ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary

ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ST-Elevation Myocardial Infarction& Cardiogenic Shock
- What Should We Do?
Advanced Angioplasty 2008
Dan Blackman
Leeds General Infirmary

Conflicts of interest
• Advisory Boards– Cordis– Boston Scientific– Medtronic– Nycomed– Lilly– St Jude
• Travel/Sponsorship– Cordis– Boston Scientific– Medtronic– Abbott– St Jude
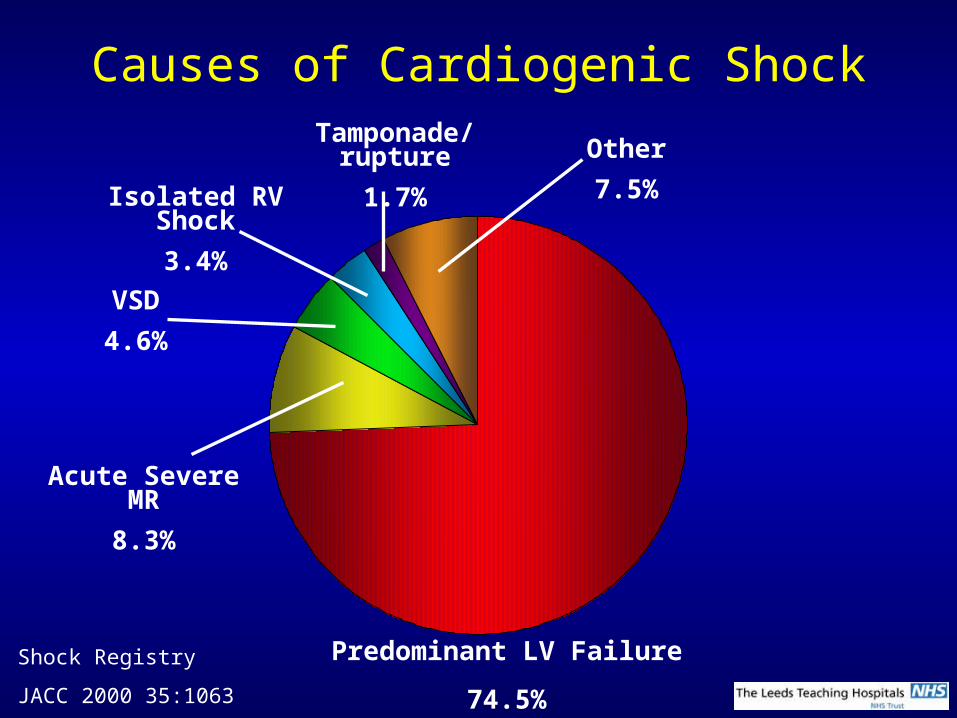
Causes of Cardiogenic Shock
Predominant LV Failure
74.5%
Acute Severe MR
8.3%
VSD
4.6%
Isolated RV Shock
3.4%
Tamponade/rupture
1.7%Other
7.5%
Shock Registry
JACC 2000 35:1063
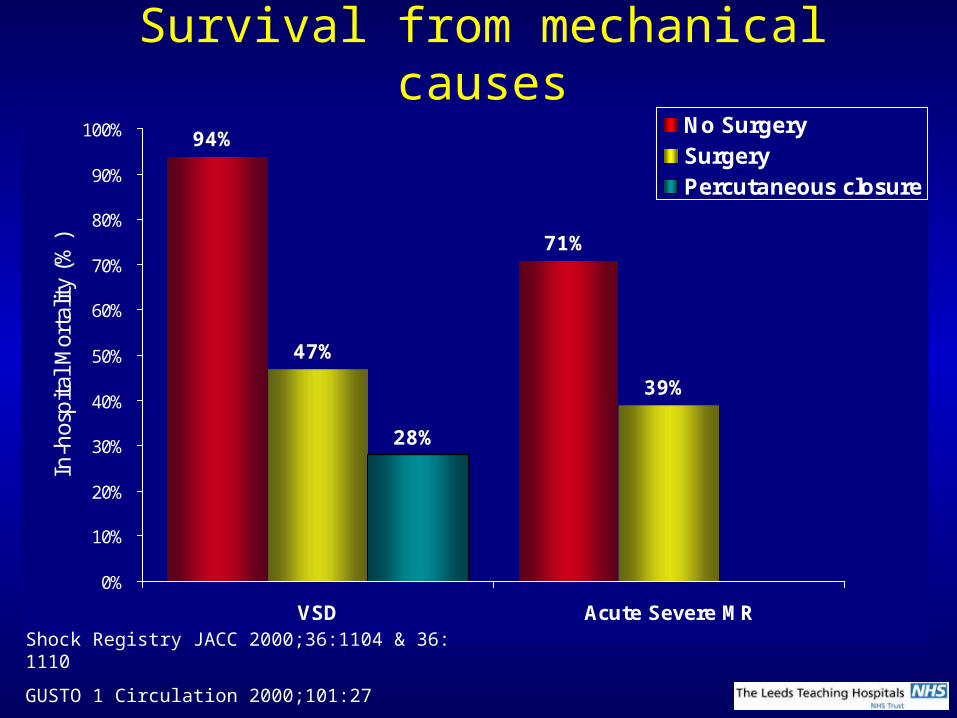
Survival from mechanical causes
94%
71%
47%
39%
28%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
VSD Acute Severe MR
In-h
ospi
tal M
orta
lity
(%)
No SurgerySurgeryPercutaneous closure
Shock Registry JACC 2000;36:1104 & 36: 1110
GUSTO 1 Circulation 2000;101:27
Holzer R CCI 2004;61:196
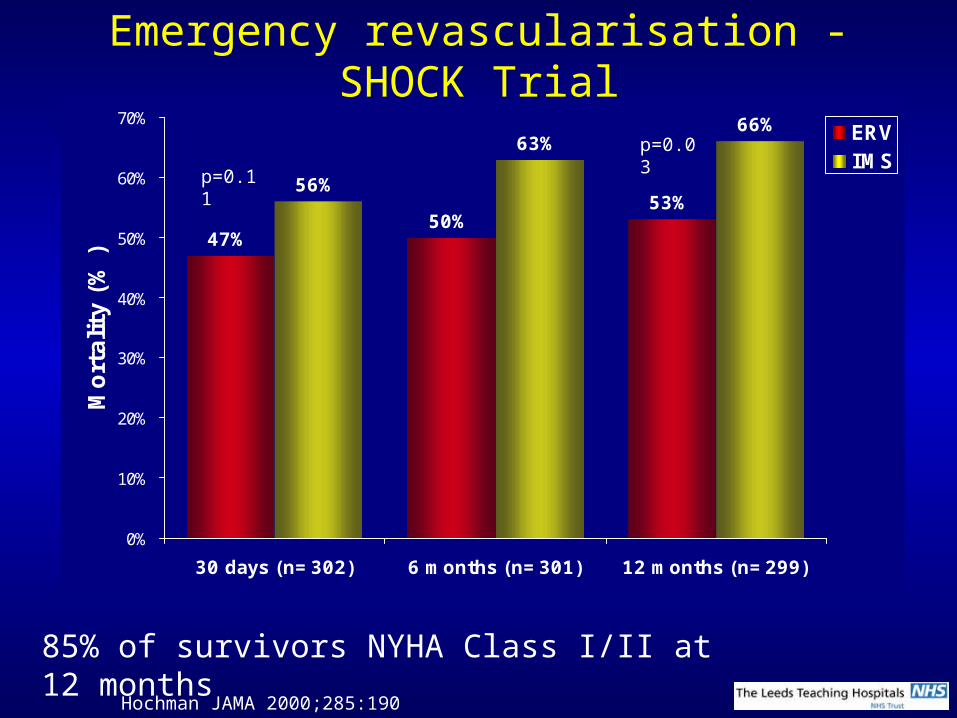
Emergency revascularisation - SHOCK Trial
47%50%
53%56%
63%66%
0%
10%
20%
30%
40%
50%
60%
70%
30 days (n=302) 6 months (n=301) 12 months (n=299)
Mort
ality
(%
)
ERVIMS
85% of survivors NYHA Class I/II at 12 months
Hochman JAMA 2000;285:190
p=0.11
p=0.03

Emergency revascularisation in the Elderly- SHOCK Trial
41%
75%
57%53%
0%
10%
20%
30%
40%
50%
60%
70%
80%
<75 years (n=246) >75 years (n=56)
30-d
ay M
ort
ality
(%
)ERVIMS
• >75 years ERV vs IMS baseline characteristics– LVEF 28% vs 36% p=0.051– Anterior MI 63% vs 41% p=0.18– Female 54% vs 31% p=0.11
p=0.01
p=0.01
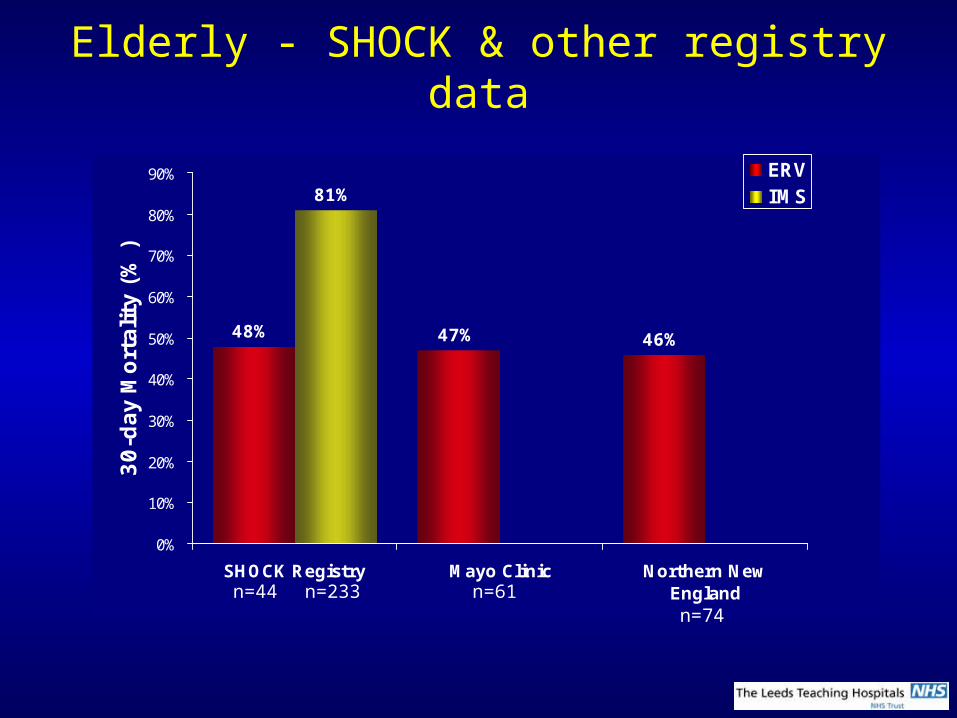
Elderly - SHOCK & other registry data
48% 47% 46%
81%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
SHOCK Registry Mayo Clinic Northern NewEngland
30-d
ay M
ort
ality
(%
)
ERVIMS
n=44 n=233 n=61n=74
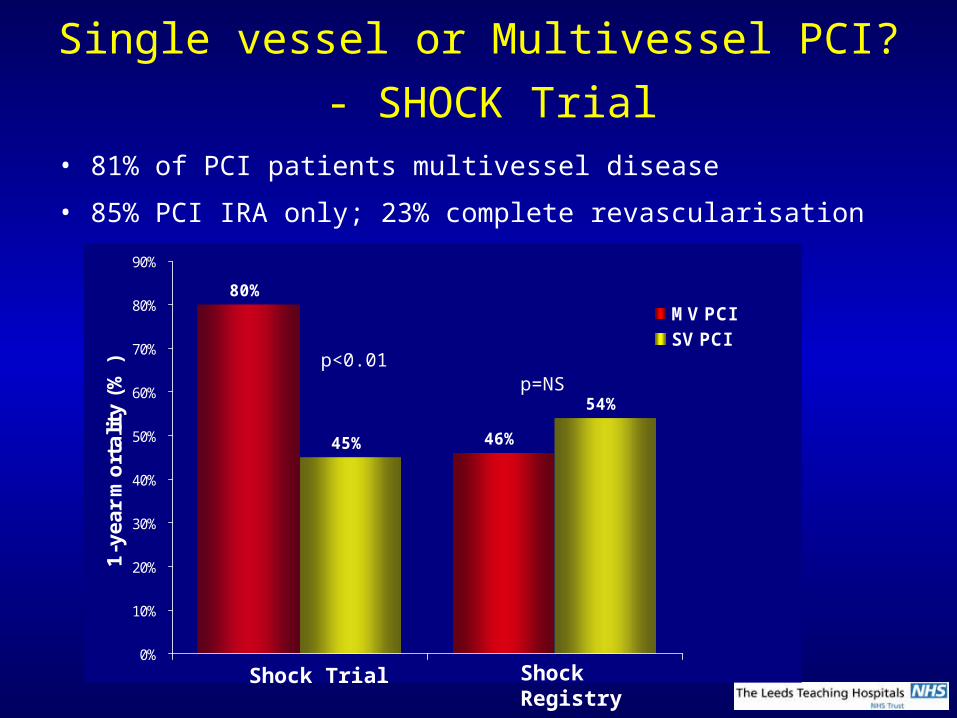
Single vessel or Multivessel PCI?
- SHOCK Trial• 81% of PCI patients multivessel disease
• 85% PCI IRA only; 23% complete revascularisation
80%
46%45%
54%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1-y
ear
mort
alit
y (%
)
MV PCISV PCI
p<0.01
Shock Trial Shock Registry
p=NS
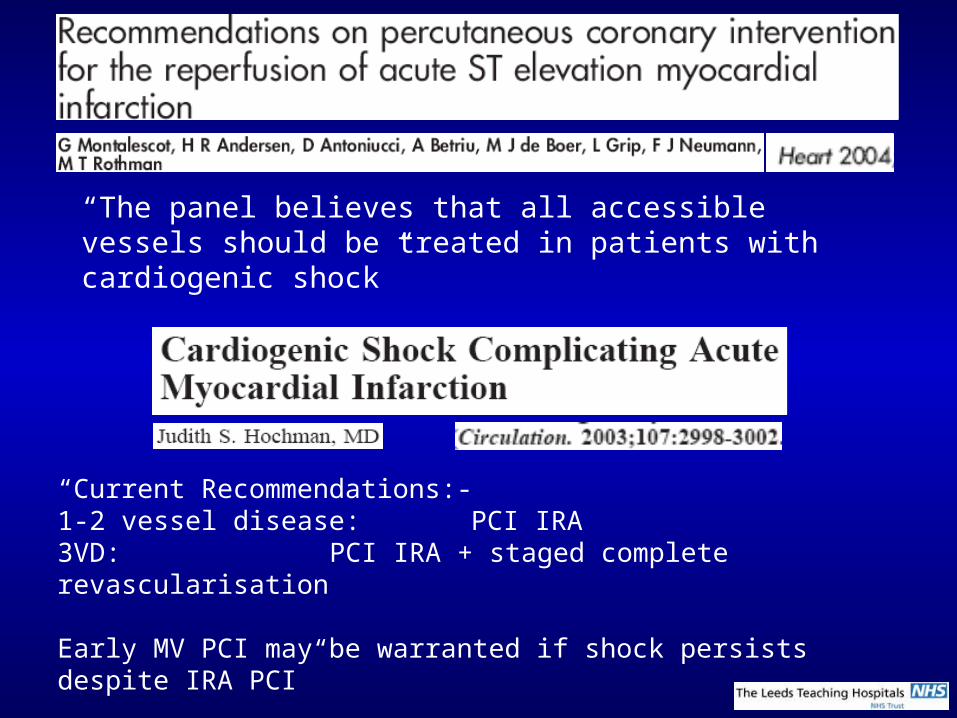
“The panel believes that all accessible vessels should be treated in patients with cardiogenic shock”
“Current Recommendations:-1-2 vessel disease: PCI IRA3VD: PCI IRA + staged complete revascularisation
Early MV PCI may be warranted if shock persists despite IRA PCI”
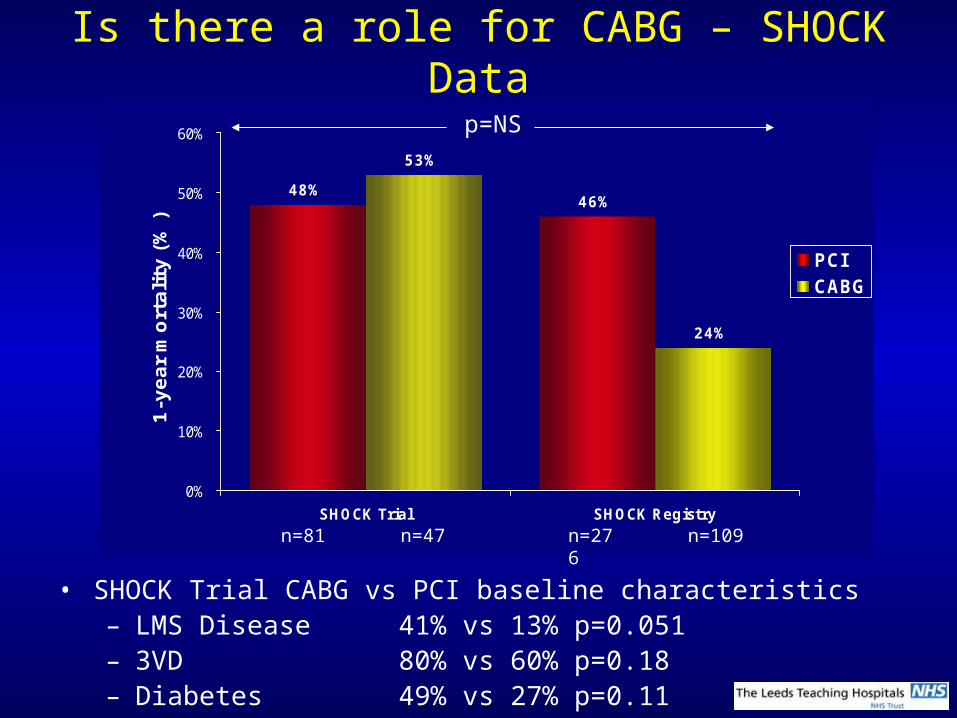
Is there a role for CABG – SHOCK Data
48%46%
53%
24%
0%
10%
20%
30%
40%
50%
60%
SHOCK Trial SHOCK Registry
1-y
ear
mort
ality
(%
)
PCICABG
p=NS
• SHOCK Trial CABG vs PCI baseline characteristics– LMS Disease 41% vs 13% p=0.051– 3VD 80% vs 60% p=0.18– Diabetes 49% vs 27% p=0.11
n=47n=81 n=276 n=109
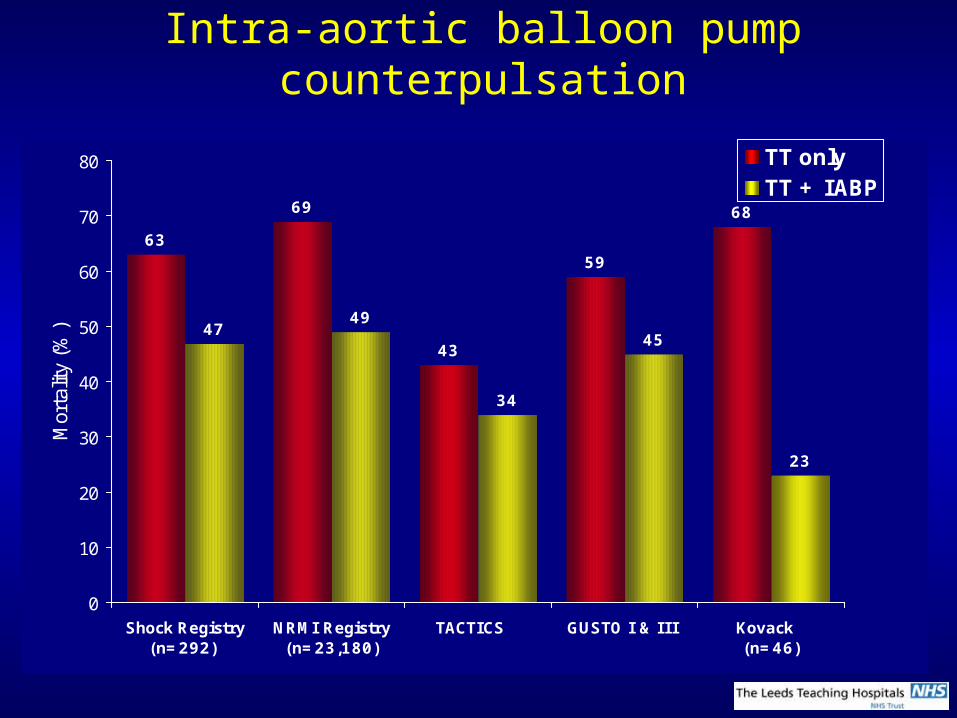
Intra-aortic balloon pump counterpulsation
63
69
43
59
68
4749
34
45
23
0
10
20
30
40
50
60
70
80
Shock Registry(n=292)
NRMI Registry(n=23,180)
TACTICS GUSTO I & III Kovack (n=46)
Mor
talit
y (%
)
TT onlyTT + IABP
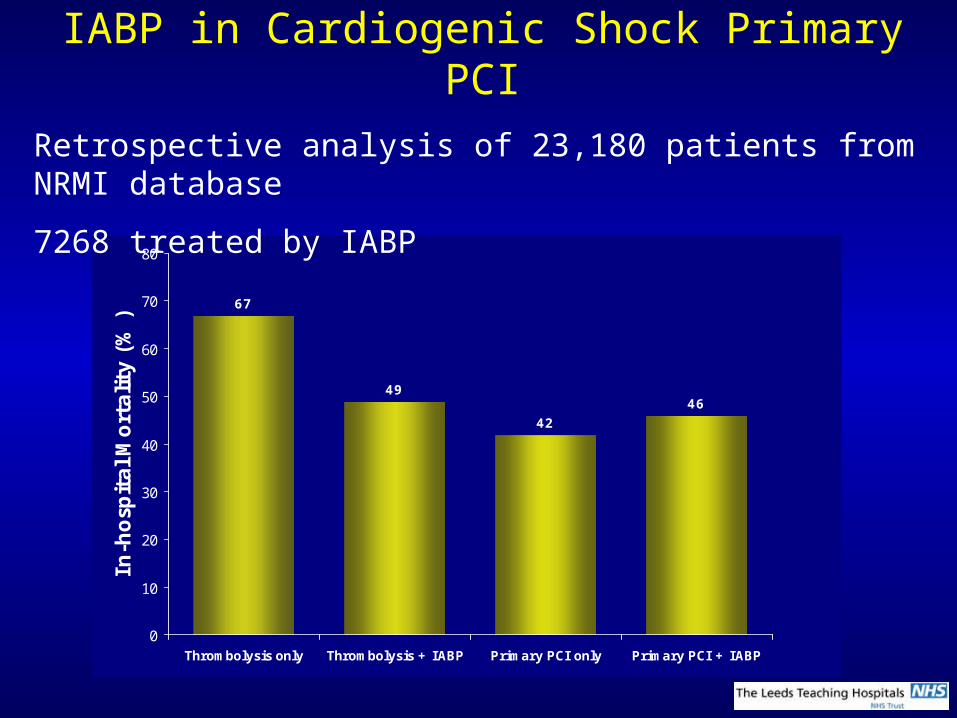
IABP in Cardiogenic Shock Primary PCI
67
49
42
46
0
10
20
30
40
50
60
70
80
Thrombolysis only Thrombolysis + IABP Primary PCI only Primary PCI + IABP
In-h
osp
ital M
ort
ality
(%
)Retrospective analysis of 23,180 patients from NRMI database
7268 treated by IABP
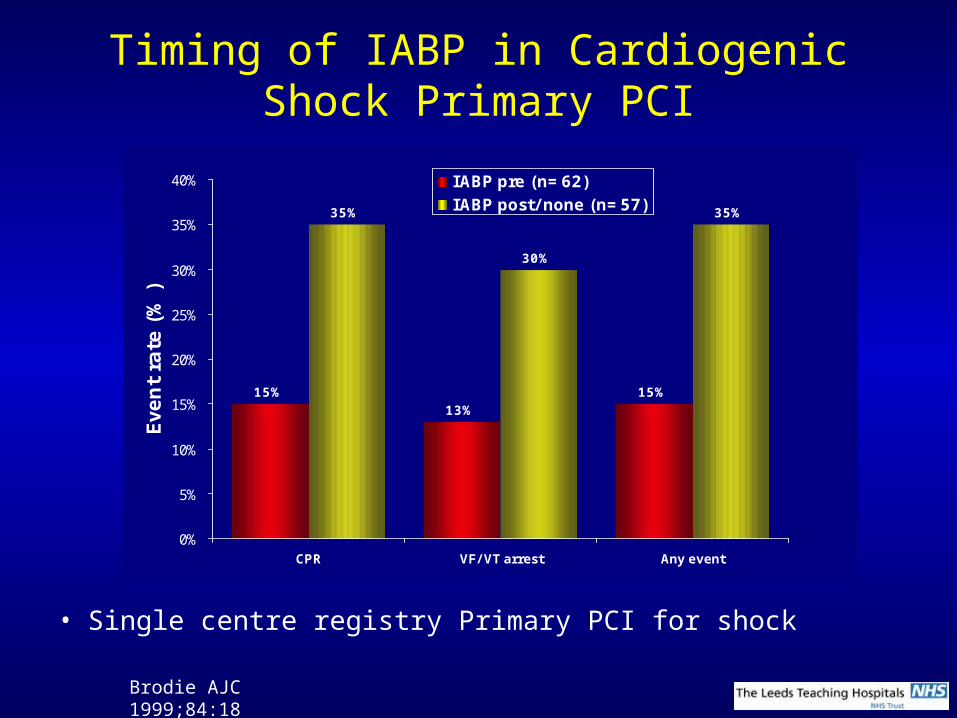
Timing of IABP in Cardiogenic Shock Primary PCI
15%13%
15%
35%
30%
35%
0%
5%
10%
15%
20%
25%
30%
35%
40%
CPR VF/ VT arrest Any event
Eve
nt
rate
(%
)
IABP pre (n=62)IABP post/ none (n=57)
• Single centre registry Primary PCI for shock
Brodie AJC 1999;84:18
Inotropes and Vasopressors
No meaningful data!
ACC/AHA Guidelines
SBP <70:-
Norepinephrine (0.5-30 g/min)
Switch to Dopamine (5-15 g/kg/min) once SBP ≥80
SBP 70-100
Dopamine (5-15 g/kg/min)
Add dobutamine (2-20 g/kg/min) once SBP ≥90

Percutaneous left ventricular assist devices
• Even with revascularisation and IABP support mortality from cardiogenic shock post STEMI remains ≥50%
• Recovery of myocardial performance following successful revascularisation may take several days. During this time many patients succumb to low cardiac output
• If effective, active cardiac support could be provided while awaiting the beneficial effects of revascularisation, survival rates may be enhanced
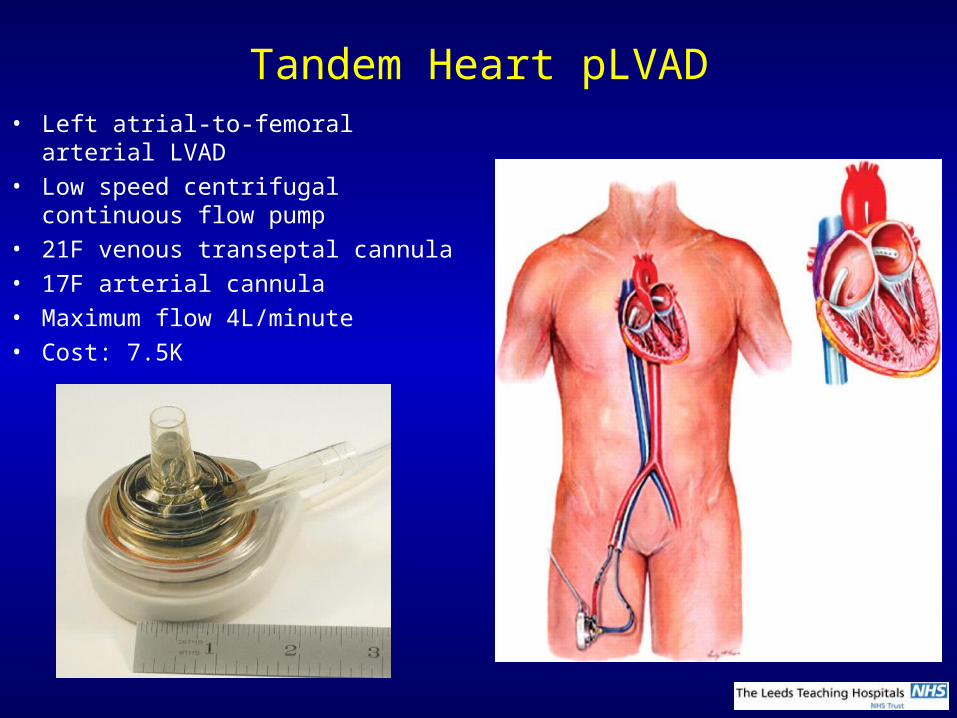
Tandem Heart pLVAD• Left atrial-to-femoral arterial LVAD• Low speed centrifugal continuous
flow pump• 21F venous transeptal cannula• 17F arterial cannula• Maximum flow 4L/minute• Cost: 7.5K
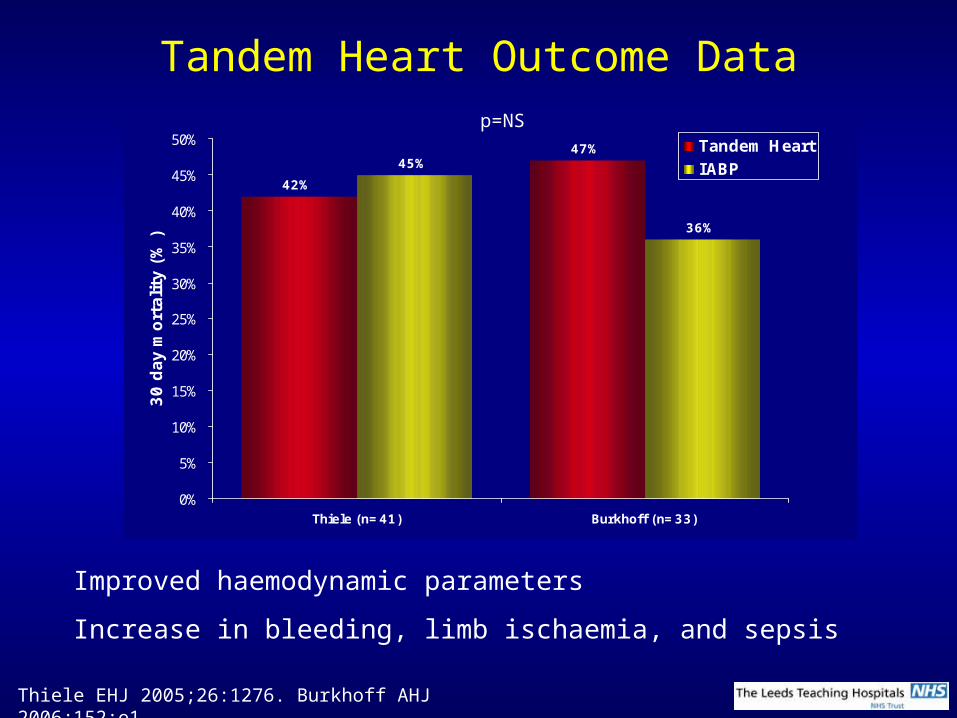
Tandem Heart Outcome Data
42%
47%45%
36%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Thiele (n=41) Burkhoff (n=33)
30 d
ay m
ort
alit
y (%
)Tandem HeartIABP
Improved haemodynamic parameters
Increase in bleeding, limb ischaemia, and sepsis
Thiele EHJ 2005;26:1276. Burkhoff AHJ 2006;152:e1
p=NS
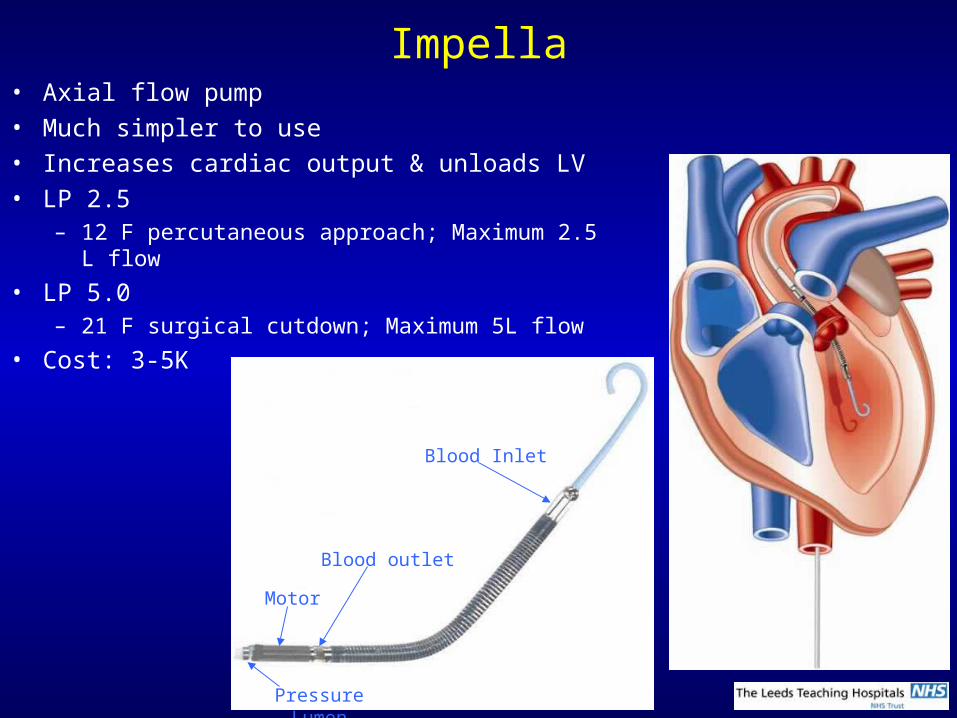
Impella• Axial flow pump• Much simpler to use• Increases cardiac output & unloads LV• LP 2.5
– 12 F percutaneous approach; Maximum 2.5 L flow
• LP 5.0– 21 F surgical cutdown; Maximum 5L flow
• Cost: 3-5K
Pressure Lumen
Motor
Blood outlet
Blood Inlet
Impella outcome data
• 1 RCT of Impella 2.5 in AMI Cardiogenic Shock
• ISAR-SHOCK
– 26 patient RCT Impella vs IABP Cardiac Index, MAP (by 10mmHg) vs IABP– Complications ≤ IABP
– No difference in mortality
What we should do about STEMI Cardiogenic Shock
• Emergency angiography and revascularisation: Primary PCI preferably– All patients <75 years
– Selected patients ≥75 years
• On-table echo to rule out mechanical defects
• Stabilise the patient in the lab before revascularisation– IABP
– Pressors if required (Norepinephrine/dopamine)
– Anaesthetic support
• Consider calling the surgeon for true surgical disease
• PCI culprit artery. Other vessels if shock persists
• Use abciximab for PCI
• Consider percutaneous LVAD if shock persists with IABP + multi-vessel
revascularisation
Related Documents











