109 症 例 北里医学 2016; 46: 109-115 Received 15 February 2016, accepted 24 June 2016 連絡先: 那須野智光 (東芝林間病院耳鼻咽喉科) 〒252-0302 神奈川県相模原市南区上鶴間7-9-1 E-mail: [email protected] 耳下腺に発生したsolitary fibrous tumor (SFT) の一例 那須野 智光 1 ,竹田 昌彦 2 ,大橋 健太郎 3 ,清野 由輩 4 , 山口 知子 5 ,岡本 牧人 4 ,山下 拓 4 1 東芝林間病院耳鼻咽喉科 2 橋本タワー耳鼻咽喉科 3 北里大学メディカルセンター耳鼻咽喉科 4 北里大学医学部耳鼻咽喉科・頭頸部外科学 5 独立行政法人国立病院機構 相模原病院耳鼻いんこう科 孤立性線維性腫瘍solitary fibrous tumor (SFT) は胸膜に発生する間葉系細胞由来の腫瘍であり, 頭頸部領域においては稀である。耳下腺に発生したSFT症例を経験したので報告する。症例は48歳 女性。右耳下部に腫瘤を触知したため当科を受診した。超音波及び造影CT画像上で右耳下腺内に 境界明瞭,血流豊富な腫瘍像が認められた。右耳下腺浅葉切除術を施行し,病理検査の結果,不規 則・不均一に増生する紡錘形の腫瘍細胞像や鹿角様と呼ばれるスリット状の血管腔が多数認めら れ,また免疫組織化学的染色においてvimentinやCD34が陽性でありSFTであると診断した。術後10 年が経過し,再発は認めていない。 Key words: 孤立性線維性腫瘍,耳下腺,免疫組織化学的検査,頭頸部領域 序 文 孤立性線維性腫瘍solitary fibrous tumor (SFT) は1931 年にKlempererとColemanによって最初に報告された間 葉系細胞由来の腫瘍である 1 。多くは胸膜に関連した胸 腔内病変として報告されてきた 2 。近年では様々な胸膜 外臓器での発生例も相次いで報告されているが,頭頸 部領域での報告は比較的稀である 3 。今回我々は耳下腺 に発生したSFTを経験したので報告する。 症 例 症例: 48歳,女性。 主訴: 右耳下部腫瘤。 既往歴: 特記すべきことなし。 現病歴 2005年末頃より右耳下部に腫瘤を触知した。2006年 4月に近医を受診したところ,右耳下腺腫瘍を疑われ, 2006年4月に当科を紹介された。 初診時所見 右耳下部に2.5 × 1.6 cm大,弾性硬で可動性良好, 圧痛のない腫瘤を触知した。顔面神経麻痺はなかっ た。 画像所見 超音波検査上,右耳下腺に1.6 × 1.3 × 1.2 cmの境 界明瞭,全体的にlowで一部isoechoicな領域が認められ た。カラードップラー像では腫瘍内部に豊富な血流シ グナルが認められた (Figure 1A,B)。頸部単純CT画像 では腫瘍性病変は周囲の耳下腺組織と同等の吸収域を 有し境界は判然とせず,石灰化像は認められなかっ た。造影CT画像では右耳下腺内に強く造影される境界 明瞭な腫瘍性病変が認められた (Figure 2A,B)。 手術所見 画像診断で良性・悪性の可能性を検討の上,手術に よる治療を選択した。腫瘍は右耳下腺浅葉に存在して いたため顔面神経本幹を同定,温存した後,右耳下腺 浅葉とともに腫瘍を摘出した。摘出した腫瘍は1.6 × 1.3 × 0.8 cm大の割面は淡赤色,内部が均一,充実性 であった (Figure 3)。 病理所見 紡錘形を呈した腫瘍細胞が特定の配列を示すことな く不規則,不均一に増生している像を認めた。拡大像 では鹿角様と呼ばれるスリット状の血管腔が多数認め

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
109
症 例 北里医学 2016; 46: 109-115
Received 15 February 2016, accepted 24 June 2016連絡先: 那須野智光 (東芝林間病院耳鼻咽喉科)〒252-0302 神奈川県相模原市南区上鶴間7-9-1E-mail: [email protected]
耳下腺に発生したsolitary fibrous tumor (SFT) の一例
那須野 智光1,竹田 昌彦2,大橋 健太郎3,清野 由輩4,
山口 知子5,岡本 牧人4,山下 拓4
1東芝林間病院耳鼻咽喉科2橋本タワー耳鼻咽喉科3北里大学メディカルセンター耳鼻咽喉科4北里大学医学部耳鼻咽喉科・頭頸部外科学5独立行政法人国立病院機構 相模原病院耳鼻いんこう科
孤立性線維性腫瘍solitary fibrous tumor (SFT) は胸膜に発生する間葉系細胞由来の腫瘍であり,
頭頸部領域においては稀である。耳下腺に発生したSFT症例を経験したので報告する。症例は48歳
女性。右耳下部に腫瘤を触知したため当科を受診した。超音波及び造影CT画像上で右耳下腺内に
境界明瞭,血流豊富な腫瘍像が認められた。右耳下腺浅葉切除術を施行し,病理検査の結果,不規
則・不均一に増生する紡錘形の腫瘍細胞像や鹿角様と呼ばれるスリット状の血管腔が多数認めら
れ,また免疫組織化学的染色においてvimentinやCD34が陽性でありSFTであると診断した。術後10年が経過し,再発は認めていない。
Key words: 孤立性線維性腫瘍,耳下腺,免疫組織化学的検査,頭頸部領域
序 文
孤立性線維性腫瘍solitary fibrous tumor (SFT) は1931
年にKlempererとColemanによって最初に報告された間
葉系細胞由来の腫瘍である1。多くは胸膜に関連した胸
腔内病変として報告されてきた2。近年では様々な胸膜
外臓器での発生例も相次いで報告されているが,頭頸
部領域での報告は比較的稀である3。今回我々は耳下腺
に発生したSFTを経験したので報告する。
症 例
症例: 48歳,女性。
主訴: 右耳下部腫瘤。
既往歴: 特記すべきことなし。
現病歴
2005年末頃より右耳下部に腫瘤を触知した。2006年
4月に近医を受診したところ,右耳下腺腫瘍を疑われ,
2006年4月に当科を紹介された。
初診時所見
右耳下部に2.5 × 1.6 cm大,弾性硬で可動性良好,
圧痛のない腫瘤を触知した。顔面神経麻痺はなかっ
た。
画像所見
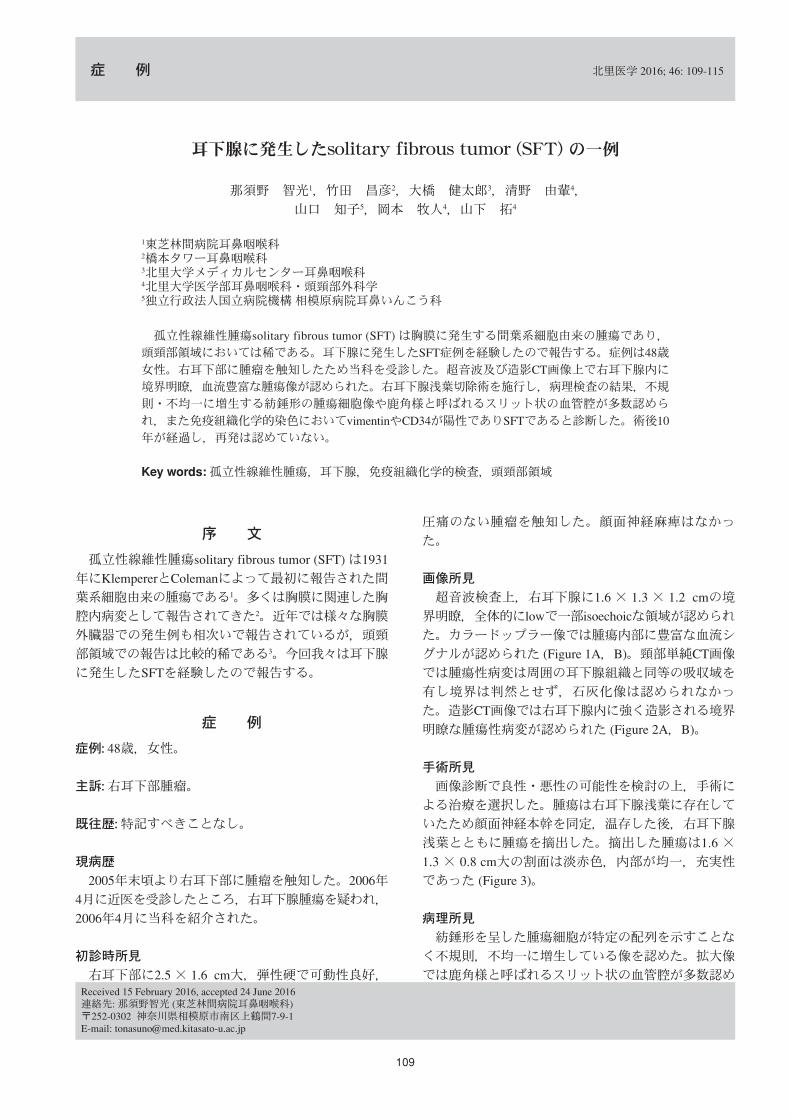
超音波検査上,右耳下腺に1.6 × 1.3 × 1.2 cmの境
界明瞭,全体的にlowで一部isoechoicな領域が認められ
た。カラードップラー像では腫瘍内部に豊富な血流シ
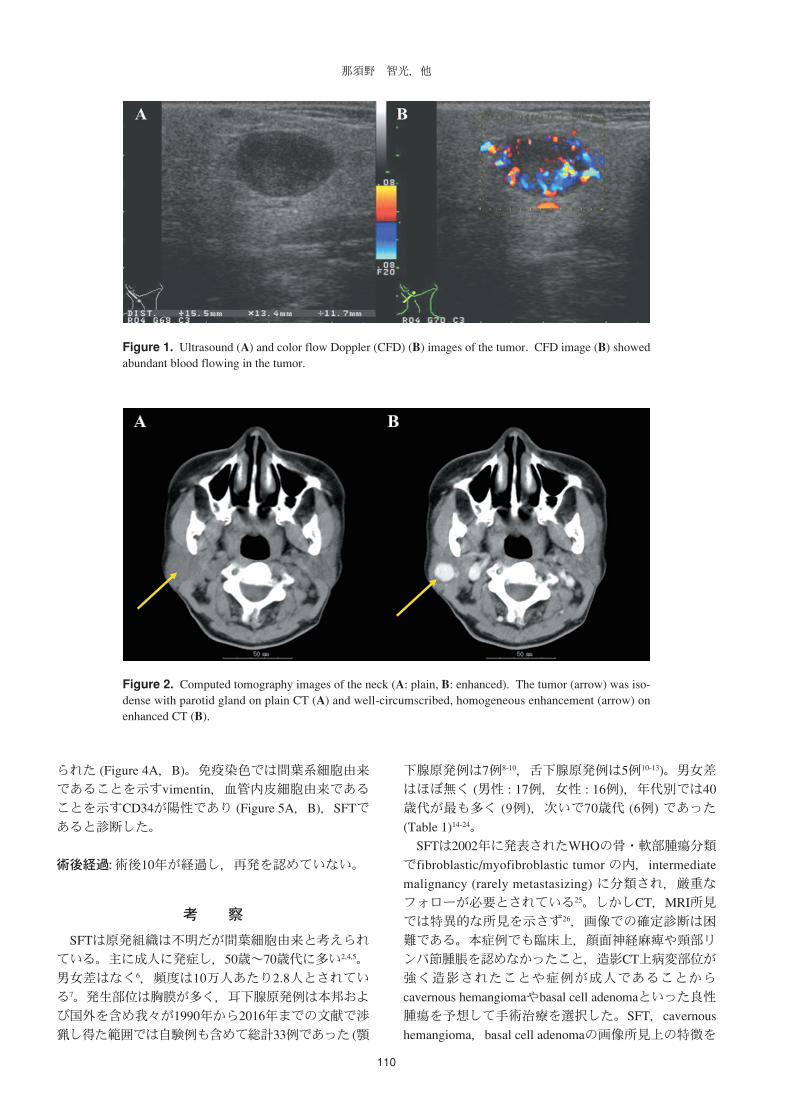
グナルが認められた (Figure 1A,B)。頸部単純CT画像
では腫瘍性病変は周囲の耳下腺組織と同等の吸収域を
有し境界は判然とせず,石灰化像は認められなかっ
た。造影CT画像では右耳下腺内に強く造影される境界
明瞭な腫瘍性病変が認められた (Figure 2A,B)。
手術所見
画像診断で良性・悪性の可能性を検討の上,手術に
よる治療を選択した。腫瘍は右耳下腺浅葉に存在して
いたため顔面神経本幹を同定,温存した後,右耳下腺
浅葉とともに腫瘍を摘出した。摘出した腫瘍は1.6 ×
1.3 × 0.8 cm大の割面は淡赤色,内部が均一,充実性
であった (Figure 3)。
病理所見
紡錘形を呈した腫瘍細胞が特定の配列を示すことな
く不規則,不均一に増生している像を認めた。拡大像
では鹿角様と呼ばれるスリット状の血管腔が多数認め
110
那須野 智光,他
Figure 1. Ultrasound (A) and color flow Doppler (CFD) (B) images of the tumor. CFD image (B) showedabundant blood flowing in the tumor.
Figure 2. Computed tomography images of the neck (A: plain, B: enhanced). The tumor (arrow) was iso-dense with parotid gland on plain CT (A) and well-circumscribed, homogeneous enhancement (arrow) onenhanced CT (B).
られた (Figure 4A,B)。免疫染色では間葉系細胞由来
であることを示すvimentin,血管内皮細胞由来である
ことを示すCD34が陽性であり (Figure 5A,B),SFTで
あると診断した。
術後経過: 術後10年が経過し,再発を認めていない。
考 察
SFTは原発組織は不明だが間葉細胞由来と考えられ
ている。主に成人に発症し,50歳〜70歳代に多い2,4,5。
男女差はなく6,頻度は10万人あたり2.8人とされてい
る7。発生部位は胸膜が多く,耳下腺原発例は本邦およ
び国外を含め我々が1990年から2016年までの文献で渉
猟し得た範囲では自験例も含めて総計33例であった (顎
下腺原発例は7例8-10,舌下腺原発例は5例10-13)。男女差
はほぼ無く (男性 : 17例,女性 : 16例),年代別では40
歳代が最も多く (9例),次いで70歳代 (6例) であった
(Table 1)14-24。
SFTは2002年に発表されたWHOの骨・軟部腫瘍分類
でfibroblastic/myofibroblastic tumor の内,intermediate
malignancy (rarely metastasizing) に分類され,厳重な
フォローが必要とされている25。しかしCT,MRI所見
では特異的な所見を示さず26,画像での確定診断は困
難である。本症例でも臨床上,顔面神経麻痺や頸部リ
ンパ節腫脹を認めなかったこと,造影CT上病変部位が
強く造影されたことや症例が成人であることから
cavernous hemangiomaやbasal cell adenomaといった良性
腫瘍を予想して手術治療を選択した。SFT,cavernous
hemangioma,basal cell adenomaの画像所見上の特徴を

111
耳下腺SFTの一例
Figure 3. The cut surface of the tumor
Figure 4. Histological images of the tumor (H&E stain, A: low-power field, B: high-power field). Lowpower photomicrograph (A) showed spindle-shaped tumor cells arranged in a haphazard or so-called patternlesspattern. High-power photomicrograph (B) showed numerous staghorn-like vessels (arrows).
Figure 5. Immunohistochemical staining of the tumor (high-power field, A: vimentin, B: CD34). Thesespindle cells are immunoactive with vimentin (A) and CD34 (B).

112
Table 1. Clinical data of 33 parotid solitary fibrous tumor cases in the current literature
症例 報告者 年度 年齢 性別 大きさ (cm) 治療 経過
1 Hanau, et al.18 1995 73 F 3.5 外科的切除 4年再発なし
2 Ferriro, et al.18 1996 78 F 1.0 外科的切除 1年再発なし
3 同上18 1996 46 M 4.4 外科的切除 0.1年再発なし
4 Sato, et al.18 1998 52 M 12.0 外科的切除 1年再発なし
5 Brunnemann, et al.18 1999 43 M 2.0 外科的切除 不明
6 同上18 1999 66 F 2.7 外科的切除 4.7年再発なし
7 Mohammed, et al.18 2001 42 F 2.2 外科的切除 0.2年再発なし
8 藤森ら14 2001 60 M 不明 外科的切除 不明
9 Guerra, et al.18 2002 37 F 7.0 外科的切除 1年再発なし
10 Kumagai, et al.18 2002 47 F 4.2 外科的切除 1.2年再発なし
11 Thompson, et al.18 2004 11 F 4.0 外科的切除 2年再発なし
12 Gerhard, et al.18 2004 34 F 4.0 外科的切除 2年再発なし
13 Suarez Roa, et al.47 2004 20 F 10.0 & 1.8 外科的切除 & 放射線治療 1年再発なし
14 立花ら16 2004 29 F 3.4 外科的切除 2.8年再発なし
15 光澤ら15 2004 65 F 不明 外科的切除 & 放射線治療 2年再発なし
16 Wiriosuparto, et al.18 2005 42 M 6.5 外科的切除 不明
17 Kim, et al.18 2005 59 M 不明 外科的切除 0.6年再発なし
18 Sreetharan, et al.18 2005 44 M 1.0 外科的切除 1年再発なし
19 Ridder, et al.18 2007 24 M 4.4 外科的切除 不明
20 平野ら17 2007 30 F 3.0 外科的切除 2.2年再発なし
21 Takahama, et al.18 2008 73 F 3.0 外科的切除 1.8年再発なし
22 Cho, et al.18 2008 58 M 6.5 外科的切除 5.6年再発なし
23 Manglik, et al.18 2008 79 M 2.4 外科的切除 0.3年再発なし
24 Yang, et al.46 2009 54 M 5.0 外科的切除 & 放射線治療 不明
25 Messa-Botero, et al.18 2011 78 F 3.9 外科的切除 0.6年再発なし
26 Iyengar, et al.19 2011 43 M 4.0 外科的切除 不明
27 Justin, et al.18 2012 66 M 4.3 外科的切除 0.8年再発なし
28 Cristofaro, et al.20 2012 38 M 3.8 外科的切除 5年再発なし
29 Sousa, et al.21 2013 42 M 4.0 外科的切除 0.8年再発なし
30 Alonso-Rodríguez, et al.24 2014 73 F 2.0 外科的切除 2年後再発あり
31 Kwok, et al.22 2015 28 M 2.7 外科的切除 不明
32 Yu, et al.23 2015 53 M 2.0 外科的手術 2年再発なし
33 本症例 2016 48 F 1.6 外科的切除 10年再発なし
Table 2. Imaging features of SFT, cavernous hemangioma and basal cell adenoma
CT MRI
単純 造影 T1 T2 T2造影
軟部組織とiso 不均一 〜 均一 iso hypo 〜 hyper 不均一 〜 均一Solitary fibrous tumor
均一 不均一 〜 均一 不均一 〜 均一
血管とiso 均一 hypo 〜 iso hyper 均一Cavernous hemangioma
均一 (時に辺縁のみ) 均一 均一
軟部組織とiso 均一 hypo hyper 均一Basal cell adenoma
均一 均一 均一
那須野 智光,他

113
後不良例の中には病理学的に悪性の所見を示すものの
他に,通常のSFTと区別できない組織像のものも存在
し,病理学的所見から予後を推測することは難しいた
め,術後も厳重なフォローが必要である。
SFTの放射線治療や化学療法の有用性は未だ確立さ
れていないが,Saynakらは外科的切除後に再発した
SFTに対し放射線治療が奏功したと報告している45。
Table 1に挙げた症例ではSuarezら及びYangらは悪性と
診断されたSFTに対し術後放射線治療を施行し46,47,光
澤らは術後再発し内頚動脈浸潤が疑われたSFTに対し
放射線治療を施行後,耳下腺全摘術を行っている15。
またParkらは切除できないSFTに対する化学療法を検
討しており,その中でdoxorubicin + ifosfamideを使用し
ている症例が最も多く,その効果はstable diseaseとする
症例が多かったと報告している48。Platelet-derived
growth factor receptor陽性の悪性SFTに対しimatinibが奏
功したとの報告もあり49,悪性度が高いと考えられる
症例においては切除術に加えて,術後補助療法を考慮
してもよいと考えられる。
文 献
1. Klemperer P, Coleman BR. Primary neoplasms of the pleura.Primary neoplasms of the pleura. A report of five cases. Am J IndMed 1992; 22: 1-31.
示す (Table 2)27-38。SFTにおいて造影効果の認められる
部位は組織学的にhigh vasucularityな部分であるという
報告や39,sizeが小さい場合は均一に,大きくなると分
葉化しcystic degenerationやcalcificationを伴うことによ
り不均一に造影されるという報告がある40。
SFTの確定診断は組織診断,特に免疫染色による鑑
別が重要である。SFTの病理組織学的特徴は卵円形〜
紡錘形の細胞が不規則に配列し,“鹿角様 (staghorn)”
と呼ばれるスリット状の血管腔が多数認められること
である。免疫組織学的特徴としてSFTの90〜95%で
CD34陽性になることが鑑別診断に特に有益である。ま
たbcl-2やMIC-2 (CD99) も高頻度に陽性に,分子遺伝学
的に特異的な融合遺伝子NAB2-STAT6を有し41,核内
でSTAT6が強く発現されるため42,STAT6が核陽性に
なる。病理組織学上の鑑別診断としてSFT以外の線維
血管組織に富む紡錘形細胞腫瘍として,①軟部血管線
維腫,②富細胞性血管線維腫,③乳腺型筋線維芽細胞
腫,④紡錘形細胞/多形脂肪腫,⑤胃腸管間質腫瘍,
⑥単相型線維性滑膜肉腫,⑦髄膜腫が挙げられる
(Table 3)43。また,悪性の基準として,①10 cm以上の
腫瘍径,②初回の播種巣,③浸潤性発育,④高細胞密
度,⑤核多形性,⑥顕微鏡下で10視野中4以上の核分
裂,⑦腫瘍壊死の存在を持つこととされている2。
治療は外科的切除術が原則であり,多くは術後良好
な経過をたどるが胸腔外SFTの場合,局所再発 : 4.3%,
転移 : 5.4%であったという報告もある44。これらの予
Table 3. Pathological and immunohistological feature of SFT and the other diseases
疾患 病理組織学的特徴
豊富な膠原線維,血管周皮腫様血管,patternlessな配列SFT
90〜95%でCD34 (+),bcl-2 (+),MIC-2 (CD99) (+),STAT6で核 (+)
膠原線維性・粘液性間質, patternlessな配列
軟部血管線維腫 分枝状小型血管網,フィブリノイド壊死,多核巨細胞
少数例でCD34 (+),約半数例でEMA (+)
豊富な線維血管組織,少量の脂肪組織,膠原線維束
富細胞性血管線維腫 壁肥厚性の小〜中型血管,血管壁の硝子化,肥満細胞
30〜60%でCD34 (+),多数例でER (+),PgR (+)
硝子様膠原線維束,脂肪組織,小型血管,多数の肥満細胞乳腺型筋繊維芽細胞腫
CD34 (+),desmin (+)
膠原線維性・粘液性基質,脂肪組織,ロープ状膠原線維,floret様多核巨細胞紡錘形細胞/多形細胞腫
CD34 (+)
腹腔内腫瘤,類上皮様腫瘍細胞,索状配列胃腸管間質腫瘍
CD34 (+),c-kit (+)
核異型,核分裂像,血管周皮腫様血管単相型線維性滑膜肉腫
CD34 (-),cytokeratin (+),EMA(+)
髄膜腫瘤,渦巻状配列,索状配列髄膜腫
CD34 (-),EMA (+)
耳下腺SFTの一例

114
2. England DM, Hochholzer L, McCarthy MJ. Localized benign andmalignant fibrous tumors of the pleura. A clinicopathologic reviewof 223 cases. Am J Surg Pathol 1989 ; 13: 640-58.
3. Ridder GJ, Kayser G, Teszler CB, et al. Solitary fibrous tumors inthe head and neck: new insights and implications for diagnosis andtreatment. Ann Otol Rhinol Laryngol 2007; 116: 265-70.
4. Cardillo G, Carbone L, Carleo F, et al. Solitary fibrous tumors ofthe pleura: an analysis of 110 patients treated in a single institution.Ann Thorac Surg 2009; 88: 1632-7.
5. Magdeleinat P, Alifano M, Petino A, et al. Solitary fibrous tumorsof the pleura: clinical characteristics, surgical treatment andoutcome. Eur J Cardiothorac Surg 2002; 21: 1087-93.
6. Penel N, Amela EY, Decanter G, et al. Solitary fibrous tumors andso-called hemangiopericytoma. Sarcoma 2012; 2012: 690251.
7. Okike N, Bernatz PE, Woolner LB. Localized mesothelioma ofthe pleura: benign and malignant variants. J Thorac CardiovascSurg 1978; 75: 363-72.
8. 苅田 健,井上小百合,片岡恵美,他. 顎下腺に発生した
Solitary fibrous tumor: SFTの一例. 日本臨床細胞学会雑誌 2014;53 (補冊2): 636.
9. 田中 宏,原澤 有,竹下 徹,他. 顎下腺に発生した
solitary fibrous tumorの1例. 日本医学放射線学会雑誌 1999;59: S422.
10. Vecina VM, Zarraonandia I, Monzon M, et al. Solitary fibroustumour of the submandibular gland. Acta Otorrinolaringológica
~Espanola 2015; 66: 302-4.11. 浦野 誠,熊澤 文,桐山 諭,他. 舌下腺に発生した
solitary fibrous tumor (SFT) の1例. 日本唾液腺学会誌 2010;51: 30.
12. Günhan O, Yildiz FR, Celasun B, et al. Solitary fibrous tumourarising from sublingual gland: report of a case. J Laryngol Otol1994; 108: 998-1000.
13. Ogawa I, Sato S, Kudo Y, et al. Solitary fibrous tumor withmalignant potential arising in sublingual gland. Pathol Int 2003;53: 40-5.
14. 藤森正登,小宮 尚,奥川真理子,他. 耳下腺solitary fibroustumorの一例. 口腔・咽頭科 2001-2002; 14: 111.
15. 光澤 知,四ノ宮隆,島田 剛,他. 耳下腺に発生した
solitary fibrous tumorの1例. 日本耳鼻咽喉科学会会報 2004;107 (Suppl 1): 52.
16. 立花哲也,千葉博茂,伊能智明,他. 耳前部に発生した孤立
性線維性腫瘍の1例. 日 本口腔外科学会雑誌 2004; 50: 239-42.
17. 平野和彦,平野和彦,山本智理子,他. 耳下腺に発生した
solitary fibrous tumorの一症例. 日本病理学会会誌 2007; 96:296.
18. Bauer JL, Miklos AZ, Thompson LD. Parotid gland solitary fibroustumor: a case report and clinicopathologic review of 22 cases fromthe literature. Head Neck Pathol 2012; 6: 21-31.
19. Iyengar JN, Atmaram M, Neeli D, et al. Solitary fibrous tumorpresenting as a mass in the parotid gland. Indian J Pathol Microbiol2011; 54: 612-3.
20. Cristofaro MG, Allegra E, Giudice M. Two new localizations ofsolitary fibrous tumor in the italian population: parotid gland andoral cavity-review of the literature. J Oral Maxillofac Surg 2012;70: 2360-7.
21. Sousa AA, Souto GR2, Sousa IA, et al. Solitary fibrous tumor ofthe parotid gland: Case report. J Clin Exp Dent 2013; 5: e208-11.
22. Kwok MM, Subramaniyan M1, Chan SW. Solitary Fibrous Tumourof the Parotid Gland: A Case Report and Review of the Literature.Case Rep Otolaryngol 2015; 2015: 741685.
23. Yu R, Rebello R. Solitary Fibrous Tumor of the Parotid Gland: ACase Report. Iran J Otorhinolaryngol 2015; 27: 401-5.
24. Alonso-Rodríguez E, González-Otero T, Castro-Calvo A, et al.Parotid gland solitary fibrous tumor with mandibular bonedestruction and aggressive behavior. J Clin Exp Dent 2014; 6:e299-302.
25. 上村明寛,朝日淳仁,野村研一郎,他. 前頸部に発生した孤
立性線維性腫瘍例. 耳鼻咽喉科臨床 2015; 108: 561-8.26. 田宮貞史,杉本英治,木村浩明,他. 骨・軟部腫瘍─臨床・
画像・病理 改訂第2版. 大塚隆信,福田国彦,小田義直編,
東京,診断と治療社,2015,p.220-1.27. Liu Y, Li K, Shi H, et al. Solitary fibrous tumours in the extracranial
head and neck region: correlation of CT and MR features withpathologic findings. Radiol Med 2014; 119: 910-9.
28. Li XM, Reng J, Zhou P, et al. Solitary fibrous tumors in abdomenand pelvis: imaging characteristics and radiologic-pathologiccorrelation. World J Gastroenterol 2014; 20: 5066-73.
29. Yang BT, Song ZL, Wang YZ, et al. Solitary fibrous tumor of thesinonasal cavity: CT and MR imaging findings. AJNR Am JNeuroradiol 2013; 34: 1248-51.
30. Papathanassiou ZG, Alberghini M, Picci P, et al. Solitary fibroustumors of the soft tissues: imaging features with histopathologiccorrelations. Clin Sarcoma Res 2013; 3: 1.
31. Ginat DT, Bokhari A, Bhatt S, et al. Imaging features of solitaryfibrous tumors. AJR Am J Roentgenol 2011; 196: 487-95.
32. Kim TA, Brunberg JA, Pearson JP, et al. Solitary fibrous tumor ofthe paranasal sinuses: CT and MR appearance. AJNR Am JNeuroradiol 1996; 17: 1767-72.
33. Hyodo R, Komada T1, Takada A, et al. Solitary fibrous tumors inthe extremities: imaging findings for six patients. Nagoya J MedSci 2015; 77: 167-78.
34. Takeshita T, Tanaka H, Harasawa A, et al. CT and MR findings ofbasal cell adenoma of the parotid gland. Radiat Med 2004; 22:260-4.
35. Yerli H1 Teksam M, Aydin E, et al. Basal cell adenoma of theparotid gland: dynamic CT and MRI findings. Br J Radiol 2005;78: 642-5.
36. Okahara M, Kiyosue H, Matsumoto S, et al. Basal cell adenoma ofthe parotid gland: MR imaging findings with pathologic correlation.AJNR Am J Neuroradio 2006; 27: 700-4.
37. Levine E, Wetzel LH, Neff JR. MR imaging and CT of extrahepaticcavernous hemangiomas. AJR Am J Roentgenol 1986; 147: 1299-304.
38. KKlotz T, Montoriol PF, Da Ines D, et al. Hepatic haemangioma:common and uncommon imaging features. Diagn Interv Imaging2013; 94: 849-59.
39. Rosado-de-Christenson ML, Abbott GF, McAdams HP, et al. Fromthe archives of the AFIP: Localized fibrous tumor of the pleura.Radiographics 2003; 23: 759-83.
40. Lee KS, Im JG, Choe KO, et al. CT findings in benign fibrousmesothelioma of the pleura: pathologic correlation in nine patients.AJR Am J Roentgenol 1992; 158: 983-6.
41. Robinson DR, Wu YM, Kalyana-Sundaram S, et al. Identificationof recurrent NAB2-STAT6 gene fusions in solitary fibrous tumorby integrative sequencing. Nat Genet 2013; 45: 180-5.
42. Doyle LA, Vivero M1, Fletcher CD, et al. Nuclear expression ofSTAT6 distinguishes solitary fibrous tumor from histologic mimics.Mod Pathol 2014; 27: 390-5.
43. 杉田真太朗,長谷川匡. 癌診療指針のための病理診断プラク
ティス. 小田義直専門編集,中山書店,東京,2013.44. Vallat-Decouvelaere AV, Dry SM, Fletcher CD. Atypical and
malignant solitary fibrous tumors in extrathoracic locations:evidence of their comparability to intra-thoracic tumors. Am JSurg Pathol 1998; 22: 1501-11.
那須野 智光,他

115
45. Saynak M, Bayir-Angin G, Kocak Z, et al. Recurrent solitaryfibrous tumor of the pleura: significant response to radiotherapy.Med Oncol 2010; 27: 45-8.
46. Yang XJ, Zheng JW, Ye WM, et al. Malignant solitary fibroustumors of the head and neck: a clinicopathological study of nineconsecutive patients. Oral Oncol 2009; 45: 678-82.
47. Suárez Roa Mde L, Ruiz Godoy Rivera LM, Meneses Garcia A, etal. Solitary fibrous tumor of the parotid region. Report of a caseand review of the literature. Med Oral 2004; 9: 82-8.
A case of solitary fibrous tumor of the parotid gland
Tomomitsu Nasuno,1 Masahiko Takeda,2 Kentaro Ohashi,3 Yutomo Seino,4
Tomoko Yamaguchi,5 Makito Okamoto,4 Taku Yamashita4
1Department of Otorhinolaryngology, Toshiba Rinkan Hospital2Hashimoto Tower Otorhinolaryngology3Department of Otorhinolaryngology, Kitasato Medical Center4Department of Otorhinolaryngology-Head and Neck Surgery, Kitasato University School of Medicine5Department of Otorhinolaryngology, Sagamihara National Hospital
Solitary fibrous tumor (SFT) is a mesenchymal neoplasm, and the most common site is the pleura. SFT in thehead and neck lesion is rare. We reported an SFT from the parotid gland. A 48-year old woman complainedof right-sided subauricular swelling. Ultrasound examination and contrast-enhanced computed tomographyrevealed a well-defined tumor with abundant blood flow. The patient underwent a right superficialparotidectomy. Histological examination revealed that the spindle cells were arranged in a random pattern,known as a "patternless pattern," and thin-walled branching vessels, "staghorn." Additionally,immunohistochemical study showed a strong positivity of vimentin and CD34. From the above findings, thistumor was diagnosed as SFT. Her postoperative course was uneventful, and she remains free from disease 10years after the surgery.
Key words: solitary fibrous tumor, parotid gland, immnohistological test, head and neck lesion
48. Park MS, Ravi V, Conley A, et al. The role of chemotherapy inadvanced solitary fibrous tumors: a retrospective analysis. ClinSarcoma Res 2013; 3: 7.
49. De Pas T, Toffalorio F, Colombo P, et al. Brief report: activity ofimatinib in a patient with platelet-derived-growth-factor receptorpositive malignant solitary fibrous tumor of the pleura. J ThoracOnco 2008; 3: 938-41.
耳下腺SFTの一例
Related Documents











