Drugs: education, prevention and policy, February 2013; 20(1): 56–66 Copyright ß 2013 Informa UK Ltd. ISSN: 0968-7637 print/1465-3370 online DOI: 10.3109/09687637.2012.696744 Social influence, health variables and criminal behaviours associated with substance use among rural Norwegian adolescents Trond Nordfjærn 1 , Hilde Dahl 2 , & Grete Flemmen 2 1 Department of Research and Development, The Drug and Alcohol Treatment Health Trust in Central Norway, The Trondheim Clinic, Trondheim, Norway and 2 Drug and Alcohol Competence Centre in Central Norway, Trondheim, Norway Aims: To investigate social influence, health, crim- inality and substance use in a sample of 1288 Norwegian rural adolescents. Relations between these factors and substance use were examined. Methods: Data were obtained from the ‘UngData’ study. A cross-sectional questionnaire survey was conducted among adolescents (n ¼ 740) in nine secondary schools and among 548 adolescents in three high schools across two counties. The response rate was 63%. Findings: Deviant behaviours had higher social status among males and adolescents in high school. The social status of deviant behaviours and partic- ipation in criminal activities were associated with alcohol and illicit substance use. Parent–adolescent trust was positively associated with alcohol use and parent involvement with friends was similarly related to illicit substance use. The social status of physical appearance and talent in sports were negatively associated with alcohol use. Conclusions: Early intervention could promote the social status of healthy activities and reduce the status of deviant behaviours. The transition between secondary school and high school may constitute a risk period for establishing problem behaviours and interventions should target this period. Research should test whether substance availability relates to differences in substance use in rural and urban settlements. INTRODUCTION Adolescence is a stage in life with a high onset risk of behaviours, such as excessive alcohol and illicit substance use (Clark, Thatcher, & Tapert, 2008). It is well established that an early onset of, for example, alcohol consumption increases the potentials of alcohol misuse over a life span (Grant & Dawson, 1997). Adolescents’ substance use may have negative impli- cations for school motivation, could damage brain pathways important for regulatory behaviours (e.g. prefrontal, thalamic and cerebellar structures) and could relate to the development of mental stress (De Bellis et al., 2005; Hawkins, Catalano, & Miller, 1992). Studies which examine the prevalence of such risk behaviours among adolescents and investigate factors associated with promoted or reduced risk of substance use in this group could have important public health implications. In most western countries, adolescence is a period where striving for more social autonomy from parents and other authorities is given priority. Adolescents do obtain information about risk behaviours from authority-like sources, such as parents, the media and teachers, but adolescent peers have important roles in shaping normative beliefs and cognitive processing of risk activities (Maxwell, 2002). Theory also argues that people tend to compare themselves to others in order to determine the appropriateness of their own behaviour (Festinger, 1954). Prospective studies have supported the assumption that substance use in adolescence is promoted by substance use in social networks (Andrews, Tildesley, Hops, & Fuzhong, 2002). However, the role of peer influence on adolescents’ substance use is not clear, and few studies have examined the perceived social peer status of different activities (e.g. status of smoking, to be good in sports) and linked this to adolescents’ alcohol and illicit substance use. Although peers have an important role in shaping risk activities such as substance use among adolescents, Correspondence: Trond Nordfjærn, Department of Research and Development, The Drug and Alcohol Treatment Health Trust in Central Norway, The Trondheim Clinic, Box 2655, 7415 Trondheim, Norway. Tel: þ47 97 68 53 62. Fax: +47 73 86 28 02. E-mail: [email protected] 56 Drugs Edu Prev Pol Downloaded from informahealthcare.com by Norges Naturvitenskapelige Universitet (NTNU) on 12/21/13 For personal use only.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Drugs: education, prevention and policy, February 2013; 20(1): 56–66
Copyright � 2013 Informa UK Ltd.
ISSN: 0968-7637 print/1465-3370 online
DOI: 10.3109/09687637.2012.696744
Social influence, health variables and criminal behavioursassociated with substance use among rural Norwegian adolescents
Trond Nordfjærn1, Hilde Dahl2, & Grete Flemmen2
1Department of Research and Development, The Drug and Alcohol Treatment Health Trust in Central Norway,The Trondheim Clinic, Trondheim, Norway and 2Drug and Alcohol Competence Centre in Central Norway,Trondheim, Norway
Aims: To investigate social influence, health, crim-inality and substance use in a sample of 1288Norwegian rural adolescents. Relations betweenthese factors and substance use were examined.Methods: Data were obtained from the ‘UngData’study. A cross-sectional questionnaire survey wasconducted among adolescents (n¼ 740) in ninesecondary schools and among 548 adolescents inthree high schools across two counties. The responserate was 63%.Findings: Deviant behaviours had higher socialstatus among males and adolescents in high school.The social status of deviant behaviours and partic-ipation in criminal activities were associated withalcohol and illicit substance use. Parent–adolescenttrust was positively associated with alcohol use andparent involvement with friends was similarlyrelated to illicit substance use. The social status ofphysical appearance and talent in sports werenegatively associated with alcohol use.Conclusions: Early intervention could promote thesocial status of healthy activities and reduce thestatus of deviant behaviours. The transition betweensecondary school and high school may constitute arisk period for establishing problem behaviours andinterventions should target this period. Researchshould test whether substance availability relates todifferences in substance use in rural and urbansettlements.
INTRODUCTION
Adolescence is a stage in life with a high onset risk ofbehaviours, such as excessive alcohol and illicitsubstance use (Clark, Thatcher, & Tapert, 2008). It is
well established that an early onset of, for example,alcohol consumption increases the potentials of alcoholmisuse over a life span (Grant & Dawson, 1997).Adolescents’ substance use may have negative impli-cations for school motivation, could damage brainpathways important for regulatory behaviours (e.g.prefrontal, thalamic and cerebellar structures) andcould relate to the development of mental stress (DeBellis et al., 2005; Hawkins, Catalano, & Miller, 1992).Studies which examine the prevalence of such riskbehaviours among adolescents and investigate factorsassociated with promoted or reduced risk of substanceuse in this group could have important public healthimplications.
In most western countries, adolescence is a periodwhere striving for more social autonomy from parents
and other authorities is given priority. Adolescents do
obtain information about risk behaviours from
authority-like sources, such as parents, the media and
teachers, but adolescent peers have important roles in
shaping normative beliefs and cognitive processing of
risk activities (Maxwell, 2002). Theory also argues that
people tend to compare themselves to others in order to
determine the appropriateness of their own behaviour
(Festinger, 1954). Prospective studies have supported
the assumption that substance use in adolescence is
promoted by substance use in social networks
(Andrews, Tildesley, Hops, & Fuzhong, 2002).
However, the role of peer influence on adolescents’
substance use is not clear, and few studies have
examined the perceived social peer status of different
activities (e.g. status of smoking, to be good in sports)
and linked this to adolescents’ alcohol and illicit
substance use.Although peers have an important role in shaping
risk activities such as substance use among adolescents,
Correspondence: Trond Nordfjærn, Department of Research and Development, The Drug and Alcohol Treatment Health Trust in
Central Norway, The Trondheim Clinic, Box 2655, 7415 Trondheim, Norway. Tel: þ47 97 68 53 62. Fax: +47 73 86 28 02.
E-mail: [email protected]
56
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.

parenting variables may also be relevant. An author-itative, responsive and involved parenting style mayreduce the risk of adolescent substance use (Baumrind,1991). Parental monitoring and involvement were alsorelated to less drinking in urban male adolescents(Griffin, Botvin, Scheier, Diaz, & Miller, 2000).However, these studies were carried out in smallurban samples including well-educated parents. Fewstudies of parenting variables related to substance usehave been carried out in less well-educated ruralcommunities. A recent review, however, argued thatparents with low education may be less authoritative,manifest less involvement and practice more severepunishment upon their children (Becona et al., 2012).Parent involvement in adolescents’ social activities andthe overall trust in the adolescent–parent relationshipcould thereby differ in rural and urban settlements.
Problem behaviour theory argued that risky healthactivities, such as cannabis smoking and drinking, andcriminal behaviours, such as vandalism, tend to beassociated (Jessor & Jessor, 1977). An explanation isthat risky health behaviours and criminal behavioursserve as replacements for healthy activities of coping.This is consistent with the behavioural choice theoryfor substance use (Bickel & Vuchinich, 2000), arguingthat substance use could be viewed as a consequence ofa lack of healthy alternative rewarding activities.Consequently, a range of criminal activities wereexpected to be associated with substance use in thisstudy.
It has also been demonstrated that additional factorssuch as mental stress is positively correlated withsubstance use (Nordfjærn, Hole, & Rundmo, 2010;Teesson & Proudfoot, 2003). The assumption thatsubstances are used as efforts to reduce mental stress isconsistent with theories such as the life-stress model(Aneshensel & Huba, 1984) and self-medicationhypothesis (Duncan, 1974; Khantzian, Mack, &Schatzberg, 1974). The role of physical activity forsubstance use is more unclear. One study showed thatadolescents who participate in team sports were morelikely to use alcohol, but less likely to use illegalsubstances such as cannabis (Wichstrøm & Wichstrøm,2009). It is also well known that anabolic steroids arerelatively common in bodybuilding and strength-demanding training (De Piccoli, Giada, Benettin,Sartori, & Piccolo, 1991). On the other hand, substanceuse is often not promoted in organized sports and theymay also reverse the positive somatic and psycholog-ical effects of physical activity.
The cited studies indicate that factors related tosocial influence, health variables and criminal behav-iours are associated with adolescent alcohol and illicitsubstance use. However, the majority of studies werecarried out in small samples in delimited urbancommunities. Few studies have examined such factorsin large samples from geographically spread ruralsettlements. The rural gradient may be importantbecause rural settlements have considerably lower
population sizes than urban settlements. Rural com-munities are also characterized by more economicalsimplicity, and lower labour diversity and less formalsocial interaction patterns than usually seen in urbansettlements (Ward, 2007). The availability of sub-stances is also usually higher in urban communities andin line with the total consumption model (Bramness &Rossow, 2010), this may cause more substance-relatedproblems in urban settlements. However, one study inthe United States showed that substance use problemswere more prevalent among adolescents in ruralcommunities (Spoth, Goldberg, Neppl, Trudeau, &Ramisetty-Mikler, 2001). More knowledge about sub-stance use in rural communities is therefore warranted.
Adolescents in Norway complete primary schooland enter secondary school at the age of 13 years.Secondary school is completed at the age of 16 years.High school is a three-year optional schooling enteredat the age of 16 and completed when the adolescentsare 19 years of age. Hence, secondary school (13–16years) and high school (16–19 years) represent twodistinct age groups. In the transition period betweensecondary school and high school, adolescentsapproach the legal age for alcohol purchase. Theadolescents often move out from their parent’s housingin this period because secondary schools tend to beallocated in the rural communities whereas the highschools are situated in the district centres. This couldmake parent monitoring of risk behaviours morecomplicated in this period. Differences in the discussedfactors could, therefore, be expected among adoles-cents attending secondary schools and high schools.
The aims of this study were to investigate socialinfluence, health variables, criminal behaviours andsubstance use among Norwegian adolescents in ruralsecondary schools and high schools. We also tested therelations between these factors with alcohol use andillicit substance use.
On the basis of the cited studies and theories, it washypothesized that increased social peer status ofdeviant behaviours would be associated with a higherrisk of substance use. Involvement in criminal behav-iours was also expected to be positively associated withsubstance use, whereas parent involvement and trustwere expected to be negatively related to use. Based onthe previous work, mental stress was hypothesized tobe associated with substance use, while physicalactivity was expected to be related to a lower risk ofsubstance use. A higher prevalence of alcohol andillicit substance use was expected among adolescents inhigh school (16–19 years) compared to adolescents insecondary school (13–16 years).
METHOD
Study setting and designCross-sectional data were obtained from theNorwegian ‘Ungdata’ investigation initiated bythe regional drug and alcohol competence centres and
SOCIAL INFLUENCE, HEALTH VARIABLES AND CRIMINAL BEHAVIOURS 57
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.

the Norwegian Social Research Institute (NOVA).During October and November 2011, all adolescentsaged between 13 and 19 years in nine municipalities inNord-Trøndelag and Sør-Trøndelag counties wereinvited to respond to an electronic questionnaire. Allnine secondary schools (pupils age 13–16 years) and allthree high schools (pupils age 16–19 years) acceptedthe invitation. At the secondary schools 740 adoles-cents responded, whereas 548 adolescents at the highschools responded to the enquiry. The response ratesranged from 39% to 93% (total response rate¼ 63%,mean response rate¼ 79%). Reasons for non-responsewere either that the adolescents were on sick leavewhen the survey was conducted or that the parentschoose not to let the adolescents participate. Thesurvey was administered by a public health coordinatorin each municipality and local contact persons in eachschool approached the adolescents together withteachers. The contact persons and teachers monitoredthat the survey procedures were followed and that theadolescents did not collaborate while responding to thesurvey. The gender distribution was 50% males and50% females. The municipalities which constituted thesampling frame are relatively homogenous provincialrural Norwegian settlements with population figures(2011) ranging from 869 to 6740 (M¼ 3255.22,Mdn¼ 3679, SD¼ 2201.25). A detailed overview ofthe sample across the different schools and municipal-ities is reported in Table I.
Ethical considerationsThe Norwegian Social Science Data Services (NSD)approved the protocol for the Ungdata study. Thisincluded full access and research rights to the central–regional data (Nord-Trøndelag and Sør-Trøndelag) forresearchers in the Drug and Alcohol Treatment inCentral Norway. All participating subjects providedwritten consent. Informed written consent was alsoobtained from the parents of all participatingadolescents.
Measurement instrumentsThe applied questionnaire was developed by an expertgroup consisting of researchers and clinicians withspecific expertise regarding risk behaviour amongadolescents. The measures were based on previouslyvalidated instruments. However, some new scales werealso developed and adjusted to local conditions inNorwegian municipalities, because no validated trans-lated Norwegian measures have been established forthe relevant psychological constructs. A pilot test of thequestionnaire was conducted in 2010, using the samemethodological procedures as described above. Thetest was carried out among 737 adolescents at second-ary schools and 545 adolescents at high schools in twomunicipalities. The pilot test indicated that the mea-surement instruments had feasible face validity in therelevant target group. However, few language revisionsof the items were conducted after feedback from thepilot test.
Mental stress was measured by an eight-item revisedversion of the Hopkins Symptom Check List-10(HSCL-10; Derogatis, Lipman, Rickels, Uhlenhuth, &Covi, 1974). The adolescents rated to which extent theyhad experienced symptoms such as ‘been angry andtense’, ‘sleep difficulties’ and ‘felt hopelessnessregarding the future’ in the last week. The instrumentwas scored on a four-point scale ranging from ‘not atall’ to ‘very much’.
Peer social status was measured by a new 10-iteminstrument asking the respondents which behavioursthey considered important to obtain social status amongtheir friends. This scale was based on the peer socialstatus instrument developed by Simons-Morton,Haynie, Crump, Eitel, and Saylor (2001). The measureincluded items such as ‘smoking cannabis’, ‘to getdrunk’, ‘to be good at sports’ and ‘to have good looks’.The items were scored on a five-point Likert scaleranging from ‘substantially reduces the status’ to‘substantially increases the status’.
Parenting variables were measured by a new six-item instrument which prompted the adolescents aboutparent involvement in their social relations and thelevels of trust in the parent–adolescent relationship.The instrument was based on the scale developed byHetherington (1992). The adolescents responded to thefollowing items: ‘my parents know the parents of myfriends’, ‘I trust my parents’, ‘my parents trust me’, ‘Itry to keep my spare time activities hidden to
Table I. Sample characteristics.
Municipality and
schools (age span)
Municipality
population
figures
(2011)
Gender
distribution
n (%)
Males Females
Flatanger 1141
Secondary school (13–16) 25 (73%) 9 (27%)
Klæbu 5930
Secondary school (13–16) 78 (56%) 62 (44%)
Namdalseid 1694
Secondary school (13–16) 24 (51%) 23 (49%)
Oppdal 6740
Secondary school (13–16) 100 (51%) 96 (49%)
High school (16–19) 116 (52%) 106 (48%)
Overhalla 3679 47 (48%) 50 (52%)
Secondary school (13–16)
Roan 987
Secondary school (13–16) 10 (31%) 22 (69%)
Selbu 4042
Secondary school (13–16) 60 (54%) 52 (46%)
High school (16–19) 72 (54%) 61 (46%)
Tydal 869
Secondary school (13–16) 16 (57%) 12 (43%)
Vikna 4215
Secondary school (13–16) 24 (45%) 29 (55%)
High school (16–19) 69 (39%) 109 (61%)
Note: n¼ 16 with missing values on the gender variable.
58 T. NORDFJÆRN ET AL.
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.

my parents’, ‘my parents know most of the friends Ispend time with during my spare time’ and ‘my parentsusually know where I am and who I am together with inthe spare time’. The items are formulated as statementsand the adolescents rated their level of agreeability on afour-point scale from ‘strongly disagree’ to ‘stronglyagree’.
Information about physical activity was obtained bysix items where the respondents rated how often theyparticipated in different physical activities. This mea-sure was based on the physical activity instrument usedin the Nord-Trøndelag Health Studies (HUNT; Holmenet al., 2003). The activities consisted of, e.g. ‘trainingin a gym or health studio’, ‘training or competing in asports team’, ‘participated in sports and trainingoutside school time’ and ‘training or exercise on yourown (running, swimming, bicycling, walking)’. Theitems were scored on a five-point Likert scale rangingfrom ‘never’ to ‘at least three times a week’.
Criminal behaviours were measured by a list of 21items asking how often during the last 12 months therespondents had conducted violations of rules andsocial norms such as ‘burglary’, ‘illegal tagging onwalls, buildings, trains or buses’, ‘deliberately dam-aged windows, bus seats, mail boxes or similar’ and‘stolen money from a friend’. The instrument wasscored on a five-point scale ranging from ‘never’ to ‘11times or more’. This measure was based on theinstrument of law obedience developed by Huba andBentler (1983).
The questionnaire also included one item asking therespondents how often they consumed alcohol (never,tasted a few times, sometimes, but not as often asmonthly, 1–3 times monthly, each week). In order toobtain sufficient statistical power and avoid a type IIerror, occasional use was dichotomized as ‘no’ andmore regular use (monthly and each week) as ‘yes’.A no/yes item which measured use of illegal substancessuch as cannabis, cocaine and amphetamine, the lastyear was also included. Previous research inNorwegian samples of adolescents showed that arelatively low proportion report regular use of illicitsubstances (Vedøy & Skretting, 2009). In order tobalance the probability of type I and type II errors, itwas considered adequate to measure illicit substanceuse during the last 12 months (see also Wichstrøm,2000).
The demographic characteristics used in this studywere gender and school type (i.e. secondary and highschool). Secondary schools (13–16 years) and highschools (16–19 years) were used as age indicators inthe study because in order to secure the confidentiallyof the respondents, the ethical committee did not acceptthe inclusion of an explicit measure of age.
Statistical proceduresPASW Statistics version 18 was used for all statisticalanalyses. Descriptive statistics were applied to yieldcharacteristics of the samples. Chi-square (�2) analyses
were carried out to investigate differences in theprevalence of substance use in demographic sub-groups. To test the underlying dimensionality of themeasurement instruments, Generalized Least Squares(GLS) factor analysis with iteration, Kaiser criterionand oblique rotation were performed. Cronbach’s alphavalues were calculated to examine the internal consis-tency of the scales.
A Multivariate Analysis of Variance (MANOVA)was carried out to test group differences in thepsychological constructs. MANOVA allows for theinclusion of several independent and dependent vari-ables into one comprehensive analysis. An advantageof one MANOVA compared to several univariateanalyses of variance (ANOVA) is that the MANOVAprotects against Type I error inflation and adjusts forcorrelations between the criterion variables. The uni-variate part of the MANOVA was consulted toinvestigate the specific independent measures whichhad significant influences on the dependent criterionvariables.
Logistic regression analyses (enter method) wereused to examine the associations between socialinfluence, health variables, criminal behavioursand substance use. Control variables (i.e. gender andschool/age range) were entered in the first block andconceptually related variables were entered in the threesubsequent blocks (i.e. social influence, criminality andhealth variables). Pseudo R-squared (Nagelkerke R2
and Cox & Snell R2) were calculated to indicate thegoodness-of-fit of the assessed models.
Factor structure and reliability of the measuresBecause this study utilized some new or adjustedversions of previously validated instruments, it wasconsidered necessary to examine the structural dimen-sionality of the items by factor analyses. As shown inTable II, peer social status segmented into twodimensions, termed Deviant Behaviours andAttractiveness. Deviant behaviours included fouritems related to the perceived peer social status ofnorm departing behaviours, such as smoking cannabisand fighting, while attractiveness related to threestatus-promoting behaviours, such as to be good insports or to wear fashionable clothing. Three itemswere removed from the instrument as they failed toload. Together, the two factors explained 64% of thevariance and the correlation between the factorswas 0.10.
Parenting variables also segmented into two factorstermed Involvement with Friends and Trust (Table II).Involvement with friends consisted of three itemsrelated to how much parent involvement the adoles-cents perceived in relation to their friends and socialnetworks. Trust included three items associated withthe perceived trust between parents and the adoles-cents. The involvement and trust factors explained atotal of 65% of the variance and the correlationbetween these factors was 0.36.
SOCIAL INFLUENCE, HEALTH VARIABLES AND CRIMINAL BEHAVIOURS 59
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.

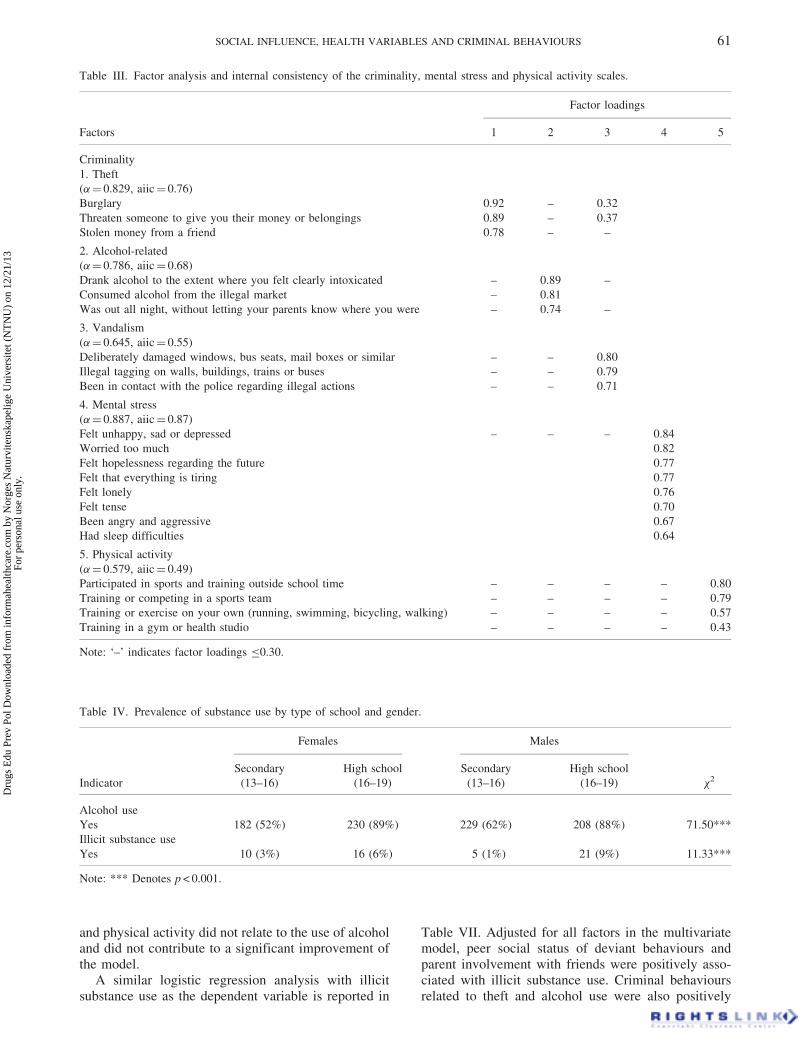
Table III illustrates GLS factor analysis and reli-ability indices of the criminality, mental stress andphysical activity scales. The test items of criminalbehaviour segmented into three factors. Theft includedthree items related to robbery and burglary and theAlcohol-related factor consisted of three items such asconsumption of alcohol obtained from the illegalmarket. Vandalism included three items concerningdeliberate damage of property. A total of 12 items wereabounded from the criminality measure because theyfailed to load. The correlation between theft and thealcohol-related factor was 0.20, whereas the correlationbetween theft and vandalism was 0.39. The alcohol-related and vandalism factors were also moderatelycorrelated (r¼ 0.26). The three factors explained 67%of the variance.
Both mental stress (56% of the variance) andphysical activity (45% of the variance) yielded unidi-mensional factors. Two items were removed from thelatter measure due to dual loadings. As shown inTables II and III, the majority of instruments had good
internal consistency reflected by � values approaching0.70 and average corrected inter-item correlations(aiic) above 0.30 (Hair, Anderson, Tatham, & Black,1998; Nunnally, 1978).
RESULTS
Differences in substance use, peer social status,parenting and health variables and criminalbehaviours by school and genderTable IV illustrates differences in substance useaccording to whether the adolescents attended second-ary or high school and by gender. Males were slightlymore likely to use alcohol in secondary school thanfemales, but the prevalence of alcohol use wasrelatively equal between the genders in high school.There was a substantially higher prevalence of alcoholuse among adolescents in high school compared tosecondary school. Illicit substance use was slightlymore common among females in secondary school, butmore common among males in high school. There wasalso an overall higher prevalence of such use amongadolescents in high school.
The outcome of a MANOVA showed a significanteffect of gender (Wilks’ �¼ 0.88, p < 0.001) and typeof school (Wilks’ �¼ 0.69, p < 0.001) on peer socialstatus, parenting, health and criminal activity variables.The interaction between school� gender failed toreach the significance (Wilks’ �¼ 0.99, ns). As illus-trated in Table V, deviant behaviours were reported tohave a higher peer social status among males(F¼ 15.69, p < 0.001) and such behaviours had astronger peer status-promoting function among adoles-cents in high school (F¼ 98.19, p < 0.001). Parentinvolvement in adolescents’ friendships was strongeramong respondents in high school (F¼ 68.57,p < 0.001) and alcohol-related criminality (F¼ 396.92,p < 0.001) was also more common in this group.Vandalism was more common among males(F¼ 25.50, p < 0.001) and a significant gen-der� school interaction effect (F¼ 6.45, p < 0.01)showed that this difference was merely found amongmales at high school level. Females reported moremental stress than males (F¼ 83.04, p < 0.001).
Associations between peer social status, parentingand health variables and criminal behaviours withsubstance useThe next step was to investigate the associationsbetween social influence, health variables, criminalbehaviours and alcohol use among the adolescents. Theoutcome of a logistic regression analysis showed thatthe social status of deviant behaviours and parent–adolescent trust were associated with an increased riskof alcohol consumption (Table VI). Peer social statusof attractiveness was related to a reduced risk ofalcohol use. Criminal behaviours related to theft,vandalism and alcohol use were also positively asso-ciated with alcohol use. The factors of mental stress
Table II. Factor analysis and internal consistency of the peer
social status and parent relation scales.
Factor loadings
Factors 1 2
Peer social status
1. Deviant behaviours
(�¼ 0.769, aiic¼ 0.71)
Smoke cigarettes 0.89 –
Smoke cannabis 0.80 –
Get drunk 0.79 –
To be good at fighting 0.57 –
2. Attractiveness
(�¼ 0.767, aiic¼ 0.68)
To have good looks – 0.88
Use fashionable clothing – 0.82
To be good at sports – 0.78
Parenting variables
1. Involvement with friends
(�¼ 0.780, aiic¼ 0.70)
My parents know most of the
friends I spend time with during
my spare time
0.88 0.36
My parents know the parents of my
friends
0.83 –
My parents usually know where I
am and who I am together with in
the spare time
0.80 0.33
2. Trust
(�¼ 0.637, aiic¼ 0.55)
I trust my parents 0.35 0.85
My parents trust me 0.32 0.85
I try to keep my spare time activities
hidden to my parents
– 0.62
Note: ‘–’ indicates factor loadings �0.30 and ‘aiic’ average
corrected inter-item correlations.
60 T. NORDFJÆRN ET AL.
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.
and physical activity did not relate to the use of alcoholand did not contribute to a significant improvement ofthe model.
A similar logistic regression analysis with illicitsubstance use as the dependent variable is reported in
Table VII. Adjusted for all factors in the multivariatemodel, peer social status of deviant behaviours andparent involvement with friends were positively asso-ciated with illicit substance use. Criminal behavioursrelated to theft and alcohol use were also positively
Table III. Factor analysis and internal consistency of the criminality, mental stress and physical activity scales.
Factors
Factor loadings
1 2 3 4 5
Criminality
1. Theft
(�¼ 0.829, aiic¼ 0.76)
Burglary 0.92 – 0.32
Threaten someone to give you their money or belongings 0.89 – 0.37
Stolen money from a friend 0.78 – –
2. Alcohol-related
(�¼ 0.786, aiic¼ 0.68)
Drank alcohol to the extent where you felt clearly intoxicated – 0.89 –
Consumed alcohol from the illegal market – 0.81
Was out all night, without letting your parents know where you were – 0.74 –
3. Vandalism
(�¼ 0.645, aiic¼ 0.55)
Deliberately damaged windows, bus seats, mail boxes or similar – – 0.80
Illegal tagging on walls, buildings, trains or buses – – 0.79
Been in contact with the police regarding illegal actions – – 0.71
4. Mental stress
(�¼ 0.887, aiic¼ 0.87)
Felt unhappy, sad or depressed – – – 0.84
Worried too much 0.82
Felt hopelessness regarding the future 0.77
Felt that everything is tiring 0.77
Felt lonely 0.76
Felt tense 0.70
Been angry and aggressive 0.67
Had sleep difficulties 0.64
5. Physical activity
(�¼ 0.579, aiic¼ 0.49)
Participated in sports and training outside school time – – – – 0.80
Training or competing in a sports team – – – – 0.79
Training or exercise on your own (running, swimming, bicycling, walking) – – – – 0.57
Training in a gym or health studio – – – – 0.43
Note: ‘–’ indicates factor loadings �0.30.
Table IV. Prevalence of substance use by type of school and gender.
Indicator
Females Males
�2Secondary
(13–16)
High school
(16–19)
Secondary
(13–16)
High school
(16–19)
Alcohol use
Yes 182 (52%) 230 (89%) 229 (62%) 208 (88%) 71.50***
Illicit substance use
Yes 10 (3%) 16 (6%) 5 (1%) 21 (9%) 11.33***
Note: *** Denotes p < 0.001.
SOCIAL INFLUENCE, HEALTH VARIABLES AND CRIMINAL BEHAVIOURS 61
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.
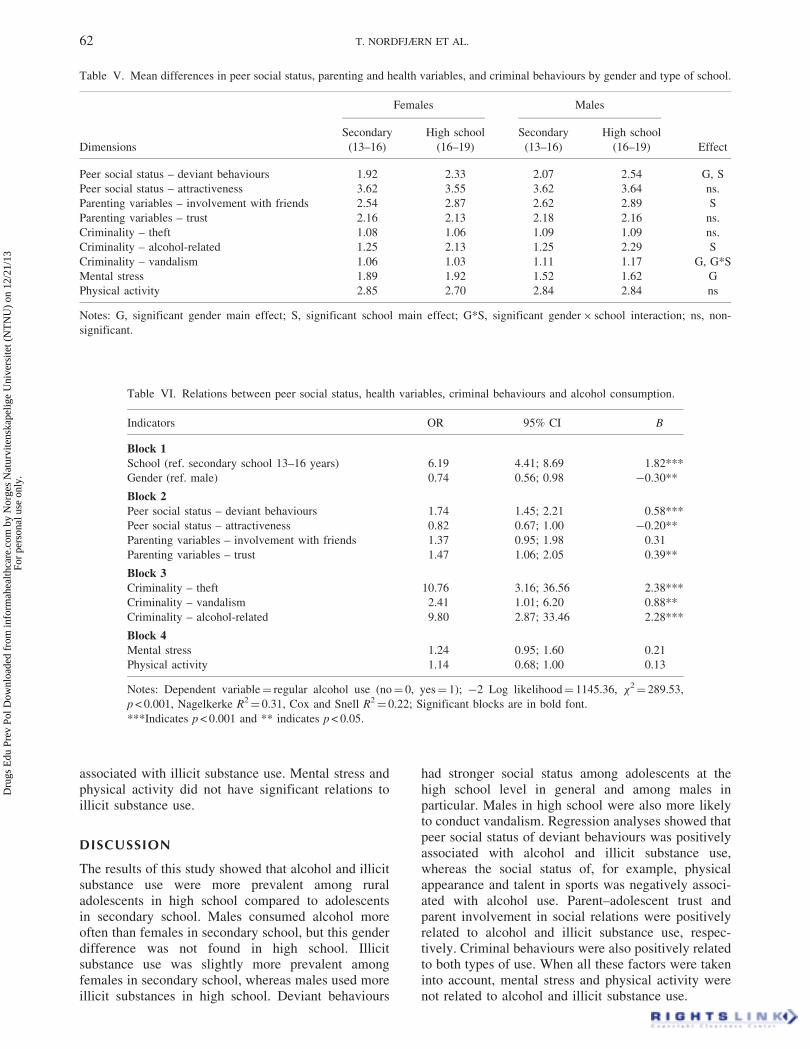
associated with illicit substance use. Mental stress andphysical activity did not have significant relations toillicit substance use.
DISCUSSION
The results of this study showed that alcohol and illicitsubstance use were more prevalent among ruraladolescents in high school compared to adolescentsin secondary school. Males consumed alcohol moreoften than females in secondary school, but this genderdifference was not found in high school. Illicitsubstance use was slightly more prevalent amongfemales in secondary school, whereas males used moreillicit substances in high school. Deviant behaviours
had stronger social status among adolescents at thehigh school level in general and among males inparticular. Males in high school were also more likelyto conduct vandalism. Regression analyses showed thatpeer social status of deviant behaviours was positivelyassociated with alcohol and illicit substance use,whereas the social status of, for example, physicalappearance and talent in sports was negatively associ-ated with alcohol use. Parent–adolescent trust andparent involvement in social relations were positivelyrelated to alcohol and illicit substance use, respec-tively. Criminal behaviours were also positively relatedto both types of use. When all these factors were takeninto account, mental stress and physical activity werenot related to alcohol and illicit substance use.
Table VI. Relations between peer social status, health variables, criminal behaviours and alcohol consumption.
Indicators OR 95% CI B
Block 1School (ref. secondary school 13–16 years) 6.19 4.41; 8.69 1.82***
Gender (ref. male) 0.74 0.56; 0.98 �0.30**
Block 2Peer social status – deviant behaviours 1.74 1.45; 2.21 0.58***
Peer social status – attractiveness 0.82 0.67; 1.00 �0.20**
Parenting variables – involvement with friends 1.37 0.95; 1.98 0.31
Parenting variables – trust 1.47 1.06; 2.05 0.39**
Block 3Criminality – theft 10.76 3.16; 36.56 2.38***
Criminality – vandalism 2.41 1.01; 6.20 0.88**
Criminality – alcohol-related 9.80 2.87; 33.46 2.28***
Block 4Mental stress 1.24 0.95; 1.60 0.21
Physical activity 1.14 0.68; 1.00 0.13
Notes: Dependent variable¼ regular alcohol use (no¼ 0, yes¼ 1); �2 Log likelihood¼ 1145.36, �2¼ 289.53,
p < 0.001, Nagelkerke R2¼ 0.31, Cox and Snell R2
¼ 0.22; Significant blocks are in bold font.
***Indicates p < 0.001 and ** indicates p < 0.05.
Table V. Mean differences in peer social status, parenting and health variables, and criminal behaviours by gender and type of school.
Dimensions
Females Males
Effect
Secondary
(13–16)
High school
(16–19)
Secondary
(13–16)
High school
(16–19)
Peer social status – deviant behaviours 1.92 2.33 2.07 2.54 G, S
Peer social status – attractiveness 3.62 3.55 3.62 3.64 ns.
Parenting variables – involvement with friends 2.54 2.87 2.62 2.89 S
Parenting variables – trust 2.16 2.13 2.18 2.16 ns.
Criminality – theft 1.08 1.06 1.09 1.09 ns.
Criminality – alcohol-related 1.25 2.13 1.25 2.29 S
Criminality – vandalism 1.06 1.03 1.11 1.17 G, G*S
Mental stress 1.89 1.92 1.52 1.62 G
Physical activity 2.85 2.70 2.84 2.84 ns
Notes: G, significant gender main effect; S, significant school main effect; G*S, significant gender� school interaction; ns, non-
significant.
62 T. NORDFJÆRN ET AL.
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.
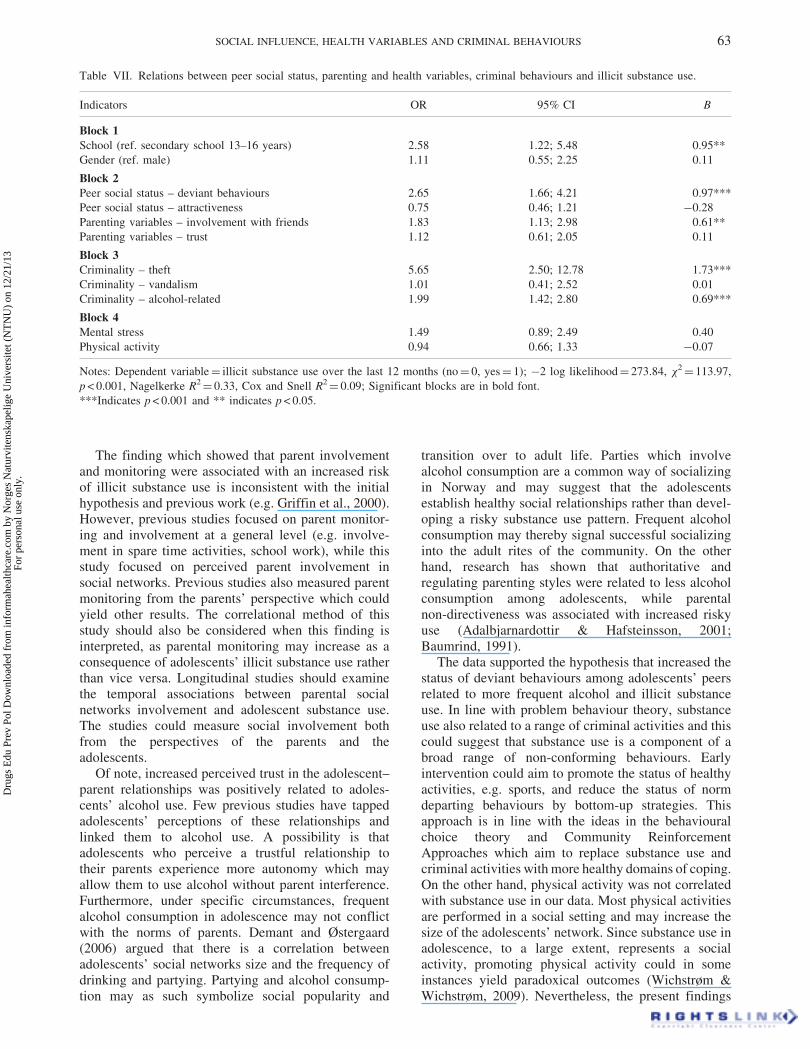
The finding which showed that parent involvementand monitoring were associated with an increased riskof illicit substance use is inconsistent with the initialhypothesis and previous work (e.g. Griffin et al., 2000).However, previous studies focused on parent monitor-ing and involvement at a general level (e.g. involve-ment in spare time activities, school work), while thisstudy focused on perceived parent involvement insocial networks. Previous studies also measured parentmonitoring from the parents’ perspective which couldyield other results. The correlational method of thisstudy should also be considered when this finding isinterpreted, as parental monitoring may increase as aconsequence of adolescents’ illicit substance use ratherthan vice versa. Longitudinal studies should examinethe temporal associations between parental socialnetworks involvement and adolescent substance use.The studies could measure social involvement bothfrom the perspectives of the parents and theadolescents.
Of note, increased perceived trust in the adolescent–parent relationships was positively related to adoles-cents’ alcohol use. Few previous studies have tappedadolescents’ perceptions of these relationships andlinked them to alcohol use. A possibility is thatadolescents who perceive a trustful relationship totheir parents experience more autonomy which mayallow them to use alcohol without parent interference.Furthermore, under specific circumstances, frequentalcohol consumption in adolescence may not conflictwith the norms of parents. Demant and Østergaard(2006) argued that there is a correlation betweenadolescents’ social networks size and the frequency ofdrinking and partying. Partying and alcohol consump-tion may as such symbolize social popularity and
transition over to adult life. Parties which involvealcohol consumption are a common way of socializingin Norway and may suggest that the adolescentsestablish healthy social relationships rather than devel-oping a risky substance use pattern. Frequent alcoholconsumption may thereby signal successful socializinginto the adult rites of the community. On the otherhand, research has shown that authoritative andregulating parenting styles were related to less alcoholconsumption among adolescents, while parentalnon-directiveness was associated with increased riskyuse (Adalbjarnardottir & Hafsteinsson, 2001;Baumrind, 1991).
The data supported the hypothesis that increased thestatus of deviant behaviours among adolescents’ peersrelated to more frequent alcohol and illicit substanceuse. In line with problem behaviour theory, substanceuse also related to a range of criminal activities and thiscould suggest that substance use is a component of abroad range of non-conforming behaviours. Earlyintervention could aim to promote the status of healthyactivities, e.g. sports, and reduce the status of normdeparting behaviours by bottom-up strategies. Thisapproach is in line with the ideas in the behaviouralchoice theory and Community ReinforcementApproaches which aim to replace substance use andcriminal activities with more healthy domains of coping.On the other hand, physical activity was not correlatedwith substance use in our data. Most physical activitiesare performed in a social setting and may increase thesize of the adolescents’ network. Since substance use inadolescence, to a large extent, represents a socialactivity, promoting physical activity could in someinstances yield paradoxical outcomes (Wichstrøm &Wichstrøm, 2009). Nevertheless, the present findings
Table VII. Relations between peer social status, parenting and health variables, criminal behaviours and illicit substance use.
Indicators OR 95% CI B
Block 1School (ref. secondary school 13–16 years) 2.58 1.22; 5.48 0.95**
Gender (ref. male) 1.11 0.55; 2.25 0.11
Block 2Peer social status – deviant behaviours 2.65 1.66; 4.21 0.97***
Peer social status – attractiveness 0.75 0.46; 1.21 �0.28
Parenting variables – involvement with friends 1.83 1.13; 2.98 0.61**
Parenting variables – trust 1.12 0.61; 2.05 0.11
Block 3Criminality – theft 5.65 2.50; 12.78 1.73***
Criminality – vandalism 1.01 0.41; 2.52 0.01
Criminality – alcohol-related 1.99 1.42; 2.80 0.69***
Block 4Mental stress 1.49 0.89; 2.49 0.40
Physical activity 0.94 0.66; 1.33 �0.07
Notes: Dependent variable¼ illicit substance use over the last 12 months (no¼ 0, yes¼ 1); �2 log likelihood¼ 273.84, �2¼ 113.97,
p < 0.001, Nagelkerke R2¼ 0.33, Cox and Snell R2
¼ 0.09; Significant blocks are in bold font.
***Indicates p < 0.001 and ** indicates p < 0.05.
SOCIAL INFLUENCE, HEALTH VARIABLES AND CRIMINAL BEHAVIOURS 63
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.

suggest that early intervention could focus particularlyon adolescent males, as the peer status of deviantbehaviours was stronger in this group. Interventions thattarget both the adolescents and their peers are alsowarranted.
As expected, adolescents in high schools usedalcohol and illicit substances more frequently thanadolescents in secondary schools. This could indicatethat the transition period between secondary school andhigh school is a risk period for the initiation of riskbehaviours. Norwegian high schools are usually allo-cated in district centres and many adolescents move outfrom their parents for the first time when starting highschool. Simultaneously, the adolescents approach thelegal purchase age for alcohol (18 years) and this couldresult in more substance use in this period. Thepreventive role of alternative activities to substanceuse should not be underestimated. Policy makersshould focus on the establishment of a wide range ofleisure facilities and health follow-up services in ruralsettlements, and inform high school adolescents thatsuch services are available. Restrictions on affordabil-ity, availability and accessibility of alcohol should bereinforced to reduce risky alcohol consumption in thisperiod (Babor et al., 2010).
Adolescent males have traditionally used alcoholand illicit substances more often than females, butresearch has shown that during the last decades,adolescent females have developed similar substanceuse patterns (Stewart, Gavric, & Collins, 2009). Thepresent findings add support to this assumption asalcohol use was fairly equal among males and femalesin high school. These findings could suggest that malestend to use alcohol somewhat more frequently insecondary school, but that females increase theirdrinking frequencies to similar patterns as males inhigh school.
On a more general level, it is noteworthy thatweekly or monthly alcohol consumption exceeded 50%and was about 88% in the secondary and high schoolsamples, respectively. An explanation is that due to therelatively high social status of behaviours such asalcohol use, the self-report measure of use may havebeen subject to social desirability. Studies have,however, shown that given a context where therespondents are provided confidentiality, such as inthis study, self-reported substance use correlatesstrongly with hair samples and urine tests (Secades-Villa & Fernandez-Hermida, 2003). Eiksund (2009)argued that Norwegian adolescents in rural communi-ties often are part of ‘party cultures’ where excessivealcohol use has strong social status and where use iscommon before the adolescents reach the legal pur-chase age. Moreover, the educational levels of peoplein the municipalities which participated in the surveyare generally low and under the average in theNorwegian population (Holmen et al., 2003). Loweducation could influence parents’ attitudes towardsalcohol use in a more liberal direction and reduce their
willingness to promote healthy attitudes towards alco-hol in their adolescents (see also Becona et al., 2012).Comparative rural–urban studies should test whetherthe educational levels among parents in these settle-ments relate to differences in adolescents’ alcohol use.
These results may suggest different substance usecultures in rural and urban settlements. The lowprevalence of illicit substance use reported in thisstudy, coupled with the relatively high prevalence ofalcohol use, may lend support to the availability-proneness theory of illicit drug abuse (Smart, 1980).An important premise of the theory is that onlysubstances which are available can be used, and thelikelihood of illicit substance use may be influenced byphysical, economic and social constraints related tohow difficult or easy it is to obtain the substances.It may be less attractive and economically lucrative toestablish a marked for illicit substances in sparselypopulated communities(Robertson, Sloboda, Boyd,Beatty, & Kozol, 1997). It could also be easier forthe police to monitor criminal activities in thesesettlements, compared to cities with higher populationfigures. Alcohol may be the preferred substance inNorwegian rural settlements because it is more avail-able than illicit substances. On the other hand, studieshave shown that rural and urban communities haverelatively equal prevalence of illicit substance use andalcohol consumption (Cronk & Sarvela, 1997). Theincreased mobility between rural and urban regionsprobably reduces the availability barrier in the ruralregions and may contribute to a more equal pattern ofsubstance use in rural and urban settlements.
Strengths and limitations of the studyThe strengths of the study include a large sampleobtained from rural communities with high geograph-ical spread and feasible response rates. However, thestudy also has some characteristics that should beconsidered when the results are interpreted. First, thestudy used a cross-sectional approach which does notallow for decisive conclusions about causality.Longitudinal studies should be conducted to test thevalidity of the present findings and conclusions.Second, the study solely obtained data from theadolescents. Respondent triangulation including theparents could have given a more accurate picture of, forexample, parent involvement in social networks. Third,some of the measurement instruments were either notvalidated by research or were modified versions ofvalidated instruments. Many validated instrumentshave not been translated and tested amongNorwegian adolescents. However, factor analyses andreliability tests indicated that the items structured inmeaningful patterns and had feasible internal consis-tency. Other limitations are that a volume measure ofalcohol was not included and that an explicit agevariable could not be accommodated into the ques-tionnaires due to ethical considerations. Nevertheless,the age range in secondary schools and high schools in
64 T. NORDFJÆRN ET AL.
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.
Norway is relatively low and due to this, the typeof schools may constitute a valid indicator of adoles-cents’ age.
ACKNOWLEDGEMENTS
The authors wish to acknowledge the work conducted by
the Norwegian regional competence centers for drug and
alcohol issues and NOVA by organizing the Ungdata
study. We are also indebted to the 1288 adolescents who
participated in the study.
Declaration of interest: The authors report no conflicts of
interest. The authors alone are responsible for the content
and writing of this article.
REFERENCES
Adalbjarnardottir, S., & Hafsteinsson, L.G. (2001). Adolescents
perceived parenting styles and their substance use: Concurrent
and longitudinal analyses. Journal of Research onAdolescence, 11, 401–423.
Andrews, J.A., Tildesley, E., Hops, H., & Fuzhong, L. (2002).
The influence of peers on young adult substance use. HealthPsychology, 21, 349–357.
Aneshensel, C.S., & Huba, G.J. (1984). An integrative causal
model of the antecedents and consequences of depression over
one year. Research in Community & Mental Health, 4, 35–72.
Babor, T., Caetano, R., Casswell, S., Edwards, G.,
Giesbrecht, N., Graham, K., . . . Rossow, I. (2010). Alcohol:No ordinary commodity. Research and public policy. Oxford,
UK: Oxford University Press.
Baumrind, D. (1991). The influence of parenting style on
adolescent competence and substance use. The Journal ofEarly Adolescence, 11, 56–95.
Becona, E., Martınez, U., Calafat, A., Juan, M., Fernandez-
Hermida, J.R., & Secades-Villa, R. (2012). Parental styles and
drug use: A review. Drugs: Education, Prevention, andPolicy, 19(1), 1–10.
Bickel, W.K., & Vuchinich, R.E. (Eds.). (2000). Reframinghealth behavior with behavioral economics. New York:
Lawrence Erlbaum.
Bramness, J.G., & Rossow, I. (2010). Can the total consumption
of a medicinal drug be used as an indicator of excessive use?
The case of carisoprodol. Drugs: Education, Prevention, andPolicy, 17, 168–180.
Clark, D.B., Thatcher, D.L., & Tapert, S.F. (2008). Alcohol,
psychological dysregulation, and adolescent brain develop-
ment. Alcoholism: Clinical and Experimental Research, 32,
375–385.
Cronk, C.E., & Sarvela, P.D. (1997). Alcohol, tobacco, and other
drug use among rural/small town and urban youth: A
secondary analysis of the monitoring the future data set.
American Journal of Public Health, 87, 760–764.
De Bellis, M.D., Narasimhan, A., Thatcher, D.L.,
Keshavan, M.S., Soloff, P., & Clark, D.B. (2005). Prefrontal
cortex, thalamus, and cerebellar volumes in adolescents and
young adults with adolescent-onset alcohol use disorders and
comorbid mental disorders. Alcoholism: Clinical andExperimental Research, 29, 1590–1600.
Demant J., & Østergaard, J. (2006). Mellem tør og vad
alkoholkultur [Between dry and wet alcohol cultures]. In
S. Bech & S. Reesen (Eds.), Rundt om rusen – En antologi omunge og rusmidler [In a frenzy of intoxication: An anthology
of youth and substance] (pp 19–26). Denmark: Komiteen for
Sundhedsoplysning (in Danish).
De Piccoli, B., Giada, F., Benettin, A., Sartori, F., & Piccolo, E.
(1991). Anabolic steroid use in body builders: An echocardio-
graphic study of left ventricle morphology and function.
International Journal of Sports Medicine, 12, 408–412.
Derogatis, L., Lipman, R.S., Rickels, K., Uhlenhuth, E.H., &
Covi, L. (1974). The Hopkins Symptom Checklist (HSCL):
A self-report symptom inventory. Behavioral Science, 19(1),
1–5.
Duncan, D.F. (1974). Reinforcement of drug abuse: Implications
for prevention. Clinical Toxicology Bulletin, 4, 69–75.
Eiksund, S. (2009). A geographical perspective on driving
attitudes and behaviour among young adults in urban and
rural Norway. Safety Science, 47, 529–536.
Festinger, L. (1954). A theory of social comparison processes.
Human Relations, 7, 117–140.
Grant, B.F., & Dawson, D.A. (1997). Age of onset of alcohol use
and its association with DSM–IV alcohol abuse and
dependence: Results from the national longitudinal alcohol
epidemiologic survey. Journal of Substance Abuse, 9,
103–110.
Griffin, K.W., Botvin, G.J., Scheier, L.M., Diaz, T., &
Miller, N.L. (2000). Parenting practices as predictors of
substance use, delinquency, and aggression among
urban minority youth: Moderating effects of family structure
and gender. Psychology of Addictive Behaviours, 14,
174–184.
Hair, J.F., Anderson, R.E., Tatham, R.L., & Black, W.C. (1998).
Multivariate data analysis. Upper Saddle River, NJ: Prentice-
Hall.
Hawkins, D.J., Catalano, R.F., & Miller, J.Y. (1992). Risk and
protective factors for alcohol and other drug problems in
adolescence and early adulthood: Implications for substance
abuse prevention. Psychological Bulletin, 112, 64–105.
Hetherington, E.M. (1992). Coping with maritial transitions: A
family systems perspective. Monographs of the Society forResearch in Child Development, 57(2–3), 1–14.
Hetherington, E.M., Clingempeel, W.G., Anderson, E.R.,
Deal, J.E., Stanley-Hagan, M., . . . Linder, M.S. (1992).
Coping with marital transition. Monographs of the Societyfor Research in Child Development, 57, 1–14.
Holmen, J., Midthjell, K., Kruger, Ø., Langhammer, A.,
Holmen, T.L., Bratberg, G.H., . . . Larsen-Lund, P.G. (2003).
The Nord-Trøndelag health study 1995–97 (HUNT 2):
Objectives, contents, methods and participation. NorskEpidemiologi, 13, 19–32.
Huba, G.J., & Bentler, P.M. (1983). Causal models of the
development of law abidance and its relationship to
psychosocial factors and drug use. In W.S. Laufer &
J.M. Day (Eds.), Personality theory, moral development,and criminal behavior (pp. 165–215). Lexington, MA:
Lexington Books.
Jessor, R., & Jessor, S.L. (1977). Problem behaviour andpsychosocial development: A longitudinal study ofyouth. New York: Academic Press.
Khantzian, E.J., Mack, J.F., & Schatzberg, A.F. (1974). Heroin
use as an attempt to cope: Clinical observations. AmericanJournal of Psychiatry, 131, 160–164.
Maxwell, K.A. (2002). Friends: The role of peer influence across
adolescent risk behaviours. Journal of Youth andAdolescence, 31, 267–277.
SOCIAL INFLUENCE, HEALTH VARIABLES AND CRIMINAL BEHAVIOURS 65
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.

Nordfjærn, T., Hole, R., & Rundmo, T. (2010). Interrelations
between patients’ personal life events, psychosocial distress
and substance use. Substance Use & Misuse, 45, 1161–1179.
Nunnally, J.C. (1978). Psychometric theory. New York:
McGraw-Hill.
Robertson, E.B., Sloboda, Z., Boyd, G.M., Beatty, L., & Kozol,
F. (1997). Rural substance abuse: State of knowledge andissues (National Institute on Drug Abuse Monograph 168,
National Institutes of Health Publication No. 97-4177).
Washington, DC: Government Printing Office.
Secades-Villa, R., & Fernandez-Hermida, J.R. (2003). The
validity of self-reports in a follow-up study with drug addicts.
Addictive Behaviours, 28, 1175–1182.
Simons-Morton, B., Haynie, D.L., Crump, A.D., Eitel, P., &
Saylor, K.E. (2001). Peer and parent influences on smoking
and drinking among early adolescents. Health, Education andBehaviour, 28, 95–107.
Smart, R.G. (1980). An availability-proness theory of illicit drug
abuse. NIDA Research Monography, 30, 46–49.
Spoth, R., Goldberg, C., Neppl, T., Trudeau, L., & Ramisetty-
Mikler, S. (2001). Rural-urban differences in the distribution
of parent-reported risk factors for substance use among young
adolescents. Journal of Substance Abuse, 13, 609–623.
Stewart, S.H., Gavric, D., & Collins., P. (2009). Women, girls
and alcohol. In K.T. Brady, S.E. Back, & S.F. Greenfield
(Eds.), Women and addiction: A comprehensive handbook(pp. 341–359). New York: The Guilford Press.
Teesson, M., & Proudfoot, H. (Eds.). (2003). Comorbidmental disorders and substance use disorders.
Canberra: Australian Government Department of Health and
Ageing.
Vedøy, T.F., & Skretting, A. (2009). Ungdom og rusmidler:Resultater fra spørreskjemaundersøkelser 1968–2008[Adolescents and substances: Results from questionnaire
surveys 1968–2008]. Oslo: SIRUS Report 5/2009 (in
Norwegian).
Ward, N.J. (2007). The culture of traffic safety in ruralAmerica. Retrieved from http://www.aaafoundation.org/pdf/
Ward.pdf
Wichstrøm, L. (2000). Predictors of adolescent suicide attempts:
A nationally representative longitudinal study of Norwegian
adolescents. Journal of the American Academy of Child andAdolescent Psychiatry, 39, 603–610.
Wichstrøm, T., & Wichstrøm, L. (2009). Does sports participa-
tion during adolescence prevent later alcohol, tobacco and
cannabis use? Addiction, 104, 138–149.
66 T. NORDFJÆRN ET AL.
Dru
gs E
du P
rev
Pol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orge
s N
atur
vite
nska
pelig
e U
nive
rsite
t (N
TN
U)
on 1
2/21
/13
For
pers
onal
use
onl
y.
Related Documents











