Yoshihisa Nakano, MD #{149} Kaori Togashi, MD #{149} Kazumasa Nishimura, MD a Kyo Itoh, MD #{149} Ichiro Fujisawa, MD #{149} Reinin Asato, MD #{149} Hideki Adachi, MD #{149} Harumi Itoh, MD #{149} Kanji Torizuka, MD Stomach and Duodenum: Radiographic Magnification Using Computed Radiography (CR)’ 383 Abdominal and Gastrointestinal Radiology We performed direct radiographic magnification (X3) using a 0.1-mm microfocal tube and computed radi- ography (CR) in air-barium double- contrast studies of the stomach and duodenum. To eliminate blurring of the image due to motion, we used the maximum kilovolt peak rate possible (102 kVp), the maximum milliampere second rate possible (64 mAs), the shortest possible exposure time (0.1 second), and a horizontal x-ray beam. With the patients in the supine position, CR provided the wide image reproduction range re- quired to obtain satisfactory radio- graphs. Image processing in the CR system produced radiographs with increased radiographic contrast and enhanced edge definition of ana- tomic borders or pathologic process- es. The duodenal villi were clearly visible in 45% of the cases. Index terms: Castrointestina! tract, radiogra- phy, 7.12 #{149} Magnification #{149} Radiography, digi- ta! Radiology 1986; 160:383-387 I From the Department of Radiology and Nu- clear Medicine, Kyoto University Medical School, Sakyo-ku, Kyoto 606, Japan. Received December 13, 1985; revision requested Febru- ary 3, 1986; revision received February 24; ac- cepted March 5. Address reprint requests to Y.N. C RSNA, 1986 T HE potential of radiographic mag- nification to facilitate diagnosis has been recognized for many years. Direct radiographic magnification has already been used to help diag- nose diseases of the breast and skele- ta! soft tissue. However, theme are in- herent differences between obtain- ing radiographic magnification im- ages of the gastrointestinal (GI) tract and obtaining images of other body systems (1). Adequate radiation pene- tration of the thickest part of the body requires the use of a limited x- ray tube current and small focal-spot size, and a short exposure time must also be employed to avoid motion am- tifact, a major problem in imaging the GI tract. In addition, a higher ki- lovolt peak (kVp) is required so that the column of barium-sulfate suspen- sion can be penetrated by the x rays. The techniques that have been suc- cessfully used in skeletal and mam- mographic magnification radiogra- phy must be modified to accom- modate these differences. We had the patients in our study assume the supine position, and we used a horizontal x-ray beam to ob- tam the magnification radiographs. With the patients in the supine posi- tion, we were able to visualize the stomach and the duodenum without their overlapping the barium-filled GI tract, the lumbar spine, and the thick muscles of the back (Fig. 1). Ad- equate radiation penetration was ob- tamed despite the system’s low gen- erator capacity, which was due to tube limitations. Although the horizontal view makes direct radiographic magnifica- tion possible, the detector system must have a wide latitude since the x ray has to penetrate the thick part of the upper abdomen and the air-filled stomach at the same time. Conse- quently, it is technically difficult to obtain optimum density using a con- ventional screen-film system . We have used the Fuji (Kanagawa, Japan) computed radiography (CR) system to obtain radiographic magnification images of the GI tract and have found it useful in helping diagnose disorders in a select group of patients in whom equivocal findings were ob- tamed in standard upper GI tract ex- aminations (2). MATERIALS AND METHODS We used an angiographic system con- sisting of a Siemens (Erlangen, West Ger- many) Tridoros i000 generator and a C- arm arrangement that employed a microfocal tube (OPTI 1 iO/ 12/50/HSG) with a nominal focal spot of 0.1 mm and an image intensifier. When the CR’s C- arm arrangement is used, the cassette with the imaging plate is attached to the front of the image intensifier (Fig. 2). After the routine upper GI examination on the tilt-table radiography-flounoscopy table was completed, each patient in our study was brought to the angiography ta- ble. The patient assumed the supine posi- tion (Fig. 2), and horizontally exposed magnification radiographs using the CR system were obtained at 102 kVp and 64 mAs, and with an exposure time of 0.i second. The image was magnified 2.5-3 times the original magnification, with a focus-film distance of 115 cm and a focus- object distance of 40 cm. In the past 2 years, we have performed upper GI tract examinations on 520 pa- tients, and we have fluoroscopically and radiographically identified equivocal findings in 95 patients. To establish more conclusively the pathologic diagnosis of these 95 patients, we obtained an addi- tional magnification radiograph using a horizontal x-ray beam. The decision to obtain an additional projection was usual- ly made during the fluoroscopic examina- tion. The demonstrability of the villi on the duodenal bulb was also evaluated in 80 patients in whom no duodenal abnormal- ities were found, since the demonstration of micromucosal patterns, such as areae gastnicae or duodenal villi, is a bench- mark by which our technique can be eval- uated (3).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Yoshihisa Nakano, MD #{149}Kaori Togashi, MD #{149}Kazumasa Nishimura, MDa Kyo Itoh, MD #{149}Ichiro Fujisawa, MD #{149}Reinin Asato, MD #{149}Hideki Adachi, MD
#{149}Harumi Itoh, MD #{149}Kanji Torizuka, MD
Stomach and Duodenum:Radiographic Magnification Using
Computed Radiography (CR)’
383
Abdominal and Gastrointestinal Radiology
We performed direct radiographicmagnification (X3) using a 0.1-mmmicrofocal tube and computed radi-ography (CR) in air-barium double-contrast studies of the stomach andduodenum. To eliminate blurring ofthe image due to motion, we usedthe maximum kilovolt peak ratepossible (102 kVp), the maximummilliampere second rate possible (64mAs), the shortest possible exposuretime (0.1 second), and a horizontalx-ray beam. With the patients in thesupine position, CR provided thewide image reproduction range re-quired to obtain satisfactory radio-graphs. Image processing in the CRsystem produced radiographs withincreased radiographic contrast andenhanced edge definition of ana-tomic borders or pathologic process-es. The duodenal villi were clearlyvisible in 45% of the cases.
Index terms: Castrointestina! tract, radiogra-
phy, 7.12 #{149}Magnification #{149}Radiography, digi-
ta!
Radiology 1986; 160:383-387
I From the Department of Radiology and Nu-clear Medicine, Kyoto University Medical
School, Sakyo-ku, Kyoto 606, Japan. ReceivedDecember 13, 1985; revision requested Febru-ary 3, 1986; revision received February 24; ac-cepted March 5. Address reprint requests toY.N.
C RSNA, 1986
T HE potential of radiographic mag-
nification to facilitate diagnosis
has been recognized for many years.
Direct radiographic magnification
has already been used to help diag-
nose diseases of the breast and skele-
ta! soft tissue. However, theme are in-
herent differences between obtain-
ing radiographic magnification im-
ages of the gastrointestinal (GI) tract
and obtaining images of other body
systems (1). Adequate radiation pene-
tration of the thickest part of the
body requires the use of a limited x-
ray tube current and small focal-spot
size, and a short exposure time must
also be employed to avoid motion am-
tifact, a major problem in imaging
the GI tract. In addition, a higher ki-
lovolt peak (kVp) is required so that
the column of barium-sulfate suspen-
sion can be penetrated by the x rays.
The techniques that have been suc-
cessfully used in skeletal and mam-
mographic magnification radiogra-
phy must be modified to accom-
modate these differences.
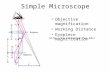
We had the patients in our study
assume the supine position, and we
used a horizontal x-ray beam to ob-
tam the magnification radiographs.
With the patients in the supine posi-
tion, we were able to visualize the
stomach and the duodenum without
their overlapping the barium-filled
GI tract, the lumbar spine, and the
thick muscles of the back (Fig. 1). Ad-
equate radiation penetration was ob-
tamed despite the system’s low gen-
erator capacity, which was due to
tube limitations.
Although the horizontal view
makes direct radiographic magnifica-
tion possible, the detector systemmust have a wide latitude since the x
ray has to penetrate the thick part of
the upper abdomen and the air-filled
stomach at the same time. Conse-
quently, it is technically difficult to
obtain optimum density using a con-
ventional screen-film system . We
have used the Fuji (Kanagawa, Japan)
computed radiography (CR) system
to obtain radiographic magnification
images of the GI tract and have
found it useful in helping diagnose
disorders in a select group of patients
in whom equivocal findings were ob-
tamed in standard upper GI tract ex-
aminations (2).
MATERIALS AND METHODS
We used an angiographic system con-sisting of a Siemens (Erlangen, West Ger-
many) Tridoros i000 generator and a C-
arm arrangement that employed a
microfocal tube (OPTI 1 iO/ 12/50/HSG)with a nominal focal spot of 0.1 mm andan image intensifier. When the CR’s C-
arm arrangement is used, the cassette
with the imaging plate is attached to the
front of the image intensifier (Fig. 2).
After the routine upper GI examinationon the tilt-table radiography-flounoscopy
table was completed, each patient in our
study was brought to the angiography ta-ble. The patient assumed the supine posi-
tion (Fig. 2), and horizontally exposed
magnification radiographs using the CR
system were obtained at 102 kVp and 64
mAs, and with an exposure time of 0.i
second. The image was magnified 2.5-3
times the original magnification, with a
focus-film distance of 115 cm and a focus-
object distance of 40 cm.
In the past 2 years, we have performed
upper GI tract examinations on 520 pa-
tients, and we have fluoroscopically and
radiographically identified equivocal
findings in 95 patients. To establish more
conclusively the pathologic diagnosis of
these 95 patients, we obtained an addi-
tional magnification radiograph using ahorizontal x-ray beam. The decision to
obtain an additional projection was usual-
ly made during the fluoroscopic examina-
tion.
The demonstrability of the villi on the
duodenal bulb was also evaluated in 80
patients in whom no duodenal abnormal-
ities were found, since the demonstration
of micromucosal patterns, such as areae
gastnicae or duodenal villi, is a bench-
mark by which our technique can be eval-
uated (3).

1. 2.
384 . Radiology August
Figures 1, 2. (1) Horizontal view of the stomach and duodenum with patient in supine position. (2) Patient in supine position on the an-
giography table. When the C-arm arrangement is used, the cassette with the imaging plate is attached to the front of the image intensifier
(arrow).
a. b.
Figure 3. (a) Magnification radiograph (X3) obtained with the CR system. (b) Close-up
view shows the fine network pattern of areae gastnicae.
Figure 4. Micromucosal pattern of duode-
nal villi.
RESULTS
Sixty-eight of the 95 magnification
radiographs obtained using the CR
system were of excellent quality, and
visualization of the mucosal pattern
was superior to that demonstrated by
the nadiographs obtained during theroutine examinations (Fig. 3). Twen-
ty-two images were acceptable for di-
agnostic use, although use was limit-
ed by mild image noise (ten studies),
slight motion artifact (eight studies),
on improper patient positioning (four
studies). Five studies were not ac-
ceptable due to movement on the
pant of the patient on technical error
(i.e., misselection of data acquisition
parameters).
We determined that duodenal villi
were demonstrated in images ob-
tamed from 36 of 80 patients (45%).
pattern that resembled a shaggy car-
pet was seen on the magnificationdiographs; that is, multiple finger-
like projections seen en face in the
duodenal bulb (Fig. 4) (1).
In 70 of the 90 patients from

c.
a. b. c.
Volume 160 Number 2 Radiology #{149}385
Figure 5. (a) The compression technique reveals a small polyp of the stomach (arrow). (b) Double-contrast study does not reveal any lesions
on the posterior wall of the stomach, so that the lesion appears to be located on the anterior wall. (c) Horizontal magnification using CR re-
veals two polyps (arrows) located on the anterior wall of the antrum of the stomach.
a. b.Figure 6. Early carcinoma on the anterior wall of the stomach. (a) Double-contrast study does not reveal the lesion. (b) The compressionmethod reveals the lesion. (c) The horizontal-magnification radiograph provides radiographic visualization of the small lesion of the anteni-or wall (arrow).
acceptable horizontal-magnification
radiographs were obtained, the pres-
ence of lesions was convincingly ex-
cluded. The presence of lesions dem-
onstrated by the CR system in the
remaining 20 patients was subse-
quently confirmed either surgically
or pathologically. The clinical and
pathologic diagnoses of all 90 pa-
tients are shown in Table 1. Horizon-
tal-magnification nadiographs ob-
tamed using the CR system proved
helpful in evaluating lesions that
were not located in the posterior wall
of the stomach (Figs. 5, 6). In one
case, the horizontal-magnification ma-
diographs also provided additional
information concerning the exact ex-
tension of stomach carcinoma
(Fig. 7).
DISCUSSION
The direct-magnification radio-
graphs (X2.5-3) obtained using the
CR system demonstrated fine detailin the small intestinal mucosa. This
detail could not be seen on the radio-
graphs obtained using the conven-
tional screen-film system. The visual-
ization of a fine, lacy, mucosal
pattern in the duodenal bulb mdi-
cates that the vilius pattern has been
successfully imaged (Fig. 4). In our
study, the villus pattern was demon-
strated in 45% of 80 images, which is
an extremely high success rate com-
pared with the 5%-iO% incidencerate reported by Glick et al. (4).
The advantages of the CR system
compared with the conventional
screen-film system are two-fold.
First, the detector of the CR system
has a wide dynamic range of
1:10,000, and a constant optimum
density can be attained whenever
any quantity of x-ray exposures are
being made. This facility to optimize
the exposure of the CR system is im-
pontant in magnification madiogra-
phy, since magnification radiogra-

phy is a technically difficult pro-
cedure. Second, the CR system allows
the images to be enhanced. Imageprocessing in the CR system incompo-
mates high-pass spatial filtering that
results in enhanced edge definition
and increased visibility of the micro-
mucosai pattern.Air-barium double-contrast radiog-
raphy of the stomach and duodenum
has gained acceptance as a routine
method of examination. This tech-nique emphasizes the en face appear-
ance of the CI mucosa for the detec-
tion of superficial abnormalities.However, the technique frequently
fails to image minute mucosal lesions
that are located in the anterior wall
or in the lesser or greater curvature
of the stomach, and that yield normalresults in the upper GI examination.
The horizontal view not only makes
direct magnification possible but also
reveals abnormalities that were not
visible in images obtained during
routine examination (Figs. 5-7).a. b. The disadvantages of CR magnifi-Figure 7. (a) Routine examination of the stomach reveals the carcinoma in the angulus of cation of the GI tract include the ex-the stomach. (b) Horizontal magnification obtained with CR shows the exact extension of pense of the CR system and of the an-the carcinoma toward the anterior wall of the stomach and along the lesser curvature (ar-
rows).
c.
;;gure 8. (a) Low spatial filtering, (b) intermediate spatial filtering, and (c) high-pass spatial filtering.
August 1986386 #{149}Radiology

a. b. c.
Volume 160 Number 2 Radiology #{149}387
Figure 9. (a) Minimum, (b) moderate, and (c) marked enhancement with intermediate spatial filtering. Marked enhanced image shows theprominent areae gastricae, suggesting chronic gastnitis.
giognaphic equipment using a small
focus tube; the limited output of the
CR system; and most important, the
problems inherent in image en-
� hancement. In Figure 8, three images
representing three kinds of spatial
filtering can be seen: low, intermedi-
ate, and high pass. Intermediate fil-
tening yields the best representation
of the areae gastnicae. In Figure 9, the
three kinds of enhancement obtained
with intermediate spatial filtering
are shown: minimum, moderate, andmarked degree of enhancement. A
moderate degree of enhancement
seems to yield the best nepresenta-
tion of areae gastnicae. Thus, image
enhancement has both advantages
and limitations. Proper image en-
hancement provides increased visu-
alization of the anatomic and patho-
logic structures, but too much
enhancement increases image noise,
resulting in a loss of diagnostic infon-
mation or even creating an artifact
that resembles a pathologic process
(Fig. 9).
In summary, we studied the effec-
tiveness of obtaining horizontal-
magnification radiographs of the
stomach and duodenum using a mi-
crofocal x-ray tube and the CR system
and having the patient assume the
supine position. Our success in visu-
alizing micromucosal patterns mayindicate that this radiographic tech-
nique could facilitate diagnosis of GI
tract disease by providing informa-
tion on mucosal structural abnormal-
ities that were not previously detect-
able by more routine methods. U
References
1. Goldberg HI, Gould R, Rosenquist J, Royal
5, Owens R, Silverman S. In vivo demon-stration of small intestinal villi in dogs andmonkeys using radiographic magnifica-tion. Radiology 1982; 142:53-58.
2. Sonoda M, Takano M, Miyahara J, Kato H.
Computed radiography utilizing scanninglaser stimulated luminescence. Radiology1983; 148:833-838.
3. Seaman WB. The areae gastricae. AJR1978; 131:554.
4. Click SN, Cohel VK, Laufer I. Mucosalsurface patterns of the duodenal bulb. Ra-diology 1984; 150:317-322.
Related Documents