Feature States’ Role in Promoting Meaningful Use of Electronic Health Records is issue of States in Action discusses the responsibilities, opportunities, and chal- lenges for state Medicaid agencies in implementing programs to encourage pro- viders to adopt electronic health records (EHRs). It focuses on the Medicaid Electronic Health Record Incentive Program, established by the Health Information Technology for Economic and Clinical Health (HITECH) Act in the American Recovery and Reinvestment Act of 2009 and jointly administered by the Centers for Medicare and Medicaid Services (CMS) and state Medicaid agencies. Rather than formal Snapshots of particular states’ efforts, the issue includes lessons from states’ early experiences in implementing the Medicaid EHR Incentive Program. e EHR Incentive Program is just one of many health information technology (HIT) initiatives supported and encouraged by the federal government. With state Medicaid agencies facing competing demands as well as limited resources, states can benefit from aligning their efforts to promote health information technology, and collaborating with other agencies, states, and stakeholders to share or reduce costs, limit duplication, and avoid confusion for providers. Health System Transformation Through HIT ree major acts passed since 2009—the Children’s Health Insurance Program Reauthorization Act, the HITECH Act, and the Affordable Care Act—expand or sustain coverage, encourage care delivery innovation and payment reform, and pro- mote the use of health information technology to improve health care safety, quality, and efficiency of (Figure 1). In particular, the HITECH Act aligns efforts to improve health care quality with adoption of HIT. e EHR Incentive Program is not merely about making paper APRIL/MAY 2011 INNOVATIONS IN STATE HEALTH POLICY I N THIS I SSUE 1 Feature: States’ Role in Promoting Meaningful Use of Electronic Health Records 10 Additional Resources 10 Related Publications 12 Upcoming Meetings 13 Editorial Advisory Board 13 About the Newsletter States in Action Published May 24, 2011 States in Action is a newsletter from The Commonwealth Fund. Published bimonthly, the newsletter is part of a Commonwealth Fund initiative on state innovations. Past issues of States in Action are available on The Commonwealth Fund Web site at commonwealthfund.org/statesinaction Authors: M. Reneé Bostick, M.P.A., Sharon Silow-Carroll, M.B.A., M.S.W., and Diana Rodin, M.P.H., Health Management Associates Editor: Ed Schor, M.D., Vice President, State Health Policy and Practices and Cara Dermody, Program Assistant, State Health Policy and Practices Managing Editor: Martha Hostetter, M.F.A.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Feature States’ Role in Promoting Meaningful Use of Electronic Health Records This issue of States in Action discusses the responsibilities, opportunities, and chal-lenges for state Medicaid agencies in implementing programs to encourage pro-viders to adopt electronic health records (EHRs). It focuses on the Medicaid Electronic Health Record Incentive Program, established by the Health Information Technology for Economic and Clinical Health (HITECH) Act in the American Recovery and Reinvestment Act of 2009 and jointly administered by the Centers for Medicare and Medicaid Services (CMS) and state Medicaid agencies. Rather than formal Snapshots of particular states’ efforts, the issue includes lessons from states’ early experiences in implementing the Medicaid EHR Incentive Program.
The EHR Incentive Program is just one of many health information technology (HIT) initiatives supported and encouraged by the federal government. With state Medicaid agencies facing competing demands as well as limited resources, states can benefit from aligning their efforts to promote health information technology, and collaborating with other agencies, states, and stakeholders to share or reduce costs, limit duplication, and avoid confusion for providers.
Health System Transformation Through HITThree major acts passed since 2009—the Children’s Health Insurance Program Reauthorization Act, the HITECH Act, and the Affordable Care Act—expand or sustain coverage, encourage care delivery innovation and payment reform, and pro-mote the use of health information technology to improve health care safety, quality, and efficiency of (Figure 1).
In particular, the HITECH Act aligns efforts to improve health care quality with adoption of HIT. The EHR Incentive Program is not merely about making paper
short survey
April/MAy 2011 innovAtions in stAte HeAltH policy
In thIs Issue
1 Feature: States’ Role in Promoting Meaningful Use of Electronic Health Records
10 Additional Resources10 Related Publications12 Upcoming Meetings13 Editorial Advisory Board13 About the Newsletter
States in Action
Published May 24, 2011
States in Action is a newsletter from The Commonwealth Fund. Published bimonthly, the newsletter is part of a Commonwealth Fund initiative on state innovations.
Past issues of States in Action are available on The Commonwealth Fund Web site atcommonwealthfund.org/statesinaction
Authors: M. Reneé Bostick, M.P.A., Sharon Silow-Carroll, M.B.A., M.S.W., and Diana Rodin, M.P.H., Health Management Associates
Editor: Ed Schor, M.D., Vice President, State Health Policy and Practices and Cara Dermody, Program Assistant, State Health Policy and Practices
Managing Editor: Martha Hostetter, M.F.A.

States in Action April/May 2011
www.commonwealthfund.org 2
processes electronic; it requires eligible providers to demonstrate the “meaningful use” of certified technology. To demonstrate meaningful use, eligible providers must use EHRs:
• in a meaningful manner, such as for electronic prescribing;
• for the electronic exchange of health information to improve quality of care (e.g., for care coordination); and
• to report clinical quality and other measures as specified by the Secretary of Health and Human Services.
Evidence of the benefits of HIT is continuing to grow. A recent evaluation of HIT projects funded through the Agency for Healthcare Research and Quality found that “grantees experienced improved efficiencies in health care delivery, improved quality of care, and increased access to care as a result of their health IT projects.”1 Ninety-two percent of recent (2007–10) articles on HIT reached positive overall conclusions about its impact, and found that “the benefits of technology are beginning to emerge in smaller practices and organizations, as well as in large orga-nizations that were early adopters.”2
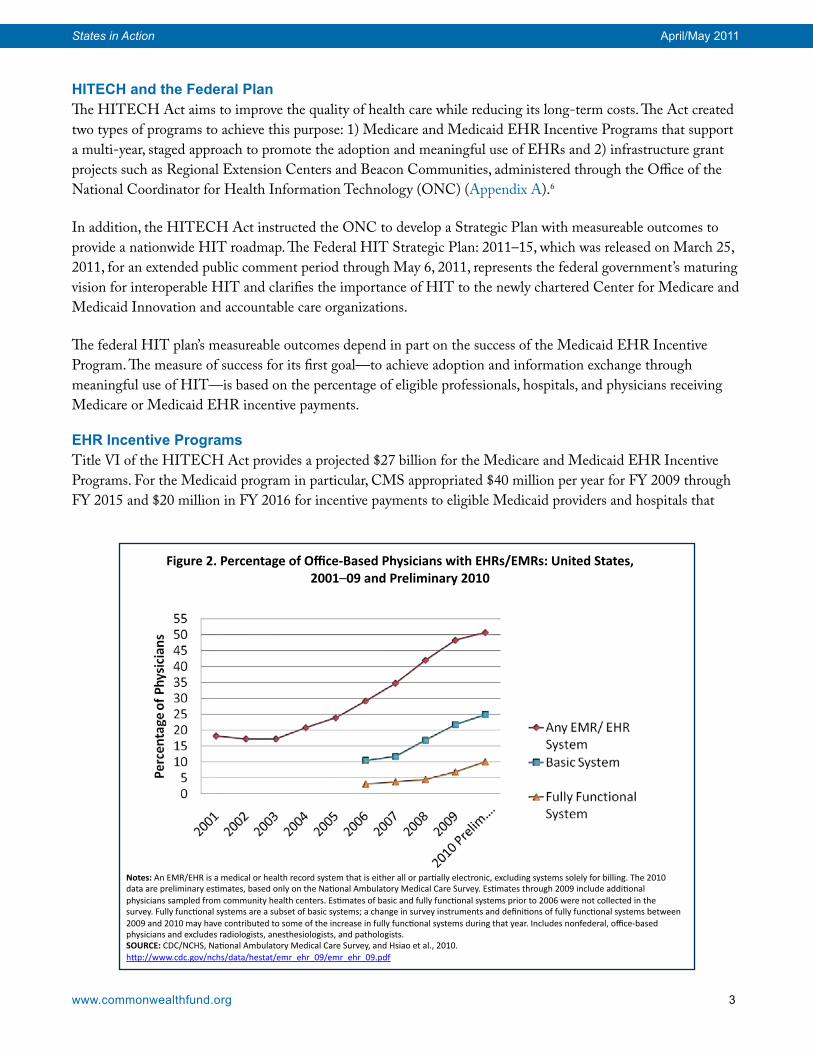
Figure 2 illustrates the increasing trend in adoption of basic or fully functional electronic health records or elec-tronic medical records by office-based physicians.3 Between 2009 and 2010, the percentage of such physicians reporting they had a basic or fully functional system increased by 14.2 percent and 46.4 percent, respectively.4 Further, 81 percent of hospitals and 41 percent of office-based physicians report they intend to apply for EHR in-centives, most of them during the first stage of the program (2011–12).5
Children’s Health Insurance Program Reauthoriza8on Act (CHIPRA) ! Expand Coverage ! Pediatric Quality Measures ! EHR Model Program
American Recovery & Reinvestment Act (ARRA – HITECH) ! Sustain Coverage ! ONC Infrastructure grants ! Medicare & Medicaid EHR IncenAve Program
Pa8ent Protec8on & Affordable Care Act (ACA) ! Expand Coverage – 16 million by 2015 ! Health Insurance Exchange ! Standardize, Streamline, & Simplify Enrollment
Source: Health Management Associates, 2011
Figure 1. Recent Legisla8on Promo8ng Health Care System Transforma8on
States in Action April/May 2011
www.commonwealthfund.org 3
HITECH and the Federal PlanThe HITECH Act aims to improve the quality of health care while reducing its long-term costs. The Act created two types of programs to achieve this purpose: 1) Medicare and Medicaid EHR Incentive Programs that support a multi-year, staged approach to promote the adoption and meaningful use of EHRs and 2) infrastructure grant projects such as Regional Extension Centers and Beacon Communities, administered through the Office of the National Coordinator for Health Information Technology (ONC) (Appendix A).6
In addition, the HITECH Act instructed the ONC to develop a Strategic Plan with measureable outcomes to provide a nationwide HIT roadmap. The Federal HIT Strategic Plan: 2011–15, which was released on March 25, 2011, for an extended public comment period through May 6, 2011, represents the federal government’s maturing vision for interoperable HIT and clarifies the importance of HIT to the newly chartered Center for Medicare and Medicaid Innovation and accountable care organizations.
The federal HIT plan’s measureable outcomes depend in part on the success of the Medicaid EHR Incentive Program. The measure of success for its first goal—to achieve adoption and information exchange through meaningful use of HIT—is based on the percentage of eligible professionals, hospitals, and physicians receiving Medicare or Medicaid EHR incentive payments.
EHR Incentive Programs Title VI of the HITECH Act provides a projected $27 billion for the Medicare and Medicaid EHR Incentive Programs. For the Medicaid program in particular, CMS appropriated $40 million per year for FY 2009 through FY 2015 and $20 million in FY 2016 for incentive payments to eligible Medicaid providers and hospitals that
Figure 2. Percentage of Office-‐Based Physicians with EHRs/EMRs: United States, 2001–09 and Preliminary 2010
Notes: An EMR/EHR is a medical or health record system that is either all or par8ally electronic, excluding systems solely for billing. The 2010 data are preliminary es8mates, based only on the Na8onal Ambulatory Medical Care Survey. Es8mates through 2009 include addi8onal physicians sampled from community health centers. Es8mates of basic and fully func8onal systems prior to 2006 were not collected in the survey. Fully func8onal systems are a subset of basic systems; a change in survey instruments and defini8ons of fully func8onal systems between 2009 and 2010 may have contributed to some of the increase in fully func8onal systems during that year. Includes nonfederal, office-‐based physicians and excludes radiologists, anesthesiologists, and pathologists. SOURCE: CDC/NCHS, Na8onal Ambulatory Medical Care Survey, and Hsiao et al., 2010. hRp://www.cdc.gov/nchs/data/hestat/emr_ehr_09/emr_ehr_09.pdf
States in Action April/May 2011
www.commonwealthfund.org 4
demonstrate they make meaningful use of EHRs, as well as for program planning and administration by state Medicaid agencies.7 The inclusion of Medicaid in the HITECH Act program demonstrates its pivotal role as the nation’s largest health care purchaser in terms of enrollment.
Under this program, state Medicaid agencies are eligible to receive 100 percent reimbursement for incentive pay-ments to eligible providers. States disburse incentive payments to professionals and hospitals “as they adopt, imple-ment, upgrade, or demonstrate meaningful use of certified EHR technology in their first year of participation and demonstrate meaningful use for up to five remaining participation years.” Eligible professionals (including physi-cians, dentists, and community health centers) can receive up to $63,750 over the six years. Hospital payments are based on various factors, beginning with a $2 million base payment.8
States also receive up to 90 percent reimbursement for operating the program, including:
• planning activities associated with designing and implementing the program and systems change;
• administering incentive payments, including tracking of meaningful use by Medicaid providers;
• oversight, including routine tracking of meaningful use evidence (attestation) and reporting mechanisms; and
• initiatives to encourage the adoption of certified EHR technology to promote health care quality and the ex-change of health care information.9
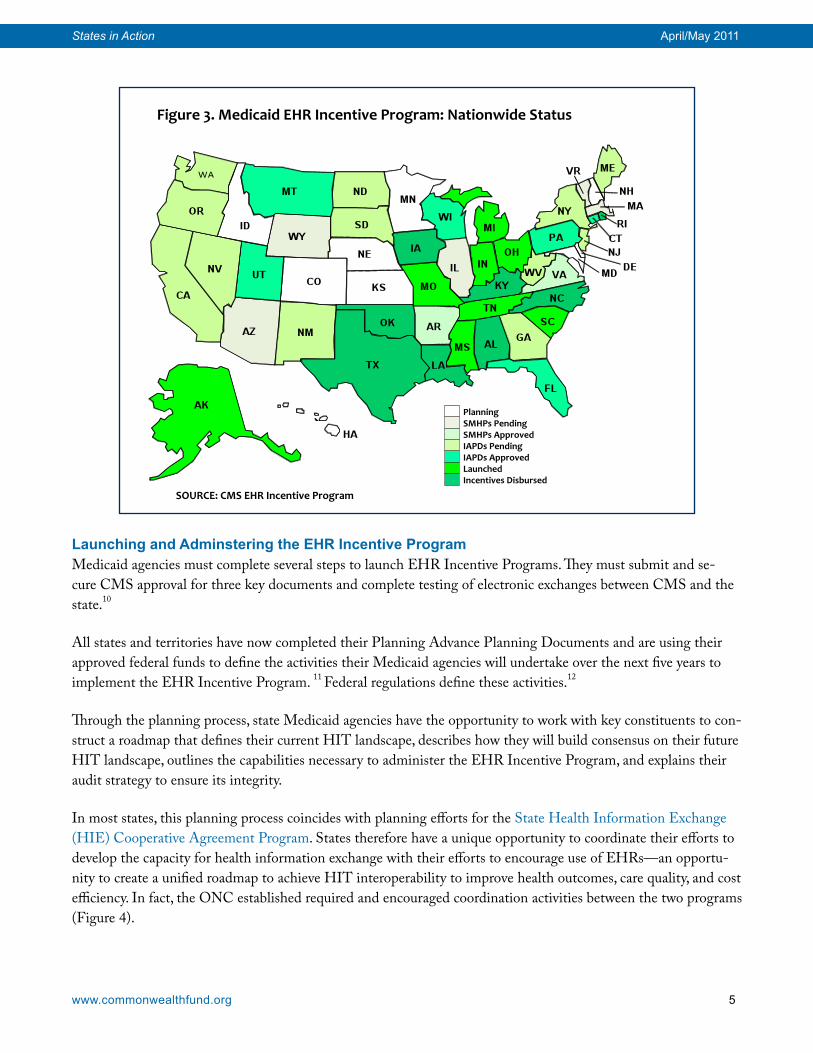
For more on the meaningful use policy priorities and goals, see Appendix B. For more information on its core objectives, see Appendix C. Eleven states launched EHR Incentive Programs on January 3, 2011, and another four states have launched programs since. Oklahoma disbursed the first incentive payment to an eligible physician practice, and Kentucky disbursed the first incentive payment to an eligible hospital. State Medicaid agencies are at varying stages in the program implementation, just as providers are at differing stages of EHR adoption and meaningful use. As of mid-April, more than 5,970 eligible professionals and 998 eligible hospitals were in the pro-cess of registering to participate. Seven states—Alabama, Iowa, Kentucky, Louisiana, North Carolina, Oklahoma, and Texas—have disbursed more than $83 million in incentive payments to eligible providers (Figure 3).
States in Action April/May 2011
www.commonwealthfund.org 5
Launching and Adminstering the EHR Incentive ProgramMedicaid agencies must complete several steps to launch EHR Incentive Programs. They must submit and se-cure CMS approval for three key documents and complete testing of electronic exchanges between CMS and the state.10
All states and territories have now completed their Planning Advance Planning Documents and are using their approved federal funds to define the activities their Medicaid agencies will undertake over the next five years to implement the EHR Incentive Program. 11 Federal regulations define these activities.12
Through the planning process, state Medicaid agencies have the opportunity to work with key constituents to con-struct a roadmap that defines their current HIT landscape, describes how they will build consensus on their future HIT landscape, outlines the capabilities necessary to administer the EHR Incentive Program, and explains their audit strategy to ensure its integrity.
In most states, this planning process coincides with planning efforts for the State Health Information Exchange (HIE) Cooperative Agreement Program. States therefore have a unique opportunity to coordinate their efforts to develop the capacity for health information exchange with their efforts to encourage use of EHRs—an opportu-nity to create a unified roadmap to achieve HIT interoperability to improve health outcomes, care quality, and cost efficiency. In fact, the ONC established required and encouraged coordination activities between the two programs (Figure 4).
Figure 3. Medicaid EHR Incentive Program: Nationwide Status
Planning SMHPs Pending SMHPs Approved IAPDs Pending IAPDs Approved Launched Incentives Disbursed
SOURCE: CMS EHR Incentive Program

States in Action April/May 2011
www.commonwealthfund.org 6
Figure 4. ONC Required and Encouraged Coordination Activities Between State Health Information Exchanges and Medicaid EHR Incentive Programs
Required Activities Encouraged Activities 1. The state’s governance structure shall include Medicaid agency representation. 2. State Level HIE shall coordinate provider outreach and communications with Medicaid.3. State Level HIE and state Medicaid agency shall identify common business or health care outcome priorities.4. State Level HIE, in collaboration with Medicaid, shall leverage, participate in, and support all Beacon Communities, Regional Extension Centers (RECs), and ONC workforce projects.5. State Level HIE shall align efforts with Medicaid to meet Medicaid requirements for meaningful use.
1. The state HIE is encouraged to obtain a letter of support from the Medicaid Director.2. Conduct joint needs assessments and environmen-tal scans.3. Collaborate with the Medicaid program and the ONC RECs to provide technical assistance to provid-ers beyond the REC scope.4. Share Help Desk or Call Center contracts and ser-vices between the State-HIE, REC, and MEHRIP. 5. Conduct statewide joint assessment and alignment of privacy policies across programs.6. Leverage current Medicaid IT infrastructure in devel-oping HIE technical architecture.7. Decide whether to integrate systems for shared objectives, i.e. share Medicaid claims and encounters with the HIE and information from non-Medicaid pro-viders with Medicaid.8. Work together to determine which specific shared services and technical services will be offered or used by Medicaid. 9. Determine which operational responsibilities Medicaid will manage. 10. Use Medicaid HIT incentives to encourage pro-vider participation in the HIE. 11. Collaborate on creation of payment incentives, such as Medicaid Pay for Performance, or encourag-ing participation of providers beyond Medicaid eligible providers.
Note: Beacon Communities are 17 innovative community collaboratives integrating certified electronic health record technologies and performance measurement into their local health care systems to improve the quality and cost effectiveness of care. Source: ONC, 2011
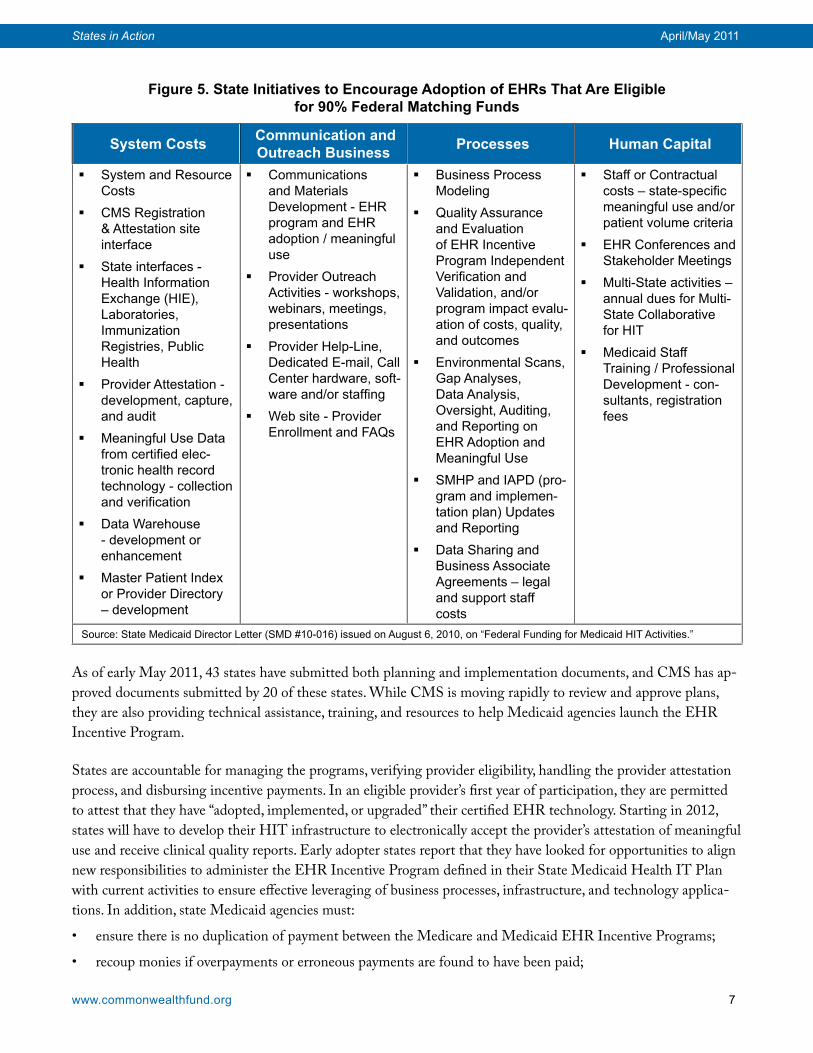
CMS has proposed regulation to guide states’ efforts in modernizing their technology infrastructure to ensure that an enhanced 90 percent federal match is provided only for changes that “provide more efficient, economical, and effective administration of the [Medicaid] plan.” Figure 5 shows the range of activities for which states may re-ceive the 90 percent federal matching funds to encourage the adoption and meaningful use of EHRs.
CMS considers the EHR Incentive Program plans to be dynamic documents that will be regularly updated by states and resubmitted to the agency, along with the HIT Implementation Advance Planning Document. The implementation document outlines the allocation or acquisition of human resources, services, and equipment that form the basis for the state’s benchmarks and transition strategies to move from the current environment to the desired future environment for HIT. States must receive approval from CMS for both documents before becom-ing eligible to receive enhanced matching funds.
States in Action April/May 2011
www.commonwealthfund.org 7
Figure 5. State Initiatives to Encourage Adoption of EHRs That Are Eligible for 90% Federal Matching Funds
System Costs Communication and Outreach Business Processes Human Capital
� System and Resource Costs
� CMS Registration & Attestation site interface
� State interfaces - Health Information Exchange (HIE), Laboratories, Immunization Registries, Public Health
� Provider Attestation - development, capture, and audit
� Meaningful Use Data from certified elec-tronic health record technology - collection and verification
� Data Warehouse - development or enhancement
� Master Patient Index or Provider Directory – development
� Communications and Materials Development - EHR program and EHR adoption / meaningful use
� Provider Outreach Activities - workshops, webinars, meetings, presentations
� Provider Help-Line, Dedicated E-mail, Call Center hardware, soft-ware and/or staffing
� Web site - Provider Enrollment and FAQs
� Business Process Modeling
� Quality Assurance and Evaluation of EHR Incentive Program Independent Verification and Validation, and/or program impact evalu-ation of costs, quality, and outcomes
� Environmental Scans, Gap Analyses, Data Analysis, Oversight, Auditing, and Reporting on EHR Adoption and Meaningful Use
� SMHP and IAPD (pro-gram and implemen-tation plan) Updates and Reporting
� Data Sharing and Business Associate Agreements – legal and support staff costs
� Staff or Contractual costs – state-specific meaningful use and/or patient volume criteria
� EHR Conferences and Stakeholder Meetings
� Multi-State activities – annual dues for Multi-State Collaborative for HIT
� Medicaid Staff Training / Professional Development - con-sultants, registration fees
Source: State Medicaid Director Letter (SMD #10-016) issued on August 6, 2010, on “Federal Funding for Medicaid HIT Activities.”
As of early May 2011, 43 states have submitted both planning and implementation documents, and CMS has ap-proved documents submitted by 20 of these states. While CMS is moving rapidly to review and approve plans, they are also providing technical assistance, training, and resources to help Medicaid agencies launch the EHR Incentive Program.
States are accountable for managing the programs, verifying provider eligibility, handling the provider attestation process, and disbursing incentive payments. In an eligible provider’s first year of participation, they are permitted to attest that they have “adopted, implemented, or upgraded” their certified EHR technology. Starting in 2012, states will have to develop their HIT infrastructure to electronically accept the provider’s attestation of meaningful use and receive clinical quality reports. Early adopter states report that they have looked for opportunities to align new responsibilities to administer the EHR Incentive Program defined in their State Medicaid Health IT Plan with current activities to ensure effective leveraging of business processes, infrastructure, and technology applica-tions. In addition, state Medicaid agencies must:
• ensure there is no duplication of payment between the Medicare and Medicaid EHR Incentive Programs;
• recoup monies if overpayments or erroneous payments are found to have been paid;
States in Action April/May 2011
www.commonwealthfund.org 8
• establish a provider appeals process for eligibility, payments, and determinations of meaningful use as part of the State Medicaid HIT Plan; and
• report estimated and actual expenditures for the program using the Medicaid Budget and Expenditure System.
Recommendations Based on States’ Early Experiences Given the requirements of health care reform and constraints on fiscal and human resources, states are well ad-vised to align their plans for HIT development among the EHR Incentive Program, HIE development, and other efforts and to collaborate with other agencies, states, and stakeholders to share or reduce costs, reuse technical ser-vices, and streamline efforts to offer providers clear direction.
Medicaid agencies could, for example, collaborate with administrators of health information exchanges on activi-ties such as fielding provider surveys, reaching out to and educating providers, creating immunization or other disease registries, and providing call center support.
To fulfill their outreach and technical assistance responsibilities, state Medicaid agencies could coordinate with regional extension centers (RECs), which are already providing outreach and technical assistance to small practices wishing to adopt EHRs and meet meaningful use criteria. Using federal funds, a few state Medicaid programs have hired RECs to expand their outreach and technical assistance to other providers (e.g., midwives and dentists) who are eligible for the Medicaid EHR Incentive Program.
Some RECs and states are working through provider associations’ established communication channels (e.g., newsletters, e-alerts, webinars, and meetings) to inform providers about the incentive program and the availability of technical assistance. In addition, a few states are offering loans to providers who cannot afford to begin the pro-cess of acquiring EHRs.
For the incentive program to succeed, states must acknowledge that EHRs are not “plug and play”: meaningful use of the technology requires education and support at the practice level. Further, to benefit from EHRs, practices need to change clinician and staff behaviors and rethink workflow. Doing so takes time and requires technical as-sistance and monitoring.
States that have been early adopters of the incentive program have learned that, instead of creating new systems to fulfill its technical requirements, they can often augment their existing systems. For example, some are using the same provider portal they use to enroll providers in Medicaid to fulfill the program’s requirement for a call center while adding new functions, such as for attesting meaningful use.
Finally, as states support and encourage development of accountable care organizations, health homes, and other innovative payment and delivery models, they should include information technology as a critical part of the pro-cess, not as an afterthought or competing priority. That is, states should integrate their policy and technology ini-tiatives by establishing goals for both and then adopting a framework and designing systems to accomplish them. There is potential for states to learn from the 17 Beacon Communities, which are integrating EHRs, HIEs, and other technologies into their local health care systems to improve quality and efficiency. The program is sharing lessons through the Health Care Transformation Has Begun site.

States in Action April/May 2011
www.commonwealthfund.org 9
Resources Contact Patty Conner, director of the Utah Health Exchange, [email protected], or see the Utah Health Exchange Web site.
Medicare and Medicaid Electronic Health Records Incentive Programs Official site
Medicare and Medicaid EHR Incentive Program Registration and Attestation System
Third Annual CMS Multi-State Medicaid HITECH Conference, May 24–5, 2011
Notes1 M. Au, S. Felt-Lisk, G. Anglin et al., Using Health IT: Eight Quality Improvement Stories (Rockville, MD: Agency
for Healthcare Research and Quality, September 2010) .2 M. Beeuwkes Buntin, M. F. Burke, M. C. Hoaglin et al., The Benefits of Health Information Technology: A
Review of the Recent Literature Shows Predominantly Positive Results, Health Affairs, 2011 30(3):464–71.3 Although the terms electronic health record (EHR) and electronic medical record (EMR) are sometimes used
interchangeably, only certified EHR systems capable of supporting interoperability are eligible for the EHR Incentive Program. EMRs often refer to information systems that are not interoperable—that is, that exchange information only within a single hospital or outpatient setting—and are not certified or eligible for such incentives.
4 C. J. Hsiao, E. Hing, T. Socey et al., Electronic Medical Record/Electronic Health Record Systems of Office-Based Physicians: United States, 2009 and Preliminary 2010 State Estimates (Hyattsville, MD, National Center for Health Statistics, December 2010).
5 D. Blumenthal, The Age of Meaningful Use: A Message from Dr. David Blumenthal, the National Coordinator for Health Information Technology, February 23, 2011, .
6 The focus of this States in Action is the Medicaid EHR Incentive Program; for more information about the Medicare EHR Incentive Program, see https://www.cms.gov/ehrincentiveprograms/ and https://www.cms.gov/apps/media/press/factsheet.asp?Counter=3792&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=6&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date.
7 Department of Health and Human Services American Recovery and Reinvestment Act, Centers for Medicare and Medicaid Services: Medicare and Medicaid Incentives and Administrative Funding, Funding Table note. Accessed at: http://www.hhs.gov/recovery/reports/plans/pdf20100610/CMS_HIT%20Implementation%20Plan%20508%20compliant.pdf.
8 Meaningful use objectives and measures are based on national Health Outcome Policy Priorities and Care Goals, and will be staged over three periods in the next five years (as highlighted earlier in Figure 3). Stage 1 (2011 and 2012) sets the baseline for electronic data capture and information sharing; meaningful use criteria and measures for Stage 1 are based on the National Health Outcome Policy Priorities (Appendix B). Stage 2 (expected to be implemented in 2013) and Stage 3 (expected to be implemented in 2015) will continue to expand on the Stage 1 baseline and be defined through future rule making.
9 §495.320-.322, Section 4201 (a)(3)(F)(i-ii).10 States must complete and obtain CMS approval for: 1) Planning Advance Planning Document; 2) State
Medicaid HIT Plan; and 3) HIT Implementation Advance Planning Document. States also must test exchanges between the Medicare and Medicaid EHR Incentive Program Registration and Attestation System and the state’s technical system for attestation and verification, and complete a number of state launch activities. See 42 CFR Parts 412, 413, 422 et al. Medicare and Medicaid Programs; Electronic Health Record Incentive Program; Final Rule 44507.

States in Action April/May 2011
www.commonwealthfund.org 10
11 See SMHP, OMB Approval Number: 0938-1088, https://www.cms.gov/MLNProducts/downloads/STATE_MEDICAID_HIT_PLAN_SMHP.pdf
12 Section 4201, Subtitle B – Medicaid Incentives, Division B: Title IV—Medicare and Medicaid Health Information Technology, HITECH of the ARRA Act; 42 CFR Parts 412, 413, 422 et al. Medicare and Medicaid Programs; Electronic Health Record Incentive Program; Final Rule; and State Medicaid Director Letters State Medicaid Director Letter SMDL# 11-002, ARRA# 8, April 8, 2011, Technical changes impacting the Medicaid EHR Incentive Program from the 2010 Medicare and Medicaid Extenders Act; SMD# 10-016, August 17, 2010, Federal Funding for Medicaid HIT Activities; SMD # 09-006, ARRA HIT # 1, September 1, 2009, Initial Guidance on Section 4201.
13 See A.-K. Fryer, M. M. Doty, and A.-M. J. Audet, Sharing Resources: Opportunities for Smaller Primary Care Practices to Increase Their Capacity for Patient Care (New York: The Commonwealth Fund, March 2011) and P. Torda, E. S. Han, and S. Hudson Scholle, Easing the Adoption and Use of Electronic Health Records in Small Practices, Health Affairs, April 2010 29(4):668–75.
Related Publications
Commonwealth Fund Publications A.-K. Fryer, M. M. Doty, and A.-M. J. Audet, Sharing Resources: Opportunities for Smaller Primary Care Practices to Increase Their Capacity for Patient Care, The Commonwealth Fund, March 2011.
N. Highsmith and J. Berenson, Driving Value in Medicaid Primary Care: The Role of Shared Support Networks for Physician Practices, The Commonwealth Fund, March 2011.
K. Purington, A. Gauthier, S. Patel et al., On the Road to Better Value: State Roles in Promoting Accountable Care Organizations, The Commonwealth Fund and the National Academy for State Health Policy, Feb. 2011.
J. Rosenthal, A. Gauthier, and A. Arons, State Strategies to Improve Quality and Efficiency: Making the Most of Opportunities in National Health Reform, The Commonwealth Fund and the National Academy for State Health Policy, December 2010.
C. Schoen, K. Stremikis, S. K. H. How, and S. R. Collins, State Trends in Premiums and Deductibles, 2003–2009: How Building on the Affordable Care Act Will Help Stem the Tide of Rising Costs and Eroding Benefits, The Commonwealth Fund, December 2010.
S. Silow-Carroll and J. N. Edwards, Intermountain Healthcare’s McKay-Dee Hospital Center: Driving Down Readmissions by Caring for Patients the “Right Way,” The Commonwealth Fund, Feb. 2011.

States in Action April/May 2011
www.commonwealthfund.org 11
M. Takach and J. Buxbaum, Developing Federally Qualified Health Centers into Community Networks to Improve State Primary Care Delivery Systems, National Academy for State Health Policy and The Commonwealth Fund, May 2011.
M. A. Zezza and S. Guterman, Perspectives on Health Reform—Achieving Accountable Care: Are We on the Right Path? The Commonwealth Fund, April 2011.
Other Related Publications
A. K. Jha, D. Doolan, D. Grandt et al., “The Use of Health Information Technology in Seven Nations,” International Journal of Medical Informatics, Dec. 2008 77(12):848–54.
L. M. Kern, A. B. Wilcox, J. Shapiro et al., “Community-Based Health Information Technology Alliances: Potential Predictors of Early Sustainability,” American Journal of Managed Care, April 2011 17(4): 290–95.
A.S. Khan, A. Fleischauer, J. Casani et al., “The Next Public Health Revolution: Public Health Information Fusion and Social Networks,” American Journal of Public Health, July 2010 100(7): 1237–42.
J. Kingsdale and J. Bertko, “Insurance Exchanges Under Health Reform: Six Design Issues for the States,” Health Affairs, June 2010 29(6):1158–63.
H. P. Rodriguez, T. von Glahn, M. N. Elliott et al., “The Effect of Performance-Based Financial Incentives on Improving Patient Care Experiences: A Statewide Evaluation,” Journal of General Internal Medicine, Dec. 2009 24(12):1281–88.
J. Roski and M. McClellan, “Measuring Health Care Performance Now, Not Tomorrow: Essential Steps to Support Effective Report,” Health Affairs, April 2011 30(4):682–89.
M. C. Shields, P. H. Patel, M. Manning et al., “A Model for Integrating Independent Physicians into Accountable Care Organizations,” Health Affairs, Dec. 2010 30(1):1–12.
M. Smith, M. R. Giuliano, and M. P. Starkowski, “In Connecticut: Improving Patient Medication Management in Primary Care,” Health Affairs, April 2011 30(4): 646–54.
D. Thompson, F. Velasco, D. Classen et al., “Reducing Clinical Costs with an EHR,” Journal of the Healthcare Financial Management Association, Oct. 2010 64(10):106–08.
P. Torda, E. S. Han, and S. Hudson Scholle, “Easing the Adoption and Use of Electronic Health Records in Small Practices,” Health Affairs, April 2010 29(4):668–75.
States in Action April/May 2011
www.commonwealthfund.org 12
Upcoming Meetings
The World Congress 2nd Leadership Summit on Accountable Care Organizations Vienna, VA May 23–4, 2011
13th Annual National Patient Safety Congress Washington, D.C. May 25–7, 2011
2011 State Health Research and Policy Interest Group Meeting Seattle, WA June 11, 2011
2011 AcademyHealth Annual Research Meeting Seattle, WA June 12–4, 2011
Sixth National Medicaid Congress: Special Health Reform Implementation Edition Washington, D.C. June 13–5, 2011
2011 National Association of Public Hospitals and Health Systems Annual Conference Chicago, IL June 22–4, 2011
Second National Accountable Care Organization (ACO) Summit Washington, D.C. June 27–9, 2011
National Association of County and City Health Official Annual 2011 Conference Hartford, CT July 20–2, 2011
National Conference of State Legislators Legislative Summit 2011 San Antonio, TX August 8–11, 2011
States in Action April/May 2011
www.commonwealthfund.org 13
Editorial Advisory BoardThe States in Action Editorial Advisory Board comprises experts from various aspects of state health policy. Members of the Editorial Advisory Board help to shape the newsletter by providing technical expertise, suggest-ing state innovations for inclusion, and by assisting in the reviewing of each issue.
John Colmers Secretary of Health and Mental Hygiene Maryland Department of Health and Mental Hygiene
Isabel Friedenzohn Senior Associate State Coverage Initiatives, AcademyHealth
Anne GauthierSenior FellowNational Academy for State Health Policy
Paul Jarris Executive Director Association of State and Territorial Health Officials
Ann KohlerDirector of Health PolicyNational Association of State Medicaid Directors
Chris Koller Health Insurance Commissioner State of Rhode Island
JoAnn Lamphere National Coordinator for State Affairs American Association of Retired Persons
Molly VorisSenior Policy Analyst, Health DivisionCenter for Best PracticesNational Governors Association
About the Newsletter
The States in Action bimonthly newsletter describes innovative state health programs from across the country. It is intended to help policymakers, administrators, and researchers as they work to stretch health care dollars and meet the needs of their residents.
States in Action is part of a Commonwealth Fund program on state health policy and practices. For more informa-tion, contact Ed Schor, Vice President, State Health Policy and Practices, at [email protected]. We welcome those involved in state efforts to expand coverage and improve care and efficiency to send an e-mail about their efforts to [email protected].
Authors: M. Reneé Bostick, M.P.A., Sharon Silow-Carroll, M.B.A., M.S.W., and Diana Rodin, M.P.H., Health Management Associates
Editor(s): Ed Schor, M.D., Vice President, State Health Policy and Practices and Cara Dermody, Program Assistant, State Health Policy and Practices.
Managing Editor: Martha Hostetter, M.F.A.
If you have a suggestion of a leader in state implementation of federal health care reform who might be a good candidate for our “Ask the Expert” column, please submit a name, organizational affiliation, and a brief explanation of why you think he or she should be featured to [email protected].
Related Documents