-
7/29/2019 Stats for Non-staticians
1/37
Statistics for
Non-Statisticians
-
7/29/2019 Stats for Non-staticians
2/37
THE BASIC IDEA
Statistics are used in clinical trials to make inferencesabout new treatments based on the evidence of thepatients in the trial E.g. New drug for treatment of lung cancer does it
work or not?
Ideally design trial that includes all patients with lungcancer Not really practical!!
Can only test the new treatment on a representativesample of the population
Statistics allow us to draw conclusions about the likelyeffect on the population using data from the sample
-
7/29/2019 Stats for Non-staticians
3/37
USING STATISTICS
But what exactly do we want the
statistics to assess:-
Assess the weight of evidence that atreatment works (ordoesnt)
Give an estimate (and likely range) of the
treatment effect Test to see how likely it is that this effect
would have been seen by chance
-
7/29/2019 Stats for Non-staticians
4/37
Statistics can neverPROVEanything
beyond anydoubt, just beyondreasonable doubt!!
BUT
-
7/29/2019 Stats for Non-staticians
5/37
STATISTICAL DATA
ANALYSIS METHODS
-
7/29/2019 Stats for Non-staticians
6/37
WHO TO INCLUDE?
In any clinical trial, one is likely to find:
Ineligible patients included by mistake
Protocol violators those who dont adhere tothe treatment regimen allocated
Patients who withdraw or get lost to follow-up
To avoid bias, keep these to a minimum
Follow-up all patients randomised into a trial
Should we include them in the analysis?
-
7/29/2019 Stats for Non-staticians
7/37
INTENTION TO TREAT ANALYSIS
As a general rule, all patients randomisedshould be analysed by treatment allocated(regardless of whether they actuallyreceived this treatment)
INTENTION TO TREAT ANALYSIS
Reasons for ITT:
Avoids or certainly minimises risk of bias
Is more pragmatic reflects real life
-
7/29/2019 Stats for Non-staticians
8/37
HYPOTHESIS TESTING
We want to compare the outcomes in differenttreatment arms (A and B)
Testing two hypotheses H0: A=B (Null hypothesis no difference) H1:AB
Calculate test statistic based on the assumption
that H0 is true (i.e. there is no real difference) Test will give us a p-value: how likely are the
collected data if H0 is true
If this is unlikely (small p-value), we reject H0
-
7/29/2019 Stats for Non-staticians
9/37
THE LURE OF THE P-VALUE
The p-value is the probability of having observed our datawhen the null hypothesis is true
Typically if the p-value is less than 0.05, people say that thetrial gives statistically significant evidence that there is a
difference
Tend to ignore results where p-value greater than 0.05
However, 0.05 is a purely arbitrary value, and not really thatsmall one time in twenty we will reject H0 wrongly! That is state difference exists, when one doesnt (false positive)
Dont become wedded to the p-value: there is not much
difference between 0.051 and 0.049
-
7/29/2019 Stats for Non-staticians
10/37
ESTIMATE OF TREATMENT EFFECT
Better still, use the data collected in the trial
to give an estimate of the treatment effectsize, together with a measure of how
certain we are of our estimate
-
7/29/2019 Stats for Non-staticians
11/37
CONFIDENCE INTERVALS (CI)
To determine the true treatment effect, we calculate theconfidence interval for our point estimate
CI is a range of values within which the true treatment effectis believed to be found, with a given level of confidence.
95% CI is a range of values within which the truetreatment effect will lie 95% of the time
Generally, 95% CI is calculated as
Sample Estimate 1.96 x Standard Error
Use the confidence interval to assess the true treatmenteffect, and not just p-values
-
7/29/2019 Stats for Non-staticians
12/37
DATA ANALYSIS
How do we do this?
What type of analysis should be performed?
Depending on the sort of outcome measure,
different types of analysis are appropriate
Because the actual analyses are now done mainlyby computer, the skill is now:-
In choosing the appropriate test
Correctly interpreting the results
-
7/29/2019 Stats for Non-staticians
13/37
COMMON OUTCOME MEASURES
Categorical
Continuous
Survival
-
7/29/2019 Stats for Non-staticians
14/37
CATEGORICAL DATA
Outcomes like good/bad, yes/no or present/absent
In testing categorical data, we are looking to see if
there is any relationship between the outcomecategory and the treatment given H0: No association between variables
H1: Association between variables
For categorical data, the chi-squared test isappropriate if the categories arent ordered
For ordered categories, use a trend test
-
7/29/2019 Stats for Non-staticians
15/37
Dead Alive Total
Aspirin 804 7783 8587
No Aspirin 1016 7584 8600
Total 1820 15,367 17,187
ISIS TRIAL OF ASPIRIN TO
PREVENT MORTALITY AFTER MI
- Use chi-squared test of association to determine whether to reject the nullhypothesis of no association between aspirin and death
-
7/29/2019 Stats for Non-staticians
16/37
Dead Alive Total
Aspirin 804 (E=909.3) 7783 (E=7677.7) 8587
No Aspirin 1016 (E=910.7) 7584 (E=7689.3) 8600
Total 1820 15,367 17,187
ISIS TRIAL OF ASPIRIN TO
PREVENT MORTALITY AFTER MI
- Use chi-squared test of association to determine whether to reject the nullhypothesis of no association between aspirin and death
- X21 = (804 909.3)2 / 909.3 + + (7584 7689.3)2 / 7689.3 = 27.26
- X21 = 27.26 (P
-
7/29/2019 Stats for Non-staticians
17/37
MEASURES OF TREATMENT EFFECT
Tested hypothesis and found strong evidence of anassociation between aspirin use and mortality
Not very informative - is aspirin harmful orbeneficial?
Various measures of treatment effect:- Absolute Risk Reduction
Number Needed to Treat
Relative Risk
Relative Risk Reduction
Odds Ratio
Odds Reduction
-
7/29/2019 Stats for Non-staticians
18/37
ODDS RATIO & ODDS REDUCTION
Odds ratio = (804 x 7584) / (7783 x 1016) = 0.77
-
7/29/2019 Stats for Non-staticians
19/37
SUMMARISING BINARY DATA IN TWO
GROUP PROSPECTIVE STUDY
Risk in standard treatment (P1) and Risk in new treatment (P2)
Term Formula ISIS Example
Absolute Risk
Reduction (ARR)
P1
- P2
0.118 0.094 = 0.024
(i.e. 2.4% in favour of new Rx)
Number needed to
treat/harm (NNT/NNH)
1 / |P1 - P2| 1 / 0.024 = 41.7, so NNT = 42
(i.e. need to treat 42 patients with
aspirin in order to prevent 1 death)
Relative Risk (RR) P2 / P1 0.094 / 0.118 = 0.80 (
-
7/29/2019 Stats for Non-staticians
20/37
CONTINUOUS DATA
Outcomes like blood pressure, weight or scores,summarised using measures of the centre and spread ofthe distribution
Measures of the centre of the distribution Mean: what we think of as an average add up all data and divide
by number of items
Median: midpoint of the data half data below median, and otherhalf above
Mode: most popular observation
Measures of spread Variance and standard deviation
Standard deviation is average distance individual observations arefrom the mean
-
7/29/2019 Stats for Non-staticians
21/37
CONTINUOUS DATA
In continuous data, we are comparing the
means in the two groups and assessing
whether the two groups come from the
same population H0: Mean A = Mean B
H1: Mean A Mean B
Use Students t-test
ANOVA if comparing >2 treatment groups
-
7/29/2019 Stats for Non-staticians
22/37
NORMAL DISTRIBUTION
T-test and ANOVA assumes data are Normally distributed However, if the data are very skew or have multiple peaks,
we use a non-parametric testwhich doesnt assume anyparticular shape for the data Wilcoxon Mann-Whitney
As a rule, non-parametric tests are more general, but lesssensitive
-
7/29/2019 Stats for Non-staticians
23/37
N Mean SDTreatment A 41 91mmHg 5.5
Treatment B 43 95mmHg 5.5
STUDY COMPARING TWO ANTI-
HYPERTENSIVE DRUGS ON BP
- Use Students t-test to assess whether means are from the same population
(i.e. Mean with Treatment A = Mean with Treatment B)
Diastolic BP compared in two groups of hypertensive patients given
two different drug treatments
-
7/29/2019 Stats for Non-staticians
24/37
TESTING FOR A DIFFERENCE
Treatment A: N=41, Mean=91mmHg, SD=5.5
Treatment B: N=43, Mean=95mmHg, SD=5.5
Use t-test to assess evidence for or against nullhypothesis (mean A = mean B)
t-test = -3.33 on 82 df (df=n1+n2-2)
P=0.0013
So there is evidence against H0 Evidence that the mean diastolic BP in the two
treatment groups are different
-
7/29/2019 Stats for Non-staticians
25/37
MEASURE OF TREATMENT EFFECT
Tested hypothesis and found evidence that mean diastolic BP in twogroups are different
Not very informative which of treatment A or B is better?
Point estimate of the treatment effect - calculate the difference betweenthe two means and the confidence interval Difference = 91 95mmHg = -4mmHg (favours treatment A)
95% CI: -6.39 to -1.61mmHg
So the difference in mean diastolic BP between groups is statistically
significant (P=0.0013) With treatment A being more effective in reducing diastolic BP
However, the observed difference of 4mmHg in favour of treatment A,could be as small as 1.6mmHg or as large as 6.4mmHg.
-
7/29/2019 Stats for Non-staticians
26/37
SURVIVAL DATA
Why are survival data different? Interested in studying the time between randomisation
and a subsequent event (say death)
These times are unlikely to be normally distributed
Cannot afford to wait until events have happened to allsubjects, for example until all are dead.
Some people may have left the study early and becomelost to follow up - only information we have about somepatients is that they were still alive at last follow-up.
Use survival analysis methods to analyse time toevent data, not just the number of events Take into account that not all patients may have had an
event
-
7/29/2019 Stats for Non-staticians
27/37
KAPLAN-MEIER SURVIVAL ANALYSIS
Basic idea: we split the trial up into distinct time
intervals
In each time interval: a certain number, N, patients
enter that time period alive and still on follow-up, andsome of these, D, have an event:
Then the probability of surviving that time interval
(assuming you live that long) is (1-D/N) Multiply all these probabilities together to give the
probability of survival up to a given time point
-
7/29/2019 Stats for Non-staticians
28/37
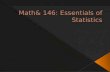
EXAMPLE SURVIVAL FUNCTION
Time in Weeks
120100806040200
1.0
.8
.6
.4
.2
0.0
Survival Function
Censored
-
7/29/2019 Stats for Non-staticians
29/37
Dead Alive Median
Survival
Total
IFN 151 187 ~4 years 338
No IFN 156 180 ~4 years 336
Total 307 367 674
AIM-HIGH TRIAL OF INTERFERON
FOR MALIGNANT MELANOMA
Want to assess whether the time to death is the same for the two treatments?
-
7/29/2019 Stats for Non-staticians
30/37
COMPARING SURVIVAL
BETWEEN GROUPS
We will have two graphs: how do we say whether
one group survives longer than the other?
Could do one test at say 1 year; compare proportions (as
before) Could keep testing at small intervals
What are the drawbacks to these methods?
Use logrank test to determine whether survival
function the same for two treatment groups
H0: Survival function/curve same for both groups
H1: Survival function/curve different across groups
-
7/29/2019 Stats for Non-staticians
31/37
SURVIVAL IN MELANOMA:
INTERFERON VS. OBSERVATION
-
7/29/2019 Stats for Non-staticians
32/37
MEASURE OF TREATMENT EFFECT
Assessed the evidence and found that there is no evidencethat time to death differs between the treatment groups
Despite lack of difference should still calculate pointestimate and confidence interval for treatment effect
Use cox regression to calculate hazard ratio andconfidence interval HR=0.94 (CI=0.75 1.18)
IFN non-significantly reduces the risk of death by 6%, withthe true treatment effect based on the confidence intervalranging from a 25% reduction in mortality to an adverse18% increase in mortality with IFN.
-
7/29/2019 Stats for Non-staticians
33/37
ANALYSES GOOD PRACTICE
Report the primary/secondary outcomes as statedin the protocol Dont give minor endpoints undue prominence in the
paper
Do not explore all endpoints until you find one thatis significant (data dredging) Looking at multiple outcomes, increases chance of
finding something significant
In 20 outcomes, just by chance 1 outcome will besignificant
Is this real, or the play of chance?
Solution: Dont have too many endpoints
-
7/29/2019 Stats for Non-staticians
34/37
ANALYSES GOOD PRACTICE
Give confidence intervals where possible,
and not just p-values
Keep subgroup analyses to a minimum
Subgroup analyses should be pre-specified
When interpreting subgroups, assess whole
picture
Do not focus upon one subgroup and
individual p-values
-
7/29/2019 Stats for Non-staticians
35/37
FINAL WORDS
The idea of statistics is to look at the strength of
the evidence for a given hypothesis and determinethe reliability of the treatment effect observed inthe trial
Calculations are based on formulas, but the
application of the formulas and the interpretationof the results is an art rather than a science
Significance is not black and white P>0.05 is not evidence of absence of effect, merely
absence of evidence of an effect
A little common sense can go a long way inmedical statistics
If in doubt, ask a statistician!
-
7/29/2019 Stats for Non-staticians
36/37
To call in the statistician after theexperiment is done may be no
more than asking him to perform a
post mortem examination: he maybe able to say what the experiment
died of.
Sir R.A. Fisher
Indian Statistical Congress, Sankhya, c. 1938
-
7/29/2019 Stats for Non-staticians
37/37
BOOK LIST
Swinscow TDV and Campbell MJ. Statistics at Square One(10th edition). BMJ Books 2002
Campbell MJ. Statistics at Square Two. BMJ Books 2001
Altman D, Machin D, Bryant T and Gardner M. Statistics
with Confidence. BMJ Books 2000
Pereira-Maxwell F.A-Z of Medical Statistics. Arnold1998