Status of Palliative Care in Lesotho A focus on essential pain medication accessibility and Pain management Sejojo Phaaroe Google+ President of LBCN Policy, Palliative care and Cancer Advocacy- -APCA

Status of Palliative care in Lesotho
Aug 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Status of Palliative
Care in Lesotho
A focus on essential pain medication
accessibility and Pain management
Sejojo Phaaroe
Google+
President of LBCN
Policy, Palliative care and Cancer Advocacy-
-APCA
Presentation layout
Goal
Concept of Palliative Care and its principles in Cancer patients and people with chronic illnesses .
continuum of care and pain management in Cancer
Tools for palliative care assessment and management
Psychological aspects of Palliative care
Structures in place for strengthening Palliative care regionally supporting Lesotho otho response/status of Palliative care
Opiods availability
Achievements
Challenges
Way forward
Advocacy
• *Palliative care services in a programme must be designed to enable change by providing Health professional and communities with tools that encourage and support those with terminal illnesses like cancer to live a functional and productive life- These are our People *- Sejojo Phaaroe 2008

There is no need to catch the Ball if you do not Know
where you are and- where you are going

Concept • •Palliative care is the total care of individuals
with incurable diseases, and their families, and embraces ….:
• •all physical,
• •Emotional
• •Social
• •Spiritual needs,
• • rather than purely Medical needs
Palliative care involves
• •Appropriate use of a range of therapies which do not aim to cure, but rather help to control symptoms, and preserve quality of life while minimizing adverse effects
• •Supporting the family and friends of the patient, and involving healthcare personel, other professionals and the community members who are skilled in communicating & helping with the psychological and social dimensions of the illness
• •Giving individuals with cancer and their families control over their own treatment and involving them in care management decisions.
Palliative care • Provides relief from pain and other distressing
symptoms;
• Affirms life and regards dying as a normal process;
• Integrates the psychological and spiritual aspects of patient care;
• Offers a support system to help patients live as actively as possible until death;
Distinctive features of palliative care • A younger affected age group in extremely emotive issues
such as sexuality, death, reproduction, guilt and loss of vitality
• Multisystem disorders more common- more than one disease process may be occurring.[
• More variable disease patterns-
• care givers must be aware of a range of new presentations of other diseases e.g Anemia
• MORE UNPREDICTABLE TERMINAL PHASE
• Greater use of multiple drug treatments, with many new therapies emerging
• Higher incidence of psychosocial problems- with often the worry of young families and loss of income and unfinished business

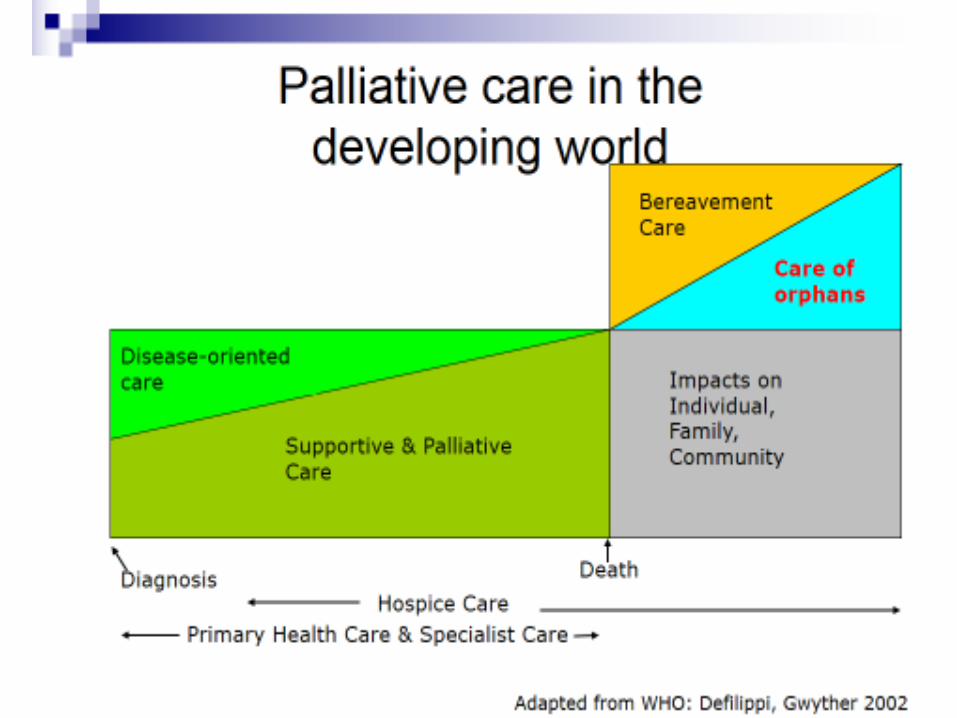
Palliative care and Pain Management
across the continuum of cancer care
Diagnosis
Death
Palliative Care
Treatments aimed at
prolonging life
Continuum of Care
Palliative care & Pain Mgt across the
continuum of care
Bereavement

Classification of Pain • Pain is generally classified as either
norciceptive or neuropathic.
• Norciceptive pain is caused by tissue injury resulting in direct stimulation of intact afferent nerve endings and it is either
• somatic or visceral.
• Somatic is usually well localised (described as dull, aching, throbbing, sharp, or gnawing in nature) whereas visceral pain is usually poorly localized (described as deep, aching, crampy, or a sensation of pressure).
Neuropathic pain
• is as a result of damage to the nerve pathways and a normal stimulus can result in an abnormal response.
• The pain may exceed observable injury and it is typically described as burning, tingling, pricking, shooting, stabbing, electrical, crawling insects, etc.
• Neuropathic pain is present in about 40% of AIDS patients the most common being painful neuropathy – predominantly sensory neuropathy (PNS).
• It is now known that several antiretroviral therapies (ARVs) e.g. Didanosine [ddI], Zalcitabine [ddC] and d4T, among others, can cause painful toxic neuropathy.
Pain in Cancer • Ninety percent (90%) of patients with
advanced cancer experience severe pain, with pain occuring in about 30% of all cancer patients, regardless of the stage of the disease.
• More than 50% of cancer patients may be undertreated for their pain and we need to remember not only that pain is rarely a sign of early cancer but that pain usually increases as cancer progresses
• Because of angiogenessis
• Most common cancer pain is as a result of tumors spreading to bones (bone metastasis).
• About 60-80% of cancer patients with bone metastasis experience pain.
• The second most common cause of cancer pain is from tumors infiltrating nerves and / or hollow viscuses.
• There is increasing evidence that tumors near nerves tend to cause the most severe pain.
• The third most common pain associated with cancer occurs as a complication of treatment given to treat the cancer: chemotherapy, radiation, or surgery.
• More than 80% of patients with cancer experience more than one distinct pain and this poses a great challenge to clinicians to effectively treat chronic cancer pain since each patient’s pain is unique.

Psychological aspects of palliative care
• Anxiety and depression are common in Cancer patients
• Signs include restlessness, insomnia, shortness of breath, numbness
• These can overshadow the psychological signs in patient with advanced disease
• A referral to a psychiatrist or other mental health professional when ever depression is suspected.
• Supportive psychotherapy and good listening is a good palliative practice
• formal psychotherapy programmes need to be established

WHO- The “Total” Pain
Concept
Spiritual
Emotional
Financial
Physical
•Guilt
•Why me?
•Life closure issues
•From disease
•From treatment
•Direct costs
•Indirect costs
•Loss of function
•Coping abilities
PAIN
opioids?

CANCER PAIN RELIEF

Comprehensive review of international conventions on
cancers • IUAC ( International union Against Cancer) • IUCR ( International Union on Cancer Research ) • IAC (International Academy of Cytology)
• WHO (2002) - • • AFROX declaration (2007) • …AU ( Maputo SRH declaration)
• …SADC
• …Lesotho Road map ( Maternal Mortality SRHR) • WHO
2. Lesotho RH Cancer Screening Guidelines WHO, 2002

Regional response
•Resolution 58.22 of the 58th World Health Assembly
echoed resolution 2005/25 of the UN’s Economic and
Social Council (ECOSOC), thereby recognising the
importance of improving the treatment of pain using
opioid analgesics and calling upon Member States to
remove barriers to ensure their medical availability.
•In an effort to advance these resolutions and to promote
the availability of essential pain medicines in Africa,
•Intensify palliative care services
•APCA held a regional essential pain medication
accessibility workshop for the southern Africa region in
February 2008

Selection criteria •Senior / Chief pharmacists;
•Drug regulatory authority and / or National Competent Authority
representatives;
•National Registrar of Drugs;
•Pharmacy Board / Council representative;
•Ministry of Health (MoH) clinical services and / or policy personnel;
•Palliative care providers – persons actively providing care;
•Senior physicians and senior nurses from teaching institutions;
•Representatives from the drug enforcement agencies;
•Heads of respective oncology , pathology and / or HIV/AIDS
treatment/ care units.
•Psychologists, and Clergies It was emphasised that the selected participants had to be willing to continue
advocating for policies that would make palliative care and essential palliative care
medicines, including opioids, available and more accessible in their espective
countries

SADC- Country teams
• INTRODUCTION OF THE COUNTRY TEAMS
• Lesotho
• Botswana
• Mozambique
• Namibia
• Kingdom of Swaziland
• Zimbabwe
• South Africa
African Palliative care support structures
ABOUT THE AFRICAN PALLIATIVE CARE ASSOCIATION
• African Palliative Care Association (APCA) was provisionally established in 2002, formally established in 2004, to be a catalyst for the scale-up of quality palliative care services across Africa.
• The mission of APCA is to promote and support culturally appropriate palliative care across the continent for people with progressive, life-limiting illnesses, such as cancer and HIV/AIDS, through education, training, advocacy
• development of standards of care, using a culturally appropriate public health approach that strives to balance quality with extended coverage.

Objectives of APCA • APCA’s broad strategic objectives are to: • Promote the availability of palliative care for all in need,
including orphans and vulnerable children (OVC); • Encourage governments across Africa to support
affordable and appropriate palliative care and to have it incorporated into the whole spectrum of existing health care services;
• Promote the availability of essential palliative care medicines (especially opioids) for all in need;
• Promote palliative care training programmes suitable for African countries;
• Develop and promote quality standards in palliative care training and service provision for the different levels of health professionals and care providers;

Palliative care Quality systems, and process control

Why Advocacy- remove
Barriers effective pain control
Patient related
Clinician related
Health system related
Political related
Cultural, religion, believes,
attitudes
Lack of knowledge on
palliative care, attitude,
Lack of services, lack of
coordination of supply chain
Lack of policies over opioid
regulation, dispensing for
nurses, prohibition at level 1

WHO- Public Health
(Stjernsward, 2007)
Oncology ?
problem
Lab
tests?

Lesotho Country Team on Palliative Care
Study

Treaties bind the entire government • Treaties are signed by a government official on behalf
of the entire nation.
• the entire government is obligated to achieve what is agreed on in any convention whereto a country is a signatory.
• In case of public health issues, this responsibility is not restricted to the Ministry of Health or even to an individual civil servant.
• Also other ministries, including the Ministry of Justice, the Ministry of Defence, the Ministry of Police, or whatever ministry is involved in drug control in a country should be dedicated to a treaty’s objectives and obligations.

The Kingdom of Lesotho • Mountain Kingdom’, gained independence from the British in
1966. • It is a landlocked country completely surrounded by South
Africa. • Lesotho is mountainous, with more than 80% of the country
being 1,800 meters above sea level. • In 2007 the population of Lesotho was estimated to be 1.8 • million compared to 1.9 million in 2004. • The population growth rate is 0.14%, with 70% of the population
being rural. • The total life expectancy at birth is 40 years. • The country is divided into 18 Health Service Areas, of which 10
are government owned and 7 are owned by the Christian Health Association of Lesotho. The doctor-to-population ratio is 1:16,298, whereas the nurse-to-population ratio is 1:2,226.
• The national literacy rate is 90.3% for females and 73.7% for males.

Situation as at 2008 •HIV and AIDS Control Policy, or the National Medicines Policy
of 2006. The Lesotho Standard Treatment Guidelines 2006
do not include palliative care either.
•However, the Drugs of Abuse Act is presently before Parliament and the
Medicines Bill is presently in draft form.
•The National Drug Policy 2006 addresses medications in general
without specifying classes (e.g. opioids).
•Most healthcare professionals (physicians, nurses, social workers,
pharmacists, and spiritual workers) are not well informed about the
concept of palliative care.
•Some of the nurses trained in IMAI and IMCI have familiarity with but
limited understanding of palliative care.
•All physicians are trained outside of Lesotho, many of whom are
foreign with language barriers and limited knowledge of culture


S.Phaaroe et al
S Phaaroe etal 2007
66.7: 100 000

Cancer Situation in Lesotho
Cervical – 40.9% - (ASIR – 66.7:100,000 (LES); (S. Phaaroe e tal MOHSW/WHO 2007)
Breast – 18% of all cancers
Prostrate – 13.5%;
Skin – 12.6%;
Lung – no estimates ( found on autopsy);
Leukemias/lymphomas – no estimates;
No cancer treatment centre; but we are strongly working on it to be established urgently
Cancer for angiogenesis

Pain Control barriers in Lesotho •‘Freedom from pain should be seen as a
right of every cancer patient and access to
pain therapy as a measure of respect for the
right in Lesotho
•There are several barriers to effective pain
control in both cancer and / or HIV/AIDS.
Such barriers could be patientrelated;
clinician-related; societal/health system;
and political and/or legal-related.

Examples of the various palliative care models not available in Lesotho are:
• Home-based care;
• Outpatient care;
• Outreach services (e.g. roadside clinics);
• Hospital-based palliative care teams;
• Day care;
• Hospice inpatient care;
• And workplace programmes.

Palliative care service management : Patients should always referred to these services
• Health education : Clarify temporary aspects of pain; acute or chronic
• palliative care advocacy focus on essential pain medication system
• Symptom management
• Pain management
• Diet management
• Non pharmacological activities –rehabilitation, physical / recreational activities, music , bathing, stress management ( comedies, , acupuncture, ocean music, meditation, motivational Talks etc)

Dietary guidelines to try and
prevent disease include
• Control weight and obesity
• Reduce consumption of total fat <30%
• Increase fibre intake
• Minimize consumption of salt-cured, salt-pickled and smoked foods
• Consume alchohol beverages in moderation if at all.
• Immune factors may interfere with recognition of tumour cell as foreign
•pain,
weakness,
• loss of appetide,
•early satiety,
•constipation,
•dry mouth,
•dyspnea
The patient ‘s wishes • •It is extremely important to involve
individuals with Cancer in the clinical decision making process wherever possible
• •This will give them a sense of control over their own life
• •Many cancer patients decline certain investigations and therapies, but take strengh from doing so
• •The wishes of the person with Terminal diseases like AIDS and Cancer should always be respected as far as is ethically possible
Medicine Formulation Strength
Pethidine Hcl Parenteral 50mg/mL
Morphine
sulphate
Tablets 10mg
Morphine Parenteral 10mg/mL
Fentanyl Parenteral 100mcg/2cc
Tramadole Tabs / caps 350 mg
Opioids Available in Lesotho are:
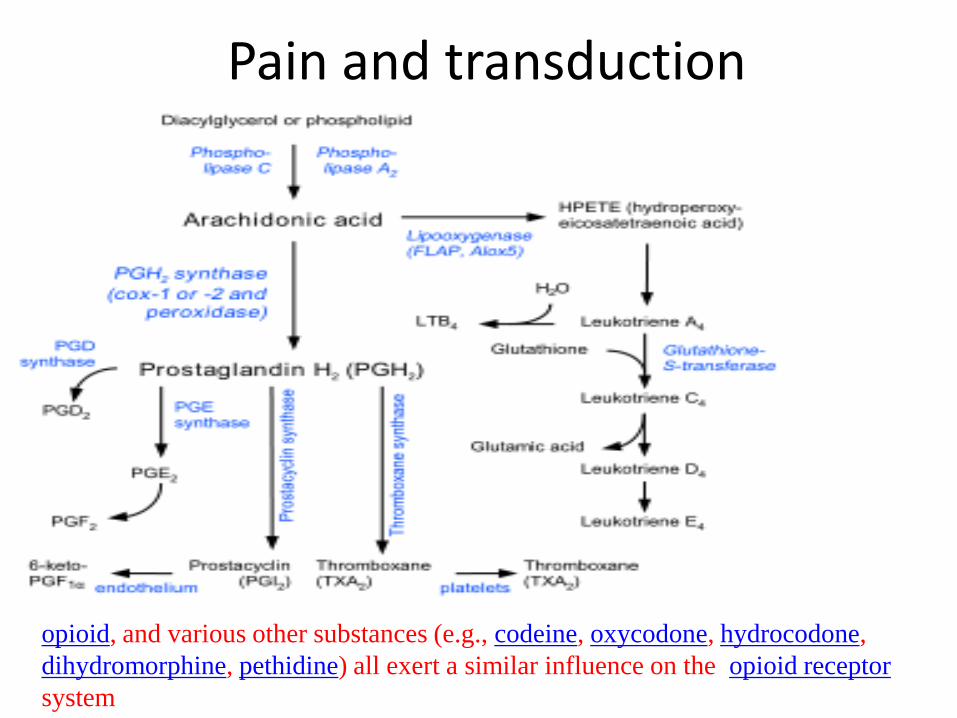
Pain and transduction
opioid, and various other substances (e.g., codeine, oxycodone, hydrocodone,
dihydromorphine, pethidine) all exert a similar influence on the opioid receptor
system

Opioids availability • Other formulations that are needed include
morphine powder for reconstitution into liquid, as well as different tablet strengths of morphine.
• In Lesotho there are no cost implication issues since all medicines are subsidised by the Government of Lesotho, with the only healthcare charge being for hospital consultations

• Opioids are bought from South Africa and abroad with only two in-country wholesale distributors: the National Drug Service Organisation (NDSO) and TriPharm (a private company).
• The Ministry of Health (MoH) is responsible for issuing importation permits, and endorses supplies received by the NDSO and orders made by public and private hospitals.
• In order to prescribe opioids, physicians only need to be actively licensed to practice with no need for separate licensure.
challenges and barriers to opioid accessibility in Lesotho
• 1. Inadequate, untimely and under-reporting from distributors to MoH thereby affecting estimates sent to INCB leading to stock-outs;
• 2. Inadequate training of MoH (the national competent authority) in estimating and reporting to the INCB;
• 3. Rapid turnover of staff in the Medical Competent Authority with poor continuity;
• 4. Lack of recommended opioid formulations and dosage forms;
• 5. Limited opioid availability for paediatric prescribing;
• 6. Opioid prescribing is limited to hospital settings (urban and rural) and urban clinics;
• 7. The mountainous terrain inhibits easy access for rural dwellers to medical facilities;

Limited use of Pain assessment tools

Pain management needs • Reassure the patient and the family that pain can be relieved.
Power of words, trust and empathy
• Explain that pain relief is not instantaneous.
• Explain that unpleasant side effects will wear off after 3 days.
• The goal of pain management is to ensure that the patient is—
• Pain-free at rest.
• Pain-free at night.
• Pain-free while active.
• Use step-by-step approach to pain relief according to the WHO analgesic ladder . The principles governing use of
analgesics are that they should be given—
• By mouth
• By the clock
• By the ladder
• By the patient
• Reassure the patient of regular visits and reassessment by health care professional.
Mild
pain
Aspirin
ibuprofen
Acetamin
ophen
+-
adjuvants
Moderate
pain
Codeaine
Oxycodain
e
Dihydroco
daine
tramadole
+-
adjuvants
Severe
pain
Morphine
Hydromor
phine
Methadon
e
Levorpha
nol
Fentayl
Oxycodai
ne +-adjuvants
• 3
2
1
Strengthen Overall Pain Management Strategy
• Empathy , care and support, Alternative
techniques in managing spiritual, emotional, and social problems may require referral to social worker or other people (medical or nonmedical).
• Determine the aim of treatment plan.
• Decide on which analgesics to use first or treatment implementation /course.
• Determine any adjuvants (i.e., co-analgesics) that may be needed to counteract side effects of the analgesics.

No- Rehabilitation services/ centres • Cancer Rehabilitation
• goal is to improve daily function and quality of life for the cancer survivor
• Fatigue
• Weakness
• Poor endurance
• Decline in balance
• Postural changes
• Joint stiffness
• Pain, pain, pain- PALLIATIVE CARE (body, mind,soul)
• Numbness in feet or hands
• Balance disorders
• Bladder and bowel management
• Multiple sclerosis
• Numbness and tingling
• Paralysis
• Parkinson's disease and other movement disorders
• Pulmonary disorders
• Sensory disorders
• Spasticity
• Speech and swallowing disorders (including apraxia)
• Walking difficulty
NO - HOSPICE
SERVICES

Corrective actions 1. Country strategy submitted for approval to DGHS
2. Approval of Technical Team and TOT Trainings to expand team carried In and Outside Country
3. Trainings of Pharmacists and Pharmacy technologists on Palliative care and in estimating and reporting to the INCB; to include Private Pharmacies
4. Curriculum review and in -cooperated in Health training institutions
5. Training of health training institutions tutors on Palliative care
6. APCA Coordination office was established in Lesotho
7. Advocacy and awareness activities , IEC, FLYERS
8. Palliative care Presentation LMA, - Mr Sibusiswe Dlamini Swaziland-

Lesotho Trainings
9. By Hospice Lady brand and APCA
10. Island Hospice Service and APCA
12. By Trainings – HPCSA and APCA
13. By Ms Sethembile Dlamini – Trainings for Nurses Swaziland
14. Dr Jenifer Johnson – USAID / SADAC Coordination-USA/ Swaziland
15 Training of health professionals on Palliative nurses –Workshops , NORTH, SOUTH, CENTRAL
16. Working with a physician provider and independently provided individual and
family assessment and care planning, adjustment counseling, grief counseling, advance care planning and long term care planning. At HOME BASED VISITS
Island Hospice Service

trainings
Follow up Achievements/ Strengths • Report of Namibia Feb 2008.doc
• ..\..\..\Sejojo Phaaroe\Desktop\PALLIATIVE CARE IN LESOTHO 5.doc
• NCDs strategic plan inclusive of palliative care
• Baseline assessment done-( reveals that there are no PALLIATIVE CARE services in Lesotho)
• VHA policy in place
• Need for Palliative care well articled in the NCD.s strategic plan and implantation plan
• Palliative care is on the Political Agenda

Community Based, multidisciplinary palliative care
Physician Initiate care plan
Oncology .
Palliative Nurses
and other nurses
Case MGT, monitor
RX
Home care Aides Bathing, toilet,
meal preparation
Social worker Psychosocial issues
Rehabilitation
therapists
Exercises,
environmental
adaptation
Psychologists, clergies
Spiritual care , church
groups, counselors
Spiritual, psychosocial,
nutrition

Palliative care Results Frameworks
5
5
Goal: Improved Health Status
And Palliative care
Objective: Improved Use of Palliative care medicines, pain assesment and management s
R1: Access/Availability R2: Quality R3: Sustainability R4: Demand
R1.1:Commodities/Facilities
R1.2: Equity
R2.2: Provider Performance
R2.3: Training/Supervision
R2.4: Information System
R3.1: Policy
R3.2: Health Care Finance
R3.3: Private Sector
R4.1: Attitude
R4.2: Knowledge
R4.3: Community Support

a Case for Palliative care M&E
The Legs (Programme Implementers):
Coordinate Implement of projects, spend the budget, report on results and leave footprints of the organisation in the community.
The Arms and Spine (M&E Champions):
Standard bearers of M&E Values and principles, concepts, methods, tools
.
Head (Senior Management):
Org Brain Machine)
Sets the Agenda. Eye, Nose, and Ears and Mouth
of the Org, break the silence

THE ROAD AHEAD NOW IS NEARLY CLEAR


Sejojo Phaaroe – Kabelo Mputsoe Cancer Radio Oncologytherapy centre


Related Documents