Spinal Orthotics Dr. Mohamed Taha Orthopedic Registrar King Fahad Hospital-Madinah KSA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Spinal Orthotics
Dr. Mohamed TahaOrthopedic Registrar
King Fahad Hospital-Madinah KSA
“A spinal orthotic device is an
external apparatus applied to the body
to limit the motion of, correct
deformity in, reduce axial loading on,
or improve the function of a
particular spinal segment of the
body”.

H i s t o r y
• 5,000 years ago ,nearly, Ancient Egyptians used first splints.
• Middle Ages armorers manufactured splints that protected as well as stabilized the body.
• Late 16th century french surgeon Ambroise Pare` developed metal corsets.
• Late 17th century Lorenz Heister is credited with developing the first spinal orthosis quite similar to the modern day Halo brace.
• Basic principles of spinal immobilization actually changed a little in past 300 years, however materials used and combination of surgery and bracing has changed tremendously.
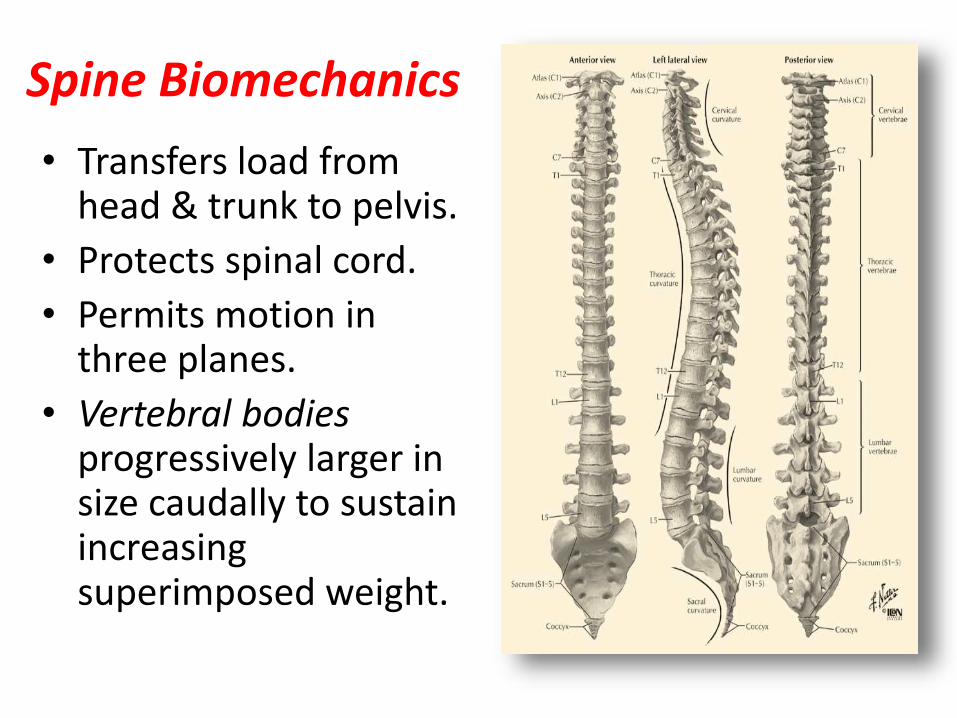
Spine Biomechanics
• Transfers load from head & trunk to pelvis.
• Protects spinal cord.
• Permits motion in three planes.
• Vertebral bodies progressively larger in size caudally to sustain increasing superimposed weight.
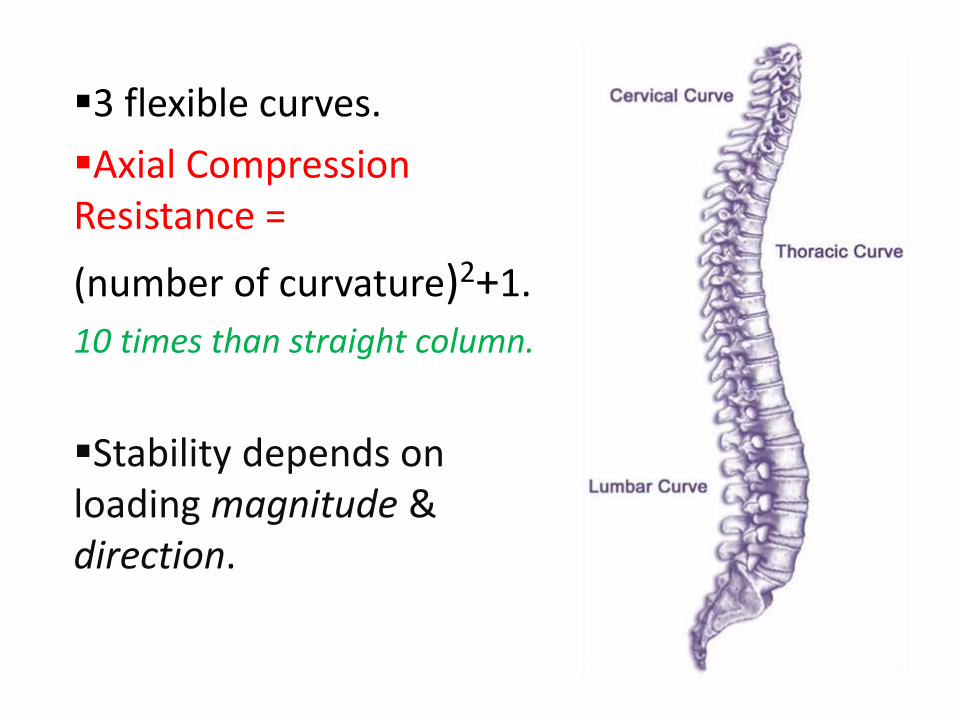
3 flexible curves.
Axial Compression Resistance =
(number of curvature)2+1.
10 times than straight column.
Stability depends on loading magnitude & direction.
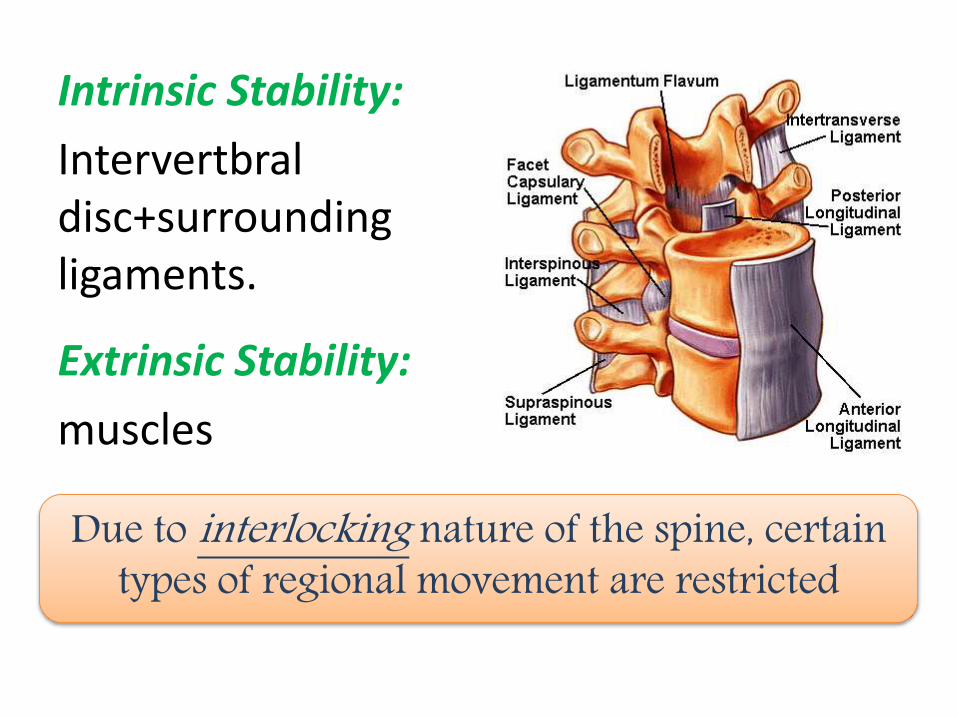
Intrinsic Stability:
Intervertbral disc+surroundingligaments.
Extrinsic Stability:
muscles
Due to interlocking nature of the spine, certain types of regional movement are restricted
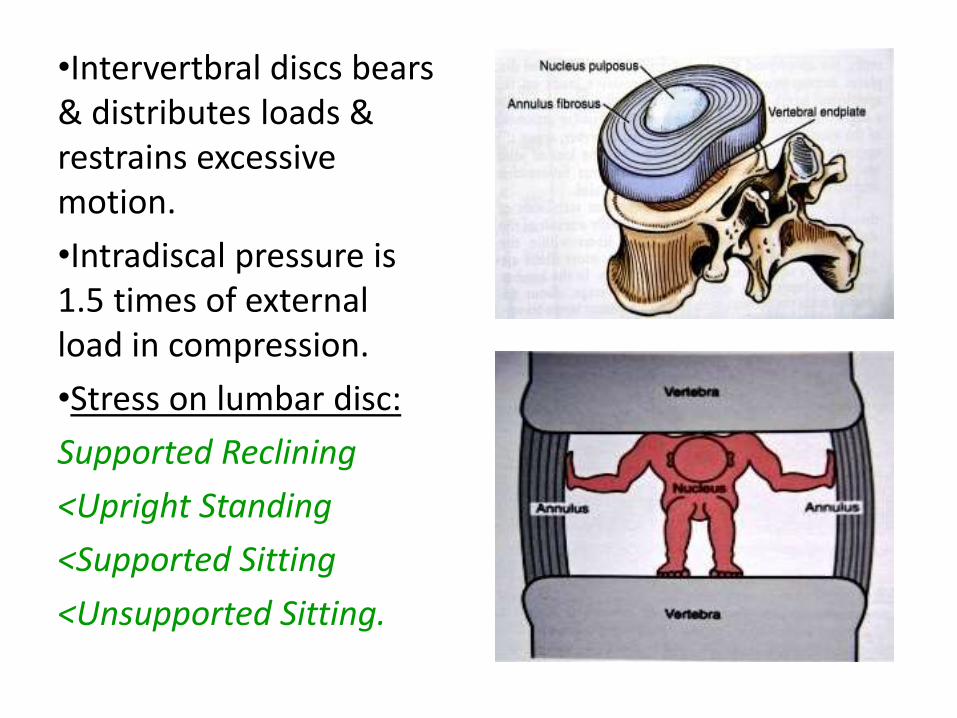
•Intervertbral discs bears & distributes loads & restrains excessive motion.
•Intradiscal pressure is 1.5 times of external load in compression.
•Stress on lumbar disc:
Supported Reclining
<Upright Standing
<Supported Sitting
<Unsupported Sitting.
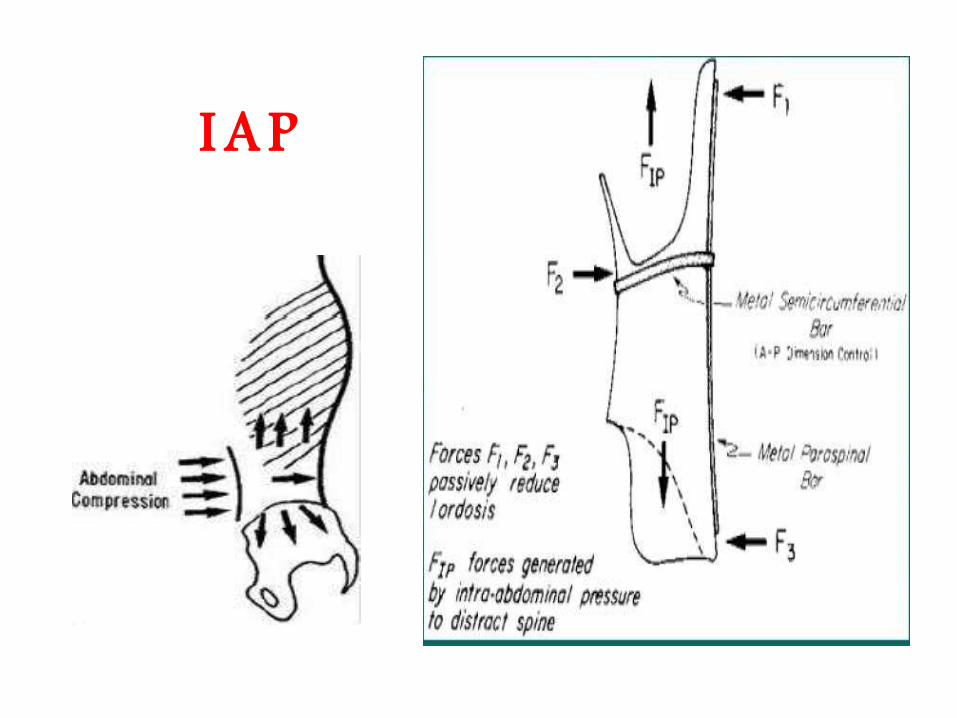
Intra Abdominal Pressure (IAP)
• IAP rises with forward bending & increasing load.
• Peak value 100mmgh in lifting heavy object.
• By activation of the muscles stabilizing the trunk the dorsal directed IAP force preventing excessive lumbar lordosis under high axial load.
• Raising IAP reduces the intra-discal pressure
(50% T12-L1 & 30% L5-S1)
S p i n a l M o t i o n
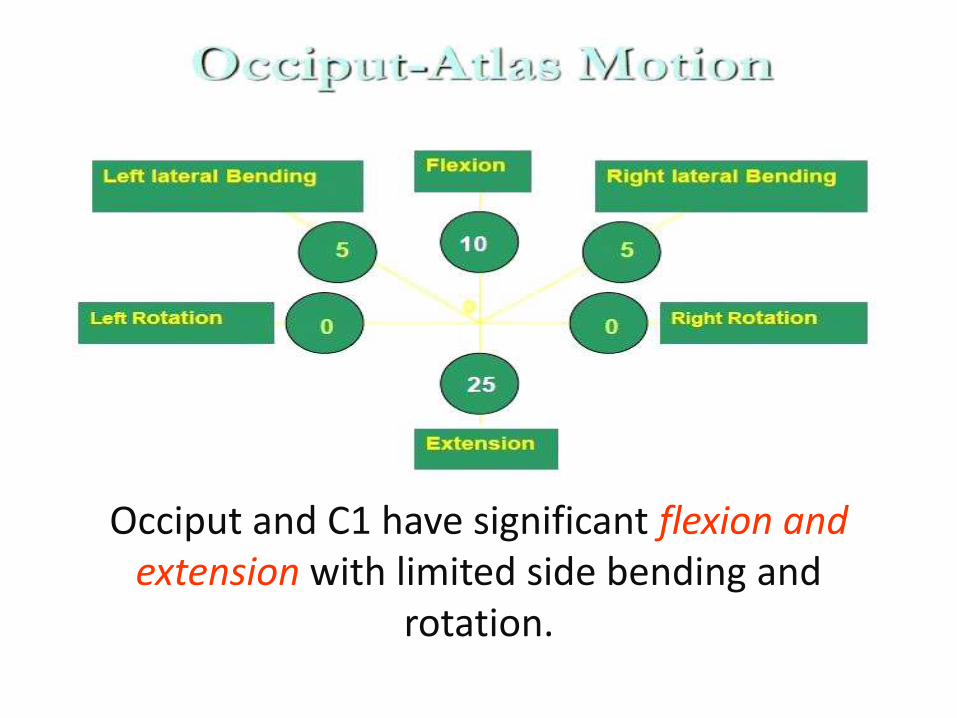
Occiput and C1 have significant flexion and extension with limited side bending and
rotation.

C1-C2 complex accounts for 50% of rotation in the cervical region
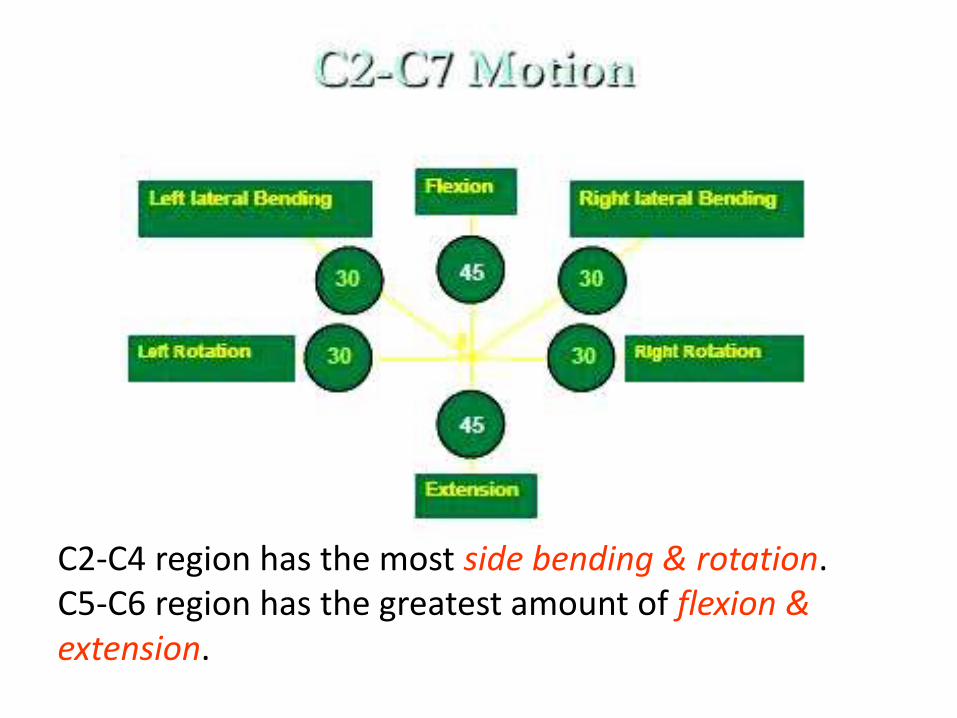
C2-C4 region has the most side bending & rotation.C5-C6 region has the greatest amount of flexion &extension.
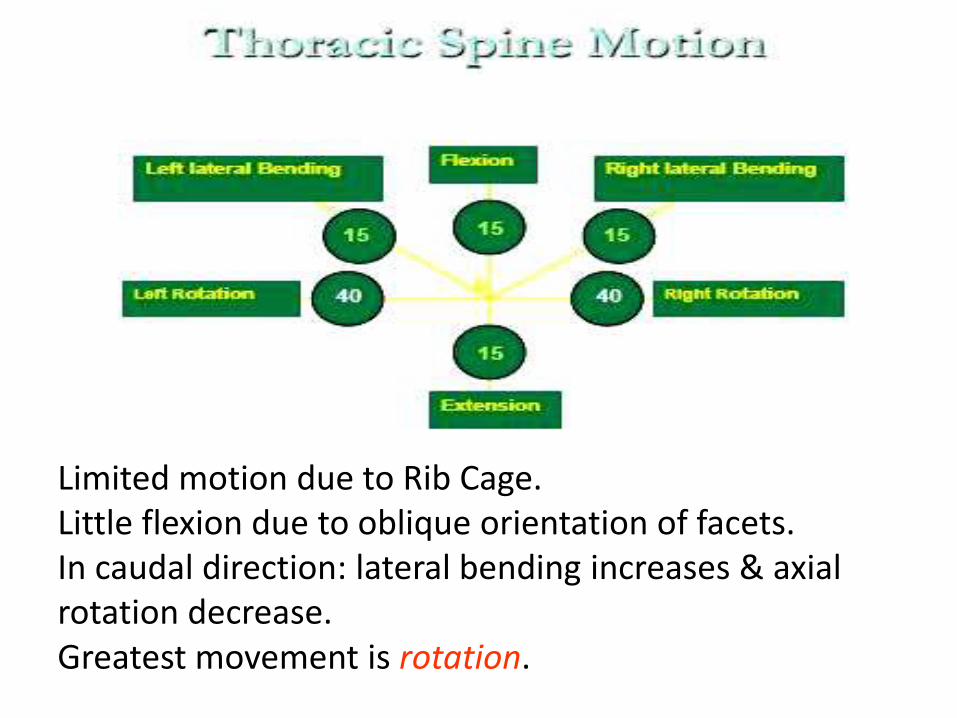
Limited motion due to Rib Cage.Little flexion due to oblique orientation of facets.In caudal direction: lateral bending increases & axial rotation decrease.Greatest movement is rotation.

•Little rotation due to vertical orientation of facets.
•Greatest movement is flexion & extension.

F u n c t i o n s
• Alignment of the spinal skeletal structure.• Protection of head from impact.• Reduction of gravitational loading.• Post-operative immobilization.• Restriction of motion.• Prevent progression of deformity.• Muscle relaxation.• Pain (back pain).
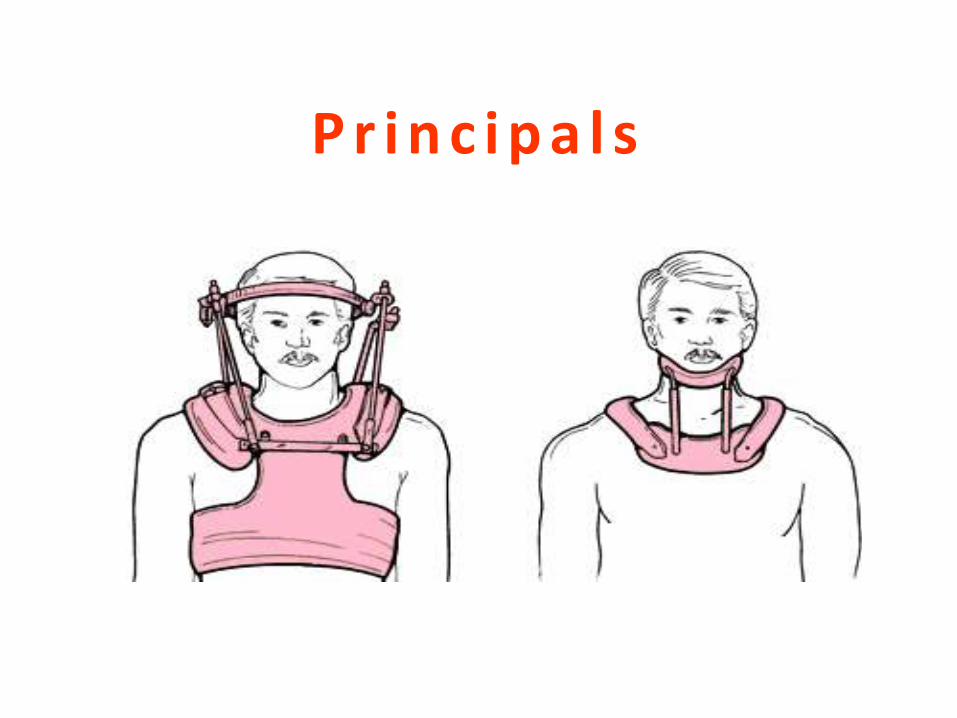
P r i n c i p a l s

Three-point reaction force can use: mandible,occiput,sternum,thorax,armpit,shoulder,back,ribcage &pelvis.
The 1ry method is the three point pressure system.
I A P
General Classifications
Flexible Orthotics or Corsetsconstructed out of strong fabrics or elastic materials with a variety of stiffer supports.
Rigid Spinal Orthotics• Used when greater control of motion or posture
is required.• Fabricated from high temperature thermoplastics
or light weight metals.• Wide varieties with a broad selection of pads and
coverings.
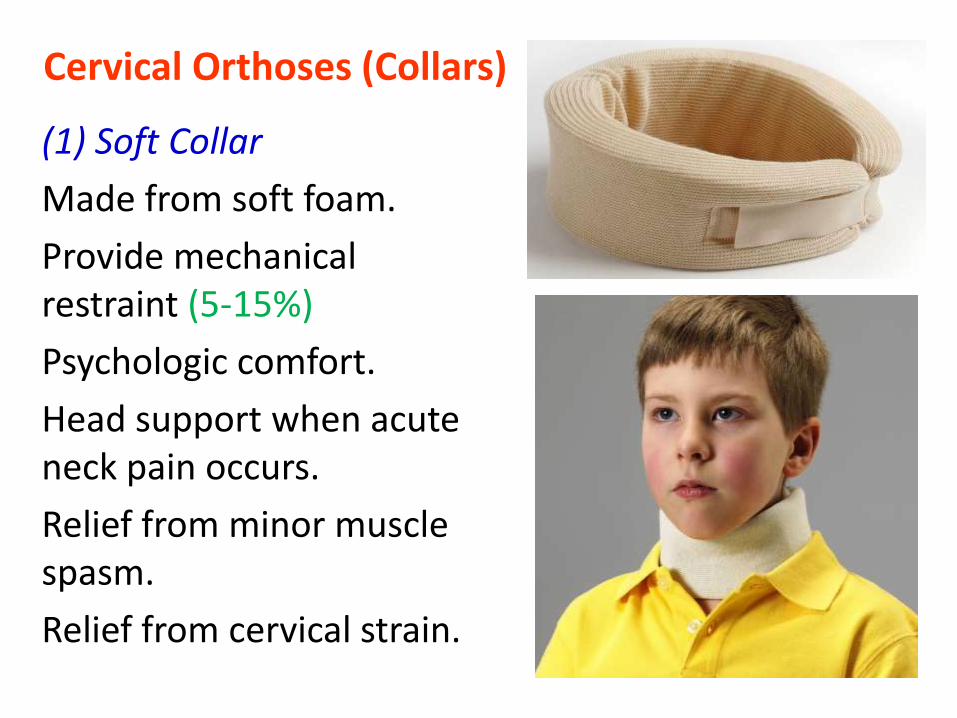
Cervical Orthoses (Collars)
(1) Soft Collar
Made from soft foam.
Provide mechanical restraint (5-15%)
Psychologic comfort.
Head support when acute neck pain occurs.
Relief from minor muscle spasm.
Relief from cervical strain.

(2) Hard collarsHead cervical orthoses (HCO)
•Semirigid and rigid plastics.
•Provide more rigid stabilization of the cervical spine.
•Include Occiput & Chin to decrease ROM.
•Used in stable spine conditions.
•Supported chin is a common place for skin breakdown.
•Clavicle is area HCOs can cause skin breakdown.
•Long-term use associated with decreased muscle function and dependency.
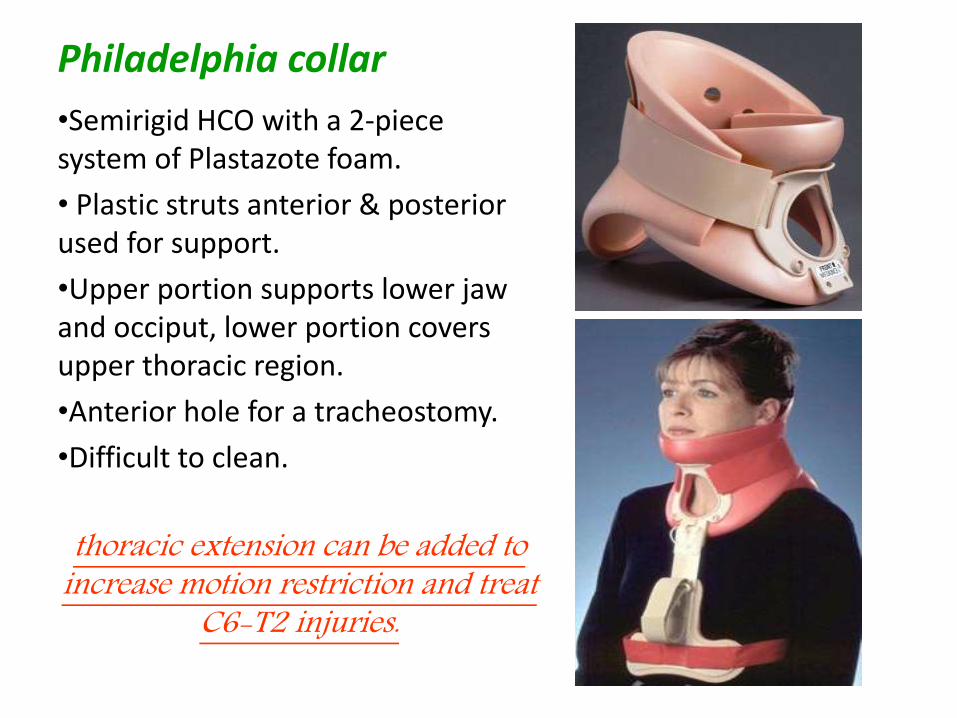
Philadelphia collar
•Semirigid HCO with a 2-piece system of Plastazote foam.
• Plastic struts anterior & posterior used for support.
•Upper portion supports lower jaw and occiput, lower portion covers upper thoracic region.
•Anterior hole for a tracheostomy.
•Difficult to clean.
thoracic extension can be added to increase motion restriction and treat
C6-T2 injuries.
Indications:
•Anterior cervical fusion.
•Halo removal.
•Dens type I cervical fractures of C2.
•Anterior diskectomy.
•Suspected cervical trauma in unconscious patients.
•Most of teardrop fracture of the vertebral body.
•Cervical strain.
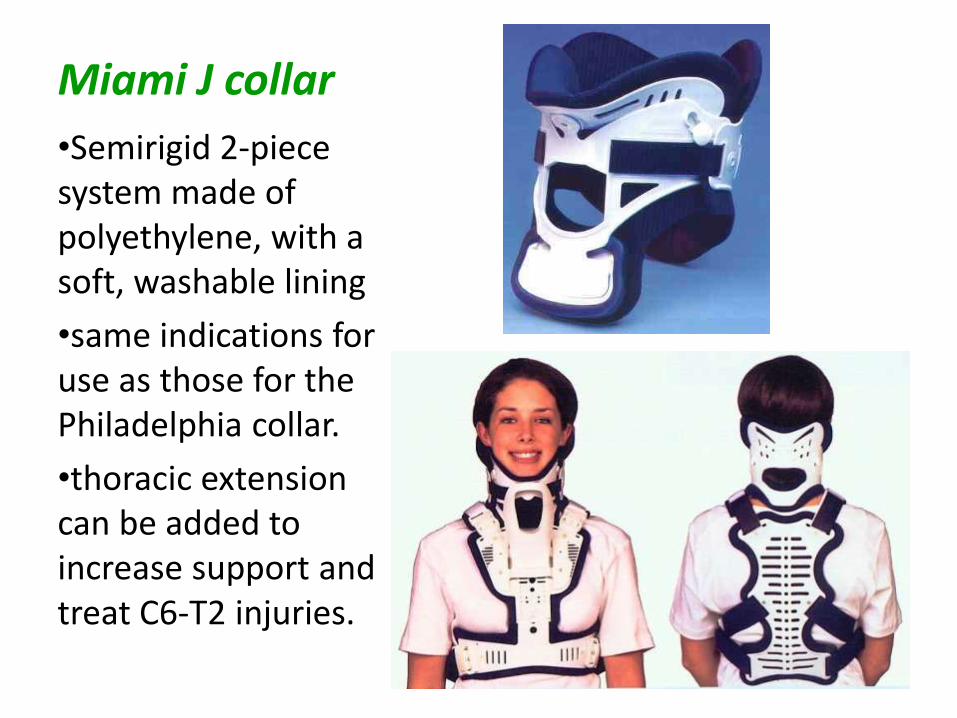
Miami J collar
•Semirigid 2-piece system made of polyethylene, with a soft, washable lining
•same indications for use as those for the Philadelphia collar.
•thoracic extension can be added to increase support and treat C6-T2 injuries.
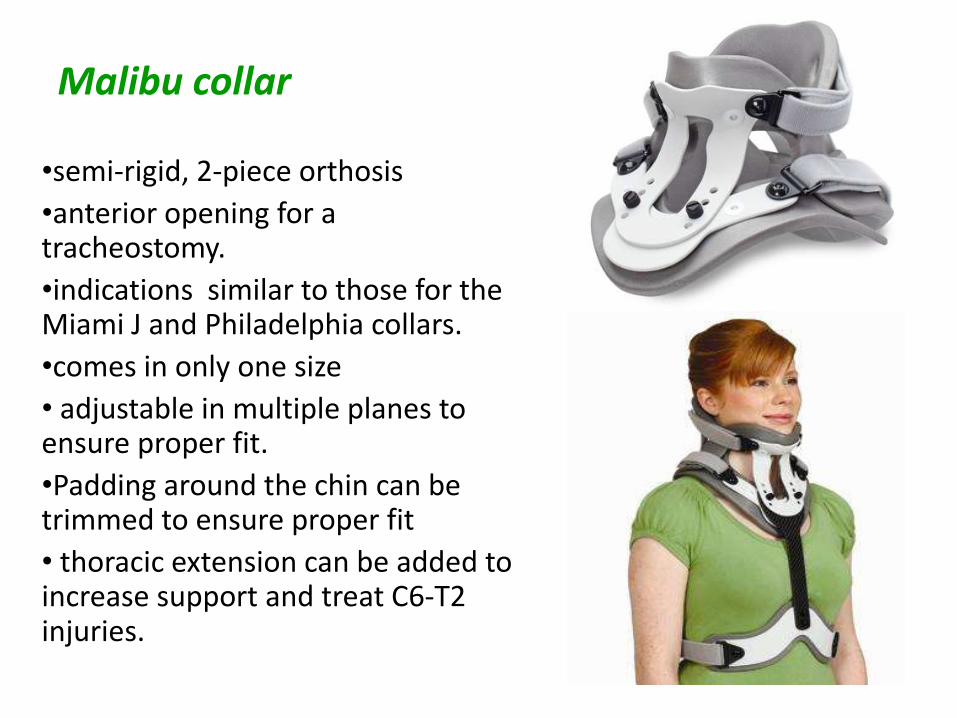
Malibu collar
•semi-rigid, 2-piece orthosis
•anterior opening for a tracheostomy.
•indications similar to those for the Miami J and Philadelphia collars.
•comes in only one size
• adjustable in multiple planes to ensure proper fit.
•Padding around the chin can be trimmed to ensure proper fit
• thoracic extension can be added to increase support and treat C6-T2 injuries.
Cervicothoracic orthoses (CTOs)
•greater motion restriction in the middle to lower cervical spine.
•upper cervical spine has less motion restriction.
•used in minimally unstable fractures.

Sternal-occipital-mandibular immobilizer (SOMI)
• CTO with anterior chest plate extending to the xiphoidprocess & metal or plastic bars curve over the shoulder.
• Straps from the bars over the shoulder & cross to opposite side of the anterior plate for fixation.
• 2-poster CTOs start from the chest plate and attach to the occipital component.
• SOMI is ideal for bedridden patients because it has no posterior rods.

•removable chin piece with an optional headpiece can be used if chin piece is removed for eating.
•Comfortable.
•Proper adjustment is crucial for motion restriction.
Indication:
•SOMI controls flexion in C1-C3 segments better than cervicothoracic brace.
•Atlantoaxial instability.
•Neural arch fractures of C2 (flexion causes instability).
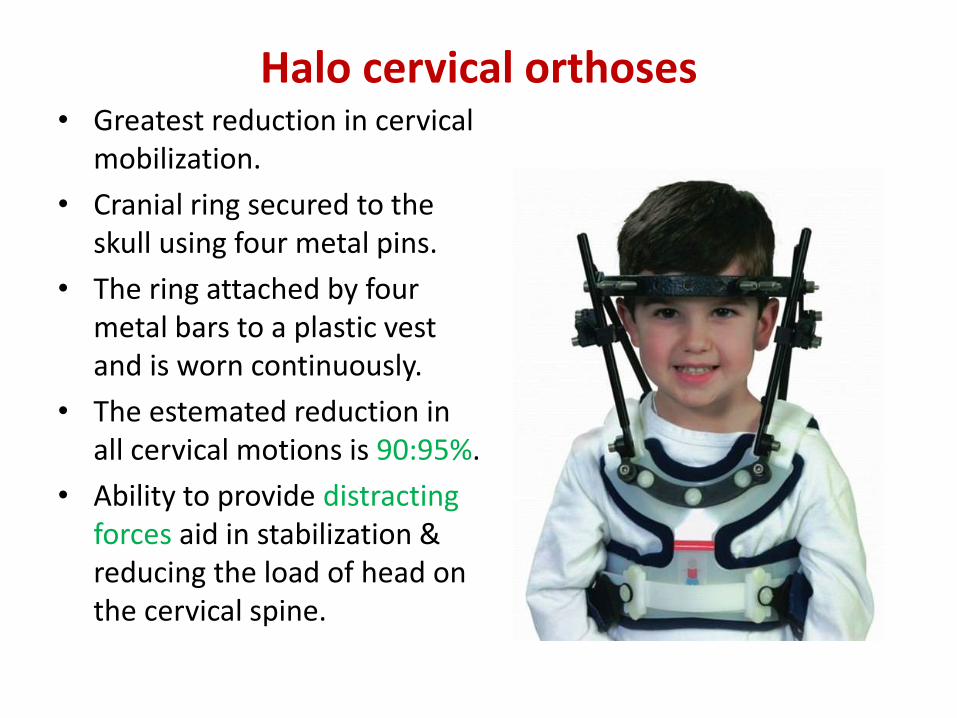
Halo cervical orthoses• Greatest reduction in cervical
mobilization.
• Cranial ring secured to the skull using four metal pins.
• The ring attached by four metal bars to a plastic vest and is worn continuously.
• The estemated reduction in all cervical motions is 90:95%.
• Ability to provide distracting forces aid in stabilization & reducing the load of head on the cervical spine.
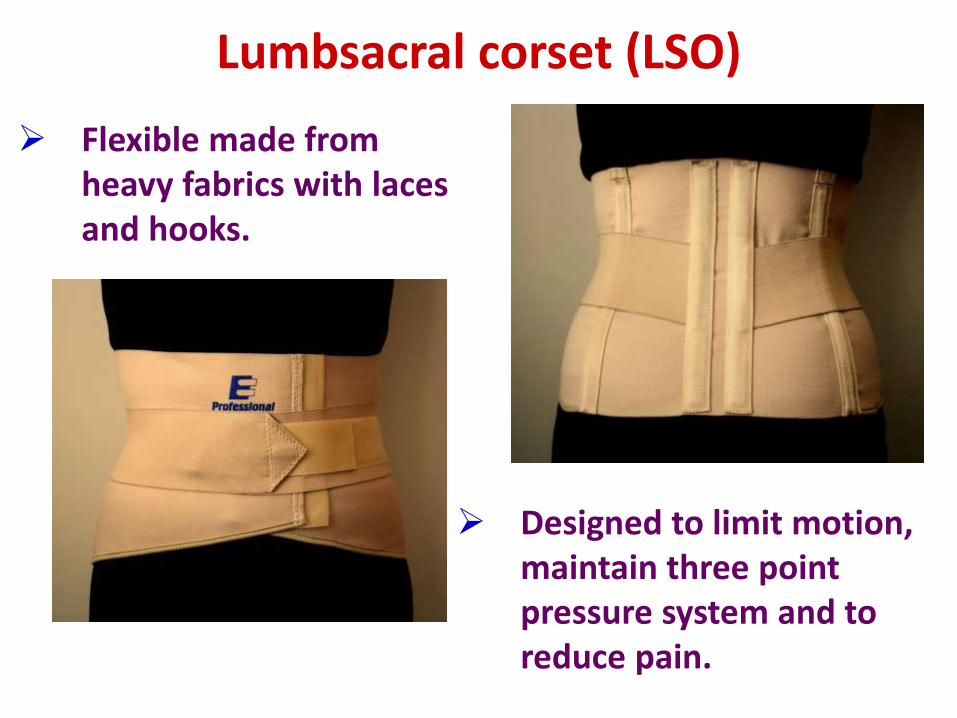
Lumbsacral corset (LSO)
Flexible made from heavy fabrics with laces and hooks.
Designed to limit motion, maintain three point pressure system and to reduce pain.

Thoracic-Lumbar-Sacral Corset
•Custom Molded Design Back Brace
•A Two-piece Foam Lined Plastic Clamshell Design With Straps.
Indications:
• Post-Operative Stabilization of the Spine.
• Lumbar Vertebrae Fractures.
• Chronic Back Pain.
• Slippage of One Vertebrae Over Another
• Stable Lumbar Fractures.
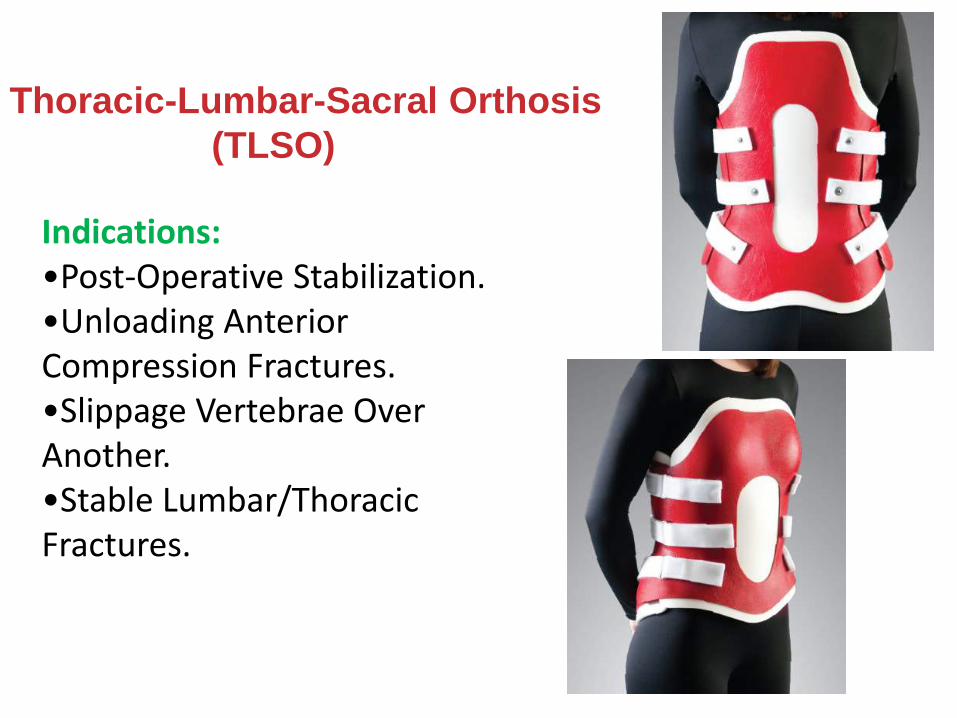
Indications:•Post-Operative Stabilization.•Unloading Anterior Compression Fractures.•Slippage Vertebrae Over Another.•Stable Lumbar/Thoracic Fractures.
Thoracic-Lumbar-Sacral Orthosis
(TLSO)
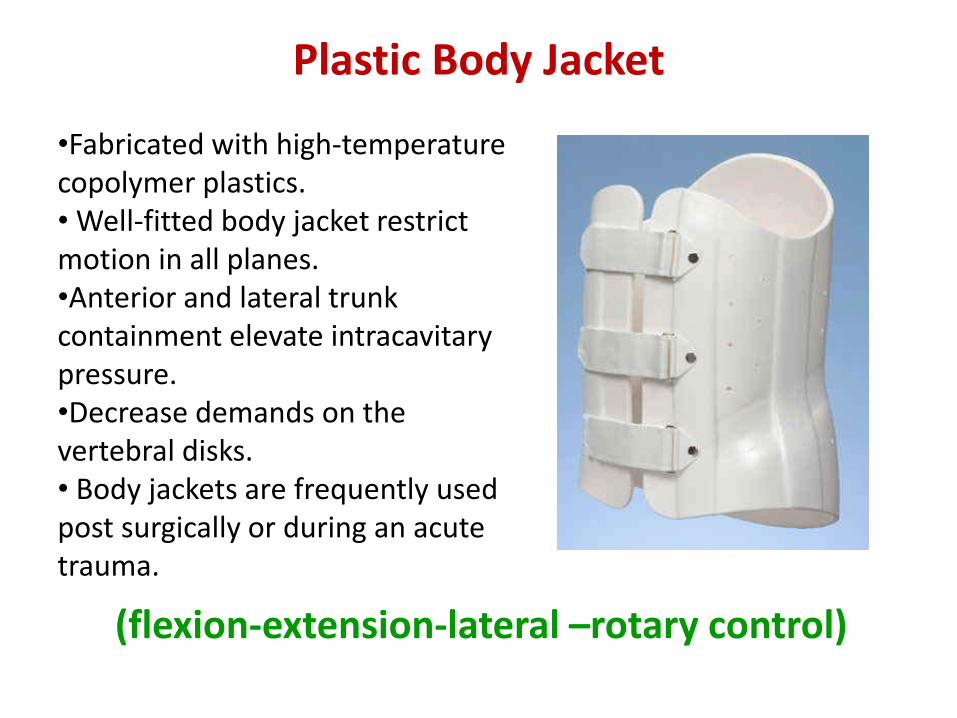
Plastic Body Jacket
•Fabricated with high-temperature copolymer plastics.• Well-fitted body jacket restrict motion in all planes. •Anterior and lateral trunk containment elevate intracavitarypressure.•Decrease demands on the vertebral disks.• Body jackets are frequently used post surgically or during an acute trauma.
(flexion-extension-lateral –rotary control)

Jewett Hyperextension Brace
Indications :
• Stable spinal compression fractures(T7:L2) without osteoporosis
• Postural kyphosis
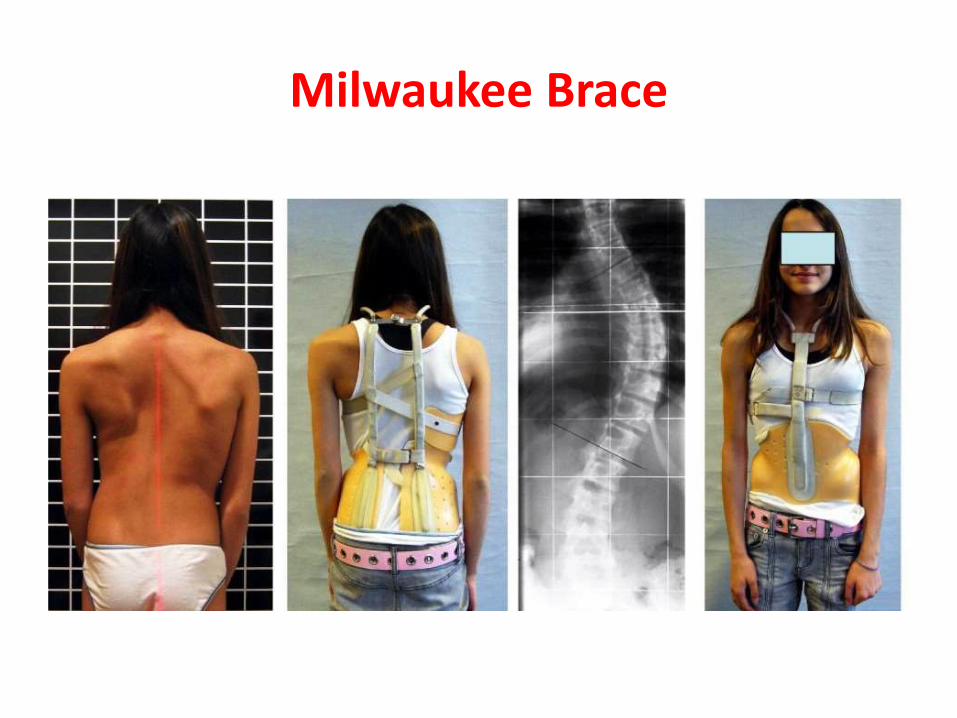
Milwaukee Brace
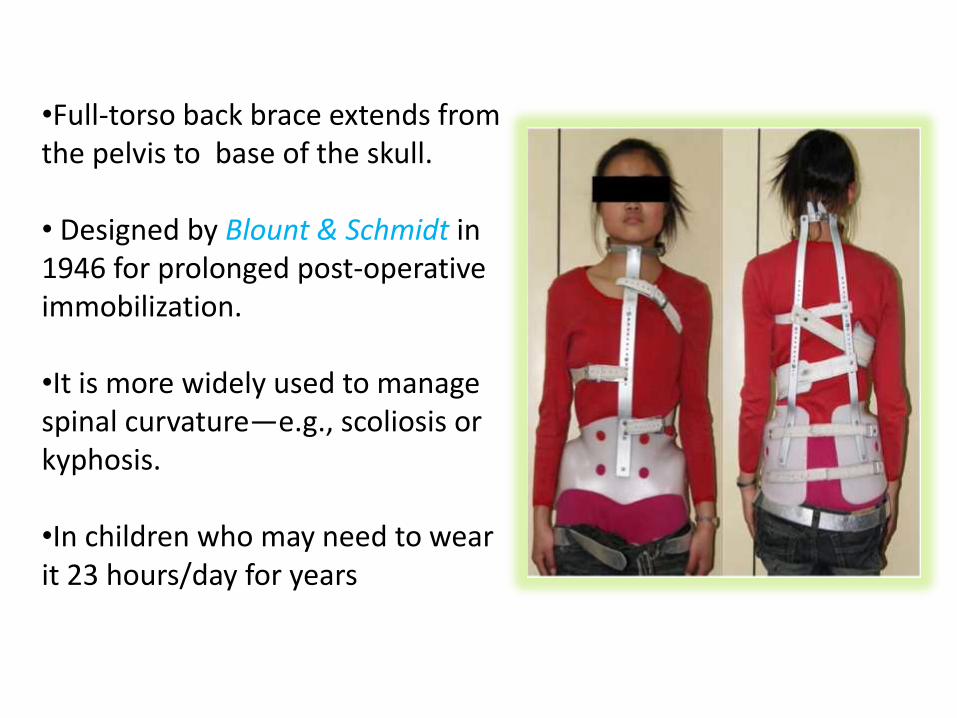
•Full-torso back brace extends from the pelvis to base of the skull.
• Designed by Blount & Schmidt in 1946 for prolonged post-operative immobilization.
•It is more widely used to manage spinal curvature—e.g., scoliosis or kyphosis.
•In children who may need to wear it 23 hours/day for years
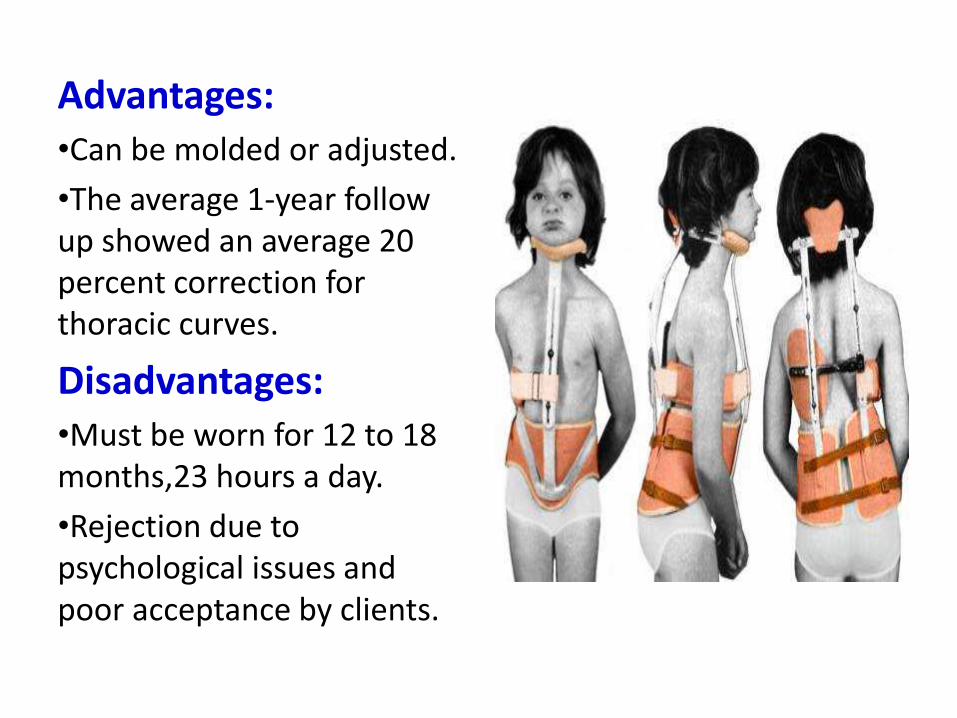
Advantages:•Can be molded or adjusted.
•The average 1-year follow up showed an average 20 percent correction for thoracic curves.
Disadvantages:•Must be worn for 12 to 18 months,23 hours a day.
•Rejection due to psychological issues and poor acceptance by clients.
Drawbacks of Spinal Orthosis
• Discomfort
• Local pain
• Osteopenia
• Skin breakdown
• Nerve compression
• Ingrown facial hair in men
• Muscle atrophy with prolonged use
• Decreased pulmonary capacity
• Difficulty in donning and doffing the orthosis
• Difficulty with transfers
• Psychologic and physical dependency
• Increased segmental motion at the ends of the orthosis
• Unsightly appearance
• Poor patient compliance
THANK YOU
Related Documents











