Soluble vascular cell adhesion molecule-1 (sVCAM-1) is an independent prognostic marker in Hodgkin’s disease I LSE C HRISTIANSEN, 1 C HRISTER S UNDSTRO ¨ M, 2 G UNILLA E NBLAD 3 AND T HOMAS H. T O ¨ TTERMAN 1 1 Department of Clinical Immunology and Transfusion Medicine, 2 Department of Pathology, and 3 Department of Oncology, University Hospital, Uppsala, Sweden Received 16 February 1998; accepted for publication 14 May 1998 Summary. Serum levels of soluble vascular cell adhesion molecule-1 (sVCAM-1, sCD106) were significantly elevated in patients with Hodgkin’s disease (HD) (n ¼ 101) compared to controls (n ¼ 31) (P < 0·0001). sVCAM-1 correlated with histology, stage, B-symptoms, and prognostic markers (sICAM-1, sCD30, sIL-2R, LDH). sVCAM-1, sICAM-1 and sCD30 added independent prognostic information for both disease-free and overall survival. 14 biopsies from 13 patients with HD were immunostained for VCAM-1 and ICAM-1. The vascular endothelium stained positive for VCAM-1 in 10/12 evaluable biopsies and for ICAM-1 in all evaluable biopsies. A stromal expression of both adhesion molecules precluded a precise evaluation of HRS-cells. This led us to investigate VCAM-1 (and ICAM-1) expression in six Hodgkin cell lines (HDLM-2, L428, L540, L591, DEV, KM- H2). Two cell lines stained positive for VCAM-1 (HDLM-2, L591). All cell lines stained positive for ICAM-1. sVCAM-1 is a new prognostic marker in HD; its predictive power equals or surpasses that of sCD30 and sICAM-1. Furthermore, two Hodgkin cell lines stained positive for VCAM-1. This indicates that VCAM-1 may be expressed by some HD tumour cells in vivo. Keywords: Hodgkin’s disease, sVCAM-1, sICAM-1, prognos- tic markers, cell lines. Adhesion molecules play a crucial role in the immune system by promoting cell–cell and cell–stroma interactions and leucocyte trafficking (Carlos & Harlan, 1994). Soluble counterparts of adhesion molecules, probably derived through proteolytic cleavage (Bazil, 1995) of the corre- sponding cellular transmembrane molecules, have been suggested to competitively inhibit the action of the receptor– ligand pairs by binding to and blocking the respective ligands (Welder et al, 1993; Becker et al, 1993; Meyer et al, 1995). This may represent a mechanism for malignant cells to escape immune surveillance and may be a possible explana- tion for tumour dissemination and metastasis (Becker et al, 1991). Vascular cell adhesion molecule-1 (VCAM-1, CD106) and intercellular adhesion molecule-1 (ICAM-1, CD54) are both members of the immunoglobulin gene superfamily. VCAM-1 is constitutively expressed at low levels by bone marrow stromal cells (Juneja et al, 1993), can be induced on vascular endothelial cells and follicular dendritic cells (FDCs), and is up-regulated on marrow stromal cells by cytokines such as tumour necrosis factor-a (TNF-a), interleukin (IL)-1, IL-4 and IL-13 (Rice et al, 1991; Carlos et al, 1990; Thornhill & Haskard, 1990; Bochner et al, 1995; Dittel et al, 1993). ICAM-1, an adhesion molecule also inducible by IL-1, TNF-a and IL-4, is widely distributed among haemopoietic and non-haemopoietic cells (Larsson & Springer, 1990; Rothlein et al, 1988). In Hodgkin’s disease (HD) the origin of the tumour cells, i.e. the Hodgkin and Reed-Sternberg (HRS) cells, is still enigmatic, although accumulating data suggest a B-cell origin (Gruss et al, 1997). In HD of nodular lymphocyte predominance (LP) histology, however, tumour cells are unequivocally of B-lymphocyte lineage (Poppema, 1992). In contrast to other primary lymph node malignancies, the tumour cells in HD constitute only a small fraction of all cells of involved nodes; the majority of cells appear to represent inflammatory cells such as eosinophils and T lymphocytes (Gruss et al, 1997). ICAM-1 is overexpressed not only by HRS-cells but also by vascular endothelium, FDCs and infiltrating macrophages (Mosmann & Sad, 1996; Sandvej et al, 1993). VCAM-1 expression in HD lymph nodes has been limited to some parts of the vascular endothelium and FDCs (Ree et al, 1994; Ruco et al, 1992). Serum levels of soluble British Journal of Haematology , 1998, 102, 701–709 701 q 1998 Blackwell Science Ltd Correspondence: Professor Thomas H. To ¨tterman, Department of Clinical Immunology and Transfusion Medicine, University Hospital, S75185 Uppsala, Sweden.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Soluble vascular cell adhesion molecule-1 (sVCAM-1)is an independent prognostic marker in Hodgkin’s disease
IL SE CHRIST IANSEN,1 CHRISTER SUNDST ROM,2 GUNILLA ENBL AD3
AND THOMAS H. TO TTERMAN1
1Department of Clinical Immunology and Transfusion Medicine, 2Department of Pathology,and 3Department of Oncology, University Hospital, Uppsala, Sweden
Received 16 February 1998; accepted for publication 14 May 1998
Summary. Serum levels of soluble vascular cell adhesionmolecule-1 (sVCAM-1, sCD106) were significantly elevatedin patients with Hodgkin’s disease (HD) (n ¼ 101) comparedto controls (n ¼ 31) (P<0·0001). sVCAM-1 correlated withhistology, stage, B-symptoms, and prognostic markers(sICAM-1, sCD30, sIL-2R, LDH). sVCAM-1, sICAM-1 andsCD30 added independent prognostic information for bothdisease-free and overall survival. 14 biopsies from 13patients with HD were immunostained for VCAM-1 andICAM-1. The vascular endothelium stained positive forVCAM-1 in 10/12 evaluable biopsies and for ICAM-1 in allevaluable biopsies. A stromal expression of both adhesionmolecules precluded a precise evaluation of HRS-cells. This
led us to investigate VCAM-1 (and ICAM-1) expression in sixHodgkin cell lines (HDLM-2, L428, L540, L591, DEV, KM-H2). Two cell lines stained positive for VCAM-1 (HDLM-2,L591). All cell lines stained positive for ICAM-1. sVCAM-1 isa new prognostic marker in HD; its predictive power equalsor surpasses that of sCD30 and sICAM-1. Furthermore, twoHodgkin cell lines stained positive for VCAM-1. This indicatesthat VCAM-1 may be expressed by some HD tumour cells invivo.
Keywords: Hodgkin’s disease, sVCAM-1, sICAM-1, prognos-tic markers, cell lines.
Adhesion molecules play a crucial role in the immunesystem by promoting cell–cell and cell–stroma interactionsand leucocyte trafficking (Carlos & Harlan, 1994). Solublecounterparts of adhesion molecules, probably derivedthrough proteolytic cleavage (Bazil, 1995) of the corre-sponding cellular transmembrane molecules, have beensuggested to competitively inhibit the action of the receptor–ligand pairs by binding to and blocking the respective ligands(Welder et al, 1993; Becker et al, 1993; Meyer et al, 1995).This may represent a mechanism for malignant cells toescape immune surveillance and may be a possible explana-tion for tumour dissemination and metastasis (Becker et al,1991). Vascular cell adhesion molecule-1 (VCAM-1, CD106)and intercellular adhesion molecule-1 (ICAM-1, CD54) areboth members of the immunoglobulin gene superfamily.VCAM-1 is constitutively expressed at low levels by bonemarrow stromal cells (Juneja et al, 1993), can be induced onvascular endothelial cells and follicular dendritic cells(FDCs), and is up-regulated on marrow stromal cells by
cytokines such as tumour necrosis factor-a (TNF-a),interleukin (IL)-1, IL-4 and IL-13 (Rice et al, 1991; Carloset al, 1990; Thornhill & Haskard, 1990; Bochner et al, 1995;Dittel et al, 1993). ICAM-1, an adhesion molecule alsoinducible by IL-1, TNF-a and IL-4, is widely distributedamong haemopoietic and non-haemopoietic cells (Larsson &Springer, 1990; Rothlein et al, 1988).
In Hodgkin’s disease (HD) the origin of the tumour cells,i.e. the Hodgkin and Reed-Sternberg (HRS) cells, is stillenigmatic, although accumulating data suggest a B-cellorigin (Gruss et al, 1997). In HD of nodular lymphocytepredominance (LP) histology, however, tumour cells areunequivocally of B-lymphocyte lineage (Poppema, 1992). Incontrast to other primary lymph node malignancies, thetumour cells in HD constitute only a small fraction of all cellsof involved nodes; the majority of cells appear to representinflammatory cells such as eosinophils and T lymphocytes(Gruss et al, 1997). ICAM-1 is overexpressed not only byHRS-cells but also by vascular endothelium, FDCs andinfiltrating macrophages (Mosmann & Sad, 1996; Sandvej etal, 1993). VCAM-1 expression in HD lymph nodes has beenlimited to some parts of the vascular endothelium and FDCs(Ree et al, 1994; Ruco et al, 1992). Serum levels of soluble
British Journal of Haematology, 1998, 102, 701–709
701q 1998 Blackwell Science Ltd
Correspondence: Professor Thomas H. Totterman, Department ofClinical Immunology and Transfusion Medicine, University Hospital,S75185 Uppsala, Sweden.
ICAM-1 (sICAM-1) are elevated in HD (Banks et al, 1993),and correlate with stage, disease activity and survival (Pizzoloet al, 1993; Christiansen et al, 1995). Elevated serum levels ofsVCAM-1 have been reported in 15 HD patients (Banks et al,1993). The present paper extends the documentation of serumlevels of sVCAM-1 in HD by elucidating the correlation tohistology, stage, other known prognostic markers, andsurvival. Further, we studied the expression and distributionof VCAM-1 and ICAM-1 in HD-involved lymph nodes in orderto clarify whether adhesion molecule tissue expression isreflected in the serum levels of the corresponding solublemolecules. This is the first report showing that VCAM-1 isexpressed by some Hodgkin cell line cells.
PATIENTS AND METHODS
Patients and control subjects. Between January 1981 andDecember 1991, serum samples were collected from 101 HDpatients at diagnosis. Sera were stored at ¹208C untilanalysis. Lymph node biopsies extirpated at diagnosis werepartly fixed in formalin, partly stored in liquid nitrogen.
Patients were followed-up until death or until 1 October,1996. For surviving patients the median follow-up periodwas 7·4 years (range 5·0-14·4 years). One patient was lostto follow-up and was censored at the time of last seen (6·3years after diagnosis). Patient characteristics are shown inTable I. Staging was performed according to the Ann Arborsystem (Carbone et al, 1971). Histopathology was re-evaluated by the same experienced pathologist to ensureuniformity. The treatment of the patients was detailedelsewhere (Enblad et al, 1993a). Briefly, early-stage patientswere treated with local extended radiotherapy and advanced-stage patients received a full course of chemotherapy (MOPP/ABVD). In intermediate-stage patients, chemotherapy wasreduced to one cycle of MOPP/ABVD followed by localextended radiotherapy.
Serum samples from 31 healthy blood donors (median 51years, range 40–60 years) were analysed for comparison.
Immunostaining procedures. 14 biopsies obtained from 13patients (one LP, seven nodular sclerosis (NS), five mixedcellularity (MC)), which had been previously snap-frozenand stored at ¹708C, were analysed. Serial sections (3 mmthick) were cut in a cryostat, air-dried and fixed in ice-coldacetone for 15 min at 48C. Subsequent incubations of thesections were carried out sequentially for 30 min followed by5 min washes in phosphate-buffered saline (PBS) betweeneach step. Incubations with monoclonal antibodies toVCAM-1 (BBIG-V1) (R&D Systems, Oxon., U.K.), ICAM-1(84H10) CD30 (HRS4) (both Immunotech, Marseilles,France), von Willebrand factor (F8/86), LMP (CS1-4), CD3(UCHT-1) and CD20 (L26) (all DAKO, Glostrup, Denmark)were followed by rabbit antimouse IgG antibody. After a finalincubation with a monoclonal alkali phosphatase-anti-alkaliphosphatase (APAAP) (DAKO, Glostrup, Denmark), optimumcolour development was achieved with 0·03% naptholAS-MX phosphate (N4875)þlevamisole (L-9756)þ Fast RedTR (F-2768) (Sigma, St Louis, U.S.A.). Slides were counter-stained in Mayers haematoxylin and mounted in Faramount(S3025, DAKO Corporation, Calif., U.S.A.).
Eosinophils were counted in haematoxylin–eosin-stainedsections (thickness 3 mm) as earlier described (Enblad et al,1993b). 10 high-power (×500) vision fields (VF) wereexamined, and the sum total of eosinophils was registered.
Reactive lymph nodes were used as controls.Flow cytometry and cytospin preparations. Hodgkin cell lines
HDLM-2 (DSMZ Department of Human and Animal Cul-tures, Braunshweig, Germany) and L428, DEV, KM-H2,L540, L591 (a kind gift from Professor Volker Diehl,Germany) (Drexler, 1993; Drexler et al, 1986; Schaadt etal, 1980), derived from bone marrow/blood (L540) orpleural effusions of patients with HD (NS), were stored inliquid nitrogen, thawed and cultured for 10 d in RPMI-1640with 20% fetal calf serum until analysis. A suspension oflymph node cells from one patient with HD (MC) wereseparated by gentle manipulation, and stored in liquidnitrogen until analysis.
For flow cytometry, cells were stained with directly labelledmonoclonal antibodies to CD45-FITC (DAKO, Glostrup,Denmark), VCAM-1-FITC, ICAM-1-FITC (both R&D Systems,Oxon., U.K.), CD30-FITC, CD3-RPE, CD4-RPE and CD8-RPE(all DAKO, Glostrup, Denmark). The cells were analysed on aBecton Dickinson FACScan flow cytometer.
Cytospin preparations were stained with monoclonal anti-bodies to VCAM-1, ICAM-1 (84H10) CD30 (HRS4), LMP (CS1–4), CD3 (UCHT-1), CD20 (L26), and CD5 as detailed above.
Serum assays. The sVCAM-1 and sICAM-1 levels in serumwere determined by enzyme immuno-assay (EIA) kitspurchased from R&D Systems Europe (Oxon, U.K.) accordingto the manufacturer’s instructions.
The sensitivity of the sVCAM-1 assay was 2 ng/ml, the inter-assay coefficient of variance (CV) was <8·5% and the intra-assay CV varied between 4·3% and 5·9%. The sensitivity of thesICAM-1 assay was 0·35 ng/ml, the inter assay CV was <7·4%and the intra-assay CV varied between 3·3% and 4·8%.
Cross reactivity between sICAM-1 and sVCAM-1 wasexcluded by adding a known concentration of sICAM-1 tothe sVCAM-1 kits and vice versa.
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 701–709
702 Ilse Christiansen et al
Table I. Patient characteristics.
No. patients
Male/Female 59/42
StageI 22II 41III 23IV 15
HistologyNodular sclerosis 67Mixed cellularity 29Lymphocyte predominance 4Lymphocyte depletion 1
Bulky disease 28B-symptoms 36Mean age (range) (years) 40 (6–87)
703sVCAM-1 is a Prognostic Marker in Hodgkin’s Disease
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 701–709
Lactate dehydrogenase (LDH), sIL-2R and sCD30 weredetermined as earlier described (Christiansen et al, 1995).
Statistical methods. Data are presented as mean andstandard deviation, unless otherwise specified. P values<0·05 were considered significant. Analysis of variance wasused to compare sVCAM-1 with Ann Arbor stage andhistology. The Bonferroni-Dunn correction was applied toexclude random significance. The unpaired Student’s t-testwas used to compare normally distributed parameters,i.e. sVCAM-1, sICAM-1 and LDH levels with bulky diseaseand B-symptoms (StatView 4.01). The Mann-Whitney U-testwas used to compare the not normally distributed sIL2Rand sCD30 levels with bulky disease, stages (IþII v IIIþIV), B-symptoms (StatView 4.01). The Spearman’s correlationcoefficient was used to determine the association betweensVCAM-1 and other serum markers (StatView 4.01). The Coxproportional hazard regression model was used in univariateand multivariate analyses of disease-free and overall survival.The multivariate analyses were performed in a stepwisemanner including B-symptoms and stage (dichotomized to IþII and IIIþIV), then testing one serum marker at a time on topof these known prognostic variables. The serum markers weretested as continuous variables in all analyses. The best cut-offvalue for sVCAM-1 was defined as the value that best dis-criminated between good and poor disease-free survival (DFS).DFS was defined as the absence of any recurrence. Patientswho never reached complete remission (CR) thus had a DFS ofzero months. A multivariate analysis was performed forsVCAM-1 and sICAM-1 when dichotomized at the level ofbest cut-off.
RESULTS
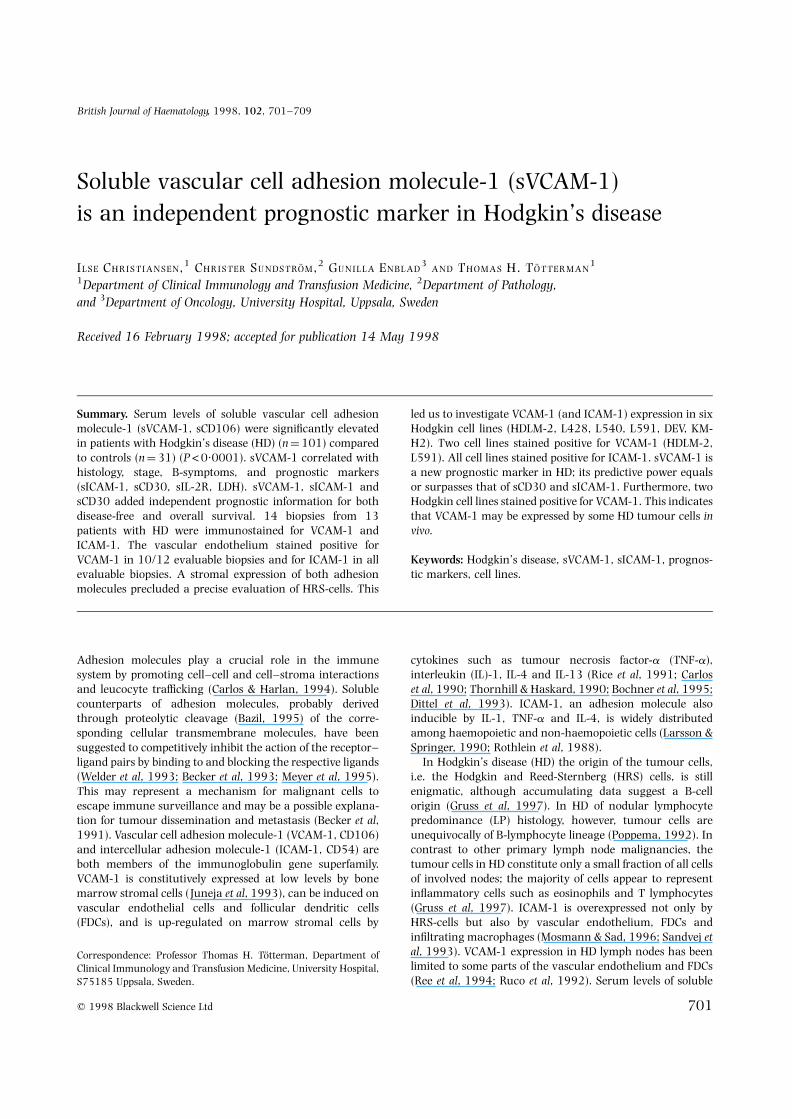
sVCAM-1 in HD patients and healthy controlsAll 101 patients with Hodgkin’s disease and all 31 controlshad detectable levels of sVCAM-1. The mean sVCAM-1 levelswere significantly elevated (P<0·0001) in the patient group(1571 6 1071 ng/ml) compared to the control group(614 6 153 ng/ml) (Fig 1).
sVCAM-1 in relation to clinical characteristicsThe levels of sVCAM-1 were significantly higher in patientswith mixed cellularity (MC) histology than in patientswith nodular sclerosis (NS) (2193 6 1521 ng/ml v 1317 6660 ng/ml; P ¼ 0·0002) (Table II). The number of patientswith the lymphocytic predominance type (LP, four patients,845 6 113 ng/ml) and lymphocytic depletion (LD, onepatient, 3427 ng/ml) histologies were too small for statisticalevaluation.
The levels of sVCAM-1 were significantly higher(P ¼ 0·0002) in patients diagnosed with advanced disease(stages IIIþIV) (2072 6 1420 ng/ml, n ¼ 38) compared topatients with localized disease (stages IþII) (1269 6 632 ng/ml, n ¼ 63) (Table II). There was a tendency towards highersVCAM-1 values between each stage, the difference beingstatistically significant between stages III and IV (P ¼
0·0015) but not between stages I and II, or stages II andIII. The presence or absence of bulky disease did not correlate
with the level of sVCAM-1 (P ¼ 0·6) (not shown). ThesVCAM-1 levels differed significantly (P ¼ 0·0002) betweenpatients with and without active disease, as reflected bypresence or absence of B-symptoms (2085 6 1349 ng/ml v1286 6 752 ng/ml) (Table II).
Fig 1. Box plot showing that serum levels of sVCAM-1 aresignificantly elevated in Hodgkin’s disease compared with controls.Horizontal lines in boxes indicate median value. Vertical linesindicate the outer quartiles.
Table II. Serum levels of sVCAM-1 and sICAM-1 (mean 6SD) differbetween early and advanced stages, histologies and presence orabsence of constitutional symptoms.
Stage
IþII IIIþIV P value*
sVCAM-1 (ng/ml) 1269 6 632 2072 6 1420 0·0002sICAM-1 (ng/ml) 418 6 198 631 6 298 <0·0001
Histology
Nodular Mixedsclerosis cellularity P value*
sVCAM-1 (ng/ml) 1317 6 660 2193 6 1521 0·0002sICAM-1 (ng/ml) 468 6 242 585 6 301 0·047
B-symptoms
Absent Present P value*
sVCAM-1 (ng/ml) 1286 6 752 2085 6 1349 0·0002sICAM-1 (ng/ml) 495 6 282 659 6 293 0·001
* Unpaired Student t-test.

sVCAM-1 compared to other serum markersAmong markers claimed to be associated with stage,B-symptoms, histology, and survival in Hodgkin’s disease, wecompared sICAM-1, LDH, sCD30 and sIL-2R to sVCAM-1.The correlation of each individual marker (apart fromsVCAM-1) to Ann Arbor stage, B-symptoms and histologicsubgroup are detailed elsewhere (Christiansen et al, 1995).All markers correlated significantly with B-symptoms andstage but only sVCAM-1, LDH and sICAM-1 correlatedwith histology (P ¼ 0·0002, P ¼ 0·01 and P ¼ 0·047,respectively).
Table III shows the correlation between the serum levels ofsVCAM-1 and sICAM-1 versus the other markers. sVCAM-1was most strongly correlated to sICAM-1 followed by sIL-2R,LDH and sCD30. The strongest correlation of all was foundbetween sICAM-1 and sIL2-R.
sVCAM-1 and prognosisIn univariate Cox regression analyses, sVCAM-1 levelsstrongly correlated with both disease-free and overall sur-vival (P<0·001 and P<0·001, respectively). In multivariateanalyses sVCAM-1, sCD30 and sICAM-1 as continuousvariables added independent prognostic information to thatof stage and B-symptoms for both disease-free and overallsurvival (Table IV), whereas LDH and sIL-2R did not.
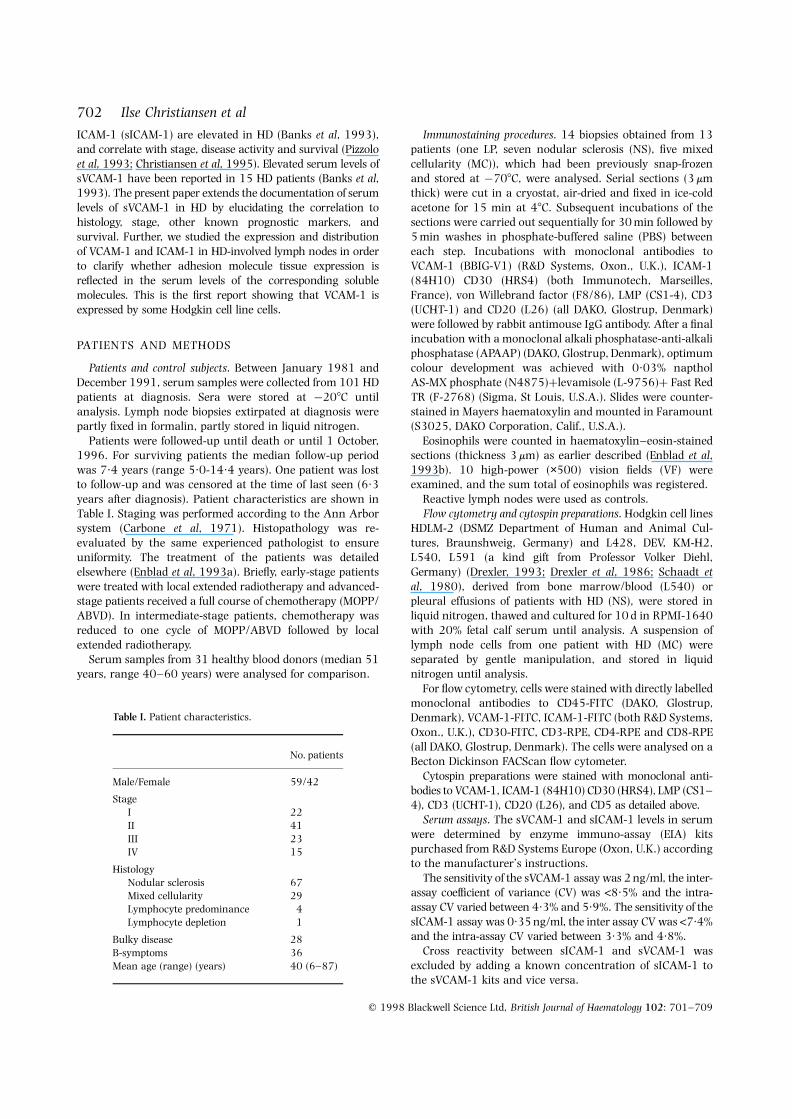
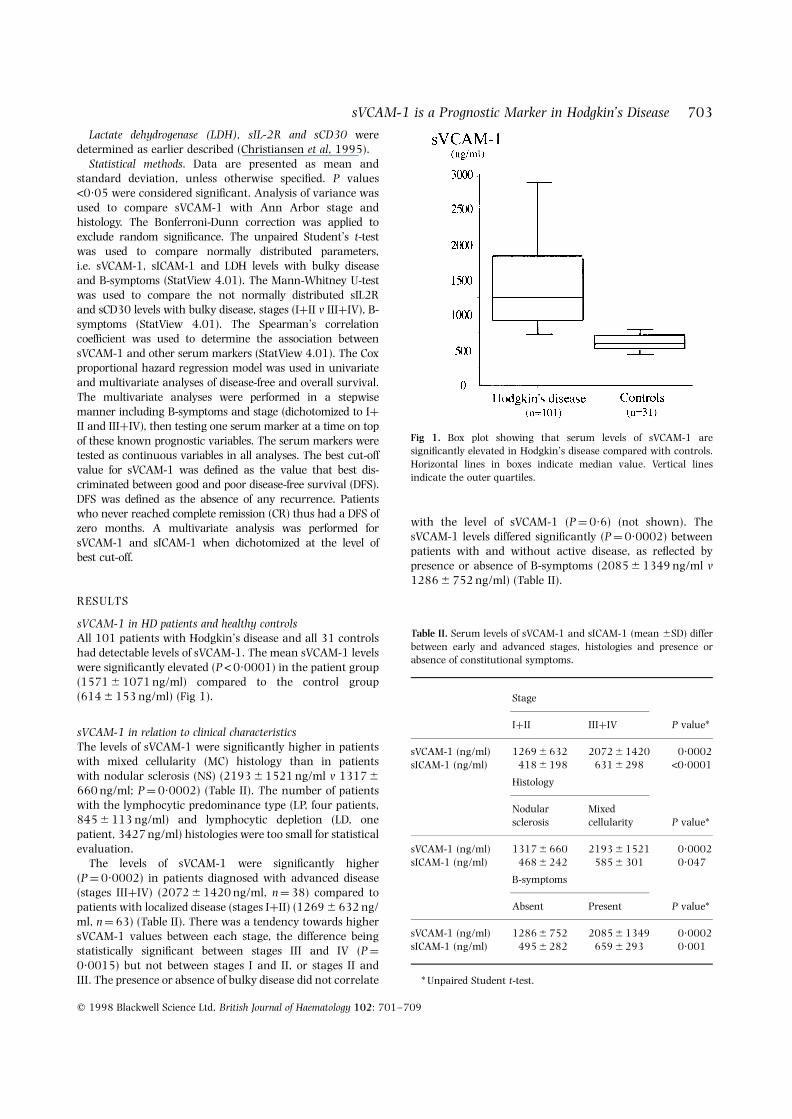
A cut-off level of sVCAM-1 at 1500 ng/ml was calculatedto optimally discriminate between good and poor disease-freeand overall survival (P<0·0001 and P<0·0001, respec-tively). The survival differences are illustrated in Figs 3 and 4.
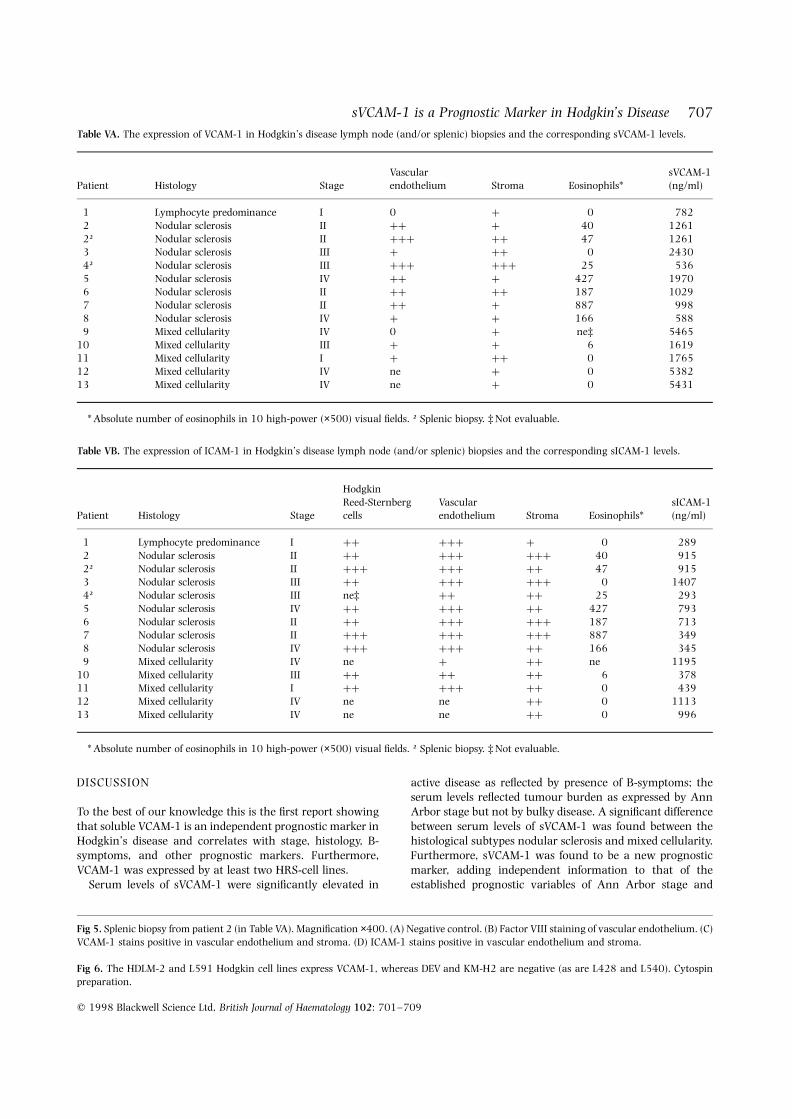
Tissue expression and serum levels of VCAM-1 and ICAM-1Tables VA and VB show the tissue expression of VCAM-1 andICAM-1 in sections of 14 biopsies from 13 patients with HDand the corresponding stage, histology, serum levels andeosinophil counts. The degree of adhesion molecule expres-sion was evaluated on an arbitrary scale from 0 (negative) to3þ (strongly positive).
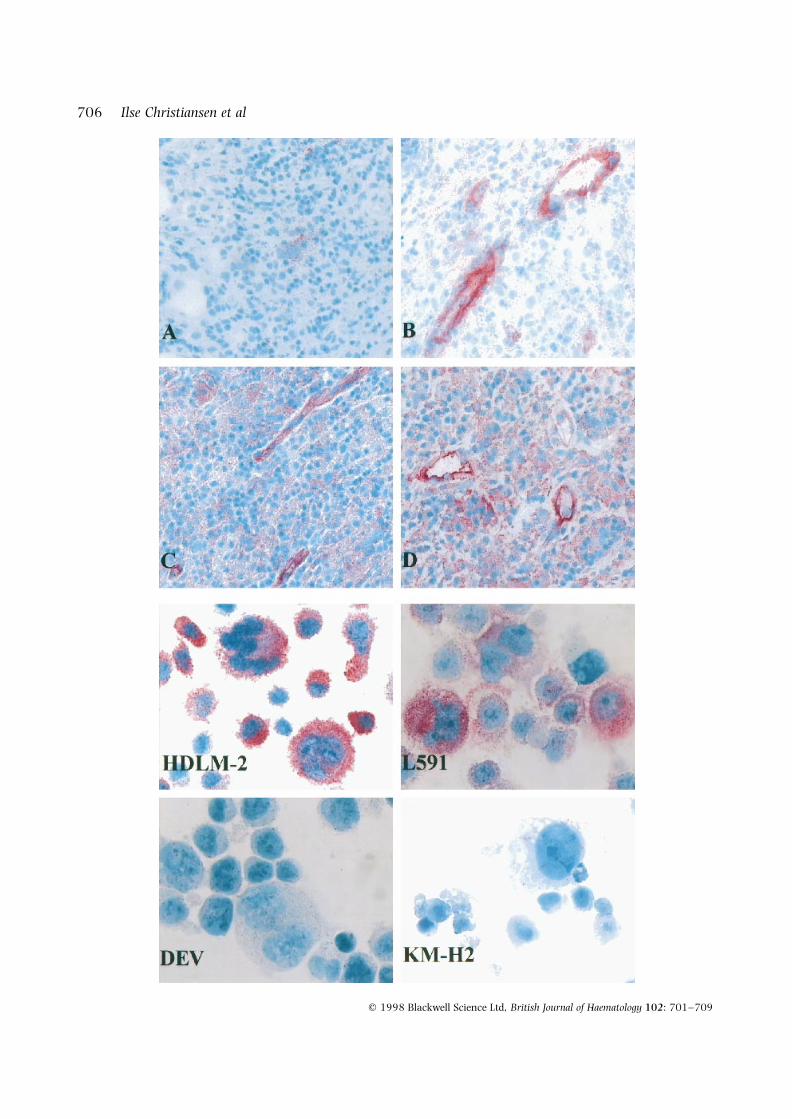
The vascular endothelium was positive for VCAM-1 (Fig 5)in 10/12 evaluable biopsies. A tendency to more extensiveinfiltration of eosinophils with more pronounced endothelialexpression of VCAM-1 was noted (Table VA). In 6/7 biopsieswith eosinophil counts >10 the expression of VCAM-1 wasþþ or more, and only one case in this group had a weakVCAM-1 expression. The three evaluable cases with eosino-phil counts <10 had weak or no VCAM-1 expression. ICAM-1expression by vascular endothelium was found in all evaluablebiopsies (Table VB). The expression was generally high andmore pronounced than for VCAM-1. No pattern betweenICAM-1 expression and eosinophil count was apparent. When
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 701–709
704 Ilse Christiansen et al
Table III. The correlation of sVCAM-1 and sICAM-1 to other serum markers inHodgkin’s disease.
sICAM-1 sIL-2R sCD30 LDH
sVCAM-1 0·60* 0·56 0·45 0·55P<0·0001 P<0·0001 P<0·0001 P<0·0001
sICAM-1 0·72 0·59 0·50P<0·0001 P<0·0001 P<0·0001
* Spearmans correlation coefficient.
Table IV. Prognostic value of sVCAM-1 and other serum markerstested in the Cox proportional hazard regression model in multi-variate analyses after inclusion of stage (IþII v IIIþIV) and B-symptoms. Serum markers as continuous variables.
Disease-free survival Overall survivalP value P value
sVCAM-1 <0·001 0·003sICAM-1 0·013 0·039sIL-2R ns nssCD30 0·005 <0·001LDH ns ns
ns: not significant.Fig 2. HDLM-2 cells express surface VCAM-1 in flow cytometricanalysis. Mean fluorescence intensity 150.
705sVCAM-1 is a Prognostic Marker in Hodgkin’s Disease
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 701–709
compared to the vascular expression of von Willebrand factor,both VCAM-1 and ICAM-1 showed a less pronounced and lessuniform expression. VCAM-1-positive cases always co-expressed ICAM-1. No correlation was evident between thevascular endothelial expression and the corresponding serumlevels of sVCAM-1 or sICAM-1, respectively.
VCAM-1 (Fig 5C) and ICAM-1 (Fig 5D) expression wasfound interstitially (stroma) but with an uneven distributionin all 14 biopsies. In one biopsy from a spleen the ICAM-1expression in stroma was restricted to the red pulp, whereasthe white pulp showed ICAM-1 expression in the T-cell area.No consistent pattern between the stromal expression andthe serum levels of the relevant adhesion moleculesappeared. The diffuse stromal expression of VCAM-1 andICAM-1 precluded an exact evaluation of the adhesionmolecule expression by HRS, B and T cells. However, in fourcases HRS cells were VCAM-1 negative, whereas in anotherfour cases no HRS cells were found in the biopsies and thus
VCAM-1 expression was not evaluable. In five cases (four NS,one MC) VCAM-1 appeared to be expressed by a variableproportion (30–100%) of HRS cells. HRS cells in all nineevaluable cases stained positive for ICAM-1. In one biopsy oflymphocytic predominance type, a 1þ expression of ICAM-1was found by the B cells. A lymph node suspension from apatient with HD (MC) was examined in cytospin smears andby FACS analysis. No expression of ICAM-1 or VCAM-1 wasfound on B or T cells (data not shown)
VCAM-1 is expressed by Hodgkin cell lines HDLM-2 and L591Six cell lines (HDLM-2, L428, DEV, KM-H2, L540, L591)were examined by staining of fixed cytospin smears and byflow cytometry. HDLM-2 and L591 expressed VCAM-1 (Fig 6)in cytospin preparations, but only HDLM-2 expressed VCAM-1 on the cell surface in flow cytometric analysis (Fig 2). Theother four cell lines did not express VCAM-1 in eithermethod. All six cell lines expressed ICAM-1 and CD30.
Fig 3. Disease-free survival of patientsaccording to cut-off level of sVCAM-1 at1500 ng/ml.
Fig 4. Overall survival of patients according tocut-off level of sVCAM-1 at 1500 ng/ml.
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 701–709
706 Ilse Christiansen et al
707sVCAM-1 is a Prognostic Marker in Hodgkin’s Disease
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 701–709
DISCUSSION
To the best of our knowledge this is the first report showingthat soluble VCAM-1 is an independent prognostic marker inHodgkin’s disease and correlates with stage, histology, B-symptoms, and other prognostic markers. Furthermore,VCAM-1 was expressed by at least two HRS-cell lines.
Serum levels of sVCAM-1 were significantly elevated in
active disease as reflected by presence of B-symptoms; theserum levels reflected tumour burden as expressed by AnnArbor stage but not by bulky disease. A significant differencebetween serum levels of sVCAM-1 was found between thehistological subtypes nodular sclerosis and mixed cellularity.Furthermore, sVCAM-1 was found to be a new prognosticmarker, adding independent information to that of theestablished prognostic variables of Ann Arbor stage and
Fig 5. Splenic biopsy from patient 2 (in Table VA). Magnification ×400. (A) Negative control. (B) Factor VIII staining of vascular endothelium. (C)VCAM-1 stains positive in vascular endothelium and stroma. (D) ICAM-1 stains positive in vascular endothelium and stroma.
Fig 6. The HDLM-2 and L591 Hodgkin cell lines express VCAM-1, whereas DEV and KM-H2 are negative (as are L428 and L540). Cytospinpreparation.
Table VA. The expression of VCAM-1 in Hodgkin’s disease lymph node (and/or splenic) biopsies and the corresponding sVCAM-1 levels.
Vascular sVCAM-1Patient Histology Stage endothelium Stroma Eosinophils* (ng/ml)
1 Lymphocyte predominance I 0 þ 0 7822 Nodular sclerosis II þþ þ 40 12612† Nodular sclerosis II þþþ þþ 47 12613 Nodular sclerosis III þ þþ 0 24304† Nodular sclerosis III þþþ þþþ 25 5365 Nodular sclerosis IV þþ þ 427 19706 Nodular sclerosis II þþ þþ 187 10297 Nodular sclerosis II þþ þ 887 9988 Nodular sclerosis IV þ þ 166 5889 Mixed cellularity IV 0 þ ne‡ 5465
10 Mixed cellularity III þ þ 6 161911 Mixed cellularity I þ þþ 0 176512 Mixed cellularity IV ne þ 0 538213 Mixed cellularity IV ne þ 0 5431
* Absolute number of eosinophils in 10 high-power (×500) visual fields. † Splenic biopsy. ‡ Not evaluable.
Table VB. The expression of ICAM-1 in Hodgkin’s disease lymph node (and/or splenic) biopsies and the corresponding sICAM-1 levels.
HodgkinReed-Sternberg Vascular sICAM-1
Patient Histology Stage cells endothelium Stroma Eosinophils* (ng/ml)
1 Lymphocyte predominance I þþ þþþ þ 0 2892 Nodular sclerosis II þþ þþþ þþþ 40 9152† Nodular sclerosis II þþþ þþþ þþ 47 9153 Nodular sclerosis III þþ þþþ þþþ 0 14074† Nodular sclerosis III ne‡ þþ þþ 25 2935 Nodular sclerosis IV þþ þþþ þþ 427 7936 Nodular sclerosis II þþ þþþ þþþ 187 7137 Nodular sclerosis II þþþ þþþ þþþ 887 3498 Nodular sclerosis IV þþþ þþþ þþ 166 3459 Mixed cellularity IV ne þ þþ ne 1195
10 Mixed cellularity III þþ þþ þþ 6 37811 Mixed cellularity I þþ þþþ þþ 0 43912 Mixed cellularity IV ne ne þþ 0 111313 Mixed cellularity IV ne ne þþ 0 996
* Absolute number of eosinophils in 10 high-power (×500) visual fields. † Splenic biopsy. ‡ Not evaluable.

B-symptoms for both disease-free and overall survival. Weconfirmed earlier reports (Christiansen et al, 1995; Gauseet al, 1991) of sICAM-1 and sCD30 as reliable independentprognostic variables whereas the prognostic information ofsIL-2R (Christiansen et al, 1995) disappeared over the longerfollow-up period.
Our results confirmed earlier reports (Sandvej et al, 1993;Ree et al, 1994; Ruco et al, 1992) showing that ICAM-1 wasexpressed by HRS cells in evaluable cases. The vascularendothelium stained positive for ICAM-1 to a variable degreein all biopsies and for VCAM-1 in 10/12 evaluable biopsies.Furthermore, all cases showed a patchy or diffuse stromalstaining for both adhesion molecules, and was mostpronounced for ICAM-1. The stromal and vascular expres-sion of VCAM-1 and ICAM-1 showed no correlation with theserum levels.
VCAM-1 in HD tumour tissue has been reported to beexpressed by follicular dendritic cells, macrophages andrarely by vascular endothelial cells but not by HRS cells(Ruco et al, 1992). We found that the stromal expression ofVCAM-1 precluded an exact evaluation of VCAM-1 expres-sion by HRS cells. However, it was our impression that someHRS cells in five cases were VCAM-1 positive. When HRS-celllines were examined 2/6 stained positive for VCAM-1. Thepresence of VCAM-1 in HRS cells of tumour biopsies needs tobe examined by, e.g., in situ hybridization (ongoing study).The HRS cell is thought to be an antigen presenting cell, butapart from the nodular LP histology the cellular origin ofHRS cells is still undetermined, although rearrangementdata suggest B- or T-lymphocyte derivation (Gruss et al,1997; Delabie et al, 1995). In the nodular LP type thetumour cells are known to be B-cell derived (Gruss et al,1997). VCAM-1 is expressed normally by dendritic cells andnot by B or T lymphocytes (Rice et al, 1991). An aberrantexpression of VCAM-1 has been reported in acute pre-B-lymphoblastic and in chronic B-lymphocytic leukaemia(Reuss-Borst et al, 1995). Therefore the presence of VCAM-1in the HRS cells would not preclude that the tumour cells maybe B-lymphocyte derived.
Although HRS cells have been shown to release sICAM-1in cell culture (Gruss et al, 1996), the cellular origin of thesoluble adhesion molecules and the mechanism behind theiroverexpression in tissues remain largely unknown atpresent. Tissue expression of both VCAM-1 and ICAM-1can be induced and up-regulated by TNF-a, IL-1 and IL-4(Carlos et al, 1990; Thornhill & Haskard, 1990; Bochner et al,1995; Dittel et al, 1993; Larsson & Springer, 1990; Rothleinet al, 1988), cytokines which are known to be dysregulatedin HD (Gruss et al, 1997; Kretchmer et al, 1990). Therefore anincreased cellular expression of the adhesion molecules andthe release of the corresponding soluble molecules could be asecondary phenomenon in HD. Furthermore, data suggestthat the soluble adhesion molecules competitively inhibit theinteraction between the cell surface adhesion molecules andtheir complementary ligands (VLA-4 and LFA-1, respec-tively) (Welder et al, 1993; Becker et al, 1993; Meyer et al,1995). These interactions are important in the normalimmune response, i.e. lymphocyte localization, traffickingand signalling between T cells and antigen-presenting cells
(Carlos & Harlan, 1994). Increased levels of the solubleadhesion molecules may be a mechanism for the tumourcells to escape immune surveillance and could promotetumour dissemination (Becker et al, 1991). VCAM-1 hasbeen shown to promote T-cell proliferation and antigenpresentation (Damle & Aruffo, 1991; Burkly et al, 1991).VCAM-1 is also involved in eosinophil adhesion (Bochneret al, 1991) and secretion of soluble VCAM-1 in broncho-alveolar lavage has been reported to coincide with eosino-philic influx in asthma patients (Zangrilli et al, 1995). In thepresent study we found a more pronounced number ofeosinophils in biopsies with high endothelial expression ofVCAM-1. A dysregulation of VCAM-1 and/or sVCAM-1could therefore be a contributory factor to the T-cell andeosinophilic-cell infiltration observed in lymph nodes affectedby HD (Enblad et al, 1993b).
In conclusion, we found that serum levels of sVCAM-1were increased in HD and correlate with stage, histology andother prognostic markers. Furthermore, sVCAM-1, sICAM-1and sCD30 are independent prognostic markers for disease-free survival, and these markers may prove valuable whenselecting patients for intensive treatment strategies. The roleof the soluble adhesion molecules in tumour growth andhost immunosuppression needs further study.
ACKNOWLEDGMENTS
We express our gratitude to J. Bring, Department of Statistics,Uppsala, for expert assistance with uni- and multivariatesurvival analyses. We thank A. Kraft, Department ofPathology, and G. Wetterberg and C. Gidlof, Department ofClinical Immunology, Uppsala University Hospital, forexcellent technical assistance.
This study was supported by grants from the SwedishCancer Society and the Lion’s Cancer Fund at the UniversityHospital, Uppsala.
REFERENCES
Banks, R.E., Gearing, A.J.H., Hemingway, I.K., Norfolk, D.R., Perren,T.J. & Selby, P.J. (1993) Circulating intercellular adhesionmolecule-1 (ICAM-1), E-selectin and vascular cell adhesionmolecule-1 (VCAM-1) in human malignancies. British Journal ofCancer, 68, 122–124.
Bazil, V. (1995) Physiological enzymatic cleavage of leukocytemembrane molecules. Immunology Today, 16, 135–140.
Becker, J.C., Dummer, R., Hartmann, A.A., Burg, G. & Schmidt, R.E.(1991) Shedding of ICAM-1 from human melanoma cell linesinduced by IFN-g and tumor necrosis factor-a: functionalconsequences on cell-mediated cytotoxicity. Journal of Immunology,147, 4398–4401.
Becker, J.C., Termeer, C., Schmidt, R.E. & Brocker, E.B. (1993)Soluble intercellular adhesion molecule-1 inhibits MHC-restricted specific T cell/tumor interaction. Journal of Immunology,151, 7224–7232.
Bochner, B.S., Klunk, D.A., Sterbinsky, S.A., Coffman, R.L. &Schleimer, R.P. (1995) IL-13 selectively induces vascular celladhesion molecule-1 expression in human endothelial cells.Journal of Immunology, 154, 799–803.
Bochner, B.S., Luscinskas, F.W., Gimbrone, M.A., Newman, W.,Sterbinsky, S.A., Derse-Anthony, C.P., Klunk, D. & Schleimer, R.P.
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 701–709
708 Ilse Christiansen et al

709sVCAM-1 is a Prognostic Marker in Hodgkin’s Disease
q 1998 Blackwell Science Ltd, British Journal of Haematology 102: 701–709
(1991) Adhesion of human basopils, eosinophils, and neutropilsto interleukin-1 activated human vascular endothelial cells:contributions of endothelial cell adhesion molecules. Journal ofExperimental Medicine, 173, 1553–1557.
Burkly, L.C., Jakubowski, A., Newman, B.M., Rosa, M.D., Chi-Rosso,G. & Lobb, R.R. (1991) Signaling by vascular cell adhesionmolecule-1 (VCAM-1) through VLA-4 promotes CD3-dependent Tcell proliferation. European Journal of Immunology, 21, 2871–2875.
Carbone, P.P., Kaplan, H.S., Musshoff, K., Smithers, D.W. & Tubiana,M. (1971) Report of the Committee on Hodgkin’s Disease StagingClassification. Cancer Research, 31, 1860–1861.
Carlos, T.M. & Harlan, J.M. (1994) Leukocyte–endothelial adhesionmolecules. Blood, 84, 2068–2101.
Carlos, T.M., Schwartz, B.R., Kovach, N.L., Yee, E., Rosso, M.,Osborn, L., Chi-Rosso, G., Newman, B., Lobb, R. & Harlan, J.M.(1990) Vascular cell adhesion molecule-1 mediates lymphocyteadherence to cytokine-activated cultured human endothelial cells.Blood, 76, 965–970.
Christiansen, I., Enblad, G., Kalkner, K.M., Gidlof, C., Glimelius, B. &Totterman, T.H. (1995) Soluble ICAM-1 in Hodgkin’s disease: apromising independent predictive marker for survival. Leukemiaand Lymphoma, 19, 243–251.
Damle, N.K. & Aruffo, A. (1991) Vascular cell adhesion molecule 1induces T-cell antigen receptor-dependent activation of CD4þ Tlymphocytes. Proceedings of the National Academy of Sciences of theUnited States of America, 88, 6403–6407.
Delabie, J., Chan, W.C., Weisenburger, D.D. & De Wolf-Peeters, C.(1995) The antigen-presenting cell function of Reed-Sternbergcells. Leukemia and Lymphoma, 18, 35–40.
Dittel, B.N., McCarthy, J.B., Wayner, E.A. & LeBien, T.W. (1993)Regulation of human B-cell precursor adhesion to bone marrowstromal cells by cytokines that exert opposing effects on theexpression of vascular cell adhesion molecule-1 (VCAM-1). Blood,81, 2272–2282.
Drexler, H.G. (1993) Recent results on the biology of Hodgkin andReed-Sternberg cells. Leukemia and Lymphoma, 9, 1–25.
Drexler, H.G., Gaedicke, G., Lok, M.S., Diehl, V. & Minowada, J.(1986) Hodgkin’s disease derived cell lines HDLM-2 and L-428:comparison of morphology, immunological and isoenzymeprofiles. Leukemia Research, 10, 487–500.
Enblad, G., Sundstrom, C. & Glimelius, B. (1993a) Immunohisto-chemical characteristics of Hodgkin and Reed-Sternberg cells inrelation to age and clinical outcome. Histopathology, 22, 535–541.
Enblad, G., Sundstrom, C. & Glimelius, B. (1993b) Infiltration ofeosinophils in Hodgkin’s disease involved lymph nodes predictsprognosis. Hematological Oncology, 11, 187–193.
Gause, A., Pohl, C., Tschiersch, A., Da Costa, L., Jung, W., Diehl, V. &Hasenclever, D. (1991) Clinical significance of soluble CD30antigen in the sera of patients with untreated Hodgkin’s disease.Blood, 77, 1983–1988.
Gruss, H.J., Pinto, A., Duyster, J., Poppema, S. & Herrmann, F. (1997)Hodgkin’s diease: a tumor with disturbed immunological path-ways. Immunology Today, 18, 156–163.
Gruss, H.J., Scheffrahn, I., Hubinger, G. & Duyster, J. (1996) TheCD30 ligand and CD40 ligand regulate CD54 surface expressionand release of its soluble form by cultured Hodgkin and Reed-Sternberg cells. Leukemia, 10, 829–835.
Juneja, H.S., Schmalsteig, F.C., Lee, S. & Chen, J. (1993) Vascular celladhesion molecule-1 and VLA-4 are obligatory adhesion proteinsin the heterotypic adherence between human leukemia/lym-phoma cells and marrow stromal cells. Experimental Hematology,21, 444–450.
Kretchmer, C., Jones, D.B., Morrison, K., Schluter, C., Feist, W.,Ulmer, A.J., Arnoldi, J., Matthes, J., Diamantstein, T., Flad, H.D. &Gerdes, J. (1990) Tumor necrosis factor-alpha and lymphotoxinproduction in Hodgkin’s disease. American Journal of Pathology,137, 341–351.
Larsson, R.S. & Springer, T.A. (1990) Structure and function ofleukocyte integrins. Immunological Reviews, 114, 181–217.
Meyer, D.M., Dustin, M.L. & Carron, C.P. (1995) Characterization ofintercellular adhesion molecule-1 ectodomain (sICAM-1) as aninhibitor of lymphocyte function-associated molecule-1 interac-tion with ICAM-1. Journal of Immunology, 155, 3578–3584.
Mosmann, T.R. & Sad, S. (1996) The expanding universe of T-cellsubsets: Th1, Th2 and more. Immunology Today, 17, 138–146.
Pizzolo, G., Vinante, F., Nadali, G., Riceti, M.M., Morosato, L.,Marrocchella, R., Vincenzi, C., Semenzato, G. & Chilosi, M. (1993)ICAM-1 tissue overexpression associated with increased serumlevels of its soluble form in Hodgkin’s disease. British Journal ofHaematology, 84, 161–162.
Poppema, S. (1992) Lymphocyte-predominance Hodgkin’s disease.Semininars in Diagnostic Pathology, 9, 257–264.
Ree, H.J., Khan, A.A., Qureshi, M.N. & Teplitz, C. (1994) Expressionof cell adhesion molecules associated with germinal center inHodgkin’s disease: an immunohistochemical study. Cancer, 73,1257–1263.
Reuss-Borst, M.A., Ning, Y., Klein, G. & Muller, C.A. (1995) Thevascular cell adhesion molecule (VCAM-1) is expressed on a subsetof lymphoid and myeloid leukaemias. British Journal of Haematol-ogy, 89, 299–305.
Rice, G.E., Munro, J.M., Corless, C. & Bevilacqua, M.P. (1991)Vascular and nonvascular expression of INCAM-110. AmericanJournal of Pathology, 138, 385–393.
Rothlein, R., Czajkowski, M., O’Neill, M.M., Marlin, S.D., Mainolfi, E.& Merluzzi, V.J. (1988) Induction of intercellular adhesionmolecule 1 on primary and continuous cell lines by pro-inflammatory cytokines. Journal of Immunology, 141, 1665–1669.
Ruco, L.P., Pomponi, D., Pigott, R., Gearing, A.J.H., Baiocchini, A. &Baroni, C.D. (1992) Expression and cell distribution of theintercellular adhesion molecule, vascular cell adhesion molecule,endothelial leukocyte adhesion molecule, and endothelial adhe-sion molecule (CD31) in reactive human lymph nodes and inHodgkin’s disease. American Journal of Pathology, 140, 1337–1344.
Sandvej, K.B., Hamilton-Duoit , S.J. & Pallesen, G. (1993) Influenceof Epstein-Barr virus encoded latent membrane protein 1 on theexpression of CD23 antigen, ICAM-1 and LFA-3 in Hodgkin andReed-Sternberg cells: a morphometric analysis. Leukemia andLymphoma, 9, 95–101.
Schaadt, M., Diehl, V., Stein, H., Fonatsch, C. & Kirchner, H.H.(1980) Two neoplastic cell lines with unique features derived fromHodgkin’s disease. International Journal of Cancer, 26, 723–731.
Thornhill, M.H. & Haskard, D.O. (1990) IL-4 regulates endothelialcell activation by IL-1, tumor necrosis factor, or IFN-g. Journal ofImmunology, 145, 865–872.
Welder, C.A., Lee, D.H.S. & Takei, F. (1993) Inhibition of celladhesion by microspheres coated with recombinant solubleintercellular adhesion molecule-1. Journal of Immunology, 150,2203–2210.
Zangrilli, J.G., Shaver, J.R., Cirelli, R.A., Kil Cho, S., Garlisi, C.G.,Falcone, A., Cuss, F.M., Fish, J.E. & Peters, S.P. (1995) sVCAM-1levels after segmental antigen challenge correlate with eosinophilinflux, IL-4, and IL-5 production, and the late phase response.American Journal of Respiratory and Critical Care Medicine, 151,1346–1353.
Related Documents











