4 STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF INFLUENZA Yes No Intoxication. CNS involvement. Acute onset of the disease with a fast t rise, headache, vomit. Resistant red dermographism, herpetic eruption on the lips. Patients can exactly indicate the time of the beginning of the disease. Children suffer from intensive headache, trashing around in their bed and broken sleep. The pain gets more intensive when turning the head, with sound and light irritants. From the first day there is repeated vomiting, not related to food intake. Children at early age have clonic-tonic convulsions frequently. Positive meningeal symptoms. In CBC: eosinofiliya, neutrophilic leukocytosis, elevated ESR. The nature of the cerebrospinal fluid: turbid, purulent, thousandth pleocytosis, neutrophilic character. Protein + + +. Low sugar and chloride levels. Meningococcal meningitis Fever syndrome, catarrh of the upper respiratory tract: profuse muco-purulent nasal discharge, mild hyperemia of posterior pharyngeal wall. Specific eye disease — purulent conjunctivitis. There is a hyperplasia of oropharyngeal lymphoid formations and lymphadenopathy of the neck. Normal CBC. Adenoviral infection Acute onset with moderate symptoms of intoxication. Catarrhal phenomena occur from the first day of illness. There is a hard, rough, dry cough, sore throat, runny nose, nasal congestion. There is a nasal discharge initially slimy, then muco-purulent. There is swelling and redness of the mucous membrane arches, soft palate, posterior pharyngeal wall. Often the first manifestation of the disease is «grits» syndrome, usually at night the child suddenly wakes up from a rough barking cough. Hoarseness, noisy breathing quickly join, laryngeal stenosis develops. Stenosis severity rarely reaches 2 nd degree. Parainfluenza The presence of purulent center (otitis, sinusitis, pneumonia) often precedes development of the disease. Sudden onset, anxiety, acute headache, hyperesthesia, repeated vomiting. Early meningeal symptoms. In young children — bulging of fontanelle, separation of sutures, increased sizes of the skull. The limb paresis, static locomotor ataxia, cranial nerve disfunction appear. Patients are pale and cyanotic, with intensive dyspnea. Hepatosplenomegaly. Frequent development of edema — brain edema, which may cause death in the first 3 days of the illness. In CBC: leukocytosis, with a sharp shift of neutrophils, high ESR. Cerebrospinal fluid analysis: turbid, purulent, greenish-gray fluid, neutrophil cell count — thousandths, a significant increase of protein level. Bacteriological test of CSF reveals diplococci of lanceolate form located extracellularly. Pneumococcal meningitis Expressed catarrhal period: purulent discharge from the nose, conjunctivitis. Dry, haunting cough. Appearance of Koplik spots. Three-stage rash: 1) maculopapular rash; 2) period of pigmentation; 3) branny olesquamation. Leukopenia in CBC. Measles Symptoms of nervous system impairment usually follow the inflammation of salivary glands, but both disorders can also occur simultaneously. Acute development of the disease with chill, headache, vomiting, weakness and myalgia. Meningeal symptoms are expressed moderately. Clear cerebrospinal fluid flows under high pressure, normal or slightly increased protein levels, lymphocyte cell count hundredths. Сhloride and sugar concentrations are not changed. Lumbar puncture makes patient feel better. Parotitic meningitis Serous meningitis of enteroviral etiology The main symptoms are: prolonged fever, headache, specific intoxication — stupor, hallucinations, delirium, loss of consciousness, pale and dry skin. There is a roseolous rash on the skin of the anterior abdominal wall. Tongue is covered with thick brown in the center, the edges are clean, red. There are imprints of the teeth. Diarrheal syndrome: «pea soup» feces up to 8–10 times a day. No nausea or vomiting. Hepatosplenomegaly. Positive Widal reaction. Typhoid The syndrome of «small disease» (short-term fever, nasopharyngitis) precedes the development of meningitis. Then the «big disease» occurs with the second wave of fever, headache, sweating, vomiting, impaired consciousness, tonic- clonic convulsions. Palpatory tenderness and tension of peripheral nerves. The paralysis develops on the 4–6 th day of the illness. The most common spinal form — flaccid paralysis of limbs, usually legs, is found. No loss of sensitivity occurs. Liquor is transparent, colorless, pressurized. Cytosis of lymphocytic character counts hundredths. Normal protein levels. Acute disease onset with high fever, chills, dizziness, weakness, fatigue, muscle and joint pain. There is pain in the temples, forehead, brow, eye area. There are delusions, hallucinations, nausea, vomiting related to food intake, medication, water. Light catarrhal conditions of the upper respiratory tract. Granulosity of posterior pharyngeal wall. X-ray pattern of segmental pulmonary edema. No clinical signs of edema. In severe cases there are convulsions, transient loss of consciousness, stiff neck. It is important to take into account the epidemiological situation. Diagnostic testing: leukopenia with lymphocytosis, liquor without T T T T T T pathological changesT T— the meningism syndromeT. TInfluenza

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

4
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF INFLUENZA
Yes No Intoxication. CNS involvement.
Acute onset of the disease with a fast t rise, headache, vomit. Resistant red dermographism, herpetic eruption on the lips. Patients can exactly indicate the time of the beginning of thedisease
. Children suffer from intensive headache, trashingaround in their bed and broken sleep. The pain gets moreintensive when turning the head, with sound and light irritants. From the first day there is repeated vomiting, not related to foodintake. Children at early age have clonic-tonic convulsions frequently. Positive meningeal symptoms. In CBC: eosinofiliya, neutrophilic leukocytosis, elevated ESR. The nature of thecerebrospinal fluid: turbid, purulent, thousandth pleocytosis, neutrophilic character. Protein + + +. Low sugar and chloridelevels.
Men
ingo
cocc
al
men
ingi
tis
Fever syndrome, catarrh of the upper respiratory tract: profuse muco-purulent nasal discharge, mild hyperemia of posterior pharyngeal wall. Specific eye disease — purulent conjunctivitis. There is a hyperplasia of oropharyngeal lymphoid formations and lymphadenopathy of the neck. Normal CBC.
Ade
novi
ral
infe
ctio
n
Acute onset with moderate symptoms of intoxication. Catarrhal phenomena occur from the first day of illness. There is a hard, rough, dry cough, sore throat, runny nose, nasal congestion. There is a nasal discharge initially slimy,
then muco-purulent. There is swelling and redness of themucous membrane arches, soft palate, posterior pharyngealwall. Often the first manifestation of the disease is «grits»syndrome, usually at night the child suddenly wakes up from a rough barking cough. Hoarseness, noisy breathing quicklyjoin, laryngeal stenosis develops. Stenosis severity rarelyreaches 2nd degree. P
arai
nflu
enza
The presence of purulent center (otitis, sinusitis, pneumonia) often precedes development of the disease. Sudden onset, anxiety, acute headache, hyperesthesia, repeated vomiting. Early meningealsymptoms. In young children — bulging of fontanelle, separationof sutures, increased sizes of the skull. The limb paresis, staticlocomotor ataxia, cranial nerve disfunction appear. Patients arepale and cyanotic, with intensive dyspnea. Hepatosplenomegaly.Frequent development of edema — brain edema, which may causedeath in the first 3 days of the illness. In CBC: leukocytosis, with a sharp shift of neutrophils, high ESR. Cerebrospinal fluid analysis:turbid, purulent, greenish-gray fluid, neutrophil cell count —thousandths, a significant increase of protein level. Bacteriological test of CSF reveals diplococci of lanceolate form locatedextracellularly.
Pne
umoc
occa
l men
ingi
tis
Expressed catarrhal period: purulent discharge from the nose, conjunctivitis. Dry, haunting cough. Appearance of Koplik spots. Three-stage rash: 1) maculopapular
rash; 2) period of pigmentation; 3) brannyolesquamation. Leukopenia in CBC.
Mea
sles
Symptoms of nervous system impairment usually follow the inflammation of salivary glands, but both disorders can also occur simultaneously. Acute development of the disease with chill, headache, vomiting, weakness and myalgia. Meningeal symptoms are expressed moderately. Clear cerebrospinal fluid flows under high pressure, normal or slightly increased proteinlevels,
lymphocyte cell count hundredths. Сhloride and sugar
concentrations are not changed. Lumbar puncture makes patientfeel better. P
arot
itic
m
enin
giti
s S
erou
s m
enin
giti
s of
en
tero
vira
l eti
olo g
y
The main symptoms are: prolonged fever, headache, specific intoxication — stupor, hallucinations, delirium, loss of consciousness, pale and dry skin. There is a roseolous rash on the skin of the anteriorabdominal wall.
Tongue is covered with thick brown inthe center, the edges are clean, red. There are imprintsof the teeth. Diarrheal syndrome: «pea soup» feces upto 8–10 times a day. No nausea or vomiting. Hepatosplenomegaly. Positive Widal reaction.
Typ
hoid
The syndrome of «small disease» (short-term fever, nasopharyngitis) precedes the development of meningitis. Then the «big disease» occurs with the second wave of fever, headache, sweating, vomiting, impaired consciousness, tonic-clonic convulsions. Palpatory tenderness and tension of peripheral nerves. The paralysis develops on the 4–6th day of the illness. The most common spinal form — flaccid paralysis of limbs, usually legs, is found. No loss of sensitivity occurs. Liquor is transparent, colorless, pressurized. Cytosis of lymphocytic character counts hundredths. Normal protein levels.
Acute disease onset with high fever, chills, dizziness, weakness, fatigue, muscle and joint pain. There is pain in the temples, forehead, brow, eye area. There are delusions, hallucinations, nausea, vomiting related to food intake, medication, water. Light catarrhal conditions of the upper respiratory tract. Granulosity of
posterior pharyngeal wall. X-ray pattern of segmental pulmonary edema. No clinical signs of edema. In severe cases there are convulsions, transient loss of consciousness, stiff neck. It isimportant to take into account the epidemiological situation. Diagnostic testing: leukopenia with lymphocytosis, liquor withoutT T T T T T
pathological changes T T— the meningism syndromeT.
TInfl
uenz
a
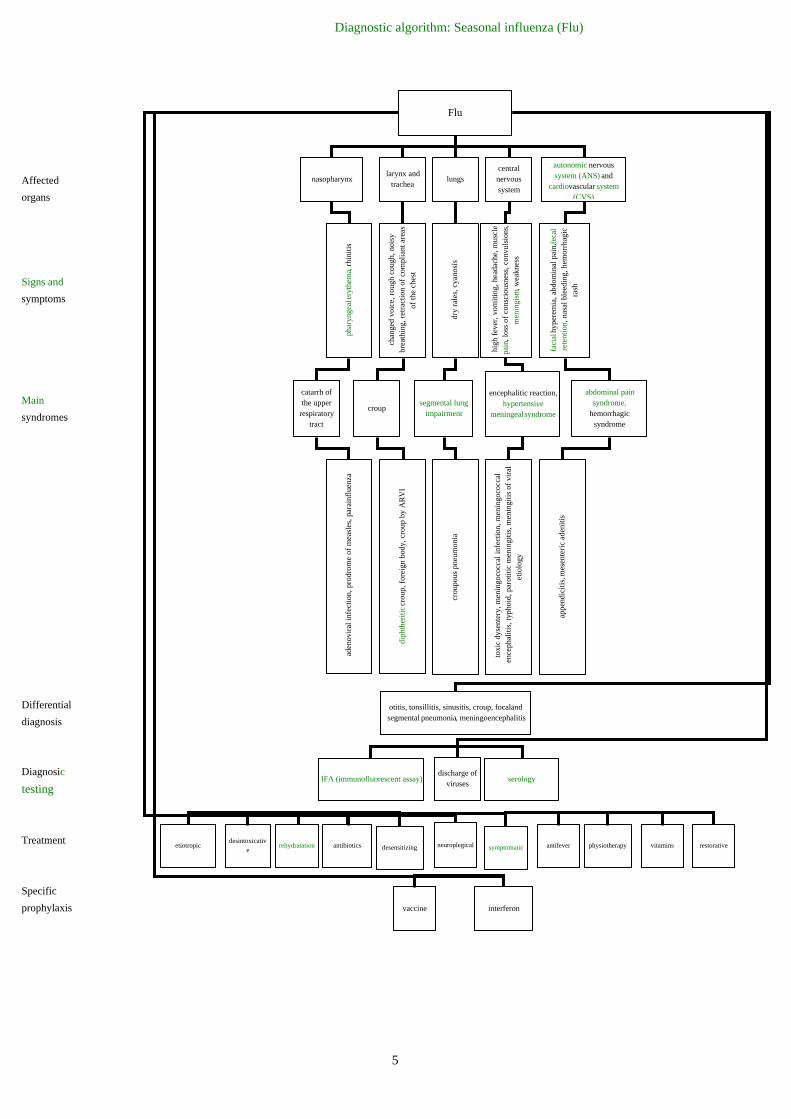
Diagnostic algorithm: Seasonal influenza (Flu)
Affected
organs
Signs and
symptoms
Main
syndromes
Differential
diagnosis
Diagnosic
testing
Treatment
Specific
prophylaxis
Flu
nasopharynxlarynx and
trachealungs
central nervous system
autonomic nervous system (ANS) and
cardiovascular system (CVS)
phar
ynge
al e
ryth
ema,
rhi
niti
s
chan
ged
voic
e, r
ough
cou
gh, n
oisy
br
eath
ing,
ret
ract
ion
of c
ompl
iant
are
as
of th
e ch
est
dry
rale
s, c
yano
sis
high
fev
er, v
omit
ing,
hea
dach
e, m
uscl
epa
in, l
oss
of c
onsc
ious
ness
, con
vuls
ions
,m
enin
gism
, wea
knes
s
faci
al h
yper
emia
, abd
omin
al p
ain,
feca
l re
tent
ion,
nas
al b
leed
ing,
hem
orrh
agic
ra
sh
catarrh of the upper
respiratory tract
croupsegmental lung
impairment
encephalitic reaction,hypertensive
meningeal syndrome
abdominal pain syndrome,
hemorrhagic syndrome
aden
ovir
al in
fect
ion,
pro
drom
e of
mea
sles
, par
ainf
luen
za
diph
ther
itic
cro
up, f
orei
gn b
ody,
cro
up b
y A
RV
I
crou
pous
pne
umon
ia
toxi
c dy
sent
ery,
men
ingo
cocc
al in
fect
ion,
men
ingo
cocc
al
ence
phal
itis
, typ
hoid
, par
otit
ic m
enin
giti
s, m
enin
giti
s of
vir
al
etio
logy
appe
ndic
itis
, mes
ente
ric
aden
itis
otitis, tonsillitis, sinusitis, croup, focal and segmental pneumonia, meningoencephalitis
discharge of viruses
IFA (immunofluorescent assay) serology
neuroplegicaldesensitizing symptomaticantibioticsrehydratationdesintoxicativ
eetiotropic antifever physiotherapy vitamins restorative
vaccine interferon
5

6
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF PARAINFLUENZA
Удалено: <sp>

Diagnostic algorithm: Paraflu
Main
syndromes
Signs and
symptoms
Differential
diagnosis
Diagnostic
criteria
Complications
Treatment
Prevention
Paraflu
catarrh of the upper respiratory tract
croup asthmatic bronchitis
slight cough, slight nasal discharge, mild
hyperemia of the fauces
sudden disease onset, barking cough, changed voice , stenosis, rapid
elimination of stenosis
cough, inspiratory dyspnea, in the lungs: hard breathing and
mixed rales
measles, influenza, adenoviral infection,
RS-infection, rhinovirus infection,
meningococcal nasopharyngitis,
enteroviral infection
foreign body, diphtheria of larynx
pertussis, attack of bronchial asthma
slight intoxicationslight catarrhal
phenomenavirus isolation IFA positive results
serology: antibodies titer increased 4
times
pneumonia otitis sinusitis croup tonsillitis
desensitizing, symptomatic, revulsive, inhalation, antispasmodic meansneuroplegical, antibiotics for complications
isolation of the patient, epidemiological actions in the spot, interferon
7

8
STEPDIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF ADENOVIRUS INFECTION
Intoxication. Catarrhal syndrome.
Gradual onset of the disease with subfeb-rile temperature. Clinical signs of croup: a rough barking cough, hoarseness, noisy breathing, stenosis of the larynx. Sore throat, rhinitis, stuffy nose. Swelling and hyperemia of the mucous oropharynx.
Yes No
Par
agri
ppe
On the 4–5 days of illness maculopapular rash appears. The first elements of the rash appear as small pink spots behind the ears and on the bridge of the nose. By the end of the first days, rash covers the entire face, neck, chest, upper back. Staging of the rash is typical. Catarrhal symptoms disappear. Face is puffy, eyelids are thickened. The eyes are red, there is pus. There are abundant rashes everywhere on the skin. The disease is called «infectious rhinitis».
Stuffiness of the nose, shortness of breath and profuse nasal watery discharge. Headache in the nasal bridge, and aches all over thebody. Herpetic eruptions on the lips and on the eve of the nose. Face is slightly pasty, excessive lacrimaion, the sclera are injected. Discomfort in the throat and a little dry cough.
Rh
inov
iru
s in
fect
ion
Increase of body temperature to 38,5–39o
C, catarrh of the upper respiratory tract. Hoarse voice, dry cough, haunting, disturbing the child. Evident bilateral conjunctivitis with bright hyperemia, conjunctival edema and discharge. Koplik spots. Enanthema in the form of small pinkish-red spots on the soft and hard palate, 1–2 days before rash.
Mea
sles
, p
erio
d o
f er
up
tion
Mea
sles
, ca
tarr
hal
per
iod
Gradual onset of the disease with a rise of temperature to subfebrile level, rhinitis, loss of appetite, dry cough. There is a pale face, conjunctival hyperemia occasionally, injection of sclera vessels. There may be headache, dizziness, chills, insomnia, sweating, pain in the eyeballs, and sometimes abdominal pain, nausea, vomiting, hepatomegaly, lymphadenopathy. In the oropharynx: pharyngitis. Symptoms of bronchitis and croup are present.
Myc
opla
smai
nfe
ctio
n «Typhoid status» (stupor, hallucinations, delusions). Symptoms of intoxication are maximal evident. Skin is pale, dry, warm, face is puffy. There is a roseolous rash on the skin of stomach, sometimes on the chest and shoulders. Icteric stained of the skin of palms and feet (Filippovich symptom) is typical. There is a Padalka symptom, hepatosplenomegaly. In CBC: leukopenia, neutropenia, aneozinofiliya, lymphocytosis, elevated erythrocyte sedimentation rate.
Typ
hoid
fev
er
Punctate macular rash covers the entire surface of the skin. There are mild catarrhal symptoms. There is a lymphadenopathy. In the blood: leukopenia, lymphocytosis, plasma cells. There is a peripheral lymph nodes enlargement, especially the occipital and back cervical. The rash is localized on extensor surfaces of the limbs around the joints, on the back and buttocks. After the elimination of the rash there is no signs of pigmentation or desquamation.
Ru
bel
la
The main signs of the disease are mild sore throat, slight dry cough, runny nose (sometimes), hyperemia of the pharynx, enanthema. Then the bubbles → erosion→ epithelization appear. By the end of the week enanthema and other manifestations of the disease completely disappear. There is a short duration of the course.
Her
pan
gin
a
Acute onset with body t over 38 C, whichpersists
o
for a long time (sometimes up to 10 days or more). Conjunctivitis, lymphadenopathy. First, the defeat of one eye, then the second. Cough is wet, mild hyperemia of the pharynx and pharyngitis. There is hepatosplenomegaly. In CBC - moderate leukocytosis with neutrophilia, lymphopenia, slightly increased ESR.
Ad
enov
iral
in
fect
ion
There is a swelling of bronchial mucosa, obstruction, bronchospasm. Cough is dry at first, then it becomes wet with discharge of mucus. Moist, dry rales are auscultated (medium, rarely fine bubbling rales). Longer process of exhalation, difficulty of breath.
Bro
nch
itis
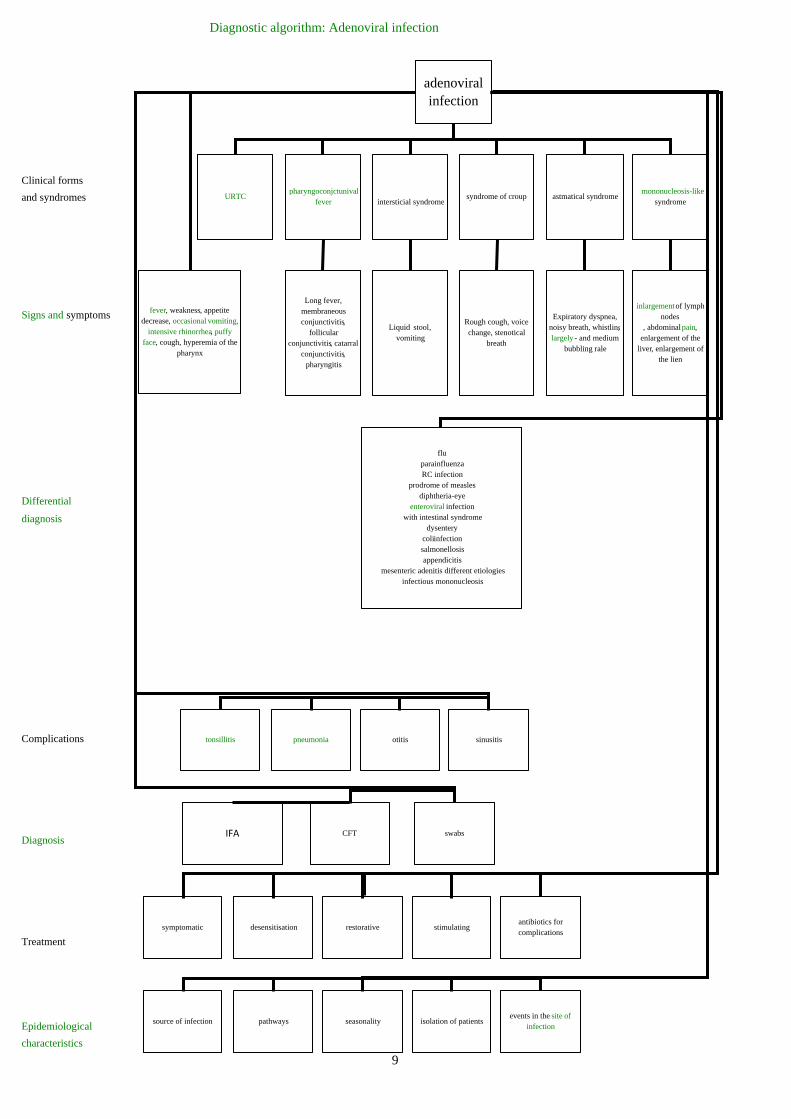
Diagnostic algorithm: Adenoviral infection
Clinical forms
and syndromes
Signs and symptoms
Differential
diagnosis
Complications
Diagnosis
Treatment
Epidemiological
characteristics
adenoviral infection
URTCpharyngoconjctunival
fever intersticial syndromesyndrome of croup astmatical syndrome
mononucleosis-like syndrome
Long fever, membraneous conjunctivitis,
follicular conjunctivitis, catarral
conjunctivitis, pharyngitis
Liquid stool, vomiting
Rough cough, voice change, stenotical
breath
Expiratory dyspnea, noisy breath, whistlinglargely - and medium
bubbling rale
inlargementof lymph nodes
, abdominal pain, enlargement of the
liver, enlargement of the lien
fever, weakness, appetite decrease, occasional vomiting,
intensive rhinorrhea, puffy face, cough, hyperemia of the
pharynx
fluparainfluenzaRC infection
prodrome of measlesdiphtheria-eye
enteroviral infectionwith intestinal syndrome
dysenterycoliinfectionsalmonellosisappendicitis
mesenteric adenitis different etiologiesinfectious mononucleosis
sinusitisotitispneumoniatonsillitis
IFA CFT swabs
symptomatic desensitisation restorative stimulatingantibiotics for complications
source of infection pathways seasonality isolation of patientsevents in the site of
infection
9

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF MYCOPLASMA INFECTION
Catarrhal symptoms. Intoxication.
Respiratory distress syndrome.
No Yes
Gradual onset of the disease with subfebrile fever. The main clinical signs are rhinitis, loss of appetite, dry cough, intoxication, pallor, conjunctival hyperemia, vascular injection of the sclera, pain in eyeballs. There is an abdominal pain, nausea, vomiting, hepatomegaly, lymphadenopathy. Symptoms of intoxication are little evident. Pharyngitis, catarrhal conditions, the symptoms of bronchitis and of croup (sometimes) develop. In the lungs there is a rough breath, inconstant scaffered rales. In CBC: moderate leukocytosis, neutrocytosis, increased ESR. M
ycop
lasm
a in
fect
ion
Bronchiolitis and bronchitis with severe bronchial obstruction are typical. There is a catarrhal syndrome, hyperemia of the fauces, subfebrile or normal temperature. There is a mild headache, chilling, chest pain, dry cough, expiratory dyspnea, perioral
infe
ctio
n
cyanosis.
RS
-
Percussion: vesiculotympanitic sound. Auscultation: crepitus fine bubbling rales.
Evident catarrhal phenomena accompanying with large nasal discharge, hyperplasia of lymphoid structures of the stomatopharynx, conjunctivitis, swollen lymph nodes, lack of changes in the peripheral blood (normal CBC). There is a wet cough, throat congestion, intoxication, possible muscle and joint pain. In young children the diarrhea of
Ad
enov
iral
in
fect
ion
enteritis character is possible.
The disease develops after contact with birds (pigeons, poultry). Acute onset with high fever and marked toxemia in the absence of catarrhal symptoms or upper respiratory tract pathology. The possibility of relapse and late myocarditis, hepatosplenomegaly, leukopenia, increased ESR, a longer course of disease. In addition, pneumonia signs can develop.
Orn
ith
osis
Acute onset with high fever, intoxication, flushing, injection of sclera vessels, puffy face, hyperemia of the tonsils and soft palate. Tracheitis, tracheobronchitis and focal pneumonia develop. There are pains in the eyeballs, muscle pain, abdominal pain, bowel disorders. Hallucinations, hepatosplenomegaly, prolonged fever, headache, insomnia and mental instability are possible. In severe
Q f
ever
cases: serous meningitis and encephalitis.
The disease proceeds with toxicosis. The onset is percute with coughing up blood, shortness of breath, sharp chest pain. The diaphragmatic pleura gets involved in the process, with pain radiating to the abdomen. There is an impaired consciousness, delirious state. Neutrophilic leukocytosis and high ESR are typical changes in CBC. Prescription of antibiotics results in rapid improvement.
Cro
up
ous
pn
eum
onia
10

Diagnostic Algorithm: mycoplasma infection
Etiology
Mechanism
of transmission
Affected organs
and tissues
Signs and
symptoms
Clinical course
Diagnostic
tests
Differential
diagnosis
Treatment
Prevention
mycoplasma infection
mycoplasmas
aerborne
broncho-pulmonary system -
nasopharyngitis, pharyngitis,
laryngitis, bronchitis,pneumonia
eye - eye damage, pain of the eyeballs
(vascular membrane)joints - arthritis liver - hepatitis
central nervous system - meningitis
kidney - nephritis, abacterial urethritis
sw
elli
ng, t
ende
rnes
s, li
mit
atio
n of
mov
emen
t
into
xica
tion
, rai
sing
the
tem
pera
ture
to f
ebri
le le
vel,
head
ache
, sor
e th
roat
, hy
pere
mia
of
the
thro
at, d
iffi
cult
y in
nas
al b
reat
hing
. Fro
m 4
-5 d
ays
scan
ty
expe
ctor
atio
n. T
here
are
som
etim
es th
e sy
mpt
oms
of c
roup
. In
the
lung
s, th
ere
is a
ha
rd b
reat
hing
, inc
onst
ant s
catt
ered
dry
ral
es. I
n pn
eum
onia
ther
e ar
e c
hest
pai
ns
pai
n in
the
eyeb
alls
, hyp
erem
ia o
f th
e co
njun
ctiv
a, i
njec
tion
ves
sels
of
scle
ra,
dam
age
to th
e ch
oroi
d
hep
atom
egal
y
hea
dach
es, m
enin
geal
sym
ptom
s
freq
uent
uri
nati
on w
ith
smal
l por
tion
s, th
e sy
mpt
oms
of n
ephr
itis
intr
aute
rine
fet
al le
sion
mis
carr
iage
, pre
mat
urit
y, g
ener
aliz
ed f
orm
of
dam
age a
nd
cent
ral n
ervo
us s
yste
m d
amag
eacute
Bacteriological: isolation of mycoplasma from pharyngeal
mucus, pus, sputum
complement fixation test and reaction of indirect
hemagglutination, latex - agglutination, diffusion in the
gel
ARVI (adenoviral, RS - infection)
ornithosis Q-fever croupous pneumonia
symptomatic therapy antibioticsdisintoxicational means,
plasmadiuretics
Early isolation of patients
common preventive measures
11

39
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF ENTEROVIRAL INFECTION
Yes No Exanthema syndrome. Intoxication.
Maculo-papular rash, first behind the ears, on the bridge of the nose with tendency to merger. On the 2 daynd — on the body and hands. On the 3rd day — on the lower limbs. Staging of the rash, Koplik spots and conjunctivitis are typical.
Mea
sles
Normal or subfebrile temperature
Macular large-spotted hemorrhagic rash appears lately (on the 6–7th day of the disease). Localization - relatively uniformly covers the whole body. There is itching of the skin. After disappearance of the rash the scaling of the skin is observed, often there is defurfuration. Kidneys are affected. Hepatosplenomegaly. CBC: leukocytosis, elevated ESR level.
Lep
tosp
iros
is
Maculo-papular rash, more abundant on the face with tendency to merger. After the disappearance of the rash pigmentation and skin exfoliation may de-velop. There is no staging of the rash. At the time of rash appearance and before there is no decrease and a new increase of body temperature. Tonsillitis is typical. CBC: atypical mononuclear cells. Lympha-denopathy develops.
Large-spotted macular rash, doesn’t merge, with no staging. With underlying fever there is swelling and puffiness of face, the muscle soreness and significant eosinophilia. From medical history: consumption of not enough processed meat 1–4 weeks before the disease.
Infe
ctio
us
mon
onu
cleo
sis
Tri
chin
osis
There is a punctuate macular pinkish-red rash on the background of unchanged skin. Elements of the rash do not merge. The rash initially appears on the face, then within a few hours it spreads throughout the body. There is a localization on the extensor surfaces of the extremities, around the joints, back and buttocks. The rash lasts for 2–3 days. It disappears without pigmentation and desquamation.
Ru
bel
la
There is at the beginning a pink-red spot of oval form on the chest with a small scaling in the center («parent plaque»). Then there is macular rash on the whole body. There are oval spots up to 15 mm, with the peeling in the center, less intensive painted with bright red border on the periphery.
Pin
k li
chen
The profuse rash, roseolic and papulous, evident on the trunk, prone to merger, is present for up to –3 weeks, then gradually pales and disappears. There is a presence of residual effects of primary syphilides (hard chancre).
Syp
hil
is
Rash appears in the first days after taking the drugs. There is an itchy skin, swollen lymph nodes and mild eosinophilia. Rash merges, there is no staging.
Med
icam
enta
l d
erm
atit
is
Abundant macular rash on the extensor surfaces of limbs with concentration in the large joints, on the buttocks. There are single elements on the body, and there is no rash on the face. Hyperemia of face and neck, vascular injection of the sclera vessels, hepatosplenomegaly are typical. R
osen
ber
g in
fect
iou
s er
yth
ema
Acute onset of the disease. Macular rash with tendency to fusion, more intense on the trunk. There is no staging. After the disappearance of the rash and pigmentation, desquamation stay. Signs of serous meningitis and epidemic myalgia were found. The rash persists for 3–4 days.
En
tero
viru
s ex
anth
ema
Enteroviral infection (Boston exanthema)

DIAGNOSTIC ALGORITHMS : ENTEROVIRAL INFECTION
Clinical forms
Signs and
symptoms
Differential
diagnosis
Principles
of treatment
Diagnostic
criteria
Epidemiology
Enteroviral Infection
serous meningitis
epidemic myalgia
exanthema herpanginaPoliomyelitis-
likeviral
diarrheaencephalo
myocarditisfe
ver,
hea
dach
e, n
ause
a, v
omit
ing,
abd
omin
al
pain
, mus
cle
pain
, m
enin
geal
sym
ptom
s
hype
rem
ia o
f th
e fa
ce, h
eada
che,
exc
ruci
atin
g m
uscl
e pa
in
feve
r, h
eada
che,
mus
cle
pain
, vom
itin
g,
mac
ulop
apul
ar r
ash
feve
r, h
eada
che,
her
pes
rash
in p
hary
nx
mus
cle
pain
, cha
nge
in m
anne
r of
wal
king
, as
ymm
etry
of
tend
on r
efle
xes,
hyp
oten
sion
cata
rrha
l syn
drom
e, v
omit
ing,
sub
febr
ile
tem
pera
ture
, ent
erit
ic f
eces
anor
exia
, som
nole
nce,
dia
rrhe
a, f
ever
, gen
eral
cy
anos
is, t
achy
card
ia, c
ardi
ac a
rrhy
thm
ias,
ca
rdia
c no
ise,
hep
atol
iena
l syn
drom
e, s
tres
s of
fo
ntan
elle
, cra
mps
Par
otit
ic m
enin
giti
s, p
olio
mye
liti
c m
enin
giti
s, m
enin
goco
ccal
m
enin
giti
s, tu
berc
ulou
s m
enin
giti
s
appe
ndic
itis
, ple
uris
y, in
flue
nza
mea
sles
, sca
rlet
fev
er, r
ubel
la,
infe
ctio
us e
xant
hem
a
herp
etic
sto
mat
itis
, aph
thou
s st
omat
itis
, ac
ute
resp
irat
ory
dise
ase
mil
d fo
rms
of p
olio
mye
litis
coli
infe
ctio
n, s
taph
yloc
occa
l en
tero
coli
tis,
sal
mon
ello
sis,
sim
ple
dysp
epsi
a
seps
is, a
cute
inte
stin
al in
fect
ions
, m
enin
gitis
desensitization
vitamin therapy
disintoxication
dehydrationanalgetics, antipyretics
hormones cardiacs
polymorphism of
clinical manifestatio
ns
prolonged fever with
severe intoxication
acute onsetepidemic anamnesis
isolation of enteroviruse
sserology
Positive immunofluore
scence
seasonalitytransmissionsource focality immunity
40

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF SPINAL FORM OF POLIOMYELITIS
No Yes Syndrome of flaccid paralysis.
Liquor syndrome.
The paralyses are characterized by acute rapid development; with period of increasing intensity from a few hours to 1-2 days. Paralyses are asymmetric, even on the same limb; different muscle groups can have different degree of damage. There are no signs of sensitivity failure, pelvic or pyramidal disorders. Typical pain syndrome: spontaneous pain in the limbs and back, painful palpation of nerve trunks. The recovery period takes 1-3 years.
Pol
iom
yeli
tis
(sp
inal
for
m)
It is characterized by sparing gait.The child tries not to step on theaffected leg, bends the knee and spares it. Passive motion and palpation are painful. Tendon reflexes and tone are preserved.Normal cerebrospinal liquid normal. In CBC: marked
som
atic
O
steo
arti
cula
r p
ath
olog
y (b
urs
itis
, art
hri
tis,
low
bac
k p
ain
, et
c.)
inflammatory changes.
Central paralysis characterized by symmetry, conduction disturbancesof sensitivity, high tonus, lively reflexes, pyramidal signs, rough and chronic pelvic disorders, trophic disorders M
yeli
tis
with the bedsoresformation.
It is often characterized by fever-freeonset, with increasing, sometimes long and wavy, development of paralyses,which are symmetrical andpredominantly distal. Polineuritic and radicular type of sensitivity impairment. CSF: increased protein with normal cell count.
Pol
yrad
icu
lon
euri
tis
Fever, catarrhal signs, herpangina, myalgia syndrome, diarrhea, exan-thema. Absent or smoothed meningoencephalitic syndrome, limited character of paresis. The normal state is of the CSF. Complete recovery of paresis is in the first 2
Pol
iom
yeli
tis-
lik
e di
seas
es
ente
rovi
ral i
nfe
ctio
n)
months of the disease.
(
12

DIAGNOSTIC ALGORITHMS: POLIOMYELITIS
Type
Clinical
forms
Signs and
symptoms
13
Differential
diagnosis
Characteristics of the
modern poliomyelitis
Stages
Diagnosis
Prevention
Therapeutic
strategies
POLIOMYELITIS
Typical Atypical
Paralytic
BulbarSpinal Pontinha
Flaccid paralysis,
asymmetry ofparalysis
Aphonia, snuffles, choke,
paradoxical breathing
Paralysis of facial nerve
AsymptomaticNon paralytic Obliterated
General infection "abortive"
Meningeal
Cough, sore throat, hyperemia of the throat, abdominal
pain, bloating, abdominal tension, frequent liquid stool
Occipital muscular rigidity, positive
Kernig's and Brudzinskiy's
symptoms
High fever, weakness, lethargy, headache, vomiting, poor appetite, hypersensitivity, pain in
the extremities, sweating, thirst, tachycardia
Poliradiculo-neuritis
OsteomyelitisDiphtheria polyneuritis
MyelitisEnteroviral infection
(paralytic)
Foreign body in airways
Peripheral neuritis of the facial nerve
FluIntestinal infections
Meningitis of different etiologies
Absence of cyclicity
Normal temperature
Good quality flow
Easy spinal paralysis
ParalyticPreparalytic ReplacementResidual effects
Complement fixation test,
neutralization
Virus isolation
Dynamics of liquorologic parameters
Quarantine DisinfectionEarly
admission to h it l
Active immunization
Miobiostimulyators
Medicaments that improve
nerve conduction
Medicaments that increase
reactivity, vitamins
EXERCISE therapy,
massage, spa, physiotherapy
Mixed forms
Hormones


STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF DISEASES ACCOMPANIED BY EXANTHEMA
Symptoms Scarlet fever Pseudotuberculosis
Measles Rubella Meningococcemia Chicken pox
Availability prodrome No No Yes, 3–4 days Absent or 1–2 days No Absent
Body temperature Febrile, 3–5 days Febrile, 4–6 days Subfebrile 3–4 days, then febrile 3 days
normal or subfebrile 2–3 days
Febrile, 5–7 days Subfebrile or febrile 3–5 days
Catarrh of the upper respiratory tract
Absent expressed expressed poorly expressed Absent Absent
Angina Typical (catarrhal, lacunar, necrotic)
Absent Catarrhal Absent Absent Absent
Conjunctivitis Absent typical typical hardly ever Absent Absent
Intoxication Moderately expressed, persists 3–5 days
Expressed, preserved more than
5 days
Moderate, persists 6–8 days slightly expressed or absent
severely expressed, persists 3–5 days
slightly expressed, persists 3–5 days
Time of the rash appearing On the 1–2 day The end of 1 week On the 4–5 day On the 1–2 day On the 1–2 day On the 1st day
Duration of the rise of the rash
1 day 1–3 days 3 days stage: face-trunk -limb
1–2 days 1–2 days 3–5 days, jerky
Character of rash Micropunctate rash, in concentarated places — petechial
with hyperemia
Micropunctate rash with hyperemia
Maculopapular, prone to merger
Predominantly spotted
Haemorrhagic, irregular shape, with central necrosis
«False» polymorphism: a spot-papule- vesicle- crust
The preferential localization of rash
Natural folds, the lateral surface of the trunk, flexion of the legs, lack
of nasolabial triangle
Symptom of «glove», «socks»,
«hood»
Does not have special localiza-tion places
The largest number in the buttocks, extensor surfaces of extremities
Mainly in the buttocks, legs Does not have special localization places
Pigmentation Absent Absent Present Absent Absent Absent
Desquamation Macroscaling — on the palms, soles,
scaly — on the trunk
macroscaling — on the palms, soles, scaly — on body
Scaly Absent Absent Absent
Enanthema Micropunctate rash, pink in color, in soft and hard palate, appears simultaneously with exanthema
Meets not permanently
1) on the buccal mucosa, gums, lips - whitish papules: Belsky –Filatov–Koplik, s spot, appear on 2–3 days of illness and persist for 2–3 days 2) on the mucosa of hard and soft palate - the pink spots appear simultaneously with exanthema
may be on the mucosa of the soft and hard
palate, appear simultaneously with
exanthema
Absent Erosion on the oral mucosa
The state of tongue Coated in the first 1–2 days, then the "strawberry"
Coated in the first 1–2 days then «strawberry»
without features without features Normal Normal
cardiovascular system and other organs impairment
1st week — the sympathetic phase: tachycardia, a tendency to the
increased blood pressure; 2nd week — vagus phase:
bradycardia, decreased blood pressure,
enlarged heart borders
Organ failure, depending on the
severity of the process
without features without features Frequent development of infective toxic shock, purulent meningitis
Normal
Lymphatic nodes increased submandibular lymph nodes
The increase in mesenteric lymph
nodes
without features increased occipital andback cervical lymph
nodes
Normal Normal

39
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF ENTEROVIRAL INFECTION
Yes No Exanthema syndrome. Intoxication.
Maculo-papular rash, first behind the ears, on the bridge of the nose with tendency to merger. On the 2 daynd — on the body and hands. On the 3rd day — on the lower limbs. Staging of the rash, Koplik spots and conjunctivitis are typical.
Mea
sles
Normal or subfebrile temperature
Macular large-spotted hemorrhagic rash appears lately (on the 6–7th day of the disease). Localization — relatively uniformly covers the whole body. There is itching of the skin. After disappearance of the rash the scaling of the skin is observed, often there is defurfuration. Kidneys are affected. Hepatosplenomegaly. CBC: leukocytosis, elevated ESR level.
Lep
tosp
iros
is
Maculo-papular rash, more abundant on the face with tendency to merger. After the disappearance of the rash pigmentation and skin exfoliation may de-velop. There is no staging of the rash. At the time of rash appearance and before there is no decrease and a new increase of body temperature. Tonsillitis is typical. CBC: atypical mononuclear cells. Lympha-denopathy develops.
Large-spotted macular rash, doesn’t merge, with no staging. With underlying fever there is swelling and puffiness of face, the muscle soreness and significant eosinophilia. From medical history: consumption of not enough processed meat 1–4 weeks before the disease.
Infe
ctio
us
mon
onu
cleo
sis
Tri
chin
osis
There is a punctuate macular pinkish-red rash on the background of unchanged skin. Elements of the rash do not merge. The rash initially appears on the face, then within a few hours it spreads throughout the body. There is a localization on the extensor surfaces of the extremities, around the joints, back and buttocks. The rash lasts for 2–3 days. It disappears without pigmentation and desquamation.
Ru
bel
la
There is at the beginning a pink-red spot of oval form on the chest with a small scaling in the center («parent plaque»). Then there is macular rash on the whole body. There are oval spots up to 15 mm, with the peeling in the center, less intensive painted with bright red border on the periphery.
Pin
k li
chen
The profuse rash, roseolic and papulous, evident on the trunk, prone to merger, is present for up to 2– weeks, then gradually pales and disappears. There is a presence of residual effects of primary syphilides (hard chancre).
Syp
hil
is
Rash appears in the first days after taking the drugs. There is an itchy skin, swollen lymph nodes and mild eosinophilia. Rash merges, there is no staging.
Med
icam
enta
l d
erm
atit
is
Abundant macular rash on the extensor surfaces of limbs with concentration in the large joints, on the buttocks. There are single elements on the body, and there is no rash on the face. Hyperemia of face and neck, vascular injection of the sclera vessels, hepatosplenomegaly are typical. R
osen
ber
g in
fect
iou
s er
yth
ema
Acute onset of the disease. Macular rash with tendency to fusion, more intense on the trunk. There is no staging. After the disappearance of the rash and pigmentation, desquamation stay. Signs of serous meningitis and epidemic myalgia were found. The rash persists for 3–4 days.
En
tero
viru
s ex
anth
ema
Enteroviral infection (Boston exanthema)

14
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF HERPETIC INFECTION (SIMPLE HERPES)
Удалено: <sp>
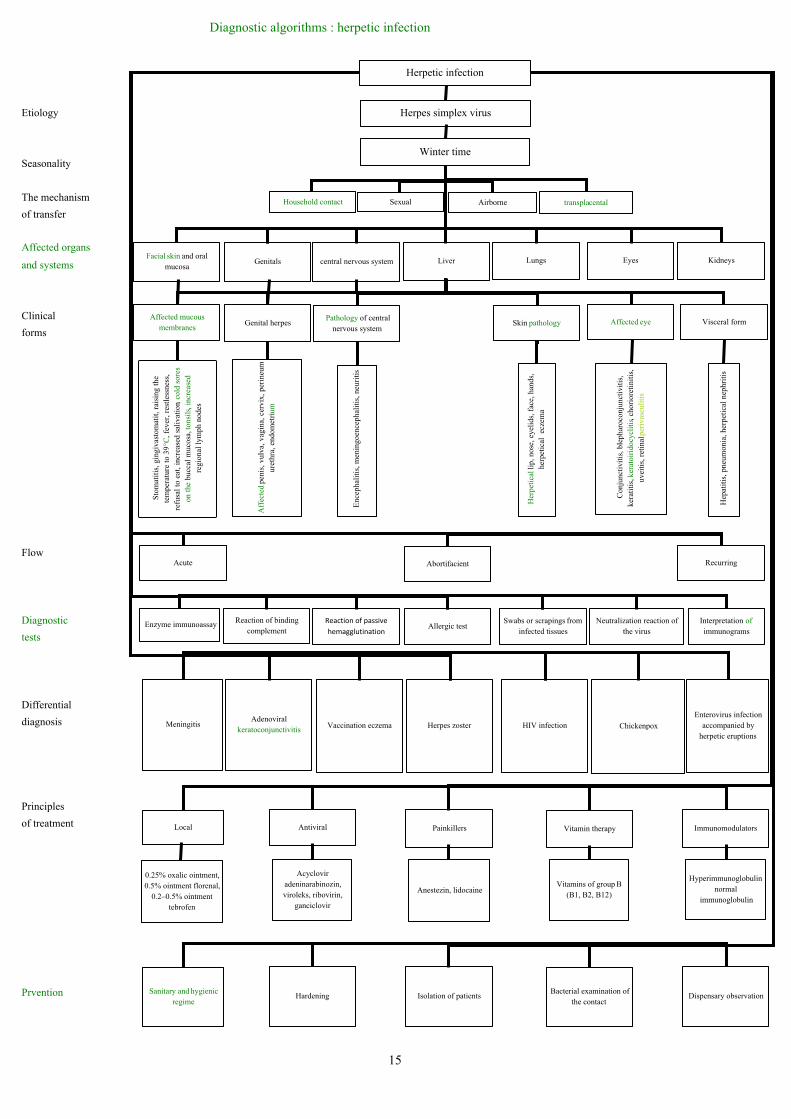
Diagnostic algorithms : herpetic infection
Etiology
Seasonality
The mechanism
of transfer
Affected organs
and systems
Clinical
forms
Flow
Diagnostic
tests
Differential
diagnosis
Principles
of treatment
Prvention
Herpetic infection
Herpes simplex virus
Winter time
Airborne transplaсentalSexual Household contact
GenitalsFacial skin and oral
mucosacentral nervous system Liver Lungs Eyes Kidneys
Affected mucous membranes
Genital herpes Pathology of central
nervous systemSkin pathology Affected eye Visceral form
Sto
mat
itis
, gin
giva
stom
atit
, rai
sing
the
tem
pera
ture
to 3
9°C
, fev
er, r
estl
essn
ess,
re
fusa
l to
eat,
incr
ease
d sa
liva
tion
, col
d so
res
on th
e bu
ccal
muc
osa,
tons
ils,
incr
ease
d re
gion
al ly
mph
nod
es
Aff
ecte
d pe
nis,
vul
va, v
agin
a, c
ervi
x, p
erin
eum
uret
hra,
end
omet
rium
Enc
epha
liti
s, m
enin
goen
ceph
alit
is, n
euri
tis
Her
peti
cal l
ip, n
ose,
eye
lids
, fac
e, h
ands
, he
rpet
ical
ecz
ema
Con
junc
tivi
tis,
ble
phar
ocon
junc
tivi
tis,
ke
rati
tis,
ker
atoi
rido
cycl
itis,
cho
rior
etin
itis
, uv
eiti
s, r
etin
al p
eriv
ascu
liti
s
Hep
atit
is, p
neum
onia
, her
peti
cal n
ephr
itis
AbortifacientAcute Recurring
Allergic testSwabs or scrapings from
infected tissuesReaction of passive
hemagglutination
Reaction of binding complement
Enzyme immunoassay Neutralization reaction of the virus
Interpretation of immunograms
Herpes zoster HIV infectionVaccination eczemaAdenoviral
keratoconjunctivitisMeningitis Chickenpox
Enterovirus infection accompanied by
herpetic eruptions
Vitamin therapy ImmunomodulatorsPainkillersAntiviralLocal
0.25% oxalic ointment, 0.5% ointment florenal,
0.2–0.5% ointment tebrofen
Hyperimmunoglobulin,normal
immunoglobulin
Vitamins of group В (В1, В2, В12)
Anestezin, lidocaine
Acyclovir adeninarabinozin, viroleks, ribovirin,
ganciclovir
Bacterial examination of the contact
Dispensary observationIsolation of patientsHardeningSanitary and hygienic
regime
15
16
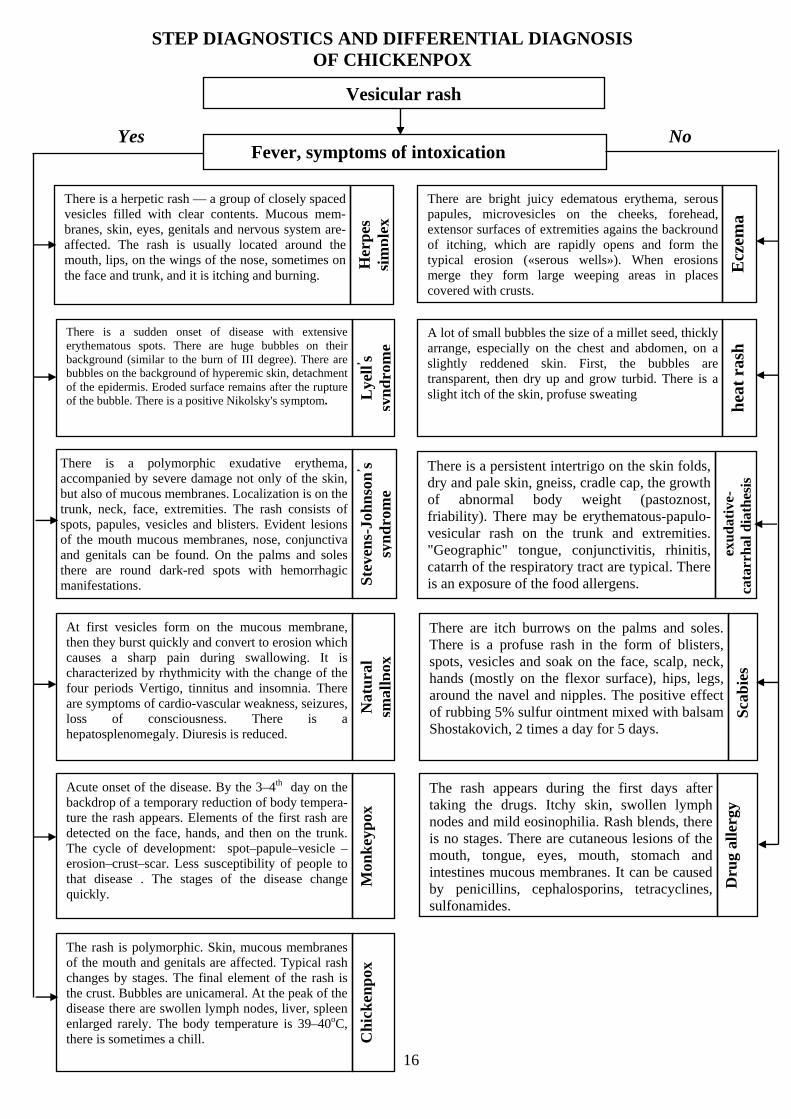
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF CHICKENPOX
Vesicular rash
Yes No Fever, symptoms of intoxication
There is a herpetic rash — a group of closely spaced vesicles filled with clear contents. Mucous mem-branes, skin, eyes, genitals and nervous system are-affected. The rash is usually located around the mouth, lips, on the wings of the nose, sometimes on the face and trunk, and it is itching and burning.
Her
pes
si
mp
lex
There are bright juicy edematous erythema, serous papules, microvesicles on the cheeks, forehead, extensor surfaces of extremities agains the backround of itching, which are rapidly opens and form the typical erosion («serous wells»). When erosions merge they form large weeping areas in places covered with crusts.
Ecz
ema
There is a sudden onset of disease with extensive erythematous spots. There are huge bubbles on their background (similar to the burn of III degree). There are bubbles on the background of hyperemic skin, detachment of the epidermis. Eroded surface remains after the rupture of the bubble. There is a positive Nikolsky's symptom.
Lye
lls ’
syn
dro
me
There is a polymorphic exudative erythema, accompanied by severe damage not only of the skin, but also of mucous membranes. Localization is on the trunk, neck, face, extremities. The rash consists of spots, papules, vesicles and blisters. Evident lesions of the mouth mucous membranes, nose, conjunctiva and genitals can be found. On the palms and soles there are round dark-red spots with hemorrhagic manifestations.
At first vesicles form on the mucous membrane, then they burst quickly and convert to erosion which causes a sharp pain during swallowing. It is characterized by rhythmicity with the change of the four periods Vertigo, tinnitus and insomnia. There are symptoms of cardio-vascular weakness, seizures, loss of consciousness. There is a hepatosplenomegaly. Diuresis is reduced.
Acute onset of the disease. By the 3–4 dayth on the backdrop of a temporary reduction of body tempera-ture the rash appears. Elements of the first rash are detected on the face, hands, and then on the trunk. The cycle of development: spot–papule–vesicle –erosion–crust–scar. Less susceptibility of people to that disease . The stages of the disease change quickly.
The rash is polymorphic. Skin, mucous membranes of the mouth and genitals are affected. Typical rash changes by stages. The final element of the rash is the crust. Bubbles are unicameral. At the peak of the disease there are swollen lymph nodes, liver, spleen enlarged rarely. The body temperature is 39–40oC, there is sometimes a chill.
Ste
ven
s-Jo
hnso
ns
s
’
ynd
rom
e N
atu
ral
smal
lpox
M
onk
eyp
ox
Ch
ick
enp
ox
A lot of small bubbles the size of a millet seed, thickly arrange, especially on the chest and abdomen, on a slightly reddened skin. First, the bubbles are transparent, then dry up and grow turbid. There is a slight itch of the skin, profuse sweating
hea
t ra
sh
There is a persistent intertrigo on the skin folds, dry and pale skin, gneiss, cradle cap, the growth of abnormal body weight (pastoznost, friability). There may be erythematous-papulo-vesicular rash on the trunk and extremities. "Geographic" tongue, conjunctivitis, rhinitis, catarrh of the respiratory tract are typical. There is an exposure of the food allergens.
exu
dat
ive-
cata
rrh
al d
iath
esis
There are itch burrows on the palms and soles. There is a profuse rash in the form of blisters, spots, vesicles and soak on the face, scalp, neck, hands (mostly on the flexor surface), hips, legs, around the navel and nipples. The positive effect of rubbing 5% sulfur ointment mixed with balsam Shostakovich, 2 times a day for 5 days.
Sca
bie
s
The rash appears during the first days after taking the drugs. Itchy skin, swollen lymph nodes and mild eosinophilia. Rash blends, there is no stages. There are cutaneous lesions of the mouth, tongue, eyes, mouth, stomach and intestines mucous membranes. It can be caused by penicillins, cephalosporins, tetracyclines, sulfonamides.
Dru
g al
lerg
y
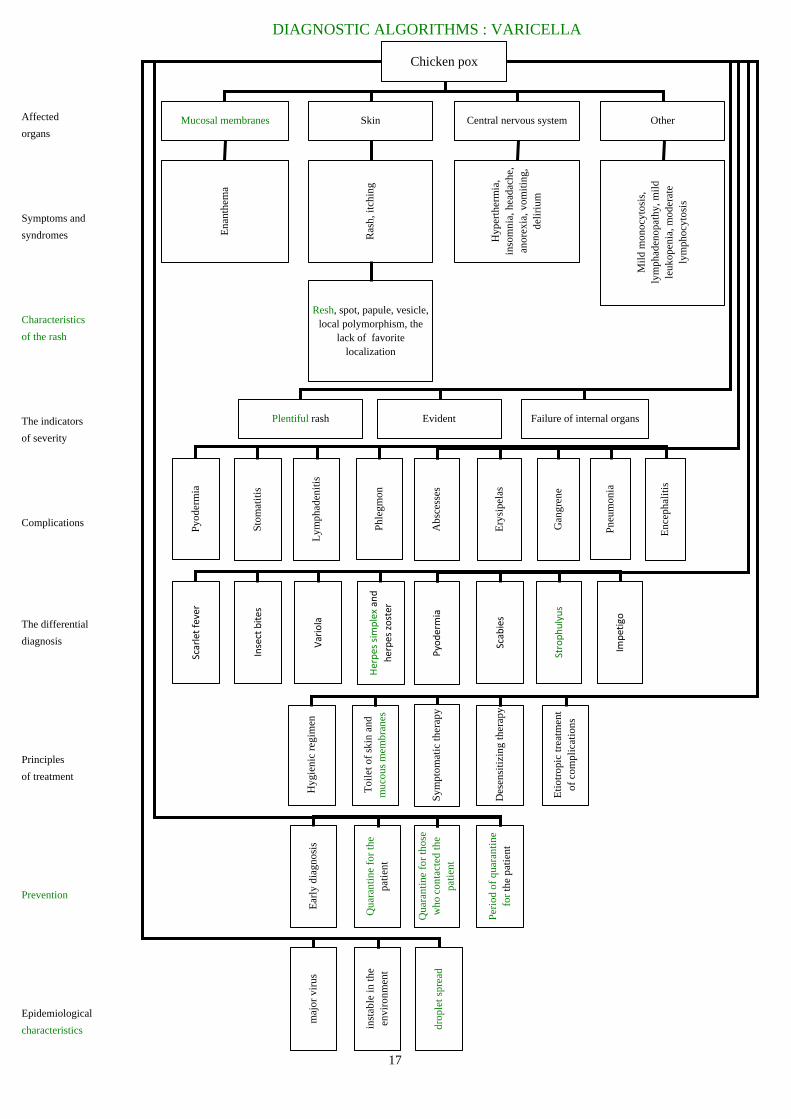
DIAGNOSTIC ALGORITHMS : VARICELLA
Affected
organs
Symptoms and
syndromes
Characteristics
of the rash
The indicators
of severity
Complications
The differential
diagnosis
Principles
of treatment
Prevention
Epidemiological
characteristics
Chicken pox
Mucosal membranes Skin Central nervous system Other
Ena
nthe
ma
Ras
h, it
chin
g
Hyp
erth
erm
ia,
inso
mni
a, h
eada
che,
an
orex
ia, v
omit
ing,
de
liri
um
Mil
d m
onoc
ytos
is,
lym
phad
enop
athy
, mil
d le
ukop
enia
, mod
erat
e ly
mph
ocyt
osis
Resh, spot, papule, vesicle, local polymorphism, the
lack of favorite localization
Plentiful rash Evident Failure of internal organs
Abs
cess
es
Phle
gmon
Ery
sipe
las
Gan
gren
e
Pneu
mon
ia
Enc
epha
liti
s
Lym
phad
enit
is
Stom
atit
is
Pyod
erm
ia
Pyodermia
Herpes sim
plex and
herpes zoster
Scabies
Strophulyus
Impetigo
Variola
Insect bites
Scarlet fever
Sym
ptom
atic
ther
apy
Toi
let o
f sk
in a
nd
muc
ous
mem
bran
es
Des
ensi
tizi
ng th
erap
y
Eti
otro
pic
trea
tmen
t of
com
plic
atio
ns
Hyg
ieni
c re
gim
en
Qua
rant
ine
for
thos
e w
ho c
onta
cted
the
pati
ent
Qua
rant
ine
for
the
pati
ent
Peri
od o
f qu
aran
tine
fo
r th
e pa
tien
t
Ear
ly d
iagn
osis
inst
able
in th
e en
viro
nmen
t
maj
or v
irus
drop
let s
prea
d
17
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSTICS OF CONGENITAL CMV INFECTION
IN CHILDREN YOUNGER THAN 1 YEAR OLD
No Yes Syndrome of intrauterine infection at fetus and newborn
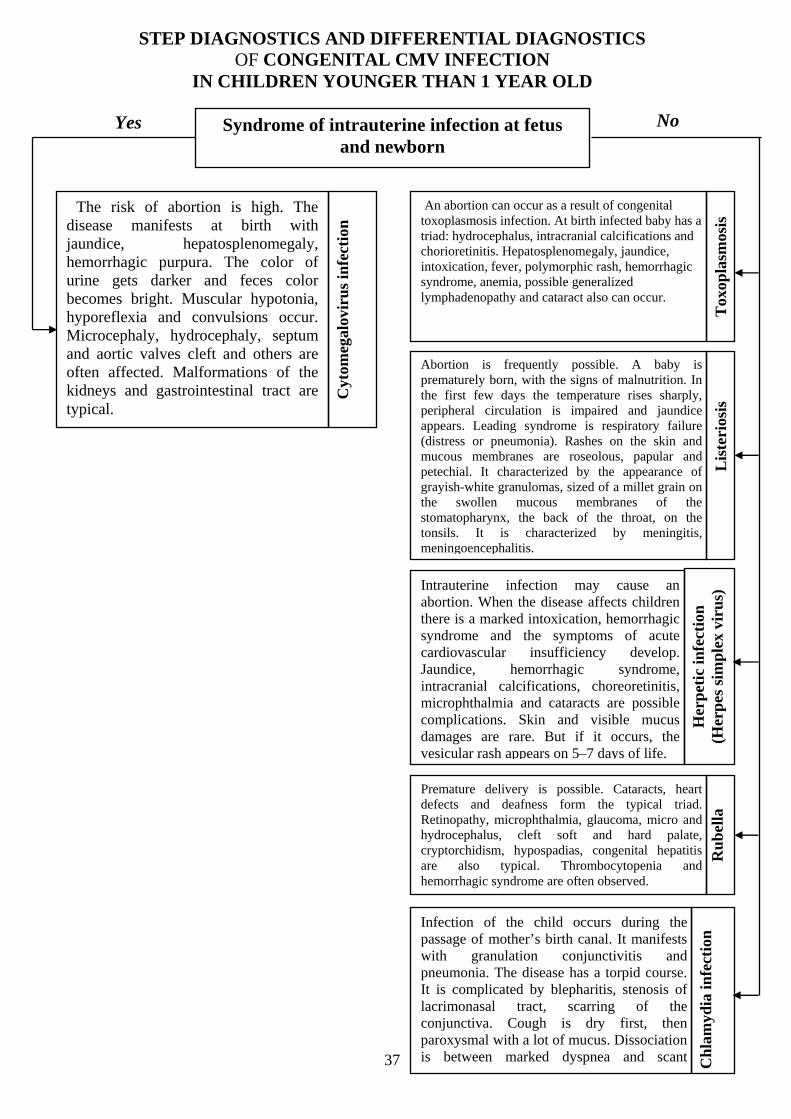
The risk of abortion is high. The disease manifests at birth with jaundice, hepatosplenomegaly, hemorrhagic purpura. The color of urine gets darker and feces color becomes bright. Muscular hypotonia, hyporeflexia and convulsions occur. Microcephaly, hydrocephaly, septum and aortic valves cleft and others are often affected. Malformations of the kidneys and gastrointestinal tract are typical.
Cyt
omeg
alov
iru
s in
fect
ion
An abortion can occur as a result of congenital toxoplasmosis infection. At birth infected baby has a triad:
Tox
opla
smos
is
hydrocephalus, intracranial calcifications and chorioretinitis. Hepatosplenomegaly, jaundice, intoxication, fever, polymorphic rash, hemorrhagic syndrome, anemia, possible generalized lymphadenopathy and cataract also can occur.
Abortion is frequently possible. A baby is prematurely born, with the signs of malnutrition. In the first few days the temperature rises sharply, peripheral circulation is impaired and jaundice appears. Leading syndrome is respiratory failure (distress or pneumonia). Rashes on the skin and mucous membranes are roseolous, papular and petechial. It characterized by the appearance of grayish-white granulomas, sized of a millet grain on the swollen mucous membranes of the stomatopharynx, the back of the throat, on the tonsils. It is characterized by meningitis, meningoencephalitis.
Lis
teri
osis
Intrauterine infection may cause an abortion. When the disease affects children there is a marked intoxication, hemorrhagic syndrome and the symptoms of acute cardiovascular insufficiency develop. Jaundice, hemorrhagic syndrome, intracranial calcifications, choreoretinitis, microphthalmia and cataracts are possible complications. Skin and visible mucus damages are rare. But if it occurs, the vesicular rash appears on 5–7 days of life.
Her
pet
ic in
fect
ion
(H
erp
es s
imp
lex
viru
s)
Premature delivery is possible. Cataracts, heart defects and deafness form the typical triad. Retinopathy, microphthalmia, glaucoma, micro and hydrocephalus, cleft soft and hard palate, cryptorchidism, hypospadias, congenital hepatitis are also typical. Thrombocytopenia and hemorrhagic syndrome are ofte
Ru
bel
la
n observed.
Infection of the child occurs during the passage of mother’s birth canal. It manifests with granulation conjunctivitis and pneumonia. The disease has a torpid course. It is complicated by blepharitis, stenosis of lacrimonasal tract, scarring of the conjunctiva. Cough is dry first, then paroxysmal with a lot of mucus. Dissociation is between marked dyspnea and scant
TCh
lam
ydia
infe
ctio
n
37h i l d

DIAGNOSTIC ALGORITHMS: CYTOMEGALOVIRAL INFECTION
Etiology
The source of infection
The mechanism
of transfer
Classification
Affected
organs and systems
Clinical forms
Methods of
diagnosis
Clinical course
Treatment
Prophylaxis
CYTOMEGALOVIRAL INFECTION
kind Herpes viridae
A sick person and virus carrier
Contagious Airborne Sexual Parenteral
Ant
ivir
al: c
yclo
fero
n,
ganc
yclo
vir,
acyc
lovi
r, V
alac
yclo
vir
Ant
ibio
tics
for
bact
eria
l in
fect
ion
stra
tifi
cati
on
Cor
tico
ster
oids
—
pred
niso
lonu
m
Vit
amin
ther
apy:
vit
amin
s B
,C
, K, PPCR
Treponema pallidum
hemagglutination
Complement fixation test
Neutralization reaction
Congenital Acquired
Detection of cytomegalovirus in the
sediments of urine, saliva, cerebrospinal fluid
LiverHemopoetic
organs Lungs Intestines KidneysHeart Salivary glands
CNS
Screening of pregnant
women for CMV
Use of condoms
During blood transfusion s:
transfusions of blood and blood
components from seronegative donors
Transplacental M
icro
ceph
aly,
miс
rogi
ria,
bra
in
arch
itect
onic
s im
pair
men
t wit
h
men
tal r
etar
datio
n de
velo
pmen
t
Atr
ial a
nd v
entr
icul
ar s
epta
l cl
eft,
end
ocar
dium
fi
broe
last
osis
, mal
form
atio
ns o
f th
e ao
rtic
val
ve a
nd p
ulm
onar
y tr
unk
Hep
atom
egal
y, ja
undi
ce
(liv
er a
cts
unde
r th
e co
stal
ar
ch o
n 3
-7 c
m)
Sple
en e
nlar
gem
ent,
hem
orrh
agic
purp
ura
(ecc
hym
osis
, pet
echi
ae
on th
e sk
in),
"vo
miti
ng, c
offe
e gr
ound
s "
Inte
rsti
tial
pne
umon
ia
(sho
rtne
ss o
f br
eath
, cy
anos
is, p
ertu
ssoi
d )
Vom
itin
g, d
iarr
hea,
ab
dom
inal
pai
n
Dar
k ur
ine
Dam
age
of th
e pa
roti
d,
subm
andi
bula
r an
d su
blin
gual
lym
ph n
odes
Localized Generalized
IFA
Acute Chronic
Imm
unom
odul
ator
s:
hype
rim
mun
oglo
buli
n, no
rmal
im
mun
oglo
buli
n hu
man
im
mun
oglo
buli
n an
ticy
tom
egal
ovir
us
Proper personal
hygiene when in contact with
a newborn
38

25
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF MEASLES
Yes No Exanthema. Intoxication syndrome. Catarrhal syndrome.
The rash appears in the first days of illness. Elements of the rash cover all the body. Rash develops simultaneously — small round pink-red spots do not merge and disappear completely after 2–3 days, with no pigmentation or desquamation. Enlargement of occipital and back cervical lymphatic nodes. Subfebrile temperature. Slightly runny nose, cough and sometimes conjunctivitis.
Ru
bel
la
Appearance of the rash is connected with taking sulfonamides, but can be due to other appointed drugs. It appears on the first days after admission. Rash is punctuate. Body temperature increases to subfebrile figures, malaise, also can be itching, swelling, peripheral lymph nodes.
med
icam
enta
l d
erm
atit
is
It begins acutely with vomiting, pain in the throat. The body temperature increases to febrile digits. On the 2nd day of onset appears punctate rash, abundant on hyperemic background, more intense on the sides of trunk, the flexors of the limbs, in the natural folds. The rash does not affect the nasolabial triangle. Peeling starts after the disappearance of the rash. Hyperemia of the stomatopharynx, clearly delimited (catarrhal, follicular, necrotic quinsy). «Strawberry» tongue.
Sca
rlet
fev
er
The disease develops gradually. Itchy nodules and vesicles appear on the skin. There are scabby tracts — linear intradermal inflammatory changes of a few millimeters, usually developing between the toes, on the flexion of the joints, the sides of the back, scrotum. No catarrhal symptoms, normal t.
En
tero
vira
l ex
anth
ema
Sudden onset of the disease, high fever, symptoms of intoxication. From the first hours there are extensive erythematous spots, with huge vesicles. Detachment of the epidermis is observed from the dermis in a large area of the hands, feet and trunk. No catarrhal symptoms.
Lye
ll, s sy
nd
rom
e
Acute onset with high fever (39–40 °C). On the 3 -4 day the temperaturerd th is critically reduced and there is a rash, spreading over the trunk, limbs, neck and head. Pale pink roseola tends to merge keeping for 2–3 days and disappear without desquamation or pigmentation. No catarrhal symptoms. It is commons in elder children.
Six
th d
isea
se
Acute onset of the disease, with the rise of body t to 39 °C and maculosis rash. Pink rash develops on unmodified skin, keeps for 1–2 days, disappears without desquamation or pigmentation. Vomiting and abdominal pain are typical. Scleritis, catarrhal conditions of the upper respiratory tract.
Acute onset of the disease, with the rise of t to 38–39 °C, maculosis papular rash, abundantly located on the face, tending to merge, with pigmentation and desquamation after disappearance. Tonsillitis, lymphadenopathy. Enlarged liver and spleen. –CBC: leukopenia, lymphocytosis, plasma cells.
Infe
ctio
us
mon
onu
cleo
sis
The disease is more frequent in adults. Sometimes it develops after ARI. Primarily, pink-red oval spot appears on the breast with desquamation in the centre. Spots can be found all over the body. Patient’s state is well. Temperature is normal or subfebrile.
Zh
iber
, s p
ink
lich
en
Acute onset of the disease with the rise of t to 38.5-39oС, development of catarrh of upper respiratory tract and conjunctivitis. Grayish-white spots appear on the buccal mucosa. After 4-5 days, maculopapular rash developsin three stages: 1 day —
st
face, neck, 2nd day — trunk, arms, 3 day —rd legs. After the disappearance of the rash brown pigmentation remains and persists up to 1.5 weeks.
Mea
sles
Sca
bie
s

Diagnostic algorithms: measles
Epidemiological
features
Affected
organs
Symptoms
Periods
of disease
Differential
diagnosis
Complications
Peculiarities in
children under 2 years
Diagnostic
Methods
Treatment
Prophylaxis
MEASLES
Instability of the virus Volatility of the virusTransmission —
airborneSource — the patient
Susceptibility - general
Nervous systemThe organs of
digestionSkin Eyes
The respiratory system
Run
ny n
ose,
cou
gh, d
yspn
ea,
retr
acti
on o
f co
mpl
iant
sit
es o
f th
e ch
est
Ena
nthe
ma,
Fil
atov
's sp
ots,
ph
aryn
geal
hyp
erem
ia, w
ater
y st
ool
Feve
r, h
eada
che,
flac
cidi
ty, v
agot
onia
Mac
ulop
apul
ar r
ash,
unc
hang
ed
back
grou
nd o
f ski
n, s
tage
s of
ras
h,
desq
uam
atio
n, p
igm
enta
tion
Phot
opho
bia,
hyp
erem
ia o
f co
njun
ctiv
a, te
arin
g an
d pa
sty
eyel
ids
EruptionProdromal Pigmentation
Flu, adenoviral infection,
paraflu, croup diphtheric
Rubella, scarlet fever, allergic
rash
Stomatitis MeningitisPneumoniaCroup Encephalitis Keratitis
Develops often, during the prodrome
Early, severe
Hemagglutinati on inhibition
reactionBlood analysis
Immunofluorescence
DesensitizationAntibiotics for complications
Care Vitamins
Air changeEarly isolation
of patients8–21 day
quarantineVaccination Gammaglobulin
Symptomatic
26

35
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSTICS OF EPIDEMIC PAROTITIS (MUMPS INFECTION)
Yes No Parotid and salivary glands. Intoxication.
It is more often seen in the elderly. Salivary gland is painful. Swelling is on the affected side. Process is unilateral. There is no fever. The stones that obstruct salivary duct can be revealed by ultrasound (US) and sialography. Normal CBC.
Sal
ivol
ith
iasi
s
Acute onset of the disease, the symptoms of intoxication are expressed slightly. The tonsils are moderately swollen, mild redness of tonsils and palatine arches. There are fibrinous coats on tonsils, «+» tissue, dirty gray, difficult to separate. The subja-cent tissue bleeds when it is removed. The membra-nous coats drown in water, are not grounded between glass slides. Regional lymph nodes are mild swollen and slight painful. In CBC: leukocytosis with neutrophilic shift.
Dip
hth
eria
of t
he
ton
sils
The lesion of the parotid salivary glands occurs due to local purulent infection (otitis, tonsillitis, and dental caries). Acute onset of the disease with high intoxication. Soreness and density are above the parotid gland. The skin over it is bright hyperemic. There is appearance of fluctuation. There is neutrophilic leukocytosis in CBC
Acu
te p
uru
len
t p
arot
itis
The lesion of the parotid glands is associated with occupational hazard. Acute and chronic poisoning by mercury and lead. Disease affects adults mostly. In children it is extremely rare. Mumps develops slowly, often accompanying with changes of the teeth and gums.
Inflammation of the salivary glands is chronic. Re-lapses occur once a year, alternating with periods of clinical well-being. The disease begins with the rise of body temperature, swelling and pain of the gland. Buccal mucosa is swelled on the affected side. Pus discharges from the parotid duct. Spontaneous disappearance of pain and swelling in 7-20 days.
Acute onset. Symptoms of intoxication. The lesion of the parotid salivary gland usually starts unilateral, after 1–2 days the process moves to the second gland. Moderately painful gland has pasty consistency. The skin above it has normal color. Positive Murso’s symptom, pain by pulling the ear up and ahead, with pressure below the outer edge of the ear canal. Vartonov’s duct is swelled. Other glands are involved in the inflammatory process: submaxillary and sublingual salivary glands, pancreas, mammary gland, gonads, thyroid gland. In clinical blood test: leukopenia and lymphocytosis.
Tox
ic p
arot
itis
P
rim
ary
chro
nic
par
otit
is
Ep
idem
ic p
arot
itis
There is intoxication, lymphadenopathy. Lesions of the tonsils are necrotic and ulcerative. It is often one-sided. Necrosis doesn’t rise above a surface of the tonsils; the surface is uneven, rough. On the 3rd–4th day of illness on necrosis place forms an ulcer crater, covered with a very thin fibrinous coat under which ulcer epithelializes for 8–12 days. Putrid smell of the breath. By microscopy in smears taken from the surface of the tonsils detected spirillum and spindle-form bacilli.
Sim
anov
sky-
Rau
hfu
s to
nsi
l-li
tis
Duration of illness is long (for months). Curve of the temperature has undulating character. Lymph nodes are swollen in all groups. Lymph nodes are enlarged to the size of V–VII, dense, fused with each other and the subjacent tissues - «potatoes in a sack.» Biopsy of lymph node shows Berezovsky–Steinberg’s cells. ly
mp
hogr
anu
lom
ath
osis
There is fever. The posterior pharyngeal wall is much hyperemic, loosened. There is a big amount of thick mucus. The tonsils are swollen, raised to II–III degree, hyperemic. Coats on the tonsils are whitish-yellow, loose, rough, rugged, easily removed and grounded between glass slides. The sharp enlargement of cervical lymph node groups, especially those located on the posterior edge of the sternocleidomastoid muscle. Lymph nodes are dense, elastic, not soldered to each other and the subjacent tissues. Nasopharyngeal tonsils are swollen. A child breathes with a half-open mouth; his voice takes on a nasal tone. Hepatosplenomegaly. In CBC: lymphocytic leukocytosis, elevatedESR, presence of atypical mononuclear cells.
Infe
ctio
us
mon
onu
cleo
sis
Disease is rare as a separate unit. Usually damage of pharynx appears due to ARI. Hypertermia, painful throat. On the tonsils, swollen and hyperemic, appears bluish overlay, rarely they can be found only in the gaps or can be like small island. Overlays partially impregnated with fibrin are difficult to remove. They are easily grounded between glass slides. Diffuse T T T T T T T T T T
bright Thyperemia of the ToropharynxT, T Twithout clear boundaries.T TExpressedT TpolyadenopathyT.
TSta
ph
yloc
occa
l an
gin
a
Diagnostic algorithms : diagnostics of mumps infection
Affected organs
and systems
Symptomsand signs
Methods of
research
36
Differential
diagnosis
Treatment
Epidemiology
and prophylaxis
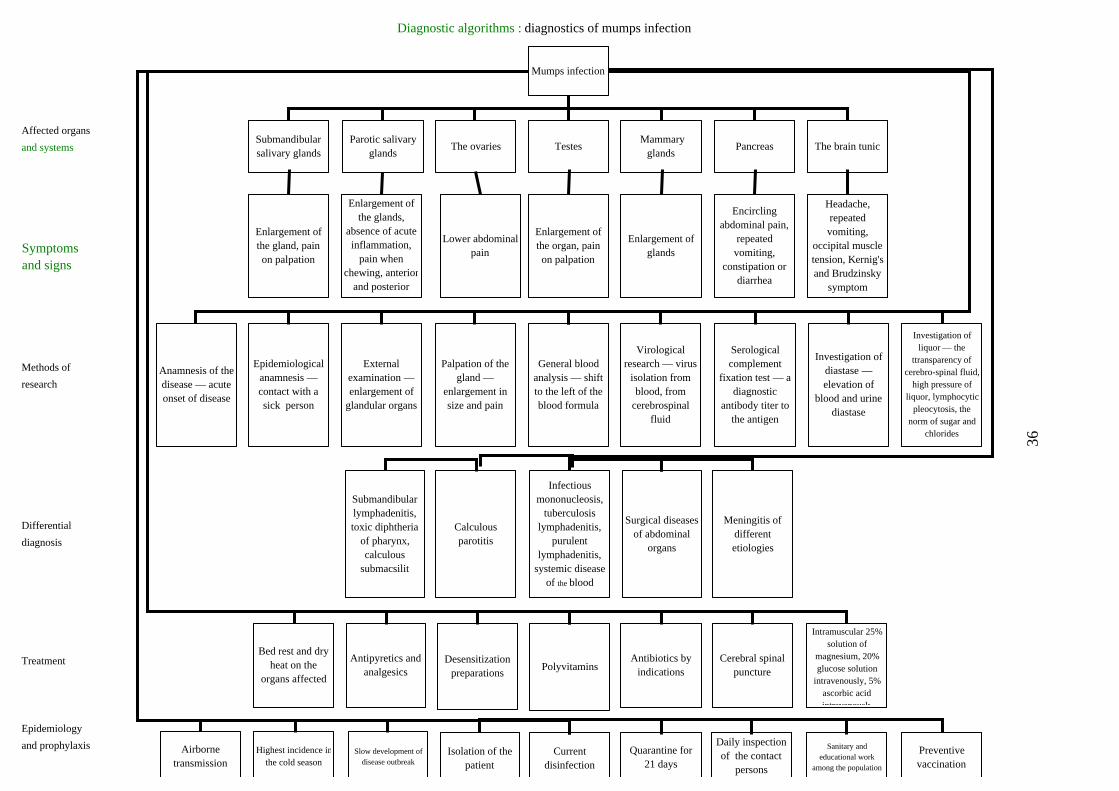
Mumps infection
Submandibular salivary glands
Parotic salivary glands
The ovaries Testes Mammary
glandsPancreas The brain tunic
Enlargement of the gland, pain on palpation
Enlargement of the glands,
absence of acute inflammation,
pain when chewing, anterior
and posterior
Lower abdominalpain
Enlargement of the organ, pain on palpation
Enlargement of glands
Encircling abdominal pain,
repeated vomiting,
constipation or diarrhea
Headache, repeated vomiting,
occipital muscle tension, Kernig's and Brudzinsky
symptom
General blood analysis — shift to the left of the blood formula
Palpation of the gland —
enlargement in size and pain
Virological research — virus
isolation from blood, from
cerebrospinal fluid
Serological complement
fixation test — a diagnostic
antibody titer to the antigen
Investigation of diastase — elevation of
blood and urine diastase
Investigation of liquor — the
ttransparency of cerebro-spinal fluid,
high pressure of liquor, lymphocytic
pleocytosis, the norm of sugar and
chlorides
External examination — enlargement of
glandular organs
Epidemiological anamnesis — contact with a sick person
Anamnesis of the disease — acute onset of disease
Infectious mononucleosis,
tuberculosis lymphadenitis,
purulent lymphadenitis,
systemic disease of the blood
Surgical diseases of abdominal
organs
Calculous parotitis
Submandibular lymphadenitis, toxic diphtheria
of pharynx, calculous
submacsilit
Meningitis of different etiologies
PolyvitaminsDesensitization
preparations
Antipyretics and analgesics
Bed rest and dry heat on the
organs affected
Antibiotics by indications
Cerebral spinal puncture
Intramuscular 25% solution of
magnesium, 20% glucose solution
intravenously, 5% ascorbic acid intravenously
Current disinfection
Isolation of the patient
Slow development of disease outbreak
Highest incidence inthe cold season
Airborne transmission
Quarantine for 21 days
Daily inspection of the contact
persons
Sanitary and educational work
among the population
Preventive vaccination

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSTICS OF STOMATOPHARYNGEAL DIPHTHERIA
Yes
No The syndrome of quinsy.
Intoxication syndrome.
The disease is caused by hemolytic streptococcus. Increased t, intoxication. Inflammation of the tonsils. Enlarged regional lymph nodes. Severe fever. Two-way process.
Ton
sill
itis
(s
trep
toc.
, st
aph
yl.)
Persons who has no immunity to streptococcal erythrogenic toxin are affected. Hyperemia of the skin
Sca
rlet
fev
er
, micropunctate rashes followed by desquamation of the skin, tachycardia, vomiting. Bright hyperemia of mucus membranes - «burning mouth»; clear, bloodshot tongue («strawberry» tongue). Desquamation is especially marked
No marked symptoms of intoxication, subfebrile t. Sore throat at swallowing is absent or not very marked. The process is usually unilateral. On the first day of mild hyperemia, swelling and an increase in one of the palatine tonsils. Then, on a background of hyperemia, a rounded greyish-white spot about 10 mm in size appears on its surface. On the 2
on the fingers.
nd–3rd day coat is forming at this place, when removing — there is an ulcer. Breath is putrid.
Sim
anov
sky-
Pla
ut-
Vin
cen
ts t
onsi
llit
is
,
Develops after hypothermia or ARI. The process is mainly on the tonsils and regional lymph nodes. Low-grade fever is in the evenings, acrocyanosis, lability of heart rate, orthostatic hypotension, unpleasant sensations in the heart. Pains in the throat. Cohesion of the tonsils with the arches, the presence of scars on the tonsils, sometimes in lacunas with caseous plugs.
Rapid rise of the t, chill, marked toxicosis. Sharp pain in throat when swallowing and even at rest, sometimes painful movement of the head. Trismus chewing muscles limits the opening of the mouth; increased salivation. Examination of the stomatopharynx is difficult. Pharyngoscopy detects unilateral swelling and bulging in the absence of coats on the mucous membrane of the tonsils.
Ch
ron
ic t
onsi
llit
is
Par
aton
sill
itis
High fever, general intoxication, an acute onset of illness. Damage of the tonsils and the enlargement of regional lymph nodes. The appearance of quinsy is lagging behind with respect to time by t increasing, symptoms of general intoxication. Pharynx involvement on the third day and later. Bilateral necrotic changes in the tonsils. Fibrinous coat on the tonsils, does not extend beyond the tonsils. Generalized lymphadenopathy. The liver and spleen may be enlarged. There are atypical mononuclear cells in the blood.
Infe
ctio
us
mon
onu
cleo
sis
The rash, usually erythematous, with the figure of the «butterfly on his face», generalized lymphadenopathy
Lis
teri
osis
, enlarged liver and spleen. There are some patients with purulent meningitis. High fever with large daily scale, septic metastases, secondary purulent foci.
The enlargement of one tonsil, its mucosa membrane is hyperemic. The regional lymph node is moderately enlarged of dense consistency, painless. No pain during swallowing. On the affected tonsil develops necrotic processes, forming a hard chancre. Low-grade fever, slight malady. Changes in the tonsils remain for a very long time without significant dynamics (up to a month or more).
Syp
hil
is
The general condition suffers a little. Body temperature remains normal, rarely subfebrile. Coat associated with the fungus is grayish-white, rarely continuous. It is usually located by separated areas, capturing not only the tonsils, but also the mucosa of the mouth, the posterior pharyngeal wall. The fever and symptoms of intoxication are absent. A common whitish coat is on the mucous membranes of the oropharynx. M
ycot
ic t
onsi
llit
is
High fever, pain at swallowing. The process is unilateral, necrotic. Coat is of grayish color, after its removal there is an ulcer. It is characterized by the formation of buboes. The regional upper anterior cervical lymph nodes are enlarged. Bubo is not soldered to the surrounding tissues, is mobile, the skin over it is not changed. Fluctuation of buboes. It may form a fistula.
Tu
lare
mia
Acute onset of the disease. Fibrinous coat is on the tonsils. Sore throat is absent or expressed only slightly. Coat is difficult to separate. Swelling of the subcutaneous fat neck. Coat is not grounded between the glass slides, drowns in the water. Body
otemperature - 37–38 P PC. When removing the coat, surface of the tonsil bleeds.
TSto
mat
oph
aryn
gea
lT Tdi
hth
eria
p
18

DIAGNOSTIC ALGORITHMS: DIPHTHERIA
Localisation
Clinical
forms
Signs
symptoms
Differential
diagnosis
Complications
Treatment
Especially
at the modern stage
Prophylaxis
Diagnostics
Diphtheria
Pharynx Nose Larynx Eyes
Tox
ic
Hyp
erto
xic
Loc
aliz
ed
Sub
toxi
c
Spr
ead
Sudd
en p
hary
nx e
dem
a, s
prea
d sc
oats
, sw
eet
brea
th, e
dem
a o
f th
e ce
rvic
al ti
ssue
Sudd
en o
nset
, dim
min
g of
con
scio
usne
ss,
wea
knes
s, h
emod
ynam
ic d
istu
rban
ces,
co
ats,
and
ede
ma
in th
e th
roat
Isla
nds
or th
e fi
lmy
coat
s on
the
tons
ils,
m
oder
ate
swel
ling
of
the
lym
ph n
odes
Coa
ts b
eyon
d th
e to
nsil
s, a
mar
ked
incr
ease
in
reg
iona
l lym
ph n
odes
Spre
ad c
oats
in
the
phar
ynx,
ede
ma
of
arou
nd t
he ly
mph
nod
es
Cat
arrh
al-
ulce
rati
ve
Mem
bran
eous
Blo
ody
disc
harg
e, e
xcor
iati
on a
roun
d th
e no
se, s
ores
in th
e th
e na
sal m
ucos
a
Film
on
the
nasa
l sep
tum
Loc
aliz
ed c
roup
Wid
espr
ead
A
Wid
espr
ead
B
Hoa
rsen
ess
to a
phon
ia, r
ough
cou
gh,
sten
osis
I
sten
osis
II
ste
nosi
s II
I
Cat
arrh
al f
orm
Cro
upou
s fo
rm
Dif
teri
tica
l fo
rm
Hyp
erem
ia o
f th
e co
njun
ctiv
a, p
urul
ent
disc
harg
e fr
om th
e ey
es
Mod
erat
e ed
ema
of th
e ey
elid
s, m
embr
anou
sco
njun
ctiv
itis
Sudd
en e
dem
a of
the
eyel
ids,
fil
ms
on
conj
unct
iva
and
on th
e ey
ebal
l
Par
aton
zill
itis
Nec
roti
c an
gina
AR
VI
Ang
ina
Sim
anov
sky
Fal
se-m
embr
anou
s an
gina
Ton
sill
itis
foll
icul
aris
Lac
unar
tons
illi
tis
Epi
dem
ic p
arot
itis
Infe
ctio
us m
omon
onuc
leos
is
Of
nose
for
eign
bod
y
Cro
up f
or A
RV
I
Cro
up in
oth
er in
fect
ions
For
eign
bod
y
Pap
pilo
mat
osis
aden
ovir
al c
onju
ncti
viti
s
Eth
moi
diti
s
Orb
ital
cel
luli
tis
Poly
radi
culo
neur
itis
Para
lysi
s an
d pa
resi
s of
cra
nial
ner
ves
Myo
card
itis
Serotherapy, desensitisation, vitamins, and plasma hormones, magnesium sulfate, strychnine, cocarboxylase, ATA, glutamic acid, dibazol, proserin,
intubation, tracheostomy
Reduction of incidence up to sporadic cases, reducing of mortality, increasing of the coefficient of severity, the prevalence of pharynx diphtheria, lack of periodic rises, the incidence in older children, the
predominant disease in rural areas, bacilli carriers are the main source of infection
Iden
tifi
cati
on o
f ca
rrie
rs o
f to
xige
nic
bact
eria
Mea
sure
s in
the
focu
s of
the
dise
ase
Con
trol
of
imm
unit
y
Tre
atm
ent o
f ca
rrie
rs
Act
ive
imm
uniz
atio
n
Bac
teri
olog
ical
res
earc
h
Ser
olog
ical
rese
arch
Bac
teri
osco
py s
wab
Pano
phta
lmia
19

Infrequent localisation
Dif
teri
tica
l fo
rmco
njun
ctiv
a an
d on
the
eyeb
all
Orb
ital
cel
luli
tis
19
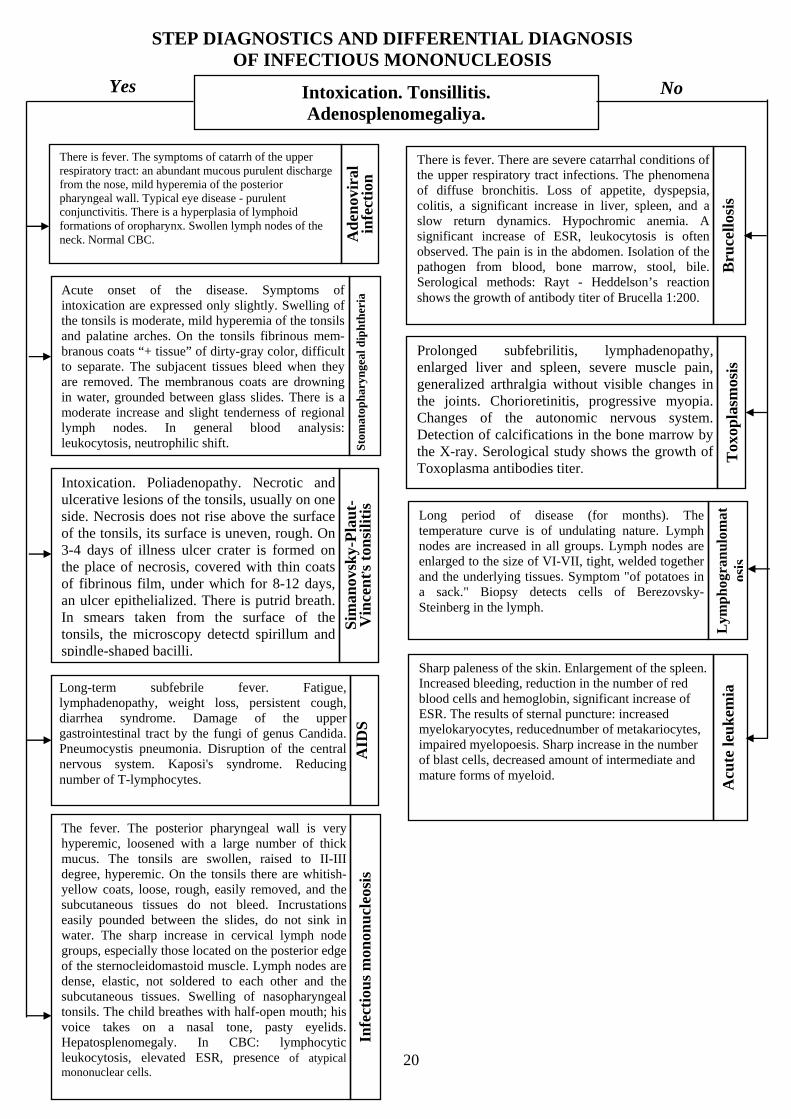
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF INFECTIOUS MONONUCLEOSIS
Yes No Intoxication. Tonsillitis.
Adenosplenomegaliya.
There is fever. The symptoms of catarrh of the upper respiratory tract: an abundant mucous purulent discharge from the nose, mild hyperemia of the posterior pharyngeal wall. Typical eye disease - purulent conjunctivitis. There is a hyperplasia of lymphoid formations of oropharynx. Swollen lymph nodes of the neck. Normal CBC. A
den
ovir
al
infe
ctio
n
There is fever. There are severe catarrhal conditions of the upper respiratory tract infections. The phenomena of diffuse bronchitis. Loss of appetite, dyspepsia, colitis, a significant increase in liver, spleen, and a slow return dynamics. Hypochromic anemia. A significant increase of ESR, leukocytosis is often observed. The pain is in the abdomen. Isolation of the pathogen from blood, bone marrow, stool, bile. Serological methods: Rayt - Heddelson’s reaction
Bru
cell
osis
shows the growth of antibody titer of Brucella 1:200. Acute onset of the disease. Symptoms of intoxication are expressed only slightly. Swelling of the tonsils is moderate, mild hyperemia of the tonsils and palatine arches. On the tonsils fibrinous mem-branous coats “+ tissue” of dirty-gray color, difficult to separate. The subjacent tissues bleed when they are removed. The membranous coats are drowning in water, grounded between glass slides. There is a moderate increase and slight tenderness of regional lymph nodes.
Prolonged subfebrilitis, lymphadenopathy, enlarged liver and spleen, severe muscle pain, generalized arthralgia without visible changes in the joints. Chorioretinitis, progressive myopia. Changes of the autonomic nervous system. Detection of calcifications in the bone marrow by the X-ray. Serological study shows the growth of Toxoplasma antibodies titer.
Tox
opla
smos
is
In general blood analysis:
dip
hth
eria
S
tom
atop
har
ynge
al
leukocytosis, neutrophilic shift.
Intoxication. Poliadenopathy. Necrotic and ulcerative lesions of the tonsils, usually on one side. Necrosis does not rise above the surface of the tonsils, its surface is uneven, rough. On 3-4 days of illness ulcer crater is formed on the place of necrosis, covered with thin coats of fibrinous film, under which for 8-12 days, an ulcer epithelialized. There is putrid breath. In smears taken from the surface of the tonsils, the microscopy detectd spirillum and spindle-shaped bacilli.
Sim
anov
sky-
Pla
ut-
Vin
cen
t, s to
nsi
liti
s
Long period of disease (for months). The temperature curve is of undulating nature. Lymph nodes are increased in all groups. Lymph nodes are enlarged to the size of VI-VII, tight, welded together and the underlying tissues. Symptom "of potatoes in a sack." Biopsy detects cells of Berezovsky-Steinberg in the lymph.
Lym
ph
ogra
nu
lom
atos
is
Sharp paleness of the skin. Enlargement of the spleen.
Long-term subfebrile fever. Fatigue, lymphadenopathy, weight loss, persistent cough, diarrhea syndrome. Damage of the upper gastrointestinal tract by the fungi of genus Candida. Pneumocystis pneumonia. Disruption of the central nervous system. Kaposi's syndrome. Reducing
Increased bleeding, reduction in the number of red blood cells and hemoglobin, significant increase of ESR.
Acu
te le
uk
emia
The results of sternal puncture: increased
AID
S
myelokaryocytes, reducednumber of metakariocytes, impaired myelopoesis. Sharp increase in the number of
number of T-lymphocytes.
blast cells, decreased amount of intermediate and mature forms of myeloid.
Infe
ctio
us
mon
onu
cleo
sis
The fever. The posterior pharyngeal wall is very hyperemic, loosened with a large number of thick mucus
20
. The tonsils are swollen, raised to II-III degree, hyperemic. On the tonsils there are whitish-yellow coats, loose, rough, easily removed, and the subcutaneous tissues do not bleed. Incrustations easily pounded between the slides, do not sink in water. The sharp increase in cervical lymph node groups, especially those located on the posterior edge of the sternocleidomastoid muscle. Lymph nodes are dense, elastic, not soldered to each other and the subcutaneous tissues. Swelling of nasopharyngeal tonsils. The child breathes with half-open mouth; his voice takes on a nasal tone, pasty eyelids. Hepatosplenomegaly. In CBC: lymphocytic leukocytosis, elevated ESR, presence of atypical mononuclear cells.

Diagnostic algorithms : Infectious mononucleosis
Affected organs
systems
Symptoms
and signs
Methods
of diagnosis
Diagnostic
features
Differential
diagnosis
Especially
in infants
Treatment
Infectious mononucleosis
Lymph nodes Nasopharynx Pharynx Parenchymal organs Blood
Enlargement of lymph nodes,
enlargement of all groups of lymph
nodes
Difficulty of nasal breathing
QuinsyEnlarged liver and
spleenFever
Palpation, external examination
Anterior and posterior rhinoscopy
Cytology of the tonsils,
pharyngoscope, bacteriological
examination
Palpation, biochemical research
General blood an alysis, leuko-concentrate,
serological reactions,thermometry
Sca
nty
runn
y no
se, e
nlar
gem
ent o
f na
soph
aryn
geal
tons
ils,
coa
ting
in th
e na
soph
aryn
x, a
typi
cal m
onon
ucle
ar c
ells
in th
e sm
ear,
cat
arrh
al p
heno
men
a, c
oatin
hin
the
phar
ynx
Min
or b
ioch
emic
al c
hang
es, m
ild
leuk
ocyt
osis
, mon
onuc
leos
is, a
typi
cal m
onon
ucle
ace
lls,
mod
erat
ely
acce
lera
ted
ES
R
The
rea
ctio
n of
Pau
l-B
unne
lya-
Dav
idso
n, th
e re
acti
on o
f T
omcz
yk, h
emag
glut
inat
io te
st w
ith
hors
e er
ythr
ocyt
es
A lo
t of
mov
ing,
wit
hout
pai
nful
lym
ph n
odes
, no
infl
amm
atio
n, c
ellu
lar
tiss
ue
past
osit
y
Acu
te o
nset
, sor
e th
roat
, sno
ring
bre
athi
ng, c
hang
es in
the
conf
igur
atio
n ne
ck, l
ong-
term
hig
h te
mpe
ratu
re
LymphadenitisTonsillitisPharynx diphtheriaAcute leukemiaLymphogranulomato
sisViral hepatitis
Adenoviral infection,HIV infection
Significant damage of nasopharynx, expressed catarrhal phenomena, skin eruptions, more atypical mononuclear cells in the blood, the absence of serological changes, insignificant coating on the tonsils
AntihistaminesAntibiotics(indicated)
AntipyreticVitaminsCorticosteroids
(indicated)
21

33
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF SCARLET FEVER
Yes No Micropunctate exanthema. Syndrome of tonsillitis. Intoxication.
The rash appears on the 3rd -4 day of onset. The skin is hyperemic. Hyperemia and expressed skin pastosity of hands and feet (the symptoms of "gloves", "socks", "hood"). There is a moderate hyperemia in the pharynx. "Strawberry" tongue. Hepatosplenomegaly. There are muscle and joint pain. Micropunctate rash is on unmodified skin, usually in the abdomen, axillary region, on the lateral surfaces of the body.
th
Pse
ud
otu
ber
culo
sis
Maculo-papular rash, maculosis, catarrhal conditions, subfebrile temperature. The rash stag-ing on the hyperemic background skin is specific. The pigmentation is after the disappearance of the rash. Filatov-Koplik,s spots, conjunctivitis. Sometimes croup syndrome may develop, rash tends to merge.
Mea
sles
It begins acutely, temperature rises, catarrhal symptoms appear. Lymphadenopathy - cervical, back cervical, located behind of sternocleidomastoid muscle like a chain. There are tonsillitis and hepatosplenomegaly. In CBC: atypical mononuclear cells, increased ALT, AST. Jaundice. Maculosis rash, and then can be pigmentation, skin desquamation.
Catarrhal symptoms. Polymorphous rash, maculopapular, hemorrhagic, often around the joints (in the hands, feet) (a symptom of "gloves", "socks", "hood"). Joint inflammation (swelling, redness, tenderness, limitation of movement). Myocarditis. Hepatosplenomegaly. Nausea, vomiting, and abdominal pain. Pouring sweat, high fever, with large daily fluctuation. Jaundice, diarrhea. Stool diluted, often with mucus, green, sometimes blood.
Infe
ctio
us
mon
onu
cleo
sis
inte
stin
al y
ersi
nio
sis
Acute onset, high fever up to 39oC and more. The rash is small maculosis -papular. Headache, muscle pain, scleritis, catarrhal symptoms. Vomiting and abdominal pain are typical. Localization of rash: face, body, sometimes arms and legs. Rash is on unmodified background skin. Rash doesn’t have staging, doesn’t leave pigmentation or desquamation.
En
tero
viru
s b
osto
n
exan
them
a
Maculosis rash associated with taking sulfonamides, antibiotics. General malaise, fever, often to subfebrile. Itching of the skin, enlargement of peripheral lymph nodes. In the blood: mild eosinophilia. The rash tends to merge, no staging. Rash appears during the first days of drug administration.
Med
ical
der
mat
itis
Normal or subfebrile t. Rash is maculosis, abundant, most marked on thetrunk. Single rosella and papules are revealed. The rash persists for a long time up to 2-3 weeks, then gradually fades and disappears without a trace. Anamnesis: the presence of primary syphilides (chancre) residual effects. Rash appears on a relatively good state of health of the patient, long-term preservation of rash without dynamic.
Syp
hil
is
The disease is most often seen in young children. The rash is micropunctate, single, with a hemorrhagic component, localized on the face, neck, upper body. Manifestations of disseminated intravascular coagulation (DIC). Diagnosis is based on severe clinic of flu. T
oxic
for
m o
f in
flu
enza
Catarrhal symptoms. Micropunctate rash is followed by desquamation of the skin. Tachycardia, frequent vomiting. Bright redness of the throat - "flaming" pharynx. Rash is on hyperemic skin, especially on fingers. Tonsillitis, lymphadenopathy, "Strawberry" tongue. Rash doesn’t leave pigmentation. Pale nasolabial triangle. Thickening of the rash on the cheeks, T T T T T
Ton the side ofT Tthe trunk,T Tabdomen,T TflexorT Tsurfaces of limbsT.
Sca
rlet
fev
er
Body temperature is subfebrile. The rash is small maculosis, sometimes papular, disappears without pigmentation, desquamation, and does not tend to merge. There is no rash staging. Lymph nodes are swollen - occipital, back cervical. slight conjunctivitis. In CBC: leukopenia, relative lymphocytosis, plasma cells (10-30%).
Ru
bel
la

DIAGNOSTIC ALGORITHMS: scarlet fever
Type of the course
Clinical
forms
Signs and
symptoms
peculiarities
in babies
Differential
diagnosis
Character of the course
Complications
Treatment
Prophylaxis
Scarlet fever
typical atypical
Severe toxic
Severe septic
Medium-severe
MildToxic-septic
Extra-pharynge
al
Hypertoxic
Hemorrhagic
Obliterated
t ris
e to
38C
, si
ngle
vo
mit
ing,
cat
arrh
al to
nsil
liti
s
t ris
e to
40
°C, r
epea
ted
vom
itin
g, n
ecro
tic
tons
illi
tis
t ris
e to
41C
,cra
mps
, del
iriu
m,
men
ingo
-enc
epha
litic
syn
drom
e
Sep
tice
mia
, phl
egm
onou
s ad
enit
is,
pyos
epti
cem
ia, e
xten
sive
nec
rosi
s in
th
e or
opha
rynx
, enl
arge
men
t of
the
live
r an
d sp
leen
Man
ifes
tati
on o
f to
xic
and
sept
ic f
orm
s
Cat
arrh
al q
uins
y,
subf
ebri
liti
s, s
atur
atio
n, s
kin
fold
s
Wou
nd s
urfa
ce, r
egio
nal
rash
, abs
ence
of
quin
sy
Unc
onsc
ious
ness
, cra
mps
, pa
raly
sis
of s
ympa
thet
ic,
coll
apse
Hem
orrh
agic
syn
drom
e,
seve
re in
toxi
cati
on
Low incidence, intoxication is weakly expressed, the absence of severe toxic forms, the severity of septic process in the acute period, the frequent development of septic
complications, rare allergic complications
Rubella MeaslesChickenp
ox rash
Allergic rash
Scarlet fever like
Far Eastern fever
Staphylococcal infection with scarlet fever like syndrome
QuinsyPharynx
diphtheriaSudamen Flu
With complications
Smooth With allergic
waves
Lym
phad
enit
is
Oti
tis
Mas
toid
itis
Sinu
siti
s
Nep
hrit
is
Syno
viti
s
Symptomatic: antipyretic, cardiacs,
antihistamines
Etiotropic: antibiotics
Liquid injection, plasma injection
One-stage filling of the chambers
QuarantineIsolation Disinfection
34

27
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF MENINGOCOCCAL INFECTION (PURULENT MENINGITIS)
Yes No Meningeal syndrome. Hypertension. Intoxication.
Acute onset of the disease with febrile fever, violent headache, hyperesthesia, repeated vomiting, and intoxication increases. A large fontanelle protrudes, sutures do not hold, size of the skull is increasing, loss of consciousness, convulsions, mono- and hemipareses. Focal lesions appear on 1-2 days of illness. Cerebrospinal fluid is muddy, often greenish, neutrophilic pleocytosis (500-1500) 106/l, increase in protein (1-10 g/l).
Pn
eum
ococ
cal
men
ingi
tis
Meningeal syndrome is developing after exanthema and is accompanied by a sharp rise in temperature to 40°C, nausea, vomiting, severe headache, hyperesthesia. Meningeal symptoms, decreased or absent tendon reflexes, especially in the lower extremities. The abdominal reflexes are absent or reduced. Cerebrospinal fluid flows under high pressure, cytosis (60-150) .106/l, lymphocytes predominate. The protein content is slightly increased (1.5 times).
Mea
sles
m
enin
goen
cep
hal
itis
Signs of meningoencephalitis appear soon after the disappearance of the rash. Low-grade fever, enlarged occipital and back cervical lymph nodes. Headache, vomiting, disturbances of consciousness, tonoclonic convulsions. Paresis, ataxia, central respiratory disorders. In cerebrospinal fluid dominated amount of lymphocytes is revealed. Virological methods - virus allocation from blood.
Ru
bel
la
men
ingo
ence
ph
alit
is
Acute onset of the disease, with a rise in t to 38-40oC. CNS damage is preceded by parotitis, an inflammation of other glandular organs. Severe headache, vomiting, weakness, myalgia, moderate meningeal syndrome. Cerebrospinal fluid flows under pressure, the protein content is normal or increased to 2.5 g/l, cytosis is from several hundreds to 2000,10 /l6 at the expense of lymphocytes, a film of fibrin may fall.
Par
otid
m
enin
giti
s
The disease begins acutely, with a rise in body temperature to 39-40oC. There is a severe headache, dizziness, repeated vomiting, restlessness, and sometimes abdominal pain, delirium, convulsions. The patient's face is hyperemic, slightly pasty, injected scleras. Mucus membranes of oropharynx are hyperemic, grain on the back wall of the pharynx and soft palate. Meningeal symptoms are from the first day, short-term. Liquor of spinal puncture is transparent, cytosis of 200-300 cells per 1 mm3 flows under the pressure; cytosis is firstly mixed, then the lymphocytic. The Pandey s reaction, is weakly positive.
En
tero
viru
s in
fect
ion
(s
erou
s m
enin
giti
s) Headache, repeated vomiting, shuddering and
twitching of individual muscle groups and limbs, and sometimes tremor, horizontal nystagmus. Meningeal symptoms are on 2-3 days of illness. In the liquor lymphocytic cell count is moderate (up to 200-300 mm3 in 1 mm), a slight increase in protein. Paralysis does not develop, but there is weakness when walking.
Pol
iom
yeli
tis
men
inge
al f
orm
It develops more often in the presence of influenza. It is characterized by an identical clinical picture of meningitis, but in contrast to recent positive dynamics is observed fast after the lumbar puncture. Liquor is diluted, from the general blood analysis - picture of a viral infection. M
enin
gism
M
enin
goco
ccal
m
enin
giti
s
Occurs on the 7 -9 day of vaccinationth th , withhigh temperature. Generalized tonoclonic convulsions, anxiety, tremors, motor automatisms, tremor of the extremities, anizoreflexia, pyramidal signs. Hallucinatory-delirium syndrome, psycho disorders, cataleptic phenomena. Normal CSF.
Pos
tvac
cin
al
men
ingo
ence
ph
alit
is
The disease begins with a rise in temperature to 39-40oC, strong chill. Severe headache, becoming worse when moving head, strong stimuli. Marked hyperesthesia, repeated vomiting, and convulsions. Meningeal symptoms for 2-3 days, red dermographism. In the spinal puncture - CSF is turbid, putrid, neutrophilic pleocytosis, measured from thousands of cells in 1 microlitre.
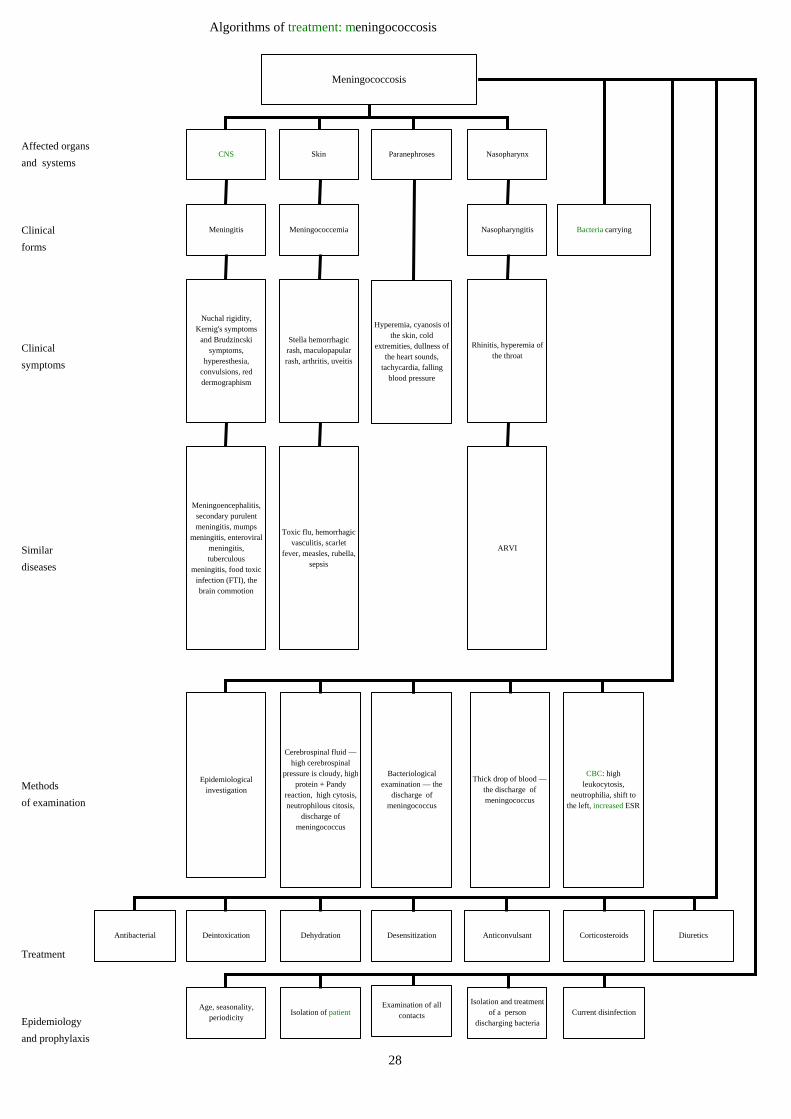
Algorithms of treatment: meningococcosis
Affected organs
and systems
Clinical
forms
Clinical
symptoms
Similar
diseases
Methods
of examination
Treatment
Epidemiology
and prophylaxis
Meningococcosis
CNS Skin Paranephroses Nasopharynx
Bacteria carryingMeningitis Meningococcemia Nasopharyngitis
Nuchal rigidity, Kernig's symptoms
and Brudzincski symptoms,
hyperesthesia, convulsions, red dermographism
Stella hemorrhagic rash, maculopapular rash, arthritis, uveitis
Hyperemia, cyanosis ofthe skin, cold
extremities, dullness of the heart sounds,
tachycardia, falling blood pressure
Rhinitis, hyperemia of the throat
Meningoencephalitis, secondary purulent meningitis, mumps
meningitis, enteroviral meningitis, tuberculous
meningitis, food toxic infection (FTI), the brain commotion
Toxic flu, hemorrhagic vasculitis, scarlet
fever, measles, rubella, sepsis
ARVI
Bacteriological examination — the
discharge of meningococcus
Cerebrospinal fluid — high cerebrospinal
pressure is cloudy, highprotein + Pandy
reaction, high cytosis, neutrophilous citosis,
discharge of meningococcus
Epidemiological investigation
Thick drop of blood — the discharge of meningococcus
CBC: high leukocytosis,
neutrophilia, shift to the left, increased ESR
DesensitizationDehydrationDeintoxication Anticonvulsant CorticosteroidsAntibacterial Diuretics
Examination of all contactsIsolation of patient
Age, seasonality, periodicity
Isolation and treatment of a person
discharging bacteriaCurrent disinfection
28
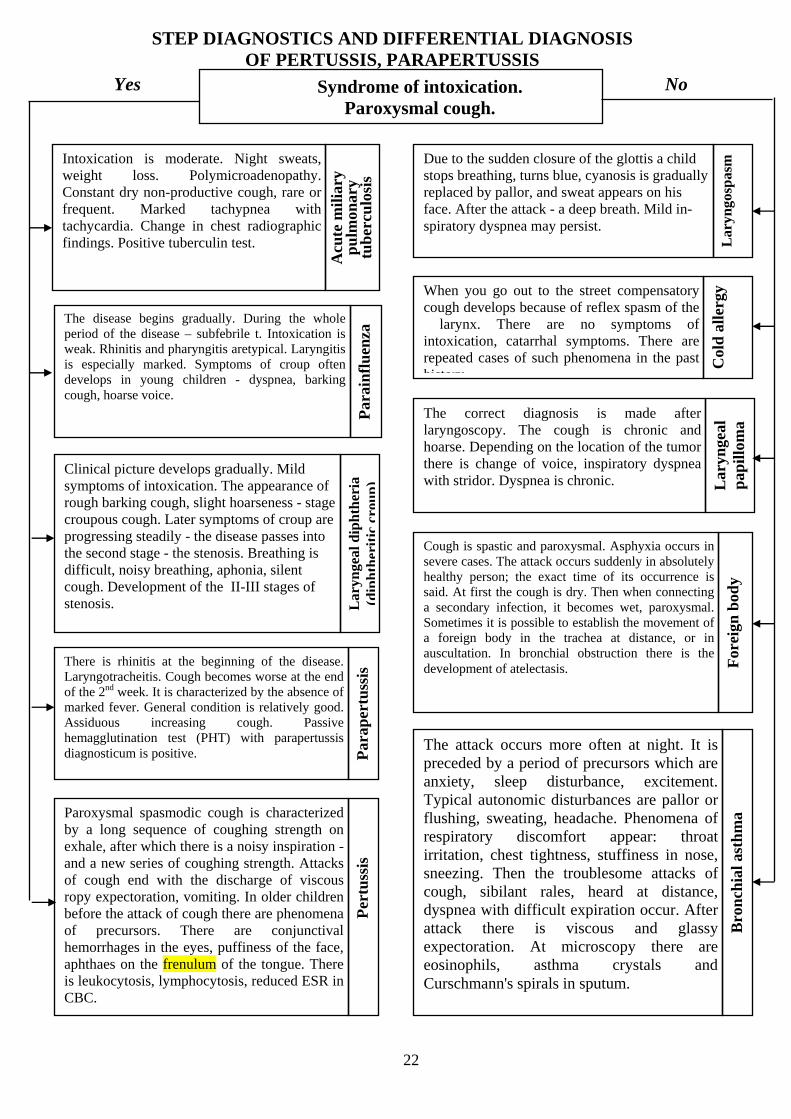
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF PERTUSSIS, PARAPERTUSSIS
Yes No
22
Syndrome of intoxication.
Paroxysmal cough.
Intoxication is moderate. Night sweats, weight loss. Polymicroadenopathy. Constant dry non-productive cough, rare or frequent. Marked tachypnea with tachycardia. Change in chest radiographic findings. Positive tuberculin test.
Acu
te m
ilia
ry
pu
lmon
ary
tub
ercu
losi
s
Due to the sudden closure of the glottis a child stops breathing, turns blue, cyanosis is gradually
Lar
yngo
spas
m
replaced by pallor, and sweat appears on his face. After the attack - a deep breath. Mild in-spiratory dyspnea may persist.
The disease begins gradually. During the whole period of the disease – subfebrile t. Intoxication is weak. Rhinitis and pharyngitis aretypical. Laryngitis is especially marked. Symptoms of croup often develops in young children - dyspnea, barking cough, hoarse voice.
Par
ain
flu
enza
The correct diagnosis is made after laryngoscopy. The cough is chronic and hoarse. Depending on the location of the tumor there is change of voice, inspiratory dyspnea with stridor. Dyspnea is chronic.
Lar
ynge
al d
iph
ther
ia
(dip
hth
erit
iccr
oup
)
Cough is spastic and paroxysmal. Asphyxia occurs in severe cases. The attack occurs suddenly in absolutely healthy person; the exact time of its occurrence is said. At first the cough is dry. Then when connecting a secondary infection, it becomes wet, paroxysmal. Sometimes it is possible to establish the movement of a foreign body in the trachea at distance, or in auscultation. In bronchial obstruction there is the development of atelectasis. F
orei
gn b
ody
The attack occurs more often at night. It is preceded by a period of precursors which are anxiety, sleep disturbance, excitement. Typical autonomic disturbances are pallor or flushing, sweating, headache. Phenomena of respiratory discomfort appear: throat irritation, chest tightness, stuffiness in nose, sneezing. Then the troublesome attacks ofcough, sibilant rales, heard at distance, dyspnea with difficult expiration occur. After attack there is viscous and glassy expectoration. At microscopy there are eosinophils, asthma crystals and Curschmann's spirals in sputum.
Bro
nch
ial a
sth
ma
Clinical picture develops gradually. Mild symptoms of intoxication. The appearance of rough barking cough, slight hoarseness - stage croupous cough. Later symptoms of croup are progressing steadily - the disease passes into the second stage - the stenosis. Breathing is difficult, noisy breathing, aphonia, silent cough. Development of the II-III stages of stenosis.
There is rhinitis at the beginning of the disease. Laryngotracheitis. Cough becomes worse at the end of the 2 weeknd . It is characterized by the absence of marked fever. General condition is relatively good. Assiduous increasing cough. Passive hemagglutination test (PHT) with parapertussis diagnosticum is positive. P
arap
ertu
ssis
When you go out to the street compensatory cough develops because of reflex spasm of the larynx. There are no symptoms of intoxication, catarrhal symptoms. There are repeated cases of such phenomena in the past C
old
all
ergy
history
Lar
ynge
al
pap
illo
ma
Paroxysmal spasmodic cough is characterized by a long sequence of coughing strength on exhale, after which there is a noisy inspiration - and a new series of coughing strength. Attacks of cough end with the discharge of viscous ropy expectoration, vomiting. In older children before the attack of cough there are phenomena of precursors. There are conjunctival hemorrhages in the eyes, puffiness of the face, aphthaes on the frenulum of the tongue. There is leukocytosis, lymphocytosis, reduced ESR in CBC.
Per
tuss
is

DIAGNOSTIC ALGORITHMS : PARA WHOOPING COUGH
Etiology
Seasonality
Mechanism
of transmission
Affected organs
and tissues
Clinical forms
Methods of diagnosis
Differential
diagnosis
Principles of treatment
Prophylaxis
PARA WHOOPING COUGH
bacillus of parawhooping cough
Autumn-winter
Airways (bronchi, trachea, alveoli)
CNSLungs
(pneumonia)Eyes
Com
puls
ive
coug
h, s
ligh
tly r
unny
nos
e , r
epri
se, t
he
paro
xysm
s, th
e di
scha
rgin
g of
vis
cous
muc
us, s
ore
offr
enul
um o
f th
e to
ngue
cere
bral
hem
orra
ge, h
ypox
ic e
ncep
halo
path
y,
conv
ulsi
ons,
men
ingi
smus
Pne
umon
ia, s
egm
enta
l ate
lect
asis
and
equ
ity,
em
phys
ema
Ble
edin
g in
the
eye
conj
unct
iva
Epidemiological (contact with
patients, bacteriocarriers)
Clinical
Haematological (leukocytosis,
lymphocytosis)
serologic (CFT, agglutination test
pertussis like Subclinical
Bacteriological (detection of
bacilli of parawhooping
cough)
Prodrome of measles
Croup Bronchial asthma Foreign body Whooping coughBronchitis PneumoniaRespiratory allergoses
ARVI
Neuroleptics Oxygen therapyAerosols: mucolytics, proteolytics (trypsin,
chymotrypsin), antispasmodics (aminophylline,
ephedrine)
Antihistamines
Aminazine 2.5%
Dimedrol, prometasine,
suprastin
Isolation of patients Sanitary-hygienic
regimen
Dispensary observation
Airborne
23
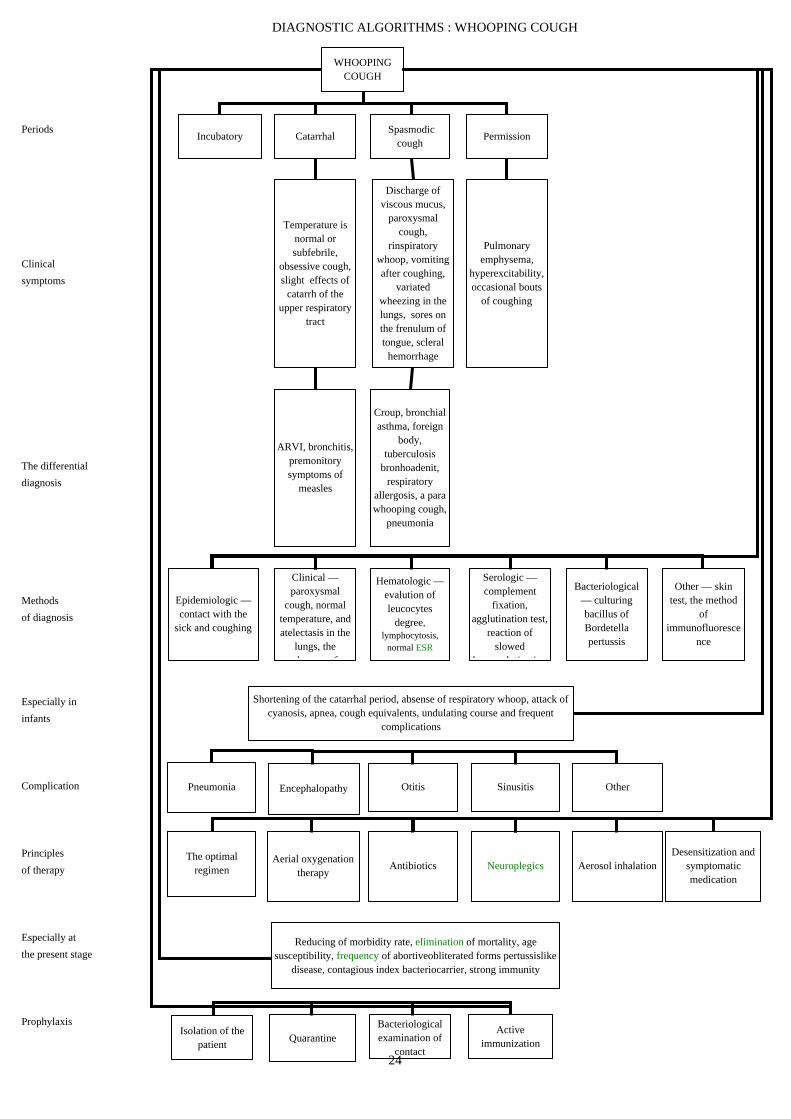
DIAGNOSTIC ALGORITHMS : WHOOPING COUGH
Periods
Clinical
symptoms
The differential
diagnosis
Methods
of diagnosis
Especially in
infants
Complication
Principles
of therapy
Especially at
the present stage
Prophylaxis
WHOOPING COUGH
Incubatory Catarrhal Spasmodic
coughPermission
Temperature is normal or subfebrile,
obsessive cough, slight effects of
catarrh of the upper respiratory
tract
Discharge of viscous mucus,
paroxysmal cough,
rinspiratory whoop, vomiting after coughing,
variated wheezing in the lungs, sores on the frenulum of tongue, scleral
hemorrhage
Pulmonary emphysema,
hyperexcitability, occasional bouts
of coughing
ARVI, bronchitis, premonitory symptoms of
measles
Croup, bronchial asthma, foreign
body, tuberculosis
bronhoadenit, respiratory
allergosis, a para whooping cough,
pneumonia
Clinical — paroxysmal
cough, normal temperature, and atelectasis in the
lungs, the b f
Epidemiologic — contact with the
sick and coughing
Hematologic — evalution of leucocytes
degree, lymphocytosis,
normal ESR
Serologic — complement
fixation, agglutination test,
reaction of slowed
h l ti ti
Bacteriological — culturing bacillus of Bordetella pertussis
Other — skin test, the method
of immunofluoresce
nce
Shortening of the catarrhal period, absense of respiratory whoop, attack of cyanosis, apnea, cough equivalents, undulating course and frequent
complications
Pneumonia Encephalopathy Otitis Sinusitis Other
The optimal regimen
Aerial oxygenation therapy
Antibiotics Neuroplegics Aerosol inhalationDesensitization and
symptomatic medication
Reducing of morbidity rate, elimination of mortality, age susceptibility, frequency of abortiveobliterated forms pertussislike
disease, contagious index bacteriocarrier, strong immunity
Isolation of the patient
QuarantineBacteriological examination of
contact
Active immunization
24
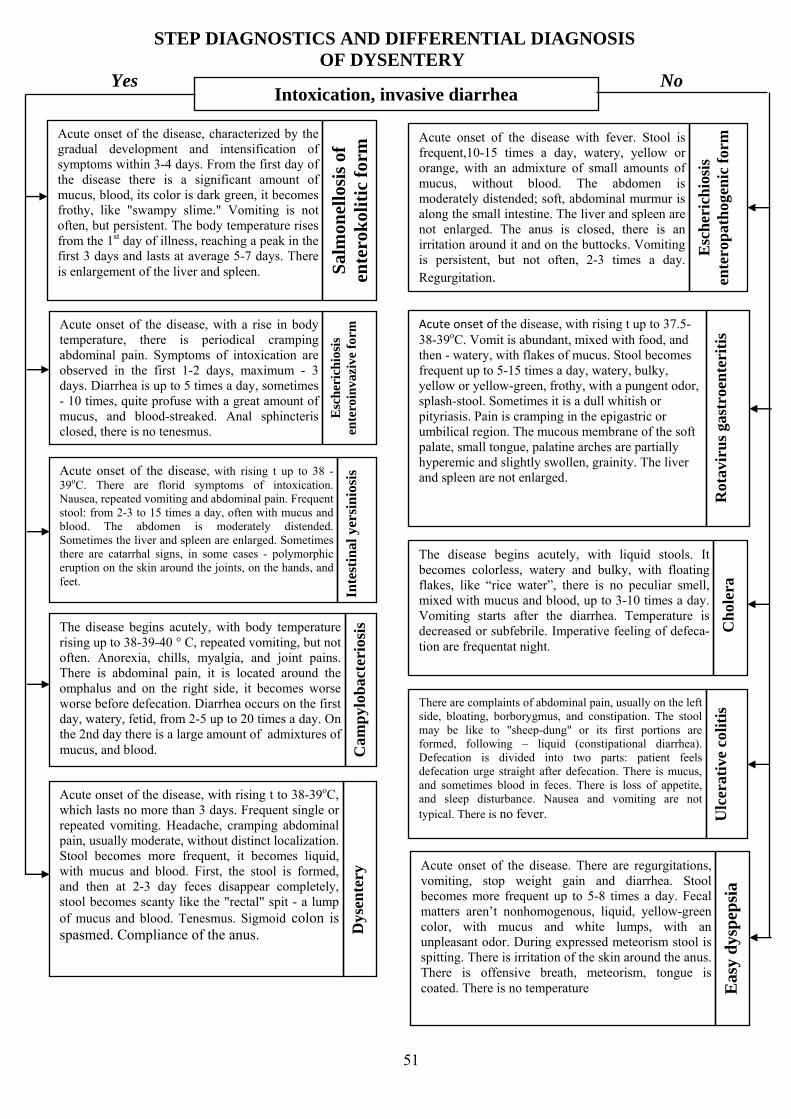
51
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF DYSENTERY
Yes No Intoxication, invasive diarrhea
Acute onset of the disease, characterized by the gradual development and intensification of symptoms within 3-4 days. From the first day of the disease there is a significant amount of mucus, blood, its color is dark green, it becomes frothy, like "swampy slime." Vomiting is not often, but persistent. The body temperature rises from the 1st day of illness, reaching a peak in the first 3 days and lasts at average 5-7 days. There is enlargement of the liver and spleen. S
alm
onel
losi
s of
en
tero
kol
itic
for
m Acute onset of the disease with fever. Stool is
frequent,10-15 times a day, watery, yellow or orange, with an admixture of small amounts of mucus, without blood. The abdomen is moderately distended; soft, abdominal murmur is along the small intestine. The liver and spleen are not enlarged. The anus is closed, there is an irritation around it and on the buttocks. Vomiting is persistent, but not often, 2-3 times a day. Regurgitation.
Esc
her
ich
iosi
s en
tero
pat
hog
enic
for
m
Acute onset of the disease, with a rise in body temperature, there is periodical cramping abdominal pain. Symptoms of intoxication are observed in the first 1-2 days, maximum - 3 days. Diarrhea is up to 5 times a day, sometimes - 10 times, quite profuse with a great amount of mucus, and blood-streaked. Anal sphincteris closed, there is no tenesmus.
Esc
her
ich
iosi
s en
tero
inva
zive
for
m
Acute onset of the disease, with rising t up to 37.5-38-39oC. Vomit is abundant, mixed with food, and then - watery, with flakes of mucus. Stool becomes frequent up to 5-15 times a day, watery, bulky, yellow or yellow-green, frothy, with a pungent odor, splash-stool. Sometimes it is a dull whitish or pityriasis. Pain is cramping in the epigastric or umbilical region. The mucous membrane of the soft palate, small tongue, palatine arches are partially hyperemic and slightly swollen, grainity. The liver and spleen are not enlarged.
The disease begins acutely, with liquid stools. It becomes colorless, watery and bulky, with floating flakes, like “rice water”, there is no peculiar smell, mixed with mucus and blood, up to 3-10 times a day. Vomiting starts after the diarrhea. Temperature is decreased or subfebrile. Imperative feeling of defeca-tion are frequentat night.
Ch
oler
a
There are complaints of abdominal pain, usually on the left side, bloating, borborygmus, and constipation. The stool may be like to "sheep-dung" or its first portions are formed, following – liquid (constipational diarrhea). Defecation is divided into two parts: patient feels defecation urge straight after defecation. There is mucus, and sometimes blood in feces. There is loss of appetite, and sleep disturbance. Nausea and vomiting are not typical. There is no fever. U
lcer
ativ
e co
liti
s
Acute onset of the disease, with rising t up to 38 -39oС. There are florid symptoms of intoxication. Nausea, repeated vomiting and abdominal pain. Frequent stool: from 2-3 to 15 times a day, often with mucus and blood. The abdomen is moderately distended. Sometimes the liver and spleen are enlarged. Sometimes there are catarrhal signs, in some cases - polymorphic eruption on the skin around the joints, on the hands, and feet.
Inte
stin
al y
ersi
nio
sis
The disease begins acutely, with body temperature rising up to 38-39-40 ° C, repeated vomiting, but not often. Anorexia, chills, myalgia, and joint pains. There is abdominal pain, it is located around the omphalus and on the right side, it becomes worse worse before defecation. Diarrhea occurs on the first day, watery, fetid, from 2-5 up to 20 times a day. On the 2nd day there is a large amount of admixtures of mucus, and blood. C
amp
ylob
acte
rios
is
Rot
avir
us
gast
roen
teri
tis
Acute onset of the disease, with rising t to 38-39oC, which lasts no more than 3 days. Frequent single or repeated vomiting. Headache, cramping abdominal pain, usually moderate, without distinct localization. Stool becomes more frequent, it becomes liquid, with mucus and blood. First, the stool is formed, and then at 2-3 day feces disappear completely, stool becomes scanty like the "rectal" spit - a lump of mucus and blood. Tenesmus. Sigmoid colon is spasmed. Compliance of the anus. D
ysen
tery
Acute onset of the disease. There are regurgitations, vomiting, stop weight gain and diarrhea. Stool becomes more frequent up to 5-8 times a day. Fecal matters aren’t nonhomogenous, liquid, yellow-green color, with mucus and white lumps, with an unpleasant odor. During expressed meteorism stool is spitting. There is irritation of the skin around the anus. There is offensive breath, meteorism, tongue is coated. There is no temperature E
asy
dys
pep
sia
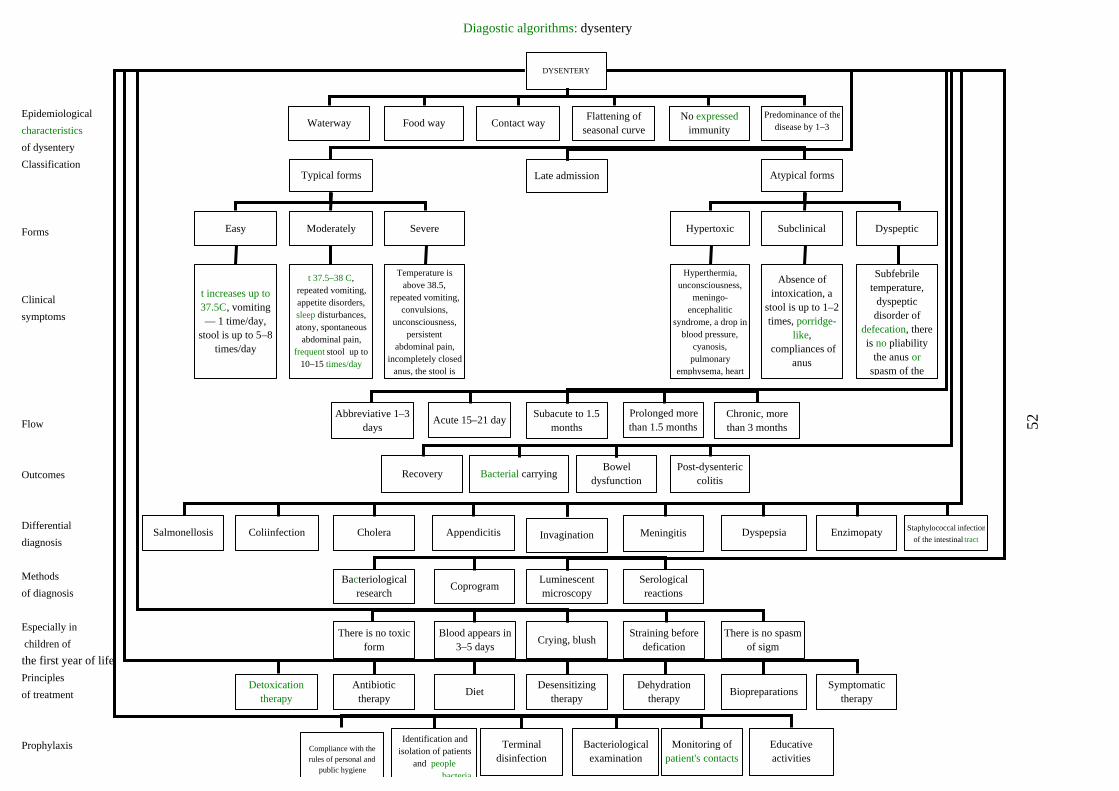
Diagostic algorithms: dysentery
Epidemiological
characteristics
of dysentery
Classification
Forms
Clinical
symptoms
Flow 52
Outcomes
Differential
diagnosis
Methods
of diagnosis
Especially in
children of
the first year of life
Principles
of treatment
Prophylaxis
DYSENTERY
Waterway Food way Contact wayFlattening of
seasonal curveNo expressed
immunity
Predominance of thedisease by 1–3
Late admissionTypical forms Atypical forms
Easy Moderately Severe
t increases up to 37.5C, vomiting — 1 time/day,
stool is up to 5–8 times/day
t 37.5–38 C, repeated vomiting, appetite disorders, sleep disturbances, atony, spontaneous
abdominal pain, frequent stool up to
10–15 times/day
Temperature is above 38.5,
repeated vomiting, convulsions,
unconsciousness, persistent
abdominal pain, incompletely closed
anus, the stool is
DyspepticSubclinicalHypertoxic
Hyperthermia, unconsciousness,
meningo-encephalitic
syndrome, a drop in blood pressure,
cyanosis, pulmonary
emphysema, heart
Absence of intoxication, a
stool is up to 1–2 times, porridge-
like, compliances of
anus
Subfebrile temperature,
dyspeptic disorder of
defecation, there is no pliability
the anus or spasm of the
Subacute to 1.5 months
Acute 15–21 dayProlonged more than 1.5 months
Chronic, more than 3 months
Abbreviative 1–3 days
Bacterial carryingBowel
dysfunctionPost-dysenteric
colitisRecovery
InvaginationAppendicitisCholeraColiinfectionSalmonellosis Meningitis Dyspepsia Enzimopaty Staphylococcal infection
of the intestinal tract
Luminescent microscopy
CoprogramBacteriological
researchSerological reactions
Crying, blushBlood appears in
3–5 daysThere is no toxic
formStraining before
deficationThere is no spasm
of sigm
Desensitizing therapy
DietAntibiotic
therapyDetoxication
therapyDehydration
therapyBiopreparations
Symptomatic therapy
Terminal disinfection
Bacteriological examination
discharging bacteria
Identification and isolation of patients
and people
Compliance with the rules of personal and
public hygiene
Monitoring of patient's contacts
Educative activities

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF INTESTINAL COLI-INFECTION IN INFANTS
Yes No The enteritis syndrome, intoxication
Disease occurs in infants and is caused by intro-ducing of supplementary food or transferring the child to bottle feeding. In such cases, when the process is too rapid, or when the quantity and quality of introduced supplementary food is not adequate to the child’s age, it leads to the functional disorders of intestines. There is no intoxication, regurgitation. Child is relatively calm. Unformedstool without pathological addi-tive. All disorders disappear after the elimination of
Temperature of the body increases from the first day of the disease to subfebrile digits. Rash is micropunctate, located in the armpits, chest, morbilliform rash in the joints. Symptoms of intoxication, nausea, vomitinggeneralized abdominal pain. Stool is porridge-like, with a small amount of mucus 3-6 times day. The disease is often accompanied by respiratory syndrome, hepatosple
Inte
stin
al
yers
inio
sis
Eas
y d
ysp
epsi
a
,
a
nomegaly.
all nutritional causes
The disease occurs in infants. It is related with mother’s disease (mastitis, sore throat, etc.). The disease develops gradually. Stool becomes more frequent, liquid, with mucus, green, often blood-streaked. The temperature is subfebrile. Clinical course is an undulating, with prolonged (for several weeks), subfebrile fever, unstable stool.
Sta
ph
yloc
occa
l en
teri
tis
Temperature increases, symptoms of intoxication, nausea, repeated vomiting, and anorexia. Abdominal pain becomes worse before defecation. Stool is liquid, watery,
Cam
pyl
obac
teri
osis
frothy, mixed with mucus and blood.
It occurs in infants, prematurity and being bottle-fed. Disease begins acutely. Vomiting, abdominal pain, loose stools with admixtures of mucus and blood. The liver is enlarged. Unlike to dysentery there is no the tenesmus and compliance of the anus.
salm
onel
losi
s,
coli
tic
form
.
The disease is more common in children younger than 2 years. The body temperature is up to 37-38°C. There are symptoms of intoxication, nausea and vomiting. Abdominal pain. Sudden imperative feel-ing of defecation ends with a loud passage of flatus and spitting stool. Stool is liquid, watery, bulky and frothy, with a pungent odor, up to 5-15 times a day. The rotavirus is more common. V
iral
dia
rrh
ea
The disease is common in infants. It is accompanied by prolonged fever, severe intoxication. Stool is liquid, yellow-green color, with mucus and fetid odor. Symptoms of dehydration develop rapidly. The liver and spleen are enlarged.
Sal
mon
ello
sis
of
ente
riti
c fo
rm
The body temperature is normal. There is moderate pain in epigastrium. Abdominal murmur. Stool is liquid, watery, without mucus and blood, mixed with undigested food. Giardia are detected in the feces. G
iard
iasi
s
The body temperature increases to 38oC. Cramping abdominal pain. Stool is loose, liq-uid with mucus, bulky, watery, bright-yellow color. The anus is closed. There is an irritation around the anus and on the buttocks. It occurs in children under 1 year.
Col
i-in
fect
ion
Body temperature increases to 38-39oC. Stool is loose with mucus and blood; abdominal pain is cramping. The abdomen is sunken, spasm of sigma. Tenesmus. "Rectal spit." There are sphincteritis and compliance of the
Dys
ente
ry
anus.
45

DIAGNOSTIC ALGORITHMS : INTESTINAL COLI INFECTION
Affected organs
and systems
Clinical
syndromes
Signs and
symptoms
Form 46
Diagnostics
The differential
diagnosis
Treatment
Course of disease
Prophylaxis
Intestinal coli infection in infants
Gastrointestinal tractCentral nervous
systemCardiovascular system Liver Kidneys Metabolism
Enteritic Toxicosis Hypovolemic shock Exsicosis Hypokalemia
Liquid watery stools, flatulence
Atony, adynamia, persistent vomiting, anorexia, prolonged
fever
Pallor of skin, cyanosis of the lips,
acrocyanosis, tachycardia, pastosity
of skin structure, hypotony
Enlargement of the liver
Oliguria, anuriaExcitation, thirst, xerosis and skin
driness, weight loss
Sleepiness, heart sounds muffled,
muscular hypotonia, changes in the electro cardiogram, paresis of
the intestine
Serological examination
Radio-immunodiffusion
Bacteriological examination of stool
Luminescent-serological studies
Syndrome of impaired intestinal absorption
Simple dyspepsia Toxic dyspepsia Dysentery SalmonellosisStaphylococcal
enterocolitisCholera
Diet therapy Antibiotic therapyDetoxification and
rehydrationStimulating and vitamin therapy
Symptomatic Biopreparations
Acute Prolonged
Sanitary-hygienic regimen
Slight Moderately Severe Coli-sepsis Bacteriologic agent
Terminal disinfectionBacteriological
examination of contactExpedited reportIsolation of the patient
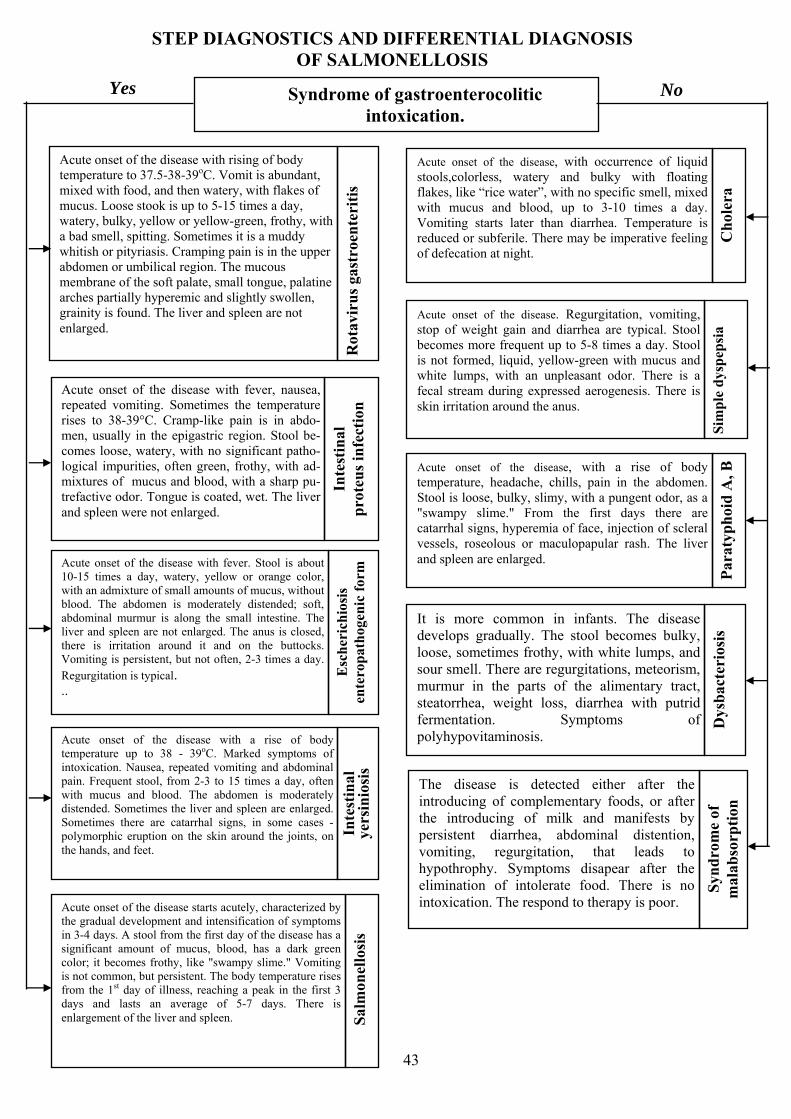
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF SALMONELLOSIS
Yes No Syndrome of gastroenterocolitic
intoxication.
Acute onset of the disease with rising of body temperature to 37.5-38-39oC. Vomit is abundant, mixed with food, and then watery, with flakes of mucus. Loose stook is up to 5-15 times a day, watery, bulky, yellow or yellow-green, frothy, with a bad smell, spitting. Sometimes it is a muddy whitish or pityriasis. Cramping pain is in the upper abdomen or umbilical region. The mucous membrane of the soft palate, small tongue, palatine arches partially hyperemic and slightly swollen, grainity is found. The liver and spleen are not enlarged.
Rot
avir
us
gast
roen
teri
tis
Acute onset of the disease, with occurrence of liquid stools,colorless, watery and bulky with floating flakes, like “rice water”, with no specific smell, mixed with mucus and blood, up to 3-10 times a day. Vomiting starts later than diarrhea. Temperature is reduced or subferile. There may be imperative feeling of defecation
Ch
oler
a
at night.
Acute onset of the disease with fever, nausea, repeated vomiting. Sometimes the temperature rises to 38-39°C. Cramp-like pain is in abdo-men, usually in the epigastric region. Stool be-comes loose, watery, with no significant patho-logical impurities, often green, frothy, with ad-mixtures of mucus and blood, with a sharp pu-trefactive odor. Tongue is coated, wet. The liver and spleen were not enlarged.
Inte
stin
al
pro
teu
s in
fect
ion
Acute onset of the disease. Regurgitation, vomiting, stop of weight gain and diarrhea are typical. Stool becomes more frequent up to 5-8 times a day. Stool is not formed, liquid, yellow-green with mucus and white lumps, with an unpleasant odor. There is a fecal stream during expressed aerogenesis. There is skin irritation around the anus.
Sim
ple
dys
pep
sia
Acute onset of the disease, with a rise of body temperature, headache, chills, pain in the abdomen. Stool is loose, bulky, slimy, with a pungent odor, as a "swampy slime." From the first days there are catarrhal signs, hyperemia of face, injection of scleral vessels, roseolous or maculopapular rash. The liver and spleen are enlarged.
Par
atyp
hoi
d А
, В
Acute onset of the disease with fever. Stool is about 10-15 times a day, watery, yellow or orange color, with an admixture of small amounts of mucus, without blood. The abdomen is moderately distended; soft, abdominal murmur is along the small intestine. The liver and spleen are not enlarged. The anus is closed, there is irritation around it and on the buttocks. Vomiting is persistent, but not often, 2-3 times a day. Regurgitation is typical. E
sch
eric
hio
sis
ente
rop
ath
ogen
icfo
rm
It is more common in infants. The disease develops gradually. The stool becomes bulky, loose, sometimes frothy, with white lumps, and sour smell. There are regurgitations, meteorism, murmur in the parts of the alimentary tract, steatorrhea, weight loss, diarrhea with putrid fermentation. Symptoms of D
ysb
acte
rios
is
..
polyhypovitaminosis. Acute onset of the disease with a rise of body temperature up to 38 - 39oС. Marked symptoms of intoxication. Nausea, repeated vomiting and abdominal pain. Frequent stool, from 2-3 to 15 times a day, often with mucus and blood. The abdomen is moderately distended. Sometimes the liver and spleen are enlarged. Sometimes there are catarrhal signs, in some cases - polymorphic eruption on the skin around the joints, on the hands, and feet.
Inte
stin
al
yers
inio
sis
Acute onset of the disease starts acutely, characterized by the gradual development and intensification of symptoms in 3-4 days. A stool from the first day of the disease has a significant amount of mucus, blood, has a dark green color; it becomes frothy, like "swampy slime." Vomiting is not common, but persistent. The body temperature rises from the 1st day of illness, reaching a peak in the first 3 days and lasts an average of 5-7 days. There is enlargement of the liver and spleen. S
alm
onel
losi
s
The disease is detected either after the introducing of complementary foods, or after the introducing of milk and manifests by persistent diarrhea, abdominal distention, vomiting, regurgitation, that leads to hypothrophy. Symptoms disapear after the elimination of intolerate food. There is no i
Syn
dro
me
of
mal
abso
rpti
on
ntoxication. The respond to therapy is poor.
43

DIAGNOSTIC ALGORITHMS : SALMONELLOSIS
Affected organs
and systems
Signs and
symptoms
Clinical
variants
Especially in children
1 year of age 44
Diagnostics
Differential
diagnosis
Flow
Treatment
Prophylaxis
SALMONELLOSIS
Gastrointestinal tract
Central nervous system
Cardiovascular system
Metabolism Liver Kidneys Spleen
Abd
omin
al p
ain,
per
sist
ent r
epea
ted
vom
itin
g, lo
ose
stoo
ls w
ith
muc
us,
bloo
d an
d gr
een,
coa
ted
tong
ue,
dist
enti
on, i
ndur
atio
n an
d te
nder
ness
of
the
colo
n
Feve
r du
ring
3-5
day
s,
flac
cidi
ty, w
eakn
ess,
an
orex
ia, c
oma,
co
nvul
sion
s
Sudd
en p
allo
r of
the
skin
, ta
chyc
ardi
a, m
uffl
ed h
ear t
soun
ds, d
ecre
ased
blo
od
pres
sure
Thi
rst,
dry
muc
ous
mem
bran
es a
nd s
kin,
w
eigh
t los
s
Enl
arge
men
t of
the
live
r,
jaun
dice
Oli
guri
a
Sple
nom
egal
y
GastricGastroenterological
EntericalGastroenterocolitic
EnterocoliticColitic
Toxico-septicalTyphoid Flu-like
ObliteratedTransient bacteriocarriers
Dyspeptic formsHigher frequency of
severe forms
Toxic-septical forms are more
common
NonpercutaneousToxicosis with
exsicosisProlonged carrying
Serologic studiesHematological
studiesCoprological examination
Bacteriological studies of feces,
vomit, blood, bile, urine
CholeraStaphylococcal enterocolitis
INTESTINAL coli infection
Dyspepsia Dysentery Viral diarrheaSyndrome of
malabsorption Typhoid fever
Chronic ProlongedAcute
Detoxificating diet, rehydration
Antibacterial Desensitization Stimulating Vitamins Biopreparations Symptomatic
Supervision of the work of nutrition
department Expedited report
Isolation of the patient
Terminal desinfection
Examination of the contact
Sanitary-hygienic regimen
Dispensary of recovered

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF CHOLERA
Yes No
Watery diarrhea, vomiting, exicсosis
Acute onset of a triad of symptoms: rising of body temperature, vomiting and diarrhea. Vomiting precedes diarrhea, repeated, lasts - 1-2 days. The number of bowel movements/ defecation - from 10 to 15 times a day. Stool is loose, yellow, without any pathologic additives, sometimes discolored or turbid pale. Dura-tion of diarrhea is 3-6 days. Rotavirus is detected by electron microscopy.
Acute onset of a triad of symptoms: the rising of temperature of the body, vomiting and diarrhea.
It begins with the appearance of vomiting and diarrhea. Slight low-grade fever. Diarrhea lasts a day, up to 10 times a day, vomiting is not profuse. From the first day, there are signs of paralytic syndrome – vision disorders, dry mouth/ xerostomia. Xerostomia is noted at early stages in all pa-tients.
Rot
avir
al
gast
roen
teri
tis
Ocular symptoms are mydriasis, unresponsive pupils, aniso-coria, ptosis and diplopia. Paresis of the facial muscles/ facial mioparesis, dysphagia - patient feels “a lump in the throat”.
Bot
uli
sm
Paresis, paralysis of skeletal muscle. Botulinum toxin de-tected in biomaterials, taken from a patient Acute onset of disease. Feces are watery, yellow
or orange in color, with an admixture of a small amount of clear mucus, bulky, unformed “porridge-like”/ "wa-ter-gruel" – excrements are mixed with water, spitting, diapers are entirely moisten with them. After liquid absorption, mucus disappears and stool often seems normal. Vomiting 1-2 times a day. The rapid development of toxicosis with exicсosis. Bacteriological confirmation/verification of the diagnosis is the growth of the colonies E. Coli
En
tero
pat
hog
enic
es
cher
ich
iosi
s
Acute onset of disease. Regurgitations, stopping of the weight gain and diarrhea are noted. Loose stool is up to 5-8 times a day. Consistence of the fecal matters is not ho-mogenous, liquid, yellow green colored, with admixtures of mucus and white flecks with bad smell. Meteorism pro-vokes streaming of the excrements during defecation. There is an irritation around anus. Offensive breath, abdominal distention, coated tongue. There is no fever. There are die-tary variations in medical history/ personal history. A
cute
dys
pep
sia
Acute onset of disease, with pain in upper ab-domen, repeated vomiting, the temperature rising to 38-40 C, general weakness. Tongue is thickly coated, dry. The abdomen is moderately distended. Stool is up to 5 times a day, porridge-like or liquid, bulky, undigested, sometimes watery or frothy, with a significant amount of spinach color like “pond scum”, foul-smelling. Develop-ing of symptoms of toxicosis and exsicosis is gradual. Salmonella is found in feces, vomit mass and other sub-stances. Increasing of salmonella antibodies level in the patient’s blood.
Guiding symptoms are abdominal and dyspeptic. Pain is moderate, localized in anticardium, around the um-bilical region. Appetite disorders, nausea, unstable stool, up to 3-4 times a day. Stool with moderate amount of mucus, without blood, with admixtures of indigested food. Loss of appetite, asthenia. Diagnosis is based on finding/detecting of cyst or vegetative form of parasite in direct smear of fe-ces.
Sal
mon
ello
sis
(gas
troe
nte
riti
ssy
nd
rom
e)
Gia
rdia
sis
Acute onset of disease with the evaluation of the temperature of the body to 38-39°C. Symptoms of intoxi-cation are manifested. Nausea, vomiting, abdominal pain. Stool is from 2-3 to 15 times a day, often with admixtures of mucus, blood. Abdomen is moderately distended. The liver and spleen are enlarged. There may be catarrhal symptoms, polymorphous eruption on the skin around the joints, on the hands and feet. Diagnosis is based on Yer-sinia detecting in patient’s biological media/ discharges.
Inte
stin
al
yers
inio
sis
The course of disease is severe and causes high mortality rate. It begins suddenly, often at night. There is severe lancinating abdominal pain (colic), uncontrollable vomiting/anacatharsis/hyperemesis, watery diarrhea. There may be admixtures of mucus, sometimes blood. Dehydration develops rapidly. Short-term remission lasts 1-2 days, but after 2-3 days patient may die. Patient is in consciousness/alert/ up to agonal/moribund state/period. consciousness to preserve agonalnog period. In patient’s personal history - fact of the agarics eating, seasonality.
Dea
th c
up
mus
hro
om (
Am
anita
ph
allo
ides
)po
ison
ing
Acute onset of disease, with increasing the tempera-
ture of the body up to 38-39°C. Headache. Abdominal pain is cramping without distinctive localization. Stool is loose, becomes watery/ liquid, with admixtures of mucus and blood. At first day, feces are formed, after 2-3 days feces mass disappear completely, stool becomes mucous as like as “rectal spitting”, scanty, with blood streaks. Tenesmus and compliances of the anus.
Acute onset of disease, temperature of the body is normal. Diarrhea starts suddenly, often at night. Defeca-tion urge is painless, there isn’t abdominal pain. At first hours, feces are formed, then - watery, bulky, turbid white, with floating flakes like “rice-water”. There aren’t pathological admixtures. Acute/severe/ sharp weakness develops, adynamia. Bulky repeated vomiting without nausea. Vomit mass like to “meat slops”. Conditions of dehydration, hypokalaemia and oliguria make rapid pro-gress. Identification of cholera vibrio/ Koch’s bacillus is based on microscopic investigations of patient’s biologi-cal media/ discharges/
Dys
ente
ry
Ch
oler
a
41

ALGORITHMS DIAGNOSTIC OF CHOLERA
Etiology
seasonality
Transmission mechanism
Affected
organs and systems
Clinical
syndromes
Clinical
symptoms
Clinical
forms
Methods of
diagnosis
Differential
diagnosis
Treatment
Clinical course
Prophylaxis
CHOLERA
GikoshimaInaba
Gastrointestinal tract Central nervous system
Cardiovascular
system Metabolism
Gastroenteritic Toxicosis with exicosis
Hypovolemic shock Hypokaliemia
Mild Medium-heavy
/severeSevere Algid state Atypical
Bacteriological of fecal culture, vomit
Luminescent-serological
Serologic methods
Escherichiosis Salmonellosis Viral diarrhea Mushroom poisoningToxicity of chemical
poisons
Antibiotics Vitamin therapy Symptomatic therapy
Alimentary
El-Tor
Summer
Ogawa
Contact-householdWater
Kidneys
Pro
fuse
vom
itin
g, w
ater
y st
ool,
abun
dant
wit
h m
uddy
-
whi
te f
lake
s fl
oati
ng r
emin
isce
nt o
f "r
ice
wat
er"
stoo
l fr
eque
ncy
3-10
tim
es a
day
and
mor
e
Hoa
rsen
ess,
low
er b
lood
pre
ssur
e, d
ry s
kin,
sev
ere
wea
knes
s, w
eakn
ess,
diz
zine
ss, h
ypot
herm
ia, t
hirs
t, w
eigh
t los
s, c
onvu
lsio
ns, m
uscl
e w
eakn
ess
Tac
hyca
rdia
, hyp
oten
sion
, cya
nosi
s of
the
naso
labi
al
tria
ngle
, acr
ocya
nosi
s
Oli
guri
a, a
nuri
a
Mus
cula
r hy
poto
nia,
dro
wsi
ness
, rap
id h
eart
sou
nds
muf
fled
obliteratedHaemorrhagicSubclinical Hypertoxic and «dry
cholera»
Disintoxication therapy
Intravenous rehydration
Fulminant With several layers of complications
Acute onset of a diseases
Isolation of the patient
Terminal disinfection Bacteriological examination of contact
Dispensary observation of
recovered
Sanitary-hygienic regimen
Alarm (emergency notification)
42
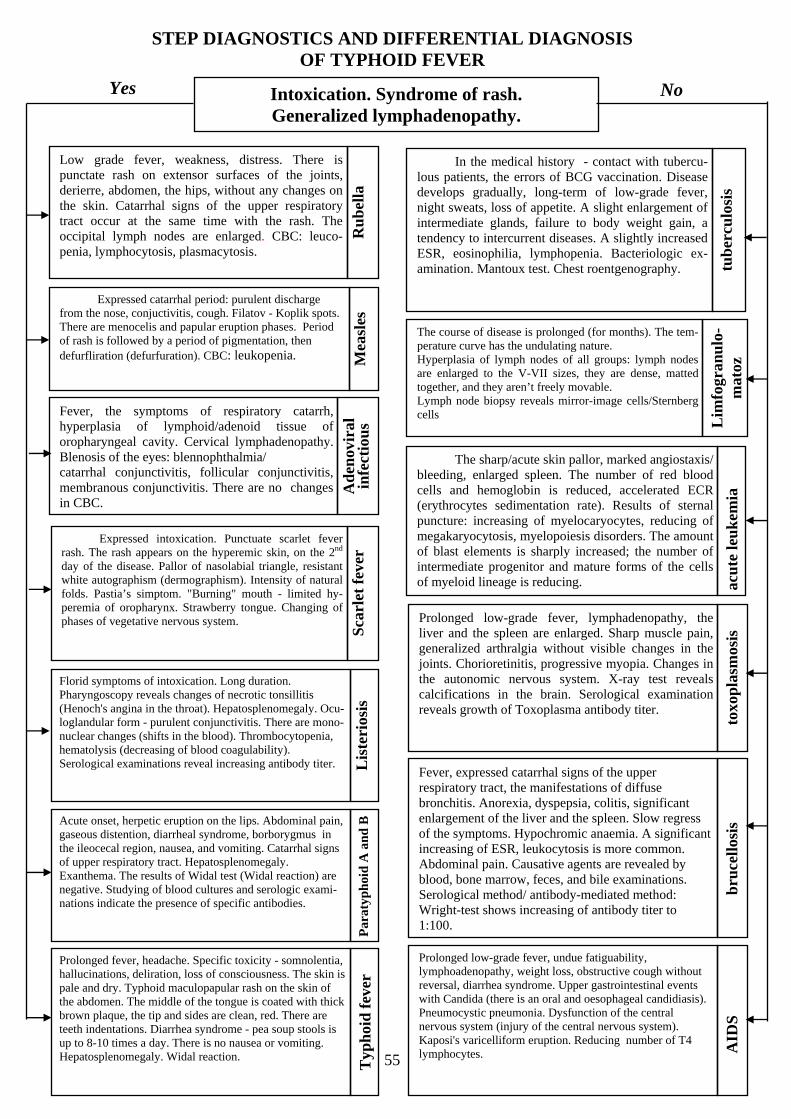
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF TYPHOID FEVER
Yes No Intoxication. Syndrome of rash.
Generalized lymphadenopathy.
Low grade fever, weakness, distress. There is punctate rash on extensor surfaces of the joints, derierre, abdomen, the hips, without any changes on the skin. Catarrhal signs of the upper respiratory tract occur at the same time with the rash. The occipital lymph nodes are enlarged. CBC: leuco-penia, lymphocytosis, plasmacytosis.
In the medical history - contact with tubercu-lous patients, the errors of BCG vaccination. Disease develops gradually, long-term of low-grade fever, night sweats, loss of appetite. A slight enlargement of intermediate glands, failure to body weight gain, a tendency to intercurrent diseases. A slightly increased ESR, eosinophilia, lymphopenia. Bacteriologic ex-amination. Mantoux test. Chest roentgenography.
Ru
bel
la
tub
ercu
losi
s
Expressed catarrhal period: purulent discharge
from the nose, conjuctivitis, cough. Filatov - Koplik spots. There are menocelis and papular eruption phases. Period of rash is followed by a period of pigmentation, then defurfliration (defurfuration). CBC: leukopenia. M
easl
es
The course of disease is prolonged (for months). The tem-perature curve has the undulating nature. Hyperplasia of lymph nodes of all groups: lymph nodes are enlarged to the V-VII sizes, they are dense, matted together, and they aren’t freely movable. Lymph node biopsy reveals mirror-image cells/Sternberg cells
Lim
fogr
anu
lo-
mat
oz
Fever, the symptoms of respiratory catarrh, hyperplasia of lymphoid/adenoid tissue of oropharyngeal cavity. Cervical lymphadenopathy. Blenosis of the eyes: blennophthalmia/ The sharp/acute skin pallor, marked angiostaxis/
bleeding, enlarged spleen. The number of red blood cells and hemoglobin is reduced, accelerated ECR (erythrocytes sedimentation rate). Results of sternal puncture: increasing of myelocaryocytes, reducing of megakaryocytosis, myelopoiesis disorders. The amount of blast elements is sharply increased; the number of intermediate progenitor and mature forms of the cells of myeloid lineage is reducing.
catarrhal conjunctivitis, follicular conjunctivitis, membranous conjunctivitis. There are no changes in CBC.
Ad
enov
iral
in
fect
iou
s
acu
te le
uk
emia
Expressed intoxication. Punctuate scarlet fever rash. The rash appears on the hyperemic skin, on the 2nd day of the disease. Pallor of nasolabial triangle, resistant white autographism (dermographism). Intensity of natural folds. Pastia’s simptom. "Burning" mouth - limited hy-peremia of oropharynx. Strawberry tongue. Changing of phases of vegetative nervous system.
Sca
rlet
fev
er
Prolonged low-grade fever, lymphadenopathy, the liver and the spleen are enlarged. Sharp muscle pain, generalized arthralgia without visible changes in the joints. Chorioretinitis, progressive myopia. Changes in the autonomic nervous system. X-ray test reveals calcifications in the brain. Serological examination reveals growth of Toxoplasma antibody titer.
toxo
pla
smos
is
Florid symptoms of intoxication. Long duration. Pharyngoscopy reveals changes of necrotic tonsillitis (Henoch's angina in the throat). Hepatosplenomegaly. Ocu-loglandular form - purulent conjunctivitis. There are mono-nuclear changes (shifts in the blood). Thrombocytopenia, hematolysis (decreasing of blood coagulability). Serological examinations reveal increasing antibody titer. L
iste
rios
is
Acute onset, herpetic eruption on the lips. Abdominal pain, gaseous distention, diarrheal syndrome, borborygmus in the ileocecal region, nausea, and vomiting. Catarrhal signs of upper respiratory tract. Hepatosplenomegaly. Exanthema. The results of Widal test (Widal reaction) are negative. Studying of blood cultures and serologic exami-nations indicate the presence of specific antibodies.
Par
atyp
hoid
A a
nd
B
Fever, expressed catarrhal signs of the upper respiratory tract, the manifestations of diffuse bronchitis. Anorexia, dyspepsia, colitis, significant enlargement of the liver and the spleen. Slow regress of the symptoms. Hypochromic anaemia. A significant increasing of ESR, leukocytosis is more common. Abdominal pain. Causative agents are revealed by blood, bone marrow, feces, and bile examinations. Serological method/ antibody-mediated method: Wright-test shows increasing of antibody titer to 1:100.
bru
cell
osis
Prolonged fever, headache. Specific toxicity - somnolentia, hallucinations, deliration, loss of consciousness. The skin is pale and dry. Typhoid maculopapular rash on the skin of the abdomen. The middle of the tongue is coated with thick brown plaque, the tip and sides are clean, red. There are teeth indentations. Diarrhea syndrome - pea soup stools is up to 8-10 times a day. There is no nausea or vomiting. Hepatosplenomegaly. Widal reaction.
Prolonged low-grade fever, undue fatiguability, lymphoadenopathy, weight loss, obstructive cough without reversal, diarrhea syndrome. Upper gastrointestinal events with Candida (there is an oral and oesophageal candidiasis).
T
yph
oid
fev
er
Pneumocystic pneumonia. Dysfunction of the central nervous system (injury of the central nervous system). Kaposi's varicelliform eruption. Reducing number of T4
TAID
S
lymphocytes.
55

Diagnostic algorithms: typhoid fever
Affected organs
Signs and
symptoms
Characteristics in
children of early
age
Complications
Methods
of diagnostics
Differential
diagnosis
Principles
of treatment
Epidemiological features
Typhoid fever
Central nervous system
Gastrointestinal tract
Cardiovascular system
Skin Blood Other organs
Feve
r, v
omit
ing,
hea
dach
e, d
elir
ium
, co
nfus
iona
l sta
te, h
allu
cina
tion
s, f
oot c
lonu
s
Ano
rexi
a, c
onst
ipat
ion
or d
iarr
hea,
blo
atin
g,a
Pada
lka'
s sy
mpt
om, c
oate
d to
ngue
Bra
dyca
rdia
, voi
cele
ss to
ne, d
icro
tic p
ulse
Dry
ski
n, F
illi
povi
ch's
sym
ptom
, ros
eola
Ney
trof
ille
sis,
incr
ease
d er
ythr
ocyt
e se
dim
enta
tion
rat
e, le
ukop
enia
Bil
e du
ct, e
nlar
ged
live
r, e
nlar
ged
sple
en
Acute onset, shortening of the period of the clinical disease, repeated vomiting, toxicosis with exsicosis, the early appearance of roseola (may be absent), dyspepsia, tachycardia, leukocytosis
Hemorrhage Rare perforation
PneumoniaParotitisStomatitisEncephalitis CholecystitisMeningitis
Urine cultureIndirect
hemagglutination test
Widal's reaction
Stool cultureBlood culture
ARDEnterovirus
infectionSalmonellosisMeningitis
Miliary tuberculosis
LeukosisDysentery
Diet Skin and
mucous careBed regimen
Etiotropic therapy
Pathogenetic and
symptomatic
Bacteria carrying control
Dispensary observation reconvalesce
nce
Antiepidemic measures
Early diagnosis
Isolation of the patient
Active immunisation
Rules of personal and
public hygiene
Sanitary and educational
activities
56
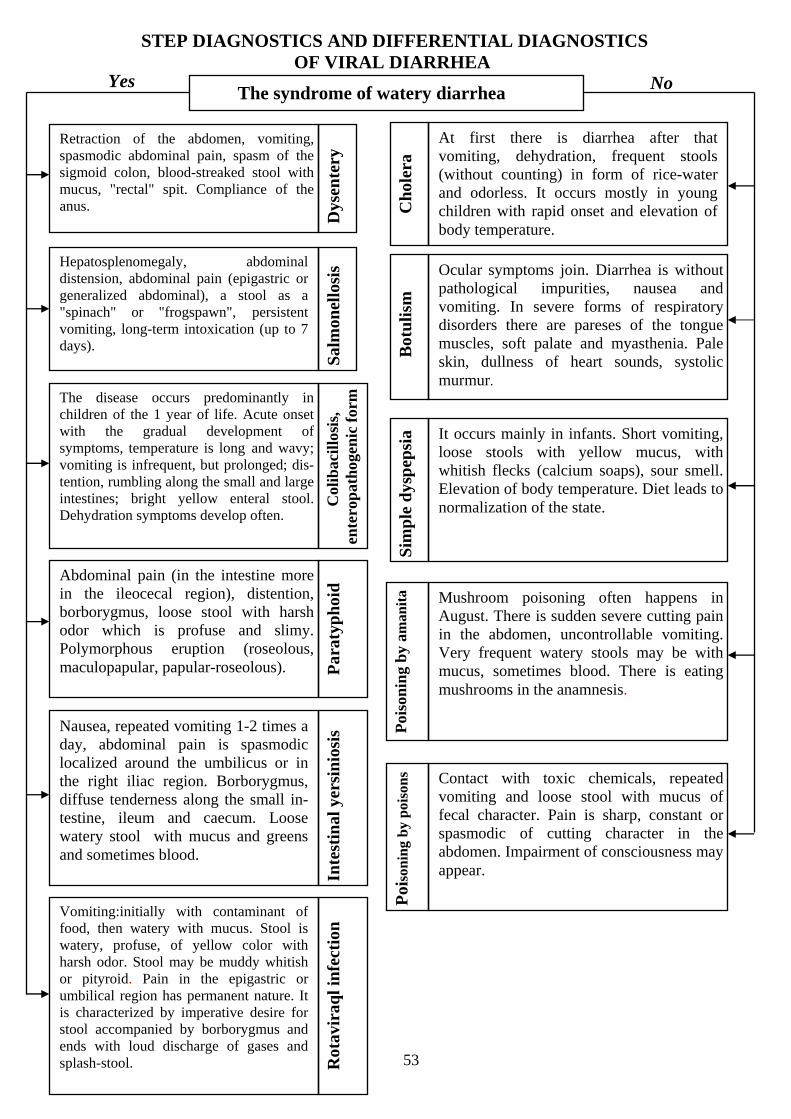
53
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSTICS OF VIRAL DIARRHEA
The syndrome of watery diarrhea
Hepatosplenomegaly, abdominal distension, abdominal pain (epigastric or generalized abdominal), a stool as a "spinach" or "frogspawn", persistent vomiting, long-term intoxication (up to 7 days).
Yes No
Sal
mon
ello
sis
At first there is diarrhea after that vomiting, dehydration, frequent stools (without counting) in form of rice-water and odorless. It occurs mostly in young children with rapid onset and elevation of body temperature.
Retraction of the abdomen, vomiting, spasmodic abdominal pain, spasm of the sigmoid colon, blood-streaked stool with mucus, "rectal" spit. Compliance of the anus.
Dys
ente
ry
Ocular symptoms join. Diarrhea is withoutpathological impurities, nausea and vomiting. In severe forms of respiratorydisorders there are pareses of the tongue muscles, soft palate and myasthenia. Pale skin, dullness of heart sounds, systolic murmur.
The disease occurs predominantly in children of the 1 year of life. Acute onset with the gradual development of symptoms, temperature is long and wavy; vomiting is infrequent, but prolonged; dis-tention, rumbling along the small and large intestines; bright yellow enteral stool. Dehydration symptoms develop often.
Col
ibac
illo
sis,
en
tero
pat
hoge
nic
for
m
Abdominal pain (in the intestine more in the ileocecal region), distention, borborygmus, loose stool with harsh odor which is profuse and slimy. Polymorphous eruption (roseolous, maculopapular, papular-roseolous).
Cho
lera
B
otu
lism
Par
atyp
hoid
Nausea, repeated vomiting 1-2 times a day, abdominal pain is spasmodic localized around the umbilicus or in the right iliac region. Borborygmus, diffuse tenderness along the small in-testine, ileum and caecum. Loose watery stool with mucus and greens and sometimes blood.
Inte
stin
al y
ersi
nio
sis
It occurs mainly in infants. Short vomiting,loose stools with yellow mucus, with whitish flecks (calcium soaps), sour smell.Elevation of body temperature. Diet leads to normalization of the state.
Sim
ple
dys
pep
sia
Mushroom poisoning often happens in August. There is sudden severe cutting pain in the abdomen, uncontrollable vomiting. Very frequent watery stools may be withmucus, sometimes blood. There is eatingmushrooms in the anamnesis.
Poi
son
ing
by
aman
ita
Contact with toxic chemicals, repeated vomiting and loose stool with mucus of fecal character. Pain is sharp, constant orspasmodic of cutting character in the abdomen. Impairment of consciousness may appear.
Poi
son
ing
by p
oiso
ns
Vomiting:initially with contaminant of food, then watery with mucus. Stool is watery, profuse, of yellow color with harsh odor. Stool may be muddy whitish or pityroid. Pain in the epigastric or umbilical region has permanent nature. It is characterized by imperative desire for stool accompanied by borborygmus and ends with loud discharge of gases and splash-stool.
TRot
avir
aql i
nfe
ctio
n

Diagnostic algorithms : viral diarrhea
Etiology
Seasonality
Forms
Characteristic
of forms
Course
Differential
diagnosis
Methods
of diagnostics
Features in children
up to one year
Principles of treatment
Prophylaxis
Viral diarrheas
Coronaviruses Calce virusesAdenoidal
virusesRotaviruses Cholera vibrio Reoviruses
Winter-spring
Typical Atypical
Easy Medium severe Severe Obliterated Asymptomatic
Tem
pera
ture
is u
p to
37,
vom
itin
g is
sev
eral
ti
mes
a d
ay, t
he li
quid
gru
el s
tool
is
2–5
tim
es a
day
Tem
pera
ture
is f
ebri
le, v
omit
ing
is
repe
ated
or
mul
tipl
e, p
ale
skin
, thi
rst,
stoo
l 8–1
6 ti
mes
Sto
ol 2
5–30
tim
es, d
ehyd
rati
on o
f th
e I
I–II
I de
gree
wit
h ex
icco
sis,
rep
eate
d vo
mit
ing,
ta
chyc
ardi
a, d
eafe
n of
the
hea
rt s
ound
s
Man
ifes
tati
ons
are
mil
d, s
hort
-ter
m c
ours
e,
reve
aled
in th
e ex
amin
atio
n of
the
cont
act
chil
dren
wit
h fo
cus
Com
plet
e ab
senc
e of
man
ifes
t sym
ptom
s,
rota
viru
s is
fou
nd in
the
chil
d , t
he
imm
unol
ogic
al s
hift
is d
eter
min
ed
Lingering With
complications Mixed infectionAcute
ShigellosisSimple
dyspepsiaSalmonellosis Colibacillosis Cholera
Virological
Specific immunological tests: indirect hemagglutination test
(IHGT), immunofluorescence test (IFT), ELISA, RIA
Rare, sometimes sporadic or group outbreaks in maternity
hospitals
More common in children of 6-12
months
Rotavirus gastroenteritis in a
form of mixed infection
It proceeds hardly through dehydration and complications
Secondary lactase deficiency is
formed
Bioremediesenzymes
Antidiarrheal remedies
Antiviral immunoglobulinDiet therapy
Rehydrationdesintoxication
Sanitary-educational work Disinfection
Following up of contact
personsFinding out isolation of
patients
Maintain of personal and public hygiene
Bacteriological
Summer
Phagotherapy of contacts
54

49
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF DYSBACTERIOSIS
Syndrome of diarrhea. Intoxication.
Hepatosplenomegaly, abdominal distension, abdominal pain (epigastric or around the abdomen), stool as "swamp slime" or "frogspawn", persistent vomiting, long-term intoxication (up to 7 days).
Yes No
Sal
mon
ello
sis
Diarrhea and then vomiting, dehydration, frequent stools (times out of number) in the form of rice-water and odorless. It is the most common in young children, with rapid onset and increase of body temperature to high numbers.
Retraction of the abdomen, vomiting, cramping abdominal pain, spasm of the sigmoid colon, stools with mucus, bloodstreaks, "rectal" spit. Compliance of the anus.
Dys
ente
ry 1. Neuroparalytic syndrome: visual impair-
ment, dry mouth, dilated pupils with a reduction or even nonreactive for the light, convergence and accommodation.Sometimes anisocoria, paralysis of accommodation may occur. The «netting»appears before the eyes. Ptosis, diplopia. 2. Paresis of the facial muscles, resulting inamimia, masklike face. Dysphagia. Thenparesis and paralysis of skeletal muscles of the trunk and extremities manifest.
It occurs predominantly in children younger than 1 year old. Acute onset with gradual development of symptoms, long, wavy temperature, infrequent, but prolonged vomiting, bloating, abdominal sounds along the small and large intestines; enteritis stool of bright yellow color, symptoms of dehydration often develop.
Col
ibac
illo
sis,
en
tero
path
ogen
ic f
orm
Children suffer from it more often than adults. It starts acutely; stool is profuse, liquid and watery, without any admixtures of mucus and blood, of dull whitish color. Vomiting is rare. Abdomen sounds are loud. The urge to defecate has an imperative character. Renal failure, acidosis. Dehydration. The pain is in the epigastrium and umbilical region. During winters.
Ch
oler
a B
otu
lism
Rot
avir
al in
fect
ion
The disease is more common in young children. It develops gradually. The stool becomes profuse, liquid, sometimes with white foamy flecks, sour smell. Posseting, meteorism, abdomen sounds in various parts, steatorrhea, weight loss, diarrhea with putrid fermentation often occur. Symptoms of polyhypovitaminosis.
Dys
bact
erio
sis
It occurs in infants and is associated usuallywith the introduction of feeding up, or transfer the child to bottle feeding. In these cases, the rapid introduction of supplementary food is not appropriate for the quality or quantity of food of the child's age, leads to functional impairment of the intestine. No intoxication, posseting. A child is relatively calm. Stool is softening, without pathological impurities. After the elimination of the nutritive cause alldisorders rapidly disappear.
Sim
ple
dys
pep
sia
The stool includes increased amounts offats. It is bulky and porous, grayish, occasionally becomes liquid, watery.Multiple stool. Loss of weight, big belly.Extended and elongated colon, which remains the same after the disappearance ofthe main symptoms. C
elia
c d
isea
se
The disease begins in newborns since birth. Belly is big, intractable, stable constipation. Subcutaneous veins are dilated, umbilicus is protruded. The child is pale, emaciated, arms and legs are disproportionate. The child stunts from peers. Digital anus examination gives a sense of increased sphincter tone of the rectum. T T T T T T
Meg
acol
on

Diagnostic algorithms: intestinal dysbacteriosis
Causes
Clinlcal
forms
Signs and
symptoms
Characteristics
in different
age groups
Methods
of diagnosis
Differential
diagnosis
Treatment
Preventive measures
Intestinal dysbacteriosis
Irrational use of antibiotics
Abnormal feeding
Presence of chronic foci of infection
Appointment of immunosuppres
sants
Radiation therapy
Malabsorption syndrome
Intestinal underdevelo
pment
Factors that reduce the
body's resistance
Compensated Subcompensated Decompensated
Baby looks healthy, normal stools, good appetite, body weight is
added gradually, disturbed intestinal microflora
Clinical symptoms are moderate, slack, pooreater, poor body weight gain, intestinal
disorders appear
Bad condition, evident intoxication, vomiting, loss of
appetite, decrease of body weight, loose stools
Disbacteriosis in young children Dysbiosis in older children
Posseting, poor weight gain, bloating, flatulence, borborygmus, steatorrhea, stool is liquid or gruel, foamy, with white lumps, profuse,
with a sour odor, undigested
Persistent usual constipation alternating with diarrhea, recurrent intestinal colic, dyskinesia of the gastrointestinal tract, belching, feeling of fullness, appetite is slightly decreased, undigested
stools
Study of stool microflora The immunological analysis
1 degree —anaerobi
c flora prevails over the aerobic flora,
opportunistic flora planted
104-102
2 degree — is an
anaerobic flora,
opportunistic
flora106–107
and replaced with atypical
variants
3 degree — dominated by aerobic
flora, opportunisti
c pathogenic
flora increases rapidly
Decrease in humoral and cellular indicators from moderate to severe
ones, depending on the degree
Diet depending on the child's age with the inclusion of preparations
with bifidobacteria
Enzyme preparations —abomin, pancreatin, festal,
smekta, mezim forte
Bifiсol, colibacterin, lactobacterin, bifidumbacterin, complex
immunodrugs, specific bacteriophages
Rational use of antibioticsRational nutrition with restriction of the use
of refined productsPrevention of intestinal infections
Opportunistic pathogenic acute intestinal infections
Acute bacterial and viral intestinal infections Nonspecific ulcerative colitis
50

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF INTESTINAL YERSINIOSIS
Yesд
No Diarrhea syndrome. Intoxication syndrome, rash.
Acute onset of the disease with fever up to 38oC. It happens most often in children younger than 2 years. Cough, runny nose, congestion of the mucous oropharynx appear. In 1-3 days pain in the abdomen and diarrhea for 5-10 times a day sometimes with mucus occur. Often there is repeated vomiting. There is the presence of multiform maculo-papular rash all over the body, and hyperemia of the body, especially of the face and neck.
The disease develops gradually. Stool is profuse
Dys
bac
teri
osis
, liquid, sometimes frothy with white
En
tero
viru
s
infe
ctio
n,
inte
stin
al f
orm
lumps. Frequent posseting, meteorism, abdominal sounds in the various parts, deficient body weight gain. There is no intoxication. The rash is absent.
Acute onset of the disease with fever up to 38-40oC, headache, chills, muscle and joint pain. Mild catarrhal signs. Nausea, vomiting, and epigastric pain. There is a loose stool 2-3 times a day enteritic-like. Rash outbreaks at once, and has either a punctate or maculosus character. It is located in the abdomen, in the axillary regions, on the lateral surfaces of the body, it is confluent around the large joints. P
seu
dot
ub
ercu
losi
s
The disease begins acutely; fever, vomiting, sore throat occur. In a few hours there is a punctate rash on unchanged skin, which spreads very rapidly on the face, neck, trunk and limbs. It is characterized by a bright localized from the hard palate hyperemia (catarrhal, follicular, necrotic tonsillitis). Diarrheal syndrome is absent.
Sca
rlet
fev
er
It begins acutely with a temperature rise to 38.5 - 39oC, upper respiratory catarrh and conjunctivitis appear. There are grayish-white spots on the buccal mucosa. Maculo-papular rash occurs in 4-5 days, which is manifested in three stages: 1 day - face, neck, 2 day - trunk, arms, 3 day - legs. Bowel disorders are not observed.
Mea
sles
The disease occurs in newborns, premature babies and infants. Acute onset of diseases, with the temperature rise. There are suppurative foci in various organs. It occurs on the background of frequent stool. Headache, vomiting, loss of appetite, bloat. Hepatosplenomegaly. Roseolous-papular rash is not
Sal
mon
ello
sis
of
sep
tic
form
Acute onset of the disease. There may be posset-ing, vomiting, deficient body weight gain, diar-rhea. Stool is more frequent up to 5-8 times a day. Consistency of feces is heterogeneous, liq-uid, slime green color, with mucus and white lumps, with an unpleasant odor. During aero-genesis stool is thrown like a jet. There is no temperature and rash.
Dys
pep
sia
severe.
Acute onset of the disease, headache, chills, pain in the abdomen. Bowel disorders, distension. From the earliest days there are catarrhal signs, hyperemia of face, injection of scleral vessels, conjunctivitis. At its height roseolous or maculopapular rash appears for several days. P
arat
yph
oid
A
Acute onset of the disease It starts acutely with short-term body temperature rise up to 38 -39oС. Symptoms of intoxication are marked. Nausea, repeated vomiting and abdominal pain. Stool is from 2-3 to 15 times a day often with mucus and blood. The abdomen is moderately distended. Sometimes the liver and spleen are enlarged. Sometimes there are catarrhal signs, in some cases there is polymorphous eruption on the skin around the joints, on the hands, feet.
Inte
stin
al
yers
inio
sis
Acute onset of the disease with temperature rise up to 38 -39oC that lasts at least for 3 days. Vomiting is single or repeated. Headache, pain in the abdomen. Stool quickens, it becomes liquid
Dys
ente
ry
, with mucus and blood. At first the stool has a fecal character, then in 2-3 day feces disappear completely, the stool becomes poor, so-called "Rectal" spit is a lump of mucus and blood. Tenesmus is marked. There is no rash.
47

DIAGNOSTIC ALGORITHMS: INTESTINAL YERSINIOSIS
Etiology
Seasonality
Mechanism of transfer
Affected organs
and systems
Clinical
forms
Course
Methods
of diagnosis
Differential
diagnosis
Principles
of treatment
Preventive measures
Intestinal yersiniosis
Iersinia enterocolitica
Winter-spring period
alimentaryaerogeniccontact-household
gastrointestinal tract
the respiratory system
Central nervous systems
livercardiovascular
systemjoints skin
gastrointerstinal pseudo-appendicular
septic erythematous hepatic articular
Into
xica
tion
, nau
sea,
vom
itin
g, f
latu
lenc
e,ab
dom
inal
pai
n in
the
ileo
ceca
lar
ea, d
iarr
hea
– pr
ofus
e w
ater
y st
ool w
ith
muc
us
and
gree
n, th
e sy
ndro
me
of e
nter
itis
and
gast
roen
teri
tis
Into
xica
tion
, vom
itin
g, a
nore
xia,
abd
omin
al p
ain
in th
e ri
ght i
liac
reg
ion,
dia
rrhe
a
Into
xica
tion
, wei
ght l
oss,
pro
long
edfe
bril
e fe
ver,
conv
ulsi
ons,
hep
atos
plen
omeg
aly,
ras
hon
the
skin
, a
rthr
itis
, abd
omin
al p
ain,
dia
rrhe
a, s
ever
e pa
llor
, dul
lnes
s of
hea
rt s
ound
s
Into
xica
tion
, pol
ymor
phou
s sk
in r
ash
arou
nd th
e jo
ints
on
the
hand
s an
d fe
et a
s p
ainf
ul p
ink
node
s w
ith
cyan
otic
ting
e
Into
xica
tion
, abd
omin
al p
ain,
he
pato
sple
nom
egal
y,ja
undi
ce, d
iarr
hea,
dar
k ur
ine,
dis
colo
red
stoo
l
Into
xica
tion
, art
hrit
is, s
wel
ling
, ten
dern
ess,
li
mit
atio
n of
mov
emen
t
relapsing
bacteriological culture of mucus from the
th t
the reaction of indirect hemagglutination
bacteriological culture of blood
bacteriological culture of urine
bacteriologic culture of feces
enzyme immunoassay
agglutination test
Shig
ello
sis
Ent
erov
irus
infe
ctio
ns
Salm
onel
losi
s
Typ
ho p
arat
hyph
oid
infe
ctio
n
Pse
udot
uber
culo
sis
Mea
sles
Rub
ella
Corticosteroids VitaminsNonsteroidal preparations
DesintoxicationAntibiotic treatment
Work in the focus with the contact
personsIsolation of patients
Early identification of sources of
infection
Sanitary and hygienic regime
Scar
let f
ever
Rhe
umat
ism
Sep
sis
Vir
us h
epat
itis
Acu
te a
bdom
en
Bru
cell
osis
Rehydration Antihistamines Diet
acute
48

31
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF PSEUDOTUBERCULOSIS
Yes No Punctate rash syndrome. Intoxication, catarrhal syndrome.
Catarrhal symptoms. Micropunctate rash is followed by peeling of the skin. Tachycardia, often vomiting. Bright redness of throat - "flaming" fauces. Lamellar skin flaking, especially on the fingers. Tonsillitis, lymphadenopathy, "strawberry" tongue. The rash does not leave the pigmentation. Pale nasolabial triangle. Rash is heavily on the cheeks, on the sides of the trunk, below abdomen, flexor surfaces of the extremities. The rash is on the hyperemic skin.
Sca
rlet
fev
er
Maculo-papular rash, large spotted rash, catarrhal symptoms, subfebrile temperature. Staging of rash on the hyperemic skin is typical. After the rash disappears, brown hyperpigmentation of the skin persists for several days. Filatov-Koplik’s spots, conjunctivitis. Sometimes croup syndrome, rash is prone to be confluent.
Mea
sles
Catarrhal signs. The rash is multiform, punctate, maculosis-papular, hemorrhagic, often around the joints, on the hands, feet (symptoms of "gloves" and "socks"). Joints inflammation (swelling, redness, tenderness and limitation of motion). Myocarditis. Hepatosplenomegaly. Nausea, vomiting, abdominal pain, heavy sweating, high fever with large daily scale, full-blown jaundice, diarrhea. Loose stool, often with mucus, green, sometimes with blood.
Inte
stin
al y
ersi
nio
sis
Body temperature is subfebrile. The rash is small maculosis, sometimes papular, not abundant, doesn’t leave pigmentation and desquamation after fading. It is not confluent. Rash hasn’t staging. Occipital and back cervical lymph nodes are swollen. Conjunctivitis is weak. In blood there is leukopenia, relative lymphocytosis, plasma cells (10-30%).
It begins acutely with temperature rise, symptoms of intoxication, abdominal pain, bloating, increased bowel sounds and pain along the intestine, in the ileocecal region. Catarrhal signs, hyperemia of face and injection of scleral vessels, conjunctivitis, herpetic eruption on the lips. Roseolous rash or maculo-papular rash, hepatosplenomegaly, sweating. In the blood there is normocytosis, neutrophilia, increased erythrocyte sedimentation rate. In severe cases complications are possible.
Par
atyp
hoi
d A
Menocelis, malaise, temperature rise, usually up to subfebrile, itchy skin, increased peripheral lymph nodes. Rash is confluent, it hasn’t any stages, it is associated with drug administration (often sulfanilamides, antibiotics, etc.). In the blood there is moderate eosinophilia. The rash is usually on the extensor surfaces. M
edic
amen
tal
der
mat
itis
Body temperature is increased, sometimes with the symptoms of intoxication. Joint pains, icteric sclerae, mucous membranes of the oropharynx, and then the skin. Aching pain is in the right hypohondrium, some person has itching. Hepatosplenomegaly. At the end of the preicteric period urine becomes dark and stool becomes discolored. Symptoms of dyspepsia occur. In the blood there is leukopenia, neutropenia, relative lympho-and monocytosis, increased direct bilirubin, thymol test is increased, prothrombin index is reduced.
Hep
atit
is A
Acute onset of the disease with fever, catarrhal signs. Lymphadenopathy - cervical, back cervical nodes, located behind sternocleidomastoid muscle by chain. Tonsillitis, hepatosplenomegaly. There are atypical mononuclear cells in blood. Alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase are increased. In the throat there are necrotic changes of tonsils. Plaque is not completely rubbed between the glass slides. It does not bleed when it is removed, can be easily removed. If you try to remove incrustations with tweezers they tear and crumble. Maculosis rash. In
fect
iou
s m
onon
ucl
eosi
s
Ru
bel
la
Acute onset of the disease, fever increases to 38-40oC, the symptoms of intoxication, muscle and joint pains, catarrhal signs. There are pains on swallowing, dizziness, nausea, vomiting, abdominal pain often in the right iliac region or in the epigastrium. Sometimes loose stool may be for 2-3 times a day. Puffiness and redness of face, neck, pale nasolabial triangle. Conjunctival hyperemia and vascular injection of sclera. Hyperemia of the pharynx, symptoms of "hood", "gloves", "socks." Micropunctate hyperemic rash occurs sometimes on unchanged skin. Skin itching. Localization is the abdomen, axillary regions, on the lateral surfaces of the body. Hepatosplenomegaly. TPse
ud
otu
ber
culo
sis
Acute onset of diseases, high fever up to 39oC and above. Rash is small maculo-papular. Headache, muscle pain, scleritis, catarrhal signs. Vomiting and abdominal pain may be often. Localization of the rash is on a face, body, sometimes on hands and feet. The rash is located on the background of unchanged skin. There is no staging, it does not leave pigmentation and desquamation.
En
tero
viru
s
(Bos
ton
exa
nth
ema)

Diagnostic algorithms : pseudotuberculosis
Etiology
Seasonality
Mechanism
of transmission
Affected organs
and systems
Clinical
forms
Clinical
symptoms
Methods
of diagnosis
Differential
diagnostics
Principles
of treatment
Course
Preventive measures
Pseudotuberculosis
Pseudotuberculosis bacteria
Winter-spring
Skin Joints LiverRespiratory system
Nau
sea,
vom
itin
g, a
bdom
inal
pai
n, b
owel
dis
orde
rs, d
ry
tong
ue c
oate
d w
ith
sabu
rra;
by
the
end
of th
e se
cond
wee
k of
illn
ess
ther
e is
a r
aspb
erry
tong
ue
Join
t pai
n, s
wol
len
join
ts, h
ot to
the
touc
h, m
ostl
y th
ey a
re
wri
st, e
lbow
, pha
lang
eal j
oint
s
Liv
er e
nlar
gem
ent,
tend
erne
ss o
n pa
lpat
ion,
icte
ric
scle
rae,
oc
hrod
erm
ia, d
ark
urin
e, in
blo
od c
onju
gate
d bi
liru
bin
frac
tion
is in
crea
sed
Com
bina
tion
of
sym
ptom
s
Sep
sis
Mal
aise
, sub
febr
ile
tem
pera
ture
, eph
emer
al r
ash
lesi
ons
of t
he o
rgan
s an
d sy
stem
s
Arthralgic Icteric Combined Generalised SepticAbdominal Suppressed SubclinicalScarlet
fever-like
Bacteriological Serological
Airborne- dust
Alimentary Droplet
Eyes Lymphatic
system
Gastro-intestinal
tract
Cardio-vascular system
Spleen
Catarrhal
Pun
ctat
e sc
arle
t fev
er r
ash
(ski
n on
the
ches
t, el
bow
, gro
in,
arm
pits
), w
hite
der
mog
raph
ism
, coa
rsel
y sp
otte
d pa
pula
r ra
sh (
on th
e fa
ce, n
asol
abia
l tri
angl
e; a
bdom
en, b
ack,
aro
und
the
join
ts),
pet
echi
al, h
emor
rhag
ic r
ash,
ery
them
a
No
clin
ical
sign
s, th
e di
agno
sis
is b
ased
on
labo
rato
ry te
sts
Cou
gh, r
unny
nos
e, s
ubfe
bril
e te
mpe
ratu
re, A
RV
IBlood
culture, culture of
feces, throat swabs
Serological reactions
Typhoid, paratyphoid
Measles Appendicitis Diarrhea HepatitisSepsisScarlet fever
Enteroviral disease
Rheumatism
Etiotropic: levomycetin
Nonsteroidalpreparations
AcuteUndulating course with
exacerbations and relapses
Proper storage of food
Bacteriological control of food products
The fight against rodents
Detoxification therapy syndromic treatment
32

29
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF VIRAL ENCEPHALITIS
Yes No Intoxication. Impaired consciousness. Convulsions. Focal symptoms.
Severe headache, especially in the fronto-temporal region, dizziness, pain in the abdomen, legs, and sometimes bleeding from the nose. Repeated vomiting, temperature is 38-40oC, impaired consciousness, sopor-comatose state, convulsions. Hyperemia of the face, chest. On the spot of the bite there is a local reaction - a little redness and infiltration of the underlying tissues with regional lymphadenitis. Enlargement of the liver, flaccid proximal paralysis or paresis of the upper limbs, the symptom of “sagging neck”, “Sprengel’s deformity”, meningeal symptoms. T
ick
bor
ne
ence
ph
alit
is It occurs usually in 7-9 days after vaccination at
high body temperature, at the height of the general and local reaction. Generalized tonoclonic spasms of varying duration - from a few seconds to several hours. Anxiety, shudder, motor automatisms, tremor of limbs, the recovery of reflexes or anisoreflexia, pyramidal signs. In older children there is a hallucinatory-delirious syndrome, psychosensorial disorder, cataleptic phenomena. CSF is not changed. E
nce
ph
alit
ic r
eact
ion
Intoxication, body temperature rise to 39-40oC, anxiety, repeated vomiting is not related to ingestion, it does not bring relief. Generalized convulsions, severe headache, dizziness, somnolentia, lethargy, hyperesthesia, positive meningeal symptoms, bulging of anterior fontanelle, position of "pointing dog", cranial nerves damage, vestibular disorders. Purulent: CSF is turbid, follows with rare drops, neutrophils predominate. Protein is increased, sugar is normal or reduced. Intracranial pressure is increased. Serous: CSFis clear, under the pressure. Initially cytosis is neutrophil-lymphocyte, then lymphocytic. Protein, sugar, chlorides usually do not elevated. Reaction is negative or weakly positive.
Ser
ous
and
pu
rule
nt
men
ingi
tis
Prolonged clinical course, prolonged fever, convulsive activity, hypertension-hydrocephalic syndrome. Child has problems with psychophysical development. Febrile reaction has the irregular wavy character. Often the secondary bacterial infection follows. Anxiety, poor sleep, weight loss, poor appetite, frequent posseting, fontanelle bulging, separation of cranial sutures, increasing of the head size. C
ytom
egal
ovir
al
ence
ph
alit
is
Acute onset of the disease, with body temperature rise, malaise, headache. Herpetic eruption appears on skin, gingivostomatitis is in the anamnesis. There are neurological symptoms. Impaired consciousness, moderate meningeal syndrome, rarely local clonic-tonic convulsions, repeated many times during the day. Hemiparesis and hemiplegia, amnesia, aphasia, neurosis-like syndrome and syndrome of liquor hypertension. There are the lesions of cranial nerves and motor oculi nerves. There is a herpes simplex virus isolated in the cerebrospinal fluid. Changes are typicalfor serous meningitis in CSF analyses.
Acu
te e
nce
ph
alit
is c
ause
d b
y h
erp
es s
imp
lex
viru
s
Loss of consciousness, nausea, vomiting, headache, cerebral symptoms. The disease manifests suddenly. Oculomotor disturbances (strabismus, "floating" eyeballs, abnormal pupillary response, size and shape of the pupils, the dissociation of reflexes, paresis of facial muscles, arterial hypertension, convulsive syndrome. C
ereb
rocr
ania
l tr
aum
a
Acute onset of the disease, with body temperature rise to 39-40oC. Chill, headache, nausea, vomiting, meningeal symptoms, scleritis, catarrhal conjunctivitis. Patients are obnubilate, indifferent, unresponsive to examination and surrounding. Rarer: excitement with delusions, hallucinations, loss of consciousness, muscle hypertension, which makes the patient lie with the throw back head and adducted towards the abdomen legs. Mono- or hemiparesis, flaccid paralysis, disturbance of breathing, swallowing, the fall of cardiovascular tone. Hyperkinesis of the facial muscles and upper limbs, sweating, and the lability of the cardiovascular system. In CBC: leukocytosis, neutrophilia, lymphopenia, eosinopenia, increased ESR. Lymphocytic cytosis, slight increase of protein.
Jap
anes
e en
cep
hal
itis
TE
pid
emic
(TTen
cep
hal
itle
thar
gic)
is
The disease is caused by injuries, aneurysms. Cerebrospinal fluid is bloody, during defecation there is a xanthosis. The pressure is 250-400 millimeter of water. Rate of fluid outflow is over 70 or like a jet. Cytosis is in the early days in accordance with red blood cells count, 5-7 days after it is 0,015-0,12. There is no sugar. Puncture brings considerable relief. S
ub
arac
hn
oid
al
hem
orrh
age
Motor excitement, impairment of consciousness, convulsions, leisure of nervous system. Flattening of the nasolabial folds, the deviation in the tongue direction, increased tendon reflexes, anizoreflexia, foot clonus, nystagmus, tremor, ataxia, light hyperkinesis, hemi-monoparesis, oculomotor disturbances. In younger children cerebral symptoms are expressed more clearly, they are often cerebellar.
TMen
ingo
ence
ph
alit
is
Catarrhal signs, body temperature rise, headache, chills, nausea, vomiting. Oropharynx is hyperemic, sleep disturbance occurs early. Patients are sleepy during the day and suffer from insomnia at night (inversion of sleep), oculomotor disturbances - ptosis, impaired convergence, diplopia, paralysis of accomodation, flac-cidity or loss of pupillary response. Face is masklike, mimic is sluggish. Vestibular disturbances are dizziness, unsteady gait, nystagmus. Vegetative disturbances are T
sweating,T Thypersalivation,T ThyperkinesisT. TIn CBC: moderate neutrophilicT Tleukocytosis, T Tincreased ESRT.
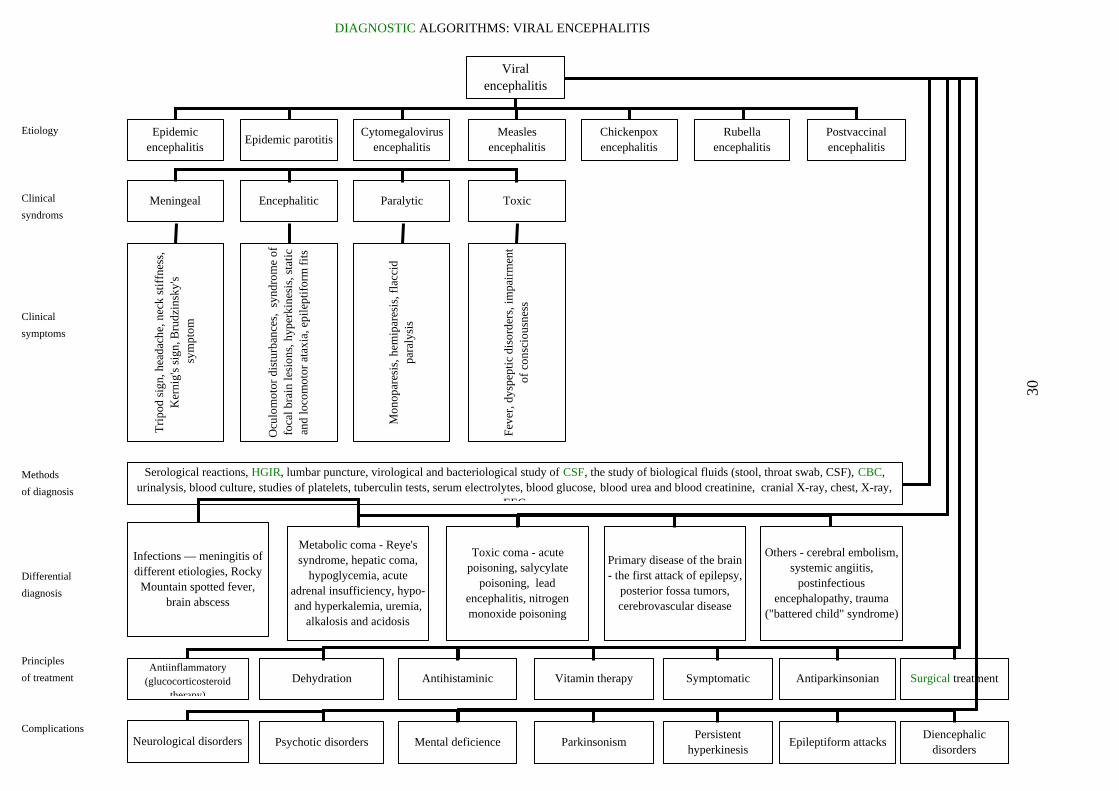
DIAGNOSTIC ALGORITHMS: VIRAL ENCEPHALITIS
Etiology
Clinical
syndroms
Clinical
symptoms
30
Methods
of diagnosis
Differential
diagnosis
Principles
of treatment
Complications
Viral encephalitis
Epidemic encephalitis
Epidemic parotitisCytomegalovirus
encephalitisMeasles
encephalitisChickenpox encephalitis
Rubella encephalitis
Postvaccinal encephalitis
Meningeal Encephalitic Paralytic Toxic
Tri
pod
sign
, hea
dach
e, n
eck
stif
fnes
s,
Ker
nig'
s si
gn, B
rudz
insk
y's
sym
ptom
Ocu
lom
otor
dis
turb
ance
s, s
yndr
ome
of
foca
l bra
in le
sion
s, h
yper
kine
sis,
sta
tic
and
loco
mot
or a
taxi
a, e
pile
ptif
orm
fit
s
Mon
opar
esis
, hem
ipar
esis
, fla
ccid
pa
raly
sis
Fev
er, d
yspe
ptic
dis
orde
rs, i
mpa
irm
ent
of c
onsc
ious
ness
Serological reactions, HGIR, lumbar puncture, virological and bacteriological study of CSF, the study of biological fluids (stool, throat swab, CSF), CBC, urinalysis, blood culture, studies of platelets, tuberculin tests, serum electrolytes, blood glucose, blood urea and blood creatinine, cranial X-ray, chest, X-ray,
EEG
Infections — meningitis of different etiologies, Rocky
Mountain spotted fever, brain abscess
Metabolic coma - Reye's syndrome, hepatic coma,
hypoglycemia, acute adrenal insufficiency, hypo-and hyperkalemia, uremia,
alkalosis and acidosis
Toxic coma - acute poisoning, salycylate
poisoning, lead encephalitis, nitrogen monoxide poisoning
Primary disease of the brain - the first attack of epilepsy,
posterior fossa tumors, cerebrovascular disease
Others - cerebral embolism, systemic angiitis,
postinfectious encephalopathy, trauma
("battered child" syndrome)
Antiinflammatory(glucocorticosteroid
therapy)
Dehydration Antihistaminic Vitamin therapy Symptomatic Antiparkinsonian Surgical treatment
Neurological disorders Psychotic disorders Mental deficience ParkinsonismPersistent
hyperkinesisEpileptiform attacks
Diencephalic disorders

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF VIRAL HEPATITIS
syndrome of jaundice
Cythemolytic icterus Hepatocellular jaundice Obstructive jaundice
Hereditary Acquired Infectious Noninfectious
Min
kow
ski-
Cha
uffa
rd’s
he
redi
tary
m
icro
sphe
rocy
tosi
s
Her
edit
ary
stom
acyt
osis
H
ered
itar
y he
mol
ytic
an
emia
cau
sed
by th
e de
fici
ency
of g
luco
se-6
-ph
osph
ate
dehy
drog
enas
e
T
hala
ssae
mia
A
utoi
mm
une
hem
olyt
ic a
nem
ia
P
arox
ysm
al n
octu
rnal
he
mog
lobi
nuri
a
Hep
atit
is A
Hep
atit
is B
Hep
atit
is C
Hepatic cirrhosis
fine
ly n
odul
ar
larg
e no
dula
r
bili
ary
Acu
te a
lcoh
olic
he
pati
tis
Dru
g-in
duce
d
hepa
titi
s
Cho
lest
atic
vi
ral h
epat
itis
Ja
undi
ce a
t tum
ors
jaun
dice
at
gall
ston
es
Jaun
dice
cau
sed
by p
aras
ites
(o
pist
horc
hias
is,
schi
stos
omia
sis,
clo
norc
hias
is)
In t
he c
lini
cal
find
ings
the
re i
s ja
undi
ce,
anem
ia,
enla
rgem
ent
of t
he s
plee
n.
THbT
Tdecr
ease
s to
eryt
hroc
ytes
40-
50 g
/ L
, bi
liru
bin
incr
ease
s (5
0-75
mcM
/ l
). T
he d
iam
eter
of
dec
reas
es,
and
the
thic
knes
s in
crea
ses.
The
for
m i
s sp
heri
cal.
The
con
-te
ntof
reti
culo
cyte
isin
crea
sed
TMar
ked
bili
rubi
ntw
o T Tcu
rved
line
s.
ane
mia
(70
-90
g / l
). E
nlar
gem
ent o
f th
e sp
leen
. Jau
ndic
e is
due
to in
dire
ct
. Def
ect i
n er
ythr
ocyt
e m
embr
ane
- co
lour
less
par
t of
the
cent
er is
lim
ited
by
TSig
nifi
cant
enl
arge
men
t of
live
r an
d sp
leen
acc
ompa
nied
by
jaun
dice
. The
incr
ease
of
Tbili
rubi
n is
Tanis
opoi
them
.
due
to th
e di
rect
fra
ctio
n. I
n th
e bl
ood
ther
e ar
e in
crea
sed
reti
culo
cyte
s,
kilo
cyto
sis,
"ta
rget
like
" er
ythr
ocyt
es a
nd m
ulti
ple
baso
phil
ic in
clus
ions
in
Jaun
dice
,ch
arac
ter
enla
rged
. Bil
irub
in is
40-
60 m
cMde
crea
sed.
sev
ere
wea
knes
s, a
rthr
algi
a, a
bdom
inal
pai
n, p
ain
in h
eart
, low
er b
ack
are
isti
c fe
atur
es T
empe
ratu
re o
f th
e bo
dy is
incr
easi
ng. T
he li
ver
and
sple
en a
re
/ l d
ue to
the
indi
rect
fra
ctio
n. H
emog
lobi
n is
T
he n
umbe
r of
ret
icul
ocyt
es is
incr
ease
d; m
acro
cyto
sis,
m
icro
sphe
rocy
tosi
s;os
mot
icre
sist
ance
ofer
ythr
ocyt
esis
redu
ced
Gra
dual
beg
inni
nghe
pato
sple
nth
e ex
acer
bati
on is
indi
rect
fto
the
abse
nce
of e
full
-blo
wn.
, wea
knes
s, m
oder
ate
jaun
dice
, hea
dach
e, a
bdom
inal
pai
n,
omeg
aly.
Exc
reti
on o
f he
mos
ider
in b
y ur
inar
y w
ay. H
emog
lobi
n du
ring
r
educ
ed to
30-
50 g
/ l.
Bil
irub
in is
incr
ease
d m
oder
atel
y du
e to
the
ract
ion.
Leu
kope
nia.
The
iron
con
tent
in b
lood
is r
educ
ed. D
ark
urin
e is
due
ry
thro
cyte
s in
it. G
rege
rsen
’s b
enzi
dine
test
is +
. Pro
tein
uria
is
In th
e an
amda
ys.
Var
impr
ovem
ES
R i
s 2-
4 m
m /
h.
Incr
ease
in
tota
l bi
liru
bin
nesi
s th
ere
is a
con
tact
wit
h th
e H
AV
pat
ient
abo
ut 1
5-30
day
s be
fore
. Pre
icte
ric
peri
od is
5-7
ia
nts
of p
reic
teri
c pe
riod
are
flu
-lik
e, d
yspe
ptic
, as
then
oveg
etat
ive.
Dur
ing
icte
ric
peri
od
ent
is o
bser
ved.
In
blo
od t
here
is
leuk
open
ia,
neut
rope
nia,
rel
ativ
e ly
mph
o-an
d m
onoc
ytos
is.
due
to t
he d
irec
t fr
acti
on.
The
thy
mol
tes
t is
inc
reas
ed.
Red
ucin
gof
PT
IIn
crea
sed
AL
TA
ST
In th
e an
amm
arke
d, o
hypo
ten
r edu
cing
of
nesi
s th
ere
is b
lood
tran
sfus
ion
and
oper
ativ
e de
ntal
pro
cedu
res.
Pre
icte
ric
peri
od is
mor
e ft
en jo
ints
are
pai
nful
. Urt
icar
ia. D
urin
g ic
teri
c pe
riod
ther
e is
det
erio
rati
on, b
rady
card
ia, a
nd
sion
. Inc
reas
ed d
irec
t bil
irub
in, i
ncre
ased
AL
T, A
ST
, dys
prot
eine
mia
, red
ucin
g of
thym
ol te
st,
PT
I. I
n bl
ood
seru
m th
ere
is H
BsA
g, H
bcA
g, a
nti H
Bc,
ant
i HB
s, a
nti H
be.
Ana
mne
sis
is th
e fa
tigu
e, a
sthe
nia,
enl
arge
men
sam
e as
that
of
HB
V (
pare
nter
al w
ay).
Oft
en it
is w
itho
ut ic
teri
c co
urse
. Gra
dual
ons
et,
t of
liv
er a
nd s
plee
n. C
lini
call
y it
is
mil
der
than
HB
V.
In t
he b
lood
ser
um
ther
eis
anti
HC
VH
CV
RN
A
TIn
the
anam
nesi
s th
ere
is a
n ac
ute
HB
V. T
he li
ver
is m
oder
atel
y en
larg
ed,
Tedge
isTan
dT Tas
the
indi
cato
rs
thic
k an
d sh
arp.
The
re a
re s
igns
of
port
al h
yper
tens
ion.
Bef
ore
asci
tic
citic
per
iods
are lo
ng-t
erm
. The
re a
re c
hang
es in
the
prot
ein
frac
tion
, of
Sub
lim
ate
and
thym
ol te
sts.
Hbs
Ag
may
be
dete
cted
.
In th
e an
amne
sis
tsp
leen
is
enla
rged
mar
ked.
here
is a
chr
onic
hep
atit
is. T
he li
ver
is e
nlar
ged.
The
edg
e is
thic
k. T
he
. T
he p
erio
d pr
ior
to t
he a
scit
ic o
ne i
s sh
ort.
Por
tal
hype
rten
sion
is
A
bdom
inal
pai
n, j
oint
pai
n, i
tchy
ski
n, d
yspe
ptic
sym
ptom
s. S
igni
fica
ntly
in
crea
sed
bili
rubi
nA
LT
AS
Tal
dola
seH
bsA
gis
dete
cted
mor
eof
ten
Fro
m a
nam
enla
rged
, sen
siti
ve, e
dges
are
ofte
n in
the
righ
t hyp
och
bili
rubi
n an
d ch
ole
nesi
s th
ere
is o
ften
cho
lest
atic
var
iant
of
HB
V. T
he li
ver
is m
oder
atel
y s
harp
. Por
tal h
yper
tens
ion
is m
oder
ate.
Abd
omin
al p
ain,
on
driu
m. W
eakn
ess,
dec
reas
ed a
ppet
ite,
itch
y sk
in. I
ncre
ased
st
erol
, alk
alin
e ph
osph
atas
e, A
ST
, AL
T, t
hym
ol te
st.
In a
nam
leuk
ocyt
osis
,B
ilir
ubin
ic a
min
otra
nsfe
rase
nesi
s th
ere
is a
lcoh
olis
m, a
lcoh
ol a
buse
. In
labo
rato
ry a
naly
sis
ther
e is
in
crea
sed
acti
vity
of
alka
line
pho
spha
tase
, cho
lest
erol
, lip
opro
tein
s-B
. d
isso
ciat
ion.
In t
he a
napr
escr
ibed
fth
e 2 Pnd
Nau
sea,
mne
sis
ther
e is
a t
reat
men
t w
ith
med
icin
es,
mor
e of
ten
whe
n th
e dr
ugs
are
or a
long
tim
e an
d in
hig
h do
ses.
Mor
e of
ten
they
are
ant
i TB
pre
para
tion
s of
s
erie
s. I
t de
velo
ps b
y th
e en
d of
the
mon
th f
rom
the
sta
rt o
f m
edic
i nes
rec
eivi
ng.
vom
itin
g, h
eart
burn
. All
ergi
c di
sord
ers.
Thy
mol
test
is
nega
tive
.
In t
he a
nam
nT
here
is
Sple
en
phos
phat
urob
ilin
esis
the
re i
s bl
ood
tran
sfus
ion
for
45-1
80 d
ays
prio
r to
the
ill
ness
. Pr
eict
eric
per
iod
is 7
-14
days
. a
fee
ling
of
heav
ines
s in
the
rig
ht h
ypoc
hond
rium
. A
rthr
algi
a is
oft
en.
Feve
r pr
eced
es b
y ja
undi
ce.
is o
ften
enl
arge
d. C
ourv
oisi
er’s
sym
ptom
is
nega
tive
. In
crea
sed
tot
al b
ilir
ubin
, A
ST
, A
LT
, al
kalin
e as
e, t
hym
ol t
est,
chol
este
rol
is d
ecre
ased
or
incr
ease
d. T
est
wit
h ga
lact
ose
is +
, ur
ine
reac
tion
to
is +
.
In t
he a
nam
nesi
s th
ere
is a
n as
then
ia b
efor
e th
e on
set
of j
aund
ice,
pai
n in
the
liv
er,
whi
ch i
s og
ress
ive
wit
h gi
rdle
sen
sati
on.
Cou
rvoi
sier
’s s
ympt
om i
s of
ten
+.
Gal
l-bl
adde
r is
not
is
inc
reas
ed d
ue t
o th
e bo
und
frac
tion
. A
lkal
ine
phos
phat
ase,
thy
mol
tes
t ar
e os
itiv
e. B
lood
cho
lest
erol
is s
harp
ly in
crea
sed,
test
wit
h ga
lact
ose
is n
egat
ive.
slow
ly p
rpa
infu
l. B
ilir
ubin
ne
gati
ve o
r w
eak
p
I In
the
ana
mne
sis
ther
e ar
e at
tack
s of
gal
lsto
ne d
isea
se. A
cute
ons
et. P
ain
in l
iver
, ful
l- p
arox
ysm
al, w
ith
typi
cal r
adia
tion
to th
e ri
ght s
houl
der
and
scap
ula.
Hig
h fe
ver
wit
h la
rge
luct
uati
ons.
Cou
rvoi
sier
’s s
ympt
om i
s of
ten
+.
Gal
l-bl
adde
r is
pai
nful
on
palp
atio
n.
Cho
lest
erol
is
norm
al o
r sl
ight
ly i
ncre
ased
. R
eact
ion
to u
robi
lin
is
Con
cret
ions
may
be
in th
e ga
ll-b
ladd
er.
blow
n,da
ily
fT
hym
ol t
est
is n
egat
ive.
nega
tive
.
Jaun
dice
is
mda
ta a
nd f
ull-
blow
n eo
sino
phil
ia
oder
ate
or w
eak,
pai
nful
epi
sode
s ar
e m
issi
ng.
It i
s im
port
ant
that
epi
dem
iolo
gica
l ar
e up
to
15-2
0% o
r m
ore.
Con
firm
atio
n is
the
det
ectio
n of
pa
rasi
tes
orth
eir
eggs
57

DIAGNOSTIC ALGORITHMS : VIRAL HEPATITIS
Etiological
forms
Epidemiological
anamnesis
Periods
Clinical
symptoms
Laboratory
data
Clinical
forms
Features in
children of the 1st
year
Differential
diagnosis
Course
Fate
Treatment
Preventive measures
VIRAL HEPATITIS
Enteral
Icteric
Parenteral
Contact Blood transfusions, surgery, injections
Preicteric Posticteric ReconvalescenceIncubation
Liv
er e
nlar
gem
ent a
nd te
nder
ness
, as
then
ia, a
bdom
inal
pai
n, f
ever
, vo
mit
ing,
poo
r ap
peti
te, c
hang
e in
ur
ine
colo
r
Into
xica
tion
, vom
itin
g, li
ver
tend
erne
ss,
hepa
tom
egal
y,
sple
nom
egal
y, o
chro
derm
ia, s
cler
al
icte
rus,
hem
orrh
agic
syn
drom
e, d
ark
urin
e, p
ale
stoo
l
Increase in direct bilirubin, increased activity of enzymes,
dysproteinemia
Bile pigments in urine
Increase of thymol test, B-
lipoproteins
Serologic identification of markers
Changes CBC
ModeratelyAcute yellow atrophy of the
liver
Typical Atypical forms
Marked Banti's syndrome
Frequent overlay of
intercurrent diseases
The prevalence of severe forms
Development of acute yellow
atrophy of the liver
Predominantly viral hepatitis B
Tox
ic h
epat
itis
Obs
truc
tive
jaun
dice
Hem
olyt
ic a
nem
ia
Och
rode
rmat
osis
AR
VI
Inte
stin
al in
fect
ions
Fun
ctio
nal
hype
rbili
rubi
nem
ia
App
endi
citi
s
Les
ion
of b
ile
pass
ages
Liv
er le
sion
s a
t oth
er
dise
ase s
Hel
min
thic
inva
sion
ChronicProlongedAcute
Chronic hepatitis
CirrhosisPosthepatic hepatomega
ly
Lethal outcome
Hyperbilirubinemia
Lesion of bile
passages
Complete clinical
recovery
Corticosteroids
VitaminsCholagogues
medicinesDietDetoxication
Symptomatic
Sparing regimen
Current and final
disinfection
Observation of the contact and the lab. survey
Gamma-globulinprophylaxis of
contact
Selection of donors
Control for the sterilization of
instruments
Isolation of the patient
Quarantine
Polymerase chainreaction (PCR)
SevereMild
58
58
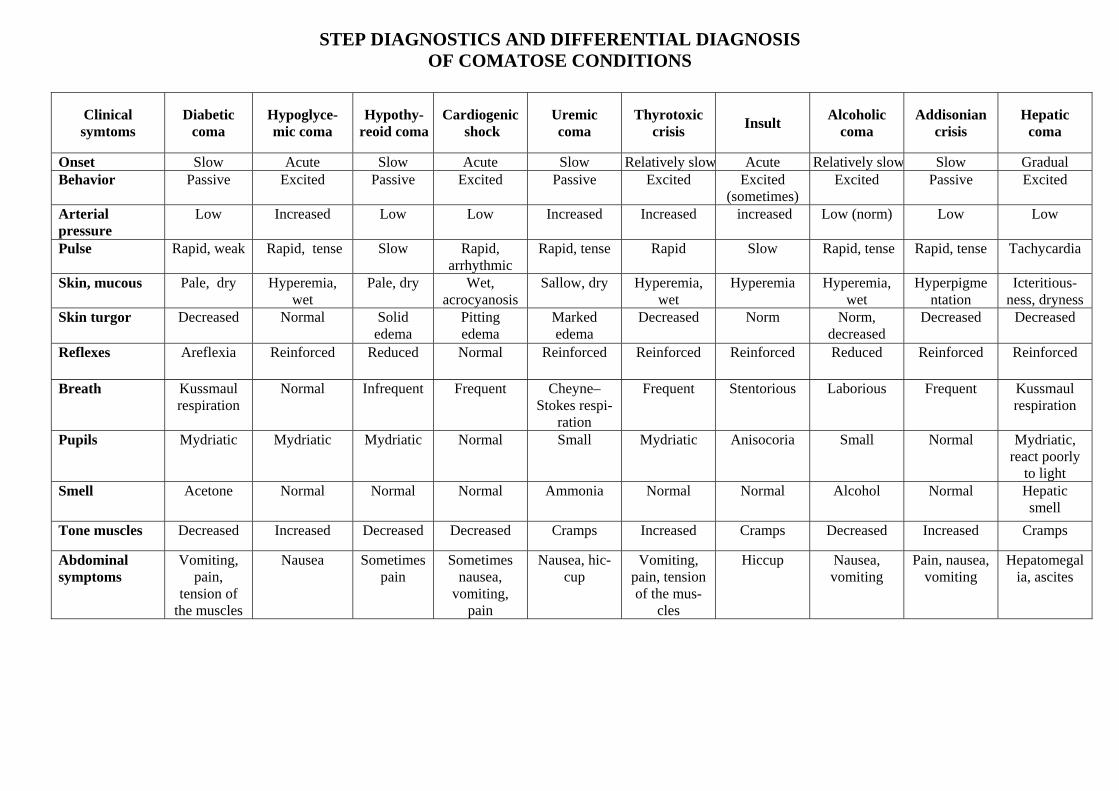
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF COMATOSE CONDITIONS
Clinical symtoms
Diabetic coma
Hypoglyce-mic coma
Hypothy-reoid coma
Cardiogenic shock
Uremic coma
Thyrotoxic crisis
Insult Alcoholic
coma Addisonian
crisis Hepatic
coma
Onset Slow Acute Slow Acute Slow Relatively slow Acute Relatively slow Slow Gradual Behavior Passive Excited Passive Excited Passive Excited Excited
(sometimes) Excited Passive Excited
Arterial pressure
Low Increased Low Low Increased Increased increased Low (norm) Low Low
Pulse
Rapid, weak Rapid, tense Slow Rapid, arrhythmic
Rapid, tense Rapid Slow Rapid, tense Rapid, tense Tachycardia
Skin, mucous Pale, dry Hyperemia, wet
Pale, dry Wet, acrocyanosis
Sallow, dry Hyperemia, wet
Hyperemia Hyperemia, wet
Hyperpigmentation
Icteritious-ness, dryness
Skin turgor Decreased Normal Solid edema
Pitting edema
Marked edema
Decreased Norm Norm, decreased
Decreased Decreased
Reflexes Areflexia Reinforced Reduced Normal Reinforced Reinforced Reinforced Reduced Reinforced Reinforced
Breath Kussmaul respiration
Normal Infrequent Frequent Cheyne–Stokes respi-
ration
Frequent Stentorious Laborious Frequent Kussmaul respiration
Pupils Mydriatic Mydriatic Mydriatic Normal Small Mydriatic Anisocoria Small Normal Mydriatic, react poorly
to light Smell Acetone Normal Normal Normal Ammonia Normal Normal Alcohol Normal Hepatic
smell
Tone muscles Decreased Increased Decreased Decreased Cramps Increased Cramps Decreased Increased Cramps
Abdominal symptoms
Vomiting, pain,
tension of the muscles
Nausea Sometimes pain
Sometimes nausea,
vomiting, pain
Nausea, hic-cup
Vomiting, pain, tension of the mus-
cles
Hiccup Nausea, vomiting
Pain, nausea, vomiting
Hepatomegalia, ascites

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF COMATOSE CONDITIONS
Impairment of consciousness (loss)
60
Signs Coma Onset
Acute Eclamptic; hypoglycemic; apoplectic Gradual Hepatic; uremic; thyrotoxic diabetic; adrenal
Antecedents Icteritiousness Hepatic; hemolitic Multiple vomiting Hepatic; diabetic; thyrotoxic
Attack of convulsions Epileptic; eclamptic; Abdominal pain Diabetic
Severe headache Meningeal; apoplectic
Tremors, sweating, Chest pain, invariable behavior
Hypokalemic; pate; apoplectic
Position in bed Opisthotonos Meningeal Lateral jack-knife position Meningeal; uremic Symptoms Marks of a blow Epileptic; posttraumatic Fever Hepatic; diabetic;
Meningeal; apoplectic Exophthalmos Thyrotoxic
Acetone-odour Diabetic
Uraroma Uremic
Arterial hypertension Eclamptic; uremic; apoplectic Attrition murmur Uremic Hepatomegaly Hepatic; uremic; anemic Splenomegaly Hepatic; anemic Diarrhea Thyrotoxic; uremic; adrenal; apoplectic
Breathing Kussmaul respiration Diabetic; uremic Biot’s respiration Uremic; meningeal Skin Pale Uremic; anemic Hyperemia Alcoholic; adrenal; apoplectic Bronze color Adrenal Icterus Hepatic; hemolitic Watery Hypoglycemic; alcoholic Dry Diabetic; uremic; adrenal Petechiae, marks of scratching Diabetic; uremic; hepatic
Guiding symptoms The absence of algesthesia
The absence of other reflexes

COMA
FOCAL SYMPTOMS
(ANISOCORIA, PTOSIS, CONVULSIONS)
YES NO ONSET OF
THE DISEASE ONSET OF
THE DISEASE
GRADUAL ACUTE
ACUTE GRADUAL
SIGNS OF AN INFECTIOUS
PROCESS
ABSCESS HYPOGLYCEMIA
ENCEPHALITIS TRAUMA
HEMORRHAGE
ISCHEMIA
TUMOR HYPOXIA
ACUTE POISONING
MENINGITIS
Yes No
ACETONEMIC UREMIC
DIABETIC HEPATIC AND OTHERS

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF CEREBRAL EDEMA’S DEGREES
Specific symptoms Degree I Degree II Degree III
Precoma: Lesion of the
middleCentral nervous system
stupefaction and inconstant
Brainstem lesion or terminal state
areas of the brain
psycho-motor agitation
Degree of consciousness manifestation
Clear, sleepiness, lethargy
No, nonreactive for intensive stimuli
No
Character of convulsions
Twitching of some muscle groups
Clonicotonic attacks
Abrupt, tonic
Severe hypertonus to the degree of
Decreased motion activity
Decreased, no motion activity
Muscular tone
opisthotonos
Tendon reflexes Brisk or norm High Not observed
Meningeal signs Induced Easily induced Not induced
Loss of vital centers (unresponsive pupilsCranial nerves
disorders ,
swallowing, respiratory response, etc.)
Focal symptoms None
Body temperature Febrile Hectic increase Hectic or hypothermia
Circulatory insufficiency
Degree I Degree I–II Degree II–III
Central venous pressure
Deeply decreased, unmeasured
High High or low
Hypoventilation, abnormal patterns of breathingRespiratory system Hyperventilation Hyperventilation to the degree of pulmonary arrest
Decreased by a third
Diuresis Oliguria Oligoanuria
Respiratory alkalosis
Uncompensated respiratory alkalosis or decompensated
metabolic acidosis
Respiratory alkalosis
or Electrolytic balance
subcompensated metabolic acidosis
Stage of hypercoagulability
or
Disseminated intravascular coagulation (DIC)
Stage of hypercoagulability Stage of
hypercoagulability or consumption coagulation
consumption coagulation
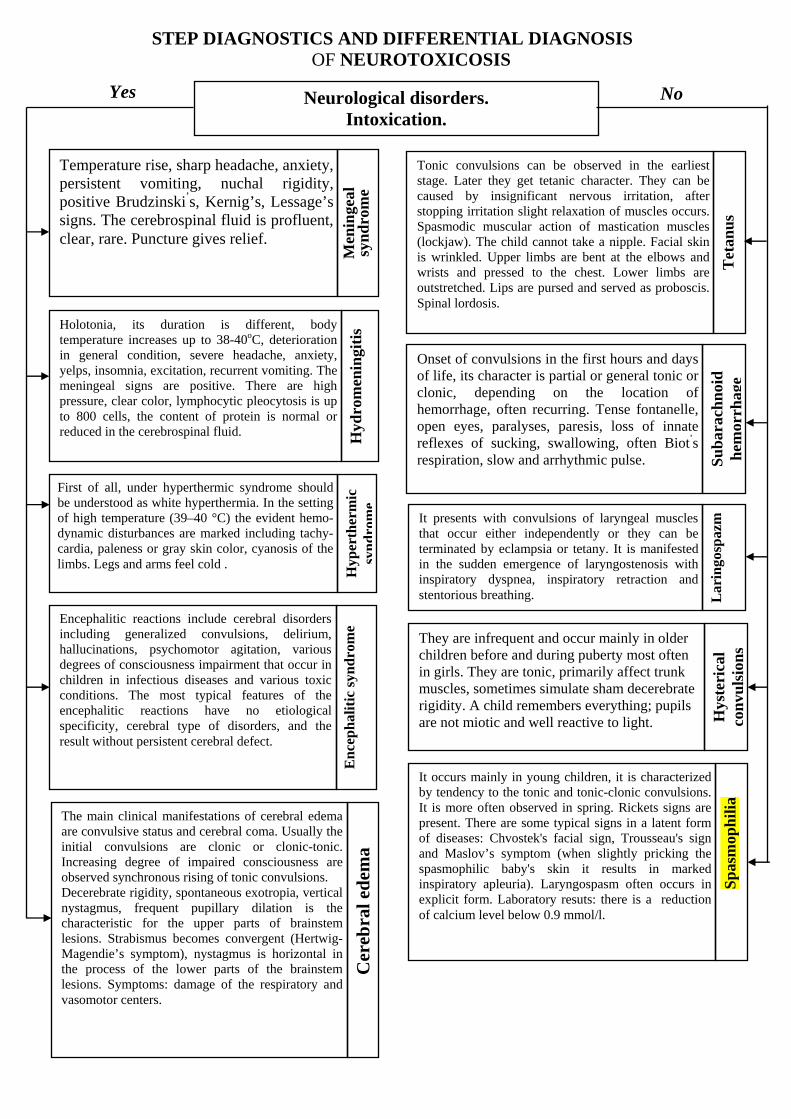
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF NEUROTOXICOSIS
Yes No Neurological disorders.
Intoxication.
Temperature rise, sharp headache, anxiety, persistent vomiting, nuchal rigidity,positive Brudzinski s’ , Kernig’s, Lessage’ssigns. The cerebrospinal fluid is profluent, clear, rare. Puncture gives relief.
Men
inge
al
syn
dro
me
Tonic convulsions can be observed in the earliest stage. Later they get tetanic character. They can be caused by insignificant nervous irritation, after stopping irritation slight relaxation of muscles occurs. Spasmodic muscular action of mastication muscles (lockjaw). The child cannot take a nipple. Facial skin is wrinkled. Upper limbs are bent at the elbows and wrists and pressed to the chest. Lower limbs are outstretched. Lips are pursed and served as proboscis. Spinal lordosis.
Tet
anu
s
Onset of convulsions in the first hours and days of life, its character is partial or general tonic or clonic, depending on the location of hemorrhage, often recurring. Tense fontanelle, open eyes, paralyses, paresis, loss of innate reflexes of sucking, swallowing, often Biot’s respiration, slow and arrhythmic pulse. S
ub
arac
hn
oid
h
emor
rhag
e
Holotonia, its duration is different, body temperature increases up to 38-40oC, deterioration in general condition, severe headache, anxiety, yelps, insomnia, excitation, recurrent vomiting. The meningeal signs are positive. There are high pressure, clear color, lymphocytic pleocytosis is up to 800 cells, the content of protein is normal or reduced in the cerebrospinal fluid.
Hyd
rom
enin
giti
s
It presents with convulsions of laryngeal muscles that occur either independently or they can be terminated by eclampsia or tetany. It is manifested in the sudden emergence of laryngostenosis with inspiratory dyspnea, inspiratory retraction and stentorious breathing. L
arin
gosp
azm
First of all, under hyperthermic syndrome should be understood as white hyperthermia. In the setting of high temperature (39–40 °C) the evident hemo-dynamic disturbances are marked including tachy-cardia, paleness or gray skin color, cyanosis of the limbs. Legs and arms feel cold .
Hyp
erth
erm
ic
syn
dro
me
En
cep
hsy
nd
al
itic
ro
me
They are infrequent and occur mainly in older children before and during puberty most often in girls. They are tonic, primarily affect trunk muscles, sometimes simulate sham decerebrate rigidity. A child remembers everything; pupils are not miotic and well reactive to light. H
yste
rica
l co
nvu
lsio
ns
It occurs mainly in young children, it is characterized by tendency to the tonic and tonic-clonic convulsions. It is more often observed in spring. Rickets signs are present. There are some typical signs in a latent form of diseases: Chvostek's facial sign, Trousseau's sign and Maslov’s symptom (when slightly pricking the spasmophilic baby's skin it results in marked inspiratory apleuria). Laryngospasm often occurs in explicit form. Laboratory resuts: there is a reduction of calcium level below 0.9 mmol/l.
Sp
asm
oph
ilia
Encephalitic reactions include cerebral disorders including generalized convulsions, delirium, hallucinations, psychomotor agitation, various degrees of consciousness impairment that occur in children in infectious diseases and various toxic conditions. The most typical features of the encephalitic reactions have no etiological specificity, cerebral type of disorders, and the result without persistent cerebral defect.
The main clinical manifestations of cerebral edema are convulsive status and cerebral coma. Usually the initial convulsions are clonic or clonic-tonic. Increasing degree of impaired consciousness are observed synchronous rising of tonic convulsions. Decerebrate rigidity, spontaneous exotropia, vertical nystagmus, frequent pupillary dilation is the characteristic for the upper parts of brainstem lesions. Strabismus becomes convergent (Hertwig-Magendie’s symptom), nystagmus is horizontal in the process of the lower parts of the brainstem lesions. Symptoms: damage of the respiratory and vasomotor centers.
Cer
ebra
l ed
ema

ALGORITHMS OF EMERGENCY MEDICAL CARE: NEUROTOXICOSIS IN CHILDREN
63
Neurotoxicosis
Antipyretic therapyTreatment of the meningeal and convulsive
disorderыTreatment of the hyperventilation, encephalitic,
cardiovascular syndromes
«Red» hyperthermia «White» hyperthermia
Physical methods of cooling, paracetamol 10 mg/kg, analgin 50% —
0.1 ml/year, diphenhydramine
hydrochloride 1% — 0.1 ml/year
Lytic cocktail, improvement of microcirculation — i/v rheopolyglucin 10 ml/kg
intravenous, detoxification
Dehydration therapy Anticonvulsant therapy
Lasix 1% — 2 mg/kg, magnesium sulfate 25% —
0.1 ml/kg,10% albumin, FFP (fresh
frozen plasma), rheopolyglucin 10 ml/ kgprednisolone 2–5 mg/ k
Seduxen - 0.5% 0.5 ml / kg,Sodium 20% - 50-100 mg / kg
Neurovegetative block:lytic cocktail (aminazin 2.5% — 1 ml,
droperidol 0.25% — 1ml, suprastin 2% — 1 ml, 0.25% novocaine — 8 ml) — 0.1–0.4
ml / kg
Ineffectively
Ganglionic blocking agent:Pentamin 5% of 1–4 mg / kg
Bеnzohexonium 2.5% of 1–2 mg / kg

EMERGENCY MEDICAL CARE ALGORITHMS: INFECTIOUS-TOXIC SHOCK
Infectious-toxic shock
Correction of the vascular syndrome Correction of the thrombohemorrhagic syndromeCorrection of the syndrome of toxic edema,
prevention of (ARF) acute renal failure
Convulsions Sodium 20% 100 mg/kgSeduxen 0,5% — 0,3–0,5 ml/kg
Dopamine 10 mcg/kg/min, rheopolyglucin 10 ml/kg IVFD
Polyglucin 3 ml/kg by stream infusion to restore blood pressure
Ineffectively
Curantyl 3–5 mg/kg«Titration» of noradrenaline
Heparin 15 U/kg/h/i/vContrykal 500–1000 U/kg i/v
FFP (fresh frozen plasma) 10 ml/kg
Broad-spectrum antibiotics, not stimulating toxicosis (levometicin-sodium succinate 100
mg/kg i/v, azithromycin 10 mg/kg i/v)Prednisolone:
Stage I. 10 mg / kgStage II. 20 mg / kgStage III. 30 mg / kg
(where 2–3 mg/kg i/v before polyglucin)Vitamin C — 10 mg/kg i/vLasix 1% — 2 mg/kg i/v
Magnesium sulfate 25% — 0.2 ml/kg i/vCocarboxylase — 4–8 mg/kg i/v
Aminophylline 2.4% — 2–4 mg/kg

69
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF INFECTIOUS-TOXIC SHOCK
IN MENINGOCOCCOSIS Yes No Acute circulatory insufficiency syndrome
and metabolic disorders
This disease develops during 1-2 days. The syn-drome of general intoxication predominates over gastrointestinal disorders. The main manifestations of shock are tachycardia in association with hypotension, diuresis decreasing. The signs of disseminated intravascular coagulation are not observed. Infectious-toxic shock occurs in the setting of isotonic hypohydration with potentiation of corresponding pathological changes.
Infe
ctio
us-
toxi
c sh
ock
in
salm
onel
losi
s
It develops in the setting of fluid loss due to profuse diarrhea and profuse recurrent vomiting. It is characterized by signs of dehydration (impairment of skin turgor, xerosis), mainly cramps in legs. Shock reaction develops less critical. Hemodynamic disorders develop with rising of dehydration. The relative density findings of plasma and hematocrit are severely increased. D
ehyd
rati
on s
hoc
k
It devolves peracutely with introducing of drugs or using of food. There are allergic reactions in the case history. Arterial hypotension, bronchospasm, pronounced respiratory failure, disorder of consciousness, skin vegetovascular reactions, clonic convulsions. Nausea, vomiting, abdominal pain, pain in the region of the heart, dizziness may be present. It is characterized by pant, dyspnea, urticarial eczema, palpebral edema, facial edema. Disseminated intravascular coagulation is not marked.
An
aph
ylac
tic
shoc
k
Infectious-toxic shock often occurs after beginning of antibacterial therapy with the bactericidal action drugs and proceeds initially like Jarish-Herxheimer reaction. Then hypotension predominates, renal failure develops soon afterwards. In
fect
iou
s-to
xic
shoc
k
in le
ptos
piro
sis
Infectious-toxic shock is observed in case of complications of bacterial pneumonia. Shock proceeds severely due to the microcirculation disturbance, severe metabolic disorders caused by hypoxia and acidosis. Acute cerebral insufficiency develops and edema - brain swelling with cerebral hypertension – develops soon afterwards.
Infe
ctio
us-
toxi
c sh
ock
in g
rip
It develops with the background of chronic heart pathology. It is characterized by acrocyanosis, jugular venous distention and dilation of cardiac borders, signs of stagnation in the pulmonary and systemic circulation. Pulse in spite of tachycardia is the sufficient strength of the pulse, arrhythmic. Arterial blood pressure decreases more slowly. Central venous pressure is increased.
Acu
te h
eart
fai
lure
Marked typical symptoms: nausea, vomiting, liquid stool. The patient has Banti's syndrome, yellowish or darkened skin.
Infe
ctio
us-
toxi
c sh
ock
in m
alar
ia
Infe
ctio
us-
toxi
c sh
ock
in
men
ingo
cocc
osis
It is characterized by abdominal pains with-out peritoneal signs. Abdominal pains occur prior to developing of arterial hypotension and breaking-out of hemorrhagic rash; they are gradually progressive, not arrested by analgesics.
Acu
te a
dre
nal
in
suff
icie
ncy
In anamnesis there is an evidence of any traumatic effect. A patient is lethargic; skin is pale and cyanotic color. Peripheral circulation is impaired. Cervical veins, limb veins arecol-lapsed. Respiratory rate slows down. Arterial blood pressure is decreased; a great drop in temperature. Diuresis is reduced up to anuria.
Wou
nd s
hoc
k
It develops during a day from the beginning of generalization. Pain is in muscles, joints and abdomen. Petechial skin rash is observed, severe punctate papular elements may be present. Hemorrhage is in the conjunctiva. Blood pressure is within normal range and slightly increased in arterial hypertension.
Отформатировано:английский (США)
Отформатировано:английский (США)
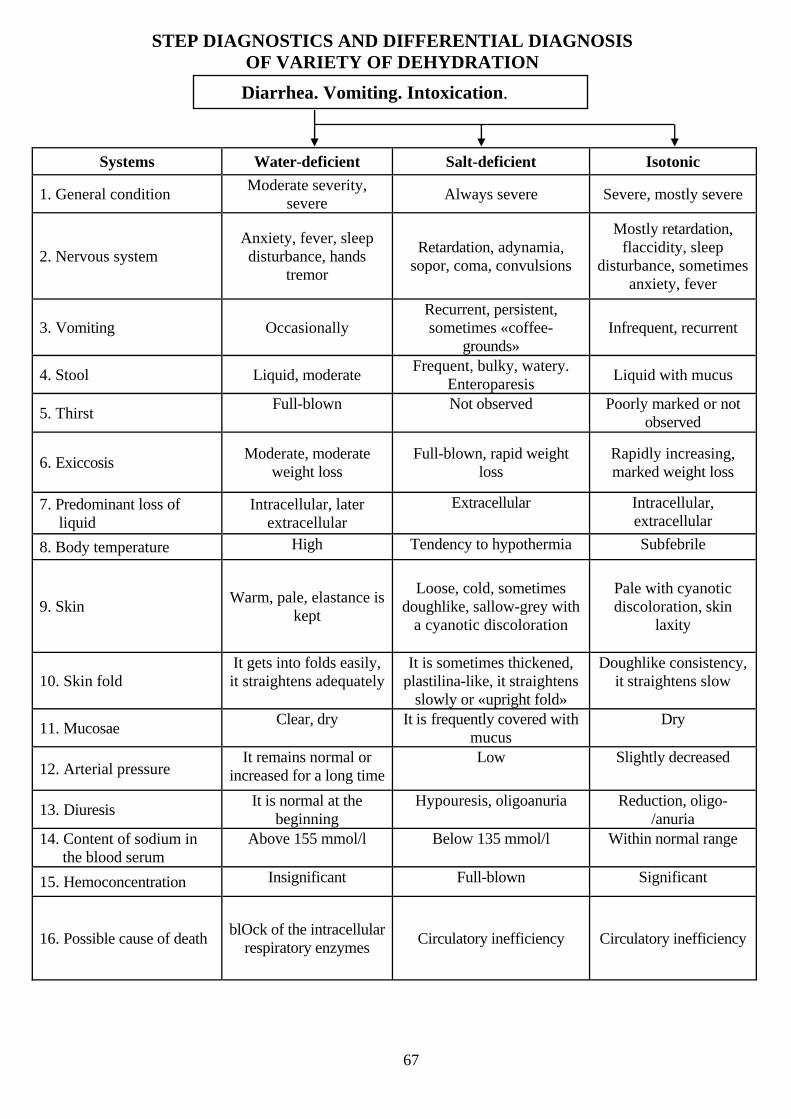
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF VARIETY OF DEHYDRATION
Diarrhea. Vomiting. Intoxication.
Systems Water-deficient Salt-deficient Isotonic
Moderate severity, severe
1. General condition Always severe Severe, mostly severe
Mostly retardation, flaccidity,
Anxiety, fever, sleep disturbance
Retardation, adynamia, sopor, coma, convulsions
sleep disturbance
2. Nervous system , hands tremor
, sometimes anxiety, fever
Recurrent, persistent, sometimes «coffee-
grounds» 3. Vomiting Occasionally Infrequent, recurrent
Frequent, bulky, watery. Enteroparesis
4. Stool Liquid, moderate Liquid with mucus
5. Thirst Full-blown Not observed Poorly marked or not observed
Moderate, moderate weight loss
Full-blown, rapid weight loss
Rapidly increasing, marked weight loss
6. Exiccosis
7. Predominant loss of liquid
Intracellular, later extracellular
Extracellular Intracellular, extracellular
8. Body temperature High Tendency to hypothermia Subfebrile
Loose, cold, sometimes doughlike, sallow-grey with
a cyanotic discoloration
Pale with cyanotic discoloration, skin
laxity
Warm, pale, elastance is kept
9. Skin
10. Skin fold It gets into folds easily, it straightens adequately
It is sometimes thickened, Doughlike consistency, plastilina-like, it straightens it straightens slow
slowly or «upright fold»
11. Mucosae Clear, dry It is frequently covered with Dry
mucus
12. Arterial pressure It remains normal or
increased for a long timeLow Slightly decreased
13. Diuresis It is normal at the
beginning Hypouresis, oligoanuria Reduction, oligo-
/anuria 14. Content of sodium in
the blood serum Above 155 mmol/l Below 135 mmol/l Within normal range
15. Hemoconcentration Insignificant Full-blown Significant
blOck of the intracellular 16. Possible cause of death
respiratory enzymes Circulatory inefficiency Circulatory inefficiency
67

STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF DEGREES OF TOXICOSIS WITH EXSICOSIS
Intoxication. Vomiting. Diarrhea.
Symptoms of exiccosis and laboratory findings
Degree I Degree II Degree III
Moderately severe From moderate severe to severe
1. Health assessment Very severe
2. Vomiting frequency 1–2 times Recurrent Multiple
Up to 10 times a day, More than 10 times, watery diarrhea
3. Stool frequency Infrequent enteritiс
4. Thirst Moderate Full-blown hydroadipsia
Quick straightening
«Upright fold» 5. Skin fold Slow straightening
6. Visible mucous Wet Slightly dry and hyperemic Dry, bright
7. Anterior fontanelle Normal Slightly sunken Sunken
8. Eyebulbs Elastic Soft Hollow eyes
9. Heart sounds Loud Slightly muffled Muffled
Normal or slightly increased
Systolic — normal, diastolic —
Decreased 10. Blood pressure increased
11. Tachycardia No Moderate Tachycardia
12. Cyanosis No Moderate Full-blown
Excitement or 13. Consciousness, environmental response
sleepiness, flaccidity
Altered state of consciousness
Normal
14. Pain reaction Significant Insignificant No observed
15. Voice Normal Leptophonia ofTen aphonia
16. Diuresis It is kept Hypouresis Oligoanuria
17. Respiration Normal Moderate dyspnea Toxic
18. Body temperature Normal Often increased Often below normal

EXICCOSIS IN CHILDREN: EMERGENCY MEDICAL CARE ALGORITHMS
Water-deficient
EXICCOSIS Salt-deficient
Isotonic
I degree
III degree
II degree
Oral rehydration (total liquid = body weight × 75)I stage 6 hours
II stage 80–100 ml/kg/day
Oral rehydration + I.V. (total liquid in kids up to 1 yeaг = body weight × 200, in older children = body weight × 170) KCl 7.5% — 2–3 ml/kg. glucose : salt = 2:1
Total liquid = body weight × 300 (up to 1 year), body weight × 220 (up to 5 years), in older children = body weight × 175.
KCl 7.5% = 2–3 ml/kg. glucose : salt = 1:1
III degree
II degree
I degree Oral rehydration (total liquid = body weight × 75)
Total liquid in kids up to 1 year = МТ × 200, in older children=body weight × 170, from 6 years = body weight × 110.
KCl 7.5% — 2–3 ml/kg. glucose : salt = 1:2
Total liquid = МТ × 300 (up to 1 year), body weight × 220(up to 5 years),
in older children=body weight × 175.
I degree
III degree
II degree
Oral rehydration (Total liquid = body weight × 75)
Total liquid = МТ × 200 (up to 1 year), body weight × 170 (up to 5 year),
in older children = body weight × 110. KCl 7 5% = 2 3 ml/kg glucose : salt = 1:1
Total liquid = body weight × 300 (up to 1 year), body weight × 220 (up to 5 year), in older children = body weight × 175.
KCl 7.5% = 2–3 ml/kg. glucose : salt = 1:1
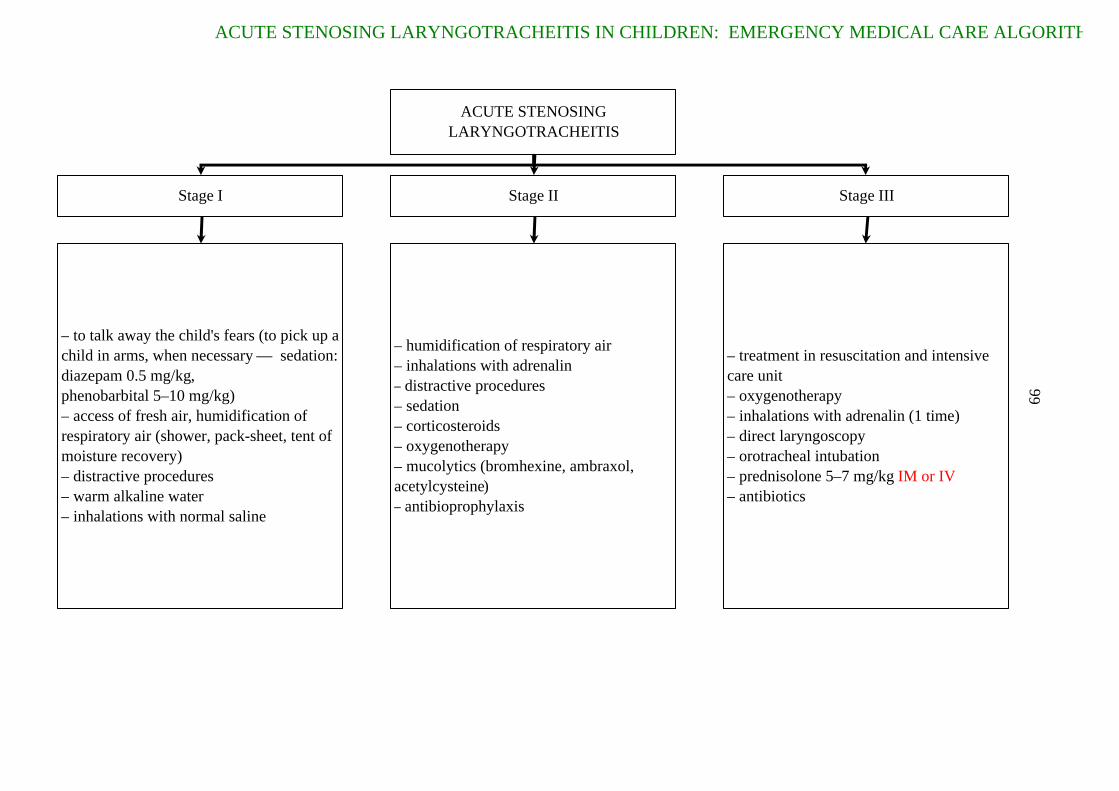
ACUTE STENOSING LARYNGOTRACHEITIS IN CHILDREN: EMERGENCY MEDICAL CARE ALGORITH
66
ACUTE STENOSING LARYNGOTRACHEITIS
Stage I Stage II Stage III
– to talk away the child's fears (to pick up a child in arms, when necessary — sedation: diazepam 0.5 mg/kg,phenobarbital 5–10 mg/kg)– access of fresh air, humidification of respiratory air (shower, pack-sheet, tent of moisture recovery)– distractive procedures– warm alkaline water– inhalations with normal saline
– humidification of respiratory air– inhalations with adrenalin– distractive procedures– sedation– corticosteroids– oxygenotherapy– mucolytics (bromhexine, ambraxol, acetylcysteine )– antibioprophylaxis
– treatment in resuscitation and intensive care unit– oxygenotherapy– inhalations with adrenalin (1 time) – direct laryngoscopy– orotracheal intubation – prednisolone 5–7 mg/kg IM or IV – antibiotics

HMS

73
STEP DIAGNOSTICS AND DIFFERENTIAL DIAGNOSIS OF VIRAL CROUP
Yes No Hoarseness. Cough. Fever.
The disease begins with moderatetemperature rise, the appearance of lowintoxication, gross "barking" cough andslight hoarseness. Then there is inspiratorydyspnea, noisy breathing, hoarse voice, up to aphonia. During inhalation there isretraction of the chest compliant places.
dip
hth
eria
of
lary
nx
(tru
e cr
oup
)
The disease begins slowly, with dry cough, slight rise of temperature, little cold. Then within 1-2 weeks cough increases, it becomesobsessive, reprises appear. During thespasmodic cough a sick person becomes red,turning blue, the veins on his neck are bulged and his eyes are engorged, his head is stuck out, the tongue is lolled out to the limit. The attack ends with viscous, ropy expectoration and vomiting.
per
tuss
is
Temperature rises up to 38.5-39.5°C,profuse runny nose, which is slimy at first, then it is slime-purulent, hoarse voice,obsessive, dry cough, photophobia, conjunctival hyperemia, eyelid edema, scleritis. There are grayish-white dots withthe size of a poppy seed, surrounded by a red border on the buccal mucosa in the molar teeth, on the mucous membrane of lips and gums.
mea
sles
The disease begins with cough, which gradually increases and sometimes becomes spasmodic with reprises. There is no hoarseness. The body temperature does not rise. Moderate
catarrhal phenomena. Par
aper
tuss
is
The disease develops gradually, with drynonproductive cough, which then becomesproductive with the mucous or muco-purulent expectoration. Prolongedexhalation, difficulty breathing. Moderateintoxication. The subfebrile temperature.
Acu
te
non
-obs
truc
tive
b
ron
chit
is
Acute onset of the disease with temperature rise, the appearance of mild symptoms of intoxication and catarrhal symptoms. The general condition suffersmoderately. Sore throat, stuffiness in nose, slimy nasal discharge, then it isslime-purulent. Among the good health,usually at night, the baby suddenly wakesup from the gross "barking" cough.Hoarseness, noisy breathing are quicklyattached and laryngeal stenosis develops.
fals
e cr
oup
(par
ain
flu
enza
)
Gradual beginning with the development of chronic obstructive bronchitis. Semicough, taking pertussis-like character, bright, not very viscous expectoration, then it is more viscous, mucopurulent. There is no hoarseness. It is characterized by chronic bilateral pneumonia with abscess formation and bronchiectasis. Symptom of respiratory and cardiovascular failure, physical development delay.
mu
covi
scid
osis
(p
ulm
onar
y fo
rm)
The disease begins with a loose tissue edema - lips, neck, eyelids, etc. (periodic edema), allergic urticaria - itching urticarial rash over the body. There is mucous discharge from nose. Cough, hoarseness. Edema of the larynx.
alle
rgic
ed
ema
of t
he
voca
l cor
ds
Long-term development of the disease.Chronic dry, hoarse cough, change of voice, often inspiratory dyspnea with stridor develops.
pap
illo
mas
of
lary
nx

VIRAL CROUP: TREATMENT ALGORITHMS
Etiological
forms
Mechanism
of transmission
Periods
Signs and
symptoms
Laboratory
tests
Clinical
forms
Clinical features in children
younger than one year old
Differential
diagnosis
Course
Outcomes
Principles
of treatment
Prevention
Syndrome of croup
False croup Membranous croup
Air-communicableAir-communicable,
contact
Stenotic coughStenosis of the I,
II, III stagesAsphyxiaCatarrhal cough
Sudden onset, absence of complete aphonia, catarrhal conditions, positive effect of the
distraction therapy
Gradual onset, complete aphonia, development of descending croup type, absence of the effect
from distraction therapy
Complement fixation test
(CFT), hemagglutination-
inhibition reaction (HGIR)
Immunofluorescence
Complete blood count
(CBC)
CBC, direct hemagglutination reaction (DHGR)
Neutralization reaction of antibodies
Bacteriological test
Moderately severe SevereMild Extremely severe
It does not appear up to 1 year
It proceeds typically after 3 months, but rate of development is fast
Cough is weak up to 3 months, stenotic breathing is not marked
Foreign body aspiration
Diphtheria of larynx
Measles Allergic edemaParaflu
ComplicatedAcute Not complicated
Residual effects Complications LethalConvalescence
Regime, diet, symptomatic therapy, antispasmodic,
distraction therapy
The injection of antidiphtheriс serum (ADS), antibiotics, detoxification,
hormone therapy, regime, diet, symptomatic therapy, antispasmodic,
distraction therapy
Quarantine Sequestration of
the patient
Current and final disinfection
Monitoring of contacts
IMMUNOLOGICAL prophylaxis of
diphtheria
Cold-water treatment
74

PULMONARY EDEMA: ALGORITHMS OF EMERGENCY AID
65
Pulmonary edema
Raised position of the upper part of the trunk and dependent position of the legs
Corticosteroids (in solution of continuity of the capillary wall by substances)
Oxygen therapy
Dehydration - furosemide - 2 mg / kg Sedative therapy (diazepam - 0.2 - 0.5 mg / kg)
Further activities
Patient transportation to the in-patient department of the
intensive therapy
Digitalization during 2-3days
Intubation and artificial pulmonary ventilation (APV) in the regime of positive end-expiratory pressure
Dopamine and dobutamine (3-5 or 5-10 mg / kg / min)
Nitroglycerin (0.1-0.7 mg / kg / min)
Other activities
Pulmonary edema causes removal Hemodialysis in case of kidney failure development Primary disease tretment
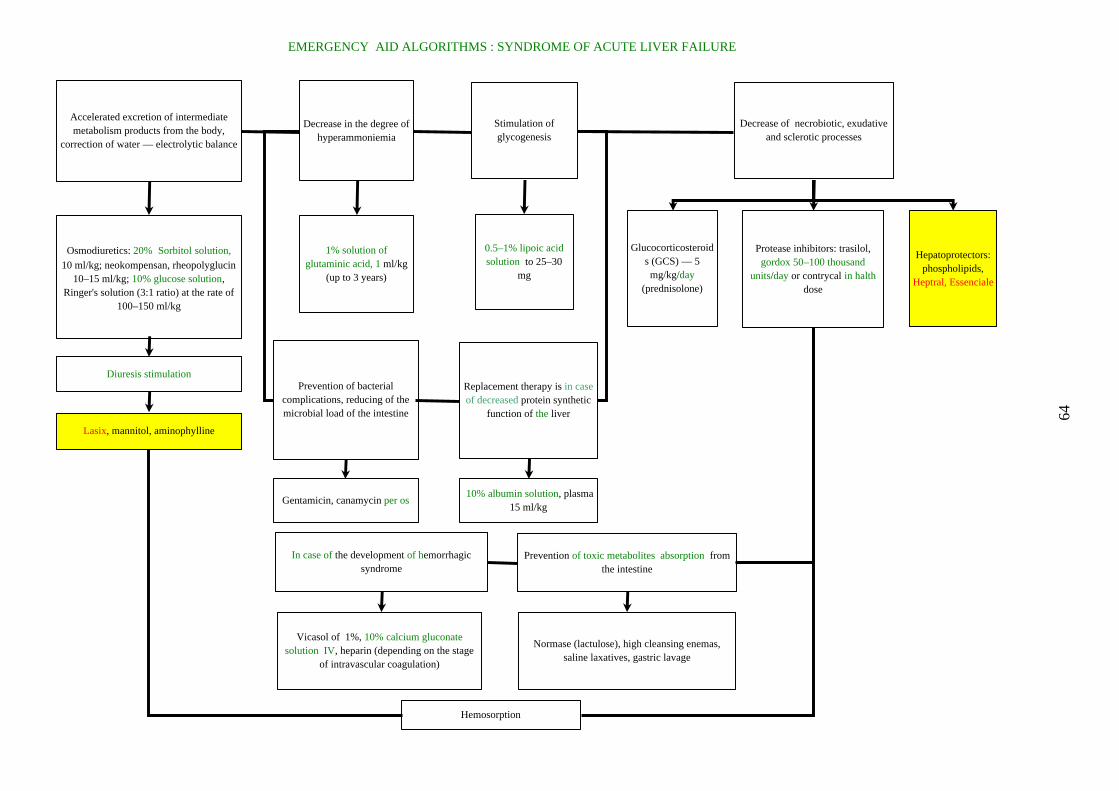
EMERGENCY AID ALGORITHMS : SYNDROME OF ACUTE LIVER FAILURE
64
Accelerated excretion of intermediate metabolism products from the body,
correction of water — electrolytic balance
Osmodiuretics: 20% Sorbitol solution,
10 ml/kg; neokompensan, rheopolyglucin 10–15 ml/kg; 10% glucose solution,
Ringer's solution (3:1 ratio) at the rate of 100–150 ml/kg
Decrease in the degree of hyperammoniemia
Stimulation of glycogenesis
Decrease of necrobiotic, exudative and sclerotic processes
1% solution of glutaminic acid, 1 ml/kg
(up to 3 years)
0.5–1% lipoic acid solution to 25–30
mg
Glucocorticosteroids (GCS) — 5 mg/kg/day
(prednisolone)
Protease inhibitors: trasilol, gordox 50–100 thousand
units/day or contrycal in halth dose
Hepatoprotectors: phospholipids,
Heptral, Essenciale
Prevention of bacterial complications, reducing of the microbial load of the intestine
Replacement therapy is in case of decreased protein synthetic
function of the liver
Diuresis stimulation
Lasix, mannitol, aminophylline
Gentamicin, canamycin per os 10% albumin solution, plasma
15 ml/kg
Prevention of toxic metabolites absorption from the intestine
In case of the development of hemorrhagic syndrome
Vicasol of 1%, 10% calcium gluconate solution IV, heparin (depending on the stage
of intravascular coagulation)
Normase (lactulose), high cleansing enemas, saline laxatives, gastric lavage
Hemosorption

The clinical features of typical and atypical community-acquired pneumonia in children during the first months of life
Sign Typical Atypical
Fever Significant, Т > 38° No or subfebrile
Dyspnea
No or imperceptible Significant
Cough
Productive Begins with cough, hard and progressive cough
Rales No or localized Diffuse
Percussion
Often shortened Box sound
X-ray pattern Often unilateral focus, or infiltration, involvement of the pleura
Ambilateral multiple foci with interstitial tissue damage
Causative agent E. coli, staphylococci, rarely pneumococci, H. influenzae
C. trachomatis. Less frequently —Pneumocystis. M. pneumoniae and U. urealysticum are arguable

Initial treatment
in hospital-aquired pneumonia
Therapy before pneumonia
Probable causative agent Recommended medication
Was not conducted Pneumococcus Mycoplasma
Parenterally: penicillin, ampicillin internally: macrolide — Sumamed
Penicillin, ampicillin
Staphylococcus, Mycoplasma Intramuscularly, intravenously: oxacillin, lincomycin, cefazolin. Per os: macrolide — Sumamed amoxicillin-clavulanate
Macrolide Resistant flora Resistant pneumococcus, H. influenzae
Per os, intramuscularly, intravenously: oxacillin, lincomycin, cefazolin
Cephalosporin-1 generation, oxacillin, lincomycin
E. Coli, other Gr (–) flora, resistant Staphylococcus
Parenterally: Augmentin, 2 –3 generation of cephalosporins
nd rd
, aminoglycoside, vancomycin, combinations of drugs
Aminoglycoside Pneumococcus, or Gr (–) flora, resistant Staphylococcus
Parenterally: penicillin, ampicillin, if it is with no effect: ureidopenicillin, rifampicin, karbopenem, vancomycin, aminoglycoside in high doses*
Aminoglycoside + cephalosporin of 2–3 generations
Resistant Gr (–) flora, resistant Staphylococcus
Parenterally: carbapenems, ureidopenicillins, rifampicin, vancomycin, aztreonam, timetin, aminoglycoside in high doses*
* Gentamicin 15 mg/kg/day, amikacin 30–50 mg/kg/day
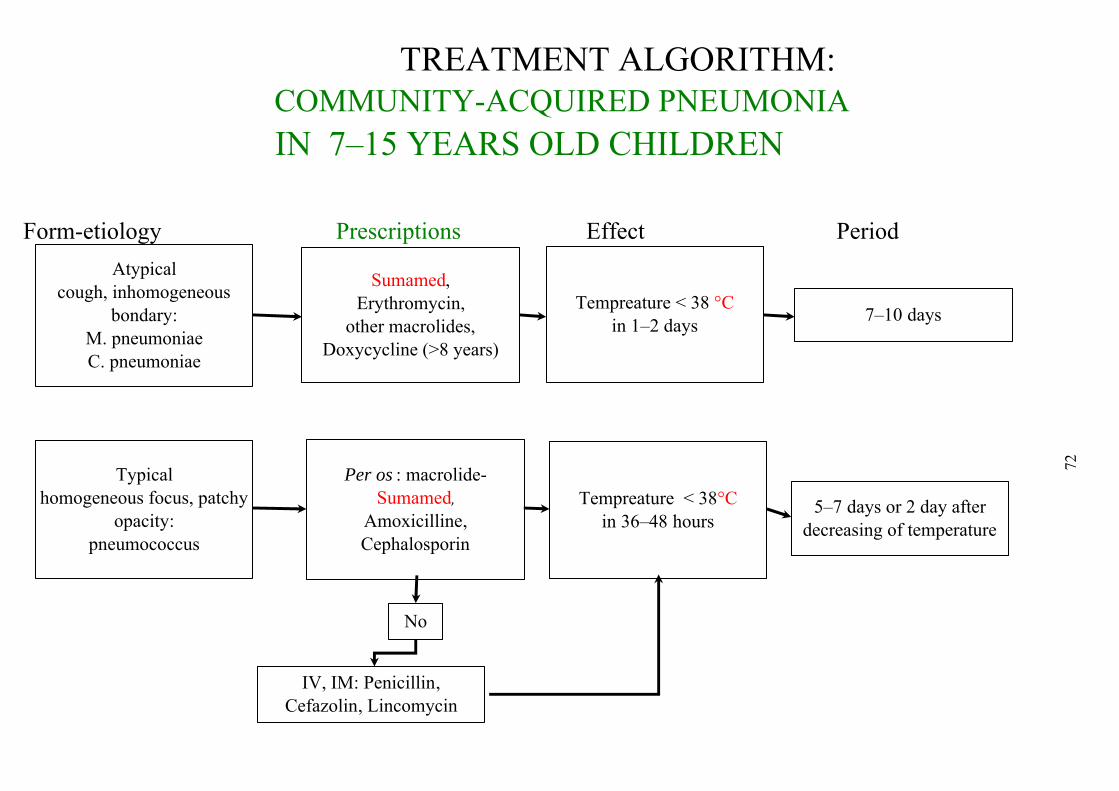
TREATMENT ALGORITHM: COMMUNITY-ACQUIRED PNEUMONIA IN 7–15 YEARS OLD CHILDREN
Form-etiology Prescriptions Effect Period
72
Atypicalcough, inhomogeneous
bondary:M. pneumoniaeC. pneumoniae
Typicalhomogeneous focus, patchy
opacity:pneumococcus
Sumamed,Erythromycin,
other macrolides,Doxycycline (>8 years)
Per os : macrolide- Sumamed,
Amoxicilline,Cephalosporin
Тempreature < 38 °Cin 1–2 days
7–10 days
Тempreature < 38°C in 36–48 hours
5–7 days or 2 day after decreasing of temperature
No
IV, IM: Penicillin, Cefazolin, Lincomycin
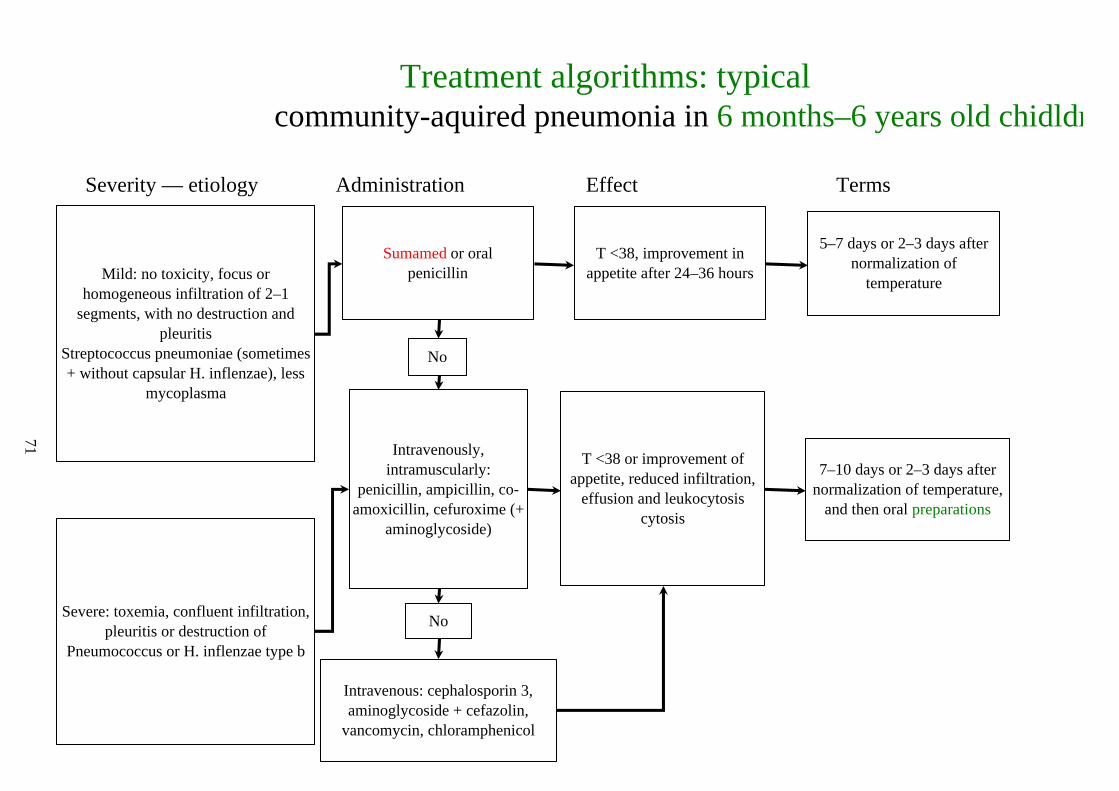
Treatment algorithms: typicalcommunity-aquired pneumonia in 6 months–6 years old chidldr
Severity — etiology Administration Effect Terms
71
Mild: no toxicity, focus or homogeneous infiltration of 2–1
segments, with no destruction and pleuritis
Streptococcus pneumoniae (sometimes + without capsular H. inflenzae), less
mycoplasma
Severe: toxemia, confluent infiltration, pleuritis or destruction of
Pneumococcus or H. inflenzae type b
Sumamed or oralpenicillin
No
Intravenously, intramuscularly:
penicillin, ampicillin, co-amoxicillin, cefuroxime (+
aminoglycoside)
No
Intravenous: cephalosporin 3, aminoglycoside + cefazolin,
vancomycin, chloramphenicol
T <38, improvement in appetite after 24–36 hours
T <38 or improvement of appetite, reduced infiltration,
effusion and leukocytosis cytosis
5–7 days or 2–3 days after normalization of
temperature
7–10 days or 2–3 days after normalization of temperature,
and then oral preparations
ren

Tretment algorithms : typicalcommunity-aquired pneumonia in 1–6 months old children
Severity, etiology Administration Effect Terms
70
Atypicaldyspnea, T <38, cough, diffuse changes
Often — C. trachomatis Rarely — Pneumocystis carinii
TypicalT <38, dyspnea> 50 per minute, toxicosis, infiltrate in the X-Ray pattern: E. Coli , other intestinal
bacteria, Staphylococcus
Sumamed
No
Per os: co-amoxicillin, Intravenous:
ampicillin + oxacillin, cefuroxime, ceftriaxone,
cefataksim
No
Cefazolin + aminoglycoside, carbapenems, vancomycin
Reduction of dyspnea after 2–3 days
T <38 after 36–48 hours, reduction the of toxicosis
3 days ofSumamed
5–7 days or 2–3 days after normalization of temperature
Co-trimoxazole Reduction of dyspnea Individually
The criteria are the same7–10 days or 3–4 days after
normalization of temperature
Related Documents