Eur Radiol (2008) 18: 2956–2966 DOI 10.1007/s00330-008-1077-8 NEURO Martin Wiesmann Veronika Schöpf Olav Jansen Hartmut Brückmann Received: 18 October 2007 Revised: 27 April 2008 Accepted: 26 May 2008 Published online: 25 July 2008 # European Society of Radiology 2008 Stent-protected angioplasty versus carotid endarterectomy in patients with carotid artery stenosis: meta-analysis of randomized trial data Abstract Stent-protected angioplasty of carotid artery stenosis may be an alternative to surgical endarterectomy. Results published so far are indeci- sive, with evidence both in favour of and against this procedure. After the recent publication of two large Eu- ropean multicentre trials (SPACE and EVA-3S) almost 3,000 patients have been included in randomized studies. For this report, we therefore con- ducted a systematic review of randomized studies that compared endovascular treatment with surgery for carotid stenosis. We evaluated seven trials including 2,973 patients. In our meta-analysis endovascular treatment seemed to carry a slightly higher risk for stroke or death within 30 days after the procedure as com- pared with surgery (8.2% vs. 6.2%; p =0.04; OR 1.35), whereas the rates of disabling stroke or death within 30 days did not differ significantly (p =0.47; n.s.). On the other hand, surgery carried a significantly higher risk for cranial nerve palsy (4.7% vs. 0.2%; p <0.0001; OR 0.17) and myo- cardial infarction (2.3% vs. 0.9%; p =0.03; OR 0.37). Long-term effects of both methods still need to be evaluated. Two other large multicentre trials (ICSS and CREST) are ongoing. Results of these studies will increase the database to about 7,000 random- ized patients. Future meta-analyses should then allow definitive treatment recommendations. Keywords Angioplasty . Carotid stenosis . Endarterectomy . Carotid stenting . Stroke prevention Introduction Substantial stenosis of the carotid artery constitutes a major risk factor for ischaemic stroke, especially in patients with recent transient ischaemic attacks or strokes (symptomatic stenosis). There is convincing evidence from large randomized trials that carotid endarterectomy significantly reduces the long-term risk of subsequent stroke from severe carotid artery stenosis [2–5]. However, surgery does have the disadvantage of requiring an incision in the neck and, in some centres, is performed under general anaesthesia. Angioplasty and, more recently, carotid artery stenting have been suggested as an alternative to carotid endarte- rectomy. The possible advantages of endovascular treat- ment include avoidance of general anaesthesia and its complications such as myocardial infarction and pulmo- nary embolism. Endovascular treatment is usually per- formed via a femoral catheter, thus avoiding an incision in The publication of first results from the SPACE study [1] has fuelled a controversial debate as to whether endovascular treatment of severe carotid artery stenosis constitutes an alternative to surgical endarterectomy— the gold-standard method so far. This article first reviews all randomized trials comparing endovascular treatment of carotid artery stenosis with surgery. In a meta-analysis the safety and efficacy of both methods are compared. Some questions arising from SPACE are then discussed separately. M. Wiesmann . V. Schöpf . H. Brückmann Department of Neuroradiology, University of Munich, Munich, Germany O. Jansen Department of Neuroradiology, UKSH Campus Kiel, Kiel, Germany M. Wiesmann (*) Abteilung für Neuroradiologie, Klinikum der Universität München – Großhadern, Marchioninistr. 15, 81377 München, Germany e-mail: [email protected] muenchen.de Tel.: +49-89-70952501 Fax: +49-89-70952509

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Eur Radiol (2008) 18: 2956–2966DOI 10.1007/s00330-008-1077-8 NEURO
Martin WiesmannVeronika SchöpfOlav JansenHartmut Brückmann
Received: 18 October 2007Revised: 27 April 2008Accepted: 26 May 2008Published online: 25 July 2008# European Society of Radiology 2008
Stent-protected angioplasty versuscarotid endarterectomy in patientswith carotid artery stenosis: meta-analysisof randomized trial data
Abstract Stent-protected angioplastyof carotid artery stenosis may be analternative to surgical endarterectomy.Results published so far are indeci-sive, with evidence both in favour ofand against this procedure. After therecent publication of two large Eu-ropean multicentre trials (SPACE andEVA-3S) almost 3,000 patients havebeen included in randomized studies.For this report, we therefore con-ducted a systematic review ofrandomized studies that comparedendovascular treatment with surgeryfor carotid stenosis. We evaluatedseven trials including 2,973 patients.In our meta-analysis endovascular
treatment seemed to carry a slightlyhigher risk for stroke or death within30 days after the procedure as com-pared with surgery (8.2% vs. 6.2%;p=0.04; OR 1.35), whereas the ratesof disabling stroke or death within30 days did not differ significantly(p=0.47; n.s.). On the other hand,surgery carried a significantly higherrisk for cranial nerve palsy (4.7% vs.0.2%; p<0.0001; OR 0.17) and myo-cardial infarction (2.3% vs. 0.9%;p=0.03; OR 0.37). Long-term effectsof both methods still need to beevaluated. Two other large multicentretrials (ICSS and CREST) are ongoing.Results of these studies will increasethe database to about 7,000 random-ized patients. Future meta-analysesshould then allow definitive treatmentrecommendations.
Keywords Angioplasty . Carotidstenosis . Endarterectomy . Carotidstenting . Stroke prevention
Introduction
Substantial stenosis of the carotid artery constitutes a majorrisk factor for ischaemic stroke, especially in patients withrecent transient ischaemic attacks or strokes (symptomaticstenosis). There is convincing evidence from largerandomized trials that carotid endarterectomy significantlyreduces the long-term risk of subsequent stroke from severecarotid artery stenosis [2–5]. However, surgery does have
the disadvantage of requiring an incision in the neck and, insome centres, is performed under general anaesthesia.
Angioplasty and, more recently, carotid artery stentinghave been suggested as an alternative to carotid endarte-rectomy. The possible advantages of endovascular treat-ment include avoidance of general anaesthesia and itscomplications such as myocardial infarction and pulmo-nary embolism. Endovascular treatment is usually per-formed via a femoral catheter, thus avoiding an incision in
The publication of first results from theSPACE study [1] has fuelled a controversialdebate as to whether endovascular treatmentof severe carotid artery stenosis constitutesan alternative to surgical endarterectomy—the gold-standard method so far. This articlefirst reviews all randomized trials comparingendovascular treatment of carotid arterystenosis with surgery. In a meta-analysis thesafety and efficacy of both methods arecompared. Some questions arising fromSPACE are then discussed separately.
M. Wiesmann . V. Schöpf .H. BrückmannDepartment of Neuroradiology,University of Munich,Munich, Germany
O. JansenDepartment of Neuroradiology,UKSH Campus Kiel,Kiel, Germany
M. Wiesmann (*)Abteilung für Neuroradiologie,Klinikum der Universität München –Großhadern,Marchioninistr. 15,81377 München, Germanye-mail: [email protected].: +49-89-70952501Fax: +49-89-70952509

the neck and subsequent cranial and cutaneous nervedamage. Hospital admission and recovery time afterendovascular treatment may be less than with surgery,therefore reducing costs. Moreover, endovascular treat-ment may be the only treatment option for patients at high-risk after surgery because of comorbidity such as ischemicheart disease or for those with surgically inaccessiblelesions.
However, stenting also carries a risk of stroke and localcomplications. As a consequence, before endovascular treat-ment can be considered as a genuine alternative to surgery, itmust be shown to be as safe and effective as surgery.
Evidence from a large number of case series hasaccumulated to suggest that this may be the case. In asystemic review published in 2005, Coward et al. hadidentified reports of more than 5,000 carotid angioplastyand stenting procedures [6–19]. The 30-day risk of strokeor death from these reports ranged from 2 to 9%, with anaverage rate of 4.7%. Thus, the complication rate forendovascular treatment from case series data were lowerthan the 30-day complication rate for surgery reported inECST (stroke rate 7.5%) [2], similar to that in NASCET(stroke rate 5.5%) [3], but greater than in the asymptomaticcarotid atherosclerosis study (stroke or death rate 2.3%)[4], or the asymptomatic carotid surgery trial (stroke ordeath rate 3.1%) [5]. In a meta-analysis published recently,Kern et al. estimated that around 50,000 patients hadalready entered mixed trial and registry data collectionsfollowing carotid artery stenting in either symptomatic orasymptomatic carotid disease [20].
However, it is mandatory that these nonrandomizedresults be confirmed in large randomized multicentre trials.This article reviews all randomized trials comparingendovascular treatment of the carotid artery with surgery.In a meta-analysis, statistical data on the 30-day risk ofstroke or death following treatment are compared. Otherrisks compared include disabling stroke, cranial nervepalsy and myocardial infarction.
Materials and methods
To identify all relevant studies and randomized trials weperformed a literature search in the following bibliographicdatabases: PubMed, EMBASE, and the Science CitationIndex. Search terms included “angioplasty”, “carotid”,“endarterectomy”, “endovascular”, “randomized”, “steno-sis” and “stenting”, in various combinations. The searchwas limited to articles published before 1 January 2008.Abstracts of retrieved citations were reviewed. Full articleswere obtained where appropriate. References of thesearticles were checked for additional material. We alsocontacted researchers in the field and balloon catheter andstent manufacturers.
We selected randomized trials of carotid endovasculartreatment compared with carotid endarterectomy in pa-
tients of any age or sex. We report trials in patients withsymptomatic as well as asymptomatic carotid arterystenosis. All trials with a minimum sample size of n=25per treatment arm were included.
Extracted outcome measures included, if available, anystroke (disabling or nondisabling) or death within 30 daysof procedure, disabling stroke or death within 30 days ofprocedure, any stroke or death within 1 year of procedure,cranial neuropathy within 30 days of procedure andmyocardial infarction within 30 days of procedure. Strokeswere classified if possible as fatal, disabling (requiring helpwith activities of daily living for >1 month after onset) ornondisabling (symptoms lasted >7 days but patient wasindependent at 30 days).
Results were reported as percentages as well as oddsratios (ORs) (i.e. the odds of an unfavourable outcomeamong patients treated by endovascular interventioncompared with the corresponding odds among patientstreated surgically). ORs were calculated using the Petofixed-effect method. Heterogeneity between trial resultswas tested for using a standard χ2 test.
Results
Between 1998 and 2004, six randomized studies comparingendovascular treatment of the carotid artery with surgerywere published (CAVATAS, Kentucky A, Kentucky B,Leicester, WALLSTENT and SAPPHIRE) [21–26]. Char-acteristics of these studies are given in Table 1, and rates ofoutcome events are listed in Table 2.
CAVATAS
The carotid and vertebral artery transluminal angioplastystudy (CAVATAS) is an international multicentre trial inwhich long-term follow-up (>5 years) is ongoing. Bothpatients with symptomatic or asymptomatic carotidstenosis could be randomized if they were equallysuitable for endovascular treatment or surgery. Ninetyper cent of patients had symptoms within 6 months beforerandomization [21].
Kentucky A/B
The Kentucky study was a single-centre randomized trialcomparing endovascular treatment (carotid angioplasty andstenting) with carotid endarterectomy. The trial compriseda symptomatic arm (Kentucky A) in which 104 patientswere included who had an ipsilateral internal carotid arterystenosis of >70% and had experienced symptoms and/orsigns of cerebral ischaemia confined to the ipsilateralcarotid artery within 3 months before randomization. Thetrial also comprised an asymptomatic arm (Kentucky B) in
2957
which 85 patients with no symptoms of cerebrovascularischemia and with internal carotid artery stenosis of >80%were randomized. In the symptomatic arm of this study,one patient died as a consequence of myocardial infarctionimmediately after carotid endarterectomy. There were noother deaths or strokes in symptomatic or asymptomaticpatients treated with stenting or surgery [22, 23].
Leicester
The Leicester study was also a single-centre trial. Onlysymptomatic patients with severe internal carotid arterystenosis (>70%) were included. The trial was stopped after
23 patients had been randomized to treatment. Only 17 ofthe randomized patients had received their allocatedtreatment at the time the trial was suspended. Ten carotidendarterectomies proceeded without complication, but 5/7patients who underwent stenting had a stroke. Allendovascular procedures were performed by the sameradiologist who, before the start of the trial, had performedeight carotid artery procedures only [24]. The Leicesterstudy has been criticized for its obviously irregular results,which were most probably due to a lack of experience ofthe involved radiologist. As a consequence, in later trialsendovascular radiologists and surgeons had to qualify interms of a minimal number of documented procedures [1,27]. Characteristics and results of the Leicester trial are
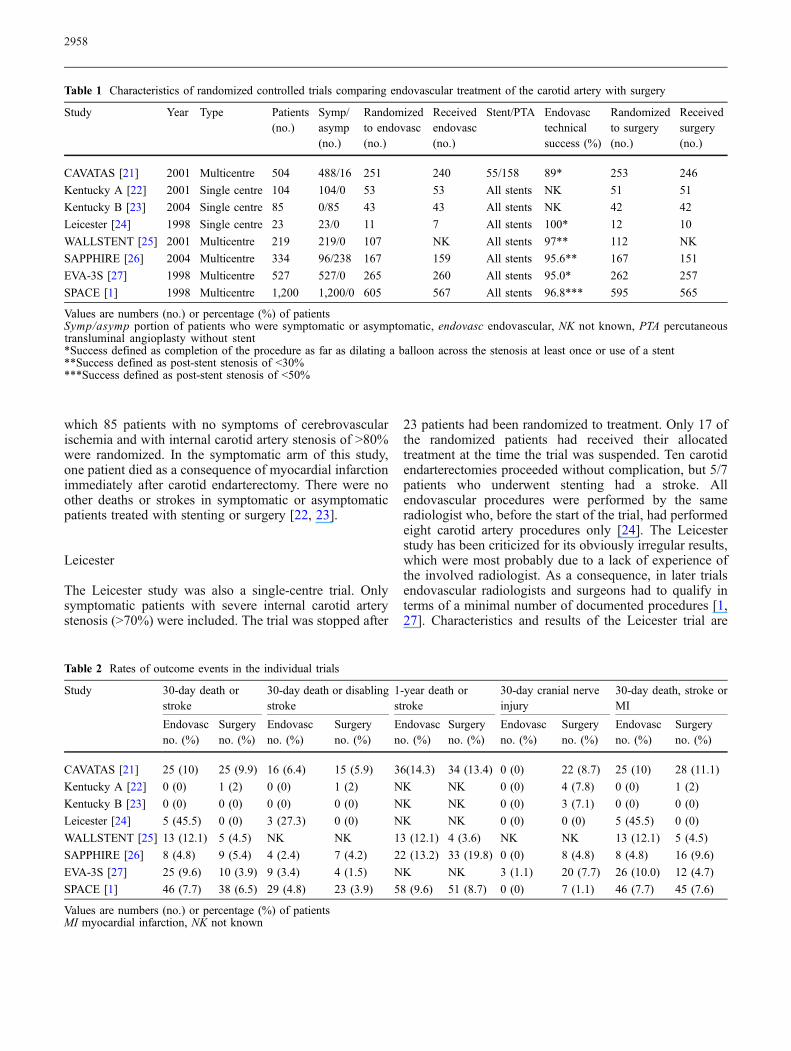
Table 1 Characteristics of randomized controlled trials comparing endovascular treatment of the carotid artery with surgery
Study Year Type Patients(no.)
Symp/asymp(no.)
Randomizedto endovasc(no.)
Receivedendovasc(no.)
Stent/PTA Endovasctechnicalsuccess (%)
Randomizedto surgery(no.)
Receivedsurgery(no.)
CAVATAS [21] 2001 Multicentre 504 488/16 251 240 55/158 89* 253 246
Kentucky A [22] 2001 Single centre 104 104/0 53 53 All stents NK 51 51
Kentucky B [23] 2004 Single centre 85 0/85 43 43 All stents NK 42 42
Leicester [24] 1998 Single centre 23 23/0 11 7 All stents 100* 12 10
WALLSTENT [25] 2001 Multicentre 219 219/0 107 NK All stents 97** 112 NK
SAPPHIRE [26] 2004 Multicentre 334 96/238 167 159 All stents 95.6** 167 151
EVA-3S [27] 1998 Multicentre 527 527/0 265 260 All stents 95.0* 262 257
SPACE [1] 1998 Multicentre 1,200 1,200/0 605 567 All stents 96.8*** 595 565
Values are numbers (no.) or percentage (%) of patientsSymp/asymp portion of patients who were symptomatic or asymptomatic, endovasc endovascular, NK not known, PTA percutaneoustransluminal angioplasty without stent*Success defined as completion of the procedure as far as dilating a balloon across the stenosis at least once or use of a stent**Success defined as post-stent stenosis of <30%***Success defined as post-stent stenosis of <50%
Table 2 Rates of outcome events in the individual trials
Study 30-day death orstroke
30-day death or disablingstroke
1-year death orstroke
30-day cranial nerveinjury
30-day death, stroke orMI
Endovascno. (%)
Surgeryno. (%)
Endovascno. (%)
Surgeryno. (%)
Endovascno. (%)
Surgeryno. (%)
Endovascno. (%)
Surgeryno. (%)
Endovascno. (%)
Surgeryno. (%)
CAVATAS [21] 25 (10) 25 (9.9) 16 (6.4) 15 (5.9) 36(14.3) 34 (13.4) 0 (0) 22 (8.7) 25 (10) 28 (11.1)
Kentucky A [22] 0 (0) 1 (2) 0 (0) 1 (2) NK NK 0 (0) 4 (7.8) 0 (0) 1 (2)
Kentucky B [23] 0 (0) 0 (0) 0 (0) 0 (0) NK NK 0 (0) 3 (7.1) 0 (0) 0 (0)
Leicester [24] 5 (45.5) 0 (0) 3 (27.3) 0 (0) NK NK 0 (0) 0 (0) 5 (45.5) 0 (0)
WALLSTENT [25] 13 (12.1) 5 (4.5) NK NK 13 (12.1) 4 (3.6) NK NK 13 (12.1) 5 (4.5)
SAPPHIRE [26] 8 (4.8) 9 (5.4) 4 (2.4) 7 (4.2) 22 (13.2) 33 (19.8) 0 (0) 8 (4.8) 8 (4.8) 16 (9.6)
EVA-3S [27] 25 (9.6) 10 (3.9) 9 (3.4) 4 (1.5) NK NK 3 (1.1) 20 (7.7) 26 (10.0) 12 (4.7)
SPACE [1] 46 (7.7) 38 (6.5) 29 (4.8) 23 (3.9) 58 (9.6) 51 (8.7) 0 (0) 7 (1.1) 46 (7.7) 45 (7.6)
Values are numbers (no.) or percentage (%) of patientsMI myocardial infarction, NK not known
2958

presented in Tables 1 and 2. However, results of the studywere excluded from the meta-analysis because the samplesize did not meet minimum requirements.
WALLSTENT
The WALLSTENT study was a multicentre trial includingpatients with symptomatic internal carotid artery stenosis of>60% stenosis [25]. In an abstract, the authors reported thatthe 30-day complication rate (any stroke or death) wassignificantly higher in the endovascular group than in thosewho underwent carotid endarterectomy (12.1% versus 4.5%;p=0.049). However, further results from this trial have notbeen published.
SAPPHIRE
The SAPPHIRE study was a multicentre randomized trialwhich compared stenting with cerebral protection to endar-terectomy in patients at high surgical risk. Patients either had>50% symptomatic stenosis or >80% asymptomatic steno-sis, plus one or more comorbidity conditions (e.g. congestiveheart failure, left ventricular dysfunction, recent myocardialinfarction or severe pulmonary disease). Most patients in thisstudy (71%) were asymptomatic. The primary endpoint ofthe trial (death, stroke or myocardial infarction within30 days of the procedure or death or ipsilateral strokebetween 31 days and 1 year) occurred in 12.2% patientsrandomized to stenting and in 20.1% patients randomized tosurgery (p=0.05, log-rank test for superiority). The trial wasterminated early because recruitment slowed after nonran-domized stent registries were established [26].
In addition to these early studies, two randomized trialshave been published recently and been intensely debated:EVA-3S (endarterectomy versus stenting in patients withsymptomatic severe carotid stenosis) [27] and SPACE(stent-protected angioplasty versus carotid endarterectomyin symptomatic patients) [1].
EVA-3S
The French randomized multicentre EVA-3S study was anoninferiority trial to assess whether endovascular treat-ment is equivalent to surgery in patients with severesymptomatic carotid artery [27]. After randomization of527 patients, the trial was stopped for reasons of both safetyand futility. After 30 days, the EVA-3S trial showed asignificantly higher periprocedural risk in the endovasculargroup, with a rate of stroke or death of 9.6%, comparedwith 3.9% in the surgery arm (relative risk 2.5, 95% CI1.2–5.1). The rates of the endpoint “any disabling stroke ordeath” were 1.5% in the endarterectomy group and 3.4% inthe stenting group. Cranial nerve injury was significantly
less common after endovascular treatment than aftersurgery, and the median duration of the hospital stay was1 day shorter in patients who underwent stenting.
This study differs from the literature in that thecomplication rates in the surgical treatment arm areunusually low, whereas the complication rates in theendovascular treatment arm are unusually high. The lowsurgical complication rates may simply be random or dueto a high level of expertise of the surgeons selected.
Reasons for the high complication rate in the endovas-cular treatment group are unclear. However, the EVA-3Strial has received criticism for two major reasons [28].Firstly, the protocol for endovascular treatment waschanged in the ongoing study. Initially, endovasculartreatment consisted of stenting with or without the use ofcerebral protection devices. After inclusion of 73 patientsin the endovascular treatment arm, the Safety Committeerecommended that the investigators stopped using un-protected stenting because the 30-day rate of stroke was 3.9times higher than that observed after stenting with cerebralprotection, although the number of cases was too small toshow significant differences. Nevertheless, as of February2003 the use of a protection device was required in theendovascular treatment arm. This decision was not onlyreached without statistical evidence, but it also meant thatinterventionalists who participated in the study and hadlittle or no experience with protection devices wererequired to use them in the ongoing trial. The secondpoint of criticism was that the level of experience differedbetween interventionalists and surgeons. Vascular surgeonswere required to have performed at least 25 CEAprocedures in the year before enrollment. Interventional-ists, however, were able to enter the study after 12 carotidprocedures or after 35 stenting procedures in the supra-aortic trunks, of which only five should have beenperformed in the carotid artery. Moreover, the EVA-3Strial allowed centres without an experienced intervention-alist to participate in the trial if all stenting procedures wereperformed under the supervision of an experienced tutoruntil the local interventional physician fulfilled thepredefined criteria.
SPACE
The SPACE trial was a multinational (Austria, Germanyand Switzerland), multicentre randomized trial that wasdesigned to test the hypothesis that CAS is not inferior toCEA in the treatment of severe symptomatic carotidstenosis [1]. It was the largest trial which has beenpublished so far and randomized 1,200 symptomaticpatients with a severe carotid artery stenosis. The use ofprotection devices was not mandatory. Of the 599 patientsin the endovascular group, 26.6% were treated using aprotection device. The 30-day results showed similar ratesof the primary endpoint “ipsilateral ischemic stroke or
2959

death” for stenting and surgery (6.84% vs. 6.34%), for “anystroke or death” (7.7% vs. 6.5%), as well as for the rate of“disabling ipsilateral stroke (modified Rankin score ≥3) ordeath” (4% vs. 2.9%). At 1 year after the procedure therates for “any stroke or death” were also similar (9.6% vs.8.7%). Thus, the SPACE trial did not find significantdifferences in favour of either of the two treatmentmodalities. The design of this noninferiority analysis wasbased on the assumption of a frequency of 5% to reach theprimary endpoint in each treatment arm. Unfortunately, thefrequency observed was higher in both arms. Thereforethe study was underpowered to establish noninferiority ofstenting versus surgery. Given the observed rates of eventsin the trial, the probability that it would achieve itsobjectives (demonstrating a statistically significant non-inferiority of stenting) was low, and it was estimated thatfor this purpose another 1,200–1,800 patients needed to berecruited. The trial was, therefore, stopped prematurely.
In 2006, two more studies were published. TheBACASS study was a Swiss prospective, randomizedsingle-centre trial including 20 symptomatic patients with astenosis > 70% of which ten patients were randomized tosurgery, and ten patients were randomized to endovasculartreatment [29]. One of the surgical patients suffered from amajor ipsilateral stroke (10%), whereas there were nocomplications in the endovascular patients.
The TESCAS-C trial was a Chinese multicentre,randomized study including 166 patients [30]. The primaryendpoint of cumulative incidence of death, stroke ormyocardial infarction within 30 days occurred in 9.8% ofpatients randomized to endovascular treatment, and in11.9% of patients randomized to surgery. Only an abstractof the study has been published in English, and details ofmethods and results are not available.
Meta-analysis of randomized studies
In 2005 Coward et al. performed a meta-analysis of sixstudies comparing endovascular treatment to surgeryinvolving 1,269 patients [31]. Analysis of 30-day safetydata found no significant difference in the odds oftreatment-related death or any stroke (odds ratio [OR],endovascular surgery, 1.33; 95% confidence interval [CI],0.86–2.04), death or disabling stroke (OR, 1.22; CI, 0.61–2.41), or death, any stroke or myocardial infarction (OR,1.04; CI, 0.69–1.57). At 1 year after randomization, therewas no significant difference between the two treatments inthe rate of any stroke or death (OR, 1.01; CI, 0.71–1.44).Endovascular treatment significantly reduced the risk ofcranial nerve injury (OR, 0.13; CI, 0.06–0.25). The authorsconcluded that although no significant difference in themajor risks of treatment was found, confidence intervalswere too wide to safely exclude a difference in favour ofone treatment. They also concluded that minor complica-tion rates favoured endovascular treatment.
In 2007 this study was updated [32] including the 30-dayresults from the EVA-3S and SPACE trials. The authorsnow concluded that the primary outcome comparison ofany stroke or death within 30 days of treatment favouredsurgery (OR, 1.39; p=0.02). On the contrary, the followingoutcome comparisons favoured endovascular treatmentover surgery: cranial neuropathy (OR, 0.07; p<0.01);30-day neurological complication or death (OR, 0.62; p=0.004). The following outcome comparisons showed littledifference between endovascular treatment and surgery:30-day stroke, myocardial infarction or death (OR, 1.11,p=0.57); stroke during long-term follow-up (OR, 1.00).
For our meta-analysis, we revisited all data, and addedthe results from the EVA-3S and SPACE trials includingthe 1-year results. Our analysis now includes randomizedstudies published between 1998 and 2007 comparingendovascular treatment and surgery of severe carotid arterystenosis. Results are presented in Figs. 1, 2, 3, 4 and 5. Thedatabase of these studies includes 2,973 patients.
Results of this meta-analysis can be summarized asfollows:
1. Endovascular treatment seems to carry a slightlyhigher risk for stroke or death within 30 days afterthe procedure as compared with surgery (8.2% vs.6.2%; p=0.04; OR 1.35). Our results indicate amoderate degree of heterogeneity between trials(Cochran Q=8.01) although this finding was notsignificant (p=0.16).
2. The rates of disabling stroke or death within 30 days donot differ significantly between endovascular treatmentand surgery (p=0.28, n.s.).
3. Surgery carries a significantly higher risk for cranialnerve palsy (4.7% vs. 0.2%; p=0.0001; OR 0.17) andmyocardial infarction (2.3%vs. 0.9%; p=0.03; OR0.37).
Discussion
This updated meta-analysis revealed significant differencesbetween endovascular and surgical treatment of severecarotid artery stenosis. Endovascular treatment carried ahigher risk for stroke or death within 30 days after theprocedure, whereas surgery carried a higher risk for cranialnerve palsy and myocardial infarction. There was nosignificant difference between both methods regarding therisk of disabling stroke or death.
Our study differs somewhat from the meta-analysispublished recently by Kern et al. [20]. Kern et al. includedthe Leicester study, which we excluded due to its irregularresults and small sample size. On the contrary, Kern et al.did not consider the results from the Kentucky B study,which were included in our analysis. The authors came tocomparable results regarding the rates of stroke or death,but did not analyse the frequency of cranial nerve palsy ormyocardial infarction.
2960
We found a moderate degree of heterogeneity betweentrials regarding the rates of stroke or death. Although notsignificant, this finding is substantiated by the study ofKern et al. in which heterogeneity between trials wasstatistically significant.
Several factors contribute to this heterogeneity:
1. Some trials include asymptomatic patients. In general,lower complication rates are found when asymptom-atic patients are treated.
2. Endovascular strategies have evolved during the timeperiod under consideration. The CAVATAS studyincluded a subgroup of patients treated by balloonangioplasty, whereas in all other studies stenting was
performed. In addition, balloon predilatation prior tostenting was used more commonly in the earlier studiesthan it is today.
3. Over recent years a number of different devices havebeen introduced that were designed to protect againstcerebral embolism during stent deployment. Theseembolic protection devices (EPD) are being increas-ingly used. Both case series from individual centresand registry data suggest that EPDs are effective. In areview of nonrandomized single-centre reports Kastrupet al. reported that the use of an EPD seems to diminishthe risk of thromboembolic complications duringendovascular treatment [33]. Recently it was alsoreported that the use of an EPD during carotid artery
CAS CEA Weights(%)
25/251 25/253 23,66
0/53 1/51 1,03
0/43 0/42 .
13/107 5/112 8,67
8/167 9/167 8,48
25/265 10/262 17,17
46/599 38/584 40,99
118/1443 89/1430 100,00
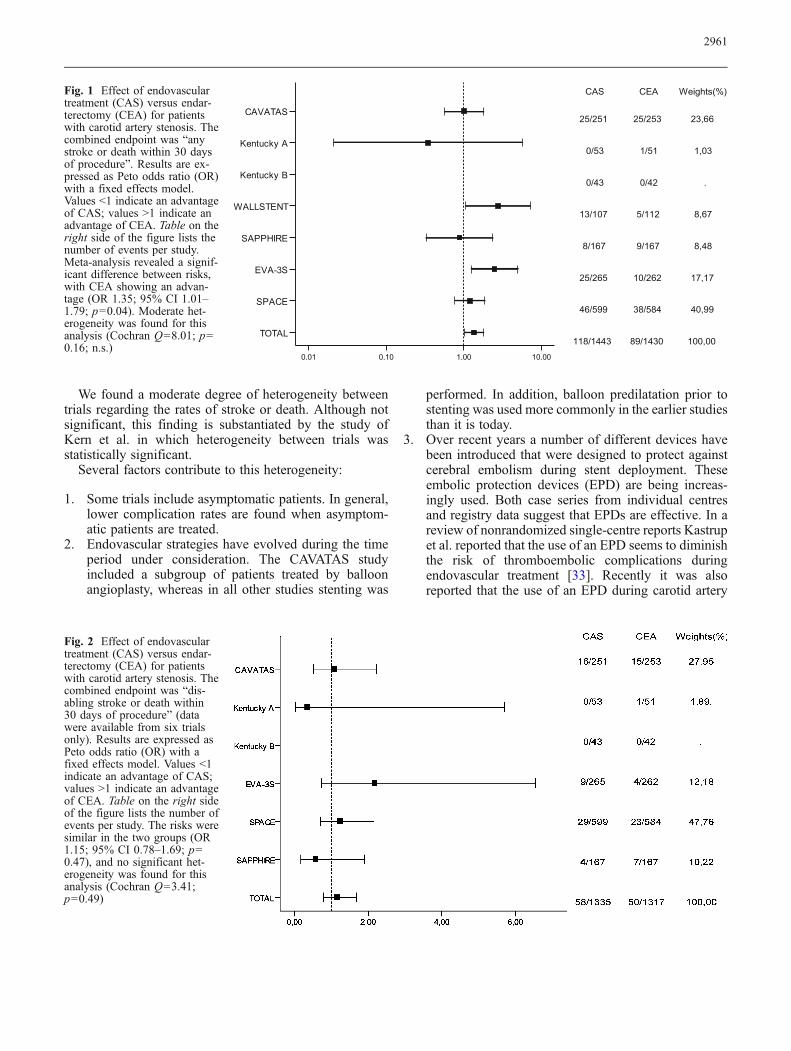
Fig. 1 Effect of endovasculartreatment (CAS) versus endar-terectomy (CEA) for patientswith carotid artery stenosis. Thecombined endpoint was “anystroke or death within 30 daysof procedure”. Results are ex-pressed as Peto odds ratio (OR)with a fixed effects model.Values <1 indicate an advantageof CAS; values >1 indicate anadvantage of CEA. Table on theright side of the figure lists thenumber of events per study.Meta-analysis revealed a signif-icant difference between risks,with CEA showing an advan-tage (OR 1.35; 95% CI 1.01–1.79; p=0.04). Moderate het-erogeneity was found for thisanalysis (Cochran Q=8.01; p=0.16; n.s.)
Fig. 2 Effect of endovasculartreatment (CAS) versus endar-terectomy (CEA) for patientswith carotid artery stenosis. Thecombined endpoint was “dis-abling stroke or death within30 days of procedure” (datawere available from six trialsonly). Results are expressed asPeto odds ratio (OR) with afixed effects model. Values <1indicate an advantage of CAS;values >1 indicate an advantageof CEA. Table on the right sideof the figure lists the number ofevents per study. The risks weresimilar in the two groups (OR1.15; 95% CI 0.78–1.69; p=0.47), and no significant het-erogeneity was found for thisanalysis (Cochran Q=3.41;p=0.49)
2961
stenting reduces the incidence of new, mostly asymp-tomatic, lesions on diffusion-weighted MRI images[34]. However, there are still no randomized trialscomparing stenting with and without use of an EPD,and so the findings remain controversial. Quite on thecontrary, EPDs may themselves cause serious compli-cations. They may dislodge emboli to the brain beforethey are in place, and the device itself may injure thevessel wall. To be able to safely use an EPD definitelyrequires some training. This may have contributed tothe results of the EVA-3S study in which all
endovascular radiologists were asked to convert toEPD-protected stenting during the ongoing trial. Inaddition, the design of an EPD seems to influence bothits efficacy to prevent cerebral emboli and its owncomplication rate [35]. Some of the first EPD designshave now disappeared from the market due to lowefficacy and poor handling but were used in the studiespublished so far. In summary, it is plausible that theprotection devices that are now available are effective,and have lower complication rates than earlier types. Itmay well be that this is not yet reflected in the
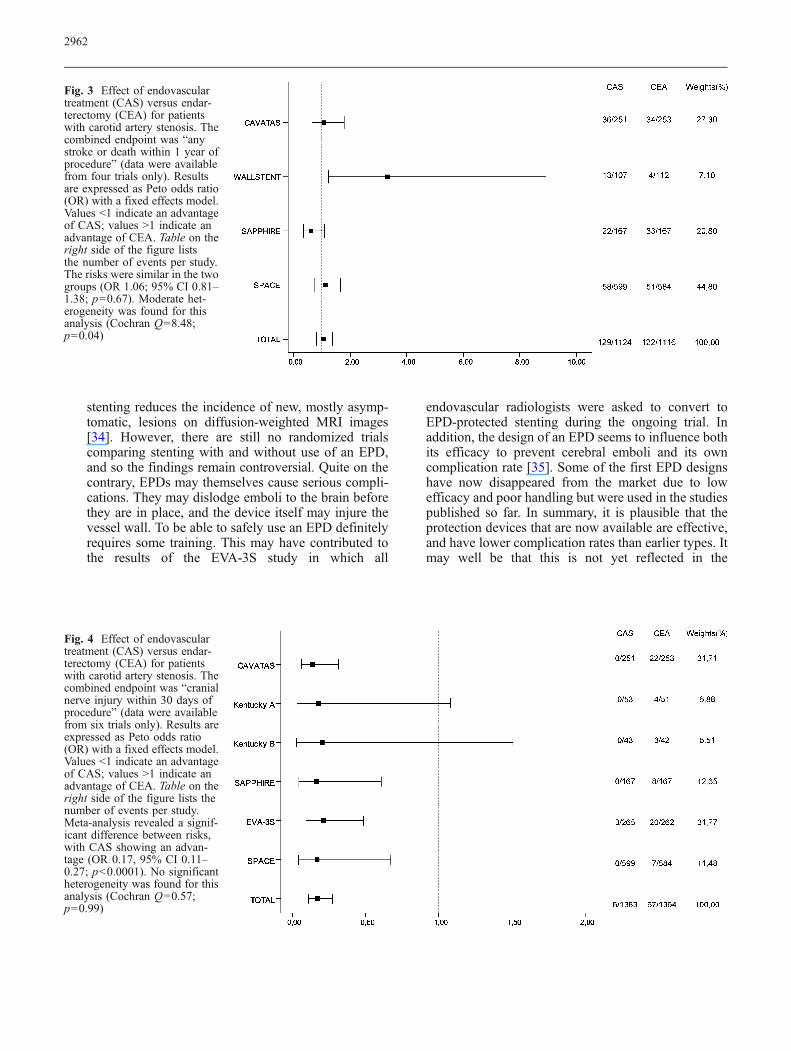
Fig. 3 Effect of endovasculartreatment (CAS) versus endar-terectomy (CEA) for patientswith carotid artery stenosis. Thecombined endpoint was “anystroke or death within 1 year ofprocedure” (data were availablefrom four trials only). Resultsare expressed as Peto odds ratio(OR) with a fixed effects model.Values <1 indicate an advantageof CAS; values >1 indicate anadvantage of CEA. Table on theright side of the figure liststhe number of events per study.The risks were similar in the twogroups (OR 1.06; 95% CI 0.81–1.38; p=0.67). Moderate het-erogeneity was found for thisanalysis (Cochran Q=8.48;p=0.04)
Fig. 4 Effect of endovasculartreatment (CAS) versus endar-terectomy (CEA) for patientswith carotid artery stenosis. Thecombined endpoint was “cranialnerve injury within 30 days ofprocedure” (data were availablefrom six trials only). Results areexpressed as Peto odds ratio(OR) with a fixed effects model.Values <1 indicate an advantageof CAS; values >1 indicate anadvantage of CEA. Table on theright side of the figure lists thenumber of events per study.Meta-analysis revealed a signif-icant difference between risks,with CAS showing an advan-tage (OR 0.17, 95% CI 0.11–0.27; p<0.0001). No significantheterogeneity was found for thisanalysis (Cochran Q=0.57;p=0.99)
2962

published studies. However, none of this can be backedup by randomized data, and the validity of theseconclusions must therefore remain speculative.
4. The stent design itself may have an influence oncomplication rates. It is plausible that closed cell cents,especially if the cell diameter is small, are superior toopen cell stents with regard to scaffolding andsupporting fractured plaque during angioplasty, thuspreventing material from embolizing to the brainduring the procedure. This hypothesis is supportedby preliminary data from a nonrandomized study inwhich 304 symptomatic patients were treated usingeither open cell or closed cell stents [35]. The eventrates (stroke, TIA, death) within 30 days after theprocedure were 2.98% for the patients treated withclosed cell stents versus 11.11% for the patients treatedwith open cell stents (p=0.014). Again, it may well bethat this is not yet reflected in the published studies.But similar to what was said regarding EPDs, as of yetthere is no randomized study comparing open cellversus closed cell stents for the carotid artery.
The results of our study are mostly in line with the meta-analysis published by Ederle et al. [32]. Differences are dueto the fact that we excluded the results from the Leicesterstudy due to its irregular results and small sample size. Wealso did not consider the results of the BACASS studybecause of its small sample size: In this single-centre studyonly ten patients were randomized per treatment arm [29].Furthermore, we did not consider the results from theChinese TESCAS-C study [30]. In this multicentre trial166 patients were randomized but the detailed results areavailable in Chinese only, and the study differs slightly
from the others in its primary and secondary endpoints. Onthe contrary, our paper is the first to include the 1-yearresults of the SPACE study.
In conclusion, according to the available trial datasurgical treatment must still be considered the standardtreatment for severe carotid artery stenosis. There is noevidence that endovascular therapy is safer than surgicalendarterectomy, nor does it provide a better outcome in theshort term (30 days). Long-term data, regarding outcome aswell as restenosis rates, are still pending. While it may bejustified to expect endovascular therapy of carotid arterystenosis to improve over time, along with gradualimprovement in endovascular materials, strategies, andanticoagulation management, this is not yet reflected in thepublished data. However, this may change soon. Firstresults from two other large trials (ICSS and CREST) areexpected in 2008. Results of these studies will increase thedatabase to about 7,000 randomized patients. Future meta-analyses should then allow definitive treatment recom-mendations.
Key points: what have we learned from the SPACEstudy?
Does the SPACE study show that surgery is superiorto endovascular treatment?
No Analysis of the results obtained 30 days after theprocedure shows slightly lower rates for ipsilateral intrace-rebral bleeding (endovascular, 0.2%; versus surgery, 0.9%)and death (0.7%vs. 0.9%) following endovascular treatment,but slightly higher rates for ipsilateral ischaemic stroke (6.5%
CAS CEA Weights(%)
0/251 3/253 19,49
0/53 0/51 .
0/43 0/42 .
4/167 10/167 65,87
1/265 2/262 14,65
6/684 16/683 100,00
Fig. 5 Effect of endovasculartreatment (CAS) versus endar-terectomy (CEA) for patientswith carotid artery stenosis. Thecombined endpoint was “myo-cardial infarction within 30 daysof procedure” (data were avail-able from five trials only). Re-sults are expressed as Peto oddsratio (OR) with a fixed effectsmodel. Values >1 indicate anadvantage of CEA. Table on theright side of the figure lists thenumber of events per study.Meta-analysis revealed a signif-icant difference between risks,with CAS showing an advan-tage (OR 0.37, 95% CI 0.16–0.89; p=0.027). No significantheterogeneity was found for thisanalysis (Cochran Q=0.36;p=0.83)
2963

vs. 5.1%) or any stroke (7.5% vs. 6.2%). All thesedifferences, however, were statistically not significant.
Does the SPACE study prove that endovasculartreatment is equivalent to surgery?
No From a statistical point of view, lack of a significantdifference between two methods does not necessarilymean that both methods are equal. Instead, the number ofpatients included may simply have been too small to showsignificant differences. The SPACE study was designed toprove that endovascular treatment is not inferior tosurgery. However, after statistical analysis of 1,200included patients it was estimated that for this purposeanother 1,200–1,800 patients needed to be recruited.Mostly for lack of financing, the study was stoppedprematurely at this point.
Are the results of the SPACE study in-linewith the literature?
Mostly, yes So far, eight randomized studies have beenpublished comparing endovascular treatment and surgery.Taken together, 2,996 patients have been randomized inthese studies. In three studies including CAVATAS (n=504), the two Kentucky trials (n=189) and SPACE (n=1,200), there was no statistical difference between the ratesof primary endpoints. In one study (SAPPHIRE, n=334)the primary endpoint was found more often after surgery.In the remaining three studies including the Leicester trial(n=23), the WALLSTENT trial (n=219) and EVA-3S (n=527) the primary endpoint was reached more often afterendovascular treatment. In the meta-analysis presented inthis paper, endovascular treatment seemed to carry ahigher risk for stroke or death within 30 days after theprocedure as compared with surgery (8.2% vs. 6.2%; p=0.04; OR 1.35). The rates of disabling stroke, however, ordeath within 30 days did not differ significantly betweenendovascular treatment and surgery (p=0.28, n.s.). On theother hand, surgery carried a significantly higher risk forcranial nerve palsy (4.7% vs. 0.2%; p=0.0001; OR 0.17)and myocardial infarction (2.3% vs. 0.9%; p=0.03; OR0.37).
Is there evidence from the SPACE study that certainsubgroups of patients benefit from either endovasculartreatment or surgery?
Maybe Subgroup analyses of the results from the SPACEstudy suggest that patients older than 75 years seem tobenefit from surgery. There was a clear difference betweenthe rates of primary endpoint events (ipsilateral stroke or
death) between endovascular treatment (11.0%) andsurgery (7.5%). In female patients there was also a higherrate of primary endpoint events following endovasculartreatment (7.7%) than after surgery (6.0%). These differ-ences, however, did not reach statistical significance.
On the contrary, there was almost no difference inprimary endpoint rates in patients younger than 75 years(endovascular treatment, 5.92% versus surgery, 5.94%),and in all male patients (6.50% vs. 6.46%).
What may be the reason for the relatively highcomplication rates after both endovascular treatmentand surgery observed in the SPACE study?
Results from the SPACE study show a high heterogeneitybetween complication rates of different centres. To find ahighly experienced interventionalist or surgeon may have ahigher influence on outcome than choosing betweenstenting or surgery.
Do the results of the SPACE study support the useof endovascular protection devices?
No In the SPACE study, protection devices were used inonly 27% of the endovascular procedures. Outcomes didnot differ significantly between those patients treated withand those treated without protection devices.
Findings may change in the future, however. Protectiondevices have been continuously improved over the years.Some devices used in previous studies would now beconsidered to have a low efficiency. Moreover, the use ofprotection devices without proper experience can lead tocomplications by itself. This may have contributed to thehigh overall endovascular complication rate reported in theEVA-3S trial. In a systematic review of single-centrestudies, however, the use of embolic protection devicesseemed to reduce thromboembolic complications [33].
When can we expect more information?
Patients treated in the SPACE and EVA-3S trials arecurrently undergoing follow-up. Two other large trials arestill recruiting patients. The ICSS (international carotidstenting study, also known as CAVATAS 2 in Europe) hasalready included more than 1,000 symptomatic patientswith carotid stenosis of >50% according to NASCETcriteria. Its sample size is estimated at 1,500 patients whowill be monitored for 5 years after randomization. EPD areused during endovascular treatment if the interventionalistthinks it can be safely deployed. CREST (carotid revascu-larization endarterectomy versus stent trial) in NorthAmerica aims to study 2,500 patients, of which more
2964

than 1,500 are currently enrolled. CREST offers inclusionto asymptomatic individuals if they have a carotid stenosisof >70%. Symptomatic patients are included with astenosis of >50%. In the endovascular arm, all patientsare treated with an EPD. The first results of these two trials
are expected in 2008. As soon as data are available meta-analyses can be performed on an overall sample size of upto 7,000 patients including sufficient sample sizes to allowvalid subgroup analysis.
References
1. SPACE Collaborative Group, RinglebPA, Allenberg J, Brückmann H, EcksteinHH, Fraedrich G, Hartmann M,Hennerici M, Jansen O, Klein G, KunzeA, Marx P, Niederkorn K, Schmiedt W,Solymosi L, Stingele R, Zeumer H,Hacke W (2006) 30 day results from theSPACE trial of stent-protected angio-plasty versus carotid endarterectomy insymptomatic patients: a randomised non-inferiority trial. Lancet 368:1239–1247
2. European Carotid Surgery Trialists’ Col-laborativeGroup (1998) Randomised trialof endarterectomy for recently symptom-atic carotid stenosis: final results of theMRC European carotid surgery trial(ECST). Lancet 351:1379–1387
3. North Am Symptomatic Carotid En-darterectomy Trial Collaborative Group(1998) The final results of the NAS-CET trial. N Engl J Med 339:1415–1425
4. Executive Committee for the Asymp-tomatic Carotid Atherosclerosis Study(1995) Endarterectomy for asymptom-atic carotid artery stenosis. JAMA273:1421–1428
5. MRC asymptomatic carotid surgerytrial (ACST) collaborative group(2004) Prevention of disabling and fatalstrokes by successful carotid endarte-rectomy in patients without recentneurological symptoms: randomisedcontrolled trial. Lancet 363:1491–1502
6. Brockenheimer S, Mathias K (1983)Percutaneous transluminal angioplastyin atherosclerotic internal carotid arterystenosis. AJNR Am J Neuroradiol4:791–792
7. Dietrich EB, Ndiaye M, Reid DB(1996) Stenting in the carotid artery.Initial experience in 110 patients. JEndovasc Surg 3:42–62
8. Freitag G, Freitag J, Koch RD, Hein-rich P, Wagemann W, Hennig HP,Deike R (1987) Transluminal angio-plasty for the treatment of carotid arterystenosis. Vasa 16:67–71
9. Gil-Peralta A, Mayol A, Marcos JR,Gonzalez A, Ruano J, Boza F, Duran F(1996) Percutaneous transluminal an-gioplasty of the symptomatic athero-sclerotic carotid arteries: results,complications and follow-up. Stroke27:2271–2273
10. Henry M, Amor M, Masson I, Henry I,Tzvetanov K, Chati Z, Khanna N(1998) Angioplasty and stenting of theextra-cranial carotid arteries. JEndovasc Surg 5:293–304
11. Kachel R, Basche S, Heerklotz I,Grossman K, Endler S (1991) Percuta-neous transluminal angioplasty (PTA)of supraaortic arteries, especially inter-nal carotid artery. Neuroradiology33:191–194
12. Mathur A, Roubin GS, Iyer SS,Piamsonboon C, Liu MW, Gomez CR,Yadav JS, Chastain HD, Fox LM, DeanLS, Vitek JJ (1998) Predictors of strokecomplicating carotid artery stenting.Circulation 97:1239–1245
13. Roubin GS, New G, Iyer SS, Vitek JJ,Al-Mubarak N, Liu MW, Yadav J,Gomez C, Kuntz RE (2001) Immediateand late clinical outcomes of carotidartery stenting in patients with symp-tomatic and asymptomatic carotid ar-tery stenosis: a 5-year prospectiveanalysis. Circulation 103:532–537
14. Theron J, Raymond J, Cascasco A,Courtheoux F (1987) Percutaneous an-gioplasty of atherosclerotic and post-surgical stenosis of carotid arteries.AJNR Am J Neuroradiol 8:495–500
15. Tsai F, Matovich V, Hieshima G (1986)Percutaneous transluminal angioplastyof the carotid artery. AJNR Am JNeuroradiol 7:349–358
16. Waigand J, Gross CM, Uhlich F,Krämer J, Tamaschke C, Vogel P, LuftFC, Dietz R (1998) Elective stenting ofcarotid artery stenosis in patients withsevere coronary artery disease. EurHeart J 19:1365–1370
17. Wholey MH, Wholey MH, Jarmo-lowski CR, Eles G, Levy D, Buecthel J(1997) Endovascular stents for carotidartery occlusive disease. J EndovascSurg 4:326–338
18. Wiggli U, Gratzl O (1983) Translumi-nal angioplasty of stenotic carotidarteries: case reports and protocol.AJNR Am J Neuroradiol 4:793–795
19. Yadav JS, Roubin GS, Iyer S, Vitek J,King P, Jordan WD, Fisher WS (1997)Elective stenting of the extracranialcarotid arteries. Circulation 95:376–381
20. Kern R, Ringleb PA, Hacke W, Mas JL,Hennerici MG (2007) Stenting forcarotid artery stenosis. Nat Clin PractNeurol 3:212–220
21. CAVATAS Investigators (2001) Endo-vascular versus surgical treatment inpatients with carotid stenosis in thecarotid and vertebral artery translumi-nal angioplasty study (CAVATAS): arandomised trial. Lancet 357:1729–1737
22. Brooks WH, McClure RR, Jones MR,Coleman TC, Breathitt L (2001) Ca-rotid angioplasty and stenting versuscarotid endarterectomy: randomizedtrial in a community hospital. J AmColl Cardiol 38:1589–1595
23. Brooks WH, McClure RR, Jones MR,Coleman TL, Breathitt L (2004) Ca-rotid angioplasty and stenting versuscarotid endarterectomy for treatment ofasymptomatic carotid stenosis: a ran-domized trial in a community hospital.Neurosurgery 54:318–325
24. Naylor RA, Bolia A, Abbott RJ, Pye IF,Smith J, Lennard N, Lloyd AJ, LondonNJM, Bell PRF (1998) Randomizedstudy of carotid angioplasty and stent-ing versus carotid endarterectomy: astopped trial. J Vasc Surg 28:326–334
25. Alberts MJ (2001) Results of a multi-center prospective randomized trial ofcarotid artery stenting vs. carotid en-darterectomy. Stroke 32:325
26. Yadav JS, Wholey MH, Kuntz RE,Fayad P, Katzen BT, Mishkel GJ,Bajwa TK, Whitlow P, Strickman NE,Jaff MR, Popma JJ, Snead DB, CutlipDE, Firth BG, Ouriel K (2004) Pro-tected carotid-artery stenting versusendarterectomy in high-risk patients. NEngl J Med 351:1493–1501
27. Mas JL, Chatellier G, Beyssen B,Branchereau A, Moulin T, BecqueminJP, Larrue V, Lièvre M, Leys D,Bonneville JF, Watelet J, Pruvo JP,Albucher JF, Viguier A, Piquet P,Garnier P, Viader F, Touzé E, GiroudM, Hosseini H, Pillet JC, Favrole P,Neau JP, Ducrocq X (2006) Endarte-rectomy versus stenting in patients withsymptomatic severe carotid stenosis. NEngl J Med 355:1660–1671
28. Brown MM, Featherstone RL, CowardLJ (2004) Carotid artery stenting withand without cerebral protection. Stroke35:2434–2435
2965
29. Hoffmann A, Taschner C, Engelter ST,Lyrer P, Rem J, Radue EW, Kirsch EC(2006) Carotid artery stenting versuscarotid endarterectomy. A prospective,randomised trial with long term followup (BACASS). Schweiz Arch NeurolPsychiatr 157:191–192
30. Ling F, Jiao LQ (2006) Preliminaryreport of trial of endarterectomy versusstenting for the treatment of carotidatherosclerotic stenosis in China (TES-CAS-C). Chin J Cerebrovascular Dis3:4–8
31. Coward LJ, Featherstone RL, BrownMM (2005) Safety and efficacy ofendovascular treatment of carotid arterystenosis compared with carotid endar-terectomy. A Cochrane systematic re-view of the randomized evidence.Stroke 36:905–911
32. Ederle J, Featherstone RL, Brown MM(2007) Percutaneous transluminal an-gioplasty and stenting for carotid arterystenosis. Cochrane Database Syst Rev4:CD000515
33. Kastrup A, Groschel K, Krapf H,Brehm BR, Dichgans J, Schulz JB(2003) Early outcome of carotid an-gioplasty and stenting with and withoutcerebral protection devices: a system-atic review of the literature. Stroke34:813–819
34. Kastrup A, Nägele T, Gröschel K,Schmidt F, Vogler E, Schulz J, Erne-mann U (2006) Incidence of new brainlesions after carotid stenting with andwithout cerebral protection. Stroke37:2312–2316
35. Bosiers M, Hart J, Deloose K, SteyaertA, Verbist J, Peeters P (2006) Dodevice characteristics impact outcomein carotid artery stenting? Presented atthe Society of Vascular Surgery AnnualMeeting, Philadelphia, 2006
2966
Related Documents











