BASIC INVESTIGATION Spectral Optical Coherence Tomography A Novel Technique for Cornea Imaging Bartlomiej J. Kaluzy, MD,* Jakub J. Kalu _ zny, MD,* Anna Szkulmowska, MSc,† Iwona Gorczyn ´ska, MSc,† Maciej Szkulmowski, MSc,† Tomasz Bajraszewski, MSc,† Maciej Wojtkowski, PhD,† and Piotr Targowski, PhD† Purpose: Spectral optical coherence tomography (SOCT) is a new, noninvasive, noncontact, high-resolution technique that provides cross-sectional images of the objects that weakly absorb and scatter light. SOCT, because of very short acquisition time and high sensitivity, is capable of providing tomograms of substantially better quality than the conventional OCT. The aim of this paper is to show the application of the SOCT to cross-sectional imaging of the cornea and its pathologies. Methods: Eleven eyes with different corneal pathologies were examined with a slit lamp and the use of a prototype SOCT instru- ment constructed in the Institute of Physics, Nicolaus Copernicus University, Torun ´, Poland. Results: Our SOCT system provides high-resolution (4 mm axial, 10 mm transversal) tomograms composed of 3000–5000 A-scans with an acquisition time of 120–200 ms. The quality of the images is adequate for detailed cross-sectional evaluation of various corneal pathologies. Objective assessment of the localization, size, shape, and light-scattering properties of the changed tissue is possible. Corneal and epithelial thickness and the depth and width of lesions can be estimated. Conclusion: SOCT technique allows acquiring clinically valuable cross-sectional optical biopsy of the cornea and its pathologies. Key Words: spectral optical coherence tomography, cornea, imaging (Cornea 2006;25:960–965) S lit-lamp biomicroscopy is a standard technique for cornea examination. Because it cannot provide all of the in- formation required for full diagnosis, many technologies have been introduced to improve clinical evaluation of the cornea. Methods such as keratometry, ultrasound pachymetry, and Placido disc-based topography systems have served ophthalmologists well for many years. Slit-scanning technol- ogy (Orbscan, Bausch and Lomb, USA) 1 and the recently introduced rotating Scheimpflug digital camera system (Pentacam, Oculus, USA) 2 have considerably improved topographic and pachymetric assessment. In addition, a tandem scanning confocal microscopy (TSCM), 3 scanning slit confocal optical system (Confoscan, Nidek, Japan), 4,5 and confocal laser microscopy (HRT II Rostock Cornea Module, Heidelberg Engineering, Germany), 6 which provide cellular- level images, can be used for en face imaging and histologic study. Unfortunately, the resolution of tomograms provided by either ultrasound biomicroscopies (UBMs) 4 or by the Scheimpflug camera 2 is not adequate for a detailed cross- sectional corneal evaluation. Recent advances in optics, fiber optics, and laser technology have enabled the development of a novel optical imaging modality—optical coherence tomography (OCT). This is a noninvasive and noncontact technique that provides high-resolution cross-sectional images of weakly absorb- ing and scattering objects. Conventional (time domain) OCT (TdOCT) has proved its usefulness in visualization of different ocular tissues, including cornea. 7 Its main disadvantage is a long acquisition time, which causes a decrease in image quality. Lately, a new variant of OCT has been developed— spectral OCT (SOCT). Because of its high sensitivity and short acquisition time, it provides tomograms of outstanding quality. 8 Therefore, SOCT seems to be the most appropriate technique for cross-sectional imaging of the cornea. SOCT- based instruments, in contrast to conventional TdOCT, are not commercially available, and only prototypes have thus far been constructed. The first in vivo low-resolution SOCT tomogram of a healthy human cornea was published in 2002. 9 Meanwhile, significant progress in this technique has been made, espe- cially in resolution enhancement. The purpose of this article is to show, for the first time to our knowledge, the application of the high-resolution SOCT prototype instrument to cross- sectional imaging of corneal pathologies. MATERIALS AND METHODS Patients Various corneal pathologies were examined in a total sample of 11 eyes. Complete ophthalmologic examination led to diagnoses of bullous keratopathy (2 eyes), scar (2 eyes), and infectious and autoimmune keratitis (2 eyes). Of the traumas, Received for publication September 27, 2005; revision received February 21, 2006; accepted for publication March 11, 2006. From the *Department of Ophthalmology, Collegium Medicum, Nicolaus Copernicus University, Bydgoszcz, Poland; and the †Institute of Physics, Nicolaus Copernicus University, Torun ´, Poland. Supported by a grant from the Polish Ministry of Education and Science. Reprints: Bartlomiej J. Kalu _ zny, MD, Department of Ophthalmology, Collegium Medicum, Nicolaus Copernicus University, Curie- Sklodowskiej 9, 85-094 Bydgoszcz, Poland (e-mail address: bartka@ by.onet.pl). Copyright Ó 2006 by Lippincott Williams & Wilkins 960 Cornea Volume 25, Number 8, September 2006 Copyright ' Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
BASIC INVESTIGATION
Spectral Optical Coherence TomographyA Novel Technique for Cornea Imaging
Bartłomiej J. Kaluzy, MD,* Jakub J. Kału_zny, MD,* Anna Szkulmowska, MSc,†
Iwona Gorczynska, MSc,† Maciej Szkulmowski, MSc,† Tomasz Bajraszewski, MSc,†
Maciej Wojtkowski, PhD,† and Piotr Targowski, PhD†
Purpose: Spectral optical coherence tomography (SOCT) is a new,
noninvasive, noncontact, high-resolution technique that provides
cross-sectional images of the objects that weakly absorb and scatter
light. SOCT, because of very short acquisition time and high
sensitivity, is capable of providing tomograms of substantially better
quality than the conventional OCT. The aim of this paper is to show
the application of the SOCT to cross-sectional imaging of the cornea
and its pathologies.
Methods: Eleven eyes with different corneal pathologies were
examined with a slit lamp and the use of a prototype SOCT instru-
ment constructed in the Institute of Physics, Nicolaus Copernicus
University, Torun, Poland.
Results: Our SOCT system provides high-resolution (4 mm axial,
10 mm transversal) tomograms composed of 3000–5000 A-scans
with an acquisition time of 120–200 ms. The quality of the images is
adequate for detailed cross-sectional evaluation of various corneal
pathologies. Objective assessment of the localization, size, shape, and
light-scattering properties of the changed tissue is possible. Corneal
and epithelial thickness and the depth and width of lesions can be
estimated.
Conclusion: SOCT technique allows acquiring clinically valuable
cross-sectional optical biopsy of the cornea and its pathologies.
Key Words: spectral optical coherence tomography, cornea, imaging
(Cornea 2006;25:960–965)
S lit-lamp biomicroscopy is a standard technique for corneaexamination. Because it cannot provide all of the in-
formation required for full diagnosis, many technologies havebeen introduced to improve clinical evaluation of the cornea.Methods such as keratometry, ultrasound pachymetry, andPlacido disc-based topography systems have served
ophthalmologists well for many years. Slit-scanning technol-ogy (Orbscan, Bausch and Lomb, USA)1 and the recentlyintroduced rotating Scheimpflug digital camera system(Pentacam, Oculus, USA)2 have considerably improvedtopographic and pachymetric assessment. In addition, a tandemscanning confocal microscopy (TSCM),3 scanning slitconfocal optical system (Confoscan, Nidek, Japan),4,5 andconfocal laser microscopy (HRT II Rostock Cornea Module,Heidelberg Engineering, Germany),6 which provide cellular-level images, can be used for en face imaging and histologicstudy. Unfortunately, the resolution of tomograms providedby either ultrasound biomicroscopies (UBMs)4 or by theScheimpflug camera2 is not adequate for a detailed cross-sectional corneal evaluation.
Recent advances in optics, fiber optics, and lasertechnology have enabled the development of a novel opticalimaging modality—optical coherence tomography (OCT).This is a noninvasive and noncontact technique that provideshigh-resolution cross-sectional images of weakly absorb-ing and scattering objects. Conventional (time domain) OCT(TdOCT) has proved its usefulness in visualization of differentocular tissues, including cornea.7 Its main disadvantage is along acquisition time, which causes a decrease in imagequality. Lately, a new variant of OCT has been developed—spectral OCT (SOCT). Because of its high sensitivity andshort acquisition time, it provides tomograms of outstandingquality.8 Therefore, SOCT seems to be the most appropriatetechnique for cross-sectional imaging of the cornea. SOCT-based instruments, in contrast to conventional TdOCT, are notcommercially available, and only prototypes have thus far beenconstructed.
The first in vivo low-resolution SOCT tomogram ofa healthy human cornea was published in 2002.9 Meanwhile,significant progress in this technique has been made, espe-cially in resolution enhancement. The purpose of this articleis to show, for the first time to our knowledge, the applicationof the high-resolution SOCT prototype instrument to cross-sectional imaging of corneal pathologies.
MATERIALS AND METHODS
PatientsVarious corneal pathologies were examined in a total
sample of 11 eyes. Complete ophthalmologic examination ledto diagnoses of bullous keratopathy (2 eyes), scar (2 eyes), andinfectious and autoimmune keratitis (2 eyes). Of the traumas,
Received for publication September 27, 2005; revision received February 21,2006; accepted for publication March 11, 2006.
From the *Department of Ophthalmology, Collegium Medicum, NicolausCopernicus University, Bydgoszcz, Poland; and the †Institute of Physics,Nicolaus Copernicus University, Torun, Poland.
Supported by a grant from the Polish Ministry of Education and Science.Reprints: Bartłomiej J. Kału _zny, MD, Department of Ophthalmology,
Collegium Medicum, Nicolaus Copernicus University, Curie-Skłodowskiej 9, 85-094 Bydgoszcz, Poland (e-mail address: [email protected]).
Copyright � 2006 by Lippincott Williams & Wilkins
960 Cornea � Volume 25, Number 8, September 2006
JOBNAME: corn 25#8 2006 PAGE: 1 OUTPUT: Friday November 3 16:01:09 2006
lww/corn/127758/ICO200320
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
3 were in corneas a few days after cataract surgery, 1 afterpenetrating keratoplasty, and 1 after foreign body removal.The slit-lamp examination was followed by SOCT measure-ments, both carried out with the patient in a sitting position.Neither topical application of anesthetics nor speculum in-sertion was necessary for the examination. To home in on thepathologic changes, the SOCT scanning beam position wasmonitored with an infrared camera. An appropriate scanningregion was located by changing the position of the SOCT heador by getting the patient to follow a fixation light.
Written informed consent was obtained from allpatients. The study was approved by the Ethics Committee ofthe Collegium Medicum in Bydgoszcz, Nicolaus CopernicusUniversity, Torun, Poland.
Spectral Optical Coherence TomographyExaminations of the corneas were performed with the
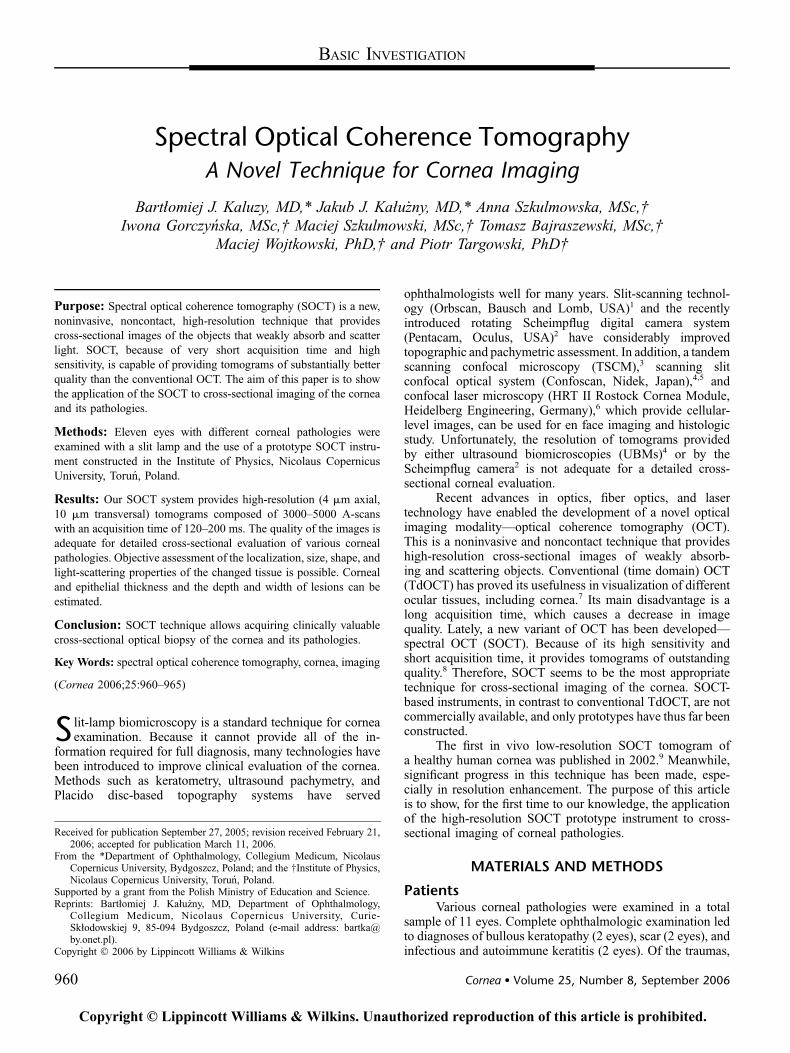
prototype SOCT instrument, constructed in the Institute ofPhysics, Nicolaus Copernicus University, Torun, Poland. Thedetails of operation of the SOCT instrument are givenelsewhere.10 In brief, the light emitted by a broadband(Dl = 70 nm, central wavelength 830 nm) superluminescentdiode light source (LS) (Fig. 1) is launched into a fiber-opticMichelson interferometer through an optical isolator (IO) andsplit into reference and object arms in a 50:50 fiber coupler(FC). The light propagating in a reference arm passes througha polarization controller (PC) and forms a semiparallel beamafter a collimator. This beam then goes through a neutraldensity filter (NDF), a block of glass acting as a dispersioncompensator (DC), and reflects from a reference mirror (RM)held in fixed position. The mirror directs the light back to thereference arm fiber and coupler (FC). The transversal scanner(X-Y) and lenses (L1.L3) in the object arm move the probingbeam across the object. This narrow beam of light penetrates
the object, scatters from the elements of its structure, and iscollected by the same optics L1...L3 back to the coupler, FC.Then it is brought to interference with the light returning fromthe reference arm. The interference signal is spectrallyanalyzed and registered by the spectrometer built of thevolume phase holographic grating (diffraction grating [DG];1200 lines/mm) and an achromatic lens that focuses spectrumon a 12-bit charge-coupled device (CCD) camera. Theresulting signal (spectral fringes) carries information on thelocations of structural interfaces in the object along the path ofthe penetrating beam. This signal after the Fourier trans-formation in the computer yields one line of the cross-sectional image (A-scan). The object beam is serially movedlaterally with the scanner X-Y to adjacent positions, and a 2-dimensional slice of the object is formed. A high-densityimage is composed of 3000 to 5000 A-scans and covers anarea of 1.1 mm in depth and 4 mm in width. The exposure time(during which the eye is illuminated) is 40 ms per singleA-scan. The total examination time is 120 to 200 ms. Thesensitivity of the system is 96 dB. The axial resolution of theinstrument is 6 mm in air (4 mm in tissue), whereas the lateralresolution is better than 10 mm (see also Fig. 6D). To calibratethe in-depth axis, the corneal group refractive index of 1.3817was used.11 Precision of geometrical thickness determinationis 3 mm. The measurement head was designed specifically foranterior segment imaging of the eye and mounted on a classicslit-lamp-like base to perform ophthalmic imaging conve-niently. The optical power of the beam incident at the cornea is750 mW. It is consistent with the American National StandardsInstitute recommended exposure limit for continuous beamviewing.12 Tomograms are presented in a grayscale—thedarker the color, the lower the reflectivity of the tissue.
An axial optical resolution is the same in SOCT, andtraditional TdOCT and depends on the light source used. Themajor difference between these techniques is the way theinformation contained in the light returning from the eye isretrieved.7 TdOCT requires that the reference mirror (or anyoptical delay line) is scanned over the imaging depth, whereasin the SOCT instrument, the mirror is held in fixed position. InSOCT, scanning is replaced by a spectral analysis of theinterference signal, and consequently, a spectrometer with aCCD camera must be used as a detector. Fourier trans-formation of spectral signal is mathematically equivalent todelay line scanning. The lack of moving parts in the referencearm makes data acquisition very fast, and high signal-to-noiseratio permits short exposition time of the CCD, even for lowirradiation of the eye.9 It can be roughly estimated that SOCTsystems are 100-fold faster than TdOCT. This advantage inspeed strongly reduces motion artifacts and is used to getA-scans of high density, with transversal scanner step muchsmaller than the lateral resolution. Such oversampled tomo-grams show increase in the sensitivity and quality by reducingthe effective speckle size and improving the delineation ofinternal structures.
RESULTSOur SOCT prototype instrument is capable of providing
cross-sectional images of the corneal inflammatory diseases.
FIGURE 1. A schematic diagram of the SOCT instrument: LS,superluminescent light source; OI, fiber isolator; FC, directionalfiber coupler; PC, polarization controller; NDF, neutral densityfilter; DC, glass block for dispersion compensation; RM,reference mirror; X-Y, galvoscanners; L, lenses; DG, diffractiongrating; CCD, line scan camera; COMP, personal computer.
q 2006 Lippincott Williams & Wilkins 961
Cornea � Volume 25, Number 8, September 2006 Spectral OCT for Corneal Imaging
JOBNAME: corn 25#8 2006 PAGE: 2 OUTPUT: Friday November 3 16:01:10 2006
lww/corn/127758/ICO200320
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
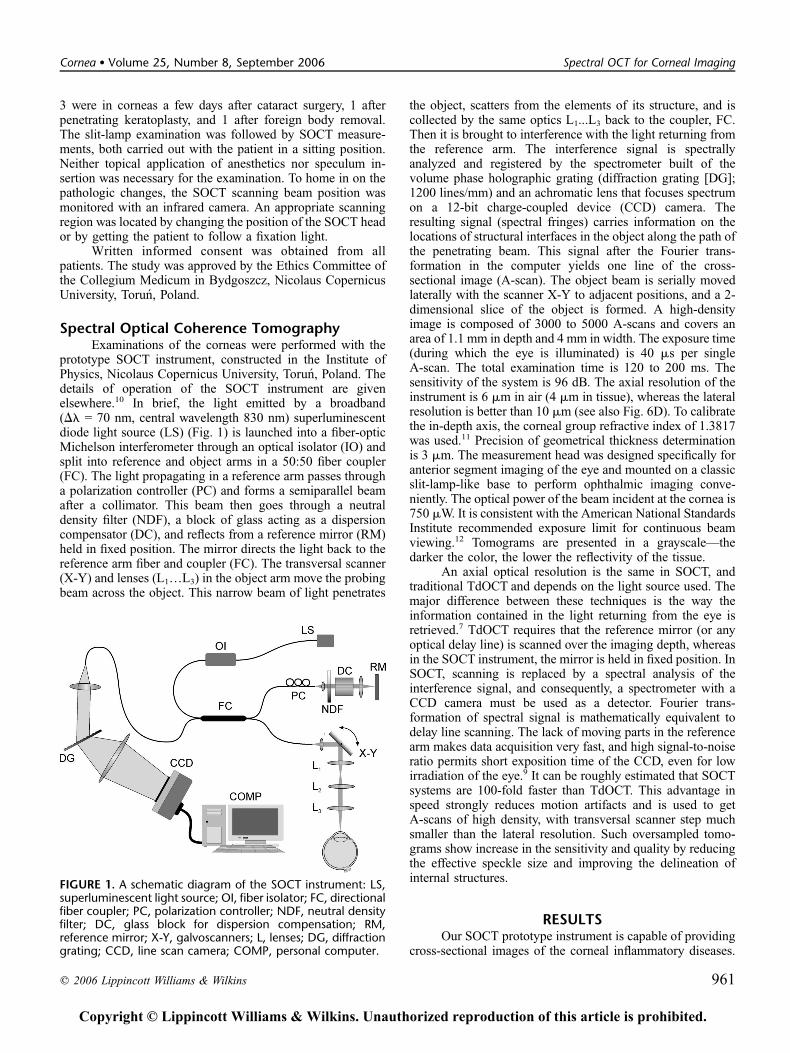
Both acute localized keratitis caused by prolonged contact lenswear (Fig. 2A) and chronic keratitis associated with ulcerativecolitis (Fig. 2B) can be clearly seen. The structure, reflectivity,and size of the lesions and surrounding tissues could beanalyzed.
Figure 3 presents the tomograms of 2 corneas in end-stage bullous keratopathy. Cross-sectional morphology ofsuperficial pathologies is visible; however, because of highscattering of the changes in the epithelium and outer stroma,the posterior part of the cornea is not seen.
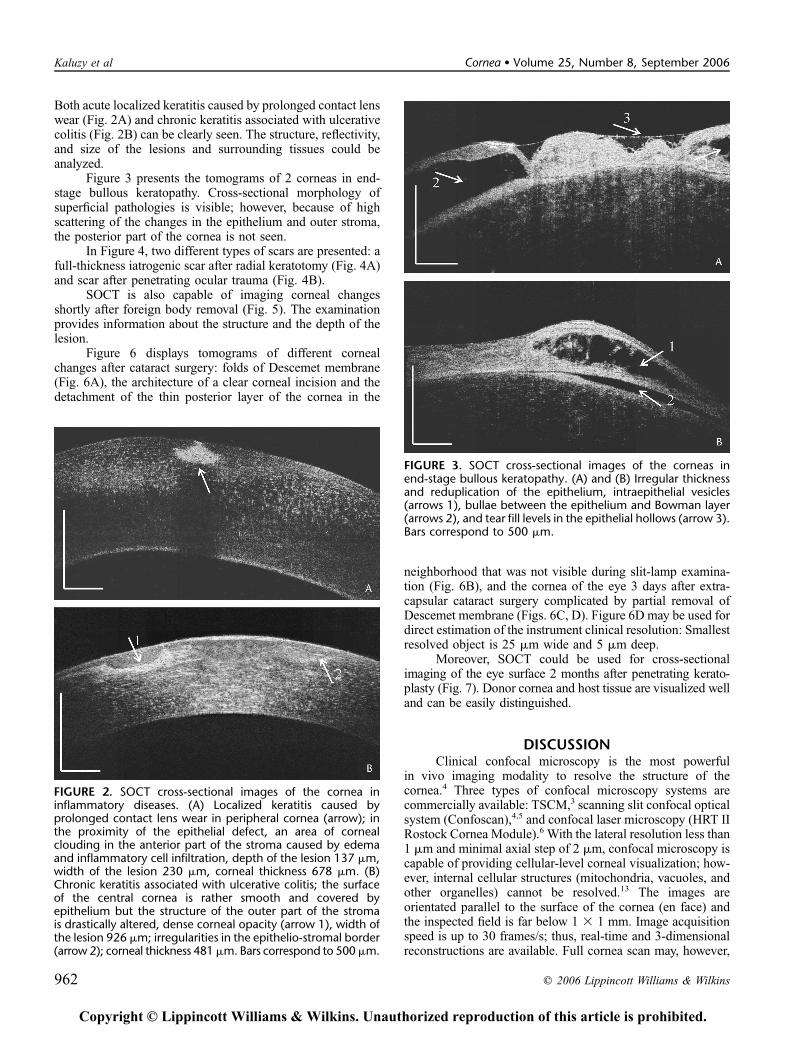
In Figure 4, two different types of scars are presented: afull-thickness iatrogenic scar after radial keratotomy (Fig. 4A)and scar after penetrating ocular trauma (Fig. 4B).
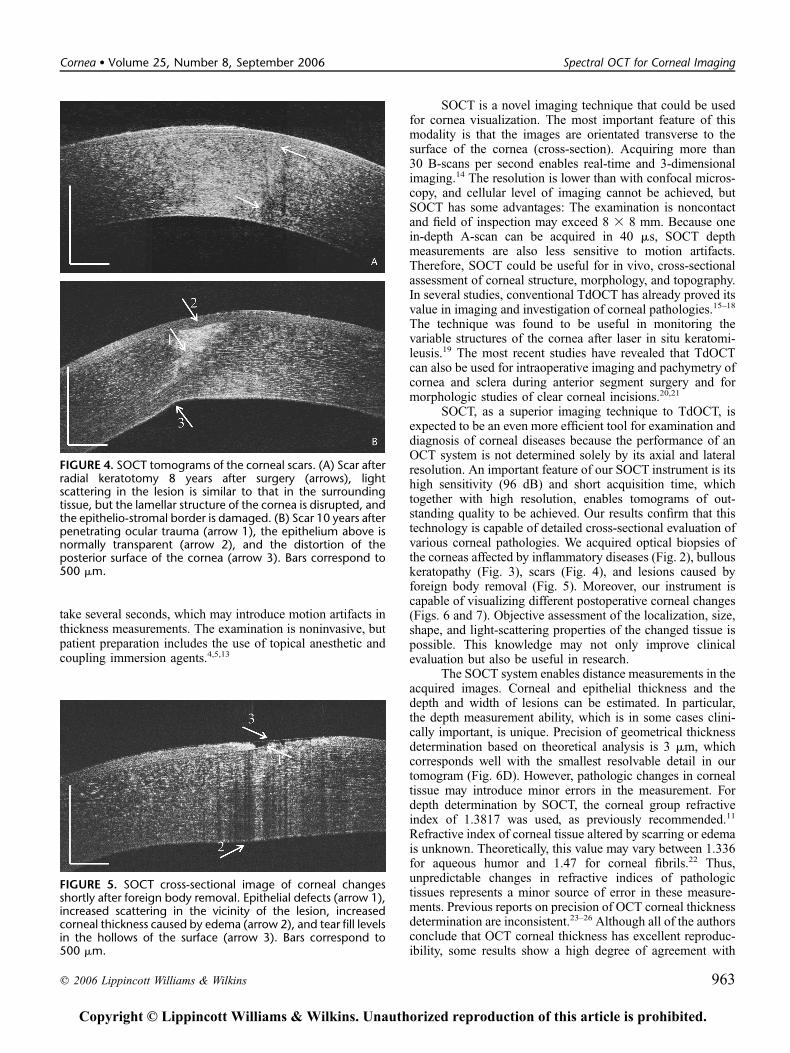
SOCT is also capable of imaging corneal changesshortly after foreign body removal (Fig. 5). The examinationprovides information about the structure and the depth of thelesion.
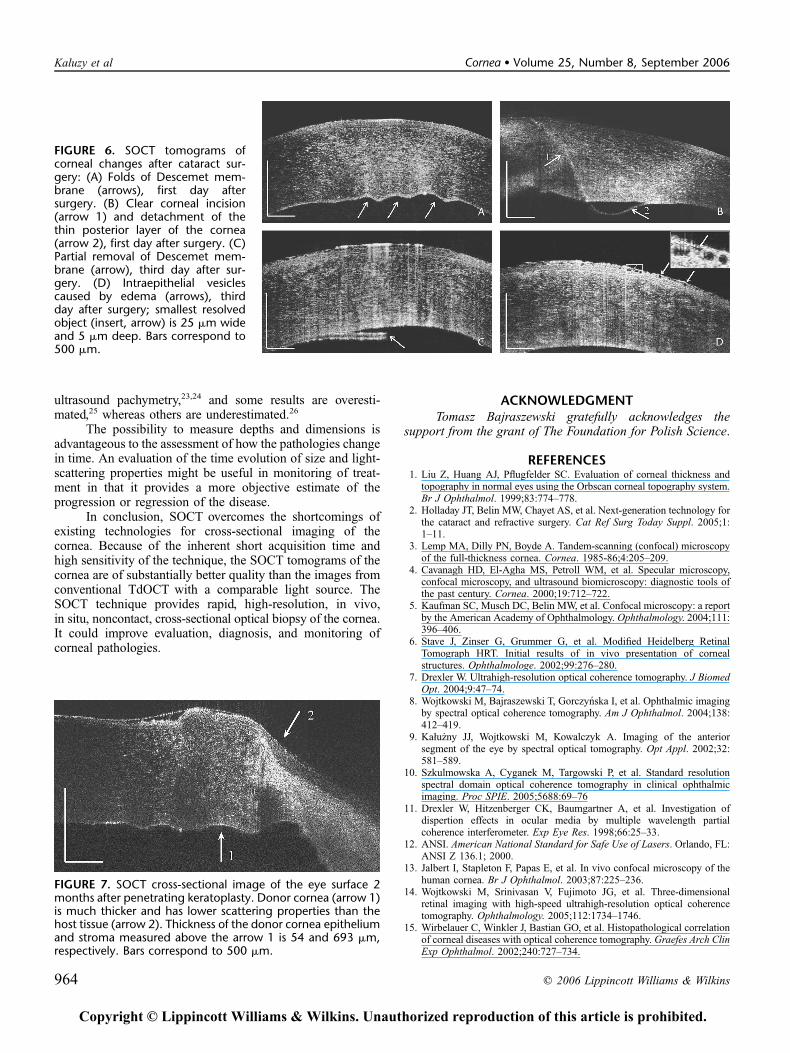
Figure 6 displays tomograms of different cornealchanges after cataract surgery: folds of Descemet membrane(Fig. 6A), the architecture of a clear corneal incision and thedetachment of the thin posterior layer of the cornea in the
neighborhood that was not visible during slit-lamp examina-tion (Fig. 6B), and the cornea of the eye 3 days after extra-capsular cataract surgery complicated by partial removal ofDescemet membrane (Figs. 6C, D). Figure 6D may be used fordirect estimation of the instrument clinical resolution: Smallestresolved object is 25 mm wide and 5 mm deep.
Moreover, SOCT could be used for cross-sectionalimaging of the eye surface 2 months after penetrating kerato-plasty (Fig. 7). Donor cornea and host tissue are visualized welland can be easily distinguished.
DISCUSSIONClinical confocal microscopy is the most powerful
in vivo imaging modality to resolve the structure of thecornea.4 Three types of confocal microscopy systems arecommercially available: TSCM,3 scanning slit confocal opticalsystem (Confoscan),4,5 and confocal laser microscopy (HRT IIRostock Cornea Module).6 With the lateral resolution less than1 mm and minimal axial step of 2 mm, confocal microscopy iscapable of providing cellular-level corneal visualization; how-ever, internal cellular structures (mitochondria, vacuoles, andother organelles) cannot be resolved.13 The images areorientated parallel to the surface of the cornea (en face) andthe inspected field is far below 1 3 1 mm. Image acquisitionspeed is up to 30 frames/s; thus, real-time and 3-dimensionalreconstructions are available. Full cornea scan may, however,
FIGURE 2. SOCT cross-sectional images of the cornea ininflammatory diseases. (A) Localized keratitis caused byprolonged contact lens wear in peripheral cornea (arrow); inthe proximity of the epithelial defect, an area of cornealclouding in the anterior part of the stroma caused by edemaand inflammatory cell infiltration, depth of the lesion 137 mm,width of the lesion 230 mm, corneal thickness 678 mm. (B)Chronic keratitis associated with ulcerative colitis; the surfaceof the central cornea is rather smooth and covered byepithelium but the structure of the outer part of the stromais drastically altered, dense corneal opacity (arrow 1), width ofthe lesion 926 mm; irregularities in the epithelio-stromal border(arrow 2); corneal thickness 481mm. Bars correspond to 500mm.
FIGURE 3. SOCT cross-sectional images of the corneas inend-stage bullous keratopathy. (A) and (B) Irregular thicknessand reduplication of the epithelium, intraepithelial vesicles(arrows 1), bullae between the epithelium and Bowman layer(arrows 2), and tear fill levels in the epithelial hollows (arrow 3).Bars correspond to 500 mm.
962 q 2006 Lippincott Williams & Wilkins
Kaluzy et al Cornea � Volume 25, Number 8, September 2006
JOBNAME: corn 25#8 2006 PAGE: 3 OUTPUT: Friday November 3 16:01:14 2006
lww/corn/127758/ICO200320
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
take several seconds, which may introduce motion artifacts inthickness measurements. The examination is noninvasive, butpatient preparation includes the use of topical anesthetic andcoupling immersion agents.4,5,13
SOCT is a novel imaging technique that could be usedfor cornea visualization. The most important feature of thismodality is that the images are orientated transverse to thesurface of the cornea (cross-section). Acquiring more than30 B-scans per second enables real-time and 3-dimensionalimaging.14 The resolution is lower than with confocal micros-copy, and cellular level of imaging cannot be achieved, butSOCT has some advantages: The examination is noncontactand field of inspection may exceed 8 3 8 mm. Because onein-depth A-scan can be acquired in 40 ms, SOCT depthmeasurements are also less sensitive to motion artifacts.Therefore, SOCT could be useful for in vivo, cross-sectionalassessment of corneal structure, morphology, and topography.In several studies, conventional TdOCT has already proved itsvalue in imaging and investigation of corneal pathologies.15–18
The technique was found to be useful in monitoring thevariable structures of the cornea after laser in situ keratomi-leusis.19 The most recent studies have revealed that TdOCTcan also be used for intraoperative imaging and pachymetry ofcornea and sclera during anterior segment surgery and formorphologic studies of clear corneal incisions.20,21
SOCT, as a superior imaging technique to TdOCT, isexpected to be an even more efficient tool for examination anddiagnosis of corneal diseases because the performance of anOCT system is not determined solely by its axial and lateralresolution. An important feature of our SOCT instrument is itshigh sensitivity (96 dB) and short acquisition time, whichtogether with high resolution, enables tomograms of out-standing quality to be achieved. Our results confirm that thistechnology is capable of detailed cross-sectional evaluation ofvarious corneal pathologies. We acquired optical biopsies ofthe corneas affected by inflammatory diseases (Fig. 2), bullouskeratopathy (Fig. 3), scars (Fig. 4), and lesions caused byforeign body removal (Fig. 5). Moreover, our instrument iscapable of visualizing different postoperative corneal changes(Figs. 6 and 7). Objective assessment of the localization, size,shape, and light-scattering properties of the changed tissue ispossible. This knowledge may not only improve clinicalevaluation but also be useful in research.
The SOCT system enables distance measurements in theacquired images. Corneal and epithelial thickness and thedepth and width of lesions can be estimated. In particular,the depth measurement ability, which is in some cases clini-cally important, is unique. Precision of geometrical thicknessdetermination based on theoretical analysis is 3 mm, whichcorresponds well with the smallest resolvable detail in ourtomogram (Fig. 6D). However, pathologic changes in cornealtissue may introduce minor errors in the measurement. Fordepth determination by SOCT, the corneal group refractiveindex of 1.3817 was used, as previously recommended.11
Refractive index of corneal tissue altered by scarring or edemais unknown. Theoretically, this value may vary between 1.336for aqueous humor and 1.47 for corneal fibrils.22 Thus,unpredictable changes in refractive indices of pathologictissues represents a minor source of error in these measure-ments. Previous reports on precision of OCT corneal thicknessdetermination are inconsistent.23–26 Although all of the authorsconclude that OCT corneal thickness has excellent reproduc-ibility, some results show a high degree of agreement with
FIGURE 4. SOCT tomograms of the corneal scars. (A) Scar afterradial keratotomy 8 years after surgery (arrows), lightscattering in the lesion is similar to that in the surroundingtissue, but the lamellar structure of the cornea is disrupted, andthe epithelio-stromal border is damaged. (B) Scar 10 years afterpenetrating ocular trauma (arrow 1), the epithelium above isnormally transparent (arrow 2), and the distortion of theposterior surface of the cornea (arrow 3). Bars correspond to500 mm.
FIGURE 5. SOCT cross-sectional image of corneal changesshortly after foreign body removal. Epithelial defects (arrow 1),increased scattering in the vicinity of the lesion, increasedcorneal thickness caused by edema (arrow 2), and tear fill levelsin the hollows of the surface (arrow 3). Bars correspond to500 mm.
q 2006 Lippincott Williams & Wilkins 963
Cornea � Volume 25, Number 8, September 2006 Spectral OCT for Corneal Imaging
JOBNAME: corn 25#8 2006 PAGE: 4 OUTPUT: Friday November 3 16:01:19 2006
lww/corn/127758/ICO200320
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
ultrasound pachymetry,23,24 and some results are overesti-mated,25 whereas others are underestimated.26
The possibility to measure depths and dimensions isadvantageous to the assessment of how the pathologies changein time. An evaluation of the time evolution of size and light-scattering properties might be useful in monitoring of treat-ment in that it provides a more objective estimate of theprogression or regression of the disease.
In conclusion, SOCT overcomes the shortcomings ofexisting technologies for cross-sectional imaging of thecornea. Because of the inherent short acquisition time andhigh sensitivity of the technique, the SOCT tomograms of thecornea are of substantially better quality than the images fromconventional TdOCT with a comparable light source. TheSOCT technique provides rapid, high-resolution, in vivo,in situ, noncontact, cross-sectional optical biopsy of the cornea.It could improve evaluation, diagnosis, and monitoring ofcorneal pathologies.
ACKNOWLEDGMENTTomasz Bajraszewski gratefully acknowledges the
support from the grant of The Foundation for Polish Science.
REFERENCES1. Liu Z, Huang AJ, Pflugfelder SC. Evaluation of corneal thickness and
topography in normal eyes using the Orbscan corneal topography system.Br J Ophthalmol. 1999;83:774–778.
2. Holladay JT, Belin MW, Chayet AS, et al. Next-generation technology forthe cataract and refractive surgery. Cat Ref Surg Today Suppl. 2005;1:1–11.
3. Lemp MA, Dilly PN, Boyde A. Tandem-scanning (confocal) microscopyof the full-thickness cornea. Cornea. 1985-86;4:205–209.
4. Cavanagh HD, El-Agha MS, Petroll WM, et al. Specular microscopy,confocal microscopy, and ultrasound biomicroscopy: diagnostic tools ofthe past century. Cornea. 2000;19:712–722.
5. Kaufman SC, Musch DC, Belin MW, et al. Confocal microscopy: a reportby the American Academy of Ophthalmology. Ophthalmology. 2004;111:396–406.
6. Stave J, Zinser G, Grummer G, et al. Modified Heidelberg RetinalTomograph HRT. Initial results of in vivo presentation of cornealstructures. Ophthalmologe. 2002;99:276–280.
7. Drexler W. Ultrahigh-resolution optical coherence tomography. J BiomedOpt. 2004;9:47–74.
8. Wojtkowski M, Bajraszewski T, Gorczynska I, et al. Ophthalmic imagingby spectral optical coherence tomography. Am J Ophthalmol. 2004;138:412–419.
9. Kału _zny JJ, Wojtkowski M, Kowalczyk A. Imaging of the anteriorsegment of the eye by spectral optical tomography. Opt Appl. 2002;32:581–589.
10. Szkulmowska A, Cyganek M, Targowski P, et al. Standard resolutionspectral domain optical coherence tomography in clinical ophthalmicimaging. Proc SPIE. 2005;5688:69–76
11. Drexler W, Hitzenberger CK, Baumgartner A, et al. Investigation ofdispertion effects in ocular media by multiple wavelength partialcoherence interferometer. Exp Eye Res. 1998;66:25–33.
12. ANSI. American National Standard for Safe Use of Lasers. Orlando, FL:ANSI Z 136.1; 2000.
13. Jalbert I, Stapleton F, Papas E, et al. In vivo confocal microscopy of thehuman cornea. Br J Ophthalmol. 2003;87:225–236.
14. Wojtkowski M, Srinivasan V, Fujimoto JG, et al. Three-dimensionalretinal imaging with high-speed ultrahigh-resolution optical coherencetomography. Ophthalmology. 2005;112:1734–1746.
15. Wirbelauer C, Winkler J, Bastian GO, et al. Histopathological correlationof corneal diseases with optical coherence tomography. Graefes Arch ClinExp Ophthalmol. 2002;240:727–734.
FIGURE 6. SOCT tomograms ofcorneal changes after cataract sur-gery: (A) Folds of Descemet mem-brane (arrows), first day aftersurgery. (B) Clear corneal incision(arrow 1) and detachment of thethin posterior layer of the cornea(arrow 2), first day after surgery. (C)Partial removal of Descemet mem-brane (arrow), third day after sur-gery. (D) Intraepithelial vesiclescaused by edema (arrows), thirdday after surgery; smallest resolvedobject (insert, arrow) is 25 mm wideand 5 mm deep. Bars correspond to500 mm.
FIGURE 7. SOCT cross-sectional image of the eye surface 2months after penetrating keratoplasty. Donor cornea (arrow 1)is much thicker and has lower scattering properties than thehost tissue (arrow 2). Thickness of the donor cornea epitheliumand stroma measured above the arrow 1 is 54 and 693 mm,respectively. Bars correspond to 500 mm.
964 q 2006 Lippincott Williams & Wilkins
Kaluzy et al Cornea � Volume 25, Number 8, September 2006
JOBNAME: corn 25#8 2006 PAGE: 5 OUTPUT: Friday November 3 16:01:24 2006
lww/corn/127758/ICO200320
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

16. Wirbelauer C, Scholz C, Hoerauf H, et al. Examination of the cornea usingoptical coherence tomography. Ophthalmologe. 2001;98:151–156.
17. Wirbelauer C, Pham DT. Imaging and quantification of calcified corneallesions with optical coherence tomography. Cornea. 2004;23:439–442.
18. Hirano K, Ito Y, Suzuki T, et al. Optical coherence tomography for thenoninvasive evaluation of the cornea. Cornea. 2001;20:281–289.
19. Wirbelauer C, Pham DT. Monitoring corneal structures with slit lamp-adapted optical coherence tomography in laser in situ keratomileusis.J Cataract Refract Surg. 2004;30:1851–1860.
20. Geerling G, Muller M, Winter C, et al. Intraoperative 2-dimensionaloptical coherence tomography as a new tool for anterior segment surgery.Arch Ophthalmol. 2005;123:253–257.
21. McDonnell PJ, Taban M, Sarayba M, et al. Dynamic morphology of clearcorneal cataract incisions. Ophthalmology. 2003;110:2342–2348.
22. Maurice DM. The structure and transparency of the cornea. J Physiol.1957;136:263–268.
23. Wirbelauer Ch, Scholz Ch, Hoerauf H, et al. Noncontact cornealpachymetry with slit lamp-adapted optical coherence tomography. Am JOphthalmol. 2002;133:444–450.
24. Fishman GR, Pons ME, Seedor JA, et al. Assessment of central cornealthickness using optical coherence tomography. J Cataract Refract Surg.2005;31:707–711.
25. Wang J, Fonn D, Simpson T, et al. Relation between optical coherencetomography and optical pachymetry measurements of corneal swellinginduced by hypoxia. Am J Ophthalmol. 2002;134:93–98.
26. Bechmann M, Thiel MJ, Neubauer AS, et al. Central corneal thicknessmeasurement with a retinal optical coherence tomography device versusstandard ultrasonic pachymetry. Cornea. 2001;20:50–54.
q 2006 Lippincott Williams & Wilkins 965
Cornea � Volume 25, Number 8, September 2006 Spectral OCT for Corneal Imaging
JOBNAME: corn 25#8 2006 PAGE: 6 OUTPUT: Friday November 3 16:01:29 2006
lww/corn/127758/ICO200320
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Related Documents











