Objectives & Background Definition Rehab Process Outcomes Nephrology Roles Conclusions Objectives S. aureus Fungal Conclusion Mycobacteria “Staph, Fungal & Tuberculous Peritonitis” Long Beach CA, (March 2017) S. Vanita Jassal Professor of Medicine, Univ. of Toronto & Staff Nephrologist, University Health Network

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles ConclusionsObjectives S. aureus Fungal ConclusionMycobacteria
“Staph, Fungal & Tuberculous Peritonitis”
Long Beach CA, (March 2017)
S. Vanita JassalProfessor of Medicine, Univ. of Toronto &
Staff Nephrologist, University Health Network
Objectives S. aureus Fungal ConclusionMycobacteria
Disclosures
• Investigator led funding from Fresenius Health Care 2015
• Salary benefits: Ontario Renal Network
Objectives
Objectives S. aureus Fungal ConclusionMycobacteria
Objectives
• To recognize and treat peritonitis caused by – Staphylococcus aureus– Fungal organisms– Mycobacteria
Objectives
Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles Conclusions
STAPHYLOCOCCUS AUREUS
Objectives S. aureus Fungal ConclusionMycobacteria
ISPD Recommendations 2016
• Empiric treatment includes antibiotics that cover S Aureus
• Treatment modified based on cultures • Cefazolin IP• Methicillen resistant organisms Vancomycin IP• Duration of treatment 3 weeks
www.ispd.org

Objectives S. aureus Fungal ConclusionMycobacteria
ISPD Recommendations 2016
• Other agents include teicoplanin and daptomycin
• +/- Rifampicin 5-7 days
• Consider rapid peritoneal lavage – severe abdominal pain – “toxic shock”-type presentation
www.ispd.org
Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles ConclusionsObjectives S. aureus Fungal ConclusionMycobacteria
ISPD Recommendations 2016
• Other adjunctive treatments to consider:– rapid peritoneal lavage for severe abdominal pain
and/or “toxic shock”-type presentation (s. aureus)– peritoneal “resting” for 2 to 3 days if bowel leak
(multiple gram negative organisms)
www.ispd.org

Objectives S. aureus Fungal ConclusionMycobacteria
ISPD Recommendations 2016Li et al, Perit Dial Int 2016; 36(5):481–508

Objectives S. aureus Fungal ConclusionMycobacteria
Relapse Risk - S Aureus
0
5
10
15
20
25
30
% Control (n = 2021) % Relapsed (n = 356)
Burke et a, AJKD 2011: 58; 429-436
Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles ConclusionsObjectives S. aureus Fungal ConclusionMycobacteria
Relapse Risk - S Aureus• High association with exit site and tunnel infections
• Consider removal of the PD catheter if little or no improvement in 4-5 days
• Consider if patient has S Aureus nasal carriage
Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles Conclusions
FUNGAL PERITONITIS

Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles ConclusionsObjectives S. aureus Fungal ConclusionMycobacteria
Prevention of Fungal Peritonitis
• Accounts for 1 – 15% of peritonitis episodes• Mortality rate 5 – 53%• Trend over time for non-Albicans Candida
• Often requires catheter removal • Leading cause of PD-peritonitis related technique failure

Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles ConclusionsObjectives S. aureus Fungal ConclusionMycobacteria
Risk Factors for Fungal Peritonitis
• frequent peritonitis **• antibiotic therapy **• immunosuppression• low serum albumin concentration• PEG tubes• peritoneo-vaginal communication

Objectives S. aureus Fungal ConclusionMycobacteria
Yeast or Fungi on the Gram Stain
TIP!
• sometimes PD fluid will be sent in someone with abdominal pain or just walking into the ER
• if there is no leukocytosis, but the gram stain shows yeast, don’t rush to take out the catheter
• repeat the sample and see if a leukocytosis is developing• sometimes yeast (indeed, other bacteria too) appears in the PD
fluid but doesn’t lead to peritonitis– be careful of drive-by cultures
Slide courtesy of Dr. Joanne Bargman

Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles ConclusionsObjectives S. aureus Fungal ConclusionMycobacteria
Prevention of Fungal Peritonitis
• Can prophylactic anti-fungal therapy at the time of antibiotic administration prevent fungal overgrowth?
• Could this therapy prevent the development of antibiotic-related fungal peritonitis?
Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles ConclusionsObjectives S. aureus Fungal ConclusionMycobacteria
Fungal Prophylaxis
• Success rate of prophylaxis will depend on baseline rate of fungal peritonitis– Units with high rates have demonstrated reduction of fungal
peritonitis rates with prophylactic anti-fungal therapy
• Oral nystatin may be inconvenient, but– it’s a safe medication– resistance not reported, but not likely a problem even if it
were
Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles ConclusionsObjectives S. aureus Fungal ConclusionMycobacteria
ISPD recommended treatmentYeast / Fungus
– PD catheter removal (1C recommendation)– Duration of Rx 2 weeks after catheter removal (2C)
– Amphotericin 25 mg IV/day plus Flucytosine for 4-6 weeks
OR– Fluconazole 150 mg IP/q2d plus oral post-removal– (case reports of intra-catheter amphotericin)
Candida and Crypotococcus
Objectives S. aureus Fungal ConclusionMycobacteria
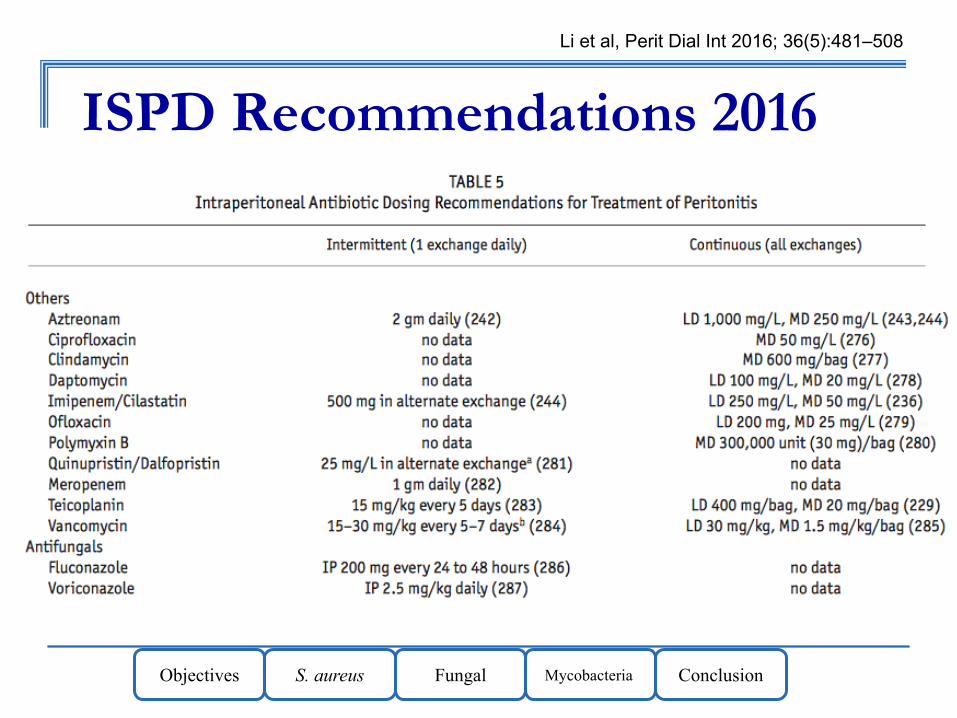
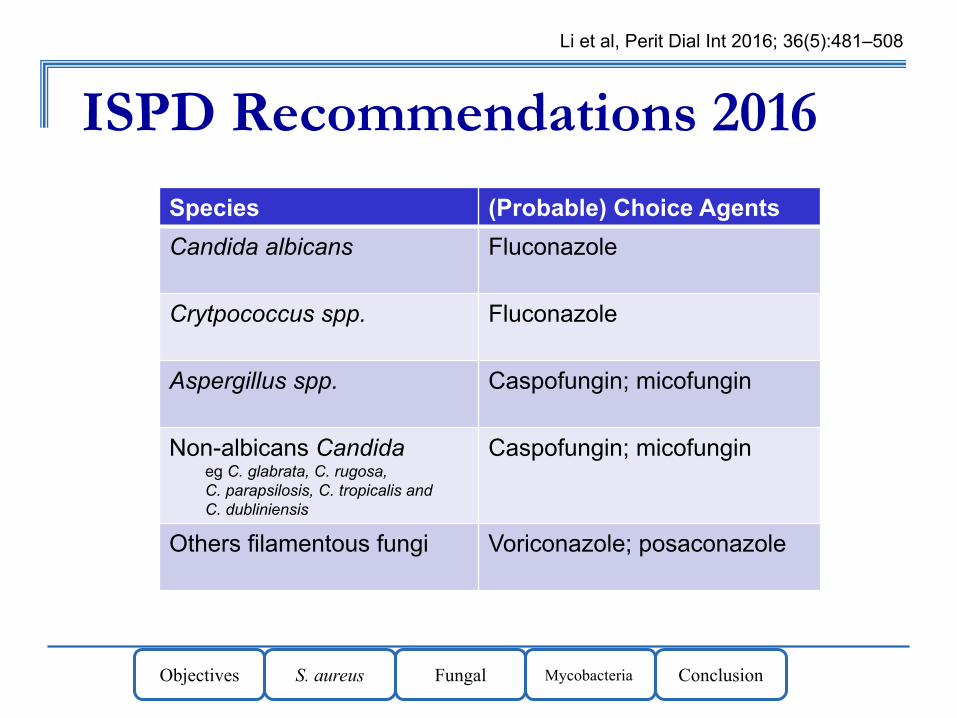
ISPD Recommendations 2016Li et al, Perit Dial Int 2016; 36(5):481–508
Objectives S. aureus Fungal ConclusionMycobacteria
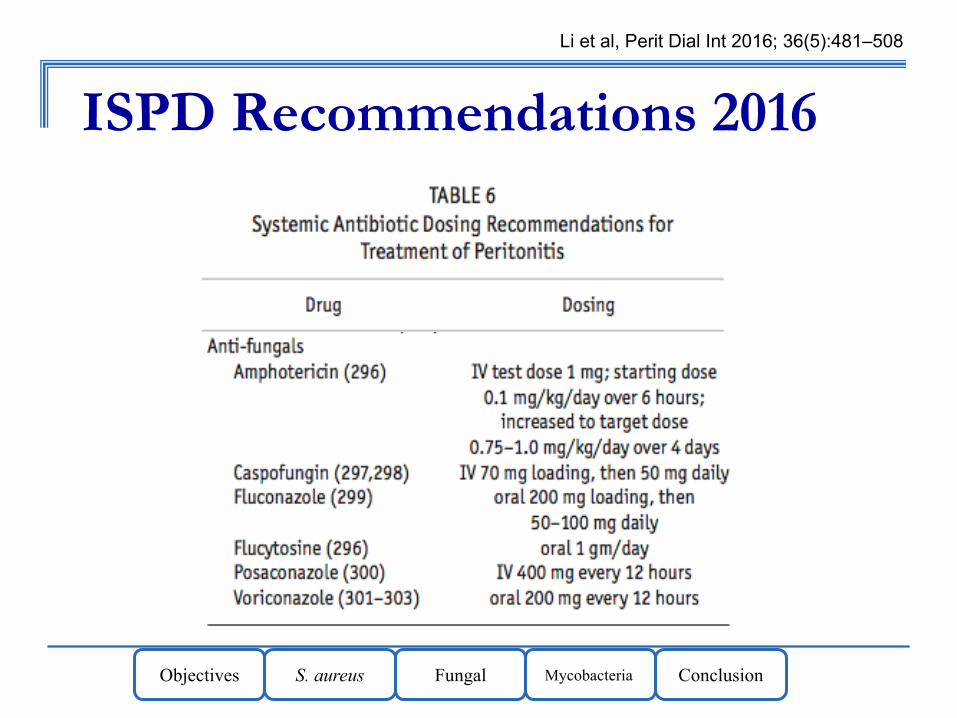
ISPD Recommendations 2016Li et al, Perit Dial Int 2016; 36(5):481–508
Objectives S. aureus Fungal ConclusionMycobacteria
ISPD Recommendations 2016Li et al, Perit Dial Int 2016; 36(5):481–508
Species (Probable) Choice AgentsCandida albicans Fluconazole
Crytpococcus spp. Fluconazole
Aspergillus spp. Caspofungin; micofungin
Non-albicans Candidaeg C. glabrata, C. rugosa, C. parapsilosis, C. tropicalis andC. dubliniensis
Caspofungin; micofungin
Others filamentous fungi Voriconazole; posaconazole

Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles ConclusionsObjectives S. aureus Fungal ConclusionMycobacteria
Yeast/Fungal Peritonitis: outcomes
• The high mortality rate is related to co-morbidity: some very ill, dying patients will get fungal peritonitis as an agonal event
• In Toronto cohort, 33% of patients were able to return to PD
Nadeau-Fredette and Bargman Perit Dial Int 2013

Objectives S. aureus Fungal ConclusionMycobacteria
Early catheter removal associated with better outcomes
• Retrospective study of 94 episodes of fungal peritonitis– Catheter removal within 24 hours in 42%– Catheter removal 2-9 days later in 45%– Mortality rate significantly higher with delayed
catheter removal (32 vs. 13%)
Chang et al, PDI 2011
Objectives S. aureus Fungal ConclusionMycobacteria
Unclear role for prophylaxis...
• Pre-procedural antibiotics– Colonoscopy, cystoscopy, hysteroscopy,
colposcopy, PD catheter manipulation– Regimens for colonoscopy should cover
enterococcus, enteric gram negatives and anaerobes
Objectives S. aureus Fungal ConclusionMycobacteria
Fungal Peritonitis
• Patients should receive fungal prophylaxis with any course of antibiotics
• Can use nystatin or fluconazole• As soon as fungal peritonitis diagnosed,
arrange early catheter removal

Objectives & Background Definition Rehab
Process Outcomes Nephrology Roles Conclusions
MYCOBACTERIAL INFECTIONS

Objectives S. aureus Fungal ConclusionMycobacteria
Mycobacteria
• Slow growing– M. tuberculosis– M. bovis– M. avium complex
• Fast growing– M. chelonae– M. fortuitum

Objectives S. aureus Fungal ConclusionMycobacteria
Consider M. tuberculosis when
• Endemic area• Culture negative, poor response• Culture positive with worsening or poor
response• Systemic illness consistent with TB
Objectives S. aureus Fungal ConclusionMycobacteria
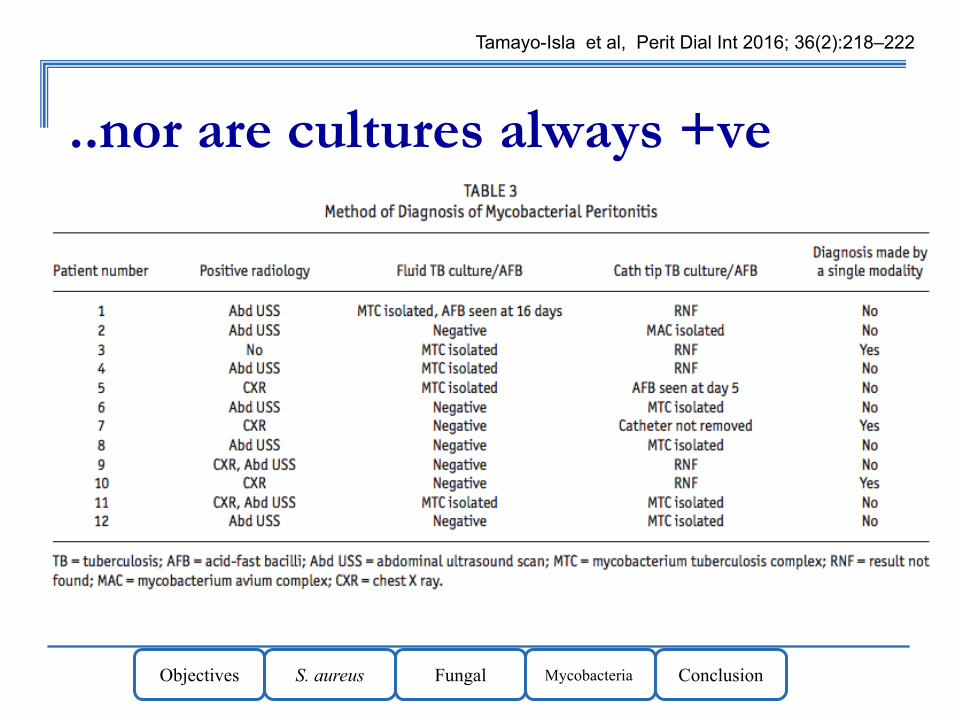
M. tuberculosis is “tricky” to find
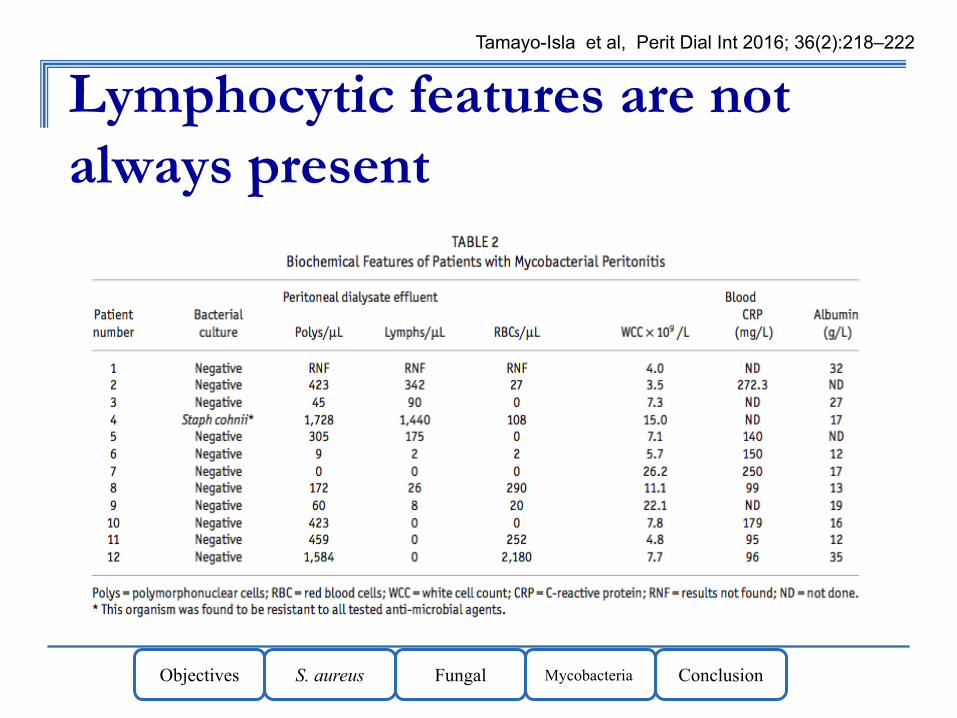
• Initial presentation is often with a neutrophil response (not lymphocytic)
• Classic ZN stains may not be sensitive– Centrifuge 50-100mls and then plate– Liquid media – Longer incubation
• DNA PCR studies have high rates of false positives
Objectives S. aureus Fungal ConclusionMycobacteria
Lymphocytic features are not always present
Tamayo-Isla et al, Perit Dial Int 2016; 36(2):218–222
Objectives S. aureus Fungal ConclusionMycobacteria
..nor are cultures always +ve
Tamayo-Isla et al, Perit Dial Int 2016; 36(2):218–222

Objectives S. aureus Fungal ConclusionMycobacteria
Treatment
• Local sensitivity and resistance patterns will influence medications used
• Often 4 drugs in combination: – rifampicin, isoniazid x 12-18 months– pyrazinamide & ofloxacin x 2 months– IP rifampicin if possible
• Pyridoxine 50-100 mg daily (with isoniazid)
www.ispd.org

Objectives S. aureus Fungal ConclusionMycobacteria
Catheter removal
• Controversial– Limpopo series – recommend it strongly– India series – not always needed
• ISPD recommendation uses the word “may” remove the catheter

Objectives S. aureus Fungal ConclusionMycobacteria
Non-tuberculous Mycobacteriae
• Emerging more commonly• Australian series 2013
– 12 cases– 1 in 1000 patient-years (0.6-1.4)– Recovery in 11 cases (3 no cath removal)
• Possible association with gentamicin– Lo et al, PDI 2013 33:267-72
Jiang et al, Int Urol Nephrol 2013 Oct;45(5):1423-8

Objectives S. aureus Fungal ConclusionMycobacteria
TreatmentsJiang et al, Int Urol Nephrol 2013 Oct;45(5):1423-8
Objectives S. aureus Fungal ConclusionMycobacteria
Conclusions
• Difficult to treat infections• All require high vigilance• Prevention is better than cure• Treatment is best with consultation with
local infectious disease specialists and use of ISPD guidelines

Objectives S. aureus Fungal ConclusionMycobacteria
University of Toronto Geriatric Nephrology Fellowship
Areas of specific focus will include one or more of the following areas: dialysis rehabilitation, care for residents in long-term care facilities, non-dialysis care and symptom management. Research
mentorship available includes Clinical Epidemiology or Translational Research
For details contact: [email protected]
Related Documents











