ST CATHERINE’S HOSPICE Primary thromboprophylaxis in advanced disease MJ Johnson

ST CATHERINE’S HOSPICE Primary thromboprophylaxis in advanced disease MJ Johnson.
Jan 01, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ST CATHERINE’SHOSPICE
Primary thromboprophylaxis in
advanced diseaseMJ Johnson

(The Mail on Sunday, 17/12/2000) 2

3

(The Sunday Telegraph, 28/1/2001)4
5

Daily Mail3/2/01
6

7
Background
• VTE : important cause of death in cancer patients • Potentially preventable with appropriate risk assessment
and prophylaxis• Therefore a healthcare priority for many countries• Some (e.g. UK) using financial incentives and targets to
drive implementation • International guidelines:
Farge D, Debourdeau P, Beckers M, Baglin C, Bauersachs RM, Brenner B, et al. International clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. J Thromb Haemost 2013 Jan;11(1):56-70.
What about palliative care?• Clinical relevance and research focus very recent in
palliative care• Moderate to high risk of VTE
– Advanced/active disease– Received ++ therapies (chemo/surgery)– Poorly mobile
• Secondary prevention is much more accepted• Still divided opinion about primary prevention
– Agreement not for those imminently dying
• But – hospice care now not just for the imminently dying

Things have changed• Hospice is no longer “the Death House”• But
– Only 7% SPC units have TP guidelines (Noble 2007)
– Not perceived as “a big problem” by clinicians– Outcome measures in studies not appropriate– Studies don’t include our patients– “A big PE is a nice way to go” (Noble 2008)
• However, difficult to keep being an ostrich…
10

11
Why prevent VTE in palliative care patients?
• High risk – Up to 50% in hospice in patients
• VTE confers a poor prognosis• Cause symptoms
– Attributable and non attributable• Challenging to treat
– Bleeding– Recurrent thrombosis– Six months of LMWH
(Noble et al Lancet Oncology 2008)

Current state of play
12
• Majority of palliative care patients admitted through medical take…
• …will be receiving PTP by default
• Some admitted to the hospice……
• ….won’t get PTP when they could benefit

Hospice VTE risk assessment project
• The utility of risk assessment tools in patients with advanced disease, and prediction of symptomatic VTE is unknown.
• Investigation: i)what is the relationship between risk of VTE and development of symptoms and, ii)what is the utility of risk assessment tools for these patients?

Method
• Retrospective consecutive admission case-note data from seven UK hospices
• Data collected during an evaluation of a VTE risk assessment protocol – Pan Birmingham Cancer Network palliative-modified
Thromboembolic Risk Factors (THRIFT) Consensus Group criteria,
– presence/absence of a temporary elevated risk (TER) of VTE.
• Symptoms/signs during admission consistent with possible VTE were documented.

Analysis plan• An exploration of the association of THRIFT, TER with
– prescription of PTP,– development of symptoms
• An estimation of the utility of THRIFT and TER in predicting symptomatic VTE during their hospice admission: – sensitivity, specificity, – predictive value (PPV and NPV), – likelihood ratios (LR(+/-)) – odds ratios
• Tests were 2-sided using a significance level of 5%, odds ratios and accuracy measures such as sensitivity are presented with 95% confidence intervals.
results• Total population: N=1164• 45 (4%) prescription of PTP on admission; (68
came on PTP; 13 of these continued; 32 new prescription)
• “Clinically relevant population” : N = 528 (45%)– The population who would have been eligible to have
PTP with LMWH– Excludes
• Contraindication to anticoagulation (bleeding, dying, thrombocytopenic) N= 496
• Already on therapeutic anticoagulation N = 139
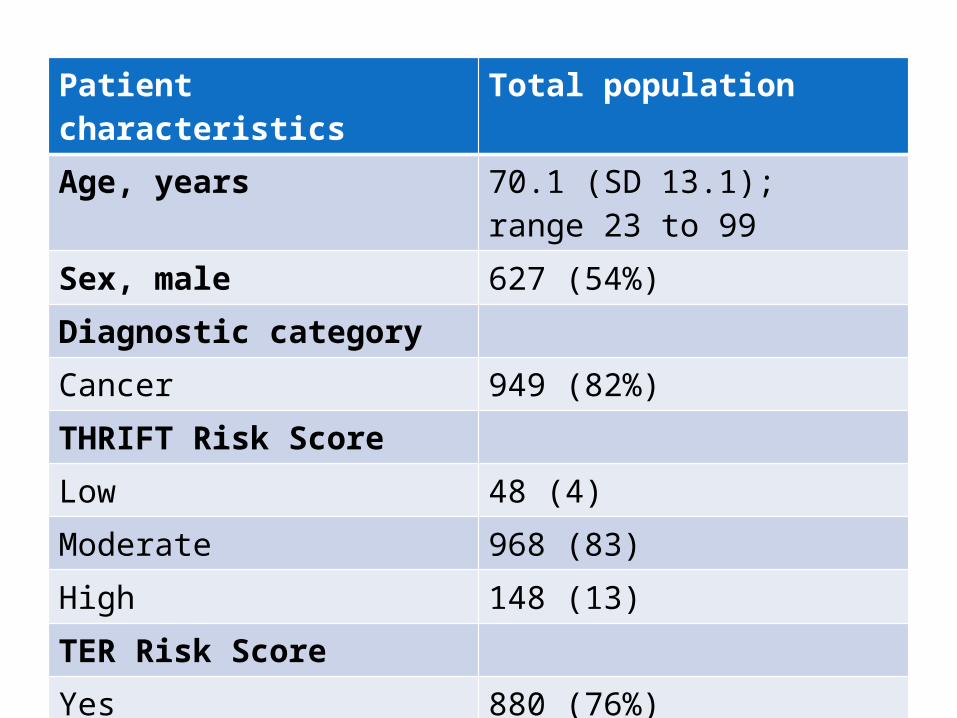
Patient characteristics Total populationAge, years 70.1 (SD 13.1); range 23 to 99 Sex, male 627 (54%)Diagnostic categoryCancer 949 (82%)THRIFT Risk Score Low 48 (4)Moderate 968 (83)High 148 (13)TER Risk ScoreYes 880 (76%)No 279 (24%)missing 5 (0%)

Symptoms (N=528)
Clinically Relevant Population
Total Population
N=528 (%) N=1164 (%)
Symptom
Pleuritic chest pain 12 (2) 21 (2)
Leg swelling 14 (3) 32 (3)Breathlessness 47 (9) 99 (9)
• Overall 12% in clinically relevant group• Those not prescribed PTP had OR 1.74, 95% CI 0.69 to
4.4, p=0.241• Too few with PTP for estimation

Symptoms by riskTHRIFT TER
symptomsN (%)
High Moderate Low Yes No Total
Yes 4 (10) 57 (12) 1 (4) 26 (21) 36 (9) 62 (12)
No 36 (90) 403 (88) 27 (96) 98 (79) 368 (91) 466 (88)
Total 40 (100) 460 (100) 28 (100) 124 (100) 404 (100) 528 (100)
•21% of those with a TER developed symptoms compared to 9% of patients without a TER (Chi-squared, p<0.001).
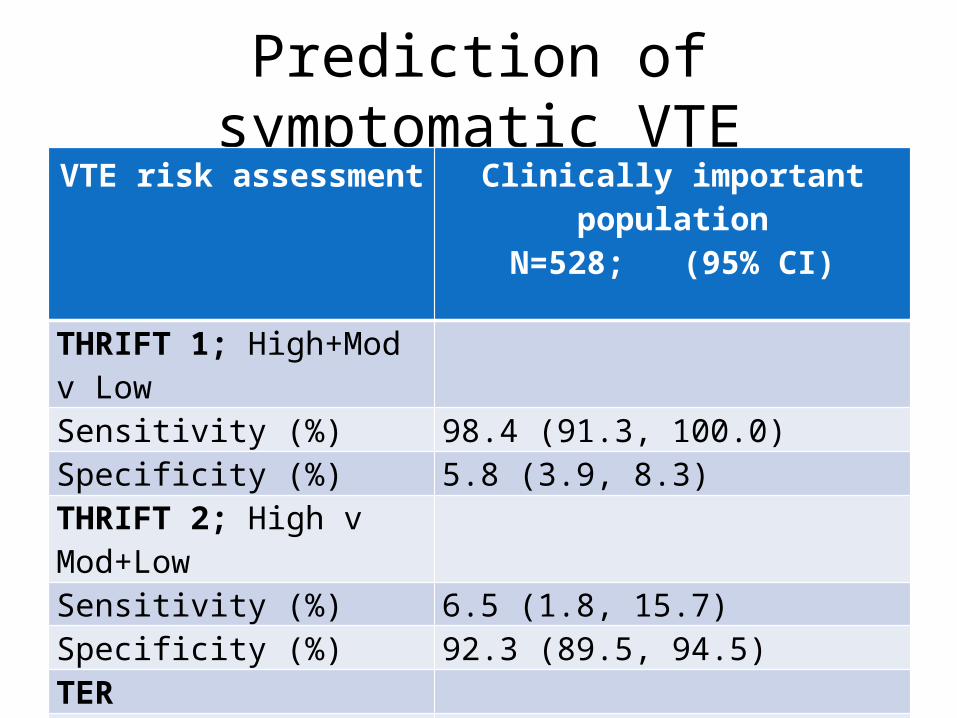
Prediction of symptomatic VTEVTE risk assessment Clinically important
populationN=528; (95% CI)
THRIFT 1; High+Mod v Low Sensitivity (%) 98.4 (91.3, 100.0)Specificity (%) 5.8 (3.9, 8.3)THRIFT 2; High v Mod+LowSensitivity (%) 6.5 (1.8, 15.7)Specificity (%) 92.3 (89.5, 94.5)TERSensitivity (%) 41.9 (29.5, 55.2)Specificity (%) 79.0 (75.0, 82.6)

Limitations
• Symptoms not routinely investigated with imaging - proxy measure
• Number caused by confirmed VTE events not known• Severity not systematically documented
– But significant enough to the patient and doctor to document in the clinical record.
• Retrospective chart review– symptoms were not systematically sought for, graded or
documented – Therefore likely to be an underestimate.
Conclusions 1: Does risk matter?
• Most patients admitted to these hospices were at moderate to high risk of developing VTE during their stay.
• Does this matter?
• There is a highly significant association between
TER and “proxy” symptoms in those who could have PTP

Conclusions 2: what should we do about it?
• Use TER rather than THRIFT for hospice patients on admission
• But…• Unknown whether PTP improves outcome • Unknown what effect symptoms have on QoL
• Therefore consider PTP in those at risk and discuss with patient
Related Documents