DOI: 10.1542/peds.2006-1486 2007;119;281 Pediatrics Alison Jacknowitz, Daniel Novillo and Laura Tiehen Infant Feeding Practices Special Supplemental Nutrition Program for Women, Infants, and Children and http://pediatrics.aappublications.org/content/119/2/281.full.html located on the World Wide Web at: The online version of this article, along with updated information and services, is of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2007 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly by guest on June 1, 2013 pediatrics.aappublications.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DOI: 10.1542/peds.2006-1486 2007;119;281Pediatrics
Alison Jacknowitz, Daniel Novillo and Laura TiehenInfant Feeding Practices
Special Supplemental Nutrition Program for Women, Infants, and Children and
http://pediatrics.aappublications.org/content/119/2/281.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2007 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from
ARTICLE
Special Supplemental Nutrition Program for Women,Infants, and Children and Infant Feeding PracticesAlison Jacknowitz, PhDa, Daniel Novillo, MPPb, Laura Tiehen, PhDc
aDepartment of Public Administration and Policy, American University, Washington, DC; bUS Government Accountability Office, Washington, DC; cEconomic ResearchService, US Department of Agriculture, Washington, DC
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE. This study examined the association between participation in the SpecialSupplemental Nutrition Program for Women, Infants, and Children (WIC) andadherence to 4 American Academy of Pediatrics recommendations on infantfeeding.
METHODS.We used data from the Early Childhood Longitudinal Study-Birth Cohort,which is nationally representative of children born in 2001. We estimated regres-sion models to assess relationships between program participation and adherenceto American Academy of Pediatrics recommendations on exclusive breastfeedingand the introduction of infant formula, cow’s milk, and solid foods.
RESULTS.Regression results indicated that WIC participation was associated with a5.9-percentage point decrease in the likelihood of exclusive breastfeeding for �4months and a 1.9-percentage point decrease in the likelihood of exclusive breast-feeding for �6 months. Program mothers were 8.5 percentage points less likelythan nonparticipants to adhere to the American Academy of Pediatrics recom-mendation to delay introduction of infant formula until month 6. Program moth-ers were 2.5 percentage points more likely than nonparticipants to delay theintroduction of cow’s milk until month 8. Program participants were 4.5 percent-age points less likely than nonparticipants to delay the introduction of solid foodsfor �4 months. However, the difference between participants and nonparticipantsdisappeared by month 6.
CONCLUSIONS.Results suggest that, although program participants are less likely tobreastfeed exclusively than eligible nonparticipants, program-provided infant for-mula is an important option for mothers who do not breastfeed exclusively. Theprogram faces the challenge to encourage breastfeeding without underminingincentives to follow other recommended infant feeding practices. Recent changesproposed to the food packages by the US Department of Agriculture Food andNutrition Service are consistent with the goal of increasing adherence to recom-mended infant feeding practices among participants.
www.pediatrics.org/cgi/doi/10.1542/peds.2006-1486
doi:10.1542/peds.2006-1486
The views and opinions expressed in thisarticle do not necessarily reflect the viewsof the Economic Research Service of the USDepartment of Agriculture or the USGovernment Accountability Office.
KeyWordsbreastfeeding, guidelines, demographiccharacteristics, infant feeding, WIC, SpecialSupplemental Nutrition Program forWomen, Infants, and Children
AbbreviationsAAP—American Academy of PediatricsECLS-B—Early Childhood LongitudinalStudy-Birth CohortWIC—Special Supplemental NutritionProgram for Women, Infants, and Children
Accepted for publication Oct 2, 2006
Address correspondence to Laura Tiehen, PhD,Economic Research Service, USDA, 1800 M StNW, Room S2076, Washington, DC 20036.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005;Online, 1098-4275). Copyright © 2007 by theAmerican Academy of Pediatrics
PEDIATRICS Volume 119, Number 2, February 2007 281 by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from

THE SPECIAL SUPPLEMENTAL Nutrition Program forWomen, Infants, and Children (WIC) provides nu-
tritious foods, nutrition counseling, and referrals tohealth services and other social services to low-incomewomen, infants, and children up to age 5. WIC wasestablished as a pilot program in 1972 and has grownfrom serving an average of 88 000 participants in 1974to an average of 8 million in 2005. The congressionallyappropriated funding for WIC was almost $5 billion dur-ing 2005, up from $10.4 million during its inauguralyear, reflecting dramatic increases in participation andspending per participant.1 Approximately one fourth(1.9 million) of WIC participants are pregnant or post-partum women.2
Through the composition of its food packages andprovision of nutritional counseling, WIC may influencethe infant feeding decisions of its participants. Infantfeeding practices are an important determinant of ma-ternal and child health outcomes,3–14 which underscoresa need to understand WIC’s influence on them. With theEarly Childhood Longitudinal Study-Birth Cohort(ECLS-B), this study examines the influence of WICparticipation on adherence to recommendations by theAmerican Academy of Pediatrics (AAP) concerning thefollowing 4 infant feeding practices: the persistence ofexclusive breastfeeding and the introduction of infantformula, cow’s milk, and solid foods.
BACKGROUND
Recommended Infant Feeding PracticesAmong the various forms of infant nourishment, breastmilk is widely considered to be the most nutritionallybeneficial during the postpartum period.3 Breast milkcontains immunologic agents that protect infants againstinfectious diseases such as bacterial meningitis, diarrhea,respiratory ailments, and urinary tract infections.4,5
Breastfeeding also has a positive impact on maternalhealth, including quicker return to prepregnancyweight6 and reduced incidence of breast and ovariancancer.7–9 The social benefits of breastfeeding includelower national health care costs and reduced costs togovernment programs such as Medicaid and WICthrough promotion of healthier mothers and infants.10
Given the benefits of breastfeeding, the AAP WorkGroup on Breastfeeding recommends exclusive breast-feeding for the first 6 months of an infant’s life.13 TheAAP defines exclusive breastfeeding as feeding infantssolely breast milk, without any form of supplementa-tion. During the second 6 months of an infant’s life, theAAP recommends that breastfeeding continue, supple-mented with other nutritional sources.
Infant formula, although not as nutrient-rich asbreast milk, contains nutrients that are important forpositive health outcomes. The high iron content in iron-fortified formula aids in infant growth and development
while reducing the risk of iron-deficiency anemia, whichcan cause abnormal cognitive, social, and motor skilldevelopment.15 Cow’s milk, in contrast, is low in ironand often is difficult for infants �9 to 12 months of ageto digest.11 The AAP recommends that infants beingweaned from breast milk, and those who are not breast-fed, receive iron-fortified formula instead of cow’s milk.Although continued breastfeeding is desirable through-out the first year, the guidelines allow for weaning after6 months, implying that mothers should refrain fromintroducing infant formula until at least that age. TheAAP advises all mothers explicitly to abstain from intro-ducing cow’s milk until their child is 12 months of age.
The AAP Work Group on Breastfeeding recommendsintroduction of solid foods at 6 months of age,13 notingthat solid foods are not necessary for optimal growthuntil month 6 and that their introduction may causesubstitution away from human milk, which continues toprovide protection against diarrhea and respiratory tractinfections. In addition, some research suggests that de-laying the introduction of solid foods until month 6decreases the probability of allergic reactions to food,such as asthma and eczema, during childhood.14 Thereare experts, however, including the AAP Committee onNutrition, who support the introduction of complemen-tary foods to infants 4 to 6 months of age who aredevelopmentally ready.12
WIC and Infant Feeding PracticesWIC provides different food packages to mother/infantpairs, depending on whether the infant is breastfeedingor not. Nonbreastfed infants receive infant formula up totheir first birthday. Concerns have been raised that thesupply of infant formula may discourage breastfeedingamong WIC participants. Therefore, since the 1990s,WIC has increased its emphasis on breastfeeding promo-tion.16 The WIC food packages have also been revised toreduce the difference in the market value of the packageprovided to participants who breastfeed and those whodo not.17 All WIC infants receive infant cereal from 4 to12 months of age.18
Research has shown that WIC participants are lesslikely to breastfeed, with or without supplementation,than nonparticipants.19–29 Recent studies used a varietyof sophisticated empirical strategies to examine whetherthis disparity in any breastfeeding is attributable to WICparticipation itself or to other characteristics associatedwith WIC participation.20,22–24
Unlike the studies examining the relationship be-tween WIC participation and any breastfeeding, researchon WIC and AAP-recommended infant feeding practiceshas focused on descriptive comparisons of WIC partici-pants and nonparticipants. However, data limitationsconstrain their ability to identify precisely those who areeligible for WIC, an important comparison group. Thestudies are also constrained in the extent to which they
282 JACKNOWITZ et al by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from

can control for the numerous other factors that couldinfluence a mother’s decision to breastfeed exclusively.
Three studies found that WIC participants were lesslikely to breastfeed exclusively than nonparticipants.27–29
Previous analyses found that WIC participation was as-sociated with greater reported use of infant formula29,30
or with higher intake of iron, which was attributed tothe use of iron-fortified infant formula.21,29,30 Most re-search found that WIC infants were less likely thaneligible nonparticipants to consume cow’s milk, on thebasis of reported feeding patterns30,31 and nutrient intakeanalysis.21,30,32 One exception was Ponza et al,29 whofound no difference between WIC and non-WIC infants7 to 11 months of age with respect to the introduction ofcow’s milk. They did find that WIC infants 4 to 6 monthsof age were more likely to have been fed cow’s milk thanwere non-WIC infants, although introduction of cow’smilk was quite rare in both groups. As noted previously,the non-WIC infants included those who were not eli-gible to receive WIC benefits.
Although an early study found that WIC participantswere more likely to delay the introduction of solid foodsuntil the child was 4 months of age,30 more-recent stud-ies found no difference between WIC participants andnonparticipants.29,31 There is some evidence that WICparticipants are less likely to introduce solid foods toinfants 4 to 11 months of age,32 but it is not possible todetermine whether the difference exists in the 4- to6-month period relevant to the AAP infant feeding rec-ommendations.
Previous research provided valuable descriptive infor-mation regarding the association between WIC partici-pation and recommended infant feeding practices. Thisstudy contributes to this body of research in severaldimensions. First, the study examines the relationshipbetween WIC and 4 infant feeding practices that havereceived significantly less attention than any breastfeed-ing. This study uses recent, nationally representativedata that are comparable to other nationally representa-tive data sets for breastfeeding outcomes.28 These dataprovide rich socioeconomic information, so that we candetermine who is eligible for WIC and compare WICparticipants with those who are eligible but do not par-ticipate. Finally, we estimate regression models and con-trol for a variety of factors in an attempt to isolate theeffect of WIC participation on adherence to recom-mended infant feeding practices.
METHODS
Data SetThe data set used in this analysis was the ECLS-B. TheECLS-B is a longitudinal data set collected by the Na-tional Center of Education Statistics. The baseline sampleof 10 688 children was designed to be nationally repre-sentative of children born in 2001. The data set contains
oversamples of children who are American Indian, Chi-nese, members of another Asian or Pacific Islandergroup, are twins, or were born with low or very lowbirth weight. The first wave of data contains informationfrom the child’s birth certificate and information on thechild and his or her parents from a household surveyadministered �9 months after the child’s birth.
The ECLS-B contains rich information on children’shealth status, growth and development, and schoolreadiness. Pertinent to this study, the ECLS-B containsinformation on WIC participation, breastfeeding andother infant feeding practices, demographic characteris-tics, income and assets, participation in other assistanceprograms, and health status and behaviors.
To perform our analysis, we constructed an analysissample of 5276 eligible mothers. Mothers needed tomeet the following 6 inclusion criteria, with the numberof observations excluded for each criterion as noted.First, only observations with state identifiers were in-cluded in the analysis (86 observations excluded). Sec-ond, only biological mothers were included (141 obser-vations excluded). Third, mothers with multiple birthswere included as single observations (794 observationsexcluded). Fourth, only mothers whose survey child was�8 months of age and �18 months of age at the time ofthe assessment were included (96 observations ex-cluded). Fifth, only observations with complete informa-tion for all relevant variables, with the exception of thevariable indicating that the child was firstborn, wereincluded (773 observations excluded). There were �200observations with missing data on whether the child wasfirstborn; therefore, we assigned them a value of 0, themodal value, for the firstborn indicator and included avariable that indicated whether the observation wasmissing data for that variable. Finally, only mothers whowere eligible for WIC were included (3522 observationsexcluded). To be eligible, a mother must have householdincome of �185% of the poverty level or participate inthe Food Stamp Program, cash welfare, or the Medicaidprogram. In addition, she must be determined to be atnutritional risk. Although the ECLS-B does not includedata to allow determination of whether a woman is atnutritional risk, research has found that nearly all in-come-eligible individuals are also at nutritional risk.33
Among eligible mothers in our analysis sample,80.6% participated in WIC, and 66.7% began participat-ing during pregnancy (Table 1). Eligible mothers whochose to participate seemed to be more disadvantagedthan those who did not participate. Mothers who par-ticipated in WIC were more likely to be non-Hispanicblack or Hispanic, to have less than a high school edu-cation, to be younger, to have never been married, toparticipate in other assistance programs, and to haveincomes below the poverty level, compared with theirnonparticipant counterparts.
PEDIATRICS Volume 119, Number 2, February 2007 283 by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from
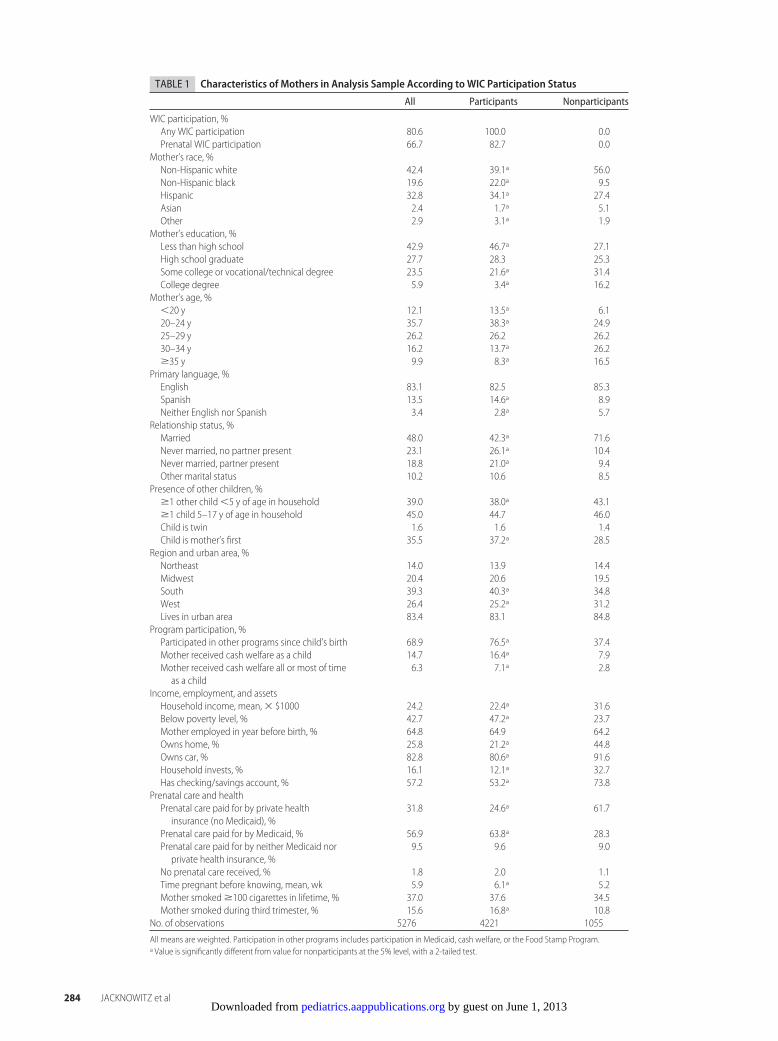
TABLE 1 Characteristics of Mothers in Analysis Sample According to WIC Participation Status
All Participants Nonparticipants
WIC participation, %Any WIC participation 80.6 100.0 0.0Prenatal WIC participation 66.7 82.7 0.0
Mother’s race, %Non-Hispanic white 42.4 39.1a 56.0Non-Hispanic black 19.6 22.0a 9.5Hispanic 32.8 34.1a 27.4Asian 2.4 1.7a 5.1Other 2.9 3.1a 1.9
Mother’s education, %Less than high school 42.9 46.7a 27.1High school graduate 27.7 28.3 25.3Some college or vocational/technical degree 23.5 21.6a 31.4College degree 5.9 3.4a 16.2
Mother’s age, %�20 y 12.1 13.5a 6.120–24 y 35.7 38.3a 24.925–29 y 26.2 26.2 26.230–34 y 16.2 13.7a 26.2�35 y 9.9 8.3a 16.5
Primary language, %English 83.1 82.5 85.3Spanish 13.5 14.6a 8.9Neither English nor Spanish 3.4 2.8a 5.7
Relationship status, %Married 48.0 42.3a 71.6Never married, no partner present 23.1 26.1a 10.4Never married, partner present 18.8 21.0a 9.4Other marital status 10.2 10.6 8.5
Presence of other children, %�1 other child �5 y of age in household 39.0 38.0a 43.1�1 child 5–17 y of age in household 45.0 44.7 46.0Child is twin 1.6 1.6 1.4Child is mother’s first 35.5 37.2a 28.5
Region and urban area, %Northeast 14.0 13.9 14.4Midwest 20.4 20.6 19.5South 39.3 40.3a 34.8West 26.4 25.2a 31.2Lives in urban area 83.4 83.1 84.8
Program participation, %Participated in other programs since child’s birth 68.9 76.5a 37.4Mother received cash welfare as a child 14.7 16.4a 7.9Mother received cash welfare all or most of timeas a child
6.3 7.1a 2.8
Income, employment, and assetsHousehold income, mean, � $1000 24.2 22.4a 31.6Below poverty level, % 42.7 47.2a 23.7Mother employed in year before birth, % 64.8 64.9 64.2Owns home, % 25.8 21.2a 44.8Owns car, % 82.8 80.6a 91.6Household invests, % 16.1 12.1a 32.7Has checking/savings account, % 57.2 53.2a 73.8
Prenatal care and healthPrenatal care paid for by private healthinsurance (no Medicaid), %
31.8 24.6a 61.7
Prenatal care paid for by Medicaid, % 56.9 63.8a 28.3Prenatal care paid for by neither Medicaid norprivate health insurance, %
9.5 9.6 9.0
No prenatal care received, % 1.8 2.0 1.1Time pregnant before knowing, mean, wk 5.9 6.1a 5.2Mother smoked �100 cigarettes in lifetime, % 37.0 37.6 34.5Mother smoked during third trimester, % 15.6 16.8a 10.8
No. of observations 5276 4221 1055
All means are weighted. Participation in other programs includes participation in Medicaid, cash welfare, or the Food Stamp Program.a Value is significantly different from value for nonparticipants at the 5% level, with a 2-tailed test.
284 JACKNOWITZ et al by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from

Statistical AnalysesWe estimated probit models, with dependent variablesthat captured the infant feeding practices recommendedby the AAP. Each mother responded to questions thatasked the age of the child (in months) when she beganfeeding her infant formula, cow’s milk, or solid foods.Exclusive breastfeeding was defined as refraining fromfeeding infant formula, cow’s milk, and solid foods. Sur-vey respondents did not provide information about feed-ing their infants other liquids, such as water or juice.Although our definition of exclusive breastfeeding wasnot as restrictive as that used by Li et al28 in their analysisof the National Immunization Survey, the exclusivebreastfeeding rates among all women were quite consis-tent. We examined the introduction of solid foods (andexclusive breastfeeding) at both 4 and 6 months becauseof the variation in the recommendations regarding theintroduction of complementary foods. Adherence tocow’s milk recommendations was measured at 8 monthsinstead of 12 months because most of the infants sur-veyed were not yet 12 months of age at the time of theassessment.
The primary independent variable of interest, WICparticipation, was defined as the mother having receivedWIC benefits during pregnancy, during the first 6months after pregnancy, or having received WIC vouch-ers to purchase food or formula for her infant in the 30days before the survey. Along with the dichotomousWIC participation variable, we included many of thecharacteristics thought to be associated with infant feed-ing decisions as control variables. The characteristics pre-sented in Table 1 were included as explanatory variables.These variables included mother’s race and ethnicity(with non-Hispanic white as the basis), mother’s educa-tion (with no high school diploma as the basis), mother’sage (with age of �20 years as the basis), mother’s pri-mary language (with English as the basis), mother’srelationship status (with married as the basis), the pres-ence of other children �5 years and between 5 and 17years of age, whether the mother has twins, andwhether the interview child is the mother’s first. We alsoincluded indicator variables for the region of residence(with residence in the West as the basis) and for living inan urban area.
We captured the women’s experience with other as-sistance programs with an indicator variable for partici-pating in cash welfare, the Food Stamp Program, orMedicaid since the birth of the child and 2 variables forthe amount of time (some of the time or at least most ofthe time) the household received cash welfare duringthe mother’s childhood (with no cash welfare receipt asthe basis). We also included household income, an in-dicator variable for household income below the povertylevel, and an indicator variable for being employed anytime during the 12 months before the child’s birth. Wecharacterized the woman’s assets with indicator vari-
ables for home ownership, car or truck ownership, hav-ing investments, and having a savings or checking ac-count.
Variables to describe characteristics related to thewomen’s pregnancy and general health were also in-cluded in the analysis. We controlled for differences inprenatal care by including indicator variables forwhether prenatal care was paid for by Medicaid, waspaid for by some other means, or was not received at all(using prenatal care paid for by private insurance as thebasis). We also included a variable for the number ofweeks into her pregnancy when the mother found outshe was pregnant, a variable that indicated that thewoman had smoked �100 cigarettes during her lifetime,and a variable that indicated whether the mother hadsmoked during her third trimester.
All probit regressions were weighted by using theweight variable W1RO, which was provided with theECLS-B data. Marginal effects evaluated with the meansof the independent variables are presented. Estimatedmarginal effects of WIC participation in unweighted re-gression analyses (available from the authors on re-quest) are quite similar to those reported. SEs wereadjusted to correct for heteroskedasticity.
RESULTSDescriptive analysis showed that 44% of WIC partici-pants and 59% of nonparticipants exclusively breastfedthrough the first 1 month after childbirth (Table 2).Rates of exclusive breastfeeding decreased steadily afterthe first month. At month 4, 15% of WIC participantsand 30% of nonparticipants exclusively breastfed; only5% of WIC participants and 10% of nonparticipants metthe stricter AAP guideline of 6 months. Although therates of exclusive breastfeeding among all mothers in theECLS-B were quite consistent with those produced byusing the National Immunization Survey,28 we foundlower rates of exclusive breastfeeding among WIC-eligi-ble mothers. This was likely attributable to differences incalculating both WIC eligibility and WIC participation.
The estimated marginal effects of WIC participationon infant feeding practices from the probit regressionanalysis are presented in Table 3. Coefficients for controlvariables for the exclusive breastfeeding models gener-ally had the expected signs. Full regression results for 4of the models are presented in the Appendix. Our re-gression analyses of exclusive breastfeeding (Table 3)showed that WIC participation was associated with a5.9-percentage point decrease in the likelihood of exclu-sive breastfeeding for �4 months (P � .01) and a 1.9-percentage point decrease in the likelihood of exclusivebreastfeeding for �6 months (P � .05). The negativeassociation between WIC participation and exclusivebreastfeeding is consistent with results from other stud-ies.27,28 However, our regression results indicated that themagnitude of the negative relationship decreased when
PEDIATRICS Volume 119, Number 2, February 2007 285 by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from

we controlled for other characteristics that influenceexclusive breastfeeding.
As shown in Table 2, WIC mothers were more likelyto initiate infant formula feeding during the first 1month after child birth (56%, compared with 41% ofnonparticipants). By month 6, 88% of participants and72% of nonparticipants had introduced infant formula.Regression results indicated that WIC mothers were 8.5percentage points less likely than non-WIC mothers (P� .01) to adhere to the AAP recommendation to delayintroduction of infant formula until month 6 (Table 3).The negative association between WIC participation anddelaying the introduction of infant formula until 6months after birth is consistent with previous studies.29,30
Consistent with our finding on exclusive breastfeeding,the regression results indicated that the measured asso-ciation between WIC participation and infant formulafeeding was much smaller when we controlled for otherexplanatory factors.
Although WIC mothers were less likely to delay the
introduction of infant formula than non-WIC mothers,they were more likely to delay the introduction of cow’smilk. It was not common for either WIC participants ornonparticipants to provide cow’s milk to their infants,with �4% of eligible women introducing it by month 8.Regression results suggested that WIC mothers were 2.5percentage points more likely (P � .01) to delay theintroduction of cow’s milk until month 8 than werenonparticipants (Table 3). The finding that WIC partici-pants were more likely to delay the introduction of cow’smilk is consistent with most previous research.21,30–32
The descriptive analysis illustrated that WIC partici-pants were more likely than nonparticipants to intro-duce solid foods to their infants by month 4 (Table 2).Our regression results corroborated the descriptive anal-ysis. WIC participants were 4.5 percentage points lesslikely than nonparticipants (P � .05) to delay the intro-duction of solid foods until their infant was �4 monthsof age (Table 3). This finding is in contrast to previousstudies on the association between WIC participation
TABLE 2 Infant Feeding Practices AmongWIC-Eligible Women According to Age of Infant
Proportion, %
Breastfed Exclusively Introduced InfantFormula
Introduced Cow’s Milk Introduced Solid Foods
WIC Non-WIC WIC Non-WIC WIC Non-WIC WIC Non-WIC
Infant age, mo1 43.6a 59.2 56.4a 40.6 0.0 0.3 0.0 0.02 29.7a 46.4 67.4a 51.7 0.3 0.7 4.5 3.43 22.5a 38.0 75.2a 59.1 0.4 0.9 10.8a 6.74 14.8a 29.6 81.0a 64.9 0.5 1.0 27.6a 20.35 7.9a 15.6 85.4a 69.2 0.7 1.3 57.8 53.46 4.7a 9.9 87.8a 72.0 0.9 1.7 72.6 70.47 1.4 1.9 90.3a 76.5 2.1 3.6 92.0 91.48 0.4 0.8 91.4a 78.1 3.1a 5.2 96.1 95.0
No. of observations 4221 1055 4221 1055 4221 1055 4221 1055
Percentage values refer to those who breastfed exclusively through the month indicated and those who introduced infant formula, cow’s milk, or solid foods before the month indicated.a Value is significantly different from value for nonparticipants at the 5% level, with a 2-tailed test.
TABLE 3 Marginal Effects From Probit Regression Analyses for Adherence to AAP Guidelines
Dependent Variable Marginal Effect (SE) for WIC Participation Among EligibleMothers
Exclusive breastfeeding for �4 mo �0.059 (0.020)a
Exclusive breastfeeding for �6 mo �0.019 (0.010)b
Did not introduce infant formula before sixth month �0.085 (0.019)a
Did not introduce cow’s milk before eighth month 0.025 (0.010)a
Did not introduce solid foods before fourth month �0.045 (0.022)b
Did not introduce solid foods before sixth month �0.029 (0.023)
The number of observations was 5276. Regressions were weighted. Robust SEs are shown in parentheses. Marginal effects were calculated withthe means of the independent variables. The full regression results are presented in the Appendix. Regression analyses included the followingcontrol variables: demographic: mother’s race, education, age, primary language, relationship status, presence of other children, and region;income-related: income, poverty status, participation in other assistance programs, childhood participation in other assistance programs, indi-cators for home ownership, car ownership, whether the mother had worked in the past 12 months, whether she invests, and whether she has achecking or savings account; health/birth-related: prenatal care payment arrangement, number of weeks the mother was pregnant beforeknowing, and indicators for whether the child is her first, whether information for the first born variable is missing, whether the child is a twin,whether the mother has smoked �100 cigarettes in her lifetime, and whether she smoked during the third trimester of pregnancy.a Value is significant at 1%.b Value is significant at 5%.
286 JACKNOWITZ et al by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from

and introduction of solid foods before month 4.29–31
However, the difference between WIC participants andnonparticipants disappeared by month 6 (Table 3),which is consistent with previous studies.29,31
DISCUSSIONWIC participation is related to most, but not all, of theinfant feeding decisions of eligible mothers. WIC partic-ipation is associated with a lower likelihood of exclusivebreastfeeding and a greater likelihood of infant formulaintroduction. Combined with WIC participants’ lowerlikelihood of introducing cow’s milk prematurely, thisfinding suggests that WIC-provided infant formulaserves as an important nutritional option for motherswho decide to breastfeed partially or not to breastfeed atall. As discussed earlier, infant formula is not as benefi-cial as breast milk. However, studies show that formulais the second best form of infant nourishment and isnutritionally superior to cow’s milk. The relatively highmarket price of infant formula would likely make such afeeding practice prohibitive for many low-income moth-ers. Therefore, if WIC stopped offering infant formula,then many nonbreastfeeding WIC mothers might opt tofeed their infants less-nutritious alternatives, includingcow’s milk.
There was also a significant negative relationship be-tween WIC participation and adherence to the recom-mendation to delay solid foods until the infant is 4months of age. However, that relationship disappearedat 6 months, and a large majority of eligible mothers hadintroduced solid foods by that time.
Limitations of the study should be noted. Given thatmothers elect to participate in the WIC program, it isdifficult to determine the causal effect of WIC participa-tion on infant feeding practices. Several recent studiesdocumented a wide array of differences between eligiblemothers who participate in WIC and those who donot.20,22,23,34 Although we have included a rich set ofcontrol variables, it is still possible that unobservablecharacteristics of the mother are associated with bothher decision to participate in the WIC program and herinfant feeding practices. If so, we may attribute, forexample, a lower rate of exclusive breastfeeding to WICparticipation when it is attributable to other character-istics that are associated strongly with WIC participation.
Two additional limitations of the study are related tothe data collection procedures. First, it was necessary toexclude mothers of infants �18 months of age becausewe could not ascertain their WIC participation status.Second, our definition of exclusive breastfeeding al-lowed the provision of juice or water, because we wereunable to account for these infant feeding practices inthe ECLS-B. Therefore, we might have overestimatedthe number of infants who were exclusively breastfed.
The promotion of recommended infant feeding prac-tices remains a challenge for WIC, particularly because
program participants have characteristics that are asso-ciated with a decreased likelihood of adherence to rec-ommended infant feeding practices. The US Departmentof Agriculture Food and Nutrition Service, which admin-isters the program at the federal level, recently proposedrevisions to the WIC food packages,35 largely based onrecommendations by the Institute of Medicine.36 Someof the proposed changes would more closely equate themarket value and nutritional value of the food packagesprovided to breastfeeding and nonbreastfeeding womenand would provide infant cereal to WIC infants at 6months, rather than 4 months, of age. These changes areconsistent with the goal of increasing adherence to AAPguidelines on infant feeding practices among WIC par-ticipants.
ACKNOWLEDGMENTSWe thank Steven Putansu for excellent research assis-tance. We also thank the participants in an EconomicResearch Service seminar and the 2006 Food Assistanceand Nutrition Research Program conference for theircomments.
REFERENCES1. US Department of Agriculture Food and Nutrition Service.
National Level Annual Summary, FY 1974–2005. Alexandria, VA:US Department of Agriculture; 2006. Available at: www.fns.usda.gov/pd/wisummary.htm. Accessed September 25, 2006
2. US Department of Agriculture Food and Nutrition Service.Monthly Data: Agency Level, FY 2005. Alexandria, VA: US Depart-ment of Agriculture; 2006. Available at: www.fns.usda.gov/pd/WIC_Monthly.htm. Accessed September 25, 2006
3. Leon-Cava N, Lutter C, Ross J, Martin L. Quantifying the Benefitsof Breastfeeding: A Summary of the Evidence. Washington, DC: PanAmerican Health Organization; 2002
4. Heinig MJ. Host defense benefits of breastfeeding for the infant:effect of breastfeeding duration and exclusivity. Pediatr ClinNorth Am. 2001;48:105–123
5. Howie PW, Forsyth JS, Ogston SA, Clark A, Florey CD. Protec-tive effect of breast feeding against infection. BMJ. 1990;300:11–16
6. Dewey KG, Heinig MJ, Nommsen LA. Maternal weight-losspatterns during prolonged lactation. Am J Clin Nutr. 1993;58:162–166
7. Labbok MH. Effects of breastfeeding on the mother. Pediatr ClinNorth Am. 2001;48:143–158
8. Newcomb PA, Storer BE, Longnecker MP, et al. Lactation anda reduced risk of premenopausal breast cancer. N Engl J Med.1994;330:81–87
9. Rosenblatt KA, Thomas DB. Lactation and the risk of epithelialovarian cancer: WHO Collaborative Study of Neoplasia andSteroid Contraceptives. Int J Epidemiol. 1993;22:192–197
10. Weimer J. The Economic Benefits of Breast Feeding: A Review andAnalysis. Washington, DC: Food and Rural Economics Division,Economic Research Service, US Department of Agriculture;2001. Food Assistance and Nutrition Research Report 13
11. American Academy of Pediatrics, Committee on Nutrition. Theuse of whole cow’s milk in infancy. Pediatrics. 1992;89:1105–1109
12. American Academy of Pediatrics, Committee on Nutrition.Supplemental foods for infants. In: Kleinman R, ed. Pediatric
PEDIATRICS Volume 119, Number 2, February 2007 287 by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from
Nutrition Handbook. 5th ed. Elk Grove Village, IL: AmericanAcademy of Pediatrics; 2004:103–119
13. American Academy of Pediatrics. Policy statement: breastfeed-ing and the use of human milk. Pediatrics. 2005;115:496–506
14. Fiocchi A, Assa’ad A, Bahna S. Food allergy and the introduc-tion of solid foods to infants: a consensus document. AnnAllergy Asthma Immunol. 2006;97:10–21
15. Grantham-McGregor S, Ani C. A review of studies on the effectof iron deficiency on cognitive development in children. J Nutr.2001;131:649S–668S
16. US Department of Agriculture Food and Nutrition Service.Legislative History of Breastfeeding Promotion. Alexandria, VA: USDepartment of Agriculture; 2006. Available at: www.fns.usda.gov/wic/Breastfeeding/bflegishistory.htm. Accessed September25, 2006
17. US Department of Agriculture Food and Nutrition Service.Revisions to the WIC Food Package. Alexandria, VA: US Depart-ment of Agriculture; 2006. Available at: www.fns.usda.gov/wic/benefitsandservices/revisionstofoodpkg-background.htm.Accessed September 25, 2006
18. US Department of Agriculture Food and Nutrition Service. WICFood Package. Alexandria, VA: US Department of Agriculture;2006. Available at: www.fns.usda.gov/wic/benefitsandservices/foodpkgtable.htm. Accessed September 25, 2006
19. Fox MK, Hamilton W, Lin B. Effects of Food Assistance andNutrition Programs on Nutrition and Health, Vol 3, Literature Re-view. Washington, DC: Food and Nutrition Service, US Depart-ment of Agriculture; 2004
20. Bitler M, Currie J. Does WIC work? The effects of WIC onpregnancy and birth outcomes. J Policy Anal Manage. 2005;24:73–91
21. Rush D, Sloan NL, Leighton J, et al. The National WICevaluation: evaluation of the Special Supplemental NutritionProgram for Women, Infants, and Children, part VI: study ofinfants and children. Am J Clin Nutr. 1988;48:484–511
22. Chatterji P, Bonuck K, Dhawan S, Deb N. WIC Participation andthe Initiation and Duration of Breastfeeding. Madison, WI: Insti-tute for Research on Poverty, University of Wisconsin-Madison; 2002. Institute for Research on Poverty DiscussionPaper 1246–02
23. Chatterji P, Brooks-Gunn J. WIC participation, breastfeedingpractices, and well-child care among unmarried, low-incomemothers. Am J Public Health. 2004;94:1324–1327
24. Schwartz JB, Popkin BM, Tognetti J, Zohoori N. Does WIC
improve breast-feeding practices? Am J Public Health. 1995;85:729–731
25. Ahluwalia IB, Morrow B, Hsia J, Grummer-Strawn LM. Who isbreastfeeding? Recent trends from the Pregnancy Risk Assess-ment and Monitoring System. J Pediatr. 2003;142:486–491
26. Ryan AS, Wenjun Z. Lower breastfeeding rates persist amongthe Special Supplemental Nutrition Program for Women, In-fants, and Children participants. Pediatrics. 2006;117:1136–1146
27. Ryan AS, Wenjun Z, Acosta A. Breastfeeding continues toincrease into the new millennium. Pediatrics. 2002;110:1103–1109
28. Li R, Darling N, Maurice E, Barker L, Grummer-Strawn LM.Breastfeeding rates in the United States by characteristics of thechild, mother, or family: the 2002 National ImmunizationSurvey.Pediatrics.2005;115(1).Availableat:www.pediatrics.org/cgi/content/full/115/1/e31
29. Ponza M, Devaney B, Ziegler P, Reidy K, Squatrito C. Nutrientintakes and food choices of infants and toddlers participating inWIC. J Am Diet Assoc. 2004;104:71–79
30. Burstein N, Fox MK, Puma MJ. Study of the Impact of WIC on theGrowth and Development of Children: Field Test: Final Report, Vol II,Preliminary Impact Estimates. Cambridge, MA: Abt Associates;1991
31. Cole N, Fox MK. Nutrition and Health Characteristics of Low-Income Populations, Vol II, WIC Participants and Nonparticipants.Washington, DC: Economic Research Service, US Departmentof Agriculture; 2004
32. Kramer-Leblanc CS, Mardis A, Gerrior S, Gaston N. Review ofthe Nutritional Status of WIC Participants. Washington, DC: Cen-ter for Nutrition Policy and Promotion, US Department ofAgriculture; 1999
33. Ver Ploeg M, Betson D. Estimating Eligibility and Participation forthe WIC Program. Washington, DC: National Research Councilof the National Academies; 2003
34. Gundersen C. A dynamic analysis of the well-being of WICrecipients and eligible non-recipients. Child Youth Serv Rev.2005;27:99–114
35. US Department of Agriculture Food and Nutrition Service.Special Supplemental Nutrition Program for Women, Infants,and Children (WIC): revisions in WIC food packages: proposedrule. Fed Regist. 2006;71:44783–44855
36. Institute of Medicine. WIC Food Packages: Time for a Change.Washington, DC: National Academies Press; 2005
288 JACKNOWITZ et al by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from
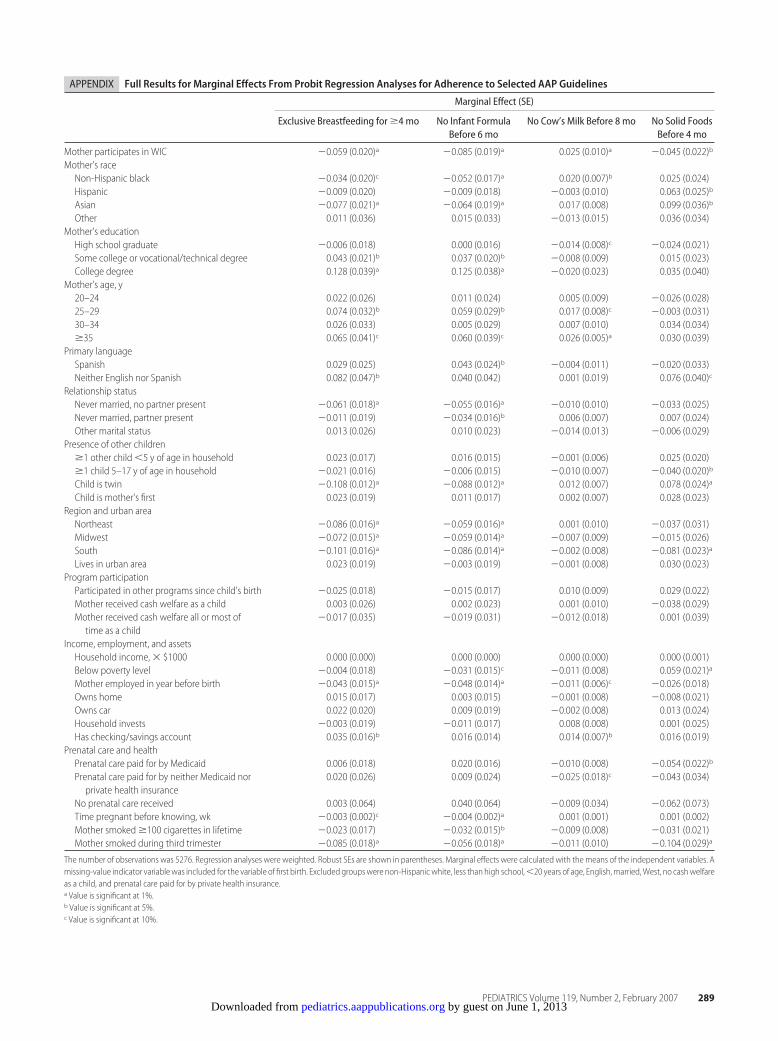
APPENDIX Full Results for Marginal Effects From Probit Regression Analyses for Adherence to Selected AAP Guidelines
Marginal Effect (SE)
Exclusive Breastfeeding for �4 mo No Infant FormulaBefore 6 mo
No Cow’s Milk Before 8 mo No Solid FoodsBefore 4 mo
Mother participates in WIC �0.059 (0.020)a �0.085 (0.019)a 0.025 (0.010)a �0.045 (0.022)b
Mother’s raceNon-Hispanic black �0.034 (0.020)c �0.052 (0.017)a 0.020 (0.007)b 0.025 (0.024)Hispanic �0.009 (0.020) �0.009 (0.018) �0.003 (0.010) 0.063 (0.025)b
Asian �0.077 (0.021)a �0.064 (0.019)a 0.017 (0.008) 0.099 (0.036)b
Other 0.011 (0.036) 0.015 (0.033) �0.013 (0.015) 0.036 (0.034)Mother’s educationHigh school graduate �0.006 (0.018) 0.000 (0.016) �0.014 (0.008)c �0.024 (0.021)Some college or vocational/technical degree 0.043 (0.021)b 0.037 (0.020)b �0.008 (0.009) 0.015 (0.023)College degree 0.128 (0.039)a 0.125 (0.038)a �0.020 (0.023) 0.035 (0.040)
Mother’s age, y20–24 0.022 (0.026) 0.011 (0.024) 0.005 (0.009) �0.026 (0.028)25–29 0.074 (0.032)b 0.059 (0.029)b 0.017 (0.008)c �0.003 (0.031)30–34 0.026 (0.033) 0.005 (0.029) 0.007 (0.010) 0.034 (0.034)�35 0.065 (0.041)c 0.060 (0.039)c 0.026 (0.005)a 0.030 (0.039)
Primary languageSpanish 0.029 (0.025) 0.043 (0.024)b �0.004 (0.011) �0.020 (0.033)Neither English nor Spanish 0.082 (0.047)b 0.040 (0.042) 0.001 (0.019) 0.076 (0.040)c
Relationship statusNever married, no partner present �0.061 (0.018)a �0.055 (0.016)a �0.010 (0.010) �0.033 (0.025)Never married, partner present �0.011 (0.019) �0.034 (0.016)b 0.006 (0.007) 0.007 (0.024)Other marital status 0.013 (0.026) 0.010 (0.023) �0.014 (0.013) �0.006 (0.029)
Presence of other children�1 other child �5 y of age in household 0.023 (0.017) 0.016 (0.015) �0.001 (0.006) 0.025 (0.020)�1 child 5–17 y of age in household �0.021 (0.016) �0.006 (0.015) �0.010 (0.007) �0.040 (0.020)b
Child is twin �0.108 (0.012)a �0.088 (0.012)a 0.012 (0.007) 0.078 (0.024)a
Child is mother’s first 0.023 (0.019) 0.011 (0.017) 0.002 (0.007) 0.028 (0.023)Region and urban areaNortheast �0.086 (0.016)a �0.059 (0.016)a 0.001 (0.010) �0.037 (0.031)Midwest �0.072 (0.015)a �0.059 (0.014)a �0.007 (0.009) �0.015 (0.026)South �0.101 (0.016)a �0.086 (0.014)a �0.002 (0.008) �0.081 (0.023)a
Lives in urban area 0.023 (0.019) �0.003 (0.019) �0.001 (0.008) 0.030 (0.023)Program participationParticipated in other programs since child’s birth �0.025 (0.018) �0.015 (0.017) 0.010 (0.009) 0.029 (0.022)Mother received cash welfare as a child 0.003 (0.026) 0.002 (0.023) 0.001 (0.010) �0.038 (0.029)Mother received cash welfare all or most oftime as a child
�0.017 (0.035) �0.019 (0.031) �0.012 (0.018) 0.001 (0.039)
Income, employment, and assetsHousehold income, � $1000 0.000 (0.000) 0.000 (0.000) 0.000 (0.000) 0.000 (0.001)Below poverty level �0.004 (0.018) �0.031 (0.015)c �0.011 (0.008) 0.059 (0.021)a
Mother employed in year before birth �0.043 (0.015)a �0.048 (0.014)a �0.011 (0.006)c �0.026 (0.018)Owns home 0.015 (0.017) 0.003 (0.015) �0.001 (0.008) �0.008 (0.021)Owns car 0.022 (0.020) 0.009 (0.019) �0.002 (0.008) 0.013 (0.024)Household invests �0.003 (0.019) �0.011 (0.017) 0.008 (0.008) 0.001 (0.025)Has checking/savings account 0.035 (0.016)b 0.016 (0.014) 0.014 (0.007)b 0.016 (0.019)
Prenatal care and healthPrenatal care paid for by Medicaid 0.006 (0.018) 0.020 (0.016) �0.010 (0.008) �0.054 (0.022)b
Prenatal care paid for by neither Medicaid norprivate health insurance
0.020 (0.026) 0.009 (0.024) �0.025 (0.018)c �0.043 (0.034)
No prenatal care received 0.003 (0.064) 0.040 (0.064) �0.009 (0.034) �0.062 (0.073)Time pregnant before knowing, wk �0.003 (0.002)c �0.004 (0.002)a 0.001 (0.001) 0.001 (0.002)Mother smoked �100 cigarettes in lifetime �0.023 (0.017) �0.032 (0.015)b �0.009 (0.008) �0.031 (0.021)Mother smoked during third trimester �0.085 (0.018)a �0.056 (0.018)a �0.011 (0.010) �0.104 (0.029)a
The number of observations was 5276. Regression analyses were weighted. Robust SEs are shown in parentheses. Marginal effects were calculated with the means of the independent variables. Amissing-value indicator variablewas included for the variable of first birth. Excluded groupswere non-Hispanicwhite, less than high school,�20 years of age, English,married,West, no cashwelfareas a child, and prenatal care paid for by private health insurance.a Value is significant at 1%.b Value is significant at 5%.c Value is significant at 10%.
PEDIATRICS Volume 119, Number 2, February 2007 289 by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2006-1486 2007;119;281Pediatrics
Alison Jacknowitz, Daniel Novillo and Laura TiehenInfant Feeding Practices
Special Supplemental Nutrition Program for Women, Infants, and Children and
ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/119/2/281.full.htincluding high resolution figures, can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/119/2/281.full.htat:This article cites 20 articles, 9 of which can be accessed free
Citations
ml#related-urlshttp://pediatrics.aappublications.org/content/119/2/281.full.htThis article has been cited by 12 HighWire-hosted articles:
Subspecialty Collections
nd_metabolismhttp://pediatrics.aappublications.org/cgi/collection/nutrition_aNutrition & Metabolismthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2007 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on June 1, 2013pediatrics.aappublications.orgDownloaded from
Related Documents











