January 1994 In two parts, part 2 volum~ 170, number 1 ETRICS AND GYNECOLOGY Copyright © 1994 bb. Mosby-Year Book, Inc. SOCIETY OF PERINATAL OBSTETRICIANS 1994 14th ANNUAL MEETING Scientific, Clinical, and Business Meeting January 24-29, 1994 Las Vegas, Nevada Published by MOSBY-YEAR BOOK, INC. St. Louis, MO 63146-3318 ISSN 0002-9378

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

January 1994 In two parts, part 2 volum~ 170, number 1
ETRICS AND GYNECOLOGY
Copyright © 1994 bb. Mosby-Year Book, Inc.
SOCIETY OF PERINATAL OBSTETRICIANS
1994 14th ANNUAL MEETING
Scientific, Clinical, and Business Meeting
January 24-29, 1994 Las Vegas, Nevada
Published by
MOSBY-YEAR BOOK, INC.
St. Louis, MO 63146-3318 ISSN 0002-9378

American Journal oy OBSTETRICS AND GYNECOLOGY Copyright © 1994 by Mosby-Year Book, Inc.
14th Annual Meeting of the
Society of Perinatal Obstetricians
January 24-29, 1994
Las Vegas, Nevada
In accordance with the wishes of the majority of the SPO membership, we ask that our
members and guests refrain from smoking in the meeting rooms. This conforms to the spirit of our society and the written procedures of our parent organization.
Table of Contents
Organization .............................................................................. iii
Letter from the Program Chair ................................................ iv
Program Committee ................................................................. v
List of Reviewers ........................................................................ vi
Acknowledgments ..................................................................... vii
Awards ........................................................................................ viii
Map of Meeting AreasmLas Vegas Hilton ............................... ix
Program ..................................................................................... x
Special Interest Group Meetings .............................................. xiii
Scientific Sessions Program ...................................................... xiv
Oral Plenary Session I .............................................................. 263
Oral Concurrent Session A ....................................................... 267
Oral Concurrent Session B ....................................................... 271
Oral Concurrent Session C ....................................................... 275
Oral Plenary Session II ............................................................. 279
Oral Concurrent Session D ...................................................... 283
Oral Concurrent Session E ....................................................... 287
Oral Concurrent Session F ....................................................... 291
Oral Plenary Session III ........................................................... 295
Poster Session I ......................................................................... 299
Poster Session II ........................................................................ 323
Poster Session III ...................................................................... 347
Poster Session IV ....................................................................... 371
Poster Session V ........................................................................ 395
Subject Index ............................................................................. 421
Author Index ............................................................................. 429
Institution Index ....................................................................... 441
ii

14th Annual Clinical, Scientific, & Business Meeting
of the
Society of Perinatal Obstetricians
January 24-29, 1994
Officers Board of Directors
President: Larry C. Gilstrap
Vice President/President Elect: Valerie M. Parisi
Secretary-Treasurer: Donald R. Coustan
Assistant Secretary-Treasurer: Mary E. D’Alton
Steven L. Clark Denise M. Main J. Peter VanDorsten Eleanor L. Capeless Frank A. Chervenak Charles M. Stedman Karin J. Blakemore Patrick Duff Roberto Romero
’94 ’94 ’94 ’95 ’95 ’95 ’96 ’96 ’96
Past Presidents
William N. Spellacy Roy M. Pitkin James A. O’Leary Donald M. Shedine Loren P. Peterson Bruce A. Work Robert H. Hayashi Roy N. Petrie John C. Morrison Amelia C. Cruz Steven G. Gabbe Robert J. Sokol Richard H. Paul Frank C. Miller Thomas J. Garite Garland D. Anderson
’77 ’78 ’79 ’80 ’81 ’82 ’83 ’84 ’85 ’86 ’87 ’88 ’89 ’90 ’91 ’92
iii

Society of Perinatal Obstetricians 409 12th STREET, SW
WASHINGTON, DC 20024
(202) 863-2476
Dear Colleagues:
Having received this issue of the American Journal, with the SPO’s supplement, I hope you are looking for- ward to the .1994 Meeting as much as those of us on the Program Committee. 1 would like to express my sincere
appreciation to all of you who submitted your work for consideration for presentation. It is a tribute to all of you that the response to our meeting has been so strong and sustained. I would also like to express my gratitude to all of the reviewers who, with very short suspenses, did a superb job in getting the information back and allowing the
timely setting of the scientific program.
This year’s meeting will follow the format established last year with both the plenary and concurrent oral sessions. We will also have posters remain on display for the entire day, however, authors will be stationed at the posters only as designated for either the morning or afternoon sessions. Also new this year, and accomplished on all abstracts submitted was an attestation statement affirming that the submitted work had not been previously pre-
sented nor published prior to the Annual Meeting of the SPO. The 1994 SPO has set another record for abstract submissions with 917. This is seven more than the 1993
Meeting and would suggest that perhaps the submissions have plateaued.
Abstracts submitted 917 Oral presentations 78 (8.5%) Plenary 30 (3.3%)
Concurrent 48 (5.2%) Poster presentations 450 (49%) Not accepted 389 (42%)
Several people require special recognition for their efforts in planning the 1994 SPO. Without the support
of Barbara Ohlstein, Linda Oriti, Karylyn Bliss, and Lauretta Stewart the meeting clearly would not be possible. These individuals devoted countless hours of time to the enormous taskings of logging in the abstracts, notifying
the authors of the receipt of their abstracts, getting each abstract out to three reviewers, ensuring that reviewers received abstracts on subjects that they had a preference to review, inputing the scores from the reviewers, and set- ting the scientific program. We were additionally very pleased to welcome Pat Stahr for a large segment of our
busiest week, the week surrounding the deadline for abstract submission. Finally, I would share with you that the
planning for this meeting began five years ago, was intensified approximately two years ago with site visits by a num- ber of individuals on the Program Committee, and has continued at an increasing pace up to and including the opening of the meeting itself.
Finally, many thanks to our President, Dr. Larry Gilstrap and the Program Committee consisting of Doctors Steven Clark, Denise Main, and Sissy Capeless. It is of enormous benefit to have as the President an individual who
has put on the Scientific Program, and who is knowledgeable in all aspects of meeting preparation and thereby able to lend great assistance to the Program Committee. Dr. Gilstrap we salute and thank you. Lastly, a very special and personal thanks to Dr. Valerie Parisi, SPO President Elect and hnmediate Past Program Chair. Her vision in making the format changes which we have carried forward to this year have truly left a mark on the SPO and elevate us to
new heights as a scientific meeting. Finally, we welcome your comments on how we might improve our upcoming meetings. Even more so, we would welcome your help.
Respectfully,
GARY D. V. HANKINS, M.D.
1994 Program Chair, SPO
Founded 1977
Education * Service * Research

1994 PROGRAM COMMITTEE
Gary D.V. Hankins, MD Program Chair
Denise M. Main, MD Poster Chair
Steven L. Clark, MD Postgraduate Course Chair
Valerie M. Parisi, MD, MPH Fundraising Chair
Eleanor L. Capeless, MD Coordinator, Special Interest Groups
The Program Chair, on behalf of the Society, is most grateful to the following people who so conscientiously and promptly judged the abstracts for this meeting.
Iffath Abbasi-Hoskins, MD
Manuel Alvarez, MD
Garland D. Anderson, MD
Robert L. Andres, MD
Joseph J. Apuzzio, MD
David A. Baker, MD
Jeffrey M. Barrett, MD
William H. Barth, Jr, MD
Laxmi Baxi, MD
ThomasJ. Benedetti, MD
Richard Berkowitz, MD
Michael D. Berkus, MD
KarinJ. Blakemore, MD
Jorge D. Blanco, MD
Barry S. Block, MD
Frank H. Boehm, MD
Alan T. Bombard, MD
Sidney F. Bottoms, MD
David W. Branch, MD
Cynthia G. Brumfield, MD
M. Shannon Burke, MD
Byron C. Calhoun, MD
Eleanor L. Capeless, MD
Steve N. Caritis, MD
RobertJ. Carpenter, MD
Robert C. Cefalo, MD
Curtis Cetrulo, MD
Frank A. Chervenak, MD
Ronald A. Chez, MD
Steven L. Clark, MD
William H. Clewell, MD
Joshua A. Copel, MD
David B. Cotton, MD
Larry Cousins, MD
Donald R. Coustan, MD
Susan M. Cox, MD
Robert K. Creasy, MD
William R. Crombleholme, MD
Dwight P. Cruikshank, MD
F. G. Cunningham, MD
Luis B. Curet, MD
Mary E. D’Alton, MD
Richard O. Davis, MD
Lawrence D. Devoe, MD
LeroyJ. Dierker, MD
Sharon L. Dooley, MD
Patrick Duff, MD
John P. Elliott, MD
Nanc3~ L. Eriksen, MD
Hossam E. Fadel, MD
James E. Ferguson, MD
Harold E. Fox, MD
Roger K. Freeman, MD
Steven G. Gabbe, MD
Harvey Gabert, MD
Stanley Gall, MD
Norman F. Gant, MD
ThomasJ. Garite, MD
Ronald S. Gibbs, MD
Larry C. Gilstrap, MD
James D. Goldberg, MD
Robert L. Goldenberg, MD
John W. Goldkrand, MD
PhillipJ. Goldstein, MD
Michael F. Greene, MD
John C. Hauth, MD
Robert H. Hayashi, MD
Durlin E. Hickok, MD
Washington C. Hill, MD
John Hobbins, MD
CalvinJ. Hobel, MD
R. H. Holbrook, MD
Robert L. Jacobson, MD
John W.C.Johnson, MD
Timothy R. Johnson, MD
Michael Katz, MD
John V. Kelly, MD
Eric Knox, MD
Robert A. Knuppel, MD
Nell K. Kochenour, MD
Oded Langer, MD
Russell K. Laros,Jr., MD
Robert P. Lorenz, MD
MichaelJ. Lucas, MD
David A. Luthy, MD
Lauren Lynch, MD
Denise M. Main, MD
Frank A. Manning, MD
James N. Martin, Jr., MD
Arthur S. Maslow, DO
PaulJ. Meis, MD
Michael T. Mennuti, MD
Frank C. Miller, MD
Kenneth J. Moise, Jr., MD
John C. Morrison, MD
Eberhard Mueller-Heubach, MD
Michael P. Nageotte, MD
Roger B. Newman, MD
Edward R. Newton, MD
Jennifer R. Niebyl, MD
Thomas E. Nolan, MD
William F. O’Brien, MD
John Owen, MD
Julian T. Parer, MD
Valerie M. Parisi, MD
Richard H. Paul, MD
Kenneth G. Perry, Jr., MD
Roy H. Petrie, MD
Jeffrey P. Phelan, MD
Lawrence D. Platt, MD
Richard P. Porreco, MD
Gerald Quirk, MD
Susan M. Ramin, MD
William F. Rayburn, MD
John A. Read, MD
Kathryn L. Reed, MD
Robert Resnik, MD
Roberto Romero, MD
Michael Ross, MD
AndrewJ. Satin, MD
Jan Schneider, MD
Harold Schulman, MD
Baha M. Sibai, MD
Michael L. Socol, MD
RobertJ. Sokol, MD
William N. Spellacy, MD
Joseph A. Spinnato, MD
Thomas H. Strong, MD
Shiraz G. Sunderji, MD
Nergesh A. Tejani, MD
Gary R. Thurnau, MD
Paul G. Tomich, MD
GuiltermoJ. Valenzuela, MD
Peter Van Dorsten, MD
Gael P. Wager, MD
RonaldJ. Wapner, MD
Steven L. Warsof, MD
Joseph R. Wax, MD
Stuart Weiner, MD
Carl P. Weiner, MD
George D. Wendel, MD
Katharine Wenstrom, MD
Isabelle A. Wilkins, MD
John Williams, III, MD
Sze-ya Yeh, MD
Edward R. Yeomans, MD
M. Lynn Yonekura, MD
Bruce K. Young, MD

ACKNOWLEDGMENTS
The Society of Perinatal Obstetricians extends sincere thanks and appreciation to the following organizations for their generous support of the 1994 Annual Meeting(*):
Acoustic Imaging
Acuson
Adeza Biomedical
Alfigen-The Genetics Institute
ATL/ADR Ultrasound
Caremark
Corometrics Medical Systems/Wyeth-Ayerst
GeneCare Labs
Genetrix
Healthdyne Perinatal Services
Hewlett Packard
Integrated Genetics
Nellcor
On-Time Medical
Ortho Pharmaceutical Corporation
Peritronics
Ross Laboratories
Tokos Medical Corporation
Toshiba Medical Corporation
Up john
Utah Medical Products
(*) This list reflects known contributors as of press deadline.

Awards On behalf of the Society of Perinatal Obstetricians, the 1994 Program Committee will announce the following awards
as outstanding contributions to this meeting at the Annual Banquet on Thursday, January 27:
Society of Perinatal Obstetricians Award Sponsored by SPO
$1000
Outstanding Research by a Fellow-in-Training Sponsored by AlfigenmThe Genetics Institute
$~000
Outstanding Community Hospital Research Sponsored by Tokos
$1000
Best Genetics Research in the Field of Perinatal Medicine Sponsored by Integrated Genetics
$500
Best Doppler Research in the Field of Perinatal Medicine Sponsored by SPO
$500
Society of Perinatal Obstetricians Achievement Award
This distinguished award has been established by the Board of Directors to honor and recognize an
individual who has contributed significantly to the SPO and its mission. The first ever such award will be presented at the 1994 Annual Banquet.
Fellowship Award of the Society of Perinatal Obstetricians Foundation
The Fellowship Award, designed to support a young investigator in maternal-fetal medicine for an additional year
of fellowship, will be presented at the Annual Banquet.
Awards for the Best Poster Presentations Sponsored by SPO
$500
An award will be given to the best poster presented at each of the five sessions. These awards will be
announced during the closing ceremony on Saturday, January 29.
viii

Ground Floor Directory LasVegas Hilton
¯ RESTAURANTS/BARS
Map Locanon #
I Restaurants ofth~World
Andlamo (ltahan)
8 Paco’s (Mexican)
¯ HOTEL FACILITIES/SERVICES
II Bell Oe~k, Check Room & Laur~dry
12 Bus Stop, Smp
13 Bus Stop~Tour and Travel
14 Elevator, Exterior
15 Elevator, Salon grates
16 Executive Offices
17 Front Desk, Registration,
20 Lobby, Mare
13
Lobby Tower
~ Elevators
\ Springs
27 Castno
28 Casino Cashier
29 Casino Marketing
30 Casino VIP Booth
31 Keno
32 Poker
33 Race and Spor~s Book
34 SuperSIot Reglstrahon Booth
18 Entrance
24 Valet Parking
CASINO FACILITIES/SERVICES
¯ ENTERTAINMENT FACILITIES 35 Arcade 36 Casino Lounge (Stage) 37 JamNrdee Animated Musical Bird Show 38 Showroom 39 Showroom Wdt Call
S
6
Casino
¯ CONVENTION/MEETING FACILITIES
40 Meeting Rooms I 14 and Board Room
41 B~.llroom
42 Package Room
43 Pavdton
44 Hdton Center
45 Salon States (2nd Floor)
Garage Parking
Kdchens
~
41
Hilton Ballroom
43
Hilton Pavilion
Hilton Center
¯ SHOPS
46 North Tower Shop~
47 EaslTower Shops
Convention Center
ix

SOCIETY OF PERINATAL OBSTETRICIANS
14th Annual MeetingmJanuary 24-29, 1994 Las Vegas Hilton ...Las Vegas, Nevada
Program Monday, January 24, 1994 6:00 pm-8:00 pm Registration
7:00 am-7:00 pm
7:00 am-7:45 am
7:00 am-10:00 pm
7:30 am-5:00 pm
8:00 am-5:00 pm
8:00 am-4:00 pm
8:00 am-5:00 pm
9:30 am-10:00 am
Noon-l:00 pm
2:30 pm-3:00 pm
4:00 pro-7:00 pm
Tuesday, January 25, 1994 Registration
Continental Breakfast
Speaker Ready Room
Child Care
Postgraduate Course I "Clinical Management of Hypertension and Diabetes in Pregnancy"
Postgraduate Course II "Preterm Rupture of the Membranes"
Postgraduate Course III "The New Genetics"
Coffee Break
Lunch
Coffee Break
Board of Directors Meeting I
Wednesday, January 26, 1994 7:00 am-6:00 pm
7:00 am-7:45 am
7:00 am-10:00 pm
7:30 am-10:00 pm
7:45 am-3:00 pm
7:45 am-3:00 pm
9:30 am-10:00 am
Noon-l:00 pm
Noon-3:00 pm
3:00 pro-5:00/6:00 pm
5:30 pm-6:30 pm
7:00 pm-10:00 pm
Registration
Continental Breakfast
Speaker Ready Room
Child Care
Postgraduate Course IV "Immunologic Disorders in Pregnancy"
Postgraduate Course V "The Brain Damaged Baby"
Coffee Break
Lunch
Board of Directors Meeting II
Special Interest Group Meetings
Program Directors Meeting
Opening Reception
Thursday, January 27, 1994 7:00 am-5:00 pm Registration
7:00 am-7:45 am Continental Breakfast
7:00 am-10:00 pm Speaker Ready Room
Ballroom Registration Desk
Ballroom Registration Desk
Ballroom Foyer
Conference Room 1
Continental/Club Salons
Ballroom A
Ballroom B
Ballroom C
Ballroom Foyer
Pavilion 9-11
Ballroom Foyer
Conference Room 4-5
Ballroom Registration Desk
Ballroom Foyer
Conference Room 1
Continental/Club Salons
Ballroom A
Ballroom B
Ballroom Foyer
Pavilion 9-11
Conference Room 4-5
(see page xiii for locations)
Ballroom C
Ballroom A-B
Ballroom Registration Desk
Ballroom Foyer/Pavilion 9
Conference Room 1

7:30 am-10:30 pm
7:45 am-8:00 am
8:00 am-10:30 am
10:30 am-Noon
Noon-l:00 pm
Noon-l:00 pm
1:00 pm-3:00 pm
1:00 pro-3:00 pm
1:00 pm-3:00 pm
3:00 pm-5:00 pm
5:00 pm-6:00 pm
5:00 pm-6:00 pm
6:30 pm-7:30 pm
7:30 pm-10:00 pm
Child Care
Welcome & Announcements Gary D. V. Hankins, MD
1994 Program Chair, SPO
Welcome Larry C. Gilstrap, MD
President, SPO
Oral Plenary Session I Moderator:
Larry C. Gilstrap, MD President, SPO
Poster Session I & Coffee
Break for Lunch
Women in Perinatology: Special Interest Group Box Lunch
Oral Concurrent Session A Maternal Fetal Physiology Moderator: John C. Hauth, MD
Oral Concurrent Session B Genetics and Teratology/Fetal Therapy/
Placental Physiology/Doppler Moderators:
Mary E. D’Alton, MD Assistant Secretary-Treasurer, SPO
Karin B. Nelson, MD Honorary Member, 1994
Oral Concurrent Session C Infectious Disease/Prematurity Moderator:
Susan M. Cox, MD
Poster Session II & Coffee
Annual SPO Business Meeting (Regular Members Only)
Associate Members Meeting (Fellow-in-Training Members and other Associate Members of SPO)
Cocktail Reception
Annual Banquet
7:00 am-5:00 pm
7:00 am-8:00 am
7:00 amo8:00 am
7:00 am-8:00 am
7:00 am-10:00 pm
7:30 am-6:00 pm
Friday, January 28, 1994 Registration
Continental Breakfast
International Society of Perinatal Obstetricians:
Special Interest Group Breakfast Meeting
Corporate Sponsor Breakfast
Speaker Ready Room
Child Care
Continental/Club Salons
Ballrooms A-C
Ballrooms A-C
Pavilion 9-11
On Your Own
Conference Room 13-14
Ballroom A
Ballroom B
Ballroom C
Pavilion 9-11
Ballroom A
Ballroom B
Ballroom Foyer
Ballrooms D-G
Ballroom Registration Desk
Ballroom Foyer/Pavilion 9
Conference Room 7-9
Conference Room 3
Conference Room 1
Continental/Club Salons

8:00 am-10:30 am
10:30 am-Noon
Noon-l:00 pm
1:00 pm-3:00 pm
1:00 pm-3:00 pm
1:00 pm-3:00 pm
3:00 pm-5:00 pm
Oral Plenary Session II Moderator:
Valerie M. Parisi, MD, MPH President-Elect, SPO
Poster Session III & Coffee
Break for Lunch
Oral Con, current Session D Labor/Intrapartum Fetal Evaluation/
Maternal Fetal Physiology
Moderator:
Sharon L. Dooley, MD
Oral Concurrent Session E Hypertensive Disease
Clinical/Operative Obstetrics Moderator:
Baha M. Sibai, MD
Oral Concurrent Session F OB Anesthesia and Pharmacology Medical Complications
Moderator:
Richard H. Paul, MD
Past President, SPO
Poster Session IV & Coffee
7:00 am-8:00 am
7:00 am-Noon
7:30 am-1:00 pm
8:00 am-10:30 am
Saturday, January 29, 1994 7:00 am-Noon Registration
Continental Breakfast
Speaker Ready Room
Child Care
Oral Plenary Session III Moderator:
Garland D. Anderson, MD
Past President, SPO
10:30 am-Noon Poster Session V & Coffee
Noon-12:30 pm Poster Session Awards
A JOtJR
Ballrooms A-C
Pavilion 9-11
On Your Own
Ballroom A
Ballroom B
Ballroom C
Pavilion 9-11
Ballroom Registration Desk
Ballroom Foyer
Conference Room 1
Continental/Club Salons
Ballroom A-C
Pavilion 9-11
Pavilion 9-11
ACCME Accreditation The American College of Obstetricians and Gynecologists is accredited by the Accreditation Council for Continuing
Medical Education (ACCME) to sponsor continuing medical education for physicians.
Continuing Medical Education Credits Postgraduate Courses I & III have been approved for 7 cognates and 7 hours in Category I and meet the criteria of the
ACOG Program for Continuing Professional Development and for the Physician’s Recognition Award of the AMA.
Postgraduate Courses II, IV & V have been approved for 6 cognates and 6 hours in Category I and meet the criteria of the ACOG Program for Continuing Professional Development and for the Physician’s Recognition Award of the AMA.
Disclosure of Financial Interests In accordance with ACOG policy, all faculty members have signed a conflict of interest statement in which they have disclosed any significant financial interests relative to topics they will discuss at this program.
At the beginning of the program faculty members are expected to disclose any such information to participants. Such disclosure allows you to make your own judgment about information presented in lectures.
Please report on your evaluation form any undisclosed conflict of interest you perceive. Thank you.
A COG Committee on Course Coordination

SPECIAL INTEREST GROUP MEETINGS Wednesday, January 26, 1994
1) COMMUNITY BASED PERINATOLOGISTS
Coordinator: John P. Elliott, MD
Time Room
3 - 5 p.m. Conference Room 9-10
2) COMPUTER USAGE IN PERINATAL MEDICINE 3 - 5 p.m.
Coordinator: Lawrence D. Devoe, MD
3) CRITICAL CARE IN PERINATAL MEDICINE 3 - 5 p.m.
Coordinator: Manuel Alvarez, MD
4) DIABETES MELLITUS IN PREGNANCY 3 - 6 p.m. Coordinator: E. Albert Reece, MD
Conference Room 11
Conference Room 12
Conference Room 13
5) GENETICS IN PERINATOLOGY 3 - 6 p.m. Ballroom D
Coordinator: Anthony Johnson, DO
6) HYPERTENSION IN PREGNANCY 3 - 6 p.m. Ballroom G
Coordinator: James Mardn, Jr., MD
7) INFECTIOUS DISEASES IN PERINATAL MEDICINE 3 - 5 p.m.
Coordinator: Susan M. Cox, MD
Conference Room 8
8) PRETERM LABOR 3 - 5 p.m. Ballroom E
Coordinator: Jay D. Iams, MD
9) RESEARCH SUPPORT PERSONNEL 3 - 5 p.m. Coordinator: Rachel Copper, RN
Conference Room 7
10) ULTRASOUND IN PERINATAL MEDICINE 3 - 5 p.m. Ballroom F
Coordinator: Michael Divon, MD
11) WOMEN IN PERINATOLOGY 5 - 7 p.m. Coordinator: Nancy Callan, MD
Conference Room 14
12)
Thursday, January 27, 1994
WOMEN IN PERINATOLOGY 12 - 1 p.m.
Coordinator: Nancy Callan, MD (Box Lunch)
Conference Room 13-14
13)
Friday, January 28, 1994
INTERNATIONAL SOCIETY OF PERINATAL
OBSTETRICIANS
Coordinator: Bruce A. Work, MD
7 - 8 a.m. Conference Room 7-9 (Continental Breakfast)
xiii

SOCIETY OF PERINATAL OBSTETRICIANS Las Vegas, NV -January 24 - 29, 1994
Schedule of Oral Presentations
Thursday, January 27, 1994
8:00 a.m. - 10:30 a.m. Oral Plenary Session I Moderator: Larry C. Gilstrap, MD
President, SPO
Ballrooms A - C
8:00 - 8:15
8:15 - 8:30
8:30 - 8:45
8:45 - 9:00
9:00 - 9:15
9:15- 9:30
9:30 - 9:45
9:45 - 10:00
OBSTETRICAL ANTECEDENTS OF NEONATAL
PERIVENTRICULAR LEUCOMALACIA (PVL)
2 FETAL CARDIOVASC~ RESPONSES TO MATERNAL
AND FETAL SEROTONIN ADMINISTRATION IN NEAR
TERM SHEEP
3
4
AMNIOTIC FLUID INTERLEUKIN-6: A SENSITIVE
TEST FOR PROSPECTIVE DIAGNOSIS OF ACUTE
INFLAMMATORY LESIONS OF THE PRETERM
PLACENTA AND PREDICTION OF PERINATAL
MORBIDITY
CYTOGENIC DISCREPANCIES IN SPONTANEOUS
ABORTIONS WITH DIRECT AND CULTURE ANALYSIS
OF CHORIONIC VILLI
OBESITY AND GLUCOSE TOLERANCE DURING
PREGNANCY
6 THE EFFECT OF PREGNANCY ON THE CONTRACTILE
RESPONSE OF THE RABBIT THORACIC AORTA
7 LOW DOSE ASPIRIN THERAPY AND PLACENTAL
PATHOLOGY IN WOMEN WITH PRIOR POOR
PREGNANCY OUTCOMES
8 SCAVENGING OF EDRF BY ERYTHROCYTES IS
ALTERED IN PREGNANCY COMPLICATED BY SICKLE
CFJ J. ANEMIA
U. Verma, N. Tejani, S. Klein,
W. Jeanty, H. Dweck, W. Zoma,
G. Comacho, E. Leikin
New York Medical College Valhalla, NY
U. Lang, R.S. Baker, K.E. Clark
Perinatal Research Institute, University of Cincinnati College
of Medicine, Cincinnati, OH
B. H. Yoon, C. K. Chun, C.J. Kim,
J. H. Lee, K. S. Kim, H. C. Syn, S. W. Kim
Seoul National University Seoul, Korea
SalvatoreJ. Lombardi, V. G. Dev
Outpatient Diagnostic Center and Genetics Associates, Nashville, TN
M. B. Landon, M. Platt, K. Osei,
T. O’Dorisio, P. Samuels, S. Gabbe
The Ohio State University College
of Medicine, Columbus, OH
G. Saade, M. Belfort, L Van den Veyver, H. Hsu, K. Moise, P. Vanhoutte
Baylor College of Medicine Houston, TX
W. Cusick, C. Salafia, J. Rodis,
W. Campbell, A. Vintzileos
University of Connecticut
Farmington, CT
L. Olmos, N. Wasserstrum,
J. V. Mombouli, P. M. Vanhoutte Baylor College of Medicine Houston, TX
xiv

10:00 - 10:15
10:15 - 10:30 10
RAPID AND ACCURATE ECHOCARDIOGRAPHIC
ASSESSMENT OF LEFT AND RIGHT HEART
HEMODYNAMICS IN CRITICALLY ILL OBSTETRIC
PATIENTS
SINGLE UMBILICAL .ARTERY: DOES IT MA’VI’ER WHICH
ARTERY IS MISSING?
M. Belfort, R. Rokey, G. Saade, K. Moise, Jr. Baylor College of Medicine Houston, TX
A. Abuhamad, W. Shaffer, G. Mari,
J. Copel, j. Hobbins, A. Evans Eastern Virginia Medical School Norfolk, VA; Yale School of
Medicine, New Haven, CT
Thursday, January 27, 1994
1:00 p.m. - 3:00 p.m. Oral Concurrent Session A
Maternal Fetal Physiology Moderator: John C. Hauth, MD
Ballroom A
1:00- 1:15
1:15 - 1:30
1:30- 1:45
1:45 - 2:00
2:00 - 2:15
2:15 - 2:30
11 NITRIC OXIDE AND INTRAUTERINE GROWTH
RETARDATION IN RATS
12 CARDIOVASCUIP~R RESPONSES TO
METHAPHETAMINE IN FETAL SHEEP
13 CARDIOVASCUI_AR RESPONSES TO NEUROMUSC~
BLOCKADE IN THE ANEMIC OVINE FETUS
14 LAPAROSCOPIC INSUFFLATION IN THE GRAVID
BABOON: MATERNAL AND FETAL EFFECTS
15
16
EVIDENCE OF TOPOGRAPHIC DIFFERENCES IN
AMNIOTIC FLUID PLASMINOGEN
ACTIVATOR/PLASMINOGEN ACTIVATOR INHIBITOR
CONCENTRATIONS DURING SPONTANEOUS ACTIVE
LABOR AT TERM
CARDIAC FUNCTION PROFILE IN FETUSES AND
NEWBORNS EXPOSED TO LOW DOSE ASPIRIN (ASA)
DURING PREGNANCY
A. L. Diket, M. t~ Pierce, U. K. Munshi, S. Eloby-Childress,
S. S. Greenberg, X.J. Zhang,
D. A. Clark, M. J. S. Miller
Louisiana State University
New Orleans, LA
A. Stek, B. Fisher, S. Baker, K. Clark University of Cincinnati
Cincinnati, OH
L. E. Shields, 1~ A. Brace University of California
San Diego, CA
H. L. Galan, M. B. Reedy, J. D. Bean,
A. Carnes, A. B. Knight, T.J. Kuehl Scott and White Clinic and
Memorial Hospital; Texas A&M University Health Science Center
College of Medicine, Temple, TX
P. Baumann, 1L Romero, R. Gonzalez,
D. B. Cotton, E. Mammen
Wayne State University, Detroit, MI;
The Perinatology Branch, NICHD, Bethesda, MD
T. Di Sessa, M. Moretti, D. Pulliam, K. Arheart, B. Sibai
University of Tennessee
Memphis, TN
×v

2:30 - 2:45
2:45 - 3:00
17 CEREBRAL OXIDATIVE METABOLISM DURING SEVERE
UMBILICAL CORD OCCLUSION
18 THE SYMPATHOADRENAL RESPONSE OF THE OVINE
FETUS TO THE DIRECT INTRAVASCULAR
ADMINISTRATION OF METHAMPHETAMINE
R. H. Ball, J. T. Parer, L. E. Caldwell,
J. Johnson CVRI, University of California
San Francisco, CA
M. M. Ramirez, R. L. Andres, V. Parisi
University of Texas Medical School
Houston, TX
Thursday, January 27, 1994
1:00 p.m. - 3:00 p.m. Oral Concurrent Session B Genetics and Teratology/Fetal Therapy/ Placental Physiology/Doppler Moderators: Mary E. D’Alton, MD
Assistant Secretary-Treasurer, SPO
Karin B. Nelson, MD Honorary Member, SPO 1994
Ballroom B
1:00 - 1:15
1:15 - 1:30
1:30- 1:45
1:45 - 2:00
2:00 - 2:15
2:15 - 2:30
19
2O
FLUORESCENCE IN SITU HYBRIDIZATION (FISH)
ANALYSIS OF UNCULTURED AMNIOCYTES FOR RAPID
DETECTION OF CHROMOSOME ANEUPLOIDIES.
EXPERIENCE WITH 10,000 PATIENTS
COMPARATIVE TRIAL OF A NEW RAPID MULTIPLE
PROBE IN SITU HYBRIDIZATION TECHNIQUE OF
UNCULTURED AMNIOCYTES FOR PRENATAL
DIAGNOSIS OF ANEUPLOIDIES
21 ASSOCIATION OF CONFINED PLACENTAL MOSAICISM
WITH INTRAUTERINE GROWTH RESTRICTION
22 IS THERE AN INCREASED INCIDENCE OF CONGENITAL
ANOMALIES IN WOMEN WITH GESTATIONAL
DIABETES?
23
24
INDUCTION OF TUMOR NECROSIS FACTOR (TNF)
AND INTERLEUKIN-6 (IL-6) mRNA IN
CYTOTROPHOBLASTS (CYTO) EXPOSED TO
LIPOPOLYSACCHARIDE (LPS)
INSULIN-LIKE GROWTH FACTORS (IGFS)AND FETAL
GROWTH
B. E. Ward, S. Gersen, M. Carelli
Integrated Genetics Framingham, MA
M. G. Martens, G. D. Anderson,
R. Chu, E. Yeomans, J. Terk, N. Prashad, W. Weber, M. Asgari
The University of Texas Medical
Branch, Galveston, TX; APROGENEX, Houston, TX
T. Cowles, S. Taylor, S. Zneimer, F. Elder
University of Texas Medical School Houston, TX; Kaiser Foundation Medical Center, Oakland, CA
O. Lancer, Robert Huff Elly Xenakis, Michael Berkus
University of Texas Health Science
Center, San Antonio, TX
B. Gonik, J. Rachmilewitz, A. Hochberg
University of Texas Medical School Houston, TX; Hebrew University
Jerusalem, Israel
Steven Roth, Ora Pescovitz,
Linda Pratt, Scott Denne, Alan Golichowski, Wei-Hua Lee
Indiana University, Indianapolis, IN
XVl
2:30 - 2:45
2:45 - 3:00
25 CHANGES IN UTERINE ARTERY BLOOD FLOW IN
RESPONSE TO CORRECTION OF AMNIOTIC FLUID
VOLUME
26 INTRAUTERINE VIDEO-ENDOSCOPIC CREATION OF
LOWER URINARY TRACT OBSTRUCTION IN THE
FETAL LAMB
N. J. Flac_k, S. Bower, W. Sepulveda, D. G. Talbert, N. M. Fisk Centre for Fetal Care; Royal Postgraduate Medical School; Institute of Obstetrics and Gynaecology; Queen Charlotte’s and Chelsea Hospital, London, UK
]. A. Deprest, F. I. Luks, IcL Vandenberghe, T. Lerut,
L A. Brosens, F. A. Van Assche Centre for Surgical Technologies, K. U. Leuven, Belgium
Thursday, January 27, 1994
1:00 p.m. - 3:00 p.m. Oral Concurrent Session C Infectious Disease/Prematurity Moderator: Susan M. Cox, MD
Ballroom C
1:00- 1:15
1:15 - 1:30
1:30- 1:45
1:45 - 2:00
2:00 - 2:15
27 AMNIOTIC FLUID PLASMINOGEN
ACTIVATOR/PLASMINOGEN ACTIVATOR INHIBITOR
CONCENTRATIONS IN PRETERM LABOR IN THE
SETrlNG OF INFECTION
28 AMNIOTIC FLUID IL-6: CORRELATION "WITH
CHORIOAMNION COLONIZATION AND GESTATIONAL
AGE IN WOMEN DELIVERED FOLLOWING
SPONTANEOUS LABOR VERSUS INDICATED DEIJVERY
29 HIV INFECTION AS A RISK FOR ADVERSE PERINATAL
OUTCOME
30 AMNIOTIC FLUID TISSUE FACTOR IN PRETERM AND
TERM PARTURITION
31 DETECTION OF INTRAUTERINE VIRAL INFECTION BY
POLYMERASE CHAIN REACTION
P. Baumann, R. Romero, R. Gonzalez,
D. B. Cotton, E. Mammen
Wayne State University, Detroit, MI;
The Perinatology Branch NICHD, Bethesda, MD
W. Andrews, J. Hauth, R. Goldenberg,
M. Mazur, R. Gomez, R. Romero,
G. Cassell
University of Alabama at
Birmingham, Birmingham, AL; Wayne State University, Detroit, MI;
The Perinatology Branch Bethesda, MD
F. Geary, M. Lindsay, W. Graves,
L. Klein
Emory University, Atlanta, GA
t2. Romero, R. Gomez, H. Munoz,
M. Galasso, L. Acosta, A. Ghidini,
D. B. Cotton, C. Lockwood Wayne State University/Hutzel Hospital, Detroit, MI; Mt Sinai
Medical School, New Yo.rk, N~ The Perinatology Branch, NICHD Bethesda, MD
L B. Van den Veyver, j. Ni, K.J. Moise,
J. A. Towbin Institute of Molecular Genetics, Baylor College of Medicine
Houston, TX
xvii
2:15 - 2:30
2:30 - 2:45
2:45 - 3:00
32 THE VALUE OF AMNIOTIC FLUID INTERLEUKIN-6
DETERMINATION IN PATIENTS WITH PRETERM
LABOR AND INTACT MEMBRANES IN THE DETECTION
OF MICROBIAL INVASION OF THE AMNIOTIC CAVITY
33 SURFACTANT REPLACEMENT THERAPY FOR
PREVENTION OF HYALINE MEMBRANE DISEASE IN
THE PRETERM BABOON
34 THE PROGNOSTIC VALUE OF AMNIOTIC FLUID
INTERLEUKIN-6 DETERMINATIONS IN PATIENTS WITH
PRETERM LABOR
L. Coultrip, J. M. Lien, A. Khoury,
J. H. Grossman Fairfax Hospital, Falls Church, VA,
George Washington Medical
Center, Washington, DC
H. L. Galan, C. Cipriani, J.J. Coalson,
J. D. Bean, G. Collier, T.J. Kuehl Scott and White Clinic; Texas A&M University Health Science Center,
Temple, TX; University of Texas Health Science Center at San
Antonio and Houston, TX
B. H. Yoon, R. Romero, C. K. Chun,
J. H. Lee, K. S. Kim, J. N. Koo, H. C. Syn, S. W. Kim
Seoul National University, Seoul, Korea; The Perinatology Branch,
NICHD, Bethesda, MD; Wayne State University/Hutzel Hospital,
Detroit, MI
Friday, January 28, 1994
8:00 a.m. - 10:30 a.m. Oral Plenary Session II Moderator: Valerie M. Parisi, MD, MPH
Vice-President and President-Elect, SPO
Ballroom C
8:00 - 8:!5
8:15 - 8:30
8:30 - 8:45
8:45 - 9:00
35 A SYSTEMATIC STUDY OF THE EFFECT OF
GESTATIONAL AGE, FETAL GENDER, INTRAUTERINE
INFECTION AND PARTURITION ON THE
BIOAVAILABILITY OF THE INTERLEUKIN-1 RECEPTOR
ANTAGONIST IN HUMAN PREGNANCY
36 THE FETAL CENTRAL VENOUS PRESSURE WAVEFORM
IN NORMAL AND COMPLICATED PREGNANCY
37 SUCCESSFUL IN UTERO TREATMENT OF FETAL HEART
BLOCK
38 FETAL CELLS IN MATERNAL BLOOD: DETERMINATION
OF PURITY AND YIELD BY QUANTITATIVE PCR
tL Romero, R. Gomez, M. Galasso,
S. Berry, M. Mazor, R. Quintero, H. Araneda, Y. Sorokin, D. B. Cotton
Wayne State University/Hutzel Hospital, Detroit, MI; The Perinatology Branch, NICHD
Bethesda, MD
A. Mori, B. Trudinger, R. Mori, V. Reed
University of Sydney, Westmead Hospital, NSW, Australia
j. A. Copd, J. P. Buyon, C. S. Kleinman Yale University, New Haven, CT; New York University, New York, NY
D. W. Bianchi, M. A. DeMaria, A. P. Shuber, A. C. Fouffner, K. W. Klinger
Tufts University School of Medicine, Boston, MA; Integrated
Genetics, Framingham, MA; Sonoscan/Genetic Sciences
Forest Hills, NY
9:00 - 9:15 39
9:15 - 9:30 40
9:30 - 9:45 41
9:45 - 10:00 42
10:00 - 10:15 43
10:15 - 10:30 44
MATERNAL AND PERINATAL OUTCOME OF 846
SINGLETON BREECH DELIVERIES AT ONE REFERRAL
CENTER
FETAL CARDIORESPIRATORY EFFECTS OF
NITROGLYCERIN IN THE NEAR TERM PREGNANT
SHEEP
THE EFFECT OF INTRAHEPATIC VEIN SAMPLING (IHV)
ON FETAL PLASMA CORTISOL AND BETA-ENDORPHIN
CONCENTRATIONS
STRATEGIES FOR THE PREVENTION OF EARLY ONSET
NEONATAL GROUP B STREPTOCOCCAL SEPSIS: A
DECISION ANALYSIS
A NEW METHOD OF DETECTION AND CONFIRMATION
OF FETAL NUCLEATED RED BLOOD CFJ J.R FROM
MATERNAL BLOOD
GESTATIONAL DIABETES: POSTPARTUM GLUCOSE
TOLERANCE TESTING
E. Schiff S. Mashiach, O. Hart,
G. Barkai, B. M. Sibai Sheba Medical Center, Tel-Aviv University, Israel; University of Tennessee, Memphis, TN
B. Bootstaylor, C. Roman,
M. A. Heymann, J. T. Parer
CVRI, University of California
San Francisco, CA
X. Giannakoulopoulos, W. Sepulveda,
P. Koutris, V. Glover, N. Fisk
Institute of OB/GYN, Royal
Postgraduate Medical School,
Queen Charlotte’s & Chelsea Hospital, London, UK
~, R. Goldenberg, S. Cliver,
G. Cutter, S. Mennemeyer, C. Fargason University of Alabama at
Birmingham, Birmingham, AL
M. G. Martens, G. D. Anderson, R. Chu, E. Yeomans, J. Terk,
N. Prashad, W. Weber, M. Asari University of Texas Medical
Branch, Galveston, TX; APROGENEX, Houston, TX
j. Dams, R. Stilson, N. Meyer, D. Muram, P. Phipps, B. Sibai
University of Tennessee
Memphis, TN
Friday, January 28, 1994
1:00 p.m. - 3:00 p.m. Oral Concurrent Session D
Labor/Intrapartum Fetal Evaluation/ Maternal Fetal Physiology Moderator: Sharon L. Dooley, MD
Ballroom A
1:00- 1:15
1:15 - 1:30
45 PHYSIOLOGICAL DOSES OF ENDOTHELIN-1 INCREASE
THE IN VITRO RESPONSE OF HUMAN MYOMETRIUM
TO OXYTOCIN
46 PROPHYLACTIC AMNIOINFUSION FOR MECON1UM
STAINED AMNIOTIC FLUID
G.J. Valenzuela, C. W. Hewitt, C. A. Ducsay
Loma Linda University, Loma Linda CA; San Bernadino County Medical Center, San Bernadino, CA
C. Y. Spon~, O. A. Ogundipe,
M. G. Ross Harbor-UCLA Medical Center
Torrance, CA
1:30- 1:45
1:45 - 2:00
,2:00 - 2:15
2:15 - 2:30
2:30 - 2:45
2:45 - 3:00
47 MANAGEMENT OF PREMATURE RUPTURE OF
MEMBRANES AT TERM: RANDOMITTJ) TRIAL
48 A PROSPECTIVE STUDY OF HIGH- VERSUS LOW-DOSE
OXYTOCIN FOR INDUCTION OF LABOR
49 NUCLEATED RED BLOOD CELLS: A MARKER FOR
FETAL ASPHYXIA
50 THE EFFECT OF ADVANCING GESTATIONAL AGE ON
FETAL ARTERIAL PRESSURE
51 FETAL HYPERINSULINISM AT 16-20 WEEKS PREDICTS
GESTATIONAL DIABETES (GDM) NOT MACROSOMIA
52 AORTIC COMPLIANCE IN EARLY PREGNANCY
R. Natale, K. Milne, K. Campbell, K. Wester, E. Halinda
St. Joseph’s Health Centre London, Ontario, Canada
A. Hourvitz, D. S. Seidman,
M. Alcalay, J. Korach, A. Lusky,
G. Barkai, B. Chayen, S. Mashiach Sheba Medical Center, Tel-Hashomer and Sackler School
of Medicine, Tel-Aviv University, Israel
j. P. Phelan, M. O. Ahn, L. Korst, G. L Martin
Pomona Valley Hospital
Pomona, CA
K.J. Moise, G. Saade, L. Goodrum, M. Belfort, R.J. Carpenter
Baylor College of Medicine Houston, TX
M. Carpenter, J. Canick, J. Star,
S. Carr, K. Shahinian, M. Tumber, M. Burke
Brown University School of Medicine, Providence, RI
j. Hibbard, A. Poppas, C. Korcarz, R. Marcus, M. Lindheimer, R. Lang
University of Chicago, Chicago, IL
Friday, January 28, 1994
1:00 p.m. - 3:00 p.m. Oral Concurrent Session E
Hypertensive Disease of Pregnancy/ Clinical/Operative Obstetrics Moderator: Baha M. Sibai, MD
Ballroom B
1:00- 1:15
1:15 - 1:30
53 NULLIPAROUS PREECLAMPSIA (PE) IS ASSOCIATED
WITH PLACENTAL EXPRESSION OF VARIANT AIJ,EI.E
OF THE NEW HISTOCOMPATIBIL1TY GENE: HLA-G
54 HOW FREQUENTLY DOES HELLP SYNDROME RECUR
IN SUBSEQUENT PREGNANCIES?
Elliott Main, Mimi Chiang,
Gail Colbern California Pacific Medical Center
San Francisco, CA
C. A. Sullivan, K. G. Perry, Jr., W. E. Roberts, E. F. Magann,
P. G. Blake, J. N. Martin, Jr.
University of Mississippi Medical
Center, Jackson, MS
×x
1:30- 1:45
1:45 - 2:00
2:00 - 2:15
2:15 - 2:30
2:30 - 2:45
2:45 - 3:00
55 RISK FACTORS FOR PREECLAMPSIA IN NULLIPAROUS
AND MULTIPAROUS WOMEN
56 THE EFFECT OF LIPID PEROXIDES ON ISOLATED
HUMAN UMBILICAL ARTERIES
THE ROLE OF NITRIC OXIDE (NO) IN THE
PATHOGENESIS OF PREECLAMPSIA
58 MATERNAL BLOOD PRESSURE RESPONSES TO
CHRONIC REDUCTION IN UTERINE BLOOD FLOW IN
PREGNANT SHEEP
59 THE IMPACT OF D~Y ROUTE ON BIRTH INJURY
IN MACROSOMIC INFANTS
60 MANAGING PREMATURE RUPTURE OF MEMBRANES
AT TERM
S. Cliver, R. Goldenberg, D. Rouse,
J. Hauth, W. Roden University of Alabama at
Birmingham, Birmingham, AL
G. Saade, M. Belfort, Y. Vedernikov, H. Hughes, K. Moise, M. Suresh,
D. Johnson Baylor College of Medicine
Houston, TX
S. P. Seligman., S. B. Abramson,
B. K. Young, J. P. Buyon New York University Medical
Center, New York, NY
U. Lan¢~, R. S. Baker, B. K. Fisher,
K. E. Clark
Perinatal Research Institute,
University of Cincinnati College of Medicine, Cincinnati, OH
C. Cook, J. Gerard, L. Zuidema,
J. Spinnato
Butterworth Hospital, Grand Rapids, MI; University of Louisville
Louisville, KY
C. E. Henderson, B. Goldman,
S. Piening, B. Sommers, M. Y. Divon
Albert Einstein College of
Medicine, Bronx, NY
Friday, January 28, 1994
1:00 p.m. - 3:00 p.m. Oral Concurrent Session F OB Anesthesia and Pharmacology/ Medical Complications of Pregnancy Moderator: Richard H. Paul, MD
Past President, SPO
Ballroom C
1:00- 1:15
1:15 - 1:30
61
62
LOW-DOSE ASPIRIN IN NULLIPAROUS WOMEN:
SAFETY OF EPIDURAL AND CORRELATION BETWEEN
BLEEDING TIME AND MATERNAL-NEONATAL
BLEEDING COMPLICATIONS
EFFECT OF ASPIRIN AND INDOMETHACIN ON
PROSTACYCLIN AND THROMBOXANE PRODUCTION
BY PLACI?2~TAL TISSUE INCUBATED WITH IgG
FRACTIONS FROM PATIENTS WITH LUPUS
ANTICOAG~T
B. Sibai, S. Caritis, E. Thorn, K. Shaw, D. McNellis NICHD MFM Network
Bethesda, MD
A. M. Peaceman, K. Rehnberg
Northwestern University Medical School, Chicago, IL

1:30- 1:45
1:45 - 2:00
2:00 - 2:15
2:15 - 2:30
2:30 - 2:45
2:45 - 3:00
63 WI~ CAN’T GOOD GLYCEMIC CONTROL OF DIABETES
IN PREGNANCY ELIMINATE THE PROBLEM OF
MACROSOMIA?
64 TOWARD UNIVERSAL CRITERIA FOR GESTATIONAL
DIABETES: THE 75 GRAM GLUCOSE TOLERANCE TEST
IN PREGNANCY
65 IS IT COST EFFECTIVE TO SCREEN TEENAGERS FOR
GESTATIONAL DIABETES?
66 CHORIOAMNIONITIS: THE ASSOCIATION OF
ABNORMAL FHR PATrERNS AND NEONATAL ACIDEMIA
67 MAGNESIUM SULFATE VERSUS PHENYTOIN (PHY) FOR
SEIZURE PREVENTION IN AMYGDALA KINDLED RATS
68 AMNIOTIC FLUID VOLUME FLUCTUATIONS REFLECT
RECENT GLYCEMIC STATUS IN GESTATIONAL
DIABETICS
B. Rosenn, M. Miodovnik, G. Holcberg, j. Khoury, R. Jaekle, T. a. Siddiqi
University of Cincinnati
Cincinnati, OH
D. Sacks, J. Greenspoon, S. Abu-Fadil,
H. Henry, G. Wolde-Tsadik, J. Yao Kaiser Foundation Hospital,
Bellflower, CA; Cedars-Sinai Medical Center, Los Angeles, CA
A. Johnson, S. Kady Wilson, L. Hosmer, K. Franko-Filipasic,
L. Chambliss
Maricopa Medical Center, The Midwifery Service, Phoenix
Memorial Hospital, Phoenix, AZ
P. Wendel, S. Cox, S. Roberts, M. Maberry, J. Dax, L. Gilstrap
University of Texas Southwestern Medical Center, Dallas, TX
C. A. Standley, S. M. Irtenkauf,
L. Stewart, B. Mason, D. B. Cotton Wayne State University/Hutzel
Hospital, Detroit, MI
I. Bar-Hava, S. A. Scarpelli, Y. Barnhard, M. Y. Divon
Albert Einstein College of Medicine, Bronx, NY
Saturday, 29 January, 1994
8:00 a.m. - 10:30 a.m. Oral Plenary Session III Moderator: Garland D. Anderson, MD
Immediate Past President, SPO
Ballrooms A - C
8:00 - 8:15
8:15 - 8:30
69 RECURRENT HYPOGLYCEMIA: A RISK FACTOR FOR
MACROSOMIA IN IDDM PREGNANCIES
70 OBSTETRICIAN’S ATTITUDE AND NEONATAL
SURVIVAL OF EXTREMELY LOW BIRTH WEIGHT
INFANTS
B. Rosenn, M. Miodovnik, T. A. Siddiqi University of Cincinnati
Cincinnati, OH
S. Bottoms, R. Paul, J. Iams, B. Mercer, D. McNellis, C. Buckley, G. Norman,
P. Jones, E. Thom NICHD MFM Network
Bethesda, MD
x×ii
8:30 - 8:45
8:45 - 9:00
9:00 - 9:15
9:15 - 9:30
9:30 - 9:45
9:45- 10:00
10:00 - 10:15
10:15 - 10:30
71
72
73
74
75
76
77
78
SONOGRAPHIC EXAMINATION OF THE UTERINE
CERVIX IS A BE~’rER PREDICTOR OF THE
LIKELIHOOD OF PRETERM DELIVERY THAN DIGITAL
EXAMINATION OF THE CERVIX IN PRETERM LABOR
WITH INTACT MEMBRANES
DOES THE CREATION OF A FETAL GASTROSCHISIS
REDUCE THE SEVERITY OF PULMONARY HYPOPLASIA
IN SHEEP WITH CONGENITAL DIAPHRAGMATIC
HERNIA?
TRANSABDOMINAL THIN-GAUGE EMBRYOFETOSCOPY
IN CONTINUING PREGNANCIES
OUTPATIENT TREATMENT OF PYELONEPHRITIS IN
PREGNANCY
EFFECT OF FETECTOMY ON MATERNAL
PITUITARY-ADRENAL FUNCTION IN PREGNANT
RHESUS MACAQUES
OPERATIVE FETOSCOPY: A NEW FRONTIER IN FETAL
MEDICINE
THE EFFECT OF PULMONARY SHUNTING (Qs/Qt) ON
FETAL ARTERIAL HEMOGLOBIN SATURATION IN THE
SHEEP MODEL
COCAINE ALTERS PLACENTAL PRODUCTION OF
THROMBOXANE AND PROSTACYCLIN
tL Gomez, M. Galasso, R. Romero,
M. Mazor, Y. Sorokin, P. Baumann, L.
Goncalves, M. Treadwell, D. B. Cotton
Wayne State University/Hutzel Hospital, Detroit, MI; The
Perinatology Branch of NICHD Bethesda, MD
M. Belfort, G. Saade, B. Baker, W. Pokorny, C. Langston, P. Minifee,
G. Jevon, I. Van den Veyver, D. Robie,
S. Longmire, Q. Palacio~,
L. Montgomery, K. Moise, Jr.
Baylor College of Medicine
Houston, TX
Ruben A. Quintero, Roberto Romero, Mordechai Bardicef, Yolanda Renfroe,
Nelson B. Isada, Mark P. Johnson, Mark L Evans, Freddy Guevara,
Roxana Lamana, David B. Cotton Wayne State University/Hutzel
Hospital, Detroit, M1; Central University of Venezuela, University
Hospital, Caracas, Venezuela; The
Perinatology Branch, NICHD Bethesda, MD
L. Millar, D. Wing, R. Paul, D. Grimes
University of Southern California
Los Angeles, CA
C. A. Ducsa,~, H. Umezaki, G. J. Valenzuela
Loma Linda University, Loma Linda, CA; San Bernadino County
Medical Center, San Bernadino, CA
Ruben A. Quintero, Harry Rdch,
Karoline S. Puder, Mordechai Bardicef,
Leonardo Acosta, David B. Cotton,
M. I. Evans, R. Romero
Wayne State University, Detroit, MI;
Wyoming Valley OB/GYN
Associates; The Perinatology Branch, NICHD, Bethesda, MD
C. J. Harry., G. D. V. Hankins
University of Texas Medical
Branch, Galveston, TX; Wilford Hall Medical .Center
San Antonio, TX
M. Monga, S. Chmielowiec,
L. R. Troyer, R. L. Andres, V. M. Parisi
University of Texas Health Science Center, Houston, TX
Oral Plenary Session I
Thursday, January 27, 1994 8:00 a.m.- 10:30 a.m.
Moderator: Larry C. Gilstrap, MD President, SPO
Ballrooms A- C Abstract Numbers 1 - 10

264 SPO Abstracts January 1994 Am J Obstet Gynecol
OBSTETRICAL ANTECEDENTS OF NEONATAL
PERIVENTRICULAR LEUCOMALACIA (PVL)
U. Verm~a, N. Tejam, S. Kleinx, W. JeantyX, H. Dweckx, W. Zoma~, G. ComachoX, E. Leikin; New York Medical College, Valhalla, NY
OBJECTIVE: PVL has a strong correlation with neurologic deficit. Since PVL takes 7 days to develop, this finding in the first 7 days (early) implies an intrauterine initiation. We correlated obstetrical factors with early PVL.
STUDY DESIGN: 73 of 911 (12.5%) neonates < 2500 gins showed early PVL. These cases were evaluated for (a) PROM >_ 24 hrs, (b) spontaneous preterm delivery without PROM > 24 hrs, and (c) delivery for maternal reasons.
Fisher’s exact test was used for comparison Additionally, feto-maternal infection, as evidenced by clinical or histopathological chorioamniomtis was evaluated.
RESULTS: No. Normal PVL "P" a) PROM 345 310 35 VS"c" .01301 b’) PTL/PTD 371 333 38 VS"c" .0001 c) Maternal 195 195 0
Indication
55 of 69 cases of PVL (88%) showed feto-maternal infection as defined. CONCLUSION: 1. PVL occurred exclusively in PROM/PTD groups and was NEVER seen in patients delivered for maternal reasons. 2 PVL was strongly associated w~th chorloamniomtis
AMN1OTIC FLUID 1NTERLEUION-6: A SENSITIVE TEST FOR
PROSPECTIVE DIAGNOSIS OF ACUTE INFLAMMATORY LESIONS
OF TIlE PRETERM PLACENTA AND PREDICTION OF PERINATAL
MORBIDITY. BH ’Yoon, CK Chu#, CJ Kim~, JH Lee’, KS Kim’, }H Lee’,
KS K~m~, HC Sya’, SW Kim’. Seoal National University, Seoul, Korea.
OBJECTIVE: To determine if amniotic fluid (AF) concentrations of
tnterleukin-6 (IL-6) are of value in the antenatal diagnosis of acute
inflammatory lesions (histologic chorlooanmonitis) of preterm pl~canta and in
the prediction of perinatal morbidity mad mortality.
STUDY DES1GN: The relattonship among the placental histologic findings,
perinatal outcome, and AF-IL-6 concentrations was examined in 32
consecutivepatieats who delivered preterm neonates (24-35 weeks) within 72
hours after transabdominal amniocentesis. IL-6 was determined by a sensitive
and specific EL1SA. Recewer operating characteristic (ROC) curve was used
for analysis.
RESULTS: 1 ) The prevalence o f histologic acute ehorio~maionitis was 72 %
(23/32). 2) Patients with acute histologic chorioamnionitis had a significantly
higher AF-IL-6 concentrations than pattents without acute chorioamnionitis
(median 70.8 ng/ml, range 0.7-499.2 vs median 2.9 ng/ml, range 0.8-16.0;
p < .005). 3) ROC curve analysis demonstrated the significant relationship
between AF-1L-6 and acute histologlc chorioamnionitis (Z ~6.8, p < .00001),
and the development of significant neonatal morbidity/mortality (defined ~
neonatal sepsis, respiratory distress syndrome, pneumonia, intraveatricul~
hemorrhage,bronchopulmonary dysplasla, or death) (Z =3.0, p < .005). 4)An
AF-1L-6 concentrations of > 17,0 ng/ml had a sensitiwty of ~3% (19123)
and a specificity of 100% (9/9) in diagnosis of ~cute hlstologic
chorioamnionitis, and had a sensitivity of 74% (17/23) ~.nd a specificity of
78% (7/9) in the prediction of sigmficant neonatal morbidity/mortallty.
CONCLUSIONS: AF-IL-6 is a sensitive test for the prospective diagnosis
of acute chorioamnlouitis and the identification of neonates at risk for
significant morbidity and mortality.
FETAL CARDIOVASCULAR RESPONSES TO MATERNAL AND FETAL
SEROTONIN ADMINISTRATION IN NEAR TERM SHEEP,
U. Lanq,~ RS Baker,~ K.E. Clark.~ Departments of Obstetrics and
Gynecology, Pediatrics and Physiology, Perinatal Research Institute,
University of C~ncinnati College of Medicine, Cincinnati, OH.
OBJECTIVE: Serotonin is a potent uterine vasoconstrictor and has been
~mp}icated in preeclampsia, The present study evaluated fetal responses
to maternal as well as fetal administration of serotonin.
STUDY DESIGN: Pregnant sheep w~th singleton fetuses were
~nstrumented between 110 and 115 days of gestation (GD) w~th femoral artery and vein catheters and tlow probes on the uterine arteries. Fetal
instrumentation consisted of hmdhmb artery and vein catheters as well as
a transonic doppler flow probe on the common umlN~ical artery. Between
GD 125 and 130 each ewe received an accumulative continuous five-
minute ~nfusion of serotonin (3, 10 and 30 ug/kg/bw) On a subsequent
day fetuses received a similar series of infusions of seroton~n (1, 3, 10 and
30 ug/kg estimated body weight).
RESULTS: Maternal administrahon of serotonm decreased uterine blood
flow (17, 59, and 78%), In response, fetal blood pressure increased (2, 3,
26%), while fetal heart rate decreased (7, 19 and 36%), Umbilical blood flow decreased (4, 15 and 35%) while umbilical vascular resistance
increased (0, 25 and 120 %) Direct fetal administrabon of serotonm
increased fetal blood pressure (1, 9, 39 and 58%), decreased fetal heart rate at the lowest three doses (I 0, ! 4, 1%) and increased it at the highest
dose (11%). During these fetal ~nfusions, umbdical blood flow decreased
(0, 6, 29 and 50%) while ur~b$cal vascular resistance =ncreased (0, 18, 117, 268%), Fetal infusions dtd not signtdcaotly change maternal blood
pressure or uterine blood flow
CONCLUSION: Seroton!n is a potent vasoconstnctor of the umb=hcal
circulabon whether given to the mother or the fetus, These data suggest
that elevations of maternal serotoNn levels could directly affect the fetal
umbilical circulation and blood pressure Supported ~n part by HD 18370,
HL 40083, HL 49901 and DFG La 660/4-1.
CYTOGENETIC DISCREPANCIES IN SPONTANEOUS ABORTIONS
WITH DIRECT AND CULTURE ANAL YSIS OF CHORIONIC VILLI. ~ V.G. Dev~ PhD. OutpatiectDiagnoslic
Center and Genetics Associates, Nashville, TN.
Objective: Recent studies report the incidence of chromosomal
abnormalities in early feted loss exceed 60%. Knowlec~e of fated
karyolype is essential for idenlificalion of women at ino’ea.sed risk for
fetal wastage. Cytogenetic evaluation of products of conceptlo~ have
been limited by high tissue culture failure and metermd cell
contamination. Cytogenelic techniques utilizing chorionic villi have
recently been applied to aborted tissue, however scant data exist
comparing the karyotype from direct verses cultured chorionic villi.
Study dealgn: Data were analyzed from 107 consecutive cases of SAB where products of conception were karyotyped using well
established laboratory protocols for direct and culture analysis of chorionic villi.
Results: All 107 chorionic villus samples were successfully
karyolype~ Direct analysis was successful in 81 caseS (76%), vs.
culture 104 (97%). Direct and culture were obtained in 78 cases (73%). Abnormal katyotypes were reported in 60 cases (56%). Abnormalities included 35% ttisomies, 10% mosaics, 21% 45,X, 32% polyploidy, and
2% with multiple ttisomies. Contradictory cylogenetic findings occurred
in ~4 cases (13%). Thirteen of these fourteen (93%) were normal in direct method and abnormal in culture, whereas one showed the converse.
Conclusion: The cytogenetic discrepancies reported in this series
were unexpected. Direct normal / culture abnormai inconsistencies are
rarely reported in clinical CVS stuc~es. The potential failure to detect a
cytogenaticaily abnormal fetus exists. A possible explanation could be
that in a 2 cell line cj/totrophoblast, postmo~em changes selectively disadvantage ~he aneuploid cell allowing the o~ploid cell in the
extraembtyonic compartment to remain viable for a longer petfod of
time and therefore more likely to be successfully analyzed.
Volume 170, Number 1, Part 2 SPO Abstracts 265 Am J Obstet Gynecol
OBESITY AND GLUCOSE TOLERANCE DURING PREGNANCY.
MB Landon, M Plattx, K Oseix, T O’Dorisiox, P Samuels, S Gabbe. Depadment of O~Gyn, The Ohio State University College of Medicine, Columbus, Ohio OBJECTIVE: Maternal obesity represents a s~gnificant risk factor for the development of cafoohydrate intolerance during pregnancy. However, many obese women do not develop OestatJonal diabetes. The purpose of this study was to determine if adipese site distribution ~ntributes to the metabolic heterogeneity found in obese pregnant women. S’I1JDYDESIGN: We performed anthropometnc measurements, 100 gm oral glucose tolerance tests (GTT), insulin, and glucagon levels in 9 lean (BMI <27) and 14 obese (BMI >_.30) women during each trimester. Obese patients were divided according to waist/hip rat~o into two categories: 8 centrally obese (CO) and 6 peripherally obese (PO). RESULTS: Maximal deterioration ~n glucose tolerance was seen in CO patients by the 2nd trimester, but not until the 3rd trimester in lean and PO subjects. No subjects developed gestational diabetes Postpartum insulin/glucose ratios increased over time within each group. Area under the GTT curve for each tnmester were s~m=lar between lean and PO groups, but greater for CO. (Third trimester values’ lean 321 +_ 49, PO 334 +_. 44, CO 428 +_70) (p< 83). Fasting insulin/~san 28 ’~ + 8 2, PO 34.3 +_ 58, CO 52 8 +_ 18.5 uU/ml) (p<.02) and postpartum insuhNglucose ral]o in late pregnancy (p< 01) were also elevated in CO compared to other groups. CONCLUSIONS: Centrally obese women exhibit alterahons in carbohydrate tolerance earlier and to a greater degree than peripherally obese women during gestation. Relative fasting and postpartum hyperinsulinem~a in centrally obese women further suggest that body fat topography can be a marker for the metabohc changes which accompany pregnancy
LOW DOSE ASPIRIN THERAPY AND PLACENTAL PATHOLOGY IN WOMEN WITH PRIOR POOR PREGNANCY OUTCOMES. W Cus~ck, C Salahax, J Rodls, W Campbell, A Vintzlleos, Un~v of CT, Farmlngton, CT. OBJECTIVE: Determine ~f low dose aspmn {~SA) thecapy ~n a subsequent pregnancy ~mproves placental h~stology =n women wdh a pnor, complicated pregnancy demonstrating defectwe placentat~on STUDY DESIGN: A retrospective chart review identified patients w(th an index pregnancy (IP) cornphceted by preeclampsla (PIH), intrauterine fetal demise (IUFD), abrupho placenta (AP), and/or preterm premature rupture of the membranes (PPROM) w~th placental changes showing defective ptacenta- t~on In the treated pregnancies (TP) 81mg/day of ASA was started prior to 10 weeks and conhnued throughout pregnancy. Pregnancy comphcahons, gestahonal age at delivery (GD), infant sex, and b=rthwe~ght (BW) were obtained from the dehvenng physic=an. Placental spec=mens from the IP and TP were rewewed by a single pathaloglst for evidence of defective placentatlon Ivascalar msufhmency and/or placental thrombos=s). The pathologist was bhnded to the prewous placental findings, pregnancy comphcatlons, or ASA therapy Only compliant pahents w~th complete follow up were ehg=bte for study The pregnancy outcomes and placental changes from the TP were compared to the ]P for each patient. Statistical analysis used included paired test for continuous data and McNemar test for categoncal data. RESULTS: Ten patients w~th a mean grawdily of 3 5 (range 1-10) and a mean par~y of 1 2/range 0-6) were enrolled. IP comphcat~ons* mdudsd IUFD (4), AP (2), and PPROM (1) TP comphcat~ons included AP (1) and PPROM (1)
l I ~P I ~P "1 P "l
Mean (+SD) ADD (weeks) ] 273(+90) i 358(+45) i <0.05| GD<36weeks I 8/10 (80%) | 2/10 (20%) | <0.05| Pregnancy Complications* ~ 10/10 (100%) ~ 2/10 (20%) | < 0.05 | Surviving infant J 2/10 (20%) | 10J10(100%) ] < 0.05 | Defective Placentation ~ 10/10(10~%) ~ 6/9(67°/o) ~ >0,05|
CONCLUSIONS: Desplt~an apparent improvement ~n pregnancy outcomes, Nstolog~c ewdence of defectwe piacentahon persists ~n women wzth a prior poor obstetrical hlston] treated with low dose ASA
THE EFFECT OF PREGNANCY ON THE CONTRACTILE RESPONSE OF THE RABBIT THORACIC AORTA. G Saadex, M Belfort=, I Van den Veyver~, H Hsux, K Moise, P Vanhoutte~ Depts Ob/Gyn and Medicine, Baylor College of Medicine, Houston, TX. OBJECTIVE: To determine the effect of pregnancy on the contractile response of female rabbit descending thoracic aorta to selected agomsts STUDY DESIGN: Vascular rings from the thoracic aortas of pregnant and non-pregnant New Zealand White rabbits were suspended in organ chambers In physiological salt solution for isometric tensLon recording. Each ring was stretched to the optimal point of its length-tension curve Cumulative dose-response curves were then determined using serotomn (5HT), phenylephrine (PE), endothelin-I (ET-I) and the thromboxane analogue U46619 in the presence of indomethacln (10-5 M) with or without N~-mtro-L-arginlne (NLA, 10-~ M). ET-1 was added only to rings without endothehum The other drugs were added to rings with and without endothehum The tensmn measured at each concentration was expressed as a percentage of the moximal tension generated Student’s t-tests were used to compare the responses at each dose, the area under the curve, the maximal tension generated and the dose producing 50% of the maximal response
(ED~0). P < 0 05 was used to denote statistical significance. RESULTS: There was no significant difference between pregnant and non-pregnant vessel responses to U46619 and PE Removal of the endothehum or pretreatment with NLA potentmted the effect of PE ~n vessels from non-pregnant animals only Serotomn was more potent in vessels from pregnant ammals (-log ED~o 4 87 __+ 0 78 vs 5 75 + 0.51, p = 0 04), but this d~fference was abohshed in vessels exposed to NLA and in those without endothehum. ET-1 was more potent in vessels from non-pregnant ammals (-log ED~o 7 72 + 0 07 vs 7.54 +_ 0 19; p = 0 03) This difference persisted m vessels treated with NLA CONCLUSION: Pregnancy has a vmable effect on the vascular response to contractile agents which cannot be totally explained by a difference in endothelial function
SCAVENGING OF EDRF BY ERYTHROCYTES IS ALTERED IN PREGNANCY COMPLICATED BY SICKLE CELL ANEMIA. L_
~ N Wassorstrum, JV Mmnbouli,~ PM vanhoutte? Baylor College cine, Houston "IX.
ORJECTIVE: Maternal and fetal morblditv m maternal stckle cell ane- rma (SSA) result m pma from the altered inicrovascular hem,ud~]cs that leads to occluszen m the utoroplacental and otN~ ma~ vascmar beds. Endothelium derived relaxmg factor (EDRF) locally rel,m~..ates tone m vascular smooth muscle and effectively controls local perfusion. Oxy- hemoglobin ~s a powerful scaveng~..of .EDRF, and rlonnal- red,.b,lood cells
~ng etr~ioncy or ~ aria. ~emo~lo,~n.(Wo) ~rem,~ ~u~ ~ (SSA grawda) with correspon~n_g samp~as ~rom normm ~awoa. STUDY DESigN: In a pe~’_fus_ Ion-supeff.us~on bloassay, E])RF ~leased from camne carotid arteries (donors) was ~tectcd by rings ~om me same vessel but denuded of eudothelima, and separated fiom the ~onors ,by.a 5 sec transfor line PreporaUons wcze contracted with .pl~y~lepg~__�, acetylchuline (ACh) ai~plied to the donor elicited stts~,ll~, EO,RP- dependent relaxatton ui both donor and de.~. tor ttssue.s. ~tana samptes~ from normal and SSA gmwda were infused ~mmedmt.ely ap. wnslream o~ the donor artery The magnitude of the. reductima in_r.e.laxat~.on .of .the d~ rector reflectud EDRF scavenging efficiency. Intact RBC and sot~ttm~s m Hb prepared from hemulysgtes were tested. .. RESULTS: Scavangin4; of EDRF by intact RBC from SSA, g~a. v~oa was only 47% as efficient as that of R.BC from normat gra~vLaa Qa<.0~2), There was no difference between EDRF scevengmg emctency or antu- Uons of Hb prepared from the 2 sets of gravida. CONCLUSIONS: The dtffere~ce in EDRF scavenging efficitmcy be- tween intact RBC from SSA gravida and normal grav~da was not evident m comparisons of their respective hemolysates. Hence, a pro ,b~bly re- flects alterattons m the cell membrane, m cell membrano-¢ndotheutno in- teractions and/or rn intracullular Hb structure in SSA. SSA is generally regjonal
blood flows winch - at rest, d_uO~- ~old stunutahon ano e.xer~se - arc elevated �ompared to black nons~ckl, e chrome anemic controts. ~ ne present results de~,~e one of the mecb.anisms for th~s hyp~rerma m .SSA. Furthermore, preliminary data suggest that the EDRF sca,v .,e~,. g of m~ta,~ RBC
from SSA grawda mcrmses’ during exposure to enaomen.um ~ue.n
an ~ncrease m EDRF scavang.mg would at least m. part explain the epi- sodic occlusion that accompmnes nocrovas~ular stas~s m SSA.

266 SPO Abstracts January 1994 Am J Obstet Gynecol
RAPID AND ACCURATE ECHOCARDIOGRAPHIC ASSESSMENT OF LEFT AND RIGHT HEART HEMODYNAMICS IN CRITICALLY ILL OBSTETRIC PATIENTS. M, Belfort,x R. Rokey x
G Saade,~ K. Moise, Jr. Departments of Obstetrms and Gynecolo.gy and Medicine, Baylor College of Medicine, Houston, Texas OBJECTIVE: We have previously shown that non-mvasive (Doppler/2D Echocardlograph~c) (DE) estimation of left ventrtcular filhng pressure (LVFP), cardiac index (CI), pulmonary artery systohc pressure (PASP), and right atrial pressure (RAP) in crittcal|y ill non-pregnant patients correlates
well w~th right heart catheter (CATH) findings. Pregnancy induces significant changes in cardiac physiology Estimates of LVFP, PASP, and RAP based on data from critically dl non-pregnant sublects may not accurately reflect cardmc pressures In equally ill pregnant patients We thus studied the correlation between DE and CATH m estimating LVFP, CI,
PASP and RAP in a heterogenous group of critically ill pregnant patients. STUDY DESIGN: Nine critically dl obstetric patients requiring invasive monitonng for chnical management were prospectively studied. S~multaneous DE and CATH readings of LVFP, C1, PASP, and RAP were subjected to regression analysis. RESULTS: The left ventricular ejection fraction as estanated by DE was 65.4% ± 15.3%. There was a good correlation between the two methods
for LVFP (R = 0 91), CI (R = 0 97), PASP (R = 95), RAP (R = 0.7) Data presented as mean +_ standard de’clarion. No serious discrepenc~es between
DE and CATH were noted.
LVFP C1 PASP RAP
(mmHg) (L/minim2) (mmHg) (mmHg)
CATH 14.1 + 6.3 436 ± 1.21 31.6 ± 11.6 53 _+_ 4.0
DE 14.8 + 7.3 4.19 _+ 1.15 323 +__ 9.3 5.4 + 3.1
CONCLUSIONS: This non-invasive technique may gave the clinician
valuabte mformaUon on cardiae hemodynamie function which may
influence therapeutic and clinical managemem
10 SINGLE UMBILICAL ARTERY: DOES IT MATTER WHICH ARTERY IS MISSING ? _A Abuh~ W Shafferx, G Manx, J Copel, J Hobbins, & A Evans. Departments of Ob/G-yn at Eastern Virginia Medical School & Yale School of Methcine, Norfolk & New Haven. Background: Single umbthcal artery (SUA), m one of the most common congeratal ranlfarmatiorts m human It is associated with an mcreused incidence of fetal anomalies, intrauterine growth retardation 0UOR),
and perinatal mortality With the advent of Color Doppler senography, the umbilical arteries can be nnaged m the fetal pelvis, thus identif3nng the side of the nussmg vessel in fetuses with SUA
Study design: During an lg month prompecttve study, the side of the missing artery was identified in all pregnancies referred w~th SUA (60). Targeted ultrasound and perinatal follow-up were obtained Statistical analysis was performed using X2& Flsher’s exact test when appropnate. Results: The left artaxV was absent (LAA) m 42160 (70%), compared with 18160 (30%) for the right arte’o (17,AA), P<0.0001 95% CI (2 5-
I2). Congemtal anomalies occurred m 18/60 (30%) pregnancies, with 14/42 (33%) m LAA and 4/18 (22%) m RAA, P=0.38 NS Complex congemtal anomalies, def’med as more than one anomaly in the fetus, occurred m 8/60 (13%) pregnaneias. All complex anomalies had LAA,
P<0 05 Cytogenelac abnormalities occurred in 4/60 (7%), al| LAA, P=0 09 NS Pregnancy loss occurred m 11/60 (18%) including 7 pregnancy termmatious, 2 stdlbirths, and 2 neonatal deaths Neonatal
follow-up was available on 45 pregnancies, with IUGR present m 3/45 (7%), 2LAA,I1LAA Six pregnancies are still ongoing Candusions: Tins is the largest prospective series of fetal SUA. The selection process of the missing vessel in SUA favors the left side We fourtd cytogenetic and complex fetal abnormalitaes exclusively with absence of the left after7 /n the absence of congenital anomalies, the incidence of 1UGR does not appear to be increased m pregnancies with SUA.
Oral Concurrent Session A Maternal Fetal Physiology
Thursday, January 27, 1994 1:00 p.m. - 3:00 p.m.
Moderator:John C. Hauth, MD
Ballroom A Abstract Numbers 11 - 18
Volume 170, Number l, Part 2 SPO Abstracts 269 Am J Obstet Gynecol
11 NITRIC OXIDE~DINTRA~FIERI~EGROWTHRETARDATION IN RATS. AL Diker, MR Pierce, UK Munshi, S Eloby-Childress, SS Greenberg, XJ Zhang, DA Clark, MJS Miller, Depts Ob/Gyn and Peds, Louisiana State University, New Orleans, LA. OBJECTI~EI The effects of nitric oxide synthase inhibition in the last third of pregnancy on maternal and fetal health were studied. STUDy DESIGN: Pregnant rats were treated with the nitric oxide synthase inhibitor, N°-nitro-L- arginine methyl ester (L-NAME), from gestational day 13 to day 20 or 21. Control animals received the inactive enantiomer D-N~A~E or no treatment. Maternal blood pressure, complete blood count (CBC), chemistry (liver and renal function) and placental and pup size as well as indices of nitric oxide formation were determined. RESULTS: L-NAME caused a dose-dependent reduc- tion in placental and pup size. Amniotic fluid levels of nitrite/nitrate were not affected by L-NAME. Hemorraghic necrosis of the pup hind- limbs occurred only with L-NAME treatment° Dgformities were dose and time-dependent. Maternal blood pressure, CBC, and blood chemistry were unaffected by L-NAME. CONCLUSION: Chronic reduction in nitric oxide production in the last third of pregnancy re- sults in significant intrauterine growth retar- dation, perhaps secondary to compromised placen- tal growth and function. Hemorrhagic necrosis of fetal hindlimbs is dependent on the duration and dose of L-NAME treatment. Maternal complications are minimal and do not mimic preeclampsia. Nitric oxide appears to be an important component of fetal growth and development.
13 CARDIOVASCULAR RESPONSES TO NEUROMUSCULAR BLOCKADE IN THE ANEMIC OVINE FETUS. L.E. Shields and R.A. Bracex, Dept. of Reproductive Medicine, Division of Perinatal Medicine, Univ. of California San Diego, CA 92103. OBJECTIVE: Currently tittle as known about the cardiovascular responses of the anemic fetus to neuromuscular blockade (NB). We hypothesized that, despite marked anemia with potentially decreased cardiac reserve, the fetal responses to pancuronium NB would differ significantly when compared with NB with atracurium (a cardiovascular sparing agen0. STUDY DESIGN: 10 fetal sheep (137_+1 (SE) days gestation) were divided into 3 groups (21 experiments): pancuronium (n=7), atracurium (n=6), and control (n=8). Fetal anemia (hct=21.8 + 0.7%) was produced by serial hemorrhage over three days (102_+3ml/day). Fetal arterial (FAP) and venous (FVP) blood pressure, heart rate (FHR), pH, pO2 and pCO2 were measured at -30, -20, 10, 20 ,30, 60, and 90 min relative to NB. NB was produced by IV injection of 0.Smg/kg of each agent. Data were analyzed by 3-way ANOVA with repeated measures. RESULTS: Pancuronium NB markedly increased FHR (p<0.0001) and decreased FAP (9<0.01). Atracurium had no effect on FHR or FAP. Both NB agents resulted in decreases in FVP (9ancuronium, p<0.001 and atracurium, p<0.03). Fetal pH and pO2 increased and pCO2 decreased in both NB groups. The blood gas changes were similar between the 2 groups while the pH increase was marginally greater with pancuronium relative to the atracurium NB (p=0.03). CONCLUSIONS: Neuromuscular blockade with atracurium produced minimal cardiovascular effects when compared to NB wnh pancuronium. Thus, because of its cardiovascular spanng effect, atracunum may be a better NB agent to use for fetal paralysis during intraul~rine transfusions, as ~ncreases in cardiac demand may be poorly tolerated by the already stressed anemic or hydropic fetus.
12 CARDIOVASCULAR RESPONSES TO METHAMPHETAMINE IN FETAL
SHEEP. A. Stek, B F~sher,x S. Baker,~ K. Clark? Dept. Ob/Gyn, Umv. of
Cincinnati, Cmcinna% OH
OBJECTIVE: Previous studies from our laboratory have demonstrated
s~gnificant alterations m fetal blood pressure (FBP), fetal heart rate (FHR),
umbilical vascular resistance (UmbVR), fetal pH (FpH) and fetal p,O2 following
maternal admimstration of 1 mg/kg of methamphetamine (Met). The present
study evaluates it these changes are due to d~rect fetal responses or due to
reductions in uterine blood flow (UBF) follow=ng Met
STUDY DESIGN: Seven late term pregnant sheep were instrumented w=th
femoral artery and vein catheters and their fetuses w~th hmdlimb atlery and
veto catheters Flow probes were placed on uterine and umbilical arteries Met
was administered intravenously to the mother (0.03, 0 1, 0 3 and 1.0 mg/kg
bw) or the fetus (0.03, 0.1, 03, 1.0, and 30 mg/kg est fw). All doses were
g=ven m increasing order and were separated by 15 mm. Maternal (M) and
fetal (F) cardiovascular parameters and fetal blood gases were determined
five ram. after each dose.
RESULTS: Maternal administration of Met increased MAP sigmficantly by 7, 14, 44 and 76% while maternal heart rate (MHF0 d~d not change, UBF
decreased by 33±8% in four animals and increased m two (7%), while uterine
vascular resistance increased significantly =n all ammals (4, 6, 51, and 140%).
In response to maternal administration, FBP increased significantly (2, 3, 10
and 28%); no significant changes were observed m FHR, UmbBF or UmbVR.
Fetal paO2 decreased significantly from 21.2±20 to 16.3±22, wh=le FpH
decreased from 7 338±0 008 to 7.294±0,028 following M administration. Direct fetal administration of Met d~d not change M parameters FBP
increased s~gnificantly 3, 5, 12, 29 and 40%, while FHR, UmbBF and UmbVR
tended to increase, but did not reach s~gnificance Following fetal
administration, fetal paO= did not change from a baseline of 20 9~_1 0 mmHg, while fetal pH decreased from 7.30120.017 to 7.157±0,085.
CONCLUSIONS; The observed changes =n fetal blood pressure and fetal pH
appear to be due to the direct action of methamphetamine on the fetus wh~le
the changes in fetal oxygenation which occur after maternal admimstration
appear to be due to decreased uterop(acenta( perfus~on
14 LAPAROSCOPIC INSUFFLATION IN THE GRAVID BABOON: MATERNAL
AND FETAL EFFECTS. HL Galan,x MB Reedy," JD Bean,x A Games," AB Kmgnt, TJ Kuehl? Scott & Wh=te Clinic and Mernonal Hospital, Texas A&M Univera=ty Health S~=ence Center College of Medicine, Temple, TX. OBJECTIVE. To test the hypothesis that intra-abdomlnet pressures (lAP)
aesoQated with abdominal insuffiatien lot laparoscopie procedures va|l alter
pulmonary and hemodynam~c parameters m the pregnant baboon and alter hemodynamic parameters in the fetus.
STtSD~/D ESIGN: Fo ur pregnant baboons at 120 + 7 days gestation underwent
general anesthesia, Swan-Ganz and adenal catheter placement, and abdominal insuttfat)on at 10 and 20 mmHg lAP for 20 min intervals at each
pressure. The following endpolnts were measured: maternal heart rate
mean artenal pressure (MAP), cardmc output (CO), pulmonary capillary wedge
pressure (PCWP), pulmonary ade~J pressure~ (PAP), cenl~alvenous pressure
(CVP), system=c vascular resistance (SVR), respiratory rate (RR), oxygen saturation, and end-tidal CO~. Fetal heart rate was recorded at each pressure
=ntervet. Umbilical artery doppler flow studies were performed immediately
before and after abdominal =nsufflation. Fetal surveillance was performed by following growth parameters before and after the procedure RESULTS: Card)ovaecular parameters: PCWP (p < 0.026), CVP (p < 0.0012),
PAP (p < 0.046) were sigmficantly increased at 20 mmHg lAP; and CO, MAP, MHR, and SVR did not vary significantly with ~r-~’vreased lAP at ~her 10 or 20
mmHg Pulmonary parameters the most etnking change was the increase in RR (from 18 to 41 breaths per mini used m an attempt to maintain adequate
oxygen saturation and end-tldal CO2 when lAP was increased to 20 mmHg. Respiratory ac=dos=s (pH < 7.35 and PaCO~ > 50 torr) was demonstrated in 3 of 4 ammals wlth=n 20 mln at an lAP of 20 mmHg. Fetal effects: Doppler flow
stud=es were unaltered immedmtely follow=ng this procedure as compared to
basehne measurements. A sigmficant fetal bradycardia occurred in one baboon whde the lAP was at 20 mmHg. Normal interval growth was shown by ultrasound two weeks follow=ng the procedure. CONCLUSIONS: Preliminary results show that both the baboon mother and
fetus may have mgnlticant morbidity associated with intra--abdom~nal pressures
of 20 mmHg Before making statements regarding the safety of laparoscopic [nsufllat~on in pregnancy, further studies assessing the effects of insufflation
are warranted.

270 SPO Abstracts January 1994 Am J Obstet Gynecol
15 EVIDENCE OF TOPOGRAPHIC DIFFERENCES IN AMNIOTIC FLUID PLASMINOGEN ACT1VATOR/PLASMINOGEN ACTIVATOR INHIBITOR CONCENTRATIONS DURING SPONTANEOUS ACTIVE LABOR AT TERM. P. Baumann= R. Romaro, R. Gonzalez~ D.B. Cotton, E. Mammen’. Dept. o~ Wayne State Univ., Detrog, MI; 8.nd tho Perinatelog?¢ Branch NICHD, Bethasda, MD. BACKGROUND/OI~JECTIVE: Tissue pla~minogen activator (tPA) and urokinase plasmino~en activator (uPA) are h gh y .specific set ne protsasas present in araniotic uuid (AF) which have been Lmplicated in the mechanisms of membrane rupture. Their activ ~y is counteracted by two soec tSc plasminogen activator mhibitors, PAI-1 and PAl-2. To determine whether there are differences in amniotic fluid concentrations of proteasas in the forebag compartment and the upper compartment of the amn ot e cavity during~abor. STUDY DESIGN: Paired samples of AF were obtained by transvaginal and .transabdominal amniocentesis from 20 women in spontaneeus labor with intact membranes at term. Protease concentrat ons were determined by chromogenic substrate based functional assay (PAl-I) and enzyme- inked immunoassay (tPA-anti~en, PAI-2, uPA) respectively. Normality was tested with the Kn[mogorov-gmirnov one sample test. Student’s paired t-test was used to detect d~ferenees between the two compartments. RESULTS: 1. Concentrations of PAId and PAI-2 in both amniotic fluid compartments were higher than the ones of tPA and uPA; 2. tPA, uPA and PAl-2 concentrations were higher in the forebag compartment than in the upper compartmentI whereas ti~e one of PAI-I was lower.
n tPA-AG PAI-I uPA [ PAI-2 Sample size 0U/ml) (IU/ml) (ng/ml) (ng/ml)
upper 20 0.70 + 33.05: 0~1.~0:1:
151 "5: compartment 0.68- 7.36 49.8
forebag 20 1.68 5: 9.45: 0.30 5: 171 5: eempartment 2.37 28.10 0.22 59 4
Values are expressed as mean + standard deviation.
CONCLUSIONS: 1. Concentrations of inhibitors of local extraeellular
~roteolysis in amniotie fluid are h gher than those of act vators; 2. The igher concentrations of tPA, uPA and PAI-2 in the forebag than in the upper compartment may be due to the effect of c)’tokiees in response to microbial products normall)! present in vaginal secrettons and 3. Metabohsm of PAI-I and PAI-2 in the fdrebag compartment appears to be differentially regulated.
17 CEREBRAL OXIDATIVE METABOLISM DURING SEVERE UMBILICAL CORD
OCCLUSION. RH Ba/I, JT Pater, LE Cak:lwelF, J Jel"�~:~’~
C’VRI. and Dept of ObiGyn erKI RS, and Anesthe~a, UCSF, San Franosca. CA. OBJECTIVE: Severe fatal asphyxia from redu~on of utedne blood Ik)w by utenne arte~ (U’,A) occlusion resuns in a decrease in cerebral oxygen consumpfJon of greater than 50%
and base factors), but oxygen d~i~y to the placenta is unaffected. The null hypothe~s
zs that 1here ~s no d=ffsrenca ~n the pattern of corbcal oxidabve metaboliem during UC ccdusi=, compered to UtA ccdus~ (i.e ut~:~p~enU insider,/). STUDY DESIGN: S~ pregnant e~es at 0 8 of gelatin were m’gicelly prq:e~ed ~ fet~ vasculer catheters, ECcG, EKG and EMG electrodes, and an inflatable cuff-type UC ocduder The fetuses were studed after 2 to 3 days of recovery Follo~ng control measurements of regional blood now (radoac~ve mKzospheres), FHR, BP, blood gases,
and acid base factors, the UC was progreseive~/ocdudad, unbl the fetal ECoG ~as Ise- elect. Ocdusion~asmaintainedferg0mins Furtherregio~albloodf~measJrements were pafm’ned at 30, 60, and 90 mm of ccduson and alt~ 3Omh of mco~
RESULTS: Umbilical ~’teej blood flow fell to 20+5% (mean_+ S[::M) of control by 60 rains and rema=md so until release ThetatalECoGbecarue~>electhcby8+15m=ns O~r the 90 min pecod of occlusico the pH fell from 7 37±0 01 to 6.82_+0.03, and BE nora ,%:1 to
-22~mEq/1 PCO2 rose from 55~2 to 96+-7 mrnHg ByABGparameterstbeaspt~
was more severe than m our UtA preperabons All differences were s~gn~f~cant, P<0 05 pJ’~OVAmdNe~euls) CaO2 fallfrem33-+04toanadrofl 6:~-04andCssO2 from
24_-K)Ato1 0~0 2 mM/I. CerlK~l blood now increased fa224%ofc~ofby30 mlnsand remained elevated. C~ebeller and m~rain blood flow increased sim~lerly Codical oxygen cons~pt~n at ~ontrcl was 110-+5 pM/100ghnin and d~d ~ot change s~n~flcan~y thoughout the perkxt of occlus~ Fefal BP and HR peranelers unde~,ent acute changes at the t~e of ocdu~ but then stabilBed at ccntrol values
CONCLUSIONS. We conclude that severe asphyxia as determined by nod base paameters produ~ by UC ocdusco, results in ma~ntenanse of cerebral 02
by approx~ataly 50%. rh~s is apparen~y due to the lesser degree of ascondng aortic hypoxia produced by UC occlusion. We speculate that thzs may help to explain why asphyxia due to partial cord occlusion (leading to variable decelerations, terminel bradycardia) =s mere benign w~th respect to neurological injury than asphyxia due to
uterol~acantal insunlc~.
16 CARDIAC FUNCTION PROFILE IN FETUSES AND NEWBORN$ EXPOSED TO LOW-
DOSE ASPIRIN (ASA) DURING PREGNANCY. T. I~ Sessa. M Moretti, D. Putl~am,x K Arheart,x B. Sibal. Dept. Ped Card and Obstetrics-Gynecology, Unlv ofTenn, Memphis,
TN OBJECTIVE: To evaluate cardiac function (CF) m fetuses exposed to low*dose ASA.
STUDY DESIGN: Aspmn 60 mg/d or a matching placebo was administered to women ~n
a double-bhnd fashion dunng the 2nd and 3rd tnmester to assess its efficacy In preventing preeclampsia. 146 echo-Doppler studies were performed on 63 fetuses from 15 to 40
weeks’gestation ParametersofCFmeasuredincluded leftventncularoutput(LVO)and
dlasteltc area (LVDA), right ventrt~tar output (RVO), and diastolic area (RVDA}, ducta[
peak velocity (DPV), mltral peak E and A wave velooty and peak tricuspid velocity. CF was
also assessed in 73 newborns In the neonates, fractional shortening (FS), cardiac output
(CO), frequency of tricuspid regurgitation (TR), and patent ductus arterlosus (PDA) were
evaluated
RESULTS: Throughout gestation, DPV, RVO (Fig.), RVDA, LVO, and LVDA increased
and were s=mllar ~n both ASA and placebo exposed fetuses Fetal diastohc flow veloot=es
were also ahke in both groups The 2 groups had s=mdar gestat=onal age at delivery
(39.2+_2 3 vs 38 7+9.6 weeks) and blrthwe~ghts (3174:t575 vs 3105:t579 grams) Table
summanzes FS, CO, TR, and frequency of patent ductus arteriosus CONCLUSIONS: The circulation of fetuses and newborns is not effected adversely by exposure to low-dose ASA during gestat!on. Supported in part by NICHD
LV FS CO TR PDA (%) (ml/min) # (%) # (%)
Aspirin (n=35) 43 7+_10 2 969+997 14 (40) 29 (82) Placebo (n=38) 45 3~.6 1009+-378 13 (34) 31 (83)
Right VentricuMr 600
Gestational Age (weeks)
18 THE SYMPATHOADRENAL RESPONSE OF THE OVINE FETUS TO THE DIRECT INTRAVASCULAR ADMINISTRATION OF METHAMPHETAMINE. M M. RamirezX, R. L Andres, V Parisi, Dept OB/GYN and Reproductive
SQences, Univ of Texas Mod Sch, Houston, TX OBJECTIVE: Previous reports have shown that rnethamphetamine
~ered to the pregnant ewe is associated ~ an acute increase in
c~rcutating fetal catecholamines. We hypothes=zed that the direct fetal adm~n~stretion of methamphetamine would result in s=milar alterations in
sympathoadrenal activity. STUDY DESIGN: 13 near-term pregnant ewes and their fetuses were chronically catheterized Methamphetamlne (1.25 mg/kg estlmatad fetal
body weight) was injected into a fetal venous catheter ovsr a 2 minute time period Fetal ertenal pH, lactate, glucose, ~nsuhn, epinephrine (E) and norepinephrine (NE~ were measured at control, 2, 5, 15, 30, 45, 60, 90, 120,
and 180 m~n. The data are presented as mean + SE and are analyzed sfet~stically by ANOVA. RESULTS: Fetal arterial pH decreased from a control value of 7 35 +_ O.01 to reach a nedtr of 7 19 + 003 at 15 m~nutas (p <0001, ANOVA). P~asma lactate increased from 75.3 ± 6.2 to 131 8 + 16.2 mg/dl over the same time
penod (p <0 05). Plasma glucose rose from 22 0 ± 3.1 to 38.0 ± 6 mg/dl at
30 min, while plasma insulin increased stesdfly from 9.1 ± 1.8 to peak at 16 8 +_ 4.6 at 180 rain. (p <0.05). Both E (control = 175 5 ± 28 0 pg/ml) and
NE (control = 229 0 + 25 53 pg/ml) =ncreased s=gnrficantiy (p <0.05) to a maximum value at 15 m=nutes (E = 8259 +356 pg/ml and NE = 7863 ±
24 9) CONCLUSION: These data suggest that dwect fetal exposure to methamphatam=ne results =n profound changes ~n sympathoadrenal activity ~ncludmg an mcreaes in circulating catacholamines. These responses may in pert explain the adverse perinatal outcome observed chn=cally in pabenta that use th~s drug
Oral Concurrent Session B Genetics and Teratology
Fetal Therapy Placental Phys~ology
Doppler Thursday, January 27, 1994
1:00 p.m. - 3:00 p.m.
Moderators: Mary E. D’Alton, MD Assistant Secretary-Treasurer, SPO
Karin B. Nelson, MD Honorary Member, SPO 1994
Ballroom B Abstract Numbers 19 - 26

Volume 170, Number 1, Part 2 sPa Abstracts 273 Am J Obstet Gynecol
19 FLUORESCENCE IN SITU HYBRIDIZATION (FISH) ANALYSIS OF UNCULTURED AMNIOCYTES FOR RAPID DETECTION OF
CHROMOSOME ANEUPLOIDIES, EXPERIENCE WITH 10,000 PATIENTS. B. E. Ward×,S. Gersen×,M. Carellix. Integrated
Genetics, Framlngham, MA. OBJECTIVE’ FISH utltlzlng chromosome specific DNA probes can Identify numerical abnormalities of chromosomes 13, 18, 21, X and Y In uncultured amnlocytes. Improvements In test performance due to expanded clinical experience and
changes In laboratory protocol were measured STUDY DESIGN. Over 10,000 r~mn~oflc fluid specimens were referred for rapid FISH aneuploidy detection and
cytogeneflcs. The numerlcml status of chromosomes 13, 18 and 21 was evaluated by single color FISH and the X and Y by
dual color FISH. The sensitivity, specificity, aneuptoldy detection rate and predictive value of FISH were determined
by compared to cytogenetics Results for the Initial 5,000 cases and the subsequent 5,000 are reported. RESULTS: FISH analysis generated Informative results In >90% of cases. 8% of cases were uninformative due to the presence
of maternal cells Cytogenetlc success rate was >99.9% For the five tested chromosomes, correlation between Informative FISH results and cytogenetlcs was 99 9%. Over 250 aneuploldles were Identified by FISH and confirmed by cytogeneflcs, The sensitivity and specificity of FISH versus cytogenetlcs was >96% and >99%. Comparison of Inlflat and subsequent cases demonstrated Improvement In aneuplold detection rate (73.3% to 79 5%), reduced false positive rate
(0.03% to 0.00%), reduced false negative rate (6.1% to 0.00%)
and reduced undetected maternal cell contamination (0.1% to 0.06%). CONCLUSION: This clinical experience demonstrates the ability of FISH to rapidly and accurately detect tdsomles and other aneuploldles of chromo<ames 13, 18, 21, X and Y In
uncultured amnlocytes, Expanded experience contributed to Improvement In reliability ,rod * mcuracy of results.
21 ASSOCIATION OF CONFZNED PLACENTAL MOSAZCZSM WITH INTRAUTERINE GROWTH RESTRICTION. T Cowles, S Taylor~ S Zneimer~ F Elder~ Dept of Peds and Path, Univ of Tx-Houston, TX; Dept of Genetics, Kaiser Foundation Medical Center-Oakland, CA.
OBJECTIVE: Confined placental mosaicism (CPM) can occur in conjunction with karyotypically normal fetuses. The purpose of this study was i) to explore the association of CPM with IUGR in fresh placentas and 2) test the feasibility of screening fixed placentas for CPM with fluorescence in situ hybridization (FISH). STUDY DESIGN: Cytogenetic analysis was performed on placental cultures from 15 prospectively identified IUGR pregnancies (<10%) and 14 normal controls. Deparaffinized nuclei from placentas of 20 fetuses/newborns with normal, trisomic or triploid karyotypes were screened in a blinded fashion with chromosome- specific DNA probes using FISH methodology. RESULTS: One abnormal case was found among the 15 fresh IUGR placentas. 30 cells from 2 primary cultures were analysed. One culture was tetraploid and the other mosaic 46,XX/92,XXXX. Placental cultures of the appropriately grown fetuses were karyotypically normal. Of the 20 fixed placentas, only 15 were correctly iden- tified with three hybridization signals present in 20-85% of the trisomic/triploid nuclei. CONCLUSION: CPM may occur more frequently in placentas of infants with unexplained IUGR. Current FISH technology is not a suitable tool for screening of CPM in fixed placental specimens.
20 COMPARATIVE TRIAL OF A NEW RAPID MULTIPLE PROBE IN-
SITU HYBRIDIZATION TECHNIQUE OF UNCULTURED AMNIOCYTES FOR PRENATAL DIAGNOSIS OF ANEUPLOIDES.
_M G Martens, G.D. Anderson, R Chux, E. Yeomans, J. Terkx, Dept of
Ob/Gyn, The Univ. of TX MedlcaI Branch, Galveston, TX. N Prashadx, W
Weberx, M. Asganx, APROGENEX, Houston, TX.
OBJECTIVE: Previous experience with prenatal d~agnosls by fluorescent
m-s~tu hybridization (FISH)) of amnlocytes has been complicated by a
number of umnformative results, (due to partial hybrld~zatmn w~thout
controls), and time consuming (approximately 16 hours) repetitive single
probe detection methodology A new rap~d (less than one hour) fluorescent
m-situ hybridization test using a single reagent containing DNA probe for the
X chromosome in combmatton wrth Y, 21-18, or X-13 was developed
(APROGENEX, Inc.) and tested for prenatal diagnosis of aneuploldles on
uncultured amnlocytes
STUDY DESIGN: The first 2cc of amnlotlc fired from 47 patients
undergoing amrnocentesls for traditional cytogenetlcS was fixed onto the
slides, and reagents containing multiple probes were applied to detect
chromosomes X,Y,21, 18, and 13 X chromosome probes were combined
w*th each of the other probes, w*th the X probe serving as an internal control.
Traditional cytogenettc studies were performed on the remaining samples
obtained Each laboratory was bhnded to the other’s results.
RESULTS: All (100%) ammotlc fluid samples gave informative results for
the five chromosomes, with 100% accuracy for four aneuploidies (2 tnsomy
18, 2 xyy), all confirmed by trad*tlonal cytogenetlcs.
CONCLUSIONS: This new method allows for a much more rapid and
accurate diagnos~s using DNA probes for chromosomal aneuploldles The
novel use of combinat*on probes allowed for the use of internal controls and
more accurate confirmatton of the eft’ic~ency of the hybndizatmn procedure
Th~s permits the analysis of fewer cells with greater accuracy, thereby providing a more rapid and specific use of DNA probes for the detection of
chromosome aneuplmdes
22 IS THERE AN INCREASED INCIDENCE OF CONGENITAL ANOMALIES IN WOMEN WITH GESTATIONAL DIABETES? 0 Lang~r_, Robert Huffx, Elly Xenak~s, Michael Berkus Dept Ob/~y~, ~Jmv TX HSC, San Anion{o, TX
OBJECTIVE: A paucity of mformaUon exists on the malformation rates In infants of gestational dlabet{c (GDM) mothers (reported
range from 3 4 to 10%), Studies on malformatlor~ rates ~n infants of GDM mothers suffer from contamination of the GDM groups with pregestatlonal diabetics and contamination of the nondla
bet~c controls w~th umdent~fied GDM subjects We sought to
determine the rate of congenital malformations In GDM when
compared to tested nondiabetlc subjects STUDY DESIGN: A prospective populanon based study compared 2,461 GDM women to a randomized group of nond~abetic
controls (4,922) who were selected from the same study t~me frame All control patients were screened for GDM and, when
appropriate (screening > 130 mg/dl), oral glucose tolerance tests (GI~) were obtained (no GDM = all values no~mal by NDDG) All
Infants were examined at dehvery for the presence of major
congemtal anomahes The GDM women were stratified by
maternal age, and level of glycemic control characterized by number of abnormal values on the GT’I’, periodioty, fasting
plasma glucose and ambulatory self monitored mean blood glucose, m order to determine the rate of congenital anomalies
RESULTS: No s~gmficant d~fference was found between the
overall rate of congemtal malformations in infants of GDM mothers (1.8%) compared to nondlabetic controls (2 2%) Prior to therapy, the GDM mothers had a mean plasma glucose of
1]6_+_2Stag/all Finally, when controlled for maternal age, a
s~mdar late of anomahes exists for each age group for both GDM
and non diabeuc sublects CONCLUSION: Women w~th gestaUonal diabetes do not have an increased rate of congemtal malformaUons ~n their offspring when compared to normoglycemlc controls

274 SPO Abstracts January 1994 Am J Obstet Gynecol
23 INDUCTION OF TUMOR NECROSIS FACTOR (TNF) AND INTERLEUKIN- 6 (IL-6) mRNA IN CYTOTROPHOBLASTS (CYTO) EXPOSED TO
LIPOPOLYSACCHARIDE (LPS) B Gomk, J Rachm~lewdzx, and A. Hechbergx, Dept OB/GYN and B~ol Chem, Un~v of Texas Med Sch, Houston,
TX and Heb Unlv, Jer~lem, IL. OBJECTIVE. The cytok~nes TNF and IL-6 have previously been ~denttfied ~n placental hs~se, and are known to be mediators of infectlon-assoQated
~nduc~on of the hset immune system Th~s study was undertaken to better
charactenze the m v~’o rogulot~on of theea cytokmes in CYTO when challenged v~th the bactanal product LPS STUDY DESIGN Term placentae (n=5) were freshly collected, d~ge~tad wth
trypsm/DNace, and subjected to per~oll gradient sentnfuga~on to isolate CYTO E~ther immediately, or after overnight incubebon, LPS (1 ug/ml) or
med~a alone was added to the cell cultures for O, 1, 2, 4, 8, 24, 48, and 72 hrs Total cellular RNA was ~solated by the guan~thn~um th~ocyanate/ces~um
cNonde methodology RNA sampMs (8 ug) were run on 1% agamse-
formaldehyde gels, and subsequently transferred to nylon filters Blots were
hybnthzed wth the appropnate P32-ratholabelled ohgonuclect~de probe RESULTS In nonLPS treated cells ram=real amounts of TNF mRNA could be
detected at zero time, or throughout the mcube~on periods. Conversely, LPS exposure resulted ~n detectable s~grml starling ot 1 hr, and peaking at 2 hrs.
after addff~on of LPS Overnight incubation gave stronger TNF s~gnals m the LPS sbmulated cells, although the kinetics of th~s response remaining s~mflar to zero time exposure IL-6 was hke~ea minimally expressed at zero hme, although nons~muloted cell cultures demonstrated progressive ~ncreaeas m
mRNA expressmn which was maximal at 16 hrs after plating LPS further augmented the transonpt~on of IL-6 mRNA, wdh peak signals seen at 4 hours after LPS s~mulabon Again, overnight =ncubot~on of the CYTO increased
basehne, and LPS-~nduced IL-6 mRNA responses Longterm constant
exposure of CYTO to LPS (untJ172 hrs ) d~d not demonstrate any ev=dence of pro}~Kjed s~gnal~ng. LPS d=d not alter mRNA express=on of the placental genes H 19 and human placental laotogen
CONCLUSION These data demonstrate the selective mduc1~on of TNF and IL-6 mRNA in CYTO wrth LPS These transcnpt~onal events are kinetically dmt]not, and short term ~n nature Overnight ~ncubatlon accentuates the TNF
and IL-6 mRNA signal, and allows for an augmented response to LPS
25 CHANGES IN UTERINE ARTERY BLOOD FLOW IN RESPONSE TO
CORRECTION OF AMNIOTIC FLUID VOLUME. N.J. Flack,~ S. Bower,"
W. Sepulveda, D.C. Talbart~ N.M. Fisk? Centre for Fetal Care, Royal
Postgraduate Medical School, Institute of Obstetrics and Gynancology, Queen
Charlotte’s and Chelsea Hospital, Goldhawk Road, London W60XG, U.K.
OBJECTIVE: Disorders of amniotie fluid volume (AFV) are amenable to
correction by ultrasound-guided drainage or infusion. It is not known whetber
associated changes in intrauterine pressure affect uteroplacental perfusion.
Color flow imaging allows reliable identification and study of the uterine
arteries. We tested the hypothesis that acute changes in amnintic fluid volume
alter uteroplacantal perfusion.
STUDY DESIGN: We studied three groups of patients of comparable
gestational age (mean 22 weeks). 1) Seven pregnancies with severe
polyhydramnios due to twin-twin transfusion syndrome (’rrl’S) undergoing
therapeutic amnioreductinn of a mean volume of 2 litres. 2) Six pregnancies
with severe oligohydramnios undergoing thagnostic amnioinfusion of a mean
volume of 265 ml. 3) A control group of six women who had lsvasive
procedures of similar duration without manipulation of AFV. Color Doppler
imaging (Aceson 12gxP, Aceson) was used to measure impedance indices and
quantitative flow, before and within one hour of the procedure in the absence
of contractions. A paired l-test was used for statistical analysis. A p value
< 0.05 was considered significant.
RESULTS: Quantitative flow measurements significantly increased after
amnioreduction (Amean velocity =23 cm/sec, CI 13-31, p <0.001) and
decreased following amnioinfusion (Amean velocity =8 cm/sec, CI 1-16, p
<0.05). Impedance indices increased significantly aster amnioinfusion
(Apulsatility index =0.2, CI 0.03-0.3, p <0.05), but did not alter with
amninreduction. Tbere were no significant changes in the control group.
CONCLUSIONS: Acute changes in AFV alter ntoroplacental porfusion.
Improvements in uteroplaceutM flow may be beneficial to fetuses in patients
undergoing serial amnloreduetion for TTTS. Conversely, in amnioinfusion the
possibility of adverse fetal effects secondary to impairment of uterine flow
warrants consideration.
24 INSULIN-LIKE GROWTH FACTORS (IGFS) AND FETAL GROW’VIi. Steven Rothx, Om Pescowlz. Linda Pratt. Scott Denne, Alan Gohchowslo. and Wel-Hua Lee Department of Ob!Gyn. Indiana Umverstty, lnthanapohs, Indiana
OBJECTIVE: Fetal macrosomm is associated v~th significant morbidity but the precise mechamsms which iegulate fetal growth are not well understood IGF-I and IGF-II are
ubiquitous peptides that share structural homology -~th insulin and have been ~mphcaled
in the fetal growth process Many studies have shown conflicting results regardmg changes in IGF levels m pregnancies comphcated by diabetes and nmesosonua Because
these studies were inconclusive and because maternal and fetal IGF levels were interpreted as representst~ve of placental effects, we set out to resolve these
inconsistencies by measunng cord serum and placental IGFs m diabetic and normal
pregnancms
STUDY DESIGN: Placentas and cord blood were collected tmmedmtely after temi
dehvenes from patients from four study groups l) non-maaresomtc (AGA)-mfants of
non<habetic mothers (non-IDM) controls, 2) macrosemlc (LGA)-IDM, 3) AGA-IDM,
and 4) grmvth retarded (SGA)-non-IDM Placental sechons were flash-fi~0zen m liquid mtrogen and stored ~,lth collected cord serum at -80"C ]GF-I and IGF-II levels were
messured m cord serum and placental tissue by radlolmmunoassay (RLA.) Exllacted total RNA was analyzed by Northern gels hybnthzed to IGF-I or IGF-II nboprobes
RESULTS: IGF-I levels m cord serum from the LGA-IDM group were slgnlfic~antly Ingher than levels from e~ther contlols or AGA-IDM There was a direct hnear
correlation between cord serum IGF-1 and infant birth weight, independent of whether DM was present (r2~)61, p<O01) IGF-II cord serum levels were elevated in [DM
when compar~ to controls but showed no correlation "Mth birth weight 02=0 04,
p=0 52) In contrast to cord blood levels, IGF-II levels were significantly decreased in the placentas from mothers ~th dmbetes (p-0 03) As ~th cord serum IGF-II levels, there
was uo correlataon ~th fetsl size IGF-I peptlde levels m placentas from both conttol and dtabehc mothers were below the seasiti,aiy of the assay IGF-I mRNA levels &d not
differ in placentas fi’om dmbetm mothers compared to controls IGF-II mRNA levels were decreased m placentas fronl diabetic mothers compared to coutro|s CONCLUSIONS: IGF-I and IGF-II levels are llacgeas~d in the cord serum of IDM The
increase in IGF-11 ts assectatod ~th the presence of maternal thabetes, independent of
fetal sine while the increase in IGF-I ts correlated v, ath the degree of macrosomla
Because there was no lucrease In saber placental IGF-I or II mRNA or peptide levels, the source of the elevated cord seruin IGFs ts most hkely fetal Ussue
26 INTRA-UTERINE VIDEO-ENDOSCOPIC CREATION OF LOWER
URINARY TRACT OBSTRUCTION IN THE FETAL LAMB. J~A
Deprestx, F I Lukex, K Vandenberghex, T Lerutx, I A Brosensx,
F A Van Ascche Centre for Surgical Technologies and Dept of
Ob/Gyn, K U Leuven, Leuven, Belgium
OBJECTIVE: To evaluate the feas~bthty of creating a fetal lamb
model for lower untaary tract obstruchon through mtra-uter~ne wdeo-
endoscopic approach
STUDY DESIGN: A lower unnary tract obstruction was created by
hgat~on of the urethra and the urachus tn 8 fetal lambs (95-105 days,
term = 145 days) The endoscopic approach consisted of 1) a 0° 5
mm telescope and CCD-camera, 2) three to four shod atraumattc 5
mm cannulas, 3) utenne distention by ammotnfuston of warmed
Hadmann solution, 4) adapted tnstrumentahon (micro-forceps,
flexible micro-scissors, b~polar cutting probe) Intra-utenne fetal
monltonng ~ncluded continuous temperature measurement and
pulse-oxtmetry
RESULTS’ The vessels of the umblhcal cord were dissected,
without fetal compromise, and the urachus isolated close to the
umbilical Inserhon (n=8) The urethra (n=7, one female subject) was
dissected in the antenor abdom{nal wall, f cm below the pents. Fetal
saturahon remained between 51 _+ 14% and 72 -+ 20%, fetal head
rate between 126 _+ 23 and 145 + 30 beats/mtn The tntra-utenne
temperature at the end of the operahon was 397 _+ 20°C All
fetuses survived the intervention
CONCLUSION: This model of mtra-utenne fetal surgery ~n the
lamb, using vtdemendoscoptc techmques and momtoring, was
successfully used to create lower urinary tract obstruction

Oral Concurrent Session C Infectious Disease
Prematurity
Thursday, January 27, 1994 1:00 p.m.- 3:00 p.m.
Moderators: Susan M. Cox, MD
Ballroom C Abstract Numbers 27 - 34

Volume 170, Number 1, Part 2 sPa Abstracts 277 Arn ] abater Gynecol
27 AMNIOTIC FLUID PLASMINOGEN ACTIVATOR/PLASMINOGEN ACTIVATOR INHIBITOR CONCENTRATIONS IN PRETERM LABOR IN THE sETrlNG OF INFECTION. P. Banmann% R. Romero, R. Gonzalez" D.B. Cotton E. MammenL Dept. of Ob/Gyn, Wayne Sta’~ ~troit, MI and t~e Perinatology Brunch, NICHD, "Beth�sale, MD. BACKGROUND/OBJECTIVE: Tissue plasminogen activator (tPA) and urokinase plasmino~en activator (uPA) are highly specific serine proteases present in amniotic nuid (AF) which have been implicated in the mechanisms of membrane .... rupture. ....... Their activity is counteracted b two specific plasmmogenactwatormhlb~tors PAl-1 andPAL2. Mmrobl~Vmvasionofthe amniotic eavi~, (MIAC) is fr~uently followed by spontaneous rupture of membranes, we ~ropose that bacterial and host si~gnals produced during the course of intrauterine infection activate i~rotease activity which in turn degrade the extraeallalar matrix and lead to membrane rupture. To determine whether there are differences in araniotic fluid concentrations of ptoteases and their inhibltors in AF of patients in preterm labor with and without MIAC. STUDY DESIGN: Ultrasound guided transabdominal amniocentesis was performed in three groups of patients: Group 1 (n=16)~ patients with preterm labor (PTL), who responded to tocol~,sis and delivered at term Group 2 (n = 14), patients with PTL without MIAC, who delivered within 48 hours; Group 3 0i = 17)~ patients with PTL and MIAC who delivered within 4g hours. MIAC was dmgnosed if at least one of the following was present positive ~ram stain, positive AF cultures white blood cell count > 50 coils/ram. Protease concentrations were determined by chromogen c substrata hasexi functional assay (PAl-l) and enzyme-linked immunoasspy (tPA-antigan, PAI-2, uPA) respectively Normality was tested with the Kolmogorov-Smirnov one sample test. Inferences were drawn by one way ANOWA followed by Duneau’~ multiple range test. RESULTS: Patients who deliveredwithln 48 hours had lower PAI-2 concentrations than those who did not. MIAC was associated with an increase in tPA, PAI-I~ and PAI-2 concentrations.
n tPA PALl uPA PAI-2
NIND 15 2 07 12 7 0 61 155 + 1.06 na ± |0 4 t~s + 0.40 us 4, 55.6 *
NID 14 2 41 12.6 1.05 I00 + 1,60 4- 7 57 ± 0 88 ± 55 7
ID 17 8.0 22 4 0.70 167 +_ 4,68 * _+771" ± 0044 na ±849*
NIND, no int~ctior~no dc, llvery; N|D, no infection-delivery; ID, infectlon-de~fivery ¯ p<0.05, ANOVA Duncan’s test; us: not significant.
CONCLUSIONS: 1) Preterm labor leading to delivery is associated with a decreased concentration of AF PAl-2, whereas PAb I eoneentrmions are not
af�ected; 2) MIAC is associated with an increase in PAl- 1 and PAl-2 concentrations.
29 HIV INFECTION AS A RISK FOR ADVERSE PERINATAL OUTCOME.
F. Geary% M. Lindsay, W. Graves% L. Klein. Dept. Gyn/Ob, Emery Unlvers=ty, Atlanta, GA.
O~JECTIVE: To determine tf HiV-mfected parturmnts are at increase
risk of adverse permatal outcome.
STUDY DESIGN= A case-control study was performed on a
population of pr@gnant women giwng birth at a large metropolitan
hospital between January 1, 1988 and December 31, 1992. The
study population consisted of 279 HIV-seropos~twe (cases) and 1171 seronegative (controls). The power of the study was 80%.
Univarlate and multiple stepwlse logistic regression analyses were
performed to identify the relationship between HIV mfeet~on and
adverse pnrmatal outcome.
RESULTS= Cases were significantly more likely than controls to
dehver tow-btrtbwetght infants (24 4% vs. 13.6%; Odds Ratio {OR)
2.1, 95% confidence interval 1.5, 2.9), preterm infants (32.6% vs.
22.9%; OR 1.6, 95% confidence interval 1 2, 2.2). and intrauterine growth retarded #nfants (15.8% vs. 8.5%, OR 2.0, 95% confidence
interval !.4, 3.0). The ask of permatal mortality and fetal
malformations were not different between the two groups. After
adjusting for confounders using the multlvanate analysis, the
mgnifmant differences prewously noted d~d not persist. HIV-
seroposltwIty was not independently associated with low blrthwelght
{OR 1.6, 95% toni)deuce interval 0,9, 2.9), preterm delivery (OR 1.2, 95% confidence interval 0.8, 1.9), or Intrauterine growth
retardatmn (OR 1,5, 95% confidence interval 0,9, 2,6}.
CONCLUSION: HIV infected parturients are not at Increase ask for
these adverse perlnatal outcomes,
28 AMNIOTIC FLUID IL-6: CORRELATION WITH CHORIOAMNION COLONIZATION AND GESTATIONAL AGE IN WOMEN DELIVERED FOLLOWING SPONTANEOUS LABOR VERSUS INDICATED DELIVERY. W. Andrews, J. Hauth, R. Goldenberg, M. Ma~J:, R. GomezL R. Romero, G. Cassell’,. Departments of Microbiology and OB/GYN, University of Alabama at Birmingham, AL, Wayne State Univ, Detroit, MI, NICHDPerinatologyS~anch, Washington, DC. HYPOTHESIS: Amniotic ~d (AF) Intedeukin-60L-6) is increased and inversely proportional to gestational age (GA) in women with chorioamnion (CA) colen~ation or in~ammatx~ and spot.neons labor vers~s women delivered for medical or obsteVical indications. STUDY DESIGN: The CA and AF were cultured at cesarean delivery for aerobes, anaerobes, ureaplasma, mycoplasrna, chlamydia andtrlchomonas in 269 singleton gestations with intact membranes. Histopathology of the CA and AF IL-6 were also determined.
Age Meeks)
RESULTS: AF IL-6 was: (1) higher in women with spontaneous labor versus those with indicated deliveries (15.8 vs 2.2 ng~nl, p=.01); (2) inversely proportional to GA in women with spontaneouslabor but notinwomenwith indicated deliveries (figure); (3) higher in women with a negative AF culture but positive CA culture (10.0 vs 3.0 ng/ml, p=.002); (4) higher in women w=th a positive AF or CA culture or histo!ogic chodoamnionitis or any combination of tt~e above (5.8 vs 1.8 ngiml, p=.001). CONCLUSION: AFIL-6 is higherand
inversely proportional to GA in women with intact membranes and spontaneous labor versus indicated delivery. AF IL-6 is reflective of CA colonization/inflammation even when the AF culture is negative. AF IL-6 may de a useful clinical marker for irffection mediated preterm lalx~’.
3O AMNIOTIC FLUID TISSUE FACTOR IN PRETERM AND TERM PARTURITION. R. Rum�to, R. Gome~, H. MunozL M. Galasso=, L. Acosta% A. GhidinP, D.B. Cotton, C. Lockwood. Dept. OB/GYN, WSU/Hutzel Hospital, Detroit, MI, Mr. Sinai Medical School, New York, NY and the PerinatololD" Branch, NICHD, Bethesda, MD. BACKGROUND/OBJECTIVEt Chorioamnionitis can lead to acuto and decompensatad disseminated intravascular coagulation (DIC). Yet, the mexhanisms responsible for DIC in the setting of intrauterine infection have not been determined. Tissue factor (TF), a potent natural procoagulant factor involved in the extrinsic pathway of blood coagulation, has been implicated in the pathogen�sis o f chorioamnionitis-iodueed DIC. The objective of this study was to determine if microbial invasion of the amniotic cavity (MIAC) is associated with changes in amniotie fluid (AF0 tissue factor immunoreaetivity. We also studied the relationship between the AF concentrations of TF and tumor necrosis factor-~x (TNF), a cytokine which induces TF gene expression and has been implicated in the host response to intrauterine infection and DIC, STUDy DESIGN: AF was retrieved by abdominal amniocentesis in patients at term (n=50), with preterm labor (n=50) and during the midtrimester of pregnancy (n=20). Amniotic fluid was cultured for aerobic, anaerobic bacteria and Mycoplasmas TF and TNF were measured using ELISA validated for amniotic fluid. Mann-Whitoey U test, KruskallWallis ANOVA and Spenrman’s rank correlation were performed for statistical analysis. RESULTS: 1) TF was present in all the AF samples; 2) AF TF concentrations increase with gastationalage (midtrimester, median 3.4 ng/ml, range 1.7-5.9 vs term no labor, median 5.4 ng/ml range 2.0-11.0 ng/ml, p<0.005); 3) Patients with preterm labor and MIAC (n=lh) had higher concentrations of AF TF than patients without MIAC (n =35), (No MIAC- term delivery: median 4.3 ng/ml, range 0.04-7.1; No M1AC-preterm delivery: median 7.5 ng/ml., range 2.g-10.3; MIAC: median 10 6ng/ml,
range 4.1-16.9; p<O.O01); 4) At term, AF concentrations of TF did not change significantly in presence of either labor or MIAC. 5) AF TF concentrations correlated with AF TNF levels in preterm patients (r= 0.6, p <0.0001). CONCLUSIONS: 1) TF is a normal ennstituent of amniotm fluid; 2) AF TF increases with advancing gestational age in AF; 3) MIAC is associated with an increase, of AF TF concentrations in pc�term patients hut not at term; 5) TF levels are correlated with TNF concentrations in AF of patients with preterm labor.
278 SPO Abstracts January 199t
Am J Obstet Gynecol
31 DETECTION OF INTRAUTERINE VIRAL INFECTION BY POLYMERASE CHAIN REACTION. I.B. Van dan VcvveP, J. Nix, K.I Morse, J.A Towbinx. Dept Pediatrics, Dept OBIGYN, h~ Mole~ Genetics, Baylor College of Medicine, Houston, TX. OBJECTIVE: To evaluate the polymerase chain reaction (PCR) as a rapid and sensitive method for dete~tion of intra-utedne viral infe~tinn.
STUDY DESIGN: 53 samples from 33 patients along with positive and negative controls were studied by PCR fur the presen~ of adonovirus, enterovirus, coxsackievirus, parvovirus Big (87% of samples),
cytomegalovknls (CMV) and herpes simplex v~us (HSV). The source of fetal tissue obtained from in-utero sampling or autopsy material was as follows blood (21), ammotic fluid (10), ascites (3), pleural fluid (1), placenta (7), cardiac tissue (6), other organs (5). RESULTS: Clinical dlagnoses were: non-immune fetal hydrops (NIH) in 14 patients (3 were twin-to-twin transfusina syndrome), fetal ascites (+/- polyhydranmios) in 4 patients, maternal viral exposure in 5 patients (4 also
had ascitas or NIFI), other or unknown in 10 patients. Viral genome was detected m 25153 analysed samples (47%) flora 15/33 patients (46%). Adenovirus was found in 9 patients (27%), parvovifus in 3 patients (10%), enterovtras in 4 patients (12%), CMV in 1 patient (3%). Of the patients
with NII-I ur isolated asdtes, 6 had adenovh’us identified (43%). PCR testing was positive in 8/21 fetal blood samples (38%), 6/10 amniofic flmds (60%), 3/7 placental Ussue samples(43%), 1/3 ascites samples(33%), 4/6 cardiac tissue samples (67%) and 4/6 other tissue samples (67%)
CONCLUSIONS: 1. PCR is a sensitive method for detection of intra-utefine viral infection 2. Although our series is small, adenovirus, a
coraraon cause of neanatal my0ca~ditis and a previously unrecognized cause of intra-utenne fetal infection w~th ~ or as~ites, was a common finding
33 SU RFACTANT REPLACEMENT THERAPY FOR PREVENTION OF HYALINE
MEMBRANE DISEASE IN THE PRETERM BABOON. HI_ Galan.,~ C Cipdani,~ dJ Coaison,x JD Bean,= G Collier,x TJ Kuehl? Seatt & White Clinic, Texas A&M University Hsatth S~ience Centre College of Medicine, Temple, TX, and The
University of Texas Health Science Cer~er at San Antonio and Houston, TX.
OBJECTIVE: Intra-amniotm administrafion of surfaetant (IAS) in pceterm rabbit fetuses has been shown to result in uptake of surfactant with changes in pulmonary mechanics. We have shown that IAS in the pretenn baboon 24 hra
prior to delivery significantly reduces clinical and pathologic aspects of hyaline membrane disease (HMD) when compared to saline controls. We next chose
to test the hypathesis that intratracheal administration of surta~tent (ITS) in the
immediate poslpartum period reduces HMD in this modal, but less than IAS.
STUDY DESIGN: 15 preterm baboons were divided into 3 trealment group~: intra-amniofic injection of saline (N = 5) 24 hrs before delivery, IAS (N = 5) 24
hrs before delivery, or intra-amniotic saline before dchvery and ITS (N = 5) at
delivery. Fetuses were delivered at 137-139 days gestation, maintained for 24 hrs using standard neonatal intensive care techniques including positive
pressure venfi~ation, and assessed for clinical, radiographic, and pathologic endpainta. Data were ana~’fzed takin0 into account repe~ted measures. RESULTS: All 15 animals completed the protocol. Compared to saline
controls, IAS and ITS treated animals had significantly better clinical courses as documented by PaO~/PAO~ (p<0.05), FiO~ (p<0.01), and PaCO~ (p<0.05). Saline controls had significantly more HMD changes than IAS and ITA treated
animals in blindly scored radiographs (p<:0.03). Using a panel of standards method to bfindly s~ore pathologic changeS in the fixed left lung, IAS and ITS
had significantly more inflation (p<0.05) than saline treated animals. Significant
differences were not found between tTS and IAS treated animals for clinical,
radiographic or pathologic endpoints. Ventilator pressures and neonatal
cardiovascular parameters did not differ between groups. Animals receiving iTS tended to have residual inflation in the central and medial aspects of oath lobe. This is in contrast to IAS treated animals which presented a more even
distribution of inflation. This observation suggests that variations in distribution of sudactant may exist depending on the route of administration.
CONCLUSIONS: IAS and ITS treatments significantly improved clinical, radiographic sPA pathologic aspects ot respiratory distress in the baboon
preterm infants, but did not completely prevent HMD in thin established model.
32 THI~ VALUE OF AMNIOTIC FLUID INTERLEUKIN-6 DETERMINATION IN PATIENTS WITH PRETERM LABOR AND INTACT MEMB~NES IN THE DI]TECTION ~ICROBIAL INVASION OF THg ANNIOTIC CAVe. ~ Couhrm. J.M.Lien, A.Khouw, J.H.Grossman. Faiff~ h~pital, Falls Church, VA and George Washington Medical Center, Washington D.C. O~B~IV~: To determine and compare the value ~ amniotic fluid (AF) IL-6 determmauon to other rapid tests to diagnosis microbial invasion of the amniotic cavity in paUents with preterm labor and intact membranes. STUDY DESIGN: AF IL-6 by ELISA was determined quantitat~�~ i~ a~nlOtlC fluid s~cl~ens obtained via amnioeentes,s in 95 patients with pretcrm labor. AF cultures for aerobes, anaerobes and mycoplasma sp. were performed. ROC analysis was pedormed. D~agnostic radices of II-6 for prediction of a ~sitive AF culture, clitoral infccuon and pretcrm delive~ were compared to thusc of gluc~e level, Gram stain, leuko~t¢ eatcras¢, and the LAL assay. RESULTS: The prevalence of ~altive AF cultures was 12.6% (12/95) but 7.4% (7/95) tf mycoplasma sp arc excluded. The median IL-6 concentration (ng/ml) in patients wtth posture AF cultures was 48.650 (range 0.268 - 48.650) in contrast to 0.29130 ng/ml (range 0.101 - 48.650) in patients with negative AF cultures (P=0.~). The highest sensit~ity was achiave~ by IL-6 and glaco~ measurement. Sensitivity and s~cffici~ of an IL6 > 10.0 ng/ml was comparable to that of gluc~e ~ 10 rag/all (~% and 8~%vs 66% and 90%) for a ~itive A~ C~S. If mycoplasma sp. are exctaded, sensitwi~ and sp¢cihci~ of an IL6 > 20.0 (1~% and 92%) were comparable to a I~ glu¢~e < 10 mg/dl (1~% and 89%) or a positwe Gram stain (100% and 96%). patients w~tk an IL6 > 30 ng/ml delivered pr¢term in contrast to of patienta with a glucose ~ 10 mg/dL L~k~se, an IL-6 > ~ rig/m1 detoeted 1~ % (~=11) of patienta destined to devetop clinical infection within 24 hours of amni~entes~s. CONCLUSIONS: AF il-6 determination rosy be a u~fal adjunct to our armam¢ntanum ~ rapid tests to exctade infection and predict d¢liv¢~ i~ patm~ta with preterm labor and intact membranes.
34 THE PROGNOSTIC VALUE OF AMNIOTIC FLUID 1NTERLEUKIN-6 DETERMINATIONS IN PATIENTS WITH PRETERM LABOR. BH YoGa. R Romero, CK Chun’, IH Lee*, KS Kir#, IN Koo’, HC Syn’, SW Kim=. Seoal National University, Seoul, Korea, the Periantology Branch, NICHD, Bethesda, MD and WSU/Hutzel Hospital, Detroit, MI. OBJECTIVE: To determine if amniotic fluid (AF) concentrations of the cytokian interlsukia-6 (IL-6) are of value in the prediction of spontaneous preterm delivery and perinatal morbidity and mortality in women with preterm labor (PTL) and intact membranes. STUDY DESIGN: Amniotic fluid was obtained by transabdominal amniocanteals in 40 consecutive patients admitted with the diagnosis of PTL and intact membranes. AF IL-6 levels were measured using a monoclonal antibody-based ELISA (sensitivity: 43 pg/ml). Receiver operating characteristic (ROC) curve analysis, stepwise logistic regression, and Cox’s proportional hazards modal were used to examine the effect of several explanatory variables on dichotomous outcomes or amnioeentesis-to-delivery interval. RESULTS: 1 ) Patlants dalivering preterm neonates had signiflcaatly higher AF-IL-6 cuncentrationsthan patients delivering at term (median 107.1 ng/ml, range 0.8-513.4 vs median 2.4 ng/ml, range 0.3-12.7, p < .0<3001). 2) ROC curve analysis demonstrated the significant relatioaship between AF-IL-6 and the occurrence of preterm delivery (< 36 weeks) (Z =9.5, p < .000001), and the devclopmeet of significant neonatal morbidity/mortality (Z~6.4, p<.000001). 3) An AF-1L*6 concentrations of > 6.0 ng/ml had a sensitivity of 90% (18/20) and a specificity of 93 % (13/14) in the prediction of preterm delivery, and had a sensitivity of 84% (16/19) and a specificity of 71% (15/21) in the prediction of significant neonatal morbidity/mortality. 4) Stepwise logistic regression analysis indicated that AF-IL-6 was the only predictor of preterta delivery (odds ratio=21.5, p<.005) and neonatal morbidity and mortality (odds ratio =7.9, p < .005) even whan gestational age was known. 5) Cox’s proportionalsurvival analysis demonstrated that AF- IL-6 added significant information to prediction of interval to delivery (hazard ratio=5.7, p<.00001) to that provided by clinical information such as gestatinnal age. CONCLUSIONS: An elevated AF-IL-6 concentration identifies patients at risk for spontaneous preterm delivery and significant neonatal morbidity/mortality.

Oral Plenary Session II
Friday, January 28, 1994 8:00 a.m.- 10:30 a.m.
Moderator: Valerie M. Parisi, MD, MPH Vice President and President-Elect, SPO
Ballrooms A- C Abstract Numbers 35 - 44

280 SPO Abstracts January 1994 Am J Obstet Gynecol
35 A SYSTEMATIC STUDY OF TIlE EFFECT OF GESTATIONAL AGE, FETAL GENDER, 1NTRAU’I~RINE INFECTION AND PARTURITION ON TIIE BIOAVAILABIL1TY OF THE INTERLEUKIN-1 RECEPTOR ANTAGONIST IN HUMAN PREGNANCY, R. Romero, R. Gomez% M. Galassox, S. Berry2 M. Mazor~, R. Qulntero, H. Aranedax, Y~.B. Cotton. Dept. OB/GYN, WSU/Hutzel Hospital, Detroit, MI, and the Perinatology I~ranch NICHD Bethesda, MD. B AC KG ,R.OUI~.!OI~JECTI~]~S: Interleakin- 1 receptor antagonist (IL- 1 ra) is a cytosine with potential value in the treatment of infectmn-assoc ated Ere, term labor (PTLJ. The behavior of this cytokine in PTL is controversial. 5ome investigators have reported no changes in amniotic fluid (AF) concentrations of IL-lra in tile setting of infe~ztion (AJOG 1992;167:863). This obsarvation is unexpected~ at variance with the known biology of IL-I ra in other tissues and also at vartance with observations made in experimental chorioamnionit~s in primates (SGI Abs #$224 1993). This stud}’ was undertaken to systematically examine the bioavailabihty of IL-lra m the maternal fetal and amniotic fluid compartments during term and preterm partur t on with and without intraamniotic infection to address the existing controvers . STUDY ~SIGN: IL-lra concentrations were determined by ELISA in
maternal and fetal btood~ amniotic fluid and fetal urine (332 determinations). The patient population mcluded women who delivered a preterm neonate (wi.th and w~thout microbial invasion of the amniotic cavi~:y [MIAC]) and pattants, at ,[term (no labor, labor without M1AC and labor with MIAC). Amntot~c naid was cultured for aerobic nnd anaerobic bacteria and
p~.l~coplasma snecies. MIAC was defined as a positive AF culture. SULTS: "1) IL-lra was normally present in fetal blood obta ned by cordoceatesis and its concentrations increase with gestational age (n= 40; r.0.61 p <0.01) 2) AF IL-lra and cord blood ~CB) concentrations were s~gnificamly higher inpatlents with PTL and MIAC than in those with PTL but without MFAC (AF: median 225.7 ng/ml, range 35.4-504.0 vs median 73.8 ng/ml, range 24.3-399.0, p <0.001"I~B: median 4.8 ng/ml range 0.3- 167.0 vs median 1.0 ng/ml range 0-]76.0 p<0.05). However, these differences were not found in patients at term; 3) In both, term and ]~reterm patients the AF and fetal urine concentrations of IL-lra were sigmficantly higher in females than in male fetuses (AF, preterm: median 227.5 ng/ml-, range 51 6-504.0 vs median 66.9 ng/ml, range 27.2-284.9, respecttvelyv p <’0.0001 ; AF, term: median 78.1 rig/!! range 28.7-264.0 vs me’finn 40.3 ng/ml, range 3.4-132.4, respectively,p <6.0001; fetal urine: median 317.0 ng/m , range 59.0-440.8 vs median "12.2 ng/ml, range 2.5-61.6, respectively ~<0 005). ’ ’ UONCLUSIONS: 1 ) Contra~ to previous reports, MIAC is associated w th an increase in AF IL- I ra in patients with preterm labor; 2) A significant fetal immune reSponse -as measured by elevated levels of [L-Ira- n preterm pat ents w tfi MIAC was observedin 41% of the cases. This observation suggests that a large fraction of fetuses born to women with MIAC are invaded by micronr~aaisms in utero and that the current methods for the dmgnosis of neonaUd infection are insensitive.
37
36 THE FET,N. C~ VENOUS PRESSURE WAVEFORM IN NORMAL AND COMPLICATED PREGNANCY A. Mon,x B Trud~le~ R. Mod,x V. ReedX Dept (7NGyn, Univ Sydney, Westmead Hospital, NSW, Australia. OBJECTIVE, Our purpose wa~ to study Ihe fetal cent’al venous pressure (CVP) ~avefom~ (fetal inferi~ veto cava [IVC]) rea:~ded r, on-inva=vdy =n
STUDY DESIGN: The changing 6ameter of the lumen of the IVC was followed
pressure ~ (coiffed by us ~n fetat lamb stu~). We stu~ 70 normal fetuses (20-40 wee~s) to dedve a normal~ve range. The complicated
ra~o). The =t s~.~/he,re de~iveff (all <10d~ys) ~as used RESULTS The fo~ co~t t~aves of the CVP ~avef~ (a,x,v,y) v,~re idenlifted and measured in the fetal recording. The a’ests of the a and v
comp~ted group was ~r~vided into three s~lxjroups. In 10 fetuses the wavefo~n ~s naffnal. In 31 there ~as a high pC~alile pattern v~h deep descentfr~ntheacresttoxlrough tn13 this ~as shallow. Clinicaloutc~me (non-reacf~ve FHR, centime I~dlw,~,ght, days NNICU) was sig~if~anb’y v,~orse in
the low compared to high pulsalite group (p<0.001, all =ndices). CONCLUSIONS: Human fela~ CVP wavef~ns can be sm~ply recorded and
38 FETAL CELLS IN MATERNAL BLOOD. DETERMINATION OF
PURITY AND YIELD BY QUANTITATIVE PCR. D.W. BianchP. M.A.
DeMariax, A.P. Shubef’, A C. Fougnef’, K.W. Klingef’. Depts of Ob/Gyn
and Pediatrics, Tufts University School of Medicine, Boston, MA,
Integrated Genetics, Framlngham, MA, and Sonoscan/Genet~c Sciences,
Forest Hills, NY.
OBJECTIVE: Aneuploidy detection by the analysis of fetal cells in the
matemal circulation has demonstrated the feasibihty of nonmvasive
prenatal diagnos~s. Fetal cells are rare in maternal blood, enrichment and
purification procedures are necessary to detect them. All current methods
of fetal cell separation also yield maternal cells. Our objective was to
develop a method of quantitative assessment of the relative numbers of
fetal and maternal cells remaining after different cell separation techniques.
STUDY DESIGN: DNA sequences from chromosomes Y (probe 49a) and
7 (probe D9) were selected for quantitative PCR (q PCR) amplification.
Standard curves were generated for known amounts of DNA. Amplification
of D9 = the numbers of chromosome 7, which is twice the number of cells
present (maternal + fetal). Amphfication of Y reflects the number of fetal
ceils originating m male fetuses. The ratio Y/(½)D9 inthcates purity of
fetal cells.
RESULTS: 40 maternal blood samples (20ml) from women carrying
kn.own males were flow sorted and analyzed by q PCR. The maximum
number of fetal cells detected was 52/1,080 maternal cells Fetal cell purity
ranged from .015 - 48% in sorted fractxons All fetuses were
chromosomally normal
CONCLUSIONS: q PCR is a sensitive new method that enables the
determination of purity and yield of all fetal cells remaining after isolation
from matemal blood. This contrasts with fluorescence in situ hybridization,
where visual screening of 10~ - l04 ceils is limited by techmcian fatigue.
This techmque will facilitate rapid comparisons between cell separation
methods, such as flow sorting and lmmunomagnetic beads

Volume 170, Number 1, Part 2 SPO Abstracts 281 Am J Obstet Gynecol
39 MATERNAL AND PERINATAL OUTCOME OF 846 SINGELTON BREECH DELIVERIES AT ONE REFFERAL CENTER. E. Schiff, S. Mashiach,x O. Hart,x G. Barkal,x BM Sibai Dept. OB/GYN Sheba Medical Center, Tel-Aviv Univ., Israel; and Univ. of Tennessee, Memphis. OBJECTIVE: To evaluate the maternal and neonatal outcome of 846 consecutive term singleton breech deliveries at one referral center. STUDY DESIGN: We reviewed the outcome of 2 groups of patients delivered between 1984 and 1991’ breech presentations f~lfillingthe criteria for trial of labor (n = 613, group 1); and breech presentations w]~o did not meet these criteria and undetwent cesarean section (C/S) (n = 233, group 2). Inclusion criteria were frank or complete breech with estimated feral weight of 2000-3500 g and no history of uterine anomaly or C/S. Pelvimetr/was not performed. Oxytocin was used in cases of hypotonic dysfunction. Two obstetricians, an anesthesiologist, and a pediatrician were present at deliver/. RESULTS: Ingroup 1,326 patients (53.2%) delivered vaginally. There was no marerna~ mortadity. In group 1, t’ebri/e morbidity and length of hospitalization were significandy increased in the women who had C/S. Among those with C/S, these outcomes were similar in groups 1 and 2 There were no stil~birrbs and 8 neonatal deaths, 6 of whom had major malformations incompatible with life (corrected perinaral mortality 0 2%). Two infants died following obstetrical comphcations: one had an uneventful vaginal dehvery and died of pneumonia, and the other died after abdominal delivery performed for a hyperextended bead. Newborns delivered vaginally in group I exhibited a h*gher rate of low Apgar scores, traumatic and respirator/complications, and ICU admissions than newborns in group 2 (table) A shght but insignificant increase in these comphcattons were found in nulliparas compared to multtparas
Group 1 floral) Group 1 (Vag) Group 2 5-rain Apgar -< 6 1.3% 1 5% 0% Traumatic complications 2 9% * 3 4% ~ 0.4% Respiratory comphcations 1.3% 1.5% 0.8% ICU admissions 4.6% 3 4% 2 2%
¯ p = .06 compared to group 2 "~ p.< 05 compared to group 2.
CONCLUSIONS: When a untform policy is applied in the selection of candidates for term vaginal breech delivery, more than half of those selected will deliver vaginally Although the short-term outcome of those delivered vaginally may appear somewhat less favorable, large-scale studies of long-term outcomes should be carrted out, since the present information is not sufficiently concluswe to warrant routine C/S for breech presentation.
41 THE EFFF-,LW OF INTRAHEPATIC VglN SAMPLING OH’V) ON FETAL
PLASMA CORTISOL AND BETA-ENDORPHIN CONCENTRATIONS.
X Gmunakonlopoulosx, W Sepulveda, P. Koutrisx, V. Gloverx & N
Ftskx. Institute of Ob/Gyn, Royal Postgraduate Medical School, Queen
Charlotte’s & Chelsea Hospital, London W60XG, UK.
OBffECTlVE It is not known whether the human fetus mounts a stress
response to mvasive procedures in the absence of hypoxaemia.
Uncomphceted fetal blood sampling (FBS) from the OC is known unt to
be associated with elevated 13-endorphin (!~-EP) concentratmns in the
fetal c~rculation The aim of this prospective study was to determine
whether puncturing the fetal abdomen, as occurs during R-IV FBS, ts
associated with elevated cortisol and ~-EP concentrattuns
STUDY DESIGN: Samples were collected at the tune of FBS for rapid
katyotypmg or for evaluation of fetal alloimmumsatlon, either from the
UC m less than 2 minutes (N=9, median gestational age 27 1 wks, range
19.7-35) or from the IHV (N=13, median time to access the vein 3 7
nuns, range 1-10, median g.a. 28.1 wks, range 19.1-34.4) The extracted
plasma samples were applied to HPLC to separate ~-EP from ~-
lipotropin, and were assayed by RIA. Only samples from fetuses with no
evidence of bradycardia were included
RESULTS: Median (range) certisol and I3-EP concentratmns were
similar (p--0.8 and p=0 58, respectively, Mann-Wlutney U-test) in the
UC group (¢orttsol, N=9. 29 9; 16-51.1 nmol 1"1, ~-EP, N=5’ 80.35;
60,7-111.1) and the lHV group (corttsol, N=13.31.6, 12.1-49 8 nmol 1"1,
[5-EP, N=6: gO 0; 55.4-100.3 pg/ml) There was un correlataon between
either corttsol or 13-EP and pH, pO2 or pCO2. There was no significant
difference in g.a, pH, pO2 and pCO2 between the two groups.
CONCLUSION: Uncomphcated IHV sampling is txot associated ,xath
an increase m fetal plasma cortlsol and ~3-EP concentrations in the f~rst
ten minutes
40 FETAL CARDIORESPIRATORY EFFECTS OF NITROGLYCERIN
IN THE NEAR TERM PREGNANT SHEEP
B Bootatavlor.x C Roman, MA Heymann, and JT Parer, CVRI, and Depts. of
Pediatrics and Ob,Gya & Reprod. Sci.,Univ. California, San Francisco, CA
OBJECTIVES: Previous studies froin our laboratory deinonstrated the
effective t0cnlytic action of nitroglycerin (NTG) in the term laboring sheep.
In this study we have determined maternal and fetal cardiorespiratory effects
of NTG, at 3 limes the minimum effective tocolytic dose.
STUDY DESIGN: Six mixed Western pregnant ewes were operated on between 128-130 d of gestation (term 145 d). Maternal and fetal vascular
catheters and an amnlotic fluid catheter were placed. A transit time Doppler
flow transdocer was placed to ineasure umbilical arterial blood flow. Studies began 2-3 days after surgery. Maternal IV infusion of NTG was given over 30
rains, at each of the following doses: 1.5, 2.5, 5.0, and 10~tg/kg inaternal
wt/min. We recorded the following variables at six different periods in each
animal: fetal femoral arterial and umbilical venous acid-base and blood gases,
hemoglobin, glucose and lactate concentrations, axterial blood pressure,
amrfiotic fluid pressure, heart rate, umbilical arterial blood flow, and fetal
regional blood flow distribution (micropberes). Fetal 02, glucose, and tactate
uptake or production were calculated by the Fick equation. Data analyzed
were by ANOVA.
RESULTS: There were no changes in fetal acid base state, blood gases, umbilical blood flow, blood pressure or heart rate with any dosage level.
Preliminary data (n=4) show no change in oxygen, glucose or lactate
metabofism. Also maternal arterial blood pressure reinalned unchanged. FETAL PRE 1.Sttg/kg 2.5ue/ke 5.0ue/ke 10ue/ke
1~ 7.37:£0.03 7.39-20.03 7.39-~-0.05 7.38:L’0.O3 7.37:£0.03 PCO2 mmItg 56.7~-6.1 64.1±15 52.3.+.5.3 54.8±4A 56.9+_5.0 PO2 mmHg 19.2±2.5 23.8£-6.1 18.9+_2.6 19.2+.3.5 18.9+_3.4 MAP mmHg 57+4 60~3 57±4 52f.3 58±6 Heart Rate 184f31 191+~8 188.+.23 184±31 200~-13 Q Uinb ml/kg/min 170~51 156~-_47 162:k43 163-~43 159±43 n---6; no significant differences
CONCLUSION: Nitroglycerin at tocolytic doses had no adverse effect on fetal cardiorespiratory function in sheep during a two hour infusion.
42 STRATEGIES FOR THE PREVENTION OF EARLY ONSET NEONATAL GROUP B STREPTOCOCCAL SEPSIS: A DECISION ANALYSIS. D J. Rousex, R. Goldenber9, S Cliver, (3. Cutter, S Mennemeyer, C. Fargason. The University of Alabama at B=rmingham, Birmingham, AL OBJECTIVE: Intrapartum maternal antibiotic therapy can significantly reduce e~rly onset neonatal group B streptococcal (GBS) seps~s. We performed a decision analysis to better understand the implications of 17 GBS prevention strategies. STUDY DESI(3N: Probability ast~mates were denved from the appropriate GBS literature. Using decision analysis, we determined the likely outcomes of 17 GBS screening and treatment strateg~as and focused on three rna~n outcomes: 1) Number of expected cases of group B streptococcal seps~s, 2) percentage of grawdas treated with =ntrapartum antibiotics, 3) total direct costs. RESULTS: Universal intrapartum antibiotic treatment (100% treatment) is the most effective strategy to reduca GBS sepsis (94% reduction) It ~s also the least costly with a reduction in total cost to 30% as compared to no screening/treatment. The ACOG has endorsed intrapartum treatment based solely on nsk factors This strategy lowers the rate of GBS seps~s to 31% of expected with an 18% maternal treatment rate and low total costs (35% of no screening/treatment costs). The strategy endorsed by the Amencan Academy of Pediatrics (universal 28 week maternal GBS culture and treatment of culture positive high risk patients in labor), is less effective at reducing neonatal seps~s (51% reducUon) and ~s costly (75% of no screening/treatment costs). Because they are ~nsens~tlve, strategies based on the available rapid GBS identification tests are ~neffect~ve at reducing neonatal sepsm and are costly. CONCLUSION: Two compelling and rational strategies for the prevenbon of early onset neonatal GBS sepsis emerge from th~s decision analysis 1) Universal maternal antibiotic treatment, and 2) maternal treatment based on risk factors alone. A high pnonty for future research should be the development of a rapid test of high sens~t~vRy and specificity.

282 SPO Abstracts January 1994
Am J Obstet Gynecol
43 A NEW METHOD OF DETECTION AND CONFIRMATION OF FETAL NUCLEATED RED BLOOD CELLS FROM MATERNAL
BLOOD. M.G. Martens. G.D.Anderson, R. Chux, E. Yeomans, J. Terkx, Dept. of Ob/Gyn, The Univ. of TX Medical Branch, Galveston, TX., N.
Prashadx, W. Weberx, M. Asarix, APROGENEX, Houston, TX. OBJECTIVE: Current diagnostic methods for the evaluatmn of fetal chromosomal abnormalitms (amniocentesis or chonomc vdlus samphng) are costly and potentially harmful to the fetus. Prenatal diagnosis utilizing fetal cells in maternal blood has been attempted in the past, but it ~s hmited by rucomplete, costly, and labor intensive methods of separation of maternal and fetal cells. A new fluorescent in-s~tu hybridization (FISH) test ut~hzing probes for messenger RNA to fetal hemoglobin has been developed which are capable of visualizing intact fetal nucleated red blood cells (RBC) distinct from maternal blood cells. STUDY DESIGN: Women between the gestat~onal ages of 5-25 weeks had 20ml of maternal blood collected The blood was centrifuged through a density gradmnt and magnetically separated m less than 90 minutes, and then mounted onto glass slides. The glass shales were probed for fetal hemoglobin messenger RNA ~n cytoplasma. Simultaneous nuclear detection of chromosomes X,Y,21,18, and 13 utdizing DNA probes was also conducted to determine if the fetal cell probe would obscure chromosome detection. RESULTS: Each blood sample produced approximately slx slides per patients with confirmation of fetal nucleated RBC by direct wsuahzat~on, resulting ~n informative results w~th 100% accuracy m detecting the six chromosomes Detection of the fetal hemoglobin probe did not obstruct visualization of nuclear DNA probes D~rect wsuahzaUon and d~scnmmatton could be made between fetal and maternal nucleated and non-nucleated red blood cells, CONCLUSIONS: The previous problem of uuhz~ng FISH for prenatal diagnos~s of aneuplmdies from maternal blood appears to be alleviated utihzing a new messenger RNA probe for fetal cell hemoglobin. Therefore, use of the fetal hemoglobin probe should allow the application of 13NA probes for specific chromosomes to be utihzed with greater specificity by ehmmatmg the problem of maternal cell contawanat~on.
44 GESTATIONAL DIABETES: POSTPARTUM GLUCOSE TOLERANCE TESTING, ,J, Oacos. R. Stdson,x N. Meyer, D. Muram,x P, Phipps,x B. Sibal. Univ. of Tenn., Memphis, TN, OBJECTIVE: To determine the incidence of and evaluate maternal dsk factors for poatpartum glucose intolerance among geslalinnal diabetic women and any identifiable characteristics within this population. STUDY DESIGN: One hundred fody-five patients diagnosed with gestational diabetes by conventk~’,al method underwent a 75 g oral glucose 2-hour glucose loierance test preceded by a 3 day diet high in carbohydralas, 5 to 10 weeks postpartum. Our study population consisted of 74% black, 23% caucasian, and 3% other (Asian, American Indian). Results were interpreted according to the National Diabetes Data Group definition of normal, diabetic, or impaired glucose tolerance. Serum glucose concentrations were measured using the glucose oxidese method. The difference among the three groups was determined by chi square analysis and probability levels d <0.05 wine carts~dered signlticant. RESULTS: Of the 145 patients te~sted in the poslpartum porJod, 14 met the criteda far diabetes and 9 showed impaired glucose tolerance for a total of 16% with abnormal glucose tolerance. Maternal age, race, 9estational age at diagnosis (<24 weeks vs >24 weeks), or obesity [body mass index (BMI) >29] did not predict abnormal poslparfum testing. The requirement of insu/in for glucose control (class ~2 during gestation was significantly associated with abnormal postpartum glucose tolerance (p=O.O001). All 14 of the patients ident~flad as diabel=c during postpartum testing were among the insulin requiring gestat~onal dmbetics (class A2). Of the 9 patients exhibiting impaired glucose tolerance on postpartum screening, 5 were diet controlled during pregr~ancy (c~ss A1) and 4 required the addition of insulin (class A2). Of the 85 patzents with d=et controlled gestational dmbetes (class A1) only 5 (7%) experienced an abnorma/postpartum lest. This ~s in contraat to 18 of 62 (30%) of insulin reduidng gestational dzabatics (class A2) with abnormal postpadum testing. CONCLUSION: Pregnancies in a predominantly black popular=on complicated by gestatlanal diabetes are at increased risk of glucose intolerance during the early postpadum period. Frank d~abetes occurs predominantly among those patients requiring insulin therapy during gestation (class A?_) whereas impaired glucose tolerance may occur following gestational d=abetes requiring diet (class A1) or dret plus insulin for control (class .~_.).

Oral Concurrent Session D Labor
Intrapartum Fetal Evaluation Maternal Fetal Physiology
Friday, January 28, 1994 1:00 p.m. - 3:00 p.m.
Moderator: Sharon L. Dooley, MD
Ballroom A Abstract Numbers 45 - 52

Volume 170, Number 1, Part 2 SPO Abstracts 285 Am J Obstet Gynecol
45 PHYSIOLOGICAL DOSES OF ENDOTHELIN-1 INCREASE
THE IN VITRO RESPONSE OF HUMAN MYOMETRIUM
TO OXYTOCIN. ~J. Valcnzuela. C.W. Hewittx, C.A. Ducsayx.
Div Perinatal Biology, Loma Linda University, and Dept. Obs~t
Gynceol, SBCMC, San Bernardino, California.
OBJECTIVE: Several potent utcrotonic hormones, including
oxytocin (OXY) and endothelin, increase only marginally before the
initiation of labor. The purpose of this study was to assess whether
physiological levels of endothelin-1 can augment the myometfial
contractile response to OXY.
STUDY DESIGN: Human myometrium was obtained from the
upper uterine margin of women undergoing elective cesarean
section at tenn. Myometfial strips were mounted in a standard muscle bath preparation in Krebs buffer at 37° C. Eight strips were pretreatcd with 10-9 M endoth¢lin while eight additional strips
from each patient served as untreated controls. All tissues were treated with increasing half-log doses of OXY (10-10 to 10"4.5M).
Contractile responses were analyzed on-line and data were
normalized to the maximal contractile response to 70 mM KC1.
RESULTS: Pretrcatment with 10"9M endothelin-1 alone did not
induce uterine contractions. However, the maximal contractile response to OXY was two-fold greater following endothelin
treatment compared to untreated controls (p<0.01).
CONCLUSIONS: Subcontractile or physiological doses of
endothelin-1 increase myometrial contractile responsiveness to
OXY. These data indicate that it may not be necessary to observe
large increases in plasma utcrotonins to stimulate uterine
contractility. The synergistic effects of physiological levels of endothelin with OXY may be sufficient to initiate labor.
47 MANAGEMENT OF PREMATURE RUPTURE OF MEMBRANES AT
TERM: RANDOMIZED TRIAL. Natale~ R.’, Milne, K?, Campbell, K?,
Wester, K.’, Halinda, E." St Joseph’s Health C~ntr~
OBJECTIVE: premature rupture of membranes (PROM) at term o~¢urs in about
10% of otherwise low risk pregnancies Historically, these patients have been
induced because of the risk of maternal, fetal and/or neonatal infections. More
recently, expectant management has been suggested to lead to a lower incidence of
cesarean birth without an increased incidence of maternal, fetal and/or neonatal
morb~thty. We hypothesize that expectant management in the presence of PROM
would result in a lower cesarean birth rate with no increase in maternal, fetal,
neonatal infection.
STUDY DESIGN: Term patients wh~ consented to the study were rendoraly allocated either to expectant management (EM) for 48 hours or to inthletion of labour (IL) aRer 8 hours of PROM. PROM was confirmed by sterile speculum examination of the vagina. All patients had endocervical cultures done. Exclusion crttema included: presence of mecomum, diabetes, pre-eclampsia, maIpresentation, IUGR, non-reactive NST, placenta previa, ~¢rvieal dilatation >3cm and > 80% effaced and patlents transferred from another centre. Patients randomized to EM were transferred to antenatal and were not examined vaginally until they went rote labour. Patients randomized to IL were stimulated with Oxytocin aRer 8 hours of PROM. RESULTS: Two hundred and fo~ty-thcee patients were randomized, 123 in the EM group and 119 in IL group. The average birth rate was similar in both groups as were the maternal weight and height The cesarean birth rate was the same in both groups (13 8% vs 12.6%, p N.S.). Chnieal diagnosis of post-partum endometfitis was also not significantly different in the two groups (14.6% in EM vs. 12.6% in IL, P N.S ). Pathologlcal diagnosis of chorioamnionitis however, was significantly greater in EM (33.3 % in EM vs. 20.2% in IL, p < 0.05), and all patients that had funisitis always had ehorioamnionitis, 10.3% of which were in the EM and 2.5% in the |L group (p < 0.0S). Eight of the 15 babies lhat land futfisitis were admitted to th~ neonatal intensive care unit for therapy (2 in IL and 6 in the EM group, p < 0 05). CONCLUSIONS: Expectant management thd not reduce the inciden¢¢ of cesarean birth and ~ncreased the pathologwal thagnos~s of funisitis and newborn requirements for N ICU. It ~s ~suggcsted that active management of labour be institsted for PROM and that newer technologies be sought to fa¢d~tate the inductlon
46 PROPHYLACTIC AMNIOINFUSION FOR MECONIUM
STAINED AMNIOTIC FLUID. CY SDongx, OA Ogundipox,
MG Ross. Dept. of OB/GYN, Harbor-UCLA Medical Center, Torrance, CA. OBJECTIVE: We hypothesize that prophylactic amnioinfusion (AI) for meconium (MEC) stained amniotic fired improves perinatal outcome. STUDY DESIGN: Eighty-two term patients w~th moderate to heavy MEC and no variable decelerations (VAR) were randomized to immediate prophylactic AI (600cc safine bolus followed by 3cc/min) or standard care (including therapeutic AI for VAR developing later). All babies were DeLee suctioned upon delivery of the head. Laryngeal cords were visualized and suctioned when meconium was seen below the cords. Statistical comparisons were performed using student’s t test, Fisher’s exact test or Chi-square analysis. RESULTS: There was no significant difference m umbilical arte~ gas values, operative delivery, incidence of fetal distress, apgar scores, or presence of MEC below the cords between the AI (38) and control (44) patients. There were 3 cases of MEC aspiration, all ~n the AI group. At delivery, meconium was visualized below the cords in only two of these. The rate of chorioammonitis was significantly higher (p<0.05) in the AI group (18%) compared to the control group (4%), although time from ruptured membranes to dehvery (8.8 hrs vs 7.5 hrs) and duration of intrauterine monitoring (6.3 hrs vs 5.4 hrs) was not different. CONCLUSIONS: Though AI does dilute amniotic MEC, prophylactic AI for MEC, in the absence of VAR, remains controversial. Together with recent reports, these data indicate a significant portion of MEC aspiration may occur prior to labor. Prophylactic AI in term pregnancies did not improve perinatal outcome and increased the risk for chonoamnionitis.
48 A PROSPECTIVE STUDY OF HIGH- VERSUS LOW-DOSE OXYTOCIN FOR
INDUCTION OF LABOR. A. Hourwtz*, D.S. Se~dm~n*,
M Alcalay*, J, Korach*, A. Lucky*, G. Barka~*, B. Chayen,
S. ~ash~ach*. Dept. OblGyn, Sheba ~ed~cal Center, Tel-
Hashomer and Sackler School of Mad., Tel-Awv Univ., Israel.
OBJECTIVES: To compare the efflcacy and safety of a hlgh-
dosage oxytocln lnductlO~ reglmen versus a commonly
recommended protocol
STUDY DESiGN: One hundred and seventy nine patients were
prospectively randomized to one of two protocols. Patients
in protocols A (n=sI) and B (n:98), received an ~nltlal dose
of 1.25 and 2.5 mu/m~n of oxytoc]n, respectively,
lncretaental increases of ] 25 and 2.5 mulmn at 30 m:nute
intervals were asslgned for protocols A and B, up to a dose
of 7 5mu/m~n Thereafter, women ~e both protocols recelved
Slml]ar incremental increases of 2.5 mu/m)n.
RESULTS: Fallure rates were not slgnlflcantly dlfferent in
protocols A and B (19.7% vs 15 3%). Time to dellvery, the
number of operatlve dellverles, cesarean sectlons, a~d
maternal anU fetal compllcat~ons were not slgnlftcantly
dlfferent However, there was a s~gnlf;cantly hlgher rate
.of uterine hyperstlmulatlon in protocol B (12.0% VS 3.t%,
p<0.05).
CONCLUSIONS: Inductlon wlth hlgher dose increments dld not
shorten tlme to dellvery. Furthermore, the hlgh-dose
protocol was assoclated w;th an Increase In uterlne
hyperst~mulatlon, although a h~gher rate of cesareans for
fetal dlstress was not observed

286 SPO Abstracts January 1094 Am J Obstet Gynecol
Jeffrey P. Phelan. M.D.; Myo~ O. Ah~# Lisa Korst, M.D. ; Gilber~ I. Mar~In, M.D.
Dept. of Ob/Gyn Pomona Valley Hospital, Pomona, CA
OBJECTIVE: Nucleated red blco~ cells (NRBC) are no~ normally encountered in newbo~ ~ are usually duced in response to fetal as~ia. ~e p~Se ~O dete~ine whe~er a relatio~hip ~is~ be~we~ presses of ~C and fe~1 asph~ia ~at ros~ pe~anen~ fetal brain ~nJ~. ~ODS : ~C da~a ~ 25 slngle~on E8~ ne~ol~- ~cally ~mpaire~ neonates (~N} were compared wi~ 85 no~l si~let~n ~e~ newbo~. ~e ~N group ~s separated a=co~ing to ~e ~ patte~ I - deceleration wi~ u~er~e ~p~e (6) 7 II - ta~ycardia (7}~ III - Persistent no~ea~ivi~ a~ission (12). The first ~d highest ~ value ~e ~e ~o ~e ~C ~isappea~nce were assessed. ~1 ~e NIN ~oup e~ited a higher initial ~C (21.2 ~ 26%) ~an did ~e group (1.2 ~ 1.8%) (p~0.001). ~ough ~e ~ between Groups I ~d II were no~ si~ficantly dif- ferent, each NIN s~group demonstrated different values and t~es ~o disappearance. ~erall, Group III e~ibited ~e highes~ ~C (39.3 ~ 47%} �o~t and ~e longest time ~o disappear~ce (244.8 ~ 183 ho~s) (p<O.05). ~e es~ate~ onset for ~e rise was closer to bi~ in Group I ~d II ~ 1ong~ in ~ime for Group III. . ~NCLUSTON: In ~is limited population, ~ ~a~ appea~s ~o aid in identifying ~e presence of asphyxia. ~en asph~ia was present, distin~ pa~erns were ~dentified ~a~ were in keeping wi~ obse~ed in~rapa~ ~ pa~e~. ~e similarity ~C findings in Groups I and II are �onsis~en~ fetal asph~la oc~ng at a s~ilar poln~ In sho~ly prior ~o bi~. In �ontrast, ~e Gro~ III ~ patte~ indicates ~at ~e asph~ia oc~ed at a nuch longer time prior ~o bi~. ~ data suggest ~a~ cord blo~ ~C co~d assist ~ ~e timing of fe~l ne~ol~i= inj~.
51 FETAL HYPERINSULINISM AT 16-20 WEEKS PREDICTS GESTATIONAL DIABETES (GDM) NOT MACROSOMIA. M. Caroenter, J. Canickx, J. Star, S. Carr, K. ShahinianX, M. Tumberx, M. Burkex. Depts. Ob/Gyn & Pathology, Brown University School of Medicine, Providence, RI. OBJECTIVE: In a prior case-control study, we noted an associ-
ation between increased amniotic fluid insulin (AFI) levels in GDM prior to 20 weeks gestational age. The present cohort study explores eady effects of maternal GDM on fetal beta cell function by examining the association of early AFI with later GDM and macrosomia. STUDY DESIGN: A cohort study of AFI assays in 317 grav=das _> 35 years who had had16-20 week amniocentesis for maternal age and subsequent glucose challenge tests for GDM. Birth weight data were available in 289. AFI distributions were compared by 2-tailed t-tests. RESULTS: The GDM incidence was 6.6 in the entire group, consistent with the advanced maternal age of the cohort. Eight of 21 GDM cases were _> 90th centile AFI values (0.91 p.U/ml, based on non- GDM subjects, 38% sensitivity, 93% specificity) and 7 of 21 GDM cases were _> 95th centile (1.33 I~U/ml, 33% sensitivity, 98% specificity). Mean AFI among GDM cases were significantly greater than non-GDM (1.16 + 1.55 v 0.51 _+ 0.66 p.U/ml, p < 0.0001 ). However, among non-GDM cases, those with babies weighing _> 4000 gins, did not have higher mean AFI compared to t.hose with lighter babies (0.46 + 0.34 v 0.53 + 0.66 p.U/ml, p = 0.48). CONCLUSIONS: Maternal glucose intolerance in GDM appears to increase fetal insulin output as early as 16-20 weeks of gestation. These data suggest that, in otherwise unselected late aged gravidas, elevated AFI identifies a high probability (26 - 23 %) of gestational diabetes. Increased early fetal beta cell function does not appear to be present in cases of fetal macrosomia in non-GDM pregnancy.
50 THE EFFECT OF ADVANCING GESTATIONAL AGE ON FETAL ARTERIAL PRESSURE.
K J Moise. G Saadex, L Goodrumx, M Belfortx, R J Carpenter. Dept ObIGyn, Baylor College
of Medicine, Houston, TX
OBJECTIVE: To evaluate the effects of gestatmual age (GA), hydrops fetahs and anemia
on the arterial pressure of the umbilical artery (UAP) m the Rh-affected fetus.
STUDY DESIGN: UAP and amniotic fluid pressure (AFP) were measured just prior to
intravascular transfusion (IVT) using an electronic blood pressure monitor (Physiocontrol
VSMXM1). The corrected UAP was obtained by subtracting the AFP from the UAP. Hydrops
fetalis was defined as the presence of ascites by ultrasound. Fetal hematocrit (HCT) was
performed using an electronic cell counter. HCT was corrected for GA by determining the
#SD from the corresponding normal mean value. Statistical techniques included multiple
regressmu and line of best fit analysis (significance: P < 0.05).
RESULTS: 12 fetuses were included (GA range 9.6 - 30.7 weeks). 4 fetuses were
hydrop~c; 8 non-hydrop=c. HCT ranged between 7.7 and 39.2 %. Multiple regression using
corrected UAP as the dependent variable and GA¢ hydrops and corrected HCT as the
=ndependent variables revealed that only GA significantly influenced the corrected UAP.
related to GA (UAP - -53.04 + 3.03 GA, R - 0.80, p - 0.001). UAP was hnearill
1~
c~=,~ ~ (~)
C0NCLgSl0NS: Fetal u~$cal a~erial pressure increases with gectatienal age. Severe
fetal anemia or hydr0ps fetahs d0 not appear to affect this pressure.
52 AORTIC COMPLIANCE IN EARLY PREGNANCY. J I-Iibbard, A Poppas, C Korcarz, R Marcus, M Lindheimer, R Lang. Dept Ob/Gyn and Mod, U of Chicago, Chicago, IL. Objective: Is there an early increase in aortic compliance during normal human pregnancy (1’)? Study design: A prospective study with tests beginning in 1st trimester; then monthly through the puerperium; then 8 wk and 6 mos postpartum. Instantaneous anVdc pressures were obtained from calibrated subclavian pulse tracings while aortic flow was acquired from continuous wave aortic Doppler and 2D echo determined aortic annular diameter. Noninvasively acquired pressure and flow data were digitalized using custom software. Aortic compliance was determined using a three-element Windkessel model. Signifieance was determined by a Student’s t- test. This study is still in progress, but here we report results in early gestation (n=10) compared to nonpregnant women (C) of similar age (n=20). Results: Age was similar (P: 31+4 v C: 32+7 yrs). Mean arterial pressure was decreased at 11.5_+1.1 wk of pregnancy (P: 74.8+6.0 v C: 87.0+11.4 nun Hg, p<0.001) while cardiac output (P: 7.42+1.62 v C: 5.43_+0.85 l/rain, p<0.001) and aortic compliance (P: 3.2-+1.1 v C: 1.4+0.3 ml/mm Hg, p<0.001) were incgeased. Conclusion: Aortic compliance is already increased in the 1st trimester. Altered aortic pressure-volume relationships in pregnancy may further explain the increased susceptibility to dissection in pregnant women. Ifbaroreceptor function is related to pulsatile elements of pressure, increased compliance may explain the sustained decrease in mean blood pressure that accompanies normal pregnancy.
Oral Concurrent Session E Hypertensive Disease of Pregnancy
Clinical/Operative Obstetrics Friday, January 28, 1994
1:00 p.~n.- 3:00 p.m.
Moderator: Baha M. Sibai, MD
Ballroom B Abstract Numbers 53 - 60
Volurne 170, Number 1, Part 2 SPO Abstracts 289 Am J Obstet Gynecol
53 NULLIPAROUS PREECLAMPSIA (PE) IS ASSOCIATED WITH PLACENTAL EXPRESSION OF A VARIANT ALLELE OF THE NEW HISTOCOMPATIBILITY GENE: HLA-G. EIhott Main. Miml CNang*,
Gall Colbern*, Dept of Ob/Gyn and Research Institute, Cahfornla
Pacific Medical Center, San Francisco, CA. 94115 OBJECTIVE: The non-classical HLA antNen, HLA-G ~s the only
htstocompatlbfllty antigen found on Invading cytotrophoblasts In maternal decldua Many authors have characterized PE as a disease
caused ~n part by poor trophoblast invasion In th~s study, we asked whether trophoblast express~on of a recently ~dent~fied polymorph~sm of HLA-G was associated w~th the elm=cat syndrome of PE. STUDY DESIGN: Placental b~opmes were taken from the dec~duab
placental interface and RNA prepared. RT-PCR was used to generate exon specific DNA sequences. Using denaturing gradient gel
electrophores=s (DGGE), a techmque that can identify single base pa~r d~fferences, two alleles in the alpha 2 domain have been ~dentff~ed the
wild type-"C" which codes a leuc[ne residue ~n pos~hon 110; and a
vanant type-"A" which codes an ~soleucme m that pos~t~on. This site
has functional s~gmficance m that rt =s ~n the pept=de binding groove of the HLA molecule Both alleles of HLA-G are expressed In
heterozygous placenta Chn~cal cases of PE were defined as per
Chesley. nulhpanty, protemurla, hyperuncemla, and normal BP at 6 weeks follow-up Normals had none of the above clmmal signs
RESULTS: HLA-G_~henotypes of the pahents are shown below:
" [ cc I AC l ~ l T°tal [ Normal | 12 ] 6 5 23 J
~_ Preeclamps a [ 4 ] 2 ] 12 ] 18 ] Preeclamptlc placenta slgmficantly differed from normals" p=0.014 by
contingency table analysis 66.6% of preeclampt~c placentas were AA
vs. 21 7% of controls CONCLUSIONS: In this initial sample of pregnancies, we identified a
strong association between the HLA-G A allele and PE. We are
currently examining a larger group of patients and controls. Supported
by NIH grant HD 24495.
55 RISK FACTORS FOR PREECLAMPSIA IN NULL|PAROUS AND
MULTIPAROUS WOMEN. S. Cllver,X R. Goldenberg, D. Rouse,~ J. Hauth,
W. Roden." University of Alabama at Birmingham, Birmingham, AL.
OBJECTIVE: To estimate the risk and attributable risk (AR) of preeclampsia
(PE) in nulliparous and multiparous women with various risk factors.
STUDY DESIGN: Risk of PE was assessed in a prospective study of 20,816
women participating in a five center prematurity prevention trial. Forty percent
of the population were nulliparous, 1.5 % were on medication for hypertension
(HTN) or had a ~reening diastolic blood pressure .~> 90 mm Hg, 3.6% were
diabetics, 1.4 % had a multiple gestation, and 13 % were obese. The overall rate
of PE was 5.2%. Univariate and multivariate estimates of risk and AR were
calculated separately for nulliparoas and multiparous women.
RESULTS: Nulliparous women were three times more likely to develop PE,
with only 10% of the cases attributable to established risk factors. Although
absolute risk of PE w~.s lower in multiparo.s, the risk attributable to HTN,
diabetes, and multiple gestation was much ~reater. Only 70% of PE occurred
in multiparous women without chronic HTN, diabetes or multiple gestation
compared to 91% of nulliparous women without those risk factors. Adjusted
risk odds ratios (ROR), 95 % confidence intervals (CI), and AR for certain risk
Nulfiparas Multiparas
Risk Factor ROR CI AR ROR CI AR
Multiple gestation 2.2 (1.2, 4.4) 1.1% 5.0 (3.0, 8.4) 4.8%
ChronicHTN 2.0 (1.1,3.6) 1.6 4.6 (2.9,7.4) 7.9
Dmbetes 1.4 (0 8, 2.3) 1.2 1.5 (0.9, 2.3) 3.5
Obesity 1.7 (1.3,2.1) 6.2 2.1 (1.6,28) 18.0
Prior PE -- 4.6 (2.8, 7.4) 6.3
Prior spun. ab. 0.8 (0.6, 1.0) 1.3 (1.0, 1.6) -
>.~.20 cigs/day 0.g (0.5, 1.2) 0.5 (0.3, 0.9) -
CONCLUSIONS’ Multiple gestation, chronic HTN and previous preeclampsia are associated with the highest risks for PE. Cigarette smoking and prior spontaneous abortion in nulliparous women is associated with lower risk. Attributable risks for negative factors are higher in multiparous women.
54 HOW FREQUENTLY DOES IlELLP SYNDROME RECUR IN
SUBSEQUENT PP-~EGNAlqCIES? C.A Sullwan~, K.G. Perry, Jr., W.E
Roberts, E F Magann, P.G. Blskex, J N Martin, Jr Dept Ob/Gyn, Univ. of
Mississippt Medical Center, Jackson, MS.
OBJECTIVE: Although an important clinical issue, accurate predtction of
recurrence risk for HELLP syndrome has been problematic due to hmited
pattent experience. This study was undertaken to determine the hkehhood that
thts form of severe preeclampsia/eclampsta would recur in a subsequent
pregmmcy
STUDY DESIGN: An extenstve retrospective analysis of the medical records
and individual patient follow-up regarding subsequent pregnancy outcome were
undertaken for the 484 patients wath HELLP syndrome managed at th~s tertiary
medical center between January 1, 1980and June30, 1993 TheMiss~ssipp~3-
class system was employed to define seventy of disease based on lowest
observed perinatal platelet count (class 1 = <__ 50,000/#L, class 2 = > 50,000
- < I00,O00/ItL, class 3 = > 100,O00 - ~ 150,O00/,aL).
RESULTS: Subsequent gestations (n = 196) occurred m 122 of 484 patients
as shown
Recurrent HELLP
Index HELLP Class # Pts # Pts / # Gest % Recur
1 25 11 12 44%
2 39 8 10 21%
3 58 17 22 29%
All 122 36 44 30%
Subsequent to class 1 and 2 HELLP gestations, 19 had recurrent dtsease for a
patient recurrence risk of 29 7 % Eight patients developed HELLP syndrome
in 2 subsequent pregnancies. If the analyses exclude any primary or
recurrent class 3 HELLP syndrome, 64 class 1 and 2 pattents had 16
subsequent class 1 or 2 HELLP gestations for a recurrence risk of 25%.
CONCLUSIONS: It appears that the risk of recurrence for HELLP
syndrome ~s approximately 1:4. This findtng is compatible with an autosomal
recessive pattern of inheritance as has been suggested prevmusly for the
parent disorder of preeclampsia/eclampsla
56 THE EFFECT OF LIPID PEROXIDES ON ISOLATED HUMAN UMBILICAL ARTERIES.
~’, M. Belfort’, Y. Vedermkov~, H. Hughes~, K. Moise, M Suresh’, D. Johnson’.
Depts. OblGyn, Medicine and Anesthesiology, Baylot College of Medicine, Houston, TX.
OBJECTIVE: To determine the effect of oxzdzzed lipids on the contractile actmty of
~solated umbihcal arteries (UAI obtained from women with uncomphcated pregnanmes.
STUDY DESIGN: Cu" and hydrogen peroxzde were used to oxidize an equimolar mixture
of arachidomc and hnole=c acids. Oxidation was assessed by hzgh pressure hquid
chromatography. UA rings were mounted in Krebs-Ringer solution (KRS) m organ baths for
isonmtrlc tension recording. After equlhbratloo at 2 gm passive tension, a stabilized
response to 60 mM KCI was obtained and used as reference. The experimental protocol
included: 1) Cumulative concentration of oxidized and non-oxidized lipid (107 to 10~ M )
and blank control solutions were added to the baths (n - 51.2) The tm~s wore incubated with oxidized or nonoxidlzed lipid (10~, 10~ or 10~ M) or control solution and then
contracted with cumulative concentrations of the thromboxane A~ analog U46619 (n - 5).
3) Rings in Ca+* free I(RS were incubated with the agents above and then Ca*"
concentraUon was increased (n - 5). Contracble responses were expressed as % of the
KCI reference contraction. Concentration,effect curves (mean _+ S E) for U46619 and Ca*+
were plotted. The effect at each concentration, the area under the curve and the
concentration causing 50% effect were used fm analyszs Stalistinal rrmthods included
ANOVA and Newman-Keuls as appropriate (significance: P < 0.05).
RESULTS: 1) The lipids had no d=rect contractile effect on any of the vessels. 2 and 3)
The hplds inhibited the response to U46619 and Ca÷* in a concentration dependent
manner, with the oxidized hpids having the most significant effect.
CONCLUSION: Contrary to their achon in adults, oxidized lip~ds lack a direct contractde
effect on isolated umbilical arteries and inhibit the response to thromboxane and calcium.

290 SPO Abstracts January 1994 An] J Obstet Gynecot
57 THE ROLE OF NITRIC OXIDE (NO) IN THE PATHOGENESIS OF PREECLAMPSIA. SP Sehgma#, SB Abramson*, BK Young, JP Buyon×. Dept. OB/GYN, NYU Medical Center, NY, NY. OBJECTIVE: Nitric oxide, a potent vasoddator re,eased by endothelial cells, inhibits platelet aggregation and adhesion to vascular endothelial surfaces. Since endothehal cell damage is considered pivotal m the pathogenes=s of preeclampsm, this study was =nibated to determine whether NO produchon is decreased in pabents with preeclampsm STUDY DESIGN: 26 patients w~th preeclampsta (as defined by a blood pressure of at least 140 mm Hg systohc and/or 90 mm Hg diastolic plus prote~nurM, >_ 300 mg/24 hours or _> 2+ by dipstick, both occurring on 2 occasions at least 4 hours apart) and 26 normotensive women w~th singleton gestabons in the third tnmester were studied. Since NO is spontaneously oxidized to both rot#to and nitrate, two analytical assays were used senally. Serum nitrite levels ware initially determined using the Greiss reagent and then the samples were further analyzed using E. C~li nitrate reductase. The Mann-Whitney two sample test was used for statistical analysis. RESULTS" Using the Greiss reagent alone, the mean + SEM of serum rotate level in 26 patients ~ath preeclampsia was significantly decreased compared to 26 normotensive pabents (3.46 + 1 43 pM vs. 4.65 ± 85 pM, P= 02). With the addition of the mtrete reductase enzyme of E Colt, the mean + SEM of serum mtnte level in 26 preeclamphc patients was again sigmficantly decreased compared to 26 normotens~ve patients (20.04 ± 125 pM vs 27 36 ± 223 pM; P=.02). One patient who developed HELLP syndrome demonstrated a concurrent decrease =n serum ndrite over a 2 week period emphasizing the relationship of NO to the pathophysMlogy of HELLP syndrome. CONCLUSIONS. Circulating levels of nitrite are decreased in patzents wth preeClamps~a. These data suppo~ the concept that diminished NO synthesis contributes to the pathophysiological changes seen m preeclampsia
59 THE IMPACT OF DELIVERY ROUTE ON BIRTH INJURY IN
MACROSOMIC INFANTS. C. Cook~, J. Gerard*, L. Zuidema, J. Spinnato.
Depts. Ob/Gyn, Batterworth Hospital, Grand Rapids, MI. and Univ. of
Louisville, Louisville, KY.
OBJECTIVE: To asse.as the impact of delivery route on significant neurologic
birth injury to the macrosomic infants of both diabetic and nondiabetic
mothers.
STUDY DESIGN: 11,047 deliveries were retrospectively reviewed for infants
with birthwalghts >4000gin. 1,282 macrosomie infants were identified
including 193 infants >4500 gin. These obstetric and newborn charts were
reviewed for birthweight, delivery route and presence of maternal diabetes. In addition, pediatric follow up was obtained for up to one year after delivery to
assess for persistence of birth injuries. Categoric variables were compare~t
using x2 analysis with Yate’s correction when appropriate
RESULTS: All birth injuries occurred in the vagiual delivery group at a rate
of 3 3% (42/1282). Tweets-nine (2.3%) were clavicular fractures that healed
without sequallac. Thirteen of 1282 (1.0%) incurred brachial plexus injuries,
with only 54% persistent to discharge and none present at one year of age.
Infants of diabetic mothers were shown to be at significantly greater risk for
brachial plexus injury (4.7 vs 0.8 %, p < .025). Nanrologic injury was not
significantly greater in the operative (versus spontaneous) vaginal (3.4 vs
1.1%, NS) or the > 4500 gm (versus 4000-4500) (2 1 vs 0.8%, NS) groups.
Vaginal delivery was successfully accomplished in 87 % (989/l 137) of the
mothers of macrosomic infants allowed to undergo labor
CONCLUSIONS: Although the rate of birth injury in vaginally delivered
macrosomic infants is significant, persistent brachial plexus deficit is st rare
occurrence and cannot justify elective cesarean delivery for all suspected
macrosomic infants. Although infants of diabetic mothers were at greater ask
for neurologie injury, no persistent injuries were identified in our review of
this or any other group. Finally, vaginal delivery can be accomplished with a
high rate of success in these infants.
58 MATERNAL BLOOD PRESSURE RESPONSES TO CHRONIC
REDUCTION IN UTERINE BLOOD FLOW IN PREGNANT SHEEP.
U. Lang,~ R.S. Baker,~ B K, Fisher,= K.E. Clark ~ Departments of Obstetrics
and Gynecology. Pediatncs and Physiology. Perinatal Research Institute,
University of Cindnnati College of Med=c=ne, Cincinnati, OH.
OBJECTIVE: To test the hypothes~s that chronic reduction in uterine
blood flow will result in increased maternal arterial blood pressure in
pregnant sheep.
STUDY DESIGN: Pregnant sheep with singleton fetuses were
instrumented on gestahonal day (GD) 110 w~th maternal and fetal femoral
artery and veto catheters and electromagnetic flow probes on the uterine
artenes as well as an externally adjustable occluder on the common
internal i~iac artery After baseline measurements on GD 115 ewes were
randomly ass=gned to a flow-restricted group (F~ where uterine blood flow
was kept between 700 and 750 ml/mm and a control group (C) where uterine peffusmn was allowed to rise with gestation Uterine blood flows
were adjusted daily and maternal arterial pressure, heart rate and utenne
blood flow were recorded for a two-hour period on GDs 117, 124, 131
and 138. On GO 138 ewes were sacrificed and fetal and placental weights
determined
RESULTS: In control animals (C) uterine blood flow increased from
866+61 ml\mm to 1520--+158 ml\mm Uterine blood flow m reduced
an=mals (R) was maintained at an average flow of 718 + 23 ml/min until
GD 138. "[his 50% reduction ~n UBF caused a 40% decrease in both fetal
and placental weight, i e intrautenne growth retardabon. C ewes
experienced a slight increase in heart rate throughout the observation
period whereas R ewes’ heart rate remained constant Initial basehne
blood pressure m C and R animals was 79+2 mmHg and 82+2 mmHg respectively, Maternal blood pressure did not change s=gn=flcantly in
response to chronic reduction ~n uterine blood flow.
CONCLUSION: Despite a 50% reduct=on in uterine blood flow which
caused severe fetal growth retardahon, changes in maternal arterial b~ood
pressure and heart rate were relatively turner. Supported m part by HD
18370, HD 20748, HL 40083, HL 49901 and DFG La 660/4-1.
6O MANAGING PREMATURE RUPTURE OF MEMBRANES AT TERM. C.E. Henderson, B. Goldman=, S. P~ening’, B. Sum,mars*, M.Y.
Divert, Dept. of Ob/Gyn. Albert Einstein College of Medicine,
Bronx, New York.
INTRODUCTION: Optimal management of premature rupture of
membranes (PROM) at term =s unclear.
OBJECTIVE: To compare cesarean seotion rates following elective
induction of labor within 24 hours (immediate) or after 24 hours
(delayed) of PROM, and expectant management of PROM.
STUDY METHOD: 2247 women with PROM at term were identified using the labor and dehvery logbook and med=cal record
computer entries (January 1981 to May 1992). Women in
spontaneous labor within 24 hours of PROM or with an intimated
induction or cesarean section were excluded. Outcome following
immed=ate =nduction (Group I) N = 171; delayed induct}on (Group II)
N=139; and expectant management (Group Ill) N=113 was
compared to a control group of the first 150 term dehverles without
PROM for each year of the study period (N = 1800).
RESULTS: Cesarean sect=ons were performed on 17.5% of the
control group, 56.7% of Group I (P=O.OOOOO1), 49.6% of Group
II (P=O.OOO001}, and 22.1% of Group III (P=NS). The mean
latency period In group III was 51.9 hours with 88% entering
spontaneous labor Wnhln 48 hours. The incidence of apgar scores
<7 st 5 minutes was 0.8% m the control group, 4% in Group ~
(P=0.O002), 2.9% =n Group II, and 2.7% (P= <0.04) in Group III.
The inmdence of Neonatal Intenswe Care Unn (NtCU) adm=ss~ons
was 1.4% in the control group, 2.9% in Group I, 3.6% in Group II,
and 6.2% (P=.OOOO1) =n Group II1. CONCLUSIONS: Cesarean sect=on rates following elective
induct=on of labor for PROM at term are double the rate observed
In the control group, whde the rates for the expectantly managed and c~ntrol groups are simder. However, the rate of NICU
admissions for the expectantly managed group was higher than
observed m any other study group.
Oral Concurrent Session F OB Anesthesia and Pharmacology
Medical Complications of Pregnancy
Friday, January 28, 1994 1:00 p.m. - 3:00 p.m.
Moderator: Richard H. Paul, MD Past President, SPO
Ballroom C Abstract Numbers 61 - 68
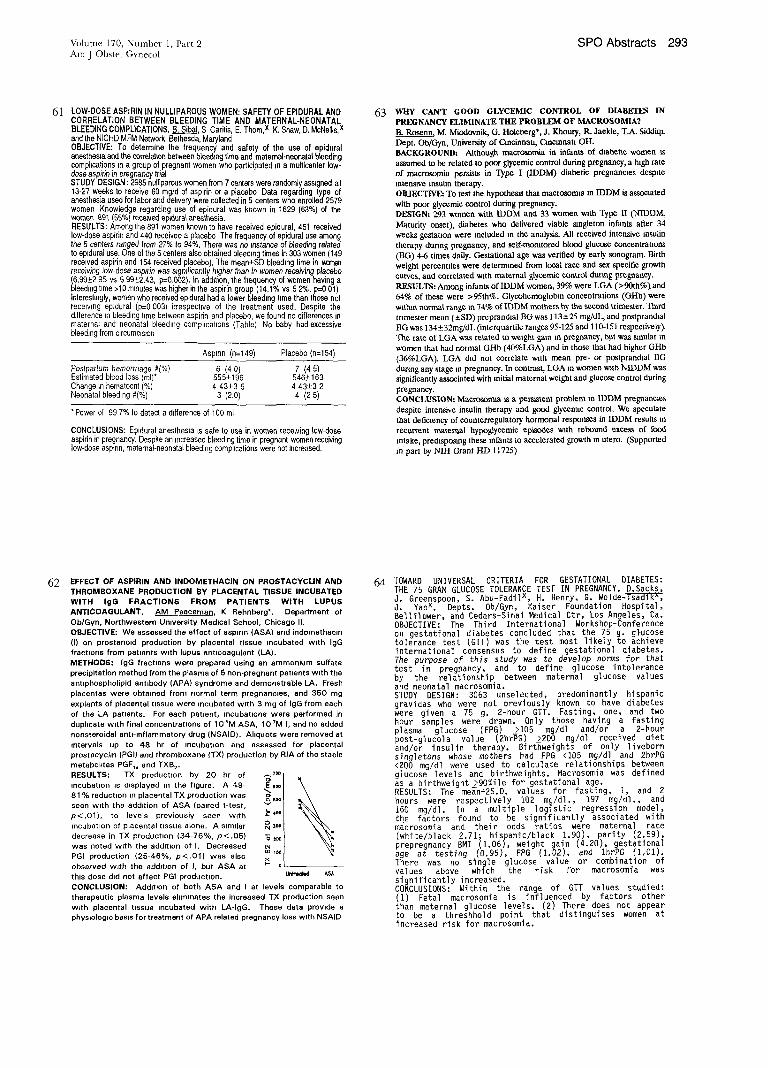
Volume I70, Number 1, Part 2 SPO Abstracts 293 Am J Obstet Gynecol
61 LOW-DOSE ASPIRIN IN NULLIPAROUS WOMEN: SAFETY OF EPIDURAL AND CORRELATION BETWEEN BLEEDING TIME AND MATERNAL-NEONATAL BLEEDING COMPLICATIONS. B. Sibai. S Caritis, E. Them,x K. Shaw, D. McNelhs,x and the NICHD MFM Network, Bethesda, Maryland OBJECTIVE: To determine the frequency and safety of the use of epidural anesthesia and the correlation between bleeding time and malemal-neonata~ bleeding comphcations ~n a group of pregnant women who participated ~n a multicenter low- dose aspirin Jn pregnancy trial STUDY DESIGN : 2985 nulliparous women from 7 centers were randomly assigned at 13-27 weeks to receive 60 mgid of aspirin or a placebo Data regarding type of anesthesia used for labor and delivery were collected in 5 centers who enrolled 2579 women Knowledge regarding use of epidural was known in 1629 (63%) of the women 891 (55%) received ep~dural anesthesia. RESULTS: Among the 891 women known to have received epidural 451 received low-dose aspirin and 440 received a placebo The frequency of epidural use among lhe 5 centers ranged from 27% to 94%, There was no instance of bleeding related to ep~dural use. One of the 5 centers also obtained bleeding times in 303 women (149 received aspirin and 154 received placebo, The mean+SD bleeding time in women receMng low-dose aspirin was s~gmfJcantly h~gher than in women receiving placebo !6, .99,+2 .95 vs .5^99+_2.43, p=,0.092). In addtlion, the frequency of women having a D=ee~mg ume >]u minutes was nigher m the aspirin group (14.1% vs 5 2%, p=0 01) Interestingly, women who received ep~dural had a lower bleeding t~me than those not rece=wng epidural (p=0 003 irrespecWe of the treatment used. Despite the difference in bleeding time between aspirin and placebo, we found no differences in maternal and neonatal bleeding comphcahons (Table) No baby had excessive bleeding from circumms~on
Aspmn (n=149) Placebo (n=154)
Postpartum hemorrhage #(%} 6 (4 O) 7 (4 5) Estimated blood loss (ml)* 555+196 546_+163 Change m hematocnt % 4 43_+3 5 4.43_+3 2 Neonatal bleeding #(%) 3 (2.0) 4 (2 5)
*Power of 99 7% to detecl a difference of 100 ml
CONCLUSIONS: Ep=dural anesthesia ts safe to use in women receMng low-dose
aspirin in pregnancy. Despite an increased bleeding time in pregnant women receiving low-dose espmn, maternal-neonatal bleeding comphcations were not increased.
63 WHY CAN’T GOOD GLYCEMIC CONTROL OF DIABETES IN
PREGNANCY ELIMINATE THE PROBLEM OF MACROSOMIA?
B. Rosenn, M. Miodovnik, G. Holcberg*, J. Khoury, R. Jaelde, T.A. Siddiqi.
Dept. Ob/C~n, University of Cincinnati, Cmeinnata OIL
BACKGROUND: Although macrosomia in infants of diabetto women ~
assumed to be related to poor glycemie control during pregnancy, a high rate
of rrmorosomia persists in Type I 0DDM) diabetic pregnancies despite
intensive insulin therapy.
OBJECTIVE= To test the hypothesis that macrosomua in IDDM is associated
with poor glyeemic control during pregnancy.
DESIGN: 293 women with IDDM and 33 women with Type II (NIDDM,
Maturity onset), diabetes who delivered viable singleton infants after 34
weeks gestaUon were included m the analysis. All received intensive insulin
therapy during pregnancy, and selfomomtored btoo~ glucose concentrations
OlG) 4-6 times daily. Gestational age was verified by early sonogram. Birth
weight percentiles were determined flom local race and sex specific growth
curves, and correlated with maternal glycemi¢ control during pregnancy.
RESULTSi Among infants of IDDM women, 39% were LGA (>90th%) and
64% of these were >95th%. Glycohemoglobln concentrations (GHb) were
within normal range m 74’70 of IDDM mothers by the second trimester. Third
trimester mean ( ± SD) preprandlal BG was 113 -+ 25 mg/dL, and postprandial
BG was 134_32ms/alL (interquartile ranges 95-125 and 110-151 respectively).
The rate of LGA was related to weight gain m pregnancy, bat was similar m
women that had normal GHb (40%LGA) and in those that had higher GHb
(36%LGA). LGA did not correlate with mean pro- or postprandial BG
during any stage in pregnancy. In contrast, LGA in women w}th NIDDM was
significantly associated with initial maternal weight and glucose control during
pregnancy.
CONCLUSION: Macrommta ~s a persistent problem tn IDDM pregnancies
despite intensive insulin therapy and good glycemic control. We speculate
that deficiency of counterregulatory hormonal responses in IDDM results in
recurrent maternal hypogtyeemie episodes ~,ath rebound excess of food
retake, predisposing these infants to accelerated growth in utero. (Supported
in part by NIH Grant HD 11725)
62 EFFECT OF ASPIRIN AND INDOMETHACIN ON PROSTACYCLIN AND
THROMBOXANE PRODUCTION BY PLACENTAL TISSUE INCUBATED WITH IgG FRACTIONS FROM PATIENTS WITH LUPUS
ANTICOAGULANT. AM Poaceman., K Rehnberg% Department of
Ob/Gyn, Northwestern University Medical School, Chicago II.
OBJECTIVE: We assessed the effect of aspmn (ASA) and indomethac=n
(I) on prostanmd production by plaoental tissue incubated w~th IgG fractmns from patmnts with lupus antmoagulant (LA).
METHODS: IgG fractions were prepared using an ammonium suffate
precipitation method from the plasma of 5 non-pregnant patmnts w~th the
ant=phospholipid ant=body (APA) syndrome and demonstrable LA. Fresh
placentas were obtained from normal term pregnancies, and 350 mg
expMnts of placental tissue were incubated with 3 mg of IgG from each
of the LA patients. For each patient, incubations were performed in duphcate with final concentrations of 105M ASA, 107M I, and no added
nonsteroidal anti-Inflammatory drug (NSAID). Ahquots were removed at
intervals up to 48 hr of incubation and assessed for placental
prostacyclm (PGI) and thromboxane (TX) production by RIA of the stable
metabohtes PGF~ and TXB2.
RESULTS: TX production by 20 hr of
incubat;on ~s displayed m the figure. A 49-
81% reduction m placental TX production was
seen with the add;tion of ASA (pmred t-test,
p<.01), to levels previously seen with
incubation of placental tissue alone. A similar
decrease in TX productmn (34-76%, p<.05)
was noted with the add=lion of I. Decreased
PGI production (25-46%, p<.01) was also
observed w~th the addmmn of I, but ASA at
this dose did not affect PG1 production.
CONCLUSION: Addition of both ASA and ~ at levels comparable to
therapeutic plasma levels ehmmates the increased TX production seen
with placental tissue incubated with LA-IgG. These data provide a phymologm basis for treatment of APA related pregnancy loss with NSAID
64 TOWARD UNIVERSAL CRITERIA FOR GESTATIONAL DIABETES: THE 75 GRAM GLUCOSE TOLERANCE TEST IN PREGNANCY. D.Sacks, J. Greenspoon, S. Abu-Fadilx, H. Henry, G. Wolde-Tsadik^, J. Yaox. Depts. Ob/Gyn, Kaiser Foundation Hospital, Bellflower, and Cedars-Sinai Medical Ctr, Los Angeles, Ca. OBJECTIVE: The Third International Workshop-Conference on gestational diabetes concluded that the 75 gl-ucose tolerance test (GTT) was the test most likely ~ achieve international consensus to define gestational diabetes. The purpose of t~is study was to develop norms for that test in pregnancy, and to define glucose intolerance by the relationship between maternal glucose values and neonatal macrosomia. STUDY DESIGN: 3063 unselected, predominantly hispanic gravidas who were not previously known to have diabetes were given a 75 g. 2-hour GTT. Fasting, one, and two hour samples were drawn. Only those having a fasting plasma glucose (FPG) >105 mg/dl and/or a 2-hour post-glucola value (2hr~G) >200 mg/dl received diet and/or insulin therapy. Birt~weights of only liveborn singletons whose mothers had FPG <105 mg/d] and 2hrPG <200 mg/dl were used to calculate relationships between glucose levels and birthweights. Macrosomia was defined as a birthweight >90%ile for gestational age. RESULTS: The me~n+2S.D, values for fasting, I, and 2 hours were respectively 102 mg/dl., 197 mg/dl., and 160 mg/dl. In a multiple logistic regression model, the factors found to be significantly associated with macrosomia and their odds ratios were maternal race (white/black 2.71; hispanic/black 1.90), parity (2.59), prepregnancy BMI (1.06), weight gain (4.20), gestational age at testing (0.95), FPG (1.02), and lhrPG (i,01). There was no single glucose value or combination of values above which the risk for macrosomia was significantly increased. CONCLUSIONS: Within the range of GTT values studied: (1) Fetal macrosomia is influenced by factors other than maternal glucose levels. (2) There does not appear to be a threshhold point that distinguises women at increased risk for macrosomia.

294 SPO Abstracts January 1994 Am J Obstet Gynecol
65 is 1T COST EFFECTIVE TO SCREEN TEENAGERS FOR
GESTATIONAL DIABETES? A.Johnsen,~ S.Kady Wilson,1 L.Hosmer,"
K.Franko-Filipasic," L.Chambliss,Dept. of Ob/Gyn, Maricopa Medical
Center, & The Midwifery Service, Phoenix Memorial Hospital, Phx. AZ.
OBJECTIVE: To detarmme the cost effectiveness of screening teenagers for
gcstntioanl diabetes.
STUDY DESIGN: We retrospectively reviewed the results of the prenatal
testing for gestatioanl diabetes in 350 women age 19 and younger who
delivered at our institutions. The results of the 1° glueela and any 30 GTTs
were recorded. Patients with an abnormal 30 GTT were identified and
assigned a class of gestational diabetes as described by White. The cost of a
1° glucola is $19.85 and for a 30 GTT is $52.00. The costs for testing this
group of 350 patients was calculated.The cost to identify each patient with
gestntional diabetes was determined by dividing the number of cases identified
by the total cost of testing.
RESULTS: 9 of the 350 patients screened had a 1° glueela > 140 rag% and
had a 30 GTT. 3 of these patients met criteria for diabetes. All 3 were Class
AI with normal fasting glucoses throughout their pregnancies on diet
alone The total cost of 350 one hour glueelas was $6,947.50. The cost of the
9 three hour GTTs was $468.00.
CONCLUSION: To screen 350 pregnant teenagers for gestational dmbetes it
cost $7,204.50 and identified only 3 gestational diabetics. All were Class A1
and none required insuhn. Lucas el. al.(1) reported that patients with Class
AI gestational diabetes did not have significant obstetrical or perinata!
morbidity. In 1991 533,483 patients 19 years and younger delivered in the
U.S,(2) The cost of testing for gestational diabetes for this group would be
approximately 11 million dollars.Given the low incidence of gestational
diabetes in pattents 19 years of age or younger coupled wtth the minimal
morbidity reported for Class A1 diabetes, it does not appear to be cost
effective to screen teenagers for gestational diabetes.
1. Lucas, M. et. al. Class A1 gestational diabetes: A Meaningful Diagnosis?
Obstet Gynecol 1993;82:260-265
2 Center for Disease Control yearly reports 1991
67 MAGNESIUM SULFATE VERSUS PHENTTOIN (PHY) FOR SEIZURE PREVENTION IN AMYGDALA KINDLED RATS.
C.A. Standley~, S.M. htenkauP, L. Stewa~, B. Mason, D.B. Cotton. Dept of Ob/Gyn, Hutzel Hospital/Wayne State University, Detroit,
MI.
OBJECTIVES: MgS04 is widely used for seizure prophylaxis in
preeclampsia-vclampsia. However, its anticonvulsant effects in other
types of seizure~ has not been proven, In the present study, we
compare the antioonvulsant effects of therapeutic blood levels of
MgSO, and PHY in amygdala kindled rats.
STUDY DESIGN: 18 male rats had a bipolar electrode stereotaxieally
implanted into the central nucleus of the amygdala. Following
recovery, an afterdischargn (seizure) threshold was determined for each rat. Rats were stimulated daily at their seizure thresholds
(=kindhng) until 3 consecutive generalized tonic-cionie seizures
occurred. Kindled rats r~mdomly received one of the foUowing
mtraveuous injections in a volume of 1.5 ml]kg: saline, MgSO, (30,
60 or 90 mg/kg) or PHY (12.5, 25 or 50 mg/kg). Doses were based
on preliminary data demonstrating blood levels of 16.2 mg/dl for 25 mg/kg PHY and 4.2 mg/dl for 60 mg/kg MgSO¢. Fifteen minutes
following injection, rats were stimulated at their seizure thresholds and seizure activity was assessed. Statislacal comparisons were done using
ANOVA and post hoc comparisons where appropriate.
RESULTS: Magnesium sulfate had no effect on any of the seizure
parameters assessed. PHY significantly reduced seizare duratton
(p< .05), duration of postictal depression (p< .05) and behavioral seizure stage (p < .05).
CONCLUSIONS: Amygdala kindled seizures are more potently
inhibited by PHY than magnesium sulfate. This suggests that
magnesium may not be a very effective treatment in situations where
repetitive seizure activity has been experienced.
66 CHO~IOAMNIONITIS: THE ASSOCIATION OF ABNORMAL FHR PATTERNS AND NEONATAL ACIDEMIA. P. Wendel, S. Cox, S. Roberts, M. Maberry, J. Dax~, L. Gilstrap. Dept Ob/Gyn, Univ. of TX Southwestern Mad. Ctr., Dallas, TX OSJECHVE: It has been previously reported that the majority of newborns with acute chorioamnionitis do not have low Ua pH’s (<7.20). We sought to determine whether selected variables, specifically FHR abnormalities, in pregnancies complicated by chorioamnionitis could predict neonatal acidemia (i.e., cord pH < 7.20). METHOOS: During a 6-month period, mothers diagnosed with chorioamnionitis were prospectively identified in tabor. Following delivery, fetal monitor strips and hospital course were reviewed for both mother and neonate. The Cox Proportional Hazards Model weighs independent variables according to their duration of exposure. Independent variables included; birthweight, loss of variability, absence of fetal heart rate accelerations, presence of fetal tachycardia, and absence of severe and late fetal heart rate decelerations. Duration of exposure for the statistical model was based upon diagnosis to delivery. RESULTS: 197 consecutive cases of chorioamnionitis were prospectively diagnosed for an incidence of 2.1% in our population. Independent variables and their relative risks for neonatal acidemia are listed below.
RR E C! (95%) Sirthweight (<2500 gms) 1.3 .60 ,5-3.3 Loss of variability .85 .77 ,3-2.5
~ bseoce 9f severe/late .84 .63 ,4-1.7 ecetera~zons NO accelerations 2.8 .01 1.3-6.1
Mild tachycardia (160-180) .8 .41 ,4-1.4
Mod/severe tachycardia (~181) 1.5 .28 ,7-3.2
The lack of fetal heart rate accelerations was the only variable slgmficantly associated with neonatal acidemia (pH < 7.20). CONCLUSION: In pregnancies complicated by chorioamnionitis, only the absence of fetal heart rate accelerations could predict neonatal acidemia, To our knowledge, this is the only report to evaluate fetal heart rate patterns according to their length of exposure.
68 ABNIOTIC FLUID VOLUME FLUCTUATIONS REFLECT RECENT GLYCEMIC STATUS IN GESTATIUMAL DIABETICS. I. Bar-Hardx, S.A. Scarpell~x, Y. Barnhardx, M.Y. Divon. Dept. Of Ob-Gyn, Albert Einstein College of Medicine, Bronx, N.Y. OBOECTIVE: To determine the association between the sonographlcally derlved amniotic fluid index (AFI) and recent glucose status in gestational diabetes mellitus (GDM). STUDY DESIGN: The following vamables were prospectively collected ~n 205 GDMs [who underwent 7 daily capillary glucose determinations w~th a memory glucometer) between 2/1/92 - 7/31/93: AFI, mean blood glucose I day prior and I week prior to the ultrasound examinations (MBG1-D and MBGI-W, respectively), and percent hyperglycemia (~120 mg~) 1 day prior and 1 week prior to the ultrasound examinations (PH1-D and PHI-W, respectively). All patients demonstrating at least 1AFI measurement within the normal range (ie, 5cm < AFI ~ 20cm) and at least I elevated measurement (ie, AFI ¯ 20cm) formed the study population. W~th each patient serving as her own control, glucose indices preceding normal and elevated AFIs (N-AFI and E-AFI, respectively) were compared w~th the use of Student’s t-test (n=39). In additlon, AFIs for each patient were plotted against gestat]onal age to determine whether there was a conslstent trend. RESULTS:
AFl(cm) MBGI-D(mg%) MBGI-W(mg%) PHI-D{%) PHI-W(%} (Mean±SD) (Mean±SD) (Mean±SD) (Mean±SD) (Mean±SD)
E-AFI 22±2 118±16 110±13 37±24 37~17 N-AFI 23±3 102±12 100±11 17±IB 18±14
p<O.O001 p<0.0032 p<O.O008 p<O.OD94 p<D.DDIB No consistent change ~n AFI was observed as a functlon of gestat~onal age. CONCLUSION: Amniotic fluid volume fluctuations reflect the preceding glycemlc status ~n GDM.

Oral Plenary Session III
Saturday, January 29, 1994 8:00 a.m. - 10:30 a.m.
Moderator: Garland D. Anderson, MD Immediate Past President, SPO
Ballrooms A- C Abstract Numbers 69 - 78
296 SPO Abstracts January 1994 Am J Obstet Gynecol
69 RECURREN’r HYPOGLYCEMIA: A RISK FACTOR FOR
MACROSOMIA IN IDDM PREGNANCIES. B. Rosen_n, M. Miodovn=k, T.A. Siddiqi. Dept. OblGyn, University of Cincinnati, Cincinnati Ohio.
OBJECTIVE: The rate of macrosomia in infants born to women with
Type-1 diabetes (IDDM) remains 30%-40% despite intensive insuhn
therapy and good glycemic control. We hypothesized that this is due to da~ent counterregulato& hormonal ?esponees to hypoglycemia: in
these women, recurrent episodes of hypoglycemia result in frequent
bouts of increased calodc intake,’ leading to fetal hypednsulmism and
macrosomia.
DESIGN: Hypoglycemia was induced in 17 women with IDDM and in 10
normal controls at 24-28 and at 32-34 weeks gestation, using the
euglycemic clamp technique with the Miles Biostator Plasma glucose
concentration was decreased to 60mg/dL and was maintained at this level for 1 hour. Blood samples were drawn every 15 minutes for
measurement of counterregulatory hormone concentrations.
RESULTS: All 17 IDDM womenhad a deficient epinephrine response to
hypogiycemia, compared to non-diabetic pregnant controls. 8 IDDM
women (non-responders) had a minimal or no response (<30pg/mL
above baseline) and 9 women (responders) had a moderate response
(45-140pg/mL). Of the 8 non-responders, 7 had large infants (b~dh
weight =n the upper quartile by local race and sex specific growth
curves), while only 3 of the 9 responders had large infants (F=sher’s exact
test: p=.05).
CONCLUStON: Recurrent hypoglycemia in pregnant lOOM women with
deficient counterregulatory responses, leading to recurrent bouts of
increased caloric intake, may be an important factor in the h~gh rate of
macrosomia in these pregnancies We speculate that tailoring the targets
of glycemic control during pregnancy to the patient’s counterregulatory
status may decrease the nsk of macrosomia and other hypoglycemia-
related complications. (Supported in part by NIH Grant HD 11725)
71 SONOGRAPHIC EXAMINATION OF THE UTERINE CERVIX IS A BETTER PREDICTOR OF TIlE LIKELIHOOD OF PRETERM DELIVERY THAN DIGITAL EXAMINATION OF THE CERVIX 1N PRETERM LABOR W1TII INTACT MEMBRANES. R. Gome#, M. Galasso~, R. Romero, M Mazor, Y. Sorokio, P. Bauman#,~. Goncalves’, M. Treadwell, D, Cotton. Dept. OB/GYN, WSU/Hutzel Hospital, Detroit, MI and the Perinatology BrancXa of NICHD, Bethasda, MD. OBJECTIVE: The purpose of this study w~ to. comp~e the d.iagnostic performance of sonogrgphie and digital examination ot the eervtx m the prediction of preterm ~]elwery in p.atients prasenting with early preterm labor. STUDY DESIGN: Endovaginal senograpi3y was ~erfdrmed in 41 consecutive patients admitted with preterm labor (20-3"5 weeks} and a eerv cald atat on of < 2 cm between 20 and 35 weeks. The following information was recorded as part of the standard so nographic examination anit pelvic examination endocervicallength (EL) funnel length (FL) funnel width (FW) cervical index ([I+FL]/EL) and cervical dilatation and effacement. Outcome ear ables were the adm ss on-to-de ivory interval and preterm deliveer~( < 36 weeks). RESULTS: The prevalence of preterm deliver’] was 43.9% (18/41). The d agnostic nd ees, pos t ve and negative predlctwe values (PPV and NPV), relative risks (RR) and 95 % confidence intarvals (CI) for preterm delivery in the different parameters were:
Cervical Index 2 0 52 78 96 93 85 6.1 2.4-15.1
EL ~; 17 6 mm 72 83 76 79 3 7 1.6-&3
FL 2 9 ram 78 74 70 81 3.7 1.4-9.2
FW ~ 7 mm 72 70 65 76 2.7 1 1-6.2
Funnehag (+) 67 78 70 75 2 8 1.3-60
Logistic regression indicated a strong and sign ficant rel.at,ioashi~ b ~etw~n. sonmtranhlc parameters and the occurrence of preterm oelivery t.p "-. u.u I lor eech,r. However, a stepw se Io~ st c.orocedura in which the cervical index was entered first, adicated thai’no significant predictive imp.rovem~e.nt was obtained by the add tlon of any odier sonographle varla/3le or algita|ly. measured carv col d atat on and effacement Survival analysis demoastratekl a shorter admissio n-to-dalive~ interval for pat eats with an abnormal eerv col index and endoeervical length (p. <0 05 for each). Controlling for gastational age, the eervlcal ndex was a better oredietor of the ad.mission-tg-dellve,ry interval (hazard ratio’ 4.2) than the findings of the d~gltal examination (p
~(~I~t~USIONS Endovag hal sonograph e exam nation of the utar ne cerv x s more aecurata than diidtal examination of the cervix ia the assessment of the risk for preterm d’elivery ia panents with preterm labor and intact membranes.
7O OBSTETRICIAN’S ATTITUDE AND NEONATAL SURVIVAL OF EXTREMELY LOW BIRTII WEIGItT INFANTS. S Bottoms, R Paul, J lams, B Mercer, D McNellisx, C Buckleyx, G Normanx, P
Jonesx, E Thornx, and the NICHD MFMU Network, Bethesda, MD.
OBJECTIVE: To determine the relationship between attitude of the obstetrician and neonatal survival of extremely low birth weight infants.
STUDY DESIGN: In an ongoing study, we evaluated 223 singleton births < 1,000 gins., excluding major anomalies, extramural delivery, antepartum stillbirth, induced abortion, and gestational age <20 wks. The obstetrician’s opinion of viabilty and plan to perform eesareen delivery in the event of fetal distress were assessed from the medical record or interview when documentation was unclear. A logistic
regression model for expected survival to hospital discharge or 120 days was developed using birth weight (BWT), gender, and presentation.
RESULTS: The total cesarean rate was 38%. Mean IBWT according to survival and the obstetrician’s opinion of viability is tabulated below.
Ohstetrieian’s Survived Died
Opinion N(%) BWT(SD) N(%) BWT(SD) Viable 111(69.8) 797(129) 48(30.2) 658(158) Nan-vlable 7(10.9) 679(152) 57(89.1) 466(102)
The obstetrician’s opinion of viability was less predictive than BWT, but still significantly improved the logistic model of survival (X2=6.5,
p=0.0105). Willingness to perform cesarean delivery was a better predictor of survival than either the obstetrician’s opinion of viability or actual cesarean birth (X2= 11.2, p=0.0008).
CONCLUSIONS: 1) Cases with errors in obstetrical assessment of viability are characterized by mean birth weights around 660 gins. 2) Even when controlled for other major determinants, neonatal survival is significantly related to the obstetrician’s opinion of viability and willingness to intervene for fetal indications.
72 DOES THE CREATION OF A FETAL GASTROSC
THE SEVERITY OF PULMONARY HYPOPLASLL) ~I~ ~IHfoE~EI~
WITH CONGENITAL DIAPHRAGMATIC HERNIA. M. l~_e!f~rt, ,
G.Saade,* B. Baker,* W Pokorny,* C. Langston,* P Mlnifee,* G Jevon,* \
I. Van den Veyver,* D Roble,* S. Longmtre,* Q Palacios,* L \
Montgomery,* K. Mmse, Jr Departments of Ob/Gyn, Surgery,~
Anesthesiology and Pathology, Baylor College of Medicine, Houston, TX |
OBJECTIVE: Pulmonary hypoplasia is a major problem rn infants with\
congemtal diaphragmatic hernia Intrauterine reparative procedures are~ associated with a high complication rate. The development of less complex !
operatmns to reduce the degree of fetal lung hypoplasia may ~mprove
neonatal survival. Our objective was to tnvest~gate the effecttveness of an
mtrogenic gastroschlsis in reducing fetal pulmonary hypoplasia in a sheep
model wtth an artificially created diaphragmatic hernia.
STUDY DESIGN: A left-sided diaphragmattc hernia (Bochdalek-type) was
created at 75 days’ gestation in an ovlne fetal model during the
pseudoglandular phase of lung development At 110 days’ gestatmn, a
left-sided gastroschlsis was created by excising part of the lower abdominal
wall and buttressing the opening w~th a rubber rmg. The fetus remained in
utero until 135 days’ gestation, at which time it was sacrificed for autopsy.
Histopatholog~c and morphometnc studies were performed on the lungs
RESULTS: Ten animals had creation of a dtaphragmatic hernia. Four
underwent the second surgery (gastroschisis) One animal completed the
entire protocol. Three fetuses were lost after the second surgery. Autopsy
confirmed effective decompression of the thoracic contents into the
amnlot~c cavity in all cases. The hmgs of the ammal that completed the
protocol were appropriately developed, while those fetuses that died soon
after gastroschisis creation had severe hypoplasla (mainly left lung).
CONCLUSIONS: We are able to

73
Volume 17q. Number 1, Part
Am J Ob~ et Gynecol
TRANSABDOMINAL THIN-GAUGE EMBRYOFETOSCOPY IN CONTINUING PREGNANCIES. Ruben A Ouintero, Roberto Romero, Mordechal Bardicef’, Yolanda Renfroe~, Nelson B. Isada, Mark P Johnson, Mark I. Evans, Freddy Guevara’, Roxana Laman#, David B. Cotton Depts of Ob/Gyn, Wayne State Umw, Hutzel Hospital, Detroit, MI, Central Univ. of Venezuela, Unwersity Hospital, Caracas, Venezuela, and the Permatology Branch, NICHD, Bethesda, MD. OBJECTIVE: TransaNlominal thin-gauge embryofetoscopy (TGEF) is a new prenatal diagnostic technique. Herewith we report our experience with TGEF in contmmng pregnancies to date
STUDY DESIGN: After careful abdominal and/or transvagmal ult~sound examinations, TGEF was performed under local or general anesthesia using an 18 gauge needle and a 0.7 mm fiberoptic endoscope. The placenta was avoided if p~ssible. For patients studied under local anesthesia, intravenous (IV) sedation was provided Patients were contacted by phone 2448 hrs later. RESULTS: Six continuing pregnancies between 11-14 week’s gestation have been evaluated. Indications for TGEF were’ maternal varicella (2), nuchal membrane (2), mass at the placental insertion of the umbilical cord in a twin gestation (1), and history of neural tube defect/maternal anxiety (1). Visualization was optimal in all cases. Observations under local anesthesia and IV sedatmn were characterized by none or slow fetal movements, which did not interfere with the examination. No obvloas lesions were seen in the patients with maternal varicella, although a small blister was thought to be present in the index finger of one of the examined fetuses. Clenched hands were noted nn one fetus with nuchal membrane dlagnosed with trlsomy 18, a finding beyond the resolutmn of transvag~nal ultrasound. Slight leakage of flud was rel~rted by 2/6 patients, but clinically appeared to be of no consequence One patient interrupted the pregnancy followmg the diagnosis of trisomy 18. There have been no complications reported in the remmning 5 ongoing pregnancies Minimal maternal dlsconfort after the procedure was reported. CONCLUSION: Experience in continuing pregnancies with TGEF is encouraging. Valuable information regarding the external anatomy of the fetus can be obtained to aid in ’the differential diagnosis of suspicious ultrasound finthngs or in the evaluation of fetuses at risk. The procedure may be performed in an outpatient setting. Continued follow-up studies are indicated to establish the actual risks/benefits of this new diagnostic tool.
SPO Abstracts 297
75 EFFECT OF FETECTOMY ON MATERNAL PITUITARY- ADRENAL FUNCTION IN PREGNANT RHESUS Mu~_CAQUES. C.A. Duesayx, H. U~x, G.J. Valenzuel~ Div. Perirtatni Biol., Depts. Ph3~siol. and Ped~., Loma Linda University, LomaLinda, Dell. Ol~/Gyn, SBCMC, San Beranrdino, CA. OliJ~CTII~: Previous studies have suggested a role for the primate fetus in parturition. This study was designed to test the hyl~thesis that fetectomy (FT) all~rs maternal pituitary-ad~nal function. STUDY DESIGN: Between 117 and 122 days of gestation (term=167d), six rhesus macaques underwent surgery for catheter implantation. At mrgery the fetuses were removed while the membranes and placenta were left in situ. Thirteen additional catheterized pregnant animals served as controls. Animals were maintained under a 12h light:dark cycle with lights on from 0700 to 1900h. Beginning at least one week after surgery, maternal arterial blood samples were collected at 3hr intervals for 24h starting at 0900h. This sampling protecol was repeated 4 times at weekly intervals until c-sectian at 151 to 157 day’s gestation. R~SIJLTS: Following FT, plasma ACTH, DHEAS, and cortisoi were significantly lower (36%, 35%, at~ 44%, respectively) compared to control animals (p<0.01). Plasma dopamine was also depressed (P<0.01) while norepinephrine and epinephrine remained unaffected. CONCLUSIONS: 1) FT resulted in decreased maternal pituitary- adrenal function. 2) The fetus plays a role in the regulation of maternal endocrine function that may intluenco the initiation of labor. (NIH HI) 228865 and Ob/Gyn and Pediatric Research Funds)
74 OUTPATIENT TREATMENT OF PYELONEPHRITIS IN PREGNANCY. L Mdlar, D. Wingx, R Paul, D. Griruesx. Dept. OB/GYN, University of Southern Cahforn~a, Los Angeles, CA OBJECTIVE: To compare the safety and efficacy of outpatient versus inpatient therapy of pyelonephrltis in pregnancy. STUDY DESIGN: A prospective blinded study randomized 120 pregnant women (<24 weeks) with pyeionephritis to inpatient or outpatient therapy Sixty Inpatlents received intravenous cefazohn until afebrlle The 60 outpatients received 1 gram of ceffnaxone intramuscularly and were released if clinically stable. Visiting nurses saw outpatients the first 3 days following release from the emergency room, gave a second injection of ceftriaxone at 18-36 hours, performed pill counts, and monitored temperature charts. All patients were educated about pyelonephritls and completed a 10 day course ofcephalexin. A urine culture was performed 5-14 days alter therapy RESULTS: The two groups were simll~ with respect to age, parity, temperature, estimated gestational age, and initial white blood cell count Escherichla cog caused 78% (93/120) of cases of pyelonephrms. Eleven percent (13/120) of bacterm were resistant to cefazohn; none were resistant to ceftnaxone Four inpatmnts (7%) and 7 outpatients (12%) had positive blood cultures at admission. At 96 hours, 6 mpatients remained fubrde necessltatlng a change in antthlotics. In contrast, all outpatients became afebrile in 72 hours (Fishers Exact p-0 03) Three outpatients (5%) were admitted to the hospital during the observation period. Twelve mpatients (20%) and 11 outpatients (18%) had positive urine cultures after therapy, Three patients in each group had recurrent pyelonephrit~s prior to documentation of sterile urine. One preterm delivery occurred in the mpatiem group at time of recurrent pyelonephritis The average cost per patient for inpatient and outpatient treatment of pyelonephritis (excluding NICU costs for premature ~nfant) was $2484.52 and $608.06 respectively CONCLUSION: Outpatient antibiotic therapy is inexpensive, safe and efficacious in pregnant women with pyelonephrltis
76 OPERATIVE FETOSCOPY: A NEW FRONTIER IN FETAL NEOICINE Ruben A. Qumtero, Harry Reich~, Karohne S Puder’, Mordechai BardiceP, Leonardo Acosta’, David B Cotton, Mark I. Evans~,,.~/ and Roberto Romero Dept of Ob Gyn, Wayne State Untv, Detroit, MI, Wyoming Valley Ob/Gyn Associates, and the Pennatology Branch, NICHD, Bethesda, MD. OBJECTIVE: Human fetal endoscopic surgery has considerable appeal because it would reduce the complications resulting from hysterotomy (i e., preterm labor and the need for cesarean section)and laparotomy How.ever, the.. h .... anmlot ..... ity p ..... ts several unique obstacles to operative endoscopy We report the development of special surgical techniques, instruments, and concepts to make tn utero fetal endoscopic surgery
~v~A ssible
TERIALS AND METHODS: Optics: Endoseopes of varying dlamet.ers (0 7-2.5 ram) and characteristics (multilens/rodlens/flbernptic, flexible/rigid, operatlng/v~ewing, ) have been compared and modified Operative Instruments: custom-designed miniature (2ram) surgical instruments have been developed and adapted including graspers, knot-pushers, trocars, and scissors, lntraanmiotic Visualization. a technique for rapid amniotic fired (AF) exchange with lactated Ringer’s (LR) solanon has been devised. An AF pressure monitoring technique to prevent sudden hydrostatic changes has been implemented. Suture material of different characteristics (absorbable/non-absorbable, color, texture, pliability) have been evaluated Ultrasuun~l-Endus~opic imaging: various methods for the simultaneous dlspla~ of the sonographic and endoscopic images have been employed to coordinate the use of 1-2 intraamntotic instrnments. RESULTS lntraanmiotlc operative endoscopic surgical procedures hav.e been successfully performed in 5 ongoing human pregnancies. Four patients have dehvered, and one pregnancy is ongoing Post-operative premature rapture of membranes has occurred in 3/5 cases, with resealing of the membranes in one of them There have been no miscarriages after the procedures R g d multdens endoscopes are preferable. Limitation of operating port size (outer diameter) to < 3 rum allows percutaneous insertion of the instruments, avoiding laparotomy or hysterotomy. AF/LR exchange has proven invaluable AF pressure pressure changes can he kept at a minimum through constant monitoring. Absorbable bright-colored suture material is preferred. Simultaneous display of ultrasound and fetoscopic nnages on a single monitor through a video-mixer is helpful for adequate instrument coordination and orientation. CONCLUSION’ Fetal endoscoplc~surgery -Operative Fetoscopy- can be performed in the human through the incorporation and adaptation of mlmmally-invasive surgery concepts into perinatology This approach represents a new frontier in fetal medicine.

298 SPO Abstracts January 1994 Am j Obstet Gyneco]
77 THE EFFECT OF PULMONARY SHUNTING (Os/Qt) ON FETAL ARTERIAL HEMOGLOBIN SATURATION IN THE SHEEP MODEL. C.J. Harveyx, G D.V. Hantdns, Dept OB/GYN, University of Texas Medial Branch, Galveston Texas and Dept OBiGYN, Willord Hall USAF Medical Center, San Antonio, Texas OBJECTIVE: The measurement of the percent ol pulmonary shunting (ce!Qt) is one of the most relaX:de in assessing efficacy ol oxygenation in the acutely ill patient. There are no da~a to rel~l the eff~ of pulmona~/shunting on fetal oxyger’,at~on The objective of th~s study was to measure the unknown effect of ino’eased maternal Qs/C~ on fetal oxygenation. STUDY DESIGN: Six pregnant ewes were placed under general anesthesia and pulmona~/a~ery, femoral ~eq and femoral vein canalization were pe,tonned. Hysterotomy was done to access and instrument fetal after/and vein. Maternal and fetal cohorts were rendered hypoxic via maternal hypoventilation. Maternal hernodynamic and pulmonary function baseline and changes were recorded. Fetal pH, pCO2.1:)02, HC03, BE, and Sa02 were measured. RESULTS: Mean steady state Os/Ot was 8.9 (+ 3.6); mean fetal Sa02 and base excess (BE) were 38°/o (.+.7%) and -2.5 ~5.8) respectively. Maternal hypoxernia produced sign~licantly elevated Qs/Ot - Maximum Os,’Qt mean ~.5 %~51) and concurrent letal Sa02 was 11%(~-S°/o). Maternal Os/Ot mean that resulted in det~able feduclions in letal I~E was 36 8% (range = 10.3%-70.7%) Mean fetal Sa02 measured at the t~rne ol BE increased was 29.5% ~13%). CONCLUSIONS: Pulmonary shunt=rig can be caused by impaired diffus=on, ventilahon-pedusion inequalit=es, anatomic shunts, and alveolar collapse. In the non pregnant he,by adult, OsiQt had a range ol 3 to 5%; in the ~Jtically ~ll patient, a shunt o115% is common, tn the pregnant ewe, QsiOt at 36% produced decreased Sa02 and raper metabe~ aademia in the fet~s. This model suggests a c~it=cal Os/Q levelthat prohbits oxygen transfer from the maternal to fetal compartment.
78 COCAINE ALTERS PLACENTAL PRODUCTION OF THROMBOXANE AND
PROSTACYCLIN. M Monga, S.Chmmlowiec×, L R.Troyer, R L.Andres,
V M.Parisi. Dept Obstet. Gynecol. & Reprod. Sci, UTH$C, Houston, T×,
Objective: We investigated the effect
of cocaine (COC) on placental production of thromboxane (IX) and prostacychn (PGI),
Study Design: Fresh placentas were obtained from 6 normal term pregnancies and 300 mg explants were incubated, in duphcate, at 37°C
with 0, 30, 300 and 3000ng/ml COC. TX and PGI production was measured
by RiA of the stable metabolites TXB2
and 6-keto-PGF1 at 0, 0 5, 1, 1.5, 2, 4,
8 and 12 hr. ANOVA wtth Newman Keul’s was used for statist=cal analysis.
Results: COC increased TX
product=on =n a dose dependent manner (p<0 001) and decreased
product=on (p<005). COC increased
the rat=o of TX/PGI product=on (p<0,05) (data shown for COC
concentration of 300ng/ml). Conclusion: COC increases TX and decreases PGI product=on by the
placenta. The increased TXiPGI ratio may result in constriction of the
uteroplacental vasculature, This may
partially explain the assoclat=on of
maternal cocaine abuse w~th IUGR, placental abruptlon, and spontaneous
abort=on and hypertension

Poster Session I
Thursday, January 27, 1994 10:30 a.m. - 12:00 p.m.
Pavilion 9 - 11
CATEGORIES
Maternal/Fetal Physiology
Antepartum Fetal Testing
Placental Physiology
POSTER NUMBERS
79-136
137-155
155164
Judges:
Nancy A. Callan, MD
Frank A. Chervenak, MD
E. Albert Reece, MD

Volume 170, Number 1, Part 2 SPO Abstracts 301 Am J Obstet Gynecol
79 FETAL BREATHING CHARACTERISTICS AND POSTNATAL
OUTCOME IN CASES OF CONGENITAL DIAPHRAGMATIC HERNIA.
H.E,Fo×, _S,S.Badalianx, C,R.Chee, I.E,Timor-Tritsch, C.J.H.Stolar~. Dcpt,
Ob/Gyn and Pediatric Surgery. Columbia University, New York, NY.
OBJECTIVE: To dctcrminecharactartsticsof fetal breathingactivity by recording
fatal nasal fluid flow velocity in ca~es of congemtal diaphragmatic hernia (CDH),
STUDY DESIGN: Records of fetal perinasal flow velocity were obtained an 45
cases at 34-41 weeks of gestation: in 14 cases of antanatally diagnosed CDH, and
in 31 cases of uncomplicated pregnancy. The records were made using a Toshiba
SSA-140A or $8A-270 ultrasound system applying color-flow and spectral
Doppler analysis The average of 25 breath cycles from each case were
determined for each of the following timing parameters" t~me of inspiration (TO,
ttme of expiration (To), breath-to-breath interval (T~.), and rmto of T, and To
(T,/T.)
RESULTS: The postnatal outcome of the 14 eases w~th CDH: one stillbtrth and
five neonatal deaths (group D, eaght survived and were discharged (group 11)
Values are mean ~+ $,E M,
Parameters Normal Group 1 Group II ANOVA P
T~(msec) 1184 1+36 2 1288,6+59,2 1068.0+72.2 0.1206
T~ (reset) 544 7+19 7 614 6+40.7 546 8_,+43.2 0.3688
To (reset) 633 6+1829 632.4__+37.7~ 493 2+34.3b 0 0039
T,/To 0.86+_.0.02’ 0.98__+0 06 I. 12__+0.05~ 0.000)
For " ~,~ ~, P < 0 05 by Student-Newman-Keuls post hoc test,
CONCLUSIONS: Observanon of fetal-breathing related nasal flmd flow velocity
m cases of antenatally diagnosed CDH prowdes a rationale for hypothesis that T,
and T,[T, may be useful in the prediction ofposmatal outcome We speculate that
the changes in the group of survivors may represent a compensatory phenomenon
by cansmg intermittent changes in the volume of fluid within the lungs.
81 NATURAL OCCURRING INSULIN AUTOANTIBODIES IN NEONATES OF NORMAL PREGNANCIES.
S. Wellikx, K Berkowltz, M de Veciana, M. Morgan, E. Arquillax Dept. of Pathology and Ob/Gyn, Univ of California, Irvine, CA.
OBJECTIVE: To determine if insulin autoantibodies (IAA) are
present in neonatal cord blood from normal pregnancies, and whether these antibody levels correlate with maternal 1AA and/or insulin
levels and neonatal cord blood insulin levels.
STUDY DESIGN: This was descripnve case series of paired
neonatal cord and maternal blood samples taken from 20 random
normal patients at delivery. Measurements of serum IAA (radio
binding assay) and msuhn (radlmmmune inhibition assay) were performed. Multiple linear regression and paired t-test were used for
data analysis.
RESULTS: No association was observed between neonatal IAA and
maternal IAA levels, nor were neonatal IAA levels associated with
maternal insulin levels (r=0.05 and 0.3 respectively). Neonatal IAA
levels (4,8 -+ 3.2 pg/ml) were significantly higher than their respective maternal IAA levels (1.6 + 2.5 pg/ml) (P< 0 005) and
positively correlated with neonatal insulin ~evels (r=0,76, P<0,00I),
/~ addition, neonatal insulin levels strongly correlated with neonatal
birthwmght (r=0.63, P<0.01). CONCLUSIONS: IAA are measurable in neonatal circulatmn at
birth and are present in significantly higher concentrations than in
their respective mothers. Since neonatal IAA are so strongly
associated with neonatal insulin, but not with maternal IAA or
insulin, it seems unlikely that maternal IAA contribute significantly
to IAA levels in fetal mrculation. These observations suggest that IAA
may be intrinsic to the fetal insuhn immune tolerance system, and
their effect on insulin bloavailability in the fetus may influence
neonatal birthweight.
8O FETAL BREATHING-RELATED NASAL FLUID FLOW
CHARACTERISTICS 1N PATIENTS WITH MATERNAL
HYPERGLYCEMIA S.S.BadallanL L.Baxi, C.R Chao, H.E Fox. Dcpt,
Ob/Gyn, Columbia University, New York, NY.
OBJECTIVE: To determine the characteristics of fetal breathing-related
nasal fluid flow in pregnancies complicated by diabetes mellitus and
hyperglycemia,
STUDY DESIGN: Fetal breathing-related nasal fluid flow velocity
waveforms were recorded using a Toshiba SSA-140A ultrasound system
combined w~th color-flow and spectral Doppler analysts. Recordings were
made in 65 women at 30-41 weeks of gestation. In 37 cases, pregnancy was
uncomplicated; in 11 cases pregnancy was comphcated by Type I diabetes
mellitus, and tn 17 cases, pregnancy was complicated by gestatiooal dtabetes
The subjects were classified into 3 groups by gestations/age: 30-33 weeks,
34-37 weeks, and 38-41 weeks. Maternal hyperglycemia was defined as a
plasma glucose value ranging from 140 to 205 mgs per 100 ml, A
continuous videotape record of the spectral Doppler tmagtng of fluid flow
velocity in the nose was made during each study session. Based on a sample
of 25 consecutive fetal breaths, the ttmmg components of breath cycles were
determined: Ume of inspiratmn (T,), time of exptration (To), breath-to-bremh
interval (T~), and ratio of T, and T. (T,/T.)
RESULTS: No relationship was found between the value of maternal blood
glucose and etther fetal T,~ (rZ=0.003), or T,/T, ratio (r~=0 0001) There
was a statistically significant d ffferance m T, (msec) at 34-37 weeks gestation
(P=0.040) tn the cases of diabetes mallitus wtth maternal hyperglycemta
(467+23 S.E.M ) and uncomplicated pregnancy with maternal normal
carbohydrate intolerance (560+28) There was a simdar tendency m the
values of T~ (465__+19 and 517+20 respecttvely) at 38-41 weeks gestatton
CONCLUSIONS: Maternal hyperglycemia m cases of diabetes melbtus
shortened the duranan of the insptratory phase of fetal breath cycle after 34
weeks of gestation This difference may be related to previously
demonstrated differences tn other breathing parameters between the normal
and hyperglycemic human fetus.
82 TUMOR NECROSIS FACTOR-e IS ELEVATED IN MATERNAL PLASMA
BUT UNDETECTED IN AMNIOTIC FLUID IN THE SECOND TRIMESTER.
M.J. Kupfermmc, A.M. Peaeeman, T.R. Wlgton, R.K. Tamure, K.A.
Rehnberg=, M.L. $ocol. Dept. Ob/Gyn, Northwestern Univ,, Chicago, IL.
OBJECTIVE: To investigate the cellular arm of the immune system in the
adaptation to pregnancy by assessing plasma and amnlotic fluid levels
of the cytok~ne tumor necrosis factor-(? (TNF-e).
STUDY DI~SIGN: Forty-six heaRhy pregnant women (~roup A) who
underwent second trimester genetic amnlocentosis at s mean gestational
age of 17.0± 1.6 weeks composed the study group. Blood was drawn
from each patient prior to smmocentesla and an ahquot of amniotlc fluid
was obtained for this study, Twenty-three healthy, non-pregnant women
of reproductive age (group B), composed the control group and blood
was drawn from each participant. All specimens were stored and
collectively assayed for TNF-o by s spemhc enzyme-linked =mmunoessay.
RESULTS: The mean age of patients In both groups was 34 years. ~n
group A, 16 patmnts were prim~grawd and 30 patients were multigravid.
All patients had a normal karyotype and uneventful pregnancy. TNF-a’
was detected in the plasma of 42/46 [91%) pregnant palmate as
compared to only 1 of 23 women (4%) in group B (p <.0001). The
madmn plasma TNF-o level for group A was 174 pg/ml (range 0-625
p.o/ml). TNF-t/was not detected In any of the amniot~c fluid specimens studied.
CONCLUSIONS: Elevated levels of TNF-a were found ~n the plasma but
not the amniotm fluid of normal pregnant patients in the second trimester. This increase in plasma concentration of TNF-a compared to
non pregnant control patients suggests involvement of the cellular
branch of the immune system In the adaptation of the mother to the
fetal allograft. G~ven Its known capacity to hm~t trophoblast proliferation,
TNF-o may be important m preventing exposure of fetal antigens to the maternal circulation. The =nubility to detect TNF-e In m~dtnmester
ammotm fluid ~mphes that the most hkely source of TNF-a is system=c
macrophages or [ymphocytes rather than those located at the maternal
fetal mterface.

302 SPO Abstracts Jan,,ary 1994 Am J Obstet Gynecol
83 B~OYCI~I~)SITIONJUIDFAT DISTRIBUTIQNIM INFANTS OF MC#EM AIIO ABIICI~NAL GLUCOSE TOLERA/ICE. P.H. CataLano, A. Th0masx, N.H. Dra9ox, S.B. Aminix, Dept, Reproductive BioLogy, NetroHeatth Hed Cir,, Case gestern Reserve University, CLeveland, OH.
O~JECTI~: Toassessbodycompositionandanthropometricmeasurements in infants of ~:~men aith nermet glucose tolerance (CTL) and gestational diabetes iGOR). Me hypothesizedthat ~o~nen aith GDR had infants aith increased and central distribution of body fat iF). SI~J~y DESlC#I: 183 infants (CTL-102 and GDN-81) had total body
electrical conductivity (TOBEC) esti!llates of body composition and anthropometricmeasurements at birth. Demographic data ~as obtairted at the time of birth. Statistical analysis mes performed using tests, chi-square analysis and analysis of covariance (ANCOVA).
RESULTS: The GDR sere significantly (mean ~ sd) older (28.9 ~ 6.6 vs 26.5 ± 5.6 yrs, p=.O09), shorter (161.8 ± 6.1 vs t64.8 ~ 7.1 cm,
p=.O02) and heavier pregravid (7~.5 ~ 23.3 vs 65.4 ~ 15.8 kg, p=.O001) as compared~ith CTL. There sere no significant differences in race, at gain during gestation, parity, s~okin9 status orpeternaL ht and at. Gestational age at delivery gas CTL 39.2 ± 1.2 vs GDH 38.2 ! 1.5 seeks, p=.O001). There sere no significant differences in neonatal sex, birth~eight (Bg), Length, fat free mess (FFH) or head and alxIominai circUmference betaeen groups. The GOH infants had greater ~F (12.9 ± 5.0 vs 10.9 ~ 4.8, p=.O06) and F mess (453 ± 231 vs 382 ± 213 gm, p=.03) as compared aith CTL. Skinfotd measurements [triceps (TR), subscapuLar iS), flank (FL), thigh(T) and abdomen (A)] sere all greater in the GDH (p=.O001) and had a more central distribution (TR+T/$+FL+A, p=.O07) as co, red
CTL. After adjusting for significant confounding factors using ANCOVA, the GDH had significantly greater Bg (p=.04), F (p=.03) and
~F (p=.01) but no significant difference in FFH as compared CTL. COI~tlS[OMS: Infants of ~ uith 6OH have significantly greater
Bg, F, gF and central distribution of F but no difference in FFH
in comparison aith CTL. These findingmey have long term implications regarding obesity and the development of diabetesmel[itus in infants of GDH. geight Catchers Four~lation and NLH 22965.
85 E~GtO!~. BLOOD FLOW OURII~ SEVERE UMBlUC~L COE) OCCLUSION. RH Ball, JT Pa~, LE Caldwallx, J Johnsenx CVRI, and Dept of O~/Gyn end R& and/~as~asia. UCSF, Sen Franc~co, C~ 06JECTIVE:We havel~=~asiypresented data attlts mee~ng, demeas~f~ng ~at severe asphyxia produced by uterine arterj (UtA) occlusion leads to organ Hood flow (BF) redstrbu~en, with probable changes =n rnetabul~m, We ~ to test oir null hypo~ess
STUDY DESIGN: S~x pregnant ewes at 0 8 of gestat~n were surg~a~y prepared v~th fetal vascular catheters, ECoG, EKG and EMG elec~odes, and an inflatable ~ff-t~/pe UC ~ccluder The fetuses were stud~ed after 2 to 3 days of recovery Followng control rneas~Rments of regional BF (ra~oad~e rnK~asp~), FHR, BP, blood gases, and add base factors, ~e UC ~as progtass~,e~y occluded unbl the fetal ECoG was isoelec~c,
at 30, 60, and 90 rn~na of occlusion and 30 rain of recovery StabslJcal anai~ was by ANOVAand Stndent-Neuman-Kedstost Stak:ddffersncesweres=gnif~cantatP<0.05 RESULTS: Llrn~ical artery BF fell to 20+5% (mean± gEM) of contro~ by 60 ~ns and rema~dso~rsk~se Thefe~ECcGbamme~-e~byS~:f.5m~ns Ov~qheD0 rn=n pedod of ocdusien ~e pH fs~l f~rn 7 37-+0 01 to 6 82~,03, and BE frmn 5_+1 to-22+_2 rnEq~ PCO2rcaeJrom55+_.2to96~:Trr~’nHg By.N~Gpa’-a’naterstheasphy~a~srnore se.,ere than m our UtA prepa’ak~s Fetol BP and HR pa’a~ u~eN~ent acuto qhenges at the trne of occlusion but then stabdEed at control values Head and gut BF dK~ not change I~enda~lSFrnorethend~ CVO, spfsen, kxlney and cercass SF fe,I to < 30% of contrd 02 delivery to the brain and adrenals rose, fe~l to the spleen, g~t,
CONCLUSIONS The fetal response to asphy’~a of sirndar seventy, as detorm~ned by add
ir, s~lt With UtA ocduson, the placenta and fetus =e e’~posed to hypo:~a, and we have shown that cardiac BF rises, as does adrenal BF W~th UC occlusion only the fetus ~s exposed to decreased 02 dal~ven./ The urnN~l wnous 02 content will be normal but the
fa~s (sta~e with UtA). We spec~te that ~e heat ~s e~x~sed to d~s char~ tn prs-
to the hypoxla w~th inaeased 02 det=~y, despite a no~nal venous 02 content This may ~rnply that severe aca~e cord (x~lu~on can have a damaging effect on cardiac function although red~stobut~on of organ BF =s other~se appropriate and s~rn~la to that seen wth
84 FACTORS AFFECTIMG FETAL GROItrH kilo Bogy COI~ITIO~I. P. Cats[enD, ~. Dragox, S. Aminix. Dept. Ob/Gyn, ~niv. of Vt. and Dept. of Reproductive Biol., Case gestern Reserve Univ., Cleveland 08JECTI¥~: To correlate gel[ recognized factors sffectir~j fetal
groath and meternat carbohydrate metabetism aith neonatal birthaeight (Bg) and bodyco~position, ge hypothesized that genetic factors primeriLy affected fat free mess (FFM) and meternal
environment affected fetal fat iF) accretion. $~JI)y DESISTS: 188 singleton infants of hmetthy non-smoking admen
had ~t and anthropemetric estimates of body composition performed aithin 24 hours of birth. Independent variables obtainedaere: (1) ~aternal ht, pPegravid at, body mess index (B~), wt gain during gestation, education, age and parity, (2) peternai ht~ at and BHl, (~) neonatal sex and gestationaL age (EGA). Additionally, 16 admen (6 control and 10 gestationat diabetes) had insulin sensitivity estimated using the glucose clamp technique. Step~ise regression analysis ~as used to correlate independent variables aith B~, LBH and F.
RESI~LTS= Hales had a significantly (p=.009) greater Bg (mean ± sd) vs females (36~5 ~ 468 vs 5467 ~ 4~ gm) as sell as length (51.8 ~ 1.9 vs 50.7 ~ 1.9 cm~ p=.0002), head circ~ference (35.5 ~ 1.1 vs ~4.9 ~ t.t cm, p=.0001) and LBH ~3157 ~ 350 vs 2~52 ~ 330 gm, p=.0001) but no difference in F (48~+ 201 vs 515 + 189 gm~ 1>=.32).
29~ of the variance ~r =.29) in Bg ~as acc~unte~ for by [EGA
(r~=.10), at gain (r~,06), pregravid at (r==,0S), P~eonataL sex
(r==.04) andperity2(r==.04)]; ]~ of the varianc~ (r==.50) in FFH by [(r~eonatal sex (r =.08), EGACj’==.09), at gMn (r==.06), pregravid at~(r==.0~) and paternal ht~tr==.0~)] and 17Y. of the variance (r~=.17) in F by [(.parity r==.08)~ EGA (r2%.04), pregravid at (r =.02), at gain (r==.02) and neonatal sex (r==.01)]. Adding insulin
sensitivity~ as a factor improved the correlations significantly. The total r= for 8g, FFH and F sere 5~, 57~ andS6%, respectively. COgCLI~IO#S: Neonatal sex, a genetic factor, had the greatest
correlation aith FFH and m eternal parity ahich ae speculate affects maternal metabolic enviror~ent had the strongest correlation F. Including insulin sensitivity as a factor improved the correlations 2 fold for LBR and~ fold for F. g[~ 22965.
86 AN EVALUATION OF T~MPANIC THERMOMETRY IN AN OBSTETRIC POPULA’RON. O. Skuaski, A. Sonnenb~ick~, W. Wagner~,
F. Chervenak. D~v. of MFM, Comell Univ. Med. Ctr.,New York, NY,
OBJECTIVE: In an obstetric population, we set out to establish normal
temper atura ranges and reproducibility for core temperatures measured
by the tympanic thermometer, compare these core temperatures to oral
electronic temperatures, and determine the tympanic thermometer’s
accuracy in recording fever.
STUDY DESIGN: Simultaneous tympanic core temperatures and oral
electronic temperatures were measured in obstetric inpatients and
outpatients, on a labor tioor, during antepartum testing, and on a post-
partum floor (73 patients). Repeat measurements weretaken 10 minutes
later.
RESULTS: Tympanic core temperatures were signdtcantly higher than
oral temperatures (p<0.OO001), with means for the two groups of 37.76
degrees Centigrade (°C) and 36.95 °C respectively. Both thermometers
showed equivalent reproduciblity between the initial and repeat
measurements, w=th Pearson’s correlation coefficients of 0.98 for
tympanic temperatures and 0.97 for oral temperatures. Using a
predetermined (eveJ of 38.0°C oral for the definit{on of fever, we found the
sensitivity, specificity, positive predictive value (PPV), and negative
predictive value (NPV) to be 100%, 93%, 75%, and 100% respectively.
CONCLUSIONS: 1) Normal temperature ranges for a pepulahon of
obstetric patients for the tympanic thermometer are demonstrated. 2)
Tympanm thermometer measurements in the normal range were shown
to be as reproducible as oral electronic measurements. 3) The mean
tympanic temperature was significantly higher, byan average of 0.81 °C,
than the mean oral temperature. 4) Acceptable sensitivity, specificity, PPV, and NPV for the diagnosis of fever were Gbtamed using the
tympanic thermometer.

Volume 170, Number 1, Part 2 SPO Abstracts 303 Am J Obstet Gynecol
87 CON’I~OL OF BEHAVIORAL STATE ORGANIZATION IN NORMAL
IILqVIAN FETUSES. LI Groome, LS Bent#, KP Singh’. University of South
Alabama, Mobile; University of Alabama, Birmingham.
OBJECTIVE: Repeated alterations in quiet sleep (QS) and active sleep (AS)
is a basic feature of behavioral state organization in human fetuses. Activation
of the reticular formation (RF) is important in the transition QS~AS, and intrinsic
changes in central nervous system activtty (CNS) govern RF activation.
Vlbroacoustic stimulation (VAS) can alter RF activation and thus delay the
occurrence of QS. Hypothesis: If intrinsic RF activation in human fetuses is
greatest just after entering AS and lowest just after entering QS, then fetu~s
ought to be m an active period longer following VAS just after entering AS then
following VAS closer to an AS-,QS transition. We wanted to test this hypothesis.
STUDY DESIGN: We examined 87 normal human fetuses at 3%41 weeks. QS
and AS were identified by the fetal heart rate pattern and the preSence or absence
of fetal eye and gross body movement. Each fetus was observed to enter AS
before randomization. After remaining in AS for 3 rain, the fetus either was not
stimulated (N=30), received a single 1-see VAS after 3-5 rain of AS (N=30),
or received a single l-see VAS after 44-46 min of AS (N =27). The study was
terminated when the fetus e~ther entered QS and remained in QS for 3 rain or did
not return to QS within 60 min.
RESULTS: Fetuses stimulated after 3-5 min of AS behaved similarly to fetuses
who had entered AS spontaneously. However, fetuses stimulated after 44-46 mln
of AS remained in an active period for a shorter length of time than fetuses who
either had been in AS for 3-5 rain before VAS (19.6 min vs 36.4 min,
p =0.0~01) or had entered AS spontaneously (19.6 min vs 44.2 rain, p =0.0001 ).
When we included our results on state organization following VAS delivered in
QS [Early Hum Develop 33 (1993) 21-7], we found that VAS near a spontaneous
AS-~QS transitlon elietted a signlficmatly dlfferent behavioral responsethan VAS
near a spontaneous QS~AS transition: regardless of whether fetuses were in AS
or QS at the time of stimulation, fetuses who were stimulated in close proximity
to an AS-~QS transition returned to QS sooner than fetuses who were stimulated
closer to a QS~AS transition (18.7 rain vs 37.2 rain, p =0.0001).
CONCLUSION: This is the first study to demonstratethet the developing CNS
places strtct requirements on the amount of AS and QS during fetal life.
89 EVALUATION OF PERIPHERAL h~RVE ~TI/~LATION IN ~SESSING PATI~TE ~S~E ~ I~S ~4 ~Y’~ w~eX, ~, ~ ~v~,~, ~pt OB~,M~ Coll ~ia,Au~sta O~To correlate ~te~al res~nses to ~ripheral nerve st~ulation (PNS) with standard clinical and laborato~ asses~ent for effects of parenteral (IV) MgS04 ~erapy. 5~ DESIGN:We studied 10 gravidas with pret~ l~or (~26-34 wks) ~d 10 with pr~l~sia (~26-41 wks). ~i r~eiv~ IV MgS0 4 4~ bolu~ ~j~ions foll~ by 2~/hr cont~uous infusions. A Paragraph~ pr~r~le p~ipheral ne~e st~lator (~ M~ical C~y) was set at a 30 ~lli~p current to simulate the ulnar nerve. ~tios of 4th to 1st twitch res~n~ (T4) were dete~ined along with ser~ Mg++ ~d Ca++ levels and patellar reflexes (~), before th~apy ~d at hourly intervals for 4 hours subse~ently. T4 ratios, ser~ Mg++ levels and DTRs were correlated with repeated ~as~es ~VA or s~le ~d ~itiple r~ressions. ~ Bo~ groups ~re s~il~ for all their data were pooled for all analyses. Ser~ Mg++ levels ~aked and reach~ a steady state after 1 hour (4.6 ~ 0.4 (SD) ~/~)~ there ~re no changes in ser~ Ca++ levels ov~ t~. ~ d~reas~ wi~ t~(p =.04). Mg++ levels were negatively correlated with DTRs(r = -.55,p =.08) T4 ratios had no significan~ ch~ges with t~ or co,elations with Mg~ levels or ~. ~USIO~ M~04 therapy execs ~ ~ibito~ effect on ~, ev~ at th~ lo~r ~d of "thera~utic r~ge," that was not ad~ately refle~ by PNS responses. PNS res~nses of ~ti~ts v~i~ unpr~i~ly once steady- state ser~ Mg~+ levels ~re attain~. The use of PNS, in this setting, appears less reliable th~ clinical ~s for ~itor~g elf--s of ~s0 4 a~istration.
88 VAGAL TONE IN NORMAL TERM FETUSES DURING QUIET SLEEP.
LJ Groome, DM Mooney’, LS Bentz’, JD WilsetP. University of South Alabama,
~obile; 13uiverslty of Arkansas, Little Rock.
OBJECTIVE: High-frequency, rhythmic fluctuations in heart period are
mediated mostly by changes in vagal activity during respiration. Considerable
success has beun achieved in neonates, infants, and older children using
parasympathetic or vagal tone (V) as a marker for individual differences in
central nervous system activity. We wanted to determine the relationship
between V during breathing and V in the absence of respiratory activity in human
fetuses during quiet sleep (QS).
STUDY DESIGN: We examined 13 normal human fetuses between 36 and 40
weeks. QS was defined by a low-variability heart rate pattern and no fetal eye
or gross body movement. Fetal breathing was monitored continuously using real-
time ultrasound. The fetal electrocardiogram was captured transebdominally in
3-rain blocks at a rate of 833 Hz and fetal R-waves were extracted using adaptive
signal processing. Fetal R-wave interbeat intervals (IBI) were converted to
equally spaced, time-based data and the low-frequency component was removed
by filtcriog the weighted IBI files in the time domain using a 21 -point third-order
moving polynomial. Amplitodes of the power densities were summed over the
frequency of spontaneous fetal breathing (0.3-1.3 Hz) and the natural logarithm
was taken to produce a single value, V.
RESULTS: 45 3-min blocks (mean 3.5, range 1-8) were colleeted during
periods of breathing and 36 3-rain blocks (meAn 2.8, range 1-6) were collected
during periods of non-breathing. Fetal breathing was associated with an
@proximately 25% increase in V as compared to non-breathing (3.25+0.45
versus 2.57+0.47, p =0.0001). When each fetus was examined separately, the
mean V during breathing was always larger than the corresponding value in the
absence of breathing. Furthermore, a significant linear relationship was found
between the mean singlc-fetas V during spontaneous respiration and the mean
single-fetus V during normally occurring apnei¢ periods (r =0.772, p =0.002).
CONCLUSION: Fetal breathing is associated with a significant increase in V,
and the linear relationship between V for periods of breathing and non-breathing
implicates a eentr~l component in the genesis of respiratory sinus arrhythmia.
90 POTENTIAL ROUTE FOR FETAL THERAPY: INTRAMEMBRANOUS
ABSORPTION OF INTRAAMNIOTICALLY INJECTED FUROSEMIDE.
W.M. Gilbert, P.S, Newmanx, R.A. Sracex. Div. of Perinatology,
Dept. of Repro. Med., Umv. of CA, San Diego.
OBJECTIVE; To determine whether mtraamntotically injected furo-
sem~de could be absorbed directly rote fetal circulation via the ovine
intramembranous pathway.
STUDY DESIGN: 5 intact fetal sheep (previously presented) and 4
w~th hgnted esophag~ were atudmd for 7 hours on two consecutive
days. Day one was a control day. On day two, 15 mg of furosemide
was in|ected Into the amnlot~c cavity after a ore hour control period.
RESULTS: On day two, intact fetuses (Figure, closed circles) demon-
strated a rapid and prolonged increase In urine flow (P < 0.0001)
as d=d the hgated fetuses (open mrcles, P < 0.001) when compared
to control day fetuses (crosses). Sodium and chloride excretion in-
creased significantly in intact (Na-591 -+ 220 (SE)% and Cb763 +-
295%) and hgated fetuses
(Na-23¢ _+ 70% and
409 +- 74%).
CONCLUSIONS: Furose-
mlde, rejected into the
owne amnlotlc cavity,
caused a rapid and pro-
longed fetal diurnals in spite
of the tnabdlty to swallow,
demonstrating absorption
of furosemide via the
intramembranous pathway,
s potentml avenue for fetal
therapy in the future.
1.2
1.0
.8
.6
.4
.2
-.2. 0 1 2 3 4 5 TiME (hr)
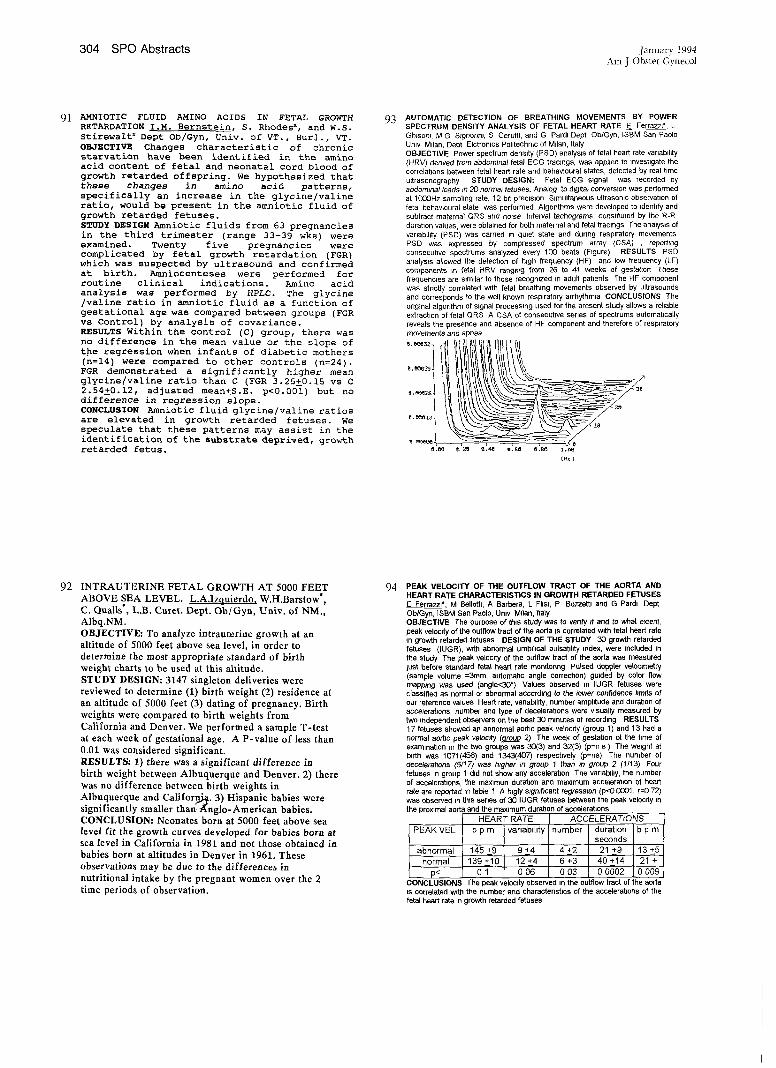
304 SPO Abstracts .Ia,mar’y 1994
Am J Obstet Gynecol
91 AMNIOTIC FLUID AMINO ACIDS IN FETAL GROWTH RETARDATION I.M. Bernstein, S. Rhodesx, and W.S. Stirewaltx Dept Ob/Gyn, Univ. of VT., Hurl., VT. OBJECTIVE Changes characteristic of chronic starvation have been identified in the amino acid content of fetal and neonatal cord blood of growth retarded offspring. We hypothesized that these changes in amino acid patterns, specifically an increase in the glycine/valine ratio, would be present in the amniotic fluid of growth retarded fetuses. STUDY DESIGN Amniotic fluids from 63 pregnancies in the third trimester (range 33-39 wks) were examined. Twenty five pregnancies were complicated by fetal growth retardation (FGR) which was suspected by ultrasound and confirmed at birth. Amniocenteses were performed for routine clinical indications. Amino acid analysis was performed by HPLC. The glycine /valine ratio in amniotic fluid as a function of gestational age was compared between groups (FGR vs Control) by analysis of covariance. RESULTS Within the control (C) group, there was no difference in the mean value or the slope of the regression when infants of diabetic mothers (n=14) were compared to other controls (n=24). FGR demonstrated a significantly higher mean glycine/valine ratio than C (FGR 3.25Z0.15 vs C 2.54Z0.12, adjusted mean±S.E, p<0.001) but no difference in regression slope. CONCLUSION Amniotic fluid glycine/valine ratios are elevated in growth retarded fetuses. We speculate that these patterns may assist in the identification of the substrate deprived, growth retarded fetus.
93 AUTOMATIC DETECTION OF BREATHING MOVEMENTS BY POWER SPECTRUM DENSITY ANALYSIS OF FETAL HEART RATE E Ferrazm*, L GNSom, M G SIgnonn~, S Ceruttl, and G Pard~ Dept Ob/Gyn, ISBM San Paolo Unlv Milan, Dept Elctronlcs Pohtechmc of Milan, Italy
OBJECTIVE Power spectrum density (PSD) analysis of fetal heart rate vanabdlfy (HRV) derived from abdominal fetal ECG tracings, was applied to investigate the correlations between fetal heart rate and behavloural states, detected by real time ultrasonography STUDY DESIGN: Fetal ECG signal was recorded by abdominal leads In 20 normal fetuses. Analog to dlgtta~ conversion was performed at l(]OOHz sampling rate, 12 bit precision S~multaneous ultrasonic observation of fetal behavloural state was performed Algorithms were developed to identify and subtract maternal QRS and noise Interval techograms, consbtuted by the R-R- duration values, were obtained for both maternal and fetal tracings The analysis of variablhty (PSD) was carried in quiet state and during respiratory movements PSD was expressed by compressed spectrum array (CSA) , reporting consecutive spectrums analyzed every 100 beats (Figure) RESULTS PSD analys~s allowed the detection of high frequency (HF) and low frequency (LF) components in fetal HRV ranging from 26 to 4f weeks ot gestat(on These frequencies are similar to those recognized in adult patients The HF component was strictly correlated with fetal breathing movements observed by ultrasounds and corresponds to the well known respiratory arrhythmla CONCLUSIONS The original algorithm of signal processing used for the present study allows a rehable extrachon of fetal QRS A CSA of consecutive s6rles of spectrums automatically reveals the presence and absence of HF component and therefore of respiratory movements and apnea
92 INTRAUTERINE FETAL GROWTH AT 5000 FEET ABOVE SEA LEVEL. L.A,Izquierdo, W.H.Barstow*, C. Qualls’, L.B. Curet. Dept. Ob/Gyn, Univ. of NM., Albq.NM. OBJECTIVE: To analyze intrauterine growth at an altitude of 5000 feet above sea level, in order to determine the most appropriate standard of birth weight charts to he used at this altitude. STUDY DESIGN: 3147 singleton deliveries were reviewed to determine (1) birth weight (2) residence at an altitude of 5000 feet (3) dating of pregnancy. Birth weights were compared to birth weights from California and Denver. We performed a sample T-test at each week of gestational age. A P-value of less than 0.01 was considered significant. RESULTS: 1) there was a significant difference in birth weight between Albuquerque and Denver. 2) there was no difference between birth weights in Albuquerque and Californ~. 3) Hispanic babies were significantly smaller than-~nglo-American babies. CONCLUSION: Neonates born at 5000 feet above sea level fit the growth curves developed for babies born at sea level in California in 1981 and not those obtained in babies born at altitudes in Denver in 1961. These observations may be due to the differences in nutritional intake by the pregnant women over the 2 time periods of observation.
94 PEAK VELOCITY OF THE OUTFLOW TRACT OF THE AORTA AND HEART RATE CHARACTERISTICS IN GROWTH RETARDED FETUSES E Ferrazzl* M 8ellottl, A Barbera, L FIIsl, P Bozzettl and G Pardi Dept Ob/Gyn, ISBM San Paolo, Umv M~lan, Italy OBJECTIVE The purpose of this study was to verify If and to what extent, peak veloc~fy of the outflow tract of the aorta is correlated w~th fetal heart rate ~n growth retarded fetuses DESIGN OF THE STUDY 30 growth retarded fetuses (~UGR), with abnormal umbilical pulsat~hty index, were included in the study The peak velocity of the outflow tract of the aorta was measured just before standard fetal heart rate momtonng Pulsed doppler velommetry (sample volume =3mm, automatic angle correcflon) guided by color flow mapping was used (angle<30°). Values observed in IUGR fetuses were classified as normal or abnormal according to the lower confidence limits of our reference values Heart rate, varlablhty, number amplitude and duration of eccelerat~ons, number and type of decelerations were visually measured by two ~ndependent observers on the best 30 m~nutes of recording RESULTS 17 fetuses showed an abnormal aortic peak velocity ro(~l~) and 13 had a normal aortic peak velocity (g£ggp~) The week of gestaflon st the time of examination ~n the two groups was 30(3) and 32(3) (p=n s ) The weight at birth was 1071(4,56) and 1343(407) respectively (p=ns) The number of decelerations (5/17~ was higher tn group 1 than m group 2 (1/13) Four fetuses in group 1 d=d not show any acceleraben The varlab~l~y, the number of accelerations, the maxlmun duration and maximum acceleretlon of heart rate are reported tn table 1 A htgly significant regressmn (p<O 1S~O1, r=O 72) was observed in this series of 30 IUGR fetuses between the peak velocity in the proximal aorta and the maximum duration of accelerabens
HEART RATE ACCELERATIONS
~-EAK VEL b p m variability number duration i b p m seconds
-~bnormal 145 +9 9 +4 4 +2 21 _+_.9 13 +_5
~normal 139 +~10 12 +4 6 +3 40 +_14 21 +
p< 0 1 0 06 0 03 0 0002 0 009
CONCLUSIONS The peak veloc~fy observed m the outflow tract of the aorta
is correlated with the number and charactenstlcs of the ecceleratlons of the fetal heart rate in growth retarded fetuses

Volume 170, Number l, [;’art 2 SPO Abstracts 305 Am J Obstet Gynecol
95 ENDOCRIMOLOGY OF TMIM PRE&MAMCY: INCREASES IN NATERMAL SERUM
AI~DRO6E~. V.Daniel Castracan~,~ Kirk Ramin,bx Gabrietla
Pridjian,~ ram Cha~[er,~ Susan Ramie,b Brad Riffe,~ Depts,
~/G~, Texas Tech Univ, HSC, ~ri[[o, TX,a Un~v, ~X South~stern
M~. Ctr., DalLas, TX,b g UR~v. Michigan Sch. M~., Ann Ar~r, M[.c ~JE~TI~: Maternal ser~ a~rogens a~rosten~ione (A) a~ testosterone (~) are e{evat~ throughout pregnancy, in early pr~na~y, this rise in ~ & A ~s thought to~ of ovarian origin. the sources of ~ternal ser~ a~rogen levels in tater pregnancy have not ~en ~[i~at~. Using twin pregnancies we ho~ to account for the c~ti~ rise in T & A in later pregna~y. STaY BESTS: Steroid levels in ra~ ~ternat bto~ sautes obtain~ fr~ twin pregnancies in ~th seco~ (n=36) a~ third (n=34) tri~sters were ~asur~. Nor~[ singleton pregnancy sables were contro[s. T & A were examined as classic a~roge~ ~ra~ters, estrio[ (E3) as a ~rker of fetal adrenal steroidogenic activity, a~estradio[ (E2) as an i~icator of ~th ~ternal a~fetal sources. Maternal ser~levets of progesterone (P) a~ h~n chorf~ic g~dotropfn (hCG) were st~i~ as i~icators of placental e~ocrino[ogy. ~E~L]S: Levels of T & A are similar in the seco~ tri~ster ~t a ~rk~ increase in twins is seen in the third tri~ster when c~r~ with singletons (T 1.33 ng/ml vs 0.8~ ~/ml a~ A 3.95 ng/m[ vs 3.28 ng/mt). Seco~ a~ third tr~ster levels of P a~ hCG in twins are e[evat~ as exactS. Mean ser~ [evets of Es ~n the seco~ tri~ster are slight[y greater in twin pregnancies; however, a ~re drastic increase is seen in the third tr~ster (213 ng/ml vs 150 ng/mt) consistent with two fetal placenta~ units. A similar ~ttern is a[so seen for ser~ E2. ~LU~S: These results i~icate that those hor~nes of placental origin are increas~ ~ twin gestation at ~th seco~ a~ third tri~ster as exactS. The ~ncrease in fetal adrenal activity in the third tri~ster corres~s to the increase in E3, The seco~ tri~ster increases ~ T g A suggests an involv~nt of the fetal adrenal a~ placenta ~n the increase of ~terna[ a~rogens in late pregnancy.
97 THE EFFECT OF SMOKING DURING PREGNANCY ON UMBILICAL
CORD BLOOD GASES Thorp JA, Meyer BA, Wlckstrom EA, Umv of MO
@ KC-St Luke’s Hospital, Kansas City, MO.
OBJECTIVE: "Co determine the effect of maternal smoking during pregnancy
on umbifical cord blood gases at the time of delivery.
STUDY D~SIG!~: A retrospectave study was performed between 1-1-87 and 6-
30-92 During this time period, there were a total of 16,470 dehveries At least
one cord blood gas parameter (venous pH) was obtained m 15,184 fetuses
dehvering during this same period, Umbilical cord blood was drawn
~mmediately after dehvery with pre-packaged, pre-hepannized syringes, placed
on ~ce and analyzed within 30 minutes of delivery.
Data are reported as mean ± SD.
RESULTS:. There is a statistically higher umbilical cord artenat pH in women
who smoked during pregnancy when compared w~th non-smokers (p = 0.0003)
*p < 0.05
pH IX)?_ ARTERY
Non-smokers 728±08 167±69
n= 12,113 n=1,444 n=1,444 n=1,449
Smokers 729±.08’ 162±78 53.7±123 24.0±3.1
n=1,538 n=202 n=203 n=202
VEIN Non-smokers
Smokers
7 36 ± .07
n=13,465
7 3~ ± .07
a=1,719
(160/I,538 vs 1,567/12,113;
pCO2 H¢Os" BE
54,0±11.6 239±2.8 -42:~40
n=1.436
-40±40
n=197
278±10.0 418±96 22.0±2.8 -36±3.6
n=1,784 n=1,785 n=1,790 n=1,771
-3 2 .~ 3.6
n=245
:ers versus non-sin(
27.2±106 42.0±94 22.3±2.8
n=245 n=246 n=245
.05) CONCLUSIONS: Compared to non-smokers, smokers have basher cord arterial
blood pH and fewer cord arterial pH values _< 7 20 These differences are
statistically, but not cfinically s~gnlficant.
96 P~OT~O~il FP~MT 1.2 ~ D-DIRER EE’~LS i~
McCattax, M. Huge, C. Green~rgx, M. Henness~, H. Kay. Dept.
~/Gyn a~ M~cine, Duke University, Durham, ~JECII~: Frag~nt 1.2 is a ~rker for thr~sis a ~rker for ffbrfnotys/s. Both are f~rtant ~rkers for coagulation. This st~ was u~ertaken to u~ersta~ the relationship of FI.2 a~ d-di~r to adverse pregnancy outc~ (i.e., preecta~sia a~ pregnancy loss).
S~f OES[~: ~(o~ was cottect~ fr~ pregnant ~tfents having
routine b[o~s drawn without evidence of disease. F1,2 was assay~
using a ~noctonat anti~-~s~ EL]SA by Organon Teknika Corp.
D-di~r was assay~ using an EL~SA fr~ A~rican Diagnostics.
Final pregnancy outc~s were determin~ fr~ chart review. Oats
a~ statistical analysis were ~rfor~ using SAS version 6.04.
RE~LTS: 340 sa~tes fr~ 249 ~tients (5.4-40.7 weeks) were
eva~uat~.
MEAN LEVELS
~r~ster Frag~nt 1.2 ~ D-di~r ~/L
Ist 1.63 ~ 2.8~ 506.2 ~ 318.4 > NS ¯ NS
2nd 2.11 $ 1.83 581.7 ± 302.7 ¯ P<O.01 > P<O.O01
3rd 4.48 ~ 11.22 I0~0.5 ~ 750.1
There was a significant decrease in F1.2 (0.68 ± 0.25 aM,
P<O,O05), I~Jt not d-dimer levels in 1st trimester losses compared
to normaL, but there were no differences in either marker in
association with subsequent preeciampsia at any trimester.
CONCLUSIONS: goth d-dimer and FI.2 increase significantly from the first trimester into the third trimester of pregnancy. These data suggest that FI.2 may be a mere sensitive marker for early pregnancy toss than d-dimer, but neither appear to be sensitive early markers for preectampsia. Further studies are indicated.
98 OXYGEN ADMINISTRATION IN THE SECOND STAGE OF LABOR
AND CORD BLOOD CO-OXIMETRY. Thoro J~, Troboughx T, Evansx
R, Hedtickx J, Yeast JD Umv ofMO @ KC-St Luke’s Hospital; Kansas C~ty,
MO
OBJE CTIVE: To determine if maternal oxygen adminstration during the 2nd
stage of labor affects cord blood co-oximetry
STUDY DESIGN_: Patients were prospectively randomized ~a~o the study at
the onset of 2nd stage. All patients had a normal term gestation and a normal
FttR tracing during the 1st stage of labor,
RESULTS: There were 67 patients randomized into the study’ 13 were
excluded t~ecause of an abnormal 2nd stage FHR tracing or requirement for
CS. Data are reported as mean ± SD Palaents randomized to the oxygen
group received 10 L/rain by mask for a mean duration of 38 ± 32 minutes.
Compliance was documented
O2 l~lemoglobln Hb CO Sat Hb 02 Sat Met Hb
Content (%) (%) (%) (%) (ml/dL)
ARTERY
Control 152 ± 1 5
~=21
Oxygen 15 7 ± 1.7 n=22
VEiN
Control 15,3 ± 1,5
~=22
Oxygen 15 7 ± 1 7
n=21
0.7±0.6 33.5±148
n=20 o=21
1 3 ± 1 6 33.8 ± 12.6
n=21 n=22
1 6 ± 1 0 65.2 ± 12.0
n=22 n=22
2.2±2.0 677±159
n=20 n=2t
07±0,1 7.0±3.0
n=21 n=21
07±02 7.5 ~: 3.0
n=22 n=22
0.7±01 13.8±2,5
0.8±0.2 14.7±35
n=21 n=21
normal labor does not affect umbilical cord blood co-ox~metry,
306 SPO Abstracts January 1994 Am ] Obstet Gynecol
99 COCAINE (COC) EFFECTS ON OVINE FETAL SWALLOWING. M.G. Ross, XL. K. Kullama, XM. I. M. Nijland, K. Chan. Dept. Ob/Gyn, Harbor-UCLA Meal Ctr, Torrance, CA.
OBJECTIVE: Fetal swallow~ng occurs primarily during low voltage (LV) ECoG activity, and fetal LV ECoG is reduced by COC. As COC
and COC me, tabolites are excreted into amniotic fluid (AF) and re- absorbed into fetal plasma via swallowing, we examined whether
cocaine alters fetal swallowing activity, and thus the resorption of AF COC. STUDY DESIGN: Six ovine fetuses (130±1 d) were chronically prepared with esophageal electrodes and an esophageal flow probe. Following a 1 hour control period, fetuses received an intravenous
injection of 1.0 mglkg COC over 30 see. Maternal and fetal blood samples were withdrawn at tuned intervals and fetal swallowing monitored for 360 rain a&es COC.
RESULTS: Basal fetal swallowing activity during the control period was 0.6+0.1 swallows/rain, with esophageal flow of 0.4+0.2 m~/min.
At 10 min following COC, fetal swallowing increased to 1.4±0.4 swallows/min though esophageal llow did not change (0.5 +0.2 ml/min). Swallowing then returned to basal levels.
CONCLUSIONS: These results demonstrate short term (10 min) stimuhtion of fetal swallowing activity. Despite suppression of LV ECoG, COC does not suppress fetal swallowing and thus may facilitate recirculation of AF
101 INVESTIGATION OF AUTONONIC CONTROL OF MA’ERNAL HEAR]
RATE IN NORFiOTENSIVE AIID HYPERTENSIVE PREGItANCIES
ONT,
p<O,O03) ~n the lov~ frequency (LF) r&~pe (O-O.O4 Hz) ~ heart
CONCLUSIONS, PSA demonstrates alterations ~ ~ear~ r~t~
100 ESTIMATION OF FLOW AND PEAK VELOCITY (PV) IN THE MAIN
PULMONARY ARTERY (1VIPA) AND RIGHT PULMONARY ARTERY (RPA) IN THE FETUS FROM 17 TO 40 VCEEKS GESTATION BY DOPPLERECHOCARDIOGRAPHY I R. Stanley,xj C Ve:lle, L. Steele.x
Dept of Ob/Gyn, Bowman Gray School of Medicine, Wlnston-Salem,
OBJECTIVE’ To describe flow characteristics of the MPA and RPA in
normal fetuses. Changes in MPA and RPA flow charactensUcs may reflect fetal pulmonary abnormahtms such as pulmonary hypoplasia. STUDY DESIGN. Fifteen normal fetuses were longitudinally studied 47
times between 17 and 40 weeks gestatlonal age (GA) using pulsed Doppler
echocardlography Waveforms were obtained from the MPA and RPA
Three to six cycles were digitahzed and averaged to determine PV and time velocity lmegral Dlamemrs of the MPA and RPA were measured u.sxng 2-D
ultrasound Flow volumes were calculated from these values and the heart
rate, Data were analyzed using linear regression GA was the independent variable RESULTS"
RPA PV (cm/sec)
RPA DIAMETER (cm)
RPA FLOW (ml/min)
MPA PV (cm/sec)
MPA DIAMETER (cm)
MPA FLOW (ml/min)
n r p
47 0 41 <0.01
46 0.87 <0 01
46 0 72 <0 01
44 0.70 <0 01
43 0 91 <0.01
43 0.83
The flow in the MPA ranged from 331 cc/m~n at 18-20 weeks GA to 1211
cc/mm at 39-40 weeks GA, while that in the RPA ranged from 8 7 cc/min to
61 8 cc/mm. The ratio of MPA to RPA flow did not change during gestation
CONCLUSIONS. The flow, PV, and vessel diameter in the MPA and RPA all increase w~th gestational age. These data m the normal fetus provide
baseline information which may be useful in identifying fetuses with
pulmonary hypoplasia.
102 UTERINE ARTERY RESISTANCE TO BLOOD FLOW DURING PUERPERIUM: A LONGITUDINAL STUDY. A.J. Jaffa,x I. Wolman, J. Sagi, J. Har-Toov, I. Gull, M.R. Peyser, Dept. of Ob/Gyn "A", Serlin Mummify Hospital, and Saclder School of Medicine, Tel Aviv University, Israel OBJECTIVE: The study was undertaken to assess the changes in the resistanco of uterine arteries during puerperium. STUDY DESIGN: In a longitudinal study, the merine arteries of 60 patients with uncomplicated pregnancy and delivery were examined transvaginally (n = 755) with computerized continuous-wave Doppler. Measurements were taken for the first 3 days after delivery, and once a week for the following 9 weeks. The control group consisted of two subgroups: 1) 220 normal pregnant women at term, and 2) 40 nongravid patients. RESULTS: The mean pulsalllity index (PI) of the first 3 puerperal days (1.2 ± 0.27) was significantly higher than that o[ ~e 3rd trimester of normal pregnancy (0.77 + 0.14). The PI decreased significantly to 1.06 + 0.19 m the’second postpartum week, and remained relatively low until week 4 postpartum (1.12 4- 0.19). Thereafter an increase in PI to 2 0 + 0.53 was observed between the 5th and 9th postpartum week. This PI was still significanlly lower than that of the nongravid controls (2.62 ± 0.59). CONCLUSIONS: Uterine vascular resistance increases soon after delivery. Vascular resistance decreases between the 2nd and 4th weeks postpartum and thereafter increases up to the 9th week, without return to the nonpregnant values.

~blutne 170, Nmnber 1, Part 2 SPO Abstracts 307 Am .10bstet OynecoI
103 A TWENTY-FOUR HOUR CORTISOL RHYTHM IS
PRESENT IN THE ItUMAN NEWBORN. GJ Valenzuela, AM
Germain, DL Hess, CA Ducsay, M Seron-Ferre. Div. Perin Biol.,
Loma Lin,l~ U, Dept Obstet and Gyn, San Bemardino County
Medical Center, Oregon Primate Center, U Oregon, and Facultad
de Ciencias Biologieas and Medicina, Pontificia Universidad
Catolica, S~ Bemardino, California, Oregon and Santiago, Chile.
OBJECTIVE. The human fetus exhibits 24-h rhythms in
physiological function such as breathing, body movement, heart rate
and adrenal function. It is unknown whether these rhythms are
passive (determinod by the mother) or endogenously generated by
the fetus. In the latter case, rhytlmm should persist after birth. To
test whether the fetal ~drenal rhythm is endogenous, we explored if
the human newborn Ires 24-h cortisol rhythm.
METHODS OF STUDY. Saliva was collected within 48 h of
birth, at 4-h intervals during a 24-h period. We collected samples
from 7 term newborn from mothers without any medical
complication. Cortisol was measured by RIA. Data was analyzed
by ANOVA with Bonferroni correctton.
RESULTS. All fetuses exhibit a 24-h cortisol rhythm. A peak of
c6rtisol occurred randomly around the clock. No rhythm was seen
in the mean data. When the individual rhythms were synchronized
there was a significant rhythm (p < 0.001). The peak value was 81.9
+ 23.8; ng/ml (SEM) while the nadir was 7.5 + 2.5.
CONCLUSIONS. This result is consistent with the presence of an
endogenous fetal rhythm of cortisol.
Supported by the San Bemardino County Medical Foundation.
105 THE EFFECT OF MULTIFETAL PREGNANCY REDUCTION
ON LUTEAL FUNCTION. L. Lynch, R.L. Berkowitz, G. Weissx,
L T Goldsmithx, R. Lapinskix, R. Weinx. Mount Sinai Medical Center. NY. NY, and New Jersey Medical School, Newark, NJ OBJECTIVE: Circulating relaxin, a marker of luteal function in pregnancy, has been implicated as a risk factor for prematurity. Our objective is to determine the effect of multifetal pregnancy reduction (MPR) on luteal function and relaxin secretion. STUDY DESIGN. 48 women w~th multifetal pregnancy after ovulation induction (26 = 3, 22 = _>4) who underwent MPR to twins were our subjects. Maternal blood was obtained on the day of MPR (10-12 wks, mean I1.6 wks) and at 14, 16, 20, 24, 30 and 36 wks. Serum rclaxin was measured by ELISA. RESULTS: For comparison, relaxin concentraton in the first trimester for nt~rmaI unsdmula~ed single,on ~e~nancies is 1.g+_~3.69 n~JmL
lVFKIWr P/M C
n = 19 25 4 Pre MPR relaxin (ng/nd) 18.25:9 12.i_+8 5.3_+3 p <.05
Post MPR relaxin (ng]rrd) 14.85:9 9.55:7 5.55:d- Last relaxin ore delivery (n~lml) 10.15:9 6.6_+7 3.0~-_2
P = Pergonal, M = Metrodin, C = Clomid Pre & post MPR relaxm levels were significamly different only in the P]M group. The difference between last and pre MPR relaxin was significant in all groups. The number of fetuses reduced did not affect the relaxm levels or changes (data not shown). The mean gestational age at delivery was 35.5+3 weeks. CONCLUSIONS: (1) Relaxin levels are highly elevated in ovulataon stimulated multifetal pregnancies. (2) Relaxm concentration is higher m IVF/GIFT > P/M > C groups, probably indicative of the initial number of follicles ovulated i.e. luteal mass. (3) Relaxin levels decrease over time during multffetal pregnancies. (4) MPR does not comistently affect relaxin concentration. (5) The number of fetuses reduced has no affect on relaxin levels. This suggests that while early pregnancy luteal rescue relies on trophoblastic hormone stimulation, luteal function in midpregnancy is quantitatively independent of ~ophoblastic function.
104 EFFECT OF PREGNANCY ON SEIZURE THRESHOLD IN
THE HIPPOCAMPUS OF RATS. C.A. Standleyx, S.M.
Irtenkaufx, D.B. Cotton, Dept of Ob/Gyn, Hutzel Hospital/Wayne
State University, Detroit, MI.
OBJECTIVE: Relatively few investigattons have examined the
effect of pregnancy on seizure suscepttbility. The present study was
designed to study changes in tnppocampal afterdischarge (AD)
thresholds to further understand epileptogenesis during pregnancy.
STUDY DESIGN: 16 female rats were surgically anesthettzed and
a btpolar electrode stereotaxlcally implanted into the dorsal
hippocampus. Fol|owmg one week recovery, baseline values for AD
(seizure) threshold were obtained on all rats. AD thresholds were
then re-determined on days 7, 14 and 21 from basehne. Rats were
then mated, and AD thresholds were re-deterrmned at days 7, 14 and
21 of pregnancy. Vaginal smears were taken 3 times weekly to
determine stage of estrus on days stimulated during non-pregnancy.
RESULTS: The amotmt of electrical current required to imtaate a
hippocampal AD (seizure) s~gnificantly decreased across each of the
three stimulations before pregnancy (p<.01). Vaginal smears
indicated that the estrus cycle did not correlate with the change m
seizure threshold. Pregnancy did not affect seizure threshold.
However, the mortality of the pups was 37.5% and tended to
correlate w~th longer seizure durahon on pregnancy day 7 and 14.
CONCLUSIONS: Pregnancy had no effect on fuppocampal seizure
thresholds in this model. Repetitive seizure actwlty during
pregnancy, however, even without behavioral manifestations leads
to a h~gh permatal wastage in pups. Gross and h~stologic
examination of the pup brains revealed micro and
macrohemorrhages. The mechamsm of these hemorrhages requires
further investigation.
106 COCAINE°S EFFECT ON OXYTOCIN IN THE BABOON DURING LATE PREGNANCY, MA Morgan. MBOM
Honnebierx, T Myersx, J Winmrx’ C Mecenasx, PW Nathanielszx’,
TJ Garite, DepL Ob/Gyn, Univ. of Calif, Irvine, Orange, CA and Laboratory for Pregnancy and Newborn Research, Comell Univ.,
Ithaca, NY. HD 21350 Objective: The mechanism of how cocaine stimulates uterine contractility, resulting m preterm labor, remains unknown. We
aimed to determine intravenous cocaine’s effect on plasma oxytocin levels in the gravid baboon. Study Design: Frye gravid baboons at 86 - 150 days’ gestation (term 180 days) had mammal femoral arterial and venous catheters surgically placed under halothane anesthesia. Five days after
surgery, cocaine hydrochlonde 0.5, 0.75 and 1.0 mg/kg by mammal weight were infused I.V. 24 hours apart into awake baboons. Arterial blood samples were obtained at -30, -15, -5, +5, +15, and
+30 minutes before and after cocaine. Plasma oxytocin levels were determined by a specific RIA. The mean baseline samples were compared to the post-cocaine samples and reported as percent change from basehne. Data are reported as mean -+ SEM. Results: Oxytocin levels s~gnificanfly increase ~ffter 1.0 mg/kg I.V.
cocaine (Figure). Conclusion: Cocaine
stimulates oxy~ocin
secretion m a dose- =~ dependent manner and c~o ,~ ~
may be an etiology for
preterm labor in those
using cocaine during
pregnancy. ~ ~,oot~,,o’,~ ..... ~

308 SPO Abstracts January 1994 Am .10bs~et Gy~ecol
107 TUMOR NECROSIS FACTORmt IN PREGNANCIES ASSOCIATED WITH PREECLAMPSIA OR SMALL-FOR-GESTATIONAL-AGE NEWBORNS. E. Sch~ff. S.A Friedman,x P. Baumann,x R Remote, and B.M. S*bai. Departments of Obstetrics and Gynecology, University of Tennessee. Memphis, and Wayne State Unive~try, Detroit OBJECTIVE: To determine the presence and concentration of mmot necrosis factot-a (TNFm0 in maternal and fetal plasma in pregnancms associated with preeclampsh (PE) or small-for-gestational-age (SGA) newborns. STUDY DESIGN: Maternal and fetal plasma TNF-~ concentrations were measured in nonpregnant women (n = 12). women with normal pregnancies (n = 24), and women with pregnancies associated with severe preeclampsia (n:23), SGA newborns (n= 14), or both pteeclampsia and SGA (n=12). TNF-~ was measured with a sensitive and specific enzyme-immunoassay RESULTS: TNF-o, was detected in 89% of the samples studied. Levels ranged from < 1.5 to 30 pg/ml. Med*an levels (pg/ml) are presented below. Maternal and fetal TNF-(~ concentrations in the group with idiopathic SGA were sJgmficantly lower than those of control group~. Similar le’~els were found in
women with severe pteeclampsia with or without SGA, women who delivered vagmally or abdominally m roe control groups, and nonpregnant women The route of delivery did not affect TNF-0t levels in both the maternal and fetal plasma Concentrations of TNF-e~ in fetal arterial plasma were s*gmfiCantly correlated with those in fetal venous plasma (r= 0 51. p = 0 01), but weakly correlated w~th those in maternal plasma (r= 0 34, p=O I f)
PE PE + SGA SGA CSVD CCS CNP Maternal 6.4 * 7.4 * 2 7 ~" 7.0 9.3 8.1 Fetal artery 3.4 8.t * 1.9 ~" 5.9 11 4 Fetal vein 5 3 * 4 2 * 2 1 y 7.5 11.7
CSVD, control with spontaneous vaginal delivery, CCS, control with cesarean section; CNP, control nonpregnant.
¯ p > 05 compared to CSVD, CCS, and CNP I p £ 01 compared to CSVD, CCS, and CNP
CONCLUSIONS: Our study demonstrates a significant decrease In maternal aud fetal plasma concentrations of TNF-~ in prel~nancies associated with idiopathic SGA newborns. This reduction Ray ha~’e e~docrmolog*c impoWance or may be reflective of widespread paracrme and autoctine events On the other hand, our findings do not support a fundamental endocrine role of TNF-~t in preedampsia
109 FETAL CARDIAC EFFECTS OF TOCOLYSIS. J Blackstone[, D Fnedman,
IA Hoskms, BK Young, Dept of OBIGYN, NYU Medical Center, NY, NY
OBJECTIVE: To ~denbfy and characterize any changes m fetal cardiac
function occumng while mothers received tocolybc therapy, utilizing the
combined ventricular shortening fraction, (CVSF), an echocard~ographic
index of fetal systohc cardiac function
STUDY DESIGN: A previous study suggested that chromc oral ntodnne
toco/ysls was asso~ated with reduced feta! systolic cardiac function
Therefore, 30 pabents diagnosed wRh pre-term labor and eligible for tocolytic
therapy were the subjects of th~s prospective non-randomized cohort study.
16 patients were treated with subcutaneous, (SQ), terbutalme, 5 with
intravenous, (IV), dtodnne, and 9 with IV magnesium sulfate, (MgSO~). All
were later maintained on oral therapy with either terbutaline or ntodnne. Each
fetus was studied on 4 sepat’ate occasions" before treatment, while on a
therapeutic Iv or SQ regimen, during oral therapy, and after beth Each
evaluation consisted of a biophysical profile, umbilical artery Doppler wave
form study, and an M-mode tracing ofventncularwall mohon generated from
a 4-chamber view of the heart to assess end diastohc, (ED), and end systolic, (ES), dimensions. The CVSF was then calculated as ED-ES/ED x
100%. Multiple analysis of vaeance was used to compare means overtime
for each vadable Means between groups were compared using the two-
tailed student t-test
RESULTS No significant change was noted in the mean CVSF of fetuses
who had been exposed to tocolytic agents, all of whom had normal studies
The mean CVSF pre-treatment was 34.8% as compared to 33.9% in patmnts treated wdh bela-mimehcs These treated with MgSO4 had an improved
mean CVSF of 37.9%.Doppler and biophysical profiles were normal, and preterm labor was successfully stopped in all cases All postnatal studies
were normal and pregnancy outcomes were good
CONCLUSION. Sho~t term treatment with commonly ubhzed tocolytlc agents
does not appear to affect fetal ventdcular funcbon m this study.
110 SLEEP PATTERNS IN PREGNANCY: A LONGITUDINAL STUDY OF
POLYSOMNOLOG¥ RECORDINGS IN PREGNANCY. S.L Sghorrx, A
Chawlax, S.P. Chanhan, C.A. Sallivanx, R.W. Nacf, Ill, J.C. Momson. Depts
Ob/Oyn and Psychiatry, Univ. of Mismsmppi Medical Center, Jackson, MS
OBJECTIVE: During pregnancy two of the most common complaints are easy
fatiganbility and excessive tiredness. Since the only known physiologic relief
for these syreptoms is increasing sleep or rest tim~, sleep patterns in pregnancy
could be very different than in nonpregnancy This study was designed to
evaluate the differences of sleep in early mad late pregnancy as compared to
nanpregnam controls.
STUDY DESIGN: Four pregnant worean were studied longitudinally during
their pregnancy. Polysomnology recordings were performed in the first
trireester m~d again late in the second trimester. Recordings were performed as
inpatients re the somnology laboratory. Measurements included
electroencephalogram, deetrocard,ogram, electroreyogram, testingofabdominal
breathingmovements, andcontmuouspulsooximotry. Fourbealthy nonpregnant
women matched for age and weight were used as controls. Each pahent was
evaluated for the time that she spent ia sleep latency, stage II latency, REM
latency, m~d total sleep time. The total sleep t~me was recorded m~d percentages
of each sleep stage generated
RESULTS: Qualitative differences m sleep between pregnancy and control
patients were evident. Control patients &splayed a normal appearance of slow
wave sleep in stage Ill and IV (delta sleep). When pregnant pauents did dmplay
delta sleep, tt appeared abnormal secondary to extensive alpha wave intrusion.
Even when including this abnormal delta sleep m a quantitative comparison,
pregnant patmnts had a significantly shorter percentage of total sleep tane spent
in delta sleep (5 8 + 8,1 versus 21.9 + 12.1, p = 0.02). There was no
significant difference in any of the other stages of sleep.
CONCLUSIONS: Sleep in pregnancy m characterized by a loss of normal slow
wave sleep. Thus, sleep stages IlI and IV are shorterned during pregnancy.
Thts sleep alteration ~s persistent when followed longitudinally in pregnancy.

Volume 170, Number 1, Part 2 SPO Abstracts 309 Am J Obstet Gynecol
111 INCREASED STROKE VOLUME IN FETUSES WITH HEART BLOCK M Alexander×, KD Wenstrom, W Johnson×. Umversity of
Alabama at Birmingham, B~rmmgham, AL OBJECTIVE: To document that the fetal heart has the capacity to increase stroke volume m the face of complete heart block. STUDY DESIGN" Measurements of left and right ventricular fractional shortening (an index of ventdcu~ar function which
correlates with stroke volume) were obtained from two fetuses w~th complete heart block and no structural defects. Measurements were obtained antepartum and postpartum using M-mode sonography, and compared to published measurements from normal fetuses (DeVoe et al., Am J Obstet Gyneco11984;150.98! -
8) No medications other than steroids for control of maternal lupus were given. RESULTS’
Fractior~al Shortening Gest. Age LV (Norman,) .RV (Normal) Stroke Volume
#1 27= 80% (33 1) 59% (32 1) .... 33’ 36% (33.1) 62% (32.1) .... 35s 36% (33.1) 63% (32 1) ....
1 month 42% .... 11.4 cc/stroke
#2 32’ 50% (33.1) 50% (32 1) .... 5 days 29% --- 12.6 cc/stroke
*Fractional shortening = (end diastolic - end systolic) + end diastohc LV = Left ventricle; RV = R~ght ventricle
CONCLUSIONS. These two fetuses were able to ~ncrease their fractional shortening (stroke volume) in response to persistent bradycardia. This supports the theory that the Frank Starling mechanism is operational in the fetal heart
113 THE ONTOGENY OF HYPERCOAGULABILITY IN NORMAL PREGNANCY AND PUERPERIUM. J Lanouettex, AA Saleh, MP Dombrowski, EF Mammenx. Grace and Hutzel Hosp., Wayne State Univ., Detroit, MI. OBJECTIVE: To evaluate changes in blood coagulation in normal pregnancy. STUDY DESIGN: We measured thrombin-antithrom- bin III complexes(TAT), prothrombin £r~gment I+2(FI+2), D-Dimer(DD), urokinase (uPA), tissue plasminogen activator(t-PA), plasmin- ogen activators inhibitors 1 and 2 (PAI-I and PAI-2), and fibronectin(FN), in non-pregnant controls (N=I5), pregnant women [<12 weeks (N=28), at 16-24 weeks(N=lg), at 24-30 weeks(N=16), at 30-36 weeks(N=27), at 36-40 weeks(N=31)], immediately postpartum(N=35), two days postpartum(N=30), and at 6 weeks pp
RESULTS: All parameters increased with gestational age (p<0.0001) except for FN. Before 12 weeks, only PAI-2 levels increased and correlated with TAT (r2=0.34, p < 0.005) and with DD (r~=0.5, p < 0.0001). F1+2 and TAT increased at 16 weeks followed by in DD at 24 weeks, PAI-I at 30 weeks, and uPA at 36 weeks. t-PA increased immediately after delivery. F1+2 increased at 2 days PP. CONCLUSIONS: l)Enhanced thrombin generation is first noted at 16 weeks, followed by enhanced fibrinolysis at 24 weeks. 2)The trophoblast modulates maternal hemostasis by increasing PAI-2 in the first and PAI-I and uPA in the third trimester. 3)PP resolution starts at 2 days and is completed by 6 weeks.
1 12 ACID-BASE STATUS AT BIRTH IN SMALL FOR GESTATIONAL AGE VS APPROPRIATE FOR GESTATIONAL AGE <1,000 GRAMS INFANTS.
FL Gaudier, RL Goldenberg, M DuBardx, KG Nelsonx, JC Hauth. University of Alabama Hospitals, Birmingham, Alabama OBJECTIVE: To examine the difference in umbilical artery acid-base status between small for gestational age (SGA) and appropriate for gestational age (AGA) extremely preterm infants. STUDY DESIGN: 664 livebom infaats < 1,000g ,109 of which were SGA, dehvcred between January 1979 and December 1991 with umbilcal cord acid-base measurements were studied. Umbilical artery blood samples were obtained at delivery from a doubly clamped segment of umbilical cord. The samples were analyzed for pH, carbon dioxide pressure (PCO2), oxygen pressure (PO2), and bicarbonate (HCO3) content. Infants were classified as SGA using the 10th percentile of Brenner et al.. RESULTS: SGA infants had lower mean umbilical a~tery pH (7.23 5: 0.10 vs 7.26 + 0.11, p <.001), higher PCO2 (54.96 ± 13.03 vs 48.00 + 13.81, p < .001), and lower 1<)2 (16.13 +_ 8.24 vs 21.47 + 9.37, p <.001) than did their AGA COUnterparts. Umbilical cord biearbenate was similar between the two groups (21.16 + 4.40 vs 20.66 5: 4.20, p = NS). The percent of SGA and AGA in various cord gas groups and the asmciated odds ratios and 95% CI for an SGA infant having that cord gas value are shown in the table. The increased incider~ze of fetal acidemia (pH -< 7.20) and lower PO2 in SGA infants remained significant in regression analyses even after controlling for gestational age, birthweight, mode of delivery, end anesthesia.
Umbilical Attar,/ SGA AGA odds rado -" 95% CI pH -< 7.20 36.7 % 21.4 % 1.99 (1.27, 3.14) PCO2 >65 18.4 % 10.3 % 1.56 (0.88, 2.77) PO2 <-14 505 % 20.8 % 3.04 (1.95, 4.74) HCO3 <17 17.6 % 13.5 % 1.66 !..0..93, 2.96)
coNcLuSION: Extremely pr~t~nn infants who are SGA at birth have a higher incidence of umbilical COrd acidemia and a lower PO2.
114 S’p-NMR SPECTROSCOPY MEASUREMENT OF
1NTRACELLULAR FREE MAG]qESIUM AND pH IN
ERYTHROCYTES OF NONPREGNANT, PREGNANT, AND
GESTATIONAL DIABETIC WOMEN. M. Bardlccf~, LM Resuickx,
O Bardic&x, Y Sorokm, DB Cotton Depts. Ob/Gyn and Int. Med.,
Wayne State Umversity, Detroit, MI
OBJECTIVE: To nosinvasively COmpare intracellular free magnesium
(MgJ) and pH 09Hi) in normal pregnancy and gestational diabetes-
STUDY DESIGN: We utilized 3~P-NMR spectrosCOpy to measure
intraeellular Mgl and pHi in red blood cells of fasting nonpregnant
(NPN, n=18), normal pregnant (PN, n=17), and diet controlled
gestatmnal diabetic (PD, n=12)~vomen.
RESULTS:
Qroup NPN P~[ PD
Mgx(ltM) 162+5 159+--7 139+--6*
pHi 7.29+0.02 7 24+__0.01" 7.23+0.01"
* sig=0.05 (ANOVA)
CONCLUSIONS: 1) Pregnancy *s associated with a shift m erythrocyte
pHi towards more acidotic values, which may be helpful m t~ssue and
placental oxygen delivery, and 2) Mgl is lower m gestational diabetes as
compared to normal pregnancy. Smce lower Mgi are also found m other
insuhn resistant disorders, ~ve hypothesize that cellular magnesium
depletion may contribute to the pathogenesis of gestationaI dmbetes.
Altogether, these data emphasize the utility of NMR as a tool in studying
cellular ion metabolism.
310 SPO Abstracts January 1994 Aru J Obstet Gynecol
115 CELLULAR MAGNESIUM DEPLETION IN
PREGNANCY
M Bardice~’, LM Resnickx, 0 Bardieet~, Y Sorokin, J Evelhochx,
BA Masonx, DB Cotton. Depts. Ob/Gyn and Int. Mad., Wayne
State University, Detroit, MI.
OBJECTIVE: To determine if tntracellular magnesium levels are
altered in pregnancy.
STUDYDESIGN: We utilized ~IP-NMR spectroscopy tomeasure
intraeellular free magnesium levels (Mgi) and intraeellular pH (pHi)
in brain, skeletal muscle, and peripheral erythrocytes of
nonpregnant (NP, n=8) and third trimester normal pregnant (P,
n=8) women.
RESULTS: Brain Sk. Morale RBC
Mgi(~tM) NP 544+78 637+45 161+5
P 357+30* 479+50* 159+7
~ NP 7.04+0.03 7.09+0.005 7.29+0.02
P 7.06+0.02 7.08+0.01 7.24+0.02
*P< 0.05 vs. NP
CONCLUSIONS: 1) Cellular magnesium depletion is a
characteristic feature of normal pregnancy; 2) Brain and skeletal
muscle Mgi, compared to RBC ]eve] s, may be more sensitive indices
of magnesium status; and 3) Since low Mgi levels are also f6und in
essential hypertension among nonpregnant populations, lower Mgi
levels in pregnancy may predispose to hypertensive disorders of
pregnancy, such as pre-eclampsia.
117 INDUCTION OF CALCIUM-DEPENDENT NITRIC OXIDE SYNTHASES (NOS) BY PREGNANCY. C Weiner, I. Lizasoainx, S. Baylisx, R. Knowiesx, L Charlesx, S. Mon~dax. Wellenme
Research Laboratory, Beckenham, Kent, England. OB,I~CTIVES: To determine the effect of pregnancy on NOS a~tixaty,
eGIV~ and endothehal (e) / neuronal (n) NOS specific- mRNA.
STUDY DESIGN: Heart, kidney, esophagus and skeletal m. were
excised from 73 time-mated pregnant guinea pigs from 0.14-0.90
gestation (term--63 days) Ten ankmals at term received 250 pg
tamoxifen (i.p. b i d. for 4 doses) prior to slaughter. NOS activity was measured by the conversion of 14C-L-arginine to 14C-L-citrulline in the
presence and absence of LNMMA and EGTA. eGMP was measured by
ILIA. Poly-A mRNA was isolated from skeletal m. by oligo dO)
chromatography, flaetionated on formaldehyde-agarose gels, and
transferred to nylon membranes The blots were hybridized with guinea
pig specific e-NOS and n-NOS mRNA probes cloned by our laboratory,
washed under stringent conditions, and autoradiographed RESULTS: Ca+2-del~ndont NOS activity had begun to rise in most
tissues by 0.14 gestation reaching 200% of the nonpregnant level by 0.30 gestation in all tissues studied. Ca+2-independent activity was
unaffected by pregnaney. NO stimulates guanylate eyelase, eGMP also
doubled with advancing gestation. But in contrast to NOS, eGMP declined in most tissues by 0.60 gestation. Tamoxifen reduced Ca+2-
dependent activity in the heart to the nonpregnant level Tamoxifen had
no affect on the other tissues tested The Northern blots revealed
increased e-NOS and n-NOS speoifie mRNA at term.
CONCLUSION: Our findings support the hypothesis that an increase in NO seeonda~ to enhanced NOS synthesis, which is at least paedally estrogen dependent, plays a role in the cardiovascular adaptations of
pregnancy. The observation that the ¢GMP response to NO is down
regulated over time may explain the rise in vascular resistance at term.
116 THE FETAL HAEMODYNAMIC RESPONSE TO 1N-UTERO
TRANSIrtJSION - AN OVINE MODEL S. MacphaiP, 1L Morrow.
Perinatal Research Unit; Mount Sinai Hospital, University of Toronto,
ONT. CANADA.
OBJECI~XcF_ To develop an urine model which would allow quantification
of the haemodynamlc changes induced in the anaemic fetus by the in-utero
transfusion of a large volume of densely packed red cells (RBC).
S~XJDY DESIGN. 6 chronically catheterised fetal sheep (124 dayg) were
made anaemic by slow haemorrhage (240mls in 2 days) (H) and then
transfused (T) rapidly with maternal RBC. Mean arterial pressure (MAP),
venous pressure (VP), heart rate (HR) umbilical placental flow (UPF) were
measured and umbilico-placental resistance (UPVR) calculated during the
H, T and until 24 hours later.
RESULTS. Data presented as mean and (1SEM).
MAP VP HR FLOW UPVR (mmHg) (mmHg) mls/mm/kg rnm/ml
preH 41,3(1.8) 2.37(0.72) 173.7(1.6) 175(2.1) 3.0696(.006)
preT 40.9(1.0) 2.67(0.36) 192.8(4.4) 211.3(1.9) ).0554(.006)
post T 55.3(2.7) 7.93(0.6) 145.8(3.5) 185.5(6.0) ].08(.01)
+6hr 47.4(3.0) 2.73(0.66) 180.8(11.8)165.4(5.1) ).0856(.013)
+24hr 47.8(4.2) 2.09(0.46) 171.01(5.4) 179.4(5) ).0798(.015) a resulted in increased HR and placental blood flow but no ~ange
in MAP or VP. During transfusion MAP increased 35% and there was a three-fold increase in VP. This was associated with a significant reduction in HR and increase in UPVR. By 24 hours there was no difference from the values obtained pre H. CONCLUSION. It was possible to develop a good ovine model of fetal anaemia and to measure the response to in-utero transfusion. This resulted in profound acute haemodynamic changes in the fetus with normal values restored by 24 hours after transfusion. The mechanisms by which the fetus withstands changes of this magnitude require further evaluation in both the sheep and in the human.
(This work was supported by an MRC(Canada) award to 1LMorrow).
118 A PRELIMINARY STUDY OF MATERNAL FETAL TRANSFER OF IgG
IN HIGH RISK PREGNANCIES
Y. Barnhard’, M. Landor=, A. NasserP, M.Y. Divon. Department of OB/GYN, Albert Einstein College of Medimne, Bronx, N.Y.
OBJECTIVE: To evaluate the effect of high risk conditions on the
transplacental passage of maternal IgG to the fetus In order to
identify pregnancies at risk for reduced neonatal IgG levels.
STUD~( DESIGN: Radial immunodiffusion was used to measure
serum IgG levels in maternal-newborn pmrs in high-risk pregnancies.
The study population included 6 premature gestations (all
<34wks), 11 chronic hypertensives at term, 10 pregestational
diabetics at term, 15 postdate gestations, and 6 lUGR gestations
>37 weeks. Control population conmsted of 28 term low-risk
gestations. Maternal blood was collected on admission to the labor
floor and fetal IgG levels were determined from the cord blood.
RESULTS: Cord IgG[Maternal IgG
Controls 1.13 + 0.22
Premature 0.79 + 0.25*
Hypertensive 1.O8 + O. 13
Diabetic 1.10 4- 0.23
Postdate 1.10 + 0.23
IUGR 0.88 + 0.21
*P<O.05 vs. controls.
CONCLUSIONS: These preliminary results suggest: (1) Transfer of
IgG is not reduced in term high-risk pregnancies compared with controls, (2) As previously shown, transplacental passage of IgG is
relatively decreased in preterro gestations, 13) Although not
statistically significant, the passive acquisiUon of maternal antibodies may be reduced In lUGR fetuses as 5/6 had IgG levels
below that of the control group. This suggests a possible inability
of the IUGR fetus to resist neonatal infecUon.

Volume 170, Number 1, Part 2 SPO Abstracts 311 Am J Obstet Gynecol
119 MAGNESIUM AND CONTRACTION OF HUMAN PLACENTAL VEINS TO ~NDOTH~LINol. SQ L~,~ N Wass~strnm. JV Mombouli,~ PM Vanhoutto? Baylor College of Medicine~ Houston TX. INTRODUCTION: Magnesium (Mg) inhibits t~e in most types of vns- cniar smooth muscle, ~md aff~ts binding of endot~lm-I (ET-I) to high affmity s~tes in blood vessels. Pharmacological doses of Mg are used m
contractile effect of (ET-1) on the placental cirealation is exerted pre- dominantly ~ya veins. Fetal levels ofET-I ar~ elevated in growth retarda- tic~ (1UGR), and maintain the high venous tone that suppmls the low fetal blood volume in this conditice. We investigated whether Mg inidb- ited th~ contractile effect of ET-1 on hmnan placental veins, in a prepmw tion ideat~cal to that in which the marked effects of extraceLlular-cal-cium
DESIGN: Rings from humafi placental veins x~re stretched to
~control), 5ram M~ o~ 10mM Mg sointi~ms. ET-I was th~n added cumu- latively (10"~°M-lCY~vI~, and ~c tensijms incased.. Dose respond_. _ curves were compo~ea with paired t-tests tbr repeateo measures al~plied
were compared by ANOVA.
rich~ solutinm did-nor alt~ the dose response curve to ET-I. CONCLUSIONS: These results
sponse of hunum placental v~ins to ET-I. Mg does not affect this re-
pressod regaxding the nee in [UGR -
t’eta] levels of ET-l-of Ca channd ,~ ¯
hibit the p .la~ntal venous ~r_esl?o~ ..to E.T-I. ,Such agents could corn av- nase the inaintenance .by ET-1 of the etu~au~, veaons tone n ~ to support the hypovolemic fetal circulative in .th~se. ~. ~,ne cur- rein .results ~.~..~st that the use of pharmacolog~.ca~.~doees of Mg m preg-
121 OBESITY, PREGNANCY AND LEFT VENTRICULAR (LV) FUNCTION. J,C. Veille, R. Hanson. Department of Ob/Gyn, Bowman Gray School of Medicine, Winston- Salem, NC. OBJECTIVE: Obesity is associated with increased maternal morbidity, increased LV wall thickness and LV mass. The purpose of this study was to investigate LV function in overweight normotensive nondiabetic patients during the 3rd trimester of pregnancy. _ STUDY DESIGN: Eight obese (O) patients (x wt. 282 + 20 lbs) had M-mode echo of the left ventricle done at 36 + 2 weeks. A group of 36 normal (N) pregnant patients at 36 + 1 weeks were used as control group. Results are expressed as mean + SEM. RESULTS:
LV EDD LVPW IVSD [ Mass CI
(nun) (nun) (nun) [.(FS%), (gin) (l/rain/m2)
~O) 52+1 114-1 124-1 414-2 2855=39 3.54-0.2
~ 504-0.7 74-0.3 84-0.3 385:1 1534-9 4.44-0.3
? NS <0.00001 <0.0001 NS 0.00001 NS
EDD = end diastolic dimension; PW = posterior wall; IVSD = interventricular septum diastole; FS = fractional shortening; CI = cardiac index. CONCLUSIONS: 1) (O) was associated with myocardial hypertrophy, increase in ventricular wall thickness, intraventricular septal thickness, and LV mass. 2) LV EDD, LV function were not different in the (O) group when compared to the (N) group. 3) Although the (O) patients had a myocardial hypertrophy, LV function was preserved.
120 EFFECTS OF ADVANCING PREGNANCY ON LEFT VENTRICULAR FUNCTION (LVF) DURING BICYCLE EXERCISE. J.C. Veille, H.K. Hellerstein, B. Cherty, A.E. Bacevice. Department of Ob/Gyn, Bowman Gray School of Medicine, Winston- Salem, NC and Department of Medicine (Cardiology), Case Western Reserve University, Cleveland, OH. OBJECTIVE: Over the last few years more women exercise during pregnancy. We previously found that vigorous bicycle exercise does not compromise LVF (Am J Cardiol 69:1506, 1992). This study examines the mechanism by which stroke volume (SV) is maintained early (E) and late (L) in gestation. STUDY DESIGN: Six pregnant patients were studied at 15 weeks and again at 33 weeks of gestation. M-mode echocardiograms were obtained at the following 3 periods: 1) Best (R), 2) maximum exercise (Ex), 3) 5th minute of recovery (Rec). RESULTS: ~ 4- EM
LV EDDmm
R (E) 45 + 4.9*
R (L). .... 48 4- 3.7
Ex (E) 46.8 4- 6.0
Ex (L) 49.6 4- 6.7
Rec (E) 50.2 4- 4.5
Ree (L) 49.5 4- 3.8
FS (%) CI (l/mirdm2)
36.1 + 6.4 2.8 4- 0.3
36.8 4- 6.0 3.8 4- 0.5
59.3 4- 8.8 8.8 4- 1.5
47.2 4- 4.4+ 7.7 4- 1.0
45.0 4- 7.5 5.0 4- 1.1
39.5 4- 7.5 4.5 4- 0.5
(*p < 0.003; +p < 0.0005; EDD = end diastolic dimension FS = fractional shortening; CI = cardiac index). CONCLUSIONS: 1) In early pregnancy the increase in SV associated with rigorous exercise is mainly due to the increase in FS (increase in contractile reserve). 2) In late gestation this increase in SV is mainly due to an increase in left ventricular size.
122 LYMPH FLOW DURING CHRONIC FETAL ANEMIA. LE Davis, AR Hohimerx, RA Bmc~x. Oregon Health Sciences
University, Portland Or. and University California San Diego,
La Jolla Ca.
OBJECTIVE: To evaluate the extent t~ which increased lymph
flow can return fluid and protein to the circulation in the
chronically anemic fetus.
STUDY DESIGN: Thoracic duct lymph flow rate (LF) over a
range of outflow pressures was measured in 5 near term fetal
sheep, 4-5 days after surgery and daily thereafter for 5 days.
After each days study 60-190 ml of blood was withdrawn at a
rate of lml/min. Regression analysis was used to establish the
lymph flow function curve. Total lymph protein (LP), plasma
protein (PP), and LF were compared by ANOVA for repeated
measures.
RESULTS: After 5 days of chronic anemia the hematoctit was
reduced from 35.6_+1.2% to 13.7_+.6% (means±se) as LF increased from .424-.03 to .864-.03 ml/r~n, p<.01. This
increase was directly related to the fall in hematocrit. PP and
LP decreased from (3.7±.1 and 2.64-.1 g/dl) to (3.54-.2 and
2.3___.1 g/dl) as the rate of total protein returned to the
circulation nearly doubled. Jugular venous pressure was not
changed.
CONCLUSIONS: During chronic fetal anemia LF increases
and thereby increases the return of protein to the circulation.
This elevated LF plays an important role in extravascular fluid
volume regulation. Supporl:ed by HL45043
312 SPO Abstracts .January 1994 Am J Obstet Gynecol
123 RIGHT VENTRICULAR FUNCTION IN CHRONIC
FETAL ANEMIA. LE Davis. GDGiraudx, AR Hohimerx,
MD Rellerx, MI Mortonx. Oregon Health Sciences University,
Portland, OR.
OBJECTIVE: To determine if the increase in extravascular
fluid in chronic fetal anemia occurs because of heart failure or
despite successful cardiac adaptation. STUDY DESIGN: Right ventricular function curves were
performed in near term chronically catheterized fetal sheep at
the start, midpoint and after 7-8 days of anemia induced by
isovolenuc daily hemorrhage. Least squares fit of the ascending
and plateau lines of stroke volume (SV) versus right atrial
pressure (RAP) were used to establish breakpoints (intersection
of the ascending and plateau lines) which were compared by
ANOVA for repeated measures. Myocardial blood flow (MBF)
was measured by microspheres.
RESULTS: After 7-8 days of chronic anemia carotid arterial
oxygen content was reduced from 6.7+_.2 to 2.1+.1 ml/dl and
the hct from 29+3 to 12.9_+1% (mean_+sem). At the
breakpoint, SV (unchanged for controls) increased from .89_+.09 to 1.24_+.07 ml/kg (p<.05). RAP remained
unchanged, 3.5_+.9 and 2.9_+.7 mmHg. Right and left
ventricular MBF were significantly increased, 1583_+298 and
1362±249 ml/min/100g. Excess fluid was present in the
abdomen and chest of most aninmls at autopsy.
CONCLUSIONS: Tzssue edema during severe anemia occurs
despite normal RAP, increased SV and markedly increased
MBF, markers of successful cardiac adaptation. Supported by
HL45043
125 PREVENTION OF LIPID PEROXIDATION IN BRAIN CELL
MEMBRANES OF FETAL GUINEA PIGS BY PHENYTOIN
DURING IN UTERO HYPOXIA. C. LamDlev. O. P. Mishrax, I.
Forouzan. Dept Ob/Gyn, Dept of Physiology, Univ. of Penn.,
Philadelphia,PA.
OBJECTIVE: To demonstrate the ability of phenytoin to protect the
membranes of fetal brain cells from hypoxic injury.
STUDY DESIGN: Studies were performed on 8 term fetal guinea pigs.
Two of these fetuses came from an untreated mother (control); two from
a mother treated with phenytoin,30 mg/kg,(treated); two from a mother placed in a 7% oxygen chamber for 60 minutes (hypoxic); two from a
treated and hypoxic mother. The fetal brains were harvested, frozen in
liquid nitrogen, and stored at -70°F. Lipid extraction was performed on
the samples. The lipide extracted were dissolved in spectrophotometric
grade heptane, and the absotbance spectra of the samples between
300 nm were me~ured. Conjugated dienes levels were calculated from
this information in p.mole/mg brain. Fluorescent products were measured by spect~ophotofluorometry. The amount of fluorescent
products present in the sample was calculated from the relative
fluorescent intensity at 435 rim.per gram of brain.
RESULTS: The level of dishes in the hypoxic animals was 72
nmol/mg tissue higher than in the control animals. There was no
significant difference between control treated and hypoxic treated
groups. The mean relative fluorescent intensity of the control; hypoxic, treated, and treated hypoxic samples were 1.33, 2.18,.2.18, and 2.04 respectively. There was a significant difference between the level of
fluorescent compounds fomid in the control and treated groups (p=.025).
No other significant differences were found. CONCLUSION: Phenytoin blocks the increase in fluorescent
coumpeunds from lipid peroxidation due to in utero hypoxia preserving
nerve cell membrane structure, which may further reduce hypoxic brain injury in the fetus.
124 OBSERVATIONS Illlll~lilll~ TI~ PATIIOPIIYSIOLflGY OF I~COWilJ AS~’IRAT I I11 SYND~flI~E. K. Ra~ninx, K. Leveno, H. Kellyx, T. Camodyx.
Dept. Ob/Gy~, Univ. of Texas Sonth~estern Ned. Ctr., DeLtas, TX. OBJECTIVE: Hypercarbis has been associated t~ith fetal gasping. We sought to determine if fetal acidemia and hypercarbia ~ere linked to the deveto~ent of meconi~la aspiration syndrome. STUOy DESI611: IJmbilicat artery blood gases in 7,7/,8 singleton
cephalic term pregnancies uith meconi~, in the amnio~ic fluid uere compared to 68 similar pregnancies ~here the infant developed meconium aspiration syndrome.
RESULTS: 7w816 pregnancies ~ith meconi~.
I Io. of infants [
Jmbit~cat arter~ blood ~:
->7.31
7.3 - 7.25
,,, ~.24 - 7.20
7.1Q - 7.10 1087 (1~) 1~
7.0~ - 7.0 1~7 (2) 7
~.~ 42 (.5) 7
~ 65 ~g or greater 822 {11) 21
4C% < 17 ~L 185 (2) 4 (6)
~CL~I~: ~e pr~se that ~c~i~ aspire significantly ass~iat~ uith h~rcarbia a~ fetal Th~ ~i~ in the ~i~ic fluid ~y ~
.,.... cx) l ,r~’ (x)IP
2536 (33) 7 (10)
2380 (31) 14 (20)
1556 (20) 17 (25)
(23)
(10)
(10)
(31)
<.0001
.07
.3
.03
<.0001
e.0001
<.0001
.08
acidemia. a fetal
"enviromlentat" hazard t~nen asphyxia supervenes rather than a result of asphyxia.
126 DECREASED Sa02 PRODUCES HIND LIMB HYPERTENSION AND REDUCED OXYGEN EXTINCTION IN THE FETAL SHEEP. G.D.V. Han~dns. CJ. Ha~eyx.
Depl OB~YN, Wilferd Hall USAF Medical Center, San Antonio, Texas and Dep~ OI~YN, Untversity d Texas Medical Branch, Galveslon, Texas. OBJECTIVE: The objective of this study was to measure fetal Sa02 and mean
~edal pressure in the fetal sheep undergoing p’ogressive hypoxemia. STUDY DESIGN: Nine pregnant sheep were administered general anesthesia and pulmonary artery, femoral artery and femoral vein were accessed. Hysferotomy was perfonnedlo expose letal hind flmbe and fetat artery and veies werecaneuiated.
Maternal and fetal units were rendered pro<3essively hypoxic and acidemic via
maternal hypoventilation. Fetal pH, IX302. p02, HC03, BE, MAP, Sa02 and limb Sv02 were measured and recorded. RESULTS: Aft nine subjects decreased arledal pH and base excess values. Hem~¥r~r~ic d~ies were cal.eo,,odzed i~o two ojoups: ~etuses that *J~v~ted
MAP, and thoselhal had no significant changein MAP. Six leluses decreased Sa02 levels <28%, significantly decreased base excess, and increased hind limb MAP.
Three subjects maintained Sa02 > 31% for the study pedod, significantly de- creased base excess levels, but did not increase MAP. Inthe increased MAP group,
all subjects subsequently reduced hind limb Sv02 and oxygen extraction ratios. CONCLUSIONS: Prugreasive hypoxemiathat results i~ fetal artedal Sa02 _< 28% is more likely to produce limb hypertension than hypoxemia that does not signifi- cantly deo’ease Sa02 (p<.01). Increases in letal hind limb MAP in response to hypoxemia, and the decreased oxygen deltvePt and extraction ratio is suggestive
ot a bemedynamic shunt. Interventionsto maintain arterial Sa02 may be beneficial even in the severely acidemic fetus to prevent preductal hypoxem ia and suboptim um oxygen extractS.

Volume 170, Number l, Part 2 SPO Abstracts 313 Am J Obstet Gynecol
127 CRITICAL OXYGEN EXTRACTION IN THE PREGNANT EWE UNDERGOING
ACUTE HYPOXEMIA. C.J. Harveyx, G.D.V, HankJns. Dept OB/GYN, University
of Texas Medical Branch, Galveston Texas and Dept OB/GYN, Wilford Hall
USAF Medical Center, San Antonio, Texas OBJECTIVE: In the nonpregnant patienL the ability of the tissue to extract
oxygen is initially independent of supply and affected by the determinants of
oxyhemoglobin diasoc~ation. No data exist confirming this physiologic phenom- ena in pregnancy, The objective of this study was to evaluate the effect of pregnancy with its resultant change in oxyhameglobin dissociation on critical
oxygen extraction.
STUDY DESIGN: Pregnant sheep (n--6) were administered general anesthesia
and pulmonary artery, femoral artery and femoral vein canalization were per- formed Maternal and fetal units were rendered progressively hypoxic and
ac~demicvia maternal hypoventilation. Maternal hemodynamic,oxygen transport
and oxygen extraction variables (MAP, MPAP, CVP, PAWP, CI SVRI, PVRI,
Sa02, Sv02, Ca02, Cv02, DO2, V02, 02ER) were recorded. RESULTS: Progressive hypoxemia increased DO2, V02 and 02ER by 25, 37,
and 64 percent, respectively. Mean critical oxygen ext~act~n ir~reased signifi-
cantly to 53% (range = 39% to 69%). Individual subjects had heterogeneous responses that could be categorized into
three groups 1). Predominant increase in DO2 (n=2); 2). increase in V02 (n=2),
or 3). and increase in 02ER (n-~2). The one subjects that had no detectable increase in 02ER bed a Hgb level 25% lower than the mean.
CONCLUSIONS: Oxygen extraction patterns in the pregnant ewe appear to be bimodal in nature. Initially, 02 extraction is 02 supply dependent. Below a crilJcal
02 supply, exf~aclion becomes delivery dependent. This response is similar to
the delivery dependent 02 consumption seen in human sepsis. A critical 02
extraction ratio of 70% bes been hypothesized in the human nonpregnant model; maximum ER measured in this study was lower with inter subject variability.
Decreased oxygen utilization may be species dependent, oxyhemoglobin disso-
ciation dependent, Hgb concentration dependent, or multJtactorial. Reduced
critical oxygen extraction in pregnancy may predispose patients to dysoxia in
acute hypoxemiC stress.
129 FETAL PULS~ O]OMETRY:"r~CHNIGAL PERFORMANCE AND INTRAPARTUM VALUES. G.D.
Anderson. C.J. Harveyx, J, Van Hook, T.N. Tabb, T.L. Shsila#, Dept. of OB/GYN, Univ. of Texas
Medical Branch, Galveston, Texas
OBJECTIVE: The objective of this study was to evaluate the perfonoanco of a newtechnobgy for the use of fetal surveillance in the intrapertum po~)c~ and to record normal SpO2 values in term
pmgnanclas. STUDY DESIGN: From October 1990 to J~ t993, term intraportom portents who presented to labor
and delivep/in a~ve labor ~h no evidence of iofection, bleeding, or placenta pravia were enrolled.
A single plane roflactanco p~ oximetar(Nellcor N-400 with N-10 sensor designed fettstal use) was applied to the presenting fetal heed dudng vaginaJ oxominat bn. Fetal pteductal pulsas were dstectsd
via computerized LCD readout and the sensor was adjusted acoo~ng to readouts. Obstetrical care
providers were blinded to the 8~oO2 recordings and data were retrospectively reviewed. Arterial and
venous umbd~cal cord dexlgases and co.oxirneWwem done on all neonstss. Maternal subjects were evsiuated for complications and neonates were examined for trauma and infection.
RESULTS: 167 rnother-tetus pa~ were o~allad. Mean gastotional age was 39.4 wks;Mean ce~vicol examinstion st the t~me of sensor piscernant was 6.cms/90% ~/-1 sts. Examiners reported mean
ease of application was 3 (s4:ais 1- 5; 5 = ve~ difficult). Sensor porfoanance (contact with fetal ~n,
~ntit~%n d pu~s whh >50% conl~nco) in all st~/s~bjec~ averaged 5"/3% (range = .5%-
952%). Performance for.<4 cm - 52%;5-7 cm - 59.7%; 8-10 crs - 63.9%. Mean fetal SpO2 during labor is helow:
CONCLUSIONS: Fetal pulse oximet~/using a noninvasive fetalre~ctance sensef podorms 58% of
monitoring time, and improves as labor progresses and greater contact is achieved between the
photodetectors and the fetal ~n. Fetal SpO~ values do not significantly change in labor, unlike
previously reported norms for pH. Variability of fetal SpO2 values during labor lend support to the
premise that fetal hemoglobin setLret~on is a dynamic process due to the ~cstion of the fetus on the oxyhemoglobin dissoc=st~on cunra.
128 THE EFFECT OF PREGNANCY ON MATERNAL Sa02 VALUES AT BIWEEKLY INTERVALS AT SEA LEVEL ,/Van Hook. C Harveyx, Depl O~letrics and Gynecology, Oepl. ol OB/GYN, University of Texas Medical Branch, Galveston, Texas, 77555 OBJECTIVE: During pregnancy, the oxyhemegiobin dissociation curve shifts to the ~ht to enhance oxygen delivery to the fetus, resulting in a chronic maternal state of compensated respiratory alkalosis. The objective el this study was to evaluate the etfecl o! dissociation shift on matemal Sa02 values throughout pregnancy. STUDY DESIGN: Pregnant petianls presenting to the obstetrical c!i~ ~ prenatal ca~e and lethe labor and delivery unit were enrolled in the study. Geetational age was established by accuracy of historical dates of ~ menstrual period, telal ultrasound examination prior to 24 weeks, or a combination of both. All subjects were sueenod for acute and chronic disease, compromise of pregnancy, and fetal complications. A Nellcor N-10pulse oximeter was used with a25L digital sensor applied lethe firsl digit otthe dominant hand Mean values over one minute were recorded. RESULTS: 881 patients were enrolled in the study at gestalional ages 8to 42 weeks. 366 of the subjects had no history or evidence of maternal ca~’diorespiratory d[seese (no hyperiension,preedampsia, asthma, pulmonary edema, heart disease, infection, fever, or smoker) and had eslablished fetal growth that met crileris for gestational age. Mean SaO2 was in the low risk group was 98.0% ($TD ±1.7) and there was no significant change at any gestationel age. CONCLUSIONS: Maternal Sa02 is a stable component of oxygen transfer during pregnancy and does not significantly change from 8 to 42 weeks gestation. Normal fetal growth is mo~ likely dependent upon the maintenance of Sa02 levels and the absence o! maternal or fetal anemia. While SaO2 appears to be stable in healthy pregnant subjects, monitoring during pathephysiologic states may be an impodant determinant of fetal 02 availability.
130 FETAL PLACENTAL BLOOD FLOW IS AFFECTED BY MATERNAL GLYCEMIC PROFILE IN DIABETIC PREGNANCIES Elhott. B D Langer, O, Valdez, M ~, Dept of Ob/Gyn, UTHSC, San Antoine, TX
OBJECTIVE. Maternal hyperglycemia has been associated with fetal hypox=a and utero placental insufficiency in pregnant d~abetlcs Fetal umbilical veto flow represents a d=stal measure of total fetal placental blood flow. We sought to investigate the effect that glucose levels have on fetal placental blood flow using this modahty in diabetm pregnanoes
STUDY DESIGN’ 89 singleton patients (26 d~abet~c, 63 normal) underwent umbilical vein velocimetry and standard biometrlc measurements to confirmgestat~onal age and fetal we=ght (Shepard) Vein diameter andpeak velocity corrected for angle of insonat=on were used to estimate flow by. Flow (cc/min) = nr2
(cm2) x Velocity (cm/sec) x 60 Maternal serum ~lucose levels were obtained in the diabetics from serial data collected by memory reflectance meter.
RESULTS A 25% difference existed m mean fetal pJacental flow between groups by Student’s t test, and normal distribution was assured by KolmogorowSm~rnov test
Flow Rate EGA EFW Peak Velocity
(cclmin) (wks) (gins} (cm/sec)
D=abetlc 438 2 29 1,458 33 6
_N_o_L~_~ .... ~_ ~_0_ ~_ ..... ~_9_ _ _~ j_,~2_s_ ..... _~_9 2_ .... p=0 01 ns ns p=0 03
Additionally, there was an ~nverse relationship ~n diabetics between fetal placental flow rates by est{mated fetal weight (EFW) and mean maternal serum glucose level
CONCLUSIONS. Fetal placental blood flow ~s increased ~n d~abetics, and is reversely related to maternal serum glucose levels We speculate that h~gher baseline flow fatal{tares glucose transport ~n d{abetes, further increasing fetal glucose load. Dkew~se, decreased flow as a result of maternal hyperglycemia may be a mechamsm by wh{ch utero-placental insufficiency evolves m the poorly controlled diabet{c.

314 SPO Abstracts Januar~ ]994 Am J Obstet Gynecol
131 THE EFFECT OF THIGH-LENGTH TED HOSE ON THE
HEMODYNAMIC RESPONSE TO PROLONGED STANDING IN
PREGNANCY. C. Hobe!, D. Rosen*, J. Greenspoon, L. Castro, D.
Miano°, S. Nessim*. Dept. OB/GYN mad Div. Biostats, Cedars-SinaiMed.
Ctr. and UCLA Sch. of Med., Los Angeles, CA.
OBJECTIVE:During pregnancy the standing position is associated with
changes in m~ternal cardiovascular p~rm~aeters due to a disturbance in
venous return from the lower extremities. The purpose of this study was
to assess the effect of TED hose on the hemodynm,ai¢ response of pregnant
women moving from the supine to the standing position.
STUDY DESIGN:We assessed the c~rdiovasculas status of 12 normal
pregnant women in the second and third trimesters using non-invasive
thoracic electrical bioimpedance (TEB) measurements of cardiac
output/cardiac index (CI) and systemic vascular resistamce/systemic
vascular resistance index (SVRI) in the supine (30 rain.) and standing (45
rain.) positions with and without support stockings (TED Hose/18 mmHg
at snide). A two factor repeated measures analysis of variance was used
to test for differences in position and stocking use.
RESULTS:Prolonged somding was associated with a s~gnifieant increase
in heart rate (HR) and blood pressure (all p values = <0.001). With the
use of TED hose there was a trend toward blunting the increase in HR that
occurred with standing. TED hose use significantly increased SVRI in the
standing position (p < .005) and was associated with a borderline decrease
in CI (p=0 054).
CONCLUSIONS:This study documents that significant cardiovascular
changes occur when pregnant women stand. Our data suggests that a
greater increase in heart rate is needed to maintain th~ BP in patients
without TED hose. TED hoso increase the total peripheral vascular
resistance, presumably by improving preload and enabling patients to
maintain BP and cardiac output during standing with smaller increases in
HR. Additional patients are being studied (supported by Kendall
Healthcare Products).
133 NORMAL VALUES OF URINARY ALBUMIN AND PROTEIN
EXCRETION DURING PREGNANCY Kenneth Hiqby, Cheryl R
Suiter’ John Y. Phelp¢, Theresa Slier Khodrx, Oded Langer, Dept.
of Ob/Gyn, The Unlv of TX Health Science Center at San Antonio,
TX and Brooke Army Medical Center, Ft Sam Houston, TX
OBJE~I’IVE: To determine the normal 24° excretion values of
urinary albumin and total prote~n In healthy pregnant women.
STUDY OESIGN: 228 healthy pregnant women -<35 years of age
without a history of or subsequent development of pre-eclamps~a,
hypertension, diabetes melhtus, renal disease or pyelonephr~tis
have been evaluated m an ongoing study. All patients gave
informed consent and were given both explicit verbal and written
instructmns regarding the 24~ collection All patients were tested
to ensure absence of a urinary tract ~nfectlon when specimens
were collected Adequacy of the collection was determined by
creatinineexcretion Creatlnlne was assayed bya modificaUon of
the Jaffe reactmn, protein by pyrogallol red, and albumin by RIA
All specimens were run in duplicate with the mean value used
RESULTS: The mean prote~n excretion ~n 24° was 98 8 mg, upper
95% confidence hm~t 261 4 mg The mean albumin excretion in
24°was 10 3 mg, upper 95% confidence hmit 34.4 mg No patient
had ewdence of m~croalbummuria defined as 24° urinary albu~mn
excretion greater than 30 mg/I
CONCLUSION: Th~s data supports 300 rag/24° of urinary protein as
the upper limit of normal dunng pregnancy. Albumin accounts
for a small fracUon of total urinary protein excretion
132 FETAL PLACENTAL BLOOD FLOW IN A POPULATION AT RISK FOR GROWTH ABNORMALITIES AND PLACENTAL INSUFFICIENCY. Elhott, B D, Langer, O Dept Ob/Gyn, Umv of Texas Health Science Center, San Antomo, Texas OBJECTIVE: Although fetal placental blood flow ~s a critical ~ssue m the evaluation of abnormal fetal growth and hypox~a, its d~rect measurement is not posslNe w~th present technology Umbd]cal veto flow by doppler veloc~metry estimates total fetal placental blood flow Our purpose was to explore this modahty m gestahons at risk for placental flow abnormalities and correlate w~th standard physiologic and Nometnc measurements STUDY DESIGN: 120 consecutive pat=ents who were at risk for flow abnormaht~es 0e hypertension, d~abetes, growth abnormaht~es, abnormal placentatlon, twins, drug abuse) were stud~ed as they presented for obstetric sonogram Umb=hcal veto peak velocity and d=ameter, and umbd=cal artery S/D ratio were obtained, =n add~hon to standard b=ometnc measurements (Shepard) Umb~hcal veto flow was calculated by Flow (cc/m~n) =~r2(cm2) x Veloclty(cm/sec) x 60 RESULTS: A s~gn~ficant assoc=at~on existed between Gestahonal Age and Umb~hcal Veto Flow (UBF) (r=0 83, p<0 0001), and between Estimated Fetal Weight and UBF (r=0 78, p<0 0001) When UBF was adjusted for Eshmated Fetal Weight, a s=gmficant ~nverse relationship w~th Gestat~onal age was demonstrated (r=-043, p<00001) L~kew~se, a s~gmficant ~nverse relat=onsh~p existed between Umbilical Artery S/D ratio and UBF (r=-0 52, p<0 0001) CONC.LUSION: Umb~hcal veto flow as a measure of fetal placental blood flow 1) increases with gestat=onal age and fetal weight, 2) decreases as a function of fetal weNht w~th increasing gestat=on, and 3) decreases w~th increased placental resistance These findings are consistent w~th current understanding of fetal and placental physiology, and suggest that tNs modahty may be a useful tool to esbmate fetal placental blood flow m research and chmcal pract=ce
134 ACCURACY LIMITS OF ULTRASONOGRAPHIC ESTIMATION OF HUMAN FETAL URINARY FLOW RATE. H L Hedriana T R Moore D~vis~on of Pennatal Medicine, Department of Reproduchve Medlc=ne, Un~vers=ty of Cahforma San D~ego, San D=ego, CA OBJECTIVE: To define m a controlled setting the accuracy of currently avadable methods of sonographmally eshmat~ng human fetal urinary flow rate (FUFR) STUDY DESIGN: 11 dem=sed fetuses were stud=ed in a water bath Sahne was infused into the bladder incrementally to s=mulate a rate of 1 ml/mm Serial fetal bladder volumes (FBV) were calculated from sonograph~c measurements using the ovoid formula reported by Campbell et al, Wlad~m~roff et al, and Rab=now~tz et al (OV=413*p~*L*W*DI8), and from a sag~ttal area volume (SAV) formula reported prewously by us (SAV=0463+1 394"SA, SGI 1993) FUFR was determined by 1) by subtracting the mean of two FBVs at the start and end of 30’ bladder filhng, or 2) regressing 3, 4, and 6 FBV observations against t~me The means of FUFR eshmates derived w~th each method were compared to the actual rate of 1 ml/m~n using the Student t test RESULTS: The volume subtract=on techmque using OV yielded FUFR=I 68 ml/mm, 95% C1=+_48% Simdar rate overpredict~on occurred us=ng regression w=th OV (1 38-1 45 ml/hr, 95% C1=+58-
66%) FUFRs from SAV (0 99-1 02 ml/hr, 95% C1=+_35-39%) were s=gn~ficantly better than those from OV, (p<0 0001) Regression w~th 3 (95% C1=±39%) or 4 points (95% C1=±37%) was marg=nally less accurate than 6 pmnts (95% Cl=_+35%,p<0 0001) CONCLUSIONS: Previously reported FUFRs based on the ovoM volume formula overest=mate the true rate by 40-70% FUFR calculated by regression of 3 or 4 measurements of the sag.ttal bladder area against t~me prowde a better esbmate of true rate with a superior margin of uncertainty Thts techmque can be used to predict human fetal urinary flow rate with an accuracy of +_ 35%
Volume 170, Number 1, Part 9 SPO Abstracts 315 Am ] Obstet Gynecol
135 137 AMNIOTIC FLUID VOLUME DOES NOT PREDICT ADVERSE FETAL OUTCOME IN DIABETES. Che~ter
B. Martin, Jr. Dept. of Ob-Gyn, University of Wisconsin,
Madison, WI. Objective: To assess the ability of abnormal amniotic fluid volume (AFV) measurements to predict adverse fetal outcome in diabetic pregnancy. Design: In a prospective observational study, AFV measurements were added to the antepartum fetal assessment protocol of 120
consecutive pregnancies of insulin-requiring diabetics (type 1, 43; type 2, 12; gestationa!, 65). Adverse outcomes assessed were operative delivery for fetal distress, low Apgar score (<5 at 1 rain ,<7 at 5 min.) and low umbilical cord blood pH (artery <7.17,
vein <7.26). Statistical comparison was by X2 analysis.
Results: Adverse fetal outcomes occurred in 22 pregnancies (18%). Pregnancies with only normal AFV measurements (4- quadrant AF index >5 <20 cm, largest vertical column >3 <8 cm)
(N=59) accounted for 16 of these (27% adverse outcomes in this group). There were 2 adverse outcomes in 12 pregnancies with 1 or more low AF measurements (17%), 1 in 9 pregnancies with
borderline measurements (AFI >5 <8 cm) (11%) and 1 in 3 pregnanmes with both high and low AF measurements (all NS vs.
normal AF measurements). There were 3 adverse outcomes in 40 pregnancies with high AF measurements (7.5%) (P=0.015 vs. normal AF measurements). The last test before delivery was low in
3 pregnancies, borderline in 6, normal in 103 and high in 8. There was no relationship between the last AF measurement and fetal outconle. Conclusion: Abnormal AF volume measurements do not identify those diabetic pregnancies at increased ask for adverse fetal outcome+
136 PLATELET ACTIVATING FACTOR ACETYL HYDROLASE (PAF-AH} ACTIVITY FOLLOWING CHORIONIC VILLUS SAMPLING (CVS) AND AM~IOCENTESIS. A.A. Saleh, J.M. Johnston,x P.G. Pryde,x N.B. Isada, M.P. Johnson, M.I. Evans, R.J. Sokol. Depts Ob/Gyn, Genetics & Pathology, Grace & Hutzel Hospitals/WSU, Detroit, MI, and Univ Texas Southwestern, Dallas, TX. OBJECTIVE: PAF is essential for embryonic development and is a potential vasodilator. It increases vascular permeability and stimulates prostaglandin E2 (PGE2) production. PAF-AH, the enzyme that degrades PAF, is synthesized by decidual macrophages. The aim of this study was to test the hypothesis that CVS and/or amniocentesis might cause an increase in maternal PAF-AH activity. STUDY DESIGN: Maternal plasma PAF-AH activity was evaluated in women before and after undergoing genetic amniocentesis (n=13) and transcervical CVS (n=29). A control group (n=9) was evaluated to study the effect of venipuncture. RESULTS: CVS caused a significant elevation in PAF-AH activity (the mean different was -2.26, 95% CI was -3.4 to -1.09, t=3.955, p<0.0001). No changes were noted in PAF-AH activity in the amnio or the control groups. CONCLUSIONS: CVS causes subclinical release of PAF-AH, possibly from decidual macrophages. Increased PAF-AH might result in decreased PAF levels. PAF decrement might lead to vasoconstriction in the placental circulation due to the lack of the vasodilator effects of PAF and possibly PGE2.
138 MODIFIED FETAL RESPONSE TO VIBRATORY ACOUSTIC
STIMULATION ASSOCIATED WITH MATERNAL INTRAVENOUS
MAGNESIUM SULFATE THERAPY, David M, Sharer, The University
of Rochester School of Medicine and Dentistry. Rochester, New York.
OBJECTIVE: Maternal intravenous magnesium sulfate (IV MgSO4)
therapy has been essocieted with decreased fetal heart rate (FHR)
variability and reactivity, resulting in an increased incidence of
nonreactive nonstress tests, frequently requiring further assessment
of fetal well-being. This study was designed to assess fetal response to vibratory acoustic stimulation (VAS) in association with maternal IV
MgSO4 therapy.
STUDY DESIGN: Five gravities with singleton gestations with normal
fetal anatomy, intact membranes, and normal amniotic fluid volume >
31 weeks, presenting with preterm labor were included. VAS was
performed prior and during IV MgSO4 such that each fetus served as
its own ~ontro|. Ultrasound was appli’ed during VAS to assess fetal
movement response. Response to VAS was considered normal if a
FHR acceleration of at least 15 bpm for at least 15 cecends occurred
within 15 seconds of VAS with prolonged fetal movements, Maternal
serum magnesium levels were obtained prior to each stimulation.
R~SULTS: All fetal responses prior to treatment were normal. All fetal
responses in association with IV MgSOa were abnormal, consisting of
blunted FHR accelerations ranging between 10-15 bpm in amplitude
for 10-15 seconds with brief fetal movements. Mean maternal serum
magnesium levels ( _+ SE) during VAS, prior to and following IV MgSO4
were 1.4_+0.1 mEq/L and 5.2_+0.4 mEqlL, respectively (p=0.008).
All five minute Apger scores were > 8. This occurrence may represent
an effect of magnesium on the fetus as either a central nervous
system depressant or a peripheral neuromuscular relaxant.
CONCLUSION: These results indicate caution should be exercised in
interpreting fetal response to VAS in the presence of therapeutic
metern~[ megnesium levels.

316 SPO Abstracts January 1994 An] J Obstet Gynecol
139 BIOPHYSICAL PROFILE TESTING IN HIGH ORDER MULTIPLE
GESTATIONS, ,L Elhott, H. FmbergL Phoemx Perinatal
Associates and Good Samaritan Regional Medical Center,
Phoenix, AZ.
OBJECTIVE: To determine the value of b~ophysical profde (BPP)
testing m preventing mtrapartum death in patients wrth h=gh
order multiple gestations (tnplets or quadruplets).
STUDY DESIGN: A retrospective rewew was performed of
pat=ents wrth triplets and quadruplets dehvered between 1988
to 1991. The ultrasound parameters of the BPP score were
used without the non-stress test (NST) component due to
technical difficulty w~th that test. A score of 6-8/8 was
therefore considered reassunng, 4/8 equivocal, and 0 or 2/8
possibly abnormal. Tests were twine per week.
RESULTS: Eighteen patients with triplets and six patients with
quads compnse the study group. The last BPP before dehvery
was evaluated. There were 0 antepartum deaths in these 78
babms. The last BPP score was 2/8 in 9 babies in 5 triplet
pregnancms and 2 bab=es in 1 quadruplet pregnancy. Six
pregnancies (25%) were dehvered based on BPP results and the
qlin~cal s~tuation. There was no morbidity or mortality in the 16
babms dehvered because of abnormal BPP testing.
CONCLUSIONS: Th=s senes produced no stdlbirths, Twenty-
five percent of these pregnancms eventually dehvered for
nonreassurmg BPP testing w~th good outcome. The BPP
appears to be a reliable antepartum test of fetal well being in
tnplets and quadruplets.
141 CHANGING OBSTETRIC OUTCOMES IN LETHAL CHROMOSOMAL ANEUPLOIDY. T. Westover~, E. Guzman, D. Day-Salvatore~ Dept. of
MFM. UMDNJ-RWJ Mad School, New Brunswick, New Jersey. OBJECTIVE: in the early 1980’s, a number of US and British
investigators reported caesarean section rates for s~ngleton tnsomy 18
infants of approximately55%. Greater than 85% of these cesareans were
performed secondary to fetal indications. We hypothesized that modern
prenatal diagnostic techmques such as high resolution ultrasound and
maternal b~ochem=cal screening would detect the vast majority of lethal
chromosomal aneuploldy and result in significant increases m the
frequency of conservaUve obstetric management as compared to the
above h~storical controls.
STU DY DESIGN: We retrospectively reviewed our cytogenetics log book
for the years 1988-m~d 1993 and correlated any lethal s~ngleton
aneuplo]dles (tnsomy 13, 18 and tnploidy) wdh a computerized medical
records search to examine the pennatal course and outcome of these
infants. The ceserean rate of our modern cohort was compared with the
previously published data using two tailed F~sher’s exact test.
RESULTS: Al133 mfants d~agnosed Jn the firat or second trimesterwere
previable (<24 weeks), were detected at amn~ocentes~s/CVS performed
for advanced maternal age, abnormal ultrasound, or abnormal AFP, and
underwent termination of pregnancy. All 8 ~nfants d~agnosed ~n the third
tnmester (4) or postnataliy (4) could have been diagnosed ~n the second
tnmester since all had at least one meier malformation easily detected on
level II ultrasound or had abnormal APP. All four =nfants dmgnosed post
natatly should have been diagnosed ~n the antepartum period s~nce
obstetric condihons mandating ultrasound evaluation developed in all
four; polyhydrammos, preeclamps=a, IUGR, or breech presentation. The
overall cesarean sectton rate was 5% (2/41). Th~a C/S rate was slgmficantly less than the historical controls (P<.01).
CONCLUSION: This data suggests that modern prenatal dmgnos~s will
detect the vast majority of lethal aneuplo~dy in the antepartum penod and
allow for conservatwe obstetncal management.
140 FETAL SMALL VESSEL DOPPLER AS A PREDICTOR OF
OUTCOME IN POST-DATES PREGNANCIES. S Nava*. J,A
Molinari. S. Weiner, A. Ludomirsky. Dept Ob!Gyn, PA Hosp, Phila, PA
OBJECTIVE: To assess whether fetal small vessel Doppler (FSVD)
analys~s is useful in predicting post-date (PD) pregnancy outcome.
STUDY DESIGN: Patients having routine PD testing after 41 weeks
were evaluated by Doppler analysis by one examiner. The pulsafihty
index (PI) of the fetal middle cerebral (MCA), common carotid (CCA),
descending aorta, renal, umbilical (UMBA) and matamal uterine (UTA)
arteries were obtained. Delivery mode, fetal distress + admission to
intensive care nursery (ICN), meconium stained amnlotic fluid (MSAF),
cord gases, Apgar scores, sex and birth weight (BW) were analysed
Pearson correlation coefficients, Spearman rank correlations and T-test
were used for statistical comparison.
RESULTS: 53 patients were evaluated at a mean of 3.3 days prior to
delivery (range 0-9) The rates of spontaneous vaginal, operative vaginal
and Cesarean (CS) deliveries were 54.7%, 13.2%, 32.1% respectively.
Four of the neonates were admitted to the ICN, 11 had fetal distress, 28
had MSAF and 19 of the newborns were female. The following
stattshcally significant eorrelattoas between PIs and outcome variables
were found: the mean CCA PI was lower m CS deliveries(1,59, SD=0,57)
than non CS deliveries (1 99, SD=0.57, p=O 04); the mean UMBA PI m
ICN fetuses was higher (0.97. SD=0 30) compared to the remaining
babies (0 75. SD=0.19; p--0 04), the mean UTA PI (SD) among fetuses
wdh MSAF was 062 (0 19) as compared to 0.44 (0 15) m deliveries
without meconium (p-0.01). There is negative correlation between
UMBA PI and the base excess (BE) values (p---O 009), and between the
CCA PI and pCO2 value in arterial cord blood (17<005). Female fetuses
had a mean MCA PI which was 15% larger then male (p--0 05) There
exists a negative correlation between UMBA PI and BW (p<O 05)
CONCLUSIONS: These positive correlations suggest that there may
be a place for FSVD in the management of PD pregnancies
142 INTRAUTERINE GROWTH RETARDATION: CONTRACTION STRESS TEST OR BIOPHYSICAL PROFILE? .JM Lien, MP Nageotte, CV Towers,
M deVeclana, JS Toohey. University of Cahfomm at Irvme, Long Beach Memorial Medical Center, Long Beach, CA
OBJECTIVE. To compare the contraction stress test (CST) and the
biophysical profile (BPP) as a back-up test for pattents with a chnlca( diagnosis of intrautenne growth retardation (lUGR) who have an equivocal
nonstress test/amnlotic fluid index (NST/AFI) STUDY DESIGN: Data collected In a prospective random=zed study was
retrospectively analyzed. The testing protocol cons=steal of twice weekly NST/AFIs. Patients with equivocal tests randomized to a CST or BPP back-
up group and remamed in that group for the rest of the pregnancy. Inclusion cntena for analys~s: (1) IUGR as the only indication for testing,
(2) singleton gestation, (3) _> 32 weeks at first test, and (4) equwocal NST/AFI randomized to CST or BPP. The CST and BPP groups were
compared for interventtons for an abnormal CST/BPP, cesarean sections,
and adverse neonatal outcomes (birth we=ght < 10%de, 5 minute Apgar
< 7, neonatal Intensive care unit admission, stdlblrth or neonatal demise). Senmtw~ty and spec=fic=ty of the CST and BPP for adverse neonatal
outcomes were calculated by evaluating interventions for abnormal tests. RESULTS:
CST (n =56) BPP
EGA at delivery (weeks) 139 I ± 1.7 39.1 +- 1.8 NS
B=rth weight (grams) 2792 :!: 638.4 2797 ± 552.6 NS
"Intervention for abnormal test,17/56 (30.4%) 4/58 (6.9%) 1=.003
Cesarean sections 116/56 (29%) 11/58 (19%) NS
Birth weight < 10%de , 8/56 (14.3%) 12/58 (20.7%) NS
Adverse neonatal outcome i 8/56 (t4.3%}
13/58 (22.4%1! NS
Sensttlwty, specfftctty 88%, 79% 17%, 96%
CONCLUSION: Although CSTs result In h~gher mtervent=on rates, they are
much more sensitive for adverse neonatal outcomes than BPPs when used
as back-up tests in paUents w~th a chn~cal dmgnosis of IUGR.
Volume 170, Number 1, Part 2 sPa Abstracts 317 Am J Obstet Gynecol
143 /~TEI~TAL FETAL ~U~ILLAW~ IN I~EGWAWCIES CONPLICATED BY FETAL VENTRAL MALL DEFECTS.Cart HHx, Asrat T, Towers CV, Nageotte MP, Free~n RK. University of California, Irvine Medical Center, Orange, CA and Long Beach Memorial Medical Center, Long Beach, CA. OBJECTIVE: To evaluate the need for antenatal fetal surveillance in pregnancies with known fetal ventral wall defects (VWD), since this issue has not been adequately addressed in the literature to date. STUOY DESI~I~: A case control stu(~/was eorw~ucted Of all inborn karyoWpica[ ty harmer fetuses with VWO’s between 1/81 and T/93. Antenatal and postnatal data from VWO cases were compared to postdates (PD) pregnancies. RESULTS: 56 cases of Vw1)’s (42 with gastroschisis and 14 with omphalocele) and B24 PO pregnancies were reviewed and compared. The mean age, gravidity and parity were similar in both groups. The incidence of antenatal a~ormal fetal surveillance tests was significantly higher in the VWE) group compared to the PD group (58.9% vs ]4.5%, 0R=2.7, p=O.O001). 41.1% of ~ cases versus 10.7% of PD cases required pregnancy intervention for abnormal fetal surveillance tests (0R=5.8, p=0.0001). ~8% of VWD cases versus 5.7% of PD cases had cesarean sections performed for fetal distress (0R=6.6, p=O.O001). The earliest delivery for fetal distress occurred at 27 weeks. IUGR occurred in 30.4% of ~ cases and 1.6% of postdates cases (0R=27.2, p=O.O001). One stillbirth occurred in esch group (at 31 weeks vs 42 weeks) (p=NS). Low Apgar scores at five minutes were reported mere frequently in the VWD group (7.1%) than in the PD group (0.~) (OR=9.0, p=O.O001). There were four neonatal deaths in the ~ group and none in the PD group (p=O.O001). COWCLUSIO#S: (1) Pregnancies con~)ticated by ventral wall defects are at significantly increased risk for antenatal compromise. (2) Fetuses with ventral wall defects also have a marked increase in the incidence of IUGR. (3) Since the earliest intervention for fetal distress occurred at 27 weeks and a stillbirth occurred at 31 weeks, we recommend initiating antenatal fetal surveillance at fetal viability.
145 IS UNEXPLAINED LOW MATERNAL SERUM ALPHAFETO PROTEIN INDICATOR OF GESTATIONAL DIABETES OR MACROSOMIA? ~_ Homsi, S. Didolkar. The Union Memorial Hosp. Baltimore MD. OBJECTIVE: To establish significance of unexplained low Maternal Serum Alpha- Fetoproteln (MS-AFP) and compare outcome between hlgh and low MS-AFP with or without pre-existing risk factors. STUDY DESIGN: All patients referred to Prena- tal Genetics Lab between Jan 1990 and Dec 1992 for abnormal MS-AFP were reviewed. 78 patients with abnormal MS-AFP and normal chromosomes were compared to 58 patients with normal MS-AFP, who were selected randomly from same population and time period and dlv~ded into 3 groups: I-Unexplained low MS- AFP (<0.4 MOM) II-Unexplained high MS-AFP (>2.0 MOM) III-Normal MS-AFP. Patlents’ char- ts were reviewed retrospectively for pre-
nancy outcome. Chi-Square analysis was used. RESULTS: There was no difference in the three groups regarding age, parity and race, al- though women in Group II delivered at an early GA-36.3 wks vs 38.3 wks (III) and 39.1 wks (I) (P<0.005) Group I showed statlstlcal- ly significant dlfference In H/O macrosomia, G.diabetes, miscarriages. During the current pregnancy, Group I had higher incldenqe of LGA/macrosomia 23.4% vs 3.22% (Group II) and 8.6~% in Group III (P<0.05). As expected, Group II was significant for IUGR, PIH, PTL, PROM. CONCLUSIONS: Unexplained low MS-AFP was asso- ciated wifh increased incidence of macrosomla, G.dlabetes and fetal distress, while high MS-AFP was associated wlth h~gher incidence of PROM, PTL, PIH, IUGR.
144 THE IMPACT OF TRANSDUCER ORIENTATION UPON THE A!MNIOTIC FLUID INDEX~ Thomas H. StronR, Jr., M.D., Glen S. Lovelace, M.D.x Phoenix Perinatal Associates - Good Samaritan Regional Medical Center, Phoenix, Arizona. OBJECTIVE: To determine the impact of the orientation of the ultrasound transducer upon the amniotic fluid index (AFI). STUDY DESIGN: Fifty consecutive gravidas received the standard AFI assessment with the ultrasound transducer held in a longitudinal plane as stipulated by the creators-of the technique. A "modified" AFI was also obtained with the transducer held transversely. For both techniques, each amniotic fluid pocket was selected by a single observer blinded to the actual measured depth of the pocket. The fluid pocket selected was measured by another observer blinded to the transducer’s orientation. Linear regression analysis was used to compare the two AFI techniques. RESULTS: A correlation coefficient (R) of 0.98 was noted. The regression equation was: modified AFI = 0.52 + 0.98 x standard AFI. The mean difference between the techniques was 0.92 +__ 0.77 era. Thirty-three (66%) had a difference between the two techniques of< 1 cm and 45 (90%) had a difference < 2 em. CONCLUSION: The two-dimensional orientation of the ultrasound transducer does not appear to impact upon AFI assessment.
146 VARIABLE DECELERATIONS DURING NONSTRESS TESTS-
CLINICAL ASSOCIATIONS. T.Tharakan, V DtBeIhP, L.V.Baxi.
Columbia University, College of Physicians and Surgeons, Columbia
Presbyterian Medical Center, New York, NY.
OBJECTIVE: To determine the clinical assoctations of variable
decelerations during nonstress tests (NSTs) with amniotic fluid volume,
m’trapaP, um complications and pen~atal outcome.
STUDY DESIGN: Patients with singleton pregnancies and intact
membranes undergoing NSTs from January 1993 onwards were enrolled
in this ongoing study NSTs were prospectively evaluated for reactivity
and the presence of decelerations, and results of Ammobe Fluid Volume
(AFV) and B~ophysical score (BPP) were recorded Intrapartum data and
perinatal outcomes were recorded. Patients/tests were divided into 3
groups -1) one or more tests showing variable decelerations (83/253), 2)
variable deceleratmns and in addition, at least one susp*eious or mm*mally
reactave test (31/202), 3) controls-all NSTs reactive (109/239).
RESULTS: To date, 223 patients undergoing 694 NSTs were evaluated.
The mean (+ SD) gestational age at last NST and at delivery were 38 44
(_t2.95) and 39.7 (+2 03) weeks, respectively Neither Group 1 or 2
showed a significant increase in the incidence of abnormal AFV or BPP,
small for gestatlona[ age infants, or low 1 or 5 min Apgar scores Patients
in Group 2 had s,gmficantly more cord eompheations (p < .005), operative
dehvencs (p= 012), emergency operaUve delivery for fetal compromise
(p<.00l) When 513 tests performed within 7 days of dehvery were
analyzed separately, simdar results were obtained In add~tmn, in this
subgroup Group 2 had increased incidence of low 1 minute Apgar scores
(p < .05)
CONCLUSIONS: Variable decelerations are associated with increased
intrapartum comphcations and adverse perlnatal outeome only when
accompamcd by minimally reachve or suspicious tracings.

318 SPO Abstracts January 1994 Am .] Obstet Gynecol
147 WHY ARE WE STILL USING THE FETAL BIOPHYSICAL
PROFILE? G. S0adex, M Belfoffx, L. Knudsenx, R. Vidalx, K. Mmse.
Dept. Ob/Gyn, Baylor College of Medicine, Houston, TX.
OBJECTIVE: To determine whether the fetal biophysical profile (BPP)
may be replaced by a simpler and less time consuming antepartum test.
STUDY DESIGN: For the last 3 years, the BPP has been used as the
primary test of fetal well-being at our center All the examinations were
performed by one of two ultrasound technicians. The patient population
consisted of women referred from outlying clinics to the tertiary care center
because of a high risk pregnancy. The examination and scoring criteria
followed the method of Manning except for the ammotic fluid component.
Instead of measuring a single pocket, the amnintic fluid index (AFI) was
determined and a score of zero given in cases where the AFI was below the
5~ percentile for gestation. The 95% limits published by Moore (1990) were
used for reference. The results of the examinations and the patients’ data
were entered into a computerized database and were reviewed
retrospectively All those with scores of 6 6r less art a scale of 8 were
identified.
RESULTS: 4022 BPP examinations were performed in 590 patients. 250
examinations had a score of 6 or less. Of these, only 19 examinations had a
score of 2 for the amniotic fluid component of the BPP. The sensitivity and
specificity of a decreased AFI in predicting a BPP of 6 or less is 92.4 and
100 %, respectively. Only 6 examinations had a score of 4 or less, all of
whom had a normal AFI. Four of these patients however had matema!
perception of decreased fetal movements (FM) Using a normal AFI
together with maternal perception of adequate fetal movements as a test of
fetal well-being would have resulted in the failure to identify 2 fetuses with
a BPP score of 4 or less. In the worst case scenario, this would have
increased the perinatal mortality rate by 3/1,000 births.
CONCLUSION: Measurement of the amniotic fluid volume appears to be a
valuable screening test. Together with the maternal evaluation of fetal
movements it represents a simpler and more cost-effective alternative to the
biophysical profile for antepartum fetal monitoring.
149 LONGITUDINAL AMNIOTIC FLUID INDEX IN TERM PREGNANCIES COMPUCATED BY OUGOHYDRAMNiOS D. W~r~x, A. Rshman and R. Paul. LAC+USC Medical Center, Los /~eles, CA. NULL HYPOTHESIS: There is no d~ereece in the penultimate amniotic flu~l index (AR) in pret~ancies destined to develop o~igchydran~ios (defined as an AR of < 5.0 cm) compared to the AR values for normal pregnan- cies as defined by Moore and Cayle (~n J Obstet Gyneco1162:1168). METHODS AND MATERIALS: During the study period of one year (January 1992 through December 1992), 11827 a~tepartum surcei~- lance tests were performed on 3378 patients. Of these patients, 576 were found to have AR’s < 5.0 cm. Of these 576 patients, 265 delivered after 36 ~geks had serial biweekly non-st~ess tests and amni- otic fluid index measurements. The amniotic fluid index was measured in the manner described by Pbelan et al (J Repred Med 32:540). The penultimate AR measurements were stratified based on estimated geatat~nel age and c(xnpared to the values defined by M~ore and Cayle. RESULTS:
EGA (wks) n USC Mean USC AFI Mean AR by
Pe~ultJrnate N:l Range(cm) Moore & Cay~e
36 17 9.3cm 5.2 - 15.7 13.8cm
37 23 8.9cm 5.5 - 11.0 13.5cm
38 22 7.7cm 5.7 - 10.7 13.2cm
39 34 9.1cm 5.2 - 13.7 12.7cm
40 30 9.0cm 5.1 - 20.3 12.3cm
41 69 8.5cm 4.7 - 15.3 11.6cm
42 50 9.0cm 4.2 - 16.8 11.0cm
At each EGA tested, the mean penultimate AR (cm) differed s~,nificantiy (p < 0.05) from the mean AR value for a normal gestation as detioeated by Moore and Cayle. The mean penultimate AR also differed sign~icantJy from similar values for matched controls. CONCLUSIONS: Them ~s a s=gnificant d=fference between the penultimate AR for pregnanmes comphcated by oligohydramn=os and the normal AR value as determined by Moore and Cay/e.
148 DISTANCE FROM THE VERTEX AS A FACTOR AFFECTING
INTRAUTERINE SOUND PRESSURE LEVELS PRODUCED
BY VAST. J. Scard~). D. El/er, A. Klei~ A. DillieS,, S. Stramd~.
Dept. OB/GYN, Medical University of SC, Charleston, SC
OBJECTIVE: The overall sound pressure level (SPL) produced by
VAST has been measured as high as 135 dB (GerhardL 1990). The
purpose of this study was to determine intrauterine sound pressure levels
produced by the VAST at specific distances from an intrantcrine
hydrophone in haman parturients.
STUDY DESIGN: Measurements of intrauterine sound were taken in 9 volunteer parturients in normal active phase labor. After informed
consent and rupture of the membranes with clear fluid, an intrauterine
hydrophone (Sparton) was placed transcervically near the fetal neck.
Ultrasound was used to confirm the location of the fetal hydrophone and to determine amniotic fluid volume. VAST was performed on the
maternal abdomen directly over the fetal hydrophone and at 5, 10, 15, 20, and 25 cm. increments from the hydrophone, as well as at the
maternal sternum. The hydrophone amplifier output was stored on a
calibrated audio tape recorder for later off-line analysis.
RESULTS:
CONCLUSION: SPLs produced by VAST at sites up to 25 cm. from the fetal vertex may minimize fetal sound and vibratory exposure and still allow for an effective test.
150 INCREASE IN AMBIENT TEMPERATURE CAN EXPLAIN DECREASE
IN AMNIOTIC FLUID INDEX (AFI). A. Sciscione,= K. Coatigan," T.
Johnson, Dept. Gyn/Ob, The Johns Hopkins Univo $cho of Mad.,
Baltimcro, MD. OBJECTIVE: In the third trimester, the AFI may be affected by
mstern~J fluid status. A~ the ambient temperature increases, there
is an increase in insonaibis fluid loss end the potential for
dehydration. We hypothesize that as temperature increases there
would be a concomitant decrease in AFI. STUDY DESIGN: From June ! ! to August f6, 19G3, 42 women
with singleton pregnancies between 27 and 40 weeks gestation
undergoing serial antenatal testing had AFI determinations recorded
st least weekly. The daily high ambient temperature in our urban
ares was subsequently obtained. A 2,3, and 4--day mean
temperature prior to the test date was compared to AFI using a
Spearman-Rank Correlation.
RESULTS: The daily high temperature ranged from 71 .F to 104.F
and AFI values ranged from 1.7 to 24.7 cm during the study period.
There Was a significant correlation between the 2,3 and 4-day mean
temperature and AFI, with the four-day mean being the most
significant (r =-0.307, p < 0.0001). This effect was most pronounced
in patients with Systemic Lupus Erythematnsus.
CONCLUSIONS: Fluctuations in ambient temperature ere inversely
correlated to changes in AFI. This relationship should he taken into
account when interpreting the AFI ss ¯ measure of fetal well-being.
Volume 170, Number 1, Part 2 SPO Abstracts 319 Am J Obstet Gynecol
151 THE SIGNIFICANCE OF UNSOLICITED PATIENT COMPLAINTS OF DECREASED FETAL MOVEMENT
J Weeks, MD, J Perlow, MD, T Asrat and C Towers, MD Dept OB/GYN University of Loulswlle, Long Beach Memonal & U C Irvme Medical
Centers Objective: To determine the hkehhood of fetal death, or need for ~mmedlate delivery following a solely patient m~t~ated visit (~ e w~thout physician prompting or sol~c~tatmn) for decreased fetal movement Study design: A cohort study of patients (n=258) who presented from
their homes, d~rectiy to ~abor & delwery w~th complaints o~ decreased fetal movement (DFM) from 5/1/89 to 3/30/93 All study patients presented beyond 20 wks gestation Patients seen for DFM in the antepartum testing canter from 1/1/81 to 12130/90 served as Nstoncal
controls (n=970) The majonty of controls presented after being questioned about fetal actiwty in their physicians office. Patients were labeled as "Ngh nsk" ~n the presence of medical comphcat~ons or red,cations for antepartum testing other than DFM Results: While there were no fetal deaths among patients seen for DFM m the antepartum testing center, 10 fetal deaths were diagnosed In the study group for an overall fetal death rate of 39 per 1000 Patients who Independently presented for DFM were s~gnificantly more hkely to have a fetal death regardless of nsk status (table 1) Immediate Cesarean delivery occurred w~th equal frequency In the study and control groups.
LOW RISK HIGH RISK I table t study consols p study controls p X2 (n=224) (n=679) (n=34) (n=29t) ,UFD
i3 1 o/o)
0 <001 ~8 8O/o) 0
<01
urgent 11 0 77 -- C/S (1 8%) (1 6%)
Conclusion: Patients who independently report to labor & delivery for DFM are s~gnlficantly more hkely to have a dead fetus than those who are referred to an antepartum testing canter Nearly 2% of all patients w~th DFM w~ll have ewdence of evolwng fetal compromise
153 FACTORS INFLUENCING MATERNAL PERCEPTION OF FETAL MOVEMENT IN THE COUNT-TO-TEN SYSTEM. HI- Hedriana., TR Moore D=ws~on of Perinatal Medicine, Unwers~ty of Califorma San Diego, San Diego, CA. OBJECTIVE. To determine which factors assessed in the rood=fled blophys=cal profile (mBPP=NST+AFI) are associated with decreased or absent fetal movement. STUDY DESIGN: 192 patients undergmng antenatal fetal testing with the mBPP also performed daffy fetal movement assessment by recording the bme to appreciate ten fetal movements (fetal movement times - FMT) The mean FMT was correlated with mBPP test results and certmn other factors including placental posRmn and IUGR/macrosomia A subgroup of 12 patients with absent fetal movements was analyzed separately RESULTS: The mean + SD FMT of patrants w~th IUGR (14+? min) or macrosom=a (16+? rain) was longer than In normals (11.+-2 rain, p=0,004) Although the FMTs associated w~th anterior placentabon (31+? vs 8_+.2 rain), NR NST (13+~ vs 11+? rain) and AFl<Scm (13+? vs 8+? rain) were prolonged compared to patients w~th a normal result, none were individually statistically sigmficant. However, the multiple regression correlation between FMT and these 3 factors was highly significant (p=.027). Among patients w~th absent fetal movement, NR NST was three times more hkely (19% vs 6%, p=0 001), and were 1 5 braes more hkely to have anterior placentat=on than normal FMT (57% vs 37%, p=0 02). CONCLUSIONS: Abnormal fetal biophysical testing is associated w~th prolonged FMT Although the combination of low AFI and anterior placentation adversely affects maternal perception of fetal actwity, the associated increase ~n NR NSTs reqmres comprehensive invesbgat~on when FMT ~s prolonged or movements are absent
152 OLIGOHYDRAMNIOS IN THE TERM GESTATION: AT WHAT LEVEL SHOULD INTERVENTION OCCUR? MC Treadwell, LJ Stacksx, SF Bottoms. Wayne State University/Hutzel Hospital, Detroit, MI OBJECTIVE: Gestational age specific nomograms have been established to define abnormal fluid volumes utilizing amniotic fluid index (AFI). The purpose of this study is to clarify the lower limit of AFI associated with increased morbidity in the term gestation. STUDY DESIGN: We evaluated 2662 anatomically normal singleton pregnancies undergoing ultrasound determination of amniotic fluid volume and delivering beyond 37 weeks gestation. Stepwise logistic regression analysis was performed to examine the relationship between AFI and morbidity, including NICU admission, primary cesarean section, and stillbirth rates. RESULTS: The only neonatal or maternal outcome measure significantly correlated with AFI was NICU admission. When analyzed at 5ram increments, there was an increased incidence of NICU admissions with AFI < 45mm. No increase in morbidity was apparent at higher fluid volumes. CONCLUSIONS: Our findings support using an AFI < 50ram as criteria for obstetrical intervention. Arbitrary use of the fifth centile for gestational age or AFI cutoffs of _<60 to 80mm to identify patients requiring immediate delivery in the absence of other factors may result in an unnecessary number of inductions.
154 MAGNETIC RESONANCE SPECTROSCOPY DETECTABLE CHANGES IN AMNIOTIC FLUID ASSOCIATED WITH
OPEN NEURAL TUBE DEFECTS. ¢.J. Sims, D.T. FujitoX,
D.R. BurholtX, D.A. WilkinsonX. Dept. Ob/Gyn, Medical
College of Pennsylvania/Allegheny Campus, Pittsburgh, PA. OBJECTIVE: This study was designed to evaluate magnetic
resonance spectroscopy (MRS) as a means of detecting
biochemical differences between normal amniotic fluid (AF)
and AF from pregnancies with open neural tube defects (NTD). STUDY DESIGN: Proton spectra were obtained at 300 MHz
on 40 normal and 10 NTD second trimester AF samples. MRS peaks were integrated and compared with the size of a
reference peak to obtain concentration estimates. Differences between the two study groups were analysed
using t-tests and the method of principal components.
RESULTS: Nine low molecular weight metabolites (acetate,
alanine, citrate, creatinine, glucose, histidine, lactate, tyrosine, and valine) were detected and quantitated using
MRS. Of these, acetate, creatinine, glucose, and histidine
were found to have mean values that were statistically different (p<.05) between normal control and NTD AF.
Acetate levels were higher while creatinine, glucose, and
histidine levels were lower in NTD samples. Differences
between normal and NTD AF were visualized using star plots
based on 2 principal components. CONCLUSIONS: Proton MRS is capable of detecting
differences in concentrations of biochemical constituents
between normal and NTD AF. This suggests that MRS could be
useful in vivo for prenatal diagnosis.
320 SPO Abstracts Jarma,’y 1994 Ant J Obstet Gynecol
155 DETERMINATION OF FETAL WRT.T.REING IN TWIN GESTATION BY DOPPLER VELO~LMETRY, NONSTRESS TE~TING, A~ 5ONOGRAPHIC GROWTh. ES Kimt MD ,x CS Croom MD, LD Devoe, MD. Dept OBGYN, Medical College of Georgia, Augusta GA. OBJECTIVE: To compare Doppler velocimetry of umbilical arteries(S:D ratio), simultaneous nonstress tests (NSTs) and ultrasonographic growth curves (UGCs) to assess individual fetal status in 3rd trimester twin gestation. STUDY DESIGN: 90 twin pairs (28-40 weeks gestation) received weekly S:D ratios (continuous wave Doppler), NSTs and AFVs. OGCs were updated every 3-4 weeks. Twins were discordant if estimated weights (EFWs) differed > 20%, and growth-retarded (IUGR) if EFWs fell below the 5th%ile for singletons. Only test data that could be consistently assigned to the sa~e twin in each pair were analyzed. Poor outcomes included perinatal mortality, fetal distress, neonatal mixed or metabolic acidosis and IUGR. Comparisons used chi-squared or t-tests. RESULTS:Test correlations with all poor outcomes are shown below as percantages;anc~alous twins are excluded.
Sensitivit7 Specificit7 +PredValue -PredValue NST 32 94 59 84 AFV 16 97 56 81 Doppler 32 95 63 84 UGC 29 94 54 84 All tests 52 85 46 87 Doppler 8:D ratios and UCGs yielded equivalent and superior prediction of IUGR and discordancy; NSTs gave better prediction of acute fetal distress and acidosis. CONCLUSIONS: Surveillance of third trimester twin gestation is best served by a ccrabined testing approach. Doppler and UCG are useful in screening for growth disturbance which, in turn, is associated with the vsst ~ajority of perinatal morbidity not attributable to anomalies or prematurity.
157 ABSENCE OF RELAXATION TO LACTATE IN HUMAN PLACENTAL VESSELS OF PREECLAMPTICS. R. Figueroa, E. Martinezx, R.P. Fayngershx, L.A. Bracero, N. Tejani, M.S. Wolinx. Depts. Physiol. & Ob/Gyn, New York Medical College, Valhalla, NY. OBJECTIVE: To determine if the observed relaxation to lactate and other agents in placental vessels of normal (N) pregnancies is altered in preeclampsia (P). STUDY DESIGN: Isolated placental vessels (1-2 mm diameter) from N and P pregnancies, incubated under 5% 02 and precontracted with 1-3 txM. PGF,,. zc~ were expose2t to lactate (1-10 mM), arachIdonIc acid (10 nM-10 /zM), nitroglycerin (1 nM-1 /zM) or forskolin (10 nM-10 ~M). T-test statistics were used. RESULTS: Relaxation to lactate was inhibited (p<0.05) in both arteries (A, n=6) and veins (V, n=7) in P vs. N (e.g. @ 5 mM lactate: N-A =54__+2%, N-V = 68__+1.4%, P-A = 3.4__+1.5%, P-V = -9.9+1.7%), whereas, responses to the other relaxing agents were not altered in the P vessels. CONCLUSION: In preeclampsia, absence of lactate- induced dilation of placental vessels may contribute to the fetal complications associated with vasospasm.
156 THE IDENTIFICATION OF A PLURIPOTENT SUBSET OF
CD34+ CELLS IN HUMAN UMBILICAL CORD BLOOD.
L. Cetrulo, M. D’Alton, D. W. Bianchi,~C. L Cetrulo, J~M. A.
DeMaria,nT. J. Vadnais,~Dept Ob/Gyn, Div. Maternal/Fetal
Medicine, Tufts University, New England Medical Center Boston,
MA.
OBJECTIVE: To identify, in cord blood, a pluripotent subset
population of CD34+ cells (CD34+, CD38-, HLADR-) that has
been shown to be capable of re-constitution of both the
haematopoietie mieroenvironment (stromal cells) and haematopoietle
stem calla.
STUDY DESIGN: Haematopoietie stem cells have been previously
identified and enriched using the CD34 + bone marrow progenitor
cell marker. This study was designed to identify CD34+ non-
lineage committed cells- particularly CD34+, CD38-, HLADR-
eelis- which have been shown to be capable of both self-renewal and
differentiation along a variety of haematopoietie lineages (Huang,
Terstappeu, Nature, Vo/. 360, 24/31, Dee. ’92). Cord blood
samples (n = 10) were eolleeted from deliveries at varying gestational
ages (range = 26~0 wks) and analyzed by flow eytometry, alIer
~mmunofluoreseent labelling with monoelonal antibodies.
RESULTS: The CD34+, CD38-, HLADR- population was
identified in every cord blood sample, with percentages ranging
from 0 01% - 0.05%.
CONCLUSION: We have identified, in cord blood, a circulating
CD34+, CD38-, HLADR- subset population that has previously
been shown m fetal bone marrow to possess full haematopoietie
reeonstitutive abdity These results suggest the possibdity of
cryopreservation of small volumes of cord blood for later use as an
alternahve or adjunct to autogenic and/or allogenic bone marrow
transplantation.
158 UMBILICAL CORD BLOOD GASES: THE EFFECT OF SMOKING ON DELAYED SAMPLING FROM THE PLACENTA. Meyer BA,
Thorp JA, Cohen GR, Yeast JD. Univ of MO @ KC - St. Luke’s Hospital;
Kansas City, MO, 64111.
OBJECTIVE: to evaluate the effect of maternal smoking on changes in
acid-base status with delayed sampling of blood from placental vessels.
STUDY DESIGN: Placentas from 40 term, uncomplicated vaginal dehveries
with clear amniofic fluid were examined. 22 non-smoking and 18 maternal
smokers were evaluated Arterial and venous cord blood gases and
hemoglobins were drawn at the lime of delivery, and from their respective
placental plate vessels at 30 and 60 minutes following delivery. Statistical
analysis was performed with two-way analysis of variance
Data are mean -+ SD
RESULTS: There were no d~fferences in hemogiobm concentrations at any
time during the study. * p < 0.05 vs Non-smoking.
pH pO2 pCO2 HCO3- Base Deficit
DELIVERY: l
Non-Smoking 7,28±~05 18,4±72 49.8±6.1 24.0±1.4 3.1 ±19
Smoking 7.30± 05 19.0±63 48.1 ±7.2 240±1.2I 28±2.4
30 MINUTES:
Non-Smoking 720±.06 158±3.9 552±9.6 22.4±2.1 6.6±2.3
’Smoking 7.13± 10" 14.0±50 70.1 ±20.6* 22.9±1.9 8.6+2.9*
60 MINUTES:
Non-Smoking 7.10±.11 13.8±4.0 706±17.5 20.8±2.1 9.9±4.1
Smoking 6.94± 10’ 11.8±28’ 94.0±310" 19.1 ±40* 17.2±4.6"
lehous blood gases were similarly altered.
CONCLUSION: In the 60 minutes after delivery: 1) there is significant
deterioration in the acid-base status of blood drawn from placental vessels,
2) there is s~gnificantly greater deterioration in the acid-base status of
smokers compared to non-smokers.

Volume 170, Number 1, Part 2 SPO Abstracts 321 Am J Obstet Gynecol
159 MID-TRIMESTER PLACENTAL VOLUMES PREDICT
BIRTH’WEIGHT AT TERM I.F Clapp*, K Rizk~, J Crass~ Depts of
Ob/Gyn and Radiology, MetroHealth Mad Ctr. and Case Western Reserve
Umversity, Cleveland, OH
OBJECTIVE: To test the hypothesis that wad-trimester placental growth is
a major deterwanant of size at bmh in acttve women.
STUDY DKSIGN: Three serial measurements of placental volume were
obtazned between the 14~ and 2@ gestatmnal week of an accurately dated
singleton pregnancy in 35 women who maintained a regular exercise
regimen throughout pregnancy Following standard fetal morphometry, a
ftxed base, articulated arm, 3 5 Ml4z B-mode transducer was used to obtain
parallel images of the placenta at 1 cm intervals and placental volume was
then calculated using the rectangular rule The method has a precision of -+
5%. Trimmed, drained placental volume and birthwelght were obtained at
dehvery and corrected for sex and gestalmnal age using institutional
normative criteria. Data were analyzed using ANOVA and least squares
regression
RESULTS: Placental volumes increased from (mean_+sd) 132_+37 cc to
247_+70 cc and 381_+96 cc at 16, 20, and 24 weeks gestation with an
average growth rate of 31_+9 cc/week over th~s time interval At term, fresh
plaeental volumes (451_+118 co) ranged between 304 and 823 cc and
blrthweight (3306_+453 gin) ranged between 2620 and 4355 gm Sigmficant
hnear correlations (r >.6500) were present at all time points between
placental volume and b~rthweight. At 20 and 24 weeks gestataon and at term
the r values between placental volume and corrected bitthwe~ght were
8441, .8798 and .8526 respeehvely and the correlabon between the wad-
trimester growth rate in placental volume and blrthwe~ght was 8778. In
contrast the correlahons between the fetal morphometnc centile ~n the nard-
trimester and at Nrth were poor in this populace (r < 4000).
CONCLUSION: In physically active women wad-trimester placental
volumes are superior to fetal morphometry m predicting size at Nrth over a
wide range of b~rthweight. Supported by NIH grants HD21268 and
HD211089
161 THE CORRELATION BETWEEN PLACENTAL HISTOLOGIC CHANGES AND HUMAN CHORIONIC GONADOTROPIN IN SMOKERS. M Fenoughtyx, HL Brown. Departments of Ob/Gyn and Pediatric Pathology, Indiana University, Indianapolis, IN. OBJECTIVE: To compare placental histolog~c changes seen in smokers with levels of Human Choriomc GonadotropNn (HCG) and infant growth status. STUDY DESIGN: Thirty five women demonstrating a sonographic Grade 2 or 3 placenta between 36 to 40 weeks gestabon and dehvering between 37-41 weeks were included. Women were divided by smoking (n=20) and nonsmoking (n=15) status and infant birthwelght, growth retardation (IUGR) and average for gestation (AGA). The maternal HCG and placentas of 12 AGA and 8 IUGR infants of smokers and 10 AGA and 5 IUGR infants of nonsmokers were compared for histologic changes including fibrin deposition (FD) syncytlal knots (SK) > 40%, and villitis and thrombos~s. Analysis was by X2 and Fisher’s exact and "t" test where appropriate. RESULTS: Mean infant birthweNht, placental weight, and volume for smokers and nonsmokers were not s~gnificantly different. HCG levels in smokers and nonsmokers were not significantly different and there was also no sign~ficant difference in HCG levels for the AGA and IUGR infants of smokers and nonsmokers. Fibrin deposition was associated w~th a significantly higher HCG level (no FD = 15028__+7916 vs FD = 21662_+5279) overall and in nonsmokers (no fibrin = 14434+_7096 vs fibrin 22,425_+4855 ) p< .05. There was no significant d~fference in HCG [eve~s and FD ~n smokers and no difference in SK or v~lhbs for smokers and nonsmokers, Unhke previous studies thrombos~s and infarction were not histologically apparent ~n the placentas of smokers whereas these findings were present in nonsmokers. There was no slgmficant relationsh=p between h~stologic vanables and IUGR, CONCLUSIONS: No specific histolog~c placental changes or hormonal levels as assessed by HCG are consistently found in smokers versus nonsmokers and the IUGR or AGA infant. Elevated HCG is associated with increased fibrin deposition.
160 AMNIOTIC FLUID ALPHA FETOPROTEIN (AFAFP) AND MATERNAL
SERUM ALPHA FETOPROTEIN (MSAFP) IN ABDOMINAL
PREGNANCIES: CORRELATION WITH EXTENT AND SITE OF
PLACENTAL IMPLANTATION AND CLINICAL IMPLICATIONS. J.
Shumwa¥~= J. Groonspoon, L. Platt, K. Blakemore, Cedars Sinai Mad
Ctr Los Angeles, CA, Johns Hopkins Univ., Bait=more, MD.
OBJECTIVE: The hypotheses are that in abdominal pregnancies 1)
elevated MSAFP ~s due to an altered maternal/ placental Interface,
and 2) differences in MSAFP levels may reflect placental location
within the maternal perltor~eal cavity.
STUDY DESIGN: A review of 1193 ectopic pregnancies from 1983-
1993 revealed 3 cases of abdominal pregnancy. A second trimester
genetm ammocentems had been performed with AFAFP and
knryotype data available in each case. Antepartum, peripartum, and
postpartum clinical courses were analyzed. Placental location was
recorded In each case.
RESULTS: MSAFP was elevated in two of the three cases (3.63 and
4.88 MoM). AFAFP was normal in all three cases. No case had an antenatal thagnosls of abdominal pregnancy. Delivery occurred at
18,19 and 37 weeks. The two cases associated with elevated
MSAFP had placentatlon involving both the bowel and uterus. The
case with normal MSAFP was implanted on the right uterine cornua.
All three cases had n normal karyotype. The two cases with elevated
MSAFP had increased maternal morbidity (mtraoperatlve thffmulty,
increased blood loss, and greater length of stay).
CONCLUSION: 1) An unexplained elevated MSAFP with normal
AFAFP and normal fetal anatomy should alert the clinician to the
poss=bdity of an abdominal pregnancy. 2) Those abdominal
pregnancies with elevated MSAFP appear to have more extensive
placental involvement of the abdominal viscera generate an increased
maternal-fetal circulatory interface; this can account for the elevated
MSAFP values given the normal AFAFP. 3) Those abdominal
pregnancies w~th elevated MSAFP may have greater maternal
morbidity.
162 HUMAN PLACENTAL GLUCOSE UPTAKE AND TRANSPORT ARE NOT ALTERED BY PHARMACOLOGIC LEVELS OF THE ORAL HYPOGLYCEMIC AGENT, GLYBURIDE Elhott, B D , Crosby Schmldt, C~, Langer, O Dept of Ob/Gyn, UTHer7 Antomo, TX
OBJECTIVE We have prevmusly demonstrated that m=mmal t=ansport of glybur~de across the human placenta =s unaffected by maternal glucose levels or dmbetes (AJOG, 1991, SPO, 1993) T|us study was undertaken to determ;ne whether glybur~de increases the placental uptake and transport of glucose to the fetus
STUDY DESIGN Maternal to fetal transport of H3 glucose was tested m the rec=rculatmg single cotyledon placental model =n normal term human placentas dually perfused for 3 hours tmmed~ately following dehvery Glybur~de (300 rig/rot) was added to the maternal perfusate in the exper=mental group and w~thheld m the control group Initial maternal glucose concentratmn was 150 mg/dl and C34 ant=pyr~ne (200 ng/ml) was added to the maternal perfusate in all experiments as an interna control L~qmd sdntdlat=on spectrometry measured the radmlabeled glucose and anttpyr=ne concentratmns in the sermlly collected samples Glucose levels ~n homogenates of the cotyledons were s~mdarly determined
RESULTS There was no s~gmficant d~fference ~n the placental transport of glucose between the experimental and control groups by the Mann Whitney U test, nor was there a d~fference in placenta/uptake
2 H[ % T[ansport GLUCOSE/ PLh.CENTAL n ANTIPYRINE UPTAKE
GLUCOSE ANTIPYRINE RATIO (ng/gm)
Glybur~de 4 14 9 17 8 83 121
Control 4 13 5 14 6 93 139
CONCLUSIONS. The oral hypoglycemic agent glybur~de in pharmacologic doses does not affect the human placental uptake of glucose, nor does ~t ~ncrease glucose transport to the fetus
322 SPO Abstracts January 1994 Am J Obstet Gynecol
163 NORMAL GLUCOSE UPTAKE AND TRANSPORT OCCUR IN THE DIABETIC PLACENTA. Elhott, B D, Crosby-Schm~t, C, Langer, O Umv of Texas Health Science Center, San Antoine, TX OBJECTIVE: There ~s a paucity of data concerning the effect maternal d~abetes and hyperglycemia have on the glucose transport mechanism of the placenta The purpose of our study ~s to characterize glucose transport m the d~abet~c human placenta STUDY DESIGN: Transport of H3-Glucose was tested m the rec~rculat~ng single cotyledon human placental model in placentas obtained ~mmedlately after dehvery from d~abet~cs w~thout vasculopathy and normal controls Each specimen was dually perfused for 3 hours w~th Krebs-Rmgers buffer at an m~tlal maternal glucose concentration of 150 mg/dl Human album~n (2 gin/all) was added to the perfusates, and C14-Antlpyrme (200 ng/ml) was added to the maternal perfusate as an ~nternal control Liquid scmhllat~on spectrometry measured levels of the rad~olabeled glucose and ant~pyrlne in the serially collected maternal and fetal samples, and homogenates of the perfused cotyledons RESULTS: No sNmficant d~fference in mean glucose transport or placental uptake existed between d~abetlc and normal placentas by Mann-Whitney U test
Placental Glucose/ Uptake Antlpyrlne --2 Hr % Transport---
..... (n~~~m) ........ Rat~o----Glucose ...... -Ant~pyrme---n---
Diabetic 131 0 94 16 8 18 0 3
Control 139 0 93 13 5 14 6 4
CONCLUSION: The d~abet~c placenta exhibits normal glucose transport and uptake
164 SERUM LYMPHOCYTOTOXIC ANTIBODIES (CYT) 1N THE UMBILICAL CIRCULATION OF TWINS WITH GROWTH DISCORDANCE. Michaal S. Edwards. Roger B. Newman, Subbi
Mathur,x Dept. Ob/~yn. Medical University of S.C., Charleston, SC.
OBJECTIVE: Fetal CYT against maternal T lymphocytes, especially
suppressors (Mathur et al., 1982; Miyagawa et al., 1982, 1983), may
play a role in the survival and maintenance of fetal allograft. This preliminary study aims to test a possible association between titers of
these antibodies and the birthweights of normal twins.
STUDY DESIGN: Serum CYT titars in the umbilical cord veins of 21
twins with disparate weights were determined by double fluorochromasia cytotoxic antibody assay (Mathur et al., 1982). Paired
’t’ test and linear regression analysis were done. RESULTS: CYT titers in the heavier twins (group A) were
significantly lowex (p = 0.013 than those in their llght~r cohorts (group
B; TABLE). CYT titers between twin cohorts significantly correlated (r = 0.753; p < 0.001), as did the birthweights (r = 0.861; p < 0.0001).
CYT t~ters and the birthweights did not correlate with each other.
TABLE. Birthweights (mean + SEM) and CYT (mean log2 + SEM) of
twins (n = 21). Twin A Twin B Paired ’t’ test
P value
Weights (gin) 2016 :t: 105 1775 ± 106 < 0.0001
CYT titers 3,7 5: 0.~ 4.5 ~: 0.4 0.01
CONCLUSION: It appears from tl~s small study of growth d~scordant
twins that the lower birthweight cotwin mounts a greater antibody d response than its counterpart. Whether these antibodies affect
placentatinn and lherefore fetal growth remains an area of interest.

Poster Session II Thursday, January 27, 1994
3:00 p.m.- 5:00 p.m.
Pavilion 9- 11
CATEGORIES
OB Anesthesia and Pharmacology
Medical Complications of Pregnancy
Clinical/Operative Obstetrics
POSTER NUMBERS
165-169
170-216
217-253
Judges:
ThomasJ. Benedetti, MD
Steven G. Gabbe, MD
Michael L. Socol, MD

324 SPO Abstracts January 1994 Am J Obstet Gynecol
165 EPIDU~LANESTHESIAANOEXTERNALCEPHALICVERSION (ECV) AT TERN.
S Caftan, N Dent, APena, P Danna0 B Richmond, D Schaefer,
Arnold Palmer Hospital for Children & Women (APH), ORHSo
Orlando, FLorida.
OBJECTIVE: To compare the effect of eptdura[ anesthesia on the
success and safety of ECV performed at term.
STLIOY DESIGN: A retrospective record review of all pregnant
women >36 weeks gestation who had attempts at ECV at APH during
4/92-4/93. Standard contraindications to ECV were observed,
Prior to and after the ECV attempt, fetal monitoring, US, and
vaginal exam was performed. Tocolytics and lumbar epidurats were
ordered by the patient’s physician based on personal preference.
RESULTS: Sixty-one patients underwent 69 attempts with 8
patients having 2 attempts. The demographics and major clinical
parameters likely to affect success were similar between the
groups with the exception of a higher percentage of epidurat
attempts by the housestaff.
EpiduraL No Epidurat P
Parameter N(%) N=32 N=37 EGA (weeks) 38 ± 1.8 38 ± 1.6 Amniotic FLuid Index (cm) 14 ± 5 14 ± 7 Cx diL at Version (cm) 2.5 ± I 2.2 ± 1.3
NS NS
Tocolysis 22 (68) 33 (89) NS Housestaff Attempt 20 (62) 10 (27) <.05 Frank Breech 23 (88) 22 ,(73) SS Success 19 (59) 9 (24) <.05 Breech at Birth 12 (37) 20 (54) NS Fetal Bradycardia 7 (21) 2 (5.4) NS Abruptio I (3) I (2.7) NS Cesarean Section (%) 46 89 <.05 Birthweight (gm) 3281 ± 582 3289 ± 531 NS pH 7.27 ± .07 7.30 ± .03 NS
Maternal Cost ($) 2354 ± 1262 3440 ± 2315 .03 The indications for cesarean delivery were similar between the epidural and no epidural groups, OnLy 15% of the E group and 11% of the NOE group were discharged without delivery. CONCLUSIONS: Regional anesthesia increases the success rate of ECV and decreases the cesarean section rate with r~ apgarent ir~:rease in fetal or maternal morbidity or mortality.
167 SIGNIFICANT FETAL N:IDENIAkSSOCIATED 9ITH REGIGNAL NIESTIIESIA Fat ELECTIVE CESAREJMI ~s:CTIGN. S.W. Robertsx, N.J. Lucas, M.A. Kellyx, M.L. Shermanx, K.J.
Leveno. Dept. of Ob/Gyn, University of Texas Southwestern, Dallas, TX. O~.IECTIVE: We sought to assess the fetal implications of the choice of anasthasta for e|ective casereansoctions in otherwise entirety normal pregnancies. S"ItlD¥ D~SIGN: Umbiticat artery (Ua) blood gases were obtained in 1601 singLeten fetuses during scheduted etective cesarean sections in ~ without eny other pregm~ncy complications. The type of anesthesia used was dependent upon patient choice and recmmerldations of the atterKling anesthesiotogist, RESULTS:
U~ pa m~m~e~L EPZlXWXL ieeloue-~-] SPI~,~L teEGZOB~L
358 252 539 176 45 7.20 (97~) (88~) (82~) (76~) (83%)
13 28 97 44 7 ~.10-7,19 (4%) (10%) (15%) (19~) (13%)
0 5 17 9 2 r.00-7.09 -- (2%) (3%) (4%) (4%)
0 1 6 2 0 6.99 -- (.4%) (.9%) (.9%) --
Significant fetal acidemia (Us pH 7.09 or tess) occurred in 42 fetuses exposed to regional anesthesia and in nonewhere general anesthesia was used (p < 0.001). These acidemias were attributed to hypercarbia. CONCLI~ION: Regional anesthesia is associatedwith significant acidemia, presumably due to acute "respiratory" uteroplacentat ineufficiency in 3 to 4~ of otherwise entirety normal fetuses.
166 DOUBLE-BLIND COMPARISON OF INTRAVENOUS BUTORPHANOL (STADOL®) AND FENTANYL
(SUBLIMAZE®) FOR ANALGESIA DURING LABOR. B.=. Atkinson,x L. Truitt,x W. Raybum, G. Tumbull,x H.D.
Christensen,x A. Wlodaver.x Dept. Obstet. GynecoL, Univ. of
Oklahoma, Health Sciences Center. Oklahoma City, OK.
OBJECTIVE: To compare analgesic properties, effects on labor,
and side effects between intravenous butorphanol and fentanyl. STUDY DESIGN: One hundred women with uncomplicated term
pregnancies in active labor were enrolled. The study was conducted in a double-bhnded manner with the patient to receive a 1-2 ml
volume of either fentanyl (50-100 mcg) or butorphanol (1-2 mg) as
often as hourly. Pain was quantitated independently by the patient
and nurse using a 10-point visual analog scale. Categorical and
measurement data were collected for comparisons of effects on labor,
maternal and fetal well-being, and neonatal outcomes. Data analysis
included Student’s t-test and chi-square testing when appropriate.
RESULTS: The fentanyl (n=50) and butorphanol (n=50) groups
were identical demographically. No change in uterine activity was
found before or during the first hour following the initial dose of
either drug. No matemal or newborn adverse effects were observed.
Greater pain relief was found w~th butorphanol than fentanyl by both
the nurses (4.10 vs. 5.86, p < .001) and patients (5.10 vs. 6.74, <
.01). Reduction m pain using butorphanol was more s~gnificant for
multiparous patients (42% vs. 17%, p < .001). When fentanyl was
given, more doses (2.06 vs. 3.14, p < .001) were necessary and
epidurals (20% vs. 32%, p < .05) were administered more frequently.
CONCLUSION: Intravenous butorphanol provided better
tempormy analgesia than fentanyl espeoally for multiparous patients.
168 AN IN-VITRO COMPARISON OF THE VASOACTIVE EFFECTS ON HUMAN
UMBILICAL ARTERY AND VEIN OF SELECTED DRUGS COMMONLY USED IN
PREGNANT PATIENTS. M. Belfort.* G.Saade,* Y. Vedernikov,* M. Suresh,* K. Mmse,
Jr., D. Johnson.* Oepts. Ob/Gyn and Anesthesiology, Baylor Coll. Medicine, Houston, TX.
OBJECTIVE: To compare the relative effects of selected vasedilators frequently used m
the management of peeclamptic patients, on human umbilical artery (UA) and vein (UV)
~n-vitro
STUDY DESIGN: Vascular rings (UA and UV - 4ram) from normotenslve pregnant women
were suspended (passive tension 2g) and bubbled at 370 C ( 2.5% 0~, 8% CO~, balance N~)
in physiological salt solution (pH - 7.25; pO~ - 35 mmHo; pCO~ - 55 mmHg) in organ
baths for isometric tension recording They were then contracted with 60mM KCI and
10 8M U46619. Concentration-relaxation curves were performed with magnesium sulfate
(MoS04), diphenylhydantom (DIPHEN), nifedlpine (NIF), nimodipme (NIM), mcardipine (NIC),
and hydralazine (HYD). The concentration of the drug (-IogM) producing 50% of the
maximal relaxation (IC~o), and the % maximal relaxation produced (%R) were calculated.
Data for KCI contracted vessels only are presented as Mean _+ SE. Szonificance; p < 0.05
RESULTS; NIF NIC NIM DIPHEN HYD MoSO.
IC5o UA 7.8+--0 1 7.5+0.1 7.1--+0 1 4.7-+0.1 4.1-+0.3 2.0-+0.1
%R -UA 58-+4 66+__3 57+--10 72+-5 10+-3 41-+8
IC~o UV 8.0--+0 2 7.5+-0 2 7.3+-0.2 4.0-+0.1 1.8+-0.1
%1~ -V 73+5 68+3 72+6 15+3 46+7 _
The stabQzed tenszon (used as the 100% contraction) obtained in UA and UV were equal
(lOg) The %R in I(CI and U46619 contracted rings were similar except for NIC
(significantly less relaxation (p < 0.05) w=th U46619 (%R-UA - 24-+9 vs 66-+3, %R-UV
- 24-+11 vs 68+3). Papavenne (3xlO~M) induced complete relaxation in the U46619
contracted vessels but not in the KCI contracted vessels
CONCLUSIONS: Calcium antagonists are significantly more potent as inhlbltors of K+
induced (but not U46619) contractions in UA and UV than the other agents. DIPHEN
causes significant arterial relaxation but requires high concentrations. MgS04 was the
least potent agent tested but still had a vasodilator effect at high concentration. NIF is the
most potent but the maximal relaxation produced is similar to that of NIC and NIM. HYD
has little vasoddator effect on the umbilical vessels and contrasts strongly with the known
pronounced vasodilator effect of HYD on adult peripheral arteries.
Volume 170, Number 1, Part 2 SPO Abstracts 325 Am J Obstet Gynecol
169 MAGNESIUM IS MORE EFFICACIOUS THAN PHENYTOIN IN REDUCING N-METHYL-D-ASPARTATE (NMDA) INDUCED SEIZURES IN RATS. B Masonx, C Standleyx, S Irtenkaufx, M Bardicefx, and D Cotton, Dept. of
OB/GYN, Hutzel Hospital, Wayne State Univ., Detroit, MI.
OBJECTIVE: The efficacy of MgSO4 in limiting seizure
achvity has been debated. Because eclamptic seizures may be
mediated by central NMDA receptors, we compared the
anticonvulsant effects of MgSO4 and phenytoin (PHY) on
NMDA-mduced seizures.
STUDY DESIGN: 17 female rats were implanted with bipolar
recording electrodes in the hippocampus and cannulae in the
lateral cerebral ventricle. After a 7 day recovery, animals
randomly received 90 mg/kg MgSO4 (n=5), 50 mg/kg PHY (n=6), or sahne (n=6) intravenously. 15 minutes after infusion,
20 #g/,~l NMDA was injected into the ventricle and seizure
activity was assessed for 20 minutes.
RESULTS: As compared to saline controls, in the MgSO4 group
the total duration of seizure activity was significantly less
(p=0.0195) and there was a significant delay in the time of onset
to first seizure (p=0.048). Rats receiving PHY showed no
significant decrease in seizure activity. The post-NMDA seizure
mortality rate was 50% for saline and 16% for PHY; none of the
rats that received MgSO4 died.
CONCLUSION: These results suggest that MgSO is 4 ’
significantly more effective as a prophylactic agent than phenytoin
in NMDA-induced seizures.
171 PLATELET-ACTIVATING FACTOR SYNTHESIS lN RESPONSE TO
ANTI~IOLI~IN ANTIBODY-POSITIVE SERUM FRACTIONS.
R.K. Silver, M.J. Lee*, P.D. O’Connell+, E.H. Sladek÷, M.S. Caplan+. Dept.
Ob/Gyn, Northwestern University, Evanston Hospital, Evanston, Il.
OBJECTIVE: Enhanced endothelial cell platelet-activating factor (PAF)
synthesis has been identified as a consequence of anticardiolipin-antibody-
positive serum exposure. While this observation suggests that PAF may
play a role in antibody-mediated vasculopathy, it has not been determined
whether the antibodies themselves are directly responsible for stimulating
PAF production. We wished to determine the degree to which extracted
immunoglobulins or non-immunoglobulin serum constituents are
responsible for the increased endothelial cell PAF production previously
observed.
STUDY DESIGN: Sera from six ACA-positive, non-pregnant women were
precipitated with ammonium sulfate and dialyzed to extract their respective
immunoglobulin fractions. IgG, A and M concentrations were measured by
nephelometry before and after precipitation and enzyme immunoassay was
used to quantify anticardiolipin antibody activity in both whole serum and
immunoglobulin suspensions. Paired endothelial cell monolayers were
incubated separately with 20% whole serum and the corresponding
immunoglobulin fraction from each patient source. After ionophore A23187
stimulation, intracellular PAF production was measured by lipid extraction
and radioiabeling. RadylPAF species were distinguished by zonal thin-layer
chromatography. Mean PAF synthesis was compared between experimental
conditions by paired T-test.
RESULTS: Significantly more endothelial cell PAF synthesis was observed
subsequent to whole serum exposure as compared to incubation with the
corresponding immunoglobulin fractions (19154+1916 vs 11785+1778; dpm,
mean+SE; p=0.007). In addition, Ig-free samples recovered after
immunoglobulin extraction retained PAF-stimulating activity (23045
+4175 dpm) in comparison to unextracted serum (19635+1266 dpm; p = 0.25).
CONCLUSION: In ACA-positive serum, non-immunoglobulin constituents
appear to provide greater stimulation of PAF synthesis than the
immunoglobulins themselves.
170 EARLY GESTATIONAL GLUCOSE SCREENING AND GF~TATIONAL
DIABETES W. Meyer, D. Gauthier. Univ. of 111., Chicago, IL.
OBJECTIVE: To determine the benefit of early gestational glucose screening
in a high risk obstetrical population.
METIIODS: A retrospective analysis of 329 patients who raceived early and
complete obstetrical care was performed. A 50 gram 1 hour glucose screen
was performed M the first prenatal visit and again, if negative, at
24-2~, weeks in all patients. All glucose screens > 135 mg/Dl were
followed by a 3 hour glucose tolerance test. Gestational diabetes was
defined as the presence of 2 or more abnormal values on the 3 hour test.
D~ta collected included maternal age, race, gravldity, presence of risk
factors, pregnancy weight gain at glucose testing and delivery, neonatal
birth weight and trauma. Risk factors included positive family history,
obesit~ (> 120% ide~ body welgl’,t), glucgsuria, prior stillborn or birth
weight > 4000 grams and hydramnios. Data was analyzed using analysis of
variance and Chi-square te~ting with P < 05 considered significant.
RESULTS: Gestational dmbetes was diagnosed in 6 1% (201329) of the study
population. Early gestational glucose testing detected 40% (8/20) of the
gestatlonaldtabetics Factors ~sociated with early development of
glucose mtolermme included maternal age > 30 (P < .001), Black race
(P < 001), and the presence of risk factors (P < .0001). Poor pregnancy
weight gain was also associated with the late development of glucose
intolerance (P < .00i) Gestational diabetes was diagnosed on repeat
testtng in 13% (6/46) of those patients who had an abnormal early glucose
screen with a norm~d 3 hour glucose tolerance test.
CONCLUSION: Early gastational glucose ~creenlng is beneficial in
detecting gestational diabetes in patients over 30 years old, who are
Black or have risk factors for diabetes. Glucose testing should be
repeated at 24-28 weeks m all patients, especially those having
abnormal early screening tests with a normal 3 hour tolerance test.
172 CALCIUI4 SU~PLENENTATION DOLES NOT INCREASE THE RISK OF IRON
DEFICIENCY ANERIA. JT Repke, J vlllar, E Berge[, JM Betizan.
Dept. Ob/Gyn, Harvard Medical school - Brigham and w~men’s Hospital,Boston, MA., Centro Rosarino de Estodios Perinatales, Roasrio, Argentina. OBJECTIVE: Iron deficiency is a coalaon nutritional co~ypiication in pregnancy. Calcium supplements may conI)ete with iron for absorptionby the gastrointestinal tract. The current investigation attempts to document whether in fact there is a biochemical or clinical|y significant effect of calcium on iron absorption. STIllY DESIGN: 874 patients enrolled in a randomized double blind placebo controlled trial of calcium supplementation were evaluated throughout pregnancy for hemoglobin concentration and hematocrit. Patients received either placebo or calcium supplementation consisting of two grams of elemental ca|cium per day. Hemoglobin concentration in each group was cow,pared at different points during gestation. RESULTS: Calciunl and placebo groups were well matched by a numl~r a variables. Overall, 35% of women in each group took iron supplementation scmetime during their pregnancy. After adjustment for initial hemoglobin value using repeated measure analysis or calculating the differences from20 week values, there was stilt no statistically significant difference in hemogiobin level between calcium and placebo groups. A life table analysis for the diagnosis of anemia (he~gtobin ~ 10 grams per deciliter or ~ 11 grams per deciliter) for the calcium and placebo groups failed to deoonstrnte a statistically significant differer~e.
~O#CLUSIO~S: 2 grams of elemental calcium supplementation per day during pregnancy does not increase the risk of clinically significant iron deficiency anemia.
326 SPO Abstracts January 1994 Am J Obstet Gynecol
173 PERINATAL OUTCOME IN WOMEN WITH ASTHMA J K Parkx, C Chazotte Dept Ob/Gyn, Albert Einstein Coil of
Med, Bronx Municipal Hosp Ctr (BMHC), Bronx, NY
OBJECTIVE: To determine if the severity and control of
asthma has an impact on maternal and fetal outcome. STUDY DESIGN: A retrospective review of patients with
asthma who delivered from Jan. 1987 to Sept. 1992 was
performed Severity of asthma was defined by medication
requirements: very mild - no medications in pregnancy, mild
- beta agonists and/or theophylline, moderate - inhaled
corticosteroids(CS) or a short course of oral CS and severe - chronic oral CS use. Pts, with antepartum asthma admission
were considered uncontrolled.
RESULTS: Of 230 patients who were identified, 210 charts
were available for review Forty pts(19%) were very mild,
111(60%) - mild, 45(24%) - moderate & 14(7%) - severe. The
prevalence of smoking and drug abuse were inversely proportional to the severity of disease (p<0.05). There were no differences in the incidence of preeclampsia, preterm
birth, birthweight, %SGA, low Apgar scores or NICU
admission by severity or control of asthma. Diabetes
developed in 25% of severe pts. Of 58(28%) with
uncontrolled asthma, exacerbations occurred in 7(12%) in 1st trimester, 27(47%) in 2nd trimester, 23(40%) in 3rd
trimester, and 4(7%) in labor. CONCLUSIONS: With modern management of asthma, we cannot confirm an increased incidence of preterm birth,
SGA, preeclampsia or poor perinatal outcome with increasing severity or poor control of asthma
175 SUPEROXIDE DISMUTASE PROTECTS MOUSE EMBRYOS
FROM HYPERGLYCEMIA-ASSOCIATED ANOMALIES:
RESULTS OF AN IN-VIVO STUDY Zion I Ha~av*. Yael
Weissix, Igor Zusman~x, LA. HAkan Borg~x, Dvora Kidron*x, Ulf J
Eriksson¶x, Yoram Groner~’X,University of Uppsala¶, Upl~sala,
Sweden, Dept. Ob/Gyn, Kaplan Hospital*, Hebrew University’, and
Weizmaim Institute of Sciencef, Rehovot, Israel. OBJECTIVE: Oxygen free radicals have been Implicated in the high
rate of fetal dysmorphogenesis associated with diabetic pregnancies.
The present investigation studies the effect of elevated levels of
superoxide dismutase (SOD) on prevention of hyperglycemia-
associated embryopathy in mouse embryos.
STUDY DESIGN: Two strains of transgenic mice carrying the human
CuZnSOD gene were used. These strains were previously shown to
exhibit a 6 (TgHS-69) and 5-fold (TgHS-70) increase in enzyme activity, as compared to non-transgemc litter mates. Diabetes was
induced by streptozotocin administration on days 6 & 7 of gestation,
hyperglycemia developed on day 8 and was maintained through day 10
(organogenesls) Fetuses were examined on day 10 for external
anomalies and their crown-rump-length (CRL) measured.
RESULTS:
CRL (ram) CRL< 25 malformation
percentile(%) &fetal loss(%)
Control
Non-diabetic 4,48+0.77a 39/156 (25)a 25/167 (15)a
Diabetic 3 65+0.64 122/171 (71) 81/223 (36)
Transgenic (TgttS-69 & TgttS-Tg)
Non-diabetic 4.72_+0.47 33/134 (25)a 35/292 (11)
Diabetic 4.45_+0.88b 79/156 (50)b 171168 (10)u
P< 0.05, non-diabetic versus diabetic group (a) and diabetic transgenic
versus diabetic control group (b) using the chi-square test. CONCLUSIONS: Elevated activity of Cu[ZnSOD confers a partial
protective effect against hyperglycemia-associated fetal growth
impairment and embryopathy.
174 UNEXPLAINED ELEVATED MATERNAL SERUM ALPHA-FETOPROTEfN
VALUES: PREGNANCY OUTCOME AND PLACENTAL PATHOLOGY !A Hoskm~s, MAA Sayed,x K Mdtal,× R Demopoulosx. Depts of Ob/Gyn-~
Pathology NYU Medical Center, NY, NY
Objective. Correlation of unexplained elevated maternal serum alpha~
fetoprote n (U-MSAFP) values, pregnancy outcome and placental pathology
Study Design Of the pal]ents who recmved MSAFP screemng from 7/1/87 to 6/30/93, maternal, neonatal and placental data were avadable for 1860
women Elevated MSAFP values were found m 175 (9 4%) ofthese patients
w~th 93 (53 1%) of them being unexplained. This consbtuted the study group
There were 279 matched control patients with normal MSAFP (N-MSAFP)
values An U~vlSAFP value was defined as > 2 5 MOM on 2 eccas~ons~.
assoc*ated w~th a normal AF AFP value and fetal anomaly scan
Results. The incidences of pregnancy complicabons in the U-MSAFP group
were fetal demise 7 9%, preterm b~rth 14 5%, severe preeclampsm 11%,
tUGR 13%, abrupbon 7%, placenta previa/accreta 7%, chonoammonlbs
4 7% There were no neonatal deaths Stepwme !oglsbc regress=on analysis
showed s=gmficant =ndependent effects of 2 factors on naks associated w~th
U-MSAFP values severe preeclampsla and/or IUGR and the presence ot
bot__~h mtervdlous fibnn and increased syncybal knots, denoting accelerated
placental maturation (odds rat~o 1 8 per abnormahty). Other placental
abnormahbes (immature/dysmature, wlht~s, mfarcbon, calc~ilca#on) were not
significantly assocmted with U-MSAFP values and adverse pregnancy
outcome. Botch, increased syncyhal knots and intervlllous fibrul OCCurred In
81% of placentas from women with Uqk, ISAFP values and preeclamps~a
and/or IUGR, vs 57% with N4VlSAFP values Ne=ther abnormahty occurred
in 6% of the study group vs 43% of the controlled (p<0 05)
Conclusions (1) Increased syncytJal knots and mtervfllous flbnn were
s~gn~ficantly associated w~th preeclamps~a andlor IUGR in women with U-
MSAFP values (2) None of the other pregnancy complmattons associated
w=th U-MSAFP values could be explained by abnormal placental pathology
Other possible explanations for these associafions require investigabon
176 ACUTE FATTY LIVER IN PREGNANCY: AN EXPERIENCE IN THE DIAGNOSIS AND MANAGEMENT OF 14 CASES. I.M. Ust&x J.R. Barton,x E.A. Amen, A. Gonzalez, B.M. Sibai, University of Tennessee, Memphis, Tennessee. OBJECTIVE. To investigate diagnostic problems and rnaternal/perinetal outcome in cases of acute fatty hver of pregnancy (AFLP). STUDY DESIGN: 14 cases with AFLP managed dunn~ the past 8-year period were studied emphasizing: presenting symptoms, adm~ting diagnos~s, laboratory findings, maternal complications and neonatal outcome. RESULTS: Mean maternal age was 27.9 yrs. The mean geetetional age at onset was 34.5 wks (range, 28-39). Admitting d~agnosis included 5 patients with definite or suspected AFLP 2 with preterrn labor or abnormal fetal testing, and 7 with preoclampsia. 9 women delivered within 24 hrs of admission; the remain ng 5 delivered within 12 days(mean 5) Coagulation findings are sumrnanzed in the table. Desp~e using an IV dextrose solution, mean serum glucose was 61 rng/dl (range, 7-84). Mean plasma ammonia was 80 grnol/L (range, 24-331). 10 had diagnosis confirmed by biopsy; 7 of these also had a CT scan with only 1 positive result. 1 patient had diagnosis by CT; the remaining 3 were diagnosed on the basis of clinioal and laboratory findings. Overall, 10 women had CT evaluation, but only 2 were positive. There were no maternal deaths; however, morbidity was frequent: 4 patients had hepatic encephalopathy, 3 pulmonary edema, 4 respiratory arrest, 2 diabetes msipidus, 1 abruptio, and 10 had transfusion of blood/blood products to correct DIG or bleeding. Mean birthweight was 2187 g (range, 980-3940); mean cord pH 7 20 (range, 6.89-7 29). There was 1 stlllNrth and 1 neonatal death from trisomy 18. CONCLUSION: Hypohbrinogenernia was present in 93% of the patients and prolonged PT ~n 86%; thus, AFLP should be suspected in all patients with preeclampsia in the presence of low hbr~nogen and prolonged PT in the absence of severe abruptio Despite lhe literature’s d~srnal prognosis, our findings indicate that rnatarnal/pennatal outcome appears favorable in well-managed pahents. CT scans are usually normal m wornan with AFLP.
TSS] # (%) Platelets <100 x 103/mm3 7 50%
Rbnnogen <300 rng/dl 13 93%
Prolonged PT (>13,4 sec) 12 86%
Prolonged PTT (>35 sec/ 11 79%

Volume 170, Nmnber 1, Part 2 SPO Abstracts 327 Am .] Obstet GynecoI
177 IIq~GI~G OF PLI[RPERAL S~PTIC THRGqBI])HLEBITIS: COVOARISOll OF
~ETIC R£~, ~TERI~ T~HY, ~ ~HY D...TwfckLe~, T. Setiawa~, R. Eva~x, M. Er~, R. StettLe¢, C. Brown, De~rt~ts of~tetrics/G~co(~y a~R~ioL~y, Univ. of TaxES S~th~estern N~ic~[ C~ter, D~{L~, TX ~JECTI~: ge s~ht to c~re the ability of ~g~tic res~e (~)~ c~teriz~ t~gPa~y (CT)~ a~ s~ra~y to ~t~t ~r~ra[ septic thr~l~itis of the ovarian veins. S~I DESi~: Forty-eight ~ ~ith ~r~rat fever for 5 days refractoPy to int~av~ antimicr~iaI therapy ~er~t NR, CT, a~ s~ra~ic i~gi~ of the ovarian vei~. Interpreters ~ePe bLi~ to ~esuIts of other st~ies. NR i~ging ~as ~rfor~ Mith ~ase rec~stP~tion. CT ]~ges of the a~n a~ ~lvis Mere ~e ~ith a~ ~ithout IV c~trast. Rea[-ti~ s~ogra~y ~as ~rfor~ ~ith ~[ex Do~[er a~ color ~LTS: HR a~ CT assess~ ~th right a~ (eft ovarian veins in a[[ cases (~8/48). U(tras~ ~ith duplex Do.Let a~ color ~ing v]sua[iz~ 2~ of ~8 right a~ 10 of ~8 taft ovarian veins. Ovarian vein thr~sis (OVT) ~as diagnos~ ~ 8 cases.
CT MR Ultraso~ +OVT 8 7 -OVT ~0 ~1
In one case CT diagnos~ right OVT, ~t ~R i~g~ng gith ~ase rec~str~ti~ ~strat~ f (og in that vesseL, suggesting a ’~tent right ovarian vein. N~trast~ CT ~as necessary diag~se an acute thr~sis in ~ case. ~CLUS~S: HR fi~ings of the ovarian veins in ~n
~er~raL fever ~ere simiLar to CT in a(~ ~t one case, ~here ~ase reconstruction i~ges provid~ ~tter evaLuation of ovarian vein fto~. s~gra~y ca~t c~sistentLy identify ovarian veins a~ recogniz~ thr~sis in ~(y 50~ of the cases.
179 PRENATAL DETECTION OF FETAL ANOMALIES ln
PREGNANCY COMPLICATED BY INSULIN - DEPENDENT
DIABETES MELLITUS (IDDM). T Albertx, M. Landon, J Whellerx,
P Samuels, R Changx, S Gabb¢. D~IX. Obfl3yn, The Ohio State Umvcrsity,
Colurnbus, OH
OBJECTIVE:To evaluate the clinical a~hty of prenatal diagnostic testing
for congenital anomahes in wuruen with IDDML
STUDY DESIGN: We analyzed data from 289 diabetic women and their
newborns from 8,87- 7/93. Our protocol included an lmtial hemoglobin Ale
(HgA t c), nmternal serum alpha-fetoprecem (MS~’TP), fetal sonography
including a "4 chamber view," and detailed fetal cchocardiography.
RESULTS: Anomalies were identified in 29 of 289 (10%)
fetuses/ncouates: 12 cardiac only, 14 non-cardiac, mid 3 combined. Overall,
21 anomalous fetuses (72%) were detected p.~natally including 12 cardiac
(80%) and I0 non-curdiac (59%) defects. Five fetuses with a cardaac defect
had an abnormal 4 chamber view, a scosidvity of oMy 33% (5/15).Thure
were no false positive 4 chamber views. The positive and negative predictive values of echocardiography were 92.3% and 99.6%, respectively.
Although the HgAlc was sigmficandy increased in 25 mothers of
anomalous fetuses (p=0 02), 4 patients had a normal (<8.0%) value.
Therefore, while 95% of women with a normal HgA lc delivered a normal
fetus, only 13% of those with an elevated tlgA lc had a malformed fetus.
MSAFP and amnlocentesis did ldentafy one case of Down syndrome.
CONCLUSION: This study demonstxates the utility of a comprehensive
program to detect feud anomalies in pregnancies of women with IDDM.
Sonography is useful an recognizing these structural defects. Due to the low
sensitivity of the four chamber view and the high proportion (-50%) of
anomalous fetuses who had a curdmc lesion, detailed echocardiography
should be offered to all &abetic gravidas. There is no apparent "threshold"
HgAlc value to select paaents with IDDM who should undergo this
178 MID-GESTATION INSULIN SENS|TIVITY AND LATE GESTATION INSULIN SECRETION DIFFERENTIATE NORMAL FROM GESTATIONAL DIABETIC (GDM) WOMEN. L. Cousins, C, Re~ R. Bergma~ M. Crawford~. Sharp
Perlnatal Center, San Dingo, CA, Dept Physlol Biophys Un~v S Cal, L.A
OBJECTIVE: Null hypotheses: There m no s~g. difference between
metabohcalty normal (C) and GDM gravtdas studied !ongituthnully in
insuhn (ins) sensitiwty or endogenous Ins secretion.
STUDY DESIGN: 13 age (+ 5 yrs) and prepregnancy body mass index
(BMI, ± 3} matched C and GDM gravldas were studied in late 2nd (25-
28 wks) and 3rd trimester (trl., 34-38 wk) and postpartum (PP, 6-15
wks}. Ins. sensitivity (measured with minimal mode~ technique), % body
fat (underwater weighing) and 1st phase and 2nd phase =ns. secretion
(frequently sampled IV glucose tolerance test) were compared.
RESULTS: There was no rag. between-group differences in gestat~onal
age at study, % body fat, or fasting glucose. See table,
’ill ’2rid Td. ] 3rd Td. Postr
BMI C (kg/m2) GDM
Insulin C
(pU/ml) GDM
S~ C
(104 min’VpUmN) GDM
1 st Phase C
{/JU/ml ° rain} GDM
2nd Phase C
~7.3+ !.8 28.8±1.9 26.3± 1.80
25,9 ±2.7 127,3 ±2.8 23.5+_2.6
10.0±1.4<> 13.5-+2.3 8.8±1.8
12.8+1.8 13.9+1.9 S,2_+1 5
3.13-+.48t 1.85±.26 ~.63 ±.44
1.56±.22 1.48±.18 3.78±.43
442±54 ~68-+130= 371 ±54
438-+86 552±114 194±42"
447± 50 ~09+127= 264_+45 <>
0JU/ml ¯ min) GDM 435-+111 503+109 173-+44
S~ - Ins. sensltlV, index, 1st )hase-lncrem. area under curve
(O - 10 rain), 2nd phase-increm, area under curve (tO - 25 mmL
o~ .1 > P > .05, <> P < .O6, * P < .O2, I"P < .005
CONCLUSIONS: 1. GDM are less Ins. sensitive in the 2nd trl,; 2.1st and 2nd phase Ins. secretion m not different in the 2nd tri. In 3rd tn. and PP
GDM have ~mpaired 1st and 2nd phase Ins. secretion.
180 BXPE~ATELET FUNCTION, ABTIPHOSPHOLIPID A~TIBODY, AND RECUP~RENT pREGNANCY LOSS. Mark E. Caine, Ronald L. Thomas, Zella R. zeiglerx, Dept Ob/Gyn and Hematology. Western Pennsylvania Hospit@l, Pittsburgh, PA. OBJEC~I~: Antiphosphollpld antlbOdleS (A~A) react agalnst n~atlVely charged phosphollpldS. T~sts for th~se antlbodles use l~unoassays for detection of antl-cardlollpln antlbodles. It is hypothesized that the mechanlsm by W~lCh antlphosphollpld antibodles cause recurrent pregnancy loss is platelet aggregatlon and adherence wlth secondary thrombcsls and placental Oamage. The present study of patlents wlth recurrent pregnancy loss attempts to measure clinical correlates between AgA and hyperplatelet functlon (HPF). HPF was established through two global measurements (circulating aggregates and spontaneous aggregation). STUDY DESIGN: In a s~rles of thirty-seven female patlents of reproduetivs age wo measured tests of HPF and APA and correlated this with the hlstory Of recurrent pregnancy lo~s (RPL). RPL was deflned as at least two pregnancy losses wlthout clear explanatlon. Patlents were considered to have ~ APA If GPL > 16~ MPL > i0 or APL > 14 (establlshed as mean ± 2 SD in 24 clinically normal patlents). HPF was deflned as abnormal if elther clrculating aggregates were > 15% (normal 0-15%, mean ± 2 SD) or spontaneous aggregation > 14%, [normal 0-14%, mean ±2 SD). Statlstlcs were performed by Chi Square. PI~ULTS: In the RPL patient groups (95 total pregnancles/19 patlents) 38 of 50 (76%) and 37 of 45 (82%) lost pregnancies in the APA ~ and APA ~ sub-groups respectlvely. In patients who were APA ~ and suffered RPL, 6 of ll (54.5%) had evldence of hyperplatelot functlon. In those wlthout RPL hlstorles but who were AgA ~, 0 of II had evidence of hyperplatelet function (P<.005). In patlents who were APA ~ but had RPL, 1 of 8 (12.5%) had evidence of hyperplatelet functlon. In the control group of APA 0 patlents wlthOUt ~PL, none had hyperplatelet function (NSl. CONCLUSIONS: Patients who are APA ~ and have a hlstory of RPL ofte~ have abnormal platelet fu~ctlo~. Patlents wlthoutA~A who have RPL may have other causes of their pregnancy loss. APAs may be a marker for HFF which may be more strongly related to BPL.

328 SPO Abstracts January 1994
Am J Obstet Gynecol
181 PREDICTORS OF COCAINE ABUSE IN PREGNANCY:
DEMOGRAPHICS AND RISK FACTORS OF PUBLIC PATIENTS IN
A MIDDLE SIZED URBAN SETI’ING. *Jon D. Lurid., xV. Daniel Castrac~ne. Department of Obstetrics and Gynecology, Texas Tech
Un~veralty Health Sciences Center, Amarillo, Texas.
OBJECTIVE: Ovar a 2Y2 year period 93 positive cocaine screens were
documented in a university public obstetrical population (Amarillo,
Texas). S~xty-five of these screens were associated with pregnancy
termination of which 59 occurred in _> 22 weeks gestation.
STUDY DESIGN: This latter group formed the bas~s for a
retmspecti’ve review evaluating material demographics and serial nsk
factors compared to our clinic population and perinatal risk factors
compared to a representative LAD population. Of this group 36 (61%)
had term deliveries an 23 {39%) had preterm deliveries,
RESULTS: The strongest association for cocaine use in these screens
was positive smoking history (90%), a prior history of drug abuse
(59%), lack of prenatal care (66%), black race (46%), preterm
deliveries (39%), low birth weight babies (49%), and a positive syphilis
or gonorrhea history (20%). An indirect association was noted with a
history of psychiatric admissions which is not a part of L & D history.
In cocaine positive nonpregnant patients, 56/143 (39%) had a h/story
of psychiatric admissions compared to only 43/560 (8%) of our general
chnic population, in the course of studying the above dsk factors, a
weighted scoring system was developed to assist in selectively
ordering laboratory confirmation.
CONCLUSIONS: This system was 92% accurate against known
positive screens and 78% accurate against know negative screens.
The risk factors observed are significant and have potential for
application in the weighted risk assessment presented. Universal
screening, not available to us, will be necessary for further evaluatlen
of this scodng system.
183 EFFICIENCY OF LOWER THRESHOLD CRITERIA FOR THE DIAGNOSIS OFGESTATIONAL DIABETES, Berkus~M, P~per, J, Langer, O Dept of Ob/Gyn, Umv of Tx Health-~cience~enter at San Antonio, TX OBJECTIVES: NDDG, ADA, ACOG, have agreed upon criteria to diagnose GDM using 2 abnormal GTT values The purpose of th=s study was to determine the =ncldence of adverse outcome m "normal" untreated grawdas, w~th mimmal hyperglycemia, classified as GDM by lower threshold crltena STUDY DESIGN: 944 consecuttve patients with glucose screening values>- 130rag/all who underwent 3 hr GT~rs comprised the study population 236 who met the NDDG criteria for GDM were excluded, 708 "normal" untreated patients were then reclassified by the criteria of Carpenter/Coustan (95,180,155,140 mg/dl), Sacks (96,172,152,131 mg/dl) or Langer (1 abnormal NDDG va~ue) RESULTS: 573 pat=ents (81%) had + screen, but were normal by all criteria The remaining 135 are compared below (Treat/LGA= #GDM treated per LGA =nfant identified)
Treat/ GDM(%) Macro LGA
LGA
Carpenter 72{10) 18 2% 23 6% 42
Sacks 101 (14) 167% 183% 55
Langer 87(12) 20 5% 24 7%* 41
Normal 0 13 3% 14 2% -- *p<03
Add=t~onally 1) of the total LGA neonates, 106 of these 708 patients, each criteria identihed Carpenter 16, Sacks 19; Langer 22; Normal-81; 2) GTT perlodlri~.y (time for GTT to return to fasting level) was s~gmhcantly increased only for the !-abnormal group, 3) there was considerable overlap between the cr~tena Langer Carpenter (56%), Langer-Sacks (63%), Carpenter Sacks (92%) (’ONL*LUSION: Using the cutena of 1 or more abnormal GTT values (NDDG) to d~agnose GDM ~s the most effective expansmn of current recommendations, =dent=fy~ng the most fetopathy for the number of patmnts comm*tted to d=abet~c management
182 GALL BLADDER DISEASE IN PREGNANCY. Kelly W!lscnx, John C.
Hisley~, Kim Haistenx, V. Daniel Castracanex. Department of Obstetrics
and Gynecology, Texas Tech University Health Sciences Center,
Amarillo, Texas.
OBJECTIVE: The incidence of gall bladder disease is higher in females
than in males and has been linked to parity in women. To our
knowledge there is no large prospective study to ascertain the true
incidence of gall bladder disease in pregnant women and therefore, that
is the purpose of the present study.
STUDY DESIGN: Random gall bladder examination in pregnancy was
performed in 189 normal patients (18 to 40 years of age) using abdominal diagnostic ultrasound, Patient accrual aimed at > 300
continues on ins study.
RESULTS; Overall the incidence of cholelithiasis was 6.9% (13/189)
which is higher than indicated by the available literature. Ethnically, the
highest incidence of stones was recorded in the hispanic population, 13%
(6/46), compared to 5.4% (6/112) in caucasians. The inddence of
cholelithiasis in blacks and orientals was low but was based on an
~nadequate patient population at this time. Of those with cholelithiasis,
36% became symptomatic and 15% with stones underwent
cholecystectomy at the end of the pregnancy.
CONCLUS|ONS: Should the incidence ot asymptomatic gall stones be
as high as suggested by this random prospective study, routine testing
seems appropriate so that one could have the opportunity to medically
or surgically treat small asymptomatic stones postpartum. The
contribution of ethnic, nutritional or geographic factors resulting in the
higher incidence in the hispanic group cannot be ruled out at this time.
It is expected that these studies will define the incidence and contribute
to the management of gall bladder disease in pregnancy.
184 INO1RECT EVIDENCE THAT TRE FETAL G~Ol~l’N PATTER~ IN IJRV~EM glTX 6ESTATIOMAL DIABETES IS =~L.= M. Lucas, T. Rowe,x L. Bowe,x D. Hclntire,x Dept. Ob/G~, Univ. TX Southwestern H~. Ctr.,
Dallas, TX ~JECH~: We us~ third tri~ster sonograms to evaluate the hy~thes~s that fetal growth associat~ with gestationa~ dia~tes differs fr~ ~tat~on nor~. Slay BESi~: 191 w~n w~th gestational dia~tes had third tr~ster fetal sonogra~; 78 ~bies (41%) were large for gestati~l age. ge c~r~ the regression lines for the ~an sonogra~ic esti~t~ fetal weights for LGA a~ AGA ~b~es in the gestationat dia~tes group to those deriv~ fr~ our obstetric ~lation. RE~LTS:
--- Population EFW, AGA
-- Population EF~N, LGA
..... Population EFW, SGA w GD AGA
-- GD LGA
GA at time of sono
CONCLUSIONS: Despite a disproportionate number of LGA neonates delivered to women with gestationat diabetes, the mean EFW within birthweight groups is virtually identical to our pol~Jlation. This suggests that LGA growth in these wofeen is "normal."

Volume 170, Number I, Part 2 SPO Abstracts 329 Am J Obstet Gynecol
185 RECOMBINANT HUMAN ERYTHROPOIETIN (rHEpo) FOR SEVERE ANEMIA IN PREGNANCIES COMPLICATED BY RENAL DISEASE. W Barth, Jr, L Lacroix~, M Goldberg~ M Greene. Depts of Ob/Gyn and Medicine, Harvard Medical School, Brigham and Women’s Hosp, Boston, MA OBJECTIVE: To study the effects of rHEpo in pregnancies complicated by severe anemia due to renal disease. STUDY DESIGN: Case series (4) and review of the literature (ii). RESULTS: rHEpo was begun prior to conception in 8 cases and during pregnancy in 7. 13/15 had chronic hypertension and i0 patients were on dialysis. Dosages ranged from 4K to 24K u/wk. 13/15 patients responded with an increase in Hct. Only 5 of 15 were transfused. In 7/13 chronic hypertension worsened. There were 2 fetal and 2 neonatal deaths. In i0 cases with data, the mean newborn hematocrit was 53% (40 to 68%). CONCLUSIONS: Use of rHEpo may decrease the need for red cell transfusions in pregnancies complicated by severe anemia due to renal disease.
187 PREGNANCY OUTCOME FOLLOWING RENAL
TRANSPLANTATION: AN UPDATE OF THE NATIONAL
TRANSPLANTATION PREGNANCY REGISTRY.
G, Maennes,=N- Silveaman, M. Moritz,* B.A. Aldswede,x V. Armentix. Division of Maternal-Fetal Medicine, Department of
Obstatzics and Gynecology,, and Department of Surgery, Jefferson
Medical College of Thomas Jefferson University, Pkiladelphie,
Pennsylvania
OBJECTIVE: To describe the otmumxe of pregnancy following maternal renal txansplantetion.
STUDY DESIGN: The National Transplantation Pregnancy
Registry was established in 1991 at Thomas Jefferson University
Hospital to study pregnancy outcome in transplant r~cipiants. Data
f~om 279 renal I~ansplant patients with 424 pregnancies were
collected by patient questionnaire, patient interview, and medical
record ~vlew.
RESULTS: The mean m~eraal age at conception was 27_3 ± 4.8
years, with a mean transplantation to conception inte~al of 4.0 _+ 3.5
years. Of the 424 pregnancies, 34 (8.0%) were therapoutically
terntinated whi~ 49 (11.6%) spontaneo~ly aboxXed prior to 20 wee.ks’ gestation. Fur Livebem infants (n--337), the mean gestational age at delivery was 35.7 ± 3.6 weeks’ with a mean birthweight of 2597 + 748
grams. Fifty-eight percent of llvebom infants delivered at less 37 weeks’, though only 18.5% of all pret~m deliveries occm~ed less than 32 wee~’. There were 12 stillbirths and 6 neonatal deaths
(all pretezm), yielding an overall parinata] mortality rate of 51 per
1000 births.
CONCLUSIONS: Pregnancies following maternal renal
t~ansplantatinn are associated with an incre~ed risk of preterm
delivery. Overall pe~natal murtsllty in these pregnancies appears to be comparable to outcomes of pregnancies in populations with
associated medically-manageable maternal illnesses.
186 CARDIAC RESERVE AFTER RECOVERY FROM
PERIPARTUM CARDIOMYOPATHY (PPCM). J Hibbard, L
Weinert, M Lampert, M Lindbeimer, R Lang. Dept Ob/Gyn and
Med, U of Chicago, Chicago, IL. Objective: We hypothesized that patients with PPCM who have recovered baseline cardiac function as determined by routine echocardiographic criteria, will demonstrate subtle abnormalities in cardiac reserve during a dobutamine challenge test. Study design: Seven well documented PPCM patients, whose echocardiographic tests demonstrated normal baseline function, underwent a load independent analysis of left ventncular (’LV) contractility. Cardiac reserve was measured by dobutamine
challenge. Seven women of similar age, race, parity and time of
dehvery, with no cardiac abnormalities comprised the control
group. Two-dimensionally targeted M-mode echo and Doppler
flow studies were performed over a wide range of loads induced by
methoxam~ne challenge. Contractile reserve was accessed after an
infusion of 5 p.g/kg/min of dobutamine, a ~ ittotrope.
Results: Baseline overall LV performance in PPCM was
indistinguishable from the control group. In contrast, contractile
reserve (described as velocity of fiber shortening units above the
baseline contractility line, cirs/sec) was significantly reduced m
the PPCM when compared to controls.
Conchision: PPCM patients, thought to have fully recovered on
routine echo, demonstrated decreased cardiac reserve when
challenged with dobutamine. This finding has important
implication in counseling of patients with PPCM who have
recovered LV function regarding future child-bearing.
188 PREGNANCY ASSOCIATED WITH APPENDICITIS RESULTS IN A
HIGHER INCIDENCE OF PULMONARY INJURYTHAN APPENDICITIS IN NONPREGNANT PATIENTS. T.Westove~, M. L~kex. Dept. of MFM,
UMDNJ RWJ Med School, New Brunswick, NJ.
OBJECTIVE: Tr~e null hypothes=s ~s that appendicitis does not
predispose to a capillary leak syndrome m pregnant patients versus
matched nonpregnant patients.
STUDY DESIGN: A retrospective chart rewew of 16 consecutive
pregnant pabents w~th appendicitis and forty consecutwe nonpregnant
aged matched fema|esw~th append~mt~s was performed to determmethe
frequency of pulmonary ~njury and any associated causative factors.
Cont=nuous varmbles were compared by two-tailed Student’s T-test and
categonc vanables were compared by two-taged Flsher’s exact test or
Wflcoxon rank sum where appropnate
RESULTS: We noted a 19% incidence of pulmonary mlury m the
pregnant pattents, documented by hypoxemta and rad~ographtc evtdence
of pulmonary edema, and a 0% mcmdence m the nonpregnant pat=ents (P= 02) No s=gnmficant dmfferences were noted in age, race,
somoeconommc status, duratmon of symptoms prior to appendectomy,
t~me from admmss~on to appendectomy, percentage of patients with temp
_>101, or percentage of patients wroth perforatmon, abscess, posit#re pentoneal culture, phlegmon or ant~b=otmc coverage.
CONCLUSION: Pregnant pat=ents with append=cit=s may be at higher
nsk for pulmonary mnjury than matched nonpregnant controls wroth the same degree of seventy of =llness.

330 SPO Abstracts Jar~u.ry 1994 Am J Obstet Gynecol
GESTATIONAL DIABETES: IS AMNIOTIC FLUID INSULIN A MIRROR
OF THE FETUS? Oded Lang_e~r, Byron Elhott, Elly Xenak~sx, Jearrna P~per Dept Ob/Gyn UmvTXHCS, SanAntomo, TX OBJECTIVE. Because maternal hyperglycemia ~s the cause of fetal hypermsuhnernla and macrosomia, we sought to evaluate whether amrnotlc fluid (AF) msuhn and glucose are associated w~th ambulatory maternal glucose profile and neonatal size STUDY DESIGN: In 276 gestat~onal d~abet~c women who measured their blood glucose using memory reflectance meters on an ambulatory bas~s, AF samples were obtamed by transabdomm~l amniocentes~s late in the third trimester Insuhn was measured by sohd phase radlolmmunoassay, and glucose was measured with a Beckman analyzer The association between maternal glucose characteristics and AF ~nsuhn and glucose levels were analyzed, as was treatment modahty The association between AF msulm and glucose and neonatal size stratified by b~rth percentile for a given gestatlonal age and macrosomla was estabhshed RESULTS: Overall, AF hypermsuhnem~a (defined as :- ISpU) was present In only 89% of the study population when maternal mean blood glucose was ~ 100 mg/dl Significantly higher levels of AF ~nsulin were found in women w~th poor glycemlc control when compared to well controlled sublects (16+-9 vs 72 7. P<0 01. respectively) Furthermore, a positive correlation exists between AF ~nsulin and maternal mean blood glucose and fasting plasma glucose (r= 31, P< 04 and r= 59, p~ 0006, respectively) NO association was found between, maternal )evel of glycem~a and AF glucose, maternal insuhn when treated and AF insulin (r= 03, p< 16); treatment modahtyandAF msuhn Infant b~rth weight and birth percentile were significantly correlated w~th fetal ammottc msuhn (r= 27, P< 000!, r= 26, P~. 0000, respectively) However, when data were d~chotom~zed by b~rth
~PnerCentlle, 66% of the LGA infants and 54% of the macrosom~c rants had normal ~nsulin levels CONCLUSION: Our data support the prewously described physiological association between maternal hyperglycemia and fetal hyper~nsuhnem~a However, due to the lack of chmcal sensitivity, ammotlc fluid Insuhn level cannot be used as a choice] marker for the presence of fetal overgrowth
191 EARLY BLOOD PRESSURE CHANGES IN DIABETIC WOMEN WHO
DEVELOP PREECLAMPSIA. A. Johannin~lx, B. Rosenn, M. M~odovmk, G. Holcbargx, J Khoury~, T.A. S~dd~ql. Unwersity of
OBJECTIVE: Women destined to develop praeclarnpsia IPRECLJ
have h~gher systolic and diastolic blood pressure (BP) values early ir~ pregnancy compared to those who do not develop PRECL. Because
msuhn-dependent d=abetes (lOOM) may affect basal vascular tone,
we hypothesized that the assocmtlon between early BP in pregnancy
end PRECL would not be evident in women with IDDM.
STUDY DESIGN; 239 IDDM women were enrolled poor to 10
weeks’ gestation, managed with intensive insulin therapy, and
followed w=th weekly measurements of BP and monthly
measurements of 24-hour urinary protein excretion. PRECL was
defined as BP -> 140/90 mmHg, or a rise in BP (after 20 weeks) of
15 mmHg in diastohc BP, 30 mmHg In systolic BP, or 20 mmHg in
mean arterial BP, with protemurla (~ 5OO rag/24 hours). Women
with chromc hypertension or nephropathy were excluded from the
analys=s.
RESULTS: 19 out of 201 women (9.4%) developed PRECLo Mean
d=astohc(D), systolic(B) and mean arterial(M) BP up to 22 weeks’
gestation are shown ~n the following table:
~< 12 W~ 13-17 Weeks 18-22 Weeks
S D M S D M S D ~
PrecL 121 72 88 117 70 86 120 71 87
No preci. 112 68 83 112 66 82 112 86 81
P-value .0001 .007 .0003 .05 .05 .02 .O01 .003.0006
CONCLUSIONS: Despite potent=el abnormaht~es In IDDM that may
affect basal vascular tone, women with IODM show the same trend
as non-IDbM women: those who go on to develop PRECL have
higher BP values early =n pregnancy, possibly allow=ng prediction of
PRECL (Supported ~n part by NIH Grant HD 11725)
190 TREATING PATIENTS Wl’rl/A SINGLE ABNORMAL 3-HOUR
G’rl" VALUE: RESULTS. D. Schwartz, G. Goyert, Y. Daoudx, J.
Copesx, P. Zazulax, D. Wright~, R. Bronsteen~, H. Epstein~. Dept
Ob/Gyn, Sinai Hospital; W.S.U., School of Medicine, Detroit, MI.
OBJECTIVE: Patients with a single abnormal value (SAV) of the
3 hour GTI" have been reported to have similar adverse perinatal
outcomes as patients with GDM. In this study, SAV patients and
gestational diabetics were managed by the same standardized
treatment protocol and perinatal outcomes were evaluated.
STUDY DESIGN: 86 SAV and GDM patients were managed by
an identical outpatient program that included current ACOG
criteria for screening, diagnosis, glycemic control and insulin
initiation. The comparsion control group excluded all diabetic
patients. Statistical assessment utilized Chi square and ANOVA.
RESULTS: Of the 86 SAV patients, 7 (8.1%) required insulin. No
significant differences were found between the SAV patients and
the control population for the following outcome measures:
gestational age at delivery, birth weight, macrosomia, LGA
neonates, shoulder dystocia, NICU admissions and PIH.
However, the primary C/S and the PNM rates were significantly
lower (P < 0.05) in the SAV patients than for control patients. In
the 7 SAV patients requiring insulin, the mean birth weight and
the rates of LGA and macrosomia were significantly less (P <
0.05) than for control patients.
CONCLUSIONS: 1. Patients with a SAV, when managed in a
protocol identical to GDM patients, had no increased risk for
adverse perinatal outcome. 2. In addition, as Insulin therapy was
required for a "significant" percentage (8.1%) of SAV patients,
these results strongly suggest the importance of close surveillance
and active management of patients with a SAV.
192 PERIPARTUM PITUITARY MASSES: DIFFERENTIAL DIAGNOSIS. E. Pressman~, S. Zeidman~, U. Reddyx, Dept. of Gyn/Ob end
Neurosurgery, Johns Hopkins Univ., Baltimore, MD.
OBJECTIVE: Lymphocytic adenohypophysitls (LAH) is an
sutoimmune disorder of the pituitary gland with a predilection for late
gestation and the postpartum period. LAH presents with acute visual
d~sturbsnee and pltuKary dysfunction with an enhancing sailer lesion
on computed tomography (CT) mimicking a p~tultary adenoma (PA).
We sought to define the clinical, endocrmologlc, and radiographic
characteristics d~fferentmtmg peripartum LAH from PA to enable non-
invaslve diagnosis and appropriate therapy.
METHODS: From pubhshed reports and our own cases, the clinical
histories, laboratory, and radiographic studms of 45 patients fulfilling
the dmgnoms of perlpartum LAH were reviewed. H~story of ~nfertihty
or menstrual irregularity, symptomatology, endocrinologm evaluation,
diagnostic imaging, end associated medmal conditions were analyzed.
For comparison, 786 patients with PA and pregnancy from published
series were evaluated.
RESULTS: Visual disturbances were s=gnificantly higher in patients
w~th LAH (64%) than PA (8.3%). The spontaneous pregnancy rate
m PA patmnts was 2.4% vs 100% m LAH patients. Maternal
prolactm levels in LAH patients ware significantly lower than for PA
patients at any point in gestation. On ~CT, there were no
distinguishing charactenstlcs; MRI may be more promising, but data
were limited. LAH was assomated with other autoimmune diseases
in 24% of patients, higher than that in PA.
CONCLUSIONS: PA typically presents w~th menstrual irregularity and
infertility. It is unlikely to have a pituitary tumor imtlally present
during gestation without pre-exist=ng menstrual dysfunction.
Spontaneous conception, low serum prolactln level, and visual
symptoms all favor the diagnosis of LAH. Though emergent surgical
decompression may be indicated in both to preserve vision, accurate
diagnosis without biopsy will allow spemfm medical therapy without
the risk of pituitary surgery.

Volume 170, Number l, Part 2 SPO Abstracts 331 Am J Obstet Gyneco|
193 PRETREATMENT GLYCOSYLATED HEMOGLOBIN AS AN
INDICATOR OF MACROSOMIA IN GESTATIONAL DIABETES
MELUTUS. S,A, Scarpslhx, D. Moskowitz=, R. Barkey-Divonx, Y.
Barnhard=, A. Anyaegbunam, M.Y. D~von. Department of Ob-Gyn, Albert Einstein College of Medicine, Bronx, NY.
OBJECTIVE: To evaluate the assomat~on between pretreatment
Gtycoaylated Hemoglobin (HbAlc) and the incidence of macrosomla
in Gestational Diabetes Melhtus (GDM|.
METHODS: HbA~c was obtained In 83 GDMs prior to initiation of
treatment. An HbA,, >-8% defined an abnormal value reflecting
prolonged pretreatment hyperglycemia. Associations between
normal and abnormal HbA~ and the Oral Glucose Tolerance Test
(OGTT)(Table I) as well as between macrosomia (BW> 90th%ile) and the mean blood glucose (BG) and the percent of hyperglycemia
(> 120mg/dl) during treatment (Table 2) were analyzed. Pat=ants
performed 7 BG tests/day using computerized meters.
RESULTS: Table 1
Hb~A,~ Fasting 1 hr 2hr 3hr Macrosomla <8%(n=66): 102+15 216_+25 198_+38 144_+46 18% _>8%(n=17): 117+_20 229_+41 238_+53 207+_41 23% p va~ua: 0.0045 O.15 O.O019 <O.0001 0.87
Table 2 Mecrosom~a HbA~ Mean BG %Hyperglycemia Present(n = 16): 6.9±1 110+_14 30_+16 Absent (n=67): 7.0_+1 102±14 26:t:14 p value: O.88 0.09 O. 1 ~ CONCLUSIONS: (1) As expected, an elevated HbA~ was associated with a significantly greater degree of OGTT abnormality.
(2) Macrosomla was associated with a higher mean BG and %
hyperglycemia, however, these differences did not reach statistical
s~gnlflcance. (3) The incidence of macr~somla was increased when
HbAI~ was elevated, however, this difference did not reach
statistical significance. Thus, an elevated pretreatment HbA~c does
not predispose to the development of macrosomle in GDM.
195 MANAGEMENT OF THROMBOEMBOLJC DISEASE ASSOCIATED
WI~’H PREGNANCY W. Evans,x S. Laifer, T. McNanley,x A.
Ruzycky,x Dept. Ob/Gyn Reprod. Sc., Univ. of Pdtsburgh,
Pittsburgh PA
OBJECTIVE: To determine the management of grav~das with a bstory of thromboembohc disease.
STUDY DESIGN: SPO members were surveyed on thaw
treatment for a gravida with a history of. 1) deep venous
thromboms (DVT) associated w=th oral contraceptives; 2)
postpartum DVT m a previous pregnancy, 3) pulmonary
embolism in a previous pregnancy; 4) mechamcal heart valve RESULTS: 550 members responsed Case 1): 73% chose
minidose heparm; 8.1% - fu~l dose heparm, 13% - no
therapy. Postpartum management’ 62% chose minidose
hepadn for 6 weeks; t3% - full dose heparin and 6 weeks of
coumadin; 8.3% no therapy. Case 2): 71 4% chose minidose heparin. Postpartum management’ 56% chose
m,]mdose hepann, 15.2% - full-dose heparin. Case 3)
56 3% chose m=mdose hepann; 38% - full dose hepar=n. Postpartum management 42% - m~mdose heparin; 19% -
full heparm dose w=th 6 weeks of coumadm. Case 4): 95%
chose to d~scontinue coumad~n and initiate full dose heparin A
majority chose partial thromboplastm times (aPTT) of 1 5- 2 0 x control as therapeutic. There was no consensus on
heparm dosing or monitoring schedule. CONCLUSION: Most respondents antlcoagulate patients with
a bstory of thromboembohc d=sease.There ~s httle agreement on dosing and monitoring of heparm therapy.
194 ARE PATIENTS WITH SICKLE CELL TRAIT AT RISK FOR PREECLAMPSIA? A. Chaudhury, M.D., S. Ahyax, E. Brown, M.D.X~ T. Patelx, C. ~eneus, M.D.x, T, Heeren, M.D.x, Boston Univ. Sch. of Med./Public Health. M. Hunter, B.A.x, L. McMahon, MoD.x, Boston Comprehensive Sickle Cell Center. OBJECTIVE: To determine the relationship of sickle cell trait (Hb AS/AC) and preeclampsia. We recently presented pilot data on 63 patients with Hb ASTAC at risk for preeclampsia at the 18th Annual Meeting, National Sickle Cell Dis. Program, Philadelphia, May, 1993. STUDY DESIGN: We report a case control study of 154 pregnancies complicated by Hb AS/AC who re- ceived prenatal care and delivered at our inst- itution from 1/1984 to 12/1990. The control group consisted of 95 pregnancies matched for age, race, gravity, parity, renal disease, hypertension and substance abuse. RESULTS: No significant differences were seen with respect to urinary tract infection, Hb status and birthweight. Hb AS/AC patients had a higher but statistically insignificant risk of preterm delivery. This group also had a higher rate of Cesarean section (23% of patients ver- sus 11% of controls, p = .056).
Preeclampsia
Hb AS/AC Group = 154 14.58%
Hb AA Control Group = 95 6.45% Relative Risk = 2.3. CONCLUSION: The relative risk of pre@clampsia is significantly higher in the Hb AS/AC group; therefore, this group of patients should be followed closely during pregnancy.
196 IS PROLONGED HOSPITAL BEDREST DURING PREGNANCY A MAJOR RISK FACTOR FOR DEVELOPING A DEEP VEIN THROMBOSIS? Carr MHx, Towers CV, Iriye BKx. Dept. of Ob/Gyn, Long Beach Memorial Women’s Hospital, Long Beach, CA and Unlverslty of Californla, Irvlne Medical Center, Orange, CA. OBJECTIVE~ Pregnancy is a reported risk factor for thrombosis as is prolonged hospital bedrest. The purpose of this study is to determlne the incidence of deep veln thrombosis (DVT) in pregnant women at prolonged bedrest. STUDY DESIGN: A retrospective review was performed of pregnant patients hospitalized at prolonged bedrest (>20 days) during the tlme period from January 198~ to July 1993. All cases of documented DVT’s associated with pregnancy during this same time period were also reviewed. RESULTS: A total of 154 pregnant women were hospitalized at bedrest for more than 20 days (mean days:34.6 ~ 14). Reasons for hospltallzatlon include prolonged premature rupture of membranes (29.9%), placenta prevla (24.7%), preterm labor (22.7%) and a variety of other medlcal compllcatlons (22.7%). None of these women developed a deep vein thrombosls(CI : 0-2.8%)and none received prophylactic heparln. In the same time perlod there were nine documented cases of DVT’s that were assoclated with pregnancy. Four occurred in the antepartum perlod and five occurred in the postpartum perlod. None of these patients had a hlstory of prolonged hospital bedrest. CONCLUSION: TO date it ~s unknown whether prolonged hospital bedrest increases the incldence of DVT’s in pregnancy. Some clinicians elect to use prophylactic heparln in this patient population. However, the risks associated with heparln antlcoagulation can include bleedlng, thrombocytopenia, hypersensltlvlty, paradoxical thrombosls and osteoporosls. Based on the above data, prophylactic heparln may not be 3ustlfled.
332 SPO Abstracts January 1994 Am J Obstet Gynecol
197 GESTATIONAL DIABETES: DOES THE PRESENCE OF RISK FACTORS INFLUENCE PERINATAL OUTCOME ? J. Weeks~C.A. Major, M. de Veciana and M.A. Morgan
Dept. of Ob/Gyn, Umv. of Cahfornia, Irvine, CA. OBJECTIVE: We hypothesize that gestational diabetics (GDM) with risk factors for GDM have a similar perinatal outcome to those without risk factOrs. STUDY DESIGN: Uruversal screening for GDM is routinely practiced at our "mstimUon. A retrospective chart review of al~ patients diagnosed with GDM from 1/90 and 12/92 was conducted. Multiple gestations and patientS with cardzae or renal thsease were excluded Risk factors
identified included: obesity, family history, previous GDM, macrosomia, bastory of stillbirth or fetal anomaly. Patients with >_ 1 risk factor (Grp.1) were compared to those without (Grp.2). A low risk non-diabetic paraents served as controls. Outcome variables included: incidence of insuhn requirement, cesarean section, neonatal macrosomia & shoulder dystocia RESULTS: 106 patxents with GDM were included: 60 with _> 1 risk factors, 46 without risk factors. 106 low risk non-diabetic controls were compased to both groups of GDM pts. (separate and combined).
VARIABLE ~ROUP 1 GROUP z tSONIROLS
A2 GDM (%) 30 Z~ O
C-secti0n rate (%) 38 35 15" B Wt >- 4000 (gin) 33 17 11" Shoulder dystooa(%) 7 13 2*
* Groups 1 & 2 combined compared to’~ontrols (p< 0.05 ~
The s~milarities between groups 1 & 2 remained after controlling for maternal age. CONCLUSION: A power analysis showed we had an 80% power to detect a 2-fold d~fference in complication rate in patients with risk racers
at a 95% confidence level. Gestahonal diabetics, with and without risk factors, have an increased inmdence of adverse outcomes compared to low risk controls. GDM with risk factors had smmilar outcome to those without. Thus selective screening for GDM using risk factors alone does not adequately identify patients at increased risk
199 CHORIOAMNIONITIS: THE INPACT OF TIHE INTERVAL FKOH DIAGNOSIS TO
DELIVERY. P. We~e_~ S. COX, S. Roberts, H. Maberry, J. Daxx, L. Gilstrap. Dept Ob/Gyn, Univ. of TX Southwestern Med. Ctr., Dallas, IX ~aECTIVE: ~e sought to determine whether the ti~r~ elal:~ed free] diagnosis to delivery played a role in neonatal outcome. METB(JOS: 197 pregnancies complicated by chorioamnionitis were prospectively followed. Mothers were treated with I~ antibiotics and antipyretics as needed for persistent fever >38"C. Neonatal outcome parameters analyzed lncluded; cord pH, develol:~nent of neonatal sepsis, oxygen requirement (ventilator, ~alo, CPAP) and
admission to the special care nursery, Exposure and outcome measures were compared with Fisher exact tests,
Interval 0-2 2-4 4-6 6-12 12-18 P (Hours) value
Number 80 57 39 18 3
Apgars @ 5
< 7 2(3) 3(5) I(3) I(61 0(0) .72
< 4 0(0) I(21 0(0; I(61 Of 0) .17
Cord gas
p~ < 7.20 25 19 17 6 I (31) (33) (44) (33) (33) .76
pH < 7.00 0 0 0 0 0
Sepsis 2(3) 0(01 0 0 0 .76
Oxyg_en 7 6 2 2 0 .85 requlrement (9) (111 (9) (11)
Ad~issien 10 10 2 2 1 .26 to SO¼ (131 (181 (5) (111 (331
There were no differences in cord pH, sepsis, admission to the
special care nursery, and oxyQen requirement in neonates, based on duration of time froa diagnosis of cherioan~ienitis to
delivery in our study. CONCLUSIOII: In pregnancies complicated by chorioamoionitis
appropriately treated with parentera[ antibiotics, an interval to delivery time of up to 12 hours appears to play little, if any, role in neonatal outcome. The number of patients in the 12-18 hour group is too sma(( to draw valid conclusions.
198 RECURRENCE OF GESTATIONAL DIABETES: WHO IS AT
RISK ? C A. Ma~ur, M. de Veciana, J. Weeks and M A. Morgan.
Dept. of Ob/Gyn, University of California, lrvine, Orange, CA.
OBJECTIVE: We hypothesized that certain risk factors may relate to
recurrence of gestatienal diabetes (GDM) in a subsequent pregnancy.
STUDY DESIGN: 66 consecutive patients with GDM were evaluated in
their subsequent pregnancy. Patients with and without recurrent GDM
were compared. Charts were abstracted for: maternal deruographi~s, pre~
pregnancy weight, body mass index (BMI), weight at delivery, risk
factors for GDM, gestational age (GA) at diagnosis of GDM, fasting
blood glucose (FBS) on 3 hr. glucose tolerance test (GTT), GDM class,
interval between pregnancies, GA and birthwmght at delivery.
RESULTS: 47 of 66 (71%) had recurrent GDM and 19 of 66 (29%) did
not recur (NO GDM).
VARIABLE
Age (~rs) -"
Pro preg wt. (lb)
BMI
Wt. @ delivery (lb)
GA@diagnoms (wk)
FBS + SD (mg/dl)
GDM risk factors (%
Class A2 GDM (%)
B Wt. (gin)
B.Wt.>- 4500gm (%)
Interval <24mos (%)
CONCISUSION: ~D
GDM NO GDM *RR (95%C.Io)
52.1_+4.9 ] 29.2-+5.3 [ p:0,03 141_+36 I 138+_29 I p=0.8 Z8.3_+6.7 [ 24.3_+4.4 [ p=0.03
171+_37,3 [ 169_+26.5 [ p=0 8
Z6.2_+5.4 I 29.8_+2.6 I p=0.007
t18-+122 I 94-+13,6 p=0,004
42 *RR=1.4(1.0-2£
77 ! 22 *RR=2.1(I.3-3.3
t851-+727 ] 3709+-500 ] 19=0.4
50 I 21 *RR=I.6(IA-2.1
¯ recurrencd is more likely m th~’~ with earl~
GDM thagnusis or insulin requirement zn the index pregnancy, > 1 risk
factor for GDM, a higher i~tial BMI, a higher FBS on GTI" and/or < 24
months interval between pregnancms. These findings facilitate
counselling of GDM patmnts.
200 PULMONARY INJURY ASSOCIATED WITH ANTEPARTUM APPENDICITIS: WHO IS AT RISK ? M. de Veciana, C.V. Towers, C.A. Major, J. M. Lien and J S. Toohey, Dept. of Ob/Gyn, Long Beach Memorial Medical Center & Univ. of California, Irvine, CA. OBJECTIVE: To review our experience with antepartum appendicit~s and evaluate if certain risk factors increase the hkelihood of developing pulmonary injury. STUDY DESIGN: We reviewed 49 consecutive cases with documented antepartum appendicitis who underwent exploratory surgery between 1/1/82 and 12/31/92 Charts were abstracted for: gestafional age at surgery, type of anesthesia, clinical factors (maximum maternal heart rate, respiratory rate and temperature prior to surgery), laboratory tests (white cell count, hematocrit, culmres and pathology findings) and treatment factors (use of tocolytics and/or antibiotics and fluid management
m the first 48 hrs). Pulmonary injurj(’ was characterized by
dyspnea, tachypnea, documented hypoxemza needing oxygen supplementation & an abnormal CXR. RESULTS: Of ~9 patients with confirmed appendicitis, 9 (18%) had pulmonary injury lARDS n=2, pulmonary edema!infiltrates n=7]. All cases with pulmonary injury 9/9 (100%) were at > 20 weeks gestation vs. 27/40 (67%) in the non-injury group (p=0 05). Univariate analysis showed that fluid overload _> 4L, maX. RR > 24, max. FIR > 110, Tmax. _> 100.4, use of general anesthesia and/or use of tocolytics were highly sigmficant (p-<0.005). A significant number of patients w*th pulmonary injury 4/9 (44%) vs only 2140 (5%) without injury received mdomethacin concurrently with other tocolyfic agents (p<0.0071. By multivariate analysis through stepwise logistic regressmn, finding fluid overload > 4L, RR > 24, Tmax -> 100 4 and tocolyt~c usage would predict
99% of cases with pulmonary injury. CONCLUSION: Pulmonary injury with m,tepartum appendic~ns can occur as has been reported wath antepartum pyelonephntis. To our knowledge this disorder has never been previously reported w~th appendicitis m pregnancy. Iatrogemc factors such as: lack of judicious fluid management and tocolytic usage can greatly increase the risk for pulmonary injury This risk may be gestatienal age dependent. Of the nine cases, seven were potentially preventable.
Volume 170, Number 1, Part 2 SPO Abstracts 333 Am J Obstet Gynecol
201 PERIPARTUMACTIVATIDII OF LUPUS. K. Ma~ee, S. Cox, J. Daxx, F, G. Cunningham. Dept Ob/Gyn, Univ. of T~ Southwestern Mad. Ctr., Dallas, TX OBJECTIVE: There are conflicting reports in the literature concerning lupus actlvity (flares) during pregnancy. We sought to ascertain pregnancy outcomes and to determine the incidence of Lupus activatlon during pregnancy and the puerperium. METRODS: Using a computerized Listing of discharge diagnoses,
pregnancies complicated by SLE were ascertained. ALL women met the American Rheumatism Association criteria for the diagnosis of
SLE. Haternal records were then reviewed. RESULTS: From 1983 to August 1993 32 pregnancies affected by SLE were identified. The incidence of SLE in pregnancy in our institution was 1:4600. Selected outcome variables are presented below: Maternal Characteristic Delivery Outcomes
Prffgnancv Induced 31% Term 41% .ypertenslon Chronic Hypertension 16% Preterm 41% Renal Insufficiency 22% Stillbirth Nephropathy 4"P/~ Termination 9% Steroid therapy 72% Incomplete Ab 3% Mortality 6%
Treatment
None
Steroid 4 (yes) n=18
Steroid 3 (no) n=9
LUPUS ACTIVITY
Antepart%m~ I ~ Postpartum (trimester) prior to (weeks)
delivery I 2 3 I 2 3 4
5 6 12 5 3 0 0 0
0 0 5 I I 0 0 0
COI~CLUSIONS: Activation of lupus during pregnancy occurred in 63% of our patients and irrespective of steroid therapy. Although this is an uncon*non pregnancy complication, pregnancy morbidity and maternal martaLity remain high. Importantly, 10 of the 20 patients who had flares did so in the week prior or the week after delivery.
203 GLUCOSE METABOLISM IN FORMER GESTATIONAL DIABETICS. ~ Bennett, P Meis. Univ of KS, KC, KS and Wake Forest Univ, Winston-Salem, NC. OBJECTIVE: Women with former gestational diabetes (FGD) have abnormal glucose metabolism frequently not evident by standard clinical glucose testing. These women are at risk for developing overt diabetes. We sought to determine the effectiveness of oral and IV GTTs in identifying aberrant glucose metabolism in FGDs. The effect of diurnal variation on these tests was also examined. STUDY DESIGN: Six FGDB and controls matched for lean body mass underwent oral GTTS. Frequently-sampled IV GTTs were also performed and insulin sensitivity (Si) was derived by the minimal modeling technique. The procedures were done twice (AM and PM) in random order. RESULTS: Glucose values were higher 60 min following oral glucose load in FGDS vs. controls (AM: 136 ~ 34 vs. 109 ± 19, PM: 178 ± 17 vs. 143 ~ 16 mg/dl, p=0.05). PM glucose values were higher than AM (prO.01). Si was slightly lower in FGDs compared to controls (AM: 4.7 + 1.8 vs. 6.7 + 1.6, PM: 2.4 + 0.8 vs. 3.7 ~--i.i xl0-4 min-1~uU/ml, p=0.16)? Si values were lower in the PM (p=0.015). CONCLUSIONS: Compared to women with similar lean body mass, FGDs demonstrate significant glucose abnormalities by oral GTT. IV GTTs show a similar trend, although insulin sensitivity is only modestly lower in FGDs. Time of day clearly effects both oral and IV GTTs.
202 ACUTE PYELONEPHRITI$: OUTCOMES AND COST EFFECTIVENESS OF
AHPICILLI~ AND GENTAMICIN THEP.APY. R. Horsa~er, S. Cox, Dept Ob/Gyn, Univ. of TX Southwestern Med. Ctr., Dallas, TX O~JECTIVE: On September I, 1992, a p~aramcy task force mandated the use of ampici[lin and gentamicin as first line agents in the treatment of antepartum pyelonephritis. T~e purpose of this study was to evaluate the results of this policy during the first
calendar year of Implementation. METHODS: One hundred and thirty pregnant women were admitted to the hospital from January I, 1992 to December 31, 1992, with a prlmary diagnosls of pyeLonephritis. Those charts were then reviewed and a descriptive analyals of outcomes compiled. RESULTS:
Mean G.~. at a~issi~n (wks) Mean IV therapy (hrs) Patients receiving > 96h of RX
Mean hospital stay (days)
Anemia at admission
Anemia at discharge
Cr ~ 0.9 mgldl
Uropathogens
Klebslella Enterobacter Proteus Citrobacter
22 Isolated uropathogens
63 E coli 89
12(9%) Klebsiel[a 5
3 Enterobacter 2 31(24%) Proteus 2 47(36~) Citrobacter I 22(17%)
Antibiotic Sensitivities
Amp Gent Mez Cefazotin 51% 100% 59% 90% 0% 100% 60% 100% 50% 100% 100% 50% 100% 100% 100% 100% 0% 100% 0% 100%
Overall 50% 100% 60% 90%
CONCLUSION: Our findings suggest that for our patient population, Cefazolin, a first generation cephalosporin, may be
a more appropriate choice of antibiotic for the treatment of antepartum pye[onephritis, This conclusion is based on urine culture sensitivities, nursing IV administration time (3 x per day vs 7), cost (¢efazoLin $12.72/day, Amp/Gent $36.02), and a decreased r~sk of renal and ototoxicity to the patient.
204 ADJUNCTIVE BEHAVIORAL THERAPY IS ASSOCIATED WITH A DECREASE IN THE INCIDENCE OF PRETERM LABOR AND DELIVERY
IN PREGNANT DRUG USERS. RL Ar]dras, PD VVdsonx, R ElkX, J Gratx~wsklx Depta of OblGyn/Repred Sm and PsycWBehav Sc~, Un~v of
Texas Med School, Houston,Tx OBJECTIVE To =nvest~gata the potanbal tmpaot of adJunctive behaworal
therapy on pennataJ outcome in pregnant drug users STUDY DESIGN A retrospective rewew of 61 patients cared for =n the
Prenatal Substance Abuse Chn~c (PSAC) at UT Houston was undertaken Group A (n=29) received no specific drug counsehng =ntervenbon whde Group B (n=32) underwent mtans=ve behaworal therapy at the same institution TI~ data were stabsbcally anayzed w~th either Ch~ Square or Student t-test RESULTS: The incidence of preterm labor requiring tocolytic agents
was greater In Grp A (34%) than in Grp B (3%) (p=0.002). Similarly,the
incidence of preterm delivery was greater in Grp A (20%) than in Grp B
(6%) (p<0.05). The groups were s~mllar with respect to drug of choice (co<;a~ne Grp A=72%, Grp B=62%), #olydrug use (Grp A=62%, Grp B=44%), alcohol use (Grp A=48%, Grp B=34%) and smoking (Grp A=55%, Grp
B=78%) There was no difference =n the ~nc=dence of SGA infants (<10th pot)
(Grp A=10%, Grp B=6.3%), preterm premature rupture of the membranes (Grp A=7%, Grp B=9%) mean prenatal vls=ts (Grp A=6 2, Grp B=9 0) or
b=rthwe=ght (Grp A=2898 + 720 gme, Grp B=2974 + 695 gms [mean _+ SD])
between groups CONCLUSION: These data suggest that =ntens=ve behavioral therapy =s associated w~th a stabstJcally s~gn~ficant decrease In the incidence of both preterm labor and dehvery The increase in direct pabent contact may play a significant role in the observed difference in preterm birth

334 SPO Abstracts January ]994 Am J Obste/Gynecol
205 CO~CURRENT DIABETES NELLITUS AND THYROID OYSFUNCTION AND PREGNANCY OUTCOHE. A.Chau, 14. Nontorox, S.Kjos. Dept of l~b/Gyn, Univ. of So~Jthern Calif, Los AngeLes, CA. 08JECTJVE: TO examine pregnancy outcome in ~:m)en with concurrent diabetes(DN; overt or gestatio~ai) and thyroid (TSY) disease, classified by status at delivery; hypothyroid (HYPO), hyperthyroid (HYPER) or euthyroid (EU). These were compsred to ~ with DR only or THY disease only. STUOY DESIGN: A cohort of 3335 ~(~))en with D~ and/or THY were followed prospectively (1/87-12/92)o study groups were: DH+TNY (N=~); DN atone; HYPER, hyperthyroid atone; HYPO, hypothyroid atone. Outcomes assesse~ were pregnancy induced (PIH) and chronic (CHTN) hypertension, delivery <37 wks (pTD), Large (LCA) and smart (SGA) for gestationai age, cesarean det ivery (CS), perinatal morta!ity (PNH). Intergroup differences were assessed by Chi SqUare analysis, RESULTS:
DM+THY HYPER NYPO DM
HYPER HYPO EU NO. 8 16 44, 56, 28 3183 ,~IN 25 33 21 20 32 11" ~,C HT N 25 6 5 5 O* 1" ,~g~TD 13 25 ~ 40* 21 21 ~SGA 0 0 0 13" 4* 0 ~LGA 14 19 27 7" O* 24 ~$ 63* 63* 43 21 39 34 %PNM 0 0 0 10" 4* 0.3 *P < 0,01 cf. other groups CONCLUSION: PIN uas increased in all groups with THY disease (HYPER, HYPO and DM~THY), A similar increase fn PTD, SGA or PNM which was fourKJ in TBY atone groups was not found in DM+THY. LGA infants were increased in aLL DM groups.
207 THE ANTIPHOSPHOLIPID SYNDROME IN PREGNANCY: IMMUNO-
GLOBULIN THERAPY. Joseph A. Spinnatu, Ann L. CI~I~ Silvia S.
Pierangeh"~ and E. Nigel HanSs*. University of Louisville Hospital, Louisville,
Kentucky.
OBJECTIVE: To study the influence of intravenous immunoglobulin (IVIG)
upon pregnancy outcome and anttcardiofipin (ACL) antibody levels in
patients with Anhphospholipid Syndrome (APS).
STUDY DESIGN: Pregnancy outcomes were evaluated in 5 consecu~ve
pataents with seventeen unsuccessful previous pregnancies. During the 5 index
pregnancies, each patient received 400 mg/kg IVIG for 5 days monthly. Four
patients with previous thromboembofic events were ~eated with heparin
prophylaxis (8,000 - 15,000 urats/day). Each patient recezved 81 mg ASA
daily. Two patients required prednisone for sepurale diagnoses. ACL IGG and
IGM levels were deterreaned before and after each course of MG.
RESULTS: St~ppresszon of ACL IGG was noted in each patienL Four
pregnancies were delivered of healthy infants at term. One patient was
delivered of a healthy infant at 32 weeks’ gestation with a diagnosis of fetal
dis~ess. There were no maternal thromboembofic events, Gestational diabetes
was observed in one patient receiving prednisone. Neither preeclampsia nor
fetal intrauterine growth retardation were observed. Significant placental
h~stologic abnormalities were not identified.
CONCLUSIONS: The outcomes suggest a benefit of MG through reduced
morbidity and cost from prematurity, withoet significant fetal or maternal side
effects, when used either as primary therapy or when other therapies raft.
Patient A~e* Parity EGA* BirthwNght~ Apgarl/5
1 29 0120 33 1786 618
2 29 0020 36 2799 7/9
3 28 0100 39 2750 8/9
4 28 0070 39 3459 8/9
5 39 0130 38 3224 8/9
* = maternal age in years, ~ = weight in grams, *birth gestational age(weeks)
206 PROFOUND DEPRESSION OF ANTI-THROMBIN llI IN ACUTE
FATTY LIVER OF PREGNANCY
M Ames, K. Shaw, T.M. Goodwin and W. McGehee, Depts. of OB/GYN
and Hematology, LAC+USC Medical Center, LA, CA
OBJECTIVE: To describe the coagulation profile in acute fatty liver of
pregnancy(AFLP).
STUDY DESIGN: A retrospective chart review was performed from
1982-1992 to identify cases of AFLP. The diagnosis was based on an
appropriate clinical picture and characteristic laboratory results in all
cases except one, in which hver biopsy was performed.
RF~ULTS: Twenty six cases of AFLP, the largest series from a single
center, were identified for an incidence of 1/6418 births No maternal
deaths occurred. There were 27 fetuses(one set of twins) with one
stillbirth and one neonatal death. Laboratory evidence of disseminated
intravascular coagulopathy(DIC) was found in 23/25 patients tested and
persisted from postpartum day(PPD)0-12. AT-III levels were drawn on
21 patrents and the average activity was 10.14%(nl 80-100%). Despite
laboratory evidence of DIC~ only 4 patients in the series had clinical
bleeding postpartum. On the premise that replacement of AT-I~ would
reverse DIC and bleeding, 7 patients were given AT-!/! concentrate
transfusions, 2 of whom were bleeding. Despite an increase m acUvity
levels of AT-HI, laboratory evidence of DIC persisted for 2-10 days and
bleeding for up to 3 days.
CONCLUSION: AFLP is almost uniformly associated w=th laboratory
evidence of DfC and profound depression of AT-U! activity. The
presence of DIC, even if it persists for days, does not seem to
s~gnificantly contribute to the outcome for the patient. AT-If1 concentrate
~nfusion probably has no place ~n the routine management of patients
with AFLP, but may be appropriate zn the rare, very seriously ill patient
in whom there was a reasonable concern that DIC was contributing to a
major hemorrhage.
208 COCAINE INDUCED RESPIRATORY FAILURE (ClRF)
M.R. Lauri~ J.E. Whitty, B.A. Mason,X and M.I. Evans. Depts
OB/GYN, MBG and Pathology, Hutzel Hospital/Wayne State
University, Detroit, MI. OBJECTIVE: 11% of Americans over 12 have used cocaine. Crack cocaine may cause CIRF through a disease continuum sta~ing with pulmonary edema (PE) and progressing to hypersensitivity pneumonitis (HP). Acute cocaine toxicity presenting with hypertensive crisis and respiratory failure (RF) in pregnancy may be confused with preeclampsia. We describe the presentation, progression, mad management of CIRF. STUDY DESIGN: Our experience and other reported cases are combined to eva/uate CIRF in pregnant and nonpregnant individuals (n=13). RESULTS: All patients included presented with sudden onset ot dyspnea temporally related to cocaine use, bilateral alveolar infiltrates with normal cardiac silhouettes on chest xray, and negative
past medical histories. 4 of 5 patients with HP underwent lung biopsy. 2 patterns were seen which differentiated HP from PE.
Fever .Resolution Local Eos Periph Eos HM Vent /rip n=5 3 >5 days 3 2 3 4
PE n=8 1 <2 days NA 0 NA 0
(Eos=Eosinophils; HM=hemosiderin macrophages; vent=mechanical ventilation)
CONCLUSIONS: All patients with RF should have a urine drug screen. Ventilator dependent crack abusers who are unresponsive within 24 hours to traditional therapy should have bronchial lavage and lung biopsy to establish the diagnosis of HP. If local eosinophilia is seen in the biopsy specimen, consideration should be given (preferably in coniunction with a clinical trial) to a course of steroids.
Volume 170, Number l, Part 2 SPO Abstracts 335 Am J Obstet Gynecol
209 GLUCOSE SCREENING IN SECOND TRIMESTER IN A HIGH RISK POPULATION. K. Adam, A. Jarolimekx. Dept. Ob/Gyn, Baylor College of Medicine, Houston, TX. OBJECTIVE: To assess whether glucose screen in second trimester is of value m the care of a non-diabetic high ~isk patient. STUDY DESIGN: 117 non-diabetic patmnts referred for high risk obstetrical care were given a one hour 50 gram glucose load screen test at 16 weeks gestation. Only 5 of these patients were referred because of history of gestadonal diabetes with previous pregnancy. Patients with glucose value of greater than 135 mg/dl were subjected to a three hour glucose tolerance test (3-hour GTF). Standard criteria for abnormal 3-hour GTI" were utilized. Patients with normal testing at 16 weeks had another glucose screen at 28 weeks gestation. Three-hour GTr was again obtained if the screen was abnormal. The incidence of glucose intolerance was evaluated. RESULTS: 29 (24%) of patiants.had an abnormal glucose screen at 16 weeks gestation. Of these patients, 14 (11% of total) met the criteria for diagnosis of gestational diabetes meltitus and initiated therapy. In this heterogenous patient population, the best predictive factors for abnormal glucose screen were a.) age greater than 30 years, b.) previous pregnancy with gestational diabetes mellitus. Of the 88 patients with normal glucose screen at 16 weeks gestation, 21 (17% of total) had abnormal screen at 28 weeks gestation. Only 3 patients were diagnosed with gestatlonal diabetes, although additional 8 patients had one abnormal value on the 3-hour GTr. Only 6 patients with abnormal glucose screen at 16 weeks and normal 3-hour GTr, had normal screen at 28 weeks gestation. CONCLUSIONS: In a high risk non-diabetic population, glucose screen at 16 weeks gestation allows for early diagnosis of majority of gestational diabetes mellitus patients. Re-screening of patients at 28 weeks allows for diagnosis of glucose metabolism impairment in additional 9% of patients. When an abnormal glucose screen is obtained at 16 weeks gestation, it is advisable to proceed directly to 3-hour GTI" at 28 weeks gestation.
211 NEONATAL HYPOGLYCEMIA IN GESTATIONAL DIABETES: REDUCTION BY TIGHT MATERNAL GLYCEM[C CONTROL. R~Ramusx, J K~tzmlller Dept of Ob/Gyn and Reproductive Sciences, Umvers~ty of California, San Francisco, San Francisco, CA OBJECTIVE: Esttmates of the frequency of neonatal hypoglycemia in women wRh gestatlonal diabetes range from 10-30% with poor maternal glycem~e control thought to be the major risk factor This mveshgatlon reviews our recent experience in women followed in a compreqaenalve diabetes and pregndncy program We examined what prenatal risk factors correlate w~th the subsequent development of neonatal hypoglycemia. STUDY DESIGN: Obstetric complications recorded prospectively in a perlnatal database were analyzed on 244 women &agnosed to have gestatlonal diabetes that delivered between July 1986 and December [991 A 50 gram one hour glucose load test >130 mg / dl was used for screening Th~s was followed by a 100 gram 3 hour GTT with abnormal defined using National Diabetes Data Group criteria Intensive dietary therapy, self-momtorlng of capillary blood glucose (BG), and selective insulin therapy were used to obtam postprandial (pp) euglycem~a (1 hour ppBG <130 mg/dl) Neonatal hypoglycemia was defined by a BG concentration of K30 mg/dl, a Dextrost~ck value <40 mg/dl, or borderline glucose values accompanied by neonatal jltterlness and increased glucose requirements RESULTS: Sixteen neonates were hypoglycemlc in the nursery (6 6%) R~sk factors found to correlate with the presence of hypoglycemia include prematunty (p<0 001), lower birth weight (p=0.066), and the need for insulin therapy (15% vs 4%, p=0 006) Maternal prepregnant body mass index, weight gain during pregnancy, mode of delivery, induction of labor, gender of the neonate, preeclampsla, maternal fasting hyperglycemia, and ethruclty were not slgmhcantly related to the development of neonatal hypoglycemm CONCLUSIONS: The overalhncldence of neonatal hypoglycemia in tl’us populabon was 6.6%, which compares favorably with prior published observations. Prematurlty and the need for msuhn therapy were the most important risk factors for hypoglycemia. The data suggest that tight glycemlc control and intensive dietary therapy are effective in reducing the incidence of neonatal hypoglycemia, which should add to the cost-effectiveness of an outpahent program designed to reduce neonatal admissions to the special care nursery
210 TItE MANAGEMENT OF IMIVlUNE TIIROMBOCYTOPENIC PURPURA
WITll PERCUTANEOUS UMBILICAL BLOOD SAMPLING.
S. GarmeP, S. Craigo~, L. Morin~, J. Crowley’, M. D’Alton, Tufts Univ., New
England Medtcal Center, Boston, MA.
OBJECTIVE: The management of immune thromboeytopanie purpura (ITP)
in pregnancy is controversial. Community obstetricians and pediatricians are
often uncomfortable managing thromboeytopet~ie pt~tients. On consultation,
percutaneous umbihcal blood sampling (PUBS) was offered to women with ITP
to determine the mode and site of delivery prior to labor.
STUDY DESIGN: Between 111989 and B/1993, 36 pregnant women underwent
PUBS. All Wbmen had a history of ITP, (+) antipl~telet antibody,
thrombocytopenia diagnosed early in pregnancy, and/or a platelet count less
than 90 thousand (K). Patients with preeclampsim and gestational
thrombocytopenia were excleded. PUBS was performed at 38 to 39 wee, ks’
gestation except m one patient with preterm labor who underwent PUBS at 31
weeks’, Patiems with normal fetM platelet cout~ta (>_ 50K) returned to their
referring physician for delivery. Records were complete in 34 pregnancies.
RESULTS: Fetal blood was successfully obtained in 32 of 34 cases (94%).
Both unsuccessful PUBS occurred early in our sartes. One patient remains
undellvered. Fetal platelet counts correlated with neonatal platelet counts in 31
of 3I cases (100%). The interval between PUBS and delivery r~nged from 0
to 31 days. Four of 31 patients (13%) had significant fetal thromboeytopenia
(< 50K), with platelets ranging from 13K to 37K. These 4 patients underwent
Cesarean section All others were allowed to labor by thelr referring physician,
except one with fetal plntaleta of 60K who was advised by her private physician
to have a Cesarean section There was one procedure-related complication in
a patient with preterm rupture of membranes and preterm labor who
experienced fetal bradycardia following PUBS. An emergent Cesarean section
was performed, resulting in a normal neonatal outcome. There were no cases
of anemia or intraventricular hemorrhage in ~ny of the neonates.
CONCLUSIONS: There is a significant incidence of feOtl thromboeytopenlain
women with ITP. PUBS reliably detects fetal thrombocytopenisand istherefore
useful in the permatal planning of mode and site of delivery.
212 llATERNAL 6LUEOSE CONTROL IN GESTATIONAL DIABETES: RELATIONSHIP TO FETAL INSULIN RESPQNSE. E. PhIl~pson. G. Hansen. C. Ingard~a. and S. Kalhan. Hartford llosp]tal, UCONN. Hartford. CT and RBC Hospital, CWRU. Cleveland. OH. OBJECTIVE: To identify the magnltude of antepartum glucose decompensaL]on that results in a helghtened fetal pancreatic B-cell response as determlned by umblllcal cord artery insulln levels. STUDY DESIgN: FaSting and 2 hour postprandial capillary blood glucose ]n response to breakfast, lunch, or dlnner were monltored }n 34 women with gesLaLiona] dlabetes (GDM) with a memory-based reflectance meter at least 3 tlmes/day for a mean of 60 days (range 50-102) prior to delivery. The mean fasting and postprandial glucose values, and the percentage of values wlthln the accepted target range (fasting ~105 mg/dl and postprandial<T20 mg/dl) were analyzed. At dellvery cord arterial insulin levels were measured. Glucose-contamlng solutions were not used durlng labor.
RESULTS: There were 8 neonates w]th an elevated (>6 mu/ml) cord
1ndex, parity, the number of daily glucose tests, and the mean
When at least 75% or more of the postprandial values were within
control (at that level) and the risk of an elevated fetal tnsulln. None of the 14 women with 275% of the postprandial glucose values and 8 of 20 women with <75% glucose control had elevated cord ~SUlm levels(p<O.02). ~ONCLUSIONS: These data indicate that postprandial glucose values need to be less than ]20 mg/dl at least 75% of the time to avoid fetal hyper~nsullnem~a. Postprandial glucose values appear to be
hyperlnsulinemla in women w~th GDM.
336 SPO Abstracts January 1994 Am J Obstet Gynecol
213 THYROID REPLACEMENT IN PREGNANCY. V. Luoo. A. Zieg*. Dept. Ob/Gyn, Hennepin County Medical Center, Mpls., MN. OBJECTIVE: Dmrted information is available regarding the need for changing doses of thyroid replacement in pregnancy STUDY DESIGN: Pahents with hypothyroidism in pregnancy were identified from the High Risk OB Chnic weekly roster and from the private practice of the senior author at Hennepin County Medical Center in MinneapOlis, MN. Maternal cha~ls were reviewed and abstracted. TSH levels were measured monthly and when elevated, increased doses of synthrmd were prescribed. RESULTS: 33 women were fotlowed through 37 pregnancies, and had 2 or more TSH levels performed. 24 patients had TSH measured pre-pregnant and 15 measured post-partum. 24/37 pregnancies (65%) required an ~ncrease in synthroid w’r~h advancing gestation. 18/20 patients (90%) wrth normal imhal TSH levels had a rise in TSH w~th advancing gestation. 1/11 (9%) with normal pregravid TSH needed a first trimester increase in dose. The mean age of increased drug requirement was 25 weeks. 6 women required multiple drug ~ncreases to suppress elevated TSH levels. 40% of women required lower doses at post-partum evaluation. Neither body mass index or underlying ehology of hypothyroidism predicts need for increased medication. Increasing weight gain with pregnancy did correlate with the need for increased synthroid dosage (P=.03) CONCLUSIONS: The majority of hypothyroid pregnant patients require additional synthroid during pregnancy. Favorable pregnancy outcomes can be expected.
215 COMPLETE OUTPATIENT MANAGEMENT OF INSULIN-
REQUIRING GESTATIONAL AND NON-INSULIN DEPENDENT
DIABETES IN PREGNANCY
C Reyes, MM Montorox, M Victorx, SL Kjos Dept of Ob/Gyn,
Umversity of Southern California, Los Angeles, Ca.
OBJECTIVE: To evaluate the efficacy of out outpatient diabetes
education program (ODEP) for m~tiating insulin therapy in women with
gestatlonal (GDM) or non-insulin dependent (NIDDM) diabetes.
STUDY DESIGN: 508 women were prospectively followed after meetang
entry criteria for ODEP. hterate, fasting serum glucose (FSG) 105-149
mg/dl, <36 weeks gestational age (GA), and no medical comphcations
All underwent intensive one day instruction in diet and insulin therapy and
in home glucose momtoring (ItGM) taught by our certified diabetes nurse
educators S ubsequent prenatal and diabetic follow-up was provded m our
d~abet~c prenatal chmc Parameters evaluated included: acceptable
glycem~c control (80% of HGM values monitored 4-6 times/day with FSG
<105 and 2 hour post-meal <120 mg/dl); antepartum or delivery admissmn
for poor glucose control, macrosomla (~_ 4000 gms) and stillbirths.
RESULTS: Subjects were predom~nately Spanish-speaking (95%) with
29% completing less than 6 years of education. 4% had NIDDM, the
remaining with A2 GDM with the highest FSG at entry of 119 + 19 mg/dl.
The mean GA at entry was 27.5 + 6.7 wks. Only 2.7% of subjects
required subsequent hospitalization for poor glucose control and 4.1% for
term delivery m poor control. Macrosomia occurred in 14%.
No stdlbtrths occurred.
CONCLUSION: A program of complete outpatient diabetes education
and management in insulin-requiring pregnant diabetics who w~re without
medical complications or severe fasting hyperglycenua was successful and
without maternal or neonatal compromise.
214 CLINICAL CONSEQUENCE~ OF LOW POSITIVE lgG ANTICARDIOLIPIN ANTIBODIES. RM Sflvet~, C Coulam’, JL Lyon’, JR Scott’, and DW Branch.
Dept Ob/Gyn and Epidemtolngy, U of Utah, ~LC, Utah.
OBJECTIVE. The presence of high levels of anticaxdiohpm antibodies (aCL)
or lupus anticoagulant (LA) axe associated with several clinical disorders,
However. the relationship between low "tlters" of these antibodies and anti-
phosphohp~d syndrome is unclear Consequently, It ~s difficult to counsel
women with low levels ofaCL regarding their hkelihood of developing chmcal
problems The purpose of our study was to determine the risk of aCL-related
disorders in women with low positive t~ters of IgG aCE STUDy DESIGN’ Medical and obstetric histories were obtained from 93
women identified b~cau~e of low positive levels of IgG aCL (8 - 19 GPL units)
determined m our lsboratory Most were test~ for pregnancy loss (54%) and
none had LA. Ag~-adjust~d raids for the development of mediead disorders
~s~oemted with aCL were then o-~leulated for the mterv~l from init’ud matlbody
t~stlng ~o t~e time of patient interview. Di~.orders In them women (low tlter
group) were compared to slmd&rly-determmedage-~ljusted rates in 130 women
with ~ 20 GPL units of lgG aCL or LA (high tlter group).
RESULTS The median interval of follow-up w~s 3.75 years. Eleven % of
women m the low titer group developed new aCL-relatod disorders, compared
to 48% m the high tlter group, P < 0.00l New dl~orders in low titer patients
included thrombosis (4), amaarosls fug~ (3), TIA’s (5), SLE (1), and ITP (2)
Low oter p~ttents developed MI of the~e comphcations at significantly lower
rates than high tlter patients. The age-~tjusted rote (per 1,000 patient years; +
SE) ~or the development of at 1coat one non-obstetricM disorder m the low tlter
group was 51 + 26, cutup&red to 288 ± 33 tn high titer p~tents; rate r~lo =
5.6 (95% CI 2.7 - 11 8). Three fet~l deaths occurred m 87 pregtmneles in low
titer pattent~, eomp~r~l to 25 of 124 in high titer petient~, P < 0
CONCLUSIONS Women with low levels of IgG aCL were only about one
fifth ~s likely to develop aCl.,-relat.ed complieationsas women with higher levels
of matlbodies. However, the risk for the development of new disorders in these
women w~s substaathdly higher titan for the general population, reinforcing the
clinical importance of identifying women with lgG aCE
216 THE PREDICTABILITY OF GLYCOSYLATED HEMOGLOBIN IN GESTATIONAL AND PREGESTATIONAL DIABETES. McFar~and, M .x Langer. O. Rodr~guez. D ,x Xenak~s, E M J . F~el~~f Texas Health Science Center at San Antonio, Texas
OBJEC-rlVE: The purpose of our study was 1) to determine the relationship between glycosylated hemoglobin (HbA1C) and ambulatory blood glucose, and 2) to ascettam the relationship between HbA1C andfetal complications.
STUDY DESIGN: ~n a prospective, [ongttudtna~ study, HbA1C was measured throughout pregnancy m 208 preexisting (PDM) and gestational (GDM) diabetics All patients momtored their blood glucose seven times a day using memory reflectance meters
RESULTS: Mean HbA~C for PDM patients prior to 20 weeks was 684 -+ 2 (coefficient of variation, 292), whereas mean thirdo tr~mesterHbA~C~nGDMwas527-+ 066(cv 12,5,p<0.02) The
PDM mean HbA1C in the third tnmester was 5 58 ± 0 8 (c v 15) Furthermore, a positive association between HbA1C and mean blood glucose was found in PDM subjects prior to 20 weeks
HbA~C PDM (< 20 weeks) HhA~C GDM (third trimester)
120 [- r~043 70 I-- r=-0 04
o .... "" o ...... 22-2 .....
80 100 120 140 160 180 80 100 120 140 160 180 Mean Blood Glucose Mean Blood Glucose
Additionally. in GDM, a strong correlation was found between the result of the glucose screen and HbA~C less than 30 weeks (r=086, p=003) No correlat~on was found between any of the HbA1C values throughout the third trimester {both PDM and GDM) and fetal weight, 5-minute Apgar, cord pH and metabohc comphcat~ons
CONCLUSIONS: HbA1C cannot be used ~n GDM asa measure of evaluation for level of glycemic control (narrow c v ) In contrast, early in pregnancy, in preexisting d~abet~cs, ~t can be used as a retrospective measure for glucose abnormahty (wide c v )

Volume 170, Number 1, Part 2 SPO Abstracts 337 Am J Obstet Gynecol
217 FETAL MEMBRANE RUPTURE IS ASSOCIATED WITH THE PRESENCE OF INSULIN-LIKE GROWTH FACTOR BINDING PROTEIN-1 (IGFBP-1) IN VAGINAL SECRETIONS. C.J. Lockwood, R. Wein~, A. Ghidini, M. Alvarez, R.L. Betkowitz. Dept. Ob/Gyn, Mr. Sinai School of Medicine, New York, NY. OBJECTIVE: The purpose of this study was to determine whether detection of IGFBP-1 in vaginal secretions was diagnostic of membrane rapture and, if so, whethe~ clinical factors affected test performance. STUDY DESIGN: Consenting patients with complaints suspicious of membrane rupture between 24 and 42 weeks were candidates for study. The diagnosis of membrane rupture required at least two of the following findings on vaginal examination: pooling of fluid; art alkaline pH; and/or microscopic ferumg. A swab of the vaginal foruix was obtained, placed m sample buffer and analyzed for IGFBP-1 by a sensitive immunoassay. Data analysis included Chi square, Mann Whitney U test, ~inear regression and Receiver Operating Characteristic (ROC) curve analysis. RESULTS: A total of 105 patients were eurolled in the study of whom 78 (74.3%) met the crirteria for membrane rapture. There was a significant difference ha mean vaginal 1GFBP-1 levels between patients with and without clinical evidence of membrane rupture, 553.6 ug/L (+__731.4) vs. 3.0 ug/L t,~_7.3); p=0.0002. The ROC curve analysis demons~ated that the optima/ cut-off for identification of patients with membrane rupture was an IGFBP-1 value > 3 ug/L [sensitivity = 74.4% (95% Confidence Interval 64.7% to 84.0%); specificity = 92.6% (82.7% to 102.5%); positive and neganve predicave values = 96.7% (92.1% to 101.2%) and 55.6% (4!.0% to 70.1%), respectwely]. Tb, ere was no correlation between maternal age, parity, gestatmnal age at rupture, the interval from membrane rupture to samplmg or sampling to delivery, cervical change, contraction frequency, or the occurrence of vaginal blee, ding or chorioanmiortitis and IGFBP-1 values. CONCLUSIONS: The presence of vaginal IGFBP-1 is highly predictive of membrane rupture, identifying 74.4% of affected patients with a very low false positive rate.
219 ’fERM PREMATURE RUPTURE OF MEMBRANES: IMMEDIATE
VERSUS DELAYED INDUCTION OF LABOR. Mordechai Halla~_,
Sidney F Bottoms Department of Ob/Gyn, Hut.zel Hospital/Wayne State
Uaiversity, Detroit, MI.
OBJECTIVE: To determine whether delayed mductlon of labor m patients
vath term PROM has beneficial effects on the mother or the infant
STUDY DESIGN: Study popui~lon mc|uded 576 pattents >37 weeks’
gestation w~th PROM and for whom we had complete data ]’he frequencies
of primary cesarean, neonatal mtenslve care umt (NICU) admissions, and
oxytocm use by the time interval elapsed between patients adunssion to the
hospital and the onset of lalmr were analyzed Onset of labor was defined as
the tune when oxytocm-mduced or sponianeous contractions started
RESULTS: Prunary cesarean rates were increased progressively by
adunsslon to onset of labor mterval Stepw~se dmcriminant function
revealed that labor duration, adrmsslon-onset of labor interval, gestational
age, and birth weight of <2500 grams were all more lmporlant determmants
than duration of PROM a~d ROM. NICU adnusslon increased from 1 9% in
<3 hours between adunsslon to onset of labor to 13.3% after >18 hours
Admissmn-onset of labor interval, bxrth weight of <2500 or >4000 grams
and mecomum were all more unportant determinants than gestatinnal age,
duration of labor, PROM, and HeM Prolonged adrmssion-onset interval
was associated wRh increased ask of variable deceleratzans (p<0 001)
CONCLUSIONS: The increased frequenctes of prtmary cesarean mid
NICU adunssion lndxcate that delayed labor induction after hospital
adm~ssmn was linked to worsened permatal outcomes These results may
have been influenced by usually performing a stngle digital examination as
part of mxtxal evaluation of term patients who present with PROM Based
on these results, we recommend tmmethate induction for term PROM ff
d~gttal exmmnatmn has been performed
218 THE EFFECT OF BETA~ETHASONE ON GLLJ~OSE SCREENS IN PREGNANT
MQ~EN. S CarLan, X Hc~eiLL, H Reis, M Jones, S Richn~nd, E
Whittington. Arnold Palmer Hospital for Children & Women (APH), ORHS, Orlando, Florida ONJECTIVE: To assess the effect of betamethasone on the stBndard g[ucose screening tests in non-diabetic pregnant wo~n. STLIO¥ DESIGN: AIL wo~en who were at risk For preterm delivery frcm 5/20/92-5/I/93 at APH, on the high risk obstetric service who were treated with betamethaaone for fetal pulmonary maturation were offered enrollment in the study. Fasting bto(x~ sugars and one-hour 50 gm plasma venous glucose challenge tests were performed pre-steroid, and 24, 72, and 96 hours after the last betamethasone injection. Patients with (asting blood sugars >I05 or a one-hour post challenge value >200 were classified as having gestationat diabetes and not challenged. Two 12mg doses of betamethasone were given intramuscularly 24 hours apart.
patient that had received a betaaimetic during the pregnancy was
included.
RES~ILTS= ~wenty-seven W~T~n were studied at a mean gestationat
age of 29 weeks, maternal weight of 143 tbs. and a mean weight
gam of 21 lbs. There was a family history of diabetes in
and previous macrosomla in 3.7% of patients, the number Of
al:~3rmet glucose screens ~as not different between the groups,
but the mean glucose values ~ere elevated in the 24-hour post-
steroid test and had returned to normal by 72 hours.
N=27 24 hr. after
Rean mp/d[ ± SD Pre-steroid last dose
FBS 80 ± 9 89 ± 10 <.05
1 hr, post 50 g 128 ~ 26 140 ± 29 .07
FBS >105 N(%) 0 0 I hr. >140 N(%) S (29) 10 (37) NS CONCLUSIONS:
t. Antenatal motert~l administration of beta/rlethasone results in
a significant increase in mean FBS at 24 hours after the last
dose but returns to normal by 72 hours.
2. The nkanber of abnormal tests using the conventional
definition of Uabnormat screens~ is unchanged by betamethasone.
220 HOW ADEQUATE IS INFORMED CONSENT AT THE TIME OF
CESAREAN DEUVERY?
K,J~.,-J=~,.~, S.R. Inglis, K.A. Eddleman, E.Q. Peeper~, LB. McCullougW, F.A. Che~venak. Diwsion of Maternal-Fetal Medicine, The
New York Hosp~taJ-Comell Medical Center, New York, NY
OBJECTIVE: A prospect=re study was undertaken =n 372 consecutive
patients undergoing non-elective cesarean dehvery (NECD) to examine
the nature and quality of reformed consent surrounding the decision to
perform operative delivery.
STUDY DESIGN: During a six month interval, all patients who
underwent NECD were asked to take part m a survey in the early post-
partum period concerning their response to recommendations for
cesarean delivery, including quest=ons pertaining to informed consent.
RESULTS: Of the 326 patients who were mterwewed, 26 (8.7%)
indicated that they did not have adequate input in the decision for N ECD.
tnd=cat~ons for NECD m these 26 patients included fetal distress(18126),
malpresentat=on(5/26), and fadure to progress(3/26). Patients w~th
inadequate input expressed s~gnificantly more concerns with regard to
the effects of surgery on thew health(p<O.01 ) as well as it’s effect on the
baby(p<0.01). There were no d~fferences between the two patient
groups w=th respect to age, grawddy, race, mantal status, employment
status, private vs chntc status, or prewous obstetnc hmtory. CONCLUSION: Thts study ts the first to provtde empinc data to
document the frequency of patient’s reservations about the reformed
consent process for N ECD. The fi’equency of 8.7% ~s high enough to be
of chn=cal concern and attention, An ~mportant observation =n the study ~s the lack of effect of such vanables as race, employment status, and
pnvate vs clinic status. This suggests that inadequacies in reformed
consent need to focus on discussion with the patient of the medical
circumstances necessitating the surgery. To prevent possible confhct,
d~scuss~on should focus on the woman’s concerns about her own health
and that of the baby’s and how those concerns can be affectively met by
avadable alternatives.
338 SPO Abstracts January 1994 Am J Obstet Gyneco!
221 ASSESSING THE COST OF A "STANDARD": HOSPITALIZED BEOREST IN TRIPLET PREGNANCY J Shall. A Bruckner×, R S11ver. S MacGregor Dept.Ob/Gyn Evanston Ho~p~Evanston IL. Northwestern Umverslty OBJECTIVE: To show the maternal and neonatal cost components that result from our pollcy of In-patient bedrest for triplets as a paradlgm for comparison, looklng for determlnable reductlons in prematur]ty. NICU use. or combined maternal/neonatal total charges STUDY DESIGN: Chart review of per~natal outcome ~n 37 triplet gestations managed between 1989-1993 was comblned with tabulation of the hospital and physlc]an charges for mothers and mfants RESULTS: Mean GA at del]very was 32.8 + 3 6 wks (N=37). the PNM was 61/1000 GA at dellvery, maternal hospT~al stay. and number of NICU days per neonate were Slmllar for patlents admitted i) w]thout/wlth cerwcal change. 2) before/after 28 weeks or 3) on/off tocolyt~cs
Electlv Cerv~xllBefore After llToco- No tocd IAdm~t Change128 wks 28 wksl lys~s lysls II Stnd
Devs ~om/neonat* N:14/41 16/48 17/51 13/38 16/48 14/41 II !GA (admlt)l 27 3 27 2 25 4 29 4 27 0 27 6 >2.2 GA (del) I 34 3 33.9 33 3 34 7 33 6 34 2 >2 3 iHosp (days) 55 6 53 4 63 2 43.0 56 3 52 4 >16 2 NICU (days) 12 1 Ii 6 13 6 i0 6 14 1 I0 4 >Ii 2
*[Excluded 7 of 37 wlth PPROM. Incomp Cx, advanced PTL, resulting in rap]d delivery (<7 days ]n hospltal)] The cost of these 30 maternal hosp]tallzatTons averaged $34,377 39. or $769 64 per day Da~ly room charges accounted for 54% of the $i 03M total. Women requiring tocolys~s accounted for 51 6% of the cost Exclusive of de~Tvery and post-partum costs, charges for In-patient bedrest in asymptomat]c cases was $315,225 65 (30 6%) Of the 104 l]veborns >24 wks GA, 75 (72%) went to the NICU for 18 5 + 21.3 days Of the 33 neonates delivered ]n 1992-93, 21 were premature, their NICU charges averaged $69.937 80 or $1719.78 per day, (medians: $48.565 and $1589) Therefore the comblned average cost per triplet neonate was ($34,377/3) + ($1589 x 18 5 days) = $40.855.50 CONCLUSIONS: Da~]y NICU costs were twice maternal da~ly charges (6x for trlplets) However early, elective hospltallzat~on d~d not appear to lengthen pregnancy nor save NICU days Outpatient care and use of ~ndlcated hosp~tal~zat~on may reduce maternal costs 30%, which our data estlmates as 8 4% of total combined charges.
223 TRENDS INxOBSTETRIC PATIENT POPULATION: AN 18 YEAR STUDY S. Amini , L. Dierker, P. Catalano, G. Ashmead, L. Mann. Dept. Epid & giostat, School of Medicine, Case Western Reserve Univer- sity, &Dept. Ob/Gyn, MetroHealth Medical Center, Cleveland, OH.
OBJECTIVE: To evaluate treads in an obstetric patient popUlation over the past 18 years using a perinatat database collected pros- pectivety since 1974. Many parameters including birthweight (BW), maternal age, length of hospital stay(LHS), mode of delivery, gestatiomal age(EGA), and socioeconomic status were fnvestigated. STUDY DESIGN: Over 65,000 deliveries (1975-1902), from a single site were used. Rates and proportions were reported for categori- cal and moans and percentiles for continuous variables. Statis- tical significance for trend tests were by Cox-Stuart, regression and time series analyses. RESULTS: The hurdler of deliveries has increased from 2,682 patients in 1975 to 4,740 in 1991, an increase of 7~. As the modian gW have reraained steady for singleton births at about 3,170 g, the 1, 5 aed 10 percentiles of gW have declined from 940, 2000, and 2,360 g in 1975 to 745, 1600, and 2,135 g in 1992. White the number of teen births (TB) did not decrease significan- t(y, the proportion of TB among staff patients (SP) has dec[ined from 43% to 25% (P<O.O01). The median maternal age has increased from 20 years in 1975 to 23 years in 1992 (P<O.O01). The proportions of C/S for private patients (pP) has declined from 37% to 26% in 1992, while it has increased for SP from 10.4% to 17.7%. During this period the proportion of twin births has increased for both the PP and sP by I%. While the premature births (PB) have increased for SP from 13,3% to 18.73;, the pro- portion of PB for PP has declined from 34.3% to 25.2%. Percent stillbirths have remained steady at about I% for SP and 1,5% for PP. Except for significant increase in the 99th percentile of LHS for neonates, other percentiles of LHS have actually declined. CONCLUSIONS: Considering the size of database and diverse back- ground of our popUlation, these treads will provide a realistic characterization of urban obstetric patient populations. We believe that examination of these trends will enhance the health care planners’ and providers ability to better prepare themselves for a changing obstetric patient population.
222 RECURRENCE RATE OF SHOULDER DYSTOCIA. R.C. Raymondx, D.F. Lewis, M.B. Perkins×, G.G. Brooksx. LSU Medical Center, Dept. OB/Gyn Shreveport, LA. OBJECTIVE: Shoulder dystocia continues to be a major complication of obstetrics. Several factors have been identified to help predict shoulder dystocia. A previous shoulder dystocia has been identified as one of these risk factor, although the recurrence rate is unknown. The purpose of this study is to establish the recurrence rate of shoulder dystocia. STUDY DESIGN: Our obstetrical data base was used to identify all vaginal deliveries between January 1983 thru December 1992. A subset of vaginal deliveries complicated by shoulder dystocia were selected from this data base. Those records were then reviewed to identify subsequent pregnancies, outcomes, risk factors, and demographic data. RESULTS: During the study period, there were 37,465 total vaginal deliveries with shoulder dystocia complicating 747 (overall rate 2%). Of these 747 cases, 140 had subsequent vaginal 4eliveries with shoulder dystocia complicating 19 of these pregnancies (13.6% recurrence rate, p < 0.0001). comparisons were made between those patients with recurrent shoulder dystocia and those without. CONCLUSION: Shoulder dystocia recurred at a rate 7 times higher than our primary rate. Whether patients with a history of shoulder dystocia should be offered an elective abdominal delivery needs further investigation.
224 SUCTION CURETTAGE IN EARLY PREGNANCY:THE RELATIONSHIP BEIWEEN HCG LEVELS AND FAILURE TO RETRIEVE CHORIONIC VILLI Mlkhall MSx, W]Imot D×, Ha GYFX, and Anyaegbnam A. Albert Einstein College of Medicine, Bronx, New York OBJECTIVE. In the presence of a subnormal increase In hCG levels, suctlon curettage is frequently employed to dlfferentlate between intra and extra-uterlne pregnancies. Failure to retrieve chor~onic wll~ (CV) on suction curettage sometimes leads to dlagnostlc errors. The purpose of this study was to examne the relatlonshlp between hCG levels and probab~llty of retr~ewng CV on suction ourettage ~n early pregnancy STUDY DESIGR. 193 patients, < 6 week gestation, who underwent suction curettage to rule out ectap~c pregnancy were stud;ed. Patients were excluded ]f they had f~brmds, congenital uterlne anomaly, or irregular uterus Of 193 patlents, 125 were found to have ~ntrauter~ne pregnancies as determined by the presence of CV on h~stopathology follow~ng one or more attempts of suction curettage. HCG levels were categorJzed and success rates of recoverlng chor~omc vlll~ ~n each category was determined; 95% confidence interval (CI) of each success ~ate was calculated based on the normal approximation to the binomial d~str~but~on. RESULTS. hCG level CV retrieved P* LCI** UCI*** <IOO 2/g 0 222 0 0.494 <200 6/17 0 352 0 125 0 590 200-499 4/13 0 307 0 056 0.558 500-999 6/12 0 500 0 217 0.782 1000-1999 15/17 0 882 0 729 1 >2000 61/66 0.924 0 860 0.988 * Probab~llty. ** Lower confldence interval *** Upper confldence interval CONCLUSIONS. When hCG levels are low, failure to retrleve CV on suctlon curettage more llkely reflects failure to curet an early pregnancy rather than the presence of an ectop]c pregnancy A repeat ~uctlon curettage may be cOnSldered prlor to unnecesaary interventlon

Volume 170, Number 1, Part 2 SPO Abstracts 339 Am J Obstet Gynecoi
225 THE EFFECT OF OBSTETRICAL TRIAGE ON RATES OF OBSTETRICAL
INTERVENTION. J LacyX, H Mornsx, T Myhrx, J Rudermanx, M Hannah,
A OhlssonL Women’s College Hospital, Toronto, ON,
OBJECTIVE: To determine if the use of an Obstetrical Triage process,
whereby women m early labour are kept out of hospital, ~s effective
in decreasing the rate of obstetrical interventions.
STUDY DESIGN: This study was a retrospective cohort comparing
1707 women who dehvered before the institution of Obstetrical Trmge
(March 90 to February 91) to 1714 women who delivered after the
institution of Tnage (September 91 to August 92). Women were
included in the study ~f they were >- 37 weeks gestation, had
singleton pregnancms, and were ~n a low or moderate risk pregnancy
category. The primary outcome (cesarean section) and the secondary
outcomes Imduction/augmentat~on of labour, operative vaginal
dehvery, ep=dural anesthesia, ep~siotomy, and admmsion to the NICU
of the infant for > 24 hrs} were analyzed using chi-square statmtics.
Log=stic regression was used to determine the effect of confounding
variables on the outcomes which were slgmficantly different for the
two groups.
RESULTS: In the Triage period, cesarean secUon rates (p=0.04), use
of ep~dural anesthesm (p=0.04) and NICU admission for > 24 hrs
(p=0.02) were reduced. However, using regression analysis,
admission during the Triage period was not predictive of cesarean
section or ep=dural rates. It was predmtive of NICU adm=sslon for
> 24 hrs.
CONCLUSIONS: Initmt~on of an Obstetrmal Triage process did not
s~gnificantly alter the rate of operative interventions. However, the
number of babms reqmring lengthy admission to the NICU was
reduced. During the Triage phase of the study, there was an increase
of 6% in the number of dehveries, but no ~ncrease in nursing staff. A
cost analysis of the benefits of an Obstetrical Triage process may be
indicated.
227 AGGRESSIVE THERAPEUTIC AMNIOCENTESIS FOR
TREATMENT OF POLYHYDRAMNIOS. ~. Elliott, T. Radinx, A. Sawyerx, Phoenix Perinatal Associates and Good Samaritan Regional Medical Center, Phoenix,
AZ, OBJECTIVE: To evaluate the safety and outcome of
aggressive therapeut=c amniocentesis (TA) in the treatment of polyhydramnios.
STUDY DESIGN: A retrospective review of therapeutic
amniocentesis was done between 1988 to 1993. Therapeutic amniocentesis was defined as an attempt to
remove enough fluid to leave a normal volume of
amniotic fluid (AFI < 25 cm). RESULTS: Ninety-four patients had 200 therapeutic
amniocentesis. The most common condition treated with TA was twin-twin transfusion syndrome (36 patients).
Complications included: one patient with ruptured membranes 1 day post TA, one patient developed
chorioamnionitis, and one patient with an anencephalic
fetus had an abruption following removal of 10,200 cc
fluid. The mean volume of fluid removed was 1666 cc
~+ 1245 cc. The fluid was removed at a mean rate of 54
cc/min +__ 22 cc. CONCLUSIONS: Aggressive therapeutic amniocentesis
can be utilized to treat polyhydramnios with a 1.5% complication rate,
226 DIGITAL VERSUS INSTRUMENTAL EXPANSION OF THE
UTERINE INCISION AT THE TIME OF A LOW SEGMENT
TRANSVERSE CESAREAN SECTI ON. Rodriguez A, Porter KB,
O’Brien WF. Dept. Ob/Gyn, Univ. of S. FL, Tampa, FL.
OBJECTIVE: The purpose of this study was to compare a difference in terms of instrumental (I) and digital (D) techniques
at the time of expansion of the uterine incision during the
performance of a low segment transverse cesarean section
(tSTC). STUDY DESIGN: A total of 264 patients who were undergoing
a LSTC were randomly assigned to one of the following surgical
techniques to extend the initial uterine incision: 1) by cutting
laterally and then upward with bandage scissors I group or 2) by inserting both index fingers into the opening and drawing them
apart with lateral and then upward pressure D group. The
primary outcome variable was the incidence of lacerations, A
laceration was defined as an unintended extension (>2cm) outside of the original line of incision, that was recognized at the
time of closure of the uterine incision.
RESULTS: 150 patients were enrolled in the I group and 142
patients were enrolled in the D group. The total rate of
lacerations was 13%. The frequencies of lacerations in the I and
D groups were 15.3% and 10.6%, respectively. The small
difference in lacerations between both groups did not reach
statistical significance (relative risk I/D = 1.5; CI 0,757 to 3,054,
p=0.3). No other measured outcome including operative time
and estimated blood loss showed a difference between groups.
CONCLUSION: I and D expansion of a LSTC incision are
equivalent in speed and complication rate.
228 LOW CESAREAN RATE AMONG ADOLESCENTS UNDER AGE 15. S.L. Lubarskv. E. Schiff, S.A. Friedman,x B.M. Sibai, B.M. Mercer. Dept. of O’B/GYN, University of Tennessee, Memphis. OBJECTIVE: To describe and analyze the obstetric characteristics of parturients under 15years of age. STUDY DESIGN: A matched cohort design was utilized. The data of all 261 nulliparous parturients under age 15"delivered at our institution between Jatiuary 1"990 and Decembgr 1992 were compared to 261 nu~liparous controls aged 20-29, marched for race, infatit gender, and year of delivery. Mu’Itiple gestation and delivery prior to hospital admission were exclusion criteria. RESULTS: The number of antepartum admissions was identical (n = 35); however, the adolescents }~ad significandy fewer clinic visits (6.5 vs. 8.3%, p =0.0001). Hypertension was more common in the adolescent rou (19 5 vs 9 2% - 0 002) There were no significant diffe ...... g~een ’the ~tu’dy ~a~-c~ntroi groups in mean-cervical
dilatation at admission, rate of induction of la[~or 02.6% for each), use
of epidur~+ anesthesia (44.4 vs. 49.4%), mean birth weight (2918_+661 vs. 2979-753 g) or delivery before 37 weeks (24.1 vs. 20.3%). Nevertheless, duration of labor, use of oxytocin, rate of cesarean delive and need for episiotomy were lower in the adolescent group (Tabl~r~.’ Subanalysis of t]~e data a~fter controlling for fetalpresentafio~i,
marital status, and insurance status did not alter these findings. The incidence of 5-rain Apgar scores <_ 6 was similar in both Rroups ~5.4 vs. 4.2%). Postpartum c’o’mphcat~ons including endometri[is and wound infection were smadar in the two groups.
< 15 years Controls i9 value
Active ph~e (h) 4.5 5.2 0.02
Second stage (ram) 52 55 NS Oxytocin use (%) 37.9 48.7 0.02
Cesarean section (%) 13.8 25,3 0.001 Cesarean due to CPD (%) 6.9 11.9 0.04
Operative delivery rate (%) 20.0 19.0 NS
~ncy Epislotomy (%) ~ 31.4 46.0 0.001
CONCLUSIONS: Pregnancy at the lower limit of reproductive age is not associated with an abnormal labor course, as is commonly believed. The lower cesarean delivery rate in this group of adolescents remains unexplained.
340 SPO Abstracts January 1994 Am J Obstet Gynecol
229 COMPLICATIONS OF ELECTIVE CERVICAL CERCLAGE. RT Edenx, TR Wigton, T Asrat, RA Pwcon, ML Socol, D Worlhmgton D~vlslons of Materna~ Fetal Medicine, Med~ca~ College of Wisconsin and
University of Wlaconsirl Mdwaukee, Milwaukee, Wisconsin, Northwestern Unwers~ty Medical School, Chicago, Bhno~s, and Women’s Memonal Hospital, Long Beach, California OBJECTIVE: To determine the frequency and Ommg of preterm premature rupture of membranes (PPROM) and mtra-amnlotlc refection (IAI) associated with elective cerwcal cerclage STUDY DESIGN: A retrospechve review of 256 elective cerwcal cerclage procedures from 1/86-12/92 was performed at two permatal centers. Patients were included if they underwent a scheduled procedure between 10-18 weeks" gestation based upon previous obstetrical history. RESULTS: Mean gestahonal age at cerclage placement was 14 4 ± 1 B weeks Mean gestatlonal age at dehvery was 35.7 _+ 6.0 weeks and 82% of patmnts dehvered at _> 32 weeks. The mc~dence and t~mm9 of PPROM and IAI are presented m the table
g 2 > 2 ~7 >7 ~28 > 28 A 24 DAYS DAYS DAYS DAYS WKS
< 24 EGA WKS EGA
PPROM 0 0 4 1.6 5.5 1 8 (%)
IAI 0 0 0.4 3.1 2 3 (%)
Neither PPROM nor IAI were related to the surgical technique for cervical cerctage (McDonald versus Shlrodkar), However, the incidence of PPROM, but not IAI, was increased with the use of silk suture compared to synthetic material (p < 0 001) CONCLUSIONS: Comphcat~ons of elechve cervical cerclage ~mmed~ateJy follow{ng the procedure are infrequent PPROM and IA[ were more common greater than 28 days after the procedure, but the contribution of the cerclage, rather than the underlying disease process, to these morbldlt~es remmns all-defined.
231 HOME-BASED PERINATAL CARE IN THE MANAGEMENT OF
THE HIGH RISK PREGNANCY: AN ALTERNATIVE TO
HOSPITALIZATION S.Ktein. D. Feustin, I. Specter*, R. DiLandro*. Madonna Perinatal Services, Mineola, NY OBJECTIVE To evaluate home-based h~gh risk pennatal ~re as an
alternative to hosp~tahzatlon, we compared a group of high risk patients
managed at home w~th a comparable group of palmers managed m the hosp=tal STUDY DESIGN’ Between May 1989 and May 1993, 118 patients admitted
w~th the d~agnos~s of preterm premature rupture of the membranes (pPROM), preterm labor (PTL), ante-partum bleeding (An), and pregnancy induced
hypertensmn (PIH), were discharged to a permatal home care program
managed by a team o( pennata~ nurses, and supervised by the patient’s obstetricians with pennatal consultation Obstetrical data were recorded
prospectively and compared with 69 control patients who were managed by
hospltahzabon Statistical analysis used the t-test, w~th a p 05 level of significance
RESULTS The gestat=onal age at dehvery showed no significant d#femnce between the two groups, except m pPROM In this sub-group, although the
gestahonal age at rupture was not significantly different (30 75 +--5 59 vs 28 0
+ 5 43 week), the gestatlonal age d~fference at delivery 95 78 + 1 74 for the home care group vs 29 40 4- 4 75 weeks for the hospitalized group was statistically s~glnlf~sant (p<0Of) The days gained in the home care and the hospital care groups for pPROM was 31 7 and 12 2 days respecbvely (p< 05) Between the two groups, there were no differences In the c-section rate, low
apgar score, pennatal and obstetnc mortahty, or senous maternal morbidity
The average dady cost for home care was 16% of the average dady cost of hospital care
CONCLUSION Home-based pennata/care of selected high risk pabents Is as safe and as efficient as convenbonal management Home-based care
yielded a s~gn~ficantly greater prolongation of pregnancy ~n the small group of
pat=ants discharged with preterm premature rupture of the membranes than continuous hospltaliza~on In addlhOn, home-based permatal care can help
reduce the high cost of m-hospital care of selected high risk pregnancies
230 PHOTO ESSAY OF NON HERPETIC VULVOVAGIN&L DISORDERS NECESSITATING CESAREAN SECTION. T WestoveP, M. Lakex. Dept
MFM, UMIDNJ, RWJ Mad School, New Brunswick, NJ.
CASE REPORT: Vulvovagmal d~sease necessitating cesarean section ~s
a d~stmctly unusual phenomena. We present the chmcal scenarros and
photographic evidence of five pafients wRh vulvovagmal d~sease so
severe as to warrant electwe cesarean section. The f~rsl patient’s vagina
was approximately 2 cm deep with a 5 mm wide, 6 cm long ep~thehahzed
tract between the cervix (palpated to be normal at cesarean section) and the d~stal vagina Vaginal dehvery was thought to be unach~evable The
precipitating traumatic event had been a vaginal delivery w~th extensive lacerabon and repair ~n a 3rd world ashen. The second pahent had a
history of permeal teratoma repair and anal reconstrucfion in childhood.
The first recurrence of this tumor was noted antepartum and elective
cesarean section was deemed necessary to preserve "neD-anal" funcfion
and to prevent uncontrollable hemorrhage at delivery. S~mple
vulvectomy was performed post partum. Elective cesarean secbon of the
last three pabents was performed since, =n the op~mon of the attending
physician, adequate hemostasls and satisfactory closure of an ep=slotomy
~nc~s~on or genital tract laceration was thought untenable The third
pabent had a history of pre-pregnancy ax=llary h=drademtls and dunng the
pregnancy developed progressively worsening vulvar hldraden~t~s
unresponsive to multiple anfib~otics The fourth pafient underwent
elective cesarean sect=on for severe and worsening painful, weeping
vulvar edema (accompamed by unnary retenfion) assocmted with
po/yhydramn~os Decompresslve amnlocentesas were unsuccessful ~n
reducing the edema. The final patient mexphcably developed huge
posterior and lateral vaginal wall vancostt~es which ti~led the mtro{tus dunng valsalva and upon assuming the upnght pos~bon. Elecfive
cesarean section was undertaken aRer peMc ultrasound revealed no
addlfional unusual pelvic varlcosltles. All patients had uncomphcated
~ntra and post-operatwe courses.
232 PREMATURE RUPTURE OF MEMBRANES AT 34-37 WEEKS’
GESTATION: AGGRESSIVE VERSUS CONSERVATIVE
MANAGEMENT. R.W. Naef~ Ill, J R. ,gilbert, B. M. Weber~, H. Roachx,
R.W. Martin, J.C. Morrlson. Dept Ob/Gyn, Univ. of Mississippi Medical
Center, Jackson, MS.
OBJECTIVE: To compare aggressive management of premature rupture of
membranes (PROM) st 34-37 weeks’ gestation (oxytocin induction of labor,
IOL) with expectant observatton.
STUDY DESIGN: In this prospectwe investigatmn, 88 gravities with singleton
pregnancies were randomtzed to receive oxytocin IOL (n = 42) or observatmn
for labor (control [C] group, n = 46). All patients had estimated gestatmnal
ages (EGA) of>__ 34.0 weeks or sonographic estimated fetal weights (SEFW)
of >__ 1800, < 2500 gm at randomization. PROM was confirmed by
visualization of fired pooling m the posterior vaginal fornix or fern arborizatton
of vaginal specimens Subjects in the study group underwent IOL using a
standard protoeoI for oxytocin inductmn Control patmnts were observed for
spontaneous labor or evidence of chortoammonitis. They underwent nonstress
tests twice weekly and ultrasound once a week until dehvery
RESULTS: Demographic characteristics were similar within each group’ EGA
at PROM (34 33 4- 1.58 weeks vs 34 46 ~+ 1.28 weeks); SEFW (2261 + 334
gm vs 2329 4- 389 gm), and b~rth weight (2352 +__ 381 gm vs 2454 4- 375 gin)
were equwalent stattsttealIy (p = t~s) Chef ~oammomtis occurred more often m
the C group (17.4% vs 2 4%, p = 0.031), but postpartum endometritts was
more common in the IOL group (9 5 % vs 0.0 %, p = 0.048). Maternal hospita|
days were similar in both groups (2 4 +__ 1.3 days vs 3 0 4- 1 7 days, p = as).
Three patleats ~n tbe IOL group and none m the C group requtred cesarean
delivery (7.1% vs 0 0%, p = as). Two neonates in the C group had culture-
proven sepsis versus none in the IOL group (4.3% vs 0.0%, p = ns). There
were no neonatal deaths
CONCLUSIONS: This data suggests that aggressive management of PROM st
~> 34 0 weeks’ gestation (or ~ 1800 gm SEFW) w~th IOL gr~d delivery at
diagnosis ~s safe and may help avoid comphcatlons of ~nfection ~n both the
mother and neoaate.

Volume 170, Number 1, Part 2 SPO Abstracts 341 Am J Obstet Gynecol
233 A RANDOMIZED STUDY OF CLOSURE OF THE PERITONEUM AT CESAREAN DELIVERY.
F. LUZUYx, O IRIONx , F. BEGUIN
Dept of Ob/Gyn, Untverstty Hospital, Geneva, Switzerland
OBJECTIVE: In general surgery reapprox~mat~on of peritoneum for
wound heahng and wound strength ~s recomzed hke non necessary We conducted tNs study to confirm that non closure of the visceral
and parietal peritoneum at low transverse cerwcal cesarean is not
associated w~th increased ~ntraoperatlve or ~mmed~ate postoperative comphoahons STUDY DESIGN: Between January and December 1992, 300
women who were to undergo cesarean dehvery were randomized to one of two categories. There were no differences In method(s) of
anesthesia, operative red,cat,on(s) or use of pertpartum eptdural narcobcs The procedures were performed by a vanety of residents,
the pahents were managed in the usual postoperaWe manner and the
nursing staff was not aware of the patient’s treatment group
RESULTS: The Incidence of fever, endometntls, or wound infection was slm=lar in both groups (7%) There were no differences In the
number of pahents requlnng parenteral narcot=c analgesia or m the number of doses per patient (control 2 70, study 2 54) There was no
difference regarding the day on wh=ch patients were advanced to
liqu=d or selected d=ets The mean operative t=me m the control group
was 53 minutes versas 47 minutes In the study group (P< 005)
Although not stat=st=cally s~gmficant, controls had slightly longer
postoperaWe hospltahzations (control group 6 77 days, study group 6 46 days)
CONCLUSIONS: Non-closure of the visceral and parietal peritoneum at low transverse cervical cesarean dehvery appears to
have no adverse effect on ~mmedlate postoperaWe recovery, and provides a slmphfied and shorter surgical procedure
235 PREVALENCE, PROTOCOLS, AND COMPLICATIONS ASSOCIATED
WITH AMNIOINFUSION KD Wenstrom: WW Andrews, JE Maher Un~vers=ty of Alabama at B~rm~ngham, B=rm=ngham, AL.
OBJECTIVE: To determine =f amn=omfusmn ~s assoc=ated w~th labor
and dehvery comphcat=ons, and if comphcatlon type and Incidence
is related to the irtfus~on method.
STUDY DESIGN: Amnmmfus~on questionnaires were sent to every
academm Ostetncs and Gynecology department =n the country (206
Res=dency D~rectors or, =f the department had a fellowsNp, to 78
Maternal-Fetal Medm=ne fellowsh=p d=rectors).
RESULTS Seventy-s~x percent (59/76) of Feltowsh=p Dwectors and
62% (127/206)of Res=dency D=rectors responded, representing
644, 910 dehvenes/year (mean 3596, range 130- 15,000) N=nety-
s~x pement of responding centers utilized amnlemfuslon (at least 22,833 amn~o~nfus=ons/year, 2 to 2,000 per center) and 79%
employed a formal protocol. Ind~cat=ons included vanable
decelerations (98%), mecon~um fluid (86%), and ohgohydramn=os
(68%) Aw~devanetyof protocols were used, the most common
revolved normal sahne (84%) and warmed flu=d (78%) adm=n=stered as a bolus followed by constant =nfus=on (64%) using an infusion
pump (69%) and e=ther a s=ngle or double lumen catheter (40% each). Ninety-one centers (49%) employed ultrasound, but only
70% of these used the ultrasound data to adjust the infusion. Forty-
nine centers (26%) reported at least one associated comphcatlon
mctud=ng uterine hypertonus (n = 27), fetal heart rate abnormaht~es
(n=17), amnlon=t=s (n=7), utenne rupture (n=4), and maternal
cardmc or respiratory compromise In=3) Two maternal deaths
were reported None of the various aspects of the many protocols
correlated w=th any comphcat~on (p=NS) The I=kehhood of
reporting a comphcat~on d=d not ~ncrease with the number of
=nfus=ons performed (p=NS) CONCLUSION Amnlolnfuslon ~s performed nationwide according to
w~ddly varying protocols wrth few associated comphcatlons. Neither
the method employed nor the number of =nfuslons performed
appears to increase the risk of having a comphcat*on.
234 APPROXIMATION OF THE SUBCUTANEOUS TISSUE LOWERS THE INCIDENCE OF WOUND COMPLICATIONS AFTER CESAREAN SECTION RW Naumann,x JC Hauth, J Owen, P Hodgkins,× T Lincoln × University of Alabama at Birm~ngham, Birmingham, AL HYPOTHESIS: Closure of the subcutaneous t~ssue in obese women decreases cesarean section post-operative wound comphcatlon8. STUDY DESIGN. Two hundred forty-five women with >2 cm of subcutaneous fat were randomized to subcutaneous tissue closure with a honzontal runrmg suture of 3-0 dexon or to no closure during cesarean section Post-operative care providers were bhnded to the method of treatment Wound complications were assessed ~n the hosp{tat, at the post-operat~ve ws~t, and patients were surveyed by telephone two weeks post-operatively. RESULTS’ One hundred seventeen women (47 8%) were randomized to closure of the subcutaneous tissue and 128 (52 2%) to no closure. The median weight for patients in the study was 203 5 Ibs (92.5 Kg). Patients in both groups had a simdar maternal weight, body mass ~ndex, subcutaneous fat thickness, inc=dence of amn~onit)s, inc=dence of preeclampsia, type of skin incision, and total time from rupture of membranes to dehvery. A wound complication was found in 24 women (9 8%) prior to discharge and ~n 27 women (11 0%) when they were examined after discharge A seroma occurred in 28 women (t 1.4%), a hematoma ~n 6 (2 5%), and a wound ~nfect~on in 17 (7 0%) Wound comphcabons were related to subcutaneous fat thickness (p=0.0001), maternal wetght (p=O 0003), and body mass ~ndex (p=O 0003) Labor pnor to cesarean section increased the nsk for wound ~nfecbon (p=0.O009), but not seroma formation Seroma formation occurred ~n 6 0% of women who had a subcutaneous closure and ~n 18 8% w~th no closure (p=0 003) Overall, the wound comphcation rate was 14.5% ~n the closure group and 26 6% when the subcutaneous t~ssue was not reapproxlmated (p=0 02). CONCLUSION Closure of the subcutaneous t~ssue reduces seroma formation and post-operative wound disruption following cesarean dehvery ~n women w~th >-2 cm of subcutaneous fat
236 ETHNICITYAND PRENATALCARE. M Gardner~, R. Goldenberg, S. Cl=ve¢, G Cutter" The Un=vers~ty of Alabama at Birm=ngham, B~rmingham, AL. OBJECTIVE: Improving pregnancy outcome for minority women is a major goal of health providers and policy makers. Most strategies involve an ~ntervent~on during the prenatal period, It ~s therefore important to know where m~nority women with various characteristics receive prenatal care and why. Our purpose was to evaluate sources of prenatal care for White (W), Black (B), Mexican-American (MA) and Puerto Rican (PR) women. STUDY DESIGN; The National Maternal and Infant Health Survey (1988) was used to ascertain age, ~ncome, marital status, education revel and source of funding ~n each ethnic group. Source of prenatal care is classified as pnvate (private physician, nurse-m~dwlfe or HMO) or public (health department, community health center, or hospital clinic) RESULTS; When categorized by ethnic group alone, 78% of W women received pnvate care compared to 44% of B women, 51% of MA women, and 37% of PR women. In those minority women reeeiwng public care, 66% of MA went to community chnics or health departments vs 33% to hospital clinics. Most PR patients (62%) went to hosp~ta)-based clinics. 52% of B women went to community clinics or health departments Private health insurance was held by 78% of W, 50% of B, 49% of MA, and 47% of PR women, Of those women with private insurance, 86% of W, 62% of B, 69% of MA, and 59% of PR received private care. Of W women with Medicaid funding, 52% received private care as opposed to a range of 20 to 42% for m~nority women with Medicaid funding. CONCLUSION; Substantial differences in sources of prenatal care exist between W and m~nonty women and between d~fferent minority groups W women are more likely to receive pnvate prenatal care regardless of socioeconomic status Many MA, B and PR women uNize public care in spite of high ~ncome and educational levels. This information Is useful when formulatin9 health po)~cy a~med at improving pregnancy outcomes in minority women.
342 SPO Abstracts January 1994 Am J Obstet Gynecol
237 ARE PREGNANCIES OVER AGE 40 AT HIGHER RISK? Y. Ezrax, P. McParlandx, D. Farine. Die. of Perinatology, Mt. Sinai Hospital, Univ. of Toronto, Ontario, Canada. OBJECTIVE: To assess the effect of maternal age and parity on intervention rate and pregnancy outcome. STUDY DESIGN: A review of 35,140 deliveries (1985-1992) included 16,030 nulliparae. Of these, 1217 were > 35 years (123 over age 40). There were 19,110 multiparae including 3,051 women >35 years (312 over age 40 ). Xz and Fisher’s exact tests were used. RESULTS: All parameters were significantly increased in nulliparae over age 35 (Table 1). These parameters did not differ in women over age 40 and between ages 35-40. The perinatal mortMity was similar in all groups.
Table 1: Odds ratio of outcome and intervention rates in nulliparae >35y when compared with nulliparae <35y (A) and multiparae >35y (B)
Variables A B Cesarean Section Rate 2.0*** 1.5"** Labor Induction 1.3"* 1.3"* Preterm Labor 1,6"** 1.9"** Instrumental Delivery 1.2" 3.2*** Pregnancy Complications 1.8"** 1.8"** CS for Maternal Disease 3.1"** 4.4*** £erinatal mortality NS NS * p<0.05 ** p<0.0005 *** p<10~ NS - not significant
CONCLUSIONS: Parturients aged >35 years and especially nulliparous women are at increased risk for interventions and complications when compared with nulliparous women <35 years and multiparous women >35 years. Women > 40 years are at similar risk as women between 35-40 years.
239 AMNIOTIC FLUID PRESSURE/VOLUME RELATIONSHIPS DURING
HUMAN PREGNANCY. D. Merrillx and C, Weiner. Dept. Ob/Gyn,
Univ. of Iowa Hospitals and Clinics, Iowa City, IA 52242.
OBJECTIVE: Although disorders of a.mniotic fluid volume are associated
with adverse perinatal outcomes, the relative contribution of the altered
volume vs altered amniotie fluid pressure (AFP) per so remains unclear.
Little is known about the regulation of amniotie fluid volume and AFP
during either normal or pathologic states and less about the relationship
betwe.~n volume mad AFP. The present study was designed to characterize
the intranmniotie pressure/volume relationship across gestation.
STUDY DESIGN: Both the AFP and a four quadrant ~rnmotie fluid index
(AFI) were measured in 116 futures undergoing n clinically indicated
eordocentesis. All results are expres~l as the mean + SEM. Multiple
linear regressinn analysis was performed with significance at p <0 05.
RESULTS: Gestational ages (GA) of the fetuses studied averaged 29.3 +
0.4 wee, ks (range = 19.0 to 38.9) . AFP and AFI averaged 9.1 + 0.4 mmHg
(range = 2-32 mmHg) and 15.1 + 0.6 cm (range = 0 to 37.5 era),
respectively. Each was positively correlated with GA. There was a
significant positive correlation between AFP and AFI independent of
gestatinnal age (A~I = .77*AFP + 8.32; R= .50; p < .00005). Intranterine
compliance (COMP) was estimated by the AFI/AFP ratio and averaged 1.8 +
0.08. COMP was unrelated to gestational age [COMP = - 03*GA + 2.83;
R=.06; p =.24].
CONCLUSION: AFP is posaively correlated with AFV (as determined by
AFI) independent of gestationM age. Intranterine compliance, however,
does not ~ppear to be altered with edvaneing gestation AFI ~ppears
elinicMly u~efal as a noninvasive ~q~proximntton of AFP over u wide range
of volume.
238 LACK OF AN ASSOCIATION BETWEEN NEONATAL HYPER-
BILIRUBINEMIAAND VACUUMASSISTED VAGINAL DELIVERY. K.M..__~.
.Wi.~eczorek~, R K. Jaekle~, B. Rosen#, D Belsky2, T.A. Sidd~qi1. Dept.
Ob/Gyn, University of Cincinnah, Cincinnati, OW and Dept. Ob/Gyn
UMDNJ, School of Osteopathic Medicine, Stratford, NJ2.
OBJECTIVE: This study was designed to test the hypothests that vacuum
assisted delivery predtsposes to an increased risk of neonatal hyper-
bilirubinemla (a controversial issue in current obstetric literature). STUDY DESIGN: 509 consecutive dehveries (gestationat age >35 weeks)
occurring over 6 months in a community hospital were reviewed retro-
spectively Hyperbdirubinemia was defined as an unconjugated bilirubin
level >10 mg/dl Results are reported as mean + SiC. Data were analyzed
with 1-way ANOVA and Chi-square analysis as appropriate (p<0.05).
RESULTS: Modes of delivery were grouped as spontaneous vaginal
dehvery (SVD)(n=339), vacuum extraction ~/ac)(n=52), forceps (n=19)
and cesarean section (C/S)(n=99). There was no differenc.e in race, ABO type, Rh, infant gender, or birth weight between delivery groups
Placement of a scalp electrode occurred more commonly m the Mac group
vs SVD and C/S groups (73%, 42% and 33%, p<0.05). Although five mm
apgar scores were statistically lower in the Vac vs SVD group (8 8+0.1 vs
9 0+_.0 03, p<0 05) this d=fference had no clinmal sign=ficance Hyper-
b~lirubinem=a rates were as follows 24/339(7 1%) infants delivered by SVD,
2/19(10.5%) with forceps, 8/52(15 4%) by Vac, and 19/99(19 2%) by C/S.
C/S was associated w=th a higher rate of hyperbil=rubinem~a compared to
SVD (p<0.001) while no stabstically s~gnlficant differences were observed
between vacuum assisted deliveries and the other modes of delivery
(p>009, SVD vs vacuum) Hyperbilirubmemia in the C/S group was not
assooated with the presence or absence of labor (p=0.32)
CONCLUSIONS: 1) Vacuum assisted vaginal delivery is not assooated
w~th h~gher rates of hyperbil=rubmemia when compared to other routes of
dehvery, 2) Cesarean delivery is associated with an increased rate of
neonatal hyperbd=rubmemia. We speculate that the association between
C/S and hyperbillrubmemia is simply the result of an observational b=as
due to the increased deltvery to the discharge interval m these infants
240 PREGNANCY OUTCOME IN ACTIVE DUTY SEAGOING
WOMEN. S. Spandorferx, E. Graham, I. Furouzan. Dept. of Ob~,;yn,
Univ. of Penn., Philadelphia, PA.
OBJECTIVE: Our objective was to examine the effect of being
assigned to naval vessels for the 1st 20 weeks of pregnancy by enhsted active duty women.
STUDY DESIGN: ~l’he antenatal and intrapartum records of 140
women on active duty for the 1st 20 weeks of their pregnancy for the 18
month period from Feb 91 to Aug 92 were reviewed. Current policy is to transfer women who conceive while on active duty to shore duty at 20
weeks gestation. This group was compared to national normative statistics
RESULTS: This population did not differ from the control group in the
incidence of anemia with hematocrit < 33 (24%), gastafional thabetes
(2%), twins (l%), postdatism (6%) or cesarean rate (22%) Among active duty women only l 1% of embryos/fetuses were exposed to
alcohol during the permatal period as compoa-ed to 60% nationally, and only 19% were exposed to tobacco as compared to 25% nationally.
There was an increased incidence when compared to controls of:
sexually transmiUed disease (STD) (24% vs 13%), urinary tract infection
(UTI) (20% vs 11%), and preeclampsia (13% vs 7%) Intrapartum
complications of failure to progress (t2%), fetal distress requiring
intervention (16%), and chorioammonitts (16%) were not different from the control group. The average birth weight was 3338 grams with 12%
delivering before 37 weeks, slrmlar to the control poputatton; however
this group differed in that 25% were large for gestational age, and 1%
were small for gestational age. The perinatal mortality rate was 2.1%,
significantly increased from the national rate of 1.47% (p<0.05).
CONCLUSIONS: Women on actave duty assigned to naval vessels
during the 1st 20 weeks of their pregnancy have an increased incidence
of STD, UTI, preeclampsia and an increased perinatal mortality rate;
however, their incidence of alcohol and tobacco use is much lower.
When compared to national data there is no difference in the incidence
of anenua, gestational diabetes, twins, postdatism, cesarean rate, or incidence of preterm delivery.
Volume 170, Nmnber 1, Part 2 SPO Abstracts 343 Am J Obstet Gynecol
241 PROST.~GI~NDIN E2 GEL PRIOR TO INDU~ION OF L,~BOR IN ~ WITH A PREVIOUS CES~ 8E~TIOM. _MA Willi~sx, DE Hickok, RW Zinghe~~, DA Luthy. Swedish Medical Center, University of Washington, Seattle, WA. O~I~ TO evaluate the efficacy and safety of preinduction intracervical prostaglandin E2 (~E2) gel (0.5 mg) in women with one previous cesarean section. S~Y DESI~ A retros~ctive cohort study design was used to c~pare 117 women with one previous cesarean section (VSACS) with 354 nulliparas. Both groups received prelnduc- tion Intracervical ~E2 gel. Student’s t, chi s~are, and l~istic regression procedures were used. ~S~TS~ The mean nu~ers of PGE2 gel applications were 2.4 and 2.5 for VBACS and controls, res~ctively (p > 0.05). Forty ~rcent of V~CS entered labor s~ntaneou~ly, as compared to 34% of controls. Mean duration of ruptured me~ranes (8.2 vs 12.1 hours) and length of labor (20.9 vs 28.4 hours) were reduced ~ong VBACS as compared with controls (p < 0.05). Overall, ~ACS had a higher cesarean section rate as compared with controls (49.6 vs 31.9%); however, the excess was attributed to a higher fre~ency of cephalo~ivic dispro~rtion ~ong VSACS. There were no differences in the occurrence of maternal and fetal morbidity. ~N~SIONS~ The efficacy and safety of 0.5 mg ~E2 gel a~inistered for preinduction cervical ri~ning in VBACS is comparable to that observed in nulliparas.
243 MATERNAL PRE-PREGNANCY WEIGHT AS A PREDICTOR OF PREECLAMPSIA C. Chambersx~ L. Nelsonx, K. Ward,. University of Utah School of Medicine and the Eccles Genetics Institute, Salt Lake City, Utah. OBJECTIVE: To determine whether pre-pregnancy weight is an independent risk factor for the development of preeclampsia. STUDY DESIGN: In this pilot study, 124 antepartum patients reported their pre-pregnancy weight (57 patients in this population were primigravid). All had no other risk factors for preeclampsia, such as diabetes, chronic hypertension or renal disease. 20% of this population had a pre-pregnancy weight of more than 160 pounds. This weight was then used as an arbitrary cutoff to determine subsequent risk of developing preeclampsia. A diagnosis of preeclampsia was made by standard ACOG criteria. Data were compared by one-way analysis of variance. RESULTS: 7 of 124 patients developed preeclampsia (6%). 19% of the patients weighing greater than 160 pounds had pregnancies affected by preeclampsia. Only 2% of patients weighing less than 160 pounds had
cy preeclampsia. (p=.0007) CONCLUSIONS: Using a cutoff of 160 pounds for pre-pregnancy weight, patients have a ten-fold increased risk of developing preeclampsia. Therefore, a pre- pregnancy weight greater than 160 pounds is an independent risk factor for preeclampsia. Data from 2,000 consecutive patients are currently being analyzed.
242 TRENDS IN THE MANAGEMENT OF MACROSOMIA 1983 VS
199h A MULTICENTER STUDY. H. Wehbeh 1.M. Fleisherx, G. C~eyx, S. Shahemx, H. Minkoff., Lutheran Medical Center, SUNY
HSC, Brooklyn, NY. OBJECTIVE: We conducted a retrospective multieentered study to
identify changes, if any, in the intrapartum management of maerosomie pregnancies (> 4500 grams) with respect to both treatment modalities
and fetal outcome for the years 1983 vs 1991. STUDY DESIGN: Data pertaining to the intrapartum management and
perinatal outcome of 160 pregnancies re.suiting in offspring weighing greater than 4500 grams during the year 1991 were compared with 124
comparable pregnancies occurring during the year 1983. These data were obtained from a birth registry maintained by SITNY Health Science Center
at Brooklyn which collects and maintains information on birth outcomes
from 4 community hospitals located in the city of New York. RESULTS: The total cesarean section rate was 49.2 % in 1983 and 53.1
% in 1991 (P-0.59). The elective cesarean section rate was lower in 1983 vs 1991 with the difference approaching statistical signifleanee (4.3
% vs 10.0 %, P=0.08). Forceps delivery was significantly higher in
1983 vs 1991 (11.3 % vs 2.5 % P < 0.(3001). We observed no difference in the rate of total fetal deaths or neonatal deaths between the years 1983 and 1991(1.6% vs 1.2%, P = 0.50 and 0.8 % vs 0.0 %, P=0.32 for total and neonatal deaths respectively). Fetal distress (5 minutes APGAR score less than 6) was lower in 1991 with the difference approaching statistical significance (22.0 % vs 15.0 %, P=0.07).
CONCLUSIONS: There appears to be a change in the management of macro~mia, with increase in elective cesarean sections coupled with the decreased use of forceps. These changes were associated with a trend
toward improving APGAR mores.
244 DEREGIONALIZATION OF CARE: IMPACT ON
BIRTHWEIGHT-SPECIFIC MORTALITY: S.Powellx,
V. Holtx, D H~ckok, T. Easterhng. Pubhc Health and C?mmumty Medicine, Univ. of Wash, Seattle, WA. OBJECTIVE: To ascertain whether there has been a shift m location of dehvery of low Nrthwe~ght infants, and whether the s~te of dehvery has produced d~fferent~al mortahty. STUDY DESIGN: Linkage of birth and death cert=ficate records m Washington State, 1980-1990, produced 43,832 hveb~rths <25009 for th~s study. Infants w~th fatal anomahes potentially diagnosed prenatally were excluded. S=gmficant differences were determined w~th ManteI-Haenzel estimates of relahve risk. RESULTS: After 1988, we detected a shift m location of birth of infants weighing 1500-1999g toward delivery at non-tertiary hospitals. For infants below 20009, dehvery at a non-tertiary hospitals was associated w~th Ngher mortality from preventable conditions (500-9999, RR=I.7, 95% CI 1.4-2.1; 1000-1499g, RR=I.5, 95% CI 0.9-2.7; 1500-1999g, RR=2.1,95% Cl 1.2-3.8)
Birthwei_ahtfa) Level I Level II Level rate* rate* rate*
500-999 615 4 583.3 353.5
1000-1499 150 9 80.0 68,6
1500-1999 27.0 56.0 21.1
2000-2499 3.5 7.6 11.2
*Death rate per 1000 births =n 1989 and 1990
CONCLUSIONS: Until popu/atmn-based mortality data mdzcate otherwise, delivery of infants ant=clpated to be less than 2000g at tertiary level centers should remain the standard of care

344 SPO Abstracts January 1994 Am J Obstet Gynecol
245 INTERNAL PODALIC VERSION FOR THE SECOND TWIN -
REPORT OF 90 CASES. G Azar,x A Khahl,x M Nabulsl,x G Khayyata,x Jr Sawaya x g~ept OB/GYN, American Umversity of
Beuut, Lebanon
OBJECTIVE To evaluate the safety regarding maternal and neonatal
outcome of 90 twin pregnancies m which internal podallc version (IPV)
was successfully performed on the second twin
STUDY DESIGN A retrospectxve survey was carried out at our center
flora 1978 to 1992. Ninety-five twin l~egnancles were identified on whom IPV was attempted on the second twul Only pregnancies with gestational
age >32 weeks, fetal weight >1500 grains, both twin members were alive on adnltsston, and absence of congemtal abnormahtles were included
Type of anesthesia, technical difficulties, matelnal comphcatlons and
neonatal data, weie all recorded
RESULTS The mean maternal age and ge~tatlonal age were 27 years and
37 weeks respectively The mean pmity was 2 with 20 patients being
prunipara InteinaI podahc velsion was successful in 90 of 95 cases Only
three of these versions were considered difficult, however, all had
satisfactory neonatal outcome. Fetal p~esentatlon for the second twin was
vertex in 47 (52%) and transveise in 43 (48%) IPV was performed with an
uitact ainmot~c fluid sac m 67 (74%) cases and following rupture of
membianes in 23 (26%) Thnty-seven (39%) lecewed epidmal anesthesia, while 37 (39%) had general anesthesia, and the reinalnmg were done under
local allc~,thesla No maternal comphcatlons were noted except for four
cases of placental abluption The mean 5 minute Apgar scores were 8 4
and 8 0, and the aveiage fetal weight was 2446 and 2452 giams for the first
and second twill ie~pectlvely Of the second twin membels, only one
neonate had an Apgar score <7 Cmd p~olapse comphcated the dehvery of
four cases~ two of which while dehvenng the f~rst twin Neonatal data
levealed no mortahty aud no evldeuce of birth trauma, except for one case
of shoulde~ dislocation
CONCLUSION This large ~etrospective study suggests the relative safety ofIPV regaiding maternal and neonatal outcome However, a double blind
prospective study Is now uutlated at urn" ceutel to further assess the role or
IPV in the lnUapartum manageinent of the second twin
247 1S MANUAL PALPATION OF UTERINE CONTRACTIONS ACCURATE?
P Arrabal, D Nagey. D~v Maternal-Fetal Med~mne, Dept OB/GYN,
Umversity of Maryland School of Medm~ne, Baltimore
Objective: The aim of tins study was to assess the accuracy of uterine
contraction palpation; determine whether the accuracy of palpation improves
with experience; determine what other factors might affect the accuracy of
palpation; and evaluate the range of intrauterine pressure (IUP) present when
an observer notes the contraction to be todd, moderate or strong
Study Design 236 observations were obtained on 46 Iabormg pauents in the
first stage of labor with water-filled intrauterine pressure catheters The
blinded observers [OB/GYN Residents, Maternal Fetal Medicine (MFM)
Fellows and Faculty and Labor and Dehvery Nurses] were asked to label a
contractlonas mild, moderateorstrong A "mild" contractlondeslgnaeunwas
accurate ff IUP~<30 mmHg;"strong" contraceon if IUP>~50mmHg,
"moderate" contraction if the IUP was intermediate. Patient’s height, weight,
parity, gestational age, use of oxytocln, use of epldural anesthesia, Iabormg
position, and the level of training of the observer were noted. Multiple loglsuc
regression was performed with accuracy as the dependent variable. Ch~-square
analysis with Yates’ correction was used for between-group comparisons.
Results " Mild" contractions had IUP=35.2+__33 8mmHg(+__2 S.D)
"Moderate" contractions had IUP=44.9+__35 4 mmHg "Strong" contractions
had IUP=55 5+28 0 mmHg The observations were accurate 49% of the
time Accuracy in designating contractions as mild or strong revealed
comparable lack of accuracy There was no improvement in accuracy with
increased physician experience. The MFM Faculty was more accurate than the
nurses (p <0 025) All physicians as a group were more aceurate than nurses
(P<0.05) Accuracy was not affected by climcal variables None of the
variables were slgmficant in predicung palpatlon accuracy.
Conclusion Manual palpation of uterine contractions is an inaccurate means
of determining contractmn strength The accuracy of contraction palpation
does not appear to improve with observer experience and does not appear to
be affected by clinical circumstances There ~s a wide range of IUP present
when palpation deslgnates a contraction as mild, moderate or strong
246 PROPHYLACTIC AMNIOINFUSION IN PREGNANCIES
COMPLICATED BY THICK MECONIUM N. Enksen, M. Hostetter*,
V. PansL Department of Obstetrics/Gynecology, University of
Texas-Houston.
OBJECTIVE: We hypothes=zed that prophylactic intrapartum
ammoinfus~on m pregnancies comphcated by thick mecomum will
not decrease the ~ncldence of fetal d~stress, cesarean section for
fetal d~stress and mecomum below the cords.
STUDY DESIGN: Patients w~th th*ck meconium were randomized
to ammomfusion (n =65) or controls (n=59). The amnio~nfus~on group received an 800 cc bolus of normal sahne followed by a
continuous infusion at 180 cc/hr. Continuous variables were
compared using students t-test end discrete variables were
compared by CN-square analysis and Fisher’s exact test as
appropriate.
RESULTS: The inmdence of fetal d=stress (16 of 65 vs 7 of 59) and
cesarean sectmn for fetal distress (7 of 65 vs 7 of 59) was not
s~gnlficantly different between the amnlolnfuslon and control
groups, respectively. The rate of mecomum below the cords (1 of
65 vs 8 of 59) was sNn~ficantly lower =n patients receiving
amn=o~nfusmn (relat=ve risk 0.09, confidence interval 0.01 and
0.82, p=0.02). Two cases of meconmm aspiration syndrome
occurred in control patients but none receiving amniolnfusion
(p = 0 22).
CONCLUSION: Prophylact=c amn=omfus=on ~n pat=ents w=th thick
meconmm decreases the incidence of meconium below the cords
and should subsequently =mpact on the incidence of mecon~um
aspiration syndrome =n larger series.
248 A RANDOMIZED PROSPECTIVE TRIAL OF TWO EXPECTANT
MANAGEMENTS OF PRE-LABOR RUPTURE OF THE MEMBRANES
~ PROM) AT 34-42 WEEKS.
L. Ladforsx, 1L~,. MattssonX,, 1M EnkssonX,, 20. Fallx, 1 Dept. Ob/-~yn ~sstra Hospital, 2Dept. Ob/Gyn M61ndal Hospital,
Un~vers=ty of Gothenburg, Sweden. OBJECTIVE: To compare obstetnc and permatal outcome between
two d=fferent expectant managements m women w=th PROM.
STUDY DESIGN: 1012 women w=th PROM at 34-42 weeks w~thout contractions two hours after admission were randomly allocated to
e=ther mduct~on w~thm 24 hours (n=502, group A) or 72 hours
(n = 510, group B). D=g~tal exam=nat=ons of the cerwx were avoided until onset of active labor. Labor was induced with oxytocln in both groups =f no spontaneous contractions occurred or if signs of
chonoamnlonltls or fetal distress were detected. Women with PROM and contractions starting within two hours after admls-
s~on(n = 373, group C) were included ~n the calculat=ons as a control
group. The malonty of women were pnm=para, group A(n = 317), group B(n=323), group C(n=228).
RESULTS: The Cesarean Sect~o(CS) rate was Iow(2-4%) and not differ between the groups. However the CS rate was h=gher ~n
pnm~paras compared to mult~paras(p =0.03). Oxytoc~n for
augmentation of labor m mult~paras was used m 58%(group A),
37%(group B), 24%(group C). In pnm~paras a lower(P=0 04) rate
of Vacuum extract~ons(VE) was found m group A (8%) compared to group B (14%). No forceps were used. S=xwomenwereglven antiNot~cs because of endometnt~s after dehvery Sixty-one(4%) of
the chddren were treated w~th antlbmt~cs and no d~fference between the three groups could be detected.
CONCLUSIONS: In tNs study a low maternal and fetal morbidity
was found when a strict protocol for the surveillance was followed including avoidance of digital examinations until onset of actwe
labor. In pnm~para the VE-rate was lower when m the 72 hours compared to 24 hours group Nodlfferencelnmfect~ousmorNdlty
could be found

Volume 170, Number 1, Part 2 SPO Abstracts 345 A~n J Obstet Gynecol
249 IANI~RLOTIC FLUID PLASMINOGEN ACTIVATORS ARE INCREASED UPTURE OF MEMBRANES AT TERM. P Banmann’, R Romero, R Gomez~, R Qulntero E Behnke" DB Cotton -E Mammen’. Dept. of Ob/Gyn, WSU/Hutzel [qosp. Detroit, MI; and the Perinatology Branch, NICHD, Bethesda, MD. ’ BACKGROUND/OBJECTIVE: Tissue plasminogen act vator (tPA) and uroklaat.e plasmmogen activator (uPA) are highly specific serine pretenses present.m amnlotlc lluid (AF) which have been lmphcated in the mechanism responsible for membrane rupture. Their act v ty s nh b ted by two se[p as. plasm~nogen activator inhibttor-I (PAI-1) and 2 (PAl-2). To determine if rupture of membranes (ROM) ts ~sociated with change in AF set ne protease/serpin concantrations. STUDY DESIGN: Transabdominal amnioeentes s was performed n 119 patients at term. These patients were arranged m four groups according to a two-by-two factorial design group 1 intact membranes-no labor N=30 ’ group2, ROM-no labor (N =25), g-roilp 3, mtact memb ...... labor ~I~=33/
group 4, ROM-labor (N=28). Pretense concentrations were determined by chromogemc substrate based functional assay (PAI-1) and enzyme-linkeit lmmuoassays (tPA-antigen (tPA-AG)t PAI-2, uPA), respect ve y Normal ty was tested with the Kolmo~orov-Smlrnov one sample test Linear contrasts (sets of t-tests) were used-to examine the association between rupture membranes, and labor and AF serlne protease/serpin concentrations. RESULTS: 1) ROM (p <0.001) as well as labor (p <0 001)were associated with all increased AF~tPA-antlgen concentrations. Moreover a sign flcant nteract on between labor and RDM in AF tPA-antigen was found w~th linear
contrasts (p<0 001); 2) ROM but notparturitton was associated with an ~ncreased AF uPA, concentration (p<0.001). 3) Neither parturition nor ROM had on effect on AF concentrations on PAI-I or PAI-2.
tPA-AG PAl- 1 uPA PAl (1U/ml) I1U/ml) (ng/ml) {ng/ml)
INL 0.51+0 42 20.1±11.0 0.37±0.38 126±38.3
RNL 1.09±0.06 16 0+9 0 0 80+0 53 109±55.4
IL I 17±0.51 16 3___10.0 0.43:1:0.29 131±52 9
RL 1 19+0 01 18 9+10.9 0 66+0.60 131+61.2 Values are expressed as mean:l: standard deviation. INL, intact-no labor, RNL, ROIM-no labor; IL, intact-labor, RL, ROM-labor CONCLUSIONS: Our data provides strong support for the concept that components of the flbrmolytic system are mvolv~l in the mechanisms of membrane rupture. We pro-pose i.hat by degrading the basement membrane and extracellular matrix of amnion and chonon the fibrmolytic system plays an ~mportent role duringphysiologic (1 e. that occurring during labor, and pathologic (i.e., pre abor~spontaneous rupture of membranes at term.
251 PRETERM DISCORDANT TWINS: WHAT BIRTHWEIGHT DIFFERENCE IS
SIGNIFICANT? V.Y.T. Cheun~, A.D. Bo~ki~, O.P. DaS~lva~. Depts. Ob/Gyn and
Paeds, University of Western Ontario, London, Ontario, Canada.
OI~ECTIVE: To determine the effect of twin discordancy on subs~uent perlnatal (PN) and noona~ (NN) outcome for d=fferent degrees of b~rthwe=ght (BW) disco, dance In
preterm twtn gestations.
STUDY DESIGN: One hundr~ and twenty-two twi~ sets, deliverad betwee~ 25 and 34
comp~etad weeks’ gestation were studied, They ware stratiflad into 5 cat.sties
acc~xding to the % d~ffarence in infant BW, which was defin~ as [(BW of larger tw~n-
BW of smaller twin}/BW of largar twin] X 100. Tha relahonsh=p between % difference in
BW and the PN and NN outcome, and the d=ffarence in outcome between the large and
small infants within each category, were betermmed.
RESULTS: Results are presant~ as % unless spec=fiad.
<10% 10-15% 15-20/o 20-30% >30% P-value
Number 102 40 46 32 24
BW (g, moan 1567 1579 1609 1529 1258 0086
+ SD) ±521 +451 +499 :~o08 :~573
C-section 42.1 35 0 36.9 34.4 79 2 0.0036
Correct~ 7.8 0.0 4.3 3.1 16.7 0,075
Infant Death
Major Conj. 6.9 5 0 2.2 9.4 37 5 0.00001
Anomalies
5rain Apgar 15.7 7 5 2.2 21.8 33.3 0,003
Score <7
PVL 1 0 25 22 6.2 167 0.000008
No d=fferences were noted among groups for maternal age, panty, gestational age at
ddivacy, and the incidar~ca of =nfant respiratory complicities, mtravant~icolar
ha, aronnhage, nocrofizmg onteroco~i6s, jaundice and patent ductus artenosus Outcomes
of [ar~ and s~alt Infan’~s ~hin catt~ones were simitar except In the >30% group,
whirs all deaths occurred in the small infants.
CONCLUSION: In i~’oterrn twin gestations, a BW disco~danca of :30% is assoc~atad
with a high advarse PN and NN outcome, despite a greatar incidence of cesarean
delivery. We suggest the use of 30% BW d=fferenca to define twin discordancy =s most
dinico~ly ralevant in idenbfymg those infants at ask for adverse outcome.
250 A COMPARATIVE STUDY OF TIlE VALUE OF AMNIOTIC FLUID INTERLEUKIN-6~ WHITE BLOOD CELL COUNT AND GRAM STAIN IN TIlE DIAGNOSIS OF MICROBIAL INVASION OF THE AMNIOTIC CAVITY IN PATIENTS MTII SPONTANEOUS LABOR AT TERM. R Romero, M Galasso’, R Gomez% M Ramirez", Y Sorokln, E Behnkd’, DB Cotton. Dept.-’i7~3~7G"~N, WSU/Hutzel Hospital, Detroit, MI, Sotero del Hospital, Santiago, Chile and the Perinatology Branch, NICHD, Bethesda, MD. BACKGROUND: Subclimcal microbial invasion of the amnlotic cavity (MIAC) occurs in 18 8 % of patients with spontaneous labor at term with intact membranes (JRM 1993;38 543) Although the ammotlc fluid (AF) white blood cell count (WBC), mterleuktn-6 ~IL-6) and glucose concentrations and the Gram stain (GS) have beet/ used for the dtagnos~s of MIAC in p~tlents with preterm labor and preterm PROM, no informatton ts available about the accuracy and specific cut-off values for these t~ in patients at term OBJECTIVE: To compare the performance of the AF GS, WBC and IL-6 in the identification of MIAC m patients with spontaneous labor at term. STUDY DESIGN: AF was retrieved from 90 patients in labor at term. AF was cultured for bacteria and Mycoplasmas species. AF GS, VVBC and IL-6 (ELISA, sens~t~vny: 43 pg/ml) were performed tn all specimens. MIAC was defined as a positive ammeter fluid culture for microorganlsms. Analysis was conducted with receiver operating characteristic curves (ROC) and logistic regression. RESULTS: The prevalence of MIAC was 15.6% (14/90). Logistic regression demonstrated a strong relationship beg’sen the results of AFWBC and IL-6 �oncentratmns -but not GS- w~th .~F culture results (p < 0.005 for both). ROC curves were constructed to determine cut-off values for the different variables Diagnostic radices, posmve (PPV) and negative (NpV) predictive values, relative risks 0~R) and 95 % confidence interval /CI) are displayed in the followin~ table:
Variable Sens Spec PPV NPV RR 95% Cl
IL-6~5 7 ng/ml 86% 79% 43% 97% 13.3 3.2-55.4
WBC~20 64% 63% 24% 91% 2.6 0.9-7.1 eells/mm3
Gram stain 28% 97% 25% 87% 1 8 0.7-5.2
Logistic regression demonstrated that when all the variables were simultaneously entered into a model, only AF 1L~i retained statistical significance. When AF IL- 6 was omitted from the analysis, the combination of the AF WBC and the GS provtded separate and importent diagnostic information. CONCLUSIONS: AF IL~ determination is the best rapid test for the detection of MIAC inpatlents in labor at term When this examination is not available, AF GS and WBC represent a reasonable approach to exclude this condition.

346 SPO Abstracts January 1994 Am J Obstet Gynecol
252 ADJUSTMENT OF BIRTH WEIGHT FOR MATERNAL
CHARACTERISTICS IMPROVES PREDICTION OF MORBIDITY AND
MORTAUTY IN THE GROWTH RETARDED INFANT. A. Sciscione
R. German,x M. Lantz,x N, Callan. Dept. Ob/Gyn, Johns Hopkins
Univ. Johns Hopkins Hospital, Baltimore, MD.
OBJECTIVE: The growth retarded infant has an =ncreased perinatal
mortality and morbidity (PNM&M). The classic definition ~s based on
oestat~one! age (GA| elone ignoring msterne| chsractertstics. We
hypothesize that maternal physical characteristics affect birth weight
(BW), and using these characteristics to adlust BW should improve
prediction of an untoward outcome.
STUDY DESIGN: The maternal pregravid weight, height, and weight
gain or loss, GA at dehvery, and infant BW were determined m 2947
normal pregnancies. Multiple regression was used to compare
maternal characteristics and BW. An equation was constructed to
calculate normal BW based on maternal characterist=cs (BW,a~). Using
the BW.~ curve, we compared the PNM&M in infants < 1Oth %ile to those ~ lOth %ile and then performed the same comparison using a
published standard curve (BW=d) based on GA.
RESULTS: Non-pregnant wmght, maternal he=ght, and weight gain
all influenced fetal we=ght significantly (p=0.001). GA and race
not differ across %des nor between BW,a~ and BW=d. Using e~ther curve, =nfants < 10th %ile were more hkely to experience PNM&M
than those _>10 %its. However, the sensitivities and relative risks
for PNM&M were h=gher for the BW,a~ curve vs BW=d curve while spsclhcltles were SllTiiter.
CONCLUSIONS: BW ~s affected by maternal height, prepregnancy
weight, and pregnancy we=ght gain. Using BW,~ as opposed to standard growth tables =reproved the prediction of PNM&M in infants
< 10th %lie.
253 PREDICI’OI~S OF FETAL MA CROSO/~A. A.Verma, N. C~unx,
D. W. Mzrrish, G Flower dew. Per inatal Unit, l~oyal Alexandra
H~pital, Uniter sity ~ff Alberta, Fxtment~n, Alta,
OKIEC~VE: To determine the r elafive impor tance of treated
gestatiatal diabetes rnellitus ((D!V~ ~g other known predictors of
f~l ~,~a
STUDY I)ESI(~’~I: 535 mether/ne-M3orn pair s voere reeru~ted 24-48
hours after delivery. Data at pre-pregnancy mad pregnancy variables v~re collected by chart r eview and interview with the mether.
Ma’phcrc~tric measures ~ere perfer meal at the newb{rns by ate of
tv~ examiner s. Univ’a~iate and rnultivar iate anaiyses were perfermed
with fetal mactosauia (bvvt:4000gms) as the dependent "¢ariable. (DM
subjects received stmadard therapy.
RESULTS: Previous histery of macresemia was the single most
po~er ful predictor. Other predictcrs in order of entry into a stepwise
logistic regressiou model were: smoking (neg ccrr elation), maternal
pr e-pr egnaacy wt, vot gain, parity, maternal birth wt, ~statioual a~
~->40 wks, mad gender. Treated (DMwas net significant by either
analysis.
CON(X,USlONS: "lhe rn~t important predictors of fetal macrosomia
appear tobe maternal and fetal censtitutienal factors. Treated (DM
does not appea¢ tohave independent significance. Recruitement is
atgnin& mad we wll present results of stepwise regress~ou analys~s
dysproportiamte fetal growth as the dependent variable.
Poster Session III Friday, January 28, 1994 10:30 a.m. - 12:00 p.m.
Pavilion 9 - 11
CATEGORIES
Genetics and Teratology
Diagnostic Ultrasound
POSTER NUMBERS
254-296
297-343
Judges:
Richard L. Berkowitz, MD
Michael T. Mennuti, MD
Wayne A. Miller, MD

348 SPO Abstracts January ]994 Ant J Obstet Gynecol
254 ADVERSE PREGNANCY OUTCOMES FOLLOWING FALSE POS- ITIVE TRI~LE SCREEN FOR DOWN SYNDROME (DS). E. Perqament,A A.K. Stein,x B. Fine,x M. 3~. Kupferminc. Department of Ob/Gyn, Northwestern University Medical School, Chicago, IL. OBJECTIVE: To prospectively assess the relative risk of adverse outcomes in pregnancies when their triple screen (AFP, uE3, hCG) indicating an increased risk for DS (1 in 250) is not con- firmed by amniocentesis (false positive). STUDY DESIGN: The study group consisted of 59 pregnancies with a false positive triple screen for DS and 118 matched controls. RESULTS: Pregnancies with false positive triple screen for DS were significantly different from their matched controls in five outcomes: fetal wastage (5.1% vs 0%); SGA (5.1% vs 0%); preterm labor (10.2% vs 2.5%); preeclampsia (6.8% vs 0%); and premature delivery (20% vs 8.5%). Gestational age at delivery was on the average 7 days earlier for pregnancies with false posi- tive triple screen for DS, compared to matched controls (38 vs 39 wks; p<.05). Overall, adverse pregnancy outcomes occurred in 20 of 59 pregnancies (34%) with a false positive risk for DS compared to 15 of 118 matched controls (12.2%); odds ratio=3.52 (Cl 1.54-8.12); p=0.002. Low uE3 was a better predictor of adverse pregnancy outcome than AFP and high hCG (odds ratios 4.1, 1.0, 0.9, respectively). CONCLUSIONS: One in 3 women with a false posi- tive triple screen for DS may experience an adverse pregnancy outcome. It now appears imperative to develop counseling strategies for informing parents about this possibility when a triple screen suggestive of an increased risk for DS is followed by normal fetal ultrasound evaluation and karyotype.
256 ABSENT FETAL SWALLOWING: A POSSIBLE ROLE IN THE PATHOGENESIS OF MICROGNATHIA David M. Sherer, Richard Jaffe, Leon A. Metlay*, James R.
Woods The University of Rochester School of Medicine and Dentistry. Rochester, New York.
OBJECTIVE: To assess the association of absent fetal swallowing in a nonrestrictive intrauterine environment and subsequent neonatal micrognathia. STUDY DESIGN: Over a five year period, fourteen fetuses with sonographic findings of massive polyhydramnios
(amniotic fluid index [AFI]>20 cm), absent mandibular "movement, and a nonvisualized fetal stomach (all consistent with absent fetal swallowing) were followed, Subsequent
mandibular development was assessed at delivery or autopsy. A group of fourteen fetuses, each with massive polyhydramnios (AFI>20 cm), yet with sonographic
evidence of active mandibular movement, and a visualized stomach, served as controls. All 28 mothers were normoglycemic throughout gestation. RESULTS: In the study group, twelve of these infants were
liveborn, and two were stillborn. Eleven of the twelve liveborn infants sustained early neonatal death. All fourteen infants of the study group demonstrated micrognathia.
None of the control infants (all of which survived) had micrognathia.
CONCLUSION: This study suggests fetal swallowing may play an important role in normal mandibular development.
255 PROCEDURE-RELATED LOSS RATE IN TRANSPLACENTAL VERSUS NON-TRANSPLACENTAL AMNIOCENTESIS. J. Finn-Powers×, S. Carter×, A. Schwartz×, A. Bombard. Dept. Ob/Gyn, Albert Elnsteln College of Medicine. Bronx, NY. OBJECTIVE: We hypothesize loss rates after ammocentes~s do not differ In transplacental versus non-transplacental procedures when performed by experlenced operators. STUDY DESIGN: Subjects were 1000 women undergoing
second trlmester amnlocentesls: 745 were referred for maternal age; 132 for poslt~ve MSAFP screens, 41
~nd]cat~ng a r~sk for fetal NTD, 91 ~nd~catlng a r~sk for fetal chromosome abnormality; 123 were referred for
other reasons. All procedures were wdeotaped. The placenta was anterior in 518 cases. In 306 of these the
needle went through the placenta. All losses were reported. The remalnder have reached EDC.
RESULTS: There were 13 losses among the 1000 procedures (1.3%). The transplacental losses occurred from 4-71 days, median 26.5 days; the non transplacental from 12 days to term, median 25 days. The loss rate was similar ]n the two categories: 6
transplacental (1.96%) and 7 non transplacenta] (1%)
[RR 1.51 (95% CL 0.83-2.73)]. CONCLUSION: Transplacental ammocentes~s does not
appear to increase the fetal loss rate ~n the hands of experienced operators. Moreover, ]n wew of the t~me span between ammocentes~s and loss ~n both groups, a
procedure-related cause seems questionable.
257 PRENATAL PATERNITY TESTING USING DNA VNTR
ANALYSIS. N. Gmsberg, S Rech~tsky, G Ennquez, C M
Strom, Reproductive Genetics Inst, Chicago, 1L
OBJE(SFIVE: To determine the feaslblhty of prenatal paternity
testing dunng the first and second trimester of pregnancy
STIJDY DESIGN: Women requesting prenatal patermty testing
prior to the 12 weeks gestation were offered CVS, and those
women greater than 12 weeks gestation were offered ammocentesis
The study analyzed the ability to obtain a complete result (paternity
index > 500 or Exclusion)
RESULTS: Ten prenatal paternity tests were performed, 5 by
CVS, 4 by ammocentesis, and 1 product of conceptmn The reasons
for this test varied from forenmc ~n 2 rape cases to cr~l nwolvmg
child support, divorce, and adoption Four women based decisions
on terminating pregnancies based on the results Complete results
(elther exclusion or nonexcluslon with a paternity index greater than
500) were obtained ~n 4 out of 5 CVS cases, 3 out of 4
ammocentes~s cases and the POC case Direct CVS results were
available within 2 weeks In 3 of the 5 CVS cases and the POC case
Anmlocyte analysis always required culturing so that results were
not available until more than 40 days in all cases
CONCLUSIONS: Recent introduction of PCR-VNTR analysis
using 3 systems has allowed us to obtain prehminary results within 7
days of CVS with a probablhty of exclusion of 0 9634 This
technique can also be apphed to direct amniocentesls specimens
The paternity index using these probes usually does not exceed 500,
however, so that Southern blot analysis is stdl necessary to provide
complete nonexclusion results CVS is the preferred method of
prenatal paternity testing because direct analysis is possible wathout
the need for tissue culture and therefore complete results are
available more rapidly than after ammocentes~s
Volume 170, Number 1, Part 2 SPO Abstracts 349 Am J Obstet Gynecol
258 MATERNAL SERUM SCREENING OF SINGLETON IN VITRO FERTILIZATION PREGNANCIES, J.A. Canickx, K.A. ShahmmnX, R V. Hamng, Jr.x, R. HackettX, L. KellnerX, D.N. Sailer, Jr. Brown Umv.AVoman & Infants Hosp., Provtdenco, RI; Winthrop-University Hosp., Mineola, NY; Strong Memorial Hosp/Univ. of Rochester, NY. OBJECTIVE: To determine whether the results of second trimester maternal serum screening (MSS) for Down syndrome (DS) and neural tube defects (NTD) m singleton in vitro ferttlizahon (IVF) pregnanmes are &fferent from those m naturally occurring singleton pregnancies. STUDY DESIGN: IVF patients at Women & Infants Hospital from 1990 through 1992 who had confirmed single viable embryos at 4 and 6 weeks and who also underwent MSS at 15-18 weeks were included m this study. Levels of alpha-fetoprotein (AFP), unconjugated estrxol (uE3), and human chorionic gonadotropin (hCG), the screening results, and medical records of all such patients were reviewed and the data tabulated. RESULTS: 32 singleton IVF pregnancies had MSS One case was lost to follow-up¯ One of the remaining 31 cases resulted in a fetal demise at 21 weeks On average, 4 embryos were transferred per pregnancy. Medran maternal age was 33 years, length of gestation was 39 weeks, birthweight was 3289 g. The 30 neonates had 5’ Apgars >7 and no significant morbidity. Median AFP was 0.86 MoM (_<0.5 MoM: 1/31; >2.0 MoM: 1/31). Me&an uE3 was 0¯93 MoM (_<04 MoM: 0/31;>1.6 MoM: 1/31)¯ Me&an hCG was 1.33 MoM (_<0.4 MoM: 1/31; _>2.5 MoM: 3/31). Ten of 31 patients (32.3%; 95% CI=17-51%) had mcreased risk of DS (>1:270 second trunester risk). One of 31 (3.2%) had increased risk of NTD (AFP = 2¯25 MoM). CONCLUSIONS: Twice as many singleton IVF pregnanmes as predicted for th~s age group were screen positive for increased risk of DS (32.3% vs 15 8%, p=.04). The increased hCG levels as well as the slightly lower AFP and uE3 levels contributed to the higher screen positave rate. Patients were screened at least 11 weeks after initial confirmataon of a singleton gestaUon. Thus, either the number of embryos transferred, the hormonal environment of the mother at the t~me of 1VF, or other as yet unknown factors might be responsible for the findrngs. These data suggest that obstetricians should be alerted that 1VF patients will have a h~gher Down syndrome screen pos~twe rate w~th second trimester maternal serum screening.
260 DUCHENNE MUSCULAR DYSTROPHY CARRIERS AND
OBSTETRIC PERFORMANCE O, Ge~fman-Hottzmanx, I M. Bernste~n,
E.L Capeless and D.W. Bianch~* D~vision of Genetics Chddren’s
Hospital and NE Medical Center, Boston MA and Dept of Ob/Gyn
Univ. of VT., Bud, VT.
OBJECTIVE Female carriers for Duchenne Muscular Dystrophy
(DMD) may demonstrate elevated serum CPK and reduction of
muscle dystroph~n m all muscle types. We hypothesize that
decreased dystrophm m utenne muscle affects the obstetnc
performance of female carners of DMD.
STUDY DESIGN We examined 38 pregnancies from 15 women
w~th documented DMD carner status, Obstetrical performance was
examined by chart rewew and patient contact. Pregnancy
outcomes were compared to 38 control (C) pregnancies. Outcome
vanables included rate of PROM, use of p~toc~n ~n labor, fetal
presentation, labor anesthesia and mode of dehvery. Statistical
analys~s was performed by t-test, X~v, and F~scher’s exact test.
RESULTS No differences were found between DMD and C
regarding race, maternal age, or panty. There were no differences
~n gestatmnal age at dehvery, ~nc~dence of PROM, use of p~tocm,
use of regional anaesthesia, or rate of vaginal operative dehvery.
Slglqlflcant differences were present in the rate of cesarean section
¯ (DMD = 21% (8/38), C = 2.6% (1/38) p = 0.001 ). Th~s resulted from
an ~ncrease m breech presentation (DMD=13% (5/38), C=0%
(0/38) p =0.03).
CONCLUSIONS There were no demographic d~fferences between
C and DMD. There was an increased rate of breech presentation
m DMD which resulted in an increased cesarean delivery rate. We
speculate the subtle changes in uterine muscle tone contnbute to
a h~gher rate of breech m carriers of the DMD gene.
259 ASSESSMENT OF BIOCHEMICAL MARKER TESTING
FOR FETAL ANEUPLOIDY ASSOCIATED WITH SECOND
TRIMESTER CHOROID PLEXUS CYSTS. A.C. Ranzini,
K. Blakemore, V. Corson*, M.G. Bhtzer*, J. Wilharns, III, D.N
Sailer, A Johnson Dlvs of MFM and Human Genetics, Jefferson Medical College of Thomas Jefferson Umv., Johna Hopkins Univ.
School of Medicine, Univ. of Maryland School of Medicine. Prenatal
D~agnosUc Ctr of Southern CA, Strong Mem Hosp. OBJECTIVE: Aneuplmdy has been reported m 0.2-3% of fetuses
wath isolated chormd plexus cysts (CPC) at 15-20 weeks. The
potential benefit of using maternal serum biochemical markers (AFP,
uE3, hCG) to refine this risk was evaluated.
STUDY DESIGN: Between May 1992 and August 1993, 127
fetuses wdh CPC at 15-20 weeks were prospectively evaluated by
detailed fetal ultrasound. Each panent was informed of the potential ~mplicatmns of the findings and offered fetal karyotyping. Maternal
serum for biochemical marker screening was requested in all cases.
RESULTS: Ten fetuses with CPC and additional anomalies were
excluded from further analysis; 9/10 were aneuploid (8, Tn-18, 1,
Tn-21). Four of 117 (34%) fetuses with isolated CPC were
aneuplold (3, Tn 18, 1, Tn-21) Maternal age range. 16-43 yrs Sertun screening was obtained in 62 isolated CPC cases; 2 of the 62
were considered at increased risk for Tri-18 (AFP <_ 0.75 M O.M..
uE3_< 060 MOM hCG <_ 0.55 M.O.M). of whom 1 hadTn-18
F~ve of the 62 had a second trimester risk of Tri-21 > 1:270; 1 had
Tn-18, whale none had Tn-21 Therefore, 2 of the 3 cases of Tri-18 with isolated CPC had abnormal biochemical testing The positive
and negaUve predictive values of serum screening for fetal
aneuplmdy with isolated CPC were 28.6% and 98.2%, respectively.
CONCLUSION: Combining multiple serum marker testing with
ultrasound findings refines the risk of fetal aneuploidy associated
w~th ~solated CPC in the second trimester. However, the negative predact~ve value frmn this series suggests that fetal karyotypmg
should still be offered
261 SECOND-TRIMESTER MATERNAL SERUM HUMAN PLACENTAL LACTOGEN AS A PREDICTOR OF DOWN’S SYNDROME. J. Har-Toovx, A.J. Jaffa, M.R. Peyser, A. Many, I. Wolman, C. Legum, Dept. 0b/Gyn "A", Serlin Maternity Hospital, and Saclder School of Medicine, Tel Aviv University, Tel Aviv, Israel OBJECTIVE: To assess the efficacy of second-trimester maternal serum human placental lactogen (HPL) in predicting the risk of Down’s Syndrome (DS). STUDY DESIGN: The study group consisted of 37 women with DS-affected fetuses, and 181 women as the control group that underwent screening for DS during the second trimester (week 15-18) with ~-fetoprotein, ~3-human chorionic
gonadotropin and unconjugated E3. The serum HPL levels were measured by radioimmunoassay. RESULTS: Thirty-seven women terminated pregnancy because of DS confirmed by amniocentesis, and all the 181 controls had healthy newborns. The results were calculated by Lan multiple of the median (MOM) and a student t test was used to analyze the difference between the two groups. Lan MOM HPL was significantly higher m the DS group (-0.253 vm’sus -O.O21; P < 0.OOO1). CONCLUSIONS: Second-trimester maternal serum HPL has a positive predictive value for DS fetuses.
350 SPO Abstracts January 1994 Am J Obstet Gynecol
262 KARYOTYPE ANALYSIS IN THE PRESENCE OF CHOROID PLEXUS CYSTS: IS THERE REALLY ANY CONTROVERSY? ~, S.
Uhrichx, T.R. Easterling, L.A. Mackx. Depart. of OB/~3YN and Radiology, University of Washington, Seattle WA 98195. OBJECTIVE: Controversy exists whether isolated choroid plexus cysts (CPC) represent sufficient indication for amniocentesis and karyotype evaluation. We hypothesize that the presence of isolated CPC is associated with an elevated risk of fetal aneuploidy and that
the risk is 2-3 times the risk associated with a maternal age of 35. STUDY DESIGN: Retrospective analysis 8474 patients referred for Prenatal Diagnosis. CPC were identified in 204 patients (2.4%) and complete data (amniocentesis and newborn outcome)
was available in 192/204 (94%). Indications for referral were abnormal ultrasound (50%), maternal age _> 35 (31%), abnormal serum screening (14%), and other (5%).
RESULTS: Isolated CPC were identified in 183/192 (95%) and multiple congenital anomalies in 9/192 (5%). Fetal aneuploidy was present in 10/183 (5.5%) (99% CI = 2.1-11.3%) patients with isolated CPC and in 14/192 (7.3%) (99% CI = 3.3-13.5%) of all patients with CPC (with and without other anomalies). Abnormal
karyotypes included trisomy 18, n=9 (71%), trisomy 21, n=l (7%), trisomy 20 mosaic n=2 (14%), Trisomy 8 mosaic n=l (7%), and one sex chromosome aneuploidy (47xyy) (7%). CONCLUSIONS: The presence of isolated CPC was associated with a risk of fetal aneuploidy of at least 2.0% (lower 99% C1). The risk of aneuploidy with isolated CPC is at least 3.5x greater
than the risk associated with a maternal age of 35 (1/180 or 0.6%). Based on our data, karyotype analysis should be offered to all patients with isolated choroid plexus cysts.
264 THE EFFECT OF FETAL SEX AND GESTATIONAL AGE ON
THE BPD/FL RATIO IN NORMAL AND DOWN SYNDROME
PREGNANCIES. J.M. Simon~, G.E. Palomaki, L.M. Neveux,
A.E. Donnenfeld. Dept. of Ob/Gyn, Pennsylvania Hospital, Phila., PA,
Foundation for Blood Research, Scarborough, ME.
OBJECTIVE: To compare the effect of fetal sex and gestational age
on the BPD/FL ratio between normal and Down syndrome pregnancies.
STUDY DESIGN: Prospectively obtained sonographic measurements
were compared between 90 Down syndrome and 870 chromosomally
normal fetuses between 13 and 21 weeks gestation. The BPD/FL ratio
was analyzed separately for males and females at 2 week gestational
age mtervals.
RESULTS: S~gnificant differences in BPD/FL between Down syn-
drome and unaffected populations were found only in the 4 groups
below (17-19 week males, 17-19 week females, 13-21 week males, and
all pregnancies). No statistical differences in BPD/FL were found
between Down syndrome and unaffected pregnancies, stratified by fetal
sex, at any other gestatlonal age interval. Mean p
Gest Age Sex Group n IIPD/FL SD value
17-18.9 male NI 76 1.565 0.143 0.04
DS 16 1 646 0.118
17-18.9 female NI 76 1.571 0.139 0.05
DS 8 1.673 0.150
13-20.9 male NI 445 1 676 0.183 0.01
DS 54 1.743 0.221
13-20.9 both N1 870 1.670 0.181 0.007
DS 90 1.720 0.203
CONCLUSION: This study confawas that BPD/FL is significantly
greater m Down syndrome than in unaffected pregnancies. This difference
is greater for males than females and appears strongest at 17-19 weeks.
263 ULTRASOUND ADJUSTED RISK OF FETAL ANEUPLOIDY IN PATIENTS WITH ELEVATED MATERNAL SERUM ALPHA-FETOPROTEIN.G MegerianX, L. Godmilow, A Doanenfeld. Dept. of OB/GYN. Pennsylvania Hosp., Phda. PA
OBJECTIVE: To determine the incidence of aneuploidy in sonographically normal fetuses undergoing ammocentesis for elevated maternal serum alpha-fetoprotein (MSAFP) STUDY DESIGN: A retrospective review of cytogenetie and sonographic data for patients undergorng amniocentesis for elevated MSAFP (>2.0 MOM) between 1988-1992 was performed The total incidence of aneuploldy and the incidence in sonographically normal fetuses was calculated. The proportion of aneuploid fetuses w~th sex chromosome abnormahties(SCA) was compared to that found in women undergoing ammocentesis for advanced maternal age by using a two tailed Fishers exact test RESULTS: 733 fetuses were sampled in 707 patients(26 twins) The mean maternal age was 28 years. Nine aneuploid fetuses (1 2%) were identified, 3 SCA’s, 2 tnsomies(13 & 21, both with fetal malformations detected sonograplacally), 2 balanced translocat~ons, 1 mosaic inversion and 1 unbalanced translocation There were a total of 31 sonographically detected fetal malformations The risk of an abnormal karyotype with a normal ultrasound was 7/702=0.99%. Excluding SCA~s, the risk of an unbalanced karyotype with a normal ultrasound was 1/702=0 14%. SCA’s were seen more often compared to the advanced maternal age group, but did not reach stat~shcal s~gnifieance (p=0.14) CONCLUSIONS: There is an increased risk of aneuploidy with elevated MSAFP, with a trend towards a higher than expected number of SCA. The total risk of an abnormal karyotype with a structurally normal fetus on ultrasound was 1% and the risk of an unbalanced karyotype,excluding SCA’s, was only 0.14% Patients should be specifically counselled about the different spectrnm of aneuploidy seen with elevated MSAFP before decidrng on ammocen~sis
265 UNEXPLAINED ELEVATED MSAFP AND PERINATAL
OUTCOME IN AN URBAN CLINIC POPULATION.
W.F. Braz~qP, A.E. Donnenfeld. Dept of Ob/Gyn, Pennsylvania
Hospital, Philadelphia, PA.
OBJECTIVE: To determine if obstetric patients with unexplained
elevated MSAFP from an indigent clinic population are at increased
risk for adverse perinatal outcome compared to similar patients with
normal MSAFP values.
STUDY DESIGN: Perinatai outcomes from inner city obstetric
patients with unexplained elevated MSAFP (>2.0 MOM) were
compared to patients from the same clinic with normal MSAFP val-
ues during 1990. The frequency of adverse outcomes in the two
groups were subjected to Z analysas.
RESULTS: Adverse perinatal outcomes occurred in 33/57 (58%)
of the subjects with unexplained elevated MSAFP levels, compared
to 163/719 (23%) of patients with normal MSAFP values
(p<0.001). Statistically significant differences were observed for
abruption (p<0.025), IUGR (p<0.025), stillbirth >20 weeks
(p<0.001), and pregnancy induced hypertension (p<0.01).
Differences in the frequency of preterm delivery, preterm rupture of
membranes, pregnancy loss <20 weeks, and congenital malforma-
tions were not statistically significant.
CONCLUSIONS: In contrast to a previous report, we found that
unexplained elevated MSAFP levels confer an increased risk of
adverse perinatal outcome in an urban clinic population, over and
above the already increased risk due to socioeconomic status.

Volume 170, Number 1, Part 2 SPO Abstracts 351 Am J Obstet Gynecol
266 MATERNAL AGE AS A FACTOR IN COUNSELING WOMEN WHO ARE
UNDERGOING MATERNAL SERUM SCREENING FOR DOWN SYNDROME.
L H Kellner*, R.R. Weiss, M. Neuer*, Z. Wemer*, G. Farmak~des
Winthrop-University Hospital, Mmeola, N.Y.
OBJECTIVE: To evaluate the effect of maternal age on 2nd tnmester
maternal serum screening (MSS) for Down syndrome (DS) w~th regard to
calculation of the initial screen positive rate end detection rate in an
unselected population.
METHOD: 7,400 women were screened using alpha-fetoproteln,
unconjugated estnol and human chorlorlic gonadotropln The mean age
was 30 years (15-44 yrs). 577 women (7.8%) were> 35 year. 40% of
the women had ultrasound dating at or before MSS A 2nd tnmester risk
~> 1/270 was considered screened pomtive Five age groups were selected and analyzed.
RESULTS: Based on the study population and its age thstrlbutlon, 10
cases of DS were expected. W~th 80% ascertmnment, 10 cases of DS
were reported Seven of the 10 were detected as a result of MSS, 4/7
under the age of 35 and 3/3 at 35 years or older. In addition, five 45,X,
1 45,X/46,XX, 1 47,XXY and 1 47,XYY karyotype were also detected
(6 m women < 35 ; 2 m women ~> 35) The overall ~n~t~al positive rate
was 8 6% Imtlal positive rates rose as a function of age associated risk,
from 2% to > 28%. Detectmn rates have also been shown to increase
with ~ncreasmg age, from 48% to greater than 85%.
CONCLUSIONS: Our results
confirm previous flndlrlgs that
biochemical markers plus age
=reproves the detection of DS and
other anomahes. Offenng MSS
to all women wdl prowde a better nsk estimate, allowing many
older womet] to avoid an
unnecessary risk of
amnlocentesls while offering it to
a more appropnate group of women.
268 MID TRIMESTER CHORION VILLUS SAMPLING : AN
ALTERNATIVE APPROACH ? AD. Cameron. KW
Murphyx, M.B. McNayx, A M Mathersx, J Kingdomx, F
Fa~rhe, S. Irenex, G. Lowtherx. The Queen Mother’s Hospital and
~iasgow Royal Maternity Hospxtal, Glasgow, Scotland
AIMS To report our experience w~th mad trimester chonon villus
sampling (CVS) for rapid karyotyptng following a positive
maternal serum screening test
STUDY DESIGN: From January 1990 untd July 1993, CVS was
offered to all women whose pregnancies were comphcated by a positive screening test for autosomal tnsomy
RESULTS. 551 mothers underwent mid trimester CVS. The mean maternal age was 31 7 years, and the mean gestatmnal age was 18 2 (SD 1 5) weeks. The mean tame taken for dtrect karyotyptng
was 4 4 (SD 0.86) days and for culture results 20 2 (SD 2 7) days
Overall, karyotype results were obtained an 99 3% of samples" both direct and culture results m 90 7%, d~rect results alone m
4 1%, culture results alone :n 4 4% There were 14 abnormal karyotypes identified and all were confirmed followang te~m~nahon of pregnancy. 5 cases of mosmc~sm were identified, 2
on d~rect testing alone and 3 on cultule alone, and all were
confined to the placenta There was a single false positwe direct test result. The overall pregnancy loss rate, excluding
terminations, was 1 7%.
CONCLUSIONS’ Mad trimester CVS ~s techmcally easter to
perform than cordocentesis and it provxdes a more rapid karyotype
t’,o ~ amnioeentes~s Our data show that the success rate xs high (99 3%), and the complicatmn rate is slmxlar to that for other
invaslve procedures.
267 FIRST TRIMESTER TRANSCERVICAL IRRIGATION: MINIMALLY INVASIVE METHOD FOR PRENATAL DIAGNOSIS. R. Bahedo-Sineh, H. Klimanx, E. Meeddoughz, T. Yeng- Feng~, J. Copel, M. Mahnnef. Yale Univ. Dept. of OB/GYN, New Haven, CT OBJECTIVE: To detomfine whether lavage of the internal os and lower uterine segment in the first trimester can yield trnphoblast for prenatal diagnosis. STUDY DESIGN: In patients presenting for pregnancy termination, a specially designed catheter (CONCORD-PORTEX) was passed under sonogrephie guidanen to the level of the internal os. Gentle lavage was performed with 3 e~a of asline. After firing the cellular material miernsenpy for trophoblast was performed. Subsquently, attempts where made to culture txophoblast cells obtained by this method. Cultured trephoblast celh were identified by anti-~hCG antibodies. RESULTS: In the first phase, trephoblasts were identified histologically in 11 of 22 eases (50%). Neither gestational age nor piacental location appeared to affect the ehane~ of sueccas. In the second phase, material retrieved by irrigation was cultured in a total of 7 cases. In 1 ease, trephoblasts were sueenssfully cultured. Results are pending in 2 cases. CONCLUSION: Trephoblasts can hn obtained and suecessfullyceltured using cervical irrigation technique as early as 7 week.,. Current genetic technology using FISH and allele specific ollgnnuclectide probes makes prenatal diagnosis possible using the method of cervical irrigation. This method does not involve significant plaeental trauma and is therefore less 1Lkely to raise concerns about enmplieatinus such as limb defects possibly associated with CVS. Compared to extraction of fetal cells from maternal blood, larger amounts of fetal cells can be obtained and cell sorting teehnlquas are not necessary. Because the trophoblasts are viable in culture, prenatal diagnosis of metabolle disorders may be possible.
269 ABNORMAL TRIPLE SCREEN AND NORMAL BIOMETRY: RISK OF FETAL ANEUPLOIDY. R. Bahado-Sin~h, I. Goldstein’, M. Inati=, T. O’Connor, M. Mabonef, J. Copel, A. Banmgarten~. Yale Univ, New Haven CT. OBJECTIVE: To determine whether normal ullxasound biometry reduces the risks of Trisomy 18 and 21 therefore the indication for anmincantesis in pregnancies at elevated risk based on combined AFP, hCG and E3 serum levels and maternal age. STUDY DESIGN: Sonographie data was generated prospectively on 352
patients with elevated risk for trisomy 21 (>1/270)or for Trisomy 18 > 1/20. Observed to expected femur (FL) and humerna lengths (HL), ecrebellar diameter TCD and BPD/FL were used to assess the fetuses. Karyotype and follow up were obtained. RESULTS: Karyotypewas obtained in 274, 40 non karyotyped eases were normal after birth, 20 are undelivered and 18 lest to follow up based on serum screening. Based on serum screening, the mean risk of trlsomy in entire study group and also in subset kar.cotyped was 1/125. Three cases of trlsomy 21 and one each of 11q- and mosaics for Trisomy 7 and XXX were found. Normal observed to expected humerus length (O/E HL > 0.gg) was most useful for predicting normal fetuses. Actual risk o f trlsomy 21 was 1/248 vs 1/13 in the normal and abnormal HL groups respectively (p < 0.025). The reiative risk was 0.05 (CI 0.005-0.53), NPV 99.64, spee. 91.18, PPV 6.90, Sons. 66.67. This is superior to simply screening for structural defects. The only structural finding was "mild hypcrechogenie" bowel in a ease of Trisomy 21. CONCLUSION: NormalHLreducesriskofTrlsomyby 95% in patients with abnormal screen. This can be used to counsel patients, in deciding on amnlocentesis.
352 SPO Abstracts January 1994 Am J Obstet Gynecol
270 DOES THE MULTIPLE MARKER SCREENING TEST IDENTIFY FETAL SEX CHROMOSOME ABNORMALITIES OR JUST CYSTIC HYGROMA/HYDROPS? KD Wenstrom LR Bootsx, P Cosperx.
University of Alabama at Birmingham, B~rm=ngham, AL. OBJECTIVE: To determine ff detect=on of feta) Turner Syndrome
with the multiple marker screening test (alpha fetoprotem, estnol,
human chononlc gonadotroph=n, and maternal age) is related to
the presence of fetal hydrops and/or cystic hygroma
STUDY DESIGN. The results of multiple marker screening tests
from 41 cases of fetal sex chromosome aneuploldy and/or cystic
hygroma/hydrops were compared" 1 ) Turner’s Group (n = 10) =
sonographlcally normal fetal Turner syndrome or Turner mosaic, 2) Sex Chromosome Group (n = 14) = other sonograph~cally
normal fetal sex chromosome aneuplo=d~es (47XXY, 47XYIY,
46XY/47XYY, 46XY/47XXY), and 3) Hygroma Group (n = 17) =
fetal cystic hygroma and/or hydrops w~th or w~thout aneuploidy.
RESULTS: Posture screening tests (Down syndrome nsk
~>1’190 or MSAFP ~> 2.5 MOM) were found in 1/10 (10%) of the Turner’s Group, 1/14 (7%) of the Sex Chromosome Group,
and 11/17(65%} of the Hygroma Group (p=.001). E~ght of the
13 total positive screens indicated an increased Down syndrome
r~sk (1:1 to 1:160), wb~le the other 5 were neural tube defect screen positive (MSAFP = 2.9 to 9.7 MOM). Screen positive
fetuses with cystic hygroma/hydrops were equally hkely to be
euplold (n=3) or aneuplold (n=8; 6 Turner S., 2 Tnsomy 21, p=l 0)
CONCLUSIONS: The multiple marker screen~n9 test ~dentff~es
fetuses with cystic hygroma/hydrops, with or w~thout fetal
aneuplo=dy Identification of sonograph~cally normal fetuses with
sex chromosome aneuploldy occurs either infrequently or
serendlp~t~ous)y.
272 PREGNANCY OUTCOME FOLLOWING EARLY VERSUS
TRADITIONAL AMNIOCENTESIS: A SINGLE INSTITUTION
CASE - CONTROLLED STUDY S ~,_mx, C Brttmficld, W Counersx,
M Dubardx, S Finleyx, R Daws Umvermty of Alabama at B~nmngham,
Birmingham, AL
OBJECTIVE: The objective of th~s case-controlled study was to
compare pregnancy outcomes following early versus traditional
alrLraocent esls
STUDY DESIGN: The case study group consisted of 314 women
undergoing early genetic anmlocentems (between 11 to 13 weeks
gestatmn) for advanced maternal age from August 1988 through December
1992 The control group consisted of 628 women who had a trachtaonal
arrunocentesls (between 16 and 18 weeks gestation) during the same t~me
period The control group was matched (2 1) vath the case group for age,
race, and number of prevmus pregnancy losses All arnmocenteses were
performed by one of 3 operators Pregnancy outcome data were obtained
by chart review and phone consultatmn vath the referring phymc~an The
data were analyzed using a F~sher Exact test StatlsUcal s~giuficance was
conmdered at p<_0 05
RESULTS: Post-procedural armnot~c flurd leakage (2 9% vs O 2%,
p= 0.03), vaginal bleeding (1 9% vs 0 2%, p= 006), and fetal loss wathm
30 days of the procedure (2 2% vs 0,2%, p=OOl) occurred more often
after ma early ammocentems The rate of fetal dermse occumng >30 days
from the procedure, preterra labor, growth retardation and neonatal deaths
were sxm~lar m both groups
CONCLUSIONS: More post procedural compiicattons occurred after
early amnlocentesls The tmme&ate fetal loss rate after early
ammocentes~s was higher than after trad~taonal ammocentes~s but was
conmstent with the published background loss rate for th~s gestatxonal age.
271 IS ELEVATED SECOND TRIMESTER hCG ASSOCIATED WITH
POOR PREGNANCY OUTCOME? K.._D Wenstrom, J Owen, L BootsX, MB Dubardx. University of Alabama at Birmingham,
B~rm~ngham, AL.
OBJECTIVE’ To determine ~f elevated second trimester human chonon~c gonadotroph~n (hCG) levels predict pregnancy outcome
after genetic arnnlocentesis. STUDY DESIGN: Multiple marker screening tests (Maternal
serum alphafetoprotem, estnol, hCG, and maternal age) were performed on stored second trimester serum from 94 women
w~th poor pregnancy outcomes excluding aneuplo~dy and structural abnormabty (H~gh Rtsk Group) and 91 matched control
women wrth normal outcomes (Low R~sk Group) who had genetic amnlocentes~s performed for advanced maternal age
(n = 129), abnormal alphafetoprotem (n = 33), famdy h~story of aneuplo~dy or neural tube defect (n= 16) or other reasons (n=7) RESULTS: The H~gh and Low R~sk Groups were matched for
age, race, panty, and gestatlonal age, and were similar w~th
regard to indication for amnlocentesls. The mean hCG level was
h~gher ~n the H=gh R=sk Group (1 41 MOM) than =n the Low R=sk
Group (0 94 MOM) (p =0.02). More H=gh Risk women had hCG
levels ~> 2.0 MOM (17/94, 18%) than Low R~sk women (4/91, 4%) (p=O.O03) An hCG ~> 2.0 MOM was s~gn~ficantly
associated w~th antenatal demise (p=O.O07), preterm dehvery
(p=0 001) and neonatal dem=se (p=0.04). Elevated hCG d=d
not ~denttfy pregnancies w~th immediate ammocentes~s
comphcabons, intrauterine growth restriction, or preeclampsla. A positive muRtple marker screening test (Down Syndrome risk >~
1 190) was not associated with any bad outcome (piNS). CONCLUSION: Elevated hCG =s S~gn=flcantly associated w~th
certain abnormal pregnancy outcomes after genetic
amnlocentesls. Despite normal amnlocentesls results, women
w~th elevated hCG should be considered at h~gh risk.
273 DOES THE MULTIPLE MARKER sCREENING TEST
IDENTIFY CHROMOSOMAL ABNORMALITIES IN THE
FIRST TRIMESTER? C Brnmfield. K Wenstrom, L, Bootsx, M
DuBardx, S Finleyx, R Daws The Umvermty of Alabama at
Bm~nB~am, B~nmngham, AL
OBJECTIVE: To determine ff the multiple marker screening test
detects c~omosomal abnormahties at 11-13 weeks
STUDY DESIGN: Multiple marker screening tests were p~fformed on
stored serum samples from women who had undergone an early
aum~ocantesxs from 1988-1993 Medians at each gestataonal age
(menstrual dates confu’med by ultrasound) 11-13 weeks were calculated
A pomtlve screemng test was a Down syndrome (DS) risk >_ 1 190 ~n the
mld-mmester The results of the serum tests were compared to the fetal
karyotype results mad pregnancy outcome data RESULTS: Three hundred eighteen samples were assayed, 300 women
(94%) were ~> age 35 at dehvery, and 294 (92%) ~vere Caucaman
There were 76 (24%) pomtxve screening tests, reflectmg the large
number of women -> 35 E~ght fetuses had abnormal karyotypes The
multiple marker screemng test identified 4/8 (50%) 2 of 2 (100%)
cases ofDS, 1 of 1 case oftnsomy 13 and 1 of 3 (33%) sex chromosome
abnornaalities T~vo unbalanced translocat~ons were not ~dentlfied The
detect~on/amn~ocentesls rate was 1/38 for DS and 1/19 overall
CONCLUSIONS: The multiple marker screerfing test appears to
detect chromosomal abnormaht~es m the first trnnester at a rate (100%
for DS, 50% for all aneuplmd~es) comparable to that reported in the
second mmester Sumlar data from other centers is needed to vahdate
this conclumort

Vo~ur,,~ ]70, ~’umber ~, Pa,-r .9 SPO Abstracts 353 Am J Obstet Gynecol
274 ADDITION OF FETAL BIOMETRY DOES NOT IMPROVE THE MULTIPLE MARKER SCREENING TEST FOR DOWN SYNDROME J Owen, KD Wenstrom, LR Bootsx, M DuBard×, P Cosper~, C Hsux. University of Alabama at B~rm~ngham, Birmingham, AL. OBJECTIVE: Because fetuses with Down Syndrome (DS) have altered blometry as compared to euploid fetuses, It has been suggested that fetal biometnc parameters can be utlhzed to estimate the nsk of aneup!o~dy We ~nvest~gated the utility of feta~ b~ometry as an adlunct to the multiple marker screen which employs MSAFP, Estnol, HCG, and maternal age to detect DS {n the m~d-tnmester (14-21 weeks). STUDY DESIGN: From our genetics and ultrasound database we identified 52 cases of confirmed DS and compared these to over 7500 structurally normal fetuses w~th complete b~ometry We found that the observed to predicted femur length rabo (FLRA) as determined from the best gestat~onal age (menstrual dates confirmed or refuted by the BPD) had the best discrim]nant value (euploid’FLRA=1.0+-+0.11 vs DS’ FLPtA=0 93+_0 13, p<0 0001 ). We then developed a quadravariate Gaussian algonthm Incorporating the 3 hormone values and the FLRA and compared ~t to the "triple screen" algonthm provided by the Foundation for Blood Research These algorithms yield a hkelihood ratio which is then used to modify the ~nherent age nsk of DS Our study populabon consisted of 38 cases of DS and 1209 euploid controls on whom hormone values and fetal biometry were available. RESULTS: Ut~hz~ng an arbitrary screen-positive rate of 6 0%, the triple screen identified 47% of the cases of DS as compared to a 50% detection rate when the FLRA was included, a difference of one case of DS The choice of other detection rates yielded s~mdar results, w~th neither model clearly outperforming the other. A 100% detection rate was obtained with a screen-positive rate of 62 5% for the tnple screen vs 66 1% for the quadravanate model CONCLUSIONS: The addition of the FLRA does not ~mprove the performance of the multiple marker screening test for DS Fetuses with DS are most readily identified by d~fferences in biochemical values.
276 CORD GASES IN FETUSES WITH ANEUPLOIDY.
A. Martinx, I. Wilkins, V. Parisi, Dept. Ob/Gyn, Univ. of Texas
Med. Sch. at Houston, Texas.
OB,NECT/VE: Fetuses with aneuploidy have an increased incidence
of caesarean section (CS) and fetal distress (FD) although the
mechanism is unknown. The purpose of this study is to investigate
the acid base status of fetuses born with chromosomal
abnormalities.
METHODS: A retrospective chart review was performed of all
newborns with aneuploid3 between January 1, 1985 and December
31, 1990. 120 records were cross referenced with labor and
delivery and medical records on the mother.
RESULTS: Of 68 cases there were 40 inborn infants (35 with cord
gases [CBG]) and 28 outborn (no CBG). A total of 60% of
neonates had trisomy (T) 21, 21% had T 18, 9% had T 13 and
10% had other chromosomal rearrangements. In T13, 83% had a
CS and 80% of these were for FD. All infants with CBG had a
respiratory acidosis. In T18, 72% had a CS and 80% were for FD.
Only 3 infants had CBG of which 2 showed acidosis, one
respiratory and one metabolic. The CS rate in T21 was 17%, of
which 57% were for FD. Of infants with CBG, 5 of 20 were
acidotic and 4 of these 5 demonstrated a respiratory pattern. Of
T21 ~nfants who had an arterial pH <7.2, 80% had congenital
heart disease compared to 46.7% of those with a pH > 7.2.
CONCLUSIONS: There is an increased CS rate in aneuploid
fetuses, particularly in T13 and T18. Of these, 76% were CS for
FD. The majority of CBG in T13 and T18 were abnormal. In
infants with acidemia, 82% had a respiratory pattern. Acidemia in
T21 was significantly associated with congenital heart disease.
275 THE USE OF POLYMERASE CHAIN REACTION |PCR) TO DETERMINE
FETAL RhD STATUS. J. Ross~ter,* K Blakemore, E. Pressman,x T.
Kinkier,x L. Kasch,* H. Kazazmn,x Johns Hopkins Umv, Bait=more, MD.
OBJECTIVE: We hypothesize that DNA amphf=cat=on of a portion of
the RhD gene present m Rh-pos=twe and absent m Rh-negat~ve indlwduels wdl allow accurate determination of fetal Rh status by
amnlocenteslS.
STUDY DESIGN: Ohgonucleot=de pnmers based on pubhshed
sequence from the RhD gene (Arce et el, 1993) were constructed
PCR performed using these primers resulted in two products: 1) a
1200 bp fragment found ~n all individuals derived from a gene
beheved to encode Rh C/c or E/e whmh was used as an internal
control for the success of the PCR reaction, and 2) a 600 bp
fragment from the RhD gene which ~s absent ~n Rh-negatwe people.
The accuracy of the assay was first confirmed by companng PCR
results w{th serological typing of 16 adult blood samples. The
method was then applied m an at-risk pregnancy. A severely Rh-
sensKized patient underwent amnlocentesm, fetal paraoentesls, and
fetal blood sampling.
RESULTS: The presence of a single 1200 bp band on agarose gel
electrophores~sconflrmedthemother’sRh-negat~vestatus Two PCR
products measuring 1200 bp and 600 bp were present in the analysis
of ammot~c fluid, fetal asmtes and fetal blood. Serologic typing of
fetal blood confirmed the RhD positive status.
CONCLUSIONS: The PCR techmque described can Identify the RhD
status of Individuals using blood, fetal aSCltes, and amnlotlc fluid.
Though the pennatal management was not altered In this case, in
24% of pregnancies to Rh-sens=tlzed women, the fetus w~ll also be
Rh-negatlve. This technique will enable rapid dmgnos~s of the fetal RhD status using amnlotlc fluid. When such testing discloses an Rh-
negative fetus, obstetrical care would be significantly altered as it
would obwate the need for serial ammocenteses or for fetal blood
sampling.
277 HYDATIDIFORM MOLE COEXISTING WITH A NORMAL FETUS: MOLECULAR ANALYSIS OF PLACENTAL
BIOPSY. JL.B Bvrnex, DW Branch, L Nelson×, J. Bakerx, K Ward University of Utah School of Medicine, Salt Lake City, Utah OBJECTIVE: To demonstrate the usefulness of placental biopsy
and molecular genetic analysis when there ~s a focal suspicious
lesion of the placenta
STUDY DESIGN: A 28 year old pnm~gravida presented with a placental abnormality on an early ultrasound By 14 weeks
gestabon, the abnormal area was felt to represent a hydatidiform mole, w~th a coexisting normal fetus A placental biopsy was
performed for karyotype and DNA flow cytometry. Parental DNA
samples were obtained for parentage determinations using short
tandem repeat polymorph=sms Cordocentes~s was performed and
senal f3-hCG titers drawn subsequently
RESULTS: Flow cytometry showed only a d~plo~d peak and the
fetal karyotype was 46,XX; however molecular testing ~ndicated the
placental t~ssue was paternal ~n origin In contrast, cordocentesis revealed a 46,XX karyotype with both parental alleles seen at every ~nformat~ve locus. 13-hCG titers have been followed, mthally fall~ng
from 39,161 to 13,651, then tncreas~ng to 41,000 at 34 weeks, while the placental mass has become less prominent. Chest CT scan is
negative Delivery is ~mm~nent, outcome and placental pathology will be presented CONCLUSIONS: Our expenence demonstrates the usefulness of
parentage testing of a les~on suspected to be a hydat~d~form mole.
The molecular genebc data was the clearest evidence of a molar gestation allowing appropriate surveillance for chonocarc~noma.

354 SPO Abstracts January 1994 Am J Obstet Gynecol
278 RELIABILITY AND PITFALLS OF PRENATAL DIAGNOSTIC CYTOGENETIC ANALYSIS BY FLUORESCENT IN SITU HYBRIDIZATION (FISH). Ennque M, Garciax, B~ Rafael Eleialde Maria M. de Elejalde*, Medical Genetics Institute, S.C. and Oept Ob/Gyn University of Wisconsin Medical School, Mdwaukee WI. OBJECTIVE: The null hypothes~s is that FiSH produces the same results as metaphase analysis for dmgnosis of normal and abnormal karyotypes m amn~ocytes. STUDY DESIGN; Slides of 25 amn~ocyte cultures were stained wrth centromenc satelhte DNA probes, for chromosomes 13/21, 18, Xand Y. 17 of the samples were chromosomalty abnormal (they included: 3 trtsom~es 21, 1 tr~somy 13, 1 47,XXY, 1 47,XXX, 1 sstellited Y, 1 46,X,t(X;Y) 1 46,X,del(X)(p22.1) and 4, 47,XY,+?(mar or ~d~;) and 8 were normal. 500 interphase nuclei were bhndly analyzed as they appeared dunng the m~croscop~c scan avoiding any selection, the observer was asked to report a diagnosis at the completion of the scanmng. All samples had standard cytogenetic analysis, RESULTS: None of the patient had single moda~ chromosome number detected by the probe/s, all had more and less chromocenters than expected from the cytogenet~c analysis All had s~gn~cant numbers of celJs that had more and less chromosomes, suggestive of a mosaic chromosome const~tubon. None of them had a mosaic constitution for standard cytogenetlc analysis. Amnlocytes from fetuses with trlscmy 21, tested w~th the 18/21 probe showed 35% nucle~ w~th 0, 17% w~th 1, 15% w~th 2, 22% w~th 3, 30% w~th 4, 26% w~th 5, and 4% wrth 6 chromocenters. They were expected to have 5 (two chromosomes 13 and three 21) ~n most of the cells. CONCLUSIONs: FISH and standard Cytogenet~ analysis do not produce the exact same results. FISH should be used w~h extreme caution or not used for chn~cal prenstai d~agnosis of cytogenet~c abnormaht~es, because of the characteristic described here.
280 DOES ISOLATED SEVERE OLIGOItYDRAMNIOS PRESAGE FETAL ANEUPLOIDY? N.M. Boe. L.P. Shulman, D.S. Emersonx. Depts. of Ob/Gyn and Radiology, University of Tennessee, Memphis. OBJECTIVE: To determine whether isolated severe oligohydramnios in the second trimester is associated with fetal aneuploidy. STUDY DESIGN: We studied 38 consecutive women, referred for genetic counseling and consideration of invasive prenatal testing in the second trimester, with severe oligohydramnios and no demonstrable fetal structural or growth abnormalities. Pregnancy outcome data were obtained from hospital and physician records. RESULTS: Eighteen of the 38 women either had historical or physical findings consistent with preterm PROM; of these 18 cases, none were found to be associated with abnormal fetal karyotypes. Among the 20 cases in which no cause for the severe oligohydramnios was apparent, fetal cytogenetic analyses again failed to yield any abnormal karyotypes. CONCLUSION: Pregnancies characterized by severe oligohydramnios and no ultrasound evidence of intrauterine growth retardation or structural abnormalities in the second trimester are not apparently associated with an increased incidence of fetal chromosome abnormalities.
279 FETAL LOSS AND TRANSPLACENTAL NEEDLE PASSAGE IN CASES OF EARLY AMNIOCENTESIS.
LP Shulman, RR Bravox, SJ Gross, S Elias. DepL Ob/Gyn, Univ.
of Tennessee, Memphis and CEMIC, Buenos Aires, Argentina. OBJECTIVE: To determine whether transplacental (TP) needle
passage presages an increased risk of fetal loss in cases of amniocentesis performed at 14.9 weeks gestation or earlier. STUDY DESIGN: 350 consecutive patients undergoing successful amniocentesis in singleton pregnancies at 14,9 weeks
gestation or earlier were divided into 2 groups: (a) those in whom transplacental needle passage occurred, and (b) those in whom
transplacenlal needle passage was avoided. Pregnancy outcome data were obtained from hospital and physician records as well as communication with patients, nurse practitioners and physicians. RESULTS: Transplacenta/(TP) needle passage occurred in 137 of the 350 cases (39.1%), Mean maternal (36.6 yrs. TP and 37.1
yrs. non-TP) and gestational (13.8 weeks TP and 13,9 weeks non- TP) ages were similar m both groups. Fourteen (10 non-TP and 4 TP) of the 350 women undergoing early amniocentesis elected to terminate their pregnancies after prenatal diagnosis because of fetal abnormalities. Frequency of fetal loss among women undergoing TP needle passage was 3 of 133 (2.2%) compared to 6 of 203 (2.9%) cases in which TP passage was avoided (p>0.05). There were also no sigmficant differences among patients experiencing losses < 24 weeks’, losses > 24 weeks’ gestation or stillbirths. CONCLUSIONS: Transplacental needle passage does not appear to presage a significantly increased risk for early or late fetal loss among women undergoing amniocentesis at or before 14.9 weeks’ gestation.
281 PREGNANCY OUTCOME IN PATIENTS ~NITH A SECOND TRIMESTER TRIPLE SCREEN POSITIVE FOR TRISOMY EIGHTEEN L C~arlegho*, W Cuslck, S Briganti*, L Feeney*, P 8enn*, J Rod,s, Univ. of Connecticut He~h Center, Farmmgton, CT OBJECTIVE: Evaluate pregnancy outcome m patients with a second trimester tnp~e screen (TS) positive for Tnsomy 18 (T18) STUDY DESIGN: Results of second tnmester maternal TS (alpha fetoprote~n (AFP), unconlugated estnol (uE3), and r~ human chonon~c gonadotropm (HcG)) performed between 9/91- 7/93 as part of the Umvers=ty of Connecticut Maternal Serum Screen for B~rlh Defects were reviewed The study group included v~able, s=ngleton pregnancies w~th a TS posrhve for T18 (AFP _< 0.75 MoM, uE3 _< 0 60 MoM, and HcG -< 0.55 MoM). Pat=ents underwent a targeted ultrasound evaluahon and were offered ammocentes~s Four serum screen normal confrere for each patient were matched for maternal age and gestat]onal age at testing. Only pahents w~th known follow up were enrolled. Pregnancy outcomes evaluated ~ncluded preterm dehvery (< 37 weeks), small for 9estatlonal age (SGA) infants, and preeclampsla (PIH). Statistical tests used included T-test for continuous data and ch= square testing wah Yates correchon for categoncal data S~gmhcance was set at p < 0.05. RESULTS: There were 17,191 TS performed ot which 23 were positive for TI& Fwe pahents have ongoing pregnancies and an add~honal pahent was lost to follow up. One case of 2nd tnmester IUFD was d~agnosed at the initial ultrasound evaluahon. Fetal chromosomal abnormalales were d~agnosed m 2/22 study patients (TI8 and Tnsomy 2t). Another infant had undateral renal agenests and a single umbthcal artery. Three infants were born pnor to 37 weeks gestahon (36.2, 35.4, 34 6) No congemtal or chromosomal abnormah- hes were d~agnosed m the control group infants.
STUDYIn=141 CONTROL!n=56} Mean _+SO dehvery age (weeks) 38 _+ 2 ~ 1 .0001 Preterm dehvery 3 0 0055 SGA infant 2 6 93 Preee~amps~a 1 0 45 CONCLUSION: A TS positive for T18 occurred m 1 3/I,000 samples. Nine percent of pahents with a TS pee~hve for T18 had chromosoma~ly abnormal ~nfants. A stahst~cally s~gn~ficant increase in the rate of preterm Ndhs was seen In patients TS positive for Tt8

Volume 170, Number 1, Part 2 SPO Abstracts 355 Am J Obstet Gynecol
282 FACTORS INFLUENCING PAIN ASSOCIATED NITHAN~IOCENTESIS
BEFORE 26 WEEKS GESTATION. K. Kennedy, S. Clark. IHC Perinatal Centers and Univ. of Utah, Salt Lake City, Utah. OBJECTIVE: Examine factors that influence pain associated wlth amniocentesis before 26 weeks gestational age. STUDY OESIG~i: 323 women having one successful ~ttempt at amniocentesis before the 26th gestational week were the subjects of this study. Age, gestational age, parity, indication, precise location of the amniocentesis, ease of procedure and use of local anesthetic were recorded. A visual analog scale (0-5) was completed by the patient before and after the procedure producing seperate scores for apprehension and pain. The data was analyzed with one and two-way analysis of variance (ANOVA), and with correlation co-efficients. RESULTS: There is a correlation between paln and apprehension (r=.33, p<.01). Higher mean pain score (MPS) is associated with nulliparity (p<.03), peripheral rather than central location (p<.01), a "d~fficult" procedure (p=<.01) and indication; the MPS for the indication increased alpha fetoprotein (MPS=2.67) or previous genetic abnormality (MPS=2.53) was different than for advanced maternal age (MPS=1.61, p<.01). Two-way ANOVA revealed indication is a significant factor effecting both pain and apprehension while location effects MPS (p=.01) only. There is no difference in MPS with use of local anesthetic. CONCLUSIONS: Indication for amniocentesis effects apprehension and reported pain. Pain is effected by location, null~parity and difficulty of the procedure but not by the use of local anesthetic.
284 FLUORESCENT IN SITU HYBRIDIZATION (FISH)
UTILIZATION FOR HIGH RISK PRENATAL DIAGNOSIS: A
TRADE-OFF AMONG SPEED, EXPENSE AND INHERENT
LIMITATIONS OF CHROMOSOME SPECIFIC PROBES (CSP).
M.I. Evans, S.A.D. Ebrahim,x S.M. Berry, W. HoLzgreve,x N.B. Isada,
R. Quintero, M.P. Johnson. Depts Ob/Gyn, Molecular Biology &
Genetics & Pathology, Hutzel Hospital/Wayne State University,
Detroit, MI, and University of Mfinster, Germany.
OBJECTIVE: The development of FISH CSP technology has allowed
the use of new fetal tissue collection techniques such as fetal cells in
maternal blood (FCMB) and coelocentesis - both of which, with
current technology, cannot generate complete karyotypes. We thus
sought to assess the potential limitations of CSP in a high risk
prenatal diagnosis center.
STUDY DESIGN: The last 24 months of fetal karyotypes from our
prenatal cytogenetics laboratory were analyzed for those
abnormalities which should be detectable by CSP and those that
would likely be missed.
RESULTS: 207 abnormalities were found in 6006 karyotypes (3.4%)
of which 104 were common trisomies, 12 triploidies and 19
monosomies which would have been detected using present probe
co ,mbinations (13,18,21,X,Y) [135/207=652%]. 72/207 abnormalities
(35%) represented other trisomies (16/207=7.7% for #9,12,15,16) and
rearrangements (inversions, translocation markers were
56/207=27.1%) which would have been missed.
CONCLUSIONS: Use of present FISH-CSP protocols would have
detected only 65% of chromosome abnormalities in our high risk
population. Incomplete ascertainment must be weighed against the
cost and speed of FISH-CSP when comparing it to karyotyping.
Whereas this new technology may prove useful in low risk scmaning
programs (FCMB), its present use in high risk populations should be
questioned until its sensitivity is expanded to identify more subtle
and less common chromosomal abnormalities.
283 ANOMALY RISK DISTRIBUTION AS A FUNCTION OF MSAFP
LEVEL. A. Reichler,x M.P. Johnson, E. Dvorin,x N.B. Isada, R.F. Hume,x J.E. O’Brien,x M. Bardicef,x A. Drugan,x M.I. Evans. Div Reproductive Genetics, Depts Ob/Gyn, Molecular Biology and Genetics, and Pathology, Hutzel Hospital/Wayne State University, Detroit, MI, and MetPath, MI. OBJECTIVE: The association of elevated MSAFP with increased risks of neural tube defects (NTDs), ventral wall anomalies and other anomalies is well appreciated, and oRen specific risks for anomalies are quoted based upon the level of MSAFP. However, review of the literature shows that most of these are mathematical formulas and not based upon actual data. Real numbers are very scant. STUDY DESIGN: Evaluations of (773) patients referzecl to our service for elevated MSAFP of whom 529 were included in the study after 244 were excluded because of twins or incorrect dates. RESULTS: There is a progressive increase in the incidence of all anomalies as a direct function of the level of MSAFP varying from 1.9% at MSAFP 2.5 to 2.9, up to 40.3% at MSAFP greater than 7.
n = 207 154 ~oM ~67..,x~. 55 52
CONCLUSIONS: Our data support the correlation between the level
of MSAFP and the risk of anomalies, but now also provide actuarial-
based data upon which to place percentage risks.
285 INTERPRETATION OF EARLY AMNIOCENTESES (EA)
REQUIRES BOTH ALPHA-FETOPROTEIN (AFP) AND
ACETYLCHOLINESTERASE (ACHE). A. Dru~anx, B. Shivers,x
A. Rcichler,x S.A.D. Ebrahim,x M.P. Johnson, R.F. Hume,x M.I.
Evans. Dept Ob/Gyn, Rambam Med Center, Haifa, Israel, and
Depts Ob/Gyn, MBG and Pathology, Hutzel Hosp/Wayne State
Univ, Detroit, MI.
OBJECTIVE: To evaluate the efficacy of early prenaud diagnosis
of fetal structural anomalies using amniotic fluid AFP (AF-AFP)
and ACHE.
STUDY DESIGN. From 1991 to 1993 we performed 281 EA’s at
11-14 weeks gestation and 2450 midtrimester amnios (15-22
gestational weeks). AF-AVP was analyzed by RIA and AChE by
gel clectrophoresis.
RESULTS The frequencies of abnormal AF-AFP in the 2 groups
were 2.5% & 1.3% respectively; positive AChE 3.6% & 1%
(p<0.0001). In midtrimester samples, a positive AChE was always
found iu association with an abnormal AF-AFP. All of these
patients had structural anomalies consistent with the biochemical diagnosis. In EA an elevated AF-AFP was observed in only 70% of
smnplcs that were AChE positive. Exencephaly, anencephaly,
acrania or hydrops with cystic hygroma were diagnosed in these 7
fetuses. Thrww cases with positive AChE and normal AF-AFP
were associated with fetal bleeding or intrauterine fetal death. Early Amniocentesis ]Vlidtrimester Amniocentesis
# Samples 281 2450
High AF-AFP 7 (2.5%) 33 (1.3%)
Positive AChE 10 (3.6%) 25 (1.0%)
CONCLUSIONS Iu midtrimester, AF-AFP may be positive when AChE is not. In EA the opposite may be observed. Interpretation of EA rcsalts can still be reliable, but requires the elevation of both AF-AFP and AChE

356 SPO Abstracts January 1994 Am J Obstet Gynecol
286 SECOND TRIMESTER FETAL ANOMALIES: FISHING LIMITS.
NB lsada, P Streicher,x PG Pryde,x A Reichler,x MP Johnson, KW
Klinger,x BE Ward,x MI Evans. Depts Ob/Gyn, Mol Biology & Genetics and Pathology, Hutzel Hospital/Wayne State Univ, Detroit, MI, and Integrated Genetics, Framingham, MA. OBJECTIVE: To assess discrepancies using fluorescent in situ hybridization (FISH) as compared to standard karyotype in patients with 2nd trimester sonographJc fetal anomalies. STUDY DESIGN: We performed a retrospective chart review of patients with sonographic fetal anomalies who underwent FISH aneuploidy screening and karyotype analysis. Chromosorae-specific probes for chromosomes 13, 18, 21, X and Y were used. Consent for FISH utilization included its investigational nature and technical limitations. RESULTS: Two cases out of 50 were identified in whom there was a discrepancy between FISH and karyotype results. Excluded were specimens with bloody Eaps or cases with less than 70% abnormal nuclei but with concordant final karyotype. Case #l was evaluated at 20 wks gestatxon for bilateral 5 mm choroid plexus cysts. FISH results were disomic; final karyotype showed a de novo unbalanced translocation for partial trisomy 13: 46,XY, -12, +der(12) t(12;13) (p13;q14.1). The region specific for the probe was not present in the translocated segment. Case #2 was evaluated at 21 wks gestation for 6 mm bilateral choroid plexus cysts. FISH results were disomic; cytogenetics showed a 10% trisomy 21 mosaicism: 46,XY/47,XY, +21. CONCLUSIONS: FISH is an effective method for rapid detection of aneuploidy in this high-risk population group. However, consistent with assay design, there are certain chromosome abnormalities (translocation and mosaicism) that cannot be detected by FISH. These cases demonstrate (1) the preliminary nature of FISH results, and (2) the continued need to require back-up karyotype, despite additional costs.
288 PROPAGATION OF MEASUREMENT UNCERTAINTY IN
MSAFP/HCG SCREENING; VARIATION OF CONFIDENCE INTERVALS FOR RISK ESTIMATES.
T. Markellox, D. J. Gloeb, D. Matt, and S. Walsh. Departments of Human
Genetics and Obstetrics and Gynecology, Medical College of Vxrginia,
lhchmond, VA.
The method using maternal serum analytes (AFP, HCG and others) developed by Cuckle and Wald et el. has become the standard for estimat-
ing the risk of Down syndmn~ in pregnancy The estimate is derived from an equation that uses many measured values, each with its own variance.
OBJECTIVE: We wish to assess the effect of experimental variance of each input measurement on the final risk estimate (confidence intervals of the estimate), and to determine how often the confidence interval overlaps
the risk of 1/350, when the recommendation of amniocentesis is made STUDY DESIGN: Variances for 12 parameters ~n the risk equation were detenmned using standard statisttcal methods. MSAFP/HCG and ges-
rational age data were obtained from pregnancies followed from 7~2 to 5193 Using a Monte Carlo technique, the variance of the individual’s risk
estimate was generated from 10,000 calculations using the ind~vxdual’s measured data, and varying it in a normally distributed random manner
RESULTS: For 2,708 patients studied, approximately 90% of the risk estimates were above or below 1/350 at the 95% confidence level. We
ldenhfied cases where significant uncertainty existed ( i e, 30%-49%) as to which side of 1/350 the true risk would have been calculated, assuming
that all measurements were errorless. CONCLUSIONS: In most cases, accounting for experimental variance
of measurements used m MSAFP/HCG screemng will not change recommendations for ammocentesls, tlowever, in approximately 10% of
cases, considerations of addxtlonal efforts may reduce variance in the measured parameters and result in a more accurate estimated risk.
287 INFLUkNCE 0E FETAL GENDER ON MID TRIMESTER TR1PLE SCREEN VALUES
C.~J. Ingardla, E.tl. Ph]tlpson. Olvlslon of Maternal/Fetal
Medicine, Hartford Hospital, Hartford, CT.
OBdECIWE: To assess the influence of fetal sex on mld-
trlmester serum levels of human chorlonlc gonadotropln
alphafetoproteln (AFP) and unconJugated estrlo!
STUDY DESIGN: A retrosgect~ve study was conducted on 1704 triple screen tests (hCG, AFP, uE3) performed by one laboratory fro~ ]0/I/91 -I/I/93. 0nly slngleton, non anomalous pregnancies were analyzed. Along wlth actual values, gestat~enal age at test, calculated risk of Down syndrome, maternal age at test and amnlocentesIs results if performed was obtalned. Information On fetal sex and outcome was obtalned vla perlnatal database. Chl SqUdre analysis and 2 Tailed Flschers Exact test when appropriate was conducted on the mean values at each gestatlonal week from 15-19 weeks.
RESULTS: The results Ind}cate that 9ravldas wlth a female fetus have a 7% lower MS-AFP level a~ross all gestat~onal age groups compared to those wlth male fetuses (p:<.002). Although mean levels of hCG appear to be sllghtly ~ncreased In women wlth female fetuses (2%) across all 9estatlonal age groups, this difference
testing (~1:270) compared w~th 7.9% w]Lha female fetus. CONCLUSIONS: Compared to other establ~shed variables (~e: maternal
289 THE IMPACT OF THE METHOD OF SECOND TRIMESTER TERMINATION UPON GENETIC COUNSELLING. S.UIremh*, A.Sc~oscm, M.Grafe×, N.Budonck", S Stoffel% D.Pretonusx. Depts
of Radiology, Med~mne, Pathology and Reproductive Medicine,
UCSD, La Jolla, CA. OBJECTIVE: To determine whether method of second trimester
termmauon(TERM), either dilatatmn and evacuat~on((3&E) or labor mduction(lNO), affects accurate pathologic dlegnos{s and/or the
ablhty to provide genetic counselling.
STUDY DESIGN: We performed a retrospect=ve cohort study of
171 genetic TERMs over 5 years, We excluded cases of
spontaneous fetal death, absent pathology(PATH) and gestations
greater than 24 weeks. Ninety-nine of the remmnmg 133
pregnancms had D&E and 34 had IND. We scored PATH as
adequate or inadequate; and compared PATH to ultrasound(US)
findings and w~th the ab~hty to prowde accurate genebc
oounsalhng.
RESULTS: Mean gestat~onal age(GA) for D&E was 18.7wk and for
IND was 21.3wk, p<O,OOOOS. The groups d~d not d~ffer with
respect to frequency of aneuplo~dy or neural tube defects(NTD).
Adequate PATH was obtained in 100% of /ND and 60% D&E,
p=O 00002. PATH was consistent w~th US m 53% w~th no
difference between the methods, but w~th D&E the relatwe nsk(RR) of unconfmmed findings was 5.15 (1.3-20.4)and the RR of
additional PATH findings was 047(0.28-0.79). PATH d~d not
eonf~rm 15% of NTDs. PATH altered counselhng {n 8%, regardless
of method. Deflmtlve counselling was prowded In 83% of cases,
but In 17% a definitive dlagnosm was not reached. The abd~ty to
provide adequate genetic counselling was not affected by method CONCLUSIONS: Although D&E hm~ts PATH findings, the abd~ty to
verify US findings and detection of other anomahes, we could not
detect an impact of the method of TERM upon genetic counselling
In our small senes.

Volume 170, Number 1, Part 2 SPO Abstracts 357 Am J Obstet Gynecol
290 TWIN BIRTH CO1V~LICATIONS, BEHAVIORAL PROBLEMS, AND READING ABILITY: A RETROSPECTIVE STUDY OF 1,398 ~ PAIRS. J.M. Meyer’, D J Gloeb, J L. Silberg~, ~ of Human Gene6cs, iv’gdical College of Virginia, Richmond, VA. OBJECTIVE: This investigation’ (1) examined the prevalence of birth complications (resusdtation, incubation, transfusion, length of hospitahzation, seizures, congenital anomalies, presemation, and mode of dehvery) as a function of twin zygoslty, birth order, and sex, and (2) analyzed the relationship between intra-pmr differences ~n bi~h compIieations, behavioral problems (hyperacli,aty, dehnquency, and neurotm behavior), and reading scores among monozygntic (MZ) twins. STUDY DESIGN: Analyses were based on data from 1,398 twin parrs, age 8-16 years, residing throughout Virginia. Retrospective reports on b~rth complications were obtained from the twins’ parents; behavioral reports (Rutter B Scale) were provided by the twius’ teachers and reading ability (Slosson Oral Reading Test) was assessed during a home visit. Multiple logistic and linear regression were used to address our two obJeCtives RESULTS: Significant associations between zygosity and Nrth order, and the twins’ presentatton, mode of delivery, and need for resuscitation were identified. Dizygotic and second born twins were more oRen deIivered by cesarean section, were breech, and needed resuscitation. In contrast, MZ and male twins were more often placed m an incubator and hospitalized longer Intra-palr differences m transfusions and length of hospitalization were positively related to differences in the hyperactivity, delinquency, and neurotic behavior of male iVIZ twins. Differences in birth complications (including presentation) were not correlated with behavioral differences in fenmle MZ twins, or reading differenees in either male or female IvlZ trans. CONCLUSIONS: Co-tvan control analyses mdieate that behavioral differ- ences among male MZ twins are in part explained by differences in perinatal transfusions and hospitalization, but not presentation. Twin differences in birth complications did not correlate with &fferences in reading ability
292 THE CLINICAL SIGNIFICANCE OF UNEXPLAINED LOW MID-
TRIMESTER MATERNAL SERUM HUMAN CHORIONIC
GONADOTROPIN (MShCG). J Samolaya, B. Burton* Dept Ob/Gyn, Univ.
of IL,Chtcago, IL.
OBJECTIVE. to determine if low second trimester MShCG is a useful
pre&ctor of comphcatlons of pregnancy.
STUDY DESIGN Between 2/1/90 and 1/31/91, 3,116 patients underwent
prenatal screening using second trimester MSAFP, MShCG and MSuE3. 244
patients with low MShCG (< .4 MoM) were matched for race, maternal age
and gestatmnal age at the time of maternal blood sampling with 261 controls
wttla normal MSAFP (>.4 and <2.5 MoM), normal MSuE3 (> 4 and <
1 6MoM) and normal MShCG( > .4 and < 2.5MoM) from the same obstetrical
population. Patients with pregestational dmbetes, chronic hypertension, or a
fetal chromosomal abnormality were excluded. Outcome information was
obtained from referring MDs Data on completed pregnancies is given The
relattve risk (R.R.) and significance level of the event to occur in the study
group was calculated
RESULTS: R.R (p value) of PIH .29(< 03); G DIAB .30(N S.) and
POL/PROM 1 I(N S ).
TABLE N LOSSES (%) R R. (p value)
CONTROL 261 7 (2.7)
MShCG < 4 MoM I60 10 (6.2) 2 3 (N.S)
MShCG .2- 4 MoM 129 5 (3 8) 1.4 (N.S.)
LOW MShCG only 144 5 (3 5) 1.3 (N.S.)
MShCG <.2 MoM 28 5 (17 9) 6 7 (<.0001)
LOW MShCG +
LOW or HIGH MSAFP
or MSuE3 16 5 (31 2) ll 7 (< 0001)
CONCLUSION. patients with very low levels of second trimester MShCG or
low MShCG with other abnormal triple screemng parameter have an tncreased
risk of pregnancy loss which is not dependent on the inmdence of PIH,
G DIABETES or POt/PROM
291 LOW UNCONJUCATED ESTRIOL LEVELS IN PREGNANT WOMEN
USING ORAL STEROIDS. L Brancazm,x S Lmfer, T
McNanley,x L Semch,x A Hogge, Dept Ob Gyn, Reprod Sc,
University of Pittsburgh, P~ttsburgh, PA
OBJECTIVE. To determine if pregnant women taking oral
stermds during the time of triple marker screening [maternal
serum alpha fetoprotein (MSAFP), chononic gonadotropm
(hCG), and unconjugated estnol (uE3) levels] have artificially
low uE3 levels. STUDY DESIGN We idenbfled patients using oral steroid
medications at the time of triple screening We compared the mean MOM (mulbple of the median for a given gestabonal
age) of each test w~th the reference MOM of 1 0. Linear
regression was performed on uE3 MOM verus steroid dose. RESULTS: We ~dentified eighteen patients using prednisone
(range 3 75mg/day to 55 mg/day). There was no s~gn~ficant difference between the reference and the subjects’ mean
MSAFP MOM (1.49 + 0 70) or the subjects’ mean hCG MOM
(1 55 +_ 1.36) [mean _+ SD]. The mean uE3 MOM (0750 _+ 0 40) was s~gn~flcantly lower than the reference (p < 0.05). The uE3 MOM was reversely correlated with prednisone dose
(R=0 650; p=0.004) No patient was found to have a fetus
w~th trisomy 21. CONCLUSIONS Gravidas using oral steroids have lower
uE3 levels when compared w~th reference values. Furthermore, there is a dose-response relatmnsh~p between
steroid dose and lower uE3 levels. Therefore, in these pabents, ~t may be inappropriate to include uE3 levels when assessing risk for tnsomy 21
293 MIDTRIMESTER TRIPLE SCREEN TESTINfiANDLATERADVERSE PERINATAL
OUTCO!4E-UTILIZATION OF SUI~IAT]ONNULTIPLE OF ME~NVALUES
C.J. Infardla, A. Fox, E. PhIllpson. DIws]on of Maternal/Fetal
Medicine, Hartford Hospital, Hartford, CT.
ORdECTIVE: To assess the associatlon of maternal serum
alphafetoprotem (AFP) and human chorlonlc gonadotrop~n (hCG)
levels wlth adverse perinatal outcome both singularly and
together through a summation of multiple of means (MOM) value.
SIgB~ O[SIGR: A retrospective study was conducted on 1704
patlentS wlth slngleton, non-anomalous pregnancles delivered at
our inst]tutlon between 12/I/91 and 6/I/93 who had a serum AFP
and hOG drawn as part of a trlple screen analysls. Adverse
perlnatal outcome measures Included: the occurrence of pregnancy
induced hypertension (PIH), small for gestation age infants
(SGA), preterm delivery, preterm labor, chor]oamnlonltls
fetal dlstress, and abruptlo placenta. Chl square analys~s was
conducted with utilization of the 2 tailed Fisher [xact Test
when appropriate.
RESULFS: The results indicate a slgnt ficant assoclatlon of
elevated MS-AFP (>2 MOM) wlth SGA infants (p=<.O001). There was also an assoclatmn of elevated hCG (>2 MOM) wlth SGA infants (p=<.O001), as well as PIH (p-<.O05) and fetal dlstress (p=<.O02). In addition, w~th summatmn of the M.O.M.S > 3,
there was an assoclat~on of SGA (p=<.O00I), PIH (p:<.O]), fetal dlstress (p:<.01) and abruptio placenta (p=<.02).
CONCLUSIONS: Elevatlon of MS-AFP > 2 MOM, hCG > 2 MOM, or sum of the two > 3 MOM, was slgnlficantly associated with later pregnancy comp]lcatlons. In the absence of fetal anomalies, these levels indlcate need for close pregnancy follow-up.

358 SPO Abstracts January 1994 Am J Obstet Gynecol
294 PRENATAL DIAGNOSIS OF FETAL HYPOTHALAMIC HYPOCORTISOLISM (HHC) WITH MATERNAL SERUM
UNCONJUGATED ESTRIOL (MSUE3).A. Druganl,x H
Mandel2,x M. Berant2,x T. Zer3,x M.I. Evans4. Dept Ob/Gyn1,
Dept Pediatrics B2, Rambam Med Ctr, Haifa, Israel; ZER Science
Based Ind Ltd3, Jerusalem, Israel; Hutzel Hosp/WSU, Detroit, MI4.
OBJECTIVE. Low MSUE3 is commonly seen with aneuploldy,
placental sulfatase deficiency, and anencephaly. Here we test MSUE3 for HJ-IC, in a consanguinous at-risk kindred.
STUDY DESIGN’ We have evaluated by serial MSUE3, four
pregnancies at-risk for fetal HHC.
RESULTS: At all gestational ages, MSUE3 was considerably lower
m pataents carrying an affected fetus (mean MOM, 0.29 v 0.96, respechvely, t=9.76, p<0.001)
MSUE3 Levels (r ml) in Affected and Normal Gestations
GA (wks) Affected Normal Normal Affected 14 -- 0.59 -- --
16 -17 0.58 1.83 1.08 0.25 18-19 0.79 2.15 2.21 0.25 22-23 -- 3.07 5.07 --
28 0.95 -- -- 31-32 1.14 8.26 -- --
Amniotic fluid E3 in affected pregnancies was also significantly
lower fl~an observed in 15 gestatlonal age matched controls (mean
0 3 v 1.97 ng/ml, t=2 55, p=O {32). Prenatal d~agnosis of fetal HHC was conhrmed at birth by undetectable levels of cortisol and
ACTH, whale fetuses predicted to be normal by MSUE3 were
confirmed to be unaffected
CONCLUSIONS- We conclude that very low levels of MSUE3
should prompt further investigation into fetal adrenal function, in
add~hon to evaluataon of fetal chromosomes and ultrasonography.
296 ABNORMAL BIOCHEMICAL SCREENING (ABS) VS 2ND
TRIMESTER ULTRASOUND (US) DETECTED MINOR
ANOMALIES (MA) AS PREDICTORS OF ANEUPLOIDY
IN LOW RISK PATIENTS. A. Drugan,x A. Reichler,x M.P.
Johnson, R.J. Sokol, S.A.D. Ebrahim,x M.I. Evans. Depts
Ob/Gyn, MBG, & Path, Hutzel Hosp/WSU, Detroit, MI, and
Rambam Meal Center, Haifa, Israel.
OBJECTIVE: To evaluate the yield of 2nd trimester US vs serum screening as indicators for chromosomal studies in
patients at presumed low risk for fetal aneuploidy.
STUDY DESIGN: From 1991 to 1993 we performed 1029
amnios for patients with ABS who were younger than 35 years, and 137 2nd trimester amnios for MA (eg, choroid
plexus cysts [CPC]) in patients without other prior genetic risks.
RESULTS: 21 chromosome anomalies were diagnosed for
ABS and 3 for MA on US. The frequency of chromosome
anomalies in study groups (2.1% & 2.3%, respectively) did not
differ significantly. (SUA=single umbilical artery) Abnormal US ABS
]~ebbed neck l’ye 1 ec.hl~ CPC SUA Total 48 34 52 3 1029
¯ Abnormals 2# 0 1" 0 21@ #=Trisomy 18; trlsomy X. *=Trksomy 18. @=-10/21 Down syndrome CONCLUSIONS: The aneuploidy detection rates of 2nd
trimester ABS and US are comparabie. However, since US
diagnosis of MA requires sophisticated equipment and
expertise, biochemical serum markers may be more suitable
for population screening. US screening may complement and
recognize another fraction of the low risk pregnant population
in need of prenatal genetic testing.
295 THE ROLE OF ULTRASONOGRAPHY (US) IN PREGNANCIES WITH MARKER CHROMOSOME (MC) ANEUPLOIDY. R.F.
Hume,x A. Drugan,x S.A.D. Ebrahim,x M.P. Johnson, N.B. Isada, A.
Reichler,x M.I. Evans. Div Reproductive Genetics, Depts Ob/Gyn, Molecular Biology & Genetics and Pathology, Hutzel Hospital/Wayne State University, Detroit, MI, and Dept Ob/Gyn, Rambam Medical Center, Haifa, Israel.
Objective: To evaluate the effect of US findings on pregnancy management in patients with MC aneuploidy ascertained through prenatal diagnosis. Study design" From 1989 through June, 1993, 15,522 prenatal diagnostic procedures were performed for accepted indications. Charts of patients with MC on amniocentesis or CVS karyotype were evaluated with respect to US anomalies, pregnancy complications, and outcome. Results: 19 cases of MC were identified. The prevalence of MC in our study was 0.12% (1:816 procedures), which is much higher than previously reported. 3 cases with incomplete records were excluded.
Pregnancies with Marker Chromosomes De hove Inherited
No’ TOP Cent N1 out No’ TOP Cent N1 Out Normal US 8 4 4 4 3 0 3 3 Abn 1 US 4 3 1 0 1 1 0 0 Conclusions: MCs are more common in pregnancies sampled for
usual genetic indications than previously reported. MCs inherited from a normal phenotypic patient do not increase the risk of fetal anomalies. The association of de hove MCs with US anomalies
confers a dismal prognosis. However, when US appears normal on initial and followup examinations, the chances for a normal phenotypic newborn are high.
297 DETECTIN(3 DEVIANT FETAL GROWTH USIN(3 THE TCD/AC
RATIO: A PROSPECTIVE, COMPARISON STUDY
W. Meyer, D. (3aathier, (3. Font’, J. Sipos~. Univ. of Ill, Chicago, IL
OBJECTIVE: To assess the accuracy of the fetal transverse cerebellar
dlameter/abdominal circumference ratio (TCD/AC) in identifying n
large or small for gestatlonal age fetus.
METIIODS: A prospective study of 250 patients having risk factors for fetal
macrosomia (n=92) or growth retardation (n = 158) was performed. Ultrasonic
evaluations were performed within 1 we.ek of birth in all patients. Biometric
parameters included the biparietal diameter (BPD), head circumference (HC),
TCD, AC, and femur length (FL). The HC/AC, TCD/AC, FL/AC ratios and
estimated fetal weight were calculated. Reference curves for biometric
parameters were created from a cross-sectional (14-42 weeks) analysis of 729
low risk, well dated, normal patients who delivered AGA infants. The
sensitivity, specificity, positive and negative predictive value, fals~
positive and negative rates for all of the above parameters in detecting the
LGA and SGA infant ware determined.
RESULTS: In the study group, there were 39 LGA and 69 SGA infants.
Inability to adequately measure the TCD occurred in 12.8% and 10.1%
of LGA and SGA infants, respectively. All other parameters were obtained in
all patients The diagnostic indices era TCD/AC ratio above or below 2 stan-
dard deviations from the mean in detecting the LGA or SGA infants follow:
n Seas. Spec. PPV. NPV. FP. FN.
LGA 34 17.6% 95.6% 75.0% 60.6% 4.4% 82.4%
SGA 62 83.9% 96.2% 94.5% 88.2% 3.8% 16.1%
The TCD/AC ratio was abnormal in 71.9% (23/32) and ia 69.2% (9113) of
symmetrically small infants with birth weights less than the tenth and third
percentile respectively. The diagnostic indices of the parameters lisW.d above,
compared to the TCD/AC ratio, in predicting deviant growth will be presented.
CONCLUSION: The TCD/AC ratio is a gestatioanl age-independent parameter
that is useful in identifying the small for gestational age fetus. The ratio
is less accurate in identifying large for gestational age infants. This parameter
is gcstational age-independent and may be particularly useful in evaluating
patients with poor gestational dating.
Volume 170, Number 1, Part 2 SPO Abstracts 359 Am J Obstet Gynecol
298 ULTRASOUND FETAL ILIAC LENGTH MEASUREMENT
IN THE SCREENING FOR DOWN SYNDROME.
A Abuhamad, P Kolmx, G Marlx, and A Evans Departments of
OB/GYN & Biostatisties at Eastern Virginia Me, heal School and
Department of OB/GYN at Yale School of Medicine, Norfolk
and New Haven.
Objective: Pelvic bone abnormalities are common in newborns
with Down Syndrome (DS). The aim of this study was to evaluate
the utility of ultrasonographic ihae bone length measurement
(ILM) for the detection of fetuses with DS in the midtrimester of
gestation.
Study design: Ultrasonographic ILM was obtained, in an axial
plane of the fetal pelvis, on 10 fetuses with DS and 180 normal
fetuses before genetic amnioccntesis. Regression equations
relating biparietal diameter (BPD) to ILM were used to calculate
ratios of observed-tu-cxpccted length, sensitivity and specificity
at various cutoff‘points.
Results: Linear regression of ILM on BPD for normal fetuses
resulted in tho fullowing equatton:ILM = - 0.2723 + 0.0333 BPD.
ILM in DS fetuses was significantly longer than normal controls
(P < 0.0001). A ratio of 1.21 for observed / expected ILM
yielded a sensitivity of 40%, a specificity of 98%, and positive
preAxctive values of 50% and 2.60% in populations at risk for
DS of 1 in 20, and 1 in 750, respectively.
Conclusions: ILM is increased in fetuses with DS. An observed /
expected ]LM of 1.21 or more has a positive predictive value of
1138 in a low risk population with a false positive rate of 2%.
This preliminary study suggests that ILM may be useful as an
ancillary screening variable in the antenatal screening for DS.
300 GROtNTH OF THE FETAL GALL BLADDER IN NORMAL PREGNANCIES. I.Goldstein, A.Tamif’, A.Weisman=, P. JakobP, J. Itskovitz% J. Copel’. Dep. OB/GYN, Rambam, Haifa, Israel, & Dep. OB/GYN,
Yale Univ., New Haven, CT." OBJECTWES: To obtain dimensions of the fetal gall bladder,
as a basis for further studies and for compansons with deviation in growth. STUDY DESIGN: The study group included 183 normal pregnant women from 13~40 weeks of gestation. Routine biometric measurements were obtained on all, including biparietal diameter, head and abdominal circumferences, measurements of the long bones, and the two diameters of the fetal gall bladder. The gall bladder area and circumference were calculated for each gestational age. RESULTS: A linear growth function was observed across gestational age, and a first degree correlation existed between gostational age and both the longitudinal (r=0.77067; p < 0.00001;y =-0.41060 + 0.0907XGA), and transverse (r = 0.602;p < 0.00001; y = 0.58567 + 0.01925xGA} diameters of the fetal gall bladder. A significant correlation was also found between gall bladder area and gestational age (r=0.6878;p<.00001), biparietal diameter (r=0.72768 ;p<.00001), abdominal cJrcumference (r=0.71363; p<.00001), and femur length (r=0.72190; p<.00001). A significant correlation was also found between gal~ b~adder circumference and gestation age (r =0.76181 ;p <.00001 }. CONCLUSIONS: These results provide normative data of the
fetal gall bladder in various dimensions and across gestational age. In addition, these data offer the potential for prenatal diagnosis of additional lesions in the extrahepatic bi[iary duct system.
299 CHOROID PLEXUS CYST(S): AN INDICATION FOR AMNIOCENTESIS. M.J. Kupferminc, R K. Tamura, R.E, Sabbaghax, E. Pergament~, T.R.
Wlgton, B.V. Parllla. Dept. Ob/Gyn, Northwestern Univ., Chicago, IL.
OBJECTIVE: To prospectively evaluate the risk of chromosomal
abnormalitms associated with chorold plexus cyst(s) in patients
undergoing second trimester ultrasound examination.
STUDY DESIGN: During a 30 month period 7790 women between 15
and 24 weeks’ gestation underwent ultrasonographm evaluation.
Patients with e dmgnosJs of a chormd plexus cyst(s) were offered
ammocentesis and a repeat ultrasound examination in 4°6 weeks.
RESULTS: A diagnosis of fetal chormd plexus cyst(s) was made in 87
patients (1.1%); in 60 fetuses (69%) the cyst was unilateral. Of the 63
patients in whom amnlocentesis was performed an abnormal karyotype
was identified in 7 fetuses (1!%); of these, 3 (4.8%) had Down syndrome, 3 (4.8%) had tnsomy 18, and 1 had an unbalanced
trsnslocation, t(3; 13). Of 24 patients not undergoing amniocentesis, 23 were dehvered of phenotypmally normal infants and 1 patient aborted a
fetus with complex cardiac lesion and multlcystlc kidneys but normal
karyotyps. Three fetuses with Down syndrome and 1 with trisomy 18,
or 87% of those w=th abnormal karyotype had no ultrasonically
detectable anomaly other than the chorold plexus cyst(s). In all 7 fetuses
with abnormal karyotype the size of the chorold plexus cyst(s) was qmte
variable with a mean of 7.2 mm +- 5.6 (2SD). Further, these cysts were
uddateral in 4/7 fetuses with abnormal karyotype. In gravidas who had
serial ultrasound examination the chormd plexus cyst(s) persisted in only
5/79 normal fetuses and In 1/4 chromosomally abnormal fetuses.
CONCLUSIONS: The presence of chorold plexus cyst(s) can be
associated with chromosomal abnormalities regardless of size, laterahty, disappearance, and absence of other structural abnormalities. The risk
of fetal chromosomal abnormality with chorold plexus cyst(s) is 1:13,
whereas the risk of Down syndrome =s 1:29. These risks are greater
than those in a woman 43 years of age and justify offering
amnlocsntesis.
301 TRANSCEREBELLAR DIAMETER MEASLrREMENT IN
THE SECOND TRIMESTER: AN ADJUNCTIVE
SONOGRAPHIC SIGN OF DOWN SYNDROME. L
Goldstein, S. Rotmenach, M. Libe~ix, T. O’Connorx, JA.
Copel. Dep OB/GYN, Yale Univ., New Haven, CT.
OBJECTIVE: To determine the utility of measurement of the
transcerebellar diameter (TCD) in the prenatal detection of
Down syndron~.
STUDY DESIGN: On the basis of gestational age, predicted
TCD was derived from 387 karyotypically normal fetuses. The
formula derived from this group was applied to 26 consecutive
Down syndrome fetuses and 774 fetuses with normal karyotype.
A ratio of measured TCD/predicted TCD was calculated for
each fetus.
RESULTS: Eight of 26 (30.8%) of fetuses with Down
syndrome exhibited a smaller TCD (measured TCD/predieted
TCD ratio <0.92), compared with 41/774 (5.3%) of fetuses
with a normal karyotype. Hence fetuses with Down syndrome
were 5.8 times more likely to exhibit small TCD than
karyotypically normal fetuses (risk ratio = 5.8; 95%
confidence interval = 3.0 - 11.1).
CONCLUSION: Prenatal ultrasonographic detection of a small
TCD increases the risk of Down syndrome. However, this
measurement may not be useful alone in a screening program.
The TCD measurement might be combined with femur and
humerus measurements, and with triple screen (maternal serum
alpha-fetoprotein, human chotionie gonadotropin, and estriol)
to further refine the risk of Down syndrome.

360 SPO Abstracts January 1994 Am J Obstet Gynecol
302 ACCURACY OF ULTRASOUND ESTIMATED FETAL WEIGHT -
A COMPARISON BY RESIDENT TRAINING LEVEL.
Mary O’Dayx, Isabelle Wilkins. D~pt. Ob/Gyn, Univ of Texas, Houston
Health Science Center Houston, Texas.
OBJECTIVE: In many labor suites, ultrasound as used by residents to
assess patients m an urgent setting. The purpose of this study was to
assess the vafidity of the estimated fetal weight (EFW) done by residents
at two training levels.
STUDY DESIGN: 150 patients with singleton pregnancies were
prospectively studied. The PGY1 and PGY3 resident each recorded a
clinical estimate of fetal weight using Leopold’s maneuvers, then an
ultrasound EFW was performed. The gestational age, patient height and
weight, and the presence or absence of oligohydramnios was recorded
All patients delivered within one week. The ultrasound EFW formula
used was from Hadlock (1985). "Correct" EFW was defined as within
10% of actual birth weight. Statistical analysis was performed using Chi-
square or Student’s T test as appropriate.
RESULTS: PGY1 clinical EFW was correct in 52% of eases, as
compared to 81% for the PGY3 resident (p<0.02). PGY1 ultrasound
EFW was correct 67% of the time as compared to 75% by the PGY3
(p>0 05). Predicted ultrasound EFW was correct most oi%en in fetuses
between 3000 and 4000 gm (81% for PGYI, 95% for PGY3) and correct
least often in fetuses weighing less than 2000 gm (55% for both years)
Maternal obesity affected the abihty of the PGYI to correctly predict both
the chmeal and ultrasound EFW. Oligohydrammos did not affect the
ability of either training level to correctly predict EFW.
CONCLUSIONS: Ability to predict clinical EFW improves with the level
of training. There is no significant difference in ultrasound estimates of
fetal weight between levels of training. Aecuraey of ultrasound EFW was
found to be within 10% of aetual birth weight 65 to 75% of the time,
consistent with previously published studies. This may obviate the need
for repeat "formal" ultrasounds to assess fetal weights.
304 PRENATAL DIAGNOSIS OF THE 2 VESSEL CORD: IMPLICATIONS FOR MANAGEMENT OF PREGNANCY. V. Catsnzarita, S. Hendricks, C. Maida~, L. Cousins, and D. Schrimmer. Maternal-Fetal Medicine, Mary Birch Hospital for Women at Sharp Memorial Hospital, and Maternal-Fetal Medicine, University of Washington, Seatt/e. OBJECTIVE: To investigate the implications of the sonographic diagnosis of the two vessel umbilical cord for pregnancy management. STUDY DESIGN: Retrospective analysis of prenatal findings and outcomes when a two vessel cord was diagnosed in utero. RESULTS: Sixty four cases of 2 vessel umbilical cord were identified and confirmed by postnatal and/or pathologic examination. Eight were aneuploid, including 6 with major structural defects. Of the remaining 56, 24 had sonographically visible anomalies, 2 were minor and 22 major. Structural defects included abnormalaies of mtracranial, thoracic, gastrointestinal, renal and limb anatomy. Nine of these 24 had additional major structural defects not seen on scan. Among the 32 sonographieally & ehremosomally normal babies, two proved to have major structural defects - one had hydrocephaly diagnosed prenatally, and one, who had early onset IUGR, has Goltz syndrome. Significant neonatal morbidity was encountered in all 6 twin pregnancies, related to IUGR in the twin with the 2 vessel cord in 5 of the 6 cases. Among chromosomally normal singletons, 6 of 18 with other anomalies and 6 of 32 with isolated 2 vessel cord had IUGR. CONCLUSIONS: 1. Karyotyping is recommended whenever a two vessel cord is seen in association with any other defect, and should be considered oven if the fetus appears otherwise normal. 2. The fetus with a 2 vessel cord and concomitant sonographically visible anomalies often has unrecognized major defects. 3. The fetus with an isolated 2 vessel cord on scan seldom has unrecognized major anomalies, but may be at risk for IUGR.
303 PROSPECTIVE EVALUATION OF ECHOGENIC FETAL BOWEL AS A PREDICTOR OF DOWN
SYNDROME. R.M. Patterson, S. Rauechx, B.G. Darbyx.
Austin, Texas. OBJECTIVE: Null Hypothesis: Ultrasonographically detected echogenic fetal bowel (EB) is not a significant predictor of fetal Down syndrome.
STUDY DESIGN: Four hundred nine consecutive patients
at increased risk for fetal Down syndrome were prospectively
examined by a single observer blinded to indication, level of risk, and concomitant ultrasonographic findings. EB was
dehned as an ochogenic outline of the fetal small intestine approaching the echogenicity of the fetal ihac crest. No management decision was based on ultrssonographic findings. Amniocentesis was performed by a separate obsever.
RESULTS:
Down Syndrome
No Yes Prev. 1.9% No 370 3 373 Sons. 62.5%
EB Opec. 92.3% Yes 31 ~ 3~6 pv+ 13.9%
pv- 99.2% 401 8 409
Fisher’s Exact Test P=.00019 One patient with trisomy 13 had EB, while a patient with 47, XXY did not. CONCLUSION: In this selected population at risk for chromosomal aneuploidy, EB was significantly associated with fetal Down syndrome. Interobserver variability and apphcation to populations of lower prevalence of aneuploidy will require further study.
305 NA%IP/~ HISICRY OF E~t~lqIC FOCI WI2HIN HEgRT. B. Pe~, M. Challeng~r , L. Wyse
COlumbia Presbyterian Medical C~nter, Babies ~h~ital, New Yozk, NY CS3EC~IVS: 2he ~ of the study is to estabish the freque~, distributicn and oTo_zse of echcg~c foci within fetal and r~natal heart. SILDY EESI~: 24 patients wh~ had intracardiac ech~g~c fcci were the subjects of the study. Initial ec!~cgraphy (E~I~) and foll~w-up BS3 ex~ticms were performed at 28, 36 w~eks ard at 3 msllths after birth. RESLLTS: ~c foci were seen in 24 fetuses out of 632 (3.8%) in the follc~ing areas: anterior papillary ~uscle of the left ventricle in 46% of fetuses, cardiac apex in 25% of fetuses, pcsterior papillary ~uscle of the left ventricle in 14% of fetuses, intraventricular s~ptun in 8% of fetuses, right ventricle in 7% of fetuses. With prcgressicn of pre~ they grew in size in 9 cases (38%), regressed in 2 cases (8%) acd re.dried the sa~ in 13 cases (54%). Ech0g~c fcci were present at all ne~mtal follcw-up~. No case of c~cpir~ cardiac tutor
CEDZSuL~ICI~3: Echcc3enic fcci within fetal heart represent infrequent b/t r~Dr~ variants of the c~=velc~t of papillary nl3scles.

Volume 170, Number 1, Part 2 SPO Abstracts 361 Am J Obstet Gynecol
306 THE SIGNIFICANCE OF PERIOPERATIVE TRANSVAGINAL
ULTRASOUND EVALUATION OF THE CERVIX IN EMERGENCY
CERCLAGE PROCEDURES. ER Guzman, C HoulihanX, J Ivanx, J Rosenbergx, R Knuppel. Division of Maternal-Fetal Medicine, UMDNJ-Robert Wood Medical School, New Brunswick, New Jersey. OBJECTIVE: To determine If perloperatlve transvaglnal sonograpbc
evaluatmn of the mcempetent cermx treated w~th emergency
cerctage procedure correlates w~th pregnancy outcome.
STUDY DESIGN: Twenty women who underwent emergency
cerv=cal cerclages had transvagmal sonographm evaluahon of the
cervix before and after surgery at 16 to 25 weeks of gestabon.
The fo~owmg measurements were taken: A) d~ameter of the mterna~
os, B) the Internal ce to the po=nt of descent of the membranes, C)
the point of descent of the membranes to the external os, and D)
internal to external es These measurements were correlated w~th
gestat~onat age at dehvery. Results are reported as mean
(centimeters) _+ 1 standard devlahon and statistical analysis was
performed w~th pmred t-test and hnear regression when approp~ate.
RESULTS: Measurements Preoperative Postoperative P value
A 13-* .7 .48-*.48 000
B 24-+12 12 _+ 6 .000
C 73 -+ .9 1 9 -+ .5 000
D 32-* .8 32 -*.6 853
Cerclage procedures resulted ~n slgnff~cent ~mprovemant m cervical
state. The average gestat~onal age at delivery was 35.4 -+ 4,2 weeks
(range 26-41). There was no correlatmn between any ultrasound
measurements obtained before and after surgery and gestat~ona~
age at dehvery
CONCLUSIONS: Pregnancy outcome m women undergoing
emergency cerclage procedures cannot be predicted by the state of
the cerv=x before or after surgery as determined by transvagmal
sonography The outcome m these pregnancies ts detarmmed by
other factors
3O8 FETAL ECIIOCARDIOGRAPiiY: INDICATIONS AND CLINICAL
VALUE. Laura Diana, MDx, Brian Koos, MD, DPhil, and Steven
Pinbeiro, MDL Depts of Ob/Gyn, Albany Medical Center, Albany, New
York, UCLA School of Medicine, Los Angeles, CA
Objectbces: To ~dentify common indmatlons for fetal echocardiography,
to estimate the incidence of abnormal scans for each lndmation, and to
determine cost-effective utlhzadon
Study Design: Medical records of gravidas referred to Albany Medical
Center Pediatric Cardiology Department for fetal echocardmgraphy were
reviewed for demographbs, reason for evaluatmn, fetal echocardiography
findings, and fetal and newborn outcome.
Results: Of 151 fetal echocardiograms, 22 (14%) were abnormal and
were assomated w~th a 64% mortality rate. Chromosome abnormalities,
cardiac malformations identified by ultrasound, noncar&ac anomalies, and
arrhythmias were h~gh yield in&cators for detecting fetal cardiac
abnormalities, whereas a prevmusly affected fetus, famdy h~story of
congenital heart d~sease, teratogen exposure, and maternal d~abetes were
low yield ~ndicators The cost of echocardlography to detect one fetal
cardiac abnormahty was about $7,650, but this expense could be lowered
42% by performing the procedure only on fetuses ~n high-ask groups and
on those in low-risk patients with cardiac abnormalities detected by
ultrasound This echocardiogram cost could be reduced further (to about
$2,890) by conducting echocardiography only on fetuses with heart
abnormalities ldent~fied by ultrasound, although some cardiac anomalies
mlght go undetected
CosehlSiOn: A reasonable approach is to reserve echoeardiography for
fetuses belonging to a high risk group and for those with cardiac
abnormalmcs detected by ultrasound.
307 KARYOTYPE OF FETUSES V¢ITH ANOMALIES DETECTED BY
SECOND TRIMESTER ULTRASOUND. R. Gonen~, H.Dar~, S. DeganP. Dept. Ob/Gyn & Winter Institute of Genetics, Bnai
Zion Hospital, Faculty of Medicine, Technion, Halfa, Israel.
OBJECTIVE: To determine the incidence of abnormal karyotype
among ~et~ses whh anoma~fies detected by second trimester
transvaglnal or abdominal ultrasonography.
STUDY DESIGN: 604 patients underwent amniocentesis following
detection of anomalies by second trimester ultrasonography.
RESULTS: 39 (6.5%) fetuses with abnormal karyotype were
detected. The most common abnormal karyotypes were: Trisomies
21 and 18 - 11 fetuses each, 45XO - 7 fetuses, trisomy 13 - 3
fetuses. The assoociation between abnormal karyotypes and anomalies is shown in the table:
Cardiac 0/18 Hydmnephrosis 0/58 Choroid plexus cyst 0/108 Mulhple 20/111 Club foot 0/7 Non immune hydrops 1/9 Cystic hygroma Nuchal thlckemng 1/38 - Not specified 13/112 Omphalocele 0/10
- Non septated 2/70 Single umblhcal artery 0/16 Duodenal atresla 2/5 Skeletal 0/10
Gastro4ntestlnal 0/7 Ventnculomegaly 0/25
CONCLUSIONS: 1. Half of the cases with abnormal karyotype
occurred in fetuses with more than one anomaly. 2. Cystic hygroma
and duodenal atresia were the isolated malformations most
commonly associated with abnormal karyotype. 3. Isolated
malformations such as choroid plexus cyst or hydronephrosis were
not associated with abnormal karyotype.
309 MIGRATION RAT~ OF ~ LYING p~AC~qTA IN TI{E TIIIRD TRIMESTER - CAN IT PREDICT OUTCC~? L.W.ODnenheimer, F. Mackenzie~, j.Girard~, A.Dabrowski×, E.~ssef~. Dept. Ob/Gyn, Univ of Ottawa and Univ of Toronto~, ONT. OBJECTIVES: TO document migration of low placentae in the third trimester and determine the correlation between the rate of migration and subsequent mode of delivery. STUDY DESI~: All patients with a placental edge lying within 3 cm or overlapping the internal cervical os on transvaginal ultrasound (TVS) were recruited into the study. The distance from the nearest point of the placental edge to the internal os was measured. TVS was repeated, on up to 4 occasions, until either the placental edge was more than 3cm from the os or the patient had delivered. Postnatally the patients were stratified into two groups according to whether or not cesarean section was performed for the indication of placenta previa. A plot of gestational age at TVS versus distance to placental edge was constructed for each group and the mean slopes (rates of migration) compared using analysis of variance. P~SULTS: The mean rates of miqration in patients with and without cesarean section- for the indication of placenta previa were 0.6 n~n/week and 5.8 rKn/week (p<0.01) Even when the placenta overlapped the os by up to 2 cm early in the third trimester, only 14% of patients required cesarean section. CONCLUSIONS: Placental migration occurs progressively throughout the third trimester The rate of migration is correlated with the subsequent mode of deliveryand as such may aid management decisions, and avoid unneccesary hospitalization, in patients w~th a low lying placenta

362 SPO Abstracts January 1994 Am J Obstet Gynecol
310 ACCURACY OF ULTRASOUND ESTIMATION OF FETAL
WEIGHT IN MULTIPLE PREGNANCIES. L. Lynch. C.I
Lockwood, R. Lapinskix, M Alvarez. Mr. Sinai School of Medicine, New York, NY
OBJECTIVE: Because of fetal crowding, the reliability of ultrasonic
esmnation of fetal weight (EFW) has been questioned. Our objective was
to assess the accuracy of EFW determination in multiple pregnmacms. STUDY DESIGN: All singleton, twin, and triplet pregnancies that
underwent EFW determinations within 1 week of delivery were
retrospectively reviewed Formulas used were Hadlock (BPD/AC/FL and
AC/FL) and Shepard (BPD/AC).
RESULTS: Smgleton Twins Triplets fetuses n 1924 464 44 Mean BW (g) 2815+920 2124+672"* 1927+555"+ Mean % absolute error
BPD/AC/FL 7.9% 9.2%** 6 9%*+ BPD/AC 8 9% 10.0% 8 5% AC/FL 8.5% 10 6%** 7 6%*+
p < 05 for **Comparison twins vs singletons, * Comparison triplet vs
singleton, and + comparison twin vs triplet
BW within 10% of EFW:
BPD/AC/FL AC/FL BPD/AC
Singleton 70% 66%* 64%+ Twins 6i% 59% 58% Triplets 71% 70% 65% BW = Birth Weight, BPD = Bipalietal Diameter, AC = Abdominal
Circumference, FL = Femur Length p <.05 for comparison * BPD/AC/FL
vs AC~L; and + BPD/AC/FL vs BPD/AC.
CONCULSIONS: (1) EFW is less accurate in twins than m singletons.
(2) EFW in mplets ~s as accurate as in singletons although this may be a
function of the small number of triplets. (3) The best formula for EFW in
singletons was BPD/AC/FL and in twins and triplets no combination of
measureruents was superior. (4) Although statistically s~gntflcant, these
differences are not hkely to be clinically s~gnificant.
312 TARGETED ULTRASONOGRAPHY VS. AMNIOCENTESIS IN EVALUATION OF ELEVATED MATERNAL SERUM ALPHA- FETOPROTEIN. G Megerianx, J Bell. Dept of OB/GYN. Pennsylvania Hospital, Phdaddphia PA. OBJECTIVE: To determine the current sensitivity of ultrasound in the detection of open neural tube defects(ONTD) and other anomalies m a population referred for high maternal serum alpha-fetoprotein (MSAFP). STUDY DESIGN: A retrospective rewew of sonographie and amniocentesis data for patients undergoing amniocentesis for elevated MSAFP (>2.0 MUM) between 1988-1992 was performed. RESULTS: 733 fetuses in 707 patients (26 twins) underwent both amniocentesis and ultrasonography. Information for analysis was available on 647 (88 2%), including all patients with elevated amniotic fluid AFP(AFAFP) and positive acetylcholinesterase (ACHE). Ultrasound identified structural abnormalities in 29/30 fetuses subsequently known to be positive for ACHE, for a sensitivity of 96.7%(95% CI:90.3- 100%). The sensitivity for detecting ONTD’s was 17118= 94.4%(95% CI. 83 8-100%) The positive predictive value for detecting all defects and ONTD’s was 85 3% (95% CI 73 4-97 2%) and 77.3%(95% CI 59.8- 94 8%), respectively The negative predictive value of ultrasound was 99 8%(95% CI 99.4-100%). Five ultrasounds were suspicious for small ONTD’s but had normal AFAFP, resulting in a specificity of 99 2% (95% CI 98 5-99 9%) None of the 5 false positive cases had intracranial changes or a definitive ONTD identified. The one missed case of ONTD had intraemmal changes associated with ONTD on retrospective review and was identified on subsequent ultrasound after positive ACHE results. In addition, ultrasound identified 2 structural abnormalities in fetuses with normal AFAFP (1 omphalocele and 1 gemtourinaty anomaly). CONCLUSIONS:Ultrasound had close to 100% sensinvity in detecting fetal anomalies and specifically ONTD’s in patients with elevated MSAFP. More experience in the interpretation of mtracranial changes associated with ONTD’s may allow for 100% sensitivity.Thus,we are currently investigating our ammocentesls loss rate in patients with unexplained high MSAFP to determine if there is justification for routine amoiocentesis
311 FETAL CONGENITAL HEART DISEASE: PERINATAL
MANAGEMENT S Smithx, M Respondek, A. Ludomirsky, S
Wei!-Chalker, S Weiner, J Huhta. MFM and Perinatal Cardiology
Sections, Pennsylvania Hospital, Philadelphia, PA
OBJECTIVE. To recommend gurdehnes for the pennatal
management of fetuses with congenital heart disease (CHD).
STUDY DESIGN: Between June 1991 and June 1993, 1365 fetal
echocarthography studres were performed on 943 fetuses. 74 fetuses vath severe CHD were identified Complete follow-up was available in
66. The following variables were analyzed retrospectively
extracardlac fetal malformations (EFM), fetal kasyotype abnormalities,
IUGR, antenatal testing (ANT) parameters, intrapartum fetal distress,
Apgar scores and umbilical artery pH. 90 patients whose fetuses had a normal echocard~ography study served as a control group (specifically, the next two consecutive normal studies for each CHD fetus reaching
viability)
RESULTS. CHD types included hypoplastic left ventricle (24), AV
septal defect (11), pelmonie stenosis/atresra (9), Tetralogy of Failer
(8), aortic stenosis (4), VSD (3), transposition of the great arteries (3),
single ventricle (2), tricuspid atresia (1), double outlet right ventricle
(1) Major EFM’s were present in 20 (38 5%) Fetal karyotype was
obtained in 52 fetuses w~th 12 trisomies identified (23 1%). !9 patients terminated their pregnancy, 47 carried to viability. The incidence of 1UGR (17% vs. 3 4%, p= .009) and non-reassunng ANT
proh~pting delivery (35% vs. 9.3%, p= 003) were significantly
increased in the CHD vs. control group. Umbilical artery pH values,
Apgar scores and the racidence of intrapartum fetal distress were not
significantly different from controls.
CONCLUSIONS" 1) Severe CHD is associated with major extracardiac malformations and/or karyotype abnormalities. A
thorough ultrasound examination, genetic ¢ounsehng. genetic
procedure are indicated. 2) Fetuses with CHD are at risk for IUGR and
ANT abnormalities Serial sonographic assessment of growth and third
trimester ANT are indicated. 3) Fetuses with normal growth and ANT
tolerate labor well.
313 INTEROBSERVER VARIABILITY OF SONOGRAPHICALLY
DETERMi~ED SECOND TRIMESTER NUCHAL SKIN-FOLD
THICKNESS MEASUREMENTS. A. E. Donnenfeld. D. Meister,
J. Allison, K. Brennan, A. Ludomirsky, D. Rightmire. Pennsylvania
HospilM, Philadelphia, PA, Acuson, Mountain View, CA, Southern
lllinois University School of Medicine, Springfield, IL.
OBJECTIVE: To determine the interobserver variability of second
trimester nuchal skin-fold (NSF) thickness.
STUDY DESIGN: Twenty recognized experts in fetal sonographic
evaluation obtained fetal NSF thickness measurements in each of 5 pregnant women between 16-18 weeks gestation. A random effects
analysis of variance model was used to explore the sources of varia-
tion in the set of measurements. The Satterthwaite approximation
method was used to derive tests of significance.
RESULTS: Ninety-six of 1130 NSF measurements were obtained.
Four measurements (all in the same patien0 were technically unob-
tainable due to fetal position. All recorded measurements were between 1.7-4.5mm. The means (and ranges) for the 5 patients were
2.7(1.7-3.6), 2.9(2.0-4.5), 2.7(2.0-4.0), 3.3(2.2-4.0), and 2.7(1.8-
4.0)ram. The standard deviation for interobserver variability, caused
by the combined effect of physician and machine imprecision, was
0.56mm and the overall coefficient of variation was 19.8%.
Interpatient differences were statistically significant (p=0.004).
Inlerphysician differences were not (p=0.11).
CONCLUSION: Among experienced sonographers using high reso-
lution ultrasound equipment, measurement of second trimester NSF
thickness was reproducible within 1.1ram of the estimated true value
with 95% probability.

Volurne 170, Number 1, Part 2 SPO Abstracts 363 Am J Obstet Gynecol
314 Sonographic Visualization of the Fetal Upper Airway
D. Richards, L. Farahx. Dept of Ob/Gya, Univ. of Florida,
Gainesville, FL.
OBJECTIVE: To determine how often the fetal upper
airway can be satisfactorily imaged with ultrasound, and to
determine the normal diameters of the trachea and larynx.
STUDY DESIGN: The fetal upper ah’way was evaluated in
120 consecutive patients. The diameter of the trachea and
pha~]nx were measured and our ability to visualize the
trachea and the larynx was evaluated. Factors which
contributed to non-visuallzation were tabulated.
RESULTS: The diameter of the trachea increased from a
mean of 2.4 mm at 18 weeks to 4.6 nun at 38 weeks. The
mean diameter of the pharynx increased from 4.4 mm at
18 weeks to 8.8 nun at 38 weeks. The fetal larynx was
adequately visualized in 67 percent of the cases, while the
entire trachea was seen in 47 percent of the cases. Our
success in visualizing the larynx and trachea was best
between 20 and 30 weeks gestation. Besides gestational
age, other factors which significantly affected our ability to
visualize the larynx were fetal chin flexion and maternal
obesity.
CONCLDSIONS: Since laryngeal obstruction is usually
associated with tracheal dilation, these nomograms should
help in establishing the diagnosis. It is possible to obtain
excellent views of the fetal airway in a high percentage of
cases.
316 MILD LATERAL VENTRICULOMEGALY IN FETUSES: CLINICAL SIGNIFICANCE AND OUTCOME. I Goldstein, J Garofalo=, R Soper=, JA CopeL Dep. OB/GYN,
Yale Univ., New Haven, CT. OBJECTWE: To evaluate outcome, including the frequency of aneuploidy and other structural abnormalities, among fetuses with mild lateral ventricular dilatation. STUDY DESIGN: The medical records of 34 consecutive fetuses with serial sonographic measurements of mild ventficulomegaly (atrial width 10-15 ram) were reviewed. Further evaluations were also undertaken. RESULTS: Information is available on 30/34 fetuses with mild ventriculomegaly. Sixteen appeared normal at birth and at one year (53%), 7 karyotypes were obtained from them and were normal. Fourteen fetuses had the following outcomes: 4 terminated their pregnancy (at autopsy 1 appeared normal, 2 confirmed hydrocephaly and 1 dechnad study). Ten dehvered with structural abnormalities and 3/10 died neonatatly. Karyotypes were available on 8/10 and 3 had abnormal chromosomes (trisomy 18, 45X, and triploidy 69XXX). Four had cardiac anomalies, 4 had mild ventriculomegaly (2 of them had seizure disorders), 1 esophageal atresia, and 1 had cleft lip and pa~ste. Spontaneous resolution of the mild ventriculomegaly occurred in-utero in 10/30 fetuses (33.3%), 7/16 of the subsequently normal infants. Data are not available in 4/34, 1 is undelivered, and 3 are lost to follow up. CONCLUSIONS: S~xteen/30 (53%) had normal outcome. The 10-15 mm atrial width of the lateral ventricles has been previously defined as abnormal, however, it resolved in one third of the fetuses in this study. In the setting of mild ventriculomegay, a normal karyotype, and the absence of other structural abnormalities the outcome may be good.
315 THE PROGNOSTIC VALUE OF PRENATAL ULTRASOUND FINDINGS IN GASTROSCHISIS. BD. Raynor, D. Richards, F. Gaudier, S. Caftan. University of FLorida st GainesviLle and Jacksonville, FL and Arnold Palmer Hospital, Orlando, O6~ECII~E: To determine if sonographic parameters are useful in predicting the neonatal course of fetuses with gastroschisis. $11JI)¥ BESION; The medical records of 38 patients and neonates with prenatally diagnosed gastroscMsis were reviewed. The number of days of hyperatimentation (HAL) and primary or staged surgical closure of the defect were chosen as the outcome variables. ULtrasound examinations were reviewed for the presence, the Location and the gestationaL age of presentation of dilated bowel, the progression of dilation, the presence of a dilated stomach, and armiotic fluid volume. Maternal records were reviewed for gestational age at delivery and type and indication for delivery. Statistical analysis was performed using chi square and Mann Whitney U tests. RE~JL[S: The mean days of HAL was 37&48 days. Primary closure was performed in 72% of neonates. Mean gestationa[ age at delivery was 36.6 ±I.9 weeks. Spontaneous vaginal delivery occurred in 30%.Dilated bowel was present in 64% of cases and 51% showed progression with time; 38%(13) had a dilated stofnach. There was one intrauterine fetal demise as a result of cord compression from a massively dilated stomach and one neonatal death from infarcted bowet fotLowingprimary closure. Fetuses with undiLatedboweL were significantly mare Likely to have a primary surgical closure (p<.05); those with primary closures tended to have fewer days of HAL (p<.07). The gestationaL age of detection, the Location and the progression of dilation did not correlate with either me[bed of closure or days of MAL; nor did amniotic fluid volume, ~ethodof delivery or gestationat age at birth. The presence of a dilated stomach did not predict a mere coa~Licated neonatal course (p<.04). CONCLUSIONS: Fetuses vith gastroschisis found onuLtrasound to have dilated bowel are Less Likely to have the defect closed primeri[y at birth. None of the other sonographic parameters studiedappear to predict neonatal outcome in terms of days of HAL or type of surgical closure, however, one intrauterine fetal death from a markedly dilated stomach was observed.
317 FEI~L BLAE~ SI~E. B.M. Pe~, H.L.
University Hcspital, Mgnhasset, NY CB3ECTIVE: ~ null hypo~ is that fetal ~is (~H) will diminish as th~ fetal bladder h~scm~s ~mptier. SIL~Y E~I6N: 53 fetuses with ~H in th~ secm~d trimester of pr~gnmcy ~re the subjects of th~ study. ~z~]~erior dieters (APD) of th~
bla~der ~ms full and when it was ~mptier.
rank order cmrrelatic~ ~cefficient. R~S~LTS: Corre]ati<z] hetwg~l the r~rml and bladler size~ are reflected ~ the follmwir~ table:
~t~ (in m~) (in~ Full 6.8 _+ 1.8 1880 _+ 1333 <0.0001
Emptier 4.8 _+ 1.6 616 _+ 114
Ctnclusic~s: There is a sigificant differen~ in the size of ~H with var?ir~ 8egrees of fetal b~ fLllin~. Enla~ ~n~l pelvises m~y appear nOZT~LI when the bladder is ~ptier. The status of th~ bl~r should he ~msidered when

364 SPO Abstracts January 1994 Am J Obstet Gynecol
Altl/~J~4L FETAL GIIOI/TH B~GIWS BEFORE THE THI~ TRIBESTER. ~ucas, T. Rowe,x Lo Bowe,x D. Mclntire,x Dept. Ob/Gyn, Univ. ~-~
Southwestern Med. Ctr.o DaLLas, TX O~JECTIV~: Estimate the gestationaL age (GA) at which fetuses at extremes of birthweight distribution diverge from average growth. STUgY DESI611: 6158 sonographic exams on 4587 singleton pregnancies were Linked to a cog~puter database of delivery information. The 10th and 90th percentiles of Brenner’s birthweight distribution were used to identify babies as smart (SGA), approprfate (AGA), or Large (LGA) for gestatfonal age. Regression lines for the means of estimated fetal weight (EFt)
for the three groups were plotted against the GA at sonography to estimate the point of divergent growth, RESULIS:
G at time of eono
The earliest GA at which the means are statistically different is 24 weeks. (~O#CLUSIOR: The rg~an sonographic estimates of fetal weight of Large and small neonates begin to diverge from average by ¯ idpregnancy. Abnormst fetal growth does not appear to be soLeLy a third trimester phenomenon: The threshold for statistically significant separation is a bioLogicaLLy iuptausibte starting Doint of divergent growth.
320 ASSESSMENT OF RISK OF ANEUPLOIDY USING THE 4 CHAMBER VIEW IN FETUSES WITH CHOROID PLEXUS CYST. R. Bahado-Singh, I. Goldstcin*, T. O’Connora, M. Mahoney, A. Baumgartcn~, C. IOeinmanx, J. CopcL Yale Univ, Dept. Ob/Gyn, New Haven, CT. OBJECTIVE: To ascertain the value o f 4 chamber cardiac view scrcaning
(4-CO) and ultrasound biomvtry in predicting the chromosomally normal fetus among those with ohoroid plexus cyst (CPC). STUDY DESIGN: A total of 134 fetuses with CPC on ultrasound wcr¢ evaluated with 4-CV and biomotry incindlng observed to expected (O/E) humerus (HL), femur lengths and transcembdlar diameter (TCD). Karyotypes wcro obtained in 85 oases.
RESULTS: Of 85 cases karyotyped, 3 had Trisomy 18 and one Tfisomy
21. A.11 four trisomi¢ fetuses had bihtcral CPC. Three had cysts < 10 mm and uric had unilocuhr cysts. Tlmm of the 4 eases had abaormal 4 CV.
Regarding ultrasound su’uctond anatomy, one Trisomy 18 was aormal on sonogram except for the preaenc¢ of the cysts. Among the 3 with abnormal 4-CV, one each had "mildly prominent" renal pelves, a two vessol cord and the third had no other abnormal anatomic finding. For normal 4-CV, spot. 97.3, NPV 98~ PPV 60.0, sens. 75 were found. Risk
of aneuploidy for normal vs abnormal 4-CV was 1/74 vs 3/5 p= 0.0005, RR 0.023 (CI 0.003-0.183). With all three parameters normal (4CV, O/E
HL > 0.89, O/E TCD > 0.92) sf~c. was 92.96, NPV 100, PPV 44.44 and sons. 100. Risk of aneuploidy with all values normal was 0/66 vs 4/9 if any of the semenlng values was abnormal; p= 0.0001 R.R. 0.017 (CI 0.001-0.285). CONCLUSION: Combined normal 4-CV, TCD, and HL vary accuratoly predicted the fetuses with CPC that had normal chromosomes. The rclativo
risk of Trisomy 18 or 21 with normal screening was sharply reduced compared to those with abnormal values. This knowledge permits moro
effective utilization of invasiv¢ prcnstal diagnosis in fetuses with CPC.
319 LEFT CARDIAC ~ DEVIATION: A MARKER FOR FETAL
ANOMALIES. R Smith, CH Comstock, JS Kirk, W Lee. William
Beaumont Hospital, Royal Oak, MI.
OBJECTIVE: To determine ff a relationship exists between left cardiac
axis deviation and abnormal fetuses.
STUDY DESIGN: Of more than 10,000 scans per year a four and five-
chamber view of the heart was attempted on all fetuses 14 weeks
gestation or more. A four-chamber view including determination of
heart axis was obtained from all fetal ultrasound scans at 17 or more
weeks gestation between 1987 to 1993. Those with heart axes greater
than 65 degrees to the left were considered to have left axis deviation.
The normal range of heart axis from 25 to 65 degrees was prevlonsly
established at our institution.1 Only cases with complete ultrasound
examinations and post delivery follow up were included.
RESULTS: 30 fetuses had left cardiac axis deviation. Of these, 8 were
normal and 22 had anomalies (positive predictive value = 73%).
Anomalies included; isolated cardiac defects (8/22), cardiac defects
~nth associated anomalies (7/22), other anomalies (5/22), and
abnormal karyotype (2/22).
CONCLUSION: Our findings suggest that left axis deviation can occur
as an isolated sonographic finding in an otherwise normal fetus.
However, a substantial number of cases will also demonstrate
additional sonographic findings especially involving the heart itself.
Occasionally, this observation will be associated with an abnormal
karyotype. The four-chamber view of the heart is an excellent
screening tool for fetal cardiac axis evaluation. If left axis deviation
is identified, we recommend a detailed ultrasound survey of the fetus.
1Comstock CH. Normal fetal heart axis and position. Obstet Gynecol
70:2, 1987.
321 THE ACCURACY AND POOR PROGNOSIS OF PRENATAL
IDENTIFICATION OF ATRIOVENTRICULAR SEPTAL DEFECTS.
CH Comstock, TW Riggsx, E Weinhousex, JS Kirk, W Lee, Divs of Fetal
Imaging and Pediatric Cardiology, William Beaumont Hospital, Royal
Oak, MI OBJECTIVE: To determine the accuracy of prenatal detection of
atrioventricular sepml defect (endocardial cushion defect) in a
predominantly screening population.
STUDY DESIGN: The study period included all scans performed over
three years at 14 wks and above. Screening exams required at least a
four-chamber view in fetuses 17 wks or more. A five-chamber view was
attempted in every fetus. The diagnosis of an atrioventficular septal
defect (AVSD) was made if part or all of the septum primum was absent
(with or without an accompanying VSD).
RESULTS: Prenatal diagnosis of AVSD occurred in 34 of 20,000 cases
(0.12%) cases; two AVSDs were found only after delivery. On prenatal
scan all 34 fetuses had absence of mitrai tricuspid valve offset and of
the septum primum. The median age at diagnosis was 18 wks. Good
outcomes occurred in 4 cases (12%). For predicting confirmed AVSD,
the sensitivity = 87.5%; specificity = 99.97%; + predictive value =
67%; negative predictive value = 99.99%. For predicting overall
congenital heart disease the PPV of prenatal AVSD was 95%. Abnormal
karyotypes occurred in 63%; trisomies 21 (41%), 18 (12%), and 13
(3%). Cases with poor outcomes and normal karyotypes included
Srmth-Lerali-Opitz (2), asplenia, chondrodystrophy, Ellis-van Creveld,
Dandy-Walker, and hydrocephalus; this is in contrast to a previous series
of referred cases in which the fetuses with normal karyotype~ almost all
had asplenia. Factors causing false positive diagnosis included persistent
left superior vena cava with a dilated coronary sinus which obscured the
septum primum (3), a VSD with abnormal mitral and tricuspid valves
(1), and VSDs in IUGR fetuses (3).
CONCLUSIONS: Prenatal diagnosis of AVSD can be accurate and highly
predictive of heart disease.
Volume 170, Number I, Part 2 SPO Abstracts 365 Am.] Obstet Gynecol
322 THE USE OF TRANSPERINEAL SONOGRAPHY TO EVALUATE THE CERVIX. S. Richey, K. Ramin, S. Cox, S. Ramin, D. Twicklerx. Dept Ob/Gyn, Univ. of TX Southwestern Mad. Ctr., Dallas, TX OBJECTIVE: We sought to determine if transperineal sonography compared with digital cervical examination in women presenting to the Labor Suite complaining of uterine contractions. METBODS: Parturients in the third trimester (n=100) were examined by one author with a General Electric Advantage 3200 ultrasound unit using a 5 mHz curvilinear transducer applied to the perineum. Ir~nediately following the study, another author performed a cervical examination, blinded to the results of the sonography. Cervical dilatation, length, and station were assessed. Results were analyzed using an Epistat statistical package. RESULTS:
MEAN ~ SEM Gestati~[ Age 37.5 .36 Dilation
Digital 2.4 .18 Transperineal 2.4 .20
Cervical Length Digital 2.04 .12
Transperineal 1,86 .11
Corrected Station Digital -1.92 .10 Transperineat -1.83 .09
Correlation Pearson’s Xapl~ Dilatation 0.87* 0.54* Cervical Length 0.80" 0.46* Corrected Station 0.69* 0.47*
* p < 0.00001
CONCLUSIONS: There is a clinically significant correlation between the diglta[ cervical examination and the sonographic assessment of cervical dilatation, length, and station. The transperineal sonographic techmque may be useful in evaluating the cervix in women in whom a digital examination is contraindicated, i.e., preterm rupture of membranes, vaginal bleeding, and placenta previa.
324 ACCURACY OF ULTRASONIC TECHNIQUES FOR THE
EVALUATION OF AMN1OTIC FLUID VOLUME IN TWINS. E F.
Magann, M.L. MortonX, S.P. Chauhan, J N Martin, Jr., N S. Whitworth,
J C. Morrisoa Dept. Ob/Gyn, Univ of Mississlppt Medical Center,
Jackson, MS.
OBJECTIVE: To determine the accuracy of ultrasonic techniques for the
evaluation of amniotie fluid volume in twin gestations.
STUDY DESIGN: This prospective, randomized study assessed the
amniotic fluid volume m 30 diamniotic twin pregnancies between 27 and 38
weeks’gestation The amniotic volume was evaluated by sonography usmg
the amniotic fired index (AFI) techmque of Phelan and Rutherford and the
2-diameter technique (2-D pocket) of Magann and Morrison The true
ammonc fluid volume (AFV) was determined by amniocentesis of each
ammotm sac followed by instillation of dye in the same manner as the dye
diluuon technique described by Charles and Jaeoby.
RESULTS: Use of the AFI and 2-D pocket techmques by the investigators
facditated correct determination of the total AFV between 500 - 2000 ml
in 16/21 (76.2%) and 17/21 (81%) of twin pregnancws, respectively (p =
ns). When the AFV was < 500 ml or > 2000 ml apphcatmn of the Alal
and 2-D pocket techniques were assomated with correct pred:ctmn of the
AFV in only 1/9 (11%) and 2/9 (22%) patients respectively (p = ns) AFV
assessments of each ammotm sac was accurate using e~ther the AFI or 2-D
pocket when true AFVs were 500 - 2000 ml, (100% and 83%) but when
AFVs were < 500 ml or > 2000 ml the AFI technique perm:tted correct
assessment in 7/29 (24%) and the 2-D pocket 13/29 (45%) (p < 0 09)
CONCLUSIONS: Use of currently avadable ultrasonic techniques to
assess AFV can be used successfully in twin pregnancies when the AFV
ranges between 500 - 2000 ml. However, use of either the AFI or 2-D
pocket by the ultrasonographer do not permit accurate assessment of tw:n
gestations complicated by AFV < 500 ml or > 2000 mi when these
figures equal the total amniotlc fluid volume or the volume of each ammotm
sac,
323 FETAL CARDIAC ASSESSMENT DECREASES THE NEED FOR INVASIVE PROCEDURES IN ISO~UNIZED PREGNANCIES.
~, G.R. Devoce, D.E. Carlson, J. Horenstein, A A.Nuhaglux, J. Platt. Dept. of Ob/Gyn., University of Southern California
School of Medicine, Los Angeles, CA. OBJECTIVE: Fetal pericardlal effumon (PE) precedes ascites (AS), skin edema (SK) and hydrops m isoimmunized pregnancies. We describe our experaence using nitrasound to assess (SK), (AS), and presence of perieardial effuston. The primary goal of this npprnach is to decrease the use of invasive diagnostic procedures (amniocenteals (AMN) and percutaneoua umbilical blood sampling (PUBS)) and optimize the timing of intrautenne transfusmn (IUT) or delivery (DEL) while maintaimng perinatal outcome. STUDY DESIGN: In a preliminary analysis of 100 randomly selected patients wlth iso~mmunization, we report the outcome of fetuses w:th normal ultcasounda contrasted with those with PE. Patients presenting with antibodies (confirmed in our labecatery) commonly causing hemolytic disease of the newborn were regularly evaluated with nitcasound including assessment for the presence of PE Frequency and type of examinabons were individualized. Factors considered were antibody blood group type, antibody t~ter, pahent~ past history of sensitization, results ot prior ultrasounds, gestatloual age, and the physician managing the patient (Authors 1,2,3,4,7) AMN was done for lung maturity. PUBS/IUT or DEL were done for the presence of PE. Descripbve statmtics and comparison of outcomes were performed for patients with and without PE. RESULTS: 60 (#) patients had an anti D t~ter, (1) C, (9) E, (2) c, (7) comblnabons w~th D, (13) other combinations and (8) Kell Median final bier and range is 8 and 1,256. 92 patients had no ewdence of AS SK or PE on ultrasoundor at delivery. 4 of these patients had initial hematsorit < 30% (22, 26, 26, 28) and 16 required one or more exchange transfusions. There were not antepartum or neonatal deaths in this group. No AMNs for OD 450 were performed except in conjunction with genetic or lung maturity Indications. One PUB was performed for blood type. GA @ DEL (37.3) with std (5.1) B~rthweight (3110) std (670). 8 patients had PE (one case PE and SK and one case of hydropa with PE, SK& AS). The fetus with hydrops expired at 18 weeks without intervention. There were no other antepartum or neonatal deaths. 3 patients had one or more successful PUIMIUTa, one PUB was unsuccessful and early DEL performed. 3 additional cases had early DEL without procedures. 3 of 7 patients required one or more exchange transfusions. GA @ DEL (34) aid (3.7). Birthweight (2618) std (865). CONCLUSIONS: We conclude that using nitrasound to assess presence of fetal pericardial efftuaon in isoimmunized pregnancies identified a group of patmnts which can safely be followed without invasive procedures. Our management approach has eliminated the use of amniocentosis for OD 450 and allows a l’Agh percentage of simultaneous initial PUB/IUTs
325 USING GESTATIONAL AGE INSENSITIVE PARAMETERS TO IDENTIFY THE LARGE FOR GESTATIONAL AGE (LGA) FETUS.Joseph M. Miller,Jr.,Fidelma B. Riqby, L.S.U. Medical Center, New Orleans, LA. OBJECTIVE:Third trimester fetal abdominal circumference (AC) and growth rate were compared to the femur length/abdominal circumference (FL/AC) ratio in assessing excessive fetal size in diabetic and nondiabetic patients. STUDY DESIGN:Ultrasounds were done after 31 weeks in 82 diabetic and 81 nondiabetic patients on 2 or more occasions at least 2 weeks apart. Initial and final scans were used. Birthwe~ght tables of Brenner defined LGA (> 90%). RESULTS:The abdominal circumference growth rate was greater zn LGA than nonLGA diabetic fetuses (1.03 vs.0,86 cm/wk, p<.000l), while nondiabetlc pregnancies did not follow thls pattern (0.89 vs 0.86 cm/wk,p=ns). With a threshold of 1.2 cm/wk for AC growth rate, sensitivity of 57%, PPV of 80%, NPV of 73% and speclflcity of 89% were obtained for LGA diabetics(p<.0001).For LGA non diabetics, sensitivity of 41%, PPV of 41%,NPV of 86% and specificity of 85% were obtained(p=.034). Using the FL/AC ratio obtained closest to term, values of sensitivity 83%,PPV 83%,NPV 87% and specificity 87%(p<.0001) were noted for LGA diabetics and sensitivity 87%,PPV 89%, specificity 56% and NPV 52%(p<.0001) were obtained for nond~abetic LGA fetuses. CONCLUSION:Accelerated fetal AC growth is present in diabetic LGA fetuses. Both FL/AC and AC growth appear to work better in diabetic pregnancies. FL/AC may be superior to the AC growth in diabetlcs.
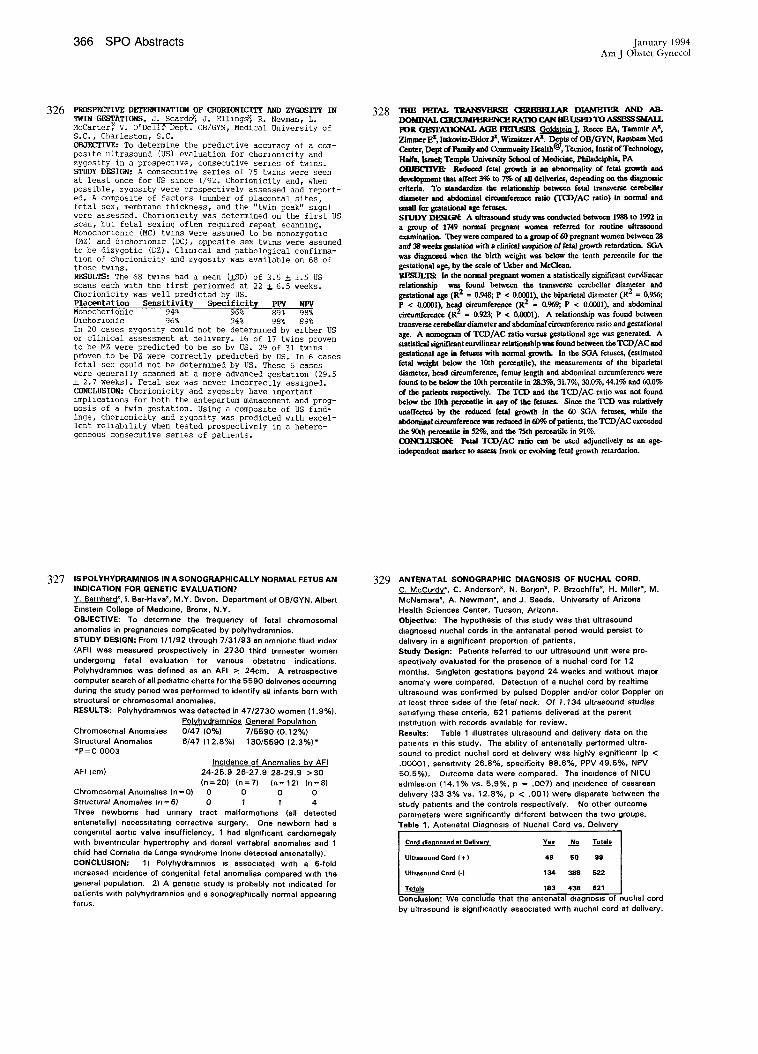
366 SPO Abstracts January 1994
Arn J Obstet Gynecol
326 P~os~c~iv~ Db’f~INATIO~ OF C~ORIONICIT~ A~D ZYGOSITY IN TWIN GESTATIONS. J. Scardo~, J. Elllngsx, R. Newman, L. McCarter~ V. O’Dell~ Dept. OB/GYN, Medical University of S.C., Charleston, S.C. OBJECTIVE: To determine the predictive accuracy of a com- posite ultrasound (US) evaluation for chorlonlcity and zygosity in a prospective, consecutive series of twins. STUDY DESIGn: A consecutive series of 75 twzns were seen at least once for US slnce 1/92. Chorionicity and, when possible, zygoszty were prospectively assessed and report- ed. A composlte of factors (number of placental sites, fetal sex, membrane thickness, and the "twin peak" slgn) were assessed. Chorlonlclty was determined on the first US scan, but fetal sexing often required repeat scannlng. Monochorlonlc (MC) twins were assumed to be monozygotlc (MZ) and dlchorlonlc (DC), opposite sex twins were assumed to be dizygotic (DZ). CllnlCal and pathological confirma- tion of chorionicity and zygoslty was available on 68 of these twlns. RESULTS: The 68 twzns had a mean (~SD) of 3.5 ~ 1.5 US scans each with the first performed at 22 ~ 6.5 weeks. Chorioniclty was well predicted by US. Placentation Sensitivity Specificity PPV NPV Monochorionic 94% 96% 89% 98% Dichorlonic 96% 94% 98% 89% In 20 cases zygoslty could not be determlned by ezther US or clinical assessment at delivery. 16 of 17 twins proven to be MZ were predicted to be so by US. 29 of 31 twins proven to be DZ were correctly predlcted by US. In 6 cases fetal sex could not be determlned by US. These 6 cases were generally scanned at a more advanced gestatzon (29.5 ~ 2.7 weeks). Fetal sex was never incorrectly assigned. CONCLUSIOn: Chorionicity and zygoslty have important lmpl~catzons for both the antepartum management and prog- nosis of a twin gestation. Using a composite of US flnd- ings, chorlonicity and zygosity was predicted w~th excel- lent relleblllty when tested prospectively in a hetero- geneous consecutive series of patlents.
328
327 IS POLYHYDRAMNIOS IN A SONOGRAPHICALLY NORMAL FETUS AN INDICATION FOR GENETIC EVALUATION?
Y. Bernhardx I. Bar-Havex, M.Y. D~von. Department of OB/GYN, Albert
Einstein College of Medicine, Bronx, N.Y. OBJECTIVE: To determine the frequency of fetal chromosomal
anomalies in pregnancies complicated by polyhydramnios.
STUDY DESIGN: From 1/1/92 through 7/31/93 an am nioUc fluid index
(AFI) was measured prospectively in 2730 third trimester women
undergoing fetal evaluauon for vamous obstetmc indications.
Polyhydramn~os was defined as an AFI ~ 24cm. A retrospscUve
computer search of all pediatric charts for the 5590 deliveries occurring
during the study pemod was performed to identify all infants born with
structural or chromosomal anomalies. RESULTS: Polyhydrammlos was detected in 47/2730 women (1.9%).
Polvhvdramnios General Population
Chromosomal Anomalies 0/47 (0%) 7/5590 (0.12%) Structural Anomalies 6/47 (12.8%) 130/5590 (2.3%)* *P=0 0003
Incidence of Anomalies by AFI
AFI (cm) 24-25,9 26-27.9 28-29.9 >30
(n=20) (n=7) (n=12) (n=8) Chromosomal Anomahes (n=0) 0 0 0 0 Structural Anomalies (n = 6) 0 1 I 4 Three newborns had urinary tract malformaUons (all detected antenatally) necessitating corrective surgery. One newborn had a
congenital aortic valve insufficiency, 1 had significant cardlomegaly
with bwentrlcular hypertrophy and dorsal vertebral anomahes and 1 chdd had Corneha de Lange syndrome (none detected antenatsllyL
CONCLUSION: 1) Polyhydremnms IS associated with a 6-fold
increased incidence of congenital fetal anomalies compared w~th the
general population. 2) A genetic study is probably not indicated for
patients w~th polyhydrsmnios and a sonographmally normal appearing
fetus.
329 ANTENATAL SONOGRAPHIC DIAGNOSIS OF NUCHAL CORD. C. McCurdy*, C. Andersonx, N. Borjonx, P. Brzechffa*, H. Mdler~, M.
McNamara*, A. Newmanx, and J. Seeds. Univers=ty of Arizona
Health Sciences Center, Tucson, Arizona.
Objective: The hypothesis of this study was that ultrasound
diagnosed nuchal cords in the antenatal period would persist to
dehvery in a mgeiflcaet proporUon of patients.
Study Design: Patients referred to our ultrasound unit were pro-
spectively evaluated for the presence of a nuchal cord for 12
months. S~ngleton gestations beyond 24 weeks and without major
anomaty were compared. Detection of a nuchal cord by realtime
ultrasound was conf~rmed by pulsed Doppler and/or color Doppler on
at least three sides of the fetal neck. Of 1,134 ultrasound studies satisfying these criteria, 621 patients delivered at the parent
institution with records available for review.
Results: Table 1 illustrates ultrasound and delivery data on the
patmnts in this study. The ability of antenatally performed ultra-
sound to predict nuchal cord at delivery was highly significant (p <
.00001, sensitivity 26.8%, specificity 88.6%, PPV 49.5%, NPV
50,5%). Outcome data were compared. The incidence of NICU
admission (14.1% vs. 5.9%, p = .O07) and incidence of cesarean
delivery (33 3% vs. 12,8%, p < .001) were disparate between the
study patients and the controls respectively, No other outcome
parameters were significantly different between the two groups.
Table 1. Antenatal Diagnos~s of Nuchal Cord vs. Dehvery
Cord diagnosed at Delivery Yes No Totals
Ultrasound Cord I +) 49 SO 99
Ultrasound Con:l (-) 134 388 522
Totals 183 438 621
Conclusion: We conclude that the antenatal dlagnos~s of nuchal cord
by ultrasound is significantly assocmted w~th nuchal cord at delivery.
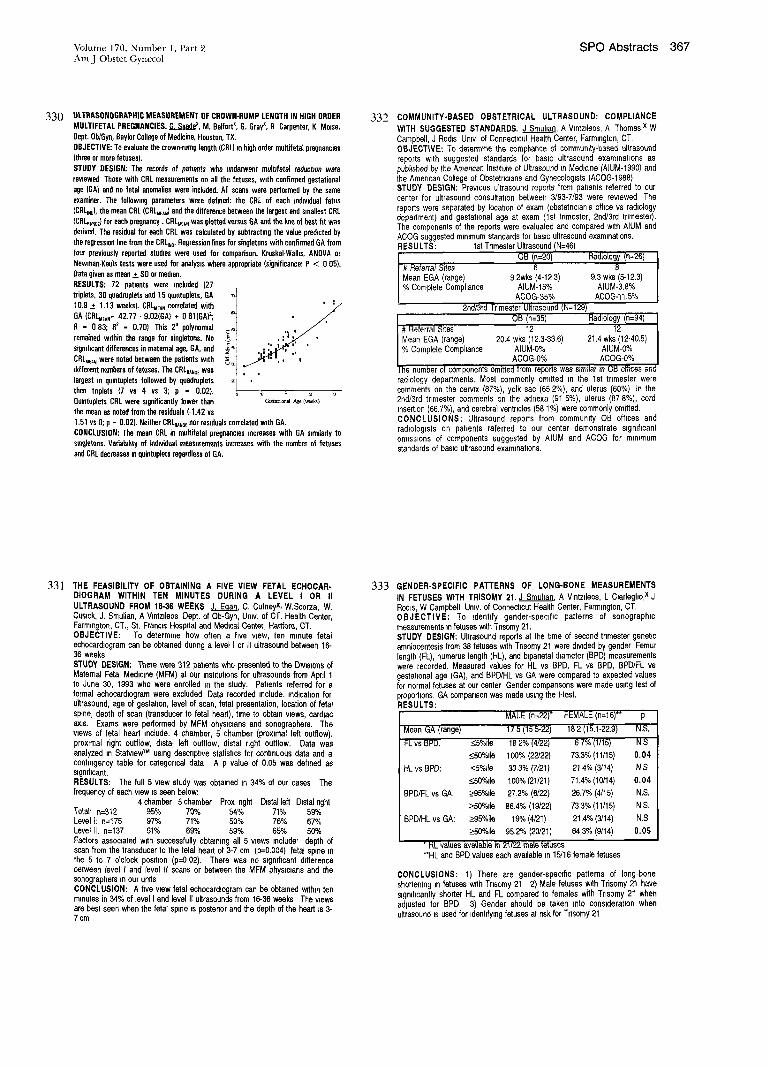
Volume 170, Number 1, Part 2 SPO Abstracts 367 Am J Obstet Gynecol
330 ULTRASONOGRAPHIC MEASUREMENT OF CROWN-RUMP LENGTH IN HIGH ORDER MULTIFETAL PREGNANCIES. G. Saadex, M. Belfortx, G. Grayx, R Carpenter, K Melee.
Dept. Ob/Gyn, 8aylor College of Medicine, Houston, TX.
OBJECTIVE: To evaluate the crown-rump length (CBL~ m high order multifetat pregnaecins
(three or mere fetuses).
STUDY DESIGN: T~ records of patmnts who underwent mult#etal reductmn were
reviewed Those with CRL measurements on all the fetuses, with confirmed gestatienal
age IGA) and no fetal anomalies were incinded. All scans were performed by the same
examiner. The following parameters were defined: the CRL of each individual fetus
(CRL~No), the mean CRL (CRLMEA,) and the difference between the largest and smallest CRL
(CRL~,~d for each pregnancy, CRLw~, was plotted versus GA and the hue of best fit was
derived. The residual for each CRL was calculated by subtracting the value predicted by
the regression line from the CRLIzo. Regression lines for singletons with confirmed GA from
four previously reported studies were used for comparison. KruskaI-Walhs, ANOVA or
Newman-Keuis tests were used for analysis where appropriate (significance: P < 0 05).
Data given as mean _+ SD or median.
RESULTS: 72 patients were included (27
triplets, 30 quadruplets and 15 qumtup[ets, GA
10.9 ± 1.13 weeks). CRLMrAN correlated with
GA (CRLMEAN- 42.77 " 9.02(GA) + 0 81(9A)2;
R - 0 83; R2 - 0.70) This 2o polynomial
remained within the range for singletons. No
significant differences in maternal age, GA, and
CRLMEAN were noted between the patients with
different numbers of fetuses. The CRLRANGE was
largest in quintuplets followed by quadruplets
then triplets {7 vs 4 vs 3; p - 0.02).
Quintuplets CRL were significantly lower than
the mean as noted from the residuals (-1.42 vs
1.51 vs O; p - 0.02). Neither CRLa~NGe nor residuals correlated with GA.
CONCLUSION: The mean CRL in multifetal pregnancies increases with GA simdarly to
smgletoes. Vsriainhty of indwidual measurements increases with the number of fetuses
and CRL decreases in quintuplets regardless of 6A.
332 COMMUNITY-BASED OBSTETRICAL ULTRASOUND: COMPLIANCE
WITH SUGGESTED STANDARDS. J Smul~an, A V~ntzdeos, A Thomas,x W Campbell, J Rod=s Un=v of Connecticut Health Center, Farmlngton, CT. OBJECTIVE: To determine the comphance of commumty-based ultrasound reports with suggested standards for basic ultrasound examinations as published by the Amencan Institute of Ultrasound In Medicine (ALUM-1990) and the American College of Obstetnc~ans and Gynecologists (AC09-1988) STUDY DESIGN: Prewous ultrasound reports from patzents referred to our center for ultrasound consultation between 3/93-7/93 were rewewed The reports were separated by location of exam (obstetnclan’s office vs rad=ology department) and gestat~onal age at exam (1st trimester, 2ndJ3rd tnmester). The components of the reports were evaluated and compared wrth AlUM and ACOG suggested m~mmum standards for basic ultrasound examinations. R ES U LTS: 1st Tnmester Ultrasound (N=46)
f OB (n=20) Radiology (n=26) # Referral Sites 6 8
|Mean EGA (range) 9 2wks (4-12 3) 9.3 wks (5-12.3) % Complete Compliance ALUM-15% ALUM-3.8%
AC09-35% AC09-11.5% 2nd/3rd I-rimester Ultrasound (N=129)
OB (n=35) Radiology (n=94) J # Referral Sites 12 12
I Mean EGA (range) 20.4 wks (12.3-33.6) 21.4 wks (12-40.5) % Complete Compliance AlUM-O% AlUM-O%
ACOG-0% ACOG-0% [he number of componenis omitted from reports was simi}ar in OB olt~cas and radiology departments. Most commonly omitted =n the 1st trimester were comments on the cervix (87%), yolk sac (65 2%), and uterus (60%) In the 2nd/3rd trimester comments on the adnexa (91 5%), uterus (87 8%), cord ~nsert~on (66.7%), and cerebral ventricles (581%) were commonly omitted. CONCLUSIONS: Ultrasound reports from community OB offices and radiologists on patients referred to our center demonstrate s~gmhcant omissions of components suggested by AlUM and ACOG for minimum standards of basic ultrasound examinations.
331 THE FEASIBILITY OF OBTAINING A FIVE VIEW FETAL ECHOCAR- DIOGRAM WITHIN TEN MINUTES DURING A LEVEL I OR II ULTRASOUND FROM 16-36 WEEKS J. Egqn, C. Cutneyx, W.Scorza, W, Cus~ck, J. Smulian, A V~ntzlteos Dept. of Ob-Gyn, Umv. of CT. Health Center, Farmmgton, CT., St. Franc~s Hosprtal and Med~.a~ Center, Hartford, CT. OBJECTIVE: To determine how often a five view, ten minute fetal echocardlogram can be obtained dunng a level I or ]1 ultrasound between 16- 36 weeks. STUDY DESIGN: There were 312 patients who presented to the D~v~s~ons of Maternal Fetal Medicine (MFM) at our inst=tut~ons for ultrasounds from April 1 to June 30, 1993 who were enrolled In the study. Patients referred for a formal echocardlogram were excluded Data recorded include, rod]cation for ultrasound, age of gestation, level of scan, fetal presentation, location of fetal spine, depth of scan (transducer to fetal heart), time to obtain views, cardiac ax~s. Exams were performed by MFM physicians and sonographers. The views of fetal heart include. 4 chamber, 5 chamber (proximal left outflow), proxtmal right outflow, d~stal left outflow, distal right outflow. Data was analyzed in StatwewTM using descriptive statistics for continuous data and a contingency table for categorical data A p value of 0.05 was defined as sNmhcant. RESULTS: The full 5 view study was obtained in 34% of our cases The frequency of each wew is seen below:
4 chamber 5 chamber Prox nght Distal left Distal right Total’ n=312 95% 70% 54% 71% 59’/o Level I: n=175 97% 71% 50% 76% 67% Level I1. n=137 91% 69% 59% 65% 50% Factors associated wdh successfully obtamng all 5 wews Include’ depth of scan from the transducer to the fetal heart of 3-7 cm (p=O.O04), fetaJ spne ~n the 5 to 7 o’clock pos~hon (p--O 02). There was no s~gmficant d~fference between level I and fever it scans or between the MFM phys~cmns and the sonographers ~n our units CONCLUSION: A five wew fetal echocard~ogram can be obtained within ten minutes in 34% of level I and level II ultrasounds from 16-36 weeks The wews are best seen when the fetal spne ~s posterior and the depth of the heart =s 3- 7 cm
333 GENDER-SPECIFIC PATTERNS OF LONG-BONE MEASUREMENTS IN FETUSES WITH TRISOMY 21. J Smultan, A Vmtzfleos, L C=arlegbo,x J Rod~s, W Campbell. Umv. of Connecticut Health Center, Farmmgton, CT. OBJECTIVE: To ~dentffy gender-specific patterns of sonograph~c measurements m fetuses w~th Tnsomy 21. STUDY DESIGN: Ultrasound reports at the t~me of second tnmester genetic amniocentesis from 38 fetuses wdh Tnsomy 21 were d~wded by gender Femur length (FL), humerus length (HL), and b~parletal diameter (BPD) measurements were recorded. Measured values for HL vs BPD, FL vs BPD, BPD/FL vs gestatlonal age (GA), and BPD/HL vs GA were compared to expected values for normal fetuses at our center Gender comparisons were made using test of proportions. GA comparison was made using the t-tast. RESULTS:
MALE (n=22)" FEMALE(nil6)** p
Mean GA (range) 17 5 (15 5-22) 18 2 (1’~.1-22.9) N.S.
FL vs BPD. <5%ile 18 2% (4/22) 6 7% (1/15) N S
_<50%de 100% (22/22) 73.3% (11/15) 0.04
HL vs BPD: _<5%11e 33 3% {7/21) 21 4% (3/14) N,S
_<50%de 100% (21/21) 71.4% (10/14) 0.04
BPD/FL vs GA: _>95%de 27.2% (6/22) 26.7% (4/15) N,S.
_>50%de 86.4% (19/22) 73 3% (11/15) N S,
BPD/HL vs GA: >95%ile 19% (4/21) 21.4% (3/14) N.S,
>50%de 95.2% (20/21) 64,3% (9/14) 0.05
* HL values available in 21/22 man fetuses **HL and BPD values each avadable in 15/16 female fetuses
CONCLUSIONS: 1) There are gender-specific patterns of long-bone sho~ening m f~uses w~th Tnsomy 21 2) Male fetuses wdh Trisomy 21 have s~gmf=canlly shorter HL and FL compared to females with Tnsomy 21 when adlusted for BPD 3) Gender should be taken into consideration when ultrasound =s used for ~dent~lng fetuses at nsk for Tnsomy 21

368 SPO Abstracts January 1994 Am J Obstet Gynecol
334 LONGITUDINAL FETAL GROWTH IN PROLONGED PRETERM PREMATURE RUPTURE OF MEMBRANES. E Miller×, W Cuslck, A V~ntzdeos, Umv of Connecticut Health Center, Farmmgton, CT. OBJECTIVE: Assess fetal Iong=tud~nal growth m pregnanc=es comphcated by prolonged preterm premature rupture of membranes (PPROM) STUDY DESIGN: Hospital records from 1/89 to 4/93 were reviewed and patients w~th PPROM were ~dent~fied. Hosp~tahzed pahents with s~ngleton pregnancies who underwent senal fetal b~ometry were ehg~ble for study. For each exam, an average estimated fetal weight (EFW) was calculated using Hadlock’s formulae (blpanetal d~ameter/abdommal mrcumference and femur length/abdominal c=rcumference), and plotted against gestatmnal age on institutionally derived normal fetal growth curves. RESULTS: A total of 71 ultrasounds from 23 patients were re- viewed. The mean number of exams/pt was 2.5 (range 2-6). The average menstrual age at the hme of exam was 27.7 weeks (range 15.4-35 4). The mean Interval between exams was 17 4 days (range 8-35). The mean average EFW was 1194 grams. When compared to inshtuhonally derived growth curves, 45% of exams fell above and 55% of exams fell be- low the mean. There ap- pears to be no d~fference ~n EFW growth curves be- tween hospltahzed pa- tients with PPROM and N normals from this instltu- hon {see figure). CONCLUSION: The long> tudmal growth of fetuses ~s unaffected by prolonged preterm premature rupture of membranes
Data points superimposed % LE on institutionally derived
ss
normal curves
i!~EAN
Gestational age (weeks)
336 YVHICH ULTRASOUND AND DOPPLER VARIABLES IN TYVIN
PREGNANCIES ARE MOST USEFUL TO PREDICT THE BIRTH
OF A SMALL FOR GESTATIONAL AGE (SGA) INFANT?
E Gazlano×, S Calvin, R Bendel, J Ney, K Pfleghaar, P Mills, B Assel,
L. Fa~rbanksx, D Brand¢, E Knox Abbott Northwestern Pennatal Center,
Mmneapohs, MN
OBJECTIVE: By multivariate analyses, determine the most m~portant
pre&ctor for SGA m twins.
STUDY DESIGN: Targeted ultrasound with anatomic survey, umbdlcal
artery (UA) Doppler veloc~metry, ammot~c flmd volume (AFV) assessment,
and b~ometry was performed for each twin ferns m 162 consecutive
pregnancies (1991-92) Excluding fetal deaths, 318 hveborn infants were
available for th~s study ARer birth, SGA was defined as a b~rth wmght of
<10th percentile for gestat~onal age Stahstmal methods used umvarmte (xz
and F~sher’s exact test) and multivariate (multiple logistic regression).
RESULTS: By umvanate analys~s, 4 of 9 ultrasound parameters were
correlated mgmficantly w~th SGA The birth of an SGA infant occurred m
only 3% of twin neonates w~th normal fetal ultrasound morphology
(N 270) compared to 35% w~th suspected growth retardahon or structural
abnormahtles (N-48) (P- 001) Those suspected by antenatal ultrasound of
growth retardation (N-24) had a 63% incidence of SGA (P-.001) The
presence of abnormal UA Doppler was also correlated w~th the bwth of an
SGA infant compared to those w~th normal Doppler (33% versus 6%)
(P- 001) Ohgohydrammos, polyhydrammos or cornbmat~ons o f AFV were
not statistically assocmted with the b~rth of an SGA infant Ultrasound
estimated fetal wmght (EFW) at <35th percentde was assocmted w~th a
60% versus 2% incidence of SGA at b~rth Stepw~se log~stlc regressmn
indicates that such fetuses are 59 t~mes more likely to be SGA at birth
compared to those at >35th percentde.
CONCLUSIONS: Ultrasound EFW at <35th percentde is the most
~mportant ultrasouud!Doppler predmtor for the b~rth of an SGA twin
335 FETAL GALLBLADDER GROWTH AND DEVELOPMENT
DURING GESTATION. L. Chan. BK Raox, YX JiangX,
B EndicottX, J CarterX, EA Reece. Departments of Ob/Gyn and Radiology, Jefferson Medical College, and Department of Ob/Gyn,
Temple University School of Medmme, Philadelphia PA. OBJECTIVE: Bile is formed after the 13th weeks of gestatton
(GA) and the fetal gallbladder (GB) ~s sonographically visible throughout the second and third trimester of pregnancy. A nomogram of the GB growth and development during gestation allows the assessment of GB abnormalities in utero. STUDY DESIGN: Normal GB ~n 193 fetuses between 15 to 40 weeks of GA were prospectively measured for length (L), anteroposterior (AP) and transverse (Tr) dimensions. GB volume
(V) was calculated usmg the prolate elhpsoid formula (0.5233 x L x AP x Tr) and the saDttal perimeter (P) was calculated using the
formula 1.57 x (L+AP). V/abdominal circumference (AC) ratio was determined. All measured data were expressed as mean +_ SEM in
mm, and V ~n mm3. RESULTS: GA N L AP T~ V V/AC P 15-20 49 8.9_+0.5 3.1_+0.1 3.7_+0.2 62_+6.4 05-+0.04 3 7_+06 20-25 37 15.8_+0 6 4 1-+0.2 5.7+0.2 206+20 1.1-+0.1 22.2_+0.7 2~-30 18 19.4+i.0 5.6_+0.4 7.5_+0.7 486_+92 2.0L-_0.3 28.2_+1 5 30-35 50 23.7_+0.8 5.7-+0.2 7.1_+0.3 557_+53 1.9+02 326-+1 1 3540 39 24.7-+1.0 5.5+03 7 1+_0.4 560-+66 1 8+_0.2 475_+1.7 CONCLUSIONS: 1) A hnear growth of the fetal GB L and P was
noted throughout gestation. 2) The AP, Tr, V, and V/AC measurements have a linear relationship to GA up to 30 weeks and plateau thereafter. 3) We established normalave dimensions of the fetal GB which will serve as a basis agmnst which abberrant growth can be evaluated prenatally.
337 THE IMPORTANCE OF BOWEL DILATATION AND ANTENATAL
TESTING IN FETUSES WITH GASTROSCHISIS A.KhouzamLx’ C, Paidas,~ K. ~lakemore, S. Sheth~, C. Gleason,~ N. Caftan, Depts
Gyn]Ob, Surgery, Radiology, & Pedmtncs, The Johns Hopkins University, Baltimore, MD.
OBJECTIVE: To determine whether the presence of bowel dilatation
(BD) in prenatal ultrasound and abnormal antenatal testing (AT) in
fetuses with gastroschlsls predicted poor perlnatal outcome
STUDY DESIGN; The prenatal and postnatal records of all 24 hveborn
infants with gastroschlsls from 1987-1993 were reviewed. Per=natal
morbidity (PM) was determined by b~rth location and mode of
delivery. In 15 of 19 prenatally diagnosed, degree of 8D and results
of AT were compared to PM. Fisher’s exact test was used for statistical analysis.
RESULTS: The mean gestat=onal age at diagnosis was 21.9 weeks
(SD 6 6), and at delivery 37 weeks (SD 1 7). All karyotypes
performed (11/24) were normal. Of 24 infants, 19 were ~nborn and
5 outborn with 12 vaginal deliveries and 12 cesarean sections (7 for
fetal distress, 1 failure to progress, 1 breech, 3 elective). Twenty-
three newborns had good surgical outcomes; there was one
postoperative death. Prenatal ultrasound data were available on 15
of 19 reborn fetuses. BD (> 1,8 cm) was noted m 11 end absent =n
4. The presence of BD did not pred=ct PM measured by fetal distress
m labor, days m the hospital, days to feed, and primary vs staged
closure. Thirteen of 19 reborn fetuses had AT performed; 4 of the
13 had abnormal AT and all 4 had mtrapartum fetal distress vs 2 of
9 w~th normal AT. When results of AT were compared to PM, fetal
distress in labor was the only mgmfmant assocmt=on (p=O.021). No
s=gniflcant d~fference in PM was found for reborn vs outborn infants
nor in those delivered by cesarean section vs vaginal delivery. CONCLUSIONS: Outcomes were good In the major=ty of infants with
gastroscNsis. The presence of BD d=d not predict PM, however, AT
was valuable m predicting intrapartum fetal distress and should be
part of the management of fetuses with gastroschlsls.

Volume 170, Number 1, Part 2 SPO Abstracts 369 Am J Obstet Gynecol
338 SEVERE OLIGOIIYDRAMNIOS WITH INTACT MEMBRANES:
AN INDICATION FOR DIAGNOSTIC AMNIO1NFUSION. P~G
_Pr~dex, M Lauriax, L Llttmanx, M Hallak, MP Johnson, SF Bottoms.
Dept. of OblGyn, Hutzel Hospltal/Wayne State University, Detroit, MI.
OBJECTIVE: To determine ~f increased identification of associated
anomalies warrants amnioinfusion in cases of severe oligohydramnms
secondary to urinary tract malformation or of unknown etiology.
STUDY DESIGN: We reviewed 17 consecutive pregnancies having
diagnostic amnioinfusion during evaluation for severe oligohydrammos,
excludingprematureruptureofthemembranes. Standardized ultrasound
examination classified 21 fetal structures as normal, abnormal, or
suboptimally visualizx’zt The finn post-infusion ultrasound report was
compared to a blinded review of pre-infusion videotapes
RESULTS: A mean of 238 ml of balanced salt solution was infused at
15-27 weeks of gestation The mean percent of organs adequately
visuahzed increased from 51% before infusion to 77% after infusion (p
< 0 0001). Brain, k~dneys, and bladder were tyDealIy visualized well
despite oligohydrammos. V~sualizahon of the umbilical cord, ventral
wall, face, spine, gemtalia, and extremities showed the greatest
improvement after amnioinfusion. Excluding abnormalities of the
urinary tract, identification of associated anomalies increased from
11 8 % to 31 3 % following d~agnostic ananioinfusion
CONCLUSION: Diagnostic amnioinfusmn significantly improves
visuali~’ation of fetal anatomy with severe oligohydramnios In cases of
severe oligohydramnios w~th intact membranes, there is a high frequency
of anomalies unrecognized without amnioinfusion. Since associated
anomalies markedly alter prognos~s a~d managemeot, we believe
amnioinfusion is indicated m those cases with inadequate visualization of
fetal anatomy.
340 EFFECT OF BLADDER VOLUME ON SONOGRAPHIC MEASUREMENT OF CERVICAL LENGTH
(~M Jackson, B Weintraub*, R Zottinger*, R Sohaey’, NK Kochenour Depts of Ob-Gyn & Radiology, University of Utah,Salt Lake City UT
The use of ultrasound for measuring cervical length ~s gaming popularity. However, measurement technique is not standardized. It is recogmzed that maternal bladder volume affects measured cerwcal length, but this effect has not been quantitated. Purpose: We sought to describe the changes in cervical length measurement due to changes m maternal bladder volume. Study Design: 20 pregnant women having a rouhne u~trasound exam between 16 and 28 weeks gestattonal age had thmr ~,~rvix measured transabdominally from internal os to external os, octh before and after voiding a measured volume of urine The change m cervical length was plotted against change in bladder volume (Vol). Results:
800T ¯ ¯ g
t * . ’* t..o, ¯ ° *
5 200~
¯ ° ° r= 63
-1 0 1 2 3 4
Length Change (cm)
Conclusion: Increasing bladder volume can increase measured cervical length. This is variable among pahents Standardization of the technique of transabdominal sonographic cerwcal measurement will be necessary before climca( data can be adequately interpreted.
339 INTRAPARTUM FETAL SUBCUTANEOUS TISSUE FEMUR LENGTH RATIO (FSCT/FL) A SONOGRAPHIC CLUE TO FETAL MACROSOMIA _J Santolaya,W Meyer, D Gauthler, D.Kahn*, V Ramakrishnan~, T Myles
Dept Ob/Gyn, Umv of ILL at Chicago OBJECTIVES fetal abdominal c~rcumferencc (AC) and esnmated fetal wmght
(EFW) are currently used for the prenatal dffferent~atmt~ of edequate (AGA) and large (LGA) fetuses Th~s study compares the lntrapartum accuracy of the AC, EFW and FSCT/FL rat~o for predlctmn of LGA fetuses STUDY DESIGN 173 normal fetases(group l)wereused~nacross-sectmnal manner to determme the normal changes of AC, FL and the FSCT/FL throughout pregnancy (FSCT me.~sured at the level of the femoral dtaphys~s) All these fetuses were dehvered at term and had approprmte wmght 101 addltlonal well dated fetuses had these same ultrasonographic measurements obtained within 24 hours of delivery (group 2). Neonatal wmght~ (NNW) of
group 2 were plotted on an approprmte nomogram and those > 90th cenule for age were designated as LGA The sensitivity and specificity for the predictmn of LGA was then calcolated using the prenatal AC > 90th ccotile, EFW (Hadlock 1984) > 90th cennle and, FSCT/FL raIm > than 2 S D. of normal RESULTS Group 1 GA 31.4 weeks +/- 5.4, range 17-41. Fetal bmmetric
parameters correlated w~th GA (FL= R-sq .89, AC= R-sq 79) FSCT also correlated w~th GA (R-sq 45, P< 000i) and wtth FL (R-sq .44, P< 0001) FSCT/FL rat~o was stable throughou’, pregnancy (R-sq (N). The mean FSCT/FL(mm) =0.06 +/- 0 01, Rangc= 0 03 0. I0). Group 2: GA 38 weeks
+/- 2 5, range 30-42 NNW (gin) was 3280 +/- 740; range 1513-4801. TABLE AGA LGA T-TEST SENS SPEC PPV NPV
N 82 19 G age 37 7 39 (N S ) NNW 3075 4165 (< O301) FL 71 0 73 (N S ) SCT 3 9 6 (< 0001) AC 328 371 (< 0001) 44% 98% 87% 89% PrdWght 3068 4029 (< 0001} 68% 85% 48% 93%
SCT/FL 005 0082 (< 0001} 82% 96% 82,% 94% CONCLUSIONS The tntrapartum determ~natmn of FSCT/FL ~s simple and,
the data suggests that ~t has a greater sens~nvittty than AC or EFW for making the dtffcrentml between AGA and LGA fetuses
341 CARDIAC AXIS: CORRELATION WFIH THE PRESENCE OF
SIGNIF|I~td~IT CONGENITAL HEAR] DISE/~SE. Lagrew DC, Randall Rx,
Steiger RM, Porto MP, Morgan MA, Umverslty of Cahforn=a, Irv~ne,
Orange, CA, Saddleback Memonal Medical Center, Laguna Hdls, CA
OBJECIWE: To evaluate the card=ac ax~s an =nd=cator of the antenatal
diagnosis of congenital heart disease (CHD)
STUDY DESIGN: Cardiac measurements were prospectively
determ=ned by echocard~ography ~n 148 normal fetuses to estabhsh
normal ax~s critena. The cardiac ax~s is the measured angle between
the mid antenor-posterior plane (spine to sternum) and the
~nterventncular septum at the four chamber cardiac view. An abnormal
cardiac ax~s was defined as <2 standard dewat~ons from the mean
card=ac axis in normal fetuses Fetuses w=th the antenatal diagnosis of
s=gmficant cardiac anomahes (n=35) had their card=ac axis
retrospechvely determ=ned. These ax=s were compared to the
estabhshed card=ac axis cntena.
RESULTS: The mean normal fetus cardiac axis was 45 + 8.7
degrees 23/35 (65 7%) fetuses with CHD had an abnormal axis. The
distribution of abhorrent ax~s "0aned by dlagnos~s: AV Canal (3/5},
Tetralogy of Fallot (3/3), Isolated ASD (0 1), Isolated VSD (4/4),
Rhabdomyoma (1/1), Hypoplast~c Left Heart (3/8), Double Outlet R~ght
Ventricle (2/5), Pulmonary Stenosis (1/2), Epstein’s Anomaly (2/2),
Dextrocard~a (4/4).
CONCLUSION: An abnormal cardiac ax~s ~s ~nd~cat~ve of a cardiac
anomaly and warrants detailed echocard~ography.
370 SPO Abstracts January 1994 Am J Obstet Gynecol
342 BORDERLINE ISOLATED MILD VENTRICULOMEGALY
IS ASSOCIATED WITH AN INCREASED INCIDENCE OF
CHROMOSOMAL ANOMALIES
M Tomlinson,x MC Treadwell, NB Roumayahx, SF Bottoms.
Wayne State University/Hutzel Hospital, Detroit, MI
OBJECTIVE: The incidence of abnormal chromosomes with
isolated mild ventriculomegaly is not well established, especially
in cases of borderline ventricular enlargement. We reviewed our
experience with patients having isolated mild ventriculomegaly to
determine the incidence of karyotypic abnormalities.
STUDY DESIGN: All patients evaluated from July 1992 to July
1993 with an atrial measurement between 10-15mm and no other
ultrasound anomalies were identified. Patients undergoing
karyotype evaluation were reviewed.
RESULTS: Seventeen patients with isolated mild
ventnculomegaly and genetic evaluation were identified. The
three abnormal karyotypes (47xxy and two 47+21) were seen in
patients with atria measurements of 11-13 mm and represented
17.6% of the total(CI=6.2-41.0%).
Atria(mm) 10 11 12 13 14
N 4 7 2 3 1
Abnormal Karyotype(%) 0 29 0 33 0
CONCLUSIONS: Isolated mild ventriculomegaly is associated
with a significantly increased incidence of chromosomal
abnormalities, even in cases of borderline atrial enlargement.
This risk far exceeds that of a 35 year old woman and these
patients should be offered genetic testing.
343 THE HUM,~N FETAd. AORTIC PHESSBRE PULSE WAVEFORM A M~,x B. Trud~, R Mo~,x V. Reed,x. DepL Ob/Gyn, Urnv. Sydney, Wes~neaa Ho~, NSW, Aus~a OBJECTIVE: To study the arterial Ixess~Jre ~aveform in the fetal desc~ng
STUDY DESIGN. The presst~e ~vefmrn propagated along the vascular f~ee
betweefl d~amel~icatly opposife points of the aodic lumen v,~s followed using a
=~er (ce~r~ ~eq~ency 3.~Hz). The ,~ samp~g ~mcy O000Hz) of
0 2turn. A cross-secbonal study of 80 nemmt fetuses between 20 and 40 ~eeks yieided nonn~ data. We stucied 58 pat~mts ~,~th evidence of pofenl~al
aoYdc ~metet ~avefonn idenld~ed Ihe mcisura of aofdc and pCrno~ry valve
RESULTS: In nonnaJ pregnancy IJ~ere was an m~ease b~ systolic and dmsto~c
I~ne and systobc.dmstolic aea mbos were constant. In ~Se fetat CCmlxo~nised group a non-reac~ve FHR Iracing (22 fetuses) ~as assoc~ed ~lh an increase
in ffmsto~ic ~.er. deQ’ease In pulse amplitude and decrease in systolic- dmstolic area ra~o (p<0.01 all measures) m cornpanso~ to I~’mse from Ihe potentially complicated ffoup ~lh a reaclJve FHR b’acmg. CONCLUSIOHS: The fetal aoCdc pressure pulse tmveform may be represented by the vessel ~mmeter waveform. In fetal comprormse an
ccm~ changes in blood pressure and we hypothe~ze are the
Poster Session IV Friday, January 28, 1994
3:00 p.m - 5:00 p.m.
Pavilion 9 - 11
CATEGORIES
Neonatology
Labor
Prematurity
Intrapartum Fetal Evaluation
POSTER NUMBERS
344352
353-377
378-419
420-434
Judges:
Thomas J. Garite, MD
Robert L. Goldenberg, MD
John E Huddleston, MD
372 SPO Abstracts January 1994 Am J Obstet Gynecol
344 ASYMMETRY CORRELATES SIGNIFICANTLY WITII ACIDOSIS AT BIRTll. M C.Wdhams,W F,O’Bnen,K B.Porter,C Lynch’,C Casanova"
Dept. of Ob/Gyn, University of South Florida, Tampa, FL 33606 OBJECTIVE: Decreased blrthwelght (BWT) for gestation is correlated
wdh fetal acidosis at dehvery among infants w~th abnormal fetal heart rate
tracings, but correlates poorly when this information is not taken into
conslderatmn. Asymmetric or lean body growth as measured by the
ponderal index (PI) also correlates with adverse birth outcomes BWT for
gestation vanes by race and gender, whde PI does not. In th~s study, we evaluated the correlation between decreased PI, decreased race adjusted
BWT and various neonatal outcome parameters
SllJDY DESIGN: Maternal and fetal database reformation from 2752
consecuhve dehvenes from July thru December, 1990 were analyzed PI
(b~rthwe~ghVcrown-hcel length3) was computed Gestahonal age (GA)
adjusted z scores were calculated for PI Z scores adjusted for race and
GA were calculated for BWT The lower 10% of the Z distributions were
defined as asymmetry (ASYM) and intrauterine growth retardatmn
(IUGR), respechvely Unpmred Student’s t-tests, Pearson chI square, and odds-ratios were performed. A P value <0 05 was considered s~gmficant.
RESULTS: Among this populahon, IUGR was significantly correlated
w~th gender (P<0 005) and maternal age (P<0 025), whde ASYM was not
correlated with these factors Both ASYM and IUGR were closely
assooated with Apgar scores < 6 at 1 min and < 7 at 5 miu (all P<0.003)
ASYM and 1UGR are closely correlated (P<0 0001), but their correlataon ~s rclahvely low by b~ologmal standards (RZ=0 03). Correlatmns w~th
decreased cord plI and increased base deficit are hsted below (O R =Odds
Ratio) pll < 7.10 Base Deficit > 8
(O R, range, P) (O R, range, P) ASYM 2 6, 1.1-6 0, <0 025 19,10-36,<0045
IUGR 2 0, 0.8-4 9, NS 1.6, 0 8-3.1, NS
CONCLUSION: ASYM is a more robust predictor of newborn status than
1UGR
346 THE RELATIONSHIP OF MATERNAL AND NEONATAL
CHARACTERISTICS TO MAJOR ItANDICAP AT > ONE YEAR OF
AGE R Goldenberg, F. Gaudier, K. Nelson, M. Paralta, M. DuBard, S
Clivcr, J. Hauth. University of Alabama at Birmingham, Birmingham, AL
OBJECTIVE: To determine the relationship between obstetrical factors, infant
characteristics arid the development of major ncurologlc handicap at >_. one year
of age.
STUDY DESIGN: The study population consists of 403 chddren born from
1979 to 1991 at 23-35 weeks gastatlonal age (GA), weighing 500-1000 grams
and seen for their last neuro-developmental evaluation at ~> one year of age
(mean 34 + 25 months), representing 78% of eligibles Major handicap (MH)
was defined as having one or more of cerebral palsy, mental retardation,
blindness or deafness
RESULTS: The overall inmdence of MH was 23 % and varied from 75 % at
23 weeks GA to 13 % (p <.001) at >__ 29 weeks B~rths at <__ 26 weeks had a
32% rate of MH compared to 17% MH at >__ 27 weeks (p=.001). In umvariate
analyses a number of other maternal and neonatal characteristics were
significantly associated (p < .05) w~th the presence or absence of MH mcledmg
steroid use (RR =0 6), preeclampsia (RR =0.6), cord pH < 7.05 (RR =2 8), cord
bicarbonate < 17 (RR=2. l), 5 minute Apgar <7 (RR=I.5), PDA (RR=I.9),
RDS (RR=I.8), NEC (RR=I 5), and IVH (RR=2 5). Regression analyms
controlling for the s~gnifieant relationship of GA to MH (p = .004) confirmed that
the use of tocolytlcs, the presence of ammonites and dehvery by cesarean section
were not significantly related to the development of MH, while maternal steroid
use tended to protect against MH [OR 0.52 (0.26, 1.04)]. In a regression
analysis evaluating the relationship of neonatal characteristics to MH, neither
blrthweight nor GA, a low 5 minute Apgar score, RDS or NEC were
sigmficantly associated with MH. However, a cord bicarbonate level < 17 [OR
2.51 (1 22, 5 16)], and the presence of IVH [OR 2.88 (1.59, 5.22)], and a PDA
][OR 2 53 (1.31, 4.90)] were strongly associated with MH.
CONCLUSIONS" When maternal factors alone are considered, increasing GA
and maternal stermd use appear to be protective against the development of MH
Acidosis at birth and the development of a PDA or IVH in the newborn period
are sigmficantly related to MH.
345 NEONATAL CONSEQUENCES OF MATERNAL PREECLAMPSlA: THE
EFFECT OF MATERNAL RISK STATUS R. Goldenberg, S. Cliver,~ D.
Rouse,x J. Hauth, W. Roden,~ R. Copper,~ & The March of Dimes Multlcenter
Study Group University of Alabama at Birmingham, Birmingham, AL.
OBJECTIVE To determine the impact of preeclampsia (PE) on neonatal
morbidity in women with compared to those without risk factors.
STUDY DESIGN: Data from the March of Dimes Multicenter Study (rate of
PE=5 2%) were used for this analysis. The population was divided into
nulliparas and multiparas and again by risk factors. Increases in the rates of
preterm birth (PTB), morbidity, and newborn length of stay (LOS) which
occurred in association with PE were determined
RESULTS: In nulhparas, 85 % of all indicated PTB secondary to PE occurred
~n low risk women, while in multiparas only 53% occurred in the low risk
group. Of the remaining indicated PTB in multlparas, 21% were in chronic
hypertensives, 8% in multiple births, and 9% each in dmbetics and women with
previous PE. The increase tn PTB and newborn LOS in association with
maternal PE by parity and risk status is shown In the Table. Rates of RDS,
IVH, NEC and neonatal death were increased proportionately.
INCREMENTAL RISE IN INCREASE IN NEONATAL PTB RATE WITH PE LOS WITH PE (DAYS)
Risk Status Nulllp Multip Nullip Multip Low Risk 5% 12% 1.5 3.6 Diabetes 3% 25% 0 1 2 7 Prewous PE --- 26% --- 1.0 Chronic HTN 12% 38% 8.4 14 0
CONCLUSIONS. In nulliparas, the vast majority of neonatal morbidity
associated with PE occurs in low risk women as does half the neonatal morbidity
in mulnparas. However, the increase m neonatal morbidity related to PE,
predominantly modulated by an increase in PTB, is substantially higher in
multlparas The greatest increase in morbidity regardless of parity occurs In
chromc hypertensives The impact of PE on neonatal outcome varies
substantially with the risk status of the mother.
347 LP.MEILARBOO¥ OENSIIYASA PREDICTOR Ot PItOSPIIOrlDYLGL¥CEROL IN
BI,~,EIICP, ND NON-DIABEtIC PREGNANCIES
C.[aSala~C. !ngdrdla, [. Ph111pson, S. ManOdvllll. A. We. Depts.
o"}’-~-/~’~’and Pathology, Hartford Hospltal. Hartford, CT.
OBJECTIVE: To correlate the lamellar body density countS (LBD)
of amnlotlc fluld wlth the presence of phosphotldylglycerol (PG)
In normal pregnancies and pregnancies compllcated by dlabeLes.
SIUB¥ BESIGR: One hundred seventy flve amnlotlc fluid speclmens
were obtained either from vaginal pool or amnlocentesis and
evaluated Vla thln layer chromatography for the determlnat~on of
the leclthln/sphmgomyelln (L/S) ratio and the presence of PG.
LBD counts were obtalned through the platelet channel of the
Coulter Counter. lhere were 27 specimens from pregnancles
complicated by dlabetes and 148 speclmens from norma! prec,,uncles.
Gestatlonai age ranged from 23-42 weeks. Excluded from analysis
were those with multlple pregnancies, growth retarded fetuses and
mothers wh~l race:red antenatal sterolds. The presence or absence
of respiratory d~stress syndrome (RDS) was recorded for all
neonates.
RES~tlS: t BD (aunts ~ 30,000 were associated wlth the
presence of PG in ~6 out of 70 patients (94%) of normal
pregnancies and 23 o~lt of 23 patleuts (i00%) whose pregnancies
were assocl~ted wlth dlubetes. In both groups there was no RDS
~n anv neonate Wlth a tBD > 30.000. Wlth a LBD - 30,000 ~n normal
pregnancies, the sensltlV~ty, speclflCIty, and posltlve predlctlve
value for the presence of PG ]s ]0%, 90%, and 95% respectlvely
$~mllarly In dlabet~c pregnancies the sens]tlvlty, speclflc~ty and
posltlve predlctlve value ]s 92%, 100% and 100% resp.
CO~EUSIORS: Lamellar body density ~s a rap~d (I0 minutes) and
inexpenslve test of fetal pulmonary maturity that correlates wlth
lhe presence Of PG and the absence of RDS when the count exceeds
30,000 In pregnancles compllcated by dlabetes.
Volume 170, Number 1, Part 2 SPO Abstracts 373 Am J Obstet Gynecol
348 SELECTED PARAMETERS OF FIBRINOLYSIS IN THE NEONATE. AA Saleh, LG Doreyx, CJ Lockwood, MP Dombrowski, EF Mammenx. Departments of OB/GYN, Wayne State Univ., Detroit, MI, and Mount Sinai Hospital, New York, NY. OBJECTIVE: To evaluate fibrinolysis in the neonate by measuring urokinase plasminogen activator (uPA) activity, a profibrinolytic factor, plasminogen activator inhibitor-2 (PAI-2), an antifibrinolytic factor, and a fibrinolytic screen (FS), an index for overall fibrinoylsis. STUDY DESIGN: We measured uPA(%) and FS(%) by chromogenic substrate technology and PAI- 2(U/ml) by ELISA, in 31 maternal-cord blood pairs. All were delivered vaginally and had no complications. Paired t tests were used for statistical analysis. RESULTS: Mean (SD)
Maternal Cord BL p
u-PA 0.5 (0.2) o.2 (0.i) <0.0001
PAI-2 120 (40) 4 (3) <0.0001
FS 116 (18) 56 (9) <0.0001 CONCLUSIONS: i) Cord blood has an overall decreased flbrinolytic activity due to lower fibrinolytic activator and inhibitor activi- ties. This predisposes the neonate to hyper- coagulability. 2) PAI-2, a unique product of the trophoblast, is poorly transferred from the placenta to the fetus.
350 TERM NEONATAL SEIZURES: EVALUATION OF OBSTETRICAL
FACTORS J.M Lmrb C.V. Towers, E.J. Qudhgan, M. deVemana, J.S
Toohey, M.A. Morgan. Umvers~ty of Cahforma at Irvme, Long Beach
Memorial Medmal Center, Long Beach, CA
OBJECTIVE: To evaluate obstetrical factors m term neonates who
developed early-onset seizures
STUDY DESIGN: A retrospective review of neonatal and obstetrical
records of infants born at ~ 37 weeks gestation between 1/8f - f/93
at Long Beach Memorial Medical Center with a diagnosis of early-onset
smzures (w=thm 72 hours of b=rth) was performed Neonatal data
reviewed included Apgar scores, EEGs, cranial ultrasounds, CT scans
and MRI results. Obstetncal data rewewed included maternal and fetal
nsk factors, mtrapartum comphcat=ons, route and mode of dehvery,
snd fetal heart rate tracings Lack of antepartum testing in high risk
pat=ents, delayed intervention with non-reassuring antepartum or
mtrapartum fetal heart rate patterns, birth trauma, and fadure to
prophylax or treat iFifectlon were the obstetrmal factors used as the
cntena for =dentdymg smzures whmh were potentially preventable.
RESULTS: 40 term neonates had early-onset seu’ures out of 60,712
hve births (0.7%). The seizures were attributed to permatsl hypoxm
events ~n 15 137.B%1, eerebra] malformations m 7 (17~5%), cerebral
infarcts in 7 (17 5%), subarachnold/mtraventrmular hemorrhage in 5
(12 5%), refection/sepsis ~n 3, and unknown etiology =n 3. Of the 23
neonates with a 5 m=nute Apgar _> 7 (cerebral malformatmns
excluded), 7 (30%) had cerebral Infarcts, In the review of all the
records, 23% of the early-onset seizures were considered potenhally
preventable. No contributing obstetrical factors were identified in any
of the cases with cerebral infarcts.
CONCLUSIONS: The majority of the term early-onset neonatal
seizures did not appear to be preventable. In addition, many of the
infants with 5 minute Apgars >_ 7 had cerebral infarcts, an ent~ty not
previously reported in the obstetric htersture as being a s~gnlflcant
etiology of term neonatal seizures.
349 ERYTHROPOIET1N FOR POST-NATAL BONE MARROW SUPPRESSION AFTER INTRAUTERINE TRANSFUSION THERAPY S R Inghs, F Chervenak, J Bussel*
New York Hosp -Comell Umv Med Center, New York, NY
OBJECTIVE: To perform a pilot study of erythropmetm for neonatal
bone marrow suppression after intrauterme transfusmn therapy
STUDY DESIGN: Ezght fetuses treated with lntrauterme transfusions
for severe Rh, Kell ~sotmmun~zatlon, or severe fetal anemia and hydops of unknown cause who developed late onset post-natal anerma were
~dentified The pahents were offered bone marrow asptratlon and erythropo~ehn 200 units per hlogram body weight SC three hmes a
week to stimulate the bone marrow on a research protocol The CBC,
retmulocyte count, and transfusion requirements were followed weekly.
Therapy was stopped when a rettculocytosis was documented and the hematocnt increased by 3%.
RESULTS: All 5 bone marrow exarmnatmns revealed marked
erythrold hypoplasla Seven of e~ght neonates appeared to respond to
e~kropomtln w~thm 2-4 weeks of treatment Two patmnts reqmred a
second course of treatment suggesting that the response was related to
the erythropomtm therapy There were no apparent s~de effects of the
treatment The patmnt who did not respond had a hypoerythrmd bone marrow desp=te 6 weeks of erythropmet~n therapy CONCLUSIONS: Intrauterine transfusions suppress the neonatal bone
marrow Erythropmetm appears to be an effective therapy for post-natal
bone marrow suppression secondary to lntrautenne transfusions Some patients may not respond to th~s therapy, possthly secondary to down
regulation of er3~hropoletm receptors or a defect early ~n erythrotd maturation Tlus therapy deserves further investigation and a
mult~eenter randomtzed double bhnded trial is underway
351 NEONATAL MORBIDITY AND MORTALITY IN THE
PREGNANT DRUG ABUSER. B. Nevils*, C. Barada=, G.
Gilson, L. Curet. University of N.M., Albuq., N.M.
OBJECTIVE: To test the null hypothesis that the pregnant
drug abuser is not at risk for adverse preg. outcome.
STUDY DESIGN: 88 patients who were followed in the
Milagro clinic and delivered at UNMH between 6/90 and 3/93
were reviewed for perinatal outcome. Three groups were
identified on the basis of urine toxicology screens throughout
pregnancy: (l)negative screen (n= 17), (2)single substance
screen (n=22), and (3)multiple substance screen (n=42).
RESULTS: 81 patients met inclusion criteria. As a group the
following characteristics were note: mean maternal age 27.59,
mean gravidity 3.98, mean birth weight 2816.0, preterm
delivery 23.75%, NICU admission 13.58%, neonatal morbidity
58.13 %, congenital anomalies 20.93 %, spontaneous abortion
3.7%, and neonatal deaths 2.47%. When the negative
toxicology group was compared to the positive toxicology
group (single and multiple substance) statistically significant
differences were seen in birth weights (p= .008), nursery days
(p= .0001), and neonatal morbidity (p= .0001). Although no
significant difference in congenital anomalies was demonstrated,
trend was noted (0.063).
CONCLUSIONS: The pregnant drug abuser with a positive
urine toxicology screen during pregnancy is at increased risk
for adverse pregnancy outcome as noted in lower birth weights,
longer nursery stays and increased neonatal morbidity. There is
a trend toward increase risk of congenital anomalies. Therefore
the null hypothesis is rejected.

374 SPO Abstracts January 1994 Am J Obstet Gyt~ecol
352 ALTERATIONS OF NEONATAL BEHAVIOR: IS IT THE COKE OR THE SMOKE? V. Delaney-Black×, C. Covingtonx Neonatology and College of Nursing, Wayne State Unlverslty, Detrolt, Michigan. OBJECTIVE: While prenatal cocaine exposure has been associated wlth alteration of neonatal behavior, prevlous studies have failed to adequately assess the effects of the covar~ates: namely, maternal smoking. We hypothesized that maternal smoklng would have slgnificant, negative impact on behavior independent of cocaine. STUDY DESIGN: Blinded Brazelton Neonatal Behavloral Assessment Scales (BNBAS) were performed on term infants. Maternal smoklng, alcohol, and cocaine exposure were documented both by history and and for cocalne by quantltatlve analysis of meconium. The effects of smoking and cocalne were assessed for each of 7 behavloral clusters: Habituatlon (H), Orientation (O), Motor (M), Range of State (}LAS), Regulation of State (ROS), Autonomic Stability (AS) and Reflexes (REF). Correlatlon coefficients and hierarchial regression models were performed. RESULTS: 57 infants (29 smoke exposed, 24 coke exposed) were studied. Smokxng correlated positively with both quantitatlve cocaine (p<0.01) and beer use (p<0.05) and negatively with birth weight (p<0.005), head circumference (p<0.02) and gestational age (p<0.05). In addltlon to prevlously reported effects of cocaine on ROS and M, smoking had a slgnificant negative impact on BNBAS 0 (f=5.14 R2 change=.099 slg f=0.014), RAS (f=4.79 R~ change=.092 slg f=0.017), AS (f=5.28 R2 change=.10, sig f=0.013) REF (f=4.64 R2 change=.ll7 sig f=.019) and M clusters (f=4.84 R2 change=.093 slg f= 016) CONCLUSION: Maternal smoklng has signiflcant, independent, negative effects on BNBAS. Since prenatal exposure to cocaine is highly correlated with smoking, evaluatlon of both behavlors is essentxal.
354 TRANSVAGINAL SONOGRAPHY AN OBJECTIVE EVALUATION OF
TIlE CERVIX IN LABOR: PRESENCE OF CERVICAL WEDGING IS
ASSOCIATED W1TII SIIORTER DURATION OF LABOR FOR
INDUCTIONS. F. Boozariomehri, I. Timor-Trltsch, C. Chao. Dept. Ob/Gyn,
Columbia University, New York, NY
OBJECTIVE: Tradttionally, the success and duration of induction have been
predicted by digital examination of the cervix. We hypothesized that assessment
of cervical wedging and cervical length as determined by transvaginal ultrasound
(TVS) would be a superior method of cervical evaluation compared to digital
examination of cervical anatomy.
STUDY DESIGN: Fifty-three patients scheduled for alect~ve induction o f labor
underwent TVS and digital cervical examinations prior to labor mducuon.
Cervical wedging was defined as an opening of the internal os creating a triangle
in the cervical canal and was assessed in a blinded fashion Cox proporttonal-
hazards multiple regression analysis was performed to determine which of these
vartables made a stgmficant contnbutton to the predictioa of latent, phase length
and ~.otal labor duration. The stattst~cal analysis controlled for the possible
confounding effects of prostaglandtn administration, parity, and previous
termiantton of pregnancy
RESULTS: Latent phase duration was significantly associated with 1) the
presence of wedging, 2) TVS-measared cervtcal length, and 3) administration of
prostaglandin, but not with digital examlnauon of cervical ddanon or effacement.
Total duratmn of labor was associated with l) the presence of wedging and 2) the
adm.nstration of prostaglandin, but not with dtgltal assessments of cervical
anatomy The presence of wedging was significantly associated wtth shorter
latent and total labor length (hours, mean + SEM)’
WEDGE NO WEDGE P
Latent Phase 16 I + 1 7 32.9 ± 3.8 <0.001
Total Duration 21.9 4- 1 9 37 9 + 3 5 <0 001
2ONCLUSIONS: Imual ultrasound assessments o f cervical length and wedging
of the internal os were better predictors of induction labor duration than tmtial
d~gltal examinations of cervical anatomy. The presence of wedging was
significantly associated wtth shorter latent phase and total labor durations.
353 OXYTOCIN ANTAGONIST INHIBITORY EFFECT ON THE BABOON AND RAT UTERUS MAY BE OVERCOME BY THE USE OF PROSTAGLANDINS.
M.D. Feigin, S.C. Pak~, G. FloureP, M. Parsons, L Wilson Jr? Dept. Ob/Gyne, Univ. of Illinois, Chicago, IL and Dept. Physiology, Northwestern Univ. Med. School, Chicago, IL. OBJECTIVE: Administration of a potent and long-acting oxytocin antagonist (OTA-III), produced in our lab, to the rat
and the pregnant baboon can inhibit uterine response to oxytocin (OT) for hours and even days. This can create an unusual
clinical problem when a need for immediate delivery may arise. The purpose of this study was to evaluate uterine response to
prostaglandins subsequent to the administration of OTA-III. STUDY DESIGN: Pregnant tethered baboons were studied between 130-160 days of pregnancy. The oxytocin antagonist was
administered into a cannula placed in the aorta. An oxytocin challenge test was performed, starting with 10 mU/min, and doubling the dose every 20 minutes up to a dose of 400 mU/min.
Once absent or minknal responsiveness to OT was established, infusion of 15-methyl-PGF2a was started. The same procedure
was performed in rats in estrous using an indwelling uterine cannula. RESULTS: Inhibition of uterine response to OT in the pregnant baboon lasted 24-48 hours. During this period the uterus
remained responsive to prostaglandins. Also, OTA did not alter
the rat uterine response to prostaglandins. CONCLUSIONS: OTA-III can inhibit rat and pregnant baboon response to OT for hours. During this period, the uterine response to prostaglandins is maintained.
355 RANDOMIZED CLINICAL TRIAL OF PGE2 GEL AND
INTRACERVICAL BALLOON IN RIPENING THE
CERVIX PRIOR TO INDUCTION OF LABOR IN
INSULIN-REQUIRING DIABETIC PATIENTS. Zion J
Haeav. Ariel. Welssman, Avl MatzkeI,~ Moshe Manor,~ Vaclav
Insler.~ Dept. Ob/Gyn, Kaplan hospital, Rehovot, affiliated with the
Hadassah School of Medicine, Israel.
OBJECTIVE: To compare the efficacy of a single application of
lntracervical prostaglandin E2 gel w~th that of intracervical
balloon catheter on the ripening of the cervix and on the
subsequent induction of labor in pattents with an unfavorable
cervix.
STUDY DESIGN’ Sixty two insulin-requiring diabetic patients at
38 weeks of gestation and with a modified Bishop score of 4 or less
were randomly assigned to receive either mtracervical PGE2 gel or
intracervical balloon catheter prior to oxytocin induction of labor.
Sixteen hours following the use of cervical ripening agent, a trial
of labor induction by oxytocin administration or/and ammotomy
(if clinically feasible) was performed.
RESULTS: No statistically significant differences were noted
prior to the use of cervical ripening agent between the two groups
with respect to maternal age, panty, and cervical score Cervical
score was significantly higher (p< 0.01) following the use of
lntracervlcal balloon as compared to the PGE2 gel (6 4+ 2 2 versus
4.1+ 3.1). The intracervical balloon group had a significantly
shorter cervical ripening-to-delivery interval (39.7+ 44.3 versus
86.5 4- 84 hours), and lower cesarean section rate (7% versus 28%)
as compared to that of the PGE2 gel group.
CONCLUSIONS: The use of intracerv~cal balloon was more
effective in ripening of the unfavorable cervix and resulted in a
lower cesarean section rate following induction of labor.

Volume 170, Number 1, Part 2 SPO Abstracts 375 Am J Obstet Gynecol
356 LOW LEVELS OF VAGINAL FETAL FIBRONECTIN (FFN)
PREDICT DELIVERIES OCCURRING AFTER 41 WEEKS.
C.J. Lockwood, R D. Moscarelhx, R. Wein1�, L. Lynch, R. Laplnskl~, and
A Ghidmi. Mr. Sinai School of Medicine, New York, NY.
OBJECTIVE: This study sought to determine whether absent or low levels of FFN m the cervical and vaginal secretions of patients at 39
weeks gestation predicted pregnancies progressing beyond 41 weeks.
STUDY DESIGN: A cohort study was undertaken utilizing cervical and vaginal samples collected from 75 consenting patients at 39 weeks
gestation Levels of FFN were measured by a sensitive immunoassay.
RESULTS: There was a 35.5-fold increase in maximal vaginal FFN
concentrations among patients delivering <41 weeks (n=52) compared with those dellvermg >_ 41 weeks (n=23). Receiver Operator
Characteristic curve analysis mdicated that the opumal FFN predictor of
rolonsed pregnancies was a vaginal FFN value < 60 ng/ml
DELIVERY > 41 weeks < 41 weeks
FFN < 60 ng/ml 22 (true+) 29 (false+) 51 FFN > 60 ng/ml 1 (false-) 23 (true-) 24
23 52 75 [sensmvlty = 95.7% (95% Confidence Interval 87.3% to 100.0%);
specificity = 44.2% (30.7% to 57.7%); positive and negative predictive
value = 43.1% (29.5% to 56.7%); and 95.8% (87.8% to I00.0%),
respectwelyl. The relative risk of a prolonged pregnancy associated w~th
a vaginal FFN value < 60 ng/ml was 10.4 (1,5 to 72.4) Among patients with a vagmal FFN > 60 ng/ml, 80.8% delivered within 7 days, and 92.3%
within 10 days, of sampling. In contrast, among patients with vaginal
FFN < 613 ng/ml, 63.3% remained undelivered after 1 week. After
centrolhng for parity and cervical dilatation, muluple logistic regression
demonstrated that vaginal FFN was a significant predictor of pregnancies
delivering at > 41 weeks [adjusted odds ratio = 6.2 (1.2 to 31.1)].
CONCLUSIONS: A vaginal FFN value < 60 ng/ml present at 39 weeks
gestauon is highly predictive of pregnancies progressing past 41 weeks
gestation This data may allow for the prediction of postdates
pregnancies, thus facilitating appropriate obstetric interventions,
358 THE MECHANISMS UNDERLYING POTASSIUM
CHLORIDE STIMULATED PHASIC MYOMETRIAL
CONTRACTIONS. M. Phillippe. E. Chienx, T. Saundersx.
Dept. Ob/Gyn, University of Chicago, Chicago, IL.
OBJECTIVE: These studies sought to test the hypothesis that KC1
stimulated phasic myometrial contractions (CTX) use cytosolic
calcium oscillation mechanisms comparable to oxytecin.
STUDY DESIGN: In vitro CTX studies were performed using
longitudinal uterine strips from proestrus/estrus Sprague Dawley
rats. Contractile activity was determined using isometric
transducers coupled to an OMEGA PCL-718 A/D beard-286 PC;
digitalized data was analyzed to determine the area under the CTX
curve for 5 minute intervals. Dose response studies were performed
using KCI (10-50 raM) with/without 2-nitro-4-carboxyphenyI-N,N-
diphenylcarbamate(NClM2), phorbol 12,13-dibutyrate, adenine,
procaine, ryanedine, nifedipine, or calcium-frec/EGTA buffer.
RESULTS: KCI (10-30 raM) produced an increase in phasic c~rx;
higher concentrations resulted in tonic CTX. The phasic KCI
aimulated CTX were significantly suppressed by inhibition of
phosphollpase C (PI-PLC) with NCDC, and activation of protein
kinase C (PKC) using phorbol dibutyrate. Inhibition of cak-ium- induced calcium release (CICR) with adenine and procaine
suppressed phasic CTX; ryanedine had no effect. Blockade of
calcium influx using nifedipine, and cak’ium-free/EGTA buffer
also markedly inhibited phasic CTX. (all p<0.05)
CONCLUSION: These studies have confirmed that PI-PLC, PKC,
CICR, and transmembrane calcium influx are important
components of the myometrlal calcium oscillator activated by KCI;
phenomena comparable to the intracellular mechanisms activated in
respon~ to oxy~.ec~n. (ftmd~! by NIH HD22063)
357 EFFECT OF PULSATILE AND CONTINUOUS RITODRINE ON THE BETA-
ADRENERGIC RECEPTOR CASCADE AND TACHYPHYLAXIS IN THE
PREGNANT SHEEP MYOMETRIUM. F Bsat., S Cantos, J Chlao*, L
Santuccl×. Dept. Ob/Gyn/Reprod.Sc , Magee-Womens Hospital,
Umverslty of P~ttsburgh, Pittsburgh, PA.
OBJECTIVE: To determine ~f down-regulatmn and tachyphylaxls are
prevented by puIsatde rttodrlne administration.
STUDY DESIGN: We placed vascular and amn=otlc flu=d catheters and
obtained a myometrml biopsy In 11 sheep at 107-117 days gestation
After 3 5 days, seven sheep rece=ved ntodrme m 6-29 mg pulses every
g0 minutes, for a total of 2-7 mg/kg]24 hours Four animals received a
continuous Infusion at 2-5 mg/kg/24 hours We quantified the uterine
response to a bolus rejection of oxytocln prior to, and after 4 and 24
hours of rltodrll~e administration by meastJrlng the area under the
amnlotle fluid pressure-time curve/AUC) After 24 hours, we obtained
a second myometrlal b~opsy We measured myometnal ~3~adrenerg~c
receptor (BAR) density and maximal adenylate cyclase actm~ty (AC-
VMAX) tO ~soproterenol st~mulatmn (10-gM-lO-4M), before and after 24
hours of ntodrme. Statistical analysis was done with ANOVA
RESULTS: See Figures
Pulsatlle Ritodrine Continuous Rltodrlne
25 50 75 100 125 1~ 25 50 75 100 125 150
CONCLUSIONS: Regardless of the mode of administration,
approximately 20 30% of BAR and AC-VMAx were lost Uterine
response to oxytocm increased approximately 20% between z~ and 24
bouts Thus pulsattle administration appears to offer no advantage over
continuous Infusion of rltodrlne.
359 A COMPUTER MODEL OF UTERINE CONTRACTIONS
BASED ON DISCRETE CONTRACTILE ELEMENTS. H F Andersen & M L Barclayx. Depts of Ob/Gyn, Loma Linda
Univ, Loma Linda, CA and Uulv of M~chigan, Ann Arbor, MI.
OBJECTIVE: Prediction of uterine contraction waveforms using
a microcomputer-based model of uterine activity based on discrete
contractile elements. We hypothesized that varying the shape of
the model, total number of cells, and pacemaker locatimts would
produce normal and abnormal contraction waveforms.
STUDY DESIGN: The model is a hollow ovoid composed of
discrete contractile dements (cells) which propagate electrical
impulses, generate pressure, and have defined contracting and
refractory periods. Each cell contacts 8 surroundang cells and
propagates impulses iteratively from cell to cell. Sample
contraction waveforms were generated based on 1000, 2000, and
4000 cells organized in ovoids of 1:1, 3:2, and 2:1 long:short a.,ds
ratios, w~th a single pacemaker at vmying positions. Contraction pressure was the sum of the pressure contributtous by contracting
cells.
RESULTS: Contraction waveforms were altered by altering ovoid
shape, but not by increasing number of contractile elements. The
vertical placement of the pacemaker had a dramatic effect on shape
and symmeUy of contractions, including the development of
patterns characteristic of "dysfunctional" uterine activity.
CONCLUSIONS. Abnormal uterine contraction patterns may
result from pacemaker actavity in unusual locations, such as mid-
uterus. Graphical analysis of generated waveforms suggest that
tins model displays chaotic behavior, a complex characteristic of
some iterative models.
376 SPO Abstracts .January 1994 Am J Obstet GynecoI
360 PROSPECTIVE COMPARISON OF EMPIRIC ANTIBIOTIC THERAPY
IN PATIENTS WITH IDIOPATHIC PRETERM LABOR. R.W. Naef, lI1,
E F. Magann, J R Allbert, W.E. Roberts, R,W Martin, J,C Morrtson. De, pt
Ob/Gyn, Univ. of Mississippi Medical Center, Jackson, MS.
OBJECTIVE: To assess the abihty of a broad spectrum antibiotic (versus
placebo) to prolong pregnancy when used in conjuneUon with intravenous
tocolytic therapy in patients wtth idiopathic preform labor (PTL)
STUDY DESIGN: All subjects in this double-blind, prospecttve investigation
had PTL (contractions with documented cervical change) with no identifiable
etiologic factors. Each patient underwent ammocentesis for determination of
amniotic fluid (AF) glucose, WBC count, gram stain, aerobtc/onaerobtc cult u res,
and Ureaplasma culture Sixty-five grav~dms were randomized to reeelve either
amptcilhn/sulhactam (AS) 3.13 gm IV q 6 h x 12 doses (AS group, n = 33) or
placebo (control group, n = 32) All patients received intravenous MgSO4
using a standard protocol for tocolysls. If the PTL was controlled with
intravenous MgSO4, patients were placed on orM tocolyhc therapy with Mg
gluconate 2 gm PO q 4 h untd 37 0 weeks’ gestation, breakthrough PTL, or
indicated delivery occurred.
RESULTS: Demographic characteristics were similar within each group AF
glucose (40 6 __+ 13.8 rag/dL vs 35.1 4- 15.5 mg/dL) and AF WBC count (124
+ 295 WBC/mm3 vs 54 + 161 WBC/mm3) were not statisttcally different (p
= ns). Lxkewtse, positive gram stains, positive aerobic/anaerobic cultures, and
poslttve Ureaplasma cultures were not statistically different. Patients receiving
AS had simdar prolongation of pregnancy compared to women in the control
group (4 69 4- 3 07 weeks vs 4.30 + 3.33 weeks, p = ns) Esttmated
gestational age at dehvery was not different between the groups (36.29 +__ 3 15
weeks vs 34.55 +__ 4 68 weeks, p = ns), as was birth weight (2751 4- 561 gm
vs 2460 4- 278 gm) Apgar scores < 7 ~t 5 minutes (25 0% vs 18 2%) and
need for neonatal intensive care (18.8% vs 12.1%) were both more common
among babies in the control group but the difference was not statistically
s~gnificant
CONCLUSIONS: These data suggest that emptrlc broad spectrum antlbtotlc
therapy Is not beneficial in treaUng the gravida with idiopathic PTL
362 NEWBORN ELECTROLYTE RESPONSES TO AMNIOINFUSION
WITII LACTATED RINGER’S VERSUS NORMAL SALINE: A
RANDOMIZED PROSPECTIVE STUDY. J.F. Washburnex, S.P
Chauhan, E F. Magann, P.H. RhodesX, P W. WilkmsX, J C. Momson.
Depts. Ob/Gyn and Pediatrics, IJnxv of Mississippi Medical Center,
Jackson, MS.
OBJECTIVE: A published study (Shields and Brace A/OG 1993;160.300)
with animal model (fetal sheep) ind~eatas that amniolnfusion with normal
saline, compared to lactated Ringer’s solution, ts associated with fetal
electrolyte imbalance, specifically hyperchloremia. The purpose of this
study was to determine if ammomfusion with normal sahne or lactated
Ringer’s is associated with electrolyte imbalance in the newborn.
STUDY DESIGN: Over two months, all partunents undergoing
amnioinfusion in the active phase of labor were randomized to receive
either normal saline (n = 37) or lactated Ringer’s (n = 30).
Amnioinfusion consisted of warmed solution (39 - 40° C) refused
transvaginally Newborn electrolytes were obtained from cord blood
samples at the time o f delivery. Maternal electrnlytes were obtained prior
to amnioinfusion Statistical analysis was performed using the Student t
test and p < 0 05 was considered slgmfieant.
RESULTS: The two groups were simdar in maternal age, ethnicity,
gr.avidity, parity, gestational age, maternal electrolyte levels prior to
amnlomfusion, amount of solutmn amniomfused, duration of labor atter
amnioinfusion, mode of delivery, and mean birth weight. At birth, the
mean (4- SD) sodium levels were not sigmficant[y different among those
who received normal saline or lactated Ringer’s (137 4- 2.3 and 136 + 2 8
retool/L, respectively; p = 0 63) The chloride concentrations were also
similar among newborns who had received normal saline or lactated
Ringer’s (102 + 2 1 and 104 + 2.4 mmot/L, respectively; p = 1 0)
CONCLUSION: Unhke the fetal sheep model, amniomfuslon with normal
sahne Is not associated with hyperehloremia in the newborn.
361 COMPARISON OF INTRAAMNIOTIC 15 - METIIYL PGF2 a AND
INTRAVAGINAL PGE2 FOR SECOND-TRIMESTER PREGNANCY
TERMINATION. D L Su|livanX, K G. Perry, Jr., E F Magann, W E.
Roberts, R.W. Naef, lit, J.C. Morrison. Dept Ob/Gyn, Univ. of
Mississippi Medical Center, Jackson, MS
OBJECTIVE: We designed this study to compare the efficacy, safety, and
frequency of s~de effects between mtraamnlotlc 15 methyl F~ <x and
mtravaginal PGE2 suppositories for therapeutic mldtnmester pregnancy
termination.
STUDY DESIGN: This retrospective study compared 59 eases of
therapeutic second-trimester pregnancy terminations: Group 1 received
PGE2 intravaginal suppositories, while group 2 received mtraamniotlc 15
methyl PGF; a Main outcomes studied were length of time from the
initiation of pregnancy termination to dehvery, side effects, and
comphcations
RESULTS: Group 1 consisted of 34 women who received intravaginal
PGE2 suppositories and group 2 consisted of 25 women receiving
mtraammotlc 15 - methyl PGF2 a. The mean gestatmnal age at the time
of termination was 19 5 + 2.6 weeks There were no differences in
maternal age, race, gravidlty, parity, or gestahonal age at termination.
Group 1 had an increase m hme to delivery (17 3 4- 8 6 hours) when
compared to group 2 (11 6 4- 6 4 hours, p = 0 008) Group 1 had a
h~gher Incidence of side effects including nausea, diarrhea, and fever
compared to group 2 (p = 0 003, 0 007, 0 025 respectively) The
eshmated blood loss was similar in both groups (159 4- 119 ml in group 1
vs 132 + 112 ml in group 2) D & C for retained placenta was required
in 26 5% of patients in group 1 compared to 12 0% of patients in group 2
(p = 0 3) There were no major complications In either group.
CONCLUSION: The use of intraamnlotlc 15 methyl PGF2 a for
therapeutic second-trimester pregnancy termination ~s safe and associated
with a more rapid evacuation of the uterine contents and less side effects
when compared to lntravagmal PGE2 suppositories.
363 ACTIVE PHASE ARREST: A RANDOMIZED TRIAL OF CHORIOAMNION MANAGEMENT .D.J. Rousex, C. McCullough*,
A. Wren~, J Owen, J C. Hauth The University of Alabama at Birmingham, B~rm~ngham, AL. OBdEOTIVE: Management of active phase arrest traditionally includes
labor augmentation with artificial membrane rupture (AROM) and oxytoc~n Our null hypothes~s was that the ~ntent to leave the
membranes intact would not affect- 1) Cesarean rate, or 2) Incidence of maternal ~nfectlous morbidity STUDY DESIGN: Prospective, randomized clinical trial of healthy, spontaneously laboring term grawdas w~th ~ntact chonoamn~on and
active phase arrest (defined as -< 1 cm of cervical change over 2 hrs
in the active phase of labor). Randomization to 1) oxytocin augmentation with ~ntact chorioamnion or 2) oxytocln augmentation
with AROM and ~nternat monitoring of uterine contract#ns and FHR
RESULTS: The AROM group (n=60) and the INTACT group (n=58) were s~mitar ~n regard to maternal age, race, nulliparity (62% in each),
labor epldural usage, gestational age, cervical dilatahon at randomization, and blrthwelght. The randomtzat~on to delivery interval
was 43 minutes longer in the INTACT group (p = 011) Other
outcome cntena include AROM (n=60) INTACT (n=58) P
C-Section (n) 5 4 1.0 Matarnal Infection
Endometritis (n) 4 0 0 06
Chonoamn~onltls (n) 3 0 0.13
Total (n) 7 0 0 007
Neonatal Infection Suspected/proven (n) 4/1 1/0 0 11
Pnor to randomization, 54 patients ~n the ARQM group vs. 52 pattents
in the INTACT group experienced complete labor arrest w~th no cervical change for at least 2 hrs All of the maternal tnfecttous
morbidity and 8 of the 9 oesarean dehvenes occurred in nulhparas. CONCLUSION: In women with active phase arrest, labor
augmentation with intact membranes lowers maternal ~nfect~ous
morbidity

Volume 170, Number 1, Part 2 SPO Abstracts 377 Am J Obstet Gynecol
364 SIGNALING BY INTERLEUKIN-1 IN HUMAN MYOMETRIAL CELLS. F. Hertelendyx, R. Romero, H. Toddx. Depts. Ob/Gyn, St, Louis University, St. Louis, MO, and Wayne State University, Detroit, MI, Perinatology Branch, NICHD, Bethesda, Maryland. OBJECTIVE: Recent evidence indicates that the human myometrium may serve as a direct target for certain cytokines. We examined further the action of IL-I on prostaglandin (PG) production and compared it to that of protein kinase C- (PKC) activating phorbol ester (TPA). STUDY DESIGN: Confluent monolayer cultures of human myometrial cells (HMC) were incubated without (control) and in the presence of human recombinant IL-I, TPA, or both together. PGs (PGE2 and 6-keto PGFIa) released into the medium were quantitated by -@pecific radioimmunoassays. Data were statistically analyzed by analysis of variance or paired t-test. RESULTS: Both IL-I and TPA elicited a time- and dose-dependent increase in PG production, which could be blocked by actinomycin D. Coincubation of HMC with both agonists provoked a highly significant synergistic response that could be suppressed by staurosporine. Downregulation of PKC by prolonged exposure to TPA did not prevent PG responses to subsequent stimulation with IL- l. However, the stimulatory action of IL-1 was reduced to about 50% by pertussis toxin, but not by cholera toxin. CONCLUSIONS: IL-I and PKC synergistically promote PG synthesis in HMC cultures by activating discrete pathways. IL-I signaling is mediated, at least in part, by a pertussis toxin-sensitive G-protein.
366 THE EFFECT OF ACTIVE MANAGEMENT OF LABOR (AMOL) ON
THE CESAREAN SECTION RATE: A REAPPRAISAL AFTER 5
YEARS A Mayesx, V. Parisi Dept Ob/Gyn, Univ of Tx,
Houston, Tx.
OBJECTIVE To determine ~f AMOL would maintain a decreased cesarean
section (c/s) rate among nulhparous women 5 years affer ~ts introduction
at our institution
METHODS The hypothesis that AMOL would decrease the c/s rate for dystocia was ong~nafly tested at our institution in 1985, The first 6 months
served as a control period, and AMOL was introduced as routine management beginning July 1, 1985 The present study reviews 378
consecutive term nulhparous deliveries in 3 different practice groups
(University, HMO, and private) in 1990, 5 years after the AMOL protocol was ~nstltuted RESULTS. The overall o/s rate was reduced from 25% to 18 5% (p < 0 01) from 1985to1990 The mc~dence of c/a for dystocia was decreased from
15% to 11% (p <0.05) dunng this time This d~fference was of equal magmtude to that reported in the 1985 AMOL penod (10%) Interestingly,
significant differences were observed among the 3 practice groups The private practice group showed a continued decline in c/s for dystocia from
the 1985 to 1990 AMOL groups, whereas the HMO prachce showed an
increase (11 0% to 14.5%) The incidence of c/s for fetal distress and other indmatmns did not s~gnificantly change and no differences =n perlnatal outcome or umbilical cord blood gases were observed
CONCLUSIONS The overall decrease in c/s observed immediately after the introductmn of AMOL m 1985 is almost entirely due to a decrease =n
quahty improvement and education have hkely contnbuted to the
at the HMO. AMOL remains a safe and effective method for reducing the
365 DOUBLE-BLIND COMPARISON OF INTRACERVICAL
AND INTRAVAGINAL PROSTAGLANDIN E2 FOR
CERVICAL RIPENING AND INDUCTION OF LABOR. K.
Hales, W Raybum, G Tumbullx, D. Christensenx, E. Patatanianx.
Dept. Obstet Gynecol U. Oklahoma Health Set Ctr, Okla Cay, OK.
OIKIECTIVE: To compare the safety and effectiveness of
prostaglandm E2 (PGE2) dehvered sequentially as an mtracervical (0.5 mg) gel or mtravagmal (2 5 rag) gel
STUDY DESIGN’ Patients with an unfavorable cervix (Bishop
score _< 4) at > 35 weeks and requmng lnductaon of labor were
assigned to recexve a 3 ml dose of gel mtracerwcally and
intravaginally m a double-blind, placebo-controlled manner. A
maximum of three doses were given every six hours untd regular
uterine contractaons occurred or there was a B~shop score change
Data were compared using a Student’s t-test or F~sher’s exact test.
RESUL’I’S. The 100 evaluahle cases recei-~ed PGE2 either
~ntracerwcally (n=52) or mtravaglnally (n=48) The two groups were
~dcnt~cal w~th respect to maternal age, race, panty, gestational age,
and predose B~shop score. Change an B~shop score ( > 3 po;nts) was
greater after using the intravag~nal than ~ntracerv~cal gel (60.4% vs.
40 4%, p < 01) regardless of panty and gestat~onal age. Regular
contractions were reduced more often w~th the mtravag,nal gel
(72 9% vs. 48 1%, p < 02). No d~fferences were found in maternal
s~de effects or fetal heart rate abnormahties, and utenne
hyperstimulat=on was present ~n only one case (xntracervlcal).
Techmcal difficulty was present w~th mtracervlcal mstillat=on only,
CONCLUSION. The mtravagma~ PGE2 ge! was eas~er to
administer, caused more cervical change, and induced labor more
often than the mtracervical gel
367 THE COURSE OF LABOR FOR PATIENTS UNDERGOING VAGINAL BIRTH
AFTER CESAREAN. AM Peaceman, S Patel*. Department of Obstetrics
and Gynecology, Northwestern Umvers~ty Medmal School, Chmago, I1.
OBJECTIVE: We evaluated the hypothems that patients delivered by
cesarean section (CS) in the second stage of labor experience shorter
labor Intervals in a subsequent vaginal trial of labor (VTOL) compared to
patients delivered by CS before or during the acnve phase of labor.
METHODS: Patients were identified whose only prior dehvery after 20
weeks’ gestation was by CS; the timing of dehvery was determined as
prior to the active phase (no labor or during latent phaseL or during the
active phase or second stage of labor The charts of 182 panents ware
reviewed In whom the subsequent pregnancy was a singleton, vertex
presentation _>37 weeks’ gestation and the onset of labor was
spontaneous. Data regarding VTOL were collected and also compared
to those of nulhparous patients (n=44) and patients with one prior
vaginal delivery (n=44)
RESULTS: For pahents w~th CS prior to the active phase (n = 45), during
the actwe phase (n= 100), or during the second stage of labor (n=37),
the rates of’ CS ~n the subsequent labor were 16°/o, 23°/0, and respectively (p = NS) There were no s~gn=ficant differences among these
three groups in maternal age, interval since the first delivery, gestatlonal
age at dehvery, birth weight In the first or second pregnancy, or usage
of epldural anesthesia or forceps. Patients with a prior second stage CS
were s~gmhcantly more dilated on admission than patients in the other
two groups (3.4 + 1,8; 3.0 ± 1.6; 4.5 ± 1.9, p < .01 ), and their labors
were less frequently augmented with oxytoc~n (67%; 73%; 46%,
p< .05). Although the mean interval from admission to vaginal dehvery
was shorter for patients with a prior second stage CS (422 + 229; 444
_+ 219; 303 + 186 ram,, p =.01), the lengths of the active phase and
second stage of labor were similar in the three groups of patler~ts. None
of the VTOL groups d~ffered from nulhparous panents ~n the lengths of
the active phase or second stage of ~abor, and al~ three groups had ~abor
intervals longer than those of patients with one prior vaginal dehvery.
CONCLUSION: For patients undergoing VTOL, progress =n the prior labor
does not influence labor intervals m the subsequent labor.

378 SPO Abstracts January 1994 Am J Obstet Gynecol
368 The Accuracy of CtJm~cat Est~lmtesof Uter~nePressures (Nantevideo
Units) in ActiveLa~or. L Appteahite~, More[ M, F[eisher dX, Minkoff
H. Oept Ob/Gyn SUNY Hearth Science Center at Brooktyn
OBJECTIVE: To determine hoe accuratety ctinicians gauge the
adequacy of contractions in patients aho are in active tabor and to
assess the determinants of accuracy,
STUDY DESIGII: A prospective study was performed at the Eings
County Hospitat Center betueen 10/92 and 7/95. Fifty pregnant
Ho~en in active tabor ~ith vertex presentations were entered after
a ctinicat diagnosis of dystocia in the active phase of tabor Has
made. Patients ~ith fete( distress or fetat compromise were
exctuded. After t~o hours Of oxytocin augmentation~ ctinicians
estimated the Montevideo Units. An internat pressure transducer
Has then ptaced and Montevideo units vere recorded. Adequate
contractions were defined as 200 Montevideo units or greater. A
data sheet containing information on ctinician experience as wett
as maternat and intrapartum factors was compteted.
RESULTS: When defining "accuracy" as pressure estimates ~ithin 10%
of the recorded pressures~ clinicians Here accurate 46% of the
time. When defining "accuracy" as correctty predicting whether
contractions ~ere adequate (>200 Montevideo units), they were
accurate 57% of the time. Junior residents were within 10% of the
recorded pressures 58% of the time while senior residents ~ere
accurate 55% (p=0.10). The sensitivity for predicting adequate
contractions was 53% ~hile the specificity was TS~ (27% of the time
patients Here fett to have achieved adequate contractions and to
need no further augmentation Hhen in fact contractions ~ere
inadequate). The ctinicianslassessment of fetat wett being (by FHR
reading) and the patients~ desire for cesarean section did not
inftuence the accuracy of ctinician estimates.
CONCLUSI(]#$: Ctinicat estimates of uterine pressures improve ~ith
experience but are often inaccurate. Without the use of pressure
transducers patients may not receive adequate oxytocin augmentation
prior to cesarean detivery for dystocia.
370 IS LABOR ABNORMAL IN PROLONGED PREGNANCY> N T F~eld, E M J Xenak~s, D Barshesx, O Langer, Dept of O~/~he Umvers~ty of Texas Health Science Center at San Antomo, TX OBJECTIVE: Controversy ex{sts as to whether labor is intrinsically abnormal or less efficient m prolonged pregnancies s~mply by wrtue of ~ts delayed onset The objechve of th~s study was to evaluate the labor charactenst~cs m post date gestat{ons STUDY DESIGN: In an ongoing prospective study, 86 consecutive prolonged pregnancies (gestat~onal age ~42 weeks) were identd~ed from all dehver~es during a 6 month period All study patients had soda.graphic confirmation of ~estatlonal age prior to the thtrd trimester Women were classified into one of three labor categories (spontaneous, augmentation, or induction) and various Intrapartum labor characteristics Including mode of dehvery were assessed Eighteen hundred term patients (gestat~onal age 37 41 weeks) who delivered w~th~n the same t~me Interval servedas a reference control population RESULTS: When matched by specific labor category, there was no d~fference ~n any of the following labor parameters between prolonged pregnancies and term controls length of labor, length of active phase, length of second stage, mean Montevideo umts m active phase, or time required for correction of labor abnormaht~es (augmentation group). The overall cesarean section rate among prolonged pregnancies was 7 2% compared to 13 7% for all deliveries at our institution during the same time period (p <0 05) Post date pregnancies had s~mJJar rates of oxytocln labor augmentation as the term control population (23% vs 28%, NS) and the Incidence of abdominal dehvery for uncorrected labor abnormahUes was 10% among prolonged gestations Although patients w~th prolonged pregnancies had a 3x higher likelihood of undergoing labor induction, only 3 6% required cesarean section for failed induction and this number was not significantly higher than the 2 8% rate seen in the control group CONCLUSION: Our data suggest that after the ~mtlat~on of labor In prolonged pregnancies, proper intrapartum management results ~n s~mllar labor characteristics, an equally low ~ncidence of uncorrected labor abnormahties, and comparably h~gh success rates of labor induction as in term pregnancies
369 EFFICACY OF HIGH DOSE VERSUS LOW DOSE OXYTOCIN IN LABORAUGMENTATION E _M-J Xenakis, N F~eld, D Barshesx, O Langer Dept of Ob/Gyn, UT~SC, San Antomo, TX OBJECTIVE To assess the efficacy of low dose versus high dose oxytocm m augmentation of labor STUDY DESIGN In an ongoing prospective study, pahents requiring oxytocin augmentation for labor abnormahtles were randomized into one of two different oxytocm protocols’ low dose oxytocm group (lmU/mln every 30 minutes) and a high dose oxytocm group (4 mU/mm every 15 minutes) Patients with abnormal presentations and absolute obstetrical contramdlcatlons to labor were excluded All patients were monitored w~th intrauterine pressure catheters RESULTS’, Both groups were comparable in demographic data (maternal age, parity gestatlona~ age, race) and maternal and neonata outcomes were similar Uterine hyperst~mulatlOn occured In only one patient in the h~gh dose protocol without adverse outcome for the mother or the fetus Comparison of multiple labor parameters bewteen the two different oxytocln protocols are shown in the table below, (mean _+ SEM)
Labor Parameters n = 35 n = 33
*p- oos
CONCLUSIONS H~gh dose oxytoc~n labor augmentation requires both less t~me for correction of labor abnormaht~es and less total time on oxytocln However, both groups had similar cesarean section rates
37! INDOMETHACIN AS A "RESCUE" TOCOLYTIC IN PRE-
TERM LABOR. B. Nevrls, L. Curet, L. Izqmerdo, M.
Chatterjee, G. Gilson, J. Macmlla, C. Barada*, Dept. of
Ob/Gyn, Umv. of N.M., Albuq., N.M.
OBJECTIVE: To test the hypothesis that ~ndomethacrn ~s an
effechve "rescue" drug rn pahents who farl other tocolytics.
STUDY DESIGN: 45 patmnts 24-34 weeks gestatron adn’utted
for pre-term labor were randomized to receive either oral
rndomethacm or rntravenous terbutaline for the imttal 48 hours
of tocolys~s. Patmnts who faded or had unacceptable side
effects on terbutabne were give ~ndomethac~n as "rescue"
therapy ~n an attempt to gain 48 hours for steroid therapy,
RESULTS: 32 patients met ~nclusmn criteria. There were no
d~fferences between pattents ~n erther the Indomethac~n (n=9)
or terbutabne (n= 13) groups. Patients m the "rescue" group
(n= I0) had stahshcally s~gmficant drfferences ~n brrth weight
(p=.001), number of nursery days (p=.0001), cervrcal ddation
(p=.0001) and number of days gamed (.0001). Maternal side
effects were more common wtth terbutahne (21.74% vs 5.26%). There were no ~nc~dence of hemodynam~cally
stgmficant constrictron of the ductus arteriosus.
CONCLUSION: lndomethacm appears to be a good "rescue"
tocolyhc to garn 48 hours to enhance fetal lung maturity with
steroids. The lower brrth werght, greater cervmal ddation,
longer nursery stays reflect patients with more advance pre-term
labor and the number of days gamed is crrtrcal to enhancing
lung maturity.
Volume 170, Number 1, Part 2 SPO Abstracts 379 Am J Obstet Gynecol
372 EVIDENCE FOR A DRAMATIC CHANGE IN Tile AVAILABILITY OF AN IMMUNE SOLUBLE CYTOKINE RECEPTOR WITII tlUMAN PARTURITION. R. Romero, M. Galassoz, R. Gomez’, S. Berry, M. Ramirez~, D.B Cotton. Dept. OB/GYN, WSU/Hutzel Hospital, Detroit, MI, the Permatology Branch, NICHD, Bethesda, MD and T-Cell Diagnostics, Cambridge, MA. BACKGROUND/OBJECTIVES: The departure of the fetus from a sterile to a non-sterile environment is major blologlcal challenge to the immune system. We have conducted a series of studtes to determine if there is any evidence of changes in the avallabdlty of potent anmano-modutators during pregnancy and parturitton in the human fetus Becaase interleukln-2 is crucial In the acttvatlon and modulation of complex immunological phenomena and exerts its actions by interacting with specific receptors, we sought to determine’ 1) the presence/concentrationsof soluble mterleukin-2 receptor (sIL-2R) in fetal blood (obtained by cordocentesls) mad amniotic fluid as a function of gestational age; 2) the effect of parturition and infection (both term and preterm) in the concentrations of sIL-2R in amniotic fluid (AF) maternal blood (MB) and cord blood (CB). STUDY DESIGN: Samples were collected from 242 patients in the following groups midtrimester (n=lS), preterm labor (n=l14) and term (n= 110). Feud serum (FS) was retrieved from 39 patients who underwent diagnostic cordocentcsis, slL-2R w~ measured by ELISA validated for AF and serum
RESULTS: 1) sIL-2R was detected in all MB and CB samples; 2) fetal serum sIL-2R �oncentraUons increased ~ a function of gesuaianal age (Spearman’s r=0.57, p<O 01); 3) AF concentrations of sIL-2R decreased with advancing ges~.tlonal age (p (0.05, Mann-Whitney U test); 4) Term parturition was associated with a s~gmflcant decrease in the AF, MB and CB concentrauon of slL-2R (p (0 05 for each compartment and comparison). A slmdar effect was also demonstrated m the AF of preterm p~tients; 5) In preterm gestation, infection w~ associated with an increase in the concentrations of sIL-2R in AF and CB, but not m MB (p (0.05 for each). CONCLUSIONS: 1) sIL-2R is a normal constituent of maternal, cord and feud blood 2) Feudal serum sIL-2R concentrations increase with gestational age m feud blood 3) Term parturaion is associated with a decrease in AF, MB and CB concentrations of the slL-2R. 4) Intrauterine infection increases the concentrauon of slL-2R in AF and CB in preterm gestation. 5) Collcctwaly, our data suggest that major changes in ~mmuno-modalation occur in preparation for human b~rth.
374 PRE-INDUCTION CERVICAL RIPENING: LOW-DOSE OXYTOClN IS AS EFFECTIVE AS
INTRACERVICAL PROSTAGLANDIN E2 GM Jackson MD. HT Sharp MD*, MW Varner MD
Dept of Ob-Gyn, University of Utah,Salt Lake City, UT Objective: To compare a low-dose oxytocin infusion (L-D Oxy) to intracerwcat prostaglandin E2 (PGE2) for cervical ripening. Study Design: A prospective, randomized, double-blind clinical trial. Patients admitted for induction of labor after 26 weeks gestational age (GA) with a Bishop score (BS) of _< 5 were eligible; exclusion criteria were vaginal bleeding, contractions ¯ 6/hour, and allergy or contraindications to PGE2. 49 patients received two doses of intracervical PGE2 (0.5 rag) s=x hours apart with an IV infus=on of saline; 48 patients received IV oxytocin (to 4 mU/min) w~th two intracervical doses of placebo gel. After 12 hours, labor was induced w~th oxytocin. Outcome variables included route of dehvery and hme from beginning ripening to delivery. Data were anatyzed w~th Student’s t-test, Chi2 test, and Fisher’s exact test. Results: Maternal age, panty, GA, and initial BS were similar [n the two treatment groups. There were no differences in cesarean section (C/S) rate, C/S for failed induct=on (CiS-FI), vaginal delivery (Vag Del) rate, and patients not dehvered (Not Del) between the two groups of pahents. L-D OXY (n=481 PGE2 (n=491 C/S (Rate) 10 (2O.8%) g (18.0%) p=NS C/S-FI (Rate) 1 (2.1%) 1 (2.O%) p=NS Not Del (Rate) 3 (6.3%) 3 (6.0%) p=NS Vag Del (Rate) 35 (72.9%) 37 (75.5%) p=NS Hours Rip-Del (mean ± SD) 26.5 +10.0 20 3 ± 7.9 p=.001 This study has >80% power to show a 300/o decrease in Vag Del rate. Conclusion: L-D Oxy is as effective as PGE2 for ensuring vaginal delivery after labor induction, although a longer interval from ripening to dehvery is necessary.
373 AMN1OINFUSION AND VAGINAL BIRTH AFTER CESAREAN SECTION. V Cook, W Roy," JA Spinnato University of Loulsvdle, Louisville, KY OBJECTIVE: The null hypothesis is that amniomfnslon (AI) may be safely performed during vaginal b~rth after cesarean section (VBAC) attempts STUDY DESIGN: A two year retrospective chart review was conducted of all VBAC attempts achieving actwe labor (cervical ddamtlon > 3cm) The outcome and compllcations of those requiring therapeutic AI for management of variable decelerations or meconium stained amniottc fluid was compared with those who dtd not RESULTS: 146 of 326 women (44 8%) recetved AI during attempted VBAC. Of those requiring AI, 108 (70 5 %) delivered vagmally versus 156 (86 7%, p < 01) of those not requtring AI for an overall 80 1% VBAC success rate. There were no uterine ruptures though 3 uterine scar separations of varying extent were noted in the non AI group and 6 in the AI group (p = NS). The incidence of chorioammonitts was nearly identical in the two groups (9 non A/vs 11 AI, p = NS). Endomyometritis developed in 12 women in the AI group (4 of whom delivered vaginally) and 3 women tn the non AI group (p = NS) Route of Apgar score Dehvery (n) 1 mm 5 min Cord arterial pH Vaginal < 4 < 7 < 7.1 mean SD w~th AI 108 1 2 5 7 24 06 without AI 156 2 3 1 7 26 06
with AI 38 4 5 7 7 18 12 without AI 23 1 0 0 7 23 06
p value NS NS < .005 < 01 Of those delivered by cesarean section, I2 of 38 recetving AI and 5 of 23 without AI underwent cesarean delivery for abnormal fetal heart rate tracing (p = NS). CONCLUSIONS: In th~s review, AI was associated with a lower VBAC success rate, an increased frequency of cord pH < 7 1, and a lower mean cord pH. These associations may be attributed to use of AI in management of protracted labor or abnormal feud heart patterns whtch predispose to the noted associations AI may be safely performed during attempted VBAC without increased risk of uterine scar disruption or infectious complications
375 .THE EFFECTS OF ACUTE COCAINE USE ON DURATION OF LABOR. A. Hacobian, MD.x, N. Oriel, MD.x, K. Park, MD.x and E. Friedman, MD.x Beth Israel Hospital, Boston, MA 02215 OBJECTIVE: The purpose of this study is to evaluate effects of acute cocaine use on labor In recent years, lay pubhc has held that cocame use makes labor faster and less painful
STUDY DESIGN: After approval by the mstttut~onal Comwattee on Chmcal hwesttgattons, the charts of 71 pahents who had used cocaine wtthm 48 hours of dehvery were revtewed The vanables recorded tnclude panty, pattern of labor progresston (sequenhal cervical ddatton and fetal statton), btrth wetght(BW) and Apgar score RESULTS: 71 pattents were admflted m acttve labor, l 6(23%) of them were dehvered by cesarean sectmn Of the remainder, only 35 had enough documentatton of labor course to be graphable accordmg to Friedman labor curves (1 e, to permtt reconstructton of the ddahon-ttme and descent-ttme curves for the purposes of calculahon of the various component parts of the labor pattern) All but 6 were mnltlparous, therefore, we hrmted our analys~s to the 29 mult~paras Mean BW for the study group was
2717+536g 9 of the 29 (24%) study group babtes had an imttal Apgar score of <7 at 1 mmute When compared to control groups(multtparas, n=500, and mulhparas w~th BW of 2500-2999g,n=94)there was no appreciable change tn overall length of labor, although the durahan of deceleratton phase and second stage was prolonged (P< 05) m the cocaine group Maxtmum slope of descent (measure of rate of fetal descent) was s~gnificantly and consastently mcreased above that of control (P< 01) CONCLUSIONS: Cocame d~d not change overall length of labor However it caused raptd fetal descent, t e precipitate descent wtuch is assoctated v~th tow tmttal Apgar sores and depressed neonates as was found m 24% of cocaine negnates

380 SPO Abstracts January 1994 Am J Obstet Gynecol
376 COMPARISON OF INTERNAL AND EXTERNAL UTERINE
ACTIVITY MONITORING IN PREGNANT RHESUS
MONKEYS. H. Umezaldx, G.J. Valenzuela, V. Pazemenasx, B
Brimmerx, C.A. Ducsayx. Div. Pednatal Blol, Loma Linda
University, Loma Lind& Dept. Ob/Gyn, SBCMC, San Bernardino,
Carelink Corp., Santa Ann, California.
OBJECTIVE. To compare the efficacy of external monitoring
(EM) with internal uterine activity monitoring (IM) during the latter
part of gestation, before labor.
METHODS. Rhesus monkeys (n=3) underwent surgery for intraamniotic catheter implantation between days 115 and 119 of
gestation (term=167days). The animals were maintained in a vest
and tether system equipped with an external tocodynomometer. We
measured uterine activity simultaneously with EM and IM
(intraamniotic pressure) between days 115 and 129 and again
between days 150 and 159 of gestalaon. We compared the number
and amplitude of contractions recorded at two time intervals (0900
to 1200h.AM and 2100 to 2400h’PM).
RESULTS, No differences were ~served m the number of
contraclaons/h recorded by IM vs. EM (AM = 5.9-~-0.9, IM vs.
5.3:~-0.8, EM; PM = 11.0~1.3, IMvs. 9.7~1.2, EM). Both methods
showed a higher number of contractions in the PM vs AM
(p<0.01). Similar trends were noted for contraction amplitude.
CONCLUSIONS. 1) Uterine activity recorded by EM was higldy
correlated with IM at two different stages of gestation, prior to labor.
2) EM may be useful for patients at high risk for preterm labor. 3)
Our studies in human and non-human primates have shown a
nocturnal increase in contractile events. The time of day of EM may
therefore be important to fully realize its predictive potential.
378 RISK FACTORS FOR SPONTANEOUS PRETERM BIRTH IN
TWIN GESTATIONS. G. Berkowitzx. R. l~kix, R. Berkowitz.
DepL Ob/Gyn, Mount Sinsl M~dical Cent~, New York N.Y. OBJECTIVE: This study was underteken to aase~ risk factort for
spontaneous preterm bkth (< 37 weeks of gestation ) and very preterm
birth (< 34 weeks of gestation) in twin pregnancies.
STUDY DESIGN: The study population coml~ised 418 ~ts of twins delivered during 1987-92 that had not undergone a multifetal pregnancy
reduction. Of these, 201 (48.1%) delivered before 37 weeks and 77 (18.4%) before 34 weeks of gestation. Categorical variables were evalaated by z2 analysis and Fisher’s exact test where appropriam and
continuous variables were compared by Student’s t-test. Logistic
regression analysis was used to evaluate which risk factors were
independently related to preterm birth.
RESULTS: There was a significant positive association (p<0.05)
between delivery before 37 weeks ami hkthweight percentile of either twin as well as a suggestion of a posidve trend (p=0.09) wi~ increasing
maternal weekly weight gain (corrected for the blrthweights of the twins).
No significant associations were observed between delivery before 37 weeks and maternal age, clinic vs. private service, racedethni¢ity, parity,
pregravld weight, a history of infertility, use of fertility medications, in viU-o-fertilization ixegna~y, or sex of the infants. For pret~m deliveay
before 3~ weeks, African Americans, Hispanies~ young woroe~ patients
on the clinic service, and twin gestations concordant for male sex were at increased risk. There was also a significant trend (p<0.001) with
increasing birthwelght percentile of either twin. Only non-white
race/ethnicity and birthweight percentile remained as independent risk
factors in the logistic regression analysis.
CONCLUSIONS: Few r~k factors were idonfified for delivery either before 3~ or 37 weeks in twin gestations. Apart from the increased risk
for non-whites of delivery before 34 weeks, traditional risk factors for
pretorm birth in singietoes do no appear to play a role in twin ge~statinns.
377 PREMATURE RUPTURE OF MEMBRANES AT TERM: INDUCTION OF LABOR WITH INTRAVAGINAL
MISOPROSTOL TABLETS (PGE1 ) OR INTRAVENOUS
OXYTOCIN. L. Sanchez-Ramos. A. Chertx, D. Brionesx, G.O.
Del Valle, F.L. Gaudier, I. DelRe. Department Obstetrics and Gynecology, University of Florida, Jacksonwlle, FL
OBJECTIVE: To evaluate the clinical effectiveness of Jntravagmal misoprostol tablets (synthetic PGE1 analog) for
cerwcal npening and labor ~nduction m patients with premature rupture of the membranes (PROM) at term.
STUDY DESIGN: This was a prospecbve randomized climcal
teal Eligible patients were randomly assigned by means of a computer-generated hst to one of two groups’ intravenous oxytocin infusion or misoprostol tablets (50 mcg) administered
~ntravaginally. Group allocation was predetermined and placed in consecuhvely numbered and sealed envelopes. Oxytoc~n was used for augmentahon in patients w~th arrest disorders in both groups. The main outcome measures included: ~nduction to vaginal
dehvery ~nterval, total length of labor, total dose of oxytoc~n, mode
of dehvery, and maternal and perinatal outcomes. RESULTS: 99 pahents were entered into the study. One patient was excluded due to refusal to participate after randomization
(m~soprostol n=47; oxytoc~n n=51). Patients recmving misoprostol were more hkely to dehver (77%) after a single dose and required s~gnificantly lower doses of oxytocin; 607.2 + 2540 mU vs 5482 8 +
9279 mU; P <.0001. The time ~nterval to vaginal dehvery was similar ~n both groups. In the m~soprostol group, 23% required operahve delivery compared to 33% m the oxytocin group; RR 0.76, 95% Cl
0.46 to 1.28. No differences were noted in the incidence of cesarean sections or maternal and pennatal complications CONCLUSIONS: Misoprostol can be used successfully to
induce labor after PROM at term with greater ease of administrahon
when compared to oxytoc{n ~nfus~on
379 A WEIGHTED RISK INDEX FOR ANTENATAL DETECTION OF PATIE NTS
UKELY TO HAVE A LOW BIRTH WEIGHT INFANT B K Young, J. Altma_n, F Innamorati, I A Hosk~ns Dept OI3/GYN, NYU Medical Center, NY, NY
OB3ECTIVE To develop an antepartum nsk sconng system that would
identity those patients at increased risk for delivery of a low birth weight
infant
METHODS Due to the relatively poor performance of existing screening
techmques a weighted nsk sconng system was dowsed empirically to
charactenze those pahents at ~ncreased nsk for low bath weight infants ~n an inner city chntc population. All patients were scored antepartum and a
threshold score for increased nsk developed based on a retrospechve
analys~s of outcome data One hundred fifty patients were then evaluated
prospechvely, employing the Risk Index to idenhty the group at highest nsk
for low birth weight No special treatment was given this group beyond standard care, mnce they were managed by physicians blinded to the Risk
Index scores No scores were changed after the onset of labor, but were
updated at each chnlc wsd The outcome studied was birth weight below
2500 grams The risk score ranged item g to 42 m md~wdua~ patients, with
a score of 6 the threshold level selected for increased risk
RESULTS W~th a level of less than 6, 70% of the population was low risk
for mulhple outcome variables. This ~s comparable to the observed
distribution in the general obstetrical populatmn at our hospital For a risk
score greater than or equal to 6, dehvery of a fetus weighing less than 2500
grams had a relative nsk of 5 1 w~th a 2 ta~led p-value of 0006 and 96%
confidence interval of 2 0-13 1. CONCLUSION A nsk scoring system was developed that was h~ghly
successful at predicting low birth weight Identification of the patient at a 5-
fold increased nsk of dehvenng an infant weighing less than 2500 grams was
achmved Tile high predictability ofth~s ~ndex compares favorably with other
radices and may allow early mtervenbon to prevent low birth weight
Identification by apphcation of the Rink Index in antenatal chmcs would select
those patients best served by intensive obstetrical care

Volume 170, Number 1, Part 2 SPO Abstracts 381 Am J Obstet Gynecol
380 ORAL SULIMDAC TO PREVENT RECURREX~OFPRETERMLABOR. S Carlaq, M Jones, S Schorr, T McNeiLl, H Rawji, K Clark. Arnold Palmer Hospital for Children & ~on)en (APH), ORHS, Orlando, Florida. OI]JECTIVE: To assess the efficacy and safety of oral suli ndac In women at risk for recurrent preterm delivery. STIJI)Y DESIGN: Prospective, placebo controlled, blinded,
randomized clinical trial. Patients were consideredeLigibLe for
the study if they had a gestationa[ age of 20 to 34 weeks, a
diagnosis of arrested preterm labor, ar~ a cervical dilatation
of <4cm. The usual contrai ndications to tocolysis were observed. All patients were having a first episode of preterm Labor and were treated with intravenous MgSO,. After a 12 hour contraction free perlod, patients were randomized to: Group I (suL1ndac 200 mg - paq12h), Group 2 (placebo, - poq12h), and treated for 7 days. Ultrasound examinations were scheduled before and at one and two weeks after the start of medication. RESULTS: Twenty-eight patients were randomized. No difference was found between the groups with respect to demographics, Cx dilatation or contraction frequency at admission, time gained in utero, or completion of 35 weeks. There were no maternal or fetal side effects, and there was no difference with regard to hourly fetal urine production, amniotic fluid index, or ductus arteriosus velocity at pre-medication, 7 days, or 14 days after. Mean ± SD Sulindac(N=13) Placebo(N=15) p EGA (weeks) 30 ± 2.4 29 ± 2.5 NS Cx di[ at randomization (cm) 2.44 ± 1.4 2.40 ± 1.2 NS US Cx Length at Rand. (cm) 2.87 ± 1.5 3.1 ± I.~ NS Read~ission for Tocotysis N(%) 5 (38) 9 (60) NS Interval from Rand.-Birth (d) 33 ± 25 26 ± 17 NS GestationaL Age at Birth (wks) 34.5 ± 3.3 33.3 * 3.8 NS Birthweight (gr) 2410 ± 688 2223 ± 766 NS Days on Ventilator .6 ± 1.9 1.2 ± 2.2 NS Days NICU 8.7 ± 19 10.9 ± IB NS CONCEUSIOW: Placebo and observation are as effective in prolonging pregnancy and preventing recurrent preterm tabor as a 7-day course of oral sulindac.
382 PLACENTAL AND NEONATAL ASSOCIATIONS WITH EARLY
INTRAVENTRICULAR HEMORRHAGE IN INFANTS BORN <32 WEEKS
GESTATION. C Salaha~, L Ernst,x J Pezzullo,x A Vintzileos, T Resenkrentz,x V
Minterx, C Kamensx, Univ. of CT Health Center Farm~ngton CT, Wayne State Univ. Medical College, Detroil MI OBJECTIVE: To s~udy relatlaesh~ps ol placental and neonatal ladors Io eady intraventricuiar hemorrhage (IVH.] STUDY DESIGN: A relrespective study o1154 singleton live born nananomalous inlanls born <32 weeks rewewed records to extract: gestational age at birth (GA), growth measures, cord venous and a~lenal pH, hernatocril and WBC (day I), and (in each ol the Isl 3 days ol life), lowesl p02 and pH and Nghest pC02, oxygen deseturation events (<B8%), lowest blood pressure, treatment with sudactant and volume expanders, mean a~rway pressures, and hypoglycemia. Paired observers, bhnded to all chrncal data except gestational age, rewewed histolngic shdes to assess lesions, including severe acute histologic acute inflammation (AI) and severe histologic ewdence ol abruption (ABR). IVH was d=agnosed by uitrasonogram <72 hours after bHh
RESULTS: AI and ABR were s~gr, iltcantly related to early IVH independent of
GA(p<0 05), Neonatal lectors associated (i)<0,05) with IVH were.need |or volume expansion m the delivery reorn (7/21 (339’0) IVH v. 17/123 (13%) non IVH), lower
systohc blood pressure (d.1, 35.7 +/- 7 IVH v. 39 +k 7 non-IVH), lower hematocrlt
on d.1 (43+/- 7 IVH v. 47+/- 7 non-IVH). Neonatal lantors associated (.0<0.05) with AI were.volume expansion at delivery, lower mean systolic blood pressure (d. 1 ; 34+/- 7 IVH v. 38 +/- 7.6 nonlVH), bwer mean I)O2 d 1 (44 8 +/- 14 IVH v. 56 8
+/- 26 non IVH), lower mean hematocrit on d. 1 (42+/- 11 IVH v. 46 +/- 6 nonlVH), and ~ncreases in cord WBC, ~mmature circulating myeloid elements, and toxic granulations of erythrecytes. Factors associated with ABR were greater number ol nucleated RBC, higher mean pCO2 (d. 1, 51 +/- 14 IMH v 45 +/- 10 non IVH), lower pH (d 1, 7 27 +/- 15 IVH v 7 32 +/- 1 nonlVH), and increased oxygen desaturahons <889’o (d 1). There were complex interactions among neonatal
ladors and AI/ABR with IVH Surlactant use was unrelated to IVH CONCLUSIONS: At andlor ABR are s~gnificanfty related to early IVH and with
early neonatal abnormal=feB in oxygenation, perlusion and blood volume. AI and ABR may be causally related to early IVH
381 INCREASED INTERLEUKIN-6 (IL-6) LEVELS IN CERVICAL
SECRETIONS ARE PREDICTIVE OF PRETERM DELIVERY BUT NOT OF INTRA-AMNIOTIC INFECTIONS.
C J Lockwood, R Welr~, A Gh~dmr~, R Lap~nsk~, M Alvarez and
D Casal~. Mount Sma~ School of Medicine, New York, NY.
OBJECTIVE: This study sought to determine whether elevated levels of
IL-6 ~n the cervical and vaginal secretions of ~niually asymptomauc
panants were predicttve of subsequent spontaneous preterm dehvary (PTD)
and/or intrapartum and postpartum mfect~ons. STUDY DESIGN: A retrospective cohort study was undertaken utihz~ng
cervical and vaginal san~ples collected from 161 consenting patients seen
at four week ~ntervals between 24 and 36 weeks Levels of IL-6 in the
sample buffer were measured by a sensitive mm~unoassay.
RESULTS: There was a 4.2~ and 3 4-fold increase m maximal cervical
and vaginal 1L-6 concenrratmns, respectively, anrong patients dehvermg preterm compared with those dehvarmg at term. Receiver Operator
Characteristic curve analys~s indicated that the optimal IL-6 predictor was
a single cervical value > 250 pg/ml present between 24 and 36 weeks
[sensmv~ty = 50 5% (95% Confidence Interval 33.2o/’o to 66.8%),
specificity = 85.0% (78 8% to 91.2%); and posture and negative
predictive value = 47.2% (30.9% to 63,5%); and 86 4% (80.4% to 92.4%),
respectively[ The opumal vaginal IL-6 cut off value (>125 pg/ml) was a
less sensitive [45.5% (28.5% to 62.4%)] but equally specific [86 6%
(807% to 92.5%)] predictor of PTD. Multiple logistic regressmn
indicated that a cervical IL-6 level > 250 pg/ml was an independent
predictor of preterm dehvery [adjusted odds ratio = 4.2 (l.6 to 10.6)]
However, there were no differences in the degree of cervical dilatauon or
effacement, the prevalence of vaginal pathogens or an alkaline vaginal pH, the mean white blood cell count or the prevalence of preterm
membrane rupture, chorioamnionitis or endomyometrltlS among patients
dehvermg preterm with cervical IL-6 values > 250 pg]ml vs. <_ 250 pg/mL
CONCLUSIONS: Cervical IL-6 determmatmns are relatively
insensitive, though h~ghly specific predictor of PTD. Moreover, among
patients dehvermg preterm, there ~s no apparent assomahon between
elevated cervical IL-6 values and subsequent mlra-ammottc refections
383 MATERNAL AND PLACENTAL ASSOCIATIONS WITH EARLY INTRAVENTRICULAR HEMORRHAGE IN INFANTS BORN AT <32 WEEKS
GESTATION: C Salafia~, L Erost,x J Pezzullo,x A Vmtzileos, T
Resenkrantz,x V Min~rx, C Kamansx, Univ. of CT Health Center Farmington
CT, Wayne State Univ. Medical Cotlnge, Detroit ML OBJECTIVE: To describe relationships among rnaterna~ and placental factors to early intraventricubr hemorrhage (IVH).
STUDY DESIGN: A retrospective study of 154 singleton liveborn nonanornalous in|ants born at <32 weeks reviewed medical records to extract, gestational age at birth(GA), mode o| delivery, use o! antenatal
steroids(AS), presence of labor and tocolytlc use, labor augmentation, fetal heart rate abnormalities, and biephysical profile score immediately before birth and its separate components. Paired obse~,ers, blinded to all clinical
data except gestat~onal age, reviewed shdes to assess decidual and placental lesions =ncludmg severe acute h~stolog~c inflammation (AI) and
severe Nstolegic evidence o| abruption (ABR). IVH was diagnosed by ultrasonogram <72 hours o! Nrth
RESULTS: 30/154 (19%) had IVH. Using multiple logistic regression
analysis, 4 factors were associated with IVH signd=cantly and independently
of GA (1) Severe variable or prolonged decelerations (10/30 (33%) IVH v 16/124 (13%) non-lVH, p<0.01), (2) Muitip/e tocotybcs (v. none or single
drug) (12/30 (40%) IVH v, 21/124 (17%) non-lVH, p<O 05), and (3) AI and/or ABR( 24/30 (80%) IVH v. 74/124 (60%) non IVH). No significant relationship was seen between AI and/or ABR and tocolytic use or fetal heart rate abnormal=hes Delivery mode (vaginal v. section, p= 0.10), presence o! labor
(p=O 12) and augmentation ot labor (p>O.20) were not related to IVH in any analyses CONCLUSIONS: (1) Use ol multiple tocelyties and severe variable or
prolonged fetal heart rate decelerations (but not labor, augmentation or
delivery mode) carry sgnificant and gestational age independent nsk o| early
IVH. (2) Acute hlstolngic inflammation and severe hisiofegic abrephon carry risk of IVH which is independent of gestational age and clinical antenatal lactors. Early IVH may be initiated in the antepartum pedod.

382 SPO Abstracts January 1994 Am J Obs[et Gynecol
384 CATALASE ACTIVITY AS A PREDICTOR OF AMNIOTIC
FLUID CULTURE RESULTS IN PRETERM LABOR OR
PREMATURE RUPTURE OF MEMBRANES,
Font Gx, Gauthier D, Meyer W, Bieniarz A, Rotmensch S, Janda W~,
University of Illinois College of Medicine, Chicago, Illinois.
OBJECTIVE: Catalase activity has been utilized as a rapid screen for
urinary tract infection. The purpose of this study was to evaluate catalase
activity as a rapid predictor of amniotic fluid cultures.
STUDY DESIGN: The ~tudy population consisted of patients ~< 36
we.~k s gestatton with preterm labor or premature rupture of membranes.
Patients were excluded if there was evidence of clinical chorioamnionltis
or feLaldlstressat tlme of admisslon. All patlent~underwent amnloeentesls
within 24 hours of admission. The arnntotie fluid was cultured for aerobic
and anaerobic bacteria and Mycoplasma species. An amniotic fluid Gram
stain was performed and stained slides were examined by microbiology
technologists Amniotic fluid catalase activity we* determined
immediately after amnioeentesis using a commercially available kit. The
sensittvity and specificity of Gram stain m~d caudt~s~ ~ctivtty were
compared wtth McNem~r’s test
RESULTS: There were 20 patients with preterm labor and 25 with
premature rupture of membranes who underwent amniocantosis to assess for
subclinical infection. Ammotic fluid cultures were positive in 40% (18/45).
The sensittvity, specificity, positive and negative predictive values of Gram
stain and catalase activity in predicting culture results are outlined below:
Sensitivity Specifictty Positive PV Negative PV Catalase actwity 94% 07118) 93% (25/27) 89% (17119) 96% (25126)
Gram stain 33% (61t8) 100% (27/27) 100% (6/6) 69% (27139) Catalase activity was significantly more sensitive than Gram stain (p <0.001)
in detecting positwe ammotic fluid cultures.
CONCLUSIONS: Catalase activtty is a rapid and simple test that is useful in
assessing for subclinical intr~xnniotic infection in preterm labor or
premature rupture of membranes.
386 THE USE OF A MODIFIED VAGINAL POUCH FOR THE DIAGNOSIS AND MANAGEMENT OF PRETERM PREMATURE RUPTURE OF THE FETAL MEMBRANES J.M. O’l~nen. B. M. Mercer, B. M. Sibai, University of Tennessee, Memph=s OBJECTIVE: This study evaluated a noninvasive method for the collection of amniotic fluid-use of a modified vaginal pouch--to assist =n the diagnosis and management of preterm premature rupture ot the fetal membranes (pPROM). STUDY DESIGN: Twenty-two women w=th confirmed or suspectedpPROM were evaluated by the use of a modified REALITyTMvag~nal pouch. The mod~hed pouch was placed within the vagina m a manner s~mdar to that of a contraceptive diaphragm. Amniotic flmd accumulating w~thin the reservoir was d=agnostic of pPROM and was sent for pulmonary maturity studies as indicated. Forty-two patients matched for gestational age at pPROM end use of prophylactic anhb~otics were randomly chosen from 96 eligible controls. Outcomes in this group were compared against those pahents requiring ammohc fluid for maturity studies (ratio 3:1). RESULTS: Of the e=ght women who were evaluated for poss=ble pPROM, the modified vag=nal pouch was helpful in establishing a diagnos~s in all patients. Of the fourteen patients in whom the modified pouch was utilized to collect amniotic fired for maturity s’tud~os, the device was effective in thirteen (93%). The pouch was in place for a median duration of six hours. The med=an volume of fluid obtained for analysis was ten milliliters. Chonoamnionitis was dtagnosed in three patients (21%) compared to ten controls (24%, p>0.1) Additionally, chor~oamniomtis was noted m only one patient prior to active labor (7.1%) versus 5 control patients (12%, p>0.1). CONCLUSIONS: The modified vaginal pouch is a simple, noninvas~ve method which a~ds in the diagnosis and management of pPROM. In add~t=on, this method does not appear to be assomated with maternal or permatal morbidity, including chorioamnionitis.
385 INFECTION AND INFLAMMATION OF THE CHORIOAMNION IN PREMATURITY. A CASE.CONTROL STUDY. DJ. Sherman, J. Tovbin, S. Arieh, I. Boldor, E. Caspi. Assaf-Harofeh Medical Center, Sackler School of Medicine, Tel Aviv Umverslty, Zenfin, Israel. OBJECTIVE: The role and microbiologlc causes of infection and inflammation of the chonoammon were studied in 85 patients with spontaneous idiopatiuc preterm bir~ (<37 weeks) and m 85 term control dehvenes. STUDY DESIGN: Spectmens for htstoiogic and microbiologic studies were obtained from the vagina upon adrmsslon, and from the chorioammotic membranes within 6 hours of delivery, ttlstologic chonoammonlus was diagnosed when significant leukocytic infiltrates were noted in a roiled strip of membranes Stanstical sigmficance was determxned by Chl-square test, the odds ratio (0.R.) was used to estimate the strength of the association. RESULTS: Microorganisms were isolated from the freshly separated chorioammon in 55% and 26% of preterm and term deliveries, respecUvely (P<0 001, O.R =3.5). Isolation rates of gram negative enteric bactena were slgnificanlly higher among preterm dehvenes than term controls (31% vs 7%, P<0 001, 0.R.=5.8), whereas differences in other species were not significant. Hlstologlc chonoamnionitis was noted xn 49% and 14% of prcterm and term dclivenes, respectively (P<0.001, O.R.=5 9), and was strongly associated with positive chorioammotic cultures xn both groups (P<0.001, 0.R.=64) Histologic chorioammom~s was noted in 94%, 54% and 4% of membranes with gram
negauve rods, other rrucroNal species, and negative cultures, respectively (P<0.001). Pretcrm dehvenes were also associated w~th s~gmficantly h~ghcr rates of bacterial vaginosis (38% vs 14%) and tsolation of vagtnal pathogens (81% vs 56%). Intrapartum or puerperal fever were noted in 7% and 1% of preterm and term deliveries, respectively (P=0 1). In only few cases were infectious neonatal complications observed. CONCLUSIONS: Gram negatave entenc rods are tmportant placental pathogens, responsible for subclimcal chorloamraonitis and prematunty Our data support the concept that rmcroorganisms ascending from the lower gemtal tract produce local lnflammanon, wluch may result tn preterm labor and delivery.
387 THE EFFECT OF BID VS. OD TRANSMISSION OF SCHEDULED HUAM RECORDINGS ON PERINATAL OUTCOMES. C.A. Beckmannx, C.R.B. BeckmannX, N. BergauerX, G. Stanzianox, C.B. Martin,Jr., Dept of OB\GYN, Univ of Wisconsin, Madrson, WI, and Healthdyne Perinatal Services, Inc., Marietta, GA. OBJECTIVE: To determine if perinatal outcomes were clinically d=fferent when women at high rrsk for preterm labor on HUAM services had scheduled (twice daily) monitoring data reviewed on a twice daily basis (BID), versus once per day (OD). STUDY DESIGN: A retrospective analysis was conducted on records of 1554 patients at risk for preterm labor that were receiving patient education and HUAM services with daily obstetrical nursing contact. Patients monitored by two perinatal centers (N = 715, N = 839) were similar in demographics, gestational age at start and stop of service, and risk factors for preterm labor, Patients received the same home monitoring device and instruction, except that one center instructed patients to transmit data after each scheduled twice daily recording session(BID), while the other group of pat=ents were instructed to record twice daily as scheduled and transmit once per day teD). RESULTS: Perinatal outcomes did not clinically differ between the groups in relation to gestational age at delivery, birthweights, or nursery days, Group(n) GA@del(mean) BW(mean) Nursery days(median)
BID(715) 36.1 wks 2798 gm 3.0 0D(839) 36.5 wks 2887 gm 3.0
A significant =ncrease in the number of physician contacts, interven~ons, and hospitalizations was found tn the BID group (p<0.05). CONCLUSIONS: This study indicates that patients at high risk for preterm labor may be effectively managed with twice daily scheduled recording and once daily teD) transmission of uterine activity data. Increased interventions and hospitalizations in the BID group may increase the cost of care for these patients.

Volume 170, Number 1, Part 2 SPO Abstracts 383 Am J Obstet Gynecol
388 ACCURACY OF MATERNAL PERCEPTION OF PRETERM UTERINE CONTRACTIONS.
C A Beckmannx, C.R.B. Bec "kmannx, G. S~zianox, N. Bergauerx
aud C.B. Martin, Jr., Dept. of OB-GYN, Univ. of Wisconsin, Madisou, WI. and Healthdyne Perinatal Services, Inc., Marietta, GA. Objective: To determine the accuracy of maternal perception of preterm uterine contracuons (UC’s). Stmty Design: Records of 778 women receiving home utenne activity monitormg (HUAM) services were analyzed retrospectively. The women were divided into multiple and singleton gestations, nulliparas and muluparas and were compared by gestational age (GA). The monitor strip recorded actual UC’s and dae mother was asked indieale when she felt a UC by means of an electronic marker.
Each woman received comprehensive education and training in self- dctcctiou of UC’s as well as re-education as necessary during daily conversatious wKh her obstetrical home care nurse. Comparisons of correct respouses, incorrect responses and missed contractions were made
Resnlts: The groups did not differ significantly in their ldentificatiou of UC’s (P=0.572). The women correctly identified only 17.4% of UC’s throughout pregnancy. Incorrect responses (i.e., identifying a UC that was not presen0 declined with increasing GA, but still averaged 44.6% over the course of pregnancy. Conclusions: These data confirm the results of previous studies that have reported the inability of gmvidas to identify their UC’s rehably. While teaching women how to identify their own UC’s has becu proposed as a method of emly detection of preterm labor, self- palpation is not a reliable tool for identification of UC’s in women
at risk lbr prelerm dehvery.
39O OBSTETRICAL DETERMINANTS OF NEONATAL SURVIVAL IN
EXTREMELY LOW BIRTH WEIGIIT INFANTS. S Bottoms, R Paul, J lares, B Mercer, D McNellisx, C Buckleyx, G Normanx, P
Jonesx, E Thomx, and the NICHD MFMU Network, Bethesda, MD.
OBJECTIVE: To identify the information available during labor most
predictive of neonatal survival for extremely low birth weight infants.
STUDY DESIGN: In an ongoing study, we evaluated 121 singleton
b~rths < 1,000 gms having complete ultrasound exams within 3 days of
delivery. Major anomalies, extramural delivery, antepartum stillbirth,
induced abortion, and gestational age <20 wks. were excluded.
Demographics, prenatal care, ultrasound results, time on the labor unit,
medical and obstetnca/ eomplicatmns, and medications were used to
develop a logistic regression model for survival to hospital discharge or
120 days.
RESULTS: 66 (54.5%) survived The best model included BPD (X2=23.7, p=0.0001), female gender (X2=12.9, ~=0.0003), MgSO4
(X2=ll.1, p=0 0009), and vertex presentation (X =8.0, p=0.0046)
BPD pcrfomed better than actual birth weight, and substantially better
than EFW or estimated gestational age. Femur length w~s useful for
unknown gender and in accurately identifying fetuses w~th no chance for
neonatal survival (femur length <38mm). Significantly improved
survival with toeolytics w~s seen only with MgSO4. This finding appeared to be unrelated to ruptured membranes, time in labor, steroids,
or complications such as preeelampsia or abruptio placenta.
CONCLUSIONS: 1) BPD and femur length are better predictors of
neonatal survival than EFW. 2) Determining gender improves the
accuracy of predicted survival. 3) The new finding of improved survival
with MgSO4 may be ~mportant and needs to be confirmed.
389 REDUCING LOW BIRTHVVEIGHT BIRTH THROUGH EVrENSIVE NURSING INTERVENTION VIA TELEPHONE. M L Moore,x P J Meis, J M Ernest. Department of Ob/Gyn, Bowman Gray School of Medicine, Wake Forest University, Winston-Salem, NC. OBJECTIVE: To examine if nursing support through 2-4 telephone calls per week from 24-37 weeks gestation will reduce rates of low birthweight (LBW) and preterm births in a high risk population. STUDY DESIGN: This preliminary report of a randomized prospective trial included 634 singleton b~rths [315 study subleCts (S), 319 control subjects (C)] All subjects received prenatal care at a clinic staffed by residents and faculty of a medical school; all were delivered at the same hospital by resident staff. Women were eligible if they were African-American and/or ~< age 18 and/or identified at risk for preterm labor on a standard risk assessment form. (S) and (C) did not d~ffer in demographic, health, and social h~story or measures of stress and support. Outcome data was also collected on women who were ehglble but did not choose to participate No subjects received home uterine ambulatory monitoring. RESULTS: All women randomized were included in the evaluation
S C p n=315 n=319
n (%) n (%)
< 2500 grams 30 (9.5) 48 (15) < 0.05
< 2000 grams 13 (4.1) 25 (7.8) < 0.10
Women ehgible but not randomized (n=417) had a rate of 14 6% for births < 2500 grams and 9.4% for births < 2000 grams,
CONCLUSIONS: Nursing telephone ~ntervention appears to offer an effective method for preventing preterm and LBW births in high risk parturients Supported by Grant #RO1-NR02410-01.
THYROID-RELEASING HORMONE (TRH) VERSUS
BETAMETHASONE OR PLACEBO IN PRETERM
PREMATURE RUPTURED MEMBRANES: A PROSPECTIVE
RANDOMIZED STUDY. D. Jackson, M. Nageotte, C. Towers, T. Asrat, R. Freeman, K. Gardner~, P. Rumney~, K. Murray~, G.
Briggs~. Long Beach Memorial Med Center, Long Beach, CA
OBJECTIVE: To evaluate the neonatal effects of antepartal
thyroid releasing hormone as compared to betamethasone or
placebo in pregnancies delivered after preterm premature
ruptured membranes (pprom).
STUDY DESIGN: Singleton pregnancies not in labor at 24
hours after pprom with gestatlonal age between 25 and 32 weeks
were randomized to receive either TRH (400 ug I.V.q. 8 hours
X 4) plus IM placebo, betamethasone (12 mg I.M.q. 24 hours X
2) plus 1V placebo, or placebo (I.V.q. 8 hours X 4 and IM q.
24 hours X 2) in a double bhnd, prospective fashion. No
tocolytms or antibiotics were utlhzed. Neonates were evaluated
for oxygen requirements, need for surfactant, length of NICU
stay, apnea, PDA and other major morbidity endpomts.
RESULTS: 24 patients received TRH (avg del 30.4wks), 25
received betamethasone (avg del 31.1 wks), and 21 received
placebo (avg del 31.8 wks). In no weight category did TRH or
betamethasone appear to decrease neonatal morbidity over
placebo m PPROM. Respiratory distress syndrome, mortahty,
and chronic lung disease were not lower in the TRH group.
CONCLUSIONS: Although antepartal TRH (when combined
with steroids) has been shown to reduce respiratory morbidity in
premature births with intact membranes, its benefit as a single
agent is not apparent in preterm ruptured membranes.

384 SPO Abstracts January 1994 Am J Obstet Gynecol
392 PREDICTION OF CERVICAL CERCLAGE OUTCOME BY
ENDOVAGINAL ULTRASOUND. H F Andersen, A Karimi, E P Sakala, R Kalugdanx. Dept Gyn-Ob, Loma Linda University,
Loma Lmda, CA.
OBJECTIVE" We hypothesized that decreasing upper cervical
segment length, measured by endovaglnal ultrasound, predicts
cervical cerclage patients at greater risk of preterm delivery (PTD).
STUDY I~ESIGN" 121 endovaginal ultrasound examinations
were performed in 32 patients following cervical cerclage.
Ultrasound measurements included length of the closed cervical
canal segments above and below the cerclage and dilatation of the
internal cervical os (funneling) with and without fundal pressure.
Rask of PTD was tested by Fisher Exact Test (two-tail).
RESULTS’ Development of funneling of the internal os and
shortening of the upper cervical segment length were the most
predictive of outcome in patients with cervical cerclage. 12
patients developed shortening of the upper cewical segment ~10 ram) prior to 30 weeks gestational (mean = 22.6 + 2.7 wks), wtule
20 patients continued to have upper cervical segment
measurements >10 ram. A short upper cervical segment prior to
30 weeks gestalaon was associated with a sigmficantly higher risk of PTD before 36 weeks (58% vs 10%, p= 006) and PTD before 34
weeks (50% vs. 5%, p=.006)
CONCLUSIONS: Endovag~nal ultrasound assessment of the
cervxx in patients with cervical cerclage xs a useful adjunct for
predictang outcome and counseling the patient. Vigorous
intervention (strict bedrest and tocolytic therapy as needed) may
have contributed to term delivery in 3 pataents with extremely short
upper cervical segments
394 CERVICAL ONCOFETAL FIBRONECTIN AS A PREDICTOR OF
PRETERM DELIVERY. O. Irionx, J. Maturex, P. Bischofx, F. B~guin Dept of Ob/Gyn, University Hospital, Geneva, Switzerland
OBJECTIVE. to evaluate the value of oncofetal ftbronecfin (FFN) as a predictor of preterm dehvery (PTD) in patients presenting with preterm
labor (PTL). STUDY DESIGN’ women adm=tted for suspicion of PTL presenting
regular uterine contrachons w=th intact membranes between 24 and 36 weeks gestation were prospectively included. A Dacron swab was sent to the laboratory to measure cervical FFN before any treatment. Values above 0.5 ng/ml were considered pos=hve. Results were
unknown to the obstetricians. RESULTS’ From september 1991 to january 1993, 64 women were included Twenty-two delivered before 37 weeks gestahon (34.4%) In
thts group, mean and median gestatlonal age were 32.2 and 33.5 weeks. FFN was positive in 15/22 women delivering preform and in
12/42 dehver~ng at term (P<0.003) Sensitivity is 68.2%, specificity 73.8%, pes=tlve predictive value 57.7%, negative predtcttve value 81 6%. The tocolytic agent Hexoprenahne was administred to 13/15 (86.7%) women m the true positive FFN group, 4/7 (57.1%) In the false negahve group, 2/11 (18 2%) in the false positive and 14/31
(45.1%) in the true negative groups Constricting only women treated by tocolysis, sens=t=wty of FFN to predict PTD is 76,5%, specificity 87,5%, pos~t=ve predictive value 86,7%, negahve pred=chve value 87,5% Mean and median FFN concentrations were respectively 483
and 88 ng/ml in the true postttve group and 86.8 and 11 in the false pos=hve group. Mean and median ~ntervals between sampling and dehvery were respectively 12 and 5 days in the true positive
compared to 29 and 23 in the false negative groups. Intervals were respectively 64 and 61 days in the false positive compared to 55 and
47 ~n the true negative groups. CONCLUSIONS: FFN is a useful test to help the clinician in discriminting true from false PTL, especialy ~n patients whith high risk
of PTD recieving toco~ysts, thus avoidmg inefficacious or dangerous treatments as well as long hospital stays.
393 CERVICOVAGINAL PROLACTIN: AN INDICATOR OF PRETERM DELIVERY, J.M. O’l~rien, G H Peeler,x D.W. Pitts,x R. Anderson,x B M Slbai, M.M Salama, B.M. Mercer Department of OB/GYN, University of Tennessee, Memphis. OBJECTIVE: To determine whether the presence of cervicovagmal prolactin is a useful predictor for subsequent preterm delivery of -<34 weeks’ gestation STUDY DESIGN: A cohort of 80 patmnts~0 mpatients receiving tocolyt~c therapy for preform labor and 40 asymptomaUc outpatients underwent speculum examination with washings obtained from the vaginal fornices and exocervix. The aspirates were stored at -70 degrees C and a batch radloimmunoassay was performed to identify the presence and concentratmn of prolactxn A prolacnn concentration of > 2 ng/ml was considered positive RESULTS: Prolactin was identified m symptomatic women more frequently than m the outpatient group (50 vs 5%, p < 0 0001) Pregnancy outcomes for each group are shown below"
% Delivered Latency Birth Weight <_ 34 weeks (days) (gins)
h~patlents
(+)Prolactm (n=20) 80* 16 + 17~" 1985 ± 729:~ (-)Prolactin (n=20) 35 34 _+ 24 2583 ± 696
Outpatients
(+)Prolactm (n=2) 5 0 17 5 + 20 5 2079 ± 664 ( )Prolactln (n=38) 3 62 4 ± 18 4 3004 ± 602
*,:~ p = 0 01 compared to prolactm (-) lnpat~ents ~" p = 0 02 compared to prolacnn (-) mpatients
The positive and negative predlcnve values of cervlcovagmal prolactxn for delivery <34 weeks were 80% and 65% respectively in the symptomatic group Prolactm was also identified in two asymptomatic women both of whom dehvered prior to term CONCLUSIONS: The presence of prolactm In the cervlcovag~nal washings is s~gnlficantly associated with delivery _<34 weeks’ gestation, a shorter latency to dehvery, and a lower b~rth weight in symptomatic women Th~s test may also prove to be a useful marker for preterm dehvery ill asymptomatlc women
395 MAJOR MORBIDITY IN PRETERM NEONATES WITII
BIOCIIEM1CAL LUNG MATURITY. MR Lauria, MP Dombrowski,
JE Uckele, SF Bottoms, Dept. of OB/GYN, Hutzel Hosp, Wayne State
Univ., Detroit, MI.
OBJECTIVE: To determine the incidence of major morbidity in
premature neonates with biochemical lung maturity.
STUDY DESIGN: Perinatal outcome was analyzed for 182 premature
neonates <35 weeks having amniocentesis during 1991-92 82 had a
lecithin sphxngomyelin ratio > 4:1 or phosphatidylglycerol ~ 1%.
RESULTS: Neorotizing enteroeolitis (NEC), intraventricular
hemorrhage (IVH), and respiratory dtstress syndrome (RDS) were
combined as a measure of major morbidity. Major morbidity was
increased among those with immature lungs, with a relative risk of 2 2
(95% confidence interval 1.3-3 9) at _<32 weeks, 3.0 (1.2-7.9) at 33-34
weeks There were no cases of necrotizing enterocolitis (NEC) among
neonates with mature lung indices. However, preterm neonates with
mature indices still had significant frequencies of RDS, IVH, and
ncooatal intensive care unit (NICU) admission.
Weeks of Gestation
_<30(n=12) 31-32(n =23) 33-34(n =47)
%(CI) %(C]) %(CI)
RDS 42(19-68) 13(5-32) 6(2-17)
IVI[ 17(5-45) 9(2-27) 6(2-17)
NICU 92(65-99) 39(22-59) 17(9-30)
CONCLUSION: The presence of mature lung indices decreases but
does not preclude major morbidity related to prematurity. Before 30
weeks, biochemical lung maturity provides little reassurance the neonate
will not develop RDS

Volume 170, Number 1, Part 2 SPO Abstracts 385 Am J Obstet Gynecol
396 PRETERM BIRTH PREDICTION IN PRIVATE NULLIPAROUS WOMEN DA Gulnnx, TR Wlgton, J (3Wen, ML Socol, MC Frederiksen.
Northwestern Univ. and Unlv of Alabama at Birmingham, Chicago IL
and B~rm~ngham AL
OBJECTIVE. To ~nvest~gate whether the Mammary Sbmulat~on Test
(MS~ in combination w~th other commonly acquired prenatal data could improve the identification of the nulhparous pabent at risk for
spontaneous preterm b{rth (SPTB)
STUDY DESIGN: 265 pnvate nulliparous pabents w~th singleton
gestations were studied The MST was performed at 26-28 weeks’
gestation The Creasy nsk sconng system (CRS) and cervical examinations were performed at the first prenatal visit and again at 26-
28 weeks Both patients and physicians were blinded to the results of
the Individual tests. Commonly acquired prenatal data (e g weight gain,
hematocnt, MSAFP, etc) were abstracted from the medical record. Summary pred~cbve values were calculated for each test and
discnm~nate analys~s was performed on selected co-vanates as
determined ~n a backward ehmlnat~on model. RESULTS. SPTB occurred at < 37 weeks In 26 of 265 (9 8%) patients.
The following variables demonstrated the best posibve pred~ct{ve value (PPV) and relative nsk (RR)" MST positive (N=49, PPV 20 0%, RR 3 0
(1 3,70)), ORS at 26-28 weeks_> 10 (N=11, PPV 363, RR 5.7
(1 5,21 0)), a soft cervix at 26-28 weeks (N=55, PPV 18%, RR 2 5 (1 1,
5 8)), and smoking tobacco throughout pregnancy (N=9, PPV 33%, RR
4 8 (1 1, 20 5)) The discnm~nate analys~s (p=0.0001) determined that
the combination of a positive MST, pnor spontaneous abortion(s),
bactenuria, current smoking, and a soft cervix at 26-28 weeks ~dent~fied
19 patients of 265 as being at nsk for SPTB Th~s combination of
vanables demonstrated a sensitivity of 35%, a specificity of 96%, and
a PPV for predlcbon of SPTB of 47%
CONCLUSION Combining routine prenatal data w~th the MST allowed
us to correctly ~danbfy 35% of the Women who were delivered preterm
w~th a PPV of 47%. Prospechve validahon of th~s model ~s warranted
398 PRETERM BIRTH SUBSEQUENTTO "SUCCESSFUL" TOCOLYTIC
TREATMENT OF IDIOPATHIC PRETERM LABOR. DA Gu~nn,×
RL Goldenberg, SP Chver,X JC Hauth. University of Alabama at
Birmingham, Birmingham AL
OBJECTIVE Our goal was to determine the risk of preterm b~rth (PTB)
at < 34 weeks’ gestation ~n the subgroup of women successfully treated
for idiopathic preterm labor (PTL) and to determine if the cervical
examination prior to ~nsbtubon of maintenance therapy enhanced the
prediction of subsequent PTB.
STUDY DESIGN: During the bme of the March of Dimes muitlcenter
prematunty prevention program (1982-1986) 486 women w~th singleton
pregnancies at less than 32 weeks’ gestation (GA) were successfully
treated for PTL w~th either IV MgSO4 or IV ritodnne and remained
undehvered at 48 hours after initiation of treatment These women, who
were placed on oral tocolyt~cs, compnsed our study populabon.
Components of the cervical examination performed at least 24 hours
after ~n~t~abon of therapy were evaluated for their ablhty to predict which
women would remain undelivered at 34 and 37 weeks’ GA.
RESULTS: Of the study populabon, 131 women (27%) dehvered at
less than 34 weeks’ GA and 245 women (50%) dehvered at < 37
weeks’ GA The following table depicts the ability of the charactenstics
of the last cervical exam to predict subsequent PTB at < 34 weeks’ GA
% PTB < 34 Week Reh Risk Sens. Spec.
Dd > 2cm 36 8 1.8 (1 3, 2.4) 51.9 67 0
Eff complete 500 21 (1.4,3.1) 198 92.8
B~shop >_ 6 30 0 7.0 (1.8, 28 6) 94.3 36 9
CONCLUSION Women successfully treated for PTL remain at
Ngh nsk for PTB Incorporating cervical characteristics ~nto risk
assessment schemes ~n tNs populahon improves our abdity to
identify those patients at highest nsk for PTB. Th~s ~nformation can
be used to design intervention tnals targeted toward a reduction in
PTB at < 34 weeks’ GA.
397 IDENTIFICATION OF INTRAUTERINE CLOT ON ULTRASOUND EXAMINATION IS ASSOCIATED WITH PRE- TERM DELIVERY. R. Davis. A. Goepfert," R. Goldenberg, M.
DuBard.X University of Alabama at Birmingham, Birmingham, AL.
OBJECTIVE: To determine the outcome of pregnancies where a retroplacental or subchonomc collection of blood was identified by an
ultrasound examination. STUDY DESIGN: A retrospective study was performed on the
outcomes of 30 pregnancies in which an intrantenne clot was coded at
the time of an ultrasound examination. Patients were divided into
groups based on the timing of the initial identification of the clot: 6-13 wks, 14-26 wks, and >26 wks. Preterm delivery was defined as
delivery <37 weeks gestation. Statistical analysis utilized Fisher’s
exact test. RESULTS: Fifteen of the 30 pregnancies delivered preterm (<37
weeks) with 10 delivering prior to 34 weeks (Table). The later the
hemorrhage was discovered the greater the likelihood of preterm delivery (p = .004). The mean gestational age at delivery in the preterm
group was 32.8 weeks (range 16-36 weeks) and the mean birthweight
was 1462 g. Three placental abruptions occurred in the preterm group.
There were also six cesarean sections, three for breech and three for fetal distress. There were no C-sectioas in the term deliveries.
Gestational Age at Ultrasound Examination
<14 weeks 14-26 weeks >26 weeks Term 10 5 0 Preterm 2 10 3
CONCLUSION: Ultrasound evidence of placental hemorrhage,
particularly after the first trimester is associated with preterm delivery.
399 WHICH CERVICAL PARAMETER BEST PREDICTS ULTIMATE PRETERM BIRTH? DA Guinn*, RL Goldenberg, SP Cliver*.
University of Alabama at Birmingham, B=rmingham AL OBJECTIVE: To determine which cervical characteristic best predicts preterm birth (PTB) in patients diagnosed and treated for preterm labor (PTL). STUDY DESIGN- Data collected dudng the time of the March of Dimes prematunty prevention program were reviewed from 574 patients w~th s~ngleton gestations and intact membranes who were diagnosed and treated for PTL pdor to 32 weeks’ gestation. Cervical d~labon (DIL), effacement (EFF), Bishop Score and Cervical Score (CS: cervical effacement in cms minus cervical dilation ~n cms) were recorded on admission to the hospital. A B~shop score of -> 6 or a CS < 0 were considered positive. Summary predictive values were calculated for each cervical charactenshc and preterm birth at < 34 weeks’ gestation. RESULTS: A total of 222 patients or 38.7% delivered at < 34 weeks gestation
Sens. S_Dec. PPV ~ Rel. Risk DIL>2 cm 63 1 62.8 43 4 79.1 2.1 (1 6,2.7) EFF 100% 25.2 93.8 64 5 73.5 2.4(1 9,3.1) B~shop>6 80.3 44.4 37.5 84.4 2.4(1.4,4.1) CS < 0 71 1 58 5 43.6 81.8 2 4(1.8,3.2)
DISCUSSION In tNs population at high risk for PTB at < 34 weeks, complete effacement on admission demonstrated the highest positive predictive value. Combining cervical characteristics in either the Bishop Score or Cervical Score will ~ncrease the sensitivity of the test whde maintaining a relabvely high positive predichve value

386 SPO Abstracts January 1994 Am J Obstet Gynecol
400 THE INTERACTION OF MATERNAL CORTICOSTEROID AND
TOCOLYTIC TREATMENT ON MORBIDI’rY AND MORTALITY RATES IN
VERY LOW BIRTHWEIGHT INFANTS MW Atklns0fl~, FL Gaudier,
SP Chver*, K NelsonX, M Peraltax, JC Hauth, RL Goldenberg Unwers~ty of Alabama at Birmingham, Birmingham, AL.
OBJECTIVES. To determine the effect and interaction of maternal admln)strat)on of cortlcoStero~ds and toco)yttcs on neonatat outcome STUDY DESIGN: 773 hveborn 500q000 gram 24-28 week infants dehvered
from 1979-91 were d~wded ~nto 4 groups those whose mothers received
1) no treatment, 2) steroids alone, 3} tocotyt~cs alone or 4) both Using unlvanate and regression analyses, the frequencies of and odds ratios (OR)
for neonatal mollahty arid vanoue morbldltleS were determined Mortah[y was defined as death before d~scharge Morbidity was evaluated in infants ahve at z 48, hours
RESULTS: The table below compares the neonatal outcome to the
maternal treatment group. An asterisk ~ndlcatas as~£nlflcant difference #ore
the no treatment group (No Rx). Regression analys~s was first performed to test the Independent effects of steroids and tocolytlcs on outcome
controlhng for gestattona~ age and mode of dehvery: steroids OR for
mortahty 0 55 (0.35-0 88), OR for IVH 0 38 (0 24-0 63), tocolyt~cs - OR for
mortahty 075 (0 54 1 04), OR for IVH 207 (1 38-3 10) Regression
analyses were repeated based on the 4 treatment groups with the results
(OR) shown in the table Belonging to any one of the therapy groups did not
affect the ~nfant’s nsk for RDS, PDA or NEC
Mortahty (%) OR (95%C0 IVH(%) OR (95%CI) No Rx 50 50 - Steroids 25* 056 (027-1 17) 30* 0.53 (025-1 14) Tocolyt~c 49 0,76 (0 53-1 07) 72* 2,3 (1 47-3 61) Both 25* 0 41 (0 24-0 72) 41 0 73 (0 43-1 24) CONCLUSION: The materna~ administration of cortlcosterolds results in lower rates of mortality and IVH in ~nfants born between 24 and 28 weeks
and weighing 500-1000 grams Tocolytlcs alone are associated w~th an
~ncrease in IVH Steroids appear to amehorate the adverse influelqce of
tocolyhcs on the development of IVH
402 ARE NEONATAL OUTCOMES BETTER IN VERY PRETERM
BIRTHS COMPLICATED BY PREECLAMPSIA ANI) PROM?
F. Gaudier, R. Goldenberg, J. Hauth, M. DuBard,~ K. Ndson?
University of Alabama at Birmingham, Bwmingham, AL.
OBJECTIVE: Very preterm births generally follow spontaneous preterm
labor (SPL), PROM, or are indicated secondary to preeclampsia (PE). We
wanted to determine if pregnancy outcome was associated with those
factors.
STUDY DESIGN 764 infants 500 to 1000g and 23 to 27 weeks
gestational age (GA) born without anomahes or other maternal
comphcatlons between 1979 and 1991 were classified as due to SPL
(n =350), PROM (n~329), or indicated PE (n=85). Survival was defmed
as being discharged alive from the hospital. In survivors at > 48 hours,
the presence of RDS, IVH, and NEC were noted.
RESULTS" The table shows the rates of survwal and morbidity for each
group Infants born because of PE had greater survwal and less morbidity
than infants m the other groups with those born following PROM having
intermediate outcomes. Regression analys~s adjusting for GA, plurality,
mode of delivery and steroid use showed that compared to the SPL group,
the odds ratio (OR) for mortality for the PROM group was 68 ( 49, .95),
while the OR for mortality for the PE group was 77 (.44, 1 4)
Outcome Variables Spontaneous PROM P_~E
Survival (%) 41 54* 64*
IVH (%) 58 57 45
RDS (%) 95 91 87*
NEC (%) 22 24 17
* Indicates sigmfieant difference from spontaneous group (p < 0.05)
CONCLUSION: Pregnancies terminating at 23 to 27 weeks complicated
by PROM have significantly lower moaality than those following SPL
while the apparent decrease in mortality associated with PE is not
statistically significant, predominantly because most of the indicated
preterm births secondary to PE occur at a later GA.
401 THE ORIGIN AND OUTCOME OF PRETERM’I’WIN PREGNANCIES.
M Gardner’, RL Goldenberg, JM Tucker, SP Chver*, K NelsonX, RL Copper*, FL Gaudier Umvers~ty of Alabama at Birmingham, Birmingham, AL OBJECTIVE. To define the et~ology of preterm twin births and determine the contribution of twin b~rths to preterm b~rth and re~atad
morbidity and mortahty. STUDY DESIGN: The March of Dimes (MOD) Mutticenter Study had
a total of 33,873 dehvenes between 1982 and 1986, 432 or 1 3% of which were sets of twins. Women were classified by reason for preterm b~rth and ethn~city Neonates were classified as to stillbirth, neonatal
death, and vanous short-term morb~d~t~es A second s~ngle inst~tuhonal data set consisting of infants < 1000 g born between 1979 - 1991 and surv~wng to one year of age (n=434, 15% twins) was used to determine ~f twins and s~ngletons born at comparable gestat~onal ages (GA) have a slmdar nsk for malor developmental handicap (MH)
RESULTS: Of the 432 twin dehvenes ~n the MOD data set, 54% were preterm compared to 10% among s~ng~etons Of those born preterm, the apparent tendency of twins to be born earher than singletons was not statistically d~fferent. Whde twins represented 2 6% of all neonates, they represented 12 8% of all preterm infants, 15.4% of all neonatal
deaths, and 9.5% of all fetal deaths Spontaneous labor accounted for 54% of twin b~rths, PROM for 22%, wh~le indicated dehveoes accounted for 23% Of the ~nd~cated b~rths, 44% were due to preeclamps~a or severe hypertension, 33% to fetal distress or IUGR, 9% to abrupt~on
and 7% to fetal death Comparing infants of s~milar GA, twins weighed
less, but after 29 weeks had a mortahty equivalent to singletons Prior to 29 weeks, twins were more hkely to d~e (OR 3 9, 95% CI 1 7, 8 8) but they d~d not have s~gnificantly more RDS, IVH, or other short term morbidity compared to s~ngletons of equivalent C~k, Twins at 500 - 1000 g who survived _> 1 yr had a rate of MH of 25% However, when GA was controlled, the rate of MH was not higher ~n twins
CONCLDSION: Twins account for a d~sproport~onal amount of preterm b~rth and associated morbidity and mortahty Less than 1000 g twins
had nearly a 4-fold ~ncrease ~n mortaht~, but d~d not have an ~ncreased prevalence of MH at 1 year of age
403 SURVIVAL AND LONG TERM NEUROLOGIC OUTCOME OF
INFANTS 23 TO 27 WEEKS, 1979-1985 VS 1996-1991. .F L Gaudier, M.P. Peraltax R.L Goldenhorg, K.G. Nelsonx, M. DuBardx,
S. Johnsonx, R. Steelex, J C. Hauth. University of Alabama Hospitals,
Birmingham, Alabama. OBJECTIVE: To determine the change in survival and neurologic
morbidity in infants delivered between 23 and 27 weeks of gestation in two
chffer ertt tmae periods. STUDY DESIGN: We reviewed the survival and long term neurologic
outcome m 785 infants 23 to 27 weeks. All were born alive without major
congenital anomalies at our institution between January 1979 and
December 1991. Gestational age was based on menslnaal history and early
fetal ultrasound parameters. Survival was defined as being discharged alive
from the hospital. The incidence of major neurologic handicap was determined for each gestational age group in 2 time periods for infants who
survived and were evaluated at -> 12 months of age. A major neurologic
handicap was def’med as one or more of cerebral palsy, mental retardation,
blindness, and deafness.
RESULTS: At each gestational age from 24 to 27 weeks there was a
significant improvement (p<.05) in survival. However, the incidence of
major neureloglc handicap in survivors was similar during both study
periods (27.0% vs 28.2%, p = NS). Due to the sma/I number of survivors
the apparent improvement in neurologic handicap over rime at 23-24 weeks
was not si[~mficant (2 = 08).
23 wks 24 wks 25 wks 26 wks 27 wks
1979-~985 . .. (N =19) (N = 55) ~N=7.4). (N=107) /N=89/
Survival 11% 9% 20% 37% 58% Handicap 100% 67% 30% 33% 19% 1986-1991 <N=31) ~N=72) ~N=l16) <N=122) <N=100)
Survival I0 % 40 % 60 % 66 % 83 %
Handicap 33 % 35 % 25 % 33 % 26 %
CONCLUSIONS: Current data on the survival and long term neurologic
morbidity of extremely premature infants is presented. This information
will be of help in parental counseling and in the decision making process of
the obstetrician.

Volume 170, Number 1, Part 2 SPO Abstracts 387 Am J Obstet Gynecol
404 INFLUENCE OF ACID-BASE STATUS AND APGAR SCORES ON
SURVIVAL IN 500 TO 1,000 g INFANTS. FL Gaudier, RL Goldenberg, M DuBardx, KG Nelsonx, JC Hanth
University of Alabama Hospitals, Birmingham, Alabama.
OBJECTIVE: To evaluate the effect of acid-base status at birth and Apgar scores on survival in extremely low birth weight infants.
STUDY DESIGN: Factors influencing survival in 1,074 infanls 500-1,000
g born alive between 1979 and 1991 were evaluated. Apgar scores were
ass~gr~ed at 1 and 5 minutes after birth. Umbilical artery blood samples
were obtained at delivery in 62% of the infants and analyzed for pH, carbon
dioxide pressure (PCO2), and bicarbonate (HCO3). Survival was defined as
being discharged alive from the hospital. Data were divided into 4
gestational age (GA) groups and analyzed with Chi-square and Inuhiple
loglstlc regression analysxs.
RESULTS: The survival (%) m GA groups by cord gases and Apgar
scores is presented in the table In every GA grouping survival was higher
with a pH>_ 7.05, and was sigmficantly so at >_ 27 weeks. There was no
consistent relat,onship between other cord gases and survival. However,
with the exception of the 1 minute Apgar score at 23-24 weeks, the
relationship of Apgar scores to survival was significant in all GA periods.
In a regression analysis conuoling for GA, birthweight, plurality, mode of
dehvery, and maternal steroid use, the only s,gnificant relationship
between any of the cord gases, Apgar scores and survival involved the 5
minute Apl~ar score [odds ratio 1.76
23 -24 wk 25-26 wk I 27 -28 wk >-29 wks
(N=179) (N-~26) (N=316) (N=153) ~H < 7.05 [_> 7.05 9%/38% 50%/59% 50%/79%* 0%/’88%*
’CO2 <65 />_65 38%/25% 61%/48% 78%/’/5% 87%/88% -ICO3 <17 /_>17 44%/35% 56%/59% 73%/79% 69%/89%*
n, pgar 1 min < 3/_>3 t20%/29% ~11%/62%* ~57%/’77%* ~/3%/92%* %p~ar 5 rain < 7 [ >_ 7 20%/38%* ~,5%/62%* 61%D9%* 70%/~6%*
* Indicates significant difference (p < 0.05).
CONCLUSION: Apgar scores are a better predxctor of survival than cord
gases in neonates <1,000 g.
406 NITRIC OXIDE METABOLITES AND PRETERM PREGNANCY
COMPLICATIONS. P.D. Lutz_, R.K. Jaekle, L Myatt, B. Rosenn, TA
Sidd=qi. Dept Ob/Gyn, University of C=ncinnati, Cincinnati, OH.
OBJECTIVE: It has been suggested that intra-amniotic bacterial infection
plays a significant role in preterm labor and preterm rupture of
membranes. Synthesis of nitric omde (NO) and its metabolites n~tnte and
nitrate are increased in infection This project was designed to evaluate
whether ptasma or urine nitdte and n~trate concentrations are increased in
patients w=th either preterm labor (PTL) or premature rupture of
membranes (PROM)
STUDY DESIGN: 25 pabents between 24-35 weeks gestation (13 with PTL,
8 w=th PROM and 4 w=th both) had blood and urine collected for mtrite and
nitrate determination after informed consent The control group consisted
of samples obtained from patients between 24-35 weeks of gestation
w~thout PTL or PROM. Nitrate in plasma and unne was reduced to nitrite
by a copper placed cadmium column and quantrtated using the Greiss
reagent RESULTS: The udne mtrate concentrations were significantly higher in only
the PTL group compared to the control (1.29+0 24 p.m/mg creatm~ne vs.
0 67~+0 05 pm/mg creatinine, p<0 02) The plasma n~trate, however, was
significantly h~gher in both the PTL and PROM groups compared to control
(400+1.5 i=m; 560+135 pm; & 126+1 2 i~m respectively, p<0.01). The
levels of n~trate m the urine or plasma did not correlate, however, w~th bme
from admmsion to delivery (P>0 2). Finally, the presence of positive
cervical or urine cultures, clinical exam consistent with chorioamnlonltls, or maternal temperature >100.4°F were not assocmted with higher levels of
nitrates.
CONCLUSION: Patients with PTL or PROM do have increased nitrates,
however, in contrast to the studies of intedeukms or other cytokines this
increased level ~s not predictive of impending delivery
405 NIFEDIPINE TO(:OLYSIS AND NEONATAL ACID-BASE STATUS AT DELIVERY D.Ra~, D,Dyson, Y.Crltes. Dept. of OB/GYN, Kaiser Permanente Med]ca] Center, Santa Clara, CA. OBJECTIVE: N]fedlp~ne has been shown to be an effectlve tocolytlc, however, reluctance to accept Its cllnlcal use exits due to concern for potential fetal effects, ]n particular acidosis suggested by animal studles. The acld-base stat~s at blrth of preterm neonates
to a group of slm]lar neonates whose mothers had not received Nlfedlplne. STUDY DESIGN: A retrospective rewew of infants with b~rth welghts (BW)~ 2000 grams and delivered following PTL and/or PROM was performed. Over 4.5 years 186 ~nfants were ]dent~fred. Of these, 126 were exposed to Riled]pine (NIF) within 24 hours of delivery. Of the 60 not exposed to N1fed~p]ne (No NIF), 11 were exposed to other tocolytlcs (MgSO~, betam~metics, Indocln) and 49 were not exposed to tocolyt~cs w~th~n 24 hours of dehvery. Mode of delivery, APGAR scores and umbilical venous cord gases were compared. RESULTS: The mean GA and BW of the NIF group was less than the No NIF group (30.9 vs. 32.0 wks, 1542 vs. 1694 gm, p = .003). There was no difference ~n the rate of C/S for delivery (NIF 43 {34~) vs. ~o RIF 22 (37~), p > ,I) and no d~ffer~nce ~n the number of C/S done for fetal dlstress INIF ]2/43 vs. No NIF 5/22, p < .1). There was no difference ~n the Incidence of I m]n. APGAR < 3 (NIF l~ vs., No NIF 8~, p > .I) or 5 m~n APGAR < 7 (NIF 11~ vs. No NIF 10~, p > The cord gas valves are compared below: ( ) = standard devrat]on.
NIF NO NIF p UvpH mean 7.34-~T~-~.07)* ~o > .05 < 7.20 4~ 7~ > .1 ~vCO~ mean 42.9(8.2)t 46.4(13.5)t .03 > 60 2.5~ 15~ .003 UvBE mean -2.2(3.3)t -2.7(3.0)1 > .I < -10 2.5~ 2~ > .i
* N = 124, t N = 119, ° N : 57, ~ N = 52
CONCLUSION: There were no cllnlcally slgnlflcant dlfferences ]n the status at dellvery of preterm neonates exposed to N~fed]p]ne ]n comparison to neonates without exposure to N~fed~p~ne. In addrtron, the umbilical venous gases compare very favorably with prevlously published normals for preterm neonates.
407
OBJECTIVE: The null hypothes/s ls that antepartum sterold treatment alone without surfactant therapy offers no clinical benefits to patlents wlth premature rupture o~ membranes. STUDY DESIGn: One hundred forty-flve maternal-neonatal concurrent palrs were studled wlth regard to therapy with antepartum steroids. There were 45 maternal-neonatal pair who received steroids after rupture of membranes during 24-35 weeks gestation. ~he two groups were identical with regard to gestatlonal age at rupture of membranes, gravity, parity, race, ~etal gender, socioeconomic stamus, smoklng, and preterm labor risk factors. Variables were examined with SYSTAT, Chi-square, and where approprlate, Fisher’s exact and Student t-test. RESULTS: Study of the stratified data revealed that maternal chorioamnionltls was less frequent in the steroid group to p<0.01. Bronchopulmonary dysplasia was less frequent in the sterozd group and was statistically of borderline significant to p<0.057. The remainder of the data revealed no statlstically slgnlflcant differences in preterm delivery rate, necrotlzing enterocolitis, respiratory distress syndrome, intraventricular hemorrhage rate or severlty of hemorrhage, hospital days, latency to delivery, or ventilator days. C’O~C~ffSIOtgS: A2though not statistlcally signifi=ant, antepartum sterold use in preterm rupture of membranes does appear to offer posslble clinical benefit in premature infants by lessenlng the rate of bronchopulmonary dysplasla in those infants receiving antepartum steroids. Larger studies with the use of antepartum steroids with premature ruptur~ oZ membranes need to be done to substantiate thzs clinical flndlng.
388 SPO Abstracts J&nu~ry 1994 Am J Obstet Gynecol
408 COCAINE USAGE ASSOCIATED WITH PRETERM PREMATURE
RUPTURE OF MEMBRANES: OBSTETRICAL AND NEONATAL
OUTCOMES. D. Mastrogiannis, G. Decaval~s~, V. Whiteman=, EA. Reece.
Dept. Ob/Oyn and RS, Temple Univ., PhiM., PA
OBJECTIVE: Co,mine usage is associated with increased incidence of
preterm premature rupture of membranes. It h~ been suggested that cocaine
may have a protective effect on the development of respiratory distress
syndrome (RDS) The purpose of our study was to investigate the obstetrical
(PPROM) is associated with cocaine abuse in pregnnncy.
STUDY DESIGN: During the years 1991-1992, we prospectively followed
MI patients with PPROM. 70 patients with PPROM had urine toxicology
examination for ¢ocnine metabolites. Of those, 26 patients tested positive for
cocaine (Group A), and 44 tested negative (Group B). Epidemlologic,
chntcM, mid laborMory data were collected from the medicM records.
Outcome variables were anMyzed using the SPSS statisticM progrmn with
w~s considered significant.
RESULTSzAge, race, gestationM age at PPROM, latency period, gestationa/
age at delivery, mode o f delivery, and in¢idertee of fetal distress were slmilar
m the two groups. Gravtdlty and parity were significantly higher and birth
weight was lower in Group A when compared to Group B (p < 05).
Neonatal complications including RDS, necrotizing enterocolitts,
intraventricular hemorrhage, sepsis, ventilatory support during
hospitalization, ventilation days, total int¢asive care nursery days and total
hospital days were similar m the newborns of the two groups
CONCLUSIONS: Cocaine usage associated with PPROM results in h=gher
incidence of low birth weight babies than expected. Nevertheless, neonatal
complications are similar In this patient population compared to patients with
PPROM without cocaine use. We did not observe a protective effect of
cocaine in the devd, opment of RDS in the cocaine positive group.
410 ARE SERUM LEVELS ACHIEVED BY ORAL SUSTAINED RELEASE
RI~OORIRE COMPARABLE 70 THOSE OBTAINED BY INTRAVENOUS AND
ORAL FORMULATIONS~. A. Hourvltz*, M. Oulltzkl*, D.S.
Seldman*, E Schlff*, J. Korach*, G Barkal*, S. Mashlach*.
Dept Ob/Gy~, Sheba Medical Center, Tel- Hashomer, Israel.
OBJECTIVE: The a~m of this study was to compare the
pharmacoklnetlcs and tolerance of r]todrlne admlnlstered
Intrave~eously (IV), and orally by plain tablets (PT) and
sustalned release (SR) capsules
STUDY DESIGN. Eleven consecutlve women wlth threatening
preterm (<35w) labor, recelved IV rltodrlne, When
contractlons ceased, IV therapy was stepped, and the patlent
started in a cross-over deslgn wlth elther PT (lOmg/2h) and
SR (4omg t i d ) Serum levels were determined after
achlevlng a steady state at 48 hours, by chromatography.
RESULTS: The mean±SD serum rltodrlne levels followlng
lnfuslon at a rate of 50ug/mln and IOOugl~ln were
34 5Z8 Ing/ml and 71 9~15 6ng/ml, respectlvely. The
meanzSD, maxlma] and mlnlmal serum concentratlons, fo]]owlng
Ingestlon of 12omg/day of rltodr]ne, were 17 6Z5 5 and
No slgnlflcant dlfferences were found in the tolerance to
CONCLUSIONS Serum levels achleved by IV r]todrlne were
slgnlflcantly hlgher than those measured followlng oral
409 NEONATAL OUTCOME AFTER DELIVERY FOR PREECLAMPSIA AT
<35 WEEKS. S.A. Fxiedman,~ E Schiff, B.M. Sibai. Department of Obstetncs and Gynecology, University of Tennessee, Memphis. OBJECTIVE: To determine whether maternal preedampsm has an adverse effect on neonatal outcome following delivery prior to 35 weeka. STUDY DESIGN: A matched cohort design was used to study 158 patients. Preeclampsm was defined as new-onset hypertension, proteinuria, and hyperuricemia. Patients delivered because ofpreedampsla at 24--35weeks (n=79) were matched for gestarional age, race, and mode of delivery to normotensive controls (n = 79) delivering preterm. Maternal and neonatal charts were reviewed for a variety of outcon~e rarebits. Results are compared using paired r test or McNemar’s test as in&cared. P values < .05 are considered s~gmficant. RESULTS: The mean gestational age at dehvery was 31 34-2 6 weeks for both
the prceclampnc and control patients. Birth weight in the preeclamptlc group was significantly lower than tn the content group (1369+433 vs. 16524-477 g, p = 0001) Except for length o~" stay in t~e intensive care umr for neonascs ~ 32weeks, no significant differences were found between the groups (Table).
All gestattonal ages < 32 weeks PPd~ Control PRE C~ontrol
(n =79) (n =79) (n = 44) (n : 44) Intensive care (%) 73.8 70 0 90.9 79.5 Intensive dare (days) 13 4±1.6 10.3±l 3 * 19 6±2.4 14 1 ±1.8 ILDS (%) 5(~ 3 58.8 79.5 68.2 Ventdauon (days) 2 7±0.8 2.6±0,6 4 7±1 4 4 1±1,1 IVH Grade III+IV (%) 3.8 1.3 6 8 2.3 NEC (%) 3.8 3 8 6 8 6.8 Bacterenua (%) 17 5 18,8 29.5 31.8 5-rain Apgar < 6 (%) 23 8 29 1 22 7 30.2 Neonataldeath (%) 6.3 5 0 11 4 6 8
PILE, prceclampsia; RDS, respiratory distress syndrome, IVH, lnterventricular hemorrhage, NEC, necrotizing enterocolins.
* p = .04
CONCLUSION: Despite lower birth weights, maternal preedampsia per se does not have a demonstrable adverse effect on the postnatal course of infants born at 24-35 weeks
411 SIlIraE-rt:NTEII I, Ni~IqIZB) PI.AC~BO CONTROLLB) TRIAL O1: ANTIMICRf]81ALS FGIi PlI~fI~TInu OF pP.ETEIIM BIRTH. S.M. Cox, V. gol~, #,k. She~x, K.a. Leveno.
Dept, Ob/Gyn, Univera|ty of Texas Southwestern, DaLLas, TX. OBJECTI~: ~e sought to determine the efficacy of antimicrobiaI therapy ~ithout other tocotytic drugs in the prevention of p~eter~birth. $IUO¥1)ESI~N: Fro~Nay 1989 to Dece~ee 1991~ 78~lo~en in labor bellmen 2g and 3~ Meek$~ gestatio~ and ~ith intact ~.~llbranes I~eee randomized to receive either antibiotics (AnlpiciLLin- $~tbacta~2 ~llever~6 hours x 8, then Augmentin 250mg po every 8h x 5 days) oe placebo. ~9 patients ~eee required i~ each a~ of the study to detect a 50g reduction in peeterm birth (po~er analysis). RESI~LT$: Sho~m betou are selected outcomes.
I,, I p~cE~o ~tmiotIcI P
total pregnancies 39 39 N$
;estatio~al ape ~ entry (~ks) ~ean ± SE~ 30.6 ± 0.3; Z9.8 ± 0,3~ gS
:ervicat dilatation ~ entry [cm) mean ± SEM 2 ± 0.16 2 ± 0.18 NS
)etivery < 37 ~eeks 25 25 NS
IntervaL0 study entry to O-ld 10 11 NS
I-2d 3 I 3-/d 1 1
8-1~d 5 3 >14d 20 23
<ean days (rnndo~izntion to ~elivery) 24.6 ± 4.0 28.7 ± 4.3 NS
tirth~eight (mean ± SEN) 2,2Z1 ¯ 118 Z,396 ± 126 qeonatal deaths 0 1
qeonatal Sepsis 0 0
COIICLU~IOII: ~r resutts do not support the use of ant 4crobiats in the prevention of preterm birth,

Volume 170, Number 1, Part 2 SPO Abstracts 389 Am J Obstet Gynecol
412 A UTERINE CONTRACTION TO CERVICAL RESISTANCE RATIO
AS A PREDICTOR OF PRETERM BIRTH FOR LOW-RISK
NULLIPARAS._C M. Stedma& R. Copper, R. Gotdenberg, M. Dubard,
J. Hauth. Dept. of OB/GYN, Ochsner Climc, New Orleans, LA and
University of Alabama at Birmingham, Birmingham, AL.
OBJECTIVE: To determine =f spontaneous preterm b~rth (SPB) w=thm
a low-risk nulhparous population could be predicted by a nsk score
directly proport=onal to the number of utenne contractions and in-
versely proporhonal to cervical resistance
STUDY DESIGN; SPB was defined as birth before 37 weeks gestation
following e~ther preterm rupture of membranes or spontaneous preterm
labor. Exclusion cntena include multffetal pregnancy, renal d~sease,
dmbetes, chronic hypeCtension, and collagen vascular disease. As part
of a randomized thai of low-dose aspinn versus placebo, 570 nulhparous
women w~th s~ngleton pregnancies underwent a cervical exam by a
study nurse and 30 minutes of tocodynometry at 28 weeks of
gestation Phys~c=ans were blinded to the results of tNs assessment
A nsk score was retrospechvely calculated as follows.
Uterine contrachons per hour
[1-%effacement] / (ddatation in cm x cerv=cal softness value)
RESULTS; The rate of SPB for the entire population was 5.5% The
rate of PTB increased as the risk score rncreased: 2 2% ~f score _<I 0,
7 7% ~f score >1.0 and <2 0, 12% if score >2.0 and <5 0; and 31.6% ~f score > 5.0. In a regression analys=s when scores of 1 to 5 and_>5 were
compared to a score of <1, the odds ratio for SPB were 2.5 (95%
confidence =nterval of .96 - 6 4) and 18.3 (95% confidence ~nterval of
5 4 - 61 5) respectively For the group with scores ->5, p = 0001. For
predicting SPB, scores >_5 had a senslt~wty of 30, a specificity of 973,
and a positive pred=chve value of 24.
CONCLUSIONS: The utenne contraction to cervical resistance rat=o,
calculated from a single evaluation at 28 weeks gestation, appears
able to identify a subset of nulliparous women at increased nsk of S PB
414 SIGNIFICANCE OF IMMATURE L/S RATIO IN THE PRESENCE OF PG IN AMNIOTIC FLUID. Dexter M Page, M D.’, Laxml Baxl, M.D., Columbm University, College of Phys=cmns and Surgeons, Sloane Hospital for Women,Columbia Presbytermn Medmal Center, N.Y., N.Y. OBJECTIVES: To investigate the slgmficance of =mmature L/S rat=o in the presence of phosphattdyiglycerol STUDY DESIGN: Lung profiles of 559 consecutive ammocentesis from September 1990, through June 1993 were retrospectively reviewed. Patients were then separated rote four groups based on L/S maturity (L.S > 2) in relation to presence of PG. 1)L:S > 2, PG + (270 patients, 48 3%); 2)L:S<2, PG- (221 pat=ents, 39.5%); 3)L:S>2, PG- (27 patients, 4.8%L 4)L:S < 2, FG + (43 patients, 7.6%L We focused on the group of 43 pat=ents wKh re]mature L/S ratios ~n the presence of PG. The varmbles that are known to alter L/S and PG values were =dentified Charts of 37 pat=ents from th=s group were avadable for addatona[ anatys~s. RESULTS: Presence of blood, mecon~um, and vaglnally collected specimens are known to lower the L/S rat~o and bacteria may contribute to a false positive PG. Amnlotlc fluid was reported as cloudy, yellow, blood or meconlum stained on 14 137 8%) occasions, one of these "cloudy" taps was diagnosed subsequently as lamellar ~cthyos~s Resp=ratory D=stress Syndrome was dmgnosed m 4 (10.8%) infants, two of which were born to mothers with chorloamnlonltls. S~gnlf~cant bacterial infectmns - group B strep, sepsis, and chonoamnlon~t=s were detected m 7(18%) pahents in our study group, Rh isolmmunlzat~on m 3(8 1%)cases, 2 fetuses had ~UGR 15.4%). Malor congenital malformahons (splna blfida, congenital d~aphragmatlc hernia, choleducta~ cyst, a ~aryngotrecbeal anomaly, cleft palate, and lamellar =cthyosls) were dmgnosed m 10 out of 37 (27.0%) infants =n our study group as opposed to 7 (8.7%) cases m 80 consecutive amnlocentems (P= 0.02). CONCLUSIONS: Infectious etiology must always be considered in the presence of L/S, PG d~ssociat~on In the present study, the presence of congenital malformations emerged as an additional factor in the setting of L/S, PG d~ssoclat~on that warrants further Investigation.
413 A RANDOMIZED PROSPECTIVE STUDY OF ADJUNCTIVE CEFTIZOXlME IN PRETERM LABOR
M. Gordonx, P J. Shubert, P. Samuels, F. Johnsonx, C Gebauerx , J b. tams Dept. of OB/GYN, The ONe State Umversity, Columbus, OH.
OBJECTIVE: To determine the role of ceft=zox~me as an adjunct m the treatment of preterm labor. STUDY DESIGN: A prospective, random=zed, double-blinded, placebo-controlled trial was conducted in patients with preterm labor between 24 and 35 weeks gestation. 485 patients with intact membranes and without chonoamnionitis who were receiving magnesium sulfate were screened. Exclusions were advanced cervical ddatatmn, penicillin allergy, current antibiotic therapy, and fadure to obtain reformed consent. 100 consecuhve, eligible, consenting pahents were randomized to receive e~ther 2 grams of ceftizoxime or a placebo every 8 hours. The primary end point was prolongahon of gestahon. Stahsbcal compansons were performed using unpaired, two-ta~led t-tests and Z2 analys~s. RESULTS: Of the 50 cefhzox=me and 50 placebo pahents, there was no drfference =n the interval to dehvery (34.8 _+ 21.1 days vs. 33.8 +_ 24.5 days, p = 0 83) and no difference in the rate of delivery before 37 weeks gestahon (60% in the ceft=zoxlme group vs. 62% m the placebo group, p = 1 0). Subanalyses of 74 subjects who received >_ 6 doses and were group B streptococcus negative, 59 pahents -< 32 weeks on presentahon and 20 sets of twins all showed no d~fferences in dehvery interval or rate of delivery < 37 weeks. The sample s~ze of th~s study was sufficient to detect a t0 day
d=fference in prolongahon of pregnancy (~z = 0.05, r~ =0.2). CONCLUSIONS: Ceftizox~me had no effect on mterva~ to delivery or durahon of pregnancy ~n women treated for preterm labor.
415 PLACENTAL TRANSFER OF SULINDAC AND ITS ACTIVE
METABOLITE IN HUMANS. W~ Kramer,* G Saade,* M Belfort,*
C-N Ou,* C Rognemd,* L Knudsen,* K Mmse, Jr Department of
Ob/Gyn, Baylor College of Medicine, Houston, TX
OBJECTIVE: To investigate the placental transfer of suhndac (SUL) and
~t’s active sulfide metabohte (SULu~x)
STUDY DESIGN: Patients undergmng cordocentesls for Rh
allolmmunlzatlon were given suhndac for tocolysls They were instructed to
take a 200 mg suhndac capsule orally 5 hours prior to the procedure Two
ml of fetal and maternal blood were placed in a plain glass tube SUL and
SULMEv serum levels were determined by high-performance hquld
chromatography Wllk-Shap~ro test was used to check for normality
Spearman correlation, paired Student t and sign-rank tests were used where
appropriate (s~gmficance P < 0 05) Data presented as median[range]
RESULTS: Eight samples from 4 fetuses were available There was a
slgmficant difference between the fetal and maternal SUL~T, (2.110 - 7 7]
v~ 14.115 2 - 18 3], P - 0 01) but not SUL levels (0.8[0.2 - 2] vs 0.5[0 1 -
2 1], P = 0 4) The ratio of SULMEr/SUL was slgmficantly higher in the
matemaI serum (26.8[7 9 - 105 7] vs 0.5[0 - 13], P < 0 01) The SULr~v
fetal/maternal ratio was significantly lower than the SUL fetal/maternal ratio
(0.2[0 - 0 8] vs 2.8[0 2 - 6], P < 0 01) Neither the SUL nor the SULr~v fetal
levels correlated with the corresponding maternal levels The SULMcr/SUL
ratio correlated w~th time from drug ingestion to samphng on the maternal (r
- 0 86, P - 0 01) but not on the fetal side (r = 0 24, P - 0 7) Although the
SUL fetal/maternal ratio increased with time (r - 0 85, P = 0 02), the same
was not noted for the SUL~r fetal/maternal ratio (r - 0 33, P - 0 5)
CONCLUSIONS: From the hmlted data available, it appears that maternal
admmlstratlon of suhndac results in re/atwely low fetal levels of Its active
form This may be the result of decreased metabolism of suhndac ~n the
fetus and/or poor placental transfer. A larger study is required to confirm
these prehmlnary findings.
390 SPO Abstracts January 1994
Am J Olostet Gynecol
416 TREATMENT OF THREATENED PRETERM LABOR. TOCOLYSIS FOR CONTRACTIONS AND NO CERVICAL CHANGE. HL Brown, AK
H=ettx, KA Bartonx, AM GolichowskL Department of Ob/Gyn, Indiana University Schoo~ of Medicine, Indianapolis, IN. OBJECTIVE: To compare the effect=veness of aggress=ve tocolys~s =n the prevent=on of preterm delivery in threatened (contractions without cerv=cal d=lat=on) and actual (contractions w~th cerv=cal change) labor. STUDY DESIGN: Tocolysis w~th intravenous magnesium sulfate was used to abort contractions in 200 women with no cerv=cal change (Group I) and in 175 women with cervical change (Group II) presenting between 24-35 weeks gestat=on. Oral tocNysls w=th terbutahne was begun after magnesium wean=ng and continued until 37 weeks gestation =n 92/200 (46%) m Group I and 115/175 (65%) women ~n Group I1. Length of gestat=on, preterm delivery rate, number of readmiss=ons for retreatment, birthwe=ght and neonatal intensive care (NICU) days was
~ oEr~al.re_,.d,, A,n.alysls was by X2 and ’t’ test when appropriate. ¯ a: r~ean gestat=on at =nitiat]on of magnesium was 29.2+3.1
weeks =n Group I and 30.6+2.8 weeks in Group II. Gestational a~ at del=very was 37 6+_.2.7 weeks ~n Group I and 36.2+--3.1 weeks in Group II. (p=NS) There was no s=gn~ficant &fference ~n age at delivery for those women on oral tocolysis versus no oral therapy in e~ther group. Delivery
less thano 35 weeks occured =n 19/200 (9.5%) ~n Group I and 40/175 (22.8Yo) ~n Group II.(p<.05) Readmisslon for one retreatment occurred =n 29/200 (14.5%) and >_ two readm=ts m 7/200 (3 5%) In Group I and in Group II 18/175 (10.2%) had one and 3/175 (1.7%) _> two readmiss=ons.(p=NS) Oral tocolys=s had no slgmhcant effect on magnesium retreatment ~n either group. Mean NICU days for Group I =nfants was 1.9+8 1 days versus 5.1+_15 3 days in Group II. (p<.05) B=rthwe=ght was 3032g for Group I =nfants and 2816g for Group II.(p=NS) CONCLUSIONS: Threatened preterm labor ~s associated with a s=gn=hcant preterm del=very rate even after aggress=ve tocolyt=c treatment. However oral therapy has no effect on the further prolongation of pregnancy in threatened or actual preterm labor.
418 ANTIBIOTIC TtlERAPY REDUCES TIlE RATE OF INFECTION- INDUCED PRETERM DELIVERY AND PERINATAL MORTALITY. R Romero, H Munoz’, R Gomez’, M Ramirez’, H Araneda=, J Cutright’, N W~B Cotton, P FideP. Dept of OB/GYN, Wayne State Universlty/Hutzel Hospital, Detroit, MI and the Pennatology Branch, NICHD, Bethesda, MD. BACKGROUND/OBJECTIVE: Strong evidence supports an association between intrauterine infection and premature labor and de’hvery. Yet, several randomized clinical trials (RCTs) of antibiotic administration to women in premature labor have found this therapy to be ineffective. Such a therapeutic l’ailure has been attributed to. 1) a dduuon of the beneficial effect of antibiotics by inclusion in RCTs of women without mtranterine infections and 2) delayed treatment of patients with proven intrauterine infections. It is essential to deteranne if antibiotics could ever be useful to eradicate an intrauterine infection and preterm labor and also the factors which determine therapeutic success or failure Since these questions cannot be answered m humans, we have resorted to animal experimentation to determine whether antibiotics can prevent preterm dehvery and reduced perinatal mortahty. STUDY DESIGN: Under hysteroscopic guidance, 69 pregnant rabbits at 70% gestation (21 days) were randomly allocated to three groups: 1) Control group: transcervical inoculation of phos.phate buffer salineO.2 ml (n =21); 2) =nrection group: transcervical inoculation of 0.2 ml of 10~ cfu of E. Coli (n=16), and 3) infection + antibiotics group: (E. Coli + ampicillin- salbactam; 150 mg/kg q 8 hours IM) (n=32). To test the consequeeeas of treatment delay animals in the latter group were randomly allocated to recewe antibiot=cs at different ntervals after barter al moculat on: 0, +6, + 11 and + 18 hr Survival analyms and chi square were used for stmtstics. RESULTS: 1) All rabb=ts inoculated with E. Coli without antlb=otics dehvered prematurely confirming that mtrauterlne infection causes premature labor and-delivery, 2) the inoculation-to-delivery interval was significantly shorter m the infection group than in the control group (median 32 hr, range 15-74.5 hr vs median 2-19.5hr, range 173-246 hr, respectwely, p<0.001), 3) antibiotic administration wlthm 12 hours of inoculation but not after 18 hours increased the duration of pregnancy (bff reducing the rate ofpreterm dehvery) and neonatal survival (from 0% to 71%,.p < 0.005). Inoculation to delivery interval in the group treated with antibiotics within 12 hours of inoculation was longer than that of the group treated aRer 12 hours (median 184 hr, range 68-222 vs median 44 hr, range 18-78, respectively, p <0.05). CONCLUSIONS: 1) Antibiotic administration can prolong pregnancy and reduce perinatal mortality after an ascending intrauterine in fectlun. However, antibiotics are effective only during a narrow therapeutic window (< 12 hours); 2) the apparent lack of effectiveness of antiliiotic administration to
~regnant women with preterm labor may be partially due to treatment delay; ) seasitwe and rapid methods for the early dmgnosls of intrauterine refection are urgently needed to exploit the therapeutic benefits of antibiotics admunstratlon to women with preterm labor and intact membranes.
417 ACTIVE RECRUITMENT INTO HEALTH CARE AND ITS
EFFECT ON PREGNANCY OUTCOME.
G L. Olson D A. Nagey. Dept. Ob/Gyn, Univ. of Maryland School of
Me&cine, Baltimore, MD.
OBJECTIVE: To analyze the effect of door to door recruitment of
pregnant women into the health care system and to determine whether
pregnancy outcomes differ when compared to a non-solicited group
STUDY DESIGN: The Baltimore Project began in November 1989
and was conUnued unnl April 1993 when it was supplanted by
Baltmaore’s Healthy Start Project. Both projects revolved the active
door to door recrtutment of pregnant women into the health care
system. The catchment area was characterized by census tract data that
~denufied poverty, low birth weight, and perinatal mortality rates
During the study period 138 women who dehvered at our institution
had been contacted by the Baltimore Project A comparison group was derived from the same census tract catchment area but dehvered at our
~nstitut~on in the two years prior to the initiation of the project. Variables of interest mcluded gestatinnal age at the first prenatal visit,
gestanonal age at the time of delivery, and birth weight. Statisical
analys~s was performed using the Mann-Wh~mey U test. Additional variables evalua/ed ut~hzing Chi-square analysis included iintiatiun of
prenatal care < 16 weeks, gestational age < 37 weeks at dehvery, birth
weight _< 1500 and < 2500 grams.
RESULTS: No statistical d~fference was found between the two
groups concerning gestational age at first v~s~t, gestatmnal age at delivery, and birth weight. When the analysis was extended to
evaluate mttmtlon of prenatal care prior to 16 weeks, dehvery prior to
37 weeks, and specific gestational weights there was still no stanstical
difference between the groups.
CONCLUSION: Medical and non-medical factors influence
uhhzatlon of health care and ultimately pregnancy outcome. Unless
tin]e has altered the risks of late prenatal care, preterm delivery, and
low birth weight a prograra that mcludes door to door recruitment into
the health care system appears to not improve these outcome variables
419 Oral Terbutahne m the Outpatient Management of Preterm Labor H. HOW, S Allen," B Vogel," S. Gall, J Spinnato Umverslty of Louisville, Lomsville, KY OBJECTIVE: To test the hypothes~s that once preterm uterine contractions/labor are controlled with intravenous tocolysis, oral terbutahne as a maintenance drug does not prolong pregnancy STUDY DESIGN: Patients who were intially treated w~th MgSO~ to arrest preterm labor were discharged to home bed rest and randomized to receive or not receive oral terbutahne (terb) tocolysis Four groups were compared with cervical change present: Group I, terb; Group II, no terb; w~th cervical change absent: Group IIl, terb, Group IV, no terb The patients were evaluated weekly Statistical analysis employed chi-squared test, Student’s t test, and ANOVA with alpha = 0 05 RESULTS: Of the 231 patients, 28 (12%) were excluded due to non- comphance The table summarizes the climeal characteristics and pregnancy outcome for the four groups
11 Ill IV fN= 56) (N= 58) (N= 46) (N= 43)
Bishop score prior to d~scharge 6.53__+1.5 c* 5.93_.+1.0 b* 3 46__+0.7 a 3.53_.+0.5 a
% of patients readmitted 14.3 a 15 5 a 28.3 a 27.9 a
Gestatlonal age atdelivery(wks) 353+26a 359_.+23a 360+-5.5ab 376_+2.7b
% del. >_ 37 wks 28.6 a 29.3 n 56 5 b 72.1 b
Values(except for percentage) are means __. SD Means with the same letter are not statistically different * 95 % CI for the difference between group I and I1 is 0.05 to 1.16
Maternal age, paray, gestational age at enrollment, duration of intravenous MgSO4, frequency of and % of patients w~th unscheduled hospital visits, as well as the number of neonates with HMD, NEC, and IVH were not slgmficantly different among the four groups Comparison of terbutahne (1+I11) and non-terbutaline (II+IV) groups revealed no statistically significant difference in outcome variables CONCLUSIONS: Our data suggest that oral terbutaline maintenance will not improve pregnancy outcome in patients who have had successful intravenous tocolysts.

Volume 170, Number 1, Part 2 SPO Abstracts 391 Am J Obstet Gynecol
420 INTRAPARTUM FETAL PULSE OXIMETRY: FETAL
OXYGEN SATURATION TRENDS DURING LABOR WITH
NORMAL NEONATAL OUTCOME. GA Dildy~, PP van don Bergx~, M Katz~, SL Clarkt, HW Jongsmax*, JG N~jhmsx*, CA
Loucksxr. Deparanents of Ob/Gyn: University of Utah School of
Medicine, Salt Lake City*; University Hospital Nllmegen, the
Netherlands*; California Pacific Medical Center, San Francisco~.
Objectives: To study fetal arterial oxygen saturaUon (SpO2) trends
by continuous pulse oximetry during labor in subjects with normal neonalal outcomes followmg vaginal delivery.
Methods: Continuous fetal SpO2 was measured during labor usmg
a noninvasive reflectance pulse oxtmeter (Nellcor, Inc, Hayward,
CA, USA) designed for fetal application. Subjects were excluded for
any of the following conditions: poor signal quality, gestational age < 37 weeks, maternal oxygen adnumstrat~on, dehvery by cesarean
sectmn, 5-nunute Apgar < 7, umb~hcal artery pH < 7 10, bLrthwe~ght
< 2500 gm, or newborn intensive care unit admission.
Results: 291 subjects were studied: 142 m Prove, 90 ~n Nljmegen,
and 59 in San Francisco. 131 subjects were excluded from the
study, and normal neonatal outcome was considered to occur m 160
cases. Mean + SD fetal SpO2 was 57.5 + 9.5% during the
cumulative period of study. A significant decrease (paired t-test, p
< 0.0001) tn fetal SpO2 occurred from Stage I (59.3 + 9.8%) to
Stage II (53.2 + 10.2%) labor. Subdividing Stage I into early ~ 4
cm), middle (5-7 cm), and late (8-10 cm) phases, a gradual
decreasing trend in fetal SpO2 was observed: 62.0 + 9,1%, 60.3 +
11.4%, and 57.5 + 10.3%.
Conclusions: Using reflectance pulse oximetry, a statistically
significant decrease in fetal SpO2 was observed during labor in
women with normal neonam/outcome.
422 THE IMPACT OF A POLICY OF AMNIOINFUSION FOR MECONIUM-STAINED
AMNIOTIC FLUID. I M Usta,x B M Mercer, N.K. Aswad,x B M Slba~, Univ. of Ten&, MempNs, TN.
O~JECTIVE. To evaluate the effects of a policy of amnlolnfusion {AI) for thick or moderate meconium-sta=ned amniohc fluid (MSAF) on the prevention of mecon=urn
aspirat=on syndrome (MAS) and ~ts comphcat=ons. STUDY DESIGN: We reviewed maternal and neonatal charts of all vertex, singleton
pregnancies (w~lhout congenital anomalies) complicated by moderate or thick meconium dunng a three-year penod All infants had Delee suction at time of delivery
of the head. Intubat~on and vocal cord visualizalion was reserved for depressed =nfants Analyzed data included the use of amnioinfus~on, maternal demographic
=nformat=on and pregnancy outcome, as well as neonatal outcomes, part=cularty MAS. RESULTS’ A total of 440 patianls of 937 (47%) received amnieinfus~on, whereas 497 (53%) d~d not receive amnioinfus=on for the following reasons. Imminent delivery
(n=310), occult mocon~um (n=141), and emergency cesarean section (n=46).TNrty- nine infants (4.2%) developed MAS. 20 (4 5%) tn the amn=o=nfusion group and 19
(3,8%) =n the no amn=oinfuslon group. The table below compares important neonatal characteristics between the two groups
CONCLUSION: With the policy of routine amnioinfus~on for moderate or tNck mecon=um-stalning of the ammot~c flu=d, AI was not clinically feasible in 53% of
cases Even ~n those who received ammo=nfus=on, 4 5% had MAS and the syndrome
wa~ a~, severe as m infants of mothers who d~d not receive such an ~nterventlon. No Amn~o=nfusion Amnioinfuslon
Variable {n=497) (n:440)
Gestalional age (wks)* 39 4 +2 0 39,9 + 1 7
Birthwe~ght (grams)* 3224 + 469 3301 _+ 505
Mecenium >trace below cords 28/97 (28 9%) 31/112 (27.8%) Apgar score at 1 min, <5 68 (13 7%) 71 (161%)
Apgar score at 5 ram, < 7 35 (7 0%) 36 (81%) Neonatal seizures 7 (1.4%) 5 (1 1%) Ventilation requ.~emenl 12 (2 4°./o) 19 {4.3%)
Venhlahon (days) 5 29 _+ 6 57 (0 5-23) 5,03 + 8 23 (0 5-33)
Neonatal death 1 (0.2%) 3 (0 7%)
ECMOt 1 (0 2%) 3 (0 7%}
¯ p <0 05,1" ECMO = Extracorporeal membrane oxygenation
421 THE EFFECT OF SAMPLING TECHNIQUE ON MEASUREMENT OF FETAL BLOOD pH AND GASES - AN IN-VITRO SYSTEM. DJ. Sherman,
S. Anali, A. Raz~el, I. Bukovski, E. Caspi. Dept. Ob/Gyn, Assaf-Harofeh Medical Center, Sackler SchooI of MOd., Zerifin, israel OBJECTIVE: Fetal scalp blood for lntrapanum pH monitoring is usually collected aeroNcolly in small volumes and may therefore be affected by the sampling mode. The effect of specimen collecuon on measured indices of fetal blood acid-base balance was evaluated in an in-vitro simulated system STUDY DESIGN: The system consisted of an air-tight syringe filled with
either arterial or venous fresh cord blood, and an attached needle with a blunted tip. The rate of blood drop formation at the np was determined by a vanable
speed infusion pump. Control acid-base values were measured directly on syringe specimens before and immediately after completion of each test. Two techniques, simulating actual scalp blood sampling, were evaluated: 1) Commonly Used Technique (CUT) - after collec’aon, sample is transferred into a syringe and subsequently measured. 2) Direct Technique (DIR) - specimen collected directly into capillary for measurement RESULTS: Control arterial and venous acid-base values did not change slgmficanfly throughout the test. Significant changes, however, were noted when sampling was by CUT: mean arterial pH increased from 7.21 to 7.26 and PO2 from 19 to 25 mmHg, while PC02 decreased from 56 to 44 mmHg (P<0.01). Changes in venous blood samples were el similar direction and magaitude.When sampling by CUT, absolute changes from control averaged 21_+2% and 15_+1% (_+SEM) for slow and fast drop rate, respecuvely (P<0.01). On the other hand, DIR sampling did not have a sigmficant effect on measured acid-base values. Differences between slow and fast drop rate were not significant: absolute changes from control averaged 4.5_+0.4% and 4 7_+1.3%, respectively (_+SEIvl).
CONCLUSIONS: The mode of fetal scalp blood sampling and handhng affects measured acid-base indices. Such changes reflect aeration of small blood
volumes, and may result in falsely elevated capillary scalp pH This effect may
be prominent when blood drops are slow-fornung or difficult to obtain.
423 THE IMPACT OF AMNIOTIC FLUID VOLUME ON
PERINATAL OUTCOME. CM Baron-x, MA Morgan, TJ Game.
Dept. Ob/Gyn, Univ. of Calif., Irvlne, Orange, CA. Objective: To determine the value of routine ammouc £uid volume assessment in patients admitted for antimpated delivery on mtrapartum comphcauons. Study Design: 767 pauents were enrolled into the study from January 1988 to June 1989. Inclusion criteria; admission to L & D with ultkmate delivery and gestat~onal age > 26 weeks. Amniotic fluid index (AFI) determined by four-quadrant techmque on admission to L &D. Ohgohydramnios (Oli) was defined as AFI _< 5 cm (n=lT0); bortierhne (BdOli) as AFI 5.1 to 8.(I cm (n=26l); normal (N) as AFI 8.1 to 20.0 cm (n=336), 9 patients with AFI > 20
were excluded. The Oli and BdOII groups were compared to the N group with regard to antenatal, ~ntrapartum and postpartum variables. Results: These groups had similar maternal age, panty, delivery gestauonal age and antenatal complications. There was no difference in apgar scores, or neonatal comphcatIons between groups. Oli predicting cesarean for fetal distress" senslUv~ty (78%), specificity (74%), positive predictive value (33%) and negauve predicUve value (95%). Data expressed as relanve risk (95%
Confidence Interval.). Parameter Oh to N BdOh to N
Meconmm stained fluid 0.67 ((! 49-0.92) 1.06 (0.94-1.20)
Variable deceleratmns 1.,~4 (1.12-1.87) 0.97 (0.75-1.27)
Cesarean, fetal distress 6.83 (1.55-30.4) 1.71 (0.17-17.3)
Conclusion: AFI detecting Oh on admission to L & D ~s a valuable sereemng test for subsequent fetal dislress reqmrrng cesarean delivery.

392 SPO Abstracts ,January 1994 Am J Obstet Gynecol
424 INTRAPARTUM FETAL PULSE OXIMETRy: THE EFFECTS
OF 40% MATERNAL OXYGEN ADMINISTRATION ON
FETAL ARTERIAL OXYGEN SATURATION. GA DtIdy,
Clark, CA Loucksx Department of Ob/Gyn, Unlverstty of Utah
School of Medicine, Salt Lake City
Objective:To observe the effects of prolonged maternal oxygen
(02) adnnmstratlon at FIef, - 0 40 on human fetal oxygen
saturation
Study Design: 10 healthy women m active labor were studied
Continuous fetal arterial oxygen saturation (SpO2) was measured
using a noninvastve reflectance pulse oxtmeter designed for fetal
application Baseline fetal SpO2 was obtained, then O2 was
administered by face mask at FrO2 - 0 40 for 45 minutes, SpO2
was measured after discontinuation of supplemental O
Differences between groups were analyzed by ANOVA,
significance was considered at p<0 05
Results: Mean 4- SD SpO2 before O2 administration was 57 3 4-
11 8% SpO~after 15, 30, and 45 minutes of 40%O2were 586
~: I4 9%, 56 8 :L 9 2%, and 62 9 ± 10 7%, respectively SpOz was
53 6 4- 12 6% and 57 I% ± 11 0% at 15 and 30 minutes followtng
disconttnuatlon of supplemental O~ No significant difference was
determined among the groups
Conclusions: Prolonged maternal administration of 40% O
resulted m uo significant cb~ange ~n fetal SpO~, determined by
reflectance pulse oxlmetry Since the adtnImstration of O2 by
standard mask techniques rarely results In 40% FIe:, fetal benefits
of such lntrapartum maternal oxygen administration are doubtful
426 PROSPECTIVE, RANDOMIZED ASSESSMENT OF AMN1OTIC FLUID
INDEX AS FETAL ADMISSION TEST. S.P. Chauhan, E.F. Magann, J.F
W~hburneX, K.G Perry, Jr., J.N. Martin, Jr , J.C. Morrlson. Dept. Ob/Gyn,
Univ of Mississippi Medleal Center, Jackson, MS.
OBJECTIVE: The null hypothesis is that there m no difference in the incidence
of abdominal dehvery for presumed fetal distress m the patient group who had
the intrapartum ammotic fluid index (IAFI) assessed and the control group who
did not.
STUDY DESIGN: Over a 7-month period, partarients at > 26 weeks’
gestation who presented in labor were randomized to the study (IAFI) or control
group. The labor and delivery staff managing the patients were aware of the
1AFI results, especially if oligohydramnios (IAFI ~< 5.0 cm) was present. All
patients had continuous electromc fetal monitoring and none had an abnormal
tracing on admission Student t test or Fisher exact test was used where
approprtata mid p < 0 05 was considered significant.
RESULTS: Maternal demographics and the incidence of med~cal/obstetrieal
complications were similar among the patients who underwent assessment of
IAFI (n = 447) and those who did not (n = 436) In the IAFI group of
patients, the incidence of abdominal delivery for presumed fetal distress (29/447)
was significantly higher than in the control group (14/436, p = 0.02, RR I 3,
95 % CI 1.1 - 1.72) The incidence of abdominal delivery for cephalopelvlc
disproportion was s~milar in both groups as was the mean birth weight,
incidence of very low birth weight, low birth weight, macrosomia, Apgar score
< 7 at 1 or 5 minutes, and admission to the neonatal intensive care unit.
Among parturients who had abdominal delivery for presumed fetal distress, the
decision-incision time was simdar regardless of whether parturients had IAFI or
not (38.5 + 14 7 versus 32 5 +__ 14.7 minutes, respectively; p = l 0).
CONCLUSIONS: We reject the null hypothes~s and accept that patients who
have an IAFI as a fetal assessment test have a significantly higher incidence of
abdominal delivery for presumed fetal distress. The decision-recision time is not
decreased and perinatal outcome is not improved if parturients undergo
assessment of IAFI in early labor.
425 FE*rAL HEART RATE TRACING INTERPRETATION: EFFECT OF NEONATAL OUTCOME. J. Wright, H. Zain’, G. Parnsh’. New Hanover Regional Medical C~nter, Coastal AHEC, Wilmington, NC and Dept. of Ob/Gyn, UNC at Chapel I-hll. OBJECTIV~ The purpose of thin study was to determine If knowledge of neonatal outcorr~ influenced physicians’ retrospective interpretation of fetal heart rate monitoring strips and opinion of appropriateness of care. STUDY i)E~IGN~ We selected 10 eases from morning rounds that involved a critical judgement by the managing physanan. We assembled prenatal histo~’, labor course, delwery, and neonatal outcome into a concise format. We photooopted fetal heart rate tracings, and removed written information to conceal true outcome. Each case contained a point In the patient’s labor at which the physician made an important judgement regarding route and timing of delivery. We marked these points on the monitor tracings for reviewer evaluation. For each ease, we created duplicate histories v, ath opposite neonatal outcomes, and each reviewer evaluated 2 ease pairs with opposite neonatal outcome. The individual cases from each pair were sent to the reviewer with one month’s time intervening. Reviewers evaluated tracings for: varlabihty, late deeelerattons, and evidence of hypoxia. They also judged whether the decision regarding dehvery verst~ COntinued labor had been appropriate.
RESULTS: Good outcome Poor outcome P-value (N= 70) (N~ 70) McNemar’s test
Reduced varmbdlty 43 (61.4%) 49 (70.0%) NS Late decelerations 39 (55.7%) 45 (64.3%) NS Evidence of hypoxm 34 (49.3%) 47 (68.1%)* .007 Decision incorrect 25 (35.7%) 41 (58.6%) .0004
NS ~ not significant * 1 response missing Re’,aewer~’ tendency to dmgnose hypoxia and to judge the management incorrect did not consistently correspond w~th n change in d~agnos~s of late deceleration~ or reduced variability. CONCLUSIONS: Our data confirm that physicians are biased by neonatal outcome when retrospectively rev~e,~ang labor management.
427 INTRAPARTUM ASSESSMENT OF BIRTIi WEIGilT: CLINICAL
VERSUSE1GHTSONOGRAPHICMODELS. S P. Chauhan W.E Roberts,
J 1:. Washburnex, C.A Sulhvan% E F Magann, J.C. Morrisen. Dept
Ob/Gyn, Univ. of Mississippi Medical Center, Jackson, MS
OBJECTIVE: To compare the relative accuracy of predicting birth weight
(BW) clinically versus sonographically
STUDY DESIGN: In the latent phase of labor, 834 partunents underwent a
clitoral esttm~e of BW followed by sonogeaphie measur~ton of bipartetal
diameter (BPD), head circumference (HC), abdominal circumference (AC) and
femur length (FL) The sonographtc estimate of the birth weight (SEBW) was
derived by using eight different models which use either one parameter (AC or
FL) or a combination of two, three, or four fetal parameters Analysis of
varmnce, followed by Dunett’s test, was used to determine which sonograph~c
models were significantly superior to clinical estimate. Linear regression
analysis was performed to determine the correlation and prediction limits for the
chnical eshmate and the sonographlc model with the highest accuracy as they
correlated with actual BW
RESULTS: The mean ~ SD) gestattonal age at delivery of the 834 patients
was 37 4 + 4 I weeks mad the mean birth weight was 2941 + 856 gm. The
mean standardized absolute error was s~gnlficantly lower w~th the prediction
derived from measurements of three (BPD, AC, FL; 10.7 + 9 1 gm/kg) or four
(BPD, HC, AC, FL, 10 7 + 8.9 gm/kg) fetal parameters and there was no
difference between these two models. Chmcal estimates of the birth weight had
a s~mdar mean standardized absolute error (12 7 +__ 14.3 gm/kg) as those
derived sonograph~cally after measuring one or any combination of two fetal
parts. Fifty-six percent of the estimates were within +__ 10% of the actual birth
weight with chmeal as well as soaographlc estimates based on three or four
fetal parameters Linear regression analysis between an estimate o f birth weight
(derived chnleally or using three or four fetal parameters) reveals correlatmn
coefficients of 0 77, 0 81, and 0.81, respectively, with the relationship being
significant (p = 0 0001) ~n each case
CONCLUSION: To improve on chnlcal estimate of birth weight, the
sonographlc prediction of newborn’s weight must be based on measurement of
three (BPD, AC, FL) or four fetal parameters (BPD, HC, AC, FL)

Volume 170, Number 1, Part 2 SPO Abstracts 393 Am J Obstet Gynecol
428 INTRAPARTUM DETECTION OF A MACROSOMIC FETUS:
CLINICAL VERSUS EIGHT SONOGRAPHIC MODELS. S P Chauhan,
E F. Magann, W E. Roberts, J.N. Martin, Jr , B.D Cowan, J.C. Morrisoa
Dept Ob/Gyn, Umv. of Miss~ss~pp~ Medtc~d Center, Jackson, MS.
OBJECTIVE: Compare the relative accuracy of eight sonographlc models that
predict a macrosomic fetus (birth weight >.~ 4000 gm)
STUDY DESIGN: Prospectively, 623 consecutwe parturients who dehvered a
newborn at >__ 37 weeks and with a birth weight > 2500 gm were analyzed
All of these patients had a clinical estimate of birth weight a,~d sonographic
measurements of fetal p~.rts--bip~neud diameter (BPD), head circumference
(HC), abdominal c~rcumference (AC), and femur length (FL)--in early labor by
the same examiner Sonographic estimate of birth weight was derived by using
eight different models which use e~ther one parameter (AC or FL) or a
combmatma of two, three or four fetal parameters Nme receiver operator
characteristic curves (ROCC) were constructed for an estimate >__ 2500 gm to
correctly identify a newborn with birth weight __> 4000 gm The area under each ROCC and the respectwe standard error was calculated The area under
tile curves were then compared by the critical ratio z-test P < 0 05 was consxdcred s~gm ficant
RESULTS: The incidence of mt~crosorma was 10.7 % (67 of 623) and the mean
(4- SD) birth weight among these 67 newborns was 4265 __+ 228 gm. Chntcal,
not sonographie, estimate of birth weight had the lowest mean standardized
’absolute error (9 9 + 7 0 gin) and the highest percent of eshmates wnh*n 4‘
10% of the actual birth weight (54%) among rnacrosom~c newborns
Comparisons of the area under the curve revealed that ehnlcal estimates of birth
weight were superior to sonographtc estimates that were based on femur length
alone There was no s*gmficant difference tn the ablhty to detect the
macrosomlc fetus chmcally or sonographically with seven other pubhshed
models wh,ch use AC alone or use combinations of two or more fetal parameters
to derwe the b~rth weight
CONCLUSIONS: Estitnates of birth weight derived chmcally or
sonograph~cally have slmdar accuracy in detecting the macrosom*c fetus
Rchnwe operating curve analysis of permatal predictive data ~s a valuable
adjunct to estabhsh mtormed decisions regarding the "best test "
430 ESTIMATE OF BIRTil WEIGHT AMONG TWINS: COMPARISON OF
EIGiIT SONOGRAPIIlC MODELS. S P Chauhan, J N. Martin, Jr , J F. Washburne~, B.C. Brostx, E F Magann, J.C. Morrtson Dept Ob/Gyn, Umv.
of Misstssippi Medtcal Center, Jackson, MS
OBJECTIVES: The accuracy o f sonographlcally estimated singleton b~rth weight
improves as an increasing number of fetal parameters are available for
computation. The purpose of thts study was to investigate and compare the
relative accuracy of eight different sonographic models which employ 1 to 4
feud biometnc measurements to derive the birth weight.
STUDY DESIGN: During a 3-year period, 181 twin gestations with
stanographic mensuration of biparietal dmmeter (BPD). head circumferet~ce
(HC), abdotmnal circumference (AC), and femur length (FL) within 96 hours
of dehvery were analyzed. Analysis of variance, followed by Student-Newman
KeuI’s test or chl-square, was used to determine the accuracy of the eight
models A receiver-operator curve was constructed to determine the
soaographlc estimate which would consistently ~dentify nonvertex twin B with
a birth weight __< 1500 gm Regression analysis of the estimated birth weight
and the actual b~rth weight for twins A and B were calculated which would
permu 90th and 95th percentde pred~ctmn of the neonatal birth weight.
RESULTS: The mean gestatlonal age (~_ SD) of the 181 twins was 32 4 4- 4.3
weeks, and the mean btrth weights of twins A and B were 1851 q- 676 gm and
1883 __+ 655 gin, respectively Analysts of variance followed by Student-
Newman Keal’s test revealed that the mean standardized absolute error was
sigmficantly higher for estimates based on one fetal parameters (AC or FL).
Regardless of presentation (A or B, vertex or nonvertex) or whether the actual
b~rth weight < 1500 or > 1500 gm, the accuracy was simdar among the six
models which utdtze >_.. 2 feud parameters to predict birth weight. For twins A
and B, the correlation coefficients for linear regression analysis for esBmated
and actual birth weight were O gl and 0 83, respectwely (p < 0 0001 for both
equatmns) Receiver-operator characteristic analysis reveals that for nonvertex
twin B, an estimate of birth weight (based on BPD and AC) ~< 1600 gm will
permit identification of all newborns wnh a birth weight <__ 1500 gm
CONCLUSIONS: Sonographlc modals which include two feud parameters are
sufficiently adequate to permit assessment of twin birth weights
429 INTRAPARTUM AMNIOTIC FLUID INDEX AND ADVERSE
OUTCOME: EXPERIENCE~VITH 1000 PARTURIENTS. S P Chauhan
B D. Cowan, E.F Magann, W E. Roberts, J.C. Morrison, J N Martin, Jr
Dept. Ob/Gyn, Univ. of Mississippi Medical Center, Jackson, MS
OBJECTIVE: To determine ff an imrapartum arnntotIc fluid index (IAFI) __<
5 0 cm is associated with abdominal delivery for presumed feud distress
(ADPFD) or Apg~r scores < 7 ~t 1 or 5 minutes.
STUDY DESIGN: Prospectively, IAFI was obtained in the latent phase of
labor mmong 1000 pn.rtunents with nonanomalous singleton pregnancy and a
gestatmnal age > 26 weeks. A relative operating characteristic curve (ROCC)
was used to determine ff any 1AFI predicts adverse outcome among 1)
compttcated (chrome hypertension, pregnancy-induced hypertension, insulin-
dependent diabetes, dehvery at <.~ 34 or >_. 42 weeks) versus uncomphcated and
(2) preterm (< 37 weeks) or term (37 to 4i+~ weeks) delivery
RESULTS: The incidence of Apgar scores < 7 at 1 or 5 minutes were simdar
among the partunents with IAFI __< 5 0 cm (n = 288) versus those with IAF1
> 5 0 cm. The mean IAFI was similar among the 69 partunents who had
ADPFD (9 1 4‘ 9 I era) and the 931 patients who did not (9 4 4- 6.2, p =
0 70) Sumlarly, the mean IAFI was not significantly different ~nong 28
patients whose newborns had Apgar scores < 7 at 5 minutes and the 972
patients whose newborns had Apgar scores >__ 7 at 5 minutes (7 4 4- 6 5 and 9 5 4- 6 5 cm, respectively, p = 0 09). Among high-risk parturients w~th IAFI <~
5 0 (n = 131) versus those w~th IAFI > 5 0 (n = 241), the mcideace of
ADPFD and low Apgar scores were not significantly different The ROCC
indicates that whether a pregnancy is comphcated (n = 372) or uncomphcated
(n = 628), preterm (n = 215) or term (n = 785), an IAFI is a poor predictor
of ADPFD or Apgo.r score < 7 at 1 or 5 minutes At all the discriminatory
]AFI values tested (0 - 20 cm), the false-positive rate was wrtually identical to
the true positive rate of the population.
CONCLUSIONS: AFI <__ 5 0 ts n~t associated with ADPFD or low Apgar
scores, regardless of whether pregnancy is term or preterm, comphcated or
uncomphcnted Moreover, the ROCC indicates that there ts no IAFI value
between 0 and 20 cm which can be used to rehably predict which parturient ~s
at ask for ADPFD or which newborn IS hkely to have low Apgar scores
431 SONOGRA.PIIIC ESTIMATE OF BIRTH WEIGHT IN LABOR AT
TERM: FACTORS INFLUENCING ITS ACCURACY. S P Chauhan
E.F Meydreehx, C A Sullivanx, K.G. Perry, Jr, E.F Magann, J C.
Morrison. Dept Ob/Gyn, Univ. of Mississippi Medical Center, Jackson,
MS.
OBJECTIVE: To study the maternal and neonatal factors that influence
the accuracy of a sonographie estimate of birth weight.
STUDY DESIGN: Sonograph~c estimate of birth weight (using abdominal
circumference and femur length) was determined among 79 women m the
latent phase of labor at term An estxmate wIthm + 10 % o f the actual b~h
we@~t was considered accurate; > 10% &sparity was deemed inaccurate
Using umvariate analys~s, the two groups were compared with respect to 11
maternal characteristics, four sonograph~c estimates of fetal btometry, and
five neonatal measurements
RESULTS: Among the 79 newborns, the mean birth weight was 3585 __+
472 g and the incidence of macrosomia (birth weight __> 4000 g) was 20%
(16/79) Ofthe79sonographieestimates, 33(41 8%)oftheestxmateswere
+ 10% of the b~rth weight while 46 (58 2%) were inaccurate. Between
these two groups of patients, univanate analysis did not identify matemal
age, gravid~ty, parity, maternal height, pre-pregnancy weight, maternal
mass index (MMI) at the hme of dehvery, change in MMI during
pregnancy, gestatlonal age at sonography, intrapartum amniotic fluid index,
in utero ponderal index, or the newborn’~ weight, length, anthropometric
measurements, and ponderal index as sigmficantly correlating with the
accuracy of sonograph~cally predicted birth weight. On the basis of
stepwise logistic regression analysis, sonographtc measurement of
abdominal circumference (p < 0 0007) and newborn’s lengt~ (p < 0 0384)
were the best combmatmn for prediction of birth weight
CONCLUSIONS: An accurate sonographic emmate o f birth weight among
laboring women at term ts not s~gmficantly influenced by maternal/neonatal
habltus or amniotie fluid volume However, in utero determination of fetal
length may ~mprove the accuracy of a sonographtc estimate of birth weight

394 SPO Abstracts January 1994 Am J Obstet Gynecol
432 THE EFFECT OF OLIGOHYDRAMNIOS ON THE ACCURACY OF
INTRAPARTUM ESTIMATES OF FETAL WEIGHT. Y Bernhard% I. Bar-Havex, M,Y. Dlvon. Department of OB/GYN,
Albert Einstein College of Medtcme, Bronx, N.Y.
OBJECTIVE: To study the effects of ohgohydramnms on the
accuracy of mtrapartum chmcal and sonographlc estimates of fetal
we=ght (EFW).
STUDY DESIGN: An mtrapartum clinical EFW by abdominal
palpation, as well as sonograph=c EFW (based on measuring the b=panetal dmmeter, abdominal mrcumference, and femur length)
and amn=ot=c fluid index (AFI) were obtained on 124 consecutive
laboring women at term Ohgohydrammos was defined as an AFI
< 5cm. Percent error of EFW was calculated as follows: 100(BW- EFW)/BW. SonograpNc end chmcal estimates were compared to
b=rthwmghts (BW) using the Student t-test.
RESULTS: Impact of AFI on EFW
Normal Fluid (n = 92) Ohgohydrammos (n = 32)
Within W~th=n % Error of EFW _+ 10% _+ 10% P Chnmal EFW 75.7% 52.3% .O29 Song EFW 78.5% 48.4% .024 Both sonographm and chnmal EFWs underest=mated BW m women
w=th ohgohydramn~os,
Clinical vs Sonographic EFW (Independent of AFI)
%Error of EFW _+ 5% -+ 10% _+15% P ChnJca~ EFW 37.9% 70.1% 86.8% NS Song EFW 42.5% 68 4% 87.8% NS CONCLUSIONS; 1) The presence of ohgohydramnlos slgn#lcantly
influenced the accuracy of both =ntrapartum chmcal and sonographlc estimates of fetal weight. Therefore, we suggest that
mtrapartum EFWs be obtained prior to artificial rupture of
membranes whenever poss=ble. 2) In term patmnts, mtrapartum
sonographlc predlctlon of blrthwe~ght offers no advantage over an est=mated fetal weight obtained by chmcal abdominal palpal=on.
434 EVALUATION OF THE APT TEST AND WRIGHT STAIN FOR THE DE- TECTION OF FETAL BLOOD. T Harstad, D Warex, J Alman,x Dept of
Obstetncs and Gynecology, Medical College of Wlsccnsln, Milwaukee, Wl OBJECTIVE. To determine If obstetnc residents (OBR) could rehably inter-
pret the APT Test (APT) and Wnght Stain (WS) to defect fetal blood on simulated vag=nal blood specimens and what effect formal instruction has
on the accuracy of interpretation STUDY DESIGN: The APT and WS were pedormed on 4 samples of fetal/ adult blood mixtures conta=n=ng 0%, 25%, 75%, or 100% fetal blood Eight
test stations were estabhshed ENhteen OBR (1992) and 17 OBR (1993)
were allowed 30 seconds at each station to interpret the APT and WS for the
amount of fetal blood The residents’ assessment was done In 1992 without
demonstration or =nstruct~on ~n the tests’ mterpretat=on and repeated m 1993
after such demonstrat=on and =nstruct=on Each response was recorded as
none (1), small (2), moderate (3), or large (4) and assNned the number in
parentheses to perform hnear regression of the response against the actual
concentrat=on of fetal blood Seventy-two and slxty-e~ght responses from
1992 and 1993 respectively were analyzed RESULTS: O~3R response correlated poorly w~th the actual amount of fetal
blood before and after demonstrat=on and instruct=on =n interpreting the re-
sults APT TEST WRIGHT STAIN
Percent Fetal Blood Percent Fetal Blood
CONCLUSIONS: Obstetnc residents could not interpret accurately the
amount of fetal blood for either the APT test or Wnght Stare The chn~cal
usefulness and ease of interpretatton as stated ~n most texts may be over-
stated
433 THE PREDICTIVE VALUE OF INTRAPARTUM FETAL
HEART RATE (FHR) ABNORMALITIES IN THE
EXTREMELY PREMATURE INFANT David Burrus,x T.
Michael O’Shea,x Jean-Claude Vedle, Eberhard Mueller-Heubach. Departments of Ob/Gyn and Pediatrics, Bowman Gray School of
Medicine, Winston-Salem, NC. OBJECTIVE: To evaluate the vahdity of ~ntrapartum FHR
abnormaht~es for predicting short- and long-term outcomes m infants
dehvered between 24 and 26 weeks STUDY DESIGN: FHR momtor strips from fetuses dehvered at 24
to 26 weeks gestation between 1988 and 1991 at an obstetric referral center were used. Tracings of satisfactory quality during the last
hour before dehvery were reviewed by two pennatologists blinded to
outcome. Tracings were evaluated regarding the following attributes.
baseline rate and variability, presence and severity of variable and
late decelerations; and overall impressmn (reassuring, non-reassuring,
or ominous). Outcome parameters were cord blood pH, Apgar
scores, ~ntraventncular hemorrhage (IVH), bronchopulmonary
dysplasia, duration of assisted ventdat~on and hospxtalizatlon,
survival, and developmental status at one year
RESULTS: Specific abnormaht~es of the FHR tracings were not
associated with infant condition at birth (cord pH and Apgars) nor
with later outcome. However, fetuses with non-reassuring or
ormnous tracings were more hkely to have IVH, reqmred more days
on assisted ventilation, and had a lower mean Mental Developmental
Index at one year (p .~< 05).
CONCLUSIONS: Overall impression of the FHR tracing, but not
specific FHR abnormalities, was predictive of long-term outcome in
extremely premature fetuses.
Poster Session V Saturday, January 29, 1994
10:30 a.m. - 12:00 p.m.
Pavilion 9 - 11
CATEGORIES
Computers
Fetal Therapy
Doppler
Hypertensive Disease of Pregnancy
Infectious Disease
POSTER NUMBERS
435-439
440-455
456-472
473-499
500-527
Judges:
Steven L. Clark, MD
John P. Elliott, MD
Roberto Romero, MD
Volume 170, Number 1, Part 2 SPO Abstracts 397 Am J Obstet Gynecol
435 NUMERIC ANALYSIS OF FHR VARIATION IN POS3"oTERM PREGNANCY.
Z Welner*, G Farmak~des, H. Schulman, L. Kellnerx, D Mauhk Dept
Ob/Gyn, Wmthrop-Unwerslty Hosp , M~neola, N Y.
OSJECTIVE: To correlate antenatal FHR vanatlon, analyzed by a
computer, and the development of fetal acidosis at dehvery, m pest-term
pregnancy STUDY DESIGN: Three hundred and thirty seven pregnant women, who
de~wered after 41 weeks’ gestation had 610 antenatal tests Fetal tests
included a computenzed tracing of the FHR, Doppler of the umNhcal
artery, and a BPP, performed every 2-4 days Induchon of labor was
performed when FHR variation was reduced, < 30 rnsec, when FHR
deceleration appeared, and when the AFI was < 5. The results of the
fetal surveillance tests were compared to the fetal metabohc status at
dehvery
RESULTS: Ten of 12 fetuses w~th reduced FHR variation had a trial of
labor Nine of the 10 fetuses developed fetal d~stress dunng labor Seven
of the 12 fetuses w~th reduced FHR variation were acidotic at dehvery
(umNhcal artery PH < 7 2) Only 3 fetuses w~th normal FHR vanatmn
were also acidotic at delivery. Their last test, however, was performed 4
days pnor to labor Only 3 of the 10 acidotic fetuses at dehvery had AFI
_% 5, only 2 had umNhcal S/D ratio above the 95th centlle, and 5 had FHR decelerations pnor ’to
labor According to ROC curve
spemfic~ty for detecting fetal
a¢~doms at dehvery was
achieved by using a
computenzed analysis of FHR
CONCLUSIONS: A numenc
post-term pregnancy.
437 A FILEMAKER PRO DATABASE OF ABSTRACTS PRESENTED
AT THE ANNUAL MEETING OF THE SOCIETY OF PERINATAL
OBSTETRICIANS. C Stedma& D Montgomery, A. Rob~chaux III
Dept. of OB/GYN, Ochsner Chine, New Orleans, LA.
OBJECTIVE: Focusing upon the end-user perinatolog~st, we sought to
create a database of all sc~enfific abstracts presented at the annual
meeting of the Society of Pennatal Obstetnc~ans Our goals included
creabng extensive search capabfl~hes, mulhple report forms, easy
navigahon w~th buttons and menus, and cross-platform avadabflity for
both Macintosh and IBM-compatible computers.
STUDY DESIGN: We identdied the following fields as being desirable:
abstract number, htle, lead author, other authors, ~nstdution, mstituhon
c~ty, Inshtuhon state, inshtution country, objechve, study design, results,
conclusions, year of meeting, c~ty of meehng, SPO abstract category,
keywords, fellow-in-training (yes/no), community-based physician (yes/
no), and a p~cture held for grapNcal data. A personal comments held
for the user also was included for notes. We chose FfleMaker Pro 2.0
because [t is the most w~dely purchased database among Macintosh
users, and has recently offered mulhplatform capaNhty w~th a W~ndows
version, EeMaker Pro for Windows 2 0 (Clans, Santa Clara, CA) RESULTS: A database w~th a total of 34 held defimhons & 28 scnpts
was developed The template plus 500 abstracts fit on one floppy Osk.
A ma~n menu is enhrely button driven and ~s connected to submenus for
spec#~c finds Ten report formats and 17 search scnpts are available.
The program {s capable of being used w~thout reference to a manuN
Hardware requirements are a Macintosh wrth 4 megabytes of RAM or
an IBM-compahble PC w=th Windows & 4 megabytes of RAM Abstracts
from future meetings are readily Imported into the database CONCLUSIONS: A m ulhplatform database now exists for rap=d access
of SPO abstracts using multiple search cr~tena To our knowledge, the
1994 SPO Annual Meeting will be the first t~me members of a national
medical group can receive all presented abstracts on a floppy d~sk
436 A HANDHELD COMPUTER SYSTEM FOR PRENATAL RECORDS R Lowensohn, D. Zocchlx, Dept. Ob/Gyn and B~omedical
Information Commun=cations Center, Oregon Health Sciences
University, Portland OR.
OBJECTIVE: The hypothes~s was that a computer system which
approximated the ex=stmg paper system for charting obstetrical
data would be acceptable for use by busy chn=cians, whde
maintaining the advantages of a computenzed design.
STUDY DESIGN: A computerized prenatal record was designed,
built around a pen-based notebook computer system utdizing
Windows 3.1, V~sual C+ +, and a standard database engine.
The underlying forms are the Oregon Uniform Prenatal Record,
developed over five years ago by the Oregon Section of ACOG,
and currently used by over 95% of all providers of prenatal care
in Oregon. The computer form is designed to min=rnize the
amount of textual data recorded, using check boxes and drop-
down cho=ces whenever possible. The record is tied to a
centrahzed database, a~lowlng clerical input of demographic data
as well as retrieval of laboratory data from the hosp=tal
laboratory computer d[rectly into the form. This is intended to
be a part of an electronm medical record currently under
development at OHSU.
RESULTS: The current system is useable, but continues to
h=ghhght the weakness of the handwriting recogmtion algorithms
=n use at th~s t=me m pen-based computer systems. At tNs point
a keyboard is necessary on some occasions to complete the
=nput ~n a timely manner.
CONCLUSIONS: A handheld computer system functioning as a
replacement for a paper prenatal record appears to provide
s=gn=ficant advantages in informat=on management. Hardware
and software advances in the near future should make tNs an
achievable, practical system.
438 PLATYPUS: PROGRAM LISTING ABNORMALITY ON
PRENATAL ULTRASOUND A COMPUTER BASED
DIAGNOSTIC AND TEACHING TOOL FOR PRENATAL
DIAGNOSIS. D McLean, R Benz]c, F Eng Dept of Ob/Gyn U ot
Ottawa, Ottawa, Canada
OBJECTIVE:The purpose ol this project ~s to develop a computer based
application capable of assisting health care professionals in prenatal
diagnosis
METHODOLOGY:At the present time a prototype utlbzmg central
nervous system (CNS) information is currently under development The development of the CNS prototype will consist of 2 major components
The first deals with the medical mlormatlon requirements Its goals are to derive logical determination rules to be used by the PLATYPUS software
and io acqmre, edit, compile and prepare ~mages both static and real time
of the CNS abnormahtles These images will be acqmred from an
international network of individuals and ~nsmutmns The secoud
component deals with technical development The goal is to develop
PLATYPUS as a micro-computer based appficatlon only The current
platform chosen is MacintoshTM based The real time ~mages will be
digitized utlhztng QulckttmeTM technology and stored on disk. A database
will be customized to collect and store the mformatmn, and to provide a user interface so that retrieval will be Pimple and mtumve Specific
anomahes will be assigned "descriptors" and these descriptors will be
used to perform searches needed m order to derive a hst of possible
diagnoses for particular sonographlc findings The real time or static nnages can then be wewea by selecting lrom the hst As an educational
tool a list ol all the anomahes can be obtained and ~mages wowed by
selecting lrom the list This wdl provide an easily accessible example of an abnormality that may be rarely ~een rn any one center
CONCLUSIONS:PLATYPUS wall provide a new and powerful
diagnostic teaching tool for health care professionals by providing an encyclopedic database of fetal anomafies diagnosed by ultrasound it will
provide rcal time images which are more accurate and esseat~al for abnormahtles of mouon and flow eg cardiac anomahcs It also provides
a platform that allows for easdy updating the reformation

398 SPO Abstracts January 1094 Am J Obstet Gynecol
439 DECISION SUPPORT VIA CONTEXT SENSITIVE HYPERTEXT: AN
ONLINE REFERENCE TO SUPPORT LABOR MANAGEMENT. L Ch~kx, MP Dombrowsk~, RJ Sokol, Depts of Ob/Gyn, Hutzel Hosp./Wayne
State Univ., Detroit, MI 48201 OBJECTIVE: Personal computer (PC) hypertext ’help’ appears useful for chnlcal mformat~on retrmval from computerized manuscripts. We revised an extensively vahdated program for labor d~agnos~s with famlhar graphic user interface and built-in context sensitive hypertext
help windows. TNs new m-depth help reference plays the role of a ’consultant’ for clinical decision support.
STUDY DESIGN: A chapter on abnormal labor management by 2 of
the authors (Danforth, m press) was converted into hypertext using
a PC Windows help compder. Program generated index hsts expedited the process.
RESULTS: The labor analys~s program based on a complex algorithm for labor diagnosis is enriched by onhne, hterature consultations oi3 abnormal labor management from ’experts’ via the manuscript.
GrapNcs and ~mages, as well as sample labor graphs appear helpful
in decision support. CONCLUSIONS: Hypertext can be used by chn=c~ans to broaden thmr
multl-d~sclphnary knowledge through literature search of electronic
designs, both in per~natal
medicine and other fields.
441 DOES AMNIOINFUSION AFFECT FETAL ACIO-BASE STATUS? J Blackstone, B K. Young, J Baut=sta, S Ordonca, I A Hosklns. Oept
OB/GYN, NYU Medical Center. NY, NY OBJECTIVE To evaluate the effects of amnlomfuslon on fetal scalp pH and
umbdical blood gas and pH values with vanable decelerahons m labor.
STUDY DESIGN Labodng pahents with vadable decelerahons, or mixed
patterns consmhng of vanable deceleratmns with fetal tachycardm or bradycardm were evaluated Excluding patmnts w~th chonoamnmnihs,
mulhple gestatmn, vaginal bleeding, meconmm, fetal anomalies, & breeches, 71 cases were stud~ed 26 were treated with amnmmfusion uhl~zmg normal
sahne A scalp pH was performed before ammoinfusmn. A repeat scalp pH measurement was obtained after amnlolllfuslon was begun, and additional
measurements were performed as climcally indicated Fetal heart rate (FHR)
tracings were evaluated by a blinded observer for ~mprovement or
deterioration of deceleretmn patterns Scalp pH & umbilical cord blood pH & gases, mode of delivery, and Apgar scores were compared to those of a
control group of 45 patients wRh similar FHR patterns who had standard
treatmentw=th oxygen, IV fluid, and change of poslhon, but no ammomfusion
RESULTS Amelmrat~on of abnormal FHR patterns was seen in 12/26 in the
ammo~nfumon group, and 8/45 in tne controls This change was not
accompanied by a concomRant rise 113 fetal scalp pH values or improvement
in umbilical cord blood values Apgar scores were comparable ~n both groups
a,s were rates of maternal complications and operahve dehvenes. No
differences between ammo~nfusmn & control groups were found in pH or
blood gases, mlhally and at delivery At dehvery the values were
Amnlomfuslon Control P Value
Umbdlcal Artery pH 7 22 + .08 7 23 ~: .074 NS
Umbdlcal Artery C0~ 51.75 4. 9.05 51 17:1:10 81 NS
Umbilical Artery 0~ 20 10 + 6.94 19 43 + 7 9 NS
Umbilical Artery BE -5.56 + 3.76 4.28 4- 6A NS
Weight 3365 464.637 62 3570.094.663 65 NS
CONCLUSION Ammomfusion may ~mpreve the FHR pattern, but no
significant effect on the fetal metabolic state was obsented
440 FETAL STEMCELL TRANSPLANTATION IN FETAL ~t AND
~ THALAS SAEMIA.
Westgren M, Brubakk AM, Bm TH, Eik-Nes S, Ek S,
Markling L, Orlandi F, Maggio A, Pchera H, Seiger /~.,
Sundstr6m E, & Ringden O.
Huddinge University Hospital, Karolinska lnsututet,
Stockholm, Sweden, National Center for Fetal Diagnosis
and Therapy and Pedtatrics, Trondheim, Norway. Servizio Autonomo Di Diagnosi Prenatale, Palermo. Italy.
The use of fetal haematopoietic stem ceils
transplantation with the purpose to achieve a permanent
haematochimeria has brought new hope in the field of
fetal medicine. Recently, Touraine et al published five
cases of fetal stem cells transplantation performed in-
utero in humans, and were able to demonstrate
engraftment in three surviving infants.
Results: At the Karolinska Institut we have during the
last year performed two fetal to fetal transplantations.
In one case of homozygous c~ thalassaemia and in on case
of [~ thalassaemia. The child with ct thalassaemia was
born in January 1993. At one week of age donor HLA
type (B35) could be isolated from leucocytes but
karyotype and blood group antigen failed to prove
chimensm. The child is anaemic and transfusion
dependent and has a normal growth and neuro-
development. The other mother is expected to deliver in
October 93. These two cases will be presented in detail.
442 FETAL ERYTHROPOIETIN IN TWIN PREGNANCIES WITH + , A Serr~, B DISCORDANT GROWTH. D. Lemery, J Santolava
.+ Jacquet~n. Dept OB/GYN, Clermont-Ferrand, France and Umv 11,
Chicago, IL*.
OBJECTIVE: To compare fetal serum Erythropolenn (Epo)
concentration ~n discordant twxns due to AGA & SGA and twin-
twin transfusion syndrome (TTTS). STUDY DESIGN: 7 sets of
well dated twins w~th d~scordant growth (EFW d~fference >25%)
were assessed for Epo concentratmn. All 14 fetuses had a
PUBS performed between 23 and 33 weeks CA. Two sets were of &fferent sex and 1 had a b~chonomc placenta confirmed
postpartum. In 4 sets w~th ~denl~cal sex, TTTS was
demonstrated by repeating the PUBS ~n the large co-twin
and detecUng adult erythrocytes prewously transfused to the
small fetus. No cytogenetic
abnormahty or xnfect~on was
found ~n rather group.
RESULTS: F~gure shows Epo
at the ~nltial PUBS plotted
against mstutlonally de-
rived nomogram.
CONCLUSION: The small
fetus will always have Ingh
Epo. Determmatmn of fetal
Epo m the large twin can
make the dffferentml be-
tween d~scordant twins due
to AGA & SGA or TTTS.
twin to lwm Transfuston AGA & SGA co-twins
(Closed="~ma£" fctm open="blg" fetus)
Volume 170, Number 1, Part 2 SPO Abstracts 399 Am J Obstet Gynecol
443 FETAL LUNG LESIONS: MANAGEMENT AND OUTCOME. Scott Adz~ckx, Michael Hamsonx, A~an F~akex, Roy F~lyx, James Gotdberg, Lori Howellx. UCSF Fetal Treatment Center, San Francisco CA. OBJECTIVE: To review our experience with fetal congenital cystic adenomato~d malformet~on (CCAM) and pulmonary sequestration emphasizing natural history, management, and outcome. STUDY DESIGN: Retrospective review of 55 fetal lung lesions diagnosed by antenatal ultrasound (US). RESULTS: There were 41 CCAM cases. Fifteen CCAM cases without hydrops were successfully resected after birth, and 3 of these les~ons had decreased in size on serial prenatal US. Of 26 large CCAMs that were assocmtsd with non-immune hydrops, 5 underwent TAB, 10 died perinatally, and 11 underwent fetal therapy since hydrops is a predictor of fetal or neonatal demise. Fetal surgical resecbon of the tumor (fetal Iobectomy) was performed at 21-27 weeks gestation in 8 cases w=th 5 fetuses showing hydrops resolution, impresswe in utero lung growth, and neonatal survival. In 3 other fetuses with a large sohtary lung cyst, a thoraco-amniot~c shunt was placed and 2 survived. Pulmonary sequestrations are echodense lesions that have a systemic arterial blood supply arming from the aorta that is detectable by color flow doppler. Of 14 sequestrabons, 9 "disappeared" on serial prenatal US and were only detectable by CT scan or MRI postnatally (no resection required), 1 underwent TAB, 2 were successfully resected after Nrth, and 2 lesions had an associated tension hydrothorax with secondary hydrops that was successfully treated w~th fetal thoracenteses or thoraco-amniotic shunting. CONCLUSIONS: The natural history of prenatally d~agnosed lung masses is vanable. Fetal therapy is now an option for lung lesions associated w~th non-immune hydrops.
445 MISLEADING TESTS IN THE DIAGNOSIS OF TWIN-TWIN
TRANSFUSION SYNDROME (TTTS). G Ryan, JFR Barrett", _E
MantayI, B Mullen, D Fanne, RJ Morrow Pennatal Unit, Mt S~nax
Hospital, University of Toronto
Objective: To report that the suggested dxagnoshc tests~’2 for the
demonstration of vascular communications in a twin pregnancy may be
misleading.
Case Illslory: A 28 year old Gt P0 presented at 22 weeks gestation with a
spontaneous twin pregnancy, of whom one was noted to have non-immune
hydrops The twins (both male) were &ammoUc and the placentae appeared
separate FOal anatomy, including echoeardiography, was otherwise normal
and both weights were on the 40~%11e A fetal blood sample (FBS) for the
hydroplc twin A revealed a Hb of 70 g/l and i v vecuromum (0 2mg)
promptly paralysed the hydroplc twin whereas the non-hydroplc twin B
remained active throughout Twin A was transfused with 20 ml of adult
blood to give a Hb of 119 g/l 30 manutes later, an FBS from twin B
revealed a HB of 186 g/l and a Betke-Klu~hauer test for adult cells was
negatwe Viral and karyotype studies on both twins were normal Follow
up ultrasound revealed persistent hydrops and 6 weeks after the transfusion
pre-tenn labour resulted in the dehvery of an hydroplc twin A (BW 750g)
with a cord Hb of 90g/l who d~ed at 3 hours of age Twin B (BW 1100g)
was born with a cord Hb of 224 g/l and survived intact The cord blood
Klelhauer tests showed 7% adult ceils m twin A and 8% In twin B
Pathology revealed a dlammohc monocbonomc placenta and rejection studies
demollstrated a patent vascular anastamosls
Conclusion; Th~s case suggests that the use of neuromuscular blockade and
the detecUon ol transfused adult cells in the fetal circulation cannot be rched
upon for the diagnosis of qTITS~’~ Blood flow through vascular anastamoses
may be intermittent (especially ~f these are arterial) and w~dely disparate
levels of Hb in twins should remain suggestive of a shared circulation
Refs ] Fisk NM Arch Dts Chdd. 1990 65(7), 657 2 Tananal~ M Fetal Dtag & Ther 1992 7(1)36
444 FETAL MEAN CORPUSCULAR VOLUMES AND RETICULOCYTE
COUNTS PREDICT NEED FOR INTRAUTERINE TRANSFUSION IN
Rh ISOIMMUNIZED PREGNANCIES. JE Uckelex, SM Berry, SF
Bottoms, KS Puderx, MP Dombrowsk=, and DB Cotton. Dept.
OB/GYN, Hutzel Hospital/Wayne State University, Detroit, MI.
OBJECTIVE: Fetal intrauterine transfusions (IUT) ~n Rh iso-
immunized pregnanmes are performed based upon hemoglobin
/hematocnt levels and a positive fetal direct Coombs (Coombs).
Fetuses with mild anemia may requ=re multiple diagnostic
cordocenteses to detect subsequent severe anemia. Our
objective was to compare initial fetal and maternal hematologic
values from two groups of Rh =soimmumzed pregnancies to
pred=ct seventy of d=sease and subsequent need for IUT.
STUDY DESIGN: We compared fetal mean corpuscular volume
(MCV), Coombs, reticulocyte count (RC), and maternal Rh
antibody tiler (Rhabl in 12 fetuses with mild and 13 fetuses
with severe anemia (adjusted for gestatmnal age). Statistical
analys~s was performed using logistic regression.
RESULTS: Fetal MCV Ip <0.021, maternal Rhab |p <0.03), and
fetal RC (p<O.05) were strongly correlated to severity of
d=sease, but strength of Coombs was not (p=0.2). Logistic
regression of data without Coombs results showed MCV (F =
7.6) to be most pred=ct=ve of the future need for IUT, followed
by maternal Rhab (F = 6.2) and RC (F = 4.8).
CONCLUSION: On initial cordocentes=s, fetal MCV, maternal
Rhab, and fetal RC were most predmtive of subsequent severe
anem=a. These parameters may be helpful in avoiding IUT in
those fetuses who have a strongly positive Coombs, but are
only mildly anem=c. We hypothes=ze that the presence of a low
affinity (luGs) Rh antibody =s respons=ble for many of these
cases of mild anemia.
446 FETO-PLACI~TAL BLOOD VOLUME - HAVE WE CKIT IT RIGHT yL:r£7. S. MacphmP, P Stone, G. Ryan, R. Morrow Pennatal Unit; Mount Sinai Hospital, University of Toronto, ONT. CANADA. O ,II/ECII%’~ The correct pre-transfuslon feto-placental volume (V~) m ~so- lmmunlsed fetuses remains uncertain. Current estimates have been obtained indirectly from the dilution of packed red cells after transfusion but this assumes no fluid loss dunng the transfusion. However data from an ovme model suggest that only 63% of the volume remains in the Clrculatton by the end of the transfusion~. A s~mdar s~tuatlon m the human fetus would reslult m underestimating the V~ which would influence the determination of volume to be transfused. Comparison of the final calculated and measured haematocrlts from each method w~th and wtthout the ovme correction factor apphed may suggest which estimate of V~ ~s most appropriate in the human fetus DESIGN. V~ was esttmated by five pubhshed methods ~,~,~,,,AI in 61 m- utero transfusions for red cell iso-lmmunlsatlon. The expected final Hct~ was then calculated for each fetus (Hct~ = (HcqV~ + Hct~V~)/(V~ + Vt)) ~nth and v~thout the correction factor (0.632) apphed to the volume transfused (Vt) Results expressed as mean (SEM). RESULTS. The mean measured post-transfusion Hcto was 0.482 (0 008) and
the estimated values were all s~gmfleantly lower (p<001)
Author (1) !(2) ~3) (4) (5)
1 lct~ D 452 0.453 ).416 0.443 D.464
Hcb (Vtx0.632) 0.519 1.520 3.463 0.504 0.538"=
Hct~ (Vtx0.8) 0.486" ) 488" 3.440 0.474" 0.501
Appl3nng the ovine correction factor resulted m a stgnifieant (p< 5) overestimate Using an lntermedmte correction (0.8) there was no difference between the measured and esumated haematocnts m three of the formulae
(*) CONCLUSION. Current cllmcally used methods for determmatton of V~ all result in an underestimate of final Hct. The estimation of Hct~ agrees more closely with Hct, ff ~t is assumed that only 80°/o of the transfused volume remains in the c~rculatlon at the end of the transfusion. Consideration of the fluid lost during transfusion should be incorporated into the calculation of pre-transfuslon feto-placental volume, i)McGregor et al 1988 2)Leduc et al I990 3)Mandelbrot et al 1988 4)Brace 1989 5)Nlcolmdes et al 1987

400 SPO Abstracts January 1994
Am J Obstet Gynecol
447 DIGOXIN AND THERAPEUTIC AMNIOCENTESIS IN THE
TREATMENT OF IDIOPATHIC NON-IMMUNE HYDROPS
FETALIS. M.G. pipette. Y. Pan, S.C. Pmette, J. Blackstone Dept. OB/GYN, Maine Medica~ Center, Portland, ME. OBJECTIVE: To attempt to improve neonatal outcome ~n
cases of idiopathic non-immune hydrops using early aggressive therapeutic amniecentesis and d~goxm.
STUDY DESIGN: Three patmnts diagnosed w~th idiopathic
non-immune hydrops ~n their second and third tnmesters were treated usm9 the same regimen. Hydrops was defined as polyhydrammos and subcutaneous edema with pleural and/or perlcardial effusions or abdominal asc~tes. Pahent evaluation consisted of a fetal echocard~ogram, maternal CBC, Kle~hauer -Betke stare, ABe and Rh typing, indirect Coombs test, VDRL,
acute t~ters for cytomegalowrus, toxoplasmos=s, parvowrus
and herpes, and G6PD dehclency screen. Amniotlc fluid (AF)
tests included karyotype and viral cultures. Each patient underwent 1-3 therapeuhc amniocentesies. Up to 2 liters of AF was drained on each occasion. Mothers were placed on
d=goxin, dosages htrated to therapeutic maternal levels. RESULTS: In all cases serial sonograms revealed a gradual
dechne in the AF index. Fetal ascites and effusions were seen
to resolve. Two fetuses delivered at term w~th no ewdence of hydrops or cardiac anomalies. All neonates have done well with no complications.
CONCLUSIONS: Treatment regimens for non-immune
hydrops vary depending on the underlying etiology of the con- d~hon. In cases where no cause can be identified digox~n and
therapeutic ammocentesm may reduce perinata~ mortality
449 INTRAUTERINE HEMATOLOGIC FINDINGS IN TWINS WITit
NORMAL AND ABNORMAL GROWTII. KS Puderx, SM Berry, SF
Bottoms, JE Uckelex, DB Cotton. Dept. of OB/GYN, Hutzel Hosp ,
Wayne State Univ., Detroit, MI.
OBJECTIVE: The difference in hemoglobin in twin pairs is used as
one of the diagnostic criteria for twin-twin transfusion syndrome (TIT).
The objectwe of this study was to evaluate differences in hematologic
values obtained by cordocentesis in twin pairs with and without TIT.
STUDY DESIGN: Cordocentesis was performed on 27 twin pairs for
rapid karyotype, evaluation of infection or assessment of fetal well-
being. The assignment to the T/T group was based on ultrasound
findings of twins with discordant size, concordant gender, single
placenta and polyhydrammos in one sac with oligo-/anhydramnios in the
other Differences in hematologic values were analyzed by differences in
eshmated fetal weight (EFW) and by twin group (’I’Fr, other). A
receiver-operator characteristic (ROC) curve was used to determine the
hemoglobin difference which would identify those gestations with TIT
RESULTS: Gestational age at evaluation differed between the groups,
with a mean of 22.3 weeks (range 19.0 - 26.1) in the TT’I" group and
28 9 weeks (range 20 4 - 35.3) in the group of other twins. We found
significant (p <0 05) rater-twin differences in hemoglobin (AHgb) in the
TIT group (mean 5.2 mg/dL; range 0.5 - 14.2 mg/dL) as compared to
the other twin group (mean 0.77mg/dL; range 0.0 - 2 4mg/dL) In all
~ cases the larger twin had the higher hemoglobin. With a
AHgb>2.4 mg/dL all cases had clinical ~ (sees.=50%,
spec.=100%, PPV=100%, NPV=83%) We found no significant
correlation between AHgb and percent difference in EFW.
CONCLUSION: At cordoeentesis, an inter-twin difference in
hemoglobin greater than 2 4 mg;dL is ¢~nsistent with a d~agnosis of
TIW, though smaller differences do not exclude this syndrome. A very
large AHgb may be seen in TFT, even in the second trimester.
448 THE EFFECT OF INTRAUTERINE TRANSFUSIONS ON FETAL SERUM BILIRUBIN IN
RED CELL ALLOIMMUNIZATION. L. Goodrumx, G. Saadex, M Belfortx, L. Knudsen×, R.
Carpenter, K Molse. Dept. 0blGyn, Baylor College ef Medicine, Houston, TX.
OBJECTIVE’ To evaluate t~ chaege ~e fetal serum h~l~ruhin levels in respuese to
letrautenee transfusion (IUT) for red cell allmmmunizatmn.
STUDY DESIGN: The records of 38 patients who underwent ~> 2 IUT’s for red cell
allolmmumzahon were rewewed. The following parameters were extracted, pro- and
post transfusion fetal hematocnt (Hct), total serum bdlrubln (Bil), retlculocyte count (Rte),
Klezhauer-Betke test IKD), volumes of intravascutar and intraperltoneat blood transfused
(IVTV and IPTV) The data were compared for interva].l (transfusion 1 to 2) and interval-2
(transfusion 2 to 3) where applicable. Sign-rank test and multiple regression analyus
were used wherever aRorepnate {s~gniflcance P < 0 05) Data ~s g~ven as the median.
RESULTS: The median number of IUT’s per patient was 3 with a range of 2- 8, between
22 - 37 weeks. Rd remained above normal tn 34 patients. There was a slgmhcant
decrease in Rtc (26 1 vs 8.2 vs 0.9 %) and fetal cells on KB (100 vs 30 vs 3.7 %) and an
increase ~n Hct (18 1 vs 30.2 vs 30.2 %) at the time of the hrst through the third IUT
~ncreased significantly after the first IUT (3,9 vs 5.4 rag/all) and remained elevated The
rate of change in Bd during interval-1 correlated with the rate of change in the Hct post-lUT but with nene ef the ether paramete;s stud~ed,
CONCLUSION: Fetal total serum bd~rub~n ~n erythroblastosis fetahs remains elevated despite intrauterine transfusion and suppression of feta] erythropoelsls.
450 FETAL URINARY ALPHA-1 MICROGLOBULIN (~t-lM): A NEW PREDICTOR FOR RENAL DYSPLASIA IN FETAL
OBSTRUCTIVE UROPATHIES (FOU). M.P. Johnson123, B.D.
SeifmanIx, J. Cejka3x, S.M. Berry1, M.I. Evans123, N.B. Isada1,
A. ReichlerIx, R.F. Humelx, K. Kithier3x. Depts. 1OB/GYN,
2MBG, 3pathology, Wayne State University, Detroit, MI.
Objective: To evaluate ~e levels of ~t-lM in fetal urine as an indicator of underlying renal dysplasia in FOU. Study Design: Serial urine specimens were obtained by vesicocenteses from 7 consecutive fetuses with FOU and analyzed for Na, Osm, C1, Ca, I]l-microglobulin, total protein, and o~-lM. Based on biochemical parameters, 3 were terminated for poor prognosis and confhTned to have dysplasia. 3 had good prognostic values, and are >2 yrs old with Cr_<0.7. One fetus had intermediate
values, and is 2.5 yrs old with Cr = 1.0-1.2. Results: All fetuses with confirmed dysplasia had final ct-lM values >80 mg/L and values that increased with sequential sampling. All fetuses with good prognosis had final ct-lM values <60 mg/L which decreased with sequential sampling. The intermediate prognosis fetus who has posmatal evidence of
moderate renal impairment had o~-IM values between 60-80 mg/L which minimally decreased between samplings. Conclusions: 1) Advanced renal dysplasia is reflected in fetal urine by a-lM values >80 mg/L and a pattern of progressive increase, 2) absence of significant underlying dysplasia is reflected
by ct-lM levels <60 mg/L with a pattern of progressive decrease, and 3) this prehminary study shows ~t-lM to be a reliable predictor of underlying renal dysplasia which wi/l facilitate patient selection for invasive fetal therapy via in utero vesicoamniotic shunt placement.

Volume 170, Number 1, Part 2 SPO Abstracts 401 Am J Obstet Gynecol
451 PRENATAL DIAGNOSTIC AMNIOINFUSION: DOES OLIGOHYDRAMNIOS PREDISPOSE TO INFECTION?
p,Q, Prvdex, N.B. Isada, M P. Johnson, R. Romero, A. Reichlerx,
M.I. Evans. Depts of Ob/Gyn, M.B.G., and Pathology, Hutzel Hospital/Wayne State University, Detroit, MI. OBJECTIVE: Diagnostic amnioinfusion, by improving the ultrasound acoustic window, facilitates prenatal diagnosis when
imaging ~s obscured by oligohydramnios. Despite recent enthusiasm for this procedure, there are scant data on related complications The purpose of this study was to evaluate perinatal morbidity associated w~th d~agnostio amnioinfusion. STODY DESIGN: We reviewed 22 consecutive pregnancies
(w~th intact membranes) managed on our service between 4/90 and
6/93 in wNch d~agnostic ammo~nfusion was performed. Using a closed dehvery system volumes of 200 to 500 cc’s of balanced salt solution were infused mtra-amniotioally. Data were obtained on
procedure indicahons, the number and types of other invasive pregnancy related procedures, as well as on outcomes and complications which were temporally related to the procedures. RESULTS: Twenty-two women underwent 35 amnioinfusions between 16 and 32 weeks of gestation. Adding other invasive
procedures including transabdominal CVS, genetic amniocentesis, vesicocentesis, and bladder shunt placement; these patients experienced a total of 105 procedures. Four patients developed
severe chnical chor~oammonitis within 48 hours of an amnioinfusion procedure (4/22 patients or 18 2% of patients, 4t’35 amnioinfusions
or ~ 1.4% of ammomfusion procedures). No other clinical infections occurred in procedures other than amnioinfusion.
CONCLUSIONS: Although the benefits of diagnostic amnio- infusion m cases complicated by severe oligohydramnios have been well documented, associated maternal morbidity must be considered in a decision for infusion. We speculate that the
absence of amniohc fluid (with its known bacteriostati¢ character)
may ~n part predispose to infection following diagnostic invasion of the uterine cavity.
453 HYDROLAPAROSCOPY IN THE RABBIT: AN ANIMAL
MODEL FOR THE DEVELOPMENT OF OPERATIVE
FETOSCOPY. Ruben A. Qumtero, Karohne S Puder,X
Mordechat Bardtcef,x Leonardo Acosta~, Karen Rossma~rX,, Davtd B Cotton Depts of Ob/Gyn and Div. of Laboratory Ammal
Resources, Wayne State Umv, Hutzel Hospxtal, Detrmt, MI. OBJECTIVE: To evaluate miniature surgical endoscopm
instruments and techmques ~n a small animal model s~mulatlng
mtraamnionc human condltions.
MATERIALS AND METHODS: F~ve white New Zealand rabbits underwent non-survxval CO2 laparoscopy under general
anesthesia using custom-designed mimature (2rim0 trocars and operanng instruments. The abdominal cawty was filled w~th
lactated Ringer’s solution (LR) through a second port. A thvd
accessory port was used for manipulation. A defect in the meso
of one of the uterine horns was performed wxth monopolar electrocautery. An extracorporeal knot was Ued around the uterine horn through the defect of the meso, and the suture was
cut lntraabdom~nally.
RESULTS Excellent visualization was obtained w~th~n the
mtraabdomlnal LR medium. Various surgical skills, including
grasping, cutting, electrocoagulafion and extracorporeal knot
tying were accompbshed and mastered Occasional leakage of
fired through the skin punctures was prevented with accessory clamps as needed.
CONCLUSION: Hydrolaparoscopy in the rabbit is a useful
model for operaUve fetoscopy. It ts inexpensive, s~mulates closely the condmons encountered dunng human observations,
and allows the evaluaUon of new m~mmally-invasive instrumentation and techmques necessary for the development of
operaUve fetoscopy.
452 DOPPLER ULTRASOUND IN THE ~fINAGEP,’ENT OF THE PREGNANCY COI~PLI CAT~] BY FETAL ANE}~ A. I I
.C,~{~d,x FL Ludemit~<y, A. Abuhamad,x A. Rd~g~olo,x D. Jones, JA£ooeL
Sble Uniuersity, New Havefl, Pennsylvania Hospital, Philadelphia, Eastem Vi~jinia M~dical S~ool, Norfolk. 0BJ[CIIVP [nvasp~ techmques c~nunue to be used for the diagnosis and
management of the anermc fetus. A mathematlca/ medel to recogmze the
anermc fetus with Doppler ultrasound and to reduce the number of
cordecenteses in the management ~f fetal anerma has been prevaously
described. 7he study assessed the maddle cerebral artery peak velocity (!vg2A-PV) and 3 risk of anemaa zcnes were ~denufied: no risk zane, low
risk zene, high risk zme. qhe a~m of th~s study was to test this
mathematical model in a muhicenter prospective fashien. gll.~Y I]E~II~t: ~IheIVIEA-PV was studied m 9 fetuses at risk for anemia
v¢no underv, ent 24 cordocentesls for Rh allo~mmunizatien. All Doppler
stu&es were performed prior to cordocentesis by 6 sinologists who were
not aware ct’the fetal he matocnts. Gestanmal age (C~) ranged from 18 to
35 v~eks. Anemaa was defined as 25~3 below the mean for the normal populat~an corrected f~r G,~. If the !vl2A-PV was abo’~e the no-risk zone,
the fetuses were caasldered to be at risk for anerma. RF_S~TS: "lhe fetuses were aneauc on 16 occasions and nrn-anen’uc aa 8
occas~ens. Oar test for anerma ha~ a sensitv,aty ~" 100%, a specificity of
50%, a pcelUve predicuve value of 84%, and a negau ve predictive ~alue of
100%.
CONEUJSIONS: Doppler ultrasound may be a useful tool in the dlagms~s
and management of the anemic fetus. If the IvlZ~-PV ~s in the no-risk
zcne, the fetus ~s hen-anemic and a cordocentesis cr amnlecentesis may
be safely delayed.
454 EFFECT OF ENDOSCOPIC WtlITE LIGHT ON THE
DEVELOPING VISUAL PATHWAYS. Rub6n A. Qumtero, Wllham
R Crossland, Dawd B Cotton Depts. of Ob/Gyn and Anatomy,
Wayne State Umv, Detroit, MI
OBJECTIVE To evaluate the potential teratogemc effect of endoscopic
whne hght on the visual pathway of the chicken embryo
MATERIALS AND METHODS: a) The right eye ot El0 chicken
embryos (day lO ot incuhanon) was exposed to white light fl’om a 300
W Xenon hght source for 10 minutes On El7, the rennas were tixed in
2 5 % glutaraldehyde (GA) and were stained with thmnln b) L~ght-
exposed embryos were rejected intravltreally with 5% wheatgerm
agglutmin horseradish peroxldase solution (WGA-HRP) on El6. On
El7, visual centers were fixed by transcardlac perfuslon with 2.5% GA
Shdes were reacted with tetramethylbenzldlne, c) Newly-hatched chxcks
were exposed to endoscopic light as above The chicken were allowed
to teed with both eyes open for 7 days (training phase) The unexposed
eye was then closed The time required for the chick to peck at the first
seed (latency) and the time to accurately peck 5 seeds (feeding tnne)
were compared between exposed and control animals
RESULTS Light-exposed retinas were hlstologlcally lndlstlngmshable
fiom controls, w~th no signs of gangbon cell damage or cell loss m any
pm tlon of the retina. Axonal transport of WGA-HRP to dlencephahc
and mesencephahc wsual centers was also normal Latency (mean
dlft~rence 0 1 sec, p>.05) and feeding time (mean difference 0 7 sec,
p> 05) were not thfferent between the two groups.
CONCLUSION Whae endoscopic light did not result lU anatomical or
functional changes in experimental ammals. Extrapolation of these
findings prowdes evidence for the safety of the use of endoscopic white
hght in human fetoscopy.

402 SPO Abstracts January 1994 Am J Obstet Gynecol
455 ZINC PROTOPORPHYRIN IN FETAL AND MATERNAL
ERYTHROCYTES AS INDICATOR OF NON-FUNCTIONAL HEMOGLOBIN. M.C.H. Haeusler. D. Paetzoid*, F. Kamer*, R. Winter*. Dept. Ob/Gyn
and 2nd Med. Dept., Umv. of Graz, Austria. OBJECTIVE: Z~nc protoporphyrin (ZPP) is normally bound to a small
fraction of hemoglobin in fetal and maternal erythrocytes. This hemoglobin fraction cannot brad oxygen and Js increased in the presence of iron deficiency. The purpose of this study was to determine the amount of ZPP-bound hemoglobin in fetuses undergoing
cordocentes~s and their mothers. STUDY DESIGN: A total of 21 fetal blood samples, 17 maternal blood samples and 4 samples of donor blood were obtained from 5
pregnancies w~th Rh allo~mmumzation and from 4 pregnancies with
congemtal anomalies or early growth retardation at 21 to 36 weeks’ gestation. ZPP was measured w~th a hematofluorometer. Hematocrit
and bd~rubm levels were measured ~n most cases.
RESULTS: 5 fetuses were non-anemic (hematocrit >30%) and 4 fetuses were anemic. In the non-anem~c fetuses ZPP levels were consistently than maternal levels (45-240 I~mol/mol heine vs. 13-59 i~mol). Of the 4 anemic fetuses, 2 had normal and 2 had extremely h~gh
ZPP levels (maximum 501 ~mo[). The ZPP levels were not hnked to the hematocr~t. In the course of 2 serial intrautenne transfusions (2 and 5 transfusions respectively), ZPP decreased continuously. ZPP in donor blood ranged from 19-28 p.mol (normal values m adults <_ 30 p, mol).
CONCLUSIONS: 1) As early as 21 weeks’ gestabon, fetal ZPP is
markedly h~gher than Jn adults. Thin suggests that fetal iron ~evels are normally lower than those ~n adults. 2) In anemic fetuses, ZPP levels
reflect the functional capacity of the residual hemoglobin. 3) The continuous decrease ot tetal ZPP during intrauterine transfusions
seems to result from depressed fetal erythropo~es~s and an increasing amount o4 c~rcutatmg donor blood. 4) Donor blood should contain low
levels o! ZPP to prowde hemoglobin of high oxygen transpoding ,capacity to the anemic fetus.
457 CONCORDANCE IN UMBILICAL ARTERY DOPPLER VELOCIMETRY IS AN INDICATOR OF SUCCESSFUL THERAPY IN TWIN-TWIN TRANSFUSION SYNDROME. J.E. Dickinson*, J.P. Newnham*, J.M. Philllps*, King Edward Memorial Hospital for Women, Perth~ Western Australia. OBJECTIVE: To determine if therapeutlc amniocentesis ~n twln-twin transfusion syndrome alters Doppler velocimetry and, if so, whether t~e alteration may be a marker of treatment success. STUDY DESIGN: Six consecutive cases of twln-twin transfusion syndrome, diagnosed at 20-23 weeks gestation, were examined prospectively. Umbilical artery Doppler velocimetry for each twin was performed at diagnosis and then weekly until delivery. Repeated therapeutic amniocenteses were performed as indicated to achieve normalizatlon of amniotlc fluid vol1~e in each sac. RESULTS: Fetal survival rate was 83% (i0 of 12 infants). In 4 of the 6 twln pairs, diastolic flow was absent (ADF) on initial flow velocity waveforms (FVW) in one fetus. These inlt~al FVW studies showed discordance between 5 twin pairs, wlth a difference in the S/D ratio greater than 1.0. In the sixth case~ both fetuses displayed ADF and died ~n utero without ~mprovement in amniotic fluid disparity despite amniocentesis. In 4 cases, diastolic flow returned and the S/D ratio progressively decreased to w~th~n the normal range in the twln with increased vascular resistance as normalization of amniotic fluid occurred. Prior to delivery the S/D ratio difference was less than 0.4 in this group. Doppler veloc~metry was not predictive of donor or recipient status. Augmented fetal growth occurred in the smaller "stuck twin" as amniotic fluid appeared antl Doppler velocimetry normalized. CONCLUSIONS: Successful therapy in twln-twln transfusion syndrome with normalization of amnlotic fluid volumes is associated with the development of concordance in Doppler velocimetry, lhls effect may be used as a marker to predlct outcome success in therapeutic interventions ~n twin-twin transfusion syndrome.
456 SPLENIC ARTERY VELOCITY WAVEFORMS IN THE APPROPRIATE AND SMALL FOR GESTATIONAL AGE
FETUS. A Abuhamad, G Manx, D Bogdanx, and A Evans
Departments of OB/GYN, Eastern Virgima Mechcal School, and
Yale School of Medicine, Norfolk and New Haven.
Objective: The spleen is an important organ in ~e human fetus.
It plays a central role in early fetal erythropoemls and fetal
immunoregulation. The aim of this study was to describe splenic
artery flow velocity waveforms in the appropriate (AGA) and the
small for gestatlonal age fetus (SGA).
Study design: Splemc artery flow velocity waveforms were
obtained in 95 AGA and 17 SGA fetuses with Doppler
ultrasound. The Resistance Index (RI) was used to quantify the
Doppler waveform. Gestataonal age was confirmed by a second
trimester ultrasound in all pregnancies. SGA was defined as an
estimated fetal weight below the 10th percentile for age.
Results: Gestational age ranged from 15-40 weeks (mean = 27 6
+/- 7.1 weeks). A second degree polynomial model expressed the
changes of the R! in AGA fetuses with advancing gestataon (y =
0 057 X - 0.001X2, R= 0.53, P < 0.001). In 15/17 (88 %) SGA
fetuses, the splemc artery RI was below the mean for gestational
age. In 5/17 (29%) SGA fetuses, the RI of the splexxic artery was
below 2 standards of error from the mean
Conclusions: The splenic artery RI has a parabolic pattern
during pregnancy, with peak resistance around 28-30 weeks of
gestation. The splenic artery vascular resistance is decreased in
some SGA fetuses suggesting an increase in blood flow to the
spleen. Our fin&ngs suggest that the spleen may be involved in
fetal autoregulation in a sparing effect similar to the fetal brain.
458 UMBIUCAL FLOW VELOCITY WAVEFORMS IN ANEUPLOID
FETUSES UNDERGOING PRENATAL DIAGNOSIS. S.Sen,qupta,
R A.Knuppel, M.Lake’, N Patel’. Dept Ob/Gyn, D~v Maternal-Fetal
Medicine, Umvers=ty of Medmme and Dentistry of New Jersey, Robed
Wood Johnson Medical School, New Brunswtck,NJ. OBJECTIVE: Abnormal umbilical veloc~metry assocmted with fetal
congenital anomahes has been reported by several ~nvest~gators.
Most of these studies were done m third trimester of pregnancy. It has
been ~mpl~cated that an anomalous fetus may be responsible for the
obhteratlon of the terfmry stem v~lh, resulting ~n increased placental
resmtance and decreased end-d=astohc flow Thcs Is the first large
prospective study of umb dleal flow waveforms in the second trimester
of pregnancy undergoing prenatal diagnosis for the identification of aneuploidy.
STUDYDESIGN: Between March 1992 and July 1993, all pregnancies
between 15 and 22 weeks of gestation undergoing p~enata~ d~agnos~s
by ammocentesls or cordocentesm were included in the study
Doppler flow evaluation of umblhcal artery was done at the bme of fetal
anatomical survey before performing the genetic procedure
RESU LTS: The umb~hcal flow waveforms were assessed in 598 fetuses undergoing genetic procedures. The indications for amnlocenteslsor
cordocentesls were advanced maternal age, abnormal ultrasound
findings, abnormal alpha-fetoprote~n or tnple screening values, and family or obstetne hmtory of fetal anomaly. There were 2 of 520 (0.4%) fetuses w~th normal karyotypes, none of 51 fetuses with structural
anomaly and normal karyotypes and 5 of 27 (19%) aneuplold fetuses
demonstrated absent end-ci~astol~c flow of umbd~cal adery. The
sensitivity, specificity, putative predlcbve and negative predictive value
of thts ftndtng ts 19%, 99.6%, 71% and 95% respectively.
CONCLUSION: Absent end-d~astolm flow m umb=hcal artery between
15 and 22 weeks of pregnancy ~s an abnormal finding and ~ts
association w~th aneuplo~d fetuses ~s s~gn~ficant as compared to the
fetuses w~th normal karyotypes.

Volume 170, Number 1, Part 2 SPO Abstracts 403 Am J Obstet Gynecol
459 UMBILICAL ARTERIAL VELOCITY RATIOS AND VENOUS
PULSATIONS IN FETUSES WITH LATE DECELERATIONS. DP Damron~, DG Chaffin, CF Andersor(, KL Reed. Dept. Ob/G~,
AZ Health Sciences Center, Tucson, AZ. Objective: Umbilical arterial (UA) and venous (UV) flow velocities were compared in fetuses with normal heart rate tracings and fetuses with late decelerations during labor.
Study Design: Doppler studies of UA systolic-to-diastolic (S/D) velocity ratios and UV velocities (presence or absence of
pulsations) obtained between contractions were compared with
those obtained during contractions in 20 fetuses. Ten fetuses had normal heart rate tracings and ten had late decelerations. Results: Fetuses with lates had higher UA S/D ratios between
(2,34_+0.74 vs. 1.56_+0.27, p<0.01) and during contractions (2.47_.+0.96 vs. 1.49_.+0.21, p<0.01) compared with normal. No significant changes in UA S/D ratios were seen in either group
when ratios obtained between contractions were compared with ratios obtained during contractions. Umbilical venous pulsations were not detected between or during contractions in normal fetuses, and were present only during (and not between) contractions in nine fetuses with late decelerations (p<0.00001).
Conclusions: While the increase in UA S/D ratios in fetuses with late decelerations is consistent with an abnormality in placental impedance, the development of UV pulsations during contractions in these fetuses suggests that the cardiovascular
pathophysiology of late decelerations involves abnormalities of cardiac performance as well. The presence of umbilical venous
pulsations during late decelerations is consistent with the hypoxic fetal cardiovascular changes (hypertension and
myocardial depression) previously reported from animal studies.
461 PROSPECTIVE INTRAPARTUM DETECTION OF FETAL
NUCHAL CORDS USING COLOR FLOW DOPPLER ULTRASOUND. G. MaconesJt M. Martlns,x Ro Wapner, R. Depp.
Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Jefferson Medical College of Thomas Jefferson
University, Philadelphia, Pennsylvania OBJECTIVE: To prospectively evaluate the predictive accuracy of color flow doppler ultrasound in the detection of fetal nuchal cords
during labor.
STUDY DESIGN: Intrapartom ultrasound examinations of the fetal
neck were performed over the time period of June 1 to July 6, 1993.
There were no exclusion criteria. The ultrasound prediction of a nuchal cord was made by analysis of both transverse and saglttal views of the fetal neck using color flow doppler (Ultramark 9, ATL). Predicted
nuchal cord status was then correlated with the presense or absence of a
nuchal cord at delivery.
RESULTS: Seventy-one singleton and two twin gestations underwent evaluation. The fetal neck was adequately visualized in all cases. All
patients were delivered within 24 hours of the examination.
Nuchal Cord at Delivery Yes No [ Total
Nuchal Cord Yes 14 2
I
16 Predicted No 1 58 5~
Total 15 60 75
95% Confidence Interval Sensitivity = .93 .87-.99 Specificity = .96 .92-1.00 Positive Predictive Value = .88 .81-.95 Negative Predictive Value = .98 .95 - 1.00
CONCLUSIONS: Color flow doppler ultrasound is a sensitive and specific medality for the intrapartom diagnosis of fetal nuchal cords.
460 UTERINE ARTERY VELOCITY WAVEFORHS DURING POSTPARTUM IN WUMEN
WITH SICKLE CELL DISEASE A Anyaeqbunam~ and M S Mlkhall * Dept or Ob/Gyn, Albert E]nsteln College of Medlclne, Bronx, New York OBJECTIVE:The well descrlbed changes In uterlne circulation durlng pregnancy are reflected ~n a s~g~f~cant decrease ~n systollc/d;astollc (S/D) ratlo and the dlsappearance of the d~astol]c notch The present study ~nvest]gates the changes ;n uterine Doppler velocmetry during the postpartum perlod in women wlth slckle col] (SS) d~sease METHOD:16 women wlth SS dlsease were followed from the thlrd trlmester of pregnancy untll 6 weeks postpartum All patlents had measurements of uterlne S/D ratlos blweekly from 28 weeks of pregnancy untll dellvery, flrst 24 hours postpartum and then weekly for 6 weeks RESULTS:Twelve of the IB women had normal (<2 6} uterine S/D ratios durlng pregnancy and dellvered appropriate for
gestatlonal age infants The mean S/D ratlo In the flrst 24
hours for these 12 women was 2 42 + 0 2 and increased
progressively to a mean S/D ratlo of ~ 4 ~ 0.6 at 6 weeks
postpartum with the appearance of a d]astollc notch The
remalnlng 4 women had abnormal uterlne S/D ratlos and SGA
dellverles Thelr mean S/D ratlos in f~rst 24 hrs was 3 8 +
0 3 These values also increased progresslvely to 8 2 ~ i 4 at
6 weeks postpartum The dlastollc notch were identlfled a mean
of 2 weeks earlier In these women wlth SGA de]iver~es and
abnormal uterine S/D ratlos when compared to women wlth AGA
dellverles and normal Doppler studies CONCLUSIONS: During the
postpartum perlod In women wlth SS disease, the dlastol~c notch
reappears earller In SGA compared to AGA pregmancles The non-
pregnant pattern of uterine artery veloclty waveforms whlch
leappears postpartum may reflect an increase in the
uteroplacental clrculatory impedence due to reversal of the
alterations In the splral arterles induced by trophoblast]c
462 CENTRAL AND PERIPHERAL HEMODYNAMIC CHANGES IN POST-
TERM FETUSES: CORRELATION WITH REDUCED AMNIOTIC FLUID
INDEX. Z. Welnerx, G Farmak~des, H. SchuJman, D. Mauhk
Dept Ob/Gyn, Wmthrop-Unlvers=ty Hosp. M=neola, N.Y.
OBJECTIVE. To evaluate central and peripheral hemodvnam~c
changes ~n post-term fetuses, and to correlate them w~th changes
~n AFI.
STUDY DESIGN: Doppler studies of the fetal heart, umbd~cal artery,
aorta, and m~ddle cerebral artery (MCA), were performed In 133
fetuses between 41-43 wks. Peak velocity, mean velocity, and
velocity t~me ~ntegral (VTI) were calculated from the flow velocity
waveforms obtamed from the outflow of the 4 cardmc chambers.
Pulsatd~ty ~ndex (PI) was calculated from the flow velomty
waveforms obtained from the umbd~cal artery, aorta, and MCA. The
results of the Doppler studies were compared w~th the NST and BPP
performed ~n these fetuses, and w~th the normal values obtmned ~n
term fetuses (37-41 wksl.
RESULTS: Central and peripheral flow veloc~metry d~d not change
s~gnlflcantly in post-term fetuses companng w~th term fetuses. In
12 pabents w~th AFI ~< 5, the left cardiac output (aortic VTIxHR
= 12.1 +1.2) , was s~gmficantly lower than ~n patients with normal
AFI (aortic VTIxHR= 14.9+1.6, p<O.01), The MCA PI was also
s~gnff~cantly lower (1.01+022 vs. 1.22+0.24, p<O.05) m
patients w~th AFI .~< 5. Flow veloc~metry of the right heart, aorta,
and umbilical artery was not significantly d~fferent comparing
between the 2 groups.
CONCLUSIONS: A decrease m AFI, ~n post term fetuses, is
associated w~th a decrease m left cardiac function and m MCA PI.
This is paradoxical when compared to IUGR fetuses where a
decrease m cerebral resistance ~s associated with increased left
cardmc output.

404 SPO Abstracts January ]994 Am J Obstet Gynecol
463 EARLY PREDICTION OF PREGNANCY HYPERTENSION
AND FETAL GROWTH RETARDATION BY DOPPLER
VELOCIMETRY OF THE UTERINE ARTERIES IN TIlE
FIRST TRIMESTER
I Thalc~ , A. Am~t, I. Itskovxtz . Dept. Ob/Gyn, Rambam
Medical Center, Faculty of Medmine, Technion, Israel Institute of
Technology Haifa, Israel
OBJECTIVE: To study the association between abnormal blood
flow velocity waveforms in the uterine artery during the late first
trimester and subsequent comphcatxons of pregnancy - pregnancy
~nduced hypertension and fetal growth retardation
STUDY DESIGN: Blood/Jew velocity waveforms (FVWs) m the
ascen&ng uterine arteries were obtained by an image-directed
transvaginal pulsed Doppler ultrasound. Seventy seven pregnant
women entered the study after informed consent. Doppler studies
were performed between 10-12 weeks The presence of a systolic
and/or diastolic notch in uterine arteries FVWs on both sides was
considered as a positive test
RESULTS: Twelve panents aborted in the first or early second
mmester. Of the remaining 65 women, 30 bad a positive test in the
first trimester Ten of these (33%) subsequently had pregnancy
hypertension or fetal growth retardation. Of the remaining 35
women w~th a negative test, only 3 (8.6%) later developed these
complicahons. Altogether, 10 of the 13 women with positive test
(77.7%) subsequently had pregnancy coraplication.
CONCLUSION: Doppler velocimetry of the main uterine arteries
in the first trimester can be used to screen pregnant women at risk
for subsequent pregnancy hypertension and fetal grovah
retardation.
465 TIlE INCIDENCE OF S/D RATIO DISCORDANCY BETWEEN
UMBILICAL ARTERIES IN NORMAL PREGNANCY
Sa|vatere ]. Lomhardi. M.D.. Suzanne M. Kavic, B.S.,=
Hardey Wddes, B.S., R.D.M.S.,’Vickie Matthews, R.T., R.D.M.S."
Outpatient Diagnostic Center and Meharry Medical College,
Nashville, TN.
OBJECTIVE: It is generally accepted that paired mnbilical arteries
are morphometricaLly similar and their flow velocity waveforms are
equal. However, discordant umbilical artery waveforms have been
reported. The objective of this study is to determine the incidence of
umbilical artery waveform discordancy in the same patient in normal
pregnancy.
S~ITdDY DESIGN: 302 singleton pregnancies at gestatinnal age 15-40
weeks underwent ultrasound as part of routine prenatal care.
Measurements of umbilical artery size and S/D ratios were taken for
each artery at the placental insertion, fetal abdominal insertion, and
a section of free loop of the umbihcal cord.
RESULTS: There were no statistically sign~eant differences in size
(p <.05) or S/D ratio (p <.05) b~tween intra-artery pairs at the 3 sites
interrogated for any gestational age.
CONCLUSION: We demonstrate that there is no size or S/D ratio
difference between the two umbihcal arteries in a given patient in
normal pregnancy. The S/D ratios obtained at any point along the
umbdical artery are reproduethle. We conclude that in a low risk
pregnancy random sampling of either umbilical artery at an easdy
accessible site, generates an accurate S/I) ratio. The f’mding of
umbilical artery size or waveform discordancy requires further
investigation as to pathegenesis and possible perinatal risks.
464 A PROSPECTIVE LONGITUDINAL STUDY OF HUMAN UMBILICAL ARTERIAL BLOOD ELOW. T A. S~ddiq~~, R.A Meyer=2, D Lynch-Salamon~,
B gosenn*~, R.K. Jaeklex~, I. Khoury~, G Holcberg’~, M MiodovnikL ~Div
M-F M, ~Child Hosp Med Cntr,, & ~Dtv Biostat, U. of Cmcinnati, OH
Objective: Fetal circulatory dynamics have been studied extenswely in the
chronically instrumented fetal lamb model (umbilical flow- 200cc/mm per kg
body wmght) Simdar data for the human fetus remain scarce. The current
prospective, longitudinal study was designed to quantttatwely determine
human umbd~cal artenal blood flow from 20 weeks gestation to term.
Study design: Normal women {n-34) w~th a confirmed gestational age were
enrolled at 20 or less weeks gestation. A complete ultrasound examinatmn
including measurements of the fetal biparietal diameter, head circumference,
abdominal circumference and femur length, was performed every 4 weeks
from weeks 20 through 36, and at week 40 if undehvered. These data were
used to estimate (eta/ weight by the Had/ock equation during each examination At each hme color flow Doppler (angle of insonation <200),
was used to determine mean flow velocity (cm/sec) and cross-sectional area
(cm~) m one of the two umbilical artenes. We calculated the total mean
umbilical artenal blood flow m cdmm by the equation "flow velooty x cross-
sechona[ area x 60 sec x (2)," assuming that there ~s equal volume flow ~n each of the two umbd~cal arteries All data are expressed as mean + SD
Results: The absolute mean volume flow and flow per umt (kg) estm~ated
fetal weight (EFW) m cc/mm are shown in the table.
Weeks gest. 20 24 28 32 36 40 (n=) {34) 04) (34) 04) 04) 03) Mean ilow 78+16 140~+32 206+48 300+50 338__+39 362_.+45 Flow/kgEgW 202+42 178~+36 150+34 136_.+21 112__+14 106+30
There is a hnear increase m absolute blood flow w~th advancing gestatmn
Arterial flow per kg of EFW however, decreases with increasing maturity
Conclusions: Human umbilical arterial flow ~s s~gmhcantly less than that
determined ~n the chromcally cathenzed fetal lamb model and may represent
specles d~fferences m regmnal d~strlbutlon of fetal cardiac output
(Supported m part by NIH HD 21687)
466 CONTACT MICRO DOPPLER (O~)): A MOVEL TECHMI~ FOR THI~ STUDY OF
CERVICAL MICROCIRCULATIOll TBROUGIIOUT ~E~- S. Rott~D. Na~a~ S. Lajinian~ R. Zoffe~ C. Hartle~
~JECTI~: The effective focal z~ (1.5-7 cm) of transvaginaL
pro~s carrying 5-9 HHz transducers a~ their size (1.5-2.5 cm)
are ina~ropriate for the stool surface e~ocervica[ (EC)
exoceevicaL (EX) microcircutation. Our objective uas to develop
a high fr~ue~y (HF) micropro~ for the stay of cervicaL
microcircutation throughout pregnancy.
STaY DESI~: T~ HF piez~lectric transducers (~0 micron 960 micron) ~ere ass~t~ at a 90° biptanar c~figurati~
a 22 cm x 2~pro~ a~excit~by a ~Ls~Oo~Ler syst~. EC
a~ EX bto~ flow was assess~ in 10 pregnant ~tients
~eeks gestation).
RE~LTS: An a~iosignaL was detect~ in aLL 10 ~tients in the
EC a~ EX areas. B[o~ ftov envelops repr~ucibte for s~ctPat
analysis ~ere detect~ in all 10 ~tients on the EC area (fig.
la a~ lb) a~ in 9/10 on the EX area (fig. 2).
~CLUSI~S: The ne~ bipLanar CHD pro~ has a high spatial
resolution for non-~nvasive assess~nt of cervical
mlcrocircuLat~on. It can provide data on cervical
microcircu[atory cha~es re[at~ to tinning, t~olyt/cs
tamp i~ocing agents, otherwise unavailable by other ~ans.
fig la
fig lb

Volume 170, Number 1, Part 2 SPO Abstracts 405 Am J Obstet Gynecol
467 EFFECTS OF TOBACCO USE AND TOBACCO + COCAINE USE ON
FETAL GROWTH AND UTERINE FLOW VELOCITY WAVEFORMS. D.
Ogungemi, L. Castro, R Allen, C. Hobal, K. RolP. Depts. Ob-Gyn, Cedars-
Sinai & Drew King Med Ctrs and the UCLA School of Medicine LA, CA
OBJECTIVE: The purpose of this study was to determine the effects of
velocimetry and fetal growth m the 3rd trimester.
STUDY DESIGN: We prospectively studied 3 groups of women in the 3rd
cocaine users (n=14). After informed consent all subjects underwent
ultrasound (UTZ) evaluation of the fetus for estimated fetal weight (EFW) and
doppler veloclmetry of the uterine and umbihcal arteries with the aid of color
data were obtained on all subjects at delivery.
RESULTS:
Gest Age at
UTZ (wks) UTZ EFW (gins)
No. C~g/day
Cotimne(ng/ml)
Uterine S/D
Umbd S/D
Gest Age at
delivery (wks)
Birth wetght(gms)
30.3+.4 30.8-t- 4 30.6+.6
I720_+89 1706_+97 1455_+111
0 12.2-t-l.8" 12 95:2.6"
<2 163-+20" 173-+31"
1 79+.05 2,14+_,1I" 2.21_+ 41- 2 865:.13 2 94-+ i4 3.22-+.22
39.65:,3 38 7_+.4 38 6±.8 3529+133 2916_+140" 2770_+100"
"p < .01 ;’p < .005 VS controls
CONCLUSIONS: Tobacco use does not ~ppenr to inhibit fetal growth until
after 31 weeks and is preceded by changes in the uterine ~xtery S/D conmstent
with the development of increased resistance to uteroplacental blood flow.
Cocaine + tobacco use may inhibit fetal growth e~rher m gestation than does
tobacco use alone resulting m a more pronounced decrease in birth weight.
469 ARE REALTIME ULTRASOUND AND UMBILICAL ARTERY
DOPPLER FINDINGS USEFUL IN PREDICTING SPECIALIZED CARE
FOR FETUSES FROM TWIN PREGNANCIES? _E Gaz~an~, S Calvin, R
Bende[, ./ Ney, K Pr’]eghaar, P M~lls, B Assel, L Falrbanks, D Bran~t, E
Knox Abbott Northwestern Perlnatal Center, Mmneapohs, MN
OBJECTIVE: Hypothes~s ultrasound and fetal Doppler derived observatmns
allow risk categonzahon for t~wn fetuses.
STUDY DESIGN: Targeted uRrasound w~th anatomic survey, umbfimal artery
(UA) Doppler veloc~metry, ammotm fired volume (AFV) assessment, bmmetry,
and gender ldeutlficatlou was performed for each twin fetus in 162 consecutive
pregnancies (1991-92) Excluding fetal deaths, 310 hveborn infants were
avadable fbr study Based upon lnltml evaluation, fetuses were admitted to one
oftw~ spec~ahzed care urals, mtenswe (ICU) or special care (SCU), or to the
normal nursery Stat~stmal methods used umvanate (x~ and F~sher’s exact test)
and multivariate (multiple logistic regression)
RESULTS: Adm~ssmn to ICU occurred m 19% of neonates w~th normal
ultrasound morphology (N 263) compared to 55% w~th suspected growth
retardation or structural abnormahtxes (N-47) (P 0001) "l~mse suspected of
growth retardatmn (N=24) expermnced an ICU admission rate of 37 5% while
those with a variety of ultrasound detected abnormahhes had the h~ghest ICU
admission rate (17 of 23), 79% (P<0001) Abnormal UA Doppler d~d not
predict ICU admission but was s~gmficantly associated (P- 05) with prolonged
care m the SCU Abnormal AFV 0"4-25) was s~gmficantly assocmted with ICU
adnnsslon, 60% vs 20% (P 001) Both ohgohydrammos (N 10) and
polyhydrammos (N 15) were stgmficantly associated w~th ICU admissions
(P 001) and (P 008) respechvely Although ultrasound EFW at <35th
perceutde was associated with growth retardation, It was not predictive of
specmhzed care Multivariate analys~s showed suspected growth retardahon and
fetal abnormahtles to be associated w~th odds ratios of 3 and 11 respectively
for [CU adtmsslon whde abnormal Doppler was associated w~th od.ds ratio of
3 for SCU adm~ssmn
CONCLUSIONS: In twin pregnanmes, individual uln’asound and Doppler
l~udl!ags correlate with admission to specaahzed care nurseries.
468 THE PRESENCE OF /~,NORMAL UMBILICAL VENOUS DOPPLER
FLOW IN MULTIPLE PREGNANCY COMPLICATED BY
OUGOHYDP, AMNIOS/POLYHYDRAMNIOS SEQUENCE. La,qrew DC=
Morgan MA, Stezger RM. Department of Ob/Gyn, University of
Cahfornm, Irvine, Orange, CA, Saddleback Memorial Medical Center,
Laguna Hdls, CA
OBJECTIVE: To evaluate the chn~cal findings of fetuses with patterns
of d~minished umbilical venous flow during atnal systole in multiple
pregnanciescomphcated byohgohydramn~os/polyhydramnlossequence
(ops). STUDY DESIGN: We prospectively followed five gestations with OPS (4
twin, 1 tnplet) with serial umbilical venous and arterial Doppler flow
patterns. Pulsed Doppler ultrasound studies were performed w~th a 3,5
M Hz transducer w~th simultaneous 2-dimensional wsualizabon. Samphng
volume was ~ncreased to record simultaneous umbd~cal artenal flow to
estimate cardiac t~ming Fetal and neonatal outcome data information
were collected.
RESULTS: All fetuses with polyhydramn~os clearly demonstrated late
diastohc notching of the umbd~cal venous tracings. The patterns
persisted desprte amniohc fluid volume improvement. No evidence of
tncusp~d regurgitation was seen but all had ¢ard~omegaly, and two
fetuses demonstrated hydrops. Three of five fetuses with notching
survived and two d~ed m the neonatal period. All five demonstrated
cardlomegaly and ventncular dysfunction with low ventncular fractional
shortening as neonates. None of the ohgohydrammos fetuses had
abnormal venous or artenal flow patterns w~th the excepbon of one
showing absent end d~astohc arterial flow shortly prior to dehvery. Four
of s~x fetuses without notching survived and none showed ewdence of
cardiac dysfunction.
CONCLUSION:Abnormal umbd~cal venous flow patterns w~th d~astohc
notching are predictive of poor ventncular function m the fetal and
newborn penod in pregnancies w~th OPS.
470 DOPPIER UUIRA~OLIND IN THE PREGNANCY C~IvPLICR~ED BY POL~I~DRAMNI OS-OLI GOH~RR~IN I 0S T[VI NS. 6. Maj,x & P~harna~’R. Sope ,~ B. ~ir-~hon, ~. ~auer~. va~e
Uniue~t y, East em Lirginia M~didal S~hool, Baylor College of f,~edidne. New Haven, Nolqolk, Houst on. 0B~CTIVE: Polyhydramni~-dlgohydramnms syndrome (POS) is a
complication oft’,un pregnancy with polyhydranmlcS ~n me gestatlonal
sac and ohgnhydranmlm in the other, l)agnoSlS of anenua in one fetus
~ a pregnancy ca-npllcated by POS strongly sug~sts a more specific dlagnes~s of twin-twin-transfusion syndrome (TITS). 3"he mm of this
study was to assess the ability ~ Doppler ultrasound to identify fetal
anemia m t~n pregnancies complicated by POS.
gIUOY II~$1G~ Mddle cerebral artery (IvUA) and ductus artermsus
(DA) peak vel¢oties (PC) were assessed in 17 sets of l~ans ~ith POS
within 7 days ofdehvery. (t.’stauonal age (C~) ran~ed between 20 and
34 weeks. Fetuses were defined to be at risk for anerma if the Iv~-PV and]cr DA-PVw~e ~’eater than 2 ~above the mean velocity measured
in a nermal populaucn.
RESBII$: Four fetuses wath chgOnydrammos and 1 fetus wth
polyhydramnlos were anerme at birth (@SD for the normal population).
"Ihe IVI2A-PV was 100%sensttive m detectmganemia, 84% spemfic and
it had apesltlve predlcUve value (PpV) of 55%and a negative predictive value 0N~C) of 100%. 1he DA-PV had a sensitivity of 100% a
specifi city of 87 %, a PPV of 57 % and a NPV of 100 %.
EONLIlI$1 ~ I)3ppler ultrasound may be a useful toni in the diagnosis
~ff the anemac fetuses tn twin pregnandes canaplicated by POS; if the
I~IA-PV and DA-PV are above 2 513 of the mean for the normal
population, the fetus is likely lobe anermc and amore speofic diagnos~s of TrPS ts strmgly suggested.

406 SPO Abstracts January 1994
Am J Obstet Gynecol
471 A~ ABNORMAL UMBILICAL ARTERY WAVEFORM IN TIlE
SMALL FOR GESTATIONAL AGE FETUS IS A STRONG AND
IN DE PENDENT PREDICTOR OF ADVERSE PERINATAL OUTCOME.
BH Yooii, CM Lee’, CK Chunx, KH Parkx, HC Syn% R Gomez’, SW Ktmx.
Seoul National Umversay, Seoal, Korea and the Perinatology Branch,
NICHD, Bethesda, MD.
BACKGROUND/OBJECTIVE: An abnormal umbilical artery Doppler
waveform is a risk factor for poor permatal outcome in SGA fetuses.
However, it has not been established whether th~s is due to the lower
gestanonal age at dehvcry of fetuses with abnormal Doppler findings or tf
Doppler findings are an independent predictor of perinatal outcome. To
determine if an abnormal Doppler umbilical artery waveform is associated
with adverse permatal outcome even after controlling the gestationalage at
delivery as a confounding variable in the SGA fetuses.
STUDY DESIGN: Perlnata[ outcome of 91 patients who had a SGA
newborns who had a Doppler umbilical artery velocimetry study performed
within 7 days of dehvery was examined. Adverse perinatal outcome was
defined as. fetal distress requiring cesarean delivery, Apgar score < 7 at 5
rain, NICU admisston, neonatal sepsis, intraventricular hemorrhage (Gr. 2-4),
respiratory distress syndrome, pneumonia, acute renal failure, necrotizing
enterocolit m, or perinatal death. Stepwise multiple logistic regression analysls
was used for analysts.
RESULTS: 1) The rate of preterm dehvery, cesarean section for fetal
dtstress, Apgar score < 7, NICU admission, and perinatal death was
stgmficantly htgher in patients wah an abnormal umbdlcal waveform than in
"those with normal waveform. 2) Stepwtse logisttc regression analysis
demonstrated that an abnormal umbdlcal artery waveform added sigmficantly
to the prediction of adverse permatal outcome even after correction for the
gestattonal age at delivery
Odds Ratio 95% C.I p
GA at dehvery 0.32 0.18-0.57 <.001
Abnormal waveform 10 70 2.22-51.58 < .005
CONCLUSIONS: An abnormal Doppler umbihcal artery waveform is a strong (Odds rano 10 7) and mdependent predictor of adverse permatal outcome m SGA fetuses
473 ELEVATED THROMBOMODULIN/CREATININE (TM/Cr)
RATIO AS AN POTENTIAL MARKER IN PREECLAMPSIA
C.D. Hsu~ B. Lucas~, T.R.B. Johnson, S.F. Hongx, D.W. Chanx,
Dept. OB/GYN, Johns Hopkins University School of Medicine,
Baltimore, MD and Yale University School of Medicine, New
Haven, CT.
OBJECTIVE: From our previous studies, we found serum TM
levels were significantly elevated in pregnant women with
preeclampsia (AJOG 1993;169:148). Thus, we sought to
determine whether urine TM/Cr ratio can be a useful marker in
identifying preeclampsia.
STUDY DESIGN: Thirty pregnant women with preeclampsia
were matched with 30 normotensive healthy women with singleton
pregnancies in the third trimester. Subjects were matched for
gestational age, parity, maternal age, and race. Maternal urine
TM, Cr, pH, and specific gravity were measured. Pair-
comparison t test was used for statistical analysis.
RESULTS: There was no significant differences in urine pH,
specific gravity, and TM levels between preeclampsia and their
matched controls. However, significantly decreased urine Cr and
increased urme TM/Cr ratios were noted in preeclamptic group as
compared with those in their matched controls (69.87+_ 8.62 mg/dl
vs 114.23 + 8.01 mg/dl, p=0.001, and 1.67 + 0.16 vs 1.15 _+
9.09, p=0.006, respectively).
CONCLUSIONS: Our data suggest that changes in renal function
are present in preeclamptic women and testing for urine TM/Cr
ratio may serve as a clinically meaningful marker in identifying
preeclampsia.
472 PLACENTATIONAND~ILIC~LRI~EERy DOPPLER~gLOC~Y IN TWIN GESTATION. CS Croom,MDf ES Ki~,MDx, LD Devoe,MD Dept OBGYN, Medical College of Georgia, Augusta GA O~JECTI~Et To determine the relationship of placentation to umbilical arterial Doppler velocimetry in third tri~ster twin gestation. ST~DE DESIGN: Eighty-four twin pairs had serial umbilical arterial Doppler velocimetry between 28 - 40 weeks" gestational age(GA). All ~airs were assessed for means and differences in birthweight (BW) and Doppler StD ratios and for placental type by pathologic exam (moncchorionic (MC), dichorionic (DC, fused or separate) and ultrasound diagnosis (single or dotlble placenta). Absolute means and differences in StD ratios were correlated with GA, BW, BW discordance (>20%), growth retardation <10%ile (IUGR) and placentation. Analyses used t-tests,chi-sq~ared tests a~dr~11tiple regressions. RESULTS. All placentas were diamniotic(DA);50 were DCDA and 34, MCDA. Mean BW and GA were similar(2350 g~, 36 weeks) for both groups;mean S~D ratios were higher in DCDA than MCDA sets. Discordancy rates in DCDA(24%) and MCDA (20%) groups were similar. In DCDA sets, IUGR (27% v.10%,p=.03), mean ~Ws (283 v. 194 gm, p=.04)) and AS:D ratios (.83 v..59 ,p=.08) were higher. Discordancy was also associated with higher ABWs and AS~D ratios in DCDA pairs than in MCDA paris. Sonography correctly identified 95% of nonfused DCDA sets. CONCLUSIONS: Twin placentation is related to differences in S~D ratios and risk for IUGR. It can be confirmed antenatally in nearly all separate DC types. While discordancy was ec~lally cc~on in both placental types, it had greater impact on S~D ratio differences in DCDA sets. Placental t~pe would be an important factor to consider when eval~ating Doppler velocimetry in twins.
474 PREECLAMPSIA DOES NOT INCREASE FETAL-MATERNAL
HEMORRHAGE C__.D. Hsn, C. Smlth~, T.R.B. Jotmson, S. F. Hong~, D. W. Clumx,
Dept. of OB/GYN, Johns Hopkins Unlverstty School of Medtcme,
Baltimore, MD and Dept. of OB/GYN, Yale University School of
Mexhcme, New Haven, CT.
OBJECTIVE: To determine whether fetal-maternal hemorrhage is
increased m preeclampttc pregnancy.
STUDY DESIGN: Stxty-two women wtth singleton pregnancies m the
tbtrd trimester were studted. Tturty-one of these women w~th
preeclampsm defined by Amertcan College of Obstetrtcs and
Gynecology criteria were matched wtth tlurty-one nonnotensive healthy pregnant women. Maternal serum levels of ~-fetoprotem (MSAFP)
and Kledtaner-Betke test (K-B test) were determined to reflect the degree of fetal-maternal hemorrhage. Patred-compartson t test was nsed for stattsttcal analysis.
RESULTS: There were no sigmficant differences m MSAFP, MSAFP/creatuune ratto between preeclan~ptic pregnanctes and thetr
matched controls (155.3 + 31.6 vs 160.3 +_ 15.9 ng/ml, p>.05 &
173.6 _+ 36.5 vs 203.4 + 20.7, p>.05 respecttvely). After pattents
wtth HELLP syndrome were exchtded, there was still no stgmficant
dtfference in MSAFP,MSAFP/creatmine rntto between patients wdh
a~td w~tbont preeclantpsta. Moreover, the appearance of fetal cells m
lhe maternal clrculatton (K-B test) m preeclampttc pattents (0.14 +
0.11% of fetal cells) was not stgmficantly elevated.
CONCLUSIONS: Our data reveal that felal-maternal hemorrhage ts
not increased m patients with preeclampsta. Whether fetal-maternal hemordmge can be better detected by advanced mulnparameter flow
cytometry ts under investigation.

Volume 17f3, Number 1, Part 2 SPO Abstracts 407 Ant J Obstet Gynecol
475 ALTERED CIRCULATING TIlROMBOMODULIN (TM) AND
ANTITIH/OMBIN Ill (AT Ill) LEVELS AS AN EVIDENCE OF
COAGULANT ACTIVATION IN PREECLAMPSIA
C D Hsu. T,R B Johnson, S F Hong’, D W Chan~, Johns Hopkins Unlversay
School of Medicine, Baltimore, MD & Yale University School of Medicine,
New Haven, CT
OIIJECTIVE To deteranme the correlation of coagulant activation between
circulating TM and AT 111 levels and ~ts potenaal as a marker in preeclampsia
STUDY DESIGN’ Sixty-eight women w~th singleton pregnancies in the third
trimester were studied Twenty with todd preeclampsia and 14 wah severe
preeclampsla defined by ACOG were matched with 34 normotens~ve healthy
pregnant women Maternal serum TM and AT I11 were measured by enzyme
nnmunoassay and microlatex particle-mediated immunoassay, respecnvely
(Dmgnostlca Stage, Asnlbres, France) Paired t test and conventional correlation
eoef[~clcnt, and receiver operator curve were used for statistical analyses.
RESULTS Serum TM levels were slgmficantly higher m severe but not mdd
prccclampttc group as compared w~th those m thexr matched controls (p < 005)
However, AT I11 levels were stgmficantly lower In both severe and mdd
preeclamptic women Serum TM levels were inversely correlated wnh AT 11I
lcvcls m severe preeclampsm (r=- 0 748, p=0 012), but not m mild
prcccIampsla Using the receiver operator curve, AT 111 was found to be a
bctter marker for both severe and todd preeclampsm Wuh a cutoffvalue below
270/~g/ml, AT 111 levels identify preeclampsia with a sensitivity of 93%, and
spccdqc~ty of 90%
CONCLUSIONS (1) C~rculatmg AT IlI leveIs were decreased in all
prceclmnpttc women whde TM levels were increased only m severe preeclamphc
women Th~s may reflect a different degree of coagulant activation in vascular
ct~dothehal damage between mdd and severe preeclampsm (2) The slgm ficantly
ntverse correlation between TM and AT Ill levels provides evidence for the
dysfunctlon of anUcoagulant properties of endothehal cells in the pathological
changes occurring in precclampsla
477 EFFECT OF MAGNESIUM SULFATE ON EXCITATORY AMINO ACID RECEPTORS IN THE RAT BRAIN: NMDA RECEPTOR -
CHANNEL COMPLEX. M Hallak, S M Irtenkaufx, C A Jannszx, H
Abratnovlcix, D B Cotton Depts ofOb/Gyn, Hutzel Hosptta!AVayne State
University, Detroit, IV[I, and Carmel Hospital, Hatfa, Israel
OBJECTIVE: The NMDA receptor ts tnvolved m the lmttatton and
propagation of seizures tn the mammalian CNS Smce MgSO4 ts w~dely
used for preventton and treatment of eclamptic seizures, the purpose of this
study was to determine its effect on the NMDA receptor complex
STUDY DESIGN: Two separate experiments were performed 1 Six rats
were injected tntrapentoneally with 270 mg/kg of magnesium sulfate,
followed by 27 mg/kg every 20 minute, for 4 hours Controls (n=6) recetved
sahne 2 Six rats received mtraperitoneal in, cottons of magnesium sulfate
(270 mg/kg) every 4 hours, for 24 hours while 6 received saline Rats were
subsequently perfused and sacrificed, their brains dissected, and frozen Cryostat sectmns were taken, labeled in-vitro by one of three hgands 13H]-
Glutamate, [3H]-Gtycine, and [3H]-IVlK-801 for autoradtography assay, and
mounted on Ultrofilm for 4 weeks Optical denstty measurements of
binding of 11 brmn regions on each section were performed using an image
analyzing system ANOVA and Student’s t test were used
RESULTS: M~SO4 effect on NMDA receptor comp!~x binding capacity Glutamate-agomst G~cble-agonls~ MK-8OI-Noncompetntve 1
NMDA blndln~ site Glycme btndm~ site anta[onlst, Charmel site 4 hrs NS change NS change Increased (6 regions)
24 hrs Decreased NS change Increased (g regions)
CONCLUSIONS: 1 Peripheral treatment vath MgSO4 results m a stgnlficant reduction in the NMDA receptor agomst bmdmg capacity m the
rat brain, and increased bmdmg for the noncompetitive atttagonist tn the
channel site 2 These results provide further information on the mechanism
by which magnesium’s central anttconvulsant activity ts mediated
476 MATERNAL MIDDLE GEF~BRAL VASCUI.h/:I CHANGES ASSOC.~ATED WITH ECLAMPSIK K. William% C. MaeLean. Dept. (~[Gyn, UBC, Va~. 1313. Canada. V6H 3V5.
OBJECTIVE: To compare maternal cerebral vascular changes in eclamphc
pahents with matched preeclamptlc controls. Eclampsia is associated with
severe generalized cerebral vasospasm. We attempted to show that preeclampsla, when it is assoc~atad with seizures (ecMmpsla), results in a s~gmficant increase m cerebral blood flow velocity in the middle cerebral
artery. STUDY DESIGN: Three eclamptlc women who had seizures wlthm 24 his of delivery, were matched wdb sJx preecMmpt~c controls Mothers were
matched for gestatlonal age of dehvery, antepartum blood pressure on admission, level of protemuna and grawdlty The three eclamptic patients developed seizures within the 24hrs of dehvery A~I patients had maternal middle cerebral blood flow velocity (MCBFV) assessed in early labour 24 hrs
postpartum, and 48 hrs postpartum using transcranial doppler with 2mHz pulsed probe. Statistical significance was assessed using the t test
RESULTS: There was a statistically significant increase in all mean MCBFV, antepartum andatthe24hrspostpartum (7~-g0%) A]though the 48 hr mean
MCBFV m eclampbcs was higher (36%) than m the preeclamptics, this did not
achieve statistical slgndlcance CONCLUSION: The development of eclampma is associated w~th a
statistically stgniflcant short hved rise in mean MCBFV ielated to ealebral
vasospasm which disappears wlth~n 24 hrs of the eclamptie convulsion
Ante- 24 hrs 48 hrs partum postl:m~lum
Ec{amptic Mean MCBFV cm/sec 109 _+ 6* 109 _+ 13" 102 +- 21 (N=3) Mean Arterial 116 ± 4 118 _+ g 110 _+ 12
Pressure (mmHg)
Matched Mean MCBFV cm/sec 57 -+ 6 67 -+ 14 75 -+ 15 PreedaiT=pti~ Mean Arterial 113 _+ 7 106 -+ 14 107 +- 16 (N=6) Pressure (mmHg)
* (P<.01) = compared with preedamptics
478 R.B. K~zel, S.A. R~hola=ini~, A. Au~. ~p~ ~/~ ~d Radiol~, Olive View/O.C.L.A. ~edical Center, Syltar, CA. ~: To study ~ s~ of ~ findings a~ociated wi~ ~e HELLP Syndro~ (hemlysis, elevated liver enz~s,
lo~ platele~), ie liver ch~qs, ~cits, & ple=al eff~ion. s~ D~I~: 14 ~tien~ wi~ ~ELLP Syn~om were sca~ by ~ 1-3 days ~st-~. ~ findin~ ~d ~eir pr~ession ~ere co~elatM ~i~ patient s~totatol~, mxi~ a~erial pr~e (~), mxi~ valu~ of: ~ic acid, ~d ~, ~d ~ini~ value of platele~.
Syndrom include: ple~al eff~ion * ascit~ NriN~al Mem - fatty infiltration of tN liver - liver
neffosis - liver n~sis ~i~ s~a~ular hemtom. With
in~easiN abnomlity, ~ore is in~easiN overlap of
findings. Ple~al eff~ion ~as present in 64% Ntien~, aseites in N%, and heNtic findin~ in all ~ Ntien~ wi~
[i~r fining, 89~ also had ~cites or ple~al eff~ion; an
had platele~ < 1~,~. NtienS ~i~ NriN~al Mere or
fatty infiltration an Md tran~tinas~ > ~ u/1 or > 1,~ u/! if n~is was pr~ent. ~e conveme ~ not t~e. ~e Mst co=elation ~ith ~e presence of liver findiNs Ntient co@lain~ of severe epiOs~ie or ~ pain (8/11 had liver findings win ~y d~ee of Nin, and 7/8 of ~ose with ~vere ~I~: ~e ~EL~ Syn~o~ is ~iated with si~ific~t ineidenc~ of ple~al eff~ion, ascit~, and liver pa~ol~ ~ de~nstratN by ~.
408 SPO Abstracts January 1994 Am ] Obstet Gynecol
479 PREVENTION OF PREECLAMPSIA BY CALCIUM
SUPPLEMENTATION IN ANGIOTENSIN-SENSITIVE PATIENTS.
L. Sanchez-Ramos. G O Del Valle, D Briones RNx, C Walker RNx, I
Delke, F Gaudier. Department Obstetrics and Gynecology, University of Florida, Jacksonville, FL.
OBJECTIVE: To evaluate the efficacy of oral supplemental
calcium in reducing the inc=dence of preeclampsia m angiotensin- sens~bve patients.
STUDY DESIGN: Thin randomized, double-blind, clinical trial was destgned to include at ~east 50 ang~otensin positive prlmlgravidae
(alpha .05 and beta .10; Power 90%). Sensitivity to intravenously- infused angiotensin II was determined at 24-28 weeks’ gestahon m 197 women w=th a positive roll-over test. A positive angiotensin
sensitiv=ty test lAST) was defined based on an effective pressor dose of < 10ng/kg/min. Angiotensin-sensitive women were
randomly allocated by means of a computer-generated
randomizahon hat to groups receiving 2 g/day of oral calcium gluconate or an ~dentical placebo. The tablets were dispensed by
the hosp=tat pharmacy in serially numbered computerized pill bottles so as to evaluate regimen compliance. Repeat AST was performed at 34-36 weeks’ gestabon.
RESULTS. 53 patients were found to be angiotensin-sensibve: 25 received 2 grams of calcium gluconate dady, and the remainder
received matching placebo unh] delivery. In the placebo group, 43% (95% CI 24% to 63%) developed preeclampsia compared to
16% (95% CI 5% to 36%) in the calcium group. Relative risk 0.44
(95% CI 0.18 to 1.07; P=.044). The incidence of gestational
hypertension was s=mdar in both groups; 59% and 42% respect=vely. CONCLUSIONS’ Calcium supplementation given in early
pregnancy to Ngh risk patients may offer some protection aga=nst preeclamps=a.
481 PLASMA LEVELS OF RETINOL AND RETINOL BINDING PROTEIN IN PREECLAMPSIA. Palan PRx, Mlkhall MS×, Anyaegbunam A, Wang $x, Basu jx, and
Romney SL Albert Elnsteln College of Medicine, Bronx, New York
OBJECTIVE Free radlcal mediated llpld perox~dat~on may be
~nvelved ~n preecl amps~a-assoc~ated endothei~a~ membrane damage Retlnol Is a potent llpld-soluble antloxldant that can protect cell membranes agalnst uncontrolled Inp;dperoxldatlon Retlnol is transported to target tlssues by a speclflc retlno] blndln9 proteln (RBP) The purpose of thls study was to Investigate the plasma levels of retlnol and Its blndlng proteln ~n
preeclampsla STODY DESIGN. Fastlng coded b] God samples were
collected from 18 patlents wlth preeclampsla (ACOG crlterla) and
26 women wlth normal pregnancles The crlterla for recruitment
included, age of 15-35 years, gestatlonal age between 28-37
weeks, slngleton pregnancy, intact membranes, absence of labor
contractlons, and absence of any other medlcal compllcatlon
concurrent wlth preeclampsla, Plasma retlnol levels were
determlned uslng high pressure llquld chromatography and RBP
levels were measured by a quantltatlve radial lmnlunodlffUslon
technlque RESULTS. (mean ~ SD)
Normal Preeclampsla P value (n:le) (n=26)
RetinoI (ug/dl) 32 9+8 1 25 7~12 4 <0 005
RBP (mg/dl) 3 3050.67 3 46±1 31 NS
Retinol:RBPmolar ratio 0 74~0 18 0 54~0 20 <0 005
CONCLUSIONS. Plasma retlnol levels and retlnol RBP molar ratlo
were slgnlflcantly decreased In preeclampsla compared to normal pregnancy. Although preeclampsla ~s usually associated w~th
hepatic dysfunctlon and RBP is syntheslzed ~n the llver, RBP
levels were not statlstlcally d~fferent between the two groups
and could not have accounted for the decrease In retlnol levels
observed In thls study. The flndlngs suggest that the
blologlcally actlve free fractlon of retlnol is slgnlflcantly
decreased In preeclampsla This may reflect Increased antloxldant utlllzatlon to counteract free radlcal-medlated llpld peroxldatlon resulting In a decrease in retlnol levels
480 LOW-DOSE ASPIRIN FOR THE PREVENTION OF PREGNANCY-INDUCED HYPERTENSION: A META-
ANALYSIS. L. Sanchez-Ramos. R. Wearsx, G.G.
Gaudier, D. Adair.x Department Obstetrics and Gynecology, Univers=ty of Florida, Jacksonv=lle, FL. OBJECTIVE: To estimate through meta-analysis the magmtude
of protechon of low-dose aspmn from gestational hypertension and preeclamps~a. STUDY DESIGN: After a literature search was performed, data from 12 randomized c~inical trials conducted dunng the per}~
1986-1993 were pooled and reanalyzed. For the outcomes of
gestat~onal hypertension and preeclamps~a, vanance-wmghted, pooled odds rabos, 95% confidence ~ntervals, and number needed
to treat were calculated Separate analyses were conducted for
subgroups of the pooled data: perinatal mortality, incidence of cesarean section, intrauterine growth retardation, preterm delivery and abruptio placenta RESULTS: Among 5115 obstetric subjects studied in twelve
trials, the risk of gestational hypertension among women who took aspirin was 12.7% (95% CI, 12% to 14%) compared to the placebo group’s 13.4% (95% C112% to 15%) odds rat=o .894 (95% C1.882 to 907) To prevent one case of gestahonal hypertenmon, 88
pabents needed to be treated. Among women supplemented with
aspirin, the risk of preeclampsia was 3.8% (95% CI 3% to 5%) compared to 6.5% (95% CI 6% to 7%) for the placebo group (OR
.527; 95% C1.510 to .545; P <.001) and the number needod to be treated was 32. No differences were noted in the cesarean section rate, permatal mortality, and the incidence of preterm
dehvery, IUGR, and abruptio placonta. CONCLUSIONS: This mete-analysis suggests that daily
supplementation with low-dose aspirin is associated with almost a
50% reducbon ~n preeclampsia. No differences in maternal or pennatal comphcabons were noted.
482 SERUM URIC ACID LEI/ELS IN IWIW GESTATIO¢IS RL Fischer, KW Bianculli’, ML Hediger". Department of OB/GYN, UMDNJ-RWJ Medical School at Camden, Cooper Hospital/University Medical Center, camden, NJ. OBJECTIVE: TO compare serum uric acid levels of twin gestations without preec[ampsia to those of twin gestations with preectampsia, as well as to published values for normal singleton pregnancies. STOB¥ DESIGW: Fifty-nine subjects with twin gestations and no evidence of chronic rena( insufficiency had serum uric acid levels drawn at the time of admission to Labor and Delivery. Uric acid levels were determined by colorimetric urocase assay. Eight subjects (13.6%) were diagnosed with preectampsia. ]he preeclamptlc and non-preeclamptic groups were compared with respect to age, gravidity, parity, gestational age (GA) at delivery, and serum uric acid levels. Statistical methods included the Student t test and Fisher exact test (two-tailed).
RESULTS: Preectampsia No Preectampsia ~N=8) ~N=51)
Age (years) 26.0 ± 7.5 25.5 ~ 6.0 Nul[iparous 7 (87.5%) 14 (27.5%) De[ivory GA (wks) 34.1 ± 2.2 34.3 ~ 3.9 Serum uric acid 7.9 ~ 1.7 5.5 ~ 1.4
(mg/dl)
Ser~ uric acid 8 (100%) 12 (23.5%) ~ 6.5 mg/dL
.84
.002
.90
.0001
.00006
In the non-preectamptic group, the serum uric acid level was
significantly higher in those delivering after 32 weeks than
before 32 weeks (5.7 ~ 1.4 vs 4.6 ± 0.8 mg/dl, p ¯ .05), The
mean serum uric aCid [eve[ in the non-preec[amptic twin gestation group (5.5 mg/dl) was higher than those of normal
singleton pregnancies at term reported in nine prior publications (mean 4.3 mg/dl, range 3.4 - 4.9 mg/dt).
CONCLUSIONS: 1) Non÷preectamptic twin gestations have serum
uric acid levels which are generally higher than previously
established means for non-preeclamptic singleton term pregnancies, and 2) twin gestations complicated by
preeclampsia are associated with higher serum uric acid levels
than the non-preec&tic twin group.

Volume 170, Number 1, Part 2 SPO Abstracts 409 Am J Obstet Gynecol
483 CHRONIC MAGNESIUM REDUCES SEIZURES INDUCED BY
CENTRALLY ADMINISTERED N-METHYL-D-ASPARTATE
(NMDA) IN RATS. C A. Standley’, S.M. IrtenkauP, D.B. Cotton. Dept of Ob/Gyn, Hutzel HospttaUWayne State Umversity, Detrmt,
MI.
OBJECTIVES: NMDA has been unphcated m a number of
pathophystologtcal conditions, including seizures. Magnesium is a
physiological blocker of the NMDA recel~or. As magnesmm sulfate
ts the standard trealment tbr eclamptlc seizures ~n North America, we examined the amtlconvulsant effects of MgSO4 on central NMDA-
reduced seizures. STUDY DESIGN: 17 female rats were surgically anesthetized and a
bipolar recordmg electrode was stereotax~cally implanted into the
dorsal hq~pocarnpus, whale a cannula was Implanted into the lateral cerebral ventricle for drag mjectlon. Following one week recovery,
baseline behavmr and electrical actlvffy were recorded. Rats then
received an intraperltoneal drag or control ]njectmn as follows: 270
mg/kg MgS04, followed every 20 minutes with 27 mg/kg MgS04 for
two hours. Control rats received an equal volume of salme. At two
hours, 20 ~g/#l NMDA was rejected mto the cerebral ventricle
through the mdwelhng cannula. Seizure act~wty was assessed for a
total of 20 minutes following NMDA mject]on.
RESULTS: Onset to the first seizure was s~gmficantly lengthened m vats receivmg MgS04 (p < .01). Total seizure duration and total seizure
munber were significantly reduced m the MgS04 treated rats (p < .05).
Mortality was 30% in the control group, whereas none of the rats that
received MgS04 died.
CONCLUSIONS: Magnesium sulfate reduces seizure achwty reduced by centrally administered NMDA. These results suggest that magnesmm’s anhconvulsant effects m eclanapsla may be mediated
through central NMDA receptors.
485 AGGRESSIVE VERSUS ILKPECTANT MANAGEMENT OF SEVERE PREECLAMPSIA AT 28-32 WEEKS’ GESTATION: A RANDOMIZED CONTROLLED TRIAL. 13,IM. S*bai, B M Mercer, E Schiff,
S A. Friedman x Dept of OB/GYN, University of Tennessee, Men~*~h*s OBJECTIVE: To determine whether aggresstve management (AM) or expectant management (EM) of severe prceclampsta at < 32 weeks ~s more beneficial to maternal and neonatal outcome STUDY DESIGN: Inclusion criteria were severe preeclampsta, s~ngleton pregnancy, and 28-32 weeks’ gestatlonal age. Patients with platelet count <100xl03/mm3, esumated fetal weight < 5th %de, or fetal dxstress were excluded Ninety-five eligible panents were randomly assigned to e*ther AM (n= 46) or EM (n= 49) AM patmnts were prepared for dehvery, either by cesarean or mductmn, 48 hours after glucocorncmds. EM patients were managed w*th bcdrest, oral annhypertens~ves as needed to keep DBP between 90 and 100 mmHg, serial laboratory testing, and ~ntensive antenatal fetal tesung In&cauons for debvery were fetal distress, thrombocytopema, uncontrolled severe hypertension, and attammem of 34 weeks’ gestation RESULTS: There were no dsffcrences between the two groups at rime of random*zauon m mean systohc BP (170+97vs 172+9.4 mm Hg), &astohc
BP ( 110 -+ 5 4 vs 112 + 4 2 mm Hg), protemuna (3 0 + 2.3 vs 3 6 + 2 3g/24 hr), and gestatmna/age (30 4 ± 1 6 vs 30 7 ± 1 5wks) for the AM and EM groups, respectively The percentage of patmnts randormzed at -< 30 weeks was also smular (47 vs 46) The average latency period m the EM group was 15 4 days (range 4 -36), and this pe~qod was not affected by the amount of protcinuria at tran~om*zation (16 days in those w*th < 5g/24 hr vs 14 days in those >- 5g) There was no eclampsia or permatal death m e~ther group Neonatal outcome is compared m the table The two groups had s*mdar incidences of abrupuo placentae (4 1 vs 4 3%) and HELLP syndrome (4 1 vs 2 1%)
AM (n = 46) EM (n = 49) P value
Gestational age at dehvery (wk) 30 8± 1 7 32 9+ 15 < 0 0001
lhrth weight (g) 1233±287 1622±360 0.0004
< 10th %de (~Yo) 10 9 30 l 0 04
Admitted to newborn center (%) 100 76 0 002 Days m newborn center 36 6± 17 4 20 2± 14 0 < 0.0001
Resp*ratory distress syndrome (%) 50 0 22 4 0 002
CONCLUSIONS: Expectant management w*th dose momtormg of mother and fetus at a perinatal referral center reduces neonatal comphcations, as well as neonatal stay In the newborn center (intensive + mtermed*ate care)
484 PLASMA TYPE II PHOSPHOLIPASE A2 LEVELS ARE ELEVATED IN ~jEVERE PREECLAMPSIA KH Ltm G Ricex, RN Taylorx. Dept. Ob/Gyn and Reproductive S_~ien_ces, Univ. of Cahfomta San Francisco, San Francisco, CA and The Royal Women’s Hospii~l, Carlton, Victoria, Australm. OBJECTIVE: To compare plasma concentrations of type II phosphohpase A2 (PLA2) m normal and preeclamptic pregnanmes. STUDY DESIGN: Type II PLA.2 is an ubiqmtous intracellular enzyme that hydrolyzes arachidomc acid from sn-2-ester bonds of membrane phosphohp~ds and plays a major role m the regulaUon of intracellular arachldomc acid concentrataons. Because preeclamps~a (PE) ~s characterized by thffuse endothelial cell injury and d~sturbed prostacyclin and thromboxane metabolism, we measured theplasma levels of type II PLA2 m 10 normalpregnant and 10 preeclamptm patients. The samples were obtained from volunteers between 34-40 weeks of gestation and were stored at - 80°C. The patients w~th PE were defined usmg strict criteria and the control group was matched for gestational age and parity. Plasma levels of type II PLA2 were measured by EIA. All samples were taken prior to me onset of labor. RESULTS: The mean plasma type II PLA2 level in control group was 5.3+2.2 ng/ml (n=10). This was not different from the mean value of 5.0~-1.8 ng/ml (n=6) in patients with mild preeclamps~a. However, the mean plasma level of 18.9 + 6.8 ng/ml (n=4) in patients with severe preeclampsia was significantly higher when compared to the above two groups (P<0.001, ANOVA with Scheffe’s post hoc tests). CONCLUSIONS: Increased plasma concentrations of type II phosph01ipase A2 have been associated with vascular compromise, ~nflammation and ~ncreased eicosanoid synthesis. These data suggest that ~n severe preeclampsia, the plasma concentrations of type II PLA2 is elevated, possibly reflecting diffuse endothehal cell damage andperturbed eicosanold metabohsm that have been associated w~th thxs disease.
486 FETAL PLASMA CELLULAR FIBRONECTIN LEVELS IN PREECLAMPSIA. S.A. Friedman,~ E. Schiff, J.J. Emeis,~ G.A. Dekker,~ B.M. Siba~. Department of Obstetrics and Gynecology, University of Tennessee, Memphis; Gaubms Laboratory IVVO-TNO, Leiden; and Free University Hospital, Amsterdam. OBJECTIVE: To determine whether plasma cellular fibronectin (cFN) conccntrations, which are elevated in preedampnc women, are similarly elevated iu their fetuses m comparison to those of normal controls. STUDY DESIGN: Prospective cohort study of 15 preeclamptic women and 15 normal women who delivered at the University of Tennessee, Memphis. Patients with preeclampsia had late-onset hypcrtcosion, protemuria, and hyperuncemia; normal patmnts had none of these features. Fetal blood was collected from chorionic plate artcrics and veins immediately after delivery. Maternal venous blood was collected just prior to dehvery. Blood was immediately fractionated and stored at -70°C. cFN was assayed using a sensitive and specific enzyme immunoassay (monoclonal anti-cFN antibody from S~gma, St. Louis). Results are expressed as mean _+ SEM. RESULTS: Plasma cFN levels ([ag/ml) are presented in the table below:
Preeclampsla Control P value
lYtal arterial cFN 4.7+0.6 2.8+0 3 0.007 Fetal venous cFN 4.6+0.5 2.8+0.4 0.01 Maternal venous cFN 13.3+3.1 4.6+ 1.1 0.01
Plasma cFN concentranons In the fetal arteries correlated slgmficantly w~th those in both the fetal vein (r- 0.83, p = 0.0001) and the maternal Venl (r= 0.77, p=0.0001). CONCLUSIONS: Plasma cFN coocentrations are higher ~n fetuses of
preedam )tic women than in fetuses of normal women, sug~estlng that the factor(s) responslb e for maternal endothelial involvement io prccclampsla IS operative In the fetal c~rculanon as well. Simple Irons ~laccntal passage of cFN is unlikely to explain this phenomenon due to ItS high mo ecular weight (450 kDa for the circulating heterodlmer).

410 SPO Abstracts January 1904
Am J Obstet Gynecol
487 POSTPARTUM CORTICOSTEROIDS: ACCELERATED RECOVERY
FROM ilELLP SYNDROME, E F Magaan, K.G Perry, Jr , J.E. Poistx,
R.L. Harris~, P F. Normanx, J N. Martin, Jr Dept Ob/Gyn, Univ of
Mississippi Medical Center, Jackson, MS.
OBJECTIVE: Because most morbidity and mortality associated with HELLP
syndrome is a postpartum phenomenon, we undertook this investigation to
evaluate the use ofcorticosteroids to minimize maternal morbidity and accelerate
postpartum recovery in patients with this form of severe preeclampsia
STUDY DESIGN: Into this prospective, randomized study were recrmted 40
parturtents with HELLP syndrome. HELLP syndrome was defined by the
presence of clinical and symptoms consistent with a diagnosis of severe
p r eeclamp sta/eclampsia in addition to laboratory evidence of hemolysis, hepatic
dysfunction, and thrombocytopenia Immediately postpartum, 20 of the
partunents were treated with dexamethasone 12 mg IV every 12 hours for 2
doses followed by 5 mg of dexamethasone every 12 hours for 2 doses Patients
assigned to the control group received no cortlcosterolds All study subjects
were mtensavely momtored via mean arterml pressure (MAP) and urinary output
every 2 hours, hematocru and platelei count every 6 hours, and LDH,
SGOT/AST, SGPT/ALT every 12 hours for the first 48 hours postpartum
RESULTS: The steroid-treated group had signlfieant changes over time versus
the no steroid group The MAP became significantly decreased at 22 hours (p
< 0.03), the urinary output increased significantly by 16 hours (p < 0.02), the
platelet count had increased sigmficantly by 24 hours (p < 0.05), and both the
LDH and SGOT/AST-SGPT/ALT had decreased significantly by 36 hours (p <
0 04 and p < 0 05), respectively
CONCLUSIONS: HELLP syndrome parturlents recovered more rapidly from
their disease process as measured by ur mary output, MAP, platelet count, LDH,
and SGOT/AST In this disease process which has significant morbidity and
mortalny, corncosterold therapy s~gnlficantly hastens recovery and lessens the
severity of the d~sease process Utdlzatton of this therapeunc approach could
result in shorter stays in recovery/mtanswe-care areas and overall hospitalization
with reduced medical care costs
489 ANTEPARTUM CORTICOSTEROIDS: DISEASE STABILIZATION IN PATIENTS WITH HELLP SYNDROME.
E.F. Magann, D. Bassx, S.P. Chauhan, D.L. Sullivan, R.W. Martin,
J. N. Martin, Jr. Dept. Ob/Gyn, Univ. of Mississippi Medical Center,
Jackson, MS. OBJECTIVE: To evaluate the impact of the antepartum administration
of corticosteroids on the course of HELLP syndrome in pregnancies 24-
37 weeks’ gestation. STUDY DESIGN: This prospective, randomized study was undertaken
m 25 antepartum patients with HELLP syndrome defined by the presence of clinical signs and symptoms consistent with a diagnosis of
severe preeclamps~a/eclamps~a in addition to laboratory evidence of
hemolysis, hepatic dysfunction, and thrombocytopenia. Twelve gravidas were randomized to receive dexamethasone 10 mg 1V every 12 hours
and 13 women d~d not receive any corticosteroids. Management and
dehvery decisions for all patients were based on a common protocol
w~th delivery undertaken for a deteriorating maternal or fetal condlt~on. RESULTS: Maternal urinary output was significantly greater in the
stere*d-treated group when compared to the no steroid group (p = 0.0006). In the corticosteroid-treated group, the maternal platelet count
rose s~gnifieantly (p = 0.006), the LDH s~gmficantly decreased (p = 0:03) and the SGPT/ALT significantly decreased (p = 0.005) when
compared to the 13 women who did not receive cortlcosterolds.
CONCLUSIONS: Stablhzation and s*gnificant improvement in HELLP syndrome occurred in women receiving antenatal cortlcosteroids as
measured by urinary output, maternal platelet count, SGPT/ALT, and
LDH. Antenatal steroids play a role in maternal stabilization and acceleration of fetal lung maturity m pregnancies < 34 weeks and
temporarily stabilize and improve pregnancies > 34 weeks complicated
by antepartum HELLP syndrome to permit pat*ent transfer to a tertiary care facihty and improve the maternal condition at the time of delivery.
488 PLASMA EXCIIANGE FOR PREECLAMPSIA II: UNSUCCESSFUL
ANTEPARTUM UTILIZATION FOR SEVERE PREECLAMPSIA WITH
OR WITIIOUT HELLP SYNDROME. J.N Martin, Jr , J.C. Fdesx, P.F
Normanx, P G BlakeX, J C. Morrlson, W.L Wiserx. Depts. Ob/Gyn and
Anesthesia, Univ. of Mississipp~ Medical Center, Jackson, MS
OBJECTIVE: To explore the efficacy of plasmapheres~s/plasma exchange as
single primary therapy to arrest and reverse precclampsln progression with or
without HELLP syndrome in order to improve permatal outcome m very
preterm pregnancies.
STUDY DESIGN: During a 4-year period, 7 gray,des w~th severe preterm
preeclampsm with or without HELLP syndrome underwent 1 2
plasmapherests/plasma exchange procedures using the IBM 2997 Cell Separator
with Intensive monitoring of laboratory parameters (n = 4 patients), central
cardiovascular monitoring (n = 3 patients), and continuous electronic fetal
monitoring (n = 7)
RESULTS: The 7 women (3 white, 4 black, 18-28 y/o, pare 0 = 5, pare 1,
2 = 2) presented between 24 and 31 weeks’ gestation Despite vascular
mampulat~on, the severity of each study subject’s preeclampsm faded to respond
(blood pressure, urlneoutput, proteinurm, edema, symptoms) and maternal-fetal
deterioration reqmred cesarean dehvery in all cases within < 48 (4 patients <
36) hours of therapy. No chn~cally s~gntficant adverse effect of plasma
exchange therapy was recorded during cardiovascular and laboratory monitoring,
two fetuses developed repetitive late decelerations during exchange despite fluid
preload of the mother One patient with HELLP syndrome developed eclnmpsia
as her third plasma exchange was being initmted; slgmfieant problems with fiu~d
retention and dtsplecemetu (variable araouat so pulmonary edema, pleural
effusions, asc~tes) were encountered in all patients after the exchange Four
neonates d~ed (24-27 weeks/438-820 gm) and 3 survived intact (740,950, 1280
gm). All patients recovered without long-term sequelae.
CONCLUSIONS: The apphcatlon ofplasmapheresls/plasma exchange therapy
to prolong very preterm pregnancy in the undehvered patient with severe
preeclampsia/eclampsia w~th or without HELLP syndrome Is discouraged
inasmuch as the patient ~s exposed to significant medical and surgical r~sk
w~thout a corresponding improvement in perinatal outcome
490 MATERNAL MORTALITY ASSOCIATED VglTH ItELLP SYNDROME.
E.F. Magann. K.G. Perry, Jr., R.W Naef, 1II, W E. Roberts, J.N. Martin, Jr.
Dept. Ob/Gyn, Univ. of Mississippi Medical Center, Jackson, MS
OBJECTIVE: Maternal mortality is a rare complication of HELLP syndrome.
We sought to learn if there are discernable common circumstances,
characteristics or clinical patterns unique to these deceased women that could
facilitate their identification as particularly h~gh-risk mothers
STUDY DESIGN: All SPO members were solicited by survey in July 1992 to
report any personal knowledge of a patient mortahty associated with HELLP
syndrome. Each case report was analyzed for pertinent demographic
information and chmeal information including presenting complaint, platalet
nadir, mode of delivery, and apparent cause(s) of death.
RESULTS: CompleXe reformation was available for 19 maternal mortalities
from 17 different institutions. Demographic charactar~stiea included age (mean
= 25 4 + 6 8 yrs), gravidlty (n = 15 GI, n = 2 G2 with previous preterm
infant and severe precclampsia, and n = 2 mult~gravidas without previous
hypertensive complications of pregnancy); race (black = 11, white = 6,
htspamc = 2); and mean gestat~onal age (30 2 + 4.7 wks, 63% < 30 wks).
The mean platelet nadir was 47,500 + 25,500 ttL (range 7000 - 98,000 #L; 10
patients < 50,000/#L and 9 patient never < 50,000/#L) The presenting
complaint was nausea/vomiting/right upper quadrant pare m 17 patients (89%)
and eclamptlc seizures in the other two (11%) All but one patieut were
delivered abdominally; the other patient died during preparations for emergent
cesarean dehvery. Death occurred 3.5 hours - 14 days after hospital admission.
Primary causes of death were ARDS (n = 6), DIC (n = 5), hypotansion with
cardiac arrest following cesarean delivery (n = 3), mtracerebral bleeding (n =
3), ARDS/pancreatitts (n = 3), and sepsis (n = 5). Mult~organ failure was
evident on autopsy m 4 of 19 (21%) losses. Medical/legal ectton was pending
in 8/13 patients (62%)
CONCLUSIONS: Most patients presented with a chief complaint of
nausea/vomiting/abdominal pain. Cesarean delivery did not avert ultimate
disease progression or death in th~s small patient series. Death occurred by a
variety of pathological processes usually including sepsis, shock, hemorrhage,
and/or card~opulmonary failure.

Volume 170, Number I, Part 2 SPO Abstracts 411 Am J Obstet Gynecol
491 ACCURACY OF AMBULATORY BLOOD PRESSURE
MONITORING DURING PREGNANCY USING DEVICES
DESIGNED FOR OBESE PATIENTS. W Schwartz IIIx, W Raybum, G Tumbullx, D Christensenx. Dept Obstet Gynecol, Umv
of Oklahoma, Health Sciences Center, Oklahoma City, OK
OBJECTIVE’ Blood pressure monitoring devices designed for
obese patients are now commercially available. The purpose ofth~s
study is to compare the relative accuracy of three such devices placed
at different anatomic sites on pregnant women with large arms.
STUDY DESIGN: Seventeen patients attending our prenatal clinic
were ehgible for pamc~pation as their gestational age was greater
than 20 weeks and their arm circumference was greater than 35 cm.
The three d~fferent nonmvaswe devices had cuffs which easily fit
around either the arm, wrist, or index finger. Recordings were
compared with those obtained simultaneously using a well calibrated
Dmamap 845A monitor Two readings using each device were taken
on each patient at least three minutes apart.
RESULTS: Systohc, diastohc, and mean arterial pressure readings
were not found to correlate between the Dinamap monitor and the device with the cuffaroond either the finger (r2 = .0~-, .10, .08), wrist (r2 = 14, 16, 18), and large arm (r2 = .77, .33, .64). The
percentages of recordings within 5 mm Hg for the systohc, diastohc,
and mean arterial pressures were low for the device with the cuff
around either the finger (7%, 32%, 32%), wrist (18%, 43%, 18%),
and amI (43%, 46%, 54%).
CONCLUSIONS: Despite their commercial appeal, none of these
blood pressure devices designed for obese patients was accurate for
use dunng pregnancy.
493 VOLUME LOADING, CENTRAL PRESSURES, AND THE RE- SPONSE TO NITROPRUSSIDE IN SEVERE PREECLAMPSLA. Wasserstrttm, DB Cotton Baylor College of Medacme, Houston TX OBJECTIVE: In severe preeclarnpsia (SPE), low doses of mtropru~_ide (NIP) - an agent ruth both ortenal and venous dilator actions - produce abrupt, steep reductions in~.meam arterial b!ond.pressure,(BP) ~ para- doxical falls m heart rate. Ires response, retatod to a caroaogemc aepres- sor IBezold-Jartsch] barorefl~ BJB,.R,, is rmtl.ga~.eq, by ucu.te vomm, e loading (VOL) prior to NIP mthsion ’llae cItrrenl stuay ex.,t~nas these oo- servatlonS and the hypothesis that the response to NiP (w~mont VOL) re- flects venodatatIon tm .pgsed on a cmatlation with low blood volume (BV). Specifically, we considered: 1) whether central venous pressaa’es (C~VP) correlate \vith the hypolgnsxve responses, and thereby appropriately renect BV, and 2) how VOL affected the balance of neurogemc cirenlatory con- trol between BJBR and smo-anrt~.c haroreflexes (SaSR). STUDY DESIGN Inlra-artenal and CVP hnes momtored the resp~_ ~os~/- to ~v NIP m 6 women w~th SPE, before and 30 mm after 1000 ml of 5~ alburmn m saline VOL. NIP was refused until BP other 1 ) was gradually reduced 10-20%, or 2) fell abruptly RESULTS Before VOL, relatavely small doses of NIP (0 53 +/- 42 ug/kg/mm) produced marked reductions in BP (A = -62 +1- 29 mm Hg). After VOL, even higher doses (I 69+/-066 ug/kg/mm;p< 02) prod,uced, milder reductions (ABP = -24 +/-15 mm Hg, p<.01 ) The magnitude oI hvpotenslve effect, both before and afk’r VOL, did not correlate w~th pre- ~fifusmn CVP or dose of NIP. The hypotensxve response after VOL was inversely related to pre.-mfus~on BP (r = 903, p<.01 ) In adthtxon, m tl~ 2 patients m whom It could be calculated, SaBR sensitivity rose after VOL CONCLUSIONS VOL moderated the hypotenslVe response to N~P, dersoanng the hcmodynarmc slgrfificance of th.e reduced BV and elev, aum venous tone m SPE l-bgher (normal) CVP dad not protect agmnst a, mrge, t~ll m BP. Tkese result~ cautaon against mterpretmg CVP as an maex BV, w~thont considenng the inercased v~eno..motor tone and reduced circu- latory capuc~ty m SPE The dn’ect correlation aflerVOL--between higher hasehne BP and increased senmtawty to a,qenov.e~.ens dilation w~th NIP- ~s analogotts to that prevmusly de,~-nbod (In subjects ,,~athont l~or vol- ume) between Ingher baselinq BP and.sensmvIty to ~ artona-I dqatlon x~th hydralazme The greater l~ypotensvve responses renect increase, sen- slt~,aty to the drugs (and decreased SaBR sensatmty), not Ingher doses. Hence, VOL shills cir~lato~y oantrol away from the depressor BJBR to- ward the SaBR, and appears to raise SaBR sens~lav~ty
492 MARINE FATTY ACIDS IN MATERNAL ERYTHROCYTES
AND RISK OF PREECLAMPSIA
MA Wflhamsx, RW Z~nghelmx, IB King~, AM Zebelman~, DE
HIckok. Swedish Medical Center, Seattle, WA. OBJECTIVE: To examine the hypothesized exposure-effect
relation between maternal dietary intake of marine n-3 fatty acids
(n-3 FA) and risk of preeelampsm (PET).
STUDY DESIGN: As a marker of dietary retake, we measured
FA m erythmcytes obtained (within 24 hours postpartum) from 22 women w~th PET (meehng ACOG criteria) and 40 controls.
Student’s t and Flsher’s exact tests were used to evaluate group
dlllerences Logistic regression procedures were used to estimate
odds ratios (OR) and 95% confidence intervals (CI).
RESULTS: Mean levels ot n-3 FA were mgmficantly lower among
women wah PET (6.6 _+ 0.98) as compared w~th controls (7,9 _+
I 6) (p=0,002). Women with PET had higher mean levels o[
ara~hidtmic acid (AA, n-6) compared w~th controls (p=0.006).
Women w~th the lowest levels u[ n-3 FA were 10.8 times more
hkely to have had their pregnancies comphcated by PET, compared
wah those women w~th the highest levels of n-3 FA (95% CI 2 3 -
50.1). The excess risk remained atter adlust~ng tot confounders.
.A 15% ~nclease in the ratm of n-3 FA to AA was associated with
a 46% rednctnm m risk of PET (OR=0.54, 95% Cl 0.41-0.72).
CONCLUSIONS: These data provide evidence of an association
between d~etary intake of marine n-3 FA and risk of PET.
494 SEVERE PREECLAMPSIA AND THE HELLP SYNDROME: GENETIC AND CLINICAL HETEROGENEITY T.S.Bloodx, J.L.B. Byrnex, L. Nelsonx, M. Varner, K. Ward. University of Utah School of Medicine, Salt Lake City, Utah. OBJECTIVE: To compare genetic and chnical features of severe preeclampsia and HELLP syndrome. STUDY DESIGN: Dehvery records were examined in 84 consecutive women with a confirmed chnical diagnosis of severe preeclampsta (PE). 38 of these also had the HELLP syndrome as defined by Sibai et al. (AJOG, 1986) Anglotensinogen (AGT) genotypes were determined in the 62 caucasian subjects using the polymerase chain reaction followed by allele-specific oligonucleotide hybridization. RESULTS: Patients with the HELLP syndrome were older, more likely to be parous, and presented at an earlier gestational age*; they had higher second trimester blood pressures* and were less likely to have large amounts of proteinuria* (*p<0,05). HELLP patients reported similar family histories with respect to preeclampsia, hypertension, and heart disease. Caucasian HELLP patients were less likely to show the predisposing AGT allele (T235) q=0.48 versus 0.68 for other severe PE subjects (2;~=6.14, p=0.01). CONCLUSIONS: Our chmcal observations are consistent with previous reports which suggest that HELLP syndrome is not a simple subset of severe PE. Although clinical features overlap, these data suggest that genetic risk factors and etiologies are likely to differ.

412 SPO Abstracts January 1994 Am J Obstet Gynecol
495 THE HEMODYNAMIC AND RESPIRATORY EFFECTS OF NIMODIP1NE IN PATIENTS WITH ECLAMPSIA.
J Anthony,X M Belf9~_,x R Johanson,~ G Saade,* K Molse, Jr, J
Dommlsse" Departments of Obstetrics and Gynecology, University of
Cape Town Medmal School, Cape Town, South Africa, and Baylor College
of Medicine, Houston, Texas
OBJECTIVE: To detemame the hemodynam~c and respiratory effects of
nlmodlplne, a cerebral-selective calcium channel antagonist, in patients
with eclampsm, using invaslve monitoring with a pulmonary artery
catheter
STUDY DESIGN: SIx patients received either intravenous (n - 4, 2mg/hr)
or subhngual (n - 2, 30 mgl ntmod~pme after seizure control The acute
hemodyoamlc and respiratory responses were recorded once the blood
pressure had stabdized Analysis Walk-Shapiro test for normalcy, paired
Student t test for wlthlo group comparisons RESULTS: Post
Parameter __ Baseline Nimodlnine p _95% Cl
IlR (bpm) 104 (17) 121 (22) 0 08 -38 to 4
MAP(rural lg) 140 (20) 117 (131 0.01 14 to 32
CVP (mmHg) 7 (5) 3 (2) 0 06 -0 45 to 9 3
PCWP (mmHg) 13 (4) 13 (4) 0 9 -8 to 7
CI(l/mm/m2) 38(08) 46(14) 006 -16to0,07
SVR1 (d,m~ s/cm 2) 3016 (863) 2199 (653) 0.03 114 to 1519
LVSWl (g/nun/m21 73 (161 55 (13) 0.03 2 to 32
DO21 (ml/mln/m2) 621 (180) 819 (352) 0 07 -427 to 31
VOzI (ml/m~n/m2} 13 l (29) 137 (32) 0 7 -51 to 30
CONCLUSIONS: These data suggest that mmodlplne is an effective
ant>hypertensive agent with a vasodilator effect that reduces the left
ventrlcular stroke work mdex (LVSWI) and tends to increase carthac index
and oxygen delivery There does not appear to be any detrimental effect on
oxygen consumption This drug may be useful in the penpartum
management of patients with severe preeclampsla!eclampsla
497 THE INCIDENCE OF PREGNANCY-INDUCED HYPERTENSION
IN HIV POSITIVE PATIENTS. G Sonde,* W Kramer,* M Belfort,* F
Ocon,* K Mmse, Jr, H Hammd,* Department of Ob/Gyn, Baylor College
of Medlcme, Houston, TX
OBJECTIVE: To in’vest,gate the mmdence of pregnancy-induced
hypertension (PIH) m patients known to be HIV positive
STUDY DESIGN: Data from the dehvery records of 94 H1V positive
paUents were compared to that obtamed from a computerized database
which included the records of 3481 patients dehvered at an tuner c~ty
hospital ItlV status was confirmed by positive western blot analysis
Parameters analyzed Included maternal age, gruvlddy, parity, race,
gestatmnal age at dehvery (GA) and number of fetuses Statrstical methods
used ~ncluded ,Z2 , Flsher’s Exact, contingency table random~zahon and
Mann-Whitney tests as approprmte Mulhple logistic regression was used to
evaluate the effect of HIV carrier status on the rlsk of developing PIH after
contrnlhng for other ~ndependent varmbles P < 0 05 was used to denote
statistical significance
RESULTS: None of the H1V posltwe patients developed PIH while 166
patmnts m the comparison group were d~agnosed with PIH (P = 0 02)
There was no statlstlcally slgmficant difference in maternal age, grawd~ty,
parity or number of fetuses between the two groups The HIV positive
group however had a larger proportion of Black patients (69 vs 509) and a
lower proportion of Hlspamc patmnts (10 vs 2709) as compared to the
comparison group The GA was lower m the HIV posmve group
(median[range] 39[29 - 421 vs 39.6[25 - 43], P < 0 01) Multiple log~stm
regression analysis revealed a slgmf~.cant relanonship between the patlel-~t’s
HIV status and their risk of developing PIH, even after controlling for the
other independent varmbles
CONCLUSION: The mcldence of PIH in patients with positive HIV status
~s slgmficantly lower as compared to that of the general population This
fin&ng lends support to the important role of the immune system m the
pathogenesls of pregnancy-reduced hypertension
496 NIMODIPINE AS AN ALTERNATIVE TO MAGNESIUM SULFATE
IN THE MANAGEMENT OF SEVERE PREECLAMPSIA:
MATERNAL AND FETAL EFFECTS. M_Belf0rt,~ G Saade,~ A
Cruz,~ K Adam, B Klrshon, W Krarner,~ K Mmse, Jr Dept Ob/Gyn,
Baylor College of Medlcme, Houston, Texas
~,)BJECTIVE: Preeclampsm may be associated w~th cerebral vasospasm
and ischemla Nlmodlp~ne, a dthydropyrldme calcmm antagomst, is an
effective cerebral vasoddator in non-pregnant patients with cerebral
WlSospasm and ~s also a good antlhypertenslve agent Our ob, lectlve was to
assess the maternal and fetal effects of orally adm~mstered mmodlpme on
selected maternal and fetal parameters m patients with severe preeclampsla
STUDY DESIGN: Ten consecutive patients were given 30 mg mmothplne
orally ever3’ 4 hours from the time of admission until 48 hours postpartum
Maternal and fetal cerebral blood velocW, umbthcal artery (UA) blood
velocity, fetal heart rate varlabd~ty, maternal blood pressure (BP), heart rate,
urine output, and transplacental passage of the drug were studied Data
analysls Paired Student’s t-Test Significance p < 0 05
RESULTS: N~modlpme acutely and significantly reduced the pulsatthty
index in the smaller diameter maternal cerebral arteries (ophthalmic
[I 4+_0 4 to I 12+_0 3, p<0 02] and central retmal [1 09_+0 1 to 0 79+_0 19,
p<0 0001]) and In the fetal m~ddle cerebral artery (l 43_+0 5 to 1,2+0 4, p<
0 011 There was a slgmficant reduction ~n the UA Sfl) ratio (2 67_+1 14 to
2 52_+1 08, p < 0 01) Maternal BP was controlled without the need for other
anhhypertenslve methcatlon (systohc, 166-+15 to 142+15, thastohc, 102_+9
to 81+8, p<0 005) N~modxp~ne, whmh reached significant maternal and
fetal levels within 2 hoers, was easily admlmstered and well tolerated by
both mother and fetus The maternal serum cord serum ratm was 2 4 : 1 at
dehvery There were no side effects apart from emesls in one patient
CONCLUSIONS: These data suggest that nlmo&pme is rap~dl~ absorbed
after oral administration and has slgmficant maternal and fetal cerebral
vasodllator activity It is an effective antlhypertens~ve drug tbr severe
preeclampsla and may be a safe alternative to parenteral magnesium sulfate
in the perlpartum management of patients with this disease
498 ALTERED SERUM TISSUE FACTOR PATHWAY INHIBITOR LEVELS IN THE HELLP SYNDROME.
D Lasser G Brozex Dept ofOb/Gyn, ColutnNa Umv, New York, NY and Dlv of Hem/One, Washington Umv Med Ctr, St Lows, Me OB3ECTIVE: To detect quantitative or qtmhtahve alterations of tissue factor pathway mhIb~tor (TFPI), an endogenous hpoproteIn-associated coagulation mtubitor, in pahents with the HELLP syndrome STUDY DESIGN: We studmd functxonal TFPI serum levels and protein structure m women with the HELLP syndrome arid gestattonal-age
matched normal pregnant woraen Blood specimens were collected in so&um-cltrate tubes at the hme of admission before inrtlatmn of therapy Serum levels of functmnal TFPI were measured by fm~ctlonal chromogemc substrate assay Standard curves ~vere constructed using pooled normal non-pregnant sera Western blots were performed to detect alteratmns in protein structure RESULTS:
SERUM TFPI FUNCTIONAL LEVELS VERSUS STANDARD HELLP MATCHED GESTATIONAL
SYNDROME PREGNANT AGE CONTROL
44% 234% 36 weeks 30% 141% 25 weeks
72% 232% 33 weeks 64% 179% 31 weeks
Anh-TFPI anhbodms recogmzed polypeptldes of mdistingmshable moleculur weight and conformation on Western blots of sermn samples from the study and control groups CONCLUSION: Functional levels of tissue factor pathway mhlbitor are reduced in patients w~th the HELLP syndrome at the hme of dmgnesis There is no detectable alteratmn ~n the stntcture of the prote~n itself Further studies are needed to investigate whether this reduction is an early or late event m the coagnlopathic state of the HELLP syndrome
Volume 170, Number 1, Part 2 SPO Abstracts 413 Am J Obstet Gynecol
499 INCREASED FRACTIONAL EXCRETION OF LYSOSOMAL
HYDROLASES IN PREECLAMPSIA. A. Sc~sc~one,x D. Jackson,* K.
Blakemore, R. Glew x Dept. Ob/Gyn, Johns Hopkins Un~v , Baltimore,
MD, Dept. Blochem, Unlv. of New Mexico Sch Mad, Albuquerque.
OBJECTIVE: In preeclampsla, both renal glomaru~ar and tubular
pathology hav~ been described. Lysosomal hydrotases are present
in the proximal renal tubular eplthehum, injury thereof causes re,ease
of these enzymes. The hypothes~s ~s that excretion of Iysosomal
enzymes ~s a marker of proximal tubule ~nNry in preeclampsla.
STUDY DESIGN: The study group consisted of 14 women with
preeciampsla (10 severe and 4 todd as per ACOG cntena) and 29
normotenstva controls with singleton pregnancies at 27 to 41 weeks.
Maternal serum and unne specimens were prospectively obtained and
analyzed for/?-glucuromdase (#-gluc),/~-hexosamnmdase (~-hex), o-
galactosldase (o-galL ,8-gel, and o-mannos~dase {o-man) using
fluorometry Mean serum and urine act=vltms and fractional enzyme
excretions (FEE) of each of the five hydrolases were compared
between the two study groups using students t-test
RESULTS: There were no significant differences between the two
groups for gestat~ona~ age, msterna~ age, or race. The serum enzyme
act~wty of ~=hex (p =0.002), o-gel (p<O 001), and o-man (p = 0.02)
was slgnlhcantly lower in preec~amptlc patients vs controls. Urine
enzyme activity of ~-gal (p=O.O01), o-gel (p=O.O02), ~-gal
(p<O.O01), and o-man (p=O.O03) was Ngher =n preeclamptm
patients. The FEE of all 5 lysosomal hydrolases was Ngher m
preeclamptlc patients vs controls (p<O.O01 for each enzyme).
CONCLUSIONS: Preeclampsla is associated with a s=gndlcant
decrease in serum activity in 3 of 5 hydrolases studied, a Slgmflcant
increase in urine enzyme activities in 4 of 5 hydrolases, end s
mgn=hcant increase m the FEE of all 5 lysosomal hydrolases. The
alterations In lysosomal hydrolase activities in the preeclamptm
patient most likely reflect proximal renal tubule damage consistent
with the proposed protein-renal tubule damage etiology. FEE of
lysosomal hydrotases ho~ds promise as a marker for preec~amps~a.
501 PERINATAL CflI~:~LICATIOIIS ASSOCIATED WITH VAGINAL GR,O,~
TB
STREPT~L ~I~TI~. ~, P. DUff, P. Clark , .
Kurtzerx, B. Frentzenx, P. ~ubftfs . Oe~rt~nts of ~/Gyn a~
Biostatist~cs, University of Florida, Gai~svit[e, FL 32610-0294 ~JECTI~: To determine the fr~uency of intra~rt~ a~ ~st- ~rt~ infection in ~rturients with group B streptococcal (GgS) genital coton~zati~ c~r~ to ~o[~iz~ w~n. ST~f DES~: ~e pros~ctivety screen~823 w~n with intra~rt~ vaginal cuLtures using selective broth~ia. Culture results were not utitiz~ in clinical ~nag~t ~isi~s. Vagi~[ GBS colonization a~ other risk factors for ~ri~rtat ~te#nat ~nfections ~ere assess~using un~variate a~ttivariate logistic ~eling. ~E~tIS: 216 of 823 ~n (26X) ~ere ~sitive for 68S. Chorio- a~ionitis or e~tritis occurr~ in 45 of 216 coIoniz~ ~n (21X) a~ 72 of 607 noncot~iz~ ~rturients (12X, p <.01). Ihrough univariate logistic ~etin£, ~e f~ a significant associati~ ~t~een ~ri~rtat ~ter~t infectors a~ cesarean delivery (~s ratio [ORI 6.6, 95~ eonfide~e qnter~at loll 4.3- 10.1), mternat ~nitor ptac~nt for ~re than 12 hours (OR 5.8, 95X Cl 3.4-10.1), rupture of ~ranes for ~re than 6 hours 5.5, 95X Cl 3.4-8.9), ~re than 6 ~a£inat ex~inatioma (OR 3.5, Cl 2.3-5.4), ta~r for ~re than 12 hours (OR 3.0, 95~ Cl pr~ture rupture of ~ranes ton 2.3, 95X Cl 1.~-3.6), a~ va£inat 68S colonization (~ 2.0, 95~ C[ ~.3-2.91. A subset of these univariate risk factors (cesarean delivery, vaginal exa~ >6, rupture of ~ranes ~6 hours, a~ 6BS cot~ization) r~in~ as significant prognostic variables ~hen art risk factors ~ere qomaider~ si~tta~ousty through ~ttivariate togistlc ~etin~. Consideration of chori~ionitis a~ e~tritis as serrate outc~ variables c~flr~ the ~ssoeiati~ ~t~een 6Be eotoni- zati~ a~ chorioa~ionitis (0~ 2.4, 9SX Cl 1.5-3.9); he,ever, carriage~asnot signifieanttyass~iat~ith e~tritis. There ~as a step, lee i~rease in the risk for chorioa~ionitis ~ith tight (OR 1.9, 95X Cl 1.0-3.7), ~erate (OR 2.6, 95X Cl 1.3-5.2), a~ hea~ (OR 3.2, 95X Cl 1.5-6.6) 6BS colonization as determin~ by s~iquantitati~e cultures. ~C1~I~: Intra~rt~a~ina[ co[~ization ~it# ~ro~8 stre#to- coccus is associat~ ~ith an increas~ risk for chorioa~ionitis, a~ this risk r~ins significant ~hen other risk factors are consider~ si~ktaneousty.
50O IN UTERO INFECTIOtl WITH TREPONENA PALLIDLII4 IN EARLY PREGIJANCy.
L. Nathaq, VR Bohman, pd Sanchez*, NK Lace*, GO Warm,el. Dept of
Ob/Gyn, U. Texas Southwestern Mad Ctr, Dallas, Tx.
(~JECTIV~: The early transplacental passage of Treponema
Pattid~ has been hypothesized by identification of spirochetes
by silver staining in aDortuses at nine arK~ ten weeks,
gestation. We hypothesized that transp[acental infection can
occur in continuing pregnancies. The purpose of this study was
to determine if amniotic fluid infection with I. Pa[lidt~occurs
in early pregnancy. STUOy DESI~: [nformed consent was obtained and ammocentesls
was performed under sonograp~ic guidance in gravldas (<20 weeks
EGA) wzth primary, secondary and latent syphilis. Five to ten
mL of arnniotic fluzd from each patient was used for rabbit
infectivity testing (RIT), intratesticu/ar inoculation of
rabbits, ar~t polymerase chain reactlon (PER) to diagnose
ammotic fluid infection with T. PallidLY.
RESULTS: Ten patients were included in the study. The mean age
of the participants was 21 years old (range, 15-30) and mean
gestatlonal age was 16.5 weeks (range, 14-19). F~ve women had
secondary syphilis, and fLve had latent syphilis. All fetal
ultrasounds were normal, RIT was positive in four cases (40%),
while PCR was positive in two patients (20%). Overall, f.
Pattidt~ in armzot~c f[md specimens was identified from four
participants (40%). All grawdas were treated with benzathlne
penicillin G, 2.4 million umts intramuscularly, and all the neonates were free of slgns and symptoms of congenital syphltls. CONCLUSION: T. Patlid~ can be identified in amnlotlc fluld frcm almost one in two gravidas with syphllis before 20 weeks’ gestat;on. These flndlngs confirm in utero infection wlth I. Palli~ in continuing early pregnancy, and indlcate that In utero trepone~nal infectlon Is eradicated by maternal treatment.
502 STILLBIRTH SECONDARY TO SYPHILIS: A REGIONAL
EPIDEMIC IN SOUTHWEST LOUISIANA. M. St. Amant. R Geex Loms~ana State Umversity, University Me&cal Center (UMC), Lafayette, LA OBJECTIVE: The objective of this study was to determine the incidence of stillbirth secondary to syphihs m our rural, md~gent care hospital ~n Southwest Lomsiana STUDY DESIGN: This descriptive study was done utdizmg a retrospective review of the labor and delivery logbook, the pathology laboratory autopsy log book, and the maternal c~harts The records of a)l stdlNrths occurring between July 1, 1992 and June 30, 1993 were located and analyzed The et~ology of stillbirth secondary to syph~hs was assigned if the mother was VDRL +, FTA-ABS +, and fetal hydrops and a large, pale placenta were noted RESULTS: Thirty four stillbirths were identified for the study
~eriod Etiology of stillbirth was assigned as follows: Unknown 3(38%), syphlIis 7(21%), chorioamnionitis 4(12%), cord accident
3(9%), placental abruption 2(6%), congenital anomaly 2(6%), hypertension 2 (6%), twin-twin transfusion 1(3%). Six of the 7
~hihs patients (86%) had noprenatal care NCLUSION: An mcreasedprevalence of both maternal syphd~s
and congenital syphilis has been noted in the United States in the last five years We believe ours to be the first report of a s~gmficant increase m stillbirth directly attributable to maternal Treponema palhdum infectaon It ~s even more impressive as it has occurred m a rural setting, not an inner city setting as is usually the case Despite the high incidence of no prenatal care in the syphilis group, we have instituted VDRL screening m each trimester in an effort to identify possible crossover patients We hypothesize that this effort will ~dentffy pregnancies at risk, and allow appropriate treatment

414 SPO Abstracts January 1994 Am J Obstet Gynecol
503 THE SEROPREVALENCE OF THE RUBEOLA ANTIBODY IN A PRENATAL SCREENING PROGRAM.
AG Neubert1X’ NC Rose1, A Copozello2X, I Forouzan1, P Samuals3.
I U of Pa. Medical Center, Phila, pA;2Reading Hospital, Reading,
PA; 3 Ohio State University, Columbus, OH.
OBJECTIVE: Rubeola (measles) is the most common of the communicable childhood exanthems. The manifestations during
pregnancy may affect both mother and fetus, resulting in preterm
labor, fetal death, as well as maternal pneumomtls and encephalitis.
Recent outbreaks of rubeola suggest that a significant number of
reproductive age women are lacking immunity. In an attempt to def’me
an "at risk" group which may benefit from screening and post parmm vaccination, we report the seroprevalence of the rubeola antibody in a
varied obstetrical population.
STUDY DESIGN: During 1992, 339 consecutive patients were screened for the presence of IgG antibody to the rubeola virus by
quantitauve ELISA assay. Of these, 169 presented for care to a prenatal chnic consisting of mostly low income patients (Group I).
In addition, 230 patients were screened from a clinic consisting of mid
to upper income patients (Group 1I). Chi-square analysis was used to compare the results.
RESULTS: In Group I, 21.3% (36/169) lacked the IgG antibody to
rubeola In the socioeconomically more privileged Group II, 8.3%
(19/230) lacked IgG antibody (p<0.001).
CONCLUSION: This study suggests that a significant proportion
of obstetrical patients maybe at risk for rubeola infection during gestation Based on this prehminary report, a more extensive
population screemng program may be mdicated to determine whether
routine screening and postpartum vaccination may reduce the
incidence of rubeola and its sequelae.
5O5 MATERNAL SERUM HIV-1 p24 ANTIGEN AS A MARKER
FOR TRANSMISSION OF H1V-1 FROM MOTHER TO
CHILD. RR Vlscarello. NJ DeGennarox, SM Grlfflthx. Divs of Mat.
Fet Med., Depts. of Ob/Gyn, New York Med. Coil, ~/ahalla, NY,
Stamford Hosp, Stamford, CT, Yale Umv Sch Med, New Haven, CT.
OBJECTIVE: We undertook th~s study to estimate the prevalence of
HIV-I p24 antigen in maternal serum throughout pregnancy and to
evaluate the prognostic significance of HIV-I p24 antigen m maternal
serum as a marker for transmission of HIV-I from mother to child.
STUDY DESIGN: 64 HIV-lnfected, pregnant women were followed
prospectively during pregnancy and their 69 children (including 5 sets
of twins) for a mean of 37.7 -+ 18 6 months postpartum Demographic,
medical, obstetrical, and HlV-outcome data were collected Maternal
serum samples were collected, centrifuged, frozen, and subsequently
analyzed for H1V-I p24 antigen using ELISA techniques
RESULTS: Racial breakdown included 14% Caucasian, 19%
Htspamc, and 67% Black. HIV-I risk factors included 52% IVDA, 46%
heterosexual, and 2% trarlsfuslon-related. Maternal HIV-status included 66% CDC Gr If, 26% Gr llI, and 8% Gr IV. 48% of pts received
antepartum Zldovudlne therapy. HIV-I p24 antigen was detected m serum samples from 2/11 pts during the 1st trimester, 4135 during the
2nd, 2136 during the 3rd, 6/41 at L & D, and 1/20 during the postpartum period The mean gestatlonal age at delivery was 38 + 2 6 weeks and
the mean weight was 2827 +_ 575 grams. Infant HIV-status included 60
infants who seroreverted and 9 who were infected with HIV-1 (5 CDC P2
and 4 CDC P1). The presence of HIV p24 antigen in the maternal serum was s~gmficantly associated with the development of H1V-I infection
in the infant (Flsher’s exact test; p<0 001). CONCLUSION: Our data suggests that the presence of HIV-1 p24
antigen in the maternal serum may identify a subset of women who are
at increased-risk for the dehvery of an HlV-infected child Our
findings, if confirmed by larger studies, would have considerable
implication for prenatal counseling of the HIV-lnfected woman. (This
research was partially supported by the American Foundation for AIDS
Research and the Pediatric AIDS Foundation, AmFAR/PAF #50034-7)
504 SONOGRAPHIC ASSESSMENT OF FETAL GROWTH AND DEVELOPMENT IN HIV-1 SEROPOSITIVE PREGNANT
WOMEN. RR Vlscarello, TE D~Nolfox, NJ DeGgnnarox, M Vecchlox,
C DeFd~ppex, D~vs of Mat Fet Med, Depts of Ob/Gyn, New York
Med. Coil, Valhalla, NY, Stamford Hosp., Stamford, CT, and Yale
Umv Sch of Med., New Haven, CT OBJECTIVE: To Investigate the effect of HIV-1 mfectmn on fetaI
growth and development and to determine the utility of ultrasound in
the prenatal detectmn of fetuses who are HIV-mfected versus those who ultimately serorevert
STUDY DESIGN: From December 1985 to January 1993, 270 interval ultrasound examinations were performed m 125 HIV-1
seroposltlve pregnancies. All patients were followed prospectively
and infant HIV-1 disease status was assigned according to 1987 CDC classification criteria at 18 months of age. Scans were reviewed for
fetal blometry (BPD, OFD, HC, TCD, OOD, humerus, uIna, femur, t~bla,
AC, EFW), fetal anatomy, placental grade and location, and ammotlc
fluid volume. Data from HIV-I-transmlttmg (n= 31) and non- transmitting pregnancies (n= 94) were compared using Student’s T, and
Ch~-square tests of analysis where appropriate
RESULTS: Transmlthng mothers and non-transmitting mothers were similar with respect to age, gravldrty, parity, race, HIV-I risk
behavior, alcohol, drug, and tobacco use, maternal CDC disease stage,
mean CD4+ cell count, mode of delivery, blrthweight, and gestatlonal
age at dehvery There were no significant differences between
sonographlc measurements from HIV-14nfected versus seroreverted
infants, including analysis of serial growth
CONCLUSIONS: We conclude that there is no difference in fetal growth as detected by high resolution sonography in pregnancies
which ultimately result in H1V-I infected children as compared to those
which serorevert Ultrasound, therefore, is not a useful tool in the prenatal d~agnos~s of HIV-I refection (This research was partially
supported by the American Foundation for AIDS Research and the
Pediatric AIDS Foundation, AmFAR/PAF #50034-7)
506 IS THE RATE OF PERINATAL TRANSMISSION OF HIV-1
INCREASED BY AMNIOCENTESIS.
!IR V~scarello. MT Cullen, NJ DeGennarox, SM Grlffithx. Dlvs of
Mat Fet Med, Depts. of Ob/Gyn, New York Med Coil, Vahalla, NY,
Stamford Hosp., Stamford, CT, Yale Univ. Sch. Med, New Haven, CT.
OBJECTIVES: Accurate prenatal diagnosis would facilitate more
effective patient counsehng regarding the risk of vertical transmission
of HIV-1, however, the lnfechous potential of invaslve diagnostic
methods remains controversial This study was undertaken to determine if the risk of transmission is increased by ammocentesls.
STUDY DESIGN: Two groups of HIV-1 infected pregnancies were
stud~ed Group I consisted of 48 pregnancies in which an amniocentesis had been performed. Indications were PTL-24, PROM-16, pulmonlc
maturity-2, karyotype-4, other-2. Group I1 included 117 women who
d~d not undergo an antepartum mvasive procedure. Data from H1V-1-
transmitting and non-transmitting pregnancies were compared using
Student’s T, and Ch~-square tests of analys~s where appropriate.
RESULTS: Both groups were similar with respect to maternal age,
H1V-status, race, risk behavior, CD4+ count, and HIV-I p24 antigen
status The mean gestanonal age at the procedure was 34.1 -+ 5 6 wks
for Group I pregnancies which resulted in H1V-I infected children, as
compared to 33 7 + 5.2 wks for Group 1 seroreverters The elapsed time
from procedure to dehvery was 14.2 days m Group I pregnancies which
resulted m H1V-1 infected children, as compared to 22.1 days for seroreverters The pennatal transmission rate in Group I was 23%, as
compared to 29% In Group 1I Penetration of an anterior placenta was
associated with an increased risk of perlnatal transmission.
CONCLUSIONS: Our data suggests that ammocentes~s which does
not penetrate the placenta may predict which fetuses are truly infected with HIV-1 without increasing the nsk of latrogenic infection. Further study is warranted in order to determine the safety of pennatal invas~ve
procedures In the prenatal d~agnosis of HIV-I. (Thls research was partially supported by the Amencan Foundation for AIDS Research and
the Pediatric AIDS Foundanon AmFAR/PAF #50034-7)

Volume 170, Number 1, Part 2 SPO Abstracts 415 Am J Obstet Gynecol
507 LONGER DURATION OF RUPTURED MEMBRANES IS ASSOCIATED
WITH INCREASED RISK OF VERTICAL TRANSMISSION OF HIV
INFECTION. Joan Youchah’, Howard M~nkoff, Sheldon Landesmanx,
David N Burns~, Robert Nugentx, James J. Goedertx. Albert Einstein
College of Medmme, Bronx, NY, SUNY-Downstate, Brooklyn, NY
AIDS Branch National Institute of Chdd Health and Human
Development, Rockwlle, MD. Viral Ep=dem=ology Branch, National
Cancer Institute, Rockvdle, MD.
OBJECTIVE: Intrapartum events may play a role In determining the
h, ehhood of verncal transmission of HIV-I. Timing and duration of
rupture of membranes (ROM) has been shown to modify transm=ssmn
nsk of other organisms, but has not been examined for HIV. Th~s
study was undertaken to assess the relationship between duration of
ROM, maternal ~mmune status, and transmission of HIV
STUDY DESIGN: 207 HIV pos=hve women entered the mother and
~nfants cohort study at 6 sites In Brooklyn and the Bronx between
1/86 and 1/91. 162 pmrs with complete maternal and fetal data,
including final infection status were Included in this analysis
Premature ROM (PROM) was defined as rupture prior to the onset of
labor, duratmn of ROM was the interval from rupture to dehvery.
RESULTS: 39 of the 162 infants (24%) exposed were infected.
Using a variety of cut pmnts for duration of ROM faded to reveal a
statistically significant association between these variables and
verncal transmission. Women with low CD4 levels (<20%} were
significantly more likely to transmU the wrus ~f ROM was >.~4 hours
8 of 15 were infected when ROM was~> 4 hours, whde only 2 of 17
were infected w~th ROM < 4 hours (P=O.02). The same assoc=ahon
was not observed among women with higher CD4 levels (P=0.69).
No association with duration of labor was seen. Adlustment for
gestat=onal age, mode of dehvery, drug use and PROM did not alter
these results.
CONCLUSIONS: In this urban, North American cohort, women with
low CD4 levels were significantly more hkely to transmit HIM to their
offspring =f the duranon of ROM was ~> 4 hours
509 STIMULATION OF PRETERM LABOR BY LIPOPOLYSACCHARIDE (LPS) 1S DEPENDENT ON GESTATIONAL AGE, P. GoluszkoX, B. NowlcklX, A. Kaulx,
M.G. Martens, R.E. Garfieldx, C. Yallampalllx, S. Nowtcklx, and G.D. Anderson. Department of Obstetrics & Gynecology, The Unlversay of Texas Medical Branch, Galveston, TX. OBJECTIVE: Infections of bacterial origin during pregnancy may lead to several compllcanons, including preterm labor. Bacterxal lipopolysaecharides (LPS) are considered to be revolved in the process of premature labor, however the mcchamsm Is not well understood. We hypothcsl,’cd that scnsmwty to LPS stimulation ~n preterm labor may be related to the gestatlonal age. STUDY DESIGN: Commcrcmlly avadable Salmonella entertttdts LPS was utlhzed for the experiments with Sprague- Dawley pregnant rats. Groups of 8 to 10 ammal~ were injected lntraperltoneally with the single dose of 100 ~tg LPS m sterile PBS on day 16, 17, 18, 19, and 20 of pregnancy and observed until the nine of dehvery. RESULTS: The infection of LPS on day 16 and 17 resulted m
growth retardation, intrauterine death and absorption of some fetuses Later ~njecUons on day 18 and 19 resulted in pretenn tabor which started wtthm 24 hours In eight amman re.letted on day 20, three dehvered six hours. CONCLUSIONS: The obtained results are in agreement w~th the proposed hypothesis that specific gcstauonal age, e.g., days
18-20 (correspond to human 32-36 weeks of gestation) appear to be associated with increased sens~Uvay to LPS-mduced preterm labor Whether human reproductive tract at gestauonal age 32-36 weeks ts assocmted with increased sensitivity to LPS remains to be investigated.
508 EXPRESSION OF RECEPTORS FOR ’P’ FIMBRIAE OF Eo COLI IN THE RAT KIDNEY DURING PREGNANCY. A. Kaul, R. N0w~¢k~x, P. Goluszkox, M.G. Martens, S. Now~ckix, and G.D. Anderson. Department of Obstetrics & Gynecology, The University of Texas Medical Branch, Galveston, TX. OBJECTIVE: There is a sigmficant ~ncrcase in the incidence of
pyelonephrlns in pregnant populaUon. The patbogenes~s of pyelonephrms in non-pregnant populations have been associated with bacterial wrulence factors, such as ’P’ flmbrlae, present in about 70-90% of all pyelonephntis cases We hypothesize that durmg pregnancy, there is an upregulauon of host receptors for ’P’ fimbrlae of uropathogemc E colt and th~s may increase the rate of colonization leading to increased incidence of pyelonephnt~s during pregnancy. STUDY DESIGN: Frozen k~dney secuons were obtained from pregnant (at different gestauonal ages) and non-pregnant Sprague-Dawlcy rats. Tissue sccUons, fixed in ~ce-cold acetone for 10 mm., were incubated w~th FITC labeled E colt stratus carrying different ~P’ fimbnae (pap-1 and pap-2) and ~n control
non-fimbriated strmn, for 1 hour at roo~n tcmp The secUons were nnsed w~th PBS (pH 7.4) for 2 mm (5X) and then viewed RESULTS: Significant increase m the attachment of pap-1 flmbnated E. colt m the 1st week, and pap-2-fimbnated E colt during the second half of the pregnancy, to the mt kidney was observed. Attachment of pap-I flmbrlated E colt was reduced m 3rd week of gestauon. CONCLUSIONS: Dynamic changes m the pap receptors that occurred during pregnancy appear to be m agreement w~th our hypothesis. We propose that the increased expression of receptors for the ’P’ fimbnae of E colt m the kidneys may be an important factor m the pathogeneslS of pyclonephrltiS m pregnant population.
510 PLASMID PROFILES OF ESCHERICHIA COLI ISOLATES FROM PREGNANT PATIENTS WITH PYELONEPHRITIS DURING DIFFERENT GESTATIONAL AGE. B, Nowlck~x. A, Hartx, M.G. Martens,
T. Phamx, S. Nowicktx~ and G.D Anderson. Department of
Obstemcs & Gynecology, The Umvers~ty of Texas Medical Branch, Ga!veston, TX, OBJECTIVE: E. colt-associated pyelonephntxs is a common medical comphcauon during pregnancy. They are characterized by virulence trails, such as fimbnac, hemolysin, O scrotype, and plasm~d patterns. There ts a lumted number of E colt clones
which usually develop pyclonephnns. We, therefore, mvcsugatctl whether plasmld patterns and associated virulence factors of E colt are characteristic for gestaUonal pyelonephrms. STUDY DESIGN: A plasmxd profile and selected wrulence routs were assayed on 52 E colt strains isolated froln pregnant pahcnts with pyelonephrms at different gestational ages Plasnuds were ~solated using Promega "Magic Mmlpreps DNA Purfftcauon System" according to protocol. RESULTS: A consistent pattern was observed among ~solates collected from the second mmestcr, especially from weeks 19 to 21 (9/13, 69%). The majority of these ~solates earned muluple plasm~ds of the following s~ze 23, 16 1, 9.7, 6.6, 5.4, and 4.4 Kb Among these, ’P’ flmbnated E colt predominated. However, only one out of 13 strains belonged to nephropathogemc scrotypcs CONCLUSIONS: It IS hkely that spcclhc E t.oh strains are
assocmted w~th acute pyelonephntlS during the second trimester of pregnancy. Some of these strains may be dff[?rent from pyeloncphr~togemc isolates in non-pregnant pauents. Whether
lhctors, such as altered hormonal status, may be responsible for these differences, remain to be mvcsugated
416 SPO Abstracts January 1994 Am J Obstet Gynecol
511 PERSISTENT ENIGMATIC FEVER IN THE POSTPARTUM PERIOD:
AN INDICATION FOR HEPARINIZATIONo D. Maslrngiaanls, K.
Nakisbendi’. Dept. Ob/Gyn and RS, Temple Univ., Phila., PA
OBJECTIVE: The postpartum course of few patients is complicated by
persistent fever in the face of adequate ~’ltibiotic coverage. When other
processes such as hematomas, wound infection, urinary tract or abdominal
infections are excluded there is a strong clinical suspicion for the diagnosis of
septic pelvic thrombophlabitis (SPT). Diagnostic imaging can demonstrate the
presence of ovarian vein thrombosis, however, it does not always support the
clinical diagnosis of SPT. In this study, we investigated the characteristics of
pauents with the clinical diagnosis of SPT, their response to antieoagulatton and
the rate of thrombus confirmation.
STUDY DESIGN: We reviewed the charts (1988-1992) of all patients with the
clinical diagnosis of SPT. Clinical, laboratory and radiographic data were
collected from the medlcal record charts. Patients who had on imaging studies
pelvic abscesses, significant hematomas or other diagnoses were excluded
RESULTS: In the study period, 9,000 deliveries occurred in our hospital.
Persistent febrilemorbidity complicated 0.4%. Eighteenpatients (0.2%) hadthe
clinical diagnosis of SPT. Of the 18 patmnts, 12 had CT scan imaging, 5 had
pelvic ultrasound and 1 did not have any imaging. Of those patients who had a
CT, ovarian vein thrombosis was confirmed in 2 (16%). From the patients
undergoing ultra,sound, 2 had non-diagnostic examinations 0e. the ovarian veins
were not visualized) and in 3 patients the study was normal All patients were
diagnosed imtially with endomyometritts, had persistent fever with taehycardia,
received broad spectrum antibiotics and were started on heparin on average
postpartum day six. Therapeutic levels were maintained for an average of seven
days All patients defervcsced by day number three of heparin therapy. All
patients were discharged m stable condition.
CONCLUSIONS: The clinical diagnosis of SPT is a rare entity end is supported
by imaging techniques in the minority of cases. Howevei’, the aon-coafirmad
cases resemble the symptomatology of enigmatic fever de-scribed by Dunn and
van Voorhis Therefore, persistent fever despite adequata antibiotic therapy and
negatwe findings for ovarian veto thrombosis by diagnostic imaging should still
be an indication for heparinization on clinical grounds.
513
512 POST-CESAREAN ENDOMETRITIS: ROLE OF ASYMPTOMATIC ANTENATAL COLONIZATION OF THE CHORIOAMNION WITH UREAPLASMA UREALYTICUM.
W Andrews, S Shahx, R Goldenberg, G Cassellx, J Hauth, W. Rodeax Departments of OB/GYN and Microbiology, University of
Alabama at Birmingham, AL HYPOTHESIS: Asymptomattc antenatal colonization of the chonoammon (CA) with Ureaplasma urealytlcum (Uu) is a risk
factor for development of post-cesarean endomemtis (EM). STUDY DESIGN: The CA was cultured at cesarean delivery for
aerobes, anaerobes, ureaplasma, mycoplasma, chlamydla and trtchomonas m 575 singleton gestaUons with intact membranes. Postopera~we endometntts was defined as a temperature of 100,4°F with uterine tenderness and without other nonpelvlc sources of fever RESULTS: A total of 58 (10°/0) of the 575 women developed EM,
Women with spontaneous labor developed EM twine as often as
those dehvered for medical or obstemcal mdtcattons (17% vs 8%. p=0 002) EndometntlS occurred m 28% of women with Uu present in the CA at cesarean delivery" compared to only 8,4% tf the culture was negative and 8,8% tf only bacteria were isolated (p<0 001) Gestatlonal age (GA) <34 weeks, spontaneous labor and
a vertical uterine Incision were associated with EM (p_<0.002). Regression analysis controlling for GA and incision type revealed an increased ask for EM of 4-fold tf the CA was colonized with Uu
at the tnne of cesarean (OR=3 7, 95%CI=1 4-9 9) and 8-fold (OR=7 7, 95%CI=1 9-31.5) m women with spontaneous labor
CONCLUSION: Colomzatton of the chorloamnion with Ureaplasma urealyttcum m women with intact membranes undergoing cesarean dehvery is a significant and independent predictor of subsequent endometntis.
514 THE IMPACT OF ANTENATAL SCREENING FOR GROUP B STREPTOCOCCUS ON OBSTETRIC AND NEONATAL PRACTICE. ]~M Mercer. RD Ramscyx, BM Stbal Umversxty of Tennessee, Memphis OBJECTIVE: To evaluate Group B streptococcus (GBS) screening and management practice and to assess its’ impact on neonatal treatment STUDY DESIGN: Separate quesnonnatres were sent to SPO and American Academy of Pedlatrws (AAP) members Routine practice was ascertained Responses to hypothetical climcal sltuanons were elicited based on the availabihty and results of GBS screens :n low- & high-ask circumstances RESULTS: Responses of 862 SPO and 917 AAP members were reviewed. sPo: Currently, 31% perform routine antenatal screemng whereas 66% screen only high-risk women, with preterm labor and pPROM being the most common ~ndications (94%, 98%). With a positive GBS screen, 35% would treat immediately (Rx), 34% treat all women m labor and 29% treat only for obstetric complications Knowledge of GBS carrier status increases mtrapartum prophylaxis of low-risk women but had little ~mpact on those with lntrapartum complications (Table below) However, (-) GBS status reduces treatment of low- & high-ask paUents
% Intrapartum treatment based on screen~ poor Rx and risk factors.
No culture (+) GBS (+)GBS/(+)Rx (-)GBS , No comphcatlons 2 1 59 6 40 7 0 5
Preterm labor 63 4 66 5 58 7 31 9
Preterm PROM 61 9 68 0 62 8 36 8
Prolonged ROM 43 6 47 0 46 1 21 6
AAP: 33 6% routinely g~ve antim~crob~al prophylax~s (Abx) to low bJrthwe~ght and preterm infants (77%<34 weeks, 86%<2250g) The ~mpact of GBS status and mtrapaytum prophylax~s ~e reviewed below
Neonatal Abx based on GBS status (-1+) & prophylaxis (Proph)
No culture (+) GBS (+)GBS No culture Proph(+) Proph(+/ ProphQ~ Proph(-!
Abx (%) 46 8 75 4 75 0 29.2
Abx 7-t4 days (%) 304 45 0 31 5 164
Abx D/C (%) 650 56 4 77 6 860
CONCLUSIONS: The knowledge of GBS carriage does not increase
prophylaxis in the presence of obstetric complications However, a
negative screen reduces lntrapartum therapy m both low and high ask
patients Knowledge of GBS carnage or mtrapartum prophylaxis
increases the incidence and duration of neonatal ant~m~croblal therapy

Volume 170, Number 1, Part 2 SPO Abstracts 417 Ant J Obstet Gynecol
515 ASSESSMENT OF GUIDEL RAPID SCREEN FOR DETECTION OF
GROUP f~ STREPTOCOCCI B L_tsmanx, J Egan, P Ambersonx, M
S=monelhx, W Scorza, St Franc=s Hospital and Med=cal Center, Hartford CT
OBJECTIVE. The purpose of th=s study was to evaluate Qu=del rap~d screen to detect group B, 13 hemolyhc strep METHODS: We conducted a prospective study of 200 women presenting to
the delivery floor m term or preterm labor w~th or wthout PROM Each patient had an exam w~th 3 sohd shaft rayon t~ppod swabs used to swab the vagina 2- 3 cm ~nto the ~ntro~tus The hrst swab was plated on 5% sheep blood agar for
48 hrs The second swab was used for the Quldel rapid screen m accordance
w~th the manufacturer’s mstruchons. The th=rd swab was first incubated ~n Todd-Hew~tt broth for an hour and then screened w~th the Qu~del rap~d screen Data collected =ncludes maternal age, age of gestat=on, membrane status,
quant~ficahon of colon=zatlon (1+ and 2+ was dehned as hght colonization and 3+, 4+ termed heavy) Tile results were analyzed using STATVIEW IFM w=th
descnpt=ve stahst~cs for continuous data and ch~ square for categorical data A p value of 0 05 was cons=dered agn~hcant
RESULTS. Two hundred women underwent the screemng. The maternal
age in years (_+ SD) was 25 (_+6) The mean age of gestation m weeks (_+SD) was 32 (+5) with 10% (19/200) of the patients at term E~ghty four percent
(169/200) had intact membranes The prevalence of poahve cultures was 9% (18/200) Overall, the sensitivity, specificity, positive (PPV) and negahve (NPV) predictive values of lhe rap~d screen were 11 1% (2/18), 100% (182/182),
100% (2/2) and 91 9% (182/198), respechvely (p=00001) Of the 76% (15/200) wh=ch were hghtly colon=zed none were Qu~del pos=t=ve Of the 1 5% (3/200) which were heavily colonized on blood agar plates 66 7% (2/3) were
Qu~del positive The senslhvlty, specificity, PPV and NPV for heavdy colomzed patients were 67 7% (2/3), 100% (197/197), 100% (2/2) and 99 5% (197/198)
respechvely (p=0 0001) None of the 15 hght isolates which were incubated for an hour m a selective Todd-Hew~tt ennchment broth became Qu~del positive
CONCLUSION: The Quldel rap=d screen had an overall sens=t~vlty of 11 1% for vaginal ~solates obtaned on labor and dehvery
517 LONG-TERM FOLLOW-UP OF PERINATAL
TRANSMISSION OF HEPATITIS C VIRUS. E. Leikin, J. Reinusx, H. Alter~, S. Piazzas, J. Shihx, B. Jettx, R. Sockolow~. Depts. Ob/Gyn and Pods, NY Med. Coil., Valhalla, NY; Div. GI, Montefiore Mad. Ctr., Bx, NY; Dept. of
Transfusion Meal., NIH, Bethesda, MD. OBJECTIVE: Look for evidence of HCV infection in children
of women with anti-HCV antibody (anti÷HeM) at delivery. STUDY DESIGN: From 7/1/89 to 7/23/93, we prospectively studied potential vedical transmission of HCV by testing pa~red maternal and cord blood samples by EIA for anti-HCV (Ortho Diagnostics, Raritan, N J) and for HCV RNA by nested PCR. Anti-NCV+ mothers and infants were evaluated periodically for clinical liver disease, HIV infection, abnormal ALT, serum HCV RNA and anti-HCV reactivity. RESULTS: Anti-HCV was found in serum of 57 mothers and
all but 2 of their 62 babies. 16 of 23 mothers and 1 of 24 babies tested to date were PCR+ at delivery. 25 of 31 infants evaluated after discharge from the hospital became HCV- by
3 yrs. 4 children were anti-HCV+ when lost to follow-up at 3 (n=3) or 6 (n=l) mons. 1 child became anti-HCV- by 5 mons but was anti-HCV+ again at 23 mons, and 1 child born to a mother w~th acute HCV has been persistently anti-HCV+. The latter 2 children have abnormal ALTs without clinical liver d=sease; no cause other than HCV has been identified. CONCLUSION: Perinatal transmission of HCV, while much
’less common than that of HBV, may occur, even in the absence of maternal HIV infection. Infants at dsk may have mothers with acute or active infection.
516 THE CORRELATION OF ANTEPARTUM GROUP B
STREPTOCOCCUS CULTURES WITH MATERNAL INTRAPARTUM
COLONIZATION. Wdham E $corza, Deanna DelPretx, EIhott
Rankx, James F X Egan, Dept of Ob/Gyn, Mt, Sinai Hospital, Ha~ord, CT and Untv of CT Health Center, Farmmgton, CT. OBJECTIVE: To determine the usefulness of antepartum cultures of group B streptococcus (GBS) m predicting maternal
colomzat=on at the t~me of labor and dehvery STUDY DESIGN: GBS cultures were taken from the vagina,
permeum and anus between 28-32 weeks m 148 pahents. The
patients were followed prospechvely and cultures were repeated at the t=me of admission for labor and dehvery. Patients w~th
pos~t=ve antepartum cultures were not treated prior to labor but
were treated m labor after the repeat culture was obtained
Pahents were excluded If they were treated with antlb=ot~cs for any reason from the time that the imtta~ culture was obtained at 28-32 weeks and the onset of labor Cultures were plated on selective
medium and read at 48 hrs. RESULTS: One hundred patients had antepartum GBS cultures negative and intrapartum cultures negative. Eleven had positive
antepartum cultures and positive intrapartum cultures Fourteen had positive antepartum and negative mtrapartum cultures.
Twenty three had negative antepartum cultures and positive
Intrapartum cultures The sensitivity, spec~fimty, posltwe predictive and negative predictive value were as follows" 32%,
87%, 44%, 81%, respectively. There were no cases of GBS seps~s. CONCLUSIONS: Antepartum GBS cultures have a low sensitivity and predictive value for the identlhcatlon of colomzed mothers m
labor The results of th~s study fad to support the most recent recommendation of the American Academy of Pediatrics, that all
pregnant women should be screened m the early third tnmester as
the method for selecting mtrapartum chemoprophylax~s
518 MATERNAL ANTIBIOTIC TREATMENT ABROGATES TIlE INFECTION-INDUCED INCREASE IN CYTOKINE PRODUCTION ~’~IIICII ANTECEDES I*REMATURE DELIVERY. R Romero, H Munoi¢, R Gomez’, M RamireZ’, H Araneda’, J Cutrtght~--N~g~ DB Cotton, P Fidel’. Dept. OB/GYN,WSU/Hutzel Hospital, Detroit, MI and the Permatolo~v Branch, N1CHD, Bethesda, MD. RACKGROUND/OB]ECTIVE: Evtdencederived from hum&n ~.rtd animd. stu&es (in monkeys rabbits and trace) indicates that the serum and amniotic fired concentrat=ons of macrophage derived cytok~nes mcreaseprior to m fectton-mduced premature de,very It ls unknown if ~mti-mlcrobialrherapy changes the cytokine profile observed in th~s condition. This question i’s =mportant to determine ff add=tional benefits could be obtained by the use of anwcytok=ne agents The current study was conducted to determine the cytokme profile associated w=th in fect=on-induced preterra labor/dellvery and to e~tabhsh whether ant=b=otic a&mmstrat=on has any effect on this cytokme
~rofile TUDY DESIGN: Timed pregnant rabbits at 70% gestation were randotniTed to rece=ve an intrauterine inoculation of 1) buffer (n = 16)" 2) E Cob 0 2 ml of lxl0~ cfu of E. Coil (n = 19), and 3) E. Coil and amplc~lhn q2 sulbactam at different interval times (< 12 hours and > 12 hours) after E Colt inoculation (n=12). Twenty hours after experimental treatment, ammot=c flu=d was collected. Ammotlc fluid mterleukm-1 (AF 1L-I) tumor necrosis factor (TNF) and mterleukm-6 (IL-6)-Iike bloactlvlry were measured wah rad~mmmune or bioass~ys. Statistical analysis was conducted with non- parametric ANOVA with post-hoe procedures RESULTS: Values are expressed m pg/ml (median range).
Control 0 156 362 15
E Coh 803* 0 1068" 893"
E Coli + ATB 27 0 406 42 < 12 hr 0-3606 0-571 0-5786 3-4686
E Col= + ATB 583* ’t56 7461 1352~ > 12 hr 0-2494 0-595 0~1790 4-2(XK)0
* p < 0 05 compared with control CONCLUSIONS: 1) Intrauterine infectmn wah E Colt ts associated with a s~gmficant increase in AF concentrations of IL-I TNF and IL-6-hke bloactivtty 2) early (< 12 hours) but not late (> 12 hours) antibiotic treatment prevented an increase m AF concentratlons/bioactlvity of tnacrophage derived cytok rues. 3) ant~-cytokme agents are of potential use m tile treatment of mfedtlon-mduced preterrn labor which is unresponsive to
418 SPO Abstracts January 1994 Am J Obstet Gynecol
519 ENHANCED ANTENATAL DETECTION OF GROUP B
STREPTOCOCCUS COLONIZATION. E. Phllipson, D. Palerminox,
A Robinson" Dept. Ob/Gyn and Pathology, Hartford Hospital,
Hartford, CT.
OBJECTIVE: Previous studies have ~ndlcatad that detecl~on of
group B streptococcus (GBS) can be Influenced by the culture medium and site. Since GBS remains an Important pathogen in
obstetrics, optimal culture methods must be established.
STUDY DESIGN: This study pmspestively compared the standard
culture medium, blood agar plate (BAP), to a selective culture
medium, Todd Hewltt broth with antibiotics (THBA), and cOmpared
vaginal culture with rectal culture at the first prenatal exam.
RESULTS: Of the 3~3 vaginal swabs received to evaluate culture
medium, 78 (20%) were positive for GBS. The sensitivity of the BAP
only method and the THBA was 64% and 97%, respectively. Using
the THBA method, an additional 94 patients were cultured vagine, lty and rectally, A total of 29 (31%) had positive cultures, The
sensitivity was 59% for the vaginal, 90% for the rectal, and 100% for
both culture sttas combined. A non-setective culture medium p~ired
with a vaginal only swab detected only 37% of patients colonized
with G~S. A selec~ve culture medium patted w/th a rectal oniy swab
detected 87% of patients colonized with GBS. A selective culture
medium paired with both vaginal and rectal swabs detected 97% of
the patients co~on|zed w~h GBS.
CONCLUSIONS: These data Indicate that maximal culture detection of GBS requires both a selective broth medium and a dual
vaginal/rectal culture. Obstetricians and microbiologists need to
insure that optimal methods are used to detect GBS.
52l POTENTIATION OF CELL-MEDIATED IMMUNITY AGAINST LISTERIA MONOCYTOGENES BY AMNIOTIC
FLUID E J Wolf, D S Cunnmghamx National Naval Medical
Center, Bethesda, MD OBJECTIVE We assessed the effect of midtnmester amn~otic
fluid on monocyte handling of intracellu/ar pathogens as a measure of cell-medmted ~mmumty STUDY DESIGN The effect of mldtnmester a.mnlot~c tiuld on
phagocytos~s and bactenc~dal act~wty against L monocytoqenes by
monocytes was compared w~th the monocytes’ response ~n the absence of amniot~c fluid and ~n the presence of term amn~ot~c fluid RESULTS The phagocytic mdex of L monocytoqenes by
untreated monocytes was 620 Term ammot~c flu=d enhanced the
phagocytic ~ndex (840), as d~d the add~hon of 22 of 25 m~dtnmester ammot~c fluid samples (910) In stark contrast, 3 of 25 m=dtnmester
ammottc fluid samp{es had no effect on the phagocyt}c ~ndex (590)
S~m~larly, the bactenc=dal act=wty of monocytes agamst I_
monocytoqenes was ~ncreased over control values =n the presence
of term ammotic fluid (0 69 log10 bactena k=lled vs 0 43 log1 0
bactena k~lled) The m~dtnmester amn~otlc fluid samples that
mcreased the phagocytic mc~ex a(so mcreased the bactenc~dal activity (0 73 log10 bactena k=lled), whde the rema~nmg 3 of 25
samples had no such effect (0.41 log10 bactena kdled) The
potentiation of monocyte handbag of L monocytoclenes d~d not
occur m the absence of ammohc flu=d durmg the assay--
premcubation of mononuclear cell preparations for as long as 4 hours pnor to mfechon d~d not gwe rise to mcreased monocyte
acbv~ty CONCLUSIONS Most m~dtnmester ammot~c fluid samples
enhanced the bactenc~dal and phagocytic act~wty of monocytes(a measure of cell-med=ated ~mmun~ty) These capab~ht~es may be of
chmcal s~gn~ficance m grawdas at ask for mtra-ammot~c ~nfect~on and preterm labor
52O SEXUAL BEHAVIOR AND THE ECOLOGY OF GROUP B STREPTOCOCCUS (GBS). E R Newton, M C Butler,x R Shain x Dept ofOb/Gyn, UTHSC, Sa~TX
OBJE(S~’IVE: Sexua~ behavior may promote Group B Streptococcus (GBS) colomzat~on of the genital tract from the gastromtestmal tract We sought to correlate the anatomic s~te of GBS colomzat~on w~th sexua) behavior
METHODS Consecutive Mexican American or African American patients who were enrolled in a study designed to understand and prevent recurrent STDs had detaded sexual h~stor*es taken by experienced Interviewers Each woman had separate swabs taken from the endocervlx, upper 1/3 of the vagina, lower 1/3 of the vagina and anus These were inoculated directly Into selective GBS broth Behavioral character=st~cs and coex~stmg organisms were used to predict the presence of mult~pleslte (all s~tes positive) and/or heavy GBS colonization (3-4+ at any s~te) usmg three separate stepwlse logistic regressions
RESULTS 57/162 (34 9%) had GBSat one or more s=tes, 26 9%. endocerwx, 28 3%, upper 1/3; 27 6%,lower 1/3; and 26 9%, anus 28 8% had vagmal isolat=on only and 3 1% had anal ~solat=on only The mc~dence of heavy colonization was 41/57 (72%) and multiple s~te colonization was 20/57 (35%) The prevalence of anal mtercourse (AI) was 22% The predictors of heavy or multiple s=te GBS colomzatlon are depicted below
Adjusted Odds Ratio (95th CI)
Pred=ctors Heavy Multiple-Site Either
Condoms/ NS NS 1 13(1,0 1 3)
10acts
AI 0 28 (0 1-0 8) NS 0 38 (0 1 t 0)
CONCLUSION Anal to vaginal transmission through coitus ~s not a malor factor In genital tract GBS colon~zat~o~ We speculate that bacterial characteristics, such as ability of organism to attach to mucosa or latex, play a greater role in colonization
522 MACROPIIAGE INFLAMMATORY PROTEIN-In IN TERM AND PRETERM PARTURITION AND MICROBIAL INVASION OF TilE AMNIOTIC CAVITY. R Romero, R Gomezx, M Galasso", L Acosta=, H Munoz~, M Ram~rez" BH Yocm D Svinarleh=, DB C~tton Dept. OB/GYN, WSU/Hutzel Hospital, Detrmt, MI, SeouI Nati~rsity, Seoal, Korea and the Perinatology Branch, NICND, Bethesda, MD. OBJECTIVE The neutrophll is the most common white blood cell recruited into the amnlotlc fluid (AT) during the course of intraamniotie infections. The mechamsms responsible for chemotaxis of neutrophds rote the ammouc cavity have not been determined. Macrophage mllammatory proteia-l~ (M1P- 1 a}, a novel cytokine produced by macro~bages ia response to bscterlal products, can induce neutrophll chemotaxis Thepur.pose of this study was to determine whether 1) gestational age, labor ~tndm~croblal invas=on of the amnmt~c cavity (MIAC) are associated wah changes in AF concentrations of xmmunoreactz’~e MIP-16~; 2) AF neutrophil count correlates with lmmunoreactwe MIP-1~ and interleukln-8 concentrations in AF. STUDY DESIGN: AF was retr=eved by amntocentesis from 116 patients; 54 women with preterm labor (PTL) ~nd intact membranes (no MIAC-dalivery at term, n =2 It no MIAC-preterm delivery, n = 16; MIAC-preterm dehvery, n= 17) 62 patients st term (no labor n =19; labor-no MIAC n=20; lnbor- MIAC, n=23) mad 10 patients in the mldtrimester of pregnancy. Amniotic fluid w~s cultured f6r ~terobie, ~at~erobic ~d Myeoplasm~, species. Determinations of AF MIP-1 and IL-8 were performed with immunoassays vahdated for AF (sensttwity’ 24 3 pg/ml and 3 pg/ml, respectively) Kruskal-Walhs ANOVA for censored data, Mann Wh=tney-U test and Spearman’s Rank Correlat=on were performed for analysis. RI’;SULTS’ 1) AF MIP-I was present in only 12.9% (4/31) ofpatients not ~n labor (midtrlmester and term) 2) P~ttents with PTL and MIAChad higher AF concentrations MIP-I than those w~thout MIAC (no M[AC-dehvery term: median < 24.3 pg/ml, range < 24.3-206.7; no MIAC-preterm dehvery: medmn 41.7 pg/n~l, range <24.3-459 6; MIAC, preterm delivery: median 8000.0 pg/ml range 400.6-37099 3; p <0.0000I) Also, among patients at term, MIAC was assocnxted with h~gher concentrations of AF MIP- ~1o~ than patients without MIAC (no labor: und-eteetable in all the eases; labor- no MIAC: median < 24 3 pg/ml, range < 24.3-137.4; labor-MIAC: median 103.2pg/ml, r~.nge <24.3-4640.0,p< 0.0001). 3) A strongcorrelationwas foundbetween AF �oncentrationsofMIP-lc~ and IL-8 (r= 088, p <0.00001) and between AF MIP-lt~ concentrations and AF WBC (r =0.49, p <0 01) CONCLUSIONS. 1) Microbial invasion of the ammotic eavtty- both at term and preterra- ts associated wtflt increased coneentr~tlons of immunore~,ctive MIP- c~ in AF 2) In the absence of MIAC parturition (term and preterm) is not associated with an ncrease n the AF concentration of MIP- 1~; 3) MIP- 1 c~ is not detectable in most samples of normal mldtrlmester and term human amnlotic fluid, 4) Our data suggests a role for MIP-I~ in the mechanisms responsible for recruitment of neutrophils into the amniotlc cavity durmg the course of mtrauterme infection

Volume 170, Number 1, Part 2 SPO Abstracts 419 Am.] Obstet Gynecol
523 COMPARISON OF AZITHI~3~YCIN AI~ ERYTtlROMYCIR FOR ~ C~VICITIS ~~. M. Edwards, K. Rainwater~ S. Carter~ F. Wllllamson~ R. Newman. Dept. OB/GYN, Medical University of S.C., Charleston, S.C. ~I~: Prospectively test the null hypothesls that there is no dlfference in the cllnlCal efflcacy of elther Azlthromycln or Erythromycln for treatment of chlamydia cerv~citls mn pregnancy. ~Y D~I~: All antepartum obstetrical patients unde~ent routine screening for chl~ydla cervicitls using a DNA probe assay (Gen-Probe Pace, San Dlego, Ca.). Women who tested posltlve for chl~ydla cervlcitis were prospectlvely randomized to receive either Az~thromycln 1 gram orally at enrollment, or Erythromycin 500 mE. orally four tlmes a day for seven days. Sexual partners were referred to the county health department for evaluatlon and treatment. A test of cure (TOC) was repeated in two weeks. Results were analyzed by Ch~-square analysis and F~sher’s exact test. ~: 31 women tested pos~tlve for chl~ydia cerv~citls and were randomized. ~e treatment groups exhlblted no s~gnlflcant demographic d~fferences. There was one treat- ment fallure in the Azithromycln group and three in the Erythromycln group (p = 0.25). ~ ~Itsby ~ea~nt ~oup
Positive Negative Totals Azlthromycin 1 15 16 Erythromycln 3 12 15 Totals 4 27 31 CONCLUSION: There does not appear to be any difference in the cl~nlcal e£f~cacy of a s~ngle 1 gram dose o£ kzlthro- mycln compared to a seven day course of Erythromycln. The trend toward a higher failure rate wlth Erythromycln may be related to incomplete compliance that ~s obviated by the single star dose of Azlthromycln. We are evaluating thls possibillty by contlnu~ng to enroll patients wlth chlamydla cervicitls and have determlned that 70 patlents ¯ n each treatment group w~ll provide 90% power to est,- llsh a 10% difference in cllnlcal efflcacy.
525 INTRAUTERINE INFECTION AND MYOMETRIAL CONTRACTILITY IN THE RABBIT E~R Newton, CA BImcker x Dept of Ob/Gyn, University of Texas HSC at San Antomo, TX
OBJECTIVE We sought to quantify the effect of group B streptococcus (GBS) chor~oammomt~s on uterine response to oxytocm mduct~on
STUDY DESIGN’ New Zealand White, Cambr~d@e or Cahforma rabb~ts at 28 29 days gestauon had emdocerwcal ~noculat~on wRh 0 2 cc of I0~ ~I CFUIml v~rulent type III GBS or 0 2 cc sterile sahne (control) On day 29 30 ~n both control and expenmental ammals, a sacrifice preparation was estabhshed under general anesthesla Through a laparotomy inclslon, a sponge tlpped pressure catheter was ~ntroduced ~nto the upper vagina and threaded transcerwcally Into an extra ovular position Intrauterine pressures were measured continuously on a Grass polygraph In five m~nute =ncrements, the following doses of oxytocm were admm=stered ~ntravenously 0, 18 75, 26 25, 36 7, 720, 1410,2765, and 5400 mU/mm Bmlog=c endpomts =ncluded onset of regular contractions and dehvery of pups Infect=on was confirmed by histology and dec~dual culture Utenne activity was measured as (number of contracUons x average intensity |m cm deflec¢lon]) - minutes at dose
RESULTS: Two of nine GBS inoculated animals dehvered w~th=n 24 hours All GBS =nocuMted rabb~ts had positive dec~dual and amn=ot=c fluid cultures at sacrifice The mean activity (SD) at ~-epresentatlve oxytocln doses ~s depicted in the following table
Uterine Activity at Selected Oxytocin Doses
26 25 72.0 276.5 540 0 Group (n) Baseline mU/mln mU/min mU/mln mU/mln
GBS(7) 68032) 197(133) 1210(155) 393(250) 260(154)
Control(4) 34(125) 193(188 151(135) 225(139) 284(267)
No s~gnlflcant differences were demonstrated CONCLUSION In the rabb~t model, GBS associated chor~o ammomt~s does not affect myometr~al contractility
524 STAPHYLOCOCCUS EPIDERMIDIS AND PREGNANCY COMPLICATIONS IN THE RABBIT. E.R Newton, K Kagan- HalletxC.A Blelcker,X W. Pea~rsX Depts of Ob/Gyn and Patho ogy, Umv. of Texas HSC, San Antomo, TX
OBJECTIVE: Staphylococcus epidermldis (STAPH-EPI) ~s the most common blood isolate ~n neonatal seps~s and maternal skin cultures at delivery Our purpose was to describe the permatal effects of decidmt~s caused by STAPH-EPI.
STUDY DESIGN: Using blood ~solates of STAPH-EPI from septic neonates, each uterine horn of 19 rabbits at 70%
~l estaUon was ~noculated transcerv~cally w~th 0 2 cc 078CFU/ml) of the bactenal suspension. Twenty-two
rabb~tsrecetved02ccstenlesahneperhorn At 96 hours or when preterm labor (PML) was recognized, the ammals were sacrificed for cultures and h~stology. Growth retardaUon (SGA) was defined as b~rtrhwe~ght (BW) < 10th percentile for gestat~onal age
RESULTS: At sacrff<e, 18119 bactena-treated animals had pure dec~dual cultures for STAPH-EPI. All sahne-treated animals had negative cultures. There was httle fever (2118) or PML (0118) in infected animals. Animals who received sahne remained asymptomat~c.
Group (n) BW (SO) SGA Fetal D~ath
Sahne (22) 15.7 g (3 4) 26% 6%
STAPH-EPI(19) 11.3 g (3.0)* 78%* 24%*
*P<-0 001, saline vs. STAPH-EPI
CONCLUSION: In the rabbit, decidu~tlS caused by STAPH-EPI ~s associated with severe Intrauterine growth retardation and fetal death. We speculate that subclimcal infections w~th ~ess-vlrulent organisms such as STAPH-EPI may play a role in unexplained growth retardation.

420 SPO Abstracts January 1994 Am J Obstet Gynecol
526 AMNIOTIC FLUID TUMOR NECROSIS FACTOR, LABOR DURATION AND CLINICAL INFECTIONS ATTERM E R Newton, T Sder Khodr ~ Dept of Ob/Gyn, UTHSC, San Antonio, TX
OBIECTIVE Tumor necrosis factor may change myometr~dl function through alterations in decldual prostaglandm production We sought to correlate amnlot~c fluid tumor necrosis factor (AF TNF~) w~th labor duration
STUDY DESIGN Using a crosssectlonal samphng scheme, 169 women at term had an AF specimen obtained by a transcerv~ca] catheter aspiration for culture and AF TNFo determination after 10 houts’ rupture of membranes Maternal ~nfect~on was defined as a positive amnlotlc fluid culture and intrapartum temperature 2 37 8~ (n = 97) or postpartum temperature 2 38~ (n = 16) plus two of the following uterine tenderness, foul smelhng fluid or Ioch~a, leukocytos~s, and maternal or fetal tachycard~a AFTNFc~ was measured by specific double radm~mmunoassay {assay sens~tw~ty, 0 163 ng/ml)
RESULTS The duratmn of labor at the t~me of samphng was slmdar between infected (n = 113) and uninfected groups (n = 55)
20ENolF [] P<001 1 5 IF [] 1 43
Mean 1 22 AF TNFe I 0
ng/ml
05
0 ~9 l0 16 ~17
Hours of Labor High AFTNFc~ was associated w~th more cesarean sectmns (P<0 05) and chn~cal mfect~on (P<0 01)
CONCLUSIONS In the absence of ~nfectmn, labor at term ~s not associated w~th elevated AF TNF(~ We speculate that AF TNF(~ ~s either a marker for or a causative agent m the decreases m myometnal function when infection occurs during labor
527 THE PHARMACOKINETICS OF AZTREONAM DURING PREGNANCY V Cook, S Allen,x J. Summersgfll,x S Gall. University of Loulsvdle, University of Louisvdle Hospital, Louiswlle, KY OBJECTIVE: Factors prompting the lnvestigationof the pharmncokmet~csof aztreonam during pregnancy tnclude’ bacterial resistence to traditionally used ampicillin ~nd/or cephalosporins, avoidance of amtnoglycoctde oto mad nephrotoxlc~ty, and significant increases in antibiotic metabohsm and ehmmation during pregnancy STUDY DESIGN: After informed consent, aztreonam was admimstered intravenously 2 g every 8 hours for at least 5 doses to achieve steady state levels prior to phlebotomy performed at peak (within 1S minutes post dose), midpoint (4 hours post dose), and trough 0mmed~ately predose) Clotted specimens were centrifuged and the serum frozen at minus 20 F untd s~multaneous batch analysis of all specimens A unne specimen was collected and frozen at the time of ~mtlblotlc administration Aztreon~m concentrations were determined by a standard agar disc-diffusion bioassay ustng E colt as the indicator organism Serum and urine concentrations were measured USlllg an aztreonam standard carve generated m pooled human serum or buffer RESULTS: peak mtd trough urine Cr CI EGA mat wt mean 54 2 119 4 45 2109 109 24.4 157 SD 23 4 6.1 3.06 1336 27 8.6 31 range tower 20 4.0 < I. 0 5010 60 12 I l l upper 107 23.7 10.0 475 147 34 205
Cr CI = creatinine clearance (ml/mm), EGA = esnmated gestatmnal weight, mat wt = maternal weight (pounds) Neither serum or urine levels correlated with creatmine clearance, gestatlonal age, or maternal weight Trough serum concentrations were less than the generally accepted mlninum inhibitory concentratmn (MIC) of 1 ~.ng/ml for the Enterobacterlace~e in 3 of 11 patzents and below 3 /xg/ml zn 6/11 patients Serum concentrationswere below the 10 #g/ml MIC necessary for treatment ol Pseudomon~s mfectmns m 5 of 10 patzents at the midpoint and m 10 of 11 at the trough level CONCLUSION: Compared with pubhshed data for nonpregnantwomen, the pharmokmetics of &ztreonam during pregnancy &ppe~xr to be ch~.ractar tzed by a more frequent oecurrence of trough concentrations below I ~g/ml due to more rapid elimination.
Subject Index

Volume 170, Number 1, Part 2 Subject Index 423 Am J Obstet Gynecol
Subject
Acid-Base Status - Fetal
Alphafetoprotein
Amnioinfusion
Amniotic Fluid Volume
Amniotomy
Antepartum Fetal Evaluation
Acoustic Stimulation
Amniotic Fluid Volume
Biophysical Profile
CST
Doppler
Fetal Movement
Non-Stress Testing
Other
Antiphospholipid Antibodies
Birth Trauma
Cardiovascular Hemodynamics
Cervical Examination
Cervical Ripening
Cesarean Section
Computers
Congenital Anomalies
Cordocentesis
Diagnostic
Intrauterine Transfusion
Technique
AbsWactNumber
17, 18, 77, 85, 97, 98, 112, 126, 127, 129, 158,
167,276,346,404,420,421,441
145, 160, 174, 258, 259, 263, 265, 266, 269, 270,
271,281,285,287,288,291,292,293,312
46,235,246,338,362,373,422,441,451
25,’68, 137, 149, 150, 152, 217, 239, 324, 423,
426,468
363,429
36, 92, 100, 134, 138, I39, 140, 142, 143, 144,
146, 148, 153, 154, 261, 282, 311, 339, 343, 379,
383,465
87,88,138,148
137,144,149,150,152,327,426,429,462
139
142,402,406
14,100,140,458,465
93,151,153
93,94,146,155
87,88,329
62,171,180,207,214
59,222,238,245,290
2, 6, 9, 12, 13, 16, 52, 116, 117, 120, 121, 123,
128,131,186,200,493,496
71,306,322,340,354,393,398,399,412,466
355,361,365,374,377
39, 60, 220, 222, 225, 226, 228, 230, 233, 234,
237,366,369,512
223,359,436,437,438,439
10, 20, 43, 72, 73, 79, 175, 179, 269, 274, 278,
283, 284, 285, 287, 289, 295, 304, 311, 314, 315,
317,319,320,321,341,414,443
445,452
31,210,442,444,449,452
50,349,448,455
41

424 Subject Index January 1994 Am J Obstet Oynecol
CT Scanning
Diabetes
Pathophysiology
Complications
Fetal Evaluation
Management
Other
Other Screening
Testing
Doppler
Drug Effects On
Fetal Echocardiography
Fetal Well Being
Findings/OB Complications
IUGR
Other
Physiology
Preeclampsia
Regional Fetal Blood Flow
Technical
Epidural Anesthesia
Exercise in Pregnancy
Fetal Anomalies
Fetal Growth
Fetal Growth Abnormalities
IUGR
Macrosomia
Abs~act Number
176,192,478,511
22, 44, 51, 63, 64, 69, 80, 130, 162, 163, 170, 175, 178, 183, 184, 189, 191, 193, 197. 198, 205, 212,
216,245,355
5,68,114,178,189,212
24, 59, 63, 64, 69, 183, 190, 191, 203, 205, 211, 245,492
83,137,155,179,300,325,347,458
44,63,65,69,189,190,211,212,245
5,190,198,261
197,198,209
44,64,65,170,183,203,216,218
25,79,80,102,435,456,457,462,463,464,470
109,467
16,94,100,109,111,305,308
459
9,132,238,461,468,469
336,463
79,80,461
102,459,460,464
57,176,463,476,479,480
10,130,456,464
465,466
61,165,167
120,159
4, 19, 22, 38, 72, 104, 141, 143, 154, 256, 262,
268, 278, 294, 298, 316, 320, 321, 331, 342, 438,
450
21, 81, 83, 84, 92, 108, 135, 252, 253, 300, 334,
335,378,504
108, 132, 207, 251, 253, 297, 301, 316, 318, 344,
427,431,449,472
11, 21, 91, 107, 112, 119, 135, 142, 164, 252, 297,
344,471
24,59,184,193,242,253,325,339,428

Volume 170, Number 1, Part 2 Sublect Index 425 Am J Obstet GynecoI
Su~ect
Fetal Lung Matnrity
Fetal Therapy
Genetics
Genetics-Diagnostic Technique
Glucose Metabolism
Hematology
Hemodynamic Monitoring
Hemolytic Disease of the Fetus
Hydrops Fetalis - Nonimmune
Hypertensive Disease in Pregnancy
Complications/Fetal
Complications/Maternal
Evaluation & Diagnosis
HELLP
Treatment
Hypoxia & Asphyxia - Fetal
Incompetent Cervix
Infections/Maternal
Chlamydia
Chorioamnionitis
275, 276,
289, 290, 342,494
Abs~act Number
218,347,386,391,395,407,414
13, 33, 37, 41, 72, 76, 239, 415, 441, 443, 445, 446, 447,
455,457
4, 20, 21, 22, 38, 43, 53, 73,
262, 263, 264, 266, 267, 269, 279, 280, 281, 283,
291, 293, 294, 296,
272, 273, 349, 391,
450, 452, 453, 454,
254, 255, 258, 260,
270, 271, 272, 273,
284, 286, 287, 288,
298, 299, 307, 320,
17, 49, 77, 85, 97, 98, 125, 126, 127, 129, 167,
350,420,424
229,306,363,392
3, 23, 29, 42, 74, 86, 200, 202, 234, 363, 413, 497,
500, 501, 502, 503, 507, 508, 509, 510, 511, 515,
516,517,519,520,523,524,525,526,527
523
1, 3, 28, 30, 32, 34, 47, 66, 199, 229, 248, 250,
385,418,451,512,521,524,525,526
4, 19, 20, 31, 38, 43, 136, 145, 154, 255, 259, 261,
267, 268, 272, 273, 274, 275, 277, 278, 279, 282,
283, 284, 285, 286, 292, 294, 295, 296, 301, 303,
333,450,451,506
51,84,163,178,193,203,211
8, 15, 27, 30, 61, 96, 113, 136, 156, 172, 180, 185,
195, 206, 210, 224, 249, 348, 434, 444, 455, 475,
498,505
9,131,186,224,493
50,116,122,123,275,323,349,444,446,448
31,37,270,443,445,447
2, 53, 54, 55, 56, 57, 58, 101, 115, 157, 207, 231,
243, 345, 409, 473, 474, 475, 476, 479, 480, 481,
484, 485, 486, 487, 489, 490, 492, 494, 496, 497,
498,499
345,402,409,474
54, 473, 474, 476, 481, 487, 488, 489, 490, 492,
495
53, 55, 57, 191, 194, 243, 473, 475, 478, 482, 484,
491,495,499
54,478,487,488,489,490,494,498
67, 89, 119, 169, 477, 479, 480, 483, 485, 488,
493,496
426 Subject Index January 1994 Am J Obstet Gynecol
Subject
Endometritis
Group B Streptococcus
HIV
Preterm Labor/PROM
lntrapartum Fetal Assessment
Labor
Meconium
Medical Complications
Medications in Pregnancy
kmtiepileptics
Calcium Channel Blockers
Cocaine
Corticosteroids
Other
Prostaglandin Inhibitors
Prostag|andins
Tocolytics
Multiple Gestation
Oligohydramnios
Oxytocin
Perinatal Outcome
Abs~act Number
177,512
42,501,513,514,515,516,519,520
29,497,504,505,506,507
1, 28, 32, 35, 232, 360, 384, 385,
399, 411, 413, 418, 507, 508, 509,
522,524
48, 49, 66, 148, 199, 250, 350, 390, 424,425,426,427,429,432,433,434,461
35, 39, 45, 46, 48, 75, 166, 219,
237, 238, 241, 245, 247, 248, 250,
354, 355, 356, 358, 359, 362, 365,
369, 370, 372, 373, 374, 375, 376,
431,434,439,501,518,525,526
46,124,235,246,422
386, 394, 398,
510, 518, 521,
420, 421, 423,
225, 228, 235,
260, 322, 353, 366, 367, 368,
377, 388, 425,
52, 74, 121, 171, 173, 176, 180, 182, 185, 186,
187, 188, 192, 195, 196, 200, 201, 202, 206, 208,
210, 213, 214, 234, 240, 254, 375, 460, 481, 491,
506, 511
67, 89, 169, 173, 195, 413, 477, 483, 523
67, 168, 169, 483
168, 495
78, 106, 181,208, 375, 467
201,218, 291,407
7, 12, 16, 90, 162, 166, 172, 185, 196, 213, 352
61, 62, 380
241,361,364, 374
40, 89, 138, 357, 358, 371,405, 410, 419
95, 105, 155, 164, 221, 245, 251, 290, 310, 324,
326, 330, 378, 401, 430, 442, 449, 457, 468, 472,
482
149, 280, 338, 423, 432
48, 60, 106, 232, 247, 353, 358, 365, 366, 368,
369, 370
1, 7, 29, 39, 66, 70, 124, 135, 143, 146, 151, 166,
173, 174, 187, 197, 199, 214, 216, 219, 22l, 222,
223, 225, 236, 237, 240, 246, 252, 255, 265, 271,
279, 281, 293, 329, 337, 344, 350, 351, 362, 379,
382, 387, 389, 390, 393, 395, 400, 401, 402, 403,
404, 408, 409, 417, 419, 422, 425, 433, 436, 469,
471,485,502, 505, 513
Volume 170, Number 1, Part 2 Author Index 427 Am J Obstet Gynecol
Subject
Physiology
Fetal
Maternal
Membranes/Placenta/Cord
Placenta Previa
Placental Pathology
Polyhydramnios
Post-Dates/Prolonged Pregnancy
Premature Labor
Premature Rupture of Membranes
Prematurity
Prenatal Care
Psychosocial Aspects of Pregnancy
Respiratory Distress Syndrome
Selective Fetal Reduction
Sickle Cell Hemoglobinopathies
Substance Abuse in Pregnancy
Teratology
Thyroid
Abstract Number
6, 14, 15, 23, 81, 82, 86, 96, 99, lO1, 104, 110,
113, 114, 115, 118, 122, 133, 156, 157, 348, 364,
421
2, 11, 13, 17, 18, 35, 36, 40, 41, 50, 51, 56, 77, 81,82, 83, 84, 85, 87, 88, 90, 91, 93, 94, 97, 98,
99, 103, 107, 108, 111, 116, 118, 119, 122, 123,
124, 126, 127, 129, 134, 153, 276, 343, 348, 372,
424, 446, 448, 453, 454, 459, 486
5, 6, 8, 11, 14, 40, 45, 52, 58, 75, 82, 86, 95, 96, 101, 102, 104, 105, 107, 110, 113, 114, 115, 117,
120, 121, 128, 131, 133, 182, 206, 247, 260, 282,
310,359,372,466,477,484,486,499,527
15, 23, 24, 56, 62, 78, 90, 95, 118, 130, 132, 136,
156, 157, 158, 159, 160, 162, 163, 164, 168, 217,
224,249,356,522
309
7,158,161,174,277,304,382,383,385,472
25,227,327
140,356,370,435,462
27, 28, 32, 34, 70, 71, 204, 231, 353, 357, 360,
364, 371, 380, 381, 384, 387, 388, 389, 390, 393,
394, 397, 406, 410, 411, 412, 415, 416, 418, 419,
508,509,510,518,522
47, 60, 217, 219, 229, 232, 248, 249, 334, 377,
381,384,386,391,407,408
3, 27, 30, 33, 34, 45, 55, 70, 112, 187, 244, 345,
346, 376, 378, 381, 382, 383, 387, 388, 392, 394,
395, 396, 397, 398, 399, 400, 401, 403, 404, 405,
406,411,412,414,416,417,433,514,521
19, 42, 65, 128, 133, 147, 151, 160, 170, 172, 194,
196, 201, 202, 204, 221, 223, 231, 236, 240, 243,
244, 254, 258, 265, 266, 288, 292, 332, 376, 379,
389, 396, 417, 436, 491, 503, 513, 514, 517, 519,
527
110,220,228,236,351,502
33,346,347
105,310,330
8,194,460
12, 18, 78, 99, 106, 161, 181, 204, 208, 351, 352, 408,467
256,453,454
192,205,213

428 Author Index January 1994 Am J Obstet Gynecol
Subject
Tocolytics
Ultrasound
Esmnated Fetal Weight
Fetal Anomahes
Fetal Echocardiography
Fetal Growth
Fetal Well Being
IUGR
Multiple Gestation
Other
Technical
Vaginal Sonography
Contraction Monitoring
Uterine Rupture
Vaginal Birth After Cesarean Section
AbsWact Number
109,357,360,371,380,400,405,410,415,416
10, 147, 177, 239, 264, 267, 280, 297, 298, 299,
302, 303, 305, 307, 309, 312, 313, 314, 315, 316, 317, 319, 323, 324, 328, 330, 331, 332, 333, 335, 337,340,397,428,430,431,447,456,470,504
92,302,318,427,428,432
76, 179, 256, 259, 262, 263, 264, 274, 286, 289,
295, 296, 299, 301, 303, 304, 307, 308, 312, 314, 315,317,319,327,337,338,341,342,438,458
37,111,305,308,311,321,323,331,341,435
159,184,300,318,325,328,334,339
47,134,147,150,152,326,329
58,91,161,336,471
139,251,326,336,430,442,469,470
36, 68. 73, 76, 144, 182, 268, 277, 313, 322, 332, 333,335,343
227,302,313,340,361
71,306,309,354,392
368,396
49
241,367,373
Author Index

Volume 170, Number i, Part 2 Author Index 431 Am J Obstet Gynecol
Author
Abramovlcl, H Abramson, S.B Abu-Fadd, S Abnhamad, A. Acosta, L. Adam D Adam, K
Adngnolo, A. Adz~ck, S. Aerts, L Ahlswede, B A. Ahn, M O. Ahya, S A~man,J. Albert, T. Alcalay, M Alexander, M
Allbert, J R. Allen, R. Allen, S Alhson, J. Alter, H Altman,J Alvarez, M.
Ames, M
Ammt, A. Amon, E.A. Andersen, H.F. Anderson, C Anderson, G.D Anderson, P Anderson, R. Amdres, R.L. Andrews, W.W. Anthony, J Anyaegbunam, A Applewh~te, L. Araneda, H. ka-hear t, K Aneh, S. Armenti, V
Arqmlla, E. Arrabal, P. Ashmead, G Asrat, T. Assel, B Aswad, N Atkmson, B. Atk~nson, M W Au, A. Azar, G Bacev~ce, A.E. Badahan, S S Bahado-Smgh, R. Baker, B
Baker, J Baker, R S. Ball, R.H Bar-Hava, I. Barada, C Barbera, A. Barclay, M L.
Bardlcef, M Bard~cef, O
Barkm, G. Barkey-Dwon, R. Barnhard, Y Barnn, C M Barrett, J.F R. Barshes, D Barstow, W.H
Barth,Jr, W Barton,J. R.
Abstract Number
477 57 64
10,298,452,456,470 30,76,453,522 480
209,496 452 443 135 187 49 194 434 179 48 111
232,360 467
419,527 313 517 379
217.310,381 2O6
83,84,223 463 176
359~392 329,459 20,43,129,508,509,510 515 393 18,78,204 28,235,512 495
193,224,460,481 368
35,418,518 16
385,421 187 81
247 223 143,151,229,391 336,469 422 166 40O 478 245 120
79,80 267,269,320 72 277
2,12,58 17,85 68,327,432 351,371 94 359
73,76,114,115,169,283,453 114,115 39,48,410 193
68,118,193,327,432 423 445
369,370 92 185 176
Author
Bass, D.
Basu, J.
Baumann, P
Baumgarten, A.
Bauusta,J.
Bax~, L
Bayhs, S
Bean,J D
Beckmann, C A.
Beckmann, C.R.B
Begmn, F
gehnke, E.
Belfort, M
Beh~an,J.M
Bell@
Bellotti, M
Belsky, D
Bendel, R.
Benn, P.
Bennett, T.
Bentz, L. S.
Benzm, R
Berant, M.
Bergauer, N
Bergel, E.
Bergman, R.
Berkowltz, G
Berkowm,, K.
BerkowlLz, R L.
Berkus, M.
Bernstmn, I.M.
Berry, S.
Berry,, S M.
B~anchl, D.W
Bmnculh, K.W.
Blenlarz, A.
Bishot, P
Blackstone, J.
Blake, P.G
Blakemore, K
Blelcker, C.A.
Bhtzer, M.G.
Blood, T.S.
Bockmg, A D.
Boe, N.M.
Bogdan, D
Bohman, V.R
Boldor, I
Bombard, A.
Boots, L.R.
Bootstaylor, B.
Boo~arjomehn, F.
Boqon, N.
Bottom~, S.F
Bowe, L.
Bower, S
Bo,’zem, P.
Brace, R A.
Bracero, L.A.
Branca71o, L,
Branch, D W.
Brandt, D
Bravo, R R
Brazerol, W.F
Brennan, K.
Bngantl, S.
Brlggs, G
Brimmer, B
Bnones D
Bntton, KA
Bronsteen, R
Brnoks, G.G.
Abs~actNumber
489 481
15, 27, 71, 107, 249 269, 320 441
80, 146, 414 117
14, 33 387, 388 387, 388 233, 394 249, 250 6, 9, 50, 56, 72, 147, 168, 330,415, 448,495,496, 497 172 312 94
238 336, 469 281 203 87, 88 438 294
387, 388 172 178 378 81
105,217, 378 22, 183 91,260 35,372 284, 444, 449, 450 38, 156, 260 482 384 394
109, 441,447 54, 488 160, 259, 275,337, 499 524, 525 259 494 251 280 456
411,500 385 255 270, 271,273, 274 40 354 329 70, 152, 219, 338, 342, 390, 395, 444, 449 184, 318 25 94 13, 90, 122 157 291 214, 277
336, 469 279 265 313 281 391 376 479 416 190 222

432 Author Index January 1994 Am J Obstet Gynecol
Author
Btoset~s, 1 A
Brost, B Brown, C. Brown, E Brown, H L Broze, G Brubakk, A M. Bruckner, A. Brumfield, C. Brzechffa, P Bsat, F
Buckley, C Budormk, N Bin, T H Bnkovsk~, 1 Burholt, D R Burke, M Burns, D N. Burrus, D. Burton, B.
Bussel,J. Butler, M C. Buyon, J.P Byrne,J.L.B Came, M.E. Caldwell, L.E. Calhoun, B. Callan, N Cah m, S Cameron, A D Campbell, K. Campbell, W
Camck, J Capeless, E L Caplan, M S Carelh, M Cantts, S Carlan, S Carlson, D.E. Carmody, T. Carnes, A Carpenter, M. Carpenter, R. Cart, M.H. Cart, S. Carter, J Carter, S Casal, D Casanova, C. Case)., G Casp~, E Cassell, G Castracane, V D Castro, L Catalano, P
Catazante, S
Cedka, J. Certrulo, L Cerutu, S
Cetrulo, Jr., C.L. ChMfin, D.G Challenger, M. Chambers, C Chambhss, L Chan, D W Chan, K. Chan, L. Chandler, P Chang, R Chao, C R. Charles, I
Chatteuee, M. Chau, A
Chaudhuw, A
Abstract Number
26 407,430 177 194 161,416 498 440 221 272,273 329 357
70,390 289 440 421 154 51 507 433 292 349 52O
37,57 277,494 180 17,85 407
252,337 336,469 268 47
7,332,333 51,258 260 171 19 61,357 165,218,315,380 323 124 14 51
50, 330, 448 143,196 51 335
255,523 381 344 242 385,421 28,512 95,181,182 131,467 83,84,223 3O4 45O 156 93 156 459 305 243 65 473,474,475 99 335 95 179 79,80,354 117 371 205 194
Author
Chauhan, S P.
Chawla, A. Chayen, B Chazotte, C. Chen, A. Cherry, B Chmwenak, F Cheung, V Y.T Ch~ang, M Chiao,J. Ch~en, E Chlk, L Chrnielowmc, S Chr~stensen, D Chu, R. Chun, C K C~arleglio, L. C~pnam, C. Clapp,J.F. Clark, A.L Clark, D A. Clark, tC Clark, K.E Clark, P. Clark, S.L. Cliver, S.
Coalson, JJ Cohen, G R. Cohen, H L. Colbern, G. Colher, G. Comacho, G Comstock, C.H Conners, W Cook, C Cook, V Copel,J.
Copes, J Copozello, A. Copper, R. Corson, V Cosper, P. Cosugan, tC Cotton, D B.
Coulam, C Couhnp, L. Cousins, L Cowngton, C. Cowan, B.D CoMes, T. Cox, S. Crmgo, S.
Crass,J. Crawford, M. Cntes, Y Croonl, C.8. Crosby-Schmidt, C Crossland, W R. Crowley, J. Cruz, A. Cullen, M.T. Cunmngham, D.S. Cunnlngham, F G. Cuomo, M Curet, L. Cus~ck, W Cutney, C.
Cutraght, J
Abs~act Nttmber
110, 324, 362, 426, 427, 428, 429,430,431,489 110 48 173 377 120 86,220,349 251 53 357 358 439 78
166,365, 491 20,43 3,34,471
281,333 33 159 ~07 11 380 2,12,58 501
282,420,424 42, 55, 236, 345, 346, 398, 399, 400,401 33 158 317 53 33 1 319,321 272 59
373,527 10, 37, 267, 269, 300, 301, 316, 320,452 190 503 345,401,412 259 270,274 150 15, 27, 30, 35, 67, 71, 73, 76, 104, 114, 169, 249, 250, 372, 418, 444, 449, 453, 454, 477, 483,493,518,522 214 32 178,304 352 428,429 21
66,199,201,202,322,411 210 159 178 405 155,472 162,163 454 210 496 5O6 521 201 317 92,351,371 7,281,331,334 33t
418,518

Volume 170, Number 1, Part 2 Author Index 433 Am J Obstet Gynecol
Author
(]utter, G
D’Ahou, M
Dabrowskl, A
Dacus,J
Damrun, D P
Danna, P
Daoud, Y
Dar, H
Darby, B G
DaSflva, O P
Davis, E E
Davis, R
Dax, 1
Day-Salvator, D
de Vec~ana, M
DeBard, M
Decavalas, G
DeF~hppo, C
Degam, S.
DeGennaro, N J.
Dekker, G.A
Del Valle, G O.
Delaney-Black, V
Delke, I,
DelPret, D.
DeMana, M A
Demopoulos, R
Denue, S
Dent, M
Depp, R
Deprest, J A
Dev, V G
Devoe, L D.
DeVore, G R
D~ Sessa, T
D~ana, L
D~Bella, V
Dickinson, J E
D~dolkar, S
D~erkm, L
Diker, A L
DaI.andro, R M
Dfldy, G A.
Dflhon, A
D~Nolio, T E
D~von, M Y.
Dombrowsk~, M P
Donnenfeld, A E
Dorey, L G
Drago, N.
Drugau, A.
DuBard, M
Ducsay, C A
Dutf, P
Duht~k~, M
Dvonn, E.
Dweck, H
Dyson, D
Eans, R
Easterhng, T
Ebrahma, S A D.
Eddleman, K.A.
Eden, R.T
Edwards, M
Egan, }" F X.
E~chenwald, E
E~k-Nes, S
Ek, S
Elder, F
Ele3alde. B R.
Ele.Jalde, M M
Ehas. S
Abstract Number
42,236
156,210
309
44
459
165
190
3O7
3O3
251
122,123
272,273,397
66,199,201
141
81,142,197,198,200,350
112,397
4O8
5O4
307
504,505,506
486
479,480
352
377,479
516
38,156
174
24
165
461
26
4
89,155,472
323
16
308
146
457
145
223
11
231
420,424
148
5O4
60,68,118,193,327,432
113,348,395,439,444
495
263,264,265,313
348
83,84
283,285,294,295,296
271, 272, 273, 274, 346,
403,404, 412
45,75,103,376
501
410
283
1
4O5
98
244,262
284,285,295,296
220
229
164,523
331,515,516
513
440
440
21
278
278
279
402,
Author
Elk, R
Eller, D
Elhngs,J.
Elhott, B.D
Elhott, J
Eloby-Chlldress, S.
Emels, J J
Emerson, D.S.
Eu&cott, B.
Eng, F
Ennquez, G.
Epstein, H.
Erdman, W
Enksen, N
Enksson, M
Enksson, uJ.
Eruest, M
Ernst, L
Evans, A
Evans, M I
E’~ arts, R
Evans, W
Evelhoch, J
Ezra, Y
Falrbanks, L
Falrhe, F
Farah, L
Fargason, C
Farme, D
Farmak~des, G
Faustxn, D
Fayngersh, R P
Feeney, L.
Felgm, M D
Fenough ty, M
F~del, P
Fteld, N T
F~gueroa, R
Fdes, J.C.
Fdly, R.
Fmberg, H.
Free, B.
Fmley, S.
Fmn-Powers, J.
Fischer, R.L.
F~sher, B
F~shman, A.
F~sk, N
Flack, N.J
Flake, A.
Flmsher, J M
Fhs~, L.
Flouret, G.
Flowerdew, G
Font, G
Fougner, A.C.
Fox, A
Fox, H E
Franko-F~hpas~c, K
Fredenksen, M.C.
Frentzen, B
Friedman, D
Friedman, E
Friedman, S.A.
Fngoletto, F D
Fu3~to, D.T
Gabbe, S
Galan, H.L.
Galasso, M
Abstract Number
204
148
326
130, I32,162,163,189
139,227
11
486
28O
335
438
257
190
177
246
248
175
389
382,383
10,298,456
73, 76, 136, 208, 283, 284, 285,
286, 294, 295,296,450, 45l
~77
195
115
237
336,469
268
248
314
42
237,445
266,435,462
231
157
281
353
161
93,94
418,518
216,369,370
157
488
443
139
254
272,273
255
482
12,58
149
41
25
443
242,368
94
353
253
297,384
125,240,503
38
293
79, 80
65
396
143,391
501
109
375
107,228,409,485,486
513
154
5,179
14,33
30,35,71,250,372,522

434 Author Index January 1004
Am J Obstet Gyne~ol
Author
Gall, S. Garcla, E Gardner, K. Gardner, M. Garfield, R.E.
Garite, TJ. Garmel, S. Garofalo, J. Gaudier, F.
Gauthier, D. Gaziano, E. Geary, F. Gebauer, C.
Gee, R Gelfinan-Holtzman, O. Geneus, C.
Gerard, J. Germain, A.M. Gersen, S Ghidlm, A. Ghlsoni, L.
Giannakoulopoulos, X. Gilbert, W.M. Gilson, G Gilstrap, L G~nsberg, N.
Glrard,J. G~raud, G.D. Gleason, C. Glew, R. Gloeb, DJ Glover, V. Godmilow, L.
Goedert, JJ Goepfert, A. Goldberg, J. Goldberg, M. Goldenberg, R.
Goldman, B. Goldsinith, L T Goldstein, 1. Gohchowsk~, A M. Goluszko, P. Gomez, R.
Goncalves, L. Gonen, R Gonik, B. Gonzalez, A GonzaleT, R. Goodrum, L. Goodwin, T.M. Gordon, M Gorman, R. Goyert, G.
Grabowskl, J. Grafe, M, Grahain, E Graves, W Gray, G Greenberg, C. Greenberg, S S Greene, M Greenspoon, J. Grlffith, S.M Grimes, D. Groner, Y. Groome, LJ. Gross, S:I Grossman, J H. Guevara, F.
Abstract Number
419,527 278 391 236,401 509 106,423 210 316 112, 315, 346, 377, 400, 401, 402,403,404,479,480
170,297,339,384 336, 469 29 413 5O2
260 194 59 103 19
30, 217,356, 381 93 41 9O 351,371 66,199 257 309 123 337 499
288,290 41
263 5O7 397 443 185
28, 42, 55, 112, 236, 345, 346, 397, 398, 399, 400, 401, 402, 403,404,412,512 60 105
269,300,301,316,320,328 24,416 508,509 28, 30, 35, 71, 249, 250, 372, 418,471,518,522 71 307 23 176
15,27 50,448 206 413 252 190 204 289 24O 29 330 96 11 185
64,131,160 505,506 74 175 87,88 279 32 73
Author
Gmnn, D.A
Guzman, E. Hackett, R Hacobian, A. Haeusler, M.C.H Hagay, zJ Hage, M. Haisten, IL Hakan Borg, L.A. Hales, K. Hahnda, E Hallak, M. Haminil, H Haning, RV. Hankins, G.D.V. Hannah, M. Hansen, G Hanson, R, Har-Toov, J. Harris, E.N. Harris, R.L. Harrison, M. Harstad, T Hart, A Hart, O Hardey, C. Hmwey, C.J.
Hauth,J.C.
Hediger, M L. Hedriana, H.L. Hellerstmn, H.K. Henderson, C.E.
Hendnck, J Hendricks, S. Hennessy, M Henry, H. Herren, T. Hertelendy, F.
Hess, D.L. Hewltt, C.W Heymann, M.A. Hibbard, J. Hickok, D. Hiettm, A.tL H,gby, K Hisley, J.C. Ho, G.Y.F. Hobbins, J. Hobel, C. Hochberg, A Hodgkins, P Hoff, C. Hogge, A. Hoh~mer, A.R. Holcberg, G. Holemans, K. Holt, V. Holzgreve, N.B.
Hong, S F. Honneb~er, M.B.O.M.
Horensteln, J. Horsager, R. Hosk~ns, I.A Hosmer, L. Hostetter, M. Houlihan, C. Hourvitz, A. How, H. Howell, L. Hse, H.
Abstract Number
396,398,399 102
141,306 258 375 455 175,355 96 182 175 365 47 219,338,477 497 258
77,126,127 225 212 121
102,261 207 487 443 434 510 39 466
77,126,127,128,129 28, 55, 112, 234, 345, 346, 363, 398, 400, 402, 403, 404, 412, 512 482 134,153 120 60 98 304
96 64 194 364 103 45 40 52,186 244,241,492 416 133 182 224 10 131,467 23 234 407 291
122,123 63,191,464 135 244 284 145 473,474,475 106 323 202 109,174,379,441 65 246 306 48,410 419 443
6

Volume 170, Number 1, Part 2 Author Index 435 Am J Obstet Gynecol
Author
Hsu, C. Huff, R.
Hutfaker, J. Hughes, H. Huhta, J. Hume, R.F. Iams,J. hnrie, S lnan, M. Ingardla, C. Inglis, S R lnnalnoratl, F. Insler, V. lnon, O. Inye, B.K Irtenkauf, S.M. Isada, N.B.
ltskow~, I.
ltskov~t~, J.
Itskowtz-Eldor, J. Ivan, J lzqmerdo, L.
Jackson, D Jackson, G.M. Jacqueun, B Jaekle, R
Jaffa, A.J. Jaffe, R. Jakobl, P. Janda, W. Janus�, C A Jarohmek, A Jeantv, w Jett, B Je~on, G flang, Y.X.
Johanson, R Johemfing, A Johnson, A. Johnson, D Johnson, F Johnson,J. Johnson, M P.
Johnson, S. Johnson, T.R.B. Johnson, W. Johnston, J,M. Jones, D Jones, M. Jones, P. Jongsma, H.W. Kagan-Hallet, K. Kahn, D Kainer, F Kalhan, S. Kalugdan, R Kamens, C. KaFlnn, A Kasch, L. Katz, M KauI, A. Kavic, S M Kay, El Kazazlan, H. Kellner, L. Kelly, M. Kennedy, IC Khahl, A. Khayyata, G. Khoury, A Khoury, J.
Abstract Number
274,473,474, 475
22 108
56 311
283,285,295,450 70,390,413 268 269 212,287,293,347 220, 349 379 355
233,394 196
67,104,169,477,483 73, 136, 283, 284, 450,451 463
300 328 3O6
92, 371 391,499 340,374 442 63,238,406, 464 102,261 256 30O 384 477 209 1 517 72
335 495 191
65,259 56,168 413
17,85 73, 136, 283, 284, 295,296,338,450,451 403
150,473,474,475 111 136 452 218,380 70,390 420 524 339 455 212 392
382,383 392 275 420
508,509 465 96 275 258,266,435 124,167 282 245 245 32 63,191,464 337
286,
285,
295,
286,
Author
Kickler, T Fadron, D
Klm, C.J Igam, E.S.
Km~, K.S. Klm, S.W. K~ng, I.B. Klngdom,J. Klrk, J.S. Klrshon, B. Klthier, K. Kltznnller, J. Klos, S. Klein, A. Klein, L. Klein, S Klemman, C. Khman, H.
Khnger, K.W. Kla~ght, A.B. Klmwles, R Klmx, E Klaudsen, L. Knuppel, R. Kochenour, N.K Kolm, P.
Koo, J N Koos, g.
Klirach, J Korcarz, C. Korst, L. Koutrls, P. Kl-amer, W. Kubfl~s, P Kuehl, TJ Kullama, L K Kupfermmc, MJ. Kurtzer, T Kurzel, R B l.aBerge, S Lacrolx, L.
Ladfors, L Lagrew, D C. Laffer, S. 1,ajmlan, S Lake, M
Lampert, M Lampley, C. Landesman, S Laudon, M. Landor, M.
Lang, R. Lang, U Langer, O.
Langston, C Lantz, M 1,apmskl, R. LaSala, C Lasser, D l,auna, M.R.
Le, S.Q. 1,ee, c M. Lee,J.H. Lee, M.J. Lee, W Lee, W.H. Legum, C. Lmkln, E Lemery, D, Leos, N.IL Lerut, T.
Abstract Number
275 175 3
155,472 3,34 3,34,471 492 268
319,321 470,496 450 211
205,245 148 29 1,231 37,320 267
38,286 14 117
336,469 I47,415,448 306,458 340 298 34 308 48,410 52 49 41 415,496,497 501 14,33 99
82,254,299 501 478 101 185 225 248
341,468 195,291 466 188,230,458 73 186 125 507 5,179 118
52,186 2,58 22, 130, 132, 133, 183,189,216,369,370 72 252 105,310,356,378,381 347 498
208,338,395 119 471
3,34 171
319,321 24 261 1,517 442 5OO 26
162, I63,
436 Author Index January 1994
Am J Obstet Gyneco/
Author
Lescale, K B Lesser, M
Lewis, D F L~beru, M
I mn,J.M, lain, K H~ 1,m, S Lmcoln, T Lmdhenner, M I,mdsay, M Iasman, B L~ttman, L
Lockwood, CJ Lombard,, SJ. Longnure, S. I,oucks, C A. Lovelace, G S towensohn, R. Lowther, G. Lubarsky, S. L Lucas, B Lucas, M Ludom~rsky, A Luks, F 1.
Lund, J D Lupo, V. Lusky, A Luthy, D,A Lutz, P D.
Luzu,,, F Lynch, C Lynch, I., Lynch-Salmnon, D Lyon,J.L Maberry, M. MacGregor, S.
Macmlla, J. Mack, I, A Mackenzie, F MacLean, C
Macphafl, S Magann, E.F
Magec, K Maggm, A Maher,J.E Mahoney, M. Malda, C. Mare, E Major, C.A
Mandawlh, S Mandel, 11 Mann, L Manor, M Mantay, E, Many, A,
Man, G. Markello, T Marklmg, L Martens, M.G Martm, A Martin, G 1 Martin, R W
Martm,.]r., C B Martin,Jr ,J N
Martmez, E Martins, M
Abstract Number
220 317
124,167,411 222 301 32,142,200,350 484 272 234 52,186 29 515 338 117
30,217,310,348,356,381 4,465 72 420,424 144 436 268 228 473 167,184,318 140,311,313,452 26 181 213 48 241 406 233 344
105,310,356 464 214 66,199 221 371 262 309 476 187,461 116,446 54, 324, 361), 361, 362, 426, 427, 428, 429, 430, 431, 487, 489,490 201 44O 235 267,269,320 304 53 197,198,200 113,15,27,249,348 347 294 223 355 445 261 52 10,298,452,456,470 288 44O
20,43,508,509,510 276 49 232,360,489 137,387,388 54, 324, 426, 428, 429, 430, 487,488,489,490 157 461
Author
Mashlach, S. Mason, B Mastroglanms, D Mathers, A.M Mathur, S. Matt, D Matthews, V. Mallsson, L.A.
Matute, J. Matzkel, A. Mauer, M.B. Mauhk, D. Mayes, A. Ma¢or, M. McCalla, C O McCarter, L McCullough, C McCullough, L.B McCurdy. C.
McFarland, M. McGehee, W Mclntlre, D McLean, D. McNalnara, M. McNanley, T McNay, M.B. McNefll, T McNelhs, D McParland, P
Meaddough, E. Mecenas, C Medeans, A L Megenan, G
Me~s, P, Melster, D Mcnnemeyer, S. Mercer, B
Merrill, D Metlay, L A Meydreeh, E F. Meyer, B. A Meyer, J M. Meyer, N Meyer, R A
Meyer, W.
M~khafl, M S. Millar, L Mdler, E
Miller, MJ.S. Miller, Jr.,J M
Mflne, K Mmffee, P. Mimor, V Mmkoff; H
Mmkotl,J. Mlodovmk, M. Mlshra, O.P. M~ttal, K. Mo~se, K.
Mohnarl,J A. Mombouh, J v. Moncada, S. Monga, M. MontgommT, D MontgommT, L. Montoro, M. Mooney, D M Moore, M.L Moore, T R
Abstract Number
39,48,410
67,115,169,208
408,511
268
164
288
465
248
394
355
47O
435,462
366
28,35,71
96
326
363
220
329
216
206
184,318
438
329
195,291
268
218,380
61,70,390
237
267
106
323
263,312
203,389
313
42
70, 228, 386, 390, 393, 422,
485,514
239
256
431
97,158
290
44
464
170,297,339,384
131
224,460,481
74
334
329
11
325
336,469
47
72
382,383
242,507
368
63,69,191,464
125
174
6, 9, 31, 50, 56, 72, 147, 168,
330,415, 448,495,496,497
140
8,119
117
78
437
72
205,245
88
389
134,153
Volume 170, Number 1, Part 2 Author Index 437 Am J Obstet Gynecol
Author
Morettl, M. Morgan, M
Mort, A Mort, R
Monn, L Montz, M Morns, H Mornsh, D W
Mornsmn,J C.
Morrow, R
Morton, MJ. Morton, M.L Moscarelh, R.D Moskowltz, D
Mueller-Heuback, E Mullen, B Munoz, H. Munsh~, U K Muram, D Murphy, K W Murray, K. Myatt, L Myers, T. Myhr, T Myles, T Nabuls~, M Naef, 111, R W Nageotte, M P. Nagey, D Nahum, G Nak~sbendt, K. Nanda, D. Nasserl, A. Natale, R Nathan, L. Nathamelsz, P.W. Naumaim, R W Nava, S Nelson,J Nelson, K.
Nelson, L Nesslm, S Neuberq A.G
Neuer, M Neveux, L.M Nevlls, B. Newman, A Newman, P.S. Newman, R.
Newnham, J P Newton, E R Ney, J N~,J Nqhuls, J G N~jland, MJ M Norman, G. Norman, P F Nowlckt, B. Now~ckl, S Nugent, R Nuhoglu, A A
O’Brlen,J E O’BrlelL J M O’Brlen, W.F O’Connell, P.D. O’Connor, T O’Day, M O’DelI, V. O’DorlslO O’Shea, T M
Abstract Number
16
81, I06, 197, 198, 341, 350,
423,468 36, 343 36,343 210 187 225 253 110, 232, 324, 360, 361, 362, 426, 427, 428, 429, 430, 431, 488
116,445,446 123 324 356 193 433 445
30,418,518,522 ll 44
268 391 406 106 225 339 245
110,232,360,361,490 142,143,391 247,417 108 511 466 118 47
50O 106 234 140 323 112, 346, 400, 401, t02, 403, 4O4
243,277,494 131 503 266 264
351,371 329 9O
164,326,523 457
520,524,525,526 336,469 31 420
99 70, 390 487,488
508,509,510 508,509,510 507 323 283
386,393 226,344 171
269,301,320 302 326 5 433
.Author
Ogundtpe, O A Ogunyeml, D. Ohlsson, A Okun, N.
Olmos, L. Olson, G.L. Oppenhem~er, L W Ordonca, S Onol, N. Orlando, F Osm, K Ou, C-N Owen,j. Paetzold, D Page, D.M. Pmdas, C Pak, S.C Palaoos, Q. Palan, P R Palermmo, D Palomak~, G E Pan, Y Pardi, G Parer, J.T. Parflla, B V Pansy, V.
Park, J.K. Park, K. Park, K H Parnsh, G Parsons, M. Patatanlan, E Patel, N Patel, S. Patel, T Patterson, R M Paul, R Pazemenas, V Pchera, H. Peaceman, A M Pea~rs, W Peavey, K. Peeler, G H. Peeper, E.Q Pena, A. Peralta, M Pergament, E. Perkms, M B
Perlow, J Perw, Jr, K G Pescow~, O Petnkovsky, B Peyser, M.R Pezzullo, l Pfleghaar, K Pham, T
Phelan,J.P Phelps,J Phil, D. Phlhpson, E. Phdhppe, M. Phflhps, J M Ph~ppa, P. Pmzza, S Pwnlng, S P~erangeh, S.S. Pterce, M.R. Pmette, M G Pinette, S G. Pmhe~ro, S P~per, J. P~rcon, R A. Parts, D.W
Abstract Number
497
46
467
225
253
8
417
101,309
441
375
440
5
415
234,271,274,363,396
455
414
337
353
72
481
519
264
447
93,94
17,40,85
299
18,78,246,276,366
173
375
471
425
353
365
458
367
194
303
70,74,149,390
376
440
62,82,367
524
407
393
220
165
346,400,403
254,299
222
151
54,361,426,431,487,490
24
305,317
102,261
382,383
336,469
510
49
133
308
212,287,293,347,519
358
457
44
517
6O
207
11
447
447
3O8
183,189
229
393

438 Author Index January 1994 Am J Obstet Gynecol
Author
Platt, 1 ,. Platt, M. Platt, R Po~st, J.E. Pokorny, W Poppas, A. Porter, K.B. Porto, M.P. Powell, S Pratt, L. Pressman, E Pretorlus, D Pndj~an, G. Pryde, P G. Puder, K.S. Pulliam, D.
Quails, C Qullligan, E.J.
Qulntero, R Rachmilew, tz, J. Radm, T. Rainwater, K Ramaknshnan, V. Ramin, K. Ram*n, S Ramlrez, M Ram~rez, M M Ramsey, R.D Ramus, R. Randall, R.
Rank, E. Ranzini, A.C. Rao, B K Rausch, S.
Rawfl, H Ray, D. Rayburn, W. Raymond, R.C. Raynor, B.D. Razml, A. Rea, C Rech~tsky, S Reddy, U. Reece, E.A. Reed, K.L. Reed, V Reedy, M.B. Rehnberg, K. Rmch, H. Relchler, A.
Reinus, J Rels, M Reller, M D Renfroe, Y. Repke, J T Restock, L M. Respondek, M. Reyes, C. Rhodes, P.H. Rhodes, S. Rice, G. Richards, D P~chey, S. Richmond, B Rifle, B Ragby, F B R~ggs, T W. Righmnrem D. Ringden, O. Ringer, S. Rask, N M. R~zk, K Roach, H
Abstract Number
160,323 5 513 487 72 52 226,344 341 244 24
192,275 289 95 136,286,338,451 76,444,449,453 16 92 350
35,73,76,249,284,453,454 23 227 523 339
95,124,322 95,322
250,372,418,518,522 18 514 211 341 516
259 335 303 380 4O5
166,365,491 222 315 421 178 257 192
328,335,408 459
36,343 14
62,82 76 283, 285, 286. 295, 296, 451 517 218 123 73 172 114,115 311 245 362 91 484
314,315 322 165,218 95 325 321 313 440 513 25 159 232
450,
Author
Roberts, S. Roberts, W.E.
Rob~chaux, III, A. Rob~e, D Robinson, A Roden, W.
Rodls,.], Rodnguez, A. Rodriguez, D. Rognerud, C Rokey, R. Roll, ~ Roman, C Romeny, S.L. Romero, R
Rooholamlni, S A. Rose, N.C Rosen, D. Rosenberg,.l Rosenkrantz, T Rosenn, B Ross, M.G Rosslter, J Rossman, K. Roth, S Rotmensch, S. Rottem, S. Roumayah, N.B. Rouse, D Rowe, T. Roy, W
Ruderman, J. Rumney, P. Ruzycky, A. Ryan, (; Saade, G.
Sabhagha, R.E. Sacks, D. Sag~, J. Sakala, E.P. Salatia, C. Saleh, A.A. Saller, D.N
Sailer,Jr., D.N Samuels, P
Sanche~, PJ Sanchez-Ramos, L
Santolaya, J. Santuccl, L Saunders, T. Sawaya, J Sawyer, A Sayed, M A.A. Scardo, J Scarpelh, S.A. Schaeter, D. Schiff, E.
Schorr, S.
Schorr, S.J. Schrimmer, D. Schulman, H Schwartz, A. Schwartz. D Schwartz, Ill, W. SCIOSCla, A ScisQone, A. Scorza, W. Scott, J R Seeds, J.
Abstract Number
66,167,199 54, 360, 361, 427, 428, 429, 490 437 72 519 55,345,512 7, 281,332, 333 226 216 415 9 467 40 481
15, 27, 28, 30, 34, 35. 71, 73,
76, 107, 249, 250, 364, 372, 418,451,518,522 478 503 131 3O6 382,383 63,69,191,238,406,464 46,99 275 453 24 301,384 466 342
42,55,345, 363 184,318 373 225 391 195 445,446
6, 9, 50, 56, 72, 147, 168, 330, 415, 448,495,496,497 299 64 102 392 7,382,383 113,136,348 259 258 5,179,413,503 500 377,479,480 292,339,442 357 358 245 227 174 148,326 68,193 165
39, 107, 228, 409, 410, 485, 486 38O 110 304 435,462 255 190 491 289
150,252,499 331,515,516 214 329
Volume 170, Number 1, Part 2 Author Index 439 Am J Obstet Gynecol
Author~
Se~dman, D S Seflman, B D Stager, A Sehgman, S P
Sengupta, S. Semch, L.
Sepulveda, W Seron-Ferre, M. Serre, A Setmwan, T Shaffer, W Shah, S Shahem, S. Shahm~an, K. Shaller, T L. Sham, R Sharp, H T Shaw, K Sherer, D.M.
Sherman, DJ Sherman, M.L. Sheth, S. Shields, L.E. Shlh,.] Shwers, B.
Sholl, J Shuber, A P Shubert, PJ. Shulman, L P Shumway, J Sxba~, B.M
S~ddlql, T.A S~gnorml, M.G
Sdberg, J.E. Sfler-Khodr, T Silver, R Silver, R M.
Sflverman, N. Simon, J.M. Slmonelh, M. Sunpson, N Smas, C.J. Smgh, K.P. Sipos, J Skupskl, D. Sladek, E.H. Smith, C. Smith, R Srmth, S
Smuhan,J Snelmer, S Sockolow, R Socol, M L
Sohaey, R. Sokol, RJ Sommers, B. Sonnenbhck, A Soper, R Sorokm, Y Spandorter, S Spector, I Spmnato,J. Spoer, R
Spong, C.Y. St Amant, M
Stacks, L.J. Standley, C A Stamslaw, H.
Stanley, J R. StanAano, G. Star, J Stedman, C.M.
Abstract Number
48,410 450 440 57 458 291
25,41 103 442 177
10 512 242 51,258 129 520 374
61,206 138,256 385,421 167,411 337
13, 262 517 285 221
38 413
279,280 160 16, 39. 44, 61, 107, 176, 228, 386, 393, 409, 422, 485, 486, 514
63, 69,191,238,406, 464 93 290 133,526 171,221 214 187 264 515 101 154 87 297 86 171 474 319 311
331,332,333 21 517
82,229,396 340
136,296,439 6O 86 316 35,71,114,115,250 240 231
59,207,373,419 470 46 502 152 67,104,169,483 108 100
387,388 51 412,437
Author
Steele, L. Steele, R. Stinger, R M. Stem, A K Stek, A Stet/ler, R. Stewart, g.
Stflson, R. Stlrewalt, W S. Stofl>l, S
Stolar, C J.H. Stone, P Stratum, S. Strmcher, P. Strom,. C M Swong,Jr., T.H. Sulter, C Sulhvan, C.A. Sulh~an, D L Summersgfll, J. Sundstrom, E Suresh, M Sv~nanch, D. Syn, H.C. Tahb, T N Talbert. D.G
Tamw A. Tamura, R.K. Taylor, R.N. Taylor, S. Tqam, N. Terk, J. Thaler, 1. Tharakan, T. Thorn, E Thomas, A Thomas, R.L. Thorp,J.A. T~mor-Tntsch, 1. Todd, H Tomhnson, M. Toohey, J.S. Tovbm, J. Towbin,J. A. Towers, C
Treadwell, M. Trobough, T. Troyer, L.R. Trudinger, B. Trultt, L. Tucker, J M. Tucker, Tumber, M Tuomala, R. Turnbull, G Twinkler, D. Uckele, J E Uhnch, S Umezakl, H. Usta, I.M
Vadna~s, T.J. Valdez, M. Valenzuela, G.]. Van Ascche, F A. Van den Berg, P P Van den Veyver, I. Vandenberghe, K
VanHook,J. Vanhoutte, P Varner, M Vecch~o, M. Vedermkov, Y. Vmlle, J.C
Abstract Number
lO0 403
341,468 254 12 177 67 44 9i 289 79 446 148
286 257 144 133
54,11o, 427,431 361,489 527 440 56,168 522 3,34,471 129 25
300,328 82,299 484 21 1,157 20,43 463 146
61,70,390 83,332 18o 97,98,158 79,354 364 342 142,200, 350 385 31
142, 143, 151, 391
71,152,342 98 78 36,343 166 401 4o7 51 513 166,365,491 177,322 395,444,449 262,289 75,376 176,422 156 130 45,75,1o3,376 26,135 420 6,31,72 26 128,129 6,8,119 374,494 504
56,168 100,120,121,433
196, 200, 350,

440 Author Index .January 1994 Am J Obstet Gynecol
Author
Verma, U
V~cto~, M V~dal, R
Vdlar,J. Vmwtleos, A. Vascarello, R.R. Vogel, B Wagner, W Walker, C Walsh, S. Wang, S Wapner, R. Ward, B.E. Ward, K Ware, D Ware, D.J. Washburne,J F. Wasserstrum, N. Wears, R Weber, B.M
Weeks, J Wehbeh, H. Wed-Chalkm, S. Wem, R Welner, C. Welner, S Winner, Z. Wmnert, I.. Wemhouse, g
Wemtraub, B V~elsmall, A Weiss, G Wmss, R R Wmss, Y
~,relssman, a Welhk, S Wendel, G D Wendel, P
WenstronL K.D. Wester, K Westgren, M Westover, T. Wheller,J Wtnteman, V Whittington, E Whmy,J.E. Wh~tworth, N S. W~cksn’om, E.A W~eczorek, K.M W~gton, T R. Wddes, H Wdkms, i Wllkms, P.W. Wdkmson, D A.
Wilhams, J. Wflhams, K Wdlia~ns, M A Wllhams, M.C. Wdhamson, R Wflmot, D. Wllson,J.D Wdson, K Wdson, P D. Wilson, S.K. Wdso~,.Jr., L W~ng, D Wmtcr,J Winter, R W~ser, W.L
W]odaver, A Wolde-Tsad~k, G.
Wnlt, EJ.
Absu-act Number
253 1 245 147 172 7,331,332,333,334,382,383 504,505,506 419 86 479 288 481 461
19, 286 243,277,494 434 89
362,426,427,430 8,119,493 480
232 151,197,198 242 311
105,217,356,381 117,239 140,311 266,435,462 186 321 340 3OO 105 266 175 355 81
5OO
66,199 111,235,270,271,273,274 47 440
141,188, 230 179 4O8 218 2O8 324 97 238 82,229,299,396 465
276,302 362 154 259 476
241,492 344 523 224 88 182 204 65 353 74,149 106 455 488 328 166 64 521
Author
Wolf, N. Wolin, M.S. Wolman, I.
Woods, J.R Worthington, D. Wren, A. Wright, D Wnght, J. Wu, A Wyse, L Xenak~s, E Yallam palh, C. Yancey, M.K
Yao,J. Yeast, J D. Yeng-Feng, T Yeomans, E.R. Yoon, B H. Yossef, E.
"~uchah, J. .Young, B.K. Zmn, H. Zazula, P. Zebelman, A.M. Zeidman, S. Zmgler, Z R. Zer, T. Zhang, X:]. Z~eg, A. Zimmer, E. Zmghmm, R.W. Zocchi, D Zoffer, M. Zolhnger, R. Zoma, W. Zmdema, L Zusman, I
Abstract Number
418,518 157
102, 261 256 229 363 190 425 347 305,317 22,189,216,369,370 5O9 501 64 98,158 267 20,43 3,34,471,522 309 507 57,109,379,441 425 190 492 192 180 294 11 213 328 241,492 436 466 340 1 59 175
Institution Index

442 Institution Index january 1994 Am J Obstet Gynecol
Institution
Abbott Northwestern Perinatal Center, MN
Acuson, Mountain View, CA Albany Medical Center
Albert Einstein College of Medicine
American University of Beirut Arizona Health Sciences Center
Arnold Palmer Hospital for Children & Women, Orlaudo
Assaf-Harofeh Medical Center, Israel
Babies Hospital, NY Baylor College of Medicine
Beth Israel Hospital
Bnai Zion Hospital Boston University School of Medicine/Public Health Bowman Gray School of Medicine, Winston-Salem
Brigham and Wom~n’s Hospital
Bronx Municipal Hospital Brooke Army Medical Center
Brown University School of Medicine
Butterworth Hospital, Grand Rapids California Pacific Medical Center
Carelink Corp., Santa Ana
Carmel Hospital, Israel
Case Western Reserve University Cedars-Sinai & Drew King Medical Centers,
Los Angeles Cedars-Sinai Medical Center
CEMIC, Buenos Aires Central University of Venezuela, Caracas
Centro Rosarino De Estudios Perinatales, Argentina
Children’s Hospital Medical Center, Cincinnati Children’s Hospital, Boston
Clermont-Ferrand, France College of Physicians and Surgeons, New York
Columbia Presbyterian Medical Center Columbia University, New York Cooper Hospital University Medical Center Cornell University Medical Center
Cornell University, Ithaca Duke University Eastern Virginia Medical School
Emory University Evanston Hospital Fairfax Hospital, Falls Church, VA
Foundation for Blood Research, ME Free University Hospital, Amsterdam
Gaubius Laboratory IVVO-TNO, Leiden George Washington Medical Center Good Samaritan Regional Medical Center, Phoenix
Hadassah School of Medicine, Israel Harbor-UCLA Medical Center
Hartford Hospital Harvard Medical School
Healthdyne Perinatal Services, Inc., GA Hebrew University, Israel
Hennepin County Medical Center Huddinge University Hospital, Stockholm Indiana University School of Medicine
Abstract Number
336,469 313
308
60, 68, 481,507 245 459
118, 173, 193, 224, 255, 327, 432, 460,
165,218,315,380 421 305
6, 8, 9, 31, 50, 56, 72, 119, 415,448,470,493,495,496,497 375
307 194
100,120,121,389,433
185,172,513 173
133
51,258 59
53,420 376
477
83,84,120,159,212,223
467
64,131,160 279 73
172 464
260 442
146,414
146,305,414 79,80,146,354,414 482
86,220,349 106 96
10,298,452,456,470
29 221
32 264
486 486
32
139,144,227 355
46,99
287,293,347,519 185,172 387,388
23,175 213 440
24,161,416
147, 168, 209, 330,
Volume 170, Number 1, Part 2 Institution Index 443 Am J Obstet Gyneco!
Institution
Inst Molec Genetics
Integrated Genetics, MA
ISBM San Paolo University Milan, Italy
Israel Institnte of Technology, Israel Jefferson Medical College of Thomas Jefferson
University Johns Hopkins University School of Medicine
Kaiser Foundation Hospital, Bellflower, CA
Kaiser Foundation Hospital, Los Angeles, CA
Kaiser Foundation Medical Center, Oakland, CA
Kaiser Permanente Medical Center, Santa Clara, CA
Kaplan Hospital, Israel Karolinska Institutet, Sweden
King Edward Memorial Hospital for Women, Western Australia
LAC/USC Medical Center
Loma Linda University
Long Beach Memorial Medical Center Louisiana State University
Lutheran Medical Center
Madonna Perinatal Seiwices
Maine Medical Center
Maricopa Medical Center, Phoenix
Mary Birch Hospital for Women at Sharp
Memorial Hospital
Medical College of Georgia
Medical College of Pennsylvania/Allegheny Campus
Medical College of Virginia
Medical College of Wisconsin Medical Genetics Institute, SC
Medical University of South Carolina
Meharry Medical College MetroHealth Medical Center
Montefiore Medical Center
Mount Sinai Medical Center
Mount Sinai Hospital, Hartfort, CT National Center for Fetal Diagnosis, Therapy and
Pediatrics, Norway National Institutes of Health
National Naval Medical Center
New England Medical Center
New Hanover Regional Medical Center New Jersey Medical School
New York Medical College
New York University Medical Center North Shore University Hospital
Northwestern University Medical School
Northwestern University/Evanston Hospital Ochsner Clinic, New Orleans
Ohio State University
Oregon Health Sciences University Ostra Hospital, Gothenburg, Sweden
Outpatient Diagnostic Center, Nashville
Pennsylvania Hospital
Phoenix Memorial Hospital Phoenix Perinatal Associates
Pomona Valley Hospital
Abstract Number
5,31
19, 38, 286
93 463
187,259,335,461
150, 160, 192, 252, 259, 499
64
108
21 405
175
440
275, 337, 473, 474, 475,
457
149,206
45,75,103,359,376,392
142,143,151,196,200,222,350,391
11,325,502
242
231
447 65
304
89,155,472 154
288,29O 434
278
148,164,326,523 465
83,159,223 517
30, 105, 217, 237, 446
516
310, 348, 356, 378, 381, 445,
440
15, 27, 28, 30, 34, 35, 61, 70, 71, 73, 76, 249, 250, 364,372,390,418,471,507,517,518,522
521
210,260 425 105
1,157,504,505,506,517
37,57,109,174,379,441
305,317
62,82,221,229,254,299,353,367 171
412,437
5,179,413,503
122,123,436 248
4,465 140,263,264,265,311,312,313,452
65
139,144,227 49
444 Institution Index January 1994 Am J Obstet Gynecol
Institution
Pontificia Universidad Catolica, Chili
Rambam Medical Center, Israel
Reading Hospital
Reproductive Genetics Institute, Chicago
Reproductive Science University of Pittsburgh
Royal Postgraduate Medical School, England Saddleback Memorial Medical Center
San Bernadino County Medical Center
Scott & White Clinical and Memorial Hospital Seoul National University
Servizio Autonomo Di Diagnosi Prenatale, Italy
Sharp Perinatal Center Sheba Medical Center, Israel
Sinai Hospital, Detroit
Sloane Hospital for Women Sonoscan/Genetic Sciences, Forest Hills Sotero del Rio Hospital, Chile
Southern Illinois University School of Medicine
St. Francis Hospital and Medical Center
St. Joseph’s Health Centre St. Louis University
St. Luke’s Hospital, Kansas City Stamford Hospital
Strong Memorial Hospital
SUNYHealth Science Center, Brooklyn
SUNY-Downstate, Brooklyn Swedish Medical Center, Seattle
T-Cell Diagnostics, MA Tecnion, Institute of Technology, Israel Tel Aviv University
Temple University School of Medicine
Texas A & M University Health Science Center
Texas Tech University Health Sciences Center, Amarillo
The Queen Mother’s Hospital/Glasgow Royal
Maternity Hospital The Royal Women’s Hospital, Australia
The Union Memorial Hospital, Baltimore
Tufts University School of Medicine
UMDNJ, School of Osteopathic Medicine, NJ
UMDNJ-Robert Wood Johnson Medical School
UMDNJ-Robert Wood Johnson Medical School at Camden
University of Alabama at Birmingham
University
University
University
University
University
of Alberta
of Arizona Health Sciences Center, Tucson
of Arkansas of British Columbia
of California, Irvine
University of California, Los Angeles
University of California, San Diego
University of California San Francisco University of Cape Town Medical School,
South Africa
University of Chicago
Abstract Number
103 285,294,295,296,300 503 257 291 25,41 341,468 75,103,376 14,33 3,34,471,522 440 178 39,410 190 414 38 250 313 331,515 47 364 97,98,158 504,505,506 258,259 368,466 507 492 372 328 48,102,261,385 328,335,408,511 14,33
95,181,182
268 484 145
38,156,210
238
141,188,230,306,458
482
28, 42, 55, 87, 111, 112, 234, 235, 236, 270, 271,
272, 273, 274, 345, 346, 363, 396, 397, 398, 399, 400, 401,402, 403, 404, 412, 512 253
329
88 476
81, 106, 142, 143, 151, 196, 197,
350, 423, 468
131,308, 467, 478
13, 90, 122,134, 153, 289
17, 40, 85, 211,443, 484
198, 200, 341,
495
52,186,358

Volmne 170, Number 1, Part 2 Institution Index 445 Am J Obstet Gynecol
Institution
University
University
University
University
University
University
University
of Cincinnati of Connecticut Health Center Degli Studi Di Milano of Florida at Gainesville of Florida at Jacksonville of Gothenburg, Sweden of Graz, Austria
University Hospital Gasthuisberg/K. U. Leuven,
Belgium
University Hospital, Geneva, Switzerland
University
University
University
University
University
University
University
University
University
Hospital Nijmegen, the Netherlands of Illinois at Chicago of Iowa Hospitals and Clinics of Kansas of Lonisville of Maryland School of Medicine of Medicine and Dentistry of New Jersey of Michigan of Mississippi Medical Center
University of Missouri at Kansas City University of Munster, Federal Republic of Gerinany
University of New Mexico School of Medicine
University of North Carolina at Chapel Hill
University of Oklahoma Health Science Center,
Oklahoma City
University of Oregon
University of Ottawa
University of Pennsylvania Medical Center University of Pittsburgh
University of Rochester School of Medicine
and Dentistry University of South Alabama, Mobile
University of South Florida
University of Southern California, Los kalgeles
University of Sydney, NSW, Australia
University of Tennessee
University of Texas Health Science Center, Houston University of Texas Health Science Center,
San Antonio
University of Texas Medical Branch
University of Texas Southwestern Medical Center at Dallas
University of Toronto University of Uppsala, Sweden University of Utah School of Medicine University of Vermont University of Washington University of Western Ontario, Canada University of Wisconsin Medical School, Milwaukee University of Wisconsin, Madison Viral Epidemiology Branch, National Cancer Institute Wake Forest University Washington University Medical Center
Abstract Number
2,12,58,63,69,191,238,406,464
7,212,281,331,332,333,334,382,383,516 94
314,315,501
315,377,479,480
248 455
26, 135
233, 394 420
170, 292,297, 339, 353, 384, 442 239
203
59, 151,207, 373, 419, 527
247, 259, 359, 417 458
95
54, 110, 232, 324, 360, 361,
429, 430, 431,487, 488, 489, 490
97, 98, 158 284
92,351,371,499 425
362, 426, 427, 428,
166,365,491 103
101,309,438
125,240,503
195,357
138,256 87,88,407
226,344
74,178,205,245,323 36
16, 39, 44, 107, 176, 228, 279, 280, 386, 393, 409, 422,485,486,514
18,21,23,33,78,204,246,276,302,366
22, 33, 130, 132, 133, 162, 163, 183,
369,370,520,524,525,526 20,43,77,126,127,128,129,508,509,510
66, 95, 124, 136, 167, 177, 184, 318, 322,411,500
116, 237, 309, 445, 446 175
214, 243, 277, 282, 340, 374, 420, 424, 494
84, 91,260
241,244, 262, 304
251
229, 278
137, 387, 388 507
203, 389 498
189, 216,
199, 201, 202,

446 Institution Index January 1994 Am J Obstet Gynecol
Institution
Wayne State University/Hutzel Hospital
Weizmann Institute of Science, Israel Wellcome Research Laboratory, Beckenham, England Western Pennsylvania Hospital Westmead Hospital, Australia Wilford Hall Medical Center William Beaumont Hospital Winthrop-University Hospital Women’s College Hospital, Canada Women’s Memorial Hospital, Long Beach Wyoming Valley OB/GYN Associates Yale University School of Medicine
ZER Science Based Ind Ltd, Israel
Abstract Number
15, 27, 28, 30, 34, 35, 67, 71, 73, 76, 104, 107,
113, 114, 115, 136, 152, 169, 190, 208, 219, 249,
250, 283, 284, 285, 286, 294, 295, 296, 338, 342,
348, 352, 364, 372, 382, 383, 395, 418, 439, 444,
449,450,451,453,454,477,483,5]8,522
175
117
180
343
77,126,127,185
319,321
258,266,435,462
225
229 76
10, 37, 267, 269, 298, 300, 301, 316, 320, 452,
456,470,473,474,475,504,505,506
294
Related Documents











