Acute Coronary Syndromes Ranil de Silva Senior Lecturer in Clinical Cardiology Senior Lecturer in Clinical Cardiology National Heart and Lung Institute, Imperial College London National Heart and Lung Institute, Imperial College London Consultant Cardiologist Consultant Cardiologist Royal Brompton and Royal Brompton and Harefield Harefield NHS Foundation Trust NHS Foundation Trust [email protected] [email protected] Acute Coronary Syndromes ST depression T wave inversion ST elevation ESC NSTE-ACS Guidelines 2007 or normal ECG Management Aims in ACS o Rapidly establish diagnosis o Determine risks – MACE (Death, non-fatal MI, recurrent ischaemia, heart failure, arrhythmia, re-hospitalisation, stroke) – Iatrogenic complications (bleeding) o Choose and implement treatment strategy – Timely – Reduce risk of MACE – Minimise risk of bleeding – Treat mechanical complications Case 1 o 79 Female o 4 hrs chest burning o Ex-smoker, stopped 30 years ago o Drugs – warfarin, digoxin 125 mcg, amlodipine 5mg, frusemide 40mg, simvastatin 20mg o Physical examination – BP 180/90 mm Hg (R=L) – HR 160 irreg – RR 24/min, O 2 sats 98% on rebreathe – BM 9.6 mmol/L – Bibasal creps o Bloods tests – Hb 10.8, K 4.1, Cr 126, INR 4.3, troponin pending Presenting ECG ECG Diagnosis o Acute LAD syndrome (NSTEACS), rapid AF o Acute posterior STEACS, rapid AF o Acute inferior STEACS, rapid AF o Acute infero-posterior STEACS, rapid AF o Acute pericarditis, rapid AF

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Acute Coronary Syndromes
Ranil de Silva
Senior Lecturer in Clinical CardiologySenior Lecturer in Clinical CardiologyNational Heart and Lung Institute, Imperial College LondonNational Heart and Lung Institute, Imperial College London
Consultant CardiologistConsultant CardiologistRoyal Brompton and Royal Brompton and HarefieldHarefield NHS Foundation TrustNHS Foundation Trust
[email protected]@imperial.ac.uk
Acute Coronary Syndromes
ST depression T wave inversionST elevation
ESC NSTE-ACS Guidelines 2007
or normal ECG
Management Aims in ACS
o Rapidly establish diagnosiso Determine risks
– MACE (Death, non-fatal MI, recurrent ischaemia, heart failure, arrhythmia, re-hospitalisation, stroke)
– Iatrogenic complications (bleeding)
o Choose and implement treatment strategy– Timely– Reduce risk of MACE– Minimise risk of bleeding– Treat mechanical complications
Case 1o 79 Female
o 4 hrs chest burning
o Ex-smoker, stopped 30 years ago
o Drugs
– warfarin, digoxin 125 mcg, amlodipine 5mg, frusemide 40mg, simvastatin 20mg
o Physical examination
– BP 180/90 mm Hg (R=L)
– HR 160 irreg
– RR 24/min, O2 sats 98% on rebreathe
– BM 9.6 mmol/L
– Bibasal creps
o Bloods tests
– Hb 10.8, K 4.1, Cr 126, INR 4.3, troponin pending
Presenting ECG ECG Diagnosis
o Acute LAD syndrome (NSTEACS), rapid AFo Acute posterior STEACS, rapid AFo Acute inferior STEACS, rapid AFo Acute infero-posterior STEACS, rapid AFo Acute pericarditis, rapid AF

Clinical risk assessment
o Low
o Medium
o High– >75 yo– F– >2h from symptom onset– Pulmonary oedema (Killip 3)– STEACS– Warfarin Rx (↑ bleeding risk)
Clinical Risk Scores
www.crusadebleedingscore.orgwww.outcomes-umassmed.org
Immediate Treatment Options
o ASA 300mg, Clopidogrel 300mg, UFH, thrombolysiso ASA 300mg, Clopidogrel 300mg, LMWH, thrombolysiso ASA 300mg, Clopidogrel 300mg, fondaparinux, thrombolysiso ASA 300mg, Clopidogrel 600mg, UFH, PPCI ± Gp IIbIIIao ASA 300mg, Clopidogrel 600mg, LMWH, PPCI ± Gp IIbIIIao ASA 300mg, Clopidogrel 600mg, bivalirudin, PPCI ± Gp
IIbIIIao ASA 300mg, Clopidogrel 600mg, fondaparinux, PPCI ± Gp
IIbIIIao ASA 300mg, Clopidogrel 600mg, LMWH, PPCI ± Gp IIbIIIao ASA 300mg, Clopidogrel 600mg, ½ dose abciximab bolus +
half dose lytic, transfer for PCIo I have no idea!
Immediate Rx
o Load with antiplatelets– Aspirin 300 mg + Clopidogrel 600 mg
o Treat heart failure– Morphine 4 mg – Furosemide 40mg iv– GTN ivi
o Maintain K 4-5 mmol/Lo Resolve the ischaemia!
PPCI
o Radial artery access– Minimise bleeding risk, ~2/3 of major bleeding in
ACS patients are related to femoral access
o Bivalirudino Thrombus aspirationo Avoid DES
– Triple therapy carries major bleeding risk of 7% per yr
– Aspirin + clopidogrel carries 2-3% per yr risk of major bleeding >75y
ACS
PPCITransfer <1hDTB <60 min
Cardiogenic shockCI to lysis
LysisPre-hospital
Pain to Rx <2hIf transfer >2h:Lytic+GpIIbIIIa
PCI within24h
Fail toreperfuse
Rescue PCI
Medical RxRisk Stratification
High/IntermediateRisk
Low Risk
Angiography± Revasc.within 96h
Medical Rx± Revasc.
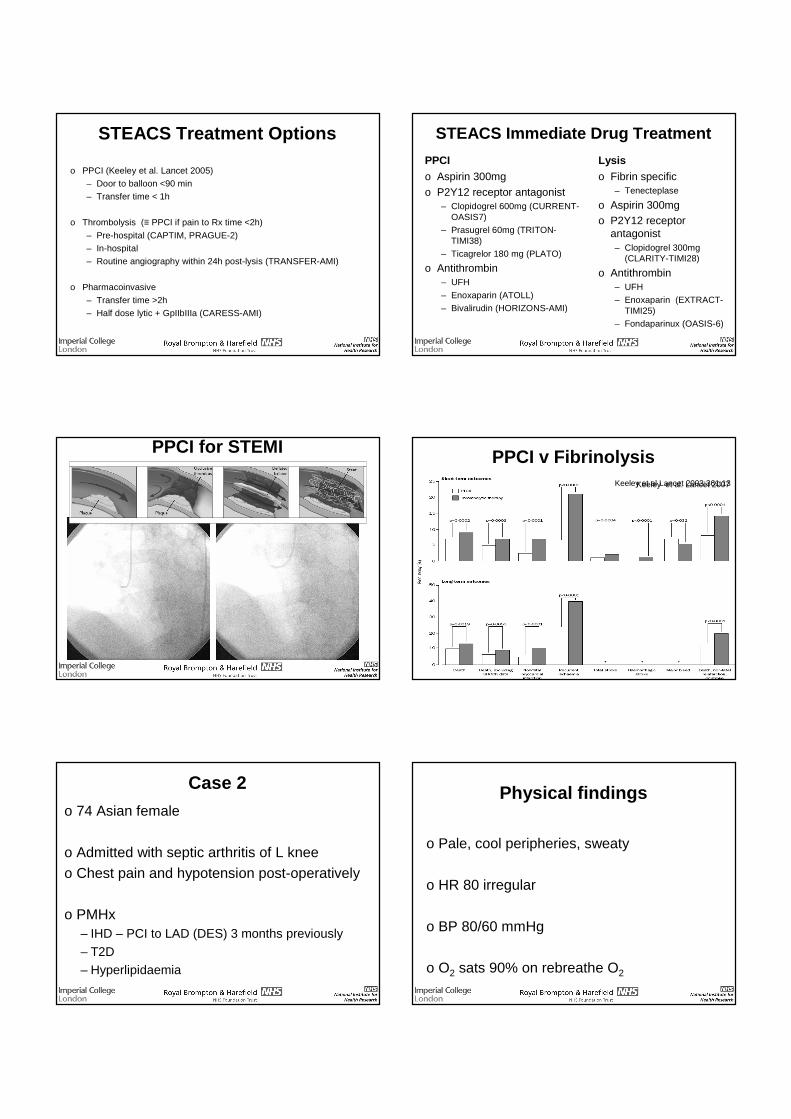
STEACS Treatment Options
o PPCI (Keeley et al. Lancet 2005)
– Door to balloon <90 min
– Transfer time < 1h
o Thrombolysis (≡ PPCI if pain to Rx time <2h)
– Pre-hospital (CAPTIM, PRAGUE-2)
– In-hospital
– Routine angiography within 24h post-lysis (TRANSFER-AMI)
o Pharmacoinvasive
– Transfer time >2h
– Half dose lytic + GpIIbIIIa (CARESS-AMI)
STEACS Immediate Drug Treatment
PPCIo Aspirin 300mgo P2Y12 receptor antagonist
– Clopidogrel 600mg (CURRENT-OASIS7)
– Prasugrel 60mg (TRITON-TIMI38)
– Ticagrelor 180 mg (PLATO)
o Antithrombin– UFH
– Enoxaparin (ATOLL)
– Bivalirudin (HORIZONS-AMI)
Lysiso Fibrin specific
– Tenecteplase
o Aspirin 300mgo P2Y12 receptor
antagonist– Clopidogrel 300mg
(CLARITY-TIMI28)
o Antithrombin– UFH
– Enoxaparin (EXTRACT-TIMI25)
– Fondaparinux (OASIS-6)
PPCI for STEMI PPCI v FibrinolysisKeeley et al Lancet 2003;361:13Keeley et al. Lancet 2007
Case 2o 74 Asian female
o Admitted with septic arthritis of L kneeo Chest pain and hypotension post-operatively
o PMHx– IHD – PCI to LAD (DES) 3 months previously– T2D– Hyperlipidaemia
Physical findings
o Pale, cool peripheries, sweaty
o HR 80 irregular
o BP 80/60 mmHg
o O2 sats 90% on rebreathe O2

12 lead ECGECG Diagnosis
o Acute inferior NSTEACS, SRo Acute inferior NSTEACS, Mobitz I AV blocko Acute inferior NSTEACS, Mobitz II AV blocko Acute anterior STEACS, SRo Acute anterior STEACS, Mobitz I AV blocko Acute anterior STEACS, Mobitz II AV block
Risk assessment
o Low
o Medium
o High
What’s happened?
o Clopidogrel stopped by admitting surgical team
o STENT THROMBOSISo ACUTE LAD STEACS + MOBITZ II AV
BLOCKo CARDIOGENIC SHOCK
Immediate Management
o Clopidogrel 600 mg stato Atropine + TPWo Intubate + ventilateo Consider inotropes
– dopamine/dobutamine– norepinephrine
o Frusemide iv infusion
o Immediate transfer to PCI capable facility– Reperfusion– Mechanical haemodyamic support
Stent Thrombosis

Management of Cardiogenic Shock
Hochman et al. NEJM 1999Hochman et al. JAMA 2000
47%50%
53%56%
63%66%
0%
10%
20%
30%
40%
50%
60%
70%
30 days (n=302) 6 months (n=301) 12 months (n=299)
Mortality (%)
ERV
IMS
Early reperfusion improves short and long term mortalityMechanical support (IABP, Impella, Tandem Heart) improves outcomes
Risk Factors for Stent Thrombosis with DES
CASE FATALITY RATE
45% !!
Iakovou et al. JAMA 2005;293:2126-2130
Learning points
o Anterior STEACS + AV block has poor prognosis, indicating proximal LAD occlusion
o Cardiogenic shock is an indication for urgent revascularisation + haemodynamic support
o Acute stent thrombosis carries ~50% mortality rate
o Do not stop clopidogrel within 1 year of DES implantation without specific consultation with a cardiologist
Case 3
o 68M Inf MI, Rx’d with tenecteplase
o R arm weakness
o CT shows small L frontal intracerebral haemorrhage
o Recurrent chest pain
o 12 lead ECG: 5mm ST↑ II, III, aVF
Options
o Transfer for rescue PCI
o Repeat thrombolysis
o Conservative
Phone a friend!o Interventional Cardiologist
– No mortality benefit from Rx’ing uncomplicated inferior MI
– Prognosis from completed inf MI better than extending ICH from further anti-thrombin and anti-platelet Rx
o Neurologist– Discontinue aspirin and clopidogrel

In the thrombolysed patient
o 20% of arteries remain occluded
o Normal coronary flow in ~65% at 90 min
o Reduced tissue perfusion in ~75%
o Increased major bleeding risk (ICH 0.6-1.4%)
o ~15% risk of recurrent ischaemia/re-infarction Post-thrombolysis
Failure to reperfuse
o <50% reduction in ST↑ at 60 min after fibrinolysis
o Look carefully at the post-fibrinolysisECGs!
o Ongoing symptoms (beware masking effect of analgesics), arrhythmia, haemodynamic instabilityGershlick et al. NEJM 2005;353:2758
■ Conservative
■ Repeat fibrinolysis
■ Rescue PCI (↓ 6 month death, rec MI, severe HF, CV event)
Options (REACT) Case 4
o 78F– Jaw and throat
discomfort– Rapidly worsening
exercise tolerance
o PMHx– Hypertension– Hyperlipidaemia
o Drugs– Aspirin 75mg OD– Amlodipine 5mg OD– Simvastatin 40mg ON
o HR 70o BP 140/70 mm Hgo Normal physical
examination
12 lead ECG
12 hr troponin I <0.04
Initial management
o Non-cardiac, discharge
o Stable angina pectoris, outpatient cardiac investigation
o Unstable angina, treat for NSTEACS

ACS
PPCITransfer <1hDTB <60 min
Cardiogenic shockCI to lysis
LysisPre-hospital
Pain to Rx <2hIf transfer >2h:Lytic+GpIIbIIIa
PCI within24h
Fail toreperfuse
Rescue PCI
Medical RxRisk Stratification
High/IntermediateRisk
Low Risk
Angiography± Revasc.within 96h
Medical Rx± Revasc.
Adjunctive Pharmacology in NSTEACS
Analgesia
O2
Oral antiplateletAspirin +
Clopidogrel/Prasugrel/Ticagrelor
Antithrombin/Xa antagonistsUFH/LMWHBivalirudin
FondaparinuxApixaban/Rivaroxaban
Intravenous antiplateletAbciximab/Tirofiban/Eptifibatide
Initial Treatment
o Clopidogrel 300mg load, 75 mg OD
o Bisoprolol 2.5 mg OD
o Atorvastatin 80 mg nocte
o Enoxaparin 1 mg/kg sc BD
NSTEACS Immediate Drug Treatment
o Aspirin 300mgo P2Y12 receptor antagonist
– Clopidogrel 300mg (CURE)• 75 mg OD for 1 year
– Clopidogrel 600mg (CURRENT-OASIS7)• 150mg OD for 7d and 75mg OD for 1 year
– Prasugrel 60mg (TRITON-TIMI38)• 10mg OD for 1 year (5mg OD in special cases)
– Ticagrelor 180 mg (PLATO)• 90 mg BD for 1 year
o Antithrombin/Xa antagonist– UFH– LMWH (ESSENCE, FRISC)
– Bivalirudin (ACUITY)
– Fondaparinux (OASIS-5)
Does the statin matter?
Wiviott et al. Circulation 2006
0
3
6
9
0 4 8 12 16Time since randomisation (weeks)
Cumulative incidence (%)
Relative risk = 0.74
(0.57-0.95), p=0.02
Atorvastatin
Placebo 8.4%
6.2%
Cannon et al NEJM 2004
Next day
Clinical progress
o Further jaw discomfort at rest
o No ECG changeso No troponin riseo HR 68o BP 130/70o Chest clear
Would you?
o Increase medical therapy– ↑Bisoprolol 5mg OD
– Perindopril 2mg OD
– ISMN MR 30mg OD
o Refer for coronary angiography
o Both of the above

NSTEACS – Timing of Angiography
o Recommended within 96h (NICE)– Mehta et al. JAMA 2005;293:2908– TIMACS NEJM 2009
o Routinely within 24h of admission is preferable– EHJ 2011;32:32
o Routine immediate angiography ± PCI provides no additional benefit v within 24h– ABOARD JAMA 2010
o Immediately if ongoing symptoms, dynamic ECG changes, haemodynamic instability, arrhythmia
Coronary Angiogram
Coronary AngiogramWhich is the culprit lesion?
oLADoIntermediateoRCAoCan’t telloDoesn’t matter – PCI to all
What next?
o IVUSo IVUS-VHo OCTo FFRo Stress echoo MPSo CMRo Any of the above
CMR
Normal LV dimensionNormal LV systolic function
No regional wall motion abnormalities

CMR
T2w STIR – Oedema/Area at Risk Late Gadolinium Enhancement - Infarction
Culprit lesion: intermediate arteryNo inducible stress perfusion defect
Novel Diagnostics in NSTEACS
o Plaque characterisationo IVUS o OCT
Stone et al. NEJM 2011
High Sensitivity Cardiac Troponin Assays
o >100-fold more sensitiveo MI defined as >99th centile of normal population
o Earlier diagnosiso ↓specificity
Keller et al NEJM 2009 Reichlin et al NEJM 2009
Progress
Clinical status
o Asymptomatico Mobile on wardo No ECG changes
What would you do?
o PCI to intermediateo Continue medical Rx
Treatment on discharge
Treatment
o Aspirin 75mg ODo Clopidogrel 75mg ODo Bisoprolol 10mg ODo ISMN MR 30mg ODo Perindopril 4mg ODo Atorvastatin 80mg ODo Omeprazole 20mg OD
Targets
o HR <60 bpmo LDL <2mmol/Lo BP <130/80 mm Hg
PROVE-IT TIMI22 Circulation 2010
Post ACS Long Term Treatment
o Beta blocker (COMMIT)
o High dose statin (MIRACL, PROVE-IT TIMI22)
o Eplerenone if associated HF (EPHESUS)
o Omacor (GISSI Prevenzione)
o ACEI (AIRE)
o LDL <2mmol/L; BP<130/80o Cardiac rehabilitation

Key Learning Points – ACS
o Incidence of STEACS is falling and NSTEACS is increasing
o PPCI within an established network to ensure timely provision of intervention is preferred option for Rx of STEACS
o Early but not immediate angiography ± PCI is indicated for NSTEACS
o Use risk scores to assess risk-benefito Individualised treatment to reduce MACE and
avoid bleeding → optimised net clinical benefit
Risk scores for prognosis in ACS
Risk of death after ACS (GRACE)
In-hospital
o High (score >140)– >3%
o Intermediate (score 109-140)– 1-3%
o Low (score ≤108)– <1%
6 months post-discharge
o High (score >118)– >8%
o Intermediate (score 89-118)– 3-8%
o Low (score ≤88)– <3%
Bleeding (CRUSADE)
Determinants of risk
o Ageo Baseline Hbo eGFRo HRo Female gendero Signs of heart failureo Prior vascular diseaseo DMo SBP <110 or >180 mm Hg
CRUSADE Bleeding Score
p<0.001 for trend; Derivation: C=0.71 Validation: C =0.70
Related Documents











