Stomas: Technical Stomas: Technical Considerations Considerations By: John N. Afthinos, By: John N. Afthinos, M.D. M.D.

Stomas: Technical Considerations By: John N. Afthinos, M.D.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Stomas: Technical Stomas: Technical ConsiderationsConsiderations
By: John N. Afthinos, M.D.By: John N. Afthinos, M.D.

Patient PreparationPatient Preparation
Patient educationPatient education– Disspell mythsDisspell myths– Confront patient’s fearsConfront patient’s fears
Enterostomal therapistEnterostomal therapist– Involvement from the pre-op period Involvement from the pre-op period
improves outcomesimproves outcomes

Patient PreparationPatient Preparation
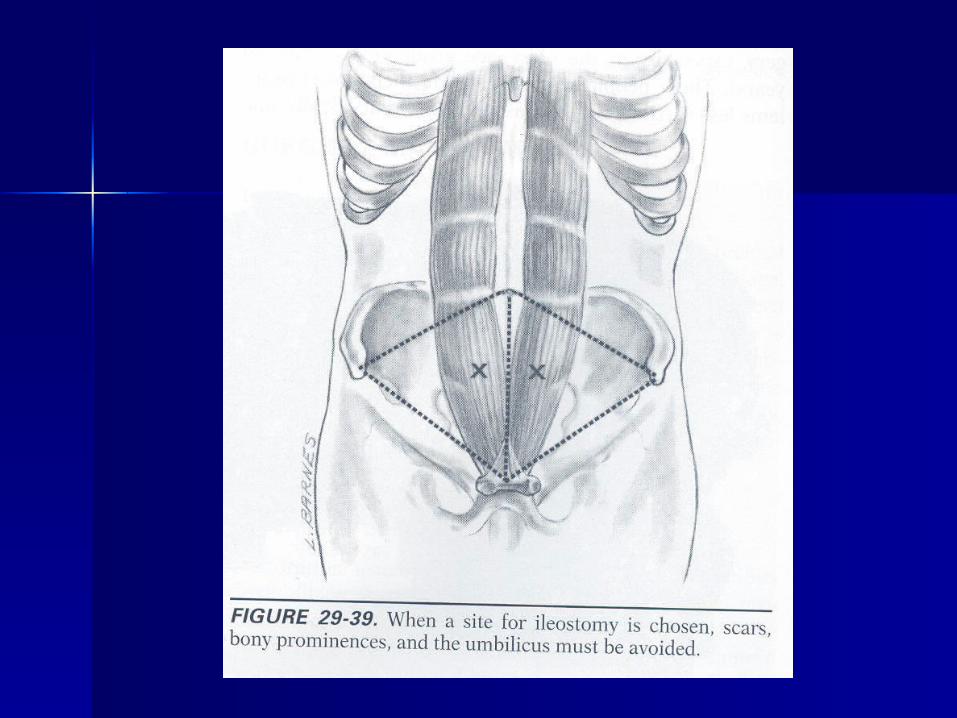
Stomal markingStomal marking– Center of triangle bounded by Center of triangle bounded by
umbilicus, ASIS, and pubisumbilicus, ASIS, and pubis Through rectus abdominusThrough rectus abdominus Have pt lie down, sit and bend forwardHave pt lie down, sit and bend forward Avoid creases, scars, bony Avoid creases, scars, bony
prominences, belt lineprominences, belt line

Types of StomasTypes of Stomas
EndEnd– Often in more permanent situations, but not Often in more permanent situations, but not
necessarilynecessarily APR APR
LoopLoop– For temporary diversions of fecal streamFor temporary diversions of fecal stream– Theoretically technically easier to restore Theoretically technically easier to restore
continuitycontinuity TechniqueTechnique
– Brooke 1952: suture mucosa directly to the Brooke 1952: suture mucosa directly to the skinskin

Basic Function and Basic Function and CareCare IleostomyIleostomy
– Begins to function @ 48 – 72 hrsBegins to function @ 48 – 72 hrs– Initially green, viscous secretionsInitially green, viscous secretions
Not a sign of true peristalsisNot a sign of true peristalsis
– Adaptation phaseAdaptation phase 1.5 – 1.8 L/d1.5 – 1.8 L/d Compensating for loss of colon and Compensating for loss of colon and
ileocecal valveileocecal valve
Basic Function and Basic Function and CareCare IleostomyIleostomy
– Stool thickens to toothpaste Stool thickens to toothpaste consistencyconsistency
– Final outputs range from 0.5 and 0.8 Final outputs range from 0.5 and 0.8 L/dL/d
Sigmoid/Descending ColostomySigmoid/Descending Colostomy– Function returns on ~POD 5Function returns on ~POD 5– Soft formed stool with a pre-op Soft formed stool with a pre-op
elimination patternelimination pattern

Basic Function and Basic Function and CareCare Ostomy ManagementOstomy Management
– Application of pouch system in ORApplication of pouch system in OR Collects secretions and protects skinCollects secretions and protects skin
– Cut aperture to 1/8” from stoma to Cut aperture to 1/8” from stoma to protect skin and prevent mucosal protect skin and prevent mucosal traumatrauma
Frequent resizing for 4 – 6 weeks post-opFrequent resizing for 4 – 6 weeks post-op
– Skin protectants limit irritation from Skin protectants limit irritation from frequent appliance changesfrequent appliance changes
NOT for use with ileostomiesNOT for use with ileostomies

Basic Function and Basic Function and CareCare Skin BarrierSkin Barrier
– Adherent porous material that Adherent porous material that protects skin from stoma output—protects skin from stoma output—especially ileostomiesespecially ileostomies
– Must preserve skin integrity so Must preserve skin integrity so appliance adheres and prevent appliance adheres and prevent leakageleakage
– Examples: karaya, StomahesiveExamples: karaya, Stomahesive PouchPouch


Basic Function and Basic Function and CareCare Frequency of ChangesFrequency of Changes
– Enough to prevent leakage and skin Enough to prevent leakage and skin irritationirritation Average of about 5 – 7 daysAverage of about 5 – 7 days

ComplicationsComplications
Stomal NecrosisStomal Necrosis– Ischemia from venous congestion, Ischemia from venous congestion,
inadequate supply, small fascial inadequate supply, small fascial openingopening
– Dusky, blue mucosa—eventually Dusky, blue mucosa—eventually black and necroticblack and necrotic
– If not corrected, the stoma may If not corrected, the stoma may retract into the abdomenretract into the abdomen

ComplicationsComplications
Retraction ~18.5% incidenceRetraction ~18.5% incidence– Usually from stomal ischemia but also Usually from stomal ischemia but also
from weight gainfrom weight gain– Can cause peritonitis, enterocutaneous Can cause peritonitis, enterocutaneous
fistula, or stricture of stomal openingfistula, or stricture of stomal opening– Repair by:Repair by:
circumcising ostomy at skin and recreationcircumcising ostomy at skin and recreation formal laparotomy and recreationformal laparotomy and recreation Panniculectomy with abdominoplastyPanniculectomy with abdominoplasty

ComplicationsComplications
ProlapseProlapse– Overall rare but seen more often Overall rare but seen more often
after loop colostomyafter loop colostomy– Oversized fascial opening, sudden Oversized fascial opening, sudden
Valsalva, redundant loop of bowel Valsalva, redundant loop of bowel leading to stomaleading to stoma
– If acute, reduce immediately either If acute, reduce immediately either with gentle pressure, or sugar if with gentle pressure, or sugar if manually irreduciblemanually irreducible
ComplicationsComplications
If occurs lateIf occurs late– Circumcise the mucosa and excise Circumcise the mucosa and excise
redundant colon redundant colon – Re-anastomose the distal mucosa to Re-anastomose the distal mucosa to
the proximalthe proximal If occurs earlyIf occurs early
– Circumcise at mucocutaneous Circumcise at mucocutaneous junctionjunction



ComplicationsComplications
Peristomal HerniaPeristomal Hernia– Reportedly, 2.8% rate if through rectusReportedly, 2.8% rate if through rectus– Causes include placement lateral to Causes include placement lateral to
rectus, too large a fascial opening, rectus, too large a fascial opening, age, chronically increased abdominal age, chronically increased abdominal pressurepressure
– If defect small, circumcise colostomy, If defect small, circumcise colostomy, repair defect and remature stoma repair defect and remature stoma
Can repair defect with meshCan repair defect with mesh

ComplicationsComplications
Peristomal HerniaPeristomal Hernia– If defect larger and no room in the If defect larger and no room in the
rectus sheath, then recreate at rectus sheath, then recreate at umbilicus or contralateral rectusumbilicus or contralateral rectus
Related Documents











