SPONDYLITIS TUBERCULOSIS vs PYOGENIC Dr. Tjuk Risantoso, SpB, SpOT(K)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SPONDYLITIS TUBERCULOSIS
vsPYOGENIC
Dr. Tjuk Risantoso, SpB, SpOT(K)
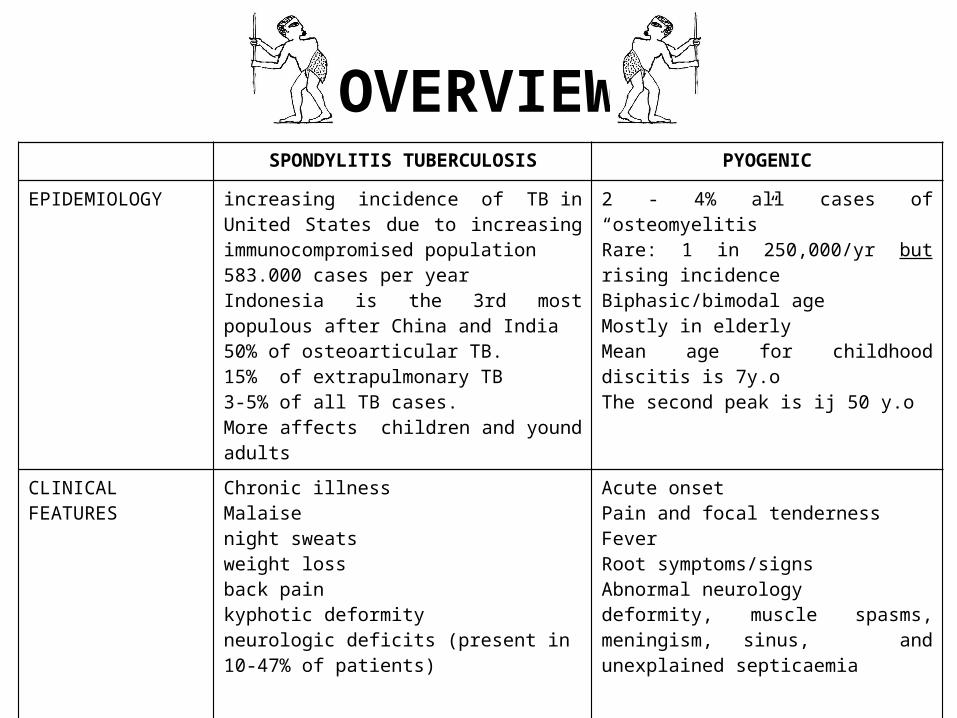
OVERVIEWSPONDYLITIS TUBERCULOSIS PYOGENIC
EPIDEMIOLOGY increasing incidence of TB in United States due to increasing immunocompromised population583.000 cases per yearIndonesia is the 3rd most populous after China and India50% of osteoarticular TB.15% of extrapulmonary TB3-5% of all TB cases.More affects children and yound adults
2 - 4% all cases of “osteomyelitis”Rare: 1 in 250,000/yr but rising incidence Biphasic/bimodal ageMostly in elderlyMean age for childhood discitis is 7y.oThe second peak is ij 50 y.o
CLINICAL FEATURES
Chronic illnessMalaisenight sweatsweight loss back pain kyphotic deformityneurologic deficits (present in 10-47% of patients)
Acute onsetPain and focal tendernessFeverRoot symptoms/signsAbnormal neurologydeformity, muscle spasms, meningism, sinus, and unexplained septicaemia
ETIOLOGY Mycobacterium tuberculosisOther Mycobacterium sp. (rare)
Staphylococcus aureus (50%)Haemophillus influenzaEscherichia coli, Pseudomonas sp. Proteus sp. Streptococcus viridans


Pathoanatomy(Spondylitis TB)
Early infection •begins in the metaphysis of the vertebral body •spreads under the anterior longitudinal ligament and leads to
•contiguous multilevel involvement •skip lesion or noncontiguous segments (15%) •paraspinal abscess formation (50%)
•usually anterior and can be quite large (much more common in TB than pyogenic infections)
•initially does not involve the disc space (distinguishes from pyogenic osteomyelitis, but can be misdiagnosed as a neoplastic lesion)
Pathogenesis(Spondylitis TB)
• Secondarily focus infection from the other organ hematogenically
• Small tubercle activate Chaperonin 10 high stimulator of bone resorption destructs anterior part of vertebrae body kyphotic deformity respiratory problem & paraplegia
• Granulomatous reaction blocks bone formation relatively avascular sequester
• Reach the soft tissue paravertebrae abscess following the fascia of psoas muscle psoas abscess ( cold abscess )
• Narrowing of adjacent disc ( being avascular )

Chronic infection leads to •severe kyphosis
•because the infection is often diagnosed late, there is often much more severe kyphosis in granulomatous spinal infections compared to pyogenic infections
•sinus formation •Pott's paraplegia
•spinal cord injury can be caused by abscess/bony sequestra or meningomyelitis •abscess/bony sequestra has a better prognosis than meningomyelitis as the cause of spinal cord injury


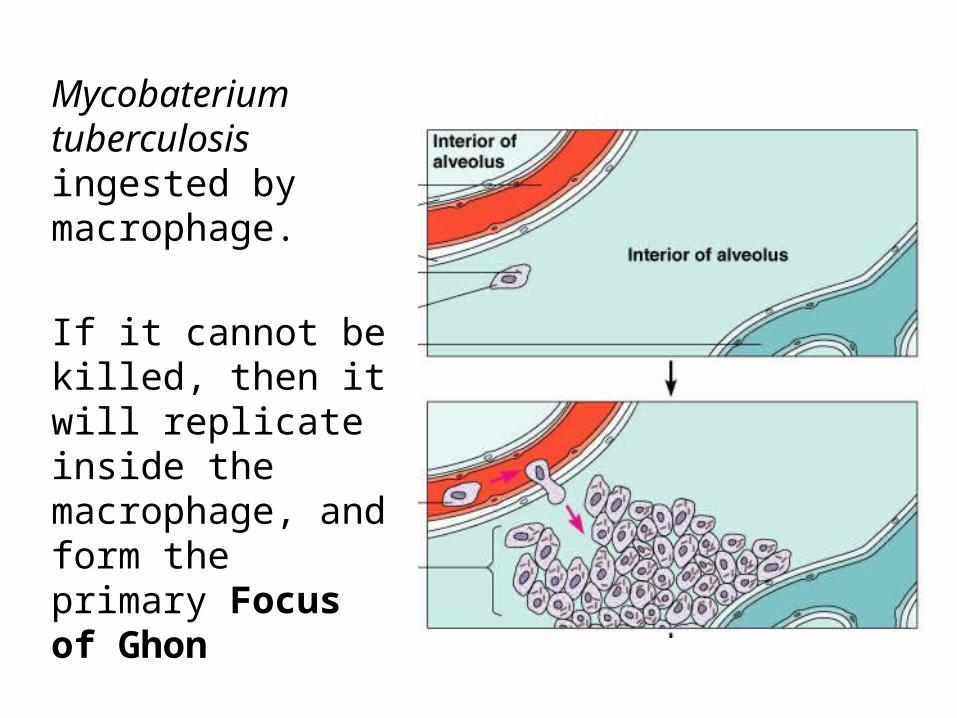
Mycobaterium tuberculosis ingested by macrophage.
If it cannot be killed, then it will replicate inside the macrophage, and form the primary Focus of Ghon
Which is tubercle formed
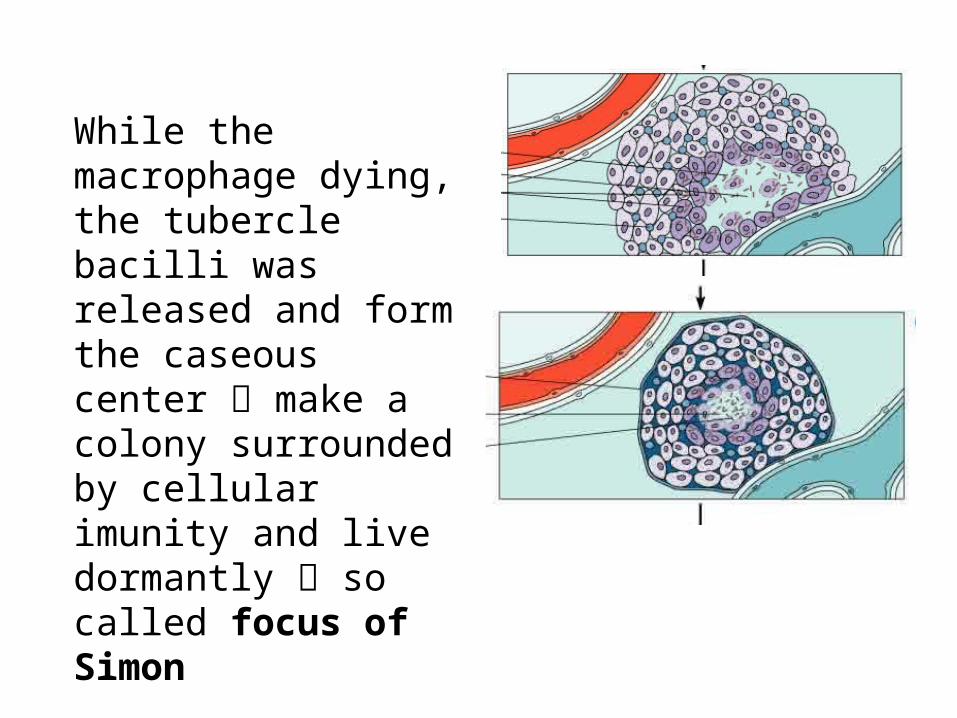
While the macrophage dying, the tubercle bacilli was released and form the caseous center make a colony surrounded by cellular imunity and live dormantly so called focus of Simon
When the immune system getting worse this focus will be activated

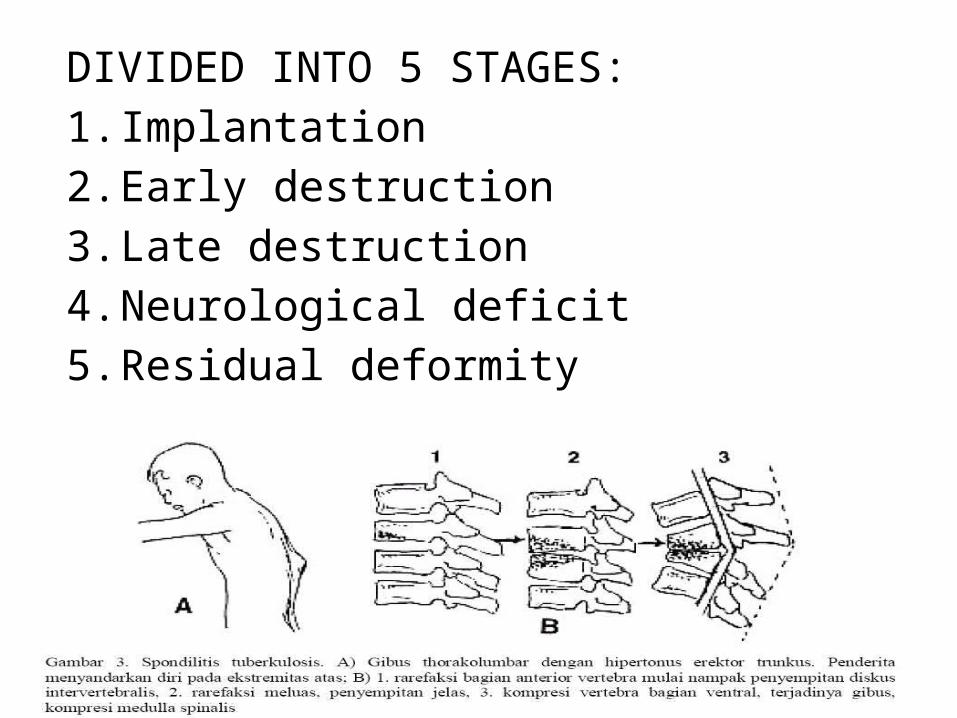
DIVIDED INTO 5 STAGES:1.Implantation2.Early destruction3.Late destruction4.Neurological deficit5.Residual deformity
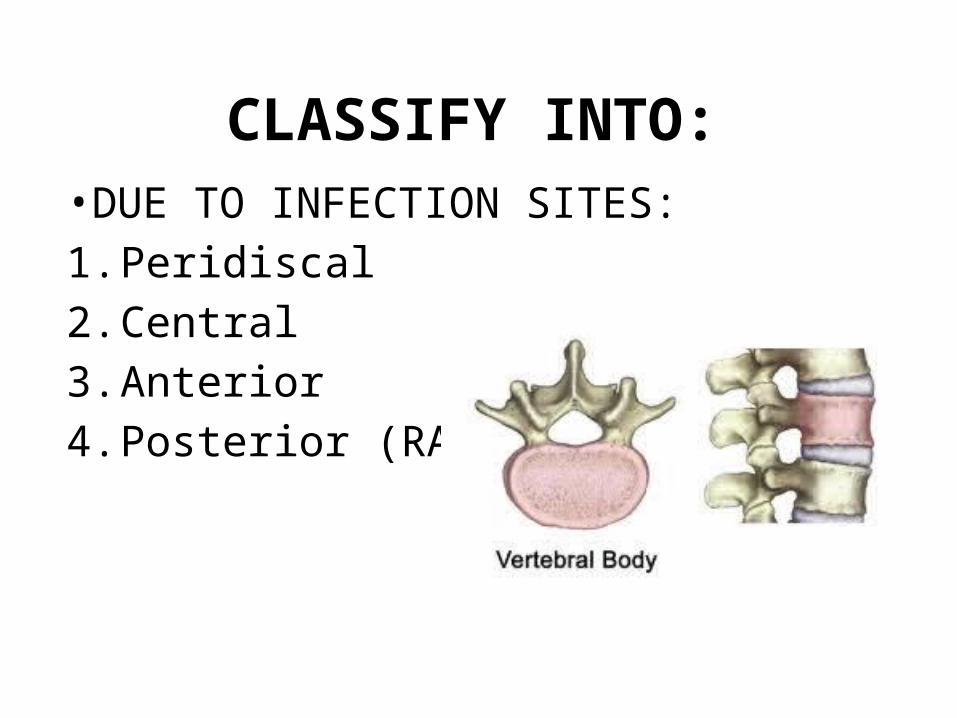
CLASSIFY INTO:•DUE TO INFECTION SITES:1.Peridiscal2.Central3.Anterior4.Posterior (RARE)
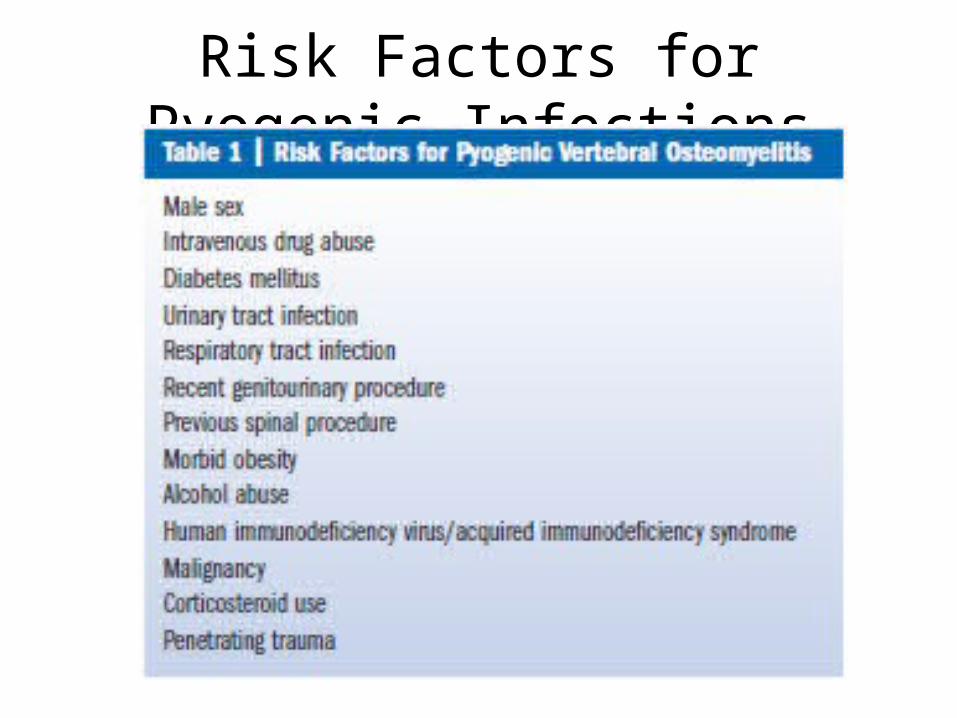
Risk Factors for Pyogenic Infections

Laboratory FindingsTB
• Leukocyte >>>• ESR is prolonged• CRP (C-reactive protein )• ELISA ( false negative >> )• PCR (95% sensitivity and 93% accuracy)
• Tuberculin test ( Mantoux )

Immunology Test
• Intradermal tuberculin test ( Mantoux )
• 67,5 – 87,5 % positive
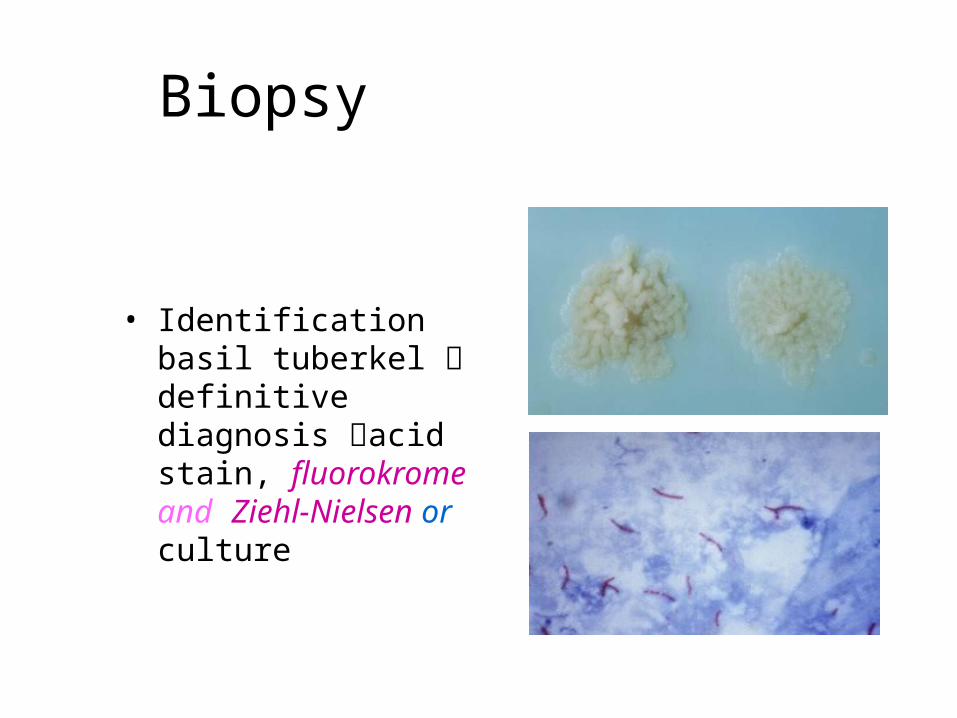
Biopsy
• Identification basil tuberkel definitive diagnosis acid stain, fluorokrome and Ziehl-Nielsen or culture


IMAGING StudiesTB
early infection shows involvement of anterior vertebral body with sparing of the disc space
late infection shows disk space destruction, lucency and compression of adjacent vertebral bodies, and development of severe kyphosis
• PYOGENIC
Vertebral metaphyseal blurring (osteolysis)
• Loss of disc height• Endplate blurring• Subchondral reactive bone formation
• Bone destruction (and deformity)
• Soft-tissue shadows e.g.psoas abscess

TB
PG
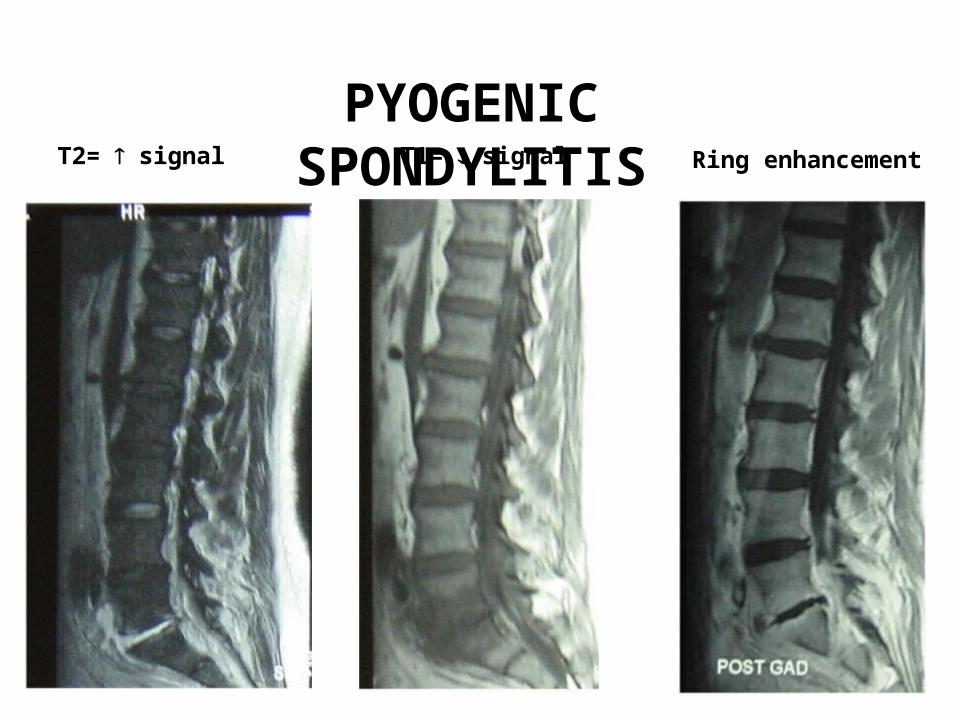
T1= signalT2= signal Ring enhancementPYOGENIC
SPONDYLITIS

Ms. SA/F/20y.o/Spondylitis
TB


TB Pyogenic
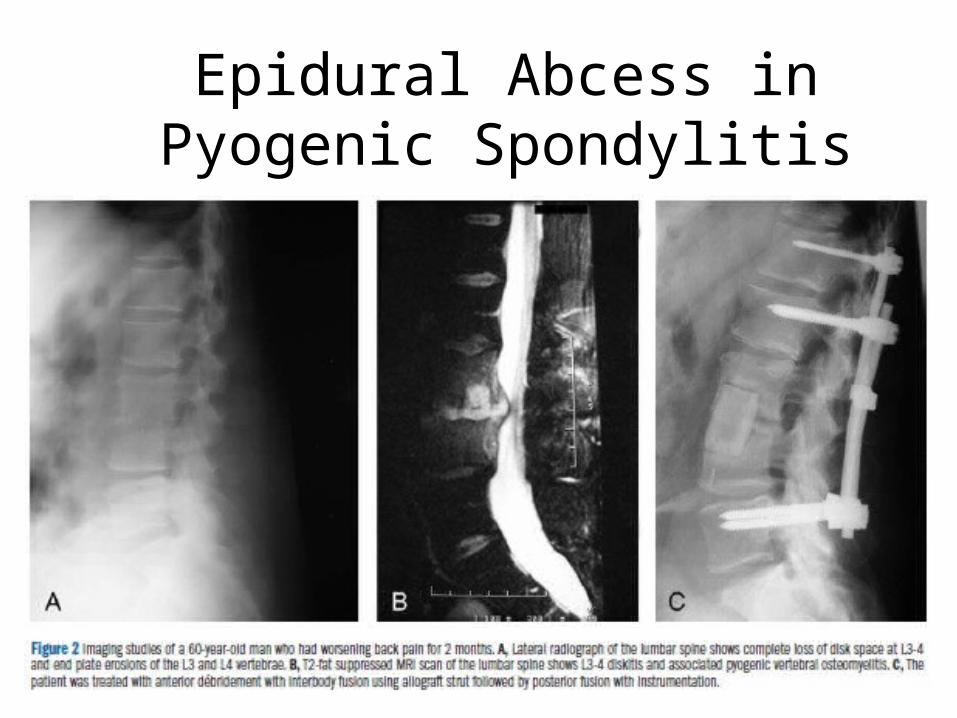
Epidural Abcess in Pyogenic Spondylitis
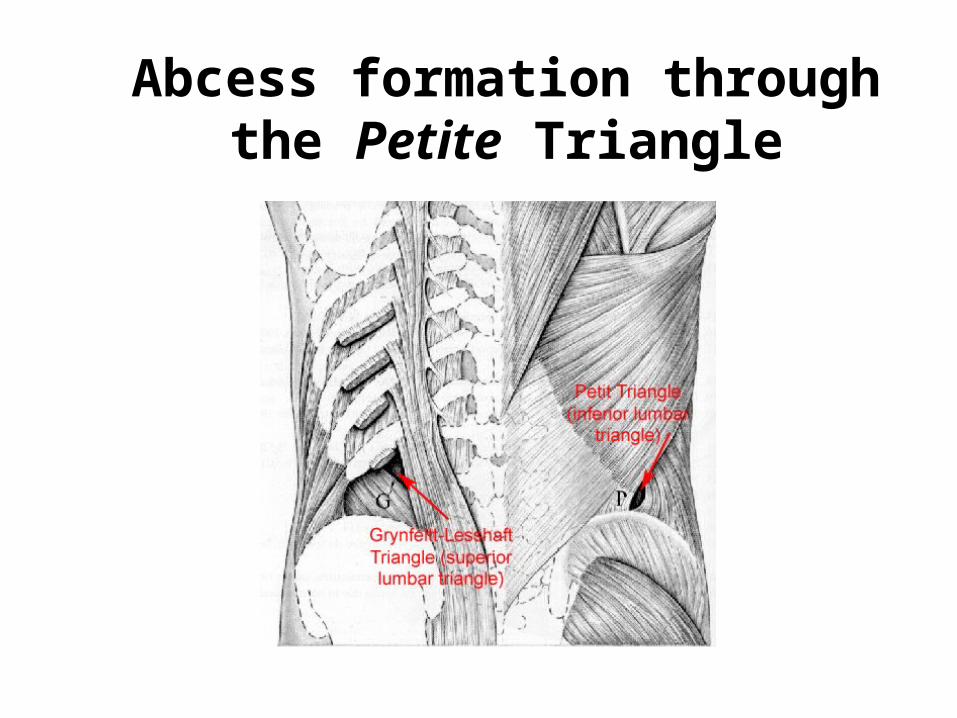
Abcess formation through the Petite Triangle
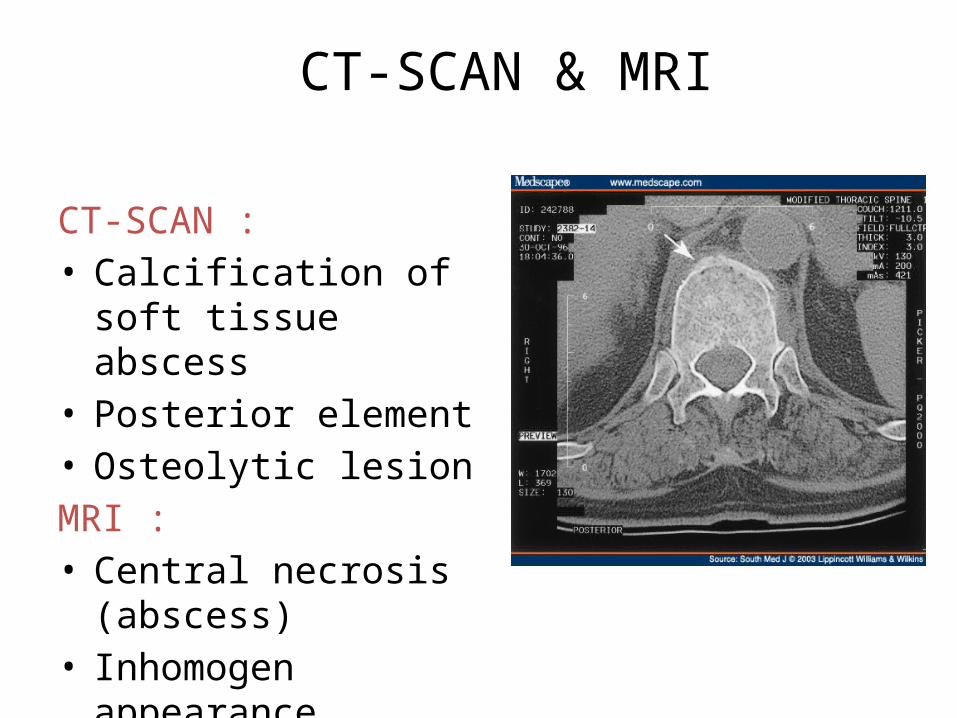
CT-SCAN & MRI
CT-SCAN :• Calcification of soft tissue abscess
• Posterior element• Osteolytic lesion MRI :• Central necrosis (abscess)
• Inhomogen appearance
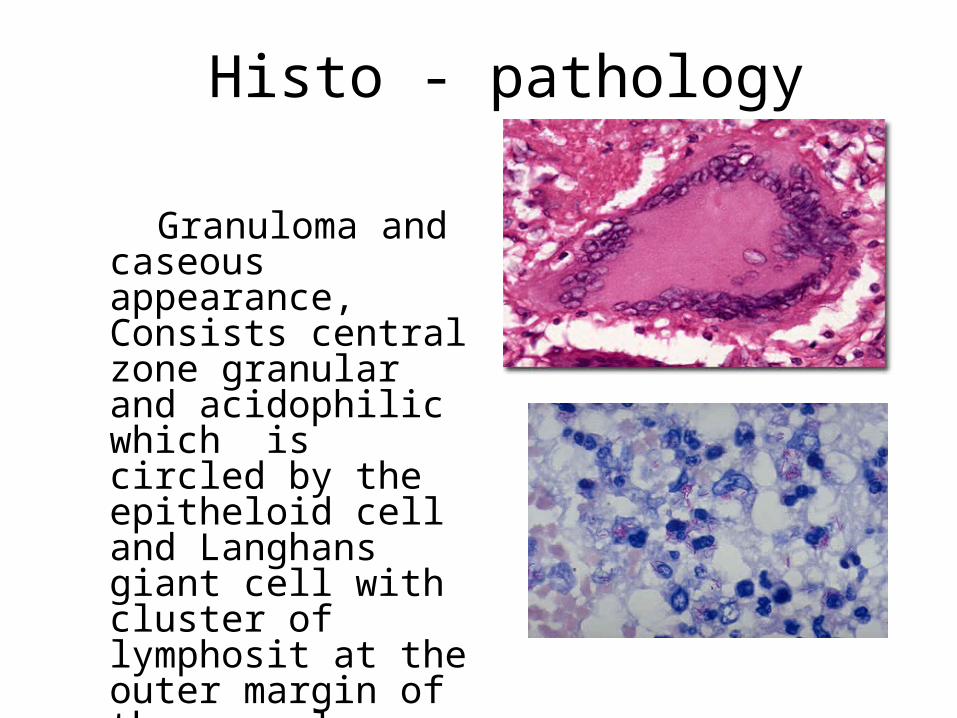
Histo - pathology
Granuloma and caseous appearance, Consists central zone granular and acidophilic which is circled by the epitheloid cell and Langhans giant cell with cluster of lymphosit at the outer margin of the granuloma.

Spinal InfectionsTreatment
Antibioticssensitivitiesadequate dose (iv then oral)ensure MBC reachedadequate duration (> 6 weeks)monitor response (clinical/ indices/ imaging)
toxicity profile and monitoring

Spinal InfectionsTreatment
Immobilisation– bed rest
– moulded orthoses (low thoracic / lumbar)
– halo-vest or orthosis (cervical / high thoracic)

Treatment for TB• The aim : eradicate the infection, stabilize the vertebrae & to correct the khypose
• The combination of chemotherapy or surgical therapy
• INH ( 5-15mg/KgBW/ day ) orally• Rifampicin ( 10-15mg/KgBW/day ) orally
• Pirazinamid ( 25-35/KgBW/day ) orally
• Ethambutol ( 15-20mg/KgBW/day ) orally
• Streptomycin ( 15-30mg/KgBW/day ) IV

Surgical TherapyThe indications :• Failed of chemotherapy treatment in 3 – 6 months
• Recurrent infection• Cervical segment abscess• Posterior lesion with abscess or sinus• Sequester formation• Vertebrae instability / progressive kyphosis
• Significant neurological deficit
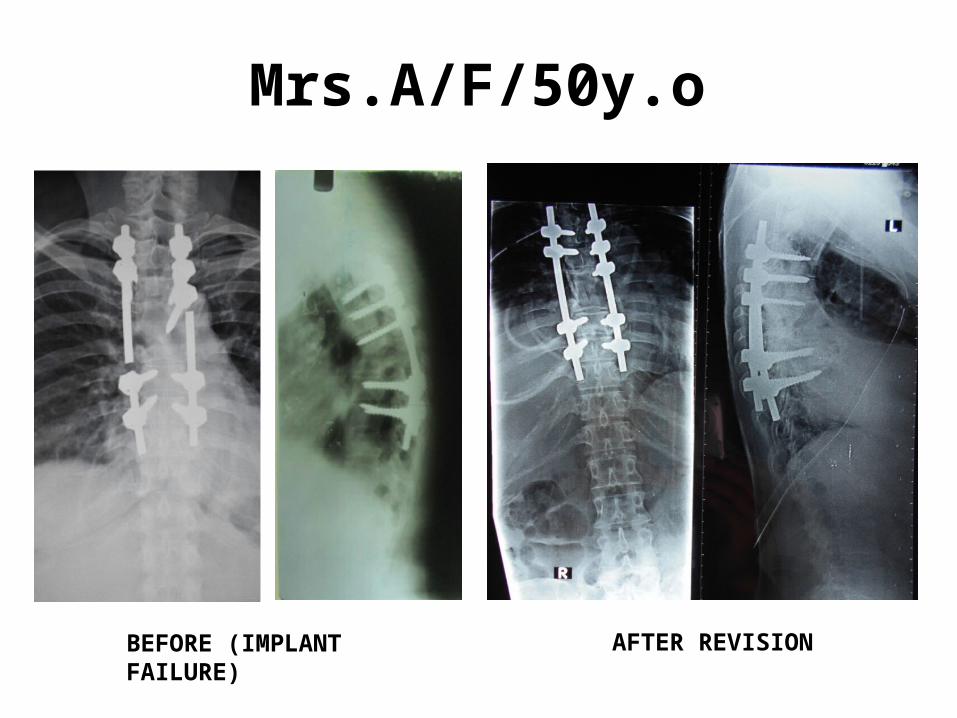
Mrs.A/F/50y.o
BEFORE (IMPLANT FAILURE)
AFTER REVISION
Surgery Techniques
• Hongkong Methods ( anterior debridement & strut grafting )
• Anterior fusion ( Upadhay et al )• Anterior instrumentation & strut graft ( Yilmaz )
• Anterior bone graft & posterior osteotomy & arthrodesis
Anterior approach Posterior approachCostotransversectomy approach
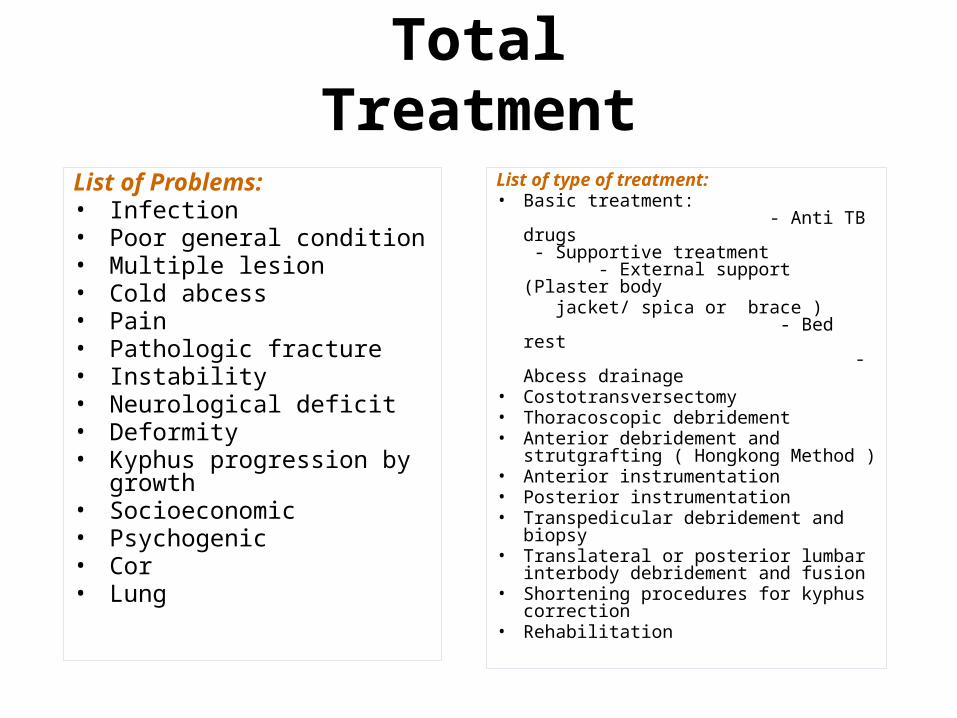
List of Problems:• Infection• Poor general condition• Multiple lesion• Cold abcess• Pain• Pathologic fracture• Instability• Neurological deficit• Deformity • Kyphus progression by
growth• Socioeconomic• Psychogenic• Cor• Lung
List of type of treatment:• Basic treatment:
- Anti TB drugs - Supportive treatment - External support (Plaster body jacket/ spica or brace ) - Bed rest - Abcess drainage
• Costotransversectomy• Thoracoscopic debridement• Anterior debridement and
strutgrafting ( Hongkong Method )• Anterior instrumentation• Posterior instrumentation• Transpedicular debridement and
biopsy• Translateral or posterior lumbar
interbody debridement and fusion• Shortening procedures for kyphus
correction• Rehabilitation
Total Treatment

Treatments alternative:1. Basic tx only2. HK methode (AD, struthgrafting, plester body
jacket)3. Antor debride (AD), fussion(F) w/wo antor
instrmt (AI)4. AD, F + PI for nonrigid kyphotic (combined
approach: antor & postor approach)5. Alternative 4 for rigid kyphotic deformity6. PD (Costotransversectomy + laminectomy), PI +
Fussion for thoracal region7. PD (laminectomy), PI + Fussion (PLIF + TLIF)
for lumbal region8. PD (Transpedicular laminectomy), PI + Fussion
for upper thoracal (Th 2, 3, 4)
9. Alternative 7 + Circumferrential decompr for kyphotic curve
60o - 90o
10. Alternative 9 for kyphotic curve >90o w/wo shorthening &
distraction

• Total treatment with 10 alternatives treat all existing problems in TB-Spine with the aim healing of the infection in stable and painless spine without unacceptable deformity with return of function, return to the society, family and occupation

• Total treatment is the most acceptable, comprehensive, rational and problem solving approach to the management of tuberculosis of the spine CURRENT TREATMENT

Related Documents











