SOFT TISSUE TUMORS COME FROM ANY TISSUE: FAT, NERVE, BV’S, SM. MUSC, SKEL. MUSC CLINICAL: SUMUCOSAL LUMPS, COVERED W/ INTACT SMOOTH EPITHELIUM BENIGN: FREELY MOVEABLE, OR IF BOUND TO BONE-HARD PALATE/GINGIVA MALIGNANT: SARCOMAS LG, BULKY ULCERATING-METAST VIA BLOOD DIFFERENTIATED BY ONE DISTINGUISHING FEATURE

SOFT TISSUE TUMORS COME FROM ANY TISSUE: FAT, NERVE, BV’S, SM. MUSC, SKEL. MUSC CLINICAL: SUMUCOSAL LUMPS, COVERED W/ INTACT SMOOTH EPITHELIUM BENIGN:
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SOFT TISSUE TUMORS
COME FROM ANY TISSUE: FAT, NERVE, BV’S, SM. MUSC, SKEL. MUSC
CLINICAL: SUMUCOSAL LUMPS, COVERED W/ INTACT SMOOTH EPITHELIUM
BENIGN: FREELY MOVEABLE, OR IF BOUND TO BONE-HARD PALATE/GINGIVA
MALIGNANT: SARCOMAS LG, BULKY ULCERATING-METAST VIA BLOOD
DIFFERENTIATED BY ONE DISTINGUISHING FEATURE

LIPOMA• COMMON MATURE ADIPOSE
• SKIN
• TRUNK, SHOULDERS, EXTREMITIES, OCCASIONALLY HEAD AND NECK
• ORAL – UNCOMMON BM AND VESTIBULE, 1-3 CM
• CLINICAL: EXOPHYTIC SOFT COMPRESSIBLE MASS W/ YELLOW CAST
• MICRO: DEMARCATED MASS OF MATURE ADIPOSE TISSUE W/ THIN FIBROUS SEPTAE

LIPOSARCOMA• MALIGNANT
• THIGH AND RETROPERITONEUM
• GROWS SLOW AND BECOMES HUGE INFILTRATING TUMOR
• DOES NOT METASTASIZE – CAN’T BE SEPARATED FROM SURROUNDING TISSUE SO IT RETURNS!
• MORE AGGRESSIVE EACH TIME IT RETURNS
• RARE IN MOUTH
• HISTO: WEIRD LOOKING FAT CELLS

SCWANNOMA/NEURILEMOMA
• BENGIN
• SCHWANN CELLS FROM NERVE
• SLOW GROWING
• FIRM ELEVATED MASS
• UNCOMMON, BUT MANY CASES IN ORAL CAVITY
• GROW CENTRALLY IN MANDIBLE, ASSOC W/ MAND. NERVE
• NOT ASSOC W/ NEUROFIBROMATOSIS
• HISTO: WELL DEMARCATED AND ENCAPSULATED
• SPINDLY CELLS W/ WAVY NUCLEI AND NO AXONS
• ANTONI A: SPINDLY CELLS, WAVY NUCLEI, VEROCAY BODIES-ORGANOIDS PALISADED
– NUCLEI AROUND CENTRAL ZONE
• ANTONI B: VACULOATED LOOSE MYXOMATOUS TISSUE

NEUROFIBROMA• COMMON BENIGN TUMOR OF PERINEURIUM
• SCHWANN CELLS AND AXONS ARISING FROM A NERVE
• SLOW GROWER, SOFT - CAN BECOME LARGE
• NOT UNCOMMON IN ORAL CAVITY
• GROW CENTRALLY IN MANDIBLE ASSOC. W/ V3 – GROWS IN CANAL AND EATS ITS WAY OUT!
• HISTO: DEMARCATED AND UNENCAPSULATED (SCWANNOMA IS ENCAPSULATED)
• INTERLACING BUNDLES OF SPINDLY WAVY CELLS MIXED W/ FIBRILLAR COLLAGEN GROUND SUBSTANCE AND AXONS (SCWANNOMA IS WAVY-ANTONI A/B)

NEUROFIBROMATOSIS 1• AUTO DOMINANT
– COMMON, COMPLETE PENETRANCE, VARIABLE EXPRESSIVITY, 50% SPONTANEOUS MUTATIONS
• PATHOGENESIS: MUTATION IN NF1 (TUMOR SUPRESSOR GENE)• NF1: MAKES NEUROFIBRIN INACTIVATING RAS, W/O RAS YOU HAVE NO NEURAL GROWTH
• CLINICAL: MULTIPLE FIBROMAS IN SKIN, BONES, ORGANS – DEVELOP THROUGHOUT CHILDHOOD– 70-90% SHOW ORAL LESIONS – CAFÉ-AU-LAIT SPOTS 6+ COAST OF CALIFORNIA-IRREGULAR– CROW SIGN – AXILLARY FRECKLING– LISCH NODULES – BROWN SPOT IN IRIS– ELEPHANTIASIS NEUROMATOSA – PENDULOUS MASSES
• SARCOMA TRANSFORMATION IN 5%• ***HISTO: PLEXIFORM NEUROFIBROMA – BAG OF WORMS

MULTIPLE ENDOCRINE NEOPLASIA III
MEN III• AUTO DOMINANT – HIGH PENETRANCE, HI EXPRESSIVITY, 50% SPONTANEOUS
MUTATIONS
• PATHOGENESIS: MUTATION OF SINGLE AMINO ACID IN RET PROTONCOGENE, CAUSING OVEREXPRESSION
• RET – PRODUCES PROTEIN PROMOTING GROWTH OF NEUROECTODERM
• C CELLS – THYROID, PHEOCHROMOCYTES – ADRENAL MEDULLA, GI GANGLION CELLS
• CLINICAL: ORAL, CONJUNCTIVA, GENITAL NEUROMAS/HAMARTOMAS, SIMILAR COWDENS
• HYPERPLASIA OF GI PARASYMPATHETIC PLEXUS – DIARRHEA
• MARFANOID HABITUS –LONG AND TALL
• PATULOUS LIPS – THICK, FULL OF NEUROMAS
• AGGRESSIVE MEDULLARY THYROID CANCERS
• PHEOCHROMOCYTOMAS, HTN, INCREASE IN CALCITONIN
• HISTO: SIMILAR TO NEUROMA
• RX: PROPHYLACTIC THYROIDECTOMY
• ASK PT IF THYROID PROBLEMS RUN IN FAMILY

GRANULAR CELL TUMOR(GRANULAR CELL MYOBLASTOMA)
• DERIVED FROM SCWANN CELLS
• TONGUE MOST COMMON LOCATION – DORSAL FEW SALIVARY GLANDS, BM AND LIP TOO
• ADULT FEMALES
• BREAST AND TIBIAL SKIN
• FIRM, SLOW GROWING LUMP COVERED W/ WHT EPITHELIUM
• CLINICALLY IT’S TOO FAR FORWARD TO BE LINGUAL THYROID
• TUMOR INFILTRATES INTO MUSCLE
• HISTO: INFILTRATIVE LG, POLYGONAL CELLS W/ DISTINCT CELL BOUNDARIES AND LG EOSINOPHILIC CYTOPLASMIC GRANULES, SM ROUND NUCLEI – INCONSPICUOUS
• ***PSEUDOEPITHELIOMATOUS HYPERPLASIA – PH, KA, EF
• RX: REMOVE, LOW RECURRENCE

CONGENITAL EPULIS• ETIOLOGY: UNKNOWN
• CLINICAL: NEWBORNS AS SMOOTH, PINK, PEDUNCULATED, POLYPOID LUMP ON ANTERIOR RIDGE – MAXILLA, 90% FEMALES
• HISTO: SHEETS OF LG, POLYGONAL GRANULAR CELLS W/ SM NUCLEI LOOKS LIKE, BUT UNRELATED TO GRANULAR CELLS IN GCT
• RX:EXCISION, NO RECURRENCE, SOMETIMES SHRINK & SPONTANEOUSLY REMIT

MELANOTIC NEUROECTOMDERMAL TUMOR OF INFANCY
• CLINICAL: ANTERIOR ALVEOLAR BONE OF NEWBORN – 1ST YR, MAXILLA• RAPIDLY GROWING MASS • INVADES BONE• LAB: URINARY VMA, PRODUCES CATECHOLAMINES• HISTO: BIPHASIC PATTERNS DUCTS- NEUROBLASTS
– SMALL DUCTS LINED W/ CUBOIDAL CELLS W/ MELANIN– CLUSTERS OF NEUROBLASTS (SM CELLS W/ HYPERCHROMATIC NUCLEI AND SCANT
CYTOPLASM– FIBROUS STROMA– NEURAL CREST ORIGIN
• TX/PX: RESCECTION, 15% RECURRENCE, 6% MALIGNANT AND METASTASIZE

HEMANGIOMA• HAMARTOMA OF BV’S• RAPID GROWER SHORTLY AFTER BIRTH OR W/IN 1 YR, GROWS FOR 6-12 MO• FEMALE PREDILECTION 3:1• HEAD & NECK
• CLINICAL: FLAT OR RAISED, RED, PURPLE OR BLUE, SM OR LG
• HISTO: CAPILLARY – PLUMP, ACTIVE ENDOTHELIAL CELLS FORMING SM VESSELS – SLOW BLD FLOW
CAVERNOUS – LG, THIN WALLED, ANASTAMOSING VESSELS, PROMINENT LUMINA
• DD: soft tissue lesion hemangioma arteriovenous malformation intraosseous lesions hemangioma ameloblastoma giant cell lesion
• TX: 90% SPONTANEOUSLY RESOLVE BY 9 YRS
NO TX UNLESS LIFE THREATENING, STEROIDS OR INTERFERON

PERIPHERAL NERVE SHEATH TUMOR(NEUROGENIC SARCOMA)
• SARCOMA – FROM PERIPHERAL NERVE
• UNCOMMON – TRANSFORMATION OF NEUROFIBROMA IN NF1
• EXTREMITIES – HEAD & NECK RARE
• PX: POOR
• HISTO: IRREGULAR SHAPED NUCLEI, SPINDLY, WAVY

VASCULAR MALFORMATIONS• OFTEN CONFUSED W/ HEMANGIOMAS CUZ:
– SEEN IN YOUNG KIDS
– RED/PURPLE LESIONS COMPOSED OF BV’S
– COMMON IN HEAD & NECK
– HAVE SIMILAR HISTO
• DIFFERENT BECUZ THEY:
– PRESENT AT BIRTH
– GROW W/ PT AND DO NOT DISAPPEAR
– LIFE THREATENING HEMORRHAGE WHEN TRAUMATIZED OR BIOPSIED – LG BLD FLOW!
– CAN OCCUR IN BONES – INCLUDING JAWS
– ASSOC. W/ GENETIC AND NON-GENETIC SYNDROMES – STURGE-WEBER SX & VON HLIPPEL-LINDAU
• TX: SURGERY, LASERS OR SCLEROSING AGENTS
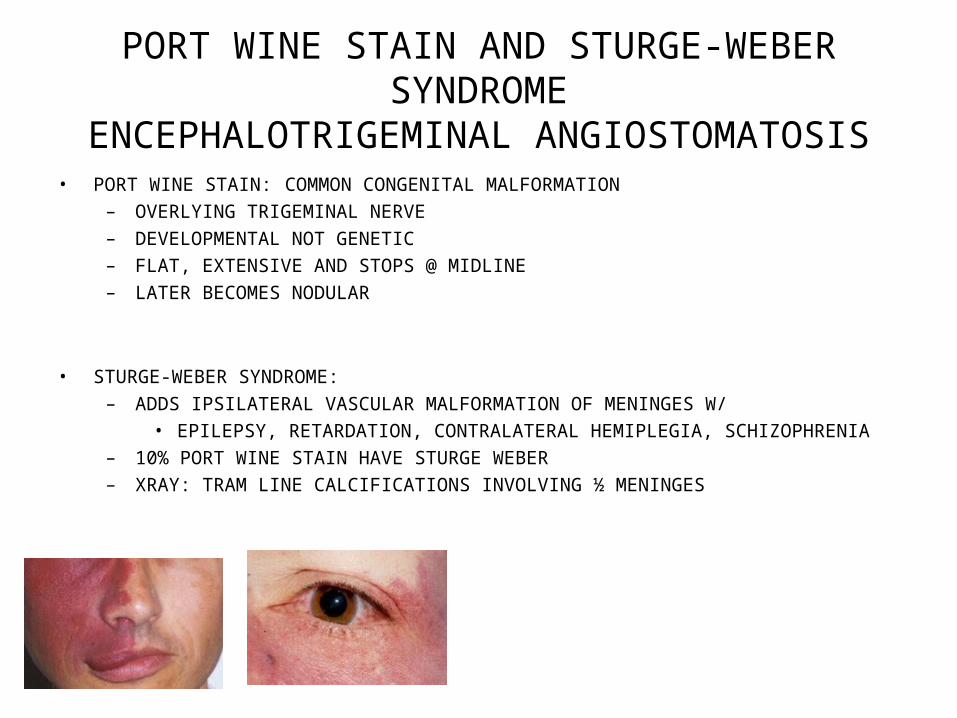
PORT WINE STAIN AND STURGE-WEBER SYNDROME
ENCEPHALOTRIGEMINAL ANGIOSTOMATOSIS• PORT WINE STAIN: COMMON CONGENITAL MALFORMATION
– OVERLYING TRIGEMINAL NERVE
– DEVELOPMENTAL NOT GENETIC
– FLAT, EXTENSIVE AND STOPS @ MIDLINE
– LATER BECOMES NODULAR
• STURGE-WEBER SYNDROME:
– ADDS IPSILATERAL VASCULAR MALFORMATION OF MENINGES W/
• EPILEPSY, RETARDATION, CONTRALATERAL HEMIPLEGIA, SCHIZOPHRENIA
– 10% PORT WINE STAIN HAVE STURGE WEBER
– XRAY: TRAM LINE CALCIFICATIONS INVOLVING ½ MENINGES

OSLER-WEBER-RENDU DZHEREDITARY HEMORRHAGIC
TELANGECTASIA(HTT)• AUTO DOMINANT
• MUTATION OF PROTEINS THAT MAINTAIN BV WALL INTEGRITY CAUSING WEAKNESS
• 1-2MM LESION ON SKIN, ORAL, GI MUCOSA
• INCREASING W/ AGE
• BLANCHE W/ PRESSURE - TELANGECTASIA
• CAUSE EPISTAXIS-CLASSIC 1ST SIGN = NOSEBLEEDS
• GI BLEEDS CAUSE ANEMIA-1 BURST SLOW BLEEDING = ANEMIA
• AV MALFORMATIONS IN LUNGS, LIVER, BRAIN
– HI CO FAILURE
– INCREASE RISK FOR BRAIN ABSCESS – FATAL – TRANSIENT BACTEREMIAS CAN GET INTO BRAIN
• ***PREMED FOR DENTAL TX

NASOPHARYNGEAL ANGIOFIBROMA
• BENIGN
• ERECTILE TISSUE – BECOMES NEOPLASTIC CUZ OF BV’S
• PTERYGOPALATINE FOSSA - MAXILLA
• ***ADOLESCENT MALES
• RISK OF FATAL HEMORRHAGE – SPONTANEOUS OR DURING SURGERY IF IT’S NICKED IT BLEEDS LIKE CRAZY
• GROWS LARGE AND FAST IS DESTRUCTIVE AND INVASIVE
• CAUSES NASAL OBSTRUCTION AND EPISTAXIS – NOSEBLEEDS
OF LG DILATED VESSELS AND DENSE FIBROUS TISSUE
• XRAY: ANT BOWING OF POSTERIOR WALL OF MAXILLA-PRESSES ON BONE AND PUSHES IT FORWARD
• RX: SURGICAL REMOVAL W/ HIGH RECURRENCE RATE

LYMPHANGIOMA• HAMARTOMA OF LYMPHATICS CONGENITAL OR W/IN 2YRS EARLY IN LIFE• HEAD AND NECK• INFILTRATE TONGUE CAUSING MACROGLOSSIA W/ PEBBLY SURFACE• ***CYSTIC HYGROMA – GIANT CONGENITAL CAVERNOUS LYMPHANGIOMA OF HEAD AND NECK
INTERFERE W/ BREATHING AND CAN BE FATAL
• LG ONES SEEN W/ INFECTION OR ALLERGY CAUSING ASPHYXIA• RX: DOESN’T DISAPPEAR & CANNOT BE SCLEROSED
SURGERY – INFILTRATES INTO MUSCLE AND RECURS
DD: lymphangioma hemangioma angiosarcoma Kaposi sarcoma

HEMANGISARCOMA• MALIGNANT TUMOR OF BLD VESSELS
• RARE 50% IN HEAD AND NECK
• NO TX
• KILLS BY LOCAL EXTENSION AND DISTANT METASTASES
• MOST ARE FATAL

LYMPHANGIOSARCOMA• MALIGNANT TUMOR OF LYMPHATICS
• AXILLA
• PTS THAT HAVE HAD LYMPH NODE DISSECTION – LYMPH HAS NO PLACE TO GO = CONSTANT SWELLING
• NOT EXPECTED IN ORAL CAVITY

KAPOSI SARCOMA• MULTI FOCAL TUMORS OF EPITHELIUM INDUCED BY HPV 8
• 3 TYPES: CLASSIC: RARE, SLOW GROWER, EXTREMITIES, OLD JEWISH/ITALIAN MEN W/ LYMPHOMAS
• ENDEMIC: AFRICAN, FASTER GROWING TUMORS OF KIDS• AIDS RELATED: AGGRESSIVE IN ORAL CAVITY, SKIN/ANAL AREA OF GAY MALES W/ AIDS
• CLINICAL: SKIN AND ORAL CAVITY, BEGIN AS FLAT, RED/BRN LESIONS – PLAQUES - NODULES
• HISTO: PROGRESSIVELY MORE ANAPLASTIC
• TX: RADIATION AND CHEMO HELP CONTROL GROWTH, AIDS RELATED KS RESPONDS TO ANTIVIRAL TX BECUZ IT CONTROLS THE HPV 8 OR/ IMMUNOSUPPRESSION
• PX: CLASSIC TYPE RARELY KILLS , AND TAKES 10 YRS, MORE AGGRESSIVE ARE VARIABLE TO TX
• YOU GET THIS IF YOU HAVE AIDS AND HPV 8
• DD: MELANOMA, hematoma hemangioma pyogenic granuloma malignant melanoma

LEIOMYOMA• BENIGN
• SMOOTH MUSCLE
• UTERUS = FIBROID
• RARE IN MOUTH – IF SO DERIVED FROM BV’S
• CLINICAL: FIRM MASS COVERED W/ EPITHELIUM
• HISTO: CELLULAR SPINDLY SMOOTH MUSCLE FASICLES W/O MITOSES
• DD: neurofibroma nodular fasciitis myxoma neurilemoma fibrous histiocytoma

RHABDOMYOMA• BENIGN TUMOR OF SKELETAL MUSCLE
• RARE
• SLOW GROWER
• MOST COMMON IN HEART, THEN HEAD AND NECK
• ORAL: FOM, SOFT PALATE, TONGUE
• HISTO: ***SPIDER WEB CELL - SKELETAL MUSCLE, NUCLEI TO THE SIDE FILLED W/ GLYCOGEN
• IF FOUND ON TONGUE YOU’D THINK GCT, NEUROFIBROMA, SCHWANNOMA FIRST!

LEIOMYOSARCOMA• MALIGNANT
• SMOOTH MUSCLE
• UNCOMMON
• UTERUS AND GI TRACT
• RARE IN ORAL CAVITY IF SO IN JAWS
• HISTO: CIGAR SHAPED NUCLEI, CELLULAR SPINDLY MUSCLE FASICLES W/ MITOSES – THIS IS KEY WHEN DECIDING BETWEEN BENIGN AND MALIGNANT
• PX: POOR

RHABDOMYOSARCOMAMALIGNANT
SKELETAL MUSCLE
ETIOLOGY: GENETIC TRANSLOCATION PRODUCING NEW PROTEIN THAT INTERRUPTS SKELETAL MUSCLE DIFFERENTIATION
COMMON SARCOMA
HISTO: STRAP LIKE CELLS W/ PLEIOMORPHIC NUCLEI
3 TYPES: EMBRYONAL: MOST COMMON, ORIFICES-NOSE MOUTH PHARYNX VAGINA, KIDS
FAST GROWER, BEST PX – CHEMO CURES 65%
ALVEOLAR: RARE, KIDS, FAST GROWER, WORST PX
PLEOMORPHIC: MOST COMMON IN ADULTS, EXTREMITIES, FAST GROWER
DD: liposarcoma neuroblastoma osteosarcoma

CLUES TO SOFT TISSUE PLAYAS!
• OFTEN ARE CONFUSED W/ FIBROMAS AND SALIVARY GLAND TUMORS
• HEMANGIOMA/VASCULAR MALFORMATION: RED/PURPLE, PRESENT MANY YEARS
• LYMPHANGIOMA: DIFFUSE, PEBBLY SOFT TONGUE LOCATION
• LIPOMA: SOFT YELLOW
• NEUROFIBROMA: SPFT
• GRANULAR CELL TUMOR(GCT): TONGUE, DORSAL
• CONGENITAL EPULIS: MAX ANTERIOR RIDGE OF NEWBORN, FEMALES
• NEUROECTODERMAL TUMOR: MAX ANT RIDGE INFANT, PIGMENTED, BONE DESTRUCTION

SALIVARY GLAND NEOPLASMS
• OCCUR IN MAJOR/MINOR SALIVARY GLANDSPAROTID MOST COMMON AND GREATEST VARIETY HISTO. 80% IN SUPERFICIAL LOBEMINOR-PALATE MOST COMMON >50%, UPPER LIP 20%, LOWER LIP LEAST COMMON, TONGUE NOT COMMON-NO SALIVARY GLANDS
FEMALESAFRICAN AMERICANS30-60 YRSPAINLESS, SLOW GROWER, SUBMUCOSA, FIRM LUMPHARD PALATE-OFF MIDLINEPAROTID-IN FRONT OF OR BELOW EAR, PHARYNGEAL MASS, DEEP LOBEMALIGNANT-SLOW GROWER, ENCAPSULATED, WELL DEMARCATED, HISTO-WELL DIFF, NO
HYPERCHROMATISM, PLEOMORPHISM, MITOTIC ACTIVITYBENIGN-INFILTRATE AND PLEOMORPHISM(OPPOSITE TO WHAT WE LEARNED),LARGER THE GLAND THE MORE BENIGN IT IS!
PAROTID/UPPER LIP – BENIGN 75-80%MALIGNANCY
SUBMANDIBULAR – 40%SUBLINGUAL – 80%PALATE/BM – 50%LOWER LIP – 70%TONGUE, FOM, RMP – 85-90%

SALIVARY GLAND NEOPLASMS
• BENIGN– BMT, PLEIOMORPHIC ADENOMA– WARTHIN’S TUMOR, PAPILLARY CYSTADENOMA,
ADENOLYMPHOMA, LYMPHOMATOSUM– CANICULAR ADENOMA– OXYPHIL ADENOMA, ONCOCYTOMA
• MALIGNANT– MUCOEPIDERMOID TUMOR– ADENOID CYSTIC CARCINOMA, CYLINDROMA– ACINIC CELL CARCINOMA– MALIGNANT MIXED TUMOR– POLYMORPHOUS LOW GRADE ADENOCARCINOMA, LOBULAR
CARCINOMA, TERMINAL DUCT CARCINOMA

BENIGN VS. MALIGNANT• THE FOLLOWING SUGGEST MALIGNANCY:
– FIXED TO UNDERLYING STRUCTURES, EXCEPT IN HARD PALATE
– ULCERATION OR INJECTION (VASCULARITY) OF SURFACE – SPONTANEOUS
– PAIN OR FACIAL PARALYSIS – PAROTID
– RAPID GROWTH
– TELANGIECTASIA OVER SURFACE

TX FOR SALIVARY GLAND TUMORS
• PAROTID LUMPS – SUPERFICIAL LOBECTOMY – DUE TO HI RECURRENCE OF BENIGN LESIONS WHEN NOT TREATED AGGRESSIVELY, EMBEDDED FACIAL NERVE COMPLICATES 2ND SURGERIES
• SUBMAXILLARY – REMOVE GLAND

BMT PLEIOMORPHIC ADENOMA
• ***MOST COMMON NEOPLASM – 70%
• PAROTID, PALATE, UPPER LIP
• ORIGIN: INTERCALATED DUCTS AND MYOEPITHELIAL CELLS
• HISTO: DUCTS, CYSTS, SHEETS OF BASALOID, SQUAMOID OR SPINDLE CELLS, HYALINE, MUCIN AND MYXOID AREAS, CHONDROID AND BONE – EASY TO MISDX ON FROZEN SECTION OR NEEDLE BIOPSY
• ONE GERM LAYER – NOT TRULY MIXED, CHONDROID, MYXOID, BONE IS MYOEPITHELIAL OR METAPLASTIC STROMAL PRODUCT
• SLOW GROWER, PERSISTENT, BENIGN
• TUMOR BUDS PENETRATE CAPSULE, HI RECURRENCE IF SHELLED OUT, LESS IN MINOR GLANDS
• 5% TURN MALIGNANT

WARTHIN’S TUMOR, PAPILLARY CYSTADENOMA ADENOLYMPHOMA, LYMPHOMATOSUM
• 6%
• IN PERIPAROTID LYMPH NODES FROM ENTRAPPED DUCTAL EPITHELIUM
• 80% MALES – CIG SMOKERS
• 8% BILATERAL
• MULTIPLE UNILATERAL PRIMARIES
• HISTO: PAPILLARY FRONDS (PROJECT INTO CYSTIC SPACE) LINED BY DBL ROW OF COLUMNAR ONCOCYTIC CELLS ON NON-NEOPLASTIC RESIDENT LYMPHOID STROMA W/ GERMINAL CENTERS
• NO RECURRENCE
• NO MALIGNANCY
• LIMITED GROWTH POTENTIAL
• MOST BENIGN TUMOR
• SOFT, BRN, FREELY MOVABLE, ENCAPSULATED

CANICULAR ADENOMA• 75% UPPER LIP
• BLUISH FROM BV’S
• SLOW GROWER
• FREELY MOVABLE, ENCAPSULATED
• HISTO: THIN LAYERS, RIBBONS OF HYPERCHROMATIC COLUMNAR DUCTAL LINING CELLS W/ LOOSE EDEMATOUS(COTTON CANDY), VASCULAR INTERVENING STROMA
• CRIBIFORM PATTERN
• SIMILAR TO ADENOID CYSTIC CARCINOMA – BAD, INFILTRATIVE

OXYPHIL ADENOMA, ONCOCYTOMA
• 1% RARE
• PAROTID
• ELDERLY
• FEMALES
• ONCOCYTES-LG PINK POLYGONAL CELLS IN SHEETS, DUCTS, RIBBONS
• NEVER GET TOO BIG
• LO RECURRENCE/MALIGNANCY
• HISTO: LG PINK, GRANULAR EOSINOPHILIC CELLS, CENTRAL HYPERCHROMATIC, PLEIOMORPHIC, PYKNOTIC NUCLEUS, DEGENERATIVE CHANGE OF DUCTAL, ACINAR CELLS, INCREASE W/ AGE

MALIGNANT

MUCOEPIDERMOID TUMOR
• KIDS MOST COMMON 11%• MOST COMMON PAROTID CANCER• ORAL SITES – RMP, PALATE – IF YOU SEE ONE AT RMP – THIS IS PROLLY IT• ORIGINATE W/IN EXCRETORY DUCTS• HISTO: INFILTRATING NESTS, LOCULES CONTAINING ADMIXTURES OF SQUAMOUS, MUCOUS
AND INTERMEDIATE CELLS• LOW GRADE = CYSTIC AND WELL DIFFERENTIATED MORE COMMON, RARE METAST• HI GRADE = SOLID, POORLY DIFFERENTIATED, MORE INTERMED/SQUAMOUS CELLS• SLOW GROWER, INFILTRATIVE = HI RECURRENCE RATE• CLINICALLY RESEMBLES MUCOCELE – BEWARE OF SOFT CYSTIC IN RMP – UNUSUAL• MOST COMMON TO ARISE AS A PRIMARY W/IN BONE W/ DENTIGEROUS CYST• XRAY: MULTIOCULAR POSTERIR MAND RADIOLUCENCY

ADENOID CYSTIC CARCINOMA, CYLINDROMA
• COMMON INTRAORAL
• PALATE - MINOR
• INFREQUENT IN PAROTID - MAJOR
• MOST COMMON MALIG IN SUBMANDIBULAR GLAND 15%, PAROTID 2%
• HALLMARK-NEUROTROPISM-TARGET AROUND NERVE - PERI &INTRANEUROINVASION, TUMOR NUGGETS FOUND ALONG NERVE = RECURRENCE
• S/S: EARLY PAIN, PAROTID, FACIAL N. PARALYSIS
• PX: 70-85%, INTRAORAL/SUBMANWORSE THAN PAROTID, 5YR SURVIVAL-70%, 15YR 20%
• IF METEST TO LUNGS – PALLIATIVE TX ONLY
• “WOLF IN SHEEP’S CLOTHING” – SLOW GROWER, HISTO LOOKS BENIGN, BUT INFILTRATIVE, BLOOD BORNE METAST(LYMPH NODE DISECTION NOT NECESSARY)
• HISTO: CRIBIFORM – SWISS CHZ MONTONOUS BASALOID CELLS COMPARTMENTALIZED INTO OVOID CYLINDERS BY HYALINIZED PINK MATERIAL. VIA MYOEPITHELIAL AND DUCTAL CELLS
• LOVES BONE, LIVER, LUNGS, EATS RIGHT THRU BONE

MALIGNANT MIXED TUMOR
• FAST GROWER
• CYTOLOGICALLY IS A BMT THAT METASTASIZES - METAST MIXED TUMOR
• CYTOLOGICALLY MALIGNANT TUMOR PRODUCING CHONDROID, HYALINE, MYXOID MATRIX, ETC. CARCINOSARCOMA –
• ***MOST COMMON - BMT UNDERGOES FOCUS OF MALIGNANT DEGENERATION, CAN BE SCCA, NON-SPECIFIC ADENOCARCINOMA, ANY TYPE OF CARCINOMA – CARCINOMA EX PLEOMORPHIC ADENOMA
• INCIDENCE: CARCINOMA EX MIXED TUMOR IS MORE COMMON AND OCCURS IN MIXED TUMORS THAT WERE PREVIUOULSY SURGERIZED ,RADIATED OR PRESENT 10-15 YRS. HX SHOWS SLOW GROWER THAT TOOK SUDDEN GROWTH SPURT= PAIN ULCERATION AND FIXATION
• PX: 5 YR 50% SURVIVAL
– 15 YR 20% SURVIVAL, DISTANT METAST USUAL

ACINIC CELL CARCINOMA
• SLOW GROWER
• PSEUDOENCAPSULATED, LOBULATED
• PAROTID
• CELLS RESEMBLE PACKED SEROUS ACINI, LOOKS BENIGN
• CLEAR CELLS TOO
• HISTO: NORMAL ACINI, BLUE DOT TUMOR, NO STRUCTS OR DUCTS, HISTO IS NOT GOOD INDICATION OF WHICH TUMORS ARE AGGRESSIVE
• TX: WIDE EXCISION PREVENTS RECURRENCES
• BLOOD BORNE METAST
• PX: 70-85% SURVIVAL

Who am I?

POLYMORPHOUS LOW GRADE ADENOCARCINOA, LOBULAR/TERMINAL DUCT CARCINOMA
• PALATE-MINOR GLANDS 65%
• SLOW GROWER, MIMICKS BMT
• ORIGIN: PROXIMAL PORTION OF INTERLOCULAR DUCT
• NON-ENCAPUSLATED
• INFILTRATIVE
• HISTO: SMALL, CLOSELY PACKED WELL DIFF PALE, DUCTAL CELLSIN CENTER OF TUMOR SHOWING POLYMORPHOUS GROWTHS-NESTS, CORDS,SHEETS, CYSTIC SPACES CRIBIFORM PATTERN***
– PERIPHERY SHOWS LINEAR, SINGLE FILE, INDIAN FILE ARRANGEMENT
– PERINEURAL INVASION-BULLS EYE AROUND NERVE SIMILAR TO ADENOCYSTIC CARCINOMA
• TX-REMOVE WIDE LOCAL EXCISION, POSSIBLE RECURRENCE 15%

SGT’S IN KIDS• PAROTID HEMANGIOMA, HEMANGIOENDOTHELIOMA – MOST COMMON
• BMT, MOST COMMON EPITHELIAL GLANDULAR TUMOR
• MUCOEPIDERMOID TUMOR – MOST COMMON MALIGNANT TUMOR

Who am I?

NECROTIZING SIALOMETAPLASIA
• PALATAL SWELLING
• 2-3 WKS LATER TISSUE NECROSIS = NON-INDURATED CRATERIFORM ULCER HEALS IN 6WKS
• ETIOLOGY: LOCAL VASCULAR INSULT = ISCHEMIC INFARCT OF SALIVARY GLAND TISSUE
• ***PEH
• HISTO: INFARCTED SALIVARY GLAND TISSUE WITH PEH OF DUCTS
• COAGULATIVE NECROSIS OF MUCOUS ACINI
• INFLAMM INFILTRATES @ PERIPHERY OF INFARCTED TISSUE
• PROLIFERATION OF DUCTS AND GLANDS
• ISLANDS OF SQUAMOUS CELLS
• DD: SCCA OR MUCOEPIDERMOID CARCINOMA
– SCCA RARE ON PALATE, INDURATED IF SEEN
– MUCOEPIDERMOID IS SLOW GROWER AND RARELY ULCERATES

MUMPS• ETIOLOGY: PARAMYXOVIRUS
• S/S: FEVER, MALAISE, INFLAMMATION, PAIN
• PAIN FROM CONSTRICTION OF DUCTS
• ACUTE BILATERAL, UNILATERAL
• ADULTS: PANCREATITIS-DIABETES, INFERTILITY

ACUTE POSTOPERATIVE PAROTITIS
• OCCURS AFTER DEBILITATING ABDOMINAL SURGERY
• PTS ARE GIVEN ATROPINE WHICH DECREASES SECRETION – INCLUDING SALIVARY GLANDS
• STENSON’S DUCT IS OBSTRUCTED
• INFECTION: S.AUREUS – LIFE THREATENING
• EXTENDS TO PARAPHARYNGEAL AREA

Who am ?

CHRONIC NONSPECIFIC SIALADENITIS, SIALOLITHIASIS
• STONE IN SALIVARY GLAND
• ETIOPATHOGENESIS: LOCAL FACTORS – DUCTAL OBSTRUCTION AND INFLAMMATION, DEHYDRATION, NOT SYSTEMIC FACTORS
• WHARTON’S DUCT FAVORED OVER STENSON CUZ ITS CURLY AND THICK SALIVA CUZ OF LOTS OF MUCOUS IN DUCT
• DX: PALPATE FOM
• RADIOGRAPHICALLY- LOOKS LIKE SOFT TISSUE RADIOOPACITY – DO NOT PROBE
• RX:INCISE ORIFICE TO REMOVE STONES, HYDRATION AND SALIVERY STIMULATION, GLAND REMOVAL, LITHOTRIPSY
• CLNICAL: STONE BLOCKS SALIVA CAUSING PAIN AND SWELLING AT MEALTIME
– IF UNTREATED=CHRONIC, SIALADENITIS CAUSING ATROPHY AND FIBROSIS OF GLAND DUE TO PRESSURE &/OR RECURRENT BACTERIAL INFECTIONS

Who am I?

SJOGRENS SYNDROME• DEF: AUTOIMMUNE, SALIVARY/LACRIMAL GLANDS DO NOT FUNCTION, IF ASSOC W/
SYSTEMIC AUTOIMMUNE DZS ITS RA, AND IT’S SECONDARY SJOGRENS, SLE, PRIMARY IS RARE!
• S/S: DRY MOUTH/EYES
• DX: MED HX, SALIVARY FLOW STUDIES, BIOPSY OF 5 LABIAL SALIVARY GLANDS, SEROLOGICAL STUDIES – INCREASE IN RF, ANA, ANTI-SS-ARO, OR BLA(SJOGRENS)
• HISTO:BENIGN LYMPHOEPITHELIAL LESION, ACINI DESTROYED BY LYMPHOCYTES INFILTRATE/REPLACE PARENCHYMA. RESIDUAL ISLANDS OF DUCTAL EPITHELIUM REMAIN
• RX: NO TX, SIALOGOGUES
• SEQUELE: 6% LYMPHOMA
• CLINICAL: XEROSTOMIA, SEROPHTHALMIA,
• 50% BILATERAL ENLARGEMENT OF SALIVARY AND LACRIMAL GLANDS, PAROTID, SUBMAN, SUBLING TOO!

SIALADENOSIS(NON-INFLAMMATORY)
• DIABETIC
• ALCOHOLIC
• IODINE/THYROID RELATED – ASSOC W/ HYPOTHYROIDISM
• MALNUTRITION, KWASHIORKOR, BULIMA, ANEOREXIA NERVOSA
• OBESITY – STROMAL INFILTRATION OF ADIPOSE TISSUE
• DRUG INDUCED - MEDS

OTHER CAUSES OF BILATERAL SWELLING
• SARCOIDOSIS – UVEOPAROTID FEVER
• TB
• LYMPHO/LEUKEMIA
• CYSTIC FIBROSIS
• UVEAL TRACTS
• BELLS PALSY, FACIAL PALSY

XEROSTOMIA• PATHOGENESIS/ETIOLOGY:
– DUCT OBSTRUCTION – VIT A DEF(SQUAMOUS META OF DUCTS), MUMPS
– NERVE DYSFUNCTION – PSYCHOGENIC-ANXIETY, DRUGS-ANTICHOLIN,HISTA,HYPER,NEURO DZS
– PARENCHYMAL REDUCTION-SENILE ATROPHY, SJOGRENS SX, RADIATION SIALADENITIS, ECTODERMAL DYSPLASIA, SARCOIDOSIS, GRAFT VS. HOST DZ
– DEHYDRATION-FEVER, DIABETES M&I, DIURETICS, CHRONIC VOMITING/DIARHHEA
• S/S: DYSGEUSIA – ALTERED/LOSS OF TASTE – CAN’T FORM BOLUS
– SPEECH AND SWALLOW DYSFUNCTION– DENTURE INTOLERANCE– BURNING, REDNESS, ATROPHY, LOSS OF LINGUAL PAPILLA, CRACKING, ULCERS – ERYTHEMA– CERVICAL CARIES AND CANDIDIASIS – GEL KAM, FL TRAYS, CHLOROHEX
• DX: MILD GLAND– ***MEASURE SALIVA FLOW– SIALOGRAPHY
• TX: SIALOGOGUES – CHOLINERGIC DRUGS, 1% PILOCARPINECEVIMELINE, EVOXAC
– ZNSO4 – STIM SALIVA, IMPROVES TASTE– ARTIFICIAL SALIVA – SJOGRENS– SUGARLESS HARD CANDY– ELIMINATE CAUSE– BIOTENE RX, TOOTHPASTE, MOUTHWASH, GEL, GUM

XEROSTOMIA

SIALORRHEA(PTYALISM)• EXCESSIVE SALIVA – SYMPTOM NOT A DZ
• ETIOLOGY: STIMULATION W/ FOOD
– STOMATITIS &ORAL SORES, ULCERS – ANUG, TEETHING, RAU, HERPES
– DRUGS – MORPHINE, IODIDES, LITHIUM, SIALOGOGUES
– DZS: PARKINSONS DZ, EPILEPSY, CEREBRAL PALSY, RABIES, CF
– HEAVY METAL POISONING – HG, PB, AU
– RETARDATION
– ESOPHAGEAL AND GASTRIC DISTURBANCES – ULCERS, SPASM, REFLUX, GERD

BACTERIAL INFECTIONSCOUGHING/FOMITES
• SCARLET FEVER• TB• SARCOIDOSIS• LYME DZ• SYPHILIS – LEUS• GONORRHEA• NOMA• ACTINOMYCOSIS• DITTRICH’S PLUGS/TONSILLAR SIALOLITHIASIS• CAT SCRATCH FEVER• NON-INFECTIOUS GRANULOMATOUS DZ
– CROHN’S– MELKERSSON-ROSENTHAL SYNDROME

Who am I?

• Etiology: group A beta hemolytic streptococci• Clinical: edematous, pus, abscess, painful, lymphaenitis. Easily
confused w/viral pharyngitis• Oral lesions: filiform papillae fall off and/or turn white = strawberry
tongue will progress to raspberry tongue • Sequelae: Rheumatic fever, poststrep glomerulonephritis• Diagnosis: instant strep test, culture• Tx: antibiotics for 3-7 days, for recurrent infections = tonsilectomy• Scarlet fever is also caused by group A beta hemolytic strep; toxins
get into blood and cause rash. Easily confused w/measles, EBV, secondary syphilis, coxsackie. Only get Scarlet fever ONCE!

• Strep pharyngitis & Scarlet fever

• Who am I?

• Etiology: Mycobacterium tuberculosis
-hominis (transferred person to person, highly infectious!
-avis (found in immunocompromised; NOT infectious
-bovinum (not seen in U.S.; transferred from cows to humans thru unpasteurized milk)
• Clinical: lupus vulgaris, scrofula, pulmonary, miliary
Lupus vulagris- TB of the skin
Scrofula- TB granulomatous ds of lymph nodes
Pulmonary – Primary: Type IV hypersensitivity. Destroys/limits organisms, which causes granulomatous areas in lungs = Ghon focus, if it drains to lymph nodes = Ghon complex (multiple, proliferating, casseous lesions in lungs) harbor for years and can reactivate = Secondary TB (commonly seen in oral cavity as chronic ulcers).
Miliary – systemic spread of TB in immunocompromised. Oral lesions• Diagnosis: AFB- Acid Fast Bacillis; stain used to test for TB;
PPD test- skin test for TB• Tx: Isoniazid- can develop acute chemical Hep
BCG- TB vaccine; will have positive PPD test• Sig to Dentists: TB is aerosol and highly contagious disease if active. DO NOT do
elective tx on active TB pt!! If emergency care needed, do under special ventilation.

• Tuberculosis


• Epidemiology: Black adults in North America• Etiology: unknown, but pine pollen suspected• Pathogenesis: Type IV hypersensitivity• Clinical features:
Skin and lymph nodes, pulmonary involvementCan be found in almost every organ
• Oral features: RareSubmucosal lumps, raised, edematous, cobblestone, can
ulcerate gingivaSalivary glands swollen and uveoparotid fever w/xerostomiaHereford’s disease- dry eyes & mouth assoc w/this ds
• Diagnosis: exclusionary, eliminate everything else and then think this. Serum findings (elevated ACE in severe ds) Kviem test, biopsy, special stains
• Tx: immunosuppressants and steroids. 95% controllable w/drugs• Prognosis: 5% fatal; usually just morbid

•Sarcoidosis

Other non-infectious granulomatous disorders
• Chron’s ds- inflammation of small bowel, anus, mouth. Cobblestone, granulomatous raised mucosa and gingiva w/aphthous superficial ulcers in linear pattern- same ulcers found in ileum.
• Pyostomatitis Vegetans- multiple lesions of lips, vestibule, gingiva, abscess looking, purulent ulcers = snail tracks. Painful. Concomitant condt of the skin= pyodermatosis vegetans. Tx: steroids, Abs. This is seen almost exclusively w/IBD (esp Chron’s ds)
• Oral facial granulomatous- face, especially lips swollen, Bell’s palsy, fissured tongue = Melkerson-Rosenthal syn. Lip lesions alone = Cheilitis Granulomatosum. Occasionally will develop Chron’s or systemic sarcoidosis. Histo: non-cesseating granulosum

MELKERSSON-ROSENTHAL SYNDROME

Wegener’s granulomatous
• Type II/III hypersens. Involving small arterioles• 3 lesions: Necrotic, granulomatous, pulmonary lesions
Necrotic, granulomatous, renal lesions – FATAL Necrotic, oronasal lesions – Strawberry gingivitis
good prog. Factor b/c less severe ds• 3 types:
1) Classic- all 3 organs; poor prog but most common type2) Limited- oronasal lesions only3) Superficial – oral & skin lesions; excellent prog
• Diagnosis: excellent clinical dx• Test: blood test (pAnca, cAnca; antineutrophilic cytoplasmic
antibody)• Tx: immunosuppression

Who am I?

• Et: Borrelia (spirochete)• Epidemiology: geographic – wooded areas from deer tick vector• Pathogenesis: Type III hypersens. To spirochetal antigens• Clinical:
Primary stage – annular rash, fever, malaise
Secondary stage – large rash, fever, malaise, migratory arthritis, meningitis, AV block, Bell’s palsy
Tertiary stage – a hypersens rxn rather than infection. Develop long term migratory arthritis
• Tx: Acute primary or secondary – Erythromycin, Tetracycline
Chronic secondary or tertiary - steroids

•Lyme Disease

Who am I?

• Et: Treponema Pallidum – this is the most invasive org. It can penetrate intact skin• Clinical:
Primary: Chancre that lasts 3-4wks and resolves or turns into secondary
Secondary (metastatic): mucocutaneous puritic rash on hands & feet also an oral lesion develops – mucus path
Tertiary: granulomatous, perivascular, bone, neurological condt. Obliterative endarteritis, gumma- a granulomatous necrotic destruction of bone (palate). NOT infectious! A type IV hypersensitivity rxn.
Congenital: uncommon, rare condt. Skull abnormalities, Hutchinson’s triad- nerve deafness, keratin on cornea, hypoplasia of
enamel (perm incisors & all primary teeth). Features of secondary ds, congenital heart ds, eye defects, saddle nose,
saber shin• Diagnosis: dark field exam
– Serology For primary – Non-specific serology: scrape lesion and look for
spirochetes. Use TPI to immobilize treponema. Look for Chancre, no serologic marker
For Secondary & tertiary- Specific tests: +VDRL+ FTA absorption

•Syphilis (lues)

Who am I?

• Et: Nissseria Gonorrhea. Has a urea receptor on it so it clings to mucosa w/urea (urinary tract). Rare in mouth
• Clinical: acute, suppurative pharyngitis• Dx: culture• Tx: broad spec antibiotics

•Gonorrhea

Who am I?

• Et: fusobacterium necrophorum or F. nucleatum and Prevotella intermedia interact w/Borrelia vincentii, S.aureus, Streptococcus
• Predisposing condts: immunodeficinecy, malnutrition, poor OH, poor sanitation, proximity to livestock, malignancy, recent illness
• Clinical: found in children ages 1-10yo. large, necrotic gingivitis and osteomyelitis. Eats away bone VERY rapidly! Begins as Necrotic infection of ANUG and progresses into deeper tissues. Fetid odor, significant pain, fever, malaise, and regional lymphadenopathy.
• Tx: broad spec antibiotics and correct situation that caused pt to become susceptible. Do NOT aggressively remove damaged area b/c it will aggravate it

•Noma

Who am I?

• Et: Actinomyces isrealii BACTERIA! Even though ds name resembles fungus
• Pathogenesis: anaerobic infection of bone after trauma• Clinical: low grade, mild swelling, sequestrum, fistulas and sinus
tract that drain into skin = lumpy jaw. It can be acute and rapidly progressing or chronic and slowly spreading. The suppurative rxn of the infection may discharge yellowish flecks that represent colonies of the bacteria = sulfur granules. In cervicofacial region it doesn’t spread thru the typical fascial planes and lymph nodes but rather directly thru the soft tissue. Pain is minimal.
• X-ray: ill-defined radiolucency = moth eaten appearance.• Cytologic/Histo: sulfur granule w/in a sea of pus, sunray fungus,
peripheral clubbing, sea of polys• Tx: hi dose antibiotics by IV for 3-6 months. Hyperbaric oxygen
chamber, surgery to remove necrotic tissue.

•Actinomycosis

DITTRICH’S PLUGS
• Need pics, see Tonsillolithiasis on pg. 167

• Hyperplastic tonsils; accumulation of dead cells, bacteria, and inflammatory cells w/in crypts. Turns yellow/white. Is painless and can become large.
• Signs/Symptoms: hallatosis• Tx: can break these off w/q-tip applicator or cotton pliars; pt can do
it at home.• Prog: if they stay there for too long, they can calcify and turn into
tonsolith, which can be seen on an x-ray

•Dittrich’s plugs
•Tonsolithiasis

Who am I?

• Et: Bartonella henselae thru unknown cat scratching a child (under 21 yo)
• Clinical: erythematous papule forms at site of scratch and then resolves. The assoc lymph node develops acute supperative lymphadenitis, which can resemble salivary gland inflammation. Fever also accompanies.
• Diagnosis: stellate abscess in lymph node; indirect fluorescent antibody assay for detecting antibodies to Bartonella henselae. Or ELISA test or PCR. Before these tests became available dx was made on 4 criteria: contact w/cat, presence of scatch, + cat-scratch ds skin test (Hangar-Rose), negative for other causes of lymphadenopathy, char histopathologic findings
• Tx: self-limiting and usually resolves w/in 4 months. Use of local heat, analgesics, and aspiration of node on suppuration is typical pattern of therapy. Antibiotics reserved for cases that have prolonged course or severe involvement.
• Variant: Bacillary angiomatosis- an unusual subcutaneous vascular proliferation, histopathologically similar to histiocytoid hemangioma that is seen in AIDS pts. The affected areas resemble Kaposi’s sarcoma and can be intraoral.

FUNGAL INFECTIONS
• BLASTOMYCOSIS• HISTOPLASMOSIS• COCCIDIOMYCOSIS• CANDIDIASIS

Who am I?

• Et: Blastomces dermatitidis, found in soil and inhaled after a rainstorm• Pathogenesis: infects immunocompromised pts thru skin and mucous
membranes.• Clinical: Spores reach lungs and grow as yeasts, in most ppl it stops here,
but in ic pts it has hematogenous spread to skin, bone, prostate, meninges, oropharyngeal mucosa and abdominal organs. Pulmonary complaints are the most freq sign/symptom. Acute ds resembles pneumonia.Chronic ds is more common and can mimic TB. Cutaneous lesions are often only sign of ds and begin as erythematous nodules that enlarge and become verrucous or ulcerated. Oral lesions result from extrapulmonary dissemination or local inoculation. They have an irregular, erythematous or white intact surface or may be ulcerations w/irregular rolled borders and varying pain, they resemble SCCa! Clinically.
• Histo: Mix of acute inflamm and granulomatous inflamm surrounding yeast cells. Has pseudoepitheliomatous hyperplasia!!!
• Tx: most pts require no tx, even if symptomatic administration of systemic amphotericin B is indicated only if: seriously ill, not improving clinically, ill for more than 2-3wks. Pts w/chronic ds or extrapulmonary lesions need tx, Itraconazole is usually recommended.

• BLASTOMYCOSIS


• Et: Histoplasma capsulatum; spores found in soil containing bird feces.• The most common systemic fungal infection in the U.S.!!• Clinical: most cases are asymptomatic or symptoms so mild the pt doesn’t
even seek tx. Expression of ds depends on quantity of spore inhaled, the immune status of host, and strain of fungus. Acute ds- self-limited pulmonary infection that develops in 1% of ppl exposed to low # of spores. If exposed to hi # spores 50-100% of ppl will develop symptoms. (fever, headache, myalgia, cough, anorexia) similar to flu symptoms, lasts about 2 weeks.Chronic ds-primarily affects lungs, but much less common than acute ds. Usually found in elderly, emphysematous white men or immunocompromised pts. Similar to TBDisseminated ds- even less common. Progressive spread to extrapulmonary sites. Usually occurs in older, debilitated, ic pts. Can affect oral mucosa (solitary, variably painful ulceration of several wks duration, but some may appear white or erythematous w/irregular surface w/rolled margins and may resemble cancer!
• Tx: usually doesn’t need tx other than analgesics and antipyretics. If chronic ds- amphotericin B (can cause sig kidney damage) use ketoconazole in nonimmunocompromised pts. Disseminated form is 90% fatal if untxed, give amphotericin B.

•Histoplasmosis

Who am I?

• Et: Coccidoides immitis, grows in alkaline, semiarid, deser soil of the SW U.S. and Mexico
• Clinical: most pts are asymptomatic, although approx 40% on infected pts experience flulike illness and pulmonary symptoms w/in 1-3 wks after inhalation. Fatigue, cough, chest pain, myalgias and headache are common. Occasionally, the immune response may trigger a hypersens rxn tht causes the development of Erythema Multiforme or Erythema nodosum. The hypersens rxn in conjunction with coccidiodomycosis = Valley fever and resolves as host immune response limits infection.
Chronic progressive pulmonary cocciddiomycosis- mimics TB and is rare
Disseminated ds - <1% of cases. Areas involved: skin, lymph nodes, bone, joints, meninges. Usually found in immunocompromised pts (hi dose corticosteroids, chemo pts, HIV). Lesions develop in area of central face, nasolabial fold but oral lesions are uncommon.
• Histo: round spherules that contain endospores
• Tx: Amphotericin B for: ic pts, severe pulmonary ds, disseminated ds, life-threatening situation. For many cases of the ds fluconazole is drug of choice

•Coccidioidomycosis• San Joaquin Valley fever; Cocci

Zygomycosis

• Et: organisms of the class Zygomycetes; grow on decaying organic materials ie. Fruit, bread
• Epidemiology: affects mostly insulin-dependent diabetics who have uncontrolled diabetes and are ketoacidic; also in immunocompromised pts
• Clinical: Rhinocerebral zygomycosis – nasal obstruction, bloody nasal discharge, facial pain, headache, facial swelling, cellulitis, visual disturbances w/concurrent proptosis. Symptoms of cranial nerve involvement (facial paralysis) are often present. If it progresses to cranial vault, blindness, lethargy, seizures may develop followed by death.If max sinus is involved: initial presentation is intraoral swelling or max alveolar process, palate. Palatal ulceration may occur- appears black and necrotic. Radiographically-opacification of sinuses results, difficult to distinguish from max sinus cancer.
• Histo: extensive necrosis w/numerous large branching nonseptate hyphae at periphery which branch out at 90 degree angles
• Tx: radical surgical debridement of infected necrotic tissue and systmeic, high dose amphotericin B. Prog is poor, often fatal.

Aspergillosis

• Fungal ds char by noninvasive and invasive forms. Noninvasive usually affects normal host, invasive form affects immunocompromised host (AIDS, chemo, transplant pts, uncontrolled diabetes mellitus).
• The spores reside in soil, water, decaying organic debris worldwide and inhaled by host resulting in opportunistic fungal infection second in frequency only to candidiasis.
• Clinical: normal host: allergy affecting sinuses or bronchopulmonary tract, asthma, low grade infection of max sinus. Can undergo dystrophic calcification, produces radioopaque body w/in sinus = antrolith.After tooth ext or endo tx: predisposes sinus to infection, results in symptoms of localized pain and tenderness w/nasal discharge. IC pts are particularly susceptible to this. Painful gingival ulcerations and diffuse soft tissue swelling w/gray or violet hue develops. If not txed extensive necrosis may occur.Disseminated ds- occurs in IC pts but symptoms are vague and difficult to diagnosis early
• Histo: varying numbers of branching septate hyphae which branch at acute angles and invade adj small blood vessels. Occlusion of vessels results in char pattern of necrosis
• Tx: IC pts w/noninvasive ds – surgical debridement allergic fungal sinusitis – debridement and corticosteroids invasive ds in normal host – debridement + systemic antibiotics invasive ds in IC pts – aggressive debridement + systemic antibiotics

Who am I?

• Incidence: ALL HIV pts will develop oral form of this disease!
• Etiology: Candida albicans overgrowth due to:– Host resistance: antibiotics, immunosuppressive drugs, systemic
debilitation– Local factors– Genetic factors: chronic familial mucocutaneous candidiasis– Endocrinopathies: Addison’s, Hypothyroid, Hypoparathyroid, Ovarian
insufficiency, Diabetes mellitus
• Pathogenesis: T & B cells usually keep this in check, but in some pts with the above condts, they will be more prone to candida mucositis. Xerostomia - increase risk b/c no Igs = no protect mucosa.
• moist enviro - increase likelihood. Org competes w/normal bacterial flora in oral cavity

• Acute pseudomembraneous candidiasis– Found in babies shortly after birth b/c they get infected thru the birth canal.– #2 oral manifestation in adults– Causes discomfort, white lesion w/surface coating (made of org) that will scrape
off to reveal red mucosa• Acute atrophic candidiasis
– Red, PAINFUL, swollen tongue, burning sensation• Chronic atrophic candidiasis
– MOST COMMON oral manifestation in adults– Red lesion, NO pain found on palate, ridge, dorsal tongue– Causes: denture sore mouth, angular cheilitis (perleche), Median Rhomboid
glossitis- midline on posterior 2/3 of tongue has PEH!!• Chronic hyperplastic candidiasis
– Uncommon– A painless white patch, hyperkeratosis w/ PEH!!– Presence of candida in this lesion doesn’t mean it is caused by candida albicans
• Histo/Cyto features– Septate pseudohypae– Can scrape off w/spatula put under microscope w/o any stain and see org– Special stains: PAS (Periodic acid-Schiff)-turns org purple; Methenamine Silver
• Tx– Antifungals (ketoconazole, Nystatin, Clortriamazole, Mycolog) Best is Diflucan 3
pills 150mg x 3, qd
Related Documents






