Speaker declaration Dr Christopher Worsnop Respiratory and Sleep Physician Austin Hospital, Melbourne. Conflict of interest – I’m an Aussie OPTIMIZING ASTHMA CONTROL

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Speaker declaration
Dr Christopher WorsnopRespiratory and Sleep Physician
Austin Hospital, Melbourne.
Conflict of interest – I’m an Aussie
OPTIMIZING ASTHMA CONTROL
Barriers to achieving asthma control
• Patients’ attitudes to their asthma
• Patient access to ICS/LABA combination therapy
• Inhaler design
• Incorrect use of devices
• Insufficient training on how to use inhalers correctly.
jh499481
These barriers should come from the case studies. Please add any others.

Down on His Luck Fred McCubbin 1889
Living with asthma
• 37-year-old gold digger• He was diagnosed with “mild” asthma 10 years ago.• He is currently on ICS via DPI device and SABA as
required.• He describes his asthma control as ‘pretty good’ and says
that it doesn’t bother him too much from day to day.• He has occasional exacerbations triggered by exercise
and cigarette smoke.• He uses his reliever several times per week.• He wakes at night with asthma every now and then.
• Is his asthma controlled?
Patients attitudes to their asthma
• People with asthma tend to expect and accept symptoms and limitations as an inevitable, normal part of having asthma.
• Patients consistently rate their asthma as well-controlled, despite having symptom levels that indicate uncontrolled asthma as assessed by guidelines.
• Patients are less likely to report symptoms to GPs if they perceive symptoms as usual for them.
• Studies have shown many patients whose asthma is poorly controlled are also under-treated.
• GPs need to show patients that effective treatments for asthma are available.
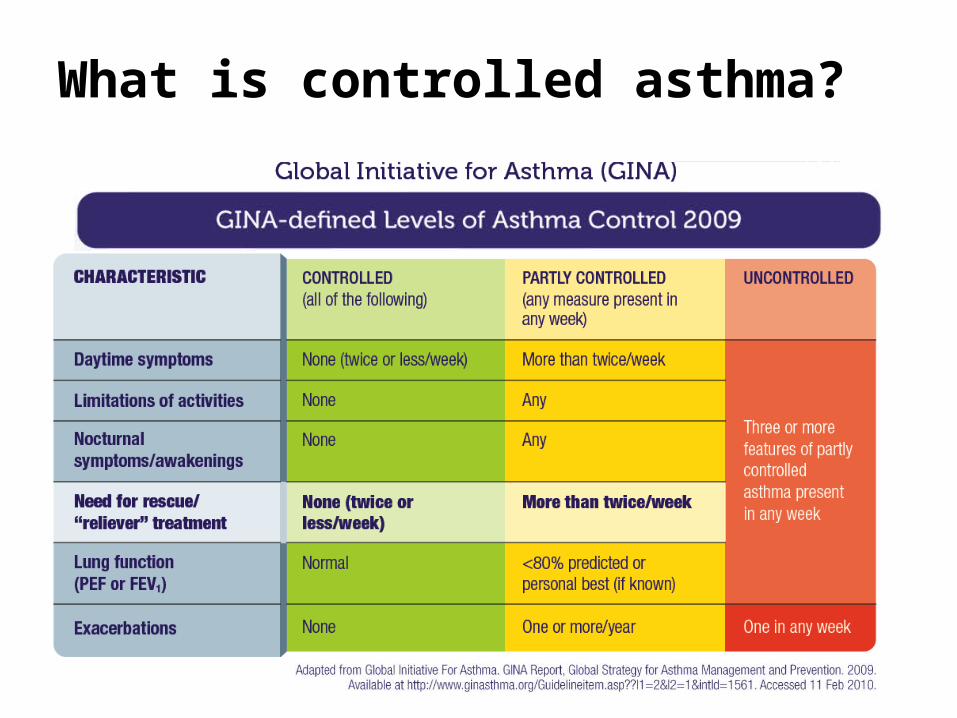
What is controlled asthma?
jh499481
Update to 2013??
Asthma Control Test (ACT)
• GINA guidelines emphasise the benefit of using asthma control, rather than asthma severity, as the way to make management decisions in asthma.
• The ACT is a validated questionnaire that can be completed by patients.
• It uses five questions to assess asthma control over the past 4 weeks, giving an overall ‘score’ of control- A score of 25 – asthma is well controlled- 20 to 24 – asthma is partially controlled- 15 to 19 – asthma is sub-optimally controlled- Below 15 – asthma uncontrolled
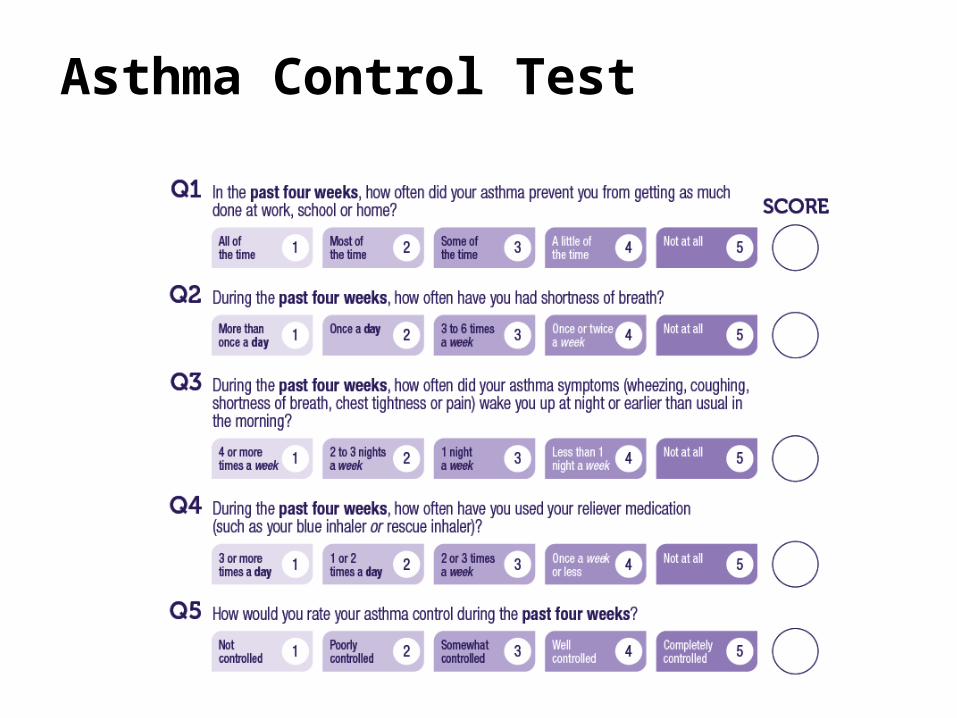
Asthma Control Test
Patients using the Asthma Control Test
• The ACT score is simple and understandable by patients in terms of their level of asthma control.
• Patients have an objective measure of the level of their asthma control.
• It can empower patients to seek control of their asthma.
• It can be used to assess control at home or in the doctor’s surgery.
• The scores can be shared with the doctor.
So is his asthma controlled?
• Occasional exacerbations. NO• He uses of his reliever several times per week. NO• He wakes at night with asthma very now and then. NO• His ACT score = 3 + 4 + 2 + 2 + 4 = 15 NO
• DON’T JUST RELY ON THE PATIENT SAYING THAT HIS/HER ASTHMA IS “OK”.
• HOW DO WE NOW IMPROVE HIS ASTHMA CONTROL?
Increasing ICS doses?
• Continual increases of ICS dose will not necessarily improve symptoms
• Higher ICS doses are more likely to increase the incidence of side-effects- dysphonia, oropharyngeal candidiasis, bruising, adrenal
suppression, BMD loss, skin thinning.• Aim to achieve asthma control with minimum ICS dose: treat
to response then step down to the lowest effective dose.• This is best achieved by combining ICS with LABA.• There is little evidence that high-dose ICS may be effective in
the acute setting of an exacerbation.
ICS / LABA combination
• Long acting beta agonists (LABA) relax bronchial smooth muscle through the stimulation of beta2 adrenoceptors.
• LABA and ICS interact with each other at a cellular level to enhance each other’s actions.
• ICS / LABA combinations are indicated for maintenance treatment of asthma.
• LABAs cannot be used as monotherapy – ICS and LABA in the one inhaler prevents patients from using the LABA alone.
• GINA guidelines recommend the addition of LABA therapy to low-dose ICS in preference to increasing ICS monotherapy.
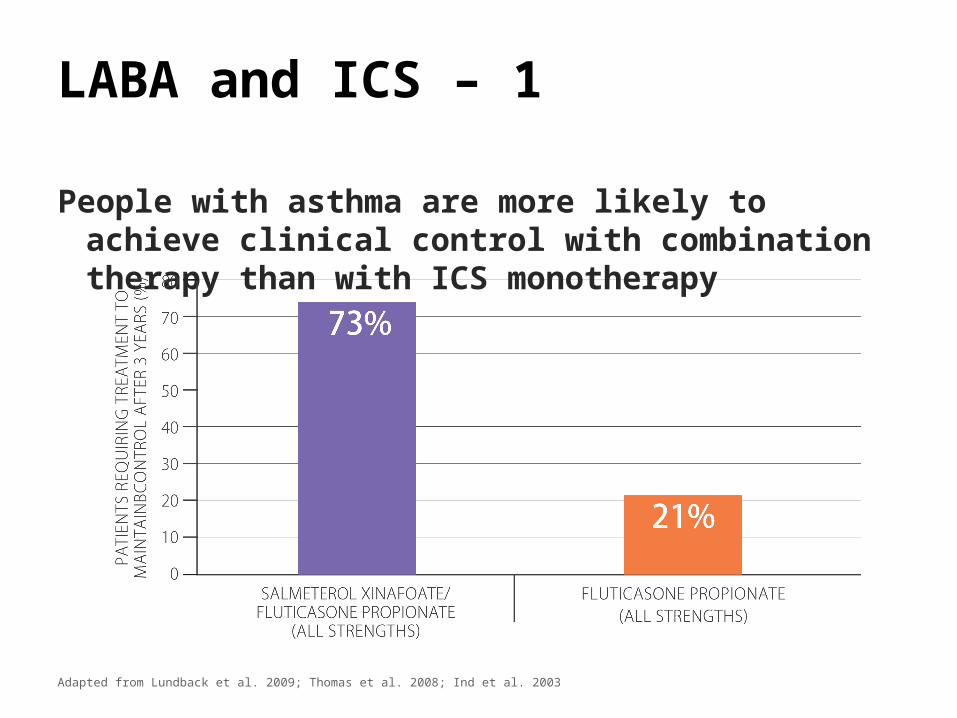
LABA and ICS – 1
People with asthma are more likely to achieve clinical control with combination therapy than with ICS monotherapy
Adapted from Lundback et al. 2009; Thomas et al. 2008; Ind et al. 2003
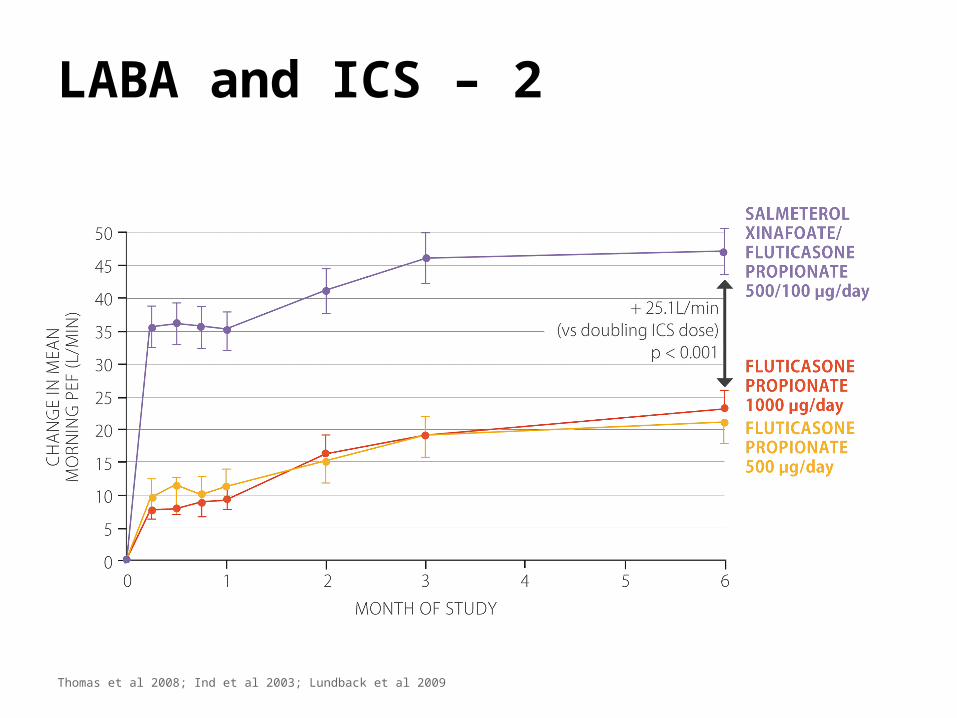
LABA and ICS – 2
Thomas et al 2008; Ind et al 2003; Lundback et al 2009
Another barrier to achieving asthma control
Living with asthma
• This patient is a female public servant.• She sleeps a lot during the day.• She has had persistent asthma since childhood.• She is taking ICS/LABA combination treatment via MDI.• She often wakes at night with asthma symptoms- and she has a morning cough and exertional
dyspnoea with chest tightness.• She has never smoked.• She says that she uses her inhaler twice per day every
day and prescription records support this.• ACT = 14
• WHAT DO YOU DO NOW?
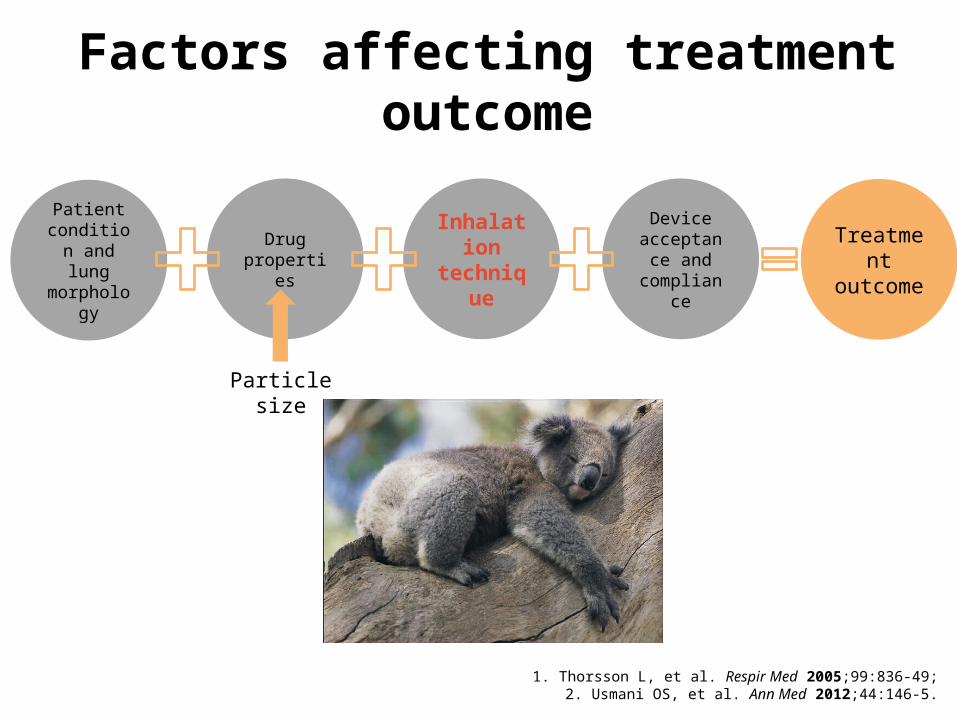
Factors influencing the treatment outcome of ICS/LABA1,2
1. Thorsson L, et al. Respir Med 2005;99:836-49;2. Usmani OS, et al. Ann Med 2012;44:146-5.
Patient condition and lung
morphology
Treatment outcome
Drug properties
Inhalation technique
Device acceptance
and compliance
ICS=inhaled corticosteroid; LABA=long-acting β2-agonist.
Particlesize
Factors affecting treatment outcome
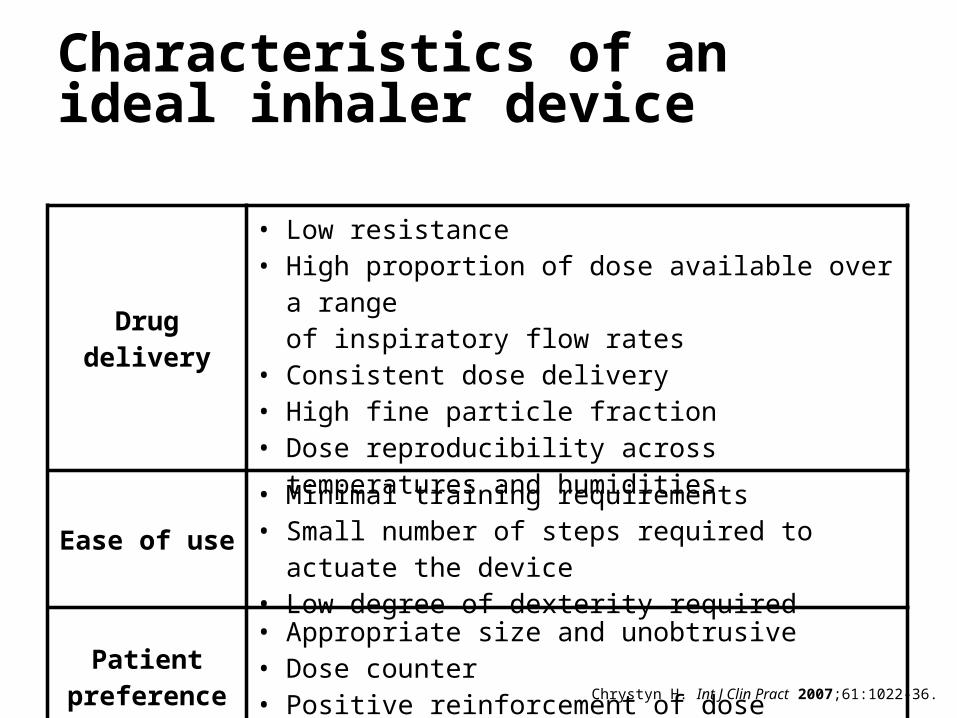
Characteristics of an ideal inhaler device
Chrystyn H. Int J Clin Pract 2007;61:1022-36.
Drug delivery
• Low resistance• High proportion of dose available over a range
of inspiratory flow rates• Consistent dose delivery• High fine particle fraction• Dose reproducibility across temperatures and humidities
Ease of use• Minimal training requirements• Small number of steps required to actuate the device• Low degree of dexterity required
Patient preference
• Appropriate size and unobtrusive• Dose counter• Positive reinforcement of dose delivery
ICS=inhaled corticosteroid; LABA=long-acting β2-agonist.
• Inhaler devices affect efficacy
• Device performance is determined by
- Resistance in the device
- The inspiratory flow rate that the patient can generate
- The proportion of particles coming out of the device that are of a respirable size (2-5 m)
Inhaler design
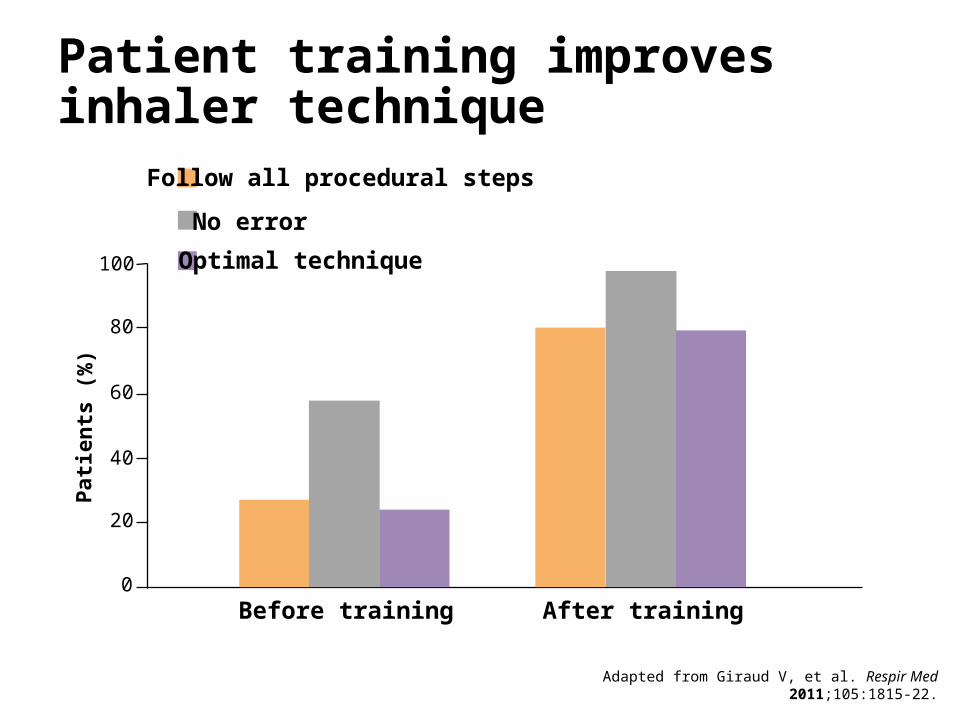
Patient training improvesinhaler technique
Adapted from Giraud V, et al. Respir Med 2011;105:1815-22.
80
100
60
40
0
Follow all procedural steps
No error
Optimal technique
Before training After training
20
Patie
nts
(%)
Proper use of the inhaler is critical
• Choose an inhaler that is going to be easy for the patient to use.
• Make sure that the patient knows how to use it.
• Repeated long tern review is necessary to maintain patients’ proper use of inhalers.
Another barrier to achieving control
Jimmy Bancks13 Nov 1923
Living with asthma
• A young male student• Prescribed Seretide MDI and spacer six months
ago when he was treated for an exacerbation of his asthma.
• No Seretide prescription since then, but several Ventolin prescriptions from locums.
• Missed 10 days of university this year.• Emergency treatment needed for night
symptoms.• Struggling with his cricket due to his asthma.• ACT = 17
• WHAT DO YOU DO NOW?
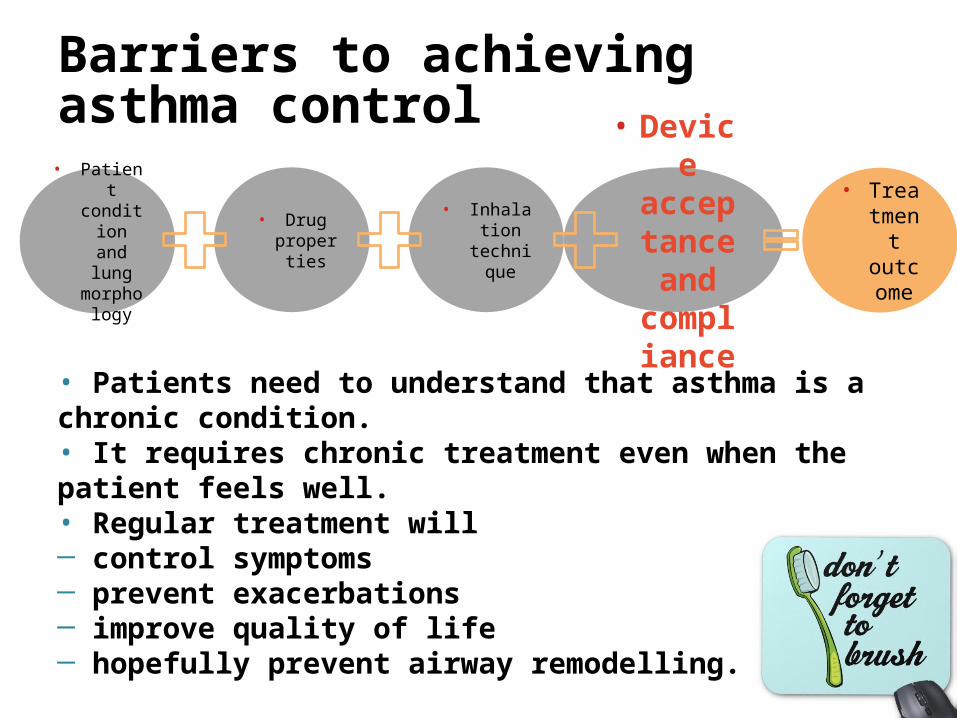
Barriers to achieving asthma control
• Patient conditio
n and lung
morphology
• Treatment
outcome
• Drug properti
es
• Inhalation
technique
• Device acceptance and complia
nce
• Patients need to understand that asthma is a chronic condition.• It requires chronic treatment even when the patient feels well.• Regular treatment will ─ control symptoms─ prevent exacerbations─ improve quality of life─ hopefully prevent airway remodelling.
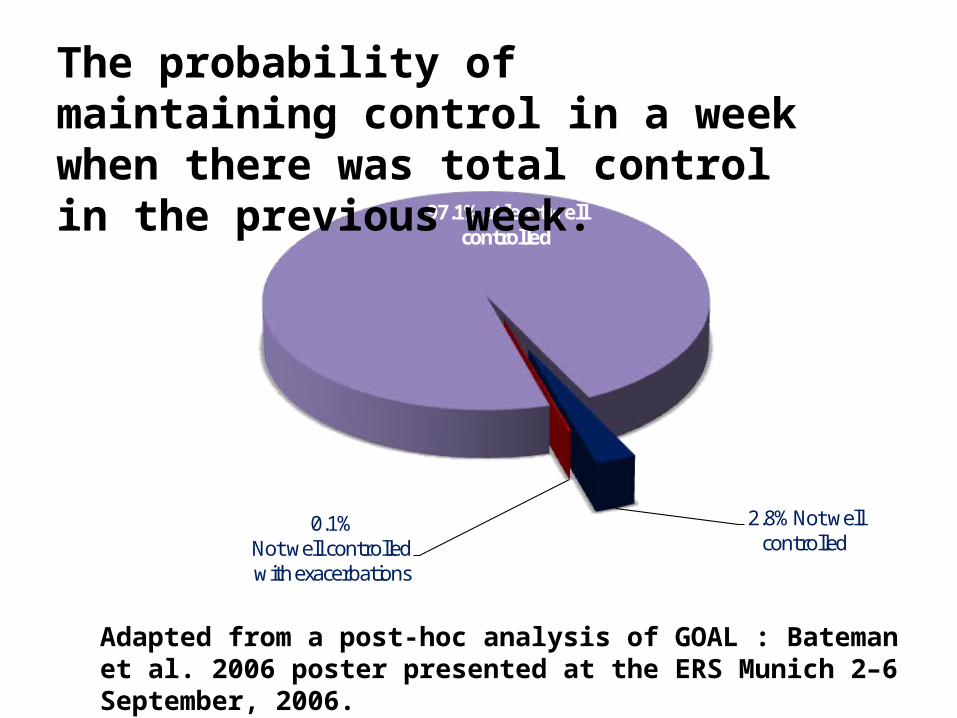
Probability of staying controlled in any week in patients on
Seretide who had total asthma control in the previous week.
97.1% at least well controlled
2.8% Not well controlled
0.1%Not well controlled with exacerbations
Adapted from a post-hoc analysis of GOAL : Bateman et al. 2006 poster presented at the ERS Munich 2–6 September, 2006.
The probability of maintaining control in a week when there was total control in the previous week.
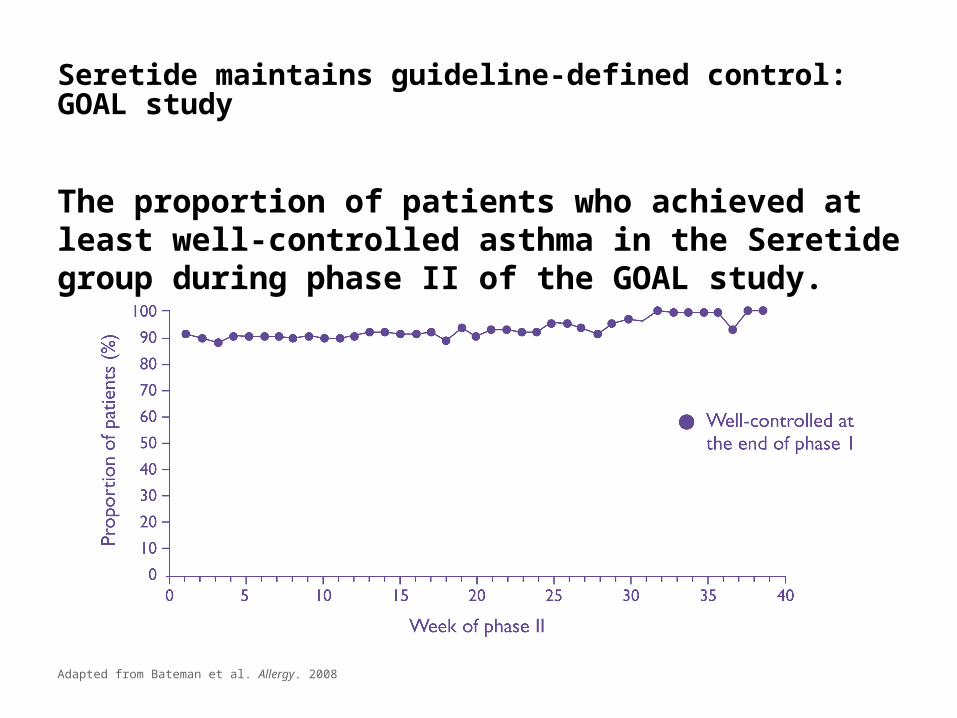
Seretide maintains guideline-defined control: GOAL study
The proportion of patients who achieved at least well-controlled asthma in the Seretide group during phase II of the GOAL study.
Adapted from Bateman et al. Allergy. 2008
Newly diagnosed asthma
A young lady presents with …
• Breathless and tight in the chest going for a run on a cold morning.
• Exercise related wheeze and cough.• Physical examination is normal.• Spirometry shows a reduced FEV1 / FVC ratio (0.6) with the
FEV1 increasing by 18 % and the ratio becoming normal after a bronchodiator.
• THE DIAGNOSIS IS ASTHMA• HOW DO YOU TREAT HER?
Initiating treatment in asthma
• Beta agonists alone? NO
• Regular twice daily ICS plus SABA as a reliever – ONE OPTION
• Start with a ICS / LABA combination plus a reliever – ANOTHER OPTION
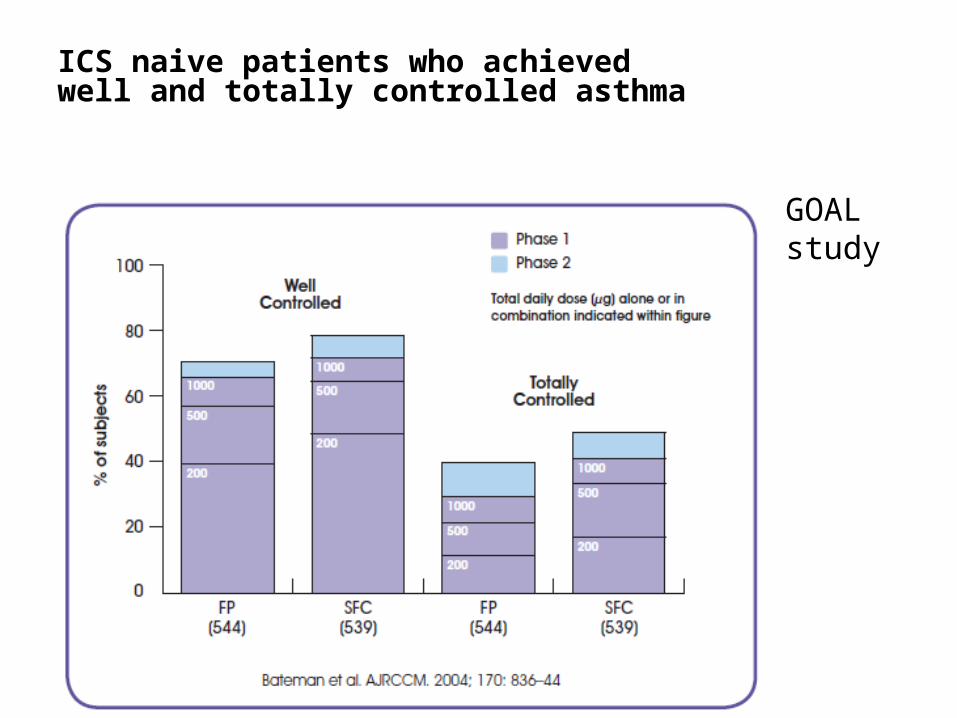
ICS naive patients who achieved well and totally controlled asthma
GOAL study
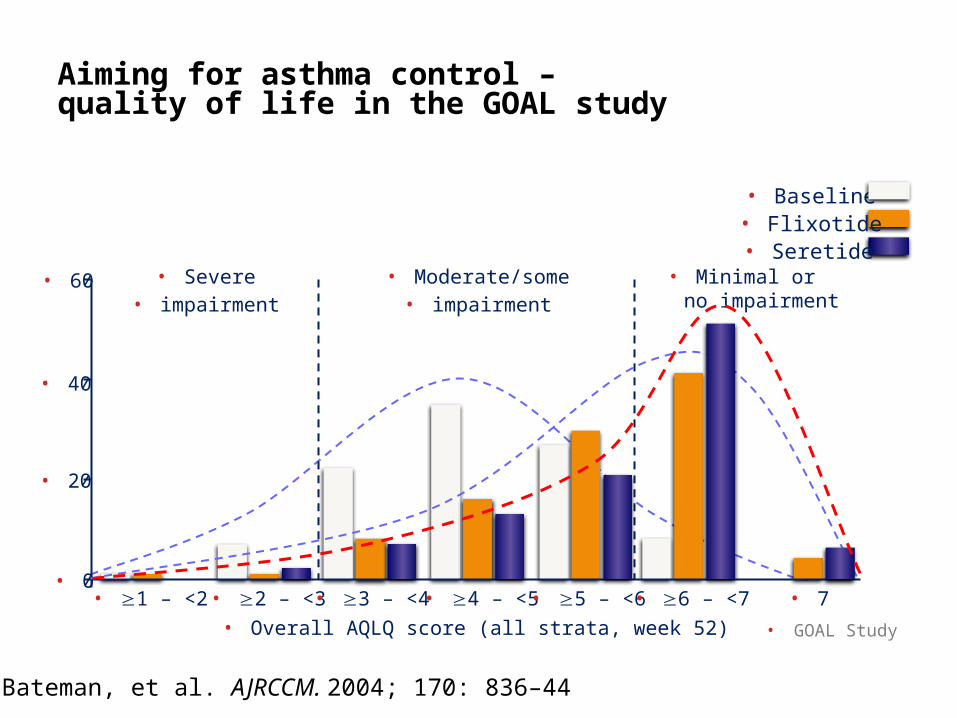
Aiming for asthma control – quality of life in the GOAL study
• Baseline
• Seretide• Flixotide
• GOAL Study
• 2 – <3 • 3 – <4
• 40
• 60
• 0• 1 – <2
• Severe• impairment
• Moderate/some• impairment
• Minimal or no impairment
• 20
• 4 – <5 • 5 – <6 • 6 – <7 • 7• Overall AQLQ score (all strata, week 52)
Bateman, et al. AJRCCM. 2004; 170: 836–44
So what have we learnt?
1. Assess asthma control carefully - the ACT can help with this. ICS / LABA combination is preferable to gain control than increasing ICS doses.
2. Choose an inhaler that is easy for the patient to use.
3. Make sure that the patient uses his/her preventer regularly.
4. ICS / LABA combination can also be used in newly diagnose asthma as an option to ICS, but beta agonists alone is not an option.
jh499481
Insert case studies as per detailed in this slide.
References – 1
1 HOLGATE S, PRICE D & VALOVIRTA E. Asthma out of control? A structured review of recent patient surveys. BMC pulmonary medicine 2006; 6.
2 HOLT S & BEASLEY R. The burden of asthma in New Zealand. Asthma and respiratory foundation of New Zealand (inc.), 2001.
jh499481
TBC once completed.
Related Documents











