STILL CROSSING THE QUALITY CHASM: A MIXED-METHODS STUDY OF PHYSICIAN DECISION-MAKING WHEN TREATING CHRONIC DISEASES by CHRISTOPHER C. LAMB Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy Weatherhead School of Management Designing Sustainable Systems CASE WESTERN RESERVE UNIVERSITY May, 2018

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
STILL CROSSING THE QUALITY CHASM: A MIXED-METHODS STUDY OF
PHYSICIAN DECISION-MAKING WHEN TREATING CHRONIC DISEASES
by
CHRISTOPHER C. LAMB
Submitted in partial fulfillment of the requirements for the degree of
Doctor of Philosophy
Weatherhead School of Management
Designing Sustainable Systems
CASE WESTERN RESERVE UNIVERSITY
May, 2018
CASE WESTERN RESERVE UNIVERSITY
SCHOOL OF GRADUATE STUDIES
We hereby approve the thesis/dissertation of
Christopher C. Lamb
candidate for the degree of Doctor of Philosophy*.
Committee Chair
Kalle Lyytinen, Ph.D., Case Reserve Western University
Committee Member
Adrian Wolfberg, Ph.D., Case Western Reserve University
Committee Member
Yunmei Wang, Ph.D., Case Western Reserve University
Committee Member
J.B. Silvers, Ph.D., Case Western Reserve University
Date of Defense
January 16, 2018
*We also certify that written approval has been obtained
for any proprietary material contained therein

© Christopher C. Lamb, 2017
All rights reserved.

Dedication
I dedicate my dissertation to my family for their unwavering support over four
years and the many times I was away from home.

v
TABLE OF CONTENTS
Table of Contents .................................................................................................................v
List of Tables ..................................................................................................................... ix
List of Figures .................................................................................................................... xi
Abstract ............................................................................................................................ xiii
Chapter 1: Introduction ........................................................................................................1
Chapter 2: Literature Review ...............................................................................................5
Overview of U.S. Healthcare Quality and Cost .............................................................7
Evolution of the Relationship between Physicians and Patients: How We Came to
Shared Decision Making (SDM) ...................................................................................9 History of SDM......................................................................................................10
Facilitators of SDM................................................................................................14
Theories Related to Clinical Decision Making ............................................................15 Decision Theory .....................................................................................................16
Power .....................................................................................................................25 Traits ......................................................................................................................28 Organizational Context ..........................................................................................34
Summary of SDM Decision Theory ......................................................................42
Summary ......................................................................................................................42
Chapter 3: Chronic Diseases ..............................................................................................45
Hemophilia ...................................................................................................................46
Primary Immunodeficiency (PID) ...............................................................................49
Analysis #1: MEPS ......................................................................................................53
Analysis #2: IDF ..........................................................................................................56 Purpose ...................................................................................................................56 Methods..................................................................................................................56 Results ....................................................................................................................57 Discussion ..............................................................................................................57
Analysis #3...................................................................................................................57 SPARCS A: PID ....................................................................................................57 SPARCS B: Hemophilia ........................................................................................59
Analysis #4...................................................................................................................60 Truven Data: PID ...................................................................................................60 Truven Data: Hemophilia ......................................................................................63
Summary ......................................................................................................................64
Chapter 4: Research Framing.............................................................................................66
vi
Theoretical Framing .....................................................................................................66 What is known?......................................................................................................66 What We Do Not Know .........................................................................................67
A Tentative Theoretical Framework ......................................................................68
Research Purpose .........................................................................................................70
Research Plan ...............................................................................................................70
Research Synopsis and Question Development ...........................................................71
Research Design...........................................................................................................74
Integration of Results ...................................................................................................77 Philosophical Lens .................................................................................................79
Summary ......................................................................................................................79
Chapter 5: Study 1: Patient-centric Vs. Physician-driven Decision Models in the
Treatment of Hemophilia ...................................................................................................80
Methodology ................................................................................................................81
Sample..........................................................................................................................82
Data Collection ............................................................................................................83
Data Analysis ...............................................................................................................84
Findings........................................................................................................................85 Findings related to Decision Theory ......................................................................86
Findings related to Power Balance ........................................................................89
Findings related to Traits .......................................................................................92
Findings related to Organizational Context ...........................................................95
Results ..........................................................................................................................95
Discussion ....................................................................................................................98 Research Gap .......................................................................................................103 Implications..........................................................................................................104
Limitations and Future Research ...............................................................................105
Conclusion .................................................................................................................106
Chapter 6: Study 2: Does Physician’s Decision-Making STYLE Effect Patient
Participation in the Treatment Choices of Primary Immunodeficiency?.........................108
Research Gaps ............................................................................................................109
Design ........................................................................................................................110 Measurement Operationalization .........................................................................110
Constructs of Interest .................................................................................................113 Physician’s Decision-Making Process Effects on Patient Participation ..............117
Mediating Effects of Treatment Approaches to Patient Participation .................117 Physician Traits ....................................................................................................118

vii
Methods......................................................................................................................121 Sample..................................................................................................................121 Data Screening .....................................................................................................122
Multivariate Assumptions ....................................................................................123 Exploratory Factor Analysis ................................................................................123 Confirmatory Factor Analysis ..............................................................................124 Mediation .............................................................................................................126 Interaction (Moderation) ......................................................................................127
Multi-group ..........................................................................................................128 Controls ................................................................................................................131 Hypotheses Results ..............................................................................................131
Discussion ..................................................................................................................136
Summary of Major Findings ......................................................................................137 Expected Findings ................................................................................................139
Unexpected Findings ...........................................................................................140 Observations that Require Future Research .........................................................142
Limitations .................................................................................................................143
Future Research ...................................................................................................144 Ethical Assurances ...............................................................................................145
Conclusions and Implications for Patient Participation .............................................145
Chapter 7: Study 3: A Qualitative Study of Immunologists that Treat PID and the Factors
that Effect Shared Decision Making with their Patients ..................................................147
Post Hoc Reanalysis ...................................................................................................148
Post Hoc Methods ................................................................................................148 Post Hoc Findings ................................................................................................150 Summary of Post Hoc ..........................................................................................152
Research Method of the Qualitative Part of the Third Study.....................................153
Findings......................................................................................................................155
Findings Related to Dual Process ........................................................................156 Findings Related to SIT and Agency Theory ......................................................159 Findings Related to Traits ....................................................................................162 Findings Related to Organizational Context ........................................................164 Findings Related to Feedback ..............................................................................166
Cross-Referencing Findings from Post Hoc and QUAL Interviews .........................168
Discussion ..................................................................................................................170
Limitations, Implications, and Future Research ........................................................171
Chapter 8: Integrative Framework ...................................................................................173
Meta-inferences..........................................................................................................175 Rational Decision Making ...................................................................................176 Patient-Centrism ..................................................................................................176
viii
Traits ....................................................................................................................177 Bias/Nudging .......................................................................................................178 Organizational Context ........................................................................................178
Implications for Practitioners .....................................................................................179
Chapter 9: Discussion, Implications, Limitations, and Contributions .............................183
Theory ........................................................................................................................184
Practice .......................................................................................................................186
Other Research Domains ...........................................................................................187
Limitations .................................................................................................................187
Conclusion .................................................................................................................189
Appendix A: Study 1 Interview Protocol and Questions .................................................190
Appendix B: Invitation Template ....................................................................................194
Appendix C: Study 2 Constructs......................................................................................195
Appendix D: Post Hoc Constructs ...................................................................................197
Appendix E: Study 3 Interview Guide .............................................................................198
Appendix F: Mixed Methods Tutorial .............................................................................202
Research and Analysis Methods ................................................................................202
Mixed Methods ....................................................................................................202 Qualitative Methods .............................................................................................203
Quantitative Methods ...........................................................................................205
References ........................................................................................................................210
ix
List of Tables
Table 1. Theories of Factors that Predict SDM .................................................................. 7
Table 2. Physicians Responsibilities when Practicing SDM (Godolphin, 2009) ............... 9
Table 3. Role of Patients in the Competing Models of Healthcare Decision-Making ..... 12
Table 4. Summary of Biases ............................................................................................. 23
Table 5. Physician Characteristics that Influences the Decision Process ......................... 29
Table 6. MEPS 2014 Item Data Summary ........................................................................ 55
Table 7. Summary of PID Inpatient Admissions and Costs (2008–2010) ........................ 62
Table 8. Summary of Hemophilia Inpatient Admissions and Costs (2008-2010) ............ 64
Table 9. Summary: Quantifying the Quality Gap ............................................................. 65
Table 10. What We Know Concerning SDM Implementation ......................................... 67
Table 11. What We Do Not Know Concerning SDM Implementation ............................ 68
Table 12. Purpose and Description of Mixed Methods .................................................... 77
Table 13. Quality Standards Used for Each Method ........................................................ 78
Table 14. Study 1: Sample Details .................................................................................... 83
Table 15. Study 1 Codes ................................................................................................... 85
Table 16. First Study: Summary of Findings .................................................................... 97
Table 17. Second Study: Summary of Hypotheses and Results ..................................... 115
Table 18. Sample Characteristics .................................................................................... 122
Table 19. Reliability and Validity ................................................................................... 125
Table 20. Descriptive Statistics and Correlations Table of Variables ............................ 126
Table 21. Mediation ........................................................................................................ 127
Table 22. Interaction Effects ........................................................................................... 128
Table 23. Multi-Group Invariance Test by Pathway ...................................................... 128
Table 24. Invariance between White and Non-white Physician Groups ........................ 129
Table 25. Invariance between Ph.D. and Non-PhD Physician Groups ........................... 130
Table 26. Influence of Physician Years of Practice ........................................................ 131
Table 27. Study 2: Expected vs Unexpected Results ...................................................... 138
Table 28. Post Hoc Abbreviations .................................................................................. 149
Table 29. Pathway Values for Figure 13 ........................................................................ 150
Table 30. Indirect Effect: Mediation of Rational Decision Making through Patient-
centrism ........................................................................................................................... 151
Table 31. Indirect Effect: Mediation of Heuristic Decision Making through Patient-
centrism ........................................................................................................................... 151
x
Table 32. Influence of Race on Patient Participation ..................................................... 152
Table 33. Influence of Immunologist Sex....................................................................... 152
Table 34. Study 3: Sample Details .................................................................................. 154
Table 35. Cross-Referencing Study 3 ............................................................................. 169
Table 36. Strengths and Weaknesses of Qualitative Methods ........................................ 204
Table 37. Strengths and Weaknesses of Quantitative Methods ...................................... 206
Table 38. Model Fit Thresholds ...................................................................................... 208
xi
List of Figures
Figure 1. Healthcare Decision Making in Transition .......................................................... 8
Figure 2. ACO Measures of Patient Care ......................................................................... 13
Figure 3. CAHPS Items of SDM ...................................................................................... 13
Figure 4. Responses to Faces ............................................................................................ 31
Figure 5. Medicare Incentive Measures (CMS, 2016) ...................................................... 38
Figure 6. Chronic Care Model (Wagner et al., 2001) ....................................................... 39
Figure 7. Theoretical Framework ..................................................................................... 69
Figure 8. Theoretical Explanations for Predicting SDM .................................................. 71
Figure 9. Overview of Study Design and Results ............................................................. 76
Figure 10. Theory Exploration ........................................................................................ 103
Figure 11. Hypothesized Model ...................................................................................... 115
Figure 12. Second Study: Structural Equation Model Result ......................................... 138
Figure 13. Model of Post-Hoc Analysis of Second Study .............................................. 149
Figure 14. Theories that Predict SDM ............................................................................ 156
Figure 15. Theoretical Framework from Chapter 4 (Revised) ....................................... 174
Figure 16. Summary of Key Findings............................................................................. 185
xii
Acknowledgements
I wish to thank committee members, Dr. Yunmei Wang, Dr. Adrian Wolfberg,
and Dr. J.B. Silvers for agreeing to serve on my committee and who graciously shared
their insights and constructive criticism. I especially thank Dr. Kalle Lyytinen, committee
chair, for his mentorship throughout my doctoral program. I also thank Marilyn Chorman
and Sue Nartker for their incredible support. I also thank Ryan Dagenais for his dedicated
assistance. Lastly, I thank those parties and individuals, both known and anonymous, for
participating in and contributing to my research.
xiii
Still Crossing the Quality Chasm: A Mixed-Methods Study of Physician Decision-
Making When Treating Chronic Diseases
Abstract
by
CHRISTOPHER C. LAMB
Overall healthcare spending in the U.S. is in the trillions and more than 15% of GDP, yet
outcomes rank below the top 25 in most quality categories when compared to other
OECD countries. The majority of spending is directed toward small patient populations
with chronic diseases. Within the context of access to insurance coverage and a certain
level of health literacy, experts believe increased patient–physician shared decision
making (SDM) should result in better care and lower cost. However, the study of the
physician’s role in facilitating SDM is limited. By understanding what factors predict
when physicians will implement SDM during the treatment of specific chronic diseases,
we can begin to understand the dynamics that most influence behaviors and offer
recommendations to improve certain aspects of healthcare in the United States. A
sequence of three studies was completed by interviewing or surveying 369 physicians
who treat hemophilia and primary immune deficiency (PID). The study used dual process
theory to explain the relationship between patient-centered care and SDM within a wider
framework of power balance, patient/physician traits, and organizational context. These
studies were supplemented by an analysis of 1) survey of 33,162 individuals across the
xiv
U.S.; 2) 25 million hospitalization records from New York State comparing two (2) five-
year periods; and 3) data from 200 million individual-level, de-identified enrollment data
and health insurance claims across a continuum of care (both inpatient and outpatient).
The first study qualitatively explored decision making between hemophilia
physicians in the U.S. and U.K. and found U.S. physicians to be more patient-centric and
less rule-based. The second study quantitatively tested the relationship between
slow/rational vs. fast/intuitive decision making by U.S. physicians treating PID and SDM
as mediated by patient-centric care; results showed a statistically significant relationship
between slow/rational decision making and SDM. The third study analyzed decision-
making by U.S. immunologists when treating PID and found a stronger association
between rational/slow decision-making, patient-centered care, and SDM but the process
is bounded by anchoring bias, power balanced by health literacy alignment, and
organizational context related to time and coordination. Overall, results show that
rational/slow decision making as predicted by dual process theory is important to achieve
SDM for patients with complex (i.e., multiple comorbidities) chronic diseases. However,
the impact of health literacy, trust, and reimbursement is much different than what is
reported in the literature. In addition, the study found evidence that information is
anchored or framed in a way that both biases and “nudges” patients as predicted by
behavioral economists. A new integrated SDM model is put forth as a result of this
research.
Combining the physician survey/interview data with an analysis of individual
surveys, hospitalization data, and insurance claims demonstrates a significant opportunity
to improve the quality of care in the U.S. through better decision making.

xv
Keywords: physician decision making; shared decision making; dual process theory;
bounded shared decision making; patient alignment; primary immunodeficiency;
hemophilia; patient-centric approach; bias; decision theory; patient participation;
physician perspective; nudge bias
1
CHAPTER 1: INTRODUCTION
I think that some people with low health knowledge just accept whatever
the doctor says and they just do it. Whereas sometimes people that are very
literate challenge you, which I enjoy, I like the challenge. And then there's
people that are very smart but really don't understand the science of what
they're talking about, and they'll argue with you with things that make no
sense, so those are the most challenging I think. (Study 3; Participant 06-
RS)
Some people don't wanna know, and they, 'cause they don't want the burden
of decision making. You still turn it into a combined decision, or collective
decision, though, because you don't want them to feel is that they're totally
left out. You want them to be involved. (Study 3; Participant 04-TH)
Crossing the Quality Chasm: A New Health System for the 21st Century, a report
prepared by the Institute of Medicine (IOM), highlighted the urgent need to address
quality gaps in the U.S. (Richardson et al., 2001). These gaps include treatment of
chronic diseases which consume 86% of healthcare resources and are commonly
associated with reduced lifespan and co-morbidities (Anderson & Horvath, 2013; CDC,
2017). More pointedly, 5% of these patients consume half the costs (Eapen & Jain, 2017).
Despite spending more per capita, the U.S. ranks below the top 20 countries in most
quality categories (Berwick & Hackbarth, 2012; Keehan et al., 2011; Schneider, Sarnak,
Squires, Shah, & Doty, 2017). To close the quality chasm, the IOM report had two
recommendations: (1) set patient-centric goals for improving the U.S. healthcare system,
meaning that patient preferences and values should guide clinical decisions, and (2) target
chronic health issues to costs (Barry & Edgman-Levitan, 2012; Gerteis et al., 2014).
One method to address both recommendations—and the subject of this paper—is
the implementation of shared decision making (SDM). SDM is a defined term in the
medical community and it relates to a process whereby patients and their healthcare
2
providers come to conclusions about patient treatment jointly (Friesen-Storms, Bours,
van der Weijden, & Beurskens, 2015). It represents a significant opportunity to improve
outcomes and lower expenses (Barry & Edgman-Levitan, 2012; Lee & Emanuel, 2013).
Physicians who incorporate SDM into their decision-making process have the potential to
provide more accurate diagnoses, improved care and better patient-perceived health
(Chambers et al., 2016; Murray, Pollack, White, & Lo, 2007; Seeborg et al., 2015).
Chronic diseases offer an excellent model to study SDM because the complex and
challenging dimensions of the disease require difficult and ongoing treatment decisions
(Abolhassani et al., 2013). Chronic diseases are those that last more than a year and
whose complexity includes multiple co-morbidities which interact in difficult to predict
and emergent ways (Parekh & Barton, 2010). However, despite several developed and
defined SDM models, implementation of SDM with chronic care is limited and little is
known about how it can serve as a useful and practical way for doctors and patients to
interact (Charles, Gafni, & Whelan, 1999; Couët et al., 2015; Légaré et al., 2014;
Stevenson, Barry, Britten, Barber, & Bradley, 2000). Some models describe the factors
that influence SDM in chronic care treatment (Légaré et al., 2013). However, these
factors have not been examined and tested within the context of specific chronic diseases
(Noonan et al., 2017). Senior U.S. policymakers have advocated for more research to fill
knowledge gaps about interventions that will benefit people with multiple chronic
conditions (Parekh, Goodman, Gordon, Koh, & Conditions, 2011; U.S. Department of
Health Human Services, 2010).
A sequence of three studies involving 369 physicians was completed to address
this knowledge gap and identify which factors most influence decision-making when
3
treating hemophilia and primary immune deficiency (PID). Hemophilia is a rare clotting
disorder that affects 10,000 people in the U.S. and is considered one of the top five most
expensive diseases to treat (Brooks, 2017). PID is a rare genetic immunological disorder
with an incidence of 32,000 diagnosed patients, although the prevalence is thought to be
much greater (Bousfiha et al., 2013; Kobrynski, Powell, & Bowen, 2014). It too is one of
the most expensive diseases to treat due to preventable hospitalizations (Gardulf et al.,
2017; Menzin, Sussman, Munsell, & Zbrozek, 2014). Hemophilia and PID represent part
of the 50% of U.S. healthcare spending driven by 5% of the population. Both are good
examples of complex chronic diseases where there is the most opportunity to improve
cost-effective care.
These studies were supplemented by an analysis of 1) survey of 33,162
individuals across the U.S.; 2) 1,425 U.S. PID patients; 3) 25 million hospitalization
records from New York State comparing two five-year periods; and 4) data from 200
million individual-level, de-identified enrollment data and health insurance claims across
a continuum of care (both inpatient and outpatient). These studies help quantify the
quality chasm and the associated cost implications.
There is no published research demonstrating an integrated model that predicts
successful implementation of SDM for chronic disorders and the potential impact on
quality of care. Therefore, theory and data were needed to understand the unique
perspectives of specific chronic diseases and the relationships between factors that
encourage physicians to use SDM in their routine practice (Alston et al., 2012). The
results from this research identified key influences which encourage and discourage
physicians to adopt SDM and should support recommendations on how these influences
4
can improve care and reduce cost. Primary influences include rational/slow decision
making and bias/nudging as predicted by dual process theory, power imbalance mitigated
by patient-centric care and health literacy, as well as organizational context related to
time and coordination of care. Recommendations include physician training on cognitive
phycology, better use of decision aids and improved systems to coordinate care between
physicians. These results can be applied more generally to other chronic disorders.
The remainder of this dissertation is organized as follows. Chapter 2 contains a
review of published literature on the clinical decision-making process. Chapter 3 presents
an analysis of patient survey data and hospitalization records to better understand the
quality gap. Chapter 4 presents the research design and purpose of the three studies.
Chapters 5–7 provide a detailed account of each study and the findings. Chapter 8
integrates the results of the analysis and three studies and discusses the implications and
contributions of this research. Finally, Chapter 9 summarizes the limitations of this
research and potential directions for future studies.
5
CHAPTER 2: LITERATURE REVIEW
There is much commentary about what ails American healthcare. In 1985, Garrett
Hardin famously wrote about the tragedy of the commons: an economic theory whereby
within a shared-resource system individual users acting independently according to their
own self-interest behave contrary to the common good of all users by depleting that
resource through their collective action (Hardin, 1985). Hardin bemoans the “U.S.
medical commons” and the “trend towards commonizing medical costs.” However,
Hardin got it wrong on two points: first, he inaccurately asserts that socializing medicine
will diminish containment of cost; and second, his notion that the psychology of life-
saving emergency acute care inexorably encourages extravagance. The fact is that
socialized single payer systems are far more cost-effective and chronic care—not acute
care—is what is driving exorbitant costs (Coghlan, 2017; Squires & Anderson, 2015).
Others more recently attribute America’s healthcare problems to a lack of access
to basic care and claim that universal coverage will eliminate health inequalities and
improve life expectancy (Ansell, 2017). Solutions include “Medicare for All” which
adherents assert will result in a simplified system that standardizes care (Fram & Freking,
2017). However, universal coverage does not address the issue that most health care is
chronic and complex. While getting more young and healthy people to buy into or be part
of an insurance pool may lower average costs, it will not address the fundamental
problem that small patient populations with chronic diseases are driving exorbitant
expenses and poor outcomes.
Too often the healthcare debate in the U.S. is about financing (public/private or
single vs. multi-payer systems) or access to coverage. However, chronic care is the real
6
problem and the U.S. has the highest percent of complex chronic care patients, meaning
those with multiple comorbidities, amongst its international peers.1
This problem is only
getting worse as baby boomers age and must be urgently addressed before costs
overwhelm business competitiveness and government expenditures. As quoted by Warren
Buffet, "The ballooning costs of healthcare act as a hungry tapeworm on the American
economy" (Hiltzik, 2018). Recent increases in overall healthcare expenditure were almost
entirely driven by increases in multiple chronic care prevalence and the high cost of
caring for these very complex patients (Gerteis et al., 2014). These increases are driven
by healthcare services prices and intensity (Dieleman et al., 2017). Shared Decision
Making (SDM) is an approach to treatment which may improve cost-effective care.
Models and confirmatory data are needed to better understand the circumstances under
which SDM can be optimally implemented.
This chapter reviews the literature related to the research question: what predicts
physician implementation of SDM. First, there is an overview of the U.S. healthcare
system and the evolution of the relationship between physicians and patients. Second,
there is an overview of clinical decision-making and theories which attempt to explain
SDM (Table 1). Using Davis’ criteria, the list of relevant theories in Table 1 were chosen
not only because they are “interesting” but because they are often cited by significant
1
Long term disorders are the main challenge facing health care systems worldwide. For example, 70% of
health service spending in the U.K. is on long term conditions Barnett, K., Mercer, S. W., Norbury, M.,
Watt, G., Wyke, S., & Guthrie, B. 2012. Epidemiology of multimorbidity and implications for health care,
research, and medical education: a cross-sectional study. The Lancet, 380(9836): 37-43, UKHCDO. 2012.
UKHCDO annual report 2012 & bleeding disorder statistics for the financial year 2011/2012.. In 2014,
68% of the U.S. population over the age of 65 have two or more chronic conditions Squires, D., &
Anderson, C. 2015. US health care from a global perspective: spending, use of services, prices, and health
in 13 countries. The Commonwealth Fund, 15: 1-16..
7
researchers in the field and there is recent scholarly work with supporting data (Davis,
1971).
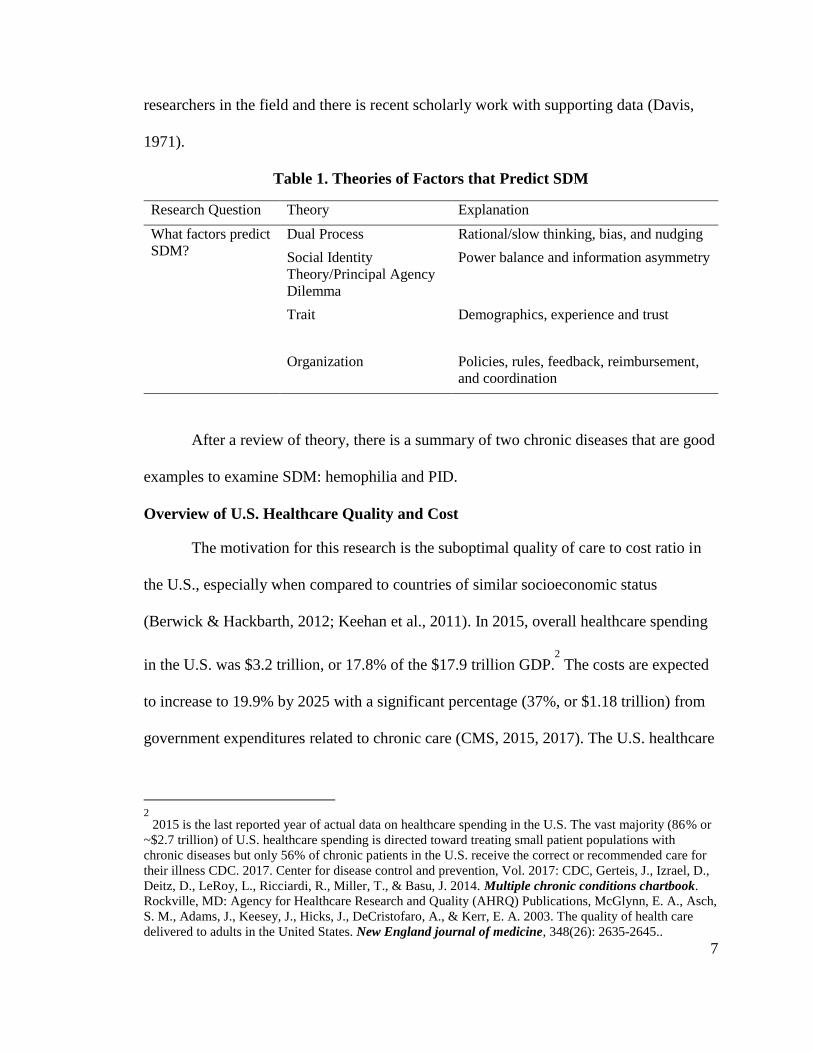
Table 1. Theories of Factors that Predict SDM
Research Question Theory Explanation
What factors predict
SDM?
Dual Process Rational/slow thinking, bias, and nudging
Social Identity
Theory/Principal Agency
Dilemma
Power balance and information asymmetry
Trait Demographics, experience and trust
Organization Policies, rules, feedback, reimbursement,
and coordination
After a review of theory, there is a summary of two chronic diseases that are good
examples to examine SDM: hemophilia and PID.
Overview of U.S. Healthcare Quality and Cost
The motivation for this research is the suboptimal quality of care to cost ratio in
the U.S., especially when compared to countries of similar socioeconomic status
(Berwick & Hackbarth, 2012; Keehan et al., 2011). In 2015, overall healthcare spending
in the U.S. was $3.2 trillion, or 17.8% of the $17.9 trillion GDP.2
The costs are expected
to increase to 19.9% by 2025 with a significant percentage (37%, or $1.18 trillion) from
government expenditures related to chronic care (CMS, 2015, 2017). The U.S. healthcare
2
2015 is the last reported year of actual data on healthcare spending in the U.S. The vast majority (86% or
~$2.7 trillion) of U.S. healthcare spending is directed toward treating small patient populations with
chronic diseases but only 56% of chronic patients in the U.S. receive the correct or recommended care for
their illness CDC. 2017. Center for disease control and prevention, Vol. 2017: CDC, Gerteis, J., Izrael, D.,
Deitz, D., LeRoy, L., Ricciardi, R., Miller, T., & Basu, J. 2014. Multiple chronic conditions chartbook.
Rockville, MD: Agency for Healthcare Research and Quality (AHRQ) Publications, McGlynn, E. A., Asch,
S. M., Adams, J., Keesey, J., Hicks, J., DeCristofaro, A., & Kerr, E. A. 2003. The quality of health care
delivered to adults in the United States. New England journal of medicine, 348(26): 2635-2645..
8
system was ranked 37th of 190 countries according to the WHO in 2000 and dropped to
50th of 55 according to Bloomberg (Du & Lu, 2016; WHO, 2000). For most health
outcomes the U.S. does not rank in the top 35 countries (OECD, 2015).
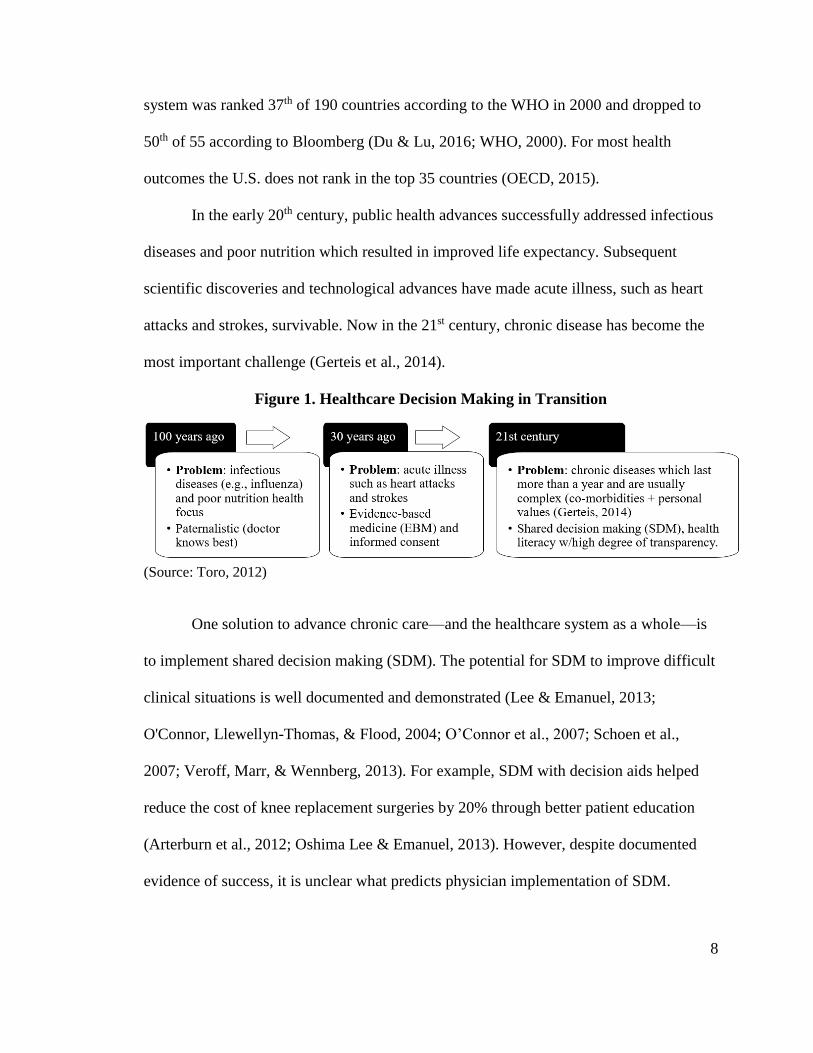
In the early 20th century, public health advances successfully addressed infectious
diseases and poor nutrition which resulted in improved life expectancy. Subsequent
scientific discoveries and technological advances have made acute illness, such as heart
attacks and strokes, survivable. Now in the 21st century, chronic disease has become the
most important challenge (Gerteis et al., 2014).
Figure 1. Healthcare Decision Making in Transition
(Source: Toro, 2012)
One solution to advance chronic care—and the healthcare system as a whole—is
to implement shared decision making (SDM). The potential for SDM to improve difficult
clinical situations is well documented and demonstrated (Lee & Emanuel, 2013;
O'Connor, Llewellyn-Thomas, & Flood, 2004; O’Connor et al., 2007; Schoen et al.,
2007; Veroff, Marr, & Wennberg, 2013). For example, SDM with decision aids helped
reduce the cost of knee replacement surgeries by 20% through better patient education
(Arterburn et al., 2012; Oshima Lee & Emanuel, 2013). However, despite documented
evidence of success, it is unclear what predicts physician implementation of SDM.
9
Evolution of the Relationship between Physicians and Patients: How We Came to
Shared Decision Making (SDM)
SDM is defined as an “approach where clinicians and patients share the best
available evidence when faced with the task of making decisions, and where patients are
supported to consider options, to achieve informed preferences” (Elwyn et al., 2010). It is
the process of integrating patient goals and concerns with medical evidence to achieve
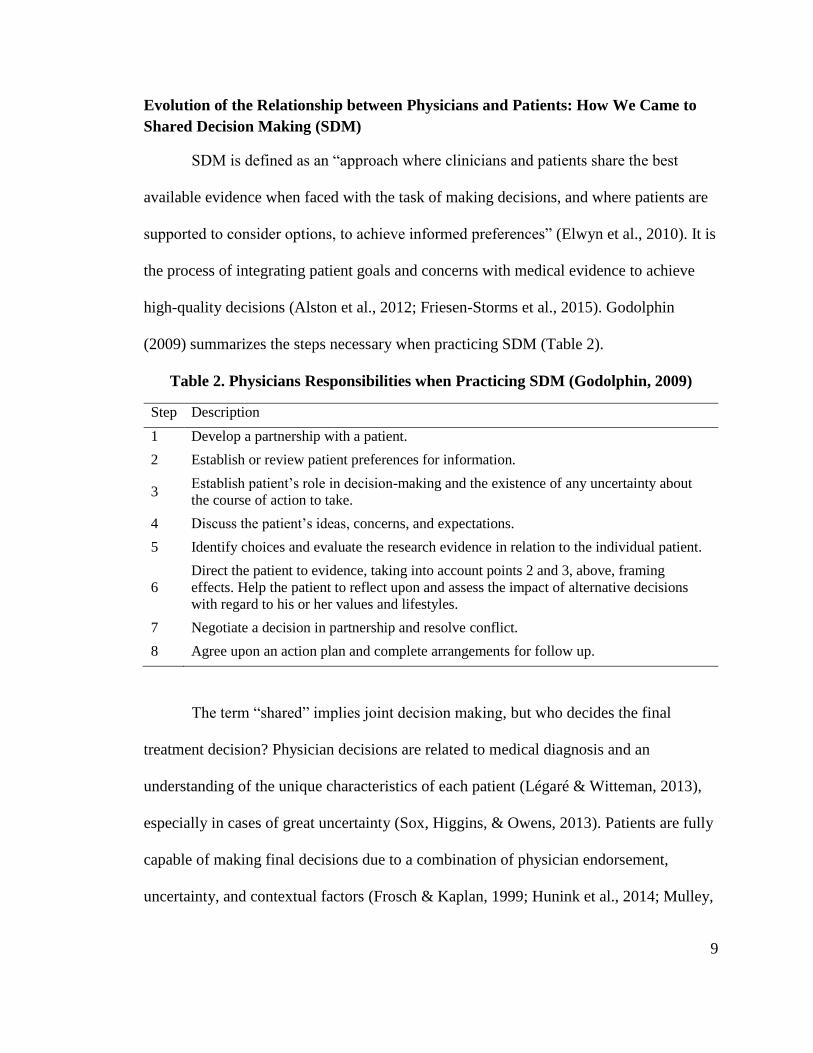
high-quality decisions (Alston et al., 2012; Friesen-Storms et al., 2015). Godolphin
(2009) summarizes the steps necessary when practicing SDM (Table 2).
Table 2. Physicians Responsibilities when Practicing SDM (Godolphin, 2009)
Step Description
1 Develop a partnership with a patient.
2 Establish or review patient preferences for information.
3 Establish patient’s role in decision-making and the existence of any uncertainty about
the course of action to take.
4 Discuss the patient’s ideas, concerns, and expectations.
5 Identify choices and evaluate the research evidence in relation to the individual patient.
6
Direct the patient to evidence, taking into account points 2 and 3, above, framing
effects. Help the patient to reflect upon and assess the impact of alternative decisions
with regard to his or her values and lifestyles.
7 Negotiate a decision in partnership and resolve conflict.
8 Agree upon an action plan and complete arrangements for follow up.
The term “shared” implies joint decision making, but who decides the final
treatment decision? Physician decisions are related to medical diagnosis and an
understanding of the unique characteristics of each patient (Légaré & Witteman, 2013),
especially in cases of great uncertainty (Sox, Higgins, & Owens, 2013). Patients are fully
capable of making final decisions due to a combination of physician endorsement,
uncertainty, and contextual factors (Frosch & Kaplan, 1999; Hunink et al., 2014; Mulley,
10
Trimble, & Elwyn, 2012; Samaan et al., 2014). However, some patients want to be
involved without making the final treatment decision, whereas other may not want any
involvement (Say & Thomson, 2003). SDM, therefore, is not about making shared
decisions but rather integrating patient-physician input into a mutually agreed upon plan
that optimizes values, preferences, cost, and outcomes.
History of SDM
Physician decision-making has been described as informed, paternalistic, or
shared (Friesen-Storms et al., 2015). These should be seen as a continuum of how much
influence is exerted by a patient or physician. Patients range from passive to active
participants in the decision-making process; meaning some patients prefer physicians to
paternalistically make decisions while others demand a decisive role (Kaba &
Sooriakumaran, 2007). Research confirms that, while there are some exceptions, there is
a clear preference on the part of patients for SDM (Kiesler & Auerbach, 2006; Légaré &
Thompson-Leduc, 2014).
Informed decision making is when physicians simply provide information that
allows patients to make all decisions. A famous example is Steve Jobs, Apple CEO, who
insisted on nine months of natural therapy to treat his cancer; unfortunately, many believe
this decision delayed effective therapy and led to a premature death (Isaacson, 2011).
Informed decision making is not applicable to chronic disorders due to disease
complexity and uncertainty of care (Friesen-Storms et al., 2015).
Prior to 2000, paternalism was the dominant decision-making approach
(Rothstein, 2014). Patients were provided minimal information about their condition and
expected to receive and follow orders (Rothstein, 2014). The introduction of “evidence-
11
based medicine” (EBM) as coined by Gordon Guyatt in 1991 was an attempt to
modernize the paternalistic model (Bensing, 2000; Djulbegovic & Guyatt, 2017; Guyatt,
1991). Evidence-based medicine (EBM) “is the conscientious, explicit and judicious use
of current best evidence in making decisions about the care of individual patients”
(Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996: 71). It is a “bottom-up approach
that integrates the best external evidence with individual clinical expertise” (Rousseau,
2012: 38). The practice of EBM was part of a movement to standardize care and reduce
variability in treatment approaches used by different physician specialties (Charles et al.,
1999; Timmermans & Berg, 2010).
After 2000, there was a shift to a patient-centered decision-making paradigm
otherwise known as SDM (Charles et al., 1999; O'Hare, Rodriguez, & Bowling, 2016).
As described in
Table 3, this shift was caused by the limitations of EBM and the recognition that
there may not be a “best” decision but rather an optimal decision based on patient values
and goals (Sturmberg & Martin, 2013: 47-49). Unlike many acute conditions like the flu
or a broken bone, chronic diseases are usually not “cured” but managed over the course
of a person’s life. Chronic disease management is complex and unpredictable and the
physician-patient interplay is crucial. Complexity results from unstable cases where
standard medical techniques cannot be applied and the “process of inquiry” is most
important: listening and exploring possible explanations (Schon, 1983). This approach is
consistent with the theory of Adaptive Health Practice, derived from Adaptive
Leadership, which recommends that physicians be mindful of not “substituting technical

12
interventions for adaptive work” with patients (Heifetz, 1994; Sturmberg & Martin, 2013:
665; Thygeson, Morrissey, & Ulstad, 2010).
Table 3. Role of Patients in the Competing Models of Healthcare Decision-Making
Paternalistic SDM
Objective Obtain relief from ailment. Make choices to alter future
probabilities of wellbeing
Information regarding (a)
medical status and (b)
medical therapy
(a) High but imperfect
(b) Low and imperfect
(a) High but imperfect
(b) High and imperfect
Capabilities Limited to observation and
feeling. Process treatment
information if packaged
appropriately.
Significant within therapies
Complex cognitive structures
involving therapy attributes,
risk, and efficacy
Preferences Not easily accessible.
Require physician effort.
Largely homogeneous within
therapies.
High motivation to express
preferences.
Heterogeneous within
therapies.
Role in physician interactions Provide information Provide and seek information
Role in decision making Passive but involved Active and engaged
Timing Crisis-induced Need- and desire-based
Motivation Prolong life, pain-free if
possible
Superior quality, not
necessarily quantity, of life
Note: Reproduced from “Toward Understanding Consumers' Role in Medical Decisions for Emerging
Treatments: Issues, Framework, and Hypotheses,” by J. Singh, L. Cuttler, and J. Silvers, 2004, Journal of
Business Research, 57(9), p. 1058. (Singh et al., 2004).
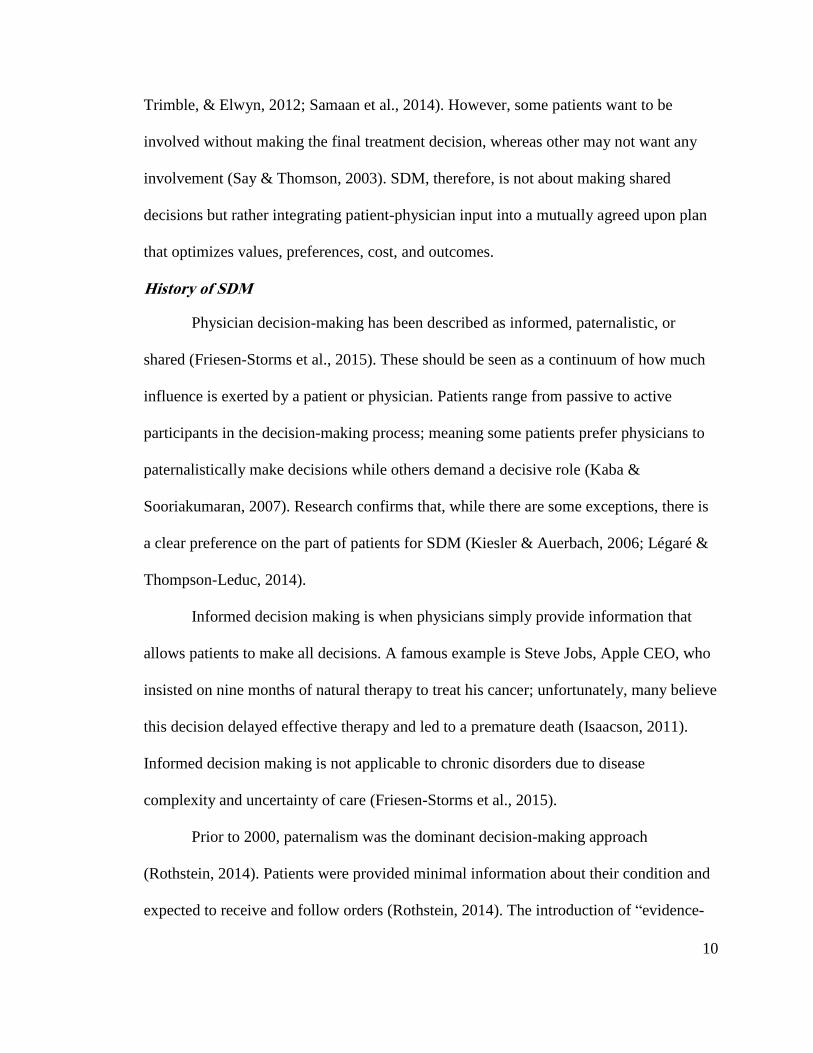
Research and official U.S. policy, enacted in the 2010 Patient Protection and
Affordable Care Act, state that SDM is best applied to chronic health issues (Friesen-
Storms et al., 2015; Frosch et al., 2011). Accountable Care Organizations (ACOs),
integrated payment and care delivery systems used by Medicare, Medicaid, and
commercial payers have developed sets of quality measures and associated financial
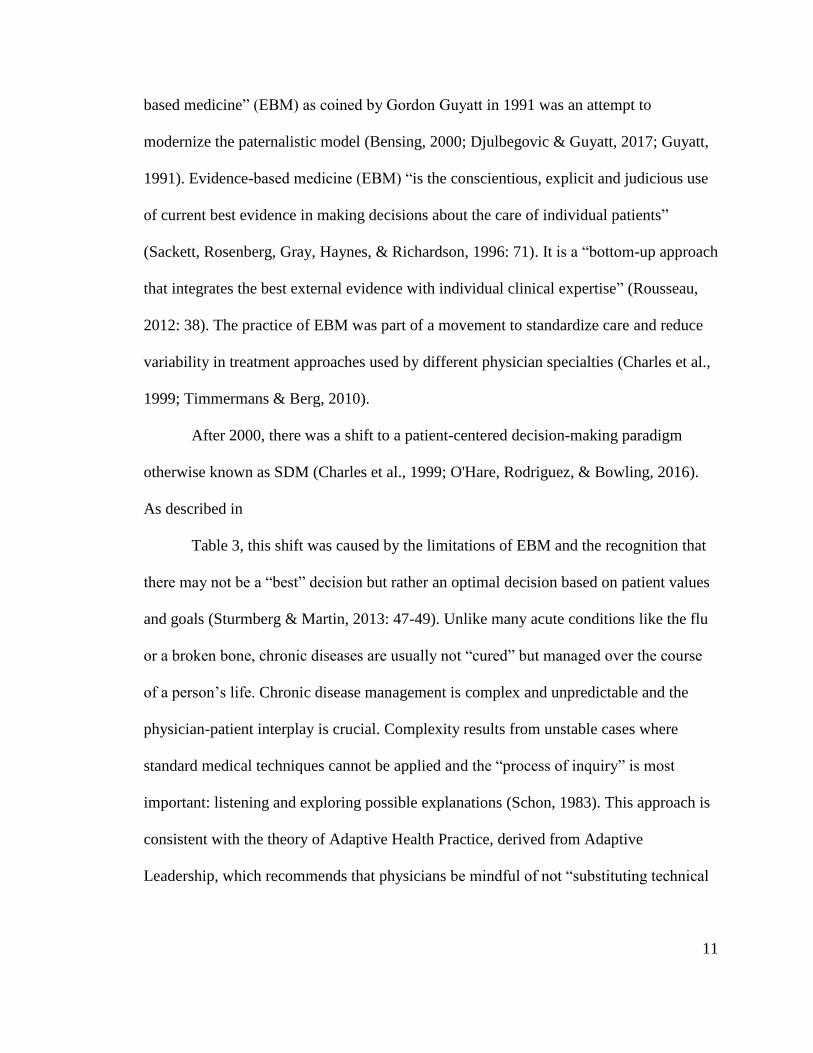
incentives and penalties tied to the use of SDM. (See Figure 2.) In addition, the SDM
consumer assessment of healthcare providers and systems (CAHPS) survey is listed
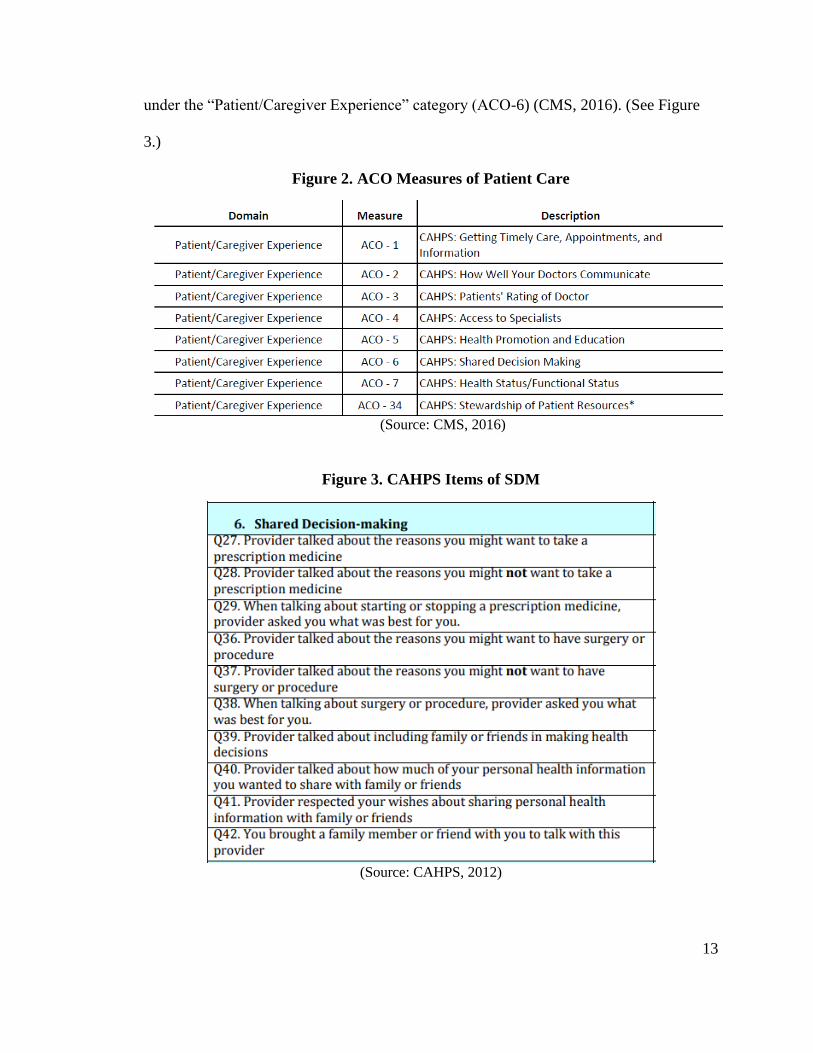
13
under the “Patient/Caregiver Experience” category (ACO-6) (CMS, 2016). (See Figure
3.)
Figure 2. ACO Measures of Patient Care
(Source: CMS, 2016)
Figure 3. CAHPS Items of SDM
(Source: CAHPS, 2012)
14
While healthcare systems are rated by patients according to their success implementing
SDM, the ratings are not linked to individual physicians. Therefore, it is very difficult to
assess physician performance and SDM.
Facilitators of SDM
By understanding what influences implementation of SDM, optimal decision-
making strategies or designs can be applied to complex chronic diseases where it is most
needed. However, despite reports suggesting the U.S. healthcare system excels at SDM,
attempts to implement and coordinate SDM into practice are scarce and poorly
understood (Desroches, 2010; Schneider et al., 2017).
Facilitators of SDM are thought to be education, appropriate training on SDM,
and improved interpersonal skills with patients (Belanger, Rodríguez, & Groleau, 2011;
Légaré et al., 2013). Barriers to SDM are thought to be conflicting practitioner roles
within healthcare systems, power imbalances between patients and practitioners,
inadequate resources, physician payment structure (quantity vs. outcomes), and time
constraints (Belanger et al., 2011; Légaré et al., 2013). Other considerations include bias
as predicted by cognitive psychologists and physicians’ relationships with stakeholders
within the larger healthcare system (Chapman, Kaatz, & Carnes, 2013; Croskerry, 2014).
The factors influencing patient participation—and SDM by extension—have been
explored on a general level, but have not been explicitly studied in the context of specific
chronic health issues (Longtin et al., 2010). Scales have been developed to measure
whether SDM is preferred by patients but do not capture the factors that predict SDM
(Giguère, Labrecque, Njoya, Thivierge, & Légaré, 2012). SDM has been measured by the
levels of perceived comfort, pain management, perceived anxiety levels, and involvement
15
of family and friends (Barry & Edgman-Levitan, 2012); but again, not the factors that
predict these perceptions. The issue is not whether SDM can be implemented but what
facilitates or predicts implementation.
As a caveat, the suspected or known consequences of SDM are also poorly
described in the literature. For example, the U.S. has been in the midst of a prescription
opioid epidemic since 2000 (Baker, 2017). The epidemic was an unforeseen consequence
of a patient-oriented approach to pain management (Manchikanti, Helm, & Janata, 2012).
The overzealous prescribing of opioids was the result of a self-reported pain scales using
standards set by the Joint Commission (Baker, 2017). The goal is to find a balance in the
decision-making process—using SDM—to provide optimal care; in other words, to avoid
under-treating and over-treating patients.
In summary, SDM is an approach that adopts the advantages of paternal and
informed approaches to care. The interpersonal aspect of this approach is best utilized for
the treatment of chronic diseases which are complex and not curable. Despite perceived
benefits, factors that predict implementation have not been adequately studied or
documented in published literature. Exploring clinical decision-making theory may
provide insight into specific factors that may facilitate or discourage SDM by physicians.
Theories Related to Clinical Decision Making
Clinical decision making is a “contextual, continuous, and evolving process,
where data are gathered, interpreted and evaluated to select the optimal choice of action”
(Tiffen, Corbridge, & Slimmer, 2014). Dual process theory has been used to explain
clinical decision making. Dual process theory is the latest iteration in a long history on
decision theory; however, it may only a partial explanation. Therefore, the following
16
sections review the literature on decision theory, the movement from classical to dual
process theory, as well as alternative theories that attempt to predict implementation of
SDM.
Decision Theory
Decision theory is the study of strategies for optimal decision-making. The best
application of decision theory to the medical community is an ongoing debate: algorithms
vs. personalized individual interviews. Some argue against the use of algorithm-based
diagnoses over traditional physician-patient in-depth interviews—specifically, recipe-like
approaches that may hinder physicians’ creativity and flexibility, often overlooking
subtle clues that can lead to the correct diagnosis (Groopman, 2008). Given that 75% of
chronic care clinical diagnostic failures are likely attributed to errors in physician
thinking, a better understanding of the medical decision-making process is necessary
(Graber, Franklin, & Gordon, 2005). Unfortunately, various studies have analyzed
characteristics of decision-making styles in a variety of settings but with mixed results
(Calder et al., 2011; Coget & Keller, 2010; Kaplan, Greenfield, Gandek, Rogers, & Ware,
1996). Further study is needed to extend decision theory into chronic care treatment
particularly since it is dominated by a mix of uncertainty, evidence-based
diagnosis/treatment and patient values (Groopman, 2008; Montgomery, 2005). This
extension of decision theory could then serve as a template for use by the medical
community for optimal SDM implementation (Croskerry, 2009a).
Classical Decision Theory
Classical decision theory is “the collection of axiomatic models of uncertainty and
risk (probability theory, including Bayesian theory), and utility (utility theory, including
17
multi-attribute utility theory)” (Beach & Lipshitz, 2017: 85). It is a method of formalizing
the alternative decision options based on existing conditions (North, 1968). However,
classical decision theory depends on two elements: an ideal decision setting and a
decision maker who can make an optimal choice after carefully evaluating all options and
possible outcomes (Beach & Lipshitz, 2017). Chronic care does not have either of these
elements; the healthcare system works best for patients with single conditions
(Grembowski et al., 2014).
Dual Process Theory for Decision Making
Dual process theory, otherwise known as prospect theory, developed from a long
history of thinkers who challenged classical decision theory (Barrett, Tugade, & Engle,
2004; Kahneman, 2011; Tversky & Kahneman, 1992). It explains how people choose
from among sub-optimal decision options based on context (Tversky & Kahneman,
1986b) and weighing costs and benefits depending on pre-existing preferences and biases
(Scott, 2000).
Dual process theory integrates two processes of thinking that can be applied to
clinical diagnoses and decisions (Croskerry, 2009b; Evans & Stanovich, 2013; Pelaccia,
Tardif, Triby, & Charlin, 2011). It categorizes how physicians think into two modes:
heuristic thinking (“System 1”) and rational thinking (“System 2”) (Djulbegovic, Hozo,
Beckstead, Tsalatsanis, & Pauker, 2012; Durning et al., 2015; Stark & Fins, 2014). The
concept of System 1 and System 2 is a modern, more robust version of Dewey’s type 1
and type 2 thinking. Dewey (1925) described “lived” experience (type 1), which is “the
result of a minimum of incidental reflection,” and “secondary” experience (type 2), which
is the result of “continued and regulated reflective inquiry” (Dewey, 1925). Simon
18
rejected Dewey’s perfect rationality and developed the concept of bounded rationality,
which takes into account environmental complexity, cognitive limits and the task-at-
hand; people satisfice by choosing what is sufficient. Bounded rationality explains how
satisficing decisions are made in the absence of information, time, and resources (Simon,
1996). Gigerenzer extended Simon’s concept of “fast and frugal” heuristics; humans
apply algorithms to achieve near-optimal decisions (Gigerenzer & Goldstein, 1996).
Heuristic decision making (System 1) is an approach that relies on experience
(Croskerry, 2009b; Kahneman, 2011). Heuristics are “strategies that ignore information
to make decisions faster, more frugally, and more accurately than more complex
methods” (Gigerenzer, 2015: 109). Physicians simplify information by forming standard
approaches to treatment-based clinical experience, otherwise known as “illness scripts”
(Borrell-Carrió, Estany, Platt, & MoralesHidalgo, 2014; Campbell, 2013). Furthermore,
physicians use “intuition” or mental cues and primers to access information from their
memory (Kahneman, 2011) However, intuition is nothing more or less than recognition
(Simon, 1996). In short, heuristic decisions are mental shortcuts based on experiences,
irrespective of supporting data (intuitive reasoning). While the ability to identify patterns
quickly may have benefits in certain settings, heuristics or fast thinking by physicians
carries certain risks, including misinterpreting conceptual relationships and introducing
bias into decision making (Campbell, 2013; Ely, Kaldjian, & D'Alessandro, 2012;
Lovallo & Sibony, 2010).
Experts have a long-standing debate between expert intuition and algorithms.
Some argue that algorithms outclass expert intuition by removing the bias and
subjectivity that comes with expert opinions, especially when involving uncertainty
19
(Kahneman, 2011). Others favor experts because algorithms cannot be applied to
dynamic, flexible real-world instances (Kahneman, 2011). Overall, algorithms may be
better than human reasoning because people rarely detect subtle valid cues in noisy
environments (Kahneman, 2011). However, expert intuition may have an advantage
when applied to a predictable environment through prolonged practice; a “less-is-more”
effect of intuitive thinking for redundant and predictable tasks (Gigerenzer, 2015). In
either case, expert intuition or heuristics, have the same risks and biases associated with
System 1 thinking (Campbell, 2013; Ely et al., 2012; Lovallo & Sibony, 2010).
Rational decision-making (System 2) is a slow and effortful process of problem-
solving by conscious analysis (Durning et al., 2015; Kahneman, 2011). This style of
thinking requires physicians to meticulously consider available options and variables
(Campbell, 2013; Croskerry, 2009b). Physicians may analyze different factors, such as
the ratio of harm to benefits, especially when there is no clear or standard procedure
given a unique or complex patient circumstances (Djulbegovic et al., 2012). Dual process
theory suggests that System 2 thinking is better able to integrate ambiguous data,
literature, and statistical algorithms (Kahneman, 2011).
Uncertainty
The presence of uncertainty plays an overarching role in the physician decision
process. Uncertainty refers to the risk that is incurred as a result of lack of definitive
answers or solutions to a problem (Jones, 1992). Physicians are usually confronted with
three types of uncertainty when making clinical decisions: limitations of medical
knowledge, the physician’s perception of the gaps in his or her medical knowledge, and
the tolerance of uncertainty (Jones, 1992). The limitations of a physician’s medical
20
knowledge are often regarded as one of the strongest influences on the decision-making
processes because of the need to use clinical skills and judgment despite incomplete
empirical support (Flynn, 2003). In some cases, physicians may have experience that
contradicts research evidence, thereby increasing their uncertainty (Timmermans & Berg,
2010: 163). Physicians have to cope with the reality that there will be gaps in their
knowledge and competencies, underscoring the importance of remaining updated and
properly trained (Flynn, 2003). Furthermore, physician tolerance to uncertainty could
affect how they treat patients; high tolerance to uncertainty may increase a physician’s
willingness to deviate from standard protocols to accommodate the patient’s lifestyle and
preferences (Flynn, 2003). Due to multiple co-morbidities, uncertainty is inherent to
chronic care and requires complex management, decision making and coordination
(Whitson & Boyd, 2016). Dual process theory suggests that greater uncertainty requires
System 2 thinking.
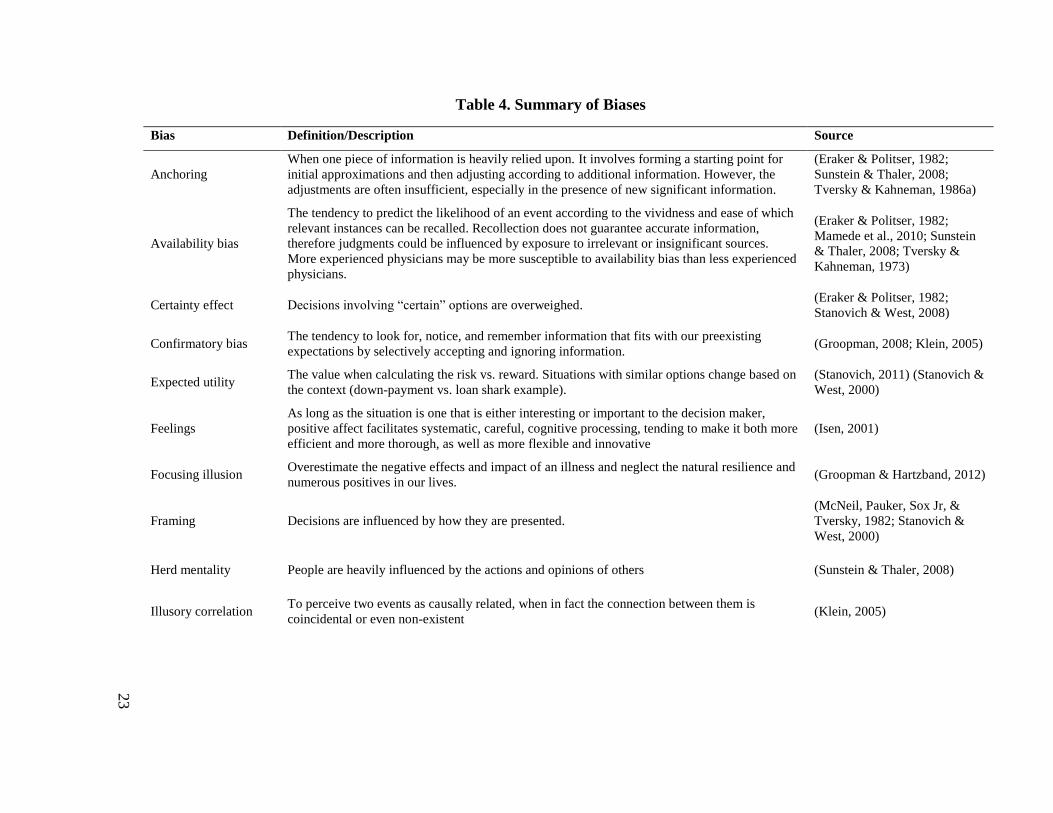
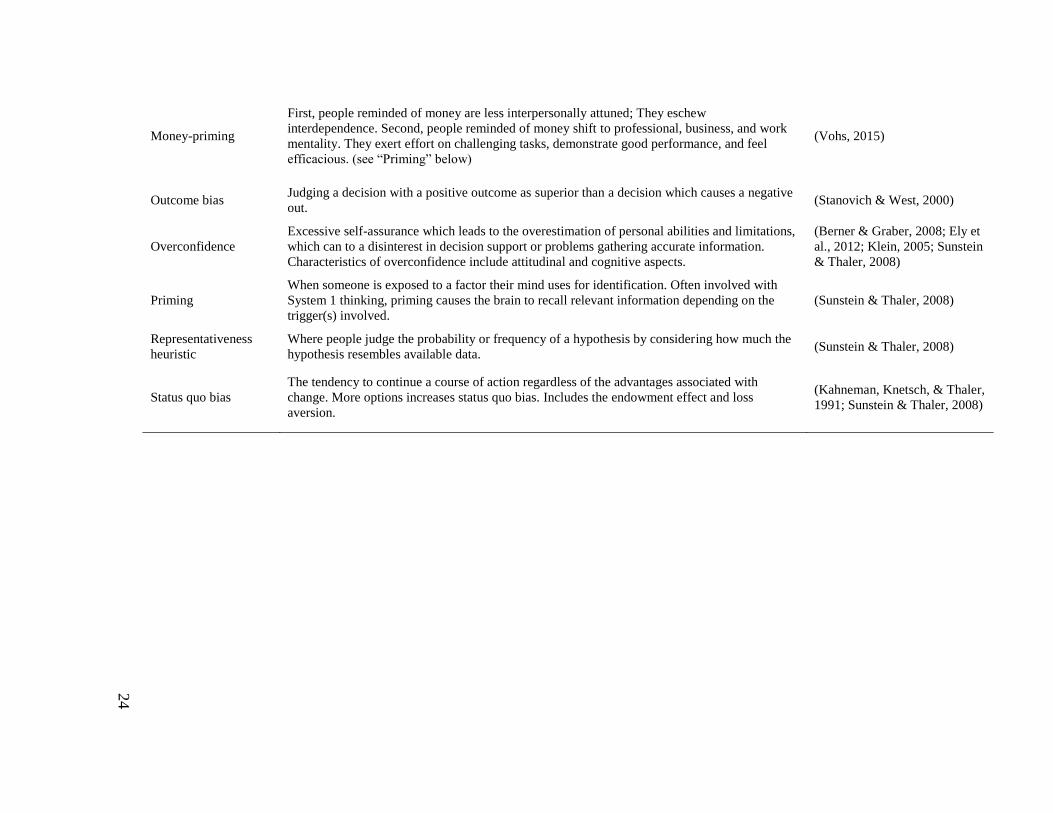
Bias
Physician decision making is susceptible to biases listed in Table 4 (Silvers,
Marinova, Mercer, Connors, & Cuttler, 2010). Bias consists of flawed evaluations of
initial information. For example, a physician may treat a new patient with the same
methods and drugs as previous patients because of similar symptoms and mentioned
insurance coverage (anchoring, availability, money-priming, and status quo bias).
Training as a resident may drastically affect how physicians think and potentially
reinforce bias: initial exposure to real patients is often the link between knowledge and
experience (Patel, Kaufman, & Arocha, 2002; Patel, Yoskowitz, & Arocha, 2009). One
21
method to combat bias is for physicians to practice meta-cognitive thinking by analyzing
how they reach conclusions (Klein, 2005).
Perhaps the most important bias related to SDM is how word framing can alter
decision making. For example, suppose patients have to decide whether to have a
hypothetical drug administered. If they are told, “This drug has a 95% survival rate,”
people are more likely to agree than when told, “This drug has a 5% death rate.” Words
have power and verbal primes impact decision making (Sapolsky, 2017: 93).
Recent studies suggest biological support for word framing bias. When patients
receive medication with a positive expectation, there is an increase in activity of the brain
area known to be involved in pain relief (regardless of whether the pain relief is from a
narcotic or placebo). Alternatively, when medication is delivered with a negative
expectation, there is reduced brain activity in this area (Ofri, 2017: 80).
Libertarian paternalism is a method of encouraging individuals to make choices
which are in their best interests while maintaining their freedom of choice (Aggarwal,
Davies, & Sullivan, 2014; Thaler & Sunstein, 2003). Physicians usually have an opinion
on the best treatment for their patients and are prone to “frame” information to nudge the
decision process in favor with aligning to their decisions (Aggarwal et al., 2014).
However, healthcare involves an immense knowledge set that patients do not normally
have access to, nor do they fully comprehend all the information (Walls, 2014).
Therefore, libertarian paternalism’s goal is to supplement the patient decision towards
effective treatment (Schiavone, De Anna, Mameli, Rebba, & Boniolo, 2014).
Both biological and behavioral theories support the hypothesis that how doctors
frame a treatment has profound effects on how patient receives, interprets and
22
experiences that treatment. One method to combat bias is for the physician to practice
meta-cognitive “slow” thinking, or to study how they reach conclusions (Klein, 2005).
However, we should consider when a bias is a negative attribute and when it is a “nudge”
which may serve as encouragement for advantageous decisions (Sunstein & Thaler,
2008).
In summary dual process theory can be a useful method for understanding
decision making and the potential for predicting SDM with chronic care. However, it is
likely that dual process theory only partially explains how clinical decisions are made.
The next section reviews alternative theories that have the potential to predict when SDM
will be implemented.
23
Table 4. Summary of Biases
Bias Definition/Description Source
Anchoring
When one piece of information is heavily relied upon. It involves forming a starting point for
initial approximations and then adjusting according to additional information. However, the
adjustments are often insufficient, especially in the presence of new significant information.
(Eraker & Politser, 1982;
Sunstein & Thaler, 2008;
Tversky & Kahneman, 1986a)
Availability bias
The tendency to predict the likelihood of an event according to the vividness and ease of which
relevant instances can be recalled. Recollection does not guarantee accurate information,
therefore judgments could be influenced by exposure to irrelevant or insignificant sources.
More experienced physicians may be more susceptible to availability bias than less experienced
physicians.
(Eraker & Politser, 1982;
Mamede et al., 2010; Sunstein
& Thaler, 2008; Tversky &
Kahneman, 1973)
Certainty effect Decisions involving “certain” options are overweighed. (Eraker & Politser, 1982;
Stanovich & West, 2008)
Confirmatory bias The tendency to look for, notice, and remember information that fits with our preexisting
expectations by selectively accepting and ignoring information. (Groopman, 2008; Klein, 2005)
Expected utility The value when calculating the risk vs. reward. Situations with similar options change based on
the context (down-payment vs. loan shark example).
(Stanovich, 2011) (Stanovich &
West, 2000)
Feelings
As long as the situation is one that is either interesting or important to the decision maker,
positive affect facilitates systematic, careful, cognitive processing, tending to make it both more
efficient and more thorough, as well as more flexible and innovative
(Isen, 2001)
Focusing illusion Overestimate the negative effects and impact of an illness and neglect the natural resilience and
numerous positives in our lives. (Groopman & Hartzband, 2012)
Framing Decisions are influenced by how they are presented.
(McNeil, Pauker, Sox Jr, &
Tversky, 1982; Stanovich &
West, 2000)
Herd mentality People are heavily influenced by the actions and opinions of others (Sunstein & Thaler, 2008)
Illusory correlation To perceive two events as causally related, when in fact the connection between them is
coincidental or even non-existent (Klein, 2005)
24
Money-priming
First, people reminded of money are less interpersonally attuned; They eschew
interdependence. Second, people reminded of money shift to professional, business, and work
mentality. They exert effort on challenging tasks, demonstrate good performance, and feel
efficacious. (see “Priming” below)
(Vohs, 2015)
Outcome bias Judging a decision with a positive outcome as superior than a decision which causes a negative
out. (Stanovich & West, 2000)
Overconfidence
Excessive self-assurance which leads to the overestimation of personal abilities and limitations,
which can to a disinterest in decision support or problems gathering accurate information.
Characteristics of overconfidence include attitudinal and cognitive aspects.
(Berner & Graber, 2008; Ely et
al., 2012; Klein, 2005; Sunstein
& Thaler, 2008)
Priming
When someone is exposed to a factor their mind uses for identification. Often involved with
System 1 thinking, priming causes the brain to recall relevant information depending on the
trigger(s) involved.
(Sunstein & Thaler, 2008)
Representativeness
heuristic
Where people judge the probability or frequency of a hypothesis by considering how much the
hypothesis resembles available data. (Sunstein & Thaler, 2008)
Status quo bias
The tendency to continue a course of action regardless of the advantages associated with
change. More options increases status quo bias. Includes the endowment effect and loss
aversion.
(Kahneman, Knetsch, & Thaler,
1991; Sunstein & Thaler, 2008)
25
Power
Power imbalance between a physician and a patient is thought to be an important
influence on clinical decision making (Topol, 2015). Social Identity Theory (SIT)
predicts that the level of imbalance is important and patient advocates claim that health
literacy is the way imbalances can be mitigated (Wald, 2015).
SIT suggests that people tend to categorize themselves and others depending on a
collection of individual roles (Ashforth & Mael, 1989). Defining social roles as part of a
performance to reinforce status and identity has been long recognized in the medical
community when, for example, doctors use an elaborate personal front such as white
coats or stages such as large desks (Goffman, 1959). Power dynamics are a fundamental
aspect of human relationships and the physician-patient dyad is no exception (Fiske,
Dupree, Nicolas, & Swencionis, 2016; Mirowsky, 2017). According to SIT, physicians
are likely to categorize themselves and colleagues as highly educated when compared to
patients. Asymmetries of information may explain why physicians are slow to adopt
SDM (Tapscott, 2010: 195). Their interactions with patients, who are likely in a different
category, affect the physician decision process depending on the categories associated
with the patient. These categories, or identities, lead to a power imbalance in the
physician-patient relationship and likely a reduction in SDM.
While the balance of power in the physician-patient relationship can affect the
overall quality of care, some believe that physicians can take measures to increase patient
empowerment which will lead to improved patient outcomes (Bravo et al., 2015). These
interventions include a patient-centered approach to care, counseling, coaching, and
addressing patient values; all of these actions are represented in SDM (Bravo et al.,
26
2015). Experienced clinicians are usually aware of power dynamics and often serve as
“guides” to patients (Hibbard, 2017; McCormack, Thomas, Lewis, & Rudd, 2017).
Nevertheless, it is clear that clinicians often use authority to “nudge” patients to do what
is best (Sunstein & Thaler, 2008).
Health literacy is a method proposed by health advocates to reduce the power
imbalance between a physician and a patient. Patient education and understanding of
medical information (“health literacy”) plays a role in the patient’s capability to make
decisions with the physicians. Information asymmetry, as described by the “agency
dilemma,” deals with the study of decisions where one party has more or better
information than the other and creates an imbalance of power (Eisenhardt, 1989).
Information asymmetries have been studied in the context of principal–agent problems
where they are a major cause of misinforming or misleading communication (Christozov,
Chukova, & Mateev, 2009).
Patient education as a source of information and empowerment is predicted to
mitigate the agency dilemma and reduce power imbalance (Nguyen, 2011). Health
literacy is seen as a necessary condition that enables SDM (Noonan et al., 2017).
Rosenthal, a Harvard-educated physician and New York Times reporter, emphatically
argues that “we must become bolder, more active and thoughtful about what we demand
of our healthcare and the people who deliver it” (Rosenthal, 2017: 329). This framework
suggests that what patients need is good data on their condition and treatment options
(Tapscott, 2010: 179). Health literacy is the ability of a patient to read and comprehend
medical information. Having this ability enables patients to contribute meaningful
additions to the physician-patient relationship and the decision process (McCormack et
27
al., 2017). According to the Picker Institute, patients can make progressively more
informed decisions with clear, specific and high-quality information (Barry & Edgman-
Levitan, 2012). The ability to make progressively more informed decisions is especially
important for patients with chronic disorders which require decisions that have lifelong
implications and consequences (Montori, Gafni, & Charles, 2006). However, one
limitation is that the data necessary to inform patients is becoming more difficult to
access and decipher (Hathi & Kocher, 2017).
One major resource likely to enable patient health literacy is the use of decisions
aids; tools that simplify information on treatments, risks, and benefits (Stacey et al.,
2014). Decision aids include pamphlets, references, or simplified graphics and have been
documented to improve options and lower costs (Arterburn et al., 2012; Légaré &
Witteman, 2013). Using decision aids, patients are more inclined to discuss and comply
with treatment regimens when they understand the goals and consequences involved in
their care (Friesen-Storms et al., 2015). There is a considerable amount of scholarly work
on the importance of decision aids to facilitate SDM (Butler, Ratner, McCreedy, Shippee,
& Kane, 2014).
The collection of professional or personal contacts and networks of patients
affected by a disease can enable SDM. Being part of a community has tremendous
benefits to patient engagement, psychological health, and physical health compared to
those “bowling alone” (Blumenthal-Barby, 2017; Putnam, 1995). The internet is a
platform to share information, deliver care and guide communities with similar chronic
disorders. Shared platforms generate vast databases to learn, collaborate and teach
(Tapscott, 2010: 184). With an interactive system in place, patients and physicians in the
28
network can be exposed to the collective experiences of patients, such as the methods of
improving day-to-day life with a chronic disease (Frost & Massagli, 2009). Patients are
part of a community, enhanced by the Internet, which disseminates information about
their disease and offer a psychological support system. (Sugawara et al., 2012). Examples
of these patient communities include the National Hemophilia Foundation and Immune
Deficiency Foundation for hemophilia and PID. The benefits of information through
these networks can extend to passive participants in virtual communities (i.e., forums),
known as “lurkers” (Leimeister & Krcmar, 2005). However, one limitation is that online
communities may not have a uniform impact on patient empowerment because of
differing levels of patient literacy and physician paternalism (Petrič, Atanasova, &
Kamin, 2017).
In summary, understanding power balance dynamics is crucial to understanding
SDM. SIT predicts that if there is a power imbalance (i.e., greater physician influence),
the likelihood of successful SDM will be lower. Health literacy is seen as the prerequisite
for successful SDM and achieved by improving literacy through knowledge, aids, and
networks. It is considered a necessary condition to balance the power relationship
between a physician and a patient as predicted by the Agency dilemma. A patient-
centered approach in combination with health literacy may explain the mechanism
through which power can be balanced and SDM is achieved.
Traits
Trait theory uses personal characteristics to predict influence. These include
demographic (sex, age, education), and experience (intelligence, knowledge) (Eysenck,
1963). Trait theory predicts that decision making is influenced by both physicians’ and
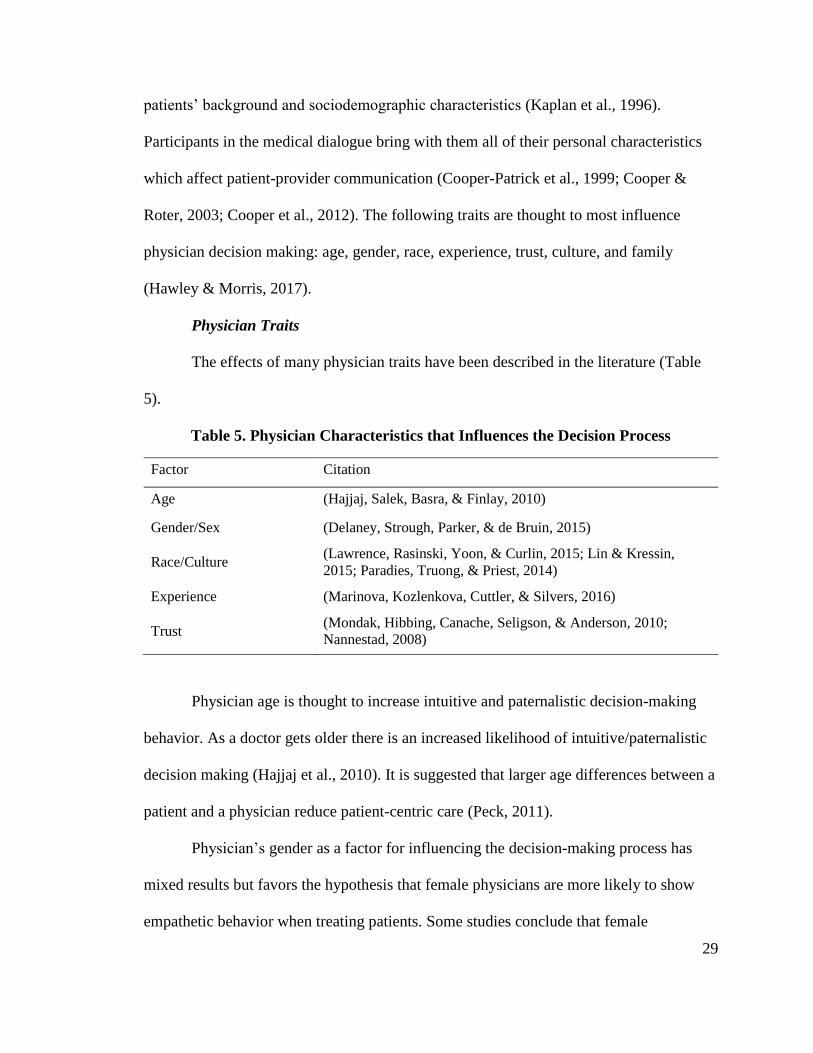
29
patients’ background and sociodemographic characteristics (Kaplan et al., 1996).
Participants in the medical dialogue bring with them all of their personal characteristics
which affect patient-provider communication (Cooper-Patrick et al., 1999; Cooper &
Roter, 2003; Cooper et al., 2012). The following traits are thought to most influence
physician decision making: age, gender, race, experience, trust, culture, and family
(Hawley & Morris, 2017).
Physician Traits
The effects of many physician traits have been described in the literature (Table
5).
Table 5. Physician Characteristics that Influences the Decision Process
Factor Citation
Age (Hajjaj, Salek, Basra, & Finlay, 2010)
Gender/Sex (Delaney, Strough, Parker, & de Bruin, 2015)
Race/Culture (Lawrence, Rasinski, Yoon, & Curlin, 2015; Lin & Kressin,
2015; Paradies, Truong, & Priest, 2014)
Experience (Marinova, Kozlenkova, Cuttler, & Silvers, 2016)
Trust (Mondak, Hibbing, Canache, Seligson, & Anderson, 2010;
Nannestad, 2008)
Physician age is thought to increase intuitive and paternalistic decision-making
behavior. As a doctor gets older there is an increased likelihood of intuitive/paternalistic
decision making (Hajjaj et al., 2010). It is suggested that larger age differences between a
patient and a physician reduce patient-centric care (Peck, 2011).
Physician’s gender as a factor for influencing the decision-making process has
mixed results but favors the hypothesis that female physicians are more likely to show
empathetic behavior when treating patients. Some studies conclude that female
30
physicians have more participatory styles related to empathy and information sharing,
adopt a more “patient-centered” behavior or spend more time with patients showing
greater concern to patient psychosocial factors (Bertakis, Franks, & Azari, 2002; Janssen
& Lagro-Janssen, 2012; Kourakos, Fradelos, Papathanasiou, Saridi, & Kafkia, 2017;
Mazzi et al., 2016; Roter, Hall, & Aoki, 2002). However, one study reports that patient
participation is a function of many complex factors and not linked to gender (Street Jr,
Gordon, Ward, Krupat, & Kravitz, 2005).
Race
There is extensive literature on the influence of race (Burgess, Van Ryn, Crowley-
Matoka, & Malat, 2006; Cooper-Patrick et al., 1999; Cooper & Roter, 2003; Cooper et
al., 2012; Lawrence et al., 2015; Schulman et al., 1999; Snipes et al., 2011; Traylor,
Schmittdiel, Uratsu, Mangione, & Subramanian, 2010). White physicians are more likely
to have different prescribing behaviors (Lawrence et al., 2015). Non-white physicians
have been reported by their patients to be less participatory (Kaplan et al., 1996). Studies
have shown that there is less conversation between physicians and patients if their races
are different (Lin & Kressin, 2015). Therefore, it is hypothesized that white physicians
are more likely to implement SDM.
Minority groups are less likely to be screened for and treated for breast cancer
than whites. One recent report documented that Black women have a 40% higher breast
cancer mortality than white women in part due to differences in diagnosis and
comorbidities (DeSantis, Ma, Goding Sauer, Newman, & Jemal, 2017). Patient
characteristics can be both explicit and non-explicit. For example, nonverbal sensitivity
(NVS) relates to how non-verbal communication is correlated with patient-centered
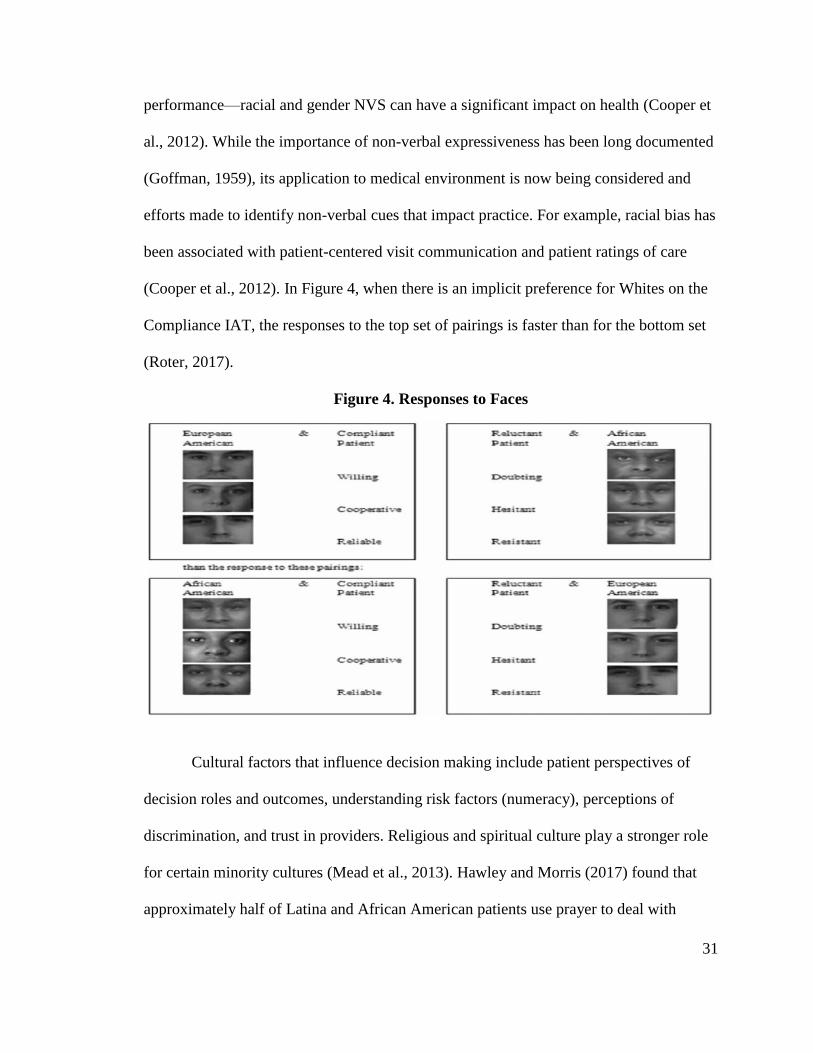
31
performance—racial and gender NVS can have a significant impact on health (Cooper et
al., 2012). While the importance of non-verbal expressiveness has been long documented
(Goffman, 1959), its application to medical environment is now being considered and
efforts made to identify non-verbal cues that impact practice. For example, racial bias has
been associated with patient-centered visit communication and patient ratings of care
(Cooper et al., 2012). In Figure 4, when there is an implicit preference for Whites on the
Compliance IAT, the responses to the top set of pairings is faster than for the bottom set
(Roter, 2017).
Figure 4. Responses to Faces
Cultural factors that influence decision making include patient perspectives of
decision roles and outcomes, understanding risk factors (numeracy), perceptions of
discrimination, and trust in providers. Religious and spiritual culture play a stronger role
for certain minority cultures (Mead et al., 2013). Hawley and Morris (2017) found that
approximately half of Latina and African American patients use prayer to deal with
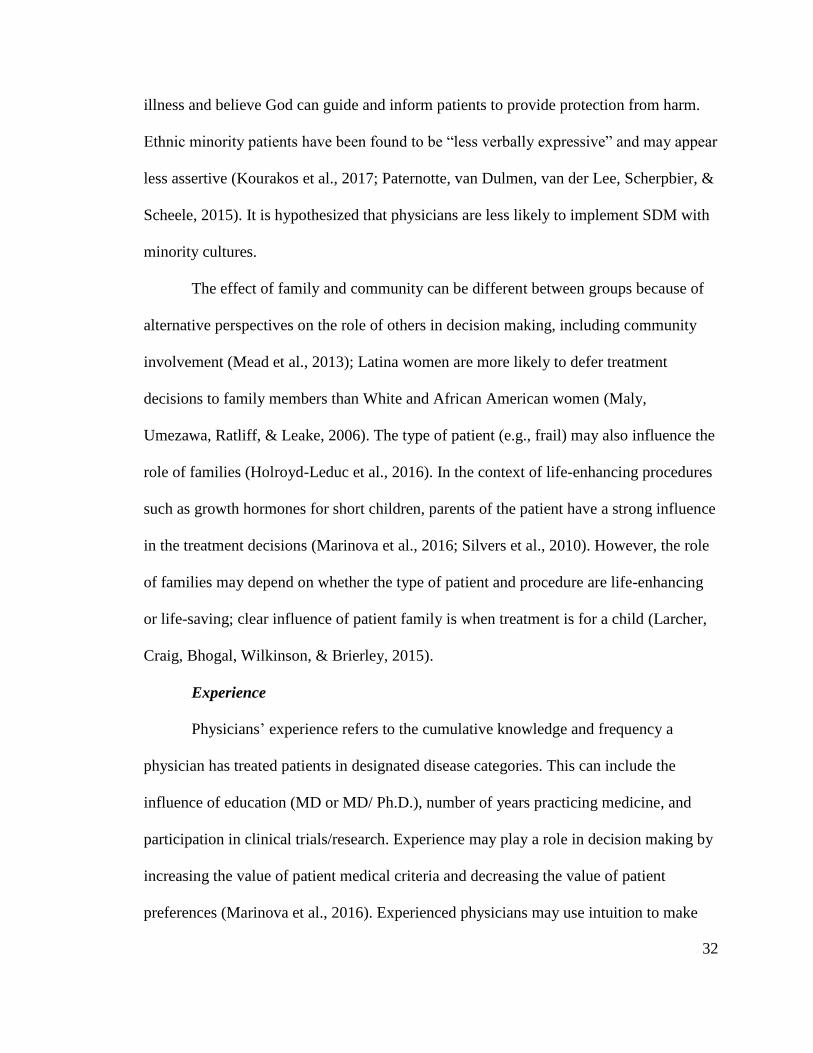
32
illness and believe God can guide and inform patients to provide protection from harm.
Ethnic minority patients have been found to be “less verbally expressive” and may appear
less assertive (Kourakos et al., 2017; Paternotte, van Dulmen, van der Lee, Scherpbier, &
Scheele, 2015). It is hypothesized that physicians are less likely to implement SDM with
minority cultures.
The effect of family and community can be different between groups because of
alternative perspectives on the role of others in decision making, including community
involvement (Mead et al., 2013); Latina women are more likely to defer treatment
decisions to family members than White and African American women (Maly,
Umezawa, Ratliff, & Leake, 2006). The type of patient (e.g., frail) may also influence the
role of families (Holroyd-Leduc et al., 2016). In the context of life-enhancing procedures
such as growth hormones for short children, parents of the patient have a strong influence
in the treatment decisions (Marinova et al., 2016; Silvers et al., 2010). However, the role
of families may depend on whether the type of patient and procedure are life-enhancing
or life-saving; clear influence of patient family is when treatment is for a child (Larcher,
Craig, Bhogal, Wilkinson, & Brierley, 2015).
Experience
Physicians’ experience refers to the cumulative knowledge and frequency a
physician has treated patients in designated disease categories. This can include the
influence of education (MD or MD/ Ph.D.), number of years practicing medicine, and
participation in clinical trials/research. Experience may play a role in decision making by
increasing the value of patient medical criteria and decreasing the value of patient
preferences (Marinova et al., 2016). Experienced physicians may use intuition to make
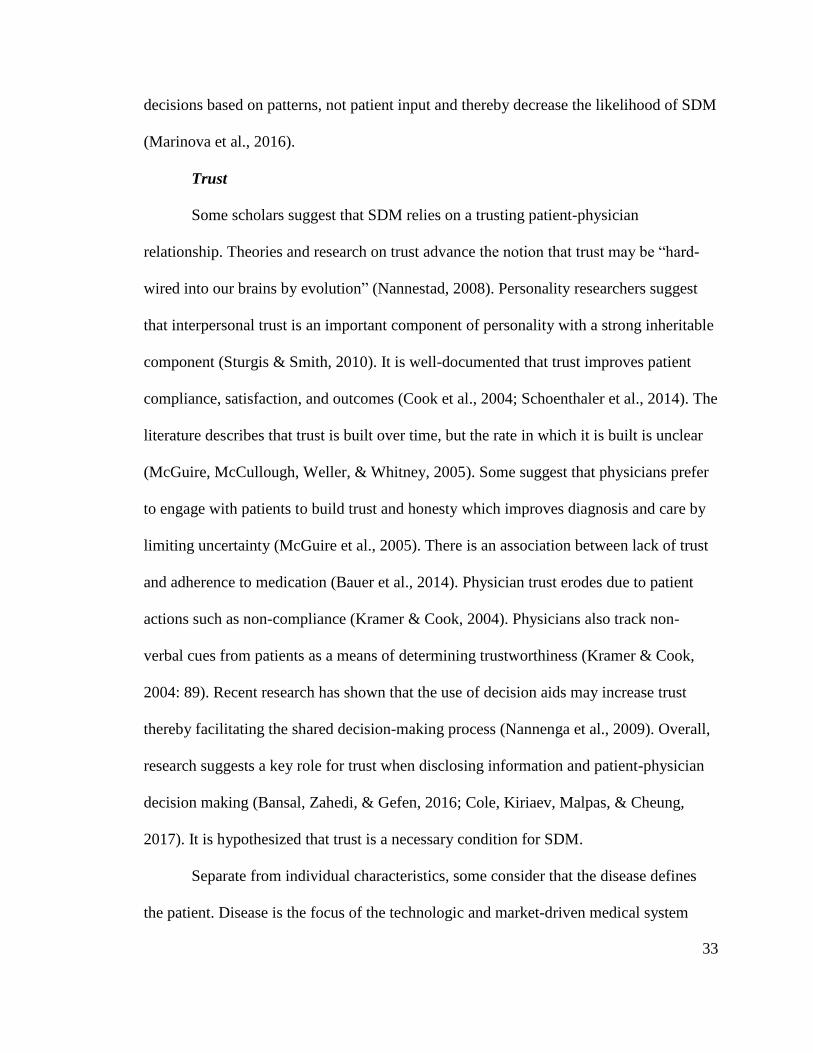
33
decisions based on patterns, not patient input and thereby decrease the likelihood of SDM
(Marinova et al., 2016).
Trust
Some scholars suggest that SDM relies on a trusting patient-physician
relationship. Theories and research on trust advance the notion that trust may be “hard-
wired into our brains by evolution” (Nannestad, 2008). Personality researchers suggest
that interpersonal trust is an important component of personality with a strong inheritable
component (Sturgis & Smith, 2010). It is well-documented that trust improves patient
compliance, satisfaction, and outcomes (Cook et al., 2004; Schoenthaler et al., 2014). The
literature describes that trust is built over time, but the rate in which it is built is unclear
(McGuire, McCullough, Weller, & Whitney, 2005). Some suggest that physicians prefer
to engage with patients to build trust and honesty which improves diagnosis and care by
limiting uncertainty (McGuire et al., 2005). There is an association between lack of trust
and adherence to medication (Bauer et al., 2014). Physician trust erodes due to patient
actions such as non-compliance (Kramer & Cook, 2004). Physicians also track non-
verbal cues from patients as a means of determining trustworthiness (Kramer & Cook,
2004: 89). Recent research has shown that the use of decision aids may increase trust
thereby facilitating the shared decision-making process (Nannenga et al., 2009). Overall,
research suggests a key role for trust when disclosing information and patient-physician
decision making (Bansal, Zahedi, & Gefen, 2016; Cole, Kiriaev, Malpas, & Cheung,
2017). It is hypothesized that trust is a necessary condition for SDM.
Separate from individual characteristics, some consider that the disease defines
the patient. Disease is the focus of the technologic and market-driven medical system
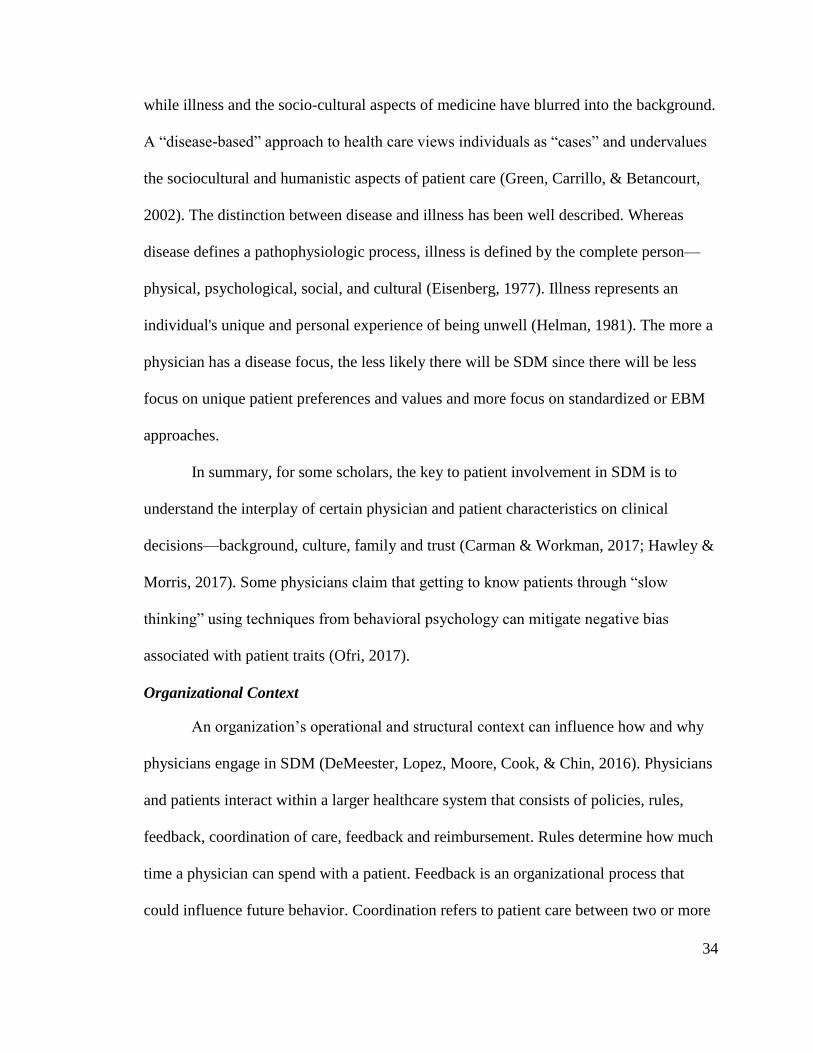
34
while illness and the socio-cultural aspects of medicine have blurred into the background.
A “disease-based” approach to health care views individuals as “cases” and undervalues
the sociocultural and humanistic aspects of patient care (Green, Carrillo, & Betancourt,
2002). The distinction between disease and illness has been well described. Whereas
disease defines a pathophysiologic process, illness is defined by the complete person—
physical, psychological, social, and cultural (Eisenberg, 1977). Illness represents an
individual's unique and personal experience of being unwell (Helman, 1981). The more a
physician has a disease focus, the less likely there will be SDM since there will be less
focus on unique patient preferences and values and more focus on standardized or EBM
approaches.
In summary, for some scholars, the key to patient involvement in SDM is to
understand the interplay of certain physician and patient characteristics on clinical
decisions—background, culture, family and trust (Carman & Workman, 2017; Hawley &
Morris, 2017). Some physicians claim that getting to know patients through “slow
thinking” using techniques from behavioral psychology can mitigate negative bias
associated with patient traits (Ofri, 2017).
Organizational Context
An organization’s operational and structural context can influence how and why
physicians engage in SDM (DeMeester, Lopez, Moore, Cook, & Chin, 2016). Physicians
and patients interact within a larger healthcare system that consists of policies, rules,
feedback, coordination of care, feedback and reimbursement. Rules determine how much
time a physician can spend with a patient. Feedback is an organizational process that
could influence future behavior. Coordination refers to patient care between two or more
35
providers. Reimbursement relates to how care is paid and who must approve treatment
costs. SDM is most likely to be optimal if aligned with organizational context
(DeMeester et al., 2016).
Policy
Physicians must take into account national policies and the structure of healthcare
system (Flynn, 2003; McMurray, Pullen, & Rhodes, 2011). The selection of one
treatment approach over another can be based on various factors such as efficacy, safety,
and cost (Liras & García-Trenchard, 2013; Peyvandi, Rosendaal, O'Mahony, &
Mannucci, 2014). The physician’s institution is a part of a larger healthcare system,
which is part of a larger macro system, which includes regulatory agencies, patient
advocacy groups, and accepted standards of care. The system as a whole is an
intermingling cluster of entities and policies that impact the boundaries within which
decisions are made. Policies are thought to reduce decision making between a patient and
physician and limit SDM options (McMurray et al., 2011).
Rules (Time)
All organizations have rules and one rule that can significantly influence SDM is
time. Lack of time is a common influence on physician decision making for chronic care
(Légaré et al., 2012; Légaré et al., 2013). Time constraints may limit the ability of
physicians to comply with preventative service recommendations (Yarnall, Pollak,
Østbye, Krause, & Michener, 2003). Schattner and Simon (2017) state that 9% (approx.
67 minutes) of the physician workday is meeting with patients. However, it is unclear
what the right amount of time is needed for patients: American physicians use more time
than British and German physicians and, according to one study, feel they spend
36
sufficient time with each patient often using more time than allocated for scheduled visits
(Konrad et al., 2010). According to the 2017 Great American Physician Survey, less than
8% of U.S. physicians believe there is not enough time to educate their patients
(Physicians Practice, 2017).
The timing of care can also affect SDM. The initial meetings likely have more
participation than subsequent check-ups. Follow-up examinations may involve minimal
changes if current treatment is satisfactory.
The alignment of physicians and SDM must fit into clinical practice and not
increase the time physicians spend during appointments (MedPAC, 2010). Specialists are
thought to be more successful in implementing SDM because of this alignment and when
decisions are most useful to a patient: cancer treatment vs. cancer screening (Medicare
Payment Advisory Commission, 2010: 192).
In summary, if chronic care requires more physician time, then the amount of
interaction may be as important as other factors. Adequate time for discussion is thought
to facilitate involvement in SDM and provide opportunities for relationship building
which is important for effective communication (Joseph-Williams, Elwyn, & Edwards,
2014). Slow vs. fast thinking may be related to the amount of time allocated to decision
making.
Coordination
Coordination of care is the organization of patient care activities between more
than two participants (McDonald et al., 2007). Effective care requires coordination
because patients with complex chronic diseases need all of their healthcare providers to
understand their unique context. For example, patients with PID have specific
37
gastrointestinal needs and procedures to avoid infections, whereas patients with
hemophilia will need extra precautions when visiting a dentist. Misinformed healthcare
providers—in other words, not coordinated with the patient’s needs—can lead to
disastrous results, nullifying any benefit of SDM. Poor coordination of care is thought to
be a barrier to SDM due to sub-optimal information flow between physicians.
Conversely, good coordination of care supports SDM (Joseph-Williams et al., 2014).
Effective coordination of care helps patients avoid the damage and cost of adverse
drug interactions, unnecessary or duplicate tests and procedures, and conflicting
information from multiple providers (McDonald et al., 2007). Furthermore, care
coordination is best applied to chronic conditions because they are “maintained” over a
lifetime rather than cured or fixed (McWilliams, 2016; Peikes, Chen, Schore, & Brown,
2009). The benefits of care coordination are recognized and incentivized by Medicare
(similar to SDM); they measure coordination of care via ACO scales (Figure 5).
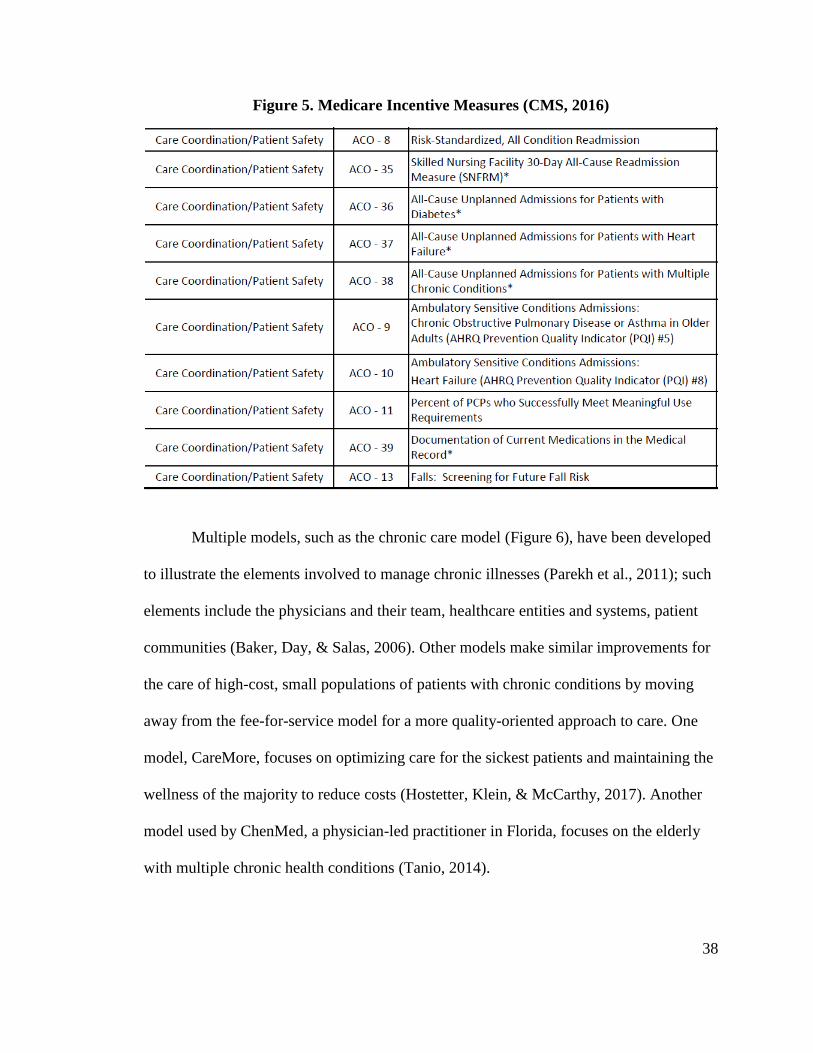
38
Figure 5. Medicare Incentive Measures (CMS, 2016)
Multiple models, such as the chronic care model (Figure 6), have been developed
to illustrate the elements involved to manage chronic illnesses (Parekh et al., 2011); such
elements include the physicians and their team, healthcare entities and systems, patient
communities (Baker, Day, & Salas, 2006). Other models make similar improvements for
the care of high-cost, small populations of patients with chronic conditions by moving
away from the fee-for-service model for a more quality-oriented approach to care. One
model, CareMore, focuses on optimizing care for the sickest patients and maintaining the
wellness of the majority to reduce costs (Hostetter, Klein, & McCarthy, 2017). Another
model used by ChenMed, a physician-led practitioner in Florida, focuses on the elderly
with multiple chronic health conditions (Tanio, 2014).
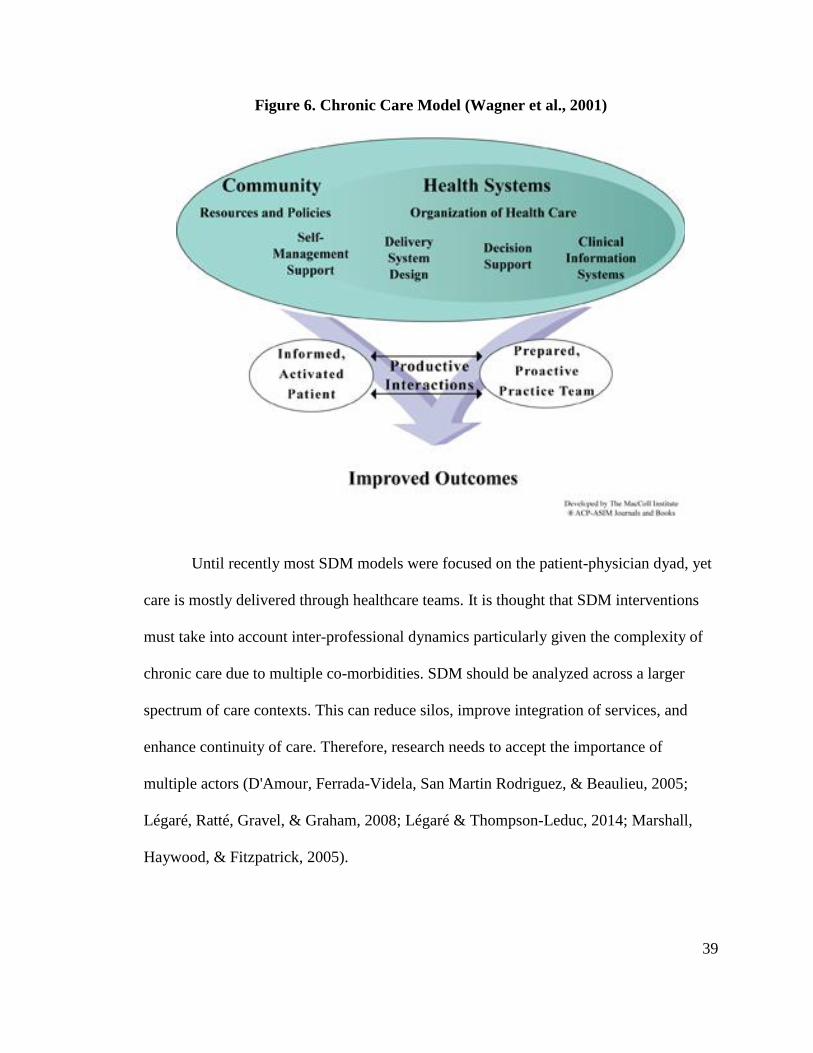
39
Figure 6. Chronic Care Model (Wagner et al., 2001)
Until recently most SDM models were focused on the patient-physician dyad, yet
care is mostly delivered through healthcare teams. It is thought that SDM interventions
must take into account inter-professional dynamics particularly given the complexity of
chronic care due to multiple co-morbidities. SDM should be analyzed across a larger
spectrum of care contexts. This can reduce silos, improve integration of services, and
enhance continuity of care. Therefore, research needs to accept the importance of
multiple actors (D'Amour, Ferrada-Videla, San Martin Rodriguez, & Beaulieu, 2005;
Légaré, Ratté, Gravel, & Graham, 2008; Légaré & Thompson-Leduc, 2014; Marshall,
Haywood, & Fitzpatrick, 2005).
40
Feedback
Feedback is an organizational factor that increases SDM by encouraging
physicians to consider their approach to patient care (Légaré et al., 2014). In the case of
Medicare ACO measures, feedback and auditing methods may make physicians consider
incorporating SDM by offering incentives similar to employee reviews. If patients do not
feel that they participated in the decision process, they respond that the physician did not
incorporate SDM, thereby reducing compensation. Feedback is thought to be an effective
method for increasing the likelihood of SDM.
Effective feedback methods can help improve how the physician and healthcare
organization meet the patient’s needs (NORC, 2014). Physicians and patients agree that
patients can evaluate healthcare providers based on infrastructure, staff, organization, and
interpersonal skills; however, both patients and physicians agree that patients cannot
evaluate the technical skills (Rothenfluh & Schulz, 2017). Feedback from the patient
allows physicians to confirm the efficacy of current treatment, whether they maintain the
regimen or make changes (Schiff, 2008). Furthermore, feedback is a possible method for
avoiding misdiagnoses by updating physicians with additional information; patients
reporting reactions and symptoms provides crucial warnings that physicians can
recognize (Schiff, 2008). Peer feedback influences the way physicians treat patients,
which reduces over/under treatment (Yeh et al., 2015). In summary, feedback is thought
to increase SDM.
Colleagues
The literature of colleague influences on the physician decision process is scarce.
It describes physicians seeking aid from colleagues when the decision is out of their
41
expertise, reconfirming knowledge, or an issue of morality (Rothman, 2017); for
instance, getting clarification for laboratory professionals (Hickner et al., 2014). The
approval of colleagues influences to physician decision making if any information of the
decision is available for colleagues to view (Godager, Henning-Schmidt, & Iversen,
2016). However, the extent of colleagues influencing the decision-making process has
little representation in the literature for the treatment of chronic diseases.
Reimbursement
Reimbursement of healthcare costs can be categorized into voluntary healthcare
insurance plans, managed care plans, and government-sponsored healthcare programs
(Casto, Layman, & Association, 2006). Approximately 40% of physicians think that there
is too much government and third-party (i.e., insurance companies) interference to
effectively and efficiently treat their patients (Physicians Practice, 2017). This view
supports the claim that insurance reimbursement is a major impediment to
implementation of SDM.
Depending on the healthcare system, the cost and method of reimbursement can
significantly influence a physician’s decision process (Flynn, 2003; Scalone, Mantovani,
Borghetti, Von Mackensen, & Gringeri, 2009). Insurance companies do their own cost-
effectiveness analysis to determine which treatment approach is the most suitable for a
patient based and what is covered under the policy (Wilson et al., 2014). For example,
when treating hemophilia, reimbursable costs are one of the main factors affecting the
decisions of physicians and patients regarding treatment (Lee et al., 2008; Scalone et al.,
2009). Reimbursement for treatment is thought to be a common barrier to SDM. The goal
of the insurance organization is to cover expenses at the lowest cost. Insurance companies
42
have criteria set for which brand, type, or method of treatment is covered (Barua et al.,
2015). Unless the physician contests the insurance and overrules the reimbursement
decision, the physician may be presented with a set of predetermined options of care for
the patient. Some states have introduced new systems to reduce the financial burden of
healthcare to insurance companies through “reinsurance” and thereby minimize coverage
issues (Johnson, 2017; Pear, 2017). However, the extent to which insurance dictates
clinical decisions is thought to be an impediment to SDM.
Summary of SDM Decision Theory
In summary, clinical decision making can be explained by different theories: dual
process, SIT and Agency, traits and organizational context. Dual process theory suggests
that cognitive thinking explains decision making. SIT and agency theory stress the role of
power imbalances resulting from role expectations and information asymmetry. Trait
theory focuses on the potential for bias associated with personal characteristics.
Organizational context represents overarching influences from the larger healthcare
system such as policies and reimbursement. How these different theories contribute to a
larger theoretical framework when treating chronic diseases is the object of this study.
Summary
The literature overwhelmingly supports SDM as an appropriate method of
improving the quality of care and reducing the cost of care for chronic diseases
(O'Connor et al., 2015; O'Connor et al., 2004; O’Connor et al., 2007; Stacey et al., 2011).
No published literature exists about factors that influence physicians to incorporate and
exercise SDM when treating hemophilia or PID, although some literature does address
support for and benefits of patient choice (Elwyn et al., 2012; Friesen-Storms et al., 2015;
43
Légaré & Witteman, 2013). One approach to explaining chronic care clinical decision
making and SDM is dual process theory; however, dual process cannot fully explain the
use of SDM. Other theories from the literature may provide alternative or complementary
explanations include power balance/agency, physician/patient traits and organizational
context.
Both the context and method by which decisions or choices are structured,
referred to by behavioral decision researchers and cognitive psychologists as “choice
architecture,” is crucial to understanding SDM as a method that encourages patients to
participate in decisions which are advantageous to their health (Kahneman, 2017;
Sunstein & Thaler, 2008). Examining physicians’ perspectives are imperative but poorly
understood. If understood, opportunities for structuring and facilitating SDM and
bridging the quality chasm may emerge (Beshears & Gino, 2015). Given the magnitude
of the problem and the impact on society, there is an urgency to understand and address
the variability, complexity, and effectiveness of chronic medical care and create decision
designs that facilitate good decision making that results in better care (Boland Jr &
Collopy, 2004; Hock, 1999: 57).
To achieve a robust understanding of SDM from the physician’s perspective, a
series of three studies were conducted to gather and analyze data and generate theory on
the physician’s role in the decision-making process. Both qualitative and quantitative
methods, “mixed methods”, were used to increase the likelihood of obtaining meaningful
results. The next chapter (Chapter 3) attempts to quantify the quality gaps with chronic
diseases in general and hemophilia and PID specifically. Chapter 4 discusses the research
question development, research methods and the results of each study. The theories
44
summarized in this Chapter 2 were used to generate and test hypotheses related to
decision theory, power imbalance, traits, and organizational context. These theories and
their hypothesized relationships to SDM have not been studied as they relate to specific
chronic diseases such as hemophilia and PID. Furthermore, very little research on these
topics has been from the physician perspective. The proposed research study should yield
better insight into what predicts physician SDM implementation.
45
CHAPTER 3: CHRONIC DISEASES
This study is focused on the treatment of chronic diseases. It is claimed that
effectiveness of SDM is optimized in the treatment of chronic diseases (Friesen-Storms et
al., 2015; Frosch et al., 2011). The goal of treatment for patients with the chronic diseases
is to return their quality of life as closely as possible to that of un-afflicted people. As
cited above, chronic diseases represent the vast expenditure of healthcare resources.
Unfortunately, Western medical training is primarily focused on acute care (Allen,
Maguire, & McKelvey, 2011a). The acute care model is more consistent with traditional
evidence-based medicine and mechanistic protocols for clinical interventions and
management. Compared to chronic care, decision making for acute care has a much
different context (Curreri & Lyytinen, 2017). The combination of longevity of treatment
(more than one year) and complexity (multiple co-morbidities) makes chronic care much
more unpredictable. There is a greater the need for co-created relational care plans and
the need to deal with uncertainty: both consistent with the need for SDM (Allen et al.,
2011a; Allen, Maguire, & McKelvey, 2011b; Letiche, 2008; Lissack & Roos, 1999).
This study explores decision-making processes of physicians who are specialists
in treating hemophilia and primary immunodeficiency. These two chronic genetic
disorders are expensive to treat and are known for their complexity (Dalton, 2015). In the
case of hemophilia, the development of inhibitors or requirement for surgery changes a
complicated disease (replace clotting factor) to a complex disease with significant
uncertainty and no standardized protocol (HFA, 2014). For PID, the disease is inherently
complex because many symptoms fall into more than one category of immunodeficiency
(Al-Herz et al., 2014). Furthermore, PID is manifested by infections, malignancy, and
46
immune dysregulation (Picard et al., 2015). Both diseases are life-long with no cure.
While hemophilia and PID are genetic diseases (not acquired), they nevertheless are good
examples to study since they affect well identified small populations and there are
specialized physicians who treat the disease that are available to survey. In addition, the
researcher has been working with these two communities for 30 years so the ability to get
access to physicians was more convenient.
Hemophilia
Hemophilia is a rare (1:10,000), extremely high cost, life-threatening genetic
disorder with minimal leeway for error and inaction because of the severity of disease if
not treated properly. Approximately $18 billion was spent for the care of hemorrhagic,
coagulation, and disorders of White Blood cells (which includes hemophilia) in 2014
(Agency for Healthcare Research and Quality, 2014a); the average cost per patient in this
category was $14,722, and approximately 78% was spent on prescribed medicines
(Agency for Healthcare Research and Quality, 2014a, f). Hemophilia is a chronic disease,
which further requires physicians to make lifelong, skilled, decisions. At $100,000–
$300,000 per year over a lifetime; it is also one of the most expensive diseases to treat
(Chen, 2016; Eldar-Lissai, Hou, & Krishnan, 2015; O’Hara et al., 2017). The disparity of
cost/outcome for hemophilia when compared to other countries is similar to the overall
disparity between healthcare systems. For example, the U.S. and the United Kingdom
(U.K.) yield similar clinical outcomes, but the cost of hemophilia care in the U.S. is 50%
or more than in the U.K.
Within hemophilia treatment, there are four basic goals at the start of a diagnosis.
First, if the patient is bleeding, the bleeding must be stopped (achieve hemostasis).
47
Second, if possible, future bleeding must be prevented (prophylaxis). Third, all of the
above are exacerbated whenever the patient requires further medical care, such as a
surgical procedure or treatment of infectious diseases (Sox et al., 2013). Fourth, if the
patient develops an antibody to the treatment (inhibitor) such that bleeding continues and
the inhibitor must be eradicated.
The current treatment of hemophilia is replacement therapy using clotting factor
products, which are categorized as either blood-derived (plasma-derived) or made
through biotechnology (recombinant). The advantage of the plasma clotting factor is its
lower cost, whereas the recombinant method eliminates the risk of a viral transmission,
such as HIV (Gringeri, 2011). Although there is less than a 1 in 1.8 million chance of
contracting HIV from plasma-derived clotting factor, the recombinant factor is generally
considered safer, due to its non-biological origins (Goodnough, Shander, & Brecher,
2003).
In recent years, long-acting recombinant factors have emerged in the current
market for clotting factors. Although more expensive, these long-acting agents allow
patients to infuse clotting factor about once a week; standard prophylactic regimens are
three or four infusions per week (Pipe, 2012). Although not yet complete with clinical
trials, therapies involving subcutaneous infusions are making product administration
easier compared to therapies that are administered intravenously (Meunier et al., 2015).
The formation of an inhibitor is one aspect of the disease’s complexity. The exact
cause of inhibitors has yet to be discovered; only a few factors have been found to
increase inhibitor risk, such as ethnicity (DiMichele, 2008). In such situations, the
physician has to approach the patient with specified protocols or adjust depending on
48
reaction to dose or tools (Minno, Minno, Capua, Cerbone, & Coppola, 2010). One
common tactic is to try immune tolerance induction (ITI), or to desensitize the patient to
his or her usual product by continuing treatment for an extended period of time; this
could involve decreasing or increasing the volume depending on patient reaction in the
hope that the efficacy will return (Zaiden, 2014a, b). More complicated treatments are
necessary if the initial treatment is ineffective. If inhibitors continue, bypassing agents
and substitutions are available, such as activated prothrombin complex concentrate
(aPCC), anti-inhibitor coagulant complex (e.g., FEIBA), recombinant clotting factor 7a
(rFVIIa), and rPorcine VIII; these options tend to be much more expensive or pose a risk
of adverse reaction in the case of rPorcine VIII because of reduced platelet counts and
allergic reactions (Gringeri, Mantovani, Scalone, & Mannucci, 2003). These products
avoid the usual coagulation cascade but achieve similar results; however, caution is often
needed because of the aforementioned adverse effects observed in some patients.
A patient’s treatment can be administered at a hemophilia treatment center (HTC),
at a hospital, or at home; self-infusion at home increases quality of life by minimizing
hospital time and expenses (Schwartz, 2013). Although self-care helps patients to manage
expenses and time, professional facilities are better suited to emergency situations and
advice for future treatment (Street, 2012). The treatments can be infused via catheters or
syringes; insertion and removal of the catheter is done by a healthcare professional.
Catheters are implanted for months to years and allow easier access to a vein for
infusions, whereas syringes, although they need precision for each infusion, pose less risk
for infection, let alone bleeding during an initial implantation.
49
Patients are generally associated with an HTC, which employs physicians, nurses,
and social workers who specialize in bleeding disorders. Approximately 150 HTCs that
treat almost all of the hemophiliacs in the U.S. and the U.K. and are closely connected to
one another through research, national and international scientific conferences, and
patient associations (Erikson, Jones, & Tilton, 2012; UKHCDO, 2014). Each HTC has
general standardized treatment protocols within which decisions are made (Srivastava et
al., 2013). Hospitals are part of a larger healthcare system that influences the overall
context in which physicians, HTCs, and hospitals make decisions.
In summary, hemophilia is a genetic disease that requires life-long maintenance,
thereby enabling patients to live full, normal lives. Key decisions for the treatment of
hemophilia involve the severity of the disease, presence of inhibitors, reaction to product
brands and types, patient lifestyles, location of therapy and reimbursement methods.
Primary Immunodeficiency (PID)
PID is a set of chronic genetic disorders resulting from a deficiency in the
immune system, typically exacerbated by increased vulnerability to infection (Costa-
Carvalho et al., 2014; Moens et al., 2014; Younger, Epland, Zampelli, & Hintermeyer,
2015). There are approximately 32,000 treated PID patients in the U.S. (Bousfiha et al.,
2013; Kobrynski et al., 2014). Better screening methods and increasing annual PID
diagnoses suggest that a substantial number of undiagnosed patients exist, particularly in
pediatrics (Ehlayel, Bener, & Laban, 2013; Espinosa-Rosales, Condino-Neto, Franco, &
Sorensen, 2016; Hernandez-Trujillo et al., 2015). Due to difficulty in identifying the
disease, it takes approximately five years from the onset of symptoms for patients to be
diagnosed with PID (Guaní-Guerra et al., 2013).
50
Inherited disorders, such as PID, cause recurrent medical problems for patients
when not treated correctly (Chapel et al., 2014; Hernandez-Trujillo et al., 2015; Jolles et
al., 2015). While manageable and curable under many circumstances, these disorders can
remain undiagnosed or be treated sub-optimally, leading to prolonged or fatal health
complications (Chapel et al., 2014; Condino-Neto et al., 2012). Approximately $28
billion was spent for the care of endocrine, nutritional & immune disorders (which
includes PID) in 2014 (Agency for Healthcare Research and Quality, 2014a); the average
cost per patient in this category was $3,195 (Agency for Healthcare Research and
Quality, 2014a, f); however, this does not reflect the cost to PID patients because the
relatively small population. Modell et al. (2011) have estimated that the annual cost for
an undiagnosed patient with PID (approximately $135,000 annually) is about two times
higher than that for a diagnosed patient (approximately $60,000 annually), which
suggests a substantial societal health care burden (CMS, 2015).
A study performed by a research group for the Immune Deficiency Foundation
approached 10,000 households (27,000 household members) and inquired regarding any
diagnosis for primary immunodeficiency for these household members (Boyle &
Buckley, 2007). This study reported a prevalence rate of 1:1200 population for the U.S.,
bringing the total U.S. PID population to 266,000 patients!
A very different approach was adopted by Joshi, Iyer, Hagan, Sauver, and Boyce
(2009). This research group utilized a cohort-based approach in calculating incidence
rates of PID in the U.S. Essentially, these investigators examined the rate of PID
diagnosis per year in a specific county (Olmsted County, MN) and tried to extrapolate
this incidence to the rest of the country. They calculated an incidence rate of 4.6
51
cases/100,000 population year. It is somewhat difficult to determine prevalence from
incidence rate because survival is a substantial element of any such
calculation. Assuming an incidence in the U.S. of 14,720 cases per year, and utilizing a
mean lifespan for these patients of 50 (assuming that most patients were diagnosed in
early age), one would reach a prevalence estimate of 736,000 patients with PID diagnosis
in the U.S. Of course, lifespan may have been substantially lower; the researchers only
determined that 93.5% of the patients were alive after 10 years. They do, however, note
that diagnosis at an older age (than <12) was significantly associated with mortality.
Thus, the mean lifespan may have been lower, leading to lower numbers for PID
prevalence in the U.S.
At about the same time, the CDC commenced a study on the prevalence and
morbidity of PID in the 2001–2007 period, examining mainly insurance records
(MarketScan databases that compile claims from insurance companies and Medicaid).
This study reported prevalence anywhere from 29.1 to 41.1 patients/100,000 population,
for a total of U.S. PID patient basis of 93,120–131,520 (Kobrynski et al., 2014). The
study determined that prevalence among whites was twice as high as among Blacks or
Hispanics and the B-cell defects predominated. The inherent bias of the CDC studies is
that it is based on health records. Obviously, it would be undercounting incidence of PID
in populations not covered by insurance companies reporting to the databases examined.
Overall, these studies indicate that PID prevalence in the U.S. is substantially
higher than numbers provided by registry-based studies. The approach by Boyle and
Buckley (2007) has been innovative; the assumptions required to calculate prevalence
from the Joshi et al. (2009) study make the very high numbers therein dubious and
52
uncertain. The CDC study by Kobrynski et al. (2014) is certainly a very solid effort and
the numbers reliable and should serve as the current baseline (U.S. PID population up to
131,520 patients), taking into account that it refers only to the period between 2001 to
2007, and that the rate of diagnosis is increasing.
Assuming the incremental care associated with an undiagnosed patient is $65,000
(referenced above) and the number of untreated patients is approximately 100,000, the
cost of missed diagnoses could be as high as $7.7 billion. Alternatively, taking the upper
CDC estimate as the baseline and assuming (a) that 50% of B-cell defects may not
require IgG treatment (very conservatively), and (b) that B-cell defects account for 75%
of all diagnoses, one can derive the estimate of approximately 50,000 patients in the U.S.
that require regular or incidental IgG treatment for their PID disorder. This would put the
cost of missed diagnosis $3.85 billion. Therefore, the likely cost of missed or poor
treatment is between $3.85 billion and $7.7 billion.
In summary, PID is a genetic disease that requires life-long maintenance that—
like hemophilia—enables patients to live full, normal lives. Key decisions for the
treatment of PID involve the severity of the disease, infection history, reaction to product
brands and types, patient lifestyles, and reimbursement methods. The impact of the
failure to properly diagnose and treat is significant.
Estimate of the Quality Gap in Chronic Care and the Implications for Hemophilia
and PID
An analysis of 1) survey data of 33,162 individuals across the U.S.; 2) 25 million
hospitalization records from New York State comparing two (2) five-year periods; and 3)
data from 200 million individual-level, de-identified enrollment data and health insurance
53
claims across a continuum of care (both inpatient and outpatient). These studies help
quantify the quality chasm and the associated cost implications. First, the MEPS data was
analyzed to understand quality gaps from the patient perspective. Second, the SPARCS
database of all New York State hospitalizations was analyzed to understand the cost of
hospitalization associated with hemophilia and PID; both diseases if properly treated
should result in very few hospitalizations. Third, a broad cross-section of U.S. health
insurance claims was analyzed to better understand the overall cost of care.
Analysis #1: MEPS
The Agency for Healthcare Research and Quality (AHRQ) conducts a survey, the
Medical Expenditure Panel Survey (MEPS), to gather data on the U.S. patient population
(Household Component) and insurance (Insurance Component). The Household
Component (HC) collects data from a nationally representative sample of families and
individuals in selected communities across the United States using a panel survey, which
features several rounds of interviewing covering two full calendar years to determine how
changes occur in respondents (Agency for Healthcare Research and Quality, 2018). Prior
MEPS published data estimates that 84% of Americans have at least one chronic
condition, wherein 31.5% of Americans have multiple chronic conditions (Gerteis et al.,
2014). This correlates well with the CDC data of which 86% of healthcare spending is on
patients with one or more chronic conditions (Gerteis et al., 2014).
The 2014 MEPS Household Component consisted of survey results from 33,162
households of which 15,158 participants were at least 18 years of age and have visited a
doctor in last 12 months. Of this sample, approximately 33% believed their healthcare
providers were not listening to them carefully (“listening”), 30% feel their healthcare
54
provider do not always respect what they have to say (“respect”), and 43% feel the
healthcare provider did not spend enough time with them (“time”); these three items were
used as the quality measures to analyze. Specific sub-samples may reflect the healthcare
quality gap. For example, participants that are older than 65 have insurance and those
with excellent perceived health rated their experiences with healthcare practitioners
significantly higher (1 standard deviation) than the average for items involving listening,
respect, and time. Whereas participants with low perceived health and no insurance were
significantly less likely to provide positive responses to the items. Table 6 was recreated
from the MEPS item data summaries, 2014.
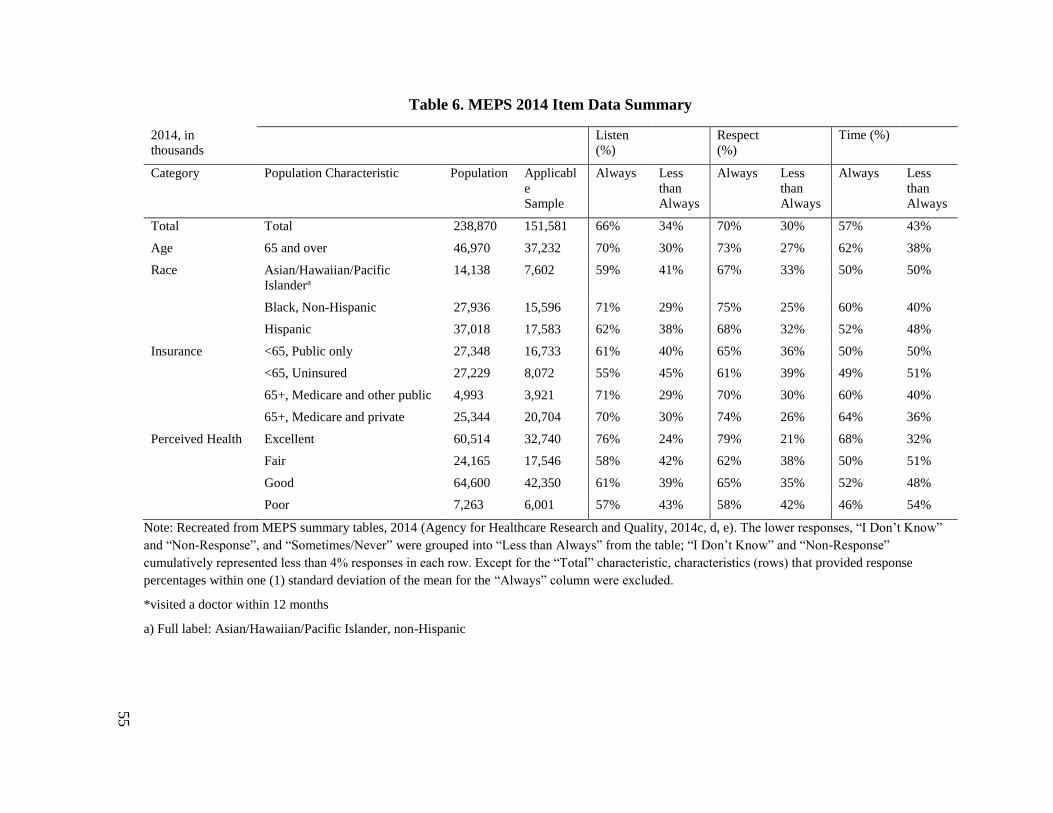
55
Table 6. MEPS 2014 Item Data Summary
2014, in
thousands
Listen
(%)
Respect
(%)
Time (%)
Category Population Characteristic Population Applicabl
e
Sample
Always Less
than
Always
Always Less
than
Always
Always Less
than
Always
Total Total 238,870 151,581 66% 34% 70% 30% 57% 43%
Age 65 and over 46,970 37,232 70% 30% 73% 27% 62% 38%
Race Asian/Hawaiian/Pacific
Islandera
14,138 7,602 59% 41% 67% 33% 50% 50%
Black, Non-Hispanic 27,936 15,596 71% 29% 75% 25% 60% 40%
Hispanic 37,018 17,583 62% 38% 68% 32% 52% 48%
Insurance <65, Public only 27,348 16,733 61% 40% 65% 36% 50% 50%
<65, Uninsured 27,229 8,072 55% 45% 61% 39% 49% 51%
65+, Medicare and other public 4,993 3,921 71% 29% 70% 30% 60% 40%
65+, Medicare and private 25,344 20,704 70% 30% 74% 26% 64% 36%
Perceived Health Excellent 60,514 32,740 76% 24% 79% 21% 68% 32%
Fair 24,165 17,546 58% 42% 62% 38% 50% 51%
Good 64,600 42,350 61% 39% 65% 35% 52% 48%
Poor 7,263 6,001 57% 43% 58% 42% 46% 54%
Note: Recreated from MEPS summary tables, 2014 (Agency for Healthcare Research and Quality, 2014c, d, e). The lower responses, “I Don’t Know”
and “Non-Response”, and “Sometimes/Never” were grouped into “Less than Always” from the table; “I Don’t Know” and “Non-Response”
cumulatively represented less than 4% responses in each row. Except for the “Total” characteristic, characteristics (rows) that provided response
percentages within one (1) standard deviation of the mean for the “Always” column were excluded.
*visited a doctor within 12 months
a) Full label: Asian/Hawaiian/Pacific Islander, non-Hispanic
56
In hemophilia3
and PID4
MEPS (2014) samples of 75 participants, there are
similar patterns around income, insurance, perceived health, and the doctor-patient
relationship (Agency for Healthcare Research and Quality, 2014b). There are 32
participants (42%) that had visited a doctor within 12 months prior to the survey; these
patients were qualified to respond to the “listen,” “respect” and “time” questions in the
MEPS. This sub-sample had 15 participants (46%) with poor perceived health and one or
more unsatisfied quality measures.
In summary, the 2014 MEPS survey data confirms that most health issues are
chronic and across three key quality indices (listening, respect and time) there are
substantial gaps: 30–43% of households give their healthcare provider low scores.
Although the numbers are small, the hemophilia and PID patients surveyed by MEPS
(total of 75) show greater quality gaps: more than half have not seen a doctor in 12
months and of those who have seen a doctor, 53% gave lower quality scores.
Analysis #2: IDF
Purpose
Seeborg et al. (2015) sought to gain a better understanding of the drivers of
perceived health (PH) among patients with PID by evaluating the data from the National
Survey of Patients with Primary Immune Deficiency Diseases in America.
Methods
The survey sample of 1,526 patients was nationally distributed and based on the
single, largest database of persons with PID in the world. Patients’ own evaluation of
3
Labeled as coagulation disorders. 4
Labeled as immunity disorders.
57
their health is a simple health metric which links to patient satisfaction and quality of life.
PH was based on the reply to the global question: “How would you describe your current
health status?”
Results
Thirty-nine percent of the patients perceived their health status as poor or very
poor. Patients who were acutely ill and hospitalized in the past 12 months, ones with
limited activity, and chronic diseases, were more likely to have poor PH. Patients with
“on demand” access to specialty care and ones on regular IVIG had higher PH. Patients
not cared for mostly by an immunologist were more likely to have poor PH.
Discussion
The occurrence of acute illness and hospitalization within the last 1 year were
significantly associated with poor PH. Multiple co-morbidities also influenced health
perception as patients with PID and morbidities such as bronchitis, malabsorption, and
recurrent infections were more likely to have poor PH.
Analysis #3
SPARCS A: PID
Purpose
This analysis compares the cost and treatment quality of PID patients from 2000–
2004 (Resnick, Bhatt, Sidi, & Cunningham-Rundles, 2013) to the most recent data from
2010–2014. Resnick et al. (2013) investigated PID in New York State (NYS) using
International Classification Codes (ICD-9).
58
Methods
The frequency and cost of hospitalization with PID in NYS was analyzed using
the Statewide Planning and Research Cooperative System (SPARCS) database, a
comprehensive data reporting system that collects ICD-9 codes patients hospitalized in
NYS. Using ICD-9 codes that classify PID patients (using 279 as the generic root code).
For the identified patients, the demographics, length of state, insurance states, chares,
charges/patients and charges/day were determined. A total of 26,132,412 hospitalizations
were reviewed.
Results
Previously published data (2000–2004) found 2,361 hospitalized patients with
PID. Identified patients were likely to be Caucasian and less likely to have Medicare
when compared to the overall NYS population. The average length of stay was 8.3 days
which was statistically longer than the general hospital population (6 days) (Resnick et
al., 2013). A review of data from 2010–2014 found 611 hospitalized patients with PID.
The racial makeup and Medicare insurance was much more consistent with the general
population. The average length of stay was 6.87 days which was statistically longer than
the general hospital population (5.5 days). The charges/patient (77,936) and charges/day
(11,342) were significantly greater than the general population (40,187 and 7,235). The
total cost PID patient hospitalizations in 2014 was $10.9 million (Resnick et al., 2013).
Conclusion
PID is a rare chronic genetic disease that affects people of all ages, sex and ethnic
groups. If properly treated, PID patients can live a normal life free of immune defects and
other complications. Diagnostic delays and different levels of treatment result in extreme
59
complications which result in unnecessary hospitalizations. The number of
hospitalizations is a surrogate measure of prevalence and cost of undertreatment amongst
diagnosed patients. NYS data suggests a significant improvement (75% reduction) in
treatment between 2000–2004 and 2010–2014. It is currently estimated that there are
32,000 treated PID patients in the U.S. Extrapolating NYS data suggests that
approximately 2,333 diagnosed patients, or 7.3% of the PID population (reduced from
24% in the prior period), are undertreated to the point of hospitalization with a total cost
impact of $181 million to the U.S. healthcare system (substantially reduced from $613
million). This estimated may be understated because NYS has the ninth-best health care
system in terms of access and only captures diagnosed patients (Bernardo, 2017).
SPARCS B: Hemophilia
Purpose
Using International Classification Codes (ICD-9) codes to investigate hemophilia
and the cost associated with under treatment in New York State (NYS). An analysis of
2014 data was performed (most recent available data).
Methods
The frequency and cost of hospitalization with hemophilia in NYS was analyzed
using the Statewide Planning and Research Cooperative System (SPARCS) database, a
comprehensive data reporting system that collects ICD-9 codes patients hospitalized in
NYS. Using ICD-9 codes that classify hemophilia patients (using 286, 287 and 289 as the
generic root codes for coagulation and hemorrhagic disorders). For the identified patients,
the demographics, length of state, insurance states, chares, charges/patients and
charges/day were determined.
60
Results
A review of 2014 data found 2,520 hospitalized patients with coagulation and
hemorrhagic disorders. The charges/patient (54,708) and charges/day (11,026) were
significantly greater than the general population (40,187 and 7,235). The total cost in
2014 for NYS was $137.8 million. While the number of hospitalized patients declined by
15% over the 5 year periods from 2010 to 2014, the charges per patient have been rising
from $44,808/patient to $54,708/patient.
Conclusion
Hemophilia is a rare chronic genetic disease that affects people of all ages, sex
and ethnic groups. If properly treated, hemophilia patients can live a normal life with
minimal bleeds and other complications. The number of hospitalizations is a surrogate
measure of prevalence and cost of under treatment. Extrapolating NYS data suggests that
the cost of under-treatment to the point of hospitalization with a total cost impact of $2.2
billion to the U.S. healthcare system. This estimate may be understated since NYS has
the ninth-best health care system in terms of access and only captures diagnosed patients
(Bernardo, 2017).
Analysis #4
Truven Data: PID
Purpose
Few studies have estimated the morbidity of PID. Data derived from the Truven
Health MarketScan medical claims databases (96,791,177 enrollees from 2001 to 2007)
were used to investigate the incidence and cost associated with undertreatment of PID
(Kobrynski et al., 2014). A comparison was made between previously published results
61
from 2001-2007 and an analysis of data between 2008 and 2010 (most recent available
data) (Truven Health MarketScan® Research Databases, 2010).
Methods
MarketScan databases comply claims from commercial health insurance plans
and Medicaid, documenting diagnoses for hospital care. The frequency and cost of
hospitalization with PID was analyzed using ICD-9 codes from hospitalized patients that
classify PID patients (using 279.0, 279.1, 279.2, 279.8, 279.9, 288.1, and 288.2 as the
generic root codes). For the identified patients, length of stay and cost was used to assess
PID-associated morbidity.
Results
Estimated prevalence 41.1/100,000 for a total U.S. PID patient population of
131,520; of which 32,000 are diagnosed (using ICD codes for immune defects) (Grifols,
2017; Kobrynski et al., 2014). Previously published data from 2001–2007 and 2008–2010
found the proportion of PID persons with hospital admission was higher each year from
2001–2005 with (13.9% to 18.6%) compared to those without a PID diagnosis (7.9 to
8.9%). Persons with PID were approximately twice as likely to be hospitalized (p<.001)
(Kobrynski et al., 2014); their significantly longer hospital stays ranged from 6 to 22 days
depending on age. Having a PID diagnosis for Medicaid patients was also related to the
mean number of admissions per person per year (1.55 versus 1.16). The hospitalization
range of 13.9%-18.6% is lower than the 24% found in New York during the period of
2000-2004. The average cost of hospitalization is estimated at $77,000 per visit for
undiagnosed PID patients; the total cost of treating one hospitalization for each of the
estimated 50,000 undiagnosed patients is as much as $3.85 billion per year.
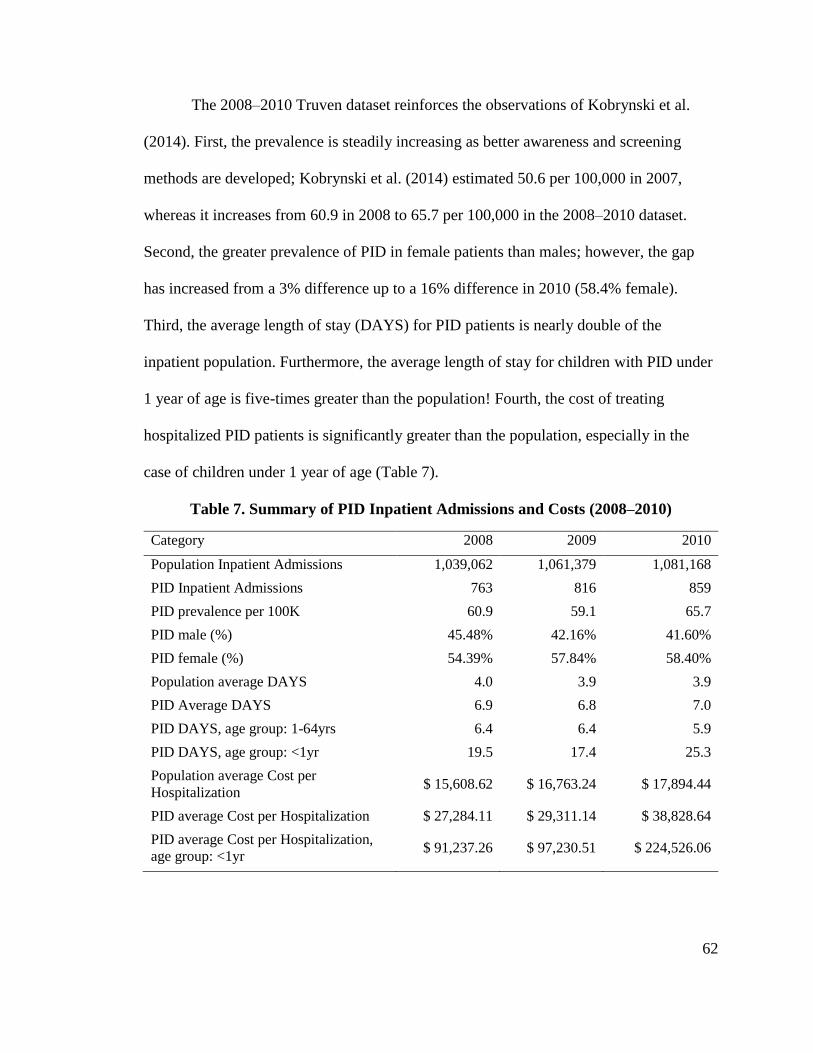
62
The 2008–2010 Truven dataset reinforces the observations of Kobrynski et al.
(2014). First, the prevalence is steadily increasing as better awareness and screening
methods are developed; Kobrynski et al. (2014) estimated 50.6 per 100,000 in 2007,
whereas it increases from 60.9 in 2008 to 65.7 per 100,000 in the 2008–2010 dataset.
Second, the greater prevalence of PID in female patients than males; however, the gap
has increased from a 3% difference up to a 16% difference in 2010 (58.4% female).
Third, the average length of stay (DAYS) for PID patients is nearly double of the
inpatient population. Furthermore, the average length of stay for children with PID under
1 year of age is five-times greater than the population! Fourth, the cost of treating
hospitalized PID patients is significantly greater than the population, especially in the
case of children under 1 year of age (Table 7).
Table 7. Summary of PID Inpatient Admissions and Costs (2008–2010)
Category 2008 2009 2010
Population Inpatient Admissions 1,039,062 1,061,379 1,081,168
PID Inpatient Admissions 763 816 859
PID prevalence per 100K 60.9 59.1 65.7
PID male (%) 45.48% 42.16% 41.60%
PID female (%) 54.39% 57.84% 58.40%
Population average DAYS 4.0 3.9 3.9
PID Average DAYS 6.9 6.8 7.0
PID DAYS, age group: 1-64yrs 6.4 6.4 5.9
PID DAYS, age group: <1yr 19.5 17.4 25.3
Population average Cost per
Hospitalization $ 15,608.62 $ 16,763.24 $ 17,894.44
PID average Cost per Hospitalization $ 27,284.11 $ 29,311.14 $ 38,828.64
PID average Cost per Hospitalization,
age group: <1yr $ 91,237.26 $ 97,230.51 $ 224,526.06
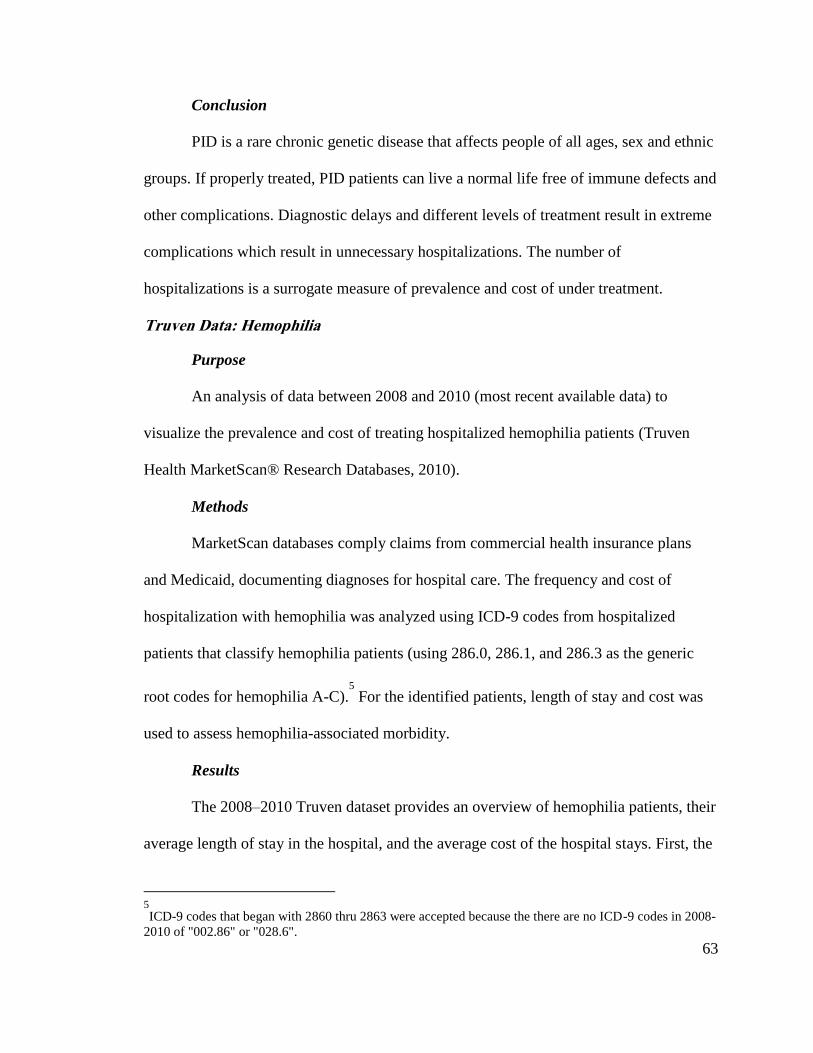
63
Conclusion
PID is a rare chronic genetic disease that affects people of all ages, sex and ethnic
groups. If properly treated, PID patients can live a normal life free of immune defects and
other complications. Diagnostic delays and different levels of treatment result in extreme
complications which result in unnecessary hospitalizations. The number of
hospitalizations is a surrogate measure of prevalence and cost of under treatment.
Truven Data: Hemophilia
Purpose
An analysis of data between 2008 and 2010 (most recent available data) to
visualize the prevalence and cost of treating hospitalized hemophilia patients (Truven
Health MarketScan® Research Databases, 2010).
Methods
MarketScan databases comply claims from commercial health insurance plans
and Medicaid, documenting diagnoses for hospital care. The frequency and cost of
hospitalization with hemophilia was analyzed using ICD-9 codes from hospitalized
patients that classify hemophilia patients (using 286.0, 286.1, and 286.3 as the generic
root codes for hemophilia A-C).5
For the identified patients, length of stay and cost was
used to assess hemophilia-associated morbidity.
Results
The 2008–2010 Truven dataset provides an overview of hemophilia patients, their
average length of stay in the hospital, and the average cost of the hospital stays. First, the
5
ICD-9 codes that began with 2860 thru 2863 were accepted because the there are no ICD-9 codes in 2008-
2010 of "002.86" or "028.6".
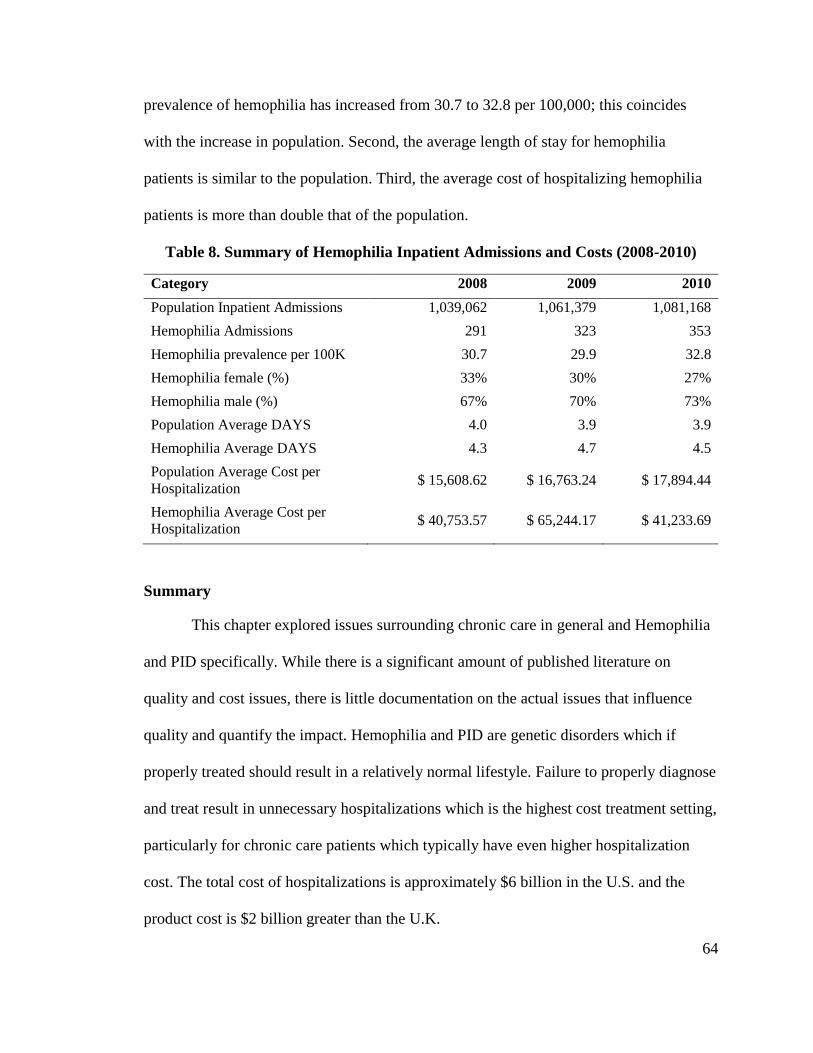
64
prevalence of hemophilia has increased from 30.7 to 32.8 per 100,000; this coincides
with the increase in population. Second, the average length of stay for hemophilia
patients is similar to the population. Third, the average cost of hospitalizing hemophilia
patients is more than double that of the population.
Table 8. Summary of Hemophilia Inpatient Admissions and Costs (2008-2010)
Category 2008 2009 2010
Population Inpatient Admissions 1,039,062 1,061,379 1,081,168
Hemophilia Admissions 291 323 353
Hemophilia prevalence per 100K 30.7 29.9 32.8
Hemophilia female (%) 33% 30% 27%
Hemophilia male (%) 67% 70% 73%
Population Average DAYS 4.0 3.9 3.9
Hemophilia Average DAYS 4.3 4.7 4.5
Population Average Cost per
Hospitalization $ 15,608.62 $ 16,763.24 $ 17,894.44
Hemophilia Average Cost per
Hospitalization $ 40,753.57 $ 65,244.17 $ 41,233.69
Summary
This chapter explored issues surrounding chronic care in general and Hemophilia
and PID specifically. While there is a significant amount of published literature on
quality and cost issues, there is little documentation on the actual issues that influence
quality and quantify the impact. Hemophilia and PID are genetic disorders which if
properly treated should result in a relatively normal lifestyle. Failure to properly diagnose
and treat result in unnecessary hospitalizations which is the highest cost treatment setting,
particularly for chronic care patients which typically have even higher hospitalization
cost. The total cost of hospitalizations is approximately $6 billion in the U.S. and the
product cost is $2 billion greater than the U.K.
65
Table 9. Summary: Quantifying the Quality Gap
Qualitative Observations Quantitative Observations
30-43% of all households give poor ratings on
the quality of interaction.
The total cost of hospitalizations: $6b
estimate (diagnosed + undiagnosed).
53% of the hemophilia and PID patients with
poor perceived health gave poor ratings.
Product cost in the U.S. is $2 billion higher
than the U.K.
Poor PH is low for almost 40% of the PID
population.
The total cost of the quality gap for PID and
hemophilia could be up to ~$8 billion
(~$80,000 per person).
An analysis of a representative sample of the U.S. population suggests that a
significant percentage of households (30–43%)—especially those with chronic care
patients—have a poor interaction with their health care provider: inadequate listening,
respect and time. While the numbers are small, this poor interaction is reflected in the
hemophilia and PID patient populations; almost 40% of the PID population reports poor
perceived health. Using hospitalization as an indicator of under treatment, the total cost
of the quality gap for PID and hemophilia could be up to ~$8 billion or $80,000 per
person. It is possible that a significant percentage of this cost could be avoided with
quality interaction/decision making proper treatment.
66
CHAPTER 4: RESEARCH FRAMING
This chapter presents the framework, research plan, and methods for the research
study.
Theoretical Framing
What is known?
From the review of published research in Chapter 2, following is a summary of
“what we know.” Dual process theory is a relevant and well-documented way of
understanding how clinical decisions are made and the associated biases with different
modes of thinking. SIT and Agency Theory predict that power influences decision
making and health literacy/patient-centric care can balance power between a physician
and patient. Physician and patient traits are thought to be relevant. In all cases, doctors
and patients operate within a wider organizational context that impacts how decisions are
made.
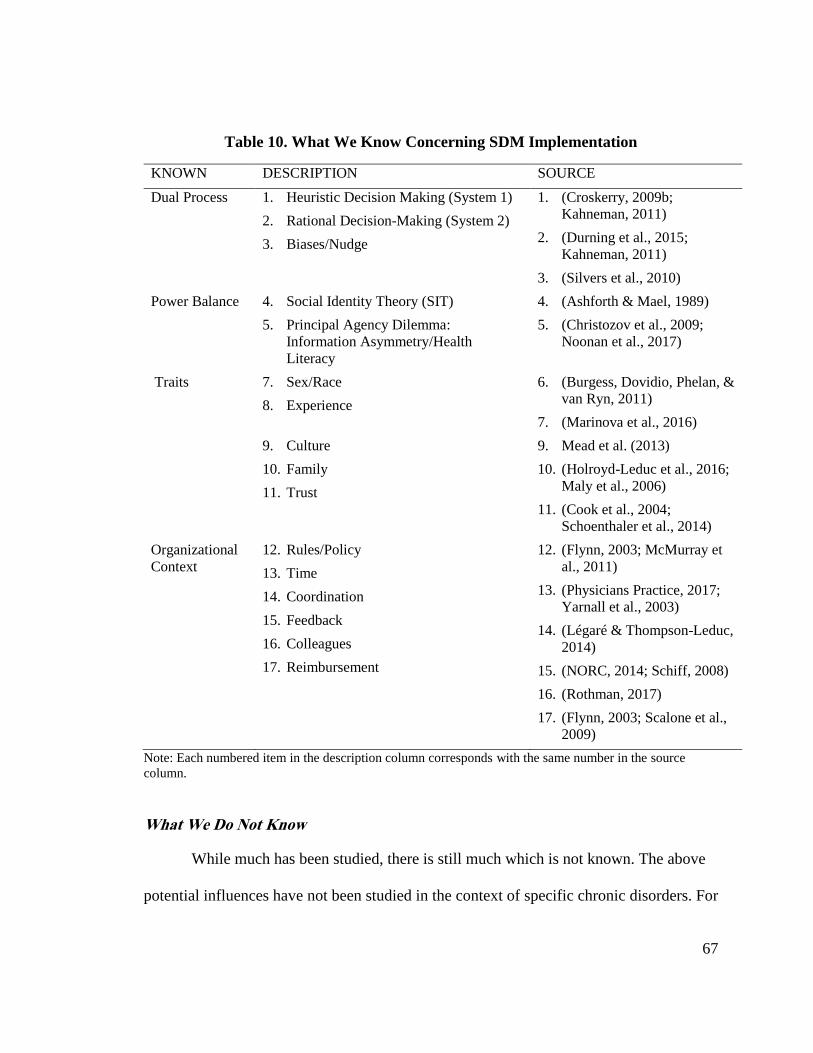
67
Table 10. What We Know Concerning SDM Implementation
KNOWN DESCRIPTION SOURCE
Dual Process 1. Heuristic Decision Making (System 1)
2. Rational Decision-Making (System 2)
3. Biases/Nudge
1. (Croskerry, 2009b;
Kahneman, 2011)
2. (Durning et al., 2015;
Kahneman, 2011)
3. (Silvers et al., 2010)
Power Balance 4. Social Identity Theory (SIT)
5. Principal Agency Dilemma:
Information Asymmetry/Health
Literacy
4. (Ashforth & Mael, 1989)
5. (Christozov et al., 2009;
Noonan et al., 2017)
Traits 7. Sex/Race
8. Experience
6. (Burgess, Dovidio, Phelan, &
van Ryn, 2011)
7. (Marinova et al., 2016)
9. Culture
10. Family
11. Trust
9. Mead et al. (2013)
10. (Holroyd-Leduc et al., 2016;
Maly et al., 2006)
11. (Cook et al., 2004;
Schoenthaler et al., 2014)
Organizational
Context
12. Rules/Policy
13. Time
14. Coordination
15. Feedback
16. Colleagues
17. Reimbursement
12. (Flynn, 2003; McMurray et
al., 2011)
13. (Physicians Practice, 2017;
Yarnall et al., 2003)
14. (Légaré & Thompson-Leduc,
2014)
15. (NORC, 2014; Schiff, 2008)
16. (Rothman, 2017)
17. (Flynn, 2003; Scalone et al.,
2009)
Note: Each numbered item in the description column corresponds with the same number in the source
column.
What We Do Not Know
While much has been studied, there is still much which is not known. The above
potential influences have not been studied in the context of specific chronic disorders. For
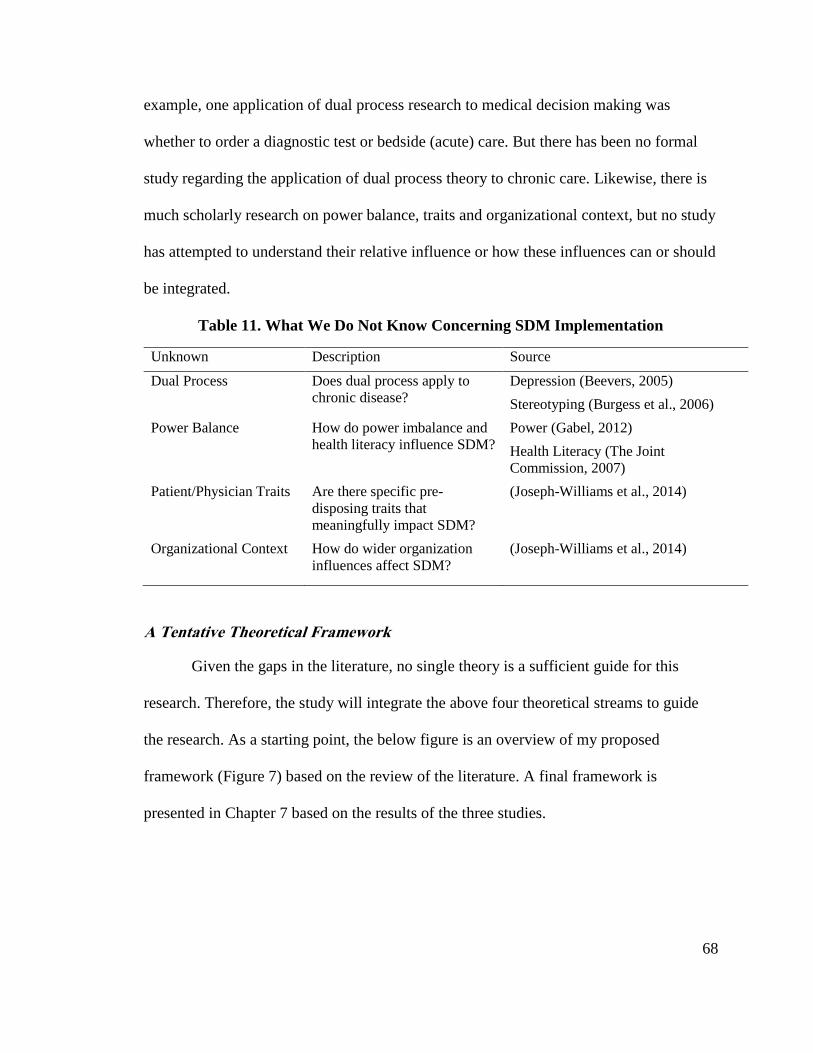
68
example, one application of dual process research to medical decision making was
whether to order a diagnostic test or bedside (acute) care. But there has been no formal
study regarding the application of dual process theory to chronic care. Likewise, there is
much scholarly research on power balance, traits and organizational context, but no study
has attempted to understand their relative influence or how these influences can or should
be integrated.
Table 11. What We Do Not Know Concerning SDM Implementation
Unknown Description Source
Dual Process Does dual process apply to
chronic disease?
Depression (Beevers, 2005)
Stereotyping (Burgess et al., 2006)
Power Balance How do power imbalance and
health literacy influence SDM?
Power (Gabel, 2012)
Health Literacy (The Joint
Commission, 2007)
Patient/Physician Traits Are there specific pre-
disposing traits that
meaningfully impact SDM?
(Joseph-Williams et al., 2014)
Organizational Context How do wider organization
influences affect SDM?
(Joseph-Williams et al., 2014)
A Tentative Theoretical Framework
Given the gaps in the literature, no single theory is a sufficient guide for this
research. Therefore, the study will integrate the above four theoretical streams to guide
the research. As a starting point, the below figure is an overview of my proposed
framework (Figure 7) based on the review of the literature. A final framework is
presented in Chapter 7 based on the results of the three studies.
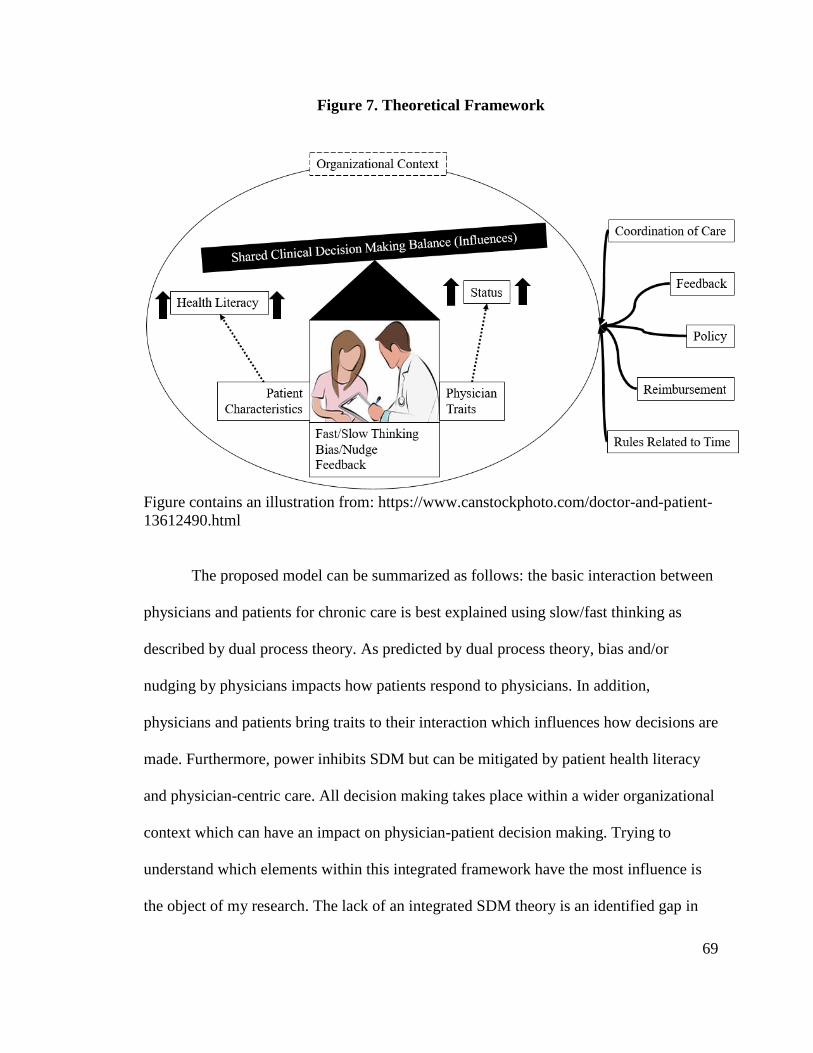
69
Figure 7. Theoretical Framework
Figure contains an illustration from: https://www.canstockphoto.com/doctor-and-patient-
13612490.html
The proposed model can be summarized as follows: the basic interaction between
physicians and patients for chronic care is best explained using slow/fast thinking as
described by dual process theory. As predicted by dual process theory, bias and/or
nudging by physicians impacts how patients respond to physicians. In addition,
physicians and patients bring traits to their interaction which influences how decisions are
made. Furthermore, power inhibits SDM but can be mitigated by patient health literacy
and physician-centric care. All decision making takes place within a wider organizational
context which can have an impact on physician-patient decision making. Trying to
understand which elements within this integrated framework have the most influence is
the object of my research. The lack of an integrated SDM theory is an identified gap in
70
the literature and if developed will contribute to enhancing the use and impact of SDM in
medical decision-making (Groot et al., 2017).
Research Purpose
The purpose of this study is to examine, identify, and analyze factors that
encourage or discourage physicians to implement SDM in the treatment of hemophilia
and PID to determine what predicts SDM. Despite greater spending on healthcare in the
U.S. than any other country, quality and cost outcomes lag far behind other OCED
countries. One potential solution is to implement SDM into the decision processes in the
treatment of chronic diseases. However, there is little evidence of how to successfully
implement SDM despite the stated intentions of physicians to adopt SDM, official U.S.
policy, and some documented SDM models.
Research Plan
The theories described in Chapter 2 were used to plan this study as described in
Figure 6 above. Starting from published theory and data, the factors that might predict
implementation of SDM were explored and tested. The study also tried to understand the
context where SDM is most applicable. Both the factors and context associated with
SDM provide an original and significant contribution to the field of clinical decision
making for chronic care. Figure 8 provides an overview of the potential theoretical
explanations for predicting SDM. The basic plan of this study is to explore and test these
theories using a mixed method design.
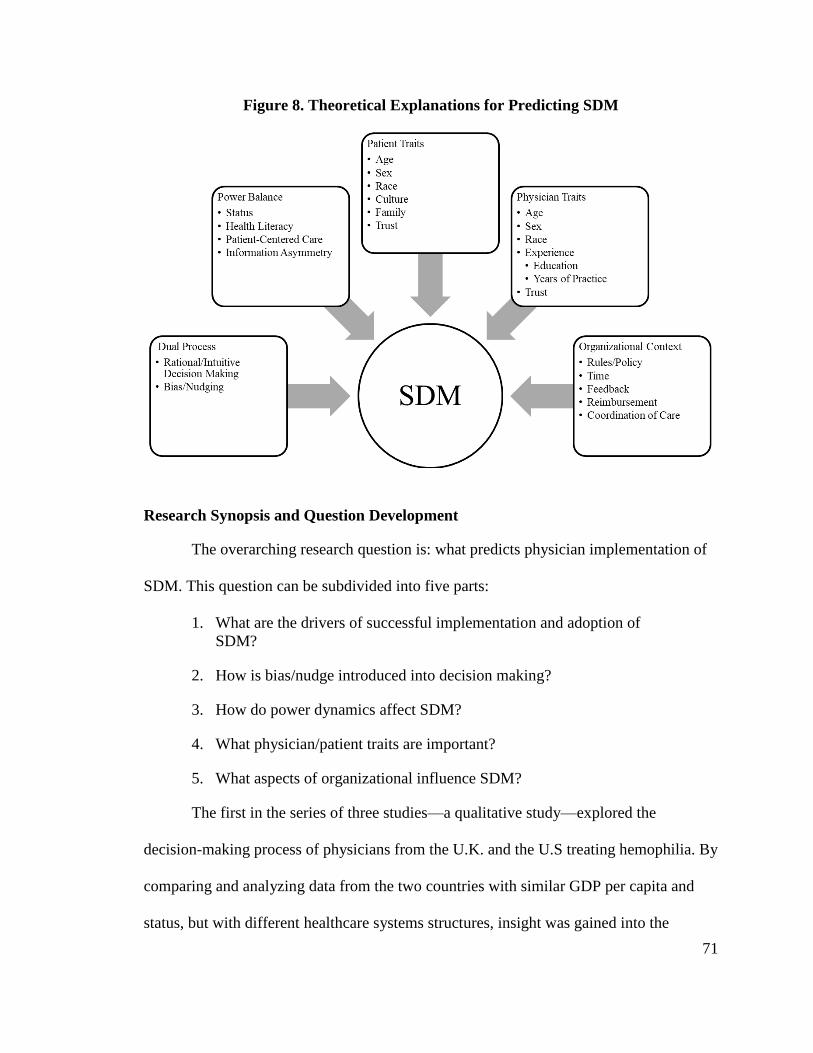
71
Figure 8. Theoretical Explanations for Predicting SDM
Research Synopsis and Question Development
The overarching research question is: what predicts physician implementation of
SDM. This question can be subdivided into five parts:
1. What are the drivers of successful implementation and adoption of
SDM?
2. How is bias/nudge introduced into decision making?
3. How do power dynamics affect SDM?
4. What physician/patient traits are important?
5. What aspects of organizational influence SDM?
The first in the series of three studies—a qualitative study—explored the
decision-making process of physicians from the U.K. and the U.S treating hemophilia. By
comparing and analyzing data from the two countries with similar GDP per capita and
status, but with different healthcare systems structures, insight was gained into the
72
decision-making process and styles implemented by physicians in each country treating
the same chronic disease. The purpose of the study was to answer the following
questions:
What are the different factors that influence the decision making of
British and American physicians regarding the treatment of
hemophilia?
How does the larger organizational network affect decision making?
Are there any discernable physician or patient traits that affect decision
making?
How do trust and health information influence decision making?
The primary finding was that U.S. physicians are more influenced by the patient (i.e.,
patient-centric) than U.K. physicians who are more influenced by Evidence-Based
Medicine (EBM). The U.K. physicians tend to make decisions in collaboration with
colleagues as guided by policies (physician-driven) rather than by patient input. A simple
model explaining the relationship between physician decision-making style (fast vs.
slow), patient-centric approach, trust and SDM was developed.
The second quantitative study was used to testing finding from the qualitative
study using hypothesizes supported by published literature. The research questions were:
Do physician decision-making styles affect patient participation in the
choice of treatment tools and protocols?
What is the role of trust and SDM?
What is the relationship between physician decision making and a
patient-centered approach?
Are there certain physician traits that influence SDM?
The primary finding was that patient participation was predicted by physician
decision-making styles for both treatment protocols and tools. It was hypothesized that
73
physicians using a rational “slow” decision-making style mediated by a patient-centric
approach increases SDM as predicted by dual process theory and SIT. It was expected
that physicians who engaged in rational decision-making would have a more patient-
centric approach than those who use a heuristic decision-making style. It was also
expected that rational decision-makers encouraged patient participation in treatment
protocols, whereas heuristic decision-making by physicians decreased participation.
However, it was unexpected to have a positive relationship between heuristic decision-
making and patient participation when selecting tools; in other words, physician use of
heuristic decision-making encouraged participation with the selection of tools, whereas
rational decision making decreased patient participation. Additionally, physician age and
sex have some influence on patient participation with protocols is this specific context;
however, other traits did not have an effect on participation.
The third study included both a post hoc analysis of the second study and a new
qualitative study. The post hoc analysis was used to better understand the unexpected
results from the second study. The second qualitative study explored other factors not
explained by the quantitative model but hypothesized in published literature: power
balance, patient traits, and organizational context. The research questions were:
What encourages or discourages physicians to adopt SDM?
What is the role of power dynamics and how does health literacy affect
these dynamics?
Do certain patient traits influence SDM?
What are the influences from the wider organization?
The results of the post hoc analysis found that immunologists using rational
decision-making and patient-centric approaches increased patient participation. In the
74
post hoc analysis patient participation was split into four DVs and tool feedback is found
to partially mediate participation with protocol management and options. Patient tool
requests were increased by rational, patient-centric decision-making, but unaffected by
the other DVs. The findings from the qualitative interviews suggest that SDM is bounded
by factors other than dual process thinking. SDM is more likely when there is a balance
of power between the patient and physician within permitted organizational boundaries
such as time and coordination of care.
Research Design
This study was an exploratory developmental mixed-methods design. The design
consisted of three sequential studies: (1) qualitative study of decision-making of
physicians in the U.S. and U.K. who treat hemophilia, (2) a quantitative study of the
decision-making style of physicians who treat PID in the U.S., and (3) a post-hoc analysis
of the second study combined with a qualitative study involving interviews with
immunologists that treat PID in the U.S. Figure 9 represents an overview of the research
design flow. Mixed methods are a robust and multifaceted approach that mitigates the
weaknesses of each method when implemented alone (Castro, Kellison, Boyd, & Kopak,
2010). This approach is particularly appropriate because the variables of interest are not
well-defined and are understudied. Furthermore, mixed methods help scholars document
the consistency of findings through triangulation between study methods, data sources,
and the literature as well as extend theory through complementarity (Gibson, 2017).
The study was initiated using a qualitative method because the overarching
research questions were about uncovering factors that influence SDM. The questions of
the first study sought to explore the influences of decision-making. Therefore, a
75
qualitative method was appropriate. Using a quantitative method, the second study used
survey questions to test theory generated from the first study using a different chronic
disorder. Following a post hoc analysis of the second study, the third study questions
explored other factors; therefore, a qualitative method was selected. The mixed method
approach for my overall multiphase design was: QUAL QUAN QUAL (Creswell,
2013b).
My research addressed five research questions over the course of three studies.
Figure 9 organizes in more detail research questions and methods associated with each
question and the overall flow of the study and related findings.
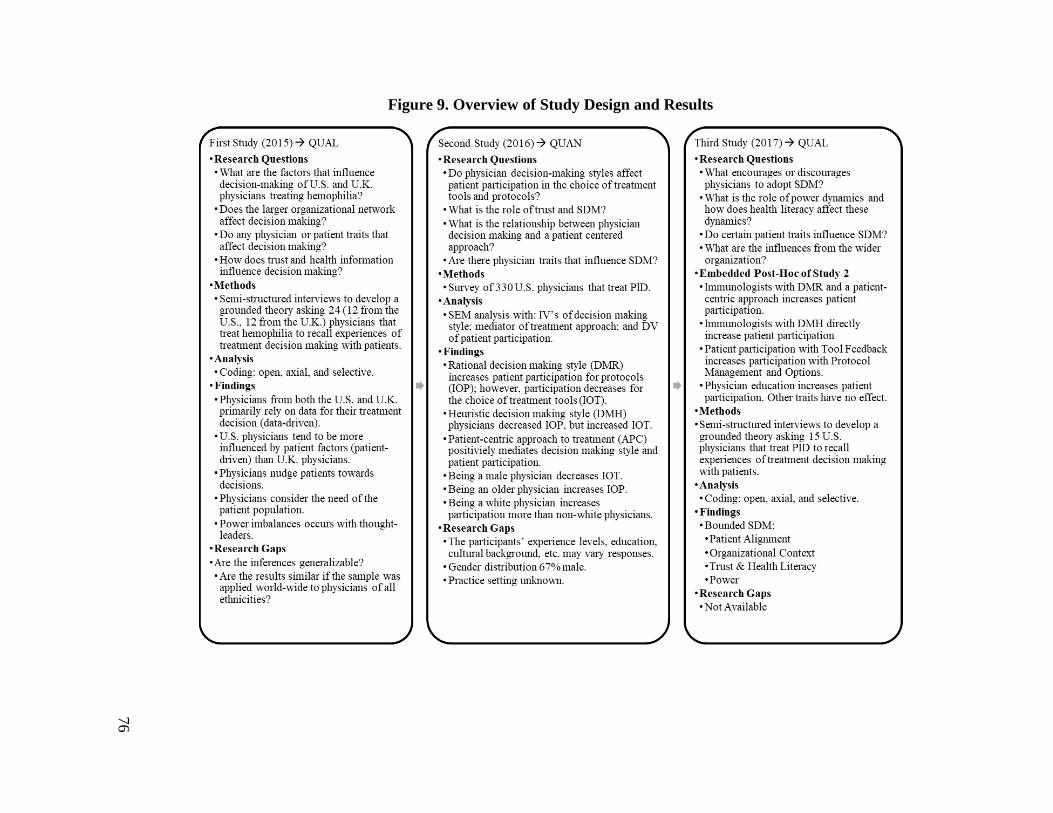
76
Figure 9. Overview of Study Design and Results
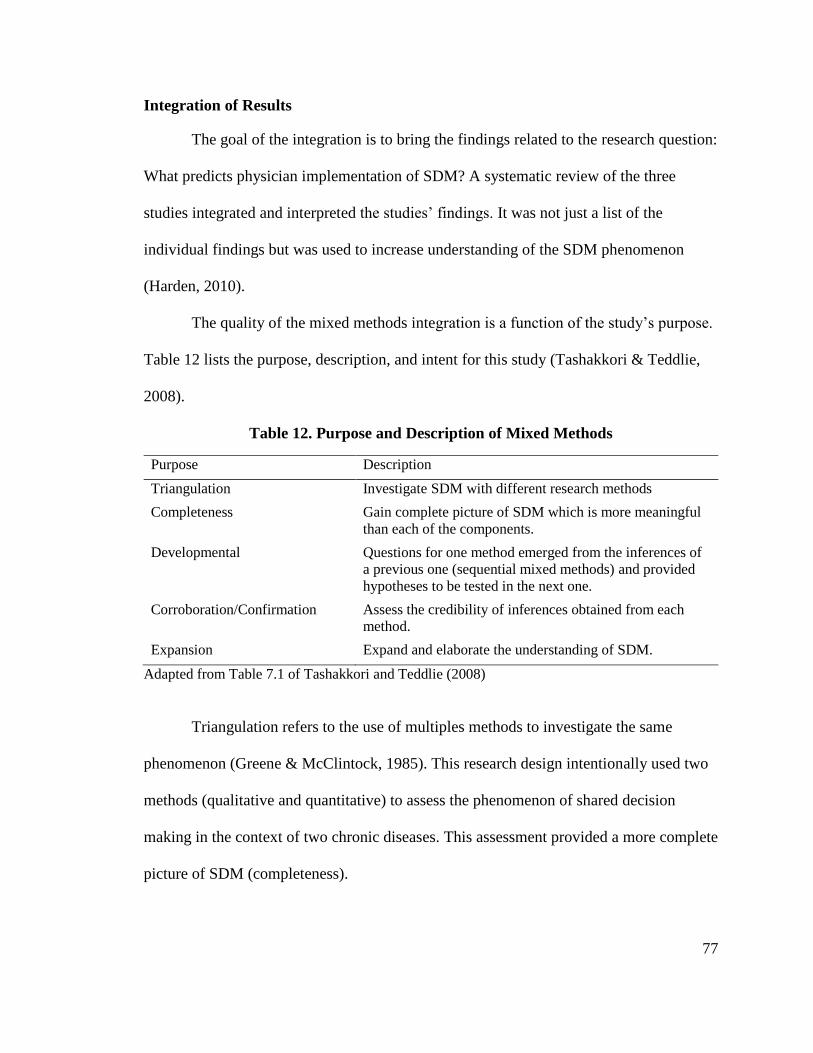
77
Integration of Results
The goal of the integration is to bring the findings related to the research question:
What predicts physician implementation of SDM? A systematic review of the three
studies integrated and interpreted the studies’ findings. It was not just a list of the
individual findings but was used to increase understanding of the SDM phenomenon
(Harden, 2010).
The quality of the mixed methods integration is a function of the study’s purpose.
Table 12 lists the purpose, description, and intent for this study (Tashakkori & Teddlie,
2008).
Table 12. Purpose and Description of Mixed Methods
Purpose Description
Triangulation Investigate SDM with different research methods
Completeness Gain complete picture of SDM which is more meaningful
than each of the components.
Developmental Questions for one method emerged from the inferences of
a previous one (sequential mixed methods) and provided
hypotheses to be tested in the next one.
Corroboration/Confirmation Assess the credibility of inferences obtained from each
method.
Expansion Expand and elaborate the understanding of SDM.
Adapted from Table 7.1 of Tashakkori and Teddlie (2008)
Triangulation refers to the use of multiples methods to investigate the same
phenomenon (Greene & McClintock, 1985). This research design intentionally used two
methods (qualitative and quantitative) to assess the phenomenon of shared decision
making in the context of two chronic diseases. This assessment provided a more complete
picture of SDM (completeness).
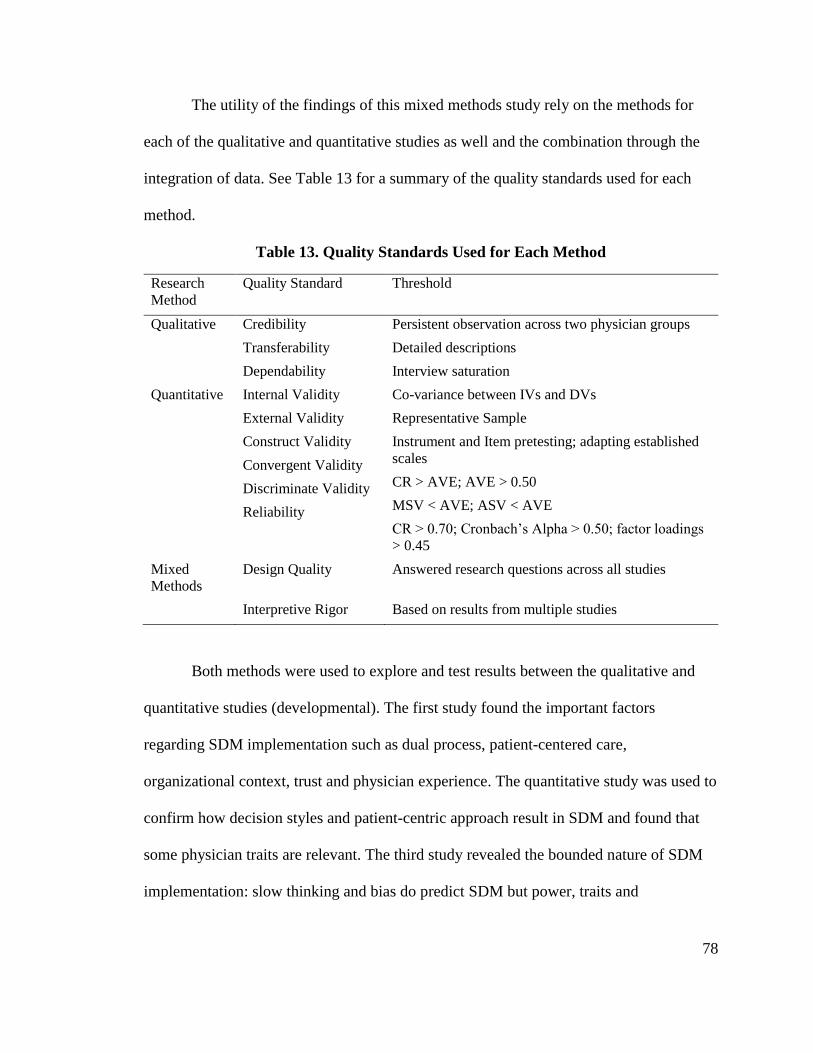
78
The utility of the findings of this mixed methods study rely on the methods for
each of the qualitative and quantitative studies as well and the combination through the
integration of data. See Table 13 for a summary of the quality standards used for each
method.
Table 13. Quality Standards Used for Each Method
Research
Method
Quality Standard Threshold
Qualitative Credibility
Transferability
Dependability
Persistent observation across two physician groups
Detailed descriptions
Interview saturation
Quantitative Internal Validity
External Validity
Construct Validity
Convergent Validity
Discriminate Validity
Reliability
Co-variance between IVs and DVs
Representative Sample
Instrument and Item pretesting; adapting established
scales
CR > AVE; AVE > 0.50
MSV < AVE; ASV < AVE
CR > 0.70; Cronbach’s Alpha > 0.50; factor loadings
> 0.45
Mixed
Methods
Design Quality Answered research questions across all studies
Interpretive Rigor Based on results from multiple studies
Both methods were used to explore and test results between the qualitative and
quantitative studies (developmental). The first study found the important factors
regarding SDM implementation such as dual process, patient-centered care,
organizational context, trust and physician experience. The quantitative study was used to
confirm how decision styles and patient-centric approach result in SDM and found that
some physician traits are relevant. The third study revealed the bounded nature of SDM
implementation: slow thinking and bias do predict SDM but power, traits and
79
organizational limits limit or bound its impact. Furthermore, both methods were able to
corroborate the results from each of the three studies.
There was also the intent to expand theory related to SDM whereby results from
the 2nd qualitative study (third study) were used to elaborate the findings found in the
quantitative study. This expansion relates to different factors influence SDM and how
these factors can be integrated into a new overall decision-making framework for chronic
care.
Philosophical Lens
This research views reality as socially constructed with the goal of understanding
what meanings physicians give to reality when making decisions (Van de Ven, 2007).
Social constructivism is founded on the idea that conclusions about human functioning
are understood based on the biological and social factors that impact behavior. All
decisions take place in a social context and is a social interpretation of reality. Social
constructivism defines decision-making process as an interaction between a physician
and a patient rather than an individual or intrapsychic process. The process “involves
negotiating, consensualizing, and, is guided by social and cultural factors in defining
what is acceptable” (Cottone, 2001, 2004).
Summary
In summary, a mixed methods research design was used to explore and test theory
related to SDM with the intent to develop a new framework that could answer the
research question: what predicts physician implementation of SDM. Chapters 5–7 review
each of the studies. Chapter 8 provides the meta-inferences derived from all three studies.
Chapter 9 details implications for the findings and suggestions for future research.
80
CHAPTER 5: STUDY 1: PATIENT-CENTRIC VS. PHYSICIAN-DRIVEN
DECISION MODELS IN THE TREATMENT OF HEMOPHILIA
The research started with an exploratory qualitative study initiated in 2015. As
described in Chapter 2, U.S. healthcare quality does not match the cost of care.
Therefore, the first study sought to understand how physicians from countries with
similar GDPs make decisions when treating a similar high-cost complex chronic disease.
In this first study, the decision-making processes of physicians that treat hemophilia were
explored. Hemophilia was chosen both because of the significant disparity of cost and
treatment between the U.S. and U.K. and the researcher’s professional experience with
this chronic disease. This cost difference is consistent with the difference in healthcare
expenses between the two countries. Overall healthcare spending is the U.K. is 50% less
than the U.S. The annual cost of treating a severe hemophiliac exceeds $300,000; in the
U.K. the cost is less than half this amount. Using grounded theory as a systematic
methodology, the goal was the construction of a theory on chronic care shared decision
making through the analysis of qualitative data.
The study started with several questions with the goal to develop operational
definitions, establish priorities, and improve the research design for future studies. The
research questions for this qualitative study were:
“What are the different factors that influence the decision-making of
British and American physicians regarding the treatment of
hemophilia?”
How does the larger organizational network affect decision making?
Are there any discernable physician or patient traits that affect decision
making?
How do trust and health information influence decision making?
81
This chapter presents the study’s design, method, results, discussion, and limitations.
Methodology
An exploratory, qualitative study was conducted based on semi-structured
interviews to compare physicians in the U.K. and U.S. and uncover key influences on the
decision process. The U.S. and the U.K. were chosen for comparison to avoid language
barriers and because both countries have similar first world status including relatively
similar per capital GDPs of $54,000 and $45,000 per annum respectively (WorldBank,
2015). The interview transcripts were analyzed using grounded theory to develop a richer
understanding of physician decision making in the treatment of hemophilia. The
transcripts were coded to extract factors and themes (Corbin & Strauss, 2014). The
methodology was appropriate for this study because physician decision-making in the
treatment of hemophilia is a poorly understood and under-theorized phenomenon.
Interviews were used “to gather rich data from people in various roles and situations”
(Myers, 2013: 119). A grounded theory approach provides guidelines for collecting and
analyzing qualitative data in order to construct theories grounded in the data, “rather than
deducing testable hypothesis from existing theories” (Charmaz, 2006: 2). A systematic
qualitative analysis can generate theory (Charmaz, 2006; Glaser & Strauss, 2017).
Qualitative research focuses on exploring the inner experiences of participants and not on
testing theories (Corbin & Strauss, 2014).
Reliability and integrity issues were addressed based on Silverman’s guidance
(2011). To ensure reliability, the interview protocol was pilot tested on the first
participant. Questions were assessed for clarity, appropriateness and relevance. Revised
interview protocols were created after the initial feedback. Data from the pilot was kept
82
in the analysis. The interviews were recorded and transcribed to ensure data integrity.
Exact quotes from participants were used to support findings.
Analytic induction, the constant comparative method, deviant-case analysis,
comprehensive data treatment, and appropriate tabulations were used to increase research
validity. Conducting counts on the data were used to confirm accuracy and identify
deviant cases (Silverman, 2011). Counts were used to keep track of repeating themes.
Moreover, quantity measurements in the qualitative study were used when possible (e.g.,
event frequency, appearance of key words, and other repeated occurrences).
Sample
Sampling was conducted “on the basis of emerging concepts, with the aim being
to explore the dimensional range or varied conditions along which the properties of
concepts vary” (Strauss & Corbin, 1998: 73). Consistent with grounded theory practice,
the sampling and interview protocol were redefined as the data was collected and
analyzed. A total of 24 physicians were interviewed; 12 with U.K. experience and 12
with U.S. experience. Participants were chosen based on availability. Participants are
described in Table 14.
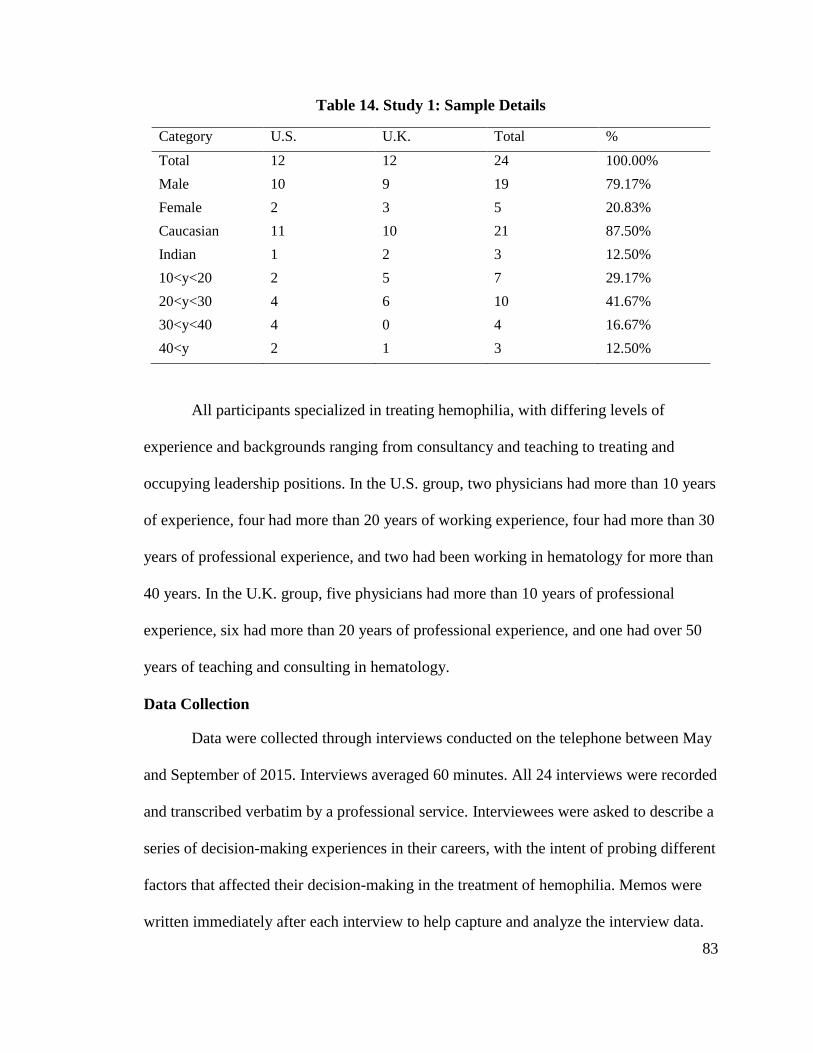
83
Table 14. Study 1: Sample Details
Category U.S. U.K. Total %
Total 12 12 24 100.00%
Male 10 9 19 79.17%
Female 2 3 5 20.83%
Caucasian 11 10 21 87.50%
Indian 1 2 3 12.50%
10<y<20 2 5 7 29.17%
20<y<30 4 6 10 41.67%
30<y<40 4 0 4 16.67%
40<y 2 1 3 12.50%
All participants specialized in treating hemophilia, with differing levels of
experience and backgrounds ranging from consultancy and teaching to treating and
occupying leadership positions. In the U.S. group, two physicians had more than 10 years
of experience, four had more than 20 years of working experience, four had more than 30
years of professional experience, and two had been working in hematology for more than
40 years. In the U.K. group, five physicians had more than 10 years of professional
experience, six had more than 20 years of professional experience, and one had over 50
years of teaching and consulting in hematology.
Data Collection
Data were collected through interviews conducted on the telephone between May
and September of 2015. Interviews averaged 60 minutes. All 24 interviews were recorded
and transcribed verbatim by a professional service. Interviewees were asked to describe a
series of decision-making experiences in their careers, with the intent of probing different
factors that affected their decision-making in the treatment of hemophilia. Memos were
written immediately after each interview to help capture and analyze the interview data.
84
After each interview was finished, the interview audio file was downloaded onto a
personal computer. The downloaded file was assigned a coded file name, and the original
file on the recording device was deleted. Both the personal computer and the stored
backup are password-protected. All printout transcript papers were stored inside a locked
file drawer. A professional commercial transcription service that follows the precaution
procedure for human subject research was used. All research materials (audio recordings,
video recordings, digital files, transcribed Word files, etc.) will be destroyed no later than
August 2018.
Data Analysis
Data analysis began immediately after the first interview and lasted throughout
the study (Corbin & Strauss, 2008). Simultaneous involvement in data collection and
analysis helped pursue those “emphases as we shape our data collections to inform our
emerging analysis” (Charmaz, 2006: 20). After careful review, the transcribed audio
recordings underwent three stages of coding:6
open, axial, and selective (Corbin &
Strauss, 2014). Codes are the categories of information found in the interview transcripts.
Table 15 summarizes the coding results.
6
NVivo 9 software package was used to code the transcripts.
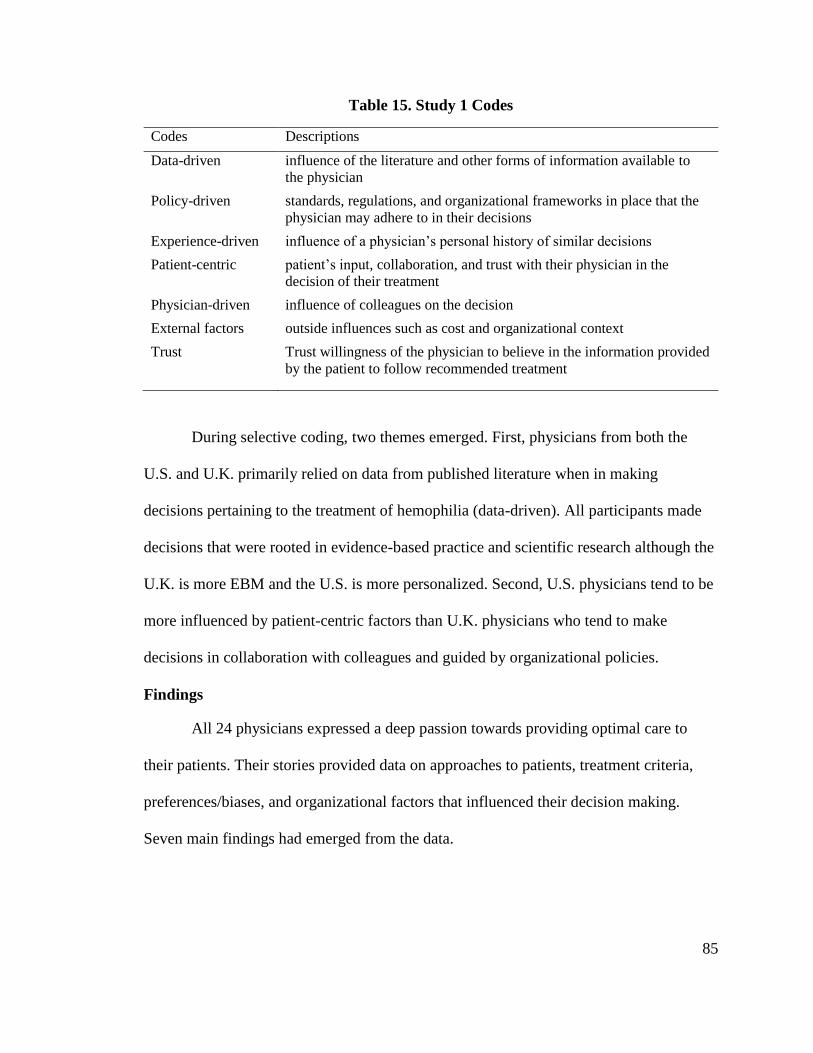
85
Table 15. Study 1 Codes
Codes Descriptions
Data-driven influence of the literature and other forms of information available to
the physician
Policy-driven standards, regulations, and organizational frameworks in place that the
physician may adhere to in their decisions
Experience-driven influence of a physician’s personal history of similar decisions
Patient-centric patient’s input, collaboration, and trust with their physician in the
decision of their treatment
Physician-driven influence of colleagues on the decision
External factors
Trust
outside influences such as cost and organizational context
Trust willingness of the physician to believe in the information provided
by the patient to follow recommended treatment
During selective coding, two themes emerged. First, physicians from both the
U.S. and U.K. primarily relied on data from published literature when in making
decisions pertaining to the treatment of hemophilia (data-driven). All participants made
decisions that were rooted in evidence-based practice and scientific research although the
U.K. is more EBM and the U.S. is more personalized. Second, U.S. physicians tend to be
more influenced by patient-centric factors than U.K. physicians who tend to make
decisions in collaboration with colleagues and guided by organizational policies.
Findings
All 24 physicians expressed a deep passion towards providing optimal care to
their patients. Their stories provided data on approaches to patients, treatment criteria,
preferences/biases, and organizational factors that influenced their decision making.
Seven main findings had emerged from the data.
86
Findings related to Decision Theory
Finding 1: Both U.S. and U.K. physicians use “slow” rational thinking but U.K.
physicians use more EBM when making decisions
For both physicians in the U.S. and U.K., their training is primarily based on
general medicine. They eventually specialized in hematology based on fellowship,
clinical experience, and personal interest. Physicians in the U.S. and U.K. had mentors
who were able to train and provide the necessary insights on how hemophiliacs are
affected by their bleeding disorder. Training outcomes appeared to be similar. Some of
the physicians engaged in cross-national training between U.K., U.S., and other countries.
Physicians from both the U.S. and U.K. primarily relied on evidence-based
medicine (EBM) in making decisions pertaining to the treatment of hemophilia (data-
driven). They valued slow, rational decision making throughout the diagnosis and
treatment process. Data acts as a boundary to decision making on two fronts: (1) the
literature offers a range of effective treatments based on context and evidence, and (2)
how each physician interprets the literature. Overall, U.K. physicians followed EBM
more than U.S. physicians
According to one U.K. participant, participating in clinical trials was less
important because their findings can be accessed in the literature, which was used as a
justification when making treatment modifications:
We did not participate in any of the recombinant trials. We basically became
aware of it from looking at the literature that the recombinant products were
available.
In the U.S., EBM is important as well. Participant US9 reported following the literature
carefully to ensure being updated with the new treatments:
87
I think as new treatments come along, we want to definitely be open-minded
about incorporating those into our practice. I follow the literature carefully.
I just came back from a big meeting where some of these drugs, including
the Roche drug were talked about quite a bit. There’s no doubt that those
will probably have some impact.
However in the U.S. evaluation of products are more nuanced and based on
individual circumstances. One participant (US3) questioned the improvements that new
products, addressing the scientific basis behind the new long-acting products:
Part of the annual visit is to vote into new products. Sometimes the patients
will bring up the question, "Doc don't you think I'd be a good candidate for
these products?" My own philosophy has been the following. … "I need to
know what your pharmacokinetics are on your current product because if
you are on the top side of the kinetic curve using the current product that
you're on, and if you have an active lifestyle so that you are going to be
active 3 out of 5 or 7 days out of the week, then I need to know how to keep
your clotting factor level over 15% at least so that you can be physically
active and I need to know how long that area under the curve is going to
be." Because the prolonged half-life products most patients don't appreciate
only talks about the prolonged area under the curve. It does not talk about
how long the peak activity is sustained. So when you begin to talk to patients
and you get them to understand that the benefits of the extended half-life
products are only at how long will you remain over 1% of Factor-8 clotting
factor activity, they begin to understand that maybe they're not the ideal
candidate to be on these products because what they really need is to have
over 30% activity so they can go out to soccer practice 3 times a week and
not have a bleed.
Finding 2: Bias/Nudging. Physicians intentionally anchor information in a way
that nudges patients to follow their recommendations.
While physicians believed that final choices are made by patients, they often
provided information to nudge the final decision to one that aligned with the physician’s
policies, evidence, or personal preference. Suggested nudges are accepted because of the
mutual trust between the physician and patient; trust is another finding describes in the
traits section below.
88
One U.K. physician (Participant UK5) explained how they approached the
national switch from plasma-derived to recombinant products, “I think it was to left to the
patient. We just gave them the whole information about the reason to move and
everything and it was completely left it to the patient to make that decision.” Other U.K.
participants (Participant UK9) explained their approach with new patients, specifying that
they generally avoid mentioning plasma-derived products with new patients.
If it's a brand-new patient, usually there are parents involved as well.
Generally speaking for hemophilia A, we would just go for recombinant
product and we'd give them information for recombinant product and
actually we wouldn't give them any information on plasma-derived. In that
space, specifically spoke about plasma-derived, wouldn't mention it.
U.S. participant (US5) specified that patients needed to know how they understood the
product options.
We always had a strong feeling that these decisions involved keeping the
patients and families well informed. In that the patient really had the choice
of what they wanted based on the best information that we could give them
… If you can use cryo rather than concentrate, do that. But of course, it
didn't matter, our patients were already infected … I think that in many
cases there really was no difference. People needed to know the pros and
the cons of how we understood it. I think that's the way you have to practice
medicine no matter whether it's hemophilia or not. Paternalism doesn't go.
During the HIV epidemic, US6 would provide input to patients switching to
recombinant despite the circumstances; the patients were adult and already potentially
exposed to HIV, making the switch potentially irrelevant in their opinion:
Adults that had been previously exposed to plasma-derived products, it
seemed very excessive to ... Not really excessive, but somewhat excessive
to switch to recombinant after they were previously exposed. Especially
when there was evidence that the plasma-derived heat treated was probably
quite safe. If the patient really wanted and specifically asked for
recombinant then we would certainly try to do that, but in general, I think
that ... Used a lot of literature to look at the safety of plasma-derived
products. I think most people were pretty convinced that they were probably
OK with heat treatment.
89
Another U.S. physician noted that after receiving all the important information, patients
can choose the best treatment for themselves:
We always had a strong feeling that these decisions involved keeping the
patients and families well informed. In that the patient really had the choice
of what they wanted based on the best information that we could give them.
Another participant shared that patients can choose whether to receive recombinant or
plasma-derived products for the treatment of hemophilia:
The program officially then and now is still patient-choice. If a patient came
in or the family came in and they wanted a recombinant product and they
were on plasma-derived, they would be switched. We weren’t necessarily
pushing one over the other. A lot of it again was patient-choice.
Findings related to Power Balance
Finding 3: Patient-centric vs Organizational-centric: As predicted by SIT, a
patient-centered approach reduces the physician-patient power imbalance and
facilitates SDM.
When making treatment decisions for hemophilia, U.S. physicians tend to be
more influenced by patient (patient-centric) factors than U.K. physicians who tend to
make decisions in collaboration with colleagues and guided by organizational policies
(organization-driven). As stated by one U.K. physician:
We didn't have the option so that's what happened, the system told us what
to do. The U.K. tender system has worked because all clinicians in the U.K.
[agreed] that all products were equal in terms of safety and efficacy. We all
had to submit information to the people doing the negotiation and we all
had to sign up to it that we all believed, and it had to be all clinicians in the
U.K.
The U.S. method of treating patients is what some referred to as a model of
“mutual participation” which expresses the benefit of a physician aiding the chronically
ill patient to self-treat (Kaba & Sooriakumaran, 2007). U.S. physicians emphasize that
90
patients have life experiences that must be taken into consideration when making
decisions. This method of treatment can be considered SDM. Participant US10 elaborates
on the importance of patient history and experiences:
I guess I'm thinking of the diagnostic puzzles of new patients and working
through diagnosis of new patients more than day-to-day treatment.
Hemophilia is more driven by individual patient's experiences and how they
respond to factor, how they respond to different things. When I use that
term, it's more for the upfront diagnostic.
[Do you let them choose the clotting factors?] There are multiple brands
and generations of factor, the factor that are recombinant or factor that is
plasma-derived. In my experience, I think that I don't have a preference of
one over another. In general, I will lean more to do the recombinant factor
and there are patients that are in certain situations and that may not be the
case but we go through the different factors, what the small differences are
in each of the generations of factor with the family.
A lot of times the family comes because they have a family history and they
have other members of the family using one factor and they know what they
want to use and that's fine but we always leave it up to the patients to decide
if they have preference. Otherwise, we use whatever we think is the easiest
product for them to administer but we always go through each of the
different options and what may be one benefit is over another or that I
always look and family knows that I think they're always equivalent in
efficacy and safety and so in the end, it's their decision.
The U.K. physicians were more likely to treat patients without taking patient input into
account.
The only other patient that this has happened to recently was a chap who's
got severe hemophilia B and he had been taking a plasma product,
Replinine, for years and years and he was our only patient on it, and it's
taken us about five years to persuade him to change. It's taken us a long time
to change his mind about it, but he has now moved over to recombinant.
U.K. decision making was primarily up to the individual treating physician or
group of physicians responsible for the patient. In the case of an inhibitor, a U.K.
physician will discuss the situation with other colleagues:
91
Most of my inhibitor patients, because it’s not that common, you tend to
discuss with colleagues, so I'd say this is a very colleague driven area of
discussion really. There was a national guideline but it doesn't say use this
one, don’t use one. It just says there's a choice, so it doesn't really tell you
what to do. So it’s colleague driven and my local colleagues particularly
didn't want to expose a patient to factor 8 because the whole idea during
that period of time not expose the patient to factor 8.
One U.K. physician mentioned the policies put in place by a board of physicians:
I think in the U.K., we make a decision on treatment on an across the board,
across the country [basis]. We have a national organization in the U.K.
called CDO. Treatment policy is decided by that body. We decided a long
time ago that recombinant factoring should be the treatment of choice for
all of our patients. We're now in a situation where we only use recombinant
Factor VIII and Factor IX for our patients with hemophilia.
Furthermore, the U.K. Physicians were more influenced by mentors and colleagues, such
as the following example from UK8:
We had a patient at the beginning of the week who had surgery on his elbow.
He is a patient, we have some of these, who never turns up, who doesn't ...
We haven't had any blood levels on him for five or six years because he just
doesn't come, or when he does come doesn't let us do any bloods on him,
helps me. Dosing him to get him up to 100 percent, he weighed 75 kilos,
he's a factor-9, and so I sort of said, "Well, we could give him 7,000 but
actually that's far too much for him. I think it's too much for him," so we
gave him less than that. We got 5,500 and that got him up to 105 percent…
Having watched [Colleague 1] and [Colleague 2] do quite a lot of it now,
they all just go, "Well, that's just a bit too much." I don't know. It just felt a
bit too much.
One U.K. physician summarized the difference with the U.S.:
It would be impossible to do something like this in the United States because
the way the United States system works and the ways of advertisement and
the way people have strong opinions that one product is better than the
other, in either efficacy or safety. People were allowed to decide one was
better than the other. If it impacted, there wasn't. That's how it was based.
There was no published evidence and it was not purely based on opinion.
There's a person who's got the strong views, it's the opinion leader and
especially someone who speaks a lot at meetings, and people get the
impression that there is evidence when really there isn't.
92
In summary, U.S. physicians are more patient-centered whereas U.K. physicians
follow organizational rules, policies, and colleagues. Organizational context likely
contributes to this difference.
Finding 4: Information asymmetry is greater with physician with more
experience.
Information asymmetry is most apparent in physicians that participated in
research studies, especially research that resulted in new products and treatment protocols
(thought-leaders). Although physicians with research experience were open to SDM,
thought leaders such as participant US3 would make sure patients knew the difference
between their current products to a new one:
Having an extended half-life product for your trough levels maintained at
1% or 5% for 3 days, that's not going to make any difference in the quality
of life unless you're sedentary. So, I think a lot of the hype and the hope of
these extended products has exceeded the educational level of the patients.
I would say that most of the hemophilia treaters and nurses who take care
of patients don't understand the concept that I just discussed. So, as a key
opinion leader, I think it's important for us to actually try and put this whole
science into perspective. In my mind, the extended half-life products are a
transition product to gene therapy, or a transition product to say the Ace 9-
10.
This pattern of stronger nudging the patient was common through the physicians who
participated in research or clinical trials.
Findings related to Traits
Finding 5: Influence of patient groups: patients are more likely viewed from a
disease perspective rather than individual traits.
Physician decisions may be impacted by the opinion/movement of an entire group
of patients (patient organization) rather than individual patient opinions. Participant UK1
discussed the influence of patient groups, “If a patient group says no to something; you
93
can't force them to have a particular type of treatment.” When the HIV epidemic
occurred, participant US6 recalled infected patients switching products, despite there
being no benefit:
Truly all the hemophilia patients as I recall, they all wanted recombinants.
I mean, why not? On the other hand, we knew, I think, there was
accumulating amount of evidence at that point that the heat treatment or
solvent-detergent or whatever was really quite effective.
Individual patient traits were less important than the views of the entire group:
The patients were allowed to comment on the safety and efficacy issue. This
was the U.K. Hemophilia Society and the patients agreed that there was no
difference in terms of the safety and efficacy in terms of the published
information. Then, but then there was another component and that was the
means of administration. Basically, the kit that came with the product, is
one kit better than the other. Patients like one kit better than another, so
there is that, they were able to, they asked a lot of patients which of those
different methods of mixing the powder and liquid they prefer. Based on
those, they came to a decision that it was actually the doctors were not
involved in that part, which of the factors did the patients prefer in terms of
administration. Interestingly, the patients came and said that one of those
products was preferable to another. They, when they came to that, it was
decided that priory the patients make that decision based on the scores they
gave the different products, the result of that will result in a price difference.
What it was decided before the bidding down of the different companies,
was that the patient preference and they did positive for one of the product,
they said they prefer the administration kit and it came to, it was decided it
would be equivalent 0.3 pence, U.K. pence, benefit…
Finding 6: Physician Trust: interpersonal trust is an important component of
physician’s personality and is often assumed at the beginning of the interaction
with patients.
The trust between physicians and patients inherently effects the decision-making
process because it is assumed and encourages patient input. Participant US9 explained
the importance of trust when making treatment decisions with patients:
I think that there's some families that, that the trust also allows some
families to say, "Look, Doctor X, I understand what you're saying. I
94
understand what you are expecting. I will just tell you that it's just really
difficult for me to do this right now. I appreciate that you're giving me the
best recommendation, but I won't be able to follow that treatment, at least
for now, and maybe in 6 months or a year, I might be able to do it better." I
think that the trusting relationship doesn't automatically mean that the
patients will do whatever I want. I think that the important thing about the
trusting relationship is that there's honesty and respect that goes both ways,
so that with somebody having all kinds of problems with their joints and
they're telling me they're dosing 3 times a week. Then I'm wracking my
brain to try and figure out why they're having all these bleeds they shouldn't
be, that would be more annoying to me to know that they've misled me as
opposed to saying, "Look, I'm not doing the prophylaxis the way you asked.
I understand that that's why I'm having these bleeds and is there some other
way we can do this?" That would be a much better conversation to have
than me trying to figure out why this kid's bleeding or why is this patient
bleeding, when the reason they're bleeding is because they're not giving the
factor but they're not telling me that. The trusting relationship really cuts
both ways. It doesn't automatically mean that they will follow what I say,
but I need them to be honest with me no matter what.
Trust is also built very quickly or assumed, which may contribute to bias and
nudging as well. Participant UK05 describes the time it takes for a trusting relationship to
form:
I don’t know how quickly it gets established. It is difficult to say that
perhaps within the, I have worked in two institutions now, I was at [London]
since 2000 and I came to [Southern England] in 2008. I do know that by the
end of 2008 I knew all my patients and they respected and talked to me after
one or two consultations.
Finding 7: Minority cultures involve family decision making.
As described by US9 above, patient culture and family status play an important
role in the decision-making process. Especially in minority groups, the patient and their
family are fully involved in the treatment decisions and education. U.S. participant
(Participant US12) educated a whole family about recombinants. It was an immigrant
family that never encountered hemophilia; the physician had to educate the family of
safety and cost differences between countries.

95
Findings related to Organizational Context
Finding 8: U.S. Physicians are not influenced by reimbursement methods.
In the U.S., insurance does not influence the physician decision process.
Physicians are often in contact with insurance companies to get coverage for specific
treatments instead of pre-approved options. However, they will not fight the insurance
company to fulfill every patient request such as switching to brands to an equivalent
product. Participant US9 recalled:
If your payer's saying you got to use Xyntha, then you got to use Xyntha."
You know what I'm saying? I will pick my battles. It would not be contrary
to my recommendation to have a patient on Xyntha. It's no problem at all. I
don't see any problem with switching. Just because a family liked Advate
or liked Baxalta, Baxter whatever, that's not a reason for me to fight with an
insurer. Now, if on the other hand, an insurer's saying, "Well, your patient
as an inhibitor and you want to use NovoSeven, but we want them to use
Feiba," that I will fight because I think inhibitor patients generally will need
both drugs. If it goes against my recommendation, I will fight for it and I
will not follow through with a treatment plan that a payer has dictated to
me. If it's, like I said, something that is really not a medical issue, such as
switching from one similar drug to another, because one is on formulary
and one is not, I'm not going to fight that battle. That's not worth fighting.
Results
The findings provide insight into the factors that influence U.S. and U.K. physician
decision making for the treatment of hemophilia (refer to the research questions on
page 80). The findings are summarized in

96
Table 16.
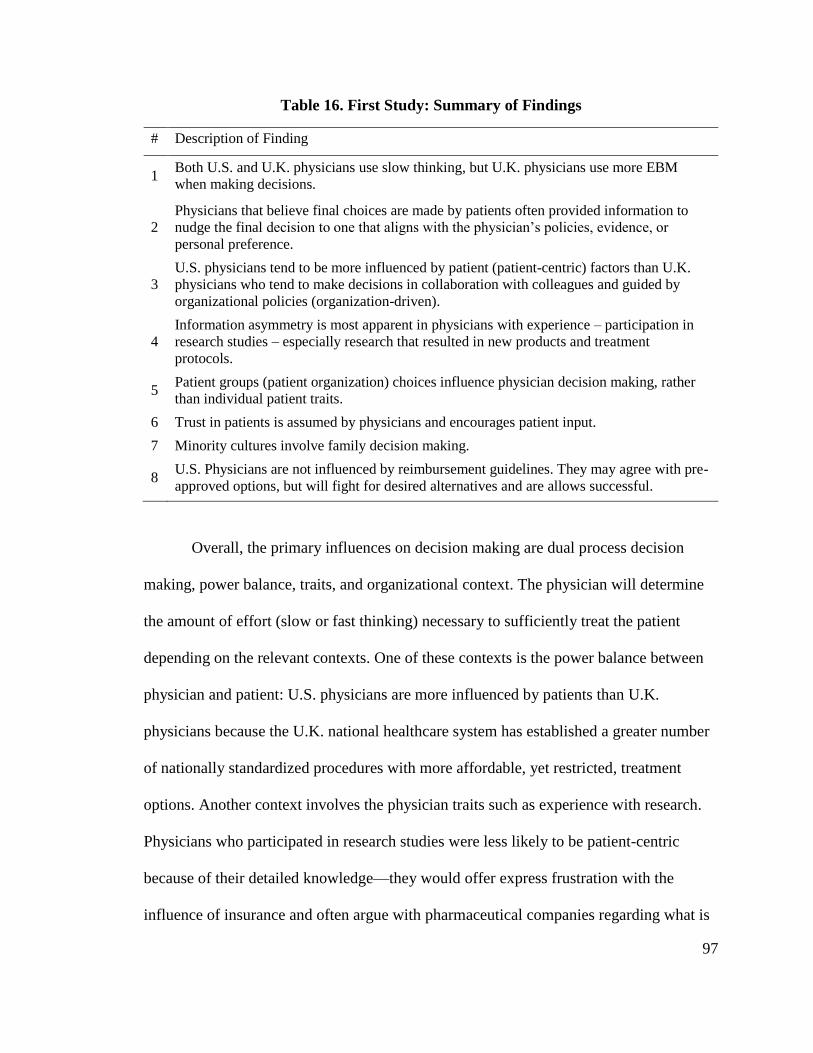
97
Table 16. First Study: Summary of Findings
# Description of Finding
1 Both U.S. and U.K. physicians use slow thinking, but U.K. physicians use more EBM
when making decisions.
2
Physicians that believe final choices are made by patients often provided information to
nudge the final decision to one that aligns with the physician’s policies, evidence, or
personal preference.
3
U.S. physicians tend to be more influenced by patient (patient-centric) factors than U.K.
physicians who tend to make decisions in collaboration with colleagues and guided by
organizational policies (organization-driven).
4
Information asymmetry is most apparent in physicians with experience – participation in
research studies – especially research that resulted in new products and treatment
protocols.
5 Patient groups (patient organization) choices influence physician decision making, rather
than individual patient traits.
6 Trust in patients is assumed by physicians and encourages patient input.
7 Minority cultures involve family decision making.
8 U.S. Physicians are not influenced by reimbursement guidelines. They may agree with pre-
approved options, but will fight for desired alternatives and are allows successful.
Overall, the primary influences on decision making are dual process decision
making, power balance, traits, and organizational context. The physician will determine
the amount of effort (slow or fast thinking) necessary to sufficiently treat the patient
depending on the relevant contexts. One of these contexts is the power balance between
physician and patient: U.S. physicians are more influenced by patients than U.K.
physicians because the U.K. national healthcare system has established a greater number
of nationally standardized procedures with more affordable, yet restricted, treatment
options. Another context involves the physician traits such as experience with research.
Physicians who participated in research studies were less likely to be patient-centric
because of their detailed knowledge—they would offer express frustration with the
influence of insurance and often argue with pharmaceutical companies regarding what is
98
the best treatment. Those who did not participate in research were more often indifferent
to the types of treatment and what insurance covered. Lastly, patient insurance—related
to organizational context—in the U.S. allows for more treatment options; despite
insurance policies, the U.S. physician will override the insurance options if suboptimal to
their desired treatment plan. U.S. hemophilia physicians are more “patient-centric” and
more likely to use SDM than U.K. physicians. The influence of the wider healthcare
organization/system was much less in the U.S. where physicians use a slow thinking style
combined with a patient-centric approach as predicted in the literature: patient-centered
care reduces power imbalance and increases SDM.
Discussion
This study provided insight into the decision processes of U.S. and U.K.
physicians. While published scientific data is a significant influence for both groups,
physicians in the U.S. are more likely to make decisions based on the needs of their
patients whereas the U.K. physicians tend to be more influenced by colleagues and
government policies.
Overall, rational/slow thinking seemed to dominate decision making. This was
less so for U.K. physicians who are more grounded in EBM and organizational policies.
The EBM focus of U.K. physicians falls in line with the literature, although described in
a general context rather than hemophilia (Campbell, 2013).
U.K. physicians are trained to develop clinical and decision-making skills. This
was supported by the first finding in which emphasized the foundational importance of
medical training for developing decision-making skills needed to treat patients with
hemophilia. In addition to formal training, physicians in both the U.S. and the U.K.
99
usually found a mentor who was able to train them and provide the necessary insights to
learn how hemophiliacs are affected by their bleeding disorder. Eventually, physicians
develop mental illness scripts to save time and energy when treating patients. If there is
uncertainty, they return to the literature to reinforce their illness script. If the physicians
from both the U.S. and U.K. rely on the data/literature for their decision process, why do
they have such different approaches to patient input?
The differences in whether the physician is patient-centric or physician-driven
likely relate to the larger healthcare system. Prior published research and study findings
support a more patient-centered and less cost sensitive approach in the U.S., whereas the
U.K. is an organization physician-driven approach (Lee et al., 2008). Kaba and
Sooriakumaran (2007) describe the U.S. patient-physician relationship is described as
“mutual participation;” the patient and physician make decisions as equals (Kaba &
Sooriakumaran, 2007). This approach is the essence of SDM. It might be that in the U.S.,
the physician is encouraged to “sell” their service to the customer. This entails the
physician to appease patient preferences and increase their chance to return as well as
ensure the treatment will be reimbursed. Patient choice is a significant value in the U.S.
system and one advocated by the U.S. patient association, the National Hemophilia
Society.
In addition, it might be that U.S. physicians are patient-centric due to the lack of
available aggregate data. As opposed to the national database in the U.K., each U.S.
physician must rely on the patient’s history and other data they have gathered in their
practice. Not only is the U.S. aggregate data limited and outdated, it is also fragmented
by the healthcare system.
100
The U.K. approach is top-down: treating chronic disorders as a whole rather than
on an individual level. The U.K. physician preference to discussing treatment with
colleagues over patients is not mentioned in the literature. This is facilitated through the
U.K National Health Service and supported by a national tender and patient registry. The
tender keeps the overall cost the treatments lower, albeit still in the $100k annual range
per hemophilia patient, and all services are free through the NHS (Mannucci, Mancuso,
& Santagostino, 2012). The tender system has also designated the most cost-effective
products and filters out more expensive therapies. Although this has lowered cost, it also
limits options. The options are chosen through the country’s physicians, who also have
access to the national hemophilia database; the database contains a vast amount of
information on every hemophiliac in the U.K., all required to participate. It may be that
the U.K. system has relieved the burden of cost and insurance from the physicians so that
they can focus on providing the highest, affordable method of care consistent with policy
and EBM.
It is clear that U.S. and U.K. physicians in hemophilia care approach treatment
decisions in part due to organizational context. The difference may result from the
system’s approach to uncertainty. The U.K. system is essentially removing as many
variables as possible in the treatment of hemophilia by limiting product options, offering
care to everyone through public financing and national guidelines, and keeping track of
all the information of each hemophiliac. U.K. physicians follow preset protocols and do
not need to worry about the individual patient need. U.S. physicians have less
organizational constraints: while insurance companies may attempt to exert control,
physicians having enough influence to get exceptions to the reimbursement policies.
101
The overall impact of influences on physician decision making was analyzed
using abductive reflection. Abductive reflection is the logical inference wherein the
simplest and most likely explanation is sought for an observation (Van de Ven, 2007). It
is clear that decision-making style and patient-centered care affect patient participation
but context matters. There must be a set of conditions that encourage and enable the
physician to implement SDM. These conditions/influences may take the form of personal
preferences in treatment approaches or overarching policies that guide the entire
treatment process.
Based on the above reflection, dual process theory was hypothesized as a possible
explanation for how hemophilia physicians make decisions within the confines of the
overall organizational context. U.K. physicians are free to maintain more of an intuitive
mode of thinking while the U.S. thinks more slowly and rationally based on patient
preferences. As the literature describes, System 1 thinking relies on experience and
illness scripts for treatment (Campbell, 2013). With the protocols in place, built using the
collaboration of the nation’s physicians and database information, they do not have to
analytically approach every single patient. This reserves their time, energy, and resources
for the more chaotic cases such as inhibitor treatment. The U.S. physicians, lacking such
protocols, must develop their own personalized approach over many years by analyzing
every patient uniquely (System 2) until patterns arise to a level safe enough for treatment
(Campbell, 2013).
Each mode of thinking (System 1 and System 2) has an impact on the treatment of
hemophilia. System 1, as implemented by the U.K., enables healthcare to be much more
affordable and yield better results in the population; one could also call this approach as
102
“disease-oriented” (Bensing, 2000). However, the protocols limit the treatment options.
For example, patients with unique pharmacokinetics (PK) may not respond well to
standard EMB techniques and require extra care. This could lead to suboptimal treatment
or multiple rounds of trial-and-error. Not only would the patient need to switch products,
but the expenses of an adverse event could be more than approaching the patient with
System 2 from the start. On the other hand, System 2 approaches have a much lower
chance of error due to the analytical nature of the mode of thinking (Campbell, 2013). By
approaching care on an individual level, unique PK patients can be distinguished and
optimally treated. This also applies to the other patient values such as lifestyle (on-
demand vs. prophylaxis) and product choice (recombinant vs. plasma-derived). Health
literacy, nudging, and trust support this practice.
One difference between U.S. and U.K. physicians was power balance. In the U.S.,
power is more balanced because the physicians use a patient-centric approach and
encourage health literacy in their patients more than the U.K. physicians. Whereas the
U.K. physicians have all the power because all treatment centers and physicians in the
U.K. provide identical/similar options to the patient.
The findings show that U.S. physicians are more likely to treat patients without
the help of colleagues and take each individual patient’s needs into consideration. These
practices may be caused by the lack of universal treatment policies and multiple
reimbursement programs in the U.S. It is also possible that without a universal data-
collection system, U.S. physicians are forced to treat patients based on their knowledge of
individual events. U.K. physicians tend to be more influenced by national policies and
procedures, limiting their ability to make personal and individual decisions. However, the
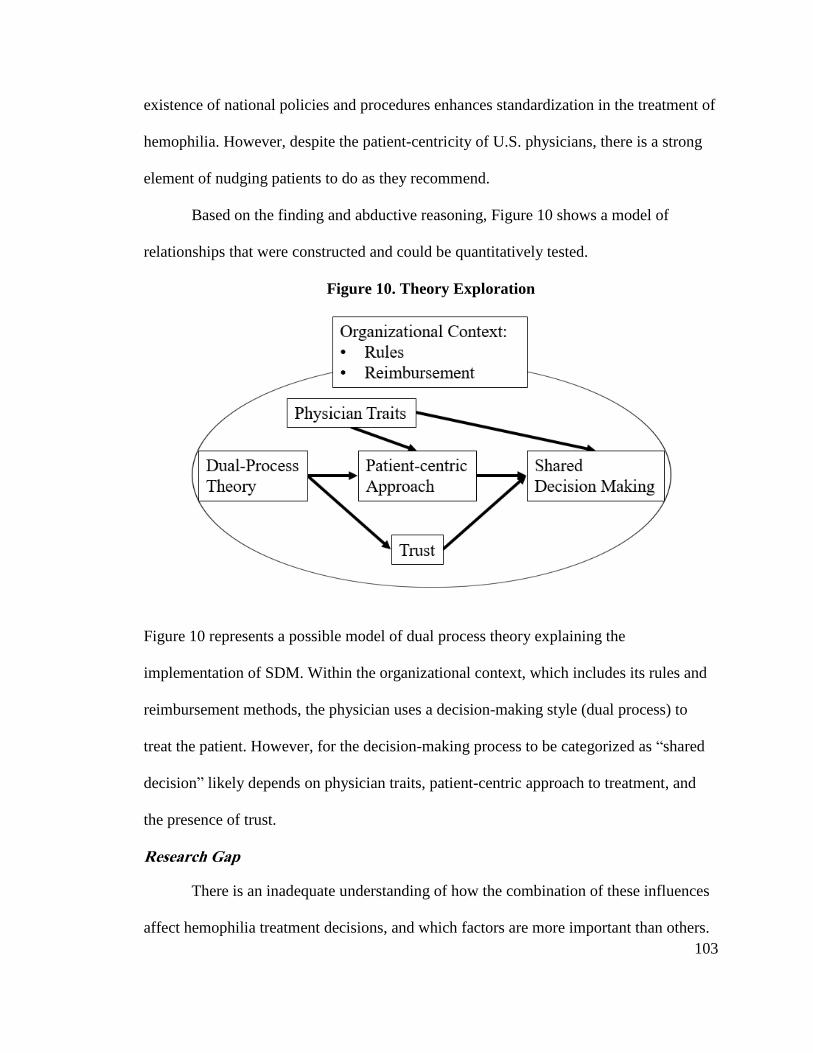
103
existence of national policies and procedures enhances standardization in the treatment of
hemophilia. However, despite the patient-centricity of U.S. physicians, there is a strong
element of nudging patients to do as they recommend.
Based on the finding and abductive reasoning, Figure 10 shows a model of
relationships that were constructed and could be quantitatively tested.
Figure 10. Theory Exploration
Figure 10 represents a possible model of dual process theory explaining the
implementation of SDM. Within the organizational context, which includes its rules and
reimbursement methods, the physician uses a decision-making style (dual process) to
treat the patient. However, for the decision-making process to be categorized as “shared
decision” likely depends on physician traits, patient-centric approach to treatment, and
the presence of trust.
Research Gap
There is an inadequate understanding of how the combination of these influences
affect hemophilia treatment decisions, and which factors are more important than others.
104
There has been no research that examined the decision-making processes of physicians
regarding the treatment of hemophilia, particularly between the U.S and the U.K. This
study addressed the gap in the literature regarding the decision-making processes
involved in the treatment of hemophilia from the perspectives of American and British
physicians.
Implications
The results of the study should be of interest to the academic community,
governments, funding agencies, and pharmaceutical company marketing departments in
understanding the influences and barriers that physicians experience when making
treatment decisions. Although the treatment of hemophilia has dramatically improved
over the past 50 years, it is likely that cost-effective treatment outcomes can be further
improved. These findings can be utilized to justify consideration of a national tendering
process in the U.S. to reduce cost while still maintaining patient-centered care to meet the
individual needs patients.
In the short-term, the role of physicians in treatment decisions and the interplay
between the physician and the wider healthcare system should be considered. American
and British physicians do not make decisions in isolation. They often have to consider
external factors such as national policies and the structure of healthcare systems. In the
longer term, thinking about how the system can be changed for new products and
protocols and how the process can be improved should be considered, particularly with
respect to the optimization of treatment of hemophilia. The decisions of American and
British physicians in the treatment of hemophilia are influenced by the literature,
105
highlighting the importance of strengthening research and participation in clinical trials.
The proposed model may be applied more broadly to other chronic diseases.
Limitations and Future Research
Limitations of this study—as with many qualitative studies—include the use of a
non-randomized, small sample with mostly participants who were Caucasian men. Given
these limitations, the homogeneity of the sample might not reflect the experiences and
perceptions of all American and British physicians who treat hemophilia. In addition,
each participant was relatively eager to participate, as opposed to those who had declined
for personal or timing issues. The results of the findings reported in this study were based
on physicians who had the time and interest to participate in this study. The open-ended
nature of the interviews may have left some important information gaps due to time
constraints so that some participants did not provide answers that truly reflect the scope
of their experiences and perceptions. In addition, the study population was mostly White
males; increasing the sample size to include a more diverse group of people and countries
would help to mitigate a potentially ethnocentric/gender point of view.
The proposed model may be applied more broadly to other chronic diseases.
Although the findings have shown divergent behavior between U.S. and U.K. physicians,
can the results be applied more generally to other chronic diseases? Do all physicians use
the data as their main influence for decisions? Is this influence similar to other physician
specialties? The question remains, is one method better than the other? Can each system
learn from each other for mutual benefit and improvement? On the surface, it appears that
the U.K. has a more cost-effective system but less SDM. In the case the U.S., the high
prices may encourage research from the pharmaceutical companies to keep pushing for
106
better, innovative treatments. Future research should examine physician decision making
in more detail.
Conclusion
In terms of the decision-making in the treatment of hemophilia for American and
British physicians, most participants tended to be more guided by empirical data and the
literature when making decisions (data-driven) although much more so in the U.K. The
U.S. physicians can be classified as more patient-centric, where most physicians in the
U.K. can be characterized as more EBM. Patient-centric physicians consider other factors
in order to individualize treatment towards a patient’s preference and values. Trust
appears to be necessary for patient-centered care. Because of the tendering process in the
U.K., physicians tend to be less collaborative with their patients in terms of their
decision-making process.
The cost of treating hemophilia A and B patients in the U.S. is approximately $2
billion more (normalizing for population) than in the U.K., with no apparent difference in
clinical outcomes. Understanding this difference within the context of physician decision
making could help professionals develop treatment strategies that could improve cost-
effective treatment for chronic diseases in the future. Policies such as the national
tendering process in the U.K. help to lower the cost of products and benefit the
manufacturers at the same time (McMurray et al., 2011). However, the tender process
operates within a system in which the options of physicians become limited. The findings
indicate that the national tendering policy can lower the costs of treatment products,
allowing U.K. physicians to be less concerned about cost. Thus, there are reinforcing
mechanisms that provide a good outcome, but simply transplanting the U.K. tender
107
system to the U.S. without the corresponding patient-centered approach may not lead to a
better care. The U.S. healthcare system has different stakeholders such as insurance
companies and patients who are already powerful actors in influencing policies and
decisions, making the establishment of national tendering process more difficult.
In summary, this study offered insight into the physician decision process for the
treatment of hemophilia in different national contexts. Furthermore, the results suggest
that slow thinking and patient-centered care are likely related to SDM. Traits also may
play a role. The next chapter, Chapter 6, discusses the subsequent quantitative study that
was conducted to test the relationships hypothesized from this study.
108
CHAPTER 6: STUDY 2: DOES PHYSICIAN’S DECISION-MAKING STYLE
EFFECT PATIENT PARTICIPATION IN THE TREATMENT CHOICES OF
PRIMARY IMMUNODEFICIENCY?
This chapter covers the methods and results of Study 2, a quantitative analysis of
physician decision-making regarding the treatment of primary immunodeficiency (PID).
This study quantified the relationships theorized based on Study 1 results. The key
findings from the first study included the role of rational decision making and patient-
centric care in the U.S. and its relationship to shared decision making. While slow
thinking may be necessary for SDM, a patient-centric approach is the mechanism through
which SMD is explained. As predicted by the SIT literature, patient-centric care reduces
power imbalance by bringing patient values and preferences into the decision process.
However, patient/physician trust must be in place for agreement on a shared treatment
plan. In addition, physician traits such as training and experience have an influence.
These findings could be tested in a quantitative model.
Because the number of physicians treating hemophilia is small and insufficient for
a quantitative analysis, I changed the target study to PID treating physicians. Similar to
hemophilia, PID is a high-cost treatment and all cases are complex due to multiple co-
morbidities. The research questions of this study were:
Do physician decision-making styles affect patient participation in the choice
of treatment tools and protocols?
Does a patient-centric approach explain the mechanism by which style
influences SDD
Does Trust explain when there is SDM?
Do certain physician traits affect patient participation?
109
This chapter presents the design, method, results, discussion, and limitations of the
second study.
Research Gaps
Some research has been done on PID patient satisfaction as well as barriers and
facilitators of SDM. However, there is very little evidence concerning how participation
is predicted by the style of physician decision-making (Gardulf & Nicolay, 2006; Gravel,
Légaré, & Graham, 2006; Légaré et al., 2008; Nicolay et al., 2005). Furthermore, there is
significant documentation that SDM improves diagnosis and treatment (Shapiro, 2013;
Shapiro, Wasserman, Bonagura, & Gupta, 2014). What is not known is whether a
physician's decision-making process affect patient participation when choosing the
protocols and tools. Does the physician’s treatment approach (patient-centricity)
encourage or inhibit patient participation?
The literature describes that trust is built over time, encourages adherence to
medication, erodes from patient actions, and is partially measured by physicians via non-
verbal cues (Kramer & Cook, 2004: 89). Is the physician trust in patient-given
information necessary for successful SDM?
Finally, there is considerable research on the impact of traits but what physician
traits play a role in patient participation?
To address gaps in the literature, and draw on published studies and related
theory, a quantitative study was designed. This study followed the qualitative study that
compared physician decision-making in the U.S. and U.K. for patients with hemophilia
(Lamb, Boland Jr, Lyytinen, & Wolfberg, 2015). The qualitative results showed how
U.S. hematologists are more likely to use “slow thinking” and be more patient-centric
110
than U.K. hematologists. Based on the earlier exploratory qualitative study, it was
theorized that differences in a physician’s decision-making style impact the level of
patient participation when influenced by a patient’s specific preferences and unique,
individual conditions. Patient-centered care is the mechanism through which SDM is
achieved: patient-centered care balances power which gives patients the opportunity to
participate. Trust plays is a potentially moderating role: it must be present for SDM.
Traits also have an impact, but it is unclear which traits matter.
Design
330 U.S. physicians who treat PID were surveyed to measure the effect of
physician decision-making style on patient participation in PID treatment. Theory
generated from the first qualitative study as well as constructs from dual process, SIT and
trait theory were applied to examine the physician decision-making process. The inquiry
linked physician decision-making style (fast vs. slow thinking) and a patient-centric
treatment approach to the level of patient participation in the decision-making process.
The role of trust and specific physician traits were also tested.
Measurement Operationalization
Constructs used measured using modified validated scales. Each item score was
set to a 5-point Likert-type scale ranging from 1 = “strongly disagree” to 5 = “strongly
agree.” The survey consisted of 76 items: 60 were adapted from other scales and 16 were
developed to collect descriptive information (i.e., age, education). Reflective scales were
used for each of the following constructs: decision-making style, approach to treatment,
patient participation with treatment protocols, patient participation with treatment tools,
111
and trust in patient-given information. With reflective constructs, the indicators are
caused by the latent variable (Kenny, 2016).
DMR & DMH
Decision-making style was measured using a scale developed by from Buck and
Daniels (1985). The scale contains 20 statements assessing a person's natural disposition
to use either an analytical (rational) or an empirical (heuristic) decision-making style
(DMH).
Patient-centric
A physician’s patient-centric approach was measured using a Physician-Patient
Orientation Scale (PPOS). The scale measures attitudes towards sharing information and
the “extent to which the respondent believes that patients desire information and should
be part of the decision making process” (Krupat et al., 2000: 51). The survey is open for
use in academic research with the condition that the original author of the survey tool
gives permission for its use before the start of the study (Krupat et al., 2000). The
instrument was originally created to evaluate doctors’, medical residents’, and patients’
views of their roles in medical care (Pereira et al., 2013). This instrument has been
regularly used and tested for validity in the U.S. and abroad (Pereira et al., 2013). Krupat
et al. (2000) determined the 0.73 reliability to be satisfactory for physician respondents.
Trust
Physician’s trust in patients to provide accurate information was measured using a
modified version of Thom’s (2011) Physician Trust in Patient Scale. The original scale
consists of 18 questions is used to measure respondents’ attitudes toward patients in the
context of prescription opioid treatment for chronic nonmalignant pain. Thom (2011)
112
trimmed the scale to 12 items and demonstrated that the items had reliability (i.e.,
construct validity) with a Cronbach’s alpha of .93 for specific self-reported behaviors.
Patient Participation
The following scales were used to measure the physician’s perception of patient’s
participation in the treatment choices: the customer participation scale from Gallan,
Jarvis, Brown, and Bitner (2013), the “Responsiveness to Patient Requests” scale from
Petroshius, Titus, and Hatch (1995), and the “Participation in Decision Making” scale
from Siegel and Ruh (1973). The scales were combined to measure patient participation
with protocols (IOP) and patient participation with tools (IOT).
Patient participation in the choice of treatment protocols was measured using
Gallan et al. (2013) participation scale and an adapted scale from Siegel and Ruh (1973).
Gallan et al. (2013) scale is a four-item tool that measures the degree to which patients
provide information to the physician and were actively involved in decision-making.
Siegel and Ruh’s (1973) scale contains five-items which concern the degree of
participation individuals have in decisions affecting their jobs.
Patient participation in choice of treatment tools was measured by the
Responsiveness to Patient Requests scale created by Petroshius et al. (1995). The scale
from Petroshius et al. (1995) contains three, five-point Likert-type statements that are
used to measure the attitude a physician has about writing prescriptions for medications
that have been specifically requested by patients.
Physician Traits
Participants were asked a series of questions to measure traits and the relationship
to the factors listed above. Physician traits include age, race, sex, and experience (years
113
of practice, education, and involvement with research). No scales were adopted from
other studies because each trait had one question for each.
Constructs of Interest
The independent variable (IV) was the physician’s decision-making process,
represented by two variables: rational decision making and heuristic decision making.
Rational decision making (DMR) involves thoughtfully attending to information, whereas
heuristic decision making (DMH) amounts to relying on simple heuristic rules or
experiences as the basis for a decision. This represents Systems 1 and 2 (fast and slow
thinking) from dual process theory. The dependent variable (DV) is patient participation,
also represented by two variables: patient participation in the choice of treatment
protocols and tools. Patient Participation with Treatment Protocols (IOP) refers to the
patient’s input on aspects of treatment such as schedules and administration methods,
whereas IOT refers to the patient’s input on the choice of treatment products.
The mediator is the physician’s approach to treatment; specifically measuring the
physician’s tendency to include a patient’s psychosocial (non-biometric) burdens in the
decision process; thus, the variable measures the physician’s “patient-centric” approach
to care (APC). APC partially mediates effects of decision making; physicians take into
account the psychosocial characteristics of the patient when making decisions which
reduce the power imbalance with patients (Bravo et al., 2015; Hibbard, 2017;
McCormack et al., 2017). Patient-centricity reduced power imbalances and enables SDM.
Therefore, a higher level of APC should increase patient participation.
114
The moderating variable is the physician’s trust in the patient to provide accurate
information and follow the treatment regimen (TIP). Patient trust must be present for a
physician to incorporate patient input and thereby increase SDM.
Multi-group variables are race, sex/gender, and education. Physician race is
thought to affect patient participation because the literature suggests white physicians
have more patient participation than non-white physicians (Lin & Kressin, 2015).
Physician gender could influence the results because some studies conclude that female
physicians have more participatory styles such as empathy and information sharing
(Bertakis et al., 2002; Janssen & Lagro-Janssen, 2012; Roter et al., 2002). Physician
education refers to the highest degree earned (MD vs. Ph.D.). Although there is no
literature—to my knowledge—measuring patient participation with physicians of
different degrees, Schnell and Currie (2017) suggest that physicians with education from
better medical schools were less likely to prescribe opioids, thereby likely to decrease
patient participation and SDM by extension.
The control variables were physician years of practice and age. Years of practice
refers to the number of years the physician has treated PID. The decision making of a
physician new to the specialty may differ from an expert. Physician age (AGE) refers
their age in years, which may reveal differences between generations of physician
decision making.
Figure 11 provides a visual representation of the variable relationships discussed.
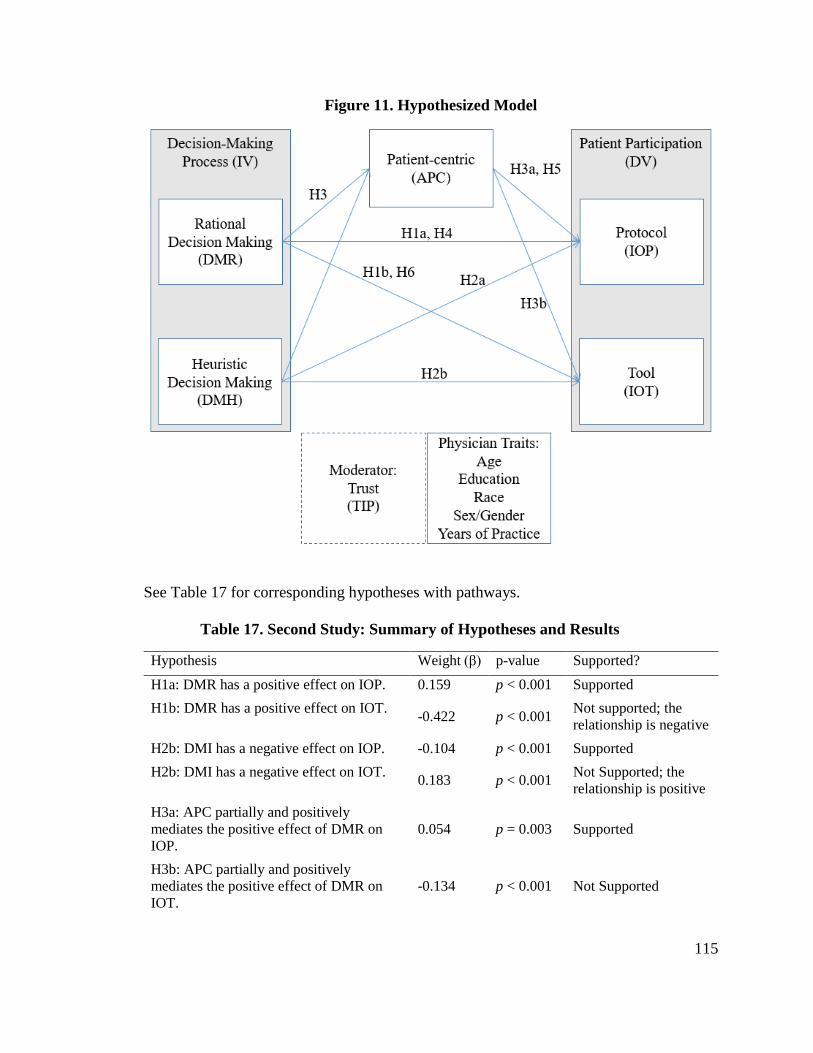
115
Figure 11. Hypothesized Model
See Table 17 for corresponding hypotheses with pathways.
Table 17. Second Study: Summary of Hypotheses and Results
Hypothesis Weight (β) p-value Supported?
H1a: DMR has a positive effect on IOP. 0.159 p < 0.001 Supported
H1b: DMR has a positive effect on IOT. -0.422 p < 0.001
Not supported; the
relationship is negative
H2b: DMI has a negative effect on IOP. -0.104 p < 0.001 Supported
H2b: DMI has a negative effect on IOT. 0.183 p < 0.001
Not Supported; the
relationship is positive
H3a: APC partially and positively
mediates the positive effect of DMR on
IOP.
0.054 p = 0.003 Supported
H3b: APC partially and positively
mediates the positive effect of DMR on
IOT.
-0.134 p < 0.001 Not Supported
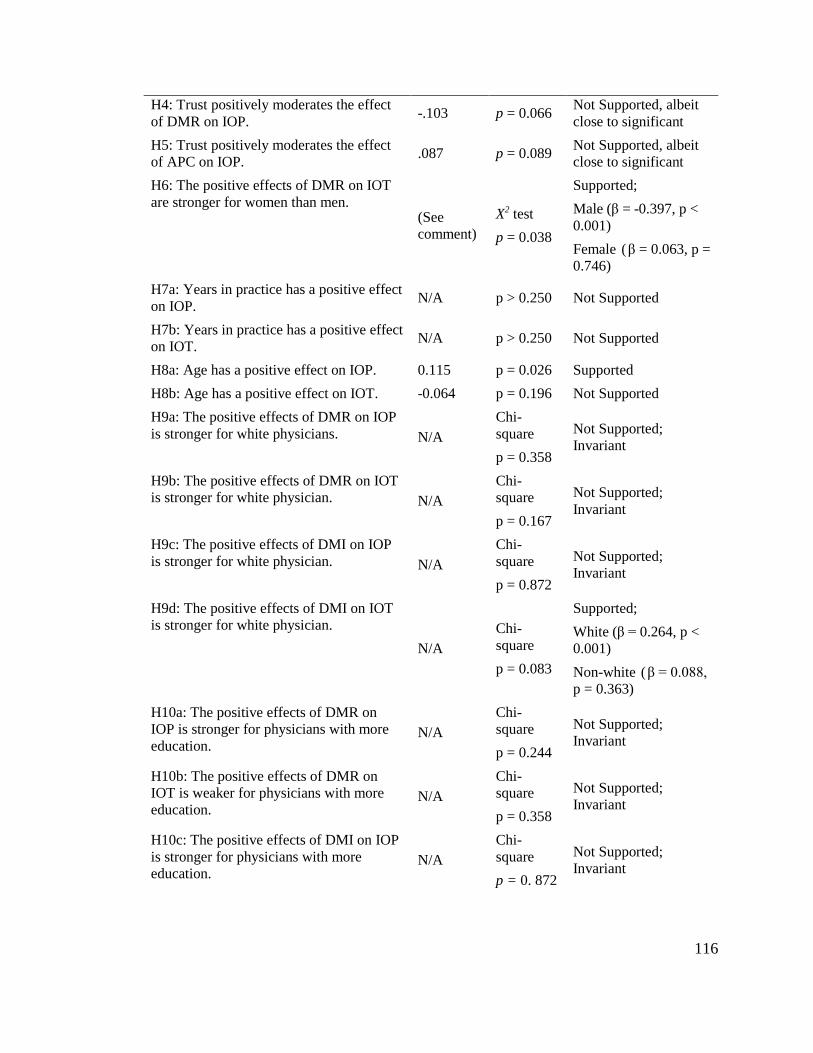
116
H4: Trust positively moderates the effect
of DMR on IOP. -.103 p = 0.066
Not Supported, albeit
close to significant
H5: Trust positively moderates the effect
of APC on IOP. .087 p = 0.089
Not Supported, albeit
close to significant
H6: The positive effects of DMR on IOT
are stronger for women than men. (See
comment)
X2 test
p = 0.038
Supported;
Male (β = -0.397, p <
0.001)
Female (β = 0.063, p =
0.746)
H7a: Years in practice has a positive effect
on IOP. N/A p > 0.250 Not Supported
H7b: Years in practice has a positive effect
on IOT. N/A p > 0.250 Not Supported
H8a: Age has a positive effect on IOP. 0.115 p = 0.026 Supported
H8b: Age has a positive effect on IOT. -0.064 p = 0.196 Not Supported
H9a: The positive effects of DMR on IOP
is stronger for white physicians. N/A
Chi-
square
p = 0.358
Not Supported;
Invariant
H9b: The positive effects of DMR on IOT
is stronger for white physician. N/A
Chi-
square
p = 0.167
Not Supported;
Invariant
H9c: The positive effects of DMI on IOP
is stronger for white physician. N/A
Chi-
square
p = 0.872
Not Supported;
Invariant
H9d: The positive effects of DMI on IOT
is stronger for white physician.
N/A
Chi-
square
p = 0.083
Supported;
White (β = 0.264, p <
0.001)
Non-white (β = 0.088,
p = 0.363)
H10a: The positive effects of DMR on
IOP is stronger for physicians with more
education. N/A
Chi-
square
p = 0.244
Not Supported;
Invariant
H10b: The positive effects of DMR on
IOT is weaker for physicians with more
education. N/A
Chi-
square
p = 0.358
Not Supported;
Invariant
H10c: The positive effects of DMI on IOP
is stronger for physicians with more
education. N/A
Chi-
square
p = 0. 872
Not Supported;
Invariant
117
H10d: The positive effects of DMI on IOT
is weaker for physicians with more
education. N/A
Chi-
square
p = 0.113
Not Supported;
Invariant
DMR= Rational Decision Making
DMI = Heuristic Decision Making
APC = Patient-centric Approach to Treatment
IOP = Patient Participation with Treatment Protocols
IOT = Patient Participation with Treatment Tools
Physician’s Decision-Making Process Effects on Patient Participation
It is expected that physicians using a rational decision-making style (DMR) are
more likely to incorporate patient input into treatment and tools; they are more likely to
incorporate the patient’s input alongside their experience with similar cases. Conversely,
it is expected that physicians with using heuristic decision making (DMH) will reduce
participation in the decision process; they should intuitively apply what they believe to be
the best approach based on their observations.
Hypothesis 1. DMR has a positive effect on IOP (H1a) and IOT (H1b).
Hypothesis 2. DMH has a negative effect on IOP (H2a) and IOT (H2b).
Mediating Effects of Treatment Approaches to Patient Participation
The relationship between the IV and DV is partially mediated by a physician’s
patient-centric approach to treatment (APC). Although a physician might have a specific
decision-making style when treating a patient, it is not sufficient to explain patient
participation. Patient-centric physicians are more likely to incorporate non-biometric
patient feedback into their decision process because a patient-centric approach to
treatment is likely to value the patient just as much as the disease when deciding
treatment (Bensing, 2000). Patient-centric physicians will “have to explore patients’
needs from a biopsychosocial model, in which psychological, and social elements are
118
valued as important as the strictly biomedical elements” (Bensing, 2000: 21). Seeborg et
al. (2015) suggests that patient perceived health is a strong indicator of future health;
therefore, addressing the patient rather than the disease enables the physician to better
access the patient’s unmet needs. A patient-centric approach reduces the power
imbalance and facilitates participation. Therefore, APC physicians with a rational
decision-making style are likely to encourage patient participation because they are
reducing the power imbalance by incorporating the patient’s physical and psychosocial
health.
Hypothesis 3. APC partially and positively mediates the positive effect of DMR on
IOP (H3a) and IOT (H3b).
Physician Traits
Age
Delaney et al. (2015) found that as people age, they are more likely to use
intuitive decision making when compared to younger people. Participants from the first
study support this observation since older physicians intuitively focused on the individual
pharmacokinetics of each hemophilia patient. Therefore, it was hypothesized that older
physicians will generally encourage more patient participation.
Hypothesis 4a. Age has a negative effect on IOP.
Hypothesis 4b. Age has a negative effect on IOT.
Gender
Published results are mixed for determining whether gender is linked to patient
participation. Results from Street Jr et al. (2005) show that patient participation is a
function of many factors, excluding gender. Other studies suggest that female physicians
take a more participatory styles, such as empathy and information sharing, than males do
119
(Bertakis et al., 2002; Janssen & Lagro-Janssen, 2012; Roter et al., 2002). The working
hypothesis for this study assumes that men and women physician’s use patient
participation differently. The differences in approach imply that, although rational
decision-making should enhance participation, the impact would be greater for women.
Hypothesis 5. The positive effects of DMR on IOT is stronger for women than
men.
Race
Lawrence et al. (2015) found that, when treating depression, white physicians are
more likely to prescribe antidepressants than black physicians, whereas black physicians
were more likely to refer the patient to a counselor or psychiatrist. Lin and Kressin (2015)
found there is less conversation between physicians and patients if their races are
different, regardless of physician race. It is expected that white physicians will have
greater participation with patients than black physicians.
Hypothesis 6a. The positive effects of DMR on IOP is stronger for White
physicians.
Hypothesis 6b. The positive effects of DMR on IOT is stronger for White
physician.
Hypothesis 6c. The positive effects of DMI on IOP is stronger for White
physician.
Hypothesis 6d. The positive effects of DMI on IOT is stronger for White
physician.
Experience
Years of Practice: Marinova et al. (2016) found that experience plays a role in
decision making by increasing the value of patient medical criteria and decreasing the
value of patient preferences; experienced physicians use intuition to make decisions
120
based on patterns, not patient input. Furthermore, the more experienced physicians are
likely older and may have paternalistic habits from before the patient-centric movement.
Hypothesis 7a. Years in practice has a positive effect on IOP.
Hypothesis 7b. Years in practice has a positive effect on IOT.
Education: Schnell and Currie (2017) found that physicians from better medical
schools were less likely to prescribe opioids to patients, suggesting there is more patient
participation and SDM by extension. Therefore, it is hypothesized that physicians with a
greater level of education, Ph.D. and MD, will have more patient participation regardless
of decision-making style.
Hypothesis 8a. The positive effects of DMR on IOP is stronger for physicians with
more education.
Hypothesis 8b. The positive effects of DMR on IOT is stronger for physicians with
more education.
Hypothesis 8c. The positive effects of DMI on IOP is stronger for physicians with
more education.
Hypothesis 8d. The positive effects of DMI on IOT is stronger for physicians with
more education.
Trust
The moderating variables in this study explain “when” decision-making style (IV)
affected patient participation (DV). If physicians trust the information provided by
patients, they are more likely to share decision-making (McGuire et al., 2005). Physicians
will not likely incorporate patient participation if the information provided by the patient
is not trusted. For example, one physician in Chapter 4 discussed that trust is assumed but
erodes if the patient is not honest thereby reducing patient participation in the treatment
decision. Therefore, trust is expected to positively moderate patient participation.
121
Hypothesis 9a. TIP positively moderates the effect of DMR on IOP.
Hypothesis 9b. TIP positively moderates the effect of APC on IOP.
Methods
I conducted a series of analyses to construct a model that most accurately
represents to data and its relationships. The following sections describe the methods I
used to create Figure 12 and extract the findings summarized in Table 27.
Sample
During a one-week period in late May 2016, a survey was sent to 16,310
physicians (67% male, 33% female) who treated PID in the U.S. The services of IMS
Health, Inc. were used to distribute the survey. Physicians were given a blinded Internet
survey consisting of 76 questions. The administration of the survey through the Internet
contributed to confidentiality for the participants. The population was selected based on
the following criteria: respondents must be physicians who treat PID in the U.S. A total
of 350 (2.1%) completed the survey. The low response rate was likely due to doctor’s
demanding schedules and the high frequency with which they receive survey requests
(Flanigan, McFarlane, & Cook, 2008). Furthermore, the surveys in this study were sent
by email, which may have decreased the response rate. After screening the respondents
based on pre-defined criteria, such as omitting unengaged respondent data, a sample size
330 was analyzed. Table 18 displays a summary of the sample demographics. The low
response rate might be a concern about the representation of the study population.
However, respondents likely represent the population of doctors who treat PID since the
330 physicians treat approximately 55% (17,500 patients) of the PID population.
Responding physicians treat an average of five PID patients per month.
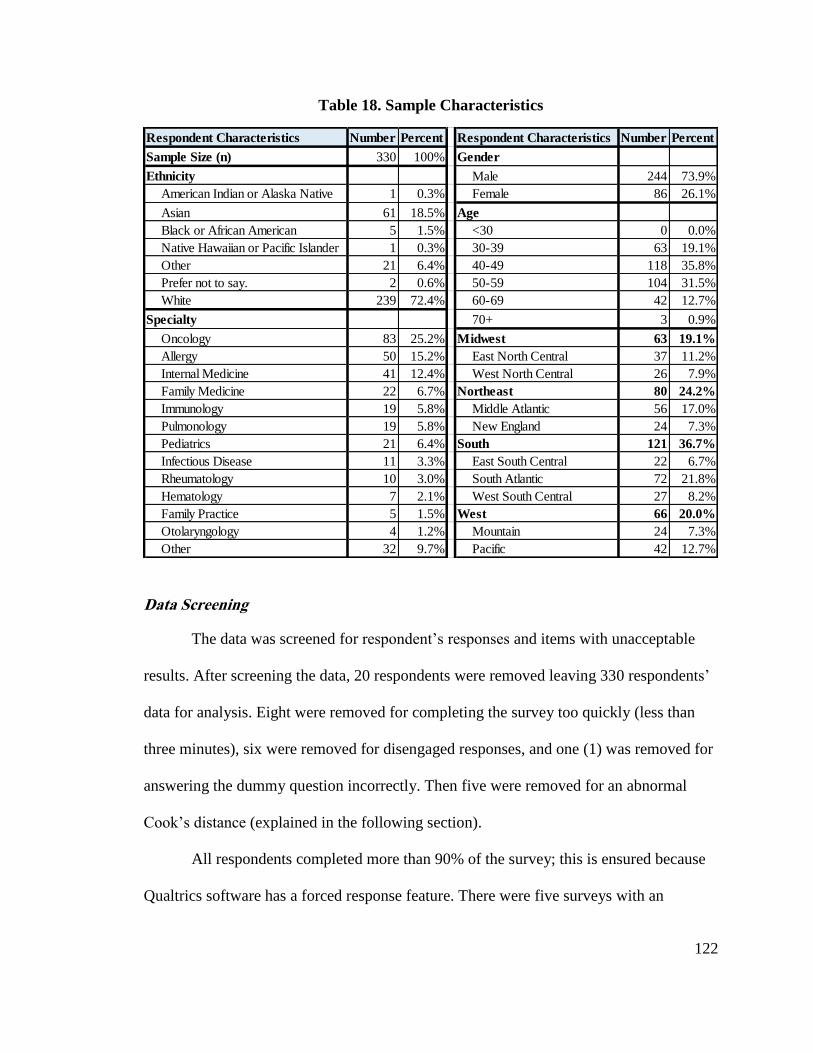
122
Table 18. Sample Characteristics
Data Screening
The data was screened for respondent’s responses and items with unacceptable
results. After screening the data, 20 respondents were removed leaving 330 respondents’
data for analysis. Eight were removed for completing the survey too quickly (less than
three minutes), six were removed for disengaged responses, and one (1) was removed for
answering the dummy question incorrectly. Then five were removed for an abnormal
Cook’s distance (explained in the following section).
All respondents completed more than 90% of the survey; this is ensured because
Qualtrics software has a forced response feature. There were five surveys with an
Respondent Characteristics Number Percent Respondent Characteristics Number Percent
Sample Size (n) 330 100% Gender
Ethnicity Male 244 73.9%
American Indian or Alaska Native 1 0.3% Female 86 26.1%
Asian 61 18.5% Age
Black or African American 5 1.5% <30 0 0.0%
Native Hawaiian or Pacific Islander 1 0.3% 30-39 63 19.1%
Other 21 6.4% 40-49 118 35.8%
Prefer not to say. 2 0.6% 50-59 104 31.5%
White 239 72.4% 60-69 42 12.7%
Specialty 70+ 3 0.9%
Oncology 83 25.2% Midwest 63 19.1%
Allergy 50 15.2% East North Central 37 11.2%
Internal Medicine 41 12.4% West North Central 26 7.9%
Family Medicine 22 6.7% Northeast 80 24.2%
Immunology 19 5.8% Middle Atlantic 56 17.0%
Pulmonology 19 5.8% New England 24 7.3%
Pediatrics 21 6.4% South 121 36.7%
Infectious Disease 11 3.3% East South Central 22 6.7%
Rheumatology 10 3.0% South Atlantic 72 21.8%
Hematology 7 2.1% West South Central 27 8.2%
Family Practice 5 1.5% West 66 20.0%
Otolaryngology 4 1.2% Mountain 24 7.3%
Other 32 9.7% Pacific 42 12.7%
123
acceptable number of missing values (<5%); the missing values were replaced with the
median because they were on an ordinal scale (Lynch, 2007). No outliers were removed,
except those with abnormal Cook’s distance (discussed in “Multivariate Assumptions”
below).
Skewness and kurtosis were measured to ensure the normality of the data. No
items were removed for skewness or kurtosis issues; those with an absolute value greater
than 1.0 had been monitored. Two items were expected to have high kurtosis values (>
3.0); therefore, they were kept and monitored for kurtosis along with three other items
with kurtosis values greater than 2.0 (Sposito, Hand, & Skarpness, 1983). The reliability
of the data was considered adequate because the Cronbach’s alphas were greater than 0.7.
Multivariate Assumptions
A Cook’s Distance test was performed to determine if any respondents’ data were
abnormally influential. Five respondents’ data were removed because their Cook’s
Distance was abnormal (> 0.05) and this may be because these respondents seemed
unengaged within each construct (i.e., answering all DMR items with “2” and APC items
with “4”, etc.). The model was tested for multicollinearity (highly correlated predictor
variables) by assessing the variable inflation factors (VIF). All predictor variables were
found to have VIF < 3.0 for both DVs, therefore, no multicollinearity was assumed (Hair,
Black, Babin, & Anderson, 2010).
Exploratory Factor Analysis
An EFA was performed to determine correlations among the variables. The
maximum likelihood extraction method was used along with a Promax (kappa=4)
rotation method. Twenty-three items were removed using EFA because they had primary
124
loadings lower than 0.5 or cross-loadings with less than 0.2 difference and two removed
items had low Cronbach’s alphas (< .60). Factor loadings represent how much a factor
explains a variable; the greater the number, the stronger the explanation.
The adequacy of the data is acceptable: the KMO is at .892 and is deemed
significant (p = .000); all the communalities are above .30 with the lowest at .31; these
six factors explain 49.02% of the variance. The eigenvalue for the six factors was 1.216
(3.685% variance; 57.748% cumulative). The factors found were: DMR, DMH, APC,
IOP, IOT, and TIP. There are 48 (9.0%) non-redundant residuals with absolute values
greater than .05; although, it is ideal to achieve less than 5% non-redundant residuals,
model fit can be met as long as there is less than 50% non-redundant residuals with
absolute values greater than .05 (Yong & Pearce, 2013). As evidence of convergent
validity, all item loadings are above .50 (Reio & Shuck, 2014). Evidence of discriminant
validity is that there were no strong cross-loadings and all cross-loadings were less than
0.20 (Costello & Osborne, 2005). The Cronbach’s Alphas for all factors are above .70;
therefore, the reliability is acceptable.
Confirmatory Factor Analysis
A confirmatory factor analysis (CFA) was conducted in SPSS AMOS version 23
using the pattern matrix from the EFA. The EFA was input into AMOS and produced
good model fit (CFI = 0.95, SRMR= 0.048, RSMEA= 0.04, PCLOSE= 1). A configural
invariance test was performed and obtained adequate goodness of fit when analyzing a
freely estimated model across two groups (CFI = 0.92, SRMR = 0.05, RSMEA = 0.04,
PCLOSE = 1). A metric invariance test was performed by constraining the two models to
be equal, and then a chi-squared difference test between the unconstrained and
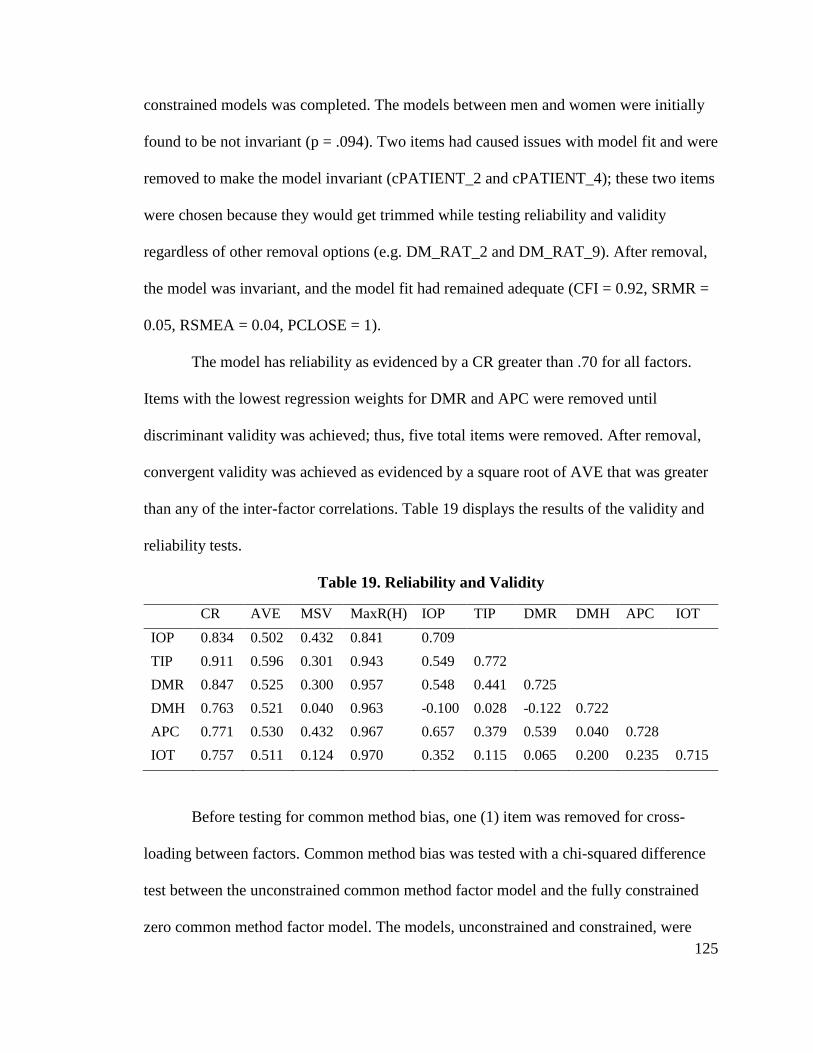
125
constrained models was completed. The models between men and women were initially
found to be not invariant (p = .094). Two items had caused issues with model fit and were
removed to make the model invariant (cPATIENT_2 and cPATIENT_4); these two items
were chosen because they would get trimmed while testing reliability and validity
regardless of other removal options (e.g. DM_RAT_2 and DM_RAT_9). After removal,
the model was invariant, and the model fit had remained adequate (CFI = 0.92, SRMR =
0.05, RSMEA = 0.04, PCLOSE = 1).
The model has reliability as evidenced by a CR greater than .70 for all factors.
Items with the lowest regression weights for DMR and APC were removed until
discriminant validity was achieved; thus, five total items were removed. After removal,
convergent validity was achieved as evidenced by a square root of AVE that was greater
than any of the inter-factor correlations. Table 19 displays the results of the validity and
reliability tests.
Table 19. Reliability and Validity
CR AVE MSV MaxR(H) IOP TIP DMR DMH APC IOT
IOP 0.834 0.502 0.432 0.841 0.709
TIP 0.911 0.596 0.301 0.943 0.549 0.772
DMR 0.847 0.525 0.300 0.957 0.548 0.441 0.725
DMH 0.763 0.521 0.040 0.963 -0.100 0.028 -0.122 0.722
APC 0.771 0.530 0.432 0.967 0.657 0.379 0.539 0.040 0.728
IOT 0.757 0.511 0.124 0.970 0.352 0.115 0.065 0.200 0.235 0.715
Before testing for common method bias, one (1) item was removed for cross-
loading between factors. Common method bias was tested with a chi-squared difference
test between the unconstrained common method factor model and the fully constrained
zero common method factor model. The models, unconstrained and constrained, were
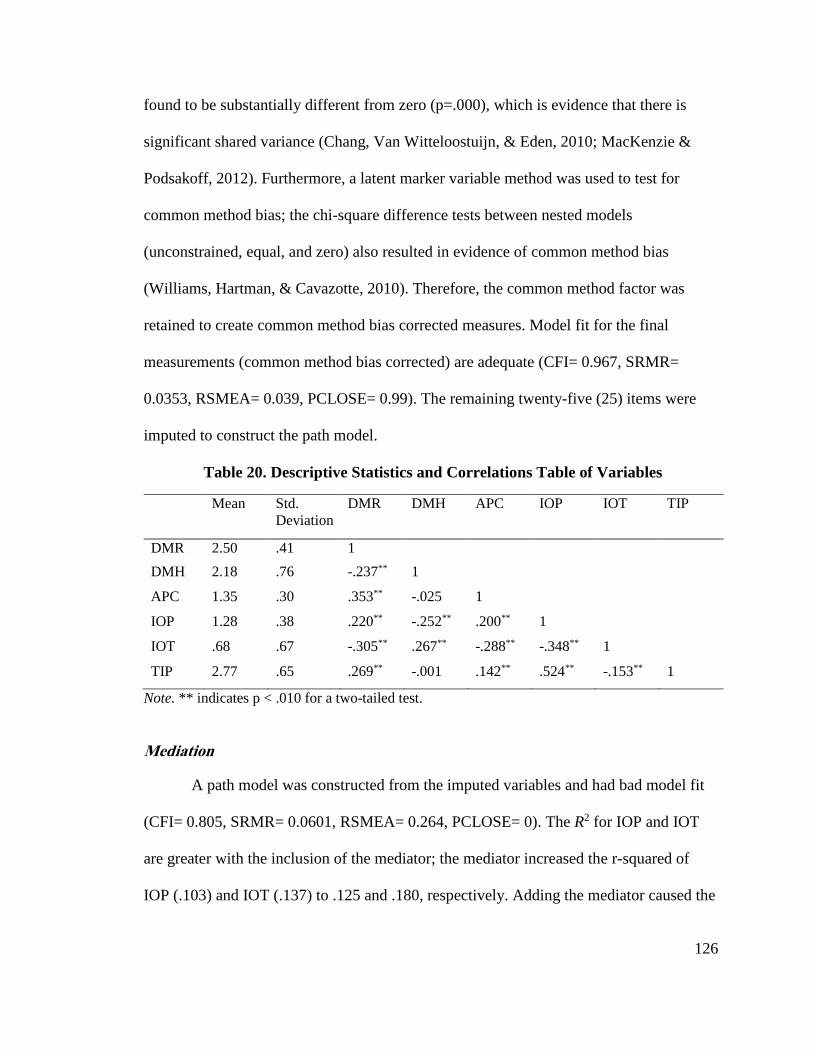
126
found to be substantially different from zero (p=.000), which is evidence that there is
significant shared variance (Chang, Van Witteloostuijn, & Eden, 2010; MacKenzie &
Podsakoff, 2012). Furthermore, a latent marker variable method was used to test for
common method bias; the chi-square difference tests between nested models
(unconstrained, equal, and zero) also resulted in evidence of common method bias
(Williams, Hartman, & Cavazotte, 2010). Therefore, the common method factor was
retained to create common method bias corrected measures. Model fit for the final
measurements (common method bias corrected) are adequate (CFI= 0.967, SRMR=
0.0353, RSMEA= 0.039, PCLOSE= 0.99). The remaining twenty-five (25) items were
imputed to construct the path model.
Table 20. Descriptive Statistics and Correlations Table of Variables
Mean Std.
Deviation
DMR DMH APC IOP IOT TIP
DMR 2.50 .41 1
DMH 2.18 .76 -.237** 1
APC 1.35 .30 .353** -.025 1
IOP 1.28 .38 .220** -.252** .200** 1
IOT .68 .67 -.305** .267** -.288** -.348** 1
TIP 2.77 .65 .269** -.001 .142** .524** -.153** 1
Note. ** indicates p < .010 for a two-tailed test.
Mediation
A path model was constructed from the imputed variables and had bad model fit
(CFI= 0.805, SRMR= 0.0601, RSMEA= 0.264, PCLOSE= 0). The R2 for IOP and IOT
are greater with the inclusion of the mediator; the mediator increased the r-squared of
IOP (.103) and IOT (.137) to .125 and .180, respectively. Adding the mediator caused the
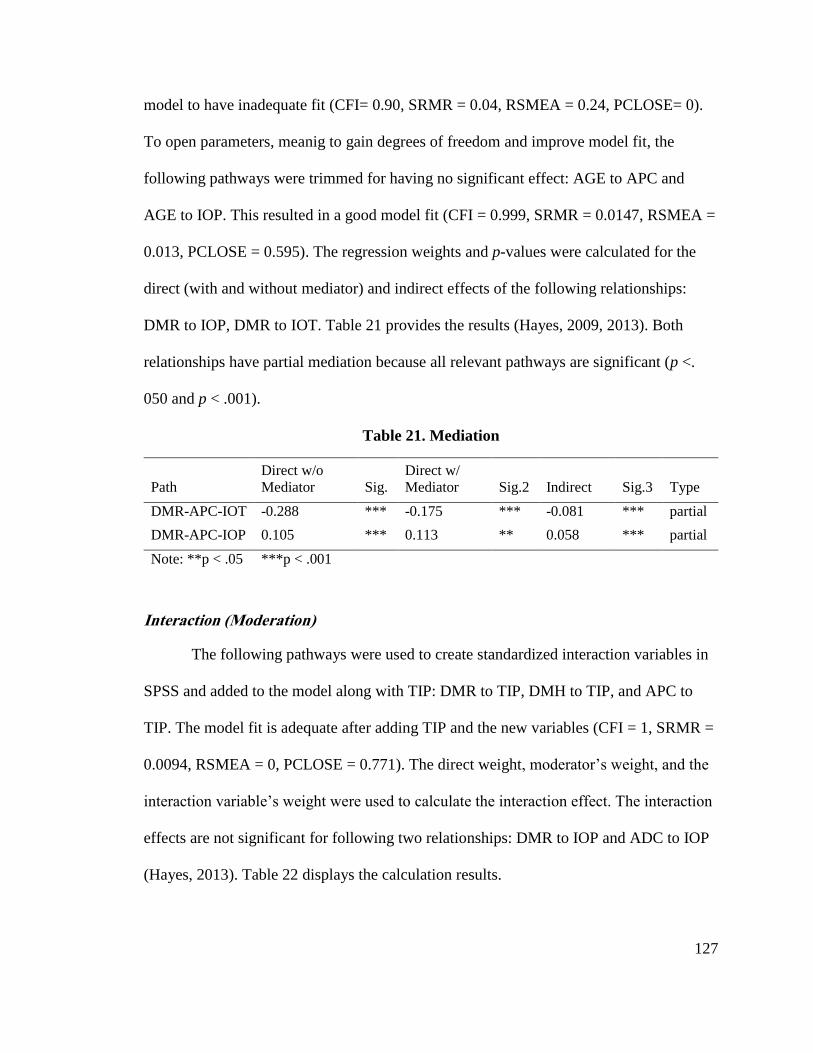
127
model to have inadequate fit (CFI= 0.90, SRMR = 0.04, RSMEA = 0.24, PCLOSE= 0).
To open parameters, meanig to gain degrees of freedom and improve model fit, the
following pathways were trimmed for having no significant effect: AGE to APC and
AGE to IOP. This resulted in a good model fit (CFI = 0.999, SRMR = 0.0147, RSMEA =
0.013, PCLOSE = 0.595). The regression weights and p-values were calculated for the
direct (with and without mediator) and indirect effects of the following relationships:
DMR to IOP, DMR to IOT. Table 21 provides the results (Hayes, 2009, 2013). Both
relationships have partial mediation because all relevant pathways are significant (p <.
050 and p < .001).
Table 21. Mediation
Path
Direct w/o
Mediator Sig.
Direct w/
Mediator Sig.2 Indirect Sig.3 Type
DMR-APC-IOT -0.288 *** -0.175 *** -0.081 *** partial
DMR-APC-IOP 0.105 *** 0.113 ** 0.058 *** partial
Note: **p < .05 ***p < .001
Interaction (Moderation)
The following pathways were used to create standardized interaction variables in
SPSS and added to the model along with TIP: DMR to TIP, DMH to TIP, and APC to
TIP. The model fit is adequate after adding TIP and the new variables (CFI = 1, SRMR =
0.0094, RSMEA = 0, PCLOSE = 0.771). The direct weight, moderator’s weight, and the
interaction variable’s weight were used to calculate the interaction effect. The interaction
effects are not significant for following two relationships: DMR to IOP and ADC to IOP
(Hayes, 2013). Table 22 displays the calculation results.
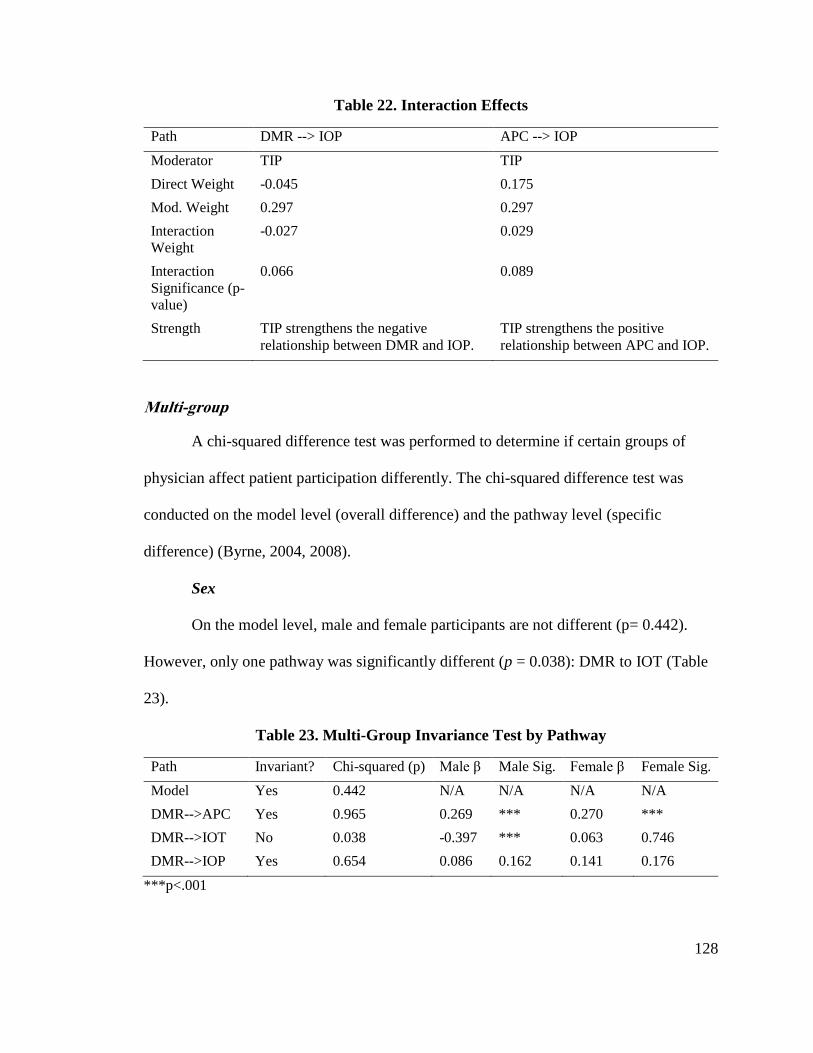
128
Table 22. Interaction Effects
Path DMR --> IOP APC --> IOP
Moderator TIP TIP
Direct Weight -0.045 0.175
Mod. Weight 0.297 0.297
Interaction
Weight
-0.027 0.029
Interaction
Significance (p-
value)
0.066 0.089
Strength TIP strengthens the negative
relationship between DMR and IOP.
TIP strengthens the positive
relationship between APC and IOP.
Multi-group
A chi-squared difference test was performed to determine if certain groups of
physician affect patient participation differently. The chi-squared difference test was
conducted on the model level (overall difference) and the pathway level (specific
difference) (Byrne, 2004, 2008).
Sex
On the model level, male and female participants are not different (p= 0.442).
However, only one pathway was significantly different (p = 0.038): DMR to IOT (Table
23).
Table 23. Multi-Group Invariance Test by Pathway
Path Invariant? Chi-squared (p) Male β Male Sig. Female β Female Sig.
Model Yes 0.442 N/A N/A N/A N/A
DMR-->APC Yes 0.965 0.269 *** 0.270 ***
DMR-->IOT No 0.038 -0.397 *** 0.063 0.746
DMR-->IOP Yes 0.654 0.086 0.162 0.141 0.176
***p<.001
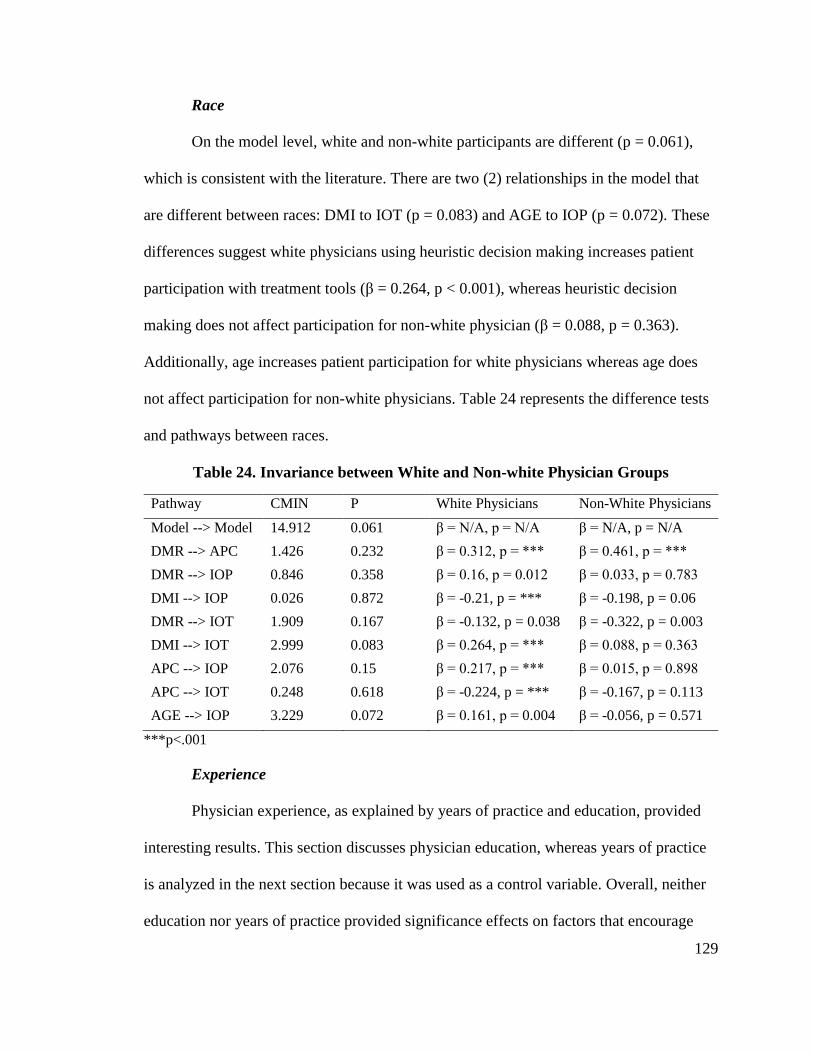
129
Race
On the model level, white and non-white participants are different (p = 0.061),
which is consistent with the literature. There are two (2) relationships in the model that
are different between races: DMI to IOT (p = 0.083) and AGE to IOP (p = 0.072). These
differences suggest white physicians using heuristic decision making increases patient
participation with treatment tools (β = 0.264, p < 0.001), whereas heuristic decision
making does not affect participation for non-white physician (β = 0.088, p = 0.363).
Additionally, age increases patient participation for white physicians whereas age does
not affect participation for non-white physicians. Table 24 represents the difference tests
and pathways between races.
Table 24. Invariance between White and Non-white Physician Groups
Pathway CMIN P White Physicians Non-White Physicians
Model --> Model 14.912 0.061 β = N/A, p = N/A β = N/A, p = N/A
DMR --> APC 1.426 0.232 β = 0.312, p = *** β = 0.461, p = ***
DMR --> IOP 0.846 0.358 β = 0.16, p = 0.012 β = 0.033, p = 0.783
DMI --> IOP 0.026 0.872 β = -0.21, p = *** β = -0.198, p = 0.06
DMR --> IOT 1.909 0.167 β = -0.132, p = 0.038 β = -0.322, p = 0.003
DMI --> IOT 2.999 0.083 β = 0.264, p = *** β = 0.088, p = 0.363
APC --> IOP 2.076 0.15 β = 0.217, p = *** β = 0.015, p = 0.898
APC --> IOT 0.248 0.618 β = -0.224, p = *** β = -0.167, p = 0.113
AGE --> IOP 3.229 0.072 β = 0.161, p = 0.004 β = -0.056, p = 0.571
***p<.001
Experience
Physician experience, as explained by years of practice and education, provided
interesting results. This section discusses physician education, whereas years of practice
is analyzed in the next section because it was used as a control variable. Overall, neither
education nor years of practice provided significance effects on factors that encourage
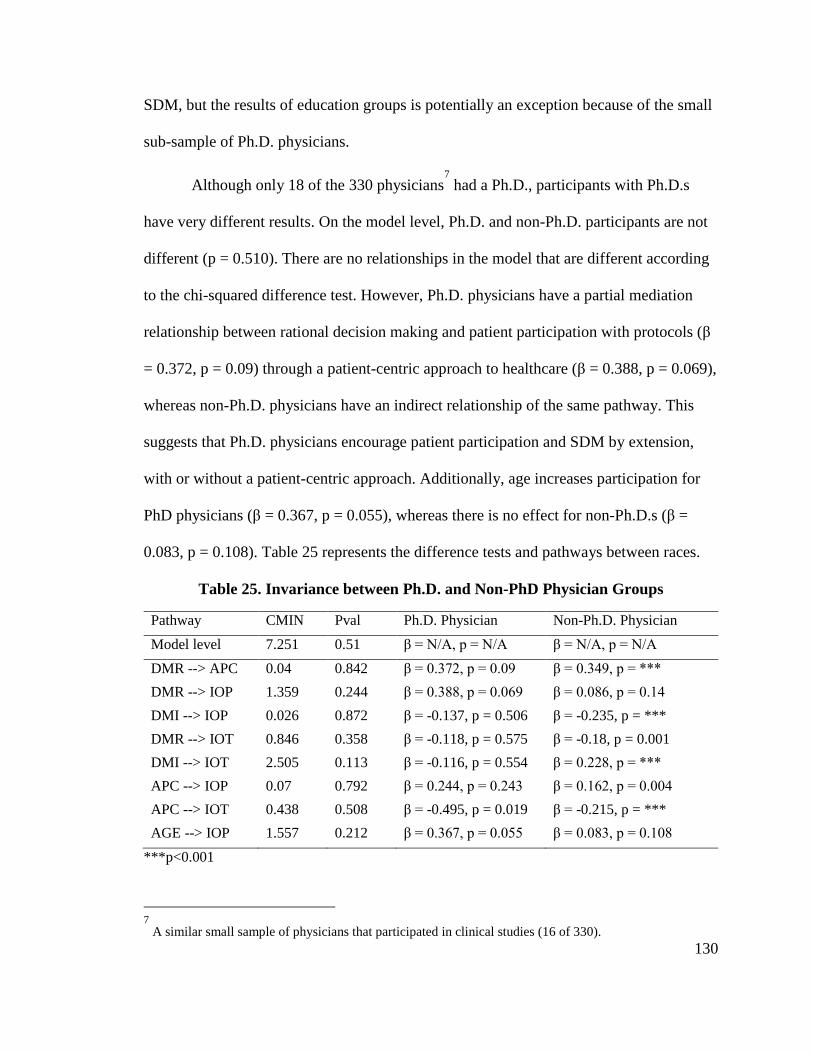
130
SDM, but the results of education groups is potentially an exception because of the small
sub-sample of Ph.D. physicians.
Although only 18 of the 330 physicians7
had a Ph.D., participants with Ph.D.s
have very different results. On the model level, Ph.D. and non-Ph.D. participants are not
different (p = 0.510). There are no relationships in the model that are different according
to the chi-squared difference test. However, Ph.D. physicians have a partial mediation
relationship between rational decision making and patient participation with protocols (β
= 0.372, p = 0.09) through a patient-centric approach to healthcare (β = 0.388, p = 0.069),
whereas non-Ph.D. physicians have an indirect relationship of the same pathway. This
suggests that Ph.D. physicians encourage patient participation and SDM by extension,
with or without a patient-centric approach. Additionally, age increases participation for
PhD physicians (β = 0.367, p = 0.055), whereas there is no effect for non-Ph.D.s (β =
0.083, p = 0.108). Table 25 represents the difference tests and pathways between races.
Table 25. Invariance between Ph.D. and Non-PhD Physician Groups
Pathway CMIN Pval Ph.D. Physician Non-Ph.D. Physician
Model level 7.251 0.51 β = N/A, p = N/A β = N/A, p = N/A
DMR --> APC 0.04 0.842 β = 0.372, p = 0.09 β = 0.349, p = ***
DMR --> IOP 1.359 0.244 β = 0.388, p = 0.069 β = 0.086, p = 0.14
DMI --> IOP 0.026 0.872 β = -0.137, p = 0.506 β = -0.235, p = ***
DMR --> IOT 0.846 0.358 β = -0.118, p = 0.575 β = -0.18, p = 0.001
DMI --> IOT 2.505 0.113 β = -0.116, p = 0.554 β = 0.228, p = ***
APC --> IOP 0.07 0.792 β = 0.244, p = 0.243 β = 0.162, p = 0.004
APC --> IOT 0.438 0.508 β = -0.495, p = 0.019 β = -0.215, p = ***
AGE --> IOP 1.557 0.212 β = 0.367, p = 0.055 β = 0.083, p = 0.108
***p<0.001
7
A similar small sample of physicians that participated in clinical studies (16 of 330).
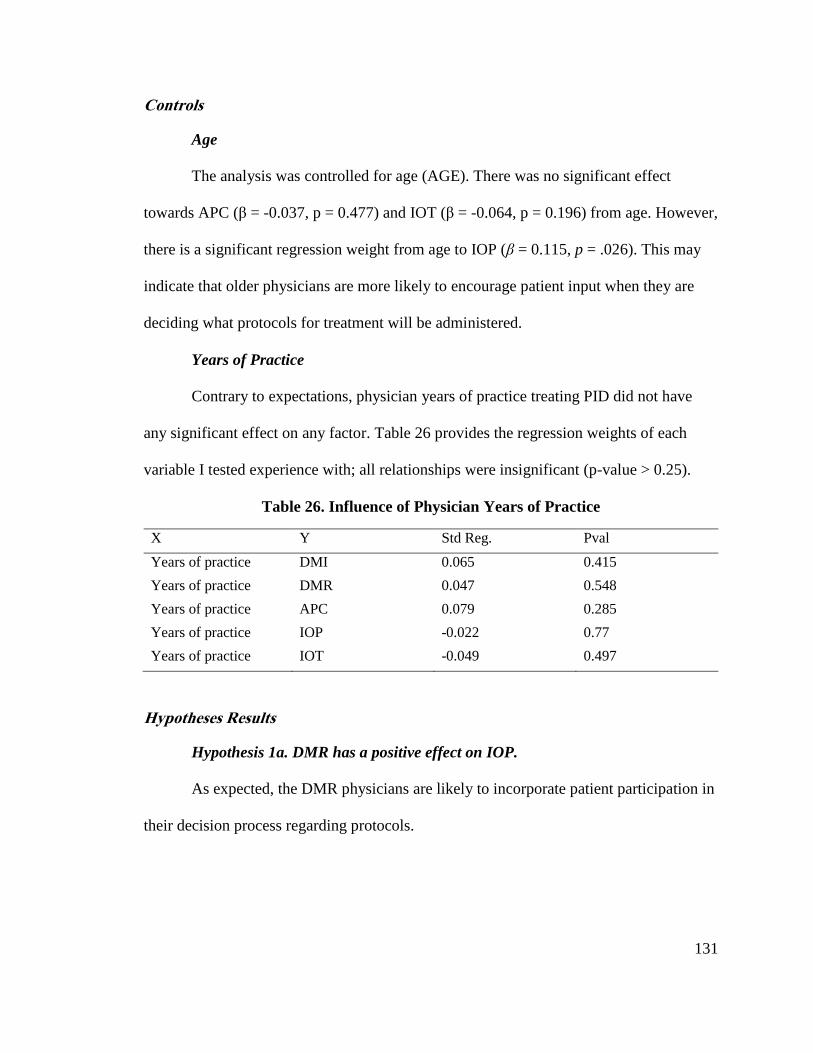
131
Controls
Age
The analysis was controlled for age (AGE). There was no significant effect
towards APC (β = -0.037, p = 0.477) and IOT (β = -0.064, p = 0.196) from age. However,
there is a significant regression weight from age to IOP (β = 0.115, p = .026). This may
indicate that older physicians are more likely to encourage patient input when they are
deciding what protocols for treatment will be administered.
Years of Practice
Contrary to expectations, physician years of practice treating PID did not have
any significant effect on any factor. Table 26 provides the regression weights of each
variable I tested experience with; all relationships were insignificant (p-value > 0.25).
Table 26. Influence of Physician Years of Practice
X Y Std Reg. Pval
Years of practice DMI 0.065 0.415
Years of practice DMR 0.047 0.548
Years of practice APC 0.079 0.285
Years of practice IOP -0.022 0.77
Years of practice IOT -0.049 0.497
Hypotheses Results
Hypothesis 1a. DMR has a positive effect on IOP.
As expected, the DMR physicians are likely to incorporate patient participation in
their decision process regarding protocols.
132
Hypothesis 1b. DMR has a positive effect on IOT.
The analysis provided counter-evidence to this hypothesis. Contrary to
expectations, DMR physicians are not likely to incorporate patient participation in their
decision process in regard to tools.
Hypothesis 2a. DMH has a negative effect on IOP.
As expected, the DMH physicians are not likely to incorporate patient
participation in their decision process regarding protocols.
Hypothesis 2b. DMH has a negative effect on IOT.
The analysis provided counter-evidence to this hypothesis. Contrary to
expectations, DMH physicians are likely to incorporate patient participation in their
decision process in regard to tools. Therefore, I reject the hypothesis.
Hypothesis 3a. APC partially and positively mediates the positive effect of DMR
on IOP.
As expected, a patient-centric treatment approach is likely to mediate the pathway
between DMR and IOP. In this case, the mediation is positive; thus, enhancing the
pathway’s effect.
Hypothesis 3b. APC partially and positively mediates the positive effect of DMR
on IOT.
As expected, a patient-centric treatment approach is likely to mediate the pathway
between DMR and IOP. Although the mediating effect is negative, the negative effect of
DMR on IOT was weakened by APC.
133
Hypothesis 4a. Age has a positive effect on IOP.
As expected, older DMR physicians have a stronger positive effect on IOP (β =
0.115, p = 0.026). Therefore, the hypothesis is supported.
Hypothesis 4b. Age has a positive effect on IOT.
Contrary to expectations, age did not have any significant effect on patient
participation with treatment tools. Therefore, this hypothesis is rejected.
Hypothesis 5. The positive effects of DMR on IOT is stronger for women than
men.
As expected, female DMR physicians have a stronger positive effect on IOT than
men. However, the results provided interesting evidence in that the female physicians did
not have a strong positive relationship between DMR and IOT (β = .063, p = .746),
whereas male physicians had a strong negative relationship (β = -.397, p < .001).
Therefore, the hypothesis is supported.
Hypothesis 6a. The positive effects of DMR on IOP is stronger for white
physicians.
Contrary to expectations, the effect of DMR on IOP is invariant between races;
the chi-squared difference test was not significant (p = 0.358). Therefore, this hypothesis
is rejected.
Hypothesis 6b. The positive effects of DMR on IOT is stronger for white
physicians.
Contrary to expectations, the effect of DMR on IOT is invariant between races;
the chi-squared difference test was not significant (p = 0.167). Therefore, this hypothesis
is rejected.
134
Hypothesis 6c. The positive effects of DMI on IOP is stronger for white
physicians.
Contrary to expectations, the effect of DMI on IOP is invariant between races; the
chi-squared difference test was not significant (p = 0.872). Therefore, this hypothesis is
rejected.
Hypothesis 6d. The positive effects of DMI on IOT is stronger for white
physicians.
The effect of DMI on IOT is not invariant between white and non-white
physicians; the chi-squared difference test was not significant (p = 0.083), confirming the
differences between races. Furthermore, white physicians had a strong, significant
pathway (β = 0.264, p < 0.001) compared to non-white physicians (β = 0.088, p = 0.363).
Therefore, this hypothesis is accepted.
Hypothesis 7a. Years of practice has a positive effect on IOP.
Contrary to expectations, years of practice did not have any significant effect on
patient participation with treatment protocols. Therefore, this hypothesis is rejected.
Hypothesis 7b. Years of practice has a positive effect on IOT.
Contrary to expectations, years of practice did not have any significant effect on
patient participation with treatment tools. Therefore, this hypothesis is rejected.
Hypothesis 8a. The positive effect of DMR on IOP is stronger for physicians
with more education.
Contrary to expectations, the effect of DMR on IOP is invariant between Ph.D.
physicians and non-PhD physicians; the chi-squared difference test was not significant (p
= 0.244). Therefore, this hypothesis is rejected. However, because the sample of Ph.D.
135
physicians is only 18, it is worth noting that the pathway for Ph.D. physicians is
significant (β = 0.388, p = 0.069) whereas it is not significant for non-Ph.D.s (β = 0.086,
p = 0.140).
Hypothesis 8b. The positive effect of DMR on IOT is weaker for physicians with
more education.
Contrary to expectations, the effect of DMR on IOT is invariant between Ph.D.
physicians and non-PhD physicians; the chi-squared difference test was not significant (p
= 0.358). Therefore, this hypothesis is rejected. However, the pathway for Ph.D.
physicians is not significant (β = -0.118, p = 0.575) whereas it is significant for non-
Ph.D.s (β = -0.180, p = 0.001).
Hypothesis 8c. The positive effects of DMI on IOP is stronger for physicians
with more education.
Contrary to expectations, the effect of DMI on IOP is invariant between Ph.D.
physicians and non-PhD physicians; the chi-squared difference test was not significant (p
= 0.872). Therefore, this hypothesis is rejected. Furthermore, the pathway for Ph.D.
physicians is not significant and negative (β = -0.137, p = 0.506) whereas it is significant
for non-PhDs (β = -0.235, p < 0.001).
Hypothesis 8d. The positive effects of DMI on IOT is weaker for physicians with
more education.
Contrary to expectations, the effect of DMI on IOP is invariant between Ph.D.
physicians and non-Ph.D. physicians; the chi-squared difference test was not significant
(p = 0.113). Therefore, this hypothesis is rejected. Furthermore, the pathway for Ph.D.
136
physicians is not significant and negative (β = -0.116, p = 0.554) whereas it is positive
and significant for non-PhDs (β = 0.228, p < 0.001).
Hypothesis 9a. TIP positively moderates the effect of DMR on IOP.
This hypothesis is not supported in the analysis; however, the analysis provided
interesting results. Trust strengthens the negative relationship between DMR and IOP, yet
the relationship is positive when trust is not present. This may suggest that DMR
physicians have lower levels of patient participation for protocols when they trust the
patient’s initial input. It is possible that DMR physicians do not feel the need to
incorporate patient participation if all the information is accurate and reliable from the
start.
Hypothesis 9b. TIP positively moderates the effect of APC on IOP.
This hypothesis is not supported in the analysis. TIP does not significantly
moderate the relationship between APC and IOP.
Discussion
Based on literature and results from the prior research, this study sought to test the
effect of physician decision-making style on patient participation. Patient participation is
often cited as an important factor to improve healthcare outcomes, so a deeper
understanding of factors that foster shared decision-making may help facilitate
improvements in the care of chronic diseases. The aim of the study was primarily focused
on quantifying the amount of patient participation in the decision process explained by a
physician’s decision-making style. As suggested by dual process theory, the results of the
study demonstrate that physicians’ decision-making style has a meaningful impact on the
patient participation in selecting treatment protocols and tools.
137
The study also focuses on the role of patient-centric care as predicted by SIT and
physician traits. Consistent with SIT theory, patient-centered care is the mechanism
through which SDM words. There are also relevant traits which impact decision making.
Summary of Major Findings
The results highlight how different decision-making styles (dual process) have the
potential to improve patient participation for tools or protocols (not both). Rational
decision making leads to participation with protocols whereas heuristic decision making
increases participation with treatment tools.
Social Identity Theory is supported because patient participation is mediated by
the patient-centric approach to healthcare, increasing patient participation likelihood
regardless of decision-making style.
There were a number of findings related to physician traits. Older physicians are
more likely to increase patient participation, yet years of practice do not affect
participation and trust has no moderating effect. Physician race provided different results
in the effects on patient participation; white physicians were more likely to increase
participation than non-white. Lastly, physician experience did not affect patient
participation; physicians with Ph.D.s were more likely to increase participation with
treatment protocols than non-Ph.D.s, but there is no statistical difference, likely caused by
the small Ph.D. population.
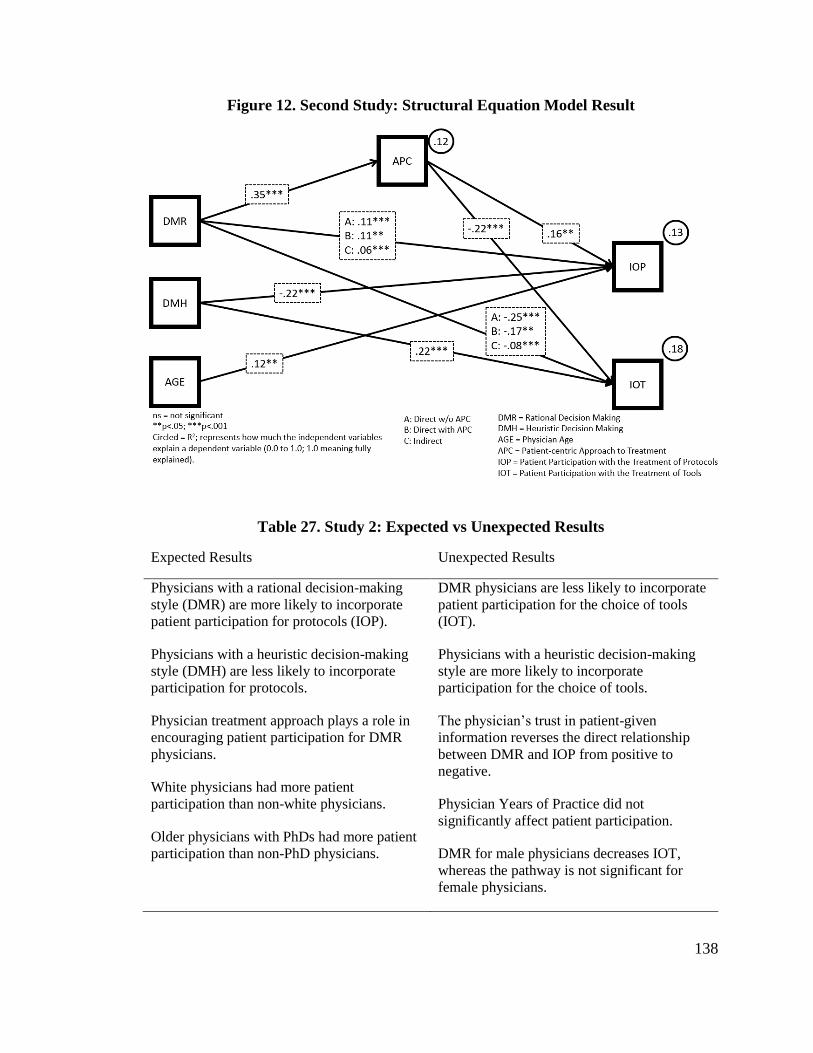
138
Figure 12. Second Study: Structural Equation Model Result
Table 27. Study 2: Expected vs Unexpected Results
Expected Results Unexpected Results
Physicians with a rational decision-making
style (DMR) are more likely to incorporate
patient participation for protocols (IOP).
Physicians with a heuristic decision-making
style (DMH) are less likely to incorporate
participation for protocols.
Physician treatment approach plays a role in
encouraging patient participation for DMR
physicians.
White physicians had more patient
participation than non-white physicians.
Older physicians with PhDs had more patient
participation than non-PhD physicians.
DMR physicians are less likely to incorporate
patient participation for the choice of tools
(IOT).
Physicians with a heuristic decision-making
style are more likely to incorporate
participation for the choice of tools.
The physician’s trust in patient-given
information reverses the direct relationship
between DMR and IOP from positive to
negative.
Physician Years of Practice did not
significantly affect patient participation.
DMR for male physicians decreases IOT,
whereas the pathway is not significant for
female physicians.
139
Expected Findings
The results suggest that physician decision-making style significantly effects
patient participation in the decision process. The results provide evidence that different
decision-making styles increase or decrease how much shared decision-making occurs. In
particular, physicians are more likely to exercise shared decision-making for treatment
protocols if they have a rational decision-making style (DMR), as opposed to the
heuristic decision-making style (DMH). This was not a surprise as we had hypothesized
that a rational decision-making style would have a positive direct effect on patient
participation with the choice of protocols (β = 0.105, p < 0.001). It was critical to
understand the fundamental differences between rational and heuristic thinkers to form
the hypotheses. We had considered hypothesizing that a rational decision-making style
would negatively affect participation with protocols (IOP), but ignoring details is the
opposite of what a rational decision maker would do. Although physicians do form
mental shortcuts, those who prefer a rational decision-making style are less likely to miss
a chance to get the patient’s perspective.
Furthermore, consistent with SIT, physicians that adopt a patient-centric approach
(APC) to treatment are more likely to incorporate patient participation in the choice of
protocols (β = 0.053, p = 0.003).
Few of the expected results involving physician traits were supported. Older
DMR physicians have a stronger positive effect on IOP. Female DMR physicians have a
stronger positive effect on IOT than men. The positive affect of DMI on IOT is stronger
for white physicians.
140
Unexpected Findings
The most interesting results of this study come from the unexpected findings.
Patient participation with tools (IOT) has provided, by far, the most results with counter-
evidence in this study. The direct relationships to IOT were significant, yet the opposite
of what was expected; DMR physicians were less likely to incorporate participation (β = -
0.288, p < 0.001), whereas DMH physicians were more likely (β = 0.195, p < 0.001).
This is the opposite of what we expected and resulted in an interesting relationship with
the mediator, patient-centric approach. We hypothesized a patient-centric approach
would positively affect DMR to IOT, but the result was significant negative mediation (β
= -0.134, p = .001). Although it is negative, the effect of APC on this relationship
actually increases the likelihood of participation by dampening the negative effect of
DMR on IOT.
The negative relationship between DMR and IOT is likely related to the overall
process of prescribing treatment tools. The physician will often prescribe a tool but be
uninvolved with the product selection (i.e., brand). When given a prescription, the patient
will go to their pharmacy to obtain the product; the pharmacist often makes the actual
brand selection. The tool may depend on various factors such as availability and type of
health insurance reimbursement.
It may be that physicians choose a decision-making style depending on how well
they know the patient and the extent of their patient-centric their healthcare approach.
New patients would be treated with a rational decision-making style, focusing on
protocols and compliance with protocols; this would involve the physician learning about
the patient lifestyle and background. The new patients may not know which brand works
141
best for them, neither does the physician. Therefore, the physician may be indifferent to
the brand of product as long as the patient follows the protocol. As the physician-patient
relationship matures, the physician would be more familiar with the patient’s lifestyle and
would not need too many to analyze it in detail. However, the patient can now provide
feedback on the brand to treat their PID. Further research would be needed to confirm
this hypothesis.
Gender had provided interesting counter-evidence to Hypothesis 6, “The positive
effect of DMR on IOT is stronger for women than men”. As expected, male DMR
physicians have a significant negative relationship to IOT (β = -0.397, p < .001);
however, female DMR physicians did not have a significant positive relationship (β =
0.105. p = 0.746). The literature suggests that female physicians are more likely to show
empathy than males. Therefore, the negative relationship between male DMR physicians
and IOT is consistent with the literature and supports the hypothesis. However, the
surprising outcome is the insignificant relationship of female DMR physicians and IOT.
This indifference may be caused by the smaller sample size of women (86) than men
(244); the sample size may provide an inadequate measure for women.
Physician traits had some influence on patient participation in specific contexts.
There was significance with physician age effecting patient participation with treatment
protocols. Physicians with Ph.D.s were more likely to have patient participation with
protocols than non-Ph.D. physicians. White physicians have more patient participation
with treatment tools than non-white physicians. Despite the other traits presenting unique
influences, years of practice does not affect patient participation.
142
The physician’s trust in patient-given information (TIP) had the most interesting
result by far. We hypothesized TIP would positively moderate the positive relationship
between DMR and IOP. However, TIP ended up reversing the relationship between DMR
and IOP; the direct relationship between DMR and IOP is positive (as expected), but
including trust in the model caused the relationship to become negative. The reason for
this reversed relationship may be related to what was discussed above; the physician may
not need to discuss protocols if the information has not changed. If a patient’s
information is accurate about his lifestyle, the physician would not need to revise the
protocols. However, if the patient provides inaccurate information, the physician may
need to compensate for any shortcomings.
Observations that Require Future Research
Certain survey items were tested for significance towards the DVs. For instance,
we asked about the physicians considering patient culture in the decision process, but
there was no significance. However, the item was part of the patient-centric factor,
suggesting they cumulatively have significance.
There were also items cut from the final model, such as those measuring if the
physician is disease-centric; meaning they approach the patient based on their disease,
not as a patient (lifestyle, etc.) with the disease. An individual item, “I tend to...Keep the
conversation focused on the disease”, was significant to participation with protocol
management (β = -0.163, p = 0.034) and nearly significant with protocol options (β = -
0.137, p = 0.073); it suggests that disease-centric patients were likely to decrease patient
participation. However, individual items are not sufficient to measure with factors
consisting of at least three (3) items.
143
Limitations
Limitations of the second study primarily relate to the use of a one-time self-
administered survey that assumes participants provided unbiased answers (Babbie,
Halley, & Zaino, 2007). The chosen sample limited potential generalization. The gender
distribution was mostly male (67%) and did not account for the practice setting (e.g.,
hospital vs doctor’s office). Participants’ experience levels, specialty, education, cultural
background, and other factors may have prompted variability in the responses.
No statistical test can assure a bias-free analysis (Podsakoff, MacKenzie, Lee, &
Podsakoff, 2003). The response rate of 2% out of 16,000 physicians was exceedingly
low. Due to the variable nature of the population (different physician specialties), the
study’s overall validity may be in question, even though doctors are treating the same
disease.
Based on the findings, the use of the dual process theory to explain physician
decision-making is limited. Although there was statistical significance between decision-
making styles and patient participation, the correlation coefficients were low. In other
words, the R squared value was less than .20 meaning patient participation is mostly
explained by other factors. Items in the analysis were mechanistically trimmed and as a
result, more than half of the items were removed (35 of 60). Future versions of the survey
must be shortened to no more than 5 items per expected factor to increase the response
rate and decrease the number of disengaged respondents.
Forming a survey of PID physicians from the findings of a qualitative research
study involving hemophilia physicians may have caused the researchers to overlook key
differences with PID (Lamb et al., 2015; Lamb, Lyytinen, & Wang, 2016). Second, the
144
results did not account for differences in physicians’ subspecialty (immunology vs.
oncology), the role of insurance in the physician decision process, and selection bias
(Certo, Busenbark, Woo, & Semadeni, 2016; Lamb et al., 2016); selection bias means the
sample randomization is limited by factors such as group (e.g race or specialty) and time
interval (e.g. summer or winter).
Another limitation of this study is related to chronic care in general. Chronic care
involves treatment and management over a long period of time, therefore a single survey
may not capture the full influence of factors affecting patient participation. A longitudinal
study would be best for future research.
Future Research
Future research can expand on the current findings by revising the model or
expanding the population. The data can be tested again by selecting different independent
variables; one variable, in particular, is trust. The survey can be administered to
physicians from other countries as well as for the treatment of other chronic diseases.
An addition to the survey could be to ask for the number of interactions the
patient has with the physician. It is apparent that—with chronic diseases—the physician-
patient interaction is not on a case-to-case basis, but a relationship that is built over time.
This information would help us observe the data as different groups of physicians and
patients based on the length of their relationships. Furthermore, this could offer insight
into how decisions are made at different stages of the relationship and the amount of
patient participation at each stage.
Multiple gaps in the second study warrant additional research.
145
Ethical Assurances
Prior to any data collection, the project was reviewed and approved by the Case
Western Reserve University Weatherhead School of Management and an institutional
review board (IRB) against the privacy and license requirements of U.S. data, protection,
and privacy rules. During the data collection process, participants were informed about
the purpose of the research, ethical procedures, and issues regarding anonymity.
Participants were also informed that use of the collected survey data was only for the
proposed study. Any specific and identifiable survey data was kept in a locked container
only accessed by the researcher. Outsiders to the dissertation process will not have access
to any specific information provided by participants to ensure privacy and to minimize
potential risk to those participating in the data collection. Participants received a standard
waiver form and assurance that they had the option of withdrawing from the study at any
point.
Conclusions and Implications for Patient Participation
“Let’s give patients the choice” is a frequent mantra in PID communities (Samaan
et al., 2014). Often cited principals of care require patient choice in treatment protocols
and tools (Chapel et al., 2014). However, patient choice must be seen in the context of
shared decision making between a doctor and patient. Using constructs and relationships
derived from the early qualitative study (First Study), a quantitative study was performed
to explore the factors that influence a physician’s decision-making process to include
patient participation in the treatment of PID. The chosen instruments provided a
systematic method for looking at the perspective of physicians by measuring attitudes
relating to shared decision-making. The sample of physicians who treat PID provided a
146
specialized perspective about the factors influencing a subset of doctors who treat a
chronic and rare disease. Structural equation modeling (SEM) is a multivariate statistical
analysis technique that was used to analyze factor relationships. As predicted by the
literature, the results showed statistically significant relationships between a physician’s
decision-making process, treatment approach, and patient participation; whereas
physician’s trust in the patient as well as the physician’s gender play less of a role than
previously stated. A physician-only trait that affects patient participation is age, wherein
older physicians increase participation with protocols; all other traits do not significantly
affect participation.
If patient participation is to be facilitated in the treatment of PID, greater attention
needs to be paid to the decision-making process of the physician. Government
policymakers, health care providers, patient organizations, and drug companies should
consider the types of interventions in which physician decision making can increase
patient participation in the treatment of PID and other chronic diseases. Furthermore,
physicians should reflect on their decision-making processes to improve patient
participation thereby improving clinical outcomes and perceived health.
147
CHAPTER 7: STUDY 3: A QUALITATIVE STUDY OF IMMUNOLOGISTS
THAT TREAT PID AND THE FACTORS THAT EFFECT SHARED DECISION
MAKING WITH THEIR PATIENTS
The results from Study 1 and Study 2 suggest: (1) physicians in the U.S. are more
patient-centric than the U.K.;8
(2) patient-centric care is the mechanism through which
SDM works; and (3) dual process theory is a relevant framework for understanding how
decision theory can be applied to SDM. However, the second study had a low explained
variance for the DVs (R2 < .2) meaning patient participation is mostly explained by other
factors, despite the significance between decision-making styles and patient participant (p
< 0.001; see Figure 12). Both a post hoc analysis of the second study and a qualitative
study of a specific subspecialty, immunology, were used to improve the understanding of
SDM.
Initial interviews to test the interview guide (discussed later in this chapter)
suggested that physician specialty may impact the relevance of significant factors found
in the second study. Focusing on immunology as a specific specialty would allow a more
focused view of the physician decision making phenomenon to better understand other
factors that influence SDM and how these factors can be integrated into an overall
decision-making framework. Therefore, I conducted a reanalysis (aka post hoc) to
analyze a sub-sample of physicians (immunologists) in the survey data of the second
study. This post hoc analysis was combined with a second qualitative study for a new
8
The U.S. performs better than other countries regarding the doctor–patient relationship, SDM, and
chronic disease management Schneider, E. C., Sarnak, D. O., Squires, D., Shah, A., & Doty, M. M. 2017.
Mirror, mirror 2017: The Commonwealth Fund, July 2017. Available from
http://www.commonwealthfund.org/publications/fund-reports/2017/jul/mirror-mirror-international-
comparisons-2017..
148
third study. The post hoc analysis was followed by a qualitative study of immunologists
to corroborate results and expand the SDM theoretical framework.
Post Hoc Reanalysis
A reanalysis was conducted to target the immunologist sub-sample to better
understand potential differences in patient participation. Instead of SPSS AMOS, the
analysis was conducted using SmartPLS software because of the small sample size
described below.
Post Hoc Methods
The sample of the quantitative reanalysis is 72 of the 330 (21.8%) completed
surveys; the physicians that specialize in allergy and immunology. Although the sample
size is quite low, it represents a significant part of the PID treating immunologists and the
treated PID population. The total PID population is approx. 32,000 (Grifols, 2017). The
sample of 72 physicians who participated in the survey treated between ~3,120 to ~9,720
patients per year (43–135 per physician). These physicians treat between 10% and 30%
of the total PID population.
Following the new factor analysis utilizing the same guidelines as the second
study, a new quantitative model was formed using revised factors. Each factor is
represented by at least three items9
and there is sufficient model fit (SRMR = 0.091)
(Iacobucci, 2010). The convergent validity was indicated by the composite reliability
loadings (CR > 0.7) despite the low average variance extracted (AVE < .5) (Wong,
2013). Lastly, the discriminant validity is sufficient according to the Heterotrait-
9
The items that form each factor are represented in Appendix D.
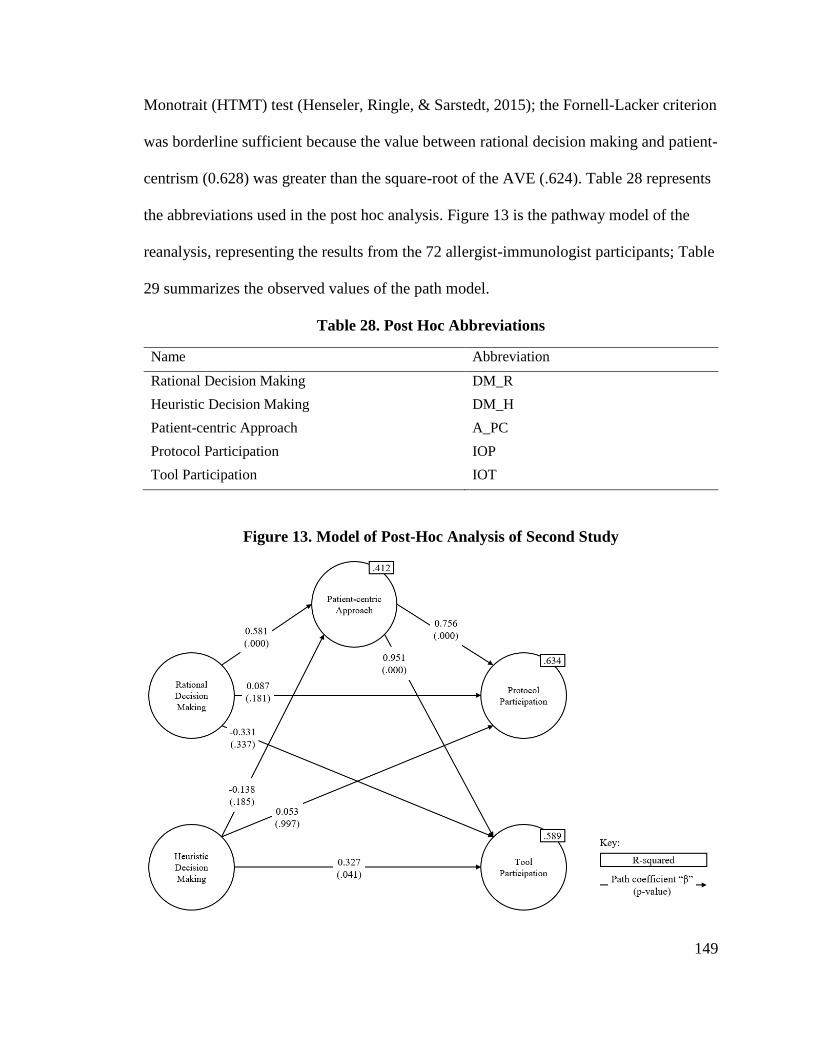
149
Monotrait (HTMT) test (Henseler, Ringle, & Sarstedt, 2015); the Fornell-Lacker criterion
was borderline sufficient because the value between rational decision making and patient-
centrism (0.628) was greater than the square-root of the AVE (.624). Table 28 represents
the abbreviations used in the post hoc analysis. Figure 13 is the pathway model of the
reanalysis, representing the results from the 72 allergist-immunologist participants; Table
29 summarizes the observed values of the path model.
Table 28. Post Hoc Abbreviations
Name Abbreviation
Rational Decision Making DM_R
Heuristic Decision Making DM_H
Patient-centric Approach A_PC
Protocol Participation IOP
Tool Participation IOT
Figure 13. Model of Post-Hoc Analysis of Second Study
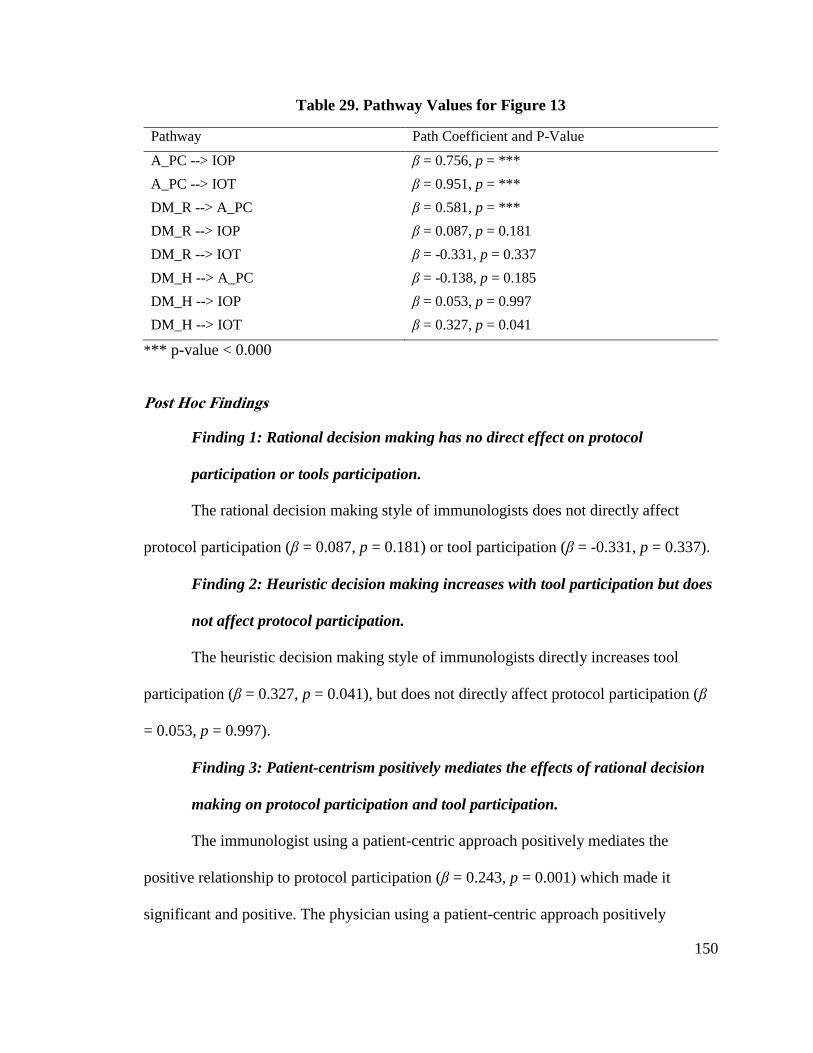
150
Table 29. Pathway Values for Figure 13
Pathway Path Coefficient and P-Value
A_PC --> IOP β = 0.756, p = ***
A_PC --> IOT β = 0.951, p = ***
DM_R --> A_PC β = 0.581, p = ***
DM_R --> IOP β = 0.087, p = 0.181
DM_R --> IOT β = -0.331, p = 0.337
DM_H --> A_PC β = -0.138, p = 0.185
DM_H --> IOP β = 0.053, p = 0.997
DM_H --> IOT β = 0.327, p = 0.041
*** p-value < 0.000
Post Hoc Findings
Finding 1: Rational decision making has no direct effect on protocol
participation or tools participation.
The rational decision making style of immunologists does not directly affect
protocol participation (β = 0.087, p = 0.181) or tool participation (β = -0.331, p = 0.337).
Finding 2: Heuristic decision making increases with tool participation but does
not affect protocol participation.
The heuristic decision making style of immunologists directly increases tool
participation (β = 0.327, p = 0.041), but does not directly affect protocol participation (β
= 0.053, p = 0.997).
Finding 3: Patient-centrism positively mediates the effects of rational decision
making on protocol participation and tool participation.
The immunologist using a patient-centric approach positively mediates the
positive relationship to protocol participation (β = 0.243, p = 0.001) which made it
significant and positive. The physician using a patient-centric approach positively
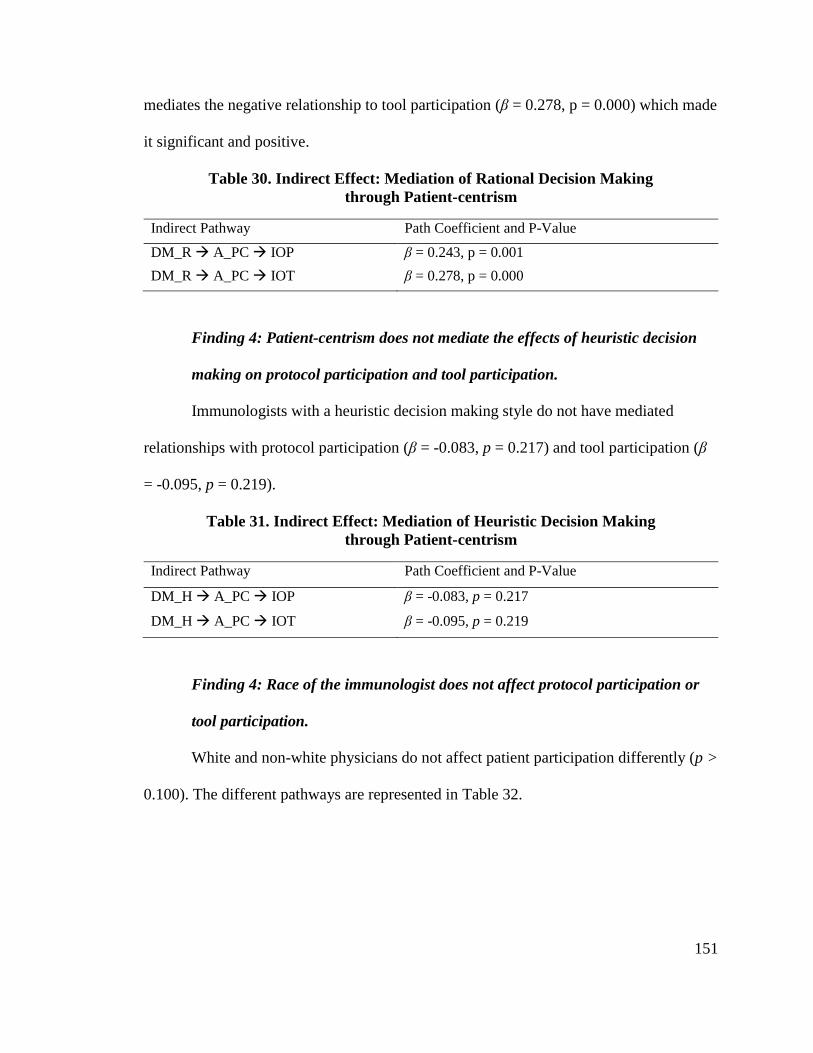
151
mediates the negative relationship to tool participation (β = 0.278, p = 0.000) which made
it significant and positive.
Table 30. Indirect Effect: Mediation of Rational Decision Making
through Patient-centrism
Indirect Pathway Path Coefficient and P-Value
DM_R A_PC IOP β = 0.243, p = 0.001
DM_R A_PC IOT β = 0.278, p = 0.000
Finding 4: Patient-centrism does not mediate the effects of heuristic decision
making on protocol participation and tool participation.
Immunologists with a heuristic decision making style do not have mediated
relationships with protocol participation (β = -0.083, p = 0.217) and tool participation (β
= -0.095, p = 0.219).
Table 31. Indirect Effect: Mediation of Heuristic Decision Making
through Patient-centrism
Indirect Pathway Path Coefficient and P-Value
DM_H A_PC IOP β = -0.083, p = 0.217
DM_H A_PC IOT β = -0.095, p = 0.219
Finding 4: Race of the immunologist does not affect protocol participation or
tool participation.
White and non-white physicians do not affect patient participation differently (p >
0.100). The different pathways are represented in Table 32.
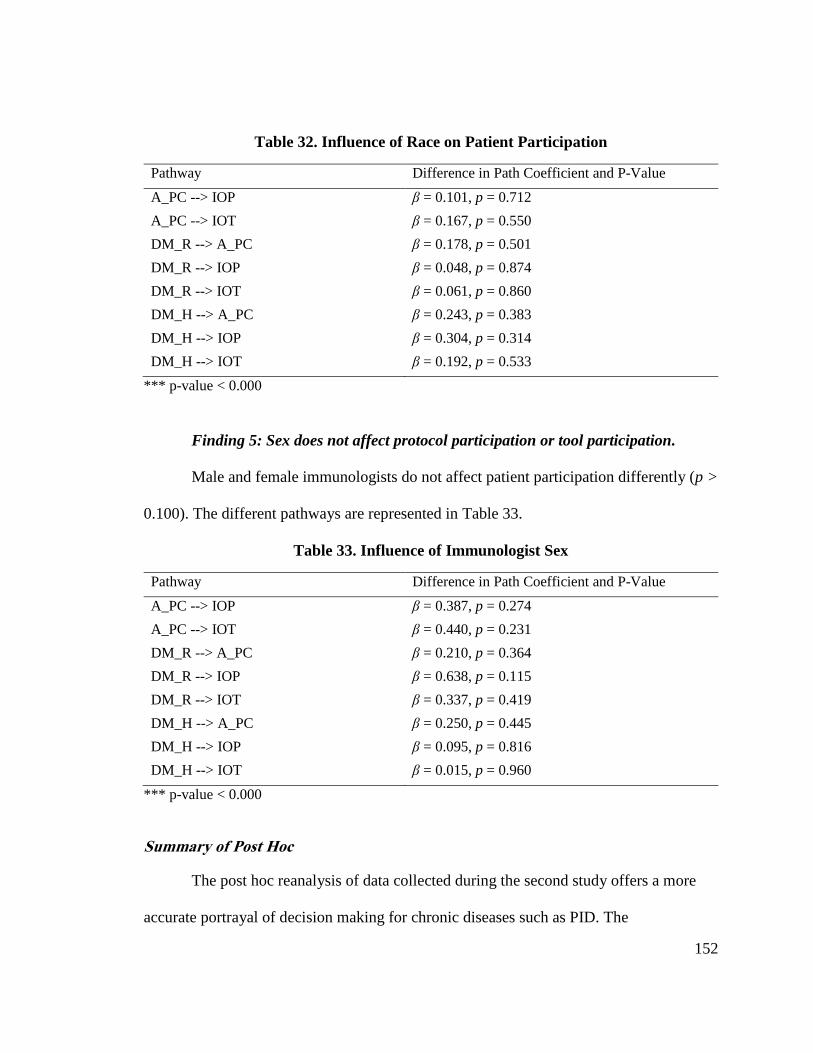
152
Table 32. Influence of Race on Patient Participation
Pathway Difference in Path Coefficient and P-Value
A_PC --> IOP β = 0.101, p = 0.712
A_PC --> IOT β = 0.167, p = 0.550
DM_R --> A_PC β = 0.178, p = 0.501
DM_R --> IOP β = 0.048, p = 0.874
DM_R --> IOT β = 0.061, p = 0.860
DM_H --> A_PC β = 0.243, p = 0.383
DM_H --> IOP β = 0.304, p = 0.314
DM_H --> IOT β = 0.192, p = 0.533
*** p-value < 0.000
Finding 5: Sex does not affect protocol participation or tool participation.
Male and female immunologists do not affect patient participation differently (p >
0.100). The different pathways are represented in Table 33.
Table 33. Influence of Immunologist Sex
Pathway Difference in Path Coefficient and P-Value
A_PC --> IOP β = 0.387, p = 0.274
A_PC --> IOT β = 0.440, p = 0.231
DM_R --> A_PC β = 0.210, p = 0.364
DM_R --> IOP β = 0.638, p = 0.115
DM_R --> IOT β = 0.337, p = 0.419
DM_H --> A_PC β = 0.250, p = 0.445
DM_H --> IOP β = 0.095, p = 0.816
DM_H --> IOT β = 0.015, p = 0.960
*** p-value < 0.000
Summary of Post Hoc
The post hoc reanalysis of data collected during the second study offers a more
accurate portrayal of decision making for chronic diseases such as PID. The
153
immunologists are the specialists responsible for treating a patient with PID throughout
most of the patient’s life, thereby providing better insight of potential SDM for this
chronic disorder. The findings suggest the following: rational decision making indirectly
increases patient participation with tools and protocols through a patient-centric
approach, heuristic decision making directly increases patient participation with tools,
and traits such as race and sex do not impact the model.
In summary, patient participation depends on a combination of decision-making
style and the approach to patient care. Rational decision makers only increase patient
participation if they incorporate a patient-centric approach to healthcare, which suggests
there is a conditional relationship involved. Therefore, the post hoc analysis was
supplemented by a qualitative study to better understand other factors associated with
SDM implementation in the immunologist population. The research questions were:
“What are the drivers of successful implementation and adoption of
SDM?
How are power and literacy balanced through health literacy
Are there patient traits that influence SDM
Are there organizational factors that influence SDM such as
coordination of care and reimbursement?
These questions guide the research to determine “when” SDM is effective, rather
than the results of SDM because the benefits are understood (Noonan et al., 2017). In this
chapter, I present the method, results, discussion, and limitations for the study.
Research Method of the Qualitative Part of the Third Study
The research is based on interviews with 15 immunologists conducted in between
May 1st and July 31st, 2017. I achieved a saturation point with 15 interviews despite
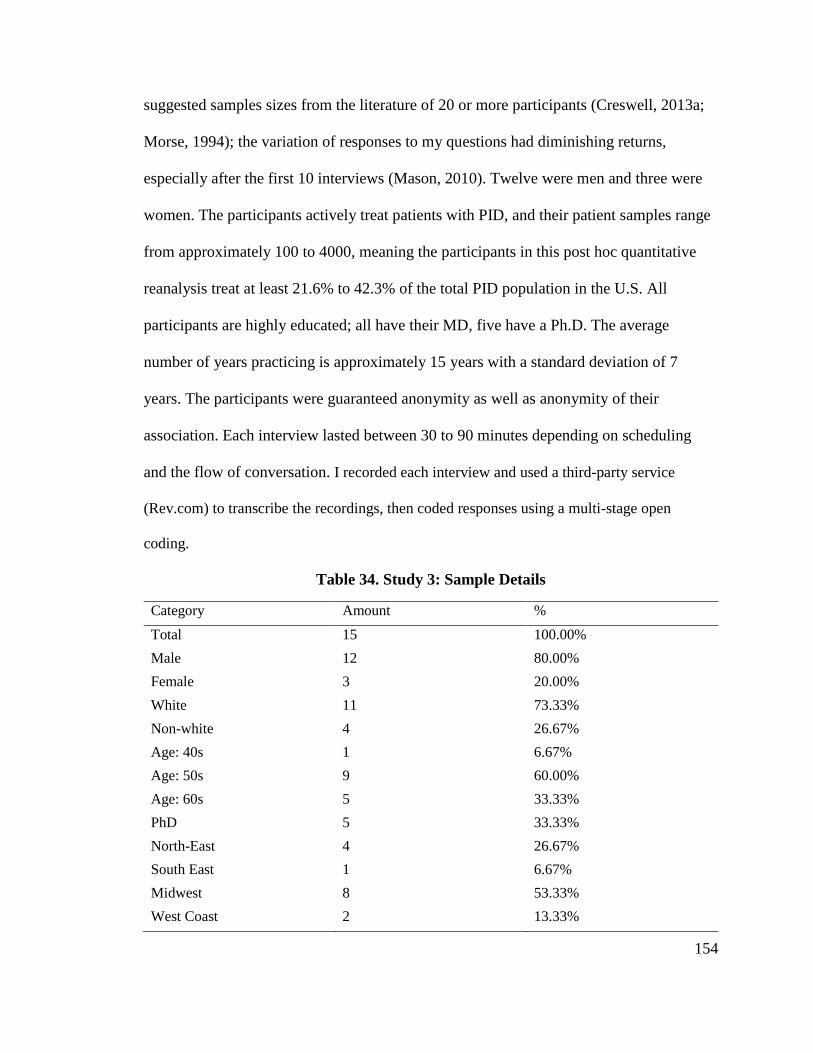
154
suggested samples sizes from the literature of 20 or more participants (Creswell, 2013a;
Morse, 1994); the variation of responses to my questions had diminishing returns,
especially after the first 10 interviews (Mason, 2010). Twelve were men and three were
women. The participants actively treat patients with PID, and their patient samples range
from approximately 100 to 4000, meaning the participants in this post hoc quantitative
reanalysis treat at least 21.6% to 42.3% of the total PID population in the U.S. All
participants are highly educated; all have their MD, five have a Ph.D. The average
number of years practicing is approximately 15 years with a standard deviation of 7
years. The participants were guaranteed anonymity as well as anonymity of their
association. Each interview lasted between 30 to 90 minutes depending on scheduling
and the flow of conversation. I recorded each interview and used a third-party service
(Rev.com) to transcribe the recordings, then coded responses using a multi-stage open
coding.
Table 34. Study 3: Sample Details
Category Amount %
Total 15 100.00%
Male 12 80.00%
Female 3 20.00%
White 11 73.33%
Non-white 4 26.67%
Age: 40s 1 6.67%
Age: 50s 9 60.00%
Age: 60s 5 33.33%
PhD 5 33.33%
North-East 4 26.67%
South East 1 6.67%
Midwest 8 53.33%
West Coast 2 13.33%
155
Reliability and validity issues were addressed based on Silverman’s guidance
(Silverman, 2015). To enhance reliability, the interview protocol was pilot tested (i.e.,
field-tested). A sample of three (3) healthcare professionals that treated PID (non-
specialists) assessed the clarity, appropriateness, and relevance of the interview
questions; revised interview protocols were created with the initial feedback. The
interviews were recorded and transcribed to ensure fidelity of the data. Exact quotes from
participants were used to state findings.
Using grounded theory as the analytic methodology to analyze the interview data,
1,389 initial codes were extracted. The coding involved primarily “identifying, analyzing
and reporting patterns (themes) within data” (p. 79) where the “a theme captures
something important about the data in relation to the research question and represents
some level of patterned response or meaning within the data set” (p. 82) (Braun &
Clarke, 2006). Codes were derived from participant's words and were added or modified
as necessary when new meanings or categories emerged. The subsequent phases
consolidated the raw data into five codes discussed in the findings section below.
Findings
The physicians interviewed acquired their knowledge and skills through a
combination of their education, training, experience, and the literature. This medical
background was similar to the hemophilia physicians in Study 1. Physicians provided an
insightful perspective to their decision-making process and potential factors that
influence their use of SDM.
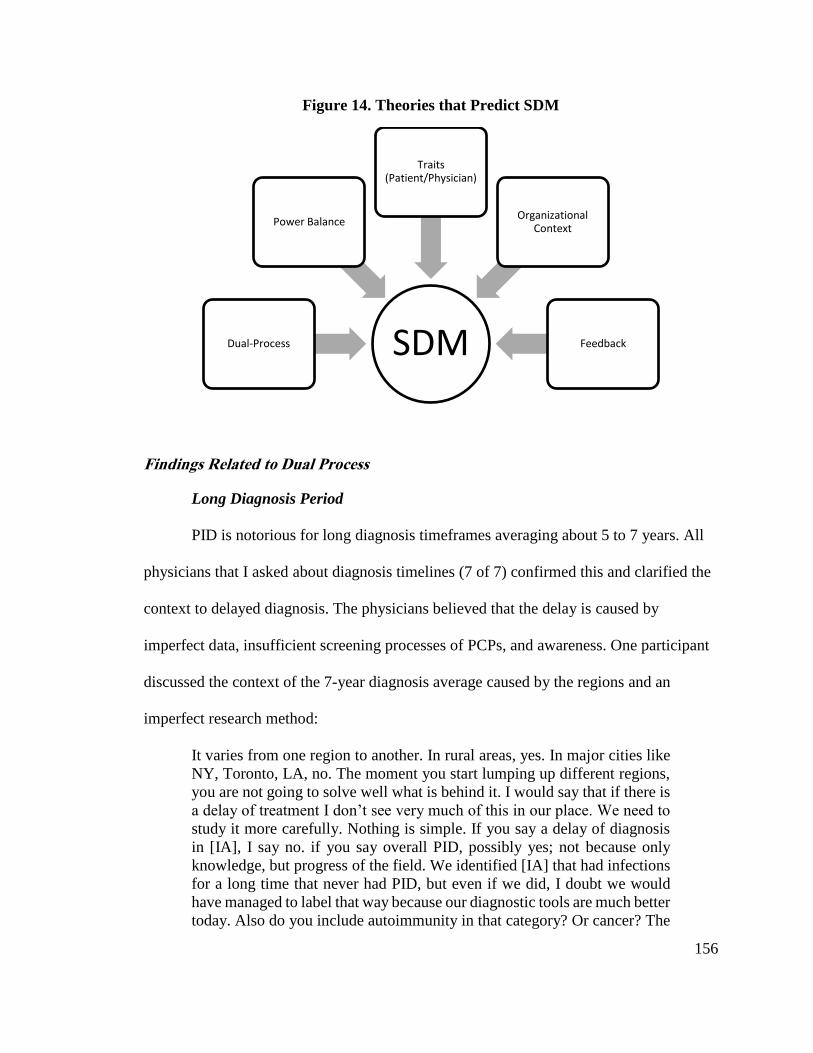
156
Figure 14. Theories that Predict SDM
Findings Related to Dual Process
Long Diagnosis Period
PID is notorious for long diagnosis timeframes averaging about 5 to 7 years. All
physicians that I asked about diagnosis timelines (7 of 7) confirmed this and clarified the
context to delayed diagnosis. The physicians believed that the delay is caused by
imperfect data, insufficient screening processes of PCPs, and awareness. One participant
discussed the context of the 7-year diagnosis average caused by the regions and an
imperfect research method:
It varies from one region to another. In rural areas, yes. In major cities like
NY, Toronto, LA, no. The moment you start lumping up different regions,
you are not going to solve well what is behind it. I would say that if there is
a delay of treatment I don’t see very much of this in our place. We need to
study it more carefully. Nothing is simple. If you say a delay of diagnosis
in [IA], I say no. if you say overall PID, possibly yes; not because only
knowledge, but progress of the field. We identified [IA] that had infections
for a long time that never had PID, but even if we did, I doubt we would
have managed to label that way because our diagnostic tools are much better
today. Also do you include autoimmunity in that category? Or cancer? The
SDMDual-Process
Power Balance
Traits (Patient/Physician)
Organizational Context
Feedback
157
delay in diagnosis for PID is hard for me to accept 7 years. It was a survey,
not a study. Part of pushing the enzyme issue. We all support it, but it is not
studied.
(CR)
Another participant believes the disease is overlooked in the primary care setting:
Often times that's because people don't get in to see a specialist in primary
immunodeficiency. I think that many patients who talk about these
diagnostic delays will talk about, "Oh, it was this breath of fresh air when I
got to see Dr. X." Well Dr. X was just somebody who's trained in this
process of true pattern recognition, and has the 90 minutes to go through
and do it, as opposed to community-based allergist that's trying to fit this
into an otherwise 20-patient workday. I also think that ... That's one reason
for diagnostic delay, getting to the true specialist. The other is that some of
these diagnoses do evolve over time, so that when you see someone at point
A, the laboratory tests may not necessarily have caught up to what their
history is, and some of that evolution does happen over time as well. So
those two reasons.
(JO)
Lastly, one participant believed the awareness of PID contributes to the delay:
I think, again, another kudos to the advocacy networks like Jeffrey Modell
Foundation, Immune Deficiency Foundation. I mean, they get the word out
to inform people and put placards up in airports, community areas that have
a lot of traffic, to tell people about these conditions. As physicians, we don't
do a good job of that. So people are becoming more aware. But I think
there's still an awareness gap. I do think patients are coming, and I've seen
it frequently. I mean, I just saw a patient who's 67 years old who actually
makes absolutely no antibody whatsoever; none whatsoever; makes no
antibody-producing cells; was actually diagnosed 35 years ago and put on
IgG replacement therapy, but then stopped due to faulty information, and
has been on antibiotics time, and time, and time again, essentially,
continually for 35 years. [How did they get to you?] She ended up seeing a
very good colleague in the community who was like, "Whoa, you've got a
big problem. You need to go to the center where they're used to taking care
of this." So they came over. Gave her her first infusion of IgG, and bridged
her with some antibiotics because she was sick, and then hopefully she's
going to do well. I think she's going to do quite well.
158
Rational/slow thinking
The physicians were more in favor of pattern recognition and experience than
evidence-based medicine. Although they expressed the importance of following the
literature for quality control purposes, they point out the inherent flaws of approaching
patients with a data-driven mindset; many study results are adequate for the population,
but not the individual.
I think that evidence-based medicine is, it's there to provide some type of
quality control and some type of guidance towards where we want to move.
But we always have to understand where evidence-based medicine comes
from. (BG)
I have a general idea of how much gamma globulin I want to give somebody
based on data but I can tell you that individual patients don't respond the
way the median response in a paper, so I can tell you that lots of people will
do fine with a gamma globulin replacement of about let's say 500 milligrams
per kilogram per month and there are other patients with exactly the same
kind of characteristics that may do fine with 400 and others who may need
1,000. (HL)
Bias and Nudging
The physicians were aware of their potential bias but knew there are some
situations where nudging the patient towards a certain treatment pathway is necessary.
For instance, on physician discussed the importance of using encouragement to help
patients choose treatments, rather than forcing options upon the patient:
I guess it's listening to the patient and offering things in a fair and objective
way. I think those are the most important factors. So if I can understand
someone and lay things out fairly and help guide them, 'cause I'm sure that
I'm biased with what I think is right, but I don't want to ever force someone
to do something, because I think it'll backfire. I'd rather encourage them and
tell them why I think they should do something and have them agree and
buy in, otherwise you don't get the compliance and outcome you want.
(RS)
Another physician described a more subtle approach to nudging patient decisions:
159
As a pediatrician, dealing with the issues, that what you did not want to have
is a scenario set up where anyone would perceive blame. So you don't want
the physician to be blamed for whatever is done, you don't want a parent,
either parent, to be blamed or feel blame. And so, what's done is a collective
decision making. Now there's sometimes when the cost of your medical
knowledge, you believe the decision should be in a certain direction. And if
the parent wants, or the patient wants, are counter to that, you try to use, for
want of better words, savvy psychology to help them understand why that
may be a preferred route to what they're thinking. Many people have mixed
perceptions of things or read testimonies that are incorrect because someone
has a grudge on one or the other. And so what you do is you lay out the
perspectives. If they're equally good, you don't add any bias to it.
(TH)
One participant acknowledges bias as inevitable. However, they believe that experience
helps mitigate the issue of bias:
I’m very sensitive to this issue. I would say if I’m unbiased, no way.
Everyone has their own ideas and experiences. Everyone is biased one way
or another. We try to present in an unbiased way. It is just human nature.
You just try and find the best way. I found that you get better over time in
dealing with being challenged by patients and ideas and being open to new
ideas. Experience gives you flexibility. I think it also has to do with egos as
well. I am definitely better than 25 years ago.
(CR)
Findings Related to SIT and Agency Theory
Power Balance
When asked about how their authority effects the patient, many (7/15) participants
stated that their authority is helpful and makes the interaction more comfortable for the
patient. They described the patients coming to them for advice, to validate their
experiences with a specialized and professional opinion.
I think when they come here to us, already they have the highest
expectations because either they can come here because they didn't get the
satisfactory treatment or approach elsewhere or they came here for unique
things we do for newborn screening, or they're just referred to us because
the other part didn't know what to do. (FS)
160
The physicians were open to SDM for treatment decisions, but not for the
diagnosis. In particular, the choice of treatment administration routes are a shared
decision to best fit the patient’s lifestyle.
I would, usually, emphasis to the patient that in order to progress along this
path of diagnosis to treatment, we need to do x, y, z. In order to understand
the problem more clearly. There isn't usually very much of a discussion
about the pro's and con's, and risk, benefit, cost, et cetera. Most of the time,
during that process. There are circumstances where, specifically, cost will
become an issue. (FB)
I mean sometimes somebody would say, "I want to try facilitated
subcutaneous, because I heard about it." That's fine. That's great. If their
insurance will let them have it, we'll get that for them. If somebody's on IV
and wants to go to subcu, that's great too. (JO)
Physicians are aware of the power balance. Some physicians try to mitigate any
intimidation by reading body language or maintaining a humble persona. However, they
try to keep a professional distance to maintain some power in the relationship for the
more difficult decisions.
That's an area that I've thought a lot about and kind of very conscious about,
so I never address an adult patient of mine by their first name, no matter,
I've known people for 30 years, I've gone to their kids' weddings or
whatever, I never ever ever address an adult patient of mine except as Mr.
or Mrs. or Ms. and I do it because I think I need to maintain a certain degree
of professional distance, maybe part of that is to protect myself but part of
that is there are certain times in a doctor-patient relationship when you have
to say to somebody, you have to give somebody bad news or you have to
say to them "I know this is what you want to do but I think this is really
wrong. (HL)
Health Literacy
The physicians mentioned how modern access to medical information is a double-
edged sword, meaning it can be beneficial or detrimental to SDM. To mitigate this risk,
many participants have taken steps to have literature, links, decision aids, and other
health information on-hand that they personally approve. One participant went as far as to
161
correct and manage Wikipedia pages to ensure their patients are exposed to the most
relevant information.
So, there are people who have read x, y, and z on the net and they may
consider themselves to be health literate but they're getting a lot of
misinformation which can really cause problems. Because now you've gotta
sort of undo what they've read and redirect them to what the actual reality
is of the treatment. (MR)
I think it's helpful; in general, I do. I think the internet is a great resource
for people. Problem is when they go to chat rooms and hear weird things
from different people, it means nothing. You have to use reputable sites, so
we actually give out our list of reputable sites for information on immune
deficiency for patients, so they can read at their leisure and look things up.
(RS)
The physicians often (7/15) mentioned that there are no guarantees of patient
compliance, despite their education and health literacy. Some participants used examples
of educated patients causing self-harm through non-compliance, whereas uneducated
compliant patients have better outcomes. Participant CCR stated, “In fact, sometimes
people who are very highly educated go out there and make up their own mind what they
want to do, and it was a pretty dumb decision.”
Patient networks are the personal and professional connections and programs that
assist in providing access to the information and care to the patient population. All
participants of this study praised the good that patient networks, especially those through
IDF and JMF, can provide. Some participants refer their patients to such networks as a
resource for the more personal needs; physicians sometimes do not have details regarding
daily life with chronic disorders.
I feel like those patients feel like they have a plan. That they can go and find
people ... I think humans, by nature, are herd animals. When they find like-
minded people that are going through the same thing, and they don't feel so
isolated, then you don't have the anxiety, depression, and all of the other
issues related to treating a child with a chronic disease or having a child
162
with a chronic disease. They can find like-minded people that have been
through the same things and can help them with the day-to-day things that
I don't necessarily have advice for because I don't live with it every day.
(LF)
Findings Related to Traits
Patient and physician traits provide inherent influence to the decision making
process. For instance, physicians approach patients as individuals or examples of the
disease (e.g. a patient with PID or a PID patient, respectively). Participant TH made this
distinction:
I think it's really good, but it's always keep telling them, take everything
with a grain of salt, because each patient is really their own individual
disease process. We look at each patient as their own individual experiment.
And so what's solely true for this other patient, and because you think the
symptoms are the same, there only telling you a fraction of the process. And
while that fraction may seem to match up, may not be the direction towards
getting the right answer type of thing. So it's very helpful, but it also helps
the patients to get guided to the right physicians to help with the thing. (TH)
Trust
Trust in the patient-physician relationship is built quickly or obtained immediately
for immunologists, rather than built over multiple visits. Some participants credited their
professional distance to the patient; usually by their formal or informal persona:
I think for my personality, and again, coming as a pediatrician, my patients
call me by my first name, and because their parents call me by my first
name, and so some of the kids will start calling me by my first name. And
I've never been pretentious about that issue, and never tried to correct people
on that. And so I think I come across, for myself, less intimidating, and so
there's a trust that builds up because I'm not trying to snow them, I'm not
trying to pull the wool over their eyes, I'm not trying to intimidate them, and
so I think happens is because they realize I'm well educated, many actually
want me to help more in the decision, not realizing that I'm psychologically
trying to help them in the process. They're actually wanting more of my
input. Even physicians I've dealt with. So I talk about the facts from a
specific patient they're dealing with, and we'll talk over the facts, talk over
163
the data. We'll talk over the different ways of potential faults of
management related issues. And then we're done, and this is what's good for
my position and what I do for providing consultative services. Then the
question comes back and says, they'll ask me, "Well what's your gut feeling?
What would you do?" And I'll say, "Okay, well let's see. That's very easy,
this is what I would do." He says, "Good, that's exactly what I was thinking
I wanted to do. And it always feels better to hear it from you.” (TH)
Other physicians recognize that some patients will try to take advantage of trust or need
to earn it depending on their intentions:
I use their noncompliance, or the dishonesty as evidence in a very
professional and transparent way, as to why I feel the way I feel, and then
I'm very clear that I'm going to document that this is my recommendation,
and they don't take it, that they're going against medical advice. That it's
their choice to go against medical advice, and if their child gets sick, they're
consequences for that. I'm very clear about that and because when you set
that expectation, in a patient that has good intentions, they will work with
you. They will understand that they have been at fault, but if their intentions
are good, and there's no secondary gain, then 9 times out of 10, they will
actually comply with you. When there is secondary gain, then I have
protected myself, and told them what the consequences would be and set
expectations. When they fail to meet my trust again, then I can take recourse
to protect the child. [What would be the secondary gain?] "My child is my
proxy-ish" kind of thing. I don't know. Parents like the attention. That's what
we consider secondary gain. For everybody, I don't know what that would
be. (LF)
Culture/Family
Cultural differences between the patient and physician influence the decision-
making process to take an alternative approach to care. One physician points out the
unique differences of many cultures such as Middle Eastern, African American, and
Hmong patients:
And so, for example, I've dealt with individuals from the Middle East, and
so one of the things we learn as being a pediatrician, obviously, is to make
contact with the individual. And so shake their hand, depending on the
severity of the process and things that are going on. Perhaps hold their hand
a while. Usually a mother, or a female, or the child type of thing for that.
Especially a child. Have them sit in your lap, you know younger children,
sit in your lap while you're doing all this and hold them, so that you reach
164
out. Some of the Middle Eastern cultures, you know, it's very offensive for
a male to touch a female, for example. And so you have to learn to know
that you can't use the same context for connecting. [Is that something you
just learned over time?] Part of that was learning, but part of it was also
when having interpreters and others that would help explain the cultural
differences on there. In the U.S., African American tends to be more
concerned about … So the African American, there is more distrust of the
healthcare system. With good reason for a variety of the things that have
occurred. And so you have to develop that trust from the very beginning,
and honesty from the very beginning on there. And establish the fact that
you recognize they're African American. You point out there's specific
items and issues that are more unique towards African Americans than to
Caucasian. And you, again, you create these, not boundaries, but openness
to that where you can generate that trust, you know?! That "I'm not gonna
be perpetrating on you things that are against your will, or that otherwise
would be harmful. That color of your skin is not a barrier to being able to
achieve the healthcare that you need." Hispanics, different cultural things.
This participant continued into an example of the decision-making process incorporating
entire families:
Hmong believe in a lot of tribalism. From Southeast Asia. Gypsies. Gypsies
are very interesting because of being sort of con artists in many of the things,
they're always very distrustful of anyone because they think everyone's
always out to get them. And usually, with the gypsies, you are in a room of
ten people, because they bring in the elders and everybody to all that.
Findings Related to Organizational Context
Coordination of Care
Many participants adopted the role of coordinator of the patient’s care because the
patient-physician relationships are often long-term when treating PID. These
immunologists, with a highly specialized knowledge-base, would assist in health-related
appointments that could have implications related to PID.
… I'm a pediatrician so there I'm much more of a coordinator, but the
continuity doesn't change, I think that's one of the really big things that we
offer in our clinic is from the time that I started and I was the junior person
with two people in the clinic, we decided the way we were going to operate
is that each of us was just going to take new patients, we would split them
up or whatever way it worked but once you had seen the patient that patient
165
was just going to be your patient and whenever they came into the clinic for
a follow-up, if it was my patient I would see that patient, if they were
admitted to the hospital, I would go to see them in the hospital. (HL)
Other physicians prefer not to be considered the coordinator, or a temporary coordinator
at most. Participant CCR was adamant about treatment roles between specialists:
…when it comes down to the therapy that I'm proposing; for example,
immunoglobulin, or gamma interferon, or Rituxan, or antibio, or anything
else, naturally, I'm going to coordinate and make that happen. I'm going to
make sure it happens. If it's a person who has a gastrointestinal condition,
it's not me. I'm not a gastrointestinal doctor. So I'm going to help them see
that other doctor. So I'm going to coordinate on one hand, and do continuity
on the other. Mine's continuity; the things that I have suggested. If I have to
send them to a rheumatologist, or to a pulmonary doctor, their pulmonary
hypertension, or their hematology, I have to send that person over to the
other quadrant for all of that. (CCR)
Rules related to Time
Most of the participants specified that they treat patients over a long period of
time (10/15) ranging from 10 years to a lifetime (5/15). Before receiving adequate
chronic care, which can take approximately five years, the participants compared their
meeting time with patients to the short appointments of primary care physicians.
Participant TH stated, “When I schedule patients, initial visit's an hour, an hour and a half
when I was doing outpatient, and the follow-ups were forty-five minutes to an hour
depending on the needs of things”. They emphasized the need for prolonged meetings to
explore the patient’s illness and lifestyle. The same participant drew concern to the state
of medicine today:
…in the ideal world, as I think you're eluding to, what we'd have are
primary care physicians that would be set up in a scenario where they would
not be having to see fifty patients a day, but be able to see twenty-five
patients a day. (TH)
166
Reimbursement
A common limitation of SDM is the reimbursement method; patients can only
afford a limited selection of treatment options. Physicians are constantly battling with
insurance companies regarding the treatment of chronic patients. Many have incorporated
strategies to “never lose” arguments with insurance, whereas others prefer to pick their
battles.
Yeah, I don't win all the time. The big issue is that the insurance companies
out there are not aware of what the evidence shows in the literature. Most
of the time what they do is they rely on "physician review" and these
physicians have absolutely no understanding of any particular field. …
Most of those cases get approved after a lot of fighting. Even then
sometimes insurance companies are like no we're not doing this. (IC)
Findings Related to Feedback
Performance Reviews
The physicians described the presence of feedback systems, but few found them
useful. One physician states the benefits of extended conversations with the patient,
which allows for direct feedback. This direct feedback increased patient confidence in the
physician:
I don't think I'm an intimidating presence. That's not my style at all. I mean,
I will tell somebody if I think they're making a bad decision, certainly. But,
I think because I really do try to make this a discussion, you know, a lot of
feedback from the patient. I think most of the time they tell me they feel
much more comfortable with the diagnosis, much more comfortable with
the treatment plan, because we've had this conversation. And I do get a lot
of referrals from people who come in and see me specifically. So, I think
they feel like they've talked to somebody who's got a lot of experience, a lot
of expertise. (MR)
However, most of the feedback is not useful or ignored. In most cases, the
feedback comes from the patients in the form of surveys, wherein patients motivated
enough to participate are often displeased with the physician; the conflict may be related
167
to their illness or irrelevant topics. One physician describes the system of feedback and
why they rarely view it anymore:
[Is there any systematic feedback?] There's not any systematic feedback.
Usually ... I've been fortunate enough that no one has lodged a complaint
against me where administration and patient advocacy have had to get
involved. I have gotten feedback when patients have said nice things to me,
nice things about me. I don't get consistent feedback and I think the only
consistent mechanism, by way that the hospital has the patients rate us is
through the Press Ganey surveys. After that incident where I had that
horrible review online, I have stopped googling myself. I'm a caretaker, I'm
a feeler. I take those things really personally because I don't want other
people, and other patients, who I take care of to read something like that
and then lose their trust in me because of something they read on the
internet. These last two years is a perfect example of seeing things on the
internet that aren't really true or not the full side of the story. They rely on
that too much… (LF)
Cost
One aspect of feedback that physicians are lacking is cost. Most physicians do not
have direct feedback regarding cost outcomes to treatment. One physician mentioned that
the insurance companies will occasionally inform them of costs.
[In the 300 patients that you have, is there any way that someone looks at
the cost of treating them over the course of the year and the outcomes? Is
there any way that someone says, "Wow, here's the 300th." And why not?]
You know, what I'll say is that there's no systematic way that is intentionally
done for my individual patients that gives me feedback. I do hear from
payers, from time to time, to say, "This patient on X asthma therapy," again,
not talking about immunodeficiency, but kind of an easier disorder to talk
about because there are just much more metrics in place to track quality and
so forth, "you might consider stepping them down from drug X to drug Y."
And I think that's based on guidelines. It's also based on cost. For sure.
There's no doubt. I mean, let's face it. We all get that. So there are some of
those things. There's also, even within our own system, like, our health plan
covers women and children who are of lower income. It's a medical
assistance, Medicaid-based payer. So we will get feedback on use of
expensive medications and lower-cost alternatives. There are some of those
things out there, but there is nothing that tracks, "Yeah, here's your 300
patients. 250 of them are optimally treated based on these outcome
measures. You're providing as cost-effective care as you can based on the
complexity level of the patient, available resources, et cetera" (NR)
168
Electronic Medical Records (EMR)
The physicians’ opinions are split regarding electronic medical records (EMRs).
One side praises their use for enabling better care coordination between physicians,
whereas the other side of the argument mentions the flaws such as accidentally nullifying
clinical trial participants. Every participant that discussed EMRs described benefits and
issues:
[Are electronic data records a good thing?] Oh yeah. I think so because I
can read everybody's notes. [Any downside to electronic records?]
Sometimes, you need to be careful what you really need to write. For
example, some of the patients, but we do sometimes research testing, of
course after getting consent, it's not ... But some other sub specialist that's
taking care of the same patient for another thing, they ... If parents tell that
to that doctor and they put it down, that's a problem because research data
cannot be in the medical records for clinical care. They happen to me a
couple of times which is difficult because then you have to addend. But, it's
not good to disappear completely. If the medical records wants to go back
and look at it, they can see it. It's going to go to the record that the other
provider will see, but it will be in the records see, there is no way you can
correct it or get rid of it. [In general terms of caring for the patient-] It makes
it very easy. (FS)
Cross-Referencing Findings from Post Hoc and QUAL Interviews
The findings of the post hoc and the QUAL interviews support each other.
Rational decision making increases participation indirectly through patient-centric care is
supported by interview responses. Of the participants, CCR was strictly rational decision
maker that did not incorporate a patient-centric approach. CCR “paternalistically”
dictated decisions for the patient and was adamant that patient lifestyle and care
coordination were not of primary concern; they had a “listen to me or go elsewhere”
perspective. On the other hand, all other participants (14/15) made an effort to coordinate,
manage, and incorporate patient input for treatment decisions; this supports the QUAN
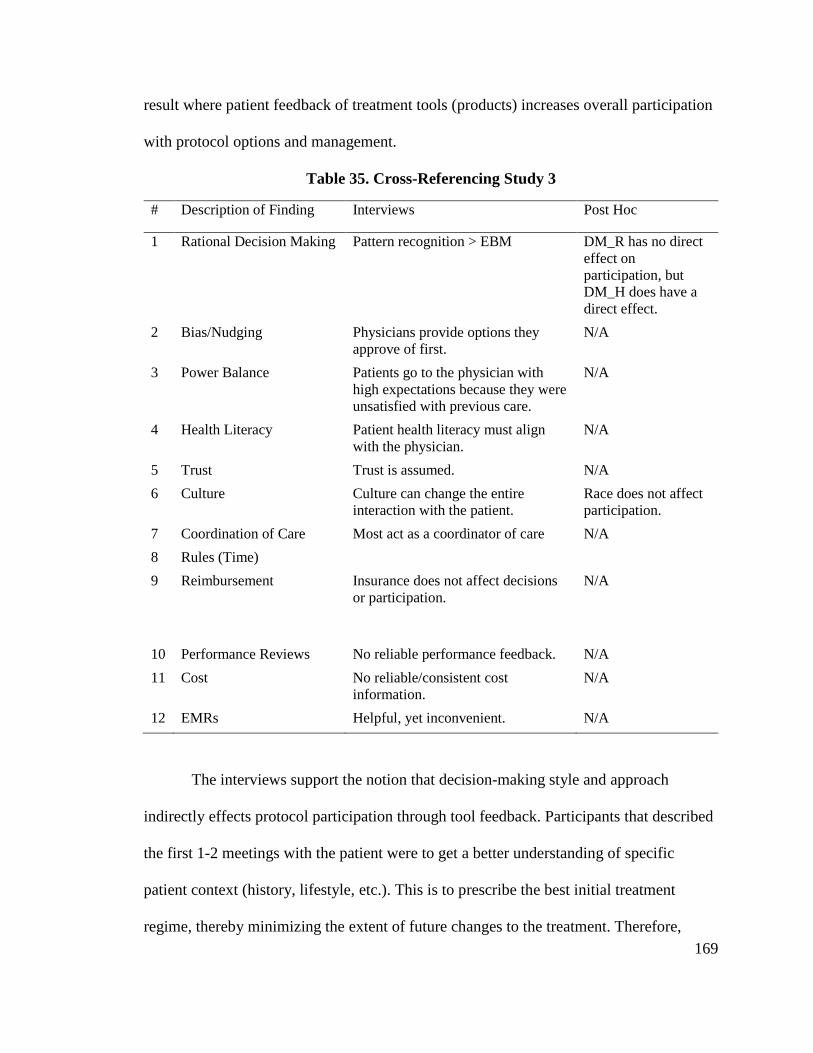
169
result where patient feedback of treatment tools (products) increases overall participation
with protocol options and management.
Table 35. Cross-Referencing Study 3
# Description of Finding Interviews Post Hoc
1 Rational Decision Making Pattern recognition > EBM DM_R has no direct
effect on
participation, but
DM_H does have a
direct effect.
2 Bias/Nudging Physicians provide options they
approve of first.
N/A
3 Power Balance Patients go to the physician with
high expectations because they were
unsatisfied with previous care.
N/A
4 Health Literacy Patient health literacy must align
with the physician.
N/A
5 Trust Trust is assumed. N/A
6 Culture Culture can change the entire
interaction with the patient.
Race does not affect
participation.
7 Coordination of Care Most act as a coordinator of care N/A
8 Rules (Time)
9 Reimbursement Insurance does not affect decisions
or participation.
N/A
10 Performance Reviews No reliable performance feedback. N/A
11 Cost No reliable/consistent cost
information.
N/A
12 EMRs Helpful, yet inconvenient. N/A
The interviews support the notion that decision-making style and approach
indirectly effects protocol participation through tool feedback. Participants that described
the first 1-2 meetings with the patient were to get a better understanding of specific
patient context (history, lifestyle, etc.). This is to prescribe the best initial treatment
regime, thereby minimizing the extent of future changes to the treatment. Therefore,
170
physicians with a patient-centric approach instigate patients to notify their physician of
the treatment efficacy (tool feedback). Furthermore, this reinforces the influence of
timing in the physician-patient relationship and how it applies to SDM; SDM is likely
most implemented in the earlier segment of the physician-patient relationship because
initial treatment is an educated guess, then refined to the patient.
Discussion
According to the findings above, physicians likely implement SDM under a set of
conditions. In other words, SDM is bounded. The physicians treat SDM similarly to the
“nudges” described in Sunstein and Thaler (2008). Nudges are the subtle suggestions in
the decision process; methods or strategies to compel limited responses. Daniel
Kahneman describes nudges as “explicitly paternalistic” because they set the “choice
architecture” (Kahneman, 2017); choice architecture means to set predetermined options.
In the case of SDM, physicians have a set of requirements to meet before
considering shared decisions with the patient. From the findings, there are four (4) main
requirements with subcategories: patient characteristics, organizational context, power
balance, and dual process. Treatment evidence refers to evidence-based medicine and the
proven treatment methods to help the patient. Power balance refers to the interactions
between the physician and patient; an imbalance could lead to patients being non-
compliant or fired in some cases, whereas others might avoid participating because of the
burden of decision-making. The system context refers to factors such as 3rd party payers;
most patients can only afford the treatment that their insurance covers. This category also
includes factors such as regulations and organizational protocols, but this I did not
explore these extensively in this study. The patient characteristics refers to factors such as
171
their health literacy and their alignment with the physicians. Patient alignment was a
consistent necessity with the participants in particular. Physicians would only implement
SDM when the patient knowledge is backed by information the physician approves.
The literature universally praises the potential benefits of SDM for being a
patient-centric approach to care that is best used for the care of chronic conditions.
However, the results suggest that SDM is parallel to nudges. Each physician has their
personal thresholds to implementing SDM. For some of these thresholds, the physicians
try to encourage particular choices such as having decision aids available for patient
learning. Therefore, contrary to the literature, paternalism is not obsolete but has shifted
to satisfy the patient-centric movement of the last 30 years.
This finding may also suggest there is an influence of time in the patient-
physician relationship. Although this study and its survey did not account for which visit
these answers are referring to (i.e., first, second, third visit, etc.), it is possible that the
immunologist sample responded to the survey items based on experiences from different
patient visits.
Limitations, Implications, and Future Research
Although I attempted to address the limitations of the first and second studies, I
acknowledge the possibility of recurring limitations. One limitation of the third study was
the lack of a demographically diverse sample of participants. Future research should
address this issue by attempting to recruit participants in a larger range of demographic
characteristics, despite the possibility that this sample accurately represents the
population of immunologists.
172
Another limitation is that the sample was selected based on availability rather than
randomized participants, thereby exposing the study to potential bias. Except for one
participant, most physicians interviewed had more than 10 years of experience in their
specialty. To overcome this limitation, future research must incorporate larger samples
with a random selection process.
Understanding physician perspectives of SDM and the encouraging factors has
practical implications for the care of patients with chronic illnesses. Therefore, leaders
and departments responsible for setting treatment policies—such as hospital standards or
insurance reimbursement policies—would benefit to encourage SDM. Forming an
environment which allows SDM can lead to better treatment and cost outcomes in the
long-term because of the known benefits of SDM (Arterburn et al., 2012; Légaré &
Witteman, 2013).
In summary, the third study offers a more refined analysis of physician decision-
making regarding chronic conditions. It expanded upon previous findings by discovering
that SDM is bounded by factors such as time, patient characteristics, system context,
power balance, and evidence. It addressed some limitations of the first and second studies
by taking physician workplace into consideration. In the next chapter, I integrate all three
studies to provide a more robust set of results with fewer limitations.
173
CHAPTER 8: INTEGRATIVE FRAMEWORK
Mixed methodologies must reconcile two standards, quantitative and qualitative,
to assess the validity and credibility of the results. An integrative framework was needed
to make meta-inferences about the SDM phenomenon beyond what each method can
explain alone (Tashakkori & Teddlie, 2008). Inferences are used to make interpretations
using a process of both interpreting findings and conclusions related to the research
question. The quality of the inferences should support the transferability of the
conclusions to other chronic disorders.
In chapter 4, an integrated framework of physician decision making for chronic
diseases was proposed. The decision-making process was described as slow or rational
(dual process) with potential for bias and nudging. Other hypothesized influences
included physician and patient traits, power imbalances, and organizational context
(Table 18). This framework has been revised based on the findings. Specifically,
influences related to organizational policy and feedback have been removed because they
were not significant or pursued; therefore, future research is necessary on these
influences.
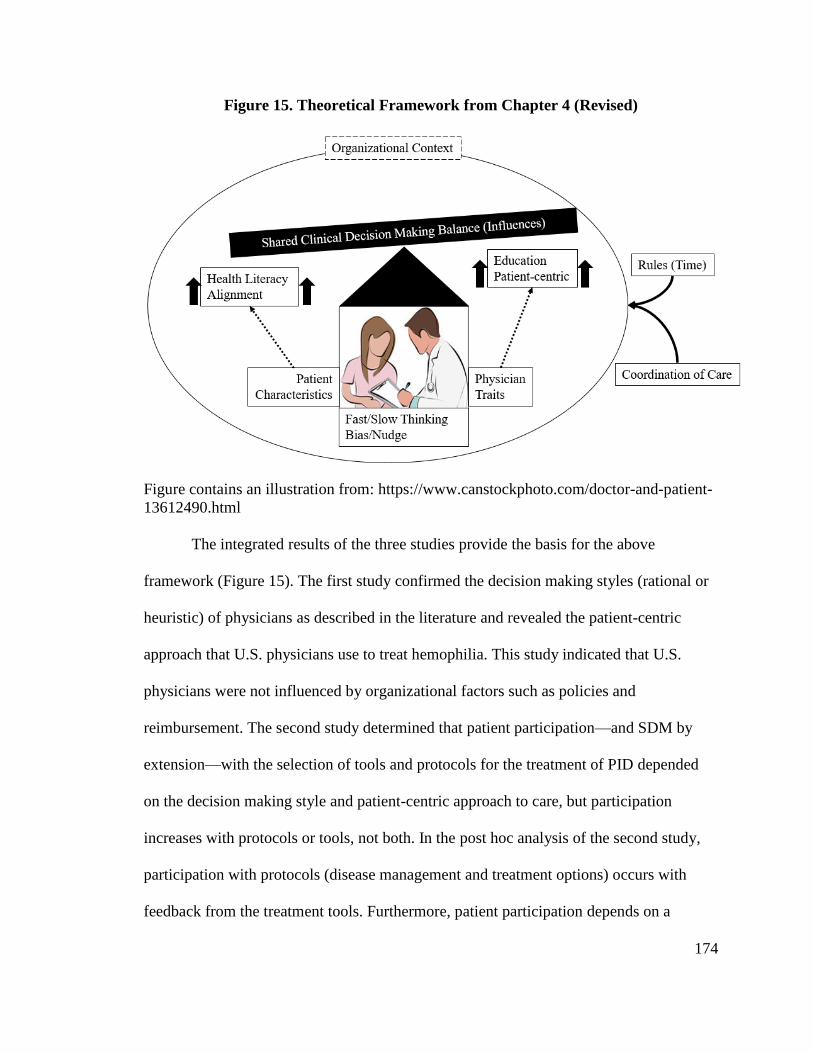
174
Figure 15. Theoretical Framework from Chapter 4 (Revised)
Figure contains an illustration from: https://www.canstockphoto.com/doctor-and-patient-
13612490.html
The integrated results of the three studies provide the basis for the above
framework (Figure 15). The first study confirmed the decision making styles (rational or
heuristic) of physicians as described in the literature and revealed the patient-centric
approach that U.S. physicians use to treat hemophilia. This study indicated that U.S.
physicians were not influenced by organizational factors such as policies and
reimbursement. The second study determined that patient participation—and SDM by
extension—with the selection of tools and protocols for the treatment of PID depended
on the decision making style and patient-centric approach to care, but participation
increases with protocols or tools, not both. In the post hoc analysis of the second study,
participation with protocols (disease management and treatment options) occurs with
feedback from the treatment tools. Furthermore, patient participation depends on a
175
rational decision-making style mediated through a patient-centric approach. The third
study provided context for when physicians implement SDM. It reinforces the influence
of rational decision making and organizational context related to time and coordination of
care.
This chapter describes the meta-inferences that emerged from the mixed methods
study which included results from 370 physicians who treat two complex chronic
diseases: hemophilia and PID. As described in Chapter 4, Research Design, these meta-
inferences provide a more complete picture of physician influence on SDM which is
more meaningful than each of the components.
Meta-inferences
This section will cover 7 meta-inferences that emerge from the multiphase mixed
methods research. Meta-inferences are “an overall conclusion, explanation or
understanding developed through an integration of the inferences obtained from the
qualitative and quantitative strands of a mixed method study” (Tashakkori & Teddlie,
2008). The purpose of these meta-inferences is to achieve a more comprehensive
understanding of what predicts physician implementation of SDM. The meta-inferences
include:
1. Rational decision making
2. Patient Centrism
3. Bias/Nudging
4. Organizational Context
5. Feedback
6. Traits
7. Power
176
Rational Decision Making
In each study, I used dual process theory to explain the physician decision
process; it partially describes the physician decision process. However, in each study, I
observe the clear reliance on rational decision making (System 2) over heuristic decision
making (System 1). Specifically, rational decision making is prioritized when the disease
is categorized as complex; hemophilia with inhibitors and PID (in general) are complex
chronic diseases. In the first study, the physicians made a transition from intuitive to
rational decision making as patient complexity increased, (i.e., if inhibitors developed);
they would consider which treatment options are best to remove the inhibitor issue.
Although heuristic decision making appeared equally significant to rational (if not better)
in the second study, the post hoc analysis found the in the population of immunologists,
rational decision making was dominant. This was further confirmed in the third study
wherein the participants all investigated the patient’s full history, especially in the initial
meetings.
Patient-Centrism
Across all studies, physicians with a patient-centric approach to care encourage
patient participation in treatment decisions. To clarify, this does not mean physicians let
patients help them diagnose the problem, but that physicians will take patient values and
preferences into consideration for treatment protocols and tools. In the post hoc, patient-
centric approaches to care reverses the negative relationship between rational decision
making and feedback with tools; meaning, physicians with a rational decision-making
style normally do not incorporate feedback, but will if they use a patient-centric approach
to providing care. A similar observation is in the third study, wherein all the physicians
177
were rational decision makers, but only a few maintained a paternalistic (non-patient-
centric) approach. As described in Chapter 6, these participants adopt an approach where
the patient accepts their decisions or gets treatment elsewhere.
Another pattern concerning patient-centrism is the mediating role it plays in
SDM. Patient participation occurs when (not “if”) the physician is patient-centric,
meaning SDM requires certain conditions to be met before implementation. The
qualitative studies reveal that a patient-centric approach to care was required for SDM to
occur because physicians dictate treatment if they did not attempt to incorporate patient
input. On the other hand, the quantitative analyses show patient-centric care to partially
mediate decision-making style and patient participation.
Traits
Physician traits did not seem to affect decisions throughout my research. In the
first study, all the physicians had similar approaches to care and patients. Although a few
outlier cases involved individuals of extraordinary expertise, they also had the similar
rational decision-making style with a patient-centric approach. The second study suggests
a few significant factors such as age and gender but these were disproven by the post hoc
analysis. Furthermore, the third study did not show differences in immunologist decisions
based on traits, either. However, these studies did not investigate physician SDM with
minority groups.
Trust was a recurring theme in the qualitative studies. In the qualitative studies,
trust was considered to be assumed or built very quickly. Based on how the physicians
described it, trust also acted as a condition for physicians to treat patients, let alone
incorporate SDM. In some cases, the physician had to “fire the patient” because certain
178
patients were non-compliant and uncooperative in providing crucial information (i.e.,
stopping treatment because X). However, when tested as a moderator in the second study,
there was no significance. This likely occurred because trust is assumed, not earned over
time. Furthermore, the patients often go to these specialists as a “last hope,” which likely
results in immediate trust.
Bias/Nudging
Throughout the qualitative studies, there are hints of nudging and bias in the
decision making process. Especially in the physician with Ph.D.s, the physician would
passionately advise and push for the treatments they prescribe. In the case of patients,
they all provide the information to the patient with the good news first, therefore priming
them to the preferred option. This adamant perspective extends to disputes with insurance
companies, wherein the physicians would fight insurance to reimburse the patient for
products the physician specifically asked for.
Organizational Context
There multiple meta-inferences related to organizational context: feedback and
reimbursement. Physicians aim to provide the best treatment on the first try, but often
need to revise based on feedback. In the first study, patients need different infusion rates
and products depending on their lifestyles and physical response to the product. If the
patient develops an inhibitor, the physician must reconsider the treatment. In the third
study, the immunologists often referred to themselves as coordinators of care. After the
extensive initial meetings, they would consistently monitor the patient and adjust the
treatment similar to hemophilia. This is also similar to the post hoc, wherein participation
with protocol options and management depended on patient feedback of tools; without
179
feedback, the physician does not need to change anything. Furthermore, the structure of
the relationships better explains patient participation because the explained variance was
about 0.25, whereas the second study was less than 0.15. In the post hoc, the relationship
between physician decision making and participation with protocols was better explained
indirectly through tool feedback. The patients providing feedback about the product
encouraged participation with decisions regarding their disease management and
treatment options.
The minimal cost feedback might relate to the minimal influence of insurance
companies. Across both qualitative studies, these specialized physicians fight insurance
companies to cover treatment costs if the pre-approved treatments do not match the
physicians’ decisions. This is not to say every case requires the physician to contest the
insurance company options; physicians will agree with the insurance option if it is
acceptable for the patient and interchangeable to that the physician preferred. If conflict
arises, the physicians all stated that they would win. Therefore, contrary to expectations
of U.S. physicians, the influence of insurance companies is minimal to non-existent.
Implications for Practitioners
This research study started with the question: what predicts physician
implementation of SDM. Using four theoretical frames, numerous findings and meta-
inferences were identified. These results have potential for healthcare practitioners to
design a better U.S. system to improve cost-effective care.
1. SDM for chronic care requires slow thinking with a patient-centric approach.
Reimbursement should support this cognitive method of thinking. Currently,
reimbursement is either fee for service, meaning billing for a visit or a test, or
180
a quality of care measure such as hospital readmissions. Greater time should
be allowed for physician-patient interaction and physicians should be paid for
this increased effort.
2. Physicians should know the cost of treating their chronic care patients. Most
hemophilia and PID doctors are specialists who treat many patients—often
dozens or hundreds. Physicians should know the cost of treating these
patients, the mean, median and range. Physicians should also have more user-
friendly electronic records which allow outcomes comparisons with their
treatment cohort. Having cost and outcomes data will allow physicians to
know the cost-effective impact of their care. Incentives can then be used to
improve cost-effective care.
3. Feedback is important. Currently, physicians do not have any formal feedback
from patients on the extent to which patients are satisfied with their
participation in the care.
4. Combining #2 and #3 above, a system which provides physicians both cost
and quality data would provide the basis for improving overall care. Such a
system could benchmark physicians.
5. The U.S. should create patient registries similar to what is done in the U.K.
This will provide national cost and outcomes data. Physicians can then be
provided with comparisons between national and local practice. This can be
used as a way to benchmark care and incentives for improvement.
6. SDM is about physician–patient interaction regarding protocols and tool
feedback. Very few physicians dictate the specific tools to be used. Therefore,
181
creating large tenders which reduce drug cost will not hinder SDM and
provide substantial system savings.
7. Coordination of care is imperative for chronic care. Defining the role of
primary care physicians and specialists is needed to provide comprehensive
treatment.
8. Health literacy is less about educating patients than it is about aligning patient
and physician understanding. Developing consistent tools which facilitate this
alignment is necessary for patient compliance. Decision aids should be
developed for hemophilia and PID to facilitate this alignment.
9. Nudging has been demonstrated to work in a variety of contexts such as
retirement planning. The role of nudging for chronic care should be
acknowledged and optimized.
10. Physician-patient health literacy alignment and nudging will likely result in a
“soft paternalism.” The concept of SDM should be revised to better define
sharing.
The results from the three studies considered in the context of the actual quality
gaps presented in Chapter 3. This analysis from several public databases on patient and
hospitalization records show:
1. 30-43% of all households give poor ratings of quality indices. Fifty-three
percent of the hemophilia and PID patients gave poor ratings on quality
indices.
2. Hospitalizations can be used as a measure of poor diagnosis and treatment.
While there has been a substantial improvement in the number. Diagnosed
182
patients hospitalized due to hemophilia and PID, the associated cost is
estimated to be around $3 billion. There is also a cost associated with
undiagnosed PID patients which is estimated to be between $3.5 and $7.7
billion. The total cost of hospitalizations is between $7 and $10 billion.
3. Given that product/tool choice is not a factor in shared decision making,
national wide tenders such as those organized by the U.K. could reduce the
cost of treatment of hemophilia and PID by up to $3 billion.
When combining the results of the analysis of patient/medical claims and
interview with physicians, there is a substantial opportunity to improve quality and
reduce cost. Quality can be improved by improving patient feedback on defined metrics
such as listening, respect, and time. Cost can be measured by looking at unnecessary
hospitalizations. Using slow thinking for the diagnosis and treatment is likely important
to achieve improvement in care and start to close the quality chasm in the U.S.
183
CHAPTER 9: DISCUSSION, IMPLICATIONS, LIMITATIONS, AND
CONTRIBUTIONS
Often medical care is viewed from the lens of acute hospital inpatients in which
informed consent and EBM are most applicable. Most medical care is now related to
chronic disorders where the setting requires a more active patient and a longer window to
make decisions. Adaption of SDM to chronic care is necessary to facilitate a patient-
physician partnership “to muster trust and mutual respect: and “create an environment
conducive to successful patient self –management” advocates for SDM believe that
chronic care requires a certain level of knowledge by the patient, a trusting relationship
with the physician and mutual engagement in setting goals based on values and
preferences Intimate engagement with patients with chronic disorders is necessary to
achieve decisions which are most advantageous to their health. SDM is a radical
departure from traditional medicine and the means through which it can be accomplished
has not been adequately understood. Once understood, the optimal choice decision
architecture can be designed to improve cost-effective care.
The results from this research reveal several important factors that influence the
adoption of SDM and how these factors can be optimized for chronic care management.
It is clear that rational decision making (System 2 thinking) as predicted by dual process
theory is important to achieve SDM, particularly with patients with complex (multiple
co-morbidities) chronic diseases. In addition, the role of health literacy, networks, EBM,
and reimbursement is more constrained than what has been reported in the literature.
Given these findings we can now better understand why some healthcare systems such as
ChenMed and CareMore are showing dramatic success and how some organizational and
184
behavioral changes can be applied more broadly to help cross the U.S. healthcare quality
chasm and build a long-term sustainable system with SDM at its core design principal
(Hathi & Kocher, 2017; Hostetter et al., 2017; Tanio, 2014). However, the impact of how
information is anchored in the decision-making process needs further research.
Theory
The most significant contribution from this research is the extension of dual
process theory as a method of analyzing the physician decision process for the treatment
of PID. All three confirmed relevance of dual process theory to examining the physician
decision process in the context of chronic health issues. However, we can learn from
other theories as well.
Nudging and libertarian paternalism are subtle methods of encouraging, not
dictating, patient choice and are present in throughout my research and the literature
(Loewenstein & Chater, 2017; Schiavone et al., 2014; Sunstein & Thaler, 2008). The
physicians would make suggested treatment options and supplemental literature for
patients, yet acknowledge the patient makes the decision (Aggarwal et al., 2014).
Status, as predicted by SIT, is relevant and health literacy as predicted by Agency
Theory is needed to balance power. Treat theory also has a contribution: certain physician
and patient traits influence SDM. Organizational context also matters. It is the integration
of all four that provides an overall framework.
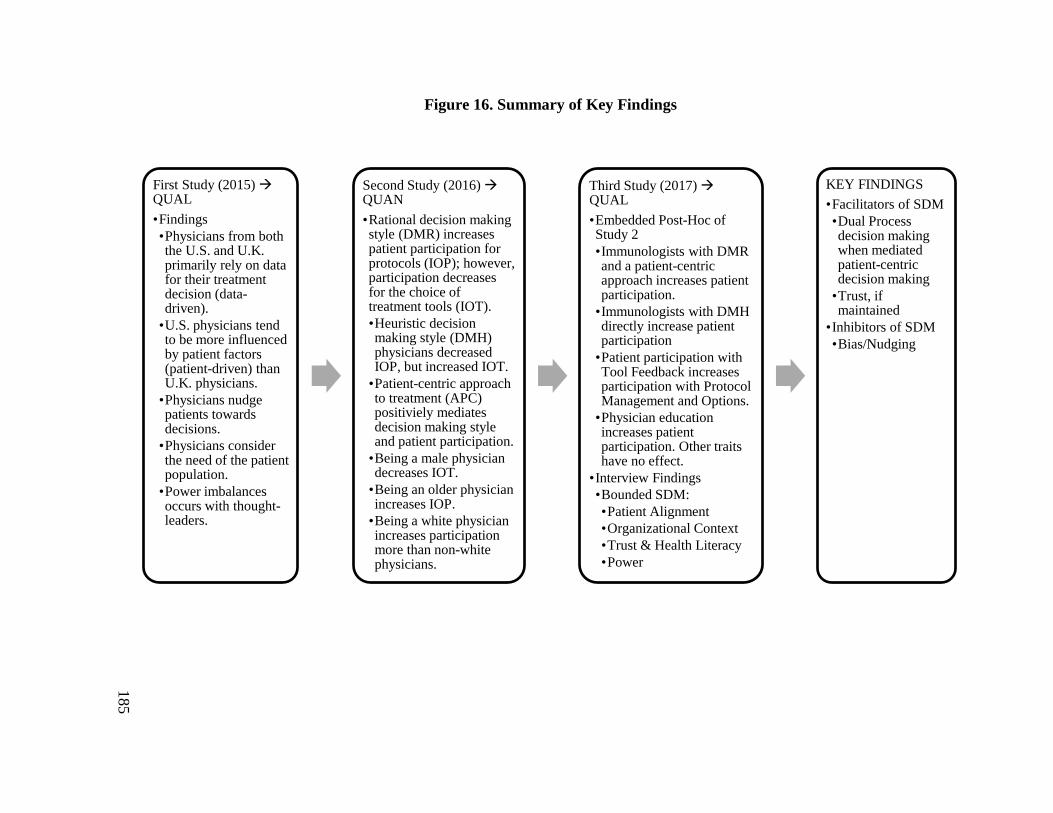
185
Figure 16. Summary of Key Findings
First Study (2015) QUAL
•Findings
•Physicians from both the U.S. and U.K. primarily rely on data for their treatment decision (data-driven).
•U.S. physicians tend to be more influenced by patient factors (patient-driven) than U.K. physicians.
•Physicians nudge patients towards decisions.
•Physicians consider the need of the patient population.
•Power imbalances occurs with thought-leaders.
Second Study (2016) QUAN
•Rational decision making style (DMR) increases patient participation for protocols (IOP); however, participation decreases for the choice of treatment tools (IOT).
•Heuristic decision making style (DMH) physicians decreased IOP, but increased IOT.
•Patient-centric approach to treatment (APC) positiviely mediates decision making style and patient participation.
•Being a male physician decreases IOT.
•Being an older physician increases IOP.
•Being a white physician increases participation more than non-white physicians.
Third Study (2017) QUAL
•Embedded Post-Hoc of Study 2
•Immunologists with DMR and a patient-centric approach increases patient participation.
•Immunologists with DMH directly increase patient participation
•Patient participation with Tool Feedback increases participation with Protocol Management and Options.
•Physician education increases patient participation. Other traits have no effect.
•Interview Findings
•Bounded SDM:
•Patient Alignment
•Organizational Context
•Trust & Health Literacy
•Power
KEY FINDINGS
•Facilitators of SDM
•Dual Process decision making when mediated patient-centric decision making
•Trust, if maintained
•Inhibitors of SDM
•Bias/Nudging
186
Practice
The findings of this study suggest the need for the development and refinement of
treatment decision aids for diagnostic procedures and recommended treatment protocols.
To our knowledge, there are no decision aids specifically for hemophilia or PID.
Decision aids would assist physicians and patients in deciding on the optimal treatment
approach; providing optimal and timely care benefits the patient both financially and
physically (Modell et al., 2011). Improving decision approaches would help physicians
and patients correctly diagnose root issues quicker, which would significantly reduce the
economic burden of misdiagnosed chronic health conditions (Modell et al., 2011).
Additionally, this paper may help physicians develop a more nuanced
understanding of their own decision-making process. Some may conduct a self-analysis
to improve or understand how they approach patient treatment and may decide to
incorporate patient participation to a greater degree. Of particular importance is the role
of nudging and to what extent it is transparently being used to facilitate decisions that are
advantageous to patient health and are consistent with SDM. Patient literacy is necessary
for decision alignment and must be sufficient such that nudging does not become another
form of paternalism.
System issues related to coordination of care and feedback need to be
implemented. Chronic care is not a dyad but a team of healthcare providers that must be
coordinated to execute SDM. Meaningful feedback loops are needed that will guide
physician in constructive ways to improve SDM behavior.
187
Other Research Domains
The application and benefits of SDM are not restricted to the treatment of
hemophilia and PID. The studies could be used as a template for additional research into
other chronic conditions. The results of the first study suggest that many U.S. physicians
treating hemophilia and PID are implementing SDM; they work with each patient to
develop individualized treatment plans that accommodate treatment to the patient’s
lifestyle. The second and third study focused on enhancing physician approaches to
chronic care with SDM; therefore, the research design is likely applicable to more
common chronic diseases such as cancer. If similar outcomes can be generalized to
chronic care (i.e., from arthritis to cancer), SDM could be the first step to improving cost-
effective care in the U.S., perhaps matching those of other OCED countries.
The application of SDM can be utilized in other professional relationships. For
instance, a lawyer and client have a similar relationship, wherein the lawyer is a
professional coordinating with the client to address legal issues. Future research can
expand into various similar contexts involving professional gaps.
Limitations
The three studies involved physicians that treat hemophilia and PID; the
specialties are unique with different issues of complexity. Therefore, the results may not
be generalizable to other chronic diseases. In addition, the analysis of quality and cost of
care for hemophilia and PID is limited to published findings.
Qualitative data relies on the use of small non-randomized samples with limited
demographic diversity. The grounded theory process mitigates these limitations,
particularly interviewing participants until saturation. The quantitative studies relied on a
188
one-time survey which had a low response rate and poor distribution of certain traits (sex
and traits). Accepted statistical techniques were used to derive meaningful results which,
although not perfect, allowed for statistically significant correlations. Mixed method rigor
was addressed by using consistent research methods for each study, consistent reference
to published research, and matching the results to similar research questions addressed in
all three studies. This research was further augmented by an analysis of patient and
hospitalization data which show substantial quality gaps and significant opportunity for
improvement.
Another limitation is the inherent meaning of shared decision making. All
participants claim to implement SDM to some extent, but the reality is different when
probing for contextual insight. Physicians are often making the decisions via nudges and
prefer aligned, compliant patients over health literate patients. However, there are some
cases where the physician wants to mitigate the risk of losing patients listening too much.
Furthermore, the definition of health literacy was not clearly defined before the research.
The degree to which each physician considers the patient as health literate greatly varied.
The quality of the information available to the patient and their ability to interpret data
also effects what can be defined as health literate.
The issues of cost and quality are a system-wide, complex problem that cannot be
solved with SDM alone. It is also focused on chronic illness and has limited application
to acute care. The impact of SDM also varies from different chronic issues; patients with
PID will have different interactions with the physicians than stroke victims.
189
Conclusion
“Nothing without us” is a frequent rallying cry by patient communities seeking
broader involvement within the healthcare system (Chu et al., 2016). As the paternalistic
approach to chronic care has lost relevance, we continue to explore influences and
barriers to SDM from the physician perspective. In our first study, we found that
physicians are willing to work with patients in forming treatment regimens that are
supported by patient-centered care using slow decision making. The second study
provided an initial picture of the application of dual process theory to the physician
decision process and some factors directly affecting patient participation. However,
neither of these studies provided a clear and complete image of the physician decision
process and the factors that influence the adoption of SDM. The third study expanded the
initial research and provided a more complete picture of SDM. The integrated results
identified significant influences on physician decision-making styles and attain a deeper
understanding of their contributions to the physician decision process. Adopting the
mixed-methods approach formed an integrated theoretical framework that may become a
new way to help implement SDM. An attempt was made to quantify the quality and cost
gaps associated with poor diagnosis and treatment which significant opportunities for
improvement. Expanding this research from individual physician-patient relationships
treating hemophilia and PID to other chronic disease categories may help healthcare to
cross the quality chasm in the U.S.
190
Appendix A: Study 1 Interview Protocol and Questions
1. Introduction and Explanation—read to the interviewee before proceeding
a. Greeting “Hello [name of participant]. Thank you for taking the time to
meet with me today. Your participation is greatly appreciated. Before
getting started, there are a couple things I would like to cover.”
b. Purpose and Format of Interview “As a current student in the Case
Western Reserve University Doctor of Management (DM) program, I am
interested in developing a greater understanding of the factors that
influence physician decision making for the treatment and management of
hemophilia. I will ask you a series of open-ended questions on this topic,
and I will ask one or more follow-up questions as you respond. The
interview will last approximately 60 to 90 minutes.”
c. Confidentiality “Everything you share in this interview will be kept in
strictest confidence, and your comments will be transcribed
anonymously—omitting your name, anyone else you refer to in this
interview, as well as the name of your current organization and/or past
organizations. Your interview responses will be included with all the other
interviews I conduct.”
d. Recording “To help me capture your responses accurately and without
being overly distracting by taking notes, I would like to record our
conversation with your permission. Again, your responses will be kept
confidential. If at any time, you are uncomfortable with this interview,
please let me know and I will turn the recorder off.”
e. “Do you have any questions before we begin?”
Introduction
1. Name
2. Education
3. Current job title and responsibilities
4. Years of practice
5. Involved with research (clinical or otherwise)
191
6. Practice setting/site of care (multiple?)
7. What is the average length of time with the patient?
8. Most have co-morbidities?
Focus in on factors that determine how you make decisions
1. Describe a typical patient
a. How do they get to you?
b. Diagnosis to treatment to maintenance
2. Describe the types of decisions you make?
a. SC vs IV
3. Do you use decision aids (describe/evidence-based?)
4. Do you find that your patients are educated or well educated on self-
management?
a. High levels of self-efficacy (I am confident I can manage my situation)
b. High levers of self-activation
c. Do you think more informed patients result in fewer health resources
and better outcomes?
d. Are you patients actively involved in patient networks (IDF, JMF,
internet networks such as patients-like-me)?
e. Do you have a patient portal where patients can review their health
history?
5. What seeing a patient: look for patterns that match past experience?
a. Tend to quickly assess symptoms and diagnosis or it it’s a slow
painstaking process that has lots of complexities (particularly with co-
morbidities)
b. Tend to spend more time on protocol or treatment
c. Would you describe yourself as patient-centric or evidence centric
(EBM)?
6. If you were to guess: do you as the physician make the final treatment
decision or leave it up to the patient
192
a. Protocols
b. Drugs
7. Does your DM style vary based on the patients’ level of understanding and
interest?
a. Does it vary based on complexity or uncertainty?
8. Do you think your status as a physician or authority figure influences how
patients respond to you in a clinical setting?
a. Is Intimidated or encouraged to share information or
b. More likely to tell you their treatment preferences or express an option
on treatment options?
9. Do you routinely ask about patient preferences: lifestyle and how treatment
will affect patient goals and values?
10. When discussing pros and cons of a potential treatment (protocol or drugs) do
you tend to lead with the pros or cons
11. How much and in what way do cost or reimbursement influence your decision
making
a. Protocol
b. Drug
12. Do patients want to play an active role in their decisions
a. Function of health literacy
b. Function of health numeracy
13. Do you see yourself a continuation of care or coordinator of care
a. Is coordination of care an issue for your PID patients
b. Are patients actively looking for you to coordinate their care?
c. Do your PID patients have problems accessing healthcare services or
getting adequate treatment?
14. Have you ever made a mistake/misdiagnosis?
a. Proper follow-up
b. Diagnostic test
c. Adequate history
193
15. Prefer face-to-face or is phone or internet possible and how often
16. Trustimpact on patient participation
17. Does DM change over time as uncertainty changes
a. Less shared decision making
18. Provider number
19. Are you rated? Do you recall your score?
20. How would you assess or describe the quality of your communication style?
a. Outgoing
b. seeking
21. Do patients tend to speak up or does it depend of the context and your
relationship
22. Impact of the organization on your decision making
a. IOM: patient-centered care: patient perspectives are now being
factored into Medicare value-based payments to hospitals
194
Appendix B: Invitation Template
Dear Dr. ___________,
My name is Christopher Lamb and I am pursuing a doctoral degree in management at
Case Western Reserve University in Cleveland, Ohio.
I am conducting interviews with experts for my qualitative research project on the
physician decision process of immunologists that treat Primary Immunodeficiency (PID).
My questions will focus largely on your experiences at work. The interviews are
conducted over the telephone for approximately 30-60 minutes and will be recorded
(audio or written notes only). You will be provided with an Amazon gift card to
compensate you for your time.
Should you be interested in being a participant in my research, please provide the best
date, time, and contact information to reach you.
The records of this research and your participation will are confidential. I will provide
additional information regarding confidentiality upon acceptance to participate (or upon
request).
If you have any questions, you are welcome to contact the Responsible Investigator, Dr.
Kalle Lyytinen, at 1-216-368 5353 or [email protected]; or the Co-Investigator,
Christopher Lamb, at (339) 440-6061 or [email protected].
Thank you in advance for consideration.
Sincerely,
Christopher Lamb
Ph.D. Candidate
Weatherhead School of Management
Case Western Reserve University
Phone # 339-440-6061
195
Appendix C: Study 2 Constructs
Patient-Centered Approach to Care (APC)
1. cPATIENT_11 I tend to... Ask patients about their quality of life status.
2. cPATIENT_12 I tend to... Ask patients about their psychological status.
3. cPATIENT_13 I tend to... Ask patients about their perceived health status.
Heuristic Decision Making (DMH)
1. DM_INT_1 I tend to...Make decisions instinctively.
2. DM_INT_2 I tend to...Quickly diagnose PID based on prior patient experience.
3. DM_INT_3 I tend to...Rely on instinct for treatment decisions based on prior
experience.
Rational Decision Making (DMR)
1. DM_RAT_1 I tend to...Be very systematic when I go about making a decision.
2. DM_RAT_3 I tend to...Take my time to think through treatment decisions.
3. DM_RAT_5 I tend to...Leave myself time to think through treatment decisions
before I act.
4. DM_RAT_6 I tend to...Carefully work out a treatment plan before making a
treatment decision.
5. DM_RAT_10 I tend to...Learn as much as I can about possible consequences
before making decisions.
Patient Participation with Treatment Protocols (IOP)
1. PROTOCOL_2 Patients tend to... Engage in discussions regarding treatment
protocol.
2. PROTOCOL_3 Patients tend to... Share with me what they understand about
their treatment protocol.
3. PROTOCOL_4 Patients tend to... Share with me what they don’t understand
about their treatment protocol
4. PROTOCOL_11 Patients tend to... Make considerable effort to discuss their
schedule with me.
Patient Participation with Treatment Tools (IOT)
196
1. TOOLS_1 Patients tend to... Influence which brand I treat them with.
2. TOOLS_9 Patients tend to...Choose the brand of IgG replacement therapy they
want.
3. TOOLS_10 Patients tend to... Actively participate in the product choice to treat
their condition.
Physician Trust in Patient Input (TIP)
1. TRUST_1 I trust the patient will... Provide accurate medical information.
2. TRUST_2 I trust the patient will... Let me know when there has been a major
change in their condition.
3. TRUST_3 I trust the patient will... Tell me about all medications they are
using.
4. TRUST_4 I trust the patient will... Follow the treatment plan exactly as I have
provided.
5. TRUST_5 I trust the patient will... Manage their condition with the prescribed
treatment plan.
6. TRUST_6 I trust the patient will... Tell me if they are not following the
treatment plan.
7. TRUST_7 I trust the patient will... Not manipulate the office visit for
secondary gain.
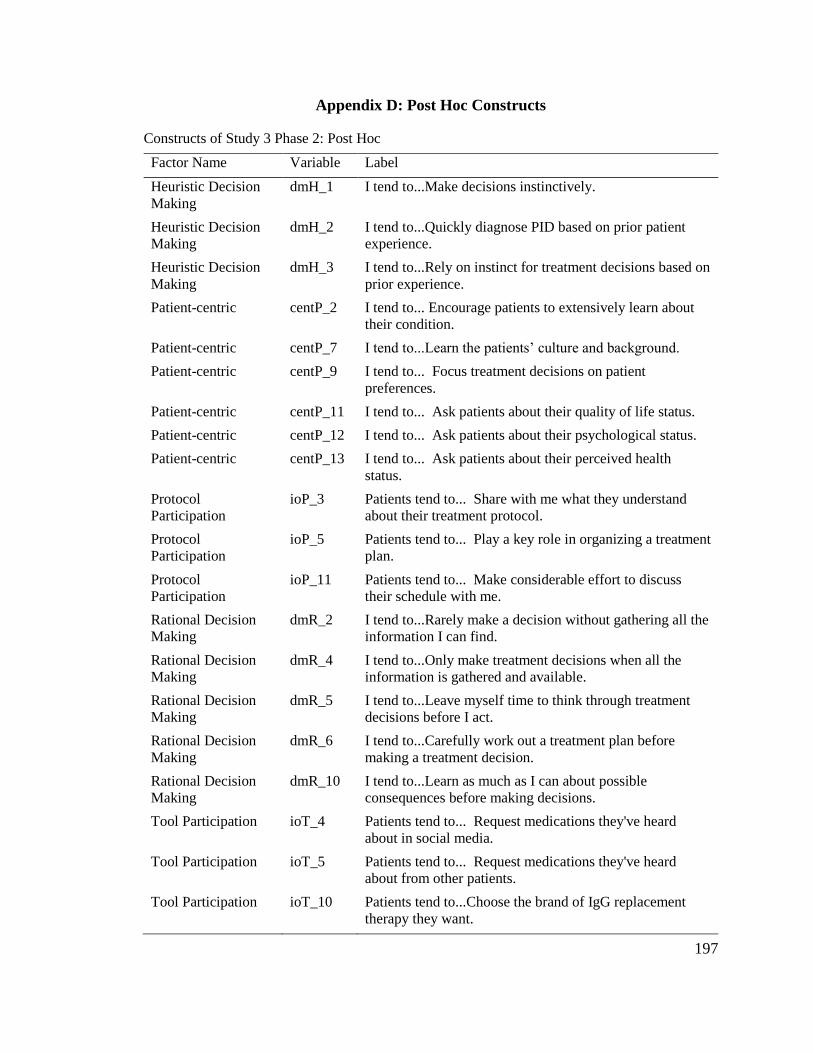
197
Appendix D: Post Hoc Constructs
Constructs of Study 3 Phase 2: Post Hoc
Factor Name Variable Label
Heuristic Decision
Making
dmH_1 I tend to...Make decisions instinctively.
Heuristic Decision
Making
dmH_2 I tend to...Quickly diagnose PID based on prior patient
experience.
Heuristic Decision
Making
dmH_3 I tend to...Rely on instinct for treatment decisions based on
prior experience.
Patient-centric centP_2 I tend to... Encourage patients to extensively learn about
their condition.
Patient-centric centP_7 I tend to...Learn the patients’ culture and background.
Patient-centric centP_9 I tend to... Focus treatment decisions on patient
preferences.
Patient-centric centP_11 I tend to... Ask patients about their quality of life status.
Patient-centric centP_12 I tend to... Ask patients about their psychological status.
Patient-centric centP_13 I tend to... Ask patients about their perceived health
status.
Protocol
Participation
ioP_3 Patients tend to... Share with me what they understand
about their treatment protocol.
Protocol
Participation
ioP_5 Patients tend to... Play a key role in organizing a treatment
plan.
Protocol
Participation
ioP_11 Patients tend to... Make considerable effort to discuss
their schedule with me.
Rational Decision
Making
dmR_2 I tend to...Rarely make a decision without gathering all the
information I can find.
Rational Decision
Making
dmR_4 I tend to...Only make treatment decisions when all the
information is gathered and available.
Rational Decision
Making
dmR_5 I tend to...Leave myself time to think through treatment
decisions before I act.
Rational Decision
Making
dmR_6 I tend to...Carefully work out a treatment plan before
making a treatment decision.
Rational Decision
Making
dmR_10 I tend to...Learn as much as I can about possible
consequences before making decisions.
Tool Participation ioT_4 Patients tend to... Request medications they've heard
about in social media.
Tool Participation ioT_5 Patients tend to... Request medications they've heard
about from other patients.
Tool Participation ioT_10 Patients tend to...Choose the brand of IgG replacement
therapy they want.
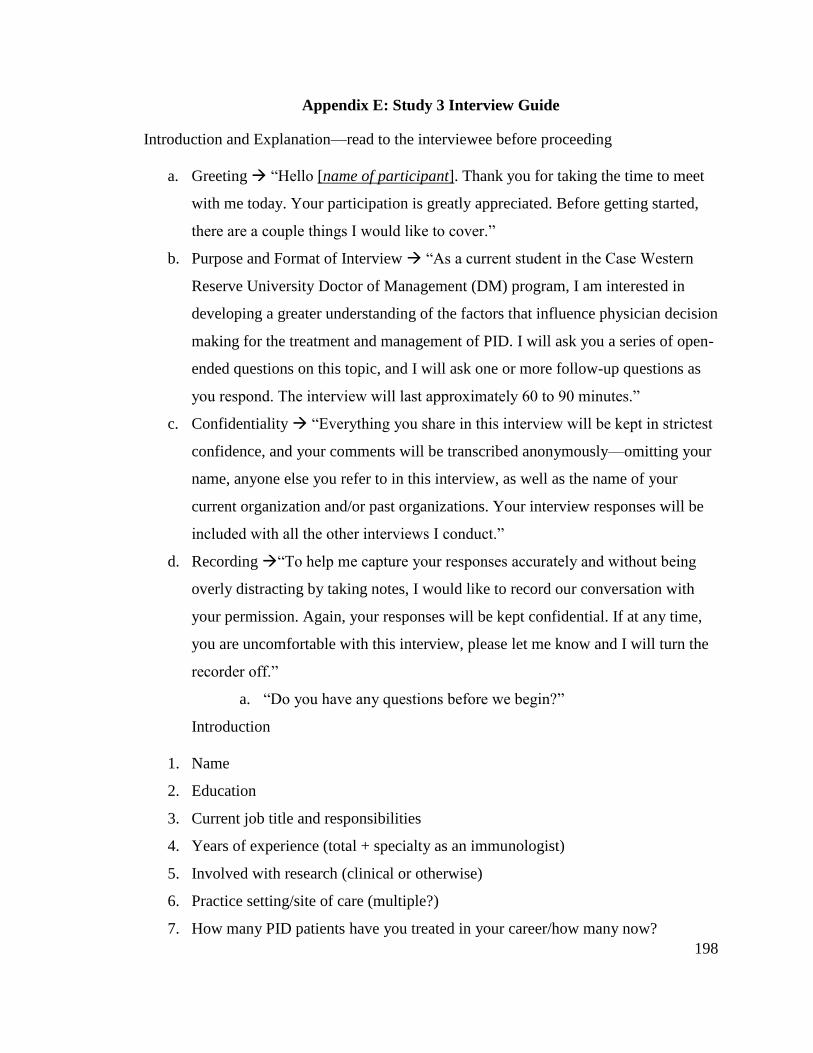
198
Appendix E: Study 3 Interview Guide
Introduction and Explanation—read to the interviewee before proceeding
a. Greeting “Hello [name of participant]. Thank you for taking the time to meet
with me today. Your participation is greatly appreciated. Before getting started,
there are a couple things I would like to cover.”
b. Purpose and Format of Interview “As a current student in the Case Western
Reserve University Doctor of Management (DM) program, I am interested in
developing a greater understanding of the factors that influence physician decision
making for the treatment and management of PID. I will ask you a series of open-
ended questions on this topic, and I will ask one or more follow-up questions as
you respond. The interview will last approximately 60 to 90 minutes.”
c. Confidentiality “Everything you share in this interview will be kept in strictest
confidence, and your comments will be transcribed anonymously—omitting your
name, anyone else you refer to in this interview, as well as the name of your
current organization and/or past organizations. Your interview responses will be
included with all the other interviews I conduct.”
d. Recording “To help me capture your responses accurately and without being
overly distracting by taking notes, I would like to record our conversation with
your permission. Again, your responses will be kept confidential. If at any time,
you are uncomfortable with this interview, please let me know and I will turn the
recorder off.”
a. “Do you have any questions before we begin?”
Introduction
1. Name
2. Education
3. Current job title and responsibilities
4. Years of experience (total + specialty as an immunologist)
5. Involved with research (clinical or otherwise)
6. Practice setting/site of care (multiple?)
7. How many PID patients have you treated in your career/how many now?
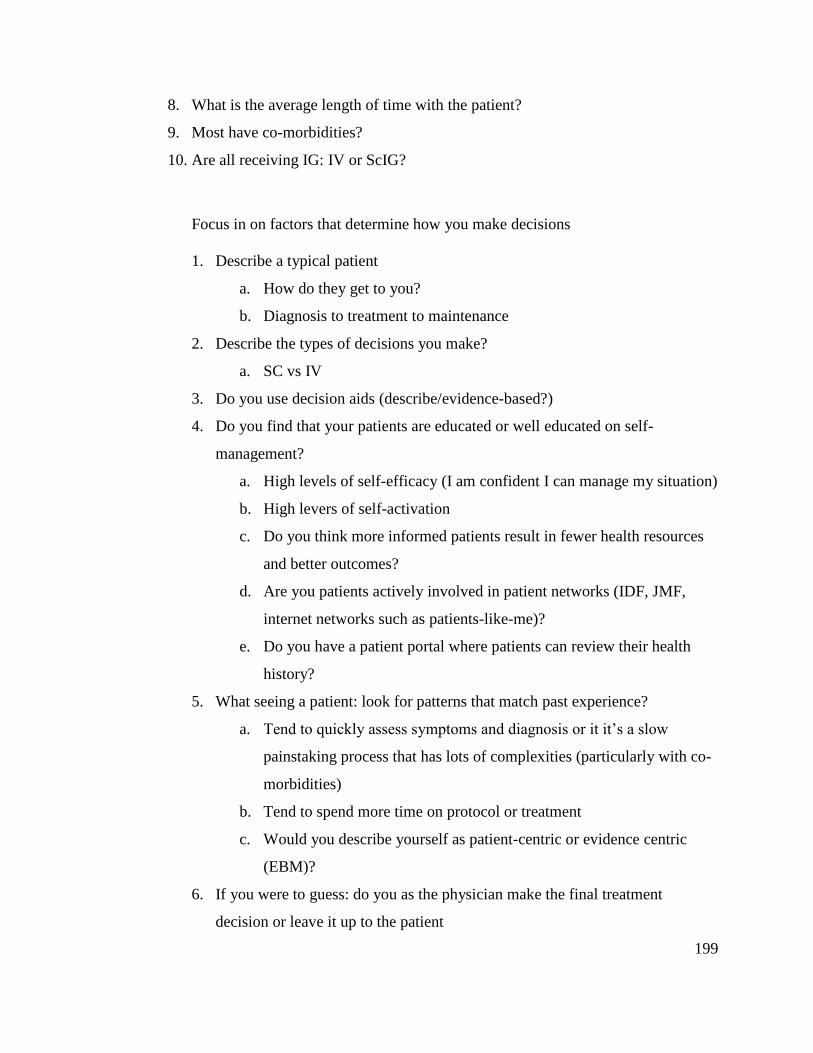
199
8. What is the average length of time with the patient?
9. Most have co-morbidities?
10. Are all receiving IG: IV or ScIG?
Focus in on factors that determine how you make decisions
1. Describe a typical patient
a. How do they get to you?
b. Diagnosis to treatment to maintenance
2. Describe the types of decisions you make?
a. SC vs IV
3. Do you use decision aids (describe/evidence-based?)
4. Do you find that your patients are educated or well educated on self-
management?
a. High levels of self-efficacy (I am confident I can manage my situation)
b. High levers of self-activation
c. Do you think more informed patients result in fewer health resources
and better outcomes?
d. Are you patients actively involved in patient networks (IDF, JMF,
internet networks such as patients-like-me)?
e. Do you have a patient portal where patients can review their health
history?
5. What seeing a patient: look for patterns that match past experience?
a. Tend to quickly assess symptoms and diagnosis or it it’s a slow
painstaking process that has lots of complexities (particularly with co-
morbidities)
b. Tend to spend more time on protocol or treatment
c. Would you describe yourself as patient-centric or evidence centric
(EBM)?
6. If you were to guess: do you as the physician make the final treatment
decision or leave it up to the patient
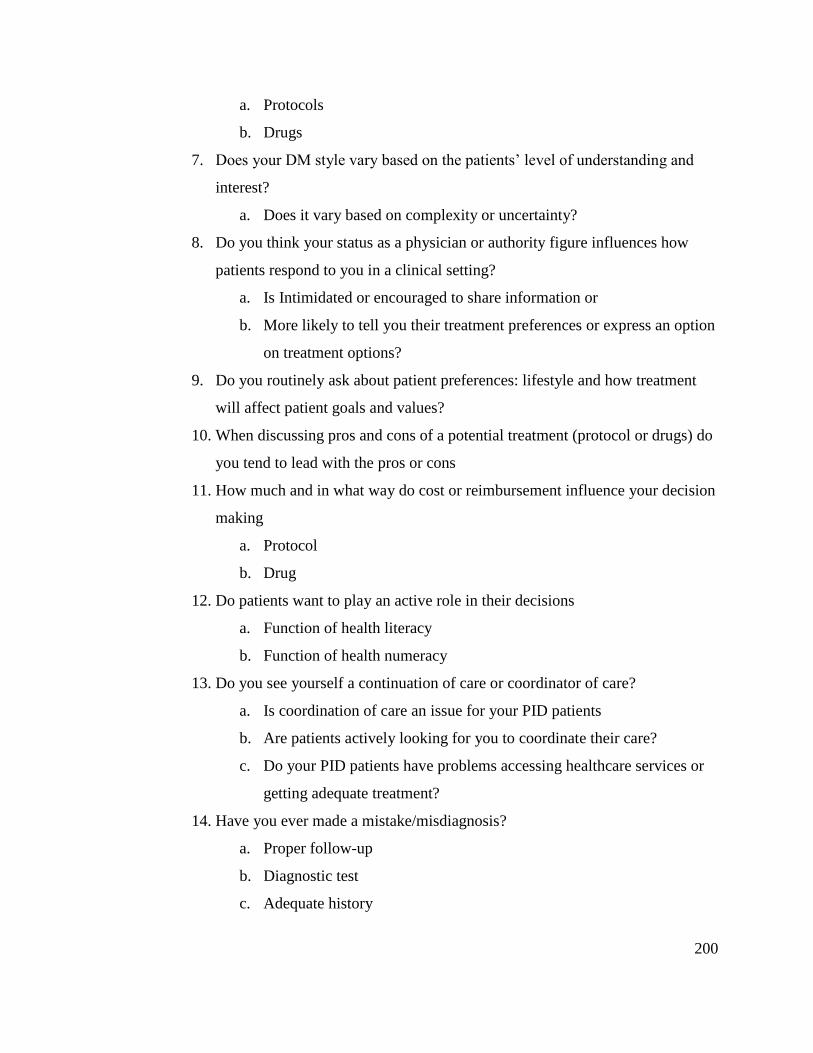
200
a. Protocols
b. Drugs
7. Does your DM style vary based on the patients’ level of understanding and
interest?
a. Does it vary based on complexity or uncertainty?
8. Do you think your status as a physician or authority figure influences how
patients respond to you in a clinical setting?
a. Is Intimidated or encouraged to share information or
b. More likely to tell you their treatment preferences or express an option
on treatment options?
9. Do you routinely ask about patient preferences: lifestyle and how treatment
will affect patient goals and values?
10. When discussing pros and cons of a potential treatment (protocol or drugs) do
you tend to lead with the pros or cons
11. How much and in what way do cost or reimbursement influence your decision
making
a. Protocol
b. Drug
12. Do patients want to play an active role in their decisions
a. Function of health literacy
b. Function of health numeracy
13. Do you see yourself a continuation of care or coordinator of care?
a. Is coordination of care an issue for your PID patients
b. Are patients actively looking for you to coordinate their care?
c. Do your PID patients have problems accessing healthcare services or
getting adequate treatment?
14. Have you ever made a mistake/misdiagnosis?
a. Proper follow-up
b. Diagnostic test
c. Adequate history
201
15. Prefer face-to-face or is phone or internet possible and how often
16. Trustimpact on patient participation
17. Does DM change over time as uncertainty changes
a. Less shared decision making
18. Provider number
19. Are you rated? Do you recall your score?
20. How would you assess or describe the quality of your communication style?
a. Outgoing
b. seeking
21. Do patients tend to speak up or does it depend of the context and your
relationship
22. Impact of the organization on your decision making
a. IOM: patient-centered care: patient perspectives are now being
factored into Medicare value-based payments to hospitals
202
Appendix F: Mixed Methods Tutorial
Research and Analysis Methods
This section summarizes the methods used in this study to gather and analyze
data. The topics are as follows: mixed-methods, qualitative methods, and then
quantitative methods.
Mixed Methods
This research follows an exploratory and developmental mixed-methods10
approach that “combines quantitative and qualitative research methods in the same
research inquiry [to] help develop rich insights that cannot be fully understood using only
[one] method” (Venkatesh et al., 2013: 21). It consists of two sequential parts:
qualitative, then quantitative. Taking a developmental approach means we adapted and
follow questions that emerge from the different parts of the study (Venkatesh et al.,
2013). A sequential approach means that each study is separate and without overlap. An
exploratory approach means that the qualitative findings were tested by the quantitative
study (Creswell & Plano Clark, 2007). The triangulation, or merging, of both the
qualitative and quantitative approaches helps to identify factors of the physician decision-
making process that facilitate or impede SDM (Creswell & Plano Clark, 2007).
Mixed methods offers a more robust foundation to this research and the results
through the triangulation of the different methods (Caracelli & Greene, 1993; Gibson,
2017). The advantage of mixed methods over single-method studies is the ability to
10
Mixed methods should not be confused with a multi-method approach; multi-method involves two or
more of the same type of research approach for an individual research inquiry (i.e., two qualitative
methods) Venkatesh, V., Brown, S. A., & Bala, H. 2013. Bridging the qualitative-quantitative divide:
Guidelines for conducting mixed methods research in information systems. Mis Quarterly, 37(1): 21-54..
203
address both exploratory and confirmatory research questions, provide stronger
inferences, reduce common method bias, and provide more divergent or complementary
views (Teddlie & Tashakkori, 2003, 2009). Additionally, mixed methods can improve the
validity and reliability of research findings and are beneficial in studies where the
research area is not well documented or previous studies yielded contradictory research
findings (Greene, Caracelli, & Graham, 1989; Silverman, 2011; Tashakkori & Teddlie,
2008). “Quantitative studies typically rely on quality criteria, such as internal validity,
generalizability, and reliability, whereas qualitative studies have roughly comparable
quality criteria of credibility, transferability, and dependability” (Wisdom, Cavaleri,
Onwuegbuzie, & Green, 2012). The triangulated results from both studies capitalizes on
the strengths of each method, likely providing a more complete understanding of
influencing factors involved in a physician’s decision process for the treatment of PID
(Wisdom et al., 2012). The following sections discuss the strengths and weaknesses of
qualitative and quantitative methods.
Qualitative Methods
Qualitative methods assume the constructivist and interpretivist paradigms, with
an emphasis on process, constant change and meaning (Tashakkori & Teddlie, 2008).
This method is very effective in identifying patterns and commonalities in participant
responses and themes of a phenomenon; interviews can be “one of the most important
data gathering techniques for qualitative researchers in business and management …
interviews allow us to gather rich data from people in various roles and situations”
(Myers, 2013: 119). Furthermore, a qualitative approach may offer a more nuanced
understanding of the treatment process of complex chronic diseases.
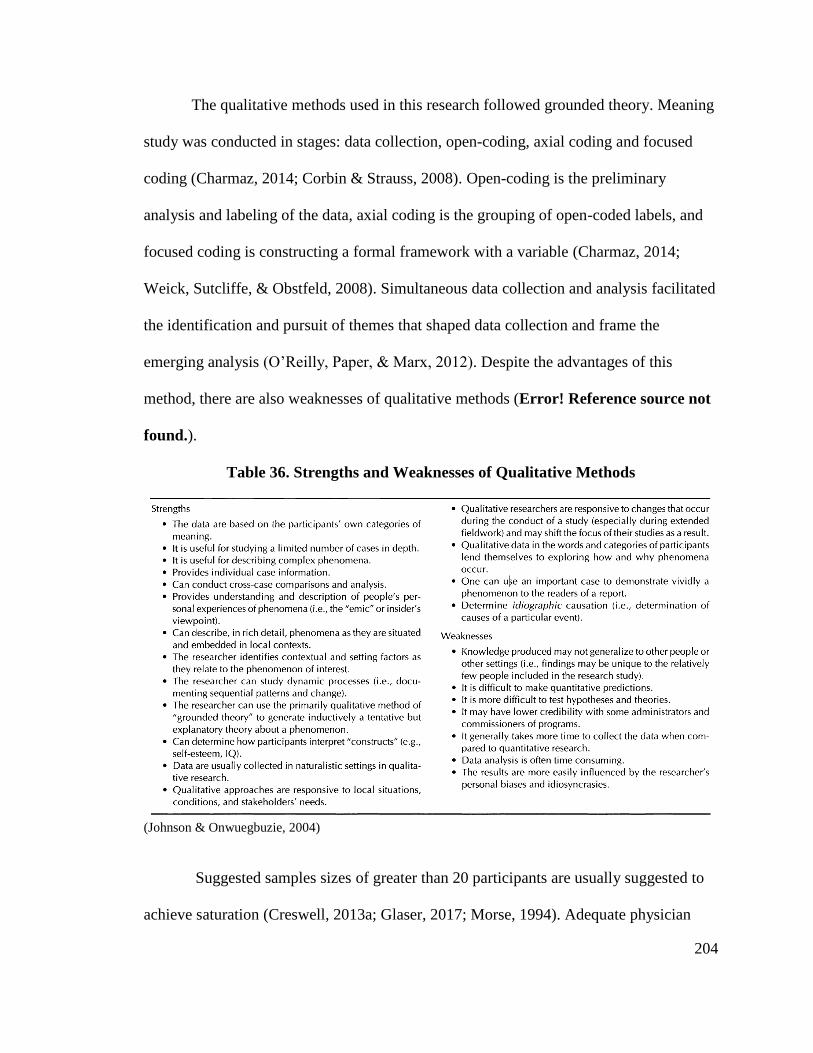
204
The qualitative methods used in this research followed grounded theory. Meaning
study was conducted in stages: data collection, open-coding, axial coding and focused
coding (Charmaz, 2014; Corbin & Strauss, 2008). Open-coding is the preliminary
analysis and labeling of the data, axial coding is the grouping of open-coded labels, and
focused coding is constructing a formal framework with a variable (Charmaz, 2014;
Weick, Sutcliffe, & Obstfeld, 2008). Simultaneous data collection and analysis facilitated
the identification and pursuit of themes that shaped data collection and frame the
emerging analysis (O’Reilly, Paper, & Marx, 2012). Despite the advantages of this
method, there are also weaknesses of qualitative methods (Error! Reference source not
found.).
Table 36. Strengths and Weaknesses of Qualitative Methods
(Johnson & Onwuegbuzie, 2004)
Suggested samples sizes of greater than 20 participants are usually suggested to
achieve saturation (Creswell, 2013a; Glaser, 2017; Morse, 1994). Adequate physician
205
response rates to surveys is a well-documented problem (Flanigan et al., 2008). The
findings of the qualitative phase will guide the instrument development and hypothesis
testing for the subsequent quantitative study, in part by validating the scales used
(Creswell, 2013b; Venkatesh et al., 2013). Completion of the qualitative interviews
occurs when the information has reached a saturation point (i.e., when additional
interviews are not providing more themes) (Charmaz, 2014; Golden-Biddle & Locke,
2007).
Quantitative Methods
Quantitative methods assume a paradigm of positivism in testing and validating
qualitative research findings in a larger context by estimating the prevalence factors and
causal links between them (Johnson & Onwuegbuzie, 2004). Despite the advantages of
this method, there are also weaknesses of quantitative methods (Error! Reference
source not found.).

206
Table 37. Strengths and Weaknesses of Quantitative Methods
(Johnson & Onwuegbuzie, 2004)
Constructs and Validity
Construct development and their validity is argued to be the most important and
significant part of any study (Podsakoff, Podsakoff, MacKenzie, & Klinger, 2013). A
scale, or set of items, can only measure a construct if (a) the [construct] exists, and (b)
variations in the [construct] causally produce variations in the outcomes of the
measurement process” (Borsboom, Cramer, Kievit, Zand Scholten, & Franić, 2009: 150).
Furthermore, the observed constructs must avoid redundancy (Shaffer, DeGeest, & Li,
2016). Strategies to increase the validity of the constructs include testing them before
207
collecting data and conducting tests during the analyses post-collection (Worthington &
Whittaker, 2006).
To increase the construct validity of the instrument, the survey items should be
pre-tested for using the Q-sort technique. Q-sort is a powerful and well-established
technique for quantitatively evaluating opinions and attitudes (Thomas & Watson, 2002).
Like other pretesting techniques, the method can be used to establish content, and
discriminant and convergent validity before the post-data collection analysis (Bolton,
1993; Krosnick, 1999). Using software such as Qualtrics, mock-participants can be asked
to drag randomized questions into categories they believe it relates to potentially unveil
cross-loading items.
After data collection, validity is measured during the analysis. The exploratory
factor analysis (EFA) was performed to conduct tests to confirm or increase the validity
of the item set; the tests include the Kaiser-Meyer-Olkin test (KMO) for adequacy,
rotation type to estimate a simple structure for the data, cross-loading analysis, and item
deletion (Worthington & Whittaker, 2006). An EFA is suitable for this study because
formal hypotheses are tested and the number of factors to be analyzed are data-driven
(Fabrigar, Wegener, MacCallum, & Strahan, 1999). Multiple EFAs were conducted if
necessary as depending on results from subsequent steps in the analysis (MacKenzie,
Podsakoff, & Podsakoff, 2011).
SEM Methods
One method of analysis for quantitative data is called structural equation
modeling (SEM) and involves the use of SPSS AMOS software version 23. SEM is a
multivariate statistical analysis technique used to analyze structural relationships by
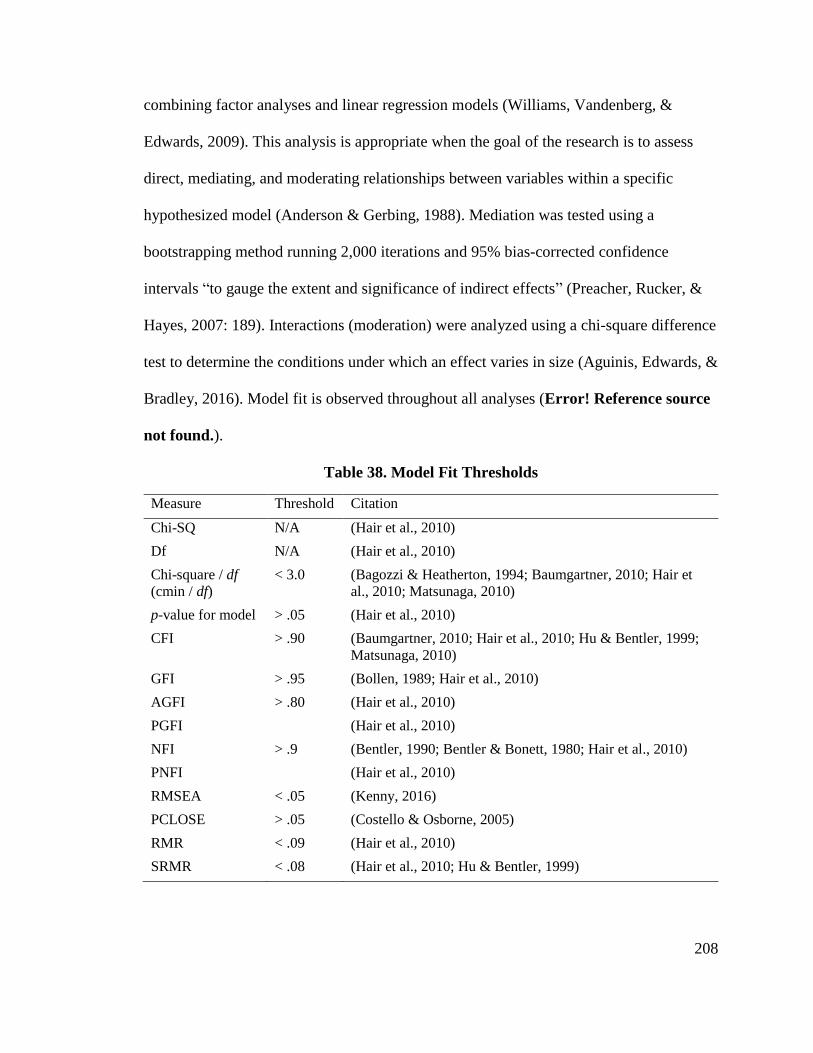
208
combining factor analyses and linear regression models (Williams, Vandenberg, &
Edwards, 2009). This analysis is appropriate when the goal of the research is to assess
direct, mediating, and moderating relationships between variables within a specific
hypothesized model (Anderson & Gerbing, 1988). Mediation was tested using a
bootstrapping method running 2,000 iterations and 95% bias-corrected confidence
intervals “to gauge the extent and significance of indirect effects” (Preacher, Rucker, &
Hayes, 2007: 189). Interactions (moderation) were analyzed using a chi-square difference
test to determine the conditions under which an effect varies in size (Aguinis, Edwards, &
Bradley, 2016). Model fit is observed throughout all analyses (Error! Reference source
not found.).
Table 38. Model Fit Thresholds
Measure Threshold Citation
Chi-SQ N/A (Hair et al., 2010)
Df N/A (Hair et al., 2010)
Chi-square / df
(cmin / df)
< 3.0 (Bagozzi & Heatherton, 1994; Baumgartner, 2010; Hair et
al., 2010; Matsunaga, 2010)
p-value for model > .05 (Hair et al., 2010)
CFI > .90 (Baumgartner, 2010; Hair et al., 2010; Hu & Bentler, 1999;
Matsunaga, 2010)
GFI > .95 (Bollen, 1989; Hair et al., 2010)
AGFI > .80 (Hair et al., 2010)
PGFI (Hair et al., 2010)
NFI > .9 (Bentler, 1990; Bentler & Bonett, 1980; Hair et al., 2010)
PNFI (Hair et al., 2010)
RMSEA < .05 (Kenny, 2016)
PCLOSE > .05 (Costello & Osborne, 2005)
RMR < .09 (Hair et al., 2010)
SRMR < .08 (Hair et al., 2010; Hu & Bentler, 1999)
209
In summary, “quantitative studies typically rely on quality criteria, such as
internal validity, generalizability, and reliability, whereas qualitative studies have roughly
comparable quality criteria of credibility, transferability, and dependability” (Wisdom et
al., 2012: 724). It is the combination of these methods that provides the best picture of the
factors that affect SDM implementation, since, through triangulation, a better
understanding of the phenomenon can be achieved. This study integrated the two
methods at the data analysis and interpretation stage after the data was collected. The
analysis for each of the three studies was done separately for each study and is provided
in Chapters 4, 5 and 6. The information was compared at the interpretation stage of the
research and is provided in Chapter 7 (Creswell & Plano Clark, 2007: 175; Hossler &
Vesper, 1993)
210
REFERENCES
Abolhassani, H., Aghamohammadi, A., Pourjabbar, S., Sadaghiani, M. S., Nikayin, S.,
Rabiee, A., Imanzadeh, A., Gharaei, J. M., Arbabi, M., & Rezaei, N. 2013.
Psychiatric aspects of primary immunodeficiency diseases: the parental study.
Iranian Journal Of Allergy, Asthma And Immunology, 12(2): 176-181.
Agency for Healthcare Research and Quality. 2014a. Mean Expenses per Person with
Care for Selected Conditions by Type of Service: United States, 2014. .
Agency for Healthcare Research and Quality. 2014b. MEPS HC-171: 2014 Full Year
Consolidated Data File. In Agency for Healthcare Research and Quality (Ed.).
Agency for Healthcare Research and Quality. 2014c. Table 4.1: Among adults age 18 and
over who reported going to a doctor's office or clinic in the last 12 months,
percent distribution of how often their health providers listened carefully to them,
United States, 2014., Medical Expenditure Panel Survey Household Component
Data, Vol. 2017.
Agency for Healthcare Research and Quality. 2014d. Table 4.5: Among adults age 18 and
over who reported going to a doctor's office or clinic in the last 12 months,
percent distribution of how often their health providers showed respect for what
they had to say, United States, 2014., Vol. 2017.
Agency for Healthcare Research and Quality. 2014e. Table 4.7: Among adults age 18 and
over who reported going to a doctor's office or clinic in the last 12 months,
percent distribution of how often their health providers spent enough time with
them, United States, 2014., Vol. 2017.
Agency for Healthcare Research and Quality. 2014f. Total Expenses and Percent
Distribution for Selected Conditions by Type of Service: United States, 2014.,
Vol. 2017.
Agency for Healthcare Research and Quality. 2018. MEPS: Survey Background, Vol.
2018.
Aggarwal, A., Davies, J., & Sullivan, R. 2014. “Nudge” in the clinical consultation–an
acceptable form of medical paternalism? BMC Medical Ethics, 15(31): 1-6.
Aguinis, H., Edwards, J. R., & Bradley, K. J. 2016. Improving our understanding of
moderation and mediation in strategic management research. Organizational
Research Methods, 20(2): 665-685.
Al-Herz, W., Bousfiha, A., Casanova, J.-L., Chatila, T., Conley, M. E., Cunningham-
Rundles, C., Etzioni, A., Franco, J. L., Gaspar, H. B., Holland, S. M., Klein, C.,
Nonoyama, S., Ochs, H. D., Oksenhendler, E., Picard, C., Puck, J. M., Sullivan,
K., & Tang, M. L. K. 2014. Primary immunodeficiency diseases: An update on
211
the classification from the international union of immunological societies expert
committee for primary immunodeficiency. Frontiers in Immunology, 5(Article
162): 1-33.
Allen, P., Maguire, S., & McKelvey, B. 2011a. The sage handbook of complexity and
management: Sage Publications.
Allen, P. M., Maguire, S., & McKelvey, B. 2011b. Complexity and management. In C.
Hooker (Ed.), Philosophy of complex systems handbook of the philosophy of
science, Vol. 10: 783-808: Elsevier.
Alston, C., Paget, L., Halvorson, G., Novelli, B., Guest, J., McCabe, P., Hoffman, K.,
Koepke, C., Simon, M., & Sutton, S. 2012. Communicating with patients on
health care evidence. Washington DC: Institute of Medicine.
Anderson, G., & Horvath, J. 2013. Chronic conditions: Making the case for ongoing
care. 2002. Princeton, NJ: Robert Wood Johnson Foundation’s Partnership for
Solutions.
Anderson, J. C., & Gerbing, D. W. 1988. Structural equation modeling in practice: A
review and recommended two-step approach. Psychological Bulletin, 103(3):
411.
Ansell, D. A. 2017. The Deah Gap: How Inequality Kills: University of Chicago Press.
Arterburn, D., Wellman, R., Westbrook, E., Rutter, C., Ross, T., McCulloch, D.,
Handley, M., & Jung, C. 2012. Introducing decision aids at Group Health was
linked to sharply lower hip and knee surgery rates and costs. Health Affairs,
31(9): 2094-2104.
Ashforth, B. E., & Mael, F. 1989. Social identity theory and the organization. Academy
of management review, 14(1): 20-39.
Babbie, E. R., Halley, F., & Zaino, J. 2007. Adventures in social research: data analysis
using SPSS 14.0 and 15.0 for Windows: Pine Forge Press.
Bagozzi, R. P., & Heatherton, T. F. 1994. A general approach to representing
multifaceted personality constructs: Application to state self‐esteem. Structural
Equation Modeling: A Multidisciplinary Journal, 1(1): 35-67.
Baker, D. P., Day, R., & Salas, E. 2006. Teamwork as an essential component of high‐
reliability organizations. Health Services Research, 41(4p2): 1576-1598.
Baker, D. W. 2017. History of The Joint Commission’s Pain Standards: Lessons for
Today’s Prescription Opioid Epidemic. JAMA, 317(11): 1117-1118.
212
Bansal, G., Zahedi, F. M., & Gefen, D. 2016. Do context and personality matter? Trust
and privacy concerns in disclosing private information online. Information &
Management, 53(1): 1-21.
Barnett, K., Mercer, S. W., Norbury, M., Watt, G., Wyke, S., & Guthrie, B. 2012.
Epidemiology of multimorbidity and implications for health care, research, and
medical education: a cross-sectional study. The Lancet, 380(9836): 37-43.
Barrett, L. F., Tugade, M. M., & Engle, R. W. 2004. Individual differences in working
memory capacity and dual-process theories of the mind. Psychological bulletin,
130(4): 553.
Barry, M. J., & Edgman-Levitan, S. 2012. Shared decision making—the pinnacle of
patient-centered care. New England Journal Of Medicine, 366(9): 780-781.
Barua, S., Greenwald, R., Grebely, J., Dore, G. J., Swan, T., & Taylor, L. E. 2015.
Restrictions for Medicaid reimbursement of Sofosbuvir for the Treatment of
Hepatitis C virus infection in the United States. Annals of Internal Medicine,
163(3): 215-223.
Bauer, A. M., Parker, M. M., Schillinger, D., Katon, W., Adler, N., Adams, A. S.,
Moffet, H. H., & Karter, A. J. 2014. Associations between antidepressant
adherence and shared decision-making, patient–provider trust, and
communication among adults with diabetes: diabetes study of northern California
(DISTANCE). Journal of general internal medicine, 29(8): 1139-1147.
Baumgartner, H. 2010. Structural Equation Modeling, Wiley International Encyclopedia
of Marketing. The Pennsylvania State University, University Park, PA, USA.
Beach, L. R., & Lipshitz, R. 2017. Why classical decision theory is an inappropriate
standard for evaluating and aiding most human decision making. In D. Harris, &
W.-C. Li (Eds.), Decision making in aviation: 85-102. London and New York:
Routledge.
Beevers, C. G. 2005. Cognitive vulnerability to depression: A dual process model.
Clinical psychology review, 25(7): 975-1002.
Belanger, E., Rodríguez, C., & Groleau, D. 2011. Shared decision-making in palliative
care: A systematic mixed studies review using narrative synthesis. Palliative
Medicine, 25(3): 242-261.
Bensing, J. 2000. Bridging the gap.: The separate worlds of evidence-based medicine and
patient-centered medicine. Patient Education And Counseling, 39(1): 17-25.
Bentler, P. M. 1990. Comparative fit indexes in structural models. Psychological
bulletin, 107(2): 238.
213
Bentler, P. M., & Bonett, D. G. 1980. Significance tests and goodness of fit in the
analysis of covariance structures. Psychological bulletin, 88(3): 588.
Bernardo, R. 2017. 2017’s Best & Worst States for Health Care, Vol. 2018: WalletHub.
Berner, E. S., & Graber, M. L. 2008. Overconfidence as a cause of diagnostic error in
medicine. The American journal of medicine, 121(5): S2-S23.
Bertakis, K. D., Franks, P., & Azari, R. 2002. Effects of physician gender on patient
satisfaction. Journal Of The American Medical Women's Association (1972),
58(2): 69-75.
Berwick, D. M., & Hackbarth, A. D. 2012. Eliminating waste in US health care. JAMA,
307(14): 1513-1516.
Beshears, J., & Gino, F. 2015. Leaders as decision architects. Harvard Business Review,
93(5): 52-62.
Blumenthal-Barby, J. 2017. ‘That’s the doctor’s job’: Overcoming patient reluctance to
be involved in medical decision making. Patient education and counseling,
100(1): 14-17.
Boland Jr, R. J., & Collopy, F. 2004. Managing as designing: Stanford University Press.
Bollen, K. A. 1989. A new incremental fit index for general structural equation models.
Sociological Methods & Research, 17(3): 303-316.
Bolton, R. N. 1993. Pretesting questionnaires: content analyses of respondents'
concurrent verbal protocols. Marketing science, 12(3): 280-303.
Borrell-Carrió, F., Estany, A., Platt, F. W., & MoralesHidalgo, V. 2014. Doctors as a
knowledge and intelligence building group: Pragmatic principles underlying
decision-making processes. Journal of Epidemiology and Community Health,
69(4): 303-305.
Borsboom, D., Cramer, A. O., Kievit, R. A., Zand Scholten, A., & Franić, S. 2009. The
end of construct validity. In R. W. Lissitz (Ed.), The concept of validity:
Revisions, new directions, and applications: 135-170. Charlotte, NC: IAP
Information Age Publishing.
Bousfiha, A. A., Jeddane, L., Ailal, F., Benhsaien, I., Mahlaoui, N., Casanova, J.-L., &
Abel, L. 2013. Primary immunodeficiency diseases worldwide: more common
than generally thought. Journal Of Clinical Immunology, 33(1): 1-7.
Boyle, J., & Buckley, R. 2007. Population prevalence of diagnosed primary
immunodeficiency diseases in the United States. Journal Of Clinical
Immunology, 27(5): 497-502.
214
Braun, V., & Clarke, V. 2006. Using thematic analysis in psychology. Qualitative
research in psychology, 3(2): 77-101.
Bravo, P., Edwards, A., Barr, P. J., Scholl, I., Elwyn, G., & McAllister, M. 2015.
Conceptualising patient empowerment: A mixed methods study. BMC Health
Services Research, 15(252): 1-14.
Brooks, M. 2017. Rare Disease Treatments Make Up Top 10 Most Costly Drugs, Vol.
2017: Medscape.
Buck, J. N., & Daniels, M. H. 1985. Assessment of Career Decision Making (ACDM):
Manual: Western Psychological Services.
Burgess, D. J., Dovidio, J., Phelan, S., & van Ryn, M. 2011. The Effect of Medical
Authoritarianism on Physicians' Treatment Decisions and Attitudes Regarding
Chronic Pain. Journal Of Applied Social Psychology, 41(6): 1399-1420.
Burgess, D. J., Van Ryn, M., Crowley-Matoka, M., & Malat, J. 2006. Understanding the
provider contribution to race/ethnicity disparities in pain treatment: insights from
dual process models of stereotyping. Pain Medicine, 7(2): 119-134.
Butler, M., Ratner, E., McCreedy, E., Shippee, N., & Kane, R. L. 2014. Decision aids for
advance care planning: an overview of the state of the ScienceDecision aids for
advance care planning. Annals of internal medicine, 161(6): 408-418.
Byrne, B. M. 2004. Testing for multigroup invariance using AMOS graphics: A road less
traveled. Structural Equation Modeling, 11(2): 272-300.
Byrne, B. M. 2008. Testing for multigroup equivalence of a measuring instrument: A
walk through the process. Psicothema, 20(4): 872-882.
CAHPS. 2012. CG CAHPS for ACOs – Field Test Survey Content by Survey Domain
Overview, Vol. 2017.
Calder, L. A., Forster, A. J., Stiell, I. G., Carr, L. K., Brehaut, J. C., Perry, J. J.,
Vaillancourt, C., & Croskerry, P. 2011. Experiential and rational decision making:
A survey to determine how emergency physicians make clinical decisions.
Emergency Medicine Journal, 29(10): 811-816.
Campbell, R. 2013. Step inside the physician's head. EHRs can enhance a physician's
cognitive processing and eliminate diagnostic errors, with some HIM-led changes.
Journal of American Health Information Management Association, 84(11): 44.
Caracelli, V. J., & Greene, J. C. 1993. Data analysis strategies for mixed-method
evaluation designs. Educational evaluation and policy analysis, 15(2): 195-207.
215
Carman, K. L., & Workman, T. A. 2017. Engaging patients and consumers in research
evidence: applying the conceptual model of patient and family engagement.
Patient education and counseling, 100(1): 25-29.
Casto, A. B., Layman, E., & Association, A. H. I. M. 2006. Principles of healthcare
reimbursement: American Health Information Management Association Chicago.
Castro, F. G., Kellison, J. G., Boyd, S. J., & Kopak, A. 2010. A methodology for
conducting integrative mixed methods research and data analyses. Journal of
mixed methods research, 4(4): 342-360.
CDC. 2017. Center for disease control and prevention, Vol. 2017: CDC.
Certo, S. T., Busenbark, J. R., Woo, H. s., & Semadeni, M. 2016. Sample selection bias
and Heckman models in strategic management research. Strategic Management
Journal, 37(13): 2639-2657.
Chambers, D., Booth, A., Baxter, S. K., Johnson, M., Dickinson, K. C., & Goyder, E. C.
2016. Evidence for models of diagnostic service provision in the community:
literature mapping exercise and focused rapid reviews. Health Services and
Delivery Research, 4(35): 1-362.
Chang, S.-J., Van Witteloostuijn, A., & Eden, L. 2010. From the editors: Common
method variance in international business research. Journal Of International
Business Studies, 41(2): 178-184.
Chapel, H., Prevot, J., Gaspar, H. B., Español, T., Bonilla, F. A., Solis, L., & Drabwell, J.
2014. Primary immune deficiencies–principles of care. Frontiers In
Immunology, 5.
Chapman, E. N., Kaatz, A., & Carnes, M. 2013. Physicians and implicit bias: how
doctors may unwittingly perpetuate health care disparities. Journal Of General
Internal Medicine, 28(11): 1504-1510.
Charles, C., Gafni, A., & Whelan, T. 1999. Decision-making in the physician–patient
encounter: revisiting the shared treatment decision-making model. Social Science
& Medicine, 49(5): 651-661.
Charmaz, K. 2006. Constructing grounded theory: A practical guide through
qualitative research. London: Sage Publications.
Charmaz, K. 2014. Constructing grounded theory: Sage.
Chen, S.-L. 2016. Economic Costs of Hemophilia and the Impact of Prophylactic
Treatment on Patient Management. The American Journal Of Managed Care,
22(5 Suppl): s126-133.
216
Christozov, D., Chukova, S., & Mateev, P. 2009. Informing processes, risks, evaluation
of the risk of misinforming, in foundations of informing science. In T. G. Gill, &
E. Cohen (Eds.), Foundations of informing science: 323-356. Santa Rosa, CA:
Informing Science Press.
Chu, L. F., Utengen, A., Kadry, B., Kucharski, S. E., Campos, H., Crockett, J., Dawson,
N., & Clauson, K. A. 2016. “Nothing about us without us”—patient partnership in
medical conferences. BMJ, 354(i3883).
CMS. 2015. National Health Expenditures 2015 Highlights: Centers for Medicare &
Medicaid Services.
CMS. 2016. Medicare Shared Savings Program quality measure benchmarks for the 2016
and 2017 reporting years, Vol. 2018.
CMS. 2017. NHE Fact Sheet, Vol. 2017: CMS.
Coget, J.-F., & Keller, E. 2010. The critical decision vortex: lessons from the emergency
room. Journal Of Management Inquiry, 19(1): 56-67.
Coghlan, A. 2017. US ranked worst healthcare system, while the NHS is the best, New
Scientist.
Cole, J., Kiriaev, O., Malpas, P., & Cheung, G. 2017. ‘Trust me, I’m a doctor’: A
qualitative study of the role of paternalism and older people in decision-making
when they have lost their capacity. Australasian Psychiatry, 25(6): 549-553.
Condino-Neto, A., Franco, J., Espinosa-Rosales, F., Leiva, L., King, A., Porras, O.,
Oleastro, M., Bezrodnik, L., Grumach, A. S., & Costa-Carvalho, B. 2012.
Advancing the management of primary immunodeficiency diseases in Latin
America: Latin American Society for Immunodeficiencies (LASID) Initiatives.
Allergologia Et Immunopathologia, 40(3): 187-193.
Cook, K., Kramer, R., Thom, D., Stepanikova, I., Bailey, S., & Cooper, R. 2004. Trust
and distrust in patient-physician relationships: Perceived determinants of high and
low trust relationships in managed care settings. In R. M. Kramer, & K. S. Cook
(Eds.), Trust and distrust in organizations: Dilemmas and approaches: 65-98.
Thousand Oaks, CA: Russell Sage Foundation.
Cooper-Patrick, L., Gallo, J. J., Gonzales, J. J., Vu, H. T., Powe, N. R., Nelson, C., &
Ford, D. E. 1999. Race, gender, and partnership in the patient-physician
relationship. JAMA, 282(6): 583-589.
Cooper, L. A., & Roter, D. 2003. Patient-provider communication: The effect of race and
ethnicity on process and outcomes of healthcare. In B. D. Smedley, A. Y. Stith, &
A. R. Nelson (Eds.), Unequal treatment: Confronting racial and ethnic
disparities in health care. Washington, DC: National Academies Press.

217
Cooper, L. A., Roter, D. L., Carson, K. A., Beach, M. C., Sabin, J. A., Greenwald, A. G.,
& Inui, T. S. 2012. The associations of clinicians’ implicit attitudes about race
with medical visit communication and patient ratings of interpersonal care.
American journal of public health, 102(5): 979-987.
Corbin, J., & Strauss, A. 2008. Basics of qualitative research (3rd ed.). London: Sage.
Corbin, J., & Strauss, A. 2014. Basics of qualitative research: Techniques and
procedures for developing grounded theory: Sage publications.
Costa-Carvalho, B. T., Grumach, A. S., Franco, J. L., Espinosa-Rosales, F. J., Leiva, L.
E., King, A., Porras, O., Bezrodnik, L., Oleastro, M., & Sorensen, R. U. 2014.
Attending to warning signs of primary immunodeficiency diseases across the
range of clinical practice. Journal Of Clinical Immunology, 34(1): 10-22.
Costello, A. B., & Osborne, J. 2005. Best practices in exploratory factor analysis: Four
recommendations for getting the most from your analysis. Practical Assessment
Research & Evaluation, 10(7): 1-9.
Cottone, R. R. 2001. A social constructivism model of ethical decision making in
counseling. Journal of Counseling & Development, 79(1): 39-45.
Cottone, R. R. 2004. Displacing the psychology of the individual in ethical decision-
making: The social constructivism model. Canadian Journal of Counselling,
38(1): 5.
Couët, N., Desroches, S., Robitaille, H., Vaillancourt, H., Leblanc, A., Turcotte, S.,
Elwyn, G., & Légaré, F. 2015. Assessments of the extent to which health‐care
providers involve patients in decision making: a systematic review of studies
using the OPTION instrument. Health Expectations, 18(4): 542-561.
Creswell, J. W. 2013a. Qualitative inquiry and research design: Choosing among five
approaches: Sage.
Creswell, J. W. 2013b. Steps in conducting a scholarly mixed methods study: DBER
Speaker Series. 48. http://digitalcommons.unl.edu/dberspeakers/48.
Creswell, J. W., & Plano Clark, V. L. 2007. Designing and conducting mixed methods
research: Sage Publications.
Croskerry, P. 2009a. Clinical cognition and diagnostic error: applications of a dual
process model of reasoning. Advances In Health Sciences Education, 14(1): 27-
35.
Croskerry, P. 2009b. A universal model of diagnostic reasoning. Academic Medicine,
84(8): 1022-1028.
218
Croskerry, P. 2014. Bias: a normal operating characteristic of the diagnosing brain.
Diagnosis, 1(1): 23-27.
Curreri, A., & Lyytinen, K. 2017. Mindfulness, Information Technology Use, and
Physicians’ Performance in Emergency Rooms. Paper presented at the Academy
of Management Proceedings.
D'Amour, D., Ferrada-Videla, M., San Martin Rodriguez, L., & Beaulieu, M.-D. 2005.
The conceptual basis for interprofessional collaboration: core concepts and
theoretical frameworks. Journal of interprofessional care, 19(sup1): 116-131.
Dalton, D. R. 2015. Hemophilia in the managed care setting. The American journal of
managed care, 21(6 Suppl): S123-130.
Davis, M. S. 1971. That's interesting! Towards a phenomenology of sociology and a
sociology of phenomenology. Philosophy of the social sciences, 1(2): 309-344.
Delaney, R., Strough, J., Parker, A. M., & de Bruin, W. B. 2015. Variations in decision-
making profiles by age and gender: A cluster-analytic approach. Personality and
individual differences, 85: 19-24.
DeMeester, R. H., Lopez, F. Y., Moore, J. E., Cook, S. C., & Chin, M. H. 2016. A model
of organizational context and shared decision making: application to LGBT racial
and ethnic minority patients. Journal of general internal medicine, 31(6): 651-
662.
DeSantis, C. E., Ma, J., Goding Sauer, A., Newman, L. A., & Jemal, A. 2017. Breast
cancer statistics, 2017, racial disparity in mortality by state. CA: A Cancer
Journal for Clinicians, 67(6): 439-448.
Desroches, S. 2010. Shared decision making and chronic diseases. Allergy, Asthma &
Clinical Immunology, 6(4): A8.
Dewey, J. 1925. Experience and nature. New York, NY: Dover Publications.
Dieleman, J. L., Squires, E., Bui, A. L., Campbell, M., Chapin, A., Hamavid, H., Horst,
C., Li, Z., Matyasz, T., & Reynolds, A. 2017. Factors Associated With Increases
in US Health Care Spending, 1996-2013. Jama, 318(17): 1668-1678.
DiMichele, D. M. 2008. Inhibitors in hemophilia: A primer (4th ed.). Montreal, Quebec:
World Federation of Hemophilia.
Djulbegovic, B., & Guyatt, G. H. 2017. Progress in evidence-based medicine: A quarter
century on. The Lancet, 390(10092): 415-423.
219
Djulbegovic, B., Hozo, I., Beckstead, J., Tsalatsanis, A., & Pauker, S. G. 2012. Dual
processing model of medical decision-making. BMC Medical Informatics And
Decision Making, 12(1): 94.
Du, L., & Lu, W. 2016. U.S. Health-Care System Ranks as One of the Least-Efficient,
Vol. 2017: Bllomberg.
Durning, S. J., Dong, T., Artino, A. R., van der Vleuten, C., Holmboe, E., & Schuwirth,
L. 2015. Dual processing theory and expertsʼ reasoning: exploring thinking on
national multiple-choice questions. Perspectives On Medical Education, 4(4):
168-175.
Eapen, Z. J., & Jain, S. H. 2017. Redesigning care for high-cost, high-risk patients,
Harvard Business Review.
Ehlayel, M. S., Bener, A., & Laban, M. A. 2013. Primary immunodeficiency diseases in
children: 15 year experience in a tertiary care medical center in Qatar. Journal Of
Clinical Immunology, 33(2): 317-324.
Eisenberg, L. 1977. Disease and illness Distinctions between professional and popular
ideas of sickness. Culture, medicine and psychiatry, 1(1): 9-23.
Eisenhardt, K. M. 1989. Agency theory: An assessment and review. Academy of
management review, 14(1): 57-74.
Eldar-Lissai, A., Hou, Q., & Krishnan, S. 2015. The changing costs of caring for
Hemophilia Patients in the US: insurers’ and patients’ perspectives. Value in
Health, 18(3): A304.
Elwyn, G., Frosch, D., Thomson, R., Joseph-Williams, N., Lloyd, A., Kinnersley, P.,
Cording, E., Tomson, D., Dodd, C., & Rollnick, S. 2012. Shared decision making:
a model for clinical practice. Journal Of General Internal Medicine, 27(10):
1361-1367.
Elwyn, G., Laitner, S., Coulter, A., Walker, E., Watson, P., & Thomson, R. 2010.
Implementing shared decision making in the NHS. BMJ, 357: j1744.
Ely, J. W., Kaldjian, L. C., & D'Alessandro, D. M. 2012. Diagnostic errors in primary
care: lessons learned. The Journal Of The American Board Of Family
Medicine, 25(1): 87-97.
Eraker, S. A., & Politser, P. 1982. How decisions are reached: physician and patient.
Annals of Internal Medicine, 97(2): 262-268.
Erikson, C., Jones, K., & Tilton, C. 2012. Physician specialty data book. Washington,
DC: Association of American Medical Colleges.
220
Espinosa-Rosales, F. J., Condino-Neto, A., Franco, J. L., & Sorensen, R. U. 2016. Into
action: Improving access to optimum care for all primary immunodeficiency
patients. Journal of Clinical Immunology, 36(5): 415-417.
Evans, J. S. B., & Stanovich, K. E. 2013. Dual-process theories of higher cognition
advancing the debate. Perspectives On Psychological Science, 8(3): 223-241.
Eysenck, H. J. 1963. Biological basis of personality. Nature, 199(4898): 1031-1034.
Fabrigar, L. R., Wegener, D. T., MacCallum, R. C., & Strahan, E. J. 1999. Evaluating the
use of exploratory factor analysis in psychological research. Psychological
methods, 4(3): 272.
Fiske, S. T., Dupree, C. H., Nicolas, G., & Swencionis, J. K. 2016. Status, power, and
intergroup relations: The personal is the societal. Current opinion in psychology,
11: 44-48.
Flanigan, T. S., McFarlane, E., & Cook, S. 2008. Conducting survey research among
physicians and other medical professionals: A review of current literature.
Paper presented at the Proceedings of the Survey Research Methods Section,
American Statistical Association.
Flynn, D. 2003. Non-medical influences upon medical decision-making and referral
behavior: an annotated bibliography: Greenwood Publishing Group.
Fram, A., & Freking, K. 2017. Sanders would make government health care role even
bigger, U.S. News & World Report.
Friesen-Storms, J. H., Bours, G. J., van der Weijden, T., & Beurskens, A. J. 2015. Shared
decision making in chronic care in the context of evidence based practice in
nursing. International Journal Of Nursing Studies, 52(1): 393-402.
Frosch, D. L., & Kaplan, R. M. 1999. Shared decision making in clinical medicine: past
research and future directions. American Journal Of Preventive Medicine, 17(4):
285-294.
Frosch, D. L., Moulton, B. W., Wexler, R. M., Holmes-Rovner, M., Volk, R. J., & Levin,
C. A. 2011. Shared decision making in the United States: policy and
implementation activity on multiple fronts. Zeitschrift Für Evidenz, Fortbildung
Und Qualität Im Gesundheitswesen, 105(4): 305-312.
Frost, J., & Massagli, M. 2009. PatientsLikeMe the case for a data-centered patient
community and how ALS patients use the community to inform treatment
decisions and manage pulmonary health. Chronic respiratory disease, 6(4): 225-
229.
221
Gabel, S. 2012. Perspective: physician leaders and their bases of power: common and
disparate elements. Academic Medicine, 87(2): 221-225.
Gallan, A. S., Jarvis, C. B., Brown, S. W., & Bitner, M. J. 2013. Customer positivity and
participation in services: an empirical test in a health care context. Journal Of
The Academy Of Marketing Science, 41(3): 338-356.
Gardulf, A., & Nicolay, U. 2006. Replacement IgG therapy and self-therapy at home
improve the health-related quality of life in patients with primary antibody
deficiencies. Current Opinion In Allergy And Clinical Immunology, 6(6): 434-
442.
Gardulf, A., Winiarski, J., Thorin, M., Arnlind, M. H., von Döbeln, U., & Hammarström,
L. 2017. Costs associated with treatment of severe combined
immunodeficiency—rationale for newborn screening in Sweden. Journal of
Allergy and Clinical Immunology, 139(5): 1713-1716. e1716.
Gerteis, J., Izrael, D., Deitz, D., LeRoy, L., Ricciardi, R., Miller, T., & Basu, J. 2014.
Multiple chronic conditions chartbook. Rockville, MD: Agency for Healthcare
Research and Quality (AHRQ) Publications.
Gibson, C. B. 2017. Elaboration, Generalization, Triangulation, and Interpretation: On
enhancing the value of mixed method research. Organizational Research
Methods, 20(2): 193-223.
Gigerenzer, G. 2015. Simply rational: Decision making in the real world: Oxford
University Press, USA.
Gigerenzer, G., & Goldstein, D. G. 1996. Reasoning the fast and frugal way: models of
bounded rationality. Psychological Review, 103(4): 650.
Giguère, A., Labrecque, M., Njoya, M., Thivierge, R., & Légaré, F. 2012. Development
of PRIDe: A tool to assess physicians’ preference of role in clinical decision
making. Patient Education And Counseling, 88(2): 277-283.
Glaser, B. 2017. Discovery of grounded theory: Strategies for qualitative research:
Routledge.
Glaser, B., & Strauss, A. 2017. Discovery of grounded theory: Strategies for qualitative
research: Routledge.
Godager, G., Henning-Schmidt, H., & Iversen, T. 2016. Does performance disclosure
influence physicians’ medical decisions? An experimental analysis. Journal of
Economic Behavior and Organization, 131: 36-46.
Godolphin, W. 2009. Shared decision-making. Healthcare Quarterly, 12(Sp): e186-e190.
222
Goffman, E. 1959. The moral career of the mental patient. Psychiatry, 22(2): 123-142.
Golden-Biddle, K., & Locke, K. 2007. Composing qualitative research: Sage.
Goodnough, L. T., Shander, A., & Brecher, M. E. 2003. Transfusion medicine: looking to
the future. The Lancet, 361(9352): 161-169.
Graber, M. L., Franklin, N., & Gordon, R. 2005. Diagnostic error in internal medicine.
Archives Of Internal Medicine, 165(13): 1493-1499.
Gravel, K., Légaré, F., & Graham, I. D. 2006. Barriers and facilitators to implementing
shared decision-making in clinical practice: A systematic review of health
professionals' perceptions. Implementation Science, 1(1): 16.
Green, A. R., Carrillo, J. E., & Betancourt, J. R. 2002. Why the disease-based model of
medicine fails our patients. Western journal of Medicine, 176(2): 141.
Greene, J., & McClintock, C. 1985. Triangulation in evaluation: Design and analysis
issues. Evaluation Review, 9(5): 523-545.
Greene, J. C., Caracelli, V. J., & Graham, W. F. 1989. Toward a conceptual framework
for mixed-method evaluation designs. Educational Evaluation And Policy
Analysis, 11(3): 255-274.
Grembowski, D., Schaefer, J., Johnson, K. E., Fischer, H., Moore, S. L., Tai-Seale, M.,
Ricciardi, R., Fraser, J. R., Miller, D., & LeRoy, L. 2014. A conceptual model of
the role of complexity in the care of patients with multiple chronic conditions.
Medical care, 52: S7-S14.
Grifols. 2017. Investors’ & Analysts’ Meeting 2017: Grifols.
Gringeri, A. 2011. Factor VIII safety: plasma-derived versus recombinant products.
Blood Transfusion, 9(4): 366.
Gringeri, A., Mantovani, L. G., Scalone, L., & Mannucci, P. M. 2003. Cost of care and
quality of life for patients with hemophilia complicated by inhibitors: the COCIS
Study Group. Blood, 102(7): 2358-2363.
Groopman, J. 2008. How doctors think: Houghton Mifflin Harcourt.
Groopman, J., & Hartzband, P. 2012. Your medical mind: How to decide what is right
for you: Penguin Books.
Groot, G., Waldron, T., Carr, T., McMullen, L., Bandura, L.-A., Neufeld, S.-M., &
Duncan, V. 2017. Development of a program theory for shared decision-making:
a realist review protocol. Systematic Reviews, 6(1): 114.
223
Guaní-Guerra, E., García-Ramírez, U. N., Jiménez-Romero, A. I., Velázquez-Ávalos, J.
M., Gallardo-Martínez, G., & Mendoza-Espinoza, F.-J. 2013. Primary
immunodeficiency diseases at reference and high-specialty hospitals in the state
of Guanajuato, Mexico. Biomed Research International, 2013(Article ID
187254).
Guyatt, G. H. 1991. Evidence-based medicine. ACP Journal Club, 114(2): A16-A16.
Hair, J. F. J., Black, W. C., Babin, B. J., & Anderson, R. E. 2010. Multivariate Data
Analysis (7th Edition ed.): Pearson Prentice Hall.
Hajjaj, F., Salek, M., Basra, M., & Finlay, A. 2010. Non-clinical influences on clinical
decision-making: a major challenge to evidence-based practice. Journal Of The
Royal Society Of Medicine, 103(5): 178-187.
Harden, A. 2010. Mixed-methods systematic reviews: Integrating quantitative and
qualitative findings. Focus, 25: 1-8.
Hardin, G. 1985. Filters against folly: Viking Books.
Hathi, S., & Kocher, R. 2017. The right way to reform health care: To cut costs, empower
patients. Foreign Affairs, 96(4): 17.
Hawley, S. T., & Morris, A. M. 2017. Cultural challenges to engaging patients in shared
decision making. Patient education and counseling, 100(1): 18-24.
Hayes, A. F. 2009. Beyond Baron and Kenny: Statistical mediation analysis in the new
millennium. Communication Monographs, 76(4): 408-420.
Hayes, A. F. 2013. Introduction to mediation, moderation, and conditional process
analysis: A regression-based approach: Guilford Press.
Heifetz, R. A. 1994. Leadership without easy answers: Harvard University Press.
Helman, C. G. 1981. Disease versus illness in general practice. Journal of the Royal
College of General Practitioners, 31(230): 548-552.
Henseler, J., Ringle, C. M., & Sarstedt, M. 2015. A new criterion for assessing
discriminant validity in variance-based structural equation modeling. Journal of
the academy of marketing science, 43(1): 115-135.
Hernandez-Trujillo, V. P., Scalchunes, C., Hernandez-Trujillo, H. S., Boyle, J., Williams,
P., Boyle, M., & Orange, J. S. 2015. Primary immunodeficiency diseases: An
opportunity in pediatrics for improving patient outcomes. Clinical Pediatrics,
54(13): 1265-1275.
HFA. 2014. Inhibitors, Vol. 2017.
224
Hibbard, J. H. 2017. Patient activation and the use of information to support informed
health decisions. Patient education and counseling, 100(1): 5-7.
Hickner, J., Thompson, P. J., Wilkinson, T., Epner, P., Shaheen, M., Pollock, A. M., Lee,
J., Duke, C. C., Jackson, B. R., & Taylor, J. R. 2014. Primary care physicians'
challenges in ordering clinical laboratory tests and interpreting results. The
Journal of the American Board of Family Medicine, 27(2): 268-274.
Hiltzik, M. 2018. Reducing healthcare costs doesn't require Bezos/Buffett/Dimon magic:
Every other country already knows how, Vol. 2018: Las Angelas Times.
Hock, D. 1999. Birth ofthe chaordic age. Los Angeles, CA: Pub Group West.
Holroyd-Leduc, J., Resin, J., Ashley, L., Barwich, D., Elliott, J., Huras, P., Légaré, F.,
Mahoney, M., Maybee, A., & McNeil, H. 2016. Giving voice to older adults
living with frailty and their family caregivers: engagement of older adults living
with frailty in research, health care decision making, and in health policy.
Research Involvement and Engagement, 2(1): 23.
Hossler, D., & Vesper, N. 1993. An exploratory study of the factors associated with
parental saving for postsecondary education. The Journal of Higher Education,
64(2): 140-165.
Hostetter, M., Klein, S., & McCarthy, D. 2017. CareMore: Improving outcomes and
controlling health care spending for high-needs patients: The Commonwealth
Fund.
Hu, L. t., & Bentler, P. M. 1999. Cutoff criteria for fit indexes in covariance structure
analysis: Conventional criteria versus new alternatives. Structural Equation
Modeling: A Multidisciplinary Journal, 6(1): 1-55.
Hunink, M. M., Weinstein, M. C., Wittenberg, E., Drummond, M. F., Pliskin, J. S.,
Wong, J. B., & Glasziou, P. P. 2014. Decision making in health and medicine:
integrating evidence and values: Cambridge University Press.
Iacobucci, D. 2010. Structural equations modeling: Fit indices, sample size, and advanced
topics. Journal of Consumer Psychology, 20(1): 90-98.
Isaacson, W. 2011. Steve Jobs: Die autorisierte Biografie des Apple-Gründers:
Verlagsgruppe Random House.
Isen, A. M. 2001. An influence of positive affect on decision making in complex
situations: Theoretical issues with practical implications. Journal of consumer
psychology, 11(2): 75-85.
225
Janssen, S. M., & Lagro-Janssen, A. L. 2012. Physician's gender, communication style,
patient preferences and patient satisfaction in gynecology and obstetrics: a
systematic review. Patient Education And Counseling, 89(2): 221-226.
Johnson, C. Y. 2017. After single payer failed, Vermont embarks on a big health care
experiment, The Washington Post.
Johnson, R. B., & Onwuegbuzie, A. J. 2004. Mixed methods research: A research
paradigm whose time has come. Educational researcher, 33(7): 14-26.
Jolles, S., Orange, J., Gardulf, A., Stein, M., Shapiro, R., Borte, M., & Berger, M. 2015.
Current treatment options with immunoglobulin G for the individualization of
care in patients with primary immunodeficiency disease. Clinical &
Experimental Immunology, 179(2): 146-160.
Jones, R. 1992. Decision-making and hospital referrals. Oxford General Practice Series,
22: 92-92.
Joseph-Williams, N., Elwyn, G., & Edwards, A. 2014. Knowledge is not power for
patients: a systematic review and thematic synthesis of patient-reported barriers
and facilitators to shared decision making. Patient education and counseling,
94(3): 291-309.
Joshi, A. Y., Iyer, V. N., Hagan, J. B., Sauver, J. L. S., & Boyce, T. G. 2009. Incidence
and temporal trends of primary immunodeficiency: A population-based cohort
study. Mayo Clinic Proceedings, 84(1): 16-22.
Kaba, R., & Sooriakumaran, P. 2007. The evolution of the doctor-patient relationship.
International Journal Of Surgery, 5(1): 57-65.
Kahneman, D. 2011. Thinking, fast and slow: Macmillan.
Kahneman, D. 2017. Less-than-Rational-Actors. In J. Christian (Ed.), Cheung Kong
Graduate School of Business. CKGSB Knowledge Magazine.
Kahneman, D., Knetsch, J. L., & Thaler, R. H. 1991. Anomalies: The endowment effect,
loss aversion, and status quo bias. The journal of economic perspectives, 5(1):
193-206.
Kaplan, S. H., Greenfield, S., Gandek, B., Rogers, W. H., & Ware, J. E. 1996.
Characteristics of physicians with participatory decision-making styles. Annals
Of Internal Medicine, 124(5): 497-504.
Keehan, S. P., Sisko, A. M., Truffer, C. J., Poisal, J. A., Cuckler, G. A., Madison, A. J.,
Lizonitz, J. M., & Smith, S. D. 2011. National health spending projections
through 2020: Economic recovery and reform drive faster spending growth.
Health Affairs, 30(8): 1594-1605.

226
Kenny, D. A. 2016. Miscellaneous Variables: Formative Variables and Second-Order
Factors.
Kiesler, D. J., & Auerbach, S. M. 2006. Optimal matches of patient preferences for
information, decision-making and interpersonal behavior: evidence, models and
interventions. Patient education and counseling, 61(3): 319-341.
Klein, J. G. 2005. Five pitfalls in decisions about diagnosis and prescribing. BMJ:
British Medical Journal, 330(7494): 781.
Kobrynski, L., Powell, R. W., & Bowen, S. 2014. Prevalence and morbidity of primary
immunodeficiency diseases, United States 2001–2007. Journal of clinical
immunology, 34(8): 954-961.
Konrad, T. R., Link, C. L., Shackelton, R. J., Marceau, L. D., von Dem Knesebeck, O.,
Siegrist, J., Arber, S., Adams, A., & McKinlay, J. B. 2010. It’s about time:
physicians’ perceptions of time constraints in primary care medical practice in
three national healthcare systems. Medical care, 48(2): 95.
Kourakos, M., Fradelos, E. C., Papathanasiou, I. V., Saridi, M., & Kafkia, T. 2017.
Communication as the Basis of Care for Patients with Chronic Diseases.
American Journal of Nursing, 7(3-1): 7-12.
Kramer, R. M., & Cook, K. S. 2004. Trust and distrust in organizations: Dilemmas and
approaches: Russell Sage Foundation.
Krosnick, J. A. 1999. Survey research. Annual review of psychology, 50(1): 537-567.
Krupat, E., Rosenkranz, S. L., Yeager, C. M., Barnard, K., Putnam, S. M., & Inui, T. S.
2000. The practice orientations of physicians and patients: the effect of doctor–
patient congruence on satisfaction. Patient Education And Counseling, 39(1):
49-59.
Lamb, C., Boland Jr, R. J., Lyytinen, K., & Wolfberg, A. 2015. Patient-driven vs.
evidence-centric decision models in the treatment of hemophilia. In W. S. o. M.
C. W. R. University (Ed.).
Lamb, C., Lyytinen, K., & Wang, Y. 2016. Does a physician’s decision making process
effect patient participation in the treatment choices of primary
immunodeficiency? In W. S. o. M. C. W. R. University (Ed.).
Larcher, V., Craig, F., Bhogal, K., Wilkinson, D., & Brierley, J. 2015. Making decisions
to limit treatment in life-limiting and life-threatening conditions in children: a
framework for practice. Archives of disease in childhood, 100(Suppl 2): s1-s23.

227
Lawrence, R. E., Rasinski, K. A., Yoon, J. D., & Curlin, F. A. 2015. Physician race and
treatment preferences for depression, anxiety, and medically unexplained
symptoms. Ethnicity & Health, 20(4): 354-364.
Lee, E., & Emanuel, E. J. 2013. Shared decision making to improve care and reduce
costs. New England Journal Of Medicine, 368(1): 6-8.
Lee, W., Joshi, A., Woolford, S., Sumner, M., Brown, M., Hadker, N., & Pashos, C.
2008. Physicians’ preferences towards coagulation factor concentrates in the
treatment of Haemophilia with inhibitors: a discrete choice experiment.
Haemophilia, 14(3): 454-465.
Légaré, F., Labrecque, M., Cauchon, M., Castel, J., Turcotte, S., & Grimshaw, J. 2012.
Training family physicians in shared decision-making to reduce the overuse of
antibiotics in acute respiratory infections: a cluster randomized trial. Canadian
Medical Association Journal, 184(13): E726-E734.
Légaré, F., Ratté, S., Gravel, K., & Graham, I. D. 2008. Barriers and facilitators to
implementing shared decision-making in clinical practice: update of a systematic
review of health professionals’ perceptions. Patient Education And Counseling,
73(3): 526-535.
Légaré, F., Stacey, D., Brière, N., Fraser, K., Desroches, S., Dumont, S., Sales, A., Puma,
C., & Aubé, D. 2013. Healthcare providers' intentions to engage in an
interprofessional approach to shared decision-making in home care programs: a
mixed methods study. Journal Of Interprofessional Care, 27(3): 214-222.
Légaré, F., Stacey, D., Turcotte, S., Cossi, M. J., Kryworuchko, J., Graham, I. D.,
Lyddiatt, A., Politi, M. C., Thomson, R., Elwyn, G., & Donner-Banzhoff, N.
2014. Interventions for improving the adoption of shared decision making by
healthcare professionals. Cochrane Database of Systematic Reviews, 9(Art. No.:
CD006732).
Légaré, F., & Thompson-Leduc, P. 2014. Twelve myths about shared decision making.
Patient education and counseling, 96(3): 281-286.
Légaré, F., & Witteman, H. O. 2013. Shared decision making: examining key elements
and barriers to adoption into routine clinical practice. Health Affairs, 32(2): 276-
284.
Leimeister, J. M., & Krcmar, H. 2005. Evaluation of a systematic design for a virtual
patient community. Journal of Computer‐Mediated Communication, 10(4): 00-
00.
Letiche, H. 2008. Making healthcare care: Managing via simple guiding principles:
IAP.
228
Lin, M.-Y., & Kressin, N. R. 2015. Race/ethnicity and Americans’ experiences with
treatment decision making. Patient Education And Counseling, 98(12): 1636-
1642.
Liras, A., & García-Trenchard, R. 2013. Treatment for hemophilia: recombinant versus
plasma-derived coagulation factors-controversy and debate forever? An ethical
medical challenge? Expert Review Of Hematology, 6(5): 489-492.
Lissack, M., & Roos, J. 1999. Words count: Viewing organizations as emerging systems
of languaging.
Loewenstein, G., & Chater, N. 2017. Putting nudges in perspective. Behavioural Public
Policy, 1(1): 26-53.
Longtin, Y., Sax, H., Leape, L. L., Sheridan, S. E., Donaldson, L., & Pittet, D. 2010.
Patient participation: current knowledge and applicability to patient safety.
Paper presented at the Mayo Clinic Proceedings.
Lovallo, D., & Sibony, O. 2010. The case for behavioral strategy. Mckinsey Quarterly,
2(1): 30-43.
Lynch, S. M. 2007. Introduction to applied Bayesian statistics and estimation for social
scientists: Springer Science & Business Media.
MacKenzie, S. B., & Podsakoff, P. M. 2012. Common method bias in marketing: causes,
mechanisms, and procedural remedies. Journal Of Retailing, 88(4): 542-555.
MacKenzie, S. B., Podsakoff, P. M., & Podsakoff, N. P. 2011. Construct measurement
and validation procedures in MIS and behavioral research: Integrating new and
existing techniques. Mis Quarterly, 35(2): 293-334.
Maly, R. C., Umezawa, Y., Ratliff, C. T., & Leake, B. 2006. Racial/ethnic group
differences in treatment decision‐making and treatment received among older
breast carcinoma patients. Cancer, 106(4): 957-965.
Mamede, S., van Gog, T., van den Berge, K., Rikers, R. M., van Saase, J. L., van
Guldener, C., & Schmidt, H. G. 2010. Effect of availability bias and reflective
reasoning on diagnostic accuracy among internal medicine residents. Jama,
304(11): 1198-1203.
Manchikanti, L., Helm, S., & Janata, J. W. 2012. Opioid epidemic in the United States.
Pain Physician, 15: ES9-ES38.
Mannucci, P. M., Mancuso, M. E., & Santagostino, E. 2012. How we choose factor VIII
to treat hemophilia. Blood, 119(18): 4108-4114.
229
Marinova, D., Kozlenkova, I. V., Cuttler, L., & Silvers, J. 2016. To Prescribe or Not to
Prescribe? Consumer Access to Life-Enhancing Products. Journal of Consumer
Research, 43(5): 806-823.
Marshall, S., Haywood, K., & Fitzpatrick, R. 2005. Patient involvement and collaboration
in shared decision making: A structured review to inform chronic disease
management: Report from the Patient-Reported Health Instruments Group to the
Department of Health.
Mason, M. 2010. Sample size and saturation in PhD studies using qualitative
interviews. Paper presented at the Forum Qualitative Sozialforschung/Forum:
Qualitative Social Research.
Matsunaga, M. 2010. How to Factor-Analyze Your Data Right: Do’s, Don’ts, and How-
To’s. International Journal Of Psychological Research, 3(1): 97-110.
Mazzi, M. A., Rimondini, M., Deveugele, M., Zimmermann, C., Deledda, G., & Bensing,
J. 2016. Does gender matter in doctor–patient communication during standard
gynaecological consultations? An analysis using mixed methods. Communication
& Medicine, 11(3): 285-298.
McCormack, L., Thomas, V., Lewis, M. A., & Rudd, R. 2017. Improving low health
literacy and patient engagement: a social ecological approach. Patient education
and counseling, 100(1): 8-13.
McDonald, K., Sundaram, V., Bravata, D., Lewis, R., Lin, N., Kraft, S., McKinnon, M.,
Paguntalan, H., & Owens, D. 2007. Closing the quality gap: A critical analysis
of quality improvement strategies. Rockville, MD: Stanford-UCSF Evidence-
based Practice Center. Agency for Healthcare Research and Quality.
McGlynn, E. A., Asch, S. M., Adams, J., Keesey, J., Hicks, J., DeCristofaro, A., & Kerr,
E. A. 2003. The quality of health care delivered to adults in the United States.
New England journal of medicine, 348(26): 2635-2645.
McGuire, A. L., McCullough, L. B., Weller, S. C., & Whitney, S. N. 2005. Missed
expectations?: physicians’ views of patients’ participation in medical decision-
making. Medical Care, 43(5): 466-470.
McMurray, R., Pullen, A., & Rhodes, C. 2011. Ethical subjectivity and politics in
organizations: A case of health care tendering. Organization, 18(4): 541-561.
McNeil, B. J., Pauker, S. G., Sox Jr, H. C., & Tversky, A. 1982. On the elicitation of
preferences for alternative therapies. New England journal of medicine, 306(21):
1259-1262.
McWilliams, J. M. 2016. Cost containment and the tale of care coordination. New
England Journal of Medicine, 375(23): 2218-2220.
230
Mead, E. L., Doorenbos, A. Z., Javid, S. H., Haozous, E. A., Alvord, L. A., Flum, D. R.,
& Morris, A. M. 2013. Shared decision-making for cancer care among racial and
ethnic minorities: a systematic review. American journal of public health,
103(12): e15-e29.
Medicare Payment Advisory Commission. 2010. Aligning incentives in Medicare. Paper
presented at the Report to the Congress: MedPAC. June 2010, Washington, DC.
MedPAC. 2010. Report to the Congress: Aligning incentives in medicine.
Menzin, J., Sussman, M., Munsell, M., & Zbrozek, A. 2014. Economic impact of
infections among patients with primary immunodeficiency disease receiving IVIG
therapy. ClinicoEconomics and Outcomes Research: CEOR, 6: 297302.
Meunier, V., Laamen, S., Harison, M., Lewis, D. R., Muraoka, S., & Walker, A. L. 2015.
Hemophilia: reshuffling the cards. Global Pharmaceuticals.
Minno, M., Minno, G., Capua, M., Cerbone, A., & Coppola, A. 2010. Cost of care of
haemophilia with inhibitors. Haemophilia, 16(1): e190-e201.
Mirowsky, J. 2017. Education, social status, and health: Routledge.
Modell, V., Gee, B., Lewis, D. B., Orange, J. S., Roifman, C. M., Routes, J. M.,
Sorensen, R. U., Notarangelo, L. D., & Modell, F. 2011. Global study of primary
immunodeficiency diseases (PI)—diagnosis, treatment, and economic impact: an
updated report from the Jeffrey Modell Foundation. Immunologic Research,
51(1): 61-70.
Moens, L. N., Falk-Sörqvist, E., Asplund, A. C., Bernatowska, E., Smith, C. E., &
Nilsson, M. 2014. Diagnostics of primary immunodeficiency diseases: a
sequencing capture approach. PLoS One, 9(12): e114901.
Mondak, J. J., Hibbing, M. V., Canache, D., Seligson, M. A., & Anderson, M. R. 2010.
Personality and civic engagement: An integrative framework for the study of trait
effects on political behavior. American Political Science Review, 104(1): 85-110.
Montgomery, K. 2005. How doctors think: Clinical judgment and the practice of
medicine: Oxford University Press.
Montori, V. M., Gafni, A., & Charles, C. 2006. A shared treatment decision‐making
approach between patients with chronic conditions and their clinicians: the case of
diabetes. Health Expectations, 9(1): 25-36.
Morse, J. M. 1994. Designing funded qualitative research. In N. K. Denzin, & Y. S.
Lincoln (Eds.), Handbook of qualitative research 220-235. Thousand Oaks, CA:
Sage Publications.
231
Mulley, A. G., Trimble, C., & Elwyn, G. 2012. Stop the silent misdiagnosis: Patients’
preferences matter. BMJ, 345: 23.
Murray, E., Pollack, L., White, M., & Lo, B. 2007. Clinical decision-making: physicians'
preferences and experiences. BMC Family Practice, 8(1): 1.
Myers, M. D. 2013. Qualitative research in business and management: Sage.
Nannenga, M. R., Montori, V. M., Weymiller, A. J., Smith, S. A., Christianson, T. J.,
Bryant, S. C., Gafni, A., Charles, C., Mullan, R. J., & Jones, L. A. 2009. A
treatment decision aid may increase patient trust in the diabetes specialist. The
Statin Choice randomized trial. Health Expectations, 12(1): 38-44.
Nannestad, P. 2008. What have we learned about generalized trust, if anything? Annual
Review of Political Science, 11: 413-436.
Nguyen, H. 2011. The principal-agent problems in health care: evidence from prescribing
patterns of private providers in Vietnam. Health Policy and Planning,
26(suppl_1): i53-i62.
Nicolay, U., Haag, S., Eichmann, F., Herget, S., Spruck, D., & Gardulf, A. 2005.
Measuring treatment satisfaction in patients with primary immunodeficiency
diseases receiving lifelong immunoglobulin replacement therapy. Quality Of Life
Research, 14(7): 1683-1691.
Noonan, V., Lyddiatt, A., Ware, P., Jaglal, S., Riopelle, R., Bingham, C., Figueiredo, S.,
Sawatzky, R., Santana, M., & Bartlett, S. 2017. Montreal accord on patient-
reported outcomes use series–paper 3: Patient reported outcomes (PRO) can
facilitate shared decision-making and guide self-management. Journal of Clinical
Epidemiology, 89: 125-135.
NORC. 2014. Demonstrating the effectiveness of patient feedback in improving the
accuracy.
North, D. W. 1968. A tutorial introduction to decision theory. Systems Science And
Cybernetics, Ieee Transactions On, 4(3): 200-210.
O'Connor, A. M., Bruine de Bruin, W., Cassels, A., Driedger, S., Greenberg, J., Gully, P.,
Kreps, G., Lemyre, L., Lofstedt, R., & North, D. 2015. Health Product Risk
Communication: Is the message getting through?: Council of Canadian
Academies.
O'Connor, A. M., Llewellyn-Thomas, H. A., & Flood, A. B. 2004. Modifying
unwarranted variations in health care: shared decision making using patient
decision aids. Health Affairs: VAR63.
232
O'Hare, A. M., Rodriguez, R. A., & Bowling, C. B. 2016. Caring for patients with kidney
disease: shifting the paradigm from evidence-based medicine to patient-centered
care. Nephrology Dialysis Transplantation, 31(3): 368-375.
O’Connor, A. M., Wennberg, J. E., Legare, F., Llewellyn-Thomas, H. A., Moulton, B.
W., Sepucha, K. R., Sodano, A. G., & King, J. S. 2007. Toward the ‘tipping
point’: decision aids and informed patient choice. Health Affairs, 26(3): 716-725.
O’Hara, J., Hughes, D., Camp, C., Burke, T., Carroll, L., & Diego, D.-A. G. 2017. The
cost of severe haemophilia in Europe: the CHESS study. Orphanet journal of
rare diseases, 12(1): 106.
O’Reilly, K., Paper, D., & Marx, S. 2012. Demystifying grounded theory for business
research. Organizational Research Methods, 15(2): 247-262.
OECD. 2015. Health at a Glance 2015, OECD Indicators, Vol. 15. OECD Publishing,
Paris.
Ofri, D. 2017. What Patients Say, what Doctors Hear: What Doctors Say, what Patients
Hear: Beacon Press.
Oshima Lee, E., & Emanuel, E. J. 2013. Shared decision making to improve care and
reduce costs. New England Journal Of Medicine, 368(1): 6-8.
Paradies, Y., Truong, M., & Priest, N. 2014. A systematic review of the extent and
measurement of healthcare provider racism. Journal Of General Internal
Medicine, 29(2): 364-387.
Parekh, A. K., & Barton, M. B. 2010. The challenge of multiple comorbidity for the US
health care system. Jama, 303(13): 1303-1304.
Parekh, A. K., Goodman, R. A., Gordon, C., Koh, H. K., & Conditions, H. I. W. o. M. C.
2011. Managing multiple chronic conditions: a strategic framework for improving
health outcomes and quality of life. Public health reports, 126(4): 460-471.
Patel, V. L., Kaufman, D. R., & Arocha, J. F. 2002. Emerging paradigms of cognition in
medical decision-making. Journal Of Biomedical Informatics, 35(1): 52-75.
Patel, V. L., Yoskowitz, N. A., & Arocha, J. F. 2009. Towards effective evaluation and
reform in medical education: a cognitive and learning sciences perspective.
Advances in Health Sciences Education, 14(5): 791-812.
Paternotte, E., van Dulmen, S., van der Lee, N., Scherpbier, A. J., & Scheele, F. 2015.
Factors influencing intercultural doctor–patient communication: A realist review.
Patient education and counseling, 98(4): 420-445.
233
Pear, R. 2017. Minnesota finds a way to slow soaring health premiums, The New York
Times.
Peck, B. M. 2011. Age-related differences in doctor-patient interaction and patient
satisfaction. Current Gerontology and Geriatrics Research, 2011(Article ID
137492).
Peikes, D., Chen, A., Schore, J., & Brown, R. 2009. Effects of care coordination on
hospitalization, quality of care, and health care expenditures among Medicare
beneficiaries: 15 randomized trials. Jama, 301(6): 603-618.
Pelaccia, T., Tardif, J., Triby, E., & Charlin, B. 2011. An analysis of clinical reasoning
through a recent and comprehensive approach: The dual-process theory. Medical
Education Online, 16(1).
Pereira, C. M., Amaral, C. F., Ribeiro, M. M., Paro, H. B., Pinto, R. M., Reis, L. E.,
Silva, C. H., & Krupat, E. 2013. Cross-cultural validation of the Patient–
Practitioner Orientation Scale (PPOS). Patient Education And Counseling,
91(1): 37-43.
Petrič, G., Atanasova, S., & Kamin, T. 2017. Impact of social processes in online health
communities on patient empowerment in relationship with the physician:
Emergence of functional and dysfunctional empowerment. Journal of Medical
Internet Research, 19(3): e74.
Petroshius, S. M., Titus, P. A., & Hatch, K. J. 1995. Physician attitudes toward
pharmaceutical drug advertising. Journal Of Advertising Research, 35(6): 41-52.
Peyvandi, F., Rosendaal, F. R., O'Mahony, B., & Mannucci, P. M. 2014. Reply to: The
importance and challenge of pediatric trials of hemophilia drugs. Nature
Medicine, 20(5): 466-466.
Physicians Practice. 2017. 2017 Great American Physician Survey, Vol. 2017: Physicians
Practice.
Picard, C., Al-Herz, W., Bousfiha, A., Casanova, J.-L., Chatila, T., Conley, M. E.,
Cunningham-Rundles, C., Etzioni, A., Holland, S. M., & Klein, C. 2015. Primary
immunodeficiency diseases: an update on the classification from the International
Union of Immunological Societies Expert Committee for Primary
Immunodeficiency 2015. Journal of clinical immunology, 35(8): 696-726.
Pipe, S. W. 2012. The hope and reality of long‐acting hemophilia products. American
Journal Of Hematology, 87(S1): S33-S39.
Podsakoff, N. P., Podsakoff, P. M., MacKenzie, S. B., & Klinger, R. L. 2013. Are we
really measuring what we say we're measuring? Using video techniques to
234
supplement traditional construct validation procedures. Journal of Applied
Psychology, 98(1): 99.
Podsakoff, P. M., MacKenzie, S. B., Lee, J.-Y., & Podsakoff, N. P. 2003. Common
Method Biases in Behavioral Research: A Critical Review of the Literature and
Recommended Remedies. Journal Of Applied Psychology, 88(5): 879-903.
Preacher, K. J., Rucker, D. D., & Hayes, A. F. 2007. Addressing moderated mediation
hypotheses: Theory, methods, and prescriptions. Multivariate Behavioral
Research, 42(1): 185-227.
Putnam, R. D. 1995. Bowling alone: America's declining social capital. Journal of
democracy, 6(1): 65-78.
Reio, T. G., & Shuck, B. 2014. Exploratory factor analysis implications for theory,
research, and practice. Advances In Developing Human Resources, 17(1): 12-25.
Resnick, E. S., Bhatt, P., Sidi, P., & Cunningham-Rundles, C. 2013. Examining the use
of ICD-9 diagnosis codes for primary immune deficiency diseases in New York
State. Journal of clinical immunology, 33(1): 40-48.
Richardson, W. C., Berwick, D. M., Bisgard, J., Bristow, L., Buck, C., & Cassel, C.
2001. Crossing the quality chasm: A new health system for the 21st century.
Washington, DC: Institute of Medicine, National Academy Press
Rosenthal, E. 2017. An American sickness: How healthcare became big business and
how you can take it back: New York, NY: Penguin Press.
Roter, D. 2017. Bridging the gap between patient-centered care and evidence-based
medicine: How and why communication matters: Kimmel Cancer Center,
Presentations and Grand Rounds. Paper 42.
http://jdc.jefferson.edu/kimmelgrandrounds/42.
Roter, D. L., Hall, J. A., & Aoki, Y. 2002. Physician gender effects in medical
communication: a meta-analytic review. Jama, 288(6): 756-764.
Rothenfluh, F., & Schulz, P. J. 2017. Physician rating websites: What aspects are
important to identify a good doctor, and are patients capable of assessing them? A
mixed-methods approach including physicians’ and health care consumers’
perspectives. Journal of Medical Internet Research, 19(5): e127.
Rothman, D. J. 2017. Strangers at the bedside: A history of how law and bioethics
transformed medical decision making: Routledge.
Rothstein, M. A. 2014. Autonomy and paternalism in health policy: currents in
contemporary bioethics. The Journal of Law, Medicine & Ethics, 42(4): 590-
594.
235
Rousseau, D. M. 2012. The Oxford handbook of evidence-based management: Oxford
University Press.
Sackett, D. L., Rosenberg, W. M., Gray, J. M., Haynes, R. B., & Richardson, W. S. 1996.
Evidence based medicine: what it is and what it isn't: British Medical Journal
Publishing Group.
Samaan, K., Levasseur, M.-C., Decaluwe, H., St-Cyr, C., Chapdelaine, H., Des Roches,
A., & Haddad, E. 2014. SCIg vs IVIg: Let's Give Patients the Choice! Journal Of
Clinical Immunology, 34(6): 611.
Sapolsky, R. M. 2017. Behave: The Biology of Humans at Our Best and Worst:
Penguin.
Say, R. E., & Thomson, R. 2003. The importance of patient preferences in treatment
decisions—challenges for doctors. BMJ: British Medical Journal, 327(7414):
542.
Scalone, L., Mantovani, L., Borghetti, F., Von Mackensen, S., & Gringeri, A. 2009.
Patients’, physicians’, and pharmacists’ preferences towards coagulation factor
concentrates to treat haemophilia with inhibitors: results from the COHIBA
Study. Haemophilia, 15(2): 473-486.
Schattner, A., & Simon, S. R. 2017. Diminishing patient face time in residencies and
patient-centered care: Elsevier.
Schiavone, G., De Anna, G., Mameli, M., Rebba, V., & Boniolo, G. 2014. Libertarian
paternalism and health care policy: a deliberative proposal. Medicine, Health
Care and Philosophy, 17(1): 103-113.
Schiff, G. D. 2008. Minimizing diagnostic error: The importance of follow-up and
feedback: Elsevier.
Schneider, E. C., Sarnak, D. O., Squires, D., Shah, A., & Doty, M. M. 2017. Mirror,
mirror 2017: The Commonwealth Fund, July 2017. Available from
http://www.commonwealthfund.org/publications/fund-reports/2017/jul/mirror-
mirror-international-comparisons-2017.
Schnell, M., & Currie, J. 2017. Addressing the opioid epidemic: Is there a role for
physician education?: National Bureau of Economic Research, NBER Working
Paper No. 23645.
Schoen, C., Guterman, S., Shih, A., Lau, J., Kasimow, S., Gauthier, A., & Davis, K.
2007. Bending the curve: options for achieving savings and improving value in
US health spending: New York: The Commonwealth Fund.
236
Schoenthaler, A., Montague, E., Baier Manwell, L., Brown, R., Schwartz, M. D., &
Linzer, M. 2014. Patient–physician racial/ethnic concordance and blood pressure
control: the role of trust and medication adherence. Ethnicity & health, 19(5):
565-578.
Schon, D. 1983. The reflective practitioner. New York, NY: Basic Books.
Schulman, K. A., Berlin, J. A., Harless, W., Kerner, J. F., Sistrunk, S., Gersh, B. J., Dube,
R., Taleghani, C. K., Burke, J. E., & Williams, S. 1999. The effect of race and sex
on physicians' recommendations for cardiac catheterization. New England
Journal of Medicine, 340(8): 618-626.
Schwartz, R. A. 2013. Factor VIII Treatment & Management.
Scott, J. 2000. Rational choice theory. In G. Browning, A. Halcli, & F. Webster (Eds.),
Understanding contemporary society: Theories of the present: 126-138: Sage
Publications.
Seeborg, F. O., Seay, R., Boyle, M., Boyle, J., Scalchunes, C., & Orange, J. S. 2015.
Perceived Health in Patients with Primary Immune Deficiency. Journal Of
Clinical Immunology, 35(7): 638-650.
Shaffer, J. A., DeGeest, D., & Li, A. 2016. Tackling the problem of construct
proliferation: A guide to assessing the discriminant validity of conceptually
related constructs. Organizational Research Methods, 19(1): 80-110.
Shapiro, R. S. 2013. Supplement: Frontiers in immunoglobulin therapy of primary
immunodeficiency disease. Journal of Clinical Immunology, 37(2): 187.
Shapiro, R. S., Wasserman, R. L., Bonagura, V., & Gupta, S. 2014. Emerging paradigm
of primary immunodeficiency disease: Individualizing immunoglobulin dose and
delivery to enhance outcomes. Journal of Clinical Immunology, 37(2): 190-196.
Siegel, A. L., & Ruh, R. A. 1973. Job involvement, participation in decision making,
personal background, and job behavior. Organizational Behavior And Human
Performance, 9: 318-327.
Silverman, D. 2011. Interpreting qualitative data: A guide to the principles of
qualitative research: SAGE Publications Limited.
Silverman, D. 2015. Interpreting qualitative data: Sage.
Silvers, J., Marinova, D., Mercer, M. B., Connors, A., & Cuttler, L. 2010. A national
study of physician recommendations to initiate and discontinue growth hormone
for short stature. Pediatrics, 126(3): 468-476.
Simon, H. A. 1996. The sciences of the artificial: MIT press.
237
Singh, J., Cuttler, L., & Silvers, J. 2004. Toward understanding consumers' role in
medical decisions for emerging treatments: Issues, framework and hypotheses.
Journal Of Business Research, 57(9): 1054-1065.
Snipes, S. A., Sellers, S. L., Tafawa, A. O., Cooper, L. A., Fields, J. C., & Bonham, V. L.
2011. Is race medically relevant? A qualitative study of physicians' attitudes about
the role of race in treatment decision-making. BMC Health Services Research,
11(1): 183.
Sox, H. C., Higgins, M. C., & Owens, D. K. 2013. Medical Decision Making (2 ed.):
Wiley-Blackwell.
Sposito, V., Hand, M., & Skarpness, B. 1983. On the efficiency of using the sample
kurtosis in selecting optimal lpestimators. Communications In Statistics-
Simulation And Computation, 12(3): 265-272.
Squires, D., & Anderson, C. 2015. US health care from a global perspective: spending,
use of services, prices, and health in 13 countries. The Commonwealth Fund, 15:
1-16.
Srivastava, A., Brewer, A., Mauser‐Bunschoten, E., Key, N. S., Kitchen, S., Llinas, A.,
Ludlam, C., Mahlangu, J., Mulder, K., & Poon, M. 2013. Guidelines for the
management of hemophilia. Haemophilia, 19(1): e1-e47.
Stacey, D., Bennett, C. L., Barry, M. J., Col, N. F., Eden, K. B., Holmes-Rovner, M.,
Llewellyn-Thomas, H., Lyddiatt, A., Légaré, F., & Thomson, R. 2011. Decision
aids for people facing health treatment or screening decisions. Cochrane
Database Syst Rev, 10(10).
Stacey, D., Légaré, F., Col, N. F., Bennett, C. L., Barry, M. J., Eden, K. B., Holmes‐
Rovner, M., Llewellyn‐Thomas, H., Lyddiatt, A., & Thomson, R. 2014. Decision
aids for people facing health treatment or screening decisions. The Cochrane
Library.
Stanovich, K. E. 2011. Rationality and the reflective mind: Oxford University Press.
Stanovich, K. E., & West, R. F. 2000. Individual differences in reasoning: Implications
for the rationality debate? Behavioral and brain sciences, 23(5): 645-665.
Stanovich, K. E., & West, R. F. 2008. On the relative independence of thinking biases
and cognitive ability. Journal of personality and social psychology, 94(4): 672.
Stark, M., & Fins, J. J. 2014. The ethical imperative to think about thinking. Cambridge
Quarterly of Healthcare Ethics, 23(04): 386-396.
238
Stevenson, F. A., Barry, C. A., Britten, N., Barber, N., & Bradley, C. P. 2000. Doctor–
patient communication about drugs: the evidence for shared decision making.
Social Science & Medicine, 50(6): 829-840.
Strauss, A., & Corbin, J. 1998. Basics of qualitative research: Procedures and
techniques for developing grounded theory. Thousand Oaks, CA: Sage
Publications.
Street, A. 2012. Developing models of haemophilia care. Haemophilia, 18(s4): 89-93.
Street Jr, R. L., Gordon, H. S., Ward, M. M., Krupat, E., & Kravitz, R. L. 2005. Patient
participation in medical consultations: why some patients are more involved than
others. Medical Care, 43(10): 960-969.
Sturgis, P., & Smith, P. 2010. Assessing the validity of generalized trust questions: what
kind of trust are we measuring? International journal of public opinion
research, 22(1): 74-92.
Sturmberg, J. P., & Martin, C. 2013. Handbook of systems and complexity in health:
Springer Science & Business Media.
Sugawara, Y., Narimatsu, H., Hozawa, A., Shao, L., Otani, K., & Fukao, A. 2012. Cancer
patients on Twitter: a novel patient community on social media. BMC Research
Notes, 5(1): 699.
Sunstein, C., & Thaler, R. 2008. Why nudge?: The politics of libertarian paternalism:
Yale University Press.
Tanio, C. 2014. Developing physician culture in new risk models, The Health Care Blog.
Tapscott, D. 2010. Macrowikinomics: New solutions for a connected planet: Atlantic
Books Ltd.
Tashakkori, A., & Teddlie, C. 2008. Quality of inferences in mixed methods research:
Calling for an integrative framework. In M. M. Bergman (Ed.), Advances in
mixed methods research: 101-119: Sage Publications.
Teddlie, C., & Tashakkori, A. 2003. Major issues and controveries in the use of mixed
methods in the social and behvioral sciences. In A. Tashakkori, & C. Teddlie
(Eds.), Handbook of Mixed Methods in Social & Behavioral Research: 3-50:
Sage Publications.
Teddlie, C., & Tashakkori, A. 2009. Foundations of mixed methods research:
Integrating quantitative and qualitative approaches in the social and behavioral
sciences: Sage Publications Inc.
239
Thaler, R., & Sunstein, C. R. 2003. Libertarian paternalism. American Economic
Review, 93(2): 175-179.
The Joint Commission. 2007. “What did the doctor say?:” Improving health literacy to
protect patient safety Available from
https://www.jointcommission.org/assets/1/18/improving_health_literacy.pdf.
Thom, D. H., Wong, S. T., Guzman, D., Wu, A., Penko, J., Miaskowski, C., & Kushel,
M. 2011. Physician trust in the patient: development and validation of a new
measure. The Annals Of Family Medicine, 9(2): 148-154.
Thomas, D. M., & Watson, R. T. 2002. Q-sorting and MIS research: A primer.
Communications Of The Association For Information Systems, 8(1): 9.
Thygeson, M., Morrissey, L., & Ulstad, V. 2010. Adaptive leadership and the practice of
medicine: a complexity‐based approach to reframing the doctor–patient
relationship. Journal of Evaluation in Clinical Practice, 16(5): 1009-1015.
Tiffen, J., Corbridge, S. J., & Slimmer, L. 2014. Enhancing clinical decision making:
development of a contiguous definition and conceptual framework. Journal of
Professional Nursing, 30(5): 399-405.
Timmermans, S., & Berg, M. 2010. The gold standard: The challenge of evidence-based
medicine and standardization in health care: Temple University Press.
Topol, E. J. 2015. The patient will see you now: the future of medicine is in your hands:
Tantor Media.
Toro, R. 2012. Leading Causes of Death in the US: 1900 - Present (Infographic),
LiveScience, Vol. 2018: LiveScience.
Traylor, A. H., Schmittdiel, J. A., Uratsu, C. S., Mangione, C. M., & Subramanian, U.
2010. The Predictors of Patient–Physician Race and Ethnic Concordance: A
Medical Facility Fixed‐Effects Approach. Health Services Research, 45(3): 792-
805.
Truven Health MarketScan® Research Databases. 2010. Commercial claims and
encounters medicare supplemental.
Tversky, A., & Kahneman, D. 1973. Availability: A heuristic for judging frequency and
probability. Cognitive psychology, 5(2): 207-232.
Tversky, A., & Kahneman, D. 1986a. Judgment under uncertainty: Heuristics and biases.
Judgment And Decision Making: An Interdisciplinary Reader: 38-55.
Tversky, A., & Kahneman, D. 1986b. Rational choice and the framing of decisions.
Journal of Business, 59(4): S251-S278.
240
Tversky, A., & Kahneman, D. 1992. Advances in prospect theory: Cumulative
representation of uncertainty. Journal of Risk and uncertainty, 5(4): 297-323.
U.S. Department of Health Human Services. 2010. Multiple chronic conditions—a
strategic framework: Optimum health and quality of life for individuals with
multiple chronic conditions. Washington, DC: US Department of Health and
Human Services.
UKHCDO. 2012. UKHCDO annual report 2012 & bleeding disorder statistics for the
financial year 2011/2012.
UKHCDO. 2014. Bleeding Disorder Statistics for April 2013 to March 2014: UKHCDO.
Van de Ven, A. H. 2007. Engaged scholarship: A guide for organizational and social
research: Oxford University Press on Demand.
Venkatesh, V., Brown, S. A., & Bala, H. 2013. Bridging the qualitative-quantitative
divide: Guidelines for conducting mixed methods research in information
systems. Mis Quarterly, 37(1): 21-54.
Veroff, D., Marr, A., & Wennberg, D. E. 2013. Enhanced support for shared decision
making reduced costs of care for patients with preference-sensitive conditions.
Health Affairs, 32(2): 285-293.
Vohs, K. D. 2015. Money priming can change people’s thoughts, feelings, motivations,
and behaviors: An update on 10 years of experiments. Journal of Experimental
Psychology: General, 144(4): e86.
Wagner, E. H., Austin, B. T., Davis, C., Hindmarsh, M., Schaefer, J., & Bonomi, A.
2001. Improving chronic illness care: translating evidence into action. Health
affairs, 20(6): 64-78.
Wald, H. S. 2015. Professional identity (trans) formation in medical education: reflection,
relationship, resilience. Academic Medicine, 90(6): 701-706.
Walls, A. N. 2014. The “when” of libertarian paternalism, Ethical Issues in Health Care:
Emory.
Weick, K. E., Sutcliffe, K. M., & Obstfeld, D. 2008. Organizing for high reliability:
Processes of collective mindfulness. Crisis management, 3(1): 81-123.
Whitson, H. E., & Boyd, C. M. 2016. Managing multiple comorbidities, UpToDate:
UpToDate, Inc. .
WHO. 2000. The world health report 2000: health systems: improving performance:
World Health Organization.
241
Williams, L. J., Hartman, N., & Cavazotte, F. 2010. Method variance and marker
variables: A review and comprehensive CFA marker technique. Organizational
Research Methods, 13(3): 477-514.
Williams, L. J., Vandenberg, R. J., & Edwards, J. R. 2009. Structural equation modeling
in management research: A guide for improved analysis. Academy of
Management Annals, 3(1): 543-604.
Wilson, L., Tang, J., Zhong, L., Balani, G., Gipson, G., Xiang, P., Yu, D., & Srinivas, S.
2014. New therapeutic options in metastatic castration-resistant prostate cancer:
Can cost-effectiveness analysis help in treatment decisions? Journal Of Oncology
Pharmacy Practice, 20(6): 417-425.
Wisdom, J. P., Cavaleri, M. A., Onwuegbuzie, A. J., & Green, C. A. 2012.
Methodological reporting in qualitative, quantitative, and mixed methods health
services research articles. Health Services Research, 47(2): 721-745.
Wong, K. K.-K. 2013. Partial least squares structural equation modeling (PLS-SEM)
techniques using SmartPLS. Marketing Bulletin, 24(1): 1-32.
WorldBank. 2015. GDP per capita (current US$), The World Bank, , Vol. 2015.
Worthington, R. L., & Whittaker, T. A. 2006. Scale development research: A content
analysis and recommendations for best practices. The Counseling Psychologist,
34(6): 806-838.
Yarnall, K. S., Pollak, K. I., Østbye, T., Krause, K. M., & Michener, J. L. 2003. Primary
care: is there enough time for prevention? American journal of public health,
93(4): 635-641.
Yeh, D. D., Naraghi, L., Larentzakis, A., Nielsen, N., Dzik, W., Bittner, E. A., Chang, Y.,
Kaafarani, H. M., Fagenholz, P., & Lee, J. 2015. Peer-to-peer physician feedback
improves adherence to blood transfusion guidelines in the surgical intensive care
unit. journal of trauma and acute care surgery, 79(1): 65-70.
Yong, A. G., & Pearce, S. 2013. A beginner’s guide to factor analysis: Focusing on
exploratory factor analysis. Tutorials In Quantitative Methods For Psychology,
9(2): 79-94.
Younger, E. M., Epland, K., Zampelli, A., & Hintermeyer, M. K. 2015. Primary
immunodeficiency diseases: A primer for PCPs. The Nurse Practitioner, 40(2):
1-7.
Zaiden, R. A. 2014a. Hemophilia A treatment & management. In S. C. Dronen (Ed.),
Medscape.
242
Zaiden, R. A. 2014b. Hemophilia B treatment & management. In S. C. Dronen (Ed.),
Medscape.
Related Documents