Stillbirth: risk factors and opportunities for prevention Vicki Flenady PhD, MMedSc (Clin Epi & Biostats) Mater Research Institute, University of Queensland

Stillbirth: risk factors and opportunities for prevention Vicki Flenady PhD, MMedSc (Clin Epi & Biostats) Mater Research Institute, University of Queensland.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Stillbirth: risk factors and opportunities for prevention
Vicki Flenady PhD, MMedSc (Clin Epi & Biostats)Mater Research Institute, University of Queensland

Content
• Brief overview of global picture • High income country picture – focussing on risk factor• The Lancet’s stillbirth series key recommendations• Stillbirth research initiatives in Australia and New Zealand

Launch April 2011
AustraliaLondonNew YorkGenevaNew DelhiFlorence, ItalyCape Town
“These papers, like no other Lancet Series before, have triggered a remarkable response not just from academia and organisations, but also from the public” - The Lancet editors
All papers can be accessed free at www.lancet.com/series/stillbirth

Global burden of stillbirth
Source: Lawn JE, Blencowe H, Pattinson R, et al, for The Lancet’s Stillbirths Series steering committee. Stillbirths: Where? When? Why? How to make the data count? Lancet 2011; published online April 14. DOI:10.1016/S0140-6736(10)62187-3.
10 countries account for 66% of the world’s stillbirths – and also 66% of neonatal deaths and over 60% of maternal deaths 1. India2. Pakistan3. Nigeria4. China5. Bangladesh6. Dem Rep Congo7. Ethiopia8. Indonesia9. Tanzania10. Afghanistan
2.65 million third
trimester stillbirths each year
98% of stillbirths occur in low-income and middle-income countries – more than two thirds are in rural families.

Stillbirths don’t count …
1. Global data NOT routinely reported to World Health Organization NOT included in the Global Burden of Disease metrics NOT measured appropriately in most national surveys
2. Global goals eg Millennium Development Goals (MDGs)Stillbirths NOT counted in the MDGs although intimately linked to:• Maternal health in MDG 5• Neonatal deaths, accounting for 41% of child deaths in MDG4• Poverty (MDG 1) and girls’ education (MDG2)
Stillbirths often missed in national or international health policy and programmes … Yet they count for families

Reality for families
Over 7200 families a day experience a stillbirth late in pregnancy…
In Australia over 2000 stillbirths each year: 7 every day (I in 130 women)
Whether they are famous or not, in a rich country or poor, the grief is overwhelming, and usually hidden
Gio
vann
i Pre
sutt
i Cia
oLap
o

Goal by 2020
Countries with a current stillbirth rate of less than 5 per 1000 births, the goal by 2020 is to eliminate all preventable stillbirths and close equity gaps.
Countries with a current stillbirth rate of more than 5 per 1000 births to reduce their stillbirth rates by at least 50% from the 2008 rates.
www.thelancet.com/series/stillbirth
PM
NC
HS
ands
UK

Stillbirths during labour – 1.2 million a year
Source: Lawn JE, Blencowe H, Pattinson R, et al, for The Lancet’s Stillbirths Series steering committee. Stillbirths: Where? When? Why? How to make the data count? Lancet 2011; published online April 14. DOI:10.1016/S0140-6736(10)62187-3.
The risk of stillbirth during labour (intrapartum) for an African woman is 50 times higher than for a woman in the UK/ANZ.
55% of all stillbirths are for rural families in Africa, South Asia

Stalled progress in high income countries
Source: Goldenberg RL, McClure EM, Bhutta ZA, et al, for The Lancet’s Stillbirths Series steering committee. Stillbirths: the vision for 2020. Lancet 2011;
published online April 14. DOI:10.1016/S0140-6736(10)62235-0.
Stillbirth rates halved 1950-1975 with improvements in infection treatment and obstetric care – rates have now stalled

Stillbirths at 28 weeks or more in high-income settings
Source: Flenady V, Middleton P, Smith GC, et al, for The Lancet’s Stillbirths Series steering committee. Stillbirths: the way forward in high-income countries. Lancet 2011; published online April 14. DOI:10.1016/S0140-6736(11)60064-0.
Differences between countries and within countries show that more reduction in stillbirth rates is achievable

Late gestation (>28weeks) stillbirth rates per 1000 births of 193 countries (Cousens et al., 2011)
Finland 2.0 (ranked 1)
Germany 2.4 (ranked 6)USA 3.0 (ranked 17)UK 3.5 (ranked 33)France 3.9 (ranked 41)
Australia 2.9 (ranked 15)
New Zealand 3.5 (ranked 34)If Australia and New Zealand achieved the stillbirth rate of the best performing country, 368 stillbirths
would be avoided each year

Potentially Modifiable Risk Factors for Stillbirth in HIC?
Maternal characteristics• Maternal/ paternal age • BMI• Smoking• Parity• Ethnicity• SES & education Adequacy of antenatal careInter-pregnancy intervalSubstance use Alcohol intakeCoffee consumption ConsanguinityStress
Medical conditions• Diabetes• Hypertensive disease Pregnancy factors• Post-term pregnancy • Multiple pregnancy• ART conceptionsPregnancy complications• FGR & SGA• BirthweightPrevious stillbirthPrevious caesarean sectionOther previous pregnancy
complications

Methodology
Study selection:Recent, population based studies (1998-Dec 2009) HIC settingsStillbirth definition of ≥20 weeks or ≥ 400 gramsMultivariate analysis controlling for important confounders (i.e. age,
BMI, smoking, medical conditions etc)Quality appraisal:Newcastle-Ottawa Scale (NOS) for cohorts and case-controls (Wells GA,
Shea B, O'Connell D, Peterson J, Welch V, Losos M & Tugwell P, 2003).
Data analysis:Random effect meta-analysis (where appropriate)Population attributable risk (PAR%)
PAR = Pe (RRe-1) / 1 + Pe (RRe-1)
19,126 studies reviewed
75 included

Maternal age > 35 years
PAR 11%
Prevalence 22%

Previous stillbirth
PAR 0.8%
Prevalence 0.5%

Potentially Modifiable Risk Factors for Stillbirth in HIC
Maternal overweight & obesity: BMI 25-30 & >30 PAR 12%: OR 1.23, 1.63 (Prevalence 40%)
(8000 stillbirths each year)
Maternal age > 35 years: PAR 11%, OR 1.65 (Prevalence 22%)
(4000 stillbirths)
Smoking: PAR 6%; OR 1.36; (Prevalence 17%) (3000 stillbirths)
30% of all stillbirths

Population attributable risk (PAR)Estimates for maternal demographics
Factor aOR 95% CI Prev % PAR%
Alcohol use
Any (<28 wk stillbirth) (single study) 1.8 1.3-2.3 50 17
1 – 3 per week 1.1 1.0- 1.2
>5 per week 1.7 1.0-3.0
Binge 1.5 1.0-2.0
Low socio-economic status (SES) 1.2 1.01-1.4 49.6 9
Low education (<10 or <8yrs) 1.7 1.4-2.0 6.9 5
Illicit drug use 1.9 1.2-3.0 2.4 2
Assisted Reproductive Technology (ART) use 2.7 1.6-4.7 3.1 3
No antenatal care 3.3 3.1-3.6 0.3 1
Caffeine intake >8 cups (SB 20-27 weeks) 2.3 1.3-3.9
Paternal age > 50 years 3.9 1.1-13.8

Population attributable risk (PAR)Estimates for medical/pregnancy complications
Factor aOR 95% CI Prev % PAR%
Small for gestational age (SGA) <10% 3.8 2.3-6.3 10.0 23
Placental abruption 18.9 16.9-12.2 1 15
Pre-existing hypertension 2.6 2.1-3.1 4.6 7
Pre-existing diabetes 2.9 2.1-4.1 2.6 5
Pre-eclampsia 1.5 1.1-2.0 5.3 3
Multiple pregnancy (any) 2.9 2.5-3.4 2 3
Pregnancy induced hypertension (PIH) 1.3 1.2-1.6 6.3 2
Multiple pregnancy (twins) 1.6 1.4-1.9 2 1
Pregnancy prolongation (≥42 weeks) 1.3 1.1-1.7 0.9 0.3
Eclampsia 2.2 1.5-3.2 0.1 0.1

Population attributable risk (PAR)Estimates for previous pregnancy history
Factor aOR 95% CI Prev % PAR%
Primiparity 1.4 1.3-1.5 42 14Caesarean section (contentious) 1.3 1.1-1.52 27 7
Stillbirth 2.7 1.6-4.6 0.5 1
SGA + preterm birth (PTB)
SGA + PTB (any) 2.1 1.6-2.8
SGA + PTB 32-36 weeks 3.4 2.1-5.6
SGA+ PTB <32 weeks 5.0 2.5-9.8

Late gestation (>28weeks) stillbirth rates per 1000 births of 193 countries (Cousens et al., 2011)
Finland 2.0 (ranked 1)
Germany 2.4 (ranked 6)USA 3.0 (ranked 17)UK 3.5 (ranked 33)France 3.9 (ranked 41)
Australia 2.9 (ranked 15)
New Zealand 3.5 (ranked 34)Indigenous Australians Ranked 56th behind Colombia
and Malaysia

Indigenous status and stillbirth adjusted analysis

Subgroup analysis: ethnic minorities
PAR%Risk factor aOR
AU IndigPAR %
CA IndigPAR%
US IndigPAR%
US Afr AmPAR %
Smoking (any) 1.7 26%(14-37)
29%(16-40)
13%(6-19)
5%(3-9)
Heavy smoking (10+) 1.9 13%(9-17)
12%(9-16)
- -
Overweight 1.315%(8-22)
23%(13-32)
21%(12-29)
25%(15-35)Obesity 1.9
Diabetes 2.9 - - - 5%(3-8)
Hazardous alcohol use 1.7 10%(0-24)
No antenatal care 3.3 8%(7-9)
- 8%(7-8)
5%(5-6)
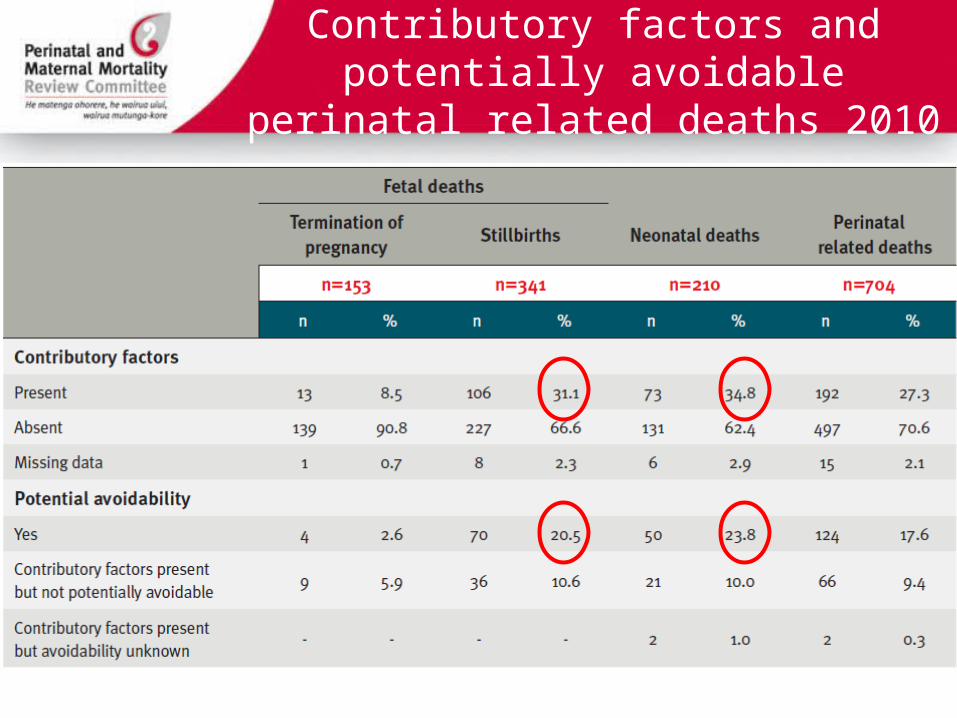
Contributory factors and potentially avoidable perinatal related deaths 2010

Action priorities in high-income countries− Reduce inequity, intentionally designing policies
and programs to reach underserved women from poorer communities or ethnic minorities
− Address lifestyle risk factors such as obesity, smoking, and advanced maternal age
− Improve data quality, Implementation high quality investigation and perinatal audit linked to practice change
− Improve detection of pregnancies at increased risk eg placental dysfunction and fetal growth restriction
Decreased fetal movements ranked in the top 10 research priorities

Stillbirths by PSANZ PDC, QLD 2000-2008

Unexplored not explained
Congenital abnormality20%
Hypertension3%
Maternal conditions6%
Specific perinatal conditions5%
Hypoxic peripartum death2%
Placenta: Other6%
Placenta: APH7%
Placenta: Insufficiency7%
Perinatal infection2%
Spontaneous preterm - chorio8%
Spontaneous preterm - no chorio3%
Spontaneous preterm - unknown chorio
4%
Unexplained stillbirth: 7%
Unexplained stillbirth: possible13%
Unknown7%

ANZ Autopsy ratesAutopsy Rates in Australia and New Zealand
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
WA SA ACT NZ TAS VIC NSW QLD NT
Region
Au
top
sy R
ate
Perinatal Mortality autopsy rateStillbirth autopsy rateNeonatal death autopsy rate

Perinatal Society of Australia and New Zealand Guidelines
Promoting a systematic approach to clinical care, including audit, around the time of a perinatal death.
• Institutional Perinatal Mortality Audit• Investigation of stillbirth• Investigation of neonatal death • Autopsy• Perinatal Mortality Classification • Psychological and social aspects of
bereavement care

Station 1: Communicating
with parents about perinatal autopsy
Station 2: Autopsy and
placental examination
Station 3: Investigation of perinatal deaths
Station 4: Examination of
babies who die in the perinatal period
Station 5: Audit and
classification of perinatal death
Station 6: Psychological and social aspects of
perinatal bereavement
SCORPIO Methodology: D.A. Hill, Medical Teacher. 1992; 14: 37-41
IMPROVE (IMproving Perinatal Mortality Review & Outcomes Via Education) Program
Study Guide
Teaching Stations
Formative Assessment

National Perinatal Death Clinical Audit Tool On-line: A platform for audit and research
1. Effective online data collection tool for maternity hospitals
2. Includes stillbirth and neonatal deaths
3. Reports automatically generated for Hospital and Health Department reporting of perinatal deaths

National prospective perinatal death data collection: Audit and research
First study: Stillbirth investigation and causes;
1,000 stillbirths – causes, contributing factors, yield of tests, costs
30 maternity hospitals
IMPROVE workshops

Decreased fetal movements− Possible adaptive response to placental dysfunction
− DFM is associated with a doubling of the risk of FGR (Flenady 2011)
− Women who reported DFM (and came to hospital with a live baby) had 4 times the risk of stillbirth compared with women who did not report DFM (Flenady 2011)
− Women perceiving a reduction in strength of fetal movements had twice the risk of stillbirth (Stacey 2010)

Women:
− 50% wait 24 hours or more to report DFM
− 60% say it is normal for movements to decrease towards term− 70% indicate awareness of FM would NOT help identify a baby at risk
Obstetricians and Midwives:
− asking women about FM is important
− define DFM most commonly by maternal perception of DFM
− lack of clinical practice guidelines
− For women with DFM :
− Suggest drink some cold/iced water
− Low level of ultrasound scan (< 10%)
DFM Reporting and Practice in Australia and New Zealand

Evidence for raising awareness (+/- kick counting)
Cochrane systematic review of Kick Counting:
INSUFFICIENT EVIDENCE
Grant trial- large Cluster RCT, methodological flaws
Lowered stillbirth rate after 28 weeks by 30%

DFM Guidelines in Australia and New Zealand
− All pregnant women should be routinely provided verbal and written information about normal FM
− All women should be advised to contact their health care provider if they have any concern about decreased or absent FM and be advised not to wait until the next day
− Maternal concern of DFM overrides any other definition
− Women should be assessed within 12 hours of reporting DFM; CTG, clinical assessment of fetal growth, risk factor
− USS if risk factors present or clinical concerns (managed a high-risk pregnancy)

DFM Information for womenTranslations: Korean, Arabic, Spanish, Hindi, Vietnamese, Chinese Simplified & Traditional

My Baby’s Movements Trial Smartphone Tool
− User-controlled− Information about fetal
movements and what to expect as pregnancy progresses
− Incudes daily fetal movement prompt (time chosen by woman)
− Includes movement monitoring option if concerned about fetal movements
− Designed to be supportive and non-directive, and minimise unnecessary anxiety and to respect women’s right to autonomy

My Baby’s Movements Trial
Primary outcome:Stillbirth 28 weeks or more
Randomisation: Assigned to timing of intervention using computer-generated random number table
Implementation schedule: 9 time periods of 4 months over 36months with groups of 3-4 hospitals in each group
27 hospitals of 3000 births/year over a 3 year period

Biophysical and biochemical tests to predict stillbirth Low predictive accuracy : fetoplacental proteins, first- and second-trimester
screening for Down syndrome, multivariable prediction models, uterine artery Doppler velocimetry, nuchal translucency, fetal growth, flow in ductus venosus, thyroid function-related tests, maternal hemoglobin levels, and cervicovaginal infection had a low predictive accuracy for stillbirth
Moderate to high predictive for stillbirth placental conditions: A pulsatility index in the uterine arteries >90th percentile and low levels of pregnancy associated plasma protein A (PAPP-A) had a moderate to high predictive accuracy for stillbirth related to placental abruption, small for gestational age or preeclampsia
Emerging evidence microRNAs derived from the placenta circulate in the maternal blood during pregnancy and may serve as non-invasive biomarkers for pregnancy complications.

Summary• Maternal overweight and obesity, smoking and advanced age are
important potentially avoidable risk factors
• Primiparity is an important risk factor. With increasing incidence of combined risk factors – stillbirth rates could increase
• Abruption, Diabetes and Hypertension remain important factors in stillbirth
• Must improve data quality including clinical audit linked to practice change
• Research to improve detection of women at risk in the antenatal period is a priority

Acknowledgements The Lancet's Stillbirth Series Steering CommitteeJ Frederik Frøen, Joy Lawn, Zulfiqar Bhutta, Robert Pattinson, Vicki Flenady, Robert Goldenberg, Monir Islam
ANZSA ResearchersAleena Wojcieszek, Annie McArdle, Cate Nagal, Ann Peacock, Paula Dillon, Debra Creedy, Jenny Gamble, Jocelyn Toohil, Tomasina Stacey, Kassam Mahomen, Julie MacPhail, Glenn Gardener, Yogesh Chadha, Ibi Ibiebele, Laura Koopmans, Dom Rossouw, Kristen Gibbons, Peter Gray
Professor Michael HumphreyQueensland Maternal Perinatal Quality Council
International Collaborators Ruth Fretts, Fredrik Frøen, Alex Haezell; Jane Norman
We also thank the women and clinicians who contributed data
MBM Trial InvestigatorsGlenn Gardener, David Ellwood, Philippa Middleton, Michael Coory, Caroline Crowther, Christine East, Emily Callander, Frances Boyle, Adrian Charles, Adrienne Gordon, Alison Kent, Belinda Jennings, Deborah Schofield, Glyn Teale, Jonathan Morris, Kassam Mahomed, Susan Vlack, Jane Norman, Fredrik Frøen,

Acknowledgements

Collaborators ANZSA Consortium hospitals and investigators
QLD: Gold Coast Hospital, Anne Sneddon; Ipswich Hospital, Kassam Mahomed; Nambour Hospital, Ted Weaver; Caboolture Hospital, Kate Kerridge; Cairns Base Hospital, Paul Howat; Logan Hospital, Janet Draper; Townville Hospital, David Watson and Anne-Maree Lawrence; Mater Mother’s Hospital Public, Mater Mother’s Hospital Private, Glenn Gardener; Royal Women’s Hospital Yogesh Chadha. NSW: Nepean Hospital, Michael Peek; Royal Prince Alfred Hospital, Sydney; Royal Hospital for Women, Leo Leader; Royal North Shore Hospital, Jonathan Morris. VIC: Sunshine Hospital, Glyn Teale; Mercy Hospital, Robyn Aldridge; Kasey and Dandenong Hospitals, Monash Medical Centre, Chris East; Royal Women’s Hospital Melbourne, Fiona Cullinane; Mercy Hospital for Women, Sue Walker. WA: King Edward Memorial, Adrian Charles and Belinda Jennings. SA: Women’s and Children’s Hospital, Rodney Petersen. NZ: Auckland City Hospital, Peter Stone and Nick Waller; Middlemore Hospital, Dr Graham Parry.

Related Documents



![[MCQS] biostats](https://static.cupdf.com/doc/110x72/544d5eb5af7959f3138b4d15/mcqs-biostats.jpg)







