Exp Brain Res (2006) 175:377–399 DOI 10.1007/s00221-006-0697-y 123 REVIEW Space motion sickness James R. Lackner · Paul DiZio Received: 1 December 2005 / Accepted: 15 August 2006 / Published online: 5 October 2006 © Springer-Verlag 2006 Abstract Motion sickness remains a persistent prob- lem in spaceXight. The present review summarizes available knowledge concerning the incidence and onset of space motion sickness and aspects of the phys- iology of motion sickness. Proposed etiological factors in the elicitation of space motion sickness are evalu- ated including Xuid shifts, head movements, visual ori- entation illusions, Coriolis cross-coupling stimulation, and otolith asymmetries. Current modes of treating space motion sickness are described. Theoretical mod- els and proposed ground-based paradigms for under- standing and studying space motion sickness are critically analyzed. Prediction tests and questionnaires for assessing susceptibility to space motion sickness and their limitations are discussed. We conclude that space motion sickness does represent a form of motion sickness and that it does not represent a unique diag- nostic entity. Motion sickness arises when movements are made during exposure to unusual force back- grounds both higher and lower in magnitude than 1 g earth gravity. Keywords Motion sickness · Sensory conXict · Fluid shift · Sensorimotor control · Weightlessness Incidence of space motion sickness A remarkable aspect of human exposure to weightless- ness for brief periods, e.g. days, is the relative paucity of severe side eVects. “Space motion sickness” and the mal de barquement that occurs after re-entry and landing are the most obvious adverse consequences. Motion sickness Wrst appeared as an operational problem in the second manned Soviet mission (Titov and Caidin 1962) and became a signiWcant concern in later missions, especially with increased Xight duration. It emerged as a problem in the American Space Program during the Apollo moon missions with the larger crew compartments then avail- able compared with the cramped crew space in the ear- lier Mercury (t1m 3 ) and Gemini missions (t1.5 m 3 ) (Graybiel 1980; Graybiel et al. 1977; Nicogossian and Uri 1994). The US missions then had the possibility, as had been present already in the Soviet Xights, of unrestricted body movements and free Xoating (Matsnev et al. 1983). The overall incidence of symptoms of motion sickness in the space shuttle program has been approximately 70% for astronauts in their Wrst space mission but is lower in experienced astronauts (Davis et al. 1988). Symptoms range in severity from drowsiness to nausea and vomiting. Since the beginning of the manned space- Xight era, our understanding of motion sickness has increased and a larger constellation of symptoms and signs is now recognized as being characteristic of motion sickness. Among these is the “sopite syndrome” which refers to the chronic drowsiness, fatigue, mood and per- sonality changes, and lack of initiative associated with long-term exposure to mildly provocative stimulation (Graybiel and Knepton 1976). Symptoms related to the sopite syndrome persist during exposure to provoca- tive situations long after more familiar features, such as J. R. Lackner (&) · P. DiZio Ashton Graybiel Spatial Orientation Laboratory and Volen Center for Complex Systems, Brandeis University, Waltham, MA 02454-9110, USA e-mail: [email protected] P. DiZio e-mail: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Exp Brain Res (2006) 175:377–399
DOI 10.1007/s00221-006-0697-yREVIEW
Space motion sickness
James R. Lackner · Paul DiZio
Received: 1 December 2005 / Accepted: 15 August 2006 / Published online: 5 October 2006© Springer-Verlag 2006
Abstract Motion sickness remains a persistent prob-lem in spaceXight. The present review summarizesavailable knowledge concerning the incidence andonset of space motion sickness and aspects of the phys-iology of motion sickness. Proposed etiological factorsin the elicitation of space motion sickness are evalu-ated including Xuid shifts, head movements, visual ori-entation illusions, Coriolis cross-coupling stimulation,and otolith asymmetries. Current modes of treatingspace motion sickness are described. Theoretical mod-els and proposed ground-based paradigms for under-standing and studying space motion sickness arecritically analyzed. Prediction tests and questionnairesfor assessing susceptibility to space motion sicknessand their limitations are discussed. We conclude thatspace motion sickness does represent a form of motionsickness and that it does not represent a unique diag-nostic entity. Motion sickness arises when movementsare made during exposure to unusual force back-grounds both higher and lower in magnitude than 1 gearth gravity.
Keywords Motion sickness · Sensory conXict · Fluid shift · Sensorimotor control · Weightlessness
Incidence of space motion sickness
A remarkable aspect of human exposure to weightless-ness for brief periods, e.g. days, is the relative paucity ofsevere side eVects. “Space motion sickness” and the malde barquement that occurs after re-entry and landing arethe most obvious adverse consequences. Motion sicknessWrst appeared as an operational problem in the secondmanned Soviet mission (Titov and Caidin 1962) andbecame a signiWcant concern in later missions, especiallywith increased Xight duration. It emerged as a problem inthe American Space Program during the Apollo moonmissions with the larger crew compartments then avail-able compared with the cramped crew space in the ear-lier Mercury (t1 m3) and Gemini missions (t1.5 m3)(Graybiel 1980; Graybiel et al. 1977; Nicogossian and Uri1994). The US missions then had the possibility, as hadbeen present already in the Soviet Xights, of unrestrictedbody movements and free Xoating (Matsnev et al. 1983).
The overall incidence of symptoms of motion sicknessin the space shuttle program has been approximately70% for astronauts in their Wrst space mission but islower in experienced astronauts (Davis et al. 1988).Symptoms range in severity from drowsiness to nauseaand vomiting. Since the beginning of the manned space-Xight era, our understanding of motion sickness hasincreased and a larger constellation of symptoms andsigns is now recognized as being characteristic of motionsickness. Among these is the “sopite syndrome” whichrefers to the chronic drowsiness, fatigue, mood and per-sonality changes, and lack of initiative associated withlong-term exposure to mildly provocative stimulation(Graybiel and Knepton 1976). Symptoms related to thesopite syndrome persist during exposure to provoca-tive situations long after more familiar features, such as
J. R. Lackner (&) · P. DiZioAshton Graybiel Spatial Orientation Laboratory and Volen Center for Complex Systems, Brandeis University, Waltham, MA 02454-9110, USAe-mail: [email protected]
P. DiZioe-mail: [email protected]
123

378 Exp Brain Res (2006) 175:377–399
nausea and pallor have abated. Aspects of the sopitesyndrome may have been experienced in the pre-Apollomissions without being recognized as being indicative ofmotion sickness. All the primary signs and symptoms ofterrestrial motion sickness, with the exception of pallor,have been observed in space motion sickness.
Symptoms of space motion sickness usually start todevelop within the Wrst several hours in weightlessness(Thornton et al. 1987a). After 72–96 h, most astronautsand cosmonauts have either recovered or begun torecover and are able to move about freely without elic-iting debilitating symptoms. In terms of incidence ofsymptoms and recovery, the American and Russianexperiences seem comparable (cf. Davis et al. 1988;Harm 1990; Jennings 1998; Matsnev et al. 1983;Homick et al. 1984).
Physiology of motion sickness
Motion sickness is a complex phenomenon. Table 1presents a diagnostic system that was developed byGraybiel et al. (1968) to rate the severity of motionsickness under laboratory and operational conditions.Nausea and vomiting are synonymous with motionsickness in most people’s minds but pallor and coldsweating are also characteristics. Pallor is not a diag-nostic sign in spaceXight, however, because of the per-sisting engorgement of the facial veins owing to thelack of a hydrostatic gradient in weightless conditions.Drowsiness is now recognized to be a common featureof low grade motion sickness, as is headache (Graybiel1969; Graybiel and Knepton 1976).
For simplicity, motion sickness can be discussedunder two primary rubrics: (1) stomach emptying and(2) stress response (cf. Money et al. 1996). The mecha-nisms of vomiting and its control have been thoroughlyexplicated by Lang (1992, 1999) and Miller and Yates(Miller 1991; Miller and Grelot 1996; Miller and Leslie1994; Miller and Wilson 1984; Yates and Miller 1996;
Yates et al. 1998). The stress response associated withmotion sickness includes psychic, endocrine, and auto-nomic changes. The conscious or psychic sensationsinclude anxiety, distress, and apprehension evenapproaching dread. The endocrine responses involveelevations of plasma levels of virtually all of the stressresponse hormones. Antidiuretic hormone levels areincreased several fold and ACTH, cortisol, epinephrine,norephinephrine, prolactin, growth hormone, betaendorphin, and thyroid hormone levels increase as well(Money et al. 1996). Most of these changes are associ-ated with elevated activity of the sympathetic nervoussystem, as is the increased blood Xow in skeletal muscleswhich may accompany motion sickness (Johnson 1974;Johnson et al. 1993; Sunahara et al. 1987).
Autonomic nervous system responses are variableand inconsistent during motion sickness. For the motionsick person, subjectively salivation seems to increase butactually salivary Xow usually decreases (Gordon et al.1989). Motion sick individuals may not swallow as muchsaliva as normal, thus producing this apparent contradic-tion. Heart rate may increase, decrease, or not changewith motion sickness and may be inXuenced by level ofseverity but this remains uncertain. Tachygastria, elec-trogastrogram activity in the 7–10 cpm range is reportedto accompany motion sickness and has been proposed asan objective measure of motion sickness (Koch 1999;Stern et al. 1985, 1987a, b; 1989, 1990). However, otherstudies have failed to conWrm this relationship and foundthat (a) tachygastria is primarily associated with height-ened anxiety levels, (b) the onset of tachygastria andonset of reported symptoms are not temporally linked,either can occur earlier, (c) motion sickness symptomscan occur without tachygastria, (d) tachygastria canoccur without motion sickness symptoms, (e) the degreeof tachygastria is not correlated with type or severity ofsymptoms, (f) tachygastria can persist long after allapparent symptoms of motion sickness have resolved(Cheung and Vaitkus 1998; Kiernan et al. 1997; Lawson1993). The R–R interval, the time between heart beats, is
Table 1 Cardinal symptoms of motion sickness and criteria for grading motion sickness severity (Graybiel et al. 1968)
Category Pathognomonic(16 points)
Major (8 points)
Minor (4 points)
Minimal (2 points)
AQS(1 point)
Nausea syndrome Vomiting or retching
Nausea II, III Nausea I Epigastric discomfort
Epigastric awareness
Skin Pallor III Pallor II Pallor I FlushingCold sweating III II IIncreased salivation III II IDrowsiness III II IPain HeadacheCentral
nervous systemDizzinessEyes closed > IIEyes open III
AQS Additional qualifying symptoms; III severe or marked; II moderate; I slight
123
Exp Brain Res (2006) 175:377–399 379
reported to become less variable, a sign of sympatheticactivity with motion sickness (Koch 1993). Blood pres-sure behaves inconsistently in motion sick individualschanging up or down or not at all (Graybiel and Lackner1980b; Johnson 1974). Facial pallor, attributable todecreased blood volume in the venous return, is a prom-inent feature of motion sickness on earth, as is sweatingdespite normal environmental temperatures (McClureand Fregly 1972).
In the laboratory, motion sickness is relatively easyto identify and to quantify because laboratory experi-ments typically involve highly provocative stimulation.The objective is to elicit symptoms quickly so thatdiVerent stimulation conditions and groups of subjectscan be compared. Under operational conditions, e.g.on shipboard or in an aircraft, it is more diYcult toassess motion sickness symptoms and severity becauseof lack of control over activity levels, environmentalconditions, and patterns of vehicle motion. There havebeen persistent attempts to identify physiological con-comitants of motion sickness that could be used toobjectively grade its severity. The success of theseendeavors has been limited because neither the centralnervous system pathways subserving motion sicknessnor the central nervous system sites involved in theevocation of nausea are fully known, although imagingstudies (Balaban 1999) implicate regions of the hypo-thalamus and frontal lobes. By contrast, through thestudies of Yates and Miller a great deal is known aboutthe CNS control and coordination of vomiting (Yates1998; Yates et al. 1998, 1999; Miller and Wilson 1984;Yates and Miller 1996), and of vestibular inXuences onautonomic function (Miller and Grelot 1996; Yates1996, 2004; Yates and Bronstein 2005; Yates et al. 1998,2000, 2002). The vestibular pathways and CNS mecha-nisms underlying motion sickness involve a multitudeof neurotransmitters and receptor types which compli-cates attempts to develop pharmacological counter-measures. Miller and Grelot (1996) and Yates et al.(1998) provide excellent reviews.
Humans with complete bilateral labyrinthine lossare usually completely insusceptible to experiencingnausea and vomiting in response to provocative physi-cal motion (Graybiel and Johnson 1963; Money 1970;Money et al. 1996; Reason and Brand 1975). They aresusceptible to fatigue but whether this is a reXection ofthe sopite syndrome is uncertain. Moreover, individu-als with one-sided loss are less susceptible than normalsubjects to provocative stimulation (Graybiel andNiven 1953). However, Johnson et al. (1999) havefound, unlike Cheung et al. (1991), that individualswith vestibular loss can experience nausea in responseto optokinetic stimulation although they have an
elevated threshold relative to people with normal ves-tibular function. Animal models of motion sicknessand nausea typically rely on vomiting as an index ofmotion sickness but some species do not vomit, e.g.,rats and rabbits. Dogs show susceptibility similaritiesto humans, but behave diVerently in terms of theirresponses to drugs that are eVective antiemetics in thehuman (Money 1990). In non-vomiting species, immo-bility and swallowing of non-nutritive substances (picabehavior) are taken as signs of motion sickness.
Etiological factors in space motion sickness
Fluid shift hypothesis
The absence of hydrostatic pressure in the circulatorysystem in weightlessness leads to a substantial rostralredistribution of blood and lymph. Lung vital capacitydecreases by hundreds of cc’s owing to the engorge-ment of the pulmonary circulation; the facies exhibit apersisting pitting edema; and, with continued exposure,the total volume of circulating blood is reduced owingto homeostatic mechanisms that interpret theincreased activity of carotid and aortic arch barorecep-tors as reXecting too large a blood volume (Moore andThornton 1987; Thornton et al. 1987a). During re-entryafter spaceXight with the return of hydrostatic pressurein the circulatory system, the decreased blood volumeproduces a tendency for vaso-vagal syncope (Noskovand Grigoriev 1994; Yates and Kerman 1998; Yateset al. 2003).
Fluid shifts are potential factors in space motionsickness because they might aVect the relative balanceof endolymphatic and perilymphatic pressures in thelabyrinth (cf. Parker et al. 1983) creating a situationakin to labyrinthine hydrops (Meneire’s disease) orthey might increase intracranial pressure (Kakurinet al. 1976; Matsnev et al. 1983; Noskov and Grigoriev1994). Both these conditions can produce nausea andvomiting. “Motion sickness” could result becauseabnormally high intralabyrinthine pressures wouldlead to unusual patterns of vestibular activity orbecause increased cerebral spinal Xuid pressures wouldactivate brainstem emetic “centers”. The Xuid shifthypothesis is appealing because shifts of hundreds ofcc’s occur in spaceXight and many investigators feelthis phenomenon cannot be without functional conse-quences. However, on earth, Xuid shifts occur when-ever an animal or human changes its orientation. Whena person is standing upright, hydrostatic pressure isgreatest because the height of the Xuid column is thendependent on the length of the major longitudinal
123

380 Exp Brain Res (2006) 175:377–399
blood vessels of the body. When the body is supine,hydrostatic pressure approaches zero because the Xuidcolumn height is eVectively the diameter of the majorblood vessels. Thus, postural changes relative to grav-ity always inXuence the regional distribution of bloodand lymph in the body.
In the course of evolution, animals have developedmechanisms of autoregulation for maintaining cerebralblood Xow within very narrow limits despite Xuctua-tions in perfusion pressure related to changes in bodyorientation. The need for autoregulation is readilyapparent in the giraVe, an animal that has been widelyused in studies of cerebral blood Xow. Without autore-gulation, cerebral blood Xow and intracranial pressurewould vary profoundly in the giraVe as it raises andlowers its head (Patterson et al. 1975; Patterson andGraybiel 1974; Van Citters et al. 1968). Tree climbingsnakes have similar demands on their cerebral bloodXow regulation and have developed mechanical spe-cializations (i.e. a more rostrally located heart and lesscompliant skin) as well as autoregulation mechanismsto control cerebral blood Xow (Badeer 1998; Lillywhite1996).
SpaceXight observations on Xuid shifts
Several spaceXight studies have addressed the issue ofXuid shifts and their role in space motion sickness.Thornton concluded from his personal observations onXuid shifts and motion sickness in space shuttle XightSTS-8 and from studies carried out under his aegis inother shuttle missions that Xuid shifts are not an impor-tant factor in space motion sickness (Thornton et al.1987a). Shifts develop after insertion into orbit andpersist until the end of the mission. They give rise todiscomfort because of sinus and facial distension butdo not aVect susceptibility to motion sickness in anyobvious way nor do they parallel the time course ofmotion sickness. Auditory evoked potentials and eyemovement recordings are normal contrary to whatwould be expected for labyrinthine hydrops orincreased intracranial pressure. Oman (1987) andOman et al. (1986, 1990) conducted systematic motionsickness monitoring in Spacelab 1. The astronauts allexperienced discomfort from the engorgement of theveins of the face which persisted throughout the mis-sion. After correlating in-Xight symptom developmentand abatement in relation both to voluntary activitylevels and to Xuid shift time courses, Oman and his col-leagues concluded that Xuid shifts are at best a minorfactor in space motion sickness. They identiWed headmovements, especially in pitch, as being particularlyprovocative. Later systematic studies by Oman on the
International Microgravity Laboratory mission led tothe same conclusions (Oman 1998). Simanonok andCharles (1994) have reported a potential positive rela-tionship between Xuid shifts and space motion sick-ness. Their correlational study did not include anassessment of astronaut activity levels in relation tosymptom development but they did Wnd that astro-nauts who were most susceptible to space motion sick-ness exhibited the largest post-Xight decreases inelectro-cardiographic measures of right ventricle, dia-stolic volume. They raise the possibility that Xuid shiftsmight decrease the threshold for vestibular stimulationto elicit motion sickness. Noskov and Grigoriev (1994)found that diuretics alleviate some of the subjectivediscomfort and congestion associated with being inweightlessness but not the motion sickness.
Ground-based studies of the Xuid shift hypothesis
Parker (1977), who monitored simultaneously endo-lymphatic pressure in a semicircular canal and cerebralspinal Xuid pressure in a ventricle of the guinea pig,found no changes related to modulations in Xuid shiftmagnitude. Parker et al. (1983) measured auditorythresholds and tympanic impedance in the human dur-ing head-down body tilt as an indirect assessment ofthe eVects of Xuid shifts on inner ear function. Using a30°, head-down, body tilt to mimic weightlessness, theyfound slight decrements in auditory sensitivity athigher frequencies and signiWcant changes in imped-ance. This magnitude of head-down tilt creates a head-ward directed hydrostatic pressure approximately 50%of that acting footward in a standing individual. Mont-gomery et al. (1993) used 6° head-down body tilts tosee how, relative to measurements at the upright,audiometric thresholds, tympanometric values, andauditory evoked potentials would be aVected. Nochanges were observed despite the congestion and dis-comfort subjects reported during the head-down tilt.
Two behavioral studies of Xuid shifts and motionsickness susceptibility involved “barbecue spit rota-tion” (Graybiel and Lackner 1977, 1979). In this situa-tion, as the body rotates, the otolith organs of the innerear are continuously re-oriented in relation to the grav-itational force vector. Such stimulation when pro-longed induces motion sickness in most subjects. Onestudy exposed blindfolded subjects to constant velocityrotation at 30 rpm while they were either in the head-horizontal, head 10° up, or head 10° down orientations,and estimated the relative magnitude of Xuid shift bymeasuring lung vital capacity (Graybiel and Lackner1977). The Xuid shifts were signiWcantly diVerent acrossall conditions and in relation to measures at the
123

Exp Brain Res (2006) 175:377–399 381
upright, but no diVerences in susceptibility or in pat-tern or severity of symptoms were present. In the otherstudy, subjects were rotated at 30 rpm while in the 10°head-down position (an orientation where the resultingXuid shift should be slightly greater than that to beexpected in weightlessness) either immediately afterbeing placed in the test position or 6 h later (Graybieland Lackner 1979). The 6-h period was chosen becausespace motion sickness is often reported within thatinterval. The experimental results showed a signiWcanttendency, P < 0.05, for subjects to tolerate rotationlonger before experiencing symptoms after havingbeen head-down for 6 h prior to the onset of rotation.
Fluid shifts and space motion sickness: conclusions
Neither spaceXight nor ground-based studies providesupport for Xuid shifts being an important factor in spacemotion sickness. Space motion sickness also does nothave the clinical characteristics that would be expected ifit were attributable to labyrinthine hydrops or abnormalcranial pressure (Reschke et al. 1994; Thornton et al.1987a). Patients with labyrinthine hydrops often havedrop attacks, elevation of auditory thresholds, acuterotary vertigo, paroxysmal episodes of dizziness, nauseaand vomiting, and nystagmus (Baloh and Honrubia1990). A paroxysmal episode may last from several min-utes to several hours, occasionally as long as 24 h.Increased cerebral spinal Xuid pressure can evoke nau-sea and vomiting irrespective of activity levels. It is alsonotable that prolonged bed rest studies which userecumbency to mimic weightlessness do not evoke thepanoply of signs and symptoms characteristic of spacemotion sickness despite the rostral Xuid shifts generated.
Role of head movements in evoking space motion sickness
Astronauts and cosmonauts have consistently reportedthat head movements tend to elicit and exacerbatesymptoms of space motion sickness. Titov Wrstreported this (Titov and Caidin 1962) and it was notedin the Apollo and Skylab missions (Graybiel 1980) andthroughout the space shuttle missions. Controlledexperiments to evaluate how diVerent kinds of naturalhead and body movements inXuence susceptibility tomotion sickness in spaceXight have not yet been car-ried out. Observations en passant (e.g. Thornton et al.1987a, b; Oman et al. 1986) indicate that at least ini-tially pitch head movements are most stressful, andyaw least, in bringing on symptoms.
Oman et al. (1986, 1990) have made key in-Xightmeasurements of motion sickness incidence in relation
to activity levels in Spacelab 1. Some of the participat-ing astronauts wore accelerometers that allowed theirhead movements to be monitored. Early in their mis-sions the astronauts found pitch and roll head move-ments to be provocative, especially pitch movements,and limited their head movements when symptomsdeveloped. The astronauts who moved their headsmost vigorously prior to symptom onset were thosewho later experienced the most severe symptoms.Establishing Wrm body contact with a surface tended toalleviate their symptoms. By mission day 4, symptomsof motion sickness abated and the astronauts wereagain able to make unrestricted head movements.
The Spacelab astronauts also found that being inunusual orientations, e.g. inverted relative to otherastronauts or to architectural features of the space-craft, could bring on or exacerbate symptoms ofmotion sickness. Episodes of sudden vomiting alsooccurred. However, as Oman et al. (1986, 1990)emphasize, prior to these episodes, prodromal signs ofsickness were usually present, i.e. the astronauts werealready sensitized. This pattern is also characteristic ofterrestrial motion sickness. Golding and Stott (1997b)found that laboratory subjects remain abnormally sen-sitive to provocative stimuli for up to 3–4 h after allapparent symptoms have abated. Following parabolicXight maneuvers, subjects who have been motion sickbut who are seemingly symptom free may exhibit sud-den vomiting when the aircraft rapidly decelerates onlanding (Lackner and Graybiel 1986a, b).
The Spacelab astronauts were tested in parabolicXight 4 days after re-entry from orbital Xight and 1-year later. In the Wrst parabolic Xight, all could makehead movements without evoking symptoms; 1 yearlater head movements did elicit symptoms. This pat-tern points to an immediate post-spaceXight desensiti-zation for certain types of stimulation. Theirensemble of in-Xight and post-Xight observations ledOman et al. (1990) to conclude that space motionsickness shares relevant features with terrestrialmotion sickness. Many tests of orientation and sen-sory function were conducted with the Spacelabastronauts pre- and post-Xight to see whether anywould be of predictive value for space motion sick-ness. None were, but Oman et al. (1990) present aninsightful analysis of the diYculties and complexitiesassociated with predicting susceptibility.
Role of head movements in evoking motion sickness in low and high force environments
The question arises whether there is something specialabout head movements eliciting motion sickness in
123

382 Exp Brain Res (2006) 175:377–399
weightless conditions or whether head movements inany non-earth force background would elicit symp-toms. In other words, is space motion sickness a uniquediagnostic entity? This issue has been systematicallyevaluated in parabolic Xight experiments where theXight path generates alternating periods of high force,approximately 1.8 g peak, and weightlessness, eachlasting about 20–25 s (Lackner and Graybiel 1984,1985). Figure 1 illustrates the Xight path and associatedforce levels. Some individuals become sick throughexposure to such cyclic alterations in force level evenwhen they are seated with head Wxed. This makes itnecessary to measure their baseline susceptibility tothe force variations per se prior to experimental obser-vations being carried out. This was done by Wrst expos-ing subjects to two, 40 parabola Xights separated byseveral days during which they were strapped in posi-tion to prevent body movements and wore orthopedicneck collars to prevent head movements. Dependingon the number of motion sickness symptoms experi-enced in their two Xights, individuals were classiWed asCategory I, insusceptible; Category II, moderately sus-ceptible; Category III, highly susceptible. After catego-rization was completed, the inXuence of yaw, pitch, androll head movements on susceptibility was evaluated
by having subjects make head movements in the 0 gphase of each parabola until nausea was reached or 40parabolas had been completed. Within and across sus-ceptibility categories, the following results wereobtained: symptoms of motion sickness appeared ear-lier and with greater overall severity when pitch headmovements were made, yaw head movements wereleast provocative, and roll movements were of interme-diate stressfulness. Movements were more provocativewhen vision was permitted.
Lackner and Graybiel (1985) had subjects makehead movements in pitch and in yaw in the 1.8 g phasesof parabolas. The experimental Wndings were similar tothose obtained in free fall. Head movements in pitchwere much more stressful than in yaw, and the pres-ence of vision further heightened susceptibility. Themain diVerence was that head movements made in1.8 g were much more stressful than those in 0 g. Manysubjects participated in both experimental series andall showed this pattern. These results demonstrate thatmotion sickness results when head movements aremade in non-1 g force environments regardlesswhether force level is increased or decreased and sug-gest that space motion sickness is not a unique diagnos-tic entity.
Fig. 1 Schematic Xight path and associated force level of an aircraft Xying parabolic maneuvers to generate periods of weightlessnessand high force
123
Exp Brain Res (2006) 175:377–399 383
Coriolis cross-coupled angular accelerations and space motion sickness
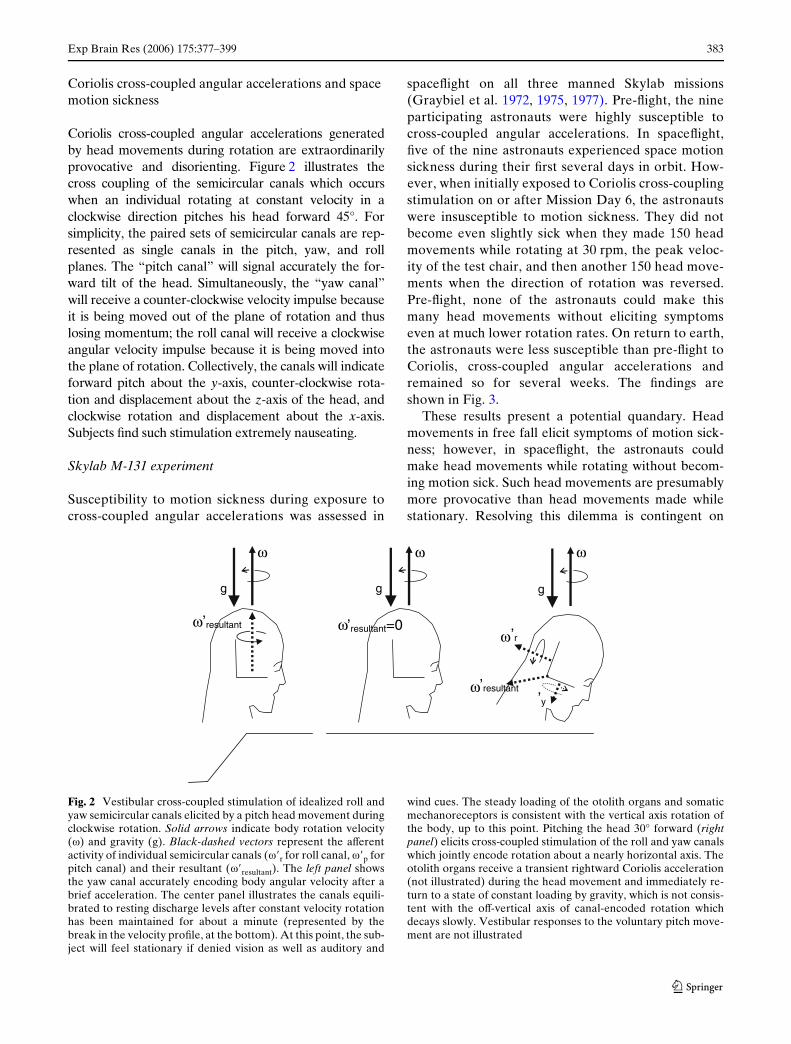
Coriolis cross-coupled angular accelerations generatedby head movements during rotation are extraordinarilyprovocative and disorienting. Figure 2 illustrates thecross coupling of the semicircular canals which occurswhen an individual rotating at constant velocity in aclockwise direction pitches his head forward 45°. Forsimplicity, the paired sets of semicircular canals are rep-resented as single canals in the pitch, yaw, and rollplanes. The “pitch canal” will signal accurately the for-ward tilt of the head. Simultaneously, the “yaw canal”will receive a counter-clockwise velocity impulse becauseit is being moved out of the plane of rotation and thuslosing momentum; the roll canal will receive a clockwiseangular velocity impulse because it is being moved intothe plane of rotation. Collectively, the canals will indicateforward pitch about the y-axis, counter-clockwise rota-tion and displacement about the z-axis of the head, andclockwise rotation and displacement about the x-axis.Subjects Wnd such stimulation extremely nauseating.
Skylab M-131 experiment
Susceptibility to motion sickness during exposure tocross-coupled angular accelerations was assessed in
spaceXight on all three manned Skylab missions(Graybiel et al. 1972, 1975, 1977). Pre-Xight, the nineparticipating astronauts were highly susceptible tocross-coupled angular accelerations. In spaceXight,Wve of the nine astronauts experienced space motionsickness during their Wrst several days in orbit. How-ever, when initially exposed to Coriolis cross-couplingstimulation on or after Mission Day 6, the astronautswere insusceptible to motion sickness. They did notbecome even slightly sick when they made 150 headmovements while rotating at 30 rpm, the peak veloc-ity of the test chair, and then another 150 head move-ments when the direction of rotation was reversed.Pre-Xight, none of the astronauts could make thismany head movements without eliciting symptomseven at much lower rotation rates. On return to earth,the astronauts were less susceptible than pre-Xight toCoriolis, cross-coupled angular accelerations andremained so for several weeks. The Wndings areshown in Fig. 3.
These results present a potential quandary. Headmovements in free fall elicit symptoms of motion sick-ness; however, in spaceXight, the astronauts couldmake head movements while rotating without becom-ing motion sick. Such head movements are presumablymore provocative than head movements made whilestationary. Resolving this dilemma is contingent on
Fig. 2 Vestibular cross-coupled stimulation of idealized roll andyaw semicircular canals elicited by a pitch head movement duringclockwise rotation. Solid arrows indicate body rotation velocity(�) and gravity (g). Black-dashed vectors represent the aVerentactivity of individual semicircular canals (��r for roll canal, ��p forpitch canal) and their resultant (��resultant). The left panel showsthe yaw canal accurately encoding body angular velocity after abrief acceleration. The center panel illustrates the canals equili-brated to resting discharge levels after constant velocity rotationhas been maintained for about a minute (represented by thebreak in the velocity proWle, at the bottom). At this point, the sub-ject will feel stationary if denied vision as well as auditory and
wind cues. The steady loading of the otolith organs and somaticmechanoreceptors is consistent with the vertical axis rotation ofthe body, up to this point. Pitching the head 30° forward (rightpanel) elicits cross-coupled stimulation of the roll and yaw canalswhich jointly encode rotation about a nearly horizontal axis. Theotolith organs receive a transient rightward Coriolis acceleration(not illustrated) during the head movement and immediately re-turn to a state of constant loading by gravity, which is not consis-tent with the oV-vertical axis of canal-encoded rotation whichdecays slowly. Vestibular responses to the voluntary pitch move-ment are not illustrated
ωω
ω
ω
ω ω ω
’resultant=0
g
’y
’r
’resultant
g
’resultant
g
123

384 Exp Brain Res (2006) 175:377–399
realizing that in the Skylab missions the Wrst headmovements during rotation were made on or after Mis-sion Day 6 when natural head movements were nolonger provocative. Other factors contributing to thedecreased sensitivity to Coriolis stimulation in space-Xight are described below.
Motion sickness and Coriolis cross-coupling stimulation in 0 and 1.8 g
Susceptibility to motion sickness during Corioliscross-coupling stimulation has been measured in thefree fall and high force phases of parabolic Xightmaneuvers to determine how background force levelaVects performance (Lackner and Graybiel 1986a, b).Subjects were tested blindfolded, while rotating at20 rpm and making pitch head movements in sets ofeight until they reached a motion sickness endpoint ofnausea, or had completed 40 sets. The experimentalresults were unequivocal: all subjects were more sus-ceptible to motion sickness during exposure to highforce levels than in free fall. The Category I and IIsubjects (see Role of head movements in evokingmotion sickness in low and high force environments)were less susceptible to motion sickness in free fallthan in the laboratory. Category III subjects, who are
susceptible during exposure to parabolas per se, wereslightly less susceptible to Coriolis stimulation in freefall than in the laboratory.
Subjects also rated the apparent intensity and pro-vocativeness of constant levels of Coriolis cross-cou-pling stimulation during parabolic Xight maneuvers.All subjects showed the same patterns: comparablephysical levels of Coriolis cross-coupling stimulationwere more intense, disorienting, and provocative in1.8 g background force levels than in 1 g, and headmovements made in 0 g were much less intense andnauseogenic than in 1 g. In addition, the aberrant headand body motion (tilt and turning about several axes)experienced when head movements were made duringstraight and level Xight was greatly enhanced in 1.8 g.In 0 g, subjects experienced pitch of their heads withlittle or no rotation about other axes. In another exper-iment, subjects made head movements during rotationin the transitions from 0 to 1.8 g or from 1.8 to 0 g(Lackner and Graybiel 1985, 1986a, b). Every subjectexperienced the same pattern. Head movements madeduring the 0 to 1.8 g transitions were more intense andprovocative than those in the 1.8 to 0 g transitions. TheinXuence of gravitoinertial force level on the apparentintensity and provocativeness of Coriolis stimulationwas thus virtually immediate.
Fig. 3 Results of the Skylab M-131 experiment for three Skylab4 astronauts. The columns represent the severity of motion sick-ness on the Graybiel scale (see Table 1). The rows of numbers
along the bottom indicate the angular velocity of body rotation,the number of head movements performed, rotation direction,and Xight day (solid line pre-Xight; R+ post-Xight)
123

Exp Brain Res (2006) 175:377–399 385
Vestibulo-ocular responses to Coriolis stimulation as a function of gravitoinertial force level
Coriolis, cross-coupling stimulation elicits reXexive eyemovements because of the impulsive stimulation of thesemicircular canals when the head is tilted out of theaxis of body rotation. DiZio et al. (1987a) measuredthe vestibulo-ocular response to constant levels ofCoriolis stimulation in straight-and-level Xight and inthe high force and free-fall phases of parabolic Xightmaneuvers. In 0 g, the average slow phase eye velocityof the nystagmus elicited decreased, as did beat fre-quency relative to 1 g values, although peak slow phasevelocity was unaVected. The time constant of nystag-mus slow phase velocity decreased in 0 and 1.8 g rela-tive to 1 g baseline values, although to a lesser extent in1.8 g than in 0 g. This modulation of reXexive eyemovement responses was systematic and highly signiW-cant statistically. Importantly, it did neither parallel thesubjective nor the motion sickness responses to Corio-lis stimulation which although likewise attenuated in0 g are greatly enhanced in 1.8 g relative to 1 g values(Lackner and Graybiel 1986a, b). This dichotomymeans that the central inXuences of semicircular canalstimulation on perception and motion sickness are dis-tinct from their inXuence on oculomotor control.
DiZio et al. (1987b) also recorded vestibulo-ocularresponses to impulsive deceleration from constantvelocity rotation in parabolic Xight. Precisely thesame angular stimulation was delivered in 0, 1, and1.8 g. The peak velocity of the resulting vestibularnystagmus was the same in all phases of parabolicXight; but, the time constant of decay of slow phaseeye velocity was lower in 1.8 g than in 1 g and lowerstill in 0 g. The value in 0 g was only slightly above theallometrically computed time constant for the hori-zontal semicircular canals. Nystagmus time constantswere shortened or “dumped” by post-rotary head tiltsin 1 and 1.8 g but not in 0 g (DiZio and Lackner1988). These Wndings indicate that velocity storage(Cohen et al. 1977), the central integration of semicir-cular canal signals, is attenuated at least during initialexposure to non-terrestrial gravitoinertial force back-grounds, and much more so in 0 g than in 1.8 g. Omanand Balkwill (1993) found similar results for nystag-mus dumping and aftereVect durations in the Spac-elab SLS-1 crew conWrming diminished velocitystorage in weightlessness. Oman et al. (1996) testedfour SLS-2 astronauts and found decreases in velocitystorage for all four. But, for two of them, the leastexperienced in spaceXight, velocity storage laterreturned toward pre-Xight levels. Head movements inpitch did not dump the velocity storage.
Altered integration of semicircular canal signals in weightlessness
Converging evidence from parabolic Xight experimentspoints to perception of the vertical and of body angulardisplacement both being aVected by exposure toweightlessness. The perception of the subjective verti-cal (Bryan et al. 2004) was tested with subjects recum-bent in a bed-like apparatus that allowed them to beset at diVerent yaw angles with respect to the gravita-tional vertical. The blindfolded subjects haptically indi-cated the vertical as an aircraft performed parabolicmaneuvers. Settings of the vertical did not diVer for 1.8and 1 g force levels. This is unlike the case for pitch androll body tilts where increased shear on the otolithorgans leads to a greater apparent body tilt relative togravity (Correia et al. 1968; Miller et al. 1965). Aftertransition into weightlessness subjects quickly felt hori-zontal and set the joystick perpendicular to their fron-tal plane (parallel to their midline). The symmetrictouch and pressure cues imposed by the restraint sys-tem of the apparatus likely account for the subjectsfeeling horizontal when weightless.
These Wndings were extended in a parabolic Xightexperiment in which recumbent subjects were dynami-cally rotated to diVerent yaw orientations relative togravity while continuously tracking the apparent verti-cal with a joystick (Lackner et al. 2006). Subjects turnedwhile in a 1 or 1.8 g force level, moved the joystick sys-tematically to the direction opposite their tilt, but whenthe aircraft entered 0 g, they moved the joystick to bevirtually perpendicular to their frontal plane (parallel totheir midline) and reported feeling horizontal. Whenthey were tilted to a new static angle while in 0 g, theyfailed to perceive a change in body orientation. Thesemicircular canal stimulation generated when subjectswere rotated to a new orientation was always at least anorder of magnitude above canal thresholds on earth foreliciting perception of a positional change. The failureto sense angular displacement indicates that spatialintegration of canal aVerent signals is disturbed or thatthe apparent vertical deWned by somatosensory infor-mation overrides the canal cues.
Implications for the skylab M-131 experiment
The experiments described above on head movementsin diVerent background force levels allow a motivatedexplanation of the Skylab results. The Skylab astro-nauts were Wrst tested with cross-coupled stimulationat a time by which natural head movements were nolonger provocative. Accordingly, one would actuallyexpect the astronauts to be unaVected by Coriolis
123

386 Exp Brain Res (2006) 175:377–399
cross-coupled stimulation because the provocativenessof Coriolis stimulation is immediately attenuated infree fall and is not much greater than that of headmovements per se. The reduced or suppressed integra-tion of canal signals in weightless conditions alsomeans that the abnormal patterns of canal activitypresent during cross coupling are not fully integratedto produce aberrant positional changes. As a result,disorientation should not be experienced, which is con-sistent with astronaut reports that head movementsduring rotation in orbit no longer “tumble their gyros”.Disorientation occurs with cross coupling in normaland high force levels because path integration of canalsignals is occurring and providing a representation ofhead motion and path which corresponds to thatexpected neither from the intended movement norfrom the otolith organs.
Otolith asymmetries and space motion sickness
Several investigators have raised the possibility thatasymmetries between the otolith organs on the twosides of the head may contribute to space motion sick-ness (Egorov and Samarin 1970; Gurovskiy et al. 1975).DiVerences in collective otoconial mass between thepaired otolith organs could in principle result in asym-metric shear forces on the otolith membranes on thetwo sides. However, compensation for asymmetries investibular function typically occurs. For example, ifone horizontal semicircular canal is destroyed, a hori-zontal nystagmus will develop, and over time will abateand Wnally disappear. If the remaining horizontal canalis destroyed, a new nystagmus of opposite sign, knownas Bechterev’s nystagmus, will appear. Its presenceindicates the existence of a central compensation thathas developed to restore normal vestibulo-ocular func-tion. Von Baumgarten and colleagues have hypothe-sized that an analogous compensatory eVect occursunder terrestrial conditions in an individual with unbal-anced peripheral inputs from the otolith organs to cre-ate concordant inputs (von Baumgarten 1986, 1987;von Baumgarten and Thumler 1979; von Baumgartenet al. 1981). Exposure to weightlessness would unmaskthe persisting central compensation and lead to thedevelopment of symptoms of motion sickness becauseof the resulting asymmetry in signals from the otolithorgans.
Ocular counterrolling is an important measure ofotolith function (Graybiel 1974; Miller and Graybiel1974). During tilt of the body in roll, the eyes counter-tort in the opposite direction by a fraction of the bodytilt. Ocular counterrolling is a relatively primitive reXex,its gain rarely exceeds 0.1 so it is inadequate to keep the
eyes aligned with the environment. By contrast, themodulation of neck, trunk, and limb musculature byotolith-spinal pathways is very important for posturaland stance control (Wilson and Melvill Jones 1979).Because of this diVerence in functional signiWcance ofocular counterrolling and vestibulo-spinal reXexes, indi-viduals with asymmetric otolith function potentiallymight exhibit asymmetric counterrolls for leftward andrightward body tilts but have centrally compensatedvestibulo-spinal pathways (Lackner et al. 1987).
To evaluate the possible role of otolith asymmetriesin evoking motion sickness, Lackner et al. (1987) ana-lyzed the ocular counterrolling scores of subjects whohad participated in parabolic Xight experiments. Thesesubjects had been categorized as insusceptible to theparabolas per se (Category I), moderately susceptible(Category II), or highly susceptible (Category III), seeRole of head movements in evoking motion sickness inlow and high force environments. On average, the Cat-egory II and III subjects had slightly smaller ocularcounterrolling amplitudes than the Category I subjects.In addition, they had signiWcantly greater asymmetriesin their counterrolls for leftward and rightward bodytilts. This Wnding shows that individuals with asymmet-ric otolith function tend to be susceptible to motionsickness during changes in gravitoinertial force level.However, these are group diVerences and some of theCategory I subjects had larger counterrolling asymme-tries than some of the Category III subjects. This pat-tern means that one cannot reliably predict a particularindividual’s susceptibility in parabolic Xight on thebasis of counterrolling scores. Diamond and Markhammeasured the ocular counterrolling of a number of vet-eran astronauts during parabolic Xight maneuvers andcalculated “torsional disconjugacies” (diVerence in tor-sion of the right eye relative to 1 g conditions minustorsion of the left eye for the 0 and 1.8 g force phases ofXight) (Diamond and Markham 1988, 1991a, b, 1992;Diamond et al. 1990; Markham and Diamond 1992,1993). The astronauts who had not been motion sick inorbital Xight overall had lower disconjugacy scores inparabolic Xight (Markham et al. 2000), but a one-to-one relationship between disconjugacy and susceptibil-ity in spaceXight cannot be drawn.
An issue of key concern is that if there is a centralasymmetry in otolith function that is “unmasked” byexposure to weightlessness, then there should be con-sequences for apparent body orientation as well as foroculomotor control. For example, astronauts shouldexperience a particular individual apparent body tiltwhenever they are not moving about because of theunmasked central compensation for the asymmetrybetween the otolith organs. Such eVects have not been
123

Exp Brain Res (2006) 175:377–399 387
reported. What is clear is that immobilizing the headseems to attenuate and hinder the development ofspace motion sickness. A signiWcant vestibular asym-metry revealed by exposure to weightlessness would beexpected to give rise to symptoms when the head is sta-tionary as well as moving, and this does not seem to bethe case.
Treatment of space motion sickness
The drugs primarily used to treat motion sickness haveantihistaminic or anticholinergic actions or a combina-tion thereof. Putcha and her colleagues have providedsummaries of the antimotion sickness drugs currentlyused in spaceXight and an analysis of the changes inpharmacodynamics potentially associated with expo-sure to weightlessness (Graebe et al. 2004; Putcha et al.1999; Putcha 1999). Oral and buccal delivery of pro-methazine has been used with some success. Baclofen,which attenuates velocity storage, is currently beingevaluated as a potential antimotion sickness therapy(Dai et al. 2006). In parabolic Xight, a combination ofscopolamine and dexedrine (“scopdex”) is often usedprophylactically. The scopolamine is used to prevent orattenuate motion sickness and the dexedrine to coun-teract the soporiWc action of the scopolamine. In USspaceXights, the commander and pilot cannot take suchmedications because of FAA regulations to which theyare subject.
Antimotion sickness drug injections
Antimotion sickness drugs given orally are oftenineVective in suppressing symptoms of motion sick-ness that have already developed. A motion sick indi-vidual may expel some of a drug dose in vomitus.Diminished gastric motility is also one of the signs ofmotion sickness; consequently, the passage of drugsto absorption sites in the small intestine may bedelayed (Money et al. 1996; Thornton et al. 1987c).Drug pharmacokinetics may also be altered in micro-gravity environments (Harm 1990; NorXeet et al. 1992;Putcha et al. 1999; Davis et al. 1993a, b; Thornton et al.1987b; Williams 2003). Parenteral administration ofantimotion sickness drugs circumvents these prob-lems and provides a rapid way of getting drugs intothe blood circulation. Subjects in parabolic Xightstudies often become severely motion sick, experienc-ing extreme nausea and multiple bouts of vomiting.Graybiel and Lackner (1987) found that most of theseindividuals could be greatly relieved of their symp-toms by intramuscular injections of promethazine or
scopolamine. Many could even resume participatingin experiments. In ground-based studies, side eVectsare usually associated with the use of scopolamineand promethazine at eVective dose levels, the mostprominent being dry mouth, drowsiness, and with sco-polamine, mydriasis (Lucot 1998; Wood et al. 1990).Motion sick subjects in parabolic Xight tended not toexperience these side eVects until after landing andthen found them preferable to experiencing repeatedbouts of nausea and vomiting. Based on these Wnd-ings, Graybiel and Lackner (1987) recommendedtreating severe space motion sickness with injectionsof promethazine.
This approach was initiated in spaceXight byBagian, himself an astronaut physician, and his col-leagues. It has proven valuable in relieving the symp-toms of astronauts disabled by motion sickness(Bagian 1991; Bagian and Ward 1994; Davis et al.1993a, b). They often recover enough to resume theiractivities and importantly do not report the severeside eVects of drowsiness that are associated withcomparable doses of promethazine under ground-based laboratory conditions. Promethazine is oftenreported to prevent adaptation or to hinder learning.Thus, there is potential concern that promethazinecould delay sensory-motor adaptation to the spaceenvironment. However, promethazine does not pre-vent the acquisition of adaptation to provocative ves-tibular stimulation if goal-directed head movementsare made (Dai et al. 2003; Lackner and Graybiel1994). Consequently, if astronauts resume their natu-ral movements while protected by promethazine, theyshould continue adapting to the weightless environ-ment. However, if they restrict their movements,adaptation to the weightless environment would bedelayed.
The use of promethazine injections to treat spacemotion sickness has been severely criticized based onlaboratory studies in which volunteer subjects havebeen exposed to tests of alertness, manual dexterity,sensorimotor coordination, and motion sickness sus-ceptibility after receiving intramuscular injections ofpromethazine (Cowings et al. 2000). Subjects showedsigniWcant decrements on the performance tasks andgreatly impaired alertness. In addition, unlike theobservations of Graybiel and Lackner (1987), andBagian and colleagues (Bagian 1991; Bagian and Ward,1994; Davis et al. 1993a, b) no protection againstmotion sickness was observed. Cowings et al. (2000)concluded that drug injections should be discontinuedin spaceXight and autogenic feedback training (AFT)substituted. It is notable, however, that in parabolicXight and spaceXight conditions, drug injections are
123

388 Exp Brain Res (2006) 175:377–399
used only when individuals are already motion sick andunable to carry on their tasks.
In the Cowings et al. (2000) study, the drug injec-tions were given at the beginning of the test day.Over the next 4.5 h, the volunteers were evaluatedon the performance measures. Then, they wereexposed to provocative vestibular stimulation byhaving them make head movements during rotation.The eVective dose duration of the promethazine usedwas speciWed to be 4.5–6 h which means that the per-formance tests were made during the period of drugeYcacy and the motion sickness tests were conductedduring the period of diminished or absent protection.The Wndings are thus not surprising. Caution is alsonecessary in comparing astronauts to laboratory sub-jects participating voluntarily for pay in activitiesthat they can terminate at any time. Astronauts oftenhave trained for years before receiving a Xight oppor-tunity. Prior to a mission they train extensively onthe speciWc tasks they will have to carry out untilthese tasks become virtually second nature. Onceinto a mission they cannot leave the situation if theybecome indisposed.
Autogenic feedback training
Autogenic feedback training has been proposed byCowings and her colleagues as a way to preventspace and terrestrial motion sickness (Cowings andToscano 1982, 2000; Cowings et al. 1977, 1986, 1995,2000; Toscano and Cowings 1982). They report that asindividuals become motion sick they show self-consis-tent patterns of physiological changes that constitutea personal trait and that remain unchanged acrossmultiple provocative exposures (Cowings et al. 1995;Staut et al. 1995). In AFT, an individual is trained torecognize various bodily sensations so as to detectchanges in heart rate, respiration, skin temperature,and other parameters. With feedback training, sub-jects learn to control these factors, and Cowings et al.report that they thereby become resistant to motionsickness.
AFT studies typically involve physical eVort on thesubject’s part, the execution of many head move-ments during rotation, thereby generating Coriolis,cross-coupling stimulation of the semicircular canals(see Coriolis cross-coupled angular accelerations andspace motion sickness). Cowings et al. have comparedAFT training to sham training on a cognitive task forsome subjects, and to no treatment for other subjects.Subjects made sets of head movements during rota-tion at progressively higher rotation velocities untilcompleting the test proWle or stopping because of
motion sickness. With repeated exposures, subjects inthe AFT group showed improvement being able to“tolerate” more rotations and head movements whilethe other groups failed to show any evidence whatso-ever of improvement over repeated exposures. Thissame pattern has been consistently reported by theCowings group using this experimental paradigm.AFT groups show improvement, non-AFT groups donot. However, it is surprising that sham and no-treat-ment control groups fail in these studies to showimprovement with repeated incremental exposure toCoriolis cross-coupling stimulation. Placebo groups indrug studies show improvement over non-treatmentgroups during this form of exposure and the latteralso improve with repeated exposures (Wood andGraybiel 1968; Wood et al. 1990). In fact, virtuallyidentical exposure conditions, but without AFT, areused in treatment programs to desensitize subjects tomotion sickness (e.g. Cramer et al. 1976; Graybielet al. 1969; Golding and Stott 1995; Reason andGraybiel 1970).
Jozsvai and Pigeau (1996) have also evaluated theeYcacy of AFT itself in suppressing symptom devel-opment. They initially exposed subjects to Corioliscross-coupling stimulation to determine their baselinesusceptibility; then divided them into three groupsmatched for susceptibility. One group received AFTwith accurate feedback about their autonomic ner-vous system responses, another AFT group receivedfalse feedback, and the third group received no treat-ment. The three groups in this comprehensive studydid not diVer in their performance, thus indicating nobeneWt of the AFT. In addition, studies in whichmotion sickness is passively induced by means of sud-den decelerations from constant velocity rotation(Graybiel and Lackner 1980a, b) or caloric stimula-tion (Costa et al. 1995) have unlike the Cowings stud-ies found no regular or self-consistent physiologicalpatterns for individuals across test situations norbetween severity of motion sickness and either aver-age values or directional variations in physiologicalparameters (Cheung and Vaitkus 1998: Cheung et al.1990; Doweck et al. 1997; Golding and Stott 1997a;Harm and Schlegel 2002; Mullen et al. 1998; Costaet al. 1995).
In summary, current studies provide little hope thatspace motion sickness can be prevented or attenuatedby AFT. This failure is disappointing because it wouldbe valuable to have an alternative to antimotion sick-ness drugs. Such an alternative is especially importantfor long duration spaceXight where the radiation lev-els encountered will diminish the shelf life of drugs(J. Clark, personal communication).
123

Exp Brain Res (2006) 175:377–399 389
Theories and ground-based models of space motion sickness
Theories of space motion sickness
We lack a fully adequate theory of why motion sick-ness occurs. “Evolutionary theories” posit that it hassurvival signiWcance (Treisman 1977). Motion sicknessby this perspective serves to empty the stomach andexpel ingested toxins, and to decrease body activity.How this response could have developed evolution-arily is unclear. The time course of the emetic responsemay also be too slow to be of functional signiWcance.Nevertheless, dogs that are surgically labyrinthectom-ized no longer show a vomiting response to some butnot all drugs that earlier induced emesis in them(Money and Cheung 1983). Vestibular overstimulationtheories have largely been abandoned because oftenthe most gentle stimuli can be more provocative thanmore intense ones, e.g. susceptibility to motion sick-ness during vertical oscillation is greater around 0.2 Hzthan 1 Hz (Guignard and McCauley 1990; O’Hanlonand McCauley 1974).
Sensory conXict theories are currently the mostaccepted explanations of motion sickness (Oman 1982,1984, 1990, 1998; Reason 1970; Reason and Brand1975). The basic notion is that motion sickness ariseswhen diVerent sensory systems give conXicting infor-mation about the ongoing motion of the body, or theexpected sensory feedback from intended movementsdoes not correspond with that actually generated. Suchtheories have great generality because motion sicknessis a disorder associated with motion and almost all situ-ations involving body motion potentially involve someform of sensory “conXict”.
Bles and Bos have proposed that all motion sicknessincluding space motion sickness result from situationsin which “... the sensed vertical as determined on thebasis of integrated information from the eyes, the ves-tibular system ... is at variance with the subjective verti-cal as expected from previous experience” (Bles et al.1998, Bles 1998; Bos and Bles 1998; de Graaf et al.1998). This sensory conXict hypothesis speciWcallyinvokes the vertical as having special signiWcance.Unfortunately, it cannot accommodate typical labora-tory conditions for studying motion sickness in whichthere is not a conXict with the vertical, e.g. passivevisual stimulation in optokinetic drums (Hu and Stern1998; Hu et al. 1999; Stern et al. 1987a; Lackner andTeixeira 1977; Teixeira and Lackner 1979), decelera-tions from constant velocity rotation (Graybiel andLackner 1980a, b), vertical oscillation (Wright et al.2005), and head mounted visual displays with visual
updating contingent on head tracking (DiZio andLackner 2000, 2002).
Although the eliciting elements in space motionsickness are not fully understood a wide range of fac-tors contribute including altered vestibular functionunder both dynamic and static conditions. Exposure toweightlessness changes the resting activity of the oto-lith organs because of the unloading of the utricularand saccular membranes. On earth, head orientationinXuences otolith activity in terms of gravity generatedshear forces. These shear forces will be absent and it isunclear what the resting patterns of utricle and sacculedischarge will be like in weightless conditions. The pat-terns of vestibular activity associated with voluntary aswell as passive head movements will also be unlikethose associated with similar changes in head orienta-tion on earth.
In addition, because the body is weightless in orbitalXight, sensory-motor control of the entire body will bedrastically altered in terms of the patterns of muscularactivation necessary to achieve changes in body conWg-uration and in the associated patterns of sensory feed-back (see Lackner and DiZio 2000a for an explanationof the physics of the situation). Body orientation andlocomotion are controlled by hand and footholds, andby pushing oV. On earth, modiWcations of the motorcontrol patterns controlling body posture and locomo-tion can, even in the presence of normal patterns ofvestibular input, produce motion sickness and posturalcontrol disruption (Lackner and DiZio 1989). Figure 4provides a schematic representation of some of the fac-tors involved in space motion sickness and adaptationto new force environments.
Ground-based models of space motion sickness
Many ground-based models of space motion sicknessinvolve creating sensory conXicts in terms of abnormalpatterns of vestibular stimulation and/or unusual visualstimulation. Such approaches include caloric irrigation,galvanic vestibular stimulation (Severac 1992), “pre-adaptation training” (Parker et al. 1985; Parker andParker 1990), and centrifugation (Albery and Martin1996; Bles et al. 1997; Ockels et al. 1990). Caloric andgalvanic studies involve stimulating the vestibularreceptors to elicit symptoms of motion sickness andpostural imbalance. Prolonged exposure to increasedg-levels has also been proposed as a model. In onestudy, test subjects including cosmonauts from MIRmissions were exposed to 3 g acceleration levels alongthe naso-occipital body axis for up to 3 h on a centri-fuge (Bles et al. 1997). Afterward, most experiencedsymptoms of motion sickness when they made head
123

390 Exp Brain Res (2006) 175:377–399
movements and were ataxic. The cosmonauts reportedthat their symptoms were comparable to those theyhad experienced in their spaceXight 3 years earlier.Motion sickness symptoms and postural imbalancewere also elicited in subjects exposed to +1.8 gz accel-eration for 90 min (Albery and Martin 1996). Subjectswho made periodic voluntary head movements whileexposed to prolonged rotation on a short arm centri-fuge also experienced symptoms of motion sicknessand exhibited post-rotational postural disturbances
(Kaufman et al. 2001). These subjects in addition toreceiving abnormal otolith stimulation because of thecentrifugal rotation also underwent Coriolis cross-cou-pling stimulation when they tilted their heads. Thus,they were exposed to multiple provocations.
The rationale for these diVerent approaches is thatmotion sickness and postural disequilibrium are associ-ated with space motion sickness and the space adapta-tion syndrome. Consequently, conditions that alsoproduce such eVects may serve as a ground-based
Fig. 4 Schematic of processes involved in space motion sickness.At the top left is the physical stimulus for the whole process, achange (open triangle) in gravitoinertial acceleration (gia), forexample, from terrestrial 1 g gravity to orbital spaceXight, 0 g.The heavy arrows embody the idea that space motion sickness isstrongly correlated with processes involved in adaptation of spa-tial orientation and sensorimotor control of whole body postureand movement and autonomic adaptation to other stressorsevoked by changes in gia. Spatial orientation and sensorimotorcontrol involve many subsystems that utilize internal models,
motor command copies, and reaVerent feedback (sensory signalscontingent on self-movement). Perturbations of orientation andmovement control activate adaptive processes that re-weight sen-sory feedback signals, recalibrate motor output, and revise inter-nal models. Motion sickness is most severe when the orientationand autonomic regulation systems are undergoing rapid recali-bration. After adaptation to 0 g orbital spaceXight a new transi-tion, for example to Martian g, artiWcial g, or re-entry to 1 gconditions can elicit motion sickness anew
Stress Adaptation
∆ gia0 gre-entryMartian gartificial gravity
Fluid dynamicsfluid levels
Cardiovascularbaroreflex
Other
Motion sickness
Pre
-dis
posi
tion
HabituationConditioningSensitization
Immediate compensation∆ anti-diuretic hormones∆
∆
∆ACTH
Recalibration∆ set points
Emetic networkVomiting
Brainstem arousal networkSopite syndrome
∆ Environment & ObjectsPhysical constraintsEnvironmental regularitiesObject/substrate connectionCanonical visual perspectivesStability of self/environmentObject inertia/weightObject weight
Adaptive recalibration
Internal models
Multisensory∆ Vestibular∆ TPK∆ Vision∆ Proprioception
Adaptive recalibration
∆Plant
Velocitystorage
Posture and MovementFix gazeVisual scanningMaintain posture
Non-supportive movementsObject wieldingInteract with tools
Spatial orientationProprioceptionStability of self/environmentMoveable objects/tools
Forward models of sensoryfeedback from motor commands
Physical constraintsEnvironmental regularitiesConnection to substrateCanonical visual perspectivesStability of self/environmentObject inertia/weightObject weight
Adaptive recalibrationControl
123
Exp Brain Res (2006) 175:377–399 391
model without the need for spaceXight. The assump-tion is that similar signs and symptoms equal similaretiology. However, similarity of symptoms of motionsickness in diVerent contexts does not necessarilyequate to similar etiology and underlying mechanismsand does not justify substitution of contexts. Anextreme example will make this clear. Patients under-going chemotherapy or radiation therapy for treatmentof cancer can exhibit many of the signs and symptomsof motion sickness and postural disequilibrium. Never-theless, one would not propose these treatments as aterrestrial model of space motion sickness. An over-night train ride through rugged terrain in a sleepercompartment also can result in postural and locomo-tory disturbances that at least superWcially share manyof the characteristics of postural re-entry disturbances.
The pre-adaptation trainer, or PAT Dome, has beenused in attempts to assess susceptibility and to pre-adapt astronauts to the unusual patterns of visual stim-ulation that they will encounter in spaceXight (Harmand Parker 1994). This device projects unusual visualscene orientations to the observer and induces orienta-tion illusions. When astronauts-free Xoat in spaceXightthey experience many body orientations in relation tothe architectural verticals and horizontals of the space-craft that would not be possible on earth. Sometimesthey also experience a compelling sense of beingupside down, and some episodes of inversion seem totrigger sudden vomiting (Oman et al. 1990). The ratio-nale for the PAT device is that pre-exposure to suchconXicting visual scenes may attenuate or eliminatespace motion sickness.
Parabolic Xight has been extensively used as aground-based approach to understanding space motionsickness. An important concern is whether informationabout motion sickness gained from parabolic Xightexperiments is directly relevant to understanding theetiology of space motion sickness and the performancechanges that occur in spaceXight. Must these factors bestudied in orbital Xight? In parabolic Xight, brief peri-ods of free fall and high gravitoinertial force level alter-nate and many individuals become motion sick as aconsequence of these periodic variations. This makes itnecessary to measure baseline susceptibility to the par-abolic maneuvers per se or it would not be possible toevaluate the relative provocativeness of diVerent formsof superimposed stimuli. The brief periods of free falland high force available also limit the measurementsthat can be made to those compatible with multiple 20–30 s intervals. With prolonged exposure to free fall inorbital Xight, a variety of adaptive changes occurs assensory-motor control and orientation mechanismsaccommodate to weightless conditions (see Fig. 4).
Those changes with relatively long time constants willbe missed in parabolic Xight experiments. By contrast,those with short time constants, e.g. seconds or min-utes, may Wrst be identiWed in the course of parabolicXight experiments.
The great advantage of spaceXight for studyingphysiological changes is the long time periods availablefor making observations. However, it takes about8 min to achieve orbital Xight after launch and a muchlonger period before systematic experimental observa-tions can be made. In ground-based studies of sensory-motor performance, adaptation can often be generatedin brief periods of time. Exposure periods are often asbrief as several minutes and rarely much longer than30–60 min because adaptation occurs so rapidly. Somesensory-motor accommodations to weightlessness mayinvolve virtually instantaneous adaptation or resetting.For example, during initial exposure to weightlessnessin parabolic Xight, individuals generally within a try ortwo are able to catch objects that are thrown to them.It is as if there is a parameter resetting for certain sen-sory-motor abilities that is extremely rapid (Lacknerand DiZio 2000a, b). In orbital Xight, the set-up ofexperimental apparatus involves unstowing and putt-ing together the test rig and instrumentation and ofteninvolves considerable head and body movementswhich can be quite provocative. In the Spacelab 1 mis-sion, astronauts found setting up the apparatus forexperiments on vestibular function to be more stressfulthan the actual experiments (von Baumgarten 1986).In some cases, setting up the apparatus may be gener-ating the sensory-motor adaptation that the experi-ment was designed to test. The ability to contrast theeVects of high and low force levels within a short timespan in parabolic Xight is thus extremely advantageousand can reveal eVects that otherwise might go unno-ticed or would be much harder to identify in space-Xight. At present, parabolic Xight constitutes the bestavailable terrestrial technique for studying etiologicalfactors in space motion sickness. The aftereVects ofprolonged exposure to +gx centrifugation (Bles et al.1997) are an intriguing phenomenon which deservesfurther exploration despite the lack of a clear link tospace motion sickness.
Prediction of susceptibility to space motion sickness
In the space shuttle missions, about 70% of the astro-nauts experience space motion sickness symptoms dur-ing the Wrst 3 days. Because the shuttle missions are ofrelatively brief duration, generally 7–14 days, 3 days ofimpaired performance represent a severe mission
123

392 Exp Brain Res (2006) 175:377–399
impact. In long duration missions lasting months suchas on the International Space Station or years such ason a projected manned mission to Mars, 3 days are lessimportant. Consequently, the ability to adapt fully tothe space environment can be as important or evenmore important than initial susceptibility in long dura-tion missions. This raises the issue whether it is possi-ble to predict how astronauts will adapt to the spaceenvironment and whether it is possible to pre-adaptastronauts to the types of provocative stimulation theywill encounter in spaceXight.
Attempts to develop predictors of motion sicknesshave included (1) trying to identify psychological orpersonality characteristics linked to motion sicknesssusceptibility, (2) motion sickness questionnaires, and(3) assessments of motion sickness susceptibility withdiVerent forms of provocative stimulation. Excellentreviews of the early literature are provided by Money(1970), Reason and Brand (1975), Reschke (1990), andTyler and Bard (1949). Despite numerous reports ofpsychological correlates of motion sickness susceptibil-ity, the correlations have little practical value for pre-dicting susceptibility. The studies show that amonghighly susceptible individuals some have speciWc per-sonality traits; however, no information is availableabout the motion sickness susceptibility of individualswith these traits in general (Wendt 1948; Tyler andBard 1949). Many investigators have suggested rela-tionships between fear, anxiety, and apprehension andmotion sickness, but Dobie (1974) has made the impor-tant observation that some instances of sickness are nottrue motion sickness but fear reactions.
Spacelab 1 prediction tests
Prior to spaceXight, the four Spacelab 1 payload crewmembers were exposed to a broad range of provoca-tive tests of motion sickness in the laboratory and inparabolic Xight (Money et al. 1984). The ground testsincluded (1) sinusoidal horizontal oscillation at 0.2 Hzalong the head y axis, (2) head-over-heels rotationabout the head y axis at 20 rpm, (3) ingestion of deute-rium oxide, “heavy water”, to render the horizontalsemicircular canals gravity sensitive, and (4) wearingprism spectacles to reverse the visual Weld. The para-bolic Xight test involved touching the head to the kneesthen to the head rest on the seat back. One cycle wascompleted each 3 s during the approximately 25 s peri-ods of weightlessness in each parabola.
The susceptibility to space motion sickness of thesefour payload specialists and the time course of theirsymptom development and abatement were carefullymonitored during the Spacelab 1 mission. Post-Xight it
was only possible to repeat the parabolic Xight suscep-tibility tests.
Three of the four astronauts vomited repeatedlyduring spaceXight, only one did not, and he like one ofthe others had taken an antimotion sickness medica-tion (scopolamine and dexedrine) before launch. Theother two were medicated after symptoms developed.Performance on the pre-Xight susceptibility tests didnot predict in-Xight susceptibility. The least susceptibleastronaut during spaceXight was the most susceptiblein the pre-Xight tests. The other three were basicallysimilar in their in-Xight performance and susceptibilitybut varied in their pre-Xight susceptibilities to thediVerent test protocols. Importantly, however, in theirpost-Xight tests in parabolic Xight, all of the astronautswere insusceptible to motion sickness when makingpitch head and trunk movements during weightless-ness. This pattern suggests a carry over of adaptationacquired in spaceXight.
The failure to Wnd a relationship between ground-based assessment tests and in-Xight susceptibility isperhaps not surprising. The test population was small,only four subjects, and the ground-based tests were notdeveloped to speciWcally mimic aspects of the factorsthat would be altered in spaceXight, but were ongoinglaboratory procedures.
Susceptibility questionnaires
Motion sickness questionnaires have been developedby the military to predict susceptibility in operationalconditions (e.g. Alexander et al. 1955; Hardacre andKennedy 1965; Miller and Graybiel 1970: Reason andBrand 1975; Lentz and Collins 1977). Subjects report-ing a past history of motion sickness generally showgreater susceptibility when tested in experimentaldevices than those who do not (Alexander et al. 1955;Miller and Graybiel 1970). Subjects who are classiWedas highly susceptible on the basis of their questionnaireanswers are also more likely to report having highlysusceptible parents or siblings. Lentz and Collins(1977) point out that this may be in part attributable tosimilar exposure histories. Bakwin (1971) and Abeet al. (1970), however, believe that motion sickness sus-ceptibility may be in part genetically determined.Asians have also been found to be more susceptiblethan Caucasians (Stern et al. 1996).
Lentz (1976) found there was no correlation betweena subject’s susceptibility score on a questionnaire andthe duration of vestibular nystagmus and sensations ofturning during and following exposure to angularacceleration despite earlier reports of a direct relation-ship between sensation and nystagmus cupulograms
123

Exp Brain Res (2006) 175:377–399 393
(plots of duration of aftersensation of rotation and nys-tagmus versus log of angular velocity impulse) and sus-ceptibility to motion sickness (de Wit 1953; Groen1957). Bles et al. (1984) and Dobie (1974) have alsofailed to conWrm a relationship between aftereVectduration and susceptibility after sudden decelerationfrom constant velocity rotation. However, DiZio andLackner (1991) found a strong correlation betweensusceptibility to motion sickness in parabolic Xight andthe extent to which post-rotary head movementsdecrease the duration of the post-rotation nystagmusunder 1 g conditions. This pattern points to a linkbetween velocity storage and space motion sickness.Cohen et al. (2003) and Dai et al. (2003) recently pro-vided strong evidence that velocity storage activity isimplicated in the evocation of motion sickness elicitedby Coriolis cross-coupled stimulation in 1 g.
Disadvantages of the questionnaire approachinclude that it is not possible to determine accuratelythe nature and intensity of a subject’s prior exposure toprovocative stimulation and that subjects diVer in theirknowledge of motion sickness symptomotology withmost simply equating motion sickness with nausea andvomiting. Two other factors are of concern: (a) ques-tionnaires provide information about past episodes ofmotion sickness and not about a subject’s ability toadapt to provocative motion nor about the rate ofrecovery from acute motion sickness, and (b) when amotion sickness questionnaire is being used as ascreening device, candidates are reluctant to revealtheir full range of motion sickness experiences. Motionsickness questionnaire evaluations also typically showgreater sickness susceptibility for women than men(Reason 1968; Reason and Brand 1975; Lentz and Col-lins 1977). However, some experimental studies con-trasting male and female susceptibility have not foundany signiWcant diVerences (Cheung and Hofer 1998;Woodman and GriYn 1997). Cheung et al. (2001) alsofailed to Wnd susceptibility variations related to thefemale’s menstrual cycle. However, others havereported females to be more susceptible than men andto also vary in their susceptibility during the menstrualcycle (Clemes and Howarth 2005; Golding et al. 2005;Grunfeld and Gresty 1998; Turner and GriYn 1995).The issue remains unresolved but any diVerences maybe relatively minor.
Reschke (1990) has provided an excellent analysis ofhow test and performance measures might be used topredict the performance of subjects in diVerent provoca-tive operational environments. The important messagefrom his large-scale study was that no ground-basedtest yet developed constituted an accurate predictor ofsusceptibility and severity in parabolic Xight or in
spaceXight. Harm and Schlegel (2002) since havefound, however, that the severity of motion sickness inparabolic Xight may correlate with higher pre-Xightbaseline levels of salivary amylase. Elevated baselineswould be consistent with a higher base level of sympa-thetic nervous system activity in these individuals. Car-diac R–R interval variations and the sympathovagalindex were also measured for the subject populationand higher values tended to be associated with moder-ate to severe susceptibility to motion sickness duringparabolic Xight.
Experimental procedures for assessing susceptibility to motion sickness
Many techniques have been used to elicit motion sick-ness under partially or fully controlled conditionsincluding (a) ships, (b) ship motion simulators, (c) ele-vators or vertical oscillators, (d) four-pole swings, (e)caloric irrigation, (f) “roll-pitch rockers”, (g) visualinversion or reversal, (h) oV-vertical axis, body rota-tion, (i) optokinetic stimulation, (j) varying angularaccelerations, (k) Coriolis and cross-coupling accelera-tions generated by active or passive head movementswhile in a rotating chair or centrifuge, (l) parabolicXight, (m) galvanic stimulation, (n) virtual environ-ments, and (o) sudden-stop stimulation. These proce-dures can elicit motion sickness symptoms in mostpeople, with the exception of labyrinthine-defectiveindividuals most of whom remain largely immuneregardless of the nature or level of the stressor environ-ment (see Physiology of motion sickness).
Miller and Graybiel (1970b, 1972) tested subjects onan extensive set of provocative procedures to deter-mine whether susceptibility to one type of provocativestimulation (e.g. oV-vertical axis rotation) would pre-dict susceptibility to another (e.g. Coriolis cross-cou-pling stimulation). They found that subjects who areextraordinarily sensitive to one form of motion tend tobe strongly susceptible to others as well. By contrast,for most individuals, susceptibility to one form of stim-ulation had little relation to susceptibility to another.Even more troubling, there was not comparablemotion sickness susceptibility for provocative condi-tions that otherwise seemed closely related, e.g. exe-cuting head movements during rotation in a slowrotation room versus in a rotating chair.
It is important to recognize that a given sign orsymptom of motion sickness may not have the samefunctional signiWcance for diVerent individuals. Forexample, some people when they experience nauseaand vomiting are basically incapacitated and unable toperform essential activities, and it may take hours after
123

394 Exp Brain Res (2006) 175:377–399
removal from the provocative situation for them torecover. By contrast, and more rarely, some subjectsmay vomit after a minute or two of exposure to provoc-ative stimulation, and then several minutes later mayhave recovered suYciently to continue exposure. Suchindividual diVerences in the relative signiWcance ofmotion sickness have not been taken into account inthe design and interpretation of questionnaires andpredictive tests of motion sickness.
Conclusions
Space motion sickness aVects nearly 70% of all astro-nauts and cosmonauts. It can develop within an hourafter launch and usually abates within 3 or 4 days. It ismost severe when the body is actively adjusting toweightlessness and sickness may reoccur upon landingduring readaptation to earth gravity. The physiologicalcharacteristics of space motion sickness parallel thoseof motion sickness on earth, except that pallor is notpresent. The engorgement of the venous return in theabsence of hydrostatic pressure in the circulatory sys-tem explains the absence of pallor in spaceXight.
The Xuid shift hypothesis has been a popular expla-nation of space motion sickness. However, neitherground-based experimental studies nor in-Xight obser-vations have provided support for it. Bed rest studiesalso do not evoke the motion sickness and disorienta-tion expected from a labyrinthine hydrops origin.Notions of increased cranial pressure are not convinc-ingly supported by available evidence, as well. The oto-lith asymmetry hypothesis, although intriguing, alsohas little experimental support. It potentially is a con-tributing factor but the other eVects one would expectfrom a central compensation for a vestibular imbalancethat is unmasked in weightlessness are absent, e.g. per-sisting sense of body tilt or displacement.
The key factor in eliciting space motion sicknessappears to be head movements, especially headmovements in pitch and roll. Both spaceXight andparabolic Xight experiments strongly support thisconclusion. The head movement contribution likelyreXects not only just an inXuence of abnormal pat-terns of vestibular input but also altered sensory-motor control of the head and body in a weightlessenvironment. Head loading during head movementson earth can evoke motion sickness in the presence ofnormal vestibular inputs. Head movements made dur-ing exposure to greater as well as less than 1 g back-ground force levels elicit motion sickness. Thispattern suggests that space motion sickness is not aunique disease entity.
Velocity storage of semicircular canal signals isaVected by exposure to weightlessness with storagebeing attenuated, at least initially, for both vestibulooc-ular reXexes as well as for generating a sense of bodyspatial displacement. Attenuation of velocity storage inweightless conditions explains why after initial adapta-tion to the space environment Coriolis cross-couplingstimulation of the semicircular canals is so much lessnauseating and disorienting. It also explains why astro-nauts and cosmonauts in spaceXight become so visuallydependent and subject to visual reorientation illusions.
Autogenic feedback training has been proposed as away of preventing and treating space motion sickness.The ground-based studies supporting this claim areseriously Xawed and carefully controlled studies fail toshow any beneWcial eVect. Treating advanced spacemotion sickness with injections of promethazine seemsthe best approach until better therapies can be devel-oped. In operational conditions, promethazine doesnot have as sedating an eVect as it does in laboratoryexperiments.
Many theories have been proposed to explain spacemotion sickness. The most adequate is the sensory con-Xict hypothesis. However, it is not a causal or mecha-nistic theory in the sense that one cannot specify inputvariables and predict a quantitative outcome. Never-theless, it is useful as a classiWcation scheme and fordesigning experiments until a more causal theory ormechanism can be developed or identiWed.
Ground-based models have been based on theassumption that situations that evoke symptoms char-acteristic of space motion sickness are potential toolsfor studying its etiology. Such analogies have little sci-entiWc merit. Parabolic Xight maneuvers to generateperiods of weightlessness are the only adequate ana-logue of spaceXight conditions. Periods of weightless-ness are brief however and alternate with periods ofhigh force. Consequently, systematic control condi-tions are essential in order to generate meaningfulresults. Any space-related events with long time con-stants will necessarily be missed.
At present, there are no adequate predictors of sus-ceptibility and severity of space motion sickness. Ques-tionnaires can identify those with a history of motionsickness under terrestrial conditions if the respondentsanswer honestly, but such protocols do not provideinsight into the individual’s ability to adapt to provoca-tive motion environments which may be more impor-tant than susceptibility given that 70% of astronautsand cosmonauts experience some degree of spacemotion sickness. This issue is particularly important forvery long duration space missions where a failure toadapt would be a major operational problem.
123

Exp Brain Res (2006) 175:377–399 395
Acknowledgments Support was provided by AFOSR grantFA9550-06-1-0102; NASA grants NAG9-1483; and NAG9-1466;NSBRI grant NA00701.
References
Abe K, Amatomi M, Kajiyama S (1970) Genetical and develop-mental aspects of susceptibility to motion sickness and frostbite. Hum Hered 30:507
Albery WB, Martin ET (1996) Development of space motionsickness in a ground-based human centrifuge. Acta Astro-naut 38:721–731
Alexander SJ, Cotzin M, Hill CJ, Ricciuti EA, Wendt GR (1955)Studies of motion sickness. X. Experimental proof that avia-tion cadets tell the truth on motion sickness history question-naires. J Psychol 39:403–409
Badeer HS (1998) Anatomical position of heart in snakes withvertical orientation: a new hypothesis. Comp Biochem Phys-iol A Mol Integr Physiol 119(1):403–405
Bagian JP (1991) First intramuscular administration in the U.S.Space Program. J Clin Pharmacol 31(10):920
Bagian JP, Ward DF (1994) A retrospective study of prometh-azine and its failure to produce the expected incidence ofsedation during space Xight. J Clin Pharmacol 34:649–651
Bakwin H (1971) Car-sickness in twins. Dev Med Child Neurol13:310
Balaban CD (1999) Vestibular autonomic regulation (includingmotion sickness and the mechanisms of vomiting). CurrOpin Neurol 12:29–33
Baloh RW, Honrubia V (1990) Clinical neurophysiology of thevestibular system. Contemporary neurology series 2nd edn.FA Davis Co, Philadelphia
von Baumgarten RJ (1986) European vestibular experiments on theSpacelab-1 mission: 1. Overview Exp Brain Res 64:239–246
von Baumgarten RJ (1987) General remarks on the role of thevestibular system in weightlessness. Arch Otorhinolaryngol244:135–142
von Baumgarten RJ, Thumler R (1979) A model for vestibularfunction in altered gravitational states. Life Sci Space Res17:161–170
von Baumgarten RJ, Vogel H, Kass JR (1981) Nauseogenic prop-erties of various dynamic and static force environments.Acta Astronaut 8:1005–1013
Bles W (1998) Coriolis eVects and motion sickness modeling.Brain Res Bull 47(5):543–549
Bles W, de Jong HAA, Oosterveld WJ (1984) Prediction of sea-sickness susceptibility. AGARD Conf Proc 372:27
Bles W, de Graaf B, Bos JE, Groen E, Krol JR (1997) A sustainedhyper-g load as a tool to simulation space motion sickness.J Gravit Physiol 4(2):p1–p4
Bles W, Bos JE, de Graaf B, Groen E, Wertheim AH (1998) Mo-tion sickness: only one provocative conXict? Brain Res Bull47(5):481–487
Bos JE, Bles W (1998) Modeling motion sickness and subjectivevertical mismatch detailed for vertical motions. Brain ResBull 47(5):537–542
Bryan A, Ventura J, Bortolami SB, DiZio P, Lackner JR (2004)Localization of subjective vertical and head midline in al-tered gravitoinertial force environments. Soc Neurosci Abst
Cheung B, Hofer K (1998) Lack of gender diVerence in motionsickness induced by vestibular Coriolis cross-coupling. J Ves-tib Res 12(4):191–200
Cheung B, Vaitkus P (1998) Perspectives of electrogastrographyand motion sickness. Brain Res Bull 47(5):421–431
Cheung BSK, Money KE, Jacobs I (1990) Motion sickness sus-ceptibility and aerobic Wtness: a longitudinal study. AviatSpace Environ Med 61:210–204
Cheung BS, Howard IP, Money KE (1991) Visually induced sick-ness in normal and bilaterally labyrinthine-defective sub-jects. Aviat Space Environ Med 62(6):527–531
Cheung B, Heskin R, Hofer K, Gagnon M (2001) The menstrualcycle and susceptibility to Coriolis-induced sickness. J VestibRes 11(2):129–136
Clemes SA, Howarth PA (2005) The menstrual cycle and suscep-tibility to virtual simulation sickness. J Biol Rhythms20(1):71–82
Cohen B, Matsuo V, Raphan T (1977) Quantitative analysis ofthe velocity characteristics of optokinetic nystagmus andoptkinetic afternystagmus. J Physiol Lond 270:321–344
Cohen B, Dai M, Raphan T (2003) The critical role of velocitystorage in production of motion sickness. Ann N Y Acad Sci1004:359–376
Correia MJ, Hixon WC, Niven JI (1968) On predictive equationsfor subjective judgments of vertical and horizon in a forceWeld. Acta Otolaryngol Suppl 230:3–20
Costa F, Lavin P, Robertson D, Biaggioni I (1995) EVect of neu-rovestibular stimulation on autonomic regulation. Clin Au-ton Res 5(5):289–293
Cowings PS, Toscano WB (1982) The relationship of motion sick-ness susceptibility to learned autonomic control for symptomsuppression. Aviat Space Environ Med 53(6):570–575
Cowings IS, Toscano WB (2000) Autogenic-feedback trainingexercise is superior to promethazine for control of motionsickness symptoms. J Clin Pharmacol 40:1154–1165
Cowings PS, Billingham J, Toscano B (1977) Learned control ofautonomic responses to compensate for the debilitatingeVects of motion sickness. Theory Psychosom Med 4:318–323
Cowings PS, Suter S, Toscano WB, Kamiya J, Naifeh K (1986)General autonomic components of motion sickness. Psycho-physiology 3:542
Cowings PS, Naifeh KH, Toscano WB (1995) The stability ofindividual patterns of autonomic response to motion sick-ness stimulation. Aviat Space Environ Med 61:399–405
Cowings PS, Toscano WB, DeRoshia C, Miller NE (2000) Pro-methazine as a motion sickness treatment: impact on humanperformance and mood states. Aviat Space Environ Med71:1013–1022
Cramer DB, Graybiel A, Oosterveld WI (1976) Successful trans-fer of adaptation acquired in a slow rotation room to motionenvironments in Navy Xight training. In: AGARD CP-203,C2-1, Recent advances in space medicine
Dai M, Kunin M, Raphan T, Cohen B (2003) The relation of mo-tion sickness to the spatial-temporal properties of velocitystorage. Exp Brain Res 151:173–189
Dai M, Raphan T, Cohen B (2006) EVects of baclofen on theangular vestibulo-ocular reXex. Exp Brain Res 171:262–271
Davis JR, Vanderploeg JM, Santy PA, Jennings RT, Stewart DF(1988) Space motion sickness during 24 Xights of the spaceshuttle. Aviat Space Environ Med 59(12):1185–1189
Davis JR, Jennings RT, Beck BG, Bagian JP (1993a) TreatmenteYcacy of intramuscular promethazine for space motionsickness. Aviat Space Environ Med 64:230–233
Davis JR, Jennings RT, Beck BG (1993b) Comparison of treat-ment strategies for space motion sickness. Acta Astronaut29:587–591
de Graaf B, Bles W, Bos JE (1998) Roll motion stimuli: sensoryconXict, perceptual weighting and motion sickness. BrainRes Bull 47(5):489–495
de Wit G (1953) Seasickness. J Am Med Assoc 86:319–324
123
396 Exp Brain Res (2006) 175:377–399
Diamond SG, Markham CH (1988) Ocular torsion in upright andtilted positions during hypo- and hypergravity of parabolicXight. Aviat Space Environ Med 59:1158–1162
Diamond SG, Markham CH (1991a) Otolith function in hypo-and hypergravity: relation to space motion sickness. ActaOtolaryngol Suppl (Stockh) 418:19–22
Diamond SG, Markham CH (1991b) Prediction of space motionsickness susceptibility by disconjugate eye torsion in para-bolic Xight. Aviat Space Environ Med 62:201–205
Diamond SG, Markham CH (1992) Validating the hypothesis ofotolith asymmetry as a cause of space motion sickness. AnnN Y Acad Sci 656:725–731
Diamond SG, Markham CH, Money KE (1990) Instability of oc-ular torsion in zero gravity: possible implications for spacemotion sickness. Aviat Space Environ Med 61:899–905
DiZio P, Lackner JR (1988) The eVects of gravitoinertial forcelevel and head movements on post-rotational nystagmus andillusory after-rotation. Exp Brain Res 70:485–495
DiZio P, Lackner JR (1991) Motion sickness susceptibility inparabolic Xight and velocity storage activity. Aviat SpaceEnviron Med 62:300–307
DiZio P, Lackner JR (2000) Motion sickness side eVects and af-ter-eVects of immersive virtual environments created withhelmet-mounted visual displays. In: NATO RTO-MP-54,The capability of virtual reality to meet military require-ments, pp 11-1–11-4
DiZio P, Lackner JR (2002) Proprioceptive adaptation and after-eVects. In: Stanney K (ed) Handbook of virtual environ-ments. Lawrence Erlbaum Associates, NY, pp 751–771
DiZio P, Lackner JR, EvanoV JN (1987a) The inXuence of gravit-ointertial force level on oculomotor and perceptual respons-es to Coriolis, cross-coupling stimulation. Aviat SpaceEnviron Med 58:A218–A223
DiZio P, Lackner JR, EvanoV JN (1987b) The inXuence of gravi-toinertial force level on oculomotor and perceptual respons-es to sudden-stop stimulation. Aviat Space Environ Med58:A224–A230
Dobie TG (1974) Airsickness in aircrew. AGARDograph No.177. Technical Editing and Reproduction Ltd, London
Doweck I, Gordon CR, Shlitner A, Spitzer O, Gonen A, Binah O,Melamed Y, Shupak A (1997) Alterations in R-R variabilityassociated with experimental motion sickness. J Auton NervSyst 67:31–37
Egorov BB, Samarin GI (1970) Possible changes in paired work-ing of the vestibular system during weightlessness. KosmBiol Med 4(2):85–86
Golding JF, Stott JR (1995) EVect of sickness severity on habitu-ation to repeated motion challenges in aircrew referred forair sickness treatment. Aviat Space Environ Med 66:625–630
Golding JF, Stott JR (1997a) Comparison of the eVects of a selec-tive muscarinic receptor antagonist and hyoscine (scopol-amine) on motion sickness, skin conductance and heart rate.Br J Clin Pharmacol 43:633–637
Golding JF, Stott JR (1997b) Objective and subjective time cours-es of recovery from motion sickness assessed by repeatedmotion challenges. J Vestib Res 7(6):421–428
Golding JF, Kadzere P, Gresty MA (2005) Motion sickness sus-ceptibility Xuctuates through the menstral cycle. Aviat SpaceEnviron Med 76(10):970–973
Gordon CR, Ben-Aryeh H, Szargel R, Attias J (1989) Salivarychanges associated with seasickness. J Auton Nerv Syst 26:37
Graebe A, Schuck EL, Lensing P, Putcha L, Derendorf H (2004)Physiological, pharmacokinetic, and pharmacodynamicchanges in space. J Clin Pharmacol 44(8):837–853
Graybiel A (1969) Structural elements in the concept of motionsickness. Aerosp Med 40:351–367
Graybiel A (1974) Measurement of otolith function in man. In:Kornhuber HH (ed) Handbook of sensory physiology, chap11. Springer, Berlin Heidelberg New York, pp 233–266
Graybiel A (1980) Space motion sickness: Skylab revisited. AviatSpace Environ Med 51:814
Graybiel A, Johnson WH (1963) A comparison of the symptom-atology experienced by healthy persons and subjects withloss of labyrinthine function when exposed to unusual pat-terns of centripetal force in a counter-rotating room. AnnOtorhinolaryngol 72:1–17
Graybiel A, Knepton J (1976) Sopite syndrome: a sometimes solemanifestation of motion sickness. Aviat Space Environ Med47(8):873–882
Graybiel A, Lackner JR (1977) Comparison of susceptibility tomotion sickness during rotation at 30 rpm in the earth-hori-zontal, 10° head-up, and 10° head-down positions. AviatSpace Environ Med 48:7–11
Graybiel A, Lackner JR (1979) Rotation at 30 rpm about the z-axis after 6 hours in the 10° head-down position: eVect onsusceptibility to motion sickness. Aviat Space Environ Med50:390–392
Graybiel A, Lackner JR (1980a) A sudden-stop vestibulovisualtest for rapid assessment of motion sickness manifestations.Aviat Space Environ Med 51:21–23
Graybiel A, Lackner JR (1980b) Evaluation of the relationshipbetween motion sickness symptomatology and blood pres-sure, heart rate, and body temperature. Aviat Space EnvironMed 51:211–214
Graybiel A, Lackner JR (1987) Treatment of severe motion sick-ness with antimotion sickness drug injections. Aviat SpaceEnviron Med 58:773–776
Graybiel A, Niven JI (1953) The absence of residual eVects attrib-utable to the otolith organs following unilateral labyrinthec-tomy in man. Laryngoscope 63:18–30
Graybiel A, Wood C, Miller E, Cramer D (1968) Diagnosticcriteria for grading the severity of acute motion sickness.Bureau of Medicine and Surgery, NASA Order R93, Pensa-cola, FL, Naval Aerospace Institute
Graybiel A, Deane FR, Colehour JK (1969) Prevention of overtmotion sickness by incremental exposure to otherwise highlystressful Coriolis accelerations. Aerosp Med 40:142–148
Graybiel A, Miller EF II, Homick JL (1972) Experiment M131:human vestibular function. In: Proceedings of the Skylab lifesciences symposium, NASA TMX-58154, vol I
Graybiel A, Miller EF II, Homick JL (1975) Individual diVerencein susceptibility to motion sickness among six Skylab astro-nauts. Acta Astronaut 2:155–174
Graybiel A, Miller EF II, Homick JL (1977) Experiment M131:human vestibular function. In: Biomedical results for Skylab,NASA SP-377, US Govt Print OYce, pp 74–103
Groen JJ (1957) Adaptation. Pract Otorhinolaryngol 19:525–530Grunfeld E, Gresty MA (1998) Relationship between motion
sickness, migraine and menstruation in crew members ofa “round the world” yacht race. Brain Res Bull 47(5):433–436
Guignard JC, McCauley ME (1990) The accelerative stimulusfor motion sickness. In: Crampton GH (ed) Motion andspace motion sickness. CRC Press, West Palm Beach, pp123–151
Gurovskiy NN, Bryanov II, Yegorov AD (1975) Changes in ves-tibular function during space Xight. Acta Astonaut 2(3–4):207–216
Hardacre LE, Kennedy RS (1965) Some issues in the develop-ment of a motion sickness questionnaire for Xight students.Bur Med Surg, Proj MR005 13-6002, Subtask 1, Report No.104, USN School Aviation Medicine, Pensacola
123

Exp Brain Res (2006) 175:377–399 397
Harm DL (1990) Physiology of motion sickness symptoms. In:Crampton GH (ed) Motion and space motion sickness, CRCPress, West Palm Beach, pp 153–177
Harm DL, Parker DE (1994) PreXight adaptation training forspatial orientation and space motion sickness. J Clin Phar-macol 34(6):618–627
Harm DL, Schlegel TT (2002) Predicting motion sickness duringparabolic Xight. Autonomic Neurosci 97:116–121
Homick JL, Reshke MF, Vanderploeg JM (1984) Space adapta-tion syndrome: incidence and operational implications forthe space transportation system program. In: Motion sick-ness: mechanisms, prediction, prevention and treatment,AGARD conference proceeding no. 372, Neuilly sur Seine,France, 36–1
Hu S, Stern RM (1998) Optokinetic nystagmus correlates withseverity of vection-induced motion sickness and gastrictachyarrhythmia. Aviat Space Environ Med 69:1162–1165
Hu S, McChesney KA, Player KA, Bahl AM, Buchanan JB, Sco-zzafava JE (1999) Systematic investigation of physiologicalcorrelates of motion sickness induced by viewing an optoki-netic rotating drum. Aviat Space Environ Med 70(8):759–765
Jennings RT (1998) Managing space motion sickness. J VestibRes 8:67–70
Johnson WH (1974) Motion sickness, Part 1. Etiology and auto-nomic eVects. In: Kornhuber HH (ed) Handbook of sensoryphysiology, vol VI/2. Springer, Berlin Heidelberg New York
Johnson WH, Sunahara FA, Landolt JP (1993) Motion sickness,vascular changes accompanying pseudo-Coriolis-inducednausea. Aviat Space Environ Med 64:367–370
Johnson WH, Sunahara FA, Landolt JP (1999) Importance of thevestibular system in visually induced nausea and self-vection.J Vestib Res 9(2):83–87
Jozsvai EE, Pigeau RA (1996) The eVects of autogenic trainingand biofeedback on motion sickness tolerance. Aviat SpaceEnviron Med 67:963–968
Kakurin LI, Kuzmin MP, Matsnev EI, Mikhailov VM (1976)Physiological eVects induced by antiorthostatic hypokinesia.Life Sci Space Res 14:101–108
Kaufman GD, Wood SJ, Gianna CC, Black FO, Paloski WH(2001) Spatial orientation and balance control changes in-duced by altered gravitoinertial force vectors. Exp Brain Res137:397–410
Kiernan BD, Soykan I, Lin Z, Dale A, McCallum RW (1997) Anew nausea model in humans produces mild nausea withoutelectrogastrogram and vasopressin changes. Neurogastroen-terol Motil 9(4):257–263
Koch KL (1993) Motion sickness. In: Sleisenger MH (ed) Hand-book of nausea and vomiting. Parthenon, NY
Koch KL (1999) Illusory self-motion and motion sickness: a mod-el for brain-gut interactions and nausea. Dig Dis Sci 44(8Suppl):53S–57S
Lackner JR, DiZio P (1989) Altered sensorimotor control of thehead as an etiological factor in space motion sickness. Per-cept Mot Skills 8:784–786
Lackner JR, DiZio P (2000a) Aspects of body self-calibration.Trends Cogn Sci 4:279–288
Lackner JR, DiZio P (2000b) ArtiWcial gravity as a countermea-sure in long duration space Xight. J Neurosci Res 62:169–176
Lackner JR, Graybiel A (1984) Elicitation of motion sickness byhead movements in the microgravity phase of parabolic Xightmaneuvers. Aviat Space Environ Med 55:513-520
Lackner JR, Graybiel A (1985) Head movements elicit motionsickness during exposure to microgravity and macrogravityacceleration levels. In: Igarashi M, Black FO (eds) Proceedingsof the VII international symposium: vestibular and visual
control of posture and locomotor equilibrium. Karger, Basel,pp 170-176
Lackner JR, Graybiel A (1986a) The eVective intensity of Corio-lis, cross-coupling stimulation is gravitoinertial force depen-dent: implications for space motion sickness. Aviat SpaceEnviron Med 57:229-235
Lackner JR, Graybiel A (1986b) Sudden emesis following para-bolic Xight maneuvers: implications for space motion sick-ness. Aviat Space Environ Med 57:343-347
Lackner JR, Graybiel A (1994) Use of promethazine to hasten adap-tation to provocative motion. J Clin Pharmacol 34:644–648
Lackner JR, Teixeira R (1977) Optokinetic motion sickness: con-tinuous head movements attenuate the visual induction ofapparent self-rotation and symptoms of motion sickness.Aviat Space Environ Med 48:248-253
Lackner JR, Graybiel A, Johnson WH, Money KE (1987) Asym-metric otolith function and increased susceptibility to motionsickness during exposure to variations in gravitoinertialacceleration level. Aviat Space Environ Med 58:652–657
Lackner JR, Ventura J, DiZio P (2006) Dynamic spatial orientationin altered gravitoinertial force environments. Soc NeurosciAbst, 244.11
Lang IM (1992) New perspectives on the mechanisms controllingvomitus expulsion. In: Bianchi AL, Grelot L, Milelr AD, KingGL (eds) Mechanisms and control of emesis, vol 223. ColloqueINSERM/John Libbey Eurotext Montrouge, France
Lang IM (1999) Noxious stimulation of emesis. Dig Dis Sci 44(8Suppl):58S–63S
Lawson BD (1993) Physiological responses to visually-inducedmotion sickness. Brandeis University PhD dissertation, Wal-tham, MA
Lentz JM (1976) Nystagmus, turning sensations, and illusorymovement in motion sickness susceptibility. Aviat SpaceEnviron Med 47(9):931–936
Lentz JM, Collins WE (1977) Motion sickness susceptibility andrelated behavioral characteristics in men and women. AviatSpace Environ Med 48(4):316–322
Lillywhite HB (1996) Gravity, blood circulation, and the adapta-tion of form and function in lower vertebrates. J Exp Zool275:217–225
Lucot JB (1998) Pharamcology of motion sickness. J Vestib Res8:61–66
Markham CH, Diamond SG (1992) Further evidence to supportdisconjugate eye torsion as a predictor of space motion sick-ness. Aviat Space Environ Med 63:118–121
Markham CH, Diamond SG (1993) A predictive test for spacemotion sickness. J Vestib Res 3(3):289–295
Markham CH, Diamond SG, Stoller DF (2000) Parabolic Xightreveals independent binocular control of otolith-induced eyetorsion. Arch Ital de Biol 138:736–86
Matsnev EI, Yakovleva IY, Tarasov IK, Alekseev VN, KornilovaLN, Mateev AD, Gorgiladze GI (1983) Space motion sick-ness: phenomenology, countermeasures, and mechanisms.Aviat Space Environ Med 54:312–317
McClure JA, Fregly AR (1972) EVect of environmental tempera-ture on sweat onset during motion sickness. Aerosp Med43:959
Miller AD (1991) Motion-induced nausea and vomiting. In: Ku-charczyk J, Steward DJ, Miller AD (eds) Nausea and vomit-ing: Recent Research and Clinical Advances, chap 2. CRCPress, Boca Raton
Miller EF II, Graybiel A (1970a) The eVect of gravitoinertialforce upon ocular counterrolling. J Appl Phsyiol 31:697–700
Miller EF II, Graybiel A (1970b) A provocative test for gradingsusceptibility to motion sickness yielding a single numericalscore. Acta Otolaryngol Stockh Suppl 274
123
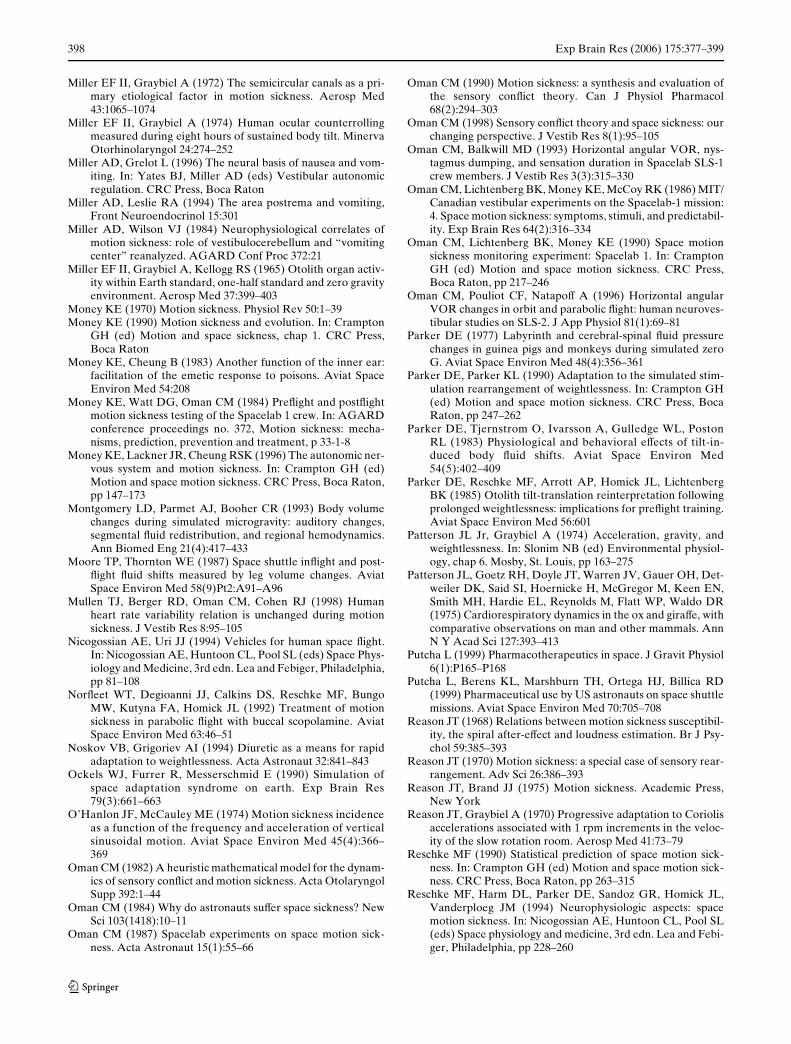
398 Exp Brain Res (2006) 175:377–399
Miller EF II, Graybiel A (1972) The semicircular canals as a pri-mary etiological factor in motion sickness. Aerosp Med43:1065–1074
Miller EF II, Graybiel A (1974) Human ocular counterrollingmeasured during eight hours of sustained body tilt. MinervaOtorhinolaryngol 24:274–252
Miller AD, Grelot L (1996) The neural basis of nausea and vom-iting. In: Yates BJ, Miller AD (eds) Vestibular autonomicregulation. CRC Press, Boca Raton
Miller AD, Leslie RA (1994) The area postrema and vomiting,Front Neuroendocrinol 15:301
Miller AD, Wilson VJ (1984) Neurophysiological correlates ofmotion sickness: role of vestibulocerebellum and “vomitingcenter” reanalyzed. AGARD Conf Proc 372:21
Miller EF II, Graybiel A, Kellogg RS (1965) Otolith organ activ-ity within Earth standard, one-half standard and zero gravityenvironment. Aerosp Med 37:399–403
Money KE (1970) Motion sickness. Physiol Rev 50:1–39Money KE (1990) Motion sickness and evolution. In: Crampton
GH (ed) Motion and space sickness, chap 1. CRC Press,Boca Raton
Money KE, Cheung B (1983) Another function of the inner ear:facilitation of the emetic response to poisons. Aviat SpaceEnviron Med 54:208
Money KE, Watt DG, Oman CM (1984) PreXight and postXightmotion sickness testing of the Spacelab 1 crew. In: AGARDconference proceedings no. 372, Motion sickness: mecha-nisms, prediction, prevention and treatment, p 33-1-8
Money KE, Lackner JR, Cheung RSK (1996) The autonomic ner-vous system and motion sickness. In: Crampton GH (ed)Motion and space motion sickness. CRC Press, Boca Raton,pp 147–173
Montgomery LD, Parmet AJ, Booher CR (1993) Body volumechanges during simulated microgravity: auditory changes,segmental Xuid redistribution, and regional hemodynamics.Ann Biomed Eng 21(4):417–433
Moore TP, Thornton WE (1987) Space shuttle inXight and post-Xight Xuid shifts measured by leg volume changes. AviatSpace Environ Med 58(9)Pt2:A91–A96
Mullen TJ, Berger RD, Oman CM, Cohen RJ (1998) Humanheart rate variability relation is unchanged during motionsickness. J Vestib Res 8:95–105
Nicogossian AE, Uri JJ (1994) Vehicles for human space Xight.In: Nicogossian AE, Huntoon CL, Pool SL (eds) Space Phys-iology and Medicine, 3rd edn. Lea and Febiger, Philadelphia,pp 81–108
NorXeet WT, Degioanni JJ, Calkins DS, Reschke MF, BungoMW, Kutyna FA, Homick JL (1992) Treatment of motionsickness in parabolic Xight with buccal scopolamine. AviatSpace Environ Med 63:46–51
Noskov VB, Grigoriev AI (1994) Diuretic as a means for rapidadaptation to weightlessness. Acta Astronaut 32:841–843
Ockels WJ, Furrer R, Messerschmid E (1990) Simulation ofspace adaptation syndrome on earth. Exp Brain Res79(3):661–663
O’Hanlon JF, McCauley ME (1974) Motion sickness incidenceas a function of the frequency and acceleration of verticalsinusoidal motion. Aviat Space Environ Med 45(4):366–369
Oman CM (1982) A heuristic mathematical model for the dynam-ics of sensory conXict and motion sickness. Acta OtolaryngolSupp 392:1–44
Oman CM (1984) Why do astronauts suVer space sickness? NewSci 103(1418):10–11
Oman CM (1987) Spacelab experiments on space motion sick-ness. Acta Astronaut 15(1):55–66
Oman CM (1990) Motion sickness: a synthesis and evaluation ofthe sensory conXict theory. Can J Physiol Pharmacol68(2):294–303
Oman CM (1998) Sensory conXict theory and space sickness: ourchanging perspective. J Vestib Res 8(1):95–105
Oman CM, Balkwill MD (1993) Horizontal angular VOR, nys-tagmus dumping, and sensation duration in Spacelab SLS-1crew members. J Vestib Res 3(3):315–330
Oman CM, Lichtenberg BK, Money KE, McCoy RK (1986) MIT/Canadian vestibular experiments on the Spacelab-1 mission:4. Space motion sickness: symptoms, stimuli, and predictabil-ity. Exp Brain Res 64(2):316–334
Oman CM, Lichtenberg BK, Money KE (1990) Space motionsickness monitoring experiment: Spacelab 1. In: CramptonGH (ed) Motion and space motion sickness. CRC Press,Boca Raton, pp 217–246
Oman CM, Pouliot CF, NatapoV A (1996) Horizontal angularVOR changes in orbit and parabolic Xight: human neuroves-tibular studies on SLS-2. J App Physiol 81(1):69–81
Parker DE (1977) Labyrinth and cerebral-spinal Xuid pressurechanges in guinea pigs and monkeys during simulated zeroG. Aviat Space Environ Med 48(4):356–361
Parker DE, Parker KL (1990) Adaptation to the simulated stim-ulation rearrangement of weightlessness. In: Crampton GH(ed) Motion and space motion sickness. CRC Press, BocaRaton, pp 247–262
Parker DE, Tjernstrom O, Ivarsson A, Gulledge WL, PostonRL (1983) Physiological and behavioral eVects of tilt-in-duced body Xuid shifts. Aviat Space Environ Med54(5):402–409
Parker DE, Reschke MF, Arrott AP, Homick JL, LichtenbergBK (1985) Otolith tilt-translation reinterpretation followingprolonged weightlessness: implications for preXight training.Aviat Space Environ Med 56:601
Patterson JL Jr, Graybiel A (1974) Acceleration, gravity, andweightlessness. In: Slonim NB (ed) Environmental physiol-ogy, chap 6. Mosby, St. Louis, pp 163–275
Patterson JL, Goetz RH, Doyle JT, Warren JV, Gauer OH, Det-weiler DK, Said SI, Hoernicke H, McGregor M, Keen EN,Smith MH, Hardie EL, Reynolds M, Flatt WP, Waldo DR(1975) Cardiorespiratory dynamics in the ox and giraVe, withcomparative observations on man and other mammals. AnnN Y Acad Sci 127:393–413
Putcha L (1999) Pharmacotherapeutics in space. J Gravit Physiol6(1):P165–P168
Putcha L, Berens KL, Marshburn TH, Ortega HJ, Billica RD(1999) Pharmaceutical use by US astronauts on space shuttlemissions. Aviat Space Environ Med 70:705–708
Reason JT (1968) Relations between motion sickness susceptibil-ity, the spiral after-eVect and loudness estimation. Br J Psy-chol 59:385–393
Reason JT (1970) Motion sickness: a special case of sensory rear-rangement. Adv Sci 26:386–393
Reason JT, Brand JJ (1975) Motion sickness. Academic Press,New York
Reason JT, Graybiel A (1970) Progressive adaptation to Coriolisaccelerations associated with 1 rpm increments in the veloc-ity of the slow rotation room. Aerosp Med 41:73–79
Reschke MF (1990) Statistical prediction of space motion sick-ness. In: Crampton GH (ed) Motion and space motion sick-ness. CRC Press, Boca Raton, pp 263–315
Reschke MF, Harm DL, Parker DE, Sandoz GR, Homick JL,Vanderploeg JM (1994) Neurophysiologic aspects: spacemotion sickness. In: Nicogossian AE, Huntoon CL, Pool SL(eds) Space physiology and medicine, 3rd edn. Lea and Febi-ger, Philadelphia, pp 228–260
123

Exp Brain Res (2006) 175:377–399 399
Severac A (1992) Electrical vestibular stimulation and space mo-tion sickness. Acta Astronaut 28:401–408
Simanonok KE, Charles JB (1994) Space sickness and Xuid shifts:a hypothesis. J Clin Pharmacol 34(6):652–663
Staut CS, Toscano WB, Cowings PS (1995) Reliability of psycho-physiological responses across multiple motion sicknessstimulation tests. J Vestib Res 5:25–33
Stern RM, Koch KL, Leibowitz HW, Linblad IM, Shupert CL,Stewart WR (1985) Tachygastria and motion sickness. AviatSpace Environ Med 56:1074–1077
Stern RM, Koch KL, Stewart WR, Lindblad IM (1987a) Spectralanalysis of tachgastria recorded during motion sickness. Gas-troenterology 92:92–97
Stern RM, Koch KL, Stewart WR, Vasey MW (1987b) Electro-gastrography: current issues in validation and methodology.Psychophysiology 24:55
Stern RM, Hu S, Vasey MW, Koch KL (1989) Adaptation to vec-tion-induced symptoms of motion sickness. Aviat SpaceEnviron Med 60:566–572
Stern RM, Koch KL, Vasey MW (1990) The gastrointestinal sys-tem. In: Cacioppo JT, Tassinary (eds) Principles of psycho-physiology (physical, social and inferential elements).Cambridge University Press, Boston, pp 554–579
Stern RM, Uijtdehaage SHJ, Muth ER, Xu LH, Koch KL (1996)Asian hypersusceptibility to motion sickness. Hum Hered46(1):7–14
Sunahara FA, Farewell J, Mintz L, Johnson WH (1987) Pharma-cological interventions for motion sickness: cardiovasculareVects. Aviat Space Environ Med 58(9Suppl):A270–A276
Teixeira RA, Lackner JR (1979) Optokinetic motion sickness:attenuation of visually-induced apparent self-rotation bypassive head movements. Aviat Space Environ Med 50:264-266
Thornton WE, Moore TP, Pool SL (1987a) Fluid shifts in weight-lessness. Aviat Space Environ Med 58(9)Pt2: A986–A980
Thornton WE, Moore TP, Pool SL, Vanderploeg J (1987b) Clin-ical characterization and etiology of space motion sickness.Aviat Space Environ Med 58:A1–A8
Thornton WE, Linder BJ, Moore TP, Pool SL (1987c) Gastroin-testinal motility in space motion sickness. Aviat Space Envi-ron Med 58:A16–21
Titov G, Caidin M (1962) I am eagle. Bobbs Merrill, IndianapolisToscano WB, Cowings PS (1982) Reducing motion sickness: a
comparison of autogenic-feedback training and an alterna-tive cognitive task. Aviat Space Environ Med 53(5):449–453
Treisman M (1977) Motion sickness: an evolutionary hypothesis.Science 197:493
Turner M, GriYn MJ (1995) Motion sickness incidence during around-the-world yacht race. Avait Space Environ Med66(9):849–856
Tyler DB, Bard P (1949) Motion sickness. Physiol Rev 29:311–369
Van Citters RL, Kemper WS, Franklin DL (1968) Blood Xow andpressure in the giraVe carotid artery. Comp Biochem Physiol24:1035–1042
Wendt GR (1948) Of what importance are psychological factorsin motion sickness? J Aviat Med 19:24–33
Williams DR (2003) The biomedical challenges of space Xight.Ann Rev Med 54:245–256
Wilson VJ, Melvill Jones G (1979) Mammalian vestibular physi-ology. Plenum, NY
Wood CD, Graybiel A (1968) Evaluation of sixteen antimotionsickness drugs under controlled laboratory conditions. Aer-osp Med 39:1341–1344
Wood CD, Stewart JJ, Wood MJ, Manno JE, Manno BR, MimsME (1990) Therapeutic eVects of antimotion sickness medi-cations on the secondary symptoms of motion sickness. Avi-at Space Environ Med 61:157–161
Woodman PD, GriYn MJ (1997) EVect of direction of headmovement on motion sickness caused by Coriolis stimula-tion. Aviat Space Environ Med 68:93–98
Wright WG, DiZio P, Lackner JR (2005) Vertical linear self-mo-tion perception during visual and actual-inertial stimulation:more than weighted summation of sensory inputs. J VestibRes 16:23–28
Yates BJ (1996) Vestibular inXuences on the autonomic nervoussystem. Ann N Y Acad Sci 781:458–473
Yates BJ (1998) Autonomic reaction to vestibular damage. Oto-laryngol Head Neck Surg 119:106–112
Yates BJ (2004) The vestibular system and cardiovascular re-sponses to altered gravity. Am J Physiol 286(1):R22
Yates BJ, Miller AD (1996) Vestibular autonomic regulation.CRC Press, Boca Raton
Yates BJ, Kerman IA (1998) Post-spaceXight orthostatic intoler-ance: possible relationship to microgravity-induced plasticityin the vestibular system. Brain Res Rev 28:73–82
Yates BJ, Bronstein AM (2005) The eVects of vestibular systemlesions on autonomic regulation: observations, mechanisms,and clinical implications. J Vestib Res 15(3):119–129
Yates BJ, Miller AD, Lucot JB (1998) Physiological basis andpharmacology of motion sickness: an update. Brain Res Bull47(5):395–406
Yates BJ, Aoki M, Burchill P, Bronstein AM, Gresty MA (1999)Cardiovascular responses elicited by linear acceleration inhumans. Exp Brain Res 125:476–484
Yates BJ, Holmes MJ, Jian BJ (2000) Adaptive plasticity in ves-tibular inXuences on cardiovascular control. Brain Res Bull53(1):3–9
Yates BJ, Billig I, Cotter LA (2002) Role of the vestibular systemin regulating respiratory muscle activity during movement.Clin Exp Pharmacol Physiol 29(1, 2):112–117
Yates BJ, Holmes MJ, Jian BJ (2003) Plastic changes in process-ing of graviceptive signals during spaceXight potentially con-tribute to post-Xight orthostatic intolerance. J Vestib Res13(4–6):395–404
123
Related Documents











