Original Contributions Social Cognitive Markers of Short-Term Clinical Outcome in First-Episode Psychosis 1 Prevention and Early Intervention Program for Psychoses (PEPP- Montreal), Douglas Mental Health University Institute, Montreal, Canada 2 Department of Psychology, Université du Québec à Montréal, Montreal, Canada 3 Department of Neurology & Neurosurgery, McGill University, Montreal, Canada 4 Department of Psychiatry, McGill University, Montreal, Canada Address for correspondence: Martin Lepage, PhD, Douglas Mental Health University Institute-FBC1, 6875 LaSalle Blvd., Verdun, Quebec, H4H 1R3, Canada Phone: 514-761-6131, x. 4393; Fax: 514-888-4064; E-mail: [email protected] Submitted: August 4, 2009; Revised: September 28, 2009; Accepted: November 11, 2009 Introduction Individuals who experience first-episode psychosis (FEP) vary in their response to treatment (1, 2), as well as in their cognitive abilities. Furthermore, there has been growing evidence that cognitive deficits are a core feature of schizophrenia (3, 4) and other psychotic disorders, and that cognitive deficits, namely verbal memory, are associated with aspects of functional outcome in chronic patients (5, 6), as well as in those experiencing their first episode (7, 8). As part of the recent attempt to establish consensus on domains of cognition in schizophrenia (Measurement and Treatment Research to Improve Cognition in Schizophrenia [MATRICS]), social cognition has been added because of Tina Montreuil 1, 2 , Michael Bodnar 1, 3 , Marie-Claude Bertrand 1 , Ashok K. Malla 1, 4 , Ridha Joober 1, 4 , Martin Lepage 1, 3, 4 Clinical Schizophrenia & Related Psychoses July 2010 • 00 Objective: In psychotic disorders, impairments in cognition have been associated with both clinical and functional outcome, while deficits in social cognition have been associated with functional outcome. As an extension to a re- cent report on neurocognition and short-term clinical outcome in first-episode psychosis (FEP), the current study explored whether social cognitive deficits could also identify poor short-term clinical outcome among FEP patients. Methods: We defined the social-cognition domain based on the scores from the Hinting Task and the Four Factor Tests of Social Intelligence. Data were collected in 45 FEP patients and 26 healthy controls. e patients were divided into good- and poor-outcome groups based on clinical data at six months following initiation of treatment. Social cognition was compared among 27 poor-outcome, 18 good-outcome, and 26 healthy-control participants. Results: Outcome groups significantly differed in the social cognition domain (z-scores: poor outcome=-2.0 [SD=1.4]; good outcome=-1.0 [SD=1.0]; p=0.005), with both groups scoring significantly lower than the control group (p<0.003). Moreover, outcome groups differed significantly only on the Cartoon Predictions subtest (z-scores: poor outcome=-2.7 [SD=2.7]; good outcome=-0.7 [SD=1.8]; p=0.001) among the five subtests used. Conclusions: Overall, social cognition appears to be compromised in all FEP patients compared to healthy controls. More interestingly, significant differences in social cognitive impairments exist between good and poor short-term clinical outcome groups, with the largest ef- fect found in the Cartoon Predictions subtest. Key Words: Social Cognition, Clinical Outcome, First-Episode Psychosis Abstract

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Original Contributions
Social Cognitive Markers of Short-Term Clinical Outcome in
First-Episode Psychosis
1 Prevention and Early Intervention Program for Psychoses (PEPP- Montreal), Douglas Mental Health University Institute, Montreal, Canada2 Department of Psychology, Université du Québec à Montréal, Montreal, Canada3 Department of Neurology & Neurosurgery, McGill University, Montreal, Canada4 Department of Psychiatry, McGill University, Montreal, Canada
Address for correspondence: Martin Lepage, PhD, Douglas Mental Health University Institute-FBC1, 6875 LaSalle Blvd., Verdun, Quebec, H4H 1R3, Canada Phone: 514-761-6131, x. 4393; Fax: 514-888-4064; E-mail: [email protected]
Submitted: August 4, 2009; Revised: September 28, 2009; Accepted: November 11, 2009
Introduction Individuals who experience first-episode psychosis(FEP)varyintheirresponsetotreatment(1,2),aswellasin their cognitive abilities. Furthermore, there has beengrowing evidence that cognitive deficits are a core featureof schizophrenia (3,4) andotherpsychoticdisorders, andthatcognitivedeficits,namelyverbalmemory,areassociatedwithaspectsoffunctionaloutcomeinchronicpatients(5,6),aswellasinthoseexperiencingtheirfirstepisode(7,8). Aspartoftherecentattempttoestablishconsensusondomainsof cognition in schizophrenia (MeasurementandTreatmentResearchtoImproveCognitioninSchizophrenia[MATRICS]), social cognition has been added because of
Tina Montreuil 1, 2, Michael Bodnar 1, 3, Marie-Claude Bertrand 1, Ashok K. Malla 1, 4, Ridha Joober 1, 4, Martin Lepage 1, 3, 4
Clinical Schizophrenia & Related PsychosesJuly2010•00
Objective:Inpsychoticdisorders,impairmentsincognitionhavebeenassociatedwithbothclinicalandfunctionaloutcome,whiledeficits insocialcognitionhavebeenassociatedwith functionaloutcome.Asanextensiontoare-cent reportonneurocognitionandshort-termclinicaloutcome infirst-episodepsychosis (FEP), thecurrent studyexploredwhethersocialcognitivedeficitscouldalsoidentifypoorshort-termclinicaloutcomeamongFEPpatients.Methods:Wedefinedthesocial-cognitiondomainbasedonthescoresfromtheHintingTaskandtheFourFactorTestsofSocialIntelligence.Datawerecollectedin45FEPpatientsand26healthycontrols.Thepatientsweredividedintogood-andpoor-outcomegroupsbasedonclinicaldataat sixmonths following initiationof treatment.Socialcognitionwascomparedamong27poor-outcome,18good-outcome,and26healthy-controlparticipants.Results:Outcomegroupssignificantlydifferedinthesocialcognitiondomain(z-scores:pooroutcome=-2.0[SD=1.4];goodoutcome=-1.0 [SD=1.0]; p=0.005), with both groups scoring significantly lower than the control group (p<0.003).Moreover,outcomegroupsdifferedsignificantlyonlyontheCartoonPredictionssubtest(z-scores:pooroutcome=-2.7[SD=2.7];goodoutcome=-0.7[SD=1.8];p=0.001)amongthefivesubtestsused.Conclusions:Overall,socialcognitionappearstobecompromisedinallFEPpatientscomparedtohealthycontrols.Moreinterestingly,significantdifferencesinsocialcognitiveimpairmentsexistbetweengoodandpoorshort-termclinicaloutcomegroups,withthelargestef-fectfoundintheCartoonPredictionssubtest.
Key Words: Social Cognition, Clinical Outcome, First-Episode Psychosis
Abstract

its relevance forclinical trialsand functionaloutcome(9).Social cognitive abilities are composed of several mentaloperations such as perception, interpretation and the pro-cessing of social information. Social cognition is bestdefinedas“theabilitytoconceptualizeotherpeople’sbeliefs,thoughtsand intentions inorder toexplainandanticipatetheirbehavior”(10). Overthepasttwodecades,studieshaveclearlyshownthat social cognition is significantly impaired in chronicschizophrenia(11,12)andinFEP(13-15).Moreinteresting-ly,thesedeficitshavebeenrelatedtoapoorerfunctionalout-comeinbothschizophrenia(11,16,17)andinFEP(13,14).Therelationshipbetweensocialcognitionperformanceandsymptomatic or short-term clinical outcome has receivedlittleattentionsofar,althoughassociationshavebeeniden-tified. Deficits in social cognition have been explained byeitheralackofdevelopmentofsuchabilitiespremorbidly,asin thecaseofpatientswithpredominantlynegativesymp-toms, or as result of a loss of such abilities consequent topositivesymptoms(18).Whethersocialcognitionisassoci-atedwithanearlyreductionofsymptoms,similar towhathas been reported for verbal memory (19), still remainsunexplored.Ifsuchanassociationdoesexist,itwillfurtherincrease the significance of assessing the domain of socialcognition as part of a cognitive battery of tests given theimportanceofafullsyndromalremissionearlyinthetreat-mentofpsychosis(20). Withpastresearchrelatingsocialcognitivedeficitstoapoorpremorbidadjustmentinpatientswithpredominantlynegativesymptomsorresultingfromalossofabilitieslinkedtopositivesymptomatology(18),itwouldbeexpectedthatdeficitsinthisdomaincouldsignificantlyaffectclinicalout-come.Basedonthisandtheabovementionedfindings,wehypothesizedthatallFEPpatientswouldshowsocialcogni-tivedeficitsincomparisontomatchedhealthycontrols.Fur-thermore,wehypothesizedthatdeficitsinsocialcognitionwouldbeassociatedwithapoorshort-termclinicaloutcomeduringtheinitialstagesoftreatmentfollowinganFEP.
Social Cognitive Markers of Clinical Outcome
00 • Clinical Schizophrenia & Related PsychosesJuly2010
Methods
Participants, Treatment Setting and Treatment Protocol All participants were part of an ongoing, longitudinalbehavioralandimagingstudybeingconductedattheDoug-lasMentalHealthUniversityInstituteinMontreal,Canada.All FEP patients were recruited and treated through thePrevention and Early Intervention Program for Psychoses(PEPP-Montreal), a specialized early-intervention servicewith integrated clinical, research, and teaching modules.The program involves a comprehensive approach with in-tensivemedicalandpsychosocialmanagement.Allpatientsare provided modified assertive case management and in-terventionstoassistintheirrecovery(forfurtherdetailsontheprogram,see[21]).Patientsaged14to30yearsfromthelocalcatchmentareasufferingfromeitheraffectiveornonaf-fectivepsychosis,whohadnottakenantipsychoticmedica-tionformorethanonemonth,wereconsecutivelyadmittedtotheprogramaseitherin-orout-patients.Thereisnocom-petingserviceandtreatmentispubliclyfunded. From PEPP-Montreal we recruited 48 patients for animagingstudy,whohadalsocompletedsupplementaryso-cialcognitivetests:theHintingTask(18)andtheFourFac-torTestsofSocial Intelligence (22).Fromour study, threepatientsweresubsequentlyremovedduetoalaterconfirmeddiagnosisofsubstance-inducedpsychosis.Inaddition,twopoor-outcome patients refused antipsychotic medicationsas a treatment option. These clients still received the psy-chosocial interventions. The remaining 45 patients weresubsequently separated into good-outcome (n=18) andpoor-outcome (n=27) groups based on six-month clinicaldata.Asperanearlierreport,goodoutcomewasdefinedbyaratingof2orless(mild)onallglobalsubscalesoftheSAPSand3orless(moderate)onallglobalsubscalesoftheSANS,excluding the subscale of “attention” (23). For the presentstudy,allFEPpatientswereincluded,whichwascomprisedof39schizophreniaspectrumdisorder(pooroutcome=24;
Clinical ImplicationsSocialcognitivedeficitshavebeenhypothesizedtoaffecttheclinicaloutcomeofpatientsbydelayingtheresponsetotreatmentorbyimpairingtheclient’smotivationtoadheretotreatmentasprescribed(7).Consequently, itwouldbeimportanttoidentifyapooroutcomeearlieronso,asclinicians,wecanpayspecialattentiontothisspecificsubgroupandpossiblyprovidemoreintensivepsychosocialinterventionsand/orintroducealternativeantipsychoticsearlieroninthetreatmentprocesstobetterbenefitalargerproportionofclients.Inaddition,studieshavefoundevidencebetweencognitiveimprovementandbetterfunctionaloutcome,suggestingthatcognitionshouldbepartofthefocusduringthetreatmentofschizophrenia(37).Ifoneoperatesonthebasisthatsocialcognitivedeficitsarelinkedtoshort-termclinicaloutcome,psychosocialinterventionsshouldincludeelementsofpsychoeducationabouttheillness,behavioractivationtoimprovemotivation,andcognitiveremediationinordertoimproveoverallareasofneurocognitioninhopeofbetteroutcome.

Clinical Schizophrenia & Related PsychosesJuly2010•00
Tina Montreuil et al.
goodoutcome=15),4affectivepsychosis(pooroutcome=2;goodoutcome=2),and2psychosisNOS(pooroutcome=1;goodoutcome=1). Twenty-six healthy controls were recruited throughadvertisementsinlocalnewspapersandtookpartinsocialcognitive testing sessions. Controls were included only iftheyhadnocurrentorpasthistoryof:1)anyAxisIdisor-ders;2)anyneurologicaldiseases;3)head traumacausinglossofconsciousness;and,4)afirst-degreefamilymembersufferingfromschizophreniaorrelatedschizophreniaspec-trumpsychosis.Controlswerealsochosenonsociodemo-graphicvariablessuchasage(attesting),gender,andparen-talsocioeconomicstatusduringchildhoodmatchedtoFEPpatientswhoweretakingpartinaneuroimagingstudy. Afteracomprehensivedescriptionofthestudy,writteninformed consent was obtained from all participants. TheDouglas Mental Health University Institute review boardapprovedtheresearchprotocols.
Clinical and Demographic Assessments PatientswerediagnosedaccordingtotheDSM-IVcrite-riabasedontheStructuredClinicalInterviewforDSM-IV
(24)andconfirmedthroughconsensusbetweentwoseniorresearchpsychiatrists(A.M.andR.J.).PositiveandnegativesymptomswereassessedwiththeScalefortheAssessmentofPositiveSymptoms(SAPS)(25)andtheScalefortheAs-sessmentofNegativeSymptoms(SANS)(26), respectively.The baseline interview session was conducted within onemonthofentryintotheprogram(mean=23.4days,SD=8.6days, range=4.8–46.2 days). The symptom ratings coveredthepreviousonemonthandwererepeatedmonthlyuntilthethirdmonthandthenagainatsixmonths,ninemonths,andtwelvemonthspastbaselineasshowninTable1.Symptomratingsareperformedbyresearchassistants(ICC=0.75forboththeSAPSandtheSANS)whohadreceivedextensivetrainingandsupervisionwithinterraterreliabilitymeasuredatleastonceayear. Medication adherence was assessed at each of theaforementionedtimepointsandaveragedoverthefirstsix-monthperiodtoprovideanoveralladherencescore.Medi-cationadherencewasbasedona5-pointscalerangingfrom0(neveradherent)to4(fullyadherent)oninformationob-tained frompatients, familymembers,casemanagers,andpsychiatrists. Duration of untreated psychosis (DUP) was
Poor Outcome (n=27)
Good Outcome (n=18)
Table 1 Characteristics and Global Symptom Ratings of Poor-Outcome and Good-Outcome Groups. (Number of participants included [n] for each variable where different from sample.)
AnalysisStatistic df p value
DUP (median, weeks)*
DUI (median, weeks)*
Antipsychotic at Testing (mg/day)
Olanzapine
Risperidone
Quetiapine
Risperidone-Injected
Haloperidol
None
Medication Adherence†
SAPS Total
Baseline
Six Months
Change
SANS Total
Baseline
Six Months
Change
38.3±44.3
277.4±250.2
11.8±5.0 (n=11)
2.3±0.8 (n=9)
350.0±173.2 (n=5)
(n=0)
(n=0)
(n=2)
3.2±1.0
28.9±16.6
12.1±11.8
16.8±12.4
28.3±13.6
25.3±11.1
3.0±13.2
93.7±148.2
295.3±260.3
10.9±8.0 (n=7)
1.5±0.8 (n=5)
775 (n=1)
25.0 (n=1)
1.5 (n=1)
(n=3)
3.5±0.8 (n=16)
35.1±17.6
1.7±2.8
33.4±17.4
27.4±13.3
14.5±18.7
12.9±17.4
t=-1.27
t=-0.24
χ2=5.31
t=0.40
t=1.80
t=-2.24
n/a
n/a
n/a
t=-1.04
t=-1.20
t=3.66
t=-3.75
t=0.22
t=2.44
t=-2.18
43
43
5
16
12
4
41
43
43
43
43
43
43
0.21
0.81
0.38
0.77
0.10
0.90
0.31
0.24
0.001‡
0.001‡
0.83
0.02‡
0.04‡
DUP=duration of untreated psychosis; DUI=duration of untreated illness; SAPS=Scale for the Assessment of Positive Symptoms; SANS=Scale for the Assessment of Negative Symptoms. *DUP and DUI are presented in raw form; however, these were analyzed using transformed data. †Medication adherence average over six months: 0 (never adherent) to 4 (always adherent). ‡Significant at 0.05 level.
Social Cognitive Markers of Clinical Outcome
00 • Clinical Schizophrenia & Related PsychosesJuly2010
calculatedasthetimeperiodfromonsetofpsychoticsymp-toms judgedtobeat threshold levelaccordingtoDSM-IVcriteriauntiltimeofadequatetreatmentwithantipsychotics(thirtydaysofcontinuoustreatmentorlessifremissionofpositivesymptomsoccurred).Durationofuntreatedillness(DUI)wasdefinedasthetimeperiodfromonsetofanypsy-chiatricsymptomstoadequatetreatmentwithantipsychot-ics(27). Parentalsocioeconomicstatus(SES)wasassessedwiththeHollingsheadsocioeconomicstatusratingscale(28).SESisanestimationthatisachievedbyconsideringtheoccupa-tionalstatusandthehighestlevelofeducationattainedbyaparent,includingotherfamilyassetsandresources.Finally,thetypeanddosageofantipsychotictakenatthetimeofthesocialcognitiveevaluationwererecorded.Allinterviewses-sions acquiring the collection and assessment of pertinentdatawereperformedbyatrainedprofessional.
Social Cognition Measures Patientswereassessedafter the initiationof treatmentandonlywheninastable,butnotnecessarilyasymptomatic,condition.AspresentedinTable1,therewasnodifferencebetween patient groups with respect to when evaluationstookplacefollowingentryintotheprogram(pooroutcome:mean=19.8 weeks, SD=9.6; good outcome: mean=18.7weeks,SD=13.0;t=0.33,df=43,p=0.74). The two social cognitive tests used were the HintingTask (18) and the Four Factor Tests of Social Intelligence(22).TheHintingTask tests theabilityof subjects to inferthe real intentions behind indirect statements. Ten shortpassagesarereadtothesubjectoneatatime,presentinganinteraction between two characters with one of the char-acters giving a very obvious hint at the end. The exam-ineemust then tellwhat the character reallymeant. If theexamineefails,thenheisaskedwhatonecharacterwantstheotheronetodo.
The Four Factor Tests of Social Intelligence measurestheabilitytounderstandthoughts,feelings,andintentionsofotherpeople.Thereare fourdifferent subtests (CartoonPredictions, Expression Grouping, Social Translation, andMissing Cartoons), of which three use pictorial stimuli(comicstripsanddrawings)andoneemploysprintedsen-tencesonly.Eachquestionisworthonepoint,yieldingfourdistinctscores(oneforeachsubtest)andaglobalcompositescore (by summing up the totals of the subtests) of socialcognition.
The Cartoon Predictions Subtest TheCartoonPredictionssubtest isa14-itemtaskthatmeasures the ability to predict social consequences byshowing a cartoon strip where the examinee must be abletoanticipatethelogicalsequenceofagivensocialsituationsimply by interpreting the cartoon characters’ emotionalreactions.Theexamineemustselect,fromfouralternativecartoon frames, the one that most likely follows from aninterpersonalsituationdepicted in thefirstcartoonframe.Acommonexampleinvolvesastripwhereamanisholdingontoaroof,whileayoungboyisstandingthere,watchingthescene.Theman’sfacialexpressionseemstodepictfear.Theexamineemustbeabletoconceivethatthemostlogi-calstripwouldshowtheboybeinghelpedbyawomanwhoiscarryinga ladderwith the intentionofhelping themancomesafelydownfromtheroof(29).
The Expression Grouping Subtest TheExpressionGroupingsubtestisa15-itemtaskthatinvolvestheabilitytoabstractcommonattributesfromdif-ferentexpressiveimages.Eachitemofthetestconsistsofagroupofthreepicturesrepresentingeitherfacialexpression,hand gestures or body posture that correspond to a com-monthought,feelingorintention.Todemonstrateacorrectunderstandingof the situation, theparticipantmust select
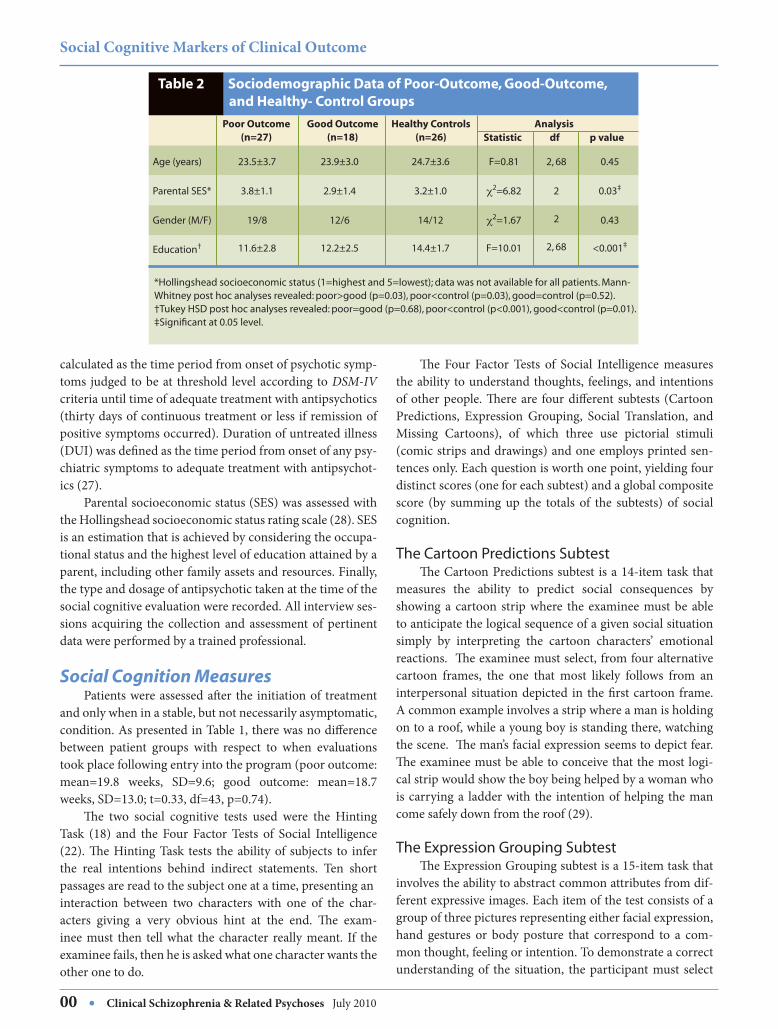
*Hollingshead socioeconomic status (1=highest and 5=lowest); data was not available for all patients. Mann-Whitney post hoc analyses revealed: poor>good (p=0.03), poor<control (p=0.03), good=control (p=0.52).†Tukey HSD post hoc analyses revealed: poor=good (p=0.68), poor<control (p<0.001), good<control (p=0.01).‡Significant at 0.05 level.
Poor Outcome (n=27)
Good Outcome (n=18)
Healthy Controls (n=26)
Table 2 Sociodemographic Data of Poor-Outcome, Good-Outcome, and Healthy- Control Groups
AnalysisStatistic df p value
Age (years)
Parental SES*
Gender (M/F)
Education†
23.5±3.7
3.8±1.1
19/8
11.6±2.8
23.9±3.0
2.9±1.4
12/6
12.2±2.5
24.7±3.6
3.2±1.0
14/12
14.4±1.7
F=0.81
χ2=6.82
χ2=1.67
F=10.01
2, 68
2
2
2, 68
0.45
0.03‡
0.43
<0.001‡
Clinical Schizophrenia & Related PsychosesJuly2010•00
Tina Montreuil et al.
onepicturerepresentingthesameemotionfromfouralter-natives.
The Social Translation Subtest TheSocialTranslationsubtestisa12-itemtaskdesignedto measure the ability to recognize changes in behavioralmeaning. Based on the principle that similar expressionalcuescanbeassociatedwithdifferentmeaningsasafunctionofdifferentcontexts,theexamineemustchooseoneofthreepossiblesentenceshavingadifferentmeaningfromthetar-getsentence.
The Missing Cartoons Subtest Finally,theMissingCartoonssubtestisa14-itemtaskmeasuringtheabilitytoconsidersocialcontext.Eachitemconsistsofanincompletecartoonstripand,afterinterpret-ing each scene, the examinee chooses, from four alterna-tives,thepanelthatbestcompletesthecartoonstrip,givingthestoryalogicalflow.
Statistical Analysis Allclinicalcharacteristicswerenormallydistributedex-ceptfordurationofuntreatedpsychosis(DUP)anddurationof untreated illness (DUI), which were normalized usinglogarithmic and square root transformations, respectively.Aone-wayanalysisofvariance (ANOVA)wasused toex-amineage(attesting)amongthethreegroups.Independentt-testswereused to comparebaselineand six-month totalsymptomratings,changesinsymptomscores,dosageofan-tipsychotic medication, medication adherence, DUP, DUI,
andPremorbidAdjustmentScale(PAS)scoresbetweenthepatient outcome groups. Parental SES and education levelamong the three groups were contrasted using a Kruskal-Wallisone-wayANOVA.Genderandtypeofantipsychoticmedicationwerecomparedusingcrosstabulationandchi-squaretests.Allof thesocialcognitivevariableswerenor-mallydistributed.Allsubtestscoresweretransformedintostandardequivalents(z-scores)usingthemeanandstandarddeviationofthehealthy-controlgroup. Forthepresentstudy,wecreatedasocialcognitiondo-mainbycombiningallfiveoftheaforementionedsubtests:that is, theHintingTaskand the four subtestsof theFourFactorTestsofSocialIntelligence.Aunivariateanalysisofcovariance (ANCOVA) was used to compare the perfor-mance of the social cognition domain among the groups,using group membership (poor outcome, good outcome,andcontrol)asthebetween-groupfactor, theglobalsocialcognitiondomainas thewithin-groupfactor,andparentalSESasacovariate.PosthocFisher’sLSDwasusedtoiden-tifyanygroupdifferences.Asubsequentandsupplementarywithin-subject multivariate analysis of covariance (MAN-COVA)wasusedtoexaminetheprofileofthefivesubtestsamong the three groups using group membership as thebetween-groupfactor,thefivesubtestsasthewithin-groupfactors,andparentalSESasacovariate.PosthocunivariateANCOVAs,alongwithFisher’sLSD,wereused to identifyanygroupdifferences.Thecriticalpvalue for thisanalysiswas set to 0.01, following the Bonferroni correction pro-cedure to control for multiple comparisons. This analysiswouldallowustoobserveiftherewereanydifferenceswith-
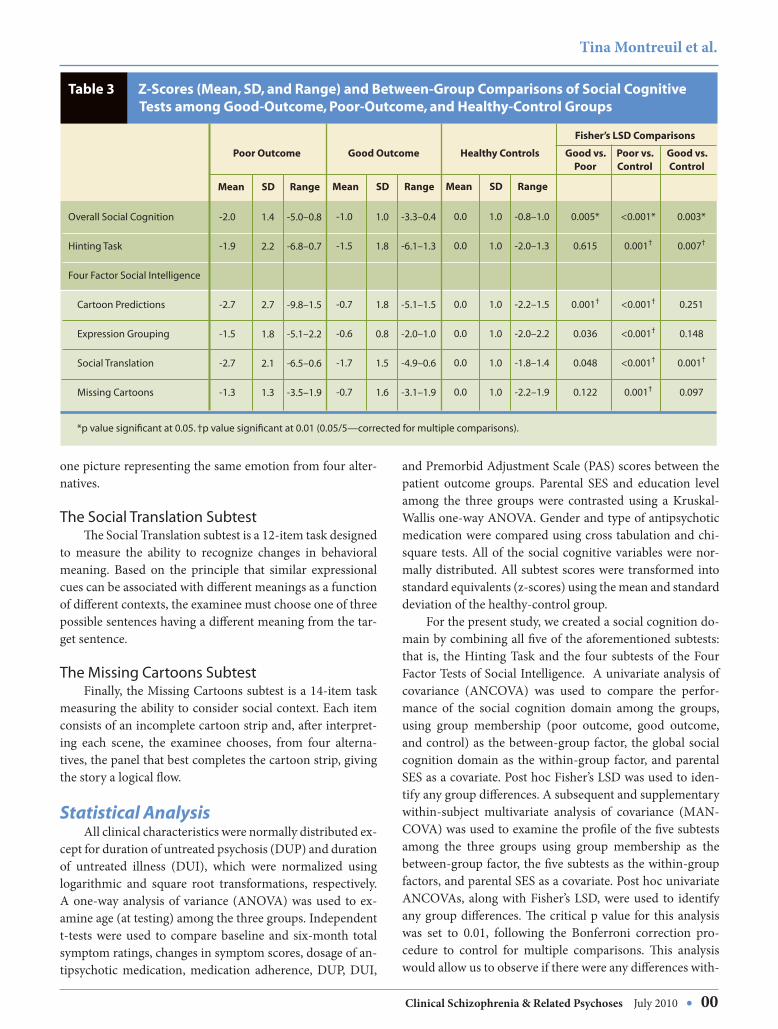
*p value significant at 0.05. †p value significant at 0.01 (0.05/5—corrected for multiple comparisons).
Poor Outcome Good Outcome Healthy Controls
Table 3 Z-Scores (Mean, SD, and Range) and Between-Group Comparisons of Social Cognitive Tests among Good-Outcome, Poor-Outcome, and Healthy-Control Groups
Fisher’s LSD Comparisons
Good vs. Poor
Poor vs. Control
Good vs. Control
Mean SD Range
-2.0
-1.9
-2.7
-1.5
-2.7
-1.3
1.4
2.2
2.7
1.8
2.1
1.3
-5.0–0.8
-6.8–0.7
-9.8–1.5
-5.1–2.2
-6.5–0.6
-3.5–1.9
Mean SD Range
-1.0
-1.5
-0.7
-0.6
-1.7
-0.7
1.0
1.8
1.8
0.8
1.5
1.6
-3.3–0.4
-6.1–1.3
-5.1–1.5
-2.0–1.0
-4.9–0.6
-3.1–1.9
Mean SD Range
0.0
0.0
0.0
0.0
0.0
0.0
1.0
1.0
1.0
1.0
1.0
1.0
-0.8–1.0
-2.0–1.3
-2.2–1.5
-2.0–2.2
-1.8–1.4
-2.2–1.9
Overall Social Cognition
Hinting Task
Four Factor Social Intelligence
Cartoon Predictions
Expression Grouping
Social Translation
Missing Cartoons
0.005*
0.615
0.001†
0.036
0.048
0.122
<0.001*
0.001†
<0.001†
<0.001†
<0.001†
0.001†
0.003*
0.007†
0.251
0.148
0.001†
0.097

Social Cognitive Markers of Clinical Outcome
00 • Clinical Schizophrenia & Related PsychosesJuly2010
ineachofthefivesubtests(thatmadeupoursocialcognitivedomain)amongthethreegroups.Finally,fortheentiresam-ple,Pearson’schi-squareandSpearman’srho(ρ)examinedthe independence and correlations, respectively, betweenthesubtestsandsymptomlevelsat the timeof theevalua-tion. Symptom data at the time of social cognitive testingwereestimatedfromthesymptomevaluationclosesttoad-ministration.Additionally, cross tabulationandchi-squaretestswereusedtoexamineiftherewasaneffectofthehet-erogeneoussampleonthesocialcognitiveprofile.Allstatis-ticaltestsweretwo-tailedwiththecriticalpvaluesetat0.05(exceptfortheMANCOVA,aspreviouslynoted),andwereperformed using the Statistical Package for the Social Sci-ences,version12(30).
Results
Clinical and Demographic Data The statistical analyses did not reveal any significantdifferencesbetweenthepoor-outcome,good-outcomeandcontrolgroupswithrespecttoageandgender.Thelevelofeducationofparticipantsdidnotsignificantlydifferamongthe experimental groups (good versus poor outcome), butthesegroupsbothdifferedfromthecontrolgroup.However,Table2showshowparentalSESdifferedbetweenthepoor-outcomeandgood-outcomegroupsandthepoor-outcomeandcontrolgroups. In lightof thesedifferences, thisvari-
ablewasincludedasacovariateinouranalysis.TherewerenodifferencesinDUP,DUI,overallmedicationadherence,andthetypeofantipsychotictakenduringsocialcognitivetestingbetweentheoutcomegroups.Finally,therewerenobetween-group differences in both positive and negativesymptoms at baseline. At six months, the poor-outcomegroup displayed significantly higher negative and positivesymptoms, as per design. In addition, over the six-monthperiod, improvements in positive and negative symptomsweresignificantlybetterforthegood-outcomegroupaspre-sentedinTable1.
Social Cognition Data The univariate ANCOVA revealed mean differencesin social cognition among the groups (F=25.51, df=2, 67,p<0.001;ES=0.81).Fisher’sLSDrevealedthepoor-outcomegroup functioned at levels significantly below the good-outcomegroup,andthatbothoutcomegroups functionedsignificantlybelowthatofthehealthy-controlgroup(Table3). The MANCOVA revealed the social cognitive profilesamong the three groups were not parallel as indicated bythesignificant(groupxsubtest)interaction(F=5.13,df=10,126,p<0.001;ES=0.64;Figure1).Thereweresignificantdif-ferencesamongthethreegroupsonallfivesubtests:Hint-ing Task (F=7.35, df=2, 67, p=0.001; ES=0.47); CartoonPredictions(F=13.06,df=2,67,p<0.001;ES=0.63);Expres-sionGrouping(F=7.99,df=2,67,p=0.001;ES=0.49);Social
Figure 1 Social Cognitive Profile of Poor-Outcome, Good-Outcome, and Healthy-Control Groups
Hinting
Task
Cartoon
Predictions
Expression
Grouping
Social
Translation
Missing
Cartoons
Poor Outcome (n=27) Good Outcome (n=18) Healthy Control (n=26)
0.0
-0.5
-1.0
-1.5
-2.0
-2.5
-3.0
-3.5
z-sc
ore
Results are displayed in z-scores with healthy controls defined with a mean of 0 and SD of 1. Error bars are equal to SD.

Discussion Thepresentstudyidentifiedadeficitinsocialcognitionasamarkerofshort-termclinicaloutcomeinfirst-episodepsychosis (FEP) patients after six months of treatment.We found a significantly lower performance in the poor-outcome patients compared to the good-outcome patientsat baseline, in addition to both outcome groups function-ingbelowthatofthecontrolgroup.Thisfindingaddstoourprevious report on nonsocial cognitive domains in whichwe reported poorer verbal memory and working memoryperformancewereassociatedwithapoorshort-termclinicaloutcomeinFEPpatients(23). Current trends in research, such as the NIMH-MATRICS,havesuggestedthat,asaseventhdomain,socialcognitionshouldincludemultiplemeasuresincluding:emo-tionalprocessing,theoryofmind,socialperception,socialknowledge and attributions (31), making it comparable totheother cognitivedomains (31).Furthermore, theMAT-RICS committee has made several recommendations, oneofwhich is touseasingle-testevaluation(Mayer-Salovey-Caruso Emotional Intelligence Test [MSCEIT]-ManagingEmotions)toevaluateoverallsocialcognitiveability.Incon-trast,theoverallsocialcognitivedomainincludedmultiplemeasures,andtheone-hourevaluationsessionforthisdo-mainissomewhattimeconsuming.Moreover,ifoneofthesubtests,whichcanbeadministeredinabouttwelveminutes,couldhavethesamepredictiveabilityastheoveralldomain,itwouldmakemoresensetohaveashortersessionifoneissolelyinterestedinpredictingoutcome.Assuch,wedecidedtoinvestigateifasingletestwashavinganoveralleffectonthedomain.OurresultssuggestedthattheCartoonPredictionssubtestwasthedrivingforcebehindtheoveralleffectofthedomain; subsequently leading to a shortened evaluation ifthegoalwastopredicttheclinicaloutcome.SimilarlytotherecommendationsmadebytheMATRICS,wearesuggest-
Poor Outcome Good Outcome Healthy Controls
Table 4 Raw Data of Social Cognitive Tests for Poor-Outcome Patients, Good- Outcome Patients, and Healthy-Control Groups
Mean SD Range
15.3
9.5
6.9
6.8
5.9
3.3
2.8
2.9
2.7
3.0
8–19
2–14
1–13
2–11
1–13
Mean SD Range
15.9
11.6
8.3
8.1
7.3
2.6
1.8
1.4
1.9
3.5
9–20
7–14
6–11
4–11
2–13
Mean SD Range
18.0
12.4
9.4
10.3
8.8
1.5
1.1
1.6
1.3
2.2
15–20
10–14
6–13
8–12
4–13
Hinting Task (max 20)
Cartoon Predictions (max 14)
Expression Grouping (max 15)
Social Translation (max 12)
Missing Cartoons (max 14)
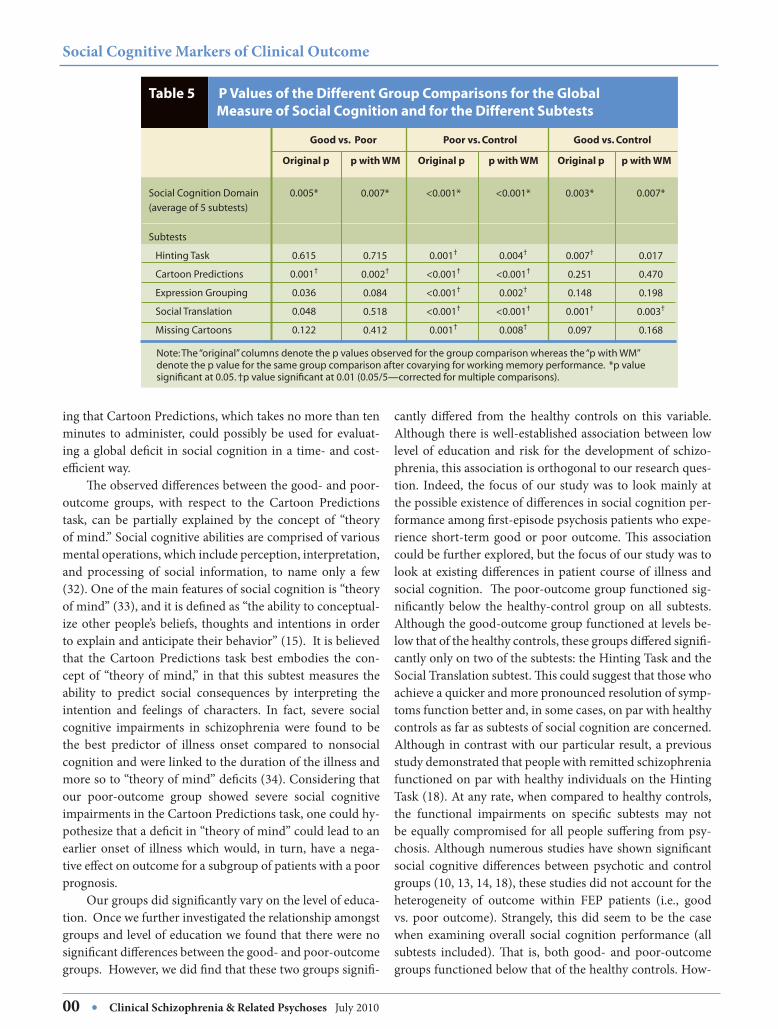
Translation (F=17.83, df=2, 67, p<0.001; ES=0.73); and,MissingCartoons(F=6.43,df=2,67,p=0.003;ES=0.44).Themean performance of the social cognition subtests revealsthese significant differences among the groups (Table 4).The good- and poor-outcome groups differed the least ontheHintingTasksubtest(mean=15.9,SD=2.6;mean=15.3,SD=3.3, respectively), while they were most discrep-ant on the Cartoon Predictions task (mean=11.6, SD=1.8;mean=9.5,SD=2.8,respectively).Fisher’sLSDrevealedthepoor-outcomegroupperformedsignificantlylowerthanthegood-outcomegroupinonlytheCartoonPredictionssub-test.Moreover,comparedtothehealthycontrols,thepoor-outcomegroupdisplayedsignificantdeficitsonallfivesub-tests, while the good-outcome group displayed significantdeficitsinonlytheHintingTaskandSocialTranslationsub-test,asshowninTable3.Inourpreviousstudyonnonsocialcognitive domains and short-term clinical outcome (23),we had observed significant group differences on verbalmemoryandworkingmemory.Weconductedthoseanaly-sesagain(ANCOVAandMANCOVA)andthenexaminedsocialcognitiveperformancewhilecovaryingeachofthesenonsocialcognitivedomains,butourresultsremainedun-changedforallthreegroups.Inparticular,thelargestgroupdifferenceonnonsocialcognitivedomainwasobservedontheworkingmemorymeasureand,ascanbeseeninTable5,covaryingforitdidnotaltertheresults. Finally, the total positive and negative symptoms atthetimeoftestingwereindependentofallthesocialcogni-tive tests (allχ2values<356.6,allpvalues>0.10)except forpositivesymptomsandSocialTranslationsubtest(χ2=195.3,p=0.04);symptomswerenotcorrelatedwithanyofthetests(-0.25<ρ<0.07,allpvalues>0.10).Chi-squaretestsrevealedno effect of diagnosis on social cognitive tests (all χ2 val-ues<19.5,allpvalues>0.53)anddiagnosiswasindependentofoutcome(χ2=0.29,p=0.87).
Clinical Schizophrenia & Related PsychosesJuly2010•00
Tina Montreuil et al.
Social Cognitive Markers of Clinical Outcome
00 • Clinical Schizophrenia & Related PsychosesJuly2010
ingthatCartoonPredictions,whichtakesnomorethantenminutes toadminister, couldpossiblybeused forevaluat-ingaglobaldeficitinsocialcognitioninatime-andcost-efficientway. Theobserveddifferencesbetweenthegood-andpoor-outcome groups, with respect to the Cartoon Predictionstask, can be partially explained by the concept of “theoryofmind.”Socialcognitiveabilitiesarecomprisedofvariousmentaloperations,whichincludeperception,interpretation,and processing of social information, to name only a few(32).Oneofthemainfeaturesofsocialcognitionis“theoryofmind”(33),anditisdefinedas“theabilitytoconceptual-izeotherpeople’sbeliefs, thoughtsand intentions inordertoexplainandanticipatetheirbehavior”(15).Itisbelievedthat the Cartoon Predictions task best embodies the con-ceptof “theoryofmind,” in that this subtestmeasures theability to predict social consequences by interpreting theintention and feelings of characters. In fact, severe socialcognitive impairments in schizophrenia were found to bethe best predictor of illness onset compared to nonsocialcognitionandwerelinkedtothedurationoftheillnessandmoresoto“theoryofmind”deficits(34).Consideringthatour poor-outcome group showed severe social cognitiveimpairmentsintheCartoonPredictionstask,onecouldhy-pothesizethatadeficitin“theoryofmind”couldleadtoanearlier onset of illness which would, in turn, have a nega-tiveeffectonoutcomeforasubgroupofpatientswithapoorprognosis. Ourgroupsdidsignificantlyvaryonthelevelofeduca-tion.Oncewefurtherinvestigatedtherelationshipamongstgroupsandlevelofeducationwefoundthattherewerenosignificantdifferencesbetweenthegood-andpoor-outcomegroups.However,wedidfindthatthesetwogroupssignifi-
Good vs. Poor Poor vs. Control Good vs. Control
Table 5 P Values of the Different Group Comparisons for the Global Measure of Social Cognition and for the Different Subtests
Original p
0.005*
0.615
0.001†
0.036
0.048
0.122
0.007*
0.715
0.002†
0.084
0.518
0.412
Social Cognition Domain
(average of 5 subtests)
Subtests
Hinting Task
Cartoon Predictions
Expression Grouping
Social Translation
Missing Cartoons
p with WM Original p
<0.001*
0.001†
<0.001†
<0.001†
<0.001†
0.001†
<0.001*
0.004†
<0.001†
0.002†
<0.001†
0.008†
p with WM Original p p with WM
0.003*
0.007†
0.251
0.148
0.001†
0.097
0.007*
0.017
0.470
0.198
0.003†
0.168
cantly differed from the healthy controls on this variable.Althoughthereiswell-establishedassociationbetweenlowlevelof educationandrisk for thedevelopmentof schizo-phrenia,thisassociationisorthogonaltoourresearchques-tion. Indeed, the focusofour studywas to lookmainlyatthepossibleexistenceofdifferencesinsocialcognitionper-formanceamongfirst-episodepsychosispatientswhoexpe-rience short-term good or poor outcome. This associationcouldbefurtherexplored,butthefocusofourstudywastolookatexistingdifferences inpatientcourseof illnessandsocialcognition.Thepoor-outcomegroupfunctionedsig-nificantly below the healthy-control group on all subtests.Althoughthegood-outcomegroupfunctionedatlevelsbe-lowthatofthehealthycontrols,thesegroupsdifferedsignifi-cantlyonlyontwoofthesubtests:theHintingTaskandtheSocialTranslationsubtest.Thiscouldsuggestthatthosewhoachieveaquickerandmorepronouncedresolutionofsymp-tomsfunctionbetterand,insomecases,onparwithhealthycontrolsasfarassubtestsofsocialcognitionareconcerned.Althoughincontrastwithourparticularresult,apreviousstudydemonstratedthatpeoplewithremittedschizophreniafunctionedonparwithhealthyindividualsontheHintingTask(18).Atanyrate,whencomparedtohealthycontrols,the functional impairments on specific subtests may notbeequallycompromisedforallpeoplesufferingfrompsy-chosis.Althoughnumerousstudieshaveshownsignificantsocial cognitive differences between psychotic and controlgroups(10,13,14,18),thesestudiesdidnotaccountfortheheterogeneity of outcome within FEP patients (i.e., goodvs. poor outcome). Strangely, this did seem to be the casewhen examining overall social cognition performance (allsubtests included). That is, both good- and poor-outcomegroupsfunctionedbelowthatofthehealthycontrols.How-
Note: The “original” columns denote the p values observed for the group comparison whereas the “p with WM” denote the p value for the same group comparison after covarying for working memory performance. *p value significant at 0.05. †p value significant at 0.01 (0.05/5—corrected for multiple comparisons).

Clinical Schizophrenia & Related PsychosesJuly2010•00
Tina Montreuil et al.
ever, we must point out that this overall effect was drivenbytwotasksinparticular:theHintingTaskandtheSocialTranslationsubtest.As such, thereappears tobeahetero-geneityofsocialcognitivefunctioningwithinthosesuffer-ing from psychosis in relation to short-term clinical out-comewithrespecttoindividualsubtests.Furthermore,evenre-runningalloftheanalysescovaryingforthesixnonsocialcognitive domains, which included working memory, didnotsignificantlychangeourresults.Assuch,itappearssafetoconcludethatnonsocialcognitionhasnosignificanteffectonsocialcognitiveabilityinrelationtoshort-termclinicaloutcome,whichwasourmainvariableofstudy. Thestrengthsofourstudyincludeawell-characterizedsampleoffirst-episodepsychosispatients.Consistently,theclinic from which the sample derives is a well-establishedprogram which offers a thorough research protocol thatincludessystematicfollow-upassessmentsandaconsistentre-evaluation and validation of diagnosis. Moreover, byusingahealthy-comparisongroup,wecontrolledforpossibledemographicdifferencesthatmayoccurwithcomparisonsmade tonormativedata.Theheterogeneityofour sample,withrespecttodiagnosis,providedamoreefficientresearchdesignforanoutcomestudy(35).Thisfollowsfromtheideathatbaselinediagnosesoffirst-episodepatientschangerath-erfrequently(36),whichcouldleadtoerroneouslydrawingconclusionstowardaspecificdiagnosticcategory. This study has some limitations. From our study, twopoor-outcomepatientsrefusedantipsychoticmedicationsasa treatmentoption.Theseclientsstill receivedthepsycho-socialinterventionandsupportallocatedthroughthePEPPclinic,andtheremovaloftheseclientsfromthesampledidnot have any effect on our results. Although our size wasadequatetodetecthighlysignificantgroupdifferences,oursmaller sample size diminishes the generalization of ourresults to thegeneralpatientpopulation.As such, replica-tionofourresultsisneededtoverifyifthereisindeedatrueeffectofsocialcognitioninrelationtoclinicaloutcome. Furthermore, our assessment of cognitive functioninginclinicalsettingsoftentakesplaceattimeswhenthepatientisinastable,butnotnecessarilyasymptomatic,condition.Astableconditioncansometimesbeachievedwithinoneortwo month post treatment. Based on these latter findings,havingsomeofthepatientstestednearthesixthmonthsep-arationtimefromenteringtheprogramtoreceivingongo-ingtreatmentforaperiodofoversixmonths,wecanassumethatpsychoticsymptomsshouldhaveverylittletonooveralleffectonourresults.Nonetheless,wecannotentirelyrejectthe possibility that psychotic symptomatology may havehadaneffectonperformanceofthesocialcognitiontasks.Social cognitionmayneed tobe further investigated;and,until then,wecannotdefine theextentofhowsymptoms,timeorclinicalstabilitywillaffectsocialcognition.
Conclusions Bothofourstudieshaveindicatedthatcognitionappearstobeareliablemarkerof short-termclinicaloutcomefol-lowingafirstepisodeofpsychosis.Thepresentstudyfoundthatpoorsocialcognition(ormorespecifically,adeficitintheability topredict social situations) isamarkerofpoorshort-termclinicaloutcomeaftersixmonthsof treatment;ourprevious study identifiedverbalmemoryandworkingmemoryinthesamecapacity.Takentogether,itwouldap-pearthatspecificimpairmentsineithersocialcognitionornonsocialcognition,namelyverbalmemory,maybeusefulfor identifying a poor prognosis early on in the treatmentprocessfollowingFEP. Socialcognitivedeficitshavebeenhypothesizedtoaffecttheclinicaloutcomeofpatientsbydelayingtheresponsetotreatmentorbyimpairingtheclient’smotivationtoadhereto treatment as prescribed (7). Consequently, it would beimportanttoidentifyapooroutcomeearlieronso,asclini-cians,wecanpayspecialattentiontothisspecificsubgroupandpossiblyprovidemoreintensivepsychosocialinterven-tionsand/orintroducealternativeantipsychoticsearlieroninthetreatmentprocesstobetterbenefitalargerproportionofclients.Inaddition,studieshavefoundevidencebetweencognitiveimprovementandbetterfunctionaloutcome,sug-gesting that cognition should be part of the focus duringthetreatmentofschizophrenia(37).Ifoneoperatesonthebasis that social cognitivedeficitsare linked to short-termclinicaloutcome,psychosocialinterventionsshouldincludeelements of psychoeducation about the illness, behavioractivationtoimprovemotivation,andcognitiveremediationinordertoimproveoverallareasofneurocognitioninhopeofbetteroutcome. We have attempted to provide evidence that specificdeficits in social cognition are possible markers of poorshort-termclinicaloutcomeinFEP,andthatnotallpatientsshowanequaldeficitonallsocialcognitivemeasures.Thatis,patientsrespondingtotreatmentfunctionatlevelssimi-lartohealthyindividualsonparticularsubtests.SimilarlytotheMATRICS,thecurrentstudyidentifiedasinglesubtestfromthesocialcognitiondomain—theCartoonPredictionstask—whichappearstobeusefulforidentifyingapoorout-comeinashort,twelve-minuteevaluationsession.However,additional studieswillbeneeded in the future inorder tosupportthecurrentfindings.
Acknowledgments
This study was supported by operating grants fromCIHR (#68961) and the Sackler Foundation to Drs. M.Lepage/A.K.Malla.M.LepageissupportedbyasalaryawardfromFRSQ.A.K.MallaissupportedbytheCanadaResearchChairsprogram.WethankthePEPP-Montrealresearchstaff

Social Cognitive Markers of Clinical Outcome
00 • Clinical Schizophrenia & Related PsychosesJuly2010
for theirhelpwithrecruitmentandclinicalassessmentsofpatients.
ReferencesLieberman J, Jody D, Geisler S, Alvir J, Loebel A, Szymanski S, et al. Timecourseandbiologiccorrelatesoftreatmentresponseinfirst-episodeschizo-phrenia.ArchGenPsychiatry1993;50(5):369-376.
Rosen K, Garety P. Predicting recovery from schizophrenia: a retrospectivecomparisonofcharacteristicsatonsetofpeoplewithsingleandmultipleepi-sodes.SchizophrBull2005;31(3):735-750.
GoldbergTE,GreenMF.Neurocognitivefunctioninginpatientswithschizo-phrenia:anoverview.In:DavisKL,CharneyD,CoyleJT,NemeroffC,editors.Neuropsychopharmacology:thefifthgenerationofprogress.Nashville(TN):AmericanCollegeofNeuropsychopharmacology;2002.p.657-669.
GoldJM,GreenMF.Neurocognitioninschizophrenia.In:SadockVA,editor.KaplanandSadock’scomprehensivetextbookofpsychiatry.8thed.Baltimore:Lippincott,Williams&Wilkins;2002.p.1426-1448.
GreenMF.Whatarethefunctionalconsequencesofneurocognitivedeficitsinschizophrenia?AmJPsychiatry1996;153(3):321-330.
GreenMF,KernRS,BraffDL,MintzJ.Neurocognitivedeficitsandfunctionaloutcomeinschizophrenia:arewemeasuringthe“rightstuff ”?SchizophrBull2000;26(1):119-136.
MallaAK,NormanRM,ManchandaR,TownsendL.Symptoms,cognition,treatmentadherenceandfunctionaloutcomeinfirst-episodepsychosis.Psy-cholMed2002;32(6):1109-1119.
AddingtonJ,SaeediH,AddingtonD.Thecourseofcognitivefunctioninginfirstepisodepsychosis:changesovertimeandimpactonoutcome.SchizophrRes2005;78(1):35-43.
NuechterleinKH,BarchDM,GoldJM,GoldbergTE,GreenMF,HeatonRK.Identificationofseparablecognitivefactorsinschizophrenia.SchizophrRes2004;72(1):29-39.
BertrandMC,AchimAM,HarveyPO,SuttonH,MallaAK,LepageM.Struc-turalneuralcorrelatesofimpairmentsinsocialcognitioninfirstepisodepsy-chosis.SocNeurosci2008;3(1):79-88.
PennDL,CorriganPW,BentallRP,RacensteinJM,NewmanL.Socialcogni-tioninschizophrenia.PsycholBull1997;121(1):114-132.
CorriganPW,PennDL.Socialcognitionandschizophrenia.Washington,DC:AmericanPsychologicalAssociation;2004.
AddingtonJ,SaeediH,AddingtonD.Influenceofsocialperceptionandsocialknowledgeoncognitiveandsocial functioning inearlypsychosis.Br JPsy-chiatry2006;189:373-378.
WilliamsLM,WhitfordTJ,FlynnG,WongW,LiddellBJ,SilversteinS,etal.Generalandsocialcognitioninfirstepisodeschizophrenia:identificationofseparablefactorsandpredictionoffunctionaloutcomeusingtheIntegNeurotestbattery.SchizophrRes2007;99(1):182-191.
BertrandMC,SuttonH,AchimAM,MallaAK,LepageM.Socialcognitiveimpairmentsinfirstepisodepsychosis.SchizophrRes2007;95(1-3):124-133.
BrekkeJ,KayDD,LeeKS,GreenMF.Biosocialpathwaystofunctionalout-comeinschizophrenia.SchizophrRes2005;80(2-3):213-225.
CoutureSM,PennDL,RobertsDL.Thefunctionalsignificanceofsocialcog-nitioninschizophrenia:areview.SchizophrBull2006;32(Suppl1):S44-63.
Corcoran R, Mercer G, Frith CD. Schizophrenia, symptomatology and so-cial inference: investigating “theoryofmind” inpeoplewith schizophrenia.SchizophrRes1995;17(1):5-13.
RubinszteinJ,MichaelA,PaykelES,SahakianJ.Cognitiveimpairmentinre-missioninbipolaraffectivedisorder.PsycholMed2000;30:1025-1036.
CassidyC,RabinovitchM,JooberR,MallaA.Acomparisonstudyofmultiplemeasuresofadherencetoantipsychoticmedicationinfirstepisodepsychosis.SchizophrRes2008;98(1):81.
MallaA,NormanR,McLeanT,ScholtenD,TownsendL.ACanadianpro-grammeforearlyinterventioninnon-affectivepsychoticdisorders.AustNZJPsychiatry2003;37(4):407-413.
O’SullivanM,GuilfordJP.Fourfactortestsofsocialintelligence(behavioralcognition):manualof instructionsandinterpretations.Orange(CA):Sheri-danPsychologicalServices,Inc.;1976.
Bodnar M, Malla A, Joober R, Lepage M. Cognitive markers of short-termclinicaloutcomeinfirst-episodepsychosis.BrJPsychiatry2008;193(4):297-304.
FirstMB,SpitzerRL,GibbonM,WilliamsJBW.StructuredclinicalinterviewforDSM-IVAxisIdisorders,patientedition(SCID-I/P&SCID-I/NP),Ver-sion2.NewYork:NewYorkPsychiatricInstitute,BiometricsResearch;1998.
AndreasenNC.Scalefortheassessmentofpositivesymptoms(SAPS).IowaCity:UniversityofIowa;1984.
Andreasen NC. Modified scale for the assessment of negative symptoms(SANS).IowaCity:UniversityofIowa;1984.
MallaA,NormanR,SchmitzN,ManchandaR,Bechard-EvansL,TakharJ,etal.Predictorsofrateandtimetoremissioninfirst-episodepsychosis:atwo-yearoutcomestudy.PsycholMed2006;36(5):649-658.
Miller DC. Handbook for research design and social measurement. 5th ed.NewburyPark(CA):SagePublications;1991.
VisserBA,AshtonMC,VernonPA.Beyondg:puttingmultipleintelligencestheorytothetest.Intelligence2006;34(5):487-502.
SPSS.SPSSforWindows,release12.0.1.Chicago,IL:SPSS;2003.
Green MF, Olivier B, Crawley JN, Penn DL, Silverstein S. Social cognitionin schizophrenia: recommendations from the measurement and treatmentresearchtoimprovecognitioninschizophrenianewapproachesconference.SchizophrBull2005;31(4):882-887.
OstromTM.Thesovereigntyofsocialcognition.In:SrullTK,editor.Hand-bookofsocialcognition.L.ErlbaumAssociates:Hillsdale(NJ);1984.p.1-37.
PremackD,WoodruffG.Chimpanzeeproblem-solving:atestforcomprehen-sion.Science1978;202:532-535.
Brüne M. Emotion recognition, ‘theory of mind,’ and social behavior inschizophrenia.PsychiatryRes2005;132(2):135-147.
VerdouxH,LiraudF,AssensF,AbalanF,vanOsJ.Socialandclinicalconse-quencesofcognitivedeficitsinearlypsychosis:atwo-yearfollow-upstudyoffirst-admittedpatients.SchizophrRes2002;56(1-2):149-159.
SchwartzJE,FennigS,Tanenberg-KarantM,CarlsonG,CraigT,GalambosN,etal.Congruenceofdiagnoses2yearsafterafirst-admissiondiagnosisofpsychosis.ArchGenPsychiatry2000;57(6):593-600.
GoldJM.Cognitivedeficitsastreatmenttargetsinschizophrenia.SchizophrRes2004;72(1):21-28.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
Related Documents











