. As a consequence of this research we gained a clearer understanding of
the advantages and disadvantages of each method of sheath removal.
Impact on literature
According to Scopus ®, this article has been cited at least 26 times in the literature,
including as part of a meta-analysis in the topic, from a journal with a 5 year impact
factor of 2.373.
25
Paper 6 (Catheter Cardiovasc Inter 2005;66:528-534)
Many of the early studies demonstrating a high incidence of vascular
complications after PCI were performed when predominantly 8 French (Fr) or larger
diameter catheters were standard. Improved guiding catheter design has resulted in
increased internal diameters, which facilitate the passage of interventional devices
without increasing their external diameter, therefore allowing coronary intervention to
be performed using smaller diameter catheters. Previous trials comparing differing
sized guiding catheters during percutaneous coronary intervention (PCI) have
revealed conflicting results with respect to the incidence of vascular complications
[13-15]. These trials were performed before the widespread use of intracoronary
stenting and had rates of stent use from 0% to 25% [13-15]. Moreover vascular
ultrasound was not routinely performed in all patients to assess asymptomatic access
site complications. To define the procedural and clinical advantages and limitations of
6 Fr compared to 7 Fr transfemoral coronary interventions in the stenting era, we
performed a randomised controlled trial and assessed vascular complications by
routine access site ultrasound, blinded to clinical outcomes. This was the basis of
Paper 6. We found that there was no reduction in peripheral vascular complications
with the use of smaller guiding catheters in percutaneous coronary intervention. There
was less contrast used in the 6 Fr group which may benefit some patient subsets;
however operators tended to prefer the larger 7 Fr system. We also concluded that the
target coronary anatomy and need for complex device intervention should mandate
the choice of guiding catheter size, rather than a perceived impact on vascular
complications.
26
Context and Implications
This work was initiated and completed by the author at Liverpool hospital in
collaboration with the department of Vascular surgery. It was the first paper to use a
blinded ultrasound determined end point to determine vascular complications
according to sheath size after coronary intervention. As a result of this research we
became less concerned about using larger sheaths when clinically necessary.
Impact on literature
According to Scopus ®, this article has been cited at least 7 times in the literature
from a journal with a 5 year impact factor of 2.373.
Paper 7 (Int J Cardiol 2007;116:321-326)
Femoral arterial sheath removal after PCI may be considered routine for health
care personnel; however this process is associated with a significant amount of
discomfort reported by patients [16,17]. Pain may be related to the removal of the
femoral sheath itself, to the pressure applied until haemostasis is achieved, or to the
need for the patient to remain supine and immobile for hours. Suboptimal pain
control may adversely affect the patients’ ability to cooperate during the femoral
sheath removal, resulting in prolonged time to haemostasis and contributing to groin
complications. The presence of pain, tissue injury and strong emotional states may
contribute to the development of vaso-vagal syncope [18,19], which may have serious
consequences (e.g., profound asystole or infarction) for patients after PCI [19,20].
Whilst the use of vascular closure devices may improve patient comfort [17]
and decrease the time to haemostasis and ambulation [17,21], there is little evidence
that they reduce the incidence of major vascular complications [4,7,11]. This,
27
together with their cost, mean that many centres including our own, remove femoral
sheaths after PCI using assisted manual compression in the majority of cases.
Published reports with respect to the use of sedation and local anaesthesia for patient
comfort during femoral sheath removal vary widely in their outcomes [22-26] and
currently there is no common consensus or practice in place with respect to their use.
We performed a randomised controlled trial on the impact of intravenous sedation and
local anaesthesia during femoral sheath removal after PCI on patient comfort and the
incidence and predictors of vaso-vagal reactions. This formed the basis of Paper 7.
We showed that special care should be taken when removing sheaths from patients in
whom the left anterior descending vessel has been treated and those on a glyceryl
trinitrate infusion as its use is associated with a higher likelihood of a vasovagal event.
We also found that the routine use of fentanyl and midazolam prior to sheath removal
leads to a reduction in pain perception and a trend to less vaso-vagal reactions. Finally
we concluded that patients given subcutaneous lignocaine prior to sheath removal
reported more pain than patients receiving no local anaesthesia and experienced more
vasovagal events; therefore the routine use of local infiltration in pain management
during sheath removal should be discouraged.
Context and Implications
This work was initiated and completed by the author at Liverpool hospital. It is the
largest study which specifically addresses the issues around analgesia and sheath
removal. As a consequence of this research we formulated a number of
recommendations for the process of femoral arterial sheath removal after
percutaneous coronary intervention consistent with our conclusions.
Impact on literature
According to Scopus ®, this article has been cited at least three times in the literature
28
to date from a journal with a 5 year impact factor of 4.111. It has been cited in the
Australian nursing clinical practice guidelines to improve care for people undergoing
percutaneous coronary interventions [27].
Paper 8 (Int J Cardiol 2008;127:252-254)
Paper 8 was a continuation of the work we started with Paper 7. Apart from
infrequent case reports [19,20] there is little published literature on potential adverse
cardiac events of vaso-vagal syncope during sheath removal particularly in the
circumstance of recent stent deployment where profound hypotension and bradycardia
may potentially lead to stent thrombosis.
We sort to determine whether vaso-vagal syncope during sheath removal after
percutaneous coronary intervention leads to a higher incidence of major adverse
cardiac events including acute stent thrombosis, in 611 patients who participated in
our previous trial assessing the impact of intravenous sedation and local anaesthesia at
this time on patient comfort.
We discovered that whilst unpleasant for patients, we concluded that vaso-
vagal syncope during sheath removal after percutaneous coronary intervention is not
associated with increased adverse cardiac events in the stent era.
Context and Implications
This work was initiated and completed by the author at Liverpool hospital and follows
on from an earlier work. To my knowledge this remains the largest study which
specifically addresses the issue of vasovagal reactions at the time of sheath removal
and was the first study to report results in the context of recent stent deployment. It
has also helped to allay concerns around this issue for our medical and nursing staff.
29
Impact on literature
According to Scopus ®, this article has been cited twice in the literature to date from a
journal with a 5 year impact factor of 4.111. This paper has also been cited in the
Australian nursing clinical practice guidelines to improve care for people undergoing
percutaneous coronary interventions [27].
30
Chapter 2 References
1. Wyman RM, Safian RD, Portway V, Skillman JJ, McKay RG, Baim DS. Current
complications of diagnostic and therapeutic cardiac catheterization. J Am Coll Cardiol
1988;12:1400-1406.
2. Moscucci M, Mansour KA, Kent KC, et al. Peripheral vascular complications of
directional coronary atherectomy and stenting: predictors, management, and outcome.
Am J Cardiol 1994;74:448-453.
3. Popma JJ, Satler LF, Pichard AD, et al Vascular complications after balloon and
new device angioplasty. Circulation 1993;88:1569-1578.
4. Kussmaul WG, III, Buchbinder M, Whitlow PL, et al. Rapid arterial hemostasis
and decreased access site complications after cardiac catheterization and angioplasty:
results of a randomized trial of a novel hemostatic device. J Am Coll Cardiol
1995;25:1685-1692.
5. Michalis LK, Rees MR, Patsouras D, et al. A prospective randomized trial
comparing the safety and efficacy of three commercially available closure devices
(Angioseal, Vasoseal and Duett). Cardiovasc Intervent Radiol 2002;25:423-429.
6. Sanborn TA, Gibbs HH, Brinker JA, Knopf WD, Kosinski EJ, Roubin GS. A
multicenter randomized trial comparing a percutaneous collagen hemostasis device
with conventional manual compression after diagnostic angiography and angioplasty.
J Am Coll Cardiol 1993;22:1273-1279.
7. Amin FR, Yousufuddin M, Stables R, et al. Femoral haemostasis after
transcatheter therapeutic intervention: a prospective randomised study of the angio-
seal device vs. the femostop device. Int J Cardiol 2000;76:235-240.
31
8. Chamberlin JR, Lardi AB, McKeever LS, et al. Use of vascular sealing devices
(VasoSeal and Perclose) versus assisted manual compression (Femostop) in
transcatheter coronary interventions requiring abciximab (ReoPro). Catheter
Cardiovasc Interv 1999;47:143-147.
9. Shammas NW, Rajendran VR, Alldredge SG, et al. Randomized comparison of
Vasoseal and Angioseal closure devices in patients undergoing coronary angiography
and angioplasty. Catheter Cardiovasc Interv 2002;55:421-425.
10. Walker SB, Cleary S, Higgins M. Comparison of the FemoStop device and
manual pressure in reducing groin puncture site complications following coronary
angioplasty and coronary stent placement. Int J Nurs Pract 2001;7:366-375.
11. Applegate RJ, Grabarczyk MA, Little WC, et al. Vascular closure devices in
patients treated with anticoagulation and IIb/IIIa receptor inhibitors during
percutaneous revascularization. J Am Coll Cardiol 2002;40:78-83.
12. Pracyk JB, Wall TC, Longabaugh JP, et al. A randomized trial of vascular
hemostasis techniques to reduce femoral vascular complications after coronary
intervention. Am J Cardiol 1998;81:970-976.
13. Metz D, Meyer P, Touati C, et al. Comparison of 6F with 7F and 8F guiding
catheters for elective coronary angioplasty: results of a prospective, multicentre,
randomized trial. Am Heart J 1997;134:131-137.
14. Talley JD, Wilkins C, Ciccone J, Hattel LJ. Comparison of 7 and 8 French guiding
catheters for elective PTCA: results of a prospective randomized trial. Cathet
Cardiovasc Diagn 1994;33:205-211.
15. Talley JD, Mauldin PD, Becker ER. A prospective randomized trial comparing the
benefits and limitations of 6 Fr and 8 Fr guiding catheters in elective coronary
32
angioplasty: Clinical, procedural, angiographic, and economic endpoints. J Interven
Cardiol 1995;8:345-353.
16. Slaughter PMP, Chetty R, Flintoft VF, et al. A single center randomized trial
assessing use of a vascular hemostasis device vs conventional manual compression
following PTCA: what are the potential resource saving? Cathet Cardiovasc Diagn
1995;34:210-214.
17. Juergens CP, Leung DYC, Crozier JA, et al. Patient tolerance and resource
utilization associated with an arterial closure versus an external compression device
after percutaneous coronary intervention. Catheter Cardiovasc Interv 2004;63:166-
170.
18. Boss BJ, Brewer L. Syncope: neuroscience nursing assessment based on an
understanding of underlying pathophysiological mechanisms. J Neurosci Nurs
1988;20:245-252.
19. Barbiere CC. Malignant vasovagal syncope after PTCA: a potential for disaster.
Crit Care Nurse 1994;14:90-93.
20. Mager A, Strasberg B, Rechavia E, et al. Clinical significance and predisposing
factors to symptomatic bradycardia and hypotension after percutaneous transluminal
coronary angioplasty. Am J Cardiol 1994;74:1085-1088.
21. Wilentz JR, Mishkel G, McDermott D, Ravi K, Fox JT, Reimers CD. Outpatient
coronary stenting using the femoral approach with vascular sealing. J Invasive
Cardiol 1999;11:709-717.
22. Peet GI, McGrath MA, Brunt JH, Hilton JD. Femoral arterial sheath removal after
PTCA: a cross-Canada survey. Can J Cardiovsc Nurs 1995;6:13-19.
23. Wadas TM, Hill J. Is lidocaine infiltration during femoral sheath removal really
necessary? Heart Lung 1998;27:31-36.
33
24. Bowden SM, Worrey JA. Assessing patient comfort: Local infiltration of
lidocaine during femoral sheath removal. Am J Crit Care 1995;4:368-369.
25. Juran NB, Smith DD, Rouse CL, DeLuca SA, Rund M. Survey of current practice
patterns for percutaneous transluminal coronary angioplasty. Am J Crit Care
1996;5:442-448.
26. Fulton TR, Peet GI, McGrath MA, et al. Effects of 3 analgesic regimens on the
perception of pain after removal of femoral artery sheaths. Am J Crit Care 2000;
9:125-129.
27. Rolley JX, Salamonson Y, Wensley C, Dennison CR, Davidson PM. Nursing
clinical practice guidelines to improve care for people undergoing percutaneous
coronary interventions. Aust Crit Care 2011; 24:18-38.
34
PAPER 5
Reprinted from Catheterization and Cardiovascular Interventions
2004;63:166-170 with permission from “John Wiley and Sons”
Patient Tolerance and Resource Utilization AssociatedWith an Arterial Closure Versus an External
Compression Device After PercutaneousCoronary Intervention
Craig P. Juergens,1*MBBS, FRACP, FACC, Dominic Y.C. Leung,1 PhD, MBBS, FRACP, FACC,John A. Crozier,2 FRACS, DDU, Adelina M. Wong,1 MClinPrac, Jacqui T.C. Robinson,2 RN, RVT, AMS,
Sidney Lo,1 MBBS, FRACP, Hashim Kachwalla,1 MBBS, and Andrew P. Hopkins1MBBS, FRACP
We assessed patient tolerance and resource utilization of using the AngioSeal closuredevice versus assisted manual compression using the Femostop device after percuta-neous coronary intervention (PCI). Patients undergoing PCI with clean arterial access andno procedural hematoma were randomized to receive the AngioSeal or Femostop deviceto achieve femoral arterial hemostasis. Times from procedure end to removal fromangiography table, hemostasis, ambulation, and hospital discharge were recorded. Bed-side nursing/medical officer care time, vascular complications, and disposable use werealso documented. Patient comfort was assessed using Present Pain Intensity and VisualAnalogue scales at baseline, 4 hr, 8 hr, and the morning after the procedure. One hundredtwenty-two patients were enrolled (62 AngioSeal, 60 Femostop). Patients in the AngioSealgroup took longer to be removed from the angiography table (11 � 4 vs. 9 � 3 min; P �0.002) compared with the Femostop group. Time to hemostasis (0.4 � 1.1 vs. 6.4 � 1.7 hr;P < 0.001) and ambulation (17 � 8 vs. 22 � 13 hr; P � 0.004) were less in the AngioSealgroup, although time to discharge was not different. Nursing and medical officer timewas no different. Disposables including device cost were higher in the AngioSeal group($209 � 13 vs. $53 � 9; P < 0.001). On a Visual Analogue scale, patients reported morepain at 4 hr (P < 0.001) and 8 hr (P < 0.001) in the Femostop group. The worst amount ofpain at any time point was also more severe in the Femostop group (P < 0.001). Similarresults were found on a Present Pain Intensity scale of pain. There were no differencesin ultrasound-determined vascular complications (two each). Femoral access site clo-sure using the AngioSeal device resulted in a small delay in leaving the angiography suiteand a higher disposable cost compared to using the Femostop device. However, patientsreceiving the AngioSeal were able to ambulate sooner and reported less pain, which mayjustify the increased costs involved. Catheter Cardiovasc Interv 2004;63:166–170.© 2004 Wiley-Liss, Inc.
Key words: AngioSealTM; FemostopTM; angioplasty; complications; pain
INTRODUCTION
Vascular access site complications result in significantmorbidity after coronary interventional procedures, withan incidence of 0.5–16.8% of cases [1–3]. Early in theexperience of intracoronary stenting, vascular complica-tions requiring surgery were seen in 5–10% of patients[2,3]. A number of vascular closure devices, includingthe AngioSeal [4,5], were developed in a bid to shortenhemostasis times and possibly reduce vascular compli-cations. The AngioSeal is a sheath-deployed, bioabsorb-able, hemostatic closure device that allows sheath re-moval at the end of the procedure while patients are stillsystemically heparinized. This device has been shown tobe a safe and effective means of obtaining vascular
hemostasis after cardiac catheterization procedures [6].Alternatively, the Femostop is an external compression
1Department of Cardiology, Liverpool Hospital, Liverpool, NewSouth Wales, Australia2Department of Vascular Surgery, University of New SouthWales, New South Wales, Australia
*Correspondence to: Craig P. Juergens, Department of Cardiology,Liverpool Hospital, Locked Bag 7103, Liverpool BC NSW 1871,Australia. E-mail: [email protected]
Received 3 October 2003; Revision accepted 9 June 2004
DOI 10.1002/ccd.20161Published online in Wiley InterScience (www.interscience.wiley.com).
Catheterization and Cardiovascular Interventions 63:166–170 (2004)
© 2004 Wiley-Liss, Inc.

device, which is cheaper but is applied after the effects ofintraprocedural heparinization have dissipated, resultingin delays in time to hemostasis, ambulation, and dis-charge when compared to the AngioSeal. Furthermore,the delay in removal of the sheath and prolonged periodof compression with the Femostop may result in morepatient discomfort than would occur using the AngioSealdevice.
While previous studies have sought to address theincidence of vascular complications comparing variousvascular closure devices [6–14], we sought to comparespecifically patient tolerance and the resource implica-tions of using the AngioSeal and Femostop devices.
MATERIALS AND METHODS
Patient Selection
All patients undergoing a percutaneous coronary in-tervention were eligible for entry into the trial. To beeligible for enrollment, patients had to have clean (singlepuncture through the anterior wall only) arterial accessand no development of hematoma during the procedure.Patients were excluded if repeat femoral access throughthe same side was likely within the ensuing 90 days. Tostandardize the arterial puncture size, only patients inwhom a 7 Fr sheath and guiding system were used wereeligible for inclusion in this trial. Patients were random-ized at the end of the procedure to either immediate groinclosure using an AngioSeal or delayed sheath removalwith the assistance of the Femostop device. The institu-tional committee on human research of our hospital ap-proved the study and all patients gave written informedconsent.
Percutaneous Coronary Intervention
Patients underwent percutaneous coronary interven-tion using standard techniques. Coronary artery stentswere implanted using standard high-pressure techniques.Heparin was administered as boluses to maintain anactivated clotting time (ACT) greater than 250 sec andglycoprotein IIb/IIIa inhibitors could be used at the op-erator’s discretion. In patients randomized to receive anAngioSeal, the device was deployed using standard tech-niques in the angiography suite at the end of the proce-dure. Femoral angiography was not performed routinelyto assess the femoral vasculature prior to device deploy-ment. For those randomized to the Femostop, the sheathwas removed when the ACT was less than 180 sec.Heparin could be restarted after sheath removal at theoperator’s discretion. All patients received at least300 mg of aspirin in the 24 hr prior to the procedure anda minimum of 100 mg per day after their procedure.Patients receiving intracoronary stents received either
ticlopidine (250 mg b.i.d.) or clopidogrel (75 mg daily)orally after standard loading doses.
Data Gathering and Follow-Up
Data were collected prospectively with respect to timefrom last angiographic image to removal from the cath-eterization laboratory table, as well as time to initialhemostasis, ambulation, and discharge. Patient comfortwas assessed based on a short form of the McGill PainQuestionnaire [15] using a Present Pain Intensity (PPI)scale and a Visual Analogue scale. First assessmentswere at the end of their percutaneous coronary interven-tion and thereafter at 4 hr, 8 hr, and the morning after theprocedure. The Present Pain Intensity scale rated painfrom 0 (no pain) to 5 (excruciating). The Visual Ana-logue scale was a scale from 1 to 10, which representedno pain to worst possible pain. The angioplasty operatoror attending physician independently made the decisionsregarding mobilization and time of discharge. Thesewere in no way mandated by the study design. Allpatients were scheduled to undergo a duplex vascularultrasound of the femoral access site the day after theprocedure, which was reported by a vascular surgeonwho was blinded to treatment assignment. The presenceof a new hematoma, pseudoaneurysm, arterovenous fis-tula, or femoral vein thrombosis was noted. The femoralaccess site was also inspected for any clinical evidence ofcomplications. Vascular complications were defined asoozing (leakage of blood from puncture site requiringdigital pressure), ecchymosis (bleeding into subcutane-ous tissue planes causing bluish-purple discoloration � 4cm in diameter), hematoma (nonpulsatile mass � 1 cm indiameter), bruit, pulsatile mass, or leg ischemia. Theneed for transfusion and hemoglobin level before andafter the procedure were also collected.
Resources consumed were also measured. The residentmedical staff and nurses attending to the patient wereasked to record the use of all disposables (such as devicecost, swabs) and pharmacological agents (such as localanesthetics, analgesics) pertaining to management of thefemoral access site. They were also asked to record timespent at the bedside in the management of the femoralaccess site.
Primary Endpoints
The primary endpoints were patient tolerance and re-source utilization. Patient tolerance was assessed by boththe Present Pain Intensity and Visual Analogue scales.The most intense pain recorded for each patient duringtheir hospital stay was compared between the twogroups. The highest score recorded on the Visual Ana-logue scale was also recorded and compared between thetwo groups. Resource utilization was determined by thecost of disposals used for both groups and amount of
Differing Femoral Access Management After PCI 167
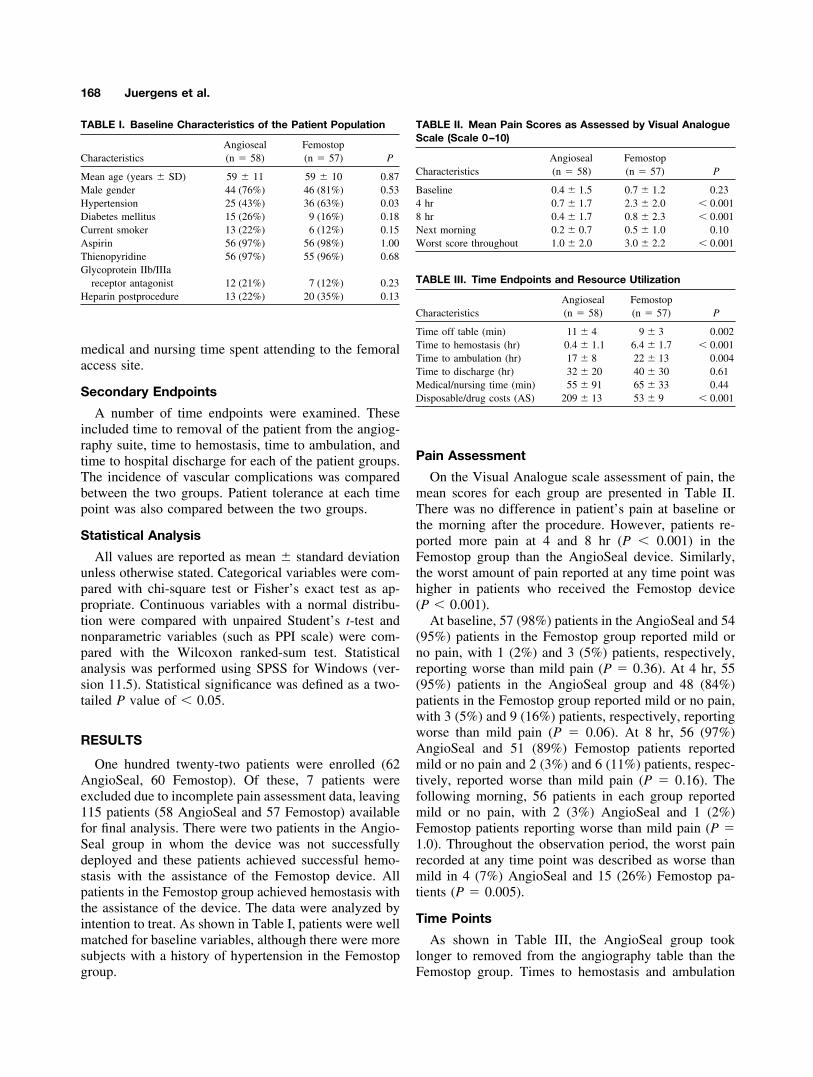
medical and nursing time spent attending to the femoralaccess site.
Secondary Endpoints
A number of time endpoints were examined. Theseincluded time to removal of the patient from the angiog-raphy suite, time to hemostasis, time to ambulation, andtime to hospital discharge for each of the patient groups.The incidence of vascular complications was comparedbetween the two groups. Patient tolerance at each timepoint was also compared between the two groups.
Statistical Analysis
All values are reported as mean � standard deviationunless otherwise stated. Categorical variables were com-pared with chi-square test or Fisher’s exact test as ap-propriate. Continuous variables with a normal distribu-tion were compared with unpaired Student’s t-test andnonparametric variables (such as PPI scale) were com-pared with the Wilcoxon ranked-sum test. Statisticalanalysis was performed using SPSS for Windows (ver-sion 11.5). Statistical significance was defined as a two-tailed P value of � 0.05.
RESULTS
One hundred twenty-two patients were enrolled (62AngioSeal, 60 Femostop). Of these, 7 patients wereexcluded due to incomplete pain assessment data, leaving115 patients (58 AngioSeal and 57 Femostop) availablefor final analysis. There were two patients in the Angio-Seal group in whom the device was not successfullydeployed and these patients achieved successful hemo-stasis with the assistance of the Femostop device. Allpatients in the Femostop group achieved hemostasis withthe assistance of the device. The data were analyzed byintention to treat. As shown in Table I, patients were wellmatched for baseline variables, although there were moresubjects with a history of hypertension in the Femostopgroup.
Pain Assessment
On the Visual Analogue scale assessment of pain, themean scores for each group are presented in Table II.There was no difference in patient’s pain at baseline orthe morning after the procedure. However, patients re-ported more pain at 4 and 8 hr (P � 0.001) in theFemostop group than the AngioSeal device. Similarly,the worst amount of pain reported at any time point washigher in patients who received the Femostop device(P � 0.001).
At baseline, 57 (98%) patients in the AngioSeal and 54(95%) patients in the Femostop group reported mild orno pain, with 1 (2%) and 3 (5%) patients, respectively,reporting worse than mild pain (P � 0.36). At 4 hr, 55(95%) patients in the AngioSeal group and 48 (84%)patients in the Femostop group reported mild or no pain,with 3 (5%) and 9 (16%) patients, respectively, reportingworse than mild pain (P � 0.06). At 8 hr, 56 (97%)AngioSeal and 51 (89%) Femostop patients reportedmild or no pain and 2 (3%) and 6 (11%) patients, respec-tively, reported worse than mild pain (P � 0.16). Thefollowing morning, 56 patients in each group reportedmild or no pain, with 2 (3%) AngioSeal and 1 (2%)Femostop patients reporting worse than mild pain (P �1.0). Throughout the observation period, the worst painrecorded at any time point was described as worse thanmild in 4 (7%) AngioSeal and 15 (26%) Femostop pa-tients (P � 0.005).
Time Points
As shown in Table III, the AngioSeal group tooklonger to removed from the angiography table than theFemostop group. Times to hemostasis and ambulation
TABLE I. Baseline Characteristics of the Patient Population
CharacteristicsAngioseal(n � 58)
Femostop(n � 57) P
Mean age (years � SD) 59 � 11 59 � 10 0.87Male gender 44 (76%) 46 (81%) 0.53Hypertension 25 (43%) 36 (63%) 0.03Diabetes mellitus 15 (26%) 9 (16%) 0.18Current smoker 13 (22%) 6 (12%) 0.15Aspirin 56 (97%) 56 (98%) 1.00Thienopyridine 56 (97%) 55 (96%) 0.68Glycoprotein IIb/IIIa
receptor antagonist 12 (21%) 7 (12%) 0.23Heparin postprocedure 13 (22%) 20 (35%) 0.13
TABLE II. Mean Pain Scores as Assessed by Visual AnalogueScale (Scale 0–10)
CharacteristicsAngioseal(n � 58)
Femostop(n � 57) P
Baseline 0.4 � 1.5 0.7 � 1.2 0.234 hr 0.7 � 1.7 2.3 � 2.0 � 0.0018 hr 0.4 � 1.7 0.8 � 2.3 � 0.001Next morning 0.2 � 0.7 0.5 � 1.0 0.10Worst score throughout 1.0 � 2.0 3.0 � 2.2 � 0.001
TABLE III. Time Endpoints and Resource Utilization
CharacteristicsAngioseal(n � 58)
Femostop(n � 57) P
Time off table (min) 11 � 4 9 � 3 0.002Time to hemostasis (hr) 0.4 � 1.1 6.4 � 1.7 � 0.001Time to ambulation (hr) 17 � 8 22 � 13 0.004Time to discharge (hr) 32 � 20 40 � 30 0.61Medical/nursing time (min) 55 � 91 65 � 33 0.44Disposable/drug costs (AS) 209 � 13 53 � 9 � 0.001
168 Juergens et al.

were less in the AngioSeal group, although time to dis-charge was no different between the two groups.
Resource Utilization
Resource usage is also shown in Table III. Nursing andmedical officer time was no different between eachgroup. Disposables including device cost were higher inthe AngioSeal group.
Vascular Complications
Vascular events are shown in Table IV. All but threepatients in the AngioSeal and two patients in the Femo-stop had a vascular ultrasound performed. In those forwhom no ultrasound was performed, there was no clin-ical suspicion of a major vascular complication. Therewas no difference in ultrasound-determined vascularcomplications (two in each group). No patient requiredtransfusion or had a decrease in hemoglobin in excess of2 g/dl.
DISCUSSION
We have demonstrated that patients whose femoralaccess site is closed with an AngioSeal device experi-enced less pain than those receiving assisted manualcompression using the Femostop device. These differ-ences were most marked at 4 and 8 hr after successfulpercutaneous coronary intervention and were no longerapparent the morning after the procedure. Potentially, thedesign of our study has biased the results against theFemostop device, which necessitates that full anticoagu-lation be allowed to diminish, whereas the AngioSealdevice is deployed immediately. However, hemostasiswas achieved with the Femostop at a mean of 6.4 hr,suggesting it was deployed after the 4-hr and removedbefore the 8-hr assessment of pain. These results aresimilar to that of Slaughter et al. [16], who demonstratedthat another collagen-based vascular closure device, theVasoseal (Datascope, Montvale, NJ), was also associatedwith less pain than traditional manual compression.
Despite ongoing anticoagulation, the time to hemosta-sis in patients receiving the AngioSeal was 15 timesfaster than found in the manual compression group inwhom heparin had been discontinued. There was a 2-mindelay in removing patients from the angiography suitewhen an AngioSeal device was deployed, a statisticallysignificant but probably clinically meaningless differ-ence. Given the different approaches to sheath removal,it is to be expected that patients receiving the AngioSealwere ambulatory sooner than those receiving the Femo-stop device. Time to discharge was similar in both groupsas all patients in our institution are routinely admittedovernight after percutaneous coronary intervention. Anumber of studies have determined that same-day dis-charge can be accomplished safely in selected patients inwhom percutaneous coronary intervention is performedvia a radial approach [17–19]. Similarly, in a study ofselected patients undergoing percutaneous interventionvia the femoral artery with the use of a vascular closuredevice, the investigators demonstrated that same-day dis-charge was feasible [20].
The incidence of minor complications was similar inboth groups, with more oozing in the AngioSeal groupand more ecchymosis in the Femostop group. There wereno differences in major vascular complications betweenthe two groups as determined by vascular ultrasound.Previous larger studies comparing the AngioSeal deviceto manual compression have shown no differences inmajor vascular complications [6,9,13] with observedrates of complications in the AngioSeal arms of 1.1–2.8%.
With respect to resource utilization, there was no dif-ference in nursing or medical officer time spent at thebedside. While the sheath can be removed relativelyquickly using the AngioSeal, the femoral access site stillneeds to be regularly observed and distal pulses assessed,which may account for the lack of difference between thetwo groups. Similarly, the higher rate of groin oozing inthe AngioSeal patients necessitated more bedside timeand manual compression. The higher cost of the Angio-Seal device led to higher disposable costs in this group ofpatients, even though there were numerically more lowcosts items utilized during removal of the sheath with theFemostop device. Due to similar times to discharge, it isunlikely we would have shown any savings with respectto hospital costs in the AngioSeal group, although we didnot specifically assess this. The potential use of theAngioSeal device to facilitate same-day discharge wouldlikely result in considerable financial benefits. However,the reduction in patient discomfort and earlier ambula-tion may justify the A$156 incremental cost of the An-gioSeal device.
Femoral access site closure using the AngioSeal de-vice resulted in a slight delay in removal from the an-
TABLE IV. Vascular Complications
CharacteristicsAngioseal(n � 58)
Femostop(n � 57) P
Clinical abnormality (any)a 26 (44.8%) 27 (47.4%) 0.79Vagal episode 2 (3.4%) 6 (10.5%) 0.162Hematoma 8 (13.8%) 9 (15.8%) 0.76Ecchymosis 8 (13.8%) 16 (28.1%) 0.06Oozing 15 (25.9%) 8 (14.0%) 0.11Bruit 1 (1.7%) 1 (1.8%) 1.0
Ultrasound abnormality 2 (3.4%) 2 (3.5%) 1.0Hematoma 2 (3.4%) 1 (1.8%) 1.0Pseudoaneursym 0 1 (1.8%) 0.5
aOne or more clinical complications.
Differing Femoral Access Management After PCI 169

giography suite and a higher disposable cost. However,patients receiving the AngioSeal achieved hemostasisfaster, were able to ambulate sooner, and reported lesspain than those patients who received assisted manualcompression with the Femostop device, outcomes thatmay substantiate the small incremental cost involved.
ACKNOWLEDGMENTS
The authors thank the nursing staff of the coronarycare unit and cardiac catheterization laboratories for theirassistance in the collection of data for this study.
REFERENCES
1. Wyman RM, Safian RD, Portway V, Skillman JJ, McKay RG,Baim DS. Current complications of diagnostic and therapeuticcardiac catheterization. J Am Coll Cardiol 1988;12:1400–1406.
2. Moscucci M, Mansour KA, Kent KC, Kuntz RE, Senerchia C,Baim DS, Carrozza JP Jr. Peripheral vascular complications ofdirectional coronary atherectomy and stenting: predictors, man-agement, and outcome. Am J Cardiol 1994;74:448–453.
3. Popma JJ, Satler LF, Pichard AD, Kent KM, Campbell A, ChuangYC, Clark C, Merritt AJ, Bucher TA, Leon MB. Vascular com-plications after balloon and new device angioplasty. Circulation1993;88:1569–1578.
4. de Swart H, Dijkman L, Hofstra L, Bar FW, Van OV, Tordoir J,Wellens HJ. A new hemostatic puncture closure device for theimmediate sealing of arterial puncture sites. Am J Cardiol 1993;72:445–449.
5. Henry M, Amor M, Allaoui M, Tricoche O. A new access sitemanagement tool: the Angio-Seal hemostatic puncture closuredevice. J Endovasc Surg 1995;2:289–296.
6. Kussmaul WG III, Buchbinder M, Whitlow PL, Aker UT, HeuserRR, King SB, Kent KM, Leon MB, Kolansky DM, Sandza JG Jr.Rapid arterial hemostasis and decreased access site complicationsafter cardiac catheterization and angioplasty: results of a random-ized trial of a novel hemostatic device. J Am Coll Cardiol 1995;25:1685–1692.
7. Michalis LK, Rees MR, Patsouras D, Katsouras CS, GoudevenosJ, Pappas S, Sourla E, Kolettis T, Sioros L, Zotou P, Gartzou-Matsouka P, Sideris DA. A prospective randomized trial compar-ing the safety and efficacy of three commercially available closuredevices (AngioSeal, Vasoseal and Duett). Cardiovasc Interv Ra-diol 2002;25:423–429.
8. Sanborn TA, Gibbs HH, Brinker JA, Knopf WD, Kosinski EJ,Roubin GS. A multicenter randomized trial comparing a percuta-neous collagen hemostasis device with conventional manual com-pression after diagnostic angiography and angioplasty. J Am CollCardiol 1993;22:1273–1279.
9. Amin FR, Yousufuddin M, Stables R, Shamim W, Al Nasser F,Coats AJ, Clague J, Sigwart U. Femoral haemostasis after trans-catheter therapeutic intervention: a prospective randomised studyof the angio-seal device vs. the femostop device. Int J Cardiol2000;76:235–240.
10. Chamberlin JR, Lardi AB, McKeever LS, Wang MH, RamaduraiG, Grunenwald P, Towne WP, Grassman ED, Leya FS, Lewis BE,Stein LH. Use of vascular sealing devices (VasoSeal and Perclose)versus assisted manual compression (Femostop) in transcathetercoronary interventions requiring abciximab (ReoPro). CatheterCardiovasc Interv 1999;47:143–147.
11. Shammas NW, Rajendran VR, Alldredge SG, Witcik WJ, RobkenJA, Lewis JR, McKinney D, Hansen CA, Kabel ME, Harris M,Jerin MJ, Bontu PR, Dippel EJ, Labroo A. Randomized compar-ison of Vasoseal and AngioSeal closure devices in patients un-dergoing coronary angiography and angioplasty. Catheter Cardio-vasc Interv 2002;55:421–425.
12. Walker SB, Cleary S, Higgins M. Comparison of the FemoStopdevice and manual pressure in reducing groin puncture site com-plications following coronary angioplasty and coronary stentplacement. Int J Nurs Pract 2001;7:366–375.
13. Applegate RJ, Grabarczyk MA, Little WC, Craven T, Walkup M,Kahl FR, Braden GA, Rankin KM, Kutcher MA. Vascular closuredevices in patients treated with anticoagulation and IIb/IIIa recep-tor inhibitors during percutaneous revascularization. J Am CollCardiol 2002;40:78–83.
14. Pracyk JB, Wall TC, Longabaugh JP, Tice FD, Hochrein J, GreenC, Cox G, Lee K, Stack RS, Tcheng JE. A randomized trial ofvascular hemostasis techniques to reduce femoral vascular com-plications after coronary intervention. Am J Cardiol 1998;81:970–976.
15. Melzack R. The short-form McGill pain questionnaire. Pain 1987;30:191–197.
16. Slaughter PM, Chetty R, Flintoft VF, Lewis S, Sykora K, BeattieDM, Schwartz L. A single center randomized trial assessing use ofa vascular hemostasis device vs. conventional manual compres-sion following PTCA: what are the potential resource savings?Cathet Cardiovasc Diagn 1995;34:210–214.
17. Gilchrist IC, Nickolaus MJ, Momplaisir T. Same-day transradialoutpatient stenting with a 6-hr course of glycoprotein IIb/IIIareceptor blockade: a feasibility study. Catheter Cardiovasc Interv2002;56:10–13.
18. Slagboom T, Kiemeneij F, Laarman GJ, van der Wieken R,Odekerken D. Actual outpatient PTCA: results of the OUTCLASpilot study. Catheter Cardiovasc Interv 2001;53:204–208.
19. Kiemeneij F, Laarman GJ, Slagboom T, van der Wieken R.Outpatient coronary stent implantation. J Am Coll Cardiol 1997;29:323–327.
20. Wilentz JR, Mishkel G, McDermott D, Ravi K, Fox JT, ReimersCD. Outpatient coronary stenting using the femoral approach withvascular sealing. J Invas Cardiol 1999;11:709–717.
170 Juergens et al.
35
PAPER 6
Reprinted from Catheterization and Cardiovascular Interventions
2005;66:528-534 with permission from “John Wiley and Sons”
Comparison of 6 and 7 French Guiding Catheters forPercutaneous Coronary Intervention: Results of a
Randomised Trial with a Vascular Ultrasound Endpoint
Craig P. Juergens,1* MBBS, FRACP, FACC, Hisham Hallani,1 MBBS, FRACP,Dominic Y.C. Leung,1 PhD, MBBS, FRACP, FACC, John A. Crozier,2 FRACS, DDU,
Jacqui T.C. Robinson,2 RN, RVT, AMS, Sidney Lo,1 MBBS, FRACP,and Andrew P. Hopkins,1 MBBS, FRACP
Objective: To perform a randomized, ultrasound controlled trial to define the proce-dural and clinical advantages and limitations of 6 French (Fr) compared with 7 Fr trans-femoral coronary intervention in the stenting era. Background: The use of 7 Fr guidingcatheters may facilitate Percutaneous Coronary Intervention (PCI), but may be asso-ciated with increased vascular complications when compared with 6 Fr catheters.Methods: Patients undergoing PCI considered suitable for either a 6 or 7 Fr sheath andguiding catheter system were included. All vascular sheaths were removed withassisted manual compression. Femoral vascular ultrasounds were performed prior tohospital discharge and interpreted by a vascular surgeon blinded to treatment assign-ment. The primary endpoint was a composite of significant vascular complicationsincluding major haematoma, retroperitoneal haematoma, pseudoaneurysm, arterio–venous fistula, or femoral venous or arterial thrombosis. Results: During the study,414 patients (mean age 61 6 11 years, 27% females) were randomly assigned to 6 Fror 7 Fr sheath groups. The incidence of major vascular complications was 5.7% inthe 6 Fr group and 3.9% in the 7 Fr group (P 5 0.383). There was no significant dif-ference in procedural or angiographic success between the groups. The use of con-trast volume was higher in the 7 Fr group (157 6 58 ml vs. 144 6 58 ml; P 5 0.029).There was a trend toward better operator satisfaction with the 7 Fr guide (P 5 0.08).Conclusions: This prospective, randomized trial indicates no reduction in major peripheralvascular complications with the use of smaller guiding catheters in PCI. There was lesscontrast used in the 6 Fr group, which may benefit some patient subsets, however opera-tors tended to prefer the larger 7 Fr system. The target coronary anatomy and need forcomplex device intervention should mandate the choice of guiding catheter size, not aperceived impact on vascular complications. ' 2005Wiley-Liss, Inc.
Key words: angioplasty; complications; size
INTRODUCTION
Local vascular complications at the access site result
in significant morbidity after coronary interventional
procedures occurring with a frequency of 1.5–16.8%
[1–3]. These earlier studies were performed with pre-
dominant use of 8 French (Fr) or larger diameter cath-
eters. Improved guiding catheter design has resulted in
increased internal diameters, which facilitate the pas-
sage of interventional devices without increasing their
external diameter, therefore, allowing coronary inter-
vention to be performed using smaller diameter Frenchcatheters. A number of studies performed during diag-nostic coronary angiography have shown no reduction
1Department of Cardiology, Liverpool Hospital, Liverpool BC,New South Wales, Australia2Department of Vascular Surgery, University of New SouthWales, Sydney, Australia
*Correspondence to: Craig P Juergens, Department of Cardiology,
Liverpool Hospital, Locked Bag 7103, Liverpool BC, NSW 1871,
Australia. E-mail: [email protected]
Received 9 March 2005; Revision accepted 21 July 2005
DOI 10.1002/ccd.20534
Published online 5 October 2005 in Wiley InterScience (www.
interscience.wiley.com).
' 2005 Wiley-Liss, Inc.
Catheterization and Cardiovascular Interventions 66:528–534 (2005)
in significant vascular complications with the use ofsmaller diameter catheters [4–8], often with compro-mised image quality and handling characteristics [4–6,8]. Previous trials comparing differently-sized guidingcatheters during percutaneous coronary intervention(PCI) have revealed conflicting results with respect tothe incidence of vascular complications [9–11]. Thesetrials were performed before the widespread use ofintracoronary stenting and had rates of stent use from0 to 25% [9–11]. Moreover, vascular ultrasound wasnot routinely performed in all patients to assess asymp-tomatic access site complications. To define the proce-dural and clinical advantages and limitations of 6 Frcompared with 7 Fr transfemoral coronary interven-tions in the stenting era, we performed a randomized,controlled trial and assessed vascular complications byroutine access site ultrasound, blinded to clinical out-comes.
METHODS
Patient Selection
Four hundred and fourteen patients undergoing aPCI between February 1999 and January 2004 wereenrolled in the study at our institution. Consecutivepatients undergoing PCI, who could provide informedconsent, were eligible for entry into the trial if the pri-mary operator felt that either a 6 Fr or a 7 Fr sheathand guiding catheter could be used safely. Patients werenot eligible, however, if a vascular ultrasound could notbe arranged prior to hospital discharge. Patients wererandomized in blocks of 10 to either 6 or 7 Fr systemsusing an opaque envelope system kept in the catheter-ization laboratory. The Institutional Committee onhuman research of our hospital approved the study andall patients gave written informed consent. Patientsinitially undergoing a diagnostic coronary angiogramwho had ‘‘nonplanned’’ or ‘‘follow-on’’ PCI were ap-proached at the end of their diagnostic study for con-sent to participate in the trial and the sheath was thenupsized to a 7 Fr if they were randomized to this arm.
Percutaneous Coronary Intervention
Patients underwent PCI using standard techniques.The brand of guiding catheter was not mandated bythe trial design. When randomization assigned a 6 Frguiding catheter size for the procedure, a Guidant(Temecula, CA) Viking 6 Fr catheter with all availableconfigurations was used in the majority of cases. Thiscatheter has an external diameter of 2.06 mm and aninternal diameter of 1.66 mm. When randomizationassigned a 7 Fr guiding catheter size for the procedure,a Boston Scientific (Maple Grove, MN) 7 Fr Wise-guide or Mach 1 catheter with all available configura-
tions was used in the majority of cases. The Mach 1catheter has an external diameter of 2.33 mm and aninternal diameter of 2.07 mm. Femoral access was ob-tained based on anatomical landmarks without routinefluoroscopic screening of the femoral head. A variety ofoperators including cardiology trainees obtained access.Coronary artery stents were implanted using standardhigh-pressure techniques. Heparin was administered asboluses to maintain an activated clotting time (ACT)greater than 250 sec and glycoprotein IIb/IIIa inhibitorscould be used at the operator’s discretion. The sheathwas removed with assisted manual compression usingthe FemostopTM device, when the ACT was less than180 sec. During working hours, a dedicated angioplastynurse removed sheaths according to an institutionalpolicy. Outside of usual working hours, a cardiologytrainee removed the sheaths according to the same pol-icy. Although heparin could be restarted after sheathremoval at the operator’s discretion, for a subset ofpatients, overnight heparin infusion was determined bysecondary randomization as part of another clinicalstudy. If heparin was to be commenced, it was com-menced 3 hr after sheath removal (without a bolusdose) and generally was continued until 6 AM the fol-lowing morning. These patients, as well as those receiv-ing glycoprotein IIb/IIIa infusions, were instructed toremain on bed rest overnight, otherwise patients weregenerally mobilized 6 hr after sheath removal, accordingto our institutional policy. All patients received at least300 mg of aspirin in the 24 hr prior to the procedureand a minimum of 100 mg per day after their proce-dure. Patients in whom intracoronary stents wereplaced received either ticlopidine (250 mg bid) or clo-pidogrel (75 mg daily) orally after loading doses of500 mg of ticlopidine or 300 mg of clopidogrel. Theloading dose was administered immediately after theprocedure and the maintenance dose was generally con-tinued for at least 1 month after the procedure, althoughthe referring cardiologist determined the duration oftherapy.
Data Gathering and Follow-Up
Data were collected prospectively, by a dedicatedangioplasty research nurse, with respect to angiogra-phic and procedural success, together with time toinitial haemostasis, ambulation, and discharge. In addi-tion, procedure duration, amount of contrast used andradiographic screening time were noted. The operatorwas asked to rank the ease of use of the guiding cathe-ter at the end of the procedure (poor, fair, and good)and the need for switch to a different sized catheterwas noted. The attending physician independently madethe decision regarding time of discharge. All patientswere scheduled to undergo a duplex vascular ultrasound
6 vs 7 Fr Guides for Percutaneous Coronary Intervention 529

of the femoral access site the day after the procedure,reported by a vascular surgeon (JAC) who was blindedto treatment assignment. The technician performing thestudy was also blinded to treatment assignment. Thepresence of a pseudoaneurysm, arterio–venous fistulaor femoral venous or arterial thrombosis, was noted. Thesubjects were also examined by our research nurse forany clinical evidence of haematoma (nonpulsatile mass>1 cm in diameter) at the femoral access site or retro-peritoneal haemorrhage. The need for transfusion andhaemoglobin level before and after the procedure werealso collected. Creatine kinase (CK) and CK-MB mea-surements were performed routinely on all patients themorning after the procedure and more frequently if therewas a clinical suspicion of an adverse cardiac event.
Endpoints
Primary endpoint. The primary endpoint was acomposite of significant vascular complications: vascu-lar ultrasound determined (pseudoaneurysm, arterio–venous fistula or femoral vein or arterial thrombosis),major haematoma (defined as presence of haematomawith decrease in haemoglobin >20 g/L or transfusionor prolongation of hospital stay due to haematoma), orretroperitoneal haemorrhage as determined by CT scan.Secondary endpoints. A number of time endpoints
were examined. These included procedure duration,time to haemostasis, time to ambulation, and time tohospital discharge for each of the patient groups. Useof contrast agents, screening time, and operators opin-ion as to ease of use of the guiding catheter were alsocompared. The combined incidence of major adversecardiac events (MACE) until day 30, including cardio-vascular death, nonfatal myocardial infarction (MI),and urgent target vessel revascularization, were alsorecorded. The diagnosis of MI was made if at least 2out of 3 of the following criteria were met: occurrenceof typical ischaemic chest pain lasting more than 30 min,abnormal Q waves not present on the baseline electro-cardiogram, or an increase in the creatinine kinase(CK) concentration to twice the upper limit of normal,with a concomitant rise in the CK- MB isoenzymeabove the upper limit of normal. The diagnosis ofrecurrent MI was determined if there was an increaseof more than 30% in the CK concentration abovebaseline. If a patient reached more than one cardiacendpoint, only the most severe endpoint was countedas a MACE for the final analysis. Occurrences ofthrombotic stent occlusion, defined angiographically asocclusion of the stented segment, were also noted.Angiographic success (achievement of less than 50%stenosis on visual assessment) and procedural success(angiographic success without 30 day death, nonfatal
MI, or need for urgent target vessel revascularisation)were also noted.
Statistical Analysis
The data were analyzed by intention to treat. Allvalues are reported as mean 6 1SD unless otherwisestated. Categorical variables were compared with v2
test or Fischer’s exact test as appropriate. Continuousvariables with a normal distribution were comparedwith unpaired Student’s t test and nonparametric varia-bles were compared with the Mann-Whitney U test.Statistical analysis was performed using SPSS for Win-dows (version 12.0). Statistical significance was de-fined as a two-tailed P value of <0.05.
RESULTS
Baseline clinical and antithrombotic details are shownin Table I. There were no significant differences inclinical features between groups. During the course ofthe study 2280 patients underwent PCI at our institu-tion of which 414 were enrolled in this study. Of allPCIs performed during the study period, �56%wereperformed using 6 Fr, 42% using 7 Fr, and 2% othersized guiding catheters.
Vascular Complications
The FemostopTM device was successfully deployed inall patients and no patients had an ipsilateral femoralvenous sheath placed during the PCI. Vascular eventsare shown in Table II. All but 5 patients in the 6 Frand 7 patients in the 7 Fr had a vascular ultrasoundperformed. In patients who did not undergo ultrasound,there was no clinical suspicion of a major vascularcomplication. There was no difference in major vascu-lar complications between the 6 Fr (5.7%) and 7 Frgroups (3.9%, P ¼ 0.383). Of the 13 pseudoaneursymsdetected during the study, five were not suspected clin-ically but were detected by ultrasound. Overall, 6patients underwent a period of compression, 1 patientreceived thrombin injection, and the remaining 6 pa-tients were discharged with subsequent ultrasoundsdetermining spontaneous resolution of the pseudo-aneurysm. Of the four arterio–venous fistulas diag-nosed, three were detected only by ultrasound and onewas associated with a large haematoma. All 4 patientswere subsequently discharged and underwent subsequentultrasound examinations, which demonstrated spontane-ous resolution. There were two nonocclusive femoralvenous thrombosis detected by ultrasound alone in the7 Fr group. Both patients were treated for a period of2 weeks with enoxaparin and subsequent ultrasoundsconfirmed resolution of the thrombus. One patient in the
530 Juergens et al.
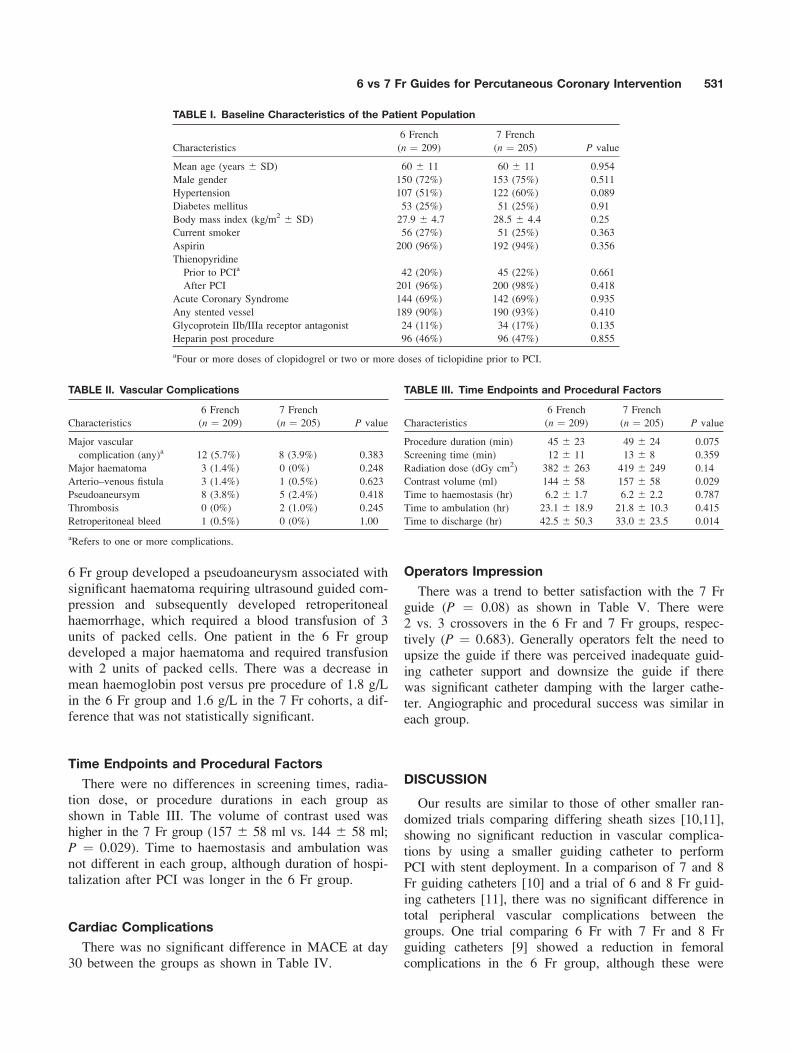
6 Fr group developed a pseudoaneurysm associated withsignificant haematoma requiring ultrasound guided com-pression and subsequently developed retroperitonealhaemorrhage, which required a blood transfusion of 3units of packed cells. One patient in the 6 Fr groupdeveloped a major haematoma and required transfusionwith 2 units of packed cells. There was a decrease inmean haemoglobin post versus pre procedure of 1.8 g/Lin the 6 Fr group and 1.6 g/L in the 7 Fr cohorts, a dif-ference that was not statistically significant.
Time Endpoints and Procedural Factors
There were no differences in screening times, radia-tion dose, or procedure durations in each group asshown in Table III. The volume of contrast used washigher in the 7 Fr group (157 6 58 ml vs. 144 6 58 ml;P ¼ 0.029). Time to haemostasis and ambulation wasnot different in each group, although duration of hospi-talization after PCI was longer in the 6 Fr group.
Cardiac Complications
There was no significant difference in MACE at day30 between the groups as shown in Table IV.
Operators Impression
There was a trend to better satisfaction with the 7 Frguide (P ¼ 0.08) as shown in Table V. There were2 vs. 3 crossovers in the 6 Fr and 7 Fr groups, respec-tively (P ¼ 0.683). Generally operators felt the need toupsize the guide if there was perceived inadequate guid-ing catheter support and downsize the guide if therewas significant catheter damping with the larger cathe-ter. Angiographic and procedural success was similar ineach group.
DISCUSSION
Our results are similar to those of other smaller ran-domized trials comparing differing sheath sizes [10,11],showing no significant reduction in vascular complica-tions by using a smaller guiding catheter to performPCI with stent deployment. In a comparison of 7 and 8Fr guiding catheters [10] and a trial of 6 and 8 Fr guid-ing catheters [11], there was no significant difference intotal peripheral vascular complications between thegroups. One trial comparing 6 Fr with 7 Fr and 8 Frguiding catheters [9] showed a reduction in femoralcomplications in the 6 Fr group, although these were
TABLE II. Vascular Complications
Characteristics
6 French
(n ¼ 209)
7 French
(n ¼ 205) P value
Major vascular
complication (any)a 12 (5.7%) 8 (3.9%) 0.383
Major haematoma 3 (1.4%) 0 (0%) 0.248
Arterio–venous fistula 3 (1.4%) 1 (0.5%) 0.623
Pseudoaneursym 8 (3.8%) 5 (2.4%) 0.418
Thrombosis 0 (0%) 2 (1.0%) 0.245
Retroperitoneal bleed 1 (0.5%) 0 (0%) 1.00
aRefers to one or more complications.
TABLE I. Baseline Characteristics of the Patient Population
Characteristics
6 French
(n ¼ 209)
7 French
(n ¼ 205) P value
Mean age (years 6 SD) 60 6 11 60 6 11 0.954
Male gender 150 (72%) 153 (75%) 0.511
Hypertension 107 (51%) 122 (60%) 0.089
Diabetes mellitus 53 (25%) 51 (25%) 0.91
Body mass index (kg/m2 6 SD) 27.9 6 4.7 28.5 6 4.4 0.25
Current smoker 56 (27%) 51 (25%) 0.363
Aspirin 200 (96%) 192 (94%) 0.356
Thienopyridine
Prior to PCIa 42 (20%) 45 (22%) 0.661
After PCI 201 (96%) 200 (98%) 0.418
Acute Coronary Syndrome 144 (69%) 142 (69%) 0.935
Any stented vessel 189 (90%) 190 (93%) 0.410
Glycoprotein IIb/IIIa receptor antagonist 24 (11%) 34 (17%) 0.135
Heparin post procedure 96 (46%) 96 (47%) 0.855
aFour or more doses of clopidogrel or two or more doses of ticlopidine prior to PCI.
TABLE III. Time Endpoints and Procedural Factors
Characteristics
6 French
(n ¼ 209)
7 French
(n ¼ 205) P value
Procedure duration (min) 45 6 23 49 6 24 0.075
Screening time (min) 12 6 11 13 6 8 0.359
Radiation dose (dGy cm2) 382 6 263 419 6 249 0.14
Contrast volume (ml) 144 6 58 157 6 58 0.029
Time to haemostasis (hr) 6.2 6 1.7 6.2 6 2.2 0.787
Time to ambulation (hr) 23.1 6 18.9 21.8 6 10.3 0.415
Time to discharge (hr) 42.5 6 50.3 33.0 6 23.5 0.014
6 vs 7 Fr Guides for Percutaneous Coronary Intervention 531
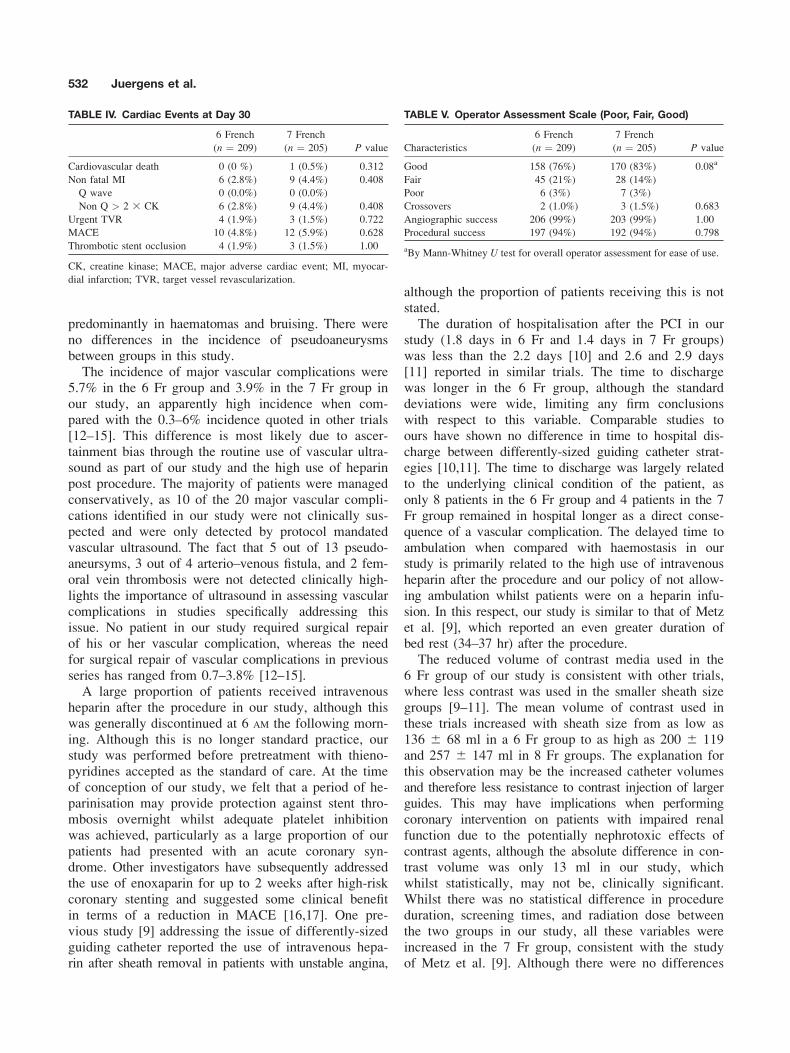
predominantly in haematomas and bruising. There wereno differences in the incidence of pseudoaneurysmsbetween groups in this study.The incidence of major vascular complications were
5.7% in the 6 Fr group and 3.9% in the 7 Fr group inour study, an apparently high incidence when com-pared with the 0.3–6% incidence quoted in other trials[12–15]. This difference is most likely due to ascer-tainment bias through the routine use of vascular ultra-sound as part of our study and the high use of heparinpost procedure. The majority of patients were managedconservatively, as 10 of the 20 major vascular compli-cations identified in our study were not clinically sus-pected and were only detected by protocol mandatedvascular ultrasound. The fact that 5 out of 13 pseudo-aneursyms, 3 out of 4 arterio–venous fistula, and 2 fem-oral vein thrombosis were not detected clinically high-lights the importance of ultrasound in assessing vascularcomplications in studies specifically addressing thisissue. No patient in our study required surgical repairof his or her vascular complication, whereas the needfor surgical repair of vascular complications in previousseries has ranged from 0.7–3.8% [12–15].A large proportion of patients received intravenous
heparin after the procedure in our study, although thiswas generally discontinued at 6 AM the following morn-ing. Although this is no longer standard practice, ourstudy was performed before pretreatment with thieno-pyridines accepted as the standard of care. At the timeof conception of our study, we felt that a period of he-parinisation may provide protection against stent thro-mbosis overnight whilst adequate platelet inhibitionwas achieved, particularly as a large proportion of ourpatients had presented with an acute coronary syn-drome. Other investigators have subsequently addressedthe use of enoxaparin for up to 2 weeks after high-riskcoronary stenting and suggested some clinical benefitin terms of a reduction in MACE [16,17]. One pre-vious study [9] addressing the issue of differently-sizedguiding catheter reported the use of intravenous hepa-rin after sheath removal in patients with unstable angina,
although the proportion of patients receiving this is notstated.The duration of hospitalisation after the PCI in our
study (1.8 days in 6 Fr and 1.4 days in 7 Fr groups)was less than the 2.2 days [10] and 2.6 and 2.9 days[11] reported in similar trials. The time to dischargewas longer in the 6 Fr group, although the standarddeviations were wide, limiting any firm conclusionswith respect to this variable. Comparable studies toours have shown no difference in time to hospital dis-charge between differently-sized guiding catheter strat-egies [10,11]. The time to discharge was largely relatedto the underlying clinical condition of the patient, asonly 8 patients in the 6 Fr group and 4 patients in the 7Fr group remained in hospital longer as a direct conse-quence of a vascular complication. The delayed time toambulation when compared with haemostasis in ourstudy is primarily related to the high use of intravenousheparin after the procedure and our policy of not allow-ing ambulation whilst patients were on a heparin infu-sion. In this respect, our study is similar to that of Metzet al. [9], which reported an even greater duration ofbed rest (34–37 hr) after the procedure.The reduced volume of contrast media used in the
6 Fr group of our study is consistent with other trials,where less contrast was used in the smaller sheath sizegroups [9–11]. The mean volume of contrast used inthese trials increased with sheath size from as low as136 6 68 ml in a 6 Fr group to as high as 200 6 119and 257 6 147 ml in 8 Fr groups. The explanation forthis observation may be the increased catheter volumesand therefore less resistance to contrast injection of largerguides. This may have implications when performingcoronary intervention on patients with impaired renalfunction due to the potentially nephrotoxic effects ofcontrast agents, although the absolute difference in con-trast volume was only 13 ml in our study, whichwhilst statistically, may not be, clinically significant.Whilst there was no statistical difference in procedureduration, screening times, and radiation dose betweenthe two groups in our study, all these variables wereincreased in the 7 Fr group, consistent with the studyof Metz et al. [9]. Although there were no differences
TABLE IV. Cardiac Events at Day 30
6 French
(n ¼ 209)
7 French
(n ¼ 205) P value
Cardiovascular death 0 (0 %) 1 (0.5%) 0.312
Non fatal MI 6 (2.8%) 9 (4.4%) 0.408
Q wave 0 (0.0%) 0 (0.0%)
Non Q > 2 3 CK 6 (2.8%) 9 (4.4%) 0.408
Urgent TVR 4 (1.9%) 3 (1.5%) 0.722
MACE 10 (4.8%) 12 (5.9%) 0.628
Thrombotic stent occlusion 4 (1.9%) 3 (1.5%) 1.00
CK, creatine kinase; MACE, major adverse cardiac event; MI, myocar-
dial infarction; TVR, target vessel revascularization.
TABLE V. Operator Assessment Scale (Poor, Fair, Good)
Characteristics
6 French
(n ¼ 209)
7 French
(n ¼ 205) P value
Good 158 (76%) 170 (83%) 0.08a
Fair 45 (21%) 28 (14%)
Poor 6 (3%) 7 (3%)
Crossovers 2 (1.0%) 3 (1.5%) 0.683
Angiographic success 206 (99%) 203 (99%) 1.00
Procedural success 197 (94%) 192 (94%) 0.798
aBy Mann-Whitney U test for overall operator assessment for ease of use.
532 Juergens et al.

in crossovers between the two groups in our study,there was a strong trend for our operators to rank the7 Fr guides easier to use than 6 Fr. This is a subjectiveassessment and as the operators were not blinded totreatment assignment this result is not robust. How-ever, it is consistent with a number of angiographyand PCI trials comparing different catheter sizes wherethe smaller size catheters were generally rated inferiorto larger ones with respect to image quality or catheterperformance [4,6,8,10,11].
Limitations
Our results are applicable to a single center in whichmultiple operators are performing PCIs in a selectpatient population with no specific needs for particu-lar-sized catheters. No vascular closure devices wereused in our trial, as all sheaths were removed using theFemostopTM device as an adjunctive manual compres-sion device. Consequently our results may not be appli-cable where sheaths are removed using closure devicesor pure manual compression. The observed event ratesof major vascular complications mean that our study isunderpowered for the primary endpoint. Whilst theinterpretation of vascular ultrasounds was blinded, theprimary operator during PCI could not be blinded tothe size of the guiding catheter and unappreciated biasmay have been present with respect to other clinicalendpoints. Similarly our dedicated research nurse whocollected the data could not be blinded to treatmentassignment with respect to sheath size. Another limita-tion of our study was that only �20% of patientsundergoing PCI during the course of the study wereenrolled. A number of these patients were not eligiblebecause they were enrolled in a concurrent vascularultrasound study [18] and many others were excludedbecause of the requirement to perform vascular ultra-sound prior to discharge and the inability to obtain thison weekends and holidays. The majority of exclusionswere however because of the operator’s reluctanceto randomize patients. There are inherent reasons whyoperators may choose a larger (e.g. bifurcation lesions,complex device intervention) or smaller (e.g. avoid catheterdamping, avoid sheath change after diagnostic angiogram,reduce complications) guiding catheter. This limits thewidespread applicability of our results, as there will alwaysbe situations where a larger or smaller guiding catheter isadvantageous. However in the absence of such occasions,we feel our study dispels the belief that a smaller guidingcatheter may reduce femoral access site complications.
CONCLUSIONS
This prospective, randomized trial indicates no re-duction in peripheral vascular complications with the
use of smaller guiding catheters in PCI. There was lesscontrast used in the 6 Fr group, which may benefitsome patient subsets; however, operators tended to pre-fer the larger 7 Fr system. The target coronary anat-omy and need for complex device intervention shouldmandate the choice of guiding catheter size, not a per-ceived impact on vascular complications.
ACKNOWLEDGMENTS
The authors thank the Nursing staff and ScientificOfficers from the Cardiac Catheterisation Laboratoriesfor their assistance in the collection of data for thisstudy and Professor John K French for his thoughtfulreview of our manuscript.
REFERENCES
1. Wyman RM, Safian RD, Portway V, Skillman JJ, McKay RG,
Baim DS. Current complications of diagnostic and therapeutic
cardiac catheterization. J Am Coll Cardiol 1988;12:1400–1406.
2. Moscucci M, Mansour KA, Kent KC, Kuntz RE, Senerchia C,
Baim DS, Carrozza JP, Jr. Peripheral vascular complications of
directional coronary atherectomy and stenting: predictors, man-
agement, and outcome. Am J Cardiol 1994;74:448–453.
3. Popma JJ, Satler LF, Pichard AD, Kent KM, Campbell A,
Chuang YC, Clark C, Merritt AJ, Bucher TA, Leon MB. Vascu-
lar complications after balloon and new device angioplasty. Cir-
culation 1993;88:1569–1578.
4. Danzi GB, Capuano C, Sesana M, Di Blasi A, Predolini S, Lat-
erza C, Quaini E. A randomized comparison of the use of 4 and
6 French diagnostic catheters: the limits of downsizing. Int J
Cardiol 2001;79:113–117.
5. Khoukaz S, Kern MJ, Bitar SR, Azrak E, Eisenhauer M, Wolf-
ord T, El-Shafei A. Coronary angiography using 4 Fr catheters
with assisted power injection: a randomized comparison to 6 Fr
manual technique and early ambulation. Cathet Cardiovasc Interv
2001;52:393–398.
6. Todd DM, Hubner PJ, Hudson N, Sarma J, McCance AJ, Caplin
J. Multicentre, prospective, randomized trial of 4 vs. 6 French
catheters in 410 patients undergoing coronary angiography. Cathet
Cardiovasc Interv 2001;54:269–275.
7. Arora P, Naik N, Bahl VK, Mishra S, Yadav R, Sharma S, Man-
chanda SC. Coronary angiography using 4 French catheters with
power injection: a randomized comparison with 6 French cathe-
ters. Indian Heart J 2002;54:184–188.
8. Hui WKK, Klinke WP, Kubac G, Talibi T. Comparison of 5F
and 7/8F catheters for left ventricular and coronary angiography.
Cathet Cardiovasc Diagn 1990;19:84–86.
9. Metz D, Meyer P, Touati C, Coste P, Petiteau PY, Durand P,
Faivre R, Lefevre T, Elaerts J. Comparison of 6F with 7F and
8F guiding catheters for elective coronary angioplasty: results of
a prospective, multicentre, randomized trail. Am Heart J 1997;
134:131–137.
10. Talley JD, Wilkins C, Ciccone J, Hattel LJ. Comparison of 7
and 8 French guiding catheters for elective PTCA: results of a
prospective randomized trial. Cathet Cardiovasc Diagn 1994;
33:205–211.
11. Talley JD, Mauldin PD, Becker ER. A prospective randomized
trial comparing the benefits and limitations of 6 Fr and 8 Fr
guiding catheters in elective coronary angioplasty. J Interv Car-
diol 1995;8:345–353.
6 vs 7 Fr Guides for Percutaneous Coronary Intervention 533

12. Applegate RJ, Grabarczyk MA, Little WC, Craven T, Walkup
M, Kahl FR, Braden GA, Rankin KM, Kutcher MA. Vascular
closure devices in patients treated with anticoagulation and IIb/
IIIa receptor inhibitors during percutaneous revascularization.
J Am Coll Cardiol 2002;40:78–83.
13. Johnson LW, Esente P, Giambartolomei A, Grant WD, Loin M,
Reger MJ, Shaw C, Walford GD. Peripheral vascular complica-
tions of coronary angioplasty by the femoral and brachial tech-
niques. Cathet Cardiovasc Diagn 1994;31:165–172.
14. Muller DWM, Shamir KJ, Ellis SG, Topol EJ. Peripheral vas-
cular complications after conventional and complex percutane-
ous coronary interventional procedures. Am J Cardiol 1992;69:
63–68.
15. Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der
Wieken R. A randomized comparison of percutaneous translumi-
nal coronary angioplasty by the radial, brachial and femoral
approaches: the access study. J Am Coll Cardiol 1997;29:1269–
1275.
16. Batchelor WB, Mahaffey KW, Berger PB, Deutsch E, Meier S,
Hasselblad V, Fry ET, Teirstein PS, Ross AM, Binanay CA,
et al, ATLAST trial investigators. A randomized, placebo-con-
trolled trial of enoxaparin after high risk coronary stenting: the
ATLAST trial. J Am Coll Cardiol 2001;38:1608–1613.
17. Daoulah A, Segev A, Leblanc K, Chisholm RJ, Strauss BH.
Postprocedural low molecular weight heparin in patients at high
risk of subacute stent thrombosis. Cardiovasc Radiat Med
2003;4:182–185.
18. Juergens CP, Leung DYC, Crozier JA, Wong AM, Robinson
JTC, Lo S, Kachwalla H, Hopkins AP. Patient tolerance and
resource utilization associated with an arterial closure versus an
external compression device after percutaneous coronary inter-
vention. Cathet Cardiovasc Interv 2004;63:166–170.
534 Juergens et al.

36
PAPER 7
Reprinted from the International Journal of Cardiology 2007;116:321-326
with permission from Elsevier
logy 116 (2007) 321–326www.elsevier.com/locate/ijcard
International Journal of Cardio
Effect of local anesthesia and intravenous sedation on pain perception andvasovagal reactions during femoral arterial sheath removal after
percutaneous coronary intervention
Choon Kiat Ang b, Dominic Y.C. Leung a, Sidney Lo a, John K. French a, Craig P. Juergens a,⁎
a Department of Cardiology, Liverpool Hospital, Locked Bag 7103, Liverpool BC NSW 1871b Department of Cardiology, Sarawak General Hospital, Kuching, Malaysia
Received 29 December 2005; accepted 1 April 2006Available online 10 August 2006
Abstract
Background: There is no consensus with respect to the use of analgesia during femoral arterial sheath removal after percutaneous coronaryintervention (PCI). We performed a randomized controlled trial to assess the impact of intravenous sedation and local anesthesia duringfemoral sheath removal after PCI on patient comfort and the incidence of vasovagal reactions.Methods: All patients undergoing PCI whose femoral sheaths were to be removed with assisted manual compression were eligible. Patientswere randomized to receive either intravenous sedation (Fentanyl and Midazolam) or local anesthesia (1% lignocaine) infiltrated around thesheath site or both or neither. The primary endpoint of the study was the patients reported worst pain according to a Visual Analogue scale(VAS) after sheath removal. The incidence and predictors of vasovagal reactions during sheath removal and occurrence of vascularcomplications was also determined.Results: A total of 611 patients were randomized into this study. The mean pain score was highest in the local anesthesia only arm ascompared to the sedation only arm, the combined local and sedation arm and the neither sedation or local arm (p=0.001). vasovagal reactionswere experienced by 35 patients (5.1%) with the highest percentage in the local anesthesia only group (9.8%). Multivariate logistic regressionanalysis identified a higher pain score (OR 1.18, 95% CI 1.12–1.24, p=0.001), use of glyceryl trinitrate during sheath removal (OR 9.05,95% CI 5.06–16.1, p<0.001), a lower body mass index (OR 1.12, 95% CI 1.08–1.18, p=0.009) and the left anterior descending artery asthe treated vessel (OR 5.2, 95% CI 3.41–7.87, p<0.001) as independent predictors of the occurrence of a vasovagal reaction. There was nosignificant difference in vascular complications between the 4 study groups.Conclusions: The routine use of fentanyl and midazolam prior to sheath removal leads to a reduction in pain perception and vasovagalincidence, whilst the routine use of local infiltration during sheath removal should be discouraged as it leads to more pain and a trend to morevasovagal reactions.© 2006 Elsevier Ireland Ltd. All rights reserved.
Keywords: Percutaneous coronary intervention; Sheath; Pain; Sedation; Analgesia
1. Introduction
Percutaneous coronary intervention (PCI) is the mostcommon revascularisation procedure performed for coronaryartery disease. Femoral arterial sheath removal after PCI maybe considered routine for health care personnel, however,
⁎ Corresponding author. Tel.: +61 2 98283074; fax: +61 2 98283054.E-mail address: [email protected] (C.P. Juergens).
0167-5273/$ - see front matter © 2006 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijcard.2006.04.045
this process is associated with a significant amount ofdiscomfort reported by patients [1,2]. Pain may be related tothe removal of the femoral sheath itself, to the pressureapplied until haemostasis is achieved, or to the need forpatient remaining supine and immobile for hours. Sub-optimal pain control may adversely affect the patients'ability to cooperate during the femoral sheath removal,resulting in prolonged time to haemostasis and contributingto groin complications. The presence of pain, tissue injury
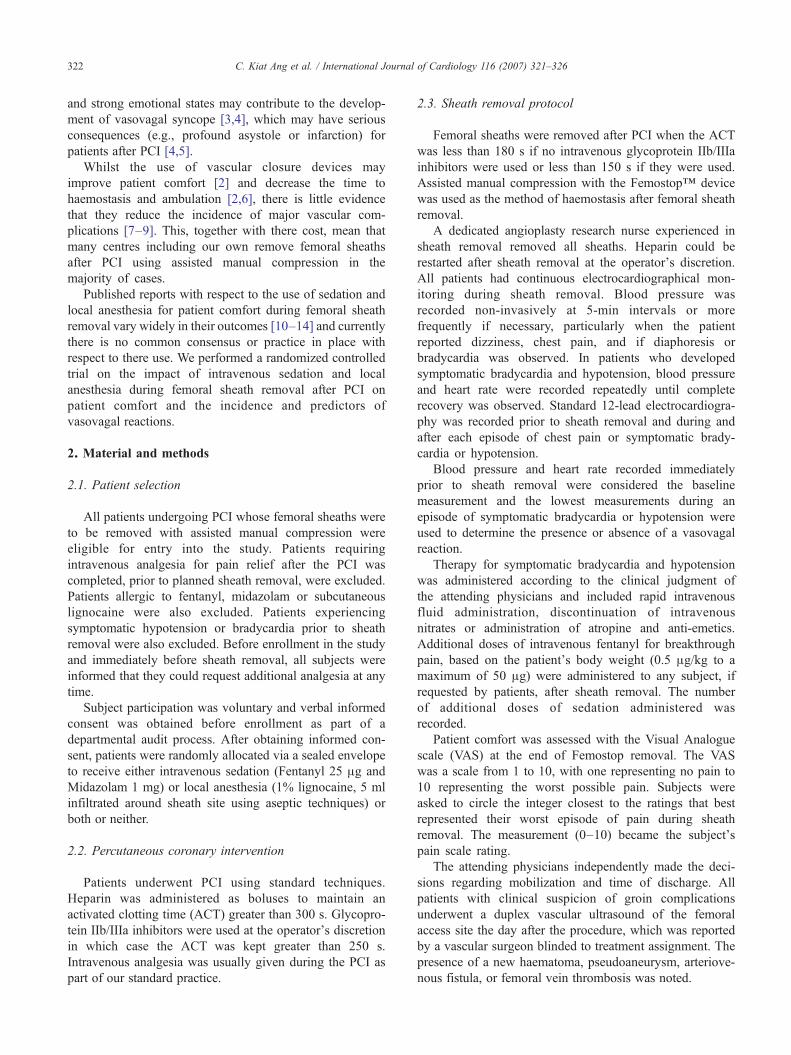
322 C. Kiat Ang et al. / International Journal of Cardiology 116 (2007) 321–326
and strong emotional states may contribute to the develop-ment of vasovagal syncope [3,4], which may have seriousconsequences (e.g., profound asystole or infarction) forpatients after PCI [4,5].
Whilst the use of vascular closure devices mayimprove patient comfort [2] and decrease the time tohaemostasis and ambulation [2,6], there is little evidencethat they reduce the incidence of major vascular com-plications [7–9]. This, together with there cost, mean thatmany centres including our own remove femoral sheathsafter PCI using assisted manual compression in themajority of cases.
Published reports with respect to the use of sedation andlocal anesthesia for patient comfort during femoral sheathremoval vary widely in their outcomes [10–14] and currentlythere is no common consensus or practice in place withrespect to there use. We performed a randomized controlledtrial on the impact of intravenous sedation and localanesthesia during femoral sheath removal after PCI onpatient comfort and the incidence and predictors ofvasovagal reactions.
2. Material and methods
2.1. Patient selection
All patients undergoing PCI whose femoral sheaths wereto be removed with assisted manual compression wereeligible for entry into the study. Patients requiringintravenous analgesia for pain relief after the PCI wascompleted, prior to planned sheath removal, were excluded.Patients allergic to fentanyl, midazolam or subcutaneouslignocaine were also excluded. Patients experiencingsymptomatic hypotension or bradycardia prior to sheathremoval were also excluded. Before enrollment in the studyand immediately before sheath removal, all subjects wereinformed that they could request additional analgesia at anytime.
Subject participation was voluntary and verbal informedconsent was obtained before enrollment as part of adepartmental audit process. After obtaining informed con-sent, patients were randomly allocated via a sealed envelopeto receive either intravenous sedation (Fentanyl 25 μg andMidazolam 1 mg) or local anesthesia (1% lignocaine, 5 mlinfiltrated around sheath site using aseptic techniques) orboth or neither.
2.2. Percutaneous coronary intervention
Patients underwent PCI using standard techniques.Heparin was administered as boluses to maintain anactivated clotting time (ACT) greater than 300 s. Glycopro-tein IIb/IIIa inhibitors were used at the operator's discretionin which case the ACT was kept greater than 250 s.Intravenous analgesia was usually given during the PCI aspart of our standard practice.
2.3. Sheath removal protocol
Femoral sheaths were removed after PCI when the ACTwas less than 180 s if no intravenous glycoprotein IIb/IIIainhibitors were used or less than 150 s if they were used.Assisted manual compression with the Femostop™ devicewas used as the method of haemostasis after femoral sheathremoval.
A dedicated angioplasty research nurse experienced insheath removal removed all sheaths. Heparin could berestarted after sheath removal at the operator's discretion.All patients had continuous electrocardiographical mon-itoring during sheath removal. Blood pressure wasrecorded non-invasively at 5-min intervals or morefrequently if necessary, particularly when the patientreported dizziness, chest pain, and if diaphoresis orbradycardia was observed. In patients who developedsymptomatic bradycardia and hypotension, blood pressureand heart rate were recorded repeatedly until completerecovery was observed. Standard 12-lead electrocardiogra-phy was recorded prior to sheath removal and during andafter each episode of chest pain or symptomatic brady-cardia or hypotension.
Blood pressure and heart rate recorded immediatelyprior to sheath removal were considered the baselinemeasurement and the lowest measurements during anepisode of symptomatic bradycardia or hypotension wereused to determine the presence or absence of a vasovagalreaction.
Therapy for symptomatic bradycardia and hypotensionwas administered according to the clinical judgment ofthe attending physicians and included rapid intravenousfluid administration, discontinuation of intravenousnitrates or administration of atropine and anti-emetics.Additional doses of intravenous fentanyl for breakthroughpain, based on the patient's body weight (0.5 μg/kg to amaximum of 50 μg) were administered to any subject, ifrequested by patients, after sheath removal. The numberof additional doses of sedation administered wasrecorded.
Patient comfort was assessed with the Visual Analoguescale (VAS) at the end of Femostop removal. The VASwas a scale from 1 to 10, with one representing no pain to10 representing the worst possible pain. Subjects wereasked to circle the integer closest to the ratings that bestrepresented their worst episode of pain during sheathremoval. The measurement (0–10) became the subject'spain scale rating.
The attending physicians independently made the deci-sions regarding mobilization and time of discharge. Allpatients with clinical suspicion of groin complicationsunderwent a duplex vascular ultrasound of the femoralaccess site the day after the procedure, which was reportedby a vascular surgeon blinded to treatment assignment. Thepresence of a new haematoma, pseudoaneurysm, arteriove-nous fistula, or femoral vein thrombosis was noted.

Table 2Pain scores of the 611 patients according to study
Study allocation Pain scores ⁎ Additional analgesics,n (%) ⁎⁎
Sedation (n=142)) 2.5±3.3 11 (7.8%)Local (n=153) 4.1±3.4 18 (11.8%)Both (n=155) 3.3±3.9 15 (9.8%)Neither (n=161) 3.6±3.5 11 (6.8%)
⁎ p=0.001.⁎⁎ p=0.44.
323C. Kiat Ang et al. / International Journal of Cardiology 116 (2007) 321–326
2.4. Endpoints
The primary endpoint of the study was the patientsreported worst pain according to VAS. A secondary endpointof the study was the incidence of vasovagal reactions. Avasovagal reaction was defined as a symptomatic bradycar-dic episode (heart rate of <60 beats per minutes) accom-panied by hypotension (systolic blood pressure of <100 mmHg or >10% drop compared with baseline) in the supineposition. The occurrence of vascular complications asconfirmed by vascular ultrasound was also sought.
2.5. Statistical analysis
All data are given as mean±one standard deviationunless otherwise stated. Categorical variables were com-pared with the Chi square test or the Fisher's Exact Testwhen appropriate. Continuous variables across two ormore groups were compared with the unpaired Student's ttest or one-way ANOVA respectively. Non-parametricvariables are compared with the Mann-Whitney U test.Multivariate logistic regression analysis was used (forwardselection, maximum likelihood ratio method) to identifyindependent predictors of the occurrence of vasovagalreaction with significant univariate predictors entered ascovariates. Statistical significance was defined as a two-tailed p value of <0.05.
3. Results
3.1. Patient characteristics
Between May 2001 and August 2004, 611 patients wereenrolled into the trial. Their baseline characteristics accord-ing to study allocation are summarized in Table 1. Apartfrom patient gender distribution, there were no significantdifferences in other baseline characteristics between the 4study groups. The use on intravenous sedation during thePCI and the time to sheath removal was no different betweenthe four groups.
Table 1Baseline characteristics of the 611 study patients according to study allocation
Sedation (n=142) Lo
Age (years) 62±12 61Male, n (%) 95 (66.9%) 11BMI (kg/m2) 27.5±4.5 27Diabetes, n (%) 34 (23.9%) 45Hypertension, n (%) 92 (64.8%) 10Vessel treated LAD 61 (43%) 62Glycoprotein IIb/IIIa inhibitor use, n (%) 23 (16.2%) 26Use of IV glyceryl trinitrate, n (%) 3 (2.1%) 6 (Dose of Midazolam during PCI (mg) 1.3±0.7 1.3Dose of Fentanyl during PCI (μg) 36.5±20 36Time from PCI start to sheath removal (min) 248±109 24Duration of PCI (min) 54±28 58
LAD=left anterior descending artery, PCI=percutaneous coronary intervention.
3.2. Pain score
The mean pain score for all patients was 3.4±3.6 and 55(9%) patients requested additional analgesia during removalof femoral sheaths. As shown in Table 2, there was asignificant difference in pain scores across the 4 study groupswith the group receiving intravenous sedation only, havingthe lowest pain scores and the group receiving localanesthetic only, having the highest pain scores. However,there was no significant difference in the number of patientsrequesting additional analgesia.
The mean pain sore of patients receiving any localanesthesia (n=307) was significantly higher (3.7±3.7)compared with patients not receiving any local anesthesia(n=307) at the vascular access site (3.07±3.4, p=0.028).However, there was no significant difference in theproportion of patient requesting additional analgesia betweenthe 2 groups (33 of 307 versus 22 of 304 patients, p=0.13).
Patients receiving any intravenous sedation (n=297) hada significantly lower mean pain score (2.92±3.6) comparedwith patients not receiving any intravenous sedation (n=314,3.83±3.4, p=0.001). Similarly, there was no significantdifference in the proportion of patient requesting additionalanalgesia between the 2 groups (26 of 297 versus 29 of 314patients, p=0.84).
3.3. Vasovagal reaction
A total of 35 (5.7%) patients experienced a vasovagalreaction. Twenty-one patients (60%) were treated with
cal (n=153) Both (n=155) Neither (n=161) p
.8±11.2 59±11.9 59.9±10.8 0.0628 (77%) 103 (66.5%) 139 (86%) <0.001.5±4.4 28.4±5.2 28±4.9 0.206(29.4%) 42 (27.3%) 36 (22.3%) 0.4882 (66.7%) 91 (59.1%) 106 (65.8%) 0.452(40.5%) 55 (35.5%) 65 (40.4%) 0.604(17.0%) 32 (20.7%) 36 (22.4%) 0.4653.9%) 6 (3.8%) 9 (5.6%) 0.49±0.8 1.2±0.6 1.3±0.8 0.39.8±21 33±18 35±19 0.367±105 245±56 244±101 0.99±26 53±22 57±24 0.22

324 C. Kiat Ang et al. / International Journal of Cardiology 116 (2007) 321–326
atropine, 31 (89%) received a bolus of intravenous fluidsand 5 (9%) received metoclopramide. There was nosignificant difference in the incidence of vasovagalreaction across the 4 study groups (Table 3). Furthermore,there was no significant difference in the incidence ofvasovagal reaction between patients receiving any localanesthesia and patients not receiving any local anesthesia(22 of 307 patients versus 13 of 304 patients, p=0.124).However, there was a trend towards a lower incidence ofvasovagal reaction for patients receiving intravenoussedation compared with those not receiving intravenoussedation (12 of 297 patients versus 23 of 314 patients,p=0.08).
Multivariate logistic regression analysis identified ahigher pain score (OR 1.18, 95% CI 1.12–1.24, p=0.001), use of glyceryl trinitrate during sheath removal(OR 9.05, 95% CI 5.06–16.1, p<0.001), a lower bodymass index (BMI) (OR 1.12, 95% CI 1.08–1.18, p=0.009)and the left anterior descending artery as the treated vessel(OR 5.2, 95% CI 3.41–7.87, p<0.001) as independentpredictors of the occurrence of a vasovagal reaction. Patientgender, age, being a smoker, diabetes, hypertension,hypercholesterolemia, use of glycoprotein IIb/IIIa inhibi-tors, sheath size, multivessel angioplasty, use of intravenoussedation and local anesthesia were not significantpredictors.
3.4. Vascular complications
The Femostop™ device was successfully deployed inall patients. Clinical suspicion of a major vascularcomplication at the femoral access site was present in 45patients (7.4%). All these 45 patients underwent vascularultrasound of the inguinal areas. Significant vascularcomplications were confirmed on ultrasound in 21 ofthese 45 patients (3.4% of total study population). Therewas no significant difference in the incidence of vascularcomplications at the femoral access site between the 4study groups (Table 3). Femoral pseudoaneursyms weredetected in 14 patients, A-V fistulas in 6 patients and anon-occlusive femoral venous thrombosis detected byultrasound in one patient. No significant univariatepredictors were identified for the occurrence of femoralaccess site vascular complications.
Table 3The occurrence of vasovagal reactions and vascular complications in the 611study patients according to study allocation
Study allocation Vasovagal reaction,n (%) ⁎
Vascular complication,n (%) ⁎⁎
Sedation only (n=142) 5 (3.5%) 6 (4.2%)Local only (n=153) 15 (9.8%) 5 (3.3%)Both (n=154) 7 (4.5%) 6 (3.9%)Neither (n=161) 8 (5.0%) 4 (2.5%)
⁎ p=0.088.⁎⁎ p=0.848.
4. Discussion
We have demonstrated that patients experience the leastamount of pain during femoral arterial sheath removal whenintravenous sedation is administered prophylactically. In asurvey of 70 US hospitals [13], 79% reported givingmedications before sheath removal with morphine beingthe most frequently prescribed medication (49%). Our resultsare different to those of Fulton et al. [14] who found nodifference in pain perception amongst 130 patients using avariety of analgesic regimens including fentanyl, morphineand lidocaine. Whilst the design of this study was similar toours, total numbers of patients were less, sheaths were larger(8 French), manual compression without a Femostop wasused and all patients had received diazepam prior to theirprocedure in this study which may have effected the patientsperception of pain at the time of sheath removal. We alsoroutinely administered midazolam with the fentanyl, whichmay have positively impacted our results. Overall 55 patients(9%) in our study requested additional analgesia forbreakthrough pain, an incidence similar to the 8% reportedby Fulton et al. [14]. The few requests for rescue analgesiatend to support the notion that sheath removal and theimmediate post-recovery phase are not perceived as painfulby most patients.
We found that the infiltration of lignocaine around thesheath insertion site prior to sheath removal actuallyincreased the amount of pain experienced by patients. Thefact that lignocaine did not reduce the perception of pain isconsistent with other smaller published studies showing aneutral effect of lignocaine use [11,12,14]. Three separatesurveys assessing practice patterns for percutaneous cor-onary intervention published in the 1990s, revealed 46–60%of hospital surveyed in the US and Canada reported the useof local anesthetic prior to sheath removal [10,12,13]. Ourresults would call into question this practice. It should beremembered that the infiltration of local anesthetic is itself aninvasive procedure and has associated risks, includingbleeding from additional puncture sites, laceration of thesheath, infection, and transient nerve injury.
Vasovagal reactions are a well-known complication ofinterventional coronary procedures with a reported incidenceof between 3.4% and 13.9% [2,5,14]. Our study is the largestto assess the occurrence and predictors of vasovagal eventspost-femoral sheath removal. Our data show an overallincidence of 5.7% of symptomatic bradycardia and hypoten-sion post-femoral sheath removal. In multivariate analysiswe identified a higher pain score, a lower BMI, receiving aglyceryl trinitrate infusion and the left anterior descendingartery as the treated vessel as predictors of an increased riskof a vasovagal event. The highest incidence of vasovagalevents (9.8%) occurred in the subgroup of patients receivinglignocaine, alone which may be explained by the higherreported pain levels in this subgroup. In a study by Mager etal. [5] of 180 patients undergoing PCI, the authors reported a13.9% incidence of at least one episode of symptomatic

325C. Kiat Ang et al. / International Journal of Cardiology 116 (2007) 321–326
bradycardia and hypotension during the early postprocedureperiod. Whilst the impact of pain and BMI was not addressedin this study the authors noted a higher incidence of thesereactions in patients undergoing PCI of the left anteriordescending artery when compared to other arteries, a resultsimilar to our own. It was also higher in patients receivingdiltiazem, verapamil and beta-blockers, especially when bothclasses of drugs were combined. We did not report data onthe use of oral medication as fasting prior to the proceduremeant usual treatment regimens were variably administered.In the study by Mager et al. [5] all patients receivedcontinuous isosorbide dinitrate limiting any conclusionsabout the impact of nitrates on the incidence of vasovagal intheir study. We actually identified the use of a glyceryltrinitrate infusion up to and beyond the time of sheathremoval as a predictor of a vasovagal event. This couldpossibly be explained by the vasodilating effect of glyceryltrinitrate in conjunction with central nervous system effectsvia nitric oxide resulting in a net increase in parasympatheticand decrease of sympathetic activity leading to a propensityfor hypotension and bradycardia [15].
Vascular complications were identified in 3.4% ofpatients in our study which is consistent with the incidencereported in other studies of between 0.3–6.0% [2,9,16–19]. There was no difference between our subgroupssuggesting patient and clinician factors other than the typeof analgesia used for sheath removal contribute to vascularcomplications.
4.1. Limitations
The major limitation of our study was that neither thepatients nor our dedicated angioplasty research nursewhere blinded to treatment assignment, which may havelead to unappreciated bias in the endpoints observed.Those receiving local anesthesia actually reported morepain than the other groups even though there may havebeen an expectation of less pain. We acknowledgehowever that placebo local anesthesia and/or sedationwould have strengthened our study. Nevertheless, thevasovagal events observed were clinically obvious neces-sitating treatment prescribed by coronary care nurses andresident medical officers who were unaware of thetreatment assigned. Our results are applicable to apopulation of patients who had generally received someintravenous sedation during their coronary intervention.Our results cannot be applied where vascular closuredevices are used to obtain haemostasis and may not bedirectly applicable where haemostasis is obtained withsimple manual compression without a Femostop™ device.In a previous study by our group [2] we found numericallyfewer vasovagal events in patients receiving an Angiosealdevice (3.4%) when compared to assisted manual com-pression using a Femostop (10.5%) although, because ofthe small sample size, this was not statistically significant.Even though our study was randomized, there were
significantly fewer males in the sedation only and sedationplus local anesthesia groups. This difference in genderdistribution could have contributed to unintentional bias inour result. A number of studies have suggested genderdifferences with respect to pain perception with womenexhibiting reduced tolerance for experimentally inducedpain when compared to men [20–22]. Whilst we had morefemales in the groups receiving any intravenous sedation,these groups actually reported less pain, and therefore anypotential bias in our study should have worked against ourresults. Finally, whilst ECG and non-invasive bloodpressure monitoring were standardized, non-pharmacologi-cal interventions such as patient education, general comfortmeasures, and family interaction were not controlled forand may have had some influence on the observedoutcomes.
5. Conclusion
The findings of this study point to a number ofrecommendations for the process of femoral arterial sheathremoval after percutaneous coronary intervention. Specialcare should be taken when removing sheaths from patientsin whom the left anterior descending vessel has beentreated and those on a glyceryl trinitrate infusion as its useare associated with a higher likelihood of a vasovagalevent. Whilst for most patients the removal femoralsheaths after PCI is a relatively painless exercise, theroutine use of fentanyl and midazolam prior to sheathremoval leads to a reduction in pain perception and a trendto less vasovagal reactions. Patients given subcutaneouslignocaine prior to sheath removal reported more pain thanpatients receiving no analgesia and experienced morevasovagal events; therefore the routine use of localinfiltration in pain management during sheath removalshould be discouraged.
Acknowledgements
The authors would like to thank Mrs. Adelina Wong forher assistance in the collection of data for this study and Dr.Andrew Hopkins for database support.
References
[1] Slaughter PMP, Chetty R, Flintoft VF, et al. A single centerrandomized trial assessing use of a vascular hemostasis device vsconventional manual compression following PTCA: what are thepotential resource saving? Cathet Cardiovasc Diagn 1995;34:210–4.
[2] Juergens CP, Leung DYC, Crozier JA, et al. Patient tolerance andresource utilization associated with an arterial closure versus anexternal compression device after percutaneous coronary intervention.Catheter Cardiovasc Interv 2004;63:166–70.
[3] Boss BJ, Brewer L. Syncope: neuroscience nursing assessment basedon an understanding of underlying pathophysiological mechanisms. JNeurosci Nurs 1988;20:245–52.
[4] Barbiere CC. Malignant vasovagal syncope after PTCA: a potential fordisaster. Crit Care Nurse 1994;14:90–3.

326 C. Kiat Ang et al. / International Journal of Cardiology 116 (2007) 321–326
[5] Mager A, Strasberg B, Rechavia E, et al. Clinical significance andpredisposing factors to symptomatic bradycardia and hypotension afterpercutaneous transluminal coronary angioplasty. Am J Cardiol1994;74:1085–8.
[6] Wilentz JR, Mishkel G, McDermott D, Ravi K, Fox JT, Reimers CD.Outpatient coronary stenting using the femoral approach with vascularsealing. J Invasive Cardiol 1999;11:709–17.
[7] Kussmaul III WG, Buchbinder M, Whitlow PL, et al. Rapid arterialhemostasis and decreased access site complications after cardiaccatheterization and angioplasty: results of a randomized trial of a novelhemostatic device. J Am Coll Cardiol 1995;25:1685–92.
[8] Amin FR, Yousufuddin M, Stables R, et al. Femoral haemostasis aftertranscatheter therapeutic intervention: a prospective randomised studyof the angio-seal device vs. the femostop device. Int J Cardiol2000;76:235–40.
[9] Applegate RJ, Grabarczyk MA, Little WC, et al. Vascular closuredevices in patients treated with anticoagulation and IIb/IIIa receptorinhibitors during percutaneous revascularization. J Am Coll Cardiol2002;40:78–83.
[10] Peet GI, McGrath MA, Brunt JH, Hilton JD. Femoral arterial sheathremoval after PTCA: a cross-Canada survey. Can J Cardiovasc Nurs1995;6:13–9.
[11] Wadas TM, Hill J. Is lidocaine infiltration during femoral sheathremoval really necessary? Heart Lung 1998;27:31–6.
[12] Bowden SM, Worrey JA. Assessing patient comfort: local infiltrationof lidocaine during femoral sheath removal. Am J Crit Care1995;4:368–9.
[13] Juran NB, Smith DD, Rouse CL, DeLuca SA, Rund M. Survey ofcurrent practice patterns for percutaneous transluminal coronaryangioplasty. Am J Crit Care 1996;5:442–8.
[14] Fulton TR, Peet GI, McGrath MA, et al. Effects of 3 analgesicregimens on the perception of pain after removal of femoral arterysheaths. Am J Crit Care 2000;9:125–9.
[15] Chowdhary S, Townend JN. Role of nitric oxide in the regulation ofcardiovascular autonomic control. Clin Sci 1999;97:5–17.
[16] Johnson LW, Esente P, Giambartolomei A, et al. Peripheral vascularcomplications of coronary angioplasty by the femoral and brachialtechniques. Cathet Cardiovasc Diagn 1994;31:165–72.
[17] Muller DWM, Shamir KJ, Ellis SG, Topol EJ. Peripheral vascularcomplications after conventional and complex percutaneous coronaryinterventional procedures. Am J Cardiol 1992;69:63–8.
[18] Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der WiekenR. A randomized comparison of percutaneous transluminal coronaryangioplasty by the radial, brachial and femoral approaches: the accessstudy. J Am Coll Cardiol 1997;29:1269–75.
[19] Juergens CP, Hallani H, Leung DYC, et al. Comparison of 6 and 7French guiding catheters for percutaneous coronary intervention:results of a randomized trial with a vascular ultrasound endpoint.Catheter Cardiovasc Interv 2005;66:528–34.
[20] Keogh E, Herdenfeldt. Gender, coping and the perception of pain. Pain2002;97:195–201.
[21] Jackson T, Iezzi T, Chen H, Ebnet S, Eglitis K. Gender, interpersonaltransactions, and the perception of pain: an experimental analysis.J Pain 2005;6:228–36.
[22] Logan HL, Gedney JJ. Sex differences in the long term stability offorehead cold pressor pain. J Pain 2004;5:406–12.

37
PAPER 8
Reprinted from the International Journal of Cardiology 2008;127:252-254
with permission from Elsevier

International Journal of Cardiology 127 (2008) 252–254www.elsevier.com/locate/ijcard
Letter to the Editor
Vaso-vagal reactions during femoral arterial sheath removal afterpercutaneous coronary intervention and impact on cardiac events
Craig P. Juergens ⁎, Sidney Lo, John K. French, Dominic Y.C. Leung
Department of Cardiology, Liverpool Hospital, and University of NSW Australia
Received 5 January 2007; accepted 17 February 2007Available online 30 April 2007
Abstract
We determined whether vaso-vagal syncope during sheath removal after percutaneous coronary intervention leads to a higher incidence ofmajor adverse cardiac events including acute stent thrombosis, in 611 patients who participated in our previous trial assessing the impact ofintravenous sedation and local anaesthesia at this time on patient comfort. A total of 35 (5.7%) patients experienced a vaso-vagal reaction.Major adverse cardiac events at day 30 occurred in 5.7% of patients experiencing vaso-vagal syncope and 7.1% of those who did not( p=1.00) with no case of stent thrombosis in the vaso-vagal group. Whilst unpleasant for patients, we conclude that vaso-vagal syncopeduring sheath removal after percutaneous coronary intervention is not associated with increased adverse cardiac events in the stent era.© 2007 Elsevier Ireland Ltd. All rights reserved.
Keywords: Vaso-vagal; Percutaneous coronary intervention; Myocardial infa
rction; StentVaso-vagal reactions are a relatively common complica-tion of interventional coronary procedures with a reportedincidence of between 3.4% and 13.9% [1–3]. The presenceof pain, tissue injury and strong emotional states maycontribute to the development of vaso-vagal syncope [4,5],which may have serious consequences (e.g., profoundasystole or infarction) for patients after percutaneouscoronary intervention (PCI) [2,5]. Apart from infrequentcase reports [2,5], there is little published literature onpotential adverse cardiac events of vaso-vagal syncopeduring sheath removal particularly in the circumstance ofrecent stent deployment where profound hypotension andbradycardia may potentially lead to stent thrombosis.
We previously reported [6] a randomized controlled trial,which assessed the impact of intravenous sedation and localanaesthesia during femoral sheath removal after PCI onpatient comfort and the incidence of vaso-vagal reactions.The aim of the present study was to evaluate whether vaso-
⁎ Corresponding author. Department of Cardiology, Liverpool Hospital,Locked Bag 7103, Liverpool, BC NSW 1871, Australia. Tel.: +61 298283074; fax: +61 2 98283054.
E-mail address: [email protected] (C.P. Juergens).
0167-5273/$ - see front matter © 2007 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijcard.2007.02.059
vagal syncope during sheath removal leads to a higherincidence of major adverse cardiac events including acutestent thrombosis.
A total of 611 patients undergoing PCI whose femoralsheaths were to be removed with assisted manual compres-sion were enrolled in our previously reported study [6].Patients were randomly allocated to receive either intrave-nous sedation (fentanyl 25 μg and midazolam 1 mg) or localanaesthesia (1% lignocaine, infiltrated around sheath siteusing aseptic techniques) or both or neither.
Patients underwent PCI using standard techniques.Femoral sheaths were removed after PCI using assistedmanual compression with the Femostop™ device by adedicated angioplasty research nurse experienced in sheathremoval. All patients had continuous electrocardiographicalmonitoring and non-invasive blood pressure recordingduring sheath removal. Blood pressure and heart raterecorded immediately prior to sheath removal were consid-ered the baseline measurement and the lowest measurementsduring an episode of symptomatic bradycardia or hypoten-sion were used to determine the presence or absence of avaso-vagal reaction. A vaso-vagal reaction was defined as asymptomatic bradycardic episode (heart rate of b60 beats/
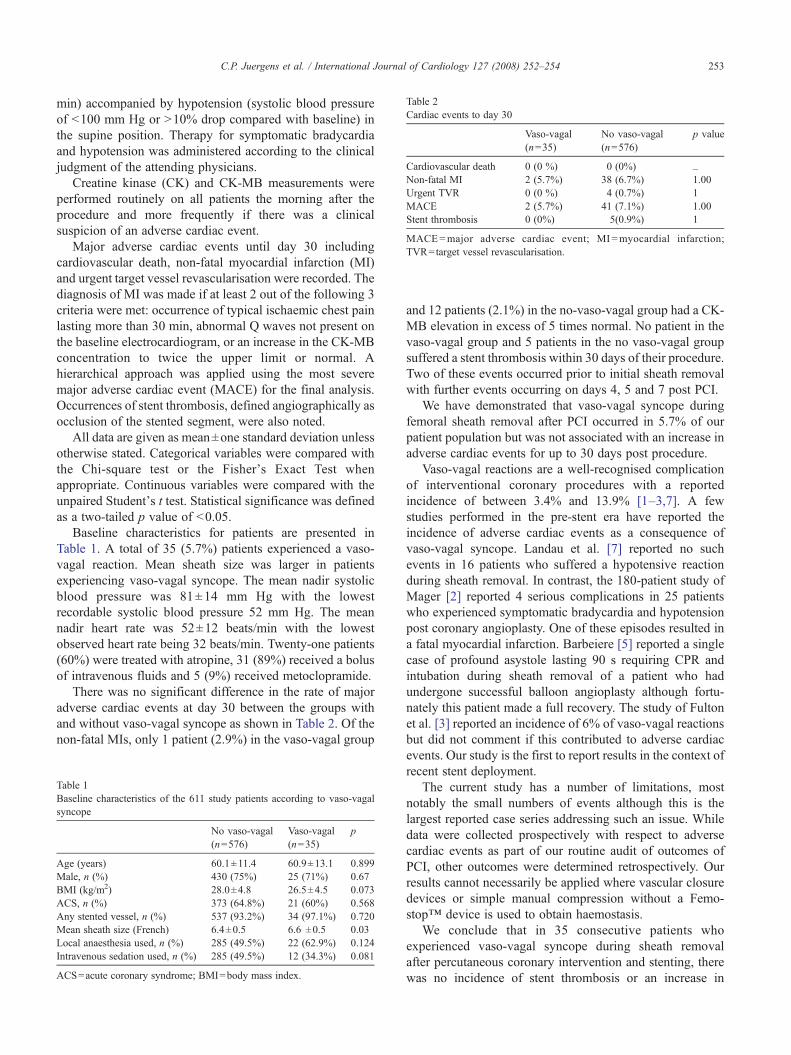
Table 2Cardiac events to day 30
Vaso-vagal(n=35)
No vaso-vagal(n=576)
p value
Cardiovascular death 0 (0 %) 0 (0%) _Non-fatal MI 2 (5.7%) 38 (6.7%) 1.00Urgent TVR 0 (0 %) 4 (0.7%) 1MACE 2 (5.7%) 41 (7.1%) 1.00Stent thrombosis 0 (0%) 5(0.9%) 1
MACE=major adverse cardiac event; MI =myocardial infarction;TVR=target vessel revascularisation.
253C.P. Juergens et al. / International Journal of Cardiology 127 (2008) 252–254
min) accompanied by hypotension (systolic blood pressureof b100 mm Hg or N10% drop compared with baseline) inthe supine position. Therapy for symptomatic bradycardiaand hypotension was administered according to the clinicaljudgment of the attending physicians.
Creatine kinase (CK) and CK-MB measurements wereperformed routinely on all patients the morning after theprocedure and more frequently if there was a clinicalsuspicion of an adverse cardiac event.
Major adverse cardiac events until day 30 includingcardiovascular death, non-fatal myocardial infarction (MI)and urgent target vessel revascularisation were recorded. Thediagnosis of MI was made if at least 2 out of the following 3criteria were met: occurrence of typical ischaemic chest painlasting more than 30 min, abnormal Q waves not present onthe baseline electrocardiogram, or an increase in the CK-MBconcentration to twice the upper limit or normal. Ahierarchical approach was applied using the most severemajor adverse cardiac event (MACE) for the final analysis.Occurrences of stent thrombosis, defined angiographically asocclusion of the stented segment, were also noted.
All data are given as mean±one standard deviation unlessotherwise stated. Categorical variables were compared withthe Chi-square test or the Fisher's Exact Test whenappropriate. Continuous variables were compared with theunpaired Student's t test. Statistical significance was definedas a two-tailed p value of b0.05.
Baseline characteristics for patients are presented inTable 1. A total of 35 (5.7%) patients experienced a vaso-vagal reaction. Mean sheath size was larger in patientsexperiencing vaso-vagal syncope. The mean nadir systolicblood pressure was 81±14 mm Hg with the lowestrecordable systolic blood pressure 52 mm Hg. The meannadir heart rate was 52±12 beats/min with the lowestobserved heart rate being 32 beats/min. Twenty-one patients(60%) were treated with atropine, 31 (89%) received a bolusof intravenous fluids and 5 (9%) received metoclopramide.
There was no significant difference in the rate of majoradverse cardiac events at day 30 between the groups withand without vaso-vagal syncope as shown in Table 2. Of thenon-fatal MIs, only 1 patient (2.9%) in the vaso-vagal group
Table 1Baseline characteristics of the 611 study patients according to vaso-vagalsyncope
No vaso-vagal(n=576)
Vaso-vagal(n=35)
p
Age (years) 60.1±11.4 60.9±13.1 0.899Male, n (%) 430 (75%) 25 (71%) 0.67BMI (kg/m2) 28.0±4.8 26.5±4.5 0.073ACS, n (%) 373 (64.8%) 21 (60%) 0.568Any stented vessel, n (%) 537 (93.2%) 34 (97.1%) 0.720Mean sheath size (French) 6.4±0.5 6.6 ±0.5 0.03Local anaesthesia used, n (%) 285 (49.5%) 22 (62.9%) 0.124Intravenous sedation used, n (%) 285 (49.5%) 12 (34.3%) 0.081
ACS=acute coronary syndrome; BMI=body mass index.
and 12 patients (2.1%) in the no-vaso-vagal group had a CK-MB elevation in excess of 5 times normal. No patient in thevaso-vagal group and 5 patients in the no vaso-vagal groupsuffered a stent thrombosis within 30 days of their procedure.Two of these events occurred prior to initial sheath removalwith further events occurring on days 4, 5 and 7 post PCI.
We have demonstrated that vaso-vagal syncope duringfemoral sheath removal after PCI occurred in 5.7% of ourpatient population but was not associated with an increase inadverse cardiac events for up to 30 days post procedure.
Vaso-vagal reactions are a well-recognised complicationof interventional coronary procedures with a reportedincidence of between 3.4% and 13.9% [1–3,7]. A fewstudies performed in the pre-stent era have reported theincidence of adverse cardiac events as a consequence ofvaso-vagal syncope. Landau et al. [7] reported no suchevents in 16 patients who suffered a hypotensive reactionduring sheath removal. In contrast, the 180-patient study ofMager [2] reported 4 serious complications in 25 patientswho experienced symptomatic bradycardia and hypotensionpost coronary angioplasty. One of these episodes resulted ina fatal myocardial infarction. Barbeiere [5] reported a singlecase of profound asystole lasting 90 s requiring CPR andintubation during sheath removal of a patient who hadundergone successful balloon angioplasty although fortu-nately this patient made a full recovery. The study of Fultonet al. [3] reported an incidence of 6% of vaso-vagal reactionsbut did not comment if this contributed to adverse cardiacevents. Our study is the first to report results in the context ofrecent stent deployment.
The current study has a number of limitations, mostnotably the small numbers of events although this is thelargest reported case series addressing such an issue. Whiledata were collected prospectively with respect to adversecardiac events as part of our routine audit of outcomes ofPCI, other outcomes were determined retrospectively. Ourresults cannot necessarily be applied where vascular closuredevices or simple manual compression without a Femo-stop™ device is used to obtain haemostasis.
We conclude that in 35 consecutive patients whoexperienced vaso-vagal syncope during sheath removalafter percutaneous coronary intervention and stenting, therewas no incidence of stent thrombosis or an increase in

254 C.P. Juergens et al. / International Journal of Cardiology 127 (2008) 252–254
adverse cardiac events when compared to those patients notexperiencing such an event.
References
[1] Juergens CP, Leung DYC, Crozier JA, et al. Patient tolerance andresource utilization associated with an arterial closure versus an externalcompression device after percutaneous coronary intervention. CatheterCardiovasc Interv 2004;63:166–70.
[2] Mager A, Strasberg B, Rechavia E, et al. Clinical significance andpredisposing factors to symptomatic bradycardia and hypotension afterpercutaneous transluminal coronary angioplasty. Am J Cardiol 1994;74:1085–8.
[3] Fulton TR, Peet GI, McGrath MA, et al. Effects of 3 analgesic regimenson the perception of pain after removal of femoral artery sheaths. Am JCrit Care 2000;9:125–9.
[4] Boss BJ, Brewer L. Syncope: neuroscience nursing assessment based onan understanding of underlying pathophysiological mechanisms.J Neurosci Nurs 1988;20:245–52.
[5] Barbiere CC. Malignant vasovagal syncope after PTCA: a potential fordisaster. Crit Care Nurse 1994;14:90–3.
[6] Ang CK, Leung DYC, Lo S, French JK, Juergens CP. Effect of localanesthesia and intravenous sedation on pain perception and vasovagalreactions during femoral arterial sheath removal after percutaneouscoronary intervention. In J Cardiol 2007;116:321–6.
[7] Landau C, Lange RA, Glamann B, Willard JE, Hills LD. Vasovagalreactions in the cardiac catheterization laboratory. Am J Cardiol 1993;73:95–7.
38
CHAPTER 3
USE OF ANTITHROMBOTIC AGENTS
Introduction
From the early beginnings of coronary intervention in the 1970s, where the
initial equipment was rudimentary, developments quickly followed reducing the
profile of equipment and facilitating easier use. Of note, most of this was on a trial
and error basis with little clinical trial data suggesting one piece of equipment was
better that any other. The use of high dose unfractionated heparin (UFH) during the
procedure and as an infusion after the procedure, if the angiographic result was
suboptimal, became standard practice despite the absence of rigorous scientific data
suggesting its benefit. Results of interventions were improved with the development
of glycoprotein IIb/IIIa inhibitors and new antiplatelet agents used together with
heparin and aspirin although at the expense of increased bleeding rates. The next
important development in the history of coronary intervention was the use of
intracoronary stents for the first time in 1987. Intracoronary stenting quickly became
an accepted treatment for vessel closure after percutaneous transluminal coronary
angioplasty (PTCA) and to reduce restenosis. Complications of stenting can occur
during the procedure itself and in the short to long term and ways to minimise these
complications remains a focus of ongoing research to which I have contributed.
Use of Unfractionated Heparin
In the early days of percutaneous coronary angioplasty acute complications
including abrupt vessel closure led many operators to routinely use an infusion of
39
intravenous unfractionated heparin for up to 12 hours post procedure to try and
minimise this complication. The development of glycoprotein IIb/IIIa antagonists
such as abciximab led to a reevaluation of this practise. The “Evaluation of 7E3 for
the prevention of ischaemic complications” (EPIC) study [1] compared three
treatment groups; a bolus and 12 hour infusion of abciximab, bolus only abciximab
and placebo in patients undergoing coronary angioplasty prior to the development of
stenting. All patients in this study were treatment with boluses of intravenous heparin
during the procedure followed by a 12 hour infusion, as was the usual practise at the
time. Vascular sheaths were maintained for at least 6 hours after the end of the
infusion of the study drug and were left in place at least 4 hours after the end of the
heparin infusion. Whilst ischaemic events were reduced with abciximab there was a
very high incidence of major bleeding episodes (7-14%) and transfusions (7-15%).
The subsequent “Evaluation in PTCA to improve long term outcomes with
abciximab GP IIb/IIIa blockade (EPILOG) study” [2] was designed to determine
whether the clinical benefits of abciximab therapy could be extended to all patients
undergoing percutaneous coronary intervention (only 2% elective stenting) and
whether the incidence of haemorrhagic complications could be reduced by adjusting
the heparin dose for body weight or reducing it. The protocol also mandated that
heparin be discontinued immediately after the procedure and the vascular sheaths be
removed when the activated clotting time was 175 seconds or less (usually 2-6 hours
later). This study showed that this strategy not only reduced ischaemic complications
but haemorrhagic events as well when compared to the earlier study although they
continued to occur in 2-3.5% of patients.
The “Enhanced suppression of the platelet IIb/IIIa receptor with Integrelin
Therapy (ESPRIT) trial” [3] examined the use of a high dose regimen of eptifibatide
40
with unfractionated heparin during the procedure as an adjunct to planned coronary
stent implantation. Further infusions of heparin after the intervention were
“discouraged” with the planned removal of sheaths within 3-4 hours of procedure
completion. Eptifibatide, continued as an infusion for a median of 18 hours, was
shown to reduce the primary composite endpoint when compared to placebo at the
expense of increased major bleeding (1.3% vs 0.4%, p=0.027).
The development of intracoronary stents whilst overcoming the issue of abrupt
vessel closure initially created another problem with respect to occasional thrombotic
occlusion of the stent. Whilst glycoprotein IIb/IIIa inhibitors were shown to reduce
ischaemic complications these agents are expensive and associated with increased
bleeding events. Therefore some operators continued to use prolonged of infusions of
unfractionated heparin post procedure after the sheath was removed if there was a
suboptimal stent result. This strategy was initially not subjected to rigorous scientific
assessment.
Paper 9 ( Heart Lung Circ 2008;127:252-254)
Paper 9 was an attempt to address some of the shortfalls in knowledge in this
area. At the time of conception of our study there was no consensus or guidelines
published about the use of postprocedural UFH after intracoronary stenting, so we
aimed to determine the incidence of vascular (using routine vascular ultrasound),
bleeding and ischaemic (including stent thrombosis) complications associated with the
use or non-use of UFH after percutaneous coronary intervention (PCI) in the stent era.
Five hundred and thirty patients undergoing a PCI between February 1999 and
January 2004 were enrolled in this study at our institution. Patients had been enrolled
in our previously published studies comparing 6 Fr and 7 Fr sheath size on the impact
41
of vascular complications [Paper 6] or patient tolerance and resource implications of
using the Angioseal™ or Femostop™ devices to facilitate vascular closure after PCI
[Paper 5]. In addition there was a subset of patients we included, whom we
randomised to the use or non use of heparin, after the previous studies had
commenced and this data had not been published previously.
We found no increase in major peripheral vascular complications when UFH
was used routinely in the stent era and routine post procedure vascular ultrasound was
performed to determine such complications. In addition we found that the use of UFH
did not appear to reduce the risk of major adverse cardiac events in this selected
patient cohort. We concluded that the choice to recommence UFH or not after
coronary intervention should be determined by individual patient factors, such as the
need for long term anticoagulation, and not on a perceived impact on vascular
complications or ischaemic complications of the procedure.
Context and Implications
This work was initiated and completed by the author at Liverpool hospital and follows
on from earlier work. Subsequent to the conception of our study the seventh ACCP
conference on antithrombotic and thrombolytic therapy recommended against a
routine postprocedural infusion of heparin after uncomplicated PCI [4], although this
recommendation was based on earlier studies performed in the prestent era. In
contradistinction, the ACC/AHA/SCAI guideline update for percutaneous coronary
intervention, does not address the use of postprocedural heparin after coronary
intervention [5]. Patients were enrolled in our study prior to the first published
guidelines suggesting that this practice was not recommended and whilst, in
retrospect, we have potentially addressed an outdated practice, our results have added
significantly to the body of evidence assessing this therapeutic intervention
42
particularly with respect to the routine use of vascular ultrasound which is unique to
our study.
Impact on literature
According to Scopus ®, this article has been cited twice in the literature from a
journal with an impact factor of 1.196.
Antiplatelet Agents
Randomised trials subsequently demonstrated that the use of the antiplatelet
regime of ticlopidine and aspirin was superior to anticoagulation therapy, with less
stent thrombosis and bleeding events when optimal stent deployment methods are
used [6-9]. As a consequence of these landmark studies, the use of ticlopidine and
aspirin after coronary stent placement became standard practice. However, because of
concerns of potentially life threatening neutropenia, which occurs in approximately
1% of patients treated for more than 2 weeks with ticlopidine, a number of centres
including our own, adopted a strategy of discontinuing therapy 2 weeks after stent
placement. A subsequent study of over 800 patients suggested this could be done
relatively safely with no case of stent thrombosis observed after ticlopidine cessation
at 14 days [10]. A concurrent study of over 19000 patients with vascular disease
showed that clopidogrel, a thienopyridine derivative closely related to ticlopidine in
chemical structure and function, reduced the frequency of adverse cardiovascular
events by 8.7% when compared to aspirin therapy [11]. The side effect profile of
clopidogrel and aspirin was similar and notably there was no increase in neutropenia.
With the widespread availability of clopidogrel and better tolerability, many
interventional cardiology centres changed to a regime of clopidogrel and aspirin in
their post coronary stenting cases. This change of practice occurred largely before the
43
publication of randomised controlled trials comparing ticlopidine and aspirin with
clopidogrel and aspirin in this group of patients.
Paper 10 (Am Heart J 2004;147;e15)
Paper 10 specifically addressed this issue in evaluating the tolerability and
efficacy of 14 days of therapy with ticlopidine in combination with aspirin compared
with clopidogrel and aspirin in patients who had undergone successful intracoronary
stenting.
We demonstrated that after 2 weeks of combination antiplatelet therapy with
aspirin, there was a trend toward improved patient tolerability of clopidogrel
compared to ticlopidine with a similarly low incidence of adverse cardiac events. We
concluded that these data may be of assistance in the management of patients
intolerant of long term therapy with thienopyridines or where costs of such treatment
are prohibitive.
Context and Implications
This work was initiated and completed by the author at Liverpool hospital.
Subsequent to the conception of our study in 1998, two large scale clinical trials
addressing the same issue were published in 2000. Patients were therefore enrolled
into our study prior to the publication of any trials suggesting switching from
ticlopidine to clopidogrel was safe after coronary stenting. Whilst a smaller study, it
does nevertheless add to the body of literature on this topic and helped guide practise
in our institution with respect to the use of clopidogrel after stenting.
Impact on literature
According to Scopus ®, this article has been cited 17 times in the literature to date,
including as part of a meta-regression, from a journal with a 5 year impact factor of
44
4.321.
Paper 11 (Heart Lung Circ 2011;20:525-531)
Drug eluting stents (DES) were the next major advance in stent design and
large trials demonstrated a reduction in in-stent restenosis and target vessel
revascularisation when compared to bare metal stents (BMS), with a similar long term
incidence of death or myocardial infarction (MI) [12,13]. However it became apparent
that DES use was associated with a higher incidence of late stent thrombosis (ST)
[14]. Furthermore these late events appeared to be related to the discontinuation of
clopidogrel therapy. Stent thrombosis continues to occur with a reported incidence at
six months to three years of between 1.3-4.1% [14-18] and leads to significant clinical
complications including a mortality rate of 19-29% and myocardial infarction in 56-
75% [14,16,19] of these patients.
Whilst thienopyridines in combination with aspirin are key in reducing the risk
of ST, The Dutch Stent Thrombosis Registry study attributed the discontinuation of
clopidogrel as one of the strongest predictors of ST [20]. Other studies have also
demonstrated an increased incidence of ST when antiplatelet therapy is withdrawn
[21,22]. Although interruption of antiplatelet therapy may explain the occurrences of
late and very late ST, it does not explain occurrences of acute and subacute ST on
treatment. More recently investigators have suggested that reduced platelet inhibition
by aspirin and thienopyridines can be seen as a potential contributor to this
phenomenon [23-25]. Although strong predictors of ST have been identified [20], the
concept of high on treatment platelet reactivity or “antiplatelet resistance” as a
predictor in itself remains contentious. Moreover, significant evidence of antiplatelet
resistance has largely been discussed with relation to DES use and stent thrombosis
45
[23,25]. Therefore we aimed to establish the significance of high on treatment platelet
reactivity across both DES and BMS thrombosis and discussed its recognition as a
strong predictor of ST. Additionally, we examined the hypothesis of potentially
reducing high on treatment antiplatelet reactivity in patients through the doubling of
the doses of aspirin and/or clopidogrel. This forms the basis of Paper 11.
Using our prospective data base of PCI procedures we identified 33 patients
experiencing 40 definite ST episodes over a 4 year period. Of these patients, 16 were
alive and willing to participate in the study. We identified a total of 40 patients who
had not experienced ST during follow up to serve as controls. Patients underwent
antiplatelet resistance testing using the point of care VerifyNow Assay (Accumetrics,
San Diego, California) to determine the platelet inhibitory effect of aspirin and
clopidogrel. In subjects found to have high on treatment platelet reactivity to aspirin
and/or clopidogrel, the daily dose of aspirin and/or clopidogrel was doubled and a
repeat platelet reactivity test was performed following a further two weeks of therapy.
We found high post treatment platelet reactivity with aspirin and/or
clopidogrel was significantly more frequent in the ST group when compared to
controls. Patients with high post treatment platelet reactivity to clopidogrel and/or
aspirin were subsequently given double dose antiplatelet therapy. After administration
of double dose therapy, 10 out of 12 subjects (83.3%) on clopidogrel and both patients
on aspirin, no longer had high on treatment platelet reactivity according to our
definition.
We concluded that high post treatment platelet reactivity with aspirin and/or
clopidogrel was common amongst patients who develop stent thrombosis.
Additionally we found that platelet reactivity can be significantly improved by
46
doubling the prior dose of antiplatelet therapy, but whether this translates into
improved outcomes awaits further study.
Context and Implications
This work was initiated and completed by the author at Liverpool hospital with the
assistance of Saissan Rajendran, a UNSW medical student who submitted the work as
part of an Independent Learning Project. Our results are consistent with the work of
others who have identified that the presence of aspirin and/or clopidogrel “resistance”
is a strong risk factor for subsequent stent thrombosis; however our study differs to
many of these in reporting the impact of doubling the dose of antiplatelet therapy in
these patients. This work has given us insight into the potential reasons for stent
thrombosis and our conclusions have already been used clinically in our institution to
help guide therapeutic decisions in the management of these patients.
Impact on literature
According to Scopus ®, this article has been cited six times in the literature to date
from a journal with an impact factor of 1.196.
Paper 12 (Expert Opin Drug Metab Toxicol 2012;8:1315-1325)
Whilst the thienopyridine clopidogrel, together with aspirin has become the
cornerstone of treatment of patients with acute coronary syndromes, a number of
newer agents have become available. One of these is ticagrelor, a cyclopentyl-
triazolo-pyrimidine, which is the first orally active reversible P2Y12 receptor
antagonist [26]. Ticagrelor’s rapid onset, reversible binding and minimal interpatient
variability make it an important alternative in the treatment of acute coronary
syndromes as it does not require conversion into an active metabolite. The PLATO
(PLATelet inhibition and clinical Outcomes) trial demonstrated superiority of
47
ticagrelor over clopidogrel in the prevention of a composite end point of death from
vascular causes, myocardial infarction or stroke with no difference between the
overall rates of major bleeding events [27].
I was asked to write a review article ( Paper 12) providing an overview of
ticagrelor’s development and chemical properties including pharmacodynamics and
pharmacokinetics. Together with two of my junior colleagues we also reviewed Phase
II and III trials looking at the safety and efficacy of ticagrelor in the management of
patients with acute coronary syndromes and discussed the future integration of this
new agent into clinical practice.
Context and Implications
This work was initiated and completed at Liverpool hospital. Whilst it is a review
article and therefore does not reflect original work, I believe it represents an excellent
overview of the most recent clinical trial data available at the time of publication. It
has also helped consolidate local knowledge about the appropriate use of ticagrelor in
our institution. It is likely the rapid onset, reversible binding and linear
pharmacokinetics of ticagrelor will result in a reduction in the use of clopidogrel in
the management of acute coronary syndromes and lead to a continued decline in the
use of glycoprotein IIb/IIIa inhibitors in the future.
Impact on literature
This paper has not been cited yet as it was only recently published in a journal with a
5 year impact factor of 3.395.
Glycoprotein IIb/IIIa inhibitors
A major advance in the use of antithrombotic agents during percutaneous
coronary intervention (PCI) was the development of intravenous glycoprotein IIb/IIIa
48
antagonists. A number of clinical trials demonstrated the use of intravenous
glycoprotein IIb/IIIa antagonists result in improved outcomes after percutaneous
transluminal coronary angioplasty (PTCA) [1,2,3,28]. Tirofiban is a highly selective
inhibitor of fibrinogen binding to the platelet glycoprotein IIb/IIIa receptor. Data from
3 large clinical trials using tirofiban comprising a total of 7288 patients demonstrated
the efficacy and tolerability of tirofiban in reducing ischaemic events in a broad range
of patients with unstable angina and non-Q wave myocardial infarction and following
high risk angioplasty in patients presenting with acute coronary syndromes [29,30].
Of note these clinical trials predated the widespread use of intracoronary stents. In the
Randomised Efficacy Study of Tirofiban for Outcomes and Restenosis (RESTORE)
trial [31] of percutaneous coronary intervention, “elective” coronary stenting was
discouraged. As a result, only 175 of the 2141 patients enrolled received intracoronary
stents. Of these, 43 (24.6%) were placed for actual or threatened closured and the rest
were placed for a suboptimal angiographic result. Since these earlier trials, the use of
aspirin in combination with a thienopyridine after intracoronary stent placement
became standard practice [6,7,32] and more placebo controlled data about the
combination of these agents with tirofiban was required.
Paper 13 (Clin Ther 2002;24:1332-1344)
Paper 13 was the first large scale randomised controlled trial which assessed
the efficacy and tolerability of tirofiban when compared to placebo, in patients
undergoing elective intracoronary stent placement in combination with aspirin and a
thienopyridine.
We found that tirofiban could be administered with a low incidence of major
bleeding to patients undergoing intracoronary stenting in combination with aspirin
49
and thienopyridines. We concluded that in patients already receiving tirofiban for
acute coronary syndromes who require coronary intervention, physicians should be
reassured that this agent can be continued throughout intracoronary stent placement
without a significant increase in life threatening bleeding complications. However in
the dosage regimen studied, patients receiving tirofiban had an increased incidence of
minor bleeding without a reduction in adverse cardiac events when compared with
placebo.
Context and Implications
This work was a multinational, multicentre trial sponsored by a pharmaceutical
company. I was a co-investigator of this study and whilst not involved in the original
trial design, I was involved in the investigator meeting and gave input into the
implementation of the trial. Liverpool hospital enrolled a large number of patients into
the trial and I wrote the initial draft of the manuscript after liaising with the
biostatiscian assigned to the trial. I sought input from my co-investigators and
subsequently revised the manuscript until it was accepted for publication. Subsequent
to the commencement of this study in 1998, a large scale clinical trial powered for
ischaemic cardiovascular endpoints comparing tirofiban with abciximab was
published in 2001. However this remains the only large scale trial comparing tirofiban
with placebo in an elective intracoronary stenting population and does contribute
important information to the scientific literature. It has also helped guide practise in
our institution with respect to the use of tirofiban during stenting.
Impact on literature
According to Scopus ®, this article has been cited in the literature on at least 12
occasions from a journal with a 5 year impact factor of 2.969. It has been included in
at least three meta-analyses on the topic and is cited in the 2011 American College of
50
Cardiology Foundation/American Heart Association/Society of Cardiovascular
Angiography and Interventions guidelines for percutaneous coronary intervention
[33].
Papers 14 (Cardiovasc Hematol Disord Drug Targets 2008;8:138-146)
& 15 (Expert Opin Biol Ther 2011;11:235-46)
Two of our Interventional Fellows and I have written review articles about the
use of the two mostly widely used glycoprotein IIb/ IIIa antagonists in Australia.
These reviews discuss the development and pharmacological characteristics of
tirofiban in the case of Paper 14 and abciximab in the case of Paper 15. We also
discuss the current evidence-base for the use of both tirofiban and abciximab in
managing patients with coronary artery disease.
Context and Implications
Both these works were initiated and completed at Liverpool hospital. Whilst they are
review articles and therefore do not reflect original work, both represent an excellent
overview of the most recent clinical trial data available at the time of publication.
They have also helped consolidate local knowledge about the appropriate use of
tirofiban and abciximab in our institution.
Impact on literature
According to Scopus ®, Paper 14 has been cited six times and Paper 15 has been cited
twice from journals with a 5 year impact factor of 2.387 and 3.395 respectively.
51
Paper 16 (Am J Cardiol 1997;80:74-75)
Whilst glycoprotein IIb/IIIa antagonists have been shown to reduce ischaemic
complications of high risk percutaneous coronary intervention (PCI) [1], the issue of
how to manage these potent antiplatelet agents in the context of a patient needing to
proceed to emergent coronary artery bypass surgery has rarely been addressed. What
was known was that these patients are at high risk of major blood loss and in hospital
mortality [34]. Paper 16 was published in 1997 during my time as an Interventional
Fellow at Stanford University Medical centre, USA. We reported a series of 4 patients
who had received abciximab and subsequently underwent coronary artery bypass
surgery within 6 hours of failed PCI. All patients received platelet transfusions
routinely and we found that all patients survived and only 2 patients required red
blood cell transfusion.
Context and Implications
The rarity, unpredictability and urgency of this complication means that randomised
controlled trials would be almost impossible to perform and therefore small single
centre experiences often help guide management. This was the first such experience
described and was conceived and written by myself with input from my supervisors at
the time. It has also helped guide practise in our institution in the rare event that
patients need to undergo coronary bypass surgery soon after receiving abciximab.
Impact on literature
According to Scopus ®, this article has been cited 44 times in the literature from a
journal with a 5 year impact factor of 3.578. This paper is cited in the Italian Society
for Haemostasis and Thrombosis guidelines for the management of bleeding and of
invasive procedures in patients with platelet disorders and/or thrombocytopaenia [35].
52
Paper 17 (Am Heart J 2012;163:649-656.e1.)
While prompt primary percutaneous coronary intervention (PCI) is a superior
reperfusion strategy to fibrinolytic therapy alone [36], in patients presenting with ST-
elevation myocardial infarction (STEMI), for several reasons many patients world-
wide receive fibrinolytic therapy as an initial reperfusion strategy [37].
Fibrinolytic-treated patients are recommended for immediate angiography and
if indicated rescue PCI, if they have failed to reperfuse, as randomised clinical trials
have shown improved outcomes compared to conservative management [38-40].
However, these trials, and more recent reports from registries, have included
significant proportions of patients who did not receive fibrin-specific therapies, stents
(including drug-eluting) or glycoprotein IIb/IIIa (GPIIb/IIIa) antagonists [38,41,42].
The use of GPIIb/IIIa inhibitors after fibrinolytic therapy in the setting of PCI in the
early hours after symptom onset has been contentious given clinician concerns about
balancing bleeding risks with risks of recurrent ischaemic events.
As patients treated at our cardiac catheterisation laboratory (CCL) and
undergoing rescue PCI have received high rates of these therapies, we studied
consecutive patients to identify factors that influence clinical outcomes. This forms
the basis of Paper 17.
We found there was a 78% rate of GPIIb/IIIa inhibitor use which was not
associated with an increased risk of TIMI major bleeding or need for transfusion. We
felt several factors may have contributed to the differences in the bleeding rate after
rescue PCI compared with older studies, such as the use of smaller arterial sheath
calibre, and improvements in pharmaco-therapies including lower heparin doses
associated with lower activated clotting times.
53
Furthermore, the mortality rate observed in our unselected patient population
without prior shock undergoing rescue PCI in the era of liberal stent use and
GPIIb/IIIa inhibitors, was similar to that of STEMI patients treated with primary PCI.
We concluded that a pharmaco-invasive approach to STEMI with rescue PCI
especially among those presenting at <3 hours is a reasonable strategy when there is
not expeditious access to primary PCI, especially in early presenting patients.
Context and Implications
This work was led by Professor John French and his PhD student Ibrahim Shugman at
Liverpool Hospital. I am the co-supervisor of Ibrahim Shugman’s PhD. I was a co-
investigator of this study and was involved in the original trial design. By establishing
a process by which coronary interventional details were routinely collected as part of
quality assurance, I believe I made a crucial contribution to this work. I was involved
in the analysis and interpretation of the data and revisions of the manuscript. We
believe this paper makes an important contribution with respect to the performance of
Rescue PCI in the modern era with the liberal use of glycoprotein IIb/IIIa antagonists.
Impact on literature
According to Scopus ®, this article has not been cited in the literature as it has only
recently been published in a journal with a 5 year impact factor of 4.321.
54
Chapter 3 References
1. The EPIC Investigators. Use of a monoclonal antibody directed against the platelet
glycoprotein IIb/IIIa receptor in high-risk coronary angioplasty. N Engl J Med 1994;
330:956-961.
2. The EPILOG Investigators. Platelet glycoprotein IIb/IIIa receptor blockade and low
dose heparin during percutaneous coronary revascularization. N Engl J Med
1997;336:1689-1696.
3. The ESPRIT Investigators. Novel dosing regimen of eptifibatide in planned
coronary stent implantation (ESPRIT) : a randomised placebo-controlled trial. Lancet
2000:356:2037-2044.
4. Popma JJ, Berger P, Ohman EM, Harrington RA, Grines C, Weitz JI.
Antithrombotic therapy during percutaneous coronary intervention. Chest
2004;126:576S-599S.
5. Smith SC, Feldman TE, Hirshfeld JW, et al. ACC/AHA/SCAI 2005 guideline
update for percutaneous coronary intervention-summary article. J Am Coll Cardiol
2006;47:216-235.
6. Colombo A, Hall P, Nakamura S, et al. Intracoronary stenting without
anticoagulation accomplished with intravascular ultrasound guidance. Circulation
1995;91:1676-1688.
7. Schomig A, Neumann F-J, Kastrati A, et al. A randomized comparison of
antiplatelet and anticoagulant therapy after the placement of coronary artery stents. N
Engl J Med 1996;334:1084-1089.
55
8. Bertrand ME, Legrand V, Boland J, et al. Randomized multicentre comparison of
conventional anticoagulation versus antiplatelet therapy in unplanned and elective
coronary stenting: the full anticoagulation versus aspirin and ticlopidine
(FANTASTIC) study. Circulation 1998;98:1597-1603.
9. Leon MB, Baim DS, Popma JJ, et al for the Stent Anticoagulation Restenosis Study
Investigators. A clinical trial comparing three antithrombotic drug regimens after
coronary artery stenting. N Engl J Med 1998;339:1665-1671.
10. Berger PB, Bell MR, Hasdai D, et al. Safety and efficacy of ticlopidine for only 2
weeks after successful intracoronary stent placement. Circulation 1999;99:248-253.
11. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus
aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996;348:1329-1339.
12. James SK, Stenestrand U, Lindback J, et al. Long-term safety and efficacy of
drug-eluting versus bare-metal stents in Sweden. N Engl J Med 2009;360:1933-1945.
13. Ko DT, Chiu M, Guo H, et al. Safety and effectiveness of drug-eluting and bare-
metal stents for patients with off- and on-label indications. J Am Coll Cardiol
2009;53:1773-1782.
14. Pfisterer M, Brunner-La Rocca HP, Buser PT, et al. Late clinical events after
clopidogrel discontinuation may limit the benefit of drug-eluting stents: an
observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol
2006;48:2584–2591.
15. Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of
thrombosis after successful implantation of drug-eluting stents. JAMA
2005;293:2126–2130.
56
16. Kuchulakanti PK, Chu WW, Torguson R, et al. Correlates and long-term
outcomes of angiographically proven stent thrombosis with sirolimus- and paclitaxel-
eluting stents. Circulation 2006;113:1108-1113.
17. Daemen J, Wenaweser P, Tsuchida K, et al. Early and late coronary stent
thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical
practice: data from a large two-institutional cohort study. Lancet 2007;369:667–678.
18. Smit JJJ, van’t Hof AWJ, de Boer MJ, et al. Incidence and predictors of subacute
thrombosis in patients undergoing primary angioplasty for an acute myocardial
infarction. Thromb Haemost 2006;96:190–195.
19. Cutlip DE, Baim DS, Ho KKL, et al. Stent thrombosis in the modern era: a pooled
analysis of multicenter coronary stent clinical trials. Circulation 2001;103:1967-1971.
20. van Werkum JW, Heestermans AA, Zomer AC, et al. Predictors of coronary stent
thrombosis: the Dutch stent thrombosis registry. J Am Coll Cardiol 2009;53:1399-
1409.
21. Waters RE, Kandzari DE, Phillips HR, Crawford LE, Sketch MH. Late
thrombosis following treatment of in-stent restenosis with drug-eluting stents after
discontinuation of antiplatelet therapy. Catheter Cardiovasc Interv 2005;65:520-524.
22. Ferrari E, Benhamou M, Cerboni P, Marcel B. Coronary syndromes following
aspirin withdrawal: a special risk for late stent thrombosis. J Am Coll Cardiol
2005;45:456-459.
23. Wang ZJ, Zhou YJ, Liu YY, et al. Impact of clopidogrel resistance on thrombotic
events after percutaneous coronary intervention with drug-eluting stent. Thrombosis
Research 2009;124:46-51.
57
24. Gurbel PA, Bliden KP, Samara W, et al. Clopidogrel effect on platelet reactivity
in patients with stent thrombosis: results of the CREST Study. J Am Coll Cardiol
2005;46:1827-1832.
25. Pinto Slottow TL, Bonello L, Gavini R, et al. Prevalence of aspirin and
clopidogrel resistance among patients with and without drug eluting stent thrombosis.
Am J Cardiol 2009;104:525-530.
26. van Giezen JJ, Humphries RG. Preclinical and clinical studies with selective
reversible direct P2Y12 antagonists. Semin Thromb Hemost 2005;31:195-204.
27. Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients
with acute coronary syndromes. N Engl J Med 2009;361:1045-1057.
28. The IMPACT II Investigators. Randomised placebo controlled trial of effect of
eptifibatide on complications of percutaneous coronary intervention: IMPACT II.
Lancet 1997;349:1422-1428.
29. The platelet receptor inhibition in ischemic syndrome management (PRISM) study
investigators. A comparison of aspirin plus tirofiban with aspirin plus heparin for
unstable angina. N Engl J Med 1998;338:1498-1505.
30. The platelet receptor inhibition in ischemic syndrome management in patients
limited by unstable signs and symptoms (PRISM-PLUS) study investigators.
Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable
angina and non-Q wave myocardial infarction. N Engl J Med 1998;338:1488-1497.
31. The RESTORE Investigators. Effects of Platelet Glycoprotein IIb/IIIa Blockade
with Tirofiban on Adverse Cardiac Events in Patients with Unstable Angina or Acute
Myocardial Infarction Undergoing Coronary Angioplasty. Circulation 1997;96:1445-
1453.
58
32. Muller C, Buttner HJ, Petersen J, Roskamm H. A randomized comparison of
clopidogrel and aspirin versus ticlopidine and aspirin after the placement of coronary
artery stents. Circulation 2000;101:590-593.
33. Levine GN, Bates ER, Blakenship JC, et al. 2011 ACCF/AHA/SCAI guideline for
percutaneous coronary intervention: a report of the American College of Cardiology
Foundation/American Heart Association task force on practice guidelines and the
Society for Cardiovascular Angiography and Interventions. Circulation
2011;124:e574-e651.
34. Boehrer JD, Kereiakes DJ, Navetta FI, Califf RM, Topol EJ, for the EPIC
investigators. Effects of profound platelet inhibition with c7E3 before coronary
angioplasty on complications of coronary bypass surgery. Am J Cardiol
1994;74:1166-1170.
35. Tosetto A, Balduini CL, Cattaneo M, et al. Management of bleeding and of
invasive procedures in patients with platelet disorders and/or thrombocytopaenia:
Guidelines of the Italian Society for Haemostasis and Thrombosis (SISET). Thromb
Res 2009;124:e13-e18.
36. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous
thrombolytic therapy for acute myocardial infarction: a quantitative review of 23
randomised trials. Lancet 2003;361:13-20.
37. Edmond JJ, Juergens CP, French JK. The pharmaco-invasive approach to STEMI:
when should fibrinolytic-treated patients go to the "cath lab"? Heart 2009;95:358-61.
59
38. Sutton AG, Campbell PG, Graham R, et al. A randomized trial of rescue
angioplasty versus a conservative approach for failed fibrinolysis in ST-segment
elevation myocardial infarction: the Middlesbrough Early Revascularization to Limit
INfarction (MERLIN) trial. J Am Coll Cardiol 2004;44:287-96.
39. Gershlick AH, Stephens-Lloyd A, Hughes S, et al. Rescue angioplasty after failed
thrombolytic therapy for acute myocardial infarction. N Engl J Med 2005;353:2758-
68.
40. Wijeysundera HC, Vijayaraghavan R, Nallamothu BK, et al. Rescue angioplasty
or repeat fibrinolysis after failed fibrinolytic therapy for ST-segment myocardial
infarction: a meta-analysis of randomized trials. J Am Coll Cardiol 2007;49:422-30.
41. Sohal M, Foo F, Sirker A, et al. Rescue angioplasty for failed fibrinolysis--long-
term follow-up of a large cohort. Catheter Cardiovasc Interv 2011;77:599-604.
42. Ko DT, Atzema CL, Donovan LR, et al. Rescue percutaneous coronary
interventions for failed fibrinolytic therapy in ST-segment elevation myocardial
infarction: A population-based study. Am Heart J 2011;161:764-70.e1.

60
PAPER 9
Reprinted from the Heart Lung and Circulation 2008;17:107-113 with
permission from Elsevier
OR
IGIN
AL
AR
TIC
LE
Original Article
Unfractionated Heparin Use After PercutaneousCoronary Intervention: Results of a Trial with a
Vascular Ultrasound EndpointCraig P. Juergens, FRACP a,∗, John A. Crozier, FRACS, DDU b,Jacqui T.C. Robinson, RN, RVT, AMS b, Sidney Lo, FRACP a,
John K. French, MBChB, PhD a and Dominic Y.C. Leung, MBBS, PhD a
a Department of Cardiology, Liverpool Hospital and University of NSW, Australiab Department of Vascular Surgery and Vascular Diagnostic Service, Liverpool Hospital, Australia
Background: Previous studies in the pre-stent era have evaluated the postprocedural use of unfractionated heparin(UFH) on clinically defined vascular complications and ischaemic cardiac complications. We prospectively evaluated thebenefits and risks of this practice, using vascular ultrasound determined endpoints in the current stent era.
Methods: Patients undergoing percutaneous coronary intervention (PCI) and enrolled in two of our previous routineand prospective vascular ultrasound studies were included in the analysis. Generally the decision to use UFH aftersheath removal was at the discretion of the operator, however a subset of patients was randomised to receive UFH ornuuve
eptf
im
K
I
Huaaoe
R2
∗HTE
©A
ot. Femoral vascular ultrasound was performed prior to hospital discharge and interpreted by an experienced vascularltrasonographer blinded to whether UFH was used or not. The primary endpoint was a composite of significant vascularltrasound determined complications including major haematoma, pseudoaneurysm, arterio-venous fistula, femoralenous or arterial thrombosis and retroperitoneal haemorrhage. Secondary endpoints included in hospital ischaemicvents, length of stay and outcome at 30 days.
Results: A total of 530 patients (43% receiving UFH) were included in the analysis. The incidence of the primaryndpoint for the entire population was 4.0% in both the UFH and no UFH groups (p = 1.00). In the 226 (43%), randomisedatient subset, the primary endpoint occurred in 5.2% in the UFH group and 4.5% in the no UFH group (p = 0.80). Time
o ambulation and discharge was similar in both groups. At 30 days, the incidence of major adverse cardiac events (4.7%or entire cohort) was similar in all groups whether randomised or not.
Conclusions: When vascular ultrasound is used to determine major vascular complications the use of UFH after PCIn the stent era was not associated with increased major vascular complications. We also failed to provide evidence of a
eaningful clinical benefit with the routine use of postprocedural heparin in this selected patient cohort.(Heart, Lung and Circulation 2008;17:107–113)
© 2007 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society of Australia andNew Zealand. Published by Elsevier Inc. All rights reserved.
eywords. Angioplasty; Complications; Unfractionated heparin
ntroduction
eparin use during urgent and elective percutaneouscoronary intervention (PCI) is well established. The
se of routine postprocedural intravenous unfraction-ted heparin (UFH) has been reported in between 39%nd 70% of interventions.1,2 Whilst this data is relativelyutdated, there is no more recent data to our knowl-dge reflecting current usage patterns. Three studies3–5
eceived 13 April 2007; received in revised form 17 July007; accepted 31 July 2007; available online 2 October 2007
Corresponding author at: Department of Cardiology, Liverpoolospital, Locked Bag 7103, Liverpool BC, NSW 1871, Australia.
el.: +61 2 9828 3078; fax: +61 2 9828 3054.-mail address: [email protected] (C.P. Juergens).
recruiting between 191 and 414 patients, have exam-ined the routine use of postprocedural UFH after PCI.Generally they have shown no reduction in ischaemicevents and an increase in bleeding complications. Nostudy routinely performed vascular ultrasound to ruleout subclinical vascular complications. These studies werepredominantly in the precoronary stent era, althoughone deployed stents in 34% of patients.5 As a conse-quence of earlier studies, the seventh ACCP conference onantithrombotic and thrombolytic therapy recommendedagainst a routine postprocedural infusion of heparin afteruncomplicated PCI.6 In contrast, the ACC/AHA/SCAIguideline update for percutaneous coronary interventiondoes not address the use of postprocedural heparin aftercoronary intervention.7 There is no data on the useful-
2007 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society ofustralia and New Zealand. Published by Elsevier Inc. All rights reserved.
1443-9506/04/$30.00doi:10.1016/j.hlc.2007.07.011

OR
IGIN
AL
AR
TIC
LE
108 Juergens et al. Heart, Lung and CirculationUnfractionated heparin use after percutaneous coronary intervention 2008;17:107–113
ness or otherwise of postprocedural UFH in the stentera, where thienopyridines are the mainstay of treatment.As the majority of patients are hospitalised overnightfollowing PCI, some operators may feel that UFH mayprevent an ‘after-hours’ stent thrombosis and the neces-sity to call back the interventional team and, with carefulmonitoring, is unlikely to be harmful. At the time ofconception of our study there was no consensus or guide-lines published about the use of postprocedural UFHafter PCI, so we aimed to determine the incidence ofvascular (using routine vascular ultrasound), bleedingand ischaemic (including stent thrombosis) complicationsassociated with the use or non-use of UFH after PCI in thestent era.
Materials and Methods
Patient SelectionFive hundred and thirty patients undergoing a PCIbetween February 1999 and January 2004 were enrolledin the study at our institution. Patients had been enrolledin our previously published studies comparing 6 Fr and 7Fr sheath size on the impact of vascular complications8 orpatient tolerance and resource implications of using theAngiosealTM or FemostopTM devices to facilitate vascu-lar closure after PCI.9 The decision to randomise a subsetof patients came after the other studies had commenced
suite at the end of the procedure. For those not receiv-ing an Angioseal, a dedicated angioplasty nurse removedsheaths during working hours according to our institu-tional policy. Outside of usual working hours, a cardiologytrainee removed the sheaths according to the same policy.Although UFH could be restarted after sheath removal atthe operator’s discretion, a subset of 226 (43%) patients,were randomised to either receive UFH or no UFH aftersheath removal via an opaque envelope system kept in thecatheterisation laboratory. If UFH was to be commenced,it was commenced three hours after sheath removal (with-out a bolus dose) and generally was continued until 6 a.m.the following morning. These patients, as well as thosereceiving glycoprotein IIb/IIIa infusions, were instructedto remain on bed rest overnight, otherwise patients weregenerally mobilised six hours after sheath removal accord-ing to our institutional policy.
All patients received at least 300 mg of aspirin in the 24hours prior to the procedure and a minimum of 100 mg perday after their procedure. Patients in whom intracoronarystents were placed received either ticlopidine (250 mg bid)or clopidogrel (75 mg daily) orally after loading doses of500 mg or 300 mg, respectively. For those not already on athienopyridine, the loading dose was administered imme-diately after the procedure and the maintenance dose wasgenerally continued for at least one month after the pro-cedure, although the referring cardiologist determined
with the first patient entered into the randomised sub-set in November 1999. The Institutional Committee onhuman research of our hospital approved the studies andall patients gave written informed consent.
Patients with cardiogenic shock, history of coagulopa-thy, requiring the sheath to be left in situ overnightor needing long-term warfarin therapy were excluded.Patients were only entered into the randomised subsetof the study if the operator felt there was no compellingindication to either prescribe postprocedural UFH (e.g.suboptimal angiographic result) or not prescribe heparin(e.g. use of glycoprotein IIb/IIIa inhibitors). Patients wereineligible if a vascular ultrasound could not be performedprior to hospital discharge.
Percutaneous Coronary InterventionPatients underwent PCI using standard techniques.Femoral arterial access was obtained based on anatomi-cal landmarks without routine fluoroscopic screening ofthe femoral head. A variety of operators, including cardi-ology trainees, obtained arterial access. Coronary arterystents (all bare metal stents) were implanted using stan-dard high-pressure techniques. Unfractionated heparinwas administered as boluses to maintain an activatedclotting time (ACT) greater than 250 s and glycoproteinIIb/IIIa inhibitors could be used at the operator’s discre-tion. For the majority of patients, the sheath was removedwith assisted manual compression using the FemostopTM
device when the ACT was less than 180 s. In the sub-set of patients who had been randomised to receive anAngiosealTM as part of our earlier study,9 the device wasdeployed using standard techniques in the angiography
duration of therapy.
Data Analysis and Follow-UpData were collected prospectively, by a dedicated angio-plasty research nurse, with respect to angiographic andprocedural success, together with time to initial haemosta-sis, ambulation and discharge. The attending physicianindependently made the decision regarding time of dis-charge. All patients were scheduled to undergo a duplexvascular ultrasound of the femoral access site the dayafter the procedure, reported by an experienced vascularsurgeon (JAC) who was blinded to treatment assign-ment. The sonographer performing the study was alsoblinded to treatment assignment. The presence of ahaematoma, pseudoaneurysm, arterio-venous fistula orfemoral venous or arterial thrombosis was noted. Thesubjects were also examined by our research nurse, forany clinical evidence of haematoma (nonpulsatile mass>1 cm in diameter) at the femoral access site or retroperi-toneal haemorrhage. The transfusion and haemoglobinlevels before and after the procedure were also collected.Creatine kinase (CK) and CK-MB measurements wereperformed routinely on all patients the morning after theprocedure and more frequently if there was a clinical sus-picion of an adverse cardiac event.
EndpointsPRIMARY ENDPOINT. The primary endpoint was a compositeof vascular ultrasound determined complications includ-ing major haematoma (defined as presence of ultrasoundevidence of haematoma with decrease in haemoglobin>20 g/L or transfusion or prolongation of hospital stay due

OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Juergens et al. 109
2008;17:107–113 Unfractionated heparin use after percutaneous coronary intervention
Table 1. Baseline Characteristics of the Entire Patient Population
Characteristics Heparin (n = 227) No Heparin (n = 303) p Value
Mean age (years ± S.D.) 60.1 ± 10.3 59.6 ± 11.3 0.61Male gender 159 (70%) 235 (78%) 0.05Hypertension 122 (54%) 168 (55%) 0.70Diabetes mellitus 64 (28%) 64 (21%) 0.06Current smoker 52 (23%) 72 (24%) 0.86Aspirin 217 (96%) 288 (95%) 0.77Thienopyridine—prior to PCIa 64 (28%) 53 (17%) <0.01Acute coronary syndrome 150 (66%) 221 (73%) 0.09Any stented vessel 212 (93%) 275 (91%) 0.27Glycoprotein IIb/IIIa receptor antagonist 3 (1%) 75 (25%) <0.001
a Four or more doses of clopidogrel or two or more doses of ticlopidine prior to PCI.
to haematoma), pseudoaneurysm, arterio-venous fistula,femoral venous or arterial thrombosis and retroperitonealhaemorrhage as determined by CT scan.
SECONDARY ENDPOINTS. The combined incidence of majoradverse cardiac events until Day 30 including cardiovascu-lar death, non-fatal myocardial infarction (MI) and urgenttarget vessel revascularisation were also recorded. Thediagnosis of MI was made if at least two out of threeof the following criteria were met: occurrence of typi-cal ischaemic chest pain lasting more than 30 minutes,abnormal Q waves not present on the baseline electro-cardiogram, or an increase in the CK concentration totwice the upper limit of normal with a concomitant risein the CK-MB isoenzyme above the upper limit of nor-mal. The diagnosis of recurrent myocardial infarction wasdetermined if there was an increase of more than 30% inthe CK concentration above baseline. If a patient reachedmore than one cardiac endpoint, a hierarchical approachwas applied using the most severe major adverse cardiacevent (MACE) for the final analysis. Occurrences of throm-botic stent occlusion (TSO), defined angiographically asocclusion of the stented segment, were also noted and inparticular, if this occurred during a UFH infusion.
A number of time endpoints were examined. Theseincluded: time to haemostasis, time to ambulation andtime to hospital discharge for each of the patient groups.
STars
variables were compared with Chi square test or Fischer’sexact test as appropriate. Continuous variables with anormal distribution were compared with unpaired Stu-dent’s t test. Statistical analysis was performed using SPSSfor Windows (version 14.0). Statistical significance wasdefined as a two-tailed p value of <0.05. Based on a sam-ple size of 530 patients and an expected event rate of 14%in the heparin group and 8% in the no heparin group [asobserved in the study of Rabah et al.3] our study wouldhave a power of 60% to detect a significant differencebetween groups at a two-tailed alpha of 0.05.
Results
During the course of the study 2280 patients underwentPCI at our institution of which 530 (23%) were enrolledin this study. Baseline clinical and antithrombotic detailsare shown in Tables 1 and 2. A subset of 226 patients (43%of the entire cohort) were randomised to receive UFH ornot after the procedure. There were slightly more patientspretreated with thienopyridines in the UFH group of theentire cohort but not in the randomised subset. The useof glycoprotein IIb/IIIa inhibitors was significantly less inthe UFH group of the non-randomised cohort.
Vascular ComplicationsThe FemostopTM device was successfully deployed inanpAe
T
C (n =
M ± 10.7M 6%)H 0%)D 3%)C 9%)A 3%)T 7%)A 1%)A 6%)G %)
a or to P
tatistical Analysishe data were analysed by intention to treat. We did sep-rate analyses for the entire patient cohort and for theandomised subset. All values are reported as mean ± onetandard deviation unless otherwise stated. Categorical
able 2. Baseline Characteristics of the Randomised Subset
haracteristics Heparin
ean age (years ± S.D.) 60.3ale gender 87 (7ypertension 58 (5iabetes mellitus 26 (2urrent smoker 33 (2spirin 107 (9hienopyridine—prior to PCIa 20 (1cute coronary syndrome 82 (7ny stented vessel 110 (9lycoprotein IIb/IIIa receptor antagonist 0 (0
Four or more doses of clopidogrel or two or more doses of ticlopidine pri
ll patients in whom it was used (472 out of 530) ando patients had an ipsilateral femoral venous sheathlaced during the PCI. In the remaining 58 patients, anngiosealTM was used to obtain haemostasis. Vascular
vents are shown in Tables 3 and 4. All but five patients
115) No Heparin (n = 111) p Value
60.7 ± 11 0.8180 (72%) 0.5566 (59%) 0.1726 (23%) 0.8827 (24%) 0.46
106 (95%) 0.4325 (23%) 0.3375 (68%) 0.5498 (88%) 0.04
1 (1%) 0.31
CI
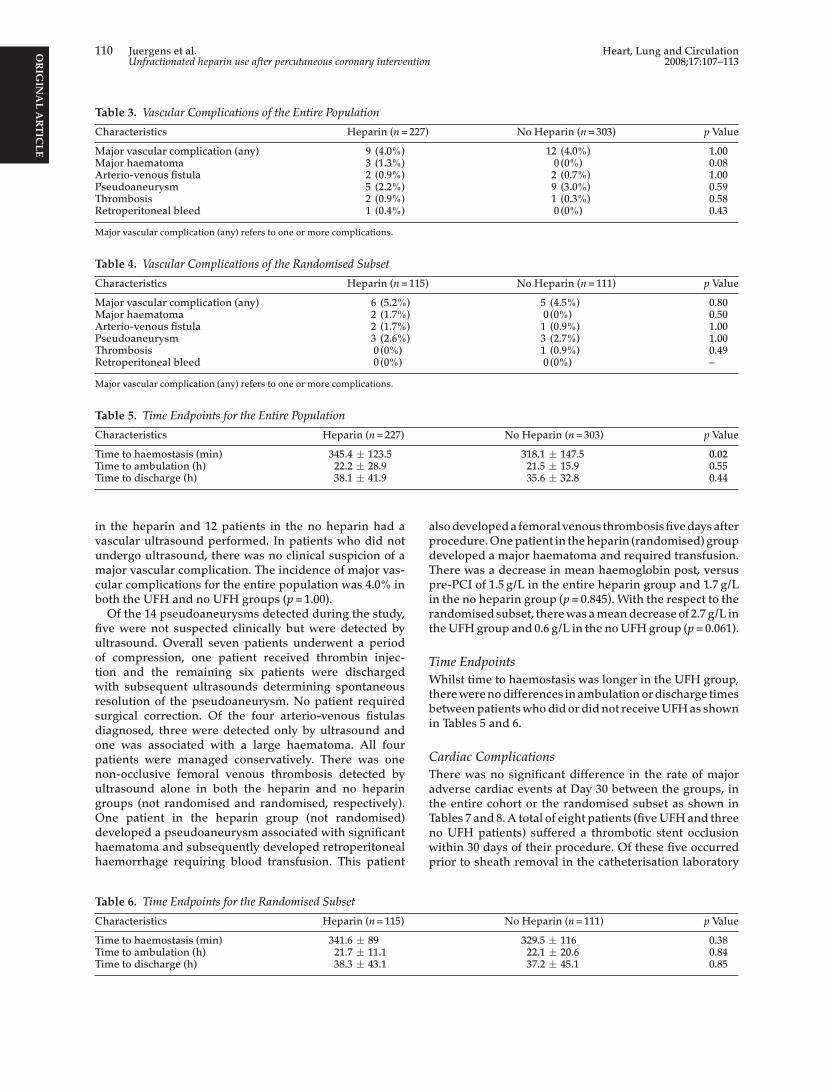
OR
IGIN
AL
AR
TIC
LE
110 Juergens et al. Heart, Lung and CirculationUnfractionated heparin use after percutaneous coronary intervention 2008;17:107–113
Table 3. Vascular Complications of the Entire Population
Characteristics Heparin (n = 227) No Heparin (n = 303) p Value
Major vascular complication (any) 9 (4.0%) 12 (4.0%) 1.00Major haematoma 3 (1.3%) 0 (0%) 0.08Arterio-venous fistula 2 (0.9%) 2 (0.7%) 1.00Pseudoaneurysm 5 (2.2%) 9 (3.0%) 0.59Thrombosis 2 (0.9%) 1 (0.3%) 0.58Retroperitoneal bleed 1 (0.4%) 0 (0%) 0.43
Major vascular complication (any) refers to one or more complications.
Table 4. Vascular Complications of the Randomised Subset
Characteristics Heparin (n = 115) No Heparin (n = 111) p Value
Major vascular complication (any) 6 (5.2%) 5 (4.5%) 0.80Major haematoma 2 (1.7%) 0 (0%) 0.50Arterio-venous fistula 2 (1.7%) 1 (0.9%) 1.00Pseudoaneurysm 3 (2.6%) 3 (2.7%) 1.00Thrombosis 0 (0%) 1 (0.9%) 0.49Retroperitoneal bleed 0 (0%) 0 (0%) –
Major vascular complication (any) refers to one or more complications.
Table 5. Time Endpoints for the Entire Population
Characteristics Heparin (n = 227) No Heparin (n = 303) p Value
Time to haemostasis (min) 345.4 ± 123.5 318.1 ± 147.5 0.02Time to ambulation (h) 22.2 ± 28.9 21.5 ± 15.9 0.55Time to discharge (h) 38.1 ± 41.9 35.6 ± 32.8 0.44
in the heparin and 12 patients in the no heparin had avascular ultrasound performed. In patients who did notundergo ultrasound, there was no clinical suspicion of amajor vascular complication. The incidence of major vas-cular complications for the entire population was 4.0% inboth the UFH and no UFH groups (p = 1.00).
Of the 14 pseudoaneurysms detected during the study,five were not suspected clinically but were detected byultrasound. Overall seven patients underwent a periodof compression, one patient received thrombin injec-tion and the remaining six patients were dischargedwith subsequent ultrasounds determining spontaneousresolution of the pseudoaneurysm. No patient requiredsurgical correction. Of the four arterio-venous fistulasdiagnosed, three were detected only by ultrasound andone was associated with a large haematoma. All fourpatients were managed conservatively. There was onenon-occlusive femoral venous thrombosis detected byultrasound alone in both the heparin and no heparingroups (not randomised and randomised, respectively).One patient in the heparin group (not randomised)developed a pseudoaneurysm associated with significanthaematoma and subsequently developed retroperitonealhaemorrhage requiring blood transfusion. This patient
also developed a femoral venous thrombosis five days afterprocedure. One patient in the heparin (randomised) groupdeveloped a major haematoma and required transfusion.There was a decrease in mean haemoglobin post, versuspre-PCI of 1.5 g/L in the entire heparin group and 1.7 g/Lin the no heparin group (p = 0.845). With the respect to therandomised subset, there was a mean decrease of 2.7 g/L inthe UFH group and 0.6 g/L in the no UFH group (p = 0.061).
Time EndpointsWhilst time to haemostasis was longer in the UFH group,there were no differences in ambulation or discharge timesbetween patients who did or did not receive UFH as shownin Tables 5 and 6.
Cardiac ComplicationsThere was no significant difference in the rate of majoradverse cardiac events at Day 30 between the groups, inthe entire cohort or the randomised subset as shown inTables 7 and 8. A total of eight patients (five UFH and threeno UFH patients) suffered a thrombotic stent occlusionwithin 30 days of their procedure. Of these five occurredprior to sheath removal in the catheterisation laboratory
Table 6. Time Endpoints for the Randomised Subset
Characteristics Heparin (n = 115)
Time to haemostasis (min) 341.6 ± 89Time to ambulation (h) 21.7 ± 11.1Time to discharge (h) 38.3 ± 43.1
No Heparin (n = 111) p Value
329.5 ± 116 0.3822.1 ± 20.6 0.8437.2 ± 45.1 0.85

OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Juergens et al. 111
2008;17:107–113 Unfractionated heparin use after percutaneous coronary intervention
Table 7. Cardiac Events at Day 30 for Entire Population
Heparin (n = 227) No Heparin (n = 303) p Value
Cardiovascular death 1 (0%) 0 (0%) 0.43Non-fatal MI 6 (2.6%) 11 (3.6%) 0.52Urgent TVR 5 (2.2%) 3 (1.0%) 0.30
MACE 11 (4.8%) 14 (4.6%) 0.90Thrombotic stent occlusion 5 (2.2%) 3 (1.0%) 0.30
MACE: major adverse cardiac event; MI: myocardial infarction; TVR: target vessel revascularisation
Table 8. Cardiac Events at Day 30 for Randomised Subset
Heparin (n = 115) No Heparin (n = 111) p Value
Cardiovascular death 0 (0%) 0 (0%) –Non-fatal MI 2 (1.7%) 3 (2.7%) 0.68Urgent TVR 3 (2.6%) 0 (0%) 0.25
MACE 5 (4.3%) 3 (2.7%) 0.72Thrombotic stent occlusion 3 (2.6%) 0 (0%) 0.25
MACE: major adverse cardiac event; MI: myocardial infarction; TVR: target vessel revascularisation.
recovery area. A further patient had an event four daysafter their procedure when they were no longer receivingUFH. One patient developed chest pain with ECG changesovernight whilst still on an UFH infusion and angiographyconfirmed stent thrombosis. The final patient experiencedstent occlusion 2.3 hours after the cessation of their UFHinfusion, the morning after the procedure.
Entire Cohort Without IIb/IIIa UseAs UFH is generally not prescribed in conjunction withglycoprotein IIb/IIIa antagonists after PCI, we performeda secondary analysis of the entire cohort after excludingthese patients. After excluding patients receiving glyco-protein IIb/IIIa antagonists there were 228 patients whodid not receive UFH after their PCI and 223 who did.The time to haemostasis was longer in the UFH groupwhen compared to the no UFH group (344 ± 134 minversus 313 ± 141 min; p = 0.012). The mean decrease inhaemoglobin after the procedure was not significantly dif-ferent in this subset of patients; 1.4 g/L in the UFH groupand 1.2 g/L in the no UFH group (p = 0.743). The incidenceof any major vascular complications was 3.1% (7 out of 228)in the no UFH group and 3.6% (8 out of 228) in the UFHgroup (p = 0.76). Any MACE occurred in 3.5% (8 out of 228)of the no UFH group and 4.3% (10 out of 223) of the UFHgroup (p = 0.60).
D
WcPdhterc
A
therapy recommended against a routine postproce-dural infusion of heparin after uncomplicated PCI,6
although this recommendation was based on earlier stud-ies performed in the pre-stent era. In contradistinctionthe ACC/AHA/SCAI guideline update for percutaneouscoronary intervention does not address the use of post-procedural heparin after coronary intervention.7 In thenon-randomised cohort of our study the operator choseto prescribe UFH in 36% of patients, a frequency similarto that reported by Juran et al.1 Patients were enrolled inour study prior to the first published guidelines which sug-gested that this practice is not recommended and whilst,in retrospect, we have potentially addressed an outdatedpractice our results have added significantly to the bodyof evidence assessing this therapeutic intervention.
In contrast to earlier studies3–5 performed in the pre-dominantly pre-stent era we found that the routine use ofpostprocedural UFH after PCI did not result in an increasein major vascular/bleeding complications. Whilst the ear-lier studies concluded there were increased bleedingcomplications these appeared to be only in haematomas,as the only study to fully define such complications,3 con-cluded there was no increase in major bleeding or vascularinjury in the postprocedural UFH group with an inci-dence of 1% in each group. In our randomised subset weobserved an incidence of major vascular complications of5.2% and 4.5% in the UFH and no UFH groups, respec-t0tmaccsvgnoa
iscussion
e have reported ultrasound determined vascular out-omes with respect to the use of postprocedural UFH afterCI, including almost half the patients who were ran-omised to this treatment strategy. As the entire cohortad been prospectively enrolled into randomised con-
rolled trials with similar endpoints, we have analysed thentire group, in order to increase the studies power, withespect to the use or non-use of postprocedural UFH afteroronary intervention in the stenting era.
Subsequent to the conception of our study the seventhCCP conference on antithrombotic and thrombolytic
ively, an apparently high incidence when compared to the.3–6% incidence quoted in other coronary interventionrials.3,10–13 This difference is most likely due to ascertain-
ent bias through the routine use of vascular ultrasounds part of our study. The majority of patients were managedonservatively as approximately half of the major vascularomplications identified in our study were not clinicallyuspected and were only detected by protocol mandatedascular ultrasound. No patient in our study required sur-ical repair of his or her vascular complication whereas theeed for surgical repair of vascular complications in previ-us series has ranged from 0.7–3.8%.10–13 We did observetrend to a greater fall in postprocedural haemoglobin in

OR
IGIN
AL
AR
TIC
LE
112 Juergens et al. Heart, Lung and CirculationUnfractionated heparin use after percutaneous coronary intervention 2008;17:107–113
the randomised UFH subset suggesting there may havebeen a difference in more minor bleeding, which we didnot specifically measure. A similar finding was noted inthe study of Rabah et al.3
We observed a delay in the time to haemostasis in theUFH group of the entire cohort. There was a higher use ofthienopyridines prior to the coronary intervention in thisgroup, although this difference would have been counter-acted by the higher use of glycoprotein IIb/IIIa inhibitorsin the no UFH group. It is important to note however, thatthis difference in time to haemostasis was not observed inthe randomised subset and did not translate into a delayto time to ambulation or discharge in the entire cohort.
Whilst our study suggests no significant hazard withrespect to vascular/bleeding complications by the routineuse of postprocedural UFH, there did not appear to beany benefit either with respect to a reduction in majorischaemic cardiac events. This is consistent with the ear-lier studies3–5 in the predominantly pre-stent era whichalso found no reduction in major adverse cardiac eventsthrough the routine use of UFH after the procedure. Whilstour study is underpowered to detect a likely impact ofthe use of UFH on the incidence of stent thrombosis, it isimportant to note that of the eight thrombotic stent occlu-sions we observed, five occurred prior to sheath removaland one occurred whilst on a heparin infusion suggest-ing it is unlikely the short-term use of UFH will reduce
are removed using closure devices or pure manual com-pression. Nevertheless our earlier study of 115 patients,9
which constitutes a subset of the current study, sug-gested no difference in vascular events between using theAngiosealTM or FemostopTM devices to facilitate vascularclosure.
Because of the observed event rates of major vascu-lar complications, our study is underpowered for theprimary and secondary endpoints and a larger samplesize may have discerned clinically meaningful differencesbetween the two UFH use strategies. Many patients werenot entered into the randomised subset because of the useof glycoprotein IIb/IIIa inhibitors, however when thesepatients were excluded and re-analysis performed, weobserved a similar incidence of the primary endpoint inboth the UFH and no UFH groups in this larger sub-group. Our dedicated research nurse who collected thedata could not be blinded to treatment assignment withrespect to UFH use and unappreciated bias may have beenpresent with respect to clinical endpoints. However theinterpretation of vascular ultrasounds was blinded whichstrengthens our primary endpoint conclusions.
Conclusions
This prospective trial indicates no increase in majorperipheral vascular complications when UFH is used rou-tinely after stent era PCI and routine after the procedure
the probability of this outcome. Our observed MACE ratewas quite low probably reflecting an element of selectionbias as only 23% of patients undergoing PCI were enteredinto the study. We cannot exclude the possibility of sometreatment benefit of heparin in a higher risk cohort, asother investigators have addressed the use of enoxaparinfor up to two weeks after high-risk coronary stenting andsuggested some clinical benefit in terms of a reduction inmajor adverse cardiac events.14,15
LimitationsOur results are applicable to a single centre in which multi-ple operators are performing PCIs in a patient populationwith no defined indication for postprocedural anticoag-ulation with UFH. Only 43% of our patients underwentrandomisation with respect to UFH use and a selectionbias in the non-randomised cohort cannot be excluded.The use of glycoprotein IIb/IIIa inhibitors was higher inthe non-randomised cohort due to our protocol of notcombining UFH infusions with these agents after the pro-cedure. All stents deployed were bare metal so our resultsmay not apply in the drug eluting era. However as wewere only investigating the short-term use of UFH, it isunlikely drug eluting stents would influence the outcome.The majority of patients were not pretreated with a load-ing dose of thienopyridines so the results with respect tovascular/bleeding complications could be different withroutine pretreatment with clopidogrel.
Vascular closure devices were used infrequently in thisstudy, with the majority of sheaths removed with assistedmanual compression using the FemostopTM device. Con-sequently our results may not be applicable where sheaths
vascular ultrasound is performed to determine complica-tions. Unfractionated heparin use however did not appearto reduce the risk of major adverse cardiac events in thisselected patient cohort. The choice to recommence UFHor not after coronary intervention should be determinedby individual patient factors, such as the need for long-term anticoagulation, and not on a perceived impact onvascular complications or ischaemic complications of theintervention.
Acknowledgement
The authors would like to thank Ms. Adelina Wong for herenormous assistance in the collection of data for this study.
References
1. Juran NB, Smith DD, Rouse CL, DeLuca SA, Rund M, theSANDBAG Nursing coordinators. Survey of current practicepatterns for percutaneous transluminal coronary angioplasty.Am J Crit Care 1996;5:442–8.
2. Ferguson JJ, Dohmen P, Wilson JM, Vaughn WK, KhoshnevisR, Kmonicek P, McKinney AA, Plachetka JR. Results of anational survey on anticoagulation for PTCA. J Invas Cardiol1995;7:136–41.
3. Rabah M, Mason D, Muller DWM, Hundley R, KugelmassAD, Weiner B, Cannon L, O’Neill WW, Safian RD. Heparinafter percutaneous coronary intervention (HAPI): a prospec-tive multicentre randomized trial of three heparin regimensafter successful coronary intervention. J Am Coll Cardiol1999;34:461–7.
4. Friedman HZ, Cragg DR, Glazier SM, Ganadharan V,Marsalese DL, Screiber TL, O’Neill WW. Randomizedprospective evaluation of prolonged versus abbreviated intra-

OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Juergens et al. 113
2008;17:107–113 Unfractionated heparin use after percutaneous coronary intervention
venous heparin therapy after coronary angioplasty. J Am CollCardiol 1994;24:1214–9.
5. Garachemani AR, Kaufmann U, Fleisch M, Meier B. Pro-longed heparin after uncomplicated coronary interventions:a prospective randomized trial. Am Heart J 1998;136:352–6.
6. Popma JJ, Berger P, Ohman EM, Harrington RA, Grines C,Weitz JI. Antithrombotic therapy during percutaneous coro-nary intervention. Chest 2004;126:576S–99S.
7. Smith SC, Feldman TE, Hirshfeld JW, Jacobs AK, Kern MJ,King SB, Morrison DA, O’Neill WW, Schaff HV, Whitlow PL,William DO. ACC/AHA/SCAI 2005 guideline update for per-cutaneous coronary intervention-summary article. J Am CollCardiol 2006;47:216–35.
8. Juergens CP, Hallani H, Leung DYC, Crozier JA, RobinsonJTC, Lo S, Hopkins AP. Comparison of 6 and 7 French guid-ing catheters for percutaneous coronary intervention: resultsof a randomized trial with a vascular ultrasound endpoint.Catheter Cardiovasc Interv 2005;66:528–34.
9. Juergens CP, Leung DYC, Crozier JA, Wong AM, RobinsonJTC, Lo S, Kachwalla H, Hopkins AP. Patient tolerance andresource utilization associated with an arterial closure versusan external compression device after percutaneous coronaryintervention. Catheter Cardiovasc Interv 2004;63:166–70.
10. Applegate RJ, Grabarczyk MA, Little WC, Craven T, WalkupM, Kahl FR, Braden GA, Rankin KM, Kutcher MA. Vascularclosure devices in patients treated with anticoagulation and
IIb/IIIa receptor inhibitors during percutaneous revascular-ization. J Am Coll Cardiol 2002;40:78–83.
11. Johnson LW, Esente P, Giambartolomei A, Grant WD, LoinM, Reger MJ, Shaw C, Walford GD. Peripheral vascu-lar complications of coronary angioplasty by the femoraland brachial techniques. Cathet Cardiovasc Diagn 1994;31:165–72.
12. Muller DWM, Shamir KJ, Ellis SG, Topol EJ. Peripheralvascular complications after conventional and complex per-cutaneous coronary interventional procedures. Am J Cardiol1992;69:63–8.
13. Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, vander Wieken R. A randomized comparison of percutaneoustransluminal coronary angioplasty by the radial, brachialand femoral approaches: the access study. J Am Coll Cardiol1997;29:1269–75.
14. Batchelor WB, Mahaffey KW, Berger PB, Deutsch E, MeierS, Hasselblad V, Fry ET, Teirstein PS, Ross AM, Binanay CA,Zidar JP, on behalf of the ATLAST trial investigators. A ran-domized, placebo controlled trial of enoxaparin after highrisk coronary stenting: the ATLAST trial. J Am Coll Cardiol2001;38:1608–13.
15. Daoulah A, Segev A, Leblanc K, Chisholm RJ, Strauss BH.Postprocedural low molecular weight heparin in patients athigh risk of subacute stent thrombosis. Cardiovasc Radiat Med2003;4:182–5.

61
PAPER 10
Reprinted from the American Heart Journal 2004;147:e15 with
permission from Elsevier
AasCSL
Bsep
Mtd
Rdate
Crot
vnIperuwwwatb
FSRLE0©d
randomized comparison of clopidogrel andspirin versus ticlopidine and aspirin after coronarytent implantation
raig P. Juergens, MBBS, Adelina M. Wong, MClinPrac, Dominic Y. C. Leung, PhD, Harry C. Lowe, PhD,idney Lo, MBBS, Clyne Fernandes, MBBS, Elizabeth F. Newland, BHlthSc, and Andrew P. Hopkins, MBBSiverpool, Australia
ackground The combination of a thienopyridine and aspirin has become the standard of care after intracoronarytenting. Clopidogrel appears to be better tolerated than ticlopidine but may be associated with more adverse cardiacvents. We assessed the tolerability and efficacy of 2 weeks of therapy with ticlopidine and aspirin in comparison to clo-idogrel and aspirin after coronary stent implantation.
ethods Patients with successful intracoronary stent implantation at our institution were randomly assigned, in addi-ion to aspirin, to receive either ticlopidine or clopidogrel. Loading doses were administered immediately after the proce-ure, and the drugs were continued for 2 weeks.
esults Three hundred seven patients were randomly assigned: 154 patients to clopidogrel and 153 to the ticlopi-ine group. The primary end point of early drug discontinuation occurred in 5 patients (3.3%) in the ticlopidine groupnd 1 patient (0.6%) in the clopidogrel group (P � .121). Within 30 days, thrombotic stent occlusion occurred in 1 pa-
ient (0.7%) in the ticlopidine group and 3 patients (1.9%) in the clopidogrel group (P � .623). A major adverse cardiacvent occurred in 3 patients (�1.9%; P � 1.00) in each group.
onclusions There was a nonsignificant trend to improved tolerability of a 2-week regimen of clopidogrel and aspi-in when compared with ticlopidine and aspirin in patients undergoing intracoronary stent implantation. The combinationf clopidogrel and aspirin results in a comparably low incidence of major adverse cardiac events when compared with
iclopidine and aspirin. (Am Heart J 2004;147:e15.)
comttstot
lCtdEdbslna
Intracoronary stenting is an accepted treatment foressel closure after percutaneous transluminal coro-ary angioplasty (PTCA)1,2 and to reduce restenosis.3,4
nitially, thrombotic occlusion of the stent, as well aseripheral vascular complications and hemorrhagicvents related to the use of aggressive anticoagulationegimes, limited the benefits of coronary stenting. These of the antiplatelet regime of ticlopidine and aspirinas shown to be superior to anticoagulation therapy,ith less stent thrombosis and bleeding events,5–8
hen optimal stent deployment methods are used. Asconsequence of these landmark studies, the use of
iclopidine and aspirin after coronary stent placementecame standard practice. However, because of con-
rom the Department of Cardiology, Liverpool Hospital, Liverpool, Australia.ubmitted June 24, 2003; accepted October 29, 2003.eprint requests: Craig Juergens, MBBS, Department of Cardiology, Liverpool Hospital,ocked Bag 7103, Liverpool BC NSW 1871, Australia.-mail: [email protected]/$ - see front matter2004, Elsevier Inc. All rights reserved.
coi:10.1016/j.ahj.2003.10.040
erns of potentially life-threatening neutropenia, whichccurs in approximately 1% of patients treated forore than 2 weeks with ticlopidine, a number of cen-
ers, including our own, adopted a strategy of discon-inuing therapy 2 weeks after stent placement. A sub-equent study of more than 800 patients suggestedhat this could be done relatively safely, with no casef stent thrombosis observed after ticlopidine cessa-ion at 14 days.9
Clopidogrel is a thienopyridine derivative closely re-ated to ticlopidine in chemical structure and function.lopidigrel has been compared with aspirin in more
han 19,000 patients with vascular disease in the clopi-ogrel versus Aspirin in Patients at Risk of Ischaemicvents (CAPRIE) study.10 In this study, clopidogrel re-uced the frequency of adverse cardiovascular eventsy 8.7% when compared with aspirin therapy. Theide effect profile of clopidogrel and aspirin was simi-ar, and, notably, there was no increase in neutrope-ia. With the widespread availability of clopidogrelnd better tolerability, many interventional cardiology
enters changed to a regime of clopidogrel and aspirin
ipdapttatireeawwd
MP
dtepddncopms
S
smpctbPctmAhd
E
wr
bbf
pai(omtlnwuttsmwrgafio
tccpp
S
cddPmouaw
R
iwtpgwgchsirpt
American Heart JournalApril 2004
K2 Juergens et al
n their post–coronary stenting cases. This change ofractice occurred largely before the publication of ran-omized, controlled trials comparing ticlopidine andspirin with clopidogrel and aspirin in this group ofatients. Subsequently, 2 large-scale, randomized, con-rolled clinical trials11,12 concluded that 1 month ofherapy with clopidogrel and aspirin was better toler-ted when compared with 1 month of therapy withiclopidine and aspirin in patients who had undergonentracoronary stent placement. However, both studiesevealed a higher number of major adverse cardiacvents in the clopidogrel groups, although the differ-nces were not statistically significant. Our trial evalu-ted the tolerability and efficacy of 14 days of therapyith ticlopidine in combination with aspirin comparedith clopidogrel and aspirin in patients who had un-ergone successful intracoronary stenting.
ethodsatient populationPatients in whom intracoronary stents were successfully
eployed (�30% residual stenosis without acute complica-ions in the catheterization laboratory resulting in death ormergency bypass surgery) at our institution were eligible toarticipate in this trial. Cardiogenic shock; unsuccessful stenteployment; known allergy to aspirin, ticlopidine, or clopi-ogrel; recent treatment with clopidogrel or ticlopidine; andeed for anticoagulants after the procedure were exclusionriteria. The institutional committee on human research ofur hospital approved the study. At the end of a successfulrocedure, patients were randomly assigned in an open-labelanner to receive clopidogrel or ticlopidine by means of a
ealed envelope system.
tents and antiplatelet regimensStents were implanted with the use of standard high-pres-
ure techniques. Heparin was administered as boluses toaintain an activated clotting time �250 seconds, and glyco-rotein IIb/IIIa inhibitors could be used at the operator’s dis-retion. The sheath was removed after the procedure whenhe activated clotting time was �180 seconds. Heparin coulde restarted after sheath removal at the operator’s discretion.atients were assigned to receive ticlopidine (250 mg bid) orlopidogrel (75 mg pd) orally for 14 days. The first dose oficlopidine (500 mg) or clopidogrel (150 mg) was given im-ediately after the procedure. Treatment was not blinded.ll patients received at least 300 mg of aspirin in the 24ours before the procedure and a minimum of 100 mg peray for the duration of the study.
nd pointsThe primary end point was the failure to complete 2eeks of initiated thienopyridine in combination with aspi-
in. The reason for discontinuation was noted.Secondary end points included hemorrhage (defined as
leeding complications requiring surgery or transfusion orleeding associated with objective evidence of organ dys-
unction); vascular end points (false aneurysms, surgical re- cair of puncture site complications or arteriovenous fistulae),nd the combined incidence of major adverse cardiac eventsncluding cardiovascular death, nonfatal myocardial infarctionMI), and urgent target vessel revascularization. The diagnosisf MI was made if at least 2 of 3 the following criteria wereet: occurrence of typical ischemic chest pain lasting more
han 30 minutes, abnormal Q waves not present on the base-ine electrocardiogram, or an increase in the creatinine ki-ase (CK) concentration to twice the upper limit of normalith a concomitant rise in the CK-MB isoenzyme above thepper limit of normal. The diagnosis of recurrent MI was de-ermined if there was an increase of �30% in the CK concen-ration above baseline. Creatinine kinase (and CK-MB) mea-urements were performed routinely on all patients theorning after the procedure and more frequently if thereas a clinical suspicion of an adverse cardiac event. Occur-
ences of thrombotic stent occlusion (TSO), defined angio-raphically as total occlusion of the stented segment, werelso noted. Routine full blood count analysis was not per-ormed as part of the trial after hospital discharge, but whenncidental blood tests were performed, we endeavored tobtain the result to ascertain any adverse hematologic events.If a patient reached more than 1 cardiac end point, only
he most severe end point was counted as a major adverseardiac event (MACE) for the final analysis. Patients wereontacted by telephone at 2 weeks and 4 weeks to assess theresence of any adverse events. MACE were verified by inde-endent chart review.
tatistical analysisThe study size was planned on the basis of estimated dis-
ontinuation rate of 9% for ticlopidine and 3% for clopi-ogrel; a sample size of 140 patients in each group was pre-icted to show a 67% relative difference, with 90% power.roportions were compared between treatment groups byeans of �2 or Fisher exact test where appropriate. Continu-
us variables in each group where compared by means of annpaired Student t test. Statistical significance was defined as2-tailed P value of �.05. Statistical analysis was performedith SPSS for Windows (version 10).
esultsAmong 307 patients who underwent successful stent
mplantation from July 1999 until January 2001, 153ere randomly assigned to receive ticlopidine and 154
o receive clopidogrel. Baseline characteristics of theatient population are shown in Tables I whilst IIives details on stent and angiographic data. Thereere no significant differences between treatment
roups with respect to demographic or lesion subsetharacteristics. The patient cohort was a relativelyigh-risk one, with a high percentage of patients pre-enting with acute coronary syndromes and the major-ty of lesions either type B2 or C. Intravenous glycop-otein IIb/IIIa antagonists were used in 23% of theatients receiving ticlopidine and 25% of patients inhe clopidogrel group. Abciximab, administered in the
ardiac catheterization laboratory, was the most fre-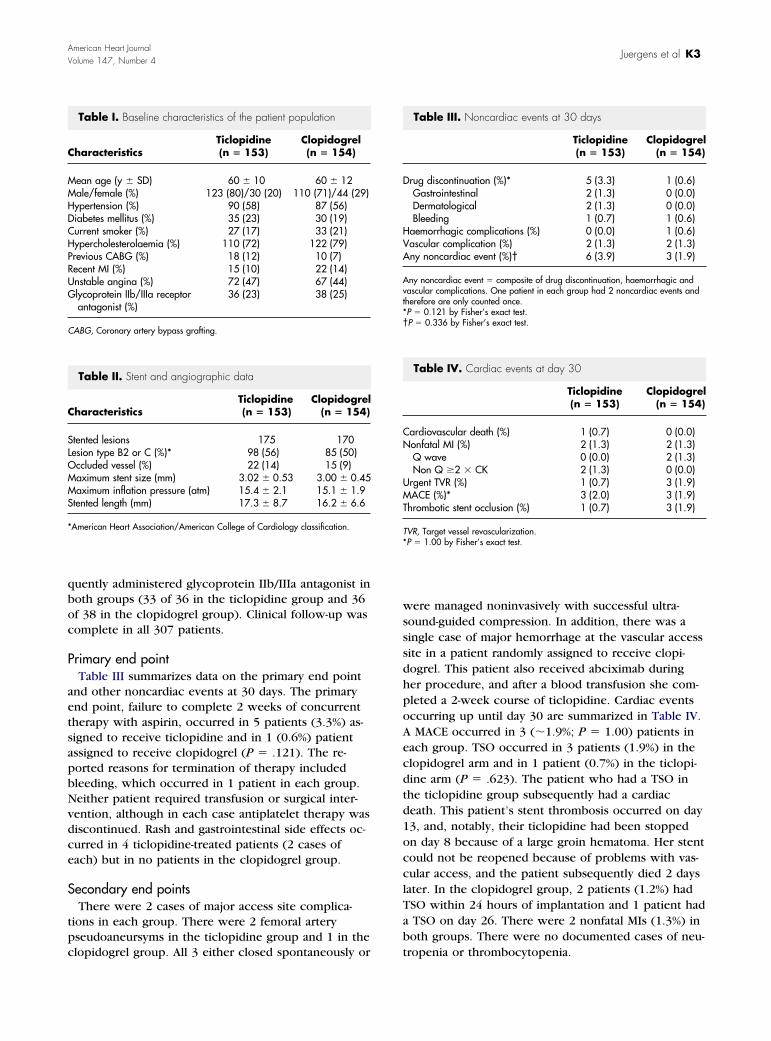
qboc
P
aetsapbNvdce
S
tpc
wsssdhpoAecdtd1occlTab
D
HVA
Avt*†
CN
UMT
T*
C
MMHDCHPRUG
C
C
SLOMMS
*
American Heart JournalVolume 147, Number 4
Juergens et al K3
uently administered glycoprotein IIb/IIIa antagonist inoth groups (33 of 36 in the ticlopidine group and 36f 38 in the clopidogrel group). Clinical follow-up wasomplete in all 307 patients.
rimary end pointTable III summarizes data on the primary end point
nd other noncardiac events at 30 days. The primarynd point, failure to complete 2 weeks of concurrentherapy with aspirin, occurred in 5 patients (3.3%) as-igned to receive ticlopidine and in 1 (0.6%) patientssigned to receive clopidogrel (P � .121). The re-orted reasons for termination of therapy includedleeding, which occurred in 1 patient in each group.either patient required transfusion or surgical inter-ention, although in each case antiplatelet therapy wasiscontinued. Rash and gastrointestinal side effects oc-urred in 4 ticlopidine-treated patients (2 cases ofach) but in no patients in the clopidogrel group.
econdary end pointsThere were 2 cases of major access site complica-
ions in each group. There were 2 femoral arteryseudoaneursyms in the ticlopidine group and 1 in the
Table I. Baseline characteristics of the patient population
haracteristicsTiclopidine(n � 153)
Clopidogrel(n � 154)
ean age (y � SD) 60 � 10 60 � 12ale/female (%) 123 (80)/30 (20) 110 (71)/44 (29)ypertension (%) 90 (58) 87 (56)iabetes mellitus (%) 35 (23) 30 (19)urrent smoker (%) 27 (17) 33 (21)ypercholesterolaemia (%) 110 (72) 122 (79)revious CABG (%) 18 (12) 10 (7)ecent MI (%) 15 (10) 22 (14)nstable angina (%) 72 (47) 67 (44)lycoprotein IIb/IIIa receptorantagonist (%)
36 (23) 38 (25)
ABG, Coronary artery bypass grafting.
Table II. Stent and angiographic data
haracteristicsTiclopidine(n � 153)
Clopidogrel(n � 154)
tented lesions 175 170esion type B2 or C (%)* 98 (56) 85 (50)ccluded vessel (%) 22 (14) 15 (9)aximum stent size (mm) 3.02 � 0.53 3.00 � 0.45aximum inflation pressure (atm) 15.4 � 2.1 15.1 � 1.9
tented length (mm) 17.3 � 8.7 16.2 � 6.6
American Heart Association/American College of Cardiology classification.
lopidogrel group. All 3 either closed spontaneously or t
ere managed noninvasively with successful ultra-ound-guided compression. In addition, there was aingle case of major hemorrhage at the vascular accessite in a patient randomly assigned to receive clopi-ogrel. This patient also received abciximab duringer procedure, and after a blood transfusion she com-leted a 2-week course of ticlopidine. Cardiac eventsccurring up until day 30 are summarized in Table IV.MACE occurred in 3 (�1.9%; P � 1.00) patients in
ach group. TSO occurred in 3 patients (1.9%) in thelopidogrel arm and in 1 patient (0.7%) in the ticlopi-ine arm (P � .623). The patient who had a TSO inhe ticlopidine group subsequently had a cardiaceath. This patient’s stent thrombosis occurred on day3, and, notably, their ticlopidine had been stoppedn day 8 because of a large groin hematoma. Her stentould not be reopened because of problems with vas-ular access, and the patient subsequently died 2 daysater. In the clopidogrel group, 2 patients (1.2%) hadSO within 24 hours of implantation and 1 patient hadTSO on day 26. There were 2 nonfatal MIs (1.3%) inoth groups. There were no documented cases of neu-
Table III. Noncardiac events at 30 days
Ticlopidine(n � 153)
Clopidogrel(n � 154)
rug discontinuation (%)* 5 (3.3) 1 (0.6)Gastrointestinal 2 (1.3) 0 (0.0)Dermatological 2 (1.3) 0 (0.0)Bleeding 1 (0.7) 1 (0.6)
aemorrhagic complications (%) 0 (0.0) 1 (0.6)ascular complication (%) 2 (1.3) 2 (1.3)ny noncardiac event (%)† 6 (3.9) 3 (1.9)
ny noncardiac event � composite of drug discontinuation, haemorrhagic andascular complications. One patient in each group had 2 noncardiac events andherefore are only counted once.P � 0.121 by Fisher’s exact test.P � 0.336 by Fisher’s exact test.
Table IV. Cardiac events at day 30
Ticlopidine(n � 153)
Clopidogrel(n � 154)
ardiovascular death (%) 1 (0.7) 0 (0.0)onfatal MI (%) 2 (1.3) 2 (1.3)Q wave 0 (0.0) 2 (1.3)Non Q �2 � CK 2 (1.3) 0 (0.0)
rgent TVR (%) 1 (0.7) 3 (1.9)ACE (%)* 3 (2.0) 3 (1.9)
hrombotic stent occlusion (%) 1 (0.7) 3 (1.9)
VR, Target vessel revascularization.P � 1.00 by Fisher’s exact test.
ropenia or thrombocytopenia.

D
taaewalras1rowsisdstsocsttws
�rTvshgrcddicsdtsopiepia
noewbwpisepturg(
tvtaiotal3dtronot
pcdsnaCvrrpgfittbmb
American Heart JournalApril 2004
K4 Juergens et al
iscussionThis single-center study provides further evidence
hat clopidogrel and aspirin is at least as well tolerateds combination therapy with ticlopidine and aspirin. Inddition, we found no significant increase in cardiacvents in the patients receiving clopidogrel and aspirinhen compared with the group receiving ticlopidine
nd aspirin. The need to discontinue study drug wasower in our study than in the larger Clopidogrel Aspi-in Stent International Cooperative Study (CLASSICS)11
nd Muller et al12 studies. Only 3.3% of patients in ourtudy stopped taking ticlopidine before the prescribed4 days of this study compared with 8.2% and 5.8%,espectively, in the aforementioned studies. Similarly,nly 0.6% of our patients stopped taking clopidogrelhen compared with 2% to 5.1% in the CLASSICS
tudy and 2.0% in the Muller study. This is not surpris-ng, given the fact that our patients were asked to taketudy drug for 14 days in our study compared with 28ays in the larger studies. Although not statisticallyignificant in our study, the trend to more discontinua-ions of ticlopidine is consistent across all studies. Atudy by Taniuchi,13which was similar in design to ourwn, compared 2 weeks of therapy with ticlopidine orlopidogrel in combination with aspirin in a broad sub-et of patients undergoing intracoronary stent implan-ation. Their reported incidence of drug discontinua-ion, 3.6% with ticlopidine and 1.6% with clopidogrel,as similar to our study, probably reflecting the
horter duration of therapy.The incidence of TSO was low in our study, at2.0% in both groups, which is consistent with that
eported in other studies of antiplatelet agents.5–8,12,13
here were 3 (1.9%) TSOs in the clopidogrel groupersus 1 (0.7%) in the ticlopidine group. Although nottatistically significant in our underpowered study, theigher rate of stent thrombosis in the clopidogrelroup observed in our study is consistent with otherandomized, controlled trials.12,13 Stent thrombosis oc-urred within in 24 hours in 2 patients in the clopi-ogrel group. This may reflect an inadequate loadingose of clopidogrel, as our protocol mandated a load-
ng dose of 150 mg and not 300 mg, which is moreommonly used currently. This loading dose was cho-en so that both groups received the same number ofoses of their respective thienopyridine, and morehan 2 doses of ticlopidine are not well tolerated. Ithould be noted, however, that 2 trials similar to ourwn mandated no loading dose of clopidogrel or ticlo-idine.11,12 The overall rate of stent thrombosis is low
n all studies, and no individual study has been largenough to specifically address this question. If appro-riately sized randomized trails were to be performed
n the future to specifically address this question, the
bsolute difference is likely to be quite small and may dot be clinically relevant, given the better tolerabilityf clopidogrel and the higher incidence of life-threat-ning hematologic disorders with ticlopidine. Thereas no statistically significant difference in the com-ined incidence of adverse cardiac events in our studyith 3 events (�1.9%) in both the ticlopidine and clo-idogrel groups (P � 1.00). Two large-scale stud-
es11,12 of 4 weeks of thienopyridine therapy havehown nonsignificant trends to more adverse cardiacvents in patients receiving clopidogrel when com-ared with those receiving ticlopidine. However, inhe Taniuchi study,13 in which therapy was discontin-ed after 14 days, the 30-day adverse cardiac eventates where nonsignificantly higher in the ticlopidineroup when compared with the clopidogrel group4.60% vs 3.85%; P � .551).A previous study has suggested that the cessation of
iclopidine after 2 weeks may be safe in terms of ad-erse cardiac events to avoid the risks of profound life-hreatening neutropenia.9 Clopidogrel is not withoutdverse hematologic sequelae, however, with a smallncidence of thrombotic thrombocytopenic purpuraccurring within 14 days of initiation of therapy,14 andhere are also the important issues of cost and compli-nce with the use of expensive antiplatelet agents foronger than 2 weeks. Although we have data on only07 patients, the occurrence of only 1 TSO betweenay 14 and day 30 in patients receiving clopidogrel oriclopidine is reassuring. In more than 1000 patientsandomly assigned, in the only other prospective studyf 2 weeks of thienopyridine therapy after intracoro-ary stent implantation,13 there was only a single casef stent thrombosis in each group occurring outside ofhe 2-week treatment period.Since our study was conceived and completed, im-ortant information has emerged from 2 large multi-enter trials addressing the issue of long-term clopi-ogrel therapy in patients who have undergoneuccessful intracoronary stenting. In both the Percuta-eous Coronary Intervention-Clopidogrel in Unstablengina to prevent Recurrent Events (PCI-CURE)15 andlopidogrel for the Reduction of Events During Obser-ation (CREDO)16 trials, patients who continued toeceive clopidogrel long-term therapy had a significanteduction in major cardiovascular events when com-ared with long-term placebo therapy. These data sug-est that there may be sustained cardiovascular bene-ts beyond reducing the risk of stent thrombosis inhe first month after intracoronary stenting. In the con-ext of this evidence, the relevance of our study coulde questioned; however, we believe that our resultsay be of assistance when treating patients who may
e intolerant of long-term therapy with thienopyri-
ines.
S
tosdtptuqmwcbautddtwwo
C
wrisTprt
Chr
R
1
1
1
1
1
1
1
American Heart JournalVolume 147, Number 4
Juergens et al K5
tudy limitationsThis study has a number of limitations, including
hose inherent in single-center studies, the nonblindingf medication use, and the small sample size. The ob-erved incidence of drug discontinuation in the ticlopi-ine group was 3.3%, which was substantially lesshan the anticipated incidence of 9%. We based ourower calculations on previous studies of 4 weeks ofherapy, as the Taniuchi study13 was not available tos at the time of commencement of our study. Conse-uently, the study is underpowered to assess the pri-ary end point. Despite this, the results are consistentith other larger-scale multicenter trials showing that
ombination therapy with clopidogrel and aspirin isetter tolerated, with efficacy similar to ticlopidine andspirin. The available data from this study do not allows to assess the risk of hematologic side effects, as rou-ine blood counts were not performed after hospitalischarge. We did not observe any severe thienopyri-ine-induced neutropenia or thrombocytopenia duringhe hospital stay, and it is likely that severe episodesould have come to our attention, but we cannot sayith absolute certainty that these events did notccur.
onclusionsIn conclusion, these data demonstrate that after 2eeks of combination antiplatelet therapy with aspi-
in, there is a trend toward improved patient tolerabil-ty of clopidogrel compared with ticlopidine, with aimilarly low incidence of adverse cardiac events.hese data may be of assistance in the treatment ofatients intolerant of long-term therapy with thienopy-idines or where costs of such treatment are prohibi-ive.
We thank the nurses and scientific officers from theardiac Catheterization laboratories at Liverpoolospital for their assistance in performing thisesearch.
eferences1. Sigwart U, Puel J, Mirkovitch V, et al. Intravascular stents to pre-
vent occlusion and restenosis after transluminal angioplasty.N Engl J Med 1987;316:701–6.
2. George BS, Voorhees WD III, Roubin GS, et al. Multicenter investi-
gation of coronary stenting to treat acute or threatened closureafter percutaneous transluminal coronary angioplasty: clinical andangiographic outcomes. J Am Coll Cardiol 1993;22:135–43.
3. Serruys PW, de Jaegere P, Kiemeneij F, et al. A comparison ofballoon expandable stent implantation with balloon angioplasty inpatients with coronary artery disease. N Engl J Med 1994;331:489–95.
4. Fischman DL, Leon MB, Baim DS, et al. A randomised comparisonof coronary stent placement and balloon angioplasty in the treat-ment of coronary artery disease. N Engl J Med 1994;331:496–501.
5. Colombo A, Hall P, Nakamura S, et al. Intracoronary stentingwithout anticoagulation accomplished with intravascular ultrasoundguidance. Circulation 1995;91:1676–88.
6. Schomig A, Neumann F-J, Kastrati A, et al. A randomized com-parison of antiplatelet and anticoagulant therapy after the place-ment of coronary artery stents. N Engl J Med 1996;334:1084–9.
7. Bertrand ME, Legrand V, Boland J, et al. Randomized multicentrecomparison of conventional anticoagulation versus antiplatelettherapy in unplanned and elective coronary stenting: the full anti-coagulation versus aspirin and ticlopidine (FANTASTIC) study. Cir-culation 1998;98:1597–603.
8. Leon MB, Baim DS, Popma JJ, et al. A clinical trial comparingthree antithrombotic drug regimens after coronary artery stenting.N Engl J Med 1998;339:1665–71.
9. Berger PB, Bell MR, Hasdai D, et al. Safety and efficacy of ticlopi-dine for only 2 weeks after successful intracoronary stent place-ment. Circulation 1999;99:248–53.
0. CAPRIE Steering Committee. A randomised, blinded, trial of clopi-dogrel versus aspirin in patients at risk of ischaemic events(CAPRIE). Lancet 1996;348:1329–39.
1. Bertrand ME, Rupprecht H-J, Urban P, et al. Double-blind study ofthe safety of clopidogrel with and without a loading dose in com-bination with aspirin compared with ticlopidine in combinationwith aspirin after coronary stenting: the clopidogrel aspirin stentinternational cooperative study (CLASSICS). Circulation 2000;102:624–9.
2. Muller C, Buttner HJ, Petersen J, et al. A randomized comparisonof clopidogrel and aspirin versus ticlopidine and aspirin after theplacement of coronary artery stents. Circulation 2000;101:590–3.
3. Taniuchi M, Kurz HI, Lasala JM. Randomized comparison of ticlo-pidine and clopidogrel after intracoronary stent implantation in abroad patient population. Circulation 2001;104:539–43.
4. Bennett CL, Connors JM, Carwile JM, et al. Thrombotic thrombocy-topenic purpura associated with clopidogrel. N Engl J Med 2000;342:1773–7.
5. Mehta SR, Yusuf S, Peters RJG, et al. Effects of pretreatment withclopidogrel and aspirin followed by long term therapy in patientsundergoing percutaneous coronary intervention: the PCI-CUREstudy. Lancet 2001;358:527–33.
6. Steinhubl SR, Berger PB, Mann JT III, et al. Early and sustaineddual oral antiplatelet therapy following percutaneous coronaryintervention: a randomized controlled trial. JAMA 2002;288:
2411–20.
62
PAPER 11
Reprinted from Heart Lung and Circulation 2011;20:525-531 with
permission from Elsevier
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright
Author's personal copy
OR
IGIN
AL
AR
TIC
LE
Original Article
High on Treatment Platelet Reactivity and StentThrombosis
Saissan Rajendran b, Devang Parikh, MBBS a, Ibrahim Shugman, MB BCh b,John K. French, MB ChB MSc PhD a,b and Craig P. Juergens, MBBS a,b,∗
a Cardiology Department, Liverpool Hospital, Australiab University of NSW, Sydney, Australia
Background: Stent thrombosis (ST) remains a major adverse outcome of percutaneous coronary intervention (PCI). Weexamined potential associations between high on treatment platelet reactivity and the risk of ST and assessed the effectsof increased antiplatelet dosage on platelet inhibition.
Methods: Differences in clinical characteristics and the effect of aspirin and clopidogrel on platelet reactivity weredetermined after angiographically proven ST in 16 patients and in 40 patients without ST. Platelet reactivity was deter-mined using the VerifyNow assays (Accumetrics Inc., San Diego, CA). Patients found with high on treatment plateletreactivity (P2Y12 Reaction Units ≥ 235 and/or Aspirin Reaction Units ≥ 550) returned following two weeks of double doseantiplatelet therapy for further analyses.
Results: High post aspirin and/or clopidogrel platelet reactivity was significantly more common in patients with STversus controls (75% vs. 2.5%, p = <0.001). Overall, ST patients were younger (52.8 ± 10.5 vs. 59 ± 9.6 years; p = 0.039), hadmore pre-existing coronary artery disease (75% vs. 42%; p = 0.028) and smaller reference vessel diameters (2.9 ± 0.36 vs.3.2 ± 0.54 mm; p = 0.047) when compared to controls. After double dose therapy, antiplatelet reactivity improved signifi-cantly in ten out of 12 subjects on clopidogrel (83.3%) and the two patients on aspirin who initially had high on treatmentplatelet reactivity.
Conclusion: This study demonstrates that high on treatment platelet reactivity with aspirin and/or clopidogrel iscommon amongst patients who develop stent thrombosis. Additionally this resistance can be improved with doublingthe prior dose of antiplatelet therapy.
(Heart, Lung and Circulation 2011;20:525–531)© 2011 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society of Australia and New Zealand.
Published by Elsevier Inc. All rights reserved.
Keywords. Stent thrombosis; Antiplatelet; Clopidogrel; Aspirin; Hyporesponsiveness
Introduction
Drug eluting stents (DES) reduce in-stent restenosisand target vessel revascularisation compared to bare
metal stents (BMS), with a similar long term incidence ofdeath or myocardial infarction (MI) [1,2]. However it hasbecome apparent that DES use is associated with a higherincidence of late stent thrombosis (ST) [3]. Furthermorethese late events appeared to be related to the discontin-uation of clopidogrel therapy. Stent thrombosis continuesto occur with a reported incidence at six months to threeyears of between 1.3 and 4.1% [3–7] and leads to significantclinical complications including a mortality rate of 19–29%and myocardial infarction in 56–75% [3,5,8] of patients.
Received 21 January 2011; received in revised form 18 March2011; accepted 13 April 2011; available online 17 May 2011
∗ Corresponding author at: Department of Cardiology, LiverpoolHospital, Elizabeth Street, Liverpool NSW 2170, Australia.Tel.: +61 2 98283078; fax: +61 2 98283054.E-mail address: [email protected] (C.P. Juergens).
Thienopyridines in combination with aspirin are key inreducing the risk of ST, with clinical trials revealing dualantiplatelet as being more effective in the prevention ofmajor cardiovascular events to aspirin alone [9]. The DutchStent Thrombosis Registry study attributed the discontin-uation of clopidogrel as one of the strongest predictors ofST along with undersizing of the coronary stents, presenceof intermediate coronary artery disease (CAD) proximalto the culprit lesion, and concomitant malignant disease[10]. Other studies have also demonstrated an increasedincidence of ST when antiplatelet therapy is withdrawn[11,12]. Although interruption of antiplatelet therapy mayexplain the occurrences of late and very late ST, it doesnot explain occurrences of acute and subacute ST on treat-ment as current clinical practice dictates the use of aspirinindefinitely and clopidogrel for ≥1 month following PCIdepending on whether a bare-metal or drug-eluting stentis used [13]. More recently investigators have suggestedthat reduced platelet inhibition by aspirin and thienopy-ridines can be seen as a potential contributor to thisphenomenon [14–16].
© 2011 Australasian Society of Cardiac and Thoracic Surgeons and the Cardiac Society ofAustralia and New Zealand. Published by Elsevier Inc. All rights reserved.
1443-9506/04/$36.00doi:10.1016/j.hlc.2011.04.004

Author's personal copy
OR
IGIN
AL
AR
TIC
LE
526 Rajendran et al. Heart, Lung and CirculationHigh on Treatment Platelet Reactivity and Stent Thrombosis 2011;20:525–531
From a clinical perspective, several key questionsrequire further clarification. Although strong predictors ofST have been identified [10], the concept of “antiplateletresistance” as a predictor in itself remains contentious.Moreover, significant evidence of antiplatelet resistancehas largely been discussed with relation to DES use andstent thrombosis [14,16]. We aimed to establish the sig-nificance of high on treatment platelet reactivity acrossboth DES and BMS thrombosis and discuss its recogni-tion as a strong predictor of ST. Additionally, we examinedthe hypothesis of potentially reducing high on treatmentantiplatelet reactivity in patients through the doubling ofthe doses of aspirin and/or clopidogrel.
Methods
Patient Population and Study DesignBetween August 2005 and July 2009, our centre performeda total of 3535 PCIs with 33 patients experiencing 40 def-inite ST episodes. This represented patients whose indexand ST procedure where performed in our hospital. Ofthese patients, 16 were alive and willing to participatein the present study. Stent thrombosis was defined inaccordance to the Academic Research Consortium (ARC)criteria for “definite” ST and acute (<24 h post index pro-cedure), subacute (24 hours to 30 days), late (30 days to1 year) and very late ST (1 year+) [17]. ST clinical criteriaincluded an acute onset of ischaemic symptoms and/ornew ischaemic ECG changes and/or a rise in cardiacbiomarkers. Angiographic criteria included both occlusiveand non-occlusive thrombi within the initial stent.
A database of clinical, procedural and outcome data forall patients undergoing PCI is prospectively maintainedat our cardiac catheterisation laboratory including proce-dural indications, patient demographics, pharmacologicaltherapy and angiographic characteristics. Angiographicdata was further reviewed by an experienced inter-ventional cardiologist. Reference vessel diameter andpercentage prestenosis were determined by quantitativecoronary analysis (QCA). Clinical follow up was per-formed by trained research staff in an interview at thehospital. Compliance and duration of antiplatelet ther-apy and other medications were also determined at studyenrolment. Further information regarding clinical out-comes such as repeated procedures was obtained frommedical records, treating physicians and general practi-tioners.
Patients who had not experienced ST during follow upwere recruited and served as controls in a planned 1:4ratio. Criteria for control subjects who were matched tocase subjects are as follows:
1. PCI of at least one coronary vessel for a de novo coro-nary lesion.
2. Same interventional cardiologist as index procedure forthe patient identified as the case of ST.
3. Undergone PCI within four weeks as the patient iden-tified as the case.
4. Alive and willing to participate in the present study.
Current usage of aspirin and clopidogrel was initiallyascertained from both cases and controls. For those com-pliant and taking aspirin (100–150 mg) and clopidogrel(75 mg) for greater than two weeks prior to enrollmentin the study, blood samples were obtained and aspirinand clopidogrel antiplatelet reactivity was determined.For those not on aspirin and/or clopidogrel, a loadingdose (300 mg aspirin, 300 mg clopidogrel) was adminis-tered and then chronic therapy commenced (≥100 mgaspirin and 75 mg clopidogrel). Such subjects returnedfollowing two weeks of therapy for antiplatelet reactiv-ity testing. In subjects found to have high on treatmentplatelet reactivity to aspirin and/or clopidogrel, the dailydose of aspirin and/or clopidogrel was doubled (aspirin200–300 mg, clopidogrel 150 mg) and a repeat plateletreactivity test was performed following a further twoweeks.
The study design was reviewed and approved by thelocal ethics committee and all patients gave informed con-sent prior to enrolment.
Procedural and Medical Therapy DetailsAll PCI’s were performed in accordance with currentclinical guidelines. Weight adjusted unfractionated hep-arin was administered during the procedure. Patientsnot on maintenance therapy were given a loading doseof at least 300 mg aspirin and/or 300 mg clopidogrelprior to PCI. Intravenous Glycoprotein IIb/IIIa inhibitorsand adjunctive PCI devices were utilised according tothe operator’s discretion. Regardless of stent type, allpatients were commenced on dual antiplatelet therapy(75 mg clopidogrel, 100–150 mg aspirin) and generallyrecommended to continue for at least 12 months postPCI.
Antiplatelet Resistance TestingThe VerifyNow Aspirin Assay (Accumetrics, San Diego,CA) was utilised to determine the platelet inhibitory effectof aspirin. Platelet aggregation is expressed in AspirinReaction Units (ARU). High post-aspirin platelet reactivitywas defined by ARU ≥ 550 based on the recommendationby the manufacturer [18]. This cut-off has also been utilisedin previous studies [19]. The VerifyNow P2Y12 Assay (Acc-umetrics) was utilised to determine high post-clopidogrelplatelet reactivity. Results are expressed in P2Y12 ReactionUnits (PRU) and high post-clopidogrel platelet reactivitywas defined by PRU ≥ 235 [20].
Statistical AnalysisStatistical analysis was performed using SPSS (SPSS Inc,Chicago) version 17.0. Categorical variables were pre-sented as numbers and percentages per cohort withthe use of the Pearson’s Chi-square test (χ2) or Fisherexact test, as appropriate, to analyse differences. Con-tinuous variables were presented as mean ± standarddeviation (SD) for normally distributed variables andmedians [interquartile range (IQR)] for skewed variables.Independent student’s t test (for normally distributedvariables) or the Mann–Whitney U test (for skewed

Author's personal copy
OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Rajendran et al. 527
2011;20:525–531 High on Treatment Platelet Reactivity and Stent Thrombosis
Table 1. Baseline Demographic Characteristics.
Characteristic ST Cases (n = 16) Controls (n = 40) p Value
Age, mean ± SD 52.8 ± 10.5 59 ± 9.6 0.039Male, n (%) 13(81.3%) 34(85%) 0.705BMI (kg/m2), mean ± SD 28.1 ± 5.8 28.7 ± 3.9 0.656History, n (%)
Systemic hypertension 14(87.5%) 26(65%) 0.114Diabetes mellitus 6(37.5%) 6(15%) 0.081Hypercholesterolaemia 14(87.5%) 25(62.5%) 0.107Moderate or severe renal insufficiencya 1(6.3%) 2(5%) 0.999Prior Known CADb 12(75%) 17(42.3%) 0.028
History of tobacco use, n (%) 11(68.8%) 26(65%) 0.789Current use 3 (18.8%) 8(20%) 0.999
BMI = body mass index; CABG = coronary artery bypass grafting; CAD = coronary artery disease; eGFR = estimated glomerular filtration rate;PCI = percutaneous coronary intervention; SD = standard deviation; ST = stent thrombosis.a Defined as eGFR < 60 ml/min pre PCI.b Included patients with prior MI, PCI and/or CABG.
variables) were used for comparisons of normally dis-tributed paired continuous variables. All tests were twotailed and p values <0.05 were considered statisticallysignificant.
Results
The baseline demographics for the 16 cases with ST and40 control patients at the time of stent implantation arepresented in Table 1. We were unable to consent fourcontrol patients for each ST patient because of our strictenrolment criteria but all ST cases had at least one con-trol patient. There were significant differences in age andpre-existing coronary artery disease (CAD) between thecases of ST and controls. Baseline angiographic charac-teristics at stent implantation between the two groups aredepicted in Table 2. Significant angiographic differencesin reference vessel diameter and percentage prestenosis
were revealed amongst ST patients but no significant dif-ference in the choice of stent (DES and mixed vs. BMS)used.
Initial ST occurred at a median of 4.5 days (range 0–40days) following implantation in the ST group. Of thesepatients 3(18.75%) had subacute ST, 12(75%) had acute STand 1(6.25%) had late ST. Furthermore 5(31.25%) patientshad recurrent ST episodes. Most ST events (75%) pre-sented as ST-elevation myocardial infarction (STEMI) and100% of patients underwent repeat revascularisation. Atthe time of thrombosis all patients were prescribed andadherent to dual antiplatelet therapy except for one whoseclopidogrel was ceased two days prior to ST due to acerebral haemorrhage, however aspirin therapy had beencontinued in this patient.
Antiplatelet reactivity measurements were performedon all subjects at a median of 643 days (range 28–1519) afterstent implantation. All but three of the control patients
Table 2. Baseline Angiographic Characteristics.
Characteristic ST Cases (n = 16) Controls (n = 40) p Value
Clinical presentation, n (%)Acute coronary syndrome 14(87.5%) 32(80%) 0.508
UA 4(28%) 5(12.5%)STEMI 4(25%) 9(22.5%)NSTEMI 6(37.5%) 18(45%)
SA/Positive functional test 2(12.5%) 8(20%) 0.508Diseased vesselsa, mean ± SD 1.44 ± 0.512 1.65 ± 0.736 0.257
Single vessel, n (%) 9(56.3%) 20(50%) 0.672Multi-vessel, n (%) 7(43.8%) 20(50%) 0.672
Reference vessel diameter (mm), mean ± SD 2.9 ± 0.36 3.2 ± 0.54 0.047Prestenosis (%), median [IQR] 97[90–100] 90[75–95] 0.011TIMI flow grade 3 before PCI, n (%) 9(56.3%) 31(77.5%) 0.189Type of stent, n (%)
DES only 7(43.8%) 18(45%) 0.932BMS only 6(37.5%) 18(45%) 0.608Mixed 3(18.8%) 4(10.0%) 0.395
Total stented length (mm), median [IQR] 30[27.3–39.5] 20[16.5–39.5] 0.061Stent diameter (mm), median [IQR] 3[2.56–3.187] 3.25[3.0–3.5] 0.543Maximal balloon pressure (atm), median [IQR] 17[14–20] 16.5[14.25–18] 0.774GP IIb/IIIa therapy, n (%) 3(18.8%) 13(32.5%) 0.350
BMS = bare metal stent; DES = drug eluting stent; GP = glycoprotein; IQR = interquartile range; NSTEMI = non-ST-segment elevation myocardialinfarction; PCI = percutaneous coronary intervention; SA = stable angina; SD = standard deviation; ST = stent thrombosis; STEMI = ST-segment elevationmyocardial infarction; TIMI = thrombolysis in myocardial infarction; UA = unstable angina.a Defined as >50% stenosis.
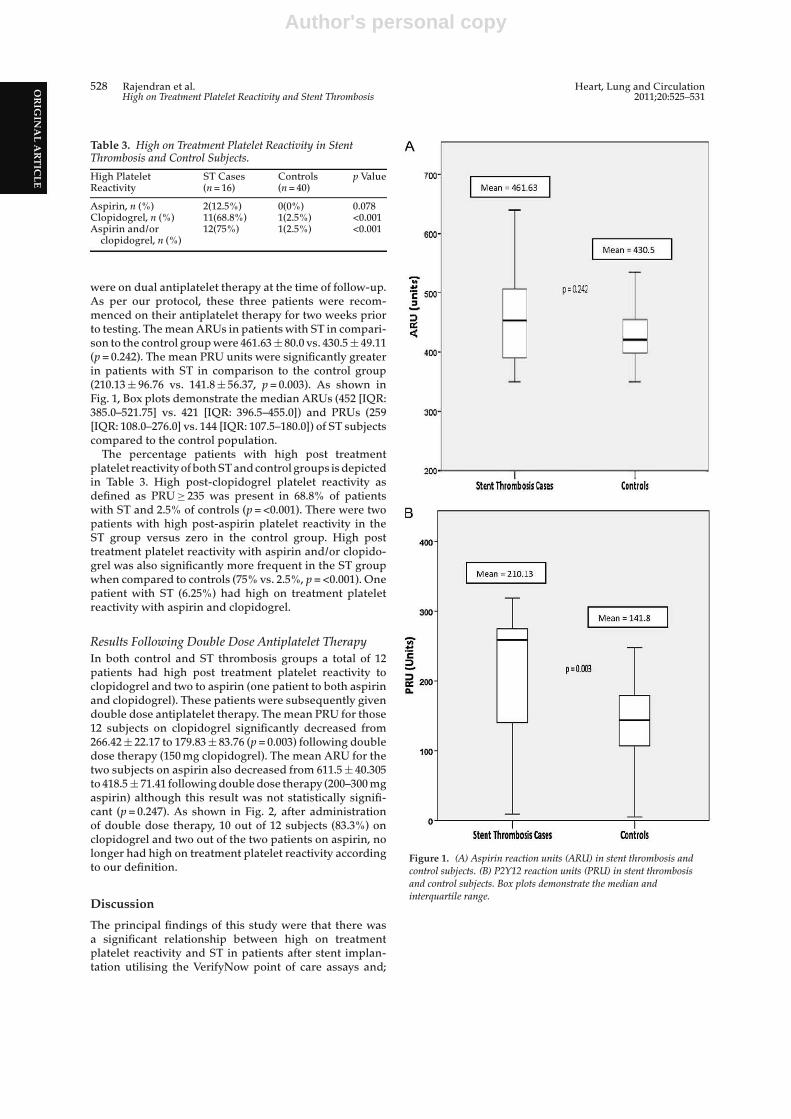
Author's personal copy
OR
IGIN
AL
AR
TIC
LE
528 Rajendran et al. Heart, Lung and CirculationHigh on Treatment Platelet Reactivity and Stent Thrombosis 2011;20:525–531
Table 3. High on Treatment Platelet Reactivity in StentThrombosis and Control Subjects.
High PlateletReactivity
ST Cases(n = 16)
Controls(n = 40)
p Value
Aspirin, n (%) 2(12.5%) 0(0%) 0.078Clopidogrel, n (%) 11(68.8%) 1(2.5%) <0.001Aspirin and/or
clopidogrel, n (%)12(75%) 1(2.5%) <0.001
were on dual antiplatelet therapy at the time of follow-up.As per our protocol, these three patients were recom-menced on their antiplatelet therapy for two weeks priorto testing. The mean ARUs in patients with ST in compari-son to the control group were 461.63 ± 80.0 vs. 430.5 ± 49.11(p = 0.242). The mean PRU units were significantly greaterin patients with ST in comparison to the control group(210.13 ± 96.76 vs. 141.8 ± 56.37, p = 0.003). As shown inFig. 1, Box plots demonstrate the median ARUs (452 [IQR:385.0–521.75] vs. 421 [IQR: 396.5–455.0]) and PRUs (259[IQR: 108.0–276.0] vs. 144 [IQR: 107.5–180.0]) of ST subjectscompared to the control population.
The percentage patients with high post treatmentplatelet reactivity of both ST and control groups is depictedin Table 3. High post-clopidogrel platelet reactivity asdefined as PRU ≥ 235 was present in 68.8% of patientswith ST and 2.5% of controls (p = <0.001). There were twopatients with high post-aspirin platelet reactivity in theST group versus zero in the control group. High posttreatment platelet reactivity with aspirin and/or clopido-grel was also significantly more frequent in the ST groupwhen compared to controls (75% vs. 2.5%, p = <0.001). Onepatient with ST (6.25%) had high on treatment plateletreactivity with aspirin and clopidogrel.
Results Following Double Dose Antiplatelet TherapyIn both control and ST thrombosis groups a total of 12patients had high post treatment platelet reactivity toclopidogrel and two to aspirin (one patient to both aspirinand clopidogrel). These patients were subsequently givendouble dose antiplatelet therapy. The mean PRU for those12 subjects on clopidogrel significantly decreased from266.42 ± 22.17 to 179.83 ± 83.76 (p = 0.003) following doubledose therapy (150 mg clopidogrel). The mean ARU for thetwo subjects on aspirin also decreased from 611.5 ± 40.305to 418.5 ± 71.41 following double dose therapy (200–300 mgaspirin) although this result was not statistically signifi-cant (p = 0.247). As shown in Fig. 2, after administrationof double dose therapy, 10 out of 12 subjects (83.3%) onclopidogrel and two out of the two patients on aspirin, nolonger had high on treatment platelet reactivity accordingto our definition.
Discussion
The principal findings of this study were that there wasa significant relationship between high on treatmentplatelet reactivity and ST in patients after stent implan-tation utilising the VerifyNow point of care assays and;
Figure 1. (A) Aspirin reaction units (ARU) in stent thrombosis andcontrol subjects. (B) P2Y12 reaction units (PRU) in stent thrombosisand control subjects. Box plots demonstrate the median andinterquartile range.
A
-.. ..
700
600
·c soo :I
400
300
Mean = 461.63
Mean =430.5
p = 0.241
200._--------~----------------~--------~
Stent Thrombosis Cases Controls
B
400
Mean = 210.13
300 Mean= 141.8
p =0.003
100
0~---------.--------------~~--------~
Stent Thrombosis cases Controls
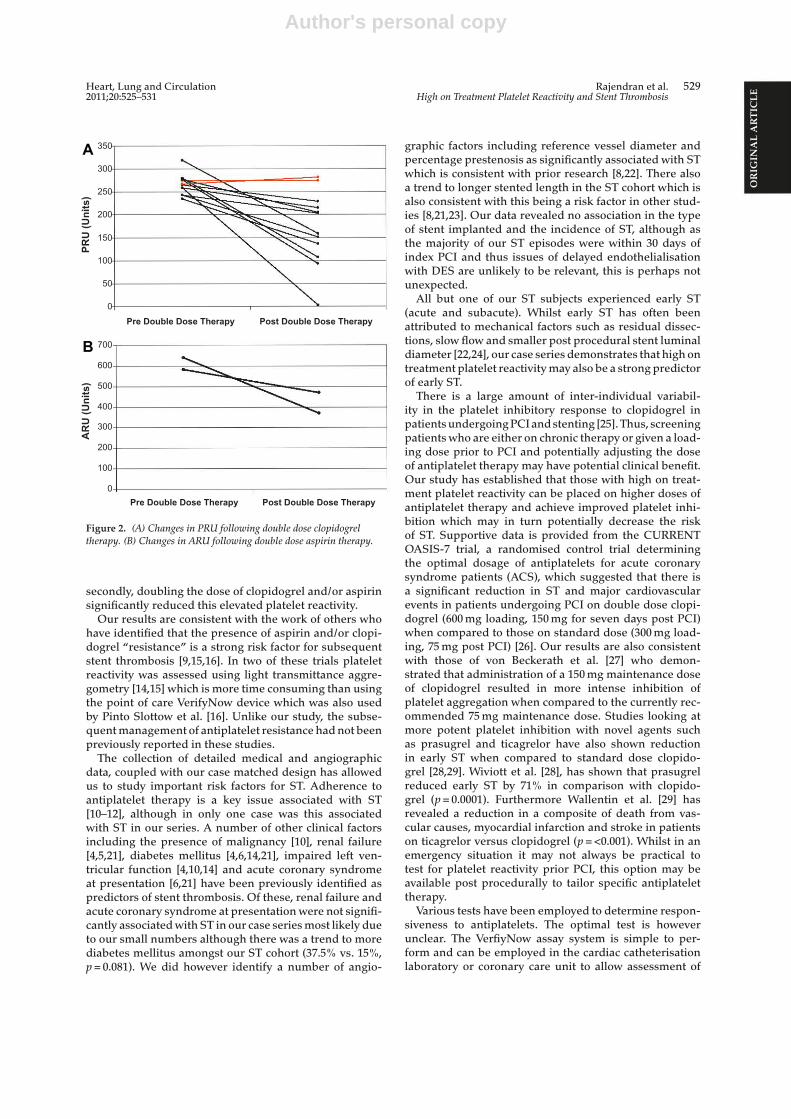
Author's personal copy
OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Rajendran et al. 529
2011;20:525–531 High on Treatment Platelet Reactivity and Stent Thrombosis
0
50
100
150
200
250
300
350
Post Double Dose TherapyPre Double Dose Therapy
PRU
(Uni
ts)
0
100
200
300
400
500
600
700
Post Double Dose TherapyPre Double Dose Therapy
AR
U (U
nits
)
A
B
Figure 2. (A) Changes in PRU following double dose clopidogreltherapy. (B) Changes in ARU following double dose aspirin therapy.
secondly, doubling the dose of clopidogrel and/or aspirinsignificantly reduced this elevated platelet reactivity.
Our results are consistent with the work of others whohave identified that the presence of aspirin and/or clopi-dogrel “resistance” is a strong risk factor for subsequentstent thrombosis [9,15,16]. In two of these trials plateletreactivity was assessed using light transmittance aggre-gometry [14,15] which is more time consuming than usingthe point of care VerifyNow device which was also usedby Pinto Slottow et al. [16]. Unlike our study, the subse-quent management of antiplatelet resistance had not beenpreviously reported in these studies.
The collection of detailed medical and angiographicdata, coupled with our case matched design has allowedus to study important risk factors for ST. Adherence toantiplatelet therapy is a key issue associated with ST[10–12], although in only one case was this associatedwith ST in our series. A number of other clinical factorsincluding the presence of malignancy [10], renal failure[4,5,21], diabetes mellitus [4,6,14,21], impaired left ven-tricular function [4,10,14] and acute coronary syndromeat presentation [6,21] have been previously identified aspredictors of stent thrombosis. Of these, renal failure andacute coronary syndrome at presentation were not signifi-cantly associated with ST in our case series most likely dueto our small numbers although there was a trend to morediabetes mellitus amongst our ST cohort (37.5% vs. 15%,p = 0.081). We did however identify a number of angio-
graphic factors including reference vessel diameter andpercentage prestenosis as significantly associated with STwhich is consistent with prior research [8,22]. There alsoa trend to longer stented length in the ST cohort which isalso consistent with this being a risk factor in other stud-ies [8,21,23]. Our data revealed no association in the typeof stent implanted and the incidence of ST, although asthe majority of our ST episodes were within 30 days ofindex PCI and thus issues of delayed endothelialisationwith DES are unlikely to be relevant, this is perhaps notunexpected.
All but one of our ST subjects experienced early ST(acute and subacute). Whilst early ST has often beenattributed to mechanical factors such as residual dissec-tions, slow flow and smaller post procedural stent luminaldiameter [22,24], our case series demonstrates that high ontreatment platelet reactivity may also be a strong predictorof early ST.
There is a large amount of inter-individual variabil-ity in the platelet inhibitory response to clopidogrel inpatients undergoing PCI and stenting [25]. Thus, screeningpatients who are either on chronic therapy or given a load-ing dose prior to PCI and potentially adjusting the doseof antiplatelet therapy may have potential clinical benefit.Our study has established that those with high on treat-ment platelet reactivity can be placed on higher doses ofantiplatelet therapy and achieve improved platelet inhi-bition which may in turn potentially decrease the riskof ST. Supportive data is provided from the CURRENTOASIS-7 trial, a randomised control trial determiningthe optimal dosage of antiplatelets for acute coronarysyndrome patients (ACS), which suggested that there isa significant reduction in ST and major cardiovascularevents in patients undergoing PCI on double dose clopi-dogrel (600 mg loading, 150 mg for seven days post PCI)when compared to those on standard dose (300 mg load-ing, 75 mg post PCI) [26]. Our results are also consistentwith those of von Beckerath et al. [27] who demon-strated that administration of a 150 mg maintenance doseof clopidogrel resulted in more intense inhibition ofplatelet aggregation when compared to the currently rec-ommended 75 mg maintenance dose. Studies looking atmore potent platelet inhibition with novel agents suchas prasugrel and ticagrelor have also shown reductionin early ST when compared to standard dose clopido-grel [28,29]. Wiviott et al. [28], has shown that prasugrelreduced early ST by 71% in comparison with clopido-grel (p = 0.0001). Furthermore Wallentin et al. [29] hasrevealed a reduction in a composite of death from vas-cular causes, myocardial infarction and stroke in patientson ticagrelor versus clopidogrel (p = <0.001). Whilst in anemergency situation it may not always be practical totest for platelet reactivity prior PCI, this option may beavailable post procedurally to tailor specific antiplatelettherapy.
Various tests have been employed to determine respon-siveness to antiplatelets. The optimal test is howeverunclear. The VerfiyNow assay system is simple to per-form and can be employed in the cardiac catheterisationlaboratory or coronary care unit to allow assessment of

Author's personal copy
OR
IGIN
AL
AR
TIC
LE
530 Rajendran et al. Heart, Lung and CirculationHigh on Treatment Platelet Reactivity and Stent Thrombosis 2011;20:525–531
individual patient response to antiplatelet agents. Unlikeother tests, an experienced technician is not requiredand results can be made available within five minutes ofsample acquisition. Some debate still exists over the opti-mal cut off levels of what is “high on treatment plateletreactivity” using the VerifyNow assay system. No stud-ies to date have challenged the aspirin cut-off value ofARU ≥ 550 provided by the manufacturer. The threshold ofa PRU ≥ 235 chosen in our study to identify potential highpost-clopidogrel platelet reactivity was identical to thatused by Price et al. [20] and in accord with that used by Pattiet al. (PRU ≥ 240) [30]. Both these studies demonstratedthat this level of impaired platelet inhibition by clopidogrelstrongly correlated with ischaemic events after stentingincluding ST.
Study LimitationsSeveral limitations of this study need to be acknowl-edged. Although our random selection case matcheddesign was able to evaluate events such as ST, it isstill vulnerable to several biases. Due to the nature ofthe study, we were only able to include patients whowere alive and had angiographically documented “def-inite” ST, leading to a potentially select group of STsurvivors. Although our design aimed at eliminating con-founding factors, unidentified confounders may still haveinfluenced the outcomes. Given that the study was a ret-rospective analysis, we cannot be certain as to the levelof antiplatelet responsiveness at the time of index PCIand ST. However testing soon after ST may not reflectthe true status quo given the thrombotic milieu and itsimpact of platelet responsiveness. Additionally, we alsocannot be certain that patients in the control arm will notexperience an ST episode in the future, although this isunlikely given the time from their index procedure. Dueto the infrequent occurrences of ST, only a small samplesize could be obtained for the present study and there-fore a multivariate analysis was not performed. To obtainconclusive evidence on alternate antiplatelet therapiesfor those with high on treatment platelet reactivity afteraspirin and/or clopidogrel, large prospective trials arerequired.
Conclusion
Our study demonstrates that high post treatment plateletreactivity with aspirin and/or clopidogrel is commonamongst patients who develop stent thrombosis. Addi-tionally platelet reactivity can be significantly improvedby doubling the prior dose of antiplatelet therapy butwhether this translates into improved outcomes awaitsfurther study.
Acknowledgements
The author wishes to thank all physicians, nurses andstaff of the Cardiology department at Liverpool hospi-tal as without their help this study could not have beenaccomplished. There was no financial assistance for thisproject.
References
[1] James SK, Stenestrand U, Lindback J, Carlsson J, ScherstenF, Nilsson T, et al. Long-term safety and efficacy of drug-eluting versus bare-metal stents in Sweden. N Engl J Med2009;360:1933–45.
[2] Ko DT, Chiu M, Guo H, Austin PC, Goeree R, Cohen E,et al. Safety and effectiveness of drug-eluting and bare-metalstents for patients with off- and on-label indications. J AmColl Cardiol 2009;53:1773–82.
[3] Pfisterer M, Brunner-La Rocca HP, Buser PT, Rickenbacher P,Hunziker P, Mueller C, et al. Late clinical events after clopi-dogrel discontinuation may limit the benefit of drug-elutingstents: an observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol 2006;48:2584–91.
[4] Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM,Stankovic G, et al. Incidence, predictors, and outcome ofthrombosis after successful implantation of drug elutingstents. JAMA 2005;293:2126–30.
[5] Kuchulakanti PK, Chu WW, Torguson R, Ge L, SangiorgiGM, Stankovic G, et al. Correlates and long-term outcomesof angiographically proven stent thrombosis with sirolimus-and paclitaxel-eluting stents. Circulation 2006;113:1108–13.
[6] Daemen J, Wenaweser P, Tsuchida K, Vaina S, Morger C,Kukreja N, et al. Early and late coronary stent thrombosisof sirolimus-eluting and paclitaxel-eluting stents in routineclinical practice: data from a large two-institutional cohortstudy. Lancet 2007;369:667–78.
[7] Smit JJJ, van’t Hof AWJ, de Boer MJ, Hoorntje JCA, DambrinkJHE, Gosselink ATM, et al. Incidence and predictors ofsubacute thrombosis in patients undergoing primary angio-plasty for an acute myocardial infarction. Thromb Haemost2006;96:190–5.
[8] Cutlip DE, Baim DS, Ho KK, Popma JJ, Lansky AJ, Cohen DJ,et al. Stent thrombosis in the modern era: a pooled analy-sis of multicenter coronary stent clinical trials. Circulation2001;103:1967–71.
[9] Hall P, Nakamura S, Maiello L, Itoh A, Blengino S, MartiniG, et al. A randomized comparison of combined ticlopidineand aspirin therapy versus aspirin therapy alone after suc-cessful intravascular-guided stent implantation. Circulation1996;93:215–22.
[10] Van Werkum JW, Heestermans AA, Zomer AC, Kelder JC,Suttorp MJ, Rensing BJ, et al. Predictors of coronary stentthrombosis: the Dutch stent thrombosis registry. J Am CollCardiol 2009;53:1399–409.
[11] Waters RE, Kandzari DE, Phillips HR, Crawford LE,Sketch MH. Late thrombosis following treatment of in-stentrestenosis with drug-eluting stents after discontinua-tion of antiplatelet therapy. Catheter Cardiovasc Interv2005;65:520–4.
[12] Ferrari E, Benhamou M, Cerboni P, Marcel B. Coronary syn-dromes following aspirin withdrawal: a special risk for latestent thrombosis. J Am Coll Cardiol 2005;45:456–9.
[13] King SB, Smith SC, Hirshfeld JW, Jakobs AK, Morrison DA,Williams DO. 2007 focused update of the ACC/AHA/SCAI2005 guideline update for percutaneous coronary interven-tion. J Am Coll Cardiol 2008;51:172–209.
[14] Wang ZJ, Zhou YJ, Liu YY, Yu M, Shi DM, Zhao YX, et al.Impact of clopidogrel resistance on thrombotic events afterpercutaneous coronary intervention with drug-eluting stent.Thromb Res 2009;124:46–51.
[15] Gurbel PA, Bliden KP, Samara W, Yoho JA, Hayes K, FisshaMZ, et al. Clopidogrel effect on platelet reactivity in patientswith stent thrombosis: results of the CREST Study. J Am CollCardiol 2005;46:1827–32.

Author's personal copy
OR
IGIN
AL
AR
TIC
LEHeart, Lung and Circulation Rajendran et al. 531
2011;20:525–531 High on Treatment Platelet Reactivity and Stent Thrombosis
[16] Pinto Slottow TL, Bonello L, Gavani R, Beauzile P, SushinskySJ, Scheinowitz M, et al. Prevalence of aspirin and clopido-grel resistance among patients with and without drug elutingstent thrombosis. Am J Cardiol 2009;104:525–30.
[17] Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, vanEs GA, et al. Clinical end points in coronary stent trials: a casefor standardized definitions. Circulation 2007;115:2344–51.
[18] VerifyNow® Aspirin Assay Product Insert. San Diego,CA: Accumetrics, revised 9/18/07. Available from: http://accumetrics.com/products/VerifyNow/docs/VerifyNowAspirin Instructions.pdf (accessed November, 2009).
[19] Nielsen HL, Kristensen SD, Thygesen SS, Mortensen J, Ped-ersen SB, Grove EL, et al. Aspirin response evaluated by theVerifyNow aspirin system and light transmission aggregom-etry. Thromb Res 2008;123:267–73.
[20] Price MJ, Endemann S, Gollapudi RR, Valencia R, Stinis CT,Levisay JP, et al. Prognostic significance of post-clopidogrelplatelet reactivity assessed by point-of-care assay on throm-botic events after drug-eluting stent implantation. Eur HeartJ 2008;29:992–1000.
[21] de la Torre-Hernandez JM, Alfonso F, Hernandez F, ElizagaJ, Sanmartin M, Pinar E, et al. Drug-eluting stent thrombo-sis: results from the multicenter Spanish registry ESTROFA(Estudio ESpanol sobre TROmbosis de stents FArmacoac-tivos). J Am Coll Cardiol 2008;51:986–90.
[22] Moussa I, Di Mario C, Di Francesco L, Reimers B, BlenginoS, Colombo A. Subacute stent thrombosis and the antico-agulation controversy: changes in drug therapy, operatortechnique, and the impact of intravascular ultrasound. Am JCardiol 1996;78(suppl 3A):13–7.
[23] Cook S, Wenaweser P, Togni M, Billinger M, Morger C, SeilerC, et al. Incomplete stent apposition and very late stentthrombosis after drug-eluting stent implantation. Circula-tion 2007;115:2426–34.
[24] Moussa I, Di Mario C, Reimers B, Akiyama T, TobisJ, Colombo A. Subacute stent thrombosis in the era ofintravascular ultrasound-guided coronary stenting withoutanticoagulation: frequency, predictors and clinical outcome.J Am Coll Cardiol 1997;29:6–12.
[25] Gurbel PA, Bliden KP, Hiatt BL, O’Connor CM. Clopidogrelfor coronary stenting: response variability, drug resistance,and the effect of pretreatment platelet reactivity. Circulation2003;107:2908–13.
[26] The C URRENT-OASIS 7 Investigators: dose comparisons ofclopidogrel and aspirin in acute coronary syndromes. N EnglJ Med 2010;363:930–42.
[27] von Beckerath N, Kastrati A, Wieczorek A, Pogatsa-MurrayG, Sibbing D, Graf I, et al. A double-blind, randomizedstudy on platelet aggregation in patients treated with a dailydose of 150 or 75 mg of clopidogrel for 30 days. Eur Heart J2007;28:1814–9.
[28] Wiviott SD, Braunwald E, McCabe CH, Horvath I, KeltaiM, Hermann JPR, et al. Intensive oral antiplatelet therapyfor reduction of ischaemic events including stent throm-bosis in patients with acute coronary syndromes treatedwith percutaneous coronary intervention and stenting in theTRITON-TIMI 38 trial: a subanalysis of a randomised trial.Lancet 2008;371:1353–63.
[29] Wallentin L, Becker RC, Budaj A, Cannon CP, EmanuelssonH, Held C, et al. Ticagrelor versus clopidogrel in patientswith acute coronary syndromes. N Engl J Med 2009;361:1045–57.
[30] Patti G, Nusca A, Mangiacapra F, Gatto L, D’Ambrosio A,Di Sciascio G. Point of care measurement of clopidogrelresponsiveness predicts clinical outcome in patients under-going percutaneous coronary intervention. J Am Coll Cardiol2008;52:1128–33.

63
PAPER 12
Reprinted from Expert Opinion Drug Metabolism and Toxicology
2012;8:1315-1325 with permission from Informa Healthcare
1. Introduction
2. The development of ticagrelor
3. Conclusion
4. Expert opinion
Drug Evaluation
Review of ticagrelor in themanagement of acute coronarysyndromesSonya Burgess, Trevor A Mallard & Craig P Juergens††University of NSW Sydney, Southwestern Sydney Clinical School, NSW, Australia
Introduction: Ticagrelor, an oral P2Y12 receptor antagonist used as part of
dual antiplatelet therapy in the treatment of acute coronary syndromes
(ACS), has many favorable characteristics when compared with the more
frequently used P2Y12 receptor antagonist clopidogrel. Ticagrelor binds
reversibly, with a rapid onset and offset of action, and produces high levels
of platelet inhibition without variation secondary to genetic polymorphism.
Ticagrelor produces increased platelet inhibition and an overall reduction in
adverse cardiac events compared with clopidogrel. Clinically relevant side
effects include an increase in non-CABG-related bleeding events as well as
off-target adverse effects including ventricular pauses and dyspnea.
Areas covered: This article details ticagrelor’s pharmacokinetic and pharma-
codynamic characteristics, development and chemical properties. The authors
review relevant clinical trials looking at the efficiency and safety of ticagrelor
focusing predominantly on the management of patients with ACS. Finally, the
review article concludes with discussion of ticagrelor’s current role and future
integration into clinical practice.
Expert opinion: Ticagrelor is a promising P2Y12 receptor antagonist with char-
acteristics that offer advantages for patients beyond those currently demon-
strated by other P2Y12 receptor antagonists. The challenge for prescribers
is to identify those most likely to benefit from ticagrelor treatment while
minimizing unnecessary bleeding events for ‘real-world’ ACS patients.
Keywords: acute coronary syndromes, aspirin, AZD6140, clopidogrel, P2Y12,
pharmacodynamics, pharmacokinetics, prasugrel, review, ticagrelor
Expert Opin. Drug Metab. Toxicol. (2012) 8(10):1315-1325
1. Introduction
Acute coronary syndromes (ACS) are a leading cause of morbidity and mortalityworldwide. In patients presenting to hospital with ACS including ST-segmentelevation myocardial infarction (STEMI), current clinical practice guidelines [1,2]
recommend dual antiplatelet treatment.Clopidogrel, a thienopyridine, is the primary P2Y12 antagonist in use; and together
with aspirin and heparin has become a cornerstone of treatment in ACS. Clopidog-rel’s limitations include slow conversion to its active metabolite, irreversible bindingand interpatient variability associated with growing evidence of increased ischemicevents [3-6].
Prasugrel, another thienopyridine, is metabolized to its active form more effi-ciently than clopidogrel and produces greater levels of platelet inhibition [7,8]. TheTRITON-TIMI 38 study (TRial to assess Improvement in Therapeutic Outcomesby optimizing platelet inhibitioN with prasugrel -- Thrombolysis In MyocardialInfarction) demonstrated improved prevention of ischemic events with prasugrelversus clopidogrel accompanied by an increased risk of major bleeding [9].
10.1517/17425255.2012.717931 © 2012 Informa UK, Ltd. ISSN 1742-5255 1315All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.
Ticagrelor (Box 1) is a cyclopentyl-triazolo-pyrimidine(CPTP), and is the first orally active reversible P2Y12 receptorantagonist [10]. Thienopyridines and CPTPs both act byblocking the P2Y12 receptor, one of two adenosine diphos-phate (ADP) receptors on platelets, to inhibit ADP-inducedplatelet activation and aggregation [11].Ticagrelor’s rapid onset, reversible binding and minimal
interpatient variability make it an important alternative inthe treatment of ACS, and unlike clopidogrel and prasugrel,it does not require conversion to an active metabolite. Tica-grelor and AR-C124910XX, its main active metabolite, havea similar potency in inhibiting the P2Y12 receptor [10]. ThePLATO (PLATelet inhibition and clinical Outcomes) trialdemonstrated superiority of ticagrelor over clopidogrel inthe prevention of a composite end point of death from vascu-lar causes, MI or stroke with no difference between the overallrates of major bleeding events [12].This article provides an overview of ticagrelor’s develop-
ment and chemical properties including pharmacodynamicsand pharmacokinetics. The authors review Phase II and IIItrials looking at the safety and efficacy of ticagrelor in themanagement of patients with ACS and conclude with a dis-cussion of ticagrelor’s future integration into clinical practice.
2. The development of ticagrelor
Ticagrelor was developed as part of a program to create stableanalogs of adenosine-5¢-triphosphate (ATP), the naturalantagonist of the P2Y12 receptor. This led first to the produc-tion of cangrelor [13], a P2Y12 antagonist which in earlyPhase II trials showed promise but large-scale trials showedno benefit over clopidogrel [14]. Cangrelor is limited by itsshort half-life and requirement for i.v. administration due torapid degradation via plasma ectonucleotidases. Subsequent
major alterations to cangrelor included changing the corepurine and sugar moiety and eliminating phosphates, whichproduced AR-C109318XX, a stable P2Y12 receptor non-phosphate antagonist [15]. Subsequent refinements to increasebioavailability resulted in the development of ticagrelor.
2.1 Chemistry and receptorTicagrelor induces conformational change and inhibits Gprotein activation by binding to the P2Y12 receptor at a siteseparate to the ADP-binding site, inhibiting signaling andreversibly rendering the P2Y12 receptor inactive [16]. This isin contrast to clopidogrel’s and prasugrel’s active metabolite,which renders the receptor non-functional for the life ofthe platelet by binding covalently to the P2Y12 receptor atthe site of ADP binding.
2.2 PharmacodynamicsTicagrelor when given as a single oral dose produces dose-related and almost complete inhibition of platelet aggregation(IPA). Maximal-extent IPA is measured by optical aggrega-tion, after the addition of ADP to a sample, and assesses theeffect on P2Y12 and P2Y1 receptors. A second measurementis made after waiting 6 min and this final-extent measurementis mediated primarily by the P2Y12 receptor [17]. In single-dose studies, final extent IPA was 88 -- 95% at 2 h, plateauedat 88 -- 100% (2 -- 8 h) and decreased to 74 -- 89% at 12 h indose ranges from 50 to 300 mg [16,18,19]. Figure 1 shows theonset and offset platelet inhibition with ticagrelor [19].
2.2.1 Off-target effectsTicagrelor is also thought to inhibit P2Y12-mediated vasocon-striction [16]. P2Y12 receptors are present in vascular smoothmuscle in concentrations greater than other ADP receptorsand stimulate vessel contraction. Contraction can be blocked
Box 1. Drug summary.
Drug name TicagrelorPhase Launched in market (Phase IV)Indication Acute coronary syndromes
Percutaneous coronary interventionPharmacology description Reversible P2Y12 receptor antagonistRoute of administration OralChemical structure
O O
S
O
O
N
N N
N
r
r
NN
Pivotal trials ONSET/OFFSET (Randomized Double-Blind Assessment of the ONSET and OFFSETof the Antiplatelet Effects of Ticagrelor Versus Clopidogrel in Patients With StableCoronary artery disease: The ONSET/OFFSET Study) [19]PLATO (The PLATelet inhibition and patient Outcomes trial) [12]
S. Burgess et al.
1316 Expert Opin. Drug Metab. Toxicol. (2012) 8(10)
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.
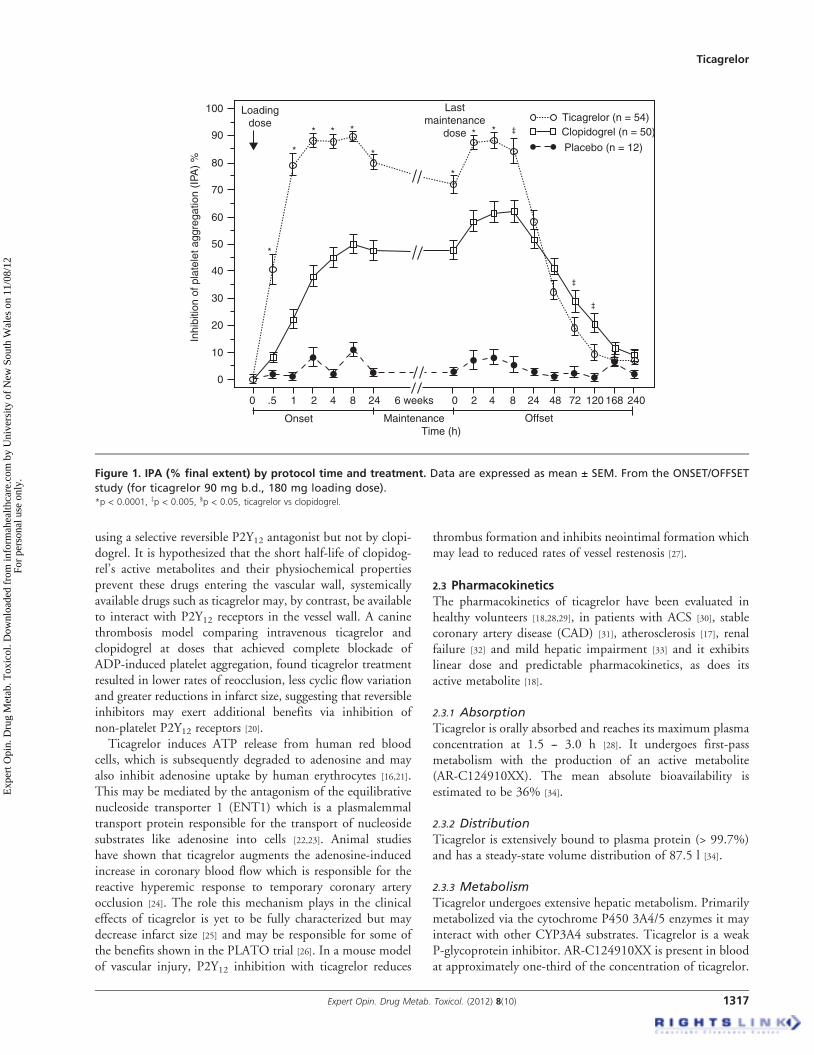
using a selective reversible P2Y12 antagonist but not by clopi-dogrel. It is hypothesized that the short half-life of clopidog-rel’s active metabolites and their physiochemical propertiesprevent these drugs entering the vascular wall, systemicallyavailable drugs such as ticagrelor may, by contrast, be availableto interact with P2Y12 receptors in the vessel wall. A caninethrombosis model comparing intravenous ticagrelor andclopidogrel at doses that achieved complete blockade ofADP-induced platelet aggregation, found ticagrelor treatmentresulted in lower rates of reocclusion, less cyclic flow variationand greater reductions in infarct size, suggesting that reversibleinhibitors may exert additional benefits via inhibition ofnon-platelet P2Y12 receptors [20].
Ticagrelor induces ATP release from human red bloodcells, which is subsequently degraded to adenosine and mayalso inhibit adenosine uptake by human erythrocytes [16,21].This may be mediated by the antagonism of the equilibrativenucleoside transporter 1 (ENT1) which is a plasmalemmaltransport protein responsible for the transport of nucleosidesubstrates like adenosine into cells [22,23]. Animal studieshave shown that ticagrelor augments the adenosine-inducedincrease in coronary blood flow which is responsible for thereactive hyperemic response to temporary coronary arteryocclusion [24]. The role this mechanism plays in the clinicaleffects of ticagrelor is yet to be fully characterized but maydecrease infarct size [25] and may be responsible for some ofthe benefits shown in the PLATO trial [26]. In a mouse modelof vascular injury, P2Y12 inhibition with ticagrelor reduces
thrombus formation and inhibits neointimal formation whichmay lead to reduced rates of vessel restenosis [27].
2.3 PharmacokineticsThe pharmacokinetics of ticagrelor have been evaluated inhealthy volunteers [18,28,29], in patients with ACS [30], stablecoronary artery disease (CAD) [31], atherosclerosis [17], renalfailure [32] and mild hepatic impairment [33] and it exhibitslinear dose and predictable pharmacokinetics, as does itsactive metabolite [18].
2.3.1 AbsorptionTicagrelor is orally absorbed and reaches its maximum plasmaconcentration at 1.5 -- 3.0 h [28]. It undergoes first-passmetabolism with the production of an active metabolite(AR-C124910XX). The mean absolute bioavailability isestimated to be 36% [34].
2.3.2 DistributionTicagrelor is extensively bound to plasma protein (> 99.7%)and has a steady-state volume distribution of 87.5 l [34].
2.3.3 MetabolismTicagrelor undergoes extensive hepatic metabolism. Primarilymetabolized via the cytochrome P450 3A4/5 enzymes it mayinteract with other CYP3A4 substrates. Ticagrelor is a weakP-glycoprotein inhibitor. AR-C124910XX is present in bloodat approximately one-third of the concentration of ticagrelor.
100 Loadingdose
*
*
* * *
*
*
* * ‡
‡
‡
Lastmaintenance
dose
Ticagrelor (n = 54)Clopidogrel (n = 50)
Placebo (n = 12)90
80
70
60
40
30
20
Inhi
bitio
n of
pla
tele
t agg
rega
tion
(IPA
) %
10
0
0 .5
Onset MaintenanceTime (h)
Offset
1 2 4 8 0 2 4 8 24 48 72 120 168 24024 6 weeks
50
Figure 1. IPA (% final extent) by protocol time and treatment. Data are expressed as mean ± SEM. From the ONSET/OFFSET
study (for ticagrelor 90 mg b.d., 180 mg loading dose).*p < 0.0001, zp < 0.005, §p < 0.05, ticagrelor vs clopidogrel.
Ticagrelor
Expert Opin. Drug Metab. Toxicol. (2012) 8(10) 1317
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.

The mean terminal half-life is approximately 7 -- 12 h forticagrelor and 8.5 -- 10 h for AR-C124910XX. Plasma levelsof ticagrelor reach steady state after 2 -- 3 days [29].
2.3.4 ExcretionBoth ticagrelor and AR-C124910XX are extensively excreted infeces via biliary secretion [29]. The primary componentsobserved in urine are the inactive metabolite AR-C133913XXand its glucuronide conjugate. Renal impairment has littleeffect on systemic exposure to the active compounds and nodose adjustment is required [32].
2.4 Clinical efficacyNotable Phase II clinical trials of ticagrelor include: Dose con-fIrmation Study assessing antiPlatelet Effects of AZD6140versus clopidogRel in non-ST segment Elevation myocardialinfarction trials (DISPERSE) [17], DISPERSE-2 [35], theONSET/OFFSET study (Randomized Double-Blind Assess-ment of the ONSET and OFFSET of the Antiplatelet Effectsof Ticagrelor Versus Clopidogrel in Patients With Stable Cor-onary artery disease: The ONSET/OFFSET Study) [19] andthe Response to Ticagrelor in Clopidogrel Non-respondersand Responders and Effect of Switching Therapies: TheRESPOND Study [36]. There has been a single pivotalPhase III efficacy study, the PLATelet inhibition and patientOutcomes (PLATO) [12]. The main clinical trials of ticagrelorare summarized in Table 1.The DISPERSE trial enrolled 200 patients with stable
artherosclerotic disease [17]. All patients received aspirin andwere randomized in a double-blind, parallel-group design toone of four ticagrelor doses (50, 100, 200 mg b.d. or 400 mgo.d.) or clopidogrel (75 mg o.d.) for 28 days. Comparison ofIPA levels between groups showed all ticagrelor-treated patientsreached their final-extent IPA 2 -- 4 h following the first dose,whereas clopidogrel-treated patients had a mean IPA of lessthan 20% at all time points on day 1. At steady state (day14), 4 h post-dose, the three higher doses of ticagrelor pro-duced comparable final-extent IPA of 90 -- 95% exceedingthat of ticagrelor 50 mg b.d. or clopidogrel 60%. A singlemajor bleeding event (gastrointestinal hemorrhage) wasreported, in a patient receiving ticagrelor 400 mg o.d. All otherbleeding events were reported to be minor.DISPERSE-2 was a randomized, double-blind, double-
dummy trial in 990 patients with non-ST-elevation ACS [35].All patients received standard ACS treatment including aspirin.Patients were randomized to ticagrelor 90 and 180 mg b.d., orclopidogrel 300 mg loading dose plus 75 mg o.d. The mediantreatment duration was 56 days. Patients receiving ticagrelorwere also randomized to either a loading dose of 270 mg or noloading dose. Those undergoing percutaneous coronary inter-vention (PCI) within 48 h of randomization could, at the discre-tion of the treating physician, receive a further 300 mg loadingdose of clopidogrel (or placebo, for ticagrelor-treated patients).Angiography was performed in 67% of patients, 42% had PCIand 9% underwent coronary artery bypass grafting (CABG).
The primary end point, major and minor bleeding at 4 weeks,was not significantly different between groups, nor was majorbleeding alone, or MI rates. In those treated with ticagrelor180mg b.d.minor bleeding at 12weeks was increased comparedwith patients treated with clopidogrel (6.1 vs 1.3%, p = 0.01). Ina substudy, optical aggregometry was used to measure IPA at4-week intervals. At 4 h post-dose, IPA was 64% (± 22%) forclopidogrel, 79% (± 22%) for ticagrelor 90 mg b.d. and 95%(± 8%) for ticagrelor 180 mg b.d. [30]. All initial doses achievedgreater IPA than a 300 mg loading dose of clopidogrel.
The ONSET/OFFSET study was a double-blind, random-ized study of 123 patients with stable CAD on aspirin [19].The ticagrelor loading dose was 180 mg followed by 90 mgb.d. (as in PLATO trial), it used a 600 mg loading dose of clo-pidogrel and 75 mg o.d., 12 patients in placebo arm were alsoincluded. Treatment was for a duration of 6 weeks. The endpoints were IPA and adverse outcomes, and included prospec-tive assessment of pulmonary function and Holter monitor-ing. The IPA was higher in ticagrelor-treated patients at alltimes measured during treatment (p < 0.0001). Two hoursafter loading 90% of the ticagrelor-treated patients and 16%of the clopidogrel-treated patients achieved IPA greaterthan > 70% (p < 0.0001; Figure 1). IPAs in the range of pla-cebo were seen on day 5 post-discontinuation of ticagrelorand on day 7 post-discontinuation of clopidogrel. Therewere no major bleeding events (PLATO study criteria), oneclinically relevant minor event in the placebo group andone in the ticagrelor group.
The RESPOND study examined the use of ticagrelor inclopidogrel non-responders with stable CAD [36]. Patientsreceived a 300 mg clopidogrel load and non-responderswere identified by light transmittance aggregometry. In atwo-way crossover design, non-responders (n = 41) and res-ponders (n = 57) randomly received clopidogrel (600/75 mgo.d.) or ticagrelor (180/90 mg b.d.) for 14 days during period1. In period 2, all non-responders switched treatment; half ofthe responders continued the same treatment, whereas theothers switched treatment. This study was the first to demon-strate that ticagrelor therapy overcomes non-responsivenessto clopidogrel therapy (Figure 2). The antiplatelet effect ofticagrelor was essentially uniform and high in clopidogrelresponders and non-responders.
The PLATO trial was an international, randomized,double-blind, Phase III trial examining the safety and efficacyof ticagrelor [12,37]. A total of 18,624 patients enrolled fromOctober 2006 to July 2008 reflected those patients whowould ordinarily received thienopyridine-based antiplatelettherapy in a clinical setting; this included patients who hadpreviously received clopidogrel and those who had not,patients with both planned invasive or non-invasive treat-ment, patients with STEMI referred for primary PCI, patientswith non-STEMI and patients who underwent bypass sur-gery, those receiving fibrinolytics were excluded. Patientswere randomized to receive either a 300 mg clopidogrelloading dose and 75 mg/day or a 180 mg loading dose of
S. Burgess et al.
1318 Expert Opin. Drug Metab. Toxicol. (2012) 8(10)
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.
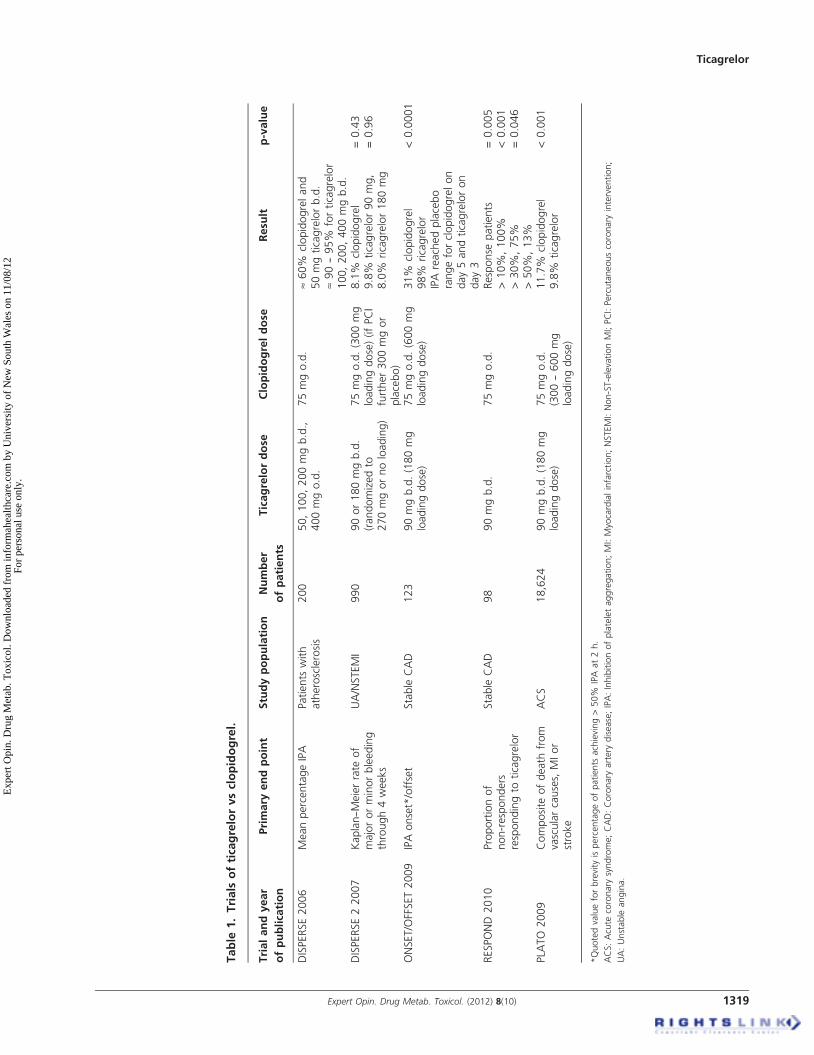
Table
1.Trials
ofticagrelorvsclopidogrel.
Trialandyear
ofpublication
Primary
endpoint
Studypopulation
Number
ofpatients
Ticagrelordose
Clopidogreldose
Resu
ltp-value
DISPERSE2006
MeanpercentageIPA
Patients
with
atherosclerosis
200
50,100,200mgb.d.,
400mgo.d.
75mgo.d.
»60%
clopidogreland
50mgticagrelorb.d.
»90--95%
forticagrelor
100,200,400mgb.d.
DISPERSE22007
Kaplan--M
eierrate
of
majororminorbleeding
through4weeks
UA/NSTEMI
990
90or180mgb.d.
(randomizedto
270mgornoloading)
75mgo.d.(300mg
loadingdose)(ifPCI
further300mgor
placebo)
8.1%
clopidogrel
9.8%
ticagrelor90mg,
8.0%
ricagrelor180mg
=0.43
=0.96
ONSET/OFFSET2009
IPAonset*/offset
Stable
CAD
123
90mgb.d.(180mg
loadingdose)
75mgo.d.(600mg
loadingdose)
31%
clopidogrel
98%
ricagrelor
IPAreachedplacebo
rangeforclopidogrelon
day5andticagreloron
day3
<0.0001
RESPOND
2010
Proportionof
non-responders
respondingto
ticagrelor
Stable
CAD
98
90mgb.d.
75mgo.d.
Response
patients
>10%
,100%
>30%
,75%
>50%
,13%
=0.005
<0.001
=0.046
PLA
TO
2009
Composite
ofdeath
from
vascularcauses,
MIor
stroke
ACS
18,624
90mgb.d.(180mg
loadingdose)
75mgo.d.
(300--600mg
loadingdose)
11.7%
clopidogrel
9.8%
ticagrelor
<0.001
*Quotedvalueforbrevity
ispercentageofpatients
achieving>50%
IPA
at2h.
ACS:Acute
coronary
syndrome;CAD:Coronary
artery
disease;IPA:Inhibitionofplateletaggregation;MI:Myocardialinfarction;NSTEMI:Non-ST-elevationMI;PCI:Percutaneouscoronary
intervention;
UA:Unstable
angina.
Ticagrelor
Expert Opin. Drug Metab. Toxicol. (2012) 8(10) 1319
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.
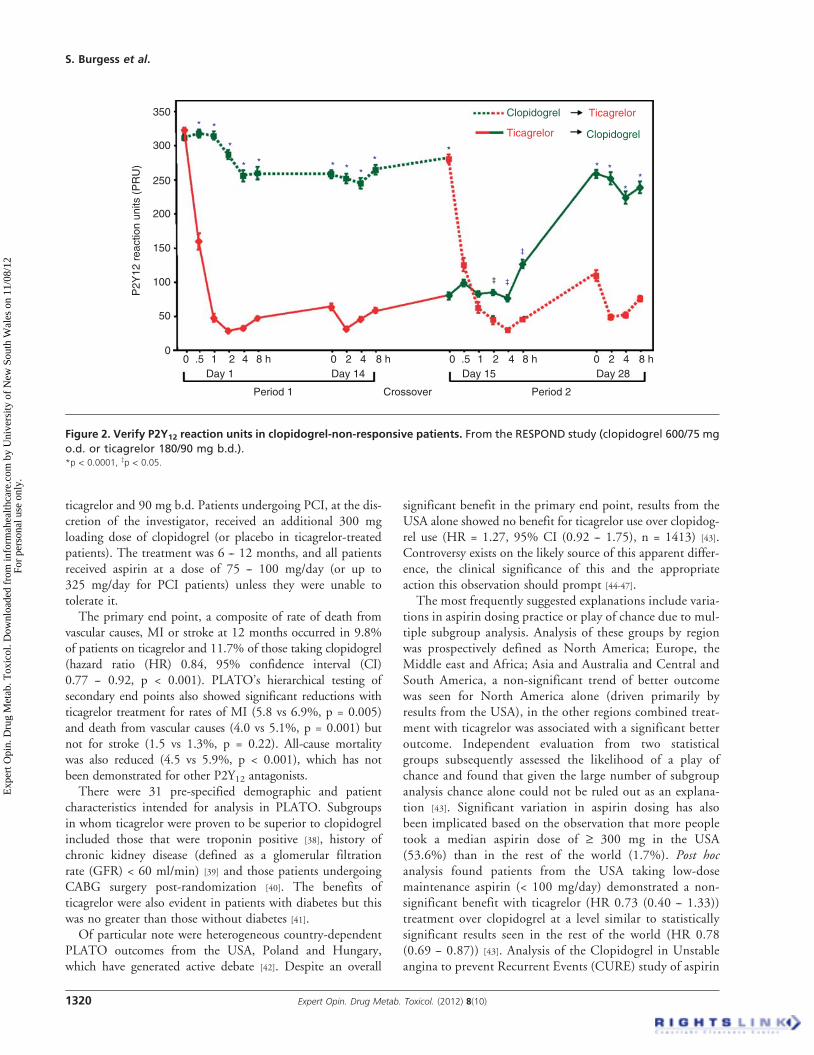
ticagrelor and 90 mg b.d. Patients undergoing PCI, at the dis-cretion of the investigator, received an additional 300 mgloading dose of clopidogrel (or placebo in ticagrelor-treatedpatients). The treatment was 6 -- 12 months, and all patientsreceived aspirin at a dose of 75 -- 100 mg/day (or up to325 mg/day for PCI patients) unless they were unable totolerate it.The primary end point, a composite of rate of death from
vascular causes, MI or stroke at 12 months occurred in 9.8%of patients on ticagrelor and 11.7% of those taking clopidogrel(hazard ratio (HR) 0.84, 95% confidence interval (CI)0.77 -- 0.92, p < 0.001). PLATO’s hierarchical testing ofsecondary end points also showed significant reductions withticagrelor treatment for rates of MI (5.8 vs 6.9%, p = 0.005)and death from vascular causes (4.0 vs 5.1%, p = 0.001) butnot for stroke (1.5 vs 1.3%, p = 0.22). All-cause mortalitywas also reduced (4.5 vs 5.9%, p < 0.001), which has notbeen demonstrated for other P2Y12 antagonists.There were 31 pre-specified demographic and patient
characteristics intended for analysis in PLATO. Subgroupsin whom ticagrelor were proven to be superior to clopidogrelincluded those that were troponin positive [38], history ofchronic kidney disease (defined as a glomerular filtrationrate (GFR) < 60 ml/min) [39] and those patients undergoingCABG surgery post-randomization [40]. The benefits ofticagrelor were also evident in patients with diabetes but thiswas no greater than those without diabetes [41].Of particular note were heterogeneous country-dependent
PLATO outcomes from the USA, Poland and Hungary,which have generated active debate [42]. Despite an overall
significant benefit in the primary end point, results from theUSA alone showed no benefit for ticagrelor use over clopidog-rel use (HR = 1.27, 95% CI (0.92 -- 1.75), n = 1413) [43].Controversy exists on the likely source of this apparent differ-ence, the clinical significance of this and the appropriateaction this observation should prompt [44-47].
The most frequently suggested explanations include varia-tions in aspirin dosing practice or play of chance due to mul-tiple subgroup analysis. Analysis of these groups by regionwas prospectively defined as North America; Europe, theMiddle east and Africa; Asia and Australia and Central andSouth America, a non-significant trend of better outcomewas seen for North America alone (driven primarily byresults from the USA), in the other regions combined treat-ment with ticagrelor was associated with a significant betteroutcome. Independent evaluation from two statisticalgroups subsequently assessed the likelihood of a play ofchance and found that given the large number of subgroupanalysis chance alone could not be ruled out as an explana-tion [43]. Significant variation in aspirin dosing has alsobeen implicated based on the observation that more peopletook a median aspirin dose of ‡ 300 mg in the USA(53.6%) than in the rest of the world (1.7%). Post hocanalysis found patients from the USA taking low-dosemaintenance aspirin (< 100 mg/day) demonstrated a non-significant benefit with ticagrelor (HR 0.73 (0.40 -- 1.33))treatment over clopidogrel at a level similar to statisticallysignificant results seen in the rest of the world (HR 0.78(0.69 -- 0.87)) [43]. Analysis of the Clopidogrel in Unstableangina to prevent Recurrent Events (CURE) study of aspirin
350* *
*
* * * *
**
* * **
*
‡
‡‡
300
250
200
150
100
P2Y
12 r
eact
ion
units
(P
RU
)
50
00 .5 1 2 4 8 h 0 .5 1 2 4 8 h
Day 1
Period 1 Period 2Crossover
Day 14 Day 15 Day 288 h420 8 h420
Clopidogrel
ClopidogrelTicagrelor
Ticagrelor
Figure 2. Verify P2Y12 reaction units in clopidogrel-non-responsive patients. From the RESPOND study (clopidogrel 600/75 mg
o.d. or ticagrelor 180/90 mg b.d.).*p < 0.0001, zp < 0.05.
S. Burgess et al.
1320 Expert Opin. Drug Metab. Toxicol. (2012) 8(10)
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.

plus clopidogrel versus aspirin alone showed no benefit ofaspirin doses above 100 mg [48]. Low-dose aspirin inhibitsthe formation of thromboxane (TXA2), a potent vasocons-trictor and platelet aggregator, while higher doses inhibitthe production of prostacyclin (PGI2), a vasodilator thatinhibits platelet aggregation. The decrease in PGI2 productionby the use of high-dose aspirin may negate the benefit ofticagrelor [49].
The ‘North American paradox’ observation was importantenough to cause the Food and Drug Administration (FDA)to delay approval for ticagrelor and to include a ‘blackbox warning’ regarding a possible attenuation of benefitwith high-dose aspiring.
2.4.1 Bleeding events in PLATONo significant difference in the primary safety end pointof major bleeding, life-threatening bleeding events or fatalbleeding was found. No significant difference in CABG-relatedmajor bleeding, or in intracranial bleeding overall, was found.However, non-CABG-related major bleeding was significantlyincreased by ticagrelor (4.5 vs 3.8%, p = 0.03) and a significantdifference in fatal intracranial bleeding was seen in the ticagrelorgroup (0.12 vs 0.03%, p = 0.02). Results favored ticagrelorwithin the subgroup ‘non-intracranial fatal bleeding’ (0.1 vs0.3%, p = 0.03) [12]. No significant difference was found whenmajor and minor bleeding events, defined using the TIMI crite-ria, were combined, however, using the PLATO study criteriafor major and minor bleeding events combined, ticagrelor-treated patients had more events than clopidogrel-treatedpatients (16.1 vs 14.6%, p = 0.008) [50].
2.4.2 Ticagrelor versus prasugrelThere are no randomized control trials comparing ticagrelorwith prasugrel, and direct comparison of major ticagrelorand prasugrel trials cannot be made due to significant differ-ences between study populations and clinical settings [51].When compared with clopidogrel, prasugrel shares with tica-grelor benefits in its faster onset (2 -- 4 h), but has a sloweroffset than ticagrelor (5 -- 7 days). Comparison of maximalIPA of prasugrel versus ticagrelor favors ticagrelor [52].
2.5 Safety and tolerabilityWhile bleeding is the major safety issue seen with ticagrelorand has been discussed previously, it is generally well toler-ated with adverse events comparable with those observedfrom o.d. clopidogrel [35]. Other notable side effects ofticagrelor reported include hypotension, ventricular pausesand dyspnea.
2.5.1 Ventricular pausesThis was first identified during post hoc analysis of theDISPERSE-2 trial data, which utilized Holter monitoring todetect recurrent ischemia. An increased frequency of ventricularpauses was found in patients given 180 mg of ticagrelorb.d. [35]. The PLATO study excluded patients at markedly
increased risk of symptomatic bradycardia without a pacemakerwhile a substudy assessed the frequency of bradyarrhythmias byperforming continuous electrocardiographic assessments on2866 patients [53]. During the first week, there was an increasedfrequency of asymptomatic ventricular pauses ‡ 3 s in the tica-grelor group (5.8 vs 3.6%, p = 0.01), which did not persist at30 days. There were no differences in the incidence of brady-cardia, syncope, heart block or pacemaker insertion. Mostpauses were due to SA node dysfunction and occurred duringthe acute phase of ACS. The mostly nocturnal pauses mayresult from increased adenosine at the SA and AV nodes at atime of increased vagal tone [53].
2.5.2 DyspneaAn increased risk of mild to moderate dyspnea has beenreported with ticagrelor [12,17,19,35]. Episodes are predomi-nantly self-limiting, mild to moderate and drug cessation isinfrequent. PLATO authors reported increased rates of dys-pnea with ticagrelor (13.8 vs 7.8%, p < 0.001) and increasedrates of cessation due to dyspnea (0.9 vs 0.1%, p < 0.001).The ONSET/OFFSET trial prospectively assessed dyspnea,electrocardiography, echocardiography, serum N-terminalpro-brain natriuretic peptide and pulmonary functiontests [54]. The incidence of dyspnea was higher than previ-ously reported and may relate to study design increasingsymptom awareness. Episodes of dyspnea were transientand no significant change in cardiac or pulmonary functionwas found. It is recognized that intravenous infusion of aden-osine to healthy volunteers can induce dyspnea without bron-choconstriction [23,55]. The inhibition of adenosine reuptakeby ticagrelor may lead to dose-related increased levels ofextracellular adenosine and stimulation of pulmonary vagalC fibers through activation of A1 receptors [56].
2.5.3 ContraindicationsTicagrelor’s listed contraindications include active patholog-ical bleeding, a history of intracranial hemorrhage, moderateto severe hepatic failure and co-administration of strongCYP3A4 inhibitors (e.g., ketoconazole, clarithromycin,nefazodone, ritonavir and atazanavir) [34].
2.6 Guidelines and regulatory affairsThe European Medicines Agency approved ticagrelor for mar-keting in the European Union from 3 December 2010 [57].The European Society of Cardiology (ESC) STEMI guide-lines 2010 recommend aspirin in combination with prasugrelor ticagrelor. Clopidogrel should be used if more effectiveagents are contraindicated or not available [58]. The ESC2011 NSTE-ACS (non-ST-segment elevation acute coronarysyndrome) guidelines also recommend ticagrelor for allpatients at moderate to high risk of ischemic events (e.g.,elevated troponins), regardless of initial treatment strategyand including those pre-treated with clopidogrel (whichshould be discontinued when ticagrelor is commenced).Prasugrel is recommended for P2Y12-inhibitor-naı̈ve patients
Ticagrelor
Expert Opin. Drug Metab. Toxicol. (2012) 8(10) 1321
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.

(especially diabetics) in whom coronary anatomy is knownand who are proceeding to PCI unless there is a high risk oflife-threatening bleeding or other contraindications. Clopi-dogrel is recommended for patients who cannot receive tica-grelor or prasugrel [59]. The US FDA approved ticagrelor forsale on 20 July 2011 [60]. The American College of Cardiol-ogy Foundation/American Heart Association (ACCF/AHA)PCI guidelines 2011 recommended aspirin in combinationwith clopidogrel, prasugrel or ticagrelor [61]. For patientswith high risk of poor clinical outcomes or with high plateletreactivity on clopidogrel, an alternative P2Y12 inhibitor maybe considered. The Australian Therapeutic Goods Adminis-tration listed ticagrelor for sale from 21 June 2011 but it isstill awaiting an approval date for a funding subsidy [62].The National Heart Foundation of Australia and NewZealand 2011 Addendum for the management of ACSrecommended consideration of prasugrel or ticagrelor as analternative to clopidogrel for subgroups of patients at highrisk of recurrent ischemic events undergoing primary PCIfor reperfusion for STEMI or revascularization for ACS [63].
3. Conclusion
Ticagrelor consistently demonstrates levels of platelet inhibi-tion beyond those seen with clopidogrel [12,17,19,35,36]. Thistogether with its rapid onset, reversible binding and linearpharmacokinetics, makes it an important addition in themanagement of patients presenting with ACS. Clinical trialshave demonstrated its superior efficacy when compared withclopidogrel in reducing adverse cardiac events. This comeswith the predictable increased bleeding risk and slightly lesspredictable off-target effects including dyspnea. Further trialsand clinical experience will clarify the future role of ticagrelorin this challenging patient subset.
4. Expert opinion
Dual antiplatelet therapy is an established means of improv-ing outcomes for ACS patients. Clopidogrel is the mostwidely used P2Y12 receptor antagonist, however data haveemerged regarding frequent high on treatment plateletreactivity and its consequences [3-6].Many of the limitations of clopidogrel treatment are not
seen with the use of ticagrelor. Ticagrelor is not a pro-drug and therefore is not prone to the interpatient variabilityattributed to genetic polymorphism increasingly reportedwith clopidogrel and associated with increased ischemicevents [3-6]. Ticagrelor more reliably produces a higher levelof platelet inhibition.Ticagrelor has a faster onset of action and it reaches pre-
dictable levels of platelet inhibition not seen with clopidogrel.This makes it a more desirable drug to use in patients presen-ting acutely. Its more rapid offset, as a result of its reversibleantagonism of the P2Y12 receptor, is advantageous forpatients requiring surgical intervention and is likely to result
in reduced lengths of stay by decreasing delay to urgent inpa-tient surgery; however, guidelines currently still recommendsurgery is postponed for 5 days which is consistent with stu-dies showing the IPA returns to the range of placebo atthis time.
In a broad range of clinical settings, treatment with ticagre-lor rather than clopidogrel should be expected to significantlydecrease adverse cardiovascular events. The subgroups whopotentially derive the most benefit include those who havethe greatest cardiovascular risk including those who are tropo-nin positive, have a history of chronic kidney disease andthose undergoing CABG, most likely due to a greater extentof disease. However, the major concern with ticagrelor is theconcomitant increased bleeding risk associated with higherlevels of platelet inhibition. In patients where there is a parti-cular risk of bleeding, especially in those with a history ofintracranial pathology or stroke, the risk:benefit ratio wouldneed to be more carefully weighed. In light of the subsetanalysis of PLATO patients enrolled in North America, themaintenance dose of concomitant aspirin should be limitedto 100 mg/day.
Clinicians are also frequently urged to consider theirpatients’ drug adherence when selecting P2Y12 receptor antag-onist as ticagrelor needs to be taken b.d. It should, however,be noted that the effect of missing a single dose of ticagrelorresults in IPA levels dropping to those seen with o.d. clopi-dogrel dosing [19]. A more important adherence issue may bethat of dyspnea. Although the dyspnea described with ticagre-lor use is frequently brief, transient and not associated withdeterioration in pulmonary function, there is a risk that,much like the myalgia issue associated with statins, real-world compliance may be challenged, negating the potentialbenefits of ticagrelor. This is particularly problematic as thedyspnea may also be a symptom of the patient’s cardiac dis-ease. For patients reporting significant dyspnea, particularlyhaving undergone interventional procedures, clinicians mayneed to consider switching to an alternative antiplatelet agentto assess for clinical improvement. For those patients with noimprovement in symptoms, further cardiovascular investiga-tions should be performed. An alternative approach may beto consider a reduction of ticagrelor maintenance dose andfurther insights into this strategy may be gained at the com-pletion of the PEGUSUS-TIMI 54 study [64], which is trial-ling the maintenance doses of 60 or 90 mg b.d. in patientswith known cardiovascular disease. The safety of ticagrelorin patients with major conduction disorders has not beenestablished and generally it should not be prescribed inpatients with known sick sinus syndrome, second- or third-degree atrioventricular (AV) conduction block or previouslydocumented syncope suspected to be due to bradycardiaunless treated with a pacemaker which were the exclusioncriteria of the PLATO trial.
Ticagrelor’s benefits are considerable, it reduces cardiacevents in a broad range of clinical settings, and it appears todo this with a reasonable separation between antithrombotic
S. Burgess et al.
1322 Expert Opin. Drug Metab. Toxicol. (2012) 8(10)
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.

effects and bleeding. Ticagrelor’s strengths are that it ismore potent and more consistent than clopidogrel, does notrequire metabolic activation, does not require platelet regene-ration to restore function and allows rapid and reversibleIPA. The greatest barrier to ticagrelor use may be cost, parti-cularly as generic forms of clopidogrel become increasinglyavailable. Given the broad indication ticagrelor has, thepotential to replace clopidogrel in a large subset of patients
presenting with ACS is significant; however, experience willbe required to anticipate and respond to the off-target effectsin real-world practice.
Declaration of interest
The authors state no conflict of interest and have received nopayment in preparation of the manuscript.
BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. Wright RS, Anderson JL, Adams CD,
et al. 2011 ACCF/AHA focused update
incorporated into the ACC/
AHA 2007 Guidelines for the
Management of Patients with Unstable
Angina/Non-ST-Elevation Myocardial
Infarction: a report of the American
College of Cardiology Foundation/
American Heart Association Task Force
on Practice Guidelines developed in
collaboration with the American
Academy of Family Physicians, Society
for Cardiovascular Angiography and
Interventions, and the Society of
Thoracic Surgeons. J Am Coll Cardiol
2011;57:e215-367
2. Kushner FG, Hand M, Smith SC Jr, et al.
2009 focused updates: ACC/
AHA guidelines for the management of
patients with ST-elevation myocardial
infarction (updating the 2004 guideline
and 2007 focused update) and ACC/AHA/
SCAI guidelines on percutaneous coronary
intervention (updating the 2005 guideline
and 2007 focused update) a report of the
American College of Cardiology
Foundation/American Heart Association
Task Force on Practice Guidelines. J Am
Coll Cardiol 2009;54:2205-41
3. Gurbel PA, Bliden KP. Durability of
platelet inhibition by clopidogrel.
Am J Cardiol 2003;91:1123-5
4. Muller I, Besta F, Schulz C, et al.
Prevalence of clopidogrel non-responders
among patients with stable angina
pectoris scheduled for elective coronary
stent placement. Thromb Haemost
2003;89:783-7
5. Serebruany VL, Steinhubl SR, Berger PB,
et al. Variability in platelet responsiveness
to clopidogrel among 544 individuals.
J Am Coll Cardiol 2005;45:246-51
6. Angiolillo DJ, Fernandez-Ortiz A,
Bernardo E, et al. Variability in
individual responsiveness to clopidogrel:
clinical implications, management, and
future perspectives. J Am Coll Cardiol
2007;49:1505-16
7. Brandt JT, Payne CD, Wiviott SD, et al.
A comparison of prasugrel and
clopidogrel loading doses on platelet
function: magnitude of platelet inhibition
is related to active metabolite formation.
Am Heart J 2007;153:66 e9-16
8. Jernberg T, Payne CD, Winters KJ, et al.
Prasugrel achieves greater inhibition of
platelet aggregation and a lower rate of
non-responders compared with
clopidogrel in aspirin-treated patients
with stable coronary artery disease.
Eur Heart J 2006;27:1166-73
9. Wiviott SD, Braunwald E, McCabe CH,
et al. Prasugrel versus clopidogrel in
patients with acute coronary syndromes.
N Engl J Med 2007;357:2001-15
10. van Giezen JJ, Humphries RG.
Preclinical and clinical studies with
selective reversible direct
P2Y12 antagonists.
Semin Thromb Hemost
2005;31:195-204
11. Storey RF. Biology and pharmacology of
the platelet P2Y12 receptor.
Curr Pharm Des 2006;12:1255-9
12. Wallentin L, Becker RC, Budaj A, et al.
Ticagrelor versus clopidogrel in patients
with acute coronary syndromes. N Engl
J Med 2009;361:1045-57.. The PLATO trial is a pivotal Phase III
randomized double-blind trial
comparing ticagrelor with clopidogrel.
It demonstrated a reduction in adverse
cardiac events with ticagrelor.
13. Ingall AH, Dixon J, Bailey A, et al.
Antagonists of the platelet P2T receptor:
a novel approach to antithrombotic
therapy. J Med Chem 1999;42:213-20
14. Ueno M, Ferreiro JL, Angiolillo DJ.
Update on the clinical development of
cangrelor. Expert Rev Cardiovasc Ther
2010;8:1069-77
15. Springthorpe B, Bailey A, Barton P,
et al. From ATP to AZD6140: the
discovery of an orally active reversible
P2Y12 receptor antagonist for the
prevention of thrombosis. Bioorg Med
Chem Lett 2007;17:6013-18
16. Husted S, van Giezen JJ. Ticagrelor: the
first reversibly binding oral
P2Y12 receptor antagonist.
Cardiovasc Ther 2009;27:259-74.. An excellent overview of the
development, chemistry,
pharmacodynamics and
pharmacokinetics of ticagrelor. It
includes animal studies, off-target
effects and early Phase II clinical trials.
17. Husted S, Emanuelsson H, Heptinstall S,
et al. Pharmacodynamics,
pharmacokinetics, and safety of the oral
reversible P2Y12 antagonist
AZD6140 with aspirin in patients with
atherosclerosis: a double-blind
comparison to clopidogrel with aspirin.
Eur Heart J 2006;27:1038-47. The DISPERSE trial was a
randomized, double-blind,
dose-finding trial of ticagrelor
compared with clopidogrel. It assessed
the antiplatelet efficacy,
pharmacokinetics and safety
of ticagrelor.
18. Teng R, Butler K. Pharmacokinetics,
pharmacodynamics, tolerability and safety
of single ascending doses of ticagrelor, a
reversibly binding oral P2Y(12) receptor
antagonist, in healthy subjects. Eur J
Clin Pharmacol 2010;66:487-96
19. Gurbel PA, Bliden KP, Butler K, et al.
Randomized double-blind assessment of
the ONSET and OFFSET of the
antiplatelet effects of ticagrelor versus
clopidogrel in patients with stable
coronary artery disease: the ONSET/
OFFSET study. Circulation
2009;120:2577-85.. This study compares the onset of
platelet inhibition with ticagrelor
against a high loading dose of
Ticagrelor
Expert Opin. Drug Metab. Toxicol. (2012) 8(10) 1323
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.

clopidogrel. It demonstrates more
rapid and greater platelet inhibition
with ticagrelor and faster recovery of
platelet function after discontinuation.
20. Wang K, Zhou X, Huang Y, et al.
Adjunctive treatment with ticagrelor, but
not clopidogrel, added to tPA enables
sustained coronary artery recanalisation
with recovery of myocardium perfusion
in a canine coronary thrombosis model.
Thromb Haemost 2010;104:609-17
21. Ohman J, Kudira R, Albinsson S, et al.
Ticagrelor induces adenosine
triphosphate release from human red
blood cells. Biochem Biophys
Res Commun 2012;418:754-8
22. Baldwin SA, Beal PR, Yao SY, et al. The
equilibrative nucleoside transporter
family, SLC29. Pflugers Arch
2004;447:735-43
23. Gan L, Wittfeldt A, Emanuelson H,
et al. Adenosine may mediate
ticagrelor-induced dyspnea. 61st Annual
Scientific Meeting American College of
Cardiology. J Am Col Cardiol
2012;59:E344
24. van Giezen JJ, Sidaway J, Glaves P, et al.
Ticagrelor inhibits adenosine uptake
in vitro and enhances
adenosine-mediated hyperemia responses
in a canine model. J Cardiovasc
Pharmacol Ther 2012;17:164-72
25. Rose JB, Naydenova Z, Bang A, et al.
Equilibrative nucleoside transporter
1 plays an essential role in
cardioprotection. Am J Physiol Heart
Circ Physiol 2010;298:H771-7
26. Serebruany VL. Mortality benefit in
PLATO cannot be explained by
antiplatelet properties of ticagrelor.
Cardiology 2010;117:231-3
27. Patil SB, Jackman LE, Francis SE, et al.
Ticagrelor effectively and reversibly
blocks murine platelet P2Y12-mediated
thrombosis and demonstrates a
requirement for sustained
P2Y12 inhibition to prevent subsequent
neointima. Arterioscler Thromb
Vasc Biol 2010;30:2385-91
28. Butler K, Teng R. Pharmacokinetics,
pharmacodynamics, safety and tolerability
of multiple ascending doses of ticagrelor
in healthy volunteers. Br J
Clin Pharmacol 2010;70:65-77
29. Teng R, Oliver S, Hayes MA, Butler K.
Absorption, distribution, metabolism,
and excretion of ticagrelor in healthy
subjects. Drug Metab Dispos
2010;38:1514-21
30. Storey RF, Husted S, Harrington RA,
et al. Inhibition of platelet aggregation
by AZD6140, a reversible oral
P2Y12 receptor antagonist, compared
with clopidogrel in patients with acute
coronary syndromes. J Am Coll Cardiol
2007;50:1852-6
31. Husted SE, Storey RF, Bliden K, et al.
Pharmacokinetics and pharmacodynamics
of ticagrelor in patients with Stable
Coronary Artery disease: results from the
ONSET-OFFSET and RESPOND
Studies. Clin Pharmacokinet
2012;51:397-409
32. Butler K, Teng R. Pharmacokinetics,
pharmacodynamics, and safety of
ticagrelor in volunteers with severe renal
impairment. J Clin Pharmacol
2011; Epub ahead of print
33. Butler K, Teng R. Pharmacokinetics,
pharmacodynamics, and safety of
ticagrelor in volunteers with mild hepatic
impairment. J Clin Pharmacol
2011;51:978-87
34. AstraZeneca. BRILINTA (Ticagrelor)
Approved Product Information. 2011
35. Cannon CP, Husted S, Harrington RA,
et al. Safety, tolerability, and initial
efficacy of AZD6140, the first reversible
oral adenosine diphosphate receptor
antagonist, compared with clopidogrel, in
patients with non-ST-segment elevation
acute coronary syndrome: primary results
of the DISPERSE-2 trial. J Am
Coll Cardiol 2007;50:1844-51. This dose-finding study demonstrated
the safety and efficacy of inhibition of
platelet activity of ticagrelor compared
with clopidogrel in patients with
non-ST-elevation ACS.
36. Gurbel PA, Bliden KP, Butler K, et al.
Response to ticagrelor in clopidogrel
nonresponders and responders and effect
of switching therapies: the RESPOND
study. Circulation 2010;121:1188-99.. This study demonstrates that switching
patients who have inadequate platelet
inhibition with clopidogrel to
ticagrelor overcomes the poor
clopidogrel response. The platelet
inhibition achieved is the same in both
clopidogrel responders and non-
responders.
37. James S, Akerblom A, Cannon CP, et al.
Comparison of ticagrelor, the first
reversible oral P2Y(12) receptor
antagonist, with clopidogrel in patients
with acute coronary syndromes: rationale,
design, and baseline characteristics of the
PLATelet inhibition and patient
Outcomes (PLATO) trial. Am Heart J
2009;157:599-605
38. Cannon CP, Harrington RA, James S,
et al. Comparison of ticagrelor with
clopidogrel in patients with a planned
invasive strategy for acute coronary
syndromes (PLATO): a randomised
double-blind study. Lancet
2010;375:283-93
39. James S, Budaj A, Aylward P, et al.
Ticagrelor versus clopidogrel in acute
coronary syndromes in relation to renal
function: results from the Platelet
Inhibition and Patient Outcomes
(PLATO) trial. Circulation
2010;122:1056-67
40. Held C, Asenblad N, Bassand JP, et al.
Ticagrelor versus clopidogrel in patients
with acute coronary syndromes
undergoing coronary artery bypass
surgery: results from the PLATO
(Platelet Inhibition and Patient
Outcomes) trial. J Am Coll Cardiol
2011;57:672-84
41. James S, Angiolillo DJ, Cornel JH, et al.
Ticagrelor vs. clopidogrel in patients with
acute coronary syndromes and diabetes:
a substudy from the PLATelet inhibition
and patient Outcomes (PLATO) trial.
Eur Heart J 2010;31:3006-16
42. Stiles S. Use low-dose aspirin with
ticagrelor, PLATO analysis suggests.
Acute Coronary Syndromes.
2011.Available from: http://www.
theheart.org/article/1244925.do [Cited
28 June 2012]
43. Mahaffey KW, Wojdyla DM, Carroll K,
et al. Ticagrelor compared with
clopidogrel by geographic region in the
Platelet Inhibition and Patient Outcomes
(PLATO) trial. Circulation
2011;124:544-54
44. Ohman EM, Roe MT. Explaining the
unexpected: insights from the PLATelet
inhibition and clinical Outcomes
(PLATO) trial comparing ticagrelor and
clopidogrel. Editorial on Serebruany
"Viewpoint: Paradoxical excess mortality
in the PLATO trial should be
independently verified" (Thromb
Haemost 2011; 105.5).
Thromb Haemost 2011;105:763-5
45. Serebruany VL. Viewpoint: paradoxical
excess mortality in the PLATO trial
S. Burgess et al.
1324 Expert Opin. Drug Metab. Toxicol. (2012) 8(10)
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.
should be independently verified.
Thromb Haemost 2011;105:752-9
46. Serebruany VL. Aspirin dose and
ticagrelor benefit in PLATO: fact or
fiction? Cardiology 2010;117:280-3
47. Wallentin L, Becker RC, James SK,
Harrington RA. The PLATO trial reveals
further opportunities to improve
outcomes in patients with acute coronary
syndrome. Editorial on serebruany.
"Viewpoint: paradoxical excess mortality
in the PLATO trial should be
independently verified" (Thromb
Haemost 2011; 105.5).
Thromb Haemost 2011;105:760-2
48. Peters RJ, Mehta SR, Fox KA, et al.
Effects of aspirin dose when used alone
or in combination with clopidogrel in
patients with acute coronary syndromes:
observations from the Clopidogrel in
Unstable angina to prevent Recurrent
Events (CURE) study. Circulation
2003;108:1682-7
49. Warner TD, Nylander S, Whatling C.
Anti-platelet therapy: cyclo-oxygenase
inhibition and the use of aspirin with
particular regard to dual anti-platelet
therapy. Br J Clin Pharmacol
2011;72:619-33
50. Becker RC, Bassand JP, Budaj A, et al.
Bleeding complications with the
P2Y12 receptor antagonists clopidogrel
and ticagrelor in the PLATelet inhibition
and patient Outcomes (PLATO) trial.
Eur Heart J 2011;32:2933-44
51. Serebruany VL. The TRITON versus
PLATO trials: differences beyond platelet
inhibition. Thromb Haemost
2010;103:259-61
52. Kirkby NS, Leadbeater PD, Chan MV,
et al. Antiplatelet effects of aspirin vary
with level of P2Y receptor blockade
supplied by either ticagrelor or prasugrel.
J Thromb Haemost 2011;9:2103-5
53. Scirica BM, Cannon CP,
Emanuelsson H, et al. The
incidence of bradyarrhythmias and
clinical bradyarrhythmic events in
patients with acute coronary syndromes
treated with ticagrelor or clopidogrel in
the PLATO (Platelet Inhibition and
Patient Outcomes) trial: results of
the continuous electrocardiographic
assessment substudy. J Am Coll Cardiol
2011;57:1908-16
54. Storey RF, Bliden KP, Patil SB, et al.
Incidence of dyspnea and assessment of
cardiac and pulmonary function in
patients with stable coronary artery
disease receiving ticagrelor, clopidogrel,
or placebo in the ONSET/OFFSET
study. J Am Coll Cardiol
2010;56:185-93
55. Burki NK, Dale WJ, Lee LY.
Intravenous adenosine and dyspnea in
humans. J Appl Physiol 2005;98:180-5
56. Hong JL, Ho CY, Kwong K, Lee LY.
Activation of pulmonary C fibres by
adenosine in anaesthetized rats: role of
adenosine A1 receptors. J Physiol
1998;508(Pt 1):109-18
57. European Medicines Agency. European
Medicines Agency. 2012.Available from:
http://www.ema.europa.eu/ema/
[Cited 06 May 2012]
58. Wijns W, Kolh P, Danchin N, et al.
Guidelines on myocardial
revascularization. Eur Heart J
2010;31:2501-55
59. Hamm CW, Bassand JP, Agewall S,
et al. ESC Guidelines for the
management of acute coronary
syndromes in patients presenting without
persistent ST-segment elevation: the Task
Force for the management of acute
coronary syndromes (ACS) in patients
presenting without persistent ST-segment
elevation of the European Society of
Cardiology (ESC). Eur Heart J
2011;32:2999-3054
60. U.S. Food and Drug Administration.
FDA. 2012.Available from:
http://www.fda.gov/default.htm
[Cited 06 May 2012]
61. Levine GN, Bates ER, Blankenship JC,
et al. 2011 ACCF/AHA/SCAI Guideline
for Percutaneous Coronary Intervention.
A report of the American College of
Cardiology Foundation/American Heart
Association Task Force on Practice
Guidelines and the Society for
Cardiovascular Angiography and
Interventions. J Am Coll Cardiol
2011;58:e44-122
62. Therapeutic Goods Administration.
Therapeutic Goods Administration.
2012.Available from: http://www.tga.gov.
au/ [Cited 06 May 2012]
63. Chew DP, Aroney CN, Aylward PE,
et al. 2011 Addendum to the National
Heart Foundation of Australia/Cardiac
Society of Australia and New Zealand
Guidelines for the management of acute
coronary syndromes (ACS) 2006.
Heart Lung Circ 2011;20:487-502
64. AstraZeneca. Prevention of
Cardiovascular Events (e.g., Death From
Heart or Vascular Disease, Heart Attack,
or Stroke) in Patients With Prior Heart
Attack Using Ticagrelor Compared to
Placebo on a Background of Aspirin
(PEGASUS). 2010.Available from:
http://clinicaltrials.gov/ct2/show/
NCT01225562 [Cited 28 June 2012]
AffiliationSonya Burgess1 MBChB BSc,
Trevor A Mallard1 BMed &
Craig P Juergens†1,2 MBBS†Author for correspondence1Department of Cardiology,
Liverpool Hospital,
Liverpool NSW,
Australia2A/Professor,
Southwestern Clinical School,
University of NSW, Sydney,
Australia
Tel: +612 98283078;
Fax: +612 98283054;
E-mail: [email protected]
Ticagrelor
Expert Opin. Drug Metab. Toxicol. (2012) 8(10) 1325
Exp
ert O
pin.
Dru
g M
etab
. Tox
icol
. Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 11
/08/
12Fo
r pe
rson
al u
se o
nly.

64
PAPER 13
Reprinted from Clinical Therapeutics 2002;24:1332-1344 with
permission from Clinical Therapeutics

CLINICAL THERAPEUTICS®fVQL. 24, NO.8, 2002
A Multicenter Study of the Tolerability of Tirofiban Versus Placebo in Patients Undergoing Planned Intracoronary Stent Placement
Craig P. Juergens, FRACP/ Harvey D. White, FRACP/ Jorge A. Belardi, MD/ Carlos Macaya, MD/ Jordi Soler-Soler, MD,S Beat]. Meyer, MD/ Richard D. Levy, FRCP/ Ton Bunt, MD,S ]oris Menten, MS, Howard C. Herrmann, MD/ AA. Jennifer Adgey, FRCP/0 and Georgia Tarnesby, MRCP8
1 Liverpool Hospital, Liverpool, Australia, 2Green Lane Hospital, Auckland, New Zealand, 3Instituto Cardiovascular de Buenos Aires, Argentina, 4Hospital Clinico Universitario San Carlos, Madrid, 5Hospital Vall d'Hebron, Barcelona, Spain, 6Swiss Cardiovascular Centre, University Hospital Inselspital, Bern, Switzerland, 7Wythenshawe Hospital, Manchester, United Kingdom, 8Merck & Co, Inc, Whitehouse Station, New Jersey, 9University of Pennsylvania Medical Center, Philadelphia, and 10Royal Victoria Hospital, Belfast, Northern Ireland, United Kingdom
ABSTRACT
Background: The use of intravenous glycoprotein lib/Ilia-receptor antagonists has been shown to improve outcomes in patients undergoing percutaneous transluminal coronary angioplasty (PICA). Tirofiban has shown benefit in a wide range of patients presenting with acute coronary syndromes. Although this agent has been used in patients undergoing percutaneous coronary intervention, a literature search identified no prospective data comparing tirofiban with placebo in patients undergoing planned intracoronary stent placement.
Objective: This study examined the tolerability of tirofiban in patients undergoing percutaneous intervention with planned intracoronary stent placement.
Methods: This was a multinational, multicenter, prospective, randomized, doubleblind, placebo-controlled trial in patients scheduled to undergo PTCA with planned intracoronary stent placement. Patients were randomized in a 3:2 ratio to receive tirofiban as an intravenous bolus (10 jJvg/kg over 3 minutes) and maintenance infusion (0.10 !Jvg/kg per minute for 36 hours) or a bolus and infusion of placebo. All patients received periprocedural aspirin and heparin and an optional postprocedural thienopyridine (ticlopidine or clopidogrel). Laboratory and safety monitoring were performed throughout the 36 hours after the procedure and at hour 40 or hospital discharge. The primary end point was the proportion of patients with bleeding, defined according to Thrombolysis in Myocardial Infarction (TIMI) trial criteria. The number of patients with cardiac events (death, myo-
Accepted for publication May 29, 2002.
Printed in the USA. Reproduction in whole or part is not permitted.
1332 0149-29181021$19.00

C.P. JUERGENS ET AL.
cardia! infarction, urgent revascularization) during the first 30 days after stent placement was also assessed.
Results: Eight hundred ninety-four patients (536 tirofiban, 358 placebo) were enrolled, all of whom received aspirin and heparin periprocedurally and optional ticlopidine or clopidogrel after the procedure. No significant between-group differences were observed in the incidence of TIMI major bleeding (0.2% tirofiban, 0.6% placebo) or any TIMI bleeding (3.2% and 1.7%, respectively). The incidence of TIMI minor bleeding was higher with tirofiban than with placebo (2.8% vs 0.6%). The 30-day incidence of the composite end point of any cardiac event was 3.9% in both groups.
Conclusions: On a background of concomitant aspirin, heparin, and a thienopyridine, tirofiban was generally well tolerated in patients undergoing PTCA with planned intracoronary stent placement. Further investigation is needed to ascertain the optimal dosing of tirofiban and heparin to achieve reductions in ischemic complications of intracoronary stenting with an acceptable incidence of bleeding complications.
Key words: intracoronary stent, percutaneous intervention, GP lib/Ilia-receptor antagonists, tirofiban. (Clin Ther. 2002; 24:1332-1344)
INTRODUCTION
Clinical trials have shown that use of intravenous glycoprotein (GP) lib/Iliareceptor antagonists results in improved outcomes after percutaneous transluminal coronary angioplasty (PTCA). 1- 3 Tirofiban is a highly selective inhibitor of the binding of fibrinogen to the platelet GP lib/Ilia receptor. Three large clinical trials
oftirofiban in a total of7288 patients have provided evidence of the efficacy and tolerability of tirofiban for reducing ischemic events in a broad range of patients, including those with unstable angina and non-Q-wave myocardial infarction (MI)4 .5
and those undergoing high-risk angioplasty after presenting with acute coronary syndromes.6 Of note, these clinical trials predated the widespread use of intracoronary stenting. In RESTORE6 (Randomized Efficacy Study of Tirofiban for Outcomes and Restenosis), planned coronary stenting was discouraged in patients undergoing percutaneous coronary intervention. As a result, only 175 of 2141 enrolled patients received an intracoronary stent. Forty-three (24.6%) of these stents were placed for actual or threatened closure, and the rest were placed for a suboptimal angiographic result. Since these earlier trials, use of aspirin in combination with a thienopyridine (ticlopidine or clopidogrel) after intracoronary stent placement has become standard practice?-9 As a result, more placebo-controlled data are required about the concomitant use of tirofiban with these agents.
The Evaluation of Platelet lib/Ilia Inhibitor for Stenting 10 (EPISTENT) was the first study to examine the use of a GP lib/Ilia-receptor antagonist ( abciximab) in patients undergoing planned intracoronary stenting. The Enhanced Suppression of the Platelet lib/lila Receptor with Integrilin Therapy 11 (ESPRIT) trial assessed the efficacy of the small-molecule GPIIb!lllareceptor antagonist eptifibatide in planned coronary stent placement. Both trials demonstrated that a strategy of using abciximab (EPISTENT) or eptifibatide (ESPRIT) with stenting was associated with a reduction in primary cardiac end points compared with placebo, with an
1333

incidence of major bleeding complications of <2%.
More recently, results have been published from TARGET12 (Do Tirofiban and ReoPro™ Give Similar Efficacy Trial), which compared tirofiban and abciximab in patients undergoing percutaneous coronary revascularization. Tirofiban was administered as a bolus dose of 10 J..Lg/kg followed by an infusion of 0.15 J..Lg/kg per minute for 18 to 24 hours. Abciximab was given as a bolus dose of 0.25 mg/kg followed by an infusion of 0.125 J..Lg/kg per minute (maximum, 10 J..Lg/kg per minute) for 12 hours. The investigators concluded that of the regimens studied, tirofiban appeared to offer less protection against major ischemic events than did abciximab. In addition, although abciximab resulted in more minor bleeding episodes and thrombocytopenia than did tirofiban, there was no significant difference in rates of major bleeding between the 2 groups.
A literature search of MEDLINE combining the terms tirofiban, stent, and placebo identified no articles published between 1966 and January 2002 that specifically addressed the comparison that is the focus of the present study. Thus, this is the first large-scale randomized controlled trial to assess the tolerability of tirofiban compared with placebo, both regimens in combination with aspirin, heparin, and a thienopyridine, in patients undergoing PTCA with planned intracoronary stent placement.
PATIENTS AND METHODS
Study Population
Patients scheduled to undergo PTCA with intracoronary stent placement at 59 centers in 24 countries were eligible for
1334
CLINICAL THERAPEUTICS~
inclusion. Patients were excluded if they had received thrombolytic therapy within 24 hours of the procedure or had elevated levels of the creatine kinase (CK)-MB isozyme at baseline; were allergic to or unable to tolerate aspirin or heparin; had received abciximab within 14 days of the procedure; had received ticlopidine, clopidogrel, or low-molecular-weight heparin within 12 to 24 hours of randomization; had undergone PTCA within 14 days or were likely to undergo planned repeat PTCA as a staged procedure; if the target vessel was an unprotected left main stenosis; had had a bleeding disorder within 3 months; had persistent systolic blood pressure > 180 mm Hg and/or persistent diastolic blood pressure > 105 mm Hg; had a history of stroke or other intracranial pathology within 1 year; had undergone recent major surgery, trauma, or cardiopulmonary resuscitation; had active peptic ulcer disease, pericarditis, significant retinopathy, suspected aortic dissection, an uncontrolled cardiac arrhythmia, other hemodynamically significant cardiac disease, or other clinically important medical illness that would make survival for the duration of the study unlikely; had a serum creatinine level >2.5 mg/dL (>220 J..Lmol/L), hemoglobin <11 g/dL, international normalized ratio > 1.5, or a platelet count <150,000/mm3; or were unable to give informed consent.
The institutional review board at each hospital approved the study protocol, and all patients gave their written informed consent for participation.
Study Design
The study design is summarized in the figure. All patients received 300 to 325 mg aspirin within 12 hours before the pro-
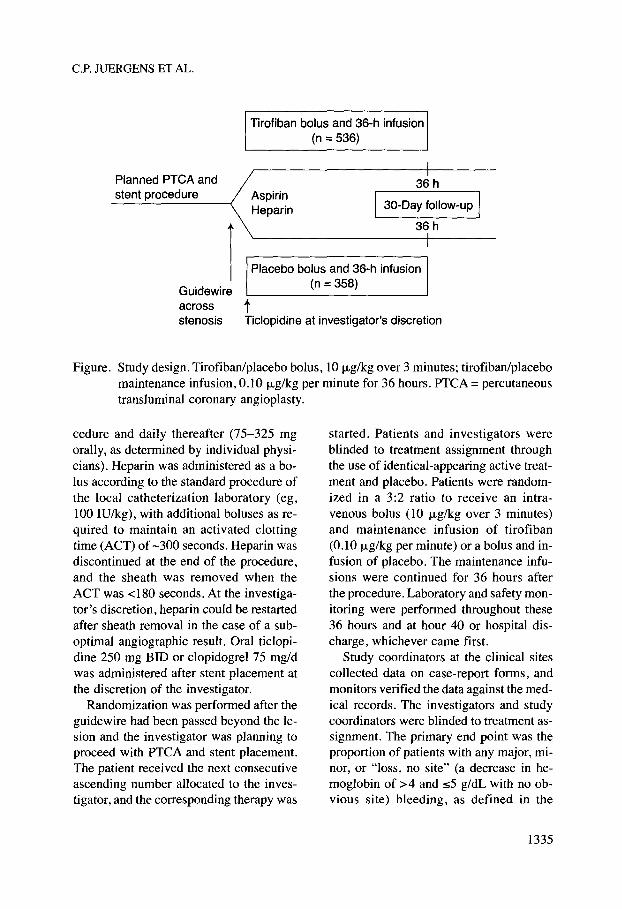
C.P. JUERGENS ET AL.
Tirofiban bolus and 36-h infusion (n = 536)
Planned PTCA and stent procedure Aspirin
Heparin
36 h
30-Day follow-up I 36 h
1 Guidewire across stenosis
Placebo bolus and 36-h infusion (n = 358)
t Ticlopidine at investigator's discretion
Figure. Study design. Tirofiban/placebo bolus, 10 ~J-g/kg over 3 minutes; tirofiban/placebo maintenance infusion, 0.10 ~J-glkg per minute for 36 hours. PTCA =percutaneous transluminal coronary angioplasty.
cedure and daily thereafter (75-325 mg orally, as determined by individual physicians). Heparin was administered as a bolus according to the standard procedure of the local catheterization laboratory ( eg, 100 IU/kg), with additional boluses as required to maintain an activated clotting time (ACT) of -300 seconds. Heparin was discontinued at the end of the procedure, and the sheath was removed when the ACT was <180 seconds. At the investigator's discretion, heparin could be restarted after sheath removal in the case of a suboptimal angiographic result. Oral ticlopidine 250 mg BID or clopidogrel 75 mg/d was administered after stent placement at the discretion of the investigator.
Randomization was performed after the guidewire had been passed beyond the lesion and the investigator was planning to proceed with PTCA and stent placement. The patient received the next consecutive ascending number allocated to the investigator, and the corresponding therapy was
started. Patients and investigators were blinded to treatment assignment through the use of identical-appearing active treatment and placebo. Patients were randomized in a 3:2 ratio to receive an intravenous bolus (10 ~J-g/kg over 3 minutes) and maintenance infusion of tirofiban (0.10 j.1g/kg per minute) or a bolus and infusion of placebo. The maintenance infusions were continued for 36 hours after the procedure. Laboratory and safety monitoring were performed throughout these 36 hours and at hour 40 or hospital discharge, whichever came first.
Study coordinators at the clinical sites collected data on case-report forms, and monitors verified the data against the medical records. The investigators and study coordinators were blinded to treatment assignment. The primary end point was the proportion of patients with any major, minor, or "loss, no site" (a decrease in hemoglobin of >4 and s5 g/dL with no obvious site) bleeding, as defined in the
1335

criteria used in the Thrombolysis in Myocardial Infarction 13 (TIMI) trial. All bleeding incidents from the start of study-drug infusion to 24 hours after completion of the infusion or hospital discharge, whichever came first, were recorded for analysis. There was no central adjudication of bleeding incidents; however, investigators were provided with definitions and were required to confirm the occurrence of these incidents on a special form.
Laboratory monitoring was performed during and after study-drug infusion, with levels of CK and CK-MB measured at 2 hours, every 6 hours for the first 24 hours, and every 8 hours until the passage of 40 hours or attainment of peak CK-MB levels, if this had not occurred by 40 hours. Hematocrit, measurement of hemoglobin, and platelet count were performed at 6, 24, and 40 hours. Thrombocytopenia, defined as a platelet count <90 ·109/L, was considered a serious adverse experience.
Although this was primarily a tolerability study, adverse cardiac outcomes were recorded in both treatment groups until 30 days after PTCA and stent placement. The following cardiac events were recorded: death, MI, urgent coronary artery bypass grafting for recurrent ischemia, and urgent repeat percutaneous intervention for recurrent ischemia in the target vessel. Cardiac events were reviewed and adjudicated by an external Event Classification Committee (ECC). Adjudicated MI events following the index procedure were subdivided into periprocedural (within 48 hours) or postprocedural (after the periprocedural period) events. A periprocedural MI was defined by either elevation in CK or CK-MB to ~3 times the upper laboratory limit for the participating hospital on ;;;,2 separate occasions or development of a new patho-
1336
CLINICAL THERAPEUTICS®
logic Q wave accompanied by an elevation in CK. A postprocedural MI was defined by either a new pathologic Q wave or an elevation in CK or CK-MB to ~2 times the upper laboratory limit for the participating hospital accompanied by chest pain and/or electrocardiographic changes. In addition to individual events, the following 2 composite adverse cardiac events were analyzed: the composite of death and MI, and the composite of all recorded cardiac events.
Statistical Analysis
All analyses were performed on an intent-to-treat basis. All statistical tests were 2-sided, with an a of0.05. P values :s0.05 were considered statistically significant. All statistical analyses were performed using SAS version 6.12 (SAS Institute Inc, Cary, N.C.) and PROC StatXact 3.11 (Cytel, Cambridge, Mass.). As most end points occurred with a low incidence, analyses were performed using exact methods, as implemented by SAS and PROC StatXact.
The comparison between treatment groups with respect to the proportion of patients with any TIMI bleeding was performed using the Fisher exact test. Treatment groups were compared for severity of bleeding complications using the Wilcoxon Mann-Whitney test. When using the latter test, the TIMI categories of minor bleeding and "loss, no site" bleeding were combined. The Fisher exact test was also used to compare the incidence of cardiac events, thrombocytopenia, and other adverse experiences between treatment groups.
This study was designed to estimate the incidence of the primary end point of any TIMI bleeding to within 3.0%, assuming
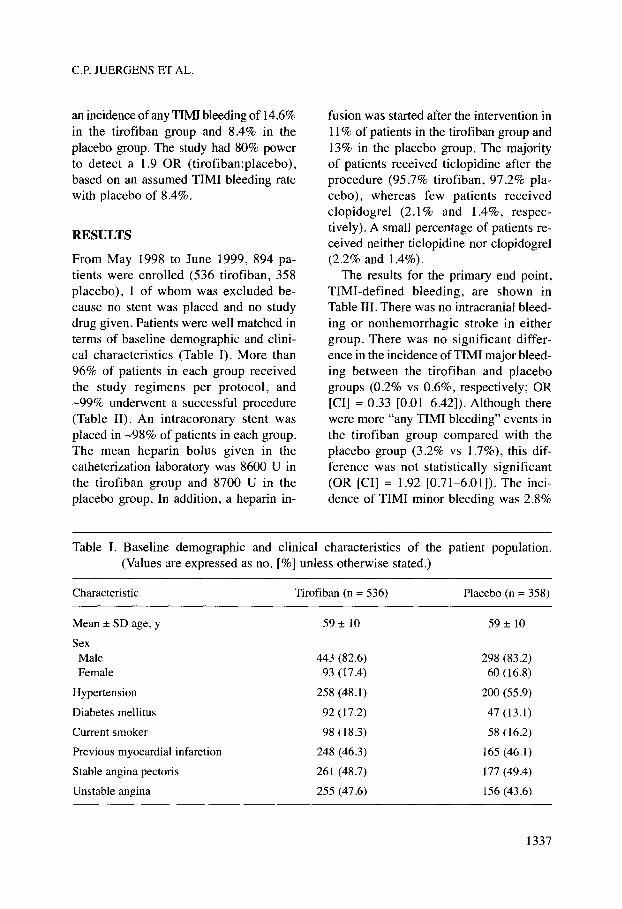
C.P. JUERGENS ET AL.
an incidence of any TIMI bleeding of 14.6% in the tirofiban group and 8.4% in the placebo group. The study had 80% power to detect a 1.9 OR (tirofiban:placebo), based on an assumed TIMI bleeding rate with placebo of 8.4%.
RESULTS
From May 1998 to June 1999, 894 patients were enrolled (536 tirofiban, 358 placebo), 1 of whom was excluded because no stent was placed and no study drug given. Patients were well matched in terms of baseline demographic and clinical characteristics (Table 1). More than 96% of patients in each group received the study regimens per protocol, and -99% underwent a successful procedure (Table II). An intracoronary stent was placed in -98% of patients in each group. The mean heparin bolus given in the catheterization laboratory was 8600 U in the tirofiban group and 8700 U in the placebo group. In addition, a heparin in-
fusion was started after the intervention in 11% of patients in the tirofiban group and 13% in the placebo group. The majority of patients received ticlopidine after the procedure (95 .7% tirofiban, 97.2% placebo), whereas few patients received clopidogrel (2.1% and 1.4%, respectively). A small percentage of patients received neither ticlopidine nor clopidogrel (2.2% and 1.4%).
The results for the primary end point, TIMI-defined bleeding, are shown in Table III. There was no intracranial bleeding or nonhemorrhagic stroke in either group. There was no significant difference in the incidence ofTIMI major bleeding between the tirofiban and placebo groups (0.2% vs 0.6%, respectively; OR [CI] = 0.33 [0.01-6.42]). Although there were more "any TIMI bleeding" events in the tirofiban group compared with the placebo group (3.2% vs 1.7%), this difference was not statistically significant (OR [CI] = 1.92 [0.71-6.01]). The incidence of TIMI minor bleeding was 2.8%
Table I. Baseline demographic and clinical characteristics of the patient population. (Values are expressed as no. [%] unless otherwise stated.)
Characteristic
Mean± SD age, y
Sex Male Female
Hypertension
Diabetes mellitus
Current smoker
Previous myocardial infarction
Stable angina pectoris
Unstable angina
Tirofiban (n = 536)
59± 10
443 (82.6) 93 (17.4)
258 (48.1)
92 (17.2)
98 (18.3)
248 (46.3)
261 (48.7)
255 (47.6)
Placebo (n = 358)
59± 10
298 (83.2) 60 (16.8)
200 (55.9)
47 (13.1)
58 (16.2)
165 (46.1)
177 (49.4)
156 (43.6)
1337
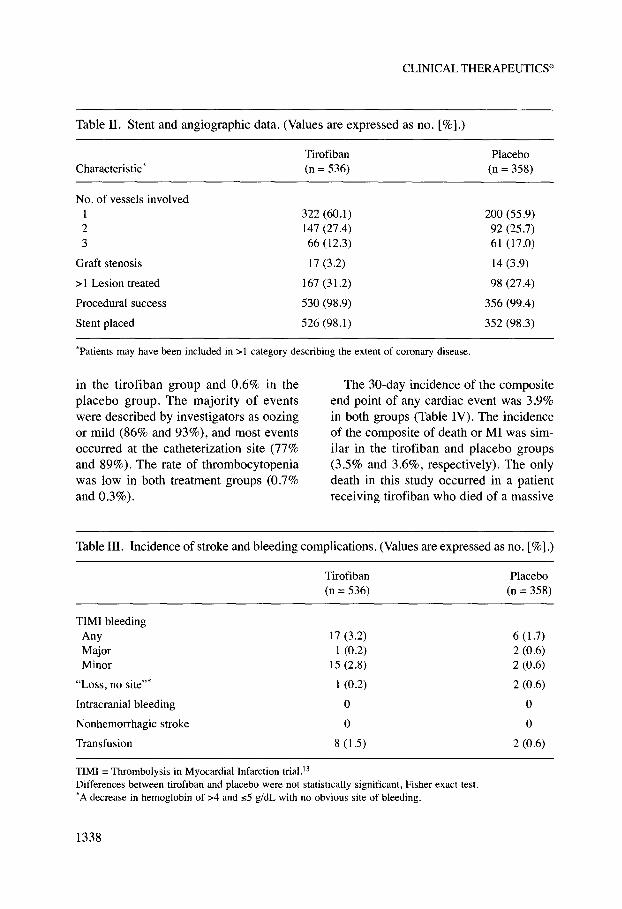
CLINICAL THERAPEUTICS®
Table II. Stent and angiographic data. (Values are expressed as no.[%].)
Tirofiban Placebo Characteristic* (n = 536) (n = 358)
No. of vessels involved I 322 (60.1) 200 (55.9) 2 147(27.4) 92 (25.7) 3 66 (12.3) 61 (17.0)
Graft stenosis 17 (3.2) 14 (3.9)
> 1 Lesion treated 167 (31.2) 98 (27 .4)
Procedural success 530 (98.9) 356 (99.4)
Stent placed 526 (98.1) 352 (98.3)
'Patients may have been included in >I category describing the extent of coronary disease.
in the tirofiban group and 0.6% in the placebo group. The majority of events were described by investigators as oozing or mild (86% and 93%), and most events occurred at the catheterization site (77% and 89%). The rate of thrombocytopenia was low in both treatment groups (0.7% and 0.3%).
The 30-day incidence of the composite end point of any cardiac event was 3.9% in both groups (Table IV). The incidence of the composite of death or MI was similar in the tirofiban and placebo groups (3.5% and 3.6%, respectively). The only death in this study occurred in a patient receiving tirofiban who died of a massive
Table III. Incidence of stroke and bleeding complications. (Values are expressed as no. [%] .)
Tirofiban (n = 536)
TIMI bleeding Any 17 (3.2) Major 1 (0.2) Minor 15 (2.8)
"Loss, no site"' I (0.2)
Intracranial bleeding 0
Nonhemorrhagic stroke 0
Transfusion 8 (1.5)
TIMI =Thrombolysis in Myocardial Infarction trial.D Differences between tirofiban and placebo were not statistically significant, Fisher exact test. 'A decrease in hemoglobin of >4 and s5 g/dL with no obvious site of bleeding.
1338
Placebo (n = 358)
6 ( 1.7) 2 (0.6) 2 (0.6)
2 (0.6)
0
0
2 (0.6)
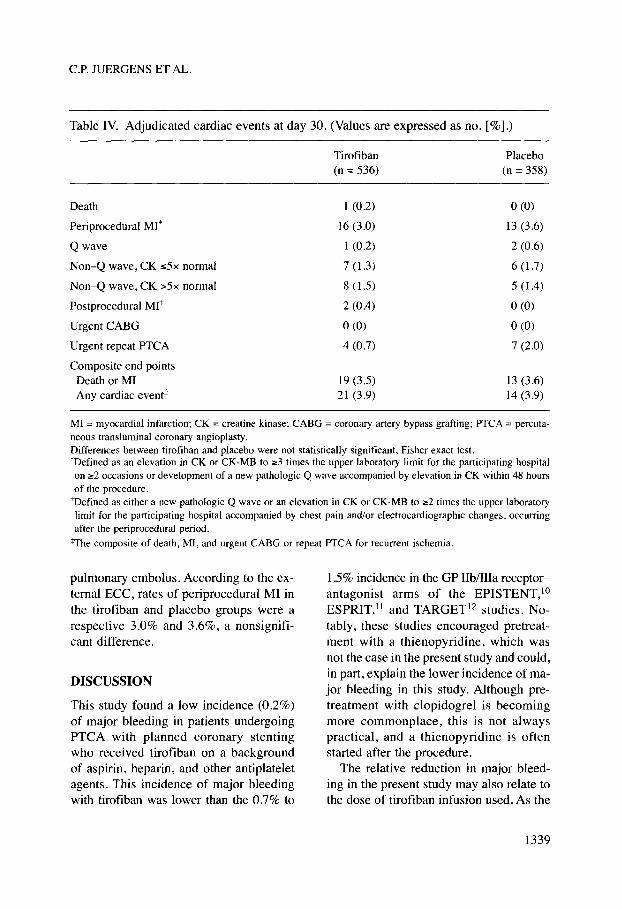
C.P. JUERGENS ET AL.
Table IV. Adjudicated cardiac events at day 30. (Values are expressed as no.[%].)
Tirofiban Placebo (n = 536) (n = 358)
Death I (0.2) 0 (0)
Periprocedural MI* 16 (3.0) 13 (3.6)
Qwave 1 (0.2) 2 (0.6)
Non-Q wave, CK s5x normal 7 (1.3) 6 (1.7)
Non-Q wave, CK >5x normal 8 ( 1.5) 5 (1.4)
Postprocedural Mit 2 (0.4) 0 (0)
Urgent CABG 0 (0) 0 (0)
Urgent repeat PTCA 4 (0.7) 7 (2.0)
Composite end points Death or MI 19 (3.5) 13 (3.6) Any cardiac event* 21 (3.9) 14 (3.9)
MI = myocardial infarction; CK = creatine kinase; CABO = coronary artery bypass grafting; PTCA = percutaneous transluminal coronary angioplasty. Differences between tirofiban and placebo were not statistically significant, Fisher exact test. 'Defined as an elevation in CK or CK-MB to ~3 times the upper laboratory limit for the participating hospital on ~2 occasions or development of a new pathologic Q wave accompanied by elevation in CK within 48 hours of the procedure.
tDefined as either a new pathologic Q wave or an elevation in CK or CK-MB to ~2 times the upper laboratory limit for the participating hospital accompanied by chest pain and/or electrocardiographic changes, occurring after the periprocedural period.
*The composite of death, MI, and urgent CABO or repeat PTCA for recurrent ischemia.
pulmonary embolus. According to the external ECC, rates of periprocedural MI in the tirofiban and placebo groups were a respective 3.0% and 3.6%, a nonsignificant difference.
DISCUSSION
This study found a low incidence (0.2%) of major bleeding in patients undergoing PTCA with planned coronary stenting who received tirofiban on a background of aspirin, heparin, and other antiplatelet agents. This incidence of major bleeding with tirofiban was lower than the 0.7% to
1.5% incidence in the GP lib/lila receptorantagonist arms of the EPISTENT, 10
ESPRIT, 11 and TARGET 12 studies. Notably, these studies encouraged pretreatment with a thienopyridine, which was not the case in the present study and could, in part, explain the lower incidence of major bleeding in this study. Although pretreatment with clopidogrel is becoming more commonplace, this is not always practical, and a thienopyridine is often started after the procedure.
The relative reduction in major bleeding in the present study may also relate to the dose of tirofiban infusion used. As the
1339
primary study objective was to establish the tolerability of tirofiban use during intracoronary stenting, we chose a conservative maintenance infusion rate of 0.10 J-Lg/kg per minute, as was used in the PRISM-PLUS5 (Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms) trial, rather than the 0.15 J-Lg/kg per minute used in RESTORE6 and TARGET.12 In the tirofiban arms of the latter 2 studies, the incidence of bleeding was 0.9% and 2.1 %, respectively, higher than in this study. It should be noted, however, that the lower incidence of major bleeding in this study occurred despite the use of higher doses of heparin than were used in TARGET. The study protocol suggested administering heparin to maintain the ACT at -300 seconds. The mean dose of heparin was >8500 U in both arms of this study, whereas the ESPRIT, EPISTENT, and TARGET investigators were encouraged to weight-adjust the heparin dose during percutaneous coronary intervention to maintain an ACT of 200 to 300 seconds. In addition, in the ESPRIT and EPISTENT protocols, the maximum total dose of heparin was mandated (6000 and 7000 U, respectively). In EPILOG2
(Evaluation in PTCA to Improve LongTerm Outcome with Abciximab GP lib/ lila Blockade), the best efficacy and bleeding outcomes with abciximab during percutaneous coronary intervention occurred when the ACT was maintained at between 200 and 300 seconds. The ESPRIT results suggested optimal outcomes with eptifibatide when the ACT was maintained at between 200 and 250 seconds. The present study did not involve prospective collection of ACT data. It is possible that the greater incidence of minor bleeding in the tirofiban arm compared with placebo
1340
CLINICAL THERAPEUTICS®
might have been reduced if the target ACT range had been lower. It is also possible that use of a higher bolus or infusion dose of tirofiban with a lower heparin dose might have resulted in an acceptable incidence of bleeding complications with a reduced incidence of adverse cardiac events compared with placebo.
The results of earlier studies in patients presenting with acute coronary syndromes suggested a reduction in cardiac events with tirofiban in those undergoing an interventional coronary procedure. In the PRISM4 (Platelet Receptor Inhibition in Ischemic Syndrome Management) trial, 21% of patients underwent percutaneous revascularization, and 34% of these received a stent. Of patients undergoing percutaneous revascularization (with or without a stent), those who received tirofiban had a reduction in the composite end point of death, Ml, or refractory ischemia at 30 days compared with those who received placebo (21% vs 27%, respectively; RR = 0.72; 95% CI, 0.53---0.98). In the PRISMPLUS5 trial, 30% of patients underwent percutaneous revascularization; in the subset of patients undergoing coronary angioplasty (with or without stenting), those who received tirofiban plus heparin also had a reduction in the same composite end point compared with those who received heparin alone (8.8% vs 15.3%; RR = 0.55; 95% CI, 0.32---0.94). The decision whether to perform a percutaneous intervention in both these studies was not randomized, there was no independent assessment of safety, and no analysis was performed based on whether stenting was performed or not. Although the present study was not powered to do so, its results do not confirm earlier observations of a reduction in cardiac events in patients receiving tirofiban who underwent planned
C.P. JUERGENS ET AL.
intracoronary stenting. This may be because of the relatively small numbers of patients enrolled and the fact that the population consisted of a relatively low-risk group of patients. It is also well established that intracoronary stenting causes more trauma to the arterial wall than does simple balloon angioplasty. 14·15 Furthermore, it is possible that the dose of tirofiban used in the present study was not sufficient to prevent ischemic complications.
In contrast to the larger EPISTENT10
(2399 patients) and ESPRIT 11 (2064 patients) trials, this study did not find a significant reduction in cardiac events in the tirofiban group compared with the placebo group. Because its primary focus was tolerability, the study was not powered to detect a clinically meaningful difference in the incidence of cardiac events. In the placebo group, the incidence of the composite end point of death, MI, or urgent revascularization was 3.9%, compared with 10.8% in EPISTENT and 9.3% in ESPRIT. The lower event rate compared with EPISTENT may be related to the greater number of patients presenting with stable angina in this trial (-50% vs 40%, respectively), the lack of pretreatment with a thienopyridine, or the more stringent definition of MI (ie, 2 blood samples with a CK or CK-MB ;::3 times the upper limit of normal). Although there was no significant difference in the rate of periprocedural MI in the tirofiban and placebo groups (3.0% vs 3.6%, respectively), use of a less stringent definition might have shown a significant difference between active treatment and placebo.
In the present study, randomization did not occur until the guidewire had been passed beyond the lesion. This was also the protocol in the RESTORE6 study, whereas abciximab and eptifibatide were
administered before commencement of the coronary intervention in EPISTENT10
and ESPRIT,ll respectively. GP lib/lilareceptor antagonists are ideally given before commencement of an intervention so that the platelets are maximally inhibited before intracoronary manipulation with a wire or balloon. There are published data confirming platelet activation and aggregation during mechanically induced vessel injury caused by balloon angioplasty.16·17 It is possible that not administering the bolus dose of tirofiban before the lesion was crossed with the guidewire may have led to platelet activation that could have been minimized if tirofiban had been given earlier.
This study had a number of limitations. The observed incidence of any TIMI bleeding with placebo was 1.7%, much lower than the anticipated incidence of 8.4%. Consequently, the study was substantially underpowered to assess the primary end point. Occurrence of the primary end point was investigator determined and subject to bias. Nonetheless, the risk of bias was reduced by the multinational, multicenter, placebo-controlled study design. The reported rates of bleeding in this trial were similar to those reported in other large-scale trials of tirofiban, including PRISM4 and TARGET,l2 and the consistency of these results suggests that they are unlikely to be the product of bias or chance. The large number of exclusion criteria necessitated by this study's primary focus on tolerability restricts the applicability of the results to the general population. Previous studies have shown that the patients who benefit most from the use of GP lib/lila-receptor antagonists are those with elevated levels of troponins. 18·19 The present study did not routinely measure troponins, but re-
1341
quiring a normal baseline CK-MB potentially excluded a number of such patients.
CONCLUSIONS
The results of this study suggest a low incidence of major bleeding when tirofiban is administered in combination with aspirin, heparin, and a thienopyridine in patients undergoing PTCA with planned intracoronary stenting. In patients who require coronary intervention and are already receiving tirofiban for acute coronary syndromes, it appears that tirofiban can be continued throughout intracoronary stent placement without a significant increase in life-threatening bleeding complications. However, in the dosage regimen studied, tirofiban use was associated with an increased incidence of minor bleeding with no reduction in adverse cardiac events compared with placebo. Further investigation is needed to ascertain the optimal dosing of tirofiban and heparin to achieve reductions in ischemic complications of intracoronary stenting with an acceptable incidence of bleeding complications.
ACKNOWLEDGMENTS
The authors thank Pam Dellea, Veerle Coenen, Keavy Gaines, and Diane Sookhu, all employees of Merck & Co, Inc, for their assistance in the preparation of this manuscript.
The names of the principal investigators in this study follow, listed by country. Argentina: Carlos B. Alvarez, Instituto Sacre Coeur, Buenos Aires; Jorge A. Belardi, Instituto Cardiovascular de Buenos Aires; Adolfo Cosentino, Hospital Britanico de Buenos Aires; Horacio J. Paella, Instituto de Cardiologia SA, Hospital Espanol, Buenos Aires; Alberto H. Sampaolesi, In-
1342
CLINICAL THERAPEUTICS®
stituto Modelo de Cardiologia Privado SRL, Cordoba; Australia: Philip E.G. Aylward, Flinders Medical Centre, Bedford Park; Craig P. Juergens, Liverpool Hospital, Liverpool; Ian T. Meredith, Monash Medical Centre, Clayton; David Muller, St. Vincent's Hospital, Darlinghurst; Austria: Heinz Drexel, Province Hospital Feldkirch; Georg B. Gaul, Hanusch Hospital 2, Vienna; Werner Klein, University Clinic Graz; Johannes Mlczoch, Hospital Vienna Lainz, Vienna; Joachim Nesser, General Public Hospital of Elisabethinen Linz, Linz; Brazil: Jose E. Sousa, Hospital Dante Pazzanese, Sao Paulo; China: Run Lin Gao, Fu Wai Hospital, Beijing; Da Yi Hu, Chao Yang Hospital, Beijing; Colombia: Luis I. Calderon, Clinica Shio, Santa Fe de Bogota; Carlos Eusse, Clinica CardioVascular Santa Maria, Medellin; Mauricio Pineda, Fundacion Cardio-Infantil, Santa Fe de Bogota; Costa Rica: Wilbert Lopez, Seccion de Cardiologia, Hospital Mexico, San Jose; Ecuador: Francisco Benitez, Hospital Metropolitano, Quito; Greece: Dennis V. Cokkinos, Onassis Cardiac Centre, Athens; Michael Kyriakidis, Laiko Hospital, Athens; George Louridas, Ahepa Thessaloniki, Thessaloniki; Lebanon: Samir Alam, American University, Beirut; Malaysia: Chim Choy Lang, University Hospital, Kuala Lumpur; Robaayah N. Zambahari, Institut Jantung Negara, Kuala Lumpur; Mexico: Jorge Gasper, Hospital Angeles, Mexico City; Jose M. Garcia y Otero, Hospital del Carmen, Guadalajara; Jose M. Palacios, Hospital de Especialidades Clinica, Monterrey; New Zealand: James Stewart, Green Lane Hospital, Auckland; Poland: Witold Ruzyllo, Institute of Cardiology, Warsaw; Portugal: Ricardo S. Gomes, Servicio de Cardiologia, Hospital Santa Cruz, Lisbon; Jorge Quininha, Servicio de Cardiologia, Hospi-
C.P. JUERGENS ET AL.
tal Santa Marta, Lisbon; Vasco G. Ribeiro, Servicio de Cardiologia, Centro Hospitalar Vila Nova de Gaia; Singapore: Lim Yean Leng, Singapore General Hospital; Peter Yan, Glenegles Hospital, Singapore; Slovenia: Peter Rakovec, Clinical Centre, Ljubljana; South Africa: Jan D. Marx, Universitas Hospital, Bloemfontein; Dirk P. Myburgh, No. 1 Military Hospital, Pretoria; Spain: Agustin Albarran, Hospital 12 de Octubre, Madrid; Inocencio Anivarro, Hospital Vall d'Hebron, Barcelona; Amadeo Betriu, Hospital Clinico y Provincial, Barcelona; Juan L. Delcan, Hospital Gregorio Maranon, Madrid; Francisco FernandezAviles, Hospital Universitario de Valladolid; Carlos Macaya, Hospital Clinico Universitario San Carlos, Madrid; Switzerland: Lukas Kappenberger, Cardiology, Centre Hospitalier Universitaire Vaudois, Lausanne; Beat J. Meyer, Swiss Cardiovascular Centre, University Hospital lnselspital, Bern; Matthias Pfisterer, Cardiology, University Hospital, Basel; Taiwan: Philip Yu-An Ding, Veterans General Hospital, Taipei; Turkey: Ferhan Ozmen, Hacettepe University, Ankara; United Kingdom: A.A. Jennifer Adgey, Royal Victoria Hospital, Belfast, Northern Ireland; Kevin Beatt, Hammersmith Hospital, London; Clifford Bucknall, St. Thomas Hospital, London; Rodney A. Foale, St. Mary's Hospital, London; Jaspal Kooner, Ealing Hospital, London; Richard D. Levy, Wythenshawe Hospital, Manchester; Douglas S. Reid, Freeman Hospital, Newcastle Upon Tyne; and Venezuela: Jose G. Loyo, Centro Medico de Caracas.
REFERENCES
I. The EPIC Investigation. Use of a monoclonal antibody directed against the platelet glycoprotein lib/Ilia receptor in
high-risk coronary angioplasty. N Engl J Med. 1994;330:956--961.
2. The EPILOG Investigators. Platelet glycoprotein lib/Ilia receptor blockade and low-dose heparin during percutaneous coronary revascularization. N Engl J Med. 1997;336: 1689-1696.
3. Integrelin to Minimise Platelet Aggregation and Coronary Thrombosis-II Investigators. Randomised placebo-controlled trial of effect of eptifibatide on complications of percutaneous coronary intervention: IMPACT-II. Lancet. 1997;349: 1422-1428.
4. Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM) Study Investigators. A comparison of aspirin plus tirofiban with aspirin plus heparin for unstable angina. N Engl J Med. 1998;338: 1498-1505.
5. Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) Study Investigators. Inhibition of the platelet glycoprotein Ilb/Illa receptor with tirofiban in unstable angina and non-Q-wave myocardial infarction. N Engl J Med. 1998;338:1488-1497.
6. The RESTORE Investigators. Effects of platelet glycoprotein lib/Ilia blockade with tirofiban on adverse cardiac events in patients with unstable angina or acute myocardial infarction undergoing coronary angioplasty. Circulation. 1997;96: 1445-1453.
7. Colombo A, Hall P, Nakamura S, et al. Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation. 1995;91: 1676--1688.
8. Schomig A, Neumann F-J, Kastrati A, et al. A randomized comparison of an-
1343
tiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Eng! J Med. 1996;334:1084--1089.
9. Muller C, Buttner HJ, Petersen J, Roskamm H. A randomized comparison of clopidogrel and aspirin versus ticlopidine and aspirin after the placement of coronary-artery stents. Circulation. 2000; 101:590-593.
10. The EPISTENT Investigators. Randomised placebo-controlled and balloonangioplasty-controlled trial to assess safety of coronary stenting with use of platelet glycoprotein-lib/lila blockade. Evaluation of Platelet lib/Ilia Inhibitor for Stenting. Lancet. 1998;352:87-92.
11. Novel dosing regimen of eptifibatide in planned coronary stent implantation (ESPRIT): A randomised, placebocontrolled trial. Lancet. 2000;356:2037-2044.
12. Topol EJ, Molitemo DJ, Herrmann HC, et al, for the TARGET Investigators. Comparison of two platelet glycoprotein lib/ Ilia inhibitors, tirofiban and abciximab, for the prevention of ischemic events with percutaneous coronary revascularization. N Eng/ J Med. 2001;344:1888-1894.
13. Rao AK, Pratt C, Berke A, et al, for the TIMI investigators. Thrombolysis in Myocardial Infarction (TIMI) Trial-phase I: Hemorrhagic manifestations and changes in plasma fibrinogen and the fibrinolytic system in patients treated with recombinant tissue plasminogen activator and streptokinase. JAm Coll Cardiol. 1988;11: 1-ll.
CLINICAL THERAPEUTICS"
14. Schwartz RS, Huber KC, Murphy JG, et a!. Restenosis and the proportional neointimal response to coronary artery injury: Results in a porcine model. J Am Coil Cardiol. 1992;19:267-274.
15. Hoffmann R, Mintz GS, Mehran R, et al. Tissue proliferation within and surrounding Palmaz-Schatz stents is dependent on the aggressiveness of stent implantation technique. Am J Cardiol. 1999;83:1170-1174.
16. Pope CF, Ezekowitz MD, Smith EO, et al. Detection of platelet deposition at the site of peripheral balloon angioplasty using indium-Ill platelet scintigraphy. Am J Cardiol. 1985;55:495-497.
17. Gasperetti CM, Gonias SL, Gimple LW, Powers ER. Platelet activation during coronary angioplasty in humans. Circulation. 1993;88:2728-2734.
18. Hamm CW, Heeschen C, Goldmann B, et al, for the c7E3 Fab Antiplatelet Therapy in Unstable Refractory Angina (CAPTURE) Study Investigators. Benefit of abciximab in patients with refractory unstable angina in relation to serum troponin T levels. N Engl J Med. 1999;340:1623-1629.
19. Heeschen C, Hamm CW, Goldmann B, et al, for the Platelet Receptor Inhibition in Ischemic Syndrome Management Study Investigators. Troponin concentrations for stratification of patients with acute coronary syndromes in relation to therapeutic efficacy of tirofiban. Lancet. 1999;354: 1757-1762.
Address correspondence to: Craig P. Juergens, FRACP, Department of Cardiology, Liverpool Hospital, Locked Bag 7103, Liverpool BC NSW 1871, Australia. E-mail: c [email protected] .au
1344

65
PAPER 14
Reprinted from Cardiovascular and Hematological Disorders- Drug
Targets 2008;8:138-146 with permission from Bentham Science
Publishers

138 Cardiol•ascular & /laematological Disorders~Drug Targets, 2008, 8, 138-146
The Role of Tirofiban in the Management of Coronary Artery Disease
Julian P. Winter and Craig P. Juergens •
Department o,{Cardiology, Liverpool!Iospital and University of NS W, Sydney, Australia
Abstract: Glycoprotein lib/III a receptor antagonists are potent anti platelet agents by inhibiting the final common pathway of platelet aggregation. Tirofiban binds specifically to the glycoprotein Ilb/IIIa receptor resulting in immediate and extensive inhibition of platelets. Studies have shown that intravenous administration of tirofiban in combination with aspirin and heparin reduces major adverse cardiac events in patients undergoing percutaneous coronary intervention and in those patients with acute coronary syndromes.
Large randomised trials using tirofiban demonstrate early clinical and long~tcnn survival benefit in all patient subgroups including high~risk patients undergoing urgent percutaneous coronary intervention, patients undergoing elective intra~ coronary stent placement and in the medical management of acute coronary syndromes. The use of high-dose bolus tirofi· ban may provide additional protection in patients at highest risk, whereas the role of tirofiban in the facilitation of primary angioplasty is less well defined.
Similar to the other glycoprotein lib/Ilia receptor antagonists, tirofiban increases the risk ofhaemorrhagic complications. However, the risk of serious bleeding, including intracranial haemorrhage, remains low and tirofiban does not appear to increase the risk of thrombocytopenia.
Overall, the use of tirofiban in coronary artery disease has been shown to be effective, has an acceptable safety profile and is potentially cost·effective.
Key Words: Tirofiban, glycoprotein Ilb!llla antagonists, percutaneous coronary intervention, acute coronary syndromes, platelets.
INTRODUCTION
Platelets play a crucial role in the pathophysiology of acute myocardial infarction and unstable angina. Disruption of an atherosclerotic plaque either spontaneously or as a con· sequence of coronary intervention exposes the underlying subendothelial matrix triggering the haemostatic pathway and platelet aggregation. Inevitably, the end result is forma~ tion of an intracoronary platelet-rich thrombus which has the potential to occlude the artery lumen [1]. Several membrane glycoprotein receptors control platelet adhesion and aggrega· tion, many of which are members of the integrin family in· eluding the glycoprotein lib/Ilia (a11b!p3 integrin) receptor which is unique to platelets [I, 2]. This major platelet surface receptor is a key mediator of platelet aggregation and is cru~ cia! to the final common pathway leading to the fonnation of platelet-rich plugs, Fig.(!). The discovery in the 1980's that a specific antibody targeted against the glycoprotein Ilblllla receptor inhibited platelet aggregation represented an impor~ taut therapeutic milestone in the management of acute coro· nary syndromes (ACS) and led to the development of a new class of potent antiplatelet agent known as glycoprotein Jib/Ilia receptor antagonists [3].
There are currently three parenteral glycoprotein Ilb/Illa receptor antagonists available for use in clinical practice and all have been extensively investigated in large randomised
*Address correspondence to this author at the Department of Cardiology, Liverpool Hospital, Elizabeth Street, Liverpool NSW, 2170, Australia; Tel: + 61 2 98283075; Fax:+ 61 2 98283064; E·mail: [email protected]
''18 $55.00+ .00
clinical trials. Although they are more potent than traditional antiplatelet drugs such as aspirin, studies show that the glycoprotein lib/Ilia receptor antagonists provide additional clinical benefit when used concomitantly with both aspirin and heparin. The trade~off for a reduction in ischemic events is a small increased risk of bleeding complications, however the incidence of serious bleeding, particularly intracranial haemorrhage, remain very low. Similarly, the use of glycoprotein Ilblllla receptor antagonists is associated with a risk of thrombocytopenia although this is rarely severe and usu~ ally does not result in major bleeding [4].
Tirofiban (Aggrastat, Merck Sharp and Dohme, Whitehouse Station, NJ) is a small (Molecular Weight: 495Da) tyrosine-derived, non-peptide molecule with high specificity for the aublp3 integrin [5]. The efficacy and safety of tirofiban has been demonstrated in patients undergoing coronary interventions (balloon angioplasty or directional coronary atherectomy) in the RESTORE (Randomised Efficacy Study of Tirofiban for Outcomes and REstenosis) trial [6]. In addition, the Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM·PLUS) trial demonstrated a reduction in ischemic events when tirofiban is administered in combina· tion with aspirin and heparin in high·risk patients with ACS [7]. The role of tirofiban in the setting of acute ST-elevation myocardial infarction (STEMI) treated with primary coronary angioplasty remains controversial [8, 9]. Moreover, results from clinical trials comparing tirofiban with other glycoprotein Ilb/llla receptor antagonists have proved disappointing with respect to tirofiban [I 0, II]. The results from
© 2008 Bentham Science Publishers Ltd.
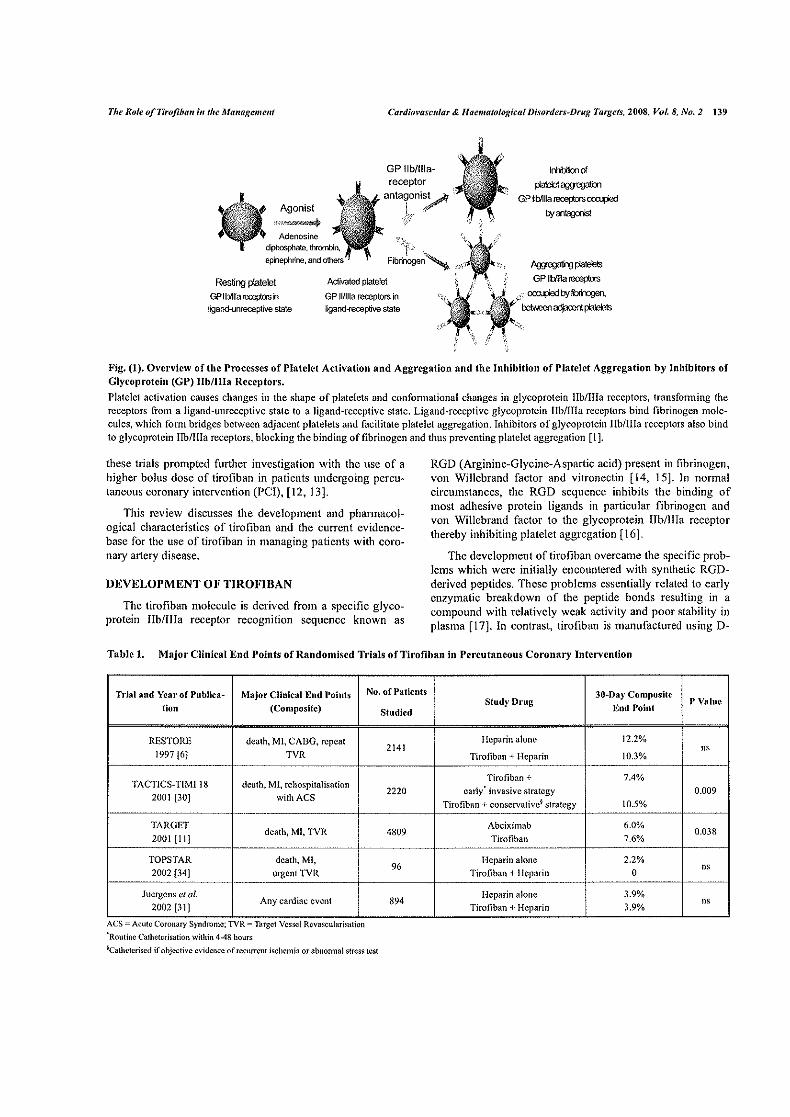
The Role ofTirofih(W in the Mattagemelll Cardi(WQSCltlar & llaematological Disorden--Drug Targets, 2008, Vol. 8, No.2 139
GPIIb/llla- lrhbilkx1 of
patrol~
GPtlt>11~-~
hy~ Agonist
'''""'-"'~
Fibrinoge~,, ~~ GPIII>11~
--~hy~. Resting platelet
GPIIbrll!a~i1
ligand-unreceptive state
Activated platelet
GP 11/llla receptors in ligand-receptive state
Fig. (1). Overview of the Processes of Platelet Activation and Aggregation and the Inhibition of Platelet Aggregation by Inhibitors of Glycoprotein (GP) lib/Ilia Receptors.
Platelet activation causes changes in the shape of platelets and confonnational changes in glycoprotein lib/Ilia receptors, transforming the receptors from a ligand-unreceptive state to a ligand-receptive state. Ligand-receptive glycoprotcitl lib/Ilia receptors bind fibrinogen molecules, which fonn bridges between adjacent platelets and facilitate platelet aggregation. Inhibitors of glycoprotein Jib/lila receptors also bind to glycoprotein IIb/IIIa receptors, blocking the binding of fibrinogen and thus preventing platelet aggregation [1 ].
these trials prompted further investigation with the use of a higher bolus dose of tirofiban in patients undergoing percutaneous coronary intervention (PCI), [12, 13].
This review discusses the development and phannacol~ ogical characteristics of tirofiban and the current evidencebase for the use of tirofiban in managing patients with coro~ nary artery disease.
DEVELOPMENT OF TIROFIBAN
The tirofiban molecule is derived from a specific glycoprotein lib/Ilia receptor recognition sequence known as
RGD (Arginine~Giycine~Aspartic acid) present in fibrinogen, von Willebrand factor and vitronectin [ 14, 15]. In normal circumstances, the RGD sequence inhibits the binding of most adhesive protein ligands in particular fibrinogen and von Willebrand factor to the glycoprotein lib/lila receptor thereby inhibiting platelet aggregation [16].
The development of tirofiban overcame the specific prob~ !ems which were initially encountered with synthetic RGD~ derived peptides. These problems essentially related to early enzymatic breakdown of the peptide bonds resulting in a compound with relatively weak activity and poor stability in plasma [17]. In contrast, tirofiban is manufactured using D~
Table 1. Major Clinical End Points of Randomised Trials of Tirofiban in Percutaneous Coronary Intervention
Trial and Year of Publica~ Major Clinical End Points
tion (Composite)
RESTORE death, MI, CABG, repeat 1997 [6] TVR
--
TACTICS-TIM! 18 death, MI, rehospita!isation 2001 [30] withACS
··--·-TARGET
2001 [It] death, Ml, TVR
TOPS TAR death, Ml, 2002 [34] urgent TVR
Juergens et al. Any cardiac event
2002 [31]
ACS- Acute Coronary Syndrome, TVR-larget Vessel Revascu!ansat10n
'Routine Cathctcrisa!ion within 4-48 hours
No. of Patients
Studied
2141
2220
4809
96
894
~Cathcteriscd if objective evidence of recurrent ischemia or abnonnal stress test
30~Day Composite Study Drug P Value
End Point
Heparin alone 12.2%
'" Tirofiban +Heparin 10.3% - --
Tirofiban + 7.4% early' invasive strategy 0.009
Tirofiban +conservative~ strategy 10.5% --
Abciximab 6.0% 0,038
Tirofiban 7.6%
Heparin alone 2.2%
Tirofiban +Heparin 0 "' Heparin alone 3.9%
Tirofiban + Heparin 3.9% ns

140 Card;ovascufar & Haematofogkal Disorders-Drug Target.\', 2008, Vol. 8, No.2 Winter and Juergens
amino acids instead of a-amino acids, therefore lacks the vulnerable peptide bonds. The overall significance of this was the production of a compound which is more resistant to enzymatic degradation and hence has an improved survival time in the circulation [I].
Tirofiban, like eptifibatide (Integrilin, COR Therapeutics, MA), the other ROD-based synthetic glycoprotein lib/lila receptor antagonist, is highly selective for the glycoprotein Jib/lila (anbP3) integrin resulting in the competitive inhibition of fibrinogen- and von Willebrand-mediated platelet aggregation by reversibly occupying the glycoprotein Ilblllla receptor binding site. This represents an important difference in the mechanism of action of tirofiban when compared to abciximab (ReoPro, Eli Lilly, IN), the Fab fragment of human-mouse monoclonal antibody. Abciximab binds with high affinity to the glycoprotein Jib/Ilia receptor but additionally can cross-react with other receptor integrins not unique to platelets such as avP3 integrin [ 18]. In contrast, tirofiban exhibits no cross-reactivity with other receptor intergrins which might explain the observed differences in results from clinical trials comparing the efficacy and safety of the glycoprotein lib/Ilia receptor antagonists [l 0].
PHARMACOKINETICS AND PHARMACODYNAMICS o•' TIROFIBAN
Tirofiban has a plasma half-life of approximately 2 hours, similar to the half-life of cptifibatidc at 2.5 hours. In comparison the plasma half-life of abciximab is significantly shorter at only 10-30 minutes [19]. However, tirofiban (and eptifibatide), has a shorter platelet bound half-life (10-15 seconds) than abciximab owing to its lower binding affinity to the glycoprotein lib/Ilia receptor. For this reason a significant proportion (approximately 35%) of the administered dose of tiro fib an will remain unbound prior to removal from the body predominantly through renal excretion. As a result of lower binding affinity, tirofiban rapidly dissociates from the glycoprotein lib/Ilia receptor with almost complete reversibility of platelet inhibition approximately four hours after cessation of therapy [20]. Despite the rapid rate of release of the tirofiban molecule from the glycoprotein Ilb/IIIa receptor, ex-vivo studies have demonstrated the extent of early inhibition of platelet aggregation with tirofiban exceeds 85-90% [21, 22]. This high level of platelet inhibition was observed after 30 seconds to 3 minutes and crucially the effect is maintained after l 0-15 minutes among patients with symptomatic coronary artery disease [21 ].
These studies demonstrate two important characteristics of the phannacodynamics of tirofiban with respect to the binding of fibrinogen to the glycoprotein lib/Ilia receptor. Firstly, the use of greater concentrations of tirofiban to achieve optimal inhibition of platelet aggregation largely overcomes the lower affinity of the tirofiban molecule for the receptor. Furthennore, binding of fibrinogen to the glycoprotein lib/Ilia receptor is biphasic, forming an initial reversible low-affinity complex followed by a second slower reaction which fonns a more stable high-affinity complex with a
smaller dissociation constant (K0 ) of 20-?0nmol/L [23 ]. The K0 for a pharmacologic agent determines the concentration that must be achieved to occupy 50% of the receptors and tirofiban has a low KD at l5nmol!L. Therefore tirofiban combines a rapid rate of dissociation with a greater association for the glycoprotein Jib/lila receptor. Importantly this binding characteristic enables tirofiban to maintain extensive inhibition of platelet aggregation during the formation of the much more stable, high-affinity complex between the glycoprotein Jib/Ilia receptor and fibrinogen [21].
In the COMparison of Platelet Inhibition with Abciximab, TiRofiban and Eptifibatidc (COMPARE) trial, 70 patients with ACS undergoing PCI were randomised to receive abciximab, tirofiban, or eptifibatide [10]. In this study, patients received tirofiban as a 0.4!lglkg/min bolus given for 30 minutes, starting lO minutes before PCI and followed by a O.IO!lglkg/min infusion for 18 hours (same dose as in the PRISM-PLUS trial), (7]. The trial was subsequently extended to assess a bolus dose of 1 O!lg/kg followed by 0.15j.tg/kg/min infusion for 18 hours (similar dosage to the RESTORE trial), [6]. These dosages of tirofiban have been shown to achieve >90% inhibition of platelet aggregation in response to 5j.lmol/L adenosine diphosphate (ADP) agonist [20]. The drug regimens for abciximab and eptifibatide in the COMPARE trial were those used in the Evaluation of Platelet Ilb/llla Inhibitor for STENTing (EPISTENT) trial (24] and the Platelet glycoprotein Ilblllla in Unstable angina Receptor Suppression Using Intergrilin Therapy (PURSUIT) trial [25J, respectively. Platelet aggregation was measured in response to a strong agonist (20j.lmol!L of ADP) using turbidimetric aggregatory at specific time intervals after drug initiation. Results from COMPARE showed early effective platelet inhibition with tirofiban as well as consistent inhibition over 12 hours. Despite both abciximab and eptifibatide performing superiorly to tirofiban in the early stages of platelet inhibition, particularly in comparison with the higherbolus dose regimen (used in RESTORE), abciximab was much less consistent over the 12 hours.
The effects of tirofiban can be reversed with haemodialysis and at least partially through a transfusion of platelets even though the new platelets are likely to be inhibited [ 19]. Instead and common to all the glycoprotein lib/lila antagonists, the primary method of reversal is somewhat inadequate which is cessation of the infusion. Significantly tirofiban can be used safely in patients with renal impairment, however because the molecule is largely removed by the kidneys, the dosage must be decreased by 50% in patients with severe renal insuffiency as defined by a creatinine clearance of <30ml/min.
TIROFIBAN IN ACUTE CORONARY SYNDROMES
Tirofiban has been extensively investigated in several major randomised controlled trials which demonstrate its efficacy and safety in patients undergoing PCI and in those patients with ACS. When tirofiban was administered to patients with ACS in combination with intravenous heparin and aspirin there was a lower incidence of ischemic events com-

The Role of Tirojiha11 ;, the Mauagemem Cardio~·ascu/ar & 1/aematological Disorders-Drug Targets, 2008, Vol. 8, No.2 141
pared to patients who received heparin and aspmn alone. The Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) trial is the main study demonstrating the clinical benefits of tirofiban in patients with ACS regardless of the subsequent pcrfonnance of PCI [7]. This was a large, multi-national, placebo-controlled, randomiscd trial evaluating tirofiban in the treatment of unstable angina and non-Q-wave myocardial infarction. Entry criteria included prolonged or repetitive anginal pain at rest or during minimal exertion in the previous 12 hours in addition to new transient or persistent ST-T ischemic changes on the electrocardiogram or elevated cardiac markers.
In total, 1915 ACS patients were enrolled with all patients receiving aspirin unless its use was contraindicated, whilst the routine usc of thienopyridines had not yet been established at the trials inception. Study drugs were infused for a mean (±SD) of 71.3±20 hours. Tirofiban was given at a dose of 0.4).lg/kg/min for 30 minutes, followed by an infusion of 0.1 ).lg/kg/min, plus adjusted-dose heparin. Whilst all patients were medically managed in the first 48 hours, coronary angiography was performed during initial hospitalisation in 89.8% of patients. Of these patients, 30.5% underwent PCI, 23.3% underwent coronary artery bypass surgery and the remainder were treated with medical management alone.
Overall the use of tirofiban in combination with aspirin and heparin showed a reduction in the frequency of the composite primary end-point of death, myocardial infarction, or refractory ischemia at 7-days compared to heparin alone (12.9% versus 17.9%, P~0.004). The clinical benefit of adjunctive tirofiban occurred early with divergence of the Kaplan-Meier survival curves apparent within hours of commencing treatment. The benefits of tirofiban-plus-heparin over heparin alone extended to 30-days (18.5% versus 22.3%, P~0.03) and 6-months (27.7% versus 32.1%, P~0.02). The reduction in the composite primary end-point in the tirofiban-plus-hcparin group was due largely to a 47% decrease in the risk of myocardial infarction and a 30% decrease in the risk of refractory ischemia as compared with the risk in the heparin-only group. Death rates were similar between both treatment groups.
In the PRISM-PLUS trial, the benefit of tirofiban-plusheparin was seen consistently across all patient subgroups, including men and women. In the 475 patients who were treated with coronary angioplasty as part of a modified early invasive strategy, there was a 44% risk reduction in death and myocardial infarction at 30-days in the tirofiban-plusheparin group when compared to heparin alone.
PRISM-PLUS has shown us that combination therapy with the addition of tiro fib an to standard care using heparin and aspirin is effective in the prevention of early major ischemic events, particularly myocardial infarction, in those patients with ACS. The clinical benefit is greatest in those patients who underwent early PCI however patients treated with medical management alone also did better.
TIROFIBAN IN PERCUTANEOUS CORONARY INTERVENTION
Balloon angioplasty inevitably disrupts atherosclerotic plaques and damages the integrity of the vascular endothelial layer and the artery wall, essentially causing coronary dissection. In addition, vessel trauma from intracoronary balloon inflation exposes the underlying subendothelial matrix to the components of blood which in turn activate the coagulation system and leads to platelet adhesion and aggregation. The formation of platelet-rich thrombus within the coronary arteries contributes to the development of acute ischemic complications both locally, at the immediate site of vascular injury, and in the distal vessels due to embolisation. The thrombogenic nature of PCI creates the most serious risks associated with this procedure, namely periprocedural myocardial infarction and death [26].
In the current stent era, mechanical repair of coronary dissection and prevention of vessel recoil has greatly reduced the incidence of abrupt vessel closure requiring emergency CABG despite an increase in high-risk patients undergoing PCI [27]. Trials performed during the earlier years of percutaneous transluminal coronary angioplasty (PTCA) prior to the use of stents as standard practice, demonstrate that treatment with aspirin and unfractionated heparin significantly decreased thrombotic complications, however these agents have not proven to be completely effective in this role [28,29]. Periprocedural ischemic events as a result of acute thrombus formation, particularly recurrent ischemia and nonfatal myocardial infarction remain a significant risk in patients undergoing PCI and the use of tirofiban in this setting has been evaluated in several clinical studies [6, 30, 31].
The Randomised Efficacy Study of Tirofiban for Outcomes and REstenosis (RESTORE) trial investigated the use of tirofiban on adverse cardiac events in patients with ACS undergoing coronary angioplasty [6]. This was a randomized, double-blind, placebo-controlled trial involving 2141 patients with ACS who went on to receive balloon angioplasty or directional atherectomy within 72 hours of presentation. After randomization, patients received a bolus dose of tiro fib an (I O).lglkg) or placebo administered intravenously over 3 minutes once the angioplasty guidcwire had crossed the lesion. Following the bolus, an intravenous infusion of tirofiban (O.l5Jlg!kg/min) or placebo was commenced and maintained for 36 hours post-procedure. In this study, intracoronary stent implantation was limited to urgent 'bailout' situations such as abrupt vessel closure which occurred in 2.5% of patients. The primary composite end-point for this study was myocardial infarction, CABG owing to angioplasty failure or recurrent ischemia, repeat target-vessel angioplasty for recurrent ischemia, insertion of a stent owing to actual or threatened abrupt closure of the target artery and death from any cause. At 30-days the primary composite endpoint showed a reduction from 12.2% in the placebo group to 10.3% in the tirofiban group (P=0.16). However, 2 days after the intervention, the tirofiban group had a 38% relative reduction in the composite endpoint (P=0.005), and at 7 days there was a 27% relative reduction (P=0.022). This reduction

142 Cunliovast·ular & llaematological Di.~ordcrs~Drug Targets, 2008, Vol. 8, No.2 Winter and Juergem
was largely due to a decrease in the rate of nonfatal myocar~ dial infarction and the need for repeat angioplasty.
In summary, this study demonstrated that whilst tirofiban was effective at preventing periprocedural ischemic complications after coronary angioplasty the smaller benefit at 30~ days with use of tiro fib an was perhaps disappointing. In particular, results at 30-days in the RESTORE trial showed less overall benefit with tirofiban compared with results similarly obtained with the use of abciximab in both the EPIC and EPILOG trials [32, 33].
The difference in the event rates at 30-days with tirofiban and abciximab between these trials might have been as a result of differences in the study methodology, particularly the definition of the composite endpoints such as myocardial infarction. One other explanation that has been hypothesized for the observed clinical difference might be with the use of an inadequate bolus-dose of tirofiban. As mentioned earlier, the COMPARE trial suggested that the tirofiban-RESTORE regimen with 1 OJ.-lglkg bolus over 3 minutes may have less effect on platelet aggregation than eptifibatide, abciximab and the tirofiban-PRISM PLUS loading regimens.
Whilst the RESTORE trial examined the role of tirofiban in PTCA, more recent trials have examined the use of tirofiban during intracoronary stent implantation. A multinational, multicentre, prospective, randomised, double-blind, placebocontrolled trial examined the tolerability of tirofiban in patients undergoing planned intracoronary stent placement [31 ]. This trial involved 894 patients who were randomised to receive tirofiban as an intravenous bolus (I Of.lglkg over 3 minutes) and maintenance infusion (O.lOf.lg/kg/min for 36 hours) or bolus and infusion of placebo. The 30-day incidence of the composite end point of any cardiac event was 3.9% in both groups. No significant differences were observed in the incidence of Thrombolysis In Myocardial Infarction (TIMI) major bleeding (0.2% in the tirofiban group compared with 0.6% in the placebo group) or the incidence of any TIMI bleeding (3.2% in the tirofiban group versus 1.7% in the placebo group). This study concluded that the use of tirofiban in combination with aspirin and heparin in patients undergoing elective PCI was safe and generally well tolerated, whilst it was not adequately powered to address its impact on major adverse cardiac events.
Similarly, the Troponin in Planned PTCA/Stent Implantation With or Without Administration of the Glycoprotein lib/Ilia Receptor Antagonist Tirofiban (TOPSTAR) trial which included 96 patients undergoing planned PTCA or stcnt implantation, showed a marked reduction in postinterventional troponin T release in patients treated with tirofiban compared with heparin-alone [34]. The risk of a major adverse cardiac event (MACE) was also lower in patients treated with tirofiban compared to heparin-alone.
The TACTICS (Treat Angina with Aggrastat and Determine Cost of Therapy with an Invasive and Conservative Strategy) TIMI-18 trial was designed to evaluate the use of upstream tirofiban in patients with high-risk ACS in combination with an early invasive treatment strategy [30]. All
patients were initially treated with aspirin, heparin and tirofiban, following which patients were randomly assigned either to undergo early diagnostic cardiac cathetcrisation within 4 to 48 hours and revascularisation as indicated, or a more conservative "selective invasive" approach with cardiac catheterisation being performed only if the patient demonstrated objective evidence of recurrent ischemia at rest or a positive stress test. At six months the risk of death and nonfatal myocardial infarction was reduced by 26% in patients who were treated with tirofiban and early PCL The greatest benefit was observed in patients who were troponin positive or who had ST-segment depression on their admission electrocardiogram [30], [35].
The TARGET (Do Tirofiban and ReoPro Give Similar Efficacy Outcomes) trial followed on from the preliminary investigations into the variability of the extent of platelet inhibition found in COMPARE and on the back of differences in results from the randomised clinical trials using tirofiban or abciximab. TARGET was a head-to-head, noninferiority study designed at the outset to demonstrate that tirofiban was not inferior to abciximab among PCI patients receiving an intracoronary stent [I 1 ]. Across 18 countries, 4809 patients undergoing elective or urgent PCI were recruited and randomly assigned to receive either a bolus and infusion of tirofiban (IOf.lg/kg bolus over 3 minutes, followed by an infusion of0.15).J.glkg/min for 18 to 24 hours), or abciximab (0.25mg/kg bolus, followed by an infusion of O.I25j.tglkg/min for 12 hours). All patients received the bolus dose of glycoprotein lib/Ilia receptor antagonist immediately before revascularisation as well as being preloaded with 250-500mg aspirin and 300mg clopidogrel. Weight-adjusted heparin was administered at the start of the procedure to achieve a target activated clotting time {ACT) of 250 seconds.
At 30-days, the primary composite end-point of death, nonfatal myocardial infarction, or urgent target-vessel revascularisation (TVR), occurred more frequently among patients in the tirofiban group than in the abciximab group (7 .6% versus 6.0%, P=0.038), predominantly due to a reduction in the incidence of myocardial infarction (6.9% in the tirofiban group versus 5.4% in the abciximab group, P=0.04). Therefore at 30~days, abciximab offered greater protection from ischemic events compared to tirofiban in patients undergoing PC!. When the follow-up period for TARGET was extended to 6-months there was no difference in the composite endpoint in patients treated with tirofiban or abciximab (14.8% versus !4.3%, P~0.591) [36]. More recently, at !-year follow-up, death occurred in 1.9% of patients who received tirofiban and 1.7% of patients who received abciximab (P=0.66), [37]. There was no difference in mortality between the two treatment groups whether patients had an ACS or not. Therefore, at 6-months tirofiban offers a similar level of overall protection from major cardiac events to abciximab and has a similar mortality benefit at 1-year.
TIROFIBAN IN PRIMARY ANGIOPLASTY
A meta·analysis which included several major randomised clinical trials has demonstrated the superiority of pri-
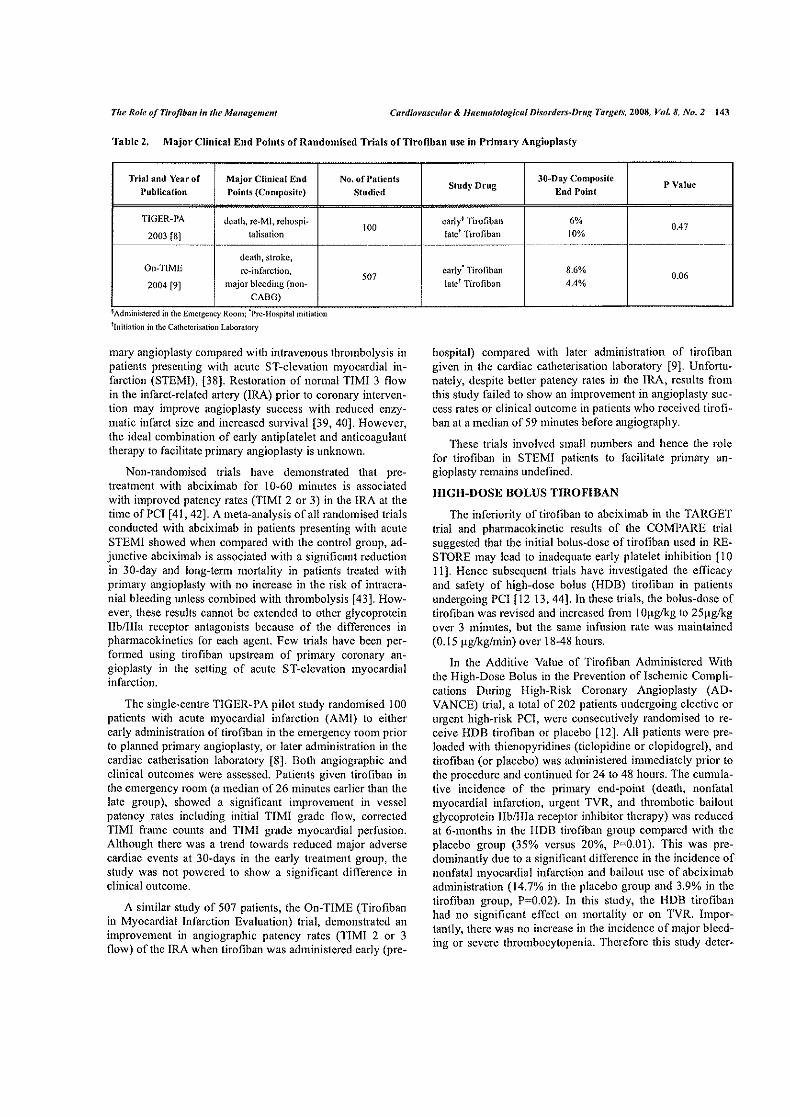
The Role of Tirojiha11 ;,, tfw Managemem Cardim•asCillar & Jlaematologicu/ Disorders~Drug Targets, 2008, Vol. 8, No.2 143
Table 2. Major Clinical End Points ofRandomiscd Trials ofTirofiban usc in Primary Angioplasty
Trial and Year of Major Clinical End Publication Points (Composite)
TJGER~PA death, re~MJ, rehospi~
2003 [8] talisation -· ........... _ .. --·
death, stroke, On-TIME re-infarction,
2004 [9] major bleeding (non-
CABO)
' Adlllnllstercd m the Emergency Room, Pre-Hosp1tal lnltl3tlon 11nitiation in the Cathctcrisation Laboratory
No. of Patients
Studied
100
-~~--~---
507
mary angioplasty compared with intravenous thrombolysis in patients presenting with acute ST-elevation myocardial infarction (STEM!), [38]. Restoration of normal TIM! 3 flow in the infarct-related artery (IRA) prior to coronary intervention may improve angioplasty success with reduced enzymatic infarct size and increased survival [39, 40]. However, the ideal combination of early antiplatelet and anticoagulant therapy to facilitate primary angioplasty is unknown.
NonRrandomised trials have demonstrated that pretreatment with abciximab for 10-60 minutes is associated with improved patency rates (TIMI 2 or 3) in the IRA at the time ofPCI [41, 42]. A meta-analysis of all randomised trials conducted with abciximab in patients presenting with acute STEM! showed when compared with the control group, adjunctive abciximab is associated with a significant reduction in 30-day and long-term mortality in patients treated with primary angioplasty with no increase in the risk of intracra~ nial bleeding unless combined with thrombolysis [43]. However, these results cannot be extended to other glycoprotein lib/Ilia receptor antagonists because of the differences in pharmacokinetics for each agent. Few trials have been performed using tirofiban upstream of primary coronary angioplasty in the setting of acute ST-elevation myocardial infarction.
The single-centre TIGER-PA pilot study randomised 100 patients with acute myocardial infarction (AMI) to either early administration of tirofiban in the emergency room prior to planned primary angioplasty, or later administration in the cardiac catherisation laboratory [8]. Both angiographic and clinical outcomes were assessed. Patients given tirofiban in the emergency room (a median of 26 minutes earlier than the late group), showed a significant improvement in vessel patency rates including initial TIMI grade flow, corrected TIMI frame counts and TIMI grade myocardial perfusion. Although there was a trend towards reduced major adverse cardiac events at 30-days in the early treatment group, the study was not powered to show a significant difference in clinical outcome.
A similar study of 507 patients, the On-TIME (Tiro fib an in Myocardial Infarction Evaluation) trial, demonstrated an improvement in angiographic patency rates (TIMI 2 or 3 flow) of the IRA when tirofiban was administered early (pre-
30~Day Composite Study Drug
End Point P Value
earlyt Tirofiban 6% 0.47
late1 Tirofiban 10% ~- ---- ·--~·-· - ----·-·-···-- ·---·-------- -----~---~~----
early' Tirofiban 8.6%
\ate1 Tirofiban 0.06
4.4%
hospital) compared with later administration of tirofiban given in the cardiac catheterisation laboratory {9]. Unfortuw nately, despite better patency rates in the IRA, results from this study failed to show an improvement in angioplasty success rates or clinical outcome in patients who received tirofiban at a median of 59 minutes before angiography.
These trials involved small numbers and hence the role for tirofiban in STEMI patients to facilitate primary angioplasty remains undefined.
HIGH-DOSE BOLUS TIROFIBAN
The inferiority of tirofiban to abciximab in the TARGET trial and pharmacokinetic results of the COMPARE trial suggested that the initial bolus-dose of tirofiban used in RESTORE may lead to inadequate early platelet inhibition [10 11]. Hence subsequent trials have investigated the efficacy and safety of high-dose bolus (HDB) tirofiban in patients undergoing PC! [12 13, 44]. In these trials, the bolus-dose of tirofiban was revised and increased from 1 O).tglkg to 25)-tg/kg over 3 minutes, but the same infusion rate was maintained (0.15 ~tgikg/min) over 18-48 hours.
In the Additive Value of Tirofiban Administered With the High-Dose Bolus in the Prevention of Ischemic Complications During High-Risk Coronary Angioplasty (ADVANCE) trial, a total of202 patients undergoing elective or urgent high~risk PCI, were consecutively randomised to receive HDB tirofiban or placebo [l2]. All patients were preloaded with thienopyridines (ticlopidine or clopidogrel), and tirofiban (or placebo) was administered immediately prior to the procedure and continued for 24 to 48 hours. The cumulative incidence of the primary end-point (death, nonfatal myocardial infarction, urgent TVR, and thrombotic bailout glycoprotein lib/Ilia receptor inhibitor therapy) was reduced at 6~months in the HDB tirofiban group compared with the placebo group (35% versus 20%, P-"='0.0 1 ). This was predominantly due to a significant difference in the incidence of nonfatal myocardial infarction and bailout use of abciximab administration (14.7% in the placebo group and 3.9% in the tirofiban group, P~0.02). In this study, the HOB tirofiban had no significant effect on mortality or on TVR. Importantly, there was no increase in the incidence of major bleeding or severe thrombocytopenia. Therefore this study deter-
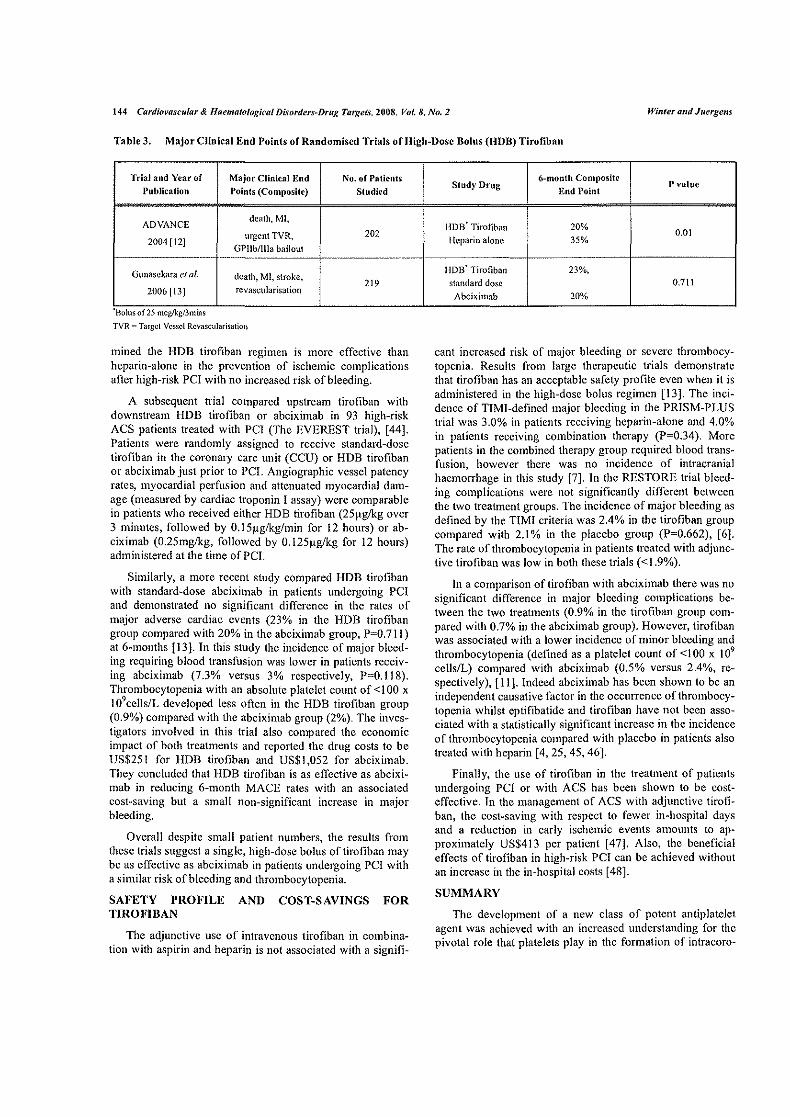
144 Cardiovascular & llaematological Disorders~Drug Target.\', 2008, Vol. 8, No.2 Wimer and Juergem
Table 3. Major Clinical End Points of Randomised Trials of HighwDose Bolus (HDB) Tirofiban
Trial and Year of Major Clinical End No. of Patients
Publication r•oints (Composite) Studied
ADVANCE death, Ml,
urgent TVR, 202 2004 [12]
GP!Ib/llla bailout ·--- ·------- ---·-·--··
Gunasckara et al. death, Ml, stroke, 219
2006 [13] rcvascularisation
Bolusof25 mcg!kg/3mms
TVR == Targcl Vessel Rcvascularisation
mined the HDB tirofiban regimen is more effective than heparinwalone in the prevention of ischemic complications after high-risk PCI with no increased risk of bleeding.
A subsequent trial compared upstream tirofiban with downstream HDB tirofiban or abciximab in 93 high-risk ACS patients treated with PCI (The EVEREST trial), [44]. Patients were randomly assigned to receive standard-dose tirofiban in the coronary care unit (CCU) or HDB tirofiban or abciximab just prior to PCI. Angiographic vessel patency rates, myocardial perfusion and attenuated myocardial damage (measured by cardiac troponin I assay) were comparable in patients who received either HDB tirofiban (25f.tglkg over 3 minutes, followed by O.l5J.lglk.g/min for 12 hours) or ab~ ciximab (0.25mg/kg, followed by O.l25~g/kg for 12 hours) administered at the time ofPCI.
Similarly, a more recent study compared HDB tirofiban with standard~dose abciximab in patients undergoing PCI and demonstrated no significant difference in the rates of major adverse cardiac events (23% in the HDB tirofiban group compared with 20% in the abciximab group, P=0.711) at 6-months [13]. In this study the incidence of major bleedw ing requiring blood transfusion was lower in patients receiv~ ing abciximab (7.3% versus 3% respectively, P=O.ll8). Thrombocytopenia with an absolute platelet count of <I 00 x I 09 cells/L developed less often in the HDB tiroiiban group (0.9%) compared with the abciximab group (2%). The investigators involved in this trial also compared the economic impact of both treatments and reported the drug costs to be US$251 for HDB tirofiban and US$1,052 for abciximab. They concluded that HDB tirofiban is as e!Tective as abcixi~ mab in reducing 6-month MACE rates with an associated cost~saving but a small non-significant increase in major bleeding.
Overall despite small patient numbers, the results from these trials suggest a single, high~dose bolus of tirofiban may be as effective as abciximab in patients undergoing PCI with a similar risk of bleeding and thrombocytopenia.
SAFETY PROFILE AND COST-SAVINGS FOR TIROFIBAN
The adjunctive usc of intravenous tirofiban in combination with aspirin and heparin is not associated with a signifi~
6~month Composite Study Drug
End Point Pvalue
HOB' Tiroflban 20% 0.01
Heparin alone 35%
IJDB' Tirofiban 23%,
standard dose 0.711
Abciximab 20%
cant increased risk of major bleeding or severe thrombocyw topcnia. Results from large therapeutic trials demonstrate that tirofiban has an acceptable safety profile even when it is administered in the high-dose bolus regimen [13]. The incidence of TIMI-defined major bleeding in the PRISM-PLUS trial was 3.0% in patients receiving heparin-alone and 4.0% in patients receiving combination therapy (P=0.34). More patients in the combined therapy group required blood trans~ fusion, however there was no incidence of intracranial haemorrhage in this study [7]. In lhe RESTORE trial bleeding complications were not significantly different between the two treatment groups. The incidence of major bleeding as defined by the TIMI criteria was 2.4% in the tirofiban group compared with 2.1% in the placebo group (P~0.662), [ 6]. The rate of thrombocytopenia in patients treated with adjunctive tirofiban was low in both these trials (<1.9%).
In a comparison of tirofiban with abciximab there was no significant difference in major bleeding complications be~ tween the two treatments (0.9% in the tirofiban group com· pared with 0.7% in the abciximab group). However, tirofiban was associated with a lower incidence of minor bleeding and thrombocytopenia (defined as a platelet count of<lOO x 109
cells/L) compared with abciximab (0.5% versus 2.4%, re~ spectively), [11]. Indeed abciximab has been shown to be an independent causative factor in the occurrence of thrombocytopenia whilst eptifibatide and tirofiban have not been associated with a statistically significant increase in the incidence of thrombocytopenia compared with placebo in patients also treated with heparin [4, 25, 45, 46].
Finally, the usc of tirofiban in the treatment of patients undergoing PCI or with ACS has been shown to be cost~ effective. In the management of ACS with adjunctive tirofi~ ban, the cost-saving with respect to fewer inwhospital days and a reduction in early ischemic events amounts to approximately US$413 per patient [47]. Also, the beneficial effects of tirofiban in high-risk PCI can be achieved without an increase in the in~hospital costs [48].
SUMMARY
The development of a new class of potent antiplatelet agent was achieved with an increased understanding for the pivotal role that platelets play in the formation of intracoro~
The Role of Tirojihan in the Ma11agemmt CardiOl'ascular & Haematofogical Disorders-Drug Targets, 2008, Vol. 8, No. l 145
nary thrombus. Tirofiban, a synthetic non-peptide molecule specifically designed to bind to the glycoprotein Ilb/llla rc~ ceptor on the platelet surface inhibits the final common pathway of platelet aggregation. As a result, adjunctive treatment with tirofiban reduces acute thrombotic complica~ lions associated with unstable coronary plaques and with the conditions of PCL
The extensive evidence~base from randomised clinical trials supports the early use oftirofiban in patients with ACS and during elective and urgent PCI. More recently, studies have suggested that patients at highest risk from ischemic complications may benefit from an increase in the initial bolus-dose of tirofiban. Currently, there is limited evidence for the use of tirofiban in patients with ST-elevation myocardial infarction prior to undergoing primary PCL
Finally, the beneficial effects observed with tirofiban can be achieved with an acceptable risk of bleeding and with potential cost-savings.
REFERENCES
[I]
[2]
[3]
[4]
[5]
[6]
[7]
[8]
[9]
[10]
Lefkovits, J.; Plow, E.F.; Topol, EJ. Platelet glycoprotein Jib/lila receptors in can:liovascular medicine. N. Engl. J. Med., 1995, 332, 1553-1559. Quinn, M.J.; Byzova, T.V.; Qin, J.; Topol, E.J.; Plow, E. F. lntegrin alphallbbcta3 and its antagonism. Arterioscler. Thromb. Vase. Bioi., 2003, 23, 945-952. Col!er, B.S.; Peerschke, IU; Scudder, LE.; Sullivan, C.A. A mur· inc monoclonal antibody that completely blocks the binding of fi. brinogcn to platelets produces a thrombasthenic-like state in nonnal platelets and binds to glycoproteins Jib and/or Ilia. J. Clin. Invest, 1983, 72, 325·338. Dasgupta, H.; Blankenship, J.C.; Wood, G.C.; Frey, C.M.; Demko, S.L; Menapace, F.J. Thrombocytopenia complicating treatment with intravenous glycoprotein lib/Ilia receptor inhibitors: a pooled analysis. Am. Heart J., 2000, 140, 206-211. Topol, E.J.; Byzova, T.V.; Plow, E. F. Platelet GPllb-llla blockers. Lancet, 1999, 353, 227-231. Effects of platelet glycoprotein lib/Ilia blockade with tirofiban on adverse cardiac events in patients with unstable angina or acute myocardial infarction undergoing coronary angioplasty. The RESTORE Investigators. Randomized Efficacy Study of Tirofiban fOr Outcomes and REstcnosis. Circulation, 1991, 96, 1445-1453. Inhibition of the platelet glycoprotein lib/Ilia receptor with tirofiban in unstable angina and non·Q-wavc myocardial infarction. Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) Sh1dy Investigators. N Engl. J. Med., 1998, 338, 1488-1497. Lee, D.P.; Hcrity, N.A.; Hiatt, B.L.; Fearon, W.F.; Rezace, M.; Cmter, A.J.; Huston, M.; Schreiber, D.; DiBattistc, P.M.; Yeung, A.C. Adjunctive platelet glycoprotein lib/Ilia receptor inhibition with tirofiban before primary angioplasty improves angiographic outcomes: results of the Tlrofibun Given in the Emergency Room before Primary Angioplasty (TIGER-PA) pilot trial. Circulation, 2003, 107, 1497-1501. van't Hof, A.W.; Emst, N.; de Boer, M.J.; de Winter, R.; Boersma, E.; Bunt, T.; Petronio, S.; Marcel Gossclink, A.T.; Jap, W.; Hollak, F.; 1-Ioomtje, J.C.; Suryapranata, H.; Dambrink, J.H.; Zijlstra, F.; On-TIME study group. Facilitation of primary coronary angioplasty by early start of a glycoprotein 2b/3a inhibitor: results of the ongoing tirofiban in myocardial infarction evaluation (OnTIME) trial. Eza: Heart J., 2004, 25, 837-846. Batchelor, W.B.; Tolleson, T.R.; Huang, Y.; Larsen, R.L.; Mantel!, R.M.; Dillard, P.; Davidian, M.; Zhang, D.; Cantor, W.J.; Sketch, M.H., Jr.; Ohman, E.M.; Zidar, J.P.; Grctler, D.; DiBalliste, P.M.; Tcheng, J.E.; Califf, R.M.; Harrington, R.A. Rundomizcd COMparison of platelet inhibition with abciximab, tiRofibun and eptifibatidc during percutaneous coronary intervention in acute coronary
syndromes: the COMPARE trial. Comparison Of Measurements of Platelet aggregation with Aggrastat, Reopro, and Eptifibatide. Circulation, 2002,106, 1470-1476.
[II] Topol, E.J.; Molitcrno, D.J.; Herrmann, H.C.; Powers, E.R.; Grines, C.L.; Cohen, D.J.; Cohen, E.A.; Bertrand, M.; Neumann, F.J.; Stone, G. W.; DiBattistc, P.M.; Demopoulos, L. TARGET lnvestigators.Do Tirofiban and ReoPro Give Similar Efficacy Trial. Comparison of two platelet glycoprotein lib/lila inhibitors, tirofiban and abciximab, for the prevention of ischemic events with percutaneous corot1ary rcvascularization. N Engl. J. Med., 2001, 344, 1888-1894.
[12] Va!gimigli, M.; Percoco, G.; Barbieri, D.; Fcrruri, F.; Guardigli, G.; Parrinello, G.; Soukhomovskaia, 0.; Ferrari, R. The additive value oftirofiban administered with the high-dose bolus in the prevention of ischemic complications during high-risk coronury angioplasty: the ADVANCE Trial. J. Am. Col/. Cardia/., 2004, 44, 14-19.
[13] Gunasckara, A.P.; Walters, D.L; Aroney, C.N. Comparison of abciximab with "high-dose" tirotiban in patients undergoing percutaneous coronary intervention. Int. J. Cardia!., 2006, 109, 16-20.
[14] Margucrie, G.A.; Plow, E.F.; Edgington, T.S. Human platelets possess an inducible and saturable receptor specific for fibrinogen. J. Bioi. Chem., 1979, 254, 5357-5363.
[15] Ruggeri, Z.M.; Bader, R.; DeMarco, L. Glanzmann thrombasthenia: deficient binding of von Willcbrand factor to thrombinstimulated platelets. Proct. Nat/. Acad. Sci. USA, 1982, 79, 6038-6041.
[16] Beacham, D.A.; Wise, R.J.; Turei, S.M.; Handin, R.I. Selective inactivation of the Arg-Gly-Asp-Scr (RGDS) binding site in von Willebrand factor by site-directed mutugcncsis. J. Bioi. Chem., 1992,267,3409-3415.
(17} Cox, D.; Aoki, T.; Scki, J.; Motoyama, Y.; Yoshida, K. The phurmacology of the intcgrins. Med. Res. Rev., 1994, 14, 195-228.
[18] Tam, S.H.; Sassoli, P.M.; Jordan, R.E.; Nakada, M.T. (RcoPro, chimeric 7E3 Fab) demonstrates equivalent affinity and functional blockade of glycoprotein lib/Ilia and alpha(v)beta3 integrins. Cir· culalion, 1998,98, 1085-1091.
[19] Gowda, R.M.; Khan, I.A.; Vasuvada, B.C.; Sacchi, T.J. Thcrapcu~ tics of platelet glycoprotein Jib/lila receptor antagonism. Am. J. The1:, 2004, If, 302-307.
[20] Kerciakes, DJ.; Kleiman, N.S.; Ambrose, J.; Cohen, M.; Rodriguez, S.; Palabrica, T.; Henmann, H.C.; Sutton, J.M.; Weaver, W.D.; McKee, D.B.; Fitzpatrick, V.; Sax, F.L. Randomized, double-blind, placebo-controlled dose-ranging study of tirofiban (MK-383) platelet lib/lila blockade in high risk patients undergoing coronary angioplasty. J. Am. Col/. Cardiol., 1996, 27, 536-542.
[21] Schneider, D.J.; Baumann, P.Q.; Whitaker, D.A.; Sobel, B.E. Variation in the ubility of glycoprotein lib-Ilia untagonists to exert and maintain their inhibitory effects on the binding of fibrinogen. J. Cardiovasc. Pharmacol., 2005,46,41-45.
[22] Schneider, D.J.; Keating, F.K.; Baumann, P.Q.; Whitaker, D.A.; Sobel, B.E. Increased ability of tirofiban to maintain its inhibitory effects on the binding of fibrinogen to platelets in blood from patients with and without diabetes mellitus. Caron. Artery Dis., 2006, 17, 57-61.
[23] Huber, W.; Hurst, J.; Schlatter, D.; Barner, R.; 1-lubschcr, J.; Kouns, W.C.; Steiner, B. Dctcnnination of kinetic constants for the interaction between the platelet glycoprotein lib-lila and fibrinogen by means of surface plasmon resonance. Eur. J. Biochem., 1995, 227,647-656.
[24] The EPISTENT Investigators. Complementary clinical benefits of coronary-artery stenting and blockade of platelet glycoprotein lib/Ilia receptors. N. Engl. J. Med., 1999, 341, 319-327.
[25] Inhibition of platelet glycoprotein llb/llla with cptifibatidc in patients with acute coronary syndromes. The PURSUIT Tria! Investigators. Platelet Glycoprotein Jlb/IIIa in Unstable Angina: Receptor Suppression Using lntegrilin Therapy. N Engl. J. Med., 1998,339, 436-443.
[26] de Fcytcr, P.J.; van den, B.M.; Laannan, OJ.; van Domburg, R.; Scm1ys, P. W., Suryapranata, H. Acute coronary artery occlusion during and uflcr percutaneous transluminal coronary angioplasty. Frequency, prediction, clinical course, manugcment, and follow-up. Circulation, 1991,83,927-936.
146 CardiowlScular & llaematological Di~·orders~Drug Targets, 2008, Vol. 8, No.2
(27) Yang, E.H.; Gumina, IU.; Lennon, IU.; Holmes, D.R.; Riha!, C.S.; Singh, M. Emergency coronmy artery bypass surgery for percutaneous coronary interventions: changes in the incidence, clinical characteristics, and indications from 1979 to 2003. J. Am. Col!. Cmdiol., 2005, 46, 2004-2009.
[28) Narins, C.R.; Hillegass, W.B.; Nelson, C.L.; Tchcng, J.E.; Harrington, R.A.; Phillips, H.R.;I Stack, R.S.; Califf, R.M. Relation between Activated Clotting Time during Angioplasty and Abrupt Closure. Circulation, 1996, 93, 667-671.
f29J Lembo, N.J.; Black, A.J.; Roubin, G.S.; Wilcntz, J.R.; Mufson, LH.; Douglas, J.S.J.; King, S.B. Effect of pretreatment with aspirin versus aspirin plus dipyridamole on frequency and type of acute comp!icatiollS of percutaneous trans!uminal coronary angioplasty. Am. J Cardia/., 1990, 65,422-426.
[30] Cannon, C.P.; Weintraub, W.S.; Demopoulos, LA.; Vicari, R.; Frey, M.J.; Lakkis, N.; Neumann, F.J.; Robertson, D.H.; DeLucca, P.T.; DiBattistc, P.M.; Gibson, C.M.; Braunwald, E. TACTICS (Treat Angina with Aggrastat and Dctenninc Cost of Therapy with an Invasive or Conservative Strategy) - TIM! 18 Investigators. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein lib/Ilia inhibitor tirofiban (TACTICS-TIM! 18. N. Engl. J. Med., 2001,344, 1879-1887.
[31) Juergens, C.P.; White, H.D.; Belardi, J.A.; Macaya, C.; Soler-Soler, J.; Meyer, B.J.; Levy, R.D.; Bunt, T.; Menten, J.; Hemnann, H.C.; Adgey, A.A.; Tamcsby, G. A multicenter study of the tolerability of tirofiban versus placebo in patients undergoing planned intra· coronary stent placement. C/in. Ther., 2002, 24, 1332-1344.
[32] The EPIC Investigators. Usc of a Monoclonal Antibody Directed against the Platelet Glycoprotein Ilb/II!a Receptor in High-Risk Corm1a1y Angioplasty. N. Engl. J. Med., 1994,330,956-961.
[33] The EPILOG Investigators. Platelet Glycoprotein lib/lila Receptor Blockade and Low-Dose Heparin during Percutaneous Coronary Revascularisation. N Engl. J. Med., 1997, 336, 1689-1696.
[34] Bonz, A. W.; Lengenfelder, B.; Stratmann, J.; Held, S.; Turschner, 0.; Barre, K.; Wacker, C.; Waller, C.; Kochsiek, N.; Mecsmann, M.; Neyses, L.; Schanzenbacher, P.; Ertl, G.; Voelker, W. Effect of additional temporary glycoprotein lib/lila receptor inhibition on troponin release in elective percutaneous coronary interventions after pretreatment with aspirin and elopidogrel (TOPS TAR trial). J. Am. Coli. Cardiol., 2002,40,662-668.
[35] McKay, R.G.; Boden, W.E. Small peptide GP lib/lila receptor inhibitors as upstream therapy in non-ST-segment elevation acute coronary syndromes: results of the PURSUIT, PRISM, PRISMPLUS, TACTICS, and PARAGON Trials. Cun-ent Opinion in Cardiology, 2001,16,364-369.
[36] Molitemo, D.J.; Yakubov, S.J.; DiBattiste, P.M.; Hemnann, H.C.; Stone, G. W.; Macaya, C.; Neumann, F.J.; Ardissino, D.; Bassand, J.P.; Borzi, L.; Yeung, A.C.; Harris, K.A.; Demopoulos, LA, Topol, E.J. TARGET, I. Outcomes at 6 months for the direct comparison of tirofiban and abciximab during percutaneous coronary revascularisation with stent placement: the TARGET follow-up study. Lancet, 2002, 360, 355-360.
[37] Mukherjee, D.; Topol, E.J.; Be11rand, M.E.; Kristensen, S.D.; Hemnann, H.C.; Neumann, F.J., Yakubov, S.J., Bassand, J.P., McClure, R.R., Stone, G. W., Ardissino, D.; Molitemo, D.J. TAR· GET, I. Mortality at I year for the direct comparison of tirofiban and abciximab during percutaneous coronary revascularization: do tirofiban and ReoPro give similar efficacy outcomes at triall-year follow-up. /:..'111: Heart J., 2005, 26, 2524-2528.
[38]
[39]
[40]
[41]
[42]
[43]
[44]
[45]
[46]
[47]
[48]
Wirrter and Juergem
Weaver, W.O.; Simes, R.J.; Bctriu, A.; Grines, C.L.; Zijlstra, F.; Garcia, E.; Grinfcld, L.; Gibbons, R.J.; Ribeiro, E.E.; DeWood, M.A.; Ribichini, F. Comparison of primary coronary angioplasty and intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review. JAMA, 1997,278,2093-2098. Stone, G.W.; Cox, D.; Garcia, E.; Brodie, B.R.; Morice, M.C.; Griffin, J.; Mattos, L.; Lansky, A.J.; O'Neill, W. W.; Grincs, C.L. Nonnal flow (TIMI-3) before mechanical repcrfusion therapy is an independent determinant of survival in acute myocardial infarction: analysis from the primary angioplasty in myocardial infarction trials. Circulation, 2001, 104, 636-641. De Luca, G.; Ernst, N.; van'! Hof, A.W.; Ottervanger, J.P.; Hoomtje, J.C.; Dambrink, J.H.E.; Gosslink, A.T.M.; de Boer, M.J.; Suryapranata, H. Preprocedural Thrombolysis In Myocardial In· farction (TlMI) flow significantly affects the extent of ST-segment resolution and myocardial blush in patients with acute anterior myocardial infarction treated by primary angiop!asty. Am. Hearl J., 2005, 150, 827-831. Gold, H.K.; Garabedian, H.D.; Dinsmore, R.E.; Guerrero, L.J.; Cigarroa, J.E.; Palacios, I. F.; Leinbach, R.C. Restoration of coro· nary flow in myocardial infarction by intravenous chimeric 7E3 antibody without exogenous plasminogen activators. Observations in animals and humans. Circulation, 1997, 95, 1755-1759. van den Merkhof, L.F.; Zijlstra, F.; Olsson, 1-1.; Grip, L.; Veen, G.; Bar, F.W.; van den Brand, M.J.; Simoons, ML; Verhcugt, F.W. Abciximab in the treatment of acute myocardial infarction eligible for primary percutaneous transluminal coronary angioplasty. Re· sults of the Glycoprotein Receptor Antagonist Patency Evaluation (GRAPE) pilot study. J. Am. Coli. Cardia/., 1999, 33, 1528-J 532. De Luca, G.; Smyapranata, H.; Stone, G. W.; Antoniucci, D.; Tchcng, J.E.; Neumann, F.J.; Van de, W.F.; Antman, E.M.; Topol, E.J. Abciximab as adjunctive therapy to reperfusion in acute STsegment elevation myocardial infarction: a meta-analysis of randomized trials. JAMA, 2005, 293, 1759-1765. Bolognese, L.; Falsini, G.; Liistro, F.; Angioli, P.; Ducci, K.; Taddei, T.; Tarducci, R.; Cosmi, F.; Baldassarre, S.; Burali, A. Ran· domised comparison of upstream tirofiban versus downstream high bolus dose tirofiban or abciximab on tissue-level perfusion and tro· ponin release in high-risk acute coronary syndromes treated with percutuncous coronary interventions: The EVEREST trial. J. Am. Coil. Cardio/., 2006, 47, 522-528. Randomised placebo-controlled trial of effect of eptifibatide on complications of percutaneous coronary intervention: IMPACT-II. lntegrilin to Minimise Platelet Aggregation and Coronary Thrombosis·ll. Lancer, 1997,349, 1422-1428. Merlini, P.A.; Rossi, M.; Menozzi, A.; Buratti, S.; Brennan, D.M.; Moliterno, D.J.; Topol, E.J.; Ardissino, D. Thrombocytopenia caused by abciximab or tirofiban and its association with clinical outcome in patients undergoing coronary stenting. Circulation, 2004,109,2203-2206. Szucs, T.D.; Meyer, B.J.; Kiowski, W. Economic assessment of tirofiban in the management of acute coronary syndromes in the hospital setting: an analysis based on the PRISM PLUS trial. Em: JfeanJ., 1999,20,1253-1260. Weintraub, W.S.; Cu!ler, S.; Boccuzzi, S.J.; Cook, J.R.; Kosinski, A.S.; Cohen, DJ.; Burnette, J. Economic impact of GPIIB/IIIA blockade after high-risk angioplasty: results from the RESTORE trial. Randomized Efficacy Study of Tirofiban for Outcomes and Restenosis. J. Am. Col!. Cardiol., 1999, 34, 1061-1066.
Received: 15 January, 2007 Revised: 03 March, 2008 Accepted: 03 March, 2008
Copyright of Cardiovascular & Haematological Disorders - Drug Targets is the property of Bentham Science Publishers Ltd. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print. download, or email articles for individual use.

66
PAPER 15
Reprinted from Expert Opinion on Biological Therapy 2011;11:235-246
with permission from Informa Healthcare
1. Introduction
2. GPIIb/IIIa receptor
3. The development of
abciximab
4. Pharmacokinetics and
pharmacodynamics of
abciximab
5. Clinical experience with
abciximab in ACS with early
revascularization
6. Abciximab in primary PCI
for ST elevation MI
7. ‘Upstream’ use of abciximab
in patients with ACS without
early revascularization
8. Alternative routes of
abciximab administration
9. Abciximab bolus only
administration
10. Adverse reactions to
abciximab therapy
11. Re-administration of
abciximab
12. Conclusion
13. Expert opinion
Drug Evaluation
Abciximab as an adjunctivetherapy for patients undergoingpercutaneous coronaryinterventionsDevang Parikh & Craig P Juergens††Liverpool Hospital, Department of Cardiology, NSW, Australia
Introduction: Platelets play a central role in the pathophysiology of acute cor-
onary syndromes (ACS) and activation of platelet glycoprotein (GP) IIb/IIIa
receptor is critical to platelet aggregation. Abciximab, a human murine chi-
meric antibody to the GPIIb/IIIa receptor, is an important biological therapy
in the management of patients presenting with ACS.
Areas covered: The objective of this review is to define the role of abciximab
in the management of ACS by interpreting the available data from random-
ized clinical trials using abciximab in various clinical scenarios, particularly in
percutaneous coronary intervention (PCI). We also review different modes
of delivery and describe the adverse effects of abciximab including thrombo-
cytopenia. Where possible, we attempt to compare abciximab to the other
available GPIIb/IIIa inhibitors. We hope the reader will gain a better under-
standing of the benefits and risks of abciximab and the important role it has
in the management of cardiology patients.
Expert opinion: Abciximab was a breakthrough drug in the management of
high risk ACS patients undergoing PCI. However, with newer available thera-
pies and improvement in PCI technology, dose and delivery of this drug have
evolved as we try to extract maximum benefit while minimizing the adverse
effects associated with it.
Keywords: abciximab, acute coronary syndromes, review, thrombocytopenia
Expert Opin. Biol. Ther. (2011) 11(2):235-246
1. Introduction
Platelets play a central role in the pathophysiology of acute coronary syndromes(ACS). During plaque rupture, spontaneously or during percutaneous coronaryintervention (PCI), platelet activation occurs, with an initial step being adhesionof the platelet to the subendothelial matrix. Intimal injury disrupts the endotheliumand leads to exposure of collagen and other subendothelial molecules. This starts thecascade of platelet adhesion, activation and aggregation, which eventually leads to aplatelet rich thrombus [1].
The main adhesion mechanism binding the platelet to the subendothelial matrixis via collagen and the platelet membrane, Glycoprotein (GP) Ia/IIa and GPVI.GPIa/IIa serves as an anchor for platelets to connect to exposed collagen whileGPVI activates adhesive receptors, including GPIa/IIa, which strengthen collagen--platelet adherence. The most potent activator of the platelet is thrombin. Theprimary platelet receptor binding thrombin is the protease-activated receptor-1.Thrombin, thromboxane A2 and ADP directly activate the platelet throughG-protein-coupled receptors (GPCRs) and lead to platelet aggregation and granulerelease. ADP receptors on the platelet are P2Y1 and P2Y12, and these separatelylead to platelet shape and functional changes [2].
10.1517/14712598.2011.551113 © 2011 Informa UK, Ltd. ISSN 1471-2598 235All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.

A final step of platelet function is aggregation to form aplatelet plug. In the resting state, platelets are freely circulat-ing, but activated platelets bound to extracellular matrix pro-teins and soluble factors initiate an inside-to-outside signal.This signal causes a conformational change in the GPIIb/IIIa receptor, allowing it to bind with specific ligands [3].The main ligand that binds to GPIIb/IIIa is fibrinogenthrough fibronectin. Von Willebrand factor and vitronectinare also able to bind to the GPIIb/IIIa receptor [1]. The bind-ing of the GPIIb/IIIa receptor initiates an outside-to-insidesignal, which causes platelets to secrete the contents of theircytoplasmic granules, including adhesive molecules, growthfactors and procoagulants as well as synthesize and releasethromboxane. This leads to further recruitment and activationof adjacent platelets. Platelet-activated second messenger sig-nals also cause a structural change in the platelet, transformingit from a discoid shape to an irregular form with multiple pro-jections. As platelets continue to aggregate, further changes inthe cytoskeleton occur [4].The understanding of the above facets of platelet biology
and pathophysiology led to the development of a new classof drugs in the 1980s known as the platelet GPIIb/IIIa antag-onists. These drugs became a cornerstone in the therapy ofACS with or without PCI.
2. GPIIb/IIIa receptor
The platelet GPIIb/IIIa receptor is a member of the integrinfamily of cell surface adhesion receptors. It consists of thea2b and b3 subunits. The a subunit is a 136 kD molecule
with a light and heavy chain. The light chain contains a shortcytoplasmic tail, a transmembrane region and a shortextracellular domain, whereas the heavy chain is entirely extra-cellular. The b subunit is an 84.5 kD molecule with a shortintracellular tail, transmembrane region and a large extracellu-lar domain. There are ~ 80,000 GPIIb/IIIa receptors on theplatelet surface [5]. During platelet activation, a conforma-tional change occurs in the GPIIb/IIIa receptor, markedlyincreasing its affinity for fibrinogen, its major ligand.
Regardless of the initiating agonist, the final commonpathway for platelet aggregation is the crosslinking of fibrin-ogen and the GPIIb/IIIa receptor. This makes the GPIIb/IIIa inhibitors many times more effective in inhibitingplatelets than other agents. Intravenous GPIIb/IIIa inhibi-tors inhibit ADP-induced platelet aggregation in vitro by ~80 -- 90%. This is in contrast to roughly 10% for aspirinand 30 -- 40% for thienopyridines. There are three paren-teral GPIIb/IIIa receptor antagonists available for use in clin-ical practice and all have been extensively investigated inlarge, randomized clinical trials. Abciximab is a humanmurine chimeric antibody to the GPIIb/IIIa receptor(Box 1), Eptifibatide is a cyclic heptapeptide inhibitor andtirofiban is a non-peptide inhibitor of the GPIIb/IIIa inhib-itor. This review focuses on abciximab (c7E3 Fab, ReoPro,Centocor, Malvern, PA, USA), the human murine chimericantibody to the GPIIb/IIIa inhibitor with a particular focuson its role in ACS.
3. The development of abciximab
Coller first described a murine mAb to the human plateletfibrinogen receptor (GPIIb/IIIa) in the 1980s. This antibody,initially known as 10E5, inhibited the binding of fibrinogento this receptor and hence prevented platelet aggregation [6].Subsequently, the Fc fragment of one such antibody 7E3 wasremoved to prevent immunogenicity and joined to the constantportion of human immunoglobulin to form the chimericcompound abciximab or c7E3.
Unlike the other available GPIIb/IIIa inhibitors, abciximabcan also crossreact with other receptor integrins not unique toplatelets known as avb3 integrin which has been reported tomediate cell attachment and spreading, cell survival, migra-tion and proliferation, intimal hyperplasia and angiogenesis [7].This has previously led to the hypothesis in clinical studiesthat abciximab may have a favorable role in reducing neo-intimal hyperplasia through its effect on this non-GPIIb/IIIareceptor. Abciximab may also interact with the neutrophil-associated integrin Mac-1 (CD11b/CD18), although themechanism and importance of this interaction are unknown.
4. Pharmacokinetics and pharmacodynamicsof abciximab
Abciximab is a high affinity GPIIb/IIIa antagonist with adissociation constant of 5 nM. The high affinity of abciximab
Box 1. Drug summary.
Drug name AbciximabPhase LaunchedIndication Acute coronary syndromesPharmacology description Glycoprotein IIb/IIIa receptor
antagonistavb3 Integrin antagonistb2 Integrin antagonistPlatelet aggregation inhibitorIntegrin antagonist
Route of administration ParenteralPivotal trial(s) EPIC
EPILOGEPISTENTCAPTUREADMIRALCADILLACRAPPORTGUSTO IV-ACSEASYBRAVE-3
Pharmaprojects -- copyright to Citeline Drug Intelligence (an Informa
business). Readers are referred to Pipeline (http://informa-pipeline.
citeline.com) and Citeline (http://informa.citeline.com).
Abciximab
236 Expert Opin. Biol. Ther. (2011) 11(2)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.

for GPIIb/IIIa allows for a high degree of association of theinitial bolus dose with the target receptor when administeredto patients. Calculations based on published data indicatethat ~ 67% of the bolus dose of abciximab used clinicallybinds to platelets, assuming that approximately a third ofplatelets are in the spleen [8]. The binding site(s) of abciximabare located at the b-chain of the GPIIb/IIIa receptor and aredifferent from the binding site for the low-molecular massinhibitors eptifibatide and tirofiban. The large-sized antibodyfragment (molecular mass about 50 kD) causes a steric hin-drance of access of ligands to their binding pocket. This alsoexplains its almost equimolar potency (kD: 7 nM) for inhibi-tion of the other b3 integrin avb3, the vitronectin receptor atthe surface of vascular cells, that is, the endothelium andvascular smooth muscle [9].
Abciximab has a short plasma half-life of 30 min. Afterbolus injection, 50% of the compound is bound to plateletswithin the first 10 min. The half-life of dissociation of abcix-imab from the platelet GPIIb/IIIa receptor is long, up to 4 h,and does not correlate with the rather short half-life of thecompound in plasma, due to rapid degradation by proteolysisof the unbound abciximab. Thus, in contrast to eptifibatideand tirofiban, abciximab has a slow off-rate. Abciximab alsore-distributes from platelet to platelet as well as from plateletsto vascular cells, that is, cells bearing the b3-chain of the het-erodimer [7]. An estimated 29 and 13% of GPIIb/IIIa recep-tors are still occupied by abciximab at 8 and 15 days aftercompletion of infusion. This long-lasting low-level receptorblockade by abciximab may be responsible for the moresubtle pharmacological effects of the compound and explainsome differences in clinical outcome as compared with otherGPIIb/IIIa antagonists [10]. In almost all the clinical trials,abciximab was given as a bolus dose of 0.25 mg/kg bodyweight followed by an infusion of 0.125 µg/kg/min up to amaximum of 10 µg/min for a total duration of 12 h. Thecharacteristics of the three commercially available intravenous(i.v.) GPIIb/IIIa inhibitors are given briefly in Table 1.
5. Clinical experience with abciximab in ACSwith early revascularization
Of all the GPIIb/IIIa inhibitors, abciximab has had the lon-gest clinical use and the most exhaustive evaluation throughrandomized clinical trials in various clinical situations(Table 2). The clinical benefits of abciximab in patients withACS undergoing early revascularization were first establishedin 1994 when the results of the EPIC trial were published [11].This was a prospective, randomized, double-blind trial inwhich coronary stenting was not performed routinely andthe patient population consisted of those who were scheduledto undergo coronary angioplasty or directional atherectomyand were considered a high risk for abrupt vessel closure.Patients were excluded if they were > 80 years old, had ableeding diathesis, recent major surgery or stroke within thelast 2 years. All patients were treated with aspirin and heparin.
Patients were randomized in a double-blind fashion to abcix-imab in a bolus dose followed by an infusion, abciximab in abolus dose followed by a placebo infusion or a placebo bolusdose and infusion. Heparin was given intravenously in an ini-tial bolus dose of 10,000 -- 12,000 U followed by incrementalbolus doses to maintain the activated clotting time (ACT)between 300 and 350 s during the procedure. Heparin infu-sion was continued for at least 12 h to maintain the acti-vated partial thromboplastin time at 1.5 -- 2.5 times thecontrol value.
When compared with placebo, a graded effect of abciximabwas found with a 10% reduction in the rate of the compositeend point in the group given the bolus alone (p = 0.43) and a35% reduction in the rate in the group given both the bolusand the infusion (p = 0.008). The patients receiving bolusand infusion had a substantial increase in both the rates ofmajor bleeding (14%) according to the thrombolysis in myo-cardial infarction (TIMI) score and transfusions of packed redblood cells (15%) compared to those in the placebo group(7 and 7%, respectively). A moderate increase was also seenin the group receiving a bolus dose alone. Bleeding was mostlyobserved at the femoral puncture site and related to coronaryartery bypass grafting (CABG). In spite of the increased riskof bleeding, this trial had important implications about thetherapy around PCI. It confirmed the importance of plateletaggregation in the occurrence of acute ischemic events inpatients undergoing PCI.
Following the results of the EPIC trial, a number of studieswere conducted on patients undergoing PCI and the use ofabciximab [12-14]. One such study was the Evaluation inPTCA to Improve Long-Term Outcome with AbciximabGPIIb/IIIa Blockade (EPILOG) [12]. Its aim was to assessthe use of abciximab in PCI with different doses of heparinto achieve clinical efficacy without increased bleeding.Approximately 50% of the patients in the study had unstableangina. High-risk patients with electrocardiographic changeswere excluded. Patients were randomly assigned in a double-blind fashion to one of three treatment groups: placebo withstandard-dose, weight-adjusted heparin (100 U/kg); abcixi-mab with standard-dose, weight-adjusted heparin; or abcixi-mab with low-dose, weight-adjusted heparin (70 U/kg). Theabciximab bolus and infusion dose were similar to thoseused in the EPIC trial. Heparin was discontinued immedi-ately after the intervention and the vascular sheath removedwhen the ACT was 175 s or less.
The EPILOG trial was terminated prematurely after enroll-ing 2792 of the planned 4800 patients. The incidence of theprimary end point was 11.7% in the placebo group, 5.2%in the group assigned to abciximab with low dose heparin(hazard ratio, 0.43; 95% CI, 0.30 -- 0.60; p < 0.001) and5.4% in the group assigned to abciximab with standard doseheparin (hazard ratio 0.45; 95% CI, 0.32 -- 0.63 p < 0.001).The treatment effect of abciximab with either heparin regi-men was homogenous among all patient groups. There wasno significant difference among the treatment groups in the
Parikh & Juergens
Expert Opin. Biol. Ther. (2011) 11(2) 237
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.
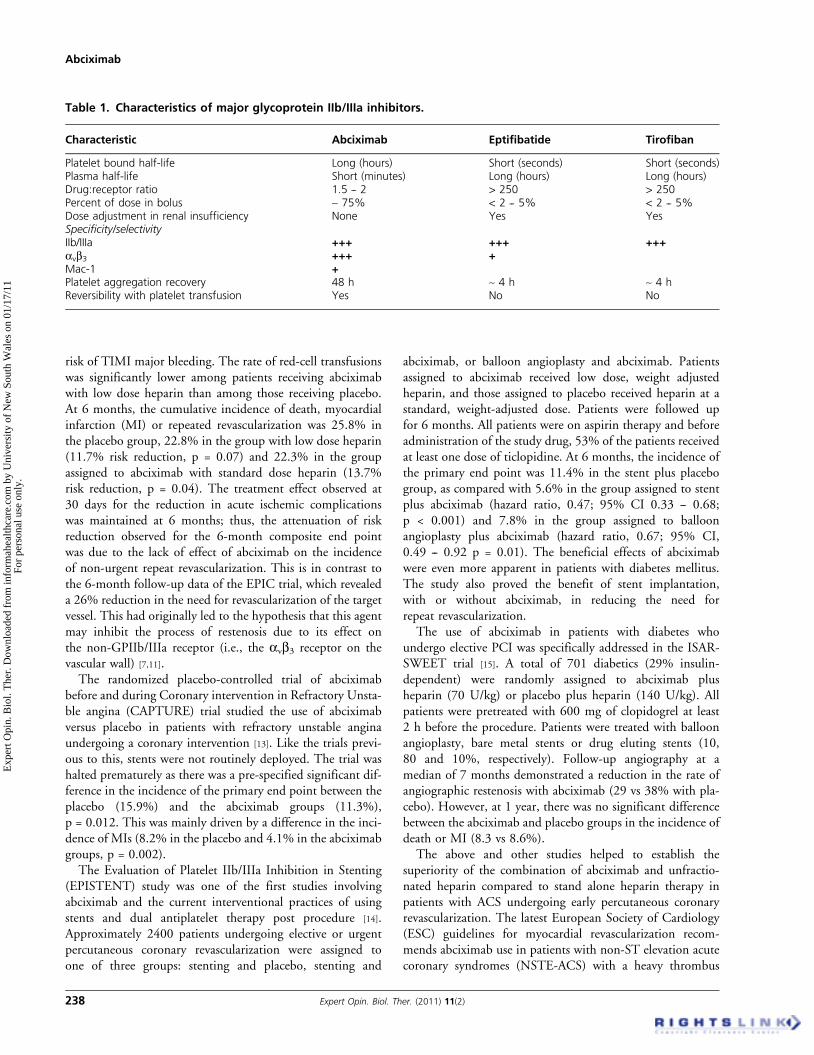
risk of TIMI major bleeding. The rate of red-cell transfusionswas significantly lower among patients receiving abciximabwith low dose heparin than among those receiving placebo.At 6 months, the cumulative incidence of death, myocardialinfarction (MI) or repeated revascularization was 25.8% inthe placebo group, 22.8% in the group with low dose heparin(11.7% risk reduction, p = 0.07) and 22.3% in the groupassigned to abciximab with standard dose heparin (13.7%risk reduction, p = 0.04). The treatment effect observed at30 days for the reduction in acute ischemic complicationswas maintained at 6 months; thus, the attenuation of riskreduction observed for the 6-month composite end pointwas due to the lack of effect of abciximab on the incidenceof non-urgent repeat revascularization. This is in contrast tothe 6-month follow-up data of the EPIC trial, which revealeda 26% reduction in the need for revascularization of the targetvessel. This had originally led to the hypothesis that this agentmay inhibit the process of restenosis due to its effect onthe non-GPIIb/IIIa receptor (i.e., the avb3 receptor on thevascular wall) [7,11].The randomized placebo-controlled trial of abciximab
before and during Coronary intervention in Refractory Unsta-ble angina (CAPTURE) trial studied the use of abciximabversus placebo in patients with refractory unstable anginaundergoing a coronary intervention [13]. Like the trials previ-ous to this, stents were not routinely deployed. The trial washalted prematurely as there was a pre-specified significant dif-ference in the incidence of the primary end point between theplacebo (15.9%) and the abciximab groups (11.3%),p = 0.012. This was mainly driven by a difference in the inci-dence of MIs (8.2% in the placebo and 4.1% in the abciximabgroups, p = 0.002).The Evaluation of Platelet IIb/IIIa Inhibition in Stenting
(EPISTENT) study was one of the first studies involvingabciximab and the current interventional practices of usingstents and dual antiplatelet therapy post procedure [14].Approximately 2400 patients undergoing elective or urgentpercutaneous coronary revascularization were assigned toone of three groups: stenting and placebo, stenting and
abciximab, or balloon angioplasty and abciximab. Patientsassigned to abciximab received low dose, weight adjustedheparin, and those assigned to placebo received heparin at astandard, weight-adjusted dose. Patients were followed upfor 6 months. All patients were on aspirin therapy and beforeadministration of the study drug, 53% of the patients receivedat least one dose of ticlopidine. At 6 months, the incidence ofthe primary end point was 11.4% in the stent plus placebogroup, as compared with 5.6% in the group assigned to stentplus abciximab (hazard ratio, 0.47; 95% CI 0.33 -- 0.68;p < 0.001) and 7.8% in the group assigned to balloonangioplasty plus abciximab (hazard ratio, 0.67; 95% CI,0.49 -- 0.92 p = 0.01). The beneficial effects of abciximabwere even more apparent in patients with diabetes mellitus.The study also proved the benefit of stent implantation,with or without abciximab, in reducing the need forrepeat revascularization.
The use of abciximab in patients with diabetes whoundergo elective PCI was specifically addressed in the ISAR-SWEET trial [15]. A total of 701 diabetics (29% insulin-dependent) were randomly assigned to abciximab plusheparin (70 U/kg) or placebo plus heparin (140 U/kg). Allpatients were pretreated with 600 mg of clopidogrel at least2 h before the procedure. Patients were treated with balloonangioplasty, bare metal stents or drug eluting stents (10,80 and 10%, respectively). Follow-up angiography at amedian of 7 months demonstrated a reduction in the rate ofangiographic restenosis with abciximab (29 vs 38% with pla-cebo). However, at 1 year, there was no significant differencebetween the abciximab and placebo groups in the incidence ofdeath or MI (8.3 vs 8.6%).
The above and other studies helped to establish thesuperiority of the combination of abciximab and unfractio-nated heparin compared to stand alone heparin therapy inpatients with ACS undergoing early percutaneous coronaryrevascularization. The latest European Society of Cardiology(ESC) guidelines for myocardial revascularization recom-mends abciximab use in patients with non-ST elevation acutecoronary syndromes (NSTE-ACS) with a heavy thrombus
Table 1. Characteristics of major glycoprotein IIb/IIIa inhibitors.
Characteristic Abciximab Eptifibatide Tirofiban
Platelet bound half-life Long (hours) Short (seconds) Short (seconds)Plasma half-life Short (minutes) Long (hours) Long (hours)Drug:receptor ratio 1.5 -- 2 > 250 > 250Percent of dose in bolus ~ 75% < 2 -- 5% < 2 -- 5%Dose adjustment in renal insufficiency None Yes YesSpecificity/selectivityIIb/IIIa +++ +++ +++avb3 +++ +Mac-1 +Platelet aggregation recovery 48 h ~ 4 h ~ 4 hReversibility with platelet transfusion Yes No No
Abciximab
238 Expert Opin. Biol. Ther. (2011) 11(2)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.
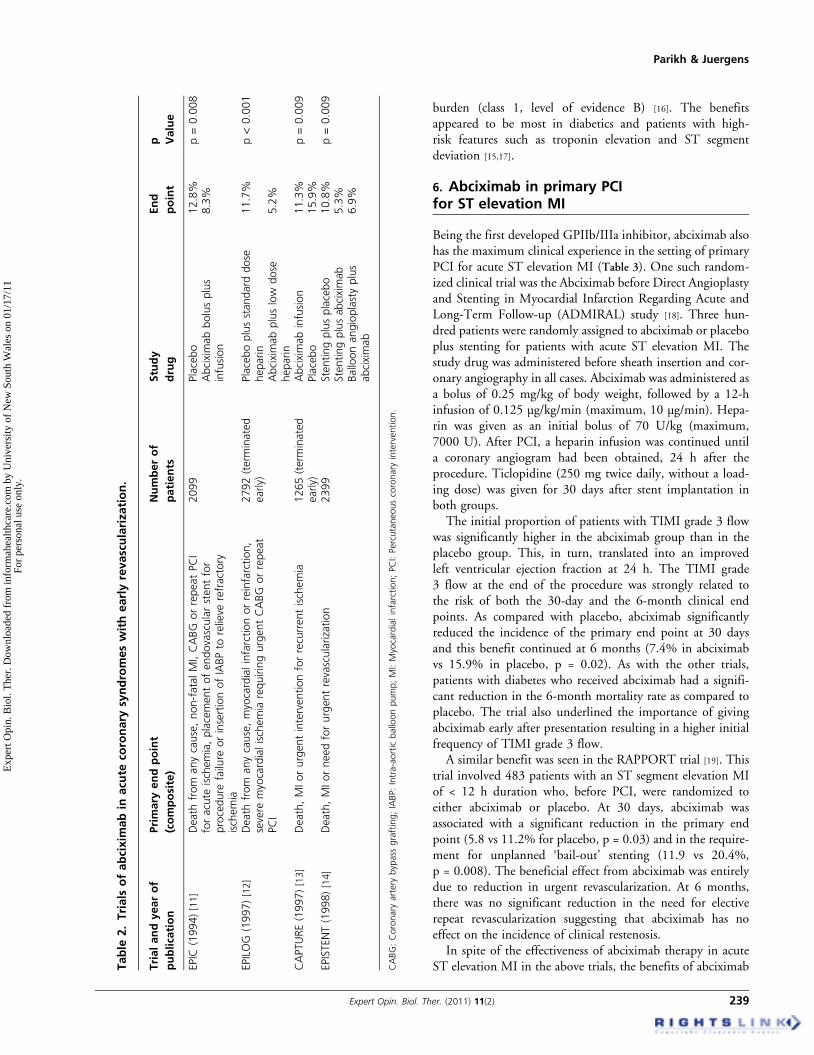
burden (class 1, level of evidence B) [16]. The benefitsappeared to be most in diabetics and patients with high-risk features such as troponin elevation and ST segmentdeviation [15,17].
6. Abciximab in primary PCIfor ST elevation MI
Being the first developed GPIIb/IIIa inhibitor, abciximab alsohas the maximum clinical experience in the setting of primaryPCI for acute ST elevation MI (Table 3). One such random-ized clinical trial was the Abciximab before Direct Angioplastyand Stenting in Myocardial Infarction Regarding Acute andLong-Term Follow-up (ADMIRAL) study [18]. Three hun-dred patients were randomly assigned to abciximab or placeboplus stenting for patients with acute ST elevation MI. Thestudy drug was administered before sheath insertion and cor-onary angiography in all cases. Abciximab was administered asa bolus of 0.25 mg/kg of body weight, followed by a 12-hinfusion of 0.125 µg/kg/min (maximum, 10 µg/min). Hepa-rin was given as an initial bolus of 70 U/kg (maximum,7000 U). After PCI, a heparin infusion was continued untila coronary angiogram had been obtained, 24 h after theprocedure. Ticlopidine (250 mg twice daily, without a load-ing dose) was given for 30 days after stent implantation inboth groups.
The initial proportion of patients with TIMI grade 3 flowwas significantly higher in the abciximab group than in theplacebo group. This, in turn, translated into an improvedleft ventricular ejection fraction at 24 h. The TIMI grade3 flow at the end of the procedure was strongly related tothe risk of both the 30-day and the 6-month clinical endpoints. As compared with placebo, abciximab significantlyreduced the incidence of the primary end point at 30 daysand this benefit continued at 6 months (7.4% in abciximabvs 15.9% in placebo, p = 0.02). As with the other trials,patients with diabetes who received abciximab had a signifi-cant reduction in the 6-month mortality rate as compared toplacebo. The trial also underlined the importance of givingabciximab early after presentation resulting in a higher initialfrequency of TIMI grade 3 flow.
A similar benefit was seen in the RAPPORT trial [19]. Thistrial involved 483 patients with an ST segment elevation MIof < 12 h duration who, before PCI, were randomized toeither abciximab or placebo. At 30 days, abciximab wasassociated with a significant reduction in the primary endpoint (5.8 vs 11.2% for placebo, p = 0.03) and in the require-ment for unplanned ‘bail-out’ stenting (11.9 vs 20.4%,p = 0.008). The beneficial effect from abciximab was entirelydue to reduction in urgent revascularization. At 6 months,there was no significant reduction in the need for electiverepeat revascularization suggesting that abciximab has noeffect on the incidence of clinical restenosis.
In spite of the effectiveness of abciximab therapy in acuteST elevation MI in the above trials, the benefits of abciximabT
able
2.Trials
ofabcixim
abin
acu
teco
ronary
syndromeswithearlyrevasculariza
tion.
Trialandyearof
publication
Primary
endpoint
(composite)
Numberof
patients
Study
drug
End
point
p Value
EPIC
(1994)[11]
Death
from
anycause,non-fatalMI,CABG
orrepeatPCI
foracute
ischemia,placementofendovascularstentfor
procedure
failure
orinsertionofIABPto
relieve
refractory
ischemia
2099
Placebo
12.8%
p=0.008
Abciximabbolusplus
infusion
8.3%
EPILOG
(1997)[12]
Death
from
anycause,myocardialinfarctionorreinfarction,
severe
myocardialischemia
requiringurgentCABG
orrepeat
PCI
2792(term
inated
early)
Placeboplusstandard
dose
heparin
11.7%
p<0.001
Abciximabpluslow
dose
heparin
5.2%
CAPTURE(1997)[13]
Death,MIorurgentinterventionforrecurrentischemia
1265(term
inated
early)
Abciximabinfusion
11.3%
p=0.009
Placebo
15.9%
EPISTENT(1998)[14]
Death,MIorneedforurgentrevascularization
2399
Stentingplusplacebo
10.8%
p=0.009
Stentingplusabciximab
5.3%
Balloonangioplastyplus
abciximab
6.9%
CABG:Coronary
artery
bypass
grafting;IABP:Intra-aortic
balloonpump;MI:Myocardialinfarction;PCI:Percutaneouscoronary
intervention.
Parikh & Juergens
Expert Opin. Biol. Ther. (2011) 11(2) 239
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.
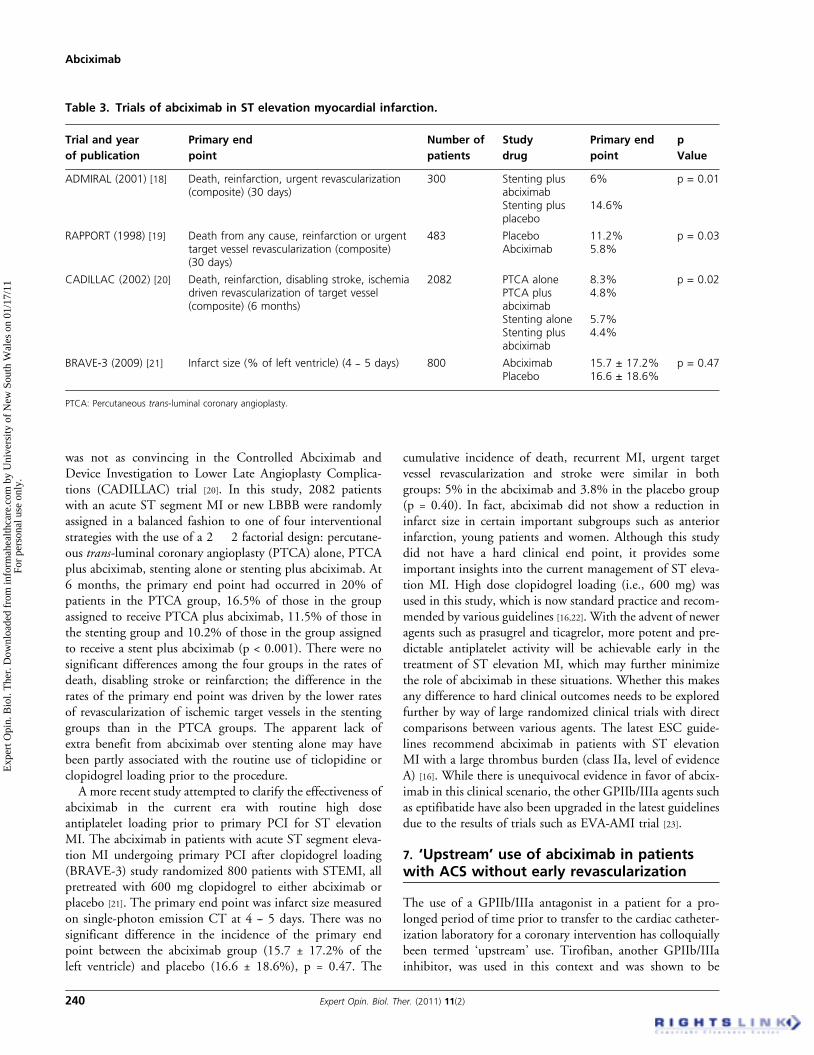
was not as convincing in the Controlled Abciximab andDevice Investigation to Lower Late Angioplasty Complica-tions (CADILLAC) trial [20]. In this study, 2082 patientswith an acute ST segment MI or new LBBB were randomlyassigned in a balanced fashion to one of four interventionalstrategies with the use of a 2 � 2 factorial design: percutane-ous trans-luminal coronary angioplasty (PTCA) alone, PTCAplus abciximab, stenting alone or stenting plus abciximab. At6 months, the primary end point had occurred in 20% ofpatients in the PTCA group, 16.5% of those in the groupassigned to receive PTCA plus abciximab, 11.5% of those inthe stenting group and 10.2% of those in the group assignedto receive a stent plus abciximab (p < 0.001). There were nosignificant differences among the four groups in the rates ofdeath, disabling stroke or reinfarction; the difference in therates of the primary end point was driven by the lower ratesof revascularization of ischemic target vessels in the stentinggroups than in the PTCA groups. The apparent lack ofextra benefit from abciximab over stenting alone may havebeen partly associated with the routine use of ticlopidine orclopidogrel loading prior to the procedure.A more recent study attempted to clarify the effectiveness of
abciximab in the current era with routine high doseantiplatelet loading prior to primary PCI for ST elevationMI. The abciximab in patients with acute ST segment eleva-tion MI undergoing primary PCI after clopidogrel loading(BRAVE-3) study randomized 800 patients with STEMI, allpretreated with 600 mg clopidogrel to either abciximab orplacebo [21]. The primary end point was infarct size measuredon single-photon emission CT at 4 -- 5 days. There was nosignificant difference in the incidence of the primary endpoint between the abciximab group (15.7 ± 17.2% of theleft ventricle) and placebo (16.6 ± 18.6%), p = 0.47. The
cumulative incidence of death, recurrent MI, urgent targetvessel revascularization and stroke were similar in bothgroups: 5% in the abciximab and 3.8% in the placebo group(p = 0.40). In fact, abciximab did not show a reduction ininfarct size in certain important subgroups such as anteriorinfarction, young patients and women. Although this studydid not have a hard clinical end point, it provides someimportant insights into the current management of ST eleva-tion MI. High dose clopidogrel loading (i.e., 600 mg) wasused in this study, which is now standard practice and recom-mended by various guidelines [16,22]. With the advent of neweragents such as prasugrel and ticagrelor, more potent and pre-dictable antiplatelet activity will be achievable early in thetreatment of ST elevation MI, which may further minimizethe role of abciximab in these situations. Whether this makesany difference to hard clinical outcomes needs to be exploredfurther by way of large randomized clinical trials with directcomparisons between various agents. The latest ESC guide-lines recommend abciximab in patients with ST elevationMI with a large thrombus burden (class IIa, level of evidenceA) [16]. While there is unequivocal evidence in favor of abcix-imab in this clinical scenario, the other GPIIb/IIIa agents suchas eptifibatide have also been upgraded in the latest guidelinesdue to the results of trials such as EVA-AMI trial [23].
7. ‘Upstream’ use of abciximab in patientswith ACS without early revascularization
The use of a GPIIb/IIIa antagonist in a patient for a pro-longed period of time prior to transfer to the cardiac catheter-ization laboratory for a coronary intervention has colloquiallybeen termed ‘upstream’ use. Tirofiban, another GPIIb/IIIainhibitor, was used in this context and was shown to be
Table 3. Trials of abciximab in ST elevation myocardial infarction.
Trial and year
of publication
Primary end
point
Number of
patients
Study
drug
Primary end
point
p
Value
ADMIRAL (2001) [18] Death, reinfarction, urgent revascularization(composite) (30 days)
300 Stenting plusabciximab
6% p = 0.01
Stenting plusplacebo
14.6%
RAPPORT (1998) [19] Death from any cause, reinfarction or urgenttarget vessel revascularization (composite)(30 days)
483 Placebo 11.2% p = 0.03Abciximab 5.8%
CADILLAC (2002) [20] Death, reinfarction, disabling stroke, ischemiadriven revascularization of target vessel(composite) (6 months)
2082 PTCA alone 8.3% p = 0.02PTCA plusabciximab
4.8%
Stenting alone 5.7%Stenting plusabciximab
4.4%
BRAVE-3 (2009) [21] Infarct size (% of left ventricle) (4 -- 5 days) 800 Abciximab 15.7 ± 17.2% p = 0.47Placebo 16.6 ± 18.6%
PTCA: Percutaneous trans-luminal coronary angioplasty.
Abciximab
240 Expert Opin. Biol. Ther. (2011) 11(2)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.

beneficial in patients with ACS irrespective of the subsequentperformance of PCI. The Platelet Receptor Inhibition inIschemic Syndrome Management in Patients Limited byUnstable Signs and Symptoms (PRISM-PLUS) trial showedthat tirofiban in combination with aspirin and heparinreduced the primary end point of death, MI or refractoryischemia at 7 days compared to heparin alone (12.9 vs17.9%, p = 0.004) [24]. The GUSTO IV-ACS study wasspecifically designed to assess the value of an i.v. abciximabfor medically treated patients with ACS [25]. A total of7800 ACS patients with high risk features (positive cardiactroponin T or I or at least 0.5 mm transient or persistentST segment depression) were randomly assigned to one ofthree treatment groups: abciximab therapy for 24 h followedby 24 h of placebo infusion; abciximab therapy for 48 h ormatching placebo (bolus and 48 h infusion). Patients with ahigh risk of bleeding, previous stroke within 2 years or aplanned coronary bypass surgery within 30 days of enrolmentwere excluded from the study. Bleeding was classified asmajor, minor or insignificant based on the TIMI criteria.The primary end point in this study was the occurrence,within 30 days after randomization, of all-cause mortalityor MI.
There was a high rate of concurrent aspirin administration.However, the use of thienopyridines was low (1 -- 2%).Around 85% patients had concomitant use of unfractionatedheparin. Revascularization was done in 30% of patientswithin 30 days after enrolment. However, only 2% patientsunderwent revascularization within 48 h while on study treat-ment. The combined primary end point was similar amongthe three treatment groups. No significant differences wereapparent in the composite end point among the three treat-ment groups at any time point (48 h, 7 days and 30 days).However, at 48 h, a higher rate of mortality was seen inpatients receiving either the 24 or 48 h abciximab infusioncompared to placebo. None of the pre-specified subgroupsshowed a significant treatment benefit with abciximab,although a significantly impaired outcome was seen inwomen. Bleeding rates were more frequent with abciximab,particularly in the 48 h treatment group.
The findings from this study were in contrast to the bene-fits of abciximab in patients with ACS undergoing coronaryinterventions [11,12,14]. They were also in contrast to the effectsof other parenteral GPIIb/IIIa inhibitors in patients withACS. Although the exact reason behind such findings is notclear, one of the hypotheses that emerged was the poten-tial paradoxical platelet activation when incomplete plate-let--receptor blockade is achieved [9]. The longer infusionperiod may have resulted in a dropping of the platelet inhibi-tion to < 80%, which is the required level to maintain efficacyof this drug. A low level of platelet-receptor blockade insome of the patients in this study might have resulted inplatelet activation and thrombotic events, offsetting a possiblebenefit in other patients whose platelet receptors were blockedadequately at that point. Following this study, abciximab
became a class III indication in patients with ACSwithout early revascularization. Consequently, abciximabwas confined to its role as a drug used mainly in the cardiaccatheterization laboratory.
8. Alternative routes of abciximabadministration
The majority of the randomized clinical trials have used an i.v.bolus and infusion of abciximab to prove its efficacy in ACS.Given its impact on plaque passivation in an acute setting, itseems intuitive that administering the drug directly into thecoronary artery (intracoronary; i.c.) would lead to betterimmediate and long-term outcomes. The randomized, Lepzigimmediate percutaneous coronary intervention abciximabi.v. versus i.c. in ST elevation MI trial, randomly assigned154 consecutive patients with an acute ST elevation MI toeither i.c. or i.v. bolus abciximab administration with subse-quent 12-h i.v. infusion [26]. The primary end point wasinfarct size and extent of microvascular obstruction as assessedby delayed enhancement magnetic resonance. The medianinfarct size was 15.1% in the i.c. versus 23.4% in the i.v.group (p = 0.01). A similar statistically significant differencewas also observed in the extent of microvascular obstruc-tion favoring the i.c. abciximab group. There was also a trendtowards a lower major adverse cardiac event rate after i.c.versus i.v. abciximab application.
Another case control study demonstrated a significantreduction in corrected TIMI frame counts (CTFC) in37 patients undergoing an emergency intervention for a rangeof ACS compared to a matched group of 37 patients receivingi.v. abciximab [27]. A recent meta-analysis compared databetween i.c. and i.v. administration of abciximab [28]. A totalof 2301 patients were analyzed of whom 984 received i.c.and 1338 received i.v. abciximab. On primary analysis, thereappeared to be a mortality benefit with i.c. compared to i.v.abciximab (odds ratio; OR 0.57, 95% CI 0.35 -- 0.94;p = 0.028). There appeared to be a nonsignificant trendtowards reduced major adverse cardiovascular events(MACE) with i.c. compared to i.v. abciximab (OR 0.62,95% CI 0.38 -- 1.03; p = 0.066). Although there appearedto be a mortality benefit with i.c. administration, the resultsshould be interpreted with caution, as the majority of thestudies were small with shorter follow-up and underpoweredto detect mortality end points.
Another theory is that i.c. administration may not allowenough time for the drug to interact with the atheromatousplaque due to the rapid coronary flow and hence local drugdelivery may be superior. This led to the development of localdelivery systems. A recent Phase II trial aimed to study thebenefits of local abciximab delivery with i.c. administrationas the control route [29]. The ClearwayRX� Therapeutic Per-fusion Catheter (Atrium Medical Corp., Hudson, NH, USA)was used to deliver abciximab. Optical coherence tomography(OCT) was used to assess the thrombus burden before and
Parikh & Juergens
Expert Opin. Biol. Ther. (2011) 11(2) 241
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.

after delivery of the drug. A total of 50 patients with ACS(40% STEMI) were randomized. The primary end pointwas the change in thrombus score after angioplasty byOCT. There was a significant reduction in the thrombus bur-den and TIMI frame count in the patients assigned to localdrug delivery. The MACE rates at 1 year were 5.9% in thelocal delivery group versus 27.2% in the i.c. infusion group(p = 0.046). This was driven by a higher target lesion revascu-larization in the i.c. infusion group. Although local deliveryappears to be a promising new mode of delivery of abciximab,larger trials with harder end points are needed before thismode of therapy becomes a part of regular practice.
9. Abciximab bolus only administration
Based on earlier randomized clinical trials, abciximab bolusonly therapy was considered to be inferior compared to abolus followed by infusion strategy [11]. This was mainlydriven by higher rates of urgent repeat revascularization inan era when stents and thienopyridines were not used rou-tinely. There was no difference in the incidence of death orMI. This led investigators to re-assess the usefulness of a bolusonly approach as about 75% of the drug is actually given inthe bolus dose. One such study was a Randomized StudyComparing Same-Day Home Discharge and AbciximabBolus and Infusion After Transradial Coronary Stent Implan-tation (EASY) study [30]. In this study, 1005 patients after abolus of abciximab and uncomplicated transradial percutane-ous coronary stent implantation, were randomized either tosame day home discharge and no infusion of abciximab orto overnight hospitalization and a standard 12-h infusion ofabciximab. Thienopyridines were used routinely in all thepatients. The patients were of moderate risk with abouttwo-thirds having unstable angina and about 20% having anelevated troponin level. The primary end point was the30-day incidence of a composite of death, MI, urgent revascu-larization, major bleeding, repeat hospitalization, access sitecomplications and severe thrombocytopenia. The incidenceof the primary end point was 20.4% in the bolus onlygroup and 18.2% in the bolus followed by infusion group(p = 0.017 for non-inferiority). This study lends weight tothe argument for a bolus only regimen in moderate riskpatients. Part of the reduction in hemorrhagic complicationscan also be explained by the transradial approach, which hasalready been proven to be superior to the transfemoralapproach in terms of bleeding risk [31].A similar retrospective analysis performed on 1001 patients
undergoing PCI and given a bolus only GPIIb/IIIa inhibitorshowed that this is an efficacious approach with the addedbenefit of reduced bleeding complications and potential forreduced cost and hospital stay [32]. While the earlier studieswere mainly based on a bolus and infusion regimen, evidenceis gradually shifting towards a bolus only approach [33]. Thisneeds to be tested further particularly in high risk patientssuch as acute ST elevation infarction.
10. Adverse reactions to abciximab therapy
Given the mechanism of action of abciximab, it perhaps notsurprising that its use has been associated with an increasedrisk of bleeding complications in patients with ACS. Bleedingcomplications can occur as a result of its effects on plateletfunction or overall count. Either way, the administration ofabciximab can become problematic leading to a reduction inthe net clinical benefit in patients with ACS. In the EPICstudy, there was a 14% risk of major bleeding in the groupwith abciximab bolus followed by an infusion, compared to7% in the placebo group (p = 0.001) [11]. The majority ofbleeding was related to access site complications followed byCABG-related bleeding which was most likely secondary tothe higher dose of heparin. Subsequently, a pooled analysisshowed no significant differences between abciximab and pla-cebo in the rates of non-CABG related major or minor bleed-ing and intracranial hemorrhage [34]. This was most likelyrelated to the practice of using weight-adjusted heparin inpatients receiving abciximab therapy. Notably in the EPICtrial, which demonstrated a statistically significant differencein bleeding rates, there was no major difference in the plateletcounts between the two groups. As the majority of the bleed-ing complications were related to the access site, abciximabuse should become safer in the future as more interventionsare done via the radial route with smaller sized devices.A study done by Philippe et al. compared the radial versusfemoral approach in 119 consecutive patients with acute STelevation MI undergoing primary PCI with abciximab [35].There was no incidence of major or minor bleeding in theradial group whereas there was a 5.4% incidence of majorbleeding in the femoral group. The results were similar to aprevious study done by Choussat et al. comparing transradialto transfemoral approach in patients undergoing PCI [31].Vascular access site bleeding complications were absent inthe transradial group while the incidence was 7.5% in theother group with two patients requiring vascular surgery. Asmentioned previously, together with a bolus only regimen,transradial access should help to reduce the bleedingcomplications from abciximab use [30].
All three currently used GPIIb/IIIa receptor blockers have aclear association with thrombocytopenia [9]. However, thegreatest association has been found with abciximab. Throm-bocytopenia, at times profound, has been observed within24 h, and occasionally within several hours after the initialdose. A pooled analysis of eight placebo-controlled, random-ized trials revealed that abciximab plus heparin resulted in asignificant risk of mild (4.2 vs 2% for placebo) or severethrombocytopenia (1 vs 0.4%) compared to placebo plusheparin [36].
A unique feature of abciximab-induced thrombocytopeniais it typically occurs within 24 h and occasionallywithin 30 min to 4 h after the initial dose. This is distinctfrom other drugs that cause thrombocytopenia mediated bydrug-dependent antiplatelet antibodies [37]. Development of
Abciximab
242 Expert Opin. Biol. Ther. (2011) 11(2)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.

antibodies with all other drugs requires a longer period ofadministration in order to induce sensitization and antibodyformation. A hypothesis to explain the rapid occurrence ofthrombocytopenia following initial exposure to GPIIb/IIIainhibitors is that patients have preformed ‘naturally occurring’antibodies against platelet neopeptides that are exposed byalteration of the GPIIb/IIIa molecule during the course ofnormal platelet reactions and senescence. These antibodiesare described as reacting with ligand-induced binding sites(‘LIBS’ effect). Although antibodies also appear to mediatethrombocytopenia induced by tirofiban and eptifibatide, therate of naturally occurring tirofiban or eptifibatide dependentantibodies appears to be lower than that seen after abciximab.
Before concluding that the thrombocytopenia is secondaryto abciximab, it is important to rule out pseudothrombocyto-penia. Platelet clumping on a peripheral smear and a differ-ence between the platelet count in blood samples obtainedusing different anticoagulants (e.g., EDTA, heparin, citrate),with one having a count at least 20% lower than that of thecomparison anticoagulant is usually enough to make a diag-nosis of this condition. Inability to diagnose pseudothrombo-cytopenia may lead to inappropriate cessation of therapy andunnecessary administration of platelets where not required.
Once pseudothrombocytopenia is ruled out, managementusually consists of cessation of abciximab. In cases of pro-found thrombocytopenia (platelet count < 10,000/µl), plate-let transfusion is usually recommended to prevent majorhemorrhagic complications. Generally, it is recommended tomeasure the platelet count within 4 h of commencing abcixi-mab therapy so that thrombocytopenia can be diagnosedearly. When the platelet count is critically low, it may bewise to cease other antiplatelet agents. The platelet count usu-ally takes a period of 3 days to 2 weeks to recover in cases ofabciximab-induced thrombocytopenia.
Besides procedure related bleeding, pulmonary alveolarhemorrhage has been reported with resulting X-ray infiltratesand hypoxia [38]. Rarely, abciximab administration may beassociated with anaphylaxis.
11. Re-administration of abciximab
As abciximab is a mAb to the platelet GPIIb/IIIa receptor andcan induce an antibody response, initial concerns had beenraised about the potential for anaphylaxis, thrombocytopeniaand reduced efficacy with repeated administration. Theseissues were further studied in the ReoPro ReadministrationRegistry [39]. This registry consisted of 500 patients whowere being treated with abciximab at least 7 days after a pre-vious treatment. Safety outcomes including bleeding, transfu-sion, allergic or anaphylactic reactions and thrombocytopeniawere measured. Platelet counts were routinely obtained 4 hafter the abciximab bolus, the morning after the procedure,at 4 weeks and as clinically indicated. Human antichimericantibody (HACA) response of patients being treated withabciximab was also measured.
Of the 500 patients in the registry, there were no cases ofanaphylactic or allergic reactions. Major bleeding occurredin eight (1.6%) of the patients. All eight required red bloodcell transfusions; one also received platelets. There was no cor-relation between major bleeding and thrombocytopenia. Thebaseline HACA status was not predictive of the developmentof thrombocytopenia nor was conversion from a negativeHACA at baseline to a positive HACA at follow-up. Withregard to efficacy, after first readministration around a quarterof patients became HACA-positive.
Profound thrombocytopenia occurred in 0.5 -- 1% patientsreceiving abciximab for the first time. The higher incidencemay be due to the persistence of antibodies that develop afterthe first exposure, an anamnestic immunological response orboth. Overall, from a clinical efficacy or anaphylaxis risk per-spective, it appears to be safe to readminister abciximab ifthere is no evidence of significant thrombocytopenia duringthe initial dose.
12. Conclusion
Due to their unique mechanism of action, platelet GPIIb/IIIainhibitors have a central role in the management of patientswith ACS. Abciximab was the first developed drug and widelystudied in randomized controlled trials. It had been shown tohave a beneficial effect in high risk patients with ACS and isrecommended as a first-line medication in patients with acuteST elevation MI undergoing emergency PCI [40]. Although ithas not proven to have any extra benefit in patients with ACSnot undergoing early revascularization, it continues to have animportant role in the cardiac catheterization laboratory forpatients undergoing PCI. Readministration has been provento be safe and in spite of the small risk of thrombocytopenia,high risk patients with diabetes will continue to derive imme-diate and potentially long-term mortality benefits withthis drug.
13. Expert opinion
Abciximab was the first GPIIb/IIIa receptor blocker to bedeveloped and undoubtedly has had the benefit of being tri-aled extensively in various clinical settings. Notably, manyof these early studies were in the pre-stent era where outcomesof PCI were less predictable due to technology constraintsand the optimal use of antiplatelet therapies had not beenwell delineated. Due to the unequivocal effects on plateletaggregation, abciximab represented breakthrough technology,which improved clinical outcomes in the setting of coronaryangioplasty, particularly with patients presenting with ACSat the highest risk of a thrombotic event during the procedure.While some may question its relevance in current day practicewhen patients are routinely treated with high dose thienopyr-idine loading, it still continues to enjoy a class I -- IIa recom-mendation for treatment of high risk ACS in currentguidelines [16,22].
Parikh & Juergens
Expert Opin. Biol. Ther. (2011) 11(2) 243
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.

Given the mechanism of action, it was somewhat intuitiveto expect a degree of hemorrhagic risk with this drug, partic-ularly in the early days of PCI where sheath sizes were largerand the majority of procedures were performed via the femo-ral route. The fact that bleeding is a real concern became obvi-ous from the EPIC trial, which had a statistically significanthigher risk of bleeding compared to placebo. This was largelyaddressed in subsequent trials, which demonstrated thatadjusting the dose of concomitant unfractionated heparinreduced this risk. Recent data suggest that bleeding eventsaround the time of procedures translate into an increasedrisk of adverse events in the future. This is most likely multi-factorial and is related to the bleeding event itself and thehemodynamic consequences thereof; the risks of blood trans-fusions where utilized; the risks of surgical procedures them-selves to deal with bleeding events; as well as interruptionsto antiplatelet therapy which places the patient at an increasedcardiac risk of events such as stent thrombosis. Notably, themajority of bleeding was access site related and as operatorsuse more radial artery access today, the risk of access sitebleeding should be minimized with abciximab use. There ismounting evidence for use of transradial access and bolusdose abciximab only to reduce overall bleeding risk [30].Within the class of GPIIb/IIIa antagonists, abciximab
seems to outperform tirofiban and eptifibatide when adminis-tered in the catheterization laboratory during PCI and cer-tainly has the most robust data in the setting of ST elevationMI. More randomized data with head to head comparisonbetween the various agents may be useful in the future tohelp refine the role of these agents in various ACS.What is less clear is the role of abciximab in the future,
as we have already seen a decline in the overall use of
GPIIb/IIIa antagonists in the stenting era where outcomesof PCI are more predictable and the use of antiplatelet agentsis ubiquitous. It is likely that as more patients are treated withmore potent oral antiplatelet agents such as prasugrel and tica-grelor that the levels of abciximab use will decline further asoperators become less concerned about adverse cardiac eventsof the procedure and more concerned about bleeding.Obviously, in keeping with the current guidelines, abciximabwill still remain invaluable in certain patient populationssuch as high risk ACS with a large thrombus burden orpatients with acute ST elevation infarction and cardiogenicshock [16,22], particularly in patients who have not been pre-treated with thienopyridines. While abciximab has beenused in a proportion of the patients who participated in trialsstudying prasugrel and ticagrelor, there is a need for specifictrials looking at the use of abciximab in the context of thesepotent oral antiplatelet agents.
To counter this are the recent intriguing data suggestingthat more targeted delivery of abciximab either through theguiding catheter or through local delivery via balloon cathe-ters may see improved cardiac outcomes with minimalincreased bleeding risk when compared to traditional i.v.use. Similarly, there has been renewed interest in the conceptof a bolus only approach rather than a bolus and infusionwhich may prove to be a safer and cost-effective strategy.This ultimately may be where the future of this fascinatingbiological therapy lies.
Declaration of interest
The authors state no conflict of interest and have received nopayment in preparation of this manuscript.
Abciximab
244 Expert Opin. Biol. Ther. (2011) 11(2)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.

Bibliography
1. Lefkovits J, Plow EF, Topol EJ. Platelet
glycoprotein IIb/IIIa receptors in
cardiovascular medicine. N Engl J Med
1995;332:1553-9
2. Kunapuli SP, Dorsam RT, Kim S,
Quinton TM. Platelet purinergic
receptors. Curr Opin Pharmacol
2003;3:175-80
3. Shattil SJ, Ginsberg MH. Integrin
signaling in vascular biology.
J Clin Invest 1997;100:1-5
4. Topol EJ, Byzova TV, Plow EF.
Platelet GPIIb-IIIa blockers. Lancet
1999;353:227-31
5. Wagner CL, Mascelli MA, Neblock DS,
et al. Analysis of GPIIb/IIIa receptor
number by quantification of 7E3
binding to human platelets. Blood
1996;88:907-14
6. Coller BS. A new murine monoclonal
antibody reports an activation-dependent
change in the conformation and/or
microenvironment of the platelet
glycoprotein IIb/IIIa complex.
J Clin Invest 1985;76:101-8
7. Tam SH, Sassoli PM, Jordan RE,
Nakada MT. Abciximab (ReoPro,
chimeric 7E3 Fab) demonstrates
equivalent affinity and functional
blockade of glycoprotein IIb/IIIa and
alpha(v)beta3 integrins. Circulation
1998;98:1085-91
8. Scarborough RM, Kleiman NS,
Phillips DR. Platelet glycoprotein
IIb/IIIa antagonists. What are the
relevant issues concerning their
pharmacology and clinical use?
Circulation 1999;100:437-44
9. Schror K, Weber AA. Comparative
pharmacology of GP IIb/IIIa
antagonists. J Thromb Thrombolysis
2003;15:71-80
10. Quinn MJ, Plow EF, Topol EJ.
Platelet glycoprotein IIb/IIIa inhibitors:
recognition of a two-edged sword?
Circulation 2002;106:379-85
11. Investigators TE. Use of a monoclonal
antibody directed against the platelet
glycoprotein IIb/IIIa receptor in
high-risk coronary angioplasty. N Engl
J Med 1994;330:956-61
12. Investigators TE. Platelet glycoprotein
IIb/IIIa receptor blockade and low-dose
heparin during percutaneous coronary
revascularization. The EPILOG
Investigators. N Engl J Med
1997;336:1689-96
13. The CAPTURE Study. Randomised
placebo-controlled trial of abciximab
before and during coronary intervention
in refractory unstable angina. Lancet
1997;349:1429-35
14. Lincoff AM, Califf RM, Moliterno DJ,
et al.; Evaluation of Platelet IIb/IIIa
Inhibition in Stenting Investigators.
Complementary clinical benefits of
coronary-artery stenting and blockade
of platelet glycoprotein IIb/IIIa
receptors. N Engl J Med
1999;341:319-27
15. Mehilli J, Kastrati A, Schuhlen H,
et al. Randomized clinical trial of
abciximab in diabetic patients
undergoing elective percutaneous
coronary interventions after treatment
with a high loading dose of clopidogrel.
Circulation 2004;110:3627-35
16. Wijns W, Kolh P, Danchin N, et al.
Guidelines on myocardial
revascularization: the Task Force on
Myocardial Revascularization of the
European Society of Cardiology (ESC)
and the European Association for
Cardio-Thoracic Surgery (EACTS).
Eur Heart J 2010;31:2501-55
17. Roffi M, Chew DP, Mukherjee D,
et al. Platelet glycoprotein IIb/IIIa
inhibitors reduce mortality in diabetic
patients with non-ST-segment-elevation
acute coronary syndromes. Circulation
2001;104:2767-71
18. Montalescot G, Barragan P,
Wittenberg O, et al. Platelet
glycoprotein IIb/IIIa inhibition with
coronary stenting for acute myocardial
infarction. N Engl J Med
2001;344:1895-903
19. Brener SJ, Barr LA, Burchenal JE,
et al. Randomized, placebo-controlled
trial of platelet glycoprotein IIb/IIIa
blockade with primary angioplasty for
acute myocardial infarction.
ReoPro and Primary PTCA
Organization and Randomized Trial
(RAPPORT) Investigators. Circulation
1998;98:734-41
20. Stone GW, Grines CL, Cox DA,
et al. Comparison of angioplasty with
stenting, with or without abciximab, in
acute myocardial infarction. N Engl
J Med 2002;346:957-66
21. Mehilli J, Kastrati A, Schulz S, et al.
Abciximab in patients with acute
ST-segment-elevation myocardial
infarction undergoing primary
percutaneous coronary intervention
after clopidogrel loading: a randomized
double-blind trial. Circulation
2009;119:1933-40
22. Kushner FG, Hand M, Smith SC Jr,
et al. 2009 focused updates: ACC/
AHA guidelines for the management
of patients with ST-elevation myocardial
infarction (updating the 2004 guideline
and 2007 focused update) and ACC/
AHA/SCAI guidelines on percutaneous
coronary intervention (updating the
2005 guideline and 2007 focused update)
a report of the American College of
Cardiology Foundation/American Heart
Association Task Force on Practice
Guidelines. J Am Coll Cardiol
2009;54:2205-41
23. Zeymer U, Margenet A, Haude M,
et al. Randomized comparison of
eptifibatide versus abciximab in primary
percutaneous coronary intervention in
patients with acute ST-segment elevation
myocardial infarction: results of the
EVA-AMI Trial. J Am Coll Cardiol
2010;56:463-9
24. Platelet Receptor Inhibition in Ischemic
Syndrome Management in Patients
Limited by Unstable Signs and
Symptoms (PRISM-PLUS) Study
Investigators. Inhibition of the platelet
glycoprotein IIb/IIIa receptor with
tirofiban in unstable angina and
non-Q-wave myocardial infarction.
N Engl J Med 1998;338:1488-97
25. Simoons ML. Effect of glycoprotein
IIb/IIIa receptor blocker abciximab on
outcome in patients with acute coronary
syndromes without early coronary
revascularisation: the GUSTO IV-ACS
randomised trial. Lancet
2001;357:1915-24
26. Thiele H, Schindler K, Friedenberger J,
et al. Intracoronary compared with
intravenous bolus abciximab application
in patients with ST-elevation myocardial
infarction undergoing primary
percutaneous coronary intervention: the
randomized Leipzig immediate
percutaneous coronary intervention
abciximab IV versus IC in ST-elevation
myocardial infarction trial. Circulation
2008;118:49-57
Parikh & Juergens
Expert Opin. Biol. Ther. (2011) 11(2) 245
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.
27. Romagnoli E, Burzotta F, Trani C,
et al. Angiographic evaluation of the
effect of intracoronary abciximab
administration in patients undergoing
urgent PCI. Int J Cardiol
2005;105:250-5
28. Hansen PR, Iversen A, Abdulla J.
Improved clinical outcomes with
intracoronary compared to intravenous
abciximab in patients with acute
coronary syndromes undergoing
percutaneous coronary intervention:
a systematic review and meta-analysis.
J Invasive Cardiol 2010;22:278-82
29. Prati F, Capodanno D, Pawlowski T,
et al. Local delivery versus
intracoronary infusion of abciximab
in patients with acute coronary
syndromes. JACC Cardiovasc Interv
2010;3:928-34
30. Bertrand OF, De Larochelliere R,
Rodes-Cabau J, et al. A randomized
study comparing same-day home
discharge and abciximab bolus only to
overnight hospitalization and abciximab
bolus and infusion after transradial
coronary stent implantation. Circulation
2006;114:2636-43
31. Choussat R, Black A, Bossi I, et al.
Vascular complications and clinical
outcome after coronary angioplasty
with platelet IIb/IIIa receptor blockade.
Comparison of transradial vs
transfemoral arterial access. Eur Heart J
2000;21:662-7
32. Marmur JD, Poludasu S, Agarwal A,
et al. Bolus-only platelet glycoprotein
IIb-IIIa inhibition during percutaneous
coronary intervention. J Invasive Cardiol
2006;18:521-6
33. Marmur JD, Poludasu S, Lazar J,
Cavusoglu E. Long-term mortality after
bolus-only administration of abciximab,
eptifibatide, or tirofiban during
percutaneous coronary intervention.
Catheter Cardiovasc Interv
2009;73:214-21
34. Cho L, Topol EJ, Balog C, et al.
Clinical benefit of glycoprotein
IIb/IIIa blockade with abciximab is
independent of gender. Pooled analysis
from EPIC, EPILOG, and EPISTENT
trials. J Am Coll Cardiol 2000;36:381-6
35. Philippe F, Larrazet F, Meziane T,
Dibie A. Comparison of transradial vs.
transfemoral approach in the treatment
of acute myocardial infarction with
primary angioplasty and abciximab.
Catheter Cardiovasc Interv
2004;61:67-73
36. Dasgupta H, Blankenship JC,
Wood GC, et al. Thrombocytopenia
complicating treatment with intravenous
glycoprotein IIb/IIIa receptor inhibitors:
a pooled analysis. Am Heart J
2000;140:206-11
37. Huxtable LM, Tafreshi MJ, Rakkar AN.
Frequency and management of
thrombocytopenia with the glycoprotein
IIb/IIIa receptor antagonists.
Am J Cardiol 2006;97:426-9
38. Conley M, Patino G, Romick B,
et al. Abciximab-induced alveolar
hemorrhage after percutaneous coronary
intervention. Can J Cardiol
2008;24:149-51
39. Tcheng JE, Kereiakes DJ, Lincoff AM,
et al. Abciximab readministration: results
of the ReoPro Readministration Registry.
Circulation 2001;104:870-5
40. Boersma E, Harrington RA,
Moliterno DJ, et al. Platelet
glycoprotein IIb/IIIa inhibitors in acute
coronary syndromes: a meta-analysis of
all major randomised clinical trials.
Lancet 2002;359:189-98
AffiliationDevang Parikh1 MBBS &
Craig P Juergens†1,2 MBBS FACC†Author for correspondence1Liverpool Hospital,
Department of Cardiology,
Elizabeth Street, Liverpool,
NSW 2170, Australia2A/Professor,
Southwestern Sydney Clinical School,
University of NSW Sydney,
NSW 2052, Australia
Tel: +612 98283078; Fax: +612 98283054;
E-mail: [email protected]
Abciximab
246 Expert Opin. Biol. Ther. (2011) 11(2)
Exp
ert O
pin.
Bio
l. T
her.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
ew S
outh
Wal
es o
n 01
/17/
11Fo
r pe
rson
al u
se o
nly.

67
PAPER 16
Reprinted from the American Journal of Cardiology 1997;80:74-75 with
permission from Elsevier
5. Ishikawa K, Kanamaru S, Yotsukura M, Tsuya T, Shirato C, Yanagisawa A. Influence of peripheral intravenous contrast injection on the QRS complex in healthy men. Cardiovasc Res 1986;20:61-66. 6. Morissette M, Gagnon RM, Lamoureux J, Lemire J. Effects of angiographic contrast media on colloid oncotic pressure. Am Heart J 1980;100:319-322. 7. Haught WH, Sokol M, Kerensky RA, Mehta JL. Decrease in hematocrit after coronary stent placement and dextran therapy. Am J Cardio/1995;76:314-315. 8. Roccario ES, Schweiger MJ, Whitfield SS, Stikley W, Weil T, Urbano A, Porway M. Hematocrit fluctuations after percutaneous transluminal coronary angioplasty. Am J Cardio/1991;68:977-978.
9. Phillips SJ, Spector M, Zeff RH, Skinner JR, Toon RS, Grignon A, Kongtahworn C. Hematocrit changes after uncomplicated percutaneous coronary angioplasty. Am J Cardio/1989;64:940. 10. Fail PS, Maniet AR, Banka VS. Subcutaneous heparin in postangioplasty management: comparative trial with intravenous heparin. Am Heart J 1993; 126:1059-1067. 11. Adelman AG, Cohen EA, Kimball BP, Bonan R, Ricci DR, Webb JG, Laramee L, Barbeau G, Traboulsi M, Corbett BN, Schwartz L, Logan AG. A comparison of directional athrectomy with balloon angioplasty for lesions of the left anterior descending coronary artery. N Eng/ J Med 1993;329:228-233.
Routine Platelet Transfusion in Patients Undergoing E1111ergency Coronary Bypass Surgery
After Receiving AIJciximaiJ Craig P. Juergens, MB BS, Alan C. Yeung, MD, and Stephen N. Oesterle, MD
The Evaluation ofllblllla platelet receptor antagonist 7E3 in Preventing Ischemic Complications (EPIC)
investigators demonstrated that the chimeric monoclonal antibody fragment c7E3 Fab fragment directed against the platelet glycoprotein llblllla receptor resulted in a 35% reduction in ischemic complications of high-risk percutaneous coronary intervention.1 This agent has subsequently come to be known as abciximab. These same investigators subsequently published the outcomes of the 58 patients who were enrolled in the original study and received emergency bypass surgery after coronary angioplasty.2 Of these 58 patients, 17 received the bolus dose plus infusion of abciximab, which has become the accepted method of administering the drug. Of these 17 patients, the all-cause mortality rate at 30 days was 29.4%, mean length of hospital stay was 15 days, and there was a 76.5% incidence of major blood loss. We could find no recent published reports on the outcome of such patients in the era of widespread use of abciximab, and consequently we present the outcomes of 4 patients who received this agent from our institution who underwent emergency surgery within 6 hours of failed coronary angioplasty.
••• The mean age of our 4 patients was 53 years (range
36 to 76), with 3 being women. The indications for angioplasty were unstable angina or non-Q-wave infarction in 3 and acute anterolateral infarction in 1. All patients had received aspirin before the attempted angioplasty and the abciximab bolus was administered before the wiring of the target lesion. Heparin was administered with the aim of maintaining the activated clotting time between the 200- and 300-second range. In our patients the mean maximum activated clotting time was 322 seconds (range 232 to 459). The indications for emergency surgery were the inability to stabilize coronary dissection in 2 patients, inability to
From the Division of Cardiovascular Medicine, Stanford University Medical Center, Stanford, California. Dr. Oesterle's address is: Division of Cardiovascular Medicine, 300 Pasteur Drive, H3563, Stanford, California 94305. Manuscript received December 31, 1996; revised manuscript received and accepted March 5, 1997.
7 4 © 1997 by Excerpta Medica, Inc. All rights reserved.
cross the lesion in a patient with unstable angina, and an inability to establish adequate anterograde flow in a patient with an evolving anterior infarction. We chose to administer platelet transfusions routinely in all4 patients to minimize perioperative bleeding. One patient received the transfusion before arrival in the operating room and the other 3 underwent transfusion as they were coming off cardiopulmonary bypass. Platelet transfusions were administered at a mean of 249 minutes (range 112 to 530) from the time of the last dose of heparin given during the angioplasty. All patients underwent full heparinization before being placed on cardiopulmonary bypass, with the average dose being 29,250 U (range 20,000 to 39,000). This was reversed at the end of the procedure with protamine. The mean time of cardiopulmonary bypass was 87 minutes (range 61 to 127). All patients underwent successful revascularization and all are alive at a mean follow-up of 5 months (range 1 to 8). Major blood loss, defined as a >5-g/dl decrease in hemoglobin occurred in only 1 of our patients, whereas only 2 patients received a red cell transfusion. No patient developed thrombocytopenia, defined as a platelet count < 100,000/mm3
• The only patient to develop new Qwave myocardial infarction was the patient who presented with an acute anterior injury pattern. Mean length of hospital stay was 7 days (range 5 to 8).
••• Although our single-center experience is small, it
does demonstrate that emergency coronary bypass surgery can be performed with acceptable bleeding complications after administration of abciximab. Despite heightened awareness of the risks of transfusion and techniques for reducing blood loss and thus reducing the need for transfusion, recent studies have shown that between 48% and 65%3
-5 of patients un
dergoing coronary bypass surgery receive at least 1 blood product before discharge. Urgent bypass surgery is associated with an even higher rate of transfusion requirement.6
•7 Aspirin use before bypass sur
gery is known to increase operative blood loss and transfusion requirements.8
•9 All patients in our small
series received aspirin before attempted angioplasty.
0002-9149/97/$17.00 Pll S0002-9149197)00287-7

In these 4 patients who underwent emergency coronary bypass surgery after receiving abciximab, we chose to ''prophylactically'' transfuse with platelets. Apart from the financial implications and use of limited blood resources, the major concern with the routine transfusion of platelets is the possible risk of viral infection. With current donor screening in the United States, the risk of contracting the human immunodeficiency virus (HIV) has been estimated to be between 1 in 450,000 and 660,000, 10 approximately 1 in 80,000 for hepatitis C virus 11 and 1 in 200,000 for hepatitis B. 12 The risk of transmission of an infectious agent is reduced by the use of single donor platelets as was the case in 3 of our patients. Although the use of autologous platelet transfusion given at the end of cardiopulmonary bypass after the reversal of heparin has been shown to reduce blood loss, 13 the routine use of platelet transfusion has not. 14 Patients in the aforementioned study had not received any antiplatelet agents for 1 week before their nonemergency bypass surgery. Consequently, their results cannot be extrapolated to our patients undergoing emergency bypass surgery who had received aspirin and this much more potent antiplatelet agent. The routine use of platelet concentrates, particularly from a single donor, may potentially reduce the amount of blood products transfused through the minimization of perioperative bleeding. Despite our patients representing a high-risk subset for perioperative bleeding, having received aspirin and undergoing emergency surgery after failed angioplasty, only 2 of the patients required red blood cell transfusion. Of these 2 patients, 1 required 2 and the other 4 U of packed red blood cells. Previous studies revealed that patients undergoing emergency bypass surgery received a mean of 4.0 and 9.7 U of blood.6
•7
•15
The routine use of platelet transfusions to reverse the effects of abciximab in patients proceeding to emergent coronary bypass surgery after failed coronary angioplasty appears reasonable.
1. The EPIC Investigators. Use of a monoclonal antibody directed against the platelet glycoprotein lib/Ilia receptor in high risk angioplasty. N Eng/ J Med 1994;330:956-961. 2. Boehrer JD, Kereiakes DJ, Navetta FI, Califf RM, Topol EJ, for the EPIC investigators. Effects of profound platelet inhibition with c7E3 before coronary angioplasty on complications of coronary bypass surgery. Am J Cardiol 1994;74:1166-1170. 3. Surgenor DM, Churchill EL, Rizzo WRJ, Chapman RH, McGurk S, Bertholf MF, Goodnough LT, Kao KJ, Koerner TAW, Olson JD, Woodson RD. Determinants of red cell, platelet, plasma and cryoprecipitate transfusions during coronary artery bypass graft surgery: the collaborative hospital transfusion study. Transfusion 1996;36:521-532. 4. Magovem JA, Sakert T, Benckart DH, Burkholder JA, Liebler GA, Magovem GJ Sr, Magovem GJ Jr. A model for predicting transfusion after coronary artery bypass grafting. Ann Thorac Surg 1996;61:27-32. 5. Kochamba GS, Pfeffer TA, Sintek CF, Khonsari S. Intraoperative autotransfusion reduces blood loss after cardiopulmonary bypass. Ann Thorac Surg 1996;61:900-903. 6. Parsonnet V, Fisch D, Gielchinsky I, Hochberg M, Hussain SM, Karanam R, Rothfeld L, Klapp L. Emergency operation after failed angioplasty. J Thorac Cardiovasc Surg 1988;96:198-203. 7. Brahos GJ, Baker NH, Ewy HG, Moore PJ, Thomas JW, Sanfelippo PM, McVicker RF, Fankhauser DJ. Aortocoronary bypass following unsuccessful PTCA: experience in 100 consecutive patients. Ann Thorac Surg 1985;40:7-10. 8. Ferraris VA, Ferraris SP, Lough FC, Berry WR. Preoperative aspirin ingestion increases operative blood loss after coronary artery bypass grafting. Ann Thorac Surg 1995;59:1036-1037. 9. Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, Doherty J, Read R, Chesler E, Sako Y, Lancaster L, Emery R, Sharma GVRK, Josa M, Pacold I, Montoya A, Parikh D, Sethi G, Holt J, Kirklin J, Shabetai R, Moores W, Aldridge J, Masud Z, DeMots H, Floten S, Haakenson C, Harker LA. Improvement in early saphenous vein graft patency after coronary artery bypass surgery with antiplatelet therapy: results of a Veterans Administration Cooperative Study. Circulation 1988;77:1324-1332. 10. Lackritz EM, Satten GA, Aberle-Grasse J, Dodd RY, Raimondi VP, Janssen RS, Lewis WF, Notari EP, Petersen LR. Estimated risk of transmission of the human immunodeficiency virus by screened blood in the United States. N Eng/ J Med 1995;333:1721-1725. 11. Busch MP, Korelitz JJ, Kleinman SH, Lee SR, AuBuchon JP, Schreiber GB, and the Retrovirus Epidemiology Donor Study. Declining value of alanine aminotransferase in screening of blood donors to prevent posttransfusion hepatitis Band C virus infection. Transfusion 1995;35:903-910. 12. Centers for Disease Control and Prevention. Public Health Service interagency guidelines for screening donors of blood, plasma, organs, tissues and semen for evidence of hepatitis B and hepatitis C. Morb Mortal Wkly Rep 1991;40(RR-4):1-17. 13. Del Rossi AJ, Cemaianu AC, Vertrees RA, Wacker CJ, Fuller SJ, Cilley JH Jr, Baldino W A. Platelet rich plasma reduces postoperative blood loss after cardiopulmonary bypass. J Tho rae Cardiovasc Surg 1990; 100:281-286. 14. Simon TL, Akl BF, Murphy W. Controlled trial of routine administration of platelet concentrates in cardiopulmonary bypass surgery. Ann Thorac Surg 1984;37:359-364. 15. Boylan MJ, Lytle BW, .Taylor PC, Loop FD, Proudfit W, Borsh JA, Cosgrove DM. Have PTCA failures requiring emergent bypass operation changed? Ann Thorac Surg 1995;59:283-287.
BRIEF REPORTS 75

68
PAPER 17
Reprinted from the American Heart Journal 2012 163:649-656.e1. with
permission from Elsevier
Safety and efficacy of rescue angioplasty forST-elevation myocardial infarction with high utilizationrates of glycoprotein IIb/IIIa inhibitorsIbrahimM. Shugman,MBBCh, VictarHsieh,MBBS, Samuel Cheng,MBBS, Devang Parikh,MBBS, Daniel Tobing,MD,Noemi Wouters, MD, Rozemarijn van der Vijver, MD, Queenie Lo, MBBS, Rohan Rajaratnam, MBBS,Andrew P. Hopkins, MBBS, Sidney Lo, MBBS, Dominic Leung, MBBS PhD, Craig P. Juergens, MBBS, andJohn K. French, MBChB, PhD New South Wales, Australia
Background Fibrinolytic therapies remain widely used for ST-elevation myocardial infarction, and for “failedreperfusion,” rescue percutaneous coronary intervention (PCI) is guideline recommended to improve outcomes. However, theserecommendations are based on data from an earlier era of pharmacotherapy and procedural techniques.
Methods and Results To determine factors affecting prognosis after rescue PCI, we studied 241 consecutivepatients (median age 55 years, interquartile range [IQR] 48-65) undergoing procedures between 2001 and 2009 (53%anterior ST-elevation myocardial infarction and 78% transferred). The median treatment-related times were 1.2 hours (IQR 0.8-2.2) from symptom onset to door, 2 hours (IQR 1.3-3.2) from symptom onset to fibrinolysis (93% tenecteplase), and 3.9 hours(IQR 3.1-5.2) from fibrinolysis to balloon. Procedural characteristics were stent deployment in 95% (11.6% drug eluting) and78% glycoprotein IIb/IIIa inhibitor use, and Thrombolysis In Myocardial Infarction (TIMI) 3 flow rates pre-PCI and post-PCI were41% and 91%, respectively (P b .001). At 30 days, TIMI major bleeding occurred in 16 (6.6%) patients, and 23 (9.5%)patients received transfusions; nonfatal stroke occurred in 4 (1.7%) patients (2 hemorrhagic). Predictors of TIMI major bleedingwere female gender (odds ratio 3.194, 95% CI 1.063-9.597; P = .039) and pre-PCI shock (odds ratio 3.619, 95% CI,1.073-12.207; P = .038). Mortality at 30 days was 6.2%, and 3.2% in patients without pre-PCI shock. One-year mortality was 8.2%(5.3% in patients without pre-PCI cardiogenic shock), 5.2% had reinfarction, and the target vessel revascularization rate was6.4% (2.6% in arteries ≥3.5 mm in diameter). Pre-PCI shock, female gender, and post-PCI TIMI flow grades ≤2 were significantpredictors of 1-year mortality on multivariable regression modeling, but TIMI major bleeding was not.
Conclusions Rescue PCI with contemporary treatments can achieve mortality rates similar to rates for contemporaryprimary PCI in patients without pre-PCI shock. Whether rates of bleeding can be reduced by different pharmacotherapies andinterventional techniques needs clarification in future studies. (Am Heart J 2012;163:649-656.e1.)
The aim of reperfusion strategies for patients with ST-elevation myocardial infarction (STEMI) is to minimizeischemic time to maximize preservation of myocytes andminimize infarct size by restoring antegrade coronaryblood flow.1-3 Although prompt primary percutaneouscoronary intervention (PCI) is a superior reperfusionstrategy to fibrinolytic therapy alone,4 for several reasons,many patients worldwide receive fibrinolytic therapy asan initial reperfusion strategy.5 In fact, early prehospital
From the Department of Cardiology, Liverpool Hospital, South Western Sydney ClinicaSchool, The University of New South Wales, Sydney, New South Wales, Australia.Submitted January 10, 2012; accepted January 10, 2012.Reprint requests: John K. French, MBChB, PhD, Cardiology Department, Liverpool HospitalElizabeth St, Liverpool, New South Wales 2170, Australia.E-mail: [email protected]/$ - see front matter© 2012, Mosby, Inc. All rights reserved.doi:10.1016/j.ahj.2012.01.014
l
,
fibrinolysis may achieve as good as, or better, late clinicaloutcomes than primary PCI if appropriately high rates ofrescue PCI and in-hospital PCI occur.6-8
Fibrinolytic-treated patients are recommended forimmediate angiography and, if indicated, rescue PCI, ifthey have failed to reperfuse, as 5 randomized clinicaltrials have shown improved outcomes compared withconservative management.5,9-11 However, these trials,and more recent reports from registries, have includedsignificant proportions of patients who did not receivefibrin-specific therapies, stents (including drug eluting), orglycoprotein IIb/IIIa (GPIIb/IIIa) antagonists.9-13 Becausepatients treated at our cardiac catheterization laboratory(CCL) and undergoing rescue PCI have received high ratesof these therapies, we studied consecutive patients toidentify factors that influence clinical outcomes, so theseinsights may provide the basis for prospective studies offuture pharmacoinvasive strategies in STEMI patients.

650 Shugman et alAmerican Heart Journal
April 2012
MethodsStudy populationWe prospectively collected clinical, demographic, and
angiographic data on consecutive patients undergoing rescuePCI at CCL at Liverpool Hospital (Sydney, Australia); details ofthe CCL database has recently been reported.14
During the study period from January 2001 to December 2009,patients with STEMI with 12 hours symptom onset, withoutcontraindications, received fibrinolytic therapy and intravenousheparin were treated with aspirin (usually 300 mg) at first medicalcontact, in the area of our CCL service (~900,000 population)except for those presenting to Liverpool Hospital during workinghours when primary PCI was usually performed until May 2006.Subsequently, a 24-hour primary PCI service was offered to patientspresenting directly to Liverpool Hospital. Failed pharmacologicreperfusion was defined b50% ST-segment recovery comparedwith baseline ST elevation at approximately 60 to 90 minutes.Patients with transient ST recovery but subsequently persistentST-segment reelevation (b12 hours post-STEMI) were alsoincluded. Assessment of outcomes after PCI was approved bythe Sydney South West Area Health Service Human ResearchEthics Committee (project no. QA2008/034). No extramuralfunding was used to support this work.
Procedural techniquesRescue PCI was performed via the femoral approach in 99% of
patients using unfractionated heparin, administered accordingto the preprocedural activated clotting time. Clopidogrelloading with 300 to 600 mg (and 75 mg daily for 12 months)was given if not administered “upstream.” The use of GPIIb/IIIareceptor inhibitors (tirofiban or abciximab) was at thediscretion of the referring physicians and/or interventionists.Deployment of drug-eluting stents (DES) was based on our CCLselective use criteria, adopted in October 2003 (applying to 89%of patients reported here) which were as follows: left mainlesions, ostial lesions in major epicardial arteries, proximal leftanterior descending lesions, lesions length ≥20 mm in vessels≤3mm, any lesion in vessels ≤2.5 mm, any lesion in diabeticpatients with vessels b3.0mm, and in-stent restenosis. Infarctartery Thrombolysis In Myocardial Infarction (TIMI) flowgrading and corrected TIMI frame counts (CTFC) pre-PCI andpost-PCI including imputation of a CTFC of 100 for TIMI 0 to 1flow were assessed by 2 cardiologists who were blinded to thepatients' history and outcomes.15
Electrocardiographic analysesAnalysis of electrocardiographs (ECGs) before and 60 to 90
minutes after fibrinolytic therapy, before and after rescue PCI, andbefore discharge were performed with callipers by 5 clinicianstrained in ST-segment recovery analysis (herein called ST recovery),blinded tooutcomes. ST recoverywas characterized as (1) complete(≥70%), (2) partial (N30% to b70%), and (3) no recovery(≤30%).16,17 Infarct size estimation by Selvester QRS scoring usedthe 32-point system (each point represents ~3% of the leftventricular myocardium).18,19 The myocardial salvage was deter-mined by subtracting infarct size frommyocardium at risk (maximalscores of baseline ST elevation) anddividing this differenceby the at-risk score.20
Clinical outcomesOutcomes were examined at 30 days and approximately 1 year
and included all-cause mortality, nonfatal myocardial infarction(MI), target vessel revascularization (TVR), stroke, and TIMI majorbleeding.10 Target vessel revascularization was defined asrepeat revascularization (PCI or coronary artery bypass graftsurgery [CABG]) of the infarct artery including proximal and distalto the target lesion. Clinical outcome data were obtainedby reviewing patients' medical records and by trained researchstaff (nurses or doctors) contacting patients, their next of kin, orlocal physicians or cardiologists by telephone. Data regardingmortality were obtained from medical records, physicians,family members, and the death registry; all patients had follow-up to 30 days, and 8 (3%) were lost to follow-up at 12 months.
Data analysesCategorical variables are reported as numbers (%) and were
compared by χ2 test or Fisher exact test as appropriate;continuous variables are reported as medians and interquartileranges (IQR). Normally distributed continuous variables werecompared by unpaired Student t tests for comparison of means,whereas skewed continuous variables were compared by Mann-Whitney U tests. Paired continuous and ordinal data werecompared by Wilcoxon signed rank tests.Univariate and multivariate analyses to determine factors
associated with clinical outcomes included the followingvariables: age, female gender, body mass index, diabetesmellitus, current smoking, prior MI, prior aspirin use,hypertension, hyperlipidemia, prior PCI, cardiogenic shock,TIMI major bleeding, symptom onset to door, symptom onsetto lytic, door to balloon, anterior MI, post-PCI TIMI flow grade,post-PCI CTFC, incomplete (b70%) ST recovery (maximal leadsand sum of leads), at-risk myocardium salvaged b50% andb70%, final QRS score N4, multivessel disease, GPIIb/IIIainhibitors, DES use, and total stent length; those with P b .2were included in the multivariate analysis. Multivariate Coxregression was used to identify independent factors associatedwith late clinical outcomes. Odds ratios (OR) and 95% CIs arereported. All statistical analyses were performed usingStatistical Package for Social Sciences version 17.0 software(SPSS, Inc, Chicago, IL). All P values b .05 (2 sided) wereconsidered statistically significant.
The authors are solely responsible for the design and conductof this study, all study analyses, the drafting and editing of themanuscript, and its final content.
ResultsClinical and procedural characteristicsBetween January 2001 and December 2009, of 241
patients undergoing rescue PCI (189 patients [78%] afterinterhospital transfer), 36 (15%) patients had PCIperformed before January 1, 2004, 102 (42.3%) hadprocedures between January 1, 2004, and May 31, 2006,and 103 (42.7%) had rescue PCIs after June 1, 2006.These patients had a median age of 55 (IQR 48-65) yearsand were hospitalized for 4 (IQR 3-5.5) days; 24 (10%)had cardiogenic shock before rescue PCI. Other patient
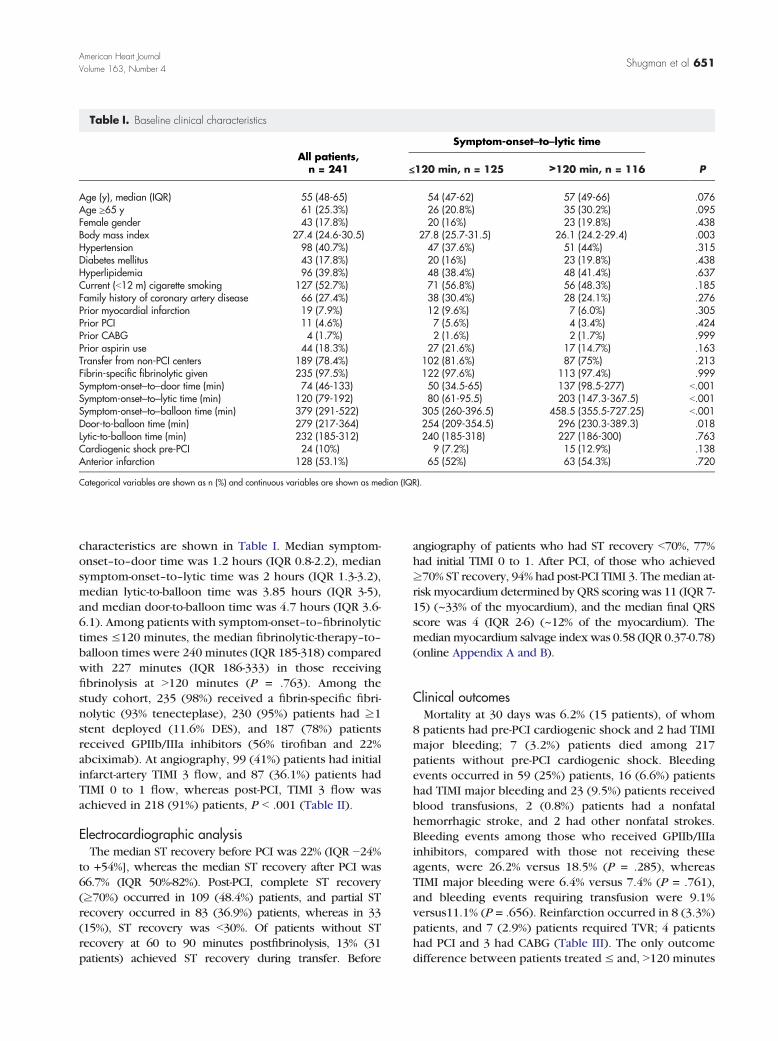
Table I. Baseline clinical characteristics
All patients,n = 241
Symptom-onset–to–lytic time
P≤120 min, n = 125 >120 min, n = 116
Age (y), median (IQR) 55 (48-65) 54 (47-62) 57 (49-66) .076Age ≥65 y 61 (25.3%) 26 (20.8%) 35 (30.2%) .095Female gender 43 (17.8%) 20 (16%) 23 (19.8%) .438Body mass index 27.4 (24.6-30.5) 27.8 (25.7-31.5) 26.1 (24.2-29.4) .003Hypertension 98 (40.7%) 47 (37.6%) 51 (44%) .315Diabetes mellitus 43 (17.8%) 20 (16%) 23 (19.8%) .438Hyperlipidemia 96 (39.8%) 48 (38.4%) 48 (41.4%) .637Current (b12 m) cigarette smoking 127 (52.7%) 71 (56.8%) 56 (48.3%) .185Family history of coronary artery disease 66 (27.4%) 38 (30.4%) 28 (24.1%) .276Prior myocardial infarction 19 (7.9%) 12 (9.6%) 7 (6.0%) .305Prior PCI 11 (4.6%) 7 (5.6%) 4 (3.4%) .424Prior CABG 4 (1.7%) 2 (1.6%) 2 (1.7%) .999Prior aspirin use 44 (18.3%) 27 (21.6%) 17 (14.7%) .163Transfer from non-PCI centers 189 (78.4%) 102 (81.6%) 87 (75%) .213Fibrin-specific fibrinolytic given 235 (97.5%) 122 (97.6%) 113 (97.4%) .999Symptom-onset–to–door time (min) 74 (46-133) 50 (34.5-65) 137 (98.5-277) b.001Symptom-onset–to–lytic time (min) 120 (79-192) 80 (61-95.5) 203 (147.3-367.5) b.001Symptom-onset–to–balloon time (min) 379 (291-522) 305 (260-396.5) 458.5 (355.5-727.25) b.001Door-to-balloon time (min) 279 (217-364) 254 (209-354.5) 296 (230.3-389.3) .018Lytic-to-balloon time (min) 232 (185-312) 240 (185-318) 227 (186-300) .763Cardiogenic shock pre-PCI 24 (10%) 9 (7.2%) 15 (12.9%) .138Anterior infarction 128 (53.1%) 65 (52%) 63 (54.3%) .720
Categorical variables are shown as n (%) and continuous variables are shown as median (IQR).
Shugman et al 651American Heart JournalVolume 163, Number 4
characteristics are shown in Table I. Median symptom-onset–to–door time was 1.2 hours (IQR 0.8-2.2), mediansymptom-onset–to–lytic time was 2 hours (IQR 1.3-3.2),median lytic-to-balloon time was 3.85 hours (IQR 3-5),and median door-to-balloon time was 4.7 hours (IQR 3.6-6.1). Among patients with symptom-onset–to–fibrinolytictimes ≤120 minutes, the median fibrinolytic-therapy–to–balloon times were 240 minutes (IQR 185-318) comparedwith 227 minutes (IQR 186-333) in those receivingfibrinolysis at N120 minutes (P = .763). Among thestudy cohort, 235 (98%) received a fibrin-specific fibri-nolytic (93% tenecteplase), 230 (95%) patients had ≥1stent deployed (11.6% DES), and 187 (78%) patientsreceived GPIIb/IIIa inhibitors (56% tirofiban and 22%abciximab). At angiography, 99 (41%) patients had initialinfarct-artery TIMI 3 flow, and 87 (36.1%) patients hadTIMI 0 to 1 flow, whereas post-PCI, TIMI 3 flow wasachieved in 218 (91%) patients, P b .001 (Table II).
Electrocardiographic analysisThe median ST recovery before PCI was 22% (IQR −24%
to +54%], whereas the median ST recovery after PCI was66.7% (IQR 50%-82%). Post-PCI, complete ST recovery(≥70%) occurred in 109 (48.4%) patients, and partial STrecovery occurred in 83 (36.9%) patients, whereas in 33(15%), ST recovery was b30%. Of patients without STrecovery at 60 to 90 minutes postfibrinolysis, 13% (31patients) achieved ST recovery during transfer. Before
angiography of patients who had ST recovery b70%, 77%had initial TIMI 0 to 1. After PCI, of those who achieved≥70% ST recovery, 94% had post-PCI TIMI 3. The median at-risk myocardium determined by QRS scoring was 11 (IQR 7-15) (~33% of the myocardium), and the median final QRSscore was 4 (IQR 2-6) (~12% of the myocardium). Themedian myocardium salvage indexwas 0.58 (IQR 0.37-0.78)(online Appendix A and B).
Clinical outcomesMortality at 30 days was 6.2% (15 patients), of whom
8 patients had pre-PCI cardiogenic shock and 2 had TIMImajor bleeding; 7 (3.2%) patients died among 217patients without pre-PCI cardiogenic shock. Bleedingevents occurred in 59 (25%) patients, 16 (6.6%) patientshad TIMI major bleeding and 23 (9.5%) patients receivedblood transfusions, 2 (0.8%) patients had a nonfatalhemorrhagic stroke, and 2 had other nonfatal strokes.Bleeding events among those who received GPIIb/IIIainhibitors, compared with those not receiving theseagents, were 26.2% versus 18.5% (P = .285), whereasTIMI major bleeding were 6.4% versus 7.4% (P = .761),and bleeding events requiring transfusion were 9.1%versus11.1% (P = .656). Reinfarction occurred in 8 (3.3%)patients, and 7 (2.9%) patients required TVR; 4 patientshad PCI and 3 had CABG (Table III). The only outcomedifference between patients treated ≤ and, N120 minutes
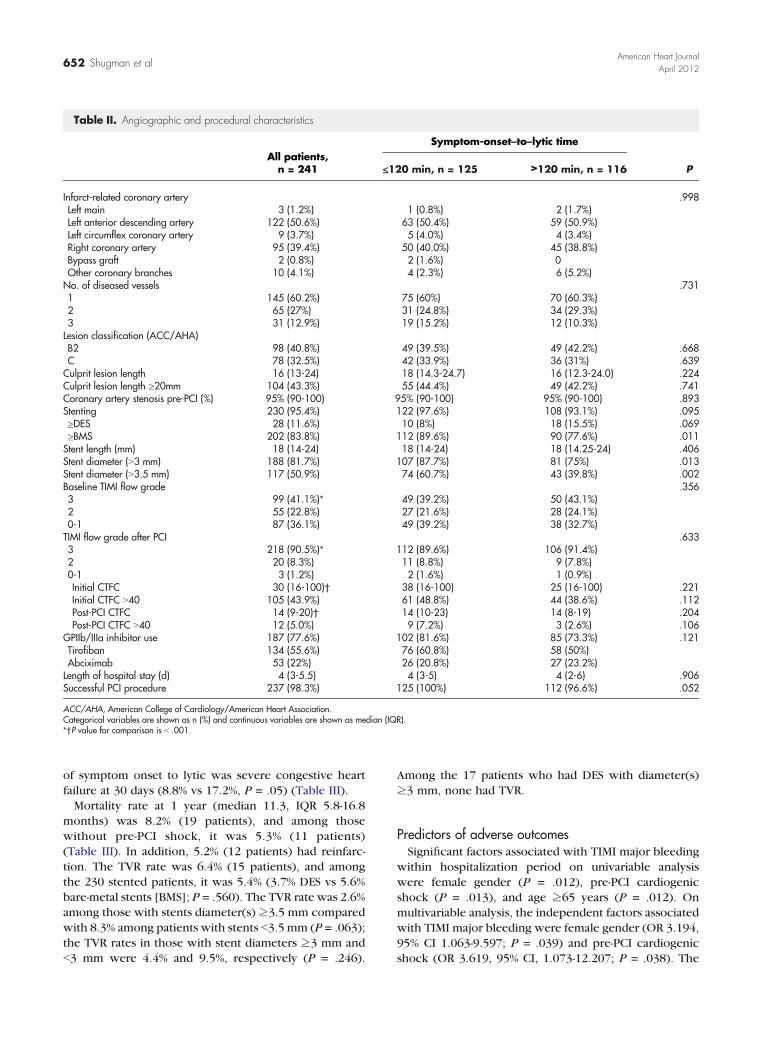
Table II. Angiographic and procedural characteristics
All patients,n = 241
Symptom-onset–to–lytic time
P≤120 min, n = 125 >120 min, n = 116
Infarct-related coronary artery .998Left main 3 (1.2%) 1 (0.8%) 2 (1.7%)Left anterior descending artery 122 (50.6%) 63 (50.4%) 59 (50.9%)Left circumflex coronary artery 9 (3.7%) 5 (4.0%) 4 (3.4%)Right coronary artery 95 (39.4%) 50 (40.0%) 45 (38.8%)Bypass graft 2 (0.8%) 2 (1.6%) 0Other coronary branches 10 (4.1%) 4 (2.3%) 6 (5.2%)No. of diseased vessels .7311 145 (60.2%) 75 (60%) 70 (60.3%)2 65 (27%) 31 (24.8%) 34 (29.3%)3 31 (12.9%) 19 (15.2%) 12 (10.3%)Lesion classification (ACC/AHA)B2 98 (40.8%) 49 (39.5%) 49 (42.2%) .668C 78 (32.5%) 42 (33.9%) 36 (31%) .639Culprit lesion length 16 (13-24) 18 (14.3-24.7) 16 (12.3-24.0) .224Culprit lesion length ≥20mm 104 (43.3%) 55 (44.4%) 49 (42.2%) .741Coronary artery stenosis pre-PCI (%) 95% (90-100) 95% (90-100) 95% (90-100) .893Stenting 230 (95.4%) 122 (97.6%) 108 (93.1%) .095≥DES 28 (11.6%) 10 (8%) 18 (15.5%) .069≥BMS 202 (83.8%) 112 (89.6%) 90 (77.6%) .011Stent length (mm) 18 (14-24) 18 (14-24) 18 (14.25-24) .406Stent diameter (N3 mm) 188 (81.7%) 107 (87.7%) 81 (75%) .013Stent diameter (N3.5 mm) 117 (50.9%) 74 (60.7%) 43 (39.8%) .002Baseline TIMI flow grade .3563 99 (41.1%)⁎ 49 (39.2%) 50 (43.1%)2 55 (22.8%) 27 (21.6%) 28 (24.1%)0-1 87 (36.1%) 49 (39.2%) 38 (32.7%)TIMI flow grade after PCI .6333 218 (90.5%)⁎ 112 (89.6%) 106 (91.4%)2 20 (8.3%) 11 (8.8%) 9 (7.8%)0-1 3 (1.2%) 2 (1.6%) 1 (0.9%)Initial CTFC 30 (16-100)† 38 (16-100) 25 (16-100) .221Initial CTFC N40 105 (43.9%) 61 (48.8%) 44 (38.6%) .112Post-PCI CTFC 14 (9-20)† 14 (10-23) 14 (8-19) .204Post-PCI CTFC N40 12 (5.0%) 9 (7.2%) 3 (2.6%) .106
GPIIb/IIIa inhibitor use 187 (77.6%) 102 (81.6%) 85 (73.3%) .121Tirofiban 134 (55.6%) 76 (60.8%) 58 (50%)Abciximab 53 (22%) 26 (20.8%) 27 (23.2%)Length of hospital stay (d) 4 (3-5.5) 4 (3-5) 4 (2-6) .906Successful PCI procedure 237 (98.3%) 125 (100%) 112 (96.6%) .052
ACC/AHA, American College of Cardiology/American Heart Association.Categorical variables are shown as n (%) and continuous variables are shown as median (IQR).⁎†P value for comparison is b .001.
652 Shugman et alAmerican Heart Journal
April 2012
of symptom onset to lytic was severe congestive heartfailure at 30 days (8.8% vs 17.2%, P = .05) (Table III).Mortality rate at 1 year (median 11.3, IQR 5.8-16.8
months) was 8.2% (19 patients), and among thosewithout pre-PCI shock, it was 5.3% (11 patients)(Table III). In addition, 5.2% (12 patients) had reinfarc-tion. The TVR rate was 6.4% (15 patients), and amongthe 230 stented patients, it was 5.4% (3.7% DES vs 5.6%bare-metal stents [BMS]; P = .560). The TVR rate was 2.6%among those with stents diameter(s) ≥3.5 mm comparedwith 8.3% among patients with stents b3.5 mm (P = .063);the TVR rates in those with stent diameters ≥3 mm andb3 mm were 4.4% and 9.5%, respectively (P = .246).
Among the 17 patients who had DES with diameter(s)≥3 mm, none had TVR.
Predictors of adverse outcomesSignificant factors associated with TIMI major bleeding
within hospitalization period on univariable analysiswere female gender (P = .012), pre-PCI cardiogenicshock (P = .013), and age ≥65 years (P = .012). Onmultivariable analysis, the independent factors associatedwith TIMI major bleeding were female gender (OR 3.194,95% CI 1.063-9.597; P = .039) and pre-PCI cardiogenicshock (OR 3.619, 95% CI, 1.073-12.207; P = .038). The
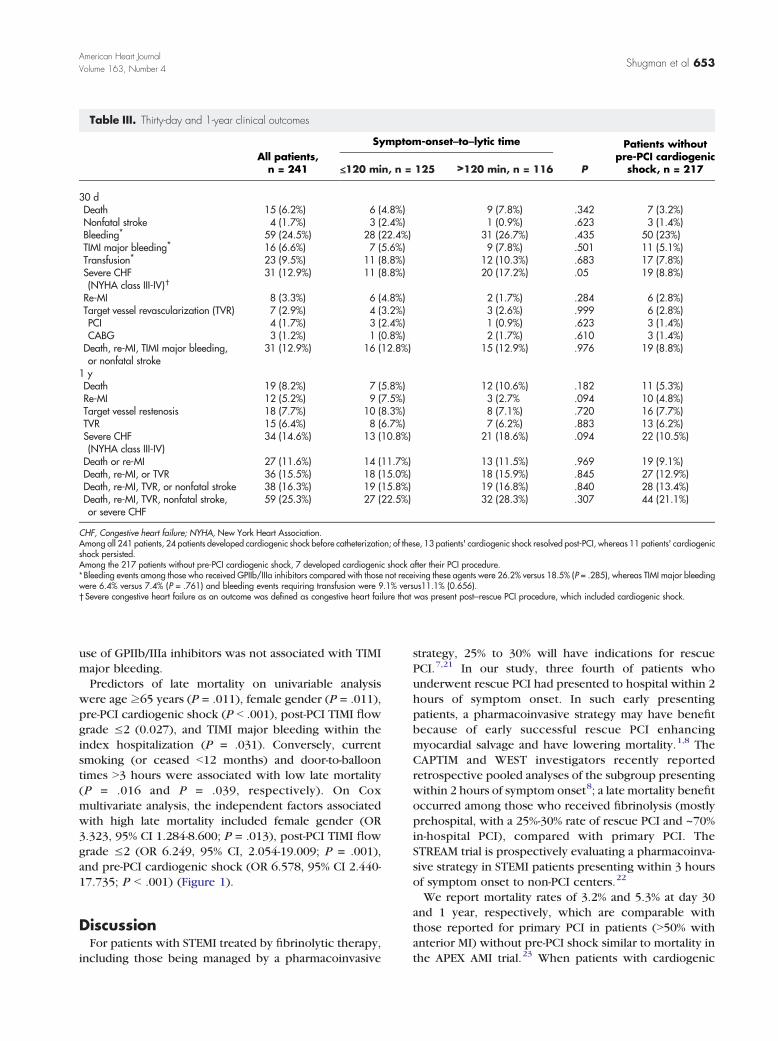
Table III. Thirty-day and 1-year clinical outcomes
All patients,n = 241
Symptom-onset–to–lytic time
P
Patients withoutpre-PCI cardiogenic
shock, n = 217≤120 min, n = 125 >120 min, n = 116
30 dDeath 15 (6.2%) 6 (4.8%) 9 (7.8%) .342 7 (3.2%)Nonfatal stroke 4 (1.7%) 3 (2.4%) 1 (0.9%) .623 3 (1.4%)Bleeding⁎ 59 (24.5%) 28 (22.4%) 31 (26.7%) .435 50 (23%)TIMI major bleeding⁎ 16 (6.6%) 7 (5.6%) 9 (7.8%) .501 11 (5.1%)Transfusion⁎ 23 (9.5%) 11 (8.8%) 12 (10.3%) .683 17 (7.8%)Severe CHF(NYHA class III-IV)†
31 (12.9%) 11 (8.8%) 20 (17.2%) .05 19 (8.8%)
Re-MI 8 (3.3%) 6 (4.8%) 2 (1.7%) .284 6 (2.8%)Target vessel revascularization (TVR) 7 (2.9%) 4 (3.2%) 3 (2.6%) .999 6 (2.8%)PCI 4 (1.7%) 3 (2.4%) 1 (0.9%) .623 3 (1.4%)CABG 3 (1.2%) 1 (0.8%) 2 (1.7%) .610 3 (1.4%)Death, re-MI, TIMI major bleeding,or nonfatal stroke
31 (12.9%) 16 (12.8%) 15 (12.9%) .976 19 (8.8%)
1 yDeath 19 (8.2%) 7 (5.8%) 12 (10.6%) .182 11 (5.3%)Re-MI 12 (5.2%) 9 (7.5%) 3 (2.7% .094 10 (4.8%)Target vessel restenosis 18 (7.7%) 10 (8.3%) 8 (7.1%) .720 16 (7.7%)TVR 15 (6.4%) 8 (6.7%) 7 (6.2%) .883 13 (6.2%)Severe CHF(NYHA class III-IV)
34 (14.6%) 13 (10.8%) 21 (18.6%) .094 22 (10.5%)
Death or re-MI 27 (11.6%) 14 (11.7%) 13 (11.5%) .969 19 (9.1%)Death, re-MI, or TVR 36 (15.5%) 18 (15.0%) 18 (15.9%) .845 27 (12.9%)Death, re-MI, TVR, or nonfatal stroke 38 (16.3%) 19 (15.8%) 19 (16.8%) .840 28 (13.4%)Death, re-MI, TVR, nonfatal stroke,or severe CHF
59 (25.3%) 27 (22.5%) 32 (28.3%) .307 44 (21.1%)
CHF, Congestive heart failure; NYHA, New York Heart Association.Among all 241 patients, 24 patients developed cardiogenic shock before catheterization; of these, 13 patients' cardiogenic shock resolved post-PCI, whereas 11 patients' cardiogenicshock persisted.Among the 217 patients without pre-PCI cardiogenic shock, 7 developed cardiogenic shock after their PCI procedure.⁎Bleeding events among those who received GPIIb/IIIa inhibitors compared with those not receiving these agents were 26.2% versus 18.5% (P = .285), whereas TIMI major bleedingwere 6.4% versus 7.4% (P = .761) and bleeding events requiring transfusion were 9.1% versus11.1% (0.656).†Severe congestive heart failure as an outcome was defined as congestive heart failure that was present post–rescue PCI procedure, which included cardiogenic shock.
Shugman et al 653American Heart JournalVolume 163, Number 4
use of GPIIb/IIIa inhibitors was not associated with TIMImajor bleeding.Predictors of late mortality on univariable analysis
were age ≥65 years (P = .011), female gender (P = .011),pre-PCI cardiogenic shock (P b .001), post-PCI TIMI flowgrade ≤2 (0.027), and TIMI major bleeding within theindex hospitalization (P = .031). Conversely, currentsmoking (or ceased b12 months) and door-to-balloontimes N3 hours were associated with low late mortality(P = .016 and P = .039, respectively). On Coxmultivariate analysis, the independent factors associatedwith high late mortality included female gender (OR3.323, 95% CI 1.284-8.600; P = .013), post-PCI TIMI flowgrade ≤2 (OR 6.249, 95% CI, 2.054-19.009; P = .001),and pre-PCI cardiogenic shock (OR 6.578, 95% CI 2.440-17.735; P b .001) (Figure 1).
DiscussionFor patients with STEMI treated by fibrinolytic therapy,
including those being managed by a pharmacoinvasive
strategy, 25% to 30% will have indications for rescuePCI.7,21 In our study, three fourth of patients whounderwent rescue PCI had presented to hospital within 2hours of symptom onset. In such early presentingpatients, a pharmacoinvasive strategy may have benefitbecause of early successful rescue PCI enhancingmyocardial salvage and have lowering mortality.1,8 TheCAPTIM and WEST investigators recently reportedretrospective pooled analyses of the subgroup presentingwithin 2 hours of symptom onset8; a late mortality benefitoccurred among those who received fibrinolysis (mostlyprehospital, with a 25%-30% rate of rescue PCI and ~70%in-hospital PCI), compared with primary PCI. TheSTREAM trial is prospectively evaluating a pharmacoinva-sive strategy in STEMI patients presenting within 3 hoursof symptom onset to non-PCI centers.22
We report mortality rates of 3.2% and 5.3% at day 30and 1 year, respectively, which are comparable withthose reported for primary PCI in patients (N50% withanterior MI) without pre-PCI shock similar to mortality inthe APEX AMI trial.23 When patients with cardiogenic
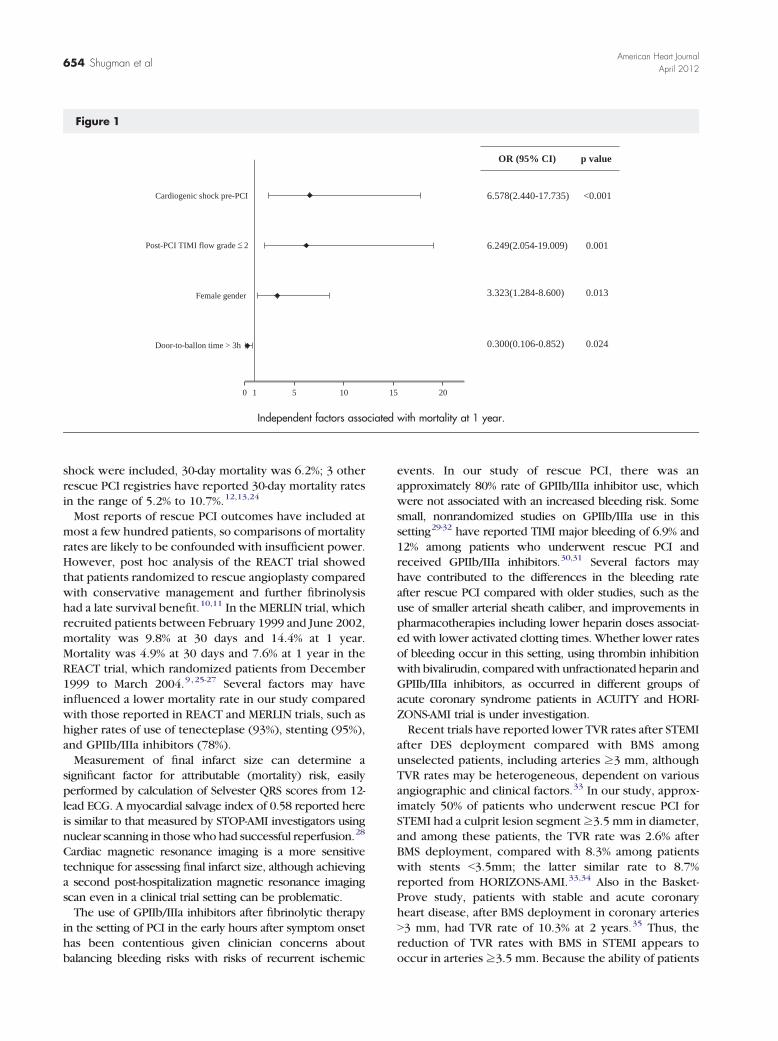
Figure 1
OR (95% CI) p value
6.578(2.440-17.735) <0.001
6.249(2.054-19.009) 0.001
3.323(1.284-8.600) 0.013
0.300(0.106-0.852) 0.024
0 1 5 10 15 20
Cardiogenic shock pre-PCI
Post-PCI TIMI flow grade 2
Female gender
Door-to-ballon time > 3h
<
Independent factors associated with mortality at 1 year.
654 Shugman et alAmerican Heart Journal
April 2012
shock were included, 30-day mortality was 6.2%; 3 otherrescue PCI registries have reported 30-day mortality ratesin the range of 5.2% to 10.7%.12,13,24
Most reports of rescue PCI outcomes have included atmost a few hundred patients, so comparisons of mortalityrates are likely to be confounded with insufficient power.However, post hoc analysis of the REACT trial showedthat patients randomized to rescue angioplasty comparedwith conservative management and further fibrinolysishad a late survival benefit.10,11 In the MERLIN trial, whichrecruited patients between February 1999 and June 2002,mortality was 9.8% at 30 days and 14.4% at 1 year.Mortality was 4.9% at 30 days and 7.6% at 1 year in theREACT trial, which randomized patients from December1999 to March 2004.9,25-27 Several factors may haveinfluenced a lower mortality rate in our study comparedwith those reported in REACT and MERLIN trials, such ashigher rates of use of tenecteplase (93%), stenting (95%),and GPIIb/IIIa inhibitors (78%).Measurement of final infarct size can determine a
significant factor for attributable (mortality) risk, easilyperformed by calculation of Selvester QRS scores from 12-lead ECG. A myocardial salvage index of 0.58 reported hereis similar to that measured by STOP-AMI investigators usingnuclear scanning in thosewho had successful reperfusion.28
Cardiac magnetic resonance imaging is a more sensitivetechnique for assessing final infarct size, although achievinga second post-hospitalization magnetic resonance imagingscan even in a clinical trial setting can be problematic.The use of GPIIb/IIIa inhibitors after fibrinolytic therapy
in the setting of PCI in the early hours after symptom onsethas been contentious given clinician concerns aboutbalancing bleeding risks with risks of recurrent ischemic
events. In our study of rescue PCI, there was anapproximately 80% rate of GPIIb/IIIa inhibitor use, whichwere not associated with an increased bleeding risk. Somesmall, nonrandomized studies on GPIIb/IIIa use in thissetting29-32 have reported TIMI major bleeding of 6.9% and12% among patients who underwent rescue PCI andreceived GPIIb/IIIa inhibitors.30,31 Several factors mayhave contributed to the differences in the bleeding rateafter rescue PCI compared with older studies, such as theuse of smaller arterial sheath caliber, and improvements inpharmacotherapies including lower heparin doses associat-ed with lower activated clotting times. Whether lower ratesof bleeding occur in this setting, using thrombin inhibitionwith bivalirudin, comparedwith unfractionated heparin andGPIIb/IIIa inhibitors, as occurred in different groups ofacute coronary syndrome patients in ACUITY and HORI-ZONS-AMI trial is under investigation.Recent trials have reported lower TVR rates after STEMI
after DES deployment compared with BMS amongunselected patients, including arteries ≥3 mm, althoughTVR rates may be heterogeneous, dependent on variousangiographic and clinical factors.33 In our study, approx-imately 50% of patients who underwent rescue PCI forSTEMI had a culprit lesion segment≥3.5 mm in diameter,and among these patients, the TVR rate was 2.6% afterBMS deployment, compared with 8.3% among patientswith stents b3.5mm; the latter similar rate to 8.7%reported from HORIZONS-AMI.33,34 Also in the Basket-Prove study, patients with stable and acute coronaryheart disease, after BMS deployment in coronary arteriesN3 mm, had TVR rate of 10.3% at 2 years.35 Thus, thereduction of TVR rates with BMS in STEMI appears tooccur in arteries ≥3.5 mm. Because the ability of patients

Shugman et al 655American Heart JournalVolume 163, Number 4
to appreciate the necessity of prolonged dual antiplatelettherapy in the setting of acute STEMI may be compro-mised,36 and the low TVR rates with BMS in vessels≥3.5 mm in diameter, future studies should specificallyaddress the necessity of DES use in this setting.This study has limitations inherent in an observational
study. There may have been unappreciated referral biasesat non-PCI hospitals, so deaths before and duringinterhospital transfer were not recorded. We found aparadoxical survivor benefit among those with door-to-balloon times N3 hours, which may represent a lower riskgroup of younger patients and lower rates of pre-PCIcardiogenic shock and/or referral bias as in the FAST-MIregistry, a higher mortality was observed in thoseundergoing rescue PCI treated ≥220 minutes comparedwith those at ≤128 minutes after fibrinolysis.6 We reportlow rates of radial access in comparison with some otherstudies, which may have influenced our rates of bleeding.Although the RIVAL trial reports that, in a subgroup ofpatients with STEMI, radial access reduces the incidenceof the primary outcome of death, MI, stroke, or majorbleeding and the secondary outcomes of death, MI, orstroke, and overall mortality within 30 days comparedwith femoral approach, this subgroup analysis warrantsfuture trial confirmation.37 In addition, we did notroutinely collect data on rates of “upstream” clopidogreladministration.In conclusion, the mortality rate of 3.2% in unselected
patients without prior shock undergoing rescue PCI in theera of liberal use of stents andGPIIb/IIIa inhibitors is similarto that of STEMI patients treated with primary PCI. Thesedata suggest that a pharmacoinvasive approach to STEMIwith rescue PCI especially among those presenting at b2hours is a reasonable strategy when there is no expeditiousaccess to primary PCI, especially in early presentingpatients. Finally, the very low TVR rate with BMS incoronary arteries ≥3.5 mm in this STEMI setting could becompared with DES use in an appropriately sized trial.
AcknowledgementsThe authors thank physicians, nurses, and staff of the
Cardiology Department at Liverpool Hospital without whosehelp this study could not have been completed. We alsothank Ingham Institute for Applied Medical Research, for anintramural departmental infrastructure grant.
DisclosuresConflict of Interest: None declared.
References1. Gersh BJ, Stone GW, White HD, et al. Pharmacological facilitation
of primary percutaneous coronary intervention for acute myocardialinfarction: is the slope of the curve the shape of the future? JAMA2005;293:979-86.
2. Kushner FG, Hand M, Smith Jr SC, et al. 2009 focused updates:ACC/AHA guidelines for the management of patients withST-elevation myocardial infarction (updating the 2004 guideline and2007 focused update) and ACC/AHA/SCAI guidelines on percu-taneous coronary intervention (updating the 2005 guideline and2007 focused update) a report of the American College ofCardiology Foundation/American Heart Association Task Force onPractice Guidelines. J Am Coll Cardiol 2009;54:2205-41.
3. Wijns W, Kolh P, Danchin N, et al. Guidelines on myocardialrevascularization: the Task Force on Myocardial Revascularization ofthe European Society of Cardiology (ESC) and the EuropeanAssociation for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2010;31:2501-55.
4. Keeley EC, Boura JA, Grines CL. Primary angioplasty versusintravenous thrombolytic therapy for acute myocardial infarction: aquantitative review of 23 randomised trials. Lancet 2003;361:13-20.
5. Edmond JJ, Juergens CP, French JK. The pharmaco-invasiveapproach to STEMI: when should fibrinolytic-treated patients go to the“cath lab”? Heart 2009;95:358-61.
6. Danchin N, Coste P, Ferrieres J, et al. Comparison of thrombolysisfollowed by broad use of percutaneous coronary intervention withprimary percutaneous coronary intervention for ST-segment-elevationacute myocardial infarction: data from the French registry on acuteST-elevation myocardial infarction (FAST-MI). Circulation 2008;118:268-76.
7. Bonnefoy E, Steg PG, Boutitie F, et al. Comparison of primaryangioplasty and pre-hospital fibrinolysis in acute myocardialinfarction (CAPTIM) trial: a 5-year follow-up. Eur Heart J 2009;30:1598-606.
8. Westerhout CM, Bonnefoy E, Welsh RC, et al. The influence of timefrom symptom onset and reperfusion strategy on 1-year survival inST-elevation myocardial infarction: a pooled analysis of an earlyfibrinolytic strategy versus primary percutaneous coronary interven-tion from CAPTIM and WEST. Am Heart J 2011;161:283-90.
9. Sutton AG, Campbell PG, Graham R, et al. A randomized trial ofrescue angioplasty versus a conservative approach for failedfibrinolysis in ST-segment elevation myocardial infarction: theMiddlesbrough Early Revascularization to Limit INfarction (MERLIN)trial. J Am Coll Cardiol 2004;44:287-96.
10. Gershlick AH, Stephens-Lloyd A, Hughes S, et al. Rescueangioplasty after failed thrombolytic therapy for acute myocardialinfarction. N Engl J Med 2005;353:2758-68.
11. Wijeysundera HC, Vijayaraghavan R, Nallamothu BK, et al. Rescueangioplasty or repeat fibrinolysis after failed fibrinolytic therapy forST-segment myocardial infarction: a meta-analysis of randomizedtrials. J Am Coll Cardiol 2007;49:422-30.
12. Sohal M, Foo F, Sirker A, et al. Rescue angioplasty for failedfibrinolysis—long-term follow-up of a large cohort. Catheter Cardi-ovasc Interv 2011;77:599-604.
13. Ko DT, Atzema CL, Donovan LR, et al. Rescue percutaneous coronaryinterventions for failed fibrinolytic therapy in ST-segment elevationmyocardial infarction: a population-based study. Am Heart J 2011;161:764e1-70e1.
14. Shugman IM, Diu P, Gohil J, et al. Evaluation of troponin T criteria forperiprocedural myocardial infarction in patients with acute coronarysyndromes. Am J Cardiol 2011;107:863-70.
15. Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: aquantitative method of assessing coronary artery flow. Circulation1996;93:879-88.
16. French JK, Andrews J, Manda SO, et al. Early ST-segment recovery,infarct artery blood flow, and long-term outcome after acutemyocardial infarction. Am Heart J 2002;143:265-71.
656 Shugman et alAmerican Heart Journal
April 2012
17. de Lemos JA, Antman EM, Giugliano RP, et al. ST-segment resolutionand infarct-related artery patency and flow after thrombolytictherapy. Thrombolysis in Myocardial Infarction (TIMI) 14 investiga-tors. Am J Cardiol 2000;85:299-304.
18. Hindman NB, Schocken DD, Widmann M, et al. Evaluation of a QRSscoring system for estimating myocardial infarct size. V. Specificityand method of application of the complete system. Am J Cardiol1985;55:1485-90.
19. Juergens CP, Fernandes C, Hasche ET, et al. Electrocardiographicmeasurement of infarct size after thrombolytic therapy. J Am CollCardiol 1996;27:617-24.
20. Barbagelata A, Di Carli MF, Califf RM, et al. Electrocardiographicinfarct size assessment after thrombolysis: insights from the AcuteMyocardial Infarction STudy ADenosine (AMISTAD) trial. Am Heart J2005;150:659-65.
21. Cantor WJ, Fitchett D, Borgundvaag B, et al. Routine earlyangioplasty after fibrinolysis for acute myocardial infarction. N Engl JMed 2009;360:2705-18.
22. Armstrong PW, Gershlick A, Goldstein P, et al. The StrategicReperfusion Early After Myocardial Infarction (STREAM) study. AmHeart J 2010;160:30 e1-5 e1.
23. Armstrong PW, Granger CB, Adams PX, et al. Pexelizumab for acuteST-elevation myocardial infarction in patients undergoing primarypercutaneous coronary intervention: a randomized controlled trial.JAMA 2007;297:43-51.
24. Perez-Berbel P, Valencia J, Ruiz-Nodar JM, et al. Rescue angioplasty:characteristics and results in a single-center experience. J IntervCardiol 2011;24:42-8.
25. Sutton AG, Campbell PG, Graham R, et al. One year results of theMiddlesbrough Early Revascularisation to Limit Infarction (MERLIN)trial. Heart 2005;91:1330-7.
26. Kunadian B, Sutton AG, Vijayalakshmi K, et al. Early invasive versusconservative treatment in patients with failed fibrinolysis–no latesurvival benefit: the final analysis of the Middlesbrough EarlyRevascularisation to Limit Infarction (MERLIN) randomized trial. AmHeart J 2007;153:763-71.
27. Carver A, Rafelt S, Gershlick AH, et al. Longer-term follow-up ofpatients recruited to the REACT (Rescue Angioplasty VersusConservative Treatment or Repeat Thrombolysis) trial. J Am CollCardiol 2009;54:118-26.
28. Dong J, Ndrepepa G, Schmitt C, et al. Early resolution of ST-segmentelevation correlates with myocardial salvage assessed by Tc-99msestamibi scintigraphy in patients with acute myocardial infarctionafter mechanical or thrombolytic reperfusion therapy. Circulation2002;105:2946-9.
29. Miller JM, Smalling R, Ohman EM, et al. Effectiveness of earlycoronary angioplasty and abciximab for failed thrombolysis(reteplase or alteplase) during acute myocardial infarction (resultsfrom the GUSTO-III trial). Global use of strategies to open occludedcoronary arteries. Am J Cardiol 1999;84:779-84.
30. Jong P, Cohen EA, Batchelor W, et al. Bleeding risks with abciximabafter full-dose thrombolysis in rescue or urgent angioplasty for acutemyocardial infarction. Am Heart J 2001;141:218-25.
31. Gruberg L, Suleiman M, Kapeliovich M, et al. Glycoprotein IIb/IIIainhibitors during rescue percutaneous coronary intervention in acutemyocardial infarction. J Invasive Cardiol 2006;18:59-62.
32. Belle L, Fourny M, Reynaud T, et al. Efficacy and safety ofglycoprotein IIb/IIIa receptor antagonists for patients undergoingpercutaneous coronary intervention within twelve hours of fibrinoly-sis. Catheter Cardiovasc Interv 2011;78:376-84.
33. Stone GW, Parise H, Witzenbichler B, et al. Selection criteria fordrug-eluting versus bare-metal stents and the impact of routineangiographic follow-up: 2-year insights from the HORIZONS-AMI(Harmonizing Outcomes With Revascularization and Stents inAcute Myocardial Infarction) trial. J Am Coll Cardiol 2010;56:1597-604.
34. Stone GW, Lansky AJ, Pocock SJ, et al. Paclitaxel-eluting stents versusbare-metal stents in acute myocardial infarction. N Engl J Med 2009;360:1946-59.
35. Kaiser C, Galatius S, Erne P, et al. Drug-eluting versus bare-metal stents in large coronary arteries. N Engl J Med 2010;363:2310-9.
36. Williams BF, French JK, White HD. Informed consent during theclinical emergency of acute myocardial infarction (HERO-2 consentsubstudy): a prospective observational study. Lancet 2003;361:918-22.
37. Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoral access forcoronary angiography and intervention in patients with acutecoronary syndromes (RIVAL): a randomised, parallel group, multi-centre trial. Lancet 2011;377:1409-20.
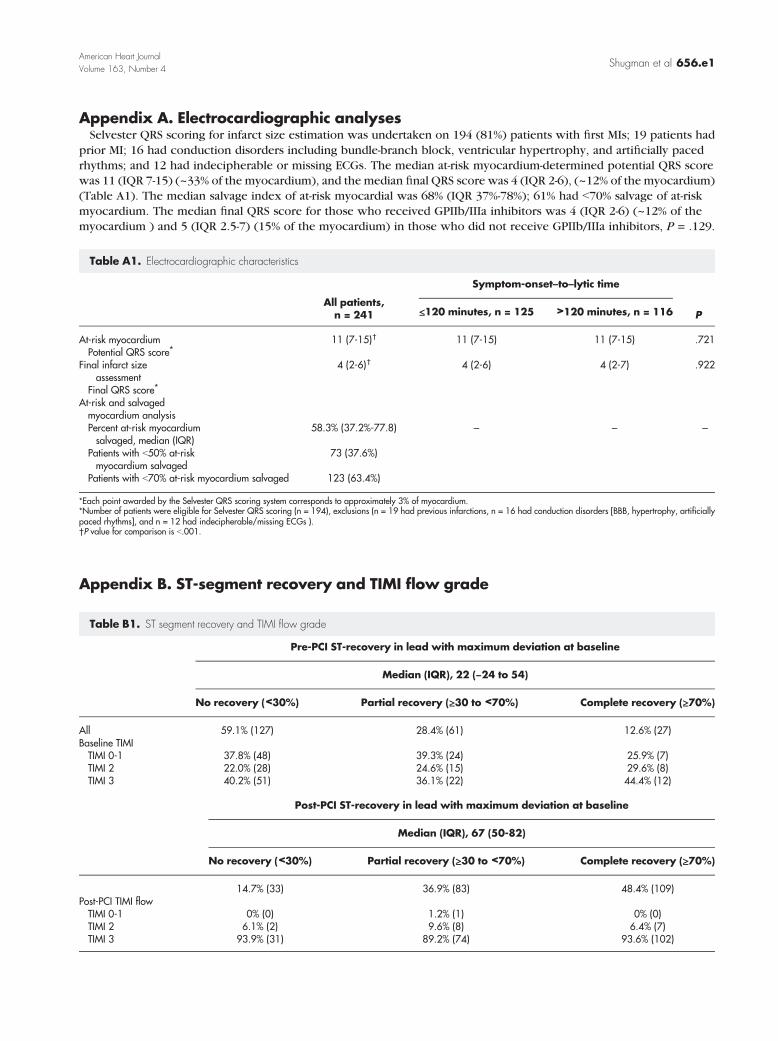
Shugman et al 656.e1American Heart JournalVolume 163, Number 4
Appendix A. Electrocardiographic analysesSelvester QRS scoring for infarct size estimation was undertaken on 194 (81%) patients with first MIs; 19 patients had
prior MI; 16 had conduction disorders including bundle-branch block, ventricular hypertrophy, and artificially pacedrhythms; and 12 had indecipherable or missing ECGs. The median at-risk myocardium-determined potential QRS scorewas 11 (IQR 7-15) (~33% of the myocardium), and the median final QRS score was 4 (IQR 2-6), (~12% of the myocardium)(Table A1). The median salvage index of at-risk myocardial was 68% (IQR 37%-78%); 61% had b70% salvage of at-riskmyocardium. The median final QRS score for those who received GPIIb/IIIa inhibitors was 4 (IQR 2-6) (~12% of themyocardium ) and 5 (IQR 2.5-7) (15% of the myocardium) in those who did not receive GPIIb/IIIa inhibitors, P = .129.
Table A1. Electrocardiographic characteristics
Symptom-onset–to–lytic time
All patients,n = 241
P ≤120 minutes, n = 125 >120 minutes, n = 116At-risk myocardium
11 (7-15)† 11 (7-15) 11 (7-15) .721 Potential QRS score⁎Final infarct sizeassessment
4 (2-6)†
4 (2-6) 4 (2-7) .922Final QRS score⁎At-risk and salvagedmyocardium analysis
Percent at-risk myocardiumsalvaged, median (IQR)58.3% (37.2%-77.8)
– – –Patients with b50% at-riskmyocardium salvaged
73 (37.6%)
Patients with b70% at-risk myocardium salvaged
123 (63.4%)⁎Each point awarded by the Selvester QRS scoring system corresponds to approximately 3% of myocardium.⁎Number of patients were eligible for Selvester QRS scoring (n = 194), exclusions (n = 19 had previous infarctions, n = 16 had conduction disorders [BBB, hypertrophy, artificiallypaced rhythms], and n = 12 had indecipherable/missing ECGs ).†P value for comparison is b.001.
Appendix B. ST-segment recovery and TIMI flow grade
Table B1. ST segment recovery and TIMI flow grade
Pre-PCI ST-recovery in lead with maximum deviation at baseline
Median (IQR), 22 (−24 to 54)
No recovery (<30%)
Partial recovery (≥30 to <70%) Complete recovery (≥70%)All
59.1% (127) 28.4% (61) 12.6% (27) Baseline TIMI TIMI 0-1 37.8% (48) 39.3% (24) 25.9% (7) TIMI 2 22.0% (28) 24.6% (15) 29.6% (8) TIMI 3 40.2% (51) 36.1% (22) 44.4% (12)Post-PCI ST-recovery in lead with maximum deviation at baseline
Median (IQR), 67 (50-82)
No recovery (<30%)
Partial recovery (≥30 to <70%) Complete recovery (≥70%)14.7% (33)
36.9% (83) 48.4% (109) Post-PCI TIMI flow TIMI 0-1 0% (0) 1.2% (1) 0% (0) TIMI 2 6.1% (2) 9.6% (8) 6.4% (7) TIMI 3 93.9% (31) 89.2% (74) 93.6% (102)
69
CHAPTER 4
REPORTING AND MANAGEMENT OF COMPLICATIONS
Introduction
Despite notable refinements in percutaneous coronary intervention (PCI)
techniques these procedures are still associated with some morbidity and mortality.
Some complications are relatively common such as peri-procedural myocardial
infarction and some are rare, such as dissection of the ascending aorta during cardiac
catheterisation.
Peri-procedural myocardial infarction
The prognostic significance of peri-procedural elevations of CKMB >3XURL
has been known for over a decade [1,2], and the importance of patterns of elevation of
blood levels of markers of myonecrosis after PCI has been emphasised in the 2000
and 2007 universal definitions of myocardial infarction (MI) [3-5]. The rapid uptake
of troponin to help risk stratify patients presenting with acute coronary syndromes has
meant that CKMB assays are less commonly performed and are often unavailable to
clinicians. When troponin levels are elevated pre-percutaneous coronary intervention
(PCI), two cardiac marker levels are required to meet the new re-MI criteria,
preferably troponin, one immediate and a second 6 hours later [3,4]. Also an increase
of ≥20% in elevated troponin levels above stabilized or falling pre-PCI levels is
needed. Changes on electrocardiograms (ECG) or imaging together with biomarkers
contribute to re-MI criteria [3,4]. As there are few data to support this troponin-based
definition of reinfarction [6,7], we examined cardiac marker levels in such patients.
70
Paper 18 (Am J Cardiol 2011;107:863-870)
When I established the PCI service at Liverpool hospital in 1997, I established
a policy that cardiac biomarkers would be routinely checked the morning after PCI
and more frequently if a complication of PCI had occurred. Initially CKMB was
measured but as troponin T became available we were in the slightly unusual situation
of having paired measurements of both CKMB and troponin T in a large cohort of
patients. We felt there was an opportunity to further examine the significance of
troponin elevations post PCI and the relationship to CKMB elevations. Initially we
examined relations between levels of creatine kinase-MB (CKMB) and troponin T
(TnT) in patients with acute coronary syndromes (ACS) and stable coronary heart
disease (CHD) to develop an algorithm for absolute increases in TnT levels above the
upper reference limit (URL). We used this algorithm in ACS patients with elevated
pre-PCI TnT levels, but normal CKMB levels, to compare percentage and absolute
increases in peri-procedural cardiac marker levels. We also examined the influence of
TnT and CKMB elevations post-PCI on late outcomes in patients with ACS,
compared to those with stable CHD. This was the basis of Paper 18.
We found a high degree of correlation between post-PCI CKMB and TnT
levels when both markers levels were elevated to >2XURL in stable CHD patients, a
finding similar to a previous report [8]. We also found a significant association
between an absolute increase in TnT levels above the stable pre-PCI elevated levels
and the absolute increase in CKMB levels above the URL. We also determined what
level of troponin rise corresponded to a CKMB levels rise to 3 times the URL both in
patients with normal and elevated troponin levels at baseline, which should be of
interest to clinicians who no longer have access to CKMB assays. We also confirmed
71
earlier work that suggested in stable coronary heart disease a rise in post-PCI cardiac
markers was associated with an adverse outcome.
Context and Implications
This work was further work led by Professor John French and Ibrahim Shugman at
Liverpool Hospital. I was a co-investigator of this study and was involved in the
original trial design. By establishing a process by which cardiac biomarkers were
routinely collected as part of quality assurance, I believe I made a crucial contribution
to this work. I was involved in the analysis and interpretation of the data and revisions
of the manuscript. We believe this paper makes an important contribution as the
diagnosis of peri-procedural myocardial infarction (MI) is often problematic in
patients with acute coronary syndromes (ACS) undergoing percutaneous coronary
intervention (PCI) when pre-PCI levels of cardiac troponin T (TnT) are elevated. This
is particularly the case as there are few data to support the new universal troponin-
based definition of reinfarction.
Impact on literature
According to Scopus ®, this article has cited twice in the literature from a journal with
a 5 year impact factor of 3.578.
Aortic Dissection
Dissection of the ascending aorta is one of the most lethal of all acute
cardiovascular conditions. Arising de novo it is associated with an in-hospital
mortality of up to 20% [9], and when recognised in time mandates immediate surgical
intervention. As a complication of cardiac catheterization it is extremely rare, with an
incidence of 0.02 to 0.03% [10-12]. PCI appears to carry greater risk than diagnostic
catheterization with a risk of 0.07% [12]. Similar to the experience with urgent
coronary bypass surgery after abciximab, catheter induced aortic dissection is a rare,
72
unpredictable event which requires swift action and not is something that lends itself
to randomised controlled trial clinical evidence.
Paper 19 (J Invasive Cardiol 2004;16:92-94)
After experiencing a case at Liverpool hospital of extensive ascending aortic
dissection caused by a percutaneous coronary intervention (PCI) procedure, we
reported a patient who was managed conservatively with a satisfactory outcome. I
wrote the case up with one of our basic physician trainees and reviewed the literature.
This was the basis of Paper 19.
Context and Implications
The rarity, unpredictability and urgency of this complication means that single case
reports such as these can help guide management. To the best of our knowledge, this
case represents the first report of catheter-induced extensive ascending aortic
dissection associated with acute ST-elevation MI to be successfully managed
conservatively and has helped guide practise in our institution. We have also used this
case frequently during our Interventional fellow training sessions as a guide to
managing this rare complication.
Impact on literature
According to Scopus ®, this article has been cited at least ten times in the literature
from a journal with an impact factor of 1.841 in 2011.
73
Chapter 4 References
1. Califf RM, Abdelmeguid AE, Kuntz RE, et al. Myonecrosis after revascularization
procedures. J Am Coll Cardiol 1998;31:241-251.
2. Abdelmeguid AE, Topol EJ. The myth of the myocardial `infarctlet' during
percutaneous coronary revascularization procedures. Circulation 1996;94:3369-3375.
3. The Joint European Society of Cardiology/American College of Cardiology
Committee. Myocardial infarction redefined - a consensus document of the Joint
European Society of Cardiology/American College of Cardiology Committee for the
redefinition of myocardial infarction. J Am Coll Cardiol 2000;36:959-969.
4. Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. J
Am Coll Cardiol 2007;50:2173-2195.
5. Alpert JS, Thygesen K, Jaffe A, White HD. The universal definition of myocardial
infarction:a consensus document. Heart 2008;94:1335-1341.
6. Gustavsson CG, Hansen O, Frennby B. Troponin must be measured before and
after PCI to diagnose procedure-related myocardial injury. Scand Cardiovasc J
2004;38:75-79.
7. Apple FS, Murakami MM. Cardiac troponin and creatine kinase MB monitoring
during in-hospital myocardial reinfarction. Clin Chem 2005;51:460-463.
8. Williams SG, Silas JH, Joseph F, Jackson M, Rittoo D, Currie P. Troponin T: how
high is high? relationship and differences between serum cardiac markers according to
level of creatine kinase and type of myocardial infarction. Postgrad Med J
2004;80:613-614.
74
9. Kazui T, Washiyama N, Bashar AHM, et al. Surgical outcome of acute type A
aortic dissection: analysis of risk factors. Ann Thorac Surg 2002;74:75-82.
10. Moles VP, Chappuis F, Simonet F, et al. Aortic dissection as complication of
percutaneous transluminal coronary angioplasty. Cathet Cardiovasc Diagn 1992;26:8-
11.
11. Dunning DW, Kahn JK, Hawkins EY, O’Neill WW. Iatrogenic coronary artery
dissections extending into and involving the aortic root. Cathet Cardiovasc Intervent
2000;51:387-393.
12. Carter AJ, Brinker JA. Dissection of the ascending aorta associated with coronary
angiography. Am J Cardiol 1994;73:922-923.

75
PAPER 18
Reprinted from the American Journal of Cardiology 2011;107:863-870
with permission from Elsevier

ar
Evaluation of Troponin T Criteria for Periprocedural MyocardialInfarction in Patients With Acute Coronary Syndromes
Ibrahim Meloud Shugman, MBBCha, Patrick Diu, MBBSa, Jayesh Gohil, MDa,Krishna Kishor Kadappu, MDa, Melissa Leung, MBiostata, Sidney Lo, MBBSa,
Dominic Y. Leung, PhDa, Andrew P. Hopkins, MBBSa, Craig P. Juergens, MBBSa, andJohn K. French, PhDa,*
In patients with acute coronary syndromes undergoing percutaneous coronary intervention(PCI), the diagnosis of periprocedural myocardial infarction is often problematic when thepre-PCI levels of cardiac troponin T (TnT) are elevated. Thus, we examined different TnTcriteria for periprocedural myocardial infarction when the pre-PCI TnT levels were ele-vated and also the associations between the post-PCI cardiac marker levels and outcomes.We established the relation between the post-PCI creatine kinase-MB (CKMB) and TnTlevels in 582 patients (315 with acute coronary syndromes and 272 with stable coronaryheart disease). A post-PCI increase in the CKMB levels to 14.7 �g/L (3� the upperreference limit [URL] in men) corresponded to a TnT of 0.23 �g/L. In the 85 patients withacute coronary syndromes and normal CKMB, but elevated post peak TnT levels beforePCI (performed at a median of 5 days, interquartile range 3 to 7), the post-PCI cardiacmarker increases were as follows: 21 (24.7%) with a >20% increase in TnT, 10 (11.8%) withan CKMB level >3� URL, and 12 (14%) with an absolute TnT increase of >0.09 �g/L(p <0.005 for both). In the patients with stable coronary heart disease and post-PCI cardiacmarkers >3� URL compared to those without markers elevations, the rate of freedomfrom death or nonfatal myocardial infarction was 88% for those with TnT elevations versus99% (p <0.001, log-rank) and 84% for those with CKMB elevations versus 98% (p <0.001,log-rank). Of the patients with acute coronary syndromes, the post-PCI marker levels didnot influence the outcomes. In conclusion, in patients with acute coronary syndromes andelevated TnT levels undergoing PCI several days later, >20% increases in TnT were morecommon than absolute increments in the TnT or CKMB levels of >3� URL. Also,periprocedural cardiac marker elevations in patients with acute coronary syndromes didnot have prognostic significance. © 2011 Elsevier Inc. All rights reserved. (Am J Cardiol
2011;107:863–870)The importance of the patterns of elevation in the bloodlevels of markers of myonecrosis has been emphasized inthe 2000 and 2007 universal definitions of myocardial in-farction (MI).1–3 When the troponin levels are elevatedbefore percutaneous coronary intervention (PCI), to meetthe recurrent MI criteria, 2 cardiac marker levels are re-quired, preferably troponin, the first immediate and thesecond 6 hours later.2,3 Also, an increase of �20% introponin levels greater than stabilized or decreasing ele-vated pre-PCI levels is needed. Changes on the electrocar-diograms or imaging findings, together with biomarkers,contribute to the recurrent MI criteria.2,3 Because few datare available to support this troponin-based definition ofeinfarction,4,5 we examined the cardiac marker levels in
such patients. Initially, we examined the relations betweenthe levels of creatine kinase-MB (CKMB) and troponin T
aDepartment of Cardiology, Liverpool Hospital, South West SydneyClinical School, University of New South Wales, Sydney, New SouthWales, Australia. Manuscript received October 15, 2010; manuscript re-ceived and accepted November 5, 2010.
*Corresponding author: Tel: (612) 9828-3069; fax: (612) 9828-3341.
E-mail address: [email protected] (J.K. French).0002-9149/11/$ – see front matter © 2011 Elsevier Inc. All rights reserved.doi:10.1016/j.amjcard.2010.11.007
(TnT) in patients with acute coronary syndromes and stablecoronary heart disease to develop an algorithm for theabsolute increases in TnT levels greater than the upperreference limit (URL). We used this algorithm in patientswith acute coronary syndromes with elevated pre-PCI TnTlevels, but normal CKMB levels, to compare the percentageand absolute increases in periprocedural cardiac markerlevels. We also examined the influence of TnT and CKMBelevations after PCI on the late outcomes in patients withacute coronary syndromes compared to those with stablecoronary heart disease.
Methods
All patients undergoing PCI have had clinical, angio-graphic, and procedural data recorded prospectively in thecardiology database at the Liverpool Hospital cardiac cath-eterization laboratory (Sydney, Australia). These data in-cluded procedural indications, patient demographics, med-ications, angiographic and lesion characteristics, and stenttype, such as drug-eluting stents. The procedural indicationswere categorized as acute coronary syndromes with or with-out ST-segment elevation. Those with angina (class II-III)
and other stable manifestations of coronary heart diseasewww.ajconline.org
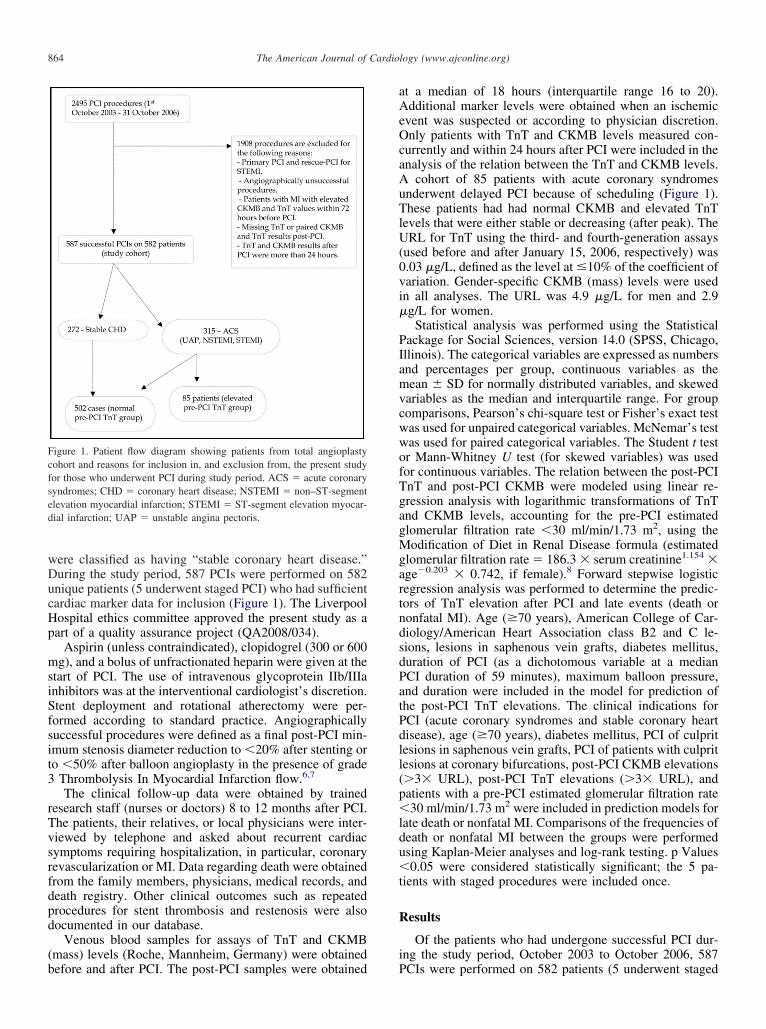
vi
MgartndsdPatPdll(p�ldu�t
R
i
s
864 The American Journal of Cardiology (www.ajconline.org)
were classified as having “stable coronary heart disease.”During the study period, 587 PCIs were performed on 582unique patients (5 underwent staged PCI) who had sufficientcardiac marker data for inclusion (Figure 1). The LiverpoolHospital ethics committee approved the present study as apart of a quality assurance project (QA2008/034).
Aspirin (unless contraindicated), clopidogrel (300 or 600mg), and a bolus of unfractionated heparin were given at thestart of PCI. The use of intravenous glycoprotein IIb/IIIainhibitors was at the interventional cardiologist’s discretion.Stent deployment and rotational atherectomy were per-formed according to standard practice. Angiographicallysuccessful procedures were defined as a final post-PCI min-imum stenosis diameter reduction to �20% after stenting orto �50% after balloon angioplasty in the presence of grade3 Thrombolysis In Myocardial Infarction flow.6,7
The clinical follow-up data were obtained by trainedresearch staff (nurses or doctors) 8 to 12 months after PCI.The patients, their relatives, or local physicians were inter-viewed by telephone and asked about recurrent cardiacsymptoms requiring hospitalization, in particular, coronaryrevascularization or MI. Data regarding death were obtainedfrom the family members, physicians, medical records, anddeath registry. Other clinical outcomes such as repeatedprocedures for stent thrombosis and restenosis were alsodocumented in our database.
Venous blood samples for assays of TnT and CKMB(mass) levels (Roche, Mannheim, Germany) were obtained
Figure 1. Patient flow diagram showing patients from total angioplastycohort and reasons for inclusion in, and exclusion from, the present studyfor those who underwent PCI during study period. ACS � acute coronaryyndromes; CHD � coronary heart disease; NSTEMI � non–ST-segment
elevation myocardial infarction; STEMI � ST-segment elevation myocar-dial infarction; UAP � unstable angina pectoris.
before and after PCI. The post-PCI samples were obtained P
at a median of 18 hours (interquartile range 16 to 20).Additional marker levels were obtained when an ischemicevent was suspected or according to physician discretion.Only patients with TnT and CKMB levels measured con-currently and within 24 hours after PCI were included in theanalysis of the relation between the TnT and CKMB levels.A cohort of 85 patients with acute coronary syndromesunderwent delayed PCI because of scheduling (Figure 1).These patients had had normal CKMB and elevated TnTlevels that were either stable or decreasing (after peak). TheURL for TnT using the third- and fourth-generation assays(used before and after January 15, 2006, respectively) was0.03 �g/L, defined as the level at �10% of the coefficient ofariation. Gender-specific CKMB (mass) levels were usedn all analyses. The URL was 4.9 �g/L for men and 2.9
�g/L for women.Statistical analysis was performed using the Statistical
Package for Social Sciences, version 14.0 (SPSS, Chicago,Illinois). The categorical variables are expressed as numbersand percentages per group, continuous variables as themean � SD for normally distributed variables, and skewedvariables as the median and interquartile range. For groupcomparisons, Pearson’s chi-square test or Fisher’s exact testwas used for unpaired categorical variables. McNemar’s testwas used for paired categorical variables. The Student t testor Mann-Whitney U test (for skewed variables) was usedfor continuous variables. The relation between the post-PCITnT and post-PCI CKMB were modeled using linear re-gression analysis with logarithmic transformations of TnTand CKMB levels, accounting for the pre-PCI estimatedglomerular filtration rate �30 ml/min/1.73 m2, using the
odification of Diet in Renal Disease formula (estimatedlomerular filtration rate � 186.3 � serum creatinine1.154 �ge�0.203 � 0.742, if female).8 Forward stepwise logisticegression analysis was performed to determine the predic-ors of TnT elevation after PCI and late events (death oronfatal MI). Age (�70 years), American College of Car-iology/American Heart Association class B2 and C le-ions, lesions in saphenous vein grafts, diabetes mellitus,uration of PCI (as a dichotomous variable at a medianCI duration of 59 minutes), maximum balloon pressure,nd duration were included in the model for prediction ofhe post-PCI TnT elevations. The clinical indications forCI (acute coronary syndromes and stable coronary heartisease), age (�70 years), diabetes mellitus, PCI of culpritesions in saphenous vein grafts, PCI of patients with culpritesions at coronary bifurcations, post-PCI CKMB elevations�3� URL), post-PCI TnT elevations (�3� URL), andatients with a pre-PCI estimated glomerular filtration rate30 ml/min/1.73 m2 were included in prediction models for
ate death or nonfatal MI. Comparisons of the frequencies ofeath or nonfatal MI between the groups were performedsing Kaplan-Meier analyses and log-rank testing. p Values0.05 were considered statistically significant; the 5 pa-
ients with staged procedures were included once.
esults
Of the patients who had undergone successful PCI dur-ng the study period, October 2003 to October 2006, 587
CIs were performed on 582 patients (5 underwent staged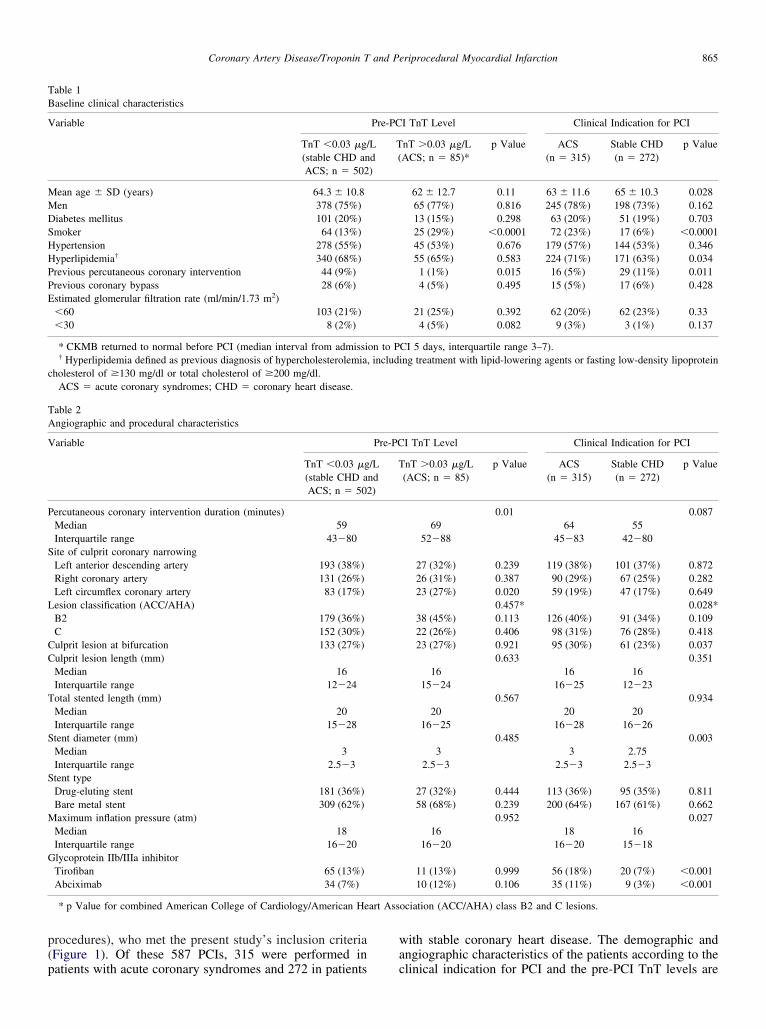
PPE
S
L
CC
T
S
S
M
G
art Ass
865Coronary Artery Disease/Troponin T and Periprocedural Myocardial Infarction
procedures), who met the present study’s inclusion criteria(Figure 1). Of these 587 PCIs, 315 were performed in
Table 1Baseline clinical characteristics
Variable
TnT �0.03 �g/(stable CHD anACS; n � 502
Mean age � SD (years) 64.3 � 10.8Men 378 (75%)Diabetes mellitus 101 (20%)Smoker 64 (13%)Hypertension 278 (55%)Hyperlipidemia† 340 (68%)
revious percutaneous coronary intervention 44 (9%)revious coronary bypass 28 (6%)stimated glomerular filtration rate (ml/min/1.73 m2)�60 103 (21%)�30 8 (2%)
* CKMB returned to normal before PCI (median interval from admissi† Hyperlipidemia defined as previous diagnosis of hypercholesterolemia,
cholesterol of �130 mg/dl or total cholesterol of �200 mg/dl.ACS � acute coronary syndromes; CHD � coronary heart disease.
Table 2Angiographic and procedural characteristics
Variable
TnT �0.03 �g(stable CHD aACS; n � 502
Percutaneous coronary intervention duration (minutes)Median 59Interquartile range 43�80ite of culprit coronary narrowingLeft anterior descending artery 193 (38%)Right coronary artery 131 (26%)Left circumflex coronary artery 83 (17%)esion classification (ACC/AHA)B2 179 (36%)C 152 (30%)ulprit lesion at bifurcation 133 (27%)ulprit lesion length (mm)Median 16Interquartile range 12�24otal stented length (mm)Median 20Interquartile range 15�28tent diameter (mm)Median 3Interquartile range 2.5�3tent typeDrug-eluting stent 181 (36%)Bare metal stent 309 (62%)aximum inflation pressure (atm)
Median 18Interquartile range 16�20lycoprotein IIb/IIIa inhibitorTirofiban 65 (13%)Abciximab 34 (7%)
* p Value for combined American College of Cardiology/American He
patients with acute coronary syndromes and 272 in patients
with stable coronary heart disease. The demographic andangiographic characteristics of the patients according to the
I TnT Level Clinical Indication for PCI
nT �0.03 �g/LACS; n � 85)*
p Value ACS(n � 315)
Stable CHD(n � 272)
p Value
62 � 12.7 0.11 63 � 11.6 65 � 10.3 0.02865 (77%) 0.816 245 (78%) 198 (73%) 0.16213 (15%) 0.298 63 (20%) 51 (19%) 0.70325 (29%) �0.0001 72 (23%) 17 (6%) �0.000145 (53%) 0.676 179 (57%) 144 (53%) 0.34655 (65%) 0.583 224 (71%) 171 (63%) 0.034
1 (1%) 0.015 16 (5%) 29 (11%) 0.0114 (5%) 0.495 15 (5%) 17 (6%) 0.428
21 (25%) 0.392 62 (20%) 62 (23%) 0.334 (5%) 0.082 9 (3%) 3 (1%) 0.137
CI 5 days, interquartile range 3–7).ing treatment with lipid-lowering agents or fasting low-density lipoprotein
I TnT Level Clinical Indication for PCI
nT �0.03 �g/L(ACS; n � 85)
p Value ACS(n � 315)
Stable CHD(n � 272)
p Value
0.01 0.08769 64 55
52�88 45�83 42�80
27 (32%) 0.239 119 (38%) 101 (37%) 0.87226 (31%) 0.387 90 (29%) 67 (25%) 0.28223 (27%) 0.020 59 (19%) 47 (17%) 0.649
0.457* 0.028*38 (45%) 0.113 126 (40%) 91 (34%) 0.10922 (26%) 0.406 98 (31%) 76 (28%) 0.41823 (27%) 0.921 95 (30%) 61 (23%) 0.037
0.633 0.35116 16 16
15�24 16�25 12�230.567 0.934
20 20 2016�25 16�28 16�26
0.485 0.0033 3 2.75
2.5�3 2.5�3 2.5�3
27 (32%) 0.444 113 (36%) 95 (35%) 0.81158 (68%) 0.239 200 (64%) 167 (61%) 0.662
0.952 0.02716 18 16
16�20 16�20 15�18
11 (13%) 0.999 56 (18%) 20 (7%) �0.00110 (12%) 0.106 35 (11%) 9 (3%) �0.001
ociation (ACC/AHA) class B2 and C lesions.
Pre-PC
Ld)
T(
on to Pinclud
Pre-PC
/Lnd)
T
clinical indication for PCI and the pre-PCI TnT levels are

opscPCo1
M�htpi1ePsdvs
wP
reem3
tl
2l
e
ee
vweep�
866 The American Journal of Cardiology (www.ajconline.org)
listed in Tables 1 and 2. Periprocedural glycoprotein IIb/IIIainhibitors were used in 20% (12.9% tirofiban and 7.5%abciximab). In 98% of PCIs, �1 stent was deployed (35%had �1 drug-eluting stent); 3 patients underwent rotationalatherectomy. The rate of peri-PCI MI for all 587 PCI proce-dures, as determined by elevated TnT and CKMB levels (both�3� URL), as recommended by the 2007 universal definitionf MI, was 23.9% and 16.7%, respectively. The independentredictors of TnT elevation after PCI on multivariate regres-ion analysis were age (�70 years; odds ratio [OR] 1.68, 95%onfidence interval [CI] 1.12 to 2.52, p � 0.011), duration ofCI (as a dichotomous variable at 59 minutes; OR 1.59, 95%I 1.07 to 2.35, p � 0.022), and American College of Cardi-logy/American Heart Association class B2 and C lesions (OR.54, 95% CI 1.00 to 2.37, p � 0.049).
Of the 502 PCIs performed in patients with normalpre-PCI TnT levels, elevated TnT levels after PCI to greaterthan the URL occurred in 188 patients (38%; 35% of pa-tients with stable coronary heart disease and 41% of patientswith acute coronary syndromes). The median level was 0.15�g/L (interquartile range 0.07 to 0.65). Elevated CKMBlevels after PCI to greater than the URL occurred in 208patients (41%; 38% with stable coronary heart disease and46% with acute coronary syndromes). The median CKMBlevel was 13 �g/L (interquartile range 7 to 38). Accordingto the increased CKMB levels to �3� URL, periprocedural
I occurred in 88 patients (18%). In contrast, TnT levels3� URL (�0.09 �g/L) indicated that periprocedural MI
ad occurred in 119 patients (24%; p �0.0001). The rela-ions between the post-PCI TnT and CKMB levels foratients with normal baseline pre-PCI TnT levels are shownn Figure 2. Of those with elevated post-PCI TnT levels,3% had normal CKMB levels. In patients without pre-PCIlevated TnT, significantly greater elevations in the post-CI TnT levels occurred in the patients with acute coronaryyndromes compared to those with stable coronary heartisease (median 0.27 �g/L, interquartile range 0.08 to 3.97s median 0.12 �g/L, interquartile range 0.06 to 0.28, re-pectively; p � 0.002).
A high correlation (r � 0.92, 95% CI 0.89 to 0.94, p �0.001)as seen between the elevated levels of TnT and CKMB after
Figure 2. CKMB and TnT levels after PCI in patients with normal TnTlevels before PCI. Stable coronary heart disease, n � 272; acute coronarysyndromes, n � 230. URL for TnT � 0.03 �g/L; URL for CKMB � 4.9�g/L for men and 2.9 �g/L for women. Numbers on top of each barrepresent number of patients in each category.
CI when the pre-PCI TnT levels were normal (Figure 3). The
egression equation describing this association is TnT (�g/L) �[(1.202[In CKMB�g/L])�4.693�0.264(if estimated glomerular filtration rate�30)],� 2.718. Using this equation and assuming an estimated glo-erular filtration rate �30 ml/min/1.73 m2, CKMB elevations to� URL (14.7 �g/L for men and to 8.7 �g/L for women)
corresponded to TnT levels of 0.23 �g/L and 0.12 �g/L respec-ively. The prediction of CKMB levels from the measured TnTevels can be obtained from the equation: CKMB level (�g/L) �e[3.737 � (0.701 [In TnT �g/L]) � 0.261 (if estimated glomerular filtration rate �30)],e � 2.718. No significant correlation was seen when either ofthese biomarker level elevations after PCI were �2� URL(r �0.11, p �0.40 for both).
A total of 85 patients with acute coronary syndromeswho underwent PCI at a median interval of 5 days (in-terquartile range 3 to 7) who had normal pre-PCI CKMBlevels but elevated TnT levels (median level 0.30 �g/L,interquartile range 0.09 to 0.86 �g/L; Table 3). Of these,
8 patients (33%) had additional increases in the TnTevels after PCI (median increase in TnT level 0.31 �g/L,
interquartile range 0.13 to 0.8 �g/L). With respect to thepost-PCI biomarker elevations, 21 patients (24.7%) had a�20% additional elevation in TnT level, 12 patients(14%) had an additional elevation in TnT level of �0.09�g/L (�3� URL), and 10 patients (11.8%) had a CKMBlevation �3� URL (p � 0.004 and p � 0.003 compar-
ing �20% TnT increases, respectively). Of the 21 pa-tients with a �20% additional TnT elevation (Table 3),none of whom had had periprocedural electrocardio-graphic changes, 9 had a CKMB elevation �3� URLafter PCI, 8 had a CKMB elevation �3� URL, and 4 hadno CKMB increase (an additional patient had a �3�URL CKMB but no TnT increase). Of the 57 patientswith no additional TnT elevation after PCI, 13 (23%) hadan elevation in CKMB levels to greater than the URL.
The correlation coefficient between the absolute in-creases in the TnT and CKMB levels is 0.75 (95% CI 0.53to 0.88, p �0.0001), and the equation describing this rela-tion is as follows: additional TnT elevation (�g/L) �
[(1.103[InCKMB�g/L])�4.821�0.406 (ifestimatedglomerularfiltrationrate�30)],� 2.718.During �1 year of follow-up, of the patients with normal
pre-PCI TnT levels, 14 died (9 with acute coronary syn-dromes [4%] and 5 with stable coronary heart disease[2%], p � 0.14), 9 had late nonfatal MI (5 with acutecoronary syndromes [2.3%] and 4 with stable coronaryheart disease [1.6%], p � 0.416), and 6 developed earlyand late stent thrombosis (3 with acute coronary syn-dromes [1.4%] and 3 with stable coronary heart disease[1.2%], p � 0.59).
Of the patients with stable coronary heart disease whohad post-PCI TnT levels and/or CKMB levels greater thanthe URL, the 1-year rate of freedom from death or nonfatalMI was lower than in those without post-PCI TnT and/orCKMB elevations (92% vs 98.8% for TnT, p � 0.006; 93%s 99% for CKMB, p � 0.012, log-rank). Of the patientsith acute coronary syndromes and either normal or
levated pre-PCI TnT and/or CKMB levels, no differ-nces were seen in event-free survival, irrespective of theost-PCI cardiac marker levels (95% vs 93% for TnT, p
0.69, and 94% vs 93% for CKMB, p � 0.81, log-rank;
Figure 4).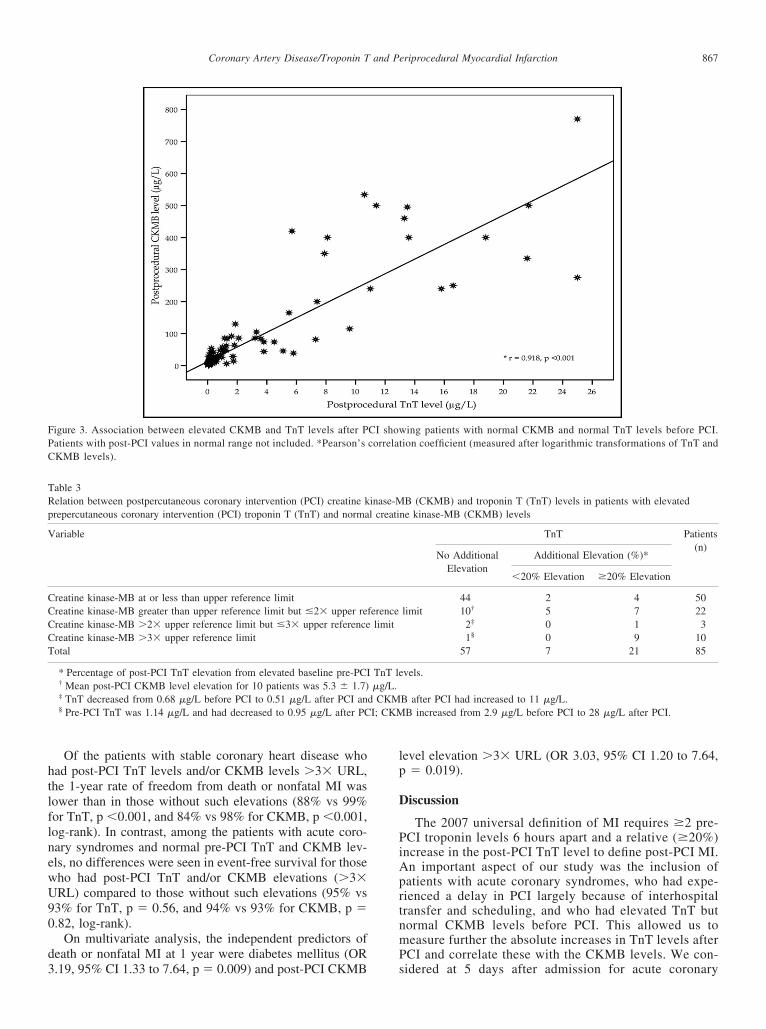
CCCCT
I; CKM
867Coronary Artery Disease/Troponin T and Periprocedural Myocardial Infarction
Of the patients with stable coronary heart disease whohad post-PCI TnT levels and/or CKMB levels �3� URL,the 1-year rate of freedom from death or nonfatal MI waslower than in those without such elevations (88% vs 99%for TnT, p �0.001, and 84% vs 98% for CKMB, p �0.001,log-rank). In contrast, among the patients with acute coro-nary syndromes and normal pre-PCI TnT and CKMB lev-els, no differences were seen in event-free survival for thosewho had post-PCI TnT and/or CKMB elevations (�3�URL) compared to those without such elevations (95% vs93% for TnT, p � 0.56, and 94% vs 93% for CKMB, p �0.82, log-rank).
On multivariate analysis, the independent predictors ofdeath or nonfatal MI at 1 year were diabetes mellitus (OR
Figure 3. Association between elevated CKMB and TnT levels after PPatients with post-PCI values in normal range not included. *Pearson’sCKMB levels).
Table 3Relation between postpercutaneous coronary intervention (PCI) creatine kprepercutaneous coronary intervention (PCI) troponin T (TnT) and norma
Variable
reatine kinase-MB at or less than upper reference limitreatine kinase-MB greater than upper reference limit but �2� upper rereatine kinase-MB �2� upper reference limit but �3� upper referencereatine kinase-MB �3� upper reference limitotal
* Percentage of post-PCI TnT elevation from elevated baseline pre-PCI† Mean post-PCI CKMB level elevation for 10 patients was 5.3 � 1.7)‡ TnT decreased from 0.68 �g/L before PCI to 0.51 �g/L after PCI an§ Pre-PCI TnT was 1.14 �g/L and had decreased to 0.95 �g/L after PC
3.19, 95% CI 1.33 to 7.64, p � 0.009) and post-PCI CKMB
level elevation �3� URL (OR 3.03, 95% CI 1.20 to 7.64,p � 0.019).
Discussion
The 2007 universal definition of MI requires �2 pre-PCI troponin levels 6 hours apart and a relative (�20%)increase in the post-PCI TnT level to define post-PCI MI.An important aspect of our study was the inclusion ofpatients with acute coronary syndromes, who had expe-rienced a delay in PCI largely because of interhospitaltransfer and scheduling, and who had elevated TnT butnormal CKMB levels before PCI. This allowed us tomeasure further the absolute increases in TnT levels afterPCI and correlate these with the CKMB levels. We con-
ing patients with normal CKMB and normal TnT levels before PCI.tion coefficient (measured after logarithmic transformations of TnT and
B (CKMB) and troponin T (TnT) levels in patients with elevatedne kinase-MB (CKMB) levels
TnT Patients(n)
No AdditionalElevation
Additional Elevation (%)*
�20% Elevation �20% Elevation
44 2 4 50limit 10† 5 7 22
2‡ 0 1 31§ 0 9 10
57 7 21 85
vels.
B after PCI had increased to 11 �g/L.B increased from 2.9 �g/L before PCI to 28 �g/L after PCI.
CI showcorrela
inase-Ml creati
ferencelimit
TnT le�g/L.
d CKM
sidered at 5 days after admission for acute coronary
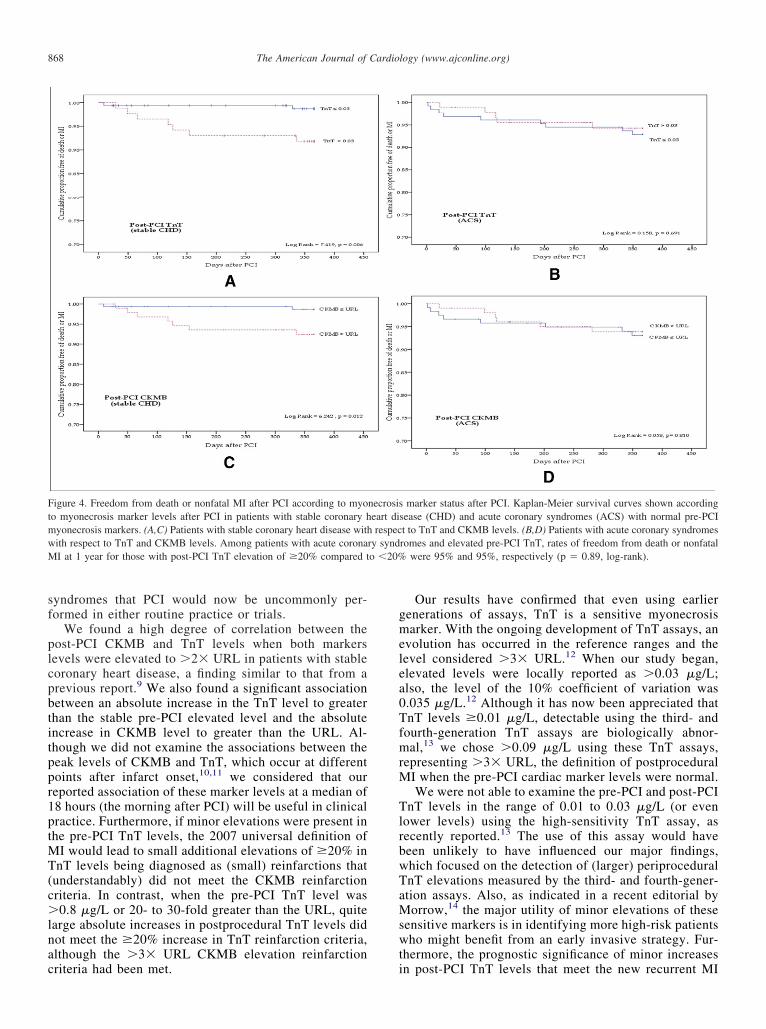
cpbtitppr1ptMT(c�
a0
swt
wM o �20%
868 The American Journal of Cardiology (www.ajconline.org)
syndromes that PCI would now be uncommonly per-formed in either routine practice or trials.
We found a high degree of correlation between thepost-PCI CKMB and TnT levels when both markerslevels were elevated to �2� URL in patients with stableoronary heart disease, a finding similar to that from arevious report.9 We also found a significant associationetween an absolute increase in the TnT level to greaterhan the stable pre-PCI elevated level and the absolutencrease in CKMB level to greater than the URL. Al-hough we did not examine the associations between theeak levels of CKMB and TnT, which occur at differentoints after infarct onset,10,11 we considered that oureported association of these marker levels at a median of8 hours (the morning after PCI) will be useful in clinicalractice. Furthermore, if minor elevations were present inhe pre-PCI TnT levels, the 2007 universal definition of
I would lead to small additional elevations of �20% innT levels being diagnosed as (small) reinfarctions that
understandably) did not meet the CKMB reinfarctionriteria. In contrast, when the pre-PCI TnT level was0.8 �g/L or 20- to 30-fold greater than the URL, quite
large absolute increases in postprocedural TnT levels didnot meet the �20% increase in TnT reinfarction criteria,although the �3� URL CKMB elevation reinfarction
Figure 4. Freedom from death or nonfatal MI after PCI according to myoto myonecrosis marker levels after PCI in patients with stable coronary hmyonecrosis markers. (A,C) Patients with stable coronary heart disease with
ith respect to TnT and CKMB levels. Among patients with acute coronaI at 1 year for those with post-PCI TnT elevation of �20% compared t
criteria had been met. i
Our results have confirmed that even using earliergenerations of assays, TnT is a sensitive myonecrosismarker. With the ongoing development of TnT assays, anevolution has occurred in the reference ranges and thelevel considered �3� URL.12 When our study began,elevated levels were locally reported as �0.03 �g/L;lso, the level of the 10% coefficient of variation was.035 �g/L.12 Although it has now been appreciated that
TnT levels �0.01 �g/L, detectable using the third- andfourth-generation TnT assays are biologically abnor-mal,13 we chose �0.09 �g/L using these TnT assays,representing �3� URL, the definition of postproceduralMI when the pre-PCI cardiac marker levels were normal.
We were not able to examine the pre-PCI and post-PCITnT levels in the range of 0.01 to 0.03 �g/L (or evenlower levels) using the high-sensitivity TnT assay, asrecently reported.13 The use of this assay would havebeen unlikely to have influenced our major findings,which focused on the detection of (larger) periproceduralTnT elevations measured by the third- and fourth-gener-ation assays. Also, as indicated in a recent editorial byMorrow,14 the major utility of minor elevations of theseensitive markers is in identifying more high-risk patientsho might benefit from an early invasive strategy. Fur-
hermore, the prognostic significance of minor increases
marker status after PCI. Kaplan-Meier survival curves shown accordingsease (CHD) and acute coronary syndromes (ACS) with normal pre-PCIt to TnT and CKMB levels. (B,D) Patients with acute coronary syndromesromes and elevated pre-PCI TnT, rates of freedom from death or nonfatal
were 95% and 95%, respectively (p � 0.89, log-rank).
necrosiseart direspec
ry synd
n post-PCI TnT levels that meet the new recurrent MI

r
o
ripnr
hpdCnm
gtblaf
ptrtt
AtlttFdsmC
869Coronary Artery Disease/Troponin T and Periprocedural Myocardial Infarction
criteria of �20%, when the pre-PCI TnT levels are �0.03�g/L and are now detected by high-sensitivity assaysequires clarification.
The prognostic significance of periprocedural elevationsf CKMB �3� URL has been known for more than a
decade,15,16 and, subsequently, similar evidence has beeneported for troponin.17 The detection of early reinfarction,ncluding periprocedural recurrent MI, using TnT- and tro-onin I-based definitions has been confounded by the ki-etic profiles of these cardiac markers with prolonged du-ation of elevation.10,11
Many investigators have reported the prognostic sig-nificance of elevated levels of CKMB after PCI.15,18
However, minor CKMB elevations, which reflect smallareas of myonecrosis identified on contrast-enhancedmagnetic resonance imaging,19 have also been shown to
ave a relation to survival. In the present study, theatients who underwent PCI for stable coronary heartisease and had any post-PCI elevated TnT and/orKMB level had a reduced rate of freedom from death oronfatal MI at 1 year compared to those without post-PCIarker elevations.The post-PCI TnT and CKMB level elevations were
reater in the acute coronary syndromes group comparedo the stable coronary heart disease group, which coulde explained by the greater frequency of American Col-ege of Cardiology/American Heart Association class B2nd C and bifurcation lesions. The data recently reportedrom the Mayo Clinic,13 which showed that among pa-
tients with acute coronary syndromes undergoing PCI,only elevated pre-PCI, and not post-PCI, cardiac markerlevels affected survival. Also periprocedural MI in pa-tients with acute coronary syndromes in the Acute Cath-eterization and Urgent intervention Triage Strategy(ACUITY) trial20 did not influence late events, although
re-PCI marker levels did. However, in the ACUITYrial, a significant fraction of patients underwent angiog-aphy and angioplasty within 12 to 18 hours of presen-ation. Also, although explicit criteria were in place forhe clinical events committee for adjudication of MI,20 a
proportion of these potential early periprocedural eventsmight not have been confirmed because of uncertaintyabout the early elevation profiles in marker levels. Incontrast, because of the cardiac marker selection criteria forour study, we did not include patients who had undergone“early” angiography and angioplasty. Also, whether theACUITY investigators made gender-specific adjustmentsfor CKMB reference ranges is not clear, although, as in ourstudy, because most patients with coronary heart disease aremen, the salient findings would likely be unaltered by thisadjustment.
Our study had limitations. Although this was a single-center study in which the PCI data were collected pro-spectively, the cardiac marker data were analyzed retro-spectively, which might have led to an unappreciatedbias. Second, because both cardiac markers were notmeasured for all patients with stable coronary heart dis-ease before PCI, we might have occasionally erroneouslyassumed the normality of the pre-PCI marker levels.Other illnesses as confounding causes of TnT elevations
other than renal impairment were not evaluated in thepresent study,10 although most patients were stable at PCI.lso, because a relatively small number of patients were in
he group with acute coronary syndromes and elevated TnTevels but normal CKMB levels, the power was insufficiento determine any (potentially modest) influence of addi-ional post-PCI TnT elevations on the 1-year outcomes.inally, we examined the composite late clinical outcome ofeath and (nonprocedural) nonfatal MI because our sampleize had limited power to examine associations between lateortality and marker levels, as reported from the Mayolinic.13
Acknowledgment: The authors thank the staff of theCardiology Department at Liverpool Hospital for theirinvaluable assistance with the present study. We alsothank Bin Jalaludin, PhD and Liza Thomas, PhD forhelpful advice.
1. The Joint European Society of Cardiology/American College ofCardiology Committee. Myocardial infarction redefined—a consen-sus document of the Joint European Society of Cardiology/Amer-ican College of Cardiology Committee for the redefinition of myo-cardial infarction. J Am Coll Cardiol 2000;36:959 –969.
2. Thygesen K, Alpert JS, White HD. Universal definition of myocardialinfarction. J Am Coll Cardiol 2007;50:2173–2195.
3. Alpert JS, Thygesen K, Jaffe A, White HD. The universal definition ofmyocardial infarction: a consensus document: ischaemic heart disease.Heart 2008;94:1335–1341.
4. Gustavsson CG, Hansen O, Frennby B. Troponin must be measuredbefore and after PCI to diagnose procedure-related myocardial injury.Scand Cardiovasc J 2004;38:75–79.
5. Apple FS, Murakami MM. Cardiac troponin and creatine kinase MBmonitoring during in-hospital myocardial reinfarction. Clin Chem2005;51:460–463.
6. Smith SC, Dove JT, Jacobs AK, Kennedy JW, Kereiakes D, Kern MJ,Kuntz RE, Popma JJ, Schaff HV, Williams DO. ACC/AHA guide-lines of percutaneous coronary interventions— executive summaryand recommendations: a report of the American College of Cardi-ology/American Heart Association Task Force on Practice Guide-lines (committee to revise the 1993 guidelines for percutaneoustransluminal coronary angioplasty). J Am Coll Cardiol 2001;37:2215–2238.
7. Smith SC, Feldman TE, Hirshfeld JW, Jacobs AK, Kern MJ, KingSB, Morrison DA, O’Neill WW, Schaff HV, Whitlow PL, WilliamsDO. ACC/AHA/SCAI guideline update for percutaneous coronaryintervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines(ACC/AHA/SCAI writing committee to update the 2001 guidelinesfor percutaneous coronary intervention). J Am Coll Cardiol 2005;2006:216 –235.
8. Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW,Hogg RJ, Perrone RD, Lau J, Eknoyan G. National Kidney Foun-dation practice guidelines for chronic kidney disease: evaluation,classification, and stratification. Ann Intern Med 2003;139:137–147.
9. Williams SG, Silas JH, Joseph F, Jackson M, Rittoo D, Currie P.Troponin T: how high is high? Relationship and differences be-tween serum cardiac markers according to level of creatine kinaseand type of myocardial infarction. Postgrad Med J 2004;80:613–614.
10. French JK, White HD. Clinical implications of the new definition ofmyocardial infarction. Heart 2004;90:99–106.
11. Jaffe AS, Babuin L, Apple FS. Biomarkers in acute cardiac disease:the present and the future. J Am Coll Cardiol 2006;48:1–11.
12. Apple FS, Wu AHB, Jaffe AS. European Society of Cardiology andAmerican College of Cardiology guidelines for redefinition of myo-cardial infarction: how to use existing assays clinically and for clinical
trials. Am Heart J 2002;144:981–986.
1
1
1
1
2
870 The American Journal of Cardiology (www.ajconline.org)
13. Prasad A, Rihal CS, Lennon RJ, Singh M, Jaffe AS, Holmes DR.Significance of periprocedural myonecrosis on outcomes after percu-taneous coronary intervention: an analysis of preintervention andpostintervention troponin T levels in 5487 patients. Circ CardiovascInterv 2008;1:10–19.
4. Morrow DA. Clinical application of sensitive troponin assays. N EnglJ Med 2009;361:913–915.
5. Califf RM, Abdelmeguid AE, Kuntz RE, Popma JJ, Davidson CJ,Cohen EA, Kleiman NS, Mahaffey KW, Topol EJ, Pepine CJ, LipickyRJ, Granger CB, Harrington RA, Tardiff BE, Crenshaw BS, BaumanRP, Zuckerman BD, Chaitman BR, Bittl JA, Ohman EM. Myonecrosisafter revascularization procedures. J Am Coll Cardiol 1998;31:241–251.
16. Abdelmeguid AE, Topol EJ. The myth of the myocardial “infarctlet”during percutaneous coronary revascularization procedures. Circula-tion 1996;94:3369–3375.
7. Nienhuis MB, Ottervanger JP, Bilo HJG, Dikkeschei BD, Zijlstra F.
Prognostic value of troponin after elective perctaneous coronary interven-tion: a meta-analysis. Catheter Cardiovasc Interv 2008;71:218–224.18. Abdelmeguid AE, Topol EJ, Whitlow PL, Sapp SK, Ellis SG.Significance of mild transient release of creatine kinase-MB frac-tion after percutaneous coronary interventions. Circulation 1996;94:1528 –1536.
9. Ricciardi MJ, Wu E, Davidson CJ, Choi KM, Klocke FJ, BonowRO, Judd RM, Kim RJ. Visualization of discrete microin-farction after percutaneous coronary intervention associated withmild creatine kinase-MB elevation. Circulation 2001;103:2780 –2783.
0. Prasad A, Gersh BJ, Bertrand ME, Lincoff AM, Moses JW, OhmanEM, White HD, Pocock SJ, McLaurin BT, Cox DA, Lansky AJ,Mehran R, Stone GW. Prognostic significance of periproceduralversus spontaneously occurring myocardial infarction after percu-taneous coronary intervention in patients with acute coronary syn-dromes: an analysis from the ACUITY (Acute Catheterization and
Urgent intervention Triage Strategy) trial. J Am Coll Cardiol 2009;54:477– 486.
76
PAPER 19
Reprinted from the Journal of Invasive Cardiology 2004;16:92-94 with
permission from the Journal of Invasive Cardiology
Document Supplied by
Ken Merten Library
"Infonnation is our Specialty"
·- ~ Health NSW South Western Sydney Pho11 e: 9828 3558 GOVVI_,., Local Health District Fax: 9828 3775
Liverpool Hospital Locked Bag 7103
Liverpool BC 1871
___A · Case Rep~orut:..J,a!:!..ml~R~edv21ie~w~----------------
Conservative Management of Ascending Aortic Dissection
Caused by Percutaneous Coronary Intervention
Brendan Doyle, MB and 'Craig Philip Juergens, MBBS
ABSTRACT: Despite nomhlt> reflnemenrs in percutaneom coronarv ilttetvention (PO) techniques. these procedun::s are still associated widt some t\mrbidity ~nd mortality. A c;,'ISe of eb::tive comnary angioplasty is described rl;ar was complicated by C(>ronaty dissection and STelevation myocardial infan:ti<m.. Subsequent dforts to recunali?.e the comna.ty arrety m;ulred in a carherer-inducc:d t(m at the origin of the vessel. with proximal extension of the dissection to involve rhe ascending anna. Lirerarure relating ro this cornplic:uion (reviewed here) suggests rhar surgical management may be indicated under the circumstances we describe. However. a conservative approach was adoptt'!l in this instance with excellem long-term re.ults.
J !NVAS CARDIOL1004; 16:92-94 Key words: aortic dissterion, coronary intervention
A case of exrens.ive ascending aon:i.c dis~ection caused by a
pcrcur.tncous coronary intervention (PCI) procedure is described. The patienr was managed conservatively wirb a sa.tis
fucrory outcome. ·me lireramre relating to this rare complication of PCI is revie\ved.
Case Report. A 64-year-old woman tV(IS referrctl r.o our department for corowny angiography. She hm:l been o.ywriencing effortrelated chest discomfort' for several month;, and a thalliu:m smn was suggc.uir>t of myocardial isdmnia. Bilateml intemt1l mrotid an'(ly stenosts of> 70% bad bcl!l7 previously dommented, udth pl.tnm:d carotid ~IUJ~1j·terrttdmy following the recent development of lift bem.ispht•ric tramient iscbnnic tat<wks. 5'he. al;o hltd symptomatic lowt·r limb V(l$CtJiar di.rt!nse, utbich w~tr non-critic:tl
CoroN(try angiography r.wealed minor lr:ft antl'tirJr descending and lift cirwmjlcx disease. The right coromJ,ry artery (RCA) was tortuous, with a 90% mid-tJessell~r>ion just beyond a marginal branch. The VtS'Sel 11!/IJ quite cak-ifod tmgiographical{y. Lift' ventriculography was normal with an tjtction fram'tm of70%.
In light of the patient'r exercise-limiting angimt and scheduled atrotid enda:rtm:cr.omy, n decision WtfS taken to proceed with PCf Despite a signifimnt degree of calcification, it was ftlt that the wssel was too rormous to consitkr high-spud rotational atberectomyofthe lesion. Therefore. elective rmgioplasty was ammged. Arterial access wt.IS obtained .from the left ftmornl army, following a foiled attempt to cannulAte the right ftmoralartery. A right ftmomlt'eitt mtheter was also imo1ed and 10.000 units if intrLl1.ti'?/Ous heparin were
From the Department of Cardiology, M~ter MiscriClltdiae Hospital, Dublin. frdand and 'tltc Departm~nt of Cardiology, Liverpool Jle-<h Service, Liverpool NSW. Austmlia.
Mmruscript received February 25, 2003, ;>ro.visional acceptance given March 25, 2003. revised mrutuscript accepted May 12,2003.
Address reprint requests to: Dr. Brendan Doyle. Deparuncnl of Caruiology, Ma~~:r l\-1lserlcordiae HosJlil.a), Eccles Street, Dublin 7,lrcland. B-mnil: [email protected],co'.uk
92
m:lmhu~>tered. \\7t had great difficulty finding a guide thai. would scat tJ.dtqr~ately in the origin rfthe RCA, rmd fi!Ul/ljt settled on an 8 French (Fr) ALl Cyber guide (Eost:ott Sciettt~fic/Sdmeri, Inc., Mapk· Grove, Minnesota), UJhic!J provided reasoJUlble but not perftct baciN.tp. A {1.014" Choice PT wt're (Boston Scient~fidScimcd. h1c.) was loaded within a 3.0 x 20 mm Bandit balloon (Bostrm Scimtific!Scimed, Inc.) and advanced into the distal part of the RCA. Quitr ttctive guide mrmiptdatirm was requited in ortkr to pas.r the balloon across the les£on. This Wtts twice inflated to 6 atmospbem and tbm withdrawn. Subscqumt angiography reveawd a significant (OYO!WJ' dissection at t!Je site of the WJion.
W'e then aumtpted to tkiiver three d[ffermt typei ofstent; without suue>s. An attempt IQ {JIISS a perfUsion balloon was also unsuccessfUL ln the course of our iflortJ·to tzdvaiU't the st:ents, wire position wa.·lost. When position Ulfzs recstnblished the lesion. wa.f dilated severn/ more times using a combination of balloons, but we were untJble to restore and maintain good amerograde flow. The p11timt developed significant che.st pain and ST segmmt elevation. At this time, it also bemme apparent that there UJt.IS a cathcter-tizduced dissection of the origin if the RCA thpt extended proxil'IWily 7 em into the ascending aorta (Figure 1). The patient's blood prmurc rose to 160190 mmHg. bur she exhibited no signs o/ cerebrm;as.~rlar (or other eru:i-orgt~.n) cJJtrtpromjst.
Tht case wt.IS discussed witb a cardia thoracic s:urg<ton. It U!tlS corPeluded that the risks ,1JsrJcirm:d witlt emergent roron<Zry a:rtay bypass grafting and aortir al'ch replamnmt in tbe context ofthe patittttt! cm·otid diseaJe and l'l!olvingmyocardiai il!fitrction werrrprohibitiue!y high and it wtu tkcidr:d shr should be treated congruatiuely. Therefore. the prHirnt WtlS transferred to thr Corona1y Gm Unit where intraHmou; wdium nitroprusside WtlJ' commmced in ortkr to optimal[y nt<UUlge her blood pressttrl!.
Serial creatine kiJII1Se fevcft peaked at 671 UIL (nomzaf range, 25-195 Ul L) atzd .serial electrocardiograms showed evolution of inferior Q-waves. The following morning, 11 transesophagcal rchocardiogram uMs cm·rird out. This sbowed tm ascending aorti.t· dissertion inwking t/1e origin of the RCA and stopping t1t the posterior margin of the !efi 111ltin cOI'01lfiiJ arwy. extending 70 mm superiorly. Most of the four lumen apperTred thnmtbosed apart ftom the superior third. There was no communication tktected between the true and jitftt lumen. There was mild cmtraL aortic regurgitation, which was known to be longstanding. A very sl'IWll region of injill'o-posterob11Sal akitmia was demonstrated
Fo1tr days later tbe study was repeated, retJealing a marked decrease in the size ofthc dissection. A third transesophagea/.echocardiogmm !IJ!fj mtried out six weeks filter; it showed no euideiWe of residtlll!aottic diJsection afu:i minimal walt mt1tion ahn(Jim.,lfitief in
The Jonmal of l11vasive Cardiology
Material may be protected by copyright law (Title 17, U.S. Code)
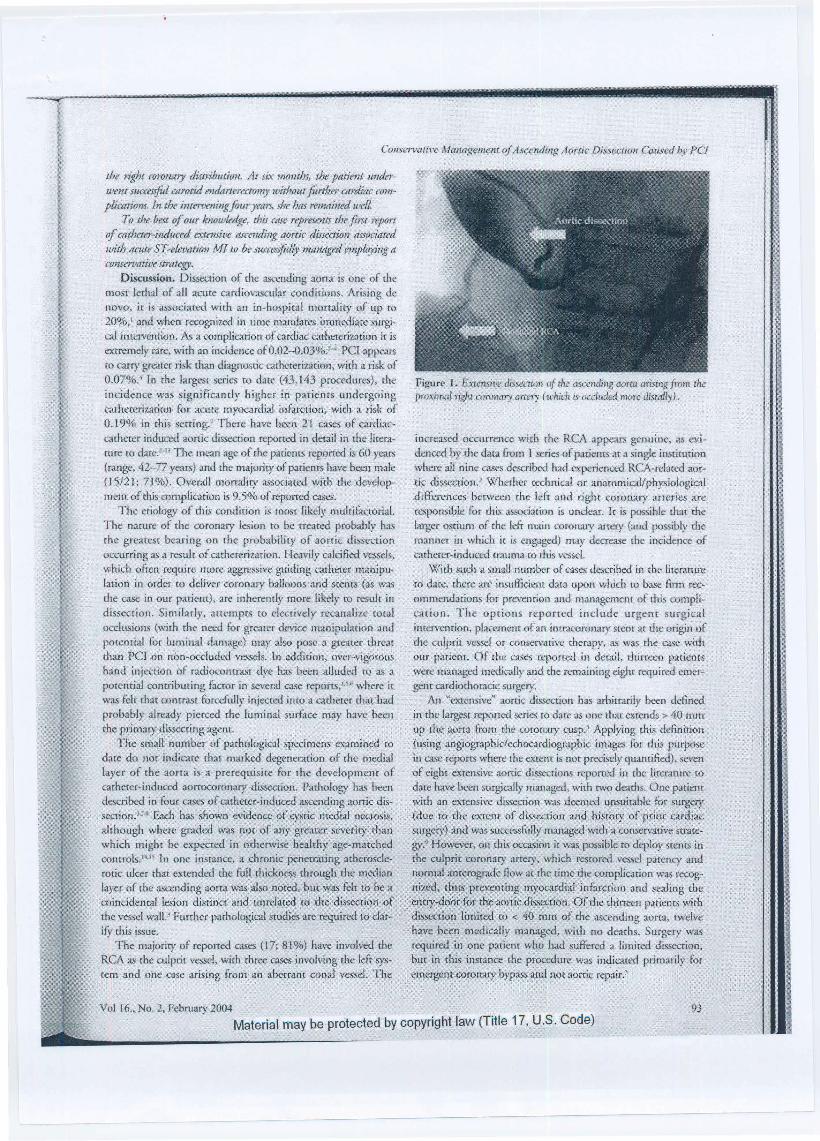
Consermti~·e Managtt~nent of Ascending Aortic DissectiOII Caused by PC!
the right coronmy distribution. At six months, the patient under· went suc('essfol carotid endanerectJJmy without further cnrditlc complicatiom. In the intm~eningjour years, she hns m1Jttined UJ<•U.
To the best of our /..·nowledge, this case represents the .first report of Mtheter-induud extensive ascending aortic dissection nssociatl'd with rtcute ST-efel!ation 1'vf! tlJ be successfid!y mrmttged enip!IJying a tonservativr strtttegy.
Discussion. Di5secrion of the ascending aorra is one of the most lethal of all acute cardiovascular conditions. Arising de novo, ic is associated with an in-hospital mortality ofup ro 20%,' and whel) rccogni7..ed in time n;andares immediate surgi· cal intervemion. As a complication of cardiac catheterization it is extremely rare, with an incidence of0.02-0.03%!"" PCl appears ro carry greater ri k than diagnostic cath .. -reri7.ation, with a risk of 0.07%:' In the largesr series ro dar~ (43,143 procedures), the incidence was significandy higher i.n pari.ems undesgoing cathereri:zarion for acute myocardial infarction, with a risk of 0.19% in rhis serring.1 There have been 21 cases of card}accathetcr induced aonic dissection reponed in derail in dte Iiterarure to dare! -" "The mean age of the patiems reported is 60 years (range, 42-77 years) and rhe majority of patients have been male (15/21; 7l%). Overall mortality associated with the development of this complication is 9.5% of reported cases.
The etiology of this condition is most likely multifactorial. The narure of the coronary [~ion to be treated probably has the greatesr bearing on the probability of aortic dissection occurring as a r~ult of catheterization. Heavily cakified vessels, which often require more aggressive guiding catheter manipulation in order to deliver coronary balloons and srents (as was the case in our patient), are inherently more likely ro resulr in dissection. Simi13rly. auemprs ro elecrively recanalize rotal occlusions (with the need for grearer device manipulation and potencial for luminal damage) may also pose a greater thr<~1.r than PCJ on non-ocehtdcd vessels. In addition, ovcr~vigorous hand injection of radioconrrast dye has been alluded ro as a porential comribut ing fucror in several case reports/~·• where it wa.~ felr char contrast forcefully injected into a catheter rhac had probably already pierced rhe luminal surface may haw been rhe primary disseccing agent.
The small number of pathological specimens examined tCJ
dare do not indic..1.re that marked degeneration of rhe media.! layer of the aorra is a prerequisite for the development of catheter-induced aorrocoronary dissection. Pathology ha.~ been d~cribed in four cases of cathet:er-induced ascending aortic disseetion.'·M Eacl1 has ~hown evid¢nce of-cystic medial necrosis, although where graded ·was not of any greater severixf·rhan which might be expected in otherwise healthy age-matched conrrols."·'l 1n one instance, a chronic penetrating atherosclerotic ulcer that extended the full rhick:ness through the median layer of rhe ascending aotta was also nored, bur was feir to be a coinc.id~ntal lesion distinct and. unrelated tO the dlssectioh o1 the vessel walJ.l Further pathological smdi~ are required to clari(y rhis issue.
The majority of reported cas~ (17; 81 %) have involved the RCA as d1c culprit vessel, wirh three cases involving the left system and one case arising from an aberrant conal vesseL The
Figure 1. Extcnsit'i:! dissection of the ascending aorra arising from r.he proximal right comllilry artLry ( !.l'hich is tKdwkd more discally).
jncreased occurrence with rhe RCA appe.trs genuine, as evidenced by the data from l series of patients at a single instirution where all nine cases d~cribed had experienced RCA-related aortic dissccrion.3 Whether technical or anatomicaVphysiological differences between rhe left and right cOJonary arrcries are
responsible for this association is unclear. lr is possible that the larger ostiwn of the !eli: main coronary arrery (:md possib~' rhe manner in which it is engaged) may dccrt.-ase rhc incidence of carhercr-indu~ trauma 1'0 rhis vessel.
\'ijith such a small number of cas~ described in the lireratmc to date, there are. in.sufficient data upon which ro base firm recommendation.~ for preve.mion and mar1agement of rhis compli· carion. The options reporred include urgent surgical ince.rvenrioo, placement of an imracoronary stem arthe origin of rhe culprit vessel or conservtttive therapy, :1!> was the CL>C widt our patient. Of dtc cases reported in detail, rhirteen patiems were manag<..xl medimlty~nd the remaining eighr required em.ergem cardiodmracic surgery.
An "extensive" aortic dissection bas arbitrarily been defined in tbe largest reponed series to date as one rhar extends > 40 rom up the .ao,rra from the coronary cusp.3 Applying rhis ddinirion (using angiographic/echocardiographic images. fDr rhis purpose in case reports w:he.re the extent is nor precisely quaruified), seven of eight extensive aortic dis.=ions reponed in the. literature to date have been surgically managed, with 1:\vo dearhs. One p.ttienr with an eXtensive dissection was deemed unsuitable for surger;• (due ~q the extent of dissection and history of p{ior cardiac surgery) and was suctessfidly managed with a conservative smnegy.• However, on this occasion it w~s possible to deploy stents in the culprit coronary artery, which rcsrored vessel patency and normal anrerograde flow ar d1e rime the complication was recognized, t~us preventing tU;yocardial infarction a.nd sealing the
'3~try-dd<:1r fOr th¢. aortic diS~.'ection, Of the rhirreen patients with dissection limited ro < 40 rum of the ascending aorta, twelve haye been medically managed, with no deaths. Surgery was required in one paricm who had suffered a limited dissecrion, but in thi> ipsrance the procedure was indicated primarily fur en1ergenr coronaty bypass and not aortic repair?
93 Vol 16 .. No. 2, Febmarv 2004 - Material may be protected by copyrighi law (Title 17, U.S . Code)
DOYLE and JUERGENS
Stenting at ~be site of d1e presumed entry-door for aortic dissection in the culprit coronal}' ves.~el has been ~ttternpted in thir
teen parients. The stcnr was successfully deployed angiographically in all of d1ese cases. All patients sutVived ro hos
pital discharge, and only 1:\VO patiems required subsequent surge!}' (in one case due co chc developmcm of hemopericardi
um, in rhe other due (0 ili.e very o:rensive nature of me diss<."C·
tion. which bad progressed to rhe aortic bifi.trcacion). Six patients did not uudergo COWQary stenting as part of me
management of mis complication. Four of these patients were
surgically treated, all of whom had suffered an extensive disseotion. "l11e remaining two patients had suffered a limited dissection. In one insrance, .steming was not available as a. treatment (ca.se report from 1973); in me orher, it was nor felt to be indi
cated since rhe culprit coronal}' ve~~el (LAD) was chronically
occluded. All six of d1ese patients survived m hospital discharge.
We did not place a srenr in our patient. With regard ro the remaining two cases in rhc lire.rarure, it is
w1dear wheilier or nor seeming was attempted prior to the emer·
gent b1J.tgery chat was required in both instances. Born of these
patients died An analysis of the case we present :.~nd those published previ
ously suggests that the differences berween spontaneous and cardiac-carherer related dissection of rhe ascending aorta may be
significant, both in rerms of pathophysiology and prognosis,
and consequently in terms of optimal managemenr. The critical difference is possibly rhe condition of rhe aorta prior to the developmern of the imimal tear. In spontaneous aortic dissec
tion, significat1t degeneration of dle media is almost universal,'" fucilitaring d1e propagation of any dissection that may occur. It would appear from the: limited data to date that this may not be rhe case in iattogenic aonic dissection. Anorher notable difference is the entry sire for rhe aortic dissccrion, and d1e setting in which this oc\;urs. The EKt that a coronary-based dissecrion
may be effectively sealed. by scenting within minutes of this complication developing should limit the potential for further
propagariou. It is possible mar ocdusiott (acute or chronic) of the coronary vessel with resultant diminished f:low across the
lesion may also efl:ecrively "seal" the entry door. The excellent results in patienrs with limited dissec.rions and successfiJI srent· ing indicate chat rhe recommended surgictl rrcatmenc for sponcaneou ascending aorcic dissection may indeed be inappropriate in these circum><ances. Careful surveillaoce with optimal blood pressure comrol and appropriate imaging could
be used ro ensure stability and healing of the dissection. Serial
transesophageal echocardiography s~udies certainly showed mis in our parienr.
In d1e case of more extensive dissection, the evidence to date indicates that a surgical approach is preferred (7/8 patients, mor
ralit}' 29% at 30 days). However, the case we report demonsn-ares rhar under unfavorable circumstances extensive ascendjng
aortic dissection may be succes.~fully managed employing a con
servative straregy.
References 1. Kazni T, Washigama N, Bashar AH, et al. Surgical oUtc;ome of a.cure <)'l>C A
•onic dissea:ion: Analysis of rt..k l~ctor~. Ann T1>tJt!JC Su/8"2002;74:75...$1 . 2. Moles VP, Olappuis JJ, Simont:r F, cr aL Aortic dis=riou: as complk:utkm of
perc~ranoota o:ansluminal <;<""'"'1)1 angioplasry. Oui;er CnrditJVtL<<: Di4gn 1992:26:8-11.
3. Dunning DW, Knhn J, Hawicins E, <! ~L Iatrogenic coronar}' a,n:ery dissecciorc~ extending to and involving the aortic tOOl. Cot/)('f (:rtrdiomK flltervenr
2000;5 1 :387 -d93. 4, C..aner AJ, 13rinkcr )A. Di'lSCcrion of the ascending aorta with <;<>ronary angio
graphy. Am} Cardio/1994;73:922-913. 5. Alfonso F, Alm<."lia C Pemandez,Ortiz. A c:t al. Aortic di.<StCrion oo:urring
duriog coronary angiopl:mr- Angingraphic and U';lnscsophageal echocan:lio· gr.tphk findings. Carkt Gtrdioua><: DiPgn 1997;42:41 2.-415.
6. &eJH, Kim Kll, Kim KS. eta!. A c-..ue of aon:ocoronary di=rion a~d <X>tn
plication during percutaueot;S n:a.nslumioal coronary angiopl.uty (PTC..A). lnt} Co.rdit•/1998;66:237-240.
7. Ahmed AA, Mmllldey.tn VS, Webb S\V, eo: .tl. Glue aonnpl:c;ty repair of aor· tic dissc:ction after: coronury angioplasty. An11 Thorar Surg 200 1;72:922-924.
8. f'ande AK, Gosselin G, kclerc Y, <t;al. Aortic dissection wmpJicaring coro-1"")' angioplasty in cystic medial nc:xrosis. Am Htxtrt j 1996;1:) 1 :1221- !223.
9. PentousisD. Toussaim M. Zlt~ng H. et al. Conservative marogemcntii>r an e-xtensive type A aortic dissection complicating coronaty angiopla~ty. j bnw CardioJ2000;l2:320-323.
!0. Se!fein HB, Missri JC, Warner MF, et .aJ. Coronary srenring ror aon:ocoronary disse<;rion foJl<Ywing balloon angiopla~ry. vttlmt Gtrdiulk1IC DiagtJ J 996;3&222-.225.
11 . Mend:tclevski B, Sigw:tn U. MatMgement of aortic dissection complicating coronary inrerwnrinn, Guh<f CmdiaL'iJse DU1g11 1997;42:491.
.12. Ochi M, Y:unau~l\i S, Yajima "f, et al. Aortic dissection extending from the left coronary mcry during pcrmuneous coronary angiopla.<ty. A1111 77Jflr.u· St<rK 19!>6;62: ll SO-l 1 8.2:
13. Geraci AR, Kcishnasw:uni V, Selman MW. AortO<::Oron"')' dissectioll oomplicaring coronary arteriography. J ThorM C!lrdiovasc Surg 197<M5:69~98.
14. Carbon ~G, Lillghei CW, f.dv;-ard JE. Cysrk medial necrosis of chc ascend· ing avrta in rdation rl) age and hyperc<:nsion. Am j Cardin/ 1?7(l;25:4J 1-415.
15. Schlahn:uu1 l]M, Becker AF. Hi!;tologk czhaJlgts in the normal ~ngaom: Implications lor diSS<"Cting aortic aneurysm. Am j Cardiul1977 ;39: 13-20.
[6. Larson tW, Et.l"'"''ls WD. Rt<k flcrors for aortic dissoction: A nc'cropsy '~udy of 16! =·Alii} Car4wl 1984:53:849.
94 The Joun.J.al of Invasive Cardiology
Material may be protected by copyright law (Title 17, U.S. Code)
77
CHAPTER 5
INVOLVEMENT IN STENT REGISTRIES
Introduction
Intracoronary stents were used for the first time in 1987. Important clinical
trials were reported in 1993 demonstrating the superiority of stenting over simple
balloon angioplasty with respect to composite clinical cardiac endpoints. Most
recently drug eluting stents (DES) have become available which reduce the frequency
of restenosis when compared to bare metal stents (BMS). Because of the rapid
obsolescence of each stent with progressing device technology, there is limited data
assessing the long term outcomes of any particular type of stent.
Paper 20 (J Inter Cardiol 1998;11:101-106)
I have been involved in a number of stent registries which have tried to collect
some long term date. With two of these registries I have actually been an author on
the published paper. The first was when I was a Fellow at Stanford University medical
centre, USA. Paper 20 reported the initial and ongoing data over the first 7 years of
experience with the Micro Stent from the original centres participating in the clinical
trial. These data suggested that the AVE Micro stents performed better than the first
generation slotted tube stents in more complex coronary anatomy.
Context and Implications
This work was a multinational, multicentre trial. Whilst I was not involved in the
original trial design, I was involved in data analysis in my role as a Fellow at Stanford
78
University where the overall analysis was performed and the first and senior author
were based. This stent and future design modifications are an integral part of the
current armentarium of interventional cardiologists today. This work was one of my
first experiences in participation in such multicentre registries which taught me a great
deal with respect to the process and benefits of such opportunities. The first and senior
authors of this paper are supportive of me reproducing this work as part of my thesis.
Impact on literature
This article has not been cited in the literature from a journal with an impact factor of
1.185.
Paper 21 (Eurointerv 2007;3:249-255)
The article that represents Paper 21 originated from work I was involved with
when I returned to take up the position as Director of the cardiac catheterisation
laboratories at Liverpool Hospital. This registry evaluated a new generation, thin strut,
stainless steel Tsunami™ coronary stent in a contemporary percutaneous coronary
intervention (PCI) practice across a wide geographical area. We concluded that in the
1437 patients studied across 82 sites, that the Tsunami™ BMS combined excellent
deliverability and safety with low MACE rates that compare favourably with DES. In
addition, longer term follow-up confirmed sustained clinical benefit.
Context and Implications
This work was a multinational, multicentre registry sponsored by a stent
manufacturer. I was a co-investigator of this study and whilst not involved in the
original trial design, I was involved in the investigator meeting and gave input into the
implementation of the trial. Liverpool hospital enrolled a large number of patients into
the registry and whilst I did not write the initial draft of the manuscript, I gave
79
significant feedback to the author of the initial draft. On behalf of the local trial
participants I also presented this paper at the annual Cardiac Society meeting of
Australia and New Zealand (CSANZ) in 2006. This work has enabled opportunities
for networking with co-investigators and may lead to more senior level participation
in future research. There may also be future potential for access to sub-analysis for the
creation of more papers. The corresponding author, Dr Gian Battista Danzi is
supportive of me reproducing this work as part of my thesis.
Impact on literature
According to Journal Citation Reports ® Science Edition (Thomson Reuters, 2012),
this article has been cited twice in the literature to date from a journal with an impact
factor of 3.285 in 2011.

80
PAPER 20
Reprinted from the Journal of Interventional Cardiology 1998;11:101-106
with permission from “John Wiley and Sons”

Microstent to GFX: Experience in 2,325 Patients
EUGENE V. POMERANTSEV, M.D., ANTONIO COLOMBO, M.D., FACC, LOUIS DE LA FUENTE, M.D.,
EBERHARD GRUBE, M.D., CRAIG JUERGENS, M.D., D. MATHEY, M.D., Ph.D., M. SCHALIJ, M.D.,
J. J. GOY, M.D., M.C. MORICE, M.D., J. SCHOFER, M.D., IRA WAN SUGENG, M.D., FACC,
and SIMON H. STERTZER, M.D., FACC, FOR THE AVE MICRO STENT STUDY GROUP
From the Division of Cardiovascular Medicine, Stanford University, Stanford, California; and the AVE Micro Stent Users Group
Introduction
The AVE Micro Stent (Arterial Vascular Engineering, Inc. Santa Rosa, CA, USA) consists of single or multiple subunits configured into zigzag crowns by processing an electropolished 316L circle of stainless steel wire 0.008" (0.2 mm) thick. I-4 The wire crosssection is circular (Micro Stent I and II), or oval (GFX, AVE, Inc.). The lengths of the subunits are 4, 3, or 2 mm (Micro Stent I or II or GFX). The number of subunits (i.e., stent lengths) implanted in this series ranged from 1 to 13. Subunits were originally unconnected (Micro Stent I), but are presently joined by a laser weld, applied helically (Micro Stent II, GFX). Diameters of 2.5, 3.0, 3.5, 4.0 and 4.5 mm, and lengths from 4 to 39 mm have now been assayed to cover a wide variety of coronary segments. The stent radiopacity is generally excellent in both the undeployed and deployed state. When deployed, the actual metallic surface area of the expanded stent is 8.4% (3.5 mm Micro Stent II device). The strut design orients the deployed stent parallel to the blood flow. The device shortens on expansion only by about 2% (3.5 mm Micro Stent II device). The mounted AVE Micro Stent displays a maximal profile of 0.062" (1.65 mm), permitting its passage comfortably through a guiding catheter of 7Fr size. A later iteration of the Micro Stent II and the GFX stent is designed for use with a 6Fr guiding system with an outer
Address for reprints: Simon H. Stertzer, M.D., FACC, Stanford University School of Medicine, H2103 300 Pasteur Drive, Stanford, CA 94305. Fax: (650) 498-7945.
See appendix for the list of participating centers.
diameter of 0.056" to 0.061 ". In addition to its low profile, the stent displays an extraordinary degree of longitudinal flexibility, such that it is expected to track wherever a percutaneous transluminal coronary angioplasty (PTCA) balloon has passed. This article reports the results of initial and ongoing data over the first 7 years of experience with the Micro Stent from 8 original centers participating in the clinical trial.
Methods and Materials
Participating Centers and Investigators. The study involved the joint participation of authors and investigators at 8 participating centers, listed in the Appendix, who carried out all study procedures. The data analysis was performed at Stanford University Hospital.
Deployment Procedure. The AVE Micro Stents are premounted on a compliant balloon delivery system. Although the stent is itself quite radiopaque, the markers on the delivery balloon also indicate the Jimits of the proximal and distal ends of the stent. A special design binds the stent to the underlying low profile balloon. The reliability of the mounting system is such that the stent is sheathless. Micro Stents and the GFX stents are available as over the wire or rapid exchange systems.
Some investigators have utilized the compliance aspects of the delivery system to deploy the Micro Stent at upwards of 10 atm, occasionally deploying up to 14 atm. When such pressure-volume relationships are attained, postdilatation by high pressure noncompliant
Vol. 11, No.2, 1998 Journal of Interventional Cardiology 101

POMERANTSEV, ET AL.
balloon was usually unnecessary. Nevertheless, intracoronary ultrasound techniques (IVUS) have shown that in some lesions that are inadequately treated, the strut apposition may be suboptimal, so that repeat higher pressure balloon dilatation does indeed improve the IVUS appearance. This phenomenon is similar to IVUS findings for other metallic stents. S-6
Because of early isolated reports of short length (e.g., 6 mm) stent displacement by an IVUS sheath or an angioplasty balloon,7 it is recommended that when deploying a device < 8 mm in length, IVUS is best avoided and high pressure postdilatation carried out. Although this short stent displacement may be the operator error in some cases, it is often due to the rigid edge of the IVUS sheath itself.
The deployment procedure in this series was performed with patients generally on oral aspirin administration (325 mg), which was continued indefnitely postprocedure ( 100-325 mg). The use of calcium antagonists was reported in 60% of cases, and ticlopidine (500 mg daily) for 3 months was reported in 76.5% patients. Coumadin (lnfimed. Inc., New York. NY, USA) under international normalized ratio (INR) control was used in 3% of patients representing early cases (e.g., prior to 1994 ). Heparin was used only during the procedure to maintain an activated clotting time (ACT) > 300 seconds.
Image Archiving and Processing. Coronary artery images of AVE Micro Stent cases were captured and archived digitally using the Apollo TM Image Manager (Seattle Systems. Bellevue, W A, USA). Cine video conversion was used for angiographic archival. Resolution of the Sony CCD camera with an optical zoom in an Arripro 35 cine video converter (Arnold & Richter Cine Technik GmbH. Munich, Germany) was 3.8 line pairs/mm, or better. For long-term archivaL highly opacified nonmagnified images for each view (usually diastolic) were selected. Analog video images were digitized using the Oculus-F/64 frame grabber board (Coreco Inc., St. Laurent, Quebec). If any coronary artery lesion was obscured at the end of diastole. the worst phasic image was used. Optically magnified pictures of the diseased segment were stored.
Quantative Coronary Arteriography. Quantitative coronary arteriography (QCA) was performed using the same hardware and QCA plus package developed and validated at Stanford University.8
-10 A single
investigator, blinded to the procedure technique. performed QCA in all cases. Each treated segment was analyzed at the following stages: preprocedure. after
the stent deployment, and after high pressure balloon dilatation. The measurements of the inflated delivery balloon and the high pressure balloon were taken. The image of a catheter was used for calibration. For subsequent analysis, minimal luminal diameter (MLD), mean diameter of the treated segment (D mean), lesion length (L), normal reference diameter (D ref). and percent diameter stenosis (%D) were used. Balloon to artery ratio (B/A) was calculated using the largest used and measured balloon and preprocedure D ref.
as: I. The percent of elastic recoil (%ELR) was defined
%ELR = DBalloon - MLDpost X 100 DBalloon
where DBalloon is the average diameter of the largest used balloon, MLDpost measured immediately postprocedure.
2. The procedural gain (PG%) was expressed as
o/oPG = MLDpost - MLDpre X I OO Drefpre
3. The amount of stretch (%S) was expressed as
o/oS = DBalloon - MLDpre X 100
Drefpre
Qualitative Lesion Description. A panel of two investigators. blinded to procedural technique, performed qualitative description of the lesion morphology. It included classification into eccentric, concentric, or total occlusion subsets. Calcifications at the lesion site and presence of border irregularity were assessed. A lesion location was considered to be on a bend point if the diseased segment was angled more than 90°. Visual estimates of discrete and diffuse disease. as well as the appearance of signifcant side branches. were recorded. Intraluminal filling defects or contrast staining before the intracoronary interventions were considered as probable signs of an intracoronary thrombus.
In addition, lesions were classifed according to Ambrose and ACC/AHA schemes. In the Ambrose 11 classification scheme, class I were concentric. smooth, focal lesions: class II. uncomplicated eccentric stenoses, focal. with smooth borders; class IlL complicated lesions. eccentric with irregular and/or overhanging borders: class IV, long (> 2.5 em) lesions, composed of several sequential narrowings counting as one complex lesion. The ACC/AHA classification was subdivided by using B 1 (when only one B-criterion was present)
102 Journal of lnterventional Cardiology Vol. II, No.2. 1998
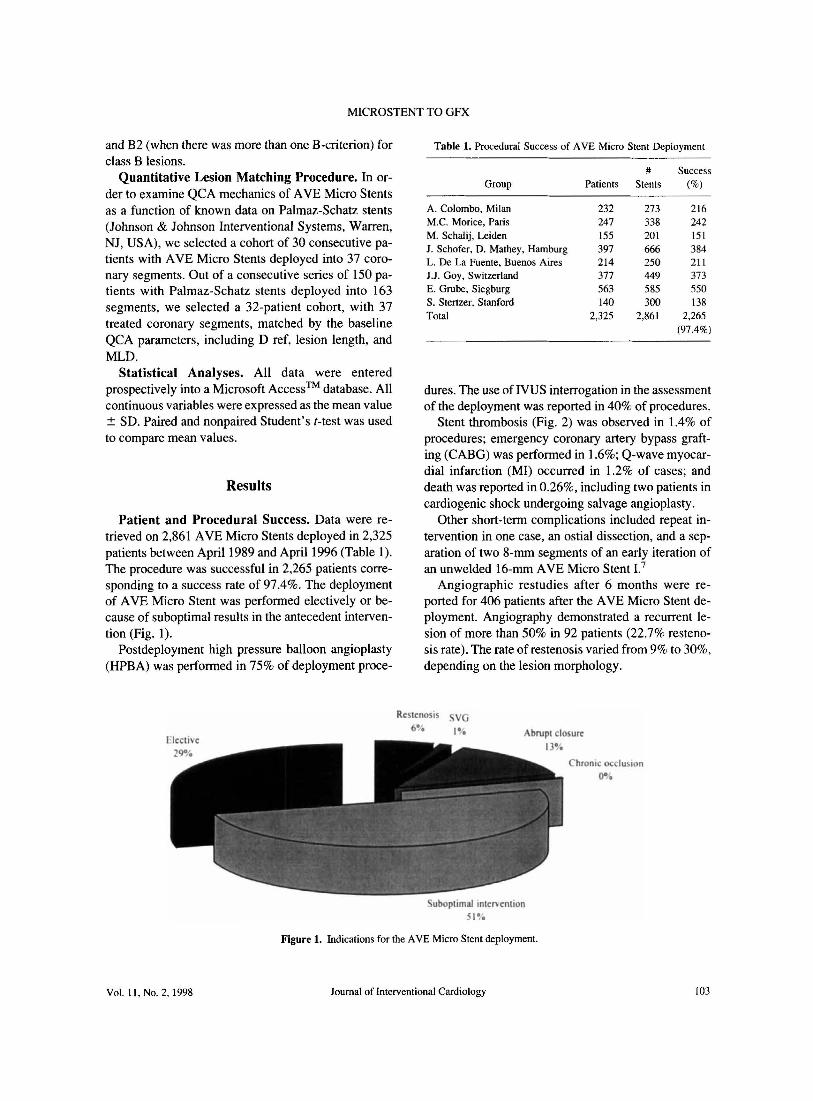
MICROSTENT TO GFX
and B2 (when there was more than one B-criterion) for class B lesions.
Quantitative Lesion Matching Procedure. In order to examine QCA mechanics of AVE Micro Stents as a function of known data on Palmaz-Schatz stents (Johnson & Johnson Interventional Systems, Warren, NJ, USA), we selected a cohort of 30 consecutive patients with AVE Micro Stents deployed into 37 coronary segments. Out of a consecutive series of 150 patients with Palmaz-Schatz stents deployed into 163 segments, we selected a 32-patient cohort, with 37 treated coronary segments, matched by the baseline QCA parameters, including D ref, lesion length, and MLD.
Statistical Analyses. All data were entered prospectively into a Microsoft Access TM database. All continuous variables were expressed as the mean value ± SD. Paired and nonpaired Student's t-test was used to compare mean values.
Results
Patient and Procedural Success. Data were retrieved on 2,861 AVE Micro Stents deployed in 2,325 patients between April 1989 and April 1996 (Table I). The procedure was successful in 2,265 patients corresponding to a success rate of 97.4%. The deployment of AVE Micro Stent was performed electively or because of suboptimal results in the antecedent intervention (Fig. 1).
Postdeployment high pressure balloon angioplasty (HPBA) was performed in 75% of deployment proce-
Table I. Procedural Success of AVE Micro Stent Deployment
# Success Group Patients Stents (%)
A. Colombo, Milan 232 273 216 M.C. Morice, Paris 247 338 242 M. Schalij, Leiden 155 201 151 J. Schofer, D. Mathey, Hamburg 397 666 384 L. De La Fuente, Buenos Aires 214 250 211 J.J. Goy, Switzerland 377 449 373 E. Grube, Siegburg 563 585 550 S. Stertzer, Stanford 140 300 138 Total 2,325 2,861 2,265
(97.4%)
dures. The use of IVUS interrogation in the assessment of the deployment was reported in 40% of procedures.
Stent thrombosis (Fig. 2) was observed in 1.4% of procedures; emergency coronary artery bypass grafting (CABG) was performed in 1.6%; Q-wave myocardial infarction (MI) occurred in 1.2% of cases; and death was reported in 0.26%, including two patients in cardiogenic shock undergoing salvage angioplasty.
Other short-term complications included repeat intervention in one case, an ostial dissection, and a separation of two 8-mrn segments of an early iteration of an unwelded 16-mm AVE Micro Stent I.7
Angiographic restudies after 6 months were reported for 406 patients after the AVE Micro Stent deployment. Angiography demonstrated a recurrent lesion of more than 50% in 92 patients (22.7% restenosis rate). The rate of restenosis varied from 9% to 30%, depending on the lesion morphology.
Restenosis VG
brupt closure
Chronic occlus1 n
oe~
Figure I. Indications for the AVE Micro Stent deployment.
Vol. II, No.2, 1998 Journal of Interventional Cardiology !03
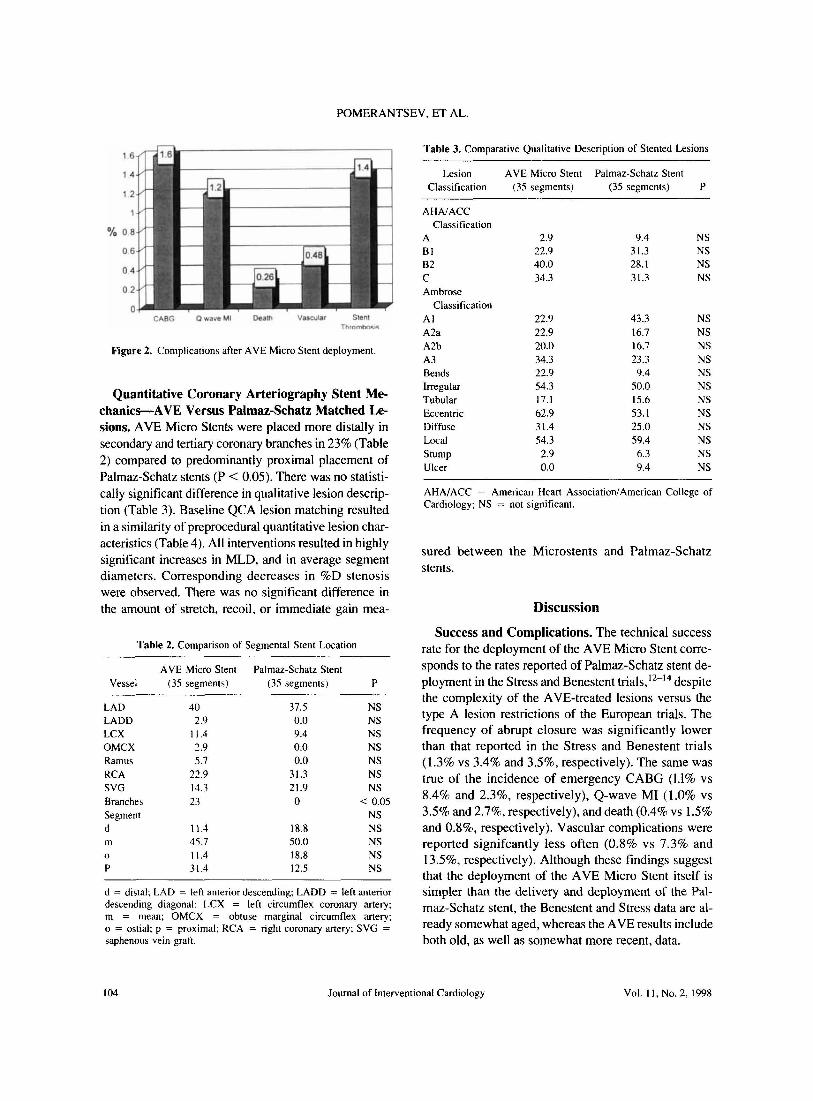
POMERANTSEV. ET AL.
% o
0
0
0
Figure 2. Complications after AVE Micro Stent deployment.
Quantitative Coronary Arteriography Stent Mechanics--AVE Versus Palmaz-Schatz Matched Lesions. AVE Micro Stents were placed more distally in secondary and tertiary coronary branches in 23% (Table 2) compared to predominantly proximal placement of Palmaz-Schatz stents (P < 0.05). There was no statistically significant difference in qualitative lesion description (Table 3). Baseline QCA lesion matching resulted in a similarity of preprocedural quantitative lesion characteristics (Table 4 ). All interventions resulted in highly significant increases in MLD, and in average segment diameters. Corresponding decreases in %0 stenosis were observed. There was no significant difference in the amount of stretch, recoil, or immediate gain mea-
Table 2. Comparison of Segmental Stent Location
AVE Micro Stent Palmaz-Schatz Stent Vessel ( 35 segments) (35 segments) p
LAD 40 37.5 NS LADD 2.9 0.0 NS LCX 11.4 9.4 NS OMCX 2.9 0.0 NS Ramus 5.7 0.0 NS RCA 22.9 31.3 NS SVG 14.3 21.9 NS Branches 23 0 < 0.05 Segment NS d 11.4 18.8 NS m 45.7 50.0 NS 0 11.4 18.8 NS p 31.4 12.5 NS
d = distal; LAD = left anterior descending; LADD = left anterior descending diagonal; LCX = left circumflex coronary artery; m = mean; OMCX = obtuse marginal circumflex artery; o = ostial; p = proximal: RCA = right coronary artery: SVG = saphenous vein graft.
Table 3. Comparative Qualitative Description of Stented Lesions
Lesion AVE Micro Stent Palmaz-Schatz Stent Classification (35 segments) (35 segments) p
AHNACC Classification
A 2.9 9.4 NS Bl 22.9 31.3 NS 82 40.0 28.1 NS c 34.3 31.3 NS Ambrose
Classification AI 22.9 43.3 NS A2a 22.9 16.7 NS A2b 20.0 16.7 NS A3 34.3 23.3 NS Bends 22.9 9.4 NS Irregular 54.3 50.0 NS Tubular 17.1 15.6 NS Eccentric 62.9 53.1 NS Diffuse 31.4 25.0 NS Local 54.3 59.4 NS Stump 2.9 6.3 NS Ulcer 0.0 9.4 NS
AHA/ACC = American Heart Association/American College of Cardiology; NS = not significant.
sured between the Microstents and Palmaz-Schatz stents.
Discussion
Success and Complications. The technical success rate for the deployment of the AVE Micro Stent corresponds to the rates reported of Palmaz-Schatz stent deployment in the Stress and Benestent trials, 12
-14 despite
the complexity of the AVE-treated lesions versus the type A lesion restrictions of the European trials. The frequency of abrupt closure was significantly lower than that reported in the Stress and Benestent trials (1.3% vs 3.4% and 3.5%, respectively). The same was true of the incidence of emergency CABG (1.1% vs 8.4% and 2.3%, respectively), Q-wave MI (1.0% vs 3.5% and 2.7%, respectively), and death (0.4% vs 1.5% and 0.8%, respectively). Vascular complications were reported signifcantly less often (0.8% vs 7.3% and 13.5%, respectively). Although these findings suggest that the deployment of the AVE Micro Stent itself is simpler than the delivery and deployment of the Palmaz-Schatz stent, the Benestent and Stress data are already somewhat aged, whereas the AVE results include both old, as well as somewhat more recent, data.
104 Journal of lnterventional Cardiology Vol. II, No.2, 1998

MICROSTENT TO GFX
Table 4. Comparative Quantitative Coronary Arteriography Data
MLD pre, mm MLD post, mm p
D avg, pre, mm D avg, post, mm p
length pre, mm D ref, pre, mm D ref, post, mm p
% D pre % D post p
stretch, % recoil,% immediate gain, %
AVE Micro Stents
(n = 35)
M SD 1.2 0.4 2.5 0.6
< 0.01 2.3 0.6 3.0 0.4
< 0.0 20.3 13.9
3.1 0.7 3.2 0.8
NS 61.6 9.6 25.7 11.0
< 0.01 51.5 43.5 11.1 47.9 62.6 22.9
Palmaz-Schatz Stent
(n = 35)
M SD 1.2 0.4 2.5 0.7
< 0.01 2.3 0.5 3.0 0.7
< 0.01 18.5 10.6 3.0 0.7 3.1 0.7
NS 59.4 10.1 21.3 12.9
< 0.01 46.7 34.6 13.9 47.3 60.6 38.9
p
NS NS
NS NS
NS NS NS
NS NS
NS NS NS
D avg = mean diameter of the treated segment; D ref = reference diameter of treated segment; MLD = minimal luminal diameter; SD = standard deviation.
AVE Microstents were generally deployed into lesions with more complicated morphology. In this regard, Nakagawa et al. 15 reported a series of 64 patients with 69 AVE Micro Stents deployed in anatomical situations inappropriate for the delivery and deployment of the Palmaz-Schatz stent, or after the deployment failure of the latter. The vessels in Nakagawa's series were generally tortuous, and the stenoses located in more distal coronary segments. This group demonstrated a lower technical success rate of 87%, with an acute stent closure rate of 1.6%. The incidence of emergency CABG was 3.1 %; acute MI, 1.5%; death, 4.7%; and vascular complications, 4.7%. The Nakagawa study 15 supports the conclusion that the deployment of AVE Micro Stent is effective even in complex lesion settings. Moreover, in a recent study in seriously unstable patients, Anwar et al.2 observed that in 68 patients (77 treated segments), there was a procedural success rate of 98.5%, with major complications seen only in 2.9%.
Recurrence Rates. Comparisons of restenosis rates between randomized and nonrandomized trials are not justifed. The Stanford group demonstrated a restenosis rate of 14.1 %. M. Schalij eta!., 16 in a consecutive series of 85 patients with 100% angiographic follow-up at 6 months, demonstrated a 12% rate of recurrence assessed by QCA. These data are more encouraging than the re-
currence rates of PICA (32%-57%), 12-
14•17
•18 direc
tional coronary atherectomy (32%-50%), 18-
21 or the Stanford series of high speed rotational atherectomy (32%). The overall rate of recurrence of 22.7% in this wide lesion spectrum compares favorably to the Stress (32% ), balloon expandable stent implantation with balloon angioplasty (Benestent) I (22%), and Benestent II (13%) data for type A lesions (Fig. 3). Yet, as stated, this is of little relevance, because Benestent I and II and Stress were limited to focal lesions, whereas the AVE cases over this 7-yearperiod were characterized by complicated lesion morphology located in distal segments of the coronary tree, in stable and unstable patients, as well as in the setting of acute MI. In the United States, the recent! y completed Study of Microstent' s Ability to Limit Restenosis Trial (SMART) ultimately does address and confmn the equivalent efficacy of the Micro Stent versus the Johnson & Johnson lnterventional Systems device (Warren, NJ, USA) in a fully randomized, prospective manner. However, the SMART data are limited to short accessible Benestent type stenosis.
QCA Mechanics. Comparative analysis of a cohort of 35 QCA matched segments treated with PalmazSchatz stent deployments versus 35 segments treated with AVE Micro Stents demonstrated no difference in qualitative lesion descriptors. AVE Micro Stents were placed into more remote and tortuous complicated coronary locations. There was no difference in the
B 811 AVE AVE S Schalij, HSRA DCA 96
Figure 3. Comparative restenosis rates in the Benestent trial (B), Stress trial (S), Benestent II trial (BII), reported resenosis rate AVE Micro Stents (AVE), AVE Mico Stents restenosis rate for the Stanford Series (AVE S), AVE Micro Stents restenosis rate reported by M.J. Schalij et al. (Schalij, 96), HSRA Multicenter registry (HSRA), and Directional Coronary Atherectomy CAVEAT study (DCA). CA YEA T = Coronary Angioplasty Versus Excisional Atherectomy trial; DCA = directional coronary atherectomy; HSRA = high speed rotational atherectomy.
Vol. II, No.2, 1998 Journal of lnterventional Cardiology 105

POMERANTSEV, ET AL.
amount of immediate gain. stretch, and elastic recoil. This study demonstrated excellent scaffolding properties for both stent models.
Conclusions
Deployment of AVE Micro Stents in distal and tortuous coronary segments as well as in clinically unstable and acute MI patients entails high success and low complication rates. Scaffolding properties of AVE Micro Stents confirm the SMART data and are comparable to the Palmaz-Schatz stent. Recurrence rates may be influenced by lesion morphology and operator deployment differences, but the passage of the AVE device in complex anatomical situations may extend its versatility beyond that previously reported for slotted tube stents.
Appendix
The following institutions and investigators participated in the AVE Micro Stent study: A. Colombo in Milan, Italy; L. De La Fuente in Buenos Aires, Argentina; J.J. Goy in Lausanne, Switzerland; E. Grube in Siegburg, Germany; M.C. Morice in Paris, France; M. Schalij and J.H.C. Reiber in Leiden, Holland; J. Schofer and D. Mathey in Hamburg, Germany; and S.H. Stertzer and E.V. Pomerantsev in Stanford, California, USA.
References
I. Ozaki Y. Keane D. Ruygrok P, et al. Acute clinical and angiographic results with the new AVE Micro coronary stent in bailout management. Am J Cardiol 1995;76: I I 2-1 I 6.
2. Anwar A. Stertzer SH, Hidalgo BO, et al. Coronary stenting with a new ultra-short balloon expandable device: Early and late animal results. Cathet Cardiovasc Diagn 1994;3I:85-89.
3. Stertzer SH, Pomerantsev EV. AVE Micro Stcnt II. In: P.W. Serruy, ed. Handbook of Coronary Stents. Rotterdam Thoraxcentre lnterventional Cardiology Group. London, United Kingdom, Martin Dunitz Ltd., 1997. pp. 41-49.
4. Steztzer S.H., Pomerantsev E. V. The AVE Micro Stents ™. In: J.H.C. Reiber. E. E. VanDer Wall, eds. Developments in Cardiovascular Medicine. Volume 186. Dodrecht/Boston/London. Kluwer Academic Publishers, I996. pp. 15-30.
5. Goldberg SL. Colombo A. Nakamura S, et al. Benefit of intra-
coronary ultrasound in the deployment of Palmaz-Schatz stents. JAm Coli Cardiol I994;24:996-1003.
6. Colombo A, Hall P, Nakamura S. et al. Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation I995;91:I676-1688.
7. Wong P, Leung WH, Wong CM. Migration of the AVE Micro coronary stent. Cathet Cardiovasc Diagn 1996;38:267-273.
8. Leung WH, Sanders W. Alderman EL. Coronary artery quantitation and data management system for paired cineangiograms. Cathet Cardiovasc Diagn 1991 ;24: 121-134.
9. Leung WH, Demopulos PA, Alderman EL, et al. Evaluation of catheters and metallic catheter markers as calibration standard for measurement of coronary dimension. Cathet Cardiovasc Diagn 1990;21:148-153.
I 0. Leung WH, Stadius ML, Alderman EL. Determinants of normal coronary artery dimensions in humans. Circulation 1991 ;84:2294-2306.
II. Ambrose JA, Winters SL, Arora RR, et al. Angiographic evolution of coronary artery morphology in unstable angina. J Am Coli Cardiol1986;7:472-478.
12. Serruys PW, de Jaegere P, Kiemeneij F, et al. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331 :489-495.
13. Serruys PW, Emanuelsson H, van der Giessen W, et al. Heparin-coated Palmaz-Schatz stents in human coronary arteries. Early outcome of the Benestent-11 Pilot Study. Circulation 1996;93:412-422.
14. Fischman DL, Leon MB. Bairn DS, et al. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators. N Engl 1 Med I 994;331 :496-501.
15. Nakagawa Y, Nakano Y, Tamura T. et al. Initial clinical experience and 6 months follow-up with AVE Micro Stent. Jpn J Interv Cardiol 1996; II :399-405.
16. Schalij MJ. Savalle LH. Tresukosol D, et al. The Micro Stent I. Initial results and six months follow-up. (abstract) J Invasive Cardiol, 1994;8:57.
I 7. Nakamura Y. Yamaoka 0. Uchida K, et al. Pravastatin reduces restenosis after coronary angioplasty of high grade stenotic lesions: Results of SHIPS (Shiga Pravastatin Study). Cardiovasc Drugs Ther 1996; 10:475-483.
18. Holmes DR Jr, Garratt KN, Isner JM, et al. Effect of subintimal resection on initial outcome and restenosis for native coronary lesions and saphenous vein graft disease treated by directional coronary athcrectomy. A report from the CAVEAT I and II investigators. Coronary Angioplasty Versus Excisional Atherectomy Trial. 1 Am Coli Cardiol 1996;28:645--651.
19. Holmes DR Jr. Topol EJ, Adelman AG, et al. Randomized trials of directional atherectomy: Implications for clinical practice and future investigation. JAm Coli Cardioll994;24:431-439.
20. Levine GN, Jacobs AK, Keeler GP, et al. Impact of diabetes mellitus on percutaneous revascularization (CAVEAT-I). CAVEAT-I Investigators. Coronary Angioplasty Versus Excisional Atherectomy Trial. Am J Cardiol I 997;79:748-755.
21. Umans VA WM, Robert A, Foley D. et al. Clinical, histologic and quantitative angiographic predictors of restenosis after directional coronary atherectomy: A multivariate analysis of the renarrowing process and late outcome. 1 Am Coli Cardiol 1994:23:49-58.
106 Journal of Interventional Cardiology Vol. II, No.2, 1998

81
PAPER 21
Reprinted from Eurointervention 2007;3:249-255 with permission from
Europa Edition

A novel ultra-thin bare metal stent (BMS): results from a worldwide registry
Didier Blanchard1, MD; Gian Battista Danzi2*, MD; Philip Urban3, MD, FESC; Morris Moseri4, MD, FESC;Craig Juergens5, MD, FACC; Philip Guyon6, MD; Bernd Nowak7, MD, FESC; Damras Tresucosol8, MD,FAPSIC; Maarten J. Suttorp9, MD, PhD; Ahmad Farshid10, MD; Ran Kornowski11, MD, FACC; Eulogio Garcia12, MD; Richard Yeend13, MD; Hirofumi Nagai14, PhD; Dragica Paunovic15, MD; on behalf of MATSURI investigators
1. St-Gatien Clinic, Tours, France; 2. Poliambulanza, Brescia, Italy (currently Ospedale Maggiore Policlinico, Milan, Italy);
3. Hôpital de La Tour, Geneva, Switzerland; 4. Hadassah Hebrew University Medical Center, Jerusalem, Israel (currently Meir
Medical Center, Kfar Saba); 5. Liverpool Hospital, Sydney, Australia; 6. Centre Cardiologique du Nord, Saint-Denis, France;
7. Cardiovascular Center Bethanien, Frankfurt/Main, Germany; 8. Siriraj Hospital, Bangkok, Thailand; 9. Sint-Antonius
Hospital, Nieuwegein, The Netherlands; 10. Canberra Hospital, Canberra, Australia; 11. Rabin Medical Center, Petah-Tikva,
Isreal; 12. Hospital Gregorio Maranon, Madrid, Spain; 13. Royal Adelaide Hospital, Adelaide, Australia; 14. Terumo
Corporation, Tokyo, Japan; 15. Terumo Europe, Leuven, Belgium
- 249 -
AbstractAims: To evaluate a new generation, thin strut, stainless steel Tsunami™ coronary stent in a contemporary
percutaneous coronary intervention (PCI) practice across a wide geographical area.
Methods and results: Patients (n=1,437) with single or multiple vessel coronary artery disease undergoing
PCI in 82 sites in Europe, Asia, and Australia were enrolled in the MATSURI registry. Clinical follow-ups
were scheduled at 1, 6 and 18 months. Primary endpoint was major adverse cardiac events (MACE) rate
at 6 months.
Diabetes was present in 25% of patients, 40% had unstable angina, 54% multivessel disease and 31%
previously underwent PCI/CABG. Procedural success was achieved in 98.1% of patients. MACE rate was
1.8%, 7.3%, and 12.6% for 1, 6 and 18 month follow-up, respectively. At 6 months, the incidence of car-
diac death, MI and TLR were 1%, 1.9% and 4.5% respectively, and confirmed stent thrombosis occurred
in 0.2% of patients. Lower risk patients (43% of registry population) had six months MACE free survival of
96.7%.
Conclusions: Based on the results of this large registry we can conclude that the Tsunami™ BMS com-
bines excellent deliverability and safety for all, together with very low MACE rates for lower risk patients.
Long term follow-up confirmed sustained clinical benefit.
KEYWORDSBare metal stent
(BMS), coronary
disease, major adverse
cardiac events,
long term follow-up
Clinical research
* Corresponding author: Ospedale Maggiore Policlinico, Divisione di Cardiologia, Via Francesco Sforza 35, 20122 Milano, Italy
E-mail: [email protected]
© Europa Edition 2007. All rights reserved.
EuroInterv.2007;3:249-255 published online ahead of print 22 May 2007
This study was supported by Terumo Europe N.V. Leuven Belgium.
None of the authors have declared any conflict of interests related to the content of this manuscript with the exception of Hirofumi Nagai
and Dragica Paunovic both of whom are employees of Terumo.

- 250 -
MATSURI registry, short and long term results
IntroductionOver the last decade coronary stents have revolutionised the field of
interventional cardiology and have become the default treatment for
percutaneous coronary intervention. However, the long-term suc-
cess of coronary stenting is hampered by exaggerated neointimal
formation resulting in in-stent restenosis. A large body of evidence
has demonstrated that stents coated with antiproliferative drugs are
the most effective way to address this problem. The efficacy of drug
eluting stents (DES) has been established in comparative studies
versus the older generation of bare metal stents (BMS) and striking
differences, mainly related to reduction of repeat revascularisation,
have completely overshadowed the latest developments in bare
metal stent technology1-4. General use of drug eluting stents, howev-
er, remains limited by their high cost and need for extended dual
antiplatelet therapy. Moreover, the antiproliferative properties of cur-
rently available DESs prevent or delay vessel healing which could be
responsible for the late stent thrombosis frequently associated with
increased incidence of myocardial infarction and death5-10.
Healthcare funding agencies and interventional cardiologists face the
challenge of properly selecting patients for this promising treatment.
Therefore, it is essential to generate further scientific evidence to iden-
tify patients/lesions with increased risk for in-stent restenosis and
contribute to adequate selection of the treatment modalities for each
individual patient. Likewise, the search for a better BMS design which
can be used as a platform for DES development is of fundamental
importance for further refinement of this breakthrough technology.
The primary aim of this large, prospective, multicentre, multi-conti-
nent, registry was to evaluate the performance of newly developed,
thin strut, Tsunami™ (Terumo Corp. Tokyo, Japan) coronary stent
system in daily clinical practice across a wide geographical area.
Methods
Patient population
Patients who were at least 18 year of age, had stable, or unstable angi-
na or silent ischaemia, were considered for enrolment. Patients were
excluded if they had left main disease, left ventricular ejection fraction
of less than 30%, bifurcation requiring stenting of a diseased side
branch, acute myocardial infarction in the preceding 48 hours, or intol-
erance to stainless steel, aspirin, clopidogrel, ticlopidine, heparin,
or contrast media. The investigators were advised to use Tsunami™
for all consecutive patients complying with inclusion criteria.
Written informed consent was obtained from all patients prior to
their inclusion into the study.
Lesions were treated with the use of standard interventional tech-
nique. Dual antiplatelet therapy with clopidogrel (75 mg once daily),
or ticlopidine (250 mg twice a day), supplemented with 80-150 mg
aspirin was recommended for four weeks. Aspirin alone was recom-
mended for at least six months.
The Tsunami™ stent system
The Tsunami™ stent system is a stainless steel tubular stent with a
double linked diamond cell structure, pre-mounted on a semi-com-
pliant, low profile balloon. Low strut thickness of only 80 µm and
short overhang of the balloon over the stent edges are designed to
reduce vessel wall injury.11,12
The Tsunami™ coronary stent system was available in 2.0, 2.25, 2.5,
3.0, 3.5 and 4.0mm diameters and 10, 15, 20, 25 and 30mm lengths.
Endpoints of the registry
The primary endpoint of this registry was a composite of major
adverse cardiac events (MACE) at six months after the procedure.
Secondary endpoints were angiographic and procedural success
rates, MACE rate at 18 months, target lesion revascularisation (TLR)
at six months and in-stent thrombosis at 30 days.
Definitions
MACE was defined as composite of cardiac death, myocardial
infarction (MI), coronary artery bypass grafting (CABG) or percuta-
neous target lesion revascularisation (TLR). Deaths were classified
as cardiac or noncardiac. Deaths from undetermined causes were
reported as cardiac. MI was defined either as the development
of pathological Q-waves in at least two contiguous leads with or
without elevated cardiac enzymes or, in the absence of pathological
Q-waves, as an elevation in creatinine kinase levels to greater than
twice the upper limit of normal in the presence of an elevated level
of CK-MB fraction. Angiographic success was defined as final resid-
ual stenosis of the target site < 50% using the assigned treatment
device alone. Procedural success was defined as angiographic suc-
cess without in-hospital major adverse cardiac events.
Stent thrombosis was defined as angiographically confirmed throm-
bus within the stented vessel or any death (without other obvious
cause), or Q-wave myocardial infarction in the territory of the stent-
ed segment within the first 30 days. It was classified as acute if it
occurred within the first 24 hours, subacute up to 30 days, and late
after 30 days. All reported re-interventions inside the stent and
5 mm proximally and distally were classified as TLRs. Other repeat-
ed PCIs in the same vessel were recorded as non-TLR target vessel
revascularisations (TVR). An independent clinical event committee
(see appendix) adjudicated all events.
Quantitative coronary angiograms obtained before and after the proce-
dure were analysed at the independent core laboratory (Corisis, Paris,
France) using a validated edge detection system (Medis-H, CMS 4.0,
Leiden, The Netherland). Baseline angiographic variables included
reference vessel diameter (RVD), minimal luminal diameter (MLD),
percent diameter stenosis, lesion length and lesion complexity as
defined by the American Heart Association/American College of
Cardiology (AHA/ACC) classification. In-stent diameter stenosis, RVD,
MLD, acute gain (final MLD-pre MLD) and the presence of dissection
were noted post-procedure. No systematic angiographic follow-up was
scheduled for this study. However, CD-ROMS for all performed repeat
angiographic procedures were provided by the sites, analysed by the
same core laboratory and adjudicated by clinical event committee.
Follow-up
All patients were scheduled to have one- and six-month clinical
follow-up. 656 patients enrolled in 34 hospitals were subsequently
re-consented for long term follow-up which took place at
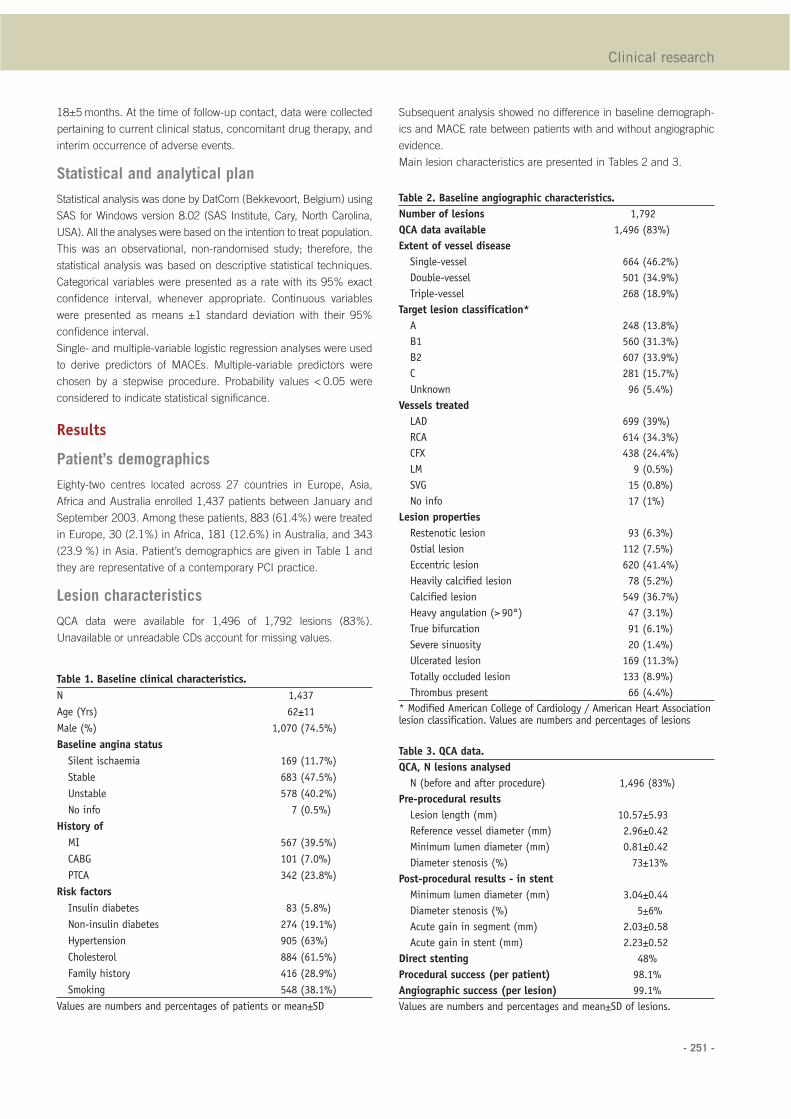
- 251 -
18±5 months. At the time of follow-up contact, data were collected
pertaining to current clinical status, concomitant drug therapy, and
interim occurrence of adverse events.
Statistical and analytical plan
Statistical analysis was done by DatCom (Bekkevoort, Belgium) using
SAS for Windows version 8.02 (SAS Institute, Cary, North Carolina,
USA). All the analyses were based on the intention to treat population.
This was an observational, non-randomised study; therefore, the
statistical analysis was based on descriptive statistical techniques.
Categorical variables were presented as a rate with its 95% exact
confidence interval, whenever appropriate. Continuous variables
were presented as means ±1 standard deviation with their 95%
confidence interval.
Single- and multiple-variable logistic regression analyses were used
to derive predictors of MACEs. Multiple-variable predictors were
chosen by a stepwise procedure. Probability values < 0.05 were
considered to indicate statistical significance.
Results
Patient’s demographics
Eighty-two centres located across 27 countries in Europe, Asia,
Africa and Australia enrolled 1,437 patients between January and
September 2003. Among these patients, 883 (61.4%) were treated
in Europe, 30 (2.1%) in Africa, 181 (12.6%) in Australia, and 343
(23.9 %) in Asia. Patient’s demographics are given in Table 1 and
they are representative of a contemporary PCI practice.
Lesion characteristics
QCA data were available for 1,496 of 1,792 lesions (83%).
Unavailable or unreadable CDs account for missing values.
Subsequent analysis showed no difference in baseline demograph-
ics and MACE rate between patients with and without angiographic
evidence.
Main lesion characteristics are presented in Tables 2 and 3.
Clinical research
Table 1. Baseline clinical characteristics.
N 1,437
Age (Yrs) 62±11
Male (%) 1,070 (74.5%)
Baseline angina status
Silent ischaemia 169 (11.7%)
Stable 683 (47.5%)
Unstable 578 (40.2%)
No info 7 (0.5%)
History of
MI 567 (39.5%)
CABG 101 (7.0%)
PTCA 342 (23.8%)
Risk factors
Insulin diabetes 83 (5.8%)
Non-insulin diabetes 274 (19.1%)
Hypertension 905 (63%)
Cholesterol 884 (61.5%)
Family history 416 (28.9%)
Smoking 548 (38.1%)
Values are numbers and percentages of patients or mean±SD
Table 2. Baseline angiographic characteristics.
Number of lesions 1,792
QCA data available 1,496 (83%)
Extent of vessel disease
Single-vessel 664 (46.2%)
Double-vessel 501 (34.9%)
Triple-vessel 268 (18.9%)
Target lesion classification*
A 248 (13.8%)
B1 560 (31.3%)
B2 607 (33.9%)
C 281 (15.7%)
Unknown 96 (5.4%)
Vessels treated
LAD 699 (39%)
RCA 614 (34.3%)
CFX 438 (24.4%)
LM 9 (0.5%)
SVG 15 (0.8%)
No info 17 (1%)
Lesion properties
Restenotic lesion 93 (6.3%)
Ostial lesion 112 (7.5%)
Eccentric lesion 620 (41.4%)
Heavily calcified lesion 78 (5.2%)
Calcified lesion 549 (36.7%)
Heavy angulation (> 90°) 47 (3.1%)
True bifurcation 91 (6.1%)
Severe sinuosity 20 (1.4%)
Ulcerated lesion 169 (11.3%)
Totally occluded lesion 133 (8.9%)
Thrombus present 66 (4.4%)
* Modified American College of Cardiology / American Heart Associationlesion classification. Values are numbers and percentages of lesions
Table 3. QCA data.
QCA, N lesions analysed
N (before and after procedure) 1,496 (83%)
Pre-procedural results
Lesion length (mm) 10.57±5.93
Reference vessel diameter (mm) 2.96±0.42
Minimum lumen diameter (mm) 0.81±0.42
Diameter stenosis (%) 73±13%
Post-procedural results - in stent
Minimum lumen diameter (mm) 3.04±0.44
Diameter stenosis (%) 5±6%
Acute gain in segment (mm) 2.03±0.58
Acute gain in stent (mm) 2.23±0.52
Direct stenting 48%
Procedural success (per patient) 98.1%
Angiographic success (per lesion) 99.1%
Values are numbers and percentages and mean±SD of lesions.
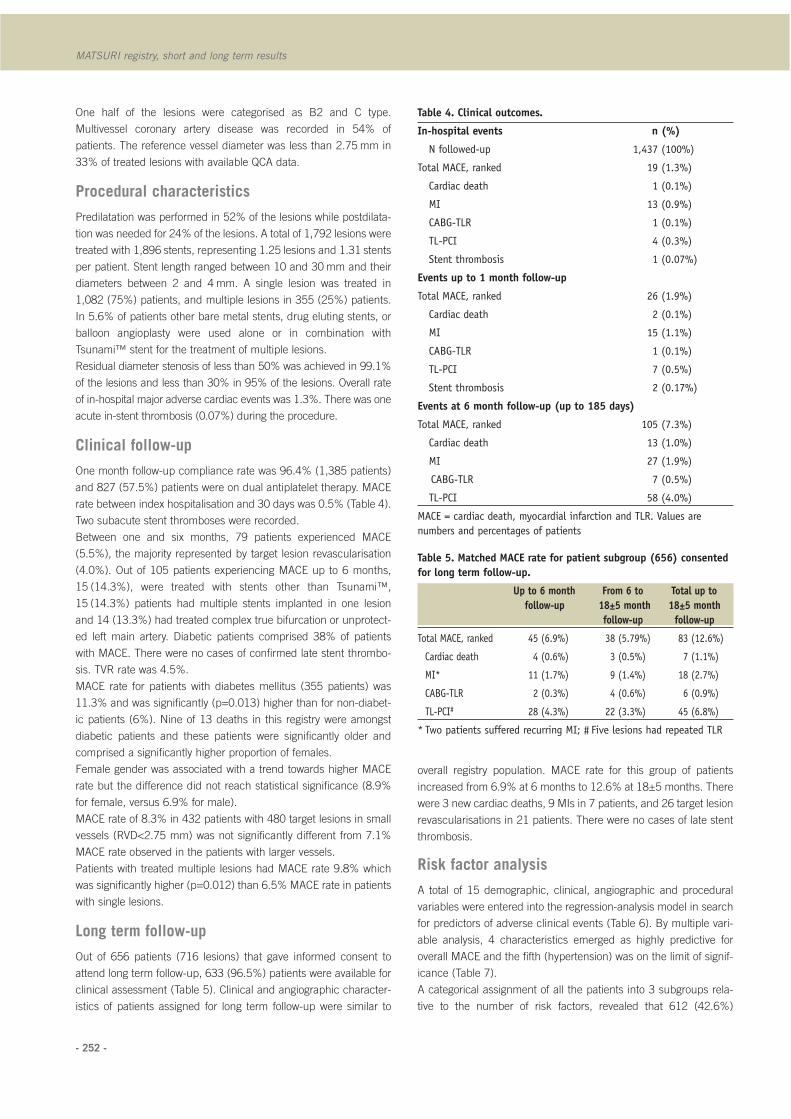
- 252 -
MATSURI registry, short and long term results
One half of the lesions were categorised as B2 and C type.
Multivessel coronary artery disease was recorded in 54% of
patients. The reference vessel diameter was less than 2.75 mm in
33% of treated lesions with available QCA data.
Procedural characteristics
Predilatation was performed in 52% of the lesions while postdilata-
tion was needed for 24% of the lesions. A total of 1,792 lesions were
treated with 1,896 stents, representing 1.25 lesions and 1.31 stents
per patient. Stent length ranged between 10 and 30 mm and their
diameters between 2 and 4 mm. A single lesion was treated in
1,082 (75%) patients, and multiple lesions in 355 (25%) patients.
In 5.6% of patients other bare metal stents, drug eluting stents, or
balloon angioplasty were used alone or in combination with
Tsunami™ stent for the treatment of multiple lesions.
Residual diameter stenosis of less than 50% was achieved in 99.1%
of the lesions and less than 30% in 95% of the lesions. Overall rate
of in-hospital major adverse cardiac events was 1.3%. There was one
acute in-stent thrombosis (0.07%) during the procedure.
Clinical follow-up
One month follow-up compliance rate was 96.4% (1,385 patients)
and 827 (57.5%) patients were on dual antiplatelet therapy. MACE
rate between index hospitalisation and 30 days was 0.5% (Table 4).
Two subacute stent thromboses were recorded.
Between one and six months, 79 patients experienced MACE
(5.5%), the majority represented by target lesion revascularisation
(4.0%). Out of 105 patients experiencing MACE up to 6 months,
15 (14.3%), were treated with stents other than Tsunami™,
15 (14.3%) patients had multiple stents implanted in one lesion
and 14 (13.3%) had treated complex true bifurcation or unprotect-
ed left main artery. Diabetic patients comprised 38% of patients
with MACE. There were no cases of confirmed late stent thrombo-
sis. TVR rate was 4.5%.
MACE rate for patients with diabetes mellitus (355 patients) was
11.3% and was significantly (p=0.013) higher than for non-diabet-
ic patients (6%). Nine of 13 deaths in this registry were amongst
diabetic patients and these patients were significantly older and
comprised a significantly higher proportion of females.
Female gender was associated with a trend towards higher MACE
rate but the difference did not reach statistical significance (8.9%
for female, versus 6.9% for male).
MACE rate of 8.3% in 432 patients with 480 target lesions in small
vessels (RVD<2.75 mm) was not significantly different from 7.1%
MACE rate observed in the patients with larger vessels.
Patients with treated multiple lesions had MACE rate 9.8% which
was significantly higher (p=0.012) than 6.5% MACE rate in patients
with single lesions.
Long term follow-up
Out of 656 patients (716 lesions) that gave informed consent to
attend long term follow-up, 633 (96.5%) patients were available for
clinical assessment (Table 5). Clinical and angiographic character-
istics of patients assigned for long term follow-up were similar to
overall registry population. MACE rate for this group of patients
increased from 6.9% at 6 months to 12.6% at 18±5 months. There
were 3 new cardiac deaths, 9 MIs in 7 patients, and 26 target lesion
revascularisations in 21 patients. There were no cases of late stent
thrombosis.
Risk factor analysis
A total of 15 demographic, clinical, angiographic and procedural
variables were entered into the regression-analysis model in search
for predictors of adverse clinical events (Table 6). By multiple vari-
able analysis, 4 characteristics emerged as highly predictive for
overall MACE and the fifth (hypertension) was on the limit of signif-
icance (Table 7).
A categorical assignment of all the patients into 3 subgroups rela-
tive to the number of risk factors, revealed that 612 (42.6%)
Table 4. Clinical outcomes.
In-hospital events n (%)
N followed-up 1,437 (100%)
Total MACE, ranked 19 (1.3%)
Cardiac death 1 (0.1%)
MI 13 (0.9%)
CABG-TLR 1 (0.1%)
TL-PCI 4 (0.3%)
Stent thrombosis 1 (0.07%)
Events up to 1 month follow-up
Total MACE, ranked 26 (1.9%)
Cardiac death 2 (0.1%)
MI 15 (1.1%)
CABG-TLR 1 (0.1%)
TL-PCI 7 (0.5%)
Stent thrombosis 2 (0.17%)
Events at 6 month follow-up (up to 185 days)
Total MACE, ranked 105 (7.3%)
Cardiac death 13 (1.0%)
MI 27 (1.9%)
CABG-TLR 7 (0.5%)
TL-PCI 58 (4.0%)
MACE = cardiac death, myocardial infarction and TLR. Values are
numbers and percentages of patients
Table 5. Matched MACE rate for patient subgroup (656) consented
for long term follow-up.
Up to 6 month From 6 to Total up to
follow-up 18±5 month 18±5 month
follow-up follow-up
Total MACE, ranked 45 (6.9%) 38 (5.79%) 83 (12.6%)
Cardiac death 4 (0.6%) 3 (0.5%) 7 (1.1%)
MI* 11 (1.7%) 9 (1.4%) 18 (2.7%)
CABG-TLR 2 (0.3%) 4 (0.6%) 6 (0.9%)
TL-PCI# 28 (4.3%) 22 (3.3%) 45 (6.8%)
* Two patients suffered recurring MI; # Five lesions had repeated TLR
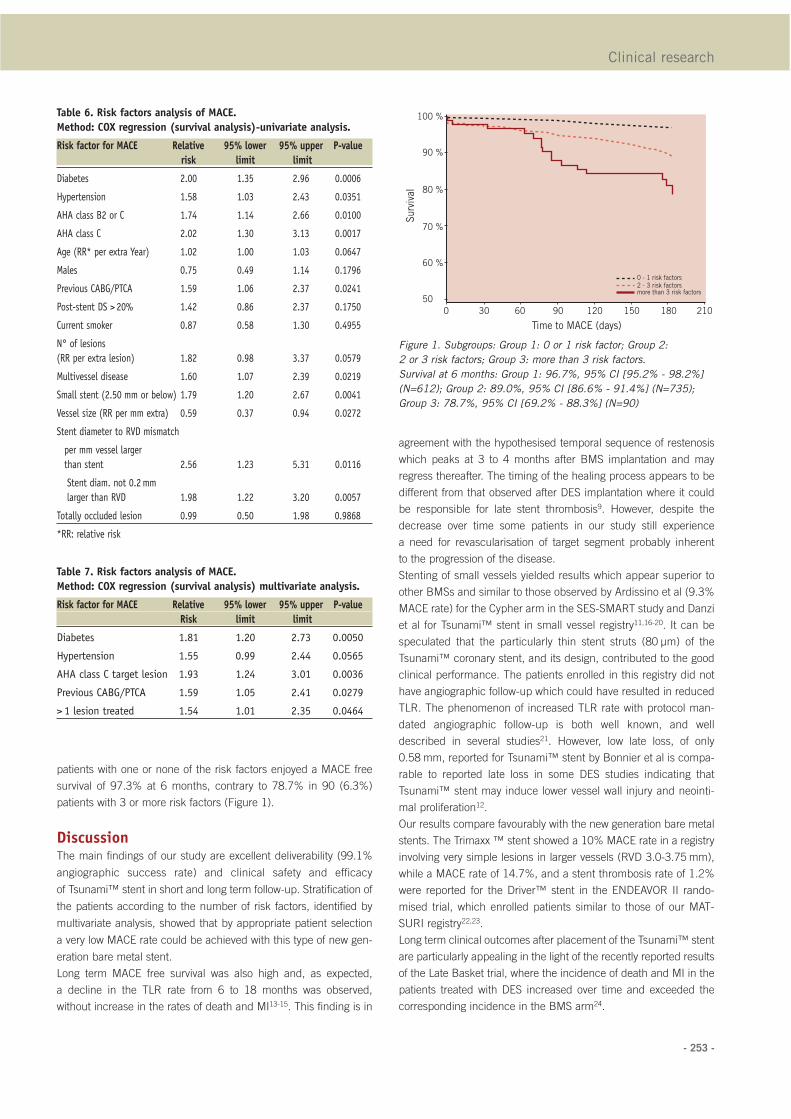
- 253 -
patients with one or none of the risk factors enjoyed a MACE free
survival of 97.3% at 6 months, contrary to 78.7% in 90 (6.3%)
patients with 3 or more risk factors (Figure 1).
DiscussionThe main findings of our study are excellent deliverability (99.1%
angiographic success rate) and clinical safety and efficacy
of Tsunami™ stent in short and long term follow-up. Stratification of
the patients according to the number of risk factors, identified by
multivariate analysis, showed that by appropriate patient selection
a very low MACE rate could be achieved with this type of new gen-
eration bare metal stent.
Long term MACE free survival was also high and, as expected,
a decline in the TLR rate from 6 to 18 months was observed,
without increase in the rates of death and MI13-15. This finding is in
agreement with the hypothesised temporal sequence of restenosis
which peaks at 3 to 4 months after BMS implantation and may
regress thereafter. The timing of the healing process appears to be
different from that observed after DES implantation where it could
be responsible for late stent thrombosis9. However, despite the
decrease over time some patients in our study still experience
a need for revascularisation of target segment probably inherent
to the progression of the disease.
Stenting of small vessels yielded results which appear superior to
other BMSs and similar to those observed by Ardissino et al (9.3%
MACE rate) for the Cypher arm in the SES-SMART study and Danzi
et al for Tsunami™ stent in small vessel registry11,16-20. It can be
speculated that the particularly thin stent struts (80 µm) of the
Tsunami™ coronary stent, and its design, contributed to the good
clinical performance. The patients enrolled in this registry did not
have angiographic follow-up which could have resulted in reduced
TLR. The phenomenon of increased TLR rate with protocol man-
dated angiographic follow-up is both well known, and well
described in several studies21. However, low late loss, of only
0.58 mm, reported for Tsunami™ stent by Bonnier et al is compa-
rable to reported late loss in some DES studies indicating that
Tsunami™ stent may induce lower vessel wall injury and neointi-
mal proliferation12.
Our results compare favourably with the new generation bare metal
stents. The Trimaxx ™ stent showed a 10% MACE rate in a registry
involving very simple lesions in larger vessels (RVD 3.0-3.75 mm),
while a MACE rate of 14.7%, and a stent thrombosis rate of 1.2%
were reported for the Driver™ stent in the ENDEAVOR II rando -
mised trial, which enrolled patients similar to those of our MAT-
SURI registry22,23.
Long term clinical outcomes after placement of the Tsunami™ stent
are particularly appealing in the light of the recently reported results
of the Late Basket trial, where the incidence of death and MI in the
patients treated with DES increased over time and exceeded the
corresponding incidence in the BMS arm24.
Clinical research
Table 6. Risk factors analysis of MACE.
Method: COX regression (survival analysis)-univariate analysis.
Risk factor for MACE Relative 95% lower 95% upper P-value
risk limit limit
Diabetes 2.00 1.35 2.96 0.0006
Hypertension 1.58 1.03 2.43 0.0351
AHA class B2 or C 1.74 1.14 2.66 0.0100
AHA class C 2.02 1.30 3.13 0.0017
Age (RR* per extra Year) 1.02 1.00 1.03 0.0647
Males 0.75 0.49 1.14 0.1796
Previous CABG/PTCA 1.59 1.06 2.37 0.0241
Post-stent DS > 20% 1.42 0.86 2.37 0.1750
Current smoker 0.87 0.58 1.30 0.4955
N° of lesions
(RR per extra lesion) 1.82 0.98 3.37 0.0579
Multivessel disease 1.60 1.07 2.39 0.0219
Small stent (2.50 mm or below) 1.79 1.20 2.67 0.0041
Vessel size (RR per mm extra) 0.59 0.37 0.94 0.0272
Stent diameter to RVD mismatch
per mm vessel larger
than stent 2.56 1.23 5.31 0.0116
Stent diam. not 0.2mm
larger than RVD 1.98 1.22 3.20 0.0057
Totally occluded lesion 0.99 0.50 1.98 0.9868
*RR: relative risk
Table 7. Risk factors analysis of MACE.
Method: COX regression (survival analysis) multivariate analysis.
Risk factor for MACE Relative 95% lower 95% upper P-value
Risk limit limit
Diabetes 1.81 1.20 2.73 0.0050
Hypertension 1.55 0.99 2.44 0.0565
AHA class C target lesion 1.93 1.24 3.01 0.0036
Previous CABG/PTCA 1.59 1.05 2.41 0.0279
> 1 lesion treated 1.54 1.01 2.35 0.0464
Figure 1. Subgroups: Group 1: 0 or 1 risk factor; Group 2:
2 or 3 risk factors; Group 3: more than 3 risk factors.
Survival at 6 months: Group 1: 96.7%, 95% CI [95.2% - 98.2%]
(N=612); Group 2: 89.0%, 95% CI [86.6% - 91.4%] (N=735);
Group 3: 78.7%, 95% CI [69.2% - 88.3%] (N=90)
50
0 30 60 90 120 150
0 - 1 risk factors2 - 3 risk factorsmore than 3 risk factors
180 210
60 %
70 %
80 %
90 %
100 %
Survival
Time to MACE (days)

- 254 -
MATSURI registry, short and long term results
The low incidence of cardiac death, myocardial infarction, and stent
thrombosis, recorded in our registry indicate that a highly deliverable,
thin strut, modern generation bare metal stents could still represent a
valuable option for the treatment of well selected patients with lower
risk of restenosis. As such, exposure of those patients to a long term
dual antiplatelet therapy, and the possible threat of late stent throm-
bosis, could be avoided without compromising clinical outcomes.
Study limitationsLack of randomisation could be considered as one of the limitations
of this study. However, despite the reliability of randomised trial
results they frequently exclude patients at the highest risk for com-
plications and those who are least likely to show benefit, reducing
as such the resemblance to real clinical practice. Absence of angio-
graphic follow-up could represent another limitation of this study
however, the value of clinical endpoints which are best assessed
through registries, such as MATSURI, may be of greater relevance
for assessing patient outcome. Similar to the other large multicenter
registries, the potential under reporting of adverse events due to the
lack of routine monitoring could be considered as one of major lim-
itation of our registry. However, previously conducted, well con-
trolled, clinical trial with Tsunami™ stent reported an incidence of
death and MI of only 2% at 6 month follow-up, suggesting that
under reporting of adverse events was not a major limitation of this
registry21. Although advised to do so, not all investigators enrolled
consecutive patients and as such biased patients selection can not
be ruled out.
ConclusionsThe relatively low MACE rate observed in this registry indicates that
modern generation thin struts bare metal stents are a safe and effi-
cient treatment option for appropriately selected patients. A large
number of participating centres and wide geographic representa-
tion assure that those results are truly representative of the real
world, instead of patients selected along strict criteria in only the
most experienced centres.
AcknowledgementsThis study was supported by Terumo Europe N.V.
Appendix Sponsor: Terumo Europe N.V.
Principal Investigator: Didier Blanchard, St. Gatien Clinic, Tours,
France
Steering Committee: Didier Blancard, St. Gatien Clinic, Tours,
France, Gian Battista Danzi, Poliambulanza , Brescia, Italy (current-
ly Ospedale Maggiore, Milan, Italy), Philip Urban, Hopital de La Tour,
Geneva, Switzerland, Eulogio Garcia, Hospital Gregorio Maranon,
Madrid, Spain, Magali Breheret, Terumo Europe, Hirofumi
Nagai Terumo, Corporation, Dragica Paunovic, Terumo Europe
Clinical Event Committee: Victor, Legrand, Centre Hospitalier
Universitaire Sart Tilman, Liege, Belgium, Thierry Lefevre, Institut
Cardiovasculaire Paris Sud, Massy, France, Nicolas Danchin,
Hopital Europeen Georges Pompidou, Paris, France.
The following investigators participated in the MATSURI study:
EUROPE: Belgium: B. Peperstraete, MD, Brussels, M. Vincent, MD,
Brussels; France: Y. Biron, MD, Rennes, D. Blanchard, MD (PI),
Tours, T. Joseph, MD, Boulogne, H. Escojido, MD, Marseille, G.
Finet, MD, Lyon, B. Glatt, MD, Saint-Denis, M. Hamon, MD, Caen,
B. Huret, MD, Caen, J. Marco, MD, Toulouse, C. Picot Bourdonnec,
MD, Rennes, V. Stratiev, MD, Paris; Germany: W. Auch-Schwelk,
MD, Heppenheim, B. Hennen, MD, Homburg, H. Sievert, MD,
Frankfurt, N. Reifart, MD, Bad Soden, K. Hauptmann, MD, Trier, T.
Schiele, MD, Muenchen, B. Nowak, MD, Frankfurt/Main, A. Klein,
MD, Ravensburg, Steindl, MD, Göppingen; Greece: D. Pentousis,
MD, Thessaloniki, G. Triantis, MD, Athens, I. Zarifis, MD, L.
Mosialos, MD, Thessaloniki; Israel: M. Mosseri, MD, Jerusalem, R.
Kornowski, MD, Petah-Tikva; Italy: G.B. Danzi, MD, Brescia; G.
Piva, MD, Ancona; M.Galli, MD, Como; C. Cernigliaro, MD, Novara;
F. Della Rovere, MD, Genova; R. Bonmassari, MD, Trento; The
Netherlands: H. Bonnier, MD, P. den Heijer, MD, Breda, M.J.
Suttorp, MD, Nieuwegein; Denmark: L. Thuesen, MD, Aarhus, H.
Kelbaeck, MD, Copenhagen, P. Thayssen, MD, Odense; Russia: V.
Chestuchin, MD, Moscow, E. Tchebotar, MD, Nizhny Novgorod, H.
Samko, MD, Moscow, V. Klimov, MD, Moscow, A. Serenko, MD,
Khanty-Mansiysk, A. Protopopov, Krasnoyarsk; Spain: M. Recio,
MD, Madrid, J. Moreu, MD, Toledo; Switzerland: P. Urban, MD,
Geneva; United Kingdom: M. Thomas, MD, London
AFRICA: Morocco: S. Ztot, MD, Rabat
ASIA: Bangladesh: S. Rahman, MD, Dhaka; China: J.B. Ge,
MDShanghai, D. Ho, Hong Kong; India: K. Punamiya, MD,
Mumbai, A. Bhat, MD, Trivandrum, L. Krishna, MD, Hyderabad,
B. Muralidhara, MD, Bangalore, S. Iyengar, MD, Bangalore;
Indonesia: T. Santoso, MD, Jakarta, O. Rachman/M. Yusak Jakarta;
Korea: SJ Park, MD, Seoul, BK Lee, MD, Seoul, JH Joon, MD, Seoul,
MH Jeong, MD, Gwan Ju; Malaysia: K. H. Sim, MD, Sarawak, O.
Ismail, MD, Penang, C. Y. Lee, MD, Johor; Philippines: E. Sison, MD,
Manila; Singapore: Y. Lim, MD, Singapore; Sri Lanka: M. Rajakaruna,
MD, Colombo; Thailand: D. Tresukosol, MD, Bangkok, W.
Udayachalerm, MD, Bangkok, S. Tansuphaswadikul, MD, Bangkok
AUSTRALIA: G. Wilkins, MD, Dunedin, G. Cope, MD, Perth, J.
Gutman, MD, Melbourne, R. Yeend, MD, Adelaide, A. Farshid, MD,
Canberra, C. Juergens, MD, Sydney, D. Eccleston, MD, Melbourne
References
1. Morice M-C, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E,
Perin M, Colombo A, Schuler G, Barragan P, Guagliumi G, Molnar F,
Falotico R. A randomized comparison of a sirolimus-eluting stent with a
standard stent for coronary revascularization. N Engl J Med.
2002;346:1773-1780.
2. Moses JW, Leon MB, Popma JJ, Fitzgerald P J, Holmes DR,
O’Shaughnessy C, Caputo RP, Kereiakes DJ, Williams DO, Teirstein PS,
Jaeger JL, Kuntz R. Sirolimus-eluting stents versus standard stents in
patients with stenosis in a native coronary artery. N Engl J Med.
2003;349:1315-1323.
3. Colombo A, Drzewiecki J, Banning A, Grube E, Hauptmann K,
Silber S, Dudek D, Fort S, Schiele F, Zmudka K, Guagliumi G, Russell EM.
Randomized study to assess the effectiveness of slow- and moderate-
release polymer-based paclitaxel-eluting stents for coronary artery lesions.
Circulation. 2003;108:788-794.

- 255 -
4. Stone GW, Ellis SG, Cox DA, Hermiller J, O’Shaughnessy C, Mann JT,
Turco M, Caputo R, Bergin P, Greenberg J, Popma JJ, Russell ME. A poly-
mer-based, paclitaxel-eluting stent in patients with coronary artery
disease. N Engl J Med. 2004;350:221-231.
5. Spertus JA, Kettelkamp R, Vance C, Decker C, Decker C,
Jones, Rumsfeld SJ, Messenger CJ, Khanal S, Peterson DE, Bach GR,
Krumholz MH, Cohen JD. Prevalence, predictors, and outcomes of pre-
mature discontinuation of thienopyridine therapy after drug-eluting stent
placement: results from the PREMIER registry. Circulation.
2006;113:2803-9.
6. Kuchulakanti PK, Chu WW, Torguson R, Ohlmann P, Rha S-W,
Clavijo CL, Kim S-W , Bui A, Gevorkian N, Xue Z, Smith K, Fournadjieva J,
Suddath OW, Satler FL, Pichard DA, Kent KM, Waksman R. Correlates
and long-term outcomes of angiographically proven stent thrombosis with
sirolimus- and paclitaxel-eluting stents. Circulation. 2006;113:1108-13.
7. Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi MG, Stankovic G,
Airoldi F, Chieffo A, Montorfano M, Carlino M, Michev I, Corvaja N,
Briguori C, Gerckens U, Grube E, Colombo A. Incidence, predictors, and
outcome of thrombosis after successful implantation of drug-eluting
stents. JAMA. 2005;293:2126-30.
8. Ong AT, McFadden EP, Regar E, de Jaegere P, van Domburg TR,
Serruys WP. Late angiographic stent thrombosis (LAST) events with drug-
eluting stents. J Am Coll Cardiol. 2005;45:2088-92.
9. Joner M, Finn AV, Farb A Mont KE, Kolodgie DF, Ladich E, Kutys R,
Skorija K, Gold KH, Virmani R. Pathology of drug-eluting stents in
humans: delayed healing and late thrombotic risk. J Am Coll Cardiol.
2006;48:193-202.
10. Farb A, Burke AP, Kolodgie FD, Virmani R. Pathological mecha-
nisms of fatal late coronary stent thrombosis in humans. Circulation.
2003;108:1701-6.
11. Danzi GB, Suryapranata H, Antoniucci D, Tresucosol D, Galli M,
Hung-Kwong DH, Tan HC. Stent Implantation in Very Small Coronary
Arteries: The Tsunami SV International Registry. Am J Cardiol
2004;94:1429-1432.
12. Bonnier HJ, van den Heuvel P, Legrand V, Tanabe K, Vos J,
Serruys PW. Clinical and angiographic outcomes after Tsunami coronary
stent placement. J Invasive Cardiol. 2004;16:252-6.
13. Kimura T, Yokoi H, Nakagawa Y, Tamura T, Kaburagi S, Sawada Y,
Sato Y, Yokoi H, Hamasaki N, Nosaka H, Nobuyoshi M. Three-year follow-
up after implantation of metallic coronary-artery stents. N Engl J Med.
1996;334:561-566.
14. Kuroda N, Kobayashi Y, Nameki M, Kuriyama N, Kinoshita T,
Okuno T, Yamamoto Y, Komiyama N, Masuda Y. Intimal hyperplasia regres-
sion from 6 to 12 months after stenting. Am J Cardiol. 2002;89:869-872.
15. Farb A, Kolodgie FD, Hwang JY, Burke A, Tefera K, Weber D,
Wight T, Virmani R. Extracellular matrix changes in stented human coro-
nary arteries. Circulation. 2004;110:940-7.
16. Kastrati A, Schomig A, Dirschinger J, Mehilli J, Dotzer F, von Welser N,
Neumann FJ for the ISAR-SMART Study Investigators A randomized trial
comparing stenting with balloon angioplasty in small vessels in patients
with symptomatic coronary artery disease. Circulation. 2000;102:2593-8.
17. Doucet S, Schalij MJ, Vrolix MC, Hilton D, Chenu P, de Bruyne B,
Udayachalerm W, Seth A, Bilodeau L, Reiber J, Harel F, Lespérance J, for
the Stent In Small Arteries (SISA) Trial Investigators. Stent placement to
prevent restenosis after angioplasty in small coronary arteries. Circulation.
2001;104:2029-33.
18. Moreno R, Fernandez C, Alfonso F Hernández R, Pérez-Vizcayno M,
Escaned J, Sabaté M, Bañuelos C, Angiolillo D, Azcona L, Macaya C.
Coronary stenting versus balloon angioplasty in small vessels: a meta-
analysis from 11 randomized studies. J Am Coll Cardiol. 2004;43:1964-72.
19. Agostoni P, Biondi-Zoccai GG, Gasparini GL, Anselmi M, Morando G,
Turril M, Abbate A, McFadden E, Vassanelli C, Zardini P, Colombo A,
Serruys PW. Is bare-metal stenting superior to balloon angioplasty for
small vessel coronary artery disease? Evidence from a meta-analysis of
randomized trials. Eur Heart J. 2005;26:881-9.
20. Ardissino D, Cavallini C, Bramucci E, Indolfi C, Marzocchi A,
Manari A, Angeloni G, Carosio G, Bonizzoni E, Colusso S, Repetto M,
Merlini PA, for the SES-SMART Investigators. Sirolimus-eluting vs uncoat-
ed stents for prevention of restenosis in small coronary arteries: a random-
ized trial. JAMA. 2004;292:2727-34.
21. Schiele F. The “angiographically correct” follow-up strategy after
stent implantation. Heart. 2001;85:363-364.
22. Abizaid A. Multicenter Clinical Trial Results with the Triple Layer
Abbott TriMaxx™ Stent. www.tctmd.com (accessed July 15th 2006).
23. Fajadet J, Wijns W, Laarman GJ, Kuck KH, Ormiston J, Münzel T,
Popma J, Fitzgerald JP, Bonan R, Kuntz ER, for the ENDEAVOR II
Investigators. Randomized, double-blind, multicenter study of the
Endeavor Zotarolimus-eluting Phosphorylcholine- encapsulated stent for
treatment of native coronary artery lesions. Clinical and angiographic
results of the ENDEAVOR II trial. Circulation. 2006;114:798-806.
24. Pfisterer M, Brunner-La Rocca HP, Buser TP, Rickenbacher P,
Hunziker P, Mueller C, Jeger R, Bader F, Osswald S, Kaiser C for the BAS-
KET-LATE Investigators. Late Clinical Events After Clopidogrel
Discontinuation May Limit the Benefit of Drug-Eluting Stents: An
Observational Study of Drug-Eluting Versus Bare-Metal Stents. J Am Coll
Cardiol. 2006;48:2584-2591.
Clinical research
82
CONCLUSION
The theme of this submission for MD by published work is the procedural
aspects of the performance of percutaneous coronary intervention, particularly with
respect to strategies to minimise adverse patient outcomes. In addition to the broader
body of work I have published, I believe the 21 papers cited here as part of a
Doctorate of Medicine by published works, has made substantial contributions in five
broad areas related to the practise of interventional cardiology including; the use of
contrast agents during invasive coronary procedures; strategies to reduce vascular
access complications; the use of antithrombotic agents during and after the procedure;
the reporting and management of complications of PCI and involvement in large stent
registries monitoring outcomes of differing types of coronary stents. Percutaneous
coronary intervention remains a rapidly evolving field and I believe I have made a
significant contribution to improving the outcomes of patients who undergo this
procedure.
83
BIBLIOGRAPHY OF PAPERS AS PART OF MD
SUBMISSION
1. Juergens CP, Khaing AM, McIntyre GJ, Leung DYC, Lo STH, Fernandes C,
Hopkins AP. Adverse reactions of low osmolar non-ionic and ionic contrast media
when used together or separately during percutaneous coronary intervention. Heart
Lung Circ 2005;14:172-177.
2. Juergens CP, Winter JP, Nguyen-Do P, Lo S, French JK, Hallani H, Fernandes C,
Jepson N, Leung DYC. Nephrotoxic effects of iodixanol and iopromide in patients
with abnormal renal function receiving N-acetylcysteine and hydration before
coronary angiography and intervention: a randomised trial. Intern Med J 2009;39:25-
31.
3. Dhawan A, Parikh D, Shugman I, French JK, Hallani H, Fernandes C, Juergens
CP. Contrast induced nephropathy in patients with pre-existing renal impairment
undergoing invasive coronary procedures – A long term follow up. Med J Aust 2011;
195:268-269.
4. Duffy SJ, Ruygrok P, Juergens CP, Sievert H, Richards M, Blake J, Whitbourn R,
Farouque HO, Pertile T, Kaye DM. Removal of contrast media from the coronary
sinus attenuates renal injury after coronary angiography and intervention. J Am Coll
Cardiol 2010;56:525-526.
5. Juergens CP, Leung DYC, Crozier JA, Wong AM, Robinson JTC, Lo S,
Kachwalla H, Hopkins AP. Patient tolerance and resource utilization associated with
an arterial closure versus an external compression device after percutaneous coronary
intervention. Catheter Cardiovasc Interv 2004;63:166-170.
6. Juergens CP, Hallani H, Leung DYC, Crozier JA, Robinson JTC, Lo S, Hopkins
AP. Comparison of 6 and 7 French guiding catheters for percutaneous coronary
84
intervention: results of a randomised trial with a vascular ultrasound endpoint.
Catheter Cardiovasc Interv 2005;66:528-534.
7. Ang CK, Leung DY, Lo S, French JK, Juergens CP. Effect of local anesthesia and
intravenous sedation on pain perception and vasovagal reactions during femoral
arterial sheath removal after percutaneous coronary intervention. Int J Cardiol
2007;116:321-326.
8. Juergens CP, Lo S, French JK, Leung DYC. Vaso-vagal reactions during femoral
arterial sheath removal after percutaneous coronary intervention and impact on
cardiac events. Int J Cardiol 2008;127:252-254.
9. Juergens CP, Crozier JA, Robinson JTC, Lo S, French JK, Leung DYC.
Unfractionated heparin use after percutaneous coronary intervention: results of a trial
with a vascular ultrasound endpoint. Heart Lung Circ 2008;17:107-113.
10. Juergens CP, Wong AM, Leung DYC, Lowe HC, Lo S, Fernandes C, Newland
EF, Hopkins AP. A randomized comparison of clopidogrel and aspirin versus
ticlopidine and aspirin after coronary stent implantation. Am Heart J 2004;147:e15.
11. Rajendran S, Parikh D, Shugman I, French JK, Juergens CP. High on treatment
platelet reactivity and stent thrombosis. Heart Lung Circ 2011;20:525-531.
12. Burgess S, Mallard TA, Juergens CP. Review of ticagrelor in the management of
acute coronary syndromes. Expert Opin Drug Metab Toxicol 2012;8:1315-1325.
13. Juergens CP, White HD, Belardi JA, Macaya C, Soler-Soler J, Meyer BJ, Levy
RD, Bunt T, Menten J, Herrmann HC, Adgey AAJ, Tarnesby G. A multicenter study
of the tolerability of tirofiban versus placebo in patients undergoing planned
intracoronary stent placement. Clin Ther 2002;24:1332-1344.
14. Winter JP, Juergens CP. The role of tirofiban in the management of coronary
artery disease. Cardiovasc Hematol Disord Drug Targets 2008;8:138-146.
85
15. Parikh D, Juergens CP. Abciximab as an adjunctive therapy for patients
undergoing percutaneous coronary intervention. Expert Opin Biol Ther 2011;11:235-
246.
16. Juergens CP, Yeung AC, Oesterle SN. Routine platelet transfusion in patients
undergoing emergent coronary bypass surgery after receiving Abciximab. Am J
Cardiol 1997;80:74-75.
17. Shugman IM, Hsieh V, Cheng S, Parikh D, Tobing D, Wouters N, van den
Vijver R, Queenie Lo, Rajaratnam R , Hopkins AP, Lo S , Leung D, Juergens CP,
French JK. Safety and efficacy of rescue angioplasty for ST-elevation myocardial
infarction with high utilization rates of glycoprotein IIb/IIIa inhibitors. Am Heart J
2012;163:649-656.e1.
18. Shugman IM, Diu P, Gohil J, Kadappu KK, Leung M, Lo S, Leung DY, Hopkins
AP, Juergens CP, French JK. Evaluation of Troponin T Criteria for Periprocedural
Myocardial Infarction in Patients with Acute Coronary Syndromes. Am J Cardiol
2011;107:863-870.
19. Doyle B, Juergens CP. Conservative management of ascending aortic dissection
caused by percutaneous coronary intervention. J Invasive Cardiol 2004;16:92-94.
20. Pomerantsev EV, Colombo A, De La Fuente L, Grube E, Juergens C, Mathey D,
Schalij M, Goy JJ, Morice MC, Schofer J, Sugeng I, Stertzer SH. Microstent to GFX:
Experience in 2325 patients. J Inter Cardiol 1998;11:101-106.
21. Blanchard D, Danzi GB, Urban P, Moseri M, Juergens C, Guyon P, Nowak B,
Tresucosol D, Suttorp MJ, Farshid A, Kornowski R, Garcia E, Yeend R, Nagai H,
Paunovic D. A novel ultra-thin bare metal stent (BMS): results from a worldwide
registry. Eurointerv 2007; 3:249-255.
86
ADDITIONAL PUBLICATIONS NOT FORMING PART
OF THESIS
1. Juergens CP, Fernandes C, Hasche ET, Meikle S, Bautovich G, Currie CA,
Freedman SB, Jeremy RW. Electrocardiographic measurement of infarct size after
thrombolytic therapy. J Am Coll Cardiol 1996;27:617-624.
2. Juergens CP, Semsarian C, Keech AC, Beller E, Harris PJ. Hemorrhagic
complications of intravenous heparin therapy. Am J Cardiol 1997;80:150-154.
3. Juergens CP, Whitbourn RJ, Yeung AC, Oesterle SN. Primary angioplasty for
acute myocardial infarction. Vasc Med 1997;2:327-334.
4. Nashed G, Juergens CP, Lowe HC. Second generation bifurcation stent: The rapid
evolution of device technology. J Invasive Cardiol 1999;11:444-446.
5. Lowe HC, Juergens CP. Use of the multifunction probing catheter as an adjunctive
device for occluded vein graft intervention. J Invasive Cardiol 1999;11:567-570.
6. Nashed G, French B, Gallagher D, Hopkins A, Juergens C, Leung D, Lowe HC.
Right ventricular perforation with cardiac tamponade associated with use of a
temporary pacing wire and abciximab during complex coronary angioplasty. Catheter
Cardiovasc Interv 1999;48:388-389.
7. Arronis C, Juergens CP, Lowe HC. A novel approach for crossing a virtually
occluded vessel using ultra low profile balloon backup. J Invasive Cardiol
2000;12:425-427.
87
8. Lowe HC, Chesterman CN, Hopkins AP, Juergens CP, Khachigian LM. Acute
local release of fibroblast growth factor-2 but not transforming growth factor-β1
following coronary stenting. Thromb Haemost 2001;85:574-576.
9. Kachwalla H, Lo ST, Tie H, Nashed G, Juergens CP, Hopkins AP, Lowe HC.
Spontaneous coronary dissection following exertion: support for a hypothesis. Intern
Med J 2001;31:501-503.
10. Boufous S, Kelleher PW, Pain CH, Dann LM, Ieraci S, Jalaludin BB, Gray AL,
Harris SE, Juergens CP. Impact of a chest pain guideline on clinical decision
making. Med J Aust 2003;178:375-380.
11. Do PN, Juergens CP. Acute stent thrombosis associated with exercise testing.
Heart Lung Circ 2004;13:198.
12. Leung DY, Lo ST, Liew CT, Wong AM, Hopkins AP, Juergens CP. Use of
functional tests before angiography in patients with normal coronary arteries. Int J
Cardiol 2005;104:326-331.
13. Shisen J, Leung DY, Juergens CP. Gender and age differences in the prevalence
of coronary artery calcification in 953 Chinese subjects. Heart Lung Circ 2005;14:69-
73.
14. Hallani H, Leung DY, Newland E, Juergens CP. Use of a quantitative point of
care test for the detection of serum cardiac troponin T in patients with suspected acute
coronary syndromes. Intern Med J 2005;35:560-562.
15. Li ZZ, Sidney L, Juergens CP, Zhu XL, Tao Y, Liu T, Wang S, Li Y. Sixty-four
cases of percutaneous coronary angioplasty on saphenous vein bypass grafts.
Zhonghua Xin Xue Guan Bing Za Zhi 2005;33:221-223. (in Chinese)
16. Ng AC, Taylor D, Juergens C. Infected left ventricular pseudoaneursym. Heart
2006;92:1237.
88
17. Fernandez RS, Griffiths R, Juergens C, Davidson P, Salamonson Y. Persistence
of coronary risk factor status in participants 12 to 18 months after percutaneous
coronary intervention. J Cardiovasc Nurs 2006;21:379-387.
18. Leung DY, Hallani H, Lo ST, Hopkins AP, Juergens CP. How compliant are we
with guidelines for coronary angiography in clinical practice? Intern Med J 2007;
37:699-704.
19. Fernandez RS, Davidson P, Salamonson Y, Griffiths R, Juergens C. The Health-
related quality of life trajectory in patients after percutaneous coronary intervention. J
Cardiopulm Rehabil Prev 2007; 27:223-226.
20. Jiang SS, Lu L, Juergens C, Gong JB, Wang LJ, Peng YP, Xu DJ, Huang ZY.
Coronary artery lesion comparison between Chinese and Australian patients with
coronary artery disease. Zhonghua Xin Xue Guan Bing Za Zhi 2007;35:447-450. (in
Chinese)
21. Gohil J, Juergens C, French J. Non-STEMI or no NSTEMI? Intern Med J
2007;37:737-738.
22. Fernandez RS, Salamonson Y, Juergens C, Griffiths R, Davidson P.
Development and preliminary testing of the Cardiac Rehabilitation Enrolment
Obstacles (CREO) scale: Implications for service development. Eur J Cardiovasc
Nurs 2008;7:96-102.
23. Fernandez RS, Salamonson Y, Juergens C, Griffiths R, Davidson P. Validation of
the revised cardiac rehabilitation preference form in patients with post-percutaneous
coronary intervention. J Cardiopulm Rehabil Prev 2007; 27:390-394.
24. Fernandez RS, Salamonson Y, Griffiths R, Juergens C, Davidson P.
Sociodemographic predictors and reasons for participation in an outpatient cardiac
89
rehabilitation programme following percutaneous coronary intervention. Int J Nurs
Pract 2008; 14:237-242.
25. Fernandez R, Davidson P, Griffiths R, Juergens C, Salamonson Y. What do we
know about the long term medication adherence in patients following percutaneous
coronary intervention? Aust J Adv Nurs 2007; 25:53-61.
26. Fernandez RS, Salamonson Y, Griffiths R, Juergens C, Davidson P. Awareness
of risk factors for coronary heart disease following interventional cardiology
procedures: A key concern for nursing practice. Int J Nurs Pract 2008; 14:435-442.
27. Jiang SS, Lv L, Juergens CP, Chen SL, Xu DJ, Huang ZY. Racial differences in
coronary artery lesions: a comparison of coronary artery lesions between mainland
Chinese and Australian patients. Angiology 2008;59:442-447.
28. Fernandez RS, Davidson P, Griffiths R, Juergens C, Stafford B, Salamonson Y.
A pilot randomised controlled trial comparing a health-related lifestyle self-
management intervention with standard cardiac rehabilitation following an acute
event: implications for a larger clinical trial. Aust Crit Care 2009; 22:17-27.
29. Edmond JJ, Juergens CP, French JK. The pharmaco-invasive approach to
STEMI: when should fibrinolytic-treated patients go to the “cath lab”? Heart
2009;95:358-361.
30. Fernandez RS, Davidson P, Griffiths R, Juergens C, Salamonson Y.
Development of a health-related lifestyle self-management intervention for patients
with coronary heart disease. Heart Lung 2009;38:491-498.
31. Aliprandi-Costa B, Ranasinghe I, Chow V, Kapila S, Juergens C, Devlin G,
Elliott J, Lefkowitz J, Brieger DB. Management and outcomes of patients with acute
coronary syndromes in Australia and New Zealand, 2000-2007. Med J Aust
2011;195:116-121.

90
32. Hee L, Mussap CJ, Yang L, Dignan R, Kadappu KK, Juergens CP, Thomas L,
French JK. Outocmes of coronary revascularization (Percutaneous or Bypass) in
patients with diabetes mellitus and multivessel coronary disease. Am J Cardiol
2012;110:643-648.
33. Hee L, Thomas L, Ang X, Yang L, Lo S, Juergens CP, Mussap CJ, Dignan R,
French JK. Risk factor modification in diabetic patients following angiographic
identification of multivessel disease. Int J Cardiol 2012; in press
Related Documents











