SPECIAL K: A LITTLE GOES A LONG WAY ALI PRYNE PHARMD, BCPS VALLEY VIEW HOSPITAL, GLENWOOD SPRINGS, CO

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
SPECIAL K: A LITTLE GOES A LONG WAY
ALI PRYNE PHARMD, BCPS
VALLEY VIEW HOSPITAL, GLENWOOD SPRINGS, CO
DISCLOSURES
• Nothing to disclose
OBJECTIVES
1. Compare differing doses of ketamine for indications such as sedation, analgesia, and depression.
2. Analyze recently published literature regarding ketamine and esketamine use.
3. Discuss treatment plans for safe administration and monitoring of ketamine.

BACKGROUND
• Administration of ketamine in Alaska limited to provider only
• RN not able to provide deep sedation
• Nursing advisory
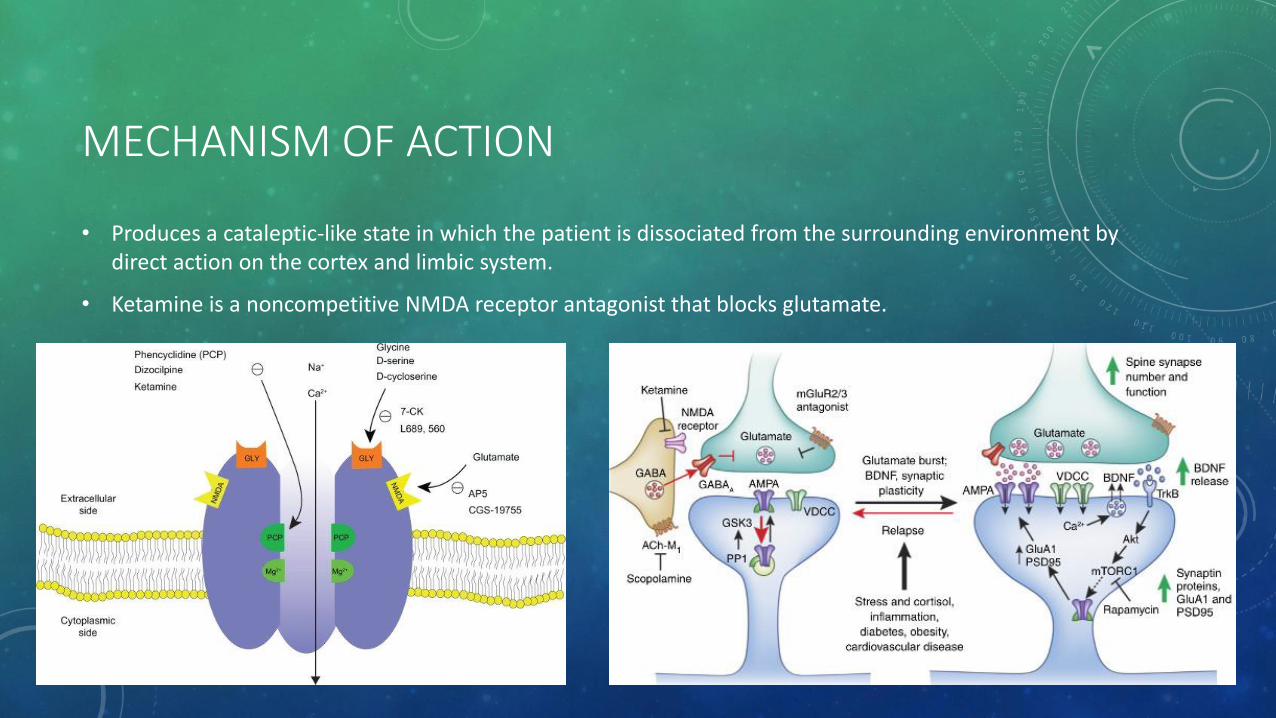
MECHANISM OF ACTION
• Produces a cataleptic-like state in which the patient is dissociated from the surrounding environment by direct action on the cortex and limbic system.
• Ketamine is a noncompetitive NMDA receptor antagonist that blocks glutamate.

MECHANISM OF ACTION
• Low (subanesthetic) doses produce analgesia, and modulate central sensitization, hyperalgesia and opioid tolerance. Reduces polysynaptic spinal reflexes.

ASSESSMENT QUESTION
Select all approved routes of administration
Intranasal
Intravenous/Intraosseous
Intramuscular
Oral
Rectal
Endotracheal
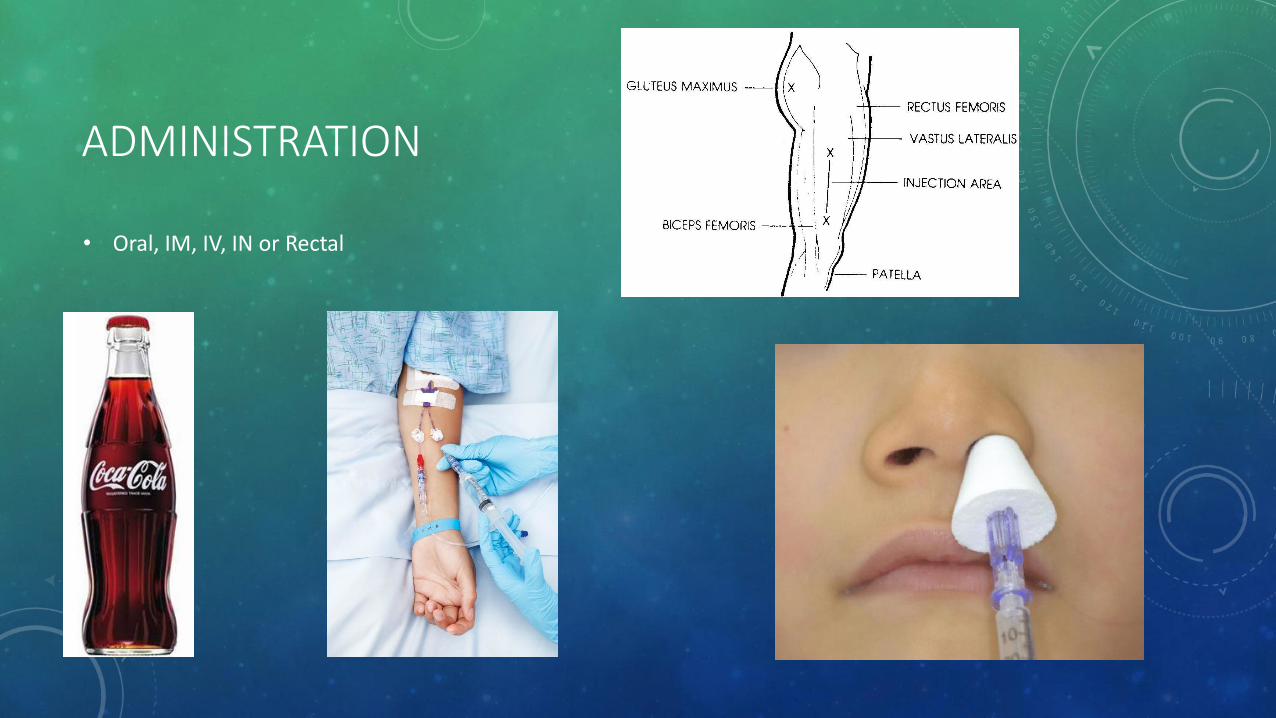
ADMINISTRATION
• Oral, IM, IV, IN or Rectal
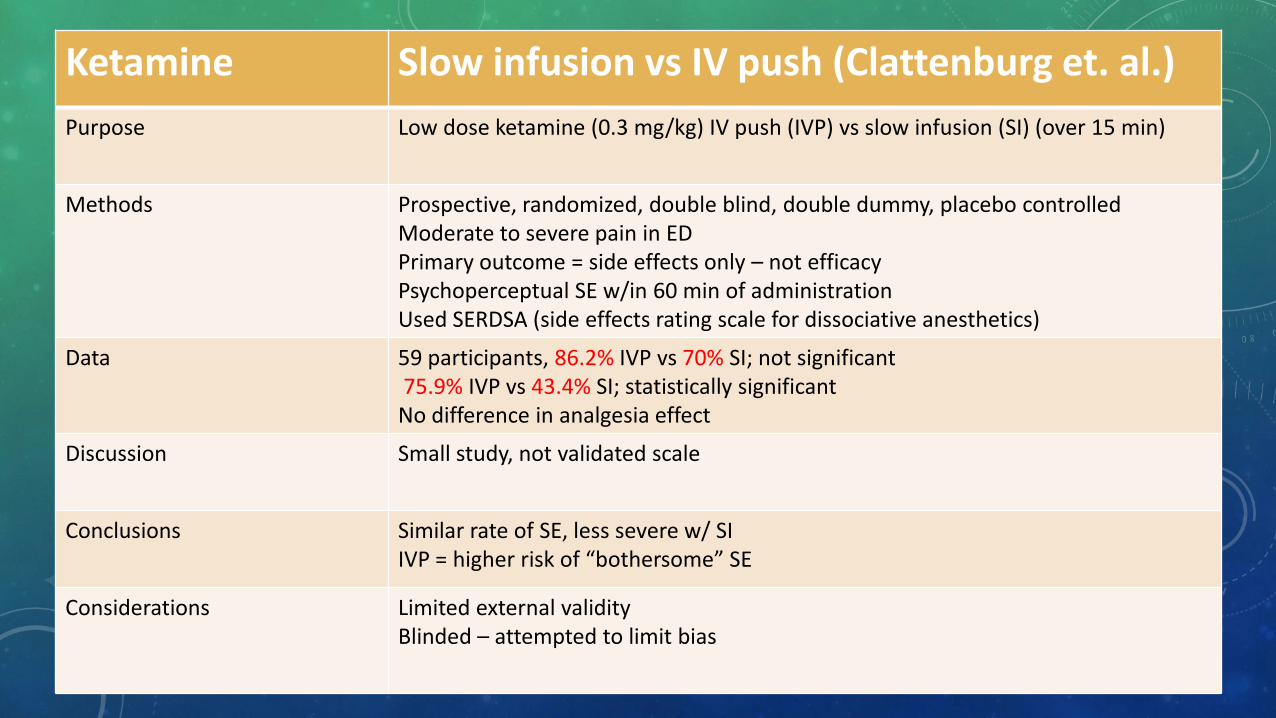
Ketamine Slow infusion vs IV push (Clattenburg et. al.)
Purpose Low dose ketamine (0.3 mg/kg) IV push (IVP) vs slow infusion (SI) (over 15 min)
Methods Prospective, randomized, double blind, double dummy, placebo controlled Moderate to severe pain in ED Primary outcome = side effects only – not efficacy Psychoperceptual SE w/in 60 min of administration Used SERDSA (side effects rating scale for dissociative anesthetics)
Data 59 participants, 86.2% IVP vs 70% SI; not significant 75.9% IVP vs 43.4% SI; statistically significant No difference in analgesia effect
Discussion Small study, not validated scale
Conclusions Similar rate of SE, less severe w/ SI IVP = higher risk of “bothersome” SE
Considerations Limited external validity Blinded – attempted to limit bias

Pharmacokinetics Onset of action: IV: 30 seconds
IM: ~4 minutes IN: ~10 minutes Oral: ~30 minutes
Duration: IV:~10 minutes IM: 15-25 minutes IN: Up to 60 minutes
Protein binding: 27 %
Metabolism: Four varying metabolites Hepatic via N-dealkylation (norketamine) - ~30 % as potent as ketamine
Bioavailability: IM: 93% IN: 35-50% Oral: 20-30%
Half-life: Alpha ~10-15 minutes, Beta 2.5 hours
Time to peak, plasma: IM: 5-30 minutes IN: 10-15 minutes Oral: ~30 minutes
Excretion: Urine 91%, feces 3%
SPECIAL CONSIDERATIONS
• Psychedelic/dissociative effects
• Nystagmus
• Protruding tongue, exaggerated mouth movements
• Hypertonia
SPECIAL CONSIDERATIONS
• Head trauma/bleeds – increases ICP and intraocular pressure
• Schizophrenia – even if stable on medications
• Cardiac decompensation
• Pharynx/larynx/bronchial abnormalities**
• Bladder dysfunction
• Tachycardia/arrythmias
ASSESSMENT QUESTION
• T/F: Ketamine is commercially available only as 50 mg/mL and 100 mg/mL.

SAFETY CONSIDERATIONS
• ISMP high risk medication
• Concentration/math errors
• “Ketofol” – mix of propofol and ketamine
• Generally 1:1

COMPOUNDING
Infusion
• Dilute 50 or 100 mg/mL with D5W or NS to final concentration of 1-2 mg/mL
• Do NOT use 10 mg/mL
• Do not mix w/ barbituates (i.e. PHENobarbital, PENTobarbital) or diazepam
• Generally send full vial for IV push, intranasal or IM routes
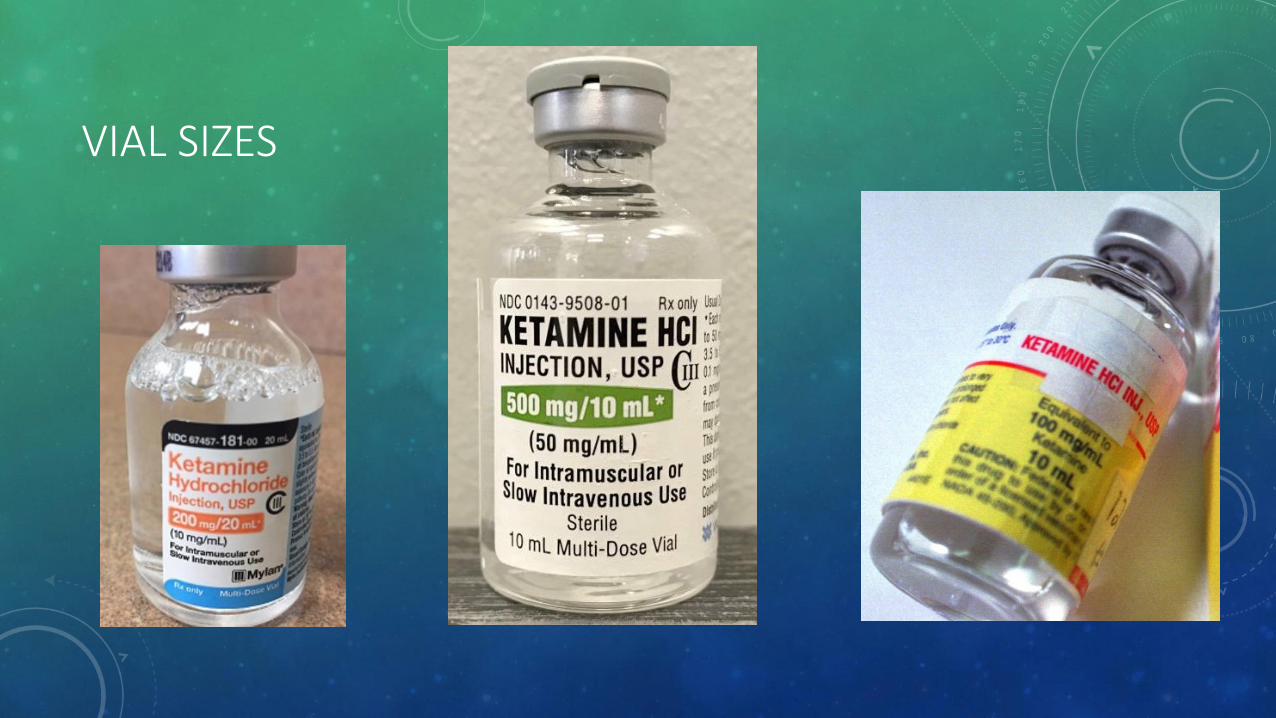
VIAL SIZES
x
x

PATIENT CASE
A 34 y/o M is transported to the ER after a MVC. No PMH and NKDA. He had a positive LOC, airbags did not deploy, GCS of 9, and is beginning to not protect his airway. MD would like to proceed with RSI and looks to you for recommendations…
• What other information do you want to know?
• Why would you advocate for/against ketamine?
ADVERSE REACTIONS
• Cardiovascular: tachycardia, hypertension
• CNS: dependence, hypertonia, increased ICP
• Dermatologic: rash
• Endocrine/metabolic: diabetes insipidus
• Gastrointestinal: nausea, sialorrhea
• Genitourinary: bladder dysfunction, cystitis, urgency
• Neuromuscular: laryngospasm
• Ophthalmic: diplopia, increased intraocular pressure, nystagmus
• Respiratory: apnea, respiratory depression

X
Ketamine Safety: PTSD (Highland et. al.)
Purpose Determine if ketamine SE increase risk for PTSD in combat casualty care.
Methods Evaluated those medically evacuated from combat (paired) PCL (PTSD checklist scores) w/in 365 days of injury, if positive and severity Ketamine >7 days before evaluation Matched cohort n(1:1, and 1:4)
Data N=1158, 107 got ketamine Primary outcome: OR=1.28 95% CI (0.48-3.47) p = .62 Secondary outcome: mean difference 1.98 95% CI (-.99 – 4.96) p = .19
Discussion Varying times between assessment, ketamine administration, and injury Low power Unknown if received in field (just at medical center post injury)
Conclusions Medical and surgical care provided in service members does not appear to increase risk for PTSD
Considerations Small sample size Accounted for confounders fairly well

SEDATION
KETAMINE DOSING: SEDATION
• Adults
• IV: 1-2 mg/kg
• IM: 4-5 mg/kg, may repeat 2-5 mg/kg if needed
• Pediatrics
• IV: 1-2 mg/kg
• IM: 4-5 mg/kg
• Intranasal: 3-6 mg/kg*
• Oral: 5 mg/kg *
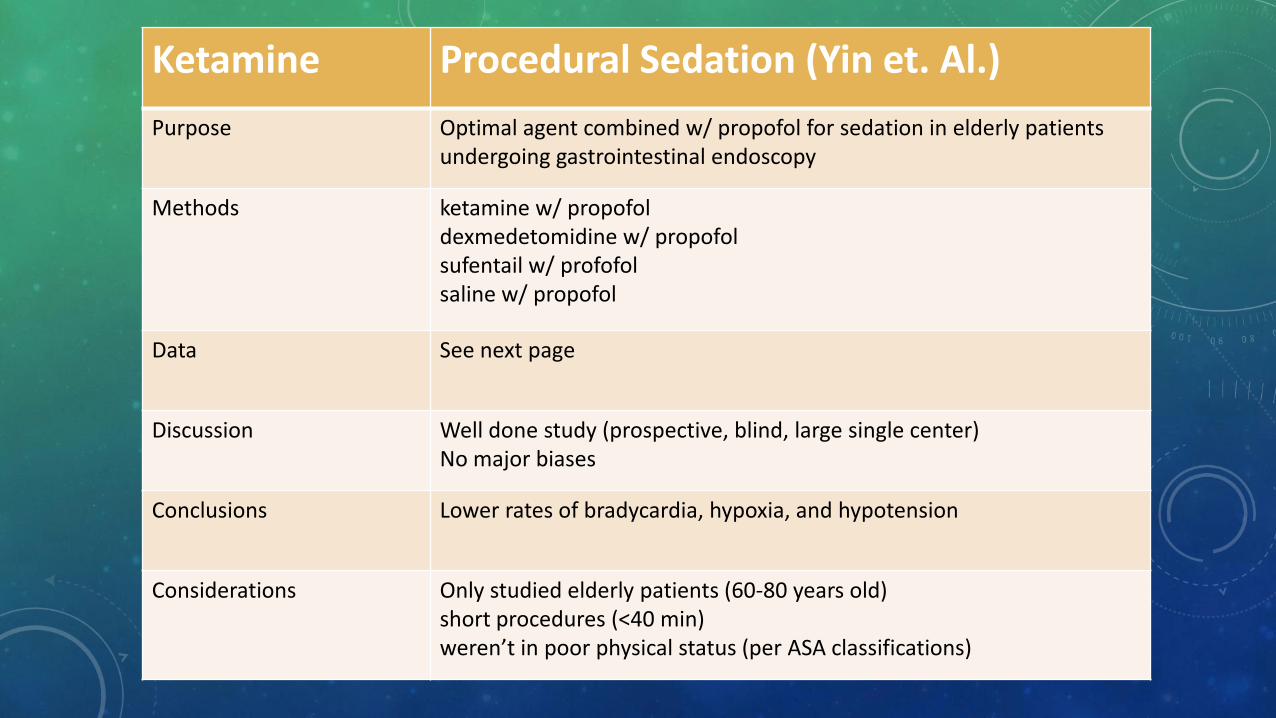
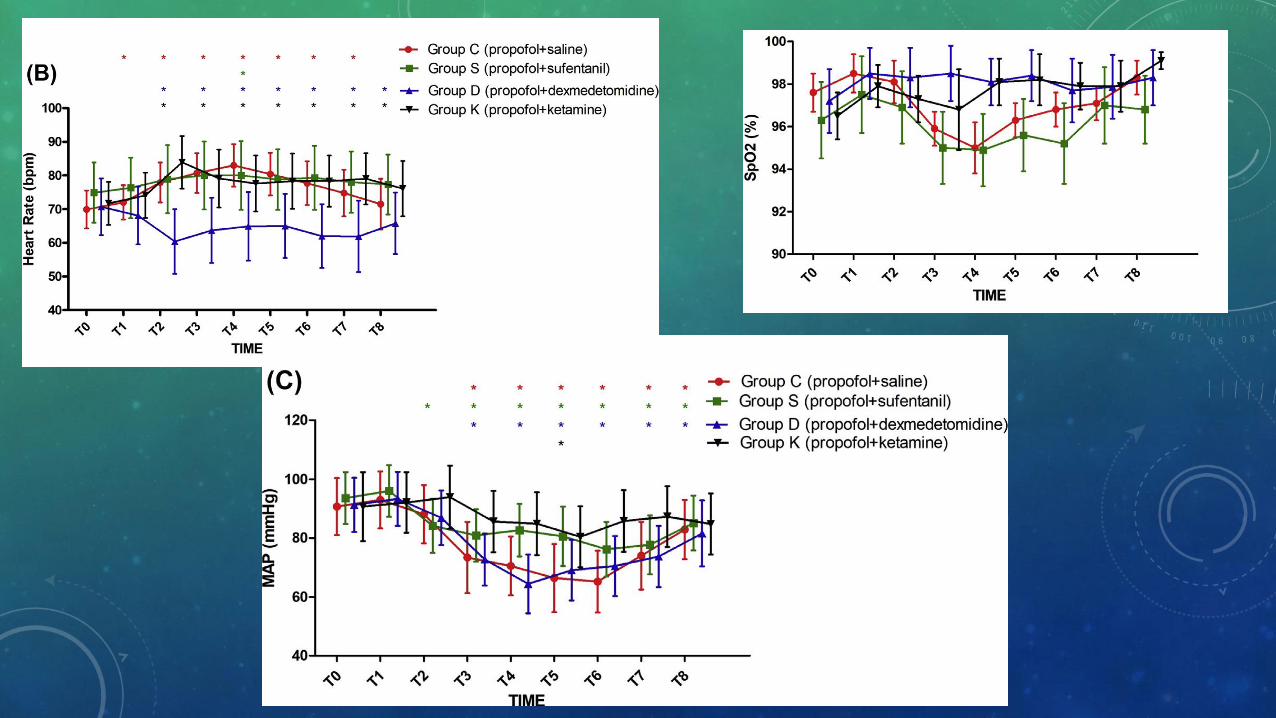
Ketamine Procedural Sedation (Yin et. Al.)
Purpose Optimal agent combined w/ propofol for sedation in elderly patients undergoing gastrointestinal endoscopy
Methods ketamine w/ propofol dexmedetomidine w/ propofol sufentail w/ profofol saline w/ propofol
Data See next page
Discussion Well done study (prospective, blind, large single center) No major biases
Conclusions Lower rates of bradycardia, hypoxia, and hypotension
Considerations Only studied elderly patients (60-80 years old) short procedures (<40 min) weren’t in poor physical status (per ASA classifications)

Ketamine Intubation sedation (Shahtahmasebi et. al.)
Purpose Does ketamine administration impact intubation rates in the transport of patients w/ behavioral disturbances
Methods Pre and post ketamine protocol introduction Selected patients transferred from remote areas of Australia Intubation rates and adverse event Ketamine failure = adverse event
Data N=340 patients, 129 had an intervention See next page for results AE = 18 ketamine and 50 I+V (difference of -0.43, p = <0.00001 CI -0.58 to -0.28)
Discussion 92.5% were mental health/substance abuse Selection bias
Conclusions Ketamine reduced intubation rates in patients w/ behavioral disturbances on transport Reduces adverse reactions, but does have risks
Considerations Included all post protocol = real life May require intubation for other illness/low GCS Lower cost?

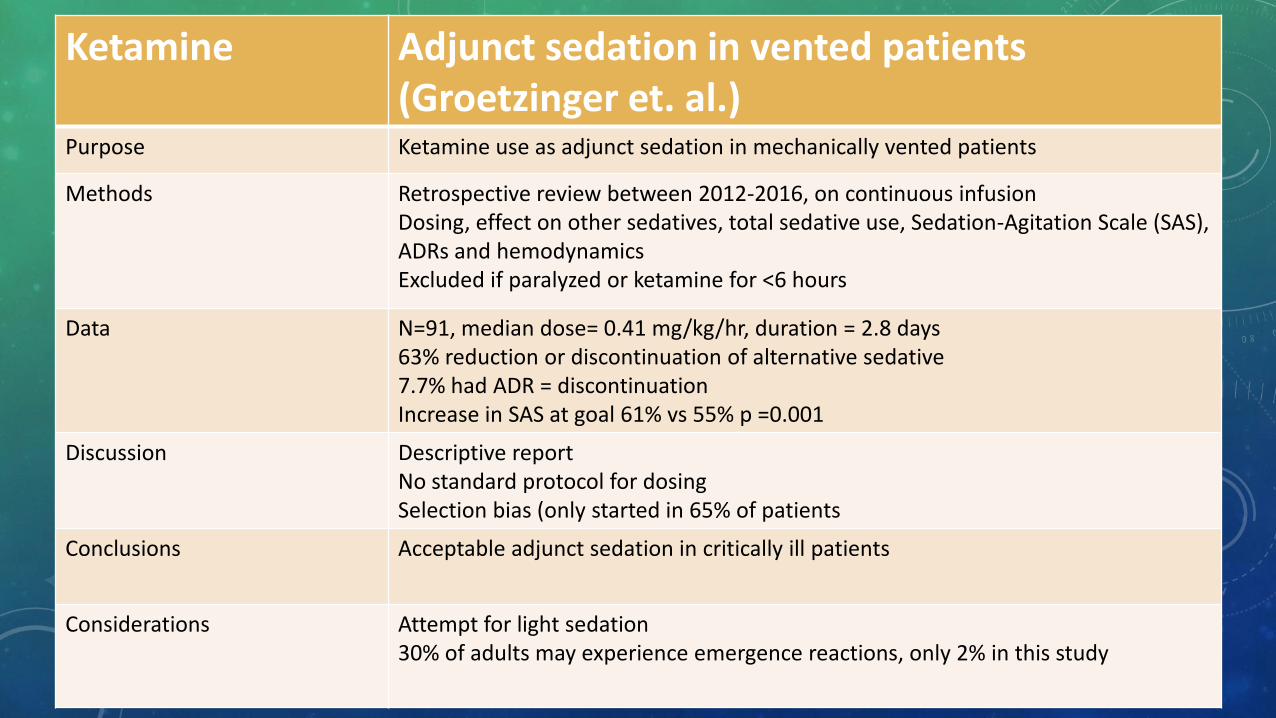
Ketamine Adjunct sedation in vented patients (Groetzinger et. al.)
Purpose Ketamine use as adjunct sedation in mechanically vented patients
Methods Retrospective review between 2012-2016, on continuous infusion Dosing, effect on other sedatives, total sedative use, Sedation-Agitation Scale (SAS), ADRs and hemodynamics Excluded if paralyzed or ketamine for <6 hours
Data N=91, median dose= 0.41 mg/kg/hr, duration = 2.8 days 63% reduction or discontinuation of alternative sedative 7.7% had ADR = discontinuation Increase in SAS at goal 61% vs 55% p =0.001
Discussion Descriptive report No standard protocol for dosing Selection bias (only started in 65% of patients
Conclusions Acceptable adjunct sedation in critically ill patients
Considerations Attempt for light sedation 30% of adults may experience emergence reactions, only 2% in this study
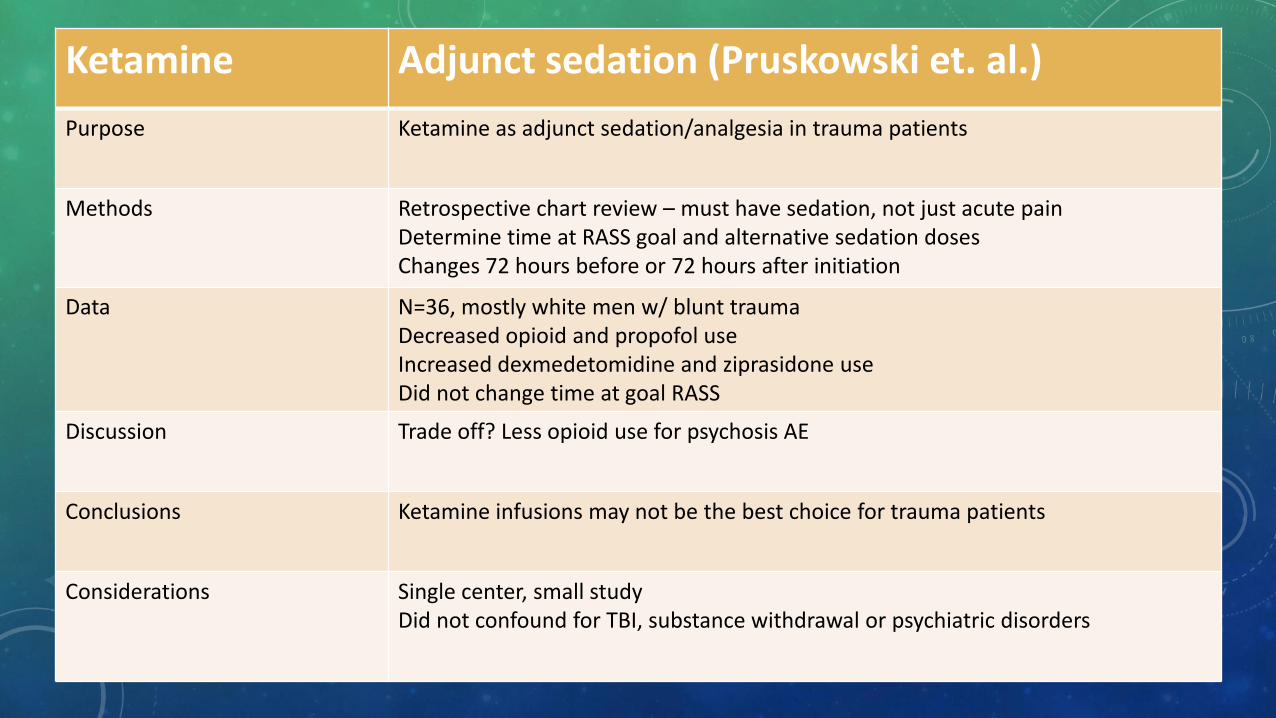
Ketamine Adjunct sedation (Pruskowski et. al.)
Purpose Ketamine as adjunct sedation/analgesia in trauma patients
Methods Retrospective chart review – must have sedation, not just acute pain Determine time at RASS goal and alternative sedation doses Changes 72 hours before or 72 hours after initiation
Data N=36, mostly white men w/ blunt trauma Decreased opioid and propofol use Increased dexmedetomidine and ziprasidone use Did not change time at goal RASS
Discussion Trade off? Less opioid use for psychosis AE
Conclusions Ketamine infusions may not be the best choice for trauma patients
Considerations Single center, small study Did not confound for TBI, substance withdrawal or psychiatric disorders

ANALGESIA
Painless

KETAMINE DOSING: ANALGESIA
• Adults
• IV: 0.2-0.8 mg/kg bolus followed by 1 mcg/kg/minute
• Intranasal: acute pain 0.5-1 mg/kg
• Pediatrics
• IV
• IM
• Intranasal
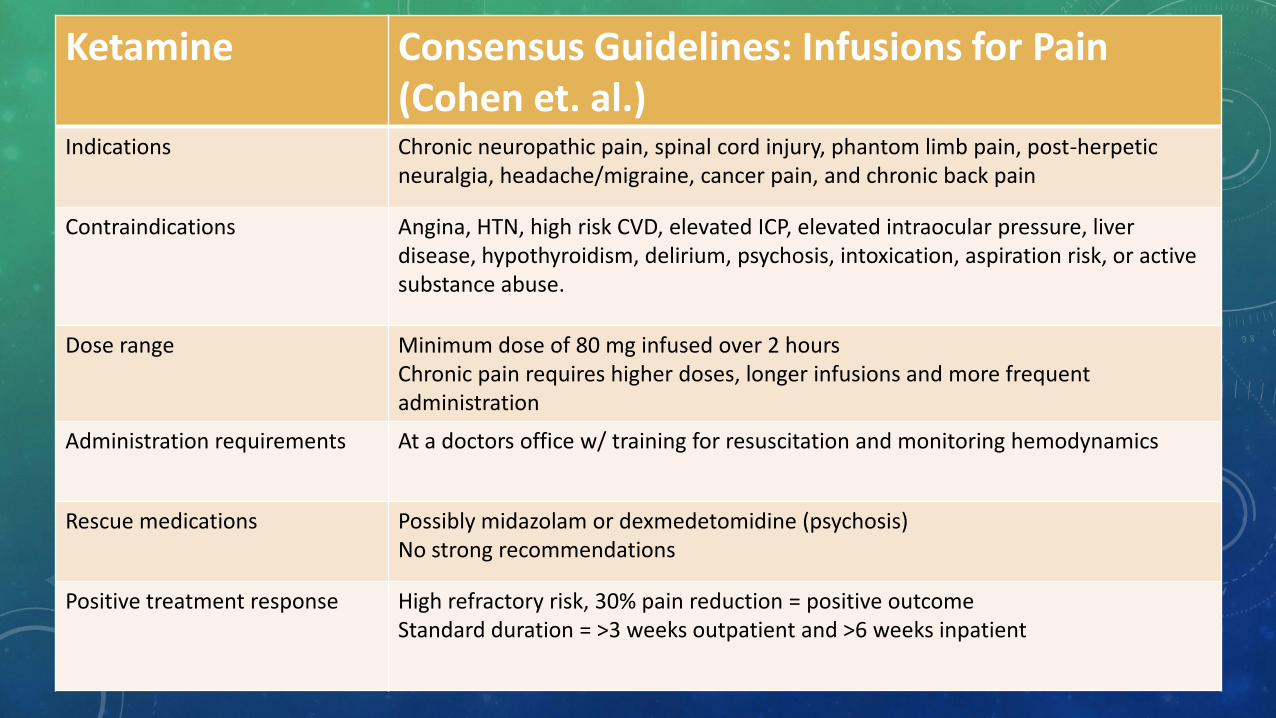
Ketamine Consensus Guidelines: Infusions for Pain (Cohen et. al.)
Indications Chronic neuropathic pain, spinal cord injury, phantom limb pain, post-herpetic neuralgia, headache/migraine, cancer pain, and chronic back pain
Contraindications Angina, HTN, high risk CVD, elevated ICP, elevated intraocular pressure, liver disease, hypothyroidism, delirium, psychosis, intoxication, aspiration risk, or active substance abuse.
Dose range Minimum dose of 80 mg infused over 2 hours Chronic pain requires higher doses, longer infusions and more frequent administration
Administration requirements At a doctors office w/ training for resuscitation and monitoring hemodynamics
Rescue medications Possibly midazolam or dexmedetomidine (psychosis) No strong recommendations
Positive treatment response High refractory risk, 30% pain reduction = positive outcome Standard duration = >3 weeks outpatient and >6 weeks inpatient

Ketamine Acute pain (Karlow et. al.)
Purpose Low dose ketamine use as alternative to opioids in ED
Methods Meta-analysis, doses <0.5 mg/kg Pain scale assessed w/in 60 minutes of administration 3 studies included N=261 patients
Data NRS or VAS scale Difference 0.42 95% CI = -0.70 to 1.54
Discussion Strict criteria for inclusion
Conclusions Low dose ketamine was non-inferior to opioids (morphine equivalents)
Considerations Only 3 studies reviewed
DEPRESSION
KETAMINE DOSING: DEPRESSION
• Adults
• IV: 0.5 mg/kg twice weekly
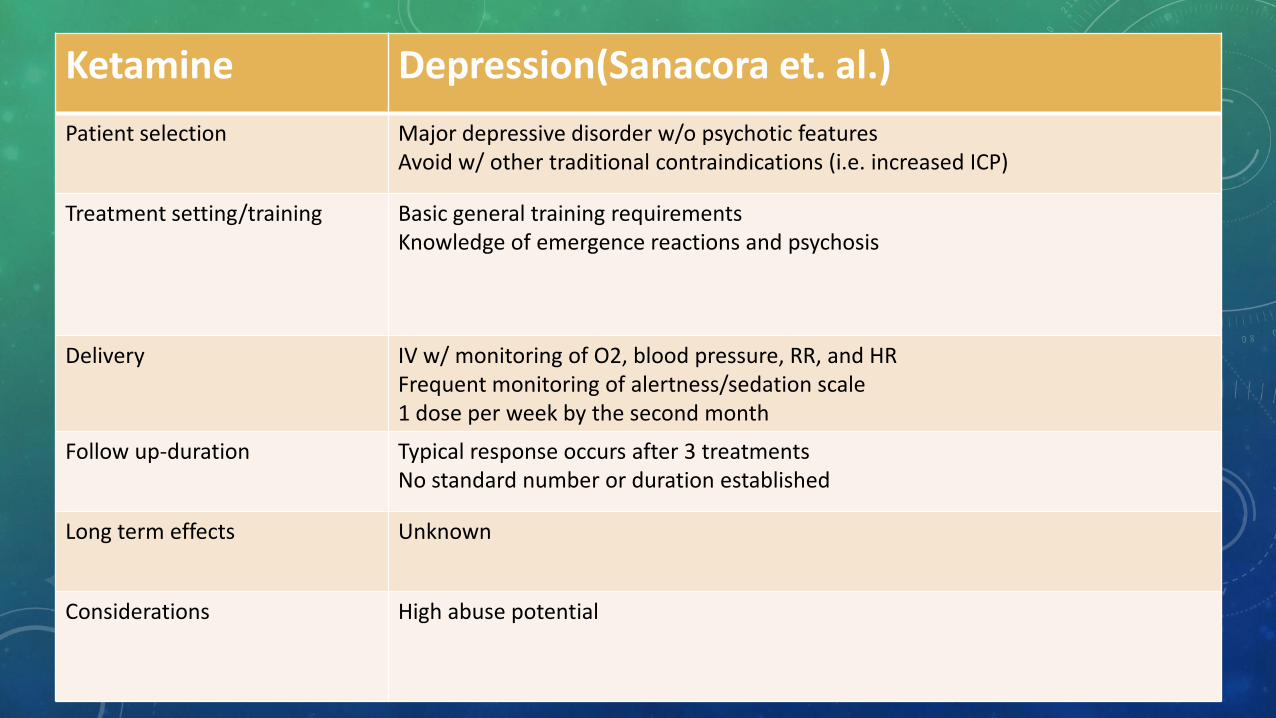
Ketamine Depression(Sanacora et. al.)
Patient selection Major depressive disorder w/o psychotic features Avoid w/ other traditional contraindications (i.e. increased ICP)
Treatment setting/training Basic general training requirements Knowledge of emergence reactions and psychosis
Delivery IV w/ monitoring of O2, blood pressure, RR, and HR Frequent monitoring of alertness/sedation scale 1 dose per week by the second month
Follow up-duration Typical response occurs after 3 treatments No standard number or duration established
Long term effects Unknown
Considerations High abuse potential
ASSESSMENT QUESTION
• Esketamine is a/an:
a. Prodrug of ketamine
b. Metabolite of ketamine
c. S-enantiomer of ketamine
d. Inactive metabolite of ketamine

MECHANISM OF ACTION
• S-enantiomer of racemic ketamine
• Non-selective, non competitive N-methyl-D-aspartate (NMDA) receptor antagonist
• Depression - unknown

PHARMACOKINETICS
Protein binding: 43 – 45 %
Metabolism: metabolized to active metabolite noresketamine via CYP450, CYP2B6, CYP3A4 and some CYP2C9/CYP2C19
Bioavailability: ~50%
Half-life: 7-12 hours, noresketamine ~8 hours
Time to peak, plasma: 20-40 minutes
Excretion: Urine <1% unchanged

ADMINISTRATION
• Intranasal only
• MD office
DEPRESSION
ESKETAMINE DOSING: DEPRESSION
• Adults
• Intranasal (induction): 56 mg twice weekly, may increase up to 84 mg twice weekly
• Evaluate after 4 weeks for continuance
• Intranasal (maintenance): At week five, continue previous dose (i.e. 56 or 84) but decrease to weekly. Evaluate every 4 weeks and decrease interval as tolerated.
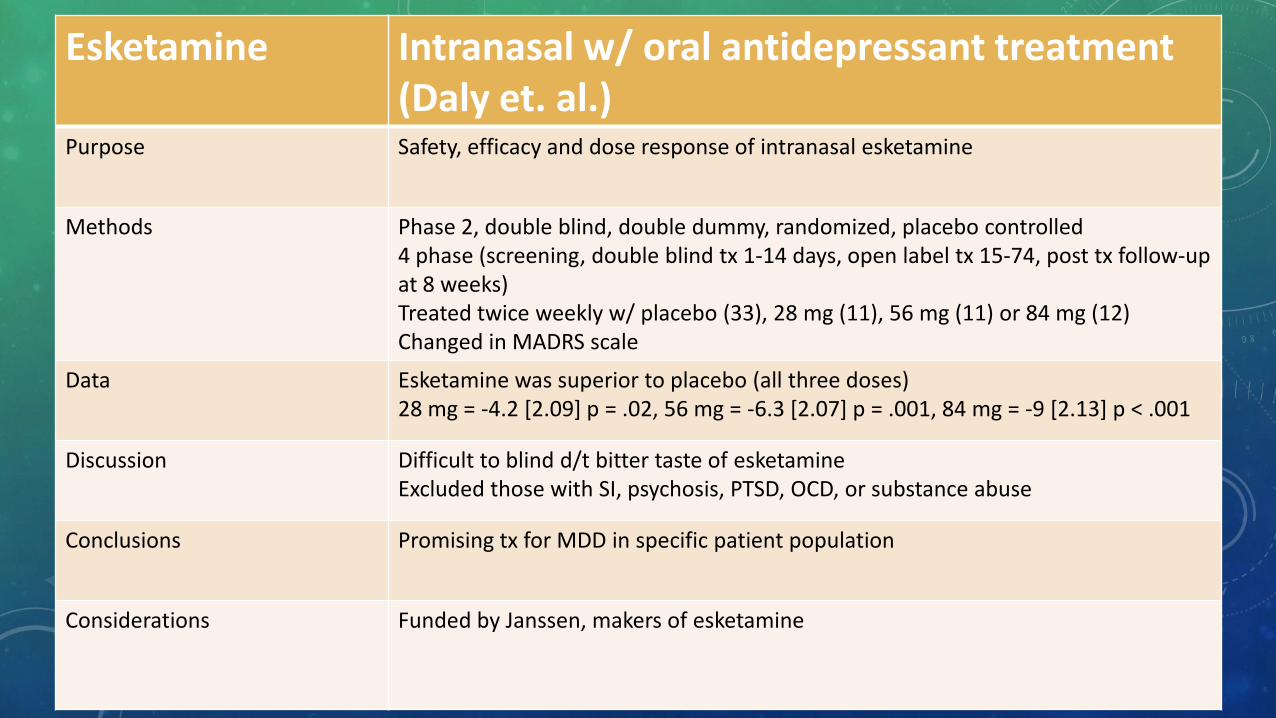
Esketamine Intranasal w/ oral antidepressant treatment (Daly et. al.)
Purpose Safety, efficacy and dose response of intranasal esketamine
Methods Phase 2, double blind, double dummy, randomized, placebo controlled 4 phase (screening, double blind tx 1-14 days, open label tx 15-74, post tx follow-up at 8 weeks) Treated twice weekly w/ placebo (33), 28 mg (11), 56 mg (11) or 84 mg (12) Changed in MADRS scale
Data Esketamine was superior to placebo (all three doses) 28 mg = -4.2 [2.09] p = .02, 56 mg = -6.3 [2.07] p = .001, 84 mg = -9 [2.13] p < .001
Discussion Difficult to blind d/t bitter taste of esketamine Excluded those with SI, psychosis, PTSD, OCD, or substance abuse
Conclusions Promising tx for MDD in specific patient population
Considerations Funded by Janssen, makers of esketamine
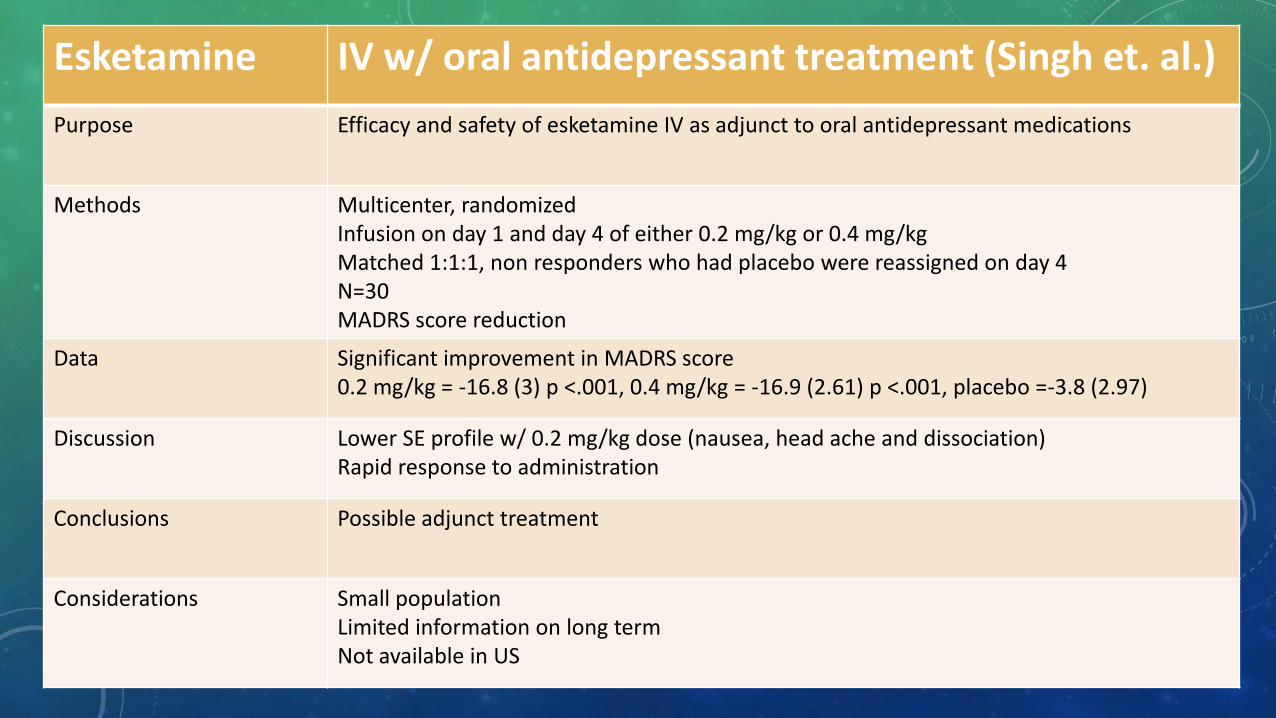
Esketamine IV w/ oral antidepressant treatment (Singh et. al.)
Purpose Efficacy and safety of esketamine IV as adjunct to oral antidepressant medications
Methods Multicenter, randomized Infusion on day 1 and day 4 of either 0.2 mg/kg or 0.4 mg/kg Matched 1:1:1, non responders who had placebo were reassigned on day 4 N=30 MADRS score reduction
Data Significant improvement in MADRS score 0.2 mg/kg = -16.8 (3) p <.001, 0.4 mg/kg = -16.9 (2.61) p <.001, placebo =-3.8 (2.97)
Discussion Lower SE profile w/ 0.2 mg/kg dose (nausea, head ache and dissociation) Rapid response to administration
Conclusions Possible adjunct treatment
Considerations Small population Limited information on long term Not available in US

ASSESSMENT QUESTION
Select all approved routes of administration
Intranasal
Intravenous/Intraosseous
Intramuscular
Oral
Rectal
Endotracheal
ASSESSMENT QUESTION
• T/F: Ketamine is commercially available only as 50 mg/mL and 100 mg/mL.
PATIENT CASE
A 34 y/o M is transported to the ER after a MVC. No PMH and NKDA. He had a positive LOC, airbags did not deploy, GCS of 9, and is beginning to not protect his airway. MD would like to proceed with RSI and looks to you for recommendations…
• What other information do you want to know?
• Why would you advocate for/against ketamine?

ASSESSMENT QUESTION
• Esketamine is a/an:
a. Prodrug of ketamine
b. Metabolite of ketamine
c. S-enantiomer of ketamine
d. Inactive metabolite of ketamine
QUESTIONS?

REFERENCES • Alaska State Board of Nursing Advisory Opinion. Link:
https://www.commerce.alaska.gov/web/portals/5/pub/nur_advisory_ketamine_administration.pdf
• ISMP's List of High-Alert Medications in Acute Care Settings. Link: https://www.ismp.org/recommendations/high-alert-medications-acute-list
• Ketamine. Lexi-Drugs. [updated 2019 Aug 6; cited 2019 Aug 12] In Lexicomp Online [Internet]. Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.
• Clattenburg E, Hailozian C, Haro D, et al. Slow infusion of low-dose ketamine reduces bothersome side effects compared to intravenous push: a double-blind, double-dummy, randomized controlled trial. Acad Emerg Med 2018;25:1048-1052.
• Highland K, Soumoff A, Spinks E, et al. Ketamine administration during hospitalization is not associated with posttraumatic stress disorder outcomes in military combat casualties: a matched cohort study. Int Anesthesiol Res Soc 2019. DOI: 10.1213/ANE.0000000000004327.
• Yin S, Hong J, Sha T, et al. Efficacy and tolerability of sufentani, dexmedetomidine, or ketamine added to propofol-based sedation for gastrointestinal endoscopy in elderly patients: a prospective, randomized, controlled trial. Clin Ther 2019; awaiting publication.
• Shahtahmasebi R, Johnson R, Shahtahmasebi S. Impact f a ketamine sedation protocol on intubation rates and undesirable outcomes in the transport of patients with acute behavioural disturbance. Emerg Med Australas 2019;29:291-296.
• Groetzinger L, Rivosecchi R, Bain W, et al. Ketamine infusion for adjunct sedation in mechanically ventilated adults. Pharmacotherapy 2018;38(2):181-188.
REFERENCES • Pruskowski K, Harbourt K, Pajoumand M, et al. Impact of ketamine use on adjunctive analgesic and sedative medications in critically
ill trauma patients. Pharmacotherapy 2017;37(12):1537-1544.
• Cohen S, Bhatia A, Buvanendran A, et al. Consensus guidelines on the use of intravenous ketamine infusions for chronic pain from the American society of regional anesthesia and pain medicine, the American academy of pain medicine, and the American society of anesthesiologists. Reg Anesth Pain Med 2018;43: 00-00.
• Karlow N, Schlaepfer CH, Stoll CR, et al. A systematic review and meta-analysis of ketamine as an alternative to opiods for acute pain in the emergency department. Acad Emerg Med 2018;25:1086-97.
• Sanacora G, Frye MA, McDonald W, et al. A consensus statement on the use of ketamine in the treatment of mood disorders. JAMA Psychiatry 2017;74:399-405.
• Bahr R, Lopez A, Rey J. Intranasal esketamine for use in treatment-resistant depression in conjunction with an oral antidepressant. Drug Forecast P&T 2019;44(6):340-347.
• Daly E, Trivedi M, Janik A, et al. A randomized withdrawal, double-blind, multicenter study of esketamine nasal spray plus an oral antidepressant for relapse prevention in treatment-resistant depression. JAMA Psychiatry 2018;75(2);139-148.
• Singh J, Fedgchin M, Daly E, et al. Intravenous esketamine in adult treatment –resistant depression: a double-blind, double-randomization, placebo-controlled study. Biol Psychiatry 2016; 80:424-431.
• Esketamine. Lexi-Drugs. [updated 2019 Aug 6; cited 2019 Aug 12] In Lexicomp Online [Internet]. Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc.
Related Documents











